Hospital Engagement Network (HEN) Measurement
|
|
|
- Irene Morris
- 6 years ago
- Views:
Transcription

1 Hospital Engagement Network (HEN) Measurement The overall CMS goal for HENs is a 40% reduction in healthcare acquired conditions (HACs) and a 20% decrease in unnecessary readmissions by the end of We know that you cannot manage what you do not measure. Toward that end, we are expected by CMS to have at least 2 outcome and one process measure in each of the 10 priority areas. Purpose. In this document, we explain how we have adapted our planned approach to meet the CMS sense of urgency. Example Success Stories show what is possible across our HEN, and run charts provide examples of how aggregate data has been reported to CMS. Specification of selected measures follows together with necessary documentation and instructions for submission. Original Plan. Our HEN subject matter experts or SMEs have worked diligently and expeditiously to identify measures that: Draw on nationally required reporting if available; Avoid the need for chart review when possible; Are meaningfully tied to identified improvement targets; and Make it easy for all hospitals to report at least one measure in each area. The awarded proposal allowed for a systematic, year-long assessment of the literature, time to harvest best-inclass improvement approaches from leading delivery systems, and a synthesis of this information in order to drive improvement through evidence-based training and aligned measures. Upon receiving the award, we learned that we could not proceed as planned and needed to markedly expedite the process with the expectation that at least 65% of our hospitals will be reporting in each of the 10 areas by December of Our SMEs have been able to expedite their content and measure identification work without compromising on quality. (We have followed finalization of key CMS required measures that begin in 2013.) Data Submission. Intermountain analysts have developed a data submission tool that makes it easy for all hospitals to submit data (about 46% of hospitals in our HEN are small, rural facilities). We have iteratively tested the tool to work out unanticipated glitches and make necessary refinements adding hospitals data as we move forward. In this document you will find aggregate run charts for selected measures. Note that we have promised to report only aggregate, de-identified data to CMS as part of our required reporting. In addition and with full participation, we will be able to provide meaningful feedback reports to hospitals. Monthly data, beginning with January, 2012 will be used. You will only see data for your hospital (and system upon request) as compared with aggregate hospitals of similar bed size and rural-urban location. Questions: If you have any questions, please contact us at admin@henlearner.org. We are working to set up calls with identified analytic personnel at all participating hospitals/systems.
2 Hospital Success Stories Early elective deliveries Innovation Profile: Standardizing the Induction Process Snapshot Summary: Dixie Regional Medical Center addressed elective inductions and length of stay in Labor & Delivery. The aim was to improve the quality of care to patients undergoing an uncomplicated vaginal delivery at DRMC. OB length of stay was identified as an area for opportunity to reduce costs. By implementing strict induction guidelines, goals for time from admission to pitocin and for time from admit to AROM, actively managing all inductions and educating physicians on appropriate active management, DRMC was able to reduce time in labor by over 1 hour average and reduce elective inductions to zero. Hospital Background: Non Profit Mixed Payer Hospital Date First Implemented: 2010 What They Did Problems Addressed The project started as a cost reduction initiative, with OB length of stay identified by the quality department as an area of opportunity. More importantly, it was an opportunity for increased standardization; they hadn t really looked at the labor and delivery care process in a long time. They focused on quality improvement knowing that lower costs would follow. Description of the Intervention Project Aims: Improve the quality of care to patients undergoing an uncomplicated vaginal delivery at DRMC by reducing variation of nurse and physician practice and improving standardization of labor management to be accomplished by September 30, 2010 (implementation by July 31, 2010). Developing the Team: The team was led by the Director of Women s & Children s Services with the OB Medical Director and several interested physicians. The group met once a week or every two weeks in the beginning, then moved to monthly meetings. Rapid Cycle Improvement: The team worked quickly. In April 2010 they pulled together the team with a goal to implement improvement by July and see results by December. Implementation Essentials: 1. Strict induction guidelines reinforced with process for scheduling and reviewing all elective and indicated inductions. Reducing time in labor begins with proper selection of good induction candidates. 2. Implement a target goal of time from admission to pitocin on all inductions. (Goal =45 minutes) 3. Educate physicians on appropriate active management requirements for all inductions regardless of time of day. 4. Active management of all inductions. 5. Decrease the amount of time from admit to AROM (artificial rupture of membrane) on all inductions. Goal of <3 4 hours. 6. Streamlining and standardizing documentation of the patient history, e.g. establishing which components of the history were required prior to the start of pitocin and which could wait. 7. Establishing a process for Group B Strep (GBS) positive patients. They receive Pitocin as per process with any other induction goal is within 45 minutes. Amniotomy on these patients is to occur after infusion of the first dose of antibiotics is in (usually at the same time as start of Pitocin). The hospital recommends that providers
3 use clinical judgment on those with advanced dilatation or history of rapid labor and not follow this early rupture care process if the patient has GBS positive status. Roll out: The team started their work with charge nurses, to create change agents for the process changes. Charge nurses then worked with mentor groups to educate, motivate and sustain the change. Ongoing communications: o The team used monthly updates in their newsletter, showing how the unit is doing and what s new. o Overall unit outcome scores were posted (admit to pitocin time, LOS) and data also reviewed individually by nurse. o Physician education for active management requirements was reinforced in department meetings every other month with Amy presenting data. o Grand rounds most recently a grand rounds on antibiotic use and Group B Strep. They presented their results outcomes, rupturing, timing and proper use of antibiotics. Challenges: o Some of the care process changes represented a culture shift for physicians and nurses, so change took time. o One big management issue was with the GBS positive patients and getting people to accept the new treatment process. The team used data to show that starting pitocin early did not make labor progress faster than the 4 hours needed to administer the second dose of antibiotics. ACOG and American College of Pediatrics guidelines could be followed. Outcomes Tracking: o Elective inductions < 39 weeks o C section rates o Admit to Pitocin o Admit to Amniotomy (AROM Artificial rupture of membranes) o Length of Stay in Labor & Delivery by physician o Cost per case for uncomplicated vaginal delivery by physician Did it Work? Results For the first quarter of full implementation there were no c sections for elective inductions that followed the protocol, indicating that the long term c section rate will either be less than or the same as the c section rate on labor induction where Pitocin start time or early AROM is promoted. Goals for reducing time in labor were met: time in labor was reduced by over 1 hour average for this population of uncomplicated vaginal delivery. Cost savings in 2011 were measured at approximately $500,000 for the hospital. See graphs below. Future Work The group is now working on admit to pitocin as a System goal. The facility average time from admit to pitocin is 48 minutes for elective induction cases, which is currently slightly above the goal of 45 minutes. Admit to amniotomy continues to be a focus as of practice pattern and culture change, as providers are shown data to support the goals. The goal is to have all patients AROM be less than 3 hours, including GBS positive status (when appropriate). With these care processes it is hoped that practice changes will continue until consistency is obtained and time in labor for elective inductions mirror those times of spontaneous labor patients (which is the trend).

4 Factors Important to Success Leadership: Team collaboration among hospital leadership, physicians, and nurses fostered an important dialogue for improved protocols and the subsequent rate improvements. Culture change: Many physicians have been receptive to changes, although participation is not 100%. The team stresses that nurses are working hard to make physicians life easier. When patient deliveries are more predictable, physicians can adjust their schedules. When physicians grumbled initially about just trying to cut costs, the team showed them studies of higher patient satisfaction with shorter labors. o The team successfully drew on the national push to improve outcomes in this area, and also argued for cost effectiveness: We are only being paid so much and those dollars have to take care of everyone. If we can accomplish more appreciated care for lower cost those dollars can be used for other things. o The team acknowledged that culture change may be more difficult at other sites. The physician group has a history of being able to stick with specific protocols and track specific outcomes. This enabled the leadership to be more firm on which patients could be induced. Intermountain Health has a national and the group knows that many improvements started at Dixie. Now we use comparative data to show that we need to go even further if we want to excel. Data Collection, Analysis, and Reporting: The team felt lucky to have a documentation system that records and tags specific elements of the process (e.g., admit to pitocin time, admit to delivery time) that could be pulled electronically. For both physicians and nurses these data were compelling: they could see that the small changes were making were having a big impact on length of stay. No competition in the community for labor and delivery. Oftentimes when a hospital is trying to work on this, physicians can posture that they will take patients somewhere else. Dixie is the only hospital in the town that provides labor and delivery services. o The team does have experience in a competitive environment, and recommends a strategy of engaging competitors in the improvement project partner with them on best practices. Selecting the right patients for induction is the key to overall quality of the experience and outcomes Data

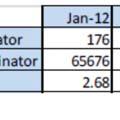
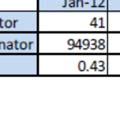
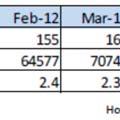
5 DRMC Admit to AROM All Inductions < 3 Hours Sept. Oct Nov. Dec. Jan Feb. Mar Apr. 11 May. Jun Jul. 11 Aug. 11 Sept. Oct Nov. Dec. Jan Feb. Mar. Apr Average time in minutes for Admit to Pitocin Jan. 10 Feb. 10 Mar. 10 Jul. 10 Aug. 10 Sept. 10 Oct. 10 Nov. 10 Dec. 10 Jan. 11 Feb. 11 Mar. 11 Apr. 11 May.11 Jun. 11 Jul. 11 Aug. 11 Sept. 11 Oct. 11 Nov. 11 Dec. 11 Jan. 12 Feb. 12 Mar. 12 Apr. 12

6 Minutes from admission to pitocin administration Elective Inductions with Pitocin Minutes Alta View American Fork Bear River Valley Cassia Regional Delta Community Dixie Regional Fillmore Community Heber Valley Intermountain Medical Center LDS Logan Regional McKay-Dee Orem Community Park City Medical Center Riverton Sanpete Valley Sevier Valley Utah Valley Valley View System
7 Falls and immobility Innovation Profile: Reducing falls in the healthcare neighborhood Snapshot Summary: The Community Living Center (CLC) within the Cheyenne VA Medical Center re organized their unit into neighborhoods, grouping similar patients and keeping consistent staff in each area. As they began a focus on fall prevention, they took steps to involve staff in the prevention effort, accommodating schedules for regular meetings and taking an empowerment approach to staff education. The unit has developed an easy to understand signage system that has served to involve multiple disciplines in fall prevention as well. Hospital Background: Long term care unit within a VA Medical Center Date first Implemented: 2009 Background The Community Living Center (CLC) of the Cheyenne VA Medical Center is an extended care unit of 50 beds, housing patients with both long term issues (e.g. cognitive decline) and short term (orthopedic) transitions. What They Did Project Origins Each year the unit has a special focus area for quality improvement. Falls reduction was this topic in 2004, amid changes in nursing leadership and movement of the facility to a more home like environment. The unit began by tracking of fall prevention issues that are not typically documented in the medical record staffing levels, patient education, communication and so on. After revisions and additions, the Info Pad tracking system now covers 90 different factors for every fall. A goal was set to have fewer than 4 falls per 1000 patient days. The Intervention The Hospital Neighborhood: The CLC decided to form their unit into three physically distinct neighborhoods of about 8 rooms (16 patients) each. The goal was to group similar patients together and to have consistent staff at each neighborhood, enhancing communication and teamwork. One neighborhood has orthopedic patients, another has longer term patients and the last encompasses hospice and dementia patients. Weekly meetings: Each week a team comprised of the unit manager, pharmacy, nurse practitioner, physical therapy, occupational therapy and the patient safety officer reviewed any falls from the previous week. They looked at common risk factors and began noticing a consistent pattern of inadequate communication across shifts and across levels of staff. In December 2011 a key change was made to include more staff in the fall review meeting by hanging the meeting time to accommodate staff needs. Participation positively rose from 4 to 8 staff per week. Data tracking: The CLC tracked all falls and falls with injury. Data were aggregated on a quarterly basis and reported across the unit by neighborhood. The data was aggregated annually and analyzed by the top 10 risk factors over the year. Specific Issues: A few years ago patients undergoing alcohol detox were experiencing falls in their first 2 days on the unit. All are now designated as a high fall risk, with bed and chair alarms and accompanying staff education specific to this high risk group.
8 Fall risk classification: Cheyenne believes that patients in nursing home environment are at high risk to fall. They began basing their signage on the transfer level (e.g., standby assist, 2 person assist, etc.). This type of signage has proved more effective at engaging all levels and types of staff. For example, a social worker who sees a 2 person assist patient getting out of bed by themselves can easily see it is time to call for assistance. The signage also informs physicians who come to the unit infrequently. Teamwork: The falls review process has given staff respect and underscored their important role. You re not just an aide, you re a part of the team and everyone has a key role to play. When staff come to team meetings they are not told what to do, they are given expectations and allowed to find a way to meet those, with freedom, respect, and accountability. As the unit experiences turnover and new staff arrive, the more experienced staff are asked to become trainers in fall prevention. Staff Education: Staff education was focused on empowerment. During initial review meetings, staffs were asked what interventions they might have tried with a patient at risk to fall, and they would usually say, more patient education. Now staff come with many more interventions already implemented a change in the transfer level, floor mats, sensor pads or posy alarms. They ve done most of the work already and individualized it to the patient, so there are fewer and fewer recommendations from the group. Everyone was encouraged to find the least restrictive ways to keep the patient safe. Patient education: Patient education was not stressed as heavily as staff education, because of the many inherent learning limitations, including poor hearing, poor eyesight, and cognitive decline. Family education was found to be more effective. Future Directions Proactive planning: In recent months there have been many weeks with no falls, so staff has become more proactive in their planning. For example, when they learned that a serious stroke patient was about to be placed on the unit, they held a meeting to brainstorm and discuss fall precautions helmet, sensor pads, and so on even before the patient arrived. Did it Work? The CLC has experienced a decline in the number of falls within their extended care unit through 2012.
9 Cheyenne VA Medical Center CLC Extended Care Unit Number of Falls Jan Feb Mar Apr May Jun Factors Important to Success Staff involvement: Moving to neighborhood teams provided the opportunity to revise weekly fall team meetings to include all neighborhood staff in fall prevention. Staff education: Weekly meetings focused on problem solving and staff accountability for individualized patient fall prevention plans. Informative signage: Fall risks identified by patients needed level of assistance served to involve other disciplines as well as outside physicians.
10 Readmissions Innovation Profile: Reducing readmissions using Project BOOST Snapshot Summary: Southwest Vermont Medical Center (SVMC) was part of the initial Society of Hospital Medicine s Project BOOST Better Outcomes for Older adults through Safe Transitions. SVMC embraced the BOOST objectives: Identify high risk patients on admission and target risk specific interventions Reduce 30 day readmission rates for general medicine patients Reduce length of stay Improve facility patient satisfaction and H CAHPS scores Improve information flow between inpatient and outpatient providers SVMC implemented a multi disciplinary set of activities from their hospital and then expanded to involve many community partners home health, assisted living/long term care, primary care, and senior housing. From a baseline rate of roughly 14% in early 2010 SVMC s 30 day all payer readmission rates are now approaching the BOOST goal of 8% and SVMC s stretch goal of 6%. Hospital Background: Not for Profit Community Hospital Licensed for 99 beds, daily occupancy patients Hospital inpatients are 60% Medicare Hospitalist discharge 85% of patients, co manage 30% of surgical population Date first Implemented: 2009 What They Did Project Origins: Reduction in 30 day readmissions is one of SVMCs strategic goals. Readmission rate was part of incentive compensation for executive and management staff Project Team: Team Leader: Jennifer Fels, RN,MS Director Health Resource Management, Social Work, Clinical Documentation Improvement. Project team: Hospital Pharmacy, Nursing, Physical Therapy, Information Technology, Physician, Medical Home, Case Management, Social Work o The project team has evolved to include other community partners: VNAs, Nursing Homes, Assisted Living Facilities and Senior Housing Care Coordinators Project Aim: Reduce 30 day readmissions from 12% to 8% with a stretch goal of 6%. Readmissions Data Analysis: In 2010 All SVMC readmissions were analyzed with the help of the Vermont Program for Health Care Quality (VPQHC). The major findings of the population with a 30 day readmission included: 66% of SVMC 30 day readmissions were over 65 years of age Readmissions occurred more frequently on Fridays The most frequent readmission diagnoses were Heart failure (10.2%), Pneumonia (13.1%) and COPD (9.9%) The average number of days to readmission was 12 days for males and 12.6 days for females
11 66% of readmissions had services in place, 31% were from a nursing facility and 31% had home health services 62% of patients readmitted from a nursing facility were from Centers for Living and Rehabilitation (CL&R) 37% of patients readmitted with home health services were from VNA& Hospice There was variation among primary care practices in the number of patients with a 30 day readmission Process Analysis and Potential Failure Modes Staff do not know when a patient leaves one setting and goes to the next Not enough information is provided when a patient transfers from one place to another Medication lists are not consistent across care settings Patients need greater access to primary care on demand (Weekends/evenings) Covering physicians do not know the patients Things go better when there is a hospital or medical home case manager involved in care management and coordination Electronic records do not connect across various care settings (example: nursing home, hospital, home health, physician offices Project BOOST BOOST provided a mentor to work with them and share lessons from other organizations that were doing this work. The mentor helped to keep on them target to implement best practices, functioning as a coach and cheerleader BOOST had tools for the discharge packet, teach back and follow up processes. We adapted the tools to fit our culture It also had list serves where other hospitals shared their experiences Participation in BOOST gave us more credibility with physicians it was one of their organizations that was sponsoring this. A few physicians trialed the BOOST approach then others wanted to do it. Project Organization The workgroup started in the hospital but expanded to include many community partners primary care medical homes, nursing homes, home health, hospice They tried to capturing all of the groups involved in transitions onto the work team; conducting interviews with other disciplines to find out what they needed from each other. They learned a lot about what is needed within each setting of care. The group took part in an IHI Expedition, and it was very collegial even though there were potential competitors involved. It was very patient centered, not going into referral patterns and business issues just looking at why patients were returning to the hospital Interventions: Development and implementation of a standard discharge packet; Patient education about their hospitalization using the teach back technique; Medication reconciliation on discharge; A follow up primary care visit within 72 hours after discharge is scheduled for the patient by SVMC staff prior to discharge A follow up phone call occurring the next business day after discharge Standardized handoffs to case managers in Medical Home Practices o There is a call from the SVMC case manager to the medical home case manager, to pull the patient back into the medical home (rather than push them out the door and to the next setting) Pharmacy consult on high risk medications warfarin, lovenox, narcotics, new insulin starts Some key specifics:



 Administration turnover Financial turn around Distractions CMS Focus on readmissions by disease Things to do differently: Use more")
12 One nursing home hired a nurse practitioner who made a difference, just being able to respond to patients when their condition changed. Throughout this facility staff began more attuned to doing good patient assessments and identifying troubling symptoms, and providing good communication in SBAR format. Hospital admissions have gone from 14 per month to 1 /month. Some sites developed protocols for management of chronic diseases. Others improved teamwork and took on the attitude that they could manage things more proactively and not just send someone to the ED Case managers in the medical home setting cite medication reconciliation as key. Old prescriptions need to be discontinued even when they are on a recurring mail ordeby facility/organization, to provide feedback, diagnose issues, system with the pharmacy Jennifer provides analyses of readmissions and motivate sitess to become best performers. Barriers: Competing priorities (CPOE) Administration turnover Financial turn around Distractions CMS Focus on readmissions by disease Things to do differently: Use more process measures earlier Earlier engagement of partners across the continuum More knowledge of reliability science Did it Work? SVMC s 30 day all payer readmission rates are approaching the BOOST goal of 8% and SVMC s stretch goal of 6% Factors Important to Success
13 Getting the entire continuum of care committed to improving transitions of care. You can do your work in the hospital but you have to engage the community. Focusing on the patient not the disease Instilling the belief that responsibility for the patient does not disappear when the patient disappears Securing executive support. Readmission reduction was a strategic goal for management. Future Work Continue work of the Improving Transitions of Care team, with specific roles and tasks for: o Primary Care o Assisted Living/LTC/Subacute Care o Home Health o Acute Care (SW Vermont) o Senior Housing Conduct another regression analysis for predictive modeling of readmissions Completion orientation of an RN Case Manager to be assigned to the ED for the hours of 12 noon 8:00 pm Implement physician dashboard incorporating 30 day readmissions, ED use and hospital admissions for one target medical group Implement the SVMC discharge Patient Passport A study is being completed on the Impact of Cardiac Rehabilitation on the Prevention on Heart Failure Readmissions. IRB approval is being obtained. Target start date July Explore collaboration with Southern Vermont College who has begun a health coach degree program. Development of an inpatient rounding process with a focus on safe transition/s
14 Pressure injuries Innovation Profile: Reducing Hospital acquired Pressure Ulcers The Power of Persistence Snapshot Summary Providence Medford Medical Center (PMMC) successfully reduced pressure ulcer prevalence after several years struggling to get attention from leadership for prevalence surveys and for nurse staff training. Taking advantage of helpful consultation from a sister Providence hospital, PMMC was able to train an RN team to assist wound ostomy care nurses in conducting the surveys. With more adequate staffing, the surveyors were able to spend time during the survey debriefing and training staff nurses on wound care. With persistence, nurse attendance at training for pressure ulcer prevention increased and the prevention effort spread throughout the hospital. The pressure ulcer champion created training notebooks for every unit, personally conducted teaching/rounding in the ICU, and promoted the use of specialized sacral dressings. Over time, pressure ulcer prevalence has declined. Hospital Background Not For Profit Mixed Payer Hospital Date First Implemented 2008 What They Did Early Concerns In 2008 hospital leadership at Providence Medford Medical Center (PMMC) became concerned about pressure ulcers, not only overall prevalence but also the ability to accurately measure hospital acquired ulcers. New reimbursement policies from CMS focused attention on the issue. Wound Care Leadership Jeanette Henault, a former rehab nurse with training in wound care (and experience working with patients on longer stays) became the unofficial champion for reducing pressure ulcers in the hospital. She began her campaign to get assistance doing quarterly NDNQI prevalence surveys and to train nurses in the essentials of pressure ulcer prevention. Conducting the Prevalence Survey Initially the NDNQI prevalence survey had to be conducted by the wound care nurse alone. To conduct the survey on the hospital s patients consumed 40 of the 56 hours allocated biweekly for wound care, leaving little time for teaching and training. Moreover, with this time pressure there was no time to debrief or train. As high pressure ulcer rates continued into the wound care nurse brought in a nurse manager from a large tertiary hospital in the Providence System, who had been overseeing pressure ulcer prevention and achieved success in reducing pressure ulcer prevalence.
15 The manager showed her how to add staff RNs to the prevalence survey team and maintain high inter rater reliability. The wound care nurse then took the NDNQI online 2 hour training, which enabled her to train other staff nurses to augment her prevalence survey team. With her persistence and the help of her sister hospital, administrators finally became convinced that the survey could not be supported only by the budget of the wound/ostomy department and that wider RN support was needed. The wound care nurse now conducts the quarterly prevalence survey with her team, and she has someone from every unit participate. The hospital is in the middle of a major remodel but they still do their best to see every patient. With refusals their rate is around 85% of patients participating. Now when the team sees a pressure ulcer during the survey, the reviewer gives the nurse a note with tips on how this patient s care might be improved (e.g., creams, heels floated, bed surface). The team also talks to staff about the importance of documentation. In the months with no prevalence survey, the wound care nurse rounds in the ICU. She goes over the Braden risk scores as well as other risk factors. She asks, What are you doing for prevention? She sometimes finds that nurses are not checking the skin, or not re checking back on the same patient. She coaches, I would consider doing. Nurses are receptive to this approach and now some stop to ask her for advice. Her message: Pressure ulcer prevention has to be part of your thinking. In Service Training The initial plan was to train 3 4 nurses each unit in 4 hour class. However there were many no shows, mostly for scheduling reasons. The scheduling was done by nurses themselves without involving their managers. If nurses didn t mark the time off their schedule their manager would schedule them for work. Others deemed it optional so they just didn t show. The wound care nurse persisted with nursing leadership that the training was NOT voluntary but required. She threatened to write nurses up as no shows if they didn t attend the training. And she refused to accept nurses who were sleep deprived after 12 hour shift. This process took 2 years to get through. Because of attrition, the wound care nurse needs to periodically train 4 5 new people each year when people leave or change units. She provides reminders to nurses and managers to attend in services. She encourages them You are making a difference! She also stresses the importance of knowing your patient and recommends to nurses that they try to get assigned to the same patient every day. She believes this continuity promotes better skin care. Specific Interventions The wound care nurse took the time to track pressure ulcer stage and body location. She found a number of ulcers related to tubing around the ear, due in part to the position of the oxygen supply in the room. She took this information to respiratory therapy, and they came up with an algorithm for when to use ear protectors. Now during the prevalence surveys team member carry these ear protectors in their pocket and hand them out wherever they are appropriate. An in service for sacral dressings was also helpful. She started using the sacral dressings for HAPU prevention in the ICU and they are still in use. They can be moved to check the skin, and some patients go to the nursing floor with them. The in service on these dressings also covered many of the comorbidities associated with skin breakdown vasopressors, cardiac arrest, shock, poor capillary refill that Jeanette can emphasize in her teaching.
16 The wound care nurse has scheduled useful vendor presentations for dressings, mattresses and beds. She made wound/ostomy training resources available in notebooks for each floor. At first they weren t used but now nurses bring them to training, maintaining and adding to them. On bigger units she has 2 nurses, on smaller she has 1. The Medical Center had one significant pressure ulcer sentinel event that raised awareness for all staff. The patient had a bad outcome for multiple reasons, but it was also clear that pressure ulcer care could have been better. This gave added impetus to the prevention effort. Did it Work? Results: The prevalence of hospital acquired pressure ulcers have declined over the past 2 years, as shown in the accompanying chart. There have been no Stage 2 or greater pressure ulcers in % of all patients Factors Important to Success 30% 20% 10.0% 10% 0% % of Inpatients with Hospital Acquired Ulcers 3.0% 14.9% 9.8% 6.9% 2008Q1 2008Q2 2008Q3 2008Q4 2009Q1 3.3% 3.4% 4.6% For PMMC 11.1% 20.0% 14.1% 14.8% 2009Q2 2009Q3 2009Q4 2010Q1 2010Q2 2010Q3 All Stages Stage 2 or Greater Stage 1 Only 2010Q4 2011Q1 2011Q2 2011Q3 2011Q4 2012Q1 2012Q2 2012Q3 Patience and persistence in getting hospital administration to support the quarterly prevalence surveys Making training on pressure ulcer prevention mandatory for all nurses Teaching and coaching during the prevalence survey Specific equipment for pressure ulcer prevention: ear protectors, sacral dressings, mattresses 5.6% 9.1% 3.8% 0.0% 0.0% 2.9% 0.0%
17 Venous thromboembolism Innovation Profile: Reducing VTE at Denver Health Snapshot Summary Denver Health Medical Center implemented changes in colorectal surgery after seeing the rate of surgical site infections peak at about 30% in By applying best practices in pre operative preparation of patients, issuing guidelines for surgeons in the operating room and providing monthly data showing progress, DHMC has been able to reduce the SSI rate to just under 5% (Q2 2012). Hospital Background Not For Profit Mixed Payer Magnet Hospital Date First Implemented 2008 What They Did Origins VTE is a major cause of morbidity and mortality 200,000 Deaths / Yr 10 40% Med/Surg Inpatients Suffer VTE VTE prophylaxis relates to Joint Commission National Patient Safety Goals on anticoagulation CMS incorporated VTE prophylaxis into SCIP, included it as part of reimbursement bundle Significant resources allocated to VTE prophylaxis Low molecular weight heparin (LMWH) was most costly line item in pharmacy budget Sequential compression devices (SCDs) cost $100,000/yr Existing clinical care standard was outdated, nonfunctional Ranked 74 th of 74 UHC hospitals in incidence of postoperative VTE Description of the Intervention Project Aim: Forming a team: Developed Goals and Strategies: o Standardize and implement risk assessment and evidence based VTE prophylaxis hospital wide o 100% Compliance o Cost savings o Lower incidence of VTE Methodology: Using Lean Methodology (Toyota Production System) Eliminate waste, improve flow to maximize value o Value Stream Analysis (VSA) o Sequence of process steps o Value assessment o Identify Ideal State
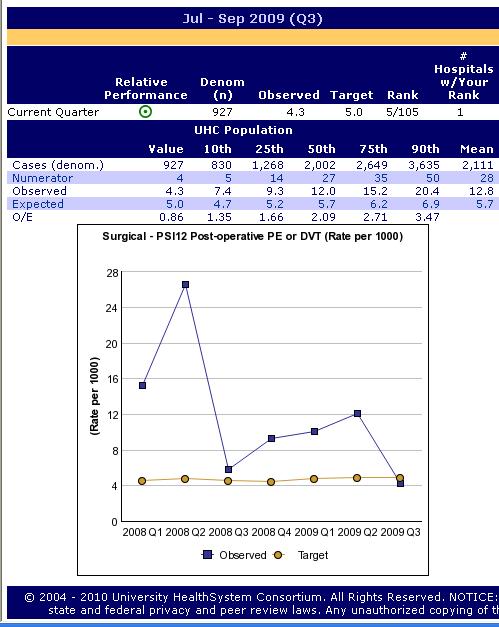
18 o o o o Gap analysis Identify achievable Future State Rapid Improvement Event (RIE) Identify multidisciplinary project team Deliverables: o Standardized risk assessment tool o ACCP Guidelines o Evidence based prophylaxis guidelines (ACCP) o CPOE order set for risk assessment and prophylaxis o Education plan o Monitoring plan Factors Important to Success Lessons Learned: Lean methodology is applicable to clinical processes Lean can cut a 6 9 month process down to weeks A Just Do It meeting 30+ days before event is helpful to identify pre work (e.g., baseline data collection, metrics) There is money to be saved by improving efficiency in the delivery of care Engaging a multidisciplinary team is critical to facilitate buy in Clinical processes should be made a part of standard work In a teaching hospital, continued education, monitoring, and feedback are essential to sustaining outcomes Challenges Sustaining This Innovatio Did it Work? Results and Run charts Outcomes: o Compliance Pharmacist s interventions improved compliance with guideline for use of LMWH to nearly 100% o Cost Savings The use of LMWH and SCDs have decreased, while use of unfractionated heparin (UFH) has increased: o Cost Savings Cumulative prophylaxis cost savings continue to rise: o VTE Incidence In the 27 months following the RIE, there has been a decrease in VTE events: o 5 th Out of 105 UHC Hospitals; O/E=0.86
19
20 Agency for Health Care Research and Quality (AHRQ) Patient Safety Indicator: Monthly Postoperative Pulmonary Embolism or Deep Vein Thrombosis (PE/DVT) Rate PE / DVT Rate per 1,000 Adult Surgical Discharges DVT/PE Rate Target Linear (DVT/PE Rate) Rapid Improvement Event occurred to change hospital DVT/PE prophylaxis practice. Jan 08 Feb 08 Mar 08 Apr 08 May 08 Jun 08 Jul 08 Aug 08 Sep 08 Oct 08 Nov 08 Dec 08 Jan 09 Feb 09 Mar 09 Apr 09 May 09 Jun 09 Jul 09 Aug 09 Sep 09 Oct 09 Nov 09 Dec 09 Jan 10 Feb 10 Mar 10 Apr 10 May 10 Jun 10 Jul 10 Aug 10 Sep 10 Discharge Month 4
21 Surgical site infections Innovation Profile: A reduction in surgical site infection rates after colorectal surgery Snapshot Summary The Providence St. Vincent Medical Center (PSVMC) implemented changes in colorectal surgery after seeing the rate of surgical site infections peak at about 24% in By applying best practices in preoperative preparation of patients, issuing guidelines for surgeons in the operating room and providing monthly data showing progress, PSVMC has been able to reduce the SSI rate to just under 5% (Q2 2012). Hospital Background Not For Profit Mixed Payer Magnet Hospital Date First Implemented 2008 What They Did Origins After joining NSQIP in 2007, PSVMC saw undeniable evidence of a peak in surgical site infections (SSI) in colorectal surgery and decided that it was time to make a change in surgical care. Description of the Intervention Project Aim: Lower infection rate in colorectal surgery to national average of 12%. Forming a team: The Chief of Surgery, Infection Preventionists, General Surgeons, members of the OR team, floor nurses, and pre surgical clinic staff were all involved in the effort to reduce surgical site infections. Developed Goals and Strategies: The team developed their own triple aim: involve direct care providers in improvement, apply best practices and give timely feedback. o The team used guidelines from the CDC and applied best practices in pre operative preparation of patients. They also looked anecdotially at surgeons who already had low rates of infections and added changing gloves after completing the bowel anastomosis to their guidelines. Provided Data: The team saturated surgeons with data and information to entice them to join the effort. o The team posted aggregate data above the scrub sinks as well as provided surgeons with individualized data. Seeing the data and outcomes pulled non participating surgeons into the projects they wanted to see how they compared. The data showed rates of both adopters and non adopters, there seemed to be a difference which made non adopters want to join up. o Individual data was sent to surgeons via inter office mail. The report was a color coded dashboard which made it easy for physicians to evaluate their own progress. Measurement: Process measure of following the steps of the bundle, in addition to the outcome measure of infection rate. What happens when there is an infection? When an infection occurred, physicians were able to see if the steps of the dashboard got followed. If an anastomotic leak occurs, it is discussed at a M&M conference.
22 Factors Important to Success Key elements of success: Leadership influence Respected chief of surgery who was heavily involved in getting surgeons on board. Buy in from all parties. Showing physicians data proved that there was a REAL issue. A continual data stream, an awareness of what s happening, keeping the issue on their radar screens and a trust of the data keeps surgeons engaged, keeping rates low. Challenges Encouraging late adopters, but receiving individualized data was a big draw. Getting surgeons to change skin prep solution had them work with IPs to show data/recent studies and saw how others were doing. Sustaining This Innovation Adopted changes into practice Got surgeon preference cards changed, became automatic Quarterly data kept in front of them to keep it going Did it Work? Results and Run charts PSVMC was able to reduce the rate of surgical site infections from a peak of about 24% in 2008 to just under 5% (Q2 2012).














23
24 Ventilator associated pneumonia Innovation Profile: A collaborative effort to reduce ventilator acquired pneumonia in the NICU. Snapshot Summary The Utah Valley Regional Medical Center, in Orem Utah, implemented a collaborative intervention aimed at reducing the incidence of Ventilator Acquired Pneumonia in the Newborn Intensive Care Unit. This began 12 years ago with an initiative to identify patients who were likely to need intubation, and then introducing nasal CPAP. This reduced the number of Ventilator Days (VD) by well over 70%. From this initiative was born a desire to address the problem of Ventilator Acquired Pneumonia with a more complete bundle of interventions. Physicians, nurses and respiratory therapists worked together to define, test and approve a bundle of interventions that ultimately saved money and, more importantly, produced healthier babies. Hospital Background Mixed Payer Non Profit Hospital Date First Implemented 2007 What They Did Description of the Intervention The Utah Valley Medical Center Newborn ICU undertook the charge to reduce Ventilator Acquired Pneumonia (VAP) in their patients about 12 years ago, when they implemented a protocol to identify patients who might need intubation, and provide them with early nasal CPAP instead. This change in workflow was very successful, reducing patient ventilator days by over 70%. After that success, they determined that the next line of defense against VAP was to develop and implement a VAP bundle of interventions. Physicians, nurses, and respiratory therapists worked together to identify components of a bundle that ultimately decreased the incidence of VAP among their delicate NICU patients. Main components of the intervention were unit specific goals, workflow analysis and bundle implementation, data collection and analysis, and a system for physician case reviews. Developed Goals and Strategies: The intervention was initially hospital specific, and then implemented system wide as a monthly measure reviewed by Intermountain. A collaborative task force group was created which addressed the issues related to the consequences of ventilator acquired pneumonia in the NICU setting. This group then developed an improvement plan. o Task Force Group: A group of MDs, nurses, and respiratory therapists worked together in the planning, implementing, and monitoring aspects of the intervention. Training and Education: Implementing various types of education enabled greater change, as the following components were crucial to reducing rates and meeting goals: o Identifying Opportunities for Improvement: physicians recognized the need to improve the incidence and severity of VAP cases among their NICU patients. o A System of Physician Case Reviews: All NICU VAP cases are reviewed every month both locally at the individual hospital level and through the system wide committee. o Staff Trainings: All physicians, nurses and respiratory therapists who work in the NICU are trained on the VAP bundle and are tasked with full implementation of it on every ventilated patient.
25 o Patient/Family Education: The families of the patients on ventilators are often extremely involved in their care, and therefore their buy in in implementing the VAP bundle and their help in ensuring all details are checked off is critical to the success of this program. Data Analysis: Baseline data from the NICU were collected from the Intermountain Electronic Data Warehouse. o Management: The Intermountain Healthcare data system was instrumental in assuring successful management of the data from this initiative. This streamlined data collection process increased the analysis speed, thus furthering the reviewing process. o Analysis: Determining and presenting reliable data and case information was essential in proper reporting to nursing teams and physicians. Did it Work? VAPs Per 1,000 Vent Days Ventilator Associated Pneumonia Per 1,000 Ventilation Days Utah Valley Regional Medical Center NICU Checklist Implemented Factors Important to Success Key elements of the planning and development process including the following: Reporting Data: Progress was enabled by routinely reporting accurate data to the team of physicians, nurses, therapists and technicians, and to the local and system committees for review. o Monthly review of all VAP patients is done by both a local, hospital based committee and on a systemwide level. This ensures that problems are addressed early and appropriately. Communication: Regular dialogue between the physicians, nurses and therapists was an integral part of the success of developing and implementing a NICU VAP bundle. Interdisciplinary collaboration among staff was a focal point of success. Challenges Scheduling: because this was implemented as a change in normal standard of care, there are always difficulties in training and implementation at the beginning.
26 Resources Used and Skills Needed Staffing: physicians, nurses, technicians and respiratory therapists were all involved in the planning and implementation of the VAP bundle. Adopting Considerations Getting Started with This Innovation Coordinate QI champions and other hospital leaders Develop a efficient data analysis system Set well defined and obtainable goals Sustaining This Innovation Report and share data amongst care providers Train new staff on VAP bundle as orientation skill Continually engage numerous leaders from the physician, nursing, and data department
27 Central line associated blood stream infections Innovation Profile: Dartmouth Hitchcock CUSP: Stop BSI Initiative Snapshot Summary The ICU is a 26 bed medical and surgical unit with a long history of working together to understand and improve bedside practices to prevent central line associated blood stream infections. A multidisciplinary team continues to receive regular performance reports to sustain and improve the process. Hospital Background Dartmouth Hitchcock Medical Center (DHMC) is New Hampshire's only academic medical center. Internationally renowned, nationally ranked, and regionally respected, we integrate high quality patient care, advanced medical education, and translational research to provide a full spectrum of health care. Date First Implemented CLABSI workgroup 2001, CUSP Stop BSI 2009, HEN 2012 What They Did Origins Why CLABSI? o Over 250,000 cases of BSI in the US hospitals each year, with 18% of those cases resulting in death o CLABSIs account for over $3 billion in excess health care costs per year o CLABSIs are often preventable and we have the science and methods to prevent them Description of the Intervention CUSP: Stop BSI o A national collaborative designed to improve the culture of patient safety and specific clinical outcomes in the intensive care unit o The specific program components include: o Implementation of the comprehensive based unit specific safety program (CUSP) and activities to measure o Eliminate central line associated blood stream infections (CLABSI) The team: o ICU nursing and physician leaders, ICU staff nurses, ICU staff physicians, pharmacists, nurse educators, measurement analyst. Goals o Decrease incidence of CLABSI to 1/1000 line days; o Increase hand hygiene compliance to 100%. o Scope: Begin in the Adult Critical Care inpatient population with expansion of relevant care processes to all areas that care for patients with central venous catheters Description of Interventions o CLABSI Bundle o Remove unnecessary lines
28 o o o o o o Hand Hygiene Maximal barrier precautions (mask, full drape, gown, gloves, and cap) Clean skin with chlorhexedine Avoid femoral line access Dressing Integrity Audits Compliance with best practice recommendations for insertion Factors Important to Success Lessons learned: Hand Hygiene, site selection and dressing change improvements were all significant in reducing infections Dialysis catheters are not antibiotic coated and remain high risk New scrub hubs will likely be a big help Challenges: Educating new nurses and house staff Hand hygiene for patients and family members Patient Acuity (immune compromised hem/onc patients) Proper line maintenance properly adhered dressing, signed and dated Sustaining This Innovation Training never stops new nurses, residents and fellows make it challenging to sustain Keep abreast of new technology/equipment Did it Work? Results 2005: 6 /1000 line days: 23 events 2006: 2.55/1000 line days: 16 events 2007: 2.05/1000 line days: 14 events 2008: 1.36/1000 line days: 9 events 2009: 1.92/1000 line days: 13 events 2010: 0.52/1000 line days: 4 events 2011: 0.92/1000 line days: 6 events 2012*:.71/1000 line days: 3 events *Qtr 1 to Qtr 3 only Savings Approximately $53,000 per infection prevented ICU Complete Central Line Bundles
29 Complete bundle: Hand hygiene performed Appropriate skin prep o Chlorhexidene gluconate (CHG) Skin prep agent has completely dried before insertion All 5 maximal sterile barriers used o Sterile gloves o Sterile gown o Cap o Mask worn o Large sterile drape % of bundles complete 100% 80% 60% 40% 20% 0% # lines placed Sep 11 Oct 11 No v 11 Dec 11 Jan 12 ICU # lines placed ICU % of bundles complete 81% 90% 90% 100% 100% 95% 94% 88% 87% 94% 98% 88% 94% Feb 12 Ma r 12 Apr 12 Ma y 12 Jun 12 Jul 12 Au g 12 Sep 12 Central Line related Bloodstream Infection Rates Oct 2001 Dec 2011
30 CRBSI /1000 Line Days 6 4 Central Line Carts 07/07 Sphinx* 12/07 Central Line Bundles 03/ *Sphinx is a clip on hand
31 Catheter associated urinary tract infections Innovation Profile: A collaborative intervention to reduce catheter acquired urinary tract infections. Snapshot Summary The Park City Medical Center, in Park City, Utah, implemented a collaborative intervention aimed at reducing the incidence of catheter acquired urinary tract infections (CAUTI). When Infection Control Practitioner Judy Rogers approached Esther Shepherd, Nurse Manager of the Medical/Surgical unit, about tracking foley catheters on her unit, Esther was more than happy to do her part to put an end to CAUTI. Together, they implemented a paper/pencil approach to tracking catheters which has resulted in no CAUTI on her unit since they began their project. Hospital Background Mixed Payer Non Profit Hospital Date First Implemented March 2011 What They Did Description of the Intervention The Park City Medical Center, in Park City, Utah, implemented a collaborative intervention aimed at reducing the incidence of catheter acquired urinary tract infections (CAUTI). When Infection Control Practitioner Judy Rogers approached Esther Shepherd, Nurse Manager of the Medical/Surgical unit, about tracking foley catheters on her unit, Esther was more than happy to do her part to put an end to CAUTI. Together, they implemented a simple paper/pencil approach to tracking catheters which has resulted in no CAUTI on her unit since they began their project. As part of her daily nurse manager rounding, Esther notes which patient has a catheter and when that catheter was inserted. If it has been more than 24 hours, Esther begins questioning why it hasn t been discontinued. Sometimes she can work with the nursing staff to get the catheter out, and sometimes it requires a call to the physician. Either way, Esther s goal is to have catheters out of her patients within 24 hour of insertion. Esther has worked out a process for checking into the status of patients even when she isn t in the hospital with the help of a health unit coordinator and her charge nurses. Bedside reporting is another way that foley catheters are observed often the nurses see them at shift change and check, once again, whether the catheter should still be in place. It s a team effort, but Esther and her nursing staff take CAUTI prevention very seriously, and it s evidenced in the results. There has been no CAUTI on her floor since this intervention was begun 18 months ago! Developed Goals and Strategies: The Infection Control Practitioner initially approached Esther, the Medical/Surgical nurse manager with the idea of tracking catheters to help prevent CAUTI. o Task Force Group Esther and Judy worked together to develop a very simple system of tracking foley catheter insertion times and initiating removal as appropriate. Once that system was working well, Esther worked with her HUC and charge nurses to develop a system of tracking, even when she is out of the hospital. Training and Education: Implementing various types of education enabled greater change, as the following components were crucial to reducing rates and meeting goals:
32 o o o Identifying Opportunities for Improvement: Infection Control first noted the opportunity for improvement, and approached the nurse manager to recruit her in working towards a lower incidence of CAUTI. Staff Trainings: nurses are trained to evaluate the necessity of catheters during their bedside rounds. Further, charge nurses are trained to act in the nurse manager s stead when she is not in the office, and be persistent in the removal of catheters that are no longer needed. Patient/Family Education: Patients and families are educated on the importance of appropriate removal of foley catheters in order to prevent CAUTI. Data Analysis: The data is recorded using a paper/pencil system, and is turned over to Infection Control monthly for analysis. Did it Work?
33 Factors Important to Success Key elements of the planning and development process including the following: Giving ownership of this process to the nurse manager, and allowing her to find a system that works well within her own workflow was critical to the sustainability of this intervention. Keeping the system simple and easy allows the tracking and evaluation of the catheters to be done on a daily basis. Having a system in place for the days when the nurse manager is out of the unit is also an important way to keep the tracking current and accurate. Challenges Scheduling: It was challenging for an already busy nurse manager to work this type of daily tracking into her schedule, but after a while, she was able to find a system that met her needs and the needs of the unit. Resources Used and Skills Needed Staffing: nurse manager, health unit coordinator, inflection control practitioner Adopting Considerations Getting Started with This Innovation Let person tracking find their own way of daily tracking that works with their schedule and working style Set well defined and obtainable goals Sustaining This Innovation Report and share data amongst care providers Make the tracking system easy and accessible.
34 FOR EACH OF THE 9 HACS and readmissions: A Summary of the interventions in the 9 HACs and readmissions is below. Following the interventions, we include run charts for each area. What to do for: Early Elective Delivery Patient Falls and Immobility Patient Readmissions Pressure Injuries Getting Started Working Harder Ahead of the Curve Identify administrative infrastructure for initiative including nursing and provider champions. Create improvement & education tools for all stakeholders including patients Implement standard Assessment tools, protocols and prevention strategies. Transitional care providers capable of performing inperson visits (e.g. home, SNF) to selected patients following hospital discharge. Identify areas needing most attention & appoint a leadership supported lead to drive improvement & education SWAT (or champion) teams that includes unit nurse/ Create a hard stop process to proactively address noncompliance by providers. Appoint leads to drive improvement & identify SWAT (or champion) teams that includes unit nurse Pharmacist-led medication management (reconciliation, regimen streamlining at discharge; post-discharge follow up regarding medication access and side effects Adopt decision algorithms for RNs to select appropriate surfaces make decisions independently of surface decisions. Create infrastructure tools for monitoring, reporting, & enforcement Implement decision algorithms and/or computerized decision support in the electronic medical record based on patient risk factors Robust readmission risk stratification tools. Establish monthly prevalence studies or incidence rates from electronic medical records then feed that data back to the SWAT teams. Adverse Drug Events Venous Thromboembolism Surgical Site Infections Ventilator Acquired Pneumonia Identify accountable teams to review all ADEs and work on performance improvement. Establish a functional, workflow friendly VTE ordering process at time of admission that complies with an institutionally agreed upon VTE prophylaxis program. CMS Core Measures: Follow SCIP guidelines for antibiotic administration, hair removal and temperature control. Track and internally report/ publicize, patient-level compliance with four VAP bundle elements in each ICU. Build in automated medication administration alerts and processes, i.e., bar coding. Develop feedback systems to ensure each patient has a VTE-P in place. Provide feedback on SCIP compliance and SSI incidence to surgeons, and encourage accountability. Integrate VAP prevention and surveillance measures as part of an ICU daily quality checklist. Automate ADE triggers and implement into pharmacy work flow with patient specific alerts. Develop a real-time VTE prophylaxis status monitoring system that allows prompt identification and correction of process gaps throughout the longitudinal course of the patient s hospital stay. Monitor antibiotic redosing in prolonged operations. Implement automated head-of-bed elevation monitors with electronic alarms to alert ICU providers/
35 What to do for: Central Line Associated Blood Stream Infections Getting Started Working Harder Ahead of the Curve Track institutional infection rates and implement the IHI central line bundle. Measure compliance with the IHI bundle and focus on catheter maintenance: Frequency and quality of dressing changes. Scrubbing the hub of access ports. Reducing access: Bundling blood draws. Appropriate IV to PO medication conversion. Catheter Acquired Urinary Tract Infections Adopt insertion and maintenance bundles. Inform all stakeholders of CAUTI definition and method used to identify. Provide monthly data to all nursing staff for CAUTI incidence. In room audits to check for maintenance compliance with just in time feedback. Track CAUTI and review where inserted-utilize practice review/update or simulation for higher rates. Nurse driven Foley catheter removal protocol. Drill down of each CAUTI for opportunity to improve. Share learning with practice council/standards team.










36 EED Run Charts













37














38 Falls & Immobility














39 Readmissions







40











41 Pressure Ulcers










42 ADE











43 VTE








44 VAP






45 CLABSI








46 CAUTI
OHA HEN 2.0 Partnership for Patients Letter of Commitment
 OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
OHA HEN 2.0 Partnership for Patients Letter of Commitment To: Re: Request to Participate in the Ohio Hospital Association Hospital Engagement Contract Date: September 24, 2015 We have reviewed the information
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
September 8, 20 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Average Daily Census (ADC)
Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health
 Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health M2 This presenter has nothing to disclose December 2012 Blue Ribbon I & II In
Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health M2 This presenter has nothing to disclose December 2012 Blue Ribbon I & II In
Medicare Value Based Purchasing August 14, 2012
 Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
CLABSI Prevention Hardwiring Improvement
 CLABSI Prevention Hardwiring Improvement Brian Koll MD, FACP, FIDSA Executive Director, Infection Prevention Mount Sinai Health System Professor of Medicine, Icahn School of Medicine September 29, 2014
CLABSI Prevention Hardwiring Improvement Brian Koll MD, FACP, FIDSA Executive Director, Infection Prevention Mount Sinai Health System Professor of Medicine, Icahn School of Medicine September 29, 2014
UI Health Hospital Dashboard September 7, 2017
 UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
SCORING METHODOLOGY APRIL 2014
 SCORING METHODOLOGY APRIL 2014 HOSPITAL SAFETY SCORE Contents What is the Hospital Safety Score?... 4 Who is The Leapfrog Group?... 4 Eligible and Excluded Hospitals... 4 Scoring Methodology... 5 Measures...
SCORING METHODOLOGY APRIL 2014 HOSPITAL SAFETY SCORE Contents What is the Hospital Safety Score?... 4 Who is The Leapfrog Group?... 4 Eligible and Excluded Hospitals... 4 Scoring Methodology... 5 Measures...
Managing Healthcare Payment Opportunity Fundamentals CENTER FOR INDUSTRY TRANSFORMATION
 Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
After reading this learning module, the nurse should be able to:
 After reading this learning module, the nurse should be able to: Identify the VTE dashboard and understand how to initiate it Identify the requirements of the VTE Core Measure and the nurse s responsibilities
After reading this learning module, the nurse should be able to: Identify the VTE dashboard and understand how to initiate it Identify the requirements of the VTE Core Measure and the nurse s responsibilities
Integrating Quality Into Your CDI Program: The Case for All-Payer Review
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Integrating Quality Into Your CDI Program: The Case for All-Payer Review Katy Good, RN, BSN, CCDS, CCS CDI Program Coordinator
7th Annual Association for Clinical Documentation Improvement Specialists Conference Integrating Quality Into Your CDI Program: The Case for All-Payer Review Katy Good, RN, BSN, CCDS, CCS CDI Program Coordinator
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
The dawn of hospital pay for quality has arrived. Hospitals have been reporting
 Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
Innovation. Successful Outpatient Management of Kidney Stone Disease. Provider HealthEast Care System
 Successful Outpatient Management of Kidney Stone Disease HealthEast Care System Many patients with kidney stones return to the ED multiple times due to recurrent symptoms. Patients then tend to receive
Successful Outpatient Management of Kidney Stone Disease HealthEast Care System Many patients with kidney stones return to the ED multiple times due to recurrent symptoms. Patients then tend to receive
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Preventing Health Care Associated Infections. PJ Brennan, MD Chief Medical Officer University of Pennsylvania Health System August 16, 2011.
 Preventing Health Care Associated Infections PJ Brennan, MD Chief Medical Officer University of Pennsylvania Health System August 16, 2011 Lind 2 Gaps in Knowldege? Pathogenesis Epidemiology Prevention
Preventing Health Care Associated Infections PJ Brennan, MD Chief Medical Officer University of Pennsylvania Health System August 16, 2011 Lind 2 Gaps in Knowldege? Pathogenesis Epidemiology Prevention
NoCVA SSI/VTE Safe Surgery Collaborative
 NoCVA SSI/VTE Safe Surgery Collaborative Orientation Webinar #3 Measures and Data Collection July 19, 2012 Presented by: Jan Mangun, MT(ASCP), MSA, CPHRM Executive Director, Quality and Patient Safety
NoCVA SSI/VTE Safe Surgery Collaborative Orientation Webinar #3 Measures and Data Collection July 19, 2012 Presented by: Jan Mangun, MT(ASCP), MSA, CPHRM Executive Director, Quality and Patient Safety
National Patient Safety Goals & Quality Measures CY 2017
 National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
Scoring Methodology FALL 2016
 Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
Improving Outcomes for High Risk and Critically Ill Patients
 Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Tell Your Story with a Well- Designed Data Plan. Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System
 Tell Your Story with a Well- Designed Data Plan Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System Purposes of Presentation Describe the elements of a well designed data plan Guidelines
Tell Your Story with a Well- Designed Data Plan Jackie McFarlin, RN, MPH,MSN, CIC VA North Texas Health Care System Purposes of Presentation Describe the elements of a well designed data plan Guidelines
University of Illinois Hospital and Clinics Dashboard May 2018
 May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
May 17, 2018 University of Illinois Hospital and Clinics Dashboard May 2018 Combined Discharges and Observation Cases for the nine months ending March 2018 are 1.6% below budget and 4.9% lower than last
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children
 Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
HOSPITAL ACQUIRED COMPLICATIONS. Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program
 HOSPITAL ACQUIRED COMPLICATIONS Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program HOSPITAL ACQUIRED COMPLICATIONS (HACS) A medical condition or complication that a patient develops during
HOSPITAL ACQUIRED COMPLICATIONS Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program HOSPITAL ACQUIRED COMPLICATIONS (HACS) A medical condition or complication that a patient develops during
Harm Across the Board Reporting: How your Hospital Can Get There
 Harm Across the Board Reporting: How your Hospital Can Get There Presentation to KHA Annual Quality Conference March 19, 2014 Jackie Conrad RN, BSN, MBA Improvement Advisor Cynosure Health Objectives Upon
Harm Across the Board Reporting: How your Hospital Can Get There Presentation to KHA Annual Quality Conference March 19, 2014 Jackie Conrad RN, BSN, MBA Improvement Advisor Cynosure Health Objectives Upon
Baptist Health System Jacksonville, FL
 Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Baptist Health System Jacksonville, FL Baptist Health System Community Leader in Healthcare Five (5) Hospital System Serving greater Jacksonville area and SE Georgia Children s Hospital Primary Care Facilities
Hospital Acquired Conditions. Tracy Blair MSN, RN
 Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
Using Care Bundles to Reduce Catheter Associated Blood Stream Infections in the NICU. Dr David Ng Paediatric Medical Officer Sarawak General Hospital
 Using Care Bundles to Reduce Catheter Associated Blood Stream Infections in the NICU Dr David Ng Paediatric Medical Officer Sarawak General Hospital Outline of Presentation Introduction Definition of CABSI
Using Care Bundles to Reduce Catheter Associated Blood Stream Infections in the NICU Dr David Ng Paediatric Medical Officer Sarawak General Hospital Outline of Presentation Introduction Definition of CABSI
Quality Improvement Plans (QIP): Progress Report for the 2016/17 QIP
: Progress Report for the 2016/17 QIP") Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Translating Evidence to Safer Care
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Greetings from Michelle & Katie QUALITY IMPROVEMENT DIVISION OF HOSPITAL MEDICINE
 IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
The Health Care Improvement Foundation 2015 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Magee Rehabilitation
 The Health Care Improvement Foundation 2015 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Magee Rehabilitation 2. Title Of Initiative Innovations to Stop Pressure Ulcers
The Health Care Improvement Foundation 2015 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Magee Rehabilitation 2. Title Of Initiative Innovations to Stop Pressure Ulcers
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Hospital Inpatient Quality Reporting (IQR) Program Measures (Calendar Year 2012 Discharges - Revised)
 Program Measures (Calendar Year 2012 Discharges - Revised)") The purpose of this document is to provide a reference guide on submission and Hospital details for Quality Improvement Organizations (QIOs) and hospitals for the Hospital Inpatient Quality Reporting (IQR)
The purpose of this document is to provide a reference guide on submission and Hospital details for Quality Improvement Organizations (QIOs) and hospitals for the Hospital Inpatient Quality Reporting (IQR)
CAMDEN CLARK MEDICAL CENTER:
 INSIGHT DRIVEN HEALTH CAMDEN CLARK MEDICAL CENTER: CARE MANAGEMENT TRANSFORMATION GENERATES SAVINGS AND ENHANCES CARE OVERVIEW Accenture helped Camden Clark Medical Center, (CCMC), a West Virginia-based
INSIGHT DRIVEN HEALTH CAMDEN CLARK MEDICAL CENTER: CARE MANAGEMENT TRANSFORMATION GENERATES SAVINGS AND ENHANCES CARE OVERVIEW Accenture helped Camden Clark Medical Center, (CCMC), a West Virginia-based
Kentucky Sepsis Summit. August 2016
 1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
1 Kentucky Sepsis Summit August 2016 St. Elizabeth Healthcare About Us: - 7 facilities & over 1200 licensed beds - Serving the NKY/Cincinnati Region in: - Orthopedic Care - Heart and Vascular Institute
Identify patients with Active Surveillance Cultures (ASC)
") MRSA CHANGE STRATEGIES The following tables include change strategies proven to be effective in healthcare settings. Implementing these changes through current or new processes may result in reducing healthcare
MRSA CHANGE STRATEGIES The following tables include change strategies proven to be effective in healthcare settings. Implementing these changes through current or new processes may result in reducing healthcare
Patient Experience of Care Survey Results Hospital Consumer Assessment of Healthcare Providers and Systems (Inpatient)
") Patient Experience of Care Survey Results Hospital Consumer Assessment of Healthcare Providers and Systems (Inpatient) HCAHPS QUESTION DESCRIPTION (April 2016 - March 2017) Patients who reported that their
Patient Experience of Care Survey Results Hospital Consumer Assessment of Healthcare Providers and Systems (Inpatient) HCAHPS QUESTION DESCRIPTION (April 2016 - March 2017) Patients who reported that their
Value-Based Purchasing & Payment Reform How Will It Affect You?
 Value-Based Purchasing & Payment Reform How Will It Affect You? HFAP Webinar September 21, 2012 Nell Buhlman, MBA VP, Product Strategy Click to view recording. Agenda Payment Reform Landscape Current &
Value-Based Purchasing & Payment Reform How Will It Affect You? HFAP Webinar September 21, 2012 Nell Buhlman, MBA VP, Product Strategy Click to view recording. Agenda Payment Reform Landscape Current &
Mohamad Fakih, MD, MPH
 Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
QUALIS HEALTH HONORS WASHINGTON HEALTHCARE PROVIDERS
 LEADERSHIP IN IMPROVING HEALTHCARE Harborview Medical Center Code Sepsis: Improving Survival in Sepsis with Early Identification and Activation of a Critical Care Team Sepsis, one of the highest causes
LEADERSHIP IN IMPROVING HEALTHCARE Harborview Medical Center Code Sepsis: Improving Survival in Sepsis with Early Identification and Activation of a Critical Care Team Sepsis, one of the highest causes
HIMSS Davies Award Enterprise Application. --- Cover Page --- IT Projects and Operations Consultant Submitter s Address: and whenever possible
 HIMSS Davies Award Enterprise Application --- Cover Page --- Name of Applicant Organization: Truman Medical Centers Organization s Address: 2301 Holmes Street, Kansas City, MO 64108 Submitter s Name: Angie
HIMSS Davies Award Enterprise Application --- Cover Page --- Name of Applicant Organization: Truman Medical Centers Organization s Address: 2301 Holmes Street, Kansas City, MO 64108 Submitter s Name: Angie
2018 Press Ganey Award Criteria
 2018 Press Ganey Award Criteria Guardian of Excellence Award SM This award honors clients who have reached the 95th percentile for patient experience, engagement or clinical quality performance. Guardian
2018 Press Ganey Award Criteria Guardian of Excellence Award SM This award honors clients who have reached the 95th percentile for patient experience, engagement or clinical quality performance. Guardian
Scoring Methodology FALL 2017
 Scoring Methodology FALL 2017 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician Order
Scoring Methodology FALL 2017 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician Order
Hospitals Face Challenges Implementing Evidence-Based Practices
 United States Government Accountability Office Report to Congressional Requesters February 2016 PATIENT SAFETY Hospitals Face Challenges Implementing Evidence-Based Practices GAO-16-308 February 2016 PATIENT
United States Government Accountability Office Report to Congressional Requesters February 2016 PATIENT SAFETY Hospitals Face Challenges Implementing Evidence-Based Practices GAO-16-308 February 2016 PATIENT
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
An academic medical center is practicing wasteology to pare time, expense,
 Quality improvement Practicing wasteology in the OR An academic medical center is practicing wasteology to pare time, expense, and hassle from its OR processes. Using lean thinking, the center is streamlining
Quality improvement Practicing wasteology in the OR An academic medical center is practicing wasteology to pare time, expense, and hassle from its OR processes. Using lean thinking, the center is streamlining
Improving Pain Center Processes utilizing a Lean Team Approach
 Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
Worth a Thousand Words: Telling a Story with Data
 A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
A5/B5 Worth a Thousand Words: Telling a Story with Data Ari Robicsek, MD Chief Medical Analytics Officer Providence St. Joseph Health Session Objectives Consider the challenges of representing patient
Catherine Porto, MPA, RHIA, CHP Executive Director HIM. Madelyn Horn Noble 3M HIM Data Analyst
 1 Catherine Porto, MPA, RHIA, CHP Executive Director HIM Madelyn Horn Noble 3M HIM Data Analyst University of New Mexico Hospitals» The state s only academic medical center» The primary teaching hospital
1 Catherine Porto, MPA, RHIA, CHP Executive Director HIM Madelyn Horn Noble 3M HIM Data Analyst University of New Mexico Hospitals» The state s only academic medical center» The primary teaching hospital
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Reducing Infections and Improving Engagement St. Luke's Nephrology Associates. Contact Information: Robert Gayner, M.D., FASN
 BEST PRACTICES Vascular Access and CLABSI Reduction Reducing Infections and Improving Engagement St. Luke's Nephrology Associates Contact Information: Robert Gayner, M.D., FASN St. Luke's Nephrology Associates
BEST PRACTICES Vascular Access and CLABSI Reduction Reducing Infections and Improving Engagement St. Luke's Nephrology Associates Contact Information: Robert Gayner, M.D., FASN St. Luke's Nephrology Associates
Improving HCAHPS with a Culture of Quiet St. Francis Hospital (Puget Sound)
") Improving HCAHPS with a Culture of Quiet St. Francis Hospital (Puget Sound) Problem: Surveys showed that the noise level made it difficult for patients to rest. Innovation: Implemented a culture of quiet.
Improving HCAHPS with a Culture of Quiet St. Francis Hospital (Puget Sound) Problem: Surveys showed that the noise level made it difficult for patients to rest. Innovation: Implemented a culture of quiet.
CMS-0044-P; Proposed Rule: Medicare and Medicaid Programs; Electronic Health Record Incentive Program Stage 2
 May 7, 2012 Submitted Electronically Ms. Marilyn Tavenner Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
May 7, 2012 Submitted Electronically Ms. Marilyn Tavenner Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
Mary Baum President & CEO BA&T September 18, 2015
 Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
Columbus Regional Hospital Pressure Ulcer Prevention
 Columbus Regional Hospital Pressure Ulcer Prevention Kathryn Jackson RN, MSN, CRRN Pressure Ulcer Prevention Columbus Regional Hospital, Columbus, IN Objectives & About Us Describe current pressure ulcer
Columbus Regional Hospital Pressure Ulcer Prevention Kathryn Jackson RN, MSN, CRRN Pressure Ulcer Prevention Columbus Regional Hospital, Columbus, IN Objectives & About Us Describe current pressure ulcer
FY 2014 Inpatient Prospective Payment System Proposed Rule
 FY 2014 Inpatient Prospective Payment System Proposed Rule Summary of Provisions Potentially Impacting EPs On April 26, 2013, the Centers for Medicare and Medicaid Services (CMS) released its Fiscal Year
FY 2014 Inpatient Prospective Payment System Proposed Rule Summary of Provisions Potentially Impacting EPs On April 26, 2013, the Centers for Medicare and Medicaid Services (CMS) released its Fiscal Year
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Tina Nelson, MBA, BSN Lisa Stepp, BSN, RN Rebecca Fyffe, BSN, RN Jessica Coughenour, LPN
 Establishing a Conservative Approach to the Prevention of Pressure Ulcers with the Utilization of Data Analytics to Monitor Effectiveness of Quality Efforts and Best Practice Models Tina Nelson, MBA, BSN
Establishing a Conservative Approach to the Prevention of Pressure Ulcers with the Utilization of Data Analytics to Monitor Effectiveness of Quality Efforts and Best Practice Models Tina Nelson, MBA, BSN
PERFORMANCE IMPROVEMENT REPORT
 PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Scoring Methodology SPRING 2018
 Scoring Methodology SPRING 2018 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 6 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician
Scoring Methodology SPRING 2018 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 6 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician
Objectives. Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004
 Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004 Session: C658 2013 ANCC National Magnet Conference Thursday, October 3, 2013
Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004 Session: C658 2013 ANCC National Magnet Conference Thursday, October 3, 2013
2014 Partnership in Prevention Award. November 21, :00-1:00PM EST. Introduction
 2014 Partnership in Prevention Award November 21, 2014 12:00-1:00PM EST Introduction Don Wright, MD, MPH Deputy Assistant Secretary for Health (Disease Prevention and Health Promotion) U.S. Department
2014 Partnership in Prevention Award November 21, 2014 12:00-1:00PM EST Introduction Don Wright, MD, MPH Deputy Assistant Secretary for Health (Disease Prevention and Health Promotion) U.S. Department
COPD & Pneumonia Readmission Reduction Program. October 25, 2017
 COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
Driving the value of health care through integration. Kaiser Permanente All Rights Reserved.
 Driving the value of health care through integration February 13, 2012 Kaiser Permanente 2010-2011. All Rights Reserved. 1 Today s agenda How Kaiser Permanente is transforming care How we re updating our
Driving the value of health care through integration February 13, 2012 Kaiser Permanente 2010-2011. All Rights Reserved. 1 Today s agenda How Kaiser Permanente is transforming care How we re updating our
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department
 Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
Benefits of Tele-ICU Management of ICU Boarders in the Emergency Department Session #309, February 22, 2017 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate
BUILDING THE PATIENT-CENTERED HOSPITAL HOME
 WHITE PAPER BUILDING THE PATIENT-CENTERED HOSPITAL HOME A New Model for Improving Hospital Care Authors Sonya Pease, MD Chief Medical Officer TeamHealth Anesthesia Kurt Ehlert, MD National Director, Orthopaedics
WHITE PAPER BUILDING THE PATIENT-CENTERED HOSPITAL HOME A New Model for Improving Hospital Care Authors Sonya Pease, MD Chief Medical Officer TeamHealth Anesthesia Kurt Ehlert, MD National Director, Orthopaedics
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Organization: Frederick Memorial Hospital. Solution Title: We Found the Missing Piece to Our CLABSI Puzzle
 Organization: Frederick Memorial Hospital Solution Title: We Found the Missing Piece to Our CLABSI Puzzle Program/Project Description: Hospitalized patients are at risk every day for contracting infections.
Organization: Frederick Memorial Hospital Solution Title: We Found the Missing Piece to Our CLABSI Puzzle Program/Project Description: Hospitalized patients are at risk every day for contracting infections.
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING
 JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
Imprinting Safety and Quality Practices on Residents and Fellows. John Szymusiak, MD Gregory M. Bump, MD
 Imprinting Safety and Quality Practices on Residents and Fellows John Szymusiak, MD Gregory M. Bump, MD Introductions 2 Gregory M. Bump, MD Associate Professor of General Internal Medicine UPMC Montefiore
Imprinting Safety and Quality Practices on Residents and Fellows John Szymusiak, MD Gregory M. Bump, MD Introductions 2 Gregory M. Bump, MD Associate Professor of General Internal Medicine UPMC Montefiore
Bold Goal PI Radar Dashboard
 Bold Goal PI Radar Dashboard Helen Macfie, Pharm.D., FABC Chief Transformation Officer Certified Lean Leader For IHI Patient Safety Executive Development Course, September, 2016 This presenter has nothing
Bold Goal PI Radar Dashboard Helen Macfie, Pharm.D., FABC Chief Transformation Officer Certified Lean Leader For IHI Patient Safety Executive Development Course, September, 2016 This presenter has nothing
Physician Performance Analytics: A Key to Cost Savings
 Physician Performance Analytics: A Key to Cost Savings Session #90, February 21, 2017 Jim Gera, SVP of Business Development, Signature Medical Group, Inc. 1 Speaker Introduction Jim Gera, MBA SVP of Business
Physician Performance Analytics: A Key to Cost Savings Session #90, February 21, 2017 Jim Gera, SVP of Business Development, Signature Medical Group, Inc. 1 Speaker Introduction Jim Gera, MBA SVP of Business
Strategies to Address All Types of Harm. Objectives. Share implementation process for a successful large scale harm reduction campaign
 C20 These presenters have nothing to disclose Strategies to Address All Types of Harm Jack Jordan, Partnership for Patients, CMMI William Conway, MD Henry Ford Health System Sam Watson, Michigan Hospital
C20 These presenters have nothing to disclose Strategies to Address All Types of Harm Jack Jordan, Partnership for Patients, CMMI William Conway, MD Henry Ford Health System Sam Watson, Michigan Hospital
Maryland Patient Safety Center s Call for Solutions Submission. Organization: Atlantic General Hospital
 Maryland Patient Safety Center s Call for Solutions Submission Organization: Atlantic General Hospital Solution Title: Using the Evolution of Data Collection Methods 2 Drive Revolution in the Reduction
Maryland Patient Safety Center s Call for Solutions Submission Organization: Atlantic General Hospital Solution Title: Using the Evolution of Data Collection Methods 2 Drive Revolution in the Reduction
EHR Enablement for Data Capture
 EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
2015 Executive Overview
 An Independent Licensee of the Blue Cross and Blue Shield Association 2015 Executive Overview Criteria for the Blue Cross and Blue Shield of Alabama Hospital Tiered Network will be updated effective January
An Independent Licensee of the Blue Cross and Blue Shield Association 2015 Executive Overview Criteria for the Blue Cross and Blue Shield of Alabama Hospital Tiered Network will be updated effective January
The Leapfrog Hospital Survey Scoring Algorithms. Scoring Details for Sections 2 9 of the 2017 Leapfrog Hospital Survey
 The Leapfrog Hospital Survey Scoring Algorithms Scoring Details for Sections 2 9 of the 2017 Leapfrog Hospital Survey 2017 Leapfrog Hospital Survey Scoring Algorithms Table of Contents 2017 Leapfrog Hospital
The Leapfrog Hospital Survey Scoring Algorithms Scoring Details for Sections 2 9 of the 2017 Leapfrog Hospital Survey 2017 Leapfrog Hospital Survey Scoring Algorithms Table of Contents 2017 Leapfrog Hospital
Key Steps in Creating & Sustaining Excellence
 Key Steps in Creating & Sustaining Excellence 1. Create a context for excellence 2. Enroll others (starting with leaders) in the vision for excellence 3. Create alignment, ownership and transparency to
Key Steps in Creating & Sustaining Excellence 1. Create a context for excellence 2. Enroll others (starting with leaders) in the vision for excellence 3. Create alignment, ownership and transparency to
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Cleveland Clinic Implementing Value-Based Care
 Cleveland Clinic Implementing Value-Based Care Overview Cleveland Clinic health system uses a systematic approach to performance improvement while simultaneously pursuing 3 goals: improving the patient
Cleveland Clinic Implementing Value-Based Care Overview Cleveland Clinic health system uses a systematic approach to performance improvement while simultaneously pursuing 3 goals: improving the patient
Ann Klein, Wound Care Specialist Brenda Mundy, Manager, Skin and Wound Program. Innovative Strategies lead to a Reduction in Pressure Ulcer Incidence
 Ann Klein, Wound Care Specialist Brenda Mundy, Manager, Skin and Wound Program Innovative Strategies lead to a Reduction in Pressure Ulcer Incidence Background Outline Innovative strategies to develop
Ann Klein, Wound Care Specialist Brenda Mundy, Manager, Skin and Wound Program Innovative Strategies lead to a Reduction in Pressure Ulcer Incidence Background Outline Innovative strategies to develop
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Quality Care Amongst Clinical Commotion: Daily Challenges in the Care Environment
 Quality Care Amongst Clinical Commotion: Daily Challenges in the Care Environment presented by Sherry Kwater, MSM,BSN,RN Chief Nursing Officer Penn State Hershey Medical Center Objectives 1. Understand
Quality Care Amongst Clinical Commotion: Daily Challenges in the Care Environment presented by Sherry Kwater, MSM,BSN,RN Chief Nursing Officer Penn State Hershey Medical Center Objectives 1. Understand
Greetings from Michelle & Katie QUALITY IMPROVEMENT DIVISION OF HOSPITAL MEDICINE
 IN THIS ISSUE: Make Sure You Are Solving the Right Problem P. 1 Are Electronic Health Records Contributing to Fraud? P. 1 Stress Ulcer Prophylaxis P. 2 Antibiotic Stewardship P. 3 APeX tips for a safe
IN THIS ISSUE: Make Sure You Are Solving the Right Problem P. 1 Are Electronic Health Records Contributing to Fraud? P. 1 Stress Ulcer Prophylaxis P. 2 Antibiotic Stewardship P. 3 APeX tips for a safe
Reducing Readmissions: Potential Measurements
 Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Reducing Readmissions: Potential Measurements Avoid Readmissions Through Collaboration October 27, 2010 Denise Remus, PhD, RN Chief Quality Officer BayCare Health System Overview Why Focus on Readmissions?
Fee: The fee for the 12-month renewal is $10,000.
 CHILDHOOD CANCER AND BLOOD DISORDERS NETWORK 2017 RENEWAL TOOLS HOW TO Renew To renew, simply submit a completed Childhood Cancer & Blood Disorders Network Renewal Form to Gena Paulk via email at gena.paulk@childrenshospitals.org.
CHILDHOOD CANCER AND BLOOD DISORDERS NETWORK 2017 RENEWAL TOOLS HOW TO Renew To renew, simply submit a completed Childhood Cancer & Blood Disorders Network Renewal Form to Gena Paulk via email at gena.paulk@childrenshospitals.org.
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Patient Experience Heart & Vascular Institute
 Patient Experience Heart & Vascular Institute Keeping patients at the center of all that Cleveland Clinic does is critical. Patients First is the guiding principle at Cleveland Clinic. Patients First is
Patient Experience Heart & Vascular Institute Keeping patients at the center of all that Cleveland Clinic does is critical. Patients First is the guiding principle at Cleveland Clinic. Patients First is
Innovative Coordinated Care Delivery
 Innovative Coordinated Care Delivery The Arizona Readmissions Summit 2015, Mesa David W. Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco February 12, 2015 OUR STRATEGIC
Innovative Coordinated Care Delivery The Arizona Readmissions Summit 2015, Mesa David W. Saÿen, MBA Regional Administrator Centers for Medicare & Medicaid Services San Francisco February 12, 2015 OUR STRATEGIC
The Triple Aim. Productivity: Digging Deep Enough 11/4/2013. quality and satisfaction); Improving the health of populations; and
; Improving the health of populations; and") NAHC Annual Conference October, 2013 Cindy Campbell, BSN, RN Associate Director Operational Consulting Fazzi Jeanie Stoker, BSN, RN, MPA, BC Director AnMed Health Home Care Context AnMed Health Home Health
NAHC Annual Conference October, 2013 Cindy Campbell, BSN, RN Associate Director Operational Consulting Fazzi Jeanie Stoker, BSN, RN, MPA, BC Director AnMed Health Home Care Context AnMed Health Home Health
Our falls rate is consistently below national
 Our falls rate is consistently below national benchmarks, but with the lessons learned from Falls Huddle rounding, we anticipate further decreases in the overall fall rate and repeater fall rate. Monica
Our falls rate is consistently below national benchmarks, but with the lessons learned from Falls Huddle rounding, we anticipate further decreases in the overall fall rate and repeater fall rate. Monica
CAUTI Reduction A Clinton Memorial Presentation
 CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
CAUTI Reduction 2016 A Clinton Memorial Presentation Clinton Memorial Statistics Rurally situated in a primarily agricultural community with a population of 42,000 The hospital is licensed for 165 beds
Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections
 C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
C10 This presenter has nothing to disclose Strategies to Reduce Readmissions, Sepsis, and Health-Care Associated Infections David Renfro, MS, RN NE BC Kelly Farnam, BSN, RN Gloria Martinez, MS, RN, NEA
Care Redesign: An Essential Feature of Bundled Payment
 Issue Brief No. 11 September 2013 Care Redesign: An Essential Feature of Bundled Payment Jett Stansbury Director, New Payment Strategies, Integrated Healthcare Association Gabrielle White, RN, CASC Executive
Issue Brief No. 11 September 2013 Care Redesign: An Essential Feature of Bundled Payment Jett Stansbury Director, New Payment Strategies, Integrated Healthcare Association Gabrielle White, RN, CASC Executive