Overall Page 1 of 215
|
|
|
- Reynard Banks
- 6 years ago
- Views:
Transcription
1 East and North Hertfordshire NHS Trust Trust Board Part I Trust Board (Part I) Lister Education Centre, Lister Hospital, Coreys Mill Lane, Stevenage, SG1 4AB 30 September :00 Overall Page 1 of 215
2 AGENDA 1 Chairman's Opening Remarks 2 Declaration of Interests 3 Questions from the Public Members of the public are reminded that Trust Board meetings are meetings held in public, not public meetings. However, the Board provides members of the public at the start of each meeting the opportunity to ask questions and/or make statements that relate to the work of the Trust. Members of the public are urged to give notice of their questions at least 48 hours before the beginning of the meeting in order that a full answer can be provided; if notice is not given, an answer will be provided whenever possible but the relevant information may not be available at the meeting. If such information is not so available, the Trust will provide a written answer to the question as soon as is practicable after the meeting. The Secretary can be contacted by (jude.archer@nhs.net), by telephone ( ), by fax ( ) or by post to: Company Secretary, Lister Hospital, Coreys Mill Lane, Stevenage, Herts, SG1 4AB. Each person will be allowed to address the meeting for no more than three minutes and will be allowed to ask only one question or make one statement. However, at the discretion of the Chair of the meeting, and if time permits, a second or subsequent question may be allowed. Generally, questions and/or statements from members of the public will not be allowed during the course of the meeting. Exceptionally, however, where an issue is of particular interest to the community, the Chairman may allow members of the public to ask questions or make comments immediately before the Board begins its deliberations on that issue, provided the Chairman s consent thereto is obtained before the meeting. 4 Apologies for Absence: DC 5 Minutes of Previous Meeting For approval 5 0 Draft July minutes pt 1.docx 5 6 Matters Arising and Actions Log 6 Pt I Actions Log to Sept 15.pdf 13 Overall Page 2 of 215

3 7 Annual Cycle Owner : Company Secretary For information 7. Board Annual Cycle pdf 15 8 Chief Executive's Report Owner : Chief Executive To Follow For consideration Chief Executive's Report and appendices.pdf 17 Floodlight Scorecare 9 Strategic Issues Ward and Emergency Department Staffing Risks Owner : Director Nursing / Acting Director of Operations For discussion 9.01 Ward Staffing and ED risk Board Sept 2015.pdf Finance and Performance 10.1 Finance and Performance Committee monthly report Owner : Chair of FPC For decision FPC Report to Board.pdf 56 14: Finance report Owner : Director of Finance Finance Report Month 5.pdf Performance Report Owner : Director of Operations Performance Report Month 5.pdf Owner : Director of Workforce and OD Workforce Report Month 5.pdf Risk and Quality Overall Page 3 of 215
4 11.1 Risk and Quality Committee report Owner : Chair of RAQC RAQC Report to Board on 30 Sept.pdf 95 15: Board Assurance Framework Owner : Company Secretary To follow 11.2 BAF framework Sept review 15.doc Charity Trust The Board will reconvene as the Charity Trustee for the following item Charity Trust Committee Report Owner : Chairman of the Charity Trust Committee 13.1 Charity Trust Committee Report.pdf : Charity Trust Committee Terms of Reference and Annual Report Owner : Chairman of the Charity Trust Committee CTC Annual Review and TOR.pdf Data pack Owner : All Directors For information Data Pack.pdf 141 HS_Metrics_AUGUST_15_v2.pdf Part II 16:00-18:00 The Trust Board resolves that under Standing Order 3.17(i) representatives of the press and other members of the public be excluded from the remainder of this meeting, having regard to the confidential nature of the matters to be transacted, publicly which would be prejudicial to the public interest Commercial-in-confidence 14.2 Governance Matters 14.3 Personnel Matters 15 Date of next meeting: 2pm - 4pm, Wednesday 28 October 2015 Room New Queen Elizabeth II Hospital, Howlands, Welwyn Garden City, AL7 4HQ Overall Page 4 of 215
5 Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 30 July 2015 at 2pm at the New Queen Elizabeth II Hospital, Welwyn Garden City. Present: Mr Ian Morfett Chairman Mrs Alison Bexfield Vice-Chairman Mr Nick Carver Chief Executive Mrs Dyan Crowther Non-Executive Director Mr John Gilham Non-Executive Director Ms Jane McCue Medical Director Mr Julian Nicholls Non-Executive Director Mr Bob Niven Non-Executive Director Mr Tony Ollis Director of Finance Mr John Watson Director of Operations From the Trust: Ms Jude Archer Ms Sarah Brierley Ms Carolyn Fowler Ms Ellen Heaney Mr Tom Simons Company Secretary Director of Business Development and Partnership Deputy Director of Nursing Deputy Company Secretary Director of Workforce and Organisational Development In attendance: Ms Sharon Webb Quality Improvement Consultant (interim) 15/168 CHAIRMAN S OPENING REMARKS ACTION 15/ The Chairman welcomed everyone to the meeting at the new Queen Elizabeth II hospital which Board Members had visited earlier in the day. It was agreed that the new building had great potential and that once the initial concerns were resolved with Community Health Partnership and Accuro it would be an asset to the community. 15/169 DECLARATIONS OF INTEREST 15/ There were no declarations of interest. 15/170 QUESTIONS FROM THE PUBLIC 15/ No questions had been submitted in advance of the meeting and the Chairman confirmed that none of the public present in the meeting had any questions they wished to raise. 15/171 APOLOGIES FOR ABSENCE 15/ Apologies for absence were received from the Deputy Chief Executive who was represented at the meeting by the Director of Business Development and Partnership and from the Director of Nursing who was represented at the meeting by the Deputy Director of Nursing. 15/172 MINUTES OF THE PREVIOUS MEETING 5 0 Draft July minutes pt 1.docx The minutes of the meeting held on 24 June 2015 were approved as an accurate record of the meeting subject to minor typographical errors being corrected. 1 Page 1 of 8 Overall Page 5 of 215
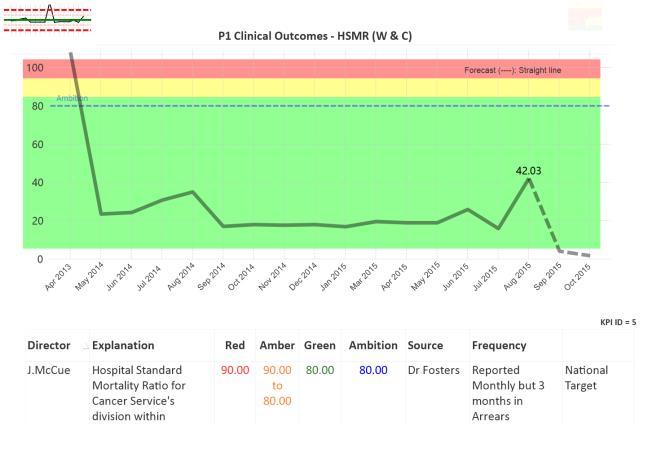
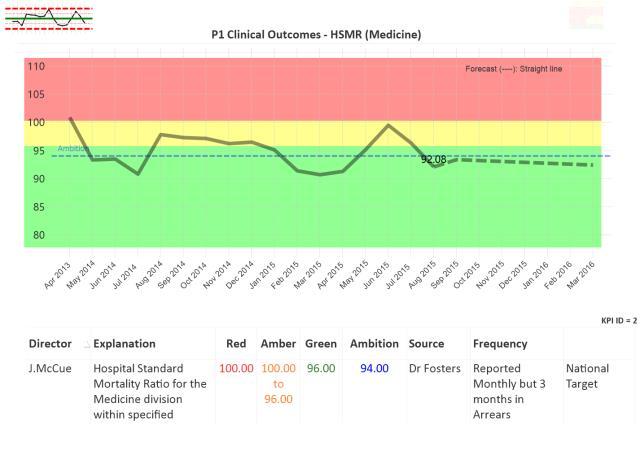
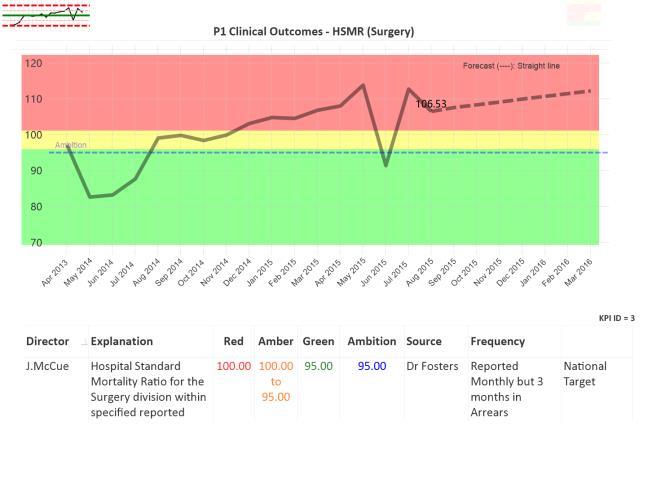
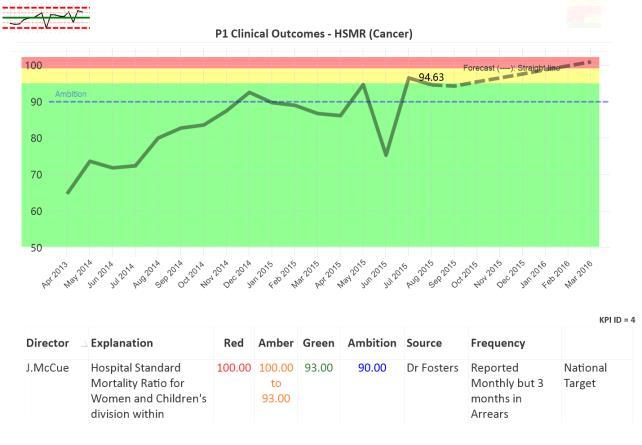
6 15/173 ACTIONS LOG 15/ The Actions Log was considered. It was noted that the Director of Finance and Director of Workforce and Organisational Development were looking at the bank and agency forecast at a more granular level and would update members of the Finance and Performance Committee on this at the special Finance and Performance Committee meeting in August. The Risk and Quality Committee had considered the impact of the reduced estates budget but had asked the Director of Estates to revise his report to focus on the potential impact on the patient experience of the budget before resubmitting. 15/ It was agreed that the prioritisation of medical equipment spending would be considered as a part of the overall capital programme and that the report should show the consequence of not being able to invest in equipment as planned. A number of reports that had been due to come to the Risk and Quality Committee had not been presented. 15/174 ANNUAL CYCLE 15/ The Annual Cycle for was noted. 15/175 CHIEF EXECUTIVE S REPORT 15/ The Chief Executive reported that the Trust s Annual General Meeting had been well received by partner organisations and the general public. He reminded Board Members that the Trust s Celebration of Excellence would be held on 25 September 2015 and encouraged everyone to attend to celebrate the areas of outstanding care and practice seen around the Trust. The Chief Executive was pleased to highlight the work carried out by the Trust and University of Hertfordshire investigating the use of technology to create white noise reducing perceived noise at night and disturbances. This had culminated in the Director of Nursing contributing to an article in the British Journal of Nursing. 15/ The Chief Executive recommended that Board Members read the briefing on the Secretary of State s speech setting out the need for a culture change in the NHS. The Board also noted the revised Floodlight Indicators and thanked the Head of Information and Chief Information Officer for their work developing an interactive tool that allowed trends over time to be reviewed. STRATEGIC ISSUES 15/176 Mortality Report /01 The Medical Director presented the Mortality Report setting out mortality rates and the work carried out to further improve mortality rates across the Trust. Crude Mortality had improved since the start of April (to 1.43% in June 2015) and the Quarter 1 crude mortality figures for was 0.13% lower than the same quarter in The Hospital Standardised Mortality Ratio (HSMR) for the twelve months up to March 2015 was (within the expected range). Despite the number of deaths and crude mortality decreasing in March the HSMR for March 2015 had increased, it was suggested that this could be a result of the loss of an experience Palliative Care 5 0 Draft July minutes pt 1.docx 2 Page 2 of 8 Overall Page 6 of 215
7 consultant and a reduction in the quality of coding following changes in senior coding staff. The Board was pleased to note that an experienced Head of Coding and Palliative Care Consultant had been recruited. Standardised Hospital Mortality Index (SHMI) had not been updated since the last Mortality Report. 15/ Stroke care continued to be an area of focus. The Trust had carried out a mortality review of 50 patients and commissioned two external reviews into Stroke provision (which confirmed that the Trust delivered high quality services) to continue to improve outcomes in this area. Recommendations from all three reports had been integrated into a unified plan. The 7 day respiratory service had opened on 1 April 2015 and was well received and the Royal College of Physicians Review of Respiratory Services had been highly positive. The Trust performed well in identifying and treating septicaemia but would recruit to a fixed term appointment to help further improve performance in this critical area. 15/ Mr Morfett (Trust Chairman) commented that the HSMR tended to oscillate but that the move in the March HSMR was away from the downtrend trend in actual and crude mortality for the month. He asked what could be done to support improvements in the Coding department. Data Quality was an ongoing concern for the Trust and often once coders were experienced they took better paid jobs in London trusts. The Finance and Performance Committee had asked to see an improvement plan with a prioritised set of actions and KPIs to monitor the backlog, depth of coding and performance against the Charleston index. The Director of Medicine was working to make junior doctors more aware of the importance of coding and to develop clinical coding links. 15/ Mr Gilham (Non-Executive Director) asked how delays in admission to ITU and HDU beds were being managed. It was noted that this was largely down to the need to discharge a patient from one of these beds before another admission could be made. The Director of Medicine offered to provide Mr Gilham with the average time taken to admit to an ITU or HDU bed outside the meeting. Dir of Med 15/177 Improving Patient Outcomes Strategy / The Medical Director presented the Improving Patient Outcome Strategy to the Board. The strategy was aligned to the Trust s Operating Plan and had been discussed throughout the organisation and at the Risk and Quality Committee meeting in July. The strategy set out five key aims aligned to four priorities (Safer Care, Effective Care, Reliable Care and Provision of Enabling Factors) the initiatives that the Trust would take to meet these aims and how they would be measured. The five aims were: Seek out and reduce harm Progressive reduction in preventable deaths Achieve the highest level of care reliability Improve capability within the workforce for continual improvement Work in partnership with staff, patients and stakeholders to improve outcomes. 5 0 Draft July minutes pt 1.docx 15/ The Board was pleased to note that this would be given to all doctors and as many nurses as possible so that everyone would 3 Page 3 of 8 Overall Page 7 of 215
8 know the Trust s aims and be able to articulate how the Trust would achieve these aims. The Board approved the Improving Patient Outcomes Strategy /178 Nursing and Midwifery Establishment Review 15/ The Nursing and Midwifery Establishment Review was presented to the Board by the Director of Nursing. The Establishment Review provided assurance that the ward establishments were safe and able to provide appropriate levels of care, that CQC requirements relating to staffing and supporting staff were adhered to was used to support the improvement of objectives and the development of the Workforce and People Strategy. 15/ The Risk and Quality Committee had discussed the original proposal in the Nursing Establishment Review (to increase the time allocated to handover) and had asked the Executive team to consider whether to increase the handover time by 5 minutes. Since the Committee meeting a series of spot checks had been completed by senior nursing team and Company Secretary. These highlighted the need to provide senior leadership at night. Given the concerns about leadership out of hours it had been felt that it would be more appropriate to allocate resources to providing senior nursing staff at night and the Executive had recommended that instead of increasing hand over time the Trust allocate resources to allow greater senior leadership presence at night. It was noted that senior leadership requirements were not considered as part of the Nursing Establishment Review (which was a ward based consideration) but would support the delivery of safe, good quality care at all times. 15/ Other recommendations as consequence of this review were: To review staffing at Mount Vernon on Wards 10, 11 and Michael Sobell House prior to October 2015 Continue to monitor the implementation of the shift hand over procedure, triangulating the data to identify any issues 15/ Mrs Crowther (Chairman of the Risk and Quality Committee) was keen to ensure that this was not a knee jerk reaction and was assured that the Director of Nursing had felt there would only be marginal benefits of extending hand over time. It was also noted that staff were entitled to record any excess working hours and take this time back and that the nursing education team would offer support and training to help wards manage their handover within 15 minutes. Mrs Crowther also expressed her disappointment that she had not been briefed of the changes to the recommendation ahead of the meeting and this was acknowledged by Trust staff. 15/ The Board noted that three wards appeared to be have a substantial deficit of substantive staff (9A, 9B, 10B) however this reflected the more flexible rostering of specials to address the changing acuity of patients on these wards. It was also noted that the Director of Nursing planned to review the profile and use of HDU beds at Mount Vernon Cancer Centre and the ward activity on Wards 10, 11 and Michael Sobell House over the summer as there may be capacity to restructure the nursing establishment in this area. 15/ The Board supported the proposal that data be collected on the use of Mount Vernon Cancer Centre s HDU beds and that the SafeCare tool (due to be implemented at Mount Vernon Cancer Centre in 5 0 Draft July minutes pt 1.docx 4 Page 4 of 8 Overall Page 8 of 215
9 October) should be used to evaluate acuity and activity and considered in this next establishment review. The Board also supported the Trust s plans to support staff to carry out efficient 15 minute handovers. FINANCE AND PERFORMANCE 15/179 Finance and Performance Committee Report 15/ Mr Nicholls (Chair of the Finance and Performance Committee) presented the Committee s report to the Board. The Committee had considered the three stroke service audits (to be discussed in Part 2 of the Board meeting) and recommended that the audits recommendations be implemented and monitored by RAQC. The Committee had asked to see a Data Quality action plan with KPIs and priorities. The Committee had received an report on the impact of the upgrade to an electronic patient record system in the ED and had asked to see a more detailed report setting out the benefits realised against the original business case 15/ Mrs Crowther asked whether the strategic projects being monitored were capital or change projects. All projects of strategic importance were monitored by the Finance and Performance Committee (FPC) and it was noted that where the FPC felt that the Risk and Quality Committee needed to be aware of issues they would continue to alert the Committee. 15/180 Finance and Performance Committee Terms of Reference and Annual Report 15/ The Chairman of the Finance and Performance Committee presented the annual report; setting out the key actions taken by the FPC over the year and recommending changes to the Committee s Terms of Reference. Mr Gilham suggested that the proposed Terms of Reference should be revised in point 6.1 to make it explicit that the Committee would approve investment within the approved budget or with reference to the Board. The Company Secretary agreed to revise the wording. The Board approved the Terms of Reference subject to the above change and confirmed that the Committee had discharged its duties. Co Sec 15/181 Finance Report Month 3. 15/ The Director of Finance presented the Finance Report. Despite pay expenditure being within budget there had been an in month adverse variance of 73k creating a year to date adverse variance of 175k. Overall the pay budget had been on target, although the Board noted a significant overspend in the Medical Division. The Division s overspend related to retrospective agency bookings being made. Actions were being put in place across the Trust to ensure that there were adequate controls and processes in place for medical agency bookings going forward. Mr Nicholls asked for the reasons behind the rising agency costs, it was noted that staff recruited from the EU needed to be supported with dual running for a period of time and that substantive recruitment to the ED was a significant concern for the Trust in line with the national picture. 15/ The Board discussed debtor / creditor management and noted that a proposal had been put to The Pathology Partnership (tpp) to mutually pay non disputed items in a similar manner to the 5 0 Draft July minutes pt 1.docx 5 Page 5 of 8 Overall Page 9 of 215
10 agreement with Hillingdon Hospital NHS Foundation Trust. The Board was pleased to note that the CCG had agreed 3.1m of support in principle (which had been assumed in the budget profile on a flat line) and that discussion were ongoing around the need for a further 12m of support. Mr Gilham asked for and received assurances that the under-spend in areas such as R&D was ring fenced. 15/182 Performance Report Month 3. 15/ The Trust had achieved the Referral to Treatment (RTT) targets and the ED 4 hour standard in May (95.13%). As previously discussed the CCG and Trust had agreed that additional RTT activity would be completed to prevent a growing backlog of patients. The significant scale of this activity meant that the Trust would need to commission some work from the independent sector and an activity tracker was being developed to ensure in house and independent sector capacity was utilised. 15/ ED targets had been met in June but the Trust had experienced more pressure in the ED in July, this was being carefully managed with regular meetings to look at recruitment plans. Demand for emergency services continued to increase, especially in the Urgent Care Centre. The level of ambulance conveyances for quarter 1 of was 12.1% higher than the same quarter in , this patient cohort represented some of the most acutely ill patients requiring more intensive support and longer stays in the ED. Despite the increasing pressure from emergency admissions the in-patient emergency length of stay had not been adversely affected. Mr Gilham asked whether the Trust had considered using pharmacists in the ED as some Trusts were piloting. The Trust had not been successful in its application for the pilot but had asked the CCG to consider pump priming a similar scheme, the results of the pilot weren t known yet but when they were the Trust would discuss them with the local health economy. 15/ Mr Niven (Non-Executive Director) asked whether waiting times for the Urgent Care Centre (UCC) were comparable to the ED and how patients could be encouraged to go there. The Director of Operations explained that staff did tell patients that the UCC waiting times were still less than that of the ED but often patients who had arrived at Lister ED were unwilling to transfer to the UCC. The UCC had seen a growth in patients with minor illnesses and injuries since the closure of the Spring House Walk In GP service. The Trust was reviewing the UCC substantive staffing to adjust to the changing case load and rising demand. 15/ The Trust had planned to temporarily close the Short Stay Unit for essential re-development work and to accommodate the displaced activity on other wards. The Trust had been aware of the time lag in international recruitment and last week had taken the decision to close a ward to maintain high standards of patient safety. This meant that the Trust was operating with 37 less beds than in May. The pressure on beds could impact on elective work and the Surgery Division was currently assessing the impact and how this could be mitigated, this information would inform the re-forecast being conducted for the special FPC meeting. 15/183 Workforce Report Month Draft July minutes pt 1.docx 6 Page 6 of 8 Overall Page 10 of 215
11 15/ The Director of Workforce and Organisational Development presented the Workforce Report. The baseline vacancy rate (based on March 2015 ledger) had reduced to 5.52% and was now expected to reduce to under 5% by August An additional 250 wte posts had been added in the May ledger and the new establishment vacancy level had increased to 10.35%. An updated Drive for Five project would be discussed by the Executive team to reduce the vacancy rate of the new establishment to under 5%. Qualified nursing recruitment continued both in the UK and abroad with 84 experienced Filipino nurses and 35 newly qualified nurses expected to join the Trust in the autumn. 15/ Mr Niven asked when the Trust would reach 5% vacancy level of the new establishment and noted that the cohort of Filipino nurses joining the Trust in the autumn would restore the vacancy level to 5% overall. The Director of Workforce and Organisational Development also highlighted developments in the Culture Change programme and his plans to develop a heat-map based on weighted indicators. RISK AND QUALITY 15/184 Risk and Quality Committee Report 15/ Mrs Crowther (Chairman of the Risk and Quality Committee) presented the Committee s report. The Committee had received a presentation from the Women and Children s Division, following this presentation the Committee had discussed its expectations for future presentations and the Company Secretary would work with the Committee Chair to set these out to the divisions. The Committee had reviewed the stroke performance audits and proposed actions. The Committee had also considered the Trust s gap analysis and action plan following the publication of the Kirkup Report. 15/ The Committee had also discussed the Annual Health and Safety Report and the Committee s own annual report and evaluation of its efficacy. Mrs Bexfield (Non-Executive Director) asked how the Trust decided whether to settle litigation in Health and Safety cases, it was noted that the Trust took the decision with the clinicians and NHS Litigation Agency on a case by case basis. Mrs Bexfield pointed out that settlement could lead to more claims being made and it was agreed that the potential impact of settling cases on both the Trust and the NHS as a whole would be discussed at the Finance and Performance Committee meeting. Dir of N 15/ The Board reflected on the Trust s response to a serious incident involving a patient with learning difficulties in 2014 and noted that the Committee had discussed the learning that had been taken from the incident. It was noted that the Annual Safeguarding Review helped the Trust to minimise the risk of such incidents re-occurring and that the roll out of the electronic observation system would significantly reduce the risk of a patient s deteriorating condition not being escalated. It was agreed that in future annual reports should discuss notable achievements and shortcomings. 15/ The Board formally noted the Kirkup Report Gap Analysis and Action Plan, Safeguarding Adults Annual Report and Annual Health and Safety Report. 5 0 Draft July minutes pt 1.docx 7 Page 7 of 8 Overall Page 11 of 215
12 15/185 Risk and Quality Committee Annual Report and Terms of Reference. 15/ The Chairman of the Risk and Quality Committee presented the annual report; setting out the key actions taken by the Committee over the year and recommending minor changes to the Committee s Terms of Reference. The Board approved the Terms of Reference and confirmed that the Committee had discharged its duties. AUDIT 15/186 Audit Committee Report 15/ Mrs Bexfield (Chairman of the Audit Committee) presented the committee s report to the Board. The Committee had supported the merge of the two policies into one & minor updates and had recommended that the Anti-Fraud and Bribery policies to the Board for final approval. The Committee had also reviewed the Board Assurance Framework process and welcomed the revised format. Mr Gilham asked how the Trust assured itself that contractors followed the Anti-Fraud and Bribery policy and noted that this was assessed during the procurement process and that the Trust could request open book accounting if there were concerns. 15/ The Board discussed the external Auditor s letter. Mr Gilham noted that the requirement to have a cumulative surplus by would be a significant challenge. Mrs Bexfield advised that this would be reviewed with the Long Term Financial Plan and when setting the budget. 15/ The Board formally approved the Anti-Fraud and Bribery Policy and noted the Annual Audit Letter. 15/187 Audit Committee Annual Report and Terms of Reference 15/ Mrs Bexfield presented the Audit Committee s annual report; setting out the key actions taken by the Committee over the year and recommending no changes to the Committee s Terms of Reference. The Board approved the Terms of Reference and confirmed that the Committee had discharged its duties. 15/188 DATA PACK 15/ The data pack was considered. There being no further business the Chairman closed the meeting at 16:20pm. Ian Morfett Trust Chairman 5 0 Draft July minutes pt 1.docx 8 Page 8 of 8 Overall Page 12 of 215
13 Action has slipped Action is not yet complete but on track Action completed * Moved with agreement Agenda item: 6 EAST AND NORTH HERTFORDSHIRE NHS TRUST TRUST BOARD ACTIONS LOG PART I TO SEPTEMBER 2015 Meeting Date 29 April 2015 Minute ref Issue Action Update Responsibility Target Date 15/95.02 Bank and Bring a detailed forecast of Bank May 2015 update: Board Director of Workforce May 2015 agency and Agency requirements over the requests to remain amber and Organisational July 2015 requirements year to the next FPC until satisfied RAQC Development. meeting. receiving regular updates. Aug Update: Included in Workforce Reports 29 April April May May /96.01 Transforming Outpatient Management Programme 15/96.03 Prioritisation of Medical Equipment 15/ Post consolidation mortality report 15/ Benefits of overseas recruitment Set out at RAQC which projects can progress in and which cannot under TOMP. Report on how resources will be prioritised to Execs and RAQC Review mortality and present a report detailing improvements made in the year following consolidation. Present a report to RAQC on the benefits, cost and retention of overseas recruitment. May 2015 update: Board requests to remain amber until RAQC received more info as per Board min 15/ July 2015 update: Responsibility changed to DoO Sept 2015: Dep. DoO to meet Chair of RAQC and agree subsequent steps. Deferred to July July 2015 update Will be considered as part of the capital process Director of Operations May 2015 July 2015 Sept 2015 ongoing Director of Operations / EBME lead Medical Director Director of Workforce and OD June 2015 July 2015 Oct 2015 November 2015 October Pt I Actions Log to Sept 15.pdf 1 Page 1 of 2 Overall Page 13 of 215
14 Action has slipped Action is not yet complete but on track Action completed * Moved with agreement Meeting Date Minute ref Issue Action Update Responsibility Target Date 24 June / Ward outliers Bring a report showing outliers by ward to the next RAQC meeting. July 2015 update deferred to September Director of Operations July 2015 Sept June / Funding streams for culture change programme Identify external funding streams with the Exec team and report back to the Risk and Quality Committee. Sept 2015 update. Director of W&OD will give verbal update to RAQC. Director of Workforce and Organisational Development September Pt I Actions Log to Sept 15.pdf 2 Page 2 of 2 Overall Page 14 of 215
15 BOARD ANNUAL CYCLE Agenda Item 7 Item Apr-15 May-15 Jun-15 Jul-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Standing Items CEO Report inc Floodlight Scorecard Data Pack Patient Testimony (part 2) Suspensions (part 2) Strategic Objectives and Annual Operating Plan 1 (final) 1 1 Long Term Financial Plan (tbc) IBP (tbc) Committee Reports Audit Committee Report CTC Report FPC Report FTC Report (as required) RAQC report Annual Reports Annual Audit Letter 1 Audit Committee TOR & Annual Report 1 Annual Report and Accounts (Trust) 1 Charity Annual Report and Accounts 1 CTC TOR and Annual Report 1 Financial Plan and Capital Plan 1 1 FPC Evaluation and TOR 1 Learning Disabilities (Adult SG) Ann. Report 1 1 Annual Floodlight Summaries 1 Health and Safety Strategy Review 1 Improving Patient Outcomes Strategy Nursing and Midwifery Strategy Review 1 Patient Experience Strategy Review 1 PQAF Assessments 1 7. Board Annual Cycle pdf Page 1 of 2 Overall Page 15 of 215
16 BOARD ANNUAL CYCLE Agenda Item 7 Item Apr-15 May-15 Jun-15 Jul-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Quality Account 1 R&D Annual Report 1 RAQC Annual Review and TOR 1 1 Revalidation Officer / Revalidation AR 1 1 Safeguarding Review (Children) 1 Other Reports SOs and SFIs 1 Raising Concerns 1 1 Market Report New floodlight scorecard format and targets 1 Board Assurance Framework Board Development Plan 1 GMC Trainee Survey Results 1 Detailed analysis of staff survey results 1 EAHSN Francis Action Plan 1 Governance and timetable for QE2 move 1 Infection Control 1 Medical Notes update 1 Mortality Report Nursing Establishment Review 1 1 SI Report (Part 2) Shareholder / Formal Contracts ENH Pharma tpp The FPC report will include the Committee report, the Finance Report, Performance Report and Workforce Report for the month. 2. The Data Pack will include: Patient Experience Dashboard, FFT, Stat & Man Exception Report, Health and Safety Indicators, Nursing Quality Indicators, Finance data, Performance Data, CQC outcomes, Workforce Data, Safer Staffing Data, Infection Control data. 7. Board Annual Cycle pdf Page 2 of 2 Overall Page 16 of 215
17 EAST AND NORTH HERTFORDSHIRE NHS TRUST 1 Celebration of excellence - staff awards CHIEF EXECUTIVE S REPORT 30 th September 2015 Over three hundred Trust staff and volunteers came together at Tewin Bury Farm on Friday, 25 September 2015 at the Trust's annual Celebration of Excellence awards. We celebrated with 30 long-serving staff their commitment of 25 years service with the Trust, with five volunteers who were recognised for 20 years of service. Awards were made to teams and individuals from across the Trust. Always moving, the public nomination award rounded off the formalities before staff had the opportunity to celebrate together. Attached to this report (Appendix C) is the text from an all staff that was sent out across the Trust on 28 September listing this year's award winners. I am sure that the Board and its members, many of whom were involved in handing out the awards on 25 September, will join me in congratulating our winners and all those nominated. 2 Mount Vernon Cancer Centre Site Development Following a number of positive meetings between myself, the Chair and our counterparts at the Hillingdon Hospitals NHS Foundation Trust (THHFT) I am pleased to report that progress has been made with regard to our agreeing to proceed with a Memorandum of Understanding (MoU). The MoU will serve to work through the process and options to secure the Trust's interests in the site and enable the Trust to work with THHFT to progress site development plans at Mount Vernon. We anticipate that, subject to any necessary board etc approvals, we will have signed an MoU by the time that we meet as a Board in October 2015, or the following month (subject to working with other stakeholders) and at this stage I expect to be in a position to provide details of a provisional timetable for developing the route to a land transfer (freehold or leasehold) and the next steps relating to a re-development plan for the site at next month's meeting. The need to invest and re-develop the site, in particular from our point of view the Mount Vernon Cancer Centre, is recognised by both organisations as is the requirement to work together to develop a coherent and strategic site strategy and development plan for the wider Mount Vernon site /15 Reference Cost Reference cost (RC) is the average unit cost to the NHS for providing healthcare to NHS patients in England. All NHS Trusts submit a mandatory return at the end of every financial year and, once submitted, the RC data is aggregated on a national basis and is used to underpin the calculation of the Payment by Results (PBR) national tariff. The DH has published draft Reference Cost Index (RCI) for the 2014/15 Return we submitted on the 29th July 2015 and ENHT has scored 96 RCI which means our cost unit is 4% less than the national average. Our Finance department is responsible for producing the annual RC submission using the patient level information and costing system (PLICS). The costing model identifies patient activity such as inpatients, outpatients, ED and assigns a cost to each activity in proportion of resources used to treat the patient that complies with Monitor s Approved Costing Guidance and HFMA Acute Health Clinical Costing Standards. Chief Executive's Report and appendices.pdf Page 1 of 30 Overall Page 17 of 215
18 These costing standards ensure all NHS Trusts are using the same costing methodology and allow effective benchmarking. 4 Trust Shortlisted for HSJ Award for Improving Environmental and Social Sustainability I am pleased to report that the Trust has been shortlisted for an award in the Improving Environmental and Social Sustainability category as part of this year s HSJ awards. This recognises the work of the Trust and its achievements to date which include: an investment in site infrastructure, implementing a Green Travel Plan, reducing carbon emissions, water consumption and the amount of waste produced together with our public health and engagement work #thefutureismembership. The teams now have a presentation and Q&A session with the judging panel in October followed by the award ceremony which will take place on 18th November Day Surgery Unit Awarded With Purple Star Award At an event held in the Trust's new day surgery unit at the Lister yesterday afternoon, representatives from Hertfordshire County Council awarded the day surgery team with a Purple Star award for the support provided to people with learning disabilities. 6 League of Friend's support for the Lister's acute medical unit I was delighted to learn of the support provided by the League of Friends, who raised funds to purchase 30 new televisions for use in the Lister's acute medical unit. They will be a great resource for our patients and we are very grateful for the efforts that the Friends went to in raising the necessary funding and purchasing the TV sets. It is another example of the great work that they do in helping our patients. 7 Westminster Diocese Lourdes Medical Team I would like to thank and recognise the work of a group of Trust staff who volunteered with the Westminster Diocese Lourdes medical team in July Staff from across the Trust regularly volunteer with pilgrimages, in their own time, to enable the sick, disabled and elderly to travel to Lourdes, France. This year nine staff including nurses, a clinical support worker, physiotherapist and consultant were part of the Westminster Diocese medical team. 8 BMJ editorial - need to improve endoscopy services In his role as chair of the British Society of Gastroenterology's clinical services and standards committee, Dr Simon Greenfield - who is one of the Trust's senior consultant gastroenterologists - has worked with colleagues at the Society publishing in the British Medical Journal outlining how NHS endoscopy services improve. Part of the evidence used to support the editorial is a paper by Dr Greenfield published previously outlining the improvements made to the Lister's endoscopy service that shows how services can be networked. An abstract of the editorial can be found on the BMJ website. 9 The National Patient Safety Suite: Diabetes E Learning Programme In January 2015, the Trust purchased The National Patient Safety Suite- Diabetes E Learning Programme, an online suite developed to provide access to comprehensive learning on The Safe Use of Insulin. Chief Executive's Report and appendices.pdf Page 2 of 30 Overall Page 18 of 215
19 The programme is owned by Virtual College and utilised by the NHS nationally. The purpose of the programme is to improve practices in the safe management of people with diabetes; primarily in the hospital clinical setting. This programme offers 8 modules on all aspects of safe and effective diabetes management with an emphasis on insulin safety, non- insulin products, managing hypoglycaemia as well as the diabetic foot and more. The programme was launched collaboratively by Nurse Education and the Diabetes Outreach Team (DOT) in March 2015 and since its inception, 265 staff members have completed and passed The Safe Use of Insulin module, with 905 modules being passed in total, in the 5 month period. East and North Herts NHS Trust is the first organisation nationally to achieve a Gold Certificate of Achievement. The certificates are based on the number of module completions when measured against the number of clinical staff in the Trust. 10 UCL Medical School's Top Teacher Awards for 2014/15 I was delighted to learn that one of the Trust's consultant radiologists, Dr William Topping, has been awarded a Top Teacher Award for 2014/15 by the School of Life and Medical Sciences at the UCL Medical School. Throughout the academic year, UCL medical students are asked, via online evaluation questionnaires, to nominate teachers who were particularly helpful or inspiring to them during their studies. During the course of the 2014/15 year, UCL Medical School's students cast over 1,000 votes, from which there were 56 people who have received a Top Teacher Award. This is a great achievement for Dr Topping and one that I welcome warmly. 11 Executive Committee Summary Report to Board Care Quality Commission Inspection of our Services October 2015 The CQC will be inspecting our services across all of our sites starting on 20 October They will look at the quality and safety of the care provided based on the things that matter to people. They will look at whether the service is: Safe Effective Caring Responsive to people s needs Well-led. We welcome this inspection and would appreciate you supporting the Trust by sharing your experiences with the CQC. The Inspectors will be running public listening events on: 14 October :00pm 7:30pm, BEST WESTERN Homestead Court Hotel Homestead Lane, Welwyn Garden City, Hertfordshire, AL7 4LX 19 October 2015, 6.00pm-7.30pm. Forum Conference & Banqueting Suite, Danestrete Stevenage, Hertfordshire, SG1 1EJ, Appendix A Public Listening Events Ward Staffing and Emergency Department Risks The Committee reviewed and considered the ward staffing risks regarding the impact of the Chief Executive's Report and appendices.pdf Page 3 of 30 Overall Page 19 of 215
20 recent closure of 20 beds on Ashwell and 6A ward and the associated risks impacting on performance and quality of service in the Emergency department. The recruitment pipeline was also taken into account. The Committee discussed and agreed contingency plans whereby additional beds would be available on other wards during periods of extreme capacity challenge. On balance of risk the decision not to re-open the closed beds until 1 November 2015 was supported. This was discussed at RAQC and will be presented at Board. Performance & Projects The Committee has continued to provide scrutiny to areas of service development, performance (quality, safety, patient experience, performance targets), operational pressures, finance, mortality, hospital acquired infections, and key strategic contracts and projects (including progress to 7 day services) and workforce planning. The focus since the Board last met has been on the financial and capacity planning for 2015/16, and monitoring the improvements in clinical coding and the contact centre. The key areas for escalation are included in the Director reports to Board and Board Committees. 12 Floodlight Scorecard The Month 5 Trust floodlight scorecard is attached as Appendix B. The Board committee executive summary reports reflect the key discussions that have taken place at both the Finance and Performance and the Risk and Quality Committees. Explanation of red indicators is provided within the appropriate accountable Director s report and the exception reports in the data pack. Chief Executive 25 th September 2015 Chief Executive's Report and appendices.pdf Page 4 of 30 Overall Page 20 of 215
21 CQC is the independent regulator of all health and social care in England. We are given powers by the government to register, monitor and inspect all health and care services Tell us about your care Come to our public listening event, meet our inspectors and share your experience of the services and care provided in the last year by: East and North Hertfordshire NHS Trust Monday 19 October 2015 Time: 6:00PM 7:30PM Forum Conference & Banqueting Suite Danestrete Stevenage, Hertfordshire SG1 1EJ, United Kingdom Share your experience anonymously at any time: - enquiries@cqc.org.uk Chief Executive's Report and appendices.pdf Page 5 of 30 Overall Page 21 of 215


22 CQC is the independent regulator of all health and social care in England. We are given powers by the government to register, monitor and inspect all health and care services Tell us about your care Come to our public listening event, meet our inspectors and share your experience of the services and care provided in the last year by: East and North Hertfordshire NHS Trust Wednesday 14 th October 2015 Time: 6:00PM 7:30PM BEST WESTERN Homestead Court Hotel Homestead Lane, Welwyn Garden City, Hertfordshire AL7 4LX Share your experience anonymously at any time: - enquiries@cqc.org.uk Chief Executive's Report and appendices.pdf Page 6 of 30 Overall Page 22 of 215

23 32 KPIS 28 KPIS 18 KPIS Chief Executive's Report and appendices.pdf Page 7 of 30 Overall Page 23 of 215

24 Dashboard Chief Executive's Report and appendices.pdf Page 8 of 30 Overall Page 24 of 215

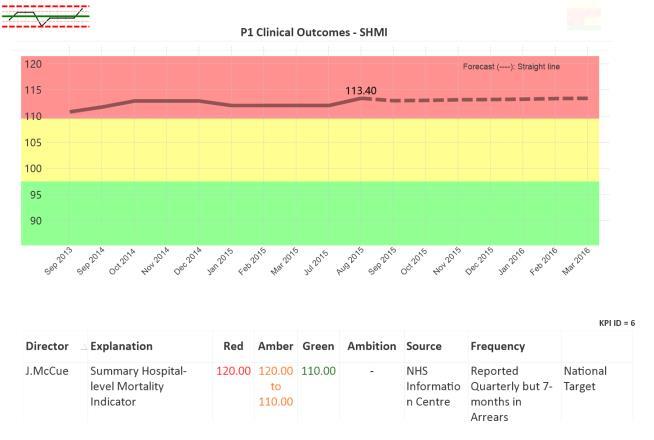
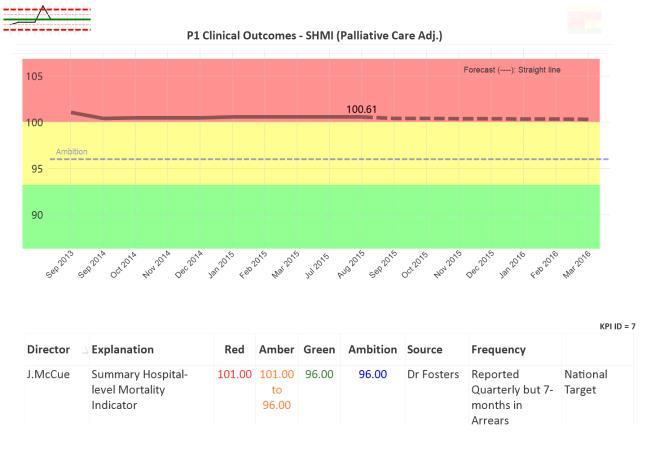
25 Mortality Chief Executive's Report and appendices.pdf Page 9 of 30 Overall Page 25 of 215



26 Governance Chief Executive's Report and appendices.pdf Page 10 of 30 Overall Page 26 of 215



27 Clinical Efficiency Chief Executive's Report and appendices.pdf Page 11 of 30 Overall Page 27 of 215


28 Patient Experience Chief Executive's Report and appendices.pdf Page 12 of 30 Overall Page 28 of 215

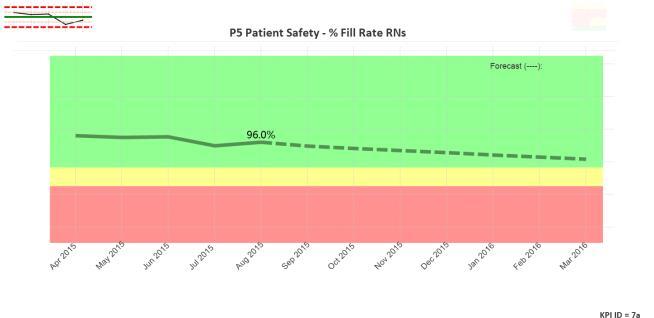
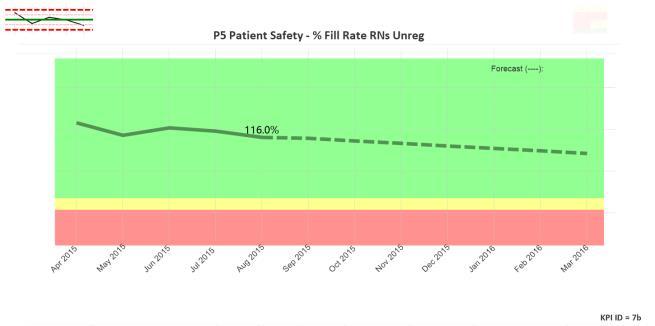

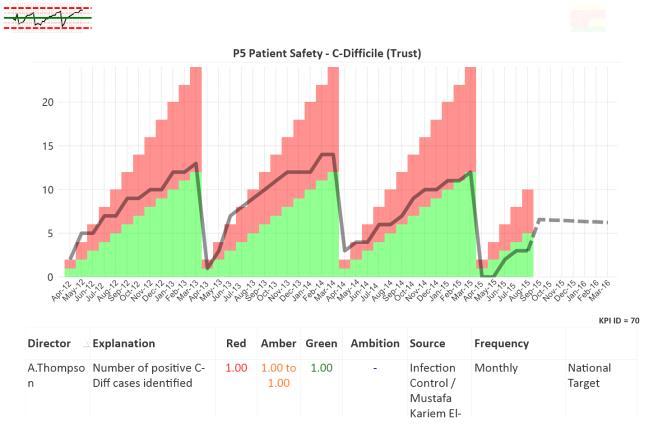
29 Patient Safety Chief Executive's Report and appendices.pdf Page 13 of 30 Overall Page 29 of 215

30 Stroke Chief Executive's Report and appendices.pdf Page 14 of 30 Overall Page 30 of 215

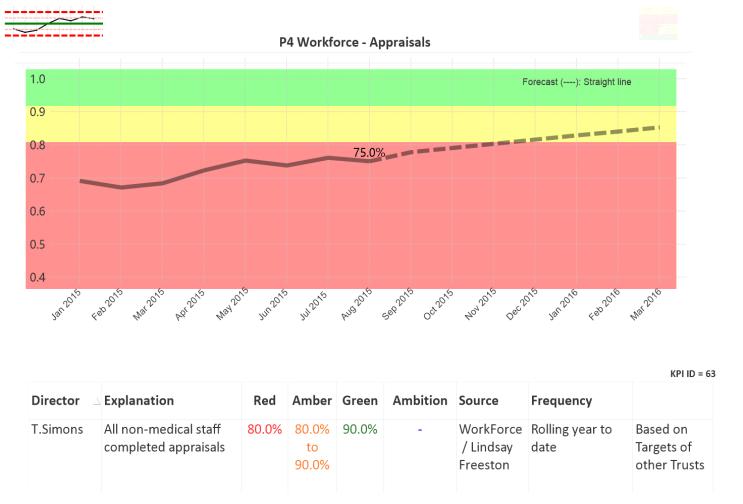
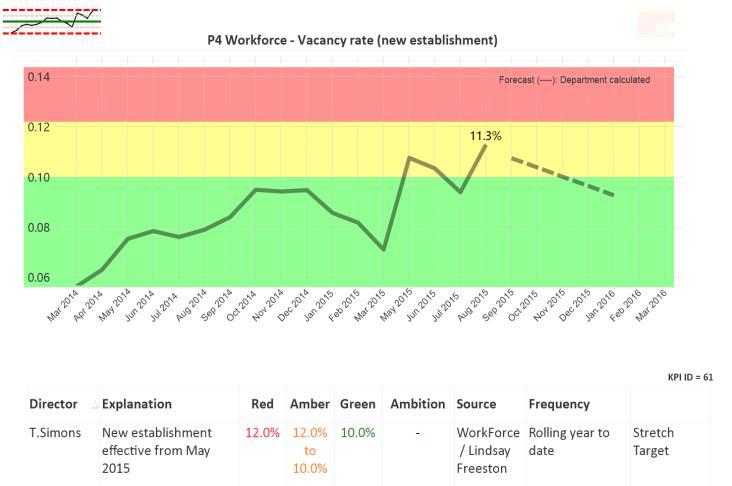
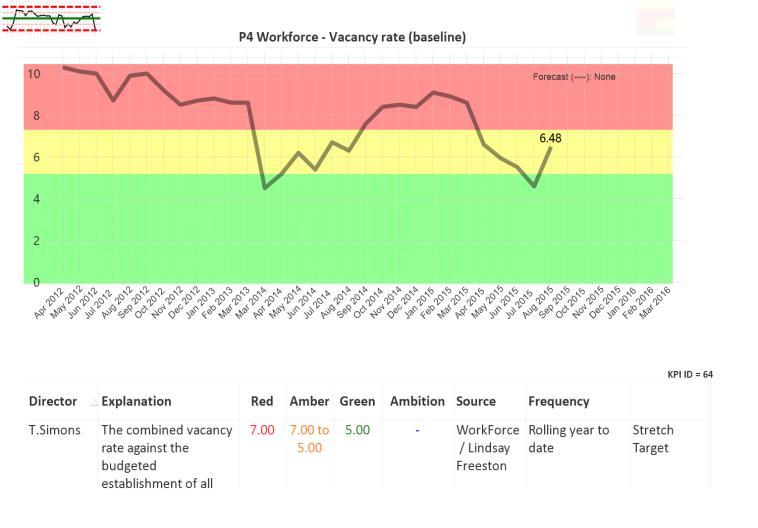

31 Workforce Chief Executive's Report and appendices.pdf Page 15 of 30 Overall Page 31 of 215




32 MCF TDA Performance Chief Executive's Report and appendices.pdf Page 16 of 30 Overall Page 32 of 215



33 Statutory Training Chief Executive's Report and appendices.pdf Page 17 of 30 Overall Page 33 of 215

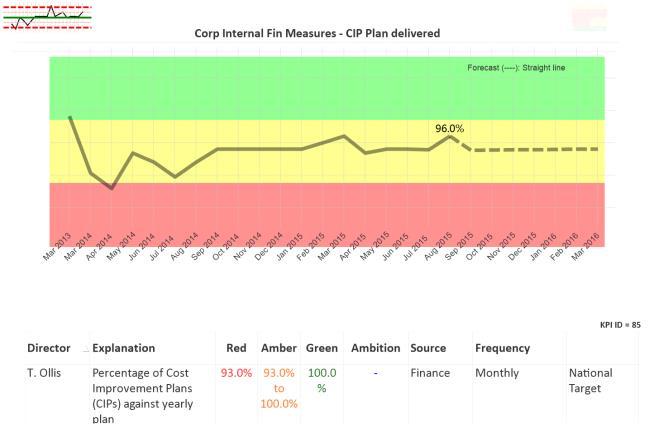
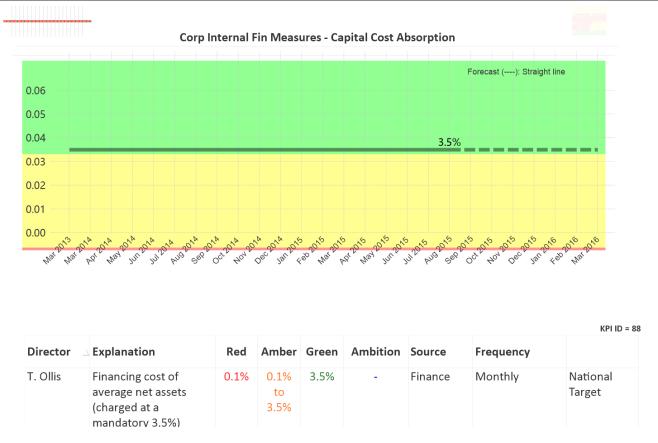
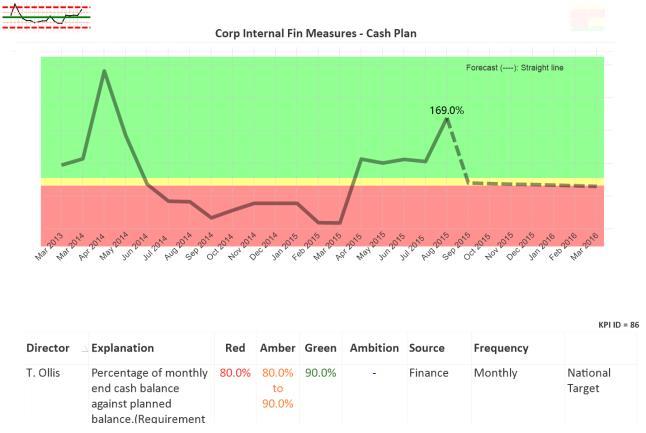

34 Financial Measures Chief Executive's Report and appendices.pdf Page 18 of 30 Overall Page 34 of 215



35 Health & Safety Chief Executive's Report and appendices.pdf Page 19 of 30 Overall Page 35 of 215
36 Nick Carver, our chief executive, has asked us to share the following message with you. Dear colleagues I would like to thank everyone who made a nomination for our annual staff awards, the Celebration of Excellence. This year, we received 167 nominations, and thank you to everyone who took the time to write in. The judging panel found it extremely difficult to make a decision. The awards ceremony was held on Friday night at Tewin Bury Farm, and attended by over 330 of our team. The winners are listed below. I would also like to congratulate everyone nominated and shortlisted for this year s awards. Thank you all for your commitment to our patients. Nick Carver Chief executive Patient experience award the Day Surgery Team Clinical Outcomes and Patient Safety award Children and Young People s Diabetes Service Continuous Improvement award Dr She Lok Team award two awards: Children and Young People s Epilepsy Service and the Health Records Team Team leader award Dagmar Louw Support Service award George Ajayi, Vinci Volunteers award Hazel Pike, Leon Ajao and Tonya Cull Public nomination award the Play Specialists Team Chief Executive's Report and appendices.pdf Page 20 of 30 Overall Page 36 of 215

37 Title: East and North Hertfordshire Integrating Care Proposition Date: January 2015 From: East and North Hertfordshire Integrated Care Programme Board Purpose: To brief the board on the development of the East and North Hertfordshire Integrating Care Proposition To request the endorsement and commitment of the board to support the proposed Integrating Care Principles 1. Background The East and North Hertfordshire Integrated Care Programme Board (ICPB) was commissioned by East and North Hertfordshire CCG in October 2014 to be responsible for the development and implementation of a whole system partnership approach to integrating care for the population of East and North Hertfordshire. Tom Cahill - Chief Executive of Hertfordshire Partnership University NHS Foundation Trust (HPFT), is designated as the provider system lead for integrated care and chair of the East and North Hertfordshire Integrated Care Programme Board (ICPB ). Appendix A describes the ICPB Membership. Engagement with the public, patients, users and staff are critical to the successful delivery of care together and this will be a priority as the programme develops. Chief Executive's Report and appendices.pdf Page 21 of 30 Overall Page 37 of 215
38 2. The Integrating Care Proposition A proposition has been developed by the Integrated Care Programme Board. The Aim The aim is to improve the care, independence and health of over 65 year olds with multiple complex needs and patients with long term chronic physical and mental health conditions. This will be achieved by ; Improving person centred and coordinated care Giving people more control over the health and care they receive Rebalancing our collective resources towards proactive and planned care to ensure a sustainable improvement in the quality of services whilst contributing to a reduction in the demand for urgent care across the health and social care system. The Approach A collaborative partnership approach by providers and commissioners will be required which recognises and brings together the innovative developments already underway across the system. A partnership approach on a locality basis with primary care providers will be a priority. The Outcome Success will be described by our patients and service users as My care is planned with people who work together to understand me and my carers, put me in control, coordinate and deliver services to achieve my best outcome Success will be described by our workforce as everyone working as a coordinated team to achieve joined-up care through a shared single person-centred care plan. We will do this by preparing, discussing, documenting and reviewing together in partnership with the person and carers rather than planning for several specific disease or care needs in isolation The delivery of the integrating care proposition will ensure that ; More people live independently in their own homes Health and care teams and services will be co-ordinated and joined-up There will be a a greater focus on proactive community care There is a move away from single disease and care management to holistic care approaches Chief Executive's Report and appendices.pdf Page 22 of 30 Overall Page 38 of 215
39 A sustainable reduction in the urgent care demand on primary care, community services, hospitals and social care services is achieved The Principles Five delivery principles have been proposed which will be embedded into current and future developments during the co-design and co-production of the integrating care delivery models. One Proactive care management by health and social care staff together will keep people as healthy as possible in the community for as long as possible Two Crisis and urgent care management in the community must be appropriately available to support the maintenance of more community proactive care management Three Coordinated and joined up care (wherever that care is provided) will make services more efficient and easier to understand and use Four Promoting more independence, choice and personalisation of the care delivered around the needs of individuals and their carers rather than around the service needs Five Promotion of health and wellbeing to help people keep well and to participate in the enjoyment of life The Commitments Alongside the principles, the following commitments to the workforce and to the service developments required have been agreed. Our Workforce Commitment We will assess comprehensively together We will share records and share goals We will proactively case find and risk stratify together We will value, respect and trust each other Together we involve and place carers and the person at the centre of care We will peer review together We will always make time for our professional supervision and support through inter professional networking We will network our care together Chief Executive's Report and appendices.pdf Page 23 of 30 Overall Page 39 of 215
40 Our Service Development Commitment We will coordinate proactive care together as an integrated team We will case manage and provide ongoing care together We will have a centralised referral, intake and staff deployment point We will share accountability for care We will appropriately co locate our services We will have one integrated directory of services We will develop person centred transfer agreements We will develop shared performance accountability and outcomes We will develop our integrated multi professional team approach We will organisationally develop together through shared values and goals Appendix B summarises the connection between the integrating care vision, principles and commitments 3. Programme Governance Integrated Governance is an essential component to enable and strengthen sustainable partnership working and decision making of the integrated care programme board. Currently the health and care system governance infrastructure for the Integrated Programme is proposed as follows : Chief Executive's Report and appendices.pdf Page 24 of 30 Overall Page 40 of 215
41 Pancounty workstream ENCCG Governing Body Direct accountability Indirect accountability Health Care Provider Boards CCG Strategic Delivery Board Health and Community Services Management Board CEO Sponsoring Group East and North Herts Integrating Care Programme Board Locality Boards Workforce Partnership Executive Group Health and Social Care Data Integration Board Workstreams Work stream implementation The implementation of the Integrating Care proposition and application of the principles will be delivered through three main work streams which have been proposed and agreed by the ICPB. These include: Work stream 1 Improving access to simplify how services are delivered through an improvement in the coordination and quality of access and assessment leading to the delivery of the appropriate care. Work stream 2 - Ensuring seamless transitions of care to improve the quality and minimise the numbers of care transfers between providers through a focus on processes with in and between providers combined with transformed coordination of admission, discharges and choice of provider. Work stream 3 - Integrating care in the community - to improve the number of people having care closer to home through a focus on transforming the approach to proactive care planning in integrated teams alongside a streamlining of the number and complexity of care pathways available to our communities and workforce. Each work stream has an assigned provider executive director (Senior Responsible Officer ) working as a system lead. All current relevant projects/ services ( 80 plus ) delivered by the providers will be Chief Executive's Report and appendices.pdf Page 25 of 30 Overall Page 41 of 215
42 reviewed within these work streams in line with the proposition principles and regrouped alongside the need for consideration of new projects and services. This will be done in conjunction with commissioners and will provide an integrated delivery foundation for the systems commitment to the Better Care Fund. APPENDIX C provides a summary of the work stream detail The balance of provider and commissioner leadership and contributions in these work streams is essential. The workstreams will work in partnership with local health and social care leaders to ensure that services are appropriately tailored and reflect the needs of the local population. Additionally there are aligned pan county work streams which will support the delivery and these include; The workforce partnership executive group The health and social care data integration board 3. TIMETABLE Oct 14 - Apr 15 Phase 1 Programme and Workstream Scoping and Initiation Mar 15 - Oct 15 Phase 2 Winter 15/16 Wins Apr 15 - Oct 16 Phase 3 Whole system model development and implementation Oct 14 Jan 15 Apr 15 Jul 15 Oct 15 Jan 16 Apr 16 Jul 16 Oct 16 The Programme is now moving at pace into the second phase of its development with work stream scoping through to implementation planning already underway. There is additionally a focus on the identification of integrated quick wins to support the system in its urgent care demand management during winter 2015/16. Whilst the overall proposition and principles are being considered and endorsed by the four provider Boards (HCT, HPFT, ENHT, HCS) and two Commissioning bodies (HCS and CCG), the programme is maintaining its focus and delivery momentum. 4. Summary & Recommendation Chief Executive's Report and appendices.pdf Page 26 of 30 Overall Page 42 of 215
43 This paper has provide an overview of the approach being taken by ENCCG, in conjunction with HCS and the four main health and social care providers to developing a new integrated delivery of care across E&N Hertfordshire. In order to deliver the benefits and outcomes outlined in this paper, commitment, ambition and partnership is required from all health and care providers and commissioners to enable the scaling up and translation of this system proposition into sustainable service delivery changes. Recommendation The Board are asked to endorse and support the direction of travel outlined in this paper; and are specifically asked to commit to the Integrating Care Principles and Commitments which are seen to be key enablers for success. Chief Executive's Report and appendices.pdf Page 27 of 30 Overall Page 43 of 215
44 APPENDIX A Chair (System Integrated Care Lead/HPFT Chief Executive Officer) ENHT Executive Lead ENHCCG / GP Lead Commissioner Integration Lead (ENCCG and HCS) Provider Partnership Programme Director HCT Executive Lead (Deputy Chair) HPFT Executive Lead HUC Chief Executive Healthwatch HCS Director lead Ambulance Trust (EEAT) ENHCCG Executive Lead Tom Cahill John Watson Dr Nicky Williams Chris Badger Alison Gilbert Julie Hoare Karen Taylor David Archur Michael Downing Earl Dutton Dave Fountain Sharn Elton Chief Executive's Report and appendices.pdf Page 28 of 30 Overall Page 44 of 215

45 APPENDIX B Chief Executive's Report and appendices.pdf Page 29 of 30 Overall Page 45 of 215
46 APPENDIX C work stream summary on a page Programme sponsor Tom Cahill Deputy: Julie Hoare Programme Manager Andrew Godfrey Programme board Programme Director Alison Gilbert WS1 Improving access SRO: Karen Taylor Deputy SRO: David Archer Clinical lead: Worksteam manager: Operations rep: WS2 Ensuring seamless transitions of care SRO: John Watson Deputy SRO: Earl Dutton Clinical lead: Worksteam manager: Operations rep: WS3 Integrating community care SRO: Julie Hoare Deputy SRO: Nicky Williams Clinical lead: Worksteam manager: Operations rep: Single Point of Access Sponsor: PM: Trusted Assessment Sponsor: PM: Home to Assess Sponsor: PM: Bed Bureau Sponsor: PM: Discharge Hubs Sponsor: PM: Integrated model Sponsor: PM: HomeFirst LLV and NH Sponsor: PM: Complex Care Premium Sponsor: PM: Prevention and self-management SRO: Sue Matthews Enabling programmes IT, data and estates SRO: Stuart Campbell Workforce Partnership Executive Group SRO: TBC Chief Executive's Report and appendices.pdf Page 30 of 30 Overall Page 46 of 215
47 Agenda Item:9.1 TRUST BOARD 30 SEPTEMBER 2015 WARD STAFFING AND OPENING TIMELINES AND LISTER EMERGENCY DEPARTMENT RISK REPORT PURPOSE PREVIOUSLY CONSIDERED BY Objective(s) to which issue relates * Risk Issues (Quality, safety, financial, HR, legal issues, equality issues) Healthcare/ National Policy (includes CQC/Monitor) To present to the Board two papers considered by RAQC regarding: - Ward Staffing risks: The predicted staffing available for the closed wards Provide proposed opening timelines Articulate contingency plans whilst wards remained closed due to staffing constraints - Lister Emergency Department risk report These papers should also be discussed in context of the overseas recruitment and TDA agency cap. Executive Committee recommendation approved. RAQC, September To continuously improve the quality of our services in order to provide the best care and optimise health outcomes for each and every individual accessing the Trust s services 2. To excel at customer service, achieving outstanding levels of communication and patient, carer and GP satisfaction 3. To provide and support the best standards of integrated care for the elderly and those with long term conditions by developing key partnerships and services 4. To consolidate services and enhance local access to specialist services in order to deliver high quality, safe, seamless, innovative and integrated services which are sustainable 5. To support the continued development of the Mount Vernon Cancer Centre and provision of leading local and tertiary cancer services 6. To improve our staff engagement and organisational culture to be amongst the best nationally Delivery of financial, operational performance and strategic objectives, FT application, CQC ratings, Governance risk Rating, Contractual performance. Achievement of Monitor, CQC, DH Operating Framework and other national and local performance standards. CRR/Board Assurance Framework * Corporate Risk Register BAF ACTION REQUIRED * For approval For discussion For decision For information DIRECTOR: DIRECTORS OF OPERATIONS, NURSING PRACTICE & WORKFORCE AND DEVELOPMENT PRESENTED BY: DIRECTOR OF OPERATIONS/ DIRECTOR OF NURSING ACTING DIRECTOR OF OPERATIONS / DEPUTY DIRECTOR OF AUTHOR: NURSING AND DEPUTY MEDICAL DIRECTOR AND COMPANY SECRETARY DATE: SEPTEMBER Page We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement 9.01 Ward Staffing and ED risk Board Sept 2015.pdf Page 1 of 9 Overall Page 47 of 215
48 Ward Staffing and Opening Timelines 1. Issue Concerns regarding the impact of recent bed closures on ED patient safety and performance. 2. Background ENHT currently has 20 acute beds closed on the Lister site due to staffing capacity issues. Significant contributory factors are the delay in recruitment of RN s from the Philippians and ongoing competency issues. Additional supportive winter planning measures on recruitment will be presented separately to DEC. The actual sequencing of events has been redacted for the purposes of this paper however at the start of August the bed base on Ashwell ward was reduced from 28 to 15, and the function of Ashwell wards team was relocated onto ward 6A south. SSU also required refurbishment and therefore the function of SSU was moved into the vacated space on Ashwell ward. The consequence of these multiple moves resulted in a loss of 20 beds across the specialities served by Ashwell and 6A. Ward 9B also has critical levels of registered substantive staff and requires support to ensure that it retains the existing workforce. If there are additional leavers on 9B then closing beds on this ward may have to be considered. Contingency arrangements have been identified to reduce some of the risk of the reduced bed capacity resulting in exit block from the ED; however these arrangements cannot completely mitigate this risk. The additional capacity identified does provide in total 4 more beds than are currently closed however it is acknowledged these are not in the ideal locations and will not be routinely available. The intention is that once appropriate staffing levels are achieved then these wards will return to their original locations and the currently closed beds across Ashwell and 6A would be open. 3. Review of Staffing Pipeline and Staffing Capabilities A joint review of the staffing pipeline and turnover was conducted with representation from Nursing, Operations and Workforce. The group have modelled the known staff leavers, starters and factored in the impact of long term sickness absence, maternity leave and any other know absence to produce a forecast of available staff through to December In addition a clinical assessment has been completed by the nursing team regarding the skill levels of the staff that are forecast to be available. The nursing workforce on Ashwell and 6A has been categorised into novice and effective nurses, those in the novice category are deemed not suitably experienced or skilled enough to independently manage a group of patients without supervision. By combining these two factors a forecast has been modelled that details the likely number of gaps in the registered and unregistered workforce per shift for each ward, see appendix 1. Taking into consideration the forecast recruitment pipeline and the clinical skills assessment, the forecasting demonstrates that on both wards they are likely to have a significant shortfall in registered nurses until the start of November. The level of substantive staff is very low during the preceding months such that even if the gaps could be filled with temporary staff there would not be sufficient critical mass of permanent staff to ensure patient safety. 2 Page We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement 9.01 Ward Staffing and ED risk Board Sept 2015.pdf Page 2 of 9 Overall Page 48 of 215
49 The consensus opinion of Operations, Nursing and Workforce was that it would be unrealistic to safely open these beds before November. However to achieve this will also require additional support from the nurse education team. The recommendation is that Ashwell and 6A remain as per the current configuration until 1 st November but then returns to 28 and 30 bed units from 1 st November. 4. Risks The forecasting is based on known staff leavers, starters and the other factors stated above. If any of those factors increase beyond the levels modelled the recovery for November could be compromised. Furthermore, ward 9B currently has significant gaps in its workforce plus an effective nursing establishment of c, 55% until November, see appendix 1. The modelling demonstrates significant gaps in the registered nursing compliment during September and October. The staffing levels on this ward are at a critical level and action is required to mitigate the risk of further staff leaving this ward. If the staffing levels deteriorate then additional beds may have to be closed to ensure patient safety on this ward. It is further recommended that ward 9B is targeted with the intention of implementing strategies to retain the existing workforce with retention packages and enhancements for taking charge of the shift. In addition the ward will require support from the nursing education team to help ensure that the existing novice workforce gains the experience and skills required to become more effective. 5. Contingency Whilst the 20 beds remain closed it is recognised that operational pressures will continue, especially in respect to patient flow out of the assessment areas, which in turn can lead to exit block from the ED, resulting in patients waiting in the ED for transfer to other parts of the hospital. Therefore during periods of extreme capacity challenge the following escalation will be established: ACU to remain at 38 beds consistently until November Swift ward to continue opening to 12 beds at the weekend Woodland View 10 additional beds are expected to be available from mid-september, whilst these are aimed at re-providing the capacity lost from Pine lodge, this does reflect an improved capacity over the last two / three months. In extremis, and with agreement from the Director of Operations or Director of Nursing, open 2 bays and 2 side rooms on Ashwell ward, creating an additional 14 beds. In order to staff the extra temporary capacity on Ashwell ward, the staff allocated to the discharge lounge would be utilised. This would result in a loss of the discharge lounge but the benefit is considered greater than the risk. Also additional nursing would be drawn from other wards so that a critical mass could be established which could in turn support temporary staff to fill any further gaps in the shift rota. In order to facilitate this Division will identify appropriate staff based on ERoster data. It is anticipated that this will be complete by 18 th September. The combined impact of the Woodland View beds and the Ashwell contingency would create 24 beds more than has been available since the closure of the 20 beds. 6. Conclusion It is the consensus view that the 20 closed beds cannot be opened safely before 1 st November. Additional contingency plans have been developed to mitigate some of the patient flow issues and reduce the likelihood of exit block in the ED, however some risk remains. Opening the closed beds in November will require focused support to ensure that the novice nurses gain the required skills and experience in a condensed timeframe. In addition ward 9B 3 Page We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement 9.01 Ward Staffing and ED risk Board Sept 2015.pdf Page 3 of 9 Overall Page 49 of 215
50 also requires focused support and a retention package to mitigate the risk of the remaining workforce leaving. This decision was approved by Executive Committee 17 September Page We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement 9.01 Ward Staffing and ED risk Board Sept 2015.pdf Page 4 of 9 Overall Page 50 of 215
51 Executive Summary PATIENT SAFETY REPORT: LISTER EMERGENCY DEPARTMENT September 2015 In March 2015, the Medical Director presented a detailed paper to Board on the Lister Emergency Department risks due to the challenge of centralisation on a background of rising Emergency attendances and difficult outflow resulting, at times, in significant departmental crowding. The paper also outlined the mitigations and actions. This was in the context of the national picture where there has been a significant rise in the number of attendances to Emergency departments across the UK. This paper provides an update and seeks to outline the current levels of risk and safety within the emergency department. Current Status During summer months within the Emergency Department (ED) there has traditionally been a reduction in crowding and associated risk. In line with other health economies, East and North Herts Trust has continued to experience winter style pressures through the summer months and the ED performance target has not been consistently met, see table below. Over the last three months however, the risk has increased with continuing demand, and a loss of 20 beds across the specialities served by Ashwell and 6A following staffing capacity issues and patient safety concerns. These beds are not currently due to reopen until 1 November 2015 following substantive recruitment. The loss of around twenty beds in the system in conjunction with no reduction in admissions and further increases in ED attendances has meant the ED has experienced crowding on the majority of days each week throughout this period. An Emergency Department is defined as crowded if: Ambulances cannot offload There are long delays for high acuity patients to see a doctor Trolley patients in the ED exceed cubicle spaces ie over occupancy Patients are waiting >2 hours for an inpatient bed after a decision to admit. Risks, Performance and Quality: In March 2015 it was reported that whilst there is evidence that crowding has adversely impacted upon patient safety and outcomes at the Lister, good standards of clinical governance in the ED, a high level of ED Consultant support and flexibility, good basic nursing care, regular Operational Centre meetings and effective whole health system working have prevented a further erosion of standards, even when subject to extreme pressure. The Division report the ongoing pressures have meant that the ongoing associated risks have remained: Reduced quality of care Increase in serious incident occurrence Ability to deliver basic nursing needs compromised Increase stress for patients/carers and ED staff Increased complaints Difficult to retain experienced staff, further reducing efficiency and quality Increased ambulance offload times Reduced ability of the ambulance service in responding to emergency calls Length of stay for non-elective admissions rise 5 Page We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement 9.01 Ward Staffing and ED risk Board Sept 2015.pdf Page 5 of 9 Overall Page 51 of 215
52 Elective activity cancellations Longer waiting times Updated performance charts: Activity Ambulance Off Load Delays Measure 01/06/ /06/ /07/ /07/2015 Ambulance off load delays 306 delays >30 mins 284 delays >30mins Standard <15 mins 10 delays >60 mins) 10 delays >60 mins Time to treatment Standard <60 mins 44 mins 35 mins 4 Hour Performance 6 Page We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement 9.01 Ward Staffing and ED risk Board Sept 2015.pdf Page 6 of 9 Overall Page 52 of 215
53 Month % Performance Quarterly Performance Jul % Aug % Sep % Q % Oct % Nov % Dec % Q % Jan % Feb % Mar % Q % Apr % May % Jun % Q % Jul % Sep % Quality Indicators Privacy & dignity - Friends and Family tests show the ED is a national outlier (continual bottom 13 for past year) & CQC outlier in 2 areas on last patient survey. Deteriorating data on quality issues e.g. sepsis screening still at very low levels (failing CQUIN). Mock CQC review this was the only area of Trust deemed inadequate (this was in 2 elements, 3 were requires improvement). The department was not overcrowded during half of visit. This was rated as overall requires improvement in August 2015 with caring rated as good. Actions have been undertaken to address the issues raised. Serious Incidents: There have not been any SIs this calendar year but all previous SI s had crowding as a factor and no. of SIs in ED out way number in any other ward areas. Four incidents are currently under review and the 72 hour investigation reports being prepared this week for forwarding to the Director of Nursing and the Medical Director for consideration. Specific Measures Employed during Periods of Crowding During periods of crowding staff adapt their practice to ensure that maintaining patient safety at these times can still remain the priority and focus. This applies within ED, throughout the wider Trust and with our external partners. Measures include: Early initiation of escalation processes to maintain patient flow and safety Whole health sector approach including regular conference calls Cohort ambulance patients in the ED using Ambulance Crew who can perform observations, interventions and intial investigations East of England Ambulance liaison officer on site from 10am to 10pm to improve offload times Deployment of additional support to ED at times of extreme demand including specialist, resuscitation and research nurses. Introduction of a rapid assessment seated area within the ED to allow earlier interventions for patients attending with majors presentations Flexing CDU capacity Weekend working from 8am to 8pm for ED Consultants to enhance decision making Focus on the SAFER bundle to improve discharge planning and clinical efficiencies. Allocation of Ward Liaison Officers (WLO) to troubleshoot and drive efficiency. Senior Manager on site seven days a week until 10pm Senior Nursing Rota 24/7 over the most challenging 7 Page We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement 9.01 Ward Staffing and ED risk Board Sept 2015.pdf Page 7 of 9 Overall Page 53 of 215
54 Progress on actions agreed in March 2015 Implement the recommendations following external review by the Royal College of Emergency Medicine on 18 th March (Positive review) Progress the development of a Frailty Unit to allow prevention of admission assessments. Further explore the feasibility of Boarding on certain wards. Consider the development of a larger assessment area. Streamline surgical and gynaecology pathways to reduce attendances. Create additional inpatient beds Further improve efficiencies around length of stay and the discharge process. Integrated working with East of England Ambulance Service, GP Partners and Commissioners to reduce demand or provide alternative pathways of care. Update In progress, awaiting update on actions Established frailty unit of 15 beds in 2014 Reviewed and agreed by Medical Director this is not a viable option viable Additional capacity currently open on ACU (4 beds), but there is not any space for further development. In progress 14 bedded additional ward scheduled to open approximately 24 December 2015 LOS and discharge processes sustained Areas and workstreams being progressed however these are yet to have an impact N/A N/A Mitigations in Progress Additional capacity additional beds are already open on ACU 8 Page We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement 9.01 Ward Staffing and ED risk Board Sept 2015.pdf Page 8 of 9 Overall Page 54 of 215
55 - Flexing into the discharge lounge for overnight stays only - 10 commissioned step down beds at Woodlands come on stream week commencing 21 September Agreed to flexibly open 14 beds on Ashwell Ward during periods of pressure (Sunday pm to Wednesday); a ward leader has been identified with substantive staff from other wards to ensure the area is not just staffed by bank and agency and to spread the risk this is currently being established - On 1 November, Ashwell and 6a will be back to capacity - 14 bedded additional ward scheduled to open approximately 24 December Continue to implement the recommendations following external review by the Royal College of Emergency Medicine and streamline pathways. Acting on recommendations from the CQC mock inspection monitored weekly at CQC Programme Board. Continued focussed recruitment and progression of business case for additional staff Continued strengthening of whole health system integrated approach to ease crowding. Formalising the winter capacity plan with clinical engagement. Continue to review information, processes and systems to support effective decision making and delivery of a quality service e.g. use of BIMs to support a live bed state, review of the operations cell and working with TPP to turn around results more timely. Conclusion: Lister ED continues to experience significant crowding on the majority of days of each week with the associated clinical risks and there has been a recent deterioration in standards of care provided. This continues to be actively monitored by the Executive Teams and the CQC Programme Board. The Board are asked to note the risks and the actions taken and planned. 9 Page We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement 9.01 Ward Staffing and ED risk Board Sept 2015.pdf Page 9 of 9 Overall Page 55 of 215
56 Our vision: To be amongst the best TRUST BOARD MEETING 30 SEPTEMBER 2015 FINANCE AND PERFORMANCE COMMITTEE 23 SEPTEMBER 2015 EXECUTIVE SUMMARY REPORT Agenda Item:10.1 PURPOSE PREVIOUSLY CONSIDERED BY Objective(s) to which issue relates * Risk Issues (Quality, safety, financial, HR, legal issues, equality issues) Healthcare/National Policy (includes CQC/Monitor) To present to the Trust Board the report from the Finance and Performance Committee (FPC) meeting of 23 September 2015 N/A 1. To continuously improve the quality of our services in order to provide the best care and optimise health outcomes for each and every individual accessing the Trust s services 2. To excel at customer service, achieving outstanding levels of communication and patient, carer and GP satisfaction 3. To provide and support the best standards of integrated care for the elderly and those with long term conditions by developing key partnerships and services 4. To consolidate services and enhance local access to specialist services in order to deliver high quality, safe, seamless, innovative and integrated services which are sustainable 5. To support the continued development of the Mount Vernon Cancer Centre and provision of leading local and tertiary cancer services 6. To improve our staff engagement and organisational culture to be amongst the best nationally Key assurance committee reporting to the Board Financial risks as outlined in paper Potential risk to CQC outcomes Key statutory requirement under SFIs, SOs. Healthcare regulation, DH Operating Framework and other national performance standards CRR/Board Assurance Framework * Corporate Risk Register BAF ACTION REQUIRED * For approval For discussion For decision For information DIRECTOR: PRESENTED BY: AUTHOR: CHAIRMAN OF FPC CHAIRMAN OF FPC BOARD COMMITTEE SECRETARY/COMPANY SECRETARY DATE: 25 SEPTEMBER 2015 We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement FPC Report to Board.pdf Page 1 of 4 Overall Page 56 of 215
57 FINANCE AND PERFORMANCE COMMITTEE 23 SEPTEMBER 2015 EXECUTIVE SUMMARY REPORT TO BOARD 30 SEPTEMBER 2015 The following members were present: Julian Nicholls (Chair), Ian Morfett, Alison Bexfield, Bob Niven, Ian Morfett Other directors in attendance: Nick Carver, Tom Simons, Sarah Brierley Tony Ollis, Angela Thompson, Stephen Posey DECISIONS MADE UNDER DELEGATED AUTHORITY: The Finance and Performance Committee (FPC) made no decisions on behalf of the Trust under the authority delegated to it within its terms of reference: OUTCOMES: Floodlight Scorecard Month 5 The FPC reviewed the floodlight scorecard for Month 5 noting indicators were in line with the previous month and key issues were reflected in the Director reports. The Committee was advised the C.difficile and MRSA information was incorrect and assured this would be updated for Trust Board. Finance Report Month 5 The FPC received the Month 5 finance report indicating an adverse variance in month of 12k, a slightly more stable position than Month 4, and potentially better than reported since additional income had been received since writing the report. Catch-up on coding and recording of non-elective admission activity from June and July delivered a positive income variance. Further key messages included: CIP delivery in month was 1,396k (103%); Five months of the 3.0 contingency had been phased into budgets and expenditure had been accrued to budget. The FPC noted the challenges to Mount Vernon Radiotherapy income, pay variances from plan by division and welcomed that agency expenditure was 51k lower than the previous month. The FPC noted the latest information relating to cashflow and supported month-end forecasts being reviewed on a daily basis Year End Financial Forecast The FPC received an update on the 2015/16 year-end forecast, including range of financial risks facing the Trust, and progress regarding agreement of strategic and transformation funding with the CCG. Due to the national financial situation, the TDA had issued all Trusts with year-end stretch targets and the Trust had responded. The FPC discussed risks and opportunities to forecast and supported next steps to ensure delivery of the year-end forecast. The FPC agreed current negotiations with the CCG would be highlighted within future monthly finance reports. The forecast would be discussed at Trust Board, Part II. TPP verbal update The FPC received a verbal update on latest information concerning TPP confirming income was in line with expectations. The FPC discussed accounting treatment for TPP. Further discussions would take place at RAQC and Trust Board, Part II FPC Report to Board.pdf Page 2 of 4 Overall Page 57 of 215
58 Income Assurance Plan The FPC received an update on the income assurance plan for revenue capture and recognition. The Committee supported the formation of an income assurance group and actions taken to stabilise and address income issues. The plan included robust governance controls, a project initiation document and also identified anticipated benefits. The Committee requested assurance at Audit Committee of the plan to review lessons learnt from the implementation of a system upgrade to avoid potential issues in the future. Further discussion would take place at Trust Board, Part II. Deloitte Project Plan The FPC received an update on the Deloitte project plan following its review of the value and coverage of the Trust s activity capture. The Deloitte report identified three areas which would create a potential improvement in average value of activity compared to other Trust s, relating to depth of coding, non-specific coding and outpatient procedures. The Committee supported next steps to identify potential opportunities to improve the Trust s income position and requested an initiative plan to monitor progress. Performance Report Months 4 and 5 The FPC received the performance report for months 4 and 5 highlighting the Trust had a TDA risk rating of band 5, standard oversight, green. The Trust achieved the Referral to Treatment (RTT) standard but did not achieve the Emergency Department (ED) 4-hour and 62-day cancer standards. The Committee noted, to achieve the additional volume of RTT activity the Trust had jointly agreed to undertake, the Trust was outsourcing to three independent sector providers. Attendance at the ED in July continued at elevated levels with volumes higher than most of the previous winter months (the usual seasonal decrease in August did not occur) and despite the growth in emergency admissions, length of stay had been maintained. The FPC noted the latest information relating to bed capacity and was assured discussions were ongoing with the CCG with regard demand and staffing. The FPC was pleased to note improvements across a number of stoke standards, specifically the 90% length of stay spent on a stroke unit. Workforce Report Month 5 The FPC received the Month 5 Workforce Report providing the latest information relating to standard monthly metrics and Trust-wide issues concerning management of the workforce. Highlights of the report included: Overseas recruitment There would be a delay to Philippine nurses commencing employment with the Trust due to language testing and certificate sponsorship; the Trust had therefore increased its number of UK and EU recruitment campaigns. Absence Assist went fully live in August. This would ensure more rigorous sickness reporting. Owing to this initiative and close monitoring, the number of staff on long-term sickness absence had decreased from 109 in July to 104 in August. Temporary staffing demand overall decreased slightly in August. Following the TDA cap on agency nursing, controls had been strengthened and agency usage had reduced from 8.3% to 2.85%; it was anticipated this would reduce further to 0% by October. Following the successful deep dive into agency nursing, the FPC requested implementation of a similar exercise for all other agency staffing. The Committee noted the latest information relating to appraisals, turnover and resourcing and discussed staff rotation. OTHER MATTERS: Health Records Benefits Realisation The FPC received an excellent benefits realisation presentation on the Health Records project from the Divisional Chair, Clinical Support Services; the project delivered on time and within budget. The Committee received assurance that following recommendations made at FPC, FPC Report to Board.pdf Page 3 of 4 Overall Page 58 of 215
59 business case and project governance processes had been strengthened. The Committee requested a review of the project financials. Data Quality Metrics The FPC received the monthly report on data quality metrics highlighting progress on recommendations made following Monitor s Payment by Results audit; the report included other data quality initiatives identifying potential training needs for clinical coders to ensure coding accuracy. The Committee noted the downward trend in average depth of coding and the Charlson Index indicators and requested a return to previous reporting methods to monitor progress of all indicators. Strategic Projects Review The FPC received the bi-monthly Strategic Projects Review detailing progress of key strategic projects; this had been updated to include the Culture Change Programme. The Committee noted responsibility for the development of Service Level Reporting/Patient Level Information and Costing Programme had been transferred to the Head of Management Accounts. The FPC discussed the review compilation and agreed it should also reflect those projects which were currently in the background and high risk. PAS Exit The FPC received a verbal briefing on the patient administration system contract conclusion; implications, timelines, potential options and next actions. This had been discussed in depth at Executive Committee when it was agreed to build a Lorenzo Investment Case. The FPC supported the recommendation to proceed with the Lorenzo system since it was tried and tested at other NHS organisations. Further discussion would take place at Trust Board, Part II. Julian Nicholls Chairman 24 September FPC Report to Board.pdf Page 4 of 4 Overall Page 59 of 215
60 TRUST BOARD MEETING 30 SEPTEMBER 2015 FINANCE REPORT MONTH 5 Agenda Item: PURPOSE PREVIOUSLY CONSIDERED BY Objective(s) to which issue relates * Risk Issues (Quality, safety, financial, HR, legal issues, equality issues) Healthcare/ National Policy (includes CQC/Monitor) To set out the Trust s financial position for the period ending 31 August 2015 Finance and Performance Committee 1. To continuously improve the quality of our services in order to provide the best care and optimise health outcomes for each and every individual accessing the Trust s services 2. To excel at customer service, achieving outstanding levels of communication and patient, carer and GP satisfaction 3. To provide and support the best standards of integrated care for the elderly and those with long term conditions by developing key partnerships and services 4. To consolidate services and enhance local access to specialist services in order to deliver high quality, safe, seamless, innovative and integrated services which are sustainable 5. To support the continued development of the Mount Vernon Cancer Centre and provision of leading local and tertiary cancer services 6. To improve our staff engagement and organisational culture to be amongst the best nationally Financial risks are described in the main report Financial and contractual compliance with Department of Health policies including the Operating Framework for 2013/14. Monitor s Financial Risk Rating metrics are used within the report and appendices. CRR/Board Assurance Framework * Corporate Risk Register BAF ACTION REQUIRED * For approval For discussion For decision For information DIRECTOR: PRESENTED BY: AUTHOR: Director of Finance Director of Finance Director of Finance DATE: September 2015 We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement * tick applicable box Finance Report Month 5.pdf May 2013 Page 1 of 14 Overall Page 60 of 215
61 Finance Report for Month 5 (to the end of August 2015) 1. Purpose of report This report sets out the financial position of the Trust at the end of August. The attached appendices provide details of the financial position for the month and the key issues are highlighted in this report. 2. Summary position The position for the month of August 2015 is summarised in the following table: 000 Plan August Actual August Variance Plan YTD Actual YTD Variance Income 31,430 31, , ,174 (1205) Expenditure (31,240) (31,408) (168) (157,713) (158,390) (678) Contingency (250) (250) 0 (1,250) (1,250) 0 EBITDA (60) (73) (13) 1,416 (466) (1,883) Depreciation and PDC (979) (968) 11 (4,901) (4,843) 58 Interest (222) (232) (10) (1,103) (1,156) (53) Net surplus/(deficit) (1,261) (1,273) (12) (4,588) (6,465) (1,878) The Trust delivered a 1,273k deficit in August against a planned deficit of 1,261k, creating an adverse in-month variance of 12k. There is a 1,878k adverse variance year to date. The key messages this month are: The Trust has delivered an adverse variance against plan of 12k in the month. Clinical income was slightly above plan in the month CIP delivery in month was 1,396k (103%) and year to date is 5,935k (96%) Five months of the 3.0m contingency has been phased into budgets and expenditure has been accrued to budget. The Continuity of Service risk rating for the month remains as a 1 and is shown in section 8 of this paper Finance Report Month 5.pdf 1 Page 2 of 14 Overall Page 61 of 215
62 3. Key issues - Month 5 income and expenditure Clinical income Clinical income relating to NHS activity was slightly ahead of Plan in August at 27,031k versus 26,894k, a positive variance of 137k (0.5%). However, the underlying position was mixed with positive variances at the Lister and QEII masking a significant shortfall at Mount Vernon. A&E activity levels were above plan with attendances at the QEII increasing by approximately 1,000 per month following the closure of the Spring House GP walk-in service on the other side of the road. This is the second month since the Spring House closure and although the activity added is significant (adding around 10% to total attendance levels) the impact on income is less so since the vast majority of these additional attendances are at the lowest A&E tariff. The CCG have agreed that a new, local, tariff will have to be calculated for the QEII since the activity pattern there does not fit well with the existing national tariff structure. Some further attention is also required to levels of coding as the case-mix at the Lister has deteriorated in the last few months. Non-elective admission levels were about in line with plan but the catch-up on coding and recording of activity from June and July delivered some additional benefit and the aggregate position for the month is a positive income variance of 344k Both Day Case and Elective Inpatient activity was very slightly under plan for the month but any negative financial impact was mitigated by the favourable mix and the adverse financial variance was negligible. Inpatient Orthopaedic and Urology activity were the main positive contributors. It should be noted that the impact of elective patient cancellations, due to lack of bed availability, was 138k in the month. Although Outpatient activity delivered a positive variance of 70k in August this was largely driven by catch-up on chemotherapy outpatient coding for prior months. The main challenge for Mount Vernon is Radiotherapy where the last few months have seen a succession of negative variances versus Plan. The total in-month shortfall for Mount Vernon was 535k (although part of this was due to assumptions made in July about activity being recovered but then not materialising). Radiotherapy activity levels have been dropping since the beginning of the year and this accounts for the majority of the cumulative Plan shortfall of 752k. Activity levels at Mount Vernon are currently under active review by the local management team. Division Expenditure Pay Expenditure against plan There has been a 240k adverse variance from the plan in the month and year to date there is a 314k adverse variance. Actual pay expenditure in the month was 19.7m compared which is a similar level to July and August. The monthly pay budget for September, however, was 200k lower than in the previous month due to an assumed reduction in RTT activity and also due to some new assumed pay cost improvement schemes Finance Report Month 5.pdf 2 Page 3 of 14 Overall Page 62 of 215
 Surgical (140) (268) Cancer (25) 44 Clinical Support 22 258 Women s & Childrens (4) (143) Corporate (101)")
63 The table below summarises the variance from plan by Division. Variance from Plan Division Pay Variance in month 000s Pay Variance YTD 000s Medical 8 (101) Surgical (140) (268) Cancer (25) 44 Clinical Support Women s & Childrens (4) (143) Corporate (101) (104) Total Pay Variance from plan (240) (314) The in-month variances from plan, by Division, have been categorised in the table below as variances due to operational, CIP and other reasons. The operational category includes variances due to changes in activity, the agreed opening of additional capacity and authorised extra staffing for quality/patient safety Finance Report Month 5.pdf 3 Page 4 of 14 Overall Page 63 of 215
64 Variance from Plan Division Operational (Capacity/ Activity) 000s CIP Other Pay Variance from plan in month 000s/ % 000s 000s Medical 0 (0) 8 8 (0.2%) Surgical (68) (8) (64) (140) (2.7%) Cancer 0 0 (25) (25) (1.3%) Clinical Support 0 (1) (1.0%) Women s & Childrens 0 (8) 4 (4) (0.2%) Corporate 0 (40) (61) (101) (5.8%) Total Pay Variance from plan (68) (57) (115) (240) (1.2%) There is a small underspend of 8k in the Medical Division, of which 140k relates to underspends on nursing staff due to vacancies in wards and ED which have not been covered. This has resulted in some bed closures due to concerns regarding patient safety. This underspend has been offset by overspends on medical staffing of 124k particularly for ED ( 48k), acute medical staff ( 57k) and Dermatology ( 31k). The Surgical Division had an overspend of 140k of pay in the month, 57k of which related to additional RTT activity, which is matched with income, and 11k for the opening of Swift ward at weekends. Of the 64k other overspend, 26k relates to anaesthetics middle grade sickness and Consultant maternity leave and 14k relates to supernumerary costs of new starters in theatres and day surgery unit. The remaining 24k is due to additional Anaesthetic locum payments to cover vacant sessions. Although the Cancer Services Division are underspent year to date on pay, there was a 25k adverse variance in August. This was due to an adjustment in pay rates of agency chemotherapy nurses, which had been backdated to December This was a result of a lack of understanding of the NHSP system by an agency which has resulted in them being underpaid. This has now been rectified on the NHSP system for future months. There is a 101k pay overspend within the Corporate departments. Of this overspend 43k is within the information department, 32k within Finance and 19k for Clinical Coding. The majority of the overspend relates to the premium costs of covering vacancies, although there are also a few additional posts where interims are being utilised to strengthen the income and information teams and to undertake various finance projects. Agency expenditure Total agency expenditure was 1,935k in August, which is 51k lower than the previous month. A breakdown of the agency expenditure is summarised in the table below: Finance Report Month 5.pdf 4 Page 5 of 14 Overall Page 64 of 215

65 Staff group Actual Agency Expenditure in month 5 000s Estimated premium in month 5 000s Medical Registered Nursing Other Clinical Non Clinical Total Agency expenditure The graph below shows the trend for agency expenditure by staff group, for the prior twelve month period. Nurse Agency Expenditure There has been a small reduction in nurse agency expenditure in the month, however, it is still the second highest month in the last twelve months. Agency registered nursing was 746k in month, which was 11.96% of the total registered nursing expenditure. The TDA have requested that the Trust agency nurse should be below 8% of total nursing expenditure from October The Trust has put in a request for a change to this ceiling due to concerns regarding patient safety and the impact of the delay in Philippine nursing. Medical Agency Expenditure There was a 43k decrease in agency expenditure in the month on medical staff. This was mainly in the Surgical and Women s and Children s Division which was partially offset by an increase in the Medical Division, particularly for ED. An internal audit of the process for Medical Locum bookings has recently been undertaken to review the governance arrangements in place across the Trust for the management of medical locum usage. The review traces the processes followed by the respective areas in securing the best options for filling the resource gap. The final report, and recommendations, has not yet been issued but this is due imminently Finance Report Month 5.pdf 5 Page 6 of 14 Overall Page 65 of 215

66 Non Clinical Agency Expenditure Non clinical agency expenditure was 297k in the month ( 54k higher than previous month) and it is at the highest level in the previous twelve months. The main departments using non clinical agency are as follows: Division Month 5 Agency Non Clinical 000s Year to Date Agency Non Clinical 000s Finance Information Clinical Coding Catering Health Records Trust Management 7 86 IT Other Total 297 1,205 The majority of the above agency expenditure relates to cover for vacancies of which recruitment plans are underway. All managers of the above departments have been requested to produce a trajectory of the agency expenditure for the remainder of the financial year. The Directors of Finance and Workforce will be conducting a detailed review of all corporate and non clinical areas to identify potential cost reduction opportunities. Non Pay Expenditure There was an adverse non pay variance against the original plan of 188k in month and year to date there is a 1,389k adverse variance. Non pay expenditure in the month was 11.7m in August, which was 0.7m lower than in July. High cost drugs, which are directly recharged to the Commissioners, accounted for all of this reduction Finance Report Month 5.pdf 6 Page 7 of 14 Overall Page 66 of 215
67 The table below summarises the variance from plan by Division. Variance from Plan Division Non-Pay Variance in month 5 000s Non Pay Variance YTD 000s Medical 6 (184) Surgical (101) (436) Cancer (41) (92) Clinical Support 14 (155) Women s & Children s (3) (94) Corporate (63) (424) Total non-pay Variance from plan (188) (1,389) The table below summarises the reasons for variance from plan by. Division Operational (Capacity/ Activity) 000s CIP Other Non Pay Variance from plan 000s/ % 000s 000s Medical (0.5%) Surgical (54) 4 (51) (101) (6.9%) Cancer (22) (10) (9) (41) (1.3%) Clinical Support (4) % Women s & Children s (2) 0 (1) (3) (1.0%) Corporate 0 22 (85) (63) (1.7%) Total non-pay Variance (82) 19 (125) (188) (1.6%) The Surgical Division has an adverse variance of 101k due partially ( 54k) to higher activity in the month than planned. Of the activity related variance, 38k relates to Endovascular stent grafts (EVARS) which is a PBR excluded device, and which should be directly recharged to Commissioners. The Division are working with the income team to ensure that these devices are captured and recharged. The remaining overspend relates to pathology guidewire charges ( 18k), minor works on wards ( 14k) and above minor variances across a number of departments. The main reason for the Cancer non pay overspend is 24 higher activity than planned in the month, in particular relating to PET scans, which is recharged directly to the commissioners and higher pathology test charges. The 10k adverse variance on non pay CIPs is offset by a favourable variance on local income CIP schemes. The other 9k relates to higher charges from Hillingdon for utilities. The Corporate Division has an adverse variance of 63k in month. Although this is an improved variance from previous months, the increase in CNST premiums has been funded from reserves/unallocated budgets from this month. The main areas of overspends includes 24k NHSP contract charges where it was anticipated that temporary staffing usage would start to reduce from July There has also been a 37k increase, above budgeted levels, for professional fees relating to VAT Finance Report Month 5.pdf 7 Page 8 of 14 Overall Page 67 of 215
68 recovery. Some of this increase is currently being queried but there has been increased VAT recovery on capital of 220k and on business activities/partial exemption 468k. Cost Improvement Programme The Trust delivered 1,396k of CIPs in month against the target of 1,349k (103%) in month. Year to date 5,935k (96%) of CIPs have been achieved against a plan of 6,182k. A summary of the month 5 performance by Division is outlined in the table below. CIP Variance in Month 000s CIP Variance year to date 000s Medical Surgical (5) (110) Cancer Clinical Support (12) 21 Women s & Childrens (32) (139) Corporate (39) (225) Total 47 (247) The main adverse variances, in month are within the Women s and Childrens and Corporate Divisions. The majority of the adverse variance within the Corporate Division ( 49k in month and 194k ytd) relates to slippage on the data capture CIP. A separate update at the FPC will be provided for this CIP scheme. The Women s & Children s in month variance is due to continued slippage on a scheme relating to a Private Maternity Partnership with United Kingdom Birth Centre (UKBC), as well as further slippage on some other smaller schemes. The Division are currently forecasting 86% CIP delivery but are working on replacement schemes to counteract the current shortfall. Over the last three months the procurement team have been working closely with the Surgical Division on a tender process for hip and knee implants. There has been strong Clinical leadership, principally by Nick De Roeck and Rajesh Sofat, and full engagement from the Surgical team and procurement. The outcome of this process is an annualised saving in excess of 300k and represents a great example of engagement and a collaborative working. All Divisions have undertaken a CIP forecast, as part of their overall year end forecast. The current forecast is for 17.0m (94% delivery), but the Trust is requesting for Divisions to develop further mitigating schemes. 4. Cashflow The cash balance at the end of August 2015 was 3.387m, well above the plan of 2.0m. However this arose due to receipt of funds after the last payment run date and is not indicative of an improvement in the Trust s underlying cash position which remains challenging Finance Report Month 5.pdf 8 Page 9 of 14 Overall Page 68 of 215
69 The Trust has been given an IRWCS (Interim Revolving Working Capital Support) facility of 19.7m and 11.0m of it has been drawn so far. 6m was drawn down in April which effectively replaced the 6.0m TBL received in 2014/15 (repaid March 2015) and the 5m drawn down in June can be linked to the deficit sustained in 2014/15. Therefore none of the additional funding received to date addresses issues arising in the current financial year. East and North Hertfordshire CCG agreed to make an advance of 5.0m against the Acute SLA in August which will be repaid in March This has been arranged to help the Trust cash position in the period leading up to the disposal of the QE2 land. BPPC performance started the year at 53.7% in April and has now improved to 58.9% for the year to date. There have been a number of significant changes to the forecast for the remainder of 2015/16, the trigger for which is a change to the anticipated month in which the Trust expects to receive the sale proceeds of the disposal of the QE2 land. This was initially planned to happen in October, but the current expectation is that the residential sale will go through in January 2016 but the care home sale may not be until March The delay has been due to protracted negotiations with an existing tenant and the inclusion of a six week judicial review period which was not previously anticipated. As a consequence the Trust will not be in a position to repay any of the IRWCS until January 2016 and the repayment of the HCA loan will also be delayed to February 2016 (i.e. 30 days after the receipt of the disposal proceeds). On 11 th September, the Trust was obliged to submit a revised financial plan for 2015/16 and this is based on an Income and Expenditure deficit of 6.1m rather than the 8m deficit in the original plan. As a consequence of this, the planned receipt of PDC of 8m that was intended to match the current year deficit has been reduced to 6.1m. It is still assumed that the PDC will be received in November, but there is a risk that this may not be permitted due to the existing draws on the IRWCS facility. The Trust is working closely with the TDA s cash team to secure either the PDC or additional IRWCS in November. The revised plan is based on a payment holiday from the Trust s Capital Investment Loans (long-term loans taken out to fund the Our Changing Hospitals programme). The Trust has yet to receive confirmation that the Department of Health will allow this, but the cashflow forecast is based on that assumption. It is too late to prevent the collection of the interest and repayment in September, so it has been assumed that these will be refunded in March 2016 and it is further assumed that the March collections will not take place. The Trust is engaging with the TDA in order to advance the payment holiday. Finally, the Trust has applied to reduce its minimum cash balance from 2.0m to 0.5m which will enable it to increase payments to suppliers at the end of each month. If this is agreed by the Department of Health, it will be effective as of October and the plans and cashflow forecasts are prepared on this basis Finance Report Month 5.pdf 9 Page 10 of 14 Overall Page 69 of 215
70 5. Top 5 Debtors over 90 days Aged debtor report as at 31 st August 2015 in 000s. Current days days days days 181+ days Total outstanding debt NHS 7, , ,628 Non NHS 2, ,375 4,089 9,537 Total 9,368 1,220 1,275 1,409 4,920 4,973 23,165 A schedule detailing the main debtors over 90 days is shown below: % of,000 s total Total aged debtors as at 30 th August ,165 Over 90 day debtors 11,303 49% Summary of top 5 debts, over 90 days old The Pathology Partnership 4,953 NHS Bedfordshire CCG 1,122 NHS Luton CCG 1,119 Hertfordshire Community NHS Trust Luton Dunstable Hospital NHS Foundation Trust Sub-total 7,995 71% The Pathology Partnership has previously advised that there will be no payment of debtor invoices whilst the Trust owes TPP more than TPP owes the Trust. A plan to mutually pay non disputed items to reduce outstanding receivables and payables has been put to TPP. A meeting has been arranged for the 17 th September to discuss this and other issues between the two organisations. NHS Bedfordshire CCG debt relates to 2014/15 forecast outturn. The income team is working on agreeing the final outturn position with the CCG. The disputes regarding NHS Luton CCG relate to queries on the monthly 2015/16 SLA invoices which are currently under investigation by the income team. Hertfordshire Community NHST is withholding payments pending resolution of disputes on creditors regarding the therapies SLA. Representatives of the two organisations have met in July 2015 to address the disputed issues. Progress is being made with resolution expected by the end of September Finance Report Month 5.pdf 10 Page 11 of 14 Overall Page 70 of 215
71 Luton and Dunstable Hospital NHS Foundation Trust debt over 90 days has reduced by 103k over August. This is expected to further reduce by the end of September 2015 as discussions regarding the debt proceed. 6. Creditors over 90 days Aged creditor report as at 31st August 2015 in 000s. Grand Current Total 8,733 11,675 3,181 2,802 1,171 10,209 37,772 A schedule detailing the main creditors over 90 days is shown below:,000 s % of total Total aged creditors as at 31st August ,772 Total over 90 days creditors 14,182 38% Summary of Top 5 Creditors, over 90 days Pathology Partnership Trust 5,844 Hillingdon Hospital NHSFT 3,164 Hertfordshire Community NHS Trust 1,330 Paul Strickland Scanner Centre 1061 Princess Alexandra Hospitals NHS Trust 534 Sub-total 11,933 85% As mentioned above a plan has been proposed to TPP in order to mutually pay non disputed items and so reduce outstanding receivables and payables. From April 2015 the Trust commenced paying 504k per month to TPP against contracted invoices and has recently agreed to increase this to 526k. Agreement has been reached with Hillingdon Hospital NHS FT regarding the level of charges being levied by them for the services we use at Mount Vernon subject to agreement on future development of the MVCC site. In the meantime progress has been made on clearing undisputed payments. Hillingdon NHS FT have agreed a process going forward to issue a single monthly invoice for the SLA s. This will prevent on account payments being made in the future. The issue with Hertfordshire Community NHS Trust concerns disputes raised regarding the amount charged for therapies and the Treatment Centre, discussions are ongoing with resolution expected by the end of September Most matters are now resolved and the over 90 day creditors has reduced in month Finance Report Month 5.pdf 11 Page 12 of 14 Overall Page 71 of 215
72 Paul Strickland Scanner Centre includes an invoice for 476k which will be cleared in September. However, a further invoice for 499k is still awaiting approval by the Cancer Division. The Divisional Director of Cancer Services is organising a swifter approval process of these invoices going forwards. The issue with Princess Alexandra Hospital NHS Trust relates to an invoice for 2014/15 Maternity Pathways not being correct. The invoice is for 1,527k of which a partial payment of 1,000k has been made, as this is the amount that the Trust agrees. The Head of Contracts is resolving the issues relating to the balancing 527k. 7. Capital Appendix 7 shows a breakdown of the Capital Programme by scheme, with a planned spend of 9,228k for the current financial year. The total spend at the end of month 5 (August 2015) is 2,194k which is 1,297k below plan. Of this, 447k relates to IM&T particularly around the Windows 7 Upgrade, Proxima and Pico Cell project, although IT has raised the orders. 8. Continuity of Service Risk Ratings The continuity of service risk rating remains a 1 this month, as predicted. Continuity of Service - Financial Risk Ratings Month Aug-15 Metric Definition Weight Risk metric Risk rating ytd Forecast rating 15/16 Liquidity ratio Working capital balance x 360 (days) Annual operating expenses 50% < Capital servicing capacity (times) Revenue available for capital service Annual debt service 50% 2.5x 1.75x 1.25x <1.25x Overall rating Overall rating Year end Forecast A year end forecast, to include risks and opportunities, will be presented as a separate paper to part two of the Trust Board This paper will also provide an update on progress with agreeing with the CCG the strategic/transformation funding. 10. Summary There is an adverse variance in month of 12k and year to date there is a 1,878k adverse variance. There are still significant challenges ahead in delivering the agreed planned deficit Finance Report Month 5.pdf 12 Page 13 of 14 Overall Page 72 of 215
73 Tony Ollis Director of Finance September Finance Report Month 5.pdf 13 Page 14 of 14 Overall Page 73 of 215
74 TRUST BOARD MEETING 30 September 2015 PERFORMANCE REPORT MONTH S 4 & 5 Agenda Item:10.04 PURPOSE PREVIOUSLY CONSIDERED BY Objective(s) to which issue relates * Risk Issues (Quality, safety, financial, HR, legal issues, equality issues) Healthcare/ National Policy (includes CQC/Monitor) To update the Trust Board on: Progress against Monitor Compliance Framework, DH Operating Standards, Contractual standards and local performance measures. Exception reports outlining action taken and next steps are provided for indicators that are either red in month, or at risk year to date. Finance and Performance Committee 1. To continuously improve the quality of our services in order to provide the best care and optimise health outcomes for each and every individual accessing the Trust s services 2. To excel at customer service, achieving outstanding levels of communication and patient, carer and GP satisfaction 3. To provide and support the best standards of integrated care for the elderly and those with long term conditions by developing key partnerships and services 4. To consolidate services and enhance local access to specialist services in order to deliver high quality, safe, seamless, innovative and integrated services which are sustainable 5. To support the continued development of the Mount Vernon Cancer Centre and provision of leading local and tertiary cancer services 6. To improve our staff engagement and organisational culture to be amongst the best nationally Delivery of financial, operational performance and strategic objectives, FT application, CQC ratings, Governance risk Rating, Contractual performance. Achievement of Monitor, CQC, DH Operating Framework and other national and local performance standards. CRR/Board Assurance Framework * Corporate Risk Register BAF ACTION REQUIRED * For approval For discussion For decision For information DIRECTOR: PRESENTED BY: AUTHOR: DIRECTOR OF OPERATIONS DIRECTOR OF OPERATIONS DEPUTY DIRECTOR OF OPERATIONS DATE: SEPTEMBER 2015 We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement Page 1 of Performance Report Month 5.pdf Page 1 of 11 Overall Page 74 of 215
75 PERFORMANCE REPORT 1. Key Headlines The Trust has a TDA risk rating of band 5, standard oversight, green. The Trust did achieve the RTT standard but did not achieve the ED 4 hour standard (see section 3) or the 62 day cancer standard (see section 4). 2. RTT 18 weeks As noted in Section 1 ENHT achieved the aggregated performance across the Open pathway standard in July and August. RTT Trust Aggregated Performance Month Non Admitted (95%) Admitted (90%) Open Pathways (92%) September 96.6% 84.1% 94.6% October 95.9% 89.4% 93.6% November 95.2% 85.9% 93.3% December 95.3% 92.0% 92.1% January 93.3% 90.8% 91.5% February 91.4% 87.8% 93.2% March 95.2% 79% 94.2% April 95.8% 90.0% 93.1% May 95.9% 90.5% 94.2% June 95.1% 90.4% 94.7% July 94.4% 87.5% 94.2% August 94.2% 82.2% 93.4% 2.1 National Reporting As reported the national reporting rules for RTT changed in June the non admitted and admitted standards have been abolished. The Trust still monitors performance against these two standards however the contractual consequence of failure has been removed. ENHT did not achieve against these two abolished standards during July & August. However this is in line with the Trusts agreed plan with the CCG to focus on reducing the number of long waiting patients and therefore whilst these patients are being treated the Trust is expecting to not achieve against the previous standards. It is important to note that ENHT continues to achieve against the Open pathway standard, the remaining RTT standard. Following the national changes to the reporting of RTT further draft guidance has subsequently been released regarding the application of pauses or suspensions on patients pathways. It is proposed that these temporary stops in the RTT clocks will be removed from 1 st October. The full potential impact on our performance is currently being modelled at the time of writing. 2.2 Additional RTT Activity As previously reported ENHT has jointly agreed to undertake additional RTT activity over this financial year and to achieve a total reduction in the number of patients waiting over 18 weeks for treatment. Page 2 of Performance Report Month 5.pdf Page 2 of 11 Overall Page 75 of 215
76 To achieve the volume of activity required ENHT is outsourcing to three independent sector providers, whilst simultaneously developing longer term strategies that would bring this activity back in house in subsequent years. The current position is showing an increase in the number of open pathways (more patients on the waiting list), which requires further analysis, therefore the information teams from both the Trust and CCG have agreed to review and monitor the assumptions used in the joint commissioning model to ensure they are holding as a variation in these would produce a change in waiting list size. The increase in open pathways is largely within outpatients, however outsourcing of referrals to the private sector commenced in September with 555 referrals passed to Pinehill across 7 surgical specialties. The IS does create risks as previously they have over committed and not delivered the volumes expected, in addition the contractual levers they have been prepared to accept are not as robust as we would have liked however they are in a strong negotiating position, knowing that our options are limited locally. A national RTT PMO has been developed and ENHT are currently exploring the mechanisms of this structure with a view to potentially utilising capacity via the national PMO; however this is a new development and requires further investigation. A further update will be provided in subsequent reports. 3. ED Performance ENHT did not achieve the 4 hour standard for July and August and is not expecting to achieve for the quarter. Month % Performance Quarterly Performance Jul % Aug % Sep % Q % Oct % Nov % Dec % Q % Jan % Feb % Mar % Q % Apr % May % Jun % Q % Jul % Aug % 3.1 Demand / Activity Attendance volumes (patients either self-presenting or conveyed to the A&E via an ambulance, this excludes patients referred to A&E) continues at the higher levels. On the Lister site, July was a very busy month in respect to attendances with volumes higher than most of the previous winter months. In addition the usual seasonal decrease in August did not occur. During August the Lister ED had 8.4% (652) more attendances than the same period last year. Page 3 of Performance Report Month 5.pdf Page 3 of 11 Overall Page 76 of 215

77 Demand at the New QEII has continued to increase as planned, in July patients transferred from Spring House to the new UCC, reflecting a step change in demand. UCC Open s Spring House Activity to New QEII Admission volumes have been very high during July and August and are comparable with the busiest months of the winter. This has created pressure on our bed capacity and will have undoubtedly led to episodes of exist block within the ED. This occurs when patients are ready to be admitted to speciality or assessment ward beds and there is no downstream bed capacity to enable the patient to be transferred from ED. The consequence is that patients remain in the ED for longer periods, if this situation is sustained then the ED becomes silted up with patients which in turn results in patients waiting over 4 hours to be seen and treated. The subsequent graph shows emergency admissions and the current length of stay (LOS) for emergency patients. The LOS data for August is not complete due to data lags and therefore should be discounted, however despite the growth in emergency admissions, LOS has been maintained. Page 4 of Performance Report Month 5.pdf Page 4 of 11 Overall Page 77 of 215

78 NB: The data excludes Mount Vernon activity and the following specialties: Midwife Episodes, Obstetrics and Well Babies. 3.2 Bed capacity At the end of July, the Trust had to close 20 emergency beds due to critical staffing levels on the wards. This has resulted in a reduction in the normal bed stock available to manage patient flow. Furthermore the CCG commissioned step down beds (10) at Pinelode had been closed earlier in the summer due to quality concerns at Pinelodge, therefore the current net reduction in bed capacity is 30. The reduction in bed stock has undoubtidly increased the pressures felt within the ED, however the level of admissions during July and August is unprecidented and therefore could not have been forecast at that time. A detailed assessment of the opportunity to open the 20 beds as early as possible has been jointly completed by the Director of Nursing, Workforce and the Deputy Director of Operations and had jointly concluded that the earliest timeframe to open is the 1 st November, based on the current shift establishment. The CCG has also commisioned a further 10 step down beds from another community facility which commences on 21 st September. In addition ACU has been increased to 38 beds, increasing by 4 beds and the discharge lounge is being used as an over night facility as required. Providing an additional 4 over night beds. Furthermore an additonal contingency plan is also being developed to allow the opening of up to 14 of the closed beds in response to critical capacity pressures. On 14 th September, 14 additional beds were opened during the evening in response to bed capacity issues. However due to staffing constraints these beds cannot remain open and need to be flexed in extremis only. At the time of writing a further paper is to be discussed at DEC which considers the risks to the ED as well as the risks to ward staffing. Whilst some mitigation has been implemented these actions do not consistently provide additional beds at the time they are required by the ED therefore flow and bottle necks will be created during surges in admission demand. 3.3 ED Staffing As stated previously ED performance is multifactorial and the current performance levels attained does not reflect the effort and hard work of the ED team that frequently run shifts short staffed or rely on their own staff working additional hours to support the current gaps in the rota. Page 5 of Performance Report Month 5.pdf Page 5 of 11 Overall Page 78 of 215
79 The ED business case supported a phased increase in staffing levels, aiming to achieve full staffing levels by October.. However until the team is fully established to the levels proposed the team will struggle with demand during peaks in activity, especially during the afternoon and early evenings. 4. Cancer Cancer performance is reported retrospectively, June and July s finalised position is shown below. In June the Trust did not achieve the 62 day referral to treatment standard or for the quarter. A significant contributing factor was the large volume of referrals that were received late in the pathway from other organisations. ENHT has written to the CEO of these hospitals reminding them of the need to ensure that patients are referred earlier in their pathway. However this wasn t the only factor that led to the failure of this standard and ENHT has identified a number of internal issues that needs to be addressed to make the pathway more efficient in the future and to ensure a sustainable delivery of this standard. Details of the recovery actions are detailed in section 4.1 Performance June 2015 Ta rge t Goal Threshold 2014/15 Target Referrals Cancer Referral to 1st Outpatient Appointment < 14 Days 93.0% 97.4% 94.6% 95.3% 95.3% Referrals with Breast Symptoms (wef January 2010) < 14 Days 93.0% 94.4% 93.5% 94.4% 94.4% Cancer Treatments Month To Date Quarter To Date Year To Date Diagnosis to 1st Definitive Treatment for all Cancers < 31 Days 96.0% 96.8% 96.2% 97.7% 97.7% Referral to Treatment from Screening (62 Day) < 62 Days 90.0% 92.8% 92.0% 89.7% 89.7% Second or Subsequent Treatment (Anti Cancer Drug Treatments) < 31 Days 98.0% 99.1% 99.3% 99.2% 99.2% Second or subsequent treatment (Radiotherapy Treatments) < 31 Days 94.0% 96.0% 95.5% 97.4% 97.4% Second or subsequent treatment (Surgery) < 31 Days 94.0% 94.5% 97.9% 96.1% 96.1% Urgent Referral to Treatment of All Cancers < 62 Days 85.0% 81.4% 76.9% 81.2% 81.2% Nat Average (June) Nat Average Qtr (Q1) 94.1% 93.6% 93.0% 93.4% 97.4% 97.5% 93.5% 93.1% 99.6% 99.6% 97.7% 97.6% 95.2% 95.0% 81.2% 81.8% In July, ENHT did not achieve the 62 day referral to treatment standard or the 31 day second or subsequent treatment (radiotherapy). It is also worth noting that the national average for Breast Screening was only 92.4% against a target of 93%. ENHT achieved 96.1% August s performance closes on Monday 5th October At this time ENHT is forecasting that it will not achieve the 62 day standard. Performance July 2015 Ta rge t Goal Threshold 2014/15 Target Referrals Cancer Referral to 1st Outpatient Appointment < 14 Days 93.0% 97.4% 96.9% 96.9% 95.8% Referrals with Breast Symptoms (wef January 2010) < 14 Days 93.0% 94.4% 96.1% 96.1% 94.8% Cancer Treatments Month To Date Quarter To Date Year To Date Decision to Treat to 1st Definitive Treatment for all Cancers < 31 Days 96.0% 96.8% 97.2% 97.2% 97.5% Referral to Treatment from Screening (62 Day) < 62 Days 90.0% 92.8% 100.0% 100.0% 91.7% Second or Subsequent Treatment (Anti Cancer Drug Treatments) < 31 Days 98.0% 99.1% 99.0% 99.0% 99.1% Second or subsequent treatment (Radiotherapy Treatments) < 31 Days 94.0% 96.0% 92.3% 92.3% 96.1% Second or subsequent treatment (Surgery) < 31 Days 94.0% 94.5% 97.4% 97.4% 96.5% Urgent Referral to Treatment of All Cancers < 62 Days 85.0% 81.4% 79.7% 79.7% 80.7% Nat Average (July) Nat Average Qtr (Q1) 93.9% 93.6% 92.4% 93.4% 97.8% 97.5% 94.4% 93.1% 99.7% 99.6% 97.9% 97.6% 95.8% 95.0% 81.7% 81.8% Page 6 of Performance Report Month 5.pdf Page 6 of 11 Overall Page 79 of 215
80 Day Recovery Actions In order to deliver a sustained and consistent performance against this key performance indicator a full pathway review at tumour site level is required. The cancer division will lead on this project which will report back to DEC fortnightly on an exception reporting basis. A copy of the current action plan has been embedded into appendix 1. The plan is a working document and is currently still in development, the intention being that the CCG and TDA will jointly agree the plan and recovery trajectory. Full sustainable and consistent performance is expected from 1 st Dec onwards. Whilst an earlier achievement trajectory would be preferable, inconsistent performance would also be equally undesirable therefore December is a realistic timeframe for completion of this extensive piece of work. 4.2 Current long waiting cancer patients ENHT currently has 11 patients that have waited over 100 days, representing 0.9% of the waiting list; the number of patients in this cohort typically fluctuates between 15 and 25 patients. The graph below demonstrates the current trend based on a four week moving average. The number of patients also waiting over 92 days has decreased over a sustained period such that the range of variation has been reduced evidencing a stable reduction in this cohort of patients. Albeit that over the last four weeks there has been a slight increase in the volume, however the number remains within the upper levels of normal variation even with the reduced range. The longest waiting patient has waited 139 days; however these are patient initiated delays which also included diagnostic delays by the patient due to their work commitments. The patient has a confirmed treatment date for 30 th September. 5. Stroke Stroke performance is reported retrospectively, therefore the latest data relates to July. Page 7 of Performance Report Month 5.pdf Page 7 of 11 Overall Page 80 of 215
81 E&NH 4 hours direct to stroke unit standard 90% 90% of time on the stroke unit standard 80% 60 minutes to scan standard 50% 60 minutes to scan urgent only standard 90% Scanned with 24 hours standard 100% TIA - high risk, not admitted, treated within 24 hours standard 60% TIA - low risk, treated within 7 days from first contact standard 65% Month Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul % 46.80% 48.70% 61.50% 29.50% 44.20% 50.00% 39.50% 70.30% 61.90% 62.50% 64.20% 71.80% 67.30% 66.70% 83.30% 78.30% 84.90% 78.40% 64.30% 86.10% 72.10% 80.90% 82.20% 52.80% 42.20% 32.40% 42.90% 31.80% 38.50% 42.90% 33.30% 57.60% 59.50% 66.70% 62.90% 80.00% 88.20% 91.70% 91.70% 81.80% 76.50% 76.20% 66.70% 85.00% 95.70% 88.90% 92.50% 94.60% % % % 95.50% 98.10% 98.00% 89.70% 97.20% 97.70% % 98.60% 54.50% 94.40% 66.70% 55.60% 56.50% 55.20% 77.80% 72.00% 58.80% 45.50% 76.20% 78.60% 82.50% 86.70% 91.70% 80.00% 89.70% 87.10% 75.90% 69.70% 68.00% 70.00% 88.60% 89.70% Page 8 of The Trust has seen improvements across a number of the standards over recent months, especially the 90% of length of stay spent on a stroke unit. This improvement commenced with the increase in beds following the ward move in October 2014, which was followed by a further increase in capacity in June Performance however remains a challenge in the 4 hour direct admission to a ward standard. This is a key indicator that continues to be challenging as it requires prompt identification of a potential stroke at presentation to the ED. This is particularly challenging for those patients that present with vague neurological symptoms, however further work in ongoing to improve performance in this area. FPC has previously received the full stroke recovery plan detailing actions being taken in this area. Each month a detailed breach analysis is carried out and a summary of the key reasons is developed. In respect to the standard for getting to the stroke unit within 4 hours of presentation the primary breach reason related to those patients presenting with an uncertain diagnosis. Breach Analysis 4 hours Clinical Need 5 Uncertain Diagnosis 15 Delay to stroke bed request 1 No capacity 3 All patients that breach as a consequence of not initially being recognised as a stroke are individually case reviewed by the stroke and ED teams to ensure that learning can be extrapolated and shared from each occurrence. 5.1 West Essex / PAH Performance Report Month 5.pdf Page 8 of 11 Overall Page 81 of 215
82 As previously mentioned West Essex CCG is not commissioning PAH to provide Hyper Acute stroke services and their intention is that from 2 nd November patients will flow to surrounding hospitals that provide HASU services (Hyper Acute Stroke Services). ENHT recognises that the services provided at PAH are not at the required standards and that their service is predominantly locum delivered which increases the risk if those staff members leave. Therefore in anticipation the Trust has already reconfigured its stroke bed base to provide some additional capacity, this has in turn reduced the capacity in elderly care which moves some risk into this area, especially if PAH cannot repatriate the Mid Essex patients within the planned timeframes. However at the time of writing, the business case between ENHT and the CCG has not been finalised and agreed, therefore ENHT will not be able to recruit and staff the stroke unit to required standards by the 2 nd November. The Trust would however be able to provide stroke services but would not be compliant with East of England staffing standards for a HASU and stroke unit. In addition the Trust is aware that one of the other hospitals that is expecting to receive patients from PAH has formally requested that Mid Essex reconsiders and defers the go live until spring of next year due to concerns about the impact on bed capacity during the winter months. ENHT will also recommend that the date is deferred until spring however if Mid Essex proceeds with the planned date the Trust has taken some steps to mitigate the impact albeit it does increase capacity risk in the elderly care areas. 6. Post-Acute Transfer Delays The graph below details all the patients awaiting transfer to other agencies and expected discharges at 11:00 hours. This graph demonstrates the operational impact on the day to day bed pressures more clearly as it shows the number of acute beds occupied by patients awaiting transfer to sub-acute areas either official or unofficial delays. Support across the health system continues in this area, however more recently the number of delays has started to increase again placing additional pressures on our bed capacity. Stakeholders have a daily telephone conference (7 days per week) to discuss every single patient and to try and reduce delays, this process also enables specific issues to be escalated to more senior managers for action. Page 9 of Performance Report Month 5.pdf Page 9 of 11 Overall Page 82 of 215

83 Notes Data taken at 11:00 each morning, prior to conference call Expected discharges = of those listed as awaiting transfer, how many are known to be being discharged that day Info includes total patients awaiting transfer to other agencies, e.g. CHC, Fast Track, Social, HCT, Self-funding Page 10 of Performance Report Month 5.pdf Page 10 of 11 Overall Page 83 of 215
84 10.03 Performance Report Month 5.pdf 11 P a g e Page 11 of 11 Overall Page 84 of 215
85 TRUST BOARD 30 SEPTEMBER 2015 WORKFORCE REPORT MONTH 5 Agenda Item: 10.4 PURPOSE PREVIOUSLY CONSIDERED BY Objective(s) to which issue relates * Risk Issues (Quality, safety, financial, HR, legal issues, equality issues) Healthcare/ National Policy (includes CQC/Monitor) To provide information on standard monthly metrics and Trust wide issues relating to management of the workforce Finance and Performance Committee, Risk and Quality Committee. 1. To continuously improve the quality of our services in order to provide the best care and optimise health outcomes for each and every individual accessing the Trust s services 2. To excel at customer service, achieving outstanding levels of communication and patient, carer and GP satisfaction 3. To provide and support the best standards of integrated care for the elderly and those with long term conditions by developing key partnerships and services 4. To consolidate services and enhance local access to specialist services in order to deliver high quality, safe, seamless, innovative and integrated services which are sustainable 5. To support the continued development of the Mount Vernon Cancer Centre and provision of leading local and tertiary cancer services 6. To improve our staff engagement and organisational culture to be amongst the best nationally Financial: increased workforce costs HR: failure to meet agreed standards Legal: failure to meet CQC and other national standards Patient Safety: failure to maintain appropriately trained workforce CQC 13 and 14 NHSLA CRR/Board Assurance Framework * Corporate Risk Register BAF ACTION REQUIRED * For approval For decision For discussion For information DIRECTOR: PRESENTED BY: AUTHOR: Director of Workforce and Organisational Development Director of Workforce and Organisational Development Head of Workforce Performance, Information & Planning DATE: September 2015 We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement * tick applicable box Workforce Report Month 5.pdf April 2014 Page 1 of 10 Overall Page 85 of 215
86 Workforce Report September 2015 (Based on data as at the end of August 2015) 1.0 Purpose This paper provides an update to the Finance and Performance/RAQC Committee for August 2015 on workforce performance. 2.0 Executive Summary The Trust took part in April 2015 a successful recruitment campaign in Philippines and 84 experienced nurses had been selected. Since the start of the Filipino campaign a number of challenges have been identified which are outside of the Trust s control that have impacted upon when the Filipino nurses will commence work in the Trust it is projected that they will arrive between Feb 2016 May To mitigate the risk caused by the Filipino delay, the Trust has increased the number of UK and EU recruitment campaigns. Absence Assist went fully live in August with the exception of Medical & Dental staff. Absence assist has introduced a more rigorous sickness reporting. The number of staff on long term sick has decreased to 104 in August from 109 in July. All long term sickness cases are now being managed through the HR Advisory Service, with additional cases under monitoring. Temporary staffing demand overall decreased slightly (1%) in August, however there was an increase in Nursing and Midwifery shifts (4%). Overall bank fill was maintained during August despite a proportion of staff being unavailable due to the holiday period. Continued work on agency controls for Nursing has reduced tier 4 (off framework) agency usage from 8.3% to 2.8% (of total agency fill) in eight weeks. It is expected that this will reduce to 0% by October meaning 100% framework compliance for Nursing and Doctors. Our Culture Ambition We want to be known as an organisation where our people feel engaged, valued and supported and empowered to deliver excellent patient care and services they are proud of. 3.1 Culture Programme - ARC In June, the Trust Board approved the Next steps ARC Programme paper, incorporating our leadership and talent strategy. Work has commenced on some workstreams in line with the milestones outlined in the strategy including: The coaching culture programme for leaders is being presented to managers at the current ARC sessions. Participants are asked to consider how the actions will enable them to meet the current challenges they are facing. Developing a leadership charter - using feedback from recent ARC sessions and centred around our values, a charter has been drafted and we are now gathering feedback at current ARC sessions Refreshing our behaviours linked to PIVOT values - these have been simplified and again, feedback is being gathered at ARC sessions Design work is being done for the next phase of our customer care training programme, working with Outpatients to develop a bespoke workshop to Workforce Report Month 5.pdf 1 Page 2 of 10 Overall Page 86 of 215
87 engage with staff in these areas to deliver excellent customer experience. 3 pilot workshops will take place in September with full roll-out from November Improving our processes to enhance our values based recruitment Recruitment processes are underway to fill posts in order to commence other key elements of the strategy including talent management, passport to leadership and a new more engaging, patient focused induction programme. The September ARC sessions are underway focusing on our Trust vision and strategic aims and preparing for CQC. So far almost 400 leaders are booked to attend. 3.2 Equality and Diversity During August the Equality and Diversity objectives for 2015/16 were refreshed. Agreement was reached regarding the notice board and ensuring the information is consistent with the Trust s approach. Work is underway for Equality week next year. The E & D newsletter is being finalised ready for communication throughout the Trust and within the Community Hub. Meal planning is in it s final stages with the Catering department with the aim of having foods in our Lister Restaurant which are representative of the diversity of both of workforce and our local community on a regular basis. 3.3 Staff Survey Quarter 2 staff Friends and Family Test (FFT) and our internal Finger on the Pulse survey has been open since early August and is due to close week commencing mid- September. Results will be able to show which areas staff feel are improving or getting worse since the previous quarters responses. The Trust have taken the decision to issue the national staff survey to all staff in 2015 and this will be run between the end of September and November. In response to staff reporting increased work related stress, some additional questions will be included to help identify and understand the underlying causes of stress so that appropriate and timely improvements can be taken forward. 3.3 Health at Work Service During July/August the Health at Work service screened 395 pre-placement questionnaires to support the Trust with ongoing recruitment plans. This compares to 389 in May/June 15. However, this is a substantial increase in activity compared to 153 in May/June 14 and 299 July/August 14. The service moved their clinical/advisor space from Woodlands clinic to the Mental Health unit, members of the team worked over the weekend to ensure there was minimal impact on service provision to the Trust and no face to face clinics were cancelled. Planning for the Flu campaign is well underway with a target of 70% clinical staff uptake. Following feedback from last year s campaign it is planned that central areas within main Trust sites will be utilised where possible to provide drop in sessions, as this is the preferred location for staff to receive vaccinations, although walkabouts and booked sessions will also be available Workforce Report Month 5.pdf 2 Page 3 of 10 Overall Page 87 of 215
88 4. Developing our people Ambition: We want to develop our people so that everyone has the skills and knowledge they need to deliver high quality patient care and so that we can build our workforce for the future. 4.1 Appraisal rate The overall appraisal rate for the Trust is 75.01% (12 month rolling) an decrease from 76.04% July but an increase from June position of 73.80%; see Appendix 1, Section 3, Table 1. The appraisal rates over a rolling 12 month period were highest in CSS (93%) and Cancer Services (88%). Medicine at 61% and surgery at 60% significantly impacted on the overall compliance rate. Surgery s performance has risen from 58% in July to 60% in August, while Medicine compliance rates have dropped from 64% in July to 61% in August. DEC has approved the switching off automatic pay progression unless staff are appraisal and statutory / mandatory training compliant, this is effective for managers who supervise staff and for all staff from 1 st November Statutory and Mandatory Training Details of statutory and mandatory training data can be found in Appendix 1, Section 3, Table People Performance Ambition: We want to ensure that we have the people we need and are clear about the standards we expect. This will enable and support the delivery of safe, consistent and high quality patient care. 5.1 Pay Position This month there was a 1.24% pay overspend on staff, with a variance over budget of 241,254. For further information on this month s pay position please refer to the Finance Paper. 5.2 Bank and Agency Spend The expenditure on agency was 1,935,264 in August; representing 9.8% of pay spend. Bank spend was 751,354 which was 3.8% of pay spend. Additional information can be found in the Finance paper. See Appendix 1, Section 4, Table 1 Bank and Agency Spend. Graph 1, Section 4 details the ledger position against worked wte. 5.3 Resourcing The Trust baseline vacancy rate increased to 6.48% (338 wte) in August 2015 from 4.58% in July and 5.52% in June. The significant rate drop in July was due to the Junior Doctor handover periods crossing across months. These percentages are based on the March ledger. An additional 250 wte posts (102 wte qualified nursing & 25 wte nursing support) were added in the May ledger, this puts the new establishment vacancy rate at 11.29% Workforce Report Month 5.pdf 3 Page 4 of 10 Overall Page 88 of 215
89 The Trust reached the projected target reduction and was on track to have a 5% baseline vacancy rate in August 15. However, 24 wte more qualified nursing staff left the Trust in July and August than started. Additionally, 11 wte more Scientific, Therapeutic & Technical staff left than started during July and August. The number of leavers is consistent with July and August last year. Appendix 1, Section 4, Table 3 compares the vacancy and turnover rates for neighbouring large acute hospitals were published information was available. There are currently in excess of 297 wte external candidates (including 50 wte medical training grades and excluding the Filipino Nurses) undergoing pre-employment checks and awaiting start date. In addition, there are almost 60 wte internal staff being appointed to other departments or promoted within their own area. Since the increase in establishment in April 2015, the original Drive to 5% project has been recast. The updated project plan (including social media initiatives) is available for review and contains a significant range of interventions to bring the vacancy rate to under 5% based on the new establishment by March 16. The Trust currently has 150 wte (9%) qualified nursing vacancies based on the March ledger but 252 wte (14%) based on the new 15/16 establishment. There are currently 88 wte in the recruitment pipeline at pre-employment (excluding the Filipino recruitment pipeline), about to start. Within the pipeline 42 wte newly qualified nursing staff are expected to join the Trust in September and October following on from successful completion of their training. It is projected with our current recruitment campaigns that the nursing qualified vacancy rate will be around 10.5% based on the new establishment by the end of December The trust took part in April 2015 a successful recruitment campaign in Philippines and 84 experienced nurses had been selected. These nurses are currently undertaking their IELTS (English test) and theoretical tests (CBT) which are an essential requirement of the NMC registration This 84 wte are in addition to the current pipeline outlined above. Since the start of the Filipino campaign a number of challenges have been identified which are outside of the Trust s control that have impacted upon when the Filipino nurses will commence work in the Trust it is projected that they will arrive between Feb 2016 May A separate paper detailing the issues will be presented to the September Board including actions that are been taken to mitigate so far as possible the operational impact. The Trust is one of a number of NHS organisations that is experiencing difficulties in having non-eu candidates entering the UK. The mitigation plans are also balancing the benefits of more EU nurses with the challenge of bringing them up to full clinical and language competency. There have been two separate recruitment open days scheduled for qualified staff nurses (one specifically for Elderly Care and Medicine; the other for nurses interested in taking up posts in surgery division). Extra UK based cohort nurse recruitment days are ongoing. There are 80 wte Clinical Support Worker (CSW) vacancies with 23 wte due to start October 15. All unqualified nursing vacancies are due to be filled by December. CSW recruitment was slowed down to accommodate the EU nurses working at Band 3 until their nursing registration is received. However given the issues with the arrival of the Filipino nurses the Trust has commenced several recruitment campaigns with the plan to fill all CSW posts by the end November In addition, 17.8 wte new CSW posts have been approved for specialing and these posts are in the process of being recruited. The attached graph in Appendix 1, Section 1, Graph 2 & 3 shows the planned vacancy level reduction over the next few months. This takes into account the recruitment pipeline (candidates currently at pre-employment checks and awaiting start date) and Workforce Report Month 5.pdf 4 Page 5 of 10 Overall Page 89 of 215
90 the projection of an average monthly attrition of 11%. Graph 2 details the vacancy levels based on the newly approved establishment for 15/16 and Graph 3 details the vacancy levels based on the March baseline establishment. The overall time to hire has increased to 9.8 weeks in August 2015 compared to 8.2 weeks in July The pre-employment checks stage of has increased by 0.6 weeks and is currently at 4 weeks see Appendix 1, Section 4, Table 2. The time to hire has increased from last month due to increased pipeline and number of applicants currently undergoing pre-employment checks. A contributing factor to this would be difficulties in obtaining references in time due to holiday period in August. The overall time to hire is predicted to be under the agreed target again in September See Appendix 1, Section 4, Table Temporary Staffing See Appendix 1, Section 4, Table 3 & 4 for NHSP Performance data. Temporary staffing demand overall decreased slightly (1%) in August, however there was an increase in Nursing and Midwifery shifts (4%) which were mainly related to sickness and escalation. Overall bank fill was maintained during August despite a proportion of staff being unavailable due to the holiday period. Agency fill dropped off by 4% which resulted in the overall fill rate going from 83% to 80% (79% to 75% in nursing alone). Continued work on agency controls for Nursing has reduced tier 4 (off framework) agency usage from 8.3% to 2.8% (of total agency fill) in eight weeks. It is expected that this will reduce to 0% by October meaning 100% framework compliance for Nursing and Doctors. A series of stake-holder engagement meeting were carried out in August as part of preparation for the tender of the Temporary Staffing Management Service. The various models for operating a Temporary Staffing Managed Service are being assessed along with service requirements so that the final specification can be confirmed by early September. The Trust has also conducted a market engagement exercise arranging to meet with all of the suppliers to discuss the procurement process. Since the introduction of the increased bank pay rate for general Registered Nurses the bank fill has picked up by an average of 55 shifts per week which is a 9% increase. There has also been an increase to bank only recruitment for Registered Nurses which is likely to be a result of the increased pay rate. The trust plans to continue to restrict the access agencies have to shifts to ensure that bank is the preferred choice of employment for temporary nurses. The Trust has partnered with NHS Professionals to carryout overseas recruitment in Italy. The workers will start in the Trust on long term bank contracts. It is expected that a total of 12 will be recruited and ready to start in January. TDA and Monitor announced that new agency rules, affecting nurses and midwives, will be introduced from September These are mandatory use of framework agencies and a ceiling on agency spending over the next three years. It has been part of the Trust s strategic goals, within temporary staffing this year, to remove the use of nonframework agency. We are currently in a very strong position to be compliant with this rule with 99% of agencies used being from an approved framework. This is a significant achievement as it has been reported that across the East of England Trusts, approximately 40% of agency usage is off framework Workforce Report Month 5.pdf 5 Page 6 of 10 Overall Page 90 of 215
91 The Trust has raised concerns with TDA and Monitor about the ceiling on agency spend being imposed it at this time and whether it would be feasible to set a limit. The agency spend limit is to be based on last year which is unrealistic for the Trust as vacancy levels have been higher since OCH. In addition, the workforce plans to significantly reduce vacancy levels have been delayed due to difficulties in recruiting overseas from the Philippines. Therefore to achieve the target the Trust would either need to close wards or impact on its nursing ratios. Appendix 2 provides an update on nursing agency spend ceilings and nurse agency trajectory. 5.4 Turnover The Trust s turnover was 13.02% in August, 13.01% in July and 13.12% in June. This annualised figure has seen increases over the year due to OCH changes. Corporate has the highest level of turnover at 17.24%, Women s and Children have the lowest level at 9.94%. Nursing unqualified have the highest staff group turnover of 15% and Medical and Dental have the lowest at 8.5%. Qualified nursing have a 13% turnover rate. Turnover remains to be a challenge at present, this month with 61 wte leaving the Trust (excluding training doctors) of which 21.5 wte were qualified nursing staff and 8 wte were unqualified nursing staff. 34 wte staff started (excluding training doctors), 5.4 wte Nurses and 8.8 wte unqualified nurses. Processes have been put in place to undertake exit interviews with members of staff who are leaving the Trust or who are thinking of leaving the Trust so that we can try to establish the reasons for attrition and take action accordingly. Action plans are now being developed by each Division. The top five reasons given at exit interviews are; 1. Retirement 2. Personal Reasons 3. Career Progression / Different role / New job 4. Relocation 5. Promotion The Medicine Division have introduced an ED band 7 Recruitment and Retention Premium for new and existing Nurse Team Managers was introduced this month. Initial market intelligence suggests this is delivering more quality applicants for the role. First phase of interviewing was carried out and from 3 applicants 2 were appointed as new Nurse Team managers. Adverts in addition to NHS recruitment in Emergency Nurse, Nursing Standard and RCN and social media including twitter will deliver candidates for the Nurse Team Manager and ENP roles. Appendix 1, Section 3, Graph 1 details the starters and leavers trend over the last year. 5.5 Medical Staffing Job Planning The collation of a central record set of job plans is ongoing. E job planning software is under overall review following the pilot at Mount Vernon Medical Recruitment Actions to tackle the recruitment difficulties include display advertising, agency recruitment, recruitment premia, Employee Referral Scheme and a forthcoming revamp Workforce Report Month 5.pdf 6 Page 7 of 10 Overall Page 91 of 215
92 of the Consultant advertisement package which will include a new format job description and departmental videos for the hard to recruit posts. Meetings with Divisional Chairs monthly to: Overview all vacancies Refine vacancy and pipeline reporting requirements Analyse and review what has taken place with identified hard to recruit posts Facilitate decisions as to next steps, their associated costs and the action plan with particular initial focus. Co-ordinate potential for shared actions across all divisions The current difficult to recruit posts are: 1 Acute Physician 2 Consultants in Dermatology 1 Senior Clinical Fellow in Emergency Medicine 1 Consultant in Emergency Medicine 1 Elderly Care Physician 1 Stroke Medicine Physician 1 Specialty Doctor in Ophthalmology 1 Consultant in Ophthalmology 1 Consultant in Microbiology 1 Consultant in Histopathology 5.6 Employee relations In August the percentage of employee relations cases within the Trust was 6.6%. The overall number of live employee relations cases increased from 338 to 353. The high number of cases is mainly due to the work the ERAS team is undertaking to record sickness cases which have been identified in departments. The customer feedback score in August for the ERAS service was 4.0 (measured on a scale of 1 to 5 with 5 being excellent). A detailed table showing the ERAS performance in all employee relations areas can be found in Appendix 1, Section 4, Table Disciplinary Cases The benchmark across five NHS organisations for the percentage of disciplinary cases of headcount is between 0.5% and 1.0%. In August the Trust percentage was 0.6% ranging from the lowest 0.3% in CSS to 0.9% in Medicine. The Trust s Key Performance Indicator is to complete all disciplinary cases within 90 days. Priority has been given to support the management of disciplinary cases that have been open for a considerable amount of time. As at 31 August 2015, there were 33 live non-medical disciplinary cases and 5 formal medical cases under the framework Maintaining High Professional Standards in the Modern NHS (MHPS) Workforce Report Month 5.pdf 7 Page 8 of 10 Overall Page 92 of 215
93 5.8 Sickness Absence The Trust annual sickness absence rate saw a slight increase 3.69% in August compared to 3.60%% in July and 3.65% in June. In month sickness saw a small increase from 3.97% in June, 3.72% in July to 4.02% in August. Short term sickness in month increased to 1.71% in August from 1.54% in July and 1.48% in June. Long term in month sickness increased to 2.32% in August from 2.21% in July but a decrease from 2.49% in June. The number of days lost to sickness in August was 5741 compared to 5436 in July and in June. Part of the reason for the increase in the sickness percentage is the more rigorous sickness reporting introduced with Absence Assist, which went fully live in August with the exception of M&D staff. The number of staff on long term sick has decreased to 104 in August from 109 in July. Currently 134 long term sickness cases (including under monitoring cases) are being managed through the HR Advisory Service, 100% of the staff on long term sick, with additional cases under monitoring. A review of all long term sickness cases continues to be undertaken. The sickness rate for nursing and midwifery is higher than the Trust average with an overall rate of 4.49%, which was days lost. Further work has been carried out by in ward areas to ensure effective sickness management and the value of having a centralised model of sickness absence reporting is currently being explored. See Appendix 1, Section 1, Graph 1, Sickness Absence. Under the new sickness policy the Trust will be managing sickness based on number of episodes rather than the Bradford score, the feedback from staff and managers is this will be a clearer and more consistent way of managing sickness. In September, the Trust launched, in a phased approach, the new central point triage sickness reporting system ELAS. The launch was originally planned for August but has been delayed on the advice of the provider. Trained sickness absence advisors will take calls 24/7, 365 days a year. Managers will be notified within 30 minutes of ELAs receiving a call. A new sickness policy is in development. 5.9 HR Policies and Procedures The following policy updates were ratified at the August Trust Partnership meeting: Trust Policy for Staff Use of Social Media Trust Policy for Removal and Associated Expenses for New Staff Sickness Absence Management Policy Two policy review meetings are planned for September, to include discussion of updates to the following policies with staff side representatives: Trust Policy for Raising Concerns at Work Trust Policy for Management of Alcohol, Drug and Substance Misuse Stress at Work Policy 5.10 Governance A review of executive director contractual documentation has taken place, to support compliance with Regulation 5 of the Health and Social Care Act 2008 (Regulated Activities) Regulations 2014 ( fit and proper person test ). 6. Making a difference in our communities Ambition: We want to transform the way we work with our local communities, making a positive difference to them and making them proud of our hospitals and services Workforce Report Month 5.pdf 8 Page 9 of 10 Overall Page 93 of 215
94 The launch of Community Hub took take place at the AGM on 14 July. The aim is to develop an engaging and interactive space in the hospital for our patients, carers, families, staff and visitors that enables access to a range of opportunities to get involved with us. The services we will be promoting will include employment, volunteering, membership, work experience and apprenticeships. We will offer a coherent and coordinated one-stop-shop to these community-facing services to help local people get the most from their local hospitals. If this approach is successful we would like to develop the hub to include some services for staff also such as the employee relations advisory service and our health and wellbeing offer to staff. The idea is that the Hub will be open core hours from 10am to 4pm Monday to Thursday. There will be a rota of staff drawn from the services represented. All participating staff will design / deliver / receive training to enable them to play an informed ambassador role for all participating services. Areas of Note 6.1 ESR The ESR eforms project team is working on changing the Trust s current paper change of circumstance, Resignation and Exit Questionnaire forms to an electronic version and will replace the Trust s eleavers system on the Knowledge Centre to the new Greenlight eleaver system. The project team having been busy working on a number of key activities and work streams over the last few months, with the following key activities having been achieved recently: The project team have briefed senior management meetings within the divisions and the central support teams, about the project and its key deliverables. The project team has completed their recruitment requirements, resulting in the project team being at its optimum capacity. (employees and managers probably not worried) The project team has completed a number of project related governance documentation and engaged with the Trust IG and Audit teams. The team have been in contact with a number of other NHS organisations to ensure this project takes on board lessons from other Trusts. Lastly, the project team have completed the extensive design and build phase for eforms to ensure it matches and enhances the Trust s current operational procedures. At present the project team have engaged with the Pharmacy and Renal teams at Lister, who have started a 5 week pilot of the new suite of eforms. This will enable eforms to be fully tested in a live environment and any required tweaks to be implemented prior to the project team rolling out the product to all departments at the Trust from October 2015 onwards. A further update will be provided in the next workforce report. 6.2 Workforce Performance Heat Maps The Performance, Information & Planning team have developed heat maps to assess the overall performance of wards and divisions and directorates against a number of key workforce performance indicators. This will aid identifying key action areas and coordinated action plans will be put in place to assist areas that are not meeting the level required Workforce Report Month 5.pdf 9 Page 10 of 10 Overall Page 94 of 215
95 def TRUST BOARD MEETING 30 SEPTEMBER 2015 RISK AND QUALITY COMMITTEE 23 SEPTEMBER 2015 EXECUTIVE SUMMARY REPORT Agenda Item:11.1 PURPOSE PREVIOUSLY CONSIDERED BY Objective(s) to which issue relates * Risk Issues (Quality, safety, financial, HR, legal issues, equality issues) Healthcare/ National Policy To present to the Trust Board the report from the Risk & Quality Committee (RAQC) meeting of 23 September N/A 1. To continuously improve the quality of our services in order to provide the best care and optimise health outcomes for each and every individual accessing the Trust s services 2. To excel at customer service, achieving outstanding levels of communication and patient, carer and GP satisfaction 3. To provide and support the best standards of integrated care for the elderly and those with long term conditions by developing key partnerships and services 4. To consolidate services and enhance local access to specialist services in order to deliver high quality, safe, seamless, innovative and integrated services which are sustainable 5. To support the continued development of the Mount Vernon Cancer Centre and provision of leading local and tertiary cancer services 6. To improve our staff engagement and organisational culture to be amongst the best nationally Key assurance committee reporting to the Board. Any major financial implications of matters considered by the RAQC are always referred to the FPC. In line with Standing Orders and best practice in corporate governance. (includes CQC/Monitor) CRR/Board Assurance Framework * Corporate Risk Register BAF ACTION REQUIRED * For approval For discussion For decision For information DIRECTOR: PRESENTED BY: AUTHOR: Chair of RAQC Chair of RAQC Corporate Governance Officer/ Company Secretary DATE: September 2015 We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement RAQC Report to Board on 30 Sept.pdf Page 1 of 31 Overall Page 95 of 215
96 RISK AND QUALITY COMMITTEE MEETING HELD ON 23 SEPTEMBER 2015 SUMMARY REPORT TO BOARD 30 SEPTEMBER 2015 The following Non-Executive Directors were present: Dyan Crowther (Chair), Bob Niven, Ian Morfett and John Gilham. The following Executive Directors were present: Angela Thompson, Jane McCue, Nick Carver, Tom Simons Outcomes: Floodlight Scorecard The Committee reviewed the floodlight scorecard for Month 5. The Committee were informed that achieving the 62 day standard for Cancer services continued to be a challenge and noted a tumour site pathway project group was being established, led by the Divisional director and Chair of cancer services, to achieve a sustainable and consistent performance by year end. Accident & Emergency performance had also proven challenging, with higher admissions than had been expected for the time of year. It was noted that the Summary Hospital-level Mortality Indicator level continued to be significantly elevated but the surgical risk had started to reduce. The Committee noted the new draft divisional scorecards. Safer Nurse Staffing Levels Report The Committee received the safer nurse staffing levels report for July and August. The Director of Nursing advised that the number of red triggers had increased slightly during August but that this was not unusual for the time with an increased number of staff taking annual leave. She advised that there had been some bed closures on Ashwell and 6A due to staffing issues. The Committee were advised that extra capacity had been added to the ACU. It was expected that the number of red shifts would decrease during September and that the situation experienced in August would be part of a national trend. The Committee noted that the key trends had not changed significantly and continued roll out of the safer care tool, which will provide data on any red flag events. Overseas Recruitment Update The Committee received an update on the current situation regarding overseas recruitment. The Director of Workforce and Organisation Development informed the Committee that a number of issues that were outside of the control of the Trust regarding the recruitment of Filipino nurses had emerged since the recruitment programme began. Those issues were: it was now more difficult for the Filipino nurses to pass the International English Language Testing System (which was part of the NMC registration process), the NMC registration process had increased from two to six weeks and it was now more difficult for the Trust to acquire certificates of sponsorship for the nurses. The impact of these issues was that the starting date for the nurses would move to the first quarter of the next calendar year. The Trust was continuing with the recruitment programme for Filipino nurses and considered that the level of risk associated with the programme would fall. Actions were also being taken to mitigate the risk of insufficient staffing levels on the wards during winter. These actions included a golden hello for UK nurses, an extension to the refer a friend scheme, an extensive advertising campaign and providing financial incentives for staff who were prepared to move to another department. The Committee supported the actions being taken and the recommendations of the report. RAQC Report to Board on 30 Sept.pdf 2 Page 2 of 31 Overall Page 96 of 215
97 Workforce Paper The Committee received the Workforce Report. The report set out that the fill rate for temporary staff was on target. In early September there had been a 9% increase in the bank fill. New rules imposing a ceiling on the amount of agency spend within a year were to be introduced by the TDA and Monitor from September The new rules also required the Trust to use only framework agencies. The Trust had requested an adjustment to the ceiling on agency staff to take account of the Filipino nurse recruitment campaign and had only employed 3 off-framework workers during the previous month. There was also a new centralised system in place for handling sickness absence, which would allow better support for the managers involved. The Committee discussed how compliance with the TDA agency cap could result in the closure of beds and agreed that patient safety was a higher priority. Ward Staffing Risks The Committee received the Ward Staffing Risks report which detailed concerns regarding the impact of the recent closure of 20 beds on Ashwell and 6A ward on patient safety. The Committee noted that contingency plans had been put in place whereby additional beds would be available on other wards during periods of extreme capacity challenge. It was the intention that, subject to appropriate staffing levels being achieved, the beds would reopen on 1 November. The Committee supported the decision regarding the closure of the 20 beds on Ashwell and 6A and noted the report. Emergency Department Risks The RAQC considered the Emergency Department Risks Report which outlined the current levels of risk and safety within the emergency department. The Trust had continued to experience winter style pressures throughout the summer months and the ED performance target had not been consistently met. The risk had increased over the last three months as a result of the loss of 20 beds across the specialities served by Ashwell and 6A following staffing capacity issues and patient safety concerns. The beds were due to reopen on 1 November, following substantive recruitment. The Committee discussed whether the current level of capacity was adequate and sustainable. It was noted that the risks associated with fully staffed ED wards filled with agency staff had been considered higher than that associated with closing 20 beds. The Committee also discussed whether the best decision makers were on shift at the busiest times and whether patients were discharged as promptly as they should be. The Committee noted the report and agreed to consider the issue in more detail at the next Trust Board alongside the ward staffing risk paper. Workforce Race Equality Standard The Committee considered a report regarding NHS England s decision to establish a Workforce Race Equality Standard (WRES) across all NHS organisations. The report set out the Trust s obligations under the WRES. It was noted that a commitment to diversity was already included within the Trust s Workforce Strategy. The Committee approved the WRES Board statement and John Gilham (Non-executive Director) agreed to act as the Board level sponsor to take the lead role in championing the WRES. The WRES Board statement is attached at Appendix 1. Divisional Presentation Children The RAQC received a presentation from the Divisional Chair, Divisional Director and Nursing Services Manager. The presentation provided the Committee with an update on the RAQC Report to Board on 30 Sept.pdf 3 Page 3 of 31 Overall Page 97 of 215
98 division s annual objectives, the divisional governance structure, detail of ongoing challenges and plans for the future. The Committee discussed the risks identified in the presentation and the steps that had been taken to mitigate them. It was noted that more information regarding the controls taken to mitigate the risks and detail of their impact would be beneficial. The RAQC asked that the wording and explanation of the risks in the presentation be revisited. The Committee noted that children s services were liaising with other divisions to ensure all their outpatient clinics separated children and adults on the lists. Safeguarding Children Annual Report The Committee reviewed the Safeguarding Children Annual Report The report provided the Committee with an overview of safeguarding children services, standards and outcomes from April 2014 to March The Trust was currently achieving a 90% rate of compliance with training for level 1 & 2 but only 70% at level 3, against an overall target of 90%. Plans were in place to address this. The Committee noted that there had been one whole system serious case review which had been a child safeguarding issue, the Trust contributed to this review. There had been a reduction in the number of Looked After Children medicals in 2014/15, which it was considered might be due to children moving more quickly through the care system to adoption. The Director of Nursing advised the Committee that the actions from the Section 11 review were now all green except for item no.2, which remained amber. The Safeguarding Children Annual Report is attached at Appendix 2. Maternity Risk Management Strategy The Committee considered the Maternity Risk Strategy 2015 which set out the principles, processes and strategic direction of clinical risk management for Maternity Services. The report included objectives for 2015/16. One of the objectives identified for 2015/16 was to achieve a rating of good in the CQC inspection and the Committee discussed the issues associated with ensuring effective dissemination of information. The RAQC discussed the importance of ensuring that learnings are taken from specific risks and incidents and that the strategies put in place are simple and effective. The Committee approved the strategy. Supervision of Midwives Annual Report The Committee received the Supervision of Midwives Report. Supervision of Midwives was a statutory responsibility which provided support and guidance to every midwife in the UK. The NMC had decided to discontinue statutory supervision in its current format in January 2015 but there had been no indication of a timescale for the withdrawal of the current format and the role was continuing as usual for the time being. The Trust had a Supervisor of Midwives ratio of approximately 1:18/1:19 but as the national SoM training courses had ceased it would not be possible to improve this ratio. An audit of the Supervisors of Midwives had returned disappointing results which had not been reflected in initial feedback on the day, so was being challenged by the Trust. It was reported that there were no plans to change the current system within the Trust at present and Supervision of Midwives would continue. Dementia and Delirium Strategy The Committee received the draft Dementia and Delirium Strategy for approval. The strategy had been developed on behalf of the Director of Nursing and Patient Experience in order to address 17 key objectives identified in the first National Dementia Strategy and to support the Hertfordshire Dementia Strategy The Committee asked for the measures of success for Ambition 3 to be expanded on and the use of charitable funds to be considered RAQC Report to Board on 30 Sept.pdf 4 Page 4 of 31 Overall Page 98 of 215
99 as a possible means of addressing that particular ambition. The Committee approved the strategy. Annual Report for the Nursing and Midwifery Ambitions The Committee received the Annual Report for the Nursing and Midwifery Ambitions which provided an evaluation of the nursing and midwifery ambitions for 2014/15. The report set out key achievements from and provided a record of the continuous delivery of initiatives to improve patient safety and experience. The Committee noted that the Trust had been the first to receive a gold star for an e-learning diabetes training module. The Director of Nursing advised that the new nursing and midwifery strategy would be updated following the publication of the national nursing and midwifery strategy. The Committee noted the report. Complaints / Patient Experience Report The RAQC considered the monthly Complaints and Patient Experience Report. The report provided an update on complaints activity and patient feedback from the preceding month. The Committee noted that there had been a decrease in the number of complaints received during August and that complaints regarding the attitude of staff had fallen to become the least frequent subject of complaints. The number of complaints regarding communication had also fallen. The Committee were advised that there had been an improvement in the number of people telephoned within one day of raising a complaint but responding within the agreed timeframe had not always been achieved. There had been two reviews of the system which had been broadly positive. The Committee asked that the possibility of picking out themes from the complaints be explored. Serious Incident Report The Committee reviewed the Serious Incident (SI) Report which covered the months of June, July and August Between the three months there had been 12 Serious Incidents, which was a decrease from the usual level. The Medical Director advised that incidents involving pressure ulcers had continued to fall and that a change to the way that they were due to be reported going forward would mean that a smaller number would be declared in future. There had also been one Never Event during the period covered by the report which had resulted in an important learning. The Medical Director also advised the Committee that there had been two never events during September (retained swabs) which were currently being investigated. The Committee noted that the number of Serious Incidents during June, July and August was almost identical to the same period last year, though there had been an overall declining trend. It was also noted that an internal audit of the SI process had received positive feedback. General Medical Council (GMC) Trust Trainee Survey The RAQC received a report detailing the results of the GMC 2015 trainee survey. The Trust scored well nationally in relation to handovers and had significantly improved year on year in 3 areas. There were a number of areas where the Trust scored lower than the national mean however. The point was made that the Our Changing Hospitals programme had only recently finished when the survey started. The Committee were also informed that positive feedback had been received following a Deanery visit. It was highlighted that the number of positive outliers was approximately double the number of negative outliers, in a reverse from last year. The Committee requested an in depth review of patient safety in Children s Services for the RAQC meeting in December. Pathology Performance Update and Recovery Plan The Committee discussed the update provided on developments and service improvement in the Pathology Partnership Performance recovery plan. The Committee were informed that the new permanent Satellite Manager was proving effective in resolving issues with the RAQC Report to Board on 30 Sept.pdf 5 Page 5 of 31 Overall Page 99 of 215
100 services provided from the Lister satellite laboratory. However, issues with electronic result transmission and process integration with the Cambridge hub remained. The Committee noted that Histology was now managed totally on site and performance had improved. Issues remained with Microbiology and the Committee discussed the importance of introducing a short term system to deal with the problem and mitigate risks. The following reports were noted by the Committee: 1. Royal College of Physicians Respiratory Report: The Committee were informed of the outcome of the invited service review of respiratory services undertaken by the Royal College of Physicians in March The review was largely positive about the Trust s respiratory service. 2. Compliance Report The Committee received an update on compliance with CQC regulation, preparedness for inspection, the CQC regulation assurance map and corporate assurance map. The Committee noted the report. 3. CQC Registration and Intelligent Monitoring Report (IMR) There had been no further change and the Trust remained band Board Assurance Framework The Committee received the updated Board Assurance Framework 2015/16 for consideration. The main strategic risks had now been identified. 5. Corporate Risk Register The Committee reviewed the latest version of the Corporate Risk Register. 6. Infection Prevention and Control The Committee were informed of the infection prevention and control performance for the period ending 31 August Annual Interpreting and Translation Services Report: The Committee were advised that there had been a year on year increase to the costs involved with interpreting and translation. Polish and Rumanian were the two languages that were most frequently requested to be translated in 2014/15. Dyan Crowther Non-Executive Director 23 September 2015 RAQC Report to Board on 30 Sept.pdf 6 Page 6 of 31 Overall Page 100 of 215
101 APPENDIX 1 Board Statement of Commitment: NHS Workforce Race Equality Standard (WRES) Equality & Inclusion NHS England s decision to establish a Race Equality Standard across all NHS organisations is reflected within this high level statement of commitment from East and North Hertfordshire NHS Trust. We are fully committed to inclusive workplaces that are free from discrimination where all staff are able to thrive and flourish based on their diverse talent. This is evidenced through our organisational values - enacted through our behaviours at all levels, robust recruitment processes; support for team working and wellbeing in the workplace; and active awareness of equality and inclusion requirements embedded within our workplace practices. Leadership of the Workforce Race Equality Standard is achieved through Board level sponsorship and support of this work and is acknowledged as crucial in driving the changes forward. Successful equality, diversity and inclusion work, including work to implement the Standard, requires specialist advice and support; it is also recognised that leadership must come from Board level. Our obligations: The Board to understand the principles of the Workforce Race Equality Standard and ensure high level reporting of findings is embedded across Senior Committees and Business Groups to enact through our business processes A Board level Sponsor to take the lead role in championing the WRES at all levels, and ensuring our organisation is embedding any learning into our practices for measurable year on year improvements Board meetings to record an annual update of WRES actions and progress The current internal WRES Briefing and regular updates are to be presented to Senior Management Teams / Senior Committees as appropriate for approval Data will be gathered across our organisation for the 9 metrics for the WRES at 1 April 2015 and annually Our workforce findings will be displayed on our website by 1 July annually for the WRES 9 workforce metrics We will analyse these annual data findings and consider any significant gaps and how we can bring in improvements where practical We will learn from the data findings to demonstrate progress against a number of indicators of workforce equality, including a specific indicator to address the low levels of BAME Board representation (Black Asian minority ethnic). An annual summary of findings and progress will be reported within our Annual Equality and Inclusion Report as an appendix of the Workforce Report, for display on our website no later than 31 January annually. The Board will ensure through overview and reporting processes that our organisation is giving due regard to: Using the indicators contained in the Workforce Race Equality Standard to help improve workplace experiences, and representation at all levels within our workforce, for Black Asian and Minority Ethnic (BAME) staff; and assurance, through the provision of evidence, that our Providers are implementing the NHS Workforce Race Equality Standard Review its workforce in relation to the metrics set out in the WRES and report annually to NHS England. RAQC Report to Board on 30 Sept.pdf Page 7 of 31 Overall Page 101 of 215
102 APPENDIX 2 We strive for excellence and continuous improvement Safeguarding Children Annual Report Christina Kelly Named Nurse for Safeguarding Children Dr Olive Hayes Named Doctor for Safeguarding Children Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 1 of 24 Page 8 of 31 Overall Page 102 of 215
103 Executive Summary Introduction Trust Safeguarding Children Leads Compliance Section Risk & Quality Assurance Risk Register Serious Case Reviews Complaints Performance Quality Audits Training Supervision & Peer Review Child Protection Medicals Child Protection Referrals Maternity Looked After Children Safeguarding Committee & Work Plan Achievements 2014/ Appendix 1 Training Action Log 2014/15 18 Appendix 2 Section 11 Action Plan..21 Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 2 of 24 Page 9 of 31 Overall Page 103 of 215
104 Executive Summary This is the 13 th Annual Safeguarding Children Report. The Safeguarding Children annual report provides the Trust Board with an overview of safeguarding children services, standards and outcomes from April 2014 March Safeguarding children services seek to promote the welfare of children and prevents them from harm. Children and Young People (CYP) are defined as children from 0-17 years up to their 18 th birthday. The Director of Nursing and Patient Experience acts as the Executive Director responsible for Safeguarding Children. Safeguarding children is everybody s business and therefore all staff within the Trust have a responsibility to safeguard children whether they work with adults or children or non-clinical duties. There are 7 main strands to East and North Hertfordshire NHS Trust (ENHT) safeguarding children s services. 1. The undertaking of child protection (CP) medicals including sexual abuse medicals 2. The provision of education for safeguarding children across the trust 3. The provision of health visitor liaison services for the East of Hertfordshire and out of area attendances. 4. The provision of Looked after Children medicals 5. The provision of supervision to trust staff 6. The provision of ad-hoc CP advice as required by any trust employee where it relates to patient care 7. Supporting staff to make referrals to children s social care and/or advice to social care relating to CP injury, abuse or neglect. The activity within the safeguarding children s team continues to be constant with notable increases in the workload of the liaison health visitor provision, section 17&47 enquiries and safeguarding children training provision. It was essential for the child protection trainer to complete a mapping exercise of all staff in the Trust to identify compliance requirements with Level 3 training in line the Intercollegiate Document March Training compliance remains a key issue for the safeguarding children s team. The East & North Hertfordshire Clinical Commissioning Group (CCG) have set a 90% compliance target for all levels of safeguarding children training. Currently the Trust is not meeting this target and although we are meeting 90% compliance for level 1 & 2, the Trust compliance for Level 3 remains around 70%. Action plans have been put in place to improve compliance. See appendix 1 There has been a marked increase in the number of referrals made by the Trust to children s social care services from 206 referrals in 2013/14 to /15. This Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 3 of 24 Page 10 of 31 Overall Page 104 of 215
105 demonstrates an increased awareness of staff in relations to identifying safeguarding children concerns. The number of child protection medicals has decreased compared to the same time period last year; however there has been a significant increase in Section 17 & Section 47 enquiries and telephone strategy meetings, specifically maternity telephone strategy meetings. The number of section 17 & section 47 requests in March 2015 has tripled since data recording commenced in April /15 April May June July Aug Sept Oct Nov Dec Jan Feb Mar TOTAL Section 17/ enquiries Mat tele -strat CP tele-strat A 0.40wte band 6 Health Visitor was recruited to the team for a six month secondment to support the team in addressing the increase in workload and a 0.46wte Band 4 administrator was employed permanently. In August 2014 the Named Nurse who had worked at the Trust for many years left the organisation to take up a role as a Designated Nurse in another area. This had a huge impact on the team dynamics. Fortunately, the Named Midwife stepped in to cover the post until a new Named Nurse for Safeguarding Children was appointed and took up the post in February The Named Midwife resumed her previous role from March Achievements Compliant with Care Quality Commission National Standards for Safeguarding Children and Section 11 assessments review 100% of Child Protection Medicals completed in accordance with RCPCH standards Monthly review of Child Protection and maternity database to evidence compliance 24% increase in referrals to Children s services reflecting an increased awareness across the organisation. Implementation of the Maternity Information Sharing meetings with a multiagency representation embedding good partnership working. Presentations within the Rolling Half Days to ensure learning is embedded back into the organisation from serious incidents and audit outcomes. Held 8th annual child protection conference with over 70 staff in attendance Safeguarding Champions to support staff in safeguarding work identified in Maternity and both the adult & children s Emergency Departments (ED). Independent Domestic Violence Advisor (IDVA) appointment to work across the organisation. Based in the Emergency Department. Completion of review and successful implementation of safeguarding children s training requirements in line with the Intercollegiate Document Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 4 of 24 Page 11 of 31 Overall Page 105 of 215
106 1.0 Introduction This is the 13 th East & North Hertfordshire NHS Trust Safeguarding Children Annual Report. It sets out the trusts compliance with its legal duties for safeguarding children and the work plan for the coming year. Safeguarding children is most effective when adhering to a partnership approach. The Trust teams work closely with Hertfordshire Children s Services, Hertfordshire Constabulary and a wide range of other agencies under the umbrella of Hertfordshire Safeguarding Children Board (HSCB) to safeguard children. Trust policies and procedures all adhere to Working Together to Safeguard Children (2015) which is the pivotal national guidance for quality and standards of safeguarding CYP, and the work plan reflects the Hertfordshire Safeguarding Children Board (HSCB) business plan. 2.0 Trust Safeguarding Children Leads Name Role Mrs Angela Thompson Director of Nursing and Executive for Safeguarding Children Dr Olive Hayes Community Paediatrician & Named Doctor Child Protection and HSCB Improving Outcomes Group Dr Jan Reiser Designated Doctor Child Protection - HSCB attendee Mrs Christina Kelly Mrs Nicole Anderson Named Nurse Child Protection - HSCB Performance Group Named Midwife Safeguarding Children, Interim Named Nurse August 2014 March 2015, HSCB Audit Group 3.0 Compliance The Trust is compliant with Section 11 of The Children Act which places a duty on ENHT organisation to ensure that all services are discharged having due regard to the need to safeguard and promote the welfare of Children and Young People (CYP). The Trust employs a Named Doctor, Named Nurse and Named Midwife who work in partnership with Hertfordshire s Designated Doctor and Designated Nurse and under the jurisdiction of Hertfordshire Safeguarding Children Board (HSCB). In March 2015, the new Working Together to Safeguard Children guidance was published. This document is considered pivotal statutory guidance for all professionals working with CYP and their parents/carers. Prior to this publication the March 2013 edition was used to underpin the work plan for the safeguarding team and trust safeguarding strategies. Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 5 of 24 Page 12 of 31 Overall Page 106 of 215
107 The child protection safeguarding training is compliant with the guidance and recommendations of the Intercollegiate Document March A mapping exercise and report was completed identifying the level of safeguarding children s training required by all staff in the trust and a review of the training programme to meet the recommendations set out in the Intercollegiate Document Section 11 Review A Section11 review was undertaken by East & North Hertfordshire CCG in November The aim of the review is to ensure compliance with standards relating to HSCB policies and national standards and guidance. This local review was undertaken by the designated team chaired by Director of Nursing for Hertfordshire CCG and Designated Safeguarding Children s Nurse. The Director of Nursing ENHT attended the meeting for ENHT with support from the named Doctor and Named Nurse. The key requirements for the section 11 review are found in the table at Appendix 2. There were seven recommendations made which the safeguarding children team has been working towards achieving. There is one action that is outside the control the safeguarding children team - Recommendation 5 HSCB are reviewing the bruising protocol. The Standard Operating procedure (SPO) is Recommendation 2 Training compliance (see section 5) Recommendation 3 - The Think Family approach aims to ensure practitioners explore who is in the family/household. This supports a holistic assessment and identification of safeguarding risks for dependants in the household. There is clear evidence that children who live in households affected by domestic violence, parental substance misuse and parental mental health are more likely to be at risk of harm therefore the recording of dependants needs to be mandatory and embedded within the assessment process. Six Monthly audits are completed to identify compliance both of which demonstrated poor compliance in recording of dependants. The audits have been fed back to the ED staff and this is also been included in mandatory safeguarding children training. We are continuing to work with the ED matron to identify safeguarding champions that will support better awareness and improved compliance around safeguarding children. 4.0 Risk and Quality Assurance The Director of Nursing is responsible for safeguarding. She presents the Annual Child Protection Report to the Trust Board and chairs Trust Safeguarding Committee. Assurance is provided to the Trust Board throughout the year by the production of compliance reports to the Risk and Quality Committee every 2 months. These compliance reports include information about performance, quality and exception reports. Assurance and strategy issues are overseen by the Director of Nursing via monthly meetings with the Named Nurse. The Division of Women and Children have responsibility for the operational management of Child Protection Service within the Trust. The Named Nurse takes the lead for the day to day management of the Children s Safeguarding Service and is supported by the Nursing Services manager for Children s Service. Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 6 of 24 Page 13 of 31 Overall Page 107 of 215
108 The Joint Adult and Children s safeguarding Committee meets six weekly. The aim is to promote shared learning for the CYP and adult safeguarding teams and enable better exploration of best practice particularly in relation to the needs of young people in the adult Emergency Department (ED) and adults with children where there are mental health, substance misuse and/or domestic violence concerns. The Director of Nursing as executive lead is notified immediately of serious case reviews, untoward incidents and identified risk to the organisation. 4.1 Risk Register There were two risks relating to safeguarding children on the risk register under a score of 15 in In summary these relate to:- 1. Percentage levels of safeguarding children training compliance rate achieved was an average 80% against a standard of 90% in Compliance with community midwives attendance at case conference, achieving 80% against target of 100%. Actions in place to mitigate the risks are reviewed at the relevant boards and committees. 4.2 Serious case reviews In accordance with national guidance, serious case reviews, partnership case reviews and domestic homicide reviews (SCR/PCR/DHR) are requested by the HSCB when a child dies or is seriously injured in circumstances where there are concerns and the case requires a whole system review. In the year, the CCG requested that all children who are seriously injured or die as a result of injuries are reported as a serious incident to the HSCB and CCG regardless without any failing being attributed to the Trust. East & North Hertfordshire NHS Trust contributed to one new review in 2014/15 1. This was in regard to a 10 month old child who died in suspicious circumstances in his mother s partners van. The Trust completed an agency reflection and learning report identifying recommendations for the Trust to promote better partnership working and improved communication within and outside the organisation. The publication of the HSCB SCR has been delayed due to legal reasons. 2. There are several on-going reviews that the Trust has contributed to and the recommendations and action plans continue to be implemented. 4.3 Complaints Three complaints were received from parents in the year 2014/15; one was due to an expectant mother not happy that a referral was made without her being informed. Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 7 of 24 Page 14 of 31 Overall Page 108 of 215
109 This was investigated and the reason for the referral was explained and why she was not notified. It was acknowledged that wherever possible the family should always be informed. The second was an on-going complaint from a parent not happy about the child protection process. The aspects of the complaint were explored and responded to which appear to have resolved the concerns raised. The third was regarding the child protection process in relation to an injury, however following the child protection (CP) medical and expert opinion it was no longer felt to be a safeguarding concern. In all cases safeguarding processes were followed. Where possible all families are offered a face to face meeting due to the complexity and emotion associated with parental complaint in safeguarding cases. 4.4 Performance Trust CP performance is monitored through the use of a comprehensive dashboard that allows the team to monitor performance and quality measures. Updated monthly, the information is used to review the work plan, and is cascaded to relevant boards and committees for monitoring purposes. The data shows:- 1. The number of referrals made to children s social care across the Trust has continued to increase with a marked increase in maternity referrals in line with the introduction of the pre-birth protocol. There were 271 referrals made to children s social care in 2014/15 an increase of 24%. 2. The number of unborn babies requiring a pre birth CP plan in 2014/15 has decreased from the previous year this is reflected by the reduction in children on a Child Protection Plan across Hertfordshire. 3. Child protection supervision with the community midwives continues to be embedded within practice. The compliance level is set at 80% and is currently being achieved. CP supervision for other disciplines is offered on either an individual or group basis and compliance is improving with a target of 90%. 4. The Trust has now implemented mandatory recording of all women/children who are seen with FGM. There have been 10 cases identified since the recording commenced in October identified through maternity assessment and one case a suspected child FGM which was referred to children s social care. 5. A reduction in the number of child protection medicals undertaken. 4.5 Quality The Child Protection team led on a number of work streams by:- 1. Contributing to the HSCB audit & performance sub group & improving outcomes sub group in order to monitor partnership working within the multiagency teams. 2. Participating in multiagency audits e.g.?children with complex needs 3. Review of documentation used for CP medicals in line with Royal College of Paediatrics and Child Health Guidance 4. Embedded the pre-birth protocol within maternity services which has reflected an increase in referrals made to children s social care. Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 8 of 24 Page 15 of 31 Overall Page 109 of 215
110 5. Key partner agency in preparing for the implementation of the National Child Protection Information Sharing Project (CP-IS) which is being cascaded across the country to improve information sharing with acute health services and children s social care agencies. Hertfordshire is one of the first counties in the country to register to implement this system enabling health organisations to check if a child is on a child protection plan or a looked after child. 6. Patient feedback is being obtained through a patient satisfaction survey which is currently on-going. 7. Trust lead for co-ordinating child death process & ensuring staff in paediatrics are aware of Rapid Response process. This includes working in partnership with the Trust bereavement team and HCT who manage the Rapid Response Team. 8. Monthly peer review among paediatricians to ensure reflection and shared learning to promote quality in child protection medical examinations. 4.6 Audits Safeguarding was included in the internal audit programme for 2014/15. There were four audits completed through the internal audit programme. 1. The Laming Audit the aim of this audit is to evidence compliance with Child Protection Medical procedures. The audit demonstrated a marked improvement in the documentation audited. A safeguarding tab was introduced into the written records last year which has been beneficial to separate CP concerns from the main body of records. 2. Think Family Audit this was first completed in November 2013 and repeated in November The aim of the audit was to identify if staff in adult ED identified adult patients with caring responsibilities for children/dependants and also if safeguarding issues were considered. Unfortunately the audit demonstrated that staff were still not routinely recording if adults were responsible for dependants. The findings have been raised with the managers and presented at the clinical governance meetings. 3. NICE the aim of this audit was to ascertain if staff are aware of what to do if they suspected a child was either at risk or being maltreated. It is reassuring to know that staff were aware of how to access information form the knowledge centre, escalation procedures and how to seek support from the safeguarding team. However due to the changes of staff in the safeguarding team not all staff were aware of who the named professionals were. 4. Fracture Audit - An audit was conducted into the biochemical investigations conducted in children who had suspicious/unexplained fractures. Overall the compliance with investigations was good with bone profiles conducted appropriately. Vitamin D levels were not checked in all cases. This was presented at peer review and at RHD. The need to conduct this was also included in doctor induction. 5.0 Training Statutory training compliance has considerably improved over the last year, with Level 1 compliance achieving 91% compliance and Level 2 90% compliance in March This is approximately a 10% increase in compliance across the Trust in Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 9 of 24 Page 16 of 31 Overall Page 110 of 215
111 the last year. Unfortunately this still needs to be reflected in the training compliance for level 3 which is currently at 71% March The compliance of all levels of safeguarding children training is monitored on a monthly basis and compliance reports are shared with divisional leads, managers & matrons. The training reports are shared with the Risk and Quality Group, the Joint Safeguarding Committee and the Women s & Children s divisional board. Additional training sessions have been offered to improve the compliance of staff however this has not been successful with attendance not being prioritised. The quality of the training continues to meet the standards of the Hertfordshire Safeguarding Children Board and Roles and Competences for Health Care Staff (2010). Training at level one and two is available via e learning & through completion of a workbook; and face to face teaching sessions. Level three continues to be delivered face to face teaching over three hours. Staff requiring level three training also need to complete an extra hour which can be achieved through e-learning, the use of reflection, supervision, attendance at strategy meetings/case conferences, peer review, psychosocial meetings and team time sessions. The Trust child protection team has contributed to multiagency training with the Hertfordshire Safeguarding Children s Board. Safeguarding Children's Training 2014/15 100% 80% 60% 40% 20% 0% Apr 14 May 14 Jun 14 Jul 14 Aug 14 Sep 14 Oct 14 Nov 14 Dec 14 Jan 15 Feb 15 Mar 15 Level 1 Level 2 Level Supervision and Peer Review Staff who work directly with child protection cases require regular supervision to reflect on practice, learn from case discussions and obtain support for the emotional aspects associated with the work. It is known that attendance at supervision increases staff knowledge, skills, and supports emotional consequences of face to face contact with child protection cases. Supervision is offered on a quarterly basis for all staff target areas including special school nurses, specialist community nurses, community paediatricians and special needs health visitors and community midwives. This is delivered as a combination of individual and group sessions as well as ad-hoc supervision on a needs case basis. The supervision compliance is monitored on a quarterly basis on the Child Protection Dashboard. Group supervision is provided at the weekly ward paediatric psycho-social meeting, paediatric & ED staff team time sessions and quarterly to Neonatal Intensive Care nurses. Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 10 of 24 Page 17 of 31 Overall Page 111 of 215
112 Peer review for junior and senior medical staff is led by the Liaison Health Visitor and Named Doctor for child protection on a monthly basis. Peer review is a training format using case discussions and is well attended by acute and community paediatricians and their medical teams. Attendance is recorded on electronic staff record (ESR) at level three. The competencies achieved are mapped on a monthly basis. 7.0 Child Protection Medicals Child protection (CP) medicals are completed adhering to Royal College of Paediatrics and Child Health standards. 100% of medicals are undertaken by a consultant. The Child Protection Companion was revised in May 2013 and the child protection medical proforma was revised in line with the RCPCH guidance. These are reviewed annually to ensure best practice. The revised companion was implemented by all paediatricians in child protection practice. There were 189 CP medicals completed in 14/15 compared to 283 in 13/14 this represents a 33% fall in numbers of children referred for a CP medical. We have requested meetings with partner agencies to identify the cause for this decline in CP medicals. re referrals. Number of CP Medicals April March 2015 Acute 29 Community 160 April March 2015 Physical Neglect Sexual Emotional Review Acute Community Total The number of children on a Child Protection Plan in Hertfordshire remained high, peaking at 1076 in April 2014 but this significantly decreased to 881 by March The majority of children are registered on a plan for Neglect followed by Emotional Abuse. This may be a contributory factor in the number of CP medicals as majority of requests for CP medicals are due to either allegations of physical abuse or sexual abuse. Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 11 of 24 Page 18 of 31 Overall Page 112 of 215
113 Children on a CP Plan in Hertfordshire st Qtr 2nd Qtr 3rd Qtr 4th Qtr Children on a CP plan 2014/2015 CP Plan Categories Q1 Q2 Q3 Q4 Neglect Emotional Sexual Physical Multiple 8.0 Child Protection Referrals Referrals are made to Children s Services when a professional considers a child or unborn baby to be at risk of significant harm. The number of referrals made to children s social care from the Trust has continued to increase with a marked increase in maternity referrals in line with the introduction of the pre-birth protocol. The referral numbers have fluctuated throughout the year peaking in December 2014 with 35 referrals made Apr 14 May 14 Jun 14 Jul 14 Aug 14 Sep 14 Oct 14 Nov 14 Dec 14 Jan 15 Feb 15 Mar 15 CP referrals Column 4 Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 12 of 24 Page 19 of 31 Overall Page 113 of 215
114 9.0 Maternity There has been a marked increase in the number of referrals to Children s services for the unborn babies over the year as recognition of the vulnerability of young babies increased. Monitoring increasing demand for the attendance of midwives at case conferences has commenced on a monthly basis and recorded on the safeguarding children dashboard. The has been a drive within maternity services to acknowledge the importance of MW attendance to CPC and core groups as the key health professional in the planning and decision making for mothers and their unborn babies Sharing information about vulnerable unborn babies has strengthened, with regular multi-agency meetings, sharing maternity database of vulnerable patients with our partners and increased collaboration with surrounding maternity units including attendance at the monthly information sharing meeting by the Named Midwife from Harlow, Essex. Liaison with our neighbouring maternity units such as Beds, Barnet and North Middlesex is improving with consideration being given to a named midwife forum to share best practice and information. The Named Midwife introduced safeguarding champions to the Maternity Unit in Champions have been identified for each area within the maternity department including the community and specific training is offered to support them in their role. On-going support is provided at regular champion meetings arranged by the Named Midwife. The champions are responsible for cascading information to their colleagues in their particular workplace. The Champions meet on a two monthly basis and have been exposed to the IDVA (Independent Domestic Violence Advisor), Female Genital Mutilation training, HALO Child Sexual Exploitation, group supervision and have contributed to policy writing. The Named Midwife provides Safeguarding supervision to community midwives and where possible in groups within the maternity unit. The Safeguarding supervision was undertaken on a four monthly basis with plans to increase to quarterly in 2015/16 inline with to best practice guidance and expectation of the CCG. The Safeguarding supervision provides support to midwives working on challenging cases, provides a managerial oversight to their safeguarding work and offers guidance where practitioners become stuck. It is also pivotal for keeping the focus on the unborn baby when there are complex parental issues involved. An evaluation of the quality of supervision is planned for 2015/16. Following the publication of Safeguarding Children and Young People Roles and Competences for Health Care Staff Intercollegiate Document in March 2014, a mapping exercise was undertaken and the need for Level Three Safeguarding Children training to Obstetricians and Gynaecologists was identified. The Named Midwife delivered specific training to them initially in November 2014 and they now attend the Trust Mandatory Level three Programme. ENHT recruited to the Named Midwife post in January 2014 with already experienced safeguarding nurse. Due to the increasing work with unborn babies the team increased the service by recruiting a part time safeguarding midwife (0.4wte). Referrals to Children s services increased for unborn babies over the year as recognition of the vulnerability of young babies increased. Monitoring increasing demand for the attendance of midwives at case conferences commenced. Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 13 of 24 Page 20 of 31 Overall Page 114 of 215

115 Sharing information about vulnerable unborn babies has strengthened, with regular multi-agency meetings, sharing maternity database of vulnerable patients with our partners and increased collaboration with surrounding maternity units. The Named midwife introduced safeguarding champions to the Maternity Unit this year. Champions were identified for each department and specific training was delivered to support them in their role. On-going support is provided at regular champion meetings arranged by the Named Midwife. The Named Midwife provided supervision to community midwives and achieved 87% compliance by April Looked-After Children (LAC) LAC children are seen on a regular basis for Health Assessments. These take place within 28 days of the child coming into care, then every 6 months (under 5 s) or annually (5+). Paediatricians carry out all LAC Initial Health Assessments (IHAs) for under 10 s and Review Health Assessments (RHA s) for all children where Adoption is in their care plan. HA s are requested by the child s social worker and arranged through the LAC team. Timescales in were that IHAs should be completed and returned to the LAC team within 15 working days of the request. From April 2015 we will be required to meet a 10 day turnaround. It is anticipated this will be a challenge as there are no additional resources to meet this shortened target. In 2014/15 RHA s need to be completed and returned within 5 weeks this is not always feasible due to late submission of paperwork from partner agencies. In 2014/15 we carried out a total of 227 LAC Medicals, 110 Initials & 117 Reviews. This compares with 2013/14 when we carried out 276 LAC medicals 102 Initials and a unusually high number of review assessments at 174. This may reflect children moving more quickly through the care system to adoption and therefore having fewer RHAs this year. Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 14 of 24 Page 21 of 31 Overall Page 115 of 215

116 This table shows the percentages of health assessments meeting timescales. Since August, we have only completed 1 Review Health Assessment outside of the timescales due to the carer refusing to attend. Early in the year we were not meeting timetables for Initial Health Assessments, action plans were implemented and compliance improved significantly towards the later part of the year. Only one initial health review was outside the time scale in January due to non-attendance Safeguarding Committee The joint Safeguarding committee met every six weeks during 2014/15. The work plan for 2014/15 was agreed through the Joint Safeguarding committee included: 1. Increase staff compliance in safeguarding training to 90% by March Update Safeguarding Children Trust Policy 3. Fully implement CQC action plan and evidence sustainability 4. Review safeguarding children training and provide standalone domestic violence training in line with 2014 Intercollegiate Document 5. Support new Independent Domestic Violence Assessor role within Emergency Department 6. Implement patient experience survey in the child protection unit 7. Continue work to embed Think family and Domestic Abuse policies in ED 8. Hold Plan 8th Annual Safeguarding Conference November Review safeguarding children training in line with the Learning and Development Team VITAL schedules 10. Contribute and/or lead on key projects and audits for HSCB as required 11. Fully implement CQC action plan 12. Prepare for section 11 review November 2014 Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 15 of 24 Page 22 of 31 Overall Page 116 of 215
117 13. Review liaison health visiting for East and North Hertfordshire with Hertfordshire Community Trust (HCT) 14. Co-operate with Health and Local Authority to implement Child Protection- Information System (CP-IS) in Hertfordshire (CP-IS is a national data sharing which aims to improve communication between agencies who come into contact with vulnerable children.) 15. Create robust sharing information agreements with neighbouring maternity units in order to share and access inter trust records 16. Increase attendance at local domestic violence forum 17. Review use of Clinical Record Viewer in Emergency Department 18. Develop systems and collate figures for Female Genital Mutilation which will be required for Department of Health from September Work plan for 2015/16 1. Liaison with Joint Child Protection Investigation Team and children s social care divisions to explore reasons for the reduction in CP medical referrals and to overcome any potential barrier to this service. 2. Review safeguarding children training and provide standalone Domestic Violence and Child Sexual Exploitation training in line with 2014 Intercollegiate Document. 3. Develop a Trust policy for Female Genital Mutilation in line with national guidance. 4. Review Trust Safeguarding Children s Policy, Child Protection Supervision policy and Domestic Violence policy. 5. Safeguarding Children level 3 Training programme/lesson plans to be reviewed in line with national and local needs. 6. Continue to review and report monthly safeguarding children training figures and identifying action plan to aid Trust compliance achieving 90% 7. Review delivery of the safeguarding children training in line with the Learning and Development Team VITAL schedules. 8. To develop a workbook to support blended learning in Safeguarding Children Level 1&2. 9. Explore possibilities of introduction of e-learning Safeguarding Children Level 3 packages. 10. Support new Independent Domestic Violence Advisor role within the Trust. 11. Review outcome of the patient experience survey in the child protection unit. 12. Continue work to embed Think family and Domestic Abuse policies in ED. 13. Organise and implement the 9th Annual Safeguarding Conference October/November Contribute to key projects and audits for HSCB as required. 15. Prepare for section 11 review November Prepare for CQC Inspection October Develop processes and implement the Child Protection-Information System ( CP-IS) within the Trust. 18. Safeguarding midwifery supervision to be increased to quarterly as opposed to four monthly 19. Safeguarding midwife to undertake and evaluate an audit of the quality of safeguarding supervision. Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 16 of 24 Page 23 of 31 Overall Page 117 of 215
118 12.0 Notable Achievements Compliant with Care Quality Commission National Standards for Safeguarding Children and Section 11 assessments review % of Child Protection Medicals completed in accordance with RCPCH standards 3. Monthly review of Child Protection and maternity database to evidence compliance 4. 24% increase in referrals to Children s services reflecting an increased awareness across the organisation. 5. Implementation of the Maternity Information Sharing meetings with a multiagency representation embedding good partnership working. 6. Presentations within the Rolling Half Days to ensure learning is embedded back into the organisation from serious incidents and audit outcomes. 7. Held 8 th annual child protection conference with over 70 staff in attendance 8. Safeguarding Champions to support staff in safeguarding work identified in Maternity and both the adult & children s Emergency Departments. 9. Independent Domestic Violence Advisor (IDVA) appointment to work across the organisation. Based in the Emergency Department. 10. Completion of review and successful implementation of safeguarding children s training requirements in line with the Intercollegiate Document Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 17 of 24 Page 24 of 31 Overall Page 118 of 215
119 Appendix 1 Training Report/Action Log 2014/15 Safeguarding Children s Training Report Month by Month 2014/15 Meets CCG requirement of 90% staff trained Between 80 89% of staff meeting requirement Less than 79% of staff meeting requirement Competence Name April May June July August September October November December January February March Level 1 82% 82% 83% 83% 85% 86% 87% 88% 87% 87% 89% 91% Level 2 80% 80% 81% 81% 83% 84% 86% 87% 86% 87% 88% 90% Level 3 70% 68% 66% 66% 66% 62% 72% 76% 76% 70% 69% 71% Trust Overall 80% 80% 81% 81% 83% 83% 86% 86% 86% 86% 87% 89% Division April May June July August September October November December January February March Cancer Services 83% 83% 85% 85% 86% 86% 86% 86% 86% 88% 90% 91% Clinical Support Services 82% 85% 87% 87% 87% 87% 86% 87% 86% 84% 88% 90% Medicine 76% 76% 77% 77% 80% 82% 84% 84% 85% 85% 86% 87% Non Clinical Support Services 77% 81% 82% 83% 84% 87% 87% 88% 88% 87% 90% 93% Surgery 77% 75% 77% 76% 78% 80% 82% 83% 82% 83% 84% 87% Women s and Children s 88% 87% 86% 86% 87% 86% 90% 92% 91% 90% 91% 92% Safeguarding Children annual report RAQC Report to Board on 30 Sept.pdf Page 25 of 31 Overall Page 119 of 215
120 % of staff compliant with all levels of safeguarding children s training Directorate April May June July August September October November December January February March Child Health 90% 90% 90% 89% 90% 89% 91% 91% 91% 89% 89% 92% Women s 86% 84% 83% 84% 85% 83% 89% 92% 92% 90% 90% 92% % of staff compliant with Level 3 safeguarding children s training Directorate April May June July August September October November December January February March Child Health 76% 77% 78% 76% 75% 72% 77% 81% 80% 76% 76% 82% Women s 66% 61% 57% 60% 62% 56% 75% 80% 82% 76% 73% 77% Medicine 69% 67% 62% 63% 60% 61% 61% 65% 61% 51% 46% 43% There is approximately 600 staff requiring level 3 training throughout the Trust, with between 60 to 90 training places available a month. Numbers of staff being trained needs to be spread across the year. Compliance with training should be monitored by managers at a staff member s appraisal non compliance needs to be raised and appraisal not signed off until completed. A list of non compliant staff with level 3 is attached please inform the relevant staff that they need to attend training. Please ensure staff are aware to book onto training if their compliance is due to be expiring. (Please note if staff have attended training in May, then they will not show as compliant until the figures have been produced beginning of June). We have to demonstrate to the CCG that we have a minimum of 90% compliant with safeguarding training this target was due by January I am willing to help your teams to achieve compliance please contact me to discuss further as to how we can do this Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 19 of 24 Page 26 of 31 Overall Page 120 of 215
121 Action has slipped Action is not yet complete but is on track Action has been completed Safeguarding Children s Training Action Log March 2015 Date Issue Update Action Responsibility Target Date Feb 2015 Safeguarding Children s level 3 compliance at 51% Medical Division (target of 90%) Feb 2015 Safeguarding Children s level 3 compliance at 76% Women s Division (Target of 90%) Monthly report sent to Divisional Director, Matron for Emergency Medicine, Matron for Practice Standards, Director for Nursing, Women s and Children s divisional Director, Named Nurse and Doctor for CP Monthly report sent to Divisional Director, clinical director, general managers and matrons All staff not booked onto training within 2 months to be identified and managers informed on non compliance. If no change to update Director for nursing. All staff not booked onto training within 2 months to be identified and managers informed on non compliance. Cheryl Lewis Divisional Director for ED March 2015 Cheryl Lewis March 2015 Feb 2015 Safeguarding Children s level 3 compliance at 76% Children s Division (target of 90%) Monthly report sent to Divisional Director, clinical director, general managers and matrons Individual non compliant staff to be ed requesting them to book onto training. All staff not booked onto training within 2 months to be identified and managers informed on non compliance. Cheryl Lewis March 2015 March 2015 Induction training programme not compliant with Intercollegiate document March 2014 Induction programme being looked at to see who will take responsibility (currently overseen between nurse education, medical education, and HR). Individual non compliant staff to be ed requesting them to book onto training. Awaiting Workbook then programme can be changed in line with intercollegiate Nurse Education/Cheryl Lewis March 2015 Workbook for all trust staff being developed (due March 2015) Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 20 of 24 Page 27 of 31 Overall Page 121 of 215
122 Appendix 2 Section 11 Review Page / no. Actions Lead Responsibility Agreed Implementation Date Comments / Progress Implementation Date 1 To update and amend the Trust Supervision Policy to include specific roles requiring supervision, frequency and in what form (Group/Individual) Named Nurse Safeguarding Children Feb 2015 Jan 15 Initial preparation to update policy for supervision has started by gathering latest research/guidance regarding safeguarding supervision July 2015 Policy has been update and sent for ratification July To improve the Safeguarding children training compliance especially for level 3 Named Nurse Safeguarding Children CP Nurse Trainer On-going Dec 14 1.Monthly monitoring of training figures 2.Non-compliance reported back to divisions to address with staff at appraisal 3. Divisions informed of monthly requirement for staff attendance to meet required target. 4.Roles and Competencies for health staff have been mapped and methods to ensure learning opportunities such as supervision, peer review and psycho social meetings to be incorporated into On-going July Action 1-4 from December 2014 remains in place. 2. Action plan implemented and reviewed monthly. 3. Extra training sessions have been provided to improve compliance levels. 4. All divisions are expected to ensure that their staff details are up to date on the Trust training record including staff on long term sick, maternity leave or extended leave. 5. Women s & Children s division have significantly improved compliance levels. Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 21 of 24 Page 28 of 31 Overall Page 122 of 215
123 Page / no. Actions Lead Responsibility Agreed Implementation Date Comments / Progress Implementation Date 3 To identify Vulnerable Adults who have children and respond appropriately i.e refer to Children Services Named Nurse Safeguarding Children Mar 2015 Jan 15 1.To extend the Safeguarding Champions idea to the Emergency Department to disseminate and support staff with safeguarding issues 2.To undertake bi-monthly Think Family audit to drive home the need to consider dependants of adults presenting who are unwell through illness, drugs & alcohol, MH or DV Audit currently taking place 3. For the Audit results to be taken back to ED staff during the rolling half day programme within ED On-going 4 To ensure children and young people who are Looked After benefit from quality, timely initial and review health assessments subject to effective quality assurance arrangements. Linda Struthers Dec 14 Dec 14 July Named Safeguarding Champions have been identified in both Ault & Children s Emergency Departments (ED). 2. Safeguarding Children Slot implemented in the ED team Time Sessions. 3. New electronic EPR system has been implemented in ED the Think Family Section is to be a mandatory field. 4. Previous Audit findings fed back to ED staff. 5. Think Family Audit to be Completed in August/September To agree with partner organisations a system to ensure clarity of standards and time frames 2.To set up robust systems for internal adherence to agreed standards and time frames 3. Monthly monitoring of health assessment timeframes on safeguarding dashboard On-going Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 22 of 24 Page 29 of 31 Overall Page 123 of 215
124 Page / no. Actions Lead Responsibility Agreed Implementation Date Comments / Progress Implementation Date 4. A new escalation policy is now in place 5. An improved database is in place to cover LAC medicals taking place both at QE2 and Danestrete clinics 6.100%target met in Dec 14 5 Care pathway for immobile babies that present at Urgent Care Centres and Minor Injury Units with suspicious bruising Arrangements need clarification for transfer to Lister ED Designated Nurse Safeguarding Children Dec Designated Nurse to take the bruising protocol back to the HSCB to discuss implications of transferring patients between URC, MIU and Emergency Departments 2. To clarify the West Herts contract regarding this issue to ensure symmetry across the county. 3. Staff in such units to be made aware of the care pathway through safeguarding supervision, team-time and training Awaiting bruising policy through HSCB July 2015 Bruising protocol is discussed in Safeguarding Children training and once the new protocol is implemented we will update the staff targeting the community staff. 6 Equity of the Health Visitor Liaison services within E&N Herts Trust. (LHV East & Out of Area employed by E&N Herts and LHV North employed by HCT) This action was set following the CQC inspection 2013 when the HV liaison service in the East was identified as good practice therefore the aim of this recommendation is E&N Herts Designated Nurse - Safeguarding Children Liaison Health Visitor Named Nurse Safeguarding Children Dec Designated Nurse to look at the equity of the service across Hertfordshire, and ensure that this is reflected in the CQC action plan return. 2. An outline of the differences within East & North Herts given to the Divisional Director with a view to eliminating the inequalities. July Telephone conference call June 2015 with HCT to discuss current service provision. HCT stated they do not have a service specification. Further meeting CCG Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 23 of 24 Page 30 of 31 Overall Page 124 of 215
125 Page / no. Actions Lead Responsibility Agreed Implementation Date Comments / Progress Implementation Date Trust to work in collaboration with HCT to aid improvement of service provided by HCT for the North. planned to establish a service specification for HV Liaison service for East & North Herts to improve inequality of service. 2. East & North Herts NHS Trust have given systems access to HV Liaison for North Hertfordshire to improve information sharing. 3. Offer made to HCT for HV Liaison North Herts to be based at hospital site to improve HVL service provision. HCT have not taken up the offer. 4. Request made to HCT for secure shared nhs.net s for health visitors & school nurses to send patient identifiable information. This will improve the timeliness of information sharing in the most secure way. Awaiting addresses. 5. There is no service specification from the CCG for either Trust for the HV liaison role. Aug 2015 removed from action plan by CCG. 7 East & North Herts NHS Trust undertake CRB checks at the beginning of employment, but do not re-check on a regular basis. This is contrary to the HSCB safe staffing policy. Designated Nurse - Safeguarding Children Director Human Resources Tom Simmons Dec Designated Nurse to explore the issue further with the CQC and the HSCB. July 2015 Process remains the same with DBS check at start of employment. Rechecked if applies for an internal vacancy in another department and DBS check over 3yrs old. Aug 2015 CCG update August 2015 No statutory requirement for 3 yearly DBS in place Safeguarding Children Annual Report 2014/15 CK/OH RAQC Report to Board on 30 Sept.pdf Page 24 of 24 Page 31 of 31 Overall Page 125 of 215
126 TRUST BOARD- September 2015 Board Assurance Framework 2015/16 Agenda Item:11.2 PURPOSE PREVIOUSLY CONSIDERED BY Objective(s) to which issue relates * Risk Issues (Quality, safety, financial, HR, legal issues, equality issues) Healthcare/ National Policy To present the Board Assurance Framework 2015/16 for consideration. Please note this continues to be developed further and is iterative. This version includes revision of descriptions of the risks, following discussion with Chair of RAQC and alignment to the new strategic objectives. New framework approved by the Audit Committee, July Draft BAF and framework Risk and Quality Committee and Board, July 2015 and reviewed September Risk descriptions and risks assessments updated following RAQC. 1. To continuously improve the quality of our services in order to provide the best care and optimise health outcomes for each and every individual accessing the Trust s services 2. To excel at customer service, achieving outstanding levels of communication and patient, carer and GP satisfaction 3. To provide and support the best standards of integrated care for the elderly and those with long term conditions by developing key partnerships and services 4. To consolidate services and enhance local access to specialist services in order to deliver high quality, safe, seamless, innovative and integrated services which are sustainable 5. To support the continued development of the Mount Vernon Cancer Centre and provision of leading local and tertiary cancer services 6. To improve our staff engagement and organisational culture to be amongst the best nationally Integral part of the Trust s Quality Governance & Risk Management Strategy As identified in the report Key element of governance and risk management structures Healthcare Regulation through CQC (includes CQC/Monitor) CRR/Board Assurance Framework * Corporate Risk Register BAF ACTION REQUIRED * For approval For discussion For decision For information DIRECTOR: PRESENTED BY: AUTHOR: Chief Executive Company Secretary Company Secretary DATE: September 2015 We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement 11.2 BAF framework Sept review 15.doc Page 1 of 4 1 Overall Page 126 of 215
127 Board Assurance Framework 2015/16 Introduction / Background The Board Assurance Framework considers the principal strategic risks associated to the achievement and delivery of the Trust Strategic and annual objectives. The Strategic objectives, from which the 2015/16 annual objectives have been framed, build on the previous work of the Trust and support the delivery of the Trust s vision: To be amongst the best and the Trust s values. In May 2015 the Board agreed three new strategic objectives. These are currently being launched to the Organisation through the ARC programme during September The three new strategic objectives are: New Strategic Objectives: 1. Keeping our promises about quality and value embedding the changes resulting from delivery of Our Changing Hospitals Programme. 2. Developing new services and ways of working delivered through working with our partner organisations 3. Delivering a positive and proactive approach to the redevelopment of the Mount Vernon Cancer Centre. The Board Assurance Framework (BAF) sets out the strategic risks against the achievements of the Trust s Business Plan and seeks to reflect the Trust s risk profile. It seeks to demonstrate the extent to which assurance can be provided on mitigating these risks and identifies where further actions are required to reduce them to an acceptable level, and also provides assurance to the Board that these are being effectively managed. The BAF is one of several mechanisms that provide supporting information for the sign-off of the effectiveness of the Trust s system of internal control in the Annual Governance Statement which is submitted to the TDA and included in the Trust s Annual Report. The format of the BAF 2015/16 was reviewed in Quarter /16 to ensure the framework remains fit for purpose for effective strategic risk management and that the strategic risks are visible to support Board Committee and Board scrutiny. The Trust s new Internal Auditor s Baker Tilly - supported this review. Following a review by the Audit Committee and RAQC, the Board approved the new format, key changes and the plans for further development during 2015/16. The BAF will continue to be iterative and reviewed on a regular basis by the Executive Directors and Company Secretary and presented to the RAQC and Board each quarter for discussion and review. Progress against achievement of the annual objectives will be reviewed for the next report. The Board are asked to note: - The updated articulation of the risks. The BAF is currently being updated to reflect the latest reports and will be circulated to all Board members. - Elements of the BAF will be tested through Internal Audit BAF framework Sept review 15.doc Page 2 of 4 2 Overall Page 127 of 215
128 The Strategic Risks: See appendix 1 for the full BAF. The revised BAF is more streamline and currently contains ten strategic risks. Eight of these were agreed at a Board development session and the other two reflect the emerging risks identified through RAQC and Board - TPP and the estate infrastructure. Risk Title/Description of Risk Previous risk rating (LxC) SR1 The risk that sudden and unforeseen changes to referral pathways impact on the delivery of our quality and financial outcomes. SR2 SR3 SR4 SR5 SR6 SR7 SR8 SR9 SR10 The risk that excess demand on services impacts on the delivery of national performance targets and quality measures. The risk that the health and social care system wide plans do not deliver the outcomes expected and further impact on capacity and demand. The risk that the clinical and non-clinical benefits of our changing hospitals are not fully realised leading to the Trust reviewing its strategy The risk that the Trust Development Authority (TDA), Clinical Commissioning Group (CCG) and public lose confidence in our plan to deliver sustainable improvements (specifically - mortality, patient survey, staff survey, A&E, finance), leading to loss of reputation, increased regulation and scrutiny, and financial penalties. The risk if we don t deliver our approved financial plan we will not be able to access further funding and invest in service developments. The risk that if we do not fully embed a value based culture we will fail to attract and retain high performing workforce and deliver our objectives. The risk of failure to maintain effective strategic relationships with partners in order to deliver integrated pathways. The risk that the Pathology Partnership (TPP) fails to perform effectively and does not deliver the operation and financial commitments, impacting on the quality outcomes for patients. The risk that the reduced available funding for the Trust estate is not sufficient to deliver the strategic outcomes for patients Current risk rating (LxC) Comment 8 (2x4) 6 (2x3) Risk and controls reassessed, evidence of planning re participated pathway changes 16 (4x4) 16 (4x4) Current impact on 62 days wait in Cancer and ED performance. Action plans in place and updates are provided within the performance report to Board 9 (3x3) 9 (3x3) 12 (3x4) 8 (2x4) Risk and controls reassessed. Post project reviews positive. 16 (4x4) 12 (3x4) Current TDA risk rating is 3, CQC IMR is band 4, Never events 4. Actions are in place and updates are provided in the director reports. 16 (4x4) 16 (4x4) Actions are in place and updates are provided in Finance report to FPC & Board 12 (3x4) 12 (3x4) Actions are in place and updates are provided in Workforce report to Board 6 (2x3) 3 (1x3) 20 (4x5) 20 (4x5) Monthly monitoring and action plans in place. Reports to RAQC, FPC and Board. 15 (3x5) 8 (2x4) Risk and controls reassessed, evidence of investment in the areas of the estate to improve quality BAF framework Sept review 15.doc Page 3 of 4 3 Overall Page 128 of 215
129 Features of the new BAF The causes and effect of the risk are clearly documented. An new strategic risk assessment 5x5 risk profiling matrix (likelihood versus consequence), providing the scores for the unmitigated risk, residual risk when taking into account the controls in place and the target risk score. See appendix 2. Assessing assurances 1. Assurances on the effectiveness of controls to manage and mitigate risks are assessed in two ways: - Whether the evidence is providing positive assurances [the controls are working effectively] identified as P+ in the BAF or negative assurance [the controls are not working effectively], identified as N- in the BAF; and - The line of assurance i.e. whether the assurance is derived from internal sources and whether it has been subject to scrutiny by the Trust s oversight function or external sources as set out below. Lines of assurance: First line of assurance (L1) i.e. Operational (Management) Second line of assurance (L2) i.e. Oversight functions (Committees, etc.) Third line of assurance (L3) i.e. Independent (Audit, Inspections, Reviews etc.) 2. Taken together, the assessments provide an indication of the adequacy of assurances and should be used to determine the actions to be taken to address gaps in controls and assurances ie. whether additional controls are needed or existing controls require strengthening or whether additional assurance is required. Further planned developments In Quarter 3 - The development of a heat map is being explored to see the Trust s risk profile on a one page map and trends/summary page. - The Quality Governance and Risk Management Strategy will be reviewed to reflect the changes. It is suggested that this is reviewed by the RAQC in September and Audit Committee at its next meeting in October. In Quarter 4 - Consider a Board Development session on strategic risk management with Baker Tilly to reflect on the changes and support further development BAF framework Sept review 15.doc Page 4 of 4 4 Overall Page 129 of 215
130 TRUST BOARD MEETING 30 SEPTEMBER 2015 CHARITY TRUSTEE COMMITTEE REPORT 14 SEPTEMBER 2015 Agenda Item:13.01 PURPOSE PREVIOUSLY CONSIDERED BY Objective(s) to which issue relates * Risk Issues (Quality, safety, financial, HR, legal issues, equality issues) Healthcare/ National Policy To present to the Board the report from the CTC meeting held on 14 May 2015 N/A 1. To continuously improve the quality of our services in order to provide the best care and optimise health outcomes for each and every individual accessing the Trust s services 2. To excel at customer service, achieving outstanding levels of communication and patient, carer and GP satisfaction 3. To provide and support the best standards of integrated care for the elderly and those with long term conditions by developing key partnerships and services 4. To consolidate services and enhance local access to specialist services in order to deliver high quality, safe, seamless, innovative and integrated services which are sustainable 5. To support the continued development of the Mount Vernon Cancer Centre and provision of leading local and tertiary cancer services 6. To improve our staff engagement and organisational culture to be amongst the best nationally Key assurance committee reporting to the Board The production of an annual report is in line with best practice in corporate governance (includes CQC/Monitor) CRR/Board Assurance Framework * Corporate Risk Register BAF ACTION REQUIRED * For approval For discussion For decision For information DIRECTOR: PRESENTED BY: AUTHOR: Chief Executive Company Secretary Board Committee Secretary/Company Secretary DATE: September 2015 We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement * tick applicable box 13.1 Charity Trust Committee Report.pdf May 2013 Page 1 of 3 Overall Page 130 of 215
131 CHARITY TRUSTEE COMMITTEE MEETING HELD 14 SEPTEMBER 2015 SUMMARY REPORT TO BOARD 30 SEPTEMBER 2015 The following members were present: Bob Niven, Ian Morfett, Tony Ollis, Stephen Posey Decisions made under delegated authority: The Charity Trustee Committee (CTC) made the following decisions on behalf of the Trust, under the authority delegated to it within its terms of reference: Transfer of Funds The CTC considered account 1212 (money from earned income through research trials) and agreed in principle the use of its funds to support research staff salaries, with the details to be determined in correspondence. Third Party Cheque Indemnity The CTC approved a third party cheque indemnity to enable the Charity to bank cheques made out in the name of individual funds or Charity appeals. Annual Report/Review of Terms of Reference Subject to minor amendments, the CTC approved the Annual Report 2014/15, demonstrating the Committee had met its terms of reference, and revised Terms of Reference, which had been updated to reflect the changes to the reporting structure of the Charity to include attendance by the Head of Engagement, and recommended final approval at Trust Board. Outcomes: Review of Charity including structure The CTC received a review of the Charity and its structure from the Interim Head of Charity. The Charity was now part of the Strategic Development directorate responsible to the Head of Engagement. The CTC noted the main changes to the structure proposed in September 2014 and supported actions to increase income, monitor expenditure, improve the fundraising database and develop the Charity s marketing on and off-line. The CTC recommended the target ratio pence in the pound be set at 25p, agreed expenditure would be patient focussed and supported that divisions would identify projects for charity funding at the beginning of the financial year. Charity Management Team Update The CTC received an update on activities of the Charity Management Team (CMT) since May 2015 and supported actions undertaken by the Interim Head of Charity to improve attendance at CMT meetings. Included within the report was a progress update in response to Kate Lampard s Lessons Learnt Report and a draft policy to address recommendations made relating to the Charity. The CTC endorsed the recommendation to update the risk register and supported suggested amendments to key performance indicators. The Committee was satisfied all Charity staff and volunteers undertook DBS checks on recruitment. Income Activity report The CTC received an update on the Charity s top line income and expenditure and main activities generating funds. Performance to the end of July 2015 was good mainly due to 13.1 Charity Trust Committee Report.pdf Page 2 of 3 Overall Page 131 of 215
132 receipt of a large amount of legacy income. The Committee discussed the Forget-me-not Appeal being behind trajectory on its target and approved the Interim Head of Charity would undertake a review of the appeal to promote visible activity across the Trust. Following the official launch of the playroom on 17 July, the Committee welcomed the continuation of the Magic of Play appeal, since its clear and recognisable brand continued to attract fundraising; the Charity was keen to continue the momentum and support further development in children s services. Charity Finance and Cash Flow Reports The Committee received an update on the financial position of the Charity. The overall position for the period ended July showed income was 3,424 (1%) above plan (including receipt of two legacies totalling 151,000) and expenditure 42,767 (12%) above. The end-year position was likely to be close to plan. Other matters: Cancer Services Division Fund Management report The CTC received an update on the Cancer Services Division charitable activities including plans for future charitable projects. As at the end of July 2015, the division held 28 funds with a total balance of 809k. Key activities supported by charitable funds included purchases to improve patient comfort, progress in recruitment of voluntary staff and improvements in the profile of the charity. Upcoming events included a House of Lords dinner for the Here if you need us campaign and a secret art sale. The Committee discussed a potential opportunity for the Trust to take over the operational and financial management of Chart Lodge, the Mount Vernon Cancer Centre patient overnight facility, and recommended the Division explore further options. The Committee was impressed by the enthusiasm of the cancer services fund raising team. Approvals of expenditure over 5k The CTC approved the following charitable expenditure: 28,214 to extend the Community Engagement Team at Mount Vernon Cancer Centre to September 2016; an update on progress would be presented at CTC before consideration of further funding to 2017; 20,000 (subject to confirmation of costs) to enhance the patient and staff environment at Nuclear Medicine, Mount Vernon; 7,500 from a staff wellbeing fund to sponsor a staff seasonal celebration at Mount Vernon; 88,700 (subject to cost control implementation) to fund a Trust-wide patient/public Wi-Fi service Investment Portfolio Update The CTC considered the latest investment portfolio to end June Performance had improved but was down on the previous year and against the market as whole. A review would be completed by the start of the next financial year. Bob Niven Chairman 22 September Charity Trust Committee Report.pdf Page 3 of 3 Overall Page 132 of 215
133 TRUST BOARD 30 SEPTEMBER 2015 CHARITY TRUSTEE COMMITTEE ANNUAL REPORT AND REVIEW OF TERMS OF REFERENCE Agenda Item:13.02 PURPOSE PREVIOUSLY CONSIDERED BY Objective(s) to which issue relates * Risk Issues (Quality, safety, financial, HR, legal issues, equality issues) Healthcare/ National Policy (includes CQC/Monitor) To present the Board the CTC Annual Report for 2014/15 and revised terms of reference for approval. The report is designed to provide an overview of the Committee s operation and its work, demonstrating the extent to which it has met its terms of reference. Charity Trustee Committee, September Minor amendments to reflect the new reporting structure of the charity and the successful delivery of the Magic of Play appeal 1. To continuously improve the quality of our services in order to provide the best care and optimise health outcomes for each and every individual accessing the Trust s services 2. To excel at customer service, achieving outstanding levels of communication and patient, carer and GP satisfaction 3. To provide and support the best standards of integrated care for the elderly and those with long term conditions by developing key partnerships and services 4. To consolidate services and enhance local access to specialist services in order to deliver high quality, safe, seamless, innovative and integrated services which are sustainable 5. To support the continued development of the Mount Vernon Cancer Centre and provision of leading local and tertiary cancer services 6. To improve our staff engagement and organisational culture to be amongst the best nationally Part of Trust assurance process The production of an annual report is in line with best practice in corporate governance CRR/Board Assurance Framework * Corporate Risk Register BAF ACTION REQUIRED * For approval For discussion For decision For information DIRECTOR: CHIEF EXECUTIVE PRESENTED BY: COMPANY SECRETARY AUTHOR: BOARD COMMITTEE SECRETARY/COMPANY SECRETARY DATE: SEPTEMBER 2015 We put our patients first We work as a team We value everybody We are open and honest We strive for excellence and continuous improvement * tick applicable box 13.2 CTC Annual Review and TOR.pdf May 2013 Page 1 of 8 Overall Page 133 of 215
134 Charity Trustee Committee Annual Review 2014/15 INTRODUCTION As set out in the terms of reference, the Charity Trustee Committee (CTC) is a committee of the Board, in its role of Corporate Trustee and with responsibility: to ensure a robust strategy for the delivery of The Charity aims and objectives; to champion The Charity and its development, providing leadership both within the Trust and externally; to provide stewardship of charitable resources and ensure compliance with relevant legislation, guidance and Trust policies. This is a delegated duty carried out on behalf of the East and North Hertfordshire NHS Trust, which is the sole Corporate Trustee of East & North Herts Hospitals Charity (registered charity no ). This is the annual review of the CTC which considers how the Committee has met its duties under its terms of reference. A review of the minutes and reports to Board, and a review of the Trust s Standing Orders and Financial Instructions have been used to inform this report. Where areas for improvement were identified, the agreed actions were noted or recommendations made. There have been some recent changes to the Chair of the Committee and the leadership of Charity. The Charity now reports to the Head of Engagement and sits in the portfolio of the Director of Strategic Development. The Committee and team are committed to continue to strengthen the charity and governance arrangements during 2015/16. The Board as Corporate Trustee is asked to note the report and approve the revised terms of reference (appendix 1 attached); these have a minor amendment and are reflective of the recent changes to the reporting of the structure of the charity. SUMMARY OF KEY FINDINGS Meetings and Membership The CTC met four times during 2014/15 and all meetings were quorate under current terms of reference. In September 2014 the CTC approved an amendment to the terms of reference; the committee quorum was reduced from three to two (one Non-executive Director plus one Director). The position of Chair of the Committee remained the same throughout 2014/15. Membership attendance was recorded in the Trust Annual Report; no issues were identified. The minutes demonstrated where scrutiny and appropriate challenge had been given during meetings. Strategic Charity Governance The CTC ensured policies and procedures were in place to allow the effective day-to-day management of The Charity and its funds. In September 2014, the Head of Hospital Charities reviewed the charity structure and this was supported by the CTC. The Charity continued to monitor ratio of costs required to generate income and apportionment percentage charges for management. The CTC is committed to reducing the ratio of costs. Throughout 2014/15 the Committee continued to develop the charity risk register and reviewed and approved Key Performance Indicators (KPI s) which were updated to reflect objectives and requirements for the year. The Charity achieved less than planned partly due to legacy income 13.2 CTC Annual Review and TOR.pdf Page 2 of 8 Overall Page 134 of 215
135 and income targets from some projects and sources not realised. The Charity recruited two fulltime fundraisers to improve performance. In December 2014 the Committee approved a new approval process for funding projects and in March 2015 recommended further strengthening of the process. This would continue to be an area of focus for 2015/16. In March 2015 the CTC received an update on the Department of Health and Association of NHS Charities outline guidance on conversion to independent status. The Committee approved the recommendation not to progress further at that time to enable the Charity time to focus on embedding its new team, cultivate income and develop its strategy; it would undertake a review in approximately two years time. Charitable Management Team (CMT) Meetings In September 2014 the CTC approved amendments to CMT terms of reference and supported the reinstatement of these meetings which were more project focussed and held at alternate Trust sites. In March 2015 the CTC approved two main capital campaigns for 2015/16; the Forget-Me-Not appeal for dementia patients and the Here If You Need Us appeal for support and information services at Mount Vernon. CMT meetings had been promoted at Divisional Executive Committee (DEC) to raise awareness of and increase attendance at these meetings, to encourage and support active fund management and new fundraising schemes. The CTC would continue to monitor attendance and effectiveness of CMT meetings. Divisional Fund Management Reports Throughout 2014/15 the CTC received divisional fund management updates on charitable activities. This new initiative was implemented to provide the Committee with information on what divisions were delivering well in terms of use of charitable funding and what was proving more challenging with reasons and next steps. The Charity supported amalgamation of dormant funds including a review of guidance on dormant funds. Annual Report and Accounts 2013/14 and 2014/15 In May 2014 the CTC considered and endorsed The Charity Annual Report and Accounts 2013/14, the Letter of Representation and External Audit Findings and recommended submission to Audit Committee on 19 May 2014, followed by final approval and sign-off at Board on 28 May 2014, in line with the Trust s Annual Report and Accounts 2013/14. External Audit findings against significant risks provided assurance the accounts were of a high standard and management action ensured no control weaknesses were identified. In May 2015 the CTC approved the Charity s annual report and accounts 2014/15. These were submitted to Audit Committee for approval on 18 May 2015, in line with the Trust s main Annual Report and Accounts. External Auditors confirmed the Charity accounts were well prepared and no significant issues were identified. Investment Policy and Portfolio In September 2014 the CTC received a full presentation by The Charity s investment adviser, who provided an update on economic growth forecasts and portfolio valuations including benchmarking of asset allocations. He confirmed in the 12-month period to September the Trust achieved an overall 7.1% return against the 8% benchmark set. The Committee was satisfied with the medium risk portfolio and the balance of investment noting that asset allocation meetings took place monthly to ensure the Trust s money was invested correctly. The CTC received a further presentation in March 2015 and, since fund performance had fallen short of the benchmark for the third quarter, agreed to implement a review of the investment policy. Operational 13.2 CTC Annual Review and TOR.pdf Page 3 of 8 Overall Page 135 of 215
136 Charity development The minutes and fundraising papers demonstrate a range of fundraising activities and new initiatives undertaken throughout the year, such as the launch of the Forget-Me-Not Appeal a fund raising campaign to improve the Trust s care for patients with dementia. During 2014/15 the capital fundraising campaign Magic of Play (to fund a new play room on the children s ward) was identified at risk of not meeting its target and this risk was reflected on the charity risk register as a 12. This was closely monitored and the appeal was successful and the play room has now been formally opened. Income activity The CTC received regular updates on top line income activity and progress of the Charity to meet income plan 2014/15. Challenges during 2014/15 related to lower than expected legacy income, delays in recruitment and variances to planned income/expenditure. The CTC supported implementation of individual targets per fundraiser and the creation of a charity staffing contingency plan to cover risks of over-spend or income underperforming. Following a drive on the staff lottery, in May 2014 the CTC was pleased to note the level of income reached its target of double the prize money for the first time since it was launched in 2012; strict monitoring continued to sustain the increase in lottery membership. The CTC supported the launch of the external Unity lottery. Throughout 2014/15 the CTC continued to raise the charity s profile throughout the local community via retail outlets, local media and major corporations. This included attendance at the Trust s Annual General Meeting as well as a presence at the annual staff ceremony for Excellence Awards. Approvals of Expenditure During 2014/15 the CTC reviewed and endorsed funding requests for the following: Treatment room refurbishment on wards 10 and 11 at Mount Vernon Hospital; Increased roll-out of refurbishment linked to outpatient changes required to enhance patient experience at Mount Vernon Hospital; A realignment of MVCC salary costs to the Charity; Purchase of 3 AccuVein hand-held vein viewing systems; Recruitment of 2 x Band 5 FTE volunteer co-ordinator at Mount Vernon; Two infusion pumps for the Neonatal Unit; Appointment of a Race Director for the Moor Park 10k and junior fun runs on 27 September Reporting to Board The Committee has reported to the Trust Board as Corporate Trustee following each meeting and the CTC actions logs provide a clear audit trail of the actions agreed through to closure. CONCLUSION The overall conclusion of this annual review is that the Committee has discharged its duties under its terms of reference during 2014/15. The CTC continues to champion and raise awareness of The Charity and its development, both externally and within the Trust, provides stewardship of charitable resources and ensures compliance with relevant legislation, guidance and Trust policies. There have been some recent changes to the Chair of the Committee and the leadership of Charity. The Charity now reports to the Head of Engagement and sits in the portfolio of the Director of Strategic Development. The Committee and team are committed to continue to strengthen the charity and governance arrangements during 2015/ CTC Annual Review and TOR.pdf Page 4 of 8 Overall Page 136 of 215
137 The Board as Corporate Trustee is asked to note the report and approve the revised terms of reference (appendix 1 attached); these have a minor amendment and are reflective of the recent changes to the reporting of the structure of the charity CTC Annual Review and TOR.pdf Page 5 of 8 Overall Page 137 of 215
138 Appendix 1 CHARITY TRUSTEE COMMITTEE TERMS OF REFERENCE 1. Purpose & Authority The purpose of the Charity Trustee Committee is: To ensure a robust strategy for the delivery of the Charity aims and objectives. To champion the charity and its development, providing leadership both within the Trust and externally To provide stewardship of charitable resources and ensure compliance with relevant legislation, guidance and Trust policies This is a delegated duty carried out on behalf of the East and North Hertfordshire NHS Trust, which is the sole Corporate Trustee of the charity, East & North Herts Hospitals Charity (registered charity no ). 2. Authority The Charitable Funds Committee is authorised: to investigate any activity within its Terms of Reference. to obtain reasonable external legal or other independent professional advice and to secure the attendance of outsiders with relevant experience or expertise, if it considers this to be necessary. 3. Membership of the Committee Membership (with voting rights): two Non-Executive Directors Director of Finance Director of Strategic Development In attendance: Head of Charities Charity Financial Accountant Company Secretary Head of Engagement additional attendees selected by the Committee as deemed necessary to fulfil its function, including the Charity Independent Investment Advisor at least annually, Trust Financial Controller and Director of Business Development and Partnerships. The Chair of the Committee shall be one of the Non-Executive Directors selected by the Board. In their absence, meetings shall be chaired by the other Non-Executive Director. If a conflict of interests is established, the above member/ attendee concerned should declare this and withdraw from the meeting and play no part in the relevant discussion or decision. 4. Quorum A minimum of two members must be present, of which one must be a Non-Executive Director and one must be an Executive Director CTC Annual Review and TOR.pdf Page 6 of 8 Overall Page 138 of 215
139 5. Meetings The Charitable Trustee Committee will meet at least four times a year (as near as practical to quarter ends). The Chair of the Committee may convene additional meetings if required to consider business that requires urgent attention. 6. Key duties and responsibilities a. To ensure a robust strategy for the delivery of The Charity aims and objectives including: To approve and monitor The Charity and Strategy and Charity Management Team Annual Plan and Priorities. b. To provide stewardship of charitable resources and ensure compliance with relevant legislation, guidance and Trust policies Ensuring policies and procedures are in place that allow the effective day to day management of the charity and its funds Ensuring The Charity satisfies all regulatory, legal and NHS compliance requirements Ensuring funding provides added value to patients and staff, above those afforded by Exchequer Funds Ensuring expenditure is in line with donors expectations of an NHS Charity Ensuring effective systems are in place to manage budget holders and ensuring they demonstrate adherence to charitable objectives in spending charitable monies To recommend the appointment of Investment Managers to provide investment advice and manage the Trusts investment portfolio through an agreed Investment Policy, so as to safeguard the charity s future while maximising income. Ensuring The Charity s financial dealings are systematically accounted for To ensure appropriate mechanisms are in place to manage restricted and designated monies, and to use monies as agreed with the donor or negotiate alternative arrangements Receive and provide scrutiny to The Charity s Annual Report and Accounts, prior to final approval by the Corporate Trustee, Encouraging a culture of expending expendable income unless there is a clear reason to accumulate Establishing a Reserves Policy and monitoring its implementation Providing assurance updates to the Audit Committee regarding the governance and risk management of the charitable funds Reviewing and approving the Fundraising and Communications Strategies and the resources required to implement them Monitoring performance against financial and other key performance targets Setting a clear framework for prioritising charitable expenditure, and establishing appropriate approval processes for agreeing new campaigns and spending existing charitable monies To ensure appropriate delegation of charitable expenditure To authorise the establishment of any new funds For charitable funds schemes with a value of 5,000 and over: - Reviewing and, if appropriate, authorising - Ensuring that the Capital Control Group, and where appropriate the Executive Committee, reviews and monitors the application and implementation of charitable funds schemes. c. To champion The Charity and its development, both externally and within the Trust to include: 13.2 CTC Annual Review and TOR.pdf Page 7 of 8 Overall Page 139 of 215
140 Providing inspiring, reflective and visible leadership of the charity, clearly communicated to all stakeholders Growing the reputation and profile of the Charity (and by association, the Trust) Advocating and being ambassadors for charitable giving to the Charity within the community Developing through high donor activities a network of seriously influential stakeholders who see themselves as business partners in the Trust s future, and personally cultivating and stewarding these relationships Leading and encouraging the Board in achieving similar and appropriate support for the Charity. 7. Reporting arrangements The Committee will report to the Trust Board, as Corporate Trustee, following each meeting. 8. Support The Company Secretary will advise the Committee on pertinent governance issues and ensure is supported administratively, including: Agreement of agenda with Chairman and attendees and collation of papers Taking the minutes Keeping a record of matters arising and issues to be carried forward 9. Review The Terms of Reference of the Committee shall be reviewed by the Trust Board (Corporate Trustee) annually CTC Annual Review and TOR.pdf Page 8 of 8 Overall Page 140 of 215
141 DATA PACK Contents 1. Data & Exception Reports: Patient Experience Dashboard FFT report Statutory & Mandatory Training Exception Report Health & Safety Indicators Nursing Quality Indicators 2. Finance Appendices 3. Performance Data: Performance Report CQC Outcomes Summary 4. Workforce Appendices 5. Risk and Quality Committee Reports: Safer Staffing Infection Control Data Data Pack.pdf Page 1 of 73 Overall Page 141 of 215
142 DATA & EXCEPTION REPORTS Patient Experience Friends and Family Test Statutory & Mandatory Training Exception Report Health and Safety Indicators Data Pack.pdf Page 2 of 73 Overall Page 142 of 215
143 Patient Experience Dashboard: August 2015 APPENDIX 3 Friends and Family Test Score (Trust) Inpatients & Day Case Community Postnatal Birth Antenatal Outpatients A&E Aug 15 Jul 15 Aug 15 Jul 15 Aug 15 Jul 15 Aug 15 Jul 15 Aug 15 Jul 15 Aug 15 Jul 15 Aug 15 Jul 15 % recommend % not recommend Neither likely/unlikely or don't know Meridian Inpatient survey question responses Enough nurses Emotional support Help with meals Understand answers nurses Know named nurse Respect & dignity 100 Involved in Understand answers doctors Rate hospital food Jul 15 0 decisions Discuss worries & fears Call bell response Pain control Noise at night staff Noise at night patients Clean ward Aug Staff Friends and Family Test Score Quarter 1 Place to work Place for care and treatment No. Patient Experience Surveys completed on Meridian (excludes FFT) Aug Friends and Family Test Response Rates Jul Data Pack.pdf Inpatients/Day Case A&E Maternity (combined) Aug 15 Jul 15 Jun 15 Jun Page 3 of 73 Overall Page 143 of 215
144 Friends and Family Test - August 2015 APPENDIX 1 Inpatients & Day Case % Would recommend % Would not recommend Extremely Likely Likely Neither Likely/ Unlikely Unlikely Extremely Unlikely Don't Know Total responses No. of Discharges Total % response rate 5A B B AN AS B B Swift Day Surgery Centre, Lister Day Surgery Treatment Centre Endoscopy, Lister Endoscopy, QEII SURGERY TOTAL SSU CLOSED CLOSED CLOSED AMU Pirton Barley A B A ACU B Ashwell NP NP B A Day Treatment, QEII Medical Day Unit Cardiac Suite MEDICINE TOTAL A Gynae Bluebell ward Bluebell day case Neonatal Unit WOMEN'S/CHILDREN TOTAL Michael Sobell House CANCER TOTAL TOTAL TRUST Data Pack.pdf Continued over.. Page 4 of 73 Overall Page 144 of 215
145 Inpatients/Day by site % Would recommend % Would not recommend Extremely Likely Likely Neither Likely/ Unlikely Unlikely Extremely Unlikely Don't Know Total responses No. of Discharges Lister QEII Mount Vernon TOTAL TRUST Total % response rate Accident & Emergency % Would recommend % Would not recommend Extremely Likely Likely Neither Likely/ Unlikely Unlikely Extremely Unlikely Don't Know Total responses No. of Discharges Total % response rate Lister A&E QEII UCC A&E TOTAL Maternity % Would recommend % Would not recommend Extremely Likely Likely Neither Likely/ Unlikely Unlikely Extremely Unlikely Don't Know Total responses No. of Discharges Antenatal Birth Postnatal Community Midwifery MATERNITY TOTAL Total % response rate Outpatients % Would recommend % Would not recommend Extremely Likely Likely Neither Likely/ Unlikely Unlikely Extremely Unlikely Don't Know Total responses Lister QEII Hertford County Mount Vernon CC Satellite Dialysis OUTPATIENTS TOTAL Trust Targets % Would recommend % response rate Inpatients/Day Case 94%> 40%> A&E 78%> 19%> Maternity (combined) 93%> 30%> Outpatients 93%> N/A Data Pack.pdf Page 5 of 73 Overall Page 145 of 215
146 Statutory Training Performance FPC Exception Report September 2015 Target / Core Standard: Trust Target: The present target for staff compliance for overall coverage and for all 9 competencies of statutory training is 90% by March Current Position and Progress: Staff compliance continues to remain steady at 87.4%, compliance in all 9 core competencies is 57.6%. Please see attached dashboard. The highest performing staff group is Nursing Qualified increasing by 5% in the last 2 month to 66%. The highest performing division is Cancer Services, at 71%, the first division to reach over 70%. Four competencies are over 90%; Conflict Resolution, Health and Safety, Moving and Handling and Safeguarding Children. The greatest challenge remains those competencies requiring yearly updates. The Safeguarding Children s team have focused on increasing compliance for the level 3 competency, with a rise by 5% to 83% in the last 2 m onths.103 staff across Medicine and Woman s and Children still require this competency. As there continues to be a number of staff not attending booked training, the work book available on the Knowledge centre now identifies those staff who did not attend for that month. This allows managers to monitor attendance. Mandatory Training The 3 new mandatory competencies have been agreed, Dementia, End of Life Care and Diabetes. Over the next two months, communication will ensure that staff are aware of the new requirements. Diabetes training is via a nationally recognised e-learning provider and staff have completed 952 modules since April 2015, with another 1125 m odules in progress. This has led to the Trust being recognised as the highest performing Trust nationally. The company Virtual Collage from Leeds visited the Trust this month to award a certificate of recognition. Prevent training Prevent training is available to staff in high risk areas. The Statutory Steering Committee have recommended an awareness element for all staff and this has now been incorporated into Vital Training. East of England Streamlining Project The Trust is in the process of mapping its training against the Core Skills Framework to allow for a training passport between Trusts. At present one area of risk is highlighted as not mapping against the agreed standard and this is Resuscitation training. This has been recognised as a regional issue and discussions are in place to reach a solution. FPC Statutory Training Exception Report Final CF Sept 15 Data Pack.pdf Page 6 of 73 Overall Page 146 of 215
147 Statutory Training September 2015 update This report provides a month-end position for August 2015 Assignments 5,095 Valid Frameworks 5,082 (99.7%) Overall Training Coverage is currently 87.4% Individual Compliance is currently 57.6% Individual Compliance by Staff Groups Nursing Other Clinical Non-Clinical Medical & Dental Competency Framework Coverage Conflict Resolution (93%) Gap analysis: Staff who are... 20% Compliant or Less 4% Safeguarding Children (90%) Equality & Diversity (84%) Over 20% but less than 40% Compliant 3% Over 40% but less than 60% Compliant 4% Safeguarding Adults (89%) Baseline Fire (77%) Over 60% but less than 80% Compliant 13% Moving and Handling (92%) Information Governance (72%) General Health & Safety (94%) Infection Prevention (89%) Over 80% but less than 100% Compliant 19% 100% Compliant 58% 0% 20% 40% 60% 80% 100% Data sources: ESR competence extract; ESR leavers extract; StatMan Compliance Database Design and visualisation concepts: ENHT InfoDept June 2015 Data Pack.pdf Page 7 of 73 Overall Page 147 of 215
148 Patient Experience Patient Safety LOS Beds NURSING & MIDWIFERY QUALITY INDICATORS: AUGUST 2015 All data is collated using nursing & midwifery establishment figures and inpatient wards only -RAG Rating for Patient Experience is Provisional SUMMARY Trust Medicine Surgery Women & Children Cancer Total Beds Bed occupancy % (at Midnight) 87.52% 88.14% 86.56% 90.54% 80.35% % E-roaster Deadline Met 81.17% 63.77% 87.38% 90.29% 83.25% Staffing e-roastering Net Hours % 0.23% 0.13% 0.66% 0.16% -0.05% Net Hours Position * % of Actual Annual Leave 14.93% 15.91% 14.59% 16.24% 12.98% Funded WTE * Actual WTE * Vacancy rate % 15.50% 20.99% 15.63% 10.28% 6.95% RN Fill Rate (day shifts) 94.82% 93.38% 93.56% 98.63% 93.70% Sickness % 4.49% 4.28% 4.28% 4.86% 5.62% Agency usage % 15.10% 21.80% 13.50% 8.40% 6.70% Bank usage % 9.50% 10.90% 7.50% 9.90% 7.20% Staff Appraised % (rolling 12 months) 71.88% 62.59% 60.08% 87.27% 83.16% Missed Breaks Nursing Overtime Statutory Mandatory Training all 9 Competency % Statutory Mandatory Training Overall Coverage % No of shifts where staffing initially triggered Red * 64.30% 58.30% 61.30% 68.42% 76.50% 90.65% 88.29% 89.45% 93.54% 92.40% % Shifts Triggered Red in Month 4.89% 6.45% 5.81% 2.15% 0.00% No. Delayed Discharges * No. Inpatient falls * No. Inpatient falls resulting in serious harm * No. of Hospital Acquired Pressure Ulcers * % News Score Completion 94.29% 90.00% 87.14% % % News Escalation * No. Medication Reported errors * % Medication administered as prescribed % Analgesia administered as prescribed 97% 96% 93% 100% 100% 96% 87% 97% 100% 100% Intentional rounding completed 92% 98% 79% Not Provided 100% Safety Thermometer Patients with harm * % of Compliance with Hand Hygiene 95.76% 93.38% 94.44% % 95.24% % Response to Inpatient Survey 29.50% 37.50% 28.50% 22.90% 35.60% Help to eat meals/infant Feeding Enough nurses on duty Respond to call bell Pain Control Understand answers from nurses Someone to talk to about worries and fears Enough emotional support from staff Know named nurse Inpatient FFT - % of patients would recommend Inpatient FFT - % of patients would not recommend 96.36% 96.51% 96.02% % 94.31% 0.70% 1.10% 0.51% 0.00% 0.81% FFT Response Rate % 38.58% 48.44% 35.12% 26.58% 45.56% No.of Complaints * * sum of division sheets Data Pack.pdf Nursing_Quality_Indicators_Report-August_FINAL_v2 Page 8 of 73 Overall Page 148 of 215
149 Patient Experience Patient Safety LOS Staffing NURSING & MIDWIFERY QUALITY INDICATORS: AUGUST 2015 CANCER Ward 10 Ward 11 Michael Sobell House e-roastering Beds Total Beds (Based on wards in this report) Bed occupancy % (at Midnight) 52.80% 50.90% 75.00% % E-roaster Deadline Met % % % Net Hours % -1.80% -0.60% 1.50% Net Hours Position % of Actual Annual Leave 16.00% 10.30% 15.30% Funded WTE Actual WTE Vacancy rate % 9.85% 14.01% 10.94% RN Fill Rate (day shifts) 82.80% 90.40% % Sickness % 2.12% 6.27% 5.01% Agency usage % 5.50% 11.20% 3.50% Bank usage % 4.30% 8.60% 8.90% Staff Appraised % (rolling 12 months) 88.00% 84.21% 89.66% Missed Breaks Nursing Overtime 0.11 Statutory Mandatory Training all 9 Competency % Statutory Mandatory Training Overall Coverage % No of shifts where staffing initially triggered Red 73.33% 56.00% 70.97% 92.74% 84.00% 90.86% % Shifts Triggered Red in Month 0.00% 0.00% 0.00% No. Delayed Discharges No. Inpatient falls No. Inpatient falls resulting in serious harm No. of Hospital Acquired Pressure Ulcers % News Score Completion Not Provided % Not Applicable News Escalation Not Provided 100 Not Applicable No. Medication Reported errors % Medication administered as prescribed % % % % Analgesia administered as prescribed % % % Data Pack.pdf Intentional rounding completed % % Not Applicable Safety Thermometer Patients with harm % of Compliance with Hand Hygiene 85.71% % % % Response to Inpatient Survey 39.40% 30.60% 42.90% Help to eat meals/infant Feeding Not Provided Enough nurses on duty Respond to call bell Pain Control Understand answers from nurses Someone to talk to about worries and fears Enough emotional support from staff Know named nurse Inpatient FFT - % of patients would recommend Inpatient FFT - % of patients would not recommend 93.67% 94.59% % 1.27% 0.00% 0.00% FFT Response Rate % 55.63% 30.58% % No.of Complaints Nursing_Quality_Indicators_Report-August_FINAL_v2 Page 9 of 73 Overall Page 149 of 215
150 Patient Experience Patient Safety LOS Staffing e-roastering Beds NURSING & MIDWIFERY QUALITY INDICATORS: AUGUST 2015 Medicine Total Beds (Based on wards in this report) Acute Medical Unit (AMU) - Ward Acute Cardiac Unit (Lister) Ashwell (AAU) Barley Pirton SSU 6A 6B 9A 9B 10B 11A Bed occupancy % (at Midnight) 85.60% 88.40% 87.30% 98.20% 87.30% 96.00% % % 97.40% 98.00% 93.50% (%) E-roster Deadline Met 66.00% 33.00% 0.00% % % 66.00% 33.00% 66.00% % 66.00% 66.00% 33.00% Net Hours % -0.50% 0.30% -0.80% -0.70% 0.80% -0.40% 1.10% 0.10% 1.60% -1.30% 0.90% 0.10% Net Hours Position % of Actual Annual Leave 22.80% 17.30% 15.10% 19.60% 16.30% 12.90% 14.60% 15.00% 14.50% 15.80% 18.30% 14.10% Funded WTE Actual WTE Vacancy rate % 37.76% 17.10% 28.05% 37.53% 12.38% 5.67% 22.39% -7.64% 31.63% 25.00% 9.85% 25.40% RN Fill Rate (day shifts) 84.70% 96.60% 92.20% 99.30% 93.20% 84.20% 96.50% 98.40% % 85.40% 95.50% 88.30% Sickness % 1.49% 6.23% 13.34% 6.79% 3.78% 6.91% 2.93% 4.92% 1.74% 6.19% 5.23% 4.51% Agency usage % 28.30% 21.80% 19.60% 27.10% 12.50% 23.10% 6.90% 2.40% 24.70% 36.80% 19.20% 23.30% Bank usage % 14.00% 12.00% 7.30% 19.30% 10.20% 11.40% 6.60% 5.70% 9.70% 7.60% 4.30% 15.00% Staff Appraised % (rolling 12 months) 55.56% 75.00% 5.56% 50.00% 81.82% 73.08% 57.14% 70.00% 33.33% 23.53% 78.26% 39.13% Missed Breaks Nursing Overtime Statutory Mandatory Training all 9 Competency % Statutory Mandatory Training Overall Coverage % No of shifts where staffing initially triggered Red 41.46% 34.69% 39.13% 66.67% 70.37% 58.82% 74.07% 68.42% 50.00% 51.72% 72.41% 71.43% 75.00% 82.82% 86.75% 94.44% 90.43% 88.73% 94.68% 92.32% 91.99% 91.67% 93.90% 95.54% % Shifts Triggered Red in Month 3.23% 3.23% 0.00% 7.53% 7.53% 13.98% 4.30% 1.08% 1.08% 11.83% 10.75% 11.83% No. Delayed Discharges No. Inpatient falls No. Inpatient falls resulting in serious harm No. of Hospital Acquired Pressure Ulcers % News Score Completion 95.00% 91.00% 82.00% 81.00% 90.00% Not Provided 85.00% % 90.00% % % 76.00% News Escalation Not Provided No. Medication Reported errors % Medication administered as prescribed % 96.00% 76.00% % % Not Provided Not Provided % 88.00% 96.00% % % % Analgesia administered as prescribed 80.00% 91.00% 90.00% 91.00% % Not Provided Not Provided % 64.00% 86.00% 94.00% 75.00% Intentional rounding completed 95.00% 96.00% 95.00% % % % Not Provided % % 96.00% % 95.00% Safety Thermometer Patients with harm % of Compliance with Hand Hygiene 91.67% 79.07% Not Provided % 97.09% % 63.04% % % % % 96.34% % Response to Inpatient Survey 34.10% 45.80% 0.00% 55.60% 51.00% Not Provided 25.40% 48.10% 5.90% 88.90% 34.60% 80.80% Help to eat meals/infant Feeding Not Provided Not Available Enough nurses on duty Not Provided Respond to call bell Not Provided Pain Control Not Provided Understand answers from nurses Not Provided Someone to talk to about worries and fears Not Provided Enough emotional support from staff Not Provided Know named nurse Not Provided Inpatient FFT - % of patients would recommend Inpatient FFT - % of patients would not recommend 96.97% 94.74% Not Provided 94.12% 92.11% Not Provided % 97.37% 90.00% 97.50% 94.44% % 0.00% 1.97% Not Provided 0.00% 0.00% Not Provided 0.00% 0.00% 10.00% 2.50% 0.00% 0.00% FFT Response Rate % 38.82% 85.88% 0.00% 62.96% 77.55% Not Provided 42.25% 48.10% 19.61% 88.89% 34.62% 80.77% No.of Complaints Data Pack.pdf Nursing_Quality_Indicators_Report-August_FINAL_v2 Page 10 of 73 Overall Page 150 of 215
151 Patient Experience Patient Safety LOS Staffing e-roastering Beds NURSING & MIDWIFERY QUALITY INDICATORS: AUGUST 2015 Surgery Total Beds (Based on wards in this report) ASCU Critical Care Swift 5A 5B 7B 8AN 8AS 8B 11B Bed occupancy % (at Midnight) % 57.70% 72.10% 93.90% 89.60% 95.10% 91.90% 91.00% 95.10% % E-roaster Deadline Met 33.00% % % % % 66.00% % % Net Hours % 4.30% -0.70% 0.50% 0.10% -0.30% -0.70% 0.40% 1.70% Net Hours Position % of Actual Annual Leave 15.70% 13.10% 14.30% 14.30% 16.40% 11.80% 15.60% 15.50% Funded WTE Actual WTE Vacancy rate % 21.63% 7.60% 23.39% 10.84% 14.22% 23.29% 10.27% 26.08% RN Fill Rate (day shifts) % 97.50% 89.00% 92.80% 85.70% 92.00% 91.50% % Sickness % 7.98% 10.94% 1.04% 7.08% 4.13% 10.02% 4.50% 3.80% Agency usage % 0.00% 11.70% 6.10% 14.00% 10.20% 10.50% 23.80% 23.90% 6.60% Bank usage % 0.00% 1.00% 10.40% 13.20% 17.00% 7.10% 9.20% 3.50% 14.30% Staff Appraised % (rolling 12 months) 32.35% 63.16% 83.33% 71.43% 88.46% 47.37% 44.44% 57.89% Missed Breaks Nursing Overtime 0.58 Statutory Mandatory Training all 9 Competency % Statutory Mandatory Training Overall Coverage % No of shifts where staffing initially triggered Red 60.64% 64.29% 58.33% 68.57% 57.14% 32.26% 64.00% 50.00% 88.56% 91.74% 91.67% 92.52% 95.00% 83.61% 92.78% 80.79% % Shifts Triggered Red in Month 1.08% 11.83% 3.23% 9.68% 5.38% 3.23% 11.83% 5.38% No. Delayed Discharges No. Inpatient falls No. Inpatient falls resulting in serious harm No. of Hospital Acquired Pressure Ulcers % News Score Completion Not Provided News Escalation Not Provided Not Applicable Not Applicable Not Provided 90.00% 80.00% % 80.00% 80.00% 80.00% % Not Provided No. Medication Reported errors % Medication administered as prescribed % Analgesia administered as prescribed 92.00% 87.00% % 95.00% 65.00% % % % Not Provided % % % % % % % 88.00% % Not Provided 89.00% Intentional rounding completed % Not Provided % % % % 10.00% 50.00% Not Provided 70.00% Safety Thermometer Patients with harm Data Pack.pdf % of Compliance with Hand Hygiene % 99.13% Not Provided % 57.14% % % % Not Provided 99.22% % Response to Inpatient Survey Help to eat meals/infant Feeding Enough nurses on duty Respond to call bell Pain Control Understand answers from nurses Someone to talk to about worries and fears Enough emotional support from staff Know named nurse Inpatient FFT - % of patients would recommend Inpatient FFT - % of patients would not recommend FFT Response Rate % Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable 18.60% 14.50% 47.50% 32.70% 35.30% 45.90% 15.30% 46.40% % 93.94% 96.55% 90.63% 94.44% 85.29% 88.89% 95.56% 2.00% 0.00% 0.00% 1.56% 0.00% 0.00% 0.00% 0.00% 22.73% 60.00% 49.15% 32.65% 35.29% 45.95% 15.25% 46.39% No.of Complaints Nursing_Quality_Indicators_Report-August_FINAL_v2 Page 11 of 73 Overall Page 151 of 215
152 LOS NURSING & MIDWIFERY QUALITY INDICATORS: AUGUST 2015 Women and Children CLU Dacre Gloucester MLU Bluebell Neonatal Unit 7A Patient Experience Patient Safety Staffing Beds Total Beds (Based on wards in this report) Bed occupancy % (at Midnight) % 47.30% % % 64.50% 43.70% % % E-roaster Deadline Met % 66.00% 66.00% % % % % e-roastering Net Hours % 0.10% 0.20% -0.20% -0.90% 0.40% -0.40% 1.90% Net Hours Position % of Actual Annual Leave 15.80% 16.90% 12.80% 16.10% 17.00% 16.00% 19.10% Funded WTE Actual WTE Vacancy rate % 22.02% 46.45% 13.88% % -2.22% 16.11% 16.68% RN Fill Rate (day shifts) 99.00% % 92.50% % 94.50% Not Provided % Sickness % 5.00% 0.00% 5.06% 11.16% 6.70% 2.55% 10.08% Agency usage % 9.90% 43.50% 15.50% 3.80% 13.10% 0.00% 4.80% Bank usage % 6.50% 14.20% 18.00% 3.10% 10.90% 15.60% 7.90% Staff Appraised % (rolling 12 months) 84.00% % 96.43% 82.35% 80.00% 93.75% 86.21% Missed Breaks Nursing Overtime Statutory Mandatory Training all 9 Competency % Statutory Mandatory Training Overall Coverage % No of shifts where staffing initially triggered Red 73.86% 80.00% 71.43% 75.00% 71.43% 75.44% 63.16% 93.96% 89.23% 93.54% 95.05% 95.88% 95.79% 93.76% % Shifts Triggered Red in Month 0.00% 0.00% 0.00% 0.00% 5.38% 0.00% 7.53% No. Delayed Discharges No. Inpatient falls No. Inpatient falls resulting in serious harm No. of Hospital Acquired Pressure Ulcers % News Score Completion Not Applicable % % Not Applicable Not Provided Not Applicable Not Applicable News Escalation Not Applicable Not Applicable Not Provided Not Applicable Not Applicable No. Medication Reported errors % Medication administered as prescribed % Analgesia administered as prescribed % % % % Not Provided Not Provided Not Provided % % % % Not Provided Not Provided Not Provided Intentional rounding completed Not Applicable Not Provided Not Provided Not Provided Safety Thermometer Patients with harm % of Compliance with Hand Hygiene % % % % Not Provided % Not Provided % Response to Inpatient Survey Not Applicable 0.90% 56.50% 21.00% Help to eat meals/infant Feeding Enough nurses on duty Not Applicable 61 Respond to call bell Not Applicable 73 Not Applicable 91 Pain Control Not Applicable 94 Data Pack.pdf Understand answers from nurses Someone to talk to about worries and fears Enough emotional support from staff 100 Not Applicable Know named nurse Not Applicable 100 Not Applicable 100 Inpatient FFT - % of patients would recommend Maternity FFT - % of patients would recommend - Antenatal Maternity FFT - % of patients would recommend - Birth Maternity FFT - % of patients would recommend - Postnatal Maternity FFT - % of patients would recommend - Community Midwifery Inpatient FFT - % of patients would not recommend Maternity FFT - % of patients would not recommend - Antenatal Maternity FFT - % of patients would not recommend - Birth Maternity FFT - % of patients would not recommend - Postnatal Maternity FFT - % of patients would not recommend - Community Midwifery % % % 0.00% 0.00% 0.00% Inpatient FFT Response Rate % Not Applicable 17.35% 95.65% 28.41% Maternity FFT Response Rate % - Combined Not Applicable 96.00% 95.88% 88.89% 96.00% Not Applicable 4.00% 1.23% 2.06% 4.00% 24.22% Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable Not Applicable No.of Complaints Nursing_Quality_Indicators_Report-August_FINAL_v2 Page 12 of 73 Overall Page 152 of 215
153 Beds e-rostering KPI Definitions DRAFT v2.4 August 2015 Theme Measure Metric Goal (at which point a Green rating is applied) Threshold (after which point a Red rating is applied) Direction Data Source / Data Owner Reporting Scope Noted Issue Comments Total beds A simple count of inpatient beds, excluding trolleys and assessment areas for each ward unit. Not applicable ` Not applicable Manual data collection/ Bed Management Team Aggregated to Trust and Division from the ward unit of analysis No thresholds set. Metric displayed for context. Bed occupancy The percentage of inpatient bed days occupied by a patient at Midnight 90% 95% Lower values are better Acumen / Information Team Aggregated to Trust and Division from the ward unit of analysis No thresholds set. Metric displayed for context. If not supplied then set as Not Applicable % E-roaster Deadline Met The percentage of approval and finalisation deadlines met in month. Each roster must be approved by the Ward Manager, Payroll and the Matron for which equal weighting is applied to when assessing full compliance. Net Hours Position The Net hour position for the last 4- week roster to fall in the month. 100% <100% Not defined MAPS / Rupert Clarke As Above As Above Not defined MAPS / Rupert Clarke Agregated to Trust and Division from the ward unit of analysis Agregated to Trust and Division from the ward unit of analysis No RAG rating thresholds have been confirmed but values If not supplied then set supplied with RAG rated as Not Provided and shading. Possible Red aggregation issue to be confirmed Definition needs to be refined. No RAG rating thresholds have been confirmed. Possible aggregation issue to be confirmed If not supplied then set as Not Provided and Red Net Hours % The % Net hour position for the last 4-week roster to fall in the month. <>2.0% swing ing the total contracted hours for the ward <>2.5% swing ing the total contracted hours for the ward MAPS / Rupert Clarke If not supplied then set as Not Provided and Red % of Actual Annual Leave The percentage for annual leave in the last four-week roster to fall in the month >=11% <=17% <10% >18% Not defined MAPS / Rupert Clarke Agregated to Trust and Division from the ward unit of analysis Definition needs to be refined. No RAG rating thresholds have been confirmed If not supplied then set as Not Provided and Red Amber = >17% <=19% Amber = >=10% <11% Funded WTE A simple count of the ward's funded working hours expressed in terms of whole time equivalents Not applicable Not applicable Not applicable ESR / Lindsay Freeston Aggregated to Trust and Division from the ward unit of analysis No thresholds set. Metric displayed for context. If not supplied then set as Not Applicable Data Pack.pdf Page 13 of 73 Overall Page 153 of 215
154 Staffing KPI Definitions DRAFT v2.4 August 2015 Theme Measure Metric Goal (at which point a Green rating is applied) Threshold (after which point a Red rating is applied) Direction Data Source / Data Owner Reporting Scope Noted Issue Comments Actual WTE A simple count of the hours worked by the ward's workforce expressed in terms of whole time equivalents Not applicable Not applicable Not applicable ESR / Lindsay Freeston Aggregated to Trust and Division from the ward unit of analysis No thresholds set. Metric displayed for context. If not supplied then set as Not Applicable Vacancy rate % The percentage of funded working hours remaining after subtracting the contracted working hours from the ward establishment. 6% 8% Lower values are better ESR / Lindsay Freeston Aggregated to Trust and Division from the ward unit of analysis Thresholds under review RH Fill Rate (day shifts) The number of actual worked hours (including overtime) divided by the total planned working hours expressed as a percentage Not defined Not defined Not defined MAPS / Rupert Clarke Agregated to Trust and Division from the ward unit of analysis Definition needs to be refined. No RAG rating thresholds have been confirmed If not supplied then set as Not Provided and Red Sickness % The number of reported sick days expressed as a percentage of the total working calendar days in month 4% 5% Lower values are better MAPS / Rupert Clarke Aggregated to Trust and Division from the ward unit of analysis Agency usage % To be confirmed 2% 5% Lower values are better General Ledger / Lisa Potter Aggregated to Trust and Division from the ward unit of analysis Definition needs to be refined. Bank usage % To be confirmed 4% 7% Lower values are better General Ledger / Lisa Potter Aggregated to Trust and Division from the ward unit of analysis Definition needs to be refined. Staff Appraised % (rolling 12 months) To be confirmed 90% 70% Higher values are better ESR / Lindsay Freeston Aggregated to Trust and Division from the ward unit of analysis Definition needs to be refined. Missed Breaks A count of the number of warnings where reported shifts of 6-hours or more do not include a 20 minute break (THIS IS NOT A %, IT S A TOTAL COUNT OF INCIDENTS) 0% 1% Not defined MAPS / Rupert Clarke Agregated to Trust and Division from the ward unit of analysis No RAG rating thresholds have been confirmed Not Yet Available Nursing Overtime To be confirmed Not defined Not defined Not defined MAPS / Rupert Clarke Agregated to Trust and Division from the ward unit of analysis Definition needs to be refined. No RAG rating thresholds have been confirmed Statutory Mandatory Training Overall Coverage % The percentage of the ward staff in post who are fully compliant with their individual Statutory Training compliance framework. 90% 80% Higher values are better ESR data extract / Lindsay Freeston. Aggregated to Trust and Division from Statutory Training the ward unit of analysis Analysis Tool / Information Team Data Pack.pdf Page 14 of 73 Overall Page 154 of 215
155 Staffing (cont.) LoS Patient Safety KPI Definitions DRAFT v2.4 August 2015 Theme Measure Metric Goal (at which point a Green rating is applied) Threshold (after which point a Red rating is applied) Direction Data Source / Data Owner Reporting Scope Noted Issue Comments Statutory Mandatory Training all 9 Competency % The percentage of the ward staff in post who are fully compliant with all 9 Statutory Training compliance framework. Never RAG Rate No of shifts where staffing initially fell below agreed levels The count of shifts on a ward where staffing initially fell below agreed levels Not applicable Not applicable Not applicable Safer Staffing Report / Adam Brown Aggregated to Trust and Division from the ward unit of analysis No thresholds set. Metric displayed for context. If not supplied then set as Not Provided and Red % Shifts Triggered Red in Month The count of shifts on wards triggering red - where staffing levels are judged to be unsafe - in month 5% 10% Lower values are better Safer Staffing Report / Adam Brown Aggregated to Trust and Division from the ward unit of analysis No RAG rating thresholds have been confirmed If not supplied then set as Not Provided and Red No. Delayed discharges Number of Delayed Discharges Not defined Not defined Lower values are better Discharge Team Aggregated to Trust and Division from the ward unit of analysis Definition needs to be refined. No RAG rating thresholds have been confirmed No. Inpatient falls The count of reported inpatient falls in month Lower values are better Manual data collection / Edna Gallagher Aggregated to Trust and Division from the ward unit of analysis. Thresholds set at Trust level only Ward-level thresholds need to be confirmed If not supplied then set as zero No. Inpatient falls resulting in serious harm The count of reported inpatient falls resulting in serious harm in month Lower values are better Manual data collection / Edna Gallagher Aggregated to Trust and Division from the ward unit of analysis. Thresholds set at Trust level only Ward-level thresholds need to be confirmed If not supplied then set as zero No. Pressure ulcers 2 The count of confirmed grade 2 and above pressure ulcers in month 8 10 Lower values are better Manual data Aggregated to Trust and Division from collection / Dianne the ward unit of analysis. Thresholds Brett set at Trust level only Ward-level thresholds need to be confirmed If not supplied then set as zero NEWS score Observations assessed against the Early Warning Score (EWS) in accordance with Trust guidelines 98% 89% Higher values are better Meridian Scores shown for wards completing required number of audits (usually 20 per month). All Audits counted towards Divisional and Trust score Scores shown for wards completing required number of audits (usually 20 per month). All Audits counted towards Divisional and Trust score If not supplied then set as Not Provided and Red. Not Applicable to Michael Sobell House, Critical Care, CLU, MLU and Neonatal Data Pack.pdf Page 15 of 73 Overall Page 155 of 215
156 Patient Safety (cont.) Patient Safety (cont.) KPI Definitions DRAFT v2.4 August 2015 Theme Measure Metric Goal (at which point a Green rating is applied) Threshold (after which point a Red rating is applied) Direction Data Source / Data Owner Reporting Scope Noted Issue Comments NEWS Escalation Documentation of referral to medical staff for patients assessed as being at risk. 98% 89% Higher values are better Meridian Aggregated to Trust and Division from the ward unit of analysis Scores shown for wards completing required number of audits (usually 20 per month). All Audits counted towards Divisional and Trust score If not supplied then set as Not Provided and Red. Not Applicable to Michael Sobell House, Critical Care, CLU, MLU and Neonatal No. Medication Reported errors The count of reported medication administration errors in month Lower values are better Electronic data collection by Datix Incident Forms / Phil James and Diane Moore Aggregated to Trust and Division from the ward unit of analysis. Thresholds set at Trust level only Ward-level thresholds need to be confirmed If not supplied then set aszero % Medication administered as prescribed Medicines administered and signed for in accordance with the prescriptoin over the last 7 days 98.00% 89.00% Higher values are better Meridian Aggregated to Trust and Division from the ward unit of analysis Scores shown for wards completing required number of audits (usually 20 per month). All Audits counted towards Divisional and Trust score If not supplied then set as Not Provided and Red % Analgesia administered as prescribed If patient experienced pain in the last 24 hours is it documented that analgesia given within 30 minutes of the complaint of pain % 89.00% Higher values are better Meridian Aggregated to Trust and Division from the ward unit of analysis Scores shown for wards completing required number of audits (usually 20 per month). All Audits counted towards Divisional and Trust score If not supplied then set as Not Provided and Red Intentional rounding completed Intentional rounding chart completed correctly for last 24 hours Higher values are better Meridian Aggregated to Trust and Division from the ward unit of analysis If not supplied then set as Not Provided and Red. Not Applicable to Michael Sobell House Safety Thermometer Patients with harm A count of patients suffering harm as defined in the Safety Thermometer audit <=381 >=382 Lower values are better Safety Thermometer Audit / Jenny Pennell Aggregated to Trust and Division from the ward unit of analysis. Thresholds set at annual Trust level only If not supplied then Not Applicable % Compliance with Hand Hygiene 100% 100% Higher values are better Meridian If not supplied then set as Not Provided and Red Data Pack.pdf Page 16 of 73 Overall Page 156 of 215
157 Patient Experience Patient Experience (cont..) KPI Definitions DRAFT v2.4 August 2015 Theme Measure Metric Goal (at which point a Green rating is applied) Threshold (after which point a Red rating is applied) Direction Data Source / Data Owner Reporting Scope Noted Issue Comments % Response rate to patient experience survey Percentage response rate to patient experience survey (inpatient, maternity, neonatal, critical care) from eligible patients >=25% <25% Higher values are better Meridian Inpatient experience Applies over all levels for Ward and survey/jenny Trust etc Pennell. Acumen / Information Team If data not supplied then set to Not Provided. Not Applicable for ASCU. Help with Meals Reported patient experience score out of 100. Inpatients & Critical Care: Did you get enough help from staff to eat your meals? Maternity: Thinking about feeding your baby (breast or bottle) did you feel midwives and other carers gave you active support and encouragement? Neonatal: If you wanted to breast feed your baby, were you given enough support to do this from the neonatal unit staff? >=67 <=56 Higher values are better Meridian Patient Aggregated to Trust and Division from Experience Survey the ward unit of analysis / Jenny Pennell Thresholds updated. If not supplied then set as Not Provided and Red. ACSU is not applicable if data not supplied. Enough nurses on duty Reported patient experience score out of 100. Inpatients: In your opinion, were there enough nurses on duty to care for you in hospital? Maternity: Were you left alone by staff at a time when it worried you? >=84 <=73 Higher values are better Meridian Patient Aggregated to Trust and Division from Experience Survey the ward unit of analysis / Jenny Pennell Thresholds updated. If not supplied then set as Not Provided and Red. Not Applicable to Critical Care and Neonatal. Respond to call bell Reported patient experience score out of 100. Inpatients and Critical Care: After you used the call button, how long did it usually take before you got help? >=68 <=61 Higher values are better Meridian Patient Aggregated to Trust and Division from Experience Survey the ward unit of analysis / Jenny Pennell Thresholds updated. If not supplied then set as Not Provided and Red. Not Applicable to Maternity and Neonatal Pain Control Reported patient experience score out of 100. Inpatients & Critical Care: Do you think the hospital staff did everything they could to help control your pain? Maternity: During labour and birth, did you feel you got the pain relief you wanted? >=86 <=79 Higher values are better Meridian Patient Aggregated to Trust and Division from Experience Survey the ward unit of analysis / Jenny Pennell Thresholds updated. If not supplied then set as Not Provided and Red. Not Applicable to Neonatal. Data Pack.pdf Page 17 of 73 Overall Page 157 of 215
158 Patient Experience (cont..) KPI Definitions DRAFT v2.4 August 2015 Theme Measure Metric Goal (at which point a Green rating is applied) Threshold (after which point a Red rating is applied) Direction Data Source / Data Owner Reporting Scope Noted Issue Comments Someone to talk to about worries and fears Reported patient experience score out of 100. Inpatients & Critical Care: Did you find someone on the hospital staff to talk to about your worries and fears? Maternity: Were you given the opportunity to discuss your birth experience? >=65 <=54 Higher values are better Meridian Patient Aggregated to Trust and Division from Experience Survey the ward unit of analysis / Jenny Pennell Thresholds updated. If not supplied then set as Not Provided and Red. Not Applicable to Neonatal Understand answers from nurses Reported patient experience score out of 100. Inpatients: When you had important questions to ask a nurse, did you get answers that you could understand? Maternity: Thinking about your care during labour and birth, were you spoken to in a way you could understand? Neonatal: When you asked questions about your baby's condition and treatment, did you get answers you could understand? >=88 <=83 Higher values are better Meridian Patient Aggregated to Trust and Division from Experience Survey the ward unit of analysis / Jenny Pennell Thresholds updated. If not supplied then set as Not Provided and Red. Not Applicable to Critical Care. Enough emotional support from staff Reported patient experience score out of 100. Inpatients: Do you feel you got enough emotional support from hospital staff during your stay? Maternity: Thinking about the care you received in hospital after the birth of your baby, were you treated with kindness and understanding by the midwives? Neonatal: Were you offered emotional support from staff caring for your baby? >=78 <=67 Higher values are better Meridian Patient Aggregated to Trust and Division from Experience Survey the ward unit of analysis / Jenny Pennell Thresholds updated. If not supplied then set as Not Provided and Red. Not Applicable to Critical Care. Know named nurse Reported patient experience score out of 100. Inpatients: Do you know who your named nurse is? Critical Care: Did the staff treating and examining you introduce themselves? Neonatal: Were you told which nurse was responsible for your baby's care each day he/she was in the neonatal unit? >=75 <=63 Higher values are better Meridian Patient Aggregated to Trust and Division from Experience Survey the ward unit of analysis / Jenny Pennell Thresholds updated. If not supplied then set as Not Provided and Red. Not applicabel to Maternity. Data Pack.pdf Page 18 of 73 Overall Page 158 of 215
159 Patient Experience (cont..) KPI Definitions DRAFT v2.4 August 2015 Theme Measure Metric Goal (at which point a Green rating is applied) Threshold (after which point a Red rating is applied) Direction Data Source / Data Owner Reporting Scope Noted Issue Comments Inpatient FFT - % of patients who would recommend The percentage of patients who are extremely likey + likely to recommend the ward to their friends and family >=93% <93% Higher values are better FFT Survey/ Jenny Pennell Aggregated to Trust and Division from the ward unit of analysis Thresholds updated. If not supplied then set as Not Provided and Red. Not Applicable for ASCU & Critical Care. Not applicable to CLU, MLU, Dacre & Gloucester as report Maternity FFT. Inpatient FFT - % of patients would not recommend The percentage of patients who are unlikey + extremely unlikely to recommend the ward to their friends and family <=2% >2% Lower values are better FFT Survey/ Jenny Pennell Aggregated to Trust and Division from the ward unit of analysis Thresholds updated. If not supplied then set as Not Provided and Red. Not Applicable for ASCU & Critical Care. Not applicable to CLU, MLU, Dacre & Gloucester as report Maternity FFT. FFT Response Rate % The percentage of patients who responded to the FFT Survey from all those eligible to respond. Maternity FFT calculated from combined response rates. >=40% <40% Higher values are better FFT Survey/ Jenny Pennell. Acumen / Information Team Thresholds updated. No.of Complaints The count of registered complaints received in month Lower values are better Datix / Jackie Martin and Jan Shrieves Aggregated to Trust and Division from the ward unit of analysis. Thresholds set at annual Trust level only Monthly and Ward-level thresholds need to be confirmed If not supplied then set as zero Data Pack.pdf Page 19 of 73 Overall Page 159 of 215
160 FINANCE APPENDICES Data Pack.pdf Page 20 of 73 Overall Page 160 of 215
161 def FINANCE REPORT MONTH 5 INDEX TO APPENDICES Page no. Appendix 1 Summary income and expenditure position 2 Appendix 2 Income and Expenditure Monthly Profile 3 Appendix 3 Contract income by patient type 4 Appendix 4 Expenditure by Division 5 Appendix 5 CIP Programme 6 Appendix 6 Rolling 12 months cashflow 7 Appendix 7 Cashflow graphs 8 Appendix 8 Capital Programme 9 Appendix 9 Balance sheet 10 Data Pack.pdf Page 1 of 9 Page 21 of 73 Overall Page 161 of 215
162 Appendix 1 def FINANCE REPORT MONTH 05 TRUST INCOME AND EXPENDITURE Current Month Year to Date F u l l Y e a r Plan Actual Variance Plan Actual Variance Plan Forecast Variance Income Income from NHS activities 26,894 27, , ,760 (1,274) 337, ,135 (638) Income from non NHS activities ,420 2, ,839 5, Other operating income 4,047 4,002 (45) 18,925 18,876 (50) 41,568 38,822 (2,746) Total Income 31,430 31, , ,174 (1,205) 385, ,915 (3,266) ` Expenditure within Divisions Pay (19,424) (19,664) (240) (97,809) (98,122) (314) (233,899) (234,884) (986) Non-Pay (11,554) (11,742) (188) (58,641) (60,030) (1,389) (139,496) (142,208) (2,712) Unallocated Budgets (261) (2) 259 (1,262) (237) 1,025 (5,875) (2,216) 3,659 Contingency (250) (250) 0 (1,250) (1,250) 0 (3,000) 0 3,000 Total expenditure within Divisions (31,490) (31,658) (169) (158,962) (159,640) (678) (382,270) (379,308) 2,962 EBITDA (60) (73) (13) 1,416 (466) (1,883) 2,910 2,607 (304) PDC Dividends payable (295) (284) 11 (1,475) (1,418) 57 (3,540) (3,406) 134 Depreciation & minor impairments (685) (685) 0 (3,426) (3,425) 1 (8,222) (8,221) 1 Profit on sale of land 3,500 4, Investment Revenue Finance Costs (223) (234) (11) (1,114) (1,170) (57) (2,673) (1,108) 1,565 NET SURPLUS / (DEFICIT) (1,261) (1,273) (12) (4,588) (6,465) (1,878) (8,000) (6,100) 1,900 Income & depreciation on donated assets Impairments NET SURPLUS / (DEFICIT) INC DONATED ASSETS/IMPAIRMENTS (1,273) (6,465) Data Pack.pdf Page 2 of 9 Page 22 of 73 Overall Page 162 of 215
163 Appendix 2 FINANCE REPORT MONTH 05 PHASED TRUST INCOME & EXPENDITURE def Apr-15 May-15 Jun-15 Q1 Jul-15 Aug-15 Sep-15 Q2 Oct-15 Nov-15 Dec-15 Q3 Jan-16 Feb-16 Mar-16 Q4 Full Year Actual Actual Actual Actual Actual Forecast Forecast Forecast Forecast Forecast Forecast Forecast Income Income from NHS activities 27,690 26,569 28,379 82,637 28,091 27,031 28,148 83,270 29,379 28,455 28,145 85,979 28,220 28,222 28,806 85, ,135 Income from non NHS activities , , , ,466 5,958 Other operating income 3,793 4,093 3,519 11,404 3,469 4,002 3,545 11,016 2,855 2,933 3,281 9,068 1,439 2,971 2,925 7,334 38,822 Total Income 31,894 31,148 32,388 95,430 32,159 31,585 32,181 95,925 32,722 31,876 31,914 96,512 30,147 31,681 32,220 94, ,915 Expenditure within Divisions Pay (19,610) (19,447) (19,702) (58,758) (19,700) (19,664) (19,500) (58,864) (19,340) (19,271) (19,444) (58,055) (19,667) (19,768) (19,772) (59,207) (234,884) Non-Pay (11,961) (11,970) (11,936) (35,868) (12,421) (11,742) (11,888) (36,051) (11,881) (11,950) (11,777) (35,608) (11,629) (11,528) (11,524) (34,681) (142,208) Unallocated Budgets (228) (50) (60) (338) 93 (2) (129) (38) (94) (94) (344) (532) (372) (472) (464) (1,308) (2,216) Contingency (250) (250) (250) (750) (250) (250) (250) (750) Total expenditure within Divisions (32,049) (31,717) (31,948) (95,714) (32,277) (31,658) (31,767) (95,703) (31,065) (31,065) (31,315) (93,445) (31,418) (31,518) (31,510) (94,446) (379,308) EBITDA (155) (569) 440 (285) (118) (73) , ,067 (1,271) (398) 2,607 PDC Dividends payable (295) (295) (295) (885) (250) (284) (284) (817) (284) (284) (284) (852) (284) (284) (284) (852) (3,406) Depreciation & minor impairments (685) (685) (685) (2,055) (685) (685) (685) (2,055) (685) (685) (685) (2,055) (685) (685) (685) (2,056) (8,221) Profit on sale of land , ,000 4,000 Investment Revenue Finance Costs (223) (223) (223) (668) (268) (234) (234) (736) (1,108) NET SURPLUS / (DEFICIT) (1,355) (1,769) (760) (3,884) (1,319) (1,273) (787) (3,379) 739 (107) (319) 314 1,478 (588) (42) 849 (6,100) 'm Income and Expenditure Position 2015/ /16 Actual surplus / (deficit) cum 2015/16 Planned surplus / (deficit) cum 2015/16 Forecast surplus / (deficit) cum Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Month Data Pack.pdf Page 3 of 9 Page 23 of 73 Overall Page 163 of 215
164 Appendix 3 FINANCE REPORT MONTH 05 ANALYSIS OF CONTRACT INCOME BY TYPE OF ACTIVITY def Income Actuals Apr-15 May-15 Jun-15 Q1 Jul-15 Aug-15 Sep-15 Q2 Oct-15 Nov-15 Dec-15 Q3 Jan-16 Feb-16 Mar-16 Q4 YTD Full Year Actual Actual Actual Actual Actual Forecast Forecast Forecast Forecast Forecast Forecast Forecast Accident & Emergency 1,348 1,358 1,513 4,219 1,273 1,462 1,467 4,202 1,513 1,467 1,513 4,493 1,513 1,421 1,513 4,447 6,954 17,361 Non-Elective Inpatients 6,215 5,867 5,445 17,527 5,766 6,445 5,778 17,989 6,088 5,895 6,088 18,071 6,088 5,702 6,114 17,904 29,738 71,491 Elective Inpatients/Day Case 3,415 3,271 3,456 10,142 4,007 3,006 3,758 10,771 3,798 3,632 3,465 10,895 3,540 3,707 3,650 10,897 17,156 42,706 Outpatient 4,393 4,616 5,399 14,408 4,902 4,584 4,946 14,432 5,363 5,127 4,891 15,381 4,891 5,127 5,127 15,145 23,894 59,366 Renal dialysis services 1, ,006 3,008 1, ,003 3,056 1,003 1,003 1,003 3,009 1,003 1,003 1,003 3,009 5,061 12,082 Maternity pathway 2,059 2,009 2,120 6,189 1,937 2,313 2,040 6,290 2,108 2,040 2,108 6,256 2,108 1,972 2,108 6,188 10,438 24,922 Drugs 1,774 1,305 1,497 4,577 1,602 1,497 1,526 4,625 1,526 1,526 1,526 4,578 1,526 1,526 1,526 4,578 7,675 18,357 Other Non-PbR cost & volume 2,569 2,546 3,011 8,126 2,627 2,548 2,709 7,885 2,709 2,709 2,709 8,127 2,709 2,709 2,709 8,127 13,302 32,265 CQUIN , , , ,356 2,427 5,591 Mount Vernon 4,446 4,125 4,513 13,084 4,341 3,690 4,469 12,500 4,819 4,604 4,390 13,813 4,390 4,603 4,604 13,597 21,115 52,994 Total Income from activities - NHS 27,690 26,569 28,379 82,637 28,091 27,031 28,148 83,270 29,379 28,455 28,145 85,979 28,220 28,222 28,806 85, , ,135 Income from Non-NHS activities , , , ,466 2,538 5,958 Other Operating Income 3,793 4,093 3,519 11,404 3,469 4,002 3,545 11,016 2,855 2,933 3,281 9,068 1,439 2,971 2,925 7,334 18,876 38,822 Grand Total 31,894 31,148 32,388 95,430 32,159 31,585 32,181 95,925 32,722 31,876 31,914 96,512 30,147 31,681 32,220 94, , ,915 Income Plan Accident & Emergency 1,365 1,409 1,365 4,139 1,409 1,490 1,446 4,344 1,490 1,446 1,490 4,425 1,490 1,402 1,490 4,381 7,037 17,290 Non-Elective Inpatients 5,870 6,088 5,873 17,831 6,086 6,101 5,888 18,075 5,957 5,744 5,957 17,658 5,957 5,531 5,957 17,445 30,017 71,008 Elective Inpatients/Day Case 3,235 3,013 3,629 9,877 3,808 3,015 3,644 10,467 3,651 3,487 3,178 10,315 3,189 3,494 3,499 10,183 16,699 40,841 Outpatient 4,783 4,390 5,328 14,502 5,565 4,514 5,500 15,579 5,572 5,340 4,899 15,810 5,214 5,421 5,407 16,042 24,581 61,934 Renal dialysis services ,084 3,004 1, ,084 3,152 1,084 1, , ,034 1,034 3,054 5,073 12,313 Maternity pathway 2,074 2,119 2,080 6,272 2,116 2,116 2,082 6,314 2,116 2,082 2,116 6,314 2,116 2,049 2,116 6,281 10,504 25,181 Drugs 1,774 1,262 1,524 4,560 1,607 1,360 1,360 4,327 1,517 1,517 1,517 4,552 1,517 1,517 1,517 4,552 7,527 17,991 Other Non-PbR cost & volume 2,589 2,582 2,751 7,922 2,851 2,683 2,784 8,318 2,822 2,747 2,741 8,310 2,745 2,726 2,798 8,269 13,457 32,820 CQUIN , , , ,363 2,272 5,452 Mount Vernon 4,546 4,078 4,516 13,140 4,501 4,226 4,635 13,362 4,478 4,407 4,407 13,292 4,335 4,407 4,407 13,149 21,867 52,943 Total Income from activities - NHS 27,677 26,330 28,602 82,609 29,530 26,894 28,878 85,302 29,140 28,259 27,744 85,143 28,003 28,035 28,681 84, , ,773 Income from Non-NHS activities , , , ,466 2,420 5,839 Other Operating Income 3,715 4,162 3,496 11,374 3,505 4,047 3,554 11,105 3,589 3,666 4,014 11, ,704 3,693 7,819 18,925 41,568 Grand Total 31,860 30,978 32,585 95,424 33,525 31,430 32,920 97,875 33,218 32,414 32,246 97,878 28,913 32,228 32,863 94, , ,180 Income Variance Vs Plan Accident & Emergency (17) (51) (136) (28) 21 (143) (83) 71 Non-Elective Inpatients 345 (220) (428) (304) (320) 344 (110) (86) (279) 483 Elective Inpatients/Day Case (173) (9) ,864 Outpatient (390) (93) (663) 70 (554) (1,147) (209) (213) (8) (429) (323) (294) (280) (897) (687) (2,568) Renal dialysis services (78) 4 (79) 63 (81) (96) (81) (31) 18 (94) 18 (31) (31) (45) (12) (231) Maternity pathway (14) (110) 41 (83) (179) 197 (42) (24) (8) (42) (8) (58) (8) (77) (8) (93) (66) (259) Drugs 0 43 (27) 17 (5) Other Non-PbR cost & volume (20) (35) (224) (135) (75) (433) (113) (38) (32) (183) (36) (17) (89) (142) (155) (555) CQUIN 0 29 (35) (6) (2) 159 (2) (2) (2) (7) (2) (2) (2) (7) Mount Vernon (100) 47 (3) (56) (161) (535) (166) (862) (17) (752) 51 Total Income from activities - NHS (224) 28 (1,439) 137 (730) (2,032) (1,274) (638) Income from Non-NHS activities (57) (0) 4 (53) Other Operating Income 77 (70) (36) (45) (9) (89) (734) (734) (734) (2,202) 1,017 (733) (768) (485) (2,746) (2,746) Grand Total (197) 6 (1,367) 155 (739) (1,950) (496) (538) (332) (1,366) 1,234 (547) (643) 44 (1,205) (3,266) Data Pack.pdf Page 4 of 9 Page 24 of 73 Overall Page 164 of 215
165 Appendix 4 FINANCE REPORT MONTH 05 EXPENDITURE BY DIVISION def Actuals by Division Apr-15 May-15 Jun-15 Q1 Jul-15 Aug-15 Sep-15 Q2 Oct-15 Nov-15 Dec-15 Q3 Jan-16 Feb-16 Mar-16 Q4 Full Year Actual Actual Actual Actual Actual Plan Plan Plan Plan Plan Plan Plan Medical Division (6,760) (6,603) (6,605) (19,968) (6,753) (6,720) (6,683) (20,157) (6,419) (6,419) (6,413) (19,251) (6,413) (6,402) (6,423) (19,237) (78,613) Surgical Division (6,787) (6,913) (6,837) (20,537) (6,981) (6,853) (6,784) (20,618) (6,694) (6,681) (6,388) (19,763) (6,358) (6,646) (6,702) (19,706) (80,625) Women's & Children's Division (2,669) (2,680) (2,695) (8,044) (2,828) (2,718) (2,672) (8,218) (2,666) (2,663) (2,662) (7,991) (2,662) (2,662) (2,667) (7,992) (32,244) Cancer Services Division (5,165) (4,727) (5,018) (14,911) (4,389) (4,751) (4,689) (13,830) (4,628) (4,628) (4,628) (13,884) (4,628) (4,628) (4,637) (13,893) (56,517) Clinical Support Division (3,838) (3,593) (3,681) (11,112) (4,356) (3,590) (3,557) (11,503) (3,526) (3,518) (3,515) (10,559) (3,514) (3,508) (3,511) (10,533) (43,706) Corporate Departments (4,573) (5,169) (5,033) (14,775) (4,911) (4,961) (4,733) (14,606) (4,770) (4,789) (4,794) (14,353) (4,806) (4,791) (4,785) (14,382) (58,116) Unallocated Budgets & R&D (542) (362) (373) (1,278) (220) (315) (613) (1,148) (1,380) (1,383) (1,383) (4,145) (1,412) (1,492) (1,418) (4,322) (10,893) Income reported in Divisions (1,716) (1,668) (1,706) (5,090) (1,839) (1,748) (1,722) (5,309) (1,722) (1,722) (1,721) (5,164) (1,721) (1,721) (1,722) (5,165) (20,728) Total Expenditure within Divisions (32,049) (31,716) (31,948) (95,713) (32,277) (31,658) (31,454) (95,388) (31,804) (31,802) (31,504) (95,110) (31,514) (31,850) (31,865) (95,229) (381,442) Plan by Division Medical Division (6,684) (6,599) (6,585) (19,868) (6,630) (6,713) (6,683) (20,026) (6,419) (6,419) (6,413) (19,251) (6,413) (6,402) (6,423) (19,237) (78,383) Surgical Division (6,669) (6,635) (6,825) (20,128) (6,823) (6,627) (6,784) (20,234) (6,694) (6,681) (6,388) (19,763) (6,358) (6,646) (6,702) (19,706) (79,832) Women's & Children's Division (2,647) (2,649) (2,671) (7,967) (2,634) (2,696) (2,672) (8,002) (2,666) (2,663) (2,662) (7,991) (2,662) (2,662) (2,667) (7,992) (31,951) Cancer Services Division (5,188) (4,710) (5,019) (14,918) (4,378) (4,701) (4,689) (13,768) (4,628) (4,628) (4,628) (13,884) (4,628) (4,628) (4,637) (13,893) (56,462) Clinical Support Division (3,949) (3,654) (3,715) (11,318) (4,334) (3,647) (3,557) (11,538) (3,526) (3,518) (3,515) (10,559) (3,514) (3,508) (3,511) (10,533) (43,948) Corporate Departments (4,606) (4,973) (4,955) (14,534) (4,816) (4,806) (4,733) (14,355) (4,770) (4,789) (4,794) (14,353) (4,806) (4,791) (4,785) (14,382) (57,624) Unallocated Budgets, contingency & R&D (677) (362) (623) (1,662) (592) (571) (613) (1,777) (1,380) (1,383) (1,383) (4,145) (1,412) (1,492) (1,418) (4,322) (11,906) Income reported in Divisions (1,721) (1,739) (1,674) (5,134) (1,737) (1,728) (1,722) (5,187) (1,722) (1,722) (1,721) (5,164) (1,721) (1,721) (1,722) (5,165) (20,650) Total Plan within Divisions (32,139) (31,321) (32,068) (95,529) (31,945) (31,488) (31,454) (94,887) (31,804) (31,802) (31,504) (95,110) (31,514) (31,850) (31,865) (95,229) (380,755) Variance by Division Medical Division (76) (4) (20) (100) (123) (8) 0 (131) (230) Surgical Division (118) (278) (12) (408) (158) (227) 0 (384) (793) Women's & Children's Division (22) (31) (24) (77) (194) (23) 0 (217) (293) Cancer Services Division 22 (16) 1 7 (11) (50) 0 (61) (54) Clinical Support Division (22) Corporate Departments 33 (196) (77) (241) (96) (155) 0 (250) (492) Unallocated Budgets & R&D 135 (0) ,013 Income reported in Divisions 5 71 (32) 45 (102) (21) 0 (122) (78) Total Variance within Divisions 90 (394) 120 (184) (332) (170) 0 (502) (686) Data Pack.pdf Page 5 of 9 Page 25 of 73 Overall Page 165 of 215
166 m Appendix 5 FINANCE REPORT MONTH 05 SUMMARY OF CIP DELIVERY BY DIVISION def Actual CIP Apr 15 May 15 Jun 15 Q1 Jul 15 Aug 15 Sep 15 Q2 Oct 15 Nov 15 Dec 15 Q3 Jan 16 Feb 16 Mar 16 Q4 Full Year Actual Actual Actual Actual Actual Forecast Forecast Forecast Forecast Forecast Forecast Forecast Medical Division , ,097 3,667 Surgical Division , , ,425 4,991 Women & Children's Division ,037 Cancer Services Division ,725 Clinical Support Division ,928 Corporate Directorates ,655 Contingency Total ,269 3,143 1,396 1,396 1,478 4,270 1,572 1,559 1,558 4,689 1,592 1,643 1,665 4,900 17,003 Plan CIP Medical Division , ,657 4,672 Surgical Division , , , ,419 5,084 Women & Children's Division ,236 Cancer Services Division ,801 Clinical Support Division ,000 Corporate Directorates , , ,227 4,477 Contingency (195) (195) (195) (585) (195) (195) (195) (585) (1,170) Total ,027 1,354 3,347 1,486 1,349 1,509 4,344 1,716 1,725 1,701 5,142 1,724 1,759 1,784 5,267 18,100 Variance Medical Division (3) (175) (199) (202) (576) (188) (186) (186) (560) (1,005) Surgical Division 7 (52) (14) (59) (46) (5) (8) (59) (5) (93) Women & Children's Division (14) (9) (41) (64) (29) (46) (32) (107) (29) (28) 0 (57) (199) Cancer Services Division (28) 14 5 (9) (1) 182 (49) (49) (40) (138) (40) (36) (35) (111) (76) Clinical Support Division (4) (6) 3 5 (14) (15) (15) (44) (15) (15) (22) (52) (72) Corporate Directorates (25) (25) (50) (100) (93) (32) (91) (216) (72) (82) (88) (242) (88) (88) (88) (264) (822) Contingency ,170 Total 000 (64) (55) (85) (204) (90) 47 (31) (74) (144) (361) (338) (453) (327) (311) (314) (367) (1,097) 20.0 CIP delivery against plan Actuals Plan Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar 16 Data Pack.pdf Page 6 of 9 Page 26 of 73 Overall Page 166 of 215
167 Appendix 6 FINANCE REPORT MONTH 5 ROLLING 12 MONTHS CASHFLOW def Mar-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul Actual Actual Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Forecast Opening Balance 648 2,054 3,387 2, Receipts NHS Acute Activity Income 39,914 34,464 27,671 26,119 28,242 27,880 27,712 29,699 32,585 27,099 27,099 27,099 27,099 Education/Merit awards/r&d 484 1, Other income 4,366 3,301 2,262 2,413 2,514 2,397 2,255 2,228 2,367 2,350 2,350 2,350 2,350 Sales proceeds QE , Interest Interim Revolving Working Capital Support (IRWCS) Interim Revenue Support PDC , Refund of interest on DH Capital Investment Loans Refund of DH Loan Repayments - CIL , PDC Received (Nurse Tech Bid & HPFT) Sub-total Receipts 45,534 38,772 30,804 29,403 37,727 31,148 46,751 32,798 37,976 30,320 30,320 30,320 30,320 PAYMENTS Salaries & Wages - Trust 9,840 9,888 9,783 9,627 9,572 9,517 9,461 9,405 9,350 9,350 9,350 9,350 9,350 Salaries & Wages - Other PAYE / Superannuation/ NI - Trust 7,007 6,975 7,014 6,974 6,934 6,894 6,853 6,813 6,773 6,773 6,773 6,700 6,700 PAYE / Superannuation/ NI - Other Creditors 14,541 19,537 8,906 13,532 19,939 13,977 26,850 10,149 18,050 13,216 13,225 13,298 13,298 Creditors - Capital 4, , , , Dividend Paid 1, , , Interest on DH Capital Investment Loans Repay TBL/IRWCS 6, , Interest on IRWCS DH Loan Repayments - CIL 1, , DH Loan Repayments - HCA , Sub-total Payments 45,582 37,439 32,191 30,903 37,727 31,148 46,751 32,798 37,976 30,320 30,320 30,320 30,320 Net in Month Cash Movement (48) 1,333 (1,387) (1,500) Closing Balance (actual and forecast) 600 3,387 2, Trust Cash plan 7,000 2,000 2,000 2,000 2,000 2,000 2,000 2,000 2,000 2,000 2,000 2,000 2,000 Data Pack.pdf Page 7 of 9 Page 27 of 73 Overall Page 167 of 215
168 Appendix 7 FINANCE REPORT MONTH 5 CAPITAL PROGRAMME 2015/16 def Scheme Description YTD Expenditure Month 1-5 YTD Plan Month 1-5 YTD Variance Forecast Expenditure Month 6-12 Forecast Expenditure to 31 March 2016 Annual plan capital spend to achieve Forecast year CRL end Variance IM&T Windows 7 Upgrade - (14/15 commitment) (30) Proxima (14/15 commitment) Pico Cell (14/15 commitment) Chemo e-prescribing (14/15 commitment) I&D Infrastructure Other 15/16 projects TOTAL IM&T ,310 1,310 0 MEDICAL EQUIPMENT Renal replacement Replacement cancer equipment at Mount Vernon 24 0 (24) /16 allocation (73) TOTAL MEDICAL EQUIPMENT (97) ESTATES Estates Allocation (21) Graveley Road - (14/15 commitment) Multi-Storey car park TOTAL ESTATES OTHER CAPITAL Capitalisation of project costs - 15/ ,700 2,470 2,230 (240) Tech Access Midwifery care Mount Vernon Voip Other 15/16 schemes Replacement Gamma Camera ESR (2) Mattresses (20) Bluebell works (65) W&C Childrens lockers (6) MVCC Lockers and chairs (25) Trust management office hub (1) Key pad locks utility room and kitchenettes (9) Wheelchairs x (3) Clock standardisation to incl day/date/time (13) Clip frames re poster standardisation (3) Cardiac arrest trolley (22) Handy Man renovations (76) Anaesthetics room reconfiguration (134) Single Sex Unit 50 0 (50) (124) TOTAL OTHER 1,111 1, ,264 4,325 3,584 (741) TOTAL - TRUST OPERATIONAL SCHEMES 1,814 2,846 1,032 5,366 7,130 6,629 (501) OCH - PHASE 4 Phase 4 slippage Additional Bed Capacity ,375 1,449 1, TOTAL - OCH ,718 2,098 2, Data Pack.pdf TOTAL - TRUST CAPITAL 2,194 3,491 1,297 7,084 9,228 9,228 0 Page 8 of 9 Page 28 of 73 Overall Page 168 of 215
169 Appendix 8 FINANCE REPORT MONTH 5 BALANCE SHEET 2015/16 def Opening Balance Balance Sheet Forecast as at 01/04/15 as at 31/08/15 as at 31/03/ FIXED ASSETS Property, Plant Equipment 185, , ,406 Trade & Other Receivables Non-Current 1,352 1,352 1,352 Other Financial Assets 2,293 2,293 2,293 TOTAL FIXED ASSETS 189, , ,051 CURRENT ASSETS Inventories 4,244 4,169 3,884 Cash & Cash Equivalents 600 3, Trade & Other Receivables - Current 40,093 43,646 39,440 Assets Held for Sale - QE2 11,913 11,913 0 TOTAL CURRENT ASSETS 56,850 63,116 43,824 Creditors: Amounts Falling Due Within One Year (68,864) (72,494) (51,475) NET CURRENT ASSETS / (LIABILITIES) (12,014) (9,378) (7,651) FIXED & NET CURRENT ASSETS LESS CURRENT LIABILITIES 177, , ,400 Creditors: Amounts Falling Due More Than One Year (68,947) (76,867) (73,655) Provisions For Liabilities & Charges (831) (777) (831) NET ASSETS 107, , ,914 FINANCED BY TAXPAYERS EQUITY: Public Dividend Capital 169, , ,016 Revaluation Reserve 43,789 43,790 49,290 Retained Earnings (106,292) (112,757) (112,392) TOTAL TAXPAYERS EQUITY 107, , ,914 Data Pack.pdf Page 9 of 9 Page 29 of 73 Overall Page 169 of 215
170 PERFORMANCE DATA Performance Report CQC outcomes summary Data Pack.pdf Page 30 of 73 Overall Page 170 of 215
171 East & North Hertfordshire NHS Trust :Board Performance Report ( ) - Month 5 Monitor Compliance Framework and SHA Provider Management Regime Monitor Compliance Framework - Performance Thresholds for Indicator Achieve Underachieve Fail Weighting Area Lead Director Q1 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Year to date PF RR Clostridium Difficile -(profiled as 1 per month) Safety AT MRSA Safety AT *All Cancers: 31-day wait from diagnosis to treatment 96% (1month in arrears) *All Cancers: 31-day wait for second or subsequent treatment - Surgery ³94% (1month in arrears) *All Cancers: 31-day wait for second or subsequent treatment - Drug ³98% (1month in arrears) *All Cancers: 31-day wait for second or subsequent treatment - Radiotherapy ³94% (1month in arrears) *All Cancers: 62-day wait for first treatment - Urgent GP referral ³85% (1month in arrears) *All Cancers: 62-day wait for first treatment - Consultant Screening Service ³90% (1month in arrears) *Cancer 2-week wait from referral to date first seen - All cancers ³93% (1month in arrears) *Cancer 2-week wait from referral to date first seen - Symptomatic breast patients ³93% (1month in arrears) Maximum Waiting Time of 18-weeks from Referral to Treatment - Admitted Maximum Waiting Time of 18-weeks from Referral to Treatment - Non-Admitted Maximum Waiting Time of 18-weeks from Referral to Treatment - Incomplete A&E: Maximum Waiting Time of four hours from Arrival to Discharge or Admission Certification against compliance with requirements regarding access to healthcare for people with a learning disability 96% - 96% 0.5 Quality JW 97.51% 98.54% 98.30% 96.20% 97.22% Not Yet Due 97.54% 0 All 3 targets met Both targets met Both targets met or more target failed 1 or more target failed 1 or more target failed 90% - 90% 1 95% - 95% 1 92% - 92% 1 1 Quality JW 96.77% 96.67% 91.30% 97.92% 97.44% Not Yet Due 96.45% 0 Quality JW % 99.01% 99.10% 99.29% 98.98% Not Yet Due 99.14% 0 Quality JW 99.18% 99.66% 97.00% 95.53% 92.31% Not Yet Due 96.05% 0 1 Quality JW 87.91% 85.89% 81.80% 76.88% 79.68% Not Yet Due 80.73% 0 Quality JW 94.74% 66.67% 92.00% 92.00% % Not Yet Due 91.67% Quality JW 99.25% 95.41% 96.13% 94.60% 96.89% Not Yet Due 95.75% 0 Quality JW 96.49% 90.80% 98.10% 93.50% 96.10% Not Yet Due 94.63% 0 Patient Experience Patient Experience Patient Experience JW 91.80% 90.00% 90.52% 90.20% 87.50% 81.95% 88.37% 0 JW 97.80% 95.83% 95.94% 95.20% 94.41% 93.39% 95.07% 0 JW 96.50% 93.10% 94.43% 94.50% 94.19% 93.39% 94.57% 0 95% - 95% 1 Quality JW 97.39% 95.31% 93.17% 95.13% 91.02% 87.92% 92.42% 0 Compliant - Non-compliant 0.5 Patient Experience AT Green Green Green Green Green Green 0 *cancer performance figures are not finalised until 6-weeks after month-end and may therefore be subject to change. Monitor Compliance Framework GRR - Quality Overrides Indicator Achieve Underachieve Fail Weighting Area Lead Director Q1 Apr-15 May-15 Jun-15 Jul-15 Aug-15 CNST Level 1-3 (Against Plan Level 1 > April 2012) Level 1 MCF Override AT Green Green Green Green Green Green Green Mandatory Services Provision MCF Override JW Green Green Green Green Green Green Green Other Certification - Financial Compliance, Cooperation with Other NHS Bodies & Local Authorities, Information MCF Override TO Green Green Green Green Green Green Green Year to date PF RR Data Pack.pdf Page 31 of 73 Overall Page 171 of 215
172 East & North Hertfordshire NHS Trust :Board Performance Report ( ) - Month 5 RED 5 5 AMBER GREEN Department of Health Operating Framework measures Indicator Achieve Underachieve Service Performance Indicators for Fail Weighting Area Lead Director Q1 Apr-15 May-15 Jun-15 Jul-15 Aug-15 RTT Delivery in all Specialties (Treatment Functions not delivered (Admitted, Non-Admitted Patient Experience JW & Incomplete Pathways) Diagnostic Test Waiting Times (patients waiting >6-weeks for 15 key diagnostic tests) 1.0% 5% 5% Patient Experience JW 1.90% 0.34% 0.33% 0.32% 0.39% 0.48% 0.37% Post Acute Transfers at Midday Quality JW Post Acute Transfers-Total Average Beds Blocked per Day Quality JW MSA breaches - Numbers of unjustified breaches 0.0% 0.5% 0.5% Patient Experience AT VTE Risk Assessment 98.0% 93% 93% Safety JM 99.57% 95.33% 94.76% 95.04% 94.52% 94.30% 94.90% Year to date Trust Clinical Efficiency KPIs Performance Thresholds for Indicator Achieve Underachieve Fail Weighting Area Lead Director Q1 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Year to date DNA rate Plan Plan +1% Plan +1% Productivity JW 7.70% 8.37% 7.52% 8.11% 8.63% 8.70% 8.08% New to Follow-up outpatient appointment ratio Productivity JW *Pre-op bed-days 6.0% 12.0% 12.0% Productivity JW 9.00% 2.17% 1.70% 2.95% 2.26% 0.00% 4.33% OCH Bed Occupancy - Elective (latest available position) 92.5% 92.5% 95.0% Resources JW 97.90% 93.40% 90.20% % 83.80% 100% OCH Bed Occupancy - Emergency (latest available position) 92.5% 92.5% 95.0% Resources JW 96.90% 96.40% 99.20% 98.18% 99.80% 98.00% Length of Stay (Overall) Resources JW Theatre Utilisation (1 month in arrears) 87.5% 75.0% 75.0% Productivity JW 93.80% 84.15% 81.73% 81.98% 79.04% Not Yet due 82.31% Resources Management numbers Data Pack.pdf Page 32 of 73 Overall Page 172 of 215
173 East & North Hertfordshire NHS Trust :Board Performance Report ( ) - Month 5 Key Contract Requirements Indicator Achieve Underachieve Fail Weighting Area Lead Director Q1 Apr-15 May-15 Jun-15 Jul-15 Aug-15 A&E Quality Indicator - Total Time in A&E (95th percentile) Quality JW >1 >1 A&E Quality Indicator - Time to initial assessment (95th 1.0 (failing >1 'Timeliness' >1 'Timeliness' >1 'Timeliness' >1 'Timeliness' Quality JW 'Timeliness' >1 'Timeliness' 'Timeliness' percentile) or more) indicator indicator indicator indicator indicator indicator achieved indicator A&E Quality Indicator - Time to treatment decision (median) OR achieved achieved achieved achieved Quality JW achieved achieved < 0.5 (failing A&E Quality Indicator - Unplanned reattendance rate 2 or Quality JW >1 'Impact' 5.30% 4.30% 4.90% 3.80% 5.50% 4.80% 1 1 less) indicator A&E Quality Indicator - Left without being seen Quality JW achieved 1.30% 1.30% 1.80% 1.10% 0.70% 1.20% Ambulance Turnaround (To Apply from Q2) 15 minutes > 15 minutes Quality JW 58.90% 75.60% 79.90% 79.70% 76.50% 73.00% Choose & Book Slot issues under 5% 5% > 5 % <EoE > EoE Avg Quality JW 12.20% 11.21% 14.24% Not Yet Available Not Yet Available Cancelled Operations - on the day 0.80% 0.8% > 1.50% Quality JW 0.64% 0.60% 0.50% 0.30% 0.00% 0.00% 0.46% Readmissions following non-elective admission 9% 13% Admissions to a Critical Care Bed <4-hours from Decision to Admit Admissions to a Stroke Bed <4-hours from Arrival at A&E (1 month in arrears)* (*Q1 50% pts, Q2 70% pts, Q3 90% pts, Q4-90% pts) > Performance Thresholds for % Activity JW TBC 10.39% 9.37% 9.37% 8.08% Not Yet Available Not Yet Available 0 >1 per month Quality JW % 81% < 81% Quality JW 40.00% 70.27% 61.90% 62.50% 64.18% Not Yet Available Year to date 14.24% 9.05% 64.43% Local Priorities Performance Thresholds for Indicator Achieve Underachieve Fail Weighting Area Lead Director Q1 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Year to date Stroke Care - % of patients spending 90% of hospital stay on a specialist stroke unit (1mth in arrears) 80% 70% Stroke Care - % patients with high risk TIA seen and scanned/treated within 24 hours (1mth in arrears) 63% 45% PPCI 150 minute call to balloon time 80% 75% Two-week wait access for Rapid Access Chest Pain Clinics. 98% MRSA Elective screening 100% 99% MRSA Emergency screening 100% 95% < < < < < < 70% Local Priority JW 83.20% 86.11% 72.09% 80.85% 92.19% TBC 80.40% 45% Local Priority JW 62.50% 57.89% 45.45% 72.73% 78.57% TBC 65.15% 75% Local Priority JW 85.70% % % % 92.00% 96.67% 97.84% 98% Local Priority JW % % % % % % % 99% Local Priority AT 99.96% TBC TBC TBC TBC TBC TBC 95% Local Priority AT 90.21% TBC TBC TBC TBC TBC TBC Data Pack.pdf Page 33 of 73 Overall Page 173 of 215
 included 5 risks.")
174 Intelligent Monitoring Report May 2015 (latest published, May 2015) Key points on the May 2015 publication: The Trust is a Band 4 (previously band 5 during 2014/15) The change in position is due to impact on 1 elevated risk and SHMI and 6 risks. The previous version (December 2014) included 5 risks. Of which - In Hospital Mortality - Gastroenterological and hepatological and Ambulance waits in excess of 60 minutes risks have now been closed. Updates on key risk areas: In Hospital Mortality - Respiratory Contitions (new)- 7 day respiratory service is in the process of being implemented. Positive recent peer review. Mortality is reported to RAQC and Board bi-monthly. Lead: Medical Director. Inpatient Survey Q23 (2014) - Help with eating meals (new) - Protected mealtimes re launched. Supported by volunteers (appropriately trained). Reported through RAQC. Lead: Director of Nursing SSNAP Domain 2, Overall team-centred rating score for key-stroke unit indicator - The data is published approximately 6 months in arrears (the data period currently reported is Q2) and it is anticipated that the postive impact of the new stroke nurse specialists employed, increased therapy cover and additional Stroke Care Consulant will show on the publication of the 2014/15 quarter 4 data. Progress against the stroke care action plan continues to be reported in the Board Committees. Lead: Director of Operations. A&E Survey Q18 Patient Privacy - This was taken at the time the A&E department was in it's 'misuse phase'; improvement expected post consolidation. Regular updates provided to RAQC in Patient Experience report. The CCG undertook an unannounced inspection on 10th February and there is a Lister A&E Friends and Family Test action plan which addresses the issues raised by patients in their feedback, privacy was not a concern. As the national A&E survey is not due this year we have provided evidence to the CQC with an aim to reducing this risk. Lead: Director of Nursing Diagnostic Waiting Times (new) - In relation to Radiology Diagnostic Performance, a series of recovery actions were undertaken in December and January which returned us to meeting the DM01 standard in February and sustaining this position to date. Additional control mechanisms have been put in place including a daily review of the PTL and a weekly performance assurance group within the division. Update provided in performance report to FPC. Lead: Director of Operations GMC Concern Regular updates provided to RAQC within Medical Directors report and this continues to be an area of focus. The latest GMC Survey results published demonstrate improvement overall; this will be reported through RAQC. Lead: Medical Director The areas of risk identified above all have full action plans in place to ensure these are addressed and are monitored through reports to RAQC and Board. Reference notes: The Intelligent Monitoring report replaces the QRP report previously provided by CQC and is updated quarterly by CQC. The full report is published on their website. Key to Banding rating: CQC has categorised trusts into one of six summary bands, with Band 1 representing highest risk and Band 6 with the lowest. These bands have been assigned based on the proportion of indicators that have been identified as risk or elevated risk or if there are known serious concerns with trusts (for example, trusts in special measures) they are categorised as Band 1. Data Pack.pdf Page 34 of 73 Overall Page 174 of 215
175 Summary of the Trust's CQC Registration Status across all Locations Fully Registered without conditions. Awaiting date of CQC new style inspection. REGULATORY ACTIVITY LISTER HOSPITAL* New QEII MVCC HERTFORD BEDFORD RENAL UNIT HARLOW RENAL UNIT Treatment of disease, disorder or injury Registered Registered Registered Registered Registered Registered Surgical procedures Registered Registered Registered Diagnostic and screening procedures Registered Registered Registered Registered Registered Maternity and midwifery services Registered Registered Registered Termination of pregnancies Registered Registered Family Planning Services Registered Registered Registered Assessment or medical treatment of people detained under the Mental Health Act 1983 Registered Registered Registered *Lister Hospital Location includes the registration for renal satelite units in St Albans Hospital and Luton and Dunstable Hospital. Data Pack.pdf Page 35 of 73 Overall Page 175 of 215
176 WORKFORCE APPENDICES Data Pack.pdf Page 36 of 73 Overall Page 176 of 215
177 EAST AND NORTH HERTS NHS TRUST Workforce Information Report Summary September Based on Month 5 Data Pack.pdf Page 37 of 73 Overall Page 177 of 215
178 APPENDIX 1: WORKFORCE INFORMATION REPORT SUMMARY Workforce Report September 2015 (Based on data as at the end of August 2015) Section 1: KPI summary position Graph 1: Sickness Rates Based On In Month Position March Baseline Vacancy Rate target, 5% Aug, 6.48% July, 4.58% 0.00% 1.00% 2.00% 3.00% 4.00% 5.00% 6.00% 7.00% New Establishment Vacancy Rate target, 5% Aug, 11.29% July, 9.40% 0.00% 2.00% 4.00% 6.00% 8.00% 10.00% 12.00% Pay Spend as % of Budget target, 100% Aug, % July, % 6.00% 5.00% 4.00% 3.00% 2.00% 1.00% 0.00% Graph 2: Vacancy Level Projection New Establishment 15/ % Short term sickness rates % Long term sickness rates % Sickness Trust% Target 3.5% Annualised sickness absence rate 99.00% 99.50% % % % Annualised Sickness Rate target, 3.50% Aug, 3.72% July, 3.60% 3.35% 3.40% 3.45% 3.50% 3.55% 3.60% 3.65% 3.70% 3.75% Vacancy % 15.00% 10.00% 5.00% 0.00% Aug Sept Oct Nov Dec Jan Nursing Qualified Nursing Unqualified Target Trust Total Turnover target, 10/ 11% Aug, 13.02% July, 13.01% 0.00% 2.00% 4.00% 6.00% 8.00% 10.00% 12.00% 14.00% Appraisal Rate target, 90.00% Aug, 75.01% July, 76.04% 65.00% 70.00% 75.00% 80.00% 85.00% 90.00% 95.00% Graph 3: Vacancy Level Projection Baseline Establishment March % Vacancy % 10.00% 5.00% 0.00% -5.00% Aug Sept Oct Nov Dec Jan Nursing Qualified Nursing Unqualified Data Pack.pdf 1 Page 38 of 73 Overall Page 178 of 215
179 APPENDIX 1: WORKFORCE INFORMATION REPORT SUMMARY Section 2: Our Culture Graph 1: FFT Trend Graph % of staff who recomend Trust for work % of staff who recomend Trust for care Average % score for comparative group - Recommend for work Average % score for comparative group - Recommend for care Table 2 Recommend for care: +ve good standards of care including personal/family/friend s experience Good facilities & services Dedicated staff Table 3 Recommend for work: +ve Friendly atmosphere, works as part of a good team Career and educational development opportunities Dedicated staff Recommend for care: -ve Inconsistent standards of care/treatment Overstretched services Understaffing and corresponding use of bank & agency Poor processes including administrative processes, medical records Recommend for work: -ve Workload/pressure/stress Feel unsupported by line manager, senior managers, non-specific Understaffing and corresponding use of bank & agency Table 1: Quarter 4 Friends and Family Test for staff Q Q Q Q Staff recommending the Trust as a place to receive treatment/care 70.08% 67% 67.82% 71.39% Staff recommending the Trust as a place to work 47.12% 50% 49.31% 49.56% Data Pack.pdf 2 Page 39 of 73 Overall Page 179 of 215
180 APPENDIX 1: WORKFORCE INFORMATION REPORT SUMMARY Section 3: Developing our people Graph 1: Starters & Leavers Graph Table 1:August 2015 Appraisal Compliance Compliance Done Not Done Not due but require review* Grand Total Completion Rate % Cancer Services Clinical Support Services Medicine Aug-14 Oct-14 Dec-14 Feb-15 Apr-15 Jun-15 Aug-15 Leavers in month FTE Starters per month FTE Corporate *New starters (first 3 mths), maternity leave returners, long term sickness returners Table 3: Training Data Research & Development Surgery Women s and Children s Source: ESR Statutory and mandatory training full compliance (Incl M&D) Statutory and mandatory training average compliance (Incl M&D) Grand Total Trust MTH Surgery Medicine CSS W & C Cancer Corporate Table 2: Appraisal Compliance by Payband Pay Band Appraisal Completion Rate % Band Band Band Band Band Band Band Band 8A Band 8B Band 8C Band 8D Band Snr Mgr Pay Tupe Grand Total Data Pack.pdf 3 Page 40 of 73 Overall Page 180 of 215
181 APPENDIX 1: WORKFORCE INFORMATION REPORT SUMMARY Section 4: People Performance Table 1:Bank & Agency Spend Graph 1: Ledger Position V Worked WTE August 2015 position Total spend Current month YTD % % Agency 1,935, ,054, Bank 751, ,812, Substantive 16,977, ,254, Agency WTE(Included in worked WTE) Bank WTE (Included in worked WTE) WTE (contracted) Total Variance against pay budget 19,664, ,122, , , Aug-14 Oct-14 Dec-14 Feb-15 Apr-15 Jun-15 Aug-15 Ledger/Budgeted Establishment WTE Table 2: Recruitment Data Table 3: Benchmarking Data Source: TRAC Target Trust MTH (weeks) Trust Last MTH (weeks) Trust vacancy rate % Trust Turnover % Qualified Nursing vacancy rate % Qualified Nursing Turnover % Time to Start: From requisition approval to start date (actual/booked) 9 weeks 9.8 weeks 8.2 weeks UCLH Imperial WHT Time to Recruit: From conditional offer to Start date (booked/actual) Time taken for approvals: From requisition being created to requisitions authorised 2.6 weeks 2 weeks 4 weeks 3.4 weeks 0.8 weeks 0.9 weeks LD Redbridge Basildon ENHT Data Pack.pdf 4 Page 41 of 73 Overall Page 181 of 215
182 APPENDIX 1: WORKFORCE INFORMATION REPORT SUMMARY Table3: NHSP Performance Staff Groups Current YTD Month & Year Net Shifts Requested Bank Filled Shifts % Bank Shift Agency Filled Shifts % Agency Filled Shifts Overall Fill Rate Unfilled Shifts % Unfilled Shifts Nursing and July ,865 3, % 2, % 79.4 % 1, % Midwifery August ,222 3, % 2, % 74.6 % 2, % Doctors July , % % 89.4 % % August , % % 85.7 % % A&C July ,929 1, % 1, % 88.5 % % August ,863 1, % 1, % 85.4 % % AHP/HCS/Support July , % 1, % 87.8 % % August , % 1, % 91.3 % % Table 4: Agency usage by tier (nursing only) Shifts Agency Tiers Data Pack.pdf 5 Page 42 of 73 Overall Page 182 of 215
183 APPENDIX 1: WORKFORCE INFORMATION REPORT SUMMARY Table 4: Performance, Employee Relations Source: ERAS Total Live Cases as at 31 July 2015 Total Live Cases as at 31 August 2015 Surgery Medicine CS W & C Cancer ( inc R&D) Corporate Headcount Number of Disciplinary Cases (excluding medical cases) % = no of cases as % of headcount Number of Grievances Number of Capability cases Number of B&H, discrimination and victimisation cases 28 (0.5%) 33 (0.6%) 7 (0.5%) 12 (0.9%) 2 (0.3%) 4 (0.5%) 4 (0.6%) (0.7%) Number of formal short term sickness cases including cases under monitoring Number of formal long term sickness cases Including cases under monitoring Number of *MHPS cases (Medical cases) Total number of cases in progress Number of suspensions/medical exclusions Number of suspensions lasting 6 months or longer Number of appeals *MHPS = Maintaining High Professional Standards Data Pack.pdf 6 Page 43 of 73 Overall Page 183 of 215
184 Report on Nurse Agency Ceiling and Nurse Agency Trajectory September 2015 (Based on data as at the end of August 2015) 1. Purpose This paper provides an update to the Finance and Performance/RAQC Committee for August 2015 on nursing agency spend ceilings and nurse agency trajectory. 2. Nurse Agency Ceiling TDA and Monitor have jointly written to the Trust confirming new regulations set out to reduce agency spend in nursing across the NHS. The regulations are set out to move staff away from agencies and back to substantive employment or working for Trust banks. The Trust has positioned itself well to be prepared for the rules to be imposed. This has been achieved by creating a strong recruitment pipeline of qualified nurses using a range of initiatives to bring the vacancy rate to below 5%. This would have been achieved by October this year however changes in legislation affecting tier 2 visas and language testing has delayed this. In addition, the Trust has set rigid controls to monitor temporary staffing demand, minimise agency usage and restrict access to tier 3 and off framework agencies. An annual limit on the agency spend as a percentage of the total nursing staff spend has been imposed from 1 st October. Detail of the ENHT target is set out below: Q3/4 2015/ / / /19 8% 6% 4% 3% Currently agency nursing spend is 10.9% of the overall nursing spend and has been at an average of 11.1% in months 1 to 4. Nursing vacancy rate is currently 14%, there are 88 nurses in the pipeline and another 84 recruited from the Philippines. 3. Nurse Agency Trajectory The planed recruitment trajectory was to reduce the nursing vacancy rate from 14% to 4% in October with the introduction of 84 nurses recruited from the Philippines on top regular recruitment activity. The first table in appendix 1 shows the projection of agency spend based on the Filipino nurses starting in October as planned. This demonstrates that with the introduction of the Filipino nurses as well as the ongoing recruitment, agency expenditure would have been 8.2% in quarter 3 and 8.8% in quarter 4. The second table in appendix 1 shows the amended agency expenditure forecast incorporating the delays with bringing the Filipino cohort to the Trust. This assumes that the majority will be in post by the end of April meaning the agency spend over quarter 3 is 10.9% and in quarter 4 is 11.9%, as this also includes the impact of the additional winter ward. The impact of the delay in Philippine recruitment is therefore expected to result in an increase of nurse agency expenditure of 1.1m and an overall increase in nurse expenditure of 140k. Data Pack.pdf Page 44 of 73 Overall Page 184 of 215
185 4. Outcome The recommendation to the executive team was that the Trust submits an application to TDA and Monitor for an adjustment to the ceiling on agency spend. The application was sent on 10 September 2015 (see appendix 2) and outlines the reasons for requesting the adjustment and details the work being complete to control the agency spend. Data Pack.pdf Page 45 of 73 Overall Page 185 of 215
186 Appendix 1 Nurse Agency trajectory with original Philippine start dates Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Total 000's 000's 000's 000's 000's 000's 000's 000's 000's 000's 000's 000's 000's Agency Nursing ,509 Total Nursing 6,325 6,474 6,280 6,459 6,245 6,327 6,437 6,171 6,242 6,244 6,257 6,278 75,739 Nursing agency % as % of total nursing Quarterly % Nurse Agency trajectory with revised Philippine start dates Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Total 000's 000's 000's 000's 000's 000's 000's 000's 000's 000's 000's 000's 000's Agency Nursing ,610 Total Nursing 6,325 6,474 6,280 6,459 6,245 6,327 6,242 6,238 6,309 6,311 6,324 6,345 75,879 Nursing agency % as % of total nursing Quarterly % Change in agency nursing - 000's 1,101 Change in total nursing expenditure - 000's Agency Nursing as a % of Total Nursing Expenditure 12 TDA ceiling - 8% 10 % Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Agency % - original start dates Agency % - revised start dates Data Pack.pdf Page 46 of 73 Overall Page 186 of 215
187 Appendix 2 Application for adjustment to ceiling trajectory To be completed by NHS Trusts and NHS Foundation Trusts, signed off by a Finance Director or Board member. Applications will be approved in exceptional circumstances Please respond to agencyrules@monitor.gov.uk by 14 September 2015 Name of Trust Completed by Job title East & North Hertfordshire NHS Trust Thomas Pounds Head of Temporary Staffing Telephone number address Thomas.pounds@nhs.net Date completed 10/09/15 Name of Board member and position 1) Why are you applying for this adjustment? (Maximum 500 words) Reducing agency spend in nursing has been one of the Trusts key strategic goals. A strong recruitment pipeline of qualified nurses has been created using a range of initiatives and rigid agency controls have been set up to manage demand, minimise agency usage, restrict access to tier 3 agencies and remove off framework agencies. The planed recruitment trajectory was to reduce the nursing vacancy rate from 14% to 4% in October with the introduction of 84 nurses recruited from the Philippines on top of intensive wider EU and local recruitment activity. The projection of agency spend based on the Filipino nurses starting in October would have reduced agency expenditure to below 8% in quarter 3 and 4. Due to the change in legislation around the approval of tier 2 visas and changes in the way the language tests are carried out, the Trust has not been able to introduce the 84 Filipino nurses as planned. The Trust will persist in recruiting the nurses however it is not expected they will start until the end of April. When the trajectory is adjusted to incorporate these delays the spend over quarter 3 and 4 is at 10.7%. Currently agency temporary staff play a crucial part in maintaining the number of staff to deliver the required level of patient care. The current number of vacancies is at 245 WTE, but with maternity and long term sickness the total shortfall in nursing establishment is 334 WTE. The total number or agency used in July to cover part of this was 158 WTE which is 47% of the shortfall in nursing establishment. To achieve the target set by TDA/Monitor in quarter 3, we would be removing an average 37.2 WTE from staffing numbers. Proportionately this would be equivalent to 1.6 in Maternity, 5.2 in specialist areas and 30.4 for wards. In quarter 4 we would be removing an average of 43.9 WTE. Proportionately this would be equivalent to 2.5 in Maternity, 8.4 in specialist areas and 32.9 for wards. It is likely that two wards would need to be closed to allow for the shortfall as well as significantly cutting back on services within specialist areas. East and North Harts have put a variety of actions and initiatives in place to manage down the agency usage in the Trust. It can be evidenced that work is being complete and significant achievement have been made so far which demonstrates that the Trust has a firm grip on the agency spend and that we are moving in the right direction to Data Pack.pdf Page 47 of 73 Overall Page 187 of 215
188 reduce agency spend. We would have been in a position of achieving the ceiling of agency spend had it not have been for the changes to legislation affecting the recruitment of nurses from overseas which has now delayed our plans. The Trust is also committed to meeting targets set for safer staffing in line with the NICE guidance and will not jeopardise patient safety or the operational running of the hospital. 2) For what period of time are you applying for an adjustment? Quarter 3 and /16 3) What is your proposed annual trajectory of nursing agency spend? Please reflect this proposal in your monthly plan for Q3 and Q4 2015/16, submitted to Monitor/TDA. If this adjustment is not approved, you will need to submit a revised monthly plan to Monitor/TDA. Y55_RWH_ NTDA Nursing Agency 4) What are your existing measures for controlling agency spend (e.g. rostering)? (Maximum 500 words) The Trust takes a very proactive approach in managing nursing agency expenditure in the Trust. Procurement works closely with the Head of Temporary Staff in the Trust and counterparts across Hertfordshire Trusts. A further competition process is run and Spend is aggregated to attract the best rates and also to ensure that neighbouring Trusts do not compete with each other inflating pay rates. These Agencies are placed in tiers in order of price and the cascade managed through the NHSP Platform, rates are validated during this process to ensure that the rates submitted during further competition are the rates invoiced. There has been a determination to eradicate the use of Non Framework Agencies with the Trust recognising that Non Framework Agencies tend to over inflate pay rates to attract workers as well as posing a governance/quality risk. The current position is 99% compliance with framework agencies with the aim of achieve 100% compliance by October. Further work has been carried out by the Trust since May 2015 to reduce the reliance on expensive tier 3 agencies. A full review of the agency cascade system was complete in order to rationalise the tier 3 usage. The outcome was that either charge rates were re-negotiated or agencies were removed all together. In addition an enhanced control was put onto the agency tier 3 meaning senior approval is required for tier 3 agencies to gain access. This has resulted in a shift in tier 3 usage going from 48% in March down to 18% in August. Safe staffing levels are actively managed on a daily basis to support patient safety while keeping a management on demand using the integrated information from Eroster, Staff Bank and Safe Care databases. A senior team including the Director of Nursing/Deputy Director of Nursing are provided with an overall view of all wards for the next three days by shift. Consideration is given to bed capacity and operational activity within the Trust which may impact on safe staffing. Actions are agreed to ensure that all areas are made safe; this may mean that a green rated ward becomes amber, due to the movement of staff to a ward that initially triggered red. Decisions are made at this time as to whether the shifts are still required or should be authorised to go to agency. Data Pack.pdf Page 48 of 73 Overall Page 188 of 215
189 Weekend look ahead meetings are held on Tuesday and Thursdays. The purpose of these meetings is to review the staffing for the weekend ahead to ensure staff are evenly distributed to minimise the need to go out to agency. On-going work is complete to ensure the Trust is making optimal use of its bank staff. A recent pay review demonstrated that the Trust was paying under the market rate therefore bank pay rates were increased. The change made in June is set out to encourage more Trust staff to working in their own Trust and encourage greater recruitment to bank. So far we have seen an 8% increase in bank fill. 5) Please confirm that this application has been discussed with, and approved by, the Nurse Director. Yes Data Pack.pdf Page 49 of 73 Overall Page 189 of 215
190 RISK AND QUALITY REPORTS Safe Staffing Nursing Infection Control Data Pack.pdf Page 50 of 73 Overall Page 190 of 215
191 PURPOSE PREVIOUSLY CONSIDERED BY Objective(s) to which issue relates * Risk Issues(Quality, safety, financial, HR, legal issues, equality issues) Healthcare/ National Policy (includes CQC/Monitor) CRR/Board Assurance Framework * * tick applicable box ACTION REQUIRED * For approval RISK & QUALITY COMMITTEE September 2015 Safe Staffing Level Report August 15 Agenda Item: To update the RAQC on monitoring of safe staffing levels by ward and cumulative position in the month of August Elements of content previously considered by the Nursing and Midwifery Executive Committee (NMEC) and Ward Sisters and Matrons Committee 1. To continuously improve the quality of our services in order to provide the best care and optimise health outcomes for each and every individual accessing the Trust s services 2. To excel at customer service, achieving outstanding levels of communication and patient, carer and GP satisfaction 3. To provide and support the best standards of integrated care for the elderly and those with long term conditions by developing key partnerships and services 4. To consolidate services and enhance local access to specialist services in order to deliver high quality, safe, seamless, innovative and integrated services which are sustainable 5. To support the continued development of the Mount Vernon Cancer Centre and provision of leading local and tertiary cancer services 6. To improve our staff engagement and organisational culture to be amongst the best nationally Poor quality patient experience Impact on safety Impact upon annual assessment ratings Non-compliance with regulatory and legislative requirements Trust reputation CQC standards, NHSLA standards, NICE Guidance Safe Staffing for nursing in adult in patient wards in acute hospitals (2014). NICE Guidance Safe midwifery staffing for maternity settings (2015). National Quality Board How to ensure the right people, with the right skills, are in the right place at the right time. (2013) Corporate Risk Register For decision For discussion X For information X DIRECTOR: Director of Nursing and Patient Experience / DIPC PRESENTED BY: Director of Nursing and Patient Experience / DIPC AUTHOR: Deputy Director of Nursing DATE: September 2015 We put our patients first we work as a team we value everybody we are open and honest We strive for excellence and continuous improvement BAF Data Pack.pdf 1 Page Page 51 of 73 Overall Page 191 of 215
192 Safe Nurse Staffing Levels August Executive Summary The purpose of this report is to provide an update on the monitoring and management of nursing and midwifery staffing in August East and North Hertfordshire NHS Trust is committed to ensuring that levels of nursing staff, which includes registered nurses, midwives and Clinical Support Workers (CSWs), match the acuity and dependency needs of patients within clinical ward areas in the Trust. This includes ensuring there is an appropriate level and skill mix of nursing staff to provide safe and effective care. These staffing levels are viewed along with reported outcome measures, registered nurse to patient ratios, the percentage skill mix ratio of registered nurses to CSWs, and the number of staff per shift required to provide safe and effective patient care. No Objective Narrative RAG 1 Executive Summary 2 Daily process to manage staffing Update report on key initiatives currently in place to improve safer staffing. Process in place to review staffing daily and take actions where indicated. 3 Unify return Monthly returns completed for August 2015 Extra capacity Staffing Specialling ACU extra capacity over shift plan due to additional open capacity. Swift Ward has remained open each weekend (12 beds) Reduction of beds: 6A 30 to 15 Ashwell 28 to 15 This is due to various staffing issues including vacancy and supporting new starter Variable across month, being tightly managed Some episodes where ward has several patients requiring support. Specialling policy awaits approval by NMEC. 4 Shifts that initially triggered red 5 E-roster and SafeCare Increase in red triggered wards (4.89%) due to improved data collection and reduction in NHSP fill rate Issues between interfaces with NHSP being resolved. SafeCare tool is being rolled out to all inpatient wards Data Pack.pdf 2 Page Page 52 of 73 Overall Page 192 of 215
193 2. Daily process to manage staffing Safe staffing levels are actively managed on a daily basis to support patient safety. At the 08:30, 12:30 and 16:00 daily bed meetings, the Director of Nursing/Deputy Director of Nursing, the Trust Temporary staffing Manager supported by the Trust Liaison Coordinator for NHS Professionals (NHSP - the organisation who coordinate providing our bank and agency nurses), in conjunction with the Nursing Services Managers and Matrons, are provided with an overall view of all wards for the next three days by shift, registered and unregistered workforce numbers and ratios. Consideration is given to bed capacity and operational activity within the Trust which may impact on safe staffing. All of these factors are considered and each ward is RAG rated as red, amber or green for each of the early, late and night periods. Actions are agreed to ensure that all areas are made safe. This may mean that a green rated ward becomes amber, due to the movement of staff to support red triggering wards. Shifts initially triggering red are usually a consequence of short term sickness or other unplanned leave. Throughout August significant changes were made to the way the Trust records ward RAG ratings, the process is now supported by the E-roster Team and this rating is recorded electronically for quicker escalation and communication. This has resulted in more accurate record keeping of both red triggered wards and the corresponding mitigating action. This live electronic record is handed over to the duty matron and night duty matron to ensure accurate record keeping. Weekend look ahead meetings are held on Tuesday and Thursdays. The purpose of these meetings is to review the staffing for the weekend ahead. The meetings are attended by Matrons from each Division, Lead Nurse (Non-Medical) Clinical Workforce, NHSP Trust Liaison Coordinator and Head of Temporary Staffing. The look ahead report is produced by the E-roster Team for these meetings and illustrates the current status of staffing for the weekend ahead. This report includes NHSP and substantive staff. Areas of risk are noted and actions identified to mitigate risk, these include: Levels of unfilled shifts, by area or specialty Levels of substantive staff Areas of extra capacity that may need to be staffed Ratio of temporary/permanent staff Ratio of agency/bank staff In the event of shortfalls of staff, or unexpected increases in patient acuity and dependency requirements, the agreed staffing levels are reviewed on a shift by shift basis and RAG rated with escalation actions specified at each level. These meetings and processes have now been formally captured in the Daily and Weekly Staffing Meeting Terms of Reference. 3. Fill rate indicator return, Staffing: Nursing, Midwifery and Care Staff (Unify) There is a requirement for all Trusts with inpatient beds to publish their staff fill rates (actual versus planned) in hours, taking into consideration day and night shifts and registered and unregistered staff. The Trusts fill rates for August 2015 has been uploaded and submitted on Unify. Patients and the public are able to see how hospitals are performing on this indicator on the NHS Choices website. This data sits alongside a range of other safety indicators. Further detail in relation to fill rate percentages is detailed below. A copy of the Trusts Unify submission is available on request. August s Unify return shows some variance in fill rate for both registered and unregistered staff. The registered nurse fill rate has dropped marginally to 94.5% from 96.5% in July. There remain a number of wards with average fill rate of clinical support workers over 100% and the combined fill rate for registered and unregistered nurses is 100.7%. The variance in fill rate can be attributed to the following: Data Pack.pdf 3 Page Page 53 of 73 Overall Page 193 of 215
194 There are currently 25 EU nurses working in the Trust awaiting their PIN and registration with the Nursing and Midwifery Council (NMC). Prior to receiving this, these staff are required to be rostered and work as a CSW. The fill rate for CSW s is high in most areas due to this factor. Throughout the month of August 6A has reduced its bed base from 30 down to 15; this was due to a combination of factors including the vacancy rate and supporting new starters. These new starters, predominantly new to nursing in the UK, have been given extended supernumerary periods to support the transition. This reduction in beds resulted in a drop in the planned hours for the month. This action saw a rise in the RN fill rate from 93.7% in July to 96.5% in August. Ashwell Ward had similar staffing challenges to 6A in terms of vacancy factor. At the end of July this ward was relocated to the North end of 6A, this ward has also reduced to 15 beds to enable the ward to stabilise staffing the RN fill rate remained steady at 92.2%. The Surgical Assessment Unit (SAU) has a flexible patient group this often results in the unit having a reduced number of patients during the early part of the day shift. Depending on acuity staff can be moved to support wards triggering red. This support provided to other areas has resulted in a significant drop in the RN fill rate for the month from 93% for registered nursing to 78.2%. Activity on wards 10 and 11 at MVCC remains below plan and less staff were required; this reflects the lower fill rates. Nursing staff are transferred between wards 10 and 11 to support activity. The Cancer Division is conducting an on-going review of activity and proposed shift plans show a reduction in required staff. As an interim measure, the planned staffing for ward 11 was reduced to reflect the predicted lower activity. Throughout August 4 additional beds were opened on ACU to allow the Trust to flex bed capacity when required, these beds were used with increased frequency throughout August due to the bed reduction on 6A and Ashwell. This increased staffing requirement is reflected in an increased fill rate for both days and nights. The proportion of shifts filled by NHSP has fallen during the month, with the shifts remaining unfilled increasing from 19.97% to 25.36%. It is likely that unfilled shifts and vacancy rates along with high reliance on temporary staffing has resulted in a reduction of RN % fill and an increase in shifts triggering red. See Appendix 1 for fill trend analysis for the month. Swift ward remains open to 12 beds over the weekend. This is therefore a cost pressure and demand on staffing resource. 4. Shifts that initially triggered red For August the number of shifts initially triggering red rose to 150 out of 3069 shifts. This equates to 4.89% from 2.67% in July (see Table 1 below). The reduced NHSP fill has had an impact on the % of wards triggering red. There are other factors that have contributed to the increase in wards triggering red these are outlined later in the paper. Data Pack.pdf 4 Page Page 54 of 73 Overall Page 194 of 215
195 Table 1 Month % of wards that triggered red in Month January 6.81% February 7.03% March 7.01% April 5.08% May 3.32% June 1.85% July 2.67% August 4.89% Out of the shifts triggering red, only 8 of the 150 (0.26%) shifts remained a challenge to mitigate. Chart 1 below shows the distribution of red triggered shifts by census period. Chart 1 % of Red triggered shifts by shift 25% 49% 26% Early Late Night Ward Analysis There were 6 wards that triggered red on over 10% of the shifts worked in August. These were Swift, 8B, 9B, SSU, 10B, 11A. There are multiple factors that contributed to the higher incidents of red triggering shifts on these wards including: Vacancy- Vacancy rates have had a significant impact on the number of shifts triggering red on 9B (25%) and 11A (25.4%). Sickness - Sickness on 9B (7.2%), 10B (4.7%), 11A (5.8%) and SSU (10.8%) have contributed to the frequency of red trigging shifts. Pre-registration nurses - 11A and 8B have had a significant number of new starters on the ward, these new registered nurse staff have been working without NMC pin numbers and therefore have been working as care support workers while waiting for their pin numbers. Additional Capacity - To support the need for additional beds, for example ACU to 38 beds and swift weekend opening. A comparison for all inpatient ward areas detailing vacancy, sickness and recruitment pipeline can be seen in Table 2 below. The total hours of reported sickness is expressed as a percentage of the total contracted hours of substantive staff out of the last four-week roster to fall in month. Table 2 also indicates the number of red shifts, both those that initially triggered red and those that remained red. Data Pack.pdf 5 Page Page 55 of 73 Overall Page 195 of 215
196 To assess whether there is any correlation between red triggered shifts and other factors and incidents Datix incidents relating to staffing issues and Friends and Family Test (FFT) scores for August are included in Table 2. Table 2 shifts that initially triggered red shifts that remained red Ward Count % Count % Staff related incidents FFT % that would recommend Vacancy rate % Sickness % on roster Pipeline recruitment in next two months 9A B Barley Pirton A B A ACU AMU-A SSU N/A AMU-W B Ashwell NP A&E A B SAU B B A B Swift Critical Care N/A ASCU N/A N/A N/A 0 7A Gynae Bluebell Dacre N/A Gloucester N/A Mat MLU N/A Mat CLU Ward Ward Michael Sobell House N/A* = areas not reported within the Inpatient/Day Case FFT results in line with NHS England guidelines ** = Establishment data requires review between Maternity and HR Data Pack.pdf 6 Page Page 56 of 73 Overall Page 196 of 215
197 Triangulation of the data is complex as incident reporting relating to staffing does not always correlate to the days that wards remained red. Equally, incidents relating to patient falls have not occurred on days where wards remained red. See Appendix 2 for details of all wards. 4.1 Datix incidents and Red Flags The overall number of Datix staffing incidents reported in August decreased compared to July. The 28 staffing related incidents raised by inpatient areas were evenly distributed between 16 clinical areas. With the exception of 10B and SSU Datix incidents did not correlate to shifts triggering shift. Some additional factors for incidents include NHSP staff not arriving for duty, vacancies, maternity leave, sickness and EU nurses awaiting NMC registration. All incidents were managed in real-time by the daily staffing scrutiny processes described in section 2. SafeCare is now being piloted to report red flag events on the ward, there were 45 red flag events raised in SafeCare on the 8 wards currently piloting the software for August. A summary of the flags raised is outlined in Table 3 below. Table 3 Red Flag Type Count of Red Flag Events Delay in providing pain relief 2 Less than 2 RNs on shift 7 Missed 'intentional rounding' 1 Patient Falls 11 Shortfall in RN time 22 Unplanned omission in providing medications 2 Grand Total 45 A sample of the pilot data for red flag report can be seen in Appendix 3. August is the first month that this red flag information has been available through SafeCare, so this data remains draft. As the project progresses these identified issues will be managed in real time by the ward, where this can t be achieved these issues are escalated to senior nursing staff. 4.2 Summary of actions taken to mitigate red shifts includes: Escalation to NHSP for staff that did not attend shift Review of other clinical areas, departments, to identify available staff Transfer of staff across Divisions where clinically appropriate and possible Increased Matron presence in areas triggering red Flexing of staff across adjacent and similar specialities Operational considerations regarding admissions and transfers Flexing bed capacity on wards such as ACU between 34 and 38 dependent on staffing levels Keeping Swift open for 12 patients over the weekend Closing 15 beds on 6A and 5 further beds on Ashwell 4.3 Friends and Family (FFT) Scores There remains no correlation between the proportion of patients who would recommend wards to their friends and family (FFT) and wards that have triggered the highest number of red shifts. It is difficult to assess the significance in the slight variance in FFT scores on wards that trigger red as it cannot be determined if staffing levels contributed to the recommendation. Further work is needed to establish what factors determine the FFT recommendation and if any of these factors 7 Page Data Pack.pdf Page 57 of 73 Overall Page 197 of 215
198 are impacted by staffing shortfalls on wards. 5. E-roster System Version 10 and SafeCare The project to introduce the SafeCare tool is now being implemented. SafeCare is an additional software component that is an extension of the e-roster system. The SafeCare tool will result in a number of benefits: Improved quality of care through effective alignment of staff to patient need, understanding patient acuity on a real time basis Improved clinical governance by providing better visibility of staffing Provision of an electronic audit trail, in real time, of staffing patient numbers and acuity Timely escalation of staffing related issues that can be remotely reviewed Recording of red flag events on wards SafeCare is now in the third phase of roll out with 8 wards (4 Surgical and 4 Medical) now actively using the system to monitor and escalate staffing issues. A further 4 wards are in the data collection phase of roll out and should be using the live system by the end of September. 6. Conclusion The provision of safe staffing levels of wards in August was supported by the falling: Continuing improvement of data collection methods and intelligence from daily staffing meetings. Formal definition of these processes has been documented in the Daily and Weekly Staffing Meeting Terms of Reference. Staffing is one of the factors in reducing the bed base on Ashwell and 6A Recruitment of overseas nurses awaiting The average fill rate for registered nurses in August was 94.5% Additional support provided by e-roster, NHSP and Temporary Staffing manager to assist wards with staffing challenges The Board are asked to note the processes in place to ensure safe staffing levels in the Trust. 7. Next Steps The current process implemented by the safer staffing team over the last 6 months have ensured the staffing issues are quickly identified actioned and where appropriate, escalated to senior staff and directors. These processes have been formalised in the Daily and Weekly Staffing meeting terms of reference approved at the Nursing and Midwifery Executive Committee in August. This document has been used to draft the Trusts Safer Staffing and Escalation Policy which will be submitted to the Nursing and Midwifery Executive Committee for ratification in September. Monitor and the Trust Development Authority (TDA) have issue a document detailing guidelines for NHS trusts with regards to the use of agency staff. The document outlines 2 key rules that the trust must adhere to from the start of quarter 3 (1 st October 2015), these are: The introduction of an annual ceiling for total nursing agency spend for each trust Mandatory use of approved frameworks for procuring agency staff The roll out of SafeCare will continue with an additional 4 wards predicted for September, further updates on progress will be supplied in the next report. Data Pack.pdf 8 Page Page 58 of 73 Overall Page 198 of 215

199 NHSP shift fill for August 2015 Appendix 1 Data Pack.pdf 9 Page Page 59 of 73 Overall Page 199 of 215
200 Shifts that initially triggered red in July 2015 Appendix 2 Month Aug-15 Days in Month Division Speciality Ward Early Late Night INITIAL REDS Number of shifts where staffing initially fell below agreed levels % of shifts where staffing fell below agreed levels and triggered a Red rating Care of the 9A Elderly 9B Stroke Barley Pirton General 6A B Respiratory 11A Cardiology ACU AMU-A Acute SSU AMU-W Renal 6B DTOC / gastro Ashwell ED A&E Total A General 8B SAU Surgical Spec 11B B A T&O 5B Swift ATCC Critical Care ASCU Total Gynae 7A Gynae Paeds Bluebell Dacre Maternity Gloucester Mat MLU Mat CLU Total Medicine Surgery Women's & Children Ward Ward Inpatient Michael Sobell House Total TRUST TOTAL Cancer Data Pack.pdf 10 Page Page 60 of 73 Overall Page 200 of 215
201 Appendix 3 Pilot Data - Red Flag Events in August Count of Red Flag Row Labels Type 10B Patient Falls 1 Shortfall in RN time 7 10B Total 8 5B Delay in providing pain relief 1 Patient Falls 3 Shortfall in RN time 7 5B Total 11 6B Patient Falls 4 Shortfall in RN time 1 Unplanned omission in providing medications 1 6B Total 6 8A Missed 'intentional rounding' 1 8A Total 1 8B Less than 2 RNs on shift 3 Patient Falls 1 Shortfall in RN time 5 8B Total 9 AMU-A Shortfall in RN time 1 AMU-A Total 1 AMU-W Delay in providing pain relief 1 Less than 2 RNs on shift 4 Patient Falls 2 Shortfall in RN time 1 Unplanned omission in providing medications 1 AMU-W Total 9 Grand Total 45 Data Pack.pdf 11 Page Page 61 of 73 Overall Page 201 of 215
202 Infection Prevention and Control Board Report Objectives & Outcomes: July & August 2015 Objective Narrative Outcome 1. Ensure that patients presenting with an infection or who acquire an infection during their care are identified promptly and receive appropriate management and treatment to reduce the risk of transmission. 1.1 In , the Trust has a target of 0 avoidable MRSA Bacteraemias 1.2 In , the Trust has a target of no more than 11 cases of hospital acquired C.difficile infection 1.3 In , the Trust has had 2 cases of hospital acquired MSSA bacteraemia year to date (no target set) 1.1 Trust reported 0 MRSA bacteraemias in July and August. One community case occurred in a renal patient and is subject to review. Year to date position is 0 cases. 1.2 Trust reported 1 hospital acquired C.difficile case in July. One community case occurred in August shortly after discharge and is subject to review. Year to date position is 3 hospital acquired cases, 2 cases below trajectory. 1.3 Trust reported 0 hospital acquired MSSA bacteraemias in July and August Year to date position is 2 hospital acquired cases (no target set) Green Green Green 1.4 In , the Trust has had 9 cases of hospital acquired E-Coli year to date (no target set) 1.4 In July there were 5 cases of hospital acquired E.coli. August figures are being reviewed. Year to date position is 9 hospital acquired cases (no target set) Green 1.7 Aim to minimise number and duration of outbreaks, eg Norovirus, through prompt identification and effective action 1.7 During July, there was a period of increased incidence of MRSA colonisation on the Neonatal Unit. There were no further incidents during July or August. Green 1.8 The Trust IPC Team uses ICNet for its identification, management and surveillance of HCAIs. 1.8 Manual work around being implemented. Additional interface support being purchased. Amber 2. Have in place and operate effective management systems for the prevention and control of HCAI which are informed by risk assessments and analysis of infection incidents 2.1 Global threat of Ebola outbreak in West Africa and impact on UK/ENHT 2.1 The Trust is maintaining vigilance for Ebola. The outbreak in West Africa appears to be subsiding. The Trust will await advice from PHE before discontinuing processes. Amber Data Pack.pdf Page 62 of 73 Overall Page 202 of 1215
203 3. Have and adhere to appropriate policies and protocols for the prevention and Control of HCAI 3.1 Fortnightly peer audits of High Impact Interventions to focus on aspects of clinical care (target over 95% for all areas). To identify good practice and any actions required will be put in place 3.1 Compliance figures for High Impact Interventions in July were all over 95% with the exception of hand hygiene (93%), PVC insertion (94.9%), PVC continuing care (86.4%), urinary catheter insertion (94.3%), urinary catheter continuing care (92.64%). Amber In August, all scores were over 95% with the exception of surgical site (93.7%), PVC continuing care (91.3%), urinary catheter insertion & continuing care (91.3%), renal dialysis line insertion (92.86%), environment & safety (86.46%), central venous catheter care (93.38%). IPC Team working with wards to agree actions to improve compliance. Data Pack.pdf Page 63 of 73 Overall Page 203 of 2215
204 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 MRSA Bacteraemias MRSA BACTERAEMIA Cumulative MRSA Bacteraemia Performance YTD MRSA bacteraemias by year NHS Year NHS Year MRSA bacteraemia by Division Division Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 YTD Cancer Medicine Surgical Women & Children Grand Total Cumulative Overview of findings from MRSA bacteraemia PIRs A patient receiving dialysis had an MRSA bacteraemia identified in August. Currently this is allocated to the community setting. A PIR is being led by the Bedfordshire CCG. Data Pack.pdf Page 64 of 73 Overall Page 204 of 3215

205 MRSA PHE Benchmarking Data (to July 2015) Data Pack.pdf Page 65 of 73 Overall Page 205 of 4215
206 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 MSSA BACTERAEMIA Cumulative MSSA Performance April March Hospital acquired MSSA by Division Total Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 YTD Cancer Medicine Surgical Women & Children MVCC Grand Total Overview of findings from MSSA bacteraemia RCAs The RCA for the May case has been completed. This was a contaminant and findings were: 1. Blood culture undertaken during emergency situation; 2. Poor documentation; 3. Non-compliance with IV devices policy. The issues identified are being fed back to junior doctors during induction and training sessions, and the Nephrology Outcomes Group is to discuss the use of central lines rather than peripheral access for all patients requiring a vascular dialysis catheter. Data Pack.pdf Page 66 of 73 Overall Page 206 of 5215

207 MSSA PHE Benchmarking Data (to July 2015) Data Pack.pdf Page 67 of 73 Overall Page 207 of 6215
208 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 No. of C. difficile cases CLOSTRIDIUM DIFFICILE Cumulative Clostridium Difficile for year 2015/16 YTD Clostridium difficile by year NHS Year C-DIFF by Division Total Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 YTD Division Cancer Medicine Surgical Women & Children Grand Total Outcomes from C.diff RCAs The RCA for the second case in June has taken place and the case was found to be unavoidable. The completed written report and action plan are awaited. A patient recently discharged from the Lister Hospital to a Hertfordshire community facility was found to be positive for a C difficile toxin. An RCA is to be held jointly with Hertfordshire Community Trust. Data Pack.pdf Page 68 of 73 Overall Page 208 of 7215

209 C.DIFFICILE PHE Benchmarking Data (to July 2015) Data Pack.pdf Page 69 of 73 Overall Page 209 of 8215
210 E.COLI BACTERAEMIA Cumulative E.Coli Performance April March Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Hospital Acquired E.Coli by Division YTD Total Division Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar Cancer Medicine Surgical Women & Children MVCC Grand Total The August figures are provisional. Review of hospital associated E.coli cases The IP&C Team are planning to introduce reviews of all hospital associated E.coli cases once the reporting process has been refined to enable the team to receive timely notification of cases. Data Pack.pdf Page 70 of 73 Overall Page 210 of 9215

211 E.COLI PHE Benchmarking Data (to July 2015) Data Pack.pdf Page 71 of 73 Overall Page 211 of 10215
EAST AND NORTH HERTFORDSHIRE NHS TRUST
 Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 24 July 2013 at 2pm in the Post Graduate Centre, QEII Hospital. Present: Mr Ian Morfett
Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 24 July 2013 at 2pm in the Post Graduate Centre, QEII Hospital. Present: Mr Ian Morfett
EAST AND NORTH HERTFORDSHIRE NHS TRUST
 Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 26 June 2013 at 2pm, Rooms 2 and 3, Hertford County Hospital Present: Mr Ian Morfett
Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 26 June 2013 at 2pm, Rooms 2 and 3, Hertford County Hospital Present: Mr Ian Morfett
Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST
 Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 25 th February 2009 at 2.00 pm in Rooms 2 and 3 at Hertford County Hospital DRAFT Present:
Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 25 th February 2009 at 2.00 pm in Rooms 2 and 3 at Hertford County Hospital DRAFT Present:
East and North Hertfordshire NHS Trust Trust Board Part I
 East and North Hertfordshire NHS Trust Trust Board Part I Rooms 2 & 3, Hertford County Hospital 1 November 2017 14:00-1 November 2017 15:30 Overall Page 1 of 359 AGENDA # Description Owner Time 1 Chair's
East and North Hertfordshire NHS Trust Trust Board Part I Rooms 2 & 3, Hertford County Hospital 1 November 2017 14:00-1 November 2017 15:30 Overall Page 1 of 359 AGENDA # Description Owner Time 1 Chair's
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016
 NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
NHS Herts Valleys Clinical Commissioning Group Board Meeting 14 April 2016 Title 2015/16 Annual Report and Accounts proposed approval process Agenda Item: 13 Purpose (tick one only) Decision or Approval
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
Newham Borough Summary report
 Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
Board Briefing. Board Briefing of Nursing and Midwifery Staffing Levels. Date of Briefing August 2017 (July 2017 data)
") Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing August 2017 (July 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author: Workforce
Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing August 2017 (July 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author: Workforce
BSUH INTEGRATED PERFORMANCE REPORT. 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain
 Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain") BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
Board Briefing. Board Briefing of Nursing and Midwifery Staffing Levels. Date of Briefing January 2018 (December 2017 data)
") Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing January 2018 (December 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author:
Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing January 2018 (December 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author:
Strategic KPI Report Performance to December 2017
 Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
Integrated Performance Report
 Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
PATIENT SAFETY, QUALITY & RISK COMMITTEE
 PATIENT SAFETY, QUALITY & RISK COMMITTEE Minutes of the Patient Safety, Quality & Risk Committee Thursday, 6 th March 2014 West Herts Meeting Room, Willow House Watford General Hospital Chair: Mahdi Hasan
PATIENT SAFETY, QUALITY & RISK COMMITTEE Minutes of the Patient Safety, Quality & Risk Committee Thursday, 6 th March 2014 West Herts Meeting Room, Willow House Watford General Hospital Chair: Mahdi Hasan
NHS Borders Feedback and Complaints Annual Report
 NHS Borders Feedback and Complaints Annual Report 2016-17 1 Introduction NHS Borders Feedback and Complaints Annual Report 2016-17 is a summary of the feedback provided by the complaints, comments, concerns
NHS Borders Feedback and Complaints Annual Report 2016-17 1 Introduction NHS Borders Feedback and Complaints Annual Report 2016-17 is a summary of the feedback provided by the complaints, comments, concerns
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
RBCH Actions to meet CQC Essential Standards
 RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
Safer Nursing and Midwifery Staffing Recommendation The Board is asked to: NOTE the report
 To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
Integrated Performance Report
 Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Nottingham University Hospitals Emergency Department Quality Issues Related to Performance
 RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
Ayrshire and Arran NHS Board
 Paper 12 Ayrshire and Arran NHS Board Monday 9 October 2017 Planned Care Performance Report Author: Fraser Doris, Performance Information Analyst Sponsoring Director: Liz Moore, Director for Acute Services
Paper 12 Ayrshire and Arran NHS Board Monday 9 October 2017 Planned Care Performance Report Author: Fraser Doris, Performance Information Analyst Sponsoring Director: Liz Moore, Director for Acute Services
Newham Borough Summary report
 Newham Borough Summary report Item K1 September 2013 Prepared on 30/09/2013 by Support team GREEN Finance and Activity Millions AMBER RED Headlines M5 Financial position M4 activity data The QIPP net savings
Newham Borough Summary report Item K1 September 2013 Prepared on 30/09/2013 by Support team GREEN Finance and Activity Millions AMBER RED Headlines M5 Financial position M4 activity data The QIPP net savings
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Quality Assurance Accreditation Scheme Assignment Report 2016/17. University Hospitals of Morecambe Bay NHS Foundation Trust
 Quality Assurance Accreditation Scheme Assignment Report 2016/17 Contents 1. Introduction 2. Executive Summary 3. Findings, Recommendations and Action Plan Appendix A: Terms of Reference Appendix B: Assurance
Quality Assurance Accreditation Scheme Assignment Report 2016/17 Contents 1. Introduction 2. Executive Summary 3. Findings, Recommendations and Action Plan Appendix A: Terms of Reference Appendix B: Assurance
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 2018
 Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE
 Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Agenda Item: 10.1 (3) HR & OD Monthly Trust Report (September 2016)
 HR & OD Monthly Trust Report (September 2016)") Agenda Item: 10.1 (3) HR & OD Monthly Trust Report (September 2016) Prepared by: Karen Taylor, Assistant Director of HR & Kyriacos Kyriacou, Interim Deputy Director of HR & OD Presented by: Louise Ludgrove,
Agenda Item: 10.1 (3) HR & OD Monthly Trust Report (September 2016) Prepared by: Karen Taylor, Assistant Director of HR & Kyriacos Kyriacou, Interim Deputy Director of HR & OD Presented by: Louise Ludgrove,
Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
 APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
FT Keogh Plans. Medway NHS Foundation Trust
 FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
Redesign of Front Door
 Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP
 COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
Strategic Risk Report 4 July 2016
 Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
Internal Audit. Health and Safety Governance. November Report Assessment
 November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
TRUST BOARD MEETING 24 JULY 2013 PERFORMANCE REPORT MONTH 3 DIRECTOR OF OPERATIONS DIRECTOR OF OPERATIONS DIRECTOR OF OPERATIONS
 TRUST BOARD MEETING 24 JULY 2013 PERFORMANCE REPORT MONTH 3 def Agenda Item: 10c PURPOSE PREVIOUSLY CONSIDERED BY Objective(s) to which issue relates * Risk Issues (Quality, safety, financial, HR, legal
TRUST BOARD MEETING 24 JULY 2013 PERFORMANCE REPORT MONTH 3 def Agenda Item: 10c PURPOSE PREVIOUSLY CONSIDERED BY Objective(s) to which issue relates * Risk Issues (Quality, safety, financial, HR, legal
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk
 Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Strategic Risk Report 12 September 2016
 Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
ENCLOSURE: J. Date of Trust Board 29 February Pressure Ulcer Clinical Improvement Programme. Purpose of Report
 ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
Performance and Quality Report Sean Morgan Director of Performance and Delivery Mary Hopper Director of Quality Dino Pardhanani, Clinical Director
 Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Improvement and assessment framework for children and young people s health services
 Improvement and assessment framework for children and young people s health services To support challenged children and young people s health services achieve a good or outstanding CQC rating February
Improvement and assessment framework for children and young people s health services To support challenged children and young people s health services achieve a good or outstanding CQC rating February
Please indicate: For Decision For Information For Discussion X Executive Summary Summary
 Governing Body 22 March 2017 Details Part 1 X Part 2 Agenda Item No. 10 Title of Paper: Board Member: Author: Presenter: PAHT Quality Improvement Plan Catherine Jackson, Executive Nurse Catherine Jackson,
Governing Body 22 March 2017 Details Part 1 X Part 2 Agenda Item No. 10 Title of Paper: Board Member: Author: Presenter: PAHT Quality Improvement Plan Catherine Jackson, Executive Nurse Catherine Jackson,
Integration Scheme. Between. Glasgow City Council. and. NHS Greater Glasgow and Clyde
 Integration Scheme Between Glasgow City Council and NHS Greater Glasgow and Clyde December 2015 Page 1 of 60 1. Introduction 1.1 The Public Bodies (Joint Working) (Scotland) Act 2014 (the Act) requires
Integration Scheme Between Glasgow City Council and NHS Greater Glasgow and Clyde December 2015 Page 1 of 60 1. Introduction 1.1 The Public Bodies (Joint Working) (Scotland) Act 2014 (the Act) requires
Safe Nurse Staffing Levels. June 2017
 Safe Nurse Staffing Levels Executive Summary June 2017 The purpose of this report is: 1. To provide an assurance with regard to the management of safe nursing and midwifery staffing for the month of June
Safe Nurse Staffing Levels Executive Summary June 2017 The purpose of this report is: 1. To provide an assurance with regard to the management of safe nursing and midwifery staffing for the month of June
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT
 NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
Hard Truths Public Board 29th September, 2016
 Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
annual report 2016/17 The Hillingdon Hospitals NHS Foundation Trust
 annual report 2016/17 The Hillingdon Hospitals NHS Foundation Trust The Hillingdon Hospitals NHS Foundation Trust Annual Report and Accounts 2016/17 Presented to Parliament pursuant to Schedule 7, paragraph
annual report 2016/17 The Hillingdon Hospitals NHS Foundation Trust The Hillingdon Hospitals NHS Foundation Trust Annual Report and Accounts 2016/17 Presented to Parliament pursuant to Schedule 7, paragraph
EAST AND NORTH HERTFORDSHIRE NHS TRUST CHIEF EXECUTIVE S REPORT
 EAST AND NORTH HERTFORDSHIRE NHS TRUST CHIEF EXECUTIVE S REPORT Agenda Item No. 7 23 rd January 2008 1. Christmas Day Visit From Mayor of Stevenage and General Secretary, Royal College of Nursing Alison
EAST AND NORTH HERTFORDSHIRE NHS TRUST CHIEF EXECUTIVE S REPORT Agenda Item No. 7 23 rd January 2008 1. Christmas Day Visit From Mayor of Stevenage and General Secretary, Royal College of Nursing Alison
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
Delivering Improvement in Practice
 v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
HERTFORDSHIRE COMMUNITY HEALTH SERVICES
 HERTFORDSHIRE COMMUNITY HEALTH SERVICES Minutes of the Hertfordshire Community Health Services Board Meeting Held on Thursday 22 nd July 2010 in the Boardroom, Howard Court Welwyn Garden City. Key Points
HERTFORDSHIRE COMMUNITY HEALTH SERVICES Minutes of the Hertfordshire Community Health Services Board Meeting Held on Thursday 22 nd July 2010 in the Boardroom, Howard Court Welwyn Garden City. Key Points
Title Open and Honest Staffing Report April 2016
 Title Open and Honest Staffing Report April 2016 File location WILJ2102 Meeting Board of Directors Date 25 th May 2016 Executive Summary This paper provides a stocktake on the position of South Tyneside
Title Open and Honest Staffing Report April 2016 File location WILJ2102 Meeting Board of Directors Date 25 th May 2016 Executive Summary This paper provides a stocktake on the position of South Tyneside
Aneurin Bevan University Health Board. Professional Revalidation
 28 th January 20 Aneurin Bevan University Health Board Professional Revalidation Purpose of the Report: The purpose of this paper is to provide the Board with an update in relation to the Nursing Revalidation
28 th January 20 Aneurin Bevan University Health Board Professional Revalidation Purpose of the Report: The purpose of this paper is to provide the Board with an update in relation to the Nursing Revalidation
Strategic Risk Report 1 March 2018
 Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
RTT Recovery Planning and Trajectory Development: A Cambridge Tale
 RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
Document Details Clinical Audit Policy
 Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
102/14(ii) Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review
 Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review") Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Ayrshire and Arran NHS Board
 Paper 12 Ayrshire and Arran NHS Board Monday 26 March 2018 Financial Management Report for the 11 months to 28 February 2018 Author: Bob Brown, Assistant Director of Finance Governance and Shared Services
Paper 12 Ayrshire and Arran NHS Board Monday 26 March 2018 Financial Management Report for the 11 months to 28 February 2018 Author: Bob Brown, Assistant Director of Finance Governance and Shared Services
Presentation to the Care Quality Commission. Dr. Lucy Moore, CEO 15 September 2015
 Presentation to the Care Quality Commission Dr. Lucy Moore, CEO 15 September 2015 Our Improvement Journey- Key Messages We have Board, Executive and Divisional leadership teams now in place with serious
Presentation to the Care Quality Commission Dr. Lucy Moore, CEO 15 September 2015 Our Improvement Journey- Key Messages We have Board, Executive and Divisional leadership teams now in place with serious
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD
 BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD") INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
Quality Improvement Scorecard March 2018
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
: Geraint Davies, Director of Commercial Services
 Report to : Trust Board of Directors Date of Report: 15/05/2015 Agenda Item: 0/15 Date of Meeting : 28 May 2015 Subject Report from Purpose : Report on Corporate Risk Register : Geraint Davies, Director
Report to : Trust Board of Directors Date of Report: 15/05/2015 Agenda Item: 0/15 Date of Meeting : 28 May 2015 Subject Report from Purpose : Report on Corporate Risk Register : Geraint Davies, Director
BOARD CLINICAL GOVERNANCE & QUALITY UPDATE MARCH 2013
 Borders NHS Board BOARD CLINICAL GOVERNANCE & QUALITY UPDATE MARCH 2013 Aim The aim of this report is to provide the Board with an overview of progress in the areas of: Patient Safety Person Centred Health
Borders NHS Board BOARD CLINICAL GOVERNANCE & QUALITY UPDATE MARCH 2013 Aim The aim of this report is to provide the Board with an overview of progress in the areas of: Patient Safety Person Centred Health
The Royal Wolverhampton NHS Trust
 Title: Safe Staffing; Planned Versus Actual Staffing by Ward September 2016 data The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 31 st October 2016 Title: Nursing Workforce Report Executive
Title: Safe Staffing; Planned Versus Actual Staffing by Ward September 2016 data The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 31 st October 2016 Title: Nursing Workforce Report Executive
Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations
 No. Domain CQC Recommendation Lead Operational Lead Current Status 1 Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations Wording in long
No. Domain CQC Recommendation Lead Operational Lead Current Status 1 Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations Wording in long
Iain Patterson. Associate Workforce Director Homerton University Hospital NHS Foundation Trust
 Iain Patterson Associate Workforce Director Homerton University Hospital NHS Foundation Trust Who we are? Who we are? North East London Sector 3,800 staff spread across Hackney and beyond c. 3,000 acute
Iain Patterson Associate Workforce Director Homerton University Hospital NHS Foundation Trust Who we are? Who we are? North East London Sector 3,800 staff spread across Hackney and beyond c. 3,000 acute
Draft Minutes. Agenda Item: 16
 Meeting of Bristol Clinical Commissioning Group Quality and Governance Committee Held on 17th December 2013 At 9:00am in Clinical Commissioning Group Meeting Room Agenda Item: 16 Draft Minutes Present:
Meeting of Bristol Clinical Commissioning Group Quality and Governance Committee Held on 17th December 2013 At 9:00am in Clinical Commissioning Group Meeting Room Agenda Item: 16 Draft Minutes Present:
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST CHIEF EXECUTIVE S REPORT. BOARD OF DIRECTORS 21 st March 2012
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST I CHIEF EXECUTIVE S REPORT BOARD OF DIRECTORS 21 st 212 1. PERFORMANCE In overall terms, the Trust continues to perform well against both regulatory and
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST I CHIEF EXECUTIVE S REPORT BOARD OF DIRECTORS 21 st 212 1. PERFORMANCE In overall terms, the Trust continues to perform well against both regulatory and
Library and Knowledge Services Annual Report
 Library and Knowledge Services Annual Report 2016-2017 West Hertfordshire Hospitals NHS Trust Katherine Teal Annual Report 2016-2017 Foreword This year has seen significant changes in the Library and Knowledge
Library and Knowledge Services Annual Report 2016-2017 West Hertfordshire Hospitals NHS Trust Katherine Teal Annual Report 2016-2017 Foreword This year has seen significant changes in the Library and Knowledge
Quality Strategy (Refreshed March 2015)
") Quality Strategy 2012-2017 (Refreshed March 2015) 1 Table of Contents 1. Executive Summary... 3 2. Drivers for improvement... 4 2.1 The Trust s ambition - vision and mission... 4 2.2 Corporate Strategy...
Quality Strategy 2012-2017 (Refreshed March 2015) 1 Table of Contents 1. Executive Summary... 3 2. Drivers for improvement... 4 2.1 The Trust s ambition - vision and mission... 4 2.2 Corporate Strategy...
NHS Greater Glasgow and Clyde Alison Noonan
 NHS Board Contact Email NHS Greater Glasgow and Clyde Alison Noonan alison.noonan@ggc.scot.nhs.uk Title Category Background/ context Problem Effective Discharge Planning and the Introduction of Delegated
NHS Board Contact Email NHS Greater Glasgow and Clyde Alison Noonan alison.noonan@ggc.scot.nhs.uk Title Category Background/ context Problem Effective Discharge Planning and the Introduction of Delegated
Welcome, Apologies for Absence and Declaration of Board Members Interest
 DRAFT Minutes of the of the Royal Cornwall Hospitals NHS Trust held on Thursday 30 March 2017 11.00 13.00 in the Knowledge Spa, Royal Cornwall Hospital Present: Mr Jim McKenna Ms Kathy Byrne Ms Catrin
DRAFT Minutes of the of the Royal Cornwall Hospitals NHS Trust held on Thursday 30 March 2017 11.00 13.00 in the Knowledge Spa, Royal Cornwall Hospital Present: Mr Jim McKenna Ms Kathy Byrne Ms Catrin
Appendix 1: Croydon Clinical Commissioning Group Risk Register and Board Assurance Framework - 9th April 2013
 Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
Developing Plans for the Better Care Fund
 Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Implementing NHS Services Seven Days a Week
 Implementing NHS Services Seven Days a Week Deborah Williams 7 Day Services Programme Manager NHS England November 2015 NHS Five Year Forward View To reduce variations in when patients receive care, we
Implementing NHS Services Seven Days a Week Deborah Williams 7 Day Services Programme Manager NHS England November 2015 NHS Five Year Forward View To reduce variations in when patients receive care, we
Above and beyond the call of duty
 E&NH0400 Above and beyond the call of duty Trust s annual nursing and midwifery awards celebrate the work of nurses, midwives and clinical support workers Stevenage 18 October 2010 The hard work and dedication
E&NH0400 Above and beyond the call of duty Trust s annual nursing and midwifery awards celebrate the work of nurses, midwives and clinical support workers Stevenage 18 October 2010 The hard work and dedication
Northumberland, Tyne and Wear NHS Foundation Trust. Board of Directors Meeting
 Agenda item 7 iv) Northumberland, Tyne and Wear NHS Foundation Trust Meeting Date: 22 February 2017 Board of Directors Meeting Title and Author of Paper: Safer Staffing Quarter 3 Report (October December,
Agenda item 7 iv) Northumberland, Tyne and Wear NHS Foundation Trust Meeting Date: 22 February 2017 Board of Directors Meeting Title and Author of Paper: Safer Staffing Quarter 3 Report (October December,
Integrated Performance Report August 2017
 Integrated Performance Report Contents Section Page High Level Dashboard Balanced scorecard 3 Domain Scorecards and Director Commentaries Operational Performance 4 Quality and Patient Safety 9 Workforce
Integrated Performance Report Contents Section Page High Level Dashboard Balanced scorecard 3 Domain Scorecards and Director Commentaries Operational Performance 4 Quality and Patient Safety 9 Workforce
Moving to 7 Day Services. Kerry Gant, Head of Finance Change Team/Debbie Freake, Executive Director of Strategy
 Report to Trust Board of Directors Date of Meeting: 24 March 2015 Enclosure Number: 12 Title of Report: Author: Executive Lead: Responsible Sub- Committee (if appropriate): Executive Summary: Moving to
Report to Trust Board of Directors Date of Meeting: 24 March 2015 Enclosure Number: 12 Title of Report: Author: Executive Lead: Responsible Sub- Committee (if appropriate): Executive Summary: Moving to
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting 16 th November 2017 2. Title of Report: 3. Key Messages: BUPA ceased to be the registered provider of Crawfords Walk Nursing Home in October. The
GOVERNING BODY REPORT 1. Date of Governing Body Meeting 16 th November 2017 2. Title of Report: 3. Key Messages: BUPA ceased to be the registered provider of Crawfords Walk Nursing Home in October. The
Delivering the Five Year Forward View Personalised Health and Care 2020
 Paper Ref: NIB 0607-006 Delivering the Five Year Forward View Personalised Health and Care 2020 INTRODUCTION The Five Year Forward View set out a clear direction for the NHS showing why change is needed
Paper Ref: NIB 0607-006 Delivering the Five Year Forward View Personalised Health and Care 2020 INTRODUCTION The Five Year Forward View set out a clear direction for the NHS showing why change is needed
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014
 Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
Sponsoring director: Purpose: Decision Assurance For information Disclosable X Non-disclosable
 TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
Governance and assurance. CATEGORY OF PAPER Specific action required: Provides Assurance: For Information:
 CATEGORY OF PAPER Specific action required: Provides Assurance: For Information: Report title: Purpose of report: Key issues: (key points of the paper, how this supports the achievement of the Trust s
CATEGORY OF PAPER Specific action required: Provides Assurance: For Information: Report title: Purpose of report: Key issues: (key points of the paper, how this supports the achievement of the Trust s
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Agenda Item The report triangulates staffing levels against appropriate quality measures. The Report is provided to the Board for:
 To: Trust Board From: Michelle Rhodes, Director of Nursing Date: 2 nd May 2017 Essential Standards: Health and Social Care Act 2008 (Regulated Activities) Regulation 18: Staffing Title: Monthly Nursing/Midwifery
To: Trust Board From: Michelle Rhodes, Director of Nursing Date: 2 nd May 2017 Essential Standards: Health and Social Care Act 2008 (Regulated Activities) Regulation 18: Staffing Title: Monthly Nursing/Midwifery
Integrated Corporate Performance Report. August Page 1 of 9
 Integrated Corporate Performance Report August Page of 9 Integrated Corporate Performance Report... Introduction The Integrated Corporate Performance Report (ICPR) includes: An Executive Summary - highlights
Integrated Corporate Performance Report August Page of 9 Integrated Corporate Performance Report... Introduction The Integrated Corporate Performance Report (ICPR) includes: An Executive Summary - highlights
Review of Inpatient Nursing Establishment, Capacity and Capability Review
 Appendix 2 Review of Inpatient Nursing Establishment, Capacity and Capability Review Mental Health Group September 2015 Review March 2016 Author: Heidi Cater, Head of Nursing, Mental Health Page 1 of 15
Appendix 2 Review of Inpatient Nursing Establishment, Capacity and Capability Review Mental Health Group September 2015 Review March 2016 Author: Heidi Cater, Head of Nursing, Mental Health Page 1 of 15
TRUST BOARD. Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director. Jo Hunter, Deputy Chief Nurse. Mary Heritage, Assistant Director of Quality
 TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING ADULT AND CHILDREN CONTINUING HEALTHCARE ANNUAL REPORT
 9.6 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING ADULT AND CHILDREN CONTINUING HEALTHCARE ANNUAL REPORT Date of the meeting 18/07/2018 Author Sponsoring Board member Purpose of Report
9.6 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING ADULT AND CHILDREN CONTINUING HEALTHCARE ANNUAL REPORT Date of the meeting 18/07/2018 Author Sponsoring Board member Purpose of Report
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April Ipswich Hospital NHS Trust NHS East of England Department of Health
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction