Anesthesia: Past, Present, Future. Kimberly Westra CRNA, MSN, DNP MBA
|
|
|
- Janice Chambers
- 6 years ago
- Views:
Transcription

1 Anesthesia: Past, Present, Future Kimberly Westra CRNA, MSN, DNP MBA
2 Anesthesia: Past Anesthesia Practices: Hospital Based Academic Hospital Based Community Private MD & CRNA group Anesthesia Management Company Locums Independent Practice
3 Anesthesia Changing Trends Past: Competition for Anesthesia Services & Contracts based in legacy, traditions & geographical factors Limited Options for Healthcare Organizations Present & Future: Competition for Anesthesia Services value based, extremely competitive markets with mergers & acquisitions the norm Numerous Anesthesia Options Local & National

4 Flexibility & Adaptability to meet Organizational needs are invaluable Collaboration & Shared Vision with Organization a must for Anesthesia Team Anesthesia Trends
5 Market Trends for CRNA s, AA, MDA Balance of Supply versus Demand: Regionally & Nationally Critical Access Areas Governmental Providers Anesthesia Trends
6 Anesthesia Activism AANA American Association of Nurse Anesthetist PANA Pennsylvania Association Nurse Anesthetist Legislators Federal & State Stewardship Essential

7 Anesthesia Professional Citizens Anesthesia Providers Professional Citizens versus Inhabitants Anesthesia Providers as Business Partners with Healthcare Organizations: Partners in Shared Vision

8 Anesthesia Professional Employment Choices Contracts Non Compete Clauses Geographic Limitations Offer Letter At Will versus Union

9 Anesthesia Professional Balance Compensation Package Scope of Practice & Practice Setting Work Life Balance
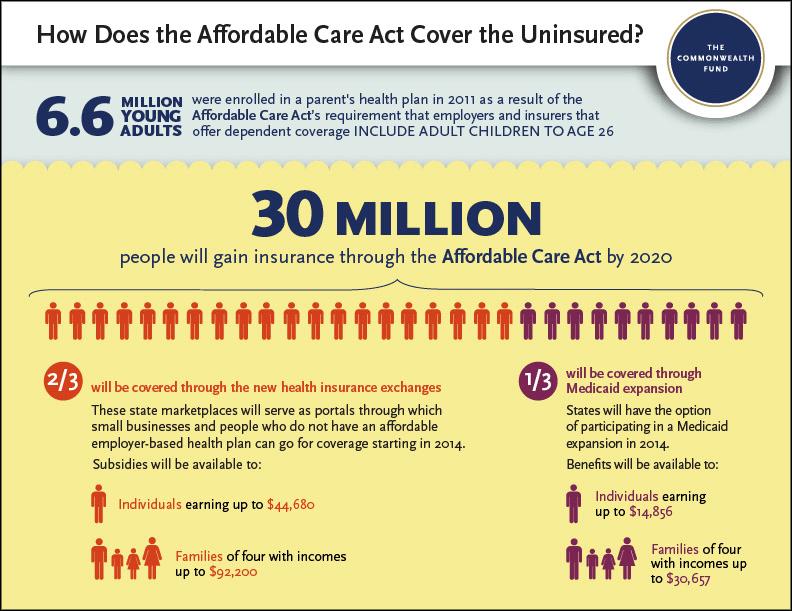
10 Anesthesia Business & Practice Healthcare Landscape Changes & Anesthesia National Trends Affordable Care Act Signed 2010 Implemented in Stages since 2011 Healthcare Exchanges Medicaid & Medicare Expansion 2011

11 New Game Changers Landscape & Environment of Healthcare Patients as Consumers Payers & Payment Innovations ACA Impacts

12 HealthCare Costs in 2040 New England Journal of Medicine projections suggest healthcare costs will encompass 26% of GDP all disciplines will play a role in the costs
13 The Business of HealthCare United States spends approximately $9366 per person on healthcare 2015 Healthcare costs increased 3.7% $2.9 TRILLION
14 HealthCare as a Business United States spends more money per capital than any other nation! Healthcare costs represent 17.8 % of Gross Domestic Product!
15 ACA

16 Affordable Care Act Politically Charged National focus on Healthcare requesting better quality for better price since to To Err is Human 1999
17 ACA, SGR, Anesthesia Sustainable Growth Rate 1997 Doc Fix Bill Since 1997 Amended multiple times to avoid reductions in Reimbursements Repealed in April 2015 with Bipartisan Support

18 ACA, SGR, Anesthesia SGR Repeal approved April 2015 focus on Value Based Reimbursement SGR repeal held off 22-25% payment cuts WHY was SGR so easily repealed by a Bipartisan Vote?

19 Goodbye SGR, ACA Pioneers Since 2011 Pioneers in Care Models & Payment Models have allowed for feedback & review of successes and failures on revolutionary changes to the healthcare system

20 Anesthesia Revenue: Metrics
21 Physician Quality Reporting System: PQRS Initially incentive based, voluntary 2015 Penalty for failure to report 2015 Decrease reimbursement for payments in (2017) 2015 payment reduction of -1.5 % Performance Years vs. Payment Years MACRA 2015 will be the new focus PQRS will evolve

22 ACA & Payments

23 Two Midnight Rule IPPS Inpatient Payment System Significant financial impact nationally on Hospital Reimbursements Anesthesia Providers must have awareness & insights to navigate with hospitals

24 Why focus on the IPPS? $539 Million Anesthesia & Surgical Issues may impact length of stay or Hospital Acquired Conditions (HAC)

25 Anesthesia & Payment Reform Alternative Payment Models: MIPS Bundle Payments ACO Payment Initiatives & Pioneer Projects

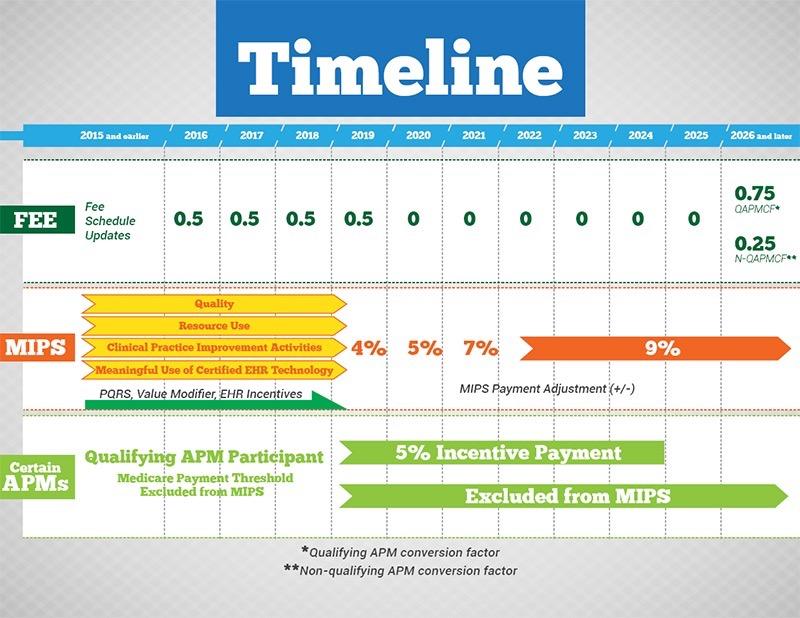
26 New Kid on the Block: MIPS Merit based incentive payment system: MIPS The roll up of PQRS, Meaningful Use, Value Based Payments 2018 Impact Year versus Performance Year: 2 year lag
 Benchmarks Data Mining Quality & Value")
27 Anesthesia Metric Reporting MIPS: Must report metrics to a qualified clinical data registry (QCDR) Benchmarks Data Mining Quality & Value
28 MIPS

29 MACRA 2015

30 Benchmarks & Bundles Benchmarks for undefined episodes of care to be compared using qualified data registries Bundles Payment Model April 2016! More Bundles to follow soon!

31 MACRA December 2015 Medicare Access & CHIP Reauthorization Act of 2015 Repeals SGR permanently & allowed input until November 2015 from Payers & Providers

32 Payer Mix Projection

33 Healthcare Exchanges & Revenue

34 Payer Mix & Revenues Payer mix with exchanges is moving target Exchanges had ACA financial incentives to mitigate financial risk but these end in 2017 Insurers are beginning to limit participation or pull out completely
35 Anesthesia Practice Anesthesia Practices as a Business are undergoing dynamic changes nationally: Anesthesia Management Companies Hospital Practice/Ownership Private Anesthesia Groups Solo Provider Locums

36 Anesthesia Clinician vs. Business The Affordable Care Act has thrust anesthesia clinicians into a myriad changes in both clinical & business aspects of anesthesia practice! Partner?

37 Anesthesia Clinician: Flexible, Adaptable Anesthesia Practice have evolved Anesthesia Providers must increase knowledge of business aspects to remain adaptable & resilient! & Resilient

38 Affordable Care Act: Change ACA was implemented in phases by year since 2011 to allow for adaptation by providers, payers, organizations & patients

39 Anesthesia Business & Practice Model Flexibility & Awareness of the new Paradigm in Anesthesia Care is extremely important Failure could result in Fiscal Insolvency
40 Evolving Changes & Anesthesia New Focus Pay for Performance P4P Volume to Value V2V Models of Care Payment Models Business

41 Anesthesia as Part of the Healthcare Healthcare organizations are evaluating the fiscal assets & liabilities. Care Organizations are determining where are the Revenue Streams, Revenue Losses, Models of Care Business
42 Anesthesia: Costs Big Picture Anesthesia Practices must ensure their business models are sound! Anesthesia accounts for 5-6% of perioperative costs in hospital settings primarily labor costs!
43 AANA Practice Data How are CRNA s practicing: 80% Team Models 37% physician group 32% hospital employee 16% Independent Contractors 3% Ambulatory Employees 36 States that allow Medicare Payment directly to CRNA 38 Blue Cross Payers that directly reimburse CRNA 22 States that mandate direct CRNA payment
44 Where is the Money?...Surgical Services Perioperative Care represents over 65% of most hospital revenue streams Significant attention & focus on Perioperative Care due to the large stake of revenue at risk!
45 Anesthesia Business Labor Costs Supply Costs Stipends Services Provided: stipends, coverage contracts (codes, OB, trauma, non elective surgery)

46 Anesthesia Business Productivity of labor Labor Models team models medical direction with 1:4 ratio Productivity: mining the data using electronic records for billable minutes per care provider versus hours paid to provider

47 Operational Efficiency Goals

48 Anesthesia Customer Service Anesthesia providers should approach both the surgeon & the patient as valued customers in the competitive market for anesthesia service!

49 Anesthesia Labor Costs Anesthesia Labor costs are a major component of the business overhead variables Staffing levels should tightly match case volume trends: Flexibility

50 Outsourcing Billing Internal costs of maintaining a billing office may be economically unfeasible. Outsource of billing to 3 rd party vendor may provide maximal billing and revenue stream bi
51 Outsourced Billing Billing Company fee for services typically are 5-6% of revenues Billing company data interface, accounts accrual & receivable must be setup to determine working cash flow.
52 Billing company should provide data on: Payer mix Metric compliance Service line revenues Bad Debt Ratio Billing Data
53 ICD 10 in use since October 2015 Tremendous increase in diagnostic codes that increase specificity of procedural description ICD 10 errors may revenue stream due to reprocessing of claims ICD 10
54 Anesthesia & Low Hanging Fruit How many anethestizing location are in use or dormant? Obtain increased locations to include NORA: CVL, EP, IR, MRI, GI* Examine the costs of beginning a new site or service line

55 Non OR Anesthesia NORA Once seen as nuisance sites have now become areas of significant revenue generation for anesthesia departments $$$

56 NORA & Revenue Streams Endoscopy reimbursements for colonoscopy screening for Population Health Initiative 100% Reimbursement mandated by ACA for screening coding can be complex.

57 Production Pressure versus Productivity Efficiency, quality, and productivity initiatives that lack care provider inclusion in systemic or infrastructure changes often result in failure
 without producing billable")
58 Productivity in Anesthesia Labor Anesthesia Care Provider Time Off Paid time off is integrated into labor cost & productivity Average CRNA vacation time: 6 weeks (30 days) without producing billable minutes $$$
 Case Cancellations or Delays Preop Clinic")
59 Anesthesia Labor & Productivity Productivity can be impaired by: Long Turn Over Times (TOT) Case Cancellations or Delays Preop Clinic Delays
60 Anesthesia Business Basics Types of Practice: Hospital Employee CRNA only group MD only group MD/CRNA private group (Blended) MD group employee Locum Tenens Independent Contractor AMC- Anesthesia Management Company
61 Anesthesia Business Organizational Type: Hospital (Type) Ambulatory Center Specialty Clinic: Pain, GI, Eye, Plastics What types of services are needed? What is the overhead? Labor, supply, medication, coverage needs, subsidization, stipends?
62 Anesthesia Care & Services Approximately 96% of Anesthesia groups require a stipend to cover cost of required services: airway, obstetrics, trauma, on call services MDA Salary ($$$) vs. CRNA Salary ($) Overall costs to Healthcare Organization must be considered Competition in Anesthesia Services*

63 Anesthesia Revenue What is the payer mix? Exchanges: Medicaid, Private, Medicare, Commercial, Federal or State Exchanges (ACA)
 Bundles Programs")
64 Anesthesia Professional Fees Fee Charged vs. Fee Collected Governmental Payers (Tricare, Medicare ) Bundles Programs Insurance Contracts Eligible Providers

65 ACA The Changing Face of Value Based Reimbursements: Adjusted Payments anesthesia metrics will promote infrastructure changes Reimbursements
 Data tracking will promote individual provider")
66 Value Based Payment & MIPS Value Based Payments will require provider compliance with Best Practices Processes (Evidence Based) Data tracking will promote individual provider accountability.
67 Anesthesia Practice Model Practice Model should fit the organizational needs: Anesthesia Care Team: Supervision or Direction RATIO s in Team Sole Provider: MD, CRNA, Blended. Misalignment of needs to care model can result in revenue loss, patient care deficiencies & safety issues!
68 Anesthesia Payment $$$ BASE UNITS + TIME UNITS (X) CONVERSION FACTOR = PAYMENT $ Remember billed versus paid fees Value Based Payments Metrics: Process and Outcome impact $$$
69 Anesthesia Payment Complexity QZ: (CRNA modifier pays 100%) non-medically directed CRNA services; CRNA is either working without medical direction or criteria was not fully met. QX: (CRNA modifier pays 50%) Medically directed CRNA services; the CRNA is being medically directed by an MD, who has met all required steps for medical direction. QK: (physician modifier { used in conjunction with QX modifier} - pays 50%) Medical direction of two, three or four concurrent procedures QY: (physician modifier { used in conjunction with QX modifier} - pays 50%) MD is medically directing one CRNA AD: (physician modifier { used in conjunction with QX modifier} - pays maximum of four units or zero) Medical supervision by a physician of more than four concurrent procedures Q6: (physician modifier- doesn t affect payment) Service furnished by locum tenens physician

70 Anesthesiologist must bill under these codes: AA Anesthesia services personally performed by MDA 100% allowable reimbursement/case Review of Billing

71 Anesthesia Billing Review Medical Supervision: AD medical supervision by MDA concurrent anesthesia services, more than 50% but less than 100% reimbursement

72 Anesthesia Billing Medical Supervision: does not meet Tefra guidelines, MD is paid 2 or 3 base units. Often avoided due to lost revenue!

73 Anesthesia Billing Review Medical Direction: QY Medical direction of one CRNA one anesthesia service, 100% of allowable reimbursement
74 TEFRA Guidelines 1. Perform a pre-anesthetic examination and evaluation and document it in the medical record. 2. Prescribe the anesthesia plan. 3. Personally participate in the most demanding procedures in the anesthesia plan including induction and emergence, if applicable and document this. 4. Ensure that any procedures in the anesthesia plan are performed by a qualified anesthetist. 5. Monitor the course of anesthesia administration at frequent intervals and document that they were present during some portion of the anesthesia monitoring. 6. Remain physically present and available for immediate diagnosis and treatment of emergencies. 7. Provide indicated-post-anesthesia care and document it.
75 Anesthesia Billing Review Medical Direction: QK Medical direction of 2, 3, 4 CRNA s concurrent procedures, 50% of allowable reimbursement per case. $$$$
76 Anesthesia Billing: Complexities Billing documents: Accuracy of Times Metric Compliance Process or Outcomes Penalty for fallouts lost revenue. Billing Process in place: Outsourced versus Internal Billing Collections Accounts Receivable for Anesthesia
77 Anesthesia Billing Internal Billing Cons: Costs of maintaining billing office & employees Mining the metrics internally difficult to provide provider dashboards Pro: Able to retain all revenues without billing fees typically 5-6% of total fees billed Interface of data from medical records simplified. Unified infrastructure

78 Anesthesia Billing Maximizing revenues is essential in the face of decreased reimbursements Documentation deficiencies result in delayed payments & are often rejected Provider documentation compliance

79 Point of Care Collections Point of care collections collecting money at the time of service or prior to initiation of service Now becoming the standard within the healthcare industry
80 Point of Care Collections Anesthesia Point of Care Collections: Collection of payments may be bundled or itemized Ethical challenge for care providers Patient education, planning and resource assistance essential.
81 Point of Care Collections Paradigm shift in revenue cycles for healthcare. Education & clear communication to patient essential to ensure NO same day cancellation of cases! Same day case cancellations result in significant fiscal losses: $ Ensure sound procedures in place, private POC area, credit care agreements & counselors in place
82 Anesthesia Revenue Anesthesia Revenue: Example: TAH 65yr. Female Medicare Length of case 1.5hrs 6 Base units + 6 Time units = 12 Units X $ $ per TAH How many cases per day? 4 x $
83 Anesthesia Business & Costs Time not Billing is lost revenue Turn over Time (TOT) Lunch, Breaks Insufficient case volumes Procedures not billed for are lost revenue Invasive lines Pain Interventions Consultations: Airway, Preop, Postoperative

84 Anesthesia Metrics: Data Driven Use of Anesthesia Metrics: Process & Outcome Based Quality of Anesthesia Care increases with use of Best Practices Evidence Based Anesthesia Care

85 Anesthesia Evidence in Practice Use of Evidence Based Care Practices Metrics Tracking Anesthesia Provider Education Infrastructure Support**
86 Anesthesia Practice: Metrics Infrastructure of metric compliance: Does the care environment support compliance? Anesthesia Provider Dashboards? Anesthesia equipment in place? Medications accessible to comply? Anesthesia Provider awareness of metrics?
87 Anesthesia Practice & Business Value NOT Volume MACRA 2015 MIPS Alternative Payment Model APM & Bonuses
88 Anesthesia Metrics & Care Setting Anesthesia Practices choose metrics based on: Type of care frequently delivered Setting of Care Acuity of Care: Preventative, Routine, Emergent Metrics change by year and should be reviewed & revised to meet care setting
89 Anesthesia Business & Practice Volume (of cases, services provided) is a MAJOR driver of a solvent practice! Value is the NEW METRIC Value added ( CRNA cost efficiency) increases job security key consideration in anesthesia provider competition MDA, CRNA, AA
90 Anesthesia Providers: The Evidence Cochrane Database an esteemed Internationally recognized database with no political, proprietary, or discipline bias! 2014 Study results: No superiority of care noted differentiating one anesthesia provider from another (MDA vs. CRNA) 6000 Literature articles total reviewed Extensive analysis

91 Cochrane Results: CRNA Care provided by CRNA s represents a cost effective, safe access to quality anesthesia care recommend CRNA s practice to the fullest scope of practice!
 Anesthesia Stipend & Contractual")
92 Anesthesia Business & Practice Anesthesia Lean Process Improvements Anesthesia Consultants Anesthesia Management Companies (AMC) Anesthesia Stipend & Contractual Analysis

93 Anesthesia Practice, Business, Lean Consultants, auditors, analysts for process improvement can provide valuable insight for efficiency but engagement, sustainable change are required to ensure fiscal solvency!

94 Anesthesia & Lean Processes Lean processes are patient centered & should ensure quality & safety are maintained or improved Lean originated with Toyota yet process improvement knowledge applicable
95 Anesthesia & Going Lean Transforms organizations using 6 main components Attitude of continuous process improvement Value creation* Unity of Purpose Respect for frontline workers Visual tracking Flexible regimentation

96 The Business Practice Model Anesthesia Providers must increase knowledge of the financial impact of practice choices, PQRS compliance, highest quality documentation, labor utilization & distribution

97 Lean & Value Stream Map Map out the entire care process from Preoperative Visit to Discharge examine areas of inefficiency, redundancy, repetition, replication. Use planned implementation science to impact sustainable change.

98 Anesthesia Providers: Value Added Anesthesia Providers must demonstrate their value added benefits to efficient care processes Integration of Services to ensure efficiencies between disciplines for the entire continuum of care

99 Anesthesia a Key Team Member Anesthesia team members a problem solvers, collaborators and expert clinicians Patient centered processes, reduction of silos, building bridges across disciplines

100 Clinical expertise alone can not solely guide the practice of anesthesia. Integration of sound interdisciplinary team processes & commitment for process improvement as a lifestyle Summary
101 Questions
4/30/2015. Our Agenda Today. Nurse Anesthesia Reimbursement: Medicare-eligible Population
 Nurse Anesthesia Reimbursement: Trends and Issues for CRNAs Frank Purcell, AANA Senior Director Federal Government Affairs Our Agenda Today What is shaping health policy? What is shaping health politics?
Nurse Anesthesia Reimbursement: Trends and Issues for CRNAs Frank Purcell, AANA Senior Director Federal Government Affairs Our Agenda Today What is shaping health policy? What is shaping health politics?
MACRA Frequently Asked Questions
 Following the release of the Quality Payment Program Interim Final Rule, the American Medical Association (AMA) conducted numerous informational and training sessions for physicians and medical societies.
Following the release of the Quality Payment Program Interim Final Rule, the American Medical Association (AMA) conducted numerous informational and training sessions for physicians and medical societies.
The Healthcare Roundtable
 The Healthcare Roundtable MACRA Update Jayme R. Matchinski Greensfelder, Hemker & Gale, P.C. April 7, 2017 New Orleans, Louisiana This presentation and outline are limited to a discussion of general principles
The Healthcare Roundtable MACRA Update Jayme R. Matchinski Greensfelder, Hemker & Gale, P.C. April 7, 2017 New Orleans, Louisiana This presentation and outline are limited to a discussion of general principles
Objectives 1. Describe the different employment options for nurse anesthetist 4/2/2012. Heidi Andruski, CRNA MS Sweet Dreams Anesthesia
 Heidi Andruski, CRNA MS Sweet Dreams Anesthesia Lessons continued Get it in writing. Every time. In every situation. Contracts protect both parties involved and let you know what the expectations are.
Heidi Andruski, CRNA MS Sweet Dreams Anesthesia Lessons continued Get it in writing. Every time. In every situation. Contracts protect both parties involved and let you know what the expectations are.
VALUE BASED ORTHOPEDIC CARE
 VALUE BASED ORTHOPEDIC CARE Becker's 14th Annual Spine, Orthopedic and Pain Management- Driven ASC Conference + The Future of Spine June 9-11, 2016 Swissotel, Chicago, IL LES JEBSON Administrator, Adjunct
VALUE BASED ORTHOPEDIC CARE Becker's 14th Annual Spine, Orthopedic and Pain Management- Driven ASC Conference + The Future of Spine June 9-11, 2016 Swissotel, Chicago, IL LES JEBSON Administrator, Adjunct
PAYMENT POLICY. Anesthesia
 IMPORTANT REMINDER This policy is current at the time of publication. Centene Corporation retains the right to change or amend this policy at any time. While this policy provides guidance regarding reimbursement,
IMPORTANT REMINDER This policy is current at the time of publication. Centene Corporation retains the right to change or amend this policy at any time. While this policy provides guidance regarding reimbursement,
5/13/2011. Background. Anesthesia Financials: An Unbalanced Equation. Understanding Anesthesia Financial Drivers
 Understanding Anesthesia Financial Drivers Becker s Hospital Review Annual Meeting, May 2011 Hugh Morgan, CMPE Director, Quality Assurance Background 17+ years healthcare management experience Military,
Understanding Anesthesia Financial Drivers Becker s Hospital Review Annual Meeting, May 2011 Hugh Morgan, CMPE Director, Quality Assurance Background 17+ years healthcare management experience Military,
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
MACRA Implementation: A Review of the Quality Payment Program
 MACRA Implementation: A Review of the Quality Payment Program Neal Logue, Kirk Sadur Centers for Medicare and Medicaid Services, Region IX, September 15, 2017 Disclaimer This presentation was prepared
MACRA Implementation: A Review of the Quality Payment Program Neal Logue, Kirk Sadur Centers for Medicare and Medicaid Services, Region IX, September 15, 2017 Disclaimer This presentation was prepared
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization. Quality Forum August 19, 2015
 The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
Describe the process for implementing an OP CDI program
 1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
10/20/2016. Working within the Value-Based World
 Working within the Value-Based World MGMA Annual Conference Roundtable Discussion Orthopedics Urology Surgery Monday, October 31, 2016 1 Learning Objectives Summarize key solutions used by other specialty
Working within the Value-Based World MGMA Annual Conference Roundtable Discussion Orthopedics Urology Surgery Monday, October 31, 2016 1 Learning Objectives Summarize key solutions used by other specialty
Here is what we know. Here is what you can do. Here is what we are doing.
 With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
APPLIES TO: x SummaCare, Inc. x Apex Health Solutions PRODUCT LINE(S): (Check all that apply)
: (Check all that apply)") POLICY NAME: ANESTHESIA PAYMENT POLICY POLICY NUMBER: ISSUING DEPT.: Claims EFFECTIVE DATE: 9/25/2017 APPROVED BY: APPLIES TO: x SummaCare, Inc. x Apex Health Solutions PRODUCT LINE(S): (Check all that
POLICY NAME: ANESTHESIA PAYMENT POLICY POLICY NUMBER: ISSUING DEPT.: Claims EFFECTIVE DATE: 9/25/2017 APPROVED BY: APPLIES TO: x SummaCare, Inc. x Apex Health Solutions PRODUCT LINE(S): (Check all that
Division C: Increasing Choice, Access, and Quality in Health Care for Americans TITLE XV: Provisions Relating to Medicare Part A
 Division C: Increasing Choice, Access, and Quality in Health Care for Americans TITLE XV: Provisions Relating to Medicare Part A Sec. 15001. Development of Medicare study for HCPCS versions of MS-DRG codes
Division C: Increasing Choice, Access, and Quality in Health Care for Americans TITLE XV: Provisions Relating to Medicare Part A Sec. 15001. Development of Medicare study for HCPCS versions of MS-DRG codes
Value-Based Reimbursements are Here: Are you Ready?
 Value-Based Reimbursements are Here: Are you Ready? White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO Published by Becker s Hospital Review April 2016 White Paper Value-Based Reimbursements are
Value-Based Reimbursements are Here: Are you Ready? White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO Published by Becker s Hospital Review April 2016 White Paper Value-Based Reimbursements are
The Quality Payment Program Overview Fact Sheet
 Quality Payment Program The Quality Payment Program Overview Background On October 14, 2016, the Department of Health and Human Services (HHS) issued its final rule with comment period implementing the
Quality Payment Program The Quality Payment Program Overview Background On October 14, 2016, the Department of Health and Human Services (HHS) issued its final rule with comment period implementing the
A Systematic Approach to Performance Improvement Under MACRA s Quality Performance Program
 A Systematic Approach to Performance Improvement Under MACRA s Quality Performance Program White Paper ELLIS MAC KNIGHT, MD, MBA Senior Vice President/CMO May 2017 CONTACT For further information about
A Systematic Approach to Performance Improvement Under MACRA s Quality Performance Program White Paper ELLIS MAC KNIGHT, MD, MBA Senior Vice President/CMO May 2017 CONTACT For further information about
MACRA Fall into Place. By Stephanie Cecchini, CPC, CEMC, CHISP, AAPC Fellow, AAPC MACRA Prof
 MACRA Fall into Place By Stephanie Cecchini, CPC, CEMC, CHISP, AAPC Fellow, AAPC MACRA Prof About the Presenter https://www.linkedin.com/in/stephaniececchini 2 Introduction Love it Hate it Don t know a
MACRA Fall into Place By Stephanie Cecchini, CPC, CEMC, CHISP, AAPC Fellow, AAPC MACRA Prof About the Presenter https://www.linkedin.com/in/stephaniececchini 2 Introduction Love it Hate it Don t know a
SVS QUALITY AND PERFORMANCE MEASURES COMMITTEE (QPMC) New Member Orientation
 New Member Orientation") SVS QUALITY AND PERFORMANCE MEASURES COMMITTEE (QPMC) New Member Orientation 2017-2018 SVS QPMC Quality and Performance Measures Committee Policy and Advocacy Council (Chair Sean Roddy) Chair: Brad Johnson,
SVS QUALITY AND PERFORMANCE MEASURES COMMITTEE (QPMC) New Member Orientation 2017-2018 SVS QPMC Quality and Performance Measures Committee Policy and Advocacy Council (Chair Sean Roddy) Chair: Brad Johnson,
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS. Amy Hancock, CEO Presented to: CPERI April 16, 2018
 DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
DRIVING VALUE-BASED POST-ACUTE COLLABORATIVE SOLUTIONS Amy Hancock, CEO Presented to: CPERI April 16, 2018 Cross-Continuum Road-Mapping Post-acute partners are beginning to utilize tools to identify new
MACRA, QPP, MIPS... more alphabet soup anyone?
 A Partner for Lifelong Health Cathy Cordova, MPS, BSN, RN, CPHIMS Director, Clinical Excellence and Value Donna McCarthy, MT (ASCP), MBA Meaningful Use Manager MACRA, QPP, MIPS... more alphabet soup anyone?
A Partner for Lifelong Health Cathy Cordova, MPS, BSN, RN, CPHIMS Director, Clinical Excellence and Value Donna McCarthy, MT (ASCP), MBA Meaningful Use Manager MACRA, QPP, MIPS... more alphabet soup anyone?
MACRA is Coming: Reimbursement for Quality and the Shift to Population-Based Care
 MACRA is Coming: Reimbursement for Quality and the Shift to Population-Based Care AMERICAN NEUROLOGICAL ASSOCIATION October 17, 2017 Marc R. Nuwer, MD PhD Professor and Vice Chair UCLA Lyell K. Jones,
MACRA is Coming: Reimbursement for Quality and the Shift to Population-Based Care AMERICAN NEUROLOGICAL ASSOCIATION October 17, 2017 Marc R. Nuwer, MD PhD Professor and Vice Chair UCLA Lyell K. Jones,
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement. Craig J. Wilson
 Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
MIPS, MACRA, & CJR: Medicare Payment Transformation. Presenter: Thomas Barber, M.D. May 31, 2016
 MIPS, MACRA, & CJR: Medicare Payment Transformation Presenter: Thomas Barber, M.D. May 31, 2016 Michael Porter- Value Based Care Delivery, Annals of Surgery 2008 Principals: Define Value as a Goal Care
MIPS, MACRA, & CJR: Medicare Payment Transformation Presenter: Thomas Barber, M.D. May 31, 2016 Michael Porter- Value Based Care Delivery, Annals of Surgery 2008 Principals: Define Value as a Goal Care
Passage of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): The Doc Fix
: The Doc Fix") April, 2015 Passage of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): The Doc Fix Author: Annemarie Wouters, Senior Advisor The President has signed into law the bipartisan bill H.R. 2,
April, 2015 Passage of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): The Doc Fix Author: Annemarie Wouters, Senior Advisor The President has signed into law the bipartisan bill H.R. 2,
Are physicians ready for macra/qpp?
 Are physicians ready for macra/qpp? Results from a KPMG-AMA Survey kpmg.com ama-assn.org Contents Summary Executive Summary 2 Background and Survey Objectives 5 What is MACRA? 5 AMA and KPMG collaboration
Are physicians ready for macra/qpp? Results from a KPMG-AMA Survey kpmg.com ama-assn.org Contents Summary Executive Summary 2 Background and Survey Objectives 5 What is MACRA? 5 AMA and KPMG collaboration
Value-Based Care Contracting and Legal Issues
 Session 4b Value-Based Care Contracting and Legal Issues Presented by: Janet Walker Farrer General Counsel and Insurance Legal Department Chair Ascension Health Leah Stewart Associate Vice President for
Session 4b Value-Based Care Contracting and Legal Issues Presented by: Janet Walker Farrer General Counsel and Insurance Legal Department Chair Ascension Health Leah Stewart Associate Vice President for
Health System Transformation, CMS Priorities, and the Medicare Access and CHIP Reauthorization Act
 Health System Transformation, CMS Priorities, and the Medicare Access and CHIP Reauthorization Act Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services
Health System Transformation, CMS Priorities, and the Medicare Access and CHIP Reauthorization Act Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services
Reimbursement Policy. Subject: Professional Anesthesia Services. Effective Date: 04/01/16. Committee Approval Obtained: 08/04/15. Section: Anesthesia
 providers.amerigroup.com Subject: Professional Anesthesia Services Effective Date: 04/01/16 Committee Approval Obtained: 08/04/15 Reimbursement Policy Section: Anesthesia ***** The most current version
providers.amerigroup.com Subject: Professional Anesthesia Services Effective Date: 04/01/16 Committee Approval Obtained: 08/04/15 Reimbursement Policy Section: Anesthesia ***** The most current version
Anesthesia Services INDIANA HEALTH COVERAGE PROGRAMS. Copyright 2017 DXC Technology Company. All rights reserved.
 INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Anesthesia Services L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 1 9 P U B L I S H E D : D E C E M B E R 1 2, 2 0 1 7 P O
INDIANA HEALTH COVERAGE PROGRAMS PROVIDER REFERENCE M ODULE Anesthesia Services L I B R A R Y R E F E R E N C E N U M B E R : P R O M O D 0 0 0 1 9 P U B L I S H E D : D E C E M B E R 1 2, 2 0 1 7 P O
Here is what we know. Here is what you can do. Here is what we are doing.
 With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
The Influence of Health Policy on Clinical Practice. Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center
 The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
LOUISIANA MEDICAID PROGRAM ISSUED: 02/01/12 REPLACED: 02/01/94 CHAPTER 5: PROFESSIONAL SERVICES SECTION 5.1: COVERED SERVICES PAGE(S) 11
 11") Anesthesia Services Surgical anesthesia services may be provided by anesthesiologists or certified registered nurse anesthetists (CRNAs). Maternity-related anesthesia services may be provided by anesthesiologists,
Anesthesia Services Surgical anesthesia services may be provided by anesthesiologists or certified registered nurse anesthetists (CRNAs). Maternity-related anesthesia services may be provided by anesthesiologists,
Reimbursement Policy. Subject: Professional Anesthesia Services
 Reimbursement Policy Subject: Professional Anesthesia Services Effective Date: 01/03/17 Committee Approval Obtained: 01/03/17 Section: Anesthesia ***** The most current version of our reimbursement policies
Reimbursement Policy Subject: Professional Anesthesia Services Effective Date: 01/03/17 Committee Approval Obtained: 01/03/17 Section: Anesthesia ***** The most current version of our reimbursement policies
TRIPLE AIM. Update on Governmental and Other Regulations Affecting Anesthesiology
 Randall M. Clark, M.D. Department of Anesthesiology University of Colorado School of Medicine Board of Directors, American Society of Anesthesiologists Chair ASA Section on Professional Standards No financial
Randall M. Clark, M.D. Department of Anesthesiology University of Colorado School of Medicine Board of Directors, American Society of Anesthesiologists Chair ASA Section on Professional Standards No financial
2017/2018. KPN Health, Inc. Quality Payment Program Solutions Guide. KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc.
 KPN Health, Inc.") 2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
Reimbursement Rate Changes for Anesthesiologists, CRNAs and/or AAs Effective for Dates of Service on or After Nov. 1, 2017
 Reimbursement Rate Changes for Anesthesiologists, CRNAs and/or AAs Effective for Dates of Service on or After Nov. 1, 2017 Information posted Oct. 25, 2017 Note: Texas Medicaid managed care organizations
Reimbursement Rate Changes for Anesthesiologists, CRNAs and/or AAs Effective for Dates of Service on or After Nov. 1, 2017 Information posted Oct. 25, 2017 Note: Texas Medicaid managed care organizations
MACRA for Critical Access Hospitals. Tuesday, July 26, 2016 Webinar
 MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
Reimbursement Policy.
 Serving Hoosier Healthwise, Healthy Indiana Plan and Hoosier Care Connect Subject: Professional Anesthesia Services Reimbursement Policy Committee Approval Obtained: Effective Date: 01/03/17 Section: Anesthesia
Serving Hoosier Healthwise, Healthy Indiana Plan and Hoosier Care Connect Subject: Professional Anesthesia Services Reimbursement Policy Committee Approval Obtained: Effective Date: 01/03/17 Section: Anesthesia
Reimbursement Policy. BadgerCare Plus. Subject: Professional Anesthesia Services. Committee Approval Obtained: Effective Date: 05/01/17
 Subject: Professional Anesthesia Services Reimbursement Policy Committee Approval Obtained: Effective Date: 05/01/17 Section: Anesthesia 01/03/17 *****The most current version of our reimbursement policies
Subject: Professional Anesthesia Services Reimbursement Policy Committee Approval Obtained: Effective Date: 05/01/17 Section: Anesthesia 01/03/17 *****The most current version of our reimbursement policies
Quality Payment Program Year 2: 2018 MIPS Participation. An Introductory Guide for CRNAs in 2018
 Quality Payment Program Year 2: 2018 MIPS Participation An Introductory Guide for CRNAs in 2018 Quality Payment Program (QPP) The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) established
Quality Payment Program Year 2: 2018 MIPS Participation An Introductory Guide for CRNAs in 2018 Quality Payment Program (QPP) The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) established
Medicare Physician Payment Reform:
 Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
MACRA Quality Payment Program
 The American College of Surgeons Resources for the New Medicare Physician System Table of Contents Understanding the... 3 Navigating MIPS in 2017... 4 MIPS Reporting: Individuals or Groups... 6 2017: The
The American College of Surgeons Resources for the New Medicare Physician System Table of Contents Understanding the... 3 Navigating MIPS in 2017... 4 MIPS Reporting: Individuals or Groups... 6 2017: The
Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment
 Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment Jeffry Peters, President Surgical Directions, LLC Joseph Bosco, MD Associate Professor;
Ensuring Your Surgical Service Line is Successful in an ACO Value-Based Purchasing and Bundled Payment Environment Jeffry Peters, President Surgical Directions, LLC Joseph Bosco, MD Associate Professor;
From Surviving to Thriving in the QPP World
 From Surviving to Thriving in the QPP World Today s Objectives Brief MACRA Overview Where are we going?: Advanced Alternative Payment Models (APMs) Where are we now? Merit Incentive-Based Payment System
From Surviving to Thriving in the QPP World Today s Objectives Brief MACRA Overview Where are we going?: Advanced Alternative Payment Models (APMs) Where are we now? Merit Incentive-Based Payment System
ORGANIZATIONAL INFORMATION BRIEF SUMMARY OF THE PROBLEM
 F E L L O W P R O J E C T Implementation of a Contractual Relationship for Anesthesia Services in an Acute Care Facility Marcia Taylor, R.N., M.B.A., FACHE, director of surgical service, Rapid City Regional
F E L L O W P R O J E C T Implementation of a Contractual Relationship for Anesthesia Services in an Acute Care Facility Marcia Taylor, R.N., M.B.A., FACHE, director of surgical service, Rapid City Regional
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM. Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017
 ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
MACRA, Implications for Physician Agreements
 MACRA, Implications for Physician Agreements Mark C Herbers, Director, AlixPartners, LLP Chicago, IL The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) creates powerful incentives for all
MACRA, Implications for Physician Agreements Mark C Herbers, Director, AlixPartners, LLP Chicago, IL The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) creates powerful incentives for all
Overview of Quality Payment Program
 Overview of Quality Payment Program Policies for 2017 & 2018 Performance Years The Medicare program has transformed how it reimburses psychiatrists and other clinicians for providing services, under the
Overview of Quality Payment Program Policies for 2017 & 2018 Performance Years The Medicare program has transformed how it reimburses psychiatrists and other clinicians for providing services, under the
Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care
 Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care Nina Marshall, MSW Senior Director, Policy and Practice Improvement NinaM@TheNationalCouncil.org Bill Hudock Senior Public
Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care Nina Marshall, MSW Senior Director, Policy and Practice Improvement NinaM@TheNationalCouncil.org Bill Hudock Senior Public
Frequently Asked Questions
 Frequently Asked Questions What is the Compass Practice Transformation Network (Compass PTN)? The Compass Practice Transformation Network (Compass PTN) was founded by the Iowa Healthcare Collaborative
Frequently Asked Questions What is the Compass Practice Transformation Network (Compass PTN)? The Compass Practice Transformation Network (Compass PTN) was founded by the Iowa Healthcare Collaborative
WELCOME. Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association
 WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
Population Health Management. Ashley Rhude RHIA, CHTS-IM HIT Practice Advisor
 Population Health Management Ashley Rhude RHIA, CHTS-IM HIT Practice Advisor Mission of OFMQ OFMQ is a not-for-profit, consulting company dedicated to advancing healthcare quality. Since 1972, we ve been
Population Health Management Ashley Rhude RHIA, CHTS-IM HIT Practice Advisor Mission of OFMQ OFMQ is a not-for-profit, consulting company dedicated to advancing healthcare quality. Since 1972, we ve been
Managed care consulting services
 Managed care consulting services WeiserMazars Health Care Consulting Services WeiserMazars LLP is an independent member firm of Mazars Group. WeiserMazars Health Care Group Managed Care consulting services
Managed care consulting services WeiserMazars Health Care Consulting Services WeiserMazars LLP is an independent member firm of Mazars Group. WeiserMazars Health Care Group Managed Care consulting services
MACRA MACRA MACRA 9/30/2015. From the Congress: A New Medicare Payment System. The Future of Medicare: A Move Toward Value Driven Healthcare W20.
 W20.8XXA The Future of Medicare: A Move Toward Value Driven Healthcare Emily L. Graham, RHIA, CCS-P VP, Regulatory Affairs, Hart Health Strategies Consultant, Coalition of State Rheumatology Organizations
W20.8XXA The Future of Medicare: A Move Toward Value Driven Healthcare Emily L. Graham, RHIA, CCS-P VP, Regulatory Affairs, Hart Health Strategies Consultant, Coalition of State Rheumatology Organizations
Alternative Payment Models and Health IT
 Alternative Payment Models and Health IT Health DataPalooza Preconference May 8, 2016 Kelly Cronin, MS, MPH, Director, Office of Care Transformation, ONC/HHS HHS Goals for Medicare Payment Reform In January
Alternative Payment Models and Health IT Health DataPalooza Preconference May 8, 2016 Kelly Cronin, MS, MPH, Director, Office of Care Transformation, ONC/HHS HHS Goals for Medicare Payment Reform In January
MANAGED CARE CONSULTING SERVICES
 CONSULTING SERVICES WeiserMazars Health Care Consulting Services THE NEW JERSEY HOSPITAL ASSOCIATION April 30,2013 WeiserMazars LLP is an independent member firm of Mazars Group. WEISERMAZARS HEALTH CARE
CONSULTING SERVICES WeiserMazars Health Care Consulting Services THE NEW JERSEY HOSPITAL ASSOCIATION April 30,2013 WeiserMazars LLP is an independent member firm of Mazars Group. WEISERMAZARS HEALTH CARE
ENHANCE HEALTHCARE CONSULTING E. COUNTRY CLUB DRIVE, SUITE 2810 AVENTURA, FL
 In today s healthcare environment, anesthesia groups have many issues to deal with, including ACO s, pressure on reimbursement, quality tracking, the surgical home, and pressure on hospital subsidies.
In today s healthcare environment, anesthesia groups have many issues to deal with, including ACO s, pressure on reimbursement, quality tracking, the surgical home, and pressure on hospital subsidies.
Anesthesia Services Policy
 Anesthesia Services Policy Policy Number Annual Approval Date 3/14/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare Medicare
Anesthesia Services Policy Policy Number Annual Approval Date 3/14/2018 Approved By Oversight Committee IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare Medicare
Highmark Reimbursement Policy Bulletin
 Highmark Reimbursement Policy Bulletin Bulletin Number: Subject: RP-033 Anesthesia Services Effective Date: March 12, 2018 End Date: Issue Date: June 11, 2018 Source: Reimbursement Policy Applicable Commercial
Highmark Reimbursement Policy Bulletin Bulletin Number: Subject: RP-033 Anesthesia Services Effective Date: March 12, 2018 End Date: Issue Date: June 11, 2018 Source: Reimbursement Policy Applicable Commercial
Is HIT a Real Tool for The Success of a Value-Based Program?
 Is HIT a Real Tool for The Success of a Value-Based Program? Sally Montes, MPH, RHIA, CCHP President, SM & Associates, Inc. smontes@sm-asociados.com (787) 306-1149 President, PR HFMA Chapter INTRODUCTION
Is HIT a Real Tool for The Success of a Value-Based Program? Sally Montes, MPH, RHIA, CCHP President, SM & Associates, Inc. smontes@sm-asociados.com (787) 306-1149 President, PR HFMA Chapter INTRODUCTION
Physician Compensation Reform: How You Will Get Paid. Alexandra A. Hall Gregory W. Moore Serene K. Zeni
 Physician Compensation Reform: How You Will Get Paid Alexandra A. Hall Gregory W. Moore Serene K. Zeni TOPICS TO COVER Sustainable Growth Rate and The Fix ICD-10 Pay-For Performance Accountable Care Organizations
Physician Compensation Reform: How You Will Get Paid Alexandra A. Hall Gregory W. Moore Serene K. Zeni TOPICS TO COVER Sustainable Growth Rate and The Fix ICD-10 Pay-For Performance Accountable Care Organizations
MACRA and the Quality Payment Program. Frequently Asked Questions Edition
 MACRA and the Quality Payment Program Frequently Asked Questions 2018 Edition What is MACRA?...3 What is the Quality Payment Program?...3 How do payments work under the QPP?...3 What is at risk under
MACRA and the Quality Payment Program Frequently Asked Questions 2018 Edition What is MACRA?...3 What is the Quality Payment Program?...3 How do payments work under the QPP?...3 What is at risk under
NACOR BASIC with Benchmarking NACOR STANDARD QUALITY REPORTING. Updated June 22, 2018
 2018 NACOR USER GUIDE A step-by-step guide to submitting data to the Anesthesia Quality Institute s National Anesthesia Clinical Outcomes Registry (NACOR).. NACOR BASIC with Benchmarking NACOR STANDARD
2018 NACOR USER GUIDE A step-by-step guide to submitting data to the Anesthesia Quality Institute s National Anesthesia Clinical Outcomes Registry (NACOR).. NACOR BASIC with Benchmarking NACOR STANDARD
Why Focus on Perioperative Services?
 1 Why Focus on Perioperative Services? 80% 60% 40% 20% 0% Perioperative Services are key to a hospital/system's success 68% % better performers revenue from perioperative services Perioperative Services
1 Why Focus on Perioperative Services? 80% 60% 40% 20% 0% Perioperative Services are key to a hospital/system's success 68% % better performers revenue from perioperative services Perioperative Services
IMPORTANT NOTICE REGARDING NEW ANESTHESIA BILLING GUIDELINES AND REIMBURSEMENT PROCEDURES November 2008
 IMPORTANT NOTICE REGARDING NEW ANESTHESIA BILLING GUIDELINES AND REIMBURSEMENT PROCEDURES November 2008 This notice will serve as an update to the August 2007Anesthesia Billing Guidelines and Reimbursement
IMPORTANT NOTICE REGARDING NEW ANESTHESIA BILLING GUIDELINES AND REIMBURSEMENT PROCEDURES November 2008 This notice will serve as an update to the August 2007Anesthesia Billing Guidelines and Reimbursement
Spring User Conference May Sandestin, FL Detailed Agenda
 Day One: Monday May 16, 2016 3 6 p.m. Conference Registration 5 6 p.m. Customer Welcome and Orientation for First-time Conference Attendees 6 8 p.m. Welcome Reception Day Two: Tuesday May 17, 2016 7 a.m.
Day One: Monday May 16, 2016 3 6 p.m. Conference Registration 5 6 p.m. Customer Welcome and Orientation for First-time Conference Attendees 6 8 p.m. Welcome Reception Day Two: Tuesday May 17, 2016 7 a.m.
BENCHMARKING FOR ORGANIZATIONAL EXCELLENCE IN ADDICTION TREATMENT
 BENCHMARKING FOR ORGANIZATIONAL EXCELLENCE IN ADDICTION TREATMENT Operational Benchmarks 1. Initial Access Initial Access Average number of calendar days between date of first contact and date of initial
BENCHMARKING FOR ORGANIZATIONAL EXCELLENCE IN ADDICTION TREATMENT Operational Benchmarks 1. Initial Access Initial Access Average number of calendar days between date of first contact and date of initial
September 6, Thank the agency for its role in permanently reversing harmful cuts.
 September 6, 2016 Andrew M. Slavitt Acting Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attn: CMS-1654-P P.O. Box 8013 7500 Security Boulevard Baltimore,
September 6, 2016 Andrew M. Slavitt Acting Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attn: CMS-1654-P P.O. Box 8013 7500 Security Boulevard Baltimore,
Centers for Medicare & Medicaid Services: Innovation Center New Direction
 Centers for Medicare & Medicaid Services: Innovation Center New Direction I. Background One of the most important goals at CMS is fostering an affordable, accessible healthcare system that puts patients
Centers for Medicare & Medicaid Services: Innovation Center New Direction I. Background One of the most important goals at CMS is fostering an affordable, accessible healthcare system that puts patients
Quality Improvement in the Advent of Population Health Management WHITE PAPER
 Quality Improvement in the Advent of Population Health Management WHITE PAPER For healthcare organizations whose reimbursement and revenue are tied to patient outcomes, achieving performance on quality
Quality Improvement in the Advent of Population Health Management WHITE PAPER For healthcare organizations whose reimbursement and revenue are tied to patient outcomes, achieving performance on quality
How to Align Quality Reporting Across PQRS, MU, and VBPM
 Health Care IT Advisor How to Align Quality Reporting Across PQRS, MU, and VBPM Anantachai (Tony) Panjamapirom Senior Consultant, Health Care IT Advisor Debe Gash CIO, St. Luke s Health System March 10,
Health Care IT Advisor How to Align Quality Reporting Across PQRS, MU, and VBPM Anantachai (Tony) Panjamapirom Senior Consultant, Health Care IT Advisor Debe Gash CIO, St. Luke s Health System March 10,
Midmark White Paper The Connected Point of Care Ecosystem: A Solid Foundation for Value-Based Care
 Midmark White Paper The Connected Point of Care Ecosystem: A Solid Foundation for Value-Based Care Introduction This white paper examines how new technologies are creating a fully connected point of care
Midmark White Paper The Connected Point of Care Ecosystem: A Solid Foundation for Value-Based Care Introduction This white paper examines how new technologies are creating a fully connected point of care
Kate Goodrich, MD MHS. Director, Center for Clinical Standards & Quality. Center for Medicare and Medicaid Services (CMS) May 6, 2016
 May 6, 2016") Kate Goodrich, MD MHS Director, Center for Clinical Standards & Quality Center for Medicare and Medicaid Services (CMS) May 6, 2016 THE MEDICARE ACCESS & CHIP REAUTHORIZATION ACT OF 2015 Quality Payment
Kate Goodrich, MD MHS Director, Center for Clinical Standards & Quality Center for Medicare and Medicaid Services (CMS) May 6, 2016 THE MEDICARE ACCESS & CHIP REAUTHORIZATION ACT OF 2015 Quality Payment
PQRS and Alignment Opportunity: Concept to Operationalization March 1, 2016
 PQRS and Alignment Opportunity: Concept to Operationalization March 1, 2016 Debe Gash/ VP & Chief Information Officer/ Saint Luke s Health System Anantachai (Tony) Panjamapirom/ Senior Consultant/ The
PQRS and Alignment Opportunity: Concept to Operationalization March 1, 2016 Debe Gash/ VP & Chief Information Officer/ Saint Luke s Health System Anantachai (Tony) Panjamapirom/ Senior Consultant/ The
THE BUSINESS OF PEDIATRICS: BETTER CARE = BETTER PAYMENT. 19 th CNHN Pediatric Practice Management Seminar Thursday, December 6, 2016
 THE BUSINESS OF PEDIATRICS: BETTER CARE = BETTER PAYMENT 19 th CNHN Pediatric Practice Management Seminar Thursday, December 6, 2016 SMALLER VS BIGGER? WHAT PRACTICE SIZE IS JUST RIGHT? Mark Weissman,
THE BUSINESS OF PEDIATRICS: BETTER CARE = BETTER PAYMENT 19 th CNHN Pediatric Practice Management Seminar Thursday, December 6, 2016 SMALLER VS BIGGER? WHAT PRACTICE SIZE IS JUST RIGHT? Mark Weissman,
Introduction. Staffing to demand increases bottom line revenue for the facility through increased volume and throughput and elimination of waste.
 Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
Learning Objectives Define a process to determine the appropriate number of rooms to run per day based on historical inpatient and outpatient case volume. Organize a team consisting of surgeons, anesthesiologists,
Health Policy Update 2017: The Evolution of Physician Payment. Declarations. Agenda 10/11/2017. Revised
 Revised 6-2000 1 Health Policy Update 2017: The Evolution of Physician Payment William P. Moran MD MS Professor and Director, General Internal Medicine and Geriatrics Medical University of South Carolina
Revised 6-2000 1 Health Policy Update 2017: The Evolution of Physician Payment William P. Moran MD MS Professor and Director, General Internal Medicine and Geriatrics Medical University of South Carolina
QUALITY PAYMENT PROGRAM
 NOTICE OF PROPOSED RULE MAKING Medicare Access and CHIP Reauthorization Act of 2015 QUALITY PAYMENT PROGRAM Executive Summary On April 27, 2016, the Department of Health and Human Services issued a Notice
NOTICE OF PROPOSED RULE MAKING Medicare Access and CHIP Reauthorization Act of 2015 QUALITY PAYMENT PROGRAM Executive Summary On April 27, 2016, the Department of Health and Human Services issued a Notice
MACRA, MIPS, and APMs What to Expect from all these Acronyms?!
 MACRA, MIPS, and APMs What to Expect from all these Acronyms?! ACP Pennsylvania Council Meeting Saturday, December 5, 2015 Shari M. Erickson, MPH Vice President, Governmental Affairs & Medical Practice
MACRA, MIPS, and APMs What to Expect from all these Acronyms?! ACP Pennsylvania Council Meeting Saturday, December 5, 2015 Shari M. Erickson, MPH Vice President, Governmental Affairs & Medical Practice
Survey of Nurse Employers in California 2014
 Survey of Nurse Employers in California 2014 Conducted by UCSF Philip R. Lee Institute for Health Policy Studies, California Institute for Nursing & Health Care, and the Hospital Association of Southern
Survey of Nurse Employers in California 2014 Conducted by UCSF Philip R. Lee Institute for Health Policy Studies, California Institute for Nursing & Health Care, and the Hospital Association of Southern
AMN Healthcare Investor Presentation
 AMN Healthcare Investor Presentation November 2016 The Innovator in Healthcare Workforce Solutions and Staffing Services Forward-Looking Statements This investor presentation contains forwardlooking statements
AMN Healthcare Investor Presentation November 2016 The Innovator in Healthcare Workforce Solutions and Staffing Services Forward-Looking Statements This investor presentation contains forwardlooking statements
April 26, Ms. Seema Verma, MPH Administrator Centers for Medicare & Medicaid Services. Dear Secretary Price and Administrator Verma:
 April 26, 2017 Thomas E. Price, MD Secretary Department of Health and Human Services Hubert H. Humphrey Building 200 Independence Avenue, SW Washington, DC 20201 Ms. Seema Verma, MPH Administrator Centers
April 26, 2017 Thomas E. Price, MD Secretary Department of Health and Human Services Hubert H. Humphrey Building 200 Independence Avenue, SW Washington, DC 20201 Ms. Seema Verma, MPH Administrator Centers
Highlights of the 2018 Medicare Physician Fee Schedule (MPFS) Final Rule
 Final Rule") Highlights of the 2018 Medicare Physician Fee Schedule (MPFS) Final Rule Physician Payment Update & Misvalued Codes Target The update to payments under the PFS in 2018 will be +0.31 percent. This reflects
Highlights of the 2018 Medicare Physician Fee Schedule (MPFS) Final Rule Physician Payment Update & Misvalued Codes Target The update to payments under the PFS in 2018 will be +0.31 percent. This reflects
CRNAs Value for Your Team and Bottom Line
 CRNAs Value for Your Team and Bottom Line Sarah Chacko, JD Assistant Director of State Government Affairs and Legal Lynn Reede, CRNA, DNP, MBA Senior Director, Professional Practice Becker s 13th Annual
CRNAs Value for Your Team and Bottom Line Sarah Chacko, JD Assistant Director of State Government Affairs and Legal Lynn Reede, CRNA, DNP, MBA Senior Director, Professional Practice Becker s 13th Annual
IMPORTANT NOTICE REGARDING NEW ANESTHESIA BILLING GUIDELINES AND REIMBURSEMENT PROCEDURES AUGUST 2007
 IMPORTANT NOTICE REGARDING NEW ANESTHESIA BILLING GUIDELINES AND REIMBURSEMENT PROCEDURES AUGUST 2007 This notice will serve as an update to the August 2005 Anesthesia Billing Guidelines and Reimbursement
IMPORTANT NOTICE REGARDING NEW ANESTHESIA BILLING GUIDELINES AND REIMBURSEMENT PROCEDURES AUGUST 2007 This notice will serve as an update to the August 2005 Anesthesia Billing Guidelines and Reimbursement
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
HFMA - Northern California. Otani Consulting Group Inc, Hawthorne Blvd, #216, Torrance, CA 90503
 1 HFMA - Northern California 2 Module 2: Departments that Impact Accounts Receivables Clinical and Technical Departments that impact Account Receivables Financial Clearance (FC) Centralized Units Case
1 HFMA - Northern California 2 Module 2: Departments that Impact Accounts Receivables Clinical and Technical Departments that impact Account Receivables Financial Clearance (FC) Centralized Units Case
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program
 March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
MACRA Open Call December 5 th, 2016
 MACRA Open Call December 5 th, 2016 Leila Volinsky, MHA, MSN, RN Quality Reporting Program Administrator This material was prepared by the New England QIN-QIO, the Medicare Quality Innovation Network-Quality
MACRA Open Call December 5 th, 2016 Leila Volinsky, MHA, MSN, RN Quality Reporting Program Administrator This material was prepared by the New England QIN-QIO, the Medicare Quality Innovation Network-Quality
Statement for the Record. American College of Physicians. Hearing before the House Energy & Commerce Subcommittee on Health
 Statement for the Record American College of Physicians Hearing before the House Energy & Commerce Subcommittee on Health A Permanent Solution to the SGR: The Time Is Now January 21-22, 2015 The American
Statement for the Record American College of Physicians Hearing before the House Energy & Commerce Subcommittee on Health A Permanent Solution to the SGR: The Time Is Now January 21-22, 2015 The American
Note: This is an outcome measure and will be calculated solely using registry data.
 Quality ID #304: Cataracts: Patient Satisfaction within 90 Days Following Cataract Surgery National Quality Strategy Domain: Person and Caregiver-Centered Experience and Outcomes 2018 OPTIONS FOR INDIVIDUAL
Quality ID #304: Cataracts: Patient Satisfaction within 90 Days Following Cataract Surgery National Quality Strategy Domain: Person and Caregiver-Centered Experience and Outcomes 2018 OPTIONS FOR INDIVIDUAL
JOHNS HOPKINS HEALTHCARE Physician Guidelines
 Page 1 of 7 ACTION New Procedure Amending Procedure Number: Superseding Procedure Number: Repealing Procedure Number: REFERENCES: AMPT Committee ASA Guidelines CMS Guidelines I. GENERAL ANESTHESIA PROCEDURE:
Page 1 of 7 ACTION New Procedure Amending Procedure Number: Superseding Procedure Number: Repealing Procedure Number: REFERENCES: AMPT Committee ASA Guidelines CMS Guidelines I. GENERAL ANESTHESIA PROCEDURE:
Improving Quality of Care in Anesthesiology Session # 182, March 7, 2018
 Improving Quality of Care in Anesthesiology Session # 182, March 7, 2018 Nilesh Chandra Partner, PA Consulting Group Paul Pomerantz CEO, American Society of Anesthesiologists 1 Conflict of Interest Nilesh
Improving Quality of Care in Anesthesiology Session # 182, March 7, 2018 Nilesh Chandra Partner, PA Consulting Group Paul Pomerantz CEO, American Society of Anesthesiologists 1 Conflict of Interest Nilesh
Practice Transformation Networks
 Practice Transformation Networks The project described was supported by Funding Opportunity Number CMS-1L1-15-003 from the U. S. Department of Health & Human Services, Centers for Medicare and Medicaid
Practice Transformation Networks The project described was supported by Funding Opportunity Number CMS-1L1-15-003 from the U. S. Department of Health & Human Services, Centers for Medicare and Medicaid
QPP in the Real Word: How Your Peers Are Achieving Success. Monday, September 25, :00 4:30 PM ET
 QPP in the Real Word: How Your Peers Are Achieving Success Monday, September 25, 2017 3:00 4:30 PM ET Meet Your Speakers Leila Volinsky MHA, MSN, RN Senior Program Administrator-Quality Payment Program
QPP in the Real Word: How Your Peers Are Achieving Success Monday, September 25, 2017 3:00 4:30 PM ET Meet Your Speakers Leila Volinsky MHA, MSN, RN Senior Program Administrator-Quality Payment Program
STATEMENT ON THE ANESTHESIA CARE TEAM
 Committee of Origin: Anesthesia Care Team (Approved by the ASA House of Delegates on October 18, 2006, and last amended on October 21, 2009) Anesthesiology is the practice of medicine including, but not
Committee of Origin: Anesthesia Care Team (Approved by the ASA House of Delegates on October 18, 2006, and last amended on October 21, 2009) Anesthesiology is the practice of medicine including, but not
Enhancing Efficiency and Communication in Perioperative Services Through Technology
 Enhancing Efficiency and Communication in Perioperative Services Through Technology Linda Yoder, RN, BSN, MBA, Clinical Director, Perioperative Services, GI Lab, Cross Creek Ambulatory Center Every driver
Enhancing Efficiency and Communication in Perioperative Services Through Technology Linda Yoder, RN, BSN, MBA, Clinical Director, Perioperative Services, GI Lab, Cross Creek Ambulatory Center Every driver
A McKesson Perspective: ICD-10-CM/PCS
 A McKesson Perspective: ICD-10-CM/PCS Its Far-Reaching Effect on the Healthcare Industry Executive Overview While many healthcare organizations are focused on qualifying for American Recovery & Reinvestment
A McKesson Perspective: ICD-10-CM/PCS Its Far-Reaching Effect on the Healthcare Industry Executive Overview While many healthcare organizations are focused on qualifying for American Recovery & Reinvestment