2014/ /17 Integrated Medium Term Plan
|
|
|
- Elwin Lawrence
- 6 years ago
- Views:
Transcription

1 2014/ /17 Integrated Medium Term Plan Our Purpose is to always put the patient first continuously improve with every action 16 th January 2014 (5 th iteration) Bwrdd Iechyd Prifysgol Aneurin Bevan yw enw gweithredol Bwrdd Iechyd Lleol Prifysgol Aneurin Bevan Aneurin Bevan University Health Board is the operational name of Aneurin Bevan University Local Health Board Page 1
2 Executive Summary We need a patient centred culture with a focus on fundamental standards, openness and transparency, candour to patients, strong cultural leadership and caring, compassionate nursing, and useful and accurate information about services. The Francis Report 2013 In order to meet the above challenges and address local health inequalities, service sustainability and future workforce requirements, we need to harness the opportunities of improving clinical pathways, technological advances and integration between services for the benefits of our patients. Status quo is clearly not an option! Changes within our healthcare system would still be required even if the current funding pressures affecting health and social care did not exist. A changing demand for our services, not least through the ageing population and increased prevalence of long term conditions and co-morbidities raise major questions about how health, social care and other partner organisations can work together in future. 1. Setting the Scene There are high expectations on us to improve the quality and care we provide to patients, quite rightly, in the aftermath of the Francis review of Mid Staffordshire Hospital public expectations for what we deliver continues to grow and we must ensure that we provide a consistent level of care 24/7. We have focused on getting the basics right, using evidence-based approaches such as Transforming Care that has improved the care we provide on our wards but we also want to deliver the basics exceptionally well. This organisation will continue to place a high importance on delivering quality care not just treatment. This is the kind of organisation we wish to be however, showing people the caring side of the NHS even at times of pressure is important to us. Since our creation four years ago, we have looked to develop our local primary and community based services and identified opportunities to integrate these with hospital based services. Some of these are captured in both our local Clinical Futures Strategy and under broader discussion in the South Wales Plan. Elements of our current models of care also appear to be outdated at a time when our population and new technologies are evolving rapidly and are changing the way in which we interact with each other. Experiences from other countries where health care organisations have already embraced new technologies indicate the shape of things to come and the potential to deliver care more effectively. We have services and facilities which need an improved environment and we have been fortunate to be able to develop some of our sites in both hospitals and GP areas, nevertheless, we still have many facilities that need significant improvement. At a practical level however, we can only manage within the funding we receive and we have a statutory responsibility to balance our budget every year. This represents a significant challenge for the organisation over the next 3 years and we will need to make savings of approximately 3-5% per year, based on current analysis and assumptions on demand. Delivering against these levels of financial savings will require us to collectively step up our approach to integrated service, workforce and financial planning in order to close the residual gap in addition to improvements in productivity and efficiency and new /existing change programmes. Page 2
3 All of us involved in the delivery of health and social care services must now look beyond current models of care to create a delivery system that really is fit for the future. Year 1 of our Three Year plan recognises that we are still in the foothills of these changes, however we must clearly evidence and articulate our priorities which align with our population, clinical, service and corporate priorities to these future goals. 2. Finance, Workforce and Performance Challenge Sustainability of the healthcare system, in the context of rising health care demands, particularly for our ageing population, is a major issue for Aneurin Bevan University Health Board. We are committed to ensuring that the resources invested in health care are vested in models of care that achieves the best outcomes for our patients. Delivering prudent healthcare means that existing services will have to be delivered at lower cost, which requires the efforts of every member of staff to reduce waste, variation and inefficiencies in our systems and processes. This Health Board has made good progress since we formed in 2009 and have improved patient services whilst operating within these challenging financial times. The funding picture for NHS Wales in the medium term however will be characterised by little or no growth for services i.e. flat cash. The next three years will therefore mean that we will need to operate within a very tight financial regime and we must continue to deliver our statutory responsibilities to break even and operate within our financial means. Details of our financial and workforce plans are detailed in Section 8 of the document. From a workforce perspective, the success of our services are directly related to the staff who provide care and services to the individuals, families and communities we serve. It is vital that we use the talents and experience of our whole workforce whilst creating future workforce sustainability. Our Clinical Futures Workforce Strategy is one of the key building blocks to delivering these changes and will ensure we have the appropriate balance of skills, competency and capabilities to meet future demands, whilst addressing the day to day challenges such as recruitment and rention, sickness, variable pay and job planning. Maintaining safe staffing levels on all of our wards and departments remain a key priority for this organisation. We have systematically reviewed our nursing workforce numbers and targeted the additional resources from the Welsh Government to improve nurse staffing levels on our medical and surgical wards. As an organisation, we also have very clear Nurse and Therapy strategies for maximising the contribution of our professional staff e.g. advanced practitioners. We know we have opportunities to improve our efficiency and productivity of our services by being as good as the Best in Wales across all of our services. If we did this we could save 43 beds by improving length of stay in 2014/15 alone, improving theatre performance would allow 1,800 more patients to be treated. By reducing outpatient demand this would release over 6,000 outpatients slots and improve waiting times. 3. Our Approach for the Next 3 Years The next 3 years will require us to focus on both operational, tactical and strategic change if we are to deliver a more sustainable high quality service for the people of Gwent and South Powys. Page 3
4 Return / scale of change Transformation typically occurs at three levels Level 3 Whole system changes across a health economy STRATEGIC CHANGE "Changing what we do" E.g. Changing the mix of services delivered Level 2 E.g. New model of The medium term TACTICAL CHANGE Developing Alternative care for A&E financial challenge "Changing the way that we do things" Operating Models Level 1 E.g. Pathway re-design for Performance improvement OPERATIONAL CHANGE Targeting Quick Wins stroke, better pharmacy stock & pay restraint "Doing things that we do now better" control & prescribing practices Time We have set out our priorities for transformational change which includes the integration of our service, workforce and financial planning to enable a step change in our approach to delivery and care for our patients. We are also creating the opportunity and capacity for our staff to lead change at all levels of the organisation, many of these small change programmes will have the greatest impact on patient experience and service s efficiency and productivity. Our key service change priorities are: Improving Quality of Care and Patient Experience Reducing Health Inequalities Strengthening Primary and Community Services Clinical Futures Remodelling (sustainable services) Workforce Change Plans Value Based Clinical Services (maximising clinical value of interventions provided to our residents) Improving Delivery Transforming Unscheduled Care Services Transforming Scheduled Care Services Delivering Financial Balance Our plans set out many of the changes that are required to re-engineer services to truly transform our healthcare system as set out in our Clincal Futures Strategy. Prioritising, sequencing and capacity to deliver this magnitude of change at the pace required represents a significant challenge going forward. Whilst complex and multi-faceted, our local system will continue to have one defining characteristic and that is to put the patient first and this should define and drive our Delivery Framework. Unfortunately, in the past, both the national and local measurement systems have not always been able to provide the evidence that this aim was being delivered. The focus from 2013 onwards will therefore be to concentrate on measuring patient outcomes and experience and demonstrating consistent improvement as noted within the Francis Report. The Health Board will continue to work in close partnership with patients, the public, our key stakeholders in Local Authorities and other public, independent and voluntary sector organisations to ensure we collectively deliver against those areas that support better quality outcomes and financial sustainability. However, we also need to draw in new areas that we think can show a further step up from previous years and set realistic but ambitious target for the next 3 years. Page 4
5 We are a learning organisation and given the work we have done on service modernisation and workforce re-design to date, we will continue to develop and refine our plans based on the best evidence available. Equally we will remain true to our purpose and values as an organisation and how these shape our strategic priorities and actions in the future. This has been represented diagrammatically overleaf: Page 5
6 Purpose Put the patient first Continually improve with every action Values Patient first Personal responsibility Passion for improvement Pride in what we do Strategic Priorities Improve patient experience and health outcomes Improve health and wellbeing Meet the needs of older people Provide more services closer to home Ensure services are sustainable Improve efficiency and effectiveness of our services 10 Strategic Change Programmes Improving Quality of Care and Patient Experience Reducing Health Inequalities Strengthening Primary and Community Services Clinical Futures Remodelling (sustainable services) Workforce Change Plans Value Based Clinical Services (maximising clinical value of interventions provided to our residents) Improving Delivery Transforming Unscheduled Care Services Transforming Scheduled Care Services Delivering Financial Balance Page 6
7 Table of Contents Chapter Heading Page Executive Summary 2 1. Setting the Scene 2 2. Finance, Workforce and Performance Challenge 3 3. Our Approach for the Next Three Years 3 1 Context and Purpose of Our 3 Year Plan 10 2 Strategic Context Our Local Strategic Direction Our Local Clinical Service Strategy Making the Service Changes Our Approach to Deliver a Sustainable Healthcare System 21 3 Health Board Profile Our Population Our Record in Improving Quality and Patient Experience Our Services Our Workforce Our Finances Our Current Performance Our Partnerships Teaching and Research 39 4 Local Needs and Challenges 41 1 Demography 41 2 Commissioning Approach 50 4 Local Pressures 55 5 Workforce Pressures 58 5 Improvement Quality of Care and Patient Experience Quality at the heart of Our Mission and Values ABUHB Approach to Quality Improvement ABUHB Components of Quality Corporate Quality Improvement Priorities 66 6 Service Change Plans and Initiatives SCP 1 Reducing Health Inequalities SCP 2 Strengthening Primary and Community Services 83 Page 7
8 Chapter Heading Page 3. SCP 3 Clinical Futures Remodelling SCP 4 - Workforce Change Plans SCP 5 Value Based Clinical Services SCP 6 Improving Delivery SCP 7 Transforming Scheduled Care Services SCP 8 Transforming Unscheduled Care Services Finance Financial Plan to The Medium Term Financial Plan Achieving Financial Sustainability Summary of Revenue Financial Plans Capital Organisational Development Purpose and Values Management Development and Leadership Aneurin Bevan Centre for Improvement (ABCi) Employee Engagement Health & Wellbeing Building Capability and Delivery Information and Communication Technology (ITC) Service and Process Improvement Capital and Estates Research and Development Health Education & Training Collaborations and Partnerships Stewardship and Governance Corporate Governance Risk Management Financial Controls, Reporting and Audit Arrangements Our Delivery Framework Our Integrated Plan Stakeholder Engagement and Support 194 Page 8
9 Appendices (separate document) to be issued. Appendix Title Annex Title Page number B.1 Tier 1 & Activity Profiles B.2 Financial Plan Summary B.3 Finance Resource Planning Assumptions B.4 Finance Statement of Comprehensive Net Expenditure 3 yrs B.5 Finance Statement of Comprehensive Net Expenditure Profiles B.6 Finance Expected Revenue Resource Limit B.7 Finance Year 1 Savings Plan B.8 Finance Years 2 & 3 Savings Plan B.9 Finance Risks and Mitigating actions B.10 Finance Cash Flow B.11 Workforce summary wte B.12 Workforce summary B.13 Asset Investment Detail B.14 Revenue Investment Detail B.15 Workforce - Recruitment Difficulties Summary B.16 Workforce Changes Summary B.17 Educational Commissioning information Page 9
10 Chapter 1 Context and Purpose of Our 3 Year Plan This integrated medium term plan, which covers the period 2014/ /17, build upon the key local themes and issues identified within our Five Year Strategic Service, Workforce and Financial Plan ( ), the Aneurin Bevan University Health Board s Clinical Futures Strategy and the UHB s Three Year Plan (2013/ /16). It has been developed in the context of the Public Health Strategic Framework Changing for the Better, the Welsh Government s Together for Health Strategy and the South Wales Programme. All of these clearly demonstrate the need for coherence between the short term and long term strategic planning of health services whilst focusing on the needs of our local population. Our plan provides the framework for how we will align the public health, service, quality, finance and workforce priorities of the organisation, within the context of a rolling three year programme of delivery and transformational change and the direction of travel described within our Clinical Futures Strategy. The purpose of our Three Year Plan is to: Emphasise that patient care remains our number one priority and that further change is necessary to provide safe, high quality services which are clinically and financially sustainable. Co-production will be at the core of our redesigned system of integrated health and social care. Communicate openly and honestly about the successes and challenges within the organisation and give a clear direction on our critical priorities for the future. Provide a robust platform for challenging the ways in which healthcare is developed and delivered for the population of Gwent and South Powys. Build on existing best practice and learn from what has worked well, whilst focusing on the key activities that can genuinely make a difference to deliver a prudent healthcare system. Detail how we will deliver the service changes required over the next 3 years that are consistent with our Clinical Futures plan, the South Wales Programme and the financially constrained environment. Deliver a balanced and sustainable service, financial and workforce plan. The UHB recognises that in order to do this we will need to: Continue to improve and deliver safe, high quality services and ensure patients experience, satisfaction and engagement remain paramount. Wherever there are unacceptable levels of variation within our services, we will ensure rapid improvement and roll-out of evidenced based practice. Learn from the outcomes and recommendations of the Francis Report with resolute commitment to: Make quality of care for every patient the first priority of each and every member of staff. Zero tolerance of poor standards of care, and care processes that are wasteful, or cause unnecessary waiting, or duplicate care for patients. Open and transparent culture within and across our healthcare system, where concerns are raised freely; is upfront when things go wrong and is transparent in showing how well, or badly we are doing. Page 10
11 Continue to focus our planning and delivery of health and social care services around the needs of vulnerable groups, particularly our frail older people, many of whom are now presenting with multiple co-morbidities and are at a substantially higher risk of falls, disability, long term care and death. Ensure better access to and integration with primary and community based services so we continue to shift resources from hospital to community based services and preventative care. As part of this agenda, we need to work with our local population to change the perception of the NHS from that of a treatment based service, to one where effective prevention and support for lifestyle choices prevails. Deliver evidenced based clinical pathways designed around individuals, consistently, 7 days a week. Where this cannot be achieved and where national standards are not being met, tough decisions will need to be made and we will use the Value Based Clinical Services 1 approach to inform these decisions. Ensure delivery of existing commitments established within the National Performance Framework, maintaining a focus on local and national performance standards remains a consistent foundation for our future success. This will drive efficiency and reduce waste, harm and variation so that within 3 years Aneurin Bevan will be (as a minimum) Best in Wales if not Best in Class, and as a minimum, will be using CHKS and NHS Benchmarking as our way of baseline comparison against core standards. Provide continued focus on the key areas identified within our Change Programmes (including, Medicines Management; Continuing Health Care; Every Day Counts for Megan (reducing reliance on inpatient beds) whilst building on key initiatives to support transformational service change (developing and implementing better service models to provide patients with the right service, at the right time, in the right place, delivered by the right person). Continue to build on the current strong foundation of partnership working with Local Authorities, the Third and Independent sectors, local universities and other partner organisations. Empower and support all our staff. 1 Our approach to Value Based Clinical Services is set out in Chapter 6 (SCP 5) Page 11
12 Chapter 2 Strategic Context National Drivers The Welsh Government has set out the national strategic direction for Health Boards and Trusts within the overarching Programme for Government and the NHS Strategy Together for Health, underpinned by more detailed strategies and plans based on key service areas or population groups and linked to the seven strategic themes of Together for Health. Together for Health A Five Year Vision for NHS Wales (2011) set out the challenge as follows: Health has improved but not for everyone and our population is ageing Improvements in health have not been shared equally. Life expectancy for the most deprived fifth of the population has risen more slowly than for any other group. For instance, people living in Monmouthshire and Ebbw Vale face a 10-year difference in average length of life. Many of the causes of poor health are deep-rooted and they are often difficult to tackle. Gwent faces an obesity epidemic and rates of smoking, drinking and substance misuse continue to cause concern. We are also facing an increase in the numbers of older people who will inevitably place more demands on our health and social care system. Older people are more likely to have at lease on chronic condition an illness such as diabetes, dementia or arthritis and have more as their age increases. Health care quality has improved but the NHS can do even better Harmful incidents in hospital are monitored better than ever before and efforts to prevent them are more rigorous. The University Health Board has a solid track record in managing hospital acquired infections and continues to see specific improvements on a range of quality targets achieving targets for reducing infection rates; we have seen falls drop and pressure sore rates whilst in hospital reduce. Our new hospital facilities have 100% single room accommodate, supporting our commitment to improved quality and safety of care. We continue to work hard to make all our services better for our patients. We recognise that people are still admitted to hospital for causes such as an asthma attack which might have been avoided had local preventative action and support been in place. Meeting the challenge of ensuring that the right service, is in the right place, at the right time is critical to delivering a safe, high quality, sustainable healthcare system for the future. Expectations are continually rising Past success and continuing improvements mean people s expectations will continue to rise. Involving communities in assessing and designing services improves those services. Involving individuals in treatment decisions and self care management improves outcomes. The challenge is to develop a new relationship with the public as co-producers in their own care will be essential, empowering the public to make informed decisions about the appropriate use of healthcare. Medical staffing is becoming a real limitation on our services Creating a sustainable workforce is a particular challenge in some specialties, including paediatrics and emergency medicine, where there are insufficient specialists than available posts across the NHS. Recruitment of medical staff is already proving to be a tough challenge. Our top priority is to provide patients with safe, high quality clinical services; our Clinical Futures model clearly sets out our plans to achieve this over the coming years. During the coming year we will look carefully at how we can sustain our existing configuration of services between now and the opening of the Specialist and Critical Care Centre. Page 12
13 We know that the key to delivering sustainable healthcare is to ensure that we use our highly skilled workforce sensibly, maximising the contribution they can make by organising the way in which we deliver services better. We believe that we can deliver more by aligning our services and our systems differently, supporting closer integration and shared responsibility for the design and delivery of care across primary, community and acute services. The shape of our workforce needs to change if we are to meet this challenge. Funding is limited The downturn in the economy and the difficult current economic outlook for public services means that the NHS in Wales faces significant and increasing financial challenges. The current system is unaffordable and in 2014/2015 the University Health Board needs to deliver savings of 27m and savings of a similar magnitude over the next few years to stay within the resources provided and to deliver the key targets expected of it. In practical financial terms this requires the delivery of approximately 2 m per month, whilst still improving services, improving quality whilst working within the resources available. Within the Health Board 3 Year Integrated Plan we have undertaken an assessment of the critical strategic priorities which will improve clinical and/or operational delivery, lead to transformational change and as a result improve our financial sustainability. The NHS Wales Planning Framework, issued in October 2013, established the planning principles which underpin the development of integrated, medium term (three year) Plans and which deliver the outcomes for catchment populations based on an alignment of key services, staff, finance and effective involvement of the public through co-production. 1. Our Local Strategic Direction Our focus over the next three years is to deliver a sustainable healthcare system, one that is coherent and aligned to the National Policy Context for NHS Wales and out local Clinical Futures strategy. We recognise that substantial service change is required to ensure that ABUHB can utilise the resources available to us to deliver health care that meets and exceeds the quality and performance targets set by Welsh Government and provides positive patient experiences. Increasingly over the three year we will: Consolidate and increase the pace of operational change to achieve Best in Organisation ; Best in Wales and Best in Class performance. Mainstream our approach to tactical change or changing the way we organise services and deploy our existing workforce to maximise clinical outcomes, productivity, and drive a value healthcare system. Harness strategic change opportunities changing what we do. Ensure that our 3 year interim service models align to our ultimate goals post completion of the SCCC in For us, this is also about a strategic shirt to enhance primary and community services. The Integrated Three Year Planning Framework is central to aligning all relevant components of our complex healthcare system to deliver our ambitious plans. Delivering the national priorities of NHS Wales is crucial to improve patient experience, safety and enhancing quality of services but sustaining and continued improvement presents challenges in some areas across the organisation. The Health Board has assessed the likely progress during 2013/14 in delivering improvement against the service and financial pressures which impact on delivery and trajectories 2014/15 and 15/16 which are illustrated in the table opposite. There remains a strong focus within the Health Board to improve year on year and these themes will Page 13
14 continue to drive achievement of plans over the next three years. Within our quality and patient experience section 2, we also identify a range of local initiatives we are taking forward to improve clinical pathways and outcomes e.g. sepsis, acute kidney injury and end of life care which are equally important to us. Over the next three years we will deliver step change in the range, capacity, quality and consistency of services delivered through integrated primary and community teams, which are built around NCN communities. We will transform our hospital based services in order to: Maximise timely access to advice, assessment, diagnosis, intervention, integrated treatment planning and delivery of care, and consequently. Minimise the need for patients to travel to hospital settings for their care. Reduce the need for patients to be admitted to hospital, and where hospital admission is necessary, to reduce their length of stay. Rebalance our system of care to a primary/community care led NHS. Developing our response to the suite of Together for Health condition based and specific service delivery plans has provided a robust vehicle to design and deliver system wide solutions to improve the health and wellbeing of our population. We will continue to use this integrated system wide approach to drive our Plan over the next three years. We have sought to map our progress against Tier 1 performance over the period and this is shown in Table Our approach to quality and patient experience is set out in Chapter 5. Page 14
15 Efficiency & Productivity Stroke Canc er Waiti ng Times Unscheduled Care Acces Mortality Rate Quality in Care Setting the Direction Table /14 PROFILED PERFORMANCE - ANEURIN BEVAN HEALTH BOARD 2013/14 tot/avg 2014/15 tot/avg 2015/16 tot/avg 2016/17 Area Source Deliverable Target performance performance performance performance All emergency deaths and discharges CHD (rolling 12 months) Number of emergency admissions¹ ³ COPD (rolling 12 months) Diabetes (rolling 12 months) Readmissions (7 day) - all patients 3.80% 3.55% 3.30% 3.20% PEDW Bed day usage for chronic conditions (rolling 12 months) Reduction CCM rate (rolling 12 months) 13.10% 12.78% 12.46% 12.12% CCM ALOS (rolling 12 months) CHD (rolling 12 months) Average Length of Stay (in days)¹ ³ COPD (rolling 12 months) Diabetes (rolling 12 months) CHKS Elimination of pressure sores² Reduction Resource Utilisation Mental Health (Wales) Measure Public Health Wales CHKS StatsWale s EDDS WAST Health Stats Delivery & Support Unit PEDW & OP MDS PEDW Further reduction in C Difficile (Persons aged over 65) - Minimum 20% improvement against baseline Further reduction in MRSA - Minimum 20% improvement against baseline Further reduction in MSSA - Minimum 20% improvement against baseline RAMI (2012 case mix) Crude Mortality % of patients waiting less than 26 weeks for treatment all specialties Number of 36 week breaches all specialities % of new patients spend no longer than 4 hours in an Emergency % of new patients Department spend no longer than 8 hours in an Emergency Reduction in Department the number of patients spending longer than 12 hours in an Emergency Department % of Cat A Ambulance responses within 8 minutes Handover performance for all patients < 15 minutes Handovers longer than 1 hour % of patients referred as non-urgent suspected cancer starting treatment % of patients within referred 31 days as urgent of diagnosis suspected cancer starting treatment 1 - First hours within bundle 62 days of referral Reduction Reduction Num to achieve 20% reduction by Mar14: Demonstrable reduction % 88.0% 91.0% 93.0% 95.0% % 92.3% 94.0% 95.0% 95.0% 99% 96.0% 96.2% 98.0% 98.0% Continuous reduction % 61.7% 63.4% 65.0% 65.0% Continuous improvement 60.0% 62.5% 65.0% 65.0% Continuous reduction 5.0% 4.8% 4.5% 4.5% 98% 98.0% 98.0% 98.0% 98.0% 95% 95.0% 95.0% 95.0% 95.0% 100.0% 100.0% 100.0% 100.0% 95% 95.0% 100.0% 100.0% 100.0% 99.4% 100.0% 100.0% 100.0% 98.2% 100.0% 100.0% 100.0% 80% 80.8% 82.3% 85.6% 85.6% 68.0% 70.0% 73.4% 73.4% General Surgery 57% 69.1% 70.5% 72.0% 72.0% Urology 71% 82.0% 83.8% 86.3% 86.3% Trauma & Orthopaedic 55% 66.0% 73.4% 78.4% 78.4% ENT 91% 86.8% 90.2% 93.1% 93.1% Ophthalmology 69% 60.0% 64.2% 69.0% 69.0% Oral Surgery 45% 67.8% 69.8% 71.9% 71.9% Gynaecology 71% 72.0% 75.3% 79.0% 79.0% General Surgery Trauma & Orthopaedic General Surgery Trauma & Orthopaedic Combined Medicine ESR Achieve annual local Sickness and Absence workforce target³ 5.08% 5.12% 4.62% 4.12% 3.62% Delivery & Support Unit 2 - First day bundle 3 - First 3 days bundle 4 - First 7 days bundle Day surgery: 80% of planned surgical procedures under the BADS50 will be treated on a day case basis¹ ³ % of surgical procedures under taken as a day case. Admission on day of surgery¹ ³ Reduce Elective AVLOS¹ ³ Reduce Emergency AVLOS¹ ³ Quality triggers & any other considerations Percentage of patients with a valid CTP - Adult Percentage of patients with a valid CTP - Older Adult Percentage of patients with a valid CTP - Forensic n/a % % % % n/a % % % % n/a % % % % n/a Page 15
16 Building on Success The ABUHB 3 year Integrated Plan sets out a bold response to the current and projected health and well being needs of its catchment population, progress against which will be measured at key points of the patient pathway and linked to feedback from our patients and other key stakeholders. Set against the challenges of population change, growing demand and cost pressures, any assessment of progress must demonstrate the impact of strategies to strengthen resource efficiency and effectiveness and further investment in NHS Wales. Achievements will be based on an integrated approach to service planning and delivery with our partner organisations, in particular our Community Health Council, Local Authorities and the Third Sector, underpinned by sustainable solutions to future, pathway based service delivery. In One Place is our joint agreement with all partner agencies to work collaborative in dealing with the accommodation needs of people with complex health and social care needs. Based on the principles of co-production, patients and the public will become equal partners in the design and delivery of services, recognising the pivotal role they must also play in achieving improved health and well being outcomes for themselves. Measured against experience of current stakeholders will be able to clearly identify where improvements are being made and the milestones against which we are assessing ourselves. In particular, patients and the public will have experienced or be aware of a discernible shift of service delivery from hospital to primary care and community settings based on integrated service models that reflect effective collaboration between ABUHB and its partner organisations. 2. Our Local Clinical Service Strategy The Health Board has a clear strategic direction for the development of clinical services and the associated development of estate and infrastructure, which has been developed by clinicians. Known as the Clinical Futures Service Strategy, this articulates this model of care and has been the framework against which service developments in the Health Board have been developed. Clinical Futures is a system vision that takes into account the role of the individual, primary, community, intermediate, secondary and tertiary care and is consistent with the Welsh Government published strategic framework for primary and community services Setting the Direction. The approach is represented on Figure 2.1 below. Figure 2.1 The concentric rings represent the various levels or settings for care within the local health community. The arrows represent the patient pathways, starting in the home or community settings, and reaching inward through local hospital care to specialist care as required. At each stage the model aims to maximise the services and care available locally that can prevent the patient needing to go further down the pathway. The key components of the whole system model are: Elective Emergency Older people, chronic conditions etc Critical Care & Specialist hospital Local hospitals Services in community Services at home Self care, promotion and prevention Mental Health Women & Children Page 16
17 Helping people to live healthy and independent lives, improving health and wellbeing and reducing health inequalities through effective health promotion and disease prevention programmes, and recognising and developing responses to the issues associated with inverse care law. Moving services into the community where it is clinically more effective to do so by increasing the range of services provided in locality communities through primary, community, social care and mental health services, with the expressed intention of reducing reliance on bed based care. Developing a network of local general hospitals to provide routine hospital based care including urgent care, day case surgery, outpatients, diagnostic and integrated care, together with mental health services. Concentrating care for our most critically unwell patients within specialist and critical care services (i.e. services that cannot be provided on multiple sites based on sustainability, clinical effectiveness, patient safety and affordability) in fewer locations to reduce risk and deliver better clinical services for patients. This underpins both our local strategies and that of the South Wales Programme. The main idea of the new system is that of a network bringing care as close to the patient as possible through different working practices, the use of new technology and the development of new facilities. This is particularly important in view of the diverse demography of the catchment area served and the complex systems that exist. All parts of this system need to work effectively together to make the best use of the resources that are available to the Gwent Healthcare Community to improve and sustain health services for decades to come. The Clinical Futures Programme transforms the basic structure for delivering health services in the area by moving from the traditional approach of concentrating healthcare in District General Hospitals to a new system which builds stronger and more comprehensive primary and community services out of hospital and at the same time develops a network of local general hospitals supporting a single specialist and critical care centre. Greater Primary & Community Care Focus The model of care highlights the need for change and supports a whole systems approach to underpin the development of sustainable health and well-being services in the area. The key to the new model of service is a re-balance of care between primary, community, secondary and tertiary services. Moreover, the model recognises that peoples needs, particularly those in vulnerable groups and older people, span organisational boundaries.. The system proposed in Setting the Direction: A Strategic Framework for Primary and Community services (2008) requires an expanded, integrated model of organised primary and community services, that focuses on the patient and not on the part of the system providing the care. The system needs to stratify risk and manage care in a proactive way for moderate to high risk patients who are being cared for in a community setting and through either increasing frailty or a deteriorating chronic condition require more complex care than may have traditionally been provided in that setting. The core elements of the new model (whilst working in a cohesive manner) were presented as: services organised in localities of 30,000 50,000; mechanisms to assess and direct people within the community; a communications hub which will fulfill both an information support (based on the GP shared record) and a care co-ordination function; core primary care services; Resource Teams (including GPs with advanced skills, community consultants and advance practitioners) operating at the previously outlined population level; Out of Hours; Page 17
18 Locality Networks reflecting multi-disciplinary teams. The Health Board, together with Local Authority partners has invested heavily in the development of Community Resource Teams, their purpose to identify and meet the needs of frail people. Moving forward into and beyond and supporting delivery of the Clinical Futures Programme and implementation of Together for Health, the Health Board recognises that a major priority and challenge for the organisation will be the need to expand and develop community based services through the development and adoption of modern, consistent and equitable models of care. The Future Model for Local General Hospital Services Our Local General Hospitals will continue to provide a broad range of services such as tests, investigations, outpatient clinics, minor injuries, minor surgery and other day case treatments, therapies and inpatient care (including physical and mental health services). They play an important role supporting primary and community services in responding to the growing population of the frail and elderly and those with co-morbidities in their local environments. LGHs also play an important role in supporting the delivery of the most efficient and effective operating model for the Specialist and Critical Care Centre and the whole system of care. They form an important part of the hub and spoke model of care that underpins the Clinical Futures. Patients access services as locally as possible where it is clinically safe and sustainable to do so. We are critically reviewing all CF service models in line with value based clinical services (see SCP 5), the challenges that the UHB now faces in delivering quality outcomes in a challenging economic climate in order to determine the optimal configuration of hospital based services through our LGH network (see SCP 3). It is becoming increasingly difficult to duplicate services across multiple sites and is not sustainable in the medium term. Delivering value based clinical services requires us to maximize clinical outcomes and minimise costs, balanced against timely access to those services. Local General Hospitals have already been opened in Ysbyty Aneurin Bevan (YAB) in Ebbw Vale and at Ysbyty Ystrad Fawr (YYF) in Ystrad Mynach. These model LGHs serve as a test bed for the future development at the Royal Gwent Hospital (RGH) and Nevill Hall Hospital (NHH) for when they become LGHs once the SCCC opens. The Future Model for Specialist and Critical Care Services The Clinical Futures Programme set out the need to consolidate those services that people access relatively infrequently but which are acute and specialised in nature at the proposed Specialist and Critical Care Centre (SCCC), located at Llanfrechfa Grange, near Cwmbran. The key services included are obstetrics, inpatient paediatric care and acute assessment, neonatal services, hyper acute medical and surgical emergencies, major trauma, critical care services and major complex surgical services. The concept of the Specialist and Critical Care Centre (SCCC) is to create a highly specialised environment to support the treatment of complex morbidity and acute emergency care. Treatment is delivered with the aim of rehabilitating the patient back to their local general hospital for on-going recovery or discharged home as appropriate. The SCCC will serve the entire Gwent catchment population for critical care and specialist services. Therefore, a key principle in the Clinical Futures model is that of access to specialist and critical care services. The Clinical Futures Programme aims to ensure that sustainable services are provided for the population, and that they deliver the best outcomes for patients by maximising the use of the resources available. The strategic objectives for these services are to: Improve the quality of care for patients in line with national standards, evidence & best practice. Page 18
.")

19 Maintain and where feasible expand the range of specialist and critical care services delivered in Gwent. Protect these scarce resources & target them at patients who most need them. Speed up access to care for patients by reducing bottlenecks in the hospital system, and improving links with Level 4 (tertiary services). Make these services more reliable and robust 24 hours a day, 7 days a week - now and in the future by developing single, integrated teams and extended working days. Help recruitment and retention in these specialist areas, and support the training and development of staff. Provide modern environments that optimise efficiency and effectiveness for patients, staff and visitors. Support the broad range of local services delivered through the Local General Hospitals. The figure below illustrates how components of the CF Hospital Network. Figure Making the Service Changes Changes continue to take place locally with the aim of aligning services and systems differently, supporting closer integration and shared responsibility for the design and delivery of care across primary, community and acute services at the following levels of care. Page 19
20 From now until 2018 ABUHB will continue to develop and implement plans to deliver the Clinical Futures Model: 1. Service Model Development The Clinical Service Models have been developed and will continue to be refined as professional guidance and practice evolves. The impact of the South Wales Programme may also influence changes to the Service Models. Review and refinement of the clinical Service Models will be ongoing over the next 3 to 5 years. Transitional service plans will also be prepared to ensure a smooth transition from the traditional District General Hospital model to the Clinical Futures model of service provision. In 2017 commissioning and implementation plans will be developed prior to the final move in 2018 /19, when the SCCC opens and the DGH s become enhanced Local General Hospitals. 2. Workforce Model Development Detailed multidisciplinary workforce plans are being developed by summer 2014 for the SCCC Full Business Case. The Service and Workforce Modelling will continue to be developed side by side. The workforce must respond to the service plans, but any expansion of the workforce must be affordable, so this will continue to be an iterative process. As new, expanded or replacement roles are identified, educational commissioning plans will be developed to ensure that there are qualified and experienced staff in post by As a whole system change in service provision is planned, discussions with the Deanery regarding the allocation and training requirements for junior doctors will continue. Changes to the working practices of all current staff will be planned, negotiated and implemented over the next 3 to 5 years as service model changes are implemented. 3. Revenue Affordability Plan As the Service and Workforce Models are developed, the revenue affordability plan will be reviewed and refined. This will also be an ongoing and cyclical process over the next 3 to 5 years. 4. Capacity Model and Performance Targets Underpinning the Clinical Futures Programme and the capital brief for the SCCC and elgh s, a capacity model, including performance improvement targets, has been developed based on current activity and compared to the performance of the best in class organisations in the UK. The Capacity Model will be re run bi-annually to check that the Health Boards planned capacity remains valid. Progress towards achievement of the performance targets year on year will also be undertaken and reported, as the Health Board moves towards 2018 and the reduction in Secondary Care bed numbers and increase in patient management in Primary and Community Care. The Capacity Model will be refine in coming years as clinical practices change and develop. Learning from other service change programmes The Clinical Futures plans will continue to respond to learning, the growing evidence and examples of best practice from changes both within Gwent (YAB and YYF and the SWP), within Wales, (The Neath Port Talbot experience and models) and across the UK. Some exciting partnering and joint learning is developing with the Northumbria Foundation Trust who are in the process of building a Specialist Emergency Centre, centralising key services form two DGHs and developing a networked approach. Page 20
21 The geography, catchment population and emerging service and estate solutions for Northumbria resonate with the CF plan and a focus on developing an ongoing clinical dialogue to understand models and challenge our assumptions will be a priority moving forward. Further details of our approach to delivering Clinical Futures are contained within SCP 2 (Strengthening Primary and Community Care) and SCP 3 (Clinical Futures Remodelled). 4. Our Approach to Deliver a Sustainable Healthcare System By putting the patient first, this plan seeks to demonstrate how the UHB will over the next three years design and deliver a sustainable healthcare system for Gwent, which reconciles with the NHS Wales policy framework and requires the UHB to deliver its ambition of achieving 'Best in Class' across of range of quality and performance measures. We recognise that this requires substantial service change at all levels within the UHB, with a more focused and continuous organisation-wide approach to service sustainability, transformational change and financial balance. We have developed our integrated medium term planning model to ensure that the UHB fully understands the implications of current and future service models, builds capacity to deliver performance, maximises the deployment of resources and delivers affordable, high quality and sustainable healthcare over the planning period. The planning model is described below and seeks to ensure that there is connectivity between the key components of the plan (Quality and Safety, Demand and Capacity Assessment, Delivery of Standards Efficiency and Effectiveness, Workforce and Finance). Figure 2.3 Integrated planning framework Model of care (Clinical Futures) Workforce modernisation Rightsizing Activity plan Service redesign Resource plan (Workforce, Capacity) Financial assessment Managing demand Benchmarking Balanced financial plan Step 1 - Model of Care The Health Board has a well articulated and understood future model of care based on a three tier model from Clinical Futures. Our emphasis will therefore be on the incremental steps required to deliver the revised models of care over the medium term within each Directorate/NCN, with a corporate overview of enabling strategies. These changes will be consistent with long term strategy and maintaining service continuity within the context of both the SCCC development and the South Wales Programme. Page 21
22 Step 2 - Activity Plans for Each Element of the System This encompasses a full description of demand and activity required to deliver core outcome targets e.g. Tier 1 targets. The demand assessment will be holistic, including health needs assessment, potential demand management opportunities (e.g. intervention threshold, INNU, variation analysis) and more traditional demand assessments. The resultant activity required will then be identified including the explicit contribution that efficiency and effectiveness benchmarks make to bridging any demand/capacity gaps. Step 3 - Aligned Resource Plan Building on the above, this describes the resource plans, bed capacity and workforce to deliver the future service model plans based on optimal performance. This will include delivery of the bed plan, development of more local health services, workforce redesign, alignment of workforce to productivity and efficiency gains and optimal utilisation of estate and other supporting infrastructure. There is also a need to understand how the culture of the organisation needs to develop and mature to manage within available resources, and how this links to values, PADRs and accountabilities. Step 4 - Balanced financial plans over the 3 years This describes how costs of the current service model will be reduced to contribute to the delivery of a sustainable healthcare system for the Aneurin Bevan University Health Board. We recognise that both internally and across the broader health and social care system we do not as yet have a sustainable model of care. Although we have a clear line of sight to the challenges and pressures over the next 3-5 years we do not as yet have a plan which will allow us to meet and balance all these priorities. This will require further internal discussions with all staff groups, the Board and external partners. The four step process allows each of the elements to be modified, tested and challenged if the proposed changes do not deliver safe and sustainable services within the available financial envelope. For example, it may be the case that the desired model of care is unaffordable. This could then be bridged by changes to the model of care, reductions in demand, further efficiency measures or a combination of the above. This is described more explicitly in the Value Based Clinical Services Change Programme and provides a vehicle to enable the Board to fulfill its ambition to become a Commissioning Board supporting the identification of fundamental choices that must be made about where we spend public monies vested in ABUHB to make maximum health gain for the population we serve. This integrated approach is consistent with best practice, and addresses one of the recommendations in the Wales Audit Office (WAO) Review of NHS Wales Finances (2012/13), specifically the strengthening of the integration of service, workforce, and financial planning. It provides a framework to ensure full clinical engagement and ownership supported by corporate departments and functions. Page 22

23 Chapter 3 Health Board Profile 1 Our Population The University Health Board serves a population of 561,400 (2009 population estimate) people and employs 13,336 staff. The Health Board was established in 2009 as an integrated Local Health Board with a primary responsibility to plan and deliver a wide range of primary, community and secondary health services to its catchment area which includes the populations of Caerphilly, Monmouthshire, Newport, Blaenau Gwent and Torfaen. Taken together with an estimate of the patients living in South Powys and other areas that are served by the Health Board for acute services, the patient population served is close to 600,000. The University Health Board covers a diverse range of population groups with different health needs and sizeable inequities in health and healthcare within and between localities. Delivery of health services has to take account of a mix of rural, urban and valley areas and a growing proportion of elderly people. The age structure of the population is similar to Wales as a whole, with slightly higher proportions of persons aged under 15 and in their forties, and lower proportions of persons in their twenties. The latest projections indicate that if current trends continue the total population across the Health Board area will remain stable, although the age profile of the population will change significantly: the numbers of persons aged 65 and over will increase by almost 50% by 2033; the proportion aged 75 and over is projected to increase between 7 and 10% (with some local authorities seeing an increase of up to 19% over the period); the percentage aged 85 and over is projected to double from between 2% and 3% to between 5% and 8% by 2033, with the exception of Monmouthshire where a sharper increase is projected with the proportion set to treble in size. Figure 3.1- Deprivation within ABUHB compared with all Wales Page 23
24 The localities of Newport, Blaenau Gwent and Caerphilly have some of the poorest health scores in Wales, with inequalities and deprivation resulting in higher levels of ill health and premature mortality as illustrated in Table 3.1 below. Table European Standardised Death Rates by Selected Causes Breast Cancer Lung Cancer Myocardial infarction Ischaemic Heart Disease Cerebrovascular disease Respiratory disease female male female male female male female male female male female Blaenau Gwent Caerphilly Monmouthshire Newport Torfaen Powys Wales Source: Office for National Statistics, European Standardised Death Rate (red = higher than Wales average ESDR) Public Health Overview Aneurin Bevan University Health Board is committed to improving health as well as treating sickness. The University Health Board is one of the pilot areas for the inverse care law programme which is one of our key transformational programmes in this Integrated Medium Term Plan. We have met the commitment in the Tackling Poverty Action Plan to identify the areas of significant need to be supported through the programme to achieve a stronger focus on preventing ill health, improved management of long term conditions in primary care and effective specialist care when needed. The programme will be integrated across the public sector with a common ambition to reduce health inequalities in our areas of greatest need. Progress has been made towards implementing the actions set out in the ABUHB Public Health Strategic Framework to achieve better health and fairer outcomes for all through addressing the causes and determinants of poor health outcomes. The aspirations of the ABUHB Public Health Strategic Framework are: Babies are born healthy. Pre-school children are safe, healthy and develop their potential. Children and young people are safe, healthy and equipped for adulthood. Working age adults live healthy lives for longer. Older people age well into retirement. Frail people are happily independent. Action taken to reduce smoking prevalence includes the implementation of a Smoke Free Environment Policy for all ABUHB premises, a pilot of a Models for Advice to Maternal Smoking Cessation Support (MAMSS), a British Heart Foundation funded Hearty Lives project to prevent young people starting to smoke and the introduction of an enhanced smoking cessation service delivered through community pharmacies. The challenge is to scale up these services to sufficient service volumes to achieve a measureable reduction in the proportion of the population who smoke, particularly in the areas of greatest need. To address the escalating problem of obesity action has been taken that is designed to increase participation rates in physical activity and reduce unhealthy eating. The action taken includes the roll out of a programme of Make Every Contact Count (MECC) training for front line clinical staff. This MECC training has been offered to all GPs and Practice Nurses through the CPD programme the University Health Board provides for primary care clinical staff. A training programme for secondary care teams is underway and will continue until training has been offered to all relevant ABUHB frontline staff. The next stage is to offer MECC training to the frontline staff Page 24
25 of partner organisations through the partnership structures that underpin the five Single Integrated Plans covering the ABUHB area. A new weight management service is being put in place for overweight and obese patients who need more than a structured brief intervention to support them to make healthier lifestyle choices. The University Health Board is working with partners on the Area Planning Board for Substance Misuse to take integrated action to stop the growth in harm from alcohol and drugs. A baseline needs assessment is nearing completion to inform the commissioning of services to prevent and treat substance misuse and to minimise harm from substance misuse. A programme of Alcohol Brief Intervention (ABI) training has started to be rolled out for frontline staff with the support of Public Health Wales and the challenge is to scale up the provision of Alcohol Brief Intervention to achieve the service volumes necessary for a measurable population impact. An innovative campaign promoting the message No Alcohol, No Risk to pregnant women is being piloted and evaluated. There has been a reduction in teenage pregnancy rates following the promotion of Long Acting Reversible Contraception (LARC) and improved access to emergency contraception services. This is a very positive improvement and the measures put in place will be continued and strengthened. Road safety initiatives to reduce accident and injury rates from Road Traffic Accidents have been taken forward through the Gwent Road Safety Group. The Gwent Frailty Programme includes a work programme to reduce injuries to older people from falls. The innovative Gwent Five Ways to Wellbeing programme to improve mental wellbeing is seen as an example of best practice in Wales and the programme is continuing to be expanded and strengthened to encompass an ever widening network of people and organisations in Gwent. As a large employer, ABUHB is leading by example and rolling out the Time for Change programme throughout the organisation to improve the work environment for ABUHB staff who have or have had a mental illness. The next stage will be to encourage and support other public sector employers in the Gwent area to follow suit. The University Health Board holds the Gold Corporate Health Award and intends to apply for the Platinum Corporate Health Award as part of its commitment to improving health at work. As part of the implementation of the Smoke Free Environment Policy staff are offered smoking cessation support if they want help to stop smoking. The planning of the Specialist Critical Care Centre provides an exciting opportunity to design a hospital that promotes the health and wellbeing of both staff and patients. The Measles Mumps Rubella campaign that was mounted in response to the recent measles emergency in Wales has lifted childhood vaccination and immunisation rates to the highest levels achieved in recent years. The challenge is to build on the success of that campaign to achieve target levels for the uptake of all the routine childhood immunisations and prevent future outbreaks of vaccine preventable diseases. Influenza vaccine uptake rates have been improving for the over 65 years, at risk groups and ABUHB staff over the last five years. There is still more to be done to achieve the target uptake rate for each of these groups and the University Health Board has systems in place to build on what has worked and to learn from what has not worked. 2. Our Record in Improving Quality and Patient Experience Aneurin Bevan University Health Board published our first Annual Quality Statement in September 2013, it sets out some of the improvements in quality of care, patient experience and safety that have been achieved in the past year, including: Page 25
26 Clostridium difficile rates have reduced by 26% compared to the previous year, following the reduction of 38% from 2010/2011 to 2011/2012. Consistent attainment of the target of treatment within 31 days for 98% of patients referred for other reasons and subsequently found to have cancer. Immunisation and vaccination rates have improved for: All infant immunisations; Teenage booster vaccinations; Influenza vaccinations for older people and for our staff; Patient satisfaction rates of 90% across all areas in our Fundamentals of Care Audit apart from Oral Health and Hygiene. Consistent achievement of mental health crisis resolution home treatment service targets, with over 95% of service users receiving assessments prior to admission to a psychiatric bed. Completed the roll-out of the National Health Service Early Warning Score to all our acute hospitals. The Surgical Site Infection rate for Caesarean Section wounds in Maternity Services in the Health Board is 3.7%, compared with an average All Wales rate of 7%. Launched our Patient Experience Framework which sets out how the organisation will actively seek the views and experiences of our patients and use their experiences to shape our services. Improved access to General Medical, General Dental and Community Optometrist services across Gwent. Fast track discharge for palliative care patients, with specialist nurses providing consistent seven day services. Dementia Intelligent Targets have improved services for people with dementia in all 5 target areas, and increased staff engagement in this important area, particularly in general acute wards. More patients than ever before coming to hospital on the day of surgery and more surgery offered through daycase procedure. Although ABUHB is doing well relative to others, there is still room for improvement. The organisation believes that improvement is part of everyone s job, wherever they work in the organisation and wholeheartedly supports the development of Improving Quality Together, which provides training in improvement methods for all staff, at all levels, whether they are clinical or nonclinical. The past year has seen the creation of ABCi, the Aneurin Bevan Centre for Improvement, to support all Health Board staff to improve the way they work, and to develop a healthy culture of patient focus across all our services. This initiative draws together people who have been working on quality and service improvement in different parts of the Health Board, and draws in further analytical and measurement expertise through a collaboration with Cardiff University, as well as building on a flourishing relationship with the 1000 Lives Plus Improvement Team. The aspiration of ABCi is to have its work driven by the needs of patients cared for by our clinical teams and to be a resource for best practice and innovation. When teams demonstrate improved practice with evidence, this practice needs to be spread to other areas in the organisation. It is a fundamental expectation that care for every patient, irrespective of setting, should be given in a way that we would want our family, friends and loved ones to be cared for. Patients are involved in their care in a variety of ways. This year, ABUHB has been a part of the Patient and Family Centred Care programme with the Kings Fund, which has used patient shadowing to help staff to see our services through the patient s eyes, so the improvements that they make to the service are designed from the patients point of view. We have also had great success in increasing the number of patients able to die in the place of their choice, through the I Want to Go Home project. It is important to listen to what patients tell us about their experience of care in a variety of ways, Page 26
27 particularly patient stories and surveys. The ABUHB Patients Panel and the Aneurin Bevan Community Health Council also give helpful feedback about what it is like to be a patient. 3 Our Services The University Health Board contracts with independent practitioners in respect of primary care services which are delivered by General Practitioners, Opticians, Pharmacists and Dentists (see Table 3.2). Outside of normal practice hours the Health Board has responsibility for and provides an Out of Hours Primary Care Service. There are 410 General Practitioners and Salaried GPs providing general medical services from 89 General Practices. Supporting these are 215 practice nurses, 170 health care support workers and a number of administrative staff, including practice managers, receptionists, secretaries and IT officers. Around 375 General Dental Practitioners provide general dental services from 84 practices. There are 128 Community Pharmacies and 69 Optometry premises across the Health Board. Table Distribution of Independent Contractor Services by Locality Locality General Practice Pharmacy Dental Optometry Blaenau Gwent Caerphilly Monmouthshire Newport Torfaen Total A wide and growing range of community based services are increasingly being delivered in patient s homes, through community hospitals, health centres and clinics (see Table 3.3 for overview). Table Overview of Community Services Service Community Nursing Community Resource Teams (Frailty) Complex Care Team Palliative Care Team Community Dental Service Distribution 29 teams across 5 Localities 5 teams across 5 localities Teams operate across all Localities 371 beds Borough Hospital Beds Blaenau Gwent YAB 96 Caerphilly YYF/N. Rhymney 88/12 Community Hospitals Monmouthshire Chepstow/Monnow Vale 44/19 Newport St Woolos 45 Torfaen County 67 The University Health Board has three acute hospitals providing a range of inpatient and outpatient services; these are The Royal Gwent Hospital, Newport; Ysbyty Ystrad Fawr, Ystrad Mynach; and Nevill Hall Hospital, Abergavenny (see Table 3.4 for configuration of inpatient services). There are a number of smaller community hospitals, integrated health and social care centres, and health centres providing important clinical services to our residents outside of hospital settings. Page 27
28 Table 3.4 Specialty Bed Configuration Specialty RGH NHH YYF Total General Surgery Urology Trauma & Orthopaedics ENT Ophthalmology 8 8 Maxillo facial surgery 2 2 General Medicine Haematology Gynaecology Adult Total Paediatrics (inc PHDU) Neonatal Unit (SCBU) Obstetrics and Midwifery Total The Health Board also provides comprehensive Mental Health and Learning Disabilities services in both hospital and community settings to the population of Gwent and South Powys. Table 3.5 Overview of Mental Health and Learning Disability services community Community Services CMHT Assertive Outreach Crisis resolution Liaison Services Early intervention psychosis PC Mental Health support Adult Older Adult Home treatment In reach Memory assessment clinics Day Hospital Learning Disability Specialist Services CLDT Intensive Support Community package Service team Eating Personality Substance Veterans Forensic disorders Disorder misuse Service Psychiatry 2 teams 2 teams Table 3.6 Overview of Mental Health and Learning Disability services inpatients Inpatient Services Adult Intensive Older Adult Forensic Learning Care Dementia Functional Disability YAB 11 YYF St Cadoc s 22 5 County Bronllys 12 YTC 13 7 Ti Siriol St Woolos Chepstow 12 Brecon 10 LLandrindod 10 Maindiff 15 Llanfrechfa Grange 34 Page 28


29 In addition, the Health Board commissions a broad range of services at an annual cost of approximately 307 million secured through a complex portfolio of contracts and contracting arrangements with English, Welsh and Third Sector Providers. Around 80m relates to hospital provided care at a secondary care level and 100m to tertiary services commissioned through Welsh Health Commissioning of Specialist Services (WHCSS). 3. Our Workforce The performance of our healthcare system is directly related to the people who provide care and services to the individuals, families and communities we serve. It is vital that we use the talents and experience of our whole workforce to provide services that improve health and improve care together, whilst creating future workforce sustainability. Achieving this balance needs a different mix of skills, competency and capabilities to the current ones. Our Clinical Futures Workforce Strategy is one of the key building blocks to delivering these changes. Primary Care Within primary care there are 1,216 FTE of which there are FTE medical posts and FTE clinical support posts which include practice nurses and health care support workers. The remaining posts include administration roles. These are shown in the pie chart below and show that medical staff and receptionists are the largest groups at 26% and 29% respectively. Figure Primary Care Workforce Admin/prescribing clerks 6% Medical Secretaries 4% Assistant Practice managers 2% IT 1% Medical 26% Data Entry Clerks 1% Receptionists 29% Nursing 13% Practice Managers 7% other 4% Pheblotmists 2% Health Care support worker 5% The variation in staff numbers by staff group between October 2012 and October 2013, along with a brief description of the reason for change is provided in Table 3.6 below. Directly Employed Workforce Overall, the Health Board employs 10,653 FTE staff with a headcount of 13,336 (as of November 2013) reflecting an increase in 71 FTE since this time last year.the breakdown of staff by banding is shown in Table 3.7. There is no appreciable difference in profile over the past 12 months. Page 29


30 Table Breakdown of staff by banding (Nov 2013) Banding (Non Number FTE Medics Number WTE medics) Band Junior Band Health Board grade doctor 2.49 Band Specialty Doctor 54.4 Band Clinical Fellow 46 Band Salaried GP/Dentist 16.1 Band General Medical Practitioner 7.92 Band Associate Specialist Band 8a 197 Consultant Band 8b 116 Band 8c 84 Band 8d 25 Band 9 10 Non A& 21 Figure 3.4 profile of Workforce 2013 Our workforce is ageing, in previous years the largest number of staff were aged years. However, this year the age profile shows that our largest age profile is years, with increasingly more staff working over the age of years. Figure Gender/full time/part time profile Female workers constitute 83% of our workforce, with a relatively equal split of full time and part time arrangments. There has been little change in this position since last years plan. Sickness and Absence Graph 3.1 The UHB has a sickness absence target of 4.99% and this has broadly been achieved in the first 6 months of 2013/14, where the rate has improved by 0.5% on the same period in the previous year. The predictable seasonality of sickness absence is such Page 30
31 however, that the delivery of 4.99% across the year will prove challenging. Volunteers Aneurin Bevan University Health Board recognises the important role which volunteering plays in complementing the work of its staff. It supports and encourages the efforts of individual volunteers and voluntary organisations for the benefit of patients and their relatives. There are over 49 volunteer schemes in operation within the organisation. Examples of such schemes include: Maternity Buddy - To act as bedside support for women who are patients on the wards within maternity. Patients' Panel - To work with the Health Board to improve health services to all patients in Gwent. Sex Matters - Peer led education on sexual health - sexual health training provided for volunteers. Gwent Cancer - To support people with a terminal illness. WRVS and League of Friends- tea bars throughout the organisation. GAVO - Wide range of schemes. Gwent Red Robins - Volunteers spend at least 4 hours a week as part of the ward team to enhance the patient's experience. Sunflower - Befriending patients to enhance socialisation, day room activities. 5. Our Finances Our Financial Allocation The University Health Board has an allocation of approximately 1 billion per annum to provide health care for our resident and registered population. This section provides a strategic overview of current resource use by programme and locality and how that compares with patterns of resource use that might be expected if factors such as reported health needs, age and deprivation are taken into account. 3 This, in turn, enables Board maturity and provides information which may support future prioritisation exercises and the development of a disinvestment framework as part of the development of the commissioning function. ABUHB spend per head is materially below Welsh average when based on crude population figures or population adjusted for health or social care need. Financial Performance Despite the challenges of its relatively lower level of funding compared to need, Aneurin Bevan University Health Board has nevertheless met its financial targets in each year since its establishment, and has delivered a significant programme of cost efficiencies. The graph below shows the actual savings delivered since 2009 compared to the performance of the former Gwent Health community. 3 The NHS Expenditure Programme Budget Statistical Report, published annually by the Welsh Government, provides an analysis of LHB expenditure by health condition for the Board s resident population. The latest publication of this data relates to financial year. Page 31
32 m Graph 3.2 Gwent Community / ABHB savings delivered / / / / / /13 Year This improvement in performance has also been a significant contributor to the Health Board s improvement in relevant and relative reference cost comparisons, as demonstrated in the graph below: Graph Summary reference cost comparison against all Wales average (100%) 160.0% 150.0% 140.0% 130.0% 120.0% 110.0% 100.0% (6th) (4th) (4th) (3rd) 90.0% 80.0% 2008 / / / / 12 Abertawe Bro Morgannwg Aneurin Bevan Betsi Cadwaladr Cardiff & Vale Cwm Taf Hywel Dda Powys None of this significant improvement in financial performance has been at the expense of the delivery of key Tier One service targets, for which the Health Board has also seen improvement, and is in fact leading the delivery across Wales, in many areas. Compared to other LHBs, ABUHB is relatively less well-resourced to meet the healthcare demands of its population. On the expectation that this relative position is unlikely to improve significantly in the immediate future, it implies an even greater emphasis is needed to prioritise the investment of funding towards those areas with the greatest relative health need. This is likely to require funding to be directed away from some existing services which might be considered of lesser benefit to the overall health of the ABUHB population. Baseline Financial Position The Health Board s baseline financial plan for identified cost pressures totalling 44.8m, with savings plans of 20m and further cost avoidance schemes of 5.8m. This left an over commitment of 19m, which the Board acknowledged in agreeing to the interim plan in March, and which would need to be managed and addressed. Page 32
33 The Board s ambition at the outset of the financial year was to set a challenging stretch for improvement based on our strong performance in previous years. Rather than accept a worse case risk assessment that would have generated a far bigger starting gap than the 19m, a strict financial governance approach was applied to create the right environment for progress to be made on finances. Financial expenditure in the first few months of indicated that the run rate was running at a higher rate than the 19m over commitment reflected in the initial financial plan. The Board therefore took the decision to revise its forecast outturn deficit to 25m in July Although this deteriorated the in year expectation, the Board s financial approach is to be very clear on the financial problem to be addressed and therefore the expectation of increased effort on further development and delivery of the financial plans. At the same time, the Board took a decision to introduce a turnaround and recovery process from within existing management resources to increase the pace of delivery. The Health Board received an additional allocation of 23.9m following the Welsh Government s announcement in October This announcement was combined with a requirement to recognise additional costs relating to the ambulance service and cardiac surgery, totalling 2.5m, leaving 21.4m to contribute towards delivering a balanced financial outturn. Following the receipt of this funding, the Board revised its forecast outturn deficit to 8.4m in October This reflected an assessment that the year end deficit could still be as high as 10m based on expenditure levels in the first half of the year, and that further action would be required to mitigate this level of risk. Following a range of plans and actions that have been agreed during the third quarter, the forecast deficit has been reduced further to 5.6m as at November This remains the current forecast outturn for , although action is continuing to chase delivery of the statutory break-even target. The recurring impact of many of the actions to deliver break-even in will be limited. The Health Board therefore enters the to planning period with an estimated underlying recurring deficit of 15 million. 6. Our Current Performance Overview of Performance (excluding Quality and Patient Experience) Progress against a range of performance measures is summarised below, augmenting those for Quality and Patient Experience section. 6.1 Immunisation rates The UHB has made incremental progress with its immunisation programmes rates in 2013/14. Influenza vaccination rates for the UHB in 2013/14 have been consistently on a par with or above the all- Wales rates for both patients aged 65+ and those <65 years of age in at risk groups. For childhood immunisation, performance is amber or green and is consistent with or, for some measures, better than average performance across Wales. A school and further education college based MMR catch up campaign has been undertaken with particular focus on the year age group, where MMR immunisation rates are lowest. 6.2 Chronic conditions management Multiple admission rates for people with chronic illness within the UHB are consistently lower that the average rates for Wales and, since December 2011, have been better than target (Graph below). The Page 33
34 Health Board average length of stay for these patients is also lower than the average for Wales and is lower than the expected standard of 5.7 days. A Primary Care divisional dashboard is nearing completion covering a range of measures related to primary care. Alongside more specific primary care measures the dashboard will also cover efforts to reduce the need for people to access acute care by improving the level and consistency of locally available services for groups such as people with chronic disease and the frail elderly. Graph % 16% 15% 14% 13% All Chronic Conditions multi-admission rate (rolling 12 months average) 12% 11% 10% Gwent target BiWales Wales 6.3 Referral to Treatment Times Despite some improvement in the first quarter of 2013/14, the 26 week standard for referral to treatment times (RTT) has deteriorated within year (Graph 3.5) with the year end forecast of approximately 90%. The number of patients with a referral to treatment time beyond the 36 week standard has increased within year and it an anticipated to be 1,400 at year end, a deterioration of approximately 1,000 within year. There are no forecast breaches of 52 weeks. This deterioration is aligned to the UHB s statutory obligation to achieve financial balance and has required to UHB to reappraise its RTT delivery profile, which is considered in greater detail below. Graph % Referral to Treatment Time 26weeks (standard = 95%) 95% 90% 85% 80% monthly target 6.4 Cancer targets The UHB has successfully maintained the 98% standard for the treatment of patients referred for reasons other than suspected cancer receiving treatment within 31 days of a diagnosis for over two and a half years. In contrast to previous years, monthly compliance with the 95% standard for patients referred with suspected cancer to receive treatment within the 62 day limit was not achieved for the first Page 34
35 five months of 2013/14 but was secured in September and subsequently maintained. Detailed action plans have been developed to maintain this performance with particular challenges in urology, breast and head and neck services. The UHB has successfully achieved compliance with the All Wales Cancer Standards across all tumour sites that are in the direct span of control of the organisation. 6.5 Day of Surgery Admission (DOSA) and Day Case Rates Improvements in DOSA rates has been sustained and the rolling 12 month average rate continues to show this. However, whilst target levels have been achieved in all surgical specialties (72%), these are short of best-in-wales (84.7%) and best-in-class (95.5%). Actions are being taken to further enhance performance, most notably with the opening of the Glan Usk suite as an admission area to facilitate improving DOSA rates in NHH with early signs of success evident. Graph % 80% 75% % Elective Operations on Day of Admission 70% 65% 60% 55% 50% abuhb monthly abuhb rolling BiWales The overall rolling 12 month day-case rate for the UHB has slowly but steadily increased within year, though this remains short of the 75% Welsh target and the 72% Best in Wales. Specialty specific daycase rate targets are being achieved in general surgery, orthopaedics, urology, ENT, ophthalmology, oral surgery and gynaecology. The British Association of Surgery (BADS) 50 performance has increased with monthly and rolling 12 month performance reaching the national target level, though there are opportunities for improvement in orthopaedics. Graph % BADs 50 Daycase Rate 80% 75% 70% monthly rolling best 6.6 Ambulance transfer times Compliance with the 15 minute ambulance handover target performance is steadily improving following a winter decline. Performance is now within the amber (10% tolerance) band and is approaching the Page 35
36 expected standard. The 60 minute handover performance has demonstrated a similar pattern but the improvement in performance has been more marked. Graph Minute Handover Time Performance 100% 95% 90% 85% 80% 75% RGH target NHH amber 6.7 Unscheduled Care Access Times UHB data, which includes Ysbyty Aneurin Bevan and Ysbyty Ystrad Fawr, shows continual improvement in the first half of 2013/2014 and is steadily approaching the target level of 95%. Over the past 12 months, ABUHB (including YAB and YYF) performed above the all Wales average 4 hour wait compliance by 1.1%. Graph % Monthly A&E 4hr Wait Performance (ABUHB v Wales) 95% 90% 85% 80% abuhb amber target Wales 75% Whilst there has been a parallel improvement in the number of patients waiting >12 hours, it falls some way short of the elimination of such waits which is the UHB s objective. 6.8 Delayed patients The increase in the numbers of patients delayed in their transfer to a more suitable care environment has continued during the first 6 months of 2013/2014. This increase has been balanced by a parallel decrease in the average delay for these patients and this has prevented any consequent increase in the total Delayed Transfer of Care (DToC) bed days. The total monthly number of days lost to DTOC has Page 36

37 fallen slightly from 2,668 in April 2013 to 2,640 in September 2013, which represents the equivalent of 88 beds and contributes to the excess emergency LOS in a number of specialities. Graph Our Partnerships It is increasingly clear that the needs of some of the most vulnerable people in our communities cannot be met by organisations working alone. Public services of the future therefore are much more likely to require strong collaborations between Statutory and Third Sector organisations to ensure that the needs of the people that we care for, and those from within their family or support networks that also fulfill a caring role, are responded to and supported. 7.1 Health Board Profile Partnerships (External) Working with the Aneurin Bevan Community Health Council Aneurin Bevan Community Health Council (CHC) forms a local link between patients and the Health Board and is an independent statutory organisation that represents the interests of the patient and the public. The CHC is the independent NHS watchdog concerned with all aspects of NHS care and treatment. The Health Board and CHC hold joint Board meetings during the year and over the last year we have continued to work closely with the CHC on a number of projects and plans particularly through a joint planning committee. The CHC has been active members providing advice and guidance on a number of our committees and programme boards to assist with shaping our plans and future services. We value the reports the CHC produces and present to each of our Public Board Meetings and the ongoing monitoring and reviewing work they undertake with regard to the operation of local health services we provide to our patients and their recommendations for improvements. Across the Aneurin Bevan Health Board area, a number of key statutory partnerships are critical for us in communicating and engaging to achieve our partnership plans across Gwent (these include Single Integrated Plans (SIPs), across the five Local Service Boards and Gwent Area Planning Board. In addition, the Health Board joint agency, Public Health and Partnership Committee, Gwent Health, Social Care & Housing Forum and the multi-agency Stakeholder Page 37
38 Reference Group provide important opportunities to align service priorities and we have an ongoing programme of work with them. As they have evolved, the SIPs have been considered by the twelve Health Board Neighbourhood Care Networks and our Clinical Leads and Primary Care Clinical Directors have led this part of the process. As a result, a range of health and social care professionals, together with representatives from Housing Associations and the Third Sector have all had the opportunity to influence the SIPs. The Communities First Clusters, building on the Welsh Government flagship community regeneration programme, are supporting the national anti-poverty priorities with a focus on education/skills, the economy and health. The clusters are based on the most deprived Lower Super Output Areas and aim to support the most disadvantaged members of the community. It will be important to join up strategic planning and service delivery initiatives set out within Single Integrated Plans and Communities First Plans. Together with Aneurin Bevan Community Health Council and other partners we have co-produced a number of strategies setting out a common vision and direction of travel for improving and strengthening delivery of our services. The Mental Health and Learning Disability Partnership Board for Gwent has been in existence for nearly three years and has representatives from across the five Local Governments in Gwent, the Aneurin Bevan University Health Board and the Voluntary Sector in Gwent but most importantly from service users and carers themselves. Together these partners have co-produced strategies for both mental health and learning disability. They have agreed a common vision, a common implementation plan and common aspirations for the services that are been delivered. These strategies have been based firmly on the views of people receiving our services and by those that care for the people who receive the services. 7.2 Partnerships (Internal) The Health Board has a number of internal mechanisms for involving its staff including our Health Professionals Forum, Staff Survey Transformation Group and Trade Union Partnership Forum. Stakeholder Reference Group The Stakeholder Reference Group was established in July 2010 and comprises representatives from a range of interests across the Gwent area and the role of the Group is to provide independent advice on any aspect of the business of the Health Board and to contribute to discussions by providing views of stakeholders from across our communities. The Group has undertaken a range of activities since that time and has agreed a programme of work to align closely with current key issues for the Health Board and the priorities of our Plans. This enables the Group to provide feedback and views to the Health Board via reports and directly through the involvement of the Chair of the Group, Mark Gardner, in Health Board discussions. The Group will continue to work closely with the Health Board to take forward our Medium Term Plan. Healthcare Professionals Forum We have also established our Healthcare Professionals Forum. The Forum comprises representatives from a range of professional groups from across the Health Board area, including hospital and community based health professionals. The Chair of the Heath Professionals Forum is Dr Sue Greening. The role of the Forum is to provide independent professional advice on any aspect of the business of the Health Board and to contribute to discussions by providing views of health professionals Page 38
39 from across our sites and services. Again the Forum has already provided input on the Health Board s Plans and we will continue to work closely with the Forum on our Medium Term Plan. Trade Union Partnership Forum The Trade Union Partnership Forum (TUPF) reports directly to the Board and has responsibility for engaging with staff organisations on key issues facing the organisation. The TUPF provides the formal mechanism for consultation, negotiation and communication between our staff and the Health Board, embracing the Trades Union Congress principles of partnership. The group is jointly chaired by the Staff Chair for Trades Unions, George Puckett and the Chief Executive Dr Andrew Goodall and is attended by Executive Directors, Senior Managers and a maximum of 30 accredited staff representatives, providing a fair range and balance of Trades Unions in the organisation. The committee offers opportunities to have detailed discussions about matters of particular importance to the Health Board such as finance, our annual and medium term plans and partnership working. The Forum has provided an excellent opportunity for managers and Trades Unions across the Health Board to meet and discuss a number of strategic issues impacting on delivery of services and workforce. The model below is intended to illustrate a range of areas where involvement and partnership can be developed to influence the performance of the Health Board. Figure 3.6 Involvement/ Partnership Increased involvement of individuals through: One to one discussion, e.g. through personal review Provision of wider development opportunities e.g. offering membership to Partnership groups Teamwork approach Innovations and suggestions teams Individual and staff representative input to local departmental issues, e.g. Review services Manage change Audit Assess & manage risk Develop local HR practices, e.g. Flexible working initiatives, where required. Strategic development Provisions of opportunities for nominated representatives and/or selected individuals to join management working groups e.g. Capital schemes & Service Planning Education & Training Workforce Planning Policy development Communication Equal opportunities Health at work Corporate responsibility & strategic direction Through participation of Staff Representatives at Health Board and Health Board-wide groups that direct the following: Corporate governance Clinical governance Performance management Health Board policy development Communication/ Information channels 8. Teaching and Research Aneurin Bevan Health Board and the Gwent Clinical School have been particularly active in the field of medical education for a number of years. The recent award of University status has formally recognised this activity which spans all facets of education and includes quality innovation and research and development. In relation to the Gwent Clinical School, University Health Board status further validates the activities which have underpinned the development of medical education as a core business of the Health Board. Our structures for education are particularly strong and encompass undergraduate and postgraduate medical education. Our Faculty has recently been strengthened through the development of Faculty Leads within postgraduate education and we have been able to bring Page 39
40 together our Health Board structures to ensure that quality issues are addressed right the way through the education spectrum. At the 2013 postgraduate Deanery commissioning meeting, the Health Board were applauded on the success of the Faculty Team and asked if they would be prepared to help other Health Boards improve their own structures. Our clinical workforce is very committed to medical education with nearly two thirds of consultant staff being formally recognised by Cardiff University with Clinical Teacher status. The Honorary Sub Dean role has raised the profile of Gwent Clinical School both within the University but more so within Aneurin Bevan Health Board which has, in turn, encouraged clinicians to engage in an educationally rich environment. This has also led to our consultants actively engaging in the development of the new C21 curriculum with many individuals leading on modules and working to ensure the success of this revolutionary curriculum. Quality Improvement is now being woven into the structures for curricula in all specialties and work is ongoing with the ABCi to target training grades to engage them in quality improvement projects at an early stage. This engagement empowers trainees to instigate changes at the coal face of patient care whilst also giving them an understanding of the wider impact of their own actions within a patient care pathway. University Health Board Status reflects a culture that places a strong emphasis on research as a core activity. University Hospitals tend to be among those that have the nation s most cutting edge medical facilities and are often the source of breakthroughs in medical care and new interventions offering their patients a higher chance of receiving the latest innovations in healthcare. For instance our planned SCCC will be one of the next generation of healthcare facilities for specialist and hyper acute care. We embrace the philosophy of Research and Development 4 (covered in more detail in Chapter 9), fostering a strong culture of research and innovation that will feed into policy and practice across our system of care. We are committed to ensuring that our university status translates into high quality research and patient care. This will encourage the best doctors, nurses and other clinicians to work within our Health Board. The Health Board has a number of jointly held health/academic posts across clinical, nursing and therapy specialties; a range of research projects being carried out collaboratively by the Health Board and Universities in Wales, and senior employees who hold Chairs at Cardiff University. We are now positioned to strengthen links with universities and support clinicians wishing to take advantage of research and development opportunities. 4 Our approach to Research and Development is set out in Chapter 9 (Section 4) Page 40
 has a resident population of around 600,000. The age structure of our population (Graph 4.")
41 Percent age change from Chapter 4 Local Needs and Challenges 1. Demography 1.1 Our population is Ageing Aneurin Bevan University Health Board (the Health Board) has a resident population of around 600,000. The age structure of our population (Graph 4.1) shows this is similar to Wales as a whole, with slightly higher proportions of persons aged under fifteen and in their forties, and lower proportions of persons in their twenties. Graph Population Pyramid ABUHB and Wales The latest projections indicate that if current trends continue the total population across the Health Board area will remain stable over the next ten years, although the age profile of the population will change significantly. Currently around 8% of the population are aged 75 years and over. Population projections predict a rise in the proportion of people over 65 years from 108,700 in 2013 (19% of the total population) to 153,500 (26% of the total population) in the next 20 years. Graph Population Projections The increase in the number of older people is likely to be associated with a rise in longterm conditions whose prevalence is strongly agerelated, such as circulatory and respiratory diseases and cancers. Older people are more likely to have at least one and often multiple chronic conditions an illness such as diabetes, dementia or arthritis and have more as their age increases. Produced by the Public Health Wales Observatory, using data from the Welsh Assembly Government Page 41
 of patients admitted to hospital with a Length of Stay (LOS) less than and more than 11 days is shown opposite in Graph 4.")
42 Graph % bed days by number of co-morbidities to 1 2 to 4 5 to 5 diseases, with 36% having 8 or more diseases. 8+ LOS >11days LOS<11 days A hospital profile (2011, ABUHB) of patients admitted to hospital with a Length of Stay (LOS) less than and more than 11 days is shown opposite in Graph 4.3 Typically for shorter lengths of stay (under 11 days) patients have an average of 3.6 diseases (co-morbidities), the profile for longer lengths of stay shows that three quarters of patients present with an average of 6.5 Ideally older people tell us that they want to live in their homes for as long as possible and have accessible health and social care services that are proportionate to their needs and minimise the likelihood of institutional based care (hospitals, residential or nursing homes).traditionally our healthcare system has not been designed to achieve this ambition, we know with some precision how to diagnose and treat certain acute diseases, but people who suffer from multiple diseases require much more individualised care, where there are equal partners working with supportive clinicians to maintain and improve their health, as illustrated below. Challenges Unsustainable stemming demand Acute centred, curative model Dealing with the parts of a person Rewarding ill-health Activity-based biomedical measures/outcomes Opportunities Sustainable managing demand Transformational, prevention model Dealing with the person Rewarding health and well-being Relational continuity measures/outcomes Our Challenge to develop new ways to use the resources we have to respond better to the changing needs of our older and ageing population. 1.2 Variation in Deprivation and Health Inequalities The population served by Aneurin Bevan Health Board covers a diverse range of population groups with different health needs and sizeable inequities in health and healthcare both within and between localities. There is new evidence of the widening gap in healthy life expectancy between the most and least deprived groups in Gwent, which can be up to 20 years difference within some localities (comparing the most deprived and least deprived people in our population), Actual life expectancy for the most deprived fifth of the population has risen more slowly than for any other group. For instance, people living in Monmouthshire and Ebbw Vale have a 10 year difference in average length of life. One of the main challenges for us and our partners is levelling up the premature mortality (death) rate from the worst to the best, by tackling health inequalities within our most deprived populations. Page 42
 shows the pattern of deprivation in Aneurin Bevan University Health Board, highlighting local authority boundaries and selected major towns. Figure 4.")

43 There are distinct areas of deprivation within Aneurin Bevan University Health Board. The map below (Figure 4.1) shows the pattern of deprivation in Aneurin Bevan University Health Board, highlighting local authority boundaries and selected major towns. Figure Map showing the pattern of multiple deprivation in ABUHB by Wales fifths of small areas (LSOA) Area of North Caerphilly, Blaenau Gwent and North Torfaen Inner city Newport Produced by the Public Health Wales Observatory The main clustering of deprivation in Aneurin Bevan University Health Board can be seen in the South Wales Valleys communities in North Caerphilly, Blaenau Gwent and North Torfaen and inner city Newport. If things stay as they are, not only will people in more deprived communities die earlier, they will also have fewer years in good health without disability than those who reside in our least deprived communities. Premature mortality is an area of considerable concern for the Health Board; Graph 4.4 shows the leading cause of premature (less than 75 years) mortality in the Aneurin Bevan area. Graph Leading causes of premature mortality in ABUHB ( , ONS) 2009 Page 43
44 Many of the causes of poor health are deep-rooted and they are often difficult to tackle. The main causes of premature mortality are cancers and circulatory diseases. The lifestyle risk factors that are precursors to these conditions are evident in our population. Gwent faces an obesity epidemic with over 60% of the population overweight or obese and our rates of smoking, and drinking to excess continue to concern because other substance misuse is a relatively small number. Addressing the Inverse Care Law The Inverse Care Law was first described by Dr Julian Tudor Hart in It states that, the availability of good medical care tends to vary inversely with the need for it in the population served. Delivering Local Health Care: Accelerating the Pace of Change, published by Welsh Government, provides a framework for action for health boards, local government and third sector partners to work together, to provide high quality, safe and sustainable services to meet the needs of local people. The plan calls for a collaborative approach to achieve a measurable closing of the gap in health outcomes between the most and least deprived areas. Aneurin Bevan University Health Board and Cwm Taf Health Board have been selected as pathfinders to develop services to improve health outcomes in areas of greatest need. Cardiovascular disease and cancer are the leading causes of premature death in Aneurin Bevan University Health Board. Rates of premature mortality from cardiovascular disease are highest in the most deprived areas of Wales and are significantly higher in males than females, as shown in Graph 4.5. The gap in the circulatory disease premature mortality rate between the most and least deprived populations is not narrowing. Graph Mortality from CVD, all persons under 75 ( ) European age-standardised rate per 100,000, by deprivation fifth, persons, Wales, ICD-10 I00-I99 Males - rate ratio 2.4 Females - rate ratio % confidence interval Least deprived Next least deprived Middle Next most deprived Most deprived Produced by Public Health Wales Observatory, using ADDE/MYE (ONS), WIMD (Welsh Government) Neighbourhood Care Networks (NCNs) have been established by Aneurin Bevan University Health Board to plan and deliver integrated out-of-hospital services. In Aneurin Bevan University Health Board there are 12 NCNs made up of around 30,000 to 50,000 people who are registered with GP practices in the catchment area. The graph below (graph 4.6) shows, for each NCN, the percentage of patients living in the most deprived fifth of areas in Wales. Of the 141,930 patients living in the most deprived fifth of areas in Wales, a total of 94,510 (66 per cent) were registered within the catchment area of the 5 NCNs. This suggests that services should be targeted in these areas to reduce premature mortality from cardiovascular disease. Page 44

45 Graph % of patients living in most deprived fifth of areas in Wales, NCN clusters in ABUHB 2013 Within Aneurin Bevan University Health Board, of the patients living in the most deprived fifth of areas in Wales, around 66 per cent were registered within the catchment area. When looking at the distribution of mortality, these areas have the highest rates of premature death from circulatory disease and all age mortality rate from coronary heart disease. Lifestyle Risk Factors The Welsh Health Survey provides information about self-reported lifestyle risk factors in adults. The chart below (Graph 4.7) shows the age-standardised percentage of risk factors for cardiovascular disease in people aged 16 and over in Wales. Graph % of reported risk factors for CVD in adults in Wales Reported risk factors for cardiovascular disease, age-standardised percentage, persons, age 16 and over, Wales, 2011 Produced by Public Health Wales Observatory, using Welsh Health Survey (WG) Physical inactivity 71 Unhealthy eating¹ 67 Overweight or obese 57 Alcohol² 43 Current smoker Obese High blood pressure³ Diabetes³ physically active on fewer than 5 days during the previous week 1 eat fewer than five fruit and vegetables during the previous day 2 drink above guidelines on at least one day during the previous week 3 currently being treated Smoking is a major risk factor for heart disease and remains a significant public health concern. In Aneurin Bevan University Health Board around 24 per cent of adult population are smokers. The percentage of adult smokers is significantly higher in Blaenau Gwent and Torfaen compared to the Wales average. The Welsh Health Survey also provides information about smoking prevalence according to socio-economic classification. The analysis of Welsh Health Survey data in 2010 showed that in households headed by someone who has never worked or who is long term unemployed, 44 per cent of adults report smoking. Obesity is another preventable risk for heart disease and is caused when energy intake from food and drink is greater than energy expenditure through the body s metabolism and physical activity Page 45
46 over a prolonged period. In Aneurin Bevan University Health Board around a quarter of adults are obese (BMI 30) with rates in Blaenau Gwent, Torfaen and Caerphilly significantly higher than the Wales average. Being physically active lowers the risk of developing CVD as regular exercise can reduce the risk of coronary heart disease by about 30% (WHO, 2009). National guidelines suggest these cardiovascular benefits can be achieved through minimum of 30 minutes of moderate activity on five or more days per week. When adults in Aneurin Bevan University Health Board were surveyed in 2009/10, the average number days per week they engaged in moderate or vigorous intensity physical activity was 2.3 days. Diet has an important role to play in the prevention of coronary heart disease. A balanced diet which is high in fruit and vegetables and low in fat, salt and sugar can help to prevent heart disease. When surveyed in 2009/10, the proportion of adults in Aneurin Bevan University Health Board who had consumed at least five portions of fruit and vegetable in the previous day was 32 per cent. Alcohol misuse is associated with an elevated risk of heart disease. In Aneurin Bevan University Health Board around 43 per cent of adults reported drinking above recommended limits in the previous week. In relation to patterns of alcohol misuse around 131,118 residents report binge drinking. Recent data suggests that middle aged males (peaking at years of age) and women (peaking at years of age) most frequently report drinking above recommended limits. Cardiovascular Disease (CVD) Risk Risk factors a recent audit of patient records on the GP clinical information systems of 49 ABUHB GP practices found only 13.44% of patients not already known to have cardiovascular disease had a formal cardiovascular disease risk assessment in the previous 5 years. This is in contrast to 81% having their smoking status, 64% their Blood Pressure (BP), 53% their cholesterol and 43% their Body Mass Index (BMI) recorded. rates for key screening information Graph % of patients (40 70 years) with recorded risk factors for CVD 43.24% 64.40% 53.25% 62.85% 81.00% 13.44% BMI BP Cholesterol CVD Risk Assess (5yrs) Smoking Status (2yrs) Smoking Status (5yrs) Produced by Public Health Wales Primary Care Quality Service and NWIS using Read Coded data on clinical information systems and extracted using Audit+ There are a number of evidence-based interventions that can prevent or postpone deaths in people with or at high risk of cardiovascular disease, cancer and diabetes, including smoking cessation and vascular risk assessment. The contribution of selected interventions will be modelled to quantify the potential impact on mortality rates and the scale of delivery required (e.g. number Page 46
47 Wales Caerphilly Blaenau Gwent Torfaen Monmouthshire Newport needed to treat) to achieve the agreed target for reduction in premature mortality. The costs of different models of care will be calculated and a balanced portfolio of interventions developed. Our Challenge to reduce pre-mature mortality in our most deprived communities. We will achieve this by initially targeting evidence based actions to close the inequality gap in premature circulatory disease mortality between the most and least deprived areas. 1.3 Improving the health of our Children and Young People Children and young people are those aged 0-24 years and constitute just over 30% of the population of Wales. Positive and negative effects on health and wellbeing accumulate through life starting before birth and vital foundations of adult health are set down in prenatal life and early childhood. Childhood inequalities in physical, mental and emotional health are strongly associated with lifetime risk of poor physical and mental health in adulthood. In terms of preventing ill-health and/or social disadvantage in the long term, the importance of promoting and protecting the health and well-being of children and young people cannot be underestimated. Table Health of Children and Young People in ABUHB Indicator (red indicates where Locality indicator is worse than the Wales average) % population aged % babies born preterm % babies breastfed at birth % children living in poverty % 5-15 year olds eligible for free school meals % year 11 leavers not in education, employment or training % 4/5 year olds overweight or obese Teenage conceptions <18s % 4 year olds up to date with immunisations Uptake for 3 complete doses of HPV vaccine Asthma prevalence (0-24 year olds) year olds with decayed missing or filled teeth Emergency admission rates (0-24 year olds) Child mortality rate (0-17 years) Source: Public Health Wales Observatory 2013 All the indicators contained in the table above have results that are higher (H) or lower (L) than average Wales for your health board area and/or one or more of its local authority areas. Page 47

48 Poor health and wellbeing in childhood is strongly associated with multiple deprivation and poverty and the table of indicators of the health of children and young people in the ABUHB area shows that in four of the Local Authority areas a high percentage of children are living in poverty. The same local authorities have high emergency admission rates for children and young people which is evidence of children and young people having poorer health and wellbeing. The fact that three of the local authority areas with high levels of deprivation now have a lower than average teenage conception rate reflects the successful development of sexual health services for young people although more still needs to be done to bring the rate down in Newport. The MMR campaign in response to the measles emergency in 2013 has boosted childhood immunisation rates for all the local authorities in Gwent and uptake at 5 years is now 92% for ABUHB as a whole. The foundation of a healthy diet and prevention of adult obesity is laid down in childhood. The table of indicators shows that children living in a deprived areas in Gwent are less likely to be breast fed and more likely to have dental caries which are both indicators of a poor diet. Conversely, Monmouthshire which has a low proportion of children living in poverty has a low percentage of 4/5 year olds who are overweight or obese indicating a healthier diet. This pattern of inequality in childhood diet and obesity needs to be urgently addressed to prevent the escalation of demand on healthcare services resulting from adult obesity. Our Challenge is to give every child the best start in life both to enable them to enjoy good health and wellbeing today and to lay down the foundations for healthy adult life in order to reduce the burden of preventable disease on the healthcare system in future. 1.4 Health Needs As noted previously, many of the challenges facing the organisation are at population level as a consequence of the changes in the demographics of our population and the legacy of the levels of social and economic deprivation that is evident in many of our communities. The increasing prevalence and incidence of dementia presents a significant challenge, as illustrated in Graph 4.9 the number of people living with dementia will rise from just over 7,000 to 12,000 by Graph Population estimates for Dementia (males and females ABUHB) Source PHW The self reported health status of our citizens indicated that for most of our localities the levels of ill-health are higher than the Wales average placing significant demands on our primary, community, mental health and secondary care services. Page 48


49 Table 4.2 Graph 4.10 The incidence and prevalence of these long term conditions are expected to rise as a result of both the predicated population ageing and our citizen s self reported unhealthy lifestyles. Local analysis of predicting increases in diabetes are shown opposite. Quality of Life Indicators are shown by Locality in Graph Table Quality of Life Indicators by Locality Our Challenge to reduce preventable morbidity resulting from unhealthy lifestyle choices and to support people to age well and live independently for as long as possible. Page 49
50 2 Commissioning Approach Strategic Approach within the Health Board Commissioning is the process of specifying, securing and monitoring services to meet individual needs at a strategic level. It involves the commitment of finite resources to evidence based interventions, particularly but not limited to health and social care sectors with the aim of improving health, reducing inequalities and enhancing patient experience. Essentially commissioning encapsulates the following key functions in order to deliver high quality and effective healthcare to patients: Assessment and Planning that demonstrates the evidence base for commissioning services captured in clear strategic and operational plans with agreed commissioning outcomes. Contracting and Procurement. This relates to agreeing, auditing, validation of contracts and ongoing financial and clinical performance of contracts. Performance management, settlement and review by ensuring providers produce timely and accurate information, benchmarking activity and costs, regular financial and performance reporting, risk sharing arrangements and establishing clear rules of engagement with service providers. Ensuring a value based approach to service provision that is focused on outcome measures, comparison to best in class and evidence based guidelines. Patient and public engagement through the establishment of mechanisms for ensuring the public, patients have an input into decision making and establishing internal and external engagement and communication strategies. In establishing a Commissioning Framework and Commissioning Strategy, the Health Board will be seen as having an investment role in four different outcomes. These are improvements in: Health outcomes: focussing on population well being and health gains for specific or general communities through service improvement or redesign (this includes promoting people s independence, reducing inequalities and promoting social inclusion). Allocation efficiency: ensure resources are aligned to areas of greater health need. Community outcomes: that could result in another part of the system improving, for instance through a regeneration programme, in ways that enable health gains. Clinical and care outcomes: the results of health and social care interventions, for example clinically effective care pathways. The statutory responsibilities and planning framework for Health Boards includes the requirement to effectively commissioning services and achieve financial balance. The current economic environment means we must use the available resources in the most cost effective way for greatest health gain for our population. ABUHB intends to develop a more structured and rigorous commissioning approach to planning and delivery of services. This approach will be informed by Value Based Healthcare principles to ensure the development of a commissioning system that prioritises resources to drive performance improvement in healthcare outcomes for patients and residents, within an ethical framework of decision making. This means ABUHB must be clear on: The strategic priorities of the Health Board described as benefits for the community. The current and future performance and aspirations of the Health Board. The tools we will require to drive improvement. The structure & culture for driving change and improvement. Page 50
51 The above elements will require the commissioning system to act as an enabler, with business intelligence and clinical evidence, along with transparency in decision making being the critical tools to success. Development of Commissioning over the next three years During 2014, the Board will be engaged in agreeing the Commissioning Framework in ABUHB. This will take a wider perspective on population need and relevant resource usage, with the aim of prioritising resources to achieve best results for the Gwent population. Aligned to this is the need to drive service design and delivery through evidence based models, structures and systems will be strengthened to align current delivery to best practice and focus on service provision on the most clinically effective care, including challenging thresholds. This Commissioning Framework will set out the process by which the Health Board will define its priorities to be explained in a Commissioning Strategy. Delivery of the Commissioning Strategy s intentions will lie with both internal divisions and external providers from all sectors, with robust monitoring of delivery to ensure best value is being delivered. The challenge is clear for ABUHB divisions and external providers have received and will continue to receive ABUHB commissioning intentions clarifying our expectations. Contributing to and leading on elements of the national approach to commissioning will be a key part of the ABUHB agenda with existing Collaborative Commissioning proposals being further developed. This will provide opportunities for shared learning, reduced duplication and development of a shared intelligent commissioner portfolio. Contracting as an element of the commissioning cycle will be developed to help act as a key catalyst to drive change with provider organisations, significant early benefits have been achieved through analysis of service delivery at a macro and micro level. Moving into the clinical challenge arena of contracting and focusing on outcomes will be the next stage of development to ensure best value is being delivered. This approach should be developed for adoption as best practice and encompass all contracts and SLA s that the Health Board commissions. Commissioning as an enabler. To ensure it is reflective of the Welsh Government s National Planning Framework requirements for commissioning and incorporates a clear, robust approach to using commissioning to integrate and enable programmes of work within and outside the organisation. Value Based Commissioning. That it builds on the concept of value based clinical services articulated within the Health Board s Three Year Framework through the introduction of value based commissioning. Driving and influencing national and regional commissioning initiatives across Wales. By developing the necessary technical expertise and business intelligence to support the wider organisation and act as a significant contributor to the supra regional and national commissioning agenda. Developing an ABUHB Commissioning Framework & Commissioning Strategy Value Based Commissioning - Prioritisation and Decision Making The Board is undertaking a significant programme of work in 2014 to develop a robust commissioning framework, arrangements and Commissioning Strategy identifying the community focused outcomes and priorities for the Health Board. In order to shift the organisation s culture and approach to decision making (in both the short and longer term) there is a need for systematic clinical and Board discussions on future priorities to ensure that resources are targeted to best effect. This decision making process will need to be based on the components of: Page 51

52 Knowledge derived from scientific or other systematic approaches (evidence). Patient and carer perspectives Clinical expertise Incorporate the wider perspective on population needs The opportunity for improvement in health outcomes, patient experience or use of resources. By applying all these components of intelligence to the commissioning of services will support the Health Board in taking an evidence based approach to decision making, support priority setting and facilitate the re-design of clinical pathways. This will require a clear policy to be developed for ABUHB including a transparent and inclusive decision framework, a clear set of criteria for determining priorities and robust monitoring, governance and information systems to be established. Decision making will need local intelligence to support cases for investment and/or disinvestment and service change will need to include patient views. It is proposed that Commissioning within the Health Board will be a whole system approach. The commissioning cycle includes several elements of activity: Needs assessment Demand/Capacity assessment Opportunity to improve clinically services and well being of our population Prioritisation Planning Setting service specifications Contracting Performance management Monitoring & review The approach within the Health Board will be for commissioning processes to recognise and coordinate the various corporate roles and responsibilities and expertise provided by different teams. With a structure that encourages joint working and optimises the outcomes sought for ABUHB and its patients. Figure Stages of the Commissioning Framework Development This will require a clear policy to be developed for ABUHB including a transparent and inclusive ethical framework, clear criteria for determining ABUHB priorities and robust structural, governance and information systems to be established. Decision making will need intelligence to support cases Page 52
53 for investment, disinvestment and service change and will need to include patient views. Key elements to be developed include: The establishment of clinical intervention prioritization - The Health Board is piloting prioritization of clinical interventions and will share our learning with other Health Boards across Wales as part of the collaborative commissioning approach. Established in July 2013, this systematic approach aims to embed evidence based care into commissioning decision making and prioritization, test the comparative clinical effectiveness of interventions and support the development of commissioning tools. The programme of work draws not only on public health and the clinical evidence base, but also on the business intelligence expertise which is described below. The triangulation of these sources of information should provide a robust assessment of current practice and identify improvements as part of a commissioning and service change decision. The initial focus has been on PCI thresholds in cardiology (linking the pathway with specialised care) and a review of gynaecology/radiology interventions for the same condition. These have been clinically driven with the project being led by the Commissioning Team. This will be evaluated and rolled out as part of evidence based commissioning and service delivery. Development of clinical leadership - The Commissioning Department is working with a wide range of professions to help support the design and delivery of service improvement through commissioning. Examples include the development of clinical champions to take forward the ongoing development of clinical prioritisation, clinical support in relation to gatekeeping and referral management, and the involvement of Public Health and Divisional Clinical Directors in key Commissioning forums such as the Commissioning Policy and Evidence Group and Commissioning Board. Ethical frameworks, prioritisation methodology and other governance frameworks - To support the application of the evidence base arising from these initiatives, it is important that the appropriate infrastructure is put in place to support ethical decision making within commissioning and to ensure the important aspects of an investment or disinvestment decision is highlighted and evaluated. Development of business intelligence to support decision making - In order to support informed decision making within ABUHB Business Intelligence will be critical. Currently there is a disparate approach to gathering and reporting information and it can be onerous to gather a comprehensive triangulated picture of service delivery and performance, both internally and externally. Improving Business Intelligence is seen as a key priority for ABUHB for commissioning, with significant early steps taken to provide improved financial and service benchmarking. Triangulating clinical evidence, patient pathway and financial information against best practice benchmarks is critical to identify opportunities for improvement. Becoming an informed commissioner is key to future decision making and has already achieved success for ABUHB during 2013/14. Programme budgeting marginal analysis - This approach to prioritization has been developed and applied internationally in various countries and within the UK. The Commissioning team will develop options for prioritization processes for the Board to consider, PBMA is one methodology being considered. Links have been made with Swansea University to identify and evaluate what has been implemented in other systems and provide informed options for the Board to consider, clearly outlining advantages and disadvantages and pragmatic options. The Commissioning Framework for ABUHB will need to be designed to handle this process with Page 53

54 resources identified to deliver this approach, particularly with regard to clinical effectiveness evaluation. Patient and carer involvement - The Commissioning Team continues to work closely with the CHC, Stakeholder and Patient Forums where required and are keen to explore other models of patient involvement to ensure the patient perspective informs future initiatives and commissioning issues at the earliest opportunity. Specific Work Programme for the Annual Commissioning Delivery Plan The ABUHB Commissioning and Contracting team have established three areas of responsibility for which an Annual Commissioning Delivery Plan will be agreed as part of the Health Board s Integrated Delivery Plan. These are external contracting, ABUHB commissioning and specialised services commissioning. These specific responsibilities include contract management of a portfolio of health service agreements including financial and activity analysis and performance management, development of outcome based indicators, supporting the programme outlined above including prioritisation process development, referral management for key initiatives and management of cross border commissioning issues. Specialised services commissioning is also a key programme of work to progress along with WHSSC partners and through other collaborative arrangements. In addition, work has commenced on improving arrangements for implementation of the Health Board s policy on procedures of Low Clinical Value such as INNUs (Interventions not Normally Undertaken), low clinical value procedures, clinical threshold developments and established guidelines developed through NICE. Aneurin Bevan University Health Board delivers the majority of routine care to our resident population within Gwent (on average 88% of hospital and community based care). We commission a broad range of services at an annual cost of approximately 307 million secured through a complex portfolio of contracts and contracting arrangements with English, Welsh and Third Sector Providers. Around 70m relates to hospital provided care at a secondary care level and 100m to tertiary services commissioned through Welsh Health Commissioning of Specialist Services (WHCSS). Figure LTA Budgets by providers English Trusts, 7 Welsh Total, 60 WHSCC, 102 Cost in millions, excludes 1.5M contingency ABUHB plans for repatriation of services or changing patient flows will be developed in partnership between external providers, delivery divisions and the Commissioning and Contracting team. Consideration of patient benefit, sustainability, relative clinical outcome performance and financial advantage will be considered as part of the process. The Commissioning Team have developed a comprehensive repatriation process and documentation to support a transparent approach to decision making, to ensure an optimal decision is made for ABUHB. Page 54
55 3. Local Pressures 3.1 Service Pressures The Health Board is required to ensure that healthcare services for the population it serves are safe, sustainable and deliver improved patient outcomes. Service delivery must be seen in the context of a range of internal and external operating pressures. It is recognised that most service plans will be devised with the intention of meeting immediate and ongoing needs. Some plans however, will require transitional arrangements in order to sustain current functionality whilst improving services in the longer term. Reconciling these short and longer term pressures presents a particular planning challenge. The external operating environment can be characterised through a range of service, financial and wider demographic contexts. It is important to understand this wider context in developing plans that are ambitious but deliverable. The external environment challenges have already been described and increasing demand, public expectations, activity of patients and a period of ongoing austerity has implications for hospital and service functioning. This includes higher levels of bed occupancy, and an increased percentage of older and co-morbid patients - which can result in increased lengths of stay. This, in turn, can present pressures on hospital front door services resulting in prolonged emergency department transit times and ambulance handover times and poorer patient experience. Overall bed occupancy for ABUHB s hospitals averages at 90.2% between April and November 2013 and it is recognised that reducing bed occupancy requires a range of demand management and patient flow process improvements. However, it is equally accepted that that reducing length of stay to improving occupancy levels requires a partnership approach, with local authority social services playing key roles as at any one time, our green list of patients suitable for discharge ranges from at any one time, however this excludes any patient that may be waiting onward transfer from our community hospitals. The wider demographic trend in terms of the aging population is reflected in the Health Boards patient case-mix, defined by an increasing requirement for chronic disease management, prolonged lengths of stay and more complex discharge and treatment processes. The ABUHB emergency length of stay currently averages 8.97 days with a Wales best at 8.75 days. With recent census data indicating that one in four of the ABUHB population expected to be over 65 years by 2030, the need to adapt services in partnership with social services and the third sector partners is evident. Overall hospital patient flow difficulties are perhaps most apparent in the provision of emergency services. These services are said to provide a barometer for overall unscheduled care functioning. Some improvement has been seen in the Health Boards Tier 1 performance recently but challenges remain - particularly with regard to the elimination of 12 hour Emergency Department transit times and 1 hour ambulance delays. Despite significant improvement in the rate of 12 hour trolley waits, recent data suggests that approximately 3 patients per day within the Health Board are waiting longer than 12 hours to be transferred or discharged and an average of just over 1 ambulance a day is delayed for 60 minutes. In addition to the Tier 1 targets, these measures are considered fundamental indicators for delivering safe emergency care and we have developed a clinical operating framework to improve our position further in coming months. The Health Boards Unscheduled Care Transformation Board will set the agenda for reform of the unscheduled care pathway through an integrated approach to planning and service improvement. In addition to pressures within unscheduled care, demand is also rising for elective services - which often compete for the same hospital bed capacity. The separation of scheduled and Page 55
56 unscheduled care patient flows will be a key planning principle going forward over the next 3 years. Scheduled Care The Health Board acknowledges that prolonged waits for outpatient appointments and elective treatments are unacceptable. Improving efficiency through theatre reform programmes, addressing clinical variation, managing demand differently and creating sufficient workforce capacity through seven day working will be central components of transformational plans for scheduled care. An example of the potential to improve elective care process may be seen in the elective average length of stay which is 3.97 days for ABUHB as compared to a Best in Wales of 2.74 days. These pressures, in the context of the current financial climate, present particular challenges in developing organisational plans. However, such constraints can also generate a greater degree of lateral thinking in designing future services, particularly when considered alongside improvements in technology, clinical leadership and reduced variation. Opportunities exist to address many of these issues through the greater integration and partnership working agenda in Wales. Locally, regionally and nationally we recognise that parts of our health and social care models are unsustainable and that a radically different model of care is required if we are to meet the needs of our population in Gwent and South Powys in the future and forms the reasoning behind Clinical Futures and our partnership involvement with the South Wales Programme. Impact of the South Wales Programme and Wider Sustainability Issues Our Board s approach to Clinical Futures has been recognised and subsequently reinforced by the South Wales Programme. One of the key driving principles is to deliver services locally but recognise that the future configuration of highly specialised services must be concentrated within fewer hospitals across South Wales. From local and national evidence, we know that the best care and treatment requires a certain volume of patients to be cared for to meet quality standards. Changes in medical training on our workforce and our collective desire to continually drive up clinical standards also reinforces the need to ensure that we plan to deliver sustainable services in the future to avoid immediate emergency action to deal with sudden crises e.g. the very recent closure of Neath Port Talbot emergency care facilities. Within Aneurin Bevan, the Board and our clinical teams know that we cannot wait until the opening of the SCCC in 5 years time to make some key decisions on the future location and configuration of certain specialist services. We will need to tackle these dilemmas directly and with purpose over the next 12 months as pressures from future demand and/or the risk from medical and clinical workforce projections could lead to certain specialties becoming increasingly unstable. Over the next three years, those services are: Obstetrics - At a national level, obstetric services have been facing up to the challenge of reducing the number of small obstetric units with less than 2,000 births for a number of years and this has led to effective service redesign such as low risk, midwifery led, birthing units, while consolidating specialist obstetric services in fewer units to comply with Royal Colleges guidance and best practice which requires senior clinical staff to be available and present in obstetric units. In order to address these clinical standard requirements, under the Clinical Futures strategy, obstetric led births will be focused at the SCCC. Although the Health Board continues to maintain obstetric services on our two District General Hospital sites, we face significant challenges in recruitment to middle grate medical positions to support rotas on both sites, and consequently our reliance on the use of locums to fill gaps. Reliance on locums compromises continuity and quality of care and also represents poor value for money. Neonatology - In our current configuration, neonatal services are delivered on a pan-gwent basis, with staff rotating across both the Royal Gwent and Nevill Hall Hospital sites. Over recent years it has become increasingly difficult to provide and equivalent level of service at both sites due to limited availability of specialist staff, this reflects experiences elsewhere in the UK. In the future, Page 56
57 neonatal services in Gwent will be consolidated at the SCCC. Whilst there is a dedicated neonatology rota at Royal Gwent, the Health Board maintains a combined rota (neonatology and paediatrics) at Nevill Hall. This has necessitated the more complex and seriously ill infants to transfer to Royal Gwent (i.e. all babies delivered before 29 weeks gestation). The Neonatology Unit at Royal Gwent has an excellent clinical reputation, survival rates for pre-term babies exceed the All Wales figures and international benchmarking; the unit is also strong in terms of research and audit. There are further benefits to be gained if the service were fully consolidated on one site, including compliance with the standards of British Association of Peri-natal Medicine. Paediatrics - There is a growing evidence and policy base that restates the need to reform children s services, with an emphasis on local where possible, specialist where necessary. This principle highlights the importance of 24 hour specialist assessment of children in emergencies and the move towards fewer inpatient paediatric units, supported by an increase in provision of children s services in the community. Workforce issues in paediatrics, including the need to comply with the European Working Time Directive pose a significant challenge, which requires fundamental changes to service organisation and delivery to ensure they are sustainable. It is becoming increasingly difficult to staff multiple paediatric inpatient services with robust round the clock medical support. This is not unique to ABUHB and is forcing changes in many paediatric services through the UK where specialist medical expertise needs to be consolidates and provided from larger units. Emergency General Surgery - Emergency general surgery services will be centralised at the SCCC site in the future. However, changes to the number of middle grade training posts (Core Surgical Trainees) at our Nevill Hall Hospital site in August 2013 present us with a real challenge in planning for covering rotas and providing the required level and quality of service. Whilst the service is making concerted efforts to explore alternative staffing options, some scenario planning is underway to assess and quantify the impact of any premature changes to this service. Within the next couple of years, it is highly likely that we will need to centralise emergency general surgery on one site whilst ring fencing elective activity. Emergency Medicine - Emergency medicine is not immune from its own specialty workforce pressures with a heavy reliance on non training grade doctors to support rotas and serve as integral service providers. The pressure on very junior doctors out of hours is also a consideration that may force some changes to the models in advance of the SCCC opening. Furthermore traditional demarcations under the emergency services provision between acute physician, A&E doctors and OOH services will need to be challenged and this is being explored in the Clinical Decision Unit models currently being implemented. The continued operation of traditional A&E services at Nevill Hall and the Royal Gwent Hospitals is dependent on being able to offer a full range of back up services such as trauma, emergency surgery, paediatrics and critical care. As described above, these services may need to be remodeled to comply with future clinical standards and workforce modernisation and are likely to have a consequent impact on the future role of the A&E Department. Stroke Services - We are making solid progress toward implementing Together for Health Stroke Delivery Plan: Our Vision and Together for Health and Stroke Delivery Plan: a Delivery Plan for the NHS and its Partners (published December 2012) which outline NHS Wales vision and the actions to achieve this by Our 2013/14 Stroke Delivery Plan was received by the Board in July 2013, where they endorsed a proposal to expedite a move to a single point of admission for hyper acute stroke care. Consideration was also given to the optimal configuration of rehabilitation resources to better meet current standards and improve patient experience. Service transformation is supported by a detailed work programme, with clear accountabilities and milestones and our approach to tackling this agenda is covered later in this document. Page 57

58 4. Workforce Pressures Workforce planning, by linking organisational strategy to people management, is essential to equipping the organisation to provide the safe patient services. The pressure to control workforce costs, and at the same time deliver a high level of services reinforces the need for detailed integrated service, workforce and financial plans. It is evident from the gaps in the workforce market and the economic downturn that workforce planning needs to assess internal and external supply and plan for reductions in the workforce and workforce costs to be realigned to the overall service strategy. This presents demanding workforce challenges over the course of the next three years and beyond. 4.1 Ageing workforce The Health Board employs 10,653 FTE staff with a headcount of 13,336 (as of November 2013). Graph Workforce profile by gender/full and part time Our workforce is ageing, this year the age profile shows that our largest age profile is years, with increasingly more staff Working over the age of years. 83% of our workforce are female and amongst female employees there is an even split between full time and part time staff. The workforce profile for General Practice is also changing Graph 4.12 illustrates the scale of the shift from a prodominantly male population amongst older GPs to female doctors within younger age groups. Graph Profile of General Practitioner workforce Other available data confirms that given the increased precalence of part time working among female doctors we should plan to recruit 1.25 wte for each wte GP retiring. 4.2 A sustainable workforce Our turnover has increased from last year and currently is projected at 5.5% which is low for a large Page 58
59 Percentage organisation but comparable to other Health Boards across Wales. Sickness/absence is 5.23% and the graph below shows the performance of recent years and that whilst sickenss still still remains a target area of workforce improved productivity, this has not increased from the same period in previous years. Graph 4.13 ABUHB Comparison 2009/10 to 2013/ April May June July Aug Sept Oct Nov Dec Jan Feb March 2013/ / / / /13 This loss of hours related to sickness equates to a monthly average of 971 wte not in work due to sickness at any one time. Bank and Agency which includes staffing for sickness, vacancy, study leave, specialing patients with additional needs and extra capacity back fill presents challenges in relation to continuity and quality of care, and is costly to the NHS, our variable pay bill in neither sustainable in the medium term or affordable in the short term, annual variable costs for nursing staff for 2013/14 will be in the region of 2.5m. As with every other public body we work within certain external constraints and considerable opportunities to maximise effectiveness and flexibility, including: Maintain safe staffing levels on all of our wards and units. As an organisation, we have very clear nurse and therapy strategies for maximising the contribution of our professional staff e.g. advanced practitioners, substitution and development roles Employment Law Infrastructure. Agenda for Change. Electronic Staff Recording System. One Wales Agreement. All Wales NHS Workforce Policies and Agreements. National Independent Contractor Framework. The majority of our workforce and consequently the majority of care is provided by our nursing staff. We have reviewed ward staffing levels against the All Wales Staffing Principles and recognise the challenge that the Health Board faces in relation to our existing ward establishments in some of our medical and surgical wards. The cost associated with the variance is 1.3m for medical wards and approximately 400k for surgical wards, which collectively is 1.8m. This has now been recognised and funded by the Welsh Government. Again, we must recognise that we need to roll out the broader nurse staffing principles to community hospitals and other units not covered by the above approach. Page 59
60 4.3 A Skilled Workforce Like many other healthcare systems in the United Kingdom, we are experiencing shortages of senior and middle grade clinicians which increasingly makes the current configuration of more specialist services unsustainable. Maintaining a sustainable workforce is a particular challenge within some specialties, including: Emergency Care; Radiology; Paediatrics and Neonates; Obstetrics and Midwifery Services; Critical Care. In some services our current staffing models need to be rebalanced with a different mix of skills, competencies and capabilities in order to deliver our ambition to provide more care in primary and community settings, and in order to improve flow across our healthcare system. These include: Medical workforce/balance of generalist to specialists (in primary, community and secondary care settings). Increasing clinical capacity to support more day and 23 hour surgery. Nursing workforce/balance and utilisation of specialist nurses and nurse practitioners. Further utilisation of extended scope/advanced practitioner allied health professional (AHP) roles Inpatient nursing workforce compliance with the All Wales Nursing Standards balanced against use of Bank and Agency. Fully integrated health and social care mental health service. In other areas our service models, and consequently staffing models need to change in order to meet the needs of our ageing population or the age profile of the workforce: Enhanced Community Services. Seven Day Services (comparable clinical capacity irrespective of time of day or day of week, including Hospital at Night models of care). GP services within Gwent and South Powys are heavily reliant on a top heavy age profile. We also need to systematically realise the benefits of investement in e-technology, re-aligning our workforce with these new technologies, including: Telemedicine; LIMS; Digital dictation; Digitised Health Records; E- rostering. Future workforce planning will need to include the current direction for collaboration across primary, community and secondary healthcare, and across Local Authorities where increasingly joint models of service delivery for vulnerable (for example, children, older people, mental health and learning disabilities) groups are being progressed; and appropriate use of the knowledge and skills of all health-care providers, including expanded role for pharmacists, nurse practitioners, therapists and other practitioners. Ultimately, our top priority is to provide patients with safe, high quality clinical services; our Clinical Futures model clearly sets out our plans to achieve this over the coming years and we will Page 60


61 increasingly be looking at how we sustain our existing configuration of services between now and the opening of the Specialist and Critical Care Centre (subject to Welsh Government approval) in the summer of An Efficient Workforce The Health Board is actively engaging in benchmarking activity to identify opportunities to maximise workforce efficiency using Iview data % of staff within ABULHB is within the Admin and Clerical staff group. Compared to the peer organisations within the benchmark it is within the lower Quartile. Graph % of staff within ABULHB is within the Registered Nursing and Midwifery staff group. Compared to the peer organisations within the benchmark is above Median. Further work will need to be undertaken as to how this information compares with each organisations bed capacity and other demand drivers. However, the majority of the Registered Nursing and Midwifery bands compared to the peer organisations are either within the Higher Quartile or above the Median. Graph % of staff within ABULHB is within the Medical and Dental staff group. Compared to the peer organisations within the benchmark is within the Lower Quartile. Compared to the peer organisations Consultants are within the Upper Quartile and other Medical and Dental grades Page 61


62 are within the lower Quartile. Graph 4.16 Graph 4.17 The information provided by benchmarking will provide useful indicators as to potential workforce modernisation opportunities, whilst acknowledging that benchmarking information will need to be further analysed to assess variabilities between benchmarked organisations. One of the most fundamental planning challenges is right-sizing the Health Board s workforce aligned to new service models. Known HR challenges within the Health Board such as medical workforce shortages, high variable pay usage and improving the alignment of job plans to operational delivery will be factored into the planning process. Addressing long-term recruitment difficulties (such as within critical care nursing and emergency medicine) through recruitment and role reform mechanisms will be a priority. Page 62
63 Chapter 5 Improvement Quality of Care and Patient Experience 1 Quality at the Heart of Our Mission and Values Quality and Patient Safety must be at the centre of our work if we are to achieve excellence in all that we do. The patient is at the heart of everything we do, we strive to improve the patients experience and quality of service with every action that we take. Our job is to use the resources we receive to reduce health inequalities and ensure the public have access to high quality services that give them a positive experience and good clinical outcomes. Our purpose is to transform patient experience and nurture a consistently person-centred approach in everyone, every day. This clear purpose is reflected in our values, which define what is important to us and the way in which we behave and deliver our services. They support a shared understanding about how staff relate to each other, as well as to patients and the public. Figure 5.1 Living Our Values Is the individual vulnerable? Did I do my best to ensure their safety and wellbeing? Was it a good and timely experience for the patient? Did I treat the patient well? Patients First Personal responsibility Passion for Improvement Pride in what we do Did I help them with their problem? Was the care I provided safe and of high quality? Every member of staff needs to be able to answer the five simple questions set out in Figure 5.1. Living these values and demonstrating this behaviour will ensure that right environment and culture is enabled in which quality will flourish, with the patient at the centre and an equal partner in their healthcare. Our thinking about quality in healthcare services in Aneurin Bevan University Health Board is guided by the Institute of Medicine s Six Aims for Improvement. We believe that an excellent patient experience results from a balanced approach to all these areas: Table 5.1 Aim Safe Effective Patient-Centred Timely Efficient Equitable This Means. Avoiding injuries to patients from the care that is intended to help them Providing services based on scientific knowledge to all who could benefit, and refraining from providing services to those not likely to benefit. Providing care that is respectful of and responsive to individual patient preferences, needs, and values, and ensuring that the patient s values guide all clinical decisions Reducing waits and sometimes harmful delays for both those who receive and those who give care Avoiding waste, including waste of equipment, supplies, ideas, and energy Providing care that does not vary in quality because of personal characteristics such as gender, ethnicity, geographic location, and socioeconomic status. Page 63
 being the framework against which we assess")
64 Providing quality services means that we need to both assure ourselves that we are meeting relevant standards and continually improving what we do. Assurance comes through having clear standards against which we can measure ourselves, with the Standards for Health Services (Doing Well, Doing Better) being the framework against which we assess all our services, to identify gaps and therefore risks and areas for improvement. The Standards are embedded at Divisional and Directorate level, and any gaps identified lead to actions taken forward through their improvement plans. NICE guidance, standards and pathways lay out the evidence base for our services which we seek to deliver reliably for all our patients. National audits, comparing our services with nationally recognised evidence based standards and good practice, show us where we need to improve. A range of external bodies, including the Community Health Council, also undertake reviews of our systems, processes and practice, which also highlights for us where we can improve. In addition to this there have been 3 National reports in 2013, all of which have implications for our service provision the Francis Report, the Keogh Report and the Berwick report. The areas that we are focusing on over the next 3 years reflect the learning from these reports. In particular, we are placing increased emphasis on engaging with patients and their families to seek their views on the care we provide to improve patient experience. We also learn locally about how we can do better from incidents, complaints and claims, from Mortality Reviews, from review of routine and CHKS data, from listening to our staff and from patient stories, patient shadowing and patient surveys. Much of this forms our Quality Triggers, so that we take action to improve our care. 2 ABUHB Approach to Quality Improvement To provide high quality care, we have to improve all the time both where we know we have gaps or risks but also where we are doing well, striving for excellence. Our fundamental approach to improvement is that all staff have two roles to do their job and to improve their job. The improvement should be based on seeing patients as equal partners in healthcare, and seeing the services we provide through their eyes. We believe that this will ensure that we have the highest quality services for the people we serve. To enable all staff to be able to do this, our staff need to learn, master and employ modern methods for quality improvement. The National Programme of Training in Quality Improvement methods, Improving Quality Together, is our core training programme, and we are working towards all staff completing the training at bronze level, and at least one member of staff in an area or team completing the silver level training. The ABCi Team and others that have a key role as champions for improvement attend the Gold Network. Our core improvement method is the Institute for Healthcare Improvement s (IHI) Model for Improvement. It is well tested and engrained in NHS Wales as the core tool used in the 1000 Lives Plus programme and taught through the Improving Quality Together programme (Figure 5.2). Figure Institute for Healthcare Improvement s Model for Improvement It requires clinical teams to be clear about: the aim of the improvement they want to make; the measures they will use; the change that will result in an improvement. They then use the Plan-Do-Study-Act cycle to test the change, starting by testing the change on just one person, and increasing the number of patients involved as the Page 64
65 iterative PDSA cycles refine the change being made. The measures are used over time to show whether the changes that are being made are reliable, and whether they are making a difference to outcomes. In the past year we have demonstrated our commitment to Quality Improvement through the creation of ABCi, the Aneurin Bevan Centre for Improvement, to support all Health Board staff to improve the way they work, and to develop a healthy culture of patient focus across all our services. This initiative draws together people working on quality and service improvement from across the UHB, and provides analytical and measurement expertise through a collaboration with Cardiff University, as well as building on a flourishing relationship with the 1000 Lives Plus Improvement Team. We want the work of ABCi to be driven by the needs of patients and to be a resource for best practice and innovation. When teams demonstrate improved practice with evidence, we want to help spread that practice to other areas in the organisation. Transparency is crucial in building our relationship with our citizens, and in driving improvement. We therefore publish data on our internet site, and in our Annual Quality Statement were open and honest about where our services should be better, and what we were doing to improve them. 3 ABUHB Components of Quality Simply put, health care quality is getting the right care to the right patient at the right time every time. There are three basic dimensions to this, structure (healthcare resources - staff, facilities, infrastructure); process (doing the right things, in the right way), and outcome (end result of care for patients). Together, these components are the foundation of providing care that is consistently safe, timely, effective, efficient, equitable, and patient-centered. Quality is a golden thread that runs through the plans of all our services in primary, secondary and community care, and in our commissioning of services. This is reflected in our strategic change plans that address structural and process deficits in our system of care the impact on quality and patient experience (as illustrated in Table 5.2 below) and in our individual service plans. Critically, we see our service change plans as vehicles to drive continuous quality improvement as illustrated in the table below. Table 5.2 Dimension of Quality Structure (Staff, skills, facilities, infrastructure) Process Key Service Change Programmes Strengthening Primary and Community Services (create capacity around NCNs to increase range of care provided in out of hospital settings). Sustainable clinical services (consolidate services to maximise timely access to specialist care - interim plans in lead up to the SCCC will be the focus of effort in the medium term) Rightsizing the workforce Value based clinical services (eliminate low value procedures, repatriation and prioritisation) Improved Delivery (Tier 1 including efficiency and productivity) Unscheduled Care Transformation Scheduled Care Transformation Intended Impact Community focused model of care for older people with complex care needs Services will deliver consistent high quality outcomes irrespective of day of week or time of day. The right staff, with the right skills, in the right place, doing the right thing at the right time, in the right way and at the right cost. Patients will have confidence that the UHB is doing the right thing, in the right way to add value to their health and wellbeing. Improving flow through the system to minimise the patient journey and maximise clinical outcomes. Page 65
66 Dimension of Quality Outcomes Key Service Change Programmes Reducing Health Inequalities / Inverse Care Law Quality and patient experience Intended Impact Reduce morbidity and mortality related to Cardiovascular Disease. Reduce avoidable harm (e.g. HCAI, RAMI). People receive compassionate care We also recognise the importance of partnership and equality across primary, community (health and social care) and secondary sectors as pivotal to delivering the model of care that the Health Board aspires to deliver; specifically shifting the balance of care provision to community settings, reducing reliance on secondary care whilst ensuring appropriate access to high quality secondary care services when needed. 4 Corporate Quality Improvement Priorities Everything we do as an organisation impacts on the quality of care, and the patient experience of that care. However, there are some areas that we prioritise as an organisation, as our assurance processes and learning have highlighted that they do not meet the standards, or are gaps or risks. The Health Board has set performance improvement trajectories for a number of patient experience and safety measures, supported by detailed delivery plans, which are summarised below. Table 5.3 Parameter 2013/ / / /17 Readmissions Pressure sores C, diff reduction MRSA reduction MSSA reduction RAMI IQT (quality together training) 25% staff 40% staff 60% staff 75% staff Some are part of our Patient Safety Improvement Plan, which aims to reduce the number of avoidable deaths and incidents of harm in the organisation. In addition, areas are prioritised on a National basis through the Delivery Framework , and we await the National Outcomes Framework. 4.1 Risk Adjusted Mortality Index (RAMI) The Health Board has been successful over the years in reducing its Risk Adjusted Mortality Index (RAMI). However, over the last year, there was an apparent slight rise in the ABUHB RAMI across the whole year. There is a seasonal pattern in the RAMI, with a higher RAMI during the winter months. Drilling down shows that the RAMI has been more or less unchanged at RGH, but is generally at a high level. It has increased at YYF to above 100. It has also increased at NHH, but is still below 100. This therefore means we need to take action across the Health Board to improve patient safety, and reduce RAMI overall to 90 or below for ABUHB, but also for each of our acute hospitals. Page 66

67 The RAMI is derived from comparing the coded data on our patients to similar data for all hospitals. How well the coding is undertaken for each patient, and how many of our patients are actually coded, compared to other organisations in England and Wales, can therefore obviously impact on our RAMI. Part of our plan to reduce the RAMI will therefore involve ensuring that our patients are all coded promptly, and accurately. This is the Improved Accuracy of Record Keeping and Coding section. In order to improve patient safety most effectively, we need to target our efforts to the areas where we can have maximum impact. We therefore need to continually review, drill down into and monitor our clinical data. We also need to review all the deaths in our hospital, to understand the system level factors that we need to improve. We need to triangulate this with information about the patient experience from our patients from concerns, patient stories and shadowing. National audits also demonstrate where we need to improve our standards. This is the Improved Surveillance and Review section. Finally, to improve our care and treatment in the areas highlighted by the data, we need to ensure that the evidence based care is provided reliably and in a timely way for all those who would benefit from it. We need clear aims for the improvement, measures of both outcome and process so we know whether we are moving towards our aim, and clear changes that we can test to see whether they make our processes more reliable. Some of these changes are national issues and are therefore part of the Delivery Targets. Some are local issues. These form the Optimise Care Delivery section of the plan. RAMI is monitored by acute hospital site and by our largest acute service areas, Scheduled and Unscheduled Care (as these are the main drivers of the RAMI). The Health Board RAMI has reduced significantly over the past four years, but this fall plateaued in 2012/13. RAMI shows seasonal variation, with higher RAMI in the winter. The RAMI across all acute and community hospital sites in the Health Board is currently stable at a value between 100 and 110. This is on a par with other Health Boards in Wales, however differences on coding practice do exist between Health Boards, and it is not statistically correct to use RAMI to compare one organisation against another. Over the last 12 months (August July2013), the median RAMI for ABUHB (2012 rebasing) is 108. Graph 5.1 Page 67
 2014-15 2015-16 2016-17 99 96 93 90 The two areas of safety improvement most likely to impact on RAMI on the Royal Gwent site are improvement of flow of emergency")

68 Graph Unscheduled Care Graph Scheduled Care Our aim is to reduce RAMI to 90 (2012 rebase) by March 2017 and to reduce/eliminate variation across our hospital sites. Table 5.4 Baseline (2013) The two areas of safety improvement most likely to impact on RAMI on the Royal Gwent site are improvement of flow of emergency patients to minimise long waits in the Emergency Department, and improvements to the care of older people. This is being addressed through planned increases in the numbers of Care of the Elderly Consultants, the reassignment of wards on the RGH site and improvement in End of Life care. Further details are provided in our Patient Safety Improvement Plan at Appendix X. Page 68
 Table 5.")

69 4.2 Healthcare Acquired Infections - MRSA and C Difficile Graph 5.4 Our aim is to reduce the incidence of hospital acquired MRSA and C difficile infections year on year (by 20% between and across the board) Table 5.5 HCAI 2013/ / / /16 Cdiff reduction MRSA reduction MSSA reduction There are detailed plans to reduce these infections. For MRSA, the key strategy is a sustained campaign of pre-emptive testing and treating patients to reduce risk. For C difficile, there is a multi strand campaign, including hand washing and cleaning schedules, fogging of wards with outbreaks using HPV, fogging cubicles after discharge of a patient with C Diff, antibiotic prescribing, isolation/cohorting. The UHB s detailed action plan is attached at Appendix x. Page 69
70 4.3 Hospital Acquired Thrombosis (HAT) Our aim is to reduce HAT by ensuring that all patients have appropriate mechanical and chemical prophylaxis. During , the measurement of the HAT rate will be implemented, and the data disseminated to all Divisions. During , the process measures of completion of the Risk Assessment tool and appropriate mechanical and chemical prophylaxis will be instituted and actions taken to improve compliance, and the target reduction set. 4.4 Sepsis Senior Doctors from our hospitals and primary care have been undertaking a review of the cases of every patient who dies in hospital at NHH and RGH, since the beginning of While these reviews often find that care was of a good standard, we do find areas where we could do better evidence of our commitment to continuous improvement. At RGH, the reviews for a period of 2012/2013 have looked particularly at patients who have or may have sepsis. The review at RGH showed that sepsis is responsible for significant mortality, with sepsis a major contributor to death in 15% of cases, and present with a minor contribution in 22% of cases. Early recognition of the Deteriorating Patient and effective treatment of sepsis is a key focus for us; similar to other healthcare providers occasionally we do not recognise and respond to patients who are deteriorating by escalating their care quickly and effectively. In the last year we have focused on putting the building blocks for recognising and responding to the deteriorating patient in place, developing a policy for physiological observations and the deteriorating patient. In addition, we have implemented a system, based on the routine, physiological observations, that supports the recognition of deterioration, called the National Health Service Early Warning Score (NEWS). To support this we have put in place one observation record chart, combined with NEWS scoring, used right across all of acute care. We have also been introducing the Rapid Response to Acute Illness Learning Set (RRAILS) care bundles from the 1000 Lives plus Programme across the Health Board, with the measurement of the reliability of the process recorded within the National Care Metrics system as part of the Fundamentals of Care System. To support this measurement, we have piloted a sepsis data base in ITU at NHH, completed by the nurses from the Outreach Team. This provides us with additional data on our response to the deteriorating patient and sepsis, and the outcomes for the patient. Graph 5.5 Percentage favourable outcomes after 24 hours - Day NHH from Oct 2011 to Nov All Wards OctNov DecJan FebMar AprMay Jun JulAugSep OctNov DecJan FebMar AprMay Jun JulAugSep OctNov Months Page 70
71 Graph 5.6 Number of patients transferred to critical care NHH from Oct 2011 to Nov All Wards OctNov Dec JanFeb MarApr May Jun JulAugSep OctNov DecJan FebMar AprMay Jun JulAugSep OctNov Months Graph 5.7 Percentage of sepsis treatment initiated by ward staff prior to outreach arriving NHH from Oct 2011 to Nov All Wards OctNov DecJan FebMar AprMay Jun JulAugSep OctNov DecJan FebMar AprMay Jun JulAugSep OctNov Months Our aim is to further improve recognition of patients with sepsis and improved outcomes for patients with Sepsis. During , the ITU sepsis data base will be spread to RGH and the data disseminated to the Divisions. It supplements the data in the care metrics. At NHH, they will ensure data is collected 24/7. Targets for improvement in outcomes will be set, based on this data. A plan will be developed for a Sepsis (and AKI) campaign. During , the data base will be spread to YYF. The Sepsis and AKI campaign will be implemented. 4.5 Acute Kidney Injury (AKI) Our aim is to further improve recognition of patients with acute kidney injury and improved outcomes for patients. In Wales, recent audits suggest that approximately 1 in 14 patients admitted to hospital have AKI and that up to 3,000 of patients dying in hospital will have AKI. The good news is that much AKI can be prevented through effective clinical management of emergency patients in the first 24 hours of hospitalization and focus on an early warning score being universally applied e.g. NEWS. During , the plan for improving recognition and treatment of AKI will be developed. This will be done in conjunction with the Sepsis campaign, as many of the measures to prevent, recognise and treat AKI are similar to the changes required for the recognition and response to sepsis. The measurement of outcomes and process will also be defined and aligned with the AKI checklist and NCEPOD report Adding Insult to Injury. Page 71
72 4.6 Pressure Damage Our aim - Zero Tolerance (through year on year reduction) Table / / / /15 Pressure sores The skin bundle has been implemented in all acute wards and has been adapted for use in all Community Hospitals and Community Services. Fortnightly Hospital Acquired Pressure Ulcer Surveillance Meetings, chaired by an Assistant Director of Nursing, continue to review all grade 3 & 4 Hospital Acquired Pressure Ulcers. The appropriate Senior Nurse has to attend and present a report outlining the investigation and if it is deemed that the PU was avoidable the Senior Nurse prepares an action plan. The implementation of action plans is also monitored by this group. During , identification of potential strategies to reduce the incidence of pressure ulcers in the community is underway. E.g. work through the Carer Strategy work streams. A part time tissue viability nurse with responsibility for nursing home patients has been appointed and started work at the end of September Each emergency admission is subject to consultant review within 12 hours. AKI is risk assessed in all areas. Education and training is in place for frontline staff (with audit compliance). Laboratory systems highlight the presence of AKI. Guidelines on transfer to tertiary treatment. 4.7 End of Life Care In-appropriate escalation of care to a District General Hospital from home, a care home or a community hospital at the end of life, are cases where the patient does not benefit from the transfer to the acute hospital, and their death would have been more dignified and peaceful if their care had not been escalated. Work is underway across the whole system of care to ensure there is anticipatory care planning for people at this stage of life, so that conversations can be held with them and their relatives in a timely way about their preferred place of death, and the appropriate arrangements made to facilitate this. Our aim is to provide appropriate and sensitive care at the end of life. Key actions patient choice around place of death, reducing preventable admissions to acute wards at the end of life through anticipatory care planning, greater understanding of a natural, anticipated and accepted death and use of the All Wales DNACPR documentation. 4.8 IQT Improving Quality Together Our aim is to make mastery of quality improvement methods part of the lifelong education and learning of all health care staff During to establish Improving Quality Together Training and train 25% of our staff During to review success and set new targets (e.g. 40% of our staff trained). During (target set in previous year, recognising that now focus will be on harder to reach groups of staff 60%) Page 72
73 4.9 Improved Patient Experience A good patient experience is at the heart of quality in healthcare as it encompasses all the dimensions of quality as illustrated in Figure 5.3. But to achieve this, we need to be able to see the patient experience through the patient s eyes, whilst recognising that every patient is an individual. Figure 5.3 Leadership and Culture Staff Experience Humanity of Care Timeliness; Safety; Equality; Clinical Effectiveness; Organisational; Efficiency. This means that the patient voice needs to be present and listened to at all levels of the organisation, and that the patient is welcomed as an equal partner in their own care and in the processes of designing and delivering care. There are high expectations on us to improve the quality and care we provide to patients, quite rightly in the aftermath of the Francis Review of Mid Staffordshire Hospital. Past success is no reason to be complacent and continuing improvements mean that people s expectations will appropriately continue to rise. Working with communities to assess and design services improves those services, whilst seeing individuals as equal partners in treatment decisions and self care management improves outcomes. The challenge is to develop a new relationship with the public as co-producers in their own care, empowering the public to make informed decisions about the appropriate use of healthcare. Our clinicians wish to provide patient-centred services, with the key challenges they face: Demands on the system: Year on year the Health Board experiences an increase in demand for our services, in 2012/13 there were: 2,500,000 GP consultations; 1,300,000 Practice Nurse consultations; 156,000 home visits by GPs; 438,378 Outpatient contacts/appointments; 310,000 Community Therapy contacts/appointments; 150,172 attendances at our Emergency Departments; 21,103 contacts with Mental Health Outpatient services; 64,442 operations; 46,503 emergency admissions; 24,795 emergency assessments that did not require a hospital admission. Page 73
74 Time: The main task in a clinical consultation is to build a relationship with the patient, collect data and agree a management plan. The time taken to gather data and agree a management plan will depend on the baseline knowledge of the patient, the health professionals and the patient's ability to communicate effectively and the complexity of the patient's problems. Within primary care for example, the average consultation in general practice lasts 7 8 minutes, these consultations are often multifaceted, with social as well as medical issues to be tackled. In hospital the average consultation time is not much longer. Our challenge is to shift the emphasis from throughput to input and quality of patient interactions. Improving the patient's experience of care is a key priority for us. A focus on what it is actually like to be a patient in the NHS - the 'patient experience' is seen as vital in the drive to improve quality in the NHS. 'Patient experience' encapsulates the totality of patients' needs and preferences. It includes both clinical and non-clinical care, and embraces everything from the success of clinical interventions to issues of access, responsiveness, choice, and the state of the physical environment of care. We have therefore reviewed and updated the driver diagram for Patient Experience that was contained within the Patient Experience Framework (Figure 5.4) and identified the key drivers. A good patient experience is influenced by a multitude of factors, some of which overlap with other areas of work within this 3 year plan, for example the priorities for improving patient safety and the OD Framework. These are the main drivers as described in the diagram: A culture that enables staff to put patients/carers first Leadership that demonstrates by example that quality of care and patient experience is at the top of their priorities Safe, effective and efficient care, so the patient outcome is good from the patient and professional s point of view A good staff experience, so staff feel positive about their experience of providing care The citizen/service user/carer voice is heard and heeded at all times and all levels of the service Some of the changes in the driver diagram will be properly defined through the aims and measures work below. Other key areas of work for patient experience, that are defined include: Clear Aims and Measures for Patient Experience During , clear aims and measures will be developed for the patient experience driver diagram, working with other department, our staff and service users/carers. The changes that will support the achievement of the aims will be identified, and combined with the aims and measures into a plan. Citizen/service user/carer voice Obtaining direct feedback from patients/service users and acting on it is essential. Our current mechanisms are listed below, covering most of the 4 quadrant framework in the Framework for Assuring Service User Experience: Patient surveys: o 1000 Lives+ surveys; o Transforming Care Patient Experience Survey; o Fundamentals of Care Patient Experience Survey. o Nutrition Reviews Observation of Care: o HIW reviews and Dignity and Essential Care Inspections (DECI); o Community Health Council spot checks and inspections; o Patient Stories. Page 74
75 Complaints Analysis. Patient/service user participation via service improvement approaches: o Kings Fund and Health Foundation Patient and Family Centred Care Programme; o Kafka Brigade Reviews. In addition to these, we will implement the WG Service User Assurance Survey (a real time survey) across all areas of the HB during , so that every Division is surveyed twice during a year. In the patient feedback methods being used will be reviewed to ensure we have full coverage across the 4 quadrants in the Framework for Assuring Service User Experience. Within the next two months we are also arranging a listening exercise to bring patients, partner organizations and staff together to further improve our response to the needs of older people. This will help shape a number of our clinical pathways going forward. In we will embed Patient and Family Centred Care in Diabetic Foot Service and Fractured Neck of femur and identify other areas to which the method can be spread. We will continue to collect and use patient stories throughout our services, to help us to see our services through the patient s eyes. We will review the evidence base/good practice related to co-production and consider ways of working at all levels across the organisation, so that we support working with patients, citizens and their carers as equal partners. Co-production Our current model of health care is based on clinicians deciding what treatment will work best for patients and requiring (sometimes supporting) their compliance with the treatment programme. Whilst this approach has served us well in the past, in the face of the rising tide of long term conditions, it has faltered and stalled. Something else is required to complement clinical expertise and health services. The answer lies in recognising what people and communities want and could do for themselves and reorienting and reshaping health and other services to support them. This new co-productive approach requires major culture change with patient s lived experience being given equal weight alongside the expertise of clinicians. The new approaches will also require a redesign of pathways around people, rather than diseases, and a reshaping of budgets and incentives. There is a growing body of evidence that coproduction improves health and produces consequent savings through reduced use of A&E, GP consultations and hospital admissions, The People Powered Health Project shows saving of between 7-20%. The potential benefits include: people gaining control over and improving their own health; clinicians increasing their job satisfaction as they visibly make a difference; UHB realising cost savings that help secure the long term future of our services. Compassionate Care During , we will develop a Volunteering Strategy with a focus on improving the patient experience. During , we will continue implementation of the Carers Strategy, and realise all the actions set out in the dignity Plans. The driver diagram (Figure 5.4) sets out the key changes/interventions that relate to the key drivers for a good patient experience, ABUHB will be progressing the actions that are clear over the medium term to improve patient experience, but some of the actions will be further refined as part of the aims and measures work. Page 75
76 Over the next three years... The views of patients, carers and the public directly inform and impact on the way we deliver care. Integrate patient stories and experiences into everything we do and our operational and key strategic decision making. All wards will be perfect wards. We will be transparent about our successes and our shortfalls and will be open and honest as to how we will respond/act. Patients will experience optimal clinical outcomes comparable with Best in Class We will operate within an organisational culture that challenges suboptimal care (including interventions of limited value), attitudes and/or behaviours. A zero tolerance to health acquired infections. Mortality rates comparable with the best Patients and their carers will be equal partners in their care Every clinical contact, procedure and/or intervention will add value to the patient. Page 76

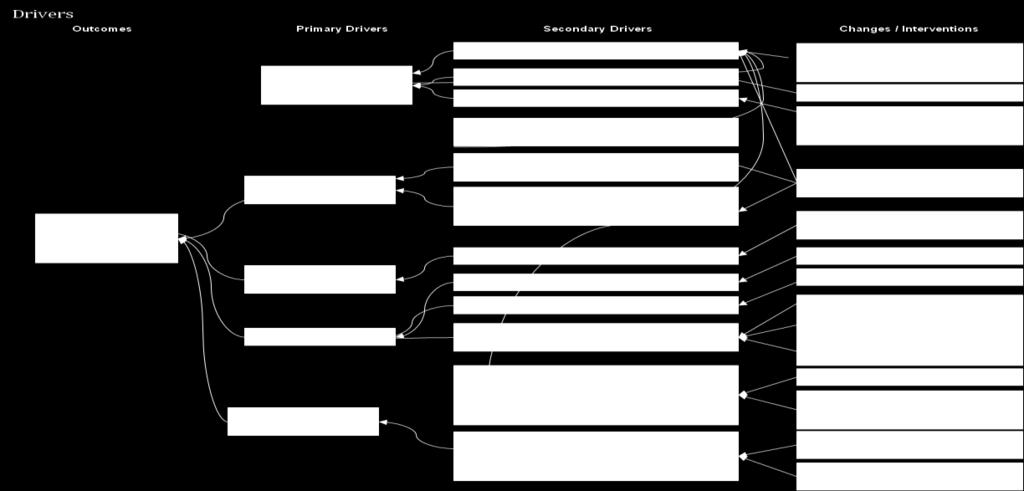
77 Figure 5.4 Page 77
78 Chapter 6 Service Change Plans and Initiatives Building on our approach to improving quality and patient outcomes, this chapter describes the service change programmes that respond to the health needs and challenges we have described. Our 3 year plans are made up in a number of ways. They include nationally led strategic change programmes, regional and organisational strategic change plans such as the South Wales Programme and Clinical Futures and existing plans and programmes carried forward from previous years. In addition each directorate has developed a local plan integrating service, workforce and financial outputs to deliver improvements in clinical effectiveness, efficiency and clinical outcomes in accordance with the new Welsh Government Planning Framework guidance. In presenting our comprehensive priority plans, we have therefore aggregated and organised these by a number of high level themes. Many of our plans involve service changes spanning more than one service area and more than one theme. The table below therefore summarises the service change plans included within each theme and described in more detail in this chapter. Table 6.1 Service Change Plan Theme Reducing Health Inequalities Strengthening Primary Care and Community Services Clinical Futures Remodelling Hospital Based Care Workforce Plans Heart disease and stroke delivery plans prevention and early detection of risk factors, including diabetes, targeted (smoking cessation and obesity work. Vascular assessment in the 5 most deprived NCN clusters under Living Well, Living Longer (addressing Inverse Care Law programme) (Public Health and Primary Care). Development of Neighbourhood Care Networks as Delivery Units. Older people. Developing integrated community services model. Maximising the efficiency of Community Hospital resources (using bed modeling). Maximising the efficiency of Complex Health Care services Frailty services. Single Integrated Plan (SIP). Delivering excellent pharmaceutical care. Making best use of medicines. Pathways: diabetes; heart disease; COPD; eye care. Bed Modelling. Sustainable Services, including: acute stroke; clinical inpatient haematology; cardiology; emergency general surgery; ambulatory breast services; obstetrics, paediatrics and neonatology. Clinical service model development. South Wales Programme. Maximising workforce efficiency. Reducing the workforce. Changing service models. Page 78
79 Service Change Plan Theme Value Based Clinical Services Improving Delivery Transforming Unscheduled Care Transforming Scheduled Care Plans Modernising the workforce (role redesign and innovation). Job planning. Organisational development. Compliance with INNU. Procedures of limited value. NICE Do not do interventions. Specialist high cost interventions. Clinical behaviours. Thresholds for intervention. Medicine effectiveness. Targeting clinical variation. Internal prioritisation and Value-based commissioning. Evidence based practice. External commissioning. Development of business intelligence aligned to benchmarking. Access to unscheduled care services. Scheduled care access (RTT, Cancer). Benchmarking. Frailty at the front door. Ambulatory emergency care. ED sustainable clinical model and workforce. Core clinical operational framework. Outpatient services. Digitalisation of Health Records. Page 79
80 SCP 1 Reducing Health Inequalities The health of individuals and the population of Gwent as a whole is affected by multiple factors including the socioeconomic environment, where we live and work, genetic makeup, the presence of risks to health, individual lifestyle choices and access to health services and support. Taken together these factors determine how healthy we are as individuals. We know that a healthier future for our population depends not just on individual lifestyle choices but also on individual life chances including education, employment prospects and the environment in which we live, work and play. The Health Board is working with all partners (the public, voluntary sector, Local Authorities, and independent sector e.g. Housing Associations) to collectively invest expertise and resources towards delivering the Gwent vision for Our Healthy Future. Action to improve the health of the population and prevent disease, illness and injury includes protecting populations from health risks and promoting healthy public policies, environments and behaviours. Achieving a better health status for the whole population and reducing demand for treatment services contributes to the sustainability of our healthcare system. Our aim is to help people stay healthy and reduce system-wide costs and deliver best value from the NHS. The Aneurin Bevan University Health Board s Public Health Strategic Framework sets out the Health Board s response to Our Healthy Future adopting a life course approach to improving population health and reducing heath inequities, starting before birth and continuing to older age. This Service Change Plan builds on the achievements of the Public Health Strategic Framework with the continued aspiration that: Babies are born healthy. Pre-school children are safe, healthy and develop their potential. Children and young people are safe, healthy and equipped for adulthood. Working age adults live healthy lives for longer. Older people age well into retirement. Frail people are happily independent. What Will We Achieve Over the Next Three Years and Beyond This Service Change Plan encompasses action over the next three years to: Increase the percentage of pregnant women who stop smoking during pregnancy and reduce inequalities in the proportion of babies born with a low birth weight. Achieve and maintain 95% uptake of routine childhood immunisations including in vulnerable groups such as Looked after Children. Achieve and maintain target uptake rates for flu immunisation in eligible groups including the new flu immunisation programme for children and young people. Continue to strengthen the Designed to Smile programme to reduce inequalities in the proportion of children who experience teeth decay and dental treatment. Develop and implement a childhood obesity pathway. Continue to reduce teenage pregnancies through accessible LARC and emergency contraception services. Implement the Inverse Care Law Programme Living Well, Living Longer to reduce premature mortality from cardiovascular disease in the 5 Neighbourhood Care Network (NCN) areas of greatest need (the Living Well Living Longer areas). We will achieve this through systematic, population scale, primary care interventions to increase the identification of people at risk of cardiovascular disease, to ensure they are on optimal treatment and to support them to make changes to their lifestyle to reduce their risk e.g. by stopping smoking. Page 80
81 Achieve 5% of smokers making a quit attempt via smoking cessation services, with at least a 40% CO validated quit rate at 4 weeks. Increase the percentage of smokers on chronic disease registers who stop smoking in the Living Well Living Longer programme areas. Increase the number of referrals to the Exercise Referral programme in the Living Well Living Longer programme areas. Implement an adult weight management pathway including a new weight management service starting in the Living Well Living Longer areas. Improve cancer outcomes in the Living Well Living Longer areas. Expand the Make Every Contact Count programme to promote healthy lifestyle choices, including a healthier diet and increased physical activity. We want to mobilize our greatest asset our staff to deliver simple and timely advice to the vast number of patients they come into contact with on a daily basis. Develop and implement an alcohol harm reduction pathway. Expand the Alcohol Brief Intervention programme so more people are aware they are drinking above the recommended guidelines and reduce their consumption. Improve access to Long Acting Reversible Contraception (LARC) for drug misusers. Promote consideration of the Five Ways to Wellbeing in the design of new services and developments, including the Specialist Critical Care Centre, through the Single Integrated Plans and the Together for Mental Health in Gwent partnership mechanisms. Embed Time for Change in the Health Board s organisational culture to promote mental wellbeing of Health Board staff. Achieve reaccreditation of the Health Board s Gold Corporate Health Award and make an application for the Platinum Corporate Health Award. Reduce accidents and injuries to older people due to repeated falls. Promote the health, well-being and independence of older people to prevent or delay their need for higher intensity or institutional care. Develop and implement an action plan to address the health needs of vulnerable groups (homeless, asylum seekers, gypsies and travelers, migrant workers, substance misusers). Protect the population from acute and chronic infectious and environmental threats to health by taking action to minimize or mitigate existing and new risks. Key Milestones for Delivery of the Reduce Health Inequalities Service Change Plan Table 6.2 Measles Mumps and Rubella campaign achieved 95% uptake of 1 st MMR by age 2 and 92% uptake of 2 nd MMR by age 5 New weight management service approved and funded Principles of the Inverse Care Law Programme agreed Costed implementation plan for Inverse Care Law programme developed Plan developed to expand ABUHB smoking cessation services Achievement of reaccreditation for Gold Corporate Health Award Gwent Alcohol Misuse Needs Assessment completed Targets for Inverse Care Law Programme developed 2013/14 Emergency campaign April-May 2013 COVER data results Agreed by ABUHB Board June 2013 Agreed by ABUHB Board 27 th November 2013 For decision by ABUHB Board Finance and Sustainability Committee 22 nd January 2014 For decision by ABUHB Board 22 nd January 2014 Assessment on 29 th January 2014 For agreement by Gwent Area Planning Board for Substance Misuse by end March 2014 For agreement by ABUHB Board by end March 2014 Page 81
82 Table /15 Phase One of Inverse Care Law programme Subject to available funding commenced in Blaenau Gwent West Smoking cessation service expanded Subject to available funding New weight management service operational April 2014 Further programmes to be added By end March 2014 Table /16 Phase One of Inverse Care Law programme Subject to available funding rolled out to other target Neighbourhood Care Network areas Further programmes to be added By end March 2014 Table /17 Phase One of Inverse Care Law programme Subject to available funding completed Further programmes to be added By end March 2014 Over the next three years we will have Implemented joint strategies with our partners to address social and physical environments that enhance wellness and promote healthier behaviours, as well as increasing access to programmes that prevent disease and injury. Increased immunisation rates, cancer screening rates to minimise the need for treatment, with actions targeted on deprived areas, decreased teenage pregnancy rates and better oral health outcomes for children in deprived areas. Increased care of vulnerable populations through better access to care and through addressing other determinants of health. Reduced rates of tobacco use, adverse effects of alcohol misuse, physical inactivity within the population will be decreased. Extended obesity services and realigned to turn the curve, and childhood obesity rates will be reducing. Decreased Health disparities across Gwent. Health outcomes will be better for everyone, especially for cardiovascular health and cancers. Page 82

83 SCP 2 Strengthening Primary and Community Services Strengthening primary and community care services is one of our top priorities. Primary care is the front door to health-care with the patient s first point of contact often being with their GP, pharmacist or dentist. The case for primary care is well established; stronger primary care leads to better health outcomes and more efficient healthcare delivery. With the ageing population and chronic diseases on the rise, it is imperative that we offer patients access to the best primary and community (health, social care and third sector) care system. This will help them maintain good health and access to the services they need when they need them. In particular we need to support older people and veterans with complex chronic conditions and individuals with addiction and mental health problems. This needs to be through co-ordinated and integrated services provided via our 12 Neighbourhood Care Networks (NCNs) and across our five Local Authority areas. We believe that the foundation for moving forward sustainably is a well evidenced Single Integrated Plan (SIP) for each Local Authority Area, one that clearly reflects the needs of the local population, and that enables local government and its partners to focus their efforts most forcefully on early intervention and prevention in order to break cycles of dependency and prevent the persistence of poor outcomes from one generation to the next. Our 12 Neighbourhood Care Networks are a clinically led, collaborative network comprising all Primary Care, health and social care community providers operating within the boundaries of the neighbourhood. The NCN Core Team is the mechanism through which plans for primary, community and where appropriate, social care services are developed. These plans are also intrinsically linked to the SIP delivery frameworks and the wider Local Service Board agenda for the community. Figure 6.1 The map shows the approximate boundaries for each Neighbourhood Care Network in Gwent. The difference in area size is due to population density because each NCN is designed to be made up of 30,000 50,000 people who are registered with GP Practices in the catchment area. The catchment areas themselves are grouped around local communities. This is in order to make it easier to plan and deliver services for particular areas, with particular health needs. Primary care, Community and Social Care teams are working together to provide better out-of-hospital services. The Health Boards Clinical Futures Strategy sets out our ambition to rebalance our healthcare system, providing care, whenever it is safe to do so, closer to people s homes, in order to avoid unnecessary hospital attendances. Achieving this is dependent on integrated models of primary and community services that will have the appropriate skills, competencies and capacity to systematically meet the diverse and growing needs of our communities. Our vision for future primary and community services in Gwent is also built around the strategic themes set out in Together for Health: Delivering Integrated Care and Shared Purpose, Shared Delivery: Sustainable Social Services for Wales. Page 83
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
Aneurin Bevan University Health Board Stroke Services Redesign Programme
 Aneurin Bevan University Health Board Services Redesign Programme 1 Introduction This report aims to update the Health Board on progress with the Services Redesign Programme of work which commenced in
Aneurin Bevan University Health Board Services Redesign Programme 1 Introduction This report aims to update the Health Board on progress with the Services Redesign Programme of work which commenced in
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aneurin Bevan Health Board. Neighbourhood Care Network. Strategic Plan
 Agenda Item: 3.8 Appendix Two Aneurin Bevan Health Board Neighbourhood Care Network Strategic Plan 2013-2018 1 CONTENTS 1 Purpose & Scope 3 2 National and Local Context 6 3 The Vision 10 4 Strategic Themes
Agenda Item: 3.8 Appendix Two Aneurin Bevan Health Board Neighbourhood Care Network Strategic Plan 2013-2018 1 CONTENTS 1 Purpose & Scope 3 2 National and Local Context 6 3 The Vision 10 4 Strategic Themes
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS
 CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Medical and Clinical Services Directorate Clinical Strategy
 www.ambulance.wales.nhs.uk Medical and Clinical Services Clinical Strategy Unique reference No: Version: 1.4 Title of author: Medical and Clinical Services No of Pages: 11 Implementation date: Next review
www.ambulance.wales.nhs.uk Medical and Clinical Services Clinical Strategy Unique reference No: Version: 1.4 Title of author: Medical and Clinical Services No of Pages: 11 Implementation date: Next review
In this edition we will showcase the work of the development of a model for GP- Paediatric Hubs
 Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Title of the Health Board Report
 AGENDA ITEM 3.2 Title of the Health Board Report IMPLEMENTING THE OUTCOME OF THE SOUTH WALES PROGRAMME THROUGH ACUTE CARE ALLIANCES AND DEVELOPMENT OF THE SOUTH WALES HEALTH COLLABORATIVE Executive Lead:
AGENDA ITEM 3.2 Title of the Health Board Report IMPLEMENTING THE OUTCOME OF THE SOUTH WALES PROGRAMME THROUGH ACUTE CARE ALLIANCES AND DEVELOPMENT OF THE SOUTH WALES HEALTH COLLABORATIVE Executive Lead:
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
IMPLEMENTING THE OUTCOME OF THE SOUTH WALES PROGRAMME THROUGH ACUTE CARE ALLIANCES AND DEVELOPMENT OF THE SOUTH WALES HEALTH COLLABORATIVE
 AGENDA ITEM 3.3 9 September 2014 IMPLEMENTING THE OUTCOME OF THE SOUTH WALES PROGRAMME THROUGH ACUTE CARE ALLIANCES AND DEVELOPMENT OF THE SOUTH WALES HEALTH COLLABORATIVE Executive Lead: Chief Executive
AGENDA ITEM 3.3 9 September 2014 IMPLEMENTING THE OUTCOME OF THE SOUTH WALES PROGRAMME THROUGH ACUTE CARE ALLIANCES AND DEVELOPMENT OF THE SOUTH WALES HEALTH COLLABORATIVE Executive Lead: Chief Executive
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Guy s and St. Thomas Healthcare Alliance. Five-year strategy
 Guy s and St. Thomas Healthcare Alliance Five-year strategy 2018-2023 Contents Contents... 2 Strategic context... 3 The current environment... 3 National response... 3 The Guy s and St Thomas Healthcare
Guy s and St. Thomas Healthcare Alliance Five-year strategy 2018-2023 Contents Contents... 2 Strategic context... 3 The current environment... 3 National response... 3 The Guy s and St Thomas Healthcare
Cranbrook a healthy new town: health and wellbeing strategy
 Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
ANEURIN BEVAN HEALTH BOARD CLINICAL FUTURES STRATEGY AND SPECIALIST CRITICAL CARE CENTRE: BRIEFING
 ANEURIN BEVAN HEALTH BOARD Aneurin Bevan Health Board CLINICAL FUTURES STRATEGY AND SPECIALIST CRITICAL CARE CENTRE: BRIEFING 1 PURPOSE The purpose of this paper to is to brief Board members on the proposed
ANEURIN BEVAN HEALTH BOARD Aneurin Bevan Health Board CLINICAL FUTURES STRATEGY AND SPECIALIST CRITICAL CARE CENTRE: BRIEFING 1 PURPOSE The purpose of this paper to is to brief Board members on the proposed
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
NHS GRAMPIAN. Local Delivery Plan - Section 2 Elective Care
 NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
NHS GRAMPIAN. Grampian Clinical Strategy - Planned Care
 NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
Integrated Medium Term Plan 2015/ /18 Summary Document
 Integrated Medium Term Plan 2015/16 2017/18 Summary Document Bwrdd Iechyd Prifysgol Aneurin Bevan yw enw gweithredol Bwrdd Iechyd Lleol Prifysgol Aneurin Bevan Aneurin Bevan University Health Board is
Integrated Medium Term Plan 2015/16 2017/18 Summary Document Bwrdd Iechyd Prifysgol Aneurin Bevan yw enw gweithredol Bwrdd Iechyd Lleol Prifysgol Aneurin Bevan Aneurin Bevan University Health Board is
Frequently Asked Questions (FAQs) Clinical Futures (including The Grange University Hospital)
 Clinical Futures (including The Grange University Hospital)") Frequently Asked Questions (FAQs) Clinical Futures (including The Grange University Hospital) What is Clinical Futures? Clinical Futures is the Health Board plan for a sustainable health care system for
Frequently Asked Questions (FAQs) Clinical Futures (including The Grange University Hospital) What is Clinical Futures? Clinical Futures is the Health Board plan for a sustainable health care system for
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report
 Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL
 DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board. Audit year: Issued: October 2015 Document reference: 491A2015
 Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
Together for Health A Delivery Plan for the Critically Ill
 Together for Health A Delivery Plan for the Critically Ill 2013-2016 March 2015 Approved at CPG Board 25 th March 2015 1. BACKGROUND AND CONTEXT Together for Health a Delivery Plan for the Critically Ill
Together for Health A Delivery Plan for the Critically Ill 2013-2016 March 2015 Approved at CPG Board 25 th March 2015 1. BACKGROUND AND CONTEXT Together for Health a Delivery Plan for the Critically Ill
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
An overview of the planning process, findings and emerging proposals for the future
 An overview of the planning process, findings and emerging proposals for the future South Wales Programme objectives Safe and high quality care for patients which matches the best elsewhere Deliverable
An overview of the planning process, findings and emerging proposals for the future South Wales Programme objectives Safe and high quality care for patients which matches the best elsewhere Deliverable
Aneurin Bevan University Health Board. Planning and Strategic Change Committee
 Aneurin Bevan University Health Board Planning and Strategic Change Committee A Meeting of the Planning and Strategic Change Committee was held on Tuesday, 19 th December 2014 in Seminar Room 4, Conference
Aneurin Bevan University Health Board Planning and Strategic Change Committee A Meeting of the Planning and Strategic Change Committee was held on Tuesday, 19 th December 2014 in Seminar Room 4, Conference
DRAFT. Rehabilitation and Enablement Services Redesign
 DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
All Wales Nursing Principles for Nursing Staff
 All Wales Nursing Principles for Nursing Staff 1 Introduction The purpose of the paper is to respond to the Welsh Governments Staffing Principles for Nurse Staffing within Wales. These principles set out
All Wales Nursing Principles for Nursing Staff 1 Introduction The purpose of the paper is to respond to the Welsh Governments Staffing Principles for Nurse Staffing within Wales. These principles set out
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
CT Scanner Replacement Nevill Hall Hospital Abergavenny. Business Justification
 CT Scanner Replacement Nevill Hall Hospital Abergavenny Business Justification Version No: 3 Issue Date: 9 July 2012 VERSION HISTORY Version Date Brief Summary of Change Owner s Name Issued Draft 21/06/12
CT Scanner Replacement Nevill Hall Hospital Abergavenny Business Justification Version No: 3 Issue Date: 9 July 2012 VERSION HISTORY Version Date Brief Summary of Change Owner s Name Issued Draft 21/06/12
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Northumberland, Tyne and Wear NHS Foundation Trust. Board of Directors Meeting. Meeting Date: 25 October Executive Lead: Rajesh Nadkarni
 Agenda item 9 ii) Northumberland, Tyne and Wear NHS Foundation Trust Board of Directors Meeting Meeting Date: 25 October 2017 Title and Author of Paper: Clinical Effectiveness (CE) Strategy update Simon
Agenda item 9 ii) Northumberland, Tyne and Wear NHS Foundation Trust Board of Directors Meeting Meeting Date: 25 October 2017 Title and Author of Paper: Clinical Effectiveness (CE) Strategy update Simon
Written Response by the Welsh Government to the report of the Health, Social Care and Sport Committee entitled Primary Care: Clusters
 Written Response by the Welsh Government to the report of the Health, Social Care and Sport Committee entitled Primary Care: Clusters I am grateful to the Committee for its inquiry into primary care. Clusters
Written Response by the Welsh Government to the report of the Health, Social Care and Sport Committee entitled Primary Care: Clusters I am grateful to the Committee for its inquiry into primary care. Clusters
The operating framework for. the NHS in England 2009/10. Background
 the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
The PCT Guide to Applying the 10 High Impact Changes. A guide from NatPaCT
 The PCT Guide to Applying the 10 High Impact Changes A guide from NatPaCT DH INFORMATION READER BOX Policy HR/Workforce Management Planning Clinical Estates Performance IM&T Finance Partnership Working
The PCT Guide to Applying the 10 High Impact Changes A guide from NatPaCT DH INFORMATION READER BOX Policy HR/Workforce Management Planning Clinical Estates Performance IM&T Finance Partnership Working
Strategic Plan for Fife ( )
") www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
Aneurin Bevan Health Board. Living Well, Living Longer: Inverse Care Law Programme
 Aneurin Bevan Health Board Living Well, Living Longer: Inverse Care Law Programme 1 Introduction The purpose of this paper is to seek the Board s agreement to a set of priority statements for an Inverse
Aneurin Bevan Health Board Living Well, Living Longer: Inverse Care Law Programme 1 Introduction The purpose of this paper is to seek the Board s agreement to a set of priority statements for an Inverse
Agenda Item 3.3 IMPLEMENTATION OF SETTING THE DIRECTION - WHOLE SYSTEMS CHANGE PROGRESS UPDATE
 FOR INFORMATION UHB Board Meeting: 17 January 2012 IMPLEMENTATION OF SETTING THE DIRECTION - WHOLE SYSTEMS CHANGE PROGRESS UPDATE Report of Paper prepared by Executive Summary Director of Public Health
FOR INFORMATION UHB Board Meeting: 17 January 2012 IMPLEMENTATION OF SETTING THE DIRECTION - WHOLE SYSTEMS CHANGE PROGRESS UPDATE Report of Paper prepared by Executive Summary Director of Public Health
Summarise the Impact of the Health Board Report Equality and diversity
 AGENDA ITEM 4.1 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact Details for further
AGENDA ITEM 4.1 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact Details for further
Vanguard Programme: Acute Care Collaboration Value Proposition
 Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Norfolk and Waveney STP - summary of key elements
 Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Health and Care Framework
 Annex 1 Health and Care Framework The NHS Grampian 2020 A Possible Future 1. NHS Grampian has agreed its Health Plan and has embarked on its Health and Care Framework (H&CF) process to determine in detail
Annex 1 Health and Care Framework The NHS Grampian 2020 A Possible Future 1. NHS Grampian has agreed its Health Plan and has embarked on its Health and Care Framework (H&CF) process to determine in detail
Driving and Supporting Improvement in Primary Care
 Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
8.1 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CLINICAL SERVICES REVIEW CONSULTATION OPTIONS. Date of the meeting 18/05/2016
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CLINICAL SERVICES REVIEW CONSULTATION OPTIONS Date of the meeting 18/05/2016 Author Sponsoring Clinician Purpose of Report Recommendation
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CLINICAL SERVICES REVIEW CONSULTATION OPTIONS Date of the meeting 18/05/2016 Author Sponsoring Clinician Purpose of Report Recommendation
COMMON GROUND EAST REGION. DEVELOPING A HEALTH AND SOCIAL CARE PLAN FOR THE EAST OF SCOTLAND Staff Briefing
 COMMON GROUND EAST REGION DEVELOPING A HEALTH AND SOCIAL CARE PLAN FOR THE EAST OF SCOTLAND Staff Briefing SEPTEMBER 2018 1 COMMON GROUND It is fitting that in the 70th anniversary year of our National
COMMON GROUND EAST REGION DEVELOPING A HEALTH AND SOCIAL CARE PLAN FOR THE EAST OF SCOTLAND Staff Briefing SEPTEMBER 2018 1 COMMON GROUND It is fitting that in the 70th anniversary year of our National
Transforming Cancer Services In South East Wales
 Transforming Cancer Services In South East Wales Clinical Service Model January 2016 Cancer survival rates are increasing. But the number of people getting cancer is increasing too. At Velindre NHS Trust
Transforming Cancer Services In South East Wales Clinical Service Model January 2016 Cancer survival rates are increasing. But the number of people getting cancer is increasing too. At Velindre NHS Trust
A Strategy for the Therapy Services 2011/2016 Mid-Term Review, May 2014
 A Strategy for the Therapy Services 2011/2016 Mid-Term Review, May 2014 1. Introduction A Strategy for the Therapy Services 2011/2016 was published in May 2011. The purpose of the Strategy was to: Describe
A Strategy for the Therapy Services 2011/2016 Mid-Term Review, May 2014 1. Introduction A Strategy for the Therapy Services 2011/2016 was published in May 2011. The purpose of the Strategy was to: Describe
Longer, healthier lives for all the people in Croydon
 D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
Your local NHS and you
 South Wales Programme Local Engagement Document Your local NHS and you Local NHS services in Cardiff and the Vale of Glamorgan are run by Cardiff and Vale University Health Board (UHB). The UHB is one
South Wales Programme Local Engagement Document Your local NHS and you Local NHS services in Cardiff and the Vale of Glamorgan are run by Cardiff and Vale University Health Board (UHB). The UHB is one
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Our Health & Care Strategy
 MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
AGENDA ITEM: JANUARY 2018 MENTAL HEALTH SERVICE REPATRIATION: PROJECT CLOSURE. Subject :
 AGENDA ITEM: 2.5 BOARD MEETING Subject : Approved and Presented by: Prepared by: Other Committees and meetings considered at: Considered by Executive Committee on: DATE OF MEETING: 31 JANUARY 2018 MENTAL
AGENDA ITEM: 2.5 BOARD MEETING Subject : Approved and Presented by: Prepared by: Other Committees and meetings considered at: Considered by Executive Committee on: DATE OF MEETING: 31 JANUARY 2018 MENTAL
2020 Objectives July 2016
 ... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
Prescription for Rural Health 2011
 Foreword Prescription for Rural Health is the Welsh NHS Confederation s contribution to the debate on health in rural Wales. This document has been published alongside Prescription for Health 2011, which
Foreword Prescription for Rural Health is the Welsh NHS Confederation s contribution to the debate on health in rural Wales. This document has been published alongside Prescription for Health 2011, which
Seven day hospital services: case study. South Warwickshire NHS Foundation Trust
 Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Health and care services in Herefordshire & Worcestershire are changing
 Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
Trust Board Meeting 05 May 2016
 Trust Board Meeting 05 May 2016 Title of the paper: Sustainability and Transformation Plan (STP) Update Agenda item: 15/37 Lead Executive: Trust objective: Purpose: Link to Board Assurance Framework (BAF)
Trust Board Meeting 05 May 2016 Title of the paper: Sustainability and Transformation Plan (STP) Update Agenda item: 15/37 Lead Executive: Trust objective: Purpose: Link to Board Assurance Framework (BAF)
Redesign of Front Door
 Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Reducing Variation in Primary Care Strategy
 Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
grampian clinical strategy
 healthfit caring listening improving consultation grampian clinical strategy 2016 to 2021 1 summary version NHS Grampian Clinical Strategy 2016 to 2021 Purpose and aims 5 Partnership working and the changing
healthfit caring listening improving consultation grampian clinical strategy 2016 to 2021 1 summary version NHS Grampian Clinical Strategy 2016 to 2021 Purpose and aims 5 Partnership working and the changing
5. Does this paper provide evidence of assurance against the Governing Body Assurance Framework?
 Item Number: 6.3 Governing Body Meeting: 4 February 2016 Report Sponsor Anthony Fitzgerald Director of Strategy and Delivery Report Author Anthony Fitzgerald Director of Strategy and Delivery 1. Title
Item Number: 6.3 Governing Body Meeting: 4 February 2016 Report Sponsor Anthony Fitzgerald Director of Strategy and Delivery Report Author Anthony Fitzgerald Director of Strategy and Delivery 1. Title
Gwent Clinical Futures
 Gwent Clinical Futures Public Consultation Document Blaenau Gwent Local Health Board Caerphilly Local Health Board Monmouthshire Local Health Board Newport Local Health Board Torfaen Local Health Board
Gwent Clinical Futures Public Consultation Document Blaenau Gwent Local Health Board Caerphilly Local Health Board Monmouthshire Local Health Board Newport Local Health Board Torfaen Local Health Board
STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby
 STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby http://nhsbetterhealth.org.uk/wp-content/uploads/2016/11/stp-draft-plan-on-page- Final-1.pdf The STP Process Q1. Version Control:
STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby http://nhsbetterhealth.org.uk/wp-content/uploads/2016/11/stp-draft-plan-on-page- Final-1.pdf The STP Process Q1. Version Control:
We plan. We achieve.
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
Aneurin Bevan Continuous Improvement
 Aneurin Bevan Continuous Improvement Creating a Health Board Centre for Quality Improvement 1. Introduction The purpose of this report is to outline a proposal for the creation of the ABCi Centre for Improvement.
Aneurin Bevan Continuous Improvement Creating a Health Board Centre for Quality Improvement 1. Introduction The purpose of this report is to outline a proposal for the creation of the ABCi Centre for Improvement.
SUMMARY. Our progress in 2013/14. Eastbourne, Hailsham and Seaford Clinical Commissioning Group.
 Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Better Healthcare in Bucks Reconfiguring acute services
 service redesign case study March 2013 No. 3 Reconfiguring acute services Key points Reach a shared understanding of the case for change across the local health economy. Start public engagement as early
service redesign case study March 2013 No. 3 Reconfiguring acute services Key points Reach a shared understanding of the case for change across the local health economy. Start public engagement as early
ANEURIN BEVAN HEALTH BOARD DELIVERING END OF LIFE CARE
 ANEURIN BEVAN HEALTH BOARD DELIVERING END OF LIFE CARE 2013-2016 1. INTRODUCTION The 5 Year NHS Plan, Together for Health, sets out the programme for health & healthcare in Wales and Together for Health
ANEURIN BEVAN HEALTH BOARD DELIVERING END OF LIFE CARE 2013-2016 1. INTRODUCTION The 5 Year NHS Plan, Together for Health, sets out the programme for health & healthcare in Wales and Together for Health
Item No: 14. Meeting Date: Wednesday 8 th November Glasgow City Integration Joint Board
 Item No: 14 Meeting Date: Wednesday 8 th November 2017 Glasgow City Integration Joint Board Report By: David Williams, Chief Officer Contact: Susanne Millar, Chief Officer, Strategy & Operations / Chief
Item No: 14 Meeting Date: Wednesday 8 th November 2017 Glasgow City Integration Joint Board Report By: David Williams, Chief Officer Contact: Susanne Millar, Chief Officer, Strategy & Operations / Chief
1000 Lives Improvement
 1000 Lives Improvement 1000 Lives Improvement is the national quality improvement service for NHS Wales delivered by Public Health Wales. Our aim is to support the NHS to improve outcomes for people using
1000 Lives Improvement 1000 Lives Improvement is the national quality improvement service for NHS Wales delivered by Public Health Wales. Our aim is to support the NHS to improve outcomes for people using
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
grampian clinical strategy
 healthfit caring listening improving grampian clinical strategy 2016 to 2021 1 summary version For full version of the Grampian Clinical Strategy, please go to www.nhsgrampian.org/clinicalstrategy Document
healthfit caring listening improving grampian clinical strategy 2016 to 2021 1 summary version For full version of the Grampian Clinical Strategy, please go to www.nhsgrampian.org/clinicalstrategy Document
A Prudent Approach to Health: Prudent Health Principles
 A Prudent Approach to Health: Prudent Health Principles 1. Summary The following paper sets out the Bevan Commission s final advice on the Prudent Health Principles to the Minister for Health and Social
A Prudent Approach to Health: Prudent Health Principles 1. Summary The following paper sets out the Bevan Commission s final advice on the Prudent Health Principles to the Minister for Health and Social
Annual Review and Evaluation of Performance 2012/2013. Torfaen County Borough Council
 Annual Review and Evaluation of Performance 2012/2013 Local Authority Name: Torfaen County Borough Council This report sets out the key areas of progress in Torfaen Social Services Department for the year
Annual Review and Evaluation of Performance 2012/2013 Local Authority Name: Torfaen County Borough Council This report sets out the key areas of progress in Torfaen Social Services Department for the year
REPORT 1 FRAIL OLDER PEOPLE
 REPORT 1 FRAIL OLDER PEOPLE Contents Vision f-3 Principles / Parameters f-4 Objectives f-6 Current Frail Older People Model f-8 ABMU Model for Frail and Older People f-11 Universal / Enabling f-12 Specialist
REPORT 1 FRAIL OLDER PEOPLE Contents Vision f-3 Principles / Parameters f-4 Objectives f-6 Current Frail Older People Model f-8 ABMU Model for Frail and Older People f-11 Universal / Enabling f-12 Specialist
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan. October 2016 submission to NHS England Public summary
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
GOULBURN VALLEY HEALTH Strategic Plan
 GOULBURN VALLEY HEALTH Strategic Plan 2014-2018 VISION Healthy communities VALUES Compassion Respect Excellence Accountability Teamwork Ethical Behaviour PRIORITIES Empowering Your Health Strengthening
GOULBURN VALLEY HEALTH Strategic Plan 2014-2018 VISION Healthy communities VALUES Compassion Respect Excellence Accountability Teamwork Ethical Behaviour PRIORITIES Empowering Your Health Strengthening
Aneurin Bevan Health Board. Improving Theatre Performance
 Aneurin Bevan Health Board Improving Theatre Performance 1 Introduction This report provides an overview on actions being taken to improve theatre performance within the Health Board. The report provides
Aneurin Bevan Health Board Improving Theatre Performance 1 Introduction This report provides an overview on actions being taken to improve theatre performance within the Health Board. The report provides
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
A Step-by-Step Guide to Tackling your Challenges
 Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
NORTH WALES CLINICAL STRATEGY. PRIMARY CARE & COMMUNITY SERVICES SBAR REPORT February 2010
 NORTH WALES CLINICAL STRATEGY PRIMARY CARE & COMMUNITY SERVICES SBAR REPORT February 2010 Situation The Primary Care & Community Services workstream had been tasked with answering the following question:
NORTH WALES CLINICAL STRATEGY PRIMARY CARE & COMMUNITY SERVICES SBAR REPORT February 2010 Situation The Primary Care & Community Services workstream had been tasked with answering the following question:
Together for Health. A Five Year Vision for the NHS in Wales
 Together for Health A Five Year Vision for the NHS in Wales WG 14021 ISBN 978 0 7504 6808 4 Crown copyright 2011 Introduction Together for Health A 5-year vision for the NHS in Wales Sustainability lies
Together for Health A Five Year Vision for the NHS in Wales WG 14021 ISBN 978 0 7504 6808 4 Crown copyright 2011 Introduction Together for Health A 5-year vision for the NHS in Wales Sustainability lies
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme. Frequently Asked Questions Second Edition
 Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
NHS GRAMPIAN. Clinical Strategy
 NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
A National Model of Care for Paediatric Healthcare Services in Ireland Chapter 4: Vision for Paediatric Health Services
 A National Model of Care for Paediatric Healthcare Services in Ireland Chapter 4: Vision for Paediatric Health Services Clinical Strategy and Programmes Division Vision for Paediatric Health Services Introduction
A National Model of Care for Paediatric Healthcare Services in Ireland Chapter 4: Vision for Paediatric Health Services Clinical Strategy and Programmes Division Vision for Paediatric Health Services Introduction
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Delivering Integrated Health and Social Care for Older People with Complex Needs across Western Bay. Statement of Intent
 Delivering Integrated Health and Social Care for Older People with Complex Needs across Western Bay Statement of Intent March 2014 1 1. Introduction This document sets out our commitment to deliver integrated
Delivering Integrated Health and Social Care for Older People with Complex Needs across Western Bay Statement of Intent March 2014 1 1. Introduction This document sets out our commitment to deliver integrated