Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday 7 th July 2016
|
|
|
- Rosamond Joanna Wiggins
- 6 years ago
- Views:
Transcription
1 Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday 7 th July pm-3.45pm Conference Room 1, Trafalgar House, King Street, Dudley DY2 8PS
2 PUBLIC MEETING OF THE TRUST BOARD 1.00pm, Thursday 7 th July 2016 Conference Room 1, Trafalgar House AGENDA Culture and Conduct Protocol We are a values-led Board. We place quality of care and safeguarding the needs of our patients at the heart of everything we do. We work consciously as a team to support and constructively challenge each other in the best interests of service users, their carers and families. We champion the interests of staff and acknowledge that they are working well in challenging times. We seek to ensure value for money at all times through efficient use of our resources in the delivery of services and achievement of standards. We welcome the rigour of debate with fellow Board members, drawing upon a range of different experiences and perspectives and applying the Nolan principles of Selflessness, Integrity, Objectivity, Accountability, Openness, Honesty and Leadership. ITEM Purpose Board Lead Format Timings 1. Expert by Experience Reflection Ms Ingram Presentation 1.00pm 2. Apologies Mr Reid Oral 1.30pm Declarations of Interest For Board members to declare any relevant interests in items on the agenda Minutes of the Previous Meeting To approve the minutes of the Board meetings held on 1 June 2016 and 22 June 2016 Summary Report of Confidential session of Trust Board held on 1 June 2016 Approval Mr Reid Mr Reid Oral Enc 1 Enc 1A 1.35pm Information Mr Reid Enc pm 6. Matters Arising/Action Schedule Continuity Mr Reid Enc 3 7. Chief Executive Officer s Overview (including written summary of strategic publications and headlines) Information Mr Axcell/PLG Enc pm 8. QUALITY, SAFETY, EFFICIENCY & EFFECTIVENESS 8.1 Trust Integrated Performance Dashboard (Month 2) Asurance Mr Davies Enc pm a b c Quality Quality and Safety Committee Chairs Report Audit Committee Chairs Report Quality Report Assurance Dr Murphy Mr Matthews Mrs Pugh Enc 6 Enc 7 Enc pm a b Finance, Performance and Workforce Finance & Performance Committee Chairs Report Finance Report Assurance Mr Higgs Mr Davies Enc 9 Enc pm
3 c d e ff ITEM Purpose Board Lead Format Timings PbR Update Contract Performance Performance Dashboard CIP PMO Report Workforce Report Mr Davies Mr Davies Mr Davies Mrs Ingram Enc 11 Enc 12 Enc 13 Enc Medical Directors Report Assurance Dr Gingell /Dr Weaver Enc pm 8.4 Director of Operations and Nursing Report Assurance Ms Pugh Enc pm 8.5 Enhancing Quality through Safer Staffing Levels - Monthly Exception Report Assurance Ms Pugh/ Enc pm 9. STRATEGIC DEVELOPMENT & DIRECTION 9.1 High Level Operational Risk Register Approval Ms Pugh Enc pm 10. LEADERSHIP, CULTURE & WORKFORCE 10.1 Agency Update 2016/17 Assurance Mr Davies / Enc pm 10.2 Service Experience Desk Annual Report 2015/16 Assurance Ms Ingram Enc pm 10.3 Annual Review of Board Committee Terms of Reference Approval Mr Lewis- Grundy Enc pm 10.4 Staff Engagement and Raising Concerns Board Update Assurance Ms Ingram Enc pm 11. FOR ASSURANCE 11.1 MExT & EMeXT Chair s Report 12. ANY OTHER BUSINESS Assurance/ Information Mr Axcell Enc pm 13. QUESTIONS FROM MEMBERS OF THE PUBLIC Oral Questions from members of the public pertaining to agenda items. 3.45pm 16. DATE AND TIME OF THE NEXT MEETING Wednesday 3 rd August 2016, The Board Room, Canalside, Bloxwich WS3 3BW
4
5 Enc 1 MINUTES OF THE TRUST BOARD MEETING OF DUDLEY AND WALSALL MENTAL HEALTH PARTNERSHIP NHS TRUST Held at 1.00pm on Wednesday, 1 st June 2016 The Board Room, Canalside, Bloxwich Present Mr B Reid Mr M Axcell Ms O Clymer Mrs G Cooper Mr R Davies Dr Gingell Mr Higgs Ms Ingram Mr D Matthews Ms W Pugh Mr Rana Dr M Weaver PUBLIC SESSION Chair Acting Chief Executive Officer Associate Non-Executive Director (non-voting) Non-Executive Director Interim Director of Finance, Performance and IM & T Joint Medical Director Non-Executive Director Director of People & Corporate Development Non-Executive Director Director of Operations, Nursing and Estates Associate Non-Executive Director (non-voting) Joint Medical Director In Attendance Mr Paul Lewis-Grundy Mrs Linda Wix Company Secretary Minute Taker ITEM ACTION WELCOME 32. The Chair welcomed the member of the public to the meeting. 33. PATIENT STORY Ms Ingram advised that the Trust took patient stories in various formats, previously this had included audio and a flipagram. The patient story presented this quarter was in written format and had been circulated with the Agenda. Posters were displayed in public areas around the Trust inviting patients and/or carers to share their experiences whether they were complimentary or complainant in nature. She provided an overview of the patient story and invited questions. The Chair advised that where possible his preference would be to invite the patient or carer to deliver their story in person to the Board. He queried the process for addressing the issues raised. The Chair stated that the patient story should be a powerful experience with the ability for the Board to Page 1 of 16
6 demonstrate action taken on issues raised. Ms Pugh confirmed that investigations into issues from patient stories were taken forward by the Quality & Safety Committee. Ms Ingram advised that the Board had recently signed off the patient story management protocol and this included feedback to the patient. RESOLVED: That the Board noted the content of the patient story. 34. APOLOGIES An apology for absence were recorded from Dr S Murphy, Non-Executive Director 35. MINUTES OF THE PREVIOUS MEETINGS The minutes of the meeting held on 5 th May 2016 were agreed as an accurate record, subject to the following amendments: Minute 24 Chief Executive Officer s Update The word citation to replace the word nomination Minute 25.1 Trust Integrated Dashboard- Finance Report 1m shortfall to be changed to 1m shortfall in income. Continuity of service was very strong and financial sustainability was sound to be added to Mr Higgs comments. The minutes of the Extraordinary Trust Board meeting held on 23rd May 2016 were agreed as an accurate record. RESOLVED: That the minutes of the meetings held on 5 May 2016 and 23 May 2016 be approved subject to the amendments outlined above and would be signed by the Chair following the completion of the above amendment. 35. SUMMARY REPORT OF CONFIDENTIAL SESSIONS OF TRUST BOARD The Board noted the summary of the business transacted in the confidential session of the Trust Board held on 5 th May MATTERS ARISING 36.1 There were no matters outstanding on the schedule. The Chair requested that realistic timelines be set for Page 2 of 16
7 completion of the actions. He understood that occasionally there may be some slippage but in the main actions should be completely in a timely manner. Mr Axcell advised that his actions with a timeframe to be advised were being taken forward by the Finance and Performance Committee. Mr Matthews referred to items 4.3 & 24 that had been closed as they were being taken forward via another Committee or Board Development Sessions. He requested, and it was agreed, that for assurance and completeness, the items would be referred to in the appropriate Chairs report or Chief Executive s report as appropriate. ACTION: Actions 4.3 & 24 that were completed and closed on the Action Schedule as being dealt with via another Committee or Board Development Sessions should be referred to in the Chief Executive s report for assurance and completeness. Mr Axcell RESOLVED: That the matters arising and the assurance given, including those above, where those actions have been completed be noted. 37. NOTIFICATIONS OF ITEMS OF ANY OTHER BUSINESS There were no notifications of any other business. 38. DECLARATIONS OF INTEREST Members were asked to disclose any interest they may have, direct or indirect, in any of the items being considered during the course of the meeting and to note that those members declaring an interest would not be allowed to participate in the consideration, discussion or vote on any issue relating to that item. No interests were declared in addition to those already recorded on the Register of Interests. 39. QUESTIONS FROM MEMBERS OF THE PUBLIC There was one members of the public present, although no questions relating to the agenda items were raised. 40. CHAIR S COMMENTS The Chair advised that after spending time in the Trust he was familiarising himself with the issues facing the Trust. The partnership working that the Trust was taking part in was imperative and would help shape the organisation over the next 2 years. Page 3 of 16
8 RESOLVED: That the Board received the Chair s update for information and assurance. 41. CHIEF EXECUTIVE OFFICER S OVERVIEW Mr Axcell referred to the following: CQC Inspection Report Mr Axcell advised that the final CQC had been received and the Trust had been rated as requiring improvement. Whilst this was disappointing it was noted that the report contained many positives. He referred to some specific areas highlighted in the report. A CQC action plan was being developed and managed through Q&S committee. A number of the actions had already been completed. Once all the actions were complete the CQC would be invited to review the areas that were rated as required improvement. A Quality Summit would be held in July with Stakeholders, Commissioners, NHS Improvement and Board members being invited to attend. Ms Pugh anticipated that the further visit from the CQC would take place approximately 6 months after the Quality Summit. The Chair stated that clarity was required on the agreed timescales and Board members needed assurance that the actions were complete and the actions taken to realise the improvements. He requested, and it was agreed, that the CQC Action Plan would be circulated to members in advance of the normal Trust Board paper circulation date to keep members up-to-date and included as an agenda item at the next meeting. Mr Axcell confirmed that this would be circulated week commencing 6 June ACTION: CQC Action Plan to be circulated to members in advance of the normal Trust Board paper circulation date week commencing 6 June 2016, and included on the agenda for the July Trust Board meeting. Ms Pugh Ms Pugh stated she would welcome feedback or comments from Board members related to the CQC Action Plan. The Chair advised Mr Matthews that time during Board Development Sessions would be identified to discuss the Action Schedule in detail, identifying recurring themes and how to do things differently. Junior Doctors Contract Mr Axcell advised that the junior doctors contract had been Page 4 of 16
9 agreed subject to a vote by BMA members and the cost implications would be discussed in depth by the Finance & Performance Committee. MERIT & Dudley CCG Vanguard The MERIT Vanguard had now received the outcome from the submitted value proposition, which had resulted in a reduced level of funding. The MERIT Vanguard Partnership had requested 3.4m of funding and had been offered 1.7m. Dudley MCP Vanguard Partnership had requested 9m of funding and had been offered 4.4m of funding. prioritisation work had been done to ensure that the Vanguard continued to meet its key aims during 2016/17. Transforming Care Together Mr Axcell confirmed that the TCT partnership board continued to meet on a monthly basis. The focus was on ensuring that the clinical workstreams were up and running after the success of the clinical stakeholder event. Further detail and greater clarity would be forthcoming over the next few months. The Board would discuss the various aspects, including resources, during Board Development sessions. Mrs Cooper requested that draft plans be shared with Board members for comment. The Chair asked that the Chief Executive s report would reflect the views of the Board on the draft plans. ACTION: Draft plans from the TCT to be shared with members for comment. The CEO s report in July to reflect the views of the Board on the draft plans. Mr Axcell RESOLVED: That the Board noted the information and actions contained with the report That the Board noted the specified actions and timescales identified throughout the report for assurance. 42. QUALITY, SAFETY, EFFICIENCY & EFFECTIVENESS 42.1 Trust Integrated Performance Dashboard Month 1 Mr Davies took the Board through the key points, issues, and risks, as set out within the Performance Report and Dashboard. For the benefit of the public member he provided an overview of the purpose of the reports. He referred to the Adverse RAG rating related to resources. Mr Higgs advised that this had been reviewed by the Finance & Performance Committee. Contract Performance Report Page 5 of 16
10 Mr Davies took the Board through the performance report drawing attention to Page 3. The red rated issues for KPIs 16 (ICD 10 diagnosis) & 18 (cluster review periods) related to Walsall and was showing an adverse trend against target with the issue reviewed by the Finance & Performance Committee. Referring to KPIs 23 (Memory Assessment Service) & 24 (Dudley & Walsall Recovery Outcomes) he advised that these were new issues. Mr Higgs said the issues related to the Memory Assessment Service and Dudley & Walsall Recovery Outcomes had been queried at Finance & Performance Committee and may be attributable to the Junior Doctors Strike. Dr Weaver and Dr Gingell stated that the services would return to normal now that the dispute had been settled. The Chair queried actions being taken to address KPIs 16 & 18. Mr Higgs stated that they were cultural issues. Dr Weaver concurred, adding that there were also logistical issues. Some teams were coping well with clustering, whilst others continued to struggle and focus was on the latter to understand the reasons and an implementation plan put in place to bring them to the required level in a short space of time. Mr Axcell stated that there had been a significant improvement over the preceding year, although there had been a dip recently. Remedial work was being undertaken with those individuals identified as struggling. Finance Report Mr Davies drew attention to the key messages The Trust had delivered a Month 01 surplus of 66k which represented an on-line trajectory with the planned surplus for the year of 700k. Pay expenditure was 29k in deficit against budget Year To Date. Bank & Agency spend equated to 579k in month (split 470k for Agency and 129k for Bank). Agency spend was ahead of plan in relation to the overall 4.05m Agency tolerance for the year (actual spend of 470k against 507k plan to date). Mr Davies confirmed that there was an action plan in place to ensure that the Trust compiled with the Agency Cap and that the Trust was committed to utilising only those agencies that applied the Cap. Non-Pay expenditure was 29k in deficit surplus against budget Year To Date. Reserves were overspent reflecting the impact of undevolved CIP yet to be allocated down to service lines. Profiling of CIP savings across the year was being developed for reporting to future Board meetings. The Trust wide activity position at year end was reflecting an under-performance of 18k. The Net position was an over-performance of 38k, however, after taking account of the impact of the CIP Page 6 of 16
11 target that had been applied to activity, being 59k, overall performance is behind target Mr Axcell advised that at Month 1 the Trust was 37k ahead of plan in terms of anticipated agency spend ( 470k spend against 507k plan). This was an improving trend although the Finance & performance Committee would keep this under review. The Chair stated that as this was a national target the Board should ensure that the Finance & performance Committee were reporting back to the Board appropriately. The Chair queried the 50% agency usage labelled as other. He was used to agency staff being utilised for clinical posts however was less clear about the use of agency staff to cover for example estates and corporate posts. For clarity he requested, and it was agreed, that the substantive posts covered by agency staff in the other category be identified and reviewed by the Finance & Performance Committee before being reported to the next Board meeting. Mr Davies ACTION: that the substantive posts covered by agency staff in the other category be identified and reviewed by the Finance & Performance Committee before being reported to the next Board meeting. In response to a query from Ms Clymer, Mr Davies reiterated that the Trust would give preference to those agencies keeping within the cap. The Chair commented that permission was required to use agencies with higher fees. Ms Ingram advised that it was not possible to state categorically that the Trust would not break the rules if there were patient safety implications. Dr Weaver advised that previously he had commented that the Trust may lose agency locums that had worked for the Trust in the long term. He was pleased to report that this had not been the case. In response to a query from Mr Rana, Mr Davies advised that the benefit of the agency cap was already having a positive impact on the Trust financially, although continuation of this was dependent on a successful recruitment programme. Mr Axcell advised Mr Higgs advised that backfill for nonrecurrent projects was under discussion with Commissioners. Quality Governance Report Ms Pugh advised that incidents related to disruptive aggressive patients had increased. A focus group to review this increase would report back to the Quality & Safety Page 7 of 16
12 Committee. There had been a number of Serious incidents, two of which related to under 18 admissions and these had been reported to specialised commissioning. Work was being undertaken on the increase in serious incidents and findings would be reported to the Quality & Safety Committee in August. An Abscond group had re-formed due to the number of absconds and failure to return from leave. Ms Pugh advised Ms Clymer that body mapping was undertaken to identify skin integrity issues and identify where these occurred. She confirmed that they had not originated within the Trust. The Trust was required to report to NHSI on any pressure ulcers that originated within the Trust. Ms Clymer drew attention to the duty of candour incident, commenting that this had not been reported in the Integrated Performance Dashboard. Mr Davies confirmed that there would be parity between the reports in future. Workforce Report: Vacancies There were 175 FTE contracted vacancies across the Trust, meaning the overall vacancy rate remained at 16%. Contracted vacancies across the Trust had reduced from 224 FTE in May The Trust had set a 10% vacancy rate target and Ms Ingram advised that it was unlikely that this target would be met by the end of quarter 1. The Trust, along with other organisations was experiencing difficulties in recruiting to some areas. There had been a useful session at the recent Director Of Nursing away day with agreement to risk assess vacancies identifying those posts to be actively recruited to. Ways in which the recruitment process could be improved would be reported to Finance & Performance Committee. Mr Higgs confirmed that issue had been discussed in detail and the Trust was recruiting to 7 posts per month, although turnover was 11 or 12 per month. Ms Clymer commented that because the Trust offered flexible working for staff however cumulatively this impacted on the Trust, affecting the number of whole time equivalent staff in post. Ms Pugh advised that a number of initiatives were being considered, including HCA progression via the LEAP programme and assisted practitioners and on-going work with Universities. Mr Rana stated that back office functions and front line staffing figures should be separated out as the trends may have differed and the approach to recruitment may also need to be different. He emphasised the benefits in employing Apprentices to particularly back office functions. ACTION: Separate front line and back office staffing figures in future reports. Ms Ingram Page 8 of 16
13 The Chair advised that there should be a co-ordinated plan in place. A change in language was required and recruitment should be to 110% to offset turnover. Employing staff in substantive posts would reduce agency spend and cost. The strategy on nursing should be specific on recruitment and upskilling. Turnover The 12 Month turnover rate at the end of month 1 had decreased to 14.86% from 15.54%. The 12 month turnover rate compared reasonably to that of MERIT partners 15.6%, 13.7% and 13.5% respectively. Sickness Absence The 12 month rolling sickness rate had decreased to 4.82% in Month 1 from 4.86% reported in Month 12. Appraisal Compliance in Month 1 had reduced to 69.1% and was below Trust target (85%). The Executive Team were implementing focussed actions to improve compliance. Mandatory Training - Mandatory Training compliance was 81.7% as at the end of Month 1, which was below the new target of 90% agreed at MEXT for all mandatory training. RESOLVED: That the Board noted the performance of the Trust as at month Medical Directors Report Dr Weaver took the Board through the Medical Directors report. Junior Doctors contract Referring to the appointment of a Guardian of Safe Working, Dr Weaver advised that the potential of having a shared arrangement for this post with the Black Country Partnership NHS Foundation Trust would be discussed. Review of how Trusts investigate and learn from deaths In line with a request from the Secretary of State, the deaths of people with learning disability or mental health problems were being reviewed by the Mortality Review Group. Local matters Dr Weaver was pleased to report that 4 Foundation trainees who were based at Bushey Fields Hospital had embarked on a career in psychiatry. At least 2 foundation trainees at the Dorothy Pattison Hospital had also obtained posts in psychiatry in the past year. Transcranial Magnetic Stimulation. This was a non-invasive treatment and feedback from patients Page 9 of 16
14 had been positive. There were private treatment centres in operation as well as within the NHS. Set up costs were quite small with a course of treatment costing between 3-4k. He would keep this under review as a potential service provision going forward. Mortality The Mortality Review Group reviewed 12 deaths during April using data received from a number of electronic sources. The Chair queried whether the Board had previously adopted policy on review of deaths, the investigation protocol, those involved and the stages undertaken and completed. Dr Gingell advised that the work undertaken by the Mortality Review Group was fast paced with a clear process and this would be outlined to the Board as part of a future Medical Directors report ACTION: The process of the review of deaths followed by the Mortality Review Group on behalf of the Trust to be included in a future Medical Directors Report Dr Gingell/Dr Weaver Mrs Cooper asked for it to be noted that every single death in the Trust was treated as serious incident, protocol followed, and reviewed by Board. In response to a question from Ms Clymer related to a suspension from ligature incident, Ms Pugh advised that the Trust had a ligature policy. Following the reported incident the Trust worked with police on the investigation and a strategy meeting was held within 72 hours of the incident. There was a full investigation with the involvement of the Trust s commissioners. RESOLVED: That the Board received the update for information and assurance Nurse Director s Report Ms Pugh took the Board through the main points within the Nurse Director s report: On the 18 May, 2016, the chief nursing officer for England announced a new four-year plan for nurses, midwives and care workers. The new framework called Leading Change, Adding Value was centered on 10 commitments. The key characteristics of those commitments would be reviewed against the 5 year plan. RESOLVED: That the Board received the update for information and assurance. Page 10 of 16
15 42.4 Monthly Ward Staffing Levels Report Ms Pugh presented the report advising that there had been two wards to note as exceptions: Malvern Ward - where the staff fill rate in part was within the lower category Clent Ward - where the fill rate was part in the high range for care staff on days and nights. She confirmed that safe staffing levels were maintained with two registered nurses on Malvern and additional care staff. due to sickness. There had been increased patient acuity and raised levels of observations. A substantial amount of time was being utilised for agency staff to be inducted, taking 3 to 4 hours. A Focus Group was working with agencies to undertake induction prior to agency staff working within the Trust. In response to Ms Clymer s comments about the commonality in the environments across different wards Ms Pugh advised that where possible the environment and for example the storage of emergency equipment was consistent across the Trust. She also confirmed that changes to the in house staff bank were beginning to have a positive impact on the safer staffing requirements. In response to Mr Axcell s question, Mrs Pugh advised that the collation of data was still manual and the data sources would be reviewed and compared to electronic rostering. Ms Pugh confirmed to Mr Higgs that the E-Rostering roll out had been successful although there were cultural difficulties and not all modules had been completed by ward managers. She anticipated a complete roll out of E-Rostering by September RESOLVED: That the Board received the report for information and assurance Cost Improvement Programme (CIP) progress Report Mr Davies advised that there were 32 projects in 2015/16 of which 30 had been delivered and closed down. Two schemes had been carried over into 2016/17 at the request of the Executive Sponsor: POD085 Catering Review POD088 Corporate Clinical Leadership Structures There were 28 project identified for 2016/17 with projected savings of 2.7m. There were 10 red RAG rated schemes in month 1 and delivery of these schemes would be challenging. Page 11 of 16
16 The impact of these schemes was limited and the Programme Board would need to ensure that the schemes moved from red to an amber/green rating. There were some amber rated schemes that may need to be altered to a red rating. There was therefore a need to ensure that new schemes were identified if required. The CIP Project Board was also focussing on schemes that overlap with the QIPP schemes for Walsall CCG. Mr Matthews stated that the commentary did not provide assurance on whether scheme would deliver the targeted saving. Mrs Cooper expressed concern that a rigorous CIP selection process had been followed with the appropriate scrutiny and risk assessments carried out and queried their inclusion in the programme if they were failing in month 1. Mr Higgs stated the red rag rated CIPs were in excess of 1m and reserves were not available to offset these. Mr Axcell understood the concern expressed by the Non-Executive Directors and advised that identification of CIPs should begin earlier in the year to enable a robust testing regime to be undertaken. Ms Ingram advised specifically that the Employment Support CIP had involved removing a management post from the structure; however the service was a priority for the West Midlands combined authority and the Executive Team had concluded that the moving the post from a small team would be counter-productive as the team did generate income. RESOLVED: That the Board received the report for information and assurance. 43. STRATEGIC DEVELOPMENT & DIRECTION 43.1 High Level Operational Risk Register Ms Pugh advised that the following risks were approved following risks for inclusion on the High Level Operational Risk Register: o 202 o 225 o 253 o FINAN 1 o HR 002 o 285 o Risk 301 The Trusts Finance and Performance Committee also reviewed the red risks which had links to the Trusts to finances and to Trust performance on 21 st March. These were Risks: 202 Page 12 of 16
17 253 FINAN 1 Risk 301 The Estates risks were being reviewed by the Quality & Safety Committee although there were no recommendations for changes to the risks at this time. The Chair requested that future reports should have narrative on the existing mitigations against the red risks and the further actions necessary, including the financial impact to mitigate the red rated risks. Ms Pugh advised that this would be considered through the appropriate Committee and report progress to the Board in July. ACTION. Future reports should have narrative on the existing mitigations against the red risks and the further actions necessary, including the financial impact to mitigate the red rated risks. Ms Pugh RESOLVED: That the Board approved the High Level Operational Risk Register and the contents therein Review of the Trust s Clinical & Social Care Strategic Vision 44. LEADERSHIP CULTURE & WORKFORCE 44.1 Health & Wellbeing Strategy Ms Ingram advised that the Trust employed over 1000 staff, including a number of volunteers and contractors, and was committed to the health and wellbeing of our staff recognising the vital role they play in progressing towards delivering high quality services and excellent patient experience. She confirmed that were Board minded to approve the strategy the implementation plan (Appendix 2) would, with the additional of appropriate timescales, become the in year delivery plan including outcomes. Mr Rana commented that had witnessed great enthusiasm and support for change within the Trust. The strategy would require funding and a further report would be received by the Board in this regard. Both Mr Axcell and Mrs Cooper expressed concern that stress, anxiety and depression were the highest reasons given for sickness absence. RESOLVED: That the Board received the report for information and assurance. approved the Health & Wellbeing Strategy Page 13 of 16
18 45. FOR ASSURANCE 45.1 Quality & Safety Committee Chair s Report The Chair noted the recommendation from the Committee that the Trust undertakes an assessment against the QGAF on a 6 monthly basis and that the next assessment was due at the end of Quarer 1. Mr Lewis-Grundy advised that this was an internal review and was an item for discussion at the Board Development session in July for reporting to the Quality & Safety Committee in August and Board in September. RESOLVED: That the Board accepted the report for assurance and endorsed the decisions and recommendations made by the Committee Finance and Performance Committee Chair s Report Mr Higgs took the Board through the Finance and Performance Committee Chair s report advising that NHS activity overall had increased by 6%. The level of overperformance in Walsall had been limited each month to 43k in line with the contractually agreed cap and collar arrangement of 500k for the financial year. Agency spend had been discussed in light of the NHSI agency cap of 4.05m. The target spend for the month was 507k across all agency staff groups and the Trust had spent 470k, reflecting a 30k favourable variance, however, it was noted that the plan was more generous in the first quarter of the year in line with the workforce plan for recruitment. Thus actions to reduce agency spending must continue throughout the year. There was concern related to cash flow which had reduced by 900k in month. The Committee noted that the level of un-clustered activity (cluster 99 s) had seen an adverse movement as compared to last month. Based on the current position the projected level of un-clustered activity would be well above the planned 700k target. RESOLVED: That the Board accepted the report for assurance and endorsed the decisions and recommendations made by the Committee MExT Chair s Report Mr Axcell asked the Board to take the report as read and there were no questions related to this item. Page 14 of 16
19 RESOLVED: That the Board received the report for information and assurance Mental Health Act Scrutiny Committee Chair s Report Mrs Cooper advised that the Committee had added a new risk to register related to training for assessments for DoLS. Policies related to the Mental Health Act code of practice required updating. RESOLVED: That the Board received the report for information and assurance MERIT Vanguard NED Assurance Group Mr Matthews advised that the Group had sought assurance on the risk on any claw back of funding. It was confirmed that this risk was considered to be relatively low, with the appropriate governance arrangements in place and audit trail to demonstrate the beneficial outcome from the work streams. There had been discussion about the requirement of partners to meet their control totals. It was confirmed, following a representation made about managing control totals within the partners, that the partnership was awaiting confirmation of this from NHS England. The Group asked for confirmation on this to be provided to the NED assurance group alongside detail of any other perceived deal breakers. RESOLVED: That the Board received the report for information and assurance Audit Committee Chair s Report Mr Matthews advised that the Audit Committee had approved the Annual Report, Accounts and Annual Governance Statement and this was endorsed by the Board at the Extraordinary Trust Board held on 23 May. The Internal Auditors had initiated changes to the team in line with the requests made by the Trust. The Older Adults service Audit had been referred to the Finance & Performance Committee. RESOLVED: That the Board received the report for information and assurance. Page 15 of 16
20 46. ANY OTHER BUSINESS The chair advised that the agendas were being re-ordered and he would be asking the Chairs of the Board Sub committees to provide an overview of any in depth discussions held by the Committee members at the beginning of each Trust Board meeting. 47. DATE AND TIME OF NEXT MEETING An Extraordinary Trust Board meeting would be held on Wednesday, 22 June 2016 at 11.30am in Conference Room 1, Trafalgar House, King Street, Dudley to sign off the quality accounts. The next Trust Board meeting would take place at 1.00pm on Thursday, 7 th July 2016 in Conference Room 1, Trafalgar House, King Street, Dudley DY2 8PS Meeting closed at Signature.. Date. Mr B Reid, on behalf of the Dudley and Walsall Mental Health Partnership NHS Trust Board Page 16 of 16
21 Enc 1A MINUTES OF THE EXTRAORDINARY TRUST BOARD MEETING OF DUDLEY AND WALSALL MENTAL HEALTH PARTNERSHIP NHS TRUST Held on Wednesday, 22nd June 2016 at 12.10pm Conference Room 1, Trafalgar House, King Street, Dudley Present Mr D Matthews Mr M Axcell Mr R Davies Ms Ingram Dr S Murphy Dr M Weaver PUBLIC SESSION Chair & Non-Executive Director Acting Chief Executive Officer Interim Director of Finance, IM&T Director of People & Corporate Development Non-Executive Director Joint Medical Director In Attendance Mr Paul Lewis-Grundy Mrs Linda Wix Company Secretary Minute Taker ITEM 48. APOLOGIES ACTION Apologies for absence were recorded for Mr Ben Reid, Chair, Mrs Gill Cooper, Non-Executive Director, Mr Mike Higgs, Non- Executive Director, Ms O Clymer, Associate Non-Executive Director, Dr Gingell, Joint Medical Director. Mr Pawiter Rana, Associate Non-Executive Director, Ms Wendy Pugh, Director of Operations and Nursing. 49. ELECTION OF CHAIR Mr Lewis-Grundy advised that apologies had been submitted by the Chair and the Deputy Chair and in accordance with the Standing Orders there was a need to appoint a Chair for the meeting. Dr Murphy nominated Mr Matthews. This was seconded by Mr Axcell. The motion was carried. MR Matthews took the Chair and sought confirmation that the meeting was quorate. Mr Lewis-Grundy confirmed this to be the case. 50. DECLARATIONS OF INTEREST Members were asked to disclose any interest they may have, direct or indirect, in any of the items being considered during the course of the meeting and to note that those members Page 1 of 3
22 declaring an interest would not be allowed to participate in the consideration, discussion or vote on any issue relating to that item. No interests were declared in addition to those already recorded on the Register of Interests /16 QUALITY ACCOUNT Ms Musson presented the item advising that the Draft Quality Account had been distributed via prior to the meeting. The process that was required to be followed in relation to the compilation of the Quality Account was referred to in the documentation. Feedback from Dudley & Walsall CCG was mandated and had been received. Whilst other stakeholders had been approached for feedback responses had been limited to comments from a Councillor from Walsall Council. The content in the Quality Account had been received by the appropriate internal committees and the Audit Committee had made a recommendation that the Trust Board approve the Quality Accounts. External Audit Opinion Mr Stocks advised that the Quality Account was an annual report to the public from providers of NHS healthcare about the quality of services they delivered. The primary purpose of the Quality Account was to encourage boards and leaders of healthcare organisations to assess quality across all the healthcare services they offered. It allowed leaders, clinicians, governors and staff to show their commitment to continuous, evidence-based quality improvement, and to explain progress to the public. The External Auditors were proposing to issue an unqualified conclusion on the Quality Account. He referred to the areas where feedback had been requested, advising that other Trusts were in a similar position and had not always received responses as requested. Mr Stocks confirmed that the data quality had been reviewed and as mandated, two indicators had been tested: enhancing the quality of life for people with long term conditions: the percentage of admissions to acute wards gate kept by the Crisis Resolution Home Treatment Team (CRHT) and preventing people from dying prematurely: the percentage of patients on Care Programme Approach (CPA) followed up within seven days of discharge. The Chair confirmed that there were no issues members wished to raise. Page 2 of 3
23 Mr Lewis-Grundy stated that subject to Board approval the Quality Account would be signed by the Mr Reid and Mr Axcell in accordance with guidance prior to publication by 30 th June RESOLVED: That the Board approved and adopted the Quality Account 2015/16 for publication. 53. ANY OTHER BUSINESS No items of any other business were raised. 54. DATE AND TIME OF NEXT MEETING The next Trust Board meeting would take place at 1.00pm on Thursday, 7 th July 2016 in Conference Room 1, Trafalgar House, King Street, Dudley DY2 9PS Meeting closed at 12.14pm Signature.. Date. Mr B Reid, on behalf of the Dudley and Walsall Mental Health Partnership NHS Trust Board Page 3 of 3
24 Board meeting date: 7 July 2016 Agenda Item number: 5 Enclosure: 2 Report Title: Summary of Confidential session of Trust Board held on 1 st June and 14 th June. Accountable Director: Author (name & title): Mr Ben Reid, Chair Paul Lewis-Grundy, Company Secretary Purpose of the report: Best practice in corporate governance requires that business considered in private session is reported into the public session as soon as possible. Given the arrangement of the Board meetings, the earliest opportunity is at the public session of the following month. This report outlines the business considered in private at the meeting of the Board held on 1 st June 2016 and 14 th June. Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: None Date reviewed: N/A Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Please give brief details: Best practice in corporate governance requires that business considered in private session is reported into the public session. Effective Well-led Safe Enc 2 Summary of confidential session 1st June 14 June (Final)(Final) Page 1 of 3
25 Title Summary of Confidential session of Trust Board held on 1 st June and 14 th June Introduction This report outlines the business considered at the meeting of the Board held in private on 1 st and 14 th June 2016 Summary of key points, issues and risks Financial Planning At the meeting held on 1 st June, the Board discussed the options available to achieve the NHSI stretch targets. A further meeting was held on 14 th June to finalise these discussions. Chief Executive s Summary The Board received information related to the financial targets for 2016/17. Service Development and Growth Progress report Mr Axcell referred members to the Service Development Projects and those projects within the Clinical and Social Care Strategic Vision. He drew attention to the Steps to Work project. The Board received an update on the in-house Payroll strategy. Director of Nursing Update report Ms Pugh provided an update on the water management issues. Estates Strategy Compliance This was being reviewed by MExT at the meeting in June and would be presented to the Board in July Mental Health Clinical Benchmarking Report Mr Davies advised that the NHS Benchmarking Network s 2015 benchmarking project summarised information provided for mental health services, with analysis performed on data for the financial year 2014/15. Data was submitted by all statutory mental health providers in the NHS in England, by all Health Boards in NHS Wales, by the largest Health Board in NHS Scotland, and by a number of independent sector providers. The information would be utilised in relation to the identification of CIPs and to support the Trust s work with its partners. Enc 2 Summary of confidential session 1st June 14 June (Final)(Final) Page 2 of 3
26 Partnership Update Mrs Axcell referred to: Walsall CCG workshops to address some of the challenges in the Walsall Health Economy MERIT Vanguard Transforming Care Together (TCT) Sustainability and Transformation Planning Resourcing Partnership Patient Story Update Dr Weaver provided an overview of the actions that had been taken since the Board had received the Patient Story in March The Board received and noted the minutes from the following meetings: Quality & Safety Committee held on 10 March 2016 Finance & Performance Committee held on 24 April 2016 MExT meeting held on 26 April 2016 and EMExT held 12 April. Mental Health Act Scrutiny Committee held on 21 April 2016 Chief Executive Vacancy The Board received an update on the process that would be followed to recruit to the substantive post of Chief Executive Officer. Recommendation The Board is invited to note the business transacted in the private session held on 1 st & 14 th June Board action required The Board is asked to receive this report for information. Enc 2 Summary of confidential session 1st June 14 June (Final)(Final) Page 3 of 3
27 MATTERS ARISING FROM PUBLIC MEETINGS Enc 4 Item No. 41 Date Added 1 June 2016 Action Responsibility Due Date Update Chief Executive s Overview CQC Action Plan to be circulated to members in advance of the normal Trust Board paper circulation date week commencing 6 June 2016, and included on the agenda for a future Trust Board meeting. Ms Pugh August 2016 Draft Action Plan has been circulated for comment to Board members in advance of the Quality Summit June 2016 Medical Directors Report The review of deaths process followed by the Mortality Review Group to be included in the Medical Directors Report in August. Dr Weaver/Dr Gingell August 2016 To be discussed at the BDS in July, including ToR Group & work done so far dTB 2 March April 2016 Workforce Report Report back to Board at its meeting in April of the Finance and Performance Committee discussions on alternative approaches to recruitment. Workforce Report Finance & Performance Committee to review appraisal completion rates in June with a report to the Board in July, with the emphasis on actions to be taken to ensure appraisal completion rates were improved by the end of the new financial year. Ms Ingram Ms Ingram August 2016 August 2016 Discussed at F&P on 27 June and will be an F&P Agenda item in July and reported to the Trust Board n August. Discussed at F&P on 27 June. Trajectories to feed into the workforce report in August. 1
28 Item No & 4.9TB Date Added 1 July March April Jan 2016 Action Responsibility Due Date Update Quality Implications should be included more prominently on Board and Committee reports and that quality impact assessments should have greater visibility within the report. Bed Review Report Mr Axcell advised that whilst action 75.1 had been completed in relation to Under 18 admissions, he was conscious that there was also an action pertaining to Older Adults and Acute and he requested that this be included on the Action Schedule. Mr Lewis- Grundy Sept 2016 Ms Pugh Sept 2016 Discussions are on-going with the Head of Nursing, Quality & Innovation with a view to implementation in September This was discussed at F&P on and due to the clear links with commissioning and contracts it was agreed a paper would go to the May F&P. Deferred to June 2016 Re the bed review paper. The older adults option paper will be presented to Junes F&P and therefore the recommended paper will be at the July Board. The adult review paper is being worked upon at present and will be taken to hopefully the July F&P and then the recommended paper to August/September board TB 2 March April 2016 Service Experience Desk Report A report to be submitted to the Board in September, to patients ability to complain, staff members ability to raise concerns, external drivers and best practice adopted by other Trusts Chief Executive s Overview It was agreed that the Quality & Safety Committee would review the documentation related to the freedom to speak up guardian in June with a report Ms Ingram Sept 2016 Ms Ingram September 2016 A draft of a new policy will be taken to the Staff Partnership Forum in June and to Policy Group in July. It will then go to Q&S in August then to Board. 2
29 Item No. Date Added Action Responsibility Due Date Update to the Board in July. Chief Executive s Overview & June st July Feb 2016 Draft plans from the TCT to be shared with members for comment. The CEO s report in July to reflect the views of the Board on the draft plans. Trust paper in response to the Mental Health Taskforce Strategy to be prepared. Mr Axcell Dr Gingell October nd Sept 2015 December 2016 To be incorporated when draft plans from work streams are available estimated October Board Dr Gingell advised that this was a significant piece of work to be undertaken and it would be preferable to await the appointment of the Research and Development Manager. The post would go out to advert in April or May. Joint working with MERIT partners would be considered. It was agreed that the completion date would be deferred until December Trust Integrated Dashboard May 2016 The Chair requested that a resolution to vacancy rate which was consistently higher than targeted be sought. The Chair requested that the resolution to the low appraisal completion rate be sought. Mr Axcell Mr Axcell To be advised To be advised & 4.7TB 6 Jan March Quality Governance Report Invite Board members to the Quality & Safety Committee when the findings of Ms Pugh Ms Pugh May 2016 June 2016 July 2016 There has been monitoring of incidents relating to this issue and no trends or patient safety concerns have been noted. Completed. 3
30 Item No. Date Added April 2016 Action Responsibility Due Date Update the incidents against occupancy were reported. (3-4 month timescale) Invite members to the spotlight session in Quality & Safety Committee diarised for June June 2016 July 2016 Closed. This will be monitored by Q&S and when we feel there is sufficient information or trends we will invite board members to that session. Completed. Closed June 2016 Matters Arising Actions 4.3 & 24 that were completed and closed on the Action Schedule as being dealt with via another Committee or Board Development Sessions should be referred to in the Chief Executive s report for assurance and completeness. Mr Lewis- Grundy July 2016 Included in Chief Executive Officer s Report. Completed. Closed June June 2016 Workforce Report Separate front line and back office staffing figures in future reports. Finance Report That the substantive posts covered by agency staff in the other category be identified and reviewed by the Finance & Performance Committee before being reported to the next Board meeting. Ms Ingram Mr Davies July 2016 July 2016 Figures separated out in workforce report. Completed. Closed. Information included in Agency Cap report Agenda item. Completed. Closed June 2016 High Level Operational Risk Register Future reports should have narrative on the existing mitigations against the red risks and the further actions necessary, including the financial impact to mitigate Ms Pugh July 2016 Discussed by Quality & Safety Committee. The Risk Register is an agenda item. Completed. Closed.. 4
31 Item No. Date Added Action Responsibility Due Date Update the red rated risks. 10.1aTB 6 April 2016 Contract Performance Report Drill down/deep dive results into clustering of activity to the Finance & Performance Committee in June with a report being provided for assurance to the Trust Board in July. Trust Integrated Dashboard Mr Davies July 2016 Update Report appended to the Finance Report. Agenda item. Completed. Closed May 2016 Action. Results of the Deep Dive into PbR issues to be reported to the Trust Board in July Mr Davies July 2016 Update Report appended to the Finance Report. Agenda item. Completed. Closed. 5
32 Board meeting date: 7 th July 2016 Agenda Item number: 7 Enclosure: 4 Report Title: CEO Strategic Overview and Horizon Scan Accountable Director: Author (name & title): Purpose of the report: Mark Axcell, Acting Chief Executive Paul Lewis-Grundy, Company Secretary This report summarises recent reports, publications and information, which are of relevance or interest to the Trust. It sets out the key points of each item and identifies the officer accountable for any action required and appraising the Board where appropriate. Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: N/A Date reviewed: Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Accountable workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Effective Please give brief details: The report provides information regarding latest news and relevant strategic developments that may impact all 5 CREWS domains. Well-led Safe Enc 4 CEO StrategicBrief-July2016-V5 Page 1 of 7
33 Introduction This report provides a summary of internal news from the Chief Executive and recently announced legislation, publications and information that is of interest and relevance to the Board. It identifies the Trust officer accountable for any action the Trust may be required to take and for appraising the Board where appropriate. Summary of key points, issues and risks CHIEF EXECUTIVE UPDATE Transforming Care Together The TCT partnership board continue to meet on a monthly basis. After the success of the launch event the Clinical workstreams are now starting to meet to develop their plans. The approach to these clinical discussions has been positive. Identifying best practice, learning from each other and identifying gaps in provision locally in line with the Mental Health Five Year Forward View has been the driver for the discussions. The clinical workstreams will report back in October on their recommendations. But if any quick wins are identified then these will be progressed sooner. In July the launch event for the non-clinical workstreams will take place. The timescale for these workstreams are the same with reports back in October on potential opportunities. Action: To Note MERIT and Dudley CCG Vanguard The Trust continues to be an integral part of both Vanguards. The MERIT Vanguard has now received the outcome from the value proposition, which has resulted in a reduced level of funding. MERIT had asked for 3.4m of funding and being offered 1.7m. Funding for the vanguard has been released now all organisations have signed up to the NHSI Control Total. All workstreams have continued to make good progress whilst waiting the funding decision. On the 29 th July the Merit Vanguard will hold its second event for all workstreams to review progress, share learning and review risks. The MERIT Vanguard will also be visited by NHS England National Director for Commissioning Strategy Ian Dodge during July. Dudley MCP Vanguard continues to develop its new model of care and MDT model. The Trust remains a positive partner in the vanguard. In June the Vanguard was visited by Don Berwick. Action: To Note Walsall CCG Healthy Walsall Partnership Board The second of the Clinical Summits was held in June, the areas of focus being Intermediate and End of Life Care. Action: To Note Enc 4 CEO StrategicBrief-July2016-V5 Page 2 of 7
34 Black Country & West Birmingham STP The STP plan continues to develop. The first submission of the plan was made at the end of April The full STP Plan needs to be submitted by 30 th June The mental health workstream will focus on variation, vanguard work and benefits from partnership working. Action: To Note Financial Implications of Partnership Working The assessment has now been completed and the outcomes are to be discussed as part of review of strategic options at the Board Development Session in July 2016 Action: To Note Monitor Deferral of Foundation Trust Application - Letter 2015 The Trust received a letter in 2015 following its application for Foundation Trust status advising that the application had been deferred for 12 months. The Board at a Development Session on 1 June 2016 reviewed the Trust s progress against the points raised by Monitor in its letter and concluded to request that the now NHS Improvement defer the Trust s application for a further 12 months particularly given the recent changes on the Trust s Board and its focus on addressing the recommendations in the recent CQC inspection report. It has been agreed with NHS Improvement that the Trust will withdraw from the FT process pending CQC re-inspection. Action: To Note Control Total /17 Following a request from NHS Improvement, the Trust at an extra-ordinary meeting of the Board held in private on 14 June 2016 agreed, based on a number of financial assumptions, to revise its financial plan 2016/17 to work to a trading surplus of 1.2 million. Action: To Note Estates Strategy and Compliance An estates department business case was considered by MExT at its meeting on 7 June The proposal concerned: The re-organisation of the Estates Department to ensure that it is fit for purpose to deliver the Trusts strategic objectives and mitigate risks that have been identified. A request for further investment in statutory areas of estates functions to ensure the Trust remains complaint The overall aim of the proposal which was supported subject to further refinement including additional work before the funding is agreed, is to improve the quality and effectiveness of the internal estates function in the Trust in support of the Trusts strategic direction, both in terms of short term requirements but also provides a stable platform for partnership working and transformation. The proposal fits with all the National policy, Health Technical Memoranda (HTM) guidance and supports compliance with the Social Care Act 2008 (Regulated Activities) Regulations 2014 (Part 3)) Care Quality Commission (Registration) Regulations 2009 (Part 4)) Regulation 15: Premises and equipment Enc 4 CEO StrategicBrief-July2016-V5 Page 3 of 7
35 It also reflects with the general approach of the organisation by providing a safe well maintained Estate, improving the experience for patients that are housed or seen in premises and will reduce the current usage of temporary staffing workforce which has benefits both financially and from quality perspective. Action: To Note NATIONAL POLICIES & STRATEGIES The following national strategies and policies have recently been issued. They are potentially relevant to the future strategic, planning and operational management of the Trust and the implications should be taken into account. Each document has been considered with the respective executive directors. This summary is not intended to incorporate all national publications, for instance those issued by National Patient Safety Agency, National Institute for Clinical Excellence or every operational directive issued by Department of Health which should be considered within the Trust by the appropriate department and necessary action taken. 1. Shaping the Future CQC Strategy for 2016 to 2021 Published by: Care Quality Commission Published on 24 May 2016 The strategy sets out an ambitious vision for a more targeted, responsive and collaborative approach to regulation so more people get high quality care Over the next five years the CQC will focus on four priorities. 1. Encouraging improvement, innovation and sustainability in care 2. Delivering an intelligence-driven approach to regulation 3. Promoting a single shared view of quality 4. Improving its efficiency and effectiveness Action: To consider implications for this Trust, particularly concerning future inspections. Web-link: Executive Director: Chief Executive / Director of Nursing, Operations and Estates Board Committee: Board and Quality and Safety Committee 2. Single Oversight Framework - Consultation Published by: NHS Improvement Published on 28 June 2016 The proposed framework which NHS Improvement is consulting on sets out: NHS I s main areas of focus in overseeing trusts How it will collect information from trusts How it will identify potential concerns with a trust s performance How it will segment the trust sector according to the level of challenge each trust faces Enc 4 CEO StrategicBrief-July2016-V5 Page 4 of 7
36 The framework also sets out how NHS I will identify where trusts may benefit from, or require, support in the key areas of quality of care, finance and use of resources, operational performance, strategic change and leadership and improvement capability. Consultation closes on 4 August 2016 at 5pm and during the consultation NHS I will run engagement events, yet to be announced, with stakeholders and to get more detailed input into the consultation. Action: Review the Consultation document and consider responding individually as a Trust or as a contribution to NHS Providers response. Clearly whether or not the Trust responds to the Consultation, there will be implications for the overall governance of the Trust as a result of the single oversight framework that will need to be worked through in due course. Web-link: _final_draft_28_06_update_cc.pdf Executive Director: Chief Executive Board Committee: Board 3. NHS Staff health and wellbeing CQUIN guidance Published by: NHS England Published on 2 June 2016 NHS England has released further guidance to help NHS organisations work towards the health and wellbeing Commissioning for Quality and Innovation (CQUIN) payment framework. To achieve the incentive, trusts are encouraged to take steps, such as introduce health and wellbeing initiatives, increase healthy food choices on premises and increase uptake of front line staff receiving the flu vaccine. Action: The guidance will be reviewed and incorporated into the implementation plan for the Staff wellbeing CQUIN, which is being led by the Associate Director of Workforce. Web-link: Executive Director: Director of People and Corporate Development Board Committee: Finance & Performance Committee 4. Freedom to Speak Up guardians purpose and key principles of the role Published by: National Guardian Office Published on 25 May 2016 The National Guardian Office has published a document to explain where a local guardian sits in an organisation and the principles which underpin their role to help to improve the culture around raising concerns. Action: To be incorporated within the Trust s plans for the Freedom to Speak Up Guardian (covered separately on this agenda) Web-link: Executive Director: Director of People and Corporate Development Board Committee: Quality & Safety Committee Enc 4 CEO StrategicBrief-July2016-V5 Page 5 of 7
37 5. Recommendations for a new Healthcare Safety Investigation Branch Published by: NHS Improvement Published on 12 May 2016 The new patient safety investigation function will help build a link between investigations and improvement. HSIB s primary purpose is to: support local NHS organisations to conduct their own consistent high quality investigations, conduct a small number of its own investigations to help establish the causality of what happened and make recommendations to enable improvements to care and patient safety. The independent Expert Advisory Group (EAG) report, advising the Secretary of State for Health on the creation of the Healthcare Safety Investigation Branch (HSIB) makes 13 recommendations: 10 aimed at the Healthcare Safety Investigation Branch and 3 for the Department of Health and the wider healthcare system. The Chief Investigator has been confirmed as Keith Conradi currently Chief Investigator for the Air Accidents Investigation Branch. He will be responsible for the initial setting up of HSIB by 1 April 2017 and for its ongoing leadership. HSIB will operate independently of government and the healthcare system. Action: To note and monitor the establishment of the HSIB over the coming months and any implications for the Trust Web-link: Executive Director: Director of Nursing Operations and Estates Board Committee: Quality & Safety Committee 6. Department of Health: Honours Nomination Form and Guidance Published by: Department of Health Published on 22 June 2016 The New Year Honours list and the Queen s Birthday Honours list acknowledge people who have made a difference in their field of work or community people who have gone that extra mile. The deadline for submitting nominations for the Queen s Birthday Honours 2017 is Wednesday 27 July Action: Trust to consider any appropriate nominations Web-link: Executive Director: Chief Executive Board Committee: Board Recommendation It is recommended that the Board consider and discuss the information contained within this report, and note for assurance the actions identified throughout the report. Enc 4 CEO StrategicBrief-July2016-V5 Page 6 of 7
38 Board action required The Board is asked to: Note the information and actions contained within the report. Identify any further specific action required and agreed timeframe for completion. Enc 4 CEO StrategicBrief-July2016-V5 Page 7 of 7
39 Board meeting date: 7 th July 2016 Agenda Item number: 8.1 Enclosure: 5 Report Title: Trust Integrated Performance Dashboard Month 2 Accountable Director: Author (name & title): Rupert Davies Interim Director of Finance and Performance Makhan Singh (Principal Consultant, Information & Performance) Purpose of the report: To update the Board on all aspects of Trust performance at month 2 of 2016/17 Quality and Safety Service User Experience Efficiency Resources Monitor and Trust Development Authority Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: Quality and Safety Committee considered elements from within the Quality and Safety domain, and the Service User Experience domain. Finance and Performance Committee considered elements from the Efficiency, Resource and Quality and Safety Domains Date reviewed Quality and Safety Committee 9 June 2016 Finance and Performance Committee 27 June 2016 Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources Enc 5 Cover Sheet 16_17 Integrated Dashboard Month 2 Page 1 of 3
40 What impact or implications does this report have on any of the following: Caring Responsive Please give brief details: The report provides an update on the performance in relation to Quality and Safety, Service User Experience, Efficiency and Resources Effective Well-led Safe Enc 5 Cover Sheet 16_17 Integrated Dashboard Month 2 Page 2 of 3
41 Title Trust Integrated Performance Dashboard Month 2 (May 2016) Introduction This paper presents the Trust s performance at the end of month two 2016/17 financial year. The 2016/17 Integrated Dashboard allows comparison and triangulation across Quality and Safety, Service User Experience, Efficiency, and Resources to give a comprehensive picture of the performance of the Trust. The 2016/17 Integrated Dashboard also includes performance, and exception commentary, by service line, so that the Board is better able to see achievements as well as any adverse performance within the overall aggregate level. Summary of key points, issues and risks Sickness - Trust Sickness in May 2016 is 4.98%, compared to 4.49% as reported in April Mandatory Training compliance is 81.9% as at the end of month two, which is below the new 90% threshold. Copies of Care Plan the Trust is below the agreed 95% threshold (94.7%). The overall Continuity of Service risk rating for the month remains green. The overall Financial Sustainability risk rating for the month remains green. Our overall Governance risk rating for the month is green with a score of 0. Further detail Please see enclosed Integrated Performance Dashboard and underpinning reports for finance, contractual performance, quality and workforce. Recommendation It is recommended that the Board note the performance of the Trust as at month two and debate accordingly. Board action required Debate the content of the reports accordingly. Enc 5 Cover Sheet 16_17 Integrated Dashboard Month 2 Page 3 of 3
42 Board meeting date: 7 th July 2016 Agenda Item number: a Enclosure: 6 Report Title: Quality and Safety Committee Summary Report Committee: Quality and Safety Committee Author (name & title): Rosie Musson Head of Nursing, Quality and Innovation Action required from the Board Decision / Approval Gain assurance Discussion Information Title Quality and Safety Chair s Report Introduction The Quality and Safety Committee met on the 9 th June 2016, where they considered and discussed the Trust s key Quality and Safety issues. Summary of key points, issues, financial impact and risks The Committee has highlighted the following key points, issues and risks to the Board: Feedback from Patient Story The Chair explained that one of the actions from the Board was around the Committee focussing specifically on the communication issues raised in the recently presented Patient s Story and to provide feedback/assurance via the Chair s Report. The Committee agreed that following the Patient s Story an Action Plan had been developed which provided assurance and that there is also a section on the Patient Story Protocol about how does the patient know that their story has made an impact and this should have been followed. The Committee agreed that the Board should be informed that the Committee is satisfied that the process for the Patient Story Protocol should address the issue and that the Committee would ensure that this is being followed. Care Quality Commission (CQC) Detailed Action Plan The Trusts detailed CQC Action Plan was presented to the Committee which includes a combination of the compliance and regulation issues picked up by the CQC and by Trust Enc 6 Quality and Safety Committee Board Report - june16 Page 1 of 5
43 staff during the course of preparation for the CQC. The Action Plan will be discussed at the Quality Summit on 12 July. It was agreed by the Committee that there should be RAG rating against the actions and if there were any reds the committee will then discuss the mitigations. The Committee will receive monthly update and any exceptions will be reported with mitigations. Quality and Safety Report Key points from the Quality report are There were 373 incidents during the month, which represents an increase of 12.9% when compared to April. There were 4 cases where Duty of Candour was considered. There was an increase in incidents in Acute & Access Services, however, disruptive aggressive behaviour type incidents had shown a decrease. Langdale Ward reported 15.8% of Disruptive/Aggressive behaviour incidents which were attributable to 2 patients who were involved in multiple incidents. There was an increase in incidents in the Older Adults Service Line and 67% of disruptive/aggressive behaviour incidents were linked to 5 patients. There was an increase in the numbers of self-harming behaviour within Early Intervention Services. One case is being investigated and the other cases are being reviewed by the individual teams. There was a decrease in incidents within Community and Recovery Service Lines. The Committee discussed the challenges within Acute Services over the last month and that work needs to be done on the Dangerous Assessment. It was agreed that a Deep Dive should be undertaken regarding the criteria for admissions from a Dangerousness point which will be presented to the Committee in July. Serious Incidents The Committee were informed that there were 4 Serious Incidents in May, two related to Under 18 s Admissions on the Acute Wards. The Committee discussed the Board decision to support Under 18 s and requested that a six month report detailing the profile of the Under 18 s be brought back to the Committee in October for review. It was agreed that the Board should be asked if the Trust should continue with this or whether the Under 18 s being admitted are too complex. Risk Register The Risk Register was presented to the Committee. It was reported that there are currently 7 operational risks on the High Level Operational Risk Register. The Compliance and Safety Department are working with the Executive Leads to look at the mitigations and ensure that there are clear timescales against the risks. This work is being driven by the Board. It was noted that the Risk in relation to Water Management now reflects that there are issues at all 3 hospital sites. Following a query from the Chair regarding how the Committee would know when an amber risk has been turned to green so that it can inform the Board, it was agreed that Enc 6 Quality and Safety Committee Board Report - june16 Page 2 of 5
44 there should be a cycle for Departmental Risks to be presented at the Committee each month. Red Risk Deep Dive A deep dive was presented to the Committee on the history of Risk 225 The risk of insufficient resilience and skills in leadership, which may result in poorly, engaged, demotivated staff and poor service quality to present day. The Committee discussed whether after the recent CQC inspection they considered that this still represent a red risk to the Trust. It was agreed that the progress made over the last 12 months had been significant, noting that sickness rates had reduced, and Staff Engagement Work had improved. However, more work was needed to be done around Leadership Development and Management Development. The Committee agreed to suggest to the Board that Risk 225 be downgraded to Amber This will be discussed under Board Agenda regarding the Risk Register. Bloxwich Hospital Assurance Plan The Committee received updated Assurance Plan which included the actions from Walsall CCGs unannounced visit. The Chair of Committee concluded that it was reassuring to see how the Assurance Plan is being implemented. The Quality and safety Committee will continue to monitor progress. DIPC/HCAI Annual Report The Committee received the Director of Infection Prevention and Control (DIPC) Annual Report for 2015/16. The DIPC reported that it had been a challenging year. The IPCC Team s main focus had been on Water Management, however, good progress and sustainability has been made across all areas. The Committee received assurance from the DIPC that it has been beneficial to have Facilities Management sitting in the same area as IPCC as it becomes more of a compliance agent. The Committee recommended the DIPC Annual Report to the Trust Board for approval. The report will be presented to the Board as part of the DONs report. Service Experience Annual Report The Service Experience Desk Annual Report was presented to the Committee which gave details about: Trust; vision, values, strategy, strategic aims and services Service Experience Activity The full picture of service experience Key achievements 2015/16 Priorities for 2016/17 The Chair asked that the role of the EBE be highlighted in the summary of key points. Enc 6 Quality and Safety Committee Board Report - june16 Page 3 of 5
45 The Committee recommended the Service Experience Annual Report to Trust Board for approval. Clinical Audit and Effectiveness Annual Summary Report 2015/16 The report highlighted to the Committee the Clinical Audits completed during 2015/16: The Committee received the report for assurance. 25 audits were identified on the Forward Audit Plan and commissioned for this reporting period 20 have been completed (2 of which are rolling audits) 2 have been deferred to the 2016/17 Forward Audit Plan 2 have been cancelled as an alternative quality improvement tool has been utilised 1 has been cancelled as no longer required due to equipment no longer in use. Performance Report Key points from the report are Copies of Care Plans have fallen below the 95% threshold.the Committee held a discussion regarding the culture around Copies of Care Plans within the Trust and how this needs to be looked at from a quality output perspective rather than a management output. It was agreed that a scoping exercise to be undertaken around Copies of Care Plan KPIs and quality output and this should be linked to the Recovery Pathway. Update to be brought back to the Committee in September. There are some data quality issues with PDRs. The Committee received assurance that this was being addressed through CARM and a Trust Wide Communication is to be sent out. Agency Spend Review internal metrics are measuring the potential impact of the Agency Spend The Committee were advised that consideration was being given to early indicators that could potentially help the bank and agency spend. The Committee agreed that an in-depth review of a Service Line should be undertaken each month, looking at sickness levels, PDRs, Mandatory Training, Agency Use and the impact on quality. The reviews will commence in September 2016 and enable the triangulation of data from internal metrics and Quality Impact Assessments to inform the Risk Register. The Chair asked whether in terms of the agency restriction there had been any impact on service delivery. From a Director of Operations and Nursing perspective it was explained that currently there has been no impact as the target for the first 2-3 of months is generous but going forward it will become more difficult. From a medical Director perspective the Committee were advised that an impact on service delivery has been seen, in that where there are vacancies to be filled by locums, however the numbers of people available are reduced. Following discussion, the Committee agreed that the risks around the filling vacancies due to the shortage of Enc 6 Quality and Safety Committee Board Report - june16 Page 4 of 5
46 locums and the shortage of Psychiatrists should be added to the Risk Register and brought back to the Committee in July Infection Prevention and Control Committee The Committee received an update on Water Management please reference DONs report to Trust Board. Policy and Procedures Focus Group The Committee were informed that the Policy and Procedures Focus Group agreed to reratify the following policy which had minor amendments. The Grievance Policy and Procedure The Standards of Business Conduct Policy was recommended to the Quality and Safety Committee for escalation to the Board for ratification. The revised Policy is currently subject to additional consultation with clinicians and staff side, after which it will be presented to Board. Interfaces with other Committees The business that was discussed by the committee interfaces with the following Committees/Groups: Audit Committee Finance and Performance Committee MExT CARM / CQR Clinical Audit and Effectiveness Committee Embedding Lessons Group Regulation and Risk Working Group Safeguarding Strategic Group Suicide Prevention Group Equality and Diversity Steering Group R&D Committee Health & Safety Committee Infection Prevention Control Committee Medicines Management Committee Mental Health Forum Policy & Procedures Group Resuscitation Committee Recommendations and requests for direction The Trust Board is asked to: Accept this report for assurance about the exercise of delegated authority by the Quality and Safety Committee. Enc 6 Quality and Safety Committee Board Report - june16 Page 5 of 5
47 Board meeting date: 7 th July 2016 Agenda Item number: b Enclosure: 7 Report Title: Audit Committee Chair s Report Committee: Audit Committee Author (name & title): David Matthews, Non-Executive Director Action required from the Board Decision / Approval Gain assurance Key issues and Risks Internal Audit Plan Discussion Information The Committee approved the internal audit plan for 2016/17 a copy is attached for the Board s information. Quality Account 2015/16 (for information only approved at Extraordinary Board Meeting on 22 nd June 2016) Ms Musson, Head of Nursing, Quality & Innovation, presented the item and advised that the content in the Quality Account had been received by the appropriate internal committees and was before the Audit Committee for a recommendation to the Trust Board for approval. Mr Stocks from Grant Thornton, referred to the External Audit Opinion. He advised that the final signed version would be submitted to the Trust, subject to the Board s approval and signature of the Chair and Chief Executive prior to submission on 30 June The Chair, on behalf of the Audit Committee, commended the Quality Account and thanked Ms Musson for her input. Following a discussion on the draft Quality Account for 2015/16 the Committee agreed to recommend it to the Trust Board for approval. Recommendations and requests for direction The Board is requested to note the internal audit plan for 2016/17. Enc 7 Audit Committee Chair Report - Audit Committee MA (Final) Page 1 of 2
 Page 2 of")
48 Appendix Summary Internal Audit Plan and Profile Enc 7 Audit Committee Chair Report - Audit Committee MA (Final) Page 2 of 2
49 Section 1 Summary of Trust Incidents and Serious Incidents
 Cause Group No.")

50 Section 1 Summary of Trust Incidents and Serious Incidents 1 May 2016 to 31 May 2016 Quality & Safety Report June INCIDENTS REPORTED 50.40% of incidents were Patient Safety Incidents (184 of 373 incidents) Cause Group No. Incidents 1 Disruptive / Aggressive Behaviour: Top Causes Physical Assault - Pt On Staff 48 incidents 4 SIs* 0 Never Events 91 SIRS** Dis Disruptive / Aggressive Behaviour Ser Serious Harming Behaviour Behavioural - Aggressive Behavioural - Disruptive 30 incidents 14 incidents Service Line No. Incidents Acute 185 Older 149 E.I. 25 Other 9 Comm & Rec 5 Service Lines Pat Patient Accident Clinical Care, Assessment And MHA Ac Access, Admission, Transfer Consent, Communication And Health & Safety Equipment Security Medication Documentation Skin Integrity Incidents by Cause Serious Harming Behaviour: Top Causes Self Harm - Cut Self Harm - Medication Overdose Self Harm - Ligature Patient Accident: Top Causes Patient - Faint/ Fit / Unwell Found With Injury Fall - Unobserved Fall Mobilising Alone 11 incidents 10 incidents 9 incidents 10 incidents 9 incidents 5 incidents Fire Incident 1 Clinical Care, Assessment And MHA: Top Causes 1 Clinical - Treatment / Care Related 20 incidents 2 Death - Natural Causes/Expected 8 incidents 3 Clinical - Difficulty In Obtaining Treatment 3 incidents 373 Total Incidents Reported Access, Admission, Transfer Discharge: Top Causes Absconded / Missing (Informal Patient) 6 incidents 28 Day Re-Admission 5 incidents * SI: Serious Incidents ** SIRS: Security Incidents Reporting System
51 Section 2 Individual Operational Service line Reports
52 Section 2 - Service Line Reports Acute & Access Service Line Quality and Safety Report June 2016 Chart Total Acute & Access incident numbers received by the Trust during the last 12 months Acute and Access Services 12 Monthly Average Mean + 2S.D. Mean - 2S.D. Incident Cause Group Acute Bed Occupancy Table Total Acute & Access incidents by Cause Group and showing a position on the previous months figures Current Month Trend analysis Position on previous month Disruptive / Aggressive Behaviour Serious Harming Behaviour Access, Admission, Transfer Discharge Clinical Care, Assessment And MHA Patient Accident 8 5 Medication 4 4 Health & Safety 4 5 Disruptive / Aggressive Behaviour 15.8% 8.5% 7.3% 4.8% 5.5% 41.8% Security 4 7 Access, Admission, Transfer Discharge 4.8% 1.8% 1.8% 1.8% 2.4% 12.7% Consent, Communication And Confidentiality 4 2 Serious Harming Behaviour 1.8% 8.5% 1.2% 4.2% 3.6% 19.4% Equipment 2 2 Clinical Care, Assessment And MHA 6.1% 3.0% 1.2% 0.0% 0.0% 10.3% Fire Incident 0 0 Patient Accident 0.6% 0.0% 2.4% 1.8% 0.0% 4.8% Documentation 3 1 Medication 0.0% 2.4% 0.0% 0.0% 0.0% 2.4% Skin Integrity 1 0 other 5.5% 0.0% 1.2% 0.6% 1.2% 8.5% Infection Control Incident 0 1 Grand Total 34.5% 24.2% 15.2% 13.3% 12.7% 100% Grand Total % 80% 60% 40% 20% 0% Bed Occupancy Last 12 months Commentary The monthly (mean) average for incidents relating to Acute & Access Services (calculated using data from the last 12 months) is Chart shows the incident numbers for Acute & Access Services have shown an increase when compared to previous month and remains above the 12 month average. Chart also offers a comparison of the bed occupancy for acute inpatient services during this period. Table shows the total number of incidents broken down by cause group. There has been a decrease in the number of Disruptive / Aggressive Behaviour type incidents There has been an increase in the number of Serious Harming behaviour type incidents. All of these incidents, apart from 1, has been reported as Low or No Harm. The 1 execption is being investigated as a Serious incident. There is no significant trend in relation to people involved with 31 different patients involved in 43 Incidents. Table shows a heat map below, where the percentage of inpatient incidents have occured and incident type. Langdale reported 15.8% of all of the Disruptive / Aggressive Behaviour type Incidents 8.5% of all inpatient self harm occured on Ambleside, this increase is in relation to 2 specific patients who were involved in multiple incidents. Table Heat Map Total Acute inpatient incidents shown by Incident Cause Group percentage and by ward Langdale Ambleside Kinver Clent Wrekin Grand Total
53 Section 2 - Service Line Reports 2.2 Older Adults Service Line Quality and Safety Report June 2016 Chart Total Older Adults incident numbers during the last 12 months Commentary Older 12 Monthly Average Mean + 2S.D. Mean - 2S.D. Older Adults exc Leave 80% 70% 60% 50% 40% 30% 20% 10% 0% Bed Occupancy The monthly (mean) average for incidents relating to Older Adults Services (calculated using data from the last 12 months) is Chart shows the number of incidents has increased when compared to the previous few months and remains above the 12 month average. Table shows the total number of incidents broken down by cause group. The most reported Incident category is Disruptive / Aggressive Behaviour which has seen an increase when compared to the previous month. 67% of all Disruptive / Aggressive Behaviour is linked to 5 patients, all of whom have care plans in place and regularly reviewed. Table Shows a heat map below showing where the percentage of inpatient incidents have occurred. Linden ward have reported 37.0% of all inpatient incident 23.7% of all inpatient incidents relate to Linden Ward and linked to incidents of Disruptive / Aggressive Behaviour 58.5% of all inpatient incident relate to Disruptive / Aggressive Behaviour Table Total Older Adults incidents by Cause Group and showing a position on the previous months figures Incident Cause Group Current Month Trend analysis Position on previous month Disruptive / Aggressive Behaviour Patient Accident Clinical Care, Assessment And MHA 14 9 Health & Safety 2 9 Last 12 months Table Heat Map Total Older Adults inpatient incidents shown by Incident Cause Group percentage and by ward Medication 3 3 Disruptive / Aggressive Behaviour 23.7% 18.5% 12.6% 3.7% 58.5% Serious Harming Behaviour 1 5 Patient Accident 8.1% 5.9% 5.9% 3.0% 23.0% Skin Integrity 1 4 Clinical Care, Assessment And MHA 1.5% 0.7% 0.7% 1.5% 4.4% Equipment 4 0 Access, Admission, Transfer Discharge 0.7% 0.0% 0.0% 2.2% 3.0% Consent, Communication And Confidentiality 2 0 Equipment 0.7% 2.2% 0.0% 0.0% 3.0% Access, Admission, Transfer Discharge 4 3 Medication 0.0% 0.7% 0.7% 0.0% 1.5% Security 2 1 Health & Safety 0.0% 0.7% 0.0% 0.7% 1.5% Infection Control Incident 0 0 Security 0.7% 0.7% 0.0% 0.0% 1.5% Documentation 1 0 Other 1.5% 1.5% 0.7% 0.0% 3.7% Fire Incident 1 1 Grand Total 37.0% 31.1% 20.7% 11.1% 100.0% Grand Total Linden Cedars Holyrood Malvern Grand Total
54 Section 2 - Service Line Reports Quality and Safety Report June Early Intervention Service line Table Total Early Intervention incidents by Cause Group and showing a position on the previous months figures Incident Cause Group Current Month Early Intervention Previous month Last 12 months Chart Total Early Intervention incident numbers during the last 12 months Serious Harming Behaviour 8 2 Disruptive / Aggressive Behaviour 6 2 Security 1 2 Clinical Care, Assessment And MHA 2 1 Consent, Communication And Confidentiality 2 4 Health & Safety 2 0 Equipment 3 1 Medication 0 0 Access, Admission, Transfer Discharge 1 0 Documentation 0 0 Fire Incident 0 2 Patient Accident 0 0 Skin Integrity 0 0 Infection Control Incident 0 0 Grand Total Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 E.I. 12 Monthly Average Commentary The monthly (mean) average for incidents relating to E.I. Services (calculated using data from the last 12 months) is Chart shows this month has seen an increase in the number of incidents for the Early Intervention Service line, with 24 incidents reported for the month. Table shows the total number of incidents broken down by Cause Group. Exceptions/Trends There has been in increase in the number of reported incidents of Serious harming behaviour. One of these cases is being investigated and other cases are being reviewed by the individual teams
55 Section 2 - Service Line Reports Quality and Safety Report June Community & Recovery Service line Chart Total Community & Recovery incident numbers during the last 12 months Table Total Community & Recovery incidents by Cause Group and showing a position on the previous months figures 25 Walsall SMS Contract End Community & Recovery 20 Incident Cause Group Current Month Previous month Last 12 months 15 Serious Harming Behaviour 1 0 Disruptive / Aggressive Behaviour 1 1 Security 3 1 Clinical Care, Assessment And MHA 0 3 Consent, Communication And Confidentiality 0 1 Health & Safety 0 1 Equipment 0 0 Medication 0 1 Access, Admission, Transfer Discharge 0 0 Documentation 0 0 Fire Incident 0 0 Patient Accident 0 0 Skin Integrity 0 0 Infection Control Incident Community & Recovery Service 12 Monthly Average Grand Total 5 8 Commentary The monthly (mean) average for incidents relating to Community & Recovery (calculated using data from the last 12 months, and as a combination of the previous individual Services) is Chart shows the incident figures which have seen a decrease since the previous month. Table shows the total number of incidents broken down by cause group. Exceptions/Trends All other incidents relate to individual services and the incidents have no specific trend.
56 Falls Analysis May 2016 Incident Number: Locality Acute or OA Where Time Object Injuries Attended A&E Staff Present? Walsall Older Adult Lounge None None Yes Dudley Older Adult Bathroom None None Yes Dudley Older Adult Kitchen None Pain in knee A&E Yes No Dudley Older Adult Bedroom None None No Dudley Older Adults Bedroom None Hit Left arm No Yes Walsall Older Adult Lounge Chairs Pain in lower back No No Walsall Older Adult Lounge None None Yes Dudley Acute Patio None None No Walsall Older Adult Bedroom None Lower back pain No No Walsall Older Adult Bedroom None Lower back pain No No Dudley Acute Bedroom Corridor Wet floor None Yes Walsall Acute Main ward area Slippery floor None Yes Walsall Older Adult Bedroom None Bruised right hip No No Findings- o o o o o 10 falls occurred in Older Adults and 3 in Acute 7 falls reported in Walsall and 6 in Dudley 5 falls occurred in Bedrooms 5 falls occurred within the early hours of the morning and 4 occurred in the evening before midnight 7 falls resulted in no injuries and 6 reported with injury No Serious Untoward Incidents reported from falls this month. 1 fall did warrant further assessment in general hospital. 1 Jackie Stevens Falls Lead
57 No of falls Acute 15 Older Adult Ealry hours Bedroom 10 Injuries Average 5 0 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 There has been an overall drop in the number of falls reported across all areas. 2 patients required further assessment at A&E. 2 Jackie Stevens Falls Lead

58 Locality Dudley OA Walsall OA Dudley Acute Walsall Acute Time of day Injuries Early morning Evening until midnight Daytime With injury without injury 3 Jackie Stevens Falls Lead

59 Section 3 Serious Incidents

60 Section Serious Incidents Quality and Safety Report June 2016 Table List of Serious Incident raised during the month of May 2016 SI Number Date of Incident Service Line Incident Description Level of Risk DoC applicable Level of response Current status 2016/ /05/2016 Acute Absconded (Sectioned Patient) moderate Yes Clinical Review Ongoing 2016/ /05/2016 Acute Under 18 Admission low No Clinical Review Ongoing 2016/ /05/2016 E.I. Self Harm - Medication Overdose low No Clinical Review Ongoing 2016/ /05/2016 Acute Self Harm - Self Injury moderate Yes Clinical Review Ongoing Chart Total number of Serious Incidents during the last 12 months Chart Summary of the Serious Incident types during the last 12 months Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 4% 2% 2% Serious Harming Behaviour Access, Admission, Transfer Discharge 47% Patient Accident 45% Clinical Care, Assessment And MHA Serious Incidents Trust Average Mean + S.D. Mean - S.D. Security Commentary The monthly (mean) average for serious incidents across the Trust (calculated using data from the last 12 months) is 4.25 Table 3.1 Shows a list of the serious incident logged on STEIS during the previous month, this includes details of the service line and nature of the incident There are 3 Serious Incident linked to Acute Services There has been 1 Serious Incident linked to the E.I. Service Chart 3.2 shows that the number of Serious Incidents has fallen when compared to the previous month and has fallen back below the 12 monthly average. Chart 3.1 illustrates the types of the Serious Incidents that have been reported over the previous 12 months. Incident Summary 2016/ This is the admission of an under 18 onto an adult acute ward. At the point of admission this patient was 10 days short of their 18th birthday. 2016/ This case is in relation to the same patient as the above, the patient had sustained an injury as a result of aggressive behaviour. The patient was being escorted to A&E for an x-ray, when the patient Abscond from staff. A full care plan is in place for this patient and the patient remains as an inpatient. 2016/ This was a medication overdose of a patient known to our CAMHS service, which resulted in hospital treatment. There is a review of this patient's ongoing care and this is being managed locally. 2016/ This patient carried out an act of self injury resulting in the patient being admitted to the Acute Trust for treatment and later an operation. This patient remains in our care and a suitable placement is being sought.
61 Section 4 National Guidance: Safety Alert Broadcasts (SAB's)


62 Section 4 Safety Alerts Quality and Safety Report June 2016 Table 4.1 Summary of Alerts received during May 2016 Type of Alert Number of Alerts in May Action not Required Assessing Relevance Action Required Circulated for Information MDA MHRA CMO DDL EFN DH EFA DH SDA NHS PSA Total During May 2016 there were 25 alerts issued via the Central Alerting System, of these 2 alerts: o 22 Alerts required no action taking. o 2 Patient Safety Alerts required action taking, this work has been subsequently completed. o The Trust is currently assessing the relevance of 1 alert. The table below (4.2) outlines a summary of the alerts issues and any action taken. Alert Number EFN/2016/07 EFN/2016/08 EFN/2016/09 EL (16)A/04 Table 4.2 Alerts issued during May via the Central Alerting System EFA/2016/001 EFN/2016/01( U) EFN/2016/10 EFN/2016/11 NHS/PSA/W/2 016/004 Alert Date Description of Alert Status Notes / action taken / assurance 03-May- High Voltage Hazard Alert - DANGEROUS INCIDENT NOTIFICATION (DIN) - Schneider Electric - Action Not The Trusts authorising officer acknowledged receipt of 2016 RN2c - Ring Main Unit Required the alert and that no action was required by the Trust 04-May- High Voltage Hazard Alert - NATIONAL EQUIPMENT DEFECT REPORT (NEDeR) - Schneider Action Not The Trusts authorising officer acknowledged receipt of 2016 Electric - VISAX - Circuit Breaker Required the alert and that no action was required by the Trust 05-May- High Voltage Hazard Alert - NATIONAL EQUIPMENT DEFECT REPORT (NEDeR) - GEC Alsthom - Action Not The Trusts authorising officer acknowledged receipt of 2016 VMX - Circuit Breaker Required the alert and that no action was required by the Trust 06-May- Drug alert class 2, action within 48 hours, aventis pharma limited trading as sanofi, rifadin 600mg Action required: All affected stock has been removed from ward level 2016 infusion Action and pharmacy at DGH, however none was held by 09-May May May May May Carbon steel press fit pipes for water heating systems: rapid corrosion and failure This Alert has been issued to highlight the issues relating to the rapid corrosion of thin-wall low carbon steel press-fit pipe due to the introduction of air (via pin holes, inadequate joints or as a result of poor installation/commissioning practices). High Voltage Hazard Alert - NATIONAL EQUIPMENT DEFECT REPORT (NEDeR) - UPDATE - Merlin Gerin - Genie - Circuit Breaker High Voltage Hazard Alert - NATIONAL EQUIPMENT DEFECT REPORT (NEDeR) - AREVA T&D Automation & Information Services - MICOM P123 - Protection Relay High Voltage Hazard Alert - DANGEROUS INCIDENT NOTIFICATION (DIN) - CG Power Systems - 11/0.433 kv Pole Mounted Transformers Risk of death and severe harm from failure to recognise acute coronary syndromes in Kawasaki disease patients This alert is to emphasise the high risk and atypical presentation of coronary artery aneurysms, coronary thrombosis and myocardial ischaemia or infarction in patients with Kawasaki disease, and to highlight the importance of specialist advice. Complete Assessing relevance Action Not Required Action Not Required Action Not Required Action required: Action Complete DWMH The Trusts Patient Safety and Compliance Team is currently working with the Estates Department to ascertain whether we have any of these devices The Trusts authorising officer acknowledged receipt of the alert and that no action was required by the Trust The Trusts authorising officer acknowledged receipt of the alert and that no action was required by the Trust The Trusts authorising officer acknowledged receipt of the alert and that no action was required by the Trust Whist it was agreed that the Trust was unlikely to be routinely diagnosing this, it was felt prudent to circulate the alert to clinicians for information.
63 Section 4 Safety Alerts Alert Number EFN/2016/12 EFN/2016/13 EFN/2016/14 EFN/2016/15 EFN/2016/16 EFN/2016/17 EFN/2016/18 EFN/2016/19 MDA/2016/006 EL (16)A/05 EFN/2016/20 EL (16)A/06 EFN/2016/21 EFN/2016/22 EFN/2016/22 EFN/2016/23 Alert Date Description of Alert Status Notes / action taken / assurance 12-May- High Voltage Hazard Alert - NATIONAL EQUIPMENT DEFECT REPORT (NEDeR) - UPDATE - Merlin Action Not The Trusts authorising officer acknowledged receipt of 2016 Gerin - Genie - Circuit Breaker Required the alert and that no action was required by the Trust 13-May- High Voltage Hazard Alert - NATIONAL EQUIPMENT DEFECT REPORT (NEDeR) - FKI - Eclipse - Action Not The Trusts authorising officer acknowledged receipt of 2016 Circuit Breaker Required the alert and that no action was required by the Trust 17-May- High Voltage Hazard Alert - DANGEROUS INCIDENT NOTIFICATION (DIN) - Schneider Electric - Action Not The Trusts authorising officer acknowledged receipt of 2016 RN6c - Ring Main Unit Required the alert and that no action was required by the Trust 17-May- High Voltage Hazard Alert - SUSPENSION OF OPERATIONAL PRACTICE (SOP) - UPDATE - Long Action Not The Trusts authorising officer acknowledged receipt of 2016 & Crawford - GF3 - Switch Required the alert and that no action was required by the Trust 18-May- High Voltage Hazard Alert - DANGEROUS INCIDENT NOTIFICATION (DIN) - Reyrolle - C7T - Circuit Action Not The Trusts authorising officer acknowledged receipt of 2016 Breaker Required the alert and that no action was required by the Trust 19-May- High Voltage Hazard Alert - DANGEROUS INCIDENT NOTIFICATION (DIN) - South Wales Action Not The Trusts authorising officer acknowledged receipt of 2016 Switchgear - D8/12X - Circuit Breaker Required the alert and that no action was required by the Trust 23-May- High Voltage Hazard Alert - NATIONAL EQUIPMENT DEFECT REPORT (NEDeR) - Siemens - S14V Action Not The Trusts authorising officer acknowledged receipt of Circuit Breaker (Retrofit) Required the alert and that no action was required by the Trust 24-May- High Voltage Hazard Alert - DANGEROUS INCIDENT NOTIFICATION (DIN) - CG Power Systems - Action Not The Trusts authorising officer acknowledged receipt of kV Transformers Required the alert and that no action was required by the Trust 24-May- CADD administration sets with Flow Stop free-flow protection manufactured by Smiths Medical ASD Action Not The Trust does not have any / use any of these 2016 risk of under-infusion Required devices. 24-May- Drug alert class 4, for information, hospira uk limited, paclitaxel 6mg/ml concentrate for solution for Action Not We are not affected by this drug alert as we only use 2016 infusion; 100mg in 16.7ml. Required the Accord branded product. 25-May- High Voltage Hazard Alert - DANGEROUS INCIDENT NOTIFICATION (DIN) - Long & Crawford - GF3 Action Not The Trusts authorising officer acknowledged receipt of Fuse Switch Required the alert and that no action was required by the Trust 25-May- Drug alert class 2, action within 48 hours, special products limited, epistatus midazolam 10mg in 1ml Action Not We are not affected by the attached drug alert as we 2016 oromucosal solution Required do not use or purchase this item. 26-May- High Voltage Hazard Alert - DANGEROUS INCIDENT NOTIFICATION (DIN) - Long & Crawford - J4 - Action Not The Trusts authorising officer acknowledged receipt of 2016 Switch Required the alert and that no action was required by the Trust 27-May- High Voltage Hazard Alert - DANGEROUS INCIDENT NOTIFICATION (DIN) - UPDATE - Schneider Action Not The Trusts authorising officer acknowledged receipt of 2016 Electric - RN2c - Ring Main Unit Required the alert and that no action was required by the Trust 27-May- High Voltage Hazard Alert - DANGEROUS INCIDENT NOTIFICATION (DIN) - UPDATE - Schneider Action Not The Trusts authorising officer acknowledged receipt of 2016 Electric - RN2c - Ring Main Unit Required the alert and that no action was required by the Trust 31-May- High Voltage Hazard Alert - NATIONAL EQUIPMENT DEFECT REPORT (NEDeR) - Areva T&D Action Not The Trusts authorising officer acknowledged receipt of 2016 Automation & Information Services - P521 Protection Relay Required the alert and that no action was required by the Trust
64 Section 5 Benchmarking The Information in this section is taken from the Department of Health's Serious Incident reporting system STEIS and shows the number of Serious Incidents reported Nationally and Regionally Table 5.1 shows total number of Serious Incidents reported during the period Jun 15- May 16, and provides the information for all Trusts across the West Midlands Region, this information is shown by Incident Type (STEIS category types) and grouped in order of highest to lowest. Table 5.2 shows total number of Serious Incidents reported during the period Jun 15- May 16, and provides the information for 53 Trusts within a Mental Health Cluster Group (as used by the NRLS/NPSA), this information is shown by Incident Type (STEIS category types) and grouped in order of highest to lowest. Key points to note: It is noted that on both tables there is no mearsure of size of Trust or Services provided. Under the category "Unauthorised absence..." which translated is the category we capture Abscond and failure to return from leave type incidents our trust is the highest when compared to other Trusts within the mental health cluster, and second highest within the West Midlands region. Under the category "Slips/Trips/Falls..." our Trust have the one lowest figures when reporting these types of incidents. There are 3 reported incidents linked to under 18's admissions, these will shortly be transferred onto specialist commissioning and will be removed from our Trust figures. Due to the Scale of the report this section is best printed in A3, copies will be made available for the various committees this paper will be presented at.
65 Section 5 - Benchmarking Quality and Safety Report June 2016 Table 5.1 Serious Incidents Reported on STEIS - West Midlands Region Grand Total The Royal Wolverhampton NHS Trust Heart of England NHS Foundation Trust The Dudley Group NHS Foundation Trust Worcestershire Health and Care NHS Trust University Hospitals Coventry and Warwickshire NHS Trust Walsall Healthcare NHS Trust Birmingham and Solihull Mental Health NHS Foundation Trust Coventry and Warwickshire Partnership NHS Trust Worcestershire Acute Hospitals Birmingham Community Healthcare NHS Trust University Hospitals Birmingham NHS Foundation Trust Sandwell and West Birmingham Hospitals NHS Trust George Eliot Hospital NHS Trust Wye Valley NHS Trust South Warwickshire NHS Foundation Trust Royal Orthopaedic Hospital NHS Foundation Trust Black Country Partnership NHS Foundation Trust Dudley and Walsall Mental Health Partnership NHS Trust West Midlands Ambulance Trust Birmingham Children's Hospital NHS Foundation Trust Birmingham Women's NHS Foundation Trust West Midlands Providers West Midlands Specialised Services 1 1 Grand Total #### Pressure ulcer meeting SI criteria Slips/trips/falls meeting SI criteria Apparent/actual/suspected self-inflicted harm meeting SI criteria HCAI/Infection control incident meeting SI criteria Diagnostic incident including delay meeting SI criteria (including failure to act on test results) Confidential information leak/information governance breach meeting SI criteria Maternity/Obstetric incident meeting SI criteria: baby only (this include foetus neonate and infant) Pending review (a category must be selected before incident is closed) Surgical/invasive procedure incident meeting SI criteria Treatment delay meeting SI criteria Sub-optimal care of the deteriorating patient meeting SI criteria Unauthorised absence meeting SI criteria Medication incident meeting SI criteria VTE meeting SI criteria Disruptive/ aggressive/ violent behaviour meeting SI criteria Maternity/Obstetric incident meeting SI criteria: mother only Accident e.g. collision/scald (not slip/trip/fall) meeting SI criteria Maternity/Obstetric incident meeting SI criteria: mother and baby (this include foetus neonate and infant) Radiation incident (including exposure when scanning) meeting SI criteria Adverse media coverage or public concern about the organisation or the wider NHS Major incident/ emergency preparedness resilience and response/ suspension of services Apparent/actual/suspected homicide meeting SI criteria Medical equipment/ devices/disposables incident meeting SI criteria Failure to obtain appropriate bed for child who needed it Abuse/alleged abuse of adult patient by staff Commissioning incident meeting SI criteria Environmental incident meeting SI criteria Abuse/alleged abuse of adult patient by third party Operation/treatment given without valid consent Abuse/alleged abuse of child patient by third party Screening issues meeting SI criteria Incident affecting patient s body after death meeting SI criteria Blood product/ transfusion incident meeting SI criteria Abuse/alleged abuse of child patient by staff Substance misuse whilst inpatient meeting SI criteria
66 Section 5 - Benchmarking Quality and Safety Report June 2016 Table 5.2 Serious Incidents Reported on STEIS - 53 Trust NRLS Mental Health Cluster Group Grand Total Southern Health NHS Foundation Trust Norfolk and Suffolk NHS Foundation Trust Kent and Medway NHS and Social Care Partnership Trust West London Mental Health NHS Trust Central and North West London Mental Health NHS Foundation Trust Solent NHS Trust Cheshire and Wirral Partnership NHS Foundation Trust Birmingham and Solihull Mental Health NHS Foundation Trust Oxford Health NHS Foundation Trust Mersey Care NHS Trust North East London NHS Foundation Trust Cornwall Partnership NHS FT Lincolnshire Partnership NHS Foundation Trust Tees Esk and Wear Valleys NHS Foundation Trust South Staffordshire and Shropshire Healthcare Foundation Trust Cambridgeshire and Peterborough NHS Foundation Trust Coventry and Warwickshire Partnership NHS Trust Avon and Wiltshire Mental Health Partnership NHS Trust Dorset Healthcare University NHS Foundation Trust Northumberland Tyne and Wear NHS Foundation Trust Bradford District Care NHS Foundation Trust Oxleas NHS Foundation Trust South London & Maudsley NHS Foundation Trust Berkshire Healthcare NHS Foundation Trust Boroughs Partnership NHS Foundation Trust Rotherham Doncaster and South Humber NHS Foundation Trust Leicestershire Partnership NHS Trust Cumbria Partnership NHS Foundation Trust Devon Partnership NHS Trust South West Yorkshire Partnership NHS Foundation Trust Camden & Islington NHS Foundation Trust North Essex Partnership NHS Foundation Trust Derbyshire Healthcare NHS Foundation Trust South West London and St George's Mental Health NHS Trust Barnet Enfield & Haringey Mental Health NHS Trust North Staffs Combined Healthcare Leeds and York Partnership NHS Foundation Trust Hertfordshire Partnership Foundation Trust Black Country Partnership NHS Foundation Trust Northamptonshire Healthcare NHS Foundation Trust Dudley and Walsall Mental Health Partnership NHS Trust Nottinghamshire Healthcare NHS Foundation Trust - Medium & High Secure Units gether NHS FT (Gloucestershire Partnership NHS FT) Somerset Partnership NHS FT Humber NHS Foundation Trust Pennine Care NHS Foundation Trust Sheffield Health and Social Care NHS Foundation Trust Manchester Mental Health and Social Care Trust Greater Manchester West Mental Health NHS Foundation Trust East London Foundation Trust - Mental Health Lancashire Care NHS Foundation Trust Tavistock and Portman NHS Foundation Trust Calderstones Partnership NHS Foundation Trust 1 1 Grand Total Apparent/actual/suspected self-inflicted harm meeting SI criteria Pressure ulcer meeting SI criteria Pending review (a category must be selected before incident is closed) Slips/trips/falls meeting SI criteria Disruptive/ aggressive/ violent behaviour meeting SI criteria Unauthorised absence meeting SI criteria Confidential information leak/information governance breach meeting SI criteria Abuse/alleged abuse of adult patient by staff Failure to obtain appropriate bed for child who needed it Apparent/actual/suspected homicide meeting SI criteria Sub-optimal care of the deteriorating patient meeting SI criteria Commissioning incident meeting SI criteria Abuse/alleged abuse of adult patient by third party Medication incident meeting SI criteria Accident e.g. collision/scald (not slip/trip/fall) meeting SI criteria HCAI/Infection control incident meeting SI criteria Treatment delay meeting SI criteria Diagnostic incident including delay meeting SI criteria (including failure to act on test results) Abuse/alleged abuse of child patient by third party Environmental incident meeting SI criteria Major incident/ emergency preparedness resilience and response/ suspension of services Adverse media coverage or public concern about the organisation or the wider NHS Abuse/alleged abuse of child patient by staff Substance misuse whilst inpatient meeting SI criteria Medical equipment/ devices/disposables incident meeting SI criteria VTE meeting SI criteria Surgical/invasive procedure incident meeting SI criteria Operation/treatment given without valid consent Screening issues meeting SI criteria Maternity/Obstetric incident meeting SI criteria: baby only (this include foetus neonate and infant) Blood product/ transfusion incident meeting SI criteria

67 DWMHT Safeguarding Performance Framework 2016/17 Section 1 Safeguarding Training Compliance Section 2 DoL's Domestic Violence Section 3 Safeguarding Children LAC - CAMH's
68 Section 1 Safeguarding Training Compliance
69 Safeguarding Training Complaince Safeguarding Performance Framework for May 2016 Compliance Target per quarter Compliant DWMH Dudley Walsall Required Compliant Compliant Required Compliant Compliant Required compliance % compliance % compliance Safeguarding Induction 100% % % % Safeguarding Adults Lvl 1 90% % % % Safeguarding Adults Lvl 2 90% % % % Safeguarding Adults Lvl 3 90% % % % Safeguarding Adults Lvl 4 90% 0 6 0% % Safeguarding Children Lvl 1 95% % % % Safeguarding Children Lvl 2 90% % % % Safeguarding Children Lvl 3 95% % % % Safeguarding Children Lvl 4 100% 0 6 0% 0 1 0% 0 2 0% Mental Capacity Act 80% % % % PREVENT 75% % % % Domestic abuse & Violence 20% % % % Compliant % Exceptions / Commentary This section shows the latest Training requirement and compliance levels as set out in the new Comissioner Contract, related to Safeguarding and Vulnerable Adults. Within the contract there are agreed trajectory requirements. Adult Safeguard Training - Childrens Safeguarding Training - Q1 - Scoping exercise to identify numbers and training levels required Compliance as detailed in the table above. Q2 - To be agreed Q3 - To be agreed Q4-90% Mental Capacity Act (MCA) and Deprivation Of Liberty (DOL s) Prevent Domestic Abuse Q1 80% Q1 75% Q1 20% Q2 80% Q2 80% Q2 30% Q3 85% Q3 90% Q3 40% Q4 90% Q4 95% Q4 50%
70 Section 2 Deprivation of Liberty (DoL's) & Domestic Violence
 - This shows the total number of active cases of DOL's, broken down by Locality 2015 2016 Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May NHS Dudley 0 2 3 0 2 1 5 1")

71 Safeguarding Performance Framework for May 2016 Section 2 - DoL's and Domestic Violence 2.1 Deprivation Of Liberties (DOL's) - This shows the total number of active cases of DOL's, broken down by Locality Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May NHS Dudley DOL's Applied For DOL's Closed NHS Walsall DOL's Applied For MARAC DOL's Closed Grand Total Grand Total Domestic Abuse Total number of cases of Domestic Violence for the current month, these include cases reported within the Trust and Externally notified by MARAC (Multi-Agency Risk Assessment Conference) Open To Mental Health Dudley Referred into MARAC Open To Mental Health Safeguarding Cases Internally reported as Domestic Abuse Walsall Referred into MARAC Apr-16 Alert Only Referral 3 10 Commentary Table 2.1 This table shows the activity in relation to cases of Deprivation Of Liberties (DOL's). This information is broken down by locality and shows the current number of Active cases, and activity for the last 12 months. There are currently 17 active cases of DoL's across the Trust Further information relating to Older Adults, health related legal restrictions / provisions Dudley - 15 patients (6 DoL's & 9 Under MHA) Walsall - 13 patients (11 DoL's & 2 Under MHA) Table 2.2 Domestic abuse cases are reported as separate figures to display the prevalence within the service. Case figures are also shown for MARAC (multi agency risk assessment conference), these figures demonstrate how many cases are heard at MARAC where the victim, perpetrator or children are open cases to mental health. The first table provides information on Cases reported Externally of the Trust which are then checked to see if these Patients are open to Dudley and Walsall Mental Health. The second table provides information on Domestic Abuse cases which have been reported internally into our Trust
72 Section 3 Safeguarding Children & Vulnerable Adults
73 Safeguarding Performance Framework for May Safeguarding Children Graph This graph provides information relating to the last 12 months and shows a breakdown of Safeguarding cases which are just for alert only and those which have been progressed to be continued under Safeguarding Table 3.1 -This shows that the number of Safeguarding cases broken down by case type and showing the locality. This also shows information on whether the case is for alert only or if it has been referred for further investigation to another agency. Table This table provides information in relation to Looked after Children (LAC), who have been referred or in receipt of our services. Table 3.1 Total number of Safeguarding Children cases for the current month Child Safeguarding Case Patient considered High Risk Position of Trust Internal Position of Trust External Under 18 Admission Under 18 Death FGM Serious Case Review (Child) Grand Total Table Looked after Children (LAC) Total number of cases of Looked after Children Dudley Walsall Grand Referral Alert Only Referral Alert Only Total Graph Total number of Safeguarding Children incidents reported during the last 12 months Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Alerts Referral Dudley Walsall Number of Looked after Number of Looked after Total Grand Total 205
74 3.2 Vulnerable Adults Safeguarding Performance Framework for May 2016 Graph 3.2 -This graph provides information relating to the last 12 months and shows a breakdown of Vulnerable Adults Cases which are just for alert only and those which have been progressed to be continued under Safeguarding. Table 3.2 This shows that the number of Vulnerable Adults cases broken down by case type and showing the locality. This also shows information on whether the case is for alert only or if it has been referred for further investigation to another agency. Investigation - Further to the reports previously in relation to concerns received relating to patient care from Bloxwich hospital. The investigation has now been concluded and the Safeguarding team are addressing the actions raised. Serious Case Reviews (SCR) - currently none Domestic Homicide Review (DHR) - currently none Table Total number of Vulnerable Adults incidents for the current month Adult Patient Considered High Risk Position Of Trust Internal Position Of Trust External Prevent Case FGM Grand Total Dudley Walsall Grand Referral Alert Only Referral Alert Only Total Graph 3.2 Total number of Vulnerable Adults incidents reported during the Last 12 Months Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Alerts Referral
75 Board meeting date: 7 th July 2016 Agenda Item number: a Enclosure: 9 Report Title: Finance and Performance Committee Chair Report Committee: Finance and Performance Committee Author (name & title): Mike Higgs Non Executive Director Action required from the Board Decision / Approval Gain assurance Key issues & risks Discussion Information The Finance and Performance committee met on the 27 th Performance information and HR position for May (Month 02). June and considered the Finance, The committee reviewed the following items of business: Performance The report was tabled and discussed. The report showed that activity was generally above expected levels, which was positive. There still remained five KPIs that were currently behind target and it was noted that failures against these KPIs could result in a 1% penalty against the total annual contract value for each month of non-achievement. A verbal update was given around an initial review into Detox activity levels and it was made clear that the reported levels, as per contracted activity, was in line with the view of clinical colleagues. All other key messages were noted and the report was approved. Finance Report 2016/17 The finance report was presented. The current financial position was reflecting a 119k surplus which was 21k ahead of the plan to date (based on the planned annual surplus of 700k). Contracted Income was over-performing by 8k which includes a 117k impact of CIPs. Before this impact the Walsall contract is actually over-performing across in-patient, CRS and EAS service lines but the level of over-performance has been limited each month to 43k in line with the contractually agreed cap and collar arrangement of 500k for the financial year, thus at Month 2 Walsall overperformance reflected a surplus of 85k. Dudley contract is now a block contract for the financial year and as such has no financial impact on the monthly position of the Trust, however, it was noted that In- Enc 9 FandP Chairs report Jul Board Meeting (M2 ) Page 1 of 3
76 Patient occupancy remained low across both Acute and Older Adults areas which could impact on the 2017/18 baseline discussions in next year s contracting round. Agency spend was discussed in light of the NHSI agency cap of 4.05m. The target spend for the month was 488k across all agency staff groups and the Trust had spent 523k, reflecting a 35k adverse variance, however, it was noted that the YTD position was almost in line with plan ( 993k spend against 995k plan). Whilst favorable at this stage we have after just two months almost spent 25% of our 4.05m target. Thus actions to reduce agency spending must continue throughout the year. The committee also noted the paper detailing the contracted income position (as summarized in the over-arching finance paper) and also received an update on Agency staffing which detailed the spending across staff groups making up the 993k spend to date and gave an overview of the agency staff aligned to Corporate budget areas, which initially had forecast an anticipated spend of circa 500k for the year. Having reviewed this further with corporate leads this position has now improved below 350k but still highlighted the need to look for substantive staff recruitment into these roles. Workforce The committee reviewed the paper. Discussions were held around Appraisals and Mandatory Training and executive leads were asked to continue their efforts to ensure that the Trust delivered to the required levels of compliance. Recruitment levels were discussed and the continuing trend of leavers outstripping the level of new starters into the Trust. Older Adults Jacky O Sullivan joined the meeting and gave a presentation on the transformation of the Older Adults service in order to meet commissioner requirements. The presentation and paper were well received by the committee but it was suggested that a visual aid/graphic be produced that will help aid understanding of the major changes involved. PBR Update The report was noted. Review of Risk Register The committee was informed that risks had been reviewed and no further updates were required at this time. Interfaces with other Committees The business that was discussed by the committee interfaces with the following Committees/Groups: MEXT Audit Committee Governance & Quality Committee CARM CQR Enc 9 FandP Chairs report Jul Board Meeting (M2 ) Page 2 of 3
77 Recommendations and requests for direction The Trust Board are asked to:- Accept this report for assurance about the exercise of delegated authority by the Finance and Performance Committee. Endorse the decisions and recommendations made by the Finance and Performance Committee. Enc 9 FandP Chairs report Jul Board Meeting (M2 ) Page 3 of 3
78 2016/17 Finance Report Month 02 1
79 2016/17 DWMHPT Finance Report Month 02 Page Key Messages 3 Overall Summary and RAG Assessment 4-5 Trust Income Statement: Functional Analysis 6-9 Cost Improvement Programme 10 Capital Programme 11 Financial Performance Metrics / NHSI Key Data Month Agency Cap 13 Cash Flow Statement 14 Debtor and Creditor Performance 15 Statement of Financial Position (Balance Sheet) 16 2
80 Key Messages : Current Performance Financial Position 119k surplus YTD The Trust has delivered a Month 02 surplus of 119k. This represents a favourable variance against plan of 21k YTD (based on a planned surplus for the year of 700k). 21k Favourable variance Expenditure Pay Expenditure Non Pay 16k Adverse variance 129k Adverse variance Pay expenditure is 16k in deficit against budget YTD. Bank & Agency spend equates to 681k in month (split 523k for Agency and 158k for Bank), which is up from the Month 01 spend of 579k. Agency spend is marginally ahead of plan in relation to the overall 4.05m Agency target for the year (actual spend of 993k against 995k plan to date). Non-Pay expenditure is 129k in deficit surplus against budget YTD. Reserves are over committed by 88k reflecting the impact of un-devolved CIP yet to be allocated down to service lines. Income & Activity 2016/17 outturn 165k Favourable variance (incl 8k contract activity over performance) The Trustwide Activity position at Month 02 is reflecting an over-performance of 8k and is explained as: Dudley CCG is now on block and so has no in-month impact Walsall CCG has over-performed by 85k Birmingham South Central CCG over-performed by 10k NCAs have over-performed against plan by 37k The activity in the Detox beds at Bushey Fields has under recovered by 9k The Net position is an over-performance of 125k, however, after taking account of the impact of the CIP target that has been applied to activity, being 117k, overall performance is marginally ahead of target. Bed days for Acute and Older Adults in Dudley continue to be low in comparison to contracted levels. Non-contracted Income such as SLA s and Education Income is ahead of plan and is adding to the current over-performance in contracted income mentioned above, giving an overall favourable income position in the month. CIP plans delivered for 2016/17 The Trust s Cost Improvement Target for the year is 2,500k and schemes have been developed for the year equating to 2,663k. The anticipated delivery of schemes taking into account the PYE of schemes starting later in the year is 2,555k which is ahead of the required target. At Month 02 CIP schemes have in the main been devolved down to budget areas with the exception of three schemes (OA Day Hospital / OA Establishment Review and Medics Establishment Review, totalling 468.3k). Income budgets also reflect 703k of CIP targets in relation Acute Wrekin beds and OA Dementia beds. Expenditure - Capital 47k spend YTD The Capital Programme has been agreed at 2,748k for the year. At present there has been minimal spend as the new financial year begins. 3
81 Overall Summary and RAG Assessment Statement of Comprehensive Income - Financial Position to 31st May 2016 Annual In Month Year To Date Plan Plan Actual Variance Plan Actual Variance Income Revenue From Activities Revenue-NHS Clinical 61,079 5,098 5,080 (18) 10,196 10, Revenue-Non NHS Clinical (9) Total Revenue From Activities 61,365 5,113 5,105 (8) 10,244 10,252 8 Other Operating Revenue Revenue-Employee Benefits Revenue-Education & Training Revenue NHS Non-Clinical Other Revenue (13) (11) Total Other Operating Revenue 2, Total Revenue 63,636 5,323 5, ,644 10, Expenditure Pay (48,642) (4,225) (4,200) 25 (8,232) (8,223) 9 Non Pay (10,745) (763) (807) (44) (1,665) (1,686) (21) Trustwide Reserves (433) (43) (112) (69) (129) (261) (131) Total Operating Expenditure (59,820) (5,031) (5,119) (88) (10,026) (10,170) (143) EBITDA 3, Depreciation (1,473) (123) (123) 0 (246) (246) 0 Amortisation (256) (21) (21) 0 (43) (43) 0 Net Operating Surplus 2, PDC (1,427) (119) (119) 0 (238) (238) 0 Interest Receivable P/L Disposal Net Surplus /(Deficit) Commentary Revenue Position The plan for the year currently reflects a planned surplus position of 700k. The Trust is reporting a surplus of 119k as at Month 02 which is 21k ahead of plan. Total Income after taking account of the impact of the applied CIP ( 703k FYE) is reflecting an over-recovery of 8k, coupled with other SLA and Educational income giving a total overrecovery of 165k on income. CIP 2016/17 Delivery The Trust has a declared plan of 2,500k for 16/17 and has schemes in place totalling 2,664k. Schemes are currently being devolved out to service lines for delivery.t the There is early indication of risks to several schemes. art of 2.143m Budgetary Reserves Trustwide Reserves are reflecting a balance of 433k for the year, and are over-committed by 131k at Month 02 this is due primarily to un-devolved CIP schemes. 4
82 Overall Summary and RAG Assessment Continued Run Rate 2016/17 Capital Programme 2016/17 '000 1, Cumulative Planned Run Rate (Surplus) Actual Run Rate '000 3,000 2,500 2,000 1,500 1, , Cumulative Planned Spend Cumulative Actual Spend CIP 2016/17 Forecast vs Actual Cash Balance 2016/17 CIP Target as per NHS Improvement 2,500 14,500 Identified Schemes (PYE) 2,555 '000 14,000 13,500 13,000 13,578 Forecast Actual Identified Schemes (FYE) 2,664 12,500 12, ,000 2,000 3,000 12,000 '000 5
83 Trust Summary Income & Expenditure Statement Including Functional Analysis Annual Plan In Month Year to Date 2016/17 Plan Actual Variance Plan Actual Variance '000 '000 '000 '000 '000 '000 '000 NHS Revenue-Activities 61,079 5,098 5, ,196 10, Revenue from LAs (9) Total Revenue from Activities 61,365 5,113 5, ,244 10,252 8 Corporate Functions Corporate Departments (12,798) (1,090) (1,109) (19) (2,140) (2,057) 83 Central Reserves (433) (43) (112) (69) (129) (261) (131) Total Corporate Functions (13,231) (1,133) (1,220) (88) (2,270) (2,318) (48) Operational Services Total Acute & Older Adults (19,520) (1,637) (1,699) (62) (3,283) (3,372) (89) Total Community Services (14,456) (1,216) (1,090) 126 (2,421) (2,294) 127 Medical Services (12,071) (979) (962) 16 (1,941) (1,919) 22 Commentary The Trust is showing an over-performance against contracted activity levels which is resulting in an favourable position of 8k. It should be noted that this is even after the impact of 117k relating to the CIP target for 2016/17. Contracted activity is over-performing in Walsall by 85k but is being offset by the impact of the CIP mentioned above. Acute and Older Adult Services are 89k overspent, which is mainly due to Inpatient area overspends (including Bank and Agency). Corporate areas are currently reflecting a surplus position which is due to surpluses within Governance, MCA DOLs, Safeguarding and Estates Maintenance. Central Reserves are reflecting the impact of CIP schemes that have yet to be devolved down to service lines. The Trust is presently reporting a surplus position for the month and for the year to date is 21k ahead of the trajectory to deliver the 700k planned surplus at year end. Total Operational Services (46,046) (3,833) (3,751) 81 (7,645) (7,585) 60 Total Expenditure (59,278) (4,965) (4,972) (6) (9,914) (9,902) 12 Sub Total 2, Interest Receivable PDC Dividend (1,427) (119) (119) 0 (238) (238) 0 Net Surplus/(Deficit)
84 Trust Income Statement Income Annual Plan In Month Year to Date 2016/17 Plan Actual Variance Plan Actual Variance '000 '000 '000 '000 '000 '000 '000 Revenue From NHS Activities Dudley CCG 28,350 2,365 2, ,730 4,730 0 Walsall CCG 27,196 2,271 2, ,542 4, NHS Walsall Sandwell & West Birmingham CCG 2, Wolverhampton CCG Birmingham Cross City CCG Birmingham South Central CCG South East Staffs & Seisdon CCG Stafford & Surrounds & E Staffs CCGs (0) Cannock Chase CCG Total Staffs CCGs Redditch & Bromsgrove CCG Wyre Forrest CCG NHS South Worcester CCG Total Worcester CCGs NCA - Adult Neuro (2) Income Generation CIP (59) (117) NCAs CAMHs Deaf 1, Total NHS Revenue-Activities 61,079 5,098 5, ,196 10, Revenue - Local Authorities Walsall MBC (8) Dudley MBC Sandwell MBC Wolverhampton MBC Stafford MBC Detox Beds (9) Dudley CRI NCA - Other HC 0 0 (0) (0) 0 (0) (0) Total Revenue from LAs (5) (9) Total Revenue from Activies 61,365 5,128 5, ,244 10,252 8 Commentary The Trust is now operating on a block contract with Dudley CCG and Walsall CCG, with the exception of C&V for Inpatients, CRS and EAS in Walsall. Neighbouring CCGs remain on block contracts with the exception of Birmingham CCGs where there is a cost per case arrangement in place for Inpatient activity that exceeds the agreed plan. Walsall activity is currently over-performing against Inpatients, CRS and EAS, however, the contract includes a cap and collar arrangement of 500k pa which limits the impact of any over/under-performance to 43k per month. Thus the chargeable activity for Month 02 is 85k, despite out-performing this cap (true over-performance is 190k). Dudley contract is under-performing at Month 02 by 85k on the traditional currency method this is due to low Inpatient activity within Older Adults (circa 157k) and Acute (circa 53k). However, as we are on a block arrangement there is no adverse financial impact in year. NCA s reflect an over-performance to date. In patient detox service at Bushey Fields has over-performed in month but is still 9k adrift against the expected activity levels to date. CIP of 703k has been applied to activity which means a required over-performance of 59k each month in order to deliver the target. Overall the Trust is over-performing to the value of 8k at Month 02 against it s contracted income. 7
85 Trust Income & Expenditure Statement - Corporate Functions Commentary Annual Plan In Month Year to Date 2016/17 Plan Actual Variance Plan Actual Variance '000 '000 '000 '000 '000 '000 '000 Corporate Functions Chief Executive (767) (69) (101) (33) (129) (138) (9) Corporate Affairs (529) (43) (41) 2 (88) (81) 7 Corporate Human Resources & Dev. & People (1,258) (108) (75) 33 (214) (172) 43 Corporate Medical (1,187) (100) (94) 5 (198) (195) 3 Corporate Estates (1,306) (109) (134) (25) (218) (235) (17) Corporate Operations (3,614) (316) (286) 31 (602) (535) 67 Corporate Finance (1,145) (96) (112) (16) (192) (194) (2) Corporate Performance & IT (2,993) (250) (265) (16) (499) (508) (8) Total Corporate Functions (12,798) (1,090) (1,109) (19) (2,140) (2,057) 83 Corp Affairs non-recurrent slippage against Business Development is currently offsetting the impact of the CDW reductions in funding from commissioners. Corp CEO - Unfunded posts within Clinical Service Dev. are currently hitting the overall CEO area. L&D slippage brought back to break even until the agreement of the service is finalised. Corp HR have been prudent and not started using LDA funds until confirmation of the allocation takes place (hence the slippage). A review of remaining CIP plans for 1617 is needed. Corp Estates Estates position has deteriorated in month due to additional Water Maintenance costs along with the premium of using Agency within the service both in Management and operational support. I anticipate that overall with some recharges that are expected, they are around a BE position. Corp Ops Additional monies have been injected into this function this month which have generated slippage along with long-standing vacancies within Ops Directorate. Corp Finance Deterioration against position due to Membership costs being due along with additional Consultancy for Hopwood. Corp IT Additional costs in month for the use of agency within the team to backfill for a managerial role. Position on target at this point of the year. 8
86 9 Trust Income & Expenditure Statement - Operational Services Operational Services Annual Plan In Month Year to Date 2016/17 Plan Actual Variance Plan Actual Variance '000 '000 '000 '000 '000 '000 '000 Acute and Older Adults Acute Access (3,440) (299) (287) 13 (601) (578) 23 Management and Administration (963) (80) (54) 26 (161) (104) 57 Acute Services (5,591) (466) (509) (43) (936) (1,041) (105) Acute Estates (2,662) (220) (217) 3 (442) (439) 3 Older Adults (6,863) (572) (632) (60) (1,143) (1,210) (66) Total Acute & Older Adults (19,520) (1,637) (1,699) (62) (3,283) (3,372) (89) Community Services Community Estates (678) (56) (61) (4) (113) (120) (7) Management and Administration 30 (2) Community Services & Recovery (5,007) (424) (387) 37 (839) (762) 77 Early Intervention (8,802) (734) (656) 78 (1,471) (1,429) 42 Recovery Services Total Community Services (14,456) (1,216) (1,090) 126 (2,421) (2,294) 127 Medical Services (12,071) (979) (962) 16 (1,941) (1,919) 22 Total Operating Services (46,046) (3,833) (3,751) 81 (7,645) (7,585) 60 Commentary Acute & Older Adult services overspent by 62k in May, including overspending of 118k on inpatients areas ( 50k Acute, 68k OA), which has been offset to some extent by management, psychology, CRHT and CMHT vacancy pay savings. The largest overspends were on Ambleside and Holyrood wards (at 34k each). Community Estates Changes in rates/rates from the previous year have contributed towards the overspend so far. Community Management CIP achievement of targets needs to be reviewed as some schemes may have changed in nature. Currently this is offset by a non-recurrent means within the Community Management Team. Community continues to generate an underspend led by the PTH/CRS group (67k) through vacancy slippage. Walsall Employment Support and Criminal Justice Team are also generating vacancy slippage Early Intervention EI teams have a number of posts vacant along with additional backfill money from LDA producing a large underspend up to M2 (36k). This is offset by the impact of the 1516 cost of Brierley Hill HC within Dudley PC which is a Cost Pressure. CAMHS across the Trust has seen new services commissioned in The slippage from this new money is supporting the usage of agency within the service. Medical services underspent by 16k in-month, due to lower than average drugs costs and the fact that training budgets are not committed in equal twelfths across the year.
87 Cost Improvement Programme Annual Schemes Schemes Transacted to Date Held Cost Improvement Programmes (by POD) Ref Plan Devolved Centrally Recurrently Non-Rec Variance FOT (slippage) Current RAG Commentary Estates - Postage CIP001 10,000 10, ,000 - Acute - Phlebotomy CIP002 12,000 12, ,000 - Acute - Wrekin Option 4 CIP , , , ,000 Community - Walsall CRS CIP , , ,810-27,953 Community - Employment Support CIP005 69,584 52,191 17, ,584-52,191 OA - Dementia Beds CIP , , , ,000 OA - Day Hosp Reconfiguration CIP007 40, , ,800-40,800 OA - Establishment Review CIP008 77, , ,500-77,500 EIA - Developments CIP , , ,800 9,200 66,680 - Medics - Establishment Review CIP , , , ,000 CEO - Admin Review CIP011 10,734 5,367 5, ,734 - CEO - Emergency Planning CIP012 10,000 10, ,000 - CEO - Office Furniture CIP013 5,000 5, , W&D - Library CIP014 1,531 1, , W&D - NonPay CIP015 8,000 8, , Corp Dev - NonPay CIP016 10,000 10, , W&D - Payroll CIP017 24,000 12,121 11,879 12, ,879 - Finance - Pay & NonPay CIP018 38,500 31,540 6,960 21,840 12,500 4,160 - CEO - PMO CIP019 33,583 33, , IM&T - Subject Access CIP020 2,400 2, , IM&T - Establishment Review CIP021 40,659 40, , Corporate - NI Savings CIP022 90,000 90, , Corporate - Savings (NP Inflation) CIP , , , Corporate - Incremental Drift CIP , , , Corporate - Reduction in Trust Surplus CIP , , , Psych Liaison Overheads CIP026 24,636 24, , MH Urgent Care Overheads CIP027 35,499 35, , Procurement CIP028 50, , ,000 - Total CIPs 2,663,916 2,103, ,299 1,102,138 33,231 1,528,547-1,251,444 Annual Target 16/17 2,500,000 Excess of Schemes Above Plan 163,916 Target for 2016/17 = 2,500k. Trust has identified schemes for the year which could deliver 2,664k FYE. As at month 02 2,104k of the schemes had been devolved to appropriate budget areas and 560k were being managed centrally in reserves. Of those devolved schemes 1,529k have been transacted to date. As at month 02 a forward look of the schemes in terms of progress/action/planning would suggest that there are several schemes still at risk on nondelivery. These have been highlighted in the table opposite under the FOT (slippage) column and currently equate to 1,251k of risk. These schemes either need to be progressed at pace or mitigating plans put forward in order to ensure the annual target is delivered. Those schemes flagged as Amber currently have mitigation plans being worked up with a view to fully deliver against target. 10
88 Capital Programme Proposed Capital Funding 2016/17 '000 Depreciation & Amortisation 1,864 Unspent Capital Monies (Capital to Revenue Transfer 2015/16) 785 Proposed Cash to capital conversion 99 Total Funding Available 2,748 Plan YTD Expenditure YTD Capital Schemes 2015/16 Plan Adj. in Year FOT Actual Accrued Total Variance '000 '000 '000 '000 '000 '000 '000 Schemes carried forward from 2015/16 Mop up of old year schemes Commentary The Trust has agreed an annual plan of 2,748k for 2016/17. There has been very little capital expenditure during the first two months of the financial year. This is to be expected as the new financial year gets underway. ESTATES Backlog Maintenance BFH - Windows Old Hill House Redecoration Halesview Roof BFH - Patient Bathroom and Bedrooms DPH - Internal Fire Doors BLX - Cleaners Rooms Life Cycle Contingency Anti-Ligature Unallocated IT Business Intelligence Electronic Patient Record 1, , ,183 Provision DocMan Hub Enterprise Wide Agreement for Windows Mobile Device Management (MDM) Solution IT Replacement Contingency Total Cost of Capital Schemes 2, , ,701 11
89 Financial Performance Metrics M01 M02 M03 Forecast Outturn subcode Plan Actual Plan Actual Plan Actual Plan Actual Liquidity Ratio Days n/a Liquidity Ratio Metric n/a Liquidity Ratio Days 25% weighting value <-14 score Capital Servicing Capacity n/a Capital Servicing Metric n/a Continuity of Services Risk Rating n/a Capital Servicing Capacity 25% weighting value <1.25 score I&E Margin n/a I&E Margin Rating n/a I&E Margin Variance n/a I&E Margin Variance from Plan Rating n/a I&E Margin 25% weighting value <=-1 I&E Margin Variance from Plan score % weighting value <=-2 Financial Sustainability Risk Rating n/a score Commentary The Trust is monitored by NHS Improvement each month in order to demonstrate Financial Sustainability through the calculation of four metrics: Capital Service Capacity (Revenue available for Debt service and or Capital service), Liquidity (Cash for Liquidity relative to turnover), I&E Margin and I&E Margin Variance from Plan. For 2016/17 the Trust Plan is a Financial Sustainability Risk Rating of 4. For Month 02 the Trust is reporting a rating of 4 in line with plan. Individually the metrics for the current month reflect: Liquidity Ratio score for Month 02 is 4 based on the number of days. This score is in line with forecast. The Capital Servicing Capacity score for Month 02 is 3. A score of 2.5 or above will deliver a maximum metric score of 4 and the Trust has achieved a score of 3. The Trust is reporting an I&E Margin ratio of 1.1 in line with forecast. A score of 1.0 or higher gives a maximum metric score of 4. In terms of I&E Margin Variance from Plan the Trust is reporting a ratio of 4 in Month 02. A score of (1.0) or above gives a metric score of 3, whilst above 0 gives a score of the maximum of 4. The four metrics are therefore combined to give a combined metric score of 4 for the period. 12
90 NHS Improvement Agency Expenditure Cap 16/17 Agency Analysis (TFR 3) ACTUALS ( 000's) Expenditure In Month as at Agency Staffing Mth 1 Mth 2 Mth 3 Mth 4 Mth 5 Mth 6 Mth 7 Mth 8 Mth 9 Mth 10 Mth 11 Mth 12 Qualified Nursing Medical Other (Incl. Admin, Estates, HCA's, AHP's) Total Agency Staffing Total Employee Benefits Total Staffing Costs (Substantive + Agency + Bank) 4,058 4, Agency as % of Total Staffing (incl Agency) 11.59% 12.34% Cumulative Position 11.59% 11.97% of which, relate to 'pilot' schemes (backfill agency costs circa): MH Urgent Care Centre Street Triage CAMHs Tier PLAN ( 000's) Expenditure In Month as at Agency Staffing Mth 1 Mth 2 Mth 3 Mth 4 Mth 5 Mth 6 Mth 7 Mth 8 Mth 9 Mth 10 Mth 11 Mth 12 Qualified Nursing Medical Other (Incl. Admin, Estates, HCA's, AHP's) Total Agency Staffing Total Employee Benefits Total Staffing Costs (Substantive + Agency + Bank) 4,122 4,160 4,173 4,136 4,135 4,125 4,125 4,124 4,123 4,126 4,119 4,122 Agency as % of Total Staffing (incl Agency) 12.30% 11.73% 10.06% 8.00% 7.88% 6.88% 6.88% 6.89% 6.84% 6.83% 6.82% 6.82% Cumulative Position 12.30% 12.01% 11.36% 10.52% 10.00% 9.48% 9.11% 8.83% 8.61% 8.44% 8.29% 8.17% Commentary For 2016/17 the Trust has been tasked with working within an overall agency expenditure cap of 4.05m for the year, which represents a circa. 35% reduction on the actual spend in 2015/16. The planned spend across the year has been profiled in line with the workforce plan based on increasing recruitment of substantive staff and the use of bank staff to offset the previously required use of agency staff. At Month 2 the Trust is 2k ahead of plan in terms of anticipated agency spend ( 993k spend against 995k plan). The Trust continues to monitor the use of agencies to ensure that only framework approved suppliers are in place and has now received responses back from all agencies currently being used and is now receiving weekly monitoring reports from agency suppliers around usage and adherence/non-adherence to price caps. Additional detail will be supplied in future reports. 13
 Trade and Other Payables have decreased over the period (a negative impact on cash) The Trust has")
 The impact of all these movements was to reduce")
91 Cash Flow Statement Commentary Cash Flow The Trust has made an operating surplus of 350k in 2016/17 and received cash of 288k in respect of depreciation and amortisation Trade and Other Receivables have increased over the period (a negative impact on cash) Trade and Other Payables have decreased over the period (a negative impact on cash) The Trust has received 7k of interest, and spent 369k on capital ( 322k on reducing capital payables from the 2015/16 year end and 47k on 2015/16 capital expenditure). Total capital expenditure in cash terms was less than the cash received for depreciation and amortisation (a negative impact on cash) The impact of all these movements was to reduce the Trust s cash balance YTD by 717k 14
92 Payables Performance & Aged Debt Commentary on Payables Better Payment Practice Code Agreed Tolerances Transactions by Number Value Non-NHS <75% 75% - 95% >95% Mth % 85.73% Mth % 93.99% Mth % 0.00% Non-NHS YTD 81.31% 88.73% NHS <75% 75% - 95% >95% Mth % 85.40% Mth % 89.71% Mth % 0.00% NHS YTD 91.76% 87.85% Debt Profile and Value Current days days days 121+ days Total ,008 Aged Debt Value % of Total Agreed Tolerances 000 Debt Over 91 days >20% 10% - 20% <10% % Over 120 days >10% 5% - 10% <5% % Commentary on Aged Debt Aged Debt as of May 2016 Current days days days 120+ days 20.4% 24.0% 0.0% 8.0% 47.6% Better Payment Practice Code The Trust has not achieved the required target for NHS invoices by number and value in both current month and YTD. It has also fallen short in terms of Non-NHS invoices being paid within 30days by both number and by value. Performance in April was impacted by the decision to hold payments at the end of March to ensure the Trusts cash balance remained within External Financing Limits at the year end. May s figures are now reflecting a favourable movement towards target. Aged Debt Profile by Value 8% of debt was aged 90 days or older at the end of April (this figure was 14% at the end of the previous month). Debt over 120 days old (totalling 81k) relates in the main to Overspill beds recharge with W ton CCG of 10.8k. Barnet CCG re NCAs of 10.5k Walsall MBC 20.2k re Nurse Specialist Pay recharge, 32.5k re CAMHs Pay recharge and 5.6k re Behaviour Support team.. 15


93 Statement of Financial Position Commentary Non Current Assets Amortisation and depreciation exceeds capital expenditure for the year decreasing the value of the Trust s Non- Current Assets in the year Final outturn against capital schemes is reviewed later in this report Current Assets Receivables have increased by 499k in 2016/17 Cash is 716k lower than the balance at 31 March 2016 An analysis of cash flows can be seen elsewhere in this report Current Liabilities Payables have reduced by 562k in the financial year. There has been a small decrease in provisions in the year. Tax Payers Equity The Current Year I&E figure reflects the surplus for the year to date of 118k. This is 20k ahead of plan for Mth /17. 16
94 PbR Briefing Paper 16/03/16. Following an external audit of PbR and clustering, 3 recommendations were made to ensure improved PbR performance. As part of 16/17 contract negotiations, both Dudley and Walsall CCG s are proposing PbR KPI s for next year contracts. Audit recommendations & actions are available within the Audit report, while CCG KPI s are detailed below (subject to change). To satisfy audit recommendations and for the Trust to achieve KPI s, the below table highlights the main issues for operations and medical teams. Proposed KPI s (16/17) Clustered Caseloads 95% (KPI) Key Issues Operations Main Issues Medical Main Issues Update 18/05/16 Trust performance currently around 90%. There are significant DQ issues within caseloads that are effecting the overall % - these have been highlighted at CARM and CPG. There are still gaps and non-adherence to processes and clustering responsibilities that mean patients are still entering services unclustered. Inpatient cluster performanceresponsibilities and process need to be agreed Data Quality issues. Ensuring clinical processes are followed to maintain accurate clustered caseloads and financial stability There remain consultant teams who are not engaged in the clustering process and clustered caseloads remain in the red zone and significantly below 90% clustered. These are mostly Older Adult Consultants There have been a number of temporary medical secretaries employed to cover gaps in the medical secretary workforce. This has resulted in a drop in cluster performance as these staff have required training and support to enter data. Data Quality issues. Ensuring clinical processes are followed to maintain accurate caseloads and financial stability Meeting with medical Directors on 09/05/16 to review all consultant teams clustering performance. Medical Directors to performance manage consultants where clustering of caseloads is low. IMT to send mthly report to all consultant teams of their clustering/ cluster review/ ICD 10 performance PbR lead to visit CRHT and EI teams as consultant caseloads are influenced directly by teams clustering performance. Ward mangers to have Cluster training during May to reduce admitted unclustered activity- this action is support by Director of Operations and will be monitored through Acute Standards meeting. Enc 10 App 1 PbR Briefing Paper (3) Page 1 of 2
95 Cluster Review 95% by Q4 Q1 70% Q2 80% Q3 90% Q4 95% Cluster review performance has improved significantly within year and is now approx. 68%. Trust remains focussed on CPA review performance reporting and KPIs. There are significantly more Non CPA patients across all teams than CPA patients. Culture shift towards Cluster review from CPA review and widening in cohort of in-scope patients Current outpatient practice and processes for those patients seen singularly by medics will not support patients being reviewed within cluster review periods due to an average DNA rate 20% and Capacity for appointments to meet demand Meeting with medical Directors on 09/05/16 to review all consultant teams cluster review performance. Medical Directors to performance manage consultants where review of clusters is low. PbR lead to attend May Community Service Standard meeting to address cluster review performance with CRS teams. ICD 10 Codes N/A An ICD 10 code needs to be updated every 12 months within OASIS for it be valid regardless of if the diagnosis has changed or not. IMT to send out monthly reports to all consultants to show patients where there is no diagnosis recorded. Communications sent by medical secretary lead instructing medical secretaries to update ICD 10 codes after every Out Patient appointment. Enc 10 App 1 PbR Briefing Paper (3) Page 2 of 2
96 Trust Contract Performance Report Month /17 1
97 Part 1 Contractual Quality Requirements Trust and CCGs (In month performance and monthly trends) KPI No KPI Detail and Target Trust Dudley CCG Walsall CCG Trust Monthly Trend Dudley CCG Trend Walsall CCG Trend 1 Percentage of Service Users on incomplete RTT pathways (yet to start treatment) waiting no more than 18 weeks from Referral. (Target: Above 92%) 100% 100% 100% 2 Care Programme Approach (CPA): The percentage of Service Users under adult mental illness specialties on CPA who were followed up within 7 days of discharge from psychiatric in-patient care. (Target: Above 95%) 96.2% 95.9% 98% 3 Completion of a valid NHS Number field in mental health and acute commissioning data sets submitted via SUS (Target: Above 99%) 99.7% 100% 99.9% 4 5 Completion of Mental Health Minimum Data Set ethnicity coding for all detained and informal Service Users. (Target: Above 90%) Completion of IAPT Minimum Data Set outcome data for all appropriate Service Users. (Target: Above 90%) 91.9% 95.2% 92.3% 96.7% 97.8% 95.3% 6 Delayed Transfer of Care (All Reasons). (Target: Below 7.5%) 0.0% 0.0% 0.0% N/A 7a 7b 8a 8b IAPT - Proportion of people who complete treatment who are moving to recovery. (Target Dudley: Above 50%) IAPT - Proportion of people who complete treatment who are moving to recovery. (Target Walsall: Above 50%) IAPT - number of people who receive psychological therapies. (Target Dudley: 5108 pa; 426 per month) IAPT - number of people who receive psychological therapies. (Target Walsall: 4328 pa; 361 per month) N/A 53.7% N/A N/A N/A N/A N/A 53.0% N/A N/A N/A 479 N/A N/A N/A N/A N/A 427 N/A N/A 9 Percentage of patients who are provided a copy of their care plan. Target: Above 95%) 94.7% 94.5% 95.3% Number of home treatment episodes by crisis teams. (Target Walsall only: 608 pa; 51 per month) Percentage of people experiencing a first episode of psychosis will be treated with a NICE approved care package within two weeks of referral. (Target: Above 50%) 54 N/A 54 N/A 63.6% 50.0% 71% 2
98 Part 1 Contractual Quality Requirements Trust and CCGs (In month performance and monthly trends) KPI No KPI Detail and Target Trust Dudley CCG Walsall CCG Trust Monthly Trend Dudley CCG Trend Walsall CCG Trend The proportion of people that wait 6 weeks or less from referral to their first IAPT treatment appointment against the number of people who enter treatment in the reporting period. (Target: Above 75%) The proportion of people that wait 18 weeks or less from referral to their first IAPT treatment appointment against the number of people who enter treatment in the reporting period. (Target: Above 95%) 89.4% 90.3% 88.4% 98.6% 100% 97.4% 14 The proportion of users on CPA who have had a review within the last 12 months. (Target: Above 95%) 96.0% 95.3% 96.6% The proportion of users on CPA with a crisis plan in place. (Target: Walsall Only: Q1 - no target; Q2-75%; Q3-85%; Q4-95%) The proportion of users with a valid ICD10 diagnosis code recorded. (Target: (Dudley: M1-75%; M2-80%; M3-85%; Q2 and Q3-90%; Q4-95%);(Walsall - TBC)) 95.2% N/A 96.0% N/A 71.6% 78.7% 68.4% 17 Proportion of in-scope patients assigned to a cluster. (Target: Above 95%) 93.6% 93.5% 95.3% 18 Proportion of patients within cluster review periods. (Target: (Dudley Q1-70%; Q2-80%; Q3-90%; Q4-95%); (Walsall Q1-70%; Q2-76.5%; Q3-83%; Q4-90%)) 69.4% 73.7% 66.1% 19 Sleeping Accommodation Breach Duty of Candour Zero tolerance RTT waits over 52 weeks for incomplete pathways IAPT DNA Rate (Target Walsall Only: Below 13.1%) N/A N/A 11% N/A N/A 23 Memory Assessment Service - Face to face initial assessment to be made within 20 days (Target Walsall Only: Above 95%) N/A N/A 98.0% N/A N/A 24 Dudley and Walsall Recovery Outcome Measure - Number of CPA patients assessed using DWROM (Target Dudley Only: Q1-65%; Q2-75%; Q3-85%; Q4-95%) N/A 58.0% N/A N/A N/A 3
99 Performance Dashboard Month 2 Presented at Trust Board 7 July 2016
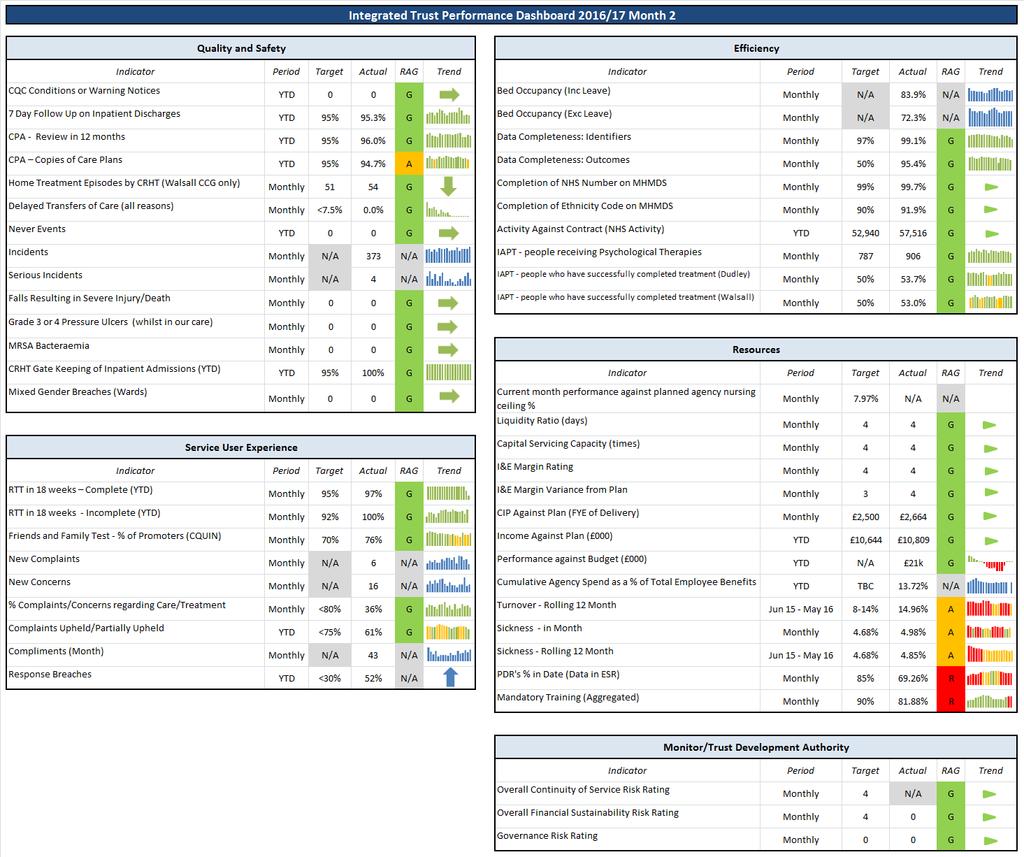
100
101 Trust Level Integrated Dashboard Commentary Quality and Safety Domain During the month of May, 373 incidents were reported by the Trust, of these 184 related to Patient Safety Incidents. This has increased from 326 reported in April. There were 4 serious incidents logged by the Trust as reported from the Safeguarding systems in May (8 reported in April). The numbers of incidents reported for non-operational teams have increased from 6 in April to 9 in May CPA Copies of Care Plan the Trust is below the 95% threshold at 94.7% at Month /17. Efficiency Domain Activity against contract (NHS Activity) NHS contracted activity remains above the target as at month two. In May, the Trust is reporting 57,516 units of activity against a target of 52,940. Activity against contract is above target for all service lines. Service User Experience There has been a decrease in the number of complaints to the Trust. 12 reported in April to 6 reported in May. Resources Domain The Trust s Cost Improvement Target for the year is 2,500k and schemes have been developed for the year equating to 2,663k. The anticipated delivery of schemes taking into account the PYE of schemes starting later in the year is 2,555k which is ahead of the required target. At Month 2 CIP schemes have in the main been devolved down to budget areas with the exception of three schemes (OA Day Hospital / OA Establishment Review and Medics Establishment Review, totalling 468.3k). Income budgets also reflect 703k of CIP targets in relation Acute Wrekin beds and Older Adults Dementia beds. Vacancies There are currently 156FTE contracted vacancies giving the Trust a vacancy rate of 14.4%. Contracted vacancies across the Trust have reduced from 187 FTE in Nov-15. Turnover The 12 Month Turnover rate has increased slightly 15.0% from 14.9%. The rate continues to be high and is attributable to the departure of individuals under TUPE. Turnover excluding TUPE employees transfers is 11.7% and is inline with other Mental Health Trusts. Sickness Absence The 12 month rolling sickness rate has remained relatively static across the last 3 months, with a current figure 4.8% in Month month sickness was 5.1% in May-15 so there has been an overall reduction in sickness over the past 12 months. Appraisal Compliance is currently 69.3% and is below Trust target. This has reduced from 87.0% in Oct-15. There are 233 employees in the Trust that haven't had an appraisal in the last 12 months. New reports are being distributed to Service leads in June to assist with when Appraisals should be completed for each member of staff. Mandatory Training - Mandatory Training compliance is 81.9% as at the end of Month 2, which is below the Trust s new target for 2016/17 of 90% (IG remains at 95%). As with the Appraisal, new reports are being distributed to Service leads in June to assist with what training individuals need to undertake over the remainder of 2016/17 in order to achieve compliance against target.
. 12 month sickness has slightly increased to 7.07% as at May 2016 (6.63% reported in month one).")
102 Service Line Summary Acute & Access Service incident figures have shown a slight increase when compared to the previous month. 178 were reported in April in comparison to 185 reported for May. Acute Services sickness in-month has increased to 6.41% in month two (5.02% reported in month one). 12 month sickness has slightly increased to 7.07% as at May 2016 (6.63% reported in month one). This remains above Target for the 12 month rolling picture due to performance throughout the year and will continue to be monitored. Performance for Mandatory Training has slightly decreased to 73.8% in month two (74.2% in month one). Appraisal performance has decreased from 72.09% in month one to 60% in month two, therefore this service remains below the 85% target. New reports are in development which will be sent to managers to facilitate planning of appraisals during 2016/17. This service line overspent by 82k up to month 2 to date. The current month variance includes an overspend of 50k on Acute ward staffing ( 118k YTD), partially offset by various non-ward vacancy savings (psychology and management posts), and non pay savings.
. Mandatory training has slightly increased to 83.")
103 Service Line Summary CPA Formal Review and Copies of Care Plan this service has remained above target for the entire 2015/16 financial year and continues to remain above target for Months 1 and /17. Community Services and Recovery in month sickness has decreased in month two and is now compliant reporting at 4.65% (6.32% in month one). Mandatory training has slightly increased to 83.76% in month two (81.94% reported in month one). Appraisals there has been a slight increase in performance in month two to 60.38% (58.82% reported in month one). New reports are in development which will be sent to managers to facilitate planning of appraisals during 2016/17. Community & Recovery Services position at month 2 is 84k underspent. The underspend continues to be driven by vacancies within the Psychological Therapy Hub and CRS.

104 Service Line Summary Early Intervention sickness has seen an decrease to 4.78% in month two (5.0% in month one). The 12 month sickness has slightly increased to 4.21% as at month 2 but still remains compliant. Mandatory training has slightly decreased from 90.14% in month one to 87.08% in month two. There has been an increase in performance for Appraisals from 76.51% in month two to 80.77% in month two therefore this service remains below the 85% target. New reports are in development which will be sent to managers to facilitate planning of appraisals during 2016/17. This service line is underspent by 42k as of month 2, again in the main due to a number of vacancies following allocation of funds from commissioners.

105 Service Line Summary Copies of Care Plan is below the 95% threshold and Head of Service is reviewing the reported exceptions with the clinical Teams. There has been an increase in incidents for this service, 120 reported in April when compared to 149 reported in May. Older Adults sickness has increased from 3.61% in month one to 5.65% in month two. The 12 month sickness has slightly decreased from 5.22% in month one to 5.26% in month two, this service remains below Target for both sickness indicators and will continue to be monitored. There has been a slight decrease in performance for appraisals from 61% in month one to 58.49% in month two and the service remains below the 85% target. New reports are in development which will be sent to managers to facilitate planning of appraisals during 2016/17. Mandatory training remains below the 90% target at 80.67% (79.45% reported in month one). This service line is overspent by 66k in month 2 which is primarily due to an overspend on staffing within Older Adult ward staffing. In-Patient budgets are currently overspent by 91k to date.
106 Board meeting date: 7 th July 2016 Agenda Item number: e Enclosure: 13 Report Title: Cost Improvement Programme (CIP) Progress Report June 2016 Accountable Director: Author (name & title): Rupert Davies, Interim Director of Finance Jacky O Sullivan, Clinical Development Director Purpose of the report: To present to the Board a summary of the current status of the Cost Improvement Programme for 2016/17 Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: CIP Programme Board & MExT Date reviewed: 22 nd June 2016 & 5 th July 2016 Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Effective Well-led Safe Please give brief details: Plans use evidence based practice to ensure improvements in quality, outcomes and patient experience. Plans are developed to ensure responsiveness to service user needs. Plans represent best value to ensure CIP plans are met through efficiency and effectiveness All transformational and service development plans have a project team approach to both development and implementation. All plans are assessed for the need for a Quality Impact Assessment and where indicated a full assessment including risks and mitigations is undertaken and monitored. Enc 13 CIP report June 16 v2 Page 1 of 15
107 CIP ideas brainstormed and scoped by Management Executive Team (MExT) and wider Review of all strategic themes by Trust Board to agree which proceed further within these parameters: High Quality Services Inclusive Partnerships Supporting Strategies Effective & Efficient Resources Leadership Culture Responsible Workforce No Idea archived Yes Idea developed and presented to MExT MExT approve/reject No Idea archived Summary of schemes including Quality Impact Assessment (QIA) & risks submitted to Trust Board Project Overview Document (POD) developed & submitted to MExT for approval & sign off including QIA, EIA, PIA & risks All projects complete POD Completed PODs & QIA signed off by Director of Nursing and Medical Directors and MExT Implementation Stage Final QIA and risks presented to MExT for project closure QIA & risks on delivered projects presented to MExT for sign off including Director of Nursing & Medical Directors Final QIA and risks presented to Trust Board for final sign off Enc 13 CIP report June 16 v2 Page 2 of 15
108 Title Cost Improvement Programme (CIP) Progress Report June 2016 Introduction The purpose of this report is to present to the Board the summary of the current status of the Cost Improvement Programme for 2016/17. Summary of key points, issues and risks 1.0 CIP 2015/16 There were 32 projects in 2015/16 of which 30 were delivered and closed down. 2 schemes have been carried over into 2016/17 at the request of the Executive Sponsor: POD085 Catering Review POD088 Corporate Clinical Leadership Structures These schemes have delivered savings; however they are being monitored for any negative impact, and will be reassessed for closure in quarter CIP 2016/ Target for 2016/17 2,500 Projects in total (full year effect) 2,594 ( 468,300 pending approval) Variance 94 CIP targets are devolved down to team budgets so any slippage is managed at team level. A full list of projects can be found in appendix 1. There are 4 schemes that will deliver savings non-recurrently; these are listed in appendix 2. There are 28 projects for the current year, of which 3 are under review and subject to approval prior to implementation, these schemes are: Redesign of Day Opportunities ( 40,800) Older Adults Establishment Review ( 77,500) Medical Services Establishment Review ( 350,000) The first two schemes link to Walsall CCG s Quality, Innovation, Productivity and Prevention (QIPP) schemes; the quality impact assessments are being completed and will be presented to the Board. The latter scheme is under review and the quality impact assessment will be presented to the Board. Of the 28 projects for the current year, 12 have delivered and will be presented to Enhanced MExT in July for closure (appendix 1.2). 1 scheme (Employment Support Services Review, value 69,584) has been closed as it will not deliver savings. The project in total value has been adjusted to reflect this. It can be seen in appendix 1.1 that there are 9 schemes with an overall project status of red. The projects are: - Postage Enc 13 CIP report June 16 v2 Page 3 of 15
109 Acute Services Wrekin Ward Beds Walsall Community Recovery Service (CRS) activity and staff establishment Older Adults Inpatient beds (Dementia) Redesign of Day Opportunities Older Adults Establishment Review Medical Services Establishment Review Payroll Performance & IM&T Establishment Changes Postage (value 10,000) The project is RAG rated red as savings have not been identified. The scheme is being monitored. Savings from waste management is being explored as an alternative scheme. Acute Services Wrekin Ward Beds (value 400,000) The project is RAG rated red due to the finance, the scheme is being progressed but there is slippage. Walsall CRS activity and staff establishment (value 111,810) The project is RAG rated red due to the finance. The scheme links to the Walsall Rehab QIPP scheme which is being progressed and expected to deliver in July. Older Adults Inpatient beds (Dementia) (value 303,000) The scheme has identified red risks, and the finance is RAG rated red. The scheme is being scoped which is looking positive in terms of this schemes development and financing. Milestones for delivery need to be developed. Redesign of Day Opportunities (value 40,800) The scheme is pending approval. The QIA is to be taken to Enhanced MExT in July. Older Adults Establishment Review (value 77,500) The scheme is pending approval. The QIA is to be taken to Enhanced MExT in July. Medical Services Establishment Review (value 350,000) The scheme is pending approval. The QIA is to be taken to Enhanced MExT in July. Payroll (value 24,000) The scheme is being progressed. There will be a part year effect which should be met in full. Performance & IM&T Establishment Changes (value 40,659) The scheme has red risks which will be monitored. The CIP has been transacted. The CIP Programme Board will be monitoring and tracking the progress of these red rated schemes to report risks, and mitigations to Enhanced MExT and the Board. The RAG rating for the forecast year end position is as follows: - RED Will not achieve full target AMBER Will not deliver full target until 17/18 GREEN Will achieve FYE by March 17 Enc 13 CIP report June 16 v2 Page 4 of 15
110 Further detail (if required) Appendix 1 and 2 contain further details of the schemes. Recommendation Trust Board members are asked to note the contents of this report and receive it for information and assurance. Board action required No action is required. Enc 13 CIP report June 16 v2 Page 5 of 15
111 Appendix /17 CIP schemes 1.1 Active Projects Operations Scheme Executive Lead Links to other projects Value Overall Project Status Plan Finance Risks QIA EIA PIA KPIs Implementation Month Quarter 1 RAG Quarter 1 Financial Position Forecast Year End RAG Forecast Year End Position Postage This project aims to reduce the overall spend on the postal costs going out of the Trust by 10k by increasing efficiency and utilising electronic methods of communication. The forecast year end position is red as savings have not been realised to date and an alternative scheme to deliver the CIP target is being explored. Wendy Pugh None 10,000 R A R A 0 N/A April 16 R 0 R 0 No impact No impact Phlebotomy The project seeks to provide the Phlebotomy service effectively and efficiently in house, rather than buying it in. A rebate from one of the SLAs has met the CIP target non recurrently whilst negotiations continue to unpick the SLA on a recurrent basis. Wendy Pugh None 12,000 A A G A 0 N/A To be confirmed G 3,000 G 12,000 No impact No impact Enc 13 CIP report June 16 v2 Page 6 of 15
112 Acute Services Wrekin Ward Walsall CRS Activity & Staff Establishment The project is an income generation scheme that aims to provide 5 acute beds on Wrekin ward to another commissioner / provider. The scheme is forecasted to achieve the CIP target, however this is dependent on having a plan in place and the scheme being progressed and monitored. Wendy Pugh None 400,000 R R R A A No impact No impact days readmission 2. The Average Length of Stay 3. 7 day follow up 4. Bed Occupancy 5. Activity against Contract 6. Delayed transfers of care July 16 R 0 G 400,000 The project is about implementing the findings from the Meridian review and therefore reducing activity and associated workforce. The scheme is linked to the QIPP Rehab service which is being progressed. There is a 3 month slippage. Wendy Pugh None 111,180 R A R A A N/A July 16 R 0 A 83,857 No impact No impact Older Adults Inpatient Beds This project is an income generation scheme to utilise existing capacity in the Dementia Wards to accommodate those patients that have a diagnosis of Dementia who are medically fit for discharge and are Delayed Transfers of Care from WMH/RHH. The scheme is forecasted to achieve the CIP target on the basis that a plan is in place and the scheme is being progressed. Enc 13 CIP report June 16 v2 Page 7 of 15
113 (Dementia) Wendy Pugh None 303,000 R A R R R N/A To be confirmed R 0 G 303,000 No impact No impact Redesign of Day Opportunities This project relates to commissioner intentions to redesign Older Adult Day Services. Savings will be realised from catering and transport. Wendy Pugh None 40,800 R R A No impact No impact N/A Pending approval R 0 Older Adults Establishment Review The project is about implementing the findings from the Meridian review and therefore reducing activity and associated workforce. Wendy Pugh None 77,500 R A A No impact No impact N/A Pending approval R 0 Early Intervention Service Line Interventions This project relates to increased efficiency and productivity in the Early Intervention Service line and associated corporate services by providing a number of new service developments within existing overheads. Wendy Pugh None 179,680 A G G A A No impact No impact N/A April 16 G 28,250 G 179,680 Enc 13 CIP report June 16 v2 Page 8 of 15
114 Medical Scheme Executive Lead Links to other projects Value Overall Project Status Plan Finance Risks QIA EIA PIA KPIs Implementation Month Quarter 1 RAG Quarter 1 Financial Position Forecast Year End RAG Forecast Year End Position Medical Services Establishment Review The scheme is about increased efficiency and productivity within the medical service line. Mark Weaver / Kate Gingell None 350,000 R A A No impact No impact N/A Pending approval R 0 Enc 13 CIP report June 16 v2 Page 9 of 15
115 Corporate Scheme Executive Lead Links to other projects Value Overall Project Status Plan Finance Risks QIA EIA PIA KPIs Implementation Month Quarter 1 RAG Quarter 1 Financial Position Forecast Year End RAG Forecast Year End Position CEO Led Admin Review This project aims to review all administration roles across the Trust, reviewing how staff could work closer together, reducing duplication across all areas. Mark Axcell None 10,734 A G G A A N/A October 16 G 0 G 5,367 No impact No impact Payroll This project delivers a more efficient payroll service through economies of scale and removal of the SBS contract. A PYE is expected from the scheme. Marsha Ingram None 24,000 R R R A A No impact 9 N/A October 16 R 0 A 12,018 Finance Department Pay & Non Pay Savings This project has identified efficiency savings in budgets across all financial services in both pay and non-pay. Rupert Davies None 38,500 A G G A A No impact No impact N/A April 16 G 5,449 G 31,540 PMO Efficiencies A review of roles within the Clinical Service Development Team has enabled the PMO facilitator post to be released for efficiencies. The scheme has delivered, however the risks are being monitored. Enc 13 CIP report June 16 v2 Page 10 of 15
116 Mark Axcell None 33,583 A G G A A No impact No impact N/A April 16 G 8,396 G 33,583 Performance & IM&T Establishment Changes Procurement & Tendering A review of roles with the Performance & IM&T team has released savings within the establishment to deliver this project. The scheme has delivered however the risks are being monitored. Rupert Davies None 40,659 R G G R A No impact No impact N/A April 16 G 10,165 G 40,659 This project will develop a process for maximising best value on non-pay spends influenced by the procurement process. Rupert Davies None 50,000 A A A G 0 No impact No impact N/A To be confirmed R 0 G 50,000 Key: QIA = Quality Impact Assessment EIA = Equality Impact Assessment PIA = Privacy Impact Assessment KPIs = Key Performance Indicators Enc 13 CIP report June 16 v2 Page 11 of 15
117 1.2 Projects presented to MExT for closure in July Scheme Executive Lead Links to other projects Value Overall Project Status Plan Finance Risks QIA EIA PIA KPIs Implementation Month Quarter 1 RAG Quarter 1 Financial Position Forecast Year End RAG Forecast Year End Position Employment Review of the Employment Support Services. Scheme closed as it will not deliver savings. Support Services Review Wendy Pugh None 69,584 Closed Healthcare Emergency Planning The Trust contributes to a regional fund as well as commission a service locally, this project proposes to cease the regional contribution and continue with local arrangements for Healthcare Emergency Planning. Mark Axcell None 10,000 G G G G 0 N/A April 16 G 2,500 G 10,000 No impact No impact Office Furniture The project aims to reduce expenditure on office furniture by setting up a page on the Intranet for staff to share spare furniture and equipment. Mark Axcell None 5,000 G G G G 0 N/A April 16 G 1,250 G 5,000 No impact No impact Library Services Library Services have identified 3 duplicate journals which can be removed and are available both as print and electronic at both Library sites. Marsha Ingram None 1,531 G G G G G No impact No impact N/A April 16 G 383 G 1,531 People & This project releases non pay savings from the People & Workforce Development budget. Enc 13 CIP report June 16 v2 Page 12 of 15
118 Workforce Development Non Pay Marsha Ingram None 8,000 G G G G 0 No impact No impact N/A April 16 G 2,000 G 8,000 Corporate Development Non Pay Savings This project releases non pay savings from the Corporate Affairs budget. Marsha Ingram None 10,000 G G G G 0 No impact No impact N/A April 16 G 2,500 G 10,000 Subject Access Requests Planned National Insurance Savings The scheme involves updating policies and procedures to charge solicitors for fulfilling subject access requests. Rupert Davies None 2,400 G G G G 0 No impact No impact An over provision for planned NI savings means the surplus can now be released for cost improvement. Rupert Davies None 90,000 G G G G 0 No impact No impact N/A April 16 G 600 G 2,400 N/A April 16 G 22,500 G 90,000 Corporate Savings Topslice Inflation Reserve by 20%. Rupert Davies None 125,000 G G G G 0 No impact No impact N/A April 16 G 31,250 G 125,000 Incremental Drift A low turnover of staff means that the budget for incremental drift will be less than planned which releases savings for cost improvement. Rupert Davies None 350,000 G G G G 0 No impact No impact N/A April 16 G 87,500 G 350,000 Reduction in This project is delivered by a reduction in the planned surplus. Enc 13 CIP report June 16 v2 Page 13 of 15
119 Planned Surplus Rupert Davies None 250,000 G G G G 0 No impact No impact N/A April 16 G 62,500 G 250,000 Psychiatric Liaison Overheads MH Urgent Care Overheads This project relates to increased efficiency and productivity in corporate services by providing Psychiatric Liaison within existing overheads. Rupert Davies None 24,636 G G G G G No impact No impact N/A April 16 G 6,159 G 24,636 This project relates to increased efficiency and productivity in corporate services by providing MHUC within existing overheads. Rupert Davies None 35,499 G G G G G No impact No impact N/A April 16 G 8,875 G 35,499 Enc 13 CIP report June 16 v2 Page 14 of 15
120 Appendix /17 Non-Recurrent CIP schemes Division Type Project Title Exec Lead Project Lead Value ( ) Delivery Corporate Transactional Band 7 reduction Rupert Davies Mark Banks 12,500 Monthly Corporate Transactional Liaison & Diversion Overheads Mark Axcell Jacky O Sullivan 54,000 Monthly Operations Transactional School Link Pilot Overheads Wendy Pugh Anne Marie Carey 9,000 Monthly Operations Transactional Walsall Activity Wendy Pugh Paul Chamberlain 85,000 Enc 13 CIP report June 16 v2 Page 15 of 15
121 Trust Board Workforce Report Month 2 1
122 Workforce Report - Contents Item Page Key Messages 3 Workforce Dashboard 5 Recruitment 6-7 Turnover 8 Sickness 9-10 Appraisal 11 Mandatory Training 12 2
123 Key Messages Vacancies There are currently 155 FTE contracted vacancies across the Trust reducing the vacancy rate to 14.3%. Contracted vacancies across the Trust have reduced from 224 FTE in May-15 There are FTE posts that are currently being recruited to. The Trust target vacancy rate is 10%. An agreed recruitment plan is being implemented, this initially projected to achieve a vacancy rate of to 11.2% by end of Q1 2016/17. However, due to slower than planned progress in the last four months, it is anticipated that the vacancy rate will be approximately 15.2% by the end of Q1 2016/17. The projection will be reviewed on the monthly basis. A Vacancy Reduction group has been established focussing on the Trust s approach to marketing and communication to recruit attract candidates to the Trust. The Trust has established a Facebook page which together with Linked in and Twitter will also be a means to advertise vacancies and attract candidates to the Trust. The Vacancy Reduction group is aligning reduction in agency usage to recruitment and positive progress is being made to recruit to vacancies. Further work is being done to review reasons for leaving to support with retention approaches. We continue to work with our formal partners to look at collaborative approaches to recruitment and retention of staff, especially in hard to recruit areas. Turnover The 12 Month Turnover rate has increased from 14.86% to 14.96%. The rate continues to be high and is attributable to the departure of individuals under TUPE. Turnover excluding TUPE employees transfers is 11.69%. Sickness Absence The 12 month rolling sickness rate has increased from 4.82% in Month 1 to 4.85% reported in Month month sickness was 5.05% in May-15 so there has been an overall reduction in sickness over the last year. In month sickness has increased from 4..49% in Month 1 to 4.98% in Month 2. A great deal of effort continues to be devoted to improving staff well-being and reducing sickness absence. A Staff Health and Well-being Strategy has been approved and an implementation plan is being developed. Preparations are underway to implement a further programme of staff well-being initiatives as part of a national CQUIN scheme for 2016/17. The Trust is collaborating with other Trusts across the region to develop peer benchmarking for sickness absence. 3
124 Key Messages Appraisal Compliance has increased from 69.1% to 72.7%, this is still below Trust target. This has reduced from 87% in Oct-15. There are 233 employees in the Trust that haven't had an appraisal recorded in the last 12 months. A trajectory is being planned for appraisal compliance in Ops to meet the required level. Mandatory Training - Mandatory Training compliance has increased from 81.7% in Month 1 to 86% in Month 2 and remains below the new target of 90% agreed at MEXT for all mandatory training (IG remains at 95%) as of 1 st April Similarly to appraisals, the Trust is developing a programme of targeted work and support to increase and sustain compliance with mandatory training. Further discussions are taking place at MEXT (5 th July) to agree plans to increase and sustain compliance. The following have been implemented: Training capacity increased to achieve the new target levels Blended training options E-learning champions, Staff guides, Support from Library in place Creation of monthly reports to Heads of service highlighting DNAs and place utilisation Routine booking of new starters onto the first available Induction day in place Exploring options to implement protected learning time Centrally allocated training places 4
125 Workforce Dashboard 445 Dudley and Walsall Mental Health Partnership NHS Trust May-16 Staff in Post Target Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Headcount Funded Establishment Staff in Post FTE (Contracted) No of Vacancies Vacancy % 10.0% 19.3% 18.0% 16.5% 15.5% 16.8% 16.8% 16.5% 15.9% 15.6% 16.0% 13.8% 14.3% Worked FTE (Substantive) Worked FTE (Temp) Worked FTE (Total) 1, , , , , , , , , , , Turnover % (12 Months) 8-14% 18.55% 18.27% 17.82% 15.02% 14.56% 14.16% 14.53% 15.07% 15.10% 15.54% 14.86% 14.96% Pay Spend Target Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Funded 4.26m 3.94m 4.08m 4.01m 3.97m 4.18m 3.92m 4.32m 4.45m 4.28m 4.06m 4.25m Substantive Spend 3.47m 3.38m 3.42m 3.44m 3.36m 3.45m 3.26m 3.32m 3.59m 3.46m 3.47m 3.56m Temp Spend 0.71m 0.69m 0.62m 0.68m 0.68m 0.61m 0.49m 0.78m 0.66m 0.76m 0.60m 0.68m Total Pay Spend 4.18m 4.07m 4.04m 4.12m 4.03m 4.06m 3.75m 4.11m 4.25m 4.22m 4.06m 4.24m Varaince - Budget to Actual 85K - 128K 35K - 104K - 62K 125K 170K 216K 194K 67K K 11K Absence Target Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Sickness % (Month) 4.68% 4.21% 4.89% 4.74% 4.17% 5.55% 5.85% 5.56% 5.22% 5.39% 4.39% 4.49% 4.98% Sickness Days Lost FTE (Month) 1,167 1,366 1,344 1,154 1,581 1,622 1,590 1,485 1,440 1,254 1,233 1,427 No of Sickness Episodes (Month) Cost of Sickness (Month) 92K 113K 113K 95K 137K 138K 138K 138K 128K 109K 104K 131K Maternity % (Month) 1.93% 2.04% 1.68% 1.68% 1.85% 1.89% 1.90% 1.80% 1.77% 1.87% 1.71% 1.53% Sickness % (12 Months) 4.68% 4.99% 4.93% 4.86% 4.80% 4.89% 4.91% 4.90% 4.90% 4.94% 4.86% 4.82% 4.85% Long Term Sickness % (12 Months) 69.0% 68.2% 65.3% 65.9% 65.9% 65.8% 66.9% 67.9% 68.0% 68.7% 67.3% 68.1% Cost of Sickness (12 Months) 1,357K 1,336K 1,316K 1,302K 1,344K 1,360K 1,366K 1,385K 1,410K 1,393K 1,386K 1,420K Development Target Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Appriasals Completed Appraisals Outstanding Appraisals Required Appraisal % 85% 77.0% 78.4% 75.6% 85.1% 86.9% 84.1% 83.2% 79.7% 74.7% 71.1% 69.1% 72.7% Mandatory Training % 90% 83.0% 82.7% 82.2% 80.7% 79.0% 79.1% 79.0% 78.9% 77.9% 80.5% 81.7% 86.0% Essential Skills Training % 90% 66.8% 73.1% 73.9% 74.7% 76.3% 76.4% 76.5% 78.0% 78.0% 80.7% 83.0% 83.5% 5
126 Recruitment DWMH Recruitment Plan Commentary Original Recruitment Plan Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Total Recruitment Pipeline Service Recruitment Plans Replacement Recruitment Total Less 15% Tolerance (Internal & Non Appointments) Recruitment Actuals New Starters Vacancy Position (Forecast) Funded FTE Staff in Post Recruitment Plan Projected Leavers No of Vacancies (Forecast) Vacancy % (Forecast) 16.8% 17.1% 15.7% 15.4% 16.0% 14.8% 15.2% Vacancy Position (Actuals) Funded FTE Staff in Post No of Vacancies Vacancy % 16.5% 15.9% 15.6% 16.1% 16.0% 14.3% Variance In Month Plan v Actuals Cumulative Plan v Actuals The revised forecast includes the 70 FTE vacancies in the current recruitment pipeline and the 63 FTE vacancies that have been identified in the latest Service Recruitment Plan. A tolerance of 15% has also been built into the the plan for internal recruits and non appoitments. Internal recruits create another vacancy and non appointments will be tracked and monitored. The plan originally predicted a 11.2% vacancy rate by the end of Q This is now predicted to be a vacancy rate of 15.2% at the end of Q new starters joined the Trust in May -16 against a target of 20.5 FTE. A summary of the projected performance against the plan is included in the following pages of this report. In month performance was 5.7 under plan, whereas the cumulative performance is now 45.6 under plan. 6
127 Recruitment Staff Group Add Prof Scientific and Additional Clinical Admin and Clerical Allied Health Professionals Estates and Ancillary Medical and Dental Nursing and Midwifery Total Vacant WTE Division Service Line Technic Services Registered Corporate CAF Corporate Affairs CDP Corporate Development and People CHX Chief Executive FIN Finance HR Human Resources OPS Operations Medical MED Medical Operations ACC Access Services ACU Acute Services AOMGT Acute & Older Adults Management COM Community Services EIN Early Intervention OAS Older Adults Total % of Total Vacancies 8% 6% 14% 3% 6% 14% 49% The table above shows the number of vacancies across the trust by Division/Service & Staff Group 49% of the 155 WTE vacancies within the Trust are Qualified Nursing positions 7
128 Turnover DWMH Turnover % by Month 23.0% 18.0% 13.0% 8.0% 3.0% Jun-15 Jul-15 Aug-15 Sep-1 5 Oct-15 Nov-15 Dec-15 Jan-16 Feb-1 6 Mar-16 Apr-16 May-16 Lower Target 8.0% 8.0% 8.0% 8.0% 8.0% 8.0% 8.0% 8.0% 8.0% 8.0% 8.0% 8.0% Turnover % 20.1% 18.3% 17.8% 15.0% 14.6% 14.2% 14.5% 15.1% 15.1% 15.5% 14.9% 15.0% Upper Target 14.0% 14.0% 14.0% 14.0% 14.0% 14.0% 14.0% 14.0% 14.0% 14.0% 14.0% 14.0% Service 445 ACU Acute Services Level AOMGT Acute & Older Adults Management Level CAF Corporate Affairs Level CDP Corporate Development and People Level CHX Chief Executive Level COM Community Services Level EIN Early Intervention Level FIN Finance Level HR Human Resources Level MED Medical Level OAS Older Adults Level OPS Operations Level Dudley and Walsall Mental Health Partnership NHS Trust Starters FTE (Month) Leavers FTE (Month) Turnover % (12 Months) % % % % % % % % % % % % % 12 Month Turnover has increased slightly to 14.96% in Month 2. Turnover continues to remain high as it includes the staff that left the Trust due to TUPE Transfers. Turnover excluding employees that left due to TUPE transfers is 11.69%. 8
129 Sickness Sickness Absence % v Trust Target 6.00% 5.50% 5.00% 4.50% 4.00% 3.50% 3.00% Jun-15 Jul-15 Aug-15 Sep-1 5 Oct-15 Nov-15 Dec-15 Jan-16 Feb-1 6 Mar-16 Apr-16 May-16 Target 4.68% 4.68% 4.68% 4.68% 4.68% 4.68% 4.68% 4.68% 4.68% 4.68% 4.68% 4.68% Sickness % 4.21% 4.89% 4.74% 4.17% 5.55% 5.85% 5.56% 5.22% 5.39% 4.39% 4.49% 4.98% Service Apr-16 May-16 Sickness % (12 Months) 445 ACU Acute Services Level % 6.41% 7.07% 445 AOMGT Acute & Older Adults Management Level % 6.31% 2.52% 445 CAF Corporate Affairs Level % 1.09% 4.35% 445 CDP Corporate Development and People Level % 3.76% 0.87% 445 CHX Chief Executive Level % 5.31% 3.36% 445 COM Community Services Level % 4.65% 5.02% 445 EIN Early Intervention Level % 4.78% 4.21% 445 FIN Finance Level HR Human Resources Level % 3.53% 6.07% 0.00% 2.10% 5.12% 445 MED Medical Level % 4.27% 4.70% 445 OAS Older Adults Level % 5.65% 5.26% 445 OPS Operations Level % 6.51% 4.36% 445 Dudley and Walsall Mental Health Partnership NHS Trust 4.49% 4.98% 4.85% The 12 month rolling sickness rate has increased slightly to 4.85% in Month 2 from 4.82% reported in Month month sickness was 5.05% in May-15 so there has been an overall reduction in sickness over the last year. Sickness has increased from 4.49% in Month 1 to 4.98% in Month 2. 9
130 Sickness Short Term/Long Term Sickness % (Rolling 12 Months) 8.00% 7.00% 6.00% 5.00% 4.00% 3.00% 2.00% 1.00% 0.00% 2.78% 1.0% 5.04% 2.0% 445 Corporate Level ACU Acute Services Level % 1.5% 1.3% 1.6% 1.9% 1.6% 445 COM Community Services Level % 445 EIN Early Intervention Level 3 ST% LT% 3.10% 445 MED Medical Level % 445 OAS Older Adults Level % 445 Dudley and Walsall Mental Health Partnership NHS Trust Long term sickness accounts for 67% of sickness for the rolling 12 month period to May-16. The number of open Long Term sickness cases is 27 in Month % 8.00% 7.00% 6.00% 5.00% 4.00% 3.00% 2.00% 1.00% 0.00% Add Prof Scientific and Technic Additional Clinical Services Sickness Absence Comparison by Staff Group Administrative and Clerical Allied Health Professionals Estates and Ancillary Medical and Dental Nursing and Midwifery Registered Apr % 6.16% 3.84% 7.87% 2.17% 4.09% 4.44% 4.49% May % 3.82% 2.96% 8.20% 7.97% 4.66% 6.96% 4.49% DWMH The top 3 reasons for sickness based on FTE days lost for Month 2 were: 1. Anxiety/Stress Injury/Fracture Gastro problems
131 Appraisal Appraisal % v Trust Target 100.0% 90.0% 80.0% 70.0% 60.0% 50.0% 40.0% Jun-15 Jul-15 Aug-15 Sep-1 5 Oct-15 Nov-15 Dec-15 Jan-16 Feb-1 6 Mar-16 Apr-16 May-16 Target 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% 85.0% Appraisal % 77.0% 76.4% 75.6% 85.1% 86.9% 84.1% 83.2% 79.7% 76.1% 71.1% 69.1% 72.7% Service Appraisals Required 445 ACU Acute Services Level AOMGT Acute & Older Adults Management Level CAF Corporate Affairs Level CDP Corporate Development and People Level CHX Chief Executive Level COM Community Services Level EIN Early Intervention Level FIN Finance Level HR Human Resources Level MED Medical Level OAS Older Adults Level OPS Operations Level Dudley and Walsall Mental Health Partnership NHS Trust 875 Apr-16 May % 62.6% 54.2% 87.0% 100.0% 100.0% 20.0% 60.0% 100.0% 100.0% 58.8% 66.3% 76.5% 84.0% 67.6% 68.8% 76.5% 82.4% 75.6% 81.0% 61.0% 60.9% 69.9% 70.8% 69.1% 72.7% +/- Appraisal compliance is tracking at 73% at the end of May-16. This has reduced significantly from 87% in Oct-15. There are 233 employees in the Trust that haven't had an appraisal in the last 12 months. 11
132 Mandatory Training 445 Dudley and Walsall Mental Health Partnership NHS Trust May-16 Training Compliance Apr-16 May-16 Competence Target Completed Required % +/- Completed Required % +/- Mandatory Training 90% % % Essential Skills 90% % % Combined Training % 90% % % Mandatory Training Apr-16 May-16 Competence Target Completed Required % +/- Completed Required % +/- Equality & Diversity 90% % % Fire Safety 90% % % Health & Safety 90% % % Infection Control (Clinical) 90% % % Infection Control (Non Clinical) 90% % % Information Governance 95% % % Moving & Handling 90% % % Safeguarding Adults Level 1 90% % % Safeguarding Children Level 1 90% % % Essential Skills Apr-16 May-16 Competence Target Completed Required % +/- Completed Required % +/- Mental Capacity Act 90% % % Prevent 90% % % Safeguarding Adults Level 2 90% % % Safeguarding Adults Level 3 90% % % Safeguarding Children Level 2 90% % % Safeguarding Children Level 3 90% % % 12
133 Board meeting date: 7 th July 2016 Agenda Item number: 8.3 Enclosure: 15 Report Title: Medical Directors Report Accountable Director: Author (name & title): Dr Gingell and Dr Weaver, Joint Medical Directors Dr Gingell and Dr Weaver, Joint Medical Directors Purpose of the report: To update the Board on matters pertaining to the joint medical directors portfolio that are of relevance and interest to the Board. This will include, but is not limited to, strategic implications of national and regulatory guidance and publications, together with local matters including risk and governance issues. Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: N/A Date reviewed: N/A N/A Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Effective Well-led Safe Please give brief details: There is potentially an impact across all the CQC domains. Enc 15 MD Board Briefing Paper Template docx DO Page 1 of 6
134 Title Medical Directors Report National and Regulatory guidance None of note to report this month. Recent Publications and Hot Topics Junior Doctors Contract Negotiations The result of the vote taken by junior doctors concerning the amendments to the new contract proposed by the Department of Health will be announced on the 6 th July. The Trust is already assessing the implications for working patterns if it is accepted, and the financial impact of the settlement. However any implementation has been paused while the vote has been taking place, apart from the appointment of the Guardian of Safe Working, which both sides have agreed is a good development. We have advertised the post in conjunction with our partners, Black Country Partnership NHS FT and are holding interviews on July 15 th, in order to have the person in post for the stipulated date of July 26 th. Major new report identifies complex factors and final events that contribute to child suicide risk Bereavement, bullying, exams and physical health conditions such as acne and asthma are some of the experiences linked to suicide in children and young people according to a new report by The University of Manchester s National Confidential Inquiry into Suicide and Homicide by People with Mental Illness (NCISH). Researchers studied the reports from a range of investigations and inquiries on 130 people under the age of 20 in England who died by suicide between January 2014 and April 2015, extracting information about their personal circumstances that the reports highlighted. This is the first time there has been a national study of suicide in children and young people in England on this scale. The researchers found that 28% of the young people who died had been bereaved, in 13% there had been a suicide by a family member or friend. 36% had a physical health condition such as acne or asthma, and 29% were facing exams or exam results when they died. Four died on the day of an exam, or the day after. Professor Louis Appleby, Director of NCISH said: Suicide is a leading cause of death in young people and the impact on families is particularly traumatic. We found the risk rose sharply from mid- to late teens and the reasons appear to be complex. There are often family problems such as drug misuse or domestic violence and more recent stresses such as bullying or bereavement, leading to a final straw factor such as an exam or relationship breakdown. Enc 15 MD Board Briefing Paper Template docx DO Page 2 of 6
135 Internet use related to suicide was found in 23% of the deaths. This was either searching for information about suicide methods, being a victim of online bullying or posting suicidal thoughts online. Bullying overall had occurred in 22% of cases, mostly face-to-face rather than online. Over twice as many males as females died by suicide and there were five deaths in those aged under 14. Hanging was the most common method, accounting for 63% of deaths followed by jumping from a height or in front of a train - methods that show a strong lethal intent. Excessive alcohol or drug use was more common in older teens, and 54% overall had previously self-harmed. In the week before they died, 10% had self-harmed and 27% had told someone of suicidal ideas. 43% had no contact with any services. Professor Nav Kapur, NCISH Head of Suicide Research said: Self-harm is strongly associated with increased future risk of suicide and is one of the main warning signs. It is crucial that there is improved help for self-harm and access to mental health care. However, with the variety of factors we found with this study, it is clear that schools, primary care, social services and youth justice all have a role to play. This study is the first phase, comprising people under 20 years of age in England and a linked academic paper is published on Thursday May 26th in The Lancet Psychiatry. A larger study widened to the UK and including those under 25 years of age will be published in 2017 and include recommendations for services. Relevance for DWMHPT With the annual increase in self harm attempts and assessments requested of our CAMHS services this information has both knowledge and service implications, informing our risk assessments and which patients will need increased monitoring. Local Matters The Care Quality Commission inspected Childrens Safeguarding processes across the Health and Social Care Economy. The draft report has been received and feedback regarding Dudley CAMHS was good, with commendations in particular for the commitment and cohesiveness of staff, and the ability to implement good safeguarding procedures for the children and young people in our care. The recommendations about crisis care provision will be addressed by the provision of a Tier 3.5 CAMHS which has finally been commissioned and recruitment is underway. It should be fully functional by September. The recent Consultants Away day held on June 15 th discussed the proposed service changes; CIP and service development opportunities. The Adult ASD/ADHD service is working very effectively, and is a model we can follow for service developments, although there are many details that need to be further assessed in the development of such services, such as medical capacity and fulfilling current commitments and obligations within the existing resources. Enc 15 MD Board Briefing Paper Template docx DO Page 3 of 6
136 Mortality Report Discussions and outcomes from the last mortality review group meeting were presented in the MDs report presented in June. Subsequently we have received information about suggested definitions: Natural deaths - ones from a recognisably incurable condition. Unexpected death - one occurs at a time that is sooner than may reasonably have been predicted Expected death - one where prognostic features have been identified leading to a reasonable expectation of death within an identified timescale Preventable death - one that should not have occurred given current medical knowledge and technology We have a teleconference scheduled with the Regional Medical Director of NHSI when we will discuss definitions and reporting mechanisms further. The most recent Trust mortality report is attached as an appendix. Recommendation To receive the report for assurance. To review and agree the actions taken in relation to incidents reported via the Trusts incident reporting system which relate to deaths of service users. Board action required The Board is asked to receive this report for assurance and review the Mortality Report appended. Enc 15 MD Board Briefing Paper Template docx DO Page 4 of 6
137 Appendix Title Mortality Information May 2016 Introduction There an ongoing requirement for Trusts to continue to take steps to understand their mortality figures, as such this report contains a review of all deaths reported during the month of May. A full list of the deaths is detailed within the report. It details: Expected or unexpected (from the descriptions and information given) Natural or unnatural/unusual in nature (from descriptions given or from coroners outcomes) Whether it has been investigated as a serious incident (and if so at what level) Summary of the root causes/contributory factors and whether the death was therefore preventable Summary of key points, issues and risks Age Gender Department Cause Group as reported on Safeguard 91 Male Woodside Death - Natural (CMHTOP) 92 Male Woodside (CMHTOP) 81 Male CMHTOP Walsall 85 Female Woodside (CMHTOP) 68 Female CMHTOP Walsall 84 Female Woodside (CMHTOP) Causes/Expected Death - Natural Causes/Expected Death - Natural Causes/Expected Death - Natural Causes/Expected Death - Natural Causes/Expected Death - Natural Causes/Expected Natural Causes / Unusual (unnatural) Expected Y/N Investigated Y/N Investigation Level Root cause Natural Causes Y N N/A Patient died of respiratory failure Probable natural causes? N N/A Patient appears to have passes away in a care home. No further details given. Patient had yet to be seen by the Trust Natural Causes Y N N/A Further information on OASIS denotes that the patient passed away as Unknown? N N/A Patient had not been seen by the Trust since 2014 Natural Causes? N N/A Informed by daughter that the patient had passed away due to a physical health issue Natural Causes Service user had been supported on a regular basis (approximately monthly) by CMHT staff for 5 years - under the care of Adult Psychiatrist. Service users had been mentally stable for some time, no mental issues recorded at time of death. Granddaughter contacted Health Care assistant to advise her grandmother had passed away. Comments Enc 15 MD Board Briefing Paper Template docx DO Page 5 of 6
138 Age Gender Department Cause Group as reported on Safeguard 47 Male Psychiatric Liaison Team - Walsall Death - Unexpected / Cause Unknown Natural Causes / Unusual (unnatural) Expected Y/N Investigated Y/N Investigation Level Root cause? N N Still awaiting further information from Coroner s office in respect to this case. A strategy meeting has however been held into the case. Comments 91 Male Woodside (CMHTOP) 85 Male Memory Services (BVC) 87 Male CMHTOP Walsall Death - Natural Causes/Expected Death - Natural Causes/Expected Death - Natural Causes/Expected Initial indications to psychiatric liaison staff were that this may be a basal skull fracture as the result of a fall. Natural Causes Y N Patient died peacefully in their sleep Natural Causes Patient passed away in Walsall Manor Hospital Probably natural causes? N N/A No further information available other than patient passed away due to a physical illness Further detail There were 10 deaths reported during April These can be analysed as follows: Age There were 10 deaths reported as incidents via the Trusts incident reported, this is broadly in line with an average of 11.6 per month reported during Male vs Female Of the above, 7 incidents were reported in respect to male patients and 3 incidents reported in relation to female patients Age Quarter Yrs Yrs Yrs Yrs Yrs Yrs Yrs Yrs Yrs Yrs Yrs Apr Reporting teams The incidents were reported by the following teams. Woodside (CMHTOP) Dudley x 5 CMHTOP Walsall 3 Memory Services Walsall (BVC) 1 Psychiatric Liaison 1 Recommendation To review and agree the actions taken in relation to incidents reported via the Trusts incident reporting system which relate to deaths of service users Action required To agree and approve the report. Enc 15 MD Board Briefing Paper Template docx DO Page 6 of 6
139 Board meeting date: 7 th July 2016 Agenda Item number: 8.4 Enclosure: 16 Report Title: Director of Operations and Nursing Report Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie Musson Head of Nursing and Quality Purpose of the report: To update the Board on matters pertaining to the Director of Operations and Nursing portfolio that are of relevance and interest to the Board. This will include, but is not limited to, strategic implications of national and regulatory guidance and publications, together with local matters including risk and governance issues. Action required from the Board Decision / Approval Gain assurance x Discussion x Information x What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: Quality and Safety Committee Date reviewed: June 2016 The Committee reviewed the long list of proposed Quality Improvement Priorities Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Effective Well-led Safe Please give brief details: The impact of the report related to all domains of quality with emphasis on promoting quality improvement. Enc 16 DONs Board Briefing Paper Public July 2016 Page 1 of 39
140 Title Director of Operations and Nursing Update Local Matters DIPC/HCAI Annual Report The DIPC Annual report is presented to the Trust Board for approval (see Appendix 1) The Quality and Safety Committee have reviewed the report and have recommended the report to Board for approval. The report demonstrates it had been a challenging year. The IPCC Team s main focus had been on Water Management, however, good progress and sustainability has been made across all areas. The Quality and Safety Committee noted the benefits to have Facilities Management sitting in the same area as IPCC as it becomes more of a compliance agent. Nurse Development and Revalidation Update Nurse Revalidation commenced on 1 April 2016 with the window for individuals to declare their fitness to practice open electronically 60 days before their due date. All nurses in the Trust with revalidation dates between April-June 2016 have now successfully revalidated. Provision continues to be in place to support nurses with their revalidation going forward. A number of nurses have written personal accounts of their revalidation journey which has been posted of the Nurse Senate section of the Nurse Development webpage to help and inspire others. Nurse Development Opportunities Nurse Development opportunities are being expanded in year beyond the 19 sessions already available to nurses to assist them with achieving the Continuous Professional Development (CPD) element of revalidation criteria of 35 hours 20 of those participatory. This includes mindfulness and dual diagnosis assisted by psychology and medical colleagues. Where appropriate sessions are offered out to other staff who may benefit from attending. This collaborative working is also seen by medical colleagues making their twice weekly education sessions available to nurses where appropriate. Professional Nurse Forum The Professional Nurse Forum continues to be held quarterly with a cross section of nurses attending regularly from right across the Trust and all service areas Recommendation As a result of the above the Board is asked to receive the update from the DONs portfolio Enc 16 DONs Board Briefing Paper Public July 2016 Page 2 of 39
141 DIRECTOR OF INFECTION PREVENTION AND CONTROL (DIPC) ANNUAL REPORT and ANNUAL WORK PROGRAMME APRIL 2015 to MARCH 2016 The DIPC annual report for Dudley and Walsall Mental Health NHS Partnership Trust AUTHORS: Emma Fulloway IPC Lead Nurse Rosie Musson Head of Nursing, Quality and Innovation PREPARED ON BEHALF OF: Wendy Pugh Director of Operations and Nursing/Director of Infection Prevention and Control DATE: April 2016 Enc 16 DONs Board Briefing Paper Public July 2016 Page 3 of 39
142 CONTENTS Section Page Number List of Abbreviations 5 List of Tables, Charts and Appendices 7 Definitions/Key Information Executive summary Introduction Infection Prevention and Control arrangements The work of the Infection Prevention and Control Committee Surveillance Outbreaks Audit Estates & Facilities Education and training Infection Prevention and Control 27 Link workers/infection Control awareness/ IPC newsletter 11.0 Occupational Health highlights Policies Conclusion 32 Enc 16 DONs Board Briefing Paper Public July 2016 Page 4 of 39
143 LIST OF ABBREVIATIONS C.diff CQC CAUTI DH Clostridium difficile The Care Quality Commission the integrated regulator of health and adult social care Catheter Associated Urinary Tract Infection Department of Health D and/or V Diarrhoea and/or Vomiting DIPC EbE E-Coli ESBL GRE HCAI HoS IPC IPCC IPCLN IPCT IPS ISS MExT MRSA MSSA Director of Infection Prevention and Control. An individual with overall responsibility for infection control and accountable to the registered provider Expert by Experience Escherichia coli Extended-Spectrum Beta-Lactamases (ESBLs) are enzymes that can be produced by bacteria making them resistant to cephalosporin s e.g. cefuroxime, cefotaxime and ceftazidime - which are the most widely used antibiotics in many hospitals. Glycopeptide-Resistant Enterococci Health Care Associated Infections Heads of Service Infection Prevention and Control Infection Prevention and Control Committee Infection Prevention and Control Lead Nurse Infection Prevention and Control Team Infection Prevention Society Integrated Services Solutions Management Executive Team Methicillin-resistant Staphylococcus aureus Methicillin-sensitive Staphylococcus aureus Enc 16 DONs Board Briefing Paper Public July 2016 Page 5 of 39
144 OHD PLACE PPE QSC SLA UTI Occupational Health Department Patient Led Assessment of the Care Environment Personal Protective Equipment Quality and Safety Committee Service Level Agreement Urinary Tract Infection Enc 16 DONs Board Briefing Paper Public July 2016 Page 6 of 39
145 LIST OF TABLES, CHARTS AND APPENDICES Table Page Number 1 Health and Social Care Act Code of Practice 11 2 Year on year comparison of Trust audit results in- patient settings 17 3 Community audit scores 18 4 Total number of mattress and pillow audits against those that have 20 failed the criteria 5 Cleaning exceptions 23 6 PLACE 2015 results 24 7 Infection Prevention and Control Mandatory Training 2015/ Nature and location of reported sharps injuries 28 9 Flu vaccines administered by staff group 2015/ Total number of staff vaccinated shown by directorate Number of flu bus visits Annual Work Programme for 2016/ Infection prevention and control audit programme for 2016/17 38 Chart 1 Surveillance data for the period April 2015 March Overall level of compliance for the Trust for Hand Hygiene, 19 PPE and Sharps observational audits 3 Trust cleaning scores for 2015/ IPC training compliance 26 5 Total number of sharps injury incidents Flu vaccines administered, by group Appendices 1 IPC Newsletter 39 Enc 16 DONs Board Briefing Paper Public July 2016 Page 7 of 39
146 DEFINITIONS / KEY INFORMATION HCAI Health Care Associated Infections HCAIs are infections acquired as a result of healthcare interventions. Whilst people are most likely to acquire HCAIs during treatment in acute hospitals, they can also occur in GP surgeries, care homes, mental health trusts, ambulances and people s own homes. MSSA BACTERAEMIA Methicillin-Sensitive Staphylococcus aureus Staphylococcus aureus is a bacterium that commonly colonises human skin and mucosa (e.g. inside the nose) without causing any problems. It can cause disease, if there is an opportunity for the bacteria to enter the body, for example through broken skin. Most strains are sensitive to the more commonly used antibiotics, and infections can be effectively treated. MRSA BACTERAEMIA Methicillin-Resistant Staphylococcus aureus MRSA is a strain of Staphylococcus aureus which is resistant to commonly used antibiotics. MRSA can be more difficult to treat and therefore infections may become more severe. MRSA can infect wounds or ulcers and more seriously if it enters the blood stream it can cause bacteraemia. C.DIFFICILE - Clostridium difficile Clostridium difficile is a bacteria that lives in the gut of about 3% of healthy adults in England. It is kept at bay by normal gut bacteria but if those bacteria are killed by antibiotics, Clostridium Difficile can proliferate. Toxins released by Difficile cause diarrhoea which can occasionally be very severe and life threatening NOROVIRUS Norovirus is the most common cause of gastroenteritis in hospital settings and outbreaks often lead to ward closure and major disruption in activity. Vomiting and short lived diarrhoea is the prominent symptom. Glycopeptide Resistant Enterococci (GRE) Enterococci are bacteria that are commonly found in the bowel of normal healthy individuals. They can cause a range of illnesses including urinary tract infections, bacteraemia (blood stream infections) and wound infections. Some strains have developed resistance to glycopeptides and these are termed glycopeptide-resistant enterococci (GRE). Enc 16 DONs Board Briefing Paper Public July 2016 Page 8 of 39
147 E-coli Escherichia coli (commonly referred to as E. coli) is a species of bacteria commonly found in the intestines of humans and animals. There are many different types of E. coli, and while some live in the intestine quite harmlessly, others may cause a variety of diseases. The bacterium is found in faeces and can survive in the environment. Alert Organism/Condition An alert organism/condition is one that is identified as having the potential to spread to others and can lead to outbreaks of infection. Enc 16 DONs Board Briefing Paper Public July 2016 Page 9 of 39
148 1.0 Executive Summary This is the seventh DIPC report for Dudley & Walsall Mental Health Partnership NHS Trust and reflects an overview of all aspects of the organisation s infection prevention and control programme for 2015/2016. This report provides assurance from the DIPC to the Board and comments that the Trust has a robust, effective and proactive infection prevention and control programme that demonstrates compliance with the Health and Social Care Act The Trust is formally registered with the Care Quality Commission (CQC) and declared as compliant with the Health and Social Care Act In July 2015 a revised code of practice was introduced for the prevention and control of health care associated infections (HCAI); The Health Act (2008), Code of Practice on the Prevention and Control of Infections and Related Guidance. The code of practice is also referred to as the Hygiene Code and is regulated by the Care Quality Commission. The areas of compliance have been updated and now include water management under Criteria 2. Criteria 3 is dedicated to antibiotic stewardship. The 10 criteria are outlined in Table 1. On 20 th August 2015 the Trust Development Authority completed a HCAI supportive visit. The objective for this was to assess the Trust s compliance with the 10 criterion within the Health and Social Care Act Following the visit an action plan was implemented to embed improvements across the Trust. The Trust remains committed to ensuring that patient safety is at the forefront of everything we do and promotes infection prevention and control as the heart of good management and clinical practice. The Trust is committed to ensuring that appropriate resources are allocated for effective protection of patients, their relatives, staff and members of the public. Enc 16 DONs Board Briefing Paper Public July 2016 Page 10 of 39
 has a pro-active Infection Prevention and Control Team (IPCT) which supports the clinical teams to deliver and")
149 Table 1 - Health and Social Care Act Code of Practice for health and adult social care on the prevention and control of infections 2.0 Introduction Dudley and Walsall Mental Health Partnership NHS Trust (the Trust) has a pro-active Infection Prevention and Control Team (IPCT) which supports the clinical teams to deliver and maintain patient safety, in relation to infection prevention & control. Infection prevention and control is the responsibility of every member of staff and must remain a high priority for all to ensure the best outcome for patients. The Trust has a zero tolerance approach to avoidable infections and a collective responsibility which places a duty on all staff to minimise the risk of infection at all times. The annual programme of work for 2015/2016 focused on ensuring on-going compliance with the Health and Social Care Act Code of Practice for health and adult social care on the prevention and control of infections. Enc 16 DONs Board Briefing Paper Public July 2016 Page 11 of 39
150 3.0 Infection Prevention and Control Arrangements The DIPC role within the Trust is located in the portfolio of the Director of Operations and Nursing. A key responsibility of the DIPC is to produce an annual report. The Head of Nursing Quality and Innovation chairs the Infection Prevention and Control Committee The Lead Nurse for Infection Prevention and Control is responsible for the operational management of the Infection Prevention and Control Team and for ensuring that the Infection Prevention and Control Strategy is embedded. The Infection Prevention and Control Nurse provide clinical infection control advice and supports Trust staff in the delivery of the Strategy. The Infection Control Doctor (ICD) is secured through a SLA with The Dudley Group NHS Foundation Trust. Director of Infection Prevention and Control Infection Control Doctor Head of Nursing, Quality and Innovation (Chair of Infection Prevention and Control Committee) IPC Lead Nurse (band 8a, 1 wte). Infection Prevention and Control Link Workers IPC Nurse (band 7, 1 wte) Team Administrator Changes within IPCT during 2015/16 The previous band 6 IPCN left the Trust in September The role banding was uplifted to a band 7. The Trust s new IPCN commenced their post in February Enc 16 DONs Board Briefing Paper Public July 2016 Page 12 of 39
151 4.0 The Work of the Infection Prevention and Control Committee (IPCC) The purpose of the Committee is to maintain an overview of Infection Prevention and Control priorities within the Trust and to link this into the governance and risk assurance processes. The Committee ensures that IPC risks are appropriately managed within Service Lines. Exception reporting is noted and managed in line with the Trust Board responsibilities and meets the requirements of the Care Quality Commission. The Committee meets bi-monthly and is chaired by the Head of Nursing, Quality and Innovation. Vice-Chair responsibility for the committee is with the IPCLN. The Committee also has service user representation from an Expert by Experience (EbE). Representatives from Public Health Walsall Metropolitan Borough Council and Dudley Metropolitan Borough Council are members of the Committee and provide assurance to the reciprocal Directors of Public Health that the infrastructure for infection prevention and control is in place. The Trusts Water Management Group feeds into the IPCC. The reporting arrangements for the IPCC of DWMHPT are as follows: DWMHPT Trust Board Quality & Safety Committee Infection Prevention & Control Committee Water Management Group Enc 16 DONs Board Briefing Paper Public July 2016 Page 13 of 39
152 5.0 Surveillance There is an on-going programme of surveillance of alert organisms and alert conditions within the Trust. Surveillance provides information for monitoring trends, comparing infection rates and evaluating effectiveness of interventions. It also acts as an early warning for potential outbreaks and a rise in the incidence of specific infections. Information is returned to the IPCNs on a weekly basis from all inpatient areas. This enables the team to identify possible outbreaks of infection and serious infections that require advice and support from them. This information is gathered through a manual process whereby the clinical in-patient teams notify the IPCNs of any issues. Access to FUSION for Walsall laboratory results and Review for Dudley laboratory results is available. This connects the IPCNs with patient data, enhances the quality of support the team is able to provide and facilitates the communication with clinical staff. The chart below indicates the number of alert organisms/conditions that have been reported to the team for this reporting period. Chart 1 Surveillance data for the period April 2015 March 2016 Month Staph Aureus Shingles/ Chicken Pox E coli MRSA Skin infections/cellulitis/ Wound Diarrhoea and/or vomiting Unexplained rashes Scabies Lice Flu Chest infection UTI - No catheter fitted C.A.U.T.I catheter assoc. UTI Patients with a catheter & no UTI April May June July Aug Sept Oct Nov Dec Jan Feb Mar Totals Patients with a cannula Enc 16 DONs Board Briefing Paper Public July 2016 Page 14 of 39
153 The surveillance data for this reporting period does not demonstrate any trends of infection. 91 cases of skin/wound infections were reported with the majority being cellulitis,self-harm wounds and the occasional leg ulcer. 70 urinary tract infections were reported; microbiological samples were not taken for all suspected cases, but antibiotics may have been administered. UTI can cause confusion in older people and people with dementia. If the person has a sudden and unexplained change in their behaviour such as increased confusion, agitation, or withdrawal, this may be caused by a UTI. 54 chest infections were reported. Microbiological samples may not have been taken for all suspected cases, but antibiotics may have been administered. 7 patients were identified to be colonised with MRSA, 5 of which were through routine MRSA screening on admission. Decolonisation treatment was administered in line with Trust policy. 2 patients isolated MRSA from wound swabs, decolonisation treatment and antibiotics were administered as required. 5 cases of diarrhoea and vomiting were identified during 2015/16. There were no outbreaks of Norovirus/diarrhoea and vomiting, during this reporting period. Urinary catheters staff reported that 18 patients had urinary catheters in-situ; staff also reported 8 instances of CAUTI. Identification of bacteria from a catheter urine specimen alone does not indicate infection, as bacteriuria (bacteria in the urine) is normal in the presence of a urinary catheter. To have true CAUTI the patient must also have other symptoms, such as: loin pain and/or a temperature. 5.1 MRSA, MSSA, GRE and E.coli Bacteraemia Mandatory Reporting During this reporting period the Trust has had zero incidents. 5.2 Clostridium difficile mandatory reporting No specific objectives were set for Clostridium difficile for the Trust for this reporting period. No cases of Clostridium difficile infection were identified during this reporting period. During this reporting period information was requested by the Dudley Office of Public Health who were undertaking a serious case review regarding a case of Clostridium difficile. A patient had a positive stool sample for Clostridium difficile 03/09/15. The patient was an in-patient at the Trust from 18/06/15-12/08/15. No risk factors (antibiotic use) were identified during their stay with the Trust. The case was not attributed to the Trust as the infection occurred after the service user was an inpatient under the Trust s care. Enc 16 DONs Board Briefing Paper Public July 2016 Page 15 of 39
154 Diphtheria Incident On the 25 th November 2015 the Trust was involved in contact tracing relating to an incident of Diphtheria led by Public Health England (PHE) The Trust participated in a multi-agency incident review and took the actions required to minimalise potential risks to service users and staff. No further cases of diphtheria were identified. 6.0 Outbreaks An outbreak is the occurrence of more cases of disease than normally expected within a specific place or group of people over a given period of time. During 2015/16 there has been no outbreaks identified. 7.0 Audit It is a requirement of the Health and Social Care Act 2008 that a programme of audit is in place to ensure that key infection control policies and practices are being implemented appropriately within the Trust. The infection prevention and control audit programme for 2016/17 can be found on page Annual audits The annual infection control audits have been completed throughout all of the inpatient wards in the Trust. The audits have been completed utilising the Trust audit tool based on the Infection Prevention Society Quality Improvement Tools. You will see in table 2 below, year on year comparison of the audit results, it is evident that the Trust still has work to do to increase compliance with the decontamination of equipment standard. In the 2015/16 annual work plan there was a work stream to promote Decontamination of Equipment; this still needs to be embedded into Trust best practise. The Medical Devices and Decontamination Committee for 2016/17 are to continue to promote policy requirements with regards to decontamination of equipment. Table 2 - Year on year comparison of Trust audit results in-patient settings Audit 2011/ / Management of Infection Control % 90% 93% Hand Hygiene 87% 93% 91% 87% 72% Environment 76% 83% 85% 88% 77% Kitchen 86% 86% 88% 91% 88% Disposal of Waste 94% 94% 92% 93% 89% Spillage and contamination 88% 85% 89% 92% 83% Personal Protective Equipment 95% 98% 100% 98% 93% Sharps 90% 93% 90% 95% 95% Linen 94% 86% 89% 92% 91% Decontamination of Equipment 81% 82% 83% 84% 85% Enc 16 DONs Board Briefing Paper Public July 2016 Page 16 of 39
155 Management of infection control has increased from last year. Hand hygiene percentage has decreased in part due to fixtures-hand wash basins not being compliant with current standards, lime scale to outlets, and access to personal alcohol hand rub. The overall percentage for the environment has decreased from last year, themes identified include: upgrade of bathroom and shower areas at Bushey Fields Hospital. Kitchens (audited are ward beverage kitchens), compliance has decreased slightly, themes include: fridge temperature recording compliance, food not labelled. Bloxwich kitchens require updating. Waste compliance has decreased themes include: signage of waste bins, stained waste bins and failure to segregate waste. Spillage and contamination compliance has decreased, themes include: accessibility to PPE using dispensers, expired spillage kits and some contamination of items identified. PPE compliance has decreased, themes include use of latex gloves, aprons in some areas not being easily accessible. Audit reports are generated by the IPCT and are distributed to the ward and the Estates and Facilities teams where action plans for areas of non-compliance are generated by the respective teams. 7.2 Community Audits A programme of community site audits have been completed, overall average scores are generated by site. Table 3 over the page gives the scores and some narrative of findings. Action plans are generated by the clinical teams for any areas of non-compliance. The Estates and Facilities teams receive a copy of the audit and generate jobs for areas of non-compliance relating to their areas of responsibility. Table 3 - Community audit scores Site Score Comments Action Plan Received Anchor Meadow 88% Worn carpets. Environment in need of repair. Hand wash facilities not available in clinical E&F YES Clinical YES room (hand rub was available) Blacken Hall 96% Staff food items not labelled E&F YES Village Centre Broadway 71% Staff on site not aware of link worker, spillage kit out of date, cleaning schedules were not displayed and environment in need of repair. Canal Side 89% Site was overall well maintained, clean and tidy. Non-compliant waste bin in clinical room. Nonsafety sharps stored in clinical room. Sharps bins not labelled. Elms 57% Site was overall well maintained, clean and tidy. Main issues identified related to processes for the decontamination of equipment, use of latex gloves staff food items not labelled Halesview 89% Environment in need of repair. High level dust noted, cleaners cupboard small and cluttered, lime scale to taps and staff kitchen microwave and fridge required cleaning. Clinical YES Due11/04/16 Clinical YES E&F YES Clinical YES E&F YES Clinical YES Enc 16 DONs Board Briefing Paper Public July 2016 Page 17 of 39
156 Kings Hill 94% Site was overall well maintained, clean and tidy. Due to lack of storage space items are stored on the floor in office areas, cleaners cupboard is also lacking in space. Ladies Walk 86% Equipment decontamination processes were not in place. Clinical room non-compliant hand wash basin. Non-safety sharps in clinical room. No access to spillage kit. Lime scale to taps. Mossley 89% Equipment decontamination processes were not in place. Clinical room was overstocked, hand wash basin not compliant with HTM 64, some high level dust noted. Some non-safety sharps were stored in clinical room. Poplars 56% Equipment decontamination processes were not in place. Cleaning schedules not displayed. many items stored on the floor, debris build up on floors in storage cupboards. Environment in need of repair. Multiple full sharps bins awaiting collection in clinical room. staff food items not labelled Woodside 88% Issues regarding external cleaning contract identified, environment was tidy and clean at the time of audit. No paper towels dispenser, some non-safety sharps in use. FULL COMPLIANCE = 95% MODERATE COMPLIANCE= 85-94% MINIMAL COMPLIANCE=66-84% NON COMPLIANT=0-65% E&F YES Clinical YES E&F YES Clinical YES E&F YES Clinical YES E&F YES Clinical YES E&F YES Clinical YES 7.3 Observational Audits Infection Prevention and Control link workers are required to submit audits on observations of clinical practice - Hand Hygiene, Sharps and Personal Protective Equipment. Inpatient areas are required to submit monthly audit results and community based teams are required to submit quarterly results. The audits are completed on paper, then are input into an Excel database. Moving forward a work stream for a more robust system is hoped to be initiated 2016/17. Chart 2 shows the overall Trust compliance for each of the observational audits for this reporting year. The minimal compliance rating is 95% which is set by the DIPC; the Trust has demonstrated compliance with the target for this year. Chart 2 - Overall level of compliance for the Trust for Hand Hygiene, PPE and Sharps observational audits Enc 16 DONs Board Briefing Paper Public July 2016 Page 18 of 39
.")

157 100% 99% Level of Compliance 2015/16 HH Sharps PPE 98% 97% 96% 95% 94% Acute Older Adult Community Early Intervention Recovery & Offender liaison 7.4 Mattress Audits Inpatient areas are required to complete an audit of mattresses against set criteria in order to identify non-compliant (damaged or soiled mattresses). The criteria utilised are based on the alert issued by Medicines and Healthcare products Regulatory Agency (MHRA) (don t judge a mattress by its cover) and the Infection Prevention Society Quality Improvement Tools. This process is designed to ensure that mattresses are clean and are in good condition, reducing the risk of infection. Any mattresses that do not meet required standards are replaced. Annual Mattress Audit Completed by Park House Healthcare August 2015 Park House Healthcare provides an annual mattress audit, all mattresses within inpatient areas are audited, as far as reasonably practicable without disrupting patient care. The auditors are accompanied by a member of the IPCT during the audit process. Table 4 below sets out the results for the Park House annual mattress audit undertaken in August Table 4 - Total number of mattresses audited against those that have not met the criteria Audit Date August Number of Mattresses Audited Number of Mattresses Failed (out of 149) 51 Total 87% 39% All mattresses identified as being noncompliant were replaced. 13% of the mattresses could not be audited due to patient use at the time of the audit. The audit reports were distributed to the clinical teams for action. Enc 16 DONs Board Briefing Paper Public July 2016 Page 19 of 39
158 7.5 Monthly mattress audit programme During 2015/16 the IPCT have led the in-patient monthly mattress audit programme with the implementation of monthly audits by ward staff; any mattresses that are identified as requiring replacement are purchased by the ward area. In addition the IPCT annual infection control audits include a spot check of mattresses and clinical staff are required to dispose of mattresses when any damage is identified. To assist the clinical teams the IPCT and Facilities Team have produced a standard operating procedure for the purchase and disposal of mattresses. 8.0 Facilities 8.1 Cleaning Services The Trust recognises its duty to provide safe and clean environments where patients, staff and other visitors can expect to be protected from the risk of infection. The Trust s cleaning services are contracted out to a specialist service provider, ISS Facility Services Healthcare (ISS) and this contract is managed through the Facilities Team. The cleaning service specification is based on recommendations from the National Specification for Cleanliness in the NHS (NSC, 2007) and the outcomes are assessed on a regular basis. All data collected from these cleaning audits are presented to the IPC Committee and a summary over the last 12 months confirms that cleaning standards have continued to consistently achieve above the 95% target. 8.2 Contractor monitoring scores (2015/2016) Cleaning scores Q1 to Q Between March 2015 and April 2016, there were 302 cleanliness audits (QA s) completed, the average results over each quarter is illustrated below and demonstrates that the Trust has continued to consistently remain 2% over the minimum standard of 95% (high risk areas as recommended in the NSC 2007) and as specified by the Trust in the Facilities Services contract. The scores, however, have indicated some areas for improvement throughout the reporting period, with a total of 10 areas reported scores between 90 and 95% (amber) and 1 area reporting lower than 90% (red). In all instances the reasons for the lower scores were fully investigated and remedial actions implemented when required. In all QA assessments, any areas identified as not meeting the required standards are uplifted as soon as possible to ensure the environment continues to meet the high standards expected by the Trust. Chart 3 - Trust cleaning scores 2015/16 Enc 16 DONs Board Briefing Paper Public July 2016 Page 20 of 39
159 Trust Cleaning Scores Trust average cleaning score Trust Target Immediate action required 97% 97% 97% 97% 95% 95% 95% 95% 90% 90% 90% 90% Q1 2015/16 Q2 2015/16 Q3 2015/16 Q4 2015/16 During the last 12 month period a number of initiatives have been developed and implemented to improve standards of cleanliness across the Trust, however much of this has focused on patient occupied areas. The majority of work has been led by Facilities Services, but working collaboratively with the cleaning contractor, IPC team, Service Lines, Heads of Service and ward based staff, as well as external observations provided through PLACE 2015 (Patient Led Assessment of the Care Environment) and the NHS TDA (NHS Trust Development Authority, now part of NHS Improvement). Improvements delivered include: Introduction of weekly descale clean for all taps and water outlets Greater attention to detail in general cleaning, corners, under tables etc. Scheduled QA audits to facilitate wider Trust participation with the cleanliness audit Wider circulation of cleanliness scores to include ward based staff More robust over-monitoring, to challenge accepted standards to drive improvement Introduction of temperature recording across all inpatient areas for catering equipment Cleaning cupboard audits, including COSHH, chemical placement, condition of equipment and storage Linen cupboard audit, both clean and dirty holding areas to ensure suitable storage facilities / containers are available at ward level Enc 16 DONs Board Briefing Paper Public July 2016 Page 21 of 39
160 Supported IPCT with the review of nurse led cleaning duties (based on NSC 2007 elements) Working with IPCT and other environment auditors, contributed to the development of an environment assurance framework, which will look to synchronise existing annual audit regimes and ensure they are scheduled together across the 12 month period and do not overlap. This planning has also enabled over-monitoring to be expanded to support clinical teams to improve their environment by reviewing actions more regularly throughout the year. Facilities services and Infection Prevention and Control have always worked collaboratively, however department restructure undertaken within the last 12 months has enabled the two services to work even more effectively together to the benefit of the Trust, its patients, staff and visitors. 8.3 Exceptions The following exceptions are currently under review and relate to cleaning services; Table 5 - Cleaning exceptions Month to IPCC Area Exception What has been done Other comments March 2016 BVC Increase in staff using the service, but no increase in cleaning provision / hours. Uplift clean to carpets completed Trial of cleaning services in place since March 2016, due to be reviewed June ISS provider, but contracted to New Horizons Early indications suggest additional cleaning hours may be required. March 2016 Bushey Fields cleaning services to Estates workshop Existing cleaning hours to be redeployed to include Estates workshop Trial completed and signed off by Head of Estates during Site Facilities March Variation to contract to be issued to ISS. Cleaning outcome for Warwick House to remain 75% in accordance with NSC 2007 recommendation for this type of area. Enc 16 DONs Board Briefing Paper Public July 2016 Page 22 of 39
161 Month to IPCC Area Exception What has been done Other comments March 2016 Seclusion room Bushey Fields Design of room different to existing; cleaning requirements to be determined. Cleaning regime defined and shared with Infection Prevention and Control and service line for comment Room is normally unoccupied. March 2016 Dorothy Pattison main kitchen Intermittent problems with access to hot water in main kitchen (pot wash area) Issues resolved Closed March 2016 Bloxwich admin area Introduction of new furniture has impacted cleaning services over time (e.g. framed beds and café style tables and chairs). Trial to redeploy existing cleaning hours to allow more hours in inpatient areas 3 month trial period. Trial commenced: 29 th Feb Trial supported by IPCT and site staff. No issues reported to date. Due to review early June Patient Led Assessment of the Care Environment (PLACE) 2015 Patient Environment The Patient Led Assessments of the Care Environment (PLACE) 2015 were completed at Bushey Fields, Dorothy Pattison and Bloxwich Hospitals. As with PLACE 2014 results, the table and graph below demonstrates how the Trust continues to out-perform the national average in three domains; with improvements identified in domain Condition, Appearance and Maintenance and Food Services. Table 6 - PLACE 2015 Results Enc 16 DONs Board Briefing Paper Public July 2016 Page 23 of 39
162 Results are provided for four domains:- Patient Led Assessment of the Care Environment (PLACE) High Level Analysis of National Results Cleanliness August 2015 Condition, Appearance and Maintenance Privacy, Dignity and Well-being Food Dementia National Average (Reported) 97.60% 90.10% 86.00% 88.50% 74.51% Trust Average 99.18% 86.02% 88.36% 84.02% 78.82% BLX 99.89% 92.24% 85.00% 88.12% 82.13% BFH 98.68% 83.14% 93.08% 86.11% 84.48% DPH 99.58% 86.71% 81.96% 89.65% 72.63% % 95.00% 90.00% 85.00% 80.00% 75.00% BLX BFH DPH National Average (Reported) Trust Average 70.00% Cleanliness Condition, Appearance and Maintenance Privacy, Dignity and Well-being Food Dementia The Quality and Safety Committee received an update in January 2016 and the committee were informed of several work streams underway to improve our in-patient environments. These work streams continue at pace and include: Assurance that minor works identified had been completed by Estates and that there were plans to maintain them being built into planned preventative maintenance. Trends identified in condition, and appearance had been reviewed, some improvements have already been implemented whilst others have now been incorporated into capital investment plans for Trends identified in food services generally related to procurement processes and choice, food safety and catering quality were scored well Partnership working with Facilities Services and the cleaning contractor to enhance standards by paying greater attention to detail on some tasks. Further improvements planned which will continue into PLACE 2016 include: Improvement in PLACE governance, to include reporting and escalation processes. Estates and Capital Planning, MExT and Quality and Safety all receive PLACE updates, which will enable requirements to be considered as part of immediate capital investment and future schemes. PLACE Lite to be incorporated into to further enhance environment assurances. 8.5 Catering All catering sites have been assessed by Environmental Health Officers (EHO); Bushey Fields Hospital holds a 5 star rating and Dorothy Pattison and Bloxwich Hospital each hold 4 star ratings. All recommendations for improvement have also been implemented. Small kitchen audits (ward level) have been introduced bi-monthly across all sites and are carried out by the catering manager / supervisors to ensure all food safety processes are in place. The completed audits are then circulated for review and actioned as required, to ensures safe working practices and food safety standards are maintained. Enc 16 DONs Board Briefing Paper Public July 2016 Page 24 of 39
163 Standard operating procedures (SOP) for fridges and dishwashers have been extended to include wards patient and ADL kitchens. This work is completed collaboratively between catering, clinical and contractor staff and recordings are taken twice daily. The Hazard Analysis and Critical Control Point plan (HACCP) review has been updated and will be rolled out across all 3 sites over the next few months; this will enable all main catering areas to be working to the same internal processes and procedures developed. Catering related Level 2 Certificate in Environmental Health (CIEH) Food Safety training has been delivered to the majority of catering staff, and others will be completing this following the release of further training dates. Level 3 CIEH Food Safety and Level 4 CIEH Food management training has been approved for all catering supervisors and managers and will be delivered once dates are finalised. A Food and Drink Strategy for the Trust has been developed and is now pending ratification prior to implementation. This will include continued service improvements based on recommendations from the Hospital Food Standards Panel s report on standards for food and drink in NHS hospitals. Catering services continue to embrace the opportunity to work closer with patients, infection prevention and control, clinical teams and the service experience desk to ensure that together catering services continue to meet the nutritional needs of individual patient as well as staff and visitors. ESTATES 8.6 Decontamination The Decontamination process continues to be led via the Decontamination Lead within the Estates Department, with support from the IPC nurses and the Electrical and Biomedical Engineering (EBME) service provider and clinical teams. The EBME service contract in 2014/15 was awarded to Avensys. There have been no known decontamination related issues reported during The Medical Devices & Decontamination Committee continues to monitor the contract. A work stream for 2016/17 is the policy review. 8.7 Water Management Following the legislative changes to the Health and Social Care Act 2008 water quality and safety has been a major focus for the Trust during Stakeholders within the Trust have been working in partnership to progress the work streams. There is now an improved governance structure, policy and water safety plan in place. The IPCLN was asked to present at a regional Public Health England conference on water management in March Enc 16 DONs Board Briefing Paper Public July 2016 Page 25 of 39
164 9.0 Education and Training Infection Prevention and Control Training is core to the Trust s approach to reducing the risk and spread of infection and is a mandatory area of training for all staff. It is compulsory for all staff clinically responsibility for patients to update training each year. For all other staff this requires updating on a 3 yearly basis. The Trusts 2015/16 target for compliance with Infection Prevention and Control Training has been 70%. This now increases to 90% from the 1 st April During 2015/16, compliance with training has exceeded the Trust s target for both clinical and non-clinical groups of staff. Monthly breakdowns are provided in the figures below. Chart 4 - IPC training compliance Figure 90% 85% 80% 75% 70% 65% 60% Infection Prevention and Control Training Compliance Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Clinical staff Non-clinical staff Table 7 - IPC mandatory training April March 2016 Infection Prevention and Control Training compliance is reported through the Trust s mandatory training dashboard. This is shared with Heads of Service on a monthly basis and reported monthly to the Finance and Performance Committee, Trust Board and through the Integrated Performance Dashboard. Information is also reviewed through quarterly Service Line Quarterly Performance Reviews and quarterly reports made to the Infection Prevention and Control Committee Infection Prevention and Control Service Promotion 10.1 Link Workers Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Clinical staff 75% 77% 77% 77% 78% 76% 73% 75% 72% 75% 75% 72% Non-clinical staff 84% 85% 84% 85% 85% 85% 83% 83% 82% 80% 79% 83% Link workers in the Trust are recognised as important components of the organisational structure whereby skills, professional practice standards and knowledge are disseminated via motivated and active staff with an interest in IPC. There is a link worker in every department both for inpatient and community areas. Link workers perform regular audits of infection control standards (see Section 7.3 Observational Audits). Enc 16 DONs Board Briefing Paper Public July 2016 Page 26 of 39
165 Quarterly forums are held for link workers in each locality which provide an invaluable opportunity to network with other colleagues Infection Control Awareness This year s focus for infection control awareness week October 2015 was promotion of the Trust decontamination processes for medical devices. The IPCT had a stand at the first Nurses Forum. The Trust policy was promoted along with the use of the orange decontamination labels and Avensys cards and cleaning product selection Save lives clean your hands The 5 th May 2015 was the annual World Health Organization s Save lives clean your hands day. To celebrate this, the IPCLN visited all three hospital sites and promoted the power of hand hygiene to reduce infections. At each hospital site staff were randomly selected to have their hand decontamination skills tested; hands were swabbed pre and post hand washing by using an ATP machine. Their participation was captured by a photograph and tweeted by the communications team IPC Newsletter During 2015/16 the IPC Team continued with the publication of a quarterly IPC Newsletter Bug Watch to raise awareness of interesting topics relating to the prevention and control of infection. The newsletter is circulated to all staff members via the Wednesday Wire. An example is attached as Appendix Occupational Health Highlights The Trust s Occupational Health (OH) service continues to be provided by Sandwell and West Birmingham NHS Trust (SWBH), and the service continues to play a key role in driving quality improvement within the areas of pre placement screening, the management/ treatment of sharps injuries, sickness absence management and the uptake of seasonal flu vaccination programme Management of Sharps Injury Policy - Injuries reported to OH From the 1 st April 2015 until 31 st March 2016, 14 injuries were reported to OH under the Management of sharps injury policy. The location and nature of the incidents along with the type of injuries are shown in Table 8. One of these injuries could have been avoided if devices with retractable or guarded needles had been used, and one if the safety device had been activated, in accordance with Health and Safety (Sharp Instruments in Healthcare) Regulations Previously in response to similar instances the IPCT in conjunction with the Procurement Team have devised a safer sharps order code list and have distributed this to clinical teams. In order to ensure safer sharps are in use the IPCT complete regular hospital visits and have updated the infection control mandatory training to include safer sharps. Two near misses fortunately did not result in injury, one of which involved a used sharp being found in a tray that had not been disposed of at the point of use, the safety device was activated. The second near miss found an over filled sharps bin with used sharps Enc 16 DONs Board Briefing Paper Public July 2016 Page 27 of 39
166 also found behind it, this has highlighted a need for staff to be vigilant in ensuring sharps bins are only filled to the fill line in accordance with Trust policy. There is focus on safe working practice at Trust induction to help instil the need, upon commencement of employment, to use safety sharps, never to re-sheath needles, and to dispose of used sharps in accordance with Trust policy. From 1 st April 2015 until 31 st March 2016 there were 14 incidents reported to OH under the Management of sharps injury policy, 2 being near misses. Table 8 - Nature and location of reported sharps injuries Date Directorate Job type Near Miss Needlestick Sharp Bite Scratch 15/04/2015 Holyrood Bank sustained when Ward Nurse patients nails sunk into arm 25/05/ /06/2015 Date 01/07/ /07/ /07/ /08/ /08/ /09/2015 Linden Ward Linden ward directorat e Infection control Malvern ward Kinver ward Langdale Ward Langdale Ward Langdale Ward 05/10/2015 Clent Ward 09/12/2015 Linden Ward Bank Nurse Staff nurse Job type Infection control nurse Staff nurse Trained Nurse Staff Nurse Staff Nurse Nursing Assistant HCA 07/01/2016 Hill House CPN 11/02/2016 Langdale Ward HCA Scratch by patient and blood splash from patient Near Miss Needlestick Sharp Bite Moved tray with sharp with activated safety in place, not disposed of. Overflowing sharps bin, when closed, found used needles behind it. Sharps injury thought safety mechanism was activated but was not. Caught thumb on needle whilst disposing into sharps bin Removed glass from patients mouth no injury Cut with knife during MAPA Scratched by patient when Graze/bite from patient Bite sustained during restraint Bite/ graze did not break skin Bite whilst feeding Enc 16 DONs Board Briefing Paper Public July 2016 Page 28 of 39
167 01/03/2016 Clent Ward Staff Nurse they grabbed staff members throat Scratched by patient when trying to get patient to return to bed Totals (14) Chart 5 - comparison of injuries reported to OH for 2013/14, 2014/15, 2015/ Needlestick Total number of incidents reported in line with the management of sharps injury policy for 2013/ /15 and 2015/ Bite Scratch Spit Sharp Blood Exposure 1 Other 2 Year 2013/14 (8) Year 2014 /15(14) Year 2015/16(14 ) 11.2 Seasonal influenza vaccination programme The 2015/16 seasonal flu vaccination programme is now complete although flu vaccines are available to staff until the end of June at which point the vaccine will reach its expiry date. As of the 31 st January 2016 OH had administered a total of 404 flu vaccines, which increases to 430 including the 26 staff who advised us that they had received a vaccine elsewhere. Table 9 provides a breakdown of staff up-take amongst different occupational groups and compares this to the up-take for the whole of 2015/2016 flu season. Of a total of 913 frontline health care workers employed with DWMHPT only 332 came forward for vaccination, this equates to 36.3% of this target group. It is recognised nationally that Mental Health Trusts have a low uptake of flu vaccines. Including all staff there was an overall uptake of 37.5%, falling short of the Trust s 50% target. Table 9 - Staff Flu vaccines administered by staff group 2015/16 Category (as per DoH uptake collection guide) Number of staff employed Number vaccinated 2015/16 Vaccinated elsewhere e.g. GP Doctor (non GP) Nurse, midwife, health visitor or school nurse Enc 16 DONs Board Briefing Paper Public July 2016 Page 29 of 39
168 Other qualified clinical worker Support to clinical staff Staff with no clinical contact/direct patient care TOTAL =430 Factors which can have an influence upon the flu vaccination up-take include a long summer and up until recently a mild winter, staff not perceiving their patients being vulnerable to contracting flu and then the associated health risks. Some staff still believe the flu vaccine gives you the flu despite all the myth busting information provided. This season was also affected by the media around the 2014/15 vaccine being less effective. Chart 6 shows the number of seasonal flu vaccines given during the 2015/2016 campaign and compares this with the number administered during the previous four seasons, it also illustrates the uptake in the different staff groups as reported on Inform. Chart 6 - Flu vaccines administered Doctor (non-gp) Nurse, midwife, health visitor or school nurse Flu vaccines given shown by group Other qualified clinical worker Support to clinical staff Staff with no clinical contact 2011/12 = /13 = /14 = /15 = /16 = 430 Building on previous experience OH broke down barriers to staff accessing the vaccine in 2015/16 by attending key events that we know high volumes of staff attend and also coincided the vaccination sessions with Team Brief sessions and The Inaugural meeting. Unfortunately OH were not advised of the timings of the Staff Awards and were unable to attend during the 2015/16 flu season. Bespoke Flu Fighters posters from NHS Employers listing the flu vaccination sessions across the Trust were distributed by The Communications Team, as this proved popular and helpful to staff last year. OH also added a flu vaccination message to September pay slips in order to reach all staff irrespective of their location and intranet access. Creating competition amongst service lines may encourage staff to come forward for vaccination. DWMHT used NHS Employers Jab-o-meter on the intranet last year but one Enc 16 DONs Board Briefing Paper Public July 2016 Page 30 of 39
169 Trust went a step further and showed vaccination up-take by service line; this proved a motivating force for their staff. During the 2015/16 season OH also advised DWMH of the number of vaccinations given in each of the Trust s Directorates. Table 10 -Total number of staff vaccinated, shown by directorate Directorate Headcount Number % vaccinated Acute Older Adults Mgt % Acute Services % Chief Executives % Community % Corporate Affairs % Corporate Development & People % Early Intervention % Finance % Human Resources % Medical % Older Adults % Operations % DWMH staff as given by ESR, not including bank staff % Please note staff numbers given by ESR for Inform do include bank staff, hence difference in % Community visits Community visits were this season covered by SWBH s flu mobile. Scheduled visits were arranged for the three trusts which OH covers; this did enable the staff of these Trusts more opportunity to access a flu vaccine during any of the stops. Remarkably the flu bus reduced the number of hours spent visiting community sites for DWMH, more vaccines were administered over more visits and over a considerably reduced length of time, this is demonstrated below in Table 11. Table 11 - Number of flu bus visits Number of visits/stops Number of hours in total (to nearest hour) Total number of vaccines for visits/stops 2014/ / The use of incentives for many trusts has also proven effective with increasing staff vaccination up-take. One trust gave out raffle tickets to those having had the flu vaccination with the chance to win an exercise bike, meal for two and numerous other items. Perhaps DWMHT could consider a similar approach. Enc 16 DONs Board Briefing Paper Public July 2016 Page 31 of 39
170 /2017 season To achieve a further increase in vaccination up-take amongst front line health care staff in 2016/17 DWMHT will need to send out really clear, firm messages to their clinical staff about professional responsibilities to ensure patient safety and the need to be protected against the flu virus by vaccination if we are to make this a reality Policies For this reporting period the following policies were developed/reviewed and ratified at Policy group Water management Decontamination 13.0 Conclusion The Trust is committed to continuous, sustainable improvement in infection prevention and control and supports zero tolerance of avoidable infection and harm to our patients and staff. Implementation of infection prevention and control standards requires a multipartnership approach. With the increasing numbers of multi-drug resistant organisms reported nationally the Trust recognises the importance of a whole health economy approach and remains committed to support this agenda. Enc 16 DONs Board Briefing Paper Public July 2016 Page 32 of 39
171 Table 12 - Infection Prevention and Cleanliness Annual Work Programme for 2016/17 Compliance Criteria 1.Systems to manage and monitor the prevention and control of infection. These systems use risk assessments and consider how susceptible service users are and any risks that their environment and other users pose to them. Programme of Work for 2016/17 Bi monthly Infection Prevention & Control Committee Meetings Ensure there is a service agreement for 24 hour access to a Microbiologist Undertake Root Cause Analysis/Post Infection Reviews following for serious incidents of HCAI and share findings within the Trust. Lead Evidence Date Risks Completion Date Director of Infection Prevention & Control (DIPC) Head of Nursing & Innovation DIPC Head of Nursing & Innovation IPCT Minuets, papers and DIPC Report Reports and Presentations March 2017 RAG Rating 2.Provide and maintain a clean and appropriate environment in managed Audit database: investigate complete electronic packages for auditing to link with Data Warehouse Annual IPC Audit programme of Clinical Facilities within Trust IPCT/IT IPCT Reports & Action Plans Enc 16 DONs Board Briefing Paper Public July 2016 Page 33 of 39
172 premises that facilitates the prevention and control of infections Monitoring processes and procedures to be enhanced to ensure cleanliness consistently meets NSC standards. This will include a more targeted overmonitoring regime to drive improvement in standards. Facilities Reports Refresh cleaning schedules to include all areas of the Trust to capture areas identified for improvement Facilities New cleaning schedules to be displayed Stakeholder group to inform specification ahead of tendering the of Facilities services contract due expire Facilities/IPC T/Procureme nt New contract Extend NSC 2007 cleanliness matrix to include elements maintained by nursing staff and estates Facilities/IPC T/HOS Reports Enc 16 DONs Board Briefing Paper Public July 2016 Page 34 of 39
173 Raise profile of catering services to include existing food hygiene assurances and exception reporting Catering Manager Reports 3.Ensure appropriate antimicrobial use to optimise patient outcomes and to reduce the risk of adverse events and antimicrobial resistance. Promote Antibiotic Stewardship during antibiotic awareness week by encouraging staff to pledge to be an Antibiotic Guardian IPCT/Pharm acy Communications to staff November n.com/test-post/ Pharmacy Team to continue to promote antibiotic formulary during induction of Doctors Pharmacy Attendance records for induction March Provide suitable accurate information on infections to service users, their visitors and any person concerned with providing further support or nursing/medical care in a timely fashion Publish Quarterly Infection Prevention & Control Newsletter Ensure any queries from staff, service users, visitors are answered in a timely fashion IPCT IPCT Newsletters Enc 16 DONs Board Briefing Paper Public July 2016 Page 35 of 39
174 IPCT to attend National & Local Healthcare Economy meetings and learning events to ensure continuing professional developmental needs are met. 5.Ensure prompt identification of people who have or are at risk of developing an infection so that they receive timely and appropriate treatment to reduce the risk of transmitting infection to other people. 6.Systems to Ensure that all care workers (including contractors and volunteers) are aware of and discharge their responsibilities in the process of preventing and controlling infection Development of IPC Risk Assessment to be completed as patient are admitted into inpatient services Ensure that Infection Prevention & Control is included within Trust Induction & Mandatory Training Programmes and annual tool box talks for Estates Team. Deliver Quarterly Infection Control Link worker sessions at both Dudley & Walsall Localities IPCT IPCT IPCT Implementation of Risk Assessment Ensure the IPCT promotes: Save Lives Clean your Hands 5 th May and Infection Control awareness week October 2016 IPCT Enc 16 DONs Board Briefing Paper Public July 2016 Page 36 of 39
175 7.Provide or secure adequate isolation facilities 8.Secure adequate access to laboratory support as appropriate 9.Have and adhere to policies, designed for the individual s care and provider organisations, which will help to prevent and control infections 10. Providers have a system in place to manage the occupational health needs and obligations of staff in relation to infection. Provide specialist infection control advice to clinical staff regarding isolation of patients with suspected or known infections Ensure laboratories with which the trust has SLAs have up to date Clinical Pathology accreditation. Revise policies as per schedule or following national updates Occupational Health Provided under contract from Sandwell & West Birmingham Hospitals IPCT - March 2017 DIPC/Procur ement IPCT/Policy Working Group Workforce SLA March 2017 Policies/IPCC Minuets March 2017 Enc 16 DONs Board Briefing Paper Public July 2016 Page 37 of 39

176 Table 13 Infection Prevention and Control Audit Programme for 2016/17 AUDIT AUDITOR FREQUENCY DATA ANALYSIS FEEDBACK TO RESULTS REPORTED TO DWMHPT Infection Annual DWMHPT Infection IPCC Prevention and Control Prevention and Control Team Team Management of Infection Control Hand Hygiene Environment Kitchen Waste Spillages PPE Sharps Linen Decontamination Hand Hygiene PPE Sharps Infection Control Link Workers (in-patient areas) Monthly DWMHPT Infection Prevention and Control Team HoS Clinical Lead Ward Manager Clinical Governance Estates Facilities Heads of Service Ward managers Clinical Leads IPCC Mattress/Pillow audit Cleaning Audits 49 elements national tool Infection Control Link Workers (community based) Clinical Leads/Ward Managers ISS QAA (Quality Audit Assistant) Quarterly Monthly DWMH IPCT Actions taken by leads at time of audit to address identified issues Monthly inpatient areas Quarterly community areas ISS Estates and Facilities HoS Clinical Lead Ward Manager IPCC monthly IPCC quarterly Enc 16 DONs Board Briefing Paper Public July 2016 Page 38 of 39

177 Appendix 1 Enc 16 DONs Board Briefing Paper Public July 2016 Page 39 of 39
178 Board meeting date: 7 th July 2016 Agenda Item number: 8.5 Enclosure: 17 Report Title: Enhancing Quality through Safer Staffing Levels - Monthly Exception Report Accountable Director: Author (name & title): Purpose of the report: Wendy Pugh Director of Operations, Nursing & Estates Rosie Musson Head of Nursing, Quality and Innovation Makhan Singh Principal Consultant, Informatics and Performance This report aims to provide the Trust Board with: 1. The summary report of planned and actual staffing which has been submitted to NHS Choices as part of a national staffing return 2. Exception reporting regarding variances provided by Heads of Service 3. Trend analysis reporting monthly average fill rate Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: Date reviewed: Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Effective Well-led Safe Please give brief details: Ensuring staffing levels are responsive to meeting patient need Ensuring staffing levels are adequate to deliver safe care Enc 17 Safer Staffing Levels on Wards - July 2016 Page 1 of 6
179 Title Safe Staffing on Inpatient Wards Introduction There is now a requirement post publication of the Francis Report 2013 and following the publication of Hard Truths that Trusts fulfill key commitments regarding publishing staffing data. This report aims to provide the Trust Board with: the summary report of planned and actual staffing which has been submitted to NHS Choices as part of a national staffing return and is available on the Trust s website. exception reporting for variances trend analysis monthly average fill rate All Trusts are required to submit data, by ward, which shows planned against actual staff fill rates for inpatient wards. This is provided by total hours for both day and night shifts. The data is broken down by registered nurse and care staff. Trust Boards are asked to receive this published data monthly. The Board will be informed by exception of those wards where staffing fell short, the reasons for the gap, the impact and the actions taken to address this gap. There has currently been no agreement on RAG rate for this data for shortfalls, or oversupply of staffing nationally, although further guidance on this tolerance is expected. However the report has used a rating based on the provisional Information Centre range thresholds which were used to identify outliers from the first submission in May Summary of key points, issues and risks This set of data indicates sustained improvement in data quality. As reported in last month s report this information is collected manually and further systems have been introduced to improve data quality and reduce the risk of double counting bank and agency staff. Across the inpatient areas the overall fill rates are 99.7%, with 96.2% for registered staff and 101.5% for care staff. Typically where our care staff rates exceed the planned numbers significantly, this is due to temporary staff being used to support patient observations or changes in skill mix. There is one ward to note as exceptions, whereby staff fill in part is within the lower category (Ambleside). An impact assessment has been completed that provides assurance safe staffing levels have not been compromised, and during May there were no reported incidents of unsafe staffing levels that relate to this ward. The Board are asked to note that the first e-rostering continues to be implemented and is making good progress line with the agreed project plan. Enc 17 Safer Staffing Levels on Wards - July 2016 Page 2 of 6
180 Recommendation To note and discuss the monthly data return submitted providing details of planned and actual staffing at ward level. Data represents May 2016 and a monthly trend analysis for a 12 month period. To note: The work underway to enable more detailed analysis of staffing data and the current complexities. The introduction of e-rostering and the safer staffing framework Board action required The Board of Directors is asked to: To note and discuss the monthly data return submitted, providing details of planned and actual staffing at ward level. Data represents May 2016 and a 12 month trend analysis. Enc 17 Safer Staffing Levels on Wards - July 2016 Page 3 of 6
181 1. Nursing and healthcare staffing fill rates May 2016 The data submission was made on 14 th June 2016 of May data. The following table provides a summary of the planned verses actual staffing levels on the inpatient wards. Day Night Day Night RMN Care Staff RMN Care Staff Planned Actual Planned Actual Planned Actual Planned Actual Average fill rate - registered nurses/midwives (%) Average fill rate - care staff (%) Average fill rate - registered nurses/midwives (%) Average fill rate - care staff (%) Cedars % 97.3% 93.2% 101.9% Linden % 98.8% 98.2% 98.3% Ambleside % 100.0% 80.9% 100.0% Langdale % 100.5% 100.0% 100.0% Clent % 114.8% 116.1% 109.5% Kinver % 100.0% 100.0% 100.0% Wrekin % 100.0% 100.0% 105.3% Holyrood % 100.7% 92.7% 102.1% Malvern % 101.5% 91.6% 101.7% Grand Total % 101.2% 95.8% 101.9% Lowest range less than 80% Highest range greater than 150% Low range greater than 80% but less than 90% High range greater than 120% but less than 150% Greater than 90% but less than 120% Across the inpatient areas the overall fill rates are 99.7%, with 96.2% for registered staff and 101.5% for care staff. The overfill result is as expected, as most of the inpatient wards do not have planned staff levels built into their rotas for increased levels of patient observation and complexity. Typically where our care staff rates exceed the planned numbers significantly, this is due to temporary staff being used to support patient observations. Enc 17 Safer Staffing Levels on Wards - July 2016 Page 4 of 6
182 2. Exception Report on Variance May 2016 For April 2016, the Trust has one exception to report to the Trust Board Exceptions Rationale Impact Remedial Actions Ambleside Ward Dorothy Safe staffing levels maintained, No action required Pattison Hospital no reported incidents 80.9% Day Average fill rate Registered Nursing (Low range) 80.9% Night Average fill rate Registered Nursing (Low range) The ward is reporting three qualified staff on sick leave and where appropriate the ward have used resource from other wards to provide additional support and accessed temporary staffing. Enc 17 Safer Staffing Levels on Wards - July 2016 Page 5 of 6

183 3. Trend Analysis average fill rate The following table shows a monthly trend of the total average fill rates planned verses actual for the Trust. It shows the improvement in the data quality and significant understanding of the capturing of planned hours of working. Enc 17 Safer Staffing Levels on Wards - July 2016 Page 6 of 6
184 Board meeting date : 7 July 2016 Agenda Item number: 9.1 Enclosure: 18 Report Title: High Level Operational Risk Register Accountable Director: Author (name & title): Wendy Pugh Neil Tong (Risk and Assurance Facilitator) Purpose of the report: The purpose of this report is to provide the Trust Board with the Red Operational Risks held on the Trusts Risk Registers for the period 7 th July The report also details the following key information: o Any new red risks Operational Risks being escalated to the High Level Operational Risk Register o Any red risks being downgraded from the High Level Operational Risk Register o Any updates to red risks currently held on the Trust High Level Operational Risk Register. Action required from the Committee Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: Quality and Safety Committee, Finance and Performance Committee and Mental Health Act Scrutiny Committee Date reviewed: 09/06/2016 (Q&S) 27/06/2016 (F&P) 23/06/2016 (MHASC) The Trusts Quality and Safety Committee Reviewed the following risks as part of the Quality and Safety Risk Register: o 202 o 225 o 253 o FINAN 1 o HR 002 o 285 o Risk 301 Following a risk spotlight session it was concluded that risk 225 could be downgraded Enc 18 High Level Op Risk Register Page 1 of 12
185 The Trusts Finance and Performance Committee also reviewed the red risks which had links to the Trusts to finances and to Trust performance on 21 st March. These were Risks: o 202 o 253 o FINAN 1 o Risk 301 The Trusts MHASC reviewed a number of risks as part of the MHASC risk register. None of these were red risks and as such no risks have been escalated to this report. Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Effective Well-led Safe Please give brief details: Some of the risks held on the register have the ability to directly or indirectly impact upon the care/services offered The High Level Operational Risk Register Provides a representation of the Trusts Red Risks and the responses to managing/action planning these risks; some (due to the nature of the risk) provide a response to a short term or long term issue Some of the risks held on the High Level Risk Register impact upon the future viability / effectiveness of the Trusts operations. Risk FINAN 1 specifically relates to the long term outlook in relation to CIP Some risks held on operational risk registers pertain to issues around service redesign and may have impacts upon leadership and staffing issues The appropriate management of risk is central to the provision of a quality, safe service. In particular CQC Outcome 16 Assessing and monitoring the quality of service provision Enc 18 High Level Op Risk Register Page 2 of 12
186 Title High Level Operational Risk Register Introduction It is the purpose of this report is to provide the Trust Board with the Red Risks Operational risks held across the Trusts Risk Registers (for the period 30 th March 2016) and in doing so provides the committee with information on: Any new red risks being escalated to the High Level Operational Risk Register. Any red risks being downgraded from the High Level Operational Risk Register Any updates to red risks currently held on the High Level Operational Risk Register. Summary of key points, issues and risks There are currently 7 risks included within this report and as such comprise the Trusts High Level Operational Risk Register. All 7 risks held on the High Level Operational Risk Register, were presented to the Trusts Quality and Safety Committee as all risks were felt to fall wholly or partially into the remit of the committee. The risks therefore presented to Quality and Safety Committee were as follows: FINAN 1 HR Following a risk spotlight session in respect to risk 225 it was agreed that this risk could be downgraded to an amber risk, as it was felt that significant progress had been made in respect to this risk and that there were a number of assurances noted in respect to this issue which were fully recognised by the CQC as part of their recent visit. In addition, the Trusts 4 red risks with links to Finance and Performance Issues were also reviewed by the Trusts Finance and Performance Committee these were risks: FINAN Enc 18 High Level Op Risk Register Page 3 of 12
187 It should also be noted that the CQC recently reviewed a copy of the Mental Health Act Scrutiny Committee risk register. No red risks were noted within the remit of the committees responsibility and as such no red risks from that committee are escalated to this report. Further detail (if required) The risks are outlined further in table 1.1, 1.2 and Appendix 1. Table 1.1 Summary of risks Risk ID Risk Description Impacts and Updates 301 There is an associated financial and quality impact Comments associated with the outcome of the current contract New risk added following discussions at Finance and negotiations with Walsall CCG in respect to the 2016/17 Performance Committee contract. The contract as it stands will result in a large Update reduction of income effective of April Whilst the risk has been generated via finance and performance committee, there are possible quality 285 Risks around legionella contamination of the Trusts water systems at Dorothy Pattison Hospital, Bushey Fields and Bloxwich Hospital 202 The Better Care Fund (BCF) involves circa 1.9bn of NHS funding being allocated to a pooled budget to provide integrated health and social care services. 253 Mental Health Currencies - Implementation of Clustering as the Currency for MH payment will impact upon data recording within the Trust and impact upon how the Trust is reimbursed going forward. implications being raised by the risk Comments Water management group are overseeing mitigations and controls to reduce contamination levels. Update Risk reviewed and updated to include issues at Bushey Fields Hospital. Hot water temperature controls at Dorothy Pattison Hospital have now been rectified Risk updated to include Bloxwich Hospital Comments There is now a national template for creation of the BCF and plans are in development. The value of the respective BCFs within each locality are now known Update Risk reviewed by Director of Finance and Performance, no updates/changes to risk Comments There is a plan to reduce the level of unclustered activity. The Trust is currently negotiating with commissioners at a local price for un-clustered work and an action plan has been developed Update Risk reviewed by Director of Finance and Performance, no changes to this risk at this time Status of risk = = = = Enc 18 High Level Op Risk Register Page 4 of 12
188 Risk ID Risk Description Impacts and Updates FINAN 1 Inability to meet CIP targets and the impact on the viability Comments of the Trust. Issues Include: Thorough quality impact assessments are undertaken Costed service plans not yet developed. against each CIP. Lack of clarity around commissioner investment plans Any high risk quality issues highlighted will be escalated and resulting CIP requirement. to the Executive Team for discussion via the Trusts CIP / Reduction in investment by Local Authorities. PMO processes N.B. Risk related to the long term picture of CIP and Update not the Trusts in year position Risk reviewed by Director of Finance and Performance. QIAs are being reviewed by Trust Board on a Quarterly basis for both in year schemes and future schemes to review progress against the CIP project and any impacts HR 002 Reduction in Local Authority Funding for Mental Health Social Care Workforce, which may impact on service delivery 225 The risk of insufficient resilience and skills in leadership, which may result in poorly engaged, demotivated staff and poor service quality. upon quality Update Risk reviewed by Director of Operations and Nursing No changes to risk aside from slight update to further actions which now reads Discussions ongoing at POG (Monthly) + Partnership Board Quarterly Update Risk reviewed following spotlight session at Quality and Safety Committee. It was agreed that this risk could be downgraded. Positive assurances had been noted in respect to this particular area by the CQC in respect to their recent assessment of the Trust. Status of risk = = Table 1.2 below outlines the source of the risks held on the High Level Operational Risk Register Table 1.2 Number of risks on the Risk Source of risk (How the risk has been identified) Register National Guidance / Initiative / Reforms 2 Feedback from stakeholders/partners 2 Finance projections/data 1 Workforce Statistics / Information 1 Risk Assessment 1 Recommendation It is recommended that the Trust Board approve the enclosed copy of the High Level Operational Risk Register and the details included within this report, which outlines the Red Risks operational risks to the organisation and approve the downgrading of risk 225 Enc 18 High Level Op Risk Register Page 5 of 12
189 Action required The board is asked to approve the High Level Operational Risk Register, approve the contents of this report and approve that risk 225 is downgraded in light of the risk spotlight session presented to the committee and its associated recommendation. Enc 18 High Level Op Risk Register Page 6 of 12


190 DWMH Red Risks Current Risks Iden tified d Governance Department Management Enc 18 High Level Op Risk Register Page 7 of 12
191 R isk N o. R isk D esc rip tion Sou rce o f R i s k D a te Iden tified P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f R ev ie Fu rthe r C o m m en ts 202 The B e tte r C a re Fund (BCF ) invo lves c irca 1.9bn o f NHS fund ing be ing a lloca ted to a poo led budge t to p rov ide in teg ra ted hea lth and soc ia l ca re se rv ices. T h is p resen ts seve ra l e le m en ts o f risk as fo llo w s : * CCG co m m iss ione rs a re like ly to have less fund ing to invest in hea lth se rv ices fro m A p ril 2014 (ave rage pe r CCG m ) - th is cou ld im pac t d irec tly on T rus t inco m e. * P a th w ay redes ign to c rea te the BCF se rv ices cou ld im pac t on D W M HP T pa th w ays and se rv ices N a tiona l In itia tive / G u idance 05 /03 /2014 M a rk A xce ll Trust Board 4 4 R ed 16 D ud ley and W a lsa ll M en ta l H ea lth P a rtne rsh ip NHS T rus t CEO is a m e m be r o f W a lsa ll's in teg ra tion boa rd, a key fo ru m to m ove fo rw a rd w ith p lans. F ina l p lans have been rec ieved fro m bo th hea lth econo m ies. D of P has es tab lished co m m un ica tio channe ls w ith bo th CCG s / M B C s rega rd ing the BCF in o rde r to be tte r unde rs tand p lans and the po ten tia l im pac t on the hea lth econo m y, pa th w ays and the T rus t R egu la r E xec leve l m ee ting es tab lished w ith D ud ley CCG w ho w il be ho ld ing the poo led budge t in D u d l e y The re is regu la r exec a ttendance a t BCF in teg ra tion m ee tings The T rus t have been invo lved in the deve lop m en ts o f the BCF s w ith in e ithe r loca lity desp ite no t be ing a s igna to ry o f e ithe r ag ree m en t. n 4 4 R ed 16 D of P to C on tinue to m ee t w ith C F O a t bo th D ud ley and W a lsa ll CCG s to fu rthe r unde rs tand p lans (O ngo ing bas is ) E s tab lish M en ta l H ea lth o f the p lann ing fra m e w o rk fo r bo th hea lth econo m ies and con tinue a ttendance a t m ee tings, beco m ing fu lly a w a re o f p lans and s tages o f deve lop m en t and risks inhe ren t w ith in (O ngo ing bas is ) 4 3 A m be r 12 R epo rts to e M E x T M ins and A c tions fro m in teg ra tion boa rd s M ins and A c tions fro m BCF s tee ring g roups 07 /12 /2015 R isk rev ie w ed by D irec to r o f F inance and P e rfo rm ance. N o changes to risk, risk to re m a in as a red risk. * The re is no w a na tiona l te m p la te fo r c rea tion o f the BCF and p lans a re in * The T rus ts ex is ting b lock con trac t a rrange m en t cou ld pu t the T rus t a t risk if p lans do no t co m e to fru ition and CCG s look to reduc ing the b lock con trac t to fund any gaps * The ex ten t o f ac tiv ity change requ ired to fund the BCF is la rge enough to cause cons ide rab le financ ia l s tress if BCF se rv ices and p lans do no t co m e to fu ll fr u iti o n. * The V a lues o f the BCF s a re kno w n to be 8 m w ith in the D ud ley loca lity and 300k w ith in W a lsa ll. The C lin ica l D eve lop m en t D irec to r is a rep resen ta tive on bo th s tee ring g roups. The va lue o f bo th the D ud ley (8 m ) and W a lsa ll (300k ) BCF s a re no w kno w n. Enc 18 High Level Op Risk Register Page 8 of 12

192 Iden tified g assu rance Enc 18 High Level Op Risk Register Page 9 of 12
193 R isk N o. R isk D esc rip tion Sou rce o f R i s k D a te Iden tifi d P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f R i Fu rthe r C o m m en ts te rm cha llenges a round C IP and no t "In Y ea r P os ition ") dec is ion m ak ing P rog ra m m e B oa rd A c tive pa rtne r o f the M en ta l H ea lth P rog ra m m e B oa rd m a in fo ru m fo r co m m iss ione r lia ison. S ens itiv ity ana lys is bu ilt in to cu rren t p lans and fu rthe r deba te had rega rd ing m on ito r assum p tions and T rus t app roach to m itiga tion. R e m ode lled e ffic iency p lan due to changes in M on ito rs requ ire m en ts, ag reed by T rus t boa rd, F inance and P e rfo rm ance co m m ittee and M E x T S trong financ ia l pe rfo rm ance to da te in yea r R epo rting a rrange m en ts to boa rd enhanced s ince A ugus t 2013 to p rov ide m o re de ta il on sche m es as w e ll as qua lity im pac t assessm en ts M on ito ring o f bank, agency and locu m s no w fo rm s pa rt o f finance repo rt and d iscuss ion a t bo th F and and M EXT. P lans in p lace fo r 2014 /15 and m a jo rity in p lace fo r 2015 /16 C IP P rog ra m B oa rd In p lace P E x te rna l bench m a rk ing o f p lans Enc 18 High Level Op Risk Register Page 10 of 12
194 R isk N o. R isk D esc rip tion Sou rce o f R i s k D a te Iden tified P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f R ev ie Fu rthe r C o m m en ts H R 002 R educ tion in Loca l Feedback F ro A u tho rity Funding fo r m S takeho lde rs M en ta l H ea lth S oc ia l / P C a re W o rk fo rce, w h ich m ay im pac t on se rv ice de live ry and on the v iab ility o f the S 75 ag ree m en ts 30 /05 /2012 W endy P ugh 4 4 R ed 16 S ec tion 75 ag ree m en ts p rov ide fo rm a l p la tfo rm as the bas is fo r any fu rthe r nego tia tions in fund ing and resou rce changes Jo in t app roach ag reed w ith W a lsa ll M B C rega rd ing im p le m en ta tion o f fund ing reduc tions. R isk A ssess m en ts on loss o f pos ts has been co m p le ted R egu la r d iscuss ions be ing he ld a t P a rtne rsh ip O pe ra tions G roup. A dd itiona l sho rt te rm capac ity has been co m m iss ioned 4 4 R ed 16 D iscuss ions ongo ing a t P O G (M on th ly ) 4 2 A m be r 8 R epo rts to M EXT U pda tes to B oa rd 11 /05 /2016 R isk rev ie w ed by G ove rnance and Q ua lity C o m m ittee. R isk to re m a in on the T rus t w ide risk reg is te r, no changes to r i s k. Enc 18 High Level Op Risk Register Page 11 of 12
195 Risk recommended for downgrading - Red to Amber R isk N o. R isk D esc rip tion Sou rce o f R i s k D a te Iden tified P r i n c i p l e O w ne r o f R i s k O t h e r C o n tri b u t o r s In itia l S co re S L C o n tr o l s S C u r r e n t S c o r e L Fu rthe r A c tions R equ ired S R e s idua l S c o r e L Sou rces o f A ssu rance D a te o f R ev ie Fu rthe r C o m m en ts 225 The risk o f insu ffic ien t res ilience and sk ills in leade rsh ip, w h ich m ay resu lt in poo rly engaged, de m o tiva ted s ta ff and poo r se rv ice qua lity. W o r k f o r c e S t a tis tic s 09 /06 /2014 M a rsha In g ra m Chief Executive Executive Directors 4 4 R ed 16 S ta ff su rveys a re unde rtaken on a regu la r bas is. T rus t has a robus t leade rsh ip p rog ra m m e The T rus t has deve loped a nu m be r o f qua lity m e trics to m easu re se rv ic e qua lity. T rus ts CQC v is it sho w ed pos itive resu lts in re la iton to S e rv ice Q ua lity. S ta ff engage m en t w o rkp lan is fu lly s igned up to by the T rus t B oa rd and is cu rren tly be ing im p le m en ted Q ua rte rly upda tes and s ta ff engage m en t p lan p resen ted to T rus t B oa rd 4 3 A m be r 12 In te rna l aud it o f s ta ff engage m en t p rog ra m (O ngo ing ) E va lua tion o f s ta ff engage m en t p lan (O ngo ing ) 4 2 A m be r 8 S ta ff S u rvey R esu lt s Q ua lity m on ito ring m e tri c s S ta ff F riends and F a m ily T e s t (Q u a rte rly ) CQC A ssess m en t 29 /06 /2016 R isk rev ie w ed fo llo w ing spo tligh t sess ion a t Q ua lity and S a fe ty C o m m ittee. It w as ag reed tha t th is risk cou ld be do w ng raded. P os itive assurances had been no ted in respect to th is pa rticu la r a rea by the CQC in respect to the ir recen t assessm en t o f the T rus t. Enc 18 High Level Op Risk Register Page 12 of 12
196 Trust Board meeting date: 7 th July 2016 Agenda Item number: 10.1 Enclosure: 19 Title Agency Update 2016/17 Accountable Director: Author (name & title): Rupert Davies, Director of Finance and Performance Mark Banks, Deputy Director of Finance Action required from the Committee: Decision / Approval Gain assurance Discussion Information What other Trust Committee has considered this report? Committee None Date reviewed Key points or recommendations Not available for this report Purpose of the report To present to members an update on the progress of Agency both in terms of monitoring and compliance in order to deliver the 4.05m agency cap target for 2016/17 as well as a position update as of Month 02.
197 Recommendation(s) to Trust Board Which key standards or assurances does this report relate to? CQC NHSLA Board Assurance Framework F&P members are asked to note the contents of the report State specific standard / outcome or BAF risk TBC TBC TBC Strategic Objective(s) to which this paper relates: / High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective & efficient resources IMPACTS & IMPLICATIONS Patient safety & experience Financial (revenue & capital) Equality & Diversity OD/Workforce What patient & public involvement has there been in this issue? The financial position of the Trust and the capital programme could have a direct impact on patient safety and experience, both adversely and positively Contained within the report Not directly applicable Establishment against budget and temporary staffing spend contained within the report Service user feedback used to inform some revenue and capital investment decisions
198 2016/17 Agency Update Monitoring and Delivery to Agency Cap Target / Month 02 Position Update 1
199 Agency Spending Profile Months 01 to 02 As of Month 02 the current spending on Agency staffing equates to 993k, which when compared to the phased plan of the 4.05m target ( 995k YTD), gives a favourable variance of just 2k. Whilst Month 01 spend of 470k was 37k favourable against the plan of 507k at that time, we have seen the Month 02 position deteriorate against the plan by 35k in month. On the current trend of spending after just two months if spend continues at the current rate then it is likely we will have spent around the 6m mark as we did as a Trust in 15/16. The analysis below shows how the agency spend is split by staff group in line with the reporting to NHSI In Mth ( 000) YTD ( 000) Plan Act Variance Plan Act Variance Agency Staffing Qualified Nursing Medical Other (Incl. Admin, Estates, HCA's, AHP's) Other' represented by: Unqualified Nursing note 1 Admin & Clerical note 2 Scientific & Technical note 3 Maint & Works note 1 note 2 note 3 Malvern 5.9 Estates 22.7 Walsall CAMHs 34.0 Wrekin 14.2 E-Rostering 19.6 Pharmacy 10.3 Clent 15.1 IM&T 14.8 Dudley CAMHs 31.2 Kinver 20.5 DPH Med Secs 13.8 Dudley Primary Care 31.0 Langdale 23.1 HR 6.3 Walsall Primary Care 4.3 Cedars 23.9 PA's Exec Office 5.6 PT Hub 6.6 Linden 36.0 Various (incl OA Malvern / OT / 19.6 Ambleside 41.6 Primary Care / Mgmt Holyrood 55.9 CAMHs / SED / HR) Adult In-Pats all the above relate to Psychology staff with the exception of Pharmacy It can be seen here that the use of Qualified Nursing is performing well against the plan to date ( 57k favourable against YTD plan), however, Other staffing has increased in month ( 40k adverse against plan) mainly across Unqualified Nursing and Scientific & Technical staff groups. Additional detail is reflected opposite as to the service line areas for the three main staff groups that make up the Other staff category. There is a risk that if the current level of spending across the staff groups opposite continues the Trust will begin to outstrip the available plan for agency spending within the next quarter. The plan for the next three months is: M03 (Jun) 420k M04 (Jul) 331k M05 (Aug) 326k 2
200 Agency Key Drivers An analysis was undertaken as to the main areas driving Agency spend across Corporate, Admin and Scientific & Technical areas. It was noted from this analysis that agency costs within corporate areas alone could potentially reach an annual cost of circa 500k for 16/17. The analysis is represented below along with actions that have been agreed to mitigate this potential cost as far as possible. Name Band Cost (Average) excl vat Week/Month Annum Switchboard Week assume 8mths till recruit 14,691 Infomatics 6 1,550 Week left end May 16,065 PA Support - CEO Week assume 8mths till recruit 20,635 Service Experience Desk (SED) Week moving onto Bank circa Sept 12,976 HR Support Week left end Apr 4,728 Staff Engagement 2,800 Month dropped to 2 days/week - finish Sept 18,434 Head of Estates 2,375 Week assume 6mths till recruit 72,181 Estates (1) Week assume 8mths till recruit 21,999 Estates (2) Week assume 8mths till recruit 29,045 Estates (3) Week assume 8mths till recruit 29,045 Estates (4) Week assume 8mths till recruit 21,999 Learning & Develop 3 Week left early Apr 605 Pharmacy 7 1,446 Week left mid-apr 9,023 Pharmacy 7 1,414 Week left early Apr 1,289 Project Lead - EPR 1,868 Week through capital 0 Project Lead - BI 1,594 Week through capital 0 Whilst the initial view for Corporate areas using agency staff had indicated a potential 2016/17 cost of around 500k, following various discussions with senior managers timelines for recruitment have been identified which has brought the likely cost down to a more realistic 344k. The same process is now being undertaken for the other staff groups/service lines in relation to Admin staff and Scientific & Technical staff. Project Lead - E-Rostering 2,379 Week E-Rostering Support Week Liaison & Diversion Week project till end Aug (funded via Cost Pressures) 49,270 project till end Aug (funded via Cost Pressures) 17,837 post recruited to - awaiting clearances 3,909 Corporate Commitments = 343,730 3

201 Agency Benefits of STAFFflow for Medics Since September 2015 the Trust has adopted the direct engagement service for Medical staff via Liaison and the STAFFflow system. Initially this was adopted to help in the recovery of VAT savings for the Trust but is now a key driver in ensuring that the use of Medical Locums falls in line with the requirements from NHS Improvement around the use of framework/price cap agency suppliers. The Finance team receive monthly updates from Liaison which clearly demonstrate the cultural shift from standard engagement from an agency supplier to one of direct engagement through the STAFFflow system. An example of how the Trusts procurement of Medical Locums has changed over the last six months can be seen below: 4
202 Agency Working Within The Agency Rules The Trust has sourced assurance from it s agency staff suppliers to confirm that they are working within the framework and pricing requirements as laid out by NHS Improvement. To gain this assurance our agency suppliers were asked to provide written confirmation that: They are signed up to a NHS Improvement approved national framework for the supply of NHS staff; and That those staff are being charged to the Trust within the price caps as prescribed by NHS Improvement, indicating the rates of pay and how they align to the prescribed rates; That agency workers supplied to the Trust are not / will not be being paid more than the maximum wage rates as from July 2016; That they will provide regular management information and reporting at shift level. 41 separate agency suppliers were contacted and all replied to the assurance questions stated above of the responses 29 said they were fully compliant (71%) and either were currently or would be moving to the prescribed pay rates. Suppliers who said that would not be able to fully comply were: Allied Healthcare no longer used by the Trust; Coyle Personnel neither on approved framework or price rates (however the use of this agency within the Trust has decreased substantially over the last several months, as detailed in our STAFFflow data reducing from a 28k spend in Sept 15 to 3k in Mar 16); DRC Locums framework compliant and will look to work to April pay rates otherwise will supply at Nov 15/Feb 16 rates (break glass); GPS Locums no longer being used by the Trust; Maxxima framework compliant but would not be applying April price rates for existing agency staff, only for new contracts; Medicare First no longer used by the Trust; Prime Time framework compliant and will only adhere to April price rates for Band 3 Nursing staff (not for Band 5 Nurses); Promedical - framework compliant but would not be applying April price rates; RIG Medical framework compliant and will look to work to July maximum wage rate awaiting further confirmation of rates for any current contracts; Robert Half not framework compliant but will look to work to April price rates; Sanctuary Personnel framework compliant and will work to April price rates for Nursing staff only will not apply for CAMHs staff (break glass) Sugarman Group framework compliant (under Cordant Group) but not adhering to April price rates The top 7 agency suppliers in use by the Trust, based on 15/16 spend, were: Sanctuary Personnel; The Flame Lily Pulse Coyle Personnel Prime Time Sugarman Group Destiny Recruitment 5
203 Risks / Moving Forward Areas of Risk Whilst the Trust is working closely with agency staff and encouraging them to come onto the staff bank or into substantive roles recently we have been informed of agencies who are evoking sign-on clauses. This could run into several thousands of pounds per agency staff as clauses often impose a % of starting salary upon recruitment into the Trust within several weeks of leaving the agency and beginning employment at the Trust. Procurement are working closely with framework organisation to minimise the risk of these fees. We are looking to compile a list by agency supplier of the potential sign-on fee terms and conditions so that recruiting managers are made aware of the potential costs. Moving Forward Allocation of all agency suppliers in use at the Trust to be ranked into tiers of those who are working to the rules fully down to those who are not fully complying the aim is to give managers a view of the preferred agency suppliers the Trust should be approaching in time of need. Proposed star chamber to review all agency staff in: Corporate departments; Admin staff working within clinical areas; Clinical areas (but not medics or nursing). Action plans will be required for all posts currently filled on an agency basis:- For posts funded recurrently a time line for recruiting to individual posts; For posts not funded plans for stopping any unfunded agency staff roles, including how the work undertaken by such staff will be managed in the future; For posts funded non-recurrently (eg, pilots) whether the trust continues with the staff on a non-recurrent basis or eliminates such posts (eg, by informing commissioners that the trust is no longer prepared to continue with activities which impact upon its agency control total set by the NHSI). 6
204 Board meeting date: 7 th July 2016 Agenda Item number: 10.3 Enclosure: 20 Report Title: Service Experience Desk Annual Report 2015/16 Accountable Director: Author (name & title): Purpose of the report: Marsha Ingram, Director of People and Corporate Development Julie Adams, Interim Service Experience Lead Mary Bytheway, Associate Director of Corporate Development To present the Trust Board with a draft Service Experience Desk Report 2015/16 for approval/comments. Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: Quality & Safety Committee Date reviewed: 9 June 2016 Very comprehensive Perhaps include a little more detail around EBEs (actioned) Present to Trust Board for approval Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Effective Please give brief details: Listening to feedback of our services and responding appropriately, providing channels for service users, carers and stakeholders to share their views with us Feedback is timely and appropriate, actions are taken to address issues Investigations and reviews are thorough and balanced. This report is considered as part of each service line s quarterly performance review Enc 20 SED Annual Report front sheet TBPage 1 of 3
205 Well-led Safe Provides information to Board and its committees in order to support effective action and decision making about service experience feedback Triangulation with Safeguarding and serious incidents supports safe service delivery and resolution Enc 20 SED Annual Report front sheet TBPage 2 of 3
206 Title Service Experience Desk Annual Report 2015/16 Introduction This report aims to provide the Trust Board with a draft Service Experience Desk Annual Report 2015/16. Summary of key points, issues and risks The annual report gives details about: Trust; vision, values, strategy, strategic aims and services Service Experience Activity The full picture of service experience Key achievements 2015/16 Priorities for 2016/17 Further detail (if required) Please see the appended Service Experience Desk Annual Report 2015/16. Recommendation The Board receives the annual report for discussion and approval. Board action required Approval. Enc 20 SED Annual Report front sheet TBPage 3 of 3
207 Service Experience Desk Annual Report 2015/16 (Incorporating Complaints, Compliments and PALs) Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 1 of 16
208 Contents 1 INTRODUCTION Chair s and Chief Executive s Foreword ABOUT THE TRUST Our Vision... ERROR! BOOKMARK NOT DEFINED. 2.2 Our Values Our Strategy Strategic Aims Our Services 5 3 SERVICE EXPERIENCE DESK ACTIVITY Celebrating Positive Feedback Complaints Management Number of formal complaints received Complaints referred to Parliamentary Health Service Ombudsman (PHSO) Nature of Complaints and concerns received Outcome of Complaints Learning from Feedback 13 4 SERVICE EXPERIENCE - THE FULL PICTURE KEY ACHIEVEMENTS 2015/ PRIORITIES FOR 2016/ JARGON BUSTER...15 Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 2 of 16
209 1 Introduction 1.1 Chair s and Chief Executive s Foreword Welcome to the Service Experience Desk annual report from Dudley and Walsall Mental Health Partnership NHS Trust. As a provider of services, we are committed to ensuring that representatives of those people who use our services and their carers are fully integrated within our decision-making and governance structures. On a day-to-day basis, we work closely with a wide range of Service User and Carer organisations across the two boroughs, seeking their views and ensuring their participation in the planning and delivery of services. Patient knowledge and experience are essential for understanding how best to improve care. The very best user and carer involvement harnesses a passion for making things better and over the past year, we have made enormous progress with implementing and expanding our involvement strategy. Our commitment to putting service users and carers at the heart of everything we do is demonstrated by the way that service user and carer involvement is taken into consideration at the forefront of new projects, initiatives and developments. We try to focus on the things that matter the most for patients, communities and staff and emphasise a culture of genuine engagement, involvement and transparency. The contents of this report specifically meet the requirements set out for Complaints Annual Reports in section 18 of the Local Authority Social Services and National Health Service Complaints (England) Regulations The requirements state that the report should specify: the number of complaints which the responsible body received the number of complaints which the responsible body decided were well-founded the number of complaints which the responsible body has been informed have been referred to the Health Service Commissioner to consider under the 1993 Act; or the Local Commissioner to consider under the Local Government Act 1974 And the report should summarise: the subject matter of complaints that the responsible body received any matters of general importance arising out of those complaints, or the way in which the complaints were handled any matters where action has been or is to be taken to improve services as a consequence of those complaints Ben Reid Chair Mark Axcell Acting Chief Executive Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 3 of 16


210 2 About the Trust The Trust is a multi-site provider (26 sites) serving the Black Country boroughs of Dudley and Walsall within the West Midlands. The Trust s headquarters are situated in Dudley, approximately 10 miles north-west of Birmingham. The Black Country region demonstrates cultural, economic and educational diversity. Walsall, along with Sandwell and Wolverhampton, experience high levels of multiple deprivation. Since formation, the Trust has made significant progress in the development of the organisation, engaging with its communities and taking stock of service quality and performance. We are proud of: Small and flexible organisation, respond to change and challenge, quickly and effectively Openness and transparency Robust relationships with commissioners and excellent local health economy knowledge Reputation for good service quality and governance Good engagement with service users, carers, agencies and community groups Consistent high performance Successful integration of two culturally and operationally different services 2.1 Our Vision The Trust s vision is one of a recovery oriented service. The vision, encapsulating the concept of the benefits arising from a single mental health trust for the populations of Dudley and Walsall, is shown below: Better Together - delivering flexible, high-quality, evidence-based services to enable people to achieve recovery. The Trust s vision has been guided by national, regional and local intelligence and strategies where there is a growing emphasis on the well-being of the population and a focus on prevention, together with early detection and intervention. 2.2 Our Values Our values are the essence of our identity. They describe what we are and what we stand for. They support our vision, shape the culture and more importantly represent the behaviours that staff value as employees. In 2015/16 we refreshed our values in close partnership with staff. This was a process that engaged all staff in revisiting what they felt were important values for us and that would shape our guiding principles and underpin the way we work. After extensive discussion and review, we chose the following new values: Figure 1 Our Values Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 4 of 16
211 These new values also reflect the NHS Constitution and are significant in that they inform attitudes and therefore behaviours of staff. Underpinning our new values is a behavioural framework that supports recruitment, personal development, performance and organisational culture. 2.3 Our Strategy The Trust has a clear, focused strategy that underpins the delivery of mental health services for the populations of Dudley and Walsall. In protecting its long term viability, the Trust explores opportunities that support the delivery of mental health services across the wider health economy, building on the skills of the Trust and meeting unmet or emerging needs. In developing its strategy, the Board stated its commitment to be flexible in its on-going consideration of the scope of services it provides in order to reflect the genuine needs of service users and carers and delivery of the Five Year Forward View (5YFV) Strategic aims The Trust s strategy has three overarching domains that together, achieve the Trust s vision: 1. Transform services to improve the patient experience and the quality of services 2. Become the preferred provider of prevention and recovery services for mental health and wellbeing within the Black Country and beyond 3. Develop the organisational culture and capabilities to support high quality service delivery 2.4 Our Services Mental health conditions are very common with 1 in 4 people experiencing some kind of mental health problem in the course of a year. These are split into two categories; common mental health problems, which include conditions such as depression and anxiety, and severe and enduring mental health problems such as schizophrenia and bipolar disorder. The Trust provides a full range of mental health treatment and rehabilitation services that manage both categories of mental health conditions. The Trust s range of services spans GP based primary care counselling and psychological therapies for common mental health problems through to the treatment and care of people detained under the Mental Health Act. Core services are provided predominately to Dudley and Walsall, but also to neighbouring Trusts in Worcestershire, Staffordshire, Birmingham and Warwickshire. We provide: Community mental health services for children, adults & older people Inpatient services for adults and older people Primary Care Mental Health services (including IAPT) Mental Health Social Care Services (via local authority partnerships) Psychological Therapies Employment, education and training support for people with mental health problems Specialist Deaf CAMHS (national hub) In 2009, the Trust was selected by the National Commissioning Group to be one of four centres in England to deliver a national Deaf Service for children up to the age of 18 and their families. Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 5 of 16
212 3 Service Experience Desk Activity The Trust s Service Experience Desk is the central point of contact for all concerns and enquiries whether these are formal or informal, complaints, compliments or requests for information. The Trust welcomes feedback about its services and considers this a valuable source of insight into the quality of our services. Being a patient, relative or carer can be a difficult, confusing and stressful time and the Service Experience Desk is there to offer advice, help and support. During the period April 2015 to March 2016, we received a total of 139 formal complaints, 215 concerns, 321 compliments and handled 792 new cases. 738 of cases are attributable to Service lines. The remaining 86 are attributable to corporate functions, trust generic or non-specific. This includes complaints, concerns, compliments, suggestions and requests for information. This feedback comes from service users, carers or their representatives and from other organisations such as commissioners or MPs. Figure 2 SED Activity by Type Case type 2015/ / /14 Compliments Informal concerns Informal enquiries Formal complaints Suggestions Table 2 above shows SED activity type for the Trust for 2015/16 along with the previous two years. The Trust is structured into four operational service lines as shown in figure 3: Acute and Access, Community and Recovery, Early Intervention and Older Adults. The service line portfolios are shown below. SED activity is proportionate to the size of the service and the nature of the service users in those services, for example, the Trust finds that older adults and young people are less likely to complain than working age adults. The Trust reports SED activity by Service Line and this is scrutinised at the quarterly performance reviews alongside all other performance data. The service lines are shown below. Figure 3 Our Service Portfolio Community Services Acute and Older Adult Services Early Intervention Services Community and Recovery Services Older Adults Acute Services Primary Care Mental Health Improving Access to Psychological Therapies Children & Adolescent Mental Health including home treatment Eating Disorders Early Intervention in Psychosis Deaf Child and Family Mental Health Community Recovery Service Teams (CRS) Therapeutic Hub Criminal Justice/Offender Liaison Liaison and Diversion Employment and Vocational services Carers service ASD assessment and diagnosis service Wards Day Services Community Mental Health Teams Memory Service Outpatients Early Access service (EAS) Wards Crisis Resolution Home Treatment Psychiatric Liaison Urgent Care Centre Outpatients Street Triage Place of Safety (136 Suite) NOTE: Service Line Structures change in April 2016 Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 6 of 16

213 Figure 4 SED Feedback Received 2015/16 Number of complaints, concerns and compliments by service line The chart above shows the number of complaints, concerns and compliments received by quarter during the year 2015/16 for the four service lines. The number of complaints received is relatively small compared to the number of patients we see and treat each year. Figure of the 321 compliments received were for the care and treatment provided by our staff The chart above shows SED activity by type for the four service lines. Compliments are the largest category, with attitude of staff as the highest cause group within that. Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 7 of 16
214 3.1 Celebrating Positive Feedback Compliments are the largest category, with attitude of staff as the highest cause group within that. Over the last twelve months we are pleased to say that we have received 321 compliments from people who have accessed our services, highlighting cases where the quality of our services has been recognised and appreciated. Examples of what they are particularly pleased with are:- Care and treatment provided by staff Quality of food Cleanliness of the wards SED shares this feedback with staff through our feature On a Happy Note which highlights the positive comments made by service users about their care by posting a selection of experiences from service users on the Trust intranet every month. Some examples of what people have said about our services are shown below. I would like to state that this ward is excellent and care provision is fantastic. It is also kept immaculately clean. This hospital is great and my health has improved hugely under the care of staff. Three weeks ago I was ready to die, I didn t want to be here anymore and I felt nothing and nobody could change that. Three weeks later and still currently in hospital, I am looking at discharge and going home to my family. I have met new people, made new friends and blossomed into the person I am now. I am stronger and more able, positive and fighting back. I want to live, I want to survive. This is all possible because I have a wonderful supportive family and a fantastic team of doctors, nurses and healthcare assistants around me to aid my recovery. Thank you each and every one of you. I like the homely environment on Kinver Ward. I would like to thank all the staff - I really enjoyed the activities. Thank you to all the staff who looked after my sister. The nurse has been a star to my sister and to us as relatives. It is the small things you do that make a difference. My therapy has been instrumental to my ongoing recovery. This combined with the mindfulness techniques gained in the course I took part in. I am confident that the therapy has been of great benefit to me and others around me and for the first time in my life I know I have the tools to enable me to be strong in the future. All members of North CRS team have been fantastic kind, helpful, non-judgemental and areal asset to the mental health service. I would like to offer my gratitude to all that have been involved in my care. I cannot compliment the doctor enough, her passion for her job and her patience is excellent. She truly cares for patients and I would be in a very dark place without her. Whenever I was seen in the clinic, I was treated with care and respect. The doctor always listened to me and took on board what I was saying and respected my wishes. I felt happy with the service and support. I would like to thank everyone in the team and hope in a nice way that I won t be back. I have found the counselling service provided to be most beneficial to me, life changing in fact. Over the past few months I have become a different person, which I have only been able to achieve by following the counsellor s advice and using the tools that I have been shown. Thank you for making me a more relaxed, calm and happy person. I just wanted to say a massive thank you for changing my life for the better. Three months ago I would never have thought I could be where I am today. I owe it all to you, thank you. The card is not really big enough for the thanks I have for you but I wanted to thank you for doing your job so well. Whilst you have just been doing your job you have just been giving me my life back. I look forward to my future. You have given me skills that now make my life much easier. Thank you from the bottom of my heart. Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 8 of 16
215 My daughter has made amazing progress. I feel every session with SAMHS has been beneficial to her. I can t fault any of the treatment she has received. I would also like to say how fantastic the practitioner has been not only for my daughter but also for me. CAMHS is an invaluable service for children who need extra help and support. I lost my husband November 2013, I hit rock bottom and felt that my word had ended, my doctor put me in touch with the mental health nurse and without his help I don t know where I would have ended up. He is very nice and talks things through. He is a credit to his work, I will always be grateful. During the past four months the doctor has played an important role in the progress made by my husband, whilst in both the Bloxwich and Manor Hospital. I would like to say that I have never experienced a doctor quite as dedicated. His dedication and professionalism goes beyond expectations from any doctor. He is the doctor everyone would want if they were ill. From my observations his patients are not just patients to him. They feel they are so important to him and he will do everything possible to aid their recovery. We would like to thank you all very much for the care and support you have given dad during his time with you. Initially, he wasn t convinced that he would benefit from attending but we have noticed a big change in him, and the fact he feels sad about leaving is a testament to your caring, friendly and skilful staff. He tells us of the good laughs he has each week not to mention the lovely meals. You provide a wonderful service. Thank you all very much. The staff nurse came through with a brilliant idea for the Malvern Ward in Dudley Hospital. She was enjoying a can of coke at the time and thought a cold drinks machine would be ideal in the garden area. What a pleasant idea she brought to mind on a beautiful sunny day. Her lovely attitude to this ward is without doubt undeniable. The great knowledge of nursing, with such dedication is truly outstanding. We would like to thank you for all of the care, support, empathy and kindness you have shown our parents. You have worked to build a special relationship with them and have gained their trust; my dad even calls you his life line. We appreciate everything you have done for us. With many thanks for everything. 3.2 Complaints Management Despite our focus on quality, we recognise that sometimes people s experience of our services is not as positive as we would hope. In October 2007, the Health Service Ombudsman published Principles for Remedy as an overall good practice guide for public bodies in dealing with complaints. Our complaints policy is based around these principles which are: 1 Getting it right 2 Being customer focused 3 Being open and accountable 4 Acting fairly and proportionately 5 Putting things right 6 Seeking continuous improvement Number of Formal Complaints Received In 2015/16, the Trust received 137 formal complaints which were attributable to the four service lines. This is shown in the chart below along with the number of informal concerns and cases referred to the Ombudsman during this year. Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 9 of 16
216 Figure /16 Complaints and Concerns Summary for the 4 service lines Informal Concerns Formal Complaints PHSO Acute & Access Community & Recovery Early Intervention Older Adults Total During the period April 2015 to March 2016, we received a total of 139 formal complaints (137 relating to the four service lines), 38 of which were withdrawn or closed. We responded to 43 cases within the target timescale; 28 cases remain open, 20 of which were still within target. These figures are correct at the time of writing Complaints referred to the Parliamentary and Health Service Ombudsman (PHSO) Four notifications were received from the Ombudsman during 2015/16 in relation to formal complaints that had been responded to by the Trust. No action was taken with two of the cases, two remain under review Nature of Complaints and Concerns Received The charts below show the primary category of the complaints and concerns received by the Trust in 2015/16. Care and treatment, like within most Trusts is the highest category of concerns with attitude of staff the next highest. Care and treatment has been drilled down as shown in figure 8 Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 10 of 16
217 Figure 7 Figure 8 Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 11 of 16
218 The chart below shows both primary and secondary categories of complaints and concerns received by the Trust in 2015/16. Primary category refers to the main concern raised and secondary categories include any additional concerns. The top 3 categories are care and treatment (clinical), communication and staff attitude. Figure Outcome of Complaints Of the cases investigated and closed, 75% of complaints were upheld or partially upheld. The decision to uphold a case or not is made following a full investigation that involves the scrutiny of notes and records, interviews with staff and service users as appropriate. The table below summarises this. Figure 10 Outcome of Complaints Number Not upheld 18 Upheld 10 *Partially Upheld 45 Withdrawn/closed 38 On-going 28 TOTAL 139 *Partially upheld outcomes are counted as upheld for KO41 reporting purposes Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 12 of 16
219 3.4 Learning from Feedback The Trust takes an active approach to resolving concerns before they escalate to formal complaints. We also provide feedback to staff about what changes have been made as a result of complaints and concerns. We receive essential and valuable feedback through the function of our Service Experience Desk. Service users, carers, staff and others contact the service experience desk for advice, support and to report concerns and complaints directly to us. Over the past twelve months our 10 Expert By Experience service users (EBE s) have been directly and significantly involved in raising awareness of Trust activities as well as gaining valuable feedback from service users and carers. The team of EBE s are aligned to special areas of interest, with each EBE bringing different skills and experience to the role. Each of our EBE s has considerable knowledge and experience of using Trust services and have helped hundreds of service users and carers in various ways, simply by listening to them and representing their interests. Our experts provide the Trust with vital knowledge gained through their experience of using mental health services or caring for someone who has. The work of our EBEs forms a significant part of the Trust s Service User and Carer Involvement Strategy, which aims to deliver our vision of involving service users and carers in all areas of our work from policy development, review patient information leaflets, carry out ward visits, attending board meetings, participate in induction, take part in the recruitment processes to the training of clinicians. Here are just a few of the selected actions that have been carried out as a result of feedback from those who use our services, their relatives and carers. Figure 11 Comments and Actions Taken You Said: I would like more information and advice about benefits, housing or finding word I am not always sure who is looking after me, staff don t always introduce themselves It s not clear who I need to contact to raise a concern or make a complaint I have dementia and often suffer from severe pain but I don t think staff notice this I miss my dog I don t feel that is much rotation of the menu We did: Provided all teams with leaflets and posters highlighting how to access advice and support. Staff are working with our Experts by Experience to raise awareness of the support and signposting we can offer We have introduced Hello my name is that encourages all our staff to introduce themselves to patients, carers and visitors Posters have been put up in all sites and staff from the complaints team have been visiting services to raise awareness. A new form has also been launched a new form on our website We have introduced a pain monitoring tool that will help staff to be able to better manage pain experienced by patients admitted to hospital with a diagnosis of dementia Team organised dog therapy where a dog comes in with an owner and patients can interact with the pet. A popular therapy sometimes used with patients who are living with memory problems Staff worked with the catering staff to offer more choice and variation Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 13 of 16
220 4 Service Experience - the full picture As well as gathering feedback about our services through SED, the Trust also has a Service Experience Coordinator who reports on other forms of service experience feedback, for example: Patient Stories for Trust Board Friends and Family Test (Net Promoter) National Surveys Local Surveys (run by teams) Focus Groups Ward and service visits buy our Experts by Experience, Community Development Workers and local mental health support groups (Walsall SUE and Dudley SAMh) Feedback from Trust members The findings of this work triangulates with SED activity and feeds into our embedding lessons process described in section Key Achievements 2015/ /16 was a busy year for the Trust s Service Experience Desk. As well as efficiently handling around 800 new cases, the team also achieved a number of improvements in how SED operates: Further improved the embedding lessons processes, actions taken as a result of recommendations and the effectiveness of those actions Shared and displayed high level Service Experience data at main sites in order to support transparency for service users and visitors Extended the number of available complaints investigating officers in order to ensure timely responses to complaints and reduce the number of breaches Promoted the vision framework from My Expectations report developed by the Parliamentary Health Service Ombudsman, Local Government Ombudsman and Healthwatch England in order to make the complaints process a good experience for our patients, families and carers Implemented recommendations from the compliments audit such as perform a monthly sample check of accuracy and timeliness of data input review and amend the SED policy 6 Priorities for 2016/17 In 2016/17 the Trust will focus on: Further improvements to the embedding lessons processes, actions taken as a result of recommendations and the effectiveness of those actions Improve our complaint response targets Further promote and embed the vision framework for concerns Make it easier for service users to give feedback Revise our website to be more transparent Trial the national complaints process survey Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 14 of 16
221 7 Jargon Buster Term CAMHS Definition Child and Adolescent Mental Health Service. A multi-agency and multi-disciplinary service specialising in the assessment and treatment of moderate to severe mental health difficulties for children and young people up to the age of 16 years. The service helps with a vast range of problems / concerns including bullying resulting in school refusal, eating disorders, Attention Deficit Hyperactivity Disorder, Autism, Psychosis and Deliberate Self-Harm. Carers (also known as informal support ) CDW Commissioners / Clinical Commissioning Groups (CCG s)/ Complaint Compliment Corporate Function EBE s Embedding Process Lessons KO41 Reporting Process Informal concern Outcome PALS PHSO A person who provides support to a partner, family member, friend or neighbour who is ill, struggling or disabled and could not manage without this help. Community Development Workers (CDW s) work in a number of different ways to challenge discrimination and stigma, and to promote mental wellbeing. Their aim is to:-help patients to access mental health services, that are appropriate to need; ensure cultural needs are met when accessing statutory services ; provide a range of self-help materials, that could help with milder forms of anxiety, depression and stress ; sign post service users of community and voluntary groups in area, that could aid recovery ; provide links to agencies, who can help with employment, benefits, child care and education; provide training / workshops regarding mental health, to Black and Minority Ethnic, and Voluntary organisations. Dudley and Walsall CCGs took over responsibility from Dudley and Walsall Primary Care Trusts in April CCG s are run by GPs and are responsible for the purchasing of healthcare for people living in Dudley and Walsall boroughs and to ensure that care services are provided effectively and that they meet the needs of the population. This process is called commissioning. An expression of dissatisfaction that requires a response. Comments received in writing about the good service received from the Trust. Services within the Trust that provide support to the clinical teams and services but do not directly provide services to patients. Service users and carers who are Experts by Experience (EBE). Our experts provide the Trust with vital knowledge gained through their experience of using mental health services or caring for someone who has. The work of our EBEs forms a significant part of the Trust s Service User and Carer Involvement Strategy, which aims to deliver our vision of involving service users and carers in all areas of our work from policy development or attending board meetings, to the training of clinicians. System through which we ensure we make sustained changes and learn lessons from the feedback we receive about our services. The KO41 data collection is the statutory based mechanism for collating written complaints data about NHS care and treatment, across all NHS organisations in England. This is mandatory and performed on behalf of the Department of Health. A concern raised that can be resolved quickly and does not require a formal response/investigation. The outcome in relation to complaints is whether the complaint was upheld or not upheld and what actions were put in place. The Patient Advice and Liaison Service (PALS) offer confidential advice, support and information on health-related matters. They provide a point of contact for patients, their families and their carers. Parliamentary and Health Service Ombudsman The Parliamentary and Health Service Ombudsman investigates complaints that individuals have been treated unfairly or have received poor service from government departments, other public organisations and the NHS in England. Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 15 of 16
222 Primary Care and IAPT Primary/Secondary/catego ry of complaint Safeguard System SED SED Activity Type Service Lines Service user Specialist Deaf CAMHS SUE and SAMh Primary Care and Improving Access to Psychological Therapies. This service aims to provide an accessible service for people experiencing mild to moderate mental health problems. Help patients identify the underlying cause of their distress or concern. They offer information and support on a range of issues including; health education and advice, redirection to appropriate services, problem solving advice, self-help advice to raise awareness about common mental health problems and the cause of distress. This service provides an opportunity to talk and to be listened to when experiencing problems. Categories of complaints refers to the specific type/cause of concern raised, for instance waiting times, staff attitude etc. Primary categories refers to the main concern raised Secondary categories, refers to all concerns raised This is the Trust s Risk Management database whereby all complaints and concerns are recorded and data extracted. Service Experience Desk. This is the central point of contact for all concerns, complaints, enquiries, suggestions and compliments. The team are on hand to offer support and guidance to patients, carers and their families when problems may arise. Type of issue raised to the Service Experience Desk Informal concern, formal complaint, compliment, suggestion. Services the Trust provides are grouped into service lines: - Acute, Community, Early Intervention, Recovery, Older Adults. A person who uses our mental health services, whether they are in their own home, in residential care or in hospital. They may also be described as patients or clients. The Deaf Child and Adolescent Mental Health Service provides a specialist mental health service for deaf and hearing impaired children with a range of emotional, behavioural and developmental problems. The team treats children with a mental health condition and either: a severe or profound hearing loss; British Sign Language (BSL) as their preferred/first language; a significant language impairment related to moderate to profound hearing loss. Mental Health Support Groups Service User Empowerment (Walsall) This service aims to improve Walsall residents access to support services and to connect people with groups and activities within the borough of Walsall, as well as provide services and activities themselves. Support Association for Mental Health (Dudley) The service aims to make sure that Mental Health services are meeting the needs of people today and the next generation. Monthly meetings are held every month for service users, their partners and carers to attend and discuss mental health services. Trust Generic / non specific Complaints that are not specific to a service line Enc 20 Appendix 1 Service Experience Desk Annual Report TB Page 16 of 16
223 Meeting date: 7 th July 2016 Agenda Item number: 10.3 Enclosure: 21 Report Title: Board Committee Review of Terms of Reference Accountable Director: Author (name & title): Purpose of the report: Marsha Ingram Director of People and Corporate Development Paul Lewis-Grundy, Company Secretary As part of good governance all Board Committee Terms of Reference should be reviewed annually. Committee members are asked to review and approve the revised Terms of Reference. Action required from MExT Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: Quality & Safety Committee on 11 May 2016 Audit Committee on 23 May 2016 Finance & Performance Committee on 23 May 2016 Mental Health Act Scrutiny Committee on 23 June 2016 MExT on 24 May 2016 Nominations and Remuneration Committee on 5 May 2016 The Nominations and Remuneration Committee discussed the role of the Associate (Non-Executive Directors) and recommended the Terms of Reference of the Board Committees be amended to reflect that Associate NED s could be members of the Committees in the same way that NED s are. All the Committees have reviewed their respective Terms of Reference, including taking account of the Nominations and Remuneration Committee recommendation. The appended Terms of Reference reflect the amendments recommended by the respective Committees. Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Responsive Effective Well-led Safe Please give brief details: The annual review of committee terms of reference by each committee and by the board is part of effective governance. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference Page 1 of 3
224 Title Board Committee Review of Terms of Reference Introduction All committees of the Board should review their terms of reference on an annual basis to ensure fitness for purpose. Summary of key points, issues and risks The Nominations and Remuneration Committee met on 5 May and discussed the role of the Associate (Non-Executive Directors). The committee noted that the position of the Associate NEDs in respect of Board Governance did not facilitate optimal use of their skills and expertise. Therefore, the committee agreed to recommend to the Trust Board that the Standing Orders should be revised to ensure that Associate NEDs have equivalent status as NEDS in all aspects except the issue of Board voting. This would include contribution to and chairing Board committees, where appropriate. Standing Orders In light of the recommendation of the Nominations and Remuneration Committee it is proposed to add the following paragraph to the Standing Orders approved by the Board at its meeting in April 2016: 2.1(2)(i) The Trust may appoint Associate Non-Executive Directors, who will have the equivalent status to the Non-Executive Directors save for voting rights at the Board, including being members of, contributing to and Chairing Board Committees, where appropriate and in accordance with national guidance and best practice. Section 2.1 concerns the Composition of the Membership of the Trust Board and (2) particularly concerns the Non-Executive Directors. Committee Terms of Reference During the annual review of the Committee Terms of Reference that was reported to the respective Board Committees through May and June 2016, they have been amended to reflect the recommendation of the Nominations and Remuneration Committee regarding the role of Associate Non-Executive Directors. The other proposed changes to the Terms of Reference, reflect any legislative changes, updated guidance, advice and best practice and have been updated where appropriate to standardise format and practice across all the Committees. The Terms of Reference of the Committees appended to the report have all been agreed through their respective meetings and have been reviewed in accordance with The Foundations of Good Governance A compendium of Good Practice, Third Edition AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference Page 2 of 3
225 Further detail The Committee Terms of Reference are attached at Appendices 1-6. Recommendation The Board is recommended to approve the Committee Terms of Reference appended. Action required The Committee Terms of Reference are presented to Board for approval. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference Page 3 of 3
226 DUDLEY AND WALSALL MENTAL HEALTH NHS PARTNERSHIP TRUST QUALITY AND SAFETY COMMITTEE Appendix 1 The Board recognises that high standards of governance throughout the Trust are essential for the delivery of the identified strategic objectives, the safety of its services the quality of service user and carer experience and the long term protection of stakeholder interests. Good governance emanates from the Board but pervades the entire organisation, being reflected in its operating practices, policies and procedures. This responsibility encompasses clinical, financial and organisational aspects of governance and enables key risks to be identified and managed, in both operational and strategic terms. This committee will therefore ensure that: The Trust has established a sound framework of clinical governance comprising those processes, systems and controls that enable NHS organisations to demonstrate accountability for continuously improving the quality of services and safeguarding high standards of care. That arrangements are in place to support staff to deliver safe and quality patient care. That consultation and involvement by service users, carers and stakeholders effectively informs continuous improvement. That clinical governance, clinical/operational risk management and safeguarding systems and processes are operating effectively, provide robust information and comply with statutory and regulatory guidance, standards and reporting requirements. That learning from feedback is embedded throughout the organisation. That all aspects of information governance relating to clinical and patient information are in place to meet IG Toolkit standards. TERMS OF REFERENCE 1. Authority 1.1 The Quality and Safety Committee is constituted as a standing committee of the Trust's board of directors. Its constitution and terms of reference shall be as set out below, subject to amendment at future board of directors meetings. 1.2 The Quality and Safety Committee is authorised by the Board of directors to instruct professional advisors and request the attendance of individuals and authorities from outside the Trust with relevant experience and expertise if it considers this necessary for or expedient to the exercise of its functions. 1.3 The Quality and Safety Committee is authorised to obtain such internal information as is necessary and expedient to the fulfilment of its functions. 2. Purpose 2.1 To enable the board to obtain assurance that high standards of care are provided by the Trust and, in particular, that adequate and appropriate governance structures, processes and controls are in place throughout the Trust to: Promote safety and excellence in the care and experience of service users and carers. Identify, prioritise and manage risk arising from clinical care. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-Q&S-Appendix1 Page 1 of 7
227 Ensure the effective and efficient use of resources through evidence-based clinical practice. Protect the health and safety of Trust employees. 3. Membership 3.1 The membership of the Quality and Safety Committee shall consist of: A minimum of 2 Non-Executive or Associate Non-Executive Directors who will act as the Chair and Vice-chair Joint Medical Directors Chief Executive Director of Nursing, Operations and EstatesNursing (also the DIPC in this Trust) Director of People and Corporate Development 3.2 The Quality and Safety Committee will be deemed quorate when 4 members are present including at least one Non- Executive / Associate Non-Executive Director and one Executive Director. 3.3 The chair Chair will be appointed by the Trust Board. 3.4 For the avoidance of doubt, Trust employees who serve as members of the Quality and Safety Committee do not do so to represent or advocate for their respective department, division or service area but to act in the interests of the Trust as a whole and as part of the Trust-wide governance structure. 3.5 Core members may nominate an appropriate deputy to attend the committee on their behalf. However, it is expected that any nominated deputy will be fully briefed and have the necessary authority to participate fully in the debate and any subsequent decisions arising. 3.6 Additional members or associates may be co-opted to attend the Committee as necessary. 4. Attendance 4.1 The following participants are required to attend meetings of the Quality and Safety Committee Chief Pharmacist Clinical Director Governance and Quality Head of Governance Head of Nursing, Quality and Innovation Director of Finance and Performance Head of Strategic Planning Trust Safeguarding Lead Deputy Director of Finance and or the Head of Business Intelligence and IM&T as appropriate ; 4.2 The Trust values the contribution of Experts by Experience to Quality and the importance of their independent role. Nominated Experts by Experience are encouraged to attend meetings and report to Quality and Safety Committee as regularly as possible Formatted: Left, Indent: Hanging: 0.54 cm Formatted: Indent: Left: 0 cm, Hanging: 1 cm AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-Q&S-Appendix1 Page 2 of 7
228 4.23 Meetings of the Quality and Safety Committee may beothers that may be invited to attend attended by the Committee: Service User and Carer Representatives/Governors Associate Director of Operations Risk and Assurance Facilitator Patient Safety Analyst The Senior Administrator for Clinical Governance, who will act as secretary. Any nominated deputy attending in place of a member of the Quality and Safety Committee. Any other person who has been invited to attend a meeting by the Quality and Safety Committee so as to assist in deliberations. 4.4 The Senior Administrator for Clinical Governance, who will act as secretary. 4.3 Other than as set out in paragraphs 4.1 and to 4.24, only members of the Quality and Safety Committee are entitled to be present at its meetings. Formatted: Indent: Left: 1.5 cm, No bullets or numbering Formatted: Indent: Left: 0 cm, Hanging: 1 cm, No bullets or numbering 4.4 Members listed at paragraph 3.1 and attendees listed at paragraph 4.1 are, respectively, required to attend at least half of the meetings held annually. 5. Frequency of Meetings 5.1 Meetings shall be held monthly. Additional meetings may be held on an exceptional basis at the request of the Chair or any three members of the Quality and Safety Committee. 6. Duties In particular, in respect of general governance arrangements: 6.1 To ensure that all statutory elements of clinical governance are adhered to within the Trust. 6.2 To agree Trust-wide clinical governance priorities and give direction to the clinical governance activities of the Trust s services, not least by reviewing and approving each service's annual clinical governance, patient safety and quality plan. 6.3 To approve the Trust's annual quality priorities and account before submission to the Board. 6.4 To approve the terms of reference and membership of its reporting sub-committees (as may be varied from time to time at the discretion of the Quality and Safety Committee) and oversee the work of those sub-committees and working groups, receiving reports from them as specified by the Quality and Safety Committee in the sub-committees terms of reference for consideration and action as necessary. 6.5 To consider matters referred to the Quality and Safety Committee by the Board. 6.6 To consider matters referred to the Quality and Safety Committee by its sub-committees AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-Q&S-Appendix1 Page 3 of 7
229 6.7 To receive and approve the annual clinical audit programme, ensuring that it is approved by the board of directors consistent with the audit needs of the Trust. 6.8 To oversee the Trust s policies and procedures with respect to the use of clinical data and patient identifiable information to ensure that this is in accordance with all relevant legislation and guidance including the Caldicott Guidelines and the Data Protection Act To make recommendations to the Audit Committee concerning the annual programme of internal audit work, to the extent that it applies to matters within these terms of reference To monitor the assessment of compliance, assurance and evidence against the Quality Governance Assurance Framework (QGAF) Well Led Framework 6.11 To review and approve clinical, governance and corporate policies and procedures relevant to these terms of reference 6.12 To foster clinical governance and quality links with primary care and other stakeholders including mental health forum members In respect of safety and excellence in patient care, in particular: To have overview responsibility for the following outcomes as described by the Care Quality Commission: Outcome 1 respecting and involving people who use the services; and Outcome 7 safeguarding people who use the services from abuse; 6.14 To agree the annual safety plan and monitor progress To ensure that internal standards are set and monitored, including (without limitation): to commission the setting of standards by the board (e.g. in Trust policies) and ensure that a mechanism exists for these standards to be monitored to ensure the standards outlined in national service frameworks are implemented and monitored. to ensure the trust complies with NHSLA standards. to ensure the registration criteria of the Care Quality Commission continue to be met. To ensure the Care Quality Commission fundamental standards are implemented and monitored 6.16 To implement an engagement programme with the leaders of clinical services to ensure regular and constructive scrutiny of activities relating to quality assurance and enhancement To promote within the Trust a culture of open and honest reporting of any situation that may threaten the quality of patient care in accordance with the trust's policy on reporting issues of concern and monitoring the implementation of that policy. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-Q&S-Appendix1 Page 4 of 7
230 6.18 To oversee processes to ensure the review of patient safety incidents (including nearmisses, complaints, claims and Rule 43 coroner reports) from within the trust and wider NHS to identify similarities or trends and areas for focused or organisation-wide learning To identify areas for improvement in respect of incident themes and complaint themes from the results of national patient survey/sed and ensure appropriate action is taken To oversee the system within the Trust for obtaining and maintaining any licenses relevant to clinical activity in the Trust, receiving such reports as the Quality and Safety Committee considers necessary To monitor the Trust s compliance with the fundamental standards of quality and safety of the Care Quality Commission that are relevant to the Quality and Safety Committee s area of responsibility, in order to provide relevant assurance to the Board so that the Board may approve the Trust s annual declaration of compliance and annual governance statement To ensure that quality and governance risks to patients are identified and minimised through the application of a comprehensive risk management system including, without limitation: To ensure that processes are in place to ensure the escalation of patient safety and quality risks from team and service line risk registers to the corporate risk register and receive reports from the Trust s risk manager. To identify areas of significant clinical risk, suggest priorities and actions to the Board. To ensure the Trust incorporates the recommendations from external bodies (e.g. the National Confidential Enquiry into Patient Outcomes and Death or Care Quality Commission, as well as those made internally e.g. in connection with serious incident reports and adverse incident reports) into practice and has mechanisms to monitor their delivery. (Assurance will be provided to the Board). To maintain and monitor the Trust s operational risk management policy To assure the Board that those areas of patient safety and quality risk within the Trust are regularly monitored and that effective disaster recovery plans are in place. To ensure implementation of the National Patient Safety Agency reporting system. To assure the Board that there are processes in place that safeguard children and adults within the Trust. To escalate to MExT and/or Audit Committee and/or Board any identified unresolved risks arising within the scope of these terms of reference that require executive action or that pose significant threats to the operation, resources or reputation of the Trust To agree the annual patient experience plan and monitor progress To assure that the Trust has reliable, real time, up-to-date information about what it is like being a patient experiencing care administered by the Trust, so as to identify areas for improvement and ensure that these improvements are effected In particular, in respect of efficient and effective use of resources through evidence-based clinical practice: To agree the annual quality plan and monitor progress. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-Q&S-Appendix1 Page 5 of 7
231 To monitor the impact on the Trust's quality of care of cost improvement programmes and any other significant re-organisations (ensuring that there is a clear process for staff to raise associated concerns and for these to be escalated to the committee) and report any concern relating to an adverse impact on quality to the board of directors. To ensure that care is based on evidence of best practice/national guidance. To assure that procedures stipulated by professional regulators of chartered practice (i.e. General Medical Council and National Midwifery Council) are in place and performed to a satisfactory standard. To ensure that there is an appropriate process in place to monitor and promote compliance across the trust with clinical standards and guidelines including but not limited to NICE guidance. To assure the implementation of all new procedures and technologies according to Trust policies. To review the implications of confidential enquiry reports for the Trust and to endorse, approve and monitor the internal action plans arising from them. To monitor trends in complaints received by the Trust and commission actions in response to adverse trends where appropriate. To monitor the development of quality indicators throughout the Trust. To generally monitor the extent to which the Trust meets the requirements of commissioners and external regulators. To help the Board identify and monitor delivery of quality improvement priorities for the Trust To identify and monitor any gaps in the delivery of effective clinical care ensuring progress is made to improve these areas, in all specialties. To ensure the research programme and governance framework is implemented and monitored. To ensure that there is an appropriate mechanism in place for action to be taken in response to the results of clinical audit and the recommendations of any relevant external reports (e.g. from the Care Quality Commission). To ensure that where practice is of high quality, that practice is recognised and propagated across the trust. To ensure the Trust is outward-looking and incorporates the recommendations from external bodies into practice with mechanisms to monitor their delivery. 7. Minutes and Reporting 7.1 The minutes of all meetings of Quality and Safety Committee shall be formally recorded. 7.2 The Quality and Safety Committee will report to the full board after each meeting. 7.3 The following reports will also be made by the Quality and Safety Committee: Quarterly quality report covering all elements of quality (including issues arising from the minutes of reporting committees and groups); Annual clinical governance and quality report including highlighting areas for improvement. Twice-yearly updates of compliance with CQC fundamental standards Service line clinical governance and quality reports at twice-yearly intervals AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-Q&S-Appendix1 Page 6 of 7
232 7.4 Sub-committees relevant to these terms of reference shall report to the Quality and Safety Committee and the effectiveness of these sub-committeess will be monitored by the Quality and Safety Committee : 7.5 Sub groups will submit their minutes to the Quality and Safety Committee and will report on progress on a monthly, quarterly or annual basis. Key issues will be reported by exception. 8. Review 8.1 The terms of reference of the Committee shall be reviewed by the Board of Directors at regular intervals, but at least annually. 8.2 The Quality and Safety Committee will undertake an assessment of its overall effectiveness and compliance with these terms of reference at least annually. This review process will be in the form of a self-assessment checklist and will include the development of the following year s reporting cycle. The terms of reference will be formally reviewed by the committee as part of this assessment. APPROVED BY THE BOARD OF DIRECTORS ON TBC AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-Q&S-Appendix1 Page 7 of 7
233 Appendix 2 DUDLEY AND WALSALL MENTAL HEALTH PARTNERSHIP NHS TRUST AUDIT COMMITTEE The Board recognises that high standards of governance throughout the Trust are essential for the delivery of the identified strategic objectives, the safety of its services the quality of service user and carer experience and the long term protection of stakeholder interests. Good governance emanates from the Board but pervades the entire organisation, being reflected in its operating practices, policies and procedures. This responsibility encompasses clinical, financial and organisational aspects of governance and enables key risks to be identified and managed, in both operational and strategic terms. The Audit committee will therefore ensure that: There is robust scrutiny of the relevance and rigour of the organisational governance structures in place and the assurances the board receives. It will support the Board in its responsibilities for issues of risk, control and governance by reviewing the comprehensiveness of assurances and reviewing the reliability and integrity of these assurances. There is an adequate and effective risk management and assurance framework in place. The scheme of reservation and delegation adequately details who the Trust empowers to take actions or make decisions on its behalf and that the standing orders (SOs) provide a comprehensive framework for carrying out activities and translation of statutory powers into a series of practical rules designed to protect the interests of both the organisation and its staff. TERMS OF REFERENCE 1. Authority 1.1 The Audit Committee is constituted as a standing Committee of the Trust's board of directors. Its constitution and terms of reference shall be as set out below, subject to amendment at future board of directors meetings. The Committee is a non-executive committee of the Board and has no executive powers, other than those specifically delegated in these terms of reference. 1.2 The Committee is authorised by the board of directors to investigate any activity within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. The Committee is authorised by the Board to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary or expedient to the carrying out its functions. 2. Purpose 2.1 The Audit Committee has primary responsibility for monitoring and reviewing financial and other risks and associated controls, corporate governance and AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-Audit-Appendix2 Page 1 of 7
234 financial assurance. The Audit Committee shall provide the Board with a means of independent and objective review of financial and corporate governance, assurance processes and risk management across the whole of the Trust s activities (clinical and non-clinical) both generally and in support of the Annual Governance Statement. 2.2 In addition the Audit Committee shall: Provide assurance of independence for external and internal audit. Ensure that appropriate standards are set and compliance with them is monitored, in non-financial, non-clinical areas that fall within the remit of the Committee. Monitor corporate governance (e.g. compliance with constitution, codes of conduct, standing orders, standing financial instructions, maintenance of registers of interests). 3. Membership 3.1 The committee shall be composed of not less than three independent nonexecutive directors / Associate Non-Executive Directors, at least one of whom should have recent and relevant financial experience. The Chair of the organisation shall not be a member of the Committee. 3.2 Any non-executive director may deputise for an appointed member of the Committee. 3.3 The appointment of the Chair of the Audit Committee will be a Non-Executive Director member of the Committee and should be made by the Governing BodyTrust s Board. 3.4 Members of the Audit Committee must attend at least three quarters of all meetings each financial year but should aim to attend all scheduled meetings. 3.5 A quorum shall be two members. One of the members, other than in exceptional circumstances will be the appointed Chair of the Audit Committee. 4. Attendance 4.1 Only members of the Audit Committee have the right to attend meetings, but the Chief Executive, Director of Finance, Performance and IM&T, Director of People and Corporate Development and appropriate internal and external audit representatives of the Trust shall generally be invited to attend routine meetings of the Audit Committee. 4.2 The Trust Chair may be invited to attend meetings of the Audit Committee as required. 4.3 A representative of the local counter anti-fraud service may be invited to attend meetings of the Audit Committee. 4.4 The Chief Executive should discuss at least annually with the Audit Committee the process for assurance that supports the annual governance statement. He or she should also attend when the Committee considers the draft internal audit plan and the annual accounts. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-Audit-Appendix2 Page 2 of 7
235 4.5 All other Trust directors and/or staff should be invited to attend those meetings in which the Committee will consider areas of risk or operation that are their responsibility. 4.6 The Director of People and Corporate Development will act as secretary to the Committee and will provide advice and ensure administrative support. The duties of the secretary in this regard include but are not limited to: Agreement of the agenda with the chair of the Audit Committee and attendees together with the collation of connected papers. Taking the minutes and keeping a record of matters arising and issues to be carried forward. Advising the Audit Committee as appropriate. 5. Frequency of Meetings 5.1 Meetings shall be held at least five times a year, with additional meetings where necessary. The Governing BodyTrust s Board, Accounting (or Accountable) Officer, external auditors or Head of Internal Audit may request an additional meeting. The internal and external auditor shall be afforded the opportunity at least once per year to meet with the Audit Committee without executive directors present. 6. Duties 6.1 The duties of the Committee can be categorised as follows: 7. Governance, Risk Management and Internal Control 7.1 To ensure the provision and maintenance of an effective system of financial risk identification and associated controls, reporting and governance. 7.2 To maintain an oversight of the Trust s general risk management structures, processes and responsibilities, including the production and issue of any risk and control related disclosure statements. 7.3 To review processes to ensure appropriate information flows to the Audit Committee from executive management and other board committees in relation to the Trust's overall internal control and risk management position. 7.4 To review the adequacy of the policies and procedures in respect of all counteranti-fraud work. 7.5 To review the effectiveness of the arrangements in place for allowing staff to raise (in confidence) concerns about possible improprieties in financial, clinical or safety matters and ensure that any such concerns are investigated proportionately and independently. 7.6 To review the adequacy of underlying assurance processes that indicate the degree of achievement of corporate objectives and the effectiveness of the management of principal risks. 7.7 To review the adequacy of policies and procedures for ensuring compliance with relevant regulatory, legal and conduct requirements. 7.8 The Committee shall seek assurance that there is an effective system of integrated governance, risk management and internal control, across the whole of the AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-Audit-Appendix2 Page 3 of 7
236 organisation s activities (both clinical and non-clinical), that supports the achievement of the organisation s objectives. 7.9 This will be evidenced through the Committee s use of an effective assurance framework to guide its work and that of the audit and assurance functions that report to it. 8. Internal Audit 8.1 The Committee shall ensure that there is an effective internal audit function that meets the Public Sector Internal Audit Standards 2013mandatory NHS Internal Audit Standards and provides appropriate independent assurance to the Audit Committee, Chief Executive and Board. This will include: Review and approval of the internal audit strategy, operational plan and more detailed programme of work, ensuring that this is consistent with the audit needs of the organisation. 8.2 Oversight on an on-going basis the effective operation of internal audit in respect of: Adequate resourcing. Its co-ordination with external audit. Meeting relevant internal audit standards. Providing adequate independence assurances. Having appropriate standing within the Trust. Meeting the internal audit needs of the Trust. 8.3 Considering the major findings of internal audit investigations and management s response and their implications and monitor progress on the implementation of recommendations. 8.4 Consideration of the provision of the internal audit service, the cost of the audit and any questions of resignation and dismissal of internal audit staff and conduct an annual review of the internal audit function. 8.5 Ensure that the internal audit function has appropriate standing within the organisation and the co-ordination between the internal and external auditors to optimise audit resources. 9. External Audit 9.1 The Committee shall review the work and findings of the external auditors and consider the implications and management s responses to their work. This will include: Consideration of the appointment and performance of the external auditors., as far as the rules governing the appointment permit. Discussion and agreement with the external audit, before the audit commences, of the nature and scope of the audit as set out in the annual plan, and ensuring coordination, as appropriate, with other external auditors in the local health economy. Discussion with the external auditors of their local evaluation of audit risks and assessment of the Trust and associated impact on the audit fee. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-Audit-Appendix2 Page 4 of 7
237 Review of all external audit reports, including the report to those charged with governance, agreement of the annual audit letter before submission to the Board and any work undertaken outside the annual audit plan, together with the appropriateness of management responses. 9.2 The Trust s separately constituted Auditor Panel carries out the functions required under the Local Audit and Accountability Act 2014, including advising Board on the appointment of external auditors, maintaining an independent relationship with the External Auditors and on any decision regarding the removal or resignation of the external auditors. 10. Annual Accounts Review 10.1 To review the annual statutory accounts, before they are presented to the board of directors, in order to determine their completeness, objectivity, integrity and accuracy. This review will cover but is not limited to: The meaning and significance of the figures, notes and significant changes. Areas where judgment has been exercised. Adherence to accounting policies and practices. Explanation of estimates or provisions having material effect. The schedule of losses and special payments. Any unadjusted statements. Any reservations and disagreements between the external auditors and management which have not been satisfactorily resolved To review the annual report and annual governance statement before they are submitted to the board of directors to determine completeness, objectivity, integrity and accuracy To review all accounting and reporting systems for reporting to the board of directors, including in respect of budgetary control. 11. Standing Orders, Standing Financial Instructions and Standards of Business Conduct 11.1 To review on behalf of the board of directors the operation of, and proposed changes to, the standing orders and standing financial instructions, the constitution, codes of conduct and standards of business conduct; including maintenance of registers To examine the circumstances of any significant departure from the requirements of any of the foregoing, and whether those departures relate to a failing, an overruling or a suspension To review the scheme of delegation. 12. Other 12.1 The Audit Committee shall review the findings of other significant assurance functions, both internal and external to the organisation, and consider the implications for the governance of the organisation To review performance indicators relevant to the remit of the Audit Committee. To examine any other matter referred to the Audit Committee by the board of directors and to initiate investigation as determined by the Audit Committee. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-Audit-Appendix2 Page 5 of 7
238 12.3 To review each year the accounting policies of the Trust and make appropriate recommendations to the board of directors To develop and use an effective assurance framework to guide the Audit Committee's work. This will include utilising and reviewing the work of the internal audit, external audit and other assurance functions as well as reports and assurances sought from directors and managers and other investigatory outcomes so as fulfill its functions in connection with these terms of reference To consider the outcomes of significant reviews carried out by other bodies which include but are not limited to regulators and inspectors within the health and social care sector and professional bodies with responsibilities that relate to staff performance and functions To review the work of all other Trust Committees in connection with the Audit Committee's assurance function. The committee may also request specific reports from individual functions within the organisation (for example, clinical audit) as they may be appropriate to the overall arrangements. 13. Minutes and Reporting 13.1 The minutes of all meetings of the Audit Committee shall formally be recorded and the ratified minutes submitted, together with recommendations where appropriate to the board of directors. The submission to the board of directors shall include details of any matters in respect of which actions or improvements are needed. This will include details of any evidence of potentially ultra vires, otherwise unlawful or improper transactions, acts, omissions or practices or any other important matters. To the extent that such matters arise, the chair of the Audit Committee shall present details to a meeting of the board of directors in addition to submission of the minutes The Audit Committee will report annually to the board of directors in respect of the fulfillment of its functions in connection with these terms of reference. Such report shall include but not be limited to functions undertaken in connection with the following: The annual governance statement The assurance framework The effectiveness of risk management within the Foundation Trust The integration of and adherence to governance arrangements Its view as to whether the self-assessment against standards for better health is appropriate. Any pertinent matters in respect of which the Audit Committee has been engaged The Trust s annual report shall include a section describing the work of the Audit Committee in discharging its responsibilities The Company Secretary will act as secretary to the Committee and will provide advice and ensure administrative support. The duties of the secretary in this regard include but are not limited to: Agreement of the agenda with the chair of the Audit Committee and attendees together with the collation of connected papers. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-Audit-Appendix2 Page 6 of 7
239 Taking the minutes and keeping a record of matters arising and issues to be carried forward. Advising the Audit Committee as appropriate. 14. Review 14.1 The Committee will undertake an assessment of its overall effectiveness and compliance with these terms of reference at least annually. This review process will be in the form of a self-assessment checklist and will include the development of the following year s reporting cycle. The terms of reference will be formally reviewed by the Committee as part of this assessment The terms of reference of the Audit Committee shall be reviewed by the board of directors at least annually. 15. Required Frequency of Attendance by Members 15.1 Members of the Audit Committee must attend at least three of all meetings each financial year but should aim to attend all scheduled meetings A quorum shall be two members. One of the members will be the appointed Chair of the Audit Committee. APPROVED BY THE BOARD OF DIRECTORS ON 1 ST APRIL 2015TBC AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-Audit-Appendix2 Page 7 of 7
240 Appendix 3 DUDLEY AND WALSALL MENTAL HEALTH PARTNERSHIP NHS TRUST FINANCE AND PERFORMANCE COMMITTEE The Board recognises that high standards of governance throughout the Trust are essential for the delivery of the identified strategic objectives, the safety of its services the quality of service user and carer experience and the long term protection of stakeholder interests. Good governance emanates from the Board but pervades the entire organisation, being reflected in its operating practices, policies and procedures. This responsibility encompasses clinical, financial and organisational aspects of governance and enables key risks to be identified and managed, in both operational and strategic terms. Finance and Performance committee will therefore ensure that: The Trust has established sound financial, performance, workforce and IT arrangements which provide robust information and comply with statutory and regulatory reporting requirements. Prime financial policies, also known as standing financial instructions, are in place and clearly set out the organisation's detailed financial procedures and responsibilities. That all staff are safe and supported to deliver quality patient care, that fair and effective management arrangements exist for all staff and there are methods in place to develop staff to meet the objectives of the organisation. That all aspects of information governance relating to finance, workforce and performance are in place to meet IG Toolkit standards. TERMS OF REFERENCE 1. Authority 1.1 The Finance & Performance Committee is constituted as a standing Committee of the Trust's board of directors. Its constitution and terms of reference shall be as set out below, subject to amendment at future Board meetings. 1.2 The Committee is authorised by the Board to investigate any activity within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. 1.3 The Committee is authorised by the Board to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary. 2. Purpose 2.1 To review the Trust s financial management arrangements and performance and make recommendations and provide advice to Trust Officers and the Trust Board. 2.2 To review the Trust s performance against key financial, operational and workforce targets. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-F&P-Appendix3 Page 1 of 6
241 2.3 To review the Trust s key financial,performance and workforce strategies, associated risks and mitigations. 2.4 To ensure appropriate financial, performance and workforce governance arrangements are in place and functioning effectively. 3. Membership 3.1 The Committee will be chaired by a Non-Executive Director of the Trust as determined by the Trust Board Membership of the Committee will consist of: T a minimum of three nnon-eexecutive / Associate NonExecutive Ddirectors of the Trust (inclusive of the Chair) as determined by the Trust Board. In addition, the Trust s Chief Executive, Director of Finance, and Performance and IM&T, Director of People and Corporate Development and Director of Nursing, Operations, Nursing and Estates will be core members of the Committee The Committee will be chaired by a Non-Executive / Associate Non-Executive Director of the Trust as determined by the Trust Board. 3.3 Any non-executive director may deputise for an appointed member of the Committee with the permission of the Chair of the Board. Core A members may nominate an appropriate deputy to attend a meeting of the Committee on their behalf. However, it is expected that the deputy will be fully briefed and have the necessary authority to participate fully in the debate and any subsequent decisions arising The Joint Medical Directors may also be in attendance, unless requested to be excluded by the Chair of the Committee, due to the nature of the business to be discussed. 3.5 A quorum will consist of at least three members, of which at least one must be a non-executive director and at least one must be an executive director. Attendance of the Joint Medical Directors does not count towards the quorum. 3.6 It is expected that members of the Committee will attend a minimum of 75% of Committee meetings each year but should aim to attend all scheduled meetings. 3.4 The Committee has the authority to require the attendance of any officers of the Trust and hold them to account for financial and operational performance. 3.5 Senior staff from the Finance Department,Performance & Informatics Department and HR department will be available to be in attendance at all meetings of the Committee, unless requested to be excluded by the Chair of the Committee, due to the nature of the business to be discussed. 3.6 Additional colleagues will be invited to attend for specific items on the agenda, as and when required. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-F&P-Appendix3 Page 2 of 6
242 4. Attendance 4.1 A quorum will consist of at least three members, of which at least one must be a non-executive director and at least one must be an executive director. 2.2 It is expected that members of the Committee will attend a minimum of 50% of Committee meetings each year but should aim to attend all scheduled meetings. 3.4 The Committee has the authority to require the attendance of any officers of the Trust and hold them to account for financial and operational performance. 3.5 Senior staff from the Finance Department,, P,Performance & Informatics Department and Human Resources department will be available to be in attendance at all meetings of the Committee, unless requested to be excluded by the Chair of the Committee, due to the nature of the business to be discussed. Formatted: Indent: Left: 0 cm, Hanging: 1 cm Formatted: Indent: Left: 0 cm, Hanging: 1 cm Additional colleagues will be invited to attend for specific items on the agenda, as and when required. 4.3 The Committee has the authority to require the attendance of any officers of the Trust and hold them to account for financial and operational performance. 5. Frequency of Meetings 5.1 The Committee will normally meet monthly during the course of the financial year. Formatted: Adjust space between Latin and Asian text, Adjust space between Asian text and numbers 5.2 The Chair of the Committee may call ad-hoc meetings of the Committee, as appropriate. 6. Duties and Responsibilities 6.1 The Committee will review all aspects of the Trust s financial management arrangements. It will receive reports from the Deputy Chief Executive Officer (and other officers of the Trust as appropriate) on the following key areas: Income and expenditure (including links to related activity and manpower targets). Cash management. Capital programme. Financial metrics. Forecasting. Working capital management. Cost improvement programme. Key financial risks. 6.2 The Committee will provide an oversight against the Trust s statutory financial targets. 6.3 The Committee will review reports from appropriate officers or any advisors engaged by the Trust regarding the efficiency of services and functions across the Trust including: Reference cost data. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-F&P-Appendix3 Page 3 of 6
243 Capacity and productivity data. Benchmarking data. Workforce data. 6.4 The Committee will also review the performance management arrangements for each service (including any shared service, agency or consortium arrangement) within the Trust. In particular it will receive reports from: The Trust s executive directors concerning the arrangements they have put in place to ensure each service meets their financial and operational targets. Appropriate senior staff from each service line concerning their financial and operational performance. 6.5 The Committee will receive reports and presentations on the financial regime within which the Trust operates and will review the Trust s arrangements for complying with the regime. 6.6 The Committee will review key financial, performance and workforce strategies, policies and plans. It will provide advice and make recommendations on these to appropriate Trust Officers and to the Trust Board. 6.7 The Committee will review the Trust s performance management arrangements and provide oversight against mandated and statutory performance targets. 6.8 The Committee will review the Trust s performance against key operational and contractual targets from appropriate officers in the Trust. Whilst not exhaustive this will encompass: Activity performance Contractual statutory KPI s reported externally as a measure of Trust performance Internal targets designed to improve/optimise performance, use of resources and clinical practice/quality Monitor KPI s Workforce KPIs 6.9 The Committee will receive and review benchmarking data and associated comparative reports The committee Committee will review the management of key risks to the delivery of financial, performance and workforce strategies, targets and duties and report to Trust Board as appropriate. 7. Minutes and Reporting 7.1 A summary report will be presented to the Trust Board following each meeting of the Committee, which will be prepared by the Director of Finance and Performance and agreed with the Chair of the Committee. 7.2 The Chair of the Committee shall draw to the attention of the Board any issues that require disclosure to the full Board, or require executive action The minutes of all meetings of the Finance & Performance Committee shall formally be recorded and the ratified minutes submitted, together with recommendations where appropriate to the board of directors. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-F&P-Appendix3 Page 4 of 6
244 The Director of Finance and Performance will act as secretary to the Committee (in conjunction with the Director of People & Corporate Development). They will ensure that the minutes of the Committee meeting shall be formally recorded, the ratified minutes submitted to the Trust Board and shall provide appropriate support to the Chair and Committee members. 7.2 The Chair of the Committee shall draw to the attention of the Board any issues that require disclosure to the full Board, or require executive action. 7.3 The agenda for meetings of the Committee will be determined by the Chair of the Committee in consultation with the Director of Finance and Performance. 7.4 The agenda for each meeting will be circulated five working days in advance, together with any supporting papers, and will be distributed by the Deputy Chief Executive Officer. 7.5 The Director of Finance and Performance will agree the minutes with the Chair of the Committee within 14 days of the meeting of the Committee having taken place. Agreed minutes would be circulated to all members of the Committee as expeditiously as possible, thereafter. 7.6 A summary report will be presented to the Trust Board following each meeting of the Committee, which will be prepared by the Director of Finance and Performance and agreed with the Chair of the Committee The Trust s Risk Manager will be appraised of any recommendations regarding changes to assurances, controls and management of risks, or any new risks, arising as a result of Committee review of risks. 7.5 The Estates and Capital Planning Group will report to the Finance and Performance Committee and the effectiveness of this sub-committee will be monitored by the Finance and Performance Committee. 7.5 The Estates and Capital Planning Group will submit their minutes to the Finance & Performance Committee and will report on progress as appropriate. 7.5 The Company Secretary will act as secretary to the Committee and will provide advice and ensure administrative support. The duties of the secretary in this regard include but are not limited to: Agreement of the agenda with the chair of the Committee and attendees together with the collation of connected papers. Taking the minutes and keeping a record of matters arising and issues to be carried forward. Advising the Finance & Performance Committee as appropriate. 7.8 Although normally decisions are reached on a consensus, in the event of a disagreement, decisions on any matter are made by the majority, with the Chair of the Committee having a second casting vote in the event of a tie. A Committee member who remains opposed to a proposal after a vote can ask for his or her dissent to be recorded in the minutes. 8. Review AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-F&P-Appendix3 Page 5 of 6
245 8.1 These terms of reference will be formally reviewed by the Committee at least annually. Any proposed amendments to the terms of reference will be approved by the Trust Board. 8.2 The work and effectiveness of the Committee will be subject to scrutiny by the Audit Committee. The Committee will also consider its effectiveness at least annually. APPROVED BY THE BOARD OF DIRECTORS ON 1 ST APRIL 2015TBC AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-F&P-Appendix3 Page 6 of 6
246 Appendix 4 DUDLEY AND WALSALL MENTAL HEALTH PARTNERSHIP NHS TRUST MANAGEMENT EXECUTIVE TEAM (MExT) The Board recognises that high standards of governance throughout the Trust are essential for the delivery of the identified strategic objectives, the safety of its services the quality of service user and carer experience and the long term protection of stakeholder interests. Good governance emanates from the Board but pervades the entire organisation, being reflected in its operating practices, policies and procedures. This responsibility encompasses clinical, financial and organisational aspects of governance and enables key risks to be identified and managed, in both operational and strategic terms. MExT will therefore ensure that: Robust policies, systems and processes exist and are appropriately applied to ensure effective and efficient operational stewardship of the organisation. It will ensure policies and processes in relation to operational management are in place and appropriately scrutinised and applied throughout the Trust. TERMS OF REFERENCE 1. Authority 1.1 The Management Executive Team reports to the Trust Board of Dudley and Walsall Mental Health Partnership NHS Trust. It is not is constituted as a standing committee of the Trust's board of directors. 2. Purpose 2.1 To oversee the operational delivery of Trust strategy within Dudley and Walsall Mental Health Partnership NHS Trust. 2.2 To provide executive and senior management input and discussion into key decisions with regard to the implementation of Trust strategy. 2.3 To oversee the interface between clinical and non-clinical services and to ensure effective operational performance. 3. Membership 3.1 The membership of MExT shall consist of the Chief Executive, all Executive Directors and Service Transformation Programme Director. The following constitutes the core membership of the MExTare members of Standard MExT Group: Chief Executive (Chair) Director of Finance, and Performance and IM&T Joint Medical Directors Director of Operations, Nursing and Estates Director of People and Corporate Development AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-MExT-Appendix4 Page 1 of 4
247 Service Transformation Programme Director MExT will be deemed quorate to the extent that 3 of the core members are present. 4. Attendance 4.1 The following participants are required to attend standard meetings of MExT Clinical Development Director Associate Director of Corporate Planning Associate Director of Operations Deputy Director of Finance Associate Director of People and Workforce Development Head of Informatics and Performance Management Head of Nursing, Quality and Innovation Head of HR Associate Director of Operations Head of Governance Head of Social Care Head of Estates & FacilitiesTechnical Services Governance Manager Strategic Planning Manager Head of Financial Planning Head of Governance Deputy Director of Finance 43.2 Enhanced meetings of MExT will also be attended bythe following are members of Enhanced MExT: All those members of Standard MExT identified in paragraph 3.1 above plus : Head of Early Intervention Services Clinical Director for Early Intervention Services Head of Recovery Services Clinical Director for Community & Recovery Services Head of Community Services Head of Older Peoples Services Clinical Director for Older Peoples Services Head of Acute Services Clinical Director for Acute Services Clinical Director for Governance & Quality Head of Estates & Facilities Chief Pharmacist Information Manager Joint Associate Director of Psychology & Psychological Therapies MExT (and E-MExT) will be deemed quorate to the extent that 3 of the Executive Directors carrying a vote at Board are present. Consultant Occupational Therapist Senior HR Manager 4.3 Meetings of MExT may be attended by: Formatted: Indent: Left: 1.54 cm, No bullets or numbering Formatted: Font: (Default) Arial, 11 pt Formatted: Normal, Indent: Left: 0.9 cm, No bullets or numbering Formatted: Font: (Default) Arial, 11 pt AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-MExT-Appendix4 Page 2 of 4
248 The PA to the Chief Executive who will act as secretary or, alternative PA in the absence of PA to the Chief Executive. Any nominated deputy attending in place of a member of MExT. Any other person who has been invited to attend a meeting by MExT so as to assist in deliberations. 4.4 A member of thethe Cororate PA teamo the Chief Executive who will act as secretary or, alternative PA in the absence of PA to the Chief Executive.. Formatted: Indent: Left: 0.5 cm, No bullets or numbering 4.45 Other Only those members than as set out in paragraphs 34.1 and 34.2, only core members of MExT are entitled to be present at its meetings Members listed at paragraphs 3.1, 4.1 and 43.2 are respectively required to attend at least half 75% of the meetings held annually. Frequency of Meetings 4.1 Meetings shall be held every two weeks on a six weekly cycle, with the following timetable: 1st meeting is an enhanced MExT (which will focus on Quality, CIP, Service Transformation and Growth). 2nd meeting is a standard MExT. 3rd meeting is a non-agenda meeting (Executive away Away dayday). 4.2 The agenda and papers will be circulated on the Thursday prior to the meeting taking place. If this is not possible, the agenda and papers will be circulated on the Friday.in line with the Trust Standing Orders. 5. Duties and Responsibilities 5.1 MExT will act as a key forum for the delivery of key strategic and operational issues. In particular, MExT will: Be the main operational board of the Trust, making the appropriate decisions that eensure the effective implementation of Trust strategy, monitoring outcomes and providing assurance of progress against key operational performance indicators. Receive reports from and monitor the work of heads of service and professional leads. Receive reports from other meetings and functional leads as appropriate to monitor progress in implementing Trust strategy. Receive and agree formal business cases to deliver strategic plans and generate business opportunities. Act as the forum in which senior managers can formally raise concerns and issues for discussion with colleagues, making decisions on these issues, where appropriate. Highlight and discuss any significant risks to operational services, the impact and the mitigating actions. Escalate to Board or relevant sub-committee as required. Oversee the operational planning and delivery of all Cost Improvement Plans and ensure sign off of quality impact assessments by the Joint Medical Directors and Director of Operations, Nursing and Estates. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-MExT-Appendix4 Page 3 of 4
249 6. Minutes and Reporting 6.1 The minutes of all Enhanced and Standard MExT meetings shall be formally recorded. 6.2 The ratified minutes of MExT meetings shall be submitted to the private session of the Trust Board. 6.3 The Chair of MExT will provide a report to the public session of board each month. 7. Review 7.1 These terms of reference will be formally reviewed by MExT at least annually. Any proposed amendments to the terms of reference will be approved by the Trust Board. 8. Links to other Committees and Groups 8.1 MExT is linked to the following: Finance and Performance Committee Quality and Safety Committee APPROVED BY THE BOARD OF DIRECTORS ON 1 ST APRIL 2015TBC AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-MExT-Appendix4 Page 4 of 4
250 Appendix 5 Formatted: Bottom: 1 cm, Footer distance from edge: 0.71 cm DUDLEY AND WALSALL MENTAL HEALTH PARTNERSHIP NHS TRUST MENTAL HEALTH ACT SCRUTINY COMMITTEE The Board recognises that high standards of governance throughout the Trust are essential for the delivery of the identified strategic objectives, the safety of its services the quality of service user and carer experience and the long term protection of stakeholder interests. Good governance emanates from the Board but pervades the entire organisation, being reflected in its operating practices, policies and procedures. This responsibility encompasses clinical, financial and organisational aspects of governance and enables key risks to be identified and managed, in both operational and strategic terms. The Mental Health Act Scrutiny committee will therefore ensure that: The organisation is working within the legal requirements of the Mental Health Act (1983), as amended by the 2007 Act and Mental Capacity Act 2005, and with reference to guiding principles as set out in the Code of Practice and associated legislation as it applies to the Mental Health Act, the Mental Capacity Act and Deprivation of Liberty. It will ensure policies and processes in relation to the Mental Health Act and Mental Capacity Act across the Trust are in place and appropriately scrutinised and applied throughout the Trust. TERMS OF REFERENCE 1. Authority 1.1 The Mental Health Act Scrutiny Committee is constituted as a standing Committee of the Trust's board of directors. Its constitution and terms of reference shall be as set out below, subject to amendment at future Board meetings. Formatted: Font: Not Italic Formatted: Font: (Default) Times New Roman, 12 pt Formatted: Normal, Left, Indent: Left: 0 cm, First line: 0 cm 1.2 The Committee is authorised by the Board to investigate any activity within its terms of reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. 1.3 The Committee is authorised by the Board to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary. 2. Purpose 2.1 To maintain an overview of the operation and application of the Act within the Trust. 2.2 To be responsible for the development, review, implementation and monitoring of Mental Health Act policies and procedures to support and ensure compliance with Mental Health Act legislation. 2.3 To review and monitor the use of the Act within the Trust, noting and ensuring investigation of any emerging trends with respect to service, age, gender, ethnicity and cultural background. 2.4 To ensure that the Trust complies with the Mental Capacity Act (MCA) and Deprivation of Liberty Safeguards (DOLS) requirements and to monitor their interface with the Mental Health Act To review and monitor statistical information on DOLs referrals from the trust. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-MHASC-Appendix5 Page 1 of 4
251 2.5 To receive and review reports from the Care Quality Commission (formerly the Mental Health Act Commission) and other relevant external bodies, ensuring that appropriate actions and responses are undertaken. 2.6 Receive the results of clinical audits and other relevant reviews of the Act and oversee the development and implementation of recommendations. 2.7 To review and oversee the implementation of any subsequent amendments to Mental Health Act legislation, guidance and best practice. 2.8 To monitor the role, functioning and performance of the Mental Health Act Lay Managers and to liaise with them on all pertinent issues. 2.9 To support the role of the Mental Health Act Administration offices The group will consider as a regular item pertinent issues arising from the Associate Lay Managers Peer Group At the discretion of the Chair, the Committee will be responsible for establishing and receiving reports from working sub-groups to investigate specific issues or trends, as required. 3. Membership 3.1 The Committee will be chaired by a Non-Executive Director of the Trust as determined by the Trust Board Membership of the Committee will consist of the following core Board members: Non-Executive Director / Associate Non-Executive Director (Chair) Non-Executive Director / Associate Non-Executive Director (Vice-chair) Director of People and Corporate Development Medical Director/s Director of Operations, Nursing, Governance & Estates 3.12 The Committee will be chaired by a Non-Executive Director / Associate Non-Executive Director of the Trust as determined by the Trust Board. 3.3 The following members will also be required to attend the Committee: Associate Director of Operations Clinical Director Acute Services Head of Acute Services Head of Older Peoples Services Head of Social Care An AMHP Lead Mental Health Act Manager Equality and Diversity Manager Learning & Development Manager Head of Nursing, Quality and Innovation Safeguarding Lead Governance Manager Formatted: Indent: Left: 2.26 cm, No bullets or numbering 3.43 Any nonnon-executive Executive directordirector / Associate Non-Executive Director may deputise for an appointed Non-Executive Director / Associate Non-Executive Director member of AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-MHASC-Appendix5 Page 2 of 4
252 the Committee with the permission of the Chair of the Board. However, it is expected that the deputy will be fully briefed and have the necessary authority to participate fully in the debate and any subsequent decisions arising. 3.4 A quorum will consist of at least two members, of which at least one must be a non-executive director and one an executive director and at least five of those required to attend listed in paragraph 4.1 below. 3.5 It is expected that members of the Committee will attend a minimum of 75% of Committee Meetings each year but should aim to attend all scheduled meetings. The attendee list will be reviewed on an annual basis and any concerns will be highlighted to the Trust Board. 3.5 Staff from the Trust or representatives from other agencies may be invited to attend the committee for specific discussions, as required. The perspectives and contributions of Expert Service Users and Carers are recognised and valued by the Trust and therefore, they may be invited to attend the Committee, at the discretion of the Chair. 4. Attendance The following members will also be required to attend the Committee: Associate Director of Operations Clinical Director Acute Services Head of Acute Services Head of Older Peoples Services Head of Social Care An AMHP Lead Mental Health Act Manager Equality and Diversity Manager Learning & Development Manager Head of Nursing, Quality and Innovation Safeguarding Lead Governance Manager Formatted: Indent: Left: 0 cm, Hanging: 1 cm Staff from the Trust or representatives from other agencies may be invited to attend the committee for specific discussions, as required. The perspectives and contributions of Expert Service Users and Carers are recognised and valued by the Trust and therefore, they may be invited to attend the Committee, at the discretion of the Chair. 4.1 A quorum will consist of at least five members, of which at least one must be a non-executive director, one an executive director and at least one must be an operational lead. 2.2 It is expected that members of the Committee will attend a minimum of three Committee Meetings each year but should aim to attend all scheduled meetings. The attendee list will be reviewed on an annual basis and any concerns will be highlighted to the Trust Board 5. Frequency of Meetings 5.1 The Committee will normally meet every other month during the course of the financial year. 5.2 The Chair of the Committee may call ad-hoc meetings of the Committee, as appropriate. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-MHASC-Appendix5 Page 3 of 4
253 6. Duties and Responsibilities Formatted: Font: Not Italic 6.1 The committee is responsible for discharging all requirements of the Mental Health Act ( the Act ), the Mental Capacity Act (MCA) and Deprivation of Liberty Safeguards (DOLS) requirements 7. Minutes and Reporting 7.1 The Company Secretary will make arrangements for the administration of the Committee. He or she will ensure that the minutes of the Committee meeting shall be formally recorded, the ratified minutes submitted to the private session of the the Trust s Board and shall provide ensure that appropriate support is provided to the Chair and Committee members. 7.2 The Chair of the Committee will report on a regular basis to the open session of the Trust Board identifying any issues that require disclosure, or require executive action. A summary report will be presented to the Trust Board following each meeting of the Committee Due to the nature of the issues considered, it may be necessary for the committee to liaise with other sub-committees, in which case specific and appropriate arrangements will be agreed. 8. Review 8.21 The terms of reference will be formally reviewed by the Committee as part of this assessment. Any proposed amendments to the terms of reference will be ratified by the Trust Board The Committee will undertake an assessment of its overall effectiveness and compliance with these terms of reference at least annually. This review process will be in the form of a selfassessment checklist and will include the development of the following year s reporting cycle. 8.2 The terms of reference will be formally reviewed by the Committee as part of this assessment. Any proposed amendments to the terms of reference will be ratified by the Trust Board. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-MHASC-Appendix5 Page 4 of 4
254 Appendix 6 DUDLEY AND WALSALL MENTAL HEALTH PARTNERSHIP NHS TRUST NOMINATIONS AND REMUNERATION COMMITTEE The Board recognises that high standards of governance throughout the Trust are essential for the delivery of the identified strategic objectives, the safety of its services the quality of service user and carer experience and the long term protection of stakeholder interests. Good governance emanates from the Board but pervades the entire organisation, being reflected in its operating practices, policies and procedures. This responsibility encompasses clinical, financial and organisational aspects of governance and enables key risks to be identified and managed, in both operational and strategic terms. This committee will therefore ensure that: There is a robust policy framework in place for establishing and reviewing the remuneration and terms and conditions for executive directors and other senior executives. People involved in the day-to-day running of the organisation do not make sensitive decisions in this area. There is appropriate consideration given to review of appointments to the Board and succession planning at senior levels within the organisation. There is robust scrutiny of compensation and early termination commitments (including pension contributions and all other elements). TERMS OF REFERENCE 1. Authority 1.1 The Nomination and Remuneration Committee (the Committee) is constituted as a standing Committee of the Trust's board of directors (the Board). Its constitution and terms of reference shall be as set out below, subject to amendment at future Board meetings. 1.2 The Committee is authorised by the Board to act within its terms of reference. All members of staff are directed to co-operate with any request made by the Committee. 1.3 The Committee is authorised by the Board to instruct professional advisors and request the attendance of individuals and authorities from outside the Trust with relevant experience and expertise if it considers this necessary for or expedient to the exercise of its functions. 1.4 The Committee is authorised to obtain such internal information as is necessary and expedient to the fulfilment of its functions. 2. Purpose 2.1 To be responsible for identifying and appointing candidates to fill all the executive director positions on the Board and for determining their remuneration and other conditions of service. 2.2 When appointing the Chief Executive, the Committee shall be the Committee described in Schedule 7, 17(3) of the National Health Service Act 2006 (the AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-N&R-Appendix6 Page 1 of 5
255 Act). When appointing the other executive directors the Committee shall be the Committee described in Schedule 7, 17(4) of the Act. 2.3 The Committee has no authority to determine remuneration arrangements for non-executive directors for whom nationally determined terms will apply. All reference to Board level posts in this document should be taken to exclude Non-Executive post holders. 3. Membership 3.1 The membership of the Committee shall consist of: The Trust Chair. The other non-executive directors, including Associate Non-Executive Directors on the Board In addition, when appointing executive directors other than the Chief Executive The Chief Executive. 3.2 The Trust Chair shall chair the Committee. 3.3 Any non-executive director may deputise for an appointed member of the Committee with the permission of the Chairman of the Board The Chief Executive should be invited to attend and should discuss the performance of the executive directors at least annually. The Committee may call the Chief Executive to speak to any item as required. 4. Attendance 4.1 Only members of the Committee have the right to attend Committee meetings. At the invitation of the Committee, meetings shall normally be attended by the Director of People and Corporate Development and or the Company Secretary. Other persons may be invited by the Committee to attend a meeting so as to assist in deliberations. 4.2 Any non-member, including the secretary to the Committee, will be asked to leave the meeting should their own conditions of employment be the subject of discussion. 4.3 A quorum shall be two members of the Committee 4.4 It is expected that members of the Committee will attend a minimum of 5075% of the Committee Meetings each year but should aim to attend all scheduled meetings. 5. Frequency of Meetings 5.1 Meetings shall be called as required but at least once in each financial year. 6. Appointments Role The Committee will: Formatted: Indent: Left: 1 cm 6.1 Regularly review the structure, size and composition (including the skills, knowledge, experience and diversity) of the Board, making use of the output of the Board evaluation process as appropriate, and make recommendations to the Board, with regard to any changes. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-N&R-Appendix6 Page 2 of 5
256 6.2 Give full consideration to and make plans for succession planning for the Chief Executive and other executive board directors taking into account the challenges and opportunities facing the Trust and the skills and expertise needed on the Board in the future. 6.3 Keep the leadership needs of the Trust under review at executive level to ensure the continued ability of the Trust to operate effectively in the health economy. 6.4 Be responsible for identifying and appointing candidates to fill posts within its remit as and when they arise. When a vacancy is identified, evaluate the balance of skills, knowledge and experience on the Board, and its diversity, and in the light of this evaluation, prepare a description of the role and capabilities required for the particular appointment. In identifying suitable candidates the Committee shall use open advertising or the services of external advisers to facilitate the search; consider candidates from a wide range of backgrounds; and consider candidates on merit against objective criteria. Ensure that a proposed executive director's other significant commitments (if applicable) are disclosed before appointment and that any changes to their commitments are reported to the Board as they arise. Ensure that proposed appointees disclose any business interests that may result in a conflict of interest prior to appointment and that any future business interests that could result in a conflict of interest are reported. 6.5 Consider any matter relating to the continuation in office of any Board executive director including the suspension or termination of service of an individual as an employee of the Trust, subject to the provisions of the law and their service contract. 7. Remuneration Role The Committee will: 7.1 Establish and keep under review a remuneration policy in respect of executive board directors. 7.2 Consult the Chief Executive about proposals relating to the remuneration of the other executive directors in accordance with all relevant laws, regulations and Trust policies, decide and keep under review the terms and conditions of office of the Trust's executive directors including: Salary, including any performance-related pay or bonus. Provisions for other benefits, including pensions and cars. Allowances. Payable expenses. Compensation payments. In adhering to all relevant laws, regulations and Trust policies the Committee will: 7.3 Establish levels of remuneration which are sufficient to attract, retain and motivate executive directors of the quality and with the skills and experience required to lead the Trust successfully, without paying more than is necessary for this purpose, and at a level which is affordable for the Trust. 7.4 Use national guidance and market benchmarking analysis in the annual determination of remuneration of executive directors, while ensuring that AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-N&R-Appendix6 Page 3 of 5
257 increases are not made where Trust or individual performance do not justify them. Be sensitive to pay and employment conditions elsewhere in the Trust. 7.5 Monitor and assess the output of the evaluation of the performance of individual executive directors, and consider this output when reviewing changes to remuneration levels. 7.6 Advise upon and oversee contractual arrangements for executive directors, including but not limited to termination payments to avoid rewarding poor performance. Ensure that there is proper calculation and scrutiny of any termination payments, ensuring appropriate authority and taking account of such national guidance as is appropriate. 7.7 To determine for all staff, under delegated powers, arrangements for any noncontractual payment, in line with NHS England guidance. The Committee shall also sign-off the payment of contractual severance payments for individual members of staff. 8. Secretary 8.1 The Company Secretary or Associate Director of People shall be secretary to the Committee. 9. Performance Evaluation 9.1 As part of the Board's annual performance review process, the Committee shall review its collective performance. This review process will be in the form of a self-assessment checklist and will include the development of the following year s reporting cycle. 10. Minutes and Reporting 10.1 Formal minutes shall be taken of all Committee meetings. The minutes of meetings shall be made available to all Committee members, the Chief Executive and the Director of People and Corporate Development. Once approved by the Committee, the minutes should be circulated to the Board unless it would be inappropriate to do so The Committee will report to the Board after each meeting and will report to the private session of the Board on the work of the Committee at least once each financial year The Committee shall receive and agree a description of the work of the Committee, its policies and all executive director emoluments in order that these are accurately reported in the required format in the Trust's annual report and accounts The Chairman of the Committee (or one other of its members) shall be available to answer questions on remuneration policy, principles and practice in respect of Board members at the Annual General Meeting of the Trust. 11. Review 11.1 The terms of reference of the Committee shall be reviewed by the Board when required, but at least annually. AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-N&R-Appendix6 Page 4 of 5
258 APPROVED BY THE BOARD OF DIRECTORS ON 1 ST APRIL 2015TBC AmendmentToStandingOrdersAndBoardCommittee-ReviewTermsOfReference-N&R-Appendix6 Page 5 of 5
259 Board meeting date: 7 th July 2016 Agenda Item number: 10.4 Enclosure: 22 Report Title: Staff Engagement and Raising Concerns Board Update Accountable Director: Author (name & title): Marsha Ingram, Director of People & Corporate Development Marsha Ingram, Director of People & Corporate Development Purpose of the report: To update the Board on the progress of staff engagement, including plans to implement the national Freedom to Speak Up guidance. Action required from the Board Decision / Approval Gain assurance Discussion Information What other Trust Committee or Group has considered the key elements of this report? Key points or recommendations from Committee: Committee: MEXT Date reviewed: 7 June 2016 Approval of proposals Strategic Objective(s) to which this paper relates: High quality services Inclusive partnerships Leadership culture Responsible workforce Supporting strategies Effective/efficient resources The CQC domains that this report relates to are: Caring Please give brief details: Responsive Effective Well-led This paper has implications for all aspects of the five CQC domains, particularly well-led. Safe Enc 22 - Staff Engagement and Raising Concerns - Board Update Page 1 of 4
260 Title Staff Engagement and Raising Concerns Board Update Introduction The Board has been receiving quarterly updates on progress against the Staff Engagement action plan, which has delivered a structured programme of work over the last two years. This has been led by an interim staff engagement lead, whose original remit was to investigate and improve the Trust s staff survey results. Following the feedback from the pilot CQC inspection in 2014, the interim staff engagement lead has also developed and implemented specific actions to help tackle bullying and harassment within the Trust. This programme of work is now coming to an end as the action plan is almost completely delivered. The only outstanding area which will be taken forward during 2016/17 is to develop and deliver a values-based management and leadership development programme. The results of the 2015 staff survey were extremely positive however, one of the key areas identified from the survey and other sources was that there are still limited pockets of the Trust where staff feel unwilling to raise concerns. Therefore, the aim of this paper is to update the Board on plans to take forward these critical areas. The Trust Board has already agreed substantive funding for a staff engagement resource as part of the 2016/17 budget-setting process. Summary of key points, issues and risks Staff Engagement and Freedom to Speak Up ( F2SU ) The Trust has placed a significant emphasis on staff engagement over the past two years. Following a period of plateau staff survey results and concerns about bullying and harassment raised in the previous CQC inspection, an independent interim Staff Engagement Lead was appointed in The remit of this post was initially to undertake staff focus groups to understand further some of the outcomes of the staff survey, and to take forward work to address bullying and harassment. A Board level action plan was agreed and has been monitored quarterly. This approach has thus far been largely successful and has achieved many positive outcomes. During this period, the Trust have introduced Workplace Advisors and Engagement Champion roles; implemented and improved results in the staff friends and family test ; developed and launched employee-led Trust values; achieved significantly improved results in the national staff survey; implemented enhanced staff communication channels; developed and implemented on-line Speak Up facility for staff to raise concerns; undertaken focus group sessions for staff which have shown improvement in many areas. The interim Staff Engagement Lead has also dealt with a number of cases where staff have approached him for confidential advice about a range of workplace concerns - giving advice, mediating resolutions and signposting. An internal audit into the Trust s staff engagement arrangements gave significant assurance and recommended that substantive resource should be identified for this area. The Trust now needs to embed a sustainable resource and overall approach for staff engagement. Whilst there is evidence that our staff experience has improved in many areas, there are pockets of evidence which would suggest that some staff are still reluctant to raise concerns about workplace issues. Whilst it may be questioned whether these views are evidence based, these perceptions Enc 22 - Staff Engagement and Raising Concerns - Board Update Page 2 of 4
261 represent very real concerns for some staff within the Trust, and clearly links to the F2SU Guardian role. Freedom to Speak Up (F2SU), one of the follow-on publications from the Francis report following the Mid-Staffs inquiry, found shortfalls in the way that NHS organisations facilitate and deal with cases where staff raise workplace concerns. The report made a series of recommendations to improve this key area, one of which was that all NHS Trusts are required to appoint a F2SU Guardian. A summary of the role is attached at Appendix 1. This development, along with the associated establishment of a national F2SU Guardian role, are seen as key developments in supporting staff to raise concerns at work and embedding a culture of openness. Trusts are required to have plans in place for the F2SU Guardian role by September 2016 and have appointed to the role by the end of March 2017 at the latest. Therefore, following a detailed debate at MEXT, it as been agreed that we combine the functions of staff engagement and F2SU Guardian within a single role within the Trust to take forward these important and over-lapping areas of work. The role description is currently under development and will be widely consulted upon before recruitment. A few other Trusts have already appointed their F2SU Guardian roles and a variety of approaches have been taken. Some Trusts have tagged the responsibility onto an existing role (senior governance role, executive director, non-executive and in one case, staff side lead). Others have taken a more similar approach to this proposal and appointed a stand-alone F2SU Guardian role, often combining this with other responsibilities. Contact has been made with a number of other Trusts to ascertain what lessons learned can be incorporated this into our plans. Raising Concerns and Whistleblowing Policy guidance In line with the national Freedom to Speak Up guidance, an NHS-wide whistleblowing policy has been developed, which all Trusts are required to adopt as a minimum standard. This was published on 1 April The Trust is using the national policy to develop a comprehensive Raising Concerns and Whistleblowing policy, which will supersede the Trust s current whistleblowing policy. This will be widely consulted upon before being presented for Board approval in September Leadership Development Programme The need for a leadership development programme to underpin the Trust s refreshed values and associated behavioural framework was a key finding of the staff engagement programme, and this was noted by the Board in March Since then, the interim Staff Engagement Lead and the L&D Manager have had extensive meetings with managers and leaders from all areas of the Trust to ascertain their views about priorities for content and delivery of such a programme. It was agreed that a priority for any programme of development would be sustainability in that it would be taken forward through appraisal and development for managers, rather than being seen as a one-off piece of work. The proposals that have resulted from this work are being presented to the Executive Team on 4 th July an update on this will be provided at the Board meeting. Recommendation The Board is asked to note the progress in these areas and support the way forward for staff engagement and raising concerns. Board action required As above. Enc 22 - Staff Engagement and Raising Concerns - Board Update Page 3 of 4

262 Appendix 1 Enc 22 - Staff Engagement and Raising Concerns - Board Update Page 4 of 4
Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday, 5 th October 2017
 Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday, 5 th October 2017 1.00pm-3.00pm Conference Room 1, Trafalgar House, King Street, Dudley PUBLIC MEETING
Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Thursday, 5 th October 2017 1.00pm-3.00pm Conference Room 1, Trafalgar House, King Street, Dudley PUBLIC MEETING
Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting
 Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Wednesday 6 th August 2014 3:00 pm 5:00 pm Board Room, 1st Floor, Canalside House, Abbotts Street, Bloxwich, Walsall,
Dudley and Walsall Mental Health Partnership NHS Trust Papers for the Trust Board Meeting Wednesday 6 th August 2014 3:00 pm 5:00 pm Board Room, 1st Floor, Canalside House, Abbotts Street, Bloxwich, Walsall,
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
 APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
Governance and Quality Committee Review. Wendy Pugh Director of Operations and Nursing. Innovation Tom Jinks - Governance Manager.
 Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
Dudley & Walsall Mental Health Partnership NHS Trust Board
 Dudley & Walsall Mental Health Partnership NHS Trust Board Date of Board Meeting: 29 th July 2 Subject: Performance Corporate Dashboard Month 3 Trust Board Lead: Jacky O Sullivan, Director of Performance
Dudley & Walsall Mental Health Partnership NHS Trust Board Date of Board Meeting: 29 th July 2 Subject: Performance Corporate Dashboard Month 3 Trust Board Lead: Jacky O Sullivan, Director of Performance
Strategic Risk Report 4 July 2016
 Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
NHS England (London) Assurance of the BEH Clinical Strategy
 Assurance of the BEH Clinical Strategy") NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
Strategic Risk Report 12 September 2016
 Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk
 Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Adults and Safeguarding Committee 19 March Implementing the Care Act 2014: Carers; Prevention; Information, Advice and Advocacy.
 Adults and Safeguarding Committee 19 March 2015 Title Report of Wards Implementing the Care Act 2014: Carers; Prevention; Information, Advice and Advocacy Dawn Wakeling (Adult and Health Commissioning
Adults and Safeguarding Committee 19 March 2015 Title Report of Wards Implementing the Care Act 2014: Carers; Prevention; Information, Advice and Advocacy Dawn Wakeling (Adult and Health Commissioning
Internal Audit. Health and Safety Governance. November Report Assessment
 November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
TRUST BOARD. Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director. Jo Hunter, Deputy Chief Nurse. Mary Heritage, Assistant Director of Quality
 TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
Primary Care Quality Assurance Framework (Medical Services)
") PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
Welcome, Apologies for Absence and Declaration of Board Members Interest
 DRAFT Minutes of the of the Royal Cornwall Hospitals NHS Trust held on Thursday 30 March 2017 11.00 13.00 in the Knowledge Spa, Royal Cornwall Hospital Present: Mr Jim McKenna Ms Kathy Byrne Ms Catrin
DRAFT Minutes of the of the Royal Cornwall Hospitals NHS Trust held on Thursday 30 March 2017 11.00 13.00 in the Knowledge Spa, Royal Cornwall Hospital Present: Mr Jim McKenna Ms Kathy Byrne Ms Catrin
Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May 2016
 Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May RAG Dark green Light green Amber Red White Definition Action complete and assurance gained Action
Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May RAG Dark green Light green Amber Red White Definition Action complete and assurance gained Action
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
NHS Workforce Race Equality Standard
 NHS Workforce Race Equality Standard (WRES) 2016 Report & Action Plan Date of Report January 2017 Subject NHS Workforce Race Equality Standard Brighton and Sussex University Hospitals NHS Trust Report
NHS Workforce Race Equality Standard (WRES) 2016 Report & Action Plan Date of Report January 2017 Subject NHS Workforce Race Equality Standard Brighton and Sussex University Hospitals NHS Trust Report
ENCLOSURE: J. Date of Trust Board 29 February Pressure Ulcer Clinical Improvement Programme. Purpose of Report
 ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
Special Measures Action Plan. Norfolk and Suffolk NHS Foundation Trust
 Special Measures Action Plan Norfolk and Suffolk NHS Foundation Trust June 2015 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver 1 Norfolk and Suffolk NHS Foundation
Special Measures Action Plan Norfolk and Suffolk NHS Foundation Trust June 2015 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver 1 Norfolk and Suffolk NHS Foundation
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
Central Alerting System (CAS) Policy
 Policy") Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Methods: Commissioning through Evaluation
 Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
: Geraint Davies, Director of Commercial Services
 Report to : Trust Board of Directors Date of Report: 15/05/2015 Agenda Item: 0/15 Date of Meeting : 28 May 2015 Subject Report from Purpose : Report on Corporate Risk Register : Geraint Davies, Director
Report to : Trust Board of Directors Date of Report: 15/05/2015 Agenda Item: 0/15 Date of Meeting : 28 May 2015 Subject Report from Purpose : Report on Corporate Risk Register : Geraint Davies, Director
Sponsoring director: Purpose: Decision Assurance For information Disclosable X Non-disclosable
 TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
Salford Integrated Care System Governance Framework: Adult Health and Care Services FINAL
 Salford Integrated Care System Governance Framework: Adult Health and Care Services FINAL 1 Background and Scope Salford is a forward thinking health and social care economy and as such has established
Salford Integrated Care System Governance Framework: Adult Health and Care Services FINAL 1 Background and Scope Salford is a forward thinking health and social care economy and as such has established
A concern means any complaint, claim or reported patient safety incident.
 PUTTING THINGS RIGHT ANNUAL REPORT -2017 Introduction The Putting Things Right Annual Report provides information on the progress and performance of Powys Teaching Local Health Board (hereafter, the health
PUTTING THINGS RIGHT ANNUAL REPORT -2017 Introduction The Putting Things Right Annual Report provides information on the progress and performance of Powys Teaching Local Health Board (hereafter, the health
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING ADULT AND CHILDREN CONTINUING HEALTHCARE ANNUAL REPORT
 9.6 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING ADULT AND CHILDREN CONTINUING HEALTHCARE ANNUAL REPORT Date of the meeting 18/07/2018 Author Sponsoring Board member Purpose of Report
9.6 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING ADULT AND CHILDREN CONTINUING HEALTHCARE ANNUAL REPORT Date of the meeting 18/07/2018 Author Sponsoring Board member Purpose of Report
TERMS OF REFERENCE. Transformation and Sustainability Committee. One per month (Second Thursday) GP Board Member (Quality) Director of Commissioning
 GP Board Member (Quality) Director of Commissioning") TERMS OF REFERENCE Committee: Frequency Of Meetings: Committee Chair: Membership: Attendance: Lead Officer: Secretary: Transformation and Sustainability Committee One per month (Second Thursday) GP Board
TERMS OF REFERENCE Committee: Frequency Of Meetings: Committee Chair: Membership: Attendance: Lead Officer: Secretary: Transformation and Sustainability Committee One per month (Second Thursday) GP Board
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP
 COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD
 BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD") INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Efficiency in mental health services
 the voice of NHS leadership briefing February 211 Issue 214 Efficiency in mental health services Supporting improvements in the acute care pathway Key points As part of the current focus on improving quality,
the voice of NHS leadership briefing February 211 Issue 214 Efficiency in mental health services Supporting improvements in the acute care pathway Key points As part of the current focus on improving quality,
Document Details Title
 Document Details Title Quality and Equalities Impact Assessment (QEIA) Process Guidance Trust Ref No 2046-45852 Local Ref (optional) Main points the document This document explains the process for QEIA,
Document Details Title Quality and Equalities Impact Assessment (QEIA) Process Guidance Trust Ref No 2046-45852 Local Ref (optional) Main points the document This document explains the process for QEIA,
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Chief Accountable Officer Director Transformation and Quality. Director Transformation and Quality Chief Accountable Officer
 Governing Body Assurance Framework (July/August 2016) Introduction The Governing Body Assurance Framework identifies the CCG s principal, strategic objectives and the principal risks to their delivery.
Governing Body Assurance Framework (July/August 2016) Introduction The Governing Body Assurance Framework identifies the CCG s principal, strategic objectives and the principal risks to their delivery.
Inpatient and Community Mental Health Patient Surveys Report written by:
 2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
CLINICAL AND CARE GOVERNANCE STRATEGY
 CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
NHS Cumbria CCG Transforming Care Programme Learning Disabilities
 NHS Cumbria CCG Governing Body Agenda Item 07 December 2016 8 NHS Cumbria CCG Transforming Care Programme Learning Disabilities Purpose of the Report To update the Governing Body on local progress with
NHS Cumbria CCG Governing Body Agenda Item 07 December 2016 8 NHS Cumbria CCG Transforming Care Programme Learning Disabilities Purpose of the Report To update the Governing Body on local progress with
WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE
 Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
The Integrated Support and Assurance Process (ISAP): guidance on assuring novel and complex contracts
: guidance on assuring novel and complex contracts") The Integrated Support and Assurance Process (ISAP): guidance on assuring novel and complex contracts Part A: Introduction Published by NHS England and NHS Improvement August 2017 First published: Friday
The Integrated Support and Assurance Process (ISAP): guidance on assuring novel and complex contracts Part A: Introduction Published by NHS England and NHS Improvement August 2017 First published: Friday
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Safeguarding Annual Assurance Self-assessment Tool. Sheffield Health and Social Care NHS Foundation Trust
 Safeguarding Annual Assurance Self-assessment Tool Sheffield Health and Social Care Foundation Trust Introduction - About this Self-assessment This self-assessment is an assessment of your own internal
Safeguarding Annual Assurance Self-assessment Tool Sheffield Health and Social Care Foundation Trust Introduction - About this Self-assessment This self-assessment is an assessment of your own internal
(Committee Chair) Chair) Interim Board Secretary (MHSA/16/25 onwards) Head of CAMHS and Childrens Learning Disability (MHSA/16/24 only)
 Chair) Interim Board Secretary (MHSA/16/25 onwards) Head of CAMHS and Childrens Learning Disability (MHSA/16/24 only)") POWYS TEACHING HEALTH BOARD MENTAL HEALTH SERVICES ASSURANCE COMMITTEE CONFIRMED MINUTES OF THE MEETING HELD ON THURSDAY 03 MARCH 2016, AT 10.00AM, GROUND CONFERENCE ROOM, NEUADD BRYCHEINIOG, BRECON Present:
POWYS TEACHING HEALTH BOARD MENTAL HEALTH SERVICES ASSURANCE COMMITTEE CONFIRMED MINUTES OF THE MEETING HELD ON THURSDAY 03 MARCH 2016, AT 10.00AM, GROUND CONFERENCE ROOM, NEUADD BRYCHEINIOG, BRECON Present:
YORKSHIRE AMBULANCE SERVICE NHS TRUST Quality Improvement Action Plan 23/05/1017 FINAL. Deputy/ Associate Director. Executive Director TRUST WIDE
 YORKSHIRE AMBULANCE SERVICE NHS TRUST Quality Improvement Action Plan 23/05/1017 FINAL CQC findings TRUST WIDE 1.1 1.2 Ensure that at all times there are qualified experienced staff (including Staff communication
YORKSHIRE AMBULANCE SERVICE NHS TRUST Quality Improvement Action Plan 23/05/1017 FINAL CQC findings TRUST WIDE 1.1 1.2 Ensure that at all times there are qualified experienced staff (including Staff communication
Safeguarding review to assist Walsall Healthcare NHS Trust
 [Type text] [Type text] [Type text] Safeguarding review to assist Walsall Healthcare NHS Trust A report for Walsall Clinical Commissioning Group April 2014 Buckley- Gray Consultancy Ltd Author: Sandra
[Type text] [Type text] [Type text] Safeguarding review to assist Walsall Healthcare NHS Trust A report for Walsall Clinical Commissioning Group April 2014 Buckley- Gray Consultancy Ltd Author: Sandra
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April Ipswich Hospital NHS Trust NHS East of England Department of Health
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
EAST AND NORTH HERTFORDSHIRE NHS TRUST
 Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 24 July 2013 at 2pm in the Post Graduate Centre, QEII Hospital. Present: Mr Ian Morfett
Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 24 July 2013 at 2pm in the Post Graduate Centre, QEII Hospital. Present: Mr Ian Morfett
Quality, Safety & Experience (QSE) Committee. Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph
 Committee. Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph") 1 Minutes QSE Public 29.3.17 V1.0 Present: Quality, Safety & Experience (QSE) Committee Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph Mrs Margaret
1 Minutes QSE Public 29.3.17 V1.0 Present: Quality, Safety & Experience (QSE) Committee Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph Mrs Margaret
PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY
 Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
UNIVERSITY HOSPITALS OF LEICESTER TRUST BOARD 2 MARCH 2017 PAGE 1 OF 6 Emergency Floor Project: Monthly Update
 UNIVERSITY HOSPITALS OF LEICESTER TRUST BOARD 2 MARCH 2017 PAGE 1 OF 6 Emergency Floor Project: Monthly Update Author: Jane Edyvean Sponsor: Richard Mitchell EXECUTIVE SUMMARY Paper J Context Construction
UNIVERSITY HOSPITALS OF LEICESTER TRUST BOARD 2 MARCH 2017 PAGE 1 OF 6 Emergency Floor Project: Monthly Update Author: Jane Edyvean Sponsor: Richard Mitchell EXECUTIVE SUMMARY Paper J Context Construction
Na. Acceptable (some apologies) x. Yes. Narrative report of the key issues of the meeting
 x. Yes. Narrative report of the key issues of the meeting") Chairpersons Report Chairpersons Name Carole Hudson Committee Name Audit Committee Date of Meeting 03.08.16 Name of Receiving Committee Trust Board Date of Receiving Committee meeting September 2016 Strategic
Chairpersons Report Chairpersons Name Carole Hudson Committee Name Audit Committee Date of Meeting 03.08.16 Name of Receiving Committee Trust Board Date of Receiving Committee meeting September 2016 Strategic
ADULT MENTAL HEALTH NHS MANAGEMENT ARRANGEMENTS. To approve. This paper supports the standards
 BOARD MEETING 25 FEBRUARY 2015 AGENDA ITEM 2.1 ADULT MENTAL HEALTH NHS MANAGEMENT ARRANGEMENTS Report of Paper prepared by Purpose of Paper Action/Decision required Link to Doing Well, Doing Better: Standards
BOARD MEETING 25 FEBRUARY 2015 AGENDA ITEM 2.1 ADULT MENTAL HEALTH NHS MANAGEMENT ARRANGEMENTS Report of Paper prepared by Purpose of Paper Action/Decision required Link to Doing Well, Doing Better: Standards
Quality and Safety Committee Terms of Reference
 Approved May 2016 Quality and Safety Committee Terms of Reference 1. Constitution The Quality and Safety Committee is established as a sub-committee of The Hillingdon Hospitals NHS Foundation Trust (THH)
Approved May 2016 Quality and Safety Committee Terms of Reference 1. Constitution The Quality and Safety Committee is established as a sub-committee of The Hillingdon Hospitals NHS Foundation Trust (THH)
Cambridgeshire and Peterborough Sustainability and Transformation Partnership
 Cambridgeshire and Peterborough Sustainability and Transformation Partnership Governance Framework November 2017 Page 1 of 28 Contents 1. Introduction 2. Sustainability and Transformation Partnership 3.
Cambridgeshire and Peterborough Sustainability and Transformation Partnership Governance Framework November 2017 Page 1 of 28 Contents 1. Introduction 2. Sustainability and Transformation Partnership 3.
Northumberland, Tyne and Wear NHS Foundation Trust. Board of Directors Meeting
 Agenda item 7 iv) Northumberland, Tyne and Wear NHS Foundation Trust Meeting Date: 22 February 2017 Board of Directors Meeting Title and Author of Paper: Safer Staffing Quarter 3 Report (October December,
Agenda item 7 iv) Northumberland, Tyne and Wear NHS Foundation Trust Meeting Date: 22 February 2017 Board of Directors Meeting Title and Author of Paper: Safer Staffing Quarter 3 Report (October December,
Primary Care Commissioning Next Steps to Delegated Commissioning September Board Paper. 2.0 Delegated Opportunities, Benefits and Risks
 Primary Care Commissioning Next Steps to Delegated Commissioning September Board Paper 1.0 Introduction This paper provides a briefing to the Wandsworth CCG Board on our progress in developing a Primary
Primary Care Commissioning Next Steps to Delegated Commissioning September Board Paper 1.0 Introduction This paper provides a briefing to the Wandsworth CCG Board on our progress in developing a Primary
Integration Scheme. Between. Glasgow City Council. and. NHS Greater Glasgow and Clyde
 Integration Scheme Between Glasgow City Council and NHS Greater Glasgow and Clyde December 2015 Page 1 of 60 1. Introduction 1.1 The Public Bodies (Joint Working) (Scotland) Act 2014 (the Act) requires
Integration Scheme Between Glasgow City Council and NHS Greater Glasgow and Clyde December 2015 Page 1 of 60 1. Introduction 1.1 The Public Bodies (Joint Working) (Scotland) Act 2014 (the Act) requires
PATIENT SAFETY AND QUALITY COMMITTEE TERMS OF REFERENCE
 PATIENT SAFETY AND QUALITY COMMITTEE TERMS OF REFERENCE Page 1 DOCUMENT CONTROL SHEET Name of Document: Patient Safety and Quality Committee Terms of Reference Version: 5 File Location / Document Name:
PATIENT SAFETY AND QUALITY COMMITTEE TERMS OF REFERENCE Page 1 DOCUMENT CONTROL SHEET Name of Document: Patient Safety and Quality Committee Terms of Reference Version: 5 File Location / Document Name:
Burton Hospitals NHS Foundation Trust. On: 30 January Review Date: November Corporate / Directorate. Department Responsible for Review:
 POLICY DOCUMENT Burton Hospitals NHS Foundation Trust MANAGEMENT OF EXTERNAL AGENCY VISITS, INSPECTIONS, ACCREDITATION AND RESULTING RECOMMENDATIONS Approved by: Trust Executive Committee On: 30 January
POLICY DOCUMENT Burton Hospitals NHS Foundation Trust MANAGEMENT OF EXTERNAL AGENCY VISITS, INSPECTIONS, ACCREDITATION AND RESULTING RECOMMENDATIONS Approved by: Trust Executive Committee On: 30 January
Present: Mr B Reid OBE Chair of the Board of Directors Mr N Summers CBE Vice Chair of the Board of Directors. Mr G McEvoy Non-executive Director
 ENC 1 MINUTES OF THE TRUST BOARD OF DIRECTORS OF WALSALL HEALTHCARE NHS TRUST HELD ON THURSDAY 25 APRIL 2013 AT 2PM IN THE MANOR LEARNING AND CONFERENCE CENTRE, WALSALL MANOR HOSPITAL Present: Mr B Reid
ENC 1 MINUTES OF THE TRUST BOARD OF DIRECTORS OF WALSALL HEALTHCARE NHS TRUST HELD ON THURSDAY 25 APRIL 2013 AT 2PM IN THE MANOR LEARNING AND CONFERENCE CENTRE, WALSALL MANOR HOSPITAL Present: Mr B Reid
Collaborative Agreement for CCGs and NHS England
 RCCG/GB/15/164 Collaborative Agreement for CCGs and NHS England East Midlands Collaborative Commissioning Oversight Group (EMCCOG) 1. Particulars 1.1. This Agreement records the particulars of the agreement
RCCG/GB/15/164 Collaborative Agreement for CCGs and NHS England East Midlands Collaborative Commissioning Oversight Group (EMCCOG) 1. Particulars 1.1. This Agreement records the particulars of the agreement
Intensive Psychiatric Care Units
 NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
QUALITY IMPROVEMENT COMMITTEE
 : 2016-002.a QUALITY IMPROVEMENT COMMITTEE Minutes of the meeting held on 11 th February 2016, Conference Room D, 1829 Building Present: Faulkner, Sarah (SF) (Chair) Lay Member, NHS West Cheshire CCG Cavanagh,
: 2016-002.a QUALITY IMPROVEMENT COMMITTEE Minutes of the meeting held on 11 th February 2016, Conference Room D, 1829 Building Present: Faulkner, Sarah (SF) (Chair) Lay Member, NHS West Cheshire CCG Cavanagh,
SUBJECT: Medical Staffing Update Report 1. PURPOSE
 Meeting of Lanarkshire NHS Board: Wednesday 25 March 2015 Lanarkshire NHS Board Kirklands Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk SUBJECT: Medical Staffing Update
Meeting of Lanarkshire NHS Board: Wednesday 25 March 2015 Lanarkshire NHS Board Kirklands Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk SUBJECT: Medical Staffing Update
NHS GRAMPIAN. Grampian Clinical Strategy - Planned Care
 NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
QUALITY COMMITTEE. Terms of Reference
 QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
Quality Assurance Accreditation Scheme Assignment Report 2016/17. University Hospitals of Morecambe Bay NHS Foundation Trust
 Quality Assurance Accreditation Scheme Assignment Report 2016/17 Contents 1. Introduction 2. Executive Summary 3. Findings, Recommendations and Action Plan Appendix A: Terms of Reference Appendix B: Assurance
Quality Assurance Accreditation Scheme Assignment Report 2016/17 Contents 1. Introduction 2. Executive Summary 3. Findings, Recommendations and Action Plan Appendix A: Terms of Reference Appendix B: Assurance
REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY PART 1
 REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY PART 1 Date of Meeting: 24 September 2015 Agenda No: 8.2 Attachment: 14 Title of Document: South West London Collaborative Commissioning programme
REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY PART 1 Date of Meeting: 24 September 2015 Agenda No: 8.2 Attachment: 14 Title of Document: South West London Collaborative Commissioning programme
Warrington CCG Operational Safeguarding Children Health Forum. Terms of Reference
 Warrington CCG Operational Safeguarding Children Health Forum 1 Introduction Terms of Reference 1.1 The Operational Safeguarding Children Health Forum (the Health Forum) is established within the Safety
Warrington CCG Operational Safeguarding Children Health Forum 1 Introduction Terms of Reference 1.1 The Operational Safeguarding Children Health Forum (the Health Forum) is established within the Safety
2017/18 Trust Balanced Scorecard
 ITEM 8b ENC 9 2017/18 Trust Balanced Scorecard Author: Performance Management Team March 2017 The purpose of this paper is to provide an update on the development of the 2017/18 Balanced Scorecard for
ITEM 8b ENC 9 2017/18 Trust Balanced Scorecard Author: Performance Management Team March 2017 The purpose of this paper is to provide an update on the development of the 2017/18 Balanced Scorecard for
REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 26 November 2015 Agenda No: 6.2 Attachment: 06 Title of Document: Adult Safeguarding Annual Report 2014/15 Purpose of Report:
REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 26 November 2015 Agenda No: 6.2 Attachment: 06 Title of Document: Adult Safeguarding Annual Report 2014/15 Purpose of Report:
Executive Workforce Report
 Executive Workforce Report (v2) Safe & Effective Kind & Caring Exceeding Expectation Agenda Item No: 9.3 The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 27 th November 2017 Title: Executive
Executive Workforce Report (v2) Safe & Effective Kind & Caring Exceeding Expectation Agenda Item No: 9.3 The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 27 th November 2017 Title: Executive
HERTFORDSHIRE COMMUNITY HEALTH SERVICES
 HERTFORDSHIRE COMMUNITY HEALTH SERVICES Minutes of the Hertfordshire Community Health Services Board Meeting Held on Thursday 22 nd July 2010 in the Boardroom, Howard Court Welwyn Garden City. Key Points
HERTFORDSHIRE COMMUNITY HEALTH SERVICES Minutes of the Hertfordshire Community Health Services Board Meeting Held on Thursday 22 nd July 2010 in the Boardroom, Howard Court Welwyn Garden City. Key Points
SPONSORSHIP AND JOINT WORKING WITH THE PHARMACEUTICAL INDUSTRY
 SPONSORSHIP AND JOINT WORKING WITH THE PHARMACEUTICAL INDUSTRY 1 SUMMARY This document sets out Haringey Clinical Commissioning Group policy and advice to employees on sponsorship and joint working with
SPONSORSHIP AND JOINT WORKING WITH THE PHARMACEUTICAL INDUSTRY 1 SUMMARY This document sets out Haringey Clinical Commissioning Group policy and advice to employees on sponsorship and joint working with
Framework for managing performer concerns NHS (Performers Lists) (England) Regulations 2013
 (England) Regulations 2013") Framework for managing performer concerns NHS (Performers Lists) (England) Regulations 2013 Information reader box NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information
Framework for managing performer concerns NHS (Performers Lists) (England) Regulations 2013 Information reader box NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information
Debbie Edwards Interim Deputy Director of Nursing Gail Naylor- Executive Director of Nursing & Midwifery. Safety & Quality Committee
 Report to Trust Board of Directors Date of Meeting: 29 July 2014 Enclosure Number: 7 Title of Report: Author: Executive Lead: Responsible Sub- Committee (if appropriate): Executive Summary: Ward Accreditation
Report to Trust Board of Directors Date of Meeting: 29 July 2014 Enclosure Number: 7 Title of Report: Author: Executive Lead: Responsible Sub- Committee (if appropriate): Executive Summary: Ward Accreditation
A Case Review Process for NHS Trusts and Foundation Trusts
 A Case Review Process for NHS Trusts and Foundation Trusts 1 1. Introduction The Francis Freedom to Speak Up review summarised the need for an independent case review system as a mechanism for external
A Case Review Process for NHS Trusts and Foundation Trusts 1 1. Introduction The Francis Freedom to Speak Up review summarised the need for an independent case review system as a mechanism for external
TITLE OF REPORT: Looked After Children Annual Report
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 13 Date of Meeting:..27 th October 2017.. TITLE OF REPORT: Looked After Children Annual Report 2016-2017 AUTHOR: Christine Dixon,
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 13 Date of Meeting:..27 th October 2017.. TITLE OF REPORT: Looked After Children Annual Report 2016-2017 AUTHOR: Christine Dixon,
Apologies Lay Member Financial Management & Audit
 Primary Care Commissioning Committee Unratified Minutes of the Public Meeting held on Thursday 2 August 2018, 09:30 10:45 Committee Room, Gedling Civic Centre, Arnot Hill Park Members Mike Wilkins (MW)
Primary Care Commissioning Committee Unratified Minutes of the Public Meeting held on Thursday 2 August 2018, 09:30 10:45 Committee Room, Gedling Civic Centre, Arnot Hill Park Members Mike Wilkins (MW)
North Cumbria University Hospitals NHS Trust Proposed Acquisition by a Foundation Trust. Stakeholder Event Wednesday, 12 October 2011
 North Cumbria University Hospitals NHS Trust Proposed Acquisition by a Foundation Trust Stakeholder Event Wednesday, 12 October 2011 Stakeholder and Foundation Trust Briefing Information 1 1. Contents
North Cumbria University Hospitals NHS Trust Proposed Acquisition by a Foundation Trust Stakeholder Event Wednesday, 12 October 2011 Stakeholder and Foundation Trust Briefing Information 1 1. Contents
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS BORDERS. Nursing & Midwifery. Rostering Policy for Nursing & Midwifery Staff in Hospitals/Wards
 NHS BORDERS Nursing & Midwifery Rostering Policy for Nursing & Midwifery Staff in Hospitals/Wards 1 CONTENTS Section Title Page 1 Purpose and Scope 3 2 Statement of Policy 3 3 Responsibilities and Organisational
NHS BORDERS Nursing & Midwifery Rostering Policy for Nursing & Midwifery Staff in Hospitals/Wards 1 CONTENTS Section Title Page 1 Purpose and Scope 3 2 Statement of Policy 3 3 Responsibilities and Organisational
Performance Evaluation Report Pembrokeshire County Council Social Services
 Performance Evaluation Report 2013 14 Pembrokeshire County Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Pembrokeshire County Council
Performance Evaluation Report 2013 14 Pembrokeshire County Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Pembrokeshire County Council
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Hard Truths Public Board 29th September, 2016
 Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Looked After Children Annual Report
 Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
Safer Nursing and Midwifery Staffing Recommendation The Board is asked to: NOTE the report
 To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
GOVERNING BODY MEETING 30 July 2014 Agenda Item 2.2
 GOVERNING BODY MEETING 30 July 2014 Report Title Purpose of report Personal Health Budgets This report provides an overview of the use of Personal Health Budgets (PHBs) within NHS Eastern Cheshire Clinical
GOVERNING BODY MEETING 30 July 2014 Report Title Purpose of report Personal Health Budgets This report provides an overview of the use of Personal Health Budgets (PHBs) within NHS Eastern Cheshire Clinical
Appendix 1: Integrated Urgent Care Service Update. 1. Purpose
 Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
James Blythe, Director of Commissioning and Strategy. Agenda item: 09 Attachment: 04
 Title of paper: Author: Exec Lead: Community Hospital Services Review Tom Elrick, Urgent Care Programme Lead James Blythe, Director of Commissioning and Strategy Date: 23 rd February 2015 Meeting: Executive
Title of paper: Author: Exec Lead: Community Hospital Services Review Tom Elrick, Urgent Care Programme Lead James Blythe, Director of Commissioning and Strategy Date: 23 rd February 2015 Meeting: Executive
Report from Quality Assurance Committee meeting held on 30 November 2017
 Report from Quality Assurance Committee meeting held on 30 November 2017 Governing Body meeting Item 18f 11 January 2018 Author(s) Sponsor Director Purpose of Paper Carol Henderson, Committee Secretary
Report from Quality Assurance Committee meeting held on 30 November 2017 Governing Body meeting Item 18f 11 January 2018 Author(s) Sponsor Director Purpose of Paper Carol Henderson, Committee Secretary
Sussex Community NHS Trust Action Plan in Response to Recommendations Made by CQC
 Sussex Community NHS Trust Action Plan in Response to Recommendations Made by CQC England s chief inspector of hospitals has rated the overall quality of services provided by Sussex Community NHS Trust
Sussex Community NHS Trust Action Plan in Response to Recommendations Made by CQC England s chief inspector of hospitals has rated the overall quality of services provided by Sussex Community NHS Trust
UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST TRUST BOARD
 UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST TRUST BOARD Date of meeting: 25 July 2012 Title / Subject: Status Internal Purpose: The attached paper provides an update of progess made in UHMB
UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST TRUST BOARD Date of meeting: 25 July 2012 Title / Subject: Status Internal Purpose: The attached paper provides an update of progess made in UHMB
Learning from Deaths Policy. This policy applies Trust wide
 Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical