KENT SURREY AND SUSSEX DEANERY QUALITY MANUAL
|
|
|
- Earl Wade
- 6 years ago
- Views:
Transcription

1 KENT SURREY AND SUSSEX DEANERY QUALITY MANUAL

2 1. Overview of the Quality Management of Education and Training Quality Management operations are regulated by the GMC and outlined in the Quality Improvement Framework, which sets out the deanery s responsibilities for quality management. The diagram below shows how the different levels of QA, QM and QC relate to each other. Currently, Medical Schools and Deaneries are the units that manage the quality of medical education and training, maintaining and improving standards over time. The GMC expects Medical Schools and Deaneries to demonstrate compliance with the standards and requirements that it sets. To do this, they will need to work in close partnership with the Medical Royal Colleges and Faculties, NHS trusts and health boards and other LEPs. This means that Quality Management should be seen as a partnership between those organisations because it is only through working together that Medical Schools, Deaneries, Royal Colleges and Faculties, with LEPs, can deliver medical education and training to the standards required. 2. Quality Management in KSS Quality management of the delivery of education and training is one of the key functions of the Deanery. The main components of the KSS quality process are visits, surveys, metrics and reports/minutes from LEPs. Data from these sources are compared and analysed to provide evidence of the quality of training provision. The quality process is underpinned by the meetings of the Deanery Quality Management Steering Group (QMSG), chaired by the Dean Director. The QMSG meets monthly and includes representation from the Quality Department, Heads of Schools, Training Programme Directors, Foundation Programme Directors, Associate Deans and the Education Department. The work of the Performance and Quality Department is reported to and approved by this group. 1
3 3. The KSS Local Quality Reporting Framework This section provides a brief summary of the KSS local quality reporting framework. Full details are set out in the Graduate Education and Assessment Regulations (GEAR). Each LEP has a Local Academic Board (LAB), which is chaired by the Director of Medical Education (DME) with the Medical Education Manager (MEM) taking up the role of Academic Registrar; and a number of Local Faculty Groups (LFGs), one for each specialty providing education and training. The LFG is the first tier of local accountability for postgraduate medical education and an effective unit for its management in LEPs. The LFG is responsible for the quality control of the local programme, ensuring the programme meets curriculum requirements, and tracking, supporting and auditing the trainees progress. Each LFG reports to the LAB. The LAB oversees the activities of the LFGs, and will aim to deal with any problems or issues arising from the LFGs. This keeps the quality control function of the LEP s activities at a local level. If there is a serious problem that cannot be dealt with at a local level, the LAB will refer to the Deanery. In this way, a local remedy can be applied to any problem area; KSS has immediate awareness of any unusual circumstances; and the KSS Head of School becomes involved only when it is necessary and appropriate. The KSS Schools and Quality Department receive the minutes from all LFG and LAB meetings and an Annual Report and Review (AAR) from each LAB and LFG. These documents feed into the Deanery Report to the GMC. 4. KSS Policies and Procedures The KSS Deanery Quality Management System is governed by a number of policies and procedures. These are being continuously produced and added to the Quality Manual as part of an on-going process of document management and control. The approved policies and procedures are stored electronically as part of the Deanery s Quality management System (QMS), which also includes work instructions and forms/templates as applicable. The KSS Quality Manual is a living document, which is reviewed and updated on a continual basis. The following section contains links to all the current KSS Policies, Procedures, Work Instructions, Forms, Templates and Guidance in the QMS. These documents are reviewed on a regular basis. Older versions are stored in the archive section. 2
4 1. Quality Structure and Terms of Reference A. KSS Organisational Structure Chart K:\QUALITY MANAGEMENT\QM Documents\Master Documents\KSS Organisational Structure Chart B. Quality Management Structure K:\QUALITY MANAGEMENT\QM Documents\Master Documents\Quality Management Structure C. Quality Management Steering Group Terms of Reference K:\QUALITY MANAGEMENT\QM Steering Group Meetings\KSS QMSG Terms of Reference D. Quality Management Operational Group Terms of Reference K:\QUALITY MANAGEMENT\QM Operational Group\KSS QMOG Terms of Reference E. Deanery Board Terms of Reference K:\QUALITY MANAGEMENT\QM Documents\Quality Manual\Deanery Board ToR F. Operational Group Terms of Reference K:\QUALITY MANAGEMENT\QM Documents\Quality Manual\Operational Group ToR G. Strategic Management Group Terms of Reference K:\QUALITY MANAGEMENT\QM Documents\Quality Manual\Strategic Management Group ToR H. Higher Specialty Training Board Terms of Reference K:\QUALITY MANAGEMENT\QM Documents\Quality Manual\ Higher Specialty Training Board ToR I. Trainee in Difficulty Committee Terms of Reference K:\QUALITY MANAGEMENT\QM Documents\Quality Manual\ Trainee in Difficulty Committee ToR J. South Thames Foundation School Board Terms of Reference K:\QUALITY MANAGEMENT\QM Documents\Quality Manual\South Thames Foundation School Board ToR K. GP School Board Terms of Reference K:\QUALITY MANAGEMENT\QM Documents\Quality Manual\ GP School Board ToR L. GP Post Certification School Terms of Reference K:\QUALITY MANAGEMENT\QM Documents\Quality Manual\ GP Post Certification School ToR M. Quality Assurance of GP Appraisal Group Terms of Reference K:\QUALITY MANAGEMENT\QM Documents\Quality Manual\ Quality Assurance of GP Appraisal Group ToR N. Joint Committee on Quality Management Terms of Reference K:\QUALITY MANAGEMENT\QM Documents\Quality Manual\ Joint Committee on Quality Management ToR 3
5 2. Deanery Report A. Guidance on Producing the KSS Deanery Report K:\QUALITY MANAGEMENT\Annual Reports\Deanery Report Documents\DR Guidance B. Deanery Report Production Flowchart K:\QUALITY MANAGEMENT\Annual Reports\Deanery Report Documents\DR Flowchart 3. LEP Metrics A. Guidance Completion of the LEP Metrics K:\QUALITY MANAGEMENT\LEP Metrics\Guidance Completion of the LEP Metrics B. LEP Metrics Template K:\QUALITY MANAGEMENT\LEP Metrics\LEP Metrics template C. LEP Metrics Signing-off Sheet K:\QUALITY MANAGEMENT\LEP Metrics\LEP Metrics Signing-off Sheet 4. GMC National Training Survey A. Process for Administering the GMC Survey K:\QUALITY MANAGEMENT\GMC Survey 2012\Process for Administering the GMC Survey 5. Specialty School Visits to LEPs A. Visiting Procedure Specialty School Visits to LEPs K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\LEP Visits Procedure version 1.6 B. Calendar for School Quality Management Visits to LEPs K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Calendar for School Quality Management Visits to LEPs C. Process for reporting Visits to Programmes K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Process for Reporting Visits to Programmes D. Visit Report Template K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Visit Report Template 4
6 E. Headline Feedback Form K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Headline feedback form F. Action Planning Template K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Action Planning Template G. DME Self Assessment Pro Forma K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\DME Self Assessment Pro Forma H. Visiting Team Pro Forma K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Visiting Team Pro Forma I. Question Prompt K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Question Prompt J. Role of the Lead Visitor overview K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Role of the Lead Visitor overview K. Visit Feedback Form (LEP) K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Visit Feedback Form (LEP) L. Visitor Feedback Form K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Visitor Feedback Form M. Visitor Guidance and Declaration K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Visitor Guidance and Declaration 6. Foundation School Visits to LEPs A. Foundation Faculty Visiting Process K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Foundation\Foundation Faculty visiting Process B. Lead Visitor checklists K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Foundation\Lead Visitor Checklists C. Guidance Notes for Lead Visitors K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Foundation\Guidance Notes for Lead Visitors D. Guidance Notes for Lead Administrators K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Foundation\Guidance Notes for Lead Administrators 5
7 E. Briefing Note K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Foundation\Briefing Note F. Headline Feedback Form K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Foundation\Headline Feedback Form 7. Pharmacy Visits A. Pharmacy Visits Procedure K:\QUALITY MANAGEMENT\Pharmacy\Pharmacy Visits\Pharmacy Visit Procedure B. Action Planning Template - Pharmacy K:\QUALITY MANAGEMENT\Pharmacy\Pharmacy Visits\Action Planning template - Pharmacy 8. GP School Visits to LEPs A. Guidance on the Quality Management of GP Specialty Training K:\QUALITY MANAGEMENT\LEP Visits\Visit Documents\Guidance to KSS GP Quality Management process - v5 9. Contract Review A. Contract Review Process 2012/13 K:\QUALITY MANAGEMENT\Contract Review\Protocol 2012 B. KSS Single Contract K:\QUALITY MANAGEMENT\Contract Review\Contract 2012 C. Quality Manual Specification K:\QUALITY MANAGEMENT\Contract Review\QM Specification PGMDE 2012 D. Education Audit K:\QUALITY MANAGEMENT\Contract Review\CR Education Audit 2012 E. Business Analysis K:\QUALITY MANAGEMENT\Contract Review\Business analysis F. LAB Strategy K:\QUALITY MANAGEMENT\Contract Review\LAB Strategy 6
8 G. Earned Autonomy Verification Report K:\QUALITY MANAGEMENT\Contract Review\Earned autonomy verification report H. Blank Verifiers Report 2012 K:\QUALITY MANAGEMENT\Contract Review\Blank Verifiers Report 2012 I. Action Plan Template 2012 K:\QUALITY MANAGEMENT\Contract Review\Action Plan Template Serious Incidents A. KSS Serious Incidents Policy K:\QUALITY MANAGEMENT\QM Documents\Master Documents\KSS Serious Incidents Policy B. Serious Incident Preliminary Notification Form K:\QUALITY MANAGEMENT\QM Documents\Master Documents\Serious Incident Preliminary Notification Form 7
9 Postgraduate Deanery for Kent, Surrey & Sussex: KSS Deanery Organisational Structure Chart October 2012 (Professor David Black) Dean Director Chair of KSS Strategic Management Group (SMG) EDUCATION Professor Zoë Playdon Head of Education PHARMACY (SEMMED) Gail Fleming Director of Pharmacy BUSINESS & SENIOR MANAGEMENT Chris Bird Chief Operating Officer Chair of Business & Senior Management Team (BSMT) GENERAL PRACTICE Professor Abdollah Tavabie Deputy Dean Director and GP Dean DENTAL Professor Stephen Lambert-Humble Dental Dean FOUNDATION Dr Jan Welch Director, South Thames Foundation School SECONDARY CARE Dr Kevin Kelleher Deputy Postgraduate Dean for Secondary Care CLINICAL LEADERSHIP Dr Lindsay Hadley Head of KSS School of Clinical Leadership Dr Clare Penlington Deputy Head of Education Karen Allman Human Resources Angela Fletcher Specialty Workforce Dr Ian McLean Deputy GP Dean and Head of KSS GP School Sandra Forster General Practice and Dental Robin Garrett I.T and Operations Marc Terry Foundation Workforce Karen Gibson Quality Management
10 Postgraduate Deanery for Kent, Surrey & Sussex: KSS Deanery Functional Structure Chart October 2012 KSS LETB Legal accountability to host organisation - CEO of BSUH Professionally accountable to - MD LETB - MD HEE - GMC KSS Deanery Board Membership includes the LETB MD Accountability to LETB through regular contract performance review meetings London Deanery Dean Director KSS Strategic Management Group STFS Board KSS Quality Management Steering Group (QMSG) Membership includes the LETB Head of Quality and Information KSS Trainee in Difficulty Group Corporate Functions Dentistry Primary Care Secondary Care Pharmacy Education Quality Management Foundation Human Resources IT and Operations Finance Primary Care Workforce Secondary care Workforce Careers Library & Knowledge Services Foundation Workforce
11 KSS Deanery Quality Management Structure KSS Quality Management Steering Group Trainees administratively managed by London KSS Quality Management Operational Group Foundation School KSS Specialty Schools Specialty Training Committees KSS or London/KSS Deanery specifies how LAB should be set up and run LABs and LFGs work according to GEAR NHS Trust Local Academic Board (LAB) (Manages Quality Control for the Trust) Trust: DME, MEM, MSM, Medical Director, HR, IT, etc. Deanery: Education Adviser and Associate Dean Trainee Rep, Lay Members Trust decides how many LFGs are required - depends on size of Trust Local Faculty Groups (LFG) E.g. Foundation Programme, Medicine, Surgery, O&G, Paediatrics, ACCS, GP, Anaesthetics, Psychiatry
12 KSS DEANERY QUALITY MANAGEMENT STEERING GROUP TERMS OF REFERENCE To design a cost effective quality management system for KSS building on current good practice and GMC direction, which is minimally disruptive to service. To implement local effective educational governance with the local education providers. To be the overall Deanery group for quality management standards, policies and problem resolution. To be the Deanery group for final recording and resolution of all issues relating to the approval of posts and programmes. To consider the wider stakeholder environment and how to involve/inform as appropriate. To lead on future GMC quality assurance visits and to act as a source of expertise to troubleshoot local problems.
13 KSS DEANERY QUALITY MANAGEMENT OPERATIONAL GROUP (QMOG) TERMS OF REFERENCE To take relevant action on matters arising from the KSS QM Steering Group as required. To facilitate communications and joint working across departments in KSS Deanery. To discuss quality management issues as they arise, and devise solutions for approval by the QM Steering Group. To provide evidence to cost the Operationalisation of QM in KSS. To provide evidence for the specifications of IT/Data Handling systems for QM in KSS. To involve/inform wider stakeholder groups as appropriate. To receive feed-back from the Schools on their QM/C activities. To lead on quality management operational issues and to act as a source of expertise to troubleshoot local problems. To call together appropriate people as necessary to deal with ad-hoc operational issues.
14 The Deanery Board will: DEANERY BOARD MEMBERSHIP AND TERMS OF REFERENCE i) promote excellence and innovation in postgraduate education and encourage and develop educational research including development and evaluation of assessment and learning ii) iii) iv) oversee the business planning process for the Deanery as a provider within the context of SHA commissioning of postgraduate medical and dental education, undergraduate and post graduate pharmacy education and possible future national commissioning add value to and promote the success of the Deanery as an organisation both nationally and regionally assure all stakeholders that work with the Deanery on a regional basis that the work of the Deanery is equitable, in particular, in its allocation of finances, quality management processes and operational contracting with Local Education Providers v) assist the Dean Director in setting strategic direction and effective educational management capacity and capability vi) vii) viii) oversee the Deanery communication strategy in order to ensure engagement of all stakeholders. take a lead role in the appointment of the senior staff review the overall performance element of the evidence required by the commissioner to meet national regulatory standards and local key performance indicators. Its principal functions are to: i) receive reports from the Dean Director and other Deans ii) iii) iv) consider and approve the Deanery strategic direction and business plan approve and review the Deanery financial plan receive and comment on the national workforce plans v) receive and approve the Deanery quality management reports vi) vii) receive and comment on GMC and other national reports appoint Appeals Committees as required viii) receive and comment on the risk register and escalate any risks to the Brighton and Sussex University Hospitals (BSUH) Board of Directors. K/DO/DD/Documents/Deanery Board/Deanery Board ToR June 2011.doc
15 The Chair will be responsible for the operation of the Deanery Board, ensuring that it makes an effective contribution to the governance of the Deanery and its pursuit of quality and excellence. The Chair will work closely with the Dean Director and the Secretary of the Deanery Board and will ensure that key and appropriate issues are discussed by the Deanery Board in a timely manner and that relevant information and advice is made available to the Deanery Board to inform the debate and decision-making process. Membership of the Deanery Board The membership of the Deanery Board will comprise: From KSS Deanery: the Dean Director, the GP Dean and the Chief Operating Officer From the Brighton and Sussex Medical School: the Dean or designated representative From KSS LETB: Managing Director From a Higher Education Institute: 2 representatives elected from the HEI college arrangement with a minimum of one place to be reserved for either the University of Kent or the University of Surrey From local acute Education Providers: 3 representatives elected through the LEP college arrangement based on the 3 counties of Kent, Surrey and Sussex From the 3 county based Mental Health Trusts: 1 representative From the 3 new county based PCT clusters: 1 representative An independent Educationalist The Deanery Board will meet monthly in the first instance. The Membership of the Deanery Board will be based on the principle of no substitutes. September 2012 K/DO/DD/Documents/Deanery Board/Deanery Board ToR June 2011.doc
16 KSS DEANERY OPERATIONAL GROUP MEMBERSHIP AND TERMS OF REFERENCE Purpose To provide day-to-day operational support to the Dean Director delivering the business of the KSS Deanery. Membership Deans Deputy Deans Associate Deans Heads of School Heads of Department Senior Business Managers Other members of staff may attend at the request of their Head of Department when discussing specific issues. Meeting Frequency Once weekly (Friday morning) chaired by the Dean Director or a nominated deputy. Meeting Functions To co-ordinate and put into operation the day-to-day management of the secondary care function. To co-ordinate, where appropriate, the work of all business functions within the Deanery. To share information of all aspects of Deanery business. To discuss KSS policy and strategy and note the business managers meetings that makes formal decisions on policies. K/DO/KSS Operational Group/ToR Oct 2012.doc
17 TERMS OF REFERENCE KSS DEANERY STRATEGIC MANAGEMENT GROUP MEMBERSHIP AND TERMS OF REFERENCE Purpose The strategy and decision making group for the Deanery. To discuss and plan the strategic direction of the Deanery. Agree the annual business plan and monitor progress against it. To debate and direct the educational direction of the Deanery. Final responsibility for the allocation and use of Deanery funds. Debate and resolution of serious or complex operational issues unresolved elsewhere. Maintain and discuss a Deanery wide top level risk register. Membership Dean Director GP Dean Dental Dean Director, South Thames Foundation School Deputy Postgraduate Dean for Secondary Care Chief Operating Officer Head of Education Head of Pharmacy Other attendees by invitation Meeting Frequency Meetings held once a month and chaired by the Dean Director. Principles of Working A forum in which all strategic leads are equally involved. A forum in which we debate and agree difficult issues, including finance, without doing backroom deals or making autocratic decisions. A forum in which we challenge arguments, but not personalise issues or re-fight old battles A forum in which we try to reach agreement by consensus, but occasionally accept a majority opinion when a decision must be made. A forum where we continually strive to be a coherent organisation with a single front to the outside world. 08 October 2012 revised K/DO/DD/Meetings/Strategic Management/ToR Oct 2012.doc
18 KSS HIGHER SPECIALTY TRAINING BOARD TERMS OF REFERENCE Remit 1. To review progress implementing the programmes which serve Higher Specialty Training (HST) in the KSS region taking account of BSUH and its allied Medical School and Departments, BSMS (as an undergraduate and postgraduate University centre) and extending to the Surrey and Kent LEPs and Academic centres. 2. To provide internal scrutiny by challenging progress to ensure minimal risk to development of new and existing programmes. Actions from scrutiny should move to the emerging LETB when appropriate. 3. To provide support in overcoming challenges and helping to meet SEC / KSS HST PGME consultation recommendations. 4. To ensure the Deanery, the Trusts, relevant Academic Institutions and other key stakeholders are all involved in the development of KSS HST Programmes. 5. To ensure high quality academic input is enhanced and maintained within KSS HST Programmes. 6. To ensure effective Communications are maintained with all Stakeholders 7. To champion and progress KSS based Higher Specialty Training Programmes by steering the delivery of key KSS HST priorities and objectives in negotiation with allied LETBs, AHSNs Deaneries and Schools. 8. To ensure alignment in Programme development meets emergent service models and by delivering expertise to emerging Clinical Commissioning Groups where appropriate. 9. To provide guidance and liaison with other allied Lead providers and Deaneries via close collaborative working 10. To take account of National and regional policy decisions relating to PGME delivery 11. To comment on future Commissioning options for PGME in the region. 12. The KSS HST Board will invite and request attendance from the following colleagues: Membership Chief Executive, Brighton and Sussex University Hospital NHS Trust Chief Executive, East Kent Hospitals University NHS Foundation Trust Chief Executive, Royal Surrey County Hospital NHS Trust Dean Director, KSS Deanery Chief Operating Officer, KSS Deanery Deputy Postgraduate Dean for Secondary Care Dean, Brighton and Sussex Medical School Chief of Medicine - BSUH Head, Division of Clinical Medicine, BSMS (academic representative) Director of Medical Education, Brighton & Sussex University Hospitals Director of Medical Education, Royal Surrey County Hospital Foundation Trust
19 Director of Medical Education, East Kent Hospitals University Foundation Trust Associate Dean (particular responsibility for Brighton), KSS Deanery Head of School of Medicine, KSS Deanery Head of ACCS, KSS Deanery Head of School of Emergency Medicine, KSS Deanery Head of School of Anaesthesia, KSS Deanery Head of School of Surgery, KSS Deanery Head of School of Obstetrics & Gynaecology, KSS Deanery Head of School of Radiology, KSS Deanery Head of School of Psychiatry, KSS Deanery Head of School of Paediatrics, KSS Deanery Head of school of Ophthalmology KSS Deanery Head of Medical Workforce, KSS Deanery Consultant Haematologist (Academic Lead) Associate Director of HR (Medical Personnel & Education), Brighton & Sussex University Hospitals MEM Representative KSS AD-Academia KSS As required: All KSS Training Programme Directors Specialty Leads from BSUH Specialty Leads from Kent based Trusts Specialty Leads from Surrey based Trusts Meetings - Every two months
20 KSS TRAINEE IN DIFFICULTY COMMITTEE TERMS OF REFERENCE 1. To act as the decision making body for the management of Trainees in Difficulty handled by KSS Deanery. 2. To discuss all Trainees in Difficulty in KSS Trusts, as well as all trainees in the South Thames Foundation Schools, including those in non-kss Trusts. 3. To offer support and advice to the Heads of Schools in managing Trainees in Difficulty. 4. To update The Trainee in Difficulty A KSS Trainee Support Guide on an annual basis. MEMBERSHIP (as at 10 May 2012) David Black (Chair), Dean Director, KSS Deanery Karen Allman, Head of Human Resources, KSS Deanery Christine Bridge, Foundation School Manager, South Thames Foundation School (Brighton Office) Geoff Bryant, Head of School of Emergency Medicine, KSS Deanery Chris Carey, Head of School of Anaesthesia and ICM, KSS Deanery Mark Cottee, Associate Director, South Thames Foundation School (Tooting Office) Graeme Dewhurst, Head of School of Medicine, KSS Deanery David Firth, Head of School of Psychiatry, KSS Deanery Sarah Flint, Lead for Obstetrics & Gynaecology, KSS Deanery Gail Fleming, Head of Pharmacy (Pharmacy Department), KSS Deanery Angela Fletcher, Head of Specialty Workforce, KSS Deanery Kevin Kelleher, Deputy Postgraduate Dean for Secondary Care, KSS Deanery Stephen Lambert-Humble, Head of Dental, KSS Deanery Nathan Nathan, GP Associate Dean, KSS Deanery Peter Martin, Head of School of Paediatrics, KSS Deanery Ian McLean, GP Deputy Dean, KSS Deanery Subir Mukherjee, Head of School of ACCS, KSS Deanery Beverley Osbourne, Foundation School Manager, South Thames Foundation School (Tooting Office) Martin Parry, Associate Director, South Thames Foundation School (Brighton Office) Simon Quy, Education Adviser, KSS Deanery Joan Reid, Senior Careers Adviser, South Thames Foundation School Humphrey Scott, Head of School of Surgery, KSS Deanery Abdol Tavabie, Dean of Postgraduate GP Education, KSS Deanery Marc Terry, Foundation School Manager, South Thames Foundation School (London Office) Jan Welch, Director, South Thames Foundation School Director David Yates, Associate Dean for Quality, KSS Deanery Camilla Sonsken / Philippa Skippage, Head of School of Radiology, KSS Deanery Geeta Menon, Head of School of Ophthalmology, KSS Deanery Edward Pickles, School of Anaesthesia representative, KSS Deanery Emma Wright, Specialist Pharmacist, Pharmacy Department, KSS Deanery
21 South Thames Foundation School South Thames Foundation School Board Terms of Reference 1 Purpose To enable Kent, Surrey and Sussex Deanery, South London sector of the London Deanery, KCL Medical School, St George s University of London and Brighton and Sussex Medical School to develop an overarching vision and direction for the South Thames Foundation School and ensure it delivers foundation training in accordance with the national Standards set by the GMC. 2 Operational Role To ensure the school has appropriate and co-ordinated processes and protocols in place in order to deliver and monitor foundation training. To co-ordinate recruitment, assessment and appeals policy and processes policy within the school and with London Deanery. To ensure there are shared and robust quality control processes to support the GMC quality assurance requirements. To review and agree expenditure for the management and administration of the school within the national financial arrangements. To ensure appropriate liaison with London Deanery and North Thames Foundation Schools. To make South Thames appointments, as appropriate, to the London foundation training board. Note: A quorum (requiring representation from both deaneries and the foundation school) would be required for the board to make formal decisions. 2.1 Frequency & Timing of Meetings 4 times per year usually in September, December, March and June 3pm usually Tuesdays 2.2 Membership Postgraduate Dean Director for KSS (Chair) Postgraduate Dean for London GP Dean for South London GP Dean for KSS Foundation School Director Foundation School Associate Director (Brighton) Foundation School Associate Director (Tooting) Principal St Georges, University of London Dean of King s College, London, School of Medicine Dean of Brighton & Sussex Medical School KSS Chief Operating Officer KSS Head of Foundation Workforce KSS Head of Education London Foundation Programme Manager Representatives from Medical Directors x 2 (1 KSS / 1 South London) Representatives from Clinical Tutors x 2 (1 KSS / 1 south London) Representative of F1 doctors Representative of F2 doctors Additional co-opted members as required Page 1 of 1 Updated: October 2012
22 KENT SURREY & SUSSEX DEANERY GENERAL PRACTICE SPECIALTY SCHOOL BOARD CONSTITUTION & TERMS OF REFERENCE Doc A A. INTRODUCTION 1. The name of the Committee shall be the KSS General Practice Specialty School Board (GP School Board) 2. The Terms of Reference shall be reviewed annually in May, or at other times if necessary. Management of the Postgraduate School of General Practice Education The school has an Executive Board which is the strategic and operational unit of the Postgraduate School of General Practice. There is representation on the Board from each of the programmes within the school. The Dean of Postgraduate GP Education is the Chair of the Executive Board. The Head of the GP School will be the Deputy GP Dean. The Executive Board also has representatives from the RCGP, LMC, GP specialty trainees, trainers, lay and university. Dean Postgraduate General Practice Education GP School Board (ARCP)Annual Review Competence Progression Head of GP School & Deputy Dean (TSC)Trainer Selection & Reselection Committee Programme Directors LMC &RCGP Regional Representative Head of Curriculum & Assessment GP Trainer Representative Others, Trainee, Lay & University A programme is a subset of the school within the deanery. Programmes are organised geographically and developed to be sensitive to local needs. Each programme has GPStRs (trainees in years ST1, ST2 and ST3), is supported by GP Programme Directors and provides a variety of training placements, in hospital, community settings and general practice. All the programmes in the KSS health economy together form the GP School. An individual programme will deliver the GP curriculum in a way congruent with local health needs, resources and expertise. Induction is a programme responsibility and it is important that trainees have an induction to the School, Trust and clinical specialty whether general practice or hospital. The first year induction is particularly important.. KSS GP Specialty School Board, Constitution & TOR v st March 2008
23 B. TERMS OF REFERENCE: 1. To advise the SEC Strategic Health Authority and its Workforce Management structure (KSS Deanery), and appropriate academic and higher education institutions: To deliver the education and training of general practitioners to meet the Royal College of General Practitioners and Postgraduate Medical and Education Training Board (PMETB) agreed curricula; to the standards set out by PMETB, and to promote excellence in all aspects of the work of the School. To implement the new MMC training programmes To manage transitions and rotations within the programmes and to manage entry to the specialty training posts in line with nationally agreed guidelines cocoordinated by the National Recruitment Office for General Practice. To ensure appropriate support for trainees in General Practice programmes who are training to be general practitioners To ensure that the delivery of training enhances the quality and safety of patient care for today s and tomorrow s patients and produces specialists fit to meet the needs of the NHS and with the skills to be able effectively to contribute to future changes in the health service. To meet workforce and patient needs by training fit for purpose general practitioners - including ensuring that all trainees gain the organisational skills, e.g. team working, leadership, change management, business management - necessary for their role as future general practitioners able to work effectively in complex organisations and able to lead and implement change in the primary care setting. To monitor the quality of training; to evaluate and review local quality control measures and reports and ensure these are used to drive continual improvement to meet the standards that will be set by the Royal College of General Practitioners and the PMETB To monitor possible discriminatory affects of any policies or procedures and steer action to promote diversity and equality of opportunity. To take part in the selection and recruitment of doctors in training to general practice training programmes and to contribute to the development of selection methodology To maintain effective formative and summative assessment processes - including the annual review of training and the process for the recommendation of the award of CCT To work with the KSS Deanery to recognise and to assess trainees in difficulty and provide them with necessary support and to implement appropriate remedial action. To manage the career development of trainees in general practice To develop academic training programmes for Academic Clinical Fellows and for Clinical Lecturers and to promote academic training for all trainees To promote excellence and innovation in training and in training methods and to encourage and develop educational research including development and evaluation of assessment methodologies To work with the KSS Head of Libraries and Knowledge Management to develop, promote and implement knowledge access and e learning KSS GP Specialty School Board, Constitution & TOR v st March 2008
24 To maintain and progress faculty development and advise the KSS Deanery of development needs and methodology for addressing these To implement procedures and practices to supports trainees who wish to train flexibly and/or who require reasonable adjustments to programmes and placements. To respond to national initiatives including those from the Department of Health, the Royal College of General Practice and the PMETB and advise the Dean of Postgraduate of GP Education on their local development and implementation. 2. Quality Management of GP Specialty training Programmes and GP Trainers: To maintain and expand a database of GP specialty training programmes, GP Trainers and training Practices, and to be responsible for the future shape and content of these programmes and placements. To approve and re-approve GP Trainers in accordance with criteria established by the RCGP/PMETB and developed by the Board. To approve and re-approve those Practices suitable to participate in the Doctors Retainer Scheme. 3. Provision of Education: To advise on the provision of GP Specialty training Programmes, ensuring a balanced programme of experience to meet the individual training needs of each trainee doctor. To advise on the appointment and reappointment of GP Programme Directors To advise on the provision of, and requirements for, training for various items of service of statutory significance, such as Child Health Surveillance, Out of Hours training provision, Minor Surgery and Family Planning. To advise on the development needs of GP educationalists (including potential GP Trainers) with an emphasis on enabling them to provide an appropriate environment for training the trainees for whom they provide supervision. To advise on the provision of a careers advisory service in General Practice to include information, advice and counseling. To advise on multi- and inter-professional learning and teaching opportunities for doctors in General Practice. To be responsible for the appointment of the members of Trainer Selection Committees, GP Programme Directors Appointments Committee, Annual Review of Competence Progression Panel.. To supervise the management of study leave budget for GPStRs. To supervise the management of the GP Retainer Scheme. To contribute to the KSS Deanery Business Plan, To supervise the management of the annual appraisal of the GP Deanery, Programme Directors and GP Trainers. To supervise the appointments and membership of Appeals Committees for GP Trainer Appointments, GP Retainer Practice Accreditation, Membership of the GP Retainer Scheme, Management of Summative Assessment. 4. Research and Audit, and Service Issues: To advise on training in audit and research methods, and management training for General Practice for doctors in training for General Practice and to identify opportunities for multidisciplinary initiatives. KSS GP Specialty School Board, Constitution & TOR v st March 2008
25 C. PRINCIPAL FUNCTIONS OF THE BOARD: Receives and comments on report from the Head of GP School Ratifies or varies recommendations for GP Trainer and Programme Directors made by appropriate Selection/Appointment Committees. Approves hospital placements selected for GP training after consideration of Deans' Visits Reports and the KSS Deanery Quality Assurance Group Receives and comments on reports by the responsible Associate GP Dean on Annual Review of Competences Progression (ARCP).(or reports from panels) Receives and comments on RCGP/PMETB documentation. Receives and comments on report from GPStR Sub Committee. Appoints Appeals Committees in relation to GP Trainer and Programme Directors appointments, and the process of the ARCP and Summative Assessment in transition. Agrees and publishes Criteria for Appointment & Reappointment of GP Trainers and Programme Directors based on recommendations published by RCGP/COGPED. Agrees and publishes Criteria for the Selection of hospital placements for GP Training in accordance with recommendations published by RCGP/COGPED D. MEMBERSHIP Ex Officio Members Postgraduate Medical Dean or his/her representative Dean of Postgraduate General Practice Education or his/her deputies Associate Deans of Postgraduate General Practice Education Professors of General Practice or Primary Care in the deanery or representatives Medical Educationalist - specialist knowledge would be sought on specific assignments as required. A Lay Representative who will also have the responsibility of chairing the Trainer Selection Committee. Representative Members: Membership Postgraduate GP Dean Chair Representation from local faculties of Royal College of General Practitioners Non Executive Director (SEC) Representatives from GP Programme Directors one per county Medical Director of PCT GP Trainee Representatives (ST1,2 &ST3) Appointment Process Nominated by KSS Deanery Nominated by the Faculties of Royal College of General Practitioners Nominated by SEC Nominated by each county Nominated by SEC From the GP Trainees Committee KSS GP Specialty School Board, Constitution & TOR v st March 2008
26 Lay/Patient Representative Brighton & Sussex Medical School Academic Representative Representative from allied clinical profession Representation from LMCs Director of Medical Education/Clinical Tutor Selected from Lay Chairs panel Nominated by Head of Primary Care BSMS Representative of University Nominated by SEC Nominated by LMCs Nominated by DME/Clinical Tutors Committee Board Members Representative members will be expected to serve for an initial period for three years, renewable at the discretion of the appointing organisation. The Board shall have the power to co-opt additional members to fulfill specific timelimited functions. A member should send a deputy if unable to attend. If an officer steps down before the end of their term, their replacement will entitled to serve for an initial period for three years, renewable at the discretion of the appointing organisation. Observers will be as follows: Deanery Staff as appropriate E. STANDING ORDERS 1. Board Meetings: The Board will normally meet four times a year. The Board is expected to meet as often as necessary to complete its business. Meetings will normally be held on Deanery premises. The Chairman will ensure that agendas and papers for meetings are circulated electronically to all members to arrive at least five working days before the meeting. One third of members shall constitute a quorum. Elections to office and changes to the constitution may only be made if declared on the agenda. Decisions of the Board will normally be reached by consensus of opinion; voting may be resorted to in certain matters at the discretion of the Chairman. In such cases, motions should be proposed and duly seconded by members of the Board, and decisions will be reached by a simple majority vote of members present. In the event of a tie, the Chairman of the meeting will have a second (or casting) vote. KSS GP Specialty School Board, Constitution & TOR v st March 2008
27 Subcommittees or Working Groups may be set up by the Board; membership will be agreed by the Board, with an individual member identified to lead and report back to the main Board. 2. Deanery Support for Board: A member of the Postgraduate General Practice Education staff will act as Secretary to the Committee. Reimbursement of travel expenses at public transport rate will be paid for members attending committee meetings. 3. Role of Chair: The Chair shall be responsible for the operation of the Board, ensuring that it makes an effective contribution to the governance of the School and its pursuit of quality and excellence. The Chair will work closely with the Head of School and the Secretary on Board business and will ensure that key and appropriate issues are discussed by the Board in a timely manner and that relevant information and advice is made available to the Board to inform the debate and decision-making process. 4. Role of Head of School: The Head of School provides leadership for the School. He reports to the Board regularly on both the delivery and quality of training and the School s pursuit of excellence. He will provide information about the process of training and aggregated information on outcomes. The information provided must enable the Board to assess and monitor progress and to advise on direction, policies and strategy. The Head of School will be responsible for producing an annual report of the School s activities and achievements which will be approved by the School Board and presented to the Deanery s Quality Management Committee. 5. Role of Members: The role of members of the Board will be to consider the key strategic and management issues facing the School in carrying out its educational governance and quality assurance functions. Member will take collective responsibility for the Board s decisions. Members will contribute to the formation of strategy by bringing a range of different perspectives and experiences. Members are responsible for taking decisions that support the School s purpose, not simply the interests of their parent or nominating organisation. Members will be expected to attend regularly, inform themselves appropriately and involve themselves actively in discussions and decision making. Whilst the nominated members are not expected formally to represent their organisations or nominated bodies, they will provide the opportunity for the views of relevant stakeholders to be considered. They may also be asked to seek the views of the nominating group. The Boards members may be asked to take specific roles if required by the Board or the GP School to support their work. KSS GP Specialty School Board, Constitution & TOR v st March 2008
28 6. Quorum: Meeting will be quorate if at least one-third of the Board is present including the Head of School or nominated deputy and at least one nominated member. 7. Voting: The Board will not routinely be required to vote but may be asked to vote on certain matters requiring an executive decision. At the discretion of the Chair, all questions put to the vote shall be determined by oral expression or by a show of hands, unless the Chair decides otherwise. Decisions made by formal vote will be determined on a majority vote which will be recorded. Proxy votes will not be accepted. Where joint members attend together, the vote of only one member will be accepted. 8. Record of Attendance: The names of the Chair and members present will be recorded. Any member fails to attend without sending a deputy; their parent organisation will be informed. 9. Open and Closed Business: The main business of the Board will concern strategy, educational governance, quality assurance/management and the pursuit of excellence. It is envisaged appeals to the GP School Board may be part of the appeal process for individual trainees exercising a right to appeal in accordance with Deanery policy. Such appeals will normally be held by a sub-committee of the Board and trainee members will not be present. Should the full Board need to discuss matters relating to individual trainees, the trainee representative will not be present. When matters concerning an individual trainer or other individuals are discussed by the Board, the Chair will determine the appropriateness of the presence of individual Board members. Confidential issues relating to individuals will not form part of publicly accessible minutes of meetings. 10. Minutes: The minutes of the meeting will be drawn up by the Board Secretary and submitted for agreement at the next meeting and signed by the Chair. Draft minutes and action points will be circulated within three weeks of each meeting. When agreed, the minutes (except for records of closed parts of the meeting) will be made available on the Deanery website. 11. Confidentiality: Board members and any staff of the Deanery attending shall not reveal or disclose confidential information including papers marked In Confidence or minutes headed Items taken in Closed Session, without the permission of the Chair. This applies to the content of any discussion as well as papers and records. KSS GP Specialty School Board, Constitution & TOR v st March 2008
29 12. Risk Register: The Head of GP School will ensure that the Boards maintain a risk register and a process for identifying and quantifying risks and liabilities 13. Recording of interests: Board members will be required, on appointment, to declare any interests of relevance to the School Board. Such interests may include: Directorships of private companies seeking to do business with the Deanery Connections with voluntary organisations contracting for NHS services If members have any doubt about the relevance of an interest, this should be discussed with the Board Chair who may bring it to the attention of the Dean Director. If a conflict of interest is identified during the course of a Board meeting, the Board member concerned should declare such an interest and withdraw from the meeting and play no part in the relevant discussion or decision. February 2008 KSS GP Specialty School Board, Constitution & TOR v st March 2008
30 Doc E KENT SURREY & SUSSEX DEANERY GENERAL PRACTICE CPD SCHOOL BOARD CONSTITUTION & TERMS OF REFERENCE A. INTRODUCTION 1. The name of the Committee shall be the KSS General Practice CPD School Board (GP CPD School Board). 2. The Terms of Reference shall be reviewed annually in May, or at other times if necessary. Management of the Post-Certificate School of General Practice Education: The School has an Executive Board which is the strategic and operational unit of the Post-Certificate School of General Practice. There is representation on the Board from each of the programme areas within the school. The Dean of Postgraduate GP Education is the Chair of the Executive Board. The Head of the Post-Certificate School will act as deputy in his absence. The Executive Board also has representatives from the RCGP, LMC, PCTs in SEC SHA, GP Tutors, KSS Remediation Services, KSS Associate Deans, Mentors and Appraisers. Dean Postgraduate General Practice CPD School Board QAWG Head of Post-Cert School KSS Remediation services GP Tutors LMC &RCGP Regional Representatives PCT Representatives Appraisers and Mentors Others, Lay & University Continuing Professional Development CPD The Post-Certification GP School is committed to the promotion of Personal Development Plans (PDPs) linked to the annual NHS appraisal process. PCT clinical governance provides a framework to monitor, review and raise the quality of care delivered by the GPs on their medical performers list. GP appraisal lies at the educational end of the spectrum of clinical governance processes. The appraisal process contributes to the overall clinical governance framework as it provides assurances that GPs are planning and reviewing their CPD in a structured way. GPs KSS GP CPD School Board, Constitution & TOR v3 1 of 10 Oct 2009
31 can include in their appraisal folder reflections on their clinical governance related activities. PCTs can also inform the appraisal process by providing where appropriate, information to GPs which can inform their own needs assessment and inform their personal and practice development planning. Appraisal and CPD are closely linked. Appraisal provides doctors with an opportunity to demonstrate the CPD they have undertaken, reflect on what they have learned from it, and plan their CPD for the following year. The learning needs identified by GPs in their personal development plans (PDPs) as part of their appraisals should inform the education and support that is available and accessible to them. Re-certification and re-licensing are being developed by the GMC and The Royal College of General Practitioners to produce the unified process of revalidation, with enhanced appraisal at its core. The Post-Certification GP School and CPD Board will work in collaboration with the PCTs in KSS to prepare GPs for revalidation and to encourage high quality professional development. The Post-Certification GP School will develop the following services: Enhanced appraisal service. Working in partnership with our PCTs the School is developing Appraisal Development Centres which will provide training and updating for new and existing appraisers and PCT personnel, preparing them for the changes required for Revalidation. Support for appraisers. In addition to the Appraisal Development Centres the School will use the GP Tutor network to provide learning sets for the appraiser network and will train lead appraisers to support their colleagues. GP Tutors will also help their PCTs organise protected learning time for GPs and practice staff and will ensure GPs in their area are fully informed about the Revalidation process. They will continue to act as a focus for educational activity and support in their localities, including support for local commissioning initiatives. The School will also collaborate with PCTs on the development of local support and performance improvement training for GPs identified through the appraisal system as needing local remediation or rehabilitation. The School will be responsible for the further development of the KSS Mentoring programme which offers additional support for GPs through a one to one, confidential relationship with a respected GP peer. This service is available to all GPs in KSS and can help with career planning and personal development as well as supporting GPs with individual or practice-based concerns. The School will also support GP Refreshers, those returning to general practice after a career break, and will try to support GPs through the transition from trainee to independent GP by encouraging learning sets for salaried doctors. KSS GP CPD School Board, Constitution & TOR v3 2 of 10 Oct 2009
32 The School will adopt new procedures to encourage effective CPD for GPs as needed in response to the further evolution of Revalidation as defined by the main regulatory bodies. B. TERMS OF REFERENCE: 1. To advise the SEC Strategic Health Authority and its Workforce Management structure (KSS Deanery), Primary Care Trusts, and appropriate academic and higher education institutions: To deliver the education and training of GP Tutors, Appraisers and Lead Appraisers to meet the Royal College of General Practitioners and General Medical Council s agreed criteria and standards for Revalidation and to promote excellence in all aspects of the work of the School. To implement the new GP Appraisal Support Programme through collaboration with individual PCTs and in response to the working of the Quality Assurance of Appraisal Working Group (QAWG). To implement the KSS Mentoring Programme to support GPs who request a peerled, confidential support programme. To ensure appropriate support for CPD for GPs in SEC SHA area through the GP Tutor network and through the promotion of effective protected learning time for GPs and their staff. To ensure that the delivery of training enhances the quality and safety of patient care for today s and tomorrow s patients and maintains and supports GP specialists, ensuring they are fit to meet the needs of the NHS and with the skills to be able effectively to contribute to future changes in the health service. To meet workforce and patient needs by ensuring CPD promotes fit for purpose general practitioners including the development of both clinical and organisational skills, (e.g. team working, leadership, change management, business management), necessary for their role as general practitioners able to work effectively in complex organisations and able to lead and implement change in the primary care setting. To monitor the quality of appraisal; to evaluate and review local quality control measures and reports and ensure these are used to drive continual improvement to meet the standards that will be set by the Royal College of General Practitioners and the GMC. KSS GP CPD School Board, Constitution & TOR v3 3 of 10 Oct 2009
33 To monitor possible discriminatory affects of any policies or procedures and steer action to promote diversity and equality of opportunity. To take part in the selection and recruitment of appraisers and mentors and to contribute to the development of selection methodology. To work with PCTs and KSS Deanery to recognise and to assess GPs in difficulty and provide them with necessary support and to implement appropriate remedial action. To promote excellence and innovation in appraisal methods and training of appraisers and mentors and to encourage and develop educational research including development and evaluation of assessment methodologies. To work with the KSS Head of Libraries and Knowledge Management to develop, promote and implement knowledge access and e learning. To implement procedures and practices to support sessional doctors and help them organize effective CPD and prepare for revalidation. To respond to national initiatives including those from the Department of Health, the Royal College of General Practice and the GMC and advise the Dean of Postgraduate of GP Education on their local development and implementation. 2. Quality Management of GP Appraisal and Appraiser Training: To maintain a database of GP Appraiser, Lead Appraisers and GP Tutors and to be responsible for the future shape and content of their training programmes and on-going skills development in response to the criteria and standards of the RCGP and GMC. To assist PCTs with the selection and re-approval of GP Appraisers in accordance with criteria established by the RCGP/GMC and developed by the Board. 3. Provision of Support for GP Education: To advise on the provision of GP support for CPD across KSS, ensuring a balanced spread of GP Tutors to meet the individual needs of each locality. To advise on the appointment and reappointment of GP Tutors. To approve and re-approve those Trainers and Practices suitable to participate in the Doctors Refresher Scheme. To advise on the development needs of GP educationalists (including potential GP Tutors and Appraisers). KSS GP CPD School Board, Constitution & TOR v3 4 of 10 Oct 2009
34 To advise on the provision of a careers advisory service in General Practice to include information, advice and counseling. To advise on multi- and inter-professional learning and teaching opportunities for doctors in General Practice. To be responsible for the appointment of the members of GP Tutor Appointment Committee. To supervise the management of the GP Refresher Scheme. To contribute to the KSS Deanery Business Plan. To supervise the management of the annual appraisal of the Deanery GP Tutors. 4. Research and Audit, and Service Issues: To advise on training in audit and research methods, and management training for General Practitioners and to identify opportunities for multidisciplinary initiatives. To encourage research and evaluation of all programmes supported by the Post- Certification GP School. C. PRINCIPAL FUNCTIONS OF THE BOARD: Receives and comments on report from the Head of Post-Certificate GP School. Ratifies or varies recommendations for GP Tutors made by appropriate Appointment Committees. Approves recommendations for Appraisal Support Programme made by Post- Certificate School and QAWG. Receives and comments on reports by the School on work undertaken by the GP Tutor network. Receives and comments on RCGP/GMC documentation concerned with appraisal, CPD and Revalidation. Receives and comments on report from QAWG. Agrees and publishes Criteria for Appointment & Reappointment of GP Tutors based on recommendations published by RCGP/GMC. D. MEMBERSHIP KSS GP CPD School Board, Constitution & TOR v3 5 of 10 Oct 2009
35 Ex Officio Members Postgraduate Medical Dean or his/her representative Dean of Postgraduate General Practice Education or his/her deputies Associate Deans of Postgraduate General Practice Education Professors of General Practice or Primary Care in the deanery or representatives Medical Educationalist - specialist knowledge would be sought on specific assignments as required. A Lay Representative who will also have the responsibility of chairing the Tutor Appointment Committee. Representative Members: Membership Postgraduate GP Dean Chair Head of Post-Certificate School Associate Dean Representative Representation from local faculties of Royal College of General Practitioners Non Executive Director (SEC) Representatives from GP Tutors one per county Responsible Officer Representatives One from each county. PCT Appraisal representatives one from each county GP Appraiser Representative Lead Appraiser Representative Mentoring Representative Lay/Patient Representative Academic Representative Representative from allied clinical profession Representation from LMCs Appointment Process Nominated by KSS Deanery Nominated by KSS Deanery Nominated by KSS Deanery Nominated by the Faculties of Royal College of General Practitioners Nominated by SEC Nominated by each county Nominated by SEC Nominated by QAWG From the Appraiser network From Appraiser network Nominated by Mentors. Selected from Lay Chairs panel Representative of University Nominated by SEC Nominated by LMCs Board Members: KSS GP CPD School Board, Constitution & TOR v3 6 of 10 Oct 2009
36 Representative members will be expected to serve for an initial period for three years, renewable at the discretion of the appointing organisation. The Board shall have the power to co-opt additional members to fulfill specific timelimited functions. A member should send a deputy if unable to attend. If an officer steps down before the end of their term, their replacement will entitled to serve for an initial period for three years, renewable at the discretion of the appointing organisation. Observers will be as follows: Deanery Staff as appropriate E. STANDING ORDERS 1. Board Meetings: The Board will normally meet four times a year. The Board is expected to meet as often as necessary to complete its business. Meetings will normally be held on Deanery premises. The Chairman will ensure that agendas and papers for meetings are circulated electronically to all members to arrive at least five working days before the meeting. One third of members shall constitute a quorum. Elections to office and changes to the constitution may only be made if declared on the agenda. Decisions of the Board will normally be reached by consensus of opinion; voting may be resorted to in certain matters at the discretion of the Chairman. In such cases, motions should be proposed and duly seconded by members of the Board, and decisions will be reached by a simple majority vote of members present. In the event of a tie, the Chairman of the meeting will have a second (or casting) vote. Subcommittees or Working Groups may be set up by the Board; membership will be agreed by the Board, with an individual member identified to lead and report back to the main Board. 2. Deanery Support for Board: A member of the Postgraduate General Practice Education staff will act as Secretary to the Committee. Reimbursement of travel expenses at public transport rate will be paid for members attending committee meetings. 3. Role of Chair: The Chair shall be responsible for the operation of the Board, ensuring that it makes an effective contribution to the governance of the School and its pursuit of quality and excellence. The Chair will work closely with the Head of School and KSS GP CPD School Board, Constitution & TOR v3 7 of 10 Oct 2009
37 the Secretary on Board business and will ensure that key and appropriate issues are discussed by the Board in a timely manner and that relevant information and advice is made available to the Board to inform the debate and decision-making process. 4. Role of Head of School: The Head of School provides leadership for the School. He reports to the Board regularly on both the delivery and quality of appraisal and CPD, and the School s pursuit of excellence. He will provide information about the process of appraisal and aggregated information on outcomes. The information provided must enable the Board to assess and monitor progress and to advise on direction, policies and strategy. The Head of School will be responsible for producing an annual report of the School s activities and achievements which will be approved by the School Board and presented to the Deanery s Quality Management Committee. 5. Role of Members: The role of members of the Board will be to consider the key strategic and management issues facing the School in carrying out its educational governance and quality assurance functions. Member will take collective responsibility for the Board s decisions. Members will contribute to the formation of strategy by bringing a range of different perspectives and experiences. Members are responsible for taking decisions that support the School s purpose, not simply the interests of their parent or nominating organisation. Members will be expected to attend regularly, inform themselves appropriately and involve themselves actively in discussions and decision making. Whilst the nominated members are not expected formally to represent their organisations or nominated bodies, they will provide the opportunity for the views of relevant stakeholders to be considered. They may also be asked to seek the views of the nominating group. The Boards members may be asked to take specific roles if required by the Board or the GP School to support their work. 6. Quorum: Meeting will be quorate if at least one-third of the Board is present and the following members are in attendance Head of School or nominated deputy At least one PCT appraisal representative At least one representative from the LMCs and / or RCGP Faculties At least one representative from the KSS Tutor and / or Mentoring network 7. Voting: The Board will not routinely be required to vote but may be asked to vote on certain matters requiring an executive decision. At the discretion of the Chair, all questions put to the vote shall be determined by oral expression or by a show of hands, unless the Chair decides otherwise. KSS GP CPD School Board, Constitution & TOR v3 8 of 10 Oct 2009
38 Decisions made by formal vote will be determined on a majority vote which will be recorded. Proxy votes will not be accepted. Where joint members attend together, the vote of only one member will be accepted. 8. Record of Attendance: The names of the Chair and members present will be recorded. Any member fails to attend without sending a deputy; their parent organisation will be informed. 9. Open and Closed Business: The main business of the Board will concern strategy, educational governance, quality assurance/management and the pursuit of excellence. When matters concerning a specific GP, Tutor, Appraiser, Mentor or other individuals are discussed by the Board, the Chair will determine the appropriateness of the presence of individual Board members. Confidential issues relating to individuals will not form part of publicly accessible minutes of meetings. 10. Minutes: The minutes of the meeting will be drawn up by the Board Secretary and submitted for agreement at the next meeting and signed by the Chair. Draft minutes and action points will be circulated within three weeks of each meeting. When agreed, the minutes (except for records of closed parts of the meeting) will be made available on the Deanery website. 11. Confidentiality: Board members and any staff of the Deanery attending shall not reveal or disclose confidential information including papers marked In Confidence or minutes headed Items taken in Closed Session, without the permission of the Chair. This applies to the content of any discussion as well as papers and records. 12. Risk Register: The Head of GP School will ensure that the Boards maintain a risk register and a process for identifying and quantifying risks and liabilities 13. Recording of interests: Board members will be required, on appointment, to declare any interests of relevance to the School Board. Such interests may include: Directorships of private companies seeking to do business with the Deanery Connections with voluntary organisations contracting for NHS services If members have any doubt about the relevance of an interest, this should be discussed with the Board Chair who may bring it to the attention of the Dean Director. KSS GP CPD School Board, Constitution & TOR v3 9 of 10 Oct 2009
39 If a conflict of interest is identified during the course of a Board meeting, the Board member concerned should declare such an interest and withdraw from the meeting and play no part in the relevant discussion or decision. February 2009 KSS GP CPD School Board, Constitution & TOR v3 10 of 10 Oct 2009
40 Doc A Constitution/Terms of Reference/Membership KSS Quality Assurance of GP Appraisal Working Group KENT, SURREY, SUSSEX (KSS) Quality Assurance of GP Appraisal Working Group (QAWG) CONSTITUTION A. INTRODUCTION 1. The name of the Committee shall be the KSS Quality Assurance of GP Appraisal Working Group (QAWG) 2. The Terms of Reference shall be reviewed annually in May, or at other times if necessary B BACKGROUND There is great variation amongst primary care trusts as to how the GP appraisal process is delivered and quality assured. This was confirmed in the recent survey of PCTs and GP Tutors across the region. Appraisal will be an integral component of relicensing and recertification when the changes to professional regulation of doctors are implemented in 2009 and beyond (revalidation process). Therefore, we need to develop a model or models of quality assurance to deliver consistency in relation to the quality of the GP appraisal process across the health economy. In addition, clinical governance provides a framework for NHS trusts and PCTs to monitor, review and raise the quality of care delivered by doctors in their employ or on their performers list. GP appraisal lies at the educational end of the spectrum of clinical governance processes. The appraisal process contributes to the overall clinical governance framework as it provides assurances that GPs are planning and reviewing their CPD in a structured way. PCTs (England) can also inform the appraisal process by providing, where appropriate, information to GPs which can inform their own needs assessment and inform their personal and practice development planning. When relicensing is introduced as part of the revalidation process, PCTs will compile information about the performance of individual GPs which the responsible officer is likely to share with GP appraisers national directions about how the relicensing process will work are awaited. C. TERMS OF REFERENCE 1. Advice to PCTs and South East Coast NHS :- 1.1 To aim for development of a model or models for the quality assurance of GP Appraisal across SEC. KSS QAWG TOR (final version).doc 8th December 08 Page 1
41 Constitution/Terms of Reference/Membership KSS Quality Assurance of GP Appraisal Working Group 1.2 To create a forum for consolidation and further development of a robust quality assurance process for GP appraisal. 1.3 To share resources including expertise and findings from PCTs activities into GP appraisal e.g. selection of GP appraisers, reselection, initial training and updating of GP appraisers, training of PCT staff key to the GP appraisal and relicensing processes, detection and clarification in relation to underperformance of doctors and feedback process 1.4 To share information relating to GP appraisal, giving and receiving feedback to PCTs 1.5 To support PCTs with their GP appraisal work on individual basis, in particular helping them to deal with performance issues uncovered in appraisal and equally providing appropriate appraisal opportunities for those subject to performance review. 1.6 To facilitate improvement in practice in the selection and reselection of GP appraisers (ie test communication skills and report writing abilities). Provide on going support and training for GP appraisers, PCT Lead appraisers, lead administrative staff. 1.7 To monitor the quality of GP appraiser training; to evaluate and review local quality control measures and reports and ensure that these are used to drive continuous improvement to meet the standards that will be set by the Royal College of General Practitioners and the GMC for recertification and relicensing respectively. 2. The KSS Deanery will: 2.1 Identify trends in the quality assurance of GP appraisal. 2.2 Develop the shared learning across the QAWG on all aspects of GP appraisal. 2.3 Pilot or put into practice initiatives related to revalidation locally and nationally as opportunities arise e.g. the national tools multisource feedback, RCGP managed CPD scheme of CPD credits. 2.4 Help with local sector meetings to look at QA process in PCTs. 2.5 Share and work with hot topics relating to GP appraisal, derived from within the group, as a means of promulgating good practice. 2.6 Facilitate delivery of appraiser training and development across the health economy. 2.7 Recognise and share good practice derived from within the group and nationally; link to national leads KSS QAWG TOR (final version).doc 8th December 08 Page 2
42 Constitution/Terms of Reference/Membership KSS Quality Assurance of GP Appraisal Working Group 2.8 Facilitate provision of a careers advisory service for general practice in connection with PCTs including information, advice and counselling targeted on doctors who need it such as those who wish to return to practice or take a career break or seek to diversify their medical careers. 3. PCTs will: 3.1 Be represented and share their appraisal activities in the QAWG meetings. 3.2 Contribute and take part in agreed QA processes. 3.3 Collate information and share with the QAWG on matters such as selection of GP appraisers, basic training, appraisers training needs, assessment and appraising the appraisers, indemnity of GP appraisers 3.4 Develop a system of needs assessment for GP appraisers with an emphasis on enabling them to provide an appropriate challenging but supportive role in GP appraisal process, working closely with the PCT s responsible officer for revalidation. 3.5 Take part in piloting the agreed national tools into different aspect of GP appraisal and revalidation process including form 4 analysis and use of tools for making judgement. 3.6 The Medical Performers list needs to be reviewed every three years and that GPs should declare issues in appraisal. 4. Research and Audit, and Service Issues: KSS Deanery staff will advise the QAWG on: 4.1 Training in audit and research methods, and management training for general practice and doctors in training for General Practice and to identify opportunities for multidisciplinary initiatives. D PRINCIPAL FUNCTIONS OF THE GROUP IN RELATION TO: 1. GP Appraisal process In essence, agree standards and processes for best practice in the quality of the appraisal process; by agreement with individual PCT monitor that quality standards are adhered to in operation of GP appraisal in individual PCTs Receives and comments on reports from the PCT staff Appraisal Leads, and PCT responsible officers (when appointed); indicate strengths, and weaknesses that PCTs may plan to rectify Receives and comments on reports from the PCT GP appraiser leads; indicate strengths, and weaknesses that PCTs may plan to rectify KSS QAWG TOR (final version).doc 8th December 08 Page 3
43 Constitution/Terms of Reference/Membership KSS Quality Assurance of GP Appraisal Working Group Receives and comments on reports by the responsible KSS Associate GP Deans and Life Long Adviser on GP appraisal process; plan for needs for remediation and reskilling of doctors about whom there are identified concerns in relation to their performance, or conduct Receives and comments on RCGP/GMC documents; subsequently advise or implement new regional systems and processes for appraisal in respect of revalidation Agrees and publishes criteria for appointment & reappointment of GP appraisers based on recommendations published by RCGP/GMC and the National Revalidation Support Group; oversee that criteria are put into practice at invitation of respective PCTs Agrees and publishes criteria for the selection process of GP appraisers in accordance with recommendations published by RCGP/GMC and the National Revalidation Support Group. 2. CPD In essence, advise PCTs about the implementation of the RCGP s managed CPD scheme and how appraisers make judgements about the CPD contents of GPs appraisal folders in line with the new CPD credit based system; monitor that quality standards are adhered to in operation of the GP credit based system within appraisal - in individual PCTs by invitation Receives and comments on report from GP Deanery. Receives and comments on report on CPD from the Convenor of the GP Tutor Working Group. E. MEMBERSHIP 1. Membership will be as follows: 1. PCT Members: GP Appraisal Lead from each PCT Responsible officer (when appointed) or manager/ administrative support lead for appraisal from each PCT 2. Deanery members: Dean of Postgraduate General Practice Education or his/her deputy Associate Deans of Postgraduate General Practice Education Lifelong learning adviser Deanery staff as appropriate 3. Representative Members Local Medical Committees RCGP 1 person from each LMC 1 person from each RCGP Faculty KSS QAWG TOR (final version).doc 8th December 08 Page 4
44 Constitution/Terms of Reference/Membership KSS Quality Assurance of GP Appraisal Working Group South East & South West Thames) appointed by the Faculties GP Tutor 1 person from each county 4. Observers will be as follows: 4.1 The QAWG shall have the power to co-opt additional members to fulfil specific time-limited functions. 4.2 A member should send a deputy if unable to attend. 5. QAWG Officers 5.1 The chair will be the Dean of Postgraduate General Practice Education. 5.2 If a representative steps down before the end of their term, their replacement will be entitled to serve for an initial period for three years, renewable for one further term. 6. QAWG Members 6.1 Representative members will be expected to serve for an initial period for three years, renewable at the discretion of the appointing organisation. F. STANDING ORDERS 1. QAWG Meetings 1.1 The QAWG will normally meet four times a year: February, May, September and December. The Group is expected to meet as often as necessary to complete its business. 1.2 Meetings will normally be held on Deanery/SHA premises. 1.3 The Chair will ensure that agendas and papers for meetings are circulated to all members to arrive at least five working days before the meeting. 1.4 One third of members across the spread of represented organisations shall constitute a quorum. 1.5 Decisions of the group will normally be reached by consensus of opinion; voting may be resorted to in certain matters at the discretion of the Chair. In such cases, motions should be proposed and duly seconded by members of the group, and decisions will be reached by a simple majority vote of members present. In the event of a tie, the Chair of the meeting will have a second (or casting) vote. KSS QAWG TOR (final version).doc 8th December 08: Page 5
45 Constitution/Terms of Reference/Membership KSS Quality Assurance of GP Appraisal Working Group 1.6 Subcommittees or working groups may be set up by the group; membership will be agreed by the QAWG, with an individual member identified to lead and report back to the main Group. 2. Deanery Support for QAWG 2.1 A member of the GP PGME staff will act as secretary to the Group. 2.2 Reimbursement of travelling expenses at public transport rate will be paid for representative members attending QAWG meetings. LMC and RCGP representatives will receive a contribution to their locum expenses. 3. Role of QAWG Chair: 3.1 Will chair the meetings of the QAWG. 3.2 Will promote and support collaborative working between PCTs and stakeholders. 3.3 Will be ultimately responsible for the operation of the quality assurance framework for GP appraisal KSS QAWG TOR (final version).doc 8th December 08: Page 6
46 (updated 3 May 2012) AGREED PROPOSAL FOR A JOINT DEANERY COMMITTEE ON QUALITY MANAGEMENT OF TRAINING BETWEEN LONDON AND KSS Background 1. Both deaneries recognise that training and trainees will continue to cross SHA/local provider boundaries as part of future programmes of training. 2. Both deaneries/shas have to assure the GMC there are comprehensive quality management arrangements in place which local education provider will want to have the minimum number of bodies, ideally one, overseeing their quality management and control arrangements. 3. Both deaneries have already agreed we continue the current position where each deanery takes responsibility for posts and the educational environment within their geographical area. Initial Terms of Reference of the Joint Deanery Committee 1. To discuss and share current quality management arrangements within the two deaneries. 2. To look for areas of agreement over commonality of process both now and in the future. 3. To share reports, results and information on issues that have arisen from Quality Management arrangements taking place within home deanery boundaries that might affect trainees in a programme being managed by another Lead Provider/Deanery. 4. To act as a source of joint support and trouble shooting for difficult or wicked problems. 5. To ensure that all such problems are escalated to the relevant Postgraduate Dean or Responsible Officer in a timely fashion. 6. To share and log information about all trainees in difficulty that cross-deanery boundaries. 7. To keep the GMC informed of all activities, usually through the Deanery Report (DR) of each organisation. Both deaneries will agree the joint exception reporting in DRs involving cross-boundary programmes. 8. Terms of Reference to be annually reviewed. Membership 1. The deans responsible for postgraduate Secondary Care education from London and KSS. 2. The Directors of the London Foundation School and the South Thames Foundation School. 3. The Associate Dean for Quality in KSS and the two Trust liaison deans in South London. 4. The Quality Managers of both Deaneries. 5. The General Practice Deans of both Deaneries. 6. KSS Education Department representative, as required. 7. A Foundation trainee representative, alternating annually between Deaneries. 8. A Specialty trainee representative, alternating annually between Deaneries. Meetings 1. The group will meet three times per year, alternating meeting venue between KSS Deanery, STFS and London Deanery offices. 2. The group will elect its own chairman on an annual basis
47 (updated 3 May 2012) 3. The Quality Managers of the two Deaneries will be responsible for administering the Committee. Primary administrative responsibility will normally alternate so that the administrating manager comes from the other deanery from that of the chair.
48 Kent, Surrey & Sussex Deanery QUALITY MANAGEMENT DEPARTMENT Guidance on producing the KSS Deanery Report The Deanery Report (DR) is the mechanism by which the Deanery provides assurance to the GMC that it is managing the quality of training in line with the GMC s standards. This document provides an overview on completing the KSS Deanery Report, and should be read in conjunction with the GMC Document, Deanery Report : Guidance for Deaneries. All deaneries are expected to report on Foundation, Specialty, and GP Training Programmes within their DR. The GMC expects all actions to be mapped against the standards, as indicated in the Deanery Report Template. Deaneries are required to demonstrate progress on actions included in the July 2011 action plan update and notify the GMC of any new actions that arose after the submission of the July 2011 update, while informing them of how the deanery is meeting standards. This revised report template maintains the principle of exception reporting, which means that describing routine management activities is not necessary. Instead, the focus should be on: a. Key areas of achievement and good practice during the previous year b. Key areas where improvement is needed to maintain standards c. Action planned (with specific timescales) to resolve issues or concerns or to disseminate good practice. Examples of exception reporting for each area have been provided in the DR template, which has been divided into three worksheets: a. Published items It is important that deaneries are able to publicly demonstrate the improvements they are securing in the quality of postgraduate medical education and training, therefore items listed on this sheet will be published on the GMC website. The report must contain open actions from the July 2011 Action Plan Update. Deaneries should also include new or other relevant items. b. Confidential items It is important that deaneries are transparent in their role in quality managing medical education and training; however, there will be a number of potential concerns or issues that require further examination or evidence. This sheet enables deaneries to keep the GMC informed about potential concerns or issues that are currently being investigated and are yet to be substantiated. c. Good practice items Good practice should include exceptional examples which have potential for wider dissemination and development, or a new approach to dealing with a problem from which other partners might learn.
49 Completing the Report The Deanery Report template is saved as a shared document on the K Drive under Genshare (see link above). The KSS Document DR Flowchart provides an overview of timelines and responsibilities for completing the report. The Quality Department is required to populate the shared report template with issues and good practice as identified in the LAB AARs, together with actions taken or planned to address the issues / disseminate good practice. The Foundation, GP and Specialty Schools are required to populate the shared report template with issues and good practice as identified in the School Reports, together with actions taken or planned to address the issues / disseminate good practice. The Education Department is required to populate the shared report template with issues and good practice as identified in the Contract Review Reports, together with actions taken or planned to address the issues / disseminate good practice. The Quality Department is required to populate the shared report template with issues and good practice as identified in exception issues and reports, together with actions taken or planned to address the issues / disseminate good practice. Where issues are generic, write Generic under the heading Programme Specialty and/or Local Education Provider, and put N/A under other column headings as appropriate. The Quality Department will be responsible for co-ordinating the drafts of the report and following up any requests for further information or clarification from the DR Project Group following the Review Meetings. The Quality Department will update/amend the report as required by the DR Project Group, produce the final report for approval by the Quality Management Steering Group and sign-off by the Dean Director, and submit the final report to the GMC. 2
50 Producing the KSS Deanery Report Timeline Mid September Task Set up a Deanery Report (DR) Project Group and arrange review meetings Responsibility Quality Department Late September Late October Populate template with issues, confidential issues and good practice as identified in LAB AARs Populate template with issues, confidential issues and good practice as identified in School Reports Quality Department All Schools - Specialty, GP, Foundation Late October Populate template with issues, confidential issues and good practice as identified in Contract Reviews Education Department Early November Produce first draft of Deanery Report including all Exception Issues Quality Department Mid November Meet to review first draft of Deanery Report DR Project Group Mid November Produce second draft of Deanery Report Quality Department Late November Meet to review second draft of Deanery Report DR Project Group Early December Produce final draft of Deanery Report Quality Department Mid December Meet to review final draft of Deanery Report (to go to December QMSG meeting) DR Project Group Late December Sign off final Deanery Report Dean Director End January Deadline for submission to the GMC Quality Department
51 Guidance - Completion of the KSS Deanery Local Education Provider Metrics Objectives To give all LEPs ability to demonstrate improvement in objective measures of processes and outcomes for Postgraduate Medical Education. For LEPs to be able to compare themselves and their process with other LEPs. To put objective information about LEPs in the public domain. To act as one source of information for the Deanery in deciding on future investment or disinvestment strategies. To assist on LEP reporting of their quality of Patient Care Mechanism An annual self assessment by the LEP that is validated through the mechanism of external quality control of Contract Review. Agreement and sign-off at the time of the educational contract with the Trust Chief Executive and other senior executives present. All measures subject to annual review, change, addition or removal. All measures generated from available LEP data. Completion 1. The Deanery will populate the document for items 2, 3, 4, 5, 10 and 11 (GMC Survey Trainers, GMC Survey Trainees, Foundation Quality, LTFT, Trainee Satisfaction and Appointing High Quality Trainees). 2. The LEPs will then be responsible for self-assessment of the other indicators and for formal sign-off for accuracy. Indicator 1 Indicator 6 Indicator 7 Indicator 8 Indicator 9 Indicator 12 QESP to be signed off by the Medical Education Manager PAs for education in the job plan to be signed off by the Director of Medical Education after discussion with the Medical Director LFG Meetings to be signed off by the Medical Education Manager Adequate tracking of training data to be signed off by the Medical Education Manager Absence of postgraduate doctors to be signed off by the Medical Staffing Manager Board-level engagement to be signed off by the Director of Medical Education 3. The relevant people need to sign the confirmation form, which is included with the metrics template. 5. The fully populated and signed metrics will then be discussed and signed off on the Contract Review visit. PLEASE NOTE: Any standard not completed by the LEP will be rated as red and will count as zero towards the overall metrics score.
52 KSS DEANERY LOCAL EDUCATION PROVIDER METRICS 2012 Standard Milestone Red Amber Green 1 QESP The proportion of LEP identified Educational Supervisors who have completed both parts of QESP or successfully completed the 'Grandparent Clause'. 2 GMC Survey for Consultant Educators 3 GMC Survey Postgraduate Doctors Percentage of LEP identified Educational Supervisors who completed the 2011 GMC National Training Survey. Percentage of postgraduate doctors who completed the 2011 GMC National Training Survey. 4 Foundation Programme Number of red flag indicators for Consent, Site Marking, and Immunosuppressants found by the most recent Foundation visiting process or by the annual STFS survey. 5 Less Than Full Time Training (LTFT) 6 PAs/SPA for Education in job plan DH wants all postgraduate doctors to have access to LTFT, so they can follow it if they wish. Thus the LEP should encourage and support LTFT. The milestone is the number of LTFT postgraduate doctors that the LEP has been offered but unable to accommodate in the past year. All consultants should have clearly designated SPAs/PA time in their job plan for their educational activities to NHS SEC's published standards. The milestone is the percentage of consultants with identified educational PAs/SPA time in job plan. 7 LFG Meetings LFGs that have not had their minimum 3 mandatory times a year meeting and produced minutes for each meeting and produced an Annual Audit and Review. 8 Adequate tracking of trainer data 9 Absence of postgraduate doctors 10 Postgraduate doctor satisfaction 11 Appointing high quality postgraduate doctors in SEC LEPs 12 Board-level Engagement in Education and Training Percentage of LEP identified Educational Supervisors where the LEP has in a database their up-to-date position on QESP, their equality and diversity training status and their status in being fully trained for workplace based assessment. Overall sickness absence for postgraduate doctors in the preceding 6 months. Overall postgraduate doctor satisfaction taken from the most recent GMC Survey. Adequate data for specialty programmes in the KSS prospectus to meet (a) the requirements of the national code of practice and (b) to attract postgraduate doctors to the programme. There must be full Board-level engagement in education and training, including a named individual and evidence that Board engagement is active. Less than 60% 61 90% More than 90% Less than 50% 51 75% 90% Less than 80% 81 90% More than 90% 3 indicators 1-2 indicators 0 indicators 2 or more % 51-90% Over 90% 2 or more 1 0 Less than 75% or failure to capture any of the 3 data sets 76-90% More than 90% 5% or over % 0-2% Less than 75% % 80% or greater Inadequate details of data to meet requirements of (a) and (b) There is no Board member and education and training has not been discussed at Board level in the preceding year. Inadequate data for either (a) or (b) or generally poor information There is a named Board member, education and training has been discussed at least once on the Board during that year; and the named Board member has attended the LAB on at least one occasion during the year. Data contains all requirements of (a) and (b) and in good detail There is a named member on the Board; postgraduate education and training is a standing item; and the named Board member has attended the LAB for the majority of meetings in the preceding year.
53 KSS Deanery Local Education Provider Metrics for signing off sheet Trust: Indicators Accuracy confirmed by: (Print name) Signature Date 6. PAs for education in job plan 12. Board-level Engagement in Education and Training Director of Medical Education 1. Qualified Educational Supervisor Programme 7. Local Faculty Group (LFG) Meetings 8. Adequate tracking of trainer data Medical Education Manager 9. Absence of postgraduate doctors Medical Staffing Manager
54 Kent, Surrey & Sussex Deanery QUALITY MANAGEMENT OF SPECIALTY TRAINING PROCESS FOR ADMINISTERING THE GMC SURVEY This document provides and overview of the KSS procedure for administering the GMC National Training Surveys, and should be read in conjunction with the GMC Survey Briefing Notes. The trainee and trainer surveys will run concurrently. The timescales shown below are subject to change year on year, and will be updated as required. GMC Timescale 17 December 2010 to 31 January 2011 Deaneries review their data (programmes, locations, post specialties and grades) and provide confirmation of data accuracy. KSS Deanery Actions By end January 2011 The Quality Manager sends the blank spreadsheets for the trainee and trainer data to the nominated administrator in each department - GP, Foundation and Specialty. 26 January 2011 The GMC sends blank spreadsheets for the trainee and trainer data to the deaneries for completion. 14 February 2011 to 28 February 2011 The administrators send the completed spreadsheets to the Quality Manager, who submits the completed spreadsheets to the GMC using Connect. 14 February 2011 to 29 April 2011 Deaneries send completed spreadsheets to the GMC using Connect. GMC validates the spreadsheets and responds to the deanery with any errors within two working days. 14 February 2011 to 29 April 2011 Quality Manager sends GMC error reports to the relevant administrator, who returns the corrected data to the Quality Manager for re-submission within two working days. 02 May 2011 to July 2011 (survey closes 22 July) Trainee and trainer survey invitations ed out to participants and the surveys go live. s are sent out over a three week period. 02 May 2011 to July 2011 The three nominated administrators validate data as required and respond to queries from trainees and trainers, liaising with the GMC where necessary. August to September 2011 Trainee and trainer survey reports validated and made available online. 31 May 2011 to July 2011 The administrators regularly monitor the GMC Survey website to check response rates, and liaise with MEMs and trainers where necessary to chase responses. October 2011 National key findings report published. Following release of preliminary reports The Assistant Quality Manager analyses the data and checks for errors, liaising with the GMC where necessary, and produces reports as required.
55 1. At the beginning of the calendar year, the managers of GP, Foundation and Specialty each nominate an individual who will administer the GMC Surveys on behalf of their department. The names of the nominated Survey Administrators are passed to the Quality Department, who will publish their contact details on the GMC Survey page of the KSS website. 2. The Survey Administrators will receive the GMC spreadsheet templates from the Quality Manager by the required deadline. They will enter the trainee and trainer data into the spreadsheets and return them to the Quality Manager for submission to the GMC via Connect by the required deadline. In exceptional circumstances, where it is necessary to obtain additional data from another department, the Survey Administrator should inform the manager of that department, and arrange to liaise with relevant staff to obtain the required data. 3. The GMC will upload any error reports to GMC Connect and inform the Quality Manager, who will forward the error report to the relevant Survey Administrator. The Administrator will make the necessary corrections and return the spreadsheet to the Quality Manager within three working days. The Quality Manager will then re-submit the corrected spreadsheet to the GMC. 4. The Survey Administrators will manage any queries or issues from trainees or trainers for their department from initiation to completion. If they are unable to resolve an issue or answer a query they refer the query to their line manager and concurrently inform the Quality Manager that there is an outstanding query. The line manager sets a timescale for resolving the query and informs the Quality Manager when it has been resolved. 5. The Survey Administrators monitor the GMC Survey website regularly to check completion rates and validate data where required. The aim is to achieve a response rate of 100%. The Administrators should be in regular contact with MEMs and trainers to encourage responses. If it becomes apparent that responses are not forthcoming from any particular area, the Survey Administrators should inform their line managers, who should reinforce the request for responses and inform the Quality Manager that they are doing so. 6. Following the release of the preliminary reports, the Assistant Quality Manager analyses the data and checks for errors, liaising with the GMC where necessary, and produces reports as required. 2
56 Doc Ref: QMV-PRO-001 Version 1.6 Kent, Surrey & Sussex Deanery VISITING PROCEDURE SPECIALTY SCHOOL VISITS TO LOCAL EDUCATION PROVIDERS Contents Page Number 1. Introduction 2 2. Objectives 2 3. LEP Visits 2 4. Routine Visits / Programme Reviews 2 5. Exception Visits 3 6. Organising the Visiting Team 3 7. The Visiting Team 4 8. Externality 5 9. Role and Requirements of Visitors Visitor Training Pre-visit Arrangements Pre-visit Documentation - The Bundle DME Self Assessment Visiting Team Pro Forma GMC Standards for Postgraduate Training The Visit Meetings with Trainees Meetings with Educational / Clinical Supervisors Feedback Preparation Meeting Feedback Session Feedback for Programme Reviews Writing the Visit Report Progressing the Visit Report Follow-up and Sign-off Document Control Change Log 12 This document was printed on 03/10/2012 at 10:08:51. Before using this document, please ensure you have the latest version by checking it against the Document Control Log located at: K:\Quality Management\QM Documents\Master Documents.
57 1. Introduction This document describes the procedure for Kent, Surrey and Sussex Postgraduate Deanery (KSS) visits to all secondary care specialties in KSS Local Education Providers (LEPs). Visits are an important part of the KSS Quality Management (QM) process. They help to assure the Deanery that LEPs providing Postgraduate Medical Education and Training meet the requirements of the General Medical Council (GMC) Standards for Postgraduate Training as set out in The Trainee Doctor: 2. Objectives The objectives of visits are to: improve the quality of education and training by identifying notable practice as well as rectifying issues; ensure that GMC standards for the delivery of postgraduate medical education are being met; investigate any matters of concern against the GMC standards; identify common issues and notable practice across the specialities; provide assurance to the GMC of the quality of training in the specialties. 3. LEP Visits Visits may be part of a planned visiting schedule (routine visits) or be triggered by specific concerns (exception visits). KSS will also undertake follow-up visits where necessary. As well as assessing training at individual LEPs, KSS will also assess the delivery of training programmes or sub-regional rotational posts in programmes. Reviews of programmes will generally be combined with LEP visits, with a single LEP acting as host for the programme review. The GMC defines a programme as a formal alignment or rotation of posts which together comprise a programme of training in a given specialty or subspecialty. A programme may either deliver the totality of the curriculum though linked stages in an entirety to CCT, or the programme may deliver different component elements of the approved curriculum. 4. Routine Visits / Programme Reviews The specialties for routine visits and programme reviews in any one year are chosen by the Heads of Schools (HoS) on a risk-based approach. The HoS decide which Schools will visit which LEPs based on information from various sources including: Trainee / Trainer Survey data and analyses; the Contract Review process; minutes of Local Academic Board (LAB) meetings; minutes of Local Faculty Group (LFG) meetings; LAB and LFG Annual Audits and Reviews (AARs); records of academic development for individual teachers within LEPs; ARCP information; findings from previous visits; correspondence and other documentation relating to individual LEPs. 2
58 When the HoS have decided which LEPs they wish to visit, the Quality Management Department (QMD) will liaise with the HoS and the LEPs Medical Education Managers (MEMs) and Directors of Medical Education (DMEs) to agree all dates for visits. They will then prepare the final visits schedule and ensure it is approved by the KSS Quality Management Steering Group (QMSG). Where a review of a programme is planned, the QMD will contact the MEMs in the host LEP to make the necessary arrangements, and send the visit schedule to all MEMs who have trainees on the programme. The MEMs at the LEPs involved in the programme review will be requested by the QMD to send representatives of their trainees and trainers to the host LEP. The QMD will prepare a draft timetable for each visit, which must be approved by the relevant HoS. The timetables and visiting teams will be reviewed by the KSS Quality Management Operational Group (QMOG) in advance of the visits to ensure any potential problems can be resolved prior to the visits taking place. The KSS Dean Director will write to the Chief Executive Officer (CEO) of each LEP, copied to the relevant Schools, to confirm formally the date of the visit and the specialties / programme / site to be visited. 5. Exception Visits Exception visits may be made to LEPs, outside the routine LEP visiting process, as a result of: a serious untoward incident, which may or may not have involved a postgraduate trainee doctor but might have implications for training; a serious trainee complaint, either directly to KSS, or via a KSS School or a London Specialty School, which raises a serious question about current training that cannot be managed through usual mechanisms; concerns raised by usual mechanisms such as GMC Surveys in small specialties or specialties not routinely covered by the KSS visiting programme; evidence from any other source raising serious questions about potential service problems that could affect trainees. The process for exception visits is: issues arising will be reviewed by the Dean Director, the Postgraduate Dean for Secondary Care, the Associate Dean for Quality, the KSS Head of School and the London Deanery Head of School if also relevant; If there is evidence of serious concern the Dean Director will make a decision for a Deanery visit and will inform the next meeting of the Quality Management Steering Group. if there is a chronic problem or there are other factors to be taken into account and it is less pressing, the matter will usually be discussed at the Quality Management Steering Group meeting before a decision is made; if it is decided that an exception visit is required, the Dean Director will inform the LEP CEO and will instruct the QMD and the relevant Specialty School(s) to prepare for a visit. 6. Organising the Visiting Team For each School visit, the Medical Workforce Project Officer (MWPO) will liaise with the HoS to determine the members of the visiting team, and will invite them accordingly, making arrangements for travel and overnight accommodation where necessary. As each visitor confirms attendance, the MWPO will enter the details on a shared master spreadsheet together with the addresses of those outside of KSS, and send the QMD the mobile telephone number of each visitor. 3
59 If any visitor entered on the master spreadsheet subsequently cancels, the MWPO must remove the details from the spreadsheet and inform the QMD of the cancellation. The QMD will start sending pre-visit information and documentation (the bundle) to the confirmed visitors six weeks before the visit, so it is essential that all visitors are added to the spreadsheet before this deadline. Any additional visitors entered onto the spreadsheet after this deadline will not have been included on the distribution list for the bundle, so the MWPO must inform the QMD immediately of the late additions to the spreadsheet and forward the bundle to any such visitors, copied to the QMD. It is essential that the master spreadsheet is kept up to date to ensure that the correct people receive all the relevant information and to enable the QMD to play an effective supporting role in coordinating the School visits. 7. The Visiting Team The visiting team will comprise the following members: Visitor Head of School, KSS Deanery Training Programme Director (TPD), KSS Deanery GP Patch Associate Dean (if GP is one of the specialties being visited) Trainee Representative External or Lay Visitor (external reps are mandatory for exception visits) A member of the KSS Specialty Workforce Department Responsibility Lead Visitor. Broad clinical context. Reporting systems and processes. Lead for own specialty. Broad clinical context. Reporting systems and processes. Lead for own specialty. Broad clinical context. Reporting systems and processes. Trainee doctor context / voice. Provide externality. Visit Officer. Provision of administrative support including preparing the report in consultation with the lead visitor. The following are optional members of the visiting team: Dean Director Deputy Dean for secondary Care GP Dean Associate Deans Assistant Dean Education Observer(s) Where GP is included in the visit to a hospital, the GP visitor(s) will see any GP trainees who are currently part of the other specialties being visited. When a visit includes consultations with trainees administratively managed by the London Deanery, the Quality Manager will send a letter from the Dean Director to the relevant Head of School in London Deanery informing of the visit, inviting a representative from the London Deanery to attend the visit, and requesting any information that may be relevant to the visit. For exception visits, the visiting team will normally comprise the same members as above, but the final members of the visiting team will be decided by the Lead Visitor based on the size of the visit and the issues to be investigated. An external College visitor is mandatory for exception visits. 4
60 8. Externality In line with GMC requirements (The Trainee Doctor, Standards for Deaneries, Standard 4), there must be external input in some circumstances for specialty and GP training, involving independent and impartial advisers. This is usually a requirement for all visits that are not routine in nature. External advisers may be medical or lay, depending on the area for advice and/or scrutiny. They must be independent of the Deanery with no conflicts of interest. Medical advisers will have expertise appropriate for the specialty programme, course or school being considered and will normally be drawn from the medical Royal Colleges, Faculties or specialty associations. The need for an external College representative and/or a lay visitor on a routine visit will depend on the issues with the LEP. It is the responsibility of the relevant HoS to decide whether or not an external College representative and/or a lay visitor is required on a particular routine visit. 9. Role and Requirements of Visitors The role involves visitors seeking to gather evidence-based information that will be used to express an opinion on the LEP s ability to ensure that the curriculum is being delivered by qualified trainers to all trainees within the LEP. This will involve verifying that robust quality control processes are in place and are followed, which allow for doctors to be trained in an environment that provides for their needs and consequently benefits patients. During the visit, the visitors will interview trainees and trainers in order to gather additional information about the training environment and curriculum delivery, triangulate this with other sources of data such as the GMC Trainee and Trainer Survey, previous visits, etc. It is essential that the trainees and trainers feel confident that the information they communicate will be handled appropriately and confidentially. 10. Visitor Training Potential future visitors without previous visiting experience will be expected to attend training sessions organised by KSS. Alternatively they may be invited to attend QM visits in an observational capacity in order to gain experience of visits. In this case they will be provided with the teaching material used in the formal training sessions. Visitors with previous experience of visiting elsewhere will be expected to familiarise themselves with the KSS visiting procedure before the visit. All visitors are required to sign the KSS Visitor Guidance and Declaration (QMV-FOR-001) before taking part in a visit. This will be sent to each visitor by the QMD, who will keep a record of the signed declarations. 11. Pre-visit Arrangements As each visit is usually conducted by more than one Specialty School, the MWPOs should decide between them who will be the lead MWPO for each visit. The MEM and/or DME will usually be the visit coordinator for the LEP, acting as the liaison point between KSS and the LEP, disseminating details of the visit within the LEP, and distributing any pre-visit questionnaires provided by the Schools. This task will sometimes be delegated to an Assistant Manager or Administrator within the LEP. 5
61 The MWPOs will inform the QMD of the trainees and trainers that the Schools wish to see on the visit. The QMD will ask the LEP visit coordinator to invite these trainers and trainees and enter their details on the attendee list sent to them with the visit timetable. This will be returned to the QMD, who will forward it to the visiting team. As the coordinator of the School QM visits, the KSS QMD needs to be aware of all matters regarding visits. It is essential that the QMD is informed of any arrangements made by the Schools regarding the LEP visits. 12. Pre-visit Documentation - The Bundle The bundle of documents, comprising information from various sources about the LEP and the specialties being visited, is collated by the QMD nine weeks before the visit. A typical bundle will contain the following documents: Contract Review - Education Management Audit Contract Review Action Plan LAB Annual Audit and Review LFG Annual Audit and Reviews (for each specialty) Last 3 LAB minutes received from Trust Last 3 LFG minutes received from Trust (for each specialty) GMC Survey analyses Last LEP Visit Reports for the specialties being visited Last Foundation Visit Report ARCP information LFG Handbooks A list of contents of the bundle is sent to the Lead Visitor for each specialty eight weeks before the visit for approval. It is essential that the Lead Visitors check the contents to ensure they are happy with the documentation. The Lead Visitors should ask the QMD to request any additional information or documentation they require from the LEP before the visit, and/or a list of documents they would like to be made available during the visit (e.g. diary cards). The QMD will send a list of contents of the bundle to the MEM eight weeks before the visit for approval by the LEP, and will ask the MEM to forward any additional documents that the LEP would like to be included in the bundle. Six weeks before the visit, each member of the visiting team is sent an with a link to the KSS website, where they can download the bundle of documents. The MWPOs are copied into the s when the bundles are sent to the visitors. The MWPOs should check the recipients to ensure all members of the visiting team have been included. If MWPOs add any visitors to the team after the bundles have been sent out, they must forward the bundle to the additional visitors straight away, and copy this to the QMD (see section 6). 13. DME Self Assessment The DME will be sent a pro forma set out under three sections; notable practice, areas of concern and details of actions planned/taken. The DME will be asked to use this pro forma to provide KSS with a self assessment of training in the LEP. The self assessment should be sent to the QMD at quality@kssdeanery.ac.uk. It will then be forwarded to the visiting team in advance of the visit. 6
62 14. Visiting Team Pro Forma Evidence for the delivery and support of appropriate education for specialty trainees will be obtained from a number of sources. The Visiting Team Pro Forma helps the visitors to review the bundle of documents and identify areas where further exploration is required. It is set out under three sections; notable practice, areas of concern and areas for clarification/further investigation. It should be used in conjunction with the GMC guidance, The Trainee Doctor. Each visitor will be asked to complete a pro forma and send it to the QMD at quality@kssdeanery.ac.uk. The QMD will then forward the pro formas to the rest of the visiting team. 15. GMC Standards for Postgraduate Training These are the set standards against which the visiting team needs to report, published in the GMC s Standards document The Trainee Doctor. As the visitors review the bundle, they use this document to help them focus on key areas and ensure adequate coverage of key issues. The GMC Standards are set out under nine Domains: 1. Patient safety 2. Quality management, review and evaluation 3. Equality, diversity and opportunity 4. Recruitment, selection and appointment 5. Delivery of approved curriculum including assessment 6. Support and development of trainees, trainers and local faculty 7. Management of education and training 8. Educational resources and capacity 9. Outcomes 16. The Visit The documentary evidence will be triangulated during the visit using interviews with trainees and those delivering and facilitating the training. The visit will include structured focus group discussions with: Trainees in hospital posts Hospital Faculty Leads Specialty Programme Directors Educational Supervisors Clinical Supervisors On the day of the visit, the visiting team should have a private meeting to divide up tasks, go through the list of issues identified as being of interest, set rules for the day, refresh understanding of the GMC Domains, and ensure that all are clear about the division of responsibilities between members. For example, different team members can lead on asking questions in different meetings. It is usual for the Lead Visitor to start the questioning and to summarise where appropriate. At the opening meeting the Lead Visitor should ensure that the LEP understands the visit process, is fully aware of the timescales and activities to be undertaken and is clear about the information requested. The Lead Visitor should communicate to the LEPs that the visit is an opportunity for them to show how well they are doing as well as to explore matters of particular concern. The DME or Faculty tutors may like to give a very brief presentation at this time. This should last in total no more than 10 minutes. 7
63 17. Meetings with Trainees The visit timetable should be constructed to include meetings with separate groups of trainees, which may be conducted in parallel. The Team should aim to meet a wide range of trainees, including full-time, academic, flexible, supernumerary trainees, trainees on different placements, trainees in difficulty, etc. Trainees should be assured of confidentiality by the Visiting Team at the beginning of each meeting. Trainees should be offered an opportunity to meet any member of the Visiting Team one-to-one should this be required. 18. Meetings with Educational / Clinical Supervisors The trainers from the specialties being visited will usually be seen together as one group. The purpose of these meetings is to discuss the trainers experience of training-related issues. Whilst the visitors may wish to explore areas raised during the meetings with the trainees, this session should not include any direct feedback from those meetings. Where a programme is being reviewed alongside a routine LEP visit, the trainers from the programme will usually be seen as a separate group. This is because the trainers in the host LEP may not wish to discuss issues in front of trainers from other LEPs. 19. Feedback Preparation Meeting The Visiting Team will meet in advance of the feedback session to discuss their headline findings, both in terms of notable practice and areas for improvement. These should be noted in brief bullet points on the feedback forms. The purpose of the feedback form is to provide the LEP with a record of the brief headline verbal feedback given to senior LEP representatives, and provide KSS with evidence of acknowledgement by the LEP of the main headlines arising from the visit. The Visiting Team should agree any issues that the LEP has to address immediately, which would primarily relate to service issues affecting patient and trainee safety, and note these on the feedback forms, using one form for each specialty being visited. The Visiting Team should ensure that all findings are based on clear evidence. Where a programme review has taken place alongside a routine LEP visit, immediate verbal feedback to senior staff at the LEP will be provided for the specialties visited at that LEP only, not for the programme review. 20. Feedback Session At the end of the visit, brief headline verbal feedback, as encapsulated in the feedback forms, will be given to the senior LEP representatives, usually the CEO accompanied by the DME and other relevant staff. (This feedback will be for the specialties visited at that LEP only, not for any programme reviews undertaken on the same day.) Any areas requiring immediate action by the LEP, particularly where patient and/or trainee safety is compromised, will be communicated to the senior LEP representatives. In addition to this, the CEO and DME will be contacted by the KSS Dean Director via by the following day. 8
64 After receiving the verbal feedback, the senior LEP representative and the Lead Visitor should sign the feedback forms. The Visit Officer should ask the MEM to photocopy the completed and signed feedback forms. One copy of each form should be left with the senior LEP representative and the other should be passed to the KSS QMD, who will save the forms with the rest of the visit documentation. The senior LEP representatives should be informed that the visit report may contain other areas of notable practice and improvement in addition to those listed on the feedback forms and communicated verbally. 21. Feedback for Programme Reviews Programme reviews involve a number of different LEPs, and it is extremely unlikely that senior representatives will be present from all LEPs involved in the programme. Therefore the lead visitor will not provide verbal feedback for the programme review. However, any patient and/or trainee safety issues identified in a programme review will be reported by telephone immediately to the relevant CEO (or senior representative), and the Dean Director will also contact the CEO and DME via by the following day. 22. Writing the Visit Report The first draft of the visit report should be written by the visiting team, coordinated by the Lead Visitor, immediately following the visit. All members of the visiting team, including lay and external representatives, are expected to contribute to the KSS visit report, to be agreed by all visitors. It is essential that visitors do not produce supplementary reports or other documents that make reference to the visit, without the express permission of the Dean Director of KSS Deanery. Where a programme review has taken place alongside a routine LEP visit, separate visit reports will be produced. A report will be produced for the LEP, and will cover the specialties visited in that LEP only. A separate report will be produced for the programme review, and will cover all LEPs involved in that programme. The Visit Officer will type the details of the report into a Visit Report Template, which is set out under the nine GMC Domains (see Section 15). The visit report should be written in conjunction with the GMC guidance, The Trainee Doctor, which sets out the standards against which the visiting team needs to report. The full report must follow the KSS Deanery reporting template and include: the detail of the visit (the name of the LEP, details of the Visiting Team, etc.) the percentage of trainees from each specialty who attended the visit LEP performance under each Domain specific examples of notable practice specific concerns indicating the evidence mandatory requirements for action with details of evidence required and suggested deadlines for correction recommendations with suggested deadlines The content of the draft and final visit reports should include issues encapsulated on the Feedback Form and communicated in verbal feedback. 9
65 Section 2 of the report (Findings against GMC Standards) should only contain matters of (reported) fact, and should not include the opinions or suggestions of the visitors. All Mandatory Requirements and Recommendations made in Section 4 of the report will be referenced back to the findings in section 2, and in the case of Mandatory Requirements will also be referenced to the relevant GMC Mandatory Requirement set out in the Standards published in The Trainee Doctor. The Visit Officer will circulate the draft report to all members of the visiting team for approval. The Visit Officer will amend the draft report as suggested by the visitors and forward it to the Quality Manager no later than 5 working days from the date of the visit. 23. Progressing the Visit Report The Quality Manager will check and amend the report as necessary, and forward to the Associate Dean for Quality (ADQ) for a consistency check. The ADQ will make any necessary amendments and return the draft report to the Quality Manager for final formatting. The draft report will then be sent to the DME for a factual accuracy check. The DME should receive the draft report no later than two weeks from the date of the visit. The Quality Manager will submit the report (with any amendments suggested by the DME) to be reviewed and formally approved at the subsequent meeting of the KSS QMSG, which meets monthly. These meetings are chaired by the Dean Director and attended by the KSS Heads of Schools. The QMSG will often suggest minor changes to reports. These changes are made by the Quality Manager before the report is signed off by the Dean Director. If substantial changes are necessary or clarification is required (and the HoS is not present at the meeting), the Quality Manager will confirm the changes with the relevant HoS (or lead visitor) before the report is sent out. The final report will be sent to the CEO (copied to the DME, MEM and other relevant stakeholders) together with a pre-populated Action Planning Template, drawn up from the requirements and recommendations in the report, to facilitate the response. The LEP will be asked to complete the action plan as part of their response to the report findings. Final reports will usually be sent out within six weeks of the visit. 24. Follow-up and Sign-off An audit trail of responses to the visit report, in the form of a tracking chart will be kept by the Quality Manager, who ensures that all actions are followed up and all requested evidence is provided to the QMSG. Any change in practice suggested that relates to a mandatory requirement in the GMC Standards is classified as a mandatory requirement, and will be followed up by the QMSG. Recommendations are suggestions that should be considered by the LEP, but do not relate to GMC mandatory requirements. These are not followed up by the QMSG; however, the LAB should discuss with the relevant LFGs what actions have been taken on any recommendations. This may then be reported to the QMSG by the LAB when responding to visit reports and will be discussed and monitored by the relevant KSS Specialty School. 10
66 All responses to mandatory requirements are reviewed and signed off by the QMSG. When all mandatory requirements are met, the Dean Director will confirm this formally in writing to the CEO. Once the report is signed off, the notable practice and mandatory requirements will be published on the KSS Deanery website together with the response(s) from the LEP and the formal sign-off date. The report will be made available to the GMC when required for their Quality Assurance processes. 25. Document Control Title: Originator: Document Owner: Document Number: Local Education Provider Visiting Process - Secondary Care Specialties Karen Gibson, Quality Manager David Yates, Associate Dean for Quality QMV-PRO-001 Version Number: V 1.6 Approved / Authorised by: KSS Quality Management Steering Group Date Issued: May 2011 Next Review Date: January 2013 Master Location: Publication Scheme: Purpose of document: K:\QUALITY MANAGEMENT\LEP Visits (LV)\Visit Documents KSS Website To set out the procedure for the KSS visiting process. 11
67 26. Change Log Version Date Revisions First draft written by Karen Gibson, Quality Manager Minor revisions made to procedure at request of Zoe Playdon, Head of Education - paragraph numbering, positioning of acronyms Additions to section 13, 14 and 15 by Karen Gibson, Quality Manager - information on feedback form added Updated to reflect consolidated standards document from the GMC - The Trainee Doctor Updated by David Yates, Associate Dean for Quality, to include information on visitor training (section 5), presentations (section 11), meetings with trainers (section 13) and report writing (section 16) Paragraph added by Karen Gibson, Quality Manager, explaining mandatory requirements and recommendations (section 16). Contents list added Updated to clarify paragraph on mandatory requirements and recommendations (section 18). Section 16 split into 3 sections Sections 5 and 18 amended to provide further clarity. Document agreed as final at May QMSG meeting Addition of Section 6, Role and Requirements of Visitors, and Section 7, Externality. Following sections renumbered to incorporate sections 6 and 7. Update to Section 8 to clarify the single point of control. Addition to Section 18 to clarify the requirement for one single visit report Updated and approved by David Black, Dean Director - minor changes to wording in Section 6 and Section Updated by Quality Manager to include information on programme reviews - additions to Sections 3, 18, 19 and 22. New section added - Section 21. Section 3 split into two sections. All numbering changed to incorporate new sections. Amendments made to clarify processes - additions to Sections 6, 7, 8 and Minor changes made to paragraph positioning by David Yates, Associate Dean for Quality, to clarify information on programme reviews Changes made to the order of paragraphs to improve the flow of information. Minor changes made to wording Document was reviewed by the QMSG on 16 December It was agreed that a headline feedback form should be used for each specialty visited rather than one single form. The procedure has been updated to reflect this, and a few minor changes were made to improve clarity. Next review date January
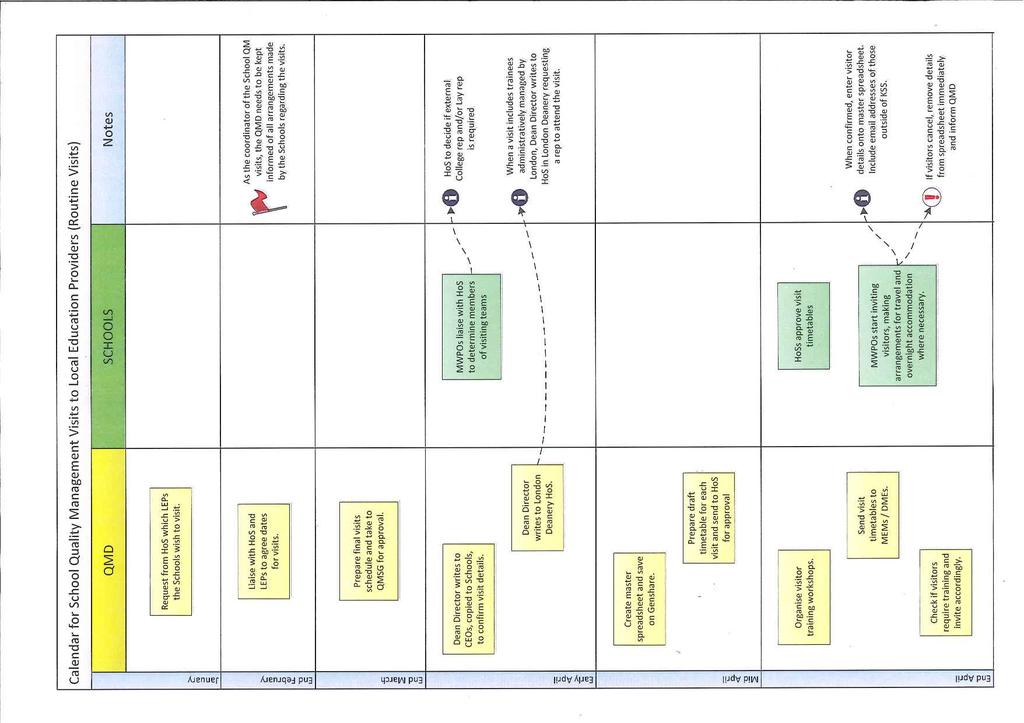
68
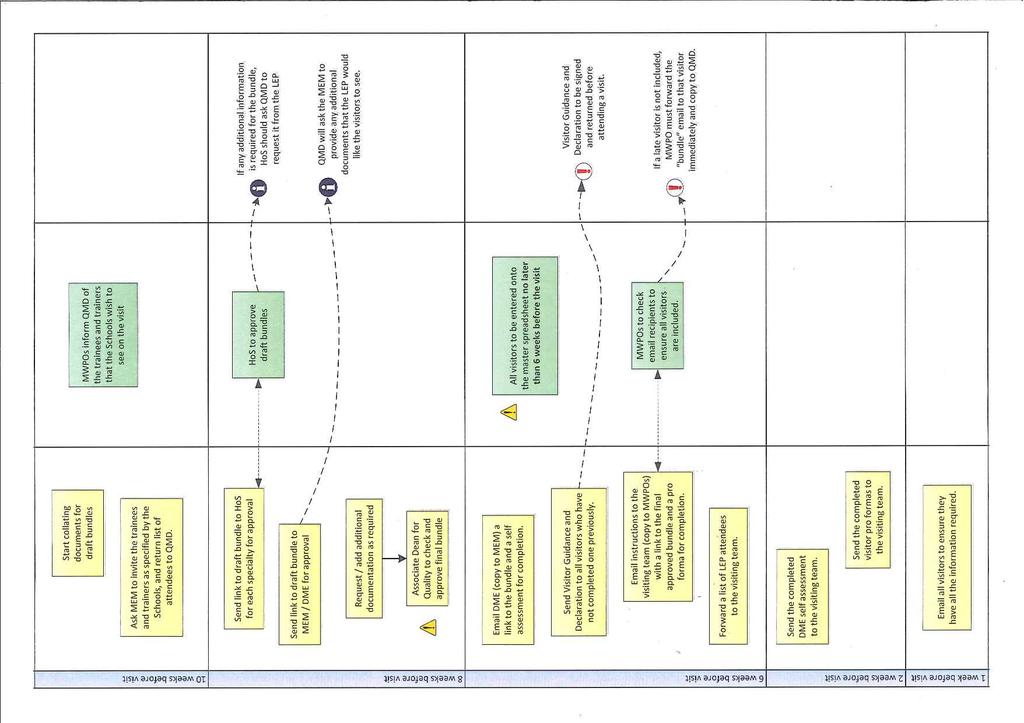
69
70
71 Kent, Surrey & Sussex Deanery Process for reporting Visits to Programmes* or sub-regional rotational posts in programmes. The KSS Deanery has a well established process for visiting Local Education providers (LEPs) to assess training posts and the educational environment. We are increasingly managing higher specialty training across Kent, Surrey and Sussex. Assessment of the quality of this training will require a wider view and we intend to look at the delivery of training programmes or sub-regional rotational posts in programmes in future. After exploring different ways of assessing programme delivery last year, we have agreed that visits to programmes or parts thereof will generally be combined with LEP visits. The process will be similar to LEP visits, but there are significant differences, summarised below: Trainees and trainers from other centres will be asked to travel to the LEP where the visit is based. Immediate verbal feedback to senior staff at the end of the visit will only be provided in relation to the specialties visited at that LEP only. Because programme visits will be considering experiences from a number of different LEPs it will not be possible to provide feedback in the same way, as senior representatives will not be present from all relevant sites. It should be noted that our current practice whereby areas requiring immediate action by the LEP (particularly those where patient and/or trainee safety is compromised) are communicated to the senior LEP representatives will apply to all sites considered in programme visits, even if no senior representatives are present. In this case telephone contact will be made, and the CEO and DME will be contacted by the KSS Dean Director via by the following day in the normal way. Separate visit reports will be produced for the LEP and programme visits. The programme visit report will be circulated to all LEPs that are involved in that programme visit. We consider the visiting process to be a vital part of quality management. We recognise that some disruption to clinical services is inevitable with any visiting process, but we hope that this way of conducting our visits will give the best outcomes with the least disruption. David Yates, Associate Dean for Quality, 20 September 2011 * GMC Definition A programme is a formal alignment or rotation of posts which together comprise a programme of training in a given specialty or subspecialty. A programme may either deliver the totality of the curriculum though linked stages in an entirety to CCT, or the programme may deliver different component elements of the approved curriculum.
72 Kent, Surrey & Sussex Deanery QUALITY MANAGEMENT OF POSTGRADUATE MEDICAL EDUCATION AND TRAINING Local Education Provider Specialty Visit Report Routine LEP Visit / Exception Visit / Follow-up Visit / Programme Review (delete as appropriate) Please note: this report is about the postgraduate medical education and training of doctors and not about the level of service provided. Purpose of Visit To ensure that national standards for the delivery of postgraduate medical education are being met To improve the quality of education and training To identify common issues and good practice across the specialities Section 1 Visit Details Local Education Provider Date of Visit Specialties / Grades Visited Percentage of trainees from each specialty who attended the visit Visiting Team Position Name address People to whom the visit report is to be sent Position Name address Chief Executive of Trust Director of Medical Education Medical Education Manager College Tutor Information and reports received prior to the visit Contract Review - Education Management audit Contract Review Action Plan LAB Annual Audit and Review LFG Annual Audit and Reviews (for each specialty) Last 3 LAB minutes received from Trust Last 3 LFG minutes received from Trust (for each specialty) GMC Survey analyses Received Page 1 of 6
73 Last LEP Visit Report Faculty Handbooks Self Assessment from Trust DME Section 2 Findings against the GMC Standards for Postgraduate Training Refer: Domain 1 - Patient safety Standard: The responsibilities, related duties, working hours and supervision of trainees must be consistent with the delivery of high-quality safe patient care. There must be clear procedures to address immediately any concerns about patient safety arising from the training of doctors. Ref: The Trainee Doctor - page 12 Specialty 1 Name Specialty 2 Name Specialty 3 Name Domain 2 - Quality management, review and evaluation Standard: Training must be quality managed, monitored, reviewed, evaluated and improved. Ref: The Trainee Doctor - page 15 Specialty 1 Name Specialty 2 Name Specialty 3 Name Page 2 of 6
74 Domain 3 - Equality, diversity and opportunity Standard: Training must be fair and based on principles of equality. Ref: The Trainee Doctor - page 16 Specialty 1 Name Specialty 2 Name Specialty 3 Name Domain 4 - Recruitment, selection and appointment Standard: Processes for recruitment, selection and appointment must be open, fair and effective. Ref: The Trainee Doctor - page 18 Specialty 1 Name Specialty 2 Name Specialty 3 Name Domain 5 - Delivery of approved curriculum including assessment Standard: The requirements set out in the approved curriculum and assessment system must be delivered and assessed. Ref: The Trainee Doctor - page 20 Specialty 1 Name Page 3 of 6
75 Specialty 2 Name Specialty 3 Name Domain 6 - Support and development of trainees, trainers and local faculty Standards: Trainees must be supported to acquire the necessary skills and experience through induction, effective educational and clinical supervision, an appropriate workload, relevant learning opportunities, personal support and time to learn. Trainers must provide a level of supervision appropriate to the competence and experience of the trainee. Trainers must be involved in, and contribute to, the learning culture in which patient care occurs. Trainers must be supported in their role by a postgraduate medical education team and have a suitable job plan with an appropriate workload and sufficient time to train, supervise, assess and provide feedback to develop trainees. Trainers must understand the structure and purpose of, and their role in, the training programme of their designated trainees. Ref: The Trainee Doctor - page 25 Specialty 1 Name Specialty 2 Name Specialty 3 Name Domain 7 - Management of education and training Standard: Education and training must be planned and managed through transparent processes that show who is responsible at each stage. Ref: The Trainee Doctor - page 32 Specialty 1 Name Specialty 2 Name Page 4 of 6
76 7.8. Specialty 3 Name Domain 8 - Educational resources and capacity Standard: The educational facilities, infrastructure and leadership must be adequate to deliver the curriculum. Ref: The Trainee Doctor - page 34 Specialty 1 Name Specialty 2 Name Specialty 3 Name Domain 9 - Outcomes Standard: The impact of the standards must be tracked against trainee outcomes and clear linkages should be made to improving the quality of training and the outcomes of the training programmes. Ref: The Trainee Doctor - page 36 Specialty 1 Name Specialty 2 Name Specialty 3 Name Page 5 of 6
77 Section Notable Practice Note as * any exceptional examples that have the potential for wider use or development elsewhere in the NHS. Section Mandatory Requirements Actions / Evidence Required Reference (Domain and paragraph no.) GMC Mandatory Req. no. Due Date Section Recommendations Reference (Domain and paragraph no.) Approved by KSS Deanery Quality Management Steering Group Signed by Professor David Black Dean of Postgraduate Education KSS Postgraduate Deanery Date: Page 6 of 6
78 Kent, Surrey & Sussex Deanery QUALITY MANAGEMENT OF SPECIALTY TRAINING Local Education Provider Specialty Visits - Headline Feedback Form The purpose of this form is to provide the LEP with a bullet-point record of the brief headline verbal feedback given to senior LEP representatives at the end of the visit, and provide KSS with evidence of acknowledgement by the LEP of the main headlines arising from the visit. A detailed report will follow in line with the KSS LEP Visiting Procedure. The report may contain other areas of notable practice and mandatory requirements / recommendations in addition to those listed below. All notes should be entered on this form, which should be signed by the senior LEP representative and the Lead Visitor after the verbal feedback is given. Once completed and signed, a copy of the form should be left with the LEP senior representative, and the original should be forwarded to the KSS Quality Management Department. LEP Visited Date of Visit Specialty Areas of Notable Practice Domain
79 Areas for Improvement Domain Areas Requiring Immediate Action (Dean Director to be notified immediately) Domain Signed by Lead Visitor for Specialty and Senior LEP Representative Position Name Signature
80 Kent, Surrey & Sussex Deanery Action Plan for Visit Reports LEP Name: Director of Medical Education: Visit Date: Medical Education Manager: The following mandatory requirements relate to the GMC Standards, and must be addressed by the LEP. All actions to address mandatory requirements will be followed up by the KSS Quality Management Steering Group (QMSG). No. Mandatory Requirements Domain Actions/Evidence Required Deadline Progress Further Action Planned
81 The following recommendations are suggestions that should be considered by the LEP, but do not relate to GMC Standards. These are not followed up by the QMSG. However, the LAB should discuss with the relevant LFGs whether or not actions should be taken on any recommendations. This may then be reported to the QMSG by the LAB when responding to visit reports and will be discussed and monitored by the relevant KSS School Committee. No. Recommendations Domain Comments
82 Kent, Surrey & Sussex Deanery QUALITY MANAGEMENT OF SPECIALTY TRAINING DME Self Assessment Pro Forma Name of Trust: Specialties being visited: Name of DME: Date of visit: As your Trust is due to be visited by a team from KSS Deanery, you are asked to complete a self assessment of training in your Trust in conjunction with the relevant Clinical Tutors. Please use this form to make a note of any areas of concern or notable practice. Please also describe any actions you have taken or are planning. A bundle of documents containing the most recent information from various sources about your Trust and the specialties that will be visited has been sent to you in the form of a online webpage. This webpage includes the GMC standards document, The Trainee Doctor, which should be used to help you focus on key areas and ensure adequate coverage of issues. Your notes will be sent to the visiting team prior to the visit. All members of the visiting team will also be provided with the bundle of documents. They will use these documents together with your self assessment to identify areas requiring further investigation, which will be followed up on the visit. Please return your completed form to quality@kssdeanery.ac.uk Please Note: This form must be typed and sent by as a Word document. Handwritten and scanned forms cannot be accepted. Areas of Notable Practice
83 Areas / Issues of Concern Actions Planned / Taken
84 Kent, Surrey & Sussex Deanery QUALITY MANAGEMENT OF SPECIALTY TRAINING Visiting Team Pro Forma Name of Trust: Specialties being visited: Name of Visitor: Date of visit: Thank you for agreeing to participate in this visit to a Local Education Provider on behalf of KSS Deanery. You have been provided with a bundle of documents containing the most recent information from various sources about the Trust and the specialties you will be visiting. As you review the bundle, please use this form to make a note of any areas/issues of concern, notable practice or issues requiring clarification/further investigation. The accompanying GMC standards document, The Trainee Doctor, should be used to help you focus on key areas and ensure adequate coverage of issues. Your notes will be sent to the other members of the Visiting Team for information. The Lead Visitor will use these notes to identify areas requiring further investigation, which will be followed up on the visit. Please return your completed form to quality@kssdeanery.ac.uk Please Note: This form must be typed and sent by as a Word document. Handwritten and scanned forms cannot be accepted. Areas of Notable Practice
85 Areas / issues of concern Issues requiring clarification / further investigation
86 Kent, Surrey & Sussex Deanery QUALITY MANAGEMENT OF SPECIALTY TRAINING Question Prompt Thank you for agreeing to participate in a visit to a Local Education Provider on behalf of KSS Deanery. For some areas, sufficient evidence may have been provided from the documentation sent to you prior to the visit, however, if the documentation indicates areas for further exploration, the areas below provide a prompt for questions to ensure adequate coverage of key issues. Domain 1 - Patient safety Areas for exploration with specialty trainees in Hospital posts Any concerns about patient safety related to the working environment/s Educational / Clinical supervision appropriate for level of responsibility Any examples of good educational / clinical supervision arrangements When help is required, is it easily available? Do the working hours/shift patterns allow adequate rest? Is the appropriate information about individual patients easily available? Do the patient records allow effective and safe management of every patient? Are shift/patient handovers adequate? Is there a hospital at night process? If so, how does it work? Any concerns about patient safety in the out of hour s placements Taking consent appropriate to level of experience. Areas for exploration with the Local Specialty Training Programme Director, Local Faculty Group Good things about specialty training in this locality Difficulties with specialty training in this locality Any trainees including GP exposed to situations that may compromise patient safety? Concerns about the provision of supervision for Specialty/ GP trainees in any location? Working rotas for trainees Any variations in the specialty placements? Organisation of patient handover in the specialty OOH arrangements, especially supervision and teaching Domain 2 - Quality Management, Review and Evaluation Areas for exploration with Local Education Provider Process to manage EWTD, Data Protection Act, and Freedom of Information Local Faculty Group management of quality control of the training posts? LFG relationship with the Local Academic Board? LFG relationship with other LFGs, where there are overlapping concerns such as GP How necessary changes are action planned, progressed and audited Compliance with EWTD Level of support from Medical Staffing Level of support from Education Centre Areas for exploration with Specialty Trainers and Programme Directors Familiarity with GMC Generic Standards for Training Familiarity with postgraduate medical educational organisational structure in KSS Familiarity with GEAR Representation of GP Trainers on the LFG What constitutes good practice in the LFG? What needs development?
87 Domain 3 - Equality, Diversity and Opportunity Areas for exploration with LEP Any examples of problems relating to these areas with any trainees? Process and practice for resolution of problems How HR/Medical Staffing department deals with issues of disability or special needs in trainees Areas for exploration with Trainees (NB individuals may not wish to disclose personal details) Seen/ experienced discrimination in the workplace? Have full information about posts, the job description, and the content and purpose of the posts? Know about, or how to get information about: o Planned absence o Unplanned absence o Training at less than full-time o Level of support offered for any disability or special needs? Areas for exploration with Specialty Educational and or Clinical Supervisors. Local Training Programme Directors / Local Faculty Group LFG monitoring processes for discrimination, either direct, or indirect Any examples of how a trainee with disability or special needs has been appropriately accommodated in training? Areas for exploration with Specialty Local Training Programme Directors / DMEs Process for monitoring that those involved in training have been trained in Equality and Diversity in the last three years Domain 4 - Recruitment, selection and appointment Areas for exploration How Trainers keep up to date with the documentation and processes that they are required to provide for the employment of trainees How the Local Faculty supports the Specialty Recruitment and Selection process carried out by the KSS Deanery on behalf of the national process Domain 5 - Delivery of curriculum including assessment Areas for exploration with Trust/DEM/ Educational and Clinical Supervisors Who carries out WPB assessments for trainee doctors How they have been trained How assessment is monitored Local curriculum audited against national curriculum framework? Curriculum individualised to meet needs of learners? Process of Educational Supervision Monitoring of Educational Supervision Process of LFG reporting to/ discussing with Educational Supervisors How Educational and Clinical Supervisors communicate with each other over trainee progression Arrangements for appropriate protected teaching for Specialty trainees Arrangements for carrying out NHS appraisal for trainees Areas for exploration with trainees How Educational or Clinical Supervisors carry out assessments How Educational or Clinical Supervisors input to Trainee Portfolio / eportfolio How their progress is discussed with Trainees Best part of the educational process How NHS appraisal is carried out
88 Areas for exploration with Local Faculty Group / Educational and or Clinical Supervisors Any problems with the hospital posts in supporting the learning outcomes of the Specialty curriculum for specialty trainees or GP trainees Any problems with the hospital posts in providing effective assessments in a timely and appropriate fashion How the LFG ensures that all are trained and moderated in the WPB assessments How the LFG supports individual Educational / Clinical Supervisor development, in the light of information from ARCP panels How the LFG ensures that it is on track to meet GMC Standards for Training and target that all Educational Supervisors will be trained by 2010 What is going well in carrying out assessments Domain 6 - Support and development of trainees, trainers and local faculty Areas for exploration with trainees The process for induction: o To the Trust o To the clinical team o In the context of on-call Nominated Clinical Supervisor/s? Nominated Educational Supervisor? o Planned or achieved Educational Supervision meetings? o Use of portfolio / eportfolio? Content and location/s of Specialty training programme Access and provision of career advice Relevance of posts for GP training [if appropriate] Any concerns about quantity or kind of work Weekly protected teaching time: o Trainee voice in choice of subjects o Consistency of attendance of teachers o Consistency of attendance of learners Learning experience in Outpatients quantity/ quality Awareness of study leave support for trainees Experienced of undue pressure or bullying Opportunities to learn from, or with, professionals other than doctors Areas for exploration with Training Programme Directors Induction of new entrants to Specialty training in the locality Allocation of Educational Supervisors to trainees How trainees are supported in their learning needs in each year How teaching time is managed and organised Study leave arrangements for trainees CPD arrangements for trainers Trainee voice in LFG and LAB Process for implementation of trainee recommendations and examples of it Support for LFG Accreditation and reaccreditation of Educational Supervisors Provision of OOH experience Areas for exploration with GP Trainers on the Local Specialty Faculty Group [if appropriate] Processes for induction for GP trainees when they come to the Practice in their ST1 year Process for induction for GP trainees when they come to the Practice for their ST3 year Study leave process for trainees in the hospital posts (the days in GP) How GP trainees are involved in audit in their GP placements How other professionals are involved in the teaching of GP trainees in the Practice and how they are monitored Deanery support processes for trainer support and continuing professional development as GP educators Provision of OOH experience
89 Domain 7 - Management of Education and Training Areas for exploration with Trust How well embedded the LFG and LAB processes are How issues from the LAB are communicated to Specialty LFG and Specialty trainees Effectiveness of communication between consultant Educational / Clinical Supervisors and Specialty Programme Directors How GP is represented on other specialty LFGs Responses to the outcomes of the GMC survey Processes for identifying and supporting trainees whose conduct, health, progress or performance give cause for concern, with examples Domain 8 - Educational resources and capacity Areas for exploration with trainees Appropriateness of learning opportunities and experience required for your specialty training Training or educational support from non-doctors Enough Supervisors (consultants, middle grades, and other professionals) to provide appropriate levels of educational support Information resources: library internet access to portfolio / eportfolio Perception of the learning environment in the Specialty/ LEP Domain 9 - Outcomes Areas for exploration with Faculty and LEP How identify a relationship between the GMC standards and the outcomes achieved by Specialty trainees? How do these outcomes feed back into changes for development of education and training for Specialty trainees and how are these shared? Areas for exploration with trainees Any information about the educational outcomes for doctors in the specialty training programme here (e.g. numbers of doctors achieving satisfactory outcomes at ARCP)?
. It should be read in conjunction with the LEP Visiting Procedure (document no. QMV-PRO-001).")
90 Overview of the role of the Lead Visitor on KSS Visits This document is intended to provide you with a brief overview of your responsibilities as a lead visitor on a KSS visit to a Local Education Provider (LEP). It should be read in conjunction with the LEP Visiting Procedure (document no. QMV-PRO-001). Pre-Visit It is the lead visitor s responsibility to check that each member of the visiting team is prepared for the visit. You should contact all members of the team a few days before the visit to ensure they have read the bundle of documents and made notes on the Visiting Team Pro Forma. You should read these notes (sent to all visitors by the Quality Department) in advance of the visit in order to identify areas requiring further investigation, which can be followed up on the visit. Visiting Team Briefing The first session of the day is the visiting team briefing, a half-hour meeting. You need to check all the team have arrived and ask them to introduce themselves. Then go through the key issues that people have picked up from the bundle and discuss the particular concerns they wish to investigate. It is helpful to allocate specific areas of questioning to visiting team members. You should run through the timetable to ensure everyone is aware of what happens in each session. There is one mistake that has been made a few times in the past; following the session with the trainees, there is a session with the faculty groups. This has sometimes turned into a feedback session, with the visitors feeding back to the consultants the issues raised by the trainees. Whilst the purpose of this session is to discuss the key issues arising from discussions with trainees together with issues identified from the bundle, the aim is to obtain the trainers views and experiences of training-related issues. This session should not involve any direct feedback from the trainee session, which has the potential to breach confidentiality. You will need to make sure the other visitors are aware of this before the start of the visit. Meeting the Trainers and Trainees At the opening meeting with the faculty leads, you should ask everyone to introduce themselves, and give a brief overview of the visit. Make sure the faculty leads understand the process, and check if they have any initial concerns. You need to make it clear that it is not an inspection but a supportive process to help them identify any areas of concern that need improving in order to meet the GMC standards. Let them know that it is also an opportunity for them to highlight areas of notable practice. At this first session, ask the DME if he will be giving a presentation (this is optional, but most LEPs choose to do so). You should ask him to keep the presentation brief, no more than 10 minutes. It is usual for the lead visitor to start the questioning for each session and to bring in the other visitors where appropriate, ensuring everyone has the opportunity to explore any issues. It is important in the trainee session to make sure the trainees understand why they are there, and to reassure them that the discussions are in confidence and no-one will be identified by their comments. You should ensure they are all encouraged to speak openly, and also give them the opportunity to speak with any of the visitors privately if they wish.
91 Visiting Team Review After the session with the faculty group, the visiting team members will meet to discuss their findings. You should note these (as brief bullet points) on the headline feedback form, or you can ask the visit secretary (usually a member of the KSS Workforce Team) to do it. The reason we have started to use this form is that there have been times in the past where LEPs have complained that a particular issue was not mentioned at the feedback session, but later appeared in the visit report. This provides us with a record of the points that were covered. Feedback Session At the feedback session, you should thank the LEP representatives for their time, and make sure you highlight all the positives as well as the areas where improvement is necessary. Tell the LEP representatives when to expect the draft report, which will be sent to the DME for a factual accuracy check. The DME should receive this within a week of the visit. The final report needs to be signed off by the KSS Quality Management Steering Group, which meets monthly. The final report will be sent to the LEP within 2 or 3 days of the Steering Group meeting. If there are any patient or trainee safety issues, which require immediate action, these must be communicated to the LEP, entered in the relevant section of the feedback form and reported straight away to the Dean Director, who will contact the Trust s CEO. The headline feedback form should be signed by you and the LEP CEO (or senior representative) at the end of the feedback session and then photocopied. One copy should be left with the LEP and the other returned to the Quality Team at the Deanery. Writing the Report After the feedback session, the visiting team will write the first draft of the report on the visit report template. The visit secretary will have populated some of the report throughout the day, but the lead visitor is responsible for ensuring each issue is captured and entered under the correct domain. Make sure all members of the visiting team contribute to the report. One thing to remember is that section 2 of the report (the main body of the report) should describe all the findings, but the visitors recommendations, requirements and comments on notable practice should not appear in this section. These should be listed in sections 3, 4 and 5. Don t worry too much about the deadlines, as these are likely to be changed or added at the Steering Group meeting, but if you decide something must be done immediately, this must be stated. The recommendations and mandatory requirements should be referenced back to section 2 of the report, and in the case of the mandatory requirements, should also be referenced to the relevant GMC standards (set out in The Trainee Doctor). Post-Visit After the visit, the visit secretary will type the report with the correct formatting and send it to you and the rest of the visitors for comments/approval, then send the final approved draft to the Quality Team. The Quality Manager will check through the report and make any minor amendments as necessary to correct errors and ensure consistency of numbering and formatting, then forward it to the DME for a factual accuracy check. The Associate Dean for Quality will check the report to ensure consistency with other reports in terms of domains, mandatory requirements and recommendations, and will make any necessary amendments. Any significant amendments will be referred back to you for approval.
92 The report will then go to the next meeting of the Quality Management Steering Group. You should attend this meeting in order to discuss the report. If you are unable to attend, it is likely that changes will be made to the report in your absence; however, if any significant queries are raised that require your input, the Quality Manager will need to contact you to request clarification. This causes unnecessary delays in processing the report, so it is important that you attend this meeting if possible. Once approved, the final report will be signed by the Dean Director and sent to the LEP. You will receive a copy of the final report. The LEP response to the mandatory requirements will be reviewed by the Steering Group. If the response is not straightforward, you will be asked to give your approval or otherwise in advance of the meeting if you are unable to attend. In this case, the Quality Manager will contact you with the details, etc. You will receive a copy of the final sign-off letter once all the requirements have been met. Karen Gibson, Quality Manager, KSS Deanery, November 2011.
93 Kent, Surrey & Sussex Deanery QUALITY MANAGEMENT OF SPECIALTY TRAINING VISIT FEEDBACK FORM Thank you for hosting a KSS Deanery Quality Management Visit. This form will be used by KSS Deanery to assist in evaluating our quality practices. We are dedicated to ensuring that our processes are robust and effective, as well as to making the visit experience a positive and productive one for everyone involved. Your comments will help us examine what worked and what didn t, and give us ideas for any future changes or improvements to the visiting process. We will keep these forms confidential and anonymise any excerpts we may use in the future. We appreciate your feedback. Local Education Provider: Date of Visit: Name of person providing feedback: Position within LEP: Once you have received the final report, please complete this form and return it to: quality@kssdeanery.ac.uk
94 Please put a X in the appropriate box after each of the following statements: Section 1: Pre-visit Strongly agree Agree Neither agree nor disagree Disagree Strongly disagree Not applicable 1. The pre-visit information was informative and useful. 2. The timing of the visit was appropriate. 3. Any questions I had regarding the visit were answered promptly and satisfactorily. 4. I knew who to contact at the Deanery for particular issues or queries. 5. We were informed of the visit date and the specialties to be visited well in advance of the visit. 6. It was clear which evidence would be used by the visit team to inform the visit. 7. I had positive interactions with Deanery staff while organising the visit. Additional comments regarding the pre-visit process:
95 Section 2: The Visit Strongly agree Agree Neither agree nor disagree Disagree Strongly disagree Not applicable 1. There were no difficulties hosting the visiting team. 2. I had confidence in the visiting team s understanding of the LEP and its quality management systems. 3. The visiting team seemed to listen to our contributions. 4. The visiting team members conducted themselves in a professional and appropriate manner throughout the visit. 5. The visiting team was an appropriate size. 6. I was confident in the Lead Visitor s ability to facilitate the visit. 7. At the conclusion of the visit, I felt that it had been a positive experience. Additional comments regarding the visit itself:
96 Section 3: Post-visit Strongly agree Agree Neither agree nor disagree Disagree Strongly disagree Not applicable 1. The visit report form is fit-for-purpose. 2. The visit report adequately reflected the discussion that took place during the visit. 3. There were no surprises present in the draft report. 4. We were given the opportunity to check the draft report for factual accuracy. 5. The report was sent at the time promised. 6. The mandatory requirements and recommendations were clear and concise. 7. The mandatory requirements and recommendations had appropriate deadlines. Additional comments on the visit report or on post-visit activities:

97 Kent, Surrey & Sussex Deanery QUALITY MANAGEMENT OF SPECIALTY TRAINING VISITOR FEEDBACK FORM Thank you for taking part in a Quality Management Visit to a Local Education Provider on behalf of KSS Deanery. This form will be used by KSS Deanery to assist in evaluating our quality practices. We are dedicated to ensuring that our processes are robust and effective, as well as to making the visit experience a positive and productive one for everyone involved. Your comments will help us examine what worked and what didn t, and give us ideas for any future changes or improvements to the visiting process. We will keep these forms confidential and anonymise any excerpts we may use in the future. We appreciate your feedback. Local Education Provider Visited: Date of Visit: Name of person providing feedback: Job Title: Please return to: quality@kssdeanery.ac.uk Please put a X in the appropriate box after each of the following statements:
98 Section 1: Pre-visit Strongly agree Agree Neither agree nor disagree Disagree Strongly disagree Not applicable 1. The timing of the visit was appropriate. 2. Any questions I had regarding the visit were answered promptly and satisfactorily. 3. I knew who to contact at the Deanery for particular issues or queries. 4. I was informed of the visit date and the specialties to be visited well in advance of the visit. 5. The with the website link to the bundle was received in good time for the visit. 6. The content of the website was clear and informative. 7. The visit pro formas were clear and easy to use. 8. The timetable was appropriate for the visit. 9. The address/directions/maps were clear and accurate. 10. The website was easy to use, and the instructions were clear and easy to understand. Additional comments regarding the pre-visit process:
99 Section 2: The Visit Strongly agree Agree Neither agree nor disagree Disagree Strongly disagree Not applicable 1. I had no problems parking at the Trust. 2. I had confidence in my fellow visitors understanding of the LEP and its quality management systems. 3. I was confident in the Lead Visitor s ability to facilitate the visit. 4. The visit team was an appropriate size. 5. The meeting rooms were an appropriate size. 6. The MEM and other staff at the Trust ensured all ran smoothly. 7. All stakeholders conducted themselves in a professional and appropriate manner throughout the visit. 8. At the conclusion of the visit, I felt that it had been a positive experience. Additional comments regarding the visit itself:
100 Section 3: Post-visit Strongly agree Agree Neither agree nor disagree Disagree Strongly disagree Not applicable 1. The visit report form was fit-for-purpose and easy to complete. 2. I was given the opportunity to contribute to the final report. 3. The visit report reflected accurately the discussion that took place during the visit. 4. The visit report reflected the views of all members of the visiting team. Additional comments on the visit report or on post-visit activities:
101 Doc Ref: QMV-FOR-001 Version 1.2 Human Resources Department LEP Visitor Guidance & Declaration 1. Introduction This guidance is intended to clarify the confidentiality requirements of visitors involved in quality visits to Local Education Providers (LEP) within Kent, Surrey and Sussex. 2. Scope The guidance relates to the full visiting panel, who will be expected to read this guidance and the KSS LEP Visiting Procedure before confirming their agreement to the requirements outlined within this guidance document and the KSS LEP Visiting Procedure. 3. Training Potential future visitors without previous visiting experience will be expected to attend training sessions organised by KSS before they can participate in a visit. Alternatively they may be invited to attend QM visits in an observational capacity in order to gain experience of visits. In this case they will be provided with the teaching material used in the formal training sessions. Visitors with previous experience of visiting elsewhere will be expected to familiarise themselves with the KSS visiting process before the visit. Visitors will be expected to confirm that they have read the KSS LEP Visiting Procedure before signing the below declaration. 4. Information Governance Visitors will also receive information in a variety of formats. Visitors will be expected to maintain the confidentiality of all information related to visits and only use the information received for this purpose. Visitors will be expected to arrange for the appropriate destruction of visit materials via confidential waste disposal or by returning information to the relevant visit secretary. 5. Role and Requirements of Visitors The role involves visitors seeking to gather evidence-based information that will be used to express an opinion on the LEP s ability to ensure that the curriculum is being delivered by qualified trainers to all trainees within the LEP. This will involve verifying that robust quality control processes are in place and are followed, which allow for doctors to be trained in an environment that provides for their needs and consequently benefits patients.
102 During the visit, the visitors will interview trainees and trainers in order to gather additional information about the training environment and curriculum delivery, triangulate this with other sources of data such as the GMC Surveys, previous visit reports, etc. It is essential that the trainees and trainers feel confident that the information they communicate will be handled appropriately and confidentially. A single report will be produced as a consequence of the visit, which will be agreed by all visitors. The report is subsequently signed off by the KSS Quality Management Steering Group, after which it can be shared with other professional organisations as appropriate. Since this process has been publicised and agreed with LEPs, it is essential that visitors do not produce supplementary reports or other documents that make reference to the visit, without the express permission of the Dean Director of KSS Deanery. Any concerns should be raised as part of the visiting process. Visitors are required to sign the below page to confirm acceptance of the requirements outlined above. 2
103 QUALITY MANAGEMENT VISITOR DECLARATION Please complete this reply slip and return it to the KSS Deanery Quality Management Department, either by post: 7 Bermondsey Street, London SE1 2DD, or by quality@kssdeanery.ac.uk I have signed below to confirm my acceptance of the requirements stated in the LEP Visitor Guidance & Declaration (QMV-FOR-001) and the requirements covered in the KSS LEP Visiting Procedure (QMV-PRO-001). I understand that I am required to comply with the confidentiality requirement, which prevents me from producing a separate report or other related documentation that relates to the LEP visit in which I have participated on behalf of KSS Deanery, without the express permission of the Dean Director of KSS Deanery. Signed forms will be held on file by the KSS Quality Management Department and may be reviewed by nominated Deanery representatives involved in the Quality Management visiting process. Signature: Full Name: Role/Post Title: Date:.... 3
.")
104 South Thames Foundation School QUALITY MANAGEMENT OF FOUNDATION TRAINING IN KSS FOUNDATION FACULTY VISITING PROCESS INTRODUCTION The GMC has defined a framework for the quality assurance of the Foundation Programme (QAFP). The South Thames Foundation School, on behalf of KSS Deanery, will need to ensure within this framework that there is a clear set of standards for trainers and training environments and that evidence of educational delivery is shared. Local foundation faculty groups will be expected to review and maintain the quality standards of foundation training within the LEP and STFS will undertake to verify and validate the process of local quality control. Any queries regarding this process or foundation quality issues should be directed to quality@stfs.org.uk 2. FOUNDATION DOCTOR ANNUAL QUESTIONNAIRE Foundation doctors will be required to complete a short questionnaire (appendix A) during November. The questionnaire is located within the foundation e-portfolio. LEPs will be responsible for ensuring completion of the questionnaire by all F1 and F2 doctors by the beginning of December. It is estimated that the form should only take approximately minutes to complete. A questionnaire response rate of less than 70% may prompt the visiting team to raise this as an item for discussion during the visit. LEPs will be able to download a summary of local responses via the e-portfolio. LEPs will be responsible for circulating the results of the questionnaire to local F1/F2 doctors. The responses will be reviewed by the STFS Director/Associate Directors for any issues of major concern which may require an earlier than scheduled visit (see 3). A summary of the responses from the relevant LEP will also be included in the visiting team pre-visit documentation (see 5). 3. VISITING CYCLE STFS visiting teams will usually visit all KSS LEPs providing foundation training programmes on a three-year cycle (see appendix B). If, however, the results of the annual trainee questionnaire indicate that there are any issues of major concern then STFS reserves the right to schedule an earlier visit. If an earlier visit is required, the LEP will be notified of this by early February and the visit will usually take place in May.
105 4. STFS VISITING TEAMS Minimum Requirement Visitor STFS Director/Associate Director A member of the KSS Education Department STFS Manager/Administrator Desirable If available Foundation doctor representative Service representative (e.g. DME/ MEM from another LEP) External visitor KSS Associate Dean Deanery Quality Manager Responsibility Lead visitor Broader clinical context. Reporting systems and processes. Signing-off the visit report. Curriculum, teacher education, supervision, learning resources, foundation doctor education experience. Administrative context. Provision of admin support including preparing the report in consultation with the lead visitor Foundation doctor context/voice Broader management and administrative aspects, including resource. Externality Local patch issues Co-ordination of visits and documentation 5. PRE-VISIT DOCUMENTATION The Bundle The following written information will be collated by the STFS quality administrator from the information already held centrally by KSS/STFS. It will be sent to the LEP (DME & MEM) 10 weeks in advance of the visit together with an LEP self-assessment which should be completed and returned within 3-weeks. The bundle, including the completed self-assessment, will be sent to the visiting team no later than 6 weeks before the visit. Doc Source 1 Quality Management of Foundation Training in KSS Foundation STFS Faculty Visiting Process Contract Review background, management audit & action plan Education Dept 3 Local foundation faculty handbook STFS 4 Most recent LFG annual audit and review STFS 5 Minutes of 3 most recent local academic board meetings. STFS 6 Minutes of 3 most recent local foundation faculty group meetings. STFS 7 National trainee survey data STFS 8 Previous foundation faculty visit report STFS 9 Summary of responses to the annual trainee questionnaire STFS 10 LEP self-assessment STFS The visiting team will review this documentation and note any areas of concern on a pro forma. Each visitor will return their pro forma to the STFS quality administrator within 2 weeks of dispatch and responses will then be forwarded to the lead visitor within 2 weeks of the visit. The faculty may be required to provide further information prior to the visit on any areas or issues that emerge from the pre-visit documentation.
106 6. VISITING TEAM TRAINING Team members will be expected to be familiar with the following documentation reference to which will be included in the training: 1. GMC The Trainee Doctor 2. GMC Outcomes for Full Registration 3. Foundation Programme Curriculum EB.pdf ulum_and_fp_reference_guide_final.pdf 4. Foundation Programme Reference Guide ulum_and_fp_reference_guide_final.pdf 5. Foundation Programme e-portfolio 6. KSS Graduate Education & Assessment Regulations (GEAR) A hard copy is available from the KSS Education Department. 7. STFS Policies/Procedures See STFS Website In particular: a. Foundation Doctor Role and Minimum Requirements for Clinical Supervision b. Delivery of the Foundation Programme Curriculum through Formal Teaching Programme Visitors will have attended a previous visit in an observer capacity before actively participating as a visitor. On the morning of the visit, the lead visitor will provide a 30-minute briefing/training session to the visiting team which will include: the aims of the day o Identify & explore patient/trainee safety issues o Qualitative assessment of the trainee experience o Exploration with trainers of any concerns raised by them o Identification of areas of faculty development and training environment needs brief review of the documentation identify the main issues to discuss/clarify agree on the distribution of questioning with appropriate regard for the experience of different members of the team 7. VISIT TIMETABLE The visit will include structured focus group discussions with: Foundation doctors Hospital faculty leads (DME, Clinical Tutor, MEM)
107 Foundation training programme directors Educational supervisors During the visit the visiting team will triangulate the documentary evidence using interviews with foundation doctors and those delivering and facilitating the training. Time Session Required 9:30 Visiting team meet and final briefing Visiting team 10:00 10:30 Meet faculty to discuss faculty DME/CT/FTPD/MEM development 10:30 11:45 Meet F1 doctors 1 As many F1s as possible (ideally including a rep from each specialty) 2 11:55 13:10 Meet F2 doctors 1 As many F2s as possible (ideally including a rep from each specialty) 2 13:10 13:40 LUNCH - 13:40 14:40 Meet focus group of FTPDs/educational hospital faculty leads/foundation supervisors (rep from programme directors/educational each dept if possible) supervisors 14:45 16:00 Collate information and prepare feedback Visiting team 16:00 Feedback session LEP Chief Executive/DME/ MEM/Medical Director/ FTPD # Tea/coffee to be available at all sessions 1 2 If a foundation doctor wishes to speak to someone confidentially about any issues/concerns they will be offered an appointment to see the STFS Director/Associate Director. Minimum 50% of all foundation doctors to attend. Local LEP administrative staff will be responsible for arranging appropriate accommodation and refreshments for the visit. They will also arrange for staff/ foundation doctors to attend the relevant sessions. Brief verbal feedback will be given to the LEP CEO and DME and other relevant staff at the end of the day. Any areas requiring an immediate response will be communicated to the LEP CEO, DME and KSS Dean Director by the lead visitor via by the end of the following day. 8. VISIT REPORT A draft written report will be produced by the lead visitor working with the relevant STFS manager/administrator within two weeks of the visit for the DME to check for factual accuracy. Once agreed, the final draft will be considered by the next scheduled monthly meeting of the KSS Quality Management Steering Group and, once signed off, the report will be formally sent to the LEP within one week. The outcome of the process will be to deliver a report highlighting examples of notable practice and the sharing of that, and mandatory and desirable developmental areas with time-limited action points.
108 The subsequent response to this report will be delivered by the local faculty group and local academic board for consideration by the KSS Deanery Quality Management Group. The report will also be available to the GMC when required for their quality assurance process. 9. SUMMARY OF THE PROCESS 10 weeks in advance of the Visit Bundle, questionnaire results and LEP self-assessment issued to LEP 7 weeks in advance of the Visit LEP self-assessment to be returned. Confirmation of visit day arrangements to be provided to STFS quality administrator. 6 weeks in advance of the Visit Bundle sent to visiting team 4 weeks in advance of the Visit Visitors return visitor pro-formas to STFS quality administrator 2 weeks in advance of the Visit STFS quality administrator forwards visiting team pro formas to lead visitor Visit By the end of the day following the Visit Lead visitor advises LEP CEO and DME of any areas requiring immediate response Within 2 weeks of the Visit Draft report provided to the LEP Next scheduled monthly meeting of QMSG Considers draft report Within 1 week of QMSG approving draft report Final report provided to the LEP with deadline for response to recommendations
109 Next Scheduled meeting of QMSG Considers LEP response to recommendations Within 1 week of QMSG considering response to recommendations Letter to trust confirming satisfactory response or additional action required 10. EXCEPTION VISITS Exception visits are visits to local education providers that are outside of the normal foundation faculty visit cycle. They may be initiated because of: A serious clinical incident which may or may not have involved a trainee but might have implications for training. A serious trainee complaint either directly to the Deanery/STFS, or via a KSS/London Specialty School which raises a serious question about current training that cannot be managed through usual mechanisms. Evidence from any other source which raises serious questions about potential service problems which could affect trainees. Concerns arising from the STFS foundation doctor annual questionnaire. Process Issues arising will be discussed by the Dean Director and the STFS Director. If there is evidence of serious concern the Dean Director will make a decision for a Deanery visit and will inform the next meeting of the Quality Management Steering Group. It there is a more complex or chronic problem or there are other factors to be taken into account and it is less pressing, the matter will usually be discussed at the Quality Management Steering Group before a decision is made. Exception visits will usually follow a similar process to that described above, however, an external/lay representative will be required to join the visiting team. The report will come to the Quality Management Steering Group for discussion and approval of action, following which the Dean Director will write to the Chief Executive of the LEP. The response of the LEP will be followed up and discussed at the Quality Management Steering Group until adequate evidence of resolution is provided. Where serious problems cannot be resolved it will be normal to approach the GMC for a trigger visit.
110 If at any stage serious problems are uncovered which put trainees or patients at risk, the Dean Director will take immediate executive action.
111 Appendix A South Thames Foundation School FOUNDATION DOCTOR ANNUAL QUESTIONNAIRE (KSS) 1. Grade (F1/F2) F1 F2 2. Which rotation are you in? Induction 3. Did you receive a contract, terms and conditions, banding notification and job description within the first 6 weeks (or earlier) of starting in the trust? Yes No 4. Did you receive an induction into your local foundation training programme? Yes No 5. Did you receive an up to date job description for your current post? Yes No 6a. Did you receive a local foundation faculty handbook? Yes No 6b. If yes, how would you rate the usefulness of the handbook? (If no, please mark "N/A") Excellent Good Average Poor N/A 7. Please rate your induction to the hospital/trust. Excellent Good Average Poor Did not happen 8. Did you have the opportunity to shadow staff before starting your post in August? Yes No 9. On the first day with your current firm, please rate your induction to your patients, other staff, duties and health and safety procedures. Excellent Good Page 1 of 7 Updated: Jan 2011
112 Average Poor Did not happen 10. Did you meet your clinical supervisor to discuss your duties in the post, expectations of your progress etc. within the first 2 weeks of starting? Yes No Supervision & Support 11. How would you rate the day-to-day level of supervision you receive from your consultant (clinical supervision)? Excellent Good Adequate Poor 12. Do you receive frequent constructive feedback on your clinical performance? Yes No 13. Do you know who your educational supervisor is? Yes No 14. Did you meet with your educational supervisor to agree educational objectives within the first 2 weeks of starting your post? Yes No 15. How many formal meetings have you had with your educational supervisor? Do you know who to approach if you are experiencing problems with your work or training? Yes No 17. Have you had problems identifying/encouraging sufficient numbers of staff to allow you to complete your foundation eportfolio? Yes No 18. Have you received, or been offered, support with your career decision making? Yes No Feedback 19. Do you know who your foundation trainee representative is on the trust faculty group? Yes No Page 2 of 7 Updated: Jan 2011
113 20. How would you rate the level of communication you receive from South Thames Foundation School? Excellent Good Average Poor Hours 21. How often do you estimate you work over your contracted hours? Never Rarely Most months Most weeks Daily Safety 22. Is there a formal hand-over period in the evening supervised by a registrar or consultant? Yes No 23a. Have you ever been asked to do anything which you felt was above your competence? Yes No 23b. If yes, did you question this? (If no to 23a, please mark "N/A") Yes No N/A 23c. If yes to 23a, did you complete the task? (If no to 23a, please mark "N/A") Yes No N/A 24. Have you ever been expected to cope alone beyond your knowledge and experience? Yes No 25. Have you ever obtained consent for a procedure with which you were unfamiliar? Yes No 26a. F1 ONLY - Have you ever prescribed, transcribed or administered cytotoxic drugs or immunosuppresants (excluding corticosteroids)? (If F2, please mark "N/A") Yes No N/A 26b. F2 ONLY - Have you ever initiated or administered cytotoxic drugs or immunosuppresants (excluding corticosteriods)? (If F1, please mark "N/A") Yes No N/A 26c. F2 ONLY - If yes to 26b, had you been trained in the relevant procedure? Page 3 of 7 Updated: Jan 2011
114 (If F1 or no to 26b, please mark "N/A") Yes No N/A 27. Have you been asked to site mark a patient without appropriate prior training (surgical posts only)? Yes No N/A 28. When help is required, is it easily available? Yes No 29. On the whole, how would you rate the level of work intensity with your current rotation? Too high High but manageable Average Low but adequate Too low Teaching & Learning 30. Are there foundation specific (weekly) formal education sessions for you as a foundation doctor? Yes No 31. If yes, are they bleep free? (If no to 30, please mark "N/A") Yes No N/A 32. Are you able to easily attend foundation specific teaching other than when you are oncall, on nights or on leave? Yes No 33. Do you usually receive 3 hours of protected teaching time for educational activity each week? (Protected time refers to the release of foundation doctors from their clinical responsibilities) Yes No 34. On the whole, how would you rate the quality and usefulness of formal education sessions? Excellent Good Average Poor For the following staff, how would you rate the informal teaching you receive e.g. discussions/teaching at bedside, in theatre, in clinics etc. either by instruction, feedback or discussion around cases? 35. Consultants Excellent Good Page 4 of 7 Updated: Jan 2011
115 Average Poor None 36. GPs (if applicable) Excellent Good Average Poor None 37. Registrars Excellent Good Average Poor None 38. ST/Trust-grade/Staff-grade/Associate Specialist level Excellent Good Average Poor None 39. Other medical professionals e.g. nurses, pharmacists etc. Excellent Good Average Poor None 40. Have you received teaching/training in equality & diversity? Yes No Educational Environment 41a. Have you ever been subjected to any forms of discrimination, bullying or harassment? Yes No 41b. If yes, please indicate by whom. Consultant GP SpR Nurse Manager Other 41c.If yes, how did you follow this through? (If no, please mark "N/A") Formal complaint Informal complaint Discussion with individual Did not take action N/A 42. Are you regularly seeing and assessing acute ill patients admitted via A&E? Yes Page 5 of 7 Updated: Jan 2011
116 No 43. How many outpatient clinics have you attended? N/A 44. How many theatre sessions have you attended? (surgical posts only) N/A 45. How many pre-assessment/pre-clerking clinics have you attended? (surgical posts only) N/A 46. How would you rate the clinical experience you are gaining in this post? Excellent Good Average Poor Facilities 47. How would you rate the phlebotomy service? Excellent Good Average Poor 48. Is there a weekend phlebotomy service? Yes No 49. How would you rate the radiology service? Excellent Good Average Poor 50. How would you rate the laboratory services? Excellent Good Average Poor 51. Do you know where your postgraduate centre is? Yes No Page 6 of 7 Updated: Jan 2011
117 52. Do you have easy access to a networked computer which you can use for online learning, research and access to relevant websites? Yes No 53. How would you rate the service provided by the postgraduate education centre? Excellent Good Average Poor 54. How would you rate the library resources and services for your learning requirements? Excellent Good Average Poor Overall 55. STFS/KSS Deanery welcomes any feedback and comments from all trainees. If you feel there is anything we have not covered in this questionnaire or you would like to raise any specific issues, please complete the comments box below. Page 7 of 7 Updated: Jan 2011
118 Appendix B Foundation Faculty Visit Schedule Trust Maidstone and Tunbridge Wells NHS Trust Royal Surrey County Hospital NHS Trust, The Dartford & Gravesham NHS Trust East Sussex Hospitals NHS Trust Date of Visit 08-Mar Mar Apr Feb-12 Ashford & St Peter's Hospitals NHS Foundation Trust 07-Feb-12 Surrey and Sussex Healthcare NHS Trust Brighton and Sussex University Hospitals NHS Trust Medway NHS Foundation Trust Western Sussex Hospitals NHS Trust Deferred Apr Feb Mar-13 East Kent Hospitals University NHS Foundation Trust 16-Apr-13 Frimley Park Hospital NHS Foundation Trust 30-Apr-13
119 DOCUMENT CONTROL Title: Originator: Manager Responsible: Quality management of foundation training in KSS Foundation faculty visiting process Marc Terry, Head of Foundation Workforce Jan Welch, Director, STFS Policy Number: Version Number: Approving Body: v.1.1 KSS Quality Management Steering Group Date Issued: December 2011 Review Date: September 2012 Date Equality Impact Assessed: Legal Advice Required/Obtained: Master Location: Publication Scheme: Purpose of document: N/A K:\South Thames Foundation School\Quality Management\Foundation Visits\KSS\Master Documents STFS e-update, STFS Website Summarise KSS/STFS process for administering foundation faculty visiting process. Document History Version Name Date Revisions/ Outcome 1.1 QMSG December 2011 Section 2 update to reflect Questionnaire included in e- portfolio Section 5 updated to include LAB minutes added to bundle requirements Section 6 updated to reflect publication of Trainee Doctor 0.1 QMSG
120 South Thames Foundation School CHECKLIST FOR USE DURING DISCUSSIONS WITH F1 DOCTORS Name of Trust Date of Visit To be completed by lead administrator and forwarded to lead visitor in advance of the visit Issue Summary from Trainee Questionnaire Visitors supplementary questions 1 Hospital Induction a) Did you have an induction to the hospital when you started work here? inc STFS slides b) What could be done to improve it? 2 Firm Induction a) Did you have an induction to your department (ward, GP surgery etc) when you started? b) Did it give you all the information you needed to start your work? What could be done to improve it? 3 Shadowing Did you have adequate time to spend shadowing the outgoing F1? (F1 only) 4 Feedback a) Do you receive regular constructive feedback? 5 Educational supervision/ Assessment/ Portfolios b) Do you receive it if you ask for it? a) Do you know who your Educational Supervisor is? b) Have you had regular meetings with your Educational Supervisor to discuss your progress? c) Does he/she look at your portfolio? d) Are you able to get your assessments carried out (e.g. DOPS, mini-cex etc?) If not, why not? If so who does them for you? 6 IT Issues Do you have convenient access to computers with Internet access to be able to access e- portfolio? 7 Clinical Supervision a) Do you feel adequately supervised and supported according to your level of experience? b) Who do you ask for clinical advice in the daytime? c) Who do you ask after hours? d) How often do you have consultant ward rounds? e) Do you work nights? If so, is this part of a Hospital at Night team? How does it work? 8 Hours Have you been asked to complete diary cards? 9 Handover/ Competence a) How often have you been asked to undertake tasks beyond your level of competence and without supervision? b) What were the tasks? Visitor Notes Updated: 23 February 2012
121 c) Do you have appropriate middle grade cover? d) How do you hand over the care of your patients to your colleagues? e) Is there a process for handing over the care of patients at the end of the shift? f) Is there time set aside in your timetable for handover? g) How often have you been asked to carry out inappropriate duties? What are these duties? h) Have you ever lost patients? (e.g. Over the weekend?) 10 Consent Have you been asked to take consent for a procedure that you are not able to perform? If yes, how often and who has asked you to do it? What did you do? 11 Cytotoxics Do you prescribe or administer cytotoxics? Have you been asked to? 12 Site Marking Have you been asked to site mark? 13 Teaching a) How much teaching time do you have during the week, other than the generic teaching programme? b) What form does it take? c) Is it bleep free? d) Is it useful to you as a Foundation Doctor? e) How often do you attend the generic teaching programme? f) Are you able to get to the sessions without difficulty? g) Do you feel that there is sufficient practical experience available so that you can obtain the competences in your curriculum? h) How could the education and training content of the programme be improved? i) Is there anything about your training programme which we have not covered that you would like to tell us about? 14 Bullying a) Have you ever been subjected to personal behaviour by others which has eroded your confidence? b) Who by? 15 Whistleblowing a) How would you feed back your concerns about a colleague who behaved unethically? b) Are you aware of any formal procedure for this? 16 Theatre/Op availability/ attendance 17 Facilities/ Support Services 18 Postgraduate Centre a) Do you have timetabled sessions when you attend theatre/op? b) Who covers your ward duties when you attend? a) Where do you access up to date clinical guidelines to which you can refer? b) Can you describe the relationship between Foundation doctors and the Radiology services? 19 Careers support a) Have you had any careers advice? b) Do you know who your careers advisors are? 20 How rate as a place to work? Would you recommend this particular post you are currently doing to a friend? Updated: 23 February 2012
122 Updated: 23 February 2012
123 South Thames Foundation School CHECKLIST FOR USE DURING DISCUSSIONS WITH F2 DOCTORS Name of Trust Date of Visit To be completed by lead administrator and forwarded to lead visitor in advance of the visit Issue Summary from Trainee Questionnaire Visitors supplementary questions 1 Hospital Induction a) Did you have an induction to the hospital when you started work here? inc STFS slides b) What could be done to improve it? 2 Firm Induction a) Did you have an induction to your department (ward, GP surgery etc) when you started? b) Did it give you all the information you needed to start your work? What could be done to improve it? 3 Feedback a) Do you receive regular constructive feedback? b) Do you receive it if you ask for it? 4 Educational supervision/ Assessment/ Portfolios a) Do you know who your Educational Supervisor is? b) Have you had regular meetings with your Educational Supervisor to discuss your progress? c) Does he/she look at your portfolio? d) Are you able to get your assessments carried out (e.g. DOPS, mini-cex etc?) If not, why not? If so who does them for you? 5 IT Issues Do you have convenient access to computers with Internet access to be able to access e- portfolio? 6 Clinical Supervision a) Do you feel adequately supervised and supported according to your level of experience? b) Who do you ask for clinical advice in the daytime? c) Who do you ask after hours? d) How often do you have consultant ward rounds? e) Do you work nights? If so, is this part of a Hospital at Night team? How does it work? 7 Hours Have you been asked to complete diary cards? 8 Handover/ Competence a) How often have you been asked to undertake tasks beyond your level of competence and without supervision? b) What were the tasks? c) Do you have appropriate middle grade cover? d) How do you hand over the care of your patients to your colleagues? e) Is there a process for handing over the care of patients at the end of the shift? Visitor Notes Updated: 23 February 2012
124 f) Is there time set aside in your timetable for handover? g) How often have you been asked to carry out inappropriate duties? What are these duties? h) Have you ever lost patients? (e.g. Over the weekend?) 9 Consent Have you been asked to take consent for a procedure that you are not able to perform? If yes, how often and who has asked you to do it? What did you do? 10 Cytotoxics Do you prescribe or administer cytotoxics? Have you been asked to? 11 Site Marking Have you been asked to site mark? 12 Teaching a) How much teaching time do you have during the week, other than the generic teaching programme? b) What form does it take? c) Is it bleep free? d) Is it useful to you as a Foundation Doctor? e) How often do you attend the generic teaching programme? f) Are you able to get to the sessions without difficulty? g) Do you feel that there is sufficient practical experience available so that you can obtain the competences in your curriculum? h) How could the education and training content of the programme be improved? i) Is there anything about your training programme which we have not covered that you would like to tell us about? 13 Bullying a) Have you ever been subjected to personal behaviour by others which has eroded your confidence? b) Who by? 14 Whistleblowing a) How would you feed back your concerns about a colleague who behaved unethically? b) Are you aware of any formal procedure for this? 15 Theatre/Op availability/ attendance 16 Facilities/ Support Services 17 Postgraduate Centre c) Do you have timetabled sessions when you attend theatre/op? d) Who covers your ward duties when you attend? a) Where do you access up to date clinical guidelines to which you can refer? b) Can you describe the relationship between Foundation doctors and the Radiology services? 18 Careers support a) Have you had any careers advice? b) Do you know who your careers advisors are? 19 How rate as a place to work? Would you recommend this particular post you are currently doing to a friend? Updated: 23 February 2012
125 South Thames Foundation School CHECKLIST FOR USE DURING DISCUSSIONS WITH FOUNDATION FACULTY (DME, FTPD, MEM) Name of Trust Date of Visit Issue 1 How are things in general? Notes 2 Any issues that the Faculty would like to bring to the attention of the Visiting Team 3 Any particular developments that the Faculty would like to bring to the attention of the Visiting Team Updated: 23 February 2012
126 4 Key Issues from the trainee pre-visit questionnaire TO BE COMPLETED BY LEAD ADMINISTRATOR 5 General Notes Updated: 23 February 2012
127 South Thames Foundation School CHECKLIST FOR USE DURING DISCUSSIONS WITH EDUCATIONAL SUPERVISORS Name of Trust Date of Visit Issue 1 How are things in general? Notes 2 Any issues that the ES would like to bring to the attention of the Visiting Team 3 Any particular developments that the ES would like to bring to the attention of the Visiting Team Updated: 23 February 2012
128 4 Key Issues from the trainee pre-visit questionnaire TO BE COMPLETED BY LEAD ADMINISTRATOR 5 General Notes Updated: 23 February 2012
129 South Thames Foundation School FOUNDATION FACULTY VISITING PROCESS GUIDANCE NOTES FOR LEAD VISITORS In advance of the visit 1. Review the bundle including the summary of trainee feedback 2. Review the lead visitor checklists (produced by lead administrator for the visit) 3. Review the summary of visiting team pro-formas with the lead administrator On the day of the visit 4. Brief the visiting team regarding the aims of the day which are: Identify & explore patient/trainee safety issues Qualitative assessment of the trainee experience Exploration with trainers of any concerns raised by them Identification of areas of faculty development and training environment needs Outline the timetable for the day 5. Circulate the lead visitor checklists and the summary of the visiting team proformas 6. As a team, identify the main issues to discuss/clarify 7. Agree on the distribution of questioning with appropriate regard for the experience of different members of the team. It is recommended that the lead visitor lead the discussions in the meetings with the faculty group, educational supervisors and feedback session bringing in the different members of the team as appropriate. 8. Remind all about the confidential nature of the visit (all have signed a confidentiality agreement). During interviews with Foundation Doctors 9. Remind Foundation Doctors that they may arrange a confidential 1:1 with the lead visitor if there are any issues that they would prefer to discuss privately. They should contact the lead administrator via to arrange either a faceto-face or telephone interview. Collate Information & prepare feedback 10. Visiting Team to agree on which items they are going to feedback on. 11. Visiting team to agree items to be included in the report, which domains they apply to and the requirements/recommendations. 12. The Headline Feedback Form (Appendix 1) needs to be completed. The purpose of this form is to provide the LEP with a record of the brief headline verbal feedback given to senior LEP representatives at the end of the visit, and provide KSS with evidence of acknowledgement by the LEP of the main headlines arising from the visit. Any areas requiring immediate action by the LEP will be noted on this form and communicated to the senior LEP Page 1 of 2 Updated: 30 th January 2012
130 representatives. In addition to this, the CEO and DME will be contacted by the KSS Dean Director via the following day. During Feedback session 13. Thank staff for their preparations for the visit as appropriate 14. Feedback positives first 15. Highlight any patient safety issues that have been identified 16. Discuss other areas for improvement/of concern 17. Confirm that a draft report will be sent to the DME within 2-wks of the visit to confirm factual content, will then be approved by KSS Quality Management Steering Group and subsequently circulated formally to Chief Executive, Medical Director, DME, FTPDs and MEM. After the Feedback Session 18. A copy of the completed and signed Headline feedback form (signed by senior LEP representative and the Lead Visitor) should be left with the Trust Senior Representative and the original should be forwarded to quality@stfs.org.uk the next day. After the Visit 19. Liaise with the lead administrator to draft/agree the report within 2-wks of the visit. Page 2 of 2 Updated: 30 th January 2012
131 South Thames Foundation School FOUNDATION FACULTY VISITING PROCESS GUIDANCE NOTES FOR LEAD ADMINISTRATORS In advance of the visit 1. Review the bundle including the summary of trainee feedback 2. Populate lead visitor checklists with data from trainee pre-visit questionnaire results 3. Review the summary of visiting team pro-formas with the lead visitor. 4. Bring copies of lead visitor checklists and collated visiting team pro-formas for members of the visiting team On the day of the visit 5. Make detailed notes of all sessions 6. Liaise with local admin staff regarding arrangements for the day 7. Contact London Bridge office ( ) if any queries 8. After the feedback session to the Foundation Faculty, visiting team to agree items to be included in the report, which domains they apply to and the requirements/recommendations. 9. After the verbal feedback is given The Headline Feedback Form (Appendix 1) needs to be completed. The purpose of this form is to provide the LEP with a record of the brief headline verbal feedback given to senior LEP representatives at the end of the visit, and provide KSS with evidence of acknowledgement by the LEP of the main headlines arising from the visit. Any areas requiring immediate action by the LEP will be noted on this form and communicated to the senior LEP representatives. In addition to this, the CEO and DME will be contacted by the KSS Dean Director via the following day. A detailed report will follow in line with the KSS LEP Visiting procedure. The report may contain other areas of notable practice and improvement in addition to those listed. After the Visit 10. A copy of the completed and signed Headline feedback form (signed by senior LEP representative and the Lead Visitor) should be left with the Trust Senior Representative and the original should be forwarded to quality@stfs.org.uk 11. Liaise with the Lead Visitor to draft/agree the report using the standard report template (R:\South Thames Foundation School\Quality Management\Foundation Visits\KSS\Master Documents\ STFS-KSS Deanery Foundation Visit Report Template) within 2-wks of the Visit 12. Forward draft report to London Bridge Office to send to the DME to confirm factual content Page 1 of 1 Updated: 30 th January 2012
132 South Thames Foundation School BRIEFING NOTE FOR FOUNDATION FACULTY VISITING TEAM Visit to: Venue: Date of visit: Trust contact: STFS LB Contact: NAME POSITION ORGANISATION CONTACT DETAILS VISITING TEAM OBSERVERS TIMETABLE Time Session Required 9:30 Visiting team meet and final briefing Visiting team 10:00 10:30 Meet faculty to discuss faculty development DME/CT/FTPD/MEM 10:30 11:45 Meet F1 doctors1 As many F1s as possible 11:55 13:10 Meet F2 doctors1 As many F2s as possible 13:10 13:40 LUNCH - 13:40 14:40 Meet focus group of hospital faculty leads/foundation programme directors/educational supervisors FTPDs/educational supervisors (rep from each dept if possible) 14:45 16:00 Collate information and prepare feedback Visiting team 16:00 Feedback session LEP Chief Executive/DME/ MEM/Medical Director/ FTPD Notes Additional Issues Page 1 of 1 Updated 18 TH April 2012
133 Appendix 1 Kent, Surrey & Sussex Deanery QUALITY MANAGEMENT OF SPECIALTY TRAINING Local Education Provider Specialty Visits - Headline Feedback Form The purpose of this form is to provide the LEP with a record of the brief headline verbal feedback given to senior LEP representatives at the end of the visit, and provide KSS with evidence of acknowledgement by the LEP of the main headlines arising from the visit. Any areas requiring immediate action by the LEP will be noted on this form and communicated to the senior LEP representatives. In addition to this, the CEO and DME will be contacted by the KSS Dean Director via by the following day. A detailed report will follow in line with the KSS LEP Visiting Procedure. The report may contain other areas of notable practice and improvement in addition to those listed below. All notes should be entered on this form, which should be signed by the senior LEP representative and the Lead Visitor after the verbal feedback is given. Once completed and signed, a copy of the form should be left with the LEP senior representative, and the original should be forwarded to: quality@stfs.org.uk LEP Visited Date of Visit Areas of Notable Practice Domain Page 1 of 2 Updated: 30 th January 2012
134 Areas for Improvement Domain Areas Requiring Immediate Action (Dean Director to be notified immediately) Domain Signed by Lead Visitor and Senior LEP Representative Position Name Signature Page 2 of 2 Updated: 30 th January 2012
135 Page 3 of 2 Updated: 30 th January 2012
136 Version 1.3 LOCAL EDUCATION PROVIDER PHARMACY VISITING PROCEDURES This document describes the procedure for Kent, Surrey and Sussex Postgraduate Deanery (KSS) visits to pharmacy departments in KSS Local Education Providers (LEPs). 1. Types of Visit There are 3 types of visits which may be made to LEPs dependent on the issues and risks:- 1. Annual verification and contract review visit 2. Developmental visit 3. Exception visit 1.1. Annual verification and contract review This is an annual process by which the Deanery reviews that the infrastructure to deliver quality pharmacy education and training is in place. The Deanery outlines a list of quality standards based on and mapped to the General Pharmaceutical Council s Standards for the Initial Education and Training of Pharmacists. Local Education Providers compile a Quality Manual which outlines procedures to ensure these standards are met and evidence to support this. In addition to this LEPs undertake an annual audit and review of their own practice against the GPhC education and training standards. Both the Quality Manual and Annual Audit and Review are submitted to the Deanery at the end of March each year. The Quality Manual content is subsequently checked during a verification visit scheduled between April and June. The findings from verification are reported and discussed at the subsequent Contract Review meeting held in May/ June each year. 1.2 A developmental visit will take place when:-: Concerns are raised through trainee surveys either by a majority of trainees or continued trends over 2 years or more have not been addressed LEP annual audit and review indicates issues that are not being addressed locally actions from contract review or annual audit and review remain unactioned over more than one year LEP reporting to the Deanery has consistently not occurred eg workforce numbers, identification of trainees in difficulty, trainee attrition This document was printed on 08/10/2012 at 15:38:23. Before using this document, please ensure you have the latest version by checking it against the Document Control Log located at: K:\Quality Management\QM Documents\Master Documents.
137 consistently low trainee progression or high attrition non compliance with Deanery: Trust Placement Agreements the LEP has requested advice or analysis of local pharmacy education and training (subject to available resources) The process for developmental visits is that the issue arising will be documented by the Head of Pharmacy and a request for a developmental visit sent to the Dean Director. If the need for a visit is agreed the KSSD Associate Dean for Quality and Quality Manager will be informed immediately and the QMSG at the next meeting. 1.3 An exception visit will take place when there is/ are:- a serious trainee complaint which raises a question about current training that cannot be managed through usual mechanisms Concern over potential patient safety / risk issues that require further investigation eg identified through o o o o Whistle blowing / concern raised LEP annual audit and review A serious untoward incident, which may or may not have involved a pharmacy trainee but might have implications for training Risks raised through other reporting mechanisms eg compliance with HCAI, aseptic audits that could impact upon the quality of training issues identified in a developmental exception visit that have not been resolved in reasonable timescales and need escalation. issues identified as high risk and require a level of clinical externality outside of the Deanery. The process for exception visits is: issues arising will be reviewed by the Dean Director and the Head of Pharmacy If there is evidence of serious concern the Dean Director will make a decision for a Deanery visit and will inform the next meeting of the Quality Management Steering Group. if there is a chronic problem or there are other factors to be taken into account and it is less pressing, the matter will usually be discussed at the Quality Management Steering Group meeting before a decision is made; if it is decided that an exception visit is required, the Dean Director will inform the LEP CEO and will instruct the QMD and Head of Pharmacy to prepare for a visit. 2. Organising the Visit The KSSD Pharmacy Department will liaise with the Trust Chief Pharmacist to inform them of the level of visit and agree a date. The KSSD Pharmacy Dept will ascertain who should take part in the visit, and will invite them accordingly, making arrangements for travel where necessary. As each visitor confirms attendance, the Pharmacy Dept will record and store confirmation and contact details. 2
138 3. The Visiting Team The visiting team will depend on the level of visit. 3.1 Verification Visits and Contract Review Verification will always be carried out by 2 verifiers. The lead verifier will be a member of the KSSD Pharmacy Department. The second verifier will be either a member of KSSD staff or a Pharmacy Educational Programme Director from another LEP. Occasionally an observer will also be present observers will generally be either KSSD staff or EPDs training to be verifiers. Contract Review visits will discuss all aspects of Deanery education i.e. medicine, dentistry, libraries and pharmacy. The Pharmacy representative will be either the Head of Pharmacy or a senior member of the KSSD Pharmacy team registered with the General Pharmaceutical Council. 3.2 Developmental visits A developmental visit team will comprise the following members: Visitor Head of Pharmacy, KSS Deanery 1-2 senior KSSD Pharmacy staff. Occasionally other LEP EPDs will act as visitors dependent on the nature of the visit e.g. if they can bring additional specialist expertise in an area. Responsibility Lead Visitor. Broad pharmacy context. Reporting systems and processes. Lead for own specialty. Broad practice context. Reporting systems and processes. Occasionally there will be observers who will normally be future visitors in training Exception visits An exception visit will comprise:- Visitor Head of Pharmacy, KSS Deanery 1-2 senior KSSD Pharmacy staff. Occasionally other LEP EPDs will act as visitors dependent on the nature of the visit e.g. if they can bring additional specialist expertise in an area. Trainee Representative (to be dictated by QMSG) External or Lay Visitor (to be dictated by QMSG) Responsibility Lead Visitor. Broad pharmacy context. Reporting systems and processes. Lead for own specialty. Broad practice context. Reporting systems and processes. Trainee context / voice. Provide externality. 3
139 4. Visitor Training Potential future visitors without previous visiting experience will be expected to attend training sessions organised by KSS. In addition they must attend at least one QM visit in an observational capacity in order to gain experience of visits. Visitors with previous experience of visiting elsewhere will be expected to familiarise themselves with the KSS visiting procedure before the visit. All visitors are required to sign the KSS Visitor Guidance and Declaration (QMV-FOR-001) before taking part in a visit. This will be sent to each visitor by the KSSD Pharmacy Department who will keep a record of the signed declarations. 5. Role and Requirements of Visitors The role involves visitors seeking to gather evidence-based information that will be used to express an opinion on the LEP s ability to ensure that the curriculum is being delivered by qualified trainers to all trainees within the LEP. This will involve verifying that robust quality control processes are in place and are followed, which allow for pharmacy trainees to be trained in an environment that provides for their needs and consequently benefits patients. During the visit, the visitors will interview trainees and trainers in order to gather additional information about the training environment and curriculum delivery, triangulate this with other sources of data such as trainee exit data, contract review reports, previous visits, etc. It is essential that the trainees and trainers feel confident that the information they communicate will be handled appropriately and confidentially. 6. Externality In any full exception visit, there must be external input involving independent and impartial advisers. External advisers may be registered pharmacy professionals or lay, depending on the area for advice and/or scrutiny. They must be independent of the Deanery with no conflicts of interest. Pharmacy advisers will have expertise appropriate for the programme and will normally be either experienced Education Programme Directors or Academic Programme Directors. 7. Pre-visit Arrangements The LEP Pharmacy Education Programme Director will usually be the visit coordinator, acting as the liaison point between the KSSD Pharmacy and the LEP, disseminating details of the visit within the Pharmacy Department. This task will sometimes be delegated to an Assistant Manager or Administrator within the LEP. The KSSD Pharmacy Department will be the single point of control at KSS for any matters regarding visits. It is essential that all communications regarding visit arrangements between KSS and the LEP go through the Pharmacy Team and the LEP Pharmacy EPD (or nominated visit coordinator for the LEP). 8. Pre-visit Documentation - The Bundle Each member of the visiting team is sent an with a link or attached bundle of documents comprising information from various sources about the LEP and the specialties being visited. The bundle of documents is collated by the Pharmacy Department at least 3 weeks before a visit. For a verification visit, visitors will be sent :- 4
140 LEP Quality Manual LEP Annual Audit and Review Contract Review action plan from the previous year Trainee feedback from the previous year Guidance on deep dive focus for verification where applicable For developmental and exception visits, a typical bundle will contain the following documents: Contract Review Action Plan LFG Annual Audit and Review Last 3 LAB minutes received from Trust Last 3 LFG minutes received from Trust Most recent trainee survey data Background to the purpose and reason for the visit 9. Visiting Team Pro Forma Evidence for the delivery and support of appropriate education for trainees will be obtained from a number of sources. The Visiting Team Pro Forma helps the visitors to review the bundle of documents and identify areas where further exploration is required. It is set out under three sections; notable practice, areas of concern and areas for clarification/further investigation. Each visitor will be asked to complete a pro forma in advance of the visit and bring it with them on the day. 10. GPhC Standards for the initial education and training of pharmacists These are the set standards against which the visiting team needs to report, published on the GPhC website. As the visitors review the bundle, they use this document to help them focus on key areas and ensure adequate coverage of key issues. The GPhC Standards are set out under ten Domains: 1. Patient and public safety 2. Monitoring, review and evaluation of initial education and training 3. Equality, diversity and fairness 4. Selection of trainees 5. Curriculum delivery and the student experience 6. Support and development of trainees 7. Support and development of academic staff and preregistration tutors 8. Management of education and training 9. Resources and capacity 10. Outcomes In developmental visits there may be a focus on specific standards and therefore not every standard might be looked at. In exception visits, all standards will be covered. 12. The Visit At verification visits, the visiting team will focus on verifying that procedures are in place to ensure compliance with GPhC education standards and that there is evidence to support this. The LEP Pharmacy Education & Training Lead must be available throughout the verification visit and should expect to be part of it. It will also be helpful but not essential for the relevant Education Programme Directors eg Preregistration Pharmacist Training Manager, Preregistration Pharmacy Technician Training Lead, NVQ Internal Verifier or PG Diploma EPD to be available if required. 5
141 In developmental and exception visits, the documentary evidence will be triangulated using interviews with trainees and those delivering and facilitating the training. The visit will include structured focus group discussions with: Trainees in hospital posts Education Programme Directors Educational Supervisors Practice Supervisors On the day of the visit, the visiting team should have a private meeting to divide up tasks, go through the list of issues identified as being of interest, set rules for the day, refresh understanding of the GPhC Domains, and ensure that all are clear about the division of responsibilities between members. For example, different team members can lead on asking questions in different meetings. It is usual for the Lead Visitor to start the questioning and to summarise where appropriate. At the opening meeting the Lead Visitor should ensure that the LEP understands the visit process, is fully aware of the timescales and activities to be undertaken and is clear about the information requested. The Lead Visitor should communicate to the LEPs that the visit is an opportunity for them to show how well they are doing as well as to explore matters of particular concern. 13. Meetings with Trainees (Developmental and Exception visits only) The visit timetable should be constructed to include meetings with trainees. The Team should aim to meet a wide range of trainees, including trainees on different placements, trainees in difficulty, etc. Trainees should be assured of confidentiality by the Visiting Team at the beginning of each meeting. Trainees should be offered an opportunity to meet any member of the Visiting Team one-to-one should this be required. 14. Meetings with Educational / Practice Supervisors (Developmental and Exception visits only) The ESs will usually be seen together as one group. The purpose of these meetings is to discuss the ESs experience of training-related issues. Whilst the visitors may wish to explore areas raised during the meetings with the trainees, this session should not include any direct feedback from those meetings. PSs may be seen as a group or occasionally individually if a specific placement is being reviewed. 15. Feedback Preparation Meeting The Visiting Team will meet in advance of the feedback session to discuss their headline findings, both in terms of notable practice and areas for improvement. These should be noted in brief bullet points on the feedback form. The purpose of the feedback form is to provide the LEP with a record of the brief headline verbal feedback given to senior LEP representatives, and provide KSS with evidence of acknowledgement by the LEP of the main headlines arising from the visit. The Visiting Team should agree any issues that the LEP has to address immediately, which would primarily relate to service issues affecting patient and trainee safety, and note these on the feedback form. The Visiting Team should ensure that all findings are based on clear evidence. 6
142 16. Feedback Session At the end of the visit, brief headline verbal feedback, as encapsulated in the feedback form, will be given to the senior LEP representatives, usually the Chief Pharmacist or Pharmacy EPD. Any areas requiring immediate action by the LEP, particularly where patient and/or trainee safety is compromised, will be communicated to the senior LEP representatives. In addition to this, the CEO will be contacted by the KSS Dean Director via by the following day. The senior LEP representatives should be informed that the visit report may contain other areas of notable practice and improvement in addition to those listed on the feedback form and communicated verbally. 17. Writing the Visit Report The first draft of the visit report should be written by the visiting team, coordinated by the Lead Visitor, immediately following the visit. All members of the visiting team, including lay and external representatives, are expected to contribute to the KSS visit report, to be agreed by all visitors. It is essential that visitors do not produce supplementary reports or other documents that make reference to the visit, without the express permission of the Dean Director of KSS Deanery Verification reports consist of a checklist of Quality Manual standards as well as notes of good practice and issues ro be taken forward and discussed at the forthcoming Contract Review meeting. The report will be sent to the KSSD Education Department for inclusion in the wider bundle of Contract Review documents covering medicine, dentistry, libraries and pharmacy. Contract Review bundles are administered and circulated by the Education Department. Responsibility for the production of the Contract Review report and action plan rests with the KSSD Education Department. The Pharmacy Lead Visitor will be responsible for producing a summary of points agreed in relation to pharmacy which will be included in the report and for checking its accuracy within the final report. The Education Department will circulate the action plan to the LEP Developmental and Exception visits are recorded on a Visit Report Template, which is set out under the 10 GPhC Domains. The full report must follow the KSS Deanery reporting template and include: the detail of the visit (the name of the LEP, details of the Visiting Team, etc.) the percentage of trainees who attended the visit LEP performance under each Domain specific examples of notable practice specific concerns indicating the evidence mandatory requirements for action with details of evidence required and suggested deadlines for correction recommendations with suggested deadlines The content of the draft and final visit reports should include issues encapsulated on the Feedback Form and communicated in verbal feedback. Section 2 of the report (Findings against GPhC Standards) should only contain matters of (reported) fact, and should not include the opinions or suggestions of the visitors. All Mandatory Requirements and Recommendations made in Section 4 of the report will be referenced back to the findings in section 2. 7
143 The Visit Secretary will circulate the draft report to all members of the visiting team for approval. The Visit Secretary will amend the draft report as suggested by the visitors and forward it to the Quality Manager no later than 5 working days from the date of the visit. 18. Progressing Developmental and Exception Visit Reports The Quality Manager will check and amend the report as necessary, and forward to the Associate Dean for Quality (ADQ) for a consistency check. The ADQ will make any necessary amendments and return the draft report to the Quality Manager for final formatting. The draft report will also be sent by KSSD Pharmacy to the Chief Pharmacist and Pharmacy EPD for a factual accuracy check. The Chief Pharmacist should receive the draft report no later than two weeks from the date of the visit. The Quality Manager will submit the report (with any amendments suggested by the Chief Pharmacist) to be reviewed and formally approved at the subsequent meeting of the KSS QMSG, which meets monthly. These meetings are chaired by the Dean Director and attended by the KSS Heads of Schools and Head of Pharmacy. Following approval by the QMSG, the final report will be sent to the CEO (copied to the Chief Pharmacist, Pharmacy EPD and other relevant stakeholders) together with a pre-populated Action Planning Template, drawn up from the requirements and recommendations in the report, to facilitate the response. The LEP will be asked to complete the action plan as part of their response to the report findings. Final reports will usually be sent out within six weeks of the visit. 19. Follow-up and Sign-off 19.1 An audit trail of responses to a Contract Review action plan in the form of a tracking chart will be kept within the KSSD Pharmacy Department and reviewed at 3 monthly intervals. If an action is not completed, a reminder will be sent. If an action continually remains outstanding, this may trigger a developmental visit An audit trail of responses to the developmental and exception visits, in the form of a tracking chart will be kept by the Quality Manager, who ensures that all actions are followed up and all requested evidence is provided to the QMSG. Any change in practice suggested that relates to a mandatory requirement will be followed up by the QMSG. Recommendations are suggestions that should be considered by the LEP. These are not followed up by the QMSG; however, the LAB should discuss with the Pharmacy LFG what actions have been taken on any recommendations. This may then be reported to the QMSG by the LAB when responding to visit reports and will be discussed and monitored by the relevant KSS School. All responses to mandatory requirements are reviewed and signed off by the QMSG. When all mandatory requirements are met, the Dean Director will confirm this formally in writing to the CEO. Once the report is signed off, the notable practice and mandatory requirements will be published on the KSS Deanery website together with the response(s) from the LEP and the formal sign-off date. 8
144 20. Document Control Title: Originator: PHARMACY EXCEPTION VISITING PROCEDURE Gail Fleming, Head of Pharmacy Date Issued: March 2012 Review Date: March
145 Kent, Surrey & Sussex Deanery Action Plan for Visit Reports - Pharmacy LEP Name: Visit Date: The following mandatory requirements relate to the GPhC Standards for Pharmacy Education and Training, and must be addressed by the LEP. All actions to address mandatory requirements will be followed up by the KSS Quality Management Steering Group (QMSG). No. Mandatory Requirements Standard Actions/Evidence Required Deadline Progress Further Action Planned The following recommendations are suggestions that should be considered by the LEP, but do not relate to mandatory standards. These are not followed up by the QMSG. However, the LAB should discuss with the LFG whether or not actions should be taken on any recommendations. This may then be reported to the QMSG when responding to visit reports and will be discussed and monitored by the KSS Pharmacy Department. No. Recommendations Standard Comments
146 Doc 1 KSS GP School Guidance on the Quality Management of GP Specialty Training in the KSS Deanery This guidance is intended for GP Specialty Programme Directors, GP Trainers, Medical Education Managers, GP Faculty Administrators and GP Training Practice Managers, but will be also helpful for GPStRs, to inform them about the context and procedures of the GP Faculty visiting process and will inform those acting as visitors and those being visited. The rationale for quality management The GMC is the statutory organisation responsible for the delivery of good quality medical training and education for all doctors in postgraduate specialty training. It sets criteria for the delivery of training, and for trainers, and approves specialty curricula. It is the body that approves GP training programmes and posts and GP Trainers, and has approved the GP curriculum. GP training is carried out in environments such as hospital and GP Training Practices, which are referred to as Local Education Providers (LEP). It is the responsibility of LEPs, and their GP Faculties (local units of the GP School) to ensure a process of quality control is in place. The Deanery is charged by GMC with the task of quality managing the quality control in all locations, and the GMC will undertake a series of processes, including visits to Deaneries, to quality assure medical education in the UK. The KSS Deanery provides guidance to all Trusts and Educators and sets out the structure of Quality Management in the Deanery in the form of the Graduate Educational and Academic Regulations (GEAR) As part of its quality management, the KSS Department of General Practice Education will seek to gain information about the delivery of GP Education and training from a number of sources including a rolling series of visits to each Trust and GP Local Faculty Group. The purpose of the visit is to review the provision of education for doctors in training against the standards set by GMC. This process is looking not just at the educational experience of GPStR doctors in hospital posts but how the local faculties support the process and in turn are supported. The visiting process is collaborative involving both Secondary, Education and General Practice Departments and all specialty schools. The visit will aim to celebrate notable practice, investigate areas of uncertainty and be formative in exploring how educational provision can be improved in any locality. In doing so, it will allow the Deanery to confirm that the GMC criteria for training and trainers are being met. Where areas of concern are identified these will be fed back to the Trust and the Local Faculty Group for action. The GMC criteria (domains) will be the common context of all parts of the visiting process and should be familiar to educators and the visitors. These form the backbone of the GP Trainer Selection evidence and also the KSS Deanery Graduate Educational and Academic Regulations (GEAR) for local Faculties and the Local Academic Board. They are available from the GMC website: and in brief are:- Domain 1: Patient safety Domain 2: Quality Assurance, Review and Evaluation Domain 3: Equality Diversity and Opportunity Domain 4: Recruitment, selection and appointment Domain 5: Delivery of curriculum including assessments Domain 6: Support and development of trainees, trainers and local faculty Domain 7: Management of Education and training Domain 8: Educational resources and capacity Domain 9: Outcomes KSS GP School QM process v.5 Page 1 of 12 Revision Date: August 2012
147 IMPORTANT NOTE FOR GPSTRS This process is about the educational support GPStRs are being given, and is NOT about their performance or progress in GP training. Appendix 4 is a letter that you may provide to your Trainees advising them about the visit. The Process This involves two parts. 1) Annual documentation check An annual information pack to be submitted by each GP LFG to consist of the following: LFG minutes and annual report to the LAB (AAR) will should incorporate: Reflection on GMC survey results Reflection on on-line Trainee Survey Feedback MRCGP examination results report (CSA, AKT and WPBA) ARCP results of all GPStRs in LFG Record of attendance of PDs at PD conferences / workshops Record of GP Trainer attendance at GP Trainer Days / Workshops Attendance registers of GP ST1/2/3 at teaching sessions Number of GPStRs defined as being in difficulty Details of Half-Day Release Course (GPStR learning sets) including dates and topics Any comments by locality PAD after reviewing LAB annual report to the Deanery Final report approved and submitted to Head of School (HoS) for sign-off. Any concerns raised will need to be explored by the HoS with the locality GP Patch Associate Dean (PAD) and GP Programme Directors (PD) if needed in order to determine what further action may be necessary. This further action may include a Deanery Exception Visit to confirm and validate any concerns. For further information please see Appendix 5. 2) 3-Yearly Routine Visit to each LEP Each GP Training Programme will be visited on a scheduled rolling programme. Large Training Programmes with more than one centre (East Kent, Brighton and Mid-Sussex, East Sussex, Maidstone and Tunbridge Wells) will rotate the visit location every three years. These visits will be timed to link with the regular Deanery Quality Management visits to LEPs for the appropriate area. This means that not all KSS Deanery Specialty School quality management visits to Trusts will include GP. Where the GP Faculty is being visited, the Visit process will take place on two days: in some cases these are consecutive days in others they are separate. If there are no GPStRs in the hospital specialty posts being visited on the second day, then there will be no need for the GP visitor to interview the specialty GPStRs. The GP visitors will obtain information from a number of sources, which include Faculty documentation, ARCP outcomes, GMC survey results, GPStR feedback from departmental on-line surveys and from direct discussion with GP educators (including hospital consultants) and GPStRs. Thus the visitors meeting with individuals are only one part of the whole process. The arrangements and organisation for the first day (GP) will be organised through the GP Department and queries concerning these arrangements will be answered by the relevant GP Patch Manager. All GP visits will run over two days, but not all Deanery Quality Management visits to Acute Hospital Trusts (LEPs) will include GP. KSS GP School QM process v.5 Page 2 of 12 Revision Date: August 2012
148 Day 1 Visit to the local GP Faculty which will involve visiting a local practice selected to represent the Faculty. This will be followed by meetings with the ST3 GPStRs and any ST1 and ST2 GPStRs currently in General Practice. The visiting team will also meet with local Trainers, Practice Managers and GP Programme Directors. Where possible this meeting will be held in a suitable GP Practice (which does not have to be the same practice as that visited). Before the visit: The local GP Programme Directors, working with the MEM or GP Faculty Administrator, will need to inform the local GP Trainer Group, and the group of GPStRs in GP placements (this will be mainly ST3 GPStRs, but will also include ST1 and ST2 doctors in GP placements, including Integrated Training Posts) of the dates and times of the meetings for the discussion groups. No preparation for these meetings will need to be done by GP Trainers or GPStRs. One GP Training Practice will, via local negotiation, need to be identified for visiting by the team of visitors. Prior to the visit, Programme Directors may be contacted by administrative lead in the GP Department (normally the Patch Manager) to provide some documentation relating to the visit if they do not already have the information. The relevant data includes: The Local Faculty Handbook that has been developed Minutes of Local Faculty Group meetings GP LFG Annual Audit and Review (AAR) Any other data which GP Faculty members locally represents good practice (for example initiatives from the GP Trainer group, the half-day release programme for GPStRs) Programme Directors do not need to specifically prepare anything for the visit, but copies of relevant documentation would be very useful to have to hand. The suggested timings of the day are given below outlining the visit programme. The timetable will be finalised in discussion with the GP Patch Manager for each locality and the GP Lead Visitor and Medical Education Manager (MEM) for the Hospital or Psychiatric Trust as this may be changed to meet local needs. The GP Patch Manager will confirm the final arrangements. Duration Session 30 minutes GP Visiting team meet for briefing 1.5 hours Practice Visit including discussion with practice members in groups, visiting team de-brief and verbal feedback to Trainer and practice team Up to 1 hour Travel/Lunch if required (depending if staying in first location or need to travel) 45 minutes Meet group of GPStRs (ST3 s and include ST1 and ST2 doctors in GP placements, including Integrated Training Posts) 15 minutes Tea break 45 minutes Meet group local GP Trainers and Practice Managers 45 minutes Meet GP Programme Directors for discussion and feedback 30 minutes Visiting Team Review visit and to start to write report 6 hours Total Visit time KSS GP School QM process v.5 Page 3 of 12 Revision Date: August 2012
149 A full visiting team will consist of: Patch Associate GP Dean from a different patch (Lead Visitor) GP Training Practice Manager from a different patch A GP Programme Director from a different patch (to provide an external input) A GPStR (preferably one who is in, or who has experienced training in a Practice placement) These visits form an excellent opportunity for GP Programme Directors to have the ability to observe and learn from their colleagues in different areas, and will provide evidence and learning opportunities for their personal development plans as Programme Directors. Evidence for each of the GMC domains will be sought from a variety of sources, as previously described, and discussion and questions will also relate to these domains. Specimen examples can be found in Appendix 1 attached to this document. You may find it helpful to visit the GMC website and refer to the section on generic standards for training and the section on standards for trainers. Guidance to the GP Training Practice visit is described in Appendix 2. GPStRs will need to ensure that they are familiar with the guidance to visits. Day 2 is a visit to the Acute Trust. Unless the Trust (LEP) is included in the GP Training Programme area that is being visited, GP will not be involved in this. If GP is involved, only the Lead GP Visitor (PAD) will be involved. This is the day in which the other Specialty Schools have the opportunity to meet with their trainees and their Supervisors in hospital posts. In each case a number of specialties will be reviewed in detail (including higher level training specialties) and if these specialties include GPStRs (in ST1 and ST2 at the time of the visit) at that location, they will be interviewed by the GP visitor/s if that LEP is also being visited for GP. Note: If there are no substantive posts used for GP training in those specialties, but the LEP is being visited as part of a GP visit, the GP visitor will support the process of the Quality Management visit, which may mean if appropriate, acting as the Lead Visitor. The roles and responsibilities of GP visitors are described in Appendix 3. Psychiatric Trusts will have separate visits as a result of their different geographical locations and they may include a GP visitor, as this specialty hosts a significant number of GPStRs who may not always manage to make the first day of a GP LFG visit. The organisation of the 2 nd day will be carried out by the KSS Deanery Quality Manager, who will liaise with the Trust via the Medical Education Manager, and ensure that the necessary documentation is shared with the GP visitor (normally accessible via a weblink). KSS GP School QM process v.5 Page 4 of 12 Revision Date: August 2012
150 An example timetable of the day is given below (the actual timetable will be the responsibility of the KSS Quality Manager and will vary according to the number of specialties being visited):- Time Session 09: Visiting Team Briefing The team meets with the Trust for final briefing session :30 Faculty Leads Meet the DME, MEM and Faculty Group Chairs (from each of the specialties being visited) as one group to discuss key issues Trainee Interviews by Specialty Coffee break Trainee Interviews by Specialty Lunch Visiting Team Review The Visiting Team meets as a group to collate information and prepare for verbal feedback Feedback session The Visitors provide brief verbal feedback to the CEO (or delegated deputy), DME and MD. Any patient safety issues must be reported and documented Report Writing The Visiting Team writes the first draft of the visit report as a group and agrees mandatory requirements and recommendations. The visiting Patch Associate GP Dean will be present only if the GP LFG is being visited at that Trust LEP, and most of the GP information will have been gained on the first day of the visit. For this day at the Trust the GP visitor will not need to meet any of the GP Educators again but at least one of the local team of Programme Directors will need be available to hear the feedback from the visitors at the end of the visit, and ideally, if possible, the Patch Associate GP Dean responsible for that area. Feedback will be given by the whole team of visitors to the Faculties and LAB in the PGMC, and will relate to the overall provision of educational support at the LEP, highlighting good practice, as well as areas for improvement in the mandatory and developmental criteria in the GMC domains. Any issues that may arise during a visit concerning GP training posts in hospital specialties that are not being formally assessed (i.e. are not any of the specialties being visited) will not be raised in the formal feedback session, but will be fed back directly to the Patch Associate GP Dean for that GP Training Programme in order to validate and resolve locally if necessary, and will not form part of the final report. The GP report will be written using the KSS quality visit report template and will relate only to the GP placements, outcomes for GP training, and the management of the GP LFG, and the learning sets, using information gathered from both days of the visit, (or from just one if there are no hospital posts to visit) and the other evidence. Issues relating specifically to specialty posts used for GP Training will be reported on only if those specialties form part of those visited on the second day. The report will be sent to the Head of the GP School and also to the specialty workforce team member who is writing the report for Secondary Care. The specialty workforce manager will combine the reports for all into the unified and integrated report which will be returned to the Deanery Quality Manager in order to then be sent to be checked for accuracy with the Trust being visited, before going to the KSS Deanery Quality Management Steering Group (QMSG). Once this is signed off by the KSS QMSG, a copy will be sent to the visited Trust with the action points. The action points will have a timescale for the LEP to address and report back on. Community issues related to general practice will be addressed by the local GP education network with reporting mechanism through the local LAB KSS GP School QM process v.5 Page 5 of 12 Revision Date: August 2012
151 APPENDIX 1 Specimen Questions Visitors may ask Programme Directors at a Faculty Visit (NB, as described above, answers to these questions will also be sought and may be provided from the other sources of evidence. These are suggested questions to help visitors that would address the GMC domains and are not considered comprehensive, exclusive, or mandatory As a result of other information visitors may consider is necessary to prioritise particular areas.) o o o o o o o o o o o o o o o o o o o o o o o o o o o Give an overview of the local faculty (hospital posts, VTS, GPStRs, trainers, the Trust LFG) good practice, developments your concerns Do you have any concerns about the working environments of GPStRs enrolled in the programme in either hospital or GP placements? Do you have any concerns about supervision in OOH training and in hospital placements? How informed are you about the wider guidance and criteria fro GP training posts? How aware are you of the GEAR guidance? How does the LFG monitor the quality of training? How does the VTS deal with issues of equality and diversity? How has the VTS dealt with any examples of direct or indirect discrimination? How do you advise GPStRs about the posts they will work in and what information do you give them? Do you know about or how to get information on sickness, maternity leave, training less than full time? How have you kept up to date with the recruitment process? How is local allocation arranged how much are GPStRs involved? How do you use feedback from the recruitment process? How have you inducted GPStRs in to all aspects of GP specialty training? How do you work with the Trust to ensure experiences relevant to the GP curriculum are delivered? How have you supported clinical supervisors in understand the WPBA assessments? How do you support doctors seeking career guidance for entry to general practice and for their future careers? How study leave is arranged locally any concerns? Are you aware of any GPStRs being bullied? How has the LFG been established? How do you ensure ST1 2 3 participation in the LFG? How does the LFG support local trainers? How have you dealt with any GPStRs in difficulty? How are you supported by the PGMC? How have your current cohorts performed in MRCGP? How do you gain feedback from GPStRs and how has this influenced your VTS? How do you manage the educational needs of the group? Similar questions will be asked of the GP Trainer group and GPStR group met by the visitors KSS GP School QM process v.5 Page 6 of 12 Revision Date: August 2012
152 Specimen questions visitors may ask the GP Trainer group at a GP Faculty Visit (NB, as described above, answers to these questions will also be sought and may be provided from the other sources of evidence. These are suggested questions to help visitors that would address the GMC domains and are not considered comprehensive, exclusive, or mandatory) o Give an overview from your perspective of how the local faculty (hospital posts, VTS, GPStRs, trainers, the Trust LFG) supports GP Specialty training. Do you have examples of good practice in your own Practice (or across the area) or concerns. o What is the experience of organizing clinical supervision of GPStRs in your Practices? o How does the Trainer group share issues or concerns about patient safety relating to any GPStRs? o Do you have any concerns about OOH training for GPStRs? o How informed are you about the wider guidance and criteria fro GP training posts? o How aware are you of the GEAR guidance? o How much do you know about the activity of the Local GP Faculty group (LFG)? o Do you attend GP LFG meetings? o Has the Trainer group dealt with any issues of equality and diversity in GP training? o Have you all had E&D training. How useful has this been? o Do you know about, or how to get information on, sickness, maternity leave, training less than full time for GPStRs? o How have you kept up to date with the recruitment process? o How do you use feedback from the recruitment process? o How much has the local Faculty / Programme Directors / Associate Dean supported you? o How have you shared good Practice for GPStR induction for GPStRs? o How do you work with GPStRs to ensure experiences relevant to the GP curriculum are delivered? o How have you supported GPStRs in understanding the WPBA assessments? o What is going well / or is difficult with MRCGP? How could it be improved? o How have local study leave arrangements worked? o How have you found the Educational supervisor role? o Have you had examples of where handover of a GPStR from each department to you has worked well / been problematic? o How do you use the Trainer group to involve and support others in your Practice involved in teaching GPStRs? o How has the Trainer group / Deanery supported your professional development? o How has the Faculty supported approval and re-approval for GP Trainers? o Are you aware of any GPStRs being bullied? o Have you had any GPStRs in difficulty? How have you and the GPStR been supported? o How do you ensure ST1 2 3 participation in the LFG? o How does the LFG support local trainers? o How have you dealt with any GPStRs in difficulty? o How do you access and use other educational resources locally? KSS GP School QM process v.5 Page 7 of 12 Revision Date: August 2012
153 APPENDIX 2 Guidance for a GP Training Practice being visited on the GP Faculty Visit GP Trainers and Training Practices are approved and re-approved in the KSS Deanery via a separate formal, evidenced process. This visit, which forms part of the Local GP Faculty quality inspection, is not meant to replicate that process, but is intended to gain further information to support and triangulate that obtained in other areas of the visit. GP Trainers and their Practices are not required to make any special preparations for the visit, apart from the practicalities of having appropriate members of the team available for the time. It is important that the information obtained from this part of the overall visit, is related to that obtained from the other sources of information. The visit provides an opportunity for visitors to informally feedback on aspects of good practice, and illuminate areas where the Trainer/s and the Practice team could consider development. Individual members of the visiting team will interview individuals in the Practice Organisation to gain this information, and a suggested scheme is described below. The visit, and the visiting team, will be coordinated by the Lead Visitor who will normally be a Patch Associate GP Dean from another area and who will have responsibility for the conduct and timetabling of the visit. Visiting team member and team members to be seen o Patch Associate GP Dean from another patch (Lead visitor) o GP Training Programme Director from another GP Training Programme o GP Training Practice Manager o GPStR from another GP Training Programme. The lead visitor should ensure that they and the other visitors are familiar with any documentation relating to the Practice (particularly the previous visit report, if any, GMC trainee surveys, and previous GPStR feedback on placement). The lead visitor should take a few minutes with the other visitors at the start of the visit to raise any particular issues that may have been indicated from the documentation or from the discussions with other groups earlier in the day, and to determine the timetable for the visit (this could be done just before leaving the Medical Education Centre, or on the journey if possible). The visit will just involve the visitors talking to the different individuals in the Practice and will not normally involve the assessment of other evidence, unless the visited Trainer and Practice wish this to be considered. Suggested timetable Visitors arrive at Practice Introductions and explanation of process 10 minutes Visitors split into groups to speak to different individuals 60 minutes Visitors meet to share and collate information 15 minutes Lead visitor gives brief verbal feedback to visited Trainer and their team 10 minutes Practice Visit concludes Total time approximately 90 minutes There will be no specific report created for the Training Practice visit, as the information gained will form part of the final Faculty report. KSS GP School QM process v.5 Page 8 of 12 Revision Date: August 2012
154 Specimen Questions Visitors may ask Trainers at a Faculty Visit o Give an overview from your perspective of how the local faculty (hospital posts, VTS, GPStRs, trainers, the Trust LFG) supports GP Specialty training. Do you have examples of good practice in your own Practice (or across the area) or concerns? o How do you arrange clinical supervision of GPStRs in your Practice? o Do you have any concerns that GPStRs in your Practice are exposed to situations that compromise patient safety? o Do you have any concerns about OOH training? o How informed are you about the wider guidance and criteria for GP training posts? o How aware are you of the GEAR guidance? o How much do you know about the activity of the Local Faculty group (LFG)? o Do you attend LFG meetings? o How does the Practice dealt with issues of equality and diversity? o How has the Practice dealt with any examples of direct or indirect discrimination? o How have you used your Equality and Diversity training? o Do you know about or how to get information on sickness, maternity leave, training less than full time? o How have you kept up to date with the recruitment process? o How is local allocation arranged how much are GPStRs/ trainers involved? o How do you use feedback from the recruitment process? o How much has the local faculty / Programme Directors / Associate Dean supported you? o How have you inducted GPStRs? o How do you work with GPStRs to ensure experiences relevant to the GP curriculum are delivered? o How have you supported GPStRs in understand the WPBA assessments? o What is going well / difficult with MRCGP? How could it be improved? o How have others in the Practice been made aware of the GP curriculum? o How have you prepared the team for undertaking multisource feedback? o How has local study leave arrangements worked? o How have you found the Educational supervisor role? o Have you had examples of where handover of a GPStR from each department to you has worked well / been problematic? o How do you involve and support others in your Practice involved in teaching GPStRs? o How has the Trainer group / Deanery supported your professional development? o Are you aware of any GPStRs being bullied? o Have you had any GPStRs in difficulty? How have you and the GPStR been supported? o How do you ensure ST1 2 3 participation in the LFG? o How does the LFG support local trainers? o How have you dealt with any GPStRs in difficulty? o How do you access and use other educational resources locally? KSS GP School QM process v.5 Page 9 of 12 Revision Date: August 2012
155 APPENDIX 3 Roles and responsibilities of visitors All visitors must understand their process of the visit and be familiar with their role. All visitors must be familiar with the GMC criteria for training and trainers. The lead visitor should speak to all visitors before the visit to ensure that this is the case, and must clarify any information needs. All visitors must adhere to principles of Equality and Diversity, and should be up to date with their training in this (with the last 3 years). All visitors must ensure that they are familiar with the documentary or electronic evidence provided prior to the visit. All other visitors will be guided by the lead visitor in terms of timing, process and areas to investigate. Lead visitor (Patch Associate GP Dean). o o o o o o o o o o o o To work with the GP Patch Manager to ensure that the date and timings are agreed and notified to the Faculty being visited. To ensure that the other visitors are contacted and have been informed about the date and time and have confirmed this To have read the provided documentation prior to the visit, and relevant feedback, such as GMC and Deanery GPStR surveys To share any appropriate and relevant information with the other members of the visiting team for the first day. To share any appropriate and relevant information with other specialty visitors pertaining the LEP To coordinate the timetable for the first day of the visit To negotiate and agree responsibilities, such as areas of questions, or individuals to interview, with the other members of the visiting team. To support the other specialty visitors in questioning GPStRs on the second day of the visit to the LEP if appropriate and indicated. To interview the group of GPStRs on the second day of the visit. To feedback to the GP Trainer and members of the Training Practice any notable outcomes from the visit to the Practice on the first day To take part in the overall feedback on the second day with a particular emphasis on the GP training To write the report with the support of the GP Patch Manager. KSS GP School QM process v.5 Page 10 of 12 Revision Date: August 2012
156 APPENDIX 4 Information and briefing letter for GPStRs being visited on GP Quality Visits To all GP Trainees in a GP Training Faculty who will be visited. Dear Doctor A team from the KSS GP School will be visiting your GP Training Programme in a few weeks. The visit is not to assess you, but is to assess the quality and appropriateness of the training environment for us to get a good idea of the educational experience provided by your department. We have a number of ways of looking at this, but in our view the best way of finding out what it is like to work in a department is to talk with the trainees. The KSS deanery has responsibility for approving all training posts in KSS on behalf of the GMC (which is the regulator for the quality of medical education), and for making sure that each post delivers a good training experience for you. Most trainees in KSS are satisfied with their posts, but there is almost always room for improvement. There are some posts which provide a truly excellent experience, and in the same way that we need to identify the weak posts we want to know about these excellent posts which can provide lessons for others. The GP visiting team will usually have up to 4 members on the first day, normally made up a a Lead Visitor, who is the Patch Associate GP Dean, a GP Training Programme Director, a GP Training Practice Manager and a GPStR. Some visits cover a number of specialties. The GP School visits GP training programmes over 2 days, with the main focus of the visit on the first day, which is located in general practice and in the community. The second day of the visit will be to the hospital, and will allow the GP visitor (only the Lead GP visitor goes to the second day) to interview those GP trainees who are undertaking hospital posts in the Specialties being visited by the secondary care visitors, who form the majority of the second day visiting team. If you wish to find out more about the areas covered in these visits and the kind of questions you can expect, you can read the guide to GP Faculty Quality Management at: On rare occasions we will identify problems which give a real concern for patient safety, and in these cases we will may ask Practices, or Trust Chief Executives (where the problem is in the hospital) to make immediate changes. More commonly there are normal developmental changes resulting from the visit, which may take a few months to be implemented. We hope you will make every effort to meet with the visitors. We recognise that not everybody can always attend, and if you are unable to attend we would ask you to share your views on your training experience with colleagues who can then speak on your behalf. Yours faithfully Ian McLean Head of KSS GP School KSS GP School QM process v.5 Page 11 of 12 Revision Date: August 2012

157 APPENDIX 5 Exception Visits Exception visits are visits to Local Education Providers that are outside of the normal year-on-year quality management processes of the Deanery. They may be initiated because of: A serious clinical incident which may or may not have involved a trainee but might have implications for training. A serious trainee complaint either directly to the Deanery, or via a KSS School or via a London Specialty School which raises a serious question about current training that cannot be managed through usual mechanisms. Concerns raised by usual mechanisms such as GMC Surveys in small specialties or specialties not routinely covered by the Deanery visiting process. An example might be Occupational Health with just 3 posts in KSS, all of which are in the private sector. Evidence from any other source which raise serious questions about potential service problems which could affect trainees. Process Issues arising will be discussed between the Dean Director and the Postgraduate Dean for Secondary care and the KSS Head of School and the London Head of School if also relevant. If there is evidence of serious concern the Dean Director will make a decision for a Deanery visit and will inform the next meeting of the Quality Management Steering Group. It there is a more complex or chronic problem or there are other factors to be taken into account and it is less pressing, the matter will usually be discussed at the Quality Management Steering Group before a decision is made. The standard KSS methodology for the visit is set out in Appendix 1. However, all visits to any LEP in KSS will be led by KSS. The report will come to the Quality Management Steering Group for discussion and approval of action, following which the Dean Director will write to the Chief Executive of the LEP. The response of the LEP will be followed up and discussed at the Quality Management Steering Group until adequate evidence of resolution is provided. Where serious problems cannot be resolved it will be normal to approach GMC for a trigger visit. If at any stage serious problems are uncovered which put trainees or patients at risk, the Dean Director will take immediate executive action. KSS GP School QM process v.5 Page 12 of 12 Revision Date: August 2012
158 7 Bermondsey Street London SE1 2DD Main Tel: Main Fax: Educational Governance: Contract Review and Development Contract Review Process 2012/13 1 Quality Manual Verification 1.1 During October the first meeting to discuss the process will take place. 1.2 KSS Education Department [Education] will be offering dates for the Contract Review meetings to the Medical Education Managers (MEM) during December. As dates are set they will be distributed by Education to the KSS Heads of Library & Knowledge Services [LKS] and Pharmacy [KSS Heads]. 1.3 As dates are confirmed, Education will ask MEMs for dates for the verification visit to take place. As dates are agreed, Education will inform KSS Heads. 1.4 If the LEP has gained Earned Autonomy for PGMDE, Internal Verification and External Review will be coordinated by Education. 1.5 If the LEP has not gained Earned Autonomy for PGMDE external verification will be organised by Education. 1.6 All verification visits for LKS and Pharmacy will be organised by KSS Heads. As dates are finalised KSS Heads will send them to Education. The LEP s MEM will be informed of these dates as a matter of continuity. 1.7 The KSS Heads will be drafting all documentation from November to early March. Once all documents are completed, they will be sent to the Head of Education at KSS. 1.8 Final versions of the documentation will be sent to the MEM, LKS Manager and Pharmacy by March for completion. 1.9 Where LEPs are to undergo the full verification visit for all departments, all QMs will be sent to Education at least two weeks before the verification visit takes place. It will be the responsibility of each of the leads to send their own documentation to Education. LKS and pharmacy leads must send a copy of their QM to either their respective KSS Heads. A copy of all documentation should also be sent to the MEM. Education will then send a printed copy to the designated verifiers two weeks before the visit. A copy of last year s Action Plan from the Contract Review meeting will also be sent to verifiers. Where Earned Autonomy has been gained for PGMDE the KSS Heads will send their QM to Education should this be appropriate MEMs will follow the Earned Autonomy process laid out in the relevant documentation provided by Education From 2011, only one verification visit per LEP will take place. Thus, only one QM per department should be produced by every Trust. These QMs must contain information from all sites and departments. Documents from sites and departments where no visit will take place should be made available electronically to Verifiers. With our partners Chair, Deanery Board - Professor Sir David Melville CBE Dean Director - Professor David Black
159 1.12 If the LEP has gained Earned Autonomy, only the LKS and Pharmacy departments will undergo the verification process. No Library and Knowledge Service verification visits will be made to Sussex Partnership Foundation LEP or Surrey and Borders Partnership LEPs as no funding flows from KSS to these LEPs for Library and Knowledge Services The purpose of the verification visit is to audit the QM. The Verifiers will: ensure that procedures are in place to meet KSS Deanery requirements; check whether the processes and procedures set out in the QM are supported by evidence provided by the department; produce a verification report (appropriate to the QM being verified) for Education. The report will provide comments on areas of good practice and areas which require development and potential changes in practice there these are considered to be required The verification visit will normally last from to for PGMDE and from for LKS and for Pharmacy An appropriate space should be made available for Verifiers to work in. Provision will be made for the verification report to be sent to the Deanery via on the day of the visit Access to all filing systems referred to in the QM must be provided. All colleagues whose files are to be viewed are to be made aware that the verifiers are working on behalf of KSS, which files should be made available, and why they need to see them. This is particularly important where there is limited access to files (for example, because they are kept by part-time staff) It would be helpful if a light lunch could be provided for the verifiers. Education should be informed if there are hospitality restrictions imposed by the LEP and therefore no lunch available The relevant lead, designated representative or manager must be available throughout the verification visit and should expect to be part of it If processes are considered to be inadequate and changes are required, the department will be requested to provide an action plan for future compliance with a realistic time line before the Contract Review visit, and verification of the QM will be delayed until then. If it is not possible for this to be done, a second verification visit will be agreed at the Contract Review visit and the contract will be signed subject to the relevant changes being made When the QM has been verified, Education will issue a formal Certificate of Verification. No QM is formally verified until the Certificate has been issued The Verification Report will be made available to the team completing the Contract Review visit and will feed into the discussion which will take place at that meeting Verifiers will provide the department leads with a copy of the Verification Report on the day of the verification visit Should a MEM, LKS or Pharmacy lead require assistance in writing the QM, they should contact Education in the first instance who will identify someone to assist with the process.
160 2 Verifiers 2.1 Verifiers will operate in pairs wherever possible. The verification teams will comprise of: a) PGMDE- a member of Education staff together with a MEM b) LKS a member of the LKS team and a senior member of LKS from another county c) Pharmacy normally a member of SEMMED and a senior pharmacy staff member from another LEP who will verify the QM for the appropriate department. 2.2 A computer will be available for verifiers to use so that the report template can be downloaded and the final Report can be ed to Education on the day (see 2.12 above). 2.3 Verification Development Meetings will be held annually in January for verifiers to develop processes and to share standards. 2.4 New verifiers will: a) Attend an Education Verifier Development meeting; b) Receive a sample QM; c) Have the opportunity to shadow experienced verifiers; d) Complete their first visit with an experienced verifier. 2.5 The verifiers provide a link between the Educational Contract signed by the Dean Director, LEP Chief Executive and Director of Medical Education/Clinical Tutor, and the operation of that Contract at daily level. 2.6 Verifiers are using their experience and knowledge to make a professional judgement in order to decide whether they can verify the procedure or not. Hold points occur when: o the Procedure does not meet the Deanery Requirement in the Quality Manual Specification; o Evidence is not available or recognised to show that the procedure is effective. If a verifier thinks there may be a hold point they should: o Discuss with their fellow verifier to agree the hold point; o discuss and explore the issue with the MEM, LKS or pharmacy lead, or a verifying colleague where there is just one verifier for the departmental verification; o agree with the MEM, LKS or pharmacy lead what corrective action will be taken; If there are more than five hold points, or one or more critical hold points, verifiers should use their judgement as to whether a second visit is required. Issues that are recognised as being addressed by the LEP are not hold points and should be noted in the Verification Report as such in the appropriate section. 2.7 Education is looking for processes that are good enough; they have to be reasonable and workable within the daily context of the LEP. The aim is to work with the LEP jointly to produce a system which works well for both the LEP and Education: this is emphatically not an inspection but is a developmental and motivational process designed to support the MEM, LKS and Pharmacy leads in the quality control of education within the LEP.
161 3 Contract Review Visits 3.1 The collated LAB Strategy must be sent to Education at least three weeks in advance of the Contract Review visit by the MEM. Where possible it should be sent together with the QM documentation. LKS and pharmacy leads must send a copy of the LEP LAB Strategy to KSS Heads. 3.2 Education will gather all documents and produce the relevant documentation for the Contract Review meetings and send them to KSS Visitors, and the LEP s MEM, at least two weeks before the visit. 3.3 The Contract Review visit must be attended by the LEP s Chief Executive, DME/Clinical Tutor, MEM, LKS and Pharmacy leads. The Medical Director of the LEP or Chair of Clinical Governance, or equivalent, will also be welcome to attend the meeting. 3.4 An Associate Dean, an Assistant Dean Education and KSS Heads will form the Visitors. Other KSS staff may be invited to attend and verifiers may attend as observers. LEPs are welcome to nominate any additional members of KSS staff whose attendance they would find helpful and such requests will be honoured whenever possible. MEMs should invite the LKS and Pharmacy leads to the meeting. 3.5 The Contract Review visit will normally take place between and The usual programme will be: DME/CT, MEM, LKS and Pharmacy meet Deanery visitors. A programme for this section of the meeting may be devised by the education leads within the LEP The Chief Executive and other staff at her/his discretion join the meeting. Where possible and/or appropriate, LEPs are asked to provide a light lunch for Visitors. 3.6 Discussion at the Contract Review visit will usually cover: issues arising from the QM Verification Reports (both verification visit and earned autonomy); a review of the Contract Review Action Plan from the previous year; discussion of the LAB Strategy. The aim is to support LEPs in taking forward their local education agendas, within regional and national guidelines. 3.7 At the end of the Contract Review visit, a draft Action Plan will be produced and forwarded to the LEP on the next working day. Each KSS visitor will write their section using the template and this will be collated by Education. Education will circulate the draft Action Plan to Visitors for signing-off and will then send it to the LEP s MEM on the next working day. The LEP s MEM will collate responses from the LEP and return an amended Action Plan, or confirmation of acceptance of the Action Plan, to Education within one week of receipt. Once agreed the Action Plan will be attached to the KSS Single Contract as a binding agreement between the LEP and KSS. All relevant parties within the LEP can expect to receive the final Action Plan one week after any comments or changes are received by Education. 3.8 The Chief Executive and DME will sign the KSS Single Contract at the Contract Review visit agreeing to comply with any required actions set out in the Action Plan.
162 4 Deadlines 4.1 Each LEP will be given two weeks in which to arrange dates for the Contract Review visit. If a LEP has not confirmed dates in that two week period, then dates will be allocated by the Deanery with which the NHS LEP will be expected to comply. 4.2 Documentation for the Contract Review visit must be received by the Deanery three weeks in advance of that visit. 4.3 Cancellation of visits by the LEP is unacceptable except for reasons beyond the control of the NHS LEP. 5 Earned Autonomy 5.1 LEPs that have been awarded Earned Autonomy will be provided with relevant documentation by Education
163 7 Bermondsey Street London SE1 2DD Main Tel: Main Fax: NHS Postgraduate Deanery for Kent, Surrey and Sussex KSS Single Contract 1 April March 2013 With our partners Chair, Deanery Advisory Board - Professor Sir David Melville CBE Dean Director - Professor Deanery David Chair Black Name
164 Contents 1. Purposes and Scope 2. Terms and Conditions 3. Required process for implementation 4. Specifications 5. Funding Arrangements 6. Management of funds issued by KSS 7. Exclusions 8. Appendices
165 Education Contract Purposes and Scope 1. Since 2010 the NHS Postgraduate Deanery for Kent, Surrey and Sussex [KSS] has issued an annual Single Contract to its Local Education Providers [LEPs] to cover all KSS Contracted Services provided by a single LEP and the LEP has managed that Contract through its Local Academic Board [LAB]. 2. This Single Contract sets out KSS s provision for quality managing and quality controlling postgraduate medical and dental education, pharmacy education and library and knowledge services and provides detail of the allocation of NHS funding related to those activities. Its purpose is to support, develop, quality manage and quality control KSS Contracted Services in LEPs in Kent, Surrey and Sussex, with the wider purpose of improving patient care. 3. This Contract is made under the conditions of Section 4 of the National Health Services and Community Care Act This Contract is subject to all national statutes, regulations and requirements that affect NHS funding and to any requirements of the NHS and the appropriate national regulatory authorities. Terms and conditions 5. In exchange for the provision of services to the specifications described below, KSS will provide funding to your LEP as detailed in the appended Schedules of Funding for 2011/ This Contract covers the period 1 April 2012 to 31 March The Dean Director of KSS, the Chief Executive of the LEP and the Chair of the LAB at the LEP will sign this Contract on completion of KSS s annual Contract Review process. Its terms and conditions will take effect automatically from 1 April 2012 unless any formal written variation to the Contract has been signed by the Dean Director of KSS, the Chief Executive of the LEP and the Chair of the LAB at the LEP. 8. The failure of the LEP to provide the services specified in this Contract will constitute noncompliance. In the event of non-compliance KSS may: 8.1. withhold 2% of the total funding in respect of postgraduate doctors salaries (as detailed on Schedule A), where mandatory GMC requirements are not met [for example, where Revalidation data for a postgraduate doctor is not submitted appropriately, or where a postgraduate doctor is not being supervised by a KSS accredited Educational Supervisor]; 8.2. withhold 2% of the total funding where the LEP is not supporting its staff to enable them to carry out duties associated with the KSS Contract [for example, where Educational Supervisors are not provided with appropriate time in their Job Plans; or where time, payments or reimbursement of expenses is not provided for duties associated with recruitment, selection, or School duties]; 8.3. require corrective action to be taken in a specified time-scale; 8.4. inform other stakeholders, in particular the General Medical Council [GMC], of the measures it is taking; 8.5. review the appropriateness of training posts in the LEP and any corresponding payments in respect of them identify and withhold specific costs to KSS of remediating non-compliance with the Contract s Specifications.
166 9. If the LEP decides to sub-contract any part of this Contract to a third party (for example, an ISTC), then the LEP must ensure that the quality of services are at least equivalent to and compatible with those specified in this Contract. 10. KSS reserves the right to inspect KSS and LEP funded posts within approved training programmes and visit postgraduate doctors and dentists and Pre-registration Pharmacists at any time. Required process for implementation 11. On receipt of this Contract, the Chief Executive must consult with the LEP s LAB Chair, Academic Registrar and Library and Knowledge Services Manager. 12. Any queries about the Single Contract should be ed immediately to the KSS Contract Review Administrator, on contractreview@kssdeanery.ac.uk who will forward it to the appropriate KSS Business Manager for a response. 13. Any agreed variations will be incorporated in the Single Contract signed at the end of the Contract Review process. 14. All queries, variations and communications concerning the Single Contract must be in written form so that they can be recorded by KSS. A copy of the record for each LEP will be provided to the Chief Executive or LAB Chair on request. 15. If circumstances change in-year, for example, due to national instruction by the DH, the SHA, GMC, GDC, or any other relevant national agency, KSS will issue Executive Letters specifying new requirements to be met. 16. In the case of dispute the Chief Executive should make direct contact with the Dean Director. Both parties will use all reasonable endeavours for resolution and, if necessary, the matter will be decided by the Chief Executive of the SHA. Specifications 17. Compliance is required in three areas: Education Programmes and Resources; Human Resources and Medical Staffing; Finance and IT. 18. Detail of the requirements for compliance is provided annually in the Quality Manual Specification and the Education Strategy Specification issued as part of Contract Review. When appropriate these requirements will be updated by KSS Executive Letters extending or modifying the requirements for compliance. 19. Compliance to specifications will be monitored by: LAB Agendas, Minutes and Reports; Local Faculty Group [LFG] Agendas, Minutes and Reports; Contract Review; KSS Visits on behalf of GMC; Other such visits and processes as KSS shall deem necessary. Funding arrangements 20. Generic funding arrangements are set out below. Schedules of Funding specific to your NHS Trust are appended to this document.
167 21. Schedule A Pay and Non-Pay Schedule A comprises funds in respect of KSS approved postgraduate doctors and dentists salary costs and a contribution to the cost of their employment. Salary costs will be as follows: F1-100% of the agreed salary point (plus London weighting where appropriate) plus an amount in respect of employers on-costs F2 50% of the agreed salary point (plus London weighting where appropriate) plus an amount in respect of employers on-costs Academic F2, Hard to fill F2 and GP F2 100% of the agreed salary point (plus London weighting where appropriate) plus an amount in respect of employers on-costs Former SpR 100% of the agreed salary point (plus London weighting where appropriate) plus an amount in respect of employers on-costs ST1/2/3/4 where created from ex-kss funded SHO posts, these posts will be funded in this financial year at the SHO rate (i.e. 50%) It should be noted that if a funded post within Schedule A is unfilled for a period of up to three months KSS will not normally take any action. However if a post remains unfilled after three months, then KSS reserves the right to withhold funds for that post until such time as it is occupied Relocation and associated expenses for all postgraduate doctors in training posts, employed by the Trust, will be centrally managed through the London Deanery. 22. Schedule B Education Centres Funds in respect of Education Centres within the NHS Trust are calculated on a historic basis (except study leave). Study leave funding will be provided for all KSS funded postgraduate doctors except: 22.1 F1 doctors 22.2 Anaesthetics Higher Speciality postgraduate doctors, where study leave will continue to be centrally managed, by Guys and St Thomas NHSFT, although this is subject to an ongoing review Those core training posts where an amount is withheld by the Head of School to facilitate centrally run training [see KSS Study Leave Guidelines for Doctors and Dentists in Training on the KSS website ]. No funds are provided in respect of capital charges. 23. Schedule C Library and Knowledge Services From April 2011 a new funding model has been implemented for the provision of Library and Knowledge Services within the LEP. This comprises a fixed cost associated with having a library presence and a variable cost based on activity, quality and collaboration. A transitional arrangement is being applied to the model, to limit the impact of the changed arrangements on Library and Knowledge Services budgetary allocations The LEP will provide equitable Library and Knowledge Services to all categories of NHS staff working in the hospital, community and primary care settings in the local health economy. Specific details of the organisations and users served as well as the services provided can be found in Schedule C It should be noted that KSS Deanery funded library and knowledge services posts cannot be frozen without the agreement of the Library and Knowledge Services Manager and the KSS Deanery KSS requires that the total sum allocated must be spent as detailed in Schedule C on Library and Knowledge Services. Any virement and or other special arrangements (for example library and knowledge services reconfigurations or staff re-gradings) must be agreed with the KSS Library and Knowledge Services Team.
168 23.4 In collaboration with the NHS Trust Finance Department the Library and Knowledge Services Manager will provide the KSS Library and Knowledge Services Team with a quarterly report on expenditure. Management of funds issued by KSS 24. All funds issued by KSS must be used for educational purposes. KSS issues these funds to the LEP expressly to support KSS Contracted Services. 25. If funds cannot be utilised for the purpose of supporting KSS Contracted Services, within the financial year that they are issued, then they must be made available to support KSS Contracted Services within the LEP in the following year, or returned to KSS. 26. It is not acceptable for the LEP to generate savings from any funds issued by KSS, or to use them for any purpose other than to support KSS Contracted Services. 27. The LAB must have formal arrangements with the LEP whereby all monies provided to the LEP by KSS are ring-fenced and can be used for purposes deemed appropriate by the LAB s Chair or Academic Registrar or Library and Knowledge Services Manager without delay. 28. Funds relating to Schedule A are used to reimburse the LEP for pay costs, which arise through the employment of postgraduate doctors and are therefore to be managed by a LEP representative. 29. Funds relating to Schedule B are to be managed by the Chair of the LAB. Funds relating to Schedule C are to be managed by the LEP s Library and Knowledge Services Manager. 30. The LEP will be expected to account for its annual expenditure against KSS funding at each Contract Review as part of the Education Audit. Annual review of funding 31. The level of funding which KSS provides to the LEP is entirely dependant upon: the rate at which the DH funds postgraduate medical education in future years and funding constraints within the NHS, which may impact upon KSS resources. KSS will, therefore, annually review its rate of funding to the LEP in light of any changes to the above. This may occur in year if DH and NHS funding arrangements are only agreed after the start of the financial year. Exclusions 32. KSS will not pay for salary supplements, such as out of hours banding, or for any element of salary protection relating to any postgraduate doctor.
169 Appendices Schedules of Funding: Schedule A Pay. Schedule B Education Centres Schedule C Library and Knowledge Services which includes a specification of users and services Quality Manual Specification Local Academic Board Education Strategy Specification
170 Signature by parties to the Education Contract The undersigned agree to comply with the terms and conditions outlined above: Local Education Provider: Signed: Name: Date: Position: NHS Trust Chief Executive or nominated officer Signed: Name: Date: Position: Chair of Local Academic Board Signed: KSS: Name: Professor David Black Position: Dean Director
171 7 Bermondsey Street London SE1 2DD Main Tel: Main Fax: Educational Governance: Contract Review and Development 2012/13 Quality Manual Specification With our partners Chair, Deanery Board - Professor Sir David Melville CBE Dean Director - Professor David Black
172 CONTENTS Glossary KSS specifications detailed by General Medical Council [GMC] Domains Domain 1: Patient safety Domain 2: Quality management, review and evaluation Domain 3: Equality, diversity and opportunity Domain 4: Recruitment, selection and appointment Domain 5: Delivery of approved curriculum including assessment Domain 6: Support and development of trainees, trainers and local faculty Domain 7: Management of education and training Domain 8: Educational resources and capacity Domain 9: Outcomes
173 Glossary of Terms ARCP Annual Review of Competence Progression AV Audio-Visual CEO Chief Executive Officer CPD Continuing Professional Development CS Clinical Supervisor DME Director of Medical Education ES Educational Supervisor EWTR European Working Time Regulations GEAR Graduate Education and Assessment Regulations GMC General Medical Council GP General Practice GPSTP General Practice Specialist Training Programme HR Human Resources HST Higher Specialty Training IT Information Technology KSS Kent, Surrey and Sussex LAB Local Academic Board LCP Local Curriculum in Practice LEP Local Education Provider LFG Local Faculty Group LKS Library and Knowledge Services LTFTT Less Than Full Time Training MEM Medical Education Manager NCF National Curriculum Framework PGMDE Postgraduate Medical and Dental Education QESP Qualified Educational Supervisor Programme QM Quality Manual SAS Staff and Associate Specialist SIG Special Interest Group SPA Supporting Professional Activities TPD Training Programme Director
174 When completing the Quality Manual, it should be noted that it is insufficient to write that a Local Education Provider (LEP) is compliant with the individual domains and their sub-criteria, it is also necessary to state how it is compliant and how this compliance is quality assured by the Local Academic Board (LAB) and Local Faculty Group (LFG) structure. Domain 1: Patient safety The duties, working hours and supervision of trainees must be consistent with the delivery of high quality, safe patient care. There must be a clear procedure to address immediately any concerns about patient safety arising from the training of doctors. 1 Induction to the Local Education Provider [LEP] Domain 1.1 [see KSS specification 27 for Induction to Programmes; KSS specification 32 for Induction to the Department] The Local Academic Board [LAB] and Local Faculty Groups [LFGs] ensure that induction to the LEP: a) Emphasises that postgraduate doctors must make the needs of patients their first concern through appropriate LEP mandatory training and as set out in the LEPs values and behaviours. b) Ensures that formal Induction into the LEP for all grades and specialties is structured, effective and inclusive (late starters, locums, etc). c) Ensures that induction includes NHS mandatory training requirements, and is recorded on NHS secure management systems. d) Ensures that incoming Foundation year 1 [F1] doctors are able to shadow their opposite number prior to taking up their first post, in order to support induction to the hospital and the post. e) Ensures that doctors from overseas receive appropriate induction to the UK and the NHS. 2 Work patterns and intensity Domain 1.2, 1.3, 1.5, 1.6, 6.9, 6.10 The LAB, linking with LFGs where appropriate must ensure that: a) Postgraduate doctors' working patterns and intensity of work, by day and by night, including on-call rotas: i) Are appropriate for learning new skills. ii) Enable access to theatre sessions, ward rounds and outpatient clinics as appropriate. iii) Provide shift and on-call rota patterns that minimise the effects of sleep deprivation in line with European Working Time Regulations [EWTR]. iv) Provide adequate time for well-organised handover arrangements, which ensure continuity of care at the start and end of periods of day or night duties. b) Working patterns are developed to ensure that: i) All postgraduate doctors and dentists are appropriately supervised according to their experience and competence. ii) Those supervising the clinical care provided by postgraduate doctors are clearly identified; competent to do so; accessible and approachable by day and by night; with sufficient time for these responsibilities clearly identified within their job plan. c) Through its Human Resources [HR] Department: i) diary card exercises are completed appropriately. ii) compliance with EWTR is monitored appropriately.
175 3 Clinical responsibility Domain 1.2, 1.4 The LAB, with LFGs where appropriate, must ensure that those supervising postgraduate doctors in the clinical setting (e.g. Educational Supervisors, Clinical Supervisors and other health care professionals): a) Carry out a realistic assessment of the competence of postgraduate doctors or dentists they are supervising and on the basis of that assessment, judge the appropriate level of exposure to clinical responsibility commensurate with delivering safe patient care. b) Ensure that before seeking consent both postgraduate doctor and supervisor are satisfied that the postgraduate doctor: i) Understands the proposed intervention and its risks. ii) Is prepared to answer associated questions the patient may ask. iii) Have access to a supervisor with the required knowledge if they are unable to answer questions asked by the patient. iv) Is able to act in accordance with GMC guidance Consent: Patients and Doctors Making Decisions Together (2008), The Michael Report: Healthcare for All (2008) and the Getting It Right Charter (2010). 4 Clinical support Domain 1.1, 6.12, 8.1 The LAB must ensure that Laboratory and Radiology services within the LEP are available on a 24- hour basis, in order to provide high quality patient care and to ensure that activities of no educational value, such as inappropriate duties, do not obstruct PGMDE.
176 Domain 2: Quality Management, review and evaluation Postgraduate education must be quality managed locally by deaneries, working with others as appropriate e.g. medical Royal Colleges/Faculties, specialty associations, education providers. 5 Graduate Education and Assessment Regulations [GEAR] Domains 2.1, 2.2, 2.3, 6.7, 6.29, 6.34, 7.1, 7.2, 7.4, 7.5 GEAR sets out the academic quality management specification for progression, review and evaluation of PGMDE in KSS. The LAB must ensure that: a) Its operation is compliant with GEAR. b) Pharmacy is incorporated into its work and represented appropriately in its management, monitoring and review of the Contract. c) Library and Knowledge Services [LKS] is incorporated into its work and represented appropriately in its management, monitoring and review of the Contract. d) LFGs are established and constituted according to the requirements of GEAR in order to manage, monitor and review all KSS programmes within the LEP including Foundation, Core and Higher Specialty Training [HST]. In accordance with GEAR LFGs are required to: i) manage, monitor, support and be held accountable for the progress of their postgraduate doctors, dentists and pharmacists, by holding formal LFG meetings at least three times each year. ii) progress any issues concerning recruitment, retention, progression, remediation or completion in order to resolve them in a timely fashion. iii) receive a summary of feedback from their postgraduates, outlining what they value in their programme and their main issues and concerns, at each meeting, and respond appropriately to it. e) All red flag issues identified within the yearly GMC surveys are progressed, resolved and reported appropriately to KSS. f) All KSS Contract Review and GMC visits, are managed appropriately and take responsibility for resulting action plans, progressing reports within the time-scale laid out following each visit. g) A record of all Quality Management visits is maintained. h) Appropriate lines of communication are maintained between KSS, relevant national authorities and the LEP by acting as a conduit for all matters concerning PGMDE. 6 Security of Information Domain 2.1 The LAB must ensure that all information concerning postgraduate education is: a) maintained securely, and in accordance with NHS Information Governance requirements, Data Protection Act and Freedom of Information Act, with appropriate policies and procedures in place for access by postgraduates if necessary. b) transferred confidentially between the LEP and KSS; and between the LEP and other LEPs.
177 7 Intrepid: postgraduate doctor and dentist data Domain 2.1, 6.20, 6.21, 9.1 The LAB, with its LEP s Information Technology [IT] Director and HR Director, must ensure that: a) The current data sets required by KSS are entered onto the Intrepid database within 4 weeks of each postgraduate taking up a new placement [ new starters ] within the LEP as required by KSS. b) The LEP has a system for ensuring that all data are current which includes details of all study leave taken by postgraduates as required by KSS. c) The LEP adheres to all KSS specifications for providing equipment and support for Intrepid. 8 Intrepid: monitoring educational supervision Domains 2.3, 9.1 The LAB, through its LFGs and with its LEP s IT Director, must record data for specialties without an e-portfolio, to show that all Education Supervisors meet their postgraduates at the start, middle and end of their post, using the appropriate section of Intrepid. 9 Short term cover for medical staffing functions Domain 2.3, 9.1 The LAB, through its LEP s HR Department, must ensure that trained short-term cover is provided for all medical staffing functions including usage of Intrepid.
178 Domain 3: Equality, diversity and opportunity Postgraduate training must be fair and based on principles of equality 10 Equality, diversity and opportunity in appointments Domain 3.1, 3.5 The LAB, through the LEP s HR Department, must ensure that: a) The LEP s local appointment processes for postgraduates adheres to the NHS equality and diversity mandatory standards and relevant legislative regulations. b) Postgraduates have access to evidence on postgraduates' recruitment, appointment, and satisfaction with the results analysed by appropriate characteristics of the Equality Act 2010, such as ethnicity, place of qualification, disability, gender and part-time training/working. 11 Equality, diversity and opportunity in education Domain 3.1, 3.2 The LAB, through its LFGs and the LEP s Human Resources Department, must ensure that: a) All educational programmes and information about them is compliant with UK Employment Law, The Human Rights Act and with the characteristics of the Equality Act 2010 and other equal opportunity legislation that may be enacted and amended in the future and is working towards best practice. b) Information about all educational and training programmes, their content and purpose, is publicly accessible either on, or via links to postgraduate deaneries and GMC websites. 12 Less than full time training [LTFTT] Domain 3.3 The LAB, through its LFGs, and the LEP s HR Department, must ensure that: a) Arrangements are in accordance with the KSS Less than Full Time Training Policy b) Programmes can be adjusted for postgraduate doctors and dentists with well-founded individual reasons for being unable to work full time to follow LTFTT. c) Its LEP accepts a fair share of LTFTT. d) Statistical data on LTFTT is provided to KSS in LAB and LFG Annual Audit and Reviews. 13 Reasonable adjustments Domain 3.4 The LAB, through its LFGs and the LEP s HR Department, must ensure that reasonable steps are taken to ensure that programmes can be adjusted for postgraduates who have disabilities, special educational or other relevant needs.
179 Domain 4: Recruitment, selection and appointment Processes for recruitment, selection and appointment must be open, fair, aid effective and those appointed must be inducted appropriately into training 14 Registration of postgraduate doctors and dentists Domain 4.1 The LAB, through its LFGs and the LEP s HR Department, must ensure that all new postgraduates: a) Have an appropriate licence to practice. b) Are fit to practice. c) Have provided appropriate references. d) Have completed appropriate CRB checks. 15 Immigration requirements Domain 4.1 The LAB, through its LEP s HR Department, must ensure compliance with requests for information from KSS to meet UK Border Agency monitoring requirements. 16 Specialty training posts Domain 4.1 The LAB, in partnership with the LFG, must ensure that: a) Posts are approved by KSS in order to allow these posts to be accredited by the GMC. b) Appropriate lines of communication must exist between Medical Education Managers [MEMs], KSS Schools, Training Programme Directors [TPDs], and medical staffing so that the correct information on numbers and nature of posts is available. 17 Selection into specialty and higher specialty programmes Domain 4.2 The LAB, through its LFGs, must ensure that postgraduate doctors are provided with appropriate opportunities to gain competencies and progress towards sign off in order to be able to demonstrate the competencies required to complete Foundation and Core and thereby be considered for entry into specialty or higher specialty programmes. (This covers candidates who have completed Foundation training, candidates who apply before completion and those who have not undertaken Foundation training, but can demonstrate the competencies in another way.) 18 Managing HST transition into KSS Specialty Schools Domain 7.2 The LAB, through its LFGs, must ensure that appropriate lines of communication are maintained with other deaneries regarding the recruitment, appointment and progress of Higher Specialty postgraduate doctors participating in programmes with the LEP.
180 19 Recruitment and selection Domain 4.3 The LAB, through its LFGs and the LEP s HR Department, must ensure that: a) Information about places on programmes, eligibility and selection criteria and the application process is made widely available in sufficient time to doctors who may be eligible to apply. b) The selection process uses criteria and processes that treat eligible candidates fairly. c) Candidates are selected on the basis of open competition. d) There is an appeals system against non-selection on the grounds that the criteria were not applied correctly, or were discriminatory. e) Only such information (apart from information sought for equalities monitoring purposes) is sought from candidates as is relevant to the published criteria and which potential candidates have been told will be required. f) Timely reports and information about recruitment, selection and appointment processes are received by KSS and its Schools. 20 Local selection panels Domain 4.4, 4.5 The LAB, through its LFGs and the LEP s HR Department, must ensure that local selection panels: a) Consist of persons who have been trained in selection principles and processes. b) Include a KSS representative where appropriate, such as the Director of Medical Education [DME], the Clinical Tutor, or a TPD. c) Include a lay representative. 21 Advertising placements locally Domain 4.3 The LAB and the LEP s HR Department, must ensure that permission is sought from the KSS Dean Director whenever it is proposed to advertise an education and training placement locally including those associated with a planned programme or rotation. 22 Contract of employment Domain 8.1 The LAB and the LEP s HR Department, must ensure that each postgraduate receives a written legal contract of employment before commencing their post, and that even under exceptional circumstances it is received no later than six weeks after commencing their post. 23 Job description Domain 8.1 The LAB and the LEP s Human Resources Department, must ensure that every placement has an up to date and accurate job description, which is given to each postgraduate when entering the LEP.
181 Domain 5: Provision of approved curriculum including assessment. The requirements set out in the approved national curriculum framework [NCF] must be provided by the local curriculum in practice [LCP]. The approved assessment system must be fit for purpose. 24 LFG Handbooks Domain 5.1, 5.2, 5.3, 5.4, 5.5, 5.6, 5.7, 5.8, 5.9, 6.8 The LAB must ensure that each of its LFGs produces an annually updated handbook that sets out in detail its LCP, in compliance with GEAR, including: a) How competencies within the approved curriculum will be achieved. b) How the posts within the programme, taken together, will meet the requirements of the approved curriculum and what must be taught within each post. c) The need for postgraduate doctors to have due regard to, and to keep up to date with, the principles of Good Medical Practice. d) How postgraduates will be able to access and be free to attend training days, courses, resources and other learning opportunities that form an intrinsic part of their programme and constitute part of their learning entitlement. e) How postgraduates requiring additional support are provided with this. f) Where postgraduates should go for career support. g) Where postgraduates should go to personal counselling. h) The approved assessment system implemented by the LFG. i) The purposes of each and all components of the approved assessment system. j) The sequence of approved assessments, matched to the learner s progression through their career pathway. k) The points at which regular feedback will be given to the postgraduate on their performance within their post i.e. supervision meetings and appraisal meetings as distinct from assessments. 25 Induction to educational programme Domain 5.1, 5.2, 5.3, 5.4, 5.6 The LAB must ensure that all its LFGs provide an induction into their educational programmes that: a) Sets out how competencies within the National Curriculum Framework (NCF) will be achieved. b) Sets out how the posts within the programme, taken together, will meet the requirements of the NCF and what must be taught within each post. c) Reminds postgraduates about the need to have due regard to, and to keep up to date with, the principles of Good Medical Practice. d) Sets out how postgraduates will be able to access and be free to attend workshops and courses, access resources and utilise other learning opportunities that form an intrinsic part of their programme and constitute part of their learning entitlement. e) Sets out how postgraduates requiring additional support are provided with this. f) Indicates where postgraduates should go for career support. g) Indicates where postgraduates should go for personal counselling. h) Sets out the approved assessment system implemented by the LFG. i) Sets out the purposes of each and all components of the approved assessment system. j) Sets out the sequence of approved assessments, matched to the postgraduate s progression through their career pathway. k) Sets out the points at which regular feedback will be given to the postgraduate on their performance within their post. l) Ensures that all postgraduates have a copy of the LFG s current handbook and that copies have been sent to KSS to the appropriate School.
182 m) Ensures all LFG handbooks are in the public domain by being available on the LEP s and KSS School s websites for reference purposes. 26 Curriculum development Domain 5.1, 5.2, 5.4, 6.17 The LAB must engage with KSS new curriculum developments and in particular ensure that: a) All Foundation doctors have access to and are released for simulation training during the course of their programme. b) Postgraduates have access to clinical audit processes, which includes participating in planning, data collection and analysis. c) Postgraduates have the opportunity to learn with, and from, other healthcare professionals. d) There is a LAB lead for new curriculum developments in: i) Simulation. ii) Careers. iii) Leadership (i.e. Leadership Pairing Scheme, Postgraduate Certificate Module in Leadership etc). iv) Patients with Learning Disabilities. v) The Role of Lay Representatives. vi) The Postgraduate Doctor s Voice. vii) Medical Humanities. viii) Co-Mentoring. ix) Curriculum mapping. 27 Educational assessment Domain 5.1, 5.5, 5.6, 5.7, 5.8, 5.9, 6.26 The LAB, through its LFGs, must ensure that: a) Appropriate opportunities for regular and timely assessment are available for postgraduates to fulfil their curriculum requirement. b) All assessments are appropriately documented to ensure that sufficient information is available for the Annual Review of Competence Progression [ARCP] process and for recruitment. c) Educational Supervisors regularly review each postgraduate's learning portfolio and meet with them at timely intervals to provide feedback and support, in order to ensure that they are progressing appropriately. d) All assessors have the practical experience and are able to use the in-work assessment tools to make judgments on the progress of postgraduates. e) All assessors record their assessments in a timely fashion, using the appropriate portfolio or e- portfolio. f) An up-to-date database of assessors, their qualification to undertake the assessment role and the date on which they qualified, is maintained by the LEP.
183 28 Study leave availability Domain 5.4, 6.19, 6.20, 6.21 The LAB, with its LEP s HR Director and its LFGs, must ensure that: a) Study leave appropriate to the career choice of each postgraduate is available, and operates within KSS Study Leave Guidance and the relevant Terms and Conditions of Service for Hospital Medical Staff, so that the process for applying for study leave is fair and transparent, and information about the KSS appeals process is readily available. b) All postgraduates are given or have access to KSS and/or the LEP local study leave guidance, including guidance on how to apply for study leave. c) All postgraduates are guided as to appropriate use of study leave funding and time, and are made aware of appropriate courses and funding within the LEP. 29 Study leave for Staff and Associate Specialist [SAS] and Trust Grade doctors Domain not applicable The LAB must ensure that: a) Where study leave and/or funding is provided by the LEP for SAS and Trust Grade doctors, whose education may be recognised by the medical Royal Colleges, similar systems must be used to those for postgraduate doctors. b) Where LABs administer those arrangements, their LEP must ensure that administrative costs are funded.
184 Domain 6: Support and development of postgraduates and local faculty Postgraduates must be supported to acquire the necessary skills, and experience through induction, effective educational supervision, and appropriate workload and time to learn. 30 lnduction to the department Domain 6.1 The LAB, through their LFGs, must ensure that: a) Every specialty, unit or department provides an induction programme which ensures postgraduates: i) understand the approved curriculum. ii) understand how their post fits within their educational programme. iii) understand their duties and reporting arrangements. iv) are told about departmental policies. v) meet key staff. vi) receive details of well-organised handover arrangements, which ensures continuity of care at the start and end of periods of day or night duties. b) Up-to-date copies of Departmental Induction Programmes are lodged with the LAB. c) Induction to the specialty, unit or department must be prioritised in order to ensure postgraduates are fully prepared to provide effective patient care in their first hours on duty. d) Induction to the specialty, unit or department provides each postgraduate with an opportunity to self assess their abilities putting patient care as their first concern. 31 Educational supervision Domain 6.3 The LAB, through its LFGs and the LEP s HR Department, must ensure that: a) All postgraduates are allocated an Educational Supervisor at the start of their programme, with name and contact details provided as part of each postgraduate doctor s induction. b) All Educational Supervisors know who their new postgraduate is, where they will initially be working, and how long they will be working within the LEP c) All Educational Supervisors have sufficient time in their job plans to undertake the Educational supervision of their postgraduates in accordance with the tariff document (.25 SPAs per postgraduate). 32 Education plans Domain 6.2, 6.4, 6.5 The LAB, through its LFGs, must ensure that: a) Within four weeks of starting post, each postgraduate has agreed with their Educational Supervisor: i) The educational framework and support systems in the post. ii) Their respective responsibilities for teaching and learning. iii) A learning agreement and educational plan setting out agreed learning and career objectives in line with the requirements of the local and national approved curriculum b) All postgraduates must have access to an appropriate log book and/or learning portfolio relevant to their current programme which they discuss with their Educational Supervisor. c) All postgraduates must have the opportunity to experience leadership at an appropriate level and to be assessed on this so that the assessment forms part of their portfolio.
185 d) Postgraduates should be allowed time to attend teaching sessions. 33 Education development meetings Domain 6.6, 6.15, 6.16 The LAB, through its LFGs, must ensure that: a) Postgraduates have further, fully documented meetings with their Educational Supervisor at least every three months, to discuss their progress in relation to their educational plan, their outstanding learning needs and how to meet them. b) Postgraduates are able to attend relevant, timetabled, organised educational meetings and have protected time for this. c) Postgraduates are able to access training in generic professional skills at all stages in their development. 34 Clinical supervision Domain 6.13, 6.25 The LAB, through its LFGs, must ensure that: a) All postgraduates are allocated a clinical supervisor for each element of their programme. b) Clinical supervisors meet their postgraduate within the first 2 weeks of their clinical placement to ensure that both the clinical supervisor and postgraduate have a mutual understanding of the expectations within the post. This may include attendance at theatre sessions, or outpatient clinics as appropriate, departmental teaching, clinical audit processes, and confirming ways in which the postgraduate can learn in the workplace. c) Clinical supervisors advise the postgraduates Educational Supervisor and the LFG if they have any concerns about the ability of their postgraduate or concern for patient safety, or any other issues or concerns for the postgraduate. d) Clinical supervisors judge the appropriate level of exposure to clinical responsibility for their postgraduate, commensurate with delivering safe patient care. e) Clinical supervisors have undertaken QESP Part 1 or as a minimum have had other education or training recognised by the LFG and LAB as stated in the KSS Recognition and Qualification for Clinical Supervisors (2010) guidelines. 35 Academic education Domain 6.22, 6.23, 6.24 The LAB, through its LFGs, must ensure that: a) Postgraduates are exposed to the academic opportunities available in their specialty. b) Postgraduates who recognise that their particular skills and aptitudes are well suited to an academic career should be encouraged and guided in that endeavour. c) Postgraduates who elect and who are competitively appointed to follow an academic path, are sited in flexible approved programmes of academic education that permit multiple entry and exit points throughout their education, from other programmes.
186 36 Workplace bullying Domain 6.11 The LAB, through its LFGs and the LEP s Human Resources Department, must ensure that: a) At commencement of employment each postgraduate receives details of the LEP s anti-workplace bullying policy and how it is implemented when necessary. b) Copies of this and other policies are maintained on the LEP s website and details of where they can be found are available within all LFG handbooks. c) All instances of workplace bullying or any behaviour which undermines postgraduates professional confidence or self-esteem are reported, reviewed and progressed in the LFGs and the LAB s Annual Audit and Review. 37 Pastoral care Domain 6.14, 6.18 The LAB, through the LEP s HR Department, must ensure that: a) Occupational health and pastoral care is readily accessible to all postgraduates and that all postgraduates know where to go for help when needed. b) Access is provided to an independent and confidential counselling service if needed by postgraduates. c) The Improving Working Lives quality standard is adhered to for postgraduates. 38 Faculty development: Selection Domain 6.32, 6.33 The LAB, through its LFGs, must ensure that: a) Faculty members with additional educational roles must be selected and demonstrate ability as an effective teacher to the standard required by KSS. b) GP trainers are trained and selected in accordance with the General and Specialist Medical Practice (Education, Training and Qualifications) Order Faculty development: CPD Domain 6.25, 6.32, 6.34 The LAB, through its LFGs, must review the CPD needs of all Faculty members at least annually to ensure that they: a) Can enable postgraduates to learn by taking responsibility for patient management within the context of clinical governance and patient safety. b) Understand and demonstrate ability in the use of the approved in-work assessment processes and be clear as to what is deemed acceptable progress. c) Have knowledge about, and comply with, national regulatory frameworks.
187 40 Faculty development: Job Plans Domain 6.30 The LAB, with its LEP s CEO, must ensure that Faculty members have adequate support and resources to undertake their educational roles. 41 Faculty development: Qualified Educational Supervisor Programme [QESP] Domain 6.27, 6.28 The LAB, through its LFGs, must ensure that all Educational Supervisors have completed or are in process of completing QESP so that they are accredited as being able to: a) Ensure that clinical care is valued for its learning opportunities. b) Ensure that learning and teaching is integrated into service provision. c) Regularly review postgraduate doctors progress. d) Adopt a constructive approach to giving feedback on performance. e) Advise on career progression. f) Understand the process for dealing with a postgraduate doctor whose progress gives cause for concern. 42 Faculty development: assessment Domain 6.26, 6.30, 6.35 The LAB, through its LFGs, must ensure that all those who provide assessment understand the requirements of the programme and are clear as to what is deemed acceptable progress. 43 Faculty development: capacity growth Domain 6.29, 6.31 The LAB, through its LFGs, must support and develop the capacity of its Faculty by: a) Identifying and supporting Faculty members who wish to follow KSS s Master s degree programmes in Education, Leadership, Careers, and Medical Humanities. b) Identifying and supporting Faculty members who wish to take on specific lead roles in KSS crosscurriculum developments. c) Supporting the creation of Special Interest Groups [SIGs] within the LEP and enabling them to share practice across LFGs and across KSS LEPs. d) Gaining ethical approval for research, development and evaluation as part of postgraduates' and their faculty's service improvement projects from the KSS Education Ethics Committee.
188 44 Faculty development: records Domain 2.3, 3.1, 6.31, 9.1 The LAB, through its LFGs and LEP s HR Department, must maintain a current, central record of: a) Faculty members currency (renewable every three years) with Equality and Diversity training. b) Faculty member s currency with Recruitment and Selection training. c) Progression of Faculty members through Assessment training. d) Progression of Faculty members through QESP, including a Register of Clinical Supervisors as per the KSS Recognition and Qualification for Clinical Supervisors (2010) guidelines, showing i) The Specialty/ies they supervise ii) The LFG/s to which they belong (with smaller specialties this may be a more generic LFG) iii) Their status as Local Recognition or KSS Qualification as appropriate iv) The date on which they entered the Register e) Compliance by Faculty members with the KSS Advice on Job Planning for Consultants. f) Completion by Faculty members of their annual appraisal and their CPD review. g) Faculty members taking lead roles on cross-curriculum developments. h) Faculty members who have completed or are engaged in KSS Master s degrees i) All Local Faculty Group meeting must be minuted and copies of all minutes must be sent to the appropriate KSS Specialty School in accordance with Point 10 (iv) page 33 of GEAR V3.
189 Domain 7: Management of education Education must be planned and maintained through transparent processes which show who is responsible for each stage. 45 Management of education a) The Chief Executive Officer [CEO] of the LEP must ensure that its Local Academic Board (LAB) is constituted according to the requirements of GEAR [which meets and exceeds GMC Standards] and that it meets formally at least three times a year. b) The LAB must ensure that non-attendance by members at its formal meetings is notified to the CEO of the LEP and to the KSS Dean Director using the Annual Audit and Review process. c) The LAB must be accountable for the management, monitoring and review of the whole of the KSS Contract signed with their LEP. d) A named member of the LEP s Board attends LAB meetings. e) The LEP s Board discusses the formal reports of the LAB three times a year. 46 Support and career advice Domain 6.8, 7.3 The LAB must: a) Coordinate the provision of career advice and support for all grades and all specialties to ensure appropriate advice is available. This includes liaison with the GP Specialty Training Programme Directors, who have responsibility for providing appropriate career advice and support to those intending or considering general practice as a career. b) With its LEP s HR Department: i) Ensure that details of how to apply for LTFTT are available to postgraduates. ii) Ensure that timely and effective support and guidance is provided to help postgraduates complete the LTFTT application and process. c) Ensure that the DME meets LFG Leads yearly for an educational appraisal. d) Ensure that the DME receives an annual educational appraisal from KSS. 47 Postgraduates requiring additional support Domain 7.3 The LAB, with its LEP s HR Department, must ensure that: a) The LEP has policies and procedures in place to support postgraduates who are experiencing difficulties with their education, their working environment or their personal lives. b) These policies and procedures are available through the LEPs intranet site and within the specialty training handbook which is given to all postgraduates to ensure they are supported at all times. c) All LFG Leads and Educational Supervisors have access to the KSS Postgraduate Doctors Requiring Additional Support guidance. d) An appropriate Occupational Health Service is readily accessible to all postgraduates, and information about this service is available to them at induction.
190 Domain 8: Educational resources and capacity The educational facilities, infrastructure and leadership must be adequate to deliver the approved curriculum. 48 Education Centre and LKS facilities Domain 7.5, 8.4, 8.5 [Cross-reference to LKS QM Section 3] The LAB must ensure that: a) Appropriate facilities are available to meet the needs of effective management of the KSS Contract, including rooms, equipment and other relevant infrastructure. b) The Education Centre is able to analyse their resources to show percentage use under the headings required by KSS s management audit, to ensure that postgraduates have appropriate access to meeting rooms and audio-visual aids. c) The LAB must ensure that Education Centres and LKS have a system for maintain communications and relationships with other local Education Centres and LKS, where the work of one centre or library affects that of others. d)staff are released to attend relevant KSS group and project meetings where appropriate and necessary to ensure continuity of communication with colleagues throughout the region. Minutes of these meetings to be provided to the LAB. 49 Teaching and learning facilities Domain 8.2 [Cross-reference to LKS QM 2.2] The LAB must ensure that: a) Appropriate facilities for teaching and learning are available within the LEP to meet all the needs of the KSS Contract. b) Quiet study space is available within the Library and where applicable in the hospital residence and common rooms to enable postgraduates to study privately. c) Clinical skills and wet lab facilities are available to enable postgraduate doctors and dentists to fulfil their curricular requirements. b) Postgraduates, qualified GP s, and dentists working in the wider health community have appropriate access to teaching rooms for education outside normal working. e) Suitable simulation facilities are available in line with KSS policy. 50 LEP facilities Domain 8.1 The LAB, with its LEP Facilities Manager, must ensure that: a) Postgraduates have access to hot food at night, during week-ends and during bank holidays. b) Postgraduates and faculty are secure when moving between parts of the LEP or when using LEP funded transport. c) Appropriate on-call/rest rooms are made available for use by postgraduates.
191 51 Education technologies Domain 8.1, , 8.5 The LAB must ensure that: a) Faculty members have access to appropriate Audio-Visual (AV) equipment, including video conferencing equipment that is able to be connected to other teaching areas, at suitable times. b) Educational Supervisors, clinical supervisors, and assessors have appropriate IT facilities to carry out their educational roles. c) AV equipment is maintained to a standard which is consistent throughout the LEP. d) There is a planned programme for upgrading all IT/AV/Video conferencing equipment informed by new curricular requirements. 52 IT facilities Domain 8.2, 8.4 [Cross-reference to LKS QM 2.3] The LAB, with its LEP s IT Department, must ensure that: a) The Education Centre and LKS are part of the LEP IT network. b) At induction, all postgraduate doctors, dentists and preregistration pharmacists are given access to clinical results systems. c) All doctors, dentists, preregistration pharmacists and Education Centre staff have access to the Internet (via NHSnet) and . d) The LEP provides IT support which is timely and effective. e) All LAB and LEP staff are able to: i) receive s and attachments from and send s and attachments to KSS and between each other without delay or difficulty. ii) utilise the IT packages and versions specified by KSS Schools. iii) fully access the KSS website without difficulty. iv) fully access KSS s web-based Virtual Learning Environment without difficulty. v) access the Intrepid database for all appropriate staff within the postgraduate and medical HR departments. vi) make full use of all of the features of the new IT and web-based Foundation/Specialty programme educational resources. vii) request hardware which is sufficient to the staff s needs within the postgraduate and medical HR department. viii) request software which is sufficient to the staff s needs within the postgraduate and medical HR departments. 53 Support staff Domain 7.5, 8.1 The LAB must ensure that appropriate support is available for: a) All LAB and LFG administration. b) Administration for Qualified General Practitioners CPD as negotiated by GP Tutor. c) The co-ordination of Qualified Dental Practitioners CPD as negotiated by Dental Tutor. d) All appropriate portering requirements.
192 54 Workforce planning Domain 8.1 The LAB, with its LEP s HR Department, must ensure that: a) The procedure for workforce planning is clearly defined and involves appropriate representation. b) A prompt and accurate response is made to all KSS requests for workforce planning data for all grades and specialties of doctors, including consultants, staff grades, overseas doctors, attachments and postgraduate doctors. 55 Appointment of DME/Clinical Tutor Domain 7.5, 8.1 The LAB, with its LEP s HR Department, must ensure that the procedure for the joint appointment of the DMEs and Clinical Tutors is in accordance with KSS guidance, which is available through the KSS HR Department. 56 Appointment of staff to the PGMDE function Domain 7.5, 8.1 The LAB, with its LEP s HR Department, must ensure that: a) There is a clearly defined, written LEP policy and procedure for the appointment of staff to all PGMDE functions: b) Processes are in place for ensuring that vacancies are filled in a timely fashion. c) Provision is made for PGMDE staff to have access to funding for overtime or time in lieu for work taking place outside normal working hours in the delivery of the PGMDE function within the LEP. d) New DMEs, Clinical Tutors and MEMs receive appropriate induction by both the LEP, and through attendance at KSS programmes. e) Provision is made for support staff within the PGMDE function to attend external meetings and courses appropriate to their role in order to develop PGMDE within the LEP. 57 Budgetary accountability Domain 7.5, 8.1 [Cross-reference to LKS QM 5.2] The LAB, with its LEP s Finance Department, must ensure that: a) DME/ Clinical Tutors are: i) Accountable for the entire Schedule A and Schedule B KSS element of the PGMDE budget. ii) Accountable to the Chief Executive for it. iii) Provide clear accountability for any delegated budgetary responsibilities to the MEM. b) Library and Knowledge Services Managers are: i) Accountable for the entire Schedule C KSS element of the PGMDE budget. ii) Aaccountable to the Chief Executive for it. iii) Provide clear accountability for any delegated budgetary responsibilities. c) Chief Pharmacists are: i) Accountable for the entire budget for Pharmacy Education. ii) Accountable to the Chief Executive for it. iii) Provide clear accountability for any delegated budgetary responsibilities.
193 58 Annual finance returns Domain 8.1 The LAB, with its LEP s Finance Department, must ensure that the LAB makes completed Annual Returns within six weeks of them being requested by KSS in respect of: i) PGMDE Budget. ii) SAS CPD Funding [by the end of March in each financial year]. iii) GPSTP funding. iv) GP education support. v) Other budgets both recurring and non-recurring, not covered by the single contract. 59 Notification of financial transfers Domain 8.1 [Cross-reference to LKS QM Section 5] The LAB, with its LEP s Finance Department, must ensure that the LAB records notifications from KSS when funds intended for the Education Centre and LKS are transferred to the LEP by KSS. 60 Expenditure of KSS monies Domain 8.1 [Cross-reference to LKS QM Section 5] The LAB, with its LEP s Finance Department, must ensure that the LAB has formal arrangements with the LEP whereby: a) All monies provided to the LAB by KSS are ring-fenced and can be used for purposes deemed appropriate by the DME/Clinical Tutor, MEM, the Library and Knowledge Services Manager [LSM] or Chief Pharmacist as appropriate without delay. b) Monies provided to the LAB by KSS are not used in LEP Cost Efficiency Savings. c) The LEP must have a facility for carrying over eligible funds from one financial year to the next as a precondition of accepting funding from KSS for educational projects which span more than one financial year. d) Educational project funding may not be vired between other KSS budget heads without specific written agreement from KSS. e) Educational project funding must be spent on the approved education project or returned to KSS.
194 Domain 9: Outcomes The impact of the standards must be tracked against outcomes and clear linkages should be reflected in developing standards. 61 Review and improvement Domain 9.1 The LAB, through its LFGs, must: a) Review the outcomes of all summative assessments and examinations results for each programme and benchmark the standards against other programmes locally and regionally. b) Provide an opportunity for programmes to share good practice, through their regular 4-monthly meetings. c) Seek to improve the provision of education by sharing good practice and seeking to identify good practice within other training organisations.
195 Educational Governance: KSS Contract Review Local Academic Board Strategy Specification The KSS Deanery 7 Bermondsey Street London SE1 2DD Tel: Fax: Dean Director Professor David Black MA MBA FRCP Head of Education Professor Zoë Playdon BA(Hons) PGCE MA PhD MEd DBA FRS
196 Name Local Address Telephone number Website Number of sites Chief Executive Medical Director Director of Medical Education Medical Education Manager Chief Pharmacist Library Services Manager Name Contact details Please give the following details for each site Clinical Tutor GP Tutor Dental Tutor Capacity of teaching rooms Simulation facilities Library facilities Education Provider [LEP] Summary
197 CONTENTS GMC Domains
198 Results of Action Plan 7, 8 Educational Management Audit 8 1 Support for Educational Roles 6 2 Attendance Audit of Local Faculty Groups [LFGs] 3, 4, 7 3 Developing Local Educational Capacity 6 4 Medical and Dental Staffing 3, 4, 7 5 External Visits and Inspections 7, 9 6 Linking Undergraduate and Postgraduate Medicine n/a 7 Appraisal and Continuous Professional Development 6 8 Education Centre Usage 3, 4, 7 9 Educational Technologies 3, 4, 7 10 LEP Management Continuity 3, 4, 7 11 LEP Management Infrastructure 3, 4, 7 12 SPOC for KSS Finance 8 13 LAB Metrics : regional RAG rating All
199 Results of Action Plan 2011 The KSS request: Please list the Action Agreed from last year s Action Plan, annotated appropriately to show progress under the following headings: Action Completed Action in Progress: a short statement of progress to date, including action discussed in your Business Analysis and Strategic Plan Action attempted: a short statement of what action was taken and why it was not carried through to completion Action not taken: a short statement explaining why action was not taken.
200 Education Management Audit 1 Support for Educational Roles In 2010 KSS re-issued formal Advice on Education and Job Planning for Consultants, setting out the usual contractual requirements necessary for consultants to undertake educational roles. Please record the numbers of consultants in your LEP compliant with this benchmark, using the format below, for the roles of: Educational Supervisor; Clinical Supervisor; Local Faculty Group Lead; Recruitment Support; STC, Head of School, or Training Programme Director; and for cross-curricular roles in Simulation; Leadership; Medical Humanities; Careers; and Undergraduate Medical Education. Numbers Compliant KSS School Total Nº ES Total Nº CS Total Nº LFG Lead Total Nº Recruit support Total Nº HoS Total Nº TPD Total N STC ACCS Anaesthetics Emergency Medicine Intensive Care Medicine Medicine Obstetrics & Gynaecology Ophthalmology Paediatrics Pathology Psychiatry Radiology Surgery Other Specialties
201 Cross-Curricular Roles Numbers Compliant Simulation Leadership Medical Humanities Careers UGME 2 Attendance audit of LFGs Please update and include your attendance chart from your LAB Annual Audit and Review to show: - the Local Faculty Groups [LFGs] that report in to the LAB showing: - the number of members of each LFG; - the number attending each LFG for its last three meetings. Please list additional LFGs that you plan for the future with their start dates 3 Developing Local Educational Capacity To support LABs in their faculty development role, in line with the requirement of Liberating the NHS: Developing the Healthcare Workforce that workforce development should be professionally informed and underpinned by strong academic links (p. 9), KSS makes available a suite of MA programmes specifically relevant to postgraduate medical education. Please report on the number of people in your LEP who have either completed or are currently attending a KSS Master s programme or an equivalent with other providers, using the following format. Programme KSS Other Provider (Please specify) Education in Clinical Settings Leadership in Clinical Settings Managing Medical Careers Medical Humanities Other Master s or Doctoral programmes (please specify) Totals 4 Medical and Dental Staffing a) the numbers of doctors and dentists currently supported by the LAB, including Trust doctors. Please explain any differences in numbers in your funding breakdown. Grades Medicine Dentistry Consultant SAS FY1
202 FY2 CM1 CM2 CS1 CS2 HST GP1 GP2 GPST3+ DF1 DF2 Clinical Attachments Undergraduates [average p.a.] Other (specify) b) Medical and dental staff turnover in the last fiscal year: this is important to establish that the LAB has sufficient permanent career grade doctors to provide robust educational supervision Grades No at start of fiscal year No at end of fiscal year No of posts filled during year Medicine Dentistry Medicine Dentistry Medicine Dentistry Consultant SAS Trust Grade c) Number of unfilled posts by grade and specialty. KSS School StR (H) StR (L) F1 F2 Foundation
203 Acute Care Common Stem Anaesthetics Emergency Medicine General Practice Intensive Care Medicine Medicine Obstetrics & Gynaecology Occupational Medicine Ophthalmology Paediatrics Pathology Psychiatry Public Health Radiology Surgery Dentistry 5 External inspections and visits KSS request: To allow us to audit our records, please report on the external visits and inspections you have received since 01 January 2010: Date & Type of visit Specialty(s) inspected Date of previous visit for specialties involved Visiting body Part of programme of visits Triggered visit YES/NO YES/NO
204 Were there actions as a result of visit YES/NO Timescale to resolve actions Date(s) of future visits Specialty(s) to be inspected 6 Linking undergraduate and postgraduate medical education Operational Relationship Yes No Does your LEP receive SIFT? Is SIFT in the DME s budget? SIFT Does the DME influence the expenditure of SIFT in collaboration with the undergraduate tutor where appropriate? Is there a LFG for undergraduate medicine? Do clinical placements: UG/PG links Have a nominated Educational Supervisor? Follow a formal written curriculum? Do Educational Supervisors meet undergraduate Tutors to discuss the programme and outcomes? 7 Appraisal and Continuous Professional Development [CPD] In line with the requirements of Liberating the NHS: Developing the Healthcare Workforce for competent and capable staff and adaptive and flexible workforce (p ), please report on your current arrangements for appraisal and CPD for your MEM team (including the Academic Registrar and LFG Administrators) and DME team (including Clinical tutors and LFG Leads) by post (not by person) Appraisal Process Current and Completed CPD Programme Agreed DME Team (please list posts) MEM Team (please list posts) Pharmacy Team (please list posts) Library and Knowledge Services Team (please list
205 posts) 8 Education Centre Usage during the last year Please provide a percentage breakdown of usage of your Education Centre using the categories provided below. It is important that you use the categories below to enable us to make comparisons between KSS LEPs. If you have more than one site, please provide data for each. Centre Users % usage Postgraduate Medical Education Undergraduate Medical Education Professions Allied to Medicine Dental Education Multi-Disciplinary Team Meetings Career Grades CPD Primary Care Education NHS Trust Management and Training Commercial lettings Other users TOTAL 9 Education Technologies Please: a) Report any problems experienced with educational technologies, including accessing e- portfolios, e-learning, and other web-based resources; b) Briefly outline the measures you have taken to deal with any problems you have experienced; c) Please state your level of satisfaction with the outcome of the measures you have taken.
206 10 LEP Management continuity In post for more than one year Yes No CEO Human Resources Director Finance Director DME MEM Library Services Manager Pre-Registration Pharmacist Training Manager Medical Director IT/Operations Director or equivalent Director of Nurse Education 11 LEP Management infrastructure Function Yes No There is an LEP Strategy Group [or equivalent] that includes at least the DME; MEM; Head of Training; Director of Nurse Education; Library Services Manager; Chief Pharmacist; and meets regularly. LEP senior executive committee regularly takes reports from the LAB and contributes to LAB Strategy. DME is a full member of the LEP senior executive committee OR has equivalent arrangements for direct, regular and frequent meetings with the CEO (please specify) DME has direct access to the CEO.
207 Medical Education Manager is a full member of an appropriate LEP senior HR committee OR has equivalent arrangements for direct, regular and frequent meetings with the senior education executive group within the LEP (please specify) Academic Registrar manages support for LAB and for all LFGs. MEM has an effective Medical Staffing Contact 12 Single Point of Contact for KSS Finance During the last year, KSS has experienced some difficulty in transferring funding for eligible educational projects to some LEPs. Please identify a named member of your LAB as your single point of contact (SPOC) for all financial transactions related to the KSS Contract. Your SPOC must have the authority to ensure that transfers of funding between KSS and your LAB are managed in a timely fashion and that their expenditure is timely and transparent. LAB SPOC for Finance Short term cover for SPOC Please provide name, post title, , address, and telephone Please provide name, post title, , address, and telephone 13 LAB Metrics : regional RAG rating The LAB Metrics provides a self-assessment for your LAB in twelve areas identified by the KSS Quality Management Steering Group [QMSG] as particularly significant performance indicators. KSS has completed your data for the first six of these areas. Please: a) Complete your data for areas 7 to 12. Any of those areas which you do not complete will automatically be rated as Red. b) Sign off your data as accurate on the proforma as follows: Indicator 1 Indicator 6 Indicator 7 Indicator 8 Indicator 9 Indicator 12 QESP to be signed off by the Medical Education Manager PAs for education in the job plan to be signed off by the Director of Medical Education after discussion with the Medical Director LFG Meetings to be signed off by the Medical Education Manager Adequate tracking of training data to be signed off by the Medical Education Manager Absence of postgraduate doctors to be signed off by the Medical Staffing Manager Board-level engagement to be signed off by the Director of Medical Education
208 7 Bermondsey Street London SE1 2DD Main Tel: Main Fax: Business Analysis 1. Your LEP s Executive Statements (Notes for Guidance 3:6) Briefly summarise the broad corporate identity, direction, and priorities of your LEP, as they relate to the KSS Contract, listing the documents where these are set out. LEP s corporate identity LEP s planned direction LEP s priorities 2. Your LAB s Executive Statements (Notes for Guidance 3:7) Briefly state your LAB s Vision (where you aim to be in three to five years time); Mission (your main means for getting there); and Unique Selling Proposition [USP] (the marketplace identity that makes you distinctive from other LABs) LAB s Vision LAB s Mission LAB s USP 3. Marketing Analysis (Notes for Guidance 3:8-14) Please provide a narrative summarising the results and implications of your Marketing Analysis and referring to the six headings set out in the Notes for Guidance and discussed in the Workshop: SWOT Analysis Marketplace Segmentation Ansoff s Planning Matrix Product Life Cycle Boston Portfolio Matrix Marketing Mix With our partners Chair, Deanery Board - Professor Sir David Melville CBE Dean Director - Professor David Black
209 In your narratives, you should tell us about areas such as: the demographics of your area what you do and what your service offers your competitors (e.g. private hospitals, other training providers) what sets you apart from them your teachers your facilities interprofessional learning use of facilities for external income generation what your LEP, faculty, and learners think of you who your partners are in achieving your goals who influences your service delivery sell your service what have you achieved in the last year? Please provide separate narratives for your internal and external markets and have available your full Marketing Analysis for reference at your Contract Review Visit. Results and implications for LAB s internal market (faculty and LEP) Results and implications for LAB s external market (learners) 4. Human Resource Analysis (Notes for Guidance 3:15-17) Please provide a narrative summarising the results and implications of your Human Resource Analysis and referring to the seven headings set out in the Notes for Guidance and discussed in the Workshop: Task Analysis Job Plans Short-term cover Multi-tasking Succession planning Appraisal CPD In your narrative, you should tell us about areas such as: your staffing structure your arrangements for short term cover for key tasks the SPA arrangements, allocations, and plans for your teaching faculty your revalidation arrangements for your teaching faculty your arrangements for succession planning your arrangements for ensuring all staff and learners are up-to-date with statutory training whether your workforce is adequate and appropriate for providing your services to the level required at present?
210 With reference to your Marketing Analysis, how you will ensure that your workforce is adequate and appropriate for providing the level and kind of services you plan for the future 5. Resource Analysis (Notes for Guidance 3:18) Please provide a narrative summarising the results and implications of your Resource Analysis and referring to the seven headings set out in the Notes for Guidance and discussed in the Workshop: Space required Technologies required Management access required Liaison required Travel and subsistence required Other essential resources 6. Management Analysis (Notes for Guidance 3:19) Please provide a narrative summarising the results and implications of your Management Analysis and referring to the six headings set out in the Notes for Guidance and discussed in the Workshop: Line Management Functional Management Autonomy Networks Partnerships Task, Role, Boundaries, Expectations for all of above 7. Finance Analysis (Notes for Guidance 3.20) Please: a) use the chart below to summarise the results of your Finance Analysis
211 Finance Long-term Recurrent Short-term Temporary Wholly funded Income generation Charitable funds Work Areas b) provide a narrative summarising the results and implications of your Finance Analysis. You should tell us about areas such as: your lines of financial management your relationship with your finance department the access you have to funds the decision-making you exercise on expenditure your ability to carry-over eligible funding from one financial year to the next your financial audit arrangements plans for major expenditure in the next year plans to manage potential budget reductions 8. Ethical Analysis (Notes for Guidance 3:21-35) Please provide a narrative summarising the results and implications of your Ethical Analysis and referring to the seven headings set out in the Notes for Guidance and discussed in the Workshop: Free exchange of expertise with other groups the Gift Economy Purchaser Supplied Programmes Pareto Principle Ethical issues and solutions Business issues and solutions Contractual reference points Participative consultation processes used Decisions on action In your narrative, you should tell us about areas such as: new collaborations development of new LFGs your use of educational programmes to develop your faculty areas for future investigation areas for immediate action areas of conflict between ethical and business imperatives proposals to resolve such conflicts
212 9. Arrangements for your LAB to review your Business Analysis (Notes for Guidance 3:34) Please state your arrangements for your LAB to review your Business Analysis on a regular basis.
213 LAB Strategy Specification 2012 Notes for Guidance 3 Business Analysis The KSS Approach 1. These Notes for Guidance describe the KSS Approach to Business Analysis. Like your Education Audit, your Business Analysis must take account of both ethical imperatives and business determinants. It must ensure that the bottom line of income and expenditure is translucent to the moral dimension encapsulated by Kant s Categorical Imperative. 2. This is particularly important since postgraduate medical and dental education [PGMDE] operates to very different business determinants from mainstream industry and commerce. In commerce, business analysis begins with the assumption that it will be possible to secure a supply of raw material of a uniform quality, in order to create products that will operate in a predictable competitive marketplace. Ethics are generally regarded as an externality, apart from concerns such as reputational risk or greenwash promotional strategies, and every marketplace is considered to be potentially accessible. By contrast, PGMDE has little control over the circumstances of learners and patients, and less control still over national and regional budget-setting. It operates at the politically volatile intersection of health and education, in a strictly limited marketplace, within a range of stringent regulatory frameworks. It is an invisible investment most people do not know that half the doctors in a hospital are postgraduate doctors and it requires a high level of tailoring to the individual needs of learners. Further, medicine and dentistry are personal services in which the professional provider is in an immediate relationship with the user. In particular, therefore, PGMDE is ethically bound, with the effects of ethical breach being experienced directly by each doctor and dentist. 3. The KSS approach to business analysis thus has a moral dimension as well as a financial one. However, it meets the same broad purposes as business analysis in commerce and industry. It provides a range of ways of understanding your business, so that you can increase your awareness and predictability, and thereby reduce risk. This sensitivity analysis also allows you to produce rapid, successful response to sudden change. Of course, it only offers hypotheses about the future and its forecasts must be reviewed regularly against actual business, and the plan adjusted accordingly. As we discussed in the Workshops, it has to be produced by an iterative process, but once it is produced, it meets a range of purposes, informing your Strategic Plan, establishing employment security, and supporting funding applications and research proposals. 4. Your Business Analysis involves working through the five business areas that you used in your Education Audit: Marketing, Human Resource, Management, Resource, and Finance. However, it also requires two additional areas of consideration, a series of Executive Statements about your Vision, Mission, and Unique Sales Proposition [USP]; and an Ethical Analysis. 5. These two additional areas the Executive Statements and the Ethical Analysis are important because the purpose of business success is to ensure ethical success. In the business of PGMDE, financial efficiency may not be achieved at the expense of educational effectiveness or clinical appropriateness. All three indicators efficiency, effectiveness, and appropriateness have to be achieved in order to ensure that learners and their patients are happy and are doing well. What is more, this is not just a matter of individuals doing well. PGMDE takes place in an integrated team context, and an important performance indicator is whether or not there are developing Communities of Practice within your organisation, such as Local Faculty Groups. It is
214 at this point that the gift economy is foregrounded, with the free exchange of expertise and experience. The first part of your Business Analysis, therefore, enables you to ensure an adequate, well-managed infrastructure for PGMDE. Your Ethical Analysis provides purpose to the rest of your Business Analysis: it tells you that you are using your resources and infrastructure to produce high quality education and best patient care. Individual Components in your Business Analysis 6. PGMDE is located within, and embodied by, the clinical services provided by your LEP to its healthcare communities. These provide the faculty, patients, and context that make up your local curriculum in action. In short, the affordances for teaching and learning PGMDE are extended or limited by your LEP s clinical engagement. Your LAB s Executive Statements, therefore, must be made within the context of your LEP s Executive Statements. So, your starting point should be the documents that set out the broad corporate identity, direction, and priorities of your LEP. 7. Within this corporate context, you need to articulate your LAB s Executive Statements: your Vision, Mission, and USP. Your USP is especially important in establishing your identity and particular strengths as a provider of PGMDE. 8. Your Marketing Analysis requires you to step back from your LEP and your LAB and to look at it critically. Each of the six key elements that we discussed in the Workshops provides a different lens for viewing your work. Your Marketing Analysis should consider: a. Your internal markets your Faculty and LEP; b. Your external markets your learners. 9. Your SWOT Analysis asks you to start with a broad overview of all the programmes you provide you will already have recorded these data in your Education Audit. Their strengths, weaknesses, opportunities and threats may be related to a range of factors: a. Your LEP s corporate identity, direction, and priorities; b. The demographics of your area; c. Competition from other education providers; d. The facilities you have; e. Your reputation, for example, reflected by GMC Surveys or KSS Visit Reports; f. Other factors reflected in your Education Audit. 10. Marketplace segmentation focuses on identifying key features of the patients and learners who currently come to your LEP. Why do they come to you? What are their alternatives? Are they the demographic that you wish to attract? 11. This Planning Matrix invites you to consider your future development. Much of what your LAB does will be Repeat Business, of course, but you will also have ideas for new developments. An example of Market Development would be setting up a new LFG, operating to existing systems, but for a new group. An example of Product Development might be Revalidation, where you will be required to provide new services to your existing faculty of learners and teachers. An example of Total Diversification might be providing Higher Specialty Training for the first time: this takes you into a relatively high risk area, since you have never provided these programmes to these learners before, and you would manage that risk by identifying resource to support it. 12. The Product Life Cycle suggests that everything has a finite life before it is taken over by new developments. New areas of education may have relatively slow uptake at first but then go through a period of growth, before having a longer-term, stable take-up. Eventually, though, they will go out of date unless they are revised, updated, and relaunched to meet contemporary requirements. The time-frame for the operation of the Product Life Cycle is likely to be different from one area of work to another, in response to policy or financial interventions. For example,
215 Leadership moved very rapidly from Launch to Growth, aided by Lord Darzi s national initiative and the funding associated with it. Strategically, it is very important not to assume that everything will continue as it always has, and the Product Life Cycle is a useful reminder to identify the areas of your work that are in decline. 13. This matrix, developed by the Boston Consulting Group, invites you to consider your portfolio of programmes by considering how many people might apply for them (Market Size) and how many people actually do apply for them (Market Share). If a lot of people wish to follow a programme and most of them prefer to follow it with you, then it is a Star. You need to consider why it is a Star what is it that you have that others don t have if you are going to retain it, since it is business that everyone else may wish to take from you. Similarly, if very few people want to follow a programme, and you can never recruit them to yours, you need to consider why that is, and why you are continuing to offer it in this form. A Prop, where only a small number of people wish to follow the programme, but they all come to you, is typical of a small or sub-specialty. It is interesting in business development terms, since if you can gain access to other markets, you might be able to develop your Prop into a Star. A Problem Area, where many people want a programme but none of them want it from you, is also interesting in business development terms. Since there is clearly a large market size, if you can fix the problem, you may be able to develop a Star. Fixing the problem very often involves considering your Marketing Mix. 14. If you are dealing with a Problem Area or setting up a new programme as part of your development strategy, it is helpful to consider the Marketing Mix, often called the 4 P s. Its aim is to analyse your programme in comparison with the provision made elsewhere, either to replicate best practice, or to compete. These comparisons concern: a. Programme content; b. Place where the programmes are offered; c. Promotional strategy you use to inform learners about them; d. Price, both as a direct, personal cost and an opportunity cost. 15. Whether you are reviewing existing Job Plans or creating new posts, the starting point for your Human Resource Analysis is a Task analysis. This will enable you to assess potential for short term cover, multi-tasking, and succession planning, provide a practical basis for appraisal, and support agreement of an appropriate plan for CPD. It is also important ethically, to ensure that staff are not overstretched or exploited, and thus to protect the learners and patients that they serve. Financially, it provides an important part of contract negotiation. 16. Task Analysis begins by identifying the time elements required for CPD and for routine meetings: these may be common across a range of staff. It then identifies the key tasks to be carried out, how long each task takes, and their frequency in the working year, identifying any key or peak dates for specific tasks. This allows you to identify the skills, knowledge, and experience required for the tasks and thus for the overall job role. It also allows you to produce a balanced Job Plan reflecting the time needed to carry out the tasks required. 17. Task Analysis can also help you to develop a flexible workforce, to provide short term cover, multitasking, and succession planning. This is especially important in complex environment, like PGMDE, where key tasks such as Revalidation must be carried out by a nationally-set, statutory, due date. As well, by identifying change and development in key tasks in a particular job role, you can agree CPD programmes with individuals that are specific to their needs. 18. If you have the staff you need, then Resource Analysis checks that you have the tools to the work that is required. This includes material resource, such as the space and the technologies required,
216 and communication systems, such as management access and lines of liaison, as well as basic items such as travel and subsistence and other essential resources. 19. Your Management Analysis aims to make sure that your business is carried on in an even, uninterrupted fashion. It is particularly important that within any activity, you are absolutely clear about the Tasks that each person will undertake; their Role in relationship to every other person involved in the Task; the Boundaries of their authority; and the Expectations that are set for their performance. 20. Your Finance Analysis is aimed at assessing the viability of your operations. It asks about the nature of the money available, and the terms on which it is available, including any penalties for non-compliance. In particular, it seeks to establish the accounting base to which you are working what counts as success within your LEP. Because this is part of a Business Analysis, it also asks about the relationship between price and quality, which is meaningful only when you compare it with other organisations providing similar programmes. Ethical Analysis 21. The focus of the Business Analysis is on the chain of contractual relationships between KSS and the LEP and the LEP and its employees, through which the business of PGMDE is transacted. But while this transactional economy is necessary to PGMDE, it is not sufficient to describe its business. Crucially, PGMDE also operates through a gift economy, in which one professional freely exchanges experience and expertise with another, for the benefit of learners, patients, and healthcare communities. This gift economy is one of the factors that defines professional environments, such as medicine, dentistry, and education, as distinct from commercial environments. The major purpose of effective and efficient management of the transactional economy, then, is to remove impediments to the gift economy and thus allow it to thrive: this is part of the meaning of professionalism. Of course, this also means that there may be a necessary tension between organisational competition and individual collaboration, and this, too, is typical of professional environments. 22. A particular kind of gift economy is represented by programmes that are supplied by KSS to its LEPs. Technically, in quality terms, these constitute what is called purchaser supplied resource - resource provided by a Purchaser to their Contractor to use in fulfillment of the Contract. The aim of purchaser-supplied resource is to provide a guaranteed quality at a favourable marketplace price and KSS meets those aims through the teacher education programmes it offers, which form part of its quality management system. Strategically, the aim is to develop educational capacity locally, as part of our collaborative continuous quality improvement. 23. Just as your financial analysis reviews the rest of your Business Analysis to see if it is affordable against the business bottom line, so your ethical analysis reviews your Business Analysis to see if it is affordable against the ethical bottom line. This illustrates the point that we kept returning to in your Workshops: the financial bottom line is indubitably necessary but in our sector, your Business Analysis is only sufficient if it protects you from moral bankruptcy. The role of the Ethical Leader, therefore, is to hold the moral vision for the organisation or group and to enact that by example. This may require negotiating with difficult people; resisting unacceptable proposals; and being creative in developing new solutions. This, in turn, will require collaboration and consultation it is not something that can be done alone. 24. The Pareto Principle, or 80/20 Rule, provides a first line of ethical analysis. This rule of thumb suggests that 80% of your business runs unproblematically but 20% may be problematic. For example, eight out of your ten LFGs might operate smoothly but the remaining two never seem to
217 form or work effectively. The 80/20 Rule goes on to suggest that, in consequence, you spend 80% of your time trying to manage this inefficient 20% of your business. Clearly, the inefficient 20% are incurring disproportionate resource and opportunity costs that are unfair to the rest of the community, which is, in effect, paying for their ineffectiveness. A first line of ethical analysis, therefore, is to identify any work area that falls into the 20% category and to plan to investigate it, with the aim of remedying the problems and thereby making a substantial business gain. 25. Often, the issues may fall into one of two categories: they are either ethical problems or they are business problems. Ethical problems are those in which compliance with the proposed action would be to the substantial disadvantage of patients, learners, the staff directly involved, or the larger healthcare community. The requirement here is to find creative ways of meeting both the ethical and the business needs of the organisation to create the Third Space so that the issues can be resolved to the reasonable satisfaction of all. The moral principle at play is the question What concession can you make in order to get on with the rest of the community? 26. Business problems are those in which a particular person or group is resistant to proposed action without being able to demonstrate any negative effects on patients, learners, staff, or the healthcare community. These issues are sometimes called cultural problems but unless they relate to a specific, recognised culture, defined by one of the protected categories in the Equality Act (2010) they are not cultural per se. They may represent an educational lacuna, perhaps an absence of information about the rationale for the action required, or an inability to appreciate the consequences of ignoring the action required. Equally, however, they may represent a powerful individual or individuals, misusing their authority, and breaching lines of management, to impose their personal views on colleagues and on the LEP. That is a kind of bullying and doubtless behind it lies fear, inadequacy, and personal anxiety, which is in itself a kind of educational problem. 27. Where the business problem is caused by an educational need, then the requirement is for an educational process, a professional conversation to explore with the individuals the issues at hand, their rationale, and their consequences for the rest of the community. Where the business problem is caused by a power struggle, there is also an educational need, since the individuals concerned are clearly focussing solely on their own defended egos, to the exclusion the needs of the rest of the community, perhaps including patients and learners. But extreme cases may also require a contractual reference point, since the work of the LAB is defined by the KSS Contract signed between the LEP and KSS, and carried out through the Contracts of Employment between the LEP and its employees. 28. It is very important to note that if a contractual reference point is needed, then your LEP s Medical Director and Head of Human Resource should be involved in your discussions and decisions. It is also very important to note that while KSS Education Department may be able to offer educational support and advice to teachers with additional needs, KSS cannot discuss the performance of any individual employed by your LEP, since this could be a violation of their employment rights: the exception, of course, is where patient safety may be compromised. Finally, such rare and extreme cases may mean that you decide that you are unable to offer training posts of a certain kind, and that a Contractual Variation is required between your LEP and KSS. Such a Contractual Variation should be discussed in detail with the relevant KSS Head of School and the KSS Chief Operating Officer by the LAB s Chair. Exceptionally, it may be necessary to involve the LEP CEO and the KSS Dean Director. 29. A second line of ethical analysis is provided by the change points you have identified in your Marketing Analysis; Human Resource Analysis; Resource Analysis; Management Analysis; and Finance Analysis. 30. Your Marketing Analysis deals with two groups, your learners and your faculty. For each group, you will have identified Repeat Business, that is, work for each that you will continue to carry out
218 as you have in previous years. You will also have identified three potential areas of change for learners and for faculty: a. Existing services that you will provide to new learners or new faculty; b. New services that you will provide to existing learners or existing faculty; c. New services that you will provide to new learners or new faculty. 31. Building on this, your Human Resource Analysis will have identified the amount of time required by staff with particular skills, knowledge, and experience, to provide the services set out in your Marketing Analysis. Your Resource Analysis will have identified the space, IT, and other resources needed by those personnel and your Management Analysis will have identified their functional and line management. Finally, your Finance Analysis will have indicated that these business ambitions are affordable within the financial bottom line. 32. Of course, this is your Business Analysis and your views and conclusions. Ethical Analysis requires that you consult fully and transparently with the people whom it will affect, both faculty and learners, through your LFG structure. The aim is to develop their participation in the design and provision of your Strategic Plan, by showing them the broad analytical basis on which you are working. 33. Typically, opportunities for participation should be offered in three ways: d. Prior documentation and a short presentation to LFG Leads, to discuss with their faculty of teachers and learners, and to feed back to you within a stated time; e. Opportunities for direct contact with the DME and MEM for individual learners or faculty members to discuss issues specific to them; f. A regular or newsletter updating everyone on how you have progressed matters in response to their views, and identifying a permanent location where they can read relevant documentation. 34. The key questions that you are asking are: g. Does this analysis and its broad directions work to the disadvantage of patients, learners, staff, or the larger healthcare community? h. If so, is the disadvantage caused by the proposals per se or by the implementation process proposed? i. What proposal do you make for an alternative course of action. It is important to note in your presentation to LFG Leads that while they are free to ask for clarification on any point, if they find the proposals problematic then an alternative proposal must be made. This could include setting up a sub-group to inquire further into the issue. 35. This process of consultation and participation should continue throughout the business year, so that each time the LFGs report in, they can indicate their progress on the work agreed for this year. In turn, the LAB should review its own progress at each meeting, making appropriate adjustments to its Business Analysis and Ethical Analysis as it implements its Strategic Plan.
219 LAB Strategic Development Quality Manual Verification Please identify action arising from your Quality Manual Verification process Target Date Target Ownership Progress RAG Education Management Audit Please identify action arising from your Education Management Audit, including your metrics Business Analysis Please identify action arising from your Business Analysis, including both cross-lep targets and targets the LAB has set for its LFGs KSS Contract Strategic Development Revalidation Notes for Guidance You MUST support the KSS Dean Director in his role as Responsible Officer by providing ALL information for Revalidation for ALL postgraduate doctors. This is a most important addition to the LAB s management responsibilities and while responsibility for its successful completion remains with the LAB Chair, its operationalization will usually form part of the role of the Academic Registrar. Draft indicative KSS Collective Exit Report and KSS Exception Exit Report forms, which may be replaced when the GMC approves a final national format, are provided at Appendix A. KSS Requirement Please identify targets in order to: a) Complete the KSS Collective Exit Report for ALL Postgraduate Doctors, indicating whether they were named in complaints or involved in conduct or formal SUI/SEA investigations, for return to KSS twice a year at the beginning of May and the beginning of November in time for the ARCP Panels. b) Complete the KSS Exception Exit Report for ALL Postgraduate Doctors named in complaints or involved in conduct or formal SUI/SEA investigations, for return to KSS twice a year, at the Target Date Target Ownership Progress RAG
220 beginning of May and the beginning of November, in time for the ARCP Panels. At the same time that a KSS Exception Exit Report is sent to KSS a copy of it should be provided to the postgraduate doctor concerned. Your return to KSS should ensure that KSS Exception Exit Reports are accompanied by the KSS Collective Exit Report c) Create a formal procedure so that the Dean Director is informed IMMEDIATELY of any significant concern about a postgraduate doctor, irrespective of when the KSS Collective Exit Report or the KSS Exception Visit Report are submitted to KSS. Educational Capacity Development Teacher Education Notes for Guidance This year s focus is on the accreditation of Educational Supervisors and Named Clinical Supervisors; and on developing and utilising educational capacity to Master s degree level. KSS Requirement Please identify targets in order to: a) Continue to manage the QESP process for Educational Supervisors and Named Clinical Supervisors. b) Identify succession planning for current Educational Supervisors and Named Clinical Supervisors. c) Audit the number of clinicians holding Master s degrees in Education in your LEP. d) Utilise to the best effect the clinicians holding Master s degrees in Education in your LEP. e) Plan to extend the number of clinicians holding Master s degrees in Education in your LEP. f) Ensure information is disseminated to all career grade doctors about the KSS part-time MA Education in Clinical Settings, including details of KSS Open Evenings. g) Provide progress reports on Teacher Education to the LAB for each of its formal meetings. Target Date Target Ownership Progress RAG Leadership Notes for Guidance This year s focus is on ensuring that the LAB manages all Leadership initiatives for KSS Contract workstreams (Medicine, Dentistry, Pharmacy, Library and Knowledge Services); has an overview of other Leadership initiatives in the LEP to reduce the possibility of duplication of effort; and on
221 developing and utilising capacity to Master s degree level. KSS Requirement Please identify targets in order to: a) Ensure that LAB membership and attendance includes a Leadership Tutor who: coordinates all Leadership initiatives for KSS Contract workstreams, including the Pairs initiative and the attendance of postgraduate doctors at the KSS Leadership Postgraduate Certificate Module Leadership in Clinical Contexts; has an overview of other Leadership initiatives in the LEP; and provides progress reports to the LAB for each of its formal meetings. b) Ensure that the LAB manages finance for all Leadership initiatives for KSS Contract workstreams. c) Audit the number of clinicians holding Master s degrees in Leadership in your LEP. d) Utilise to the best effect the clinicians holding Master s degrees in Leadership in your LEP. e) Plan to extend the number of clinicians holding Master s degrees in Leadership in your LEP. f) Ensure information is disseminated to all eligible staff about KSS part-time accredited programmes in Leadership, including details of KSS Open Evenings. Managing Medical Careers Notes for Guidance The management of medical careers is becoming increasingly professionalised and KSS is supporting that process by offering nationally a part-time Postgraduate Certificate; Postgraduate Diploma; and Master s degree in Managing Medical Careers. This year s focus is on initiating or extending that professionalisation process in your LEP. KSS Requirement Please identify targets in order to: a) Ensure that LAB membership and attendance includes a Managing Medical Careers Lead who: coordinates all Medical Careers initiatives; has an overview of other Careers initiatives in the LEP; and provides progress reports to the LAB for each of its formal meetings. b) Audit the number of staff holding Postgraduate Certificate; Postgraduate Diploma; and Master s degree qualifications in Managing Medical Careers in your LEP. c) Utilise to the best effect the staff holding Postgraduate Certificate; Postgraduate Diploma; and Master s degree qualifications in Managing Medical Careers in your LEP. d) Plan to extend the number of staff holding the KSS part-time Postgraduate Certificate;
222 Postgraduate Diploma; and Master s degree qualifications in Managing Medical Careers in your LEP. Medical Humanities Notes for Guidance KSS provides nationally a part-time Master s degree and an MPhil/PhD programme in Medical Humanities that focuses particularly on professionalism in the doctor-patient consultations and cultural features which shape those values. The focus this year is on developing a minimum level of engagement with Medical Humanities for each LAB; and on developing capacity to Master s degree level. KSS Requirement Please identify targets in order to: a) Ensure that LAB membership and attendance includes a Medical Humanities Lead who: attends two half-day KSS Medical Humanities Workshops during the year; develops Medical Humanities as a cross-curricular element in the LEP; and provides progress reports to the LAB for each of its formal meetings. b) Ensure information is disseminated to all eligible staff about KSS part-time accredited programmes in Medical Humanities, including details of KSS Open Evenings. Simulation Notes for Guidance This year s focus is on ensuring that the LAB manages all Simulation initiatives for KSS Contract workstreams (Medicine, Dentistry, Pharmacy, Library and Knowledge Services); has an overview of other Simulation initiatives in the LEP to reduce the possibility of duplication of effort; and on supporting KSS s work to develop capacity locally. KSS Requirement Please identify targets in order to: a) Ensure that LAB membership and attendance includes a Simulation Lead who: coordinates all Simulation initiatives for KSS Contract workstreams; has an overview of other Simulation initiatives in the LEP; and provides progress reports to the LAB for each of its formal meetings. b) Ensure that the LAB manages finance for all Simulation initiatives for KSS workstreams. c) Ensure LAB progress reports on Simulation are forwarded in a timely fashion to the KSS
223 Assistant Dean Education leading on Simulation (currently Alison Gisvold). d) Ensure that the Simulation Lead attends KSS Simulation meetings and events as required to enable joint development of Simulation initiatives. Curriculum Mapping Notes for Guidance Last year we asked LABs to review their LFGs to identify which ones had a Curriculum Statement for their postgraduate doctors, produced according to the best-practice model supplied by KSS from Frimley Park Hospital. The focus this year is on ensuring that the LAB manages all curriculum mapping initiatives for medicine in the LEP. KSS Requirement Please identify targets in order to: a) Ensure that LAB membership and attendance includes a Curriculum Mapping Lead who: coordinates all Curriculum Mapping initiatives for medicine; and provides progress reports to the LAB for each of its formal meetings. b) Ensure LAB progress reports on Curriculum Mapping are forwarded in a timely fashion to the KSS Assistant Dean Education leading on Curriculum Mapping (currently Dr Clare Penlington and Dr Elaine Hawkins) Patients with Learning Disabilities Notes for Guidance KSS provides Workshops to develop capacity for your postgraduate doctors and faculty to work with Patients with Learning Disabilities [PLDs]. This is an important aspect of developing professionalism, improving clinical governance, meeting the requirements of the Equality Act, and improving patient care. KSS Requirement Please identify targets in order to: a) Ensure that all LFGs include attendance at KSS PLD Workshops as part of their plan for faculty development. b) Discuss with your LEP its plans to sign up to Mencap s Getting It Right Charter and report progress at your LAB.
224 Trainees in Difficulty Notes for Guidance KSS has an ongoing commitment to supporting postgraduate doctors with additional needs and we believe that this is an important element of the LAB s management role. KSS Requirement Please identify targets in order to: a) Ensure that LAB membership and attendance includes a Trainees in Difficulty Lead who: coordinates all support for postgraduate doctors with additional needs; and provides progress reports to the LAB for each of its formal meetings. Postgraduate Doctor Representatives Notes for Guidance KSS GEAR requires all LFGs to ensure that their postgraduate doctors meet regularly to provide feedback to the Faculty, and to ensure that there is an appropriately trained Postgraduate Doctor Representative sitting on the LFG and on the LAB. The focus this year is on developing local capacity for those functions. KSS Requirement Please identify targets in order to: a) Ensure that the LAB provides at least one Workshop to train Postgraduate Doctor Representatives. b) Ensure a report on the Workshop is provided in a timely fashion to the KSS Education Department Professional Services staff managing Postgraduate Doctor Representatives (currently Jon Nodding). Lay Representatives Notes for Guidance Lay Representatives provide an important element of externality to LAB meetings and management and are required by the GMC Standards. The focus this year is on developing local capacity for that. KSS Requirement Please identify targets in order to: a) Ensure that the LAB provides at least one Lay Representative to attend the KSS Annual Forum for Lay Representatives.
225 School Specific Development General Practice School Target Date Target Ownership Progress RAG ARCP Data Notes for Guidance Since GP Trainees only attend ARCP Panels exceptionally, it is important for all assessment and other reports to be entered accurately and in a timely fashion on the INSITE database. KSS has funded administration costs for this specific purpose. KSS Requirement Please identify targets in order to manage and monitor: a) The collection of data monitoring GP Trainees progress towards their ARCP. b) GP trainees progress through the RCGP E-Portfolio. c) Arrangements for maintaining the KSS INSITE database regularly in advance of GP LFG meetings. d) Arrangements for updating INSITE according to the guidance and timescales provided annually by KSS. GP Single Employer Notes for Guidance To ensure consistency in GP Trainees employment, KSS has signed a Single Employer Service Level Agreement [ the SESLA ] with KSS LEPs. The SESLA provides a single Lead Acute Trust Employer for GP Trainees following three year programmes and identifies other LEPs where they work and learn as Host organisations. KSS Requirement Please identify targets in order to manage and monitor: a) Your compliance with the SESLA. b) Your communication systems, including regularity and frequency, with host organisations. c) Your system for ensuring accurate reports on salary and non pay expenses are made to KSS in the required format and at the prescribed times. d) Your system for collecting information and transmitting to the Single employer acute trust for ensuring accurate reports of sickness and absence are made to KSS in the required format
226 and at the prescribed times. Foundation School National Reports Notes for Guidance The Collins Report and the Psychiatry Taskforce recommendations provide national standards for Foundation for implementation locally. KSS Requirement Please identify targets in order to: a) Manage and monitor your Foundation LFG s compliance with the Collins Report. b) Manage and monitor your Foundation LFG s implementation of the Psychiatry Taskforce s recommendations. Shadowing Notes for Guidance It is best practice for LABs to provide shadowing opportunities for Foundation doctors. The focus this year is on implementing forthcoming new national requirements in shadowing. KSS Requirement Please identify targets in order to: a) Support your Foundation LFG in developing a plan to meet the new national requirements for shadowing within a month of their publication. b) Monitor progress by your Foundation LFG in implementing, reviewing, and reporting its arrangements for shadowing. School of Anaesthetics Educational Supervisors Notes for Guidance Educational Supervisors attendance at LFGs as set out in KSS GEAR is a matter of ethical educational practice, professional obligation, and contractual agreement. KSS Requirement
227 Please provide targets in order to: a) Monitor Educational Supervisor attendance at your Anaesthetics LFG. b) Address all and any issues of attendance that is not compliant with KSS GEAR. Recruitment Interviews Notes for Guidance KSS relies on its consultant body to provide expert input to the interview process in order to ensure that excellent candidates are attracted to work in this region. This year s focus is on ensuring an adequate support for this important central function. KSS Requirement Please provide targets in order to: a) Ensure that your LFG Anaesthetics is able to meet the KSS Head of School s requirements for support for recruitment interviews. School of Obstetrics and Gynaecology ARCP Data Notes for Guidance KSS requires Educational Supervisors reports to be completed and submitted 2 weeks in advance of the ARCP deadline set by the KSS School of Obstetrics and Gynaecology. KSS Requirement Please identify targets in order to: a) Manage and monitor your LFG Obstetrics and Gynaecology s completion of Educational Supervisors reports. b) Ensure that these data are submitted to KSS on deadline. Basic Ultrasound Training Notes for Guidance KSS requires all postgraduate doctors to undergo mandatory RCOG Basic Ultrasound Training. KSS Requirement Please identify targets in order to: a) Manage and monitor your LFG Obstetrics and Gynaecology s completion of mandatory RCOG
228 Basic Ultrasound Training for all of its postgraduate doctors. b) Maintain a register of completion of this training and include that in its Annual Report. Obstetric Simulation Notes for Guidance KSS requires all postgraduate doctors to engage with Obstetric Simulation, which is assessed at ARCP. KSS Requirement Please identify targets in order to: a) Manage and monitor your LFG Obstetrics and Gynaecology s provision of Basic Obstetric Simulation in the form of Skills Drills or similar activities. b) Manage and monitor your LFG Obstetrics and Gynaecology s provision of Low-Tech Simulation in areas such as perineal repair and laparoscopy. Curriculum Notes for Guidance KSS requires all postgraduate doctors to follow a planned curriculum that maximises the opportunities for practical and surgical training. KSS Requirement Please identify targets in order to: a) Manage and monitor your LFG Obstetrics and Gynaecology s production of a curriculum map. b) Review your LFG Obstetrics and Gynaecology s curriculum map to ensure that it maximises the opportunities for practical and surgical training. Tasters Notes for Guidance Provision of Taster Weeks by LFGs Obstetrics and Gynaecology is an important part of attracting the best candidates into the School. KSS Requirement Please identify targets in order to: a) Review your LFG Obstetrics and Gynaecology s capacity for providing Taster Weeks.
229 School of Opthalmology LFG Establishment Notes for Guidance The new KSS School of Opthalmology requires an LFG to be set up specifically for Opthalomology, separate from the LFG for Surgery. KSS Requirement Please provide targets in order to: a) Establish an Opthalmology LFG operating to KSS GEAR. b) Manage and monitor its progress including its reporting to your LAB and to the KSS Head of School as required by KSS GEAR. SAS Doctors Local Faculty Development Notes for Guidance KSS values highly the work of SAS doctors and KSS LABs have provided excellent support through the establishment of SAS LFGs and the utilisation of SAS doctors in educational, leadership, and service improvement roles. This year s focus is on consolidating this work. KSS Requirement Please provide targets in order to: a) Ensure that your SAS LFG continues to receive appropriate support from and management by your LAB. b) Ensure that your SAS doctors receive Study Leave and CPD as an entitlement within their Contracts of Employment. KSS Specialty Prospectuses Notes for Guidance In order to attract the highest quality applicants to the region, KSS requires regularly-updated information for its Prospectuses. A form for recording and returning these data appears at Appendix B. KSS Requirement Please identify targets in order to:
230 a) Ensure an entry per Specialty is provided to KSS Head of Specialty Workforce (Angela Fletcher in post) by October each year for Core posts and by January each year for Higher posts. b) Review content on an annual basis by October and January each year and provide updated information to KSS. Review and Reporting Notes for Guidance Regular review and reporting by LFGs to their LAB and to Schools is crucial to local quality control, especially in remediating poor performance against the GMC Surveys. Similarly, regular review and reporting of your LAB to your LEP s senior executive committee and to KSS is crucial to managing the continuous quality improvement of PGME locally. KSS Requirement Please provide targets in order to: a) Ensure LFGs meet, review progress, and report to LAB, including planning to remediate poor performance against the GMC Surveys, as required by KSS GEAR. b) Ensure your LAB regularly reviews and reports progress to your LEP s senior executive committee in order to manage and improve quality locally. c) Ensure LFG and LAB review and reporting processes are integrated into the LAB s local processes for managing KSS Visits and for producing the Annual Review. Target Date Target Ownership Progress RAG
231 Library and Knowledge Services Development Strategy (a) Library and Knowledge Services Strategy The KSS request: Please provide a copy of your current strategy and highlight your key priorities for the coming year and how your service will ensure it can deliver on them. (b) Collaborative Working The KSS request: Please describe your strategy for embedding library and knowledge services in research, education, clinical and corporate governance, service planning and direct patient care and other relevant processes in local NHS organisations. (c) Marketing and Promotion The KSS request: Please describe your strategy for raising awareness and increasing usage of your services among users and non-users in your local Trusts and amongst other stakeholders. (d) Participation in Local Academic Board and Local Faculty Groups The KSS request: Please describe your strategy for active participation with the Local Academic Board and how you engage with the Local Faculty Groups. (e) SIFT Funding The KSS request: Please report on the allocation of SIFT Library and Knowledge Services receive per capita and per Higher Education Institution. Higher Education Institution Per Capita Funding Brighton and Sussex Medical School St George s Medical School King s Medical School University of Southampton Medical School Other (f) Non-Medical Education Funding for Students on Clinical Placement The KSS request: Please report on the allocation of funding Library and Knowledge Services receive for non-medical education students on clinical placement per capita and per Higher Education Institution
232 Higher Education Institution Per Capita Funding Canterbury Christchurch University University of Brighton University of Greenwich University of Surrey Other (g) Library and Knowledge Services Staffing KSS request: Please report on any difficulty in filling posts and the impact on services that is likely to have. (h) Library and Knowledge Services Ideas and Issues KSS request: We recognise that Library and Knowledge Services are often creative in their thinking, and equally, that some Library and Knowledge Services may have particular issues that do not affect Library and Knowledge Services in general. It would be helpful if Library and Knowledge Services could report on: a) major influences on your work at present; b) major proposed developments for the future; c) local concerns and issues which are relevant to Contract Review.
233 KSS Pharmacy Local Faculty Group Annual Audit and Review. PHARMACY TRAINING TEMPLATE. Trust name: LFG Chair: Pre-registration Pharmacist EPD: Number or Pre-reg Pharmacists: Pre-registration Trainee Pharmacy Technician EPD: Number of PTPTs: Foundation Pharmacist EPD: Number of band 6 pharmacists on Foundation Programme: Local Faculty Group Meetings Date of LFG Meetings: Number of Attendees: Summary of Trainees progress Attach confidential spreadsheet
234 Domain 1 Patient Safety There must be clear procedures in place to address concerns about patient safety arising from initial pharmacy education and training. Concerns must be addressed immediately. Areas you may wish to comment on: GPhC standards of conduct, ethics and performance and trainees understanding of this. Supervision of trainees to ensure safe practice. Notable practice: Areas of concern with time bound targets for action and named responsibility:
235 Domain 2 Monitoring, review and evaluation of initial education and training. The quality of pharmacy education and training must be monitored, reviewed and evaluated in a systematic and developmental way. Areas you may wish to comment on: The whole curriculum and timetable and evaluation of it. Input from a range of internal and external stakeholders (including patients and public) into monitoring and evaluation. Trainees in difficulty and the Trainee in Difficulty policy. Notable practice: Areas of concern with time bound targets for action and named responsibility:
236 Domain 3 Equality, Diversity and fairness Pharmacy education and training must be based on the principles of equality, diversity and fairness. It must meet the needs of current legislation. Areas you may wish to comment on: Support for any trainees with additional needs. Adjustments to programmes for trainees with disabilities. Any other education and development issues. Notable practice: Areas of concern with time bound targets for action and named responsibility: Domain 4 Selection of students and trainees Selection processes must be open and fair and comply with relevant legislation. Areas you may wish to comment on: Recruitment & Selection training and support. Processes for recruitment of trainees. Notable practice: Areas of concern with time bound targets for action and named responsibility:
237 Domain 5 Curriculum delivery and student experience The local curriculum must be appropriate for national requirements. It must ensure that trainees and PG pharmacists practise safely and effectively. To ensure this, pass/ competence criteria must describe professional, safe and effective practice. Areas you may wish to comment on: The GPhC pre-reg performance standards, KSSD Pre-registration Trainee Pharmacist Handbook and local curricular response to them. Range of educational and practice activities as set out in the local curriculum. Access to training days, e-learning resources and other learning opportunities that form an intrinsic part of the training programme. Notable practice: Areas of concern with time bound targets for action and named responsibility:
238 Domain 6 Support and development for trainees Trainees on any programme managed by the Pharmacy LFG must be supported to develop as learners and professionals. They must have regular ongoing educational supervision with a timetable for supervision meetings. All LFGs must adhere to the KSSD Trainee in Difficulty policy and be able to show how this works in practice. LFGs must implement and monitor policies aqnd incidents of grievance and discipline, bullying and harassment. All trainees should have the opportunity to learn from and with other health care professionals. Areas you may wish to comment on: The range of mechanisms to support trainees to develop as learners and professionals. Bullying, harassment, grievance and disciplinary issues. Opportunities to learn with and from other healthcare professionals. Notable practice: Areas of concern with time bound targets for action and named responsibility:
239 Domain 7 Support and development for Pre-registration Trainee Pharmacist Practice Supervisors and Educational Supervisors. Practice supervisors, educational supervisors and education programme directors should have these roles clearly identified and be trained and competent to undertake them. Supervisors should have time to carry out their role and access to support and training including identified peer support. Areas you may wish to comment on: Practice Supervisor, Educational Supervisor and Educational Programme Director training and support. Notable practice: Areas of concern with time bound targets for action and named responsibility:
240 Domain 8 Management of initial education and training. There should be transparent processes which show who is responsible for each element and each stage of training programmes. Areas you may wish to comment on: The responsibilities of all staff involved in the programme. Succession planning for Practice Supervisor and Educational Supervisor roles. Notable practice: Areas of concern with time bound targets for action and named responsibility: Domain 9 Resources and capacity. Resources and capacity are sufficient to deliver outcomes. Areas you may wish to comment on: The availability of resources. Appropriateness of educational facilities. Notable practice: Areas of concern with time bound targets for action and named responsibility:
241 Domain 10 Outcomes There should be an analysis of outcomes of assessments benchmarked against others which is accessible to trainees. These should be an analysis of the outcomes of assessments benchmarked whenever possible. Areas you may wish to comment on: An analysis of outcomes of assessments. Comparators and benchmarks. Notable practice: Areas of concern with time bound targets for action and named responsibility: Comment on any difficulties in securing full membership here:
242 Comment on any issues relating to LFG procedural regulations, difficulties and steps taken to resolve them Confirm that trainees are represented on the LFG and trained for this role. Signed by Chair of Pharmacy LFG: Date:
243 Appendix A KSS Collective Exit Report for Postgraduate Doctors To be completed by the Employer/ Host Training Organisation. In the case of GP trainees in a primary care placement this Report should be completed by the PCT/ Organisation responsible for maintaining the local GP Performance List. Use an excel spread sheet or add more rows to the table below to list all the doctors employed in each organisation. Postgraduate Doctor s Name GMC Number Dates of Employment Start Date End Date Involved in conduct, capability or Formal Serious Untoward Incidents/ Significant Event Investigation or named in complaints (Please state YES or NO) I confirm that I have included an Exception Exit Report for any of the postgraduate doctors listed above who have been involved in conduct, capability or formal Serious Untoward Incidents/ Significant Event Investigation or named in complaints whilst employed by this organisation, whether as a postgraduate doctor or as a locum, on the dates specified above. Signature Full name Name of the Organisation Date Job Title Name of the Medical Director (If the signatory is not the MD)
244 KSS Exception Exit Report for Postgraduate Doctors To accompany the Collective Exit Report To be completed by the Employer/ Host Training Organisation. In the case of GP trainees in a primary care placement this Report should be filled by the PCT/ Organisation responsible for maintaining the local GP Performance List and by their Clinical/Educational Supervisor Postgraduate Doctor s Name: GMC Number: Start Date End date Details of Employment/Placements/Locum Comments Details of concerns/investigations: Conduct, Capability Investigation This trainee has been involved in a conduct, capability investigation This has been resolved satisfactorily with no unresolved concerns about this trainee s conduct. If not, please give a brief summary and the anticipated date of the outcome of the investigation: YES / NO YES / NO Serious Untoward Incident/ Significant This trainee has been involved in formal Serious Untoward Incident/Significant Event investigation This has been resolved satisfactorily with no unresolved concerns about a trainee s fitness to practice YES / NO YES / NO
245 Event investigation If not, please give a brief summary and the anticipated date of the outcome of the investigation: Complaints This trainee has been named in complaint(s) YES / NO This has been resolved satisfactorily with no unresolved concerns about a trainee s fitness to practice or conduct YES / NO If not, please give a brief summary and the anticipated date of the outcome of the investigation: Signature Full name Name of the Organisation Date Job Title Name of the Medical Director (If the signatory is not the MD)
246 Appendix B LAB Education Strategy Appendix B TRAINING PROGRAMME Trust Hospital UOA Introduction Terms of Business Include terms of business and information on workfinding service Distinction between training programme offer and employment contract Post details Specialty Grade Location within programme Type of Work Name of the position and work needing to be done Qualifications and professional registration required Attach JD Anticipated duration of programme Commencement date Standard rotation details Educational Supervisor Clinical Lead Outcome CCT/CESR/CP/Core Outcome of training programme i.e. core competencies KSS Sample Timetable: Monday Am Pm Tuesday Am Pm Wednesday Am Pm Thursday Am Pm Friday Am Pm
247 Location Info on likely locations including likely specific sites within rotations Confirmation of location including specific info on site within multi-site employer Payments/Policy Salary Scale Basic Pay referring to national salary scales Travel and relocation expenses policy
248 Educational Governance Contract Review and Development 2012 Quality Manual notification of change and verification report This form is to be used in conjunction with the Quality Manual This document is to be used for those LEPs who have been awarded Earned Autonomy for the Single Contract Review (SCR) process. It is the contractual responsibility of the LAB to ensure that the internal verification process is conducted and completed appropriately. This QM should be completed with the same rigour and robustness of all SCR documentation to ensure that Earned Autonomy can also be awarded in future SCR cycles. Please note that you are only required to note any changes to the Quality Manual which have occurred since the last single contract review cycle. However, these changes should be reported as a narrative, (not using bullet points) to ensure clarity and understanding. A member of the KSS Verification Team may contact the MEM if further clarification is needed on any of the points in this document. Local Education Provider [LEP] Medical Education Manager I confirm that the processes set out in the Quality Manual 2011 are current and any exceptions to this have been noted below. Medical Education Manager s signature Date Please prefix any changes to process with the relevant section number from the Quality Manual. Domain 1: Patient safety (1-4) Domain 2: Quality management, review and evaluation (5-9) Domain 3: Equality, diversity and opportunity (10-13) Notification of change and verification report Page 1 of 2 Created on 08/10/201216/02/2012
249 Domain 4: Recruitment, selection and appointment (14-23) Domain 5: Provision of approved curriculum including assessment (24-29) Domain 6: Support and development of postgraduate doctors and LFG (30-44) Domain 7: Management of PGMDE (45-47) Domain 8: Educational resources and capacity (48-60) Domain 9: Outcomes (61) Notification of change and verification report Page 2 of 2 Created on 08/10/201216/02/2012


250 7 Bermondsey Street London SE1 2DD Main Tel: Main Fax: KSS Deanery Contract Review and Development 2011/12 Educational Governance Quality Manual Verification Visit Location: Date: Attendance: DOMAIN 1: PATIENT SAFETY 1 INDUCTION TO THE LEP 2 Work Patterns and Intensity 3 Clinical Responsibility 4 Clinical Support Domain 2: Quality Management, Review and Evaluation 5 Graduate Education and Assessment Regulations (GEAR) 6 Security of Information 7 Intrepid: Postgraduate Doctor and Dentist Data 8 Intrepid: Monitoring Educational Supervision 9 Short Term Cover for Medical Staffing Functions With our partners Chair, Deanery Advisory Board - Professor Sir David Melville CBE Dean Director - Professor Deanery David Chair Black Name
251 Domain 3: Equality, Diversity and Opportunity 10 Equality, Diversity and Opportunity in Appointments 11 Equality, Diversity and Opportunity in Education 12 Less Than Full Time Training [LTFTT] 13 Reasonable Adjustments Domain 4: Recruitment, Selection and Appointment 14 Registration of Postgraduate Doctors and Dentists 15 Immigration Requirements 16 Specialty Training Posts 17 Selection into Specialty and Higher Specialty Programmes 18 Managing HST Transition into KSS Specialty Schools 19 Recruitment and Selection 20 Local Selection Panels 21 Advertising Placements Locally 22 Contract of Employment 23 Job Description Domain 5: Provision of Approved Curriculum Including Assessment 24 LFG Handbooks 25 Induction to Educational Programme 26 Curriculum Development 27 Educational Assessment 28 Study Leave Availability 29 Study Leave for SAS and Trust Grade Doctors Domain 6: Support and Development of Postgraduates and Local Faculty 30 Induction to the Department 31 Educational Supervision
252 32 Educational Plans 33 Educational Development Meetings 34 Clinical Supervision 35 Academic Education 36 Workplace Bullying 37 Pastoral Care 38 Faculty Development: Selection 39 Faculty Development: CPD 40 Faculty Development: Job Plans 41 Faculty Development: QESP 42 Faculty Development: Assessment 43 Faculty Development: Capacity Growth 44 Faculty Development: Records Domain 7: Management of Education 45 Management of Education 46 Support and Career Advice 47 Postgraduates requiring additional support Domain 8: Educational Resources and Capacity 48 Education Centre and LKS Facilities 49 Teaching and Learning Facilities 50 LEP Facilities 51 Education Technologies 52 IT Facilities 53 Support Staff 54 Workforce Planning 55 Appointment of DME/Clinical Tutor 56 Appointment of Staff to the PGDME Function
253 57 Budgetary Accountability 58 Annual Finance Returns 59 Notification of Financial Transfers 60 Expenditure of KSS Monies Domain 9: Outcomes 61 Review and Improvement

![Apologies: Head of Library and Knowledge Services: Chief Executive: KSS: Assistant Dean [Education]: Deputy PG Dean for Secondary Care: Dental Associate Dean for](/docs-images/71/65973090/images/254-1.jpg "Secondary Care: Head of Library and Knowledge Services: Head of KSS Pharmacy: Feedback session: as above plus Medical Director: Finance representative: HR")
254 Contract Review Visit 2012 Location: Date: Attendance: Director of Medical Education: DSM (QA) and Medical Education Manager: DSM (Ops) and MEM: Clinical Tutor: Clinical Tutor: Clinical Tutor: Dental Tutor: Knowledge Services Manager: Director of Pharmacy: Lead Pharmacist Education and Development: Education Advisor: Apologies: Head of Library and Knowledge Services: Chief Executive: KSS: Assistant Dean [Education]: Deputy PG Dean for Secondary Care: Dental Associate Dean for Secondary Care: Head of Library and Knowledge Services: Head of KSS Pharmacy: Feedback session: as above plus Medical Director: Finance representative: HR representative:
Kent, Surrey and Sussex General Practice Specialty Training School Integrated Training Posts as part of GP Speciality training in KSS
 Integrated Training Posts as part of GP Speciality training in KSS KSS ITP May 2008 updated 8/7/2008 1 of 13 Integrated Training Posts as part of GP Speciality training in KSS The regulations for GP Specialty
Integrated Training Posts as part of GP Speciality training in KSS KSS ITP May 2008 updated 8/7/2008 1 of 13 Integrated Training Posts as part of GP Speciality training in KSS The regulations for GP Specialty
Level 2: Exceptional LEP Review Visit by School Level 3: Exceptional LEP Trigger Visit by Deanery with Externality... 18
 Postgraduate Training Ongoing Quality Review and Enhancement Framework Version 1: 2010 Contents Contents... 2 PMET Quality Review Framework Introduction... 3 Introduction... 3 Postgraduate Training Quality
Postgraduate Training Ongoing Quality Review and Enhancement Framework Version 1: 2010 Contents Contents... 2 PMET Quality Review Framework Introduction... 3 Introduction... 3 Postgraduate Training Quality
Action Plan for Health Education Kent, Surrey and Sussex
 Action Plan for Health Education Kent, Surrey and Sussex Requirements Report HEKSS1 HEKSS must work with East Kent Hospitals University NHS Foundation Trust to address the patient safety concern identified
Action Plan for Health Education Kent, Surrey and Sussex Requirements Report HEKSS1 HEKSS must work with East Kent Hospitals University NHS Foundation Trust to address the patient safety concern identified
The Trainee Support Group
 Postgraduate Deanery for Kent, Surrey and Sussex Postgraduate Medical and Dental Education The Trainee Support Group Including The Trainee In Difficulty A KSS Guide November 2009 Contents 3 4 Introduction
Postgraduate Deanery for Kent, Surrey and Sussex Postgraduate Medical and Dental Education The Trainee Support Group Including The Trainee In Difficulty A KSS Guide November 2009 Contents 3 4 Introduction
ST. MARTIN S POSTGRADUATE CENTRE St. Martin s Hospital, Littlebourne Road, Canterbury, Kent
 ST. MARTIN S POSTGRADUATE CENTRE St. Martin s Hospital, Littlebourne Road, Canterbury, Kent 1. JOB DETAILS Job Title: Accountable to: Responsible to: Location: Postgraduate Administrator Director of Medical
ST. MARTIN S POSTGRADUATE CENTRE St. Martin s Hospital, Littlebourne Road, Canterbury, Kent 1. JOB DETAILS Job Title: Accountable to: Responsible to: Location: Postgraduate Administrator Director of Medical
DME Self-Assessment Template
 Health Education Kent, Surrey and Sussex QUALITY MANAGEMENT OF SPECIALTY TRAINING DME Self-Assessment Template Name of Trust: ASHFORD AND ST. PETERS Specialties being visited: A+E, ACCS,GP and Rheumatology
Health Education Kent, Surrey and Sussex QUALITY MANAGEMENT OF SPECIALTY TRAINING DME Self-Assessment Template Name of Trust: ASHFORD AND ST. PETERS Specialties being visited: A+E, ACCS,GP and Rheumatology
The GMC Quality Framework for specialty including GP training in the UK
 The GMC Quality Framework for specialty including GP training in the UK April 2010 In April 2010 the Postgraduate Medical Education and Training Board (PMETB) was merged with the General Medical Council
The GMC Quality Framework for specialty including GP training in the UK April 2010 In April 2010 the Postgraduate Medical Education and Training Board (PMETB) was merged with the General Medical Council
NHS England (Wessex) Clinical Senate and Strategic Networks. Accountability and Governance Arrangements
 Clinical Senate and Strategic Networks. Accountability and Governance Arrangements") NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
Quality Management in Pharmacy Pre-registration Training: Current Practice
 Pharmacy Education, 2013; 13 (1): 82-86 Quality Management in Pharmacy Pre-registration Training: Current Practice ELIZABETH MILLS 1*, ALISON BLENKINSOPP 2, PATRICIA BLACK 3 1 Postgraduate Academic Course
Pharmacy Education, 2013; 13 (1): 82-86 Quality Management in Pharmacy Pre-registration Training: Current Practice ELIZABETH MILLS 1*, ALISON BLENKINSOPP 2, PATRICIA BLACK 3 1 Postgraduate Academic Course
Review of Health Education Kent, Surrey and Sussex
 Kent, Surrey and Sussex regional review 2015 Review of Health Education Kent, Surrey and Sussex This visit is part of a regional review and uses a risk-based approach. For more information on this approach
Kent, Surrey and Sussex regional review 2015 Review of Health Education Kent, Surrey and Sussex This visit is part of a regional review and uses a risk-based approach. For more information on this approach
Training Hubs - Funding Allocation Paper
 Training Hubs - Funding Allocation Paper Background Health Education England (HEE), NHS England, the Royal College of General Practitioners (RCGP) and the BMA GPs Committee (GPC) are working together to
Training Hubs - Funding Allocation Paper Background Health Education England (HEE), NHS England, the Royal College of General Practitioners (RCGP) and the BMA GPs Committee (GPC) are working together to
Contents... 2 ADR Introduction... 3 Postgraduate Training Quality Governance Framework... 4 ADR Process and Documentation... 6 GMC Standards for
 Annual Deanery Report Guidance Version 1: 2010 Contents Contents... 2 ADR Introduction... 3 Postgraduate Training Quality Governance Framework... 4 ADR Process and Documentation... 6 GMC Standards for
Annual Deanery Report Guidance Version 1: 2010 Contents Contents... 2 ADR Introduction... 3 Postgraduate Training Quality Governance Framework... 4 ADR Process and Documentation... 6 GMC Standards for
Fellowships in Clinical Leadership (Darzi Fellows 2017/18)
") Fellowships in Clinical Leadership (Darzi Fellows 2017/18) Darzi Fellow job description mployer: Department: Location: Accountable to: Job Type: Job Title: Req Grade: Full-Time, Fixed Term Darzi Fellow
Fellowships in Clinical Leadership (Darzi Fellows 2017/18) Darzi Fellow job description mployer: Department: Location: Accountable to: Job Type: Job Title: Req Grade: Full-Time, Fixed Term Darzi Fellow
Supervision of Trainee Doctors
 Appendix 13 Supervision of Trainee Doctors Good Medical Practice Supervision of Trainee Doctors Teaching, training, appraising and assessing doctors and students are important for the care of patients
Appendix 13 Supervision of Trainee Doctors Good Medical Practice Supervision of Trainee Doctors Teaching, training, appraising and assessing doctors and students are important for the care of patients
The Trainee Doctor. Foundation and specialty, including GP training
 Foundation and specialty, including GP training The duties of a doctor registered with the General Medical Council Patients must be able to trust doctors with their lives and health. To justify that trust
Foundation and specialty, including GP training The duties of a doctor registered with the General Medical Council Patients must be able to trust doctors with their lives and health. To justify that trust
Royal College of Obstetricians & Gynaecologists. Principles and processes for externality in specialty education and training
 Royal College of Obstetricians & Gynaecologists Principles and processes for externality in specialty education and training Introduction 1. The aims of this document are to: explain why externality is
Royal College of Obstetricians & Gynaecologists Principles and processes for externality in specialty education and training Introduction 1. The aims of this document are to: explain why externality is
HEALTH EDUCATION NORTH WEST ANNUAL ASSESSMENT VISIT
 Health Education North West HEALTH EDUCATION NORTH WEST ANNUAL ASSESSMENT VISIT VISITORS:- Postgraduate Dean: Professor David Graham PUBLIC HEALTH ith 9" October 2013 Associate Director of Postgraduate
Health Education North West HEALTH EDUCATION NORTH WEST ANNUAL ASSESSMENT VISIT VISITORS:- Postgraduate Dean: Professor David Graham PUBLIC HEALTH ith 9" October 2013 Associate Director of Postgraduate
Reference Guide. has bee. July 2012
 Reference Guide ument This doc n has bee for updated 2014 August July 2012 Contents 1. Introduction 4 2. The purpose of the Foundation Programme 5 3. Organisation of postgraduate training 7 4. Shape of
Reference Guide ument This doc n has bee for updated 2014 August July 2012 Contents 1. Introduction 4 2. The purpose of the Foundation Programme 5 3. Organisation of postgraduate training 7 4. Shape of
Scottish Advisory Committee on Distinction Awards GUIDE TO THE SCHEME
 Scottish Advisory Committee on Distinction Awards GUIDE TO THE SCHEME 2015 This guide is available at: http://www.scclea.scot.nhs.uk/ The SACDA Online system is available at: https://awards.scclea.scot.nhs.uk/
Scottish Advisory Committee on Distinction Awards GUIDE TO THE SCHEME 2015 This guide is available at: http://www.scclea.scot.nhs.uk/ The SACDA Online system is available at: https://awards.scclea.scot.nhs.uk/
Clinical Skills and Simulation Strategy
 Clinical Skills and Simulation Strategy August 2010 Contents 2 Forward... 3 Definitions... 4 Introduction... 4 Regional context... 5 Aim... 6 Action Plan... 6 Quality Standards... 7 Regional investment
Clinical Skills and Simulation Strategy August 2010 Contents 2 Forward... 3 Definitions... 4 Introduction... 4 Regional context... 5 Aim... 6 Action Plan... 6 Quality Standards... 7 Regional investment
NW Clinical Placement Strategy. FAQs
 NW Clinical Placement Strategy FAQs What is the NW Clinical Placement Strategy? The NW Clinical Placement Strategy (2007) resulted from a Regional profession wide consultation focussing on the delivery
NW Clinical Placement Strategy FAQs What is the NW Clinical Placement Strategy? The NW Clinical Placement Strategy (2007) resulted from a Regional profession wide consultation focussing on the delivery
QUALITY COMMITTEE. Terms of Reference
 QUALITY COMMITTEE Terms of Reference CONSTITUTION 1. The Board of Directors approved the establishment of the Quality Committee (known as the Committee in these terms of reference) for the purpose of:
QUALITY COMMITTEE Terms of Reference CONSTITUTION 1. The Board of Directors approved the establishment of the Quality Committee (known as the Committee in these terms of reference) for the purpose of:
Revalidation Annual Report
 Paper 31 14 Revalidation Annual Report 2013-14 Purpose of Document: To provide the Board with a report on the first year s experience with medical revalidation in Public Health Wales. Board/Committee to-
Paper 31 14 Revalidation Annual Report 2013-14 Purpose of Document: To provide the Board with a report on the first year s experience with medical revalidation in Public Health Wales. Board/Committee to-
East Kent Hospitals University NHS Foundation Trust William Harvey Hospital
 LOCAL EDUCATION PROVIDER VISITS 2012-2013 East Kent Hospitals University NHS Foundation Trust William Harvey Hospital Friday 15 March 2013 Specialties being visited: Emergency Medicine, General Surgery,
LOCAL EDUCATION PROVIDER VISITS 2012-2013 East Kent Hospitals University NHS Foundation Trust William Harvey Hospital Friday 15 March 2013 Specialties being visited: Emergency Medicine, General Surgery,
WESSEX DEANERY OUT OF HOURS GUIDELINES (Aug 2013)
") WESSEX DEANERY OUT OF HOURS GUIDELINES (Aug 2013) Introduction 1. Emergency and unscheduled work remains an essential part of Primary Health Care services and all General Practice Trainees must gain experience
WESSEX DEANERY OUT OF HOURS GUIDELINES (Aug 2013) Introduction 1. Emergency and unscheduled work remains an essential part of Primary Health Care services and all General Practice Trainees must gain experience
An Overview for F2 Doctors of Foundation Programme attachments to General Practice
 An Overview for F2 Doctors of Foundation Programme attachments to General Practice July 2011 Contents Page GP Placements 2 Guidance on Educational Agreements 4 Key facts about F2 Placements 6 The Foundation
An Overview for F2 Doctors of Foundation Programme attachments to General Practice July 2011 Contents Page GP Placements 2 Guidance on Educational Agreements 4 Key facts about F2 Placements 6 The Foundation
North School of Pharmacy and Medicines Optimisation Strategic Plan
 North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
INTRODUCTION TO THE UK PUBLIC HEALTH REGISTER ROUTE TO REGISTRATION FOR PUBLIC HEALTH PRACTITIONERS
 INTRODUCTION TO THE UK PUBLIC HEALTH REGISTER ROUTE TO REGISTRATION FOR PUBLIC HEALTH PRACTITIONERS This introduction consists of: 1. Introduction to the UK Public Health Register 2. Process and Structures
INTRODUCTION TO THE UK PUBLIC HEALTH REGISTER ROUTE TO REGISTRATION FOR PUBLIC HEALTH PRACTITIONERS This introduction consists of: 1. Introduction to the UK Public Health Register 2. Process and Structures
Model terms and conditions of service for a salaried general practitioner employed by a GMS practice ( Practice )
") Model terms and conditions of service for a salaried general practitioner employed by a GMS practice ( Practice ) Notes These are model terms and conditions for use by GMS Practices in England and the
Model terms and conditions of service for a salaried general practitioner employed by a GMS practice ( Practice ) Notes These are model terms and conditions for use by GMS Practices in England and the
Dartford and Gravesham NHS Trust Darent Valley Hospital INDUCTION HANDBOOK FOR THE ANAESTHETIC FACULTY GROUP
 Dartford and Gravesham NHS Trust Darent Valley Hospital INDUCTION HANDBOOK FOR THE ANAESTHETIC FACULTY GROUP August 2015 Page 1 KENT SURREY AND SUSSEX POSTGRADUATE DEANERY FOR MEDICAL AND DENTAL EDUCATION
Dartford and Gravesham NHS Trust Darent Valley Hospital INDUCTION HANDBOOK FOR THE ANAESTHETIC FACULTY GROUP August 2015 Page 1 KENT SURREY AND SUSSEX POSTGRADUATE DEANERY FOR MEDICAL AND DENTAL EDUCATION
This statement should be seen as a stimulus to further discussion and development, and is not definitive policy.
 POSTGRADUATE MEDICAL CAREERS IN THE UK Cardiff Discussion Document This statement should be seen as a stimulus to further discussion and development, and is not definitive policy. Background: The Modernising
POSTGRADUATE MEDICAL CAREERS IN THE UK Cardiff Discussion Document This statement should be seen as a stimulus to further discussion and development, and is not definitive policy. Background: The Modernising
Wessex GP Fellowships Job Description
 Wessex GP Fellowships Job Description TITLE: GRADE: HOURS: Fixed Term Post for; GP Fellow GPST at appropriate increment 6 sessions per week (0.6fte) 12 months (other options may be possible) Commences:
Wessex GP Fellowships Job Description TITLE: GRADE: HOURS: Fixed Term Post for; GP Fellow GPST at appropriate increment 6 sessions per week (0.6fte) 12 months (other options may be possible) Commences:
Visit report on Royal Cornwall Hospital NHS Trust
 South West Regional Review 2016 Visit report on Royal Cornwall Hospital NHS Trust This visit is part of the South West regional review to ensure organisations are complying with the standards and requirements
South West Regional Review 2016 Visit report on Royal Cornwall Hospital NHS Trust This visit is part of the South West regional review to ensure organisations are complying with the standards and requirements
Primary Care Commissioning Committee. Terms of Reference. FINAL March 2015
 Primary Care Commissioning Committee Terms of Reference FINAL March 2015 1. Introduction 1.1. Simon Stevens, the Chief Executive of NHS England, announced on 1 May 2014 that NHS England was inviting Clinical
Primary Care Commissioning Committee Terms of Reference FINAL March 2015 1. Introduction 1.1. Simon Stevens, the Chief Executive of NHS England, announced on 1 May 2014 that NHS England was inviting Clinical
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine
 Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Supporting information for appraisal and revalidation: guidance for Supporting information for appraisal and revalidation: guidance for ophthalmology
 FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
Scotland Deanery Policy on Enhanced Monitoring Authors Quality Workstream Leads A.R.McLellan, D.Bruce & D.Pollock
 Scotland Deanery Policy on Enhanced Monitoring Authors Quality Workstream Leads A.R.McLellan, D.Bruce & D.Pollock Policy approved by MDET 14 th March 2016 Review Date 14 th March 2017 Version 1: 14 th
Scotland Deanery Policy on Enhanced Monitoring Authors Quality Workstream Leads A.R.McLellan, D.Bruce & D.Pollock Policy approved by MDET 14 th March 2016 Review Date 14 th March 2017 Version 1: 14 th
Clinical Advisory Forum DRAFT Terms of Reference
 Clinical Advisory Forum DRAFT Terms of Reference 1. Constitution 1.1. The Trust Executive Committee (TEC) hereby resolves to establish a Forum to be known as the Clinical Advisory Forum (the Forum). The
Clinical Advisory Forum DRAFT Terms of Reference 1. Constitution 1.1. The Trust Executive Committee (TEC) hereby resolves to establish a Forum to be known as the Clinical Advisory Forum (the Forum). The
Clinical Commissioning Group Governing Body Paper Summary Sheet For: PUBLIC session PRIVATE session. Date of Meeting: 24 March 2015
 Clinical Commissioning Group Governing Body Paper Summary Sheet For: PUBLIC session PRIVATE session Date of Meeting: 24 March 205 For: Decision Discussion Noting Agenda Item and title: Author: GOV/5/03/20
Clinical Commissioning Group Governing Body Paper Summary Sheet For: PUBLIC session PRIVATE session Date of Meeting: 24 March 205 For: Decision Discussion Noting Agenda Item and title: Author: GOV/5/03/20
NHS Governance Clinical Governance General Medical Council
 NHS Governance Clinical Governance General Medical Council Thank you for the opportunity to respond to this call for evidence. The GMC has a particular role in clinical governance, as outlined below, and
NHS Governance Clinical Governance General Medical Council Thank you for the opportunity to respond to this call for evidence. The GMC has a particular role in clinical governance, as outlined below, and
Review of the Defence Postgraduate Medical Deanery
 Defence Postgraduate Medical Deanery review 2013 14 Review of the Defence Postgraduate Medical Deanery This visit is part of a regional review and uses a risk-based approach. For more information on this
Defence Postgraduate Medical Deanery review 2013 14 Review of the Defence Postgraduate Medical Deanery This visit is part of a regional review and uses a risk-based approach. For more information on this
CLINICAL GOVERNANCE AND QUALITY COMMITTEE. Final - Terms of Reference - Final
 CLINICAL GOVERNANCE AND QUALITY COMMITTEE Final - Terms of Reference - Final CONSTITUTION 1. The Board of Directors approved the establishment of the Clinical Governance and Quality Committee (known as
CLINICAL GOVERNANCE AND QUALITY COMMITTEE Final - Terms of Reference - Final CONSTITUTION 1. The Board of Directors approved the establishment of the Clinical Governance and Quality Committee (known as
CURRENT AND FUTURE RECOGNITION OF THOSE HOLDING EDUCATIONAL ROLES
 DEFINITIONS, SELECTION AND MANAGEMENT (QM/QC) OF NON- GP TRAINERS (TEACHERS & SUPERVISORS) FOR UNDERGRADUATE AND POSTGRADUATE MEDICAL EDUCATION IN SCOTLAND BACKGROUND Following consultation, the GMC has
DEFINITIONS, SELECTION AND MANAGEMENT (QM/QC) OF NON- GP TRAINERS (TEACHERS & SUPERVISORS) FOR UNDERGRADUATE AND POSTGRADUATE MEDICAL EDUCATION IN SCOTLAND BACKGROUND Following consultation, the GMC has
Postgraduate Quality Assurance Visit. Report on Wales Deanery 2011/12
 Postgraduate Quality Assurance Visit Report on Wales Deanery 2011/12 Contents Executive summary... 3 Summary of key findings... 5 Good practice... 5 Requirements... 7 Recommendations... 7 The Report...
Postgraduate Quality Assurance Visit Report on Wales Deanery 2011/12 Contents Executive summary... 3 Summary of key findings... 5 Good practice... 5 Requirements... 7 Recommendations... 7 The Report...
Visit Report on NHS Grampian
 National Review of Scotland 2017 Visit Report on NHS Grampian This visit is part of our national review of undergraduate and postgraduate medical education and training in Scotland. Our visits check that
National Review of Scotland 2017 Visit Report on NHS Grampian This visit is part of our national review of undergraduate and postgraduate medical education and training in Scotland. Our visits check that
Contents. Foundation Programme Reference Guide 2016
 Reference Guide May 2016 Contents 1. Introduction and background... 5 2. Foundation Programme: policy and organisation... 6 THE UK FOUNDATION PROGRAMME OFFICE (UKFPO)... 6 UK HEALTH DEPARTMENTS... 6 HEALTH
Reference Guide May 2016 Contents 1. Introduction and background... 5 2. Foundation Programme: policy and organisation... 6 THE UK FOUNDATION PROGRAMME OFFICE (UKFPO)... 6 UK HEALTH DEPARTMENTS... 6 HEALTH
CLINICAL GOVERNANCE AND QUALITY COMMITTEE Terms of Reference
 CLINICAL GOVERNANCE AND QUALITY COMMITTEE Terms of Reference CONSTITUTION 1. The Board of Directors approved the establishment of the Clinical Governance and Quality Committee (known as the Committee in
CLINICAL GOVERNANCE AND QUALITY COMMITTEE Terms of Reference CONSTITUTION 1. The Board of Directors approved the establishment of the Clinical Governance and Quality Committee (known as the Committee in
Visit to The Queen Elizabeth Hospital King s Lynn NHS Foundation Trust
 East of England regional review 2015 Visit to The Queen Elizabeth Hospital King s Lynn NHS Foundation Trust This visit is part of a regional review and uses a risk-based approach. For more information
East of England regional review 2015 Visit to The Queen Elizabeth Hospital King s Lynn NHS Foundation Trust This visit is part of a regional review and uses a risk-based approach. For more information
JOB DESCRIPTION. Dubai, but occasional travel may be required across the UAE. Chief Medical Officer, Maudsley Health
 Job Details Job Title: Grade: JOB DESCRIPTION Consultant Psychiatry (Four posts required; CAMHS, Addictions, Forensics and Older Adults) Consultant Hours: 40 hours 2 years Fixed Term Contract initially
Job Details Job Title: Grade: JOB DESCRIPTION Consultant Psychiatry (Four posts required; CAMHS, Addictions, Forensics and Older Adults) Consultant Hours: 40 hours 2 years Fixed Term Contract initially
Independent Group Advising (NHS Digital) on the Release of Data (IGARD)
 on the Release of Data (IGARD)") Document filename: Independent Group Advising (NHS Digital) on the Release of Data (IGARD) Directorate / Programme IGSA Project IGARD Document Reference Status Final Owner Martin Severs Version 1.6 Author
Document filename: Independent Group Advising (NHS Digital) on the Release of Data (IGARD) Directorate / Programme IGSA Project IGARD Document Reference Status Final Owner Martin Severs Version 1.6 Author
Supporting information for appraisal and revalidation: guidance for psychiatry
 Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
NHS EDUCATION FOR SCOTLAND JOB DESCRIPTION
 NHS EDUCATION FOR SCOTLAND JOB DESCRIPTION 1. JOB DETAILS JOB REFERENCE JOB TITLE DEPARTMENT AND LOCATION IMMEDIATE MANAGER S TITLE NES General Practice Nursing Education Supervisor NHS Education for Scotland
NHS EDUCATION FOR SCOTLAND JOB DESCRIPTION 1. JOB DETAILS JOB REFERENCE JOB TITLE DEPARTMENT AND LOCATION IMMEDIATE MANAGER S TITLE NES General Practice Nursing Education Supervisor NHS Education for Scotland
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013
 Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
GUIDANCE ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY
 ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
Professional Support for Doctors in Training
 Professional Support for Doctors in Training Guidance and support for trainees and trainers Professional Support for Doctors in Training 1. Introduction Almost all medical and dental trainees will complete
Professional Support for Doctors in Training Guidance and support for trainees and trainers Professional Support for Doctors in Training 1. Introduction Almost all medical and dental trainees will complete
Quality and Safety Committee Terms of Reference
 Approved May 2016 Quality and Safety Committee Terms of Reference 1. Constitution The Quality and Safety Committee is established as a sub-committee of The Hillingdon Hospitals NHS Foundation Trust (THH)
Approved May 2016 Quality and Safety Committee Terms of Reference 1. Constitution The Quality and Safety Committee is established as a sub-committee of The Hillingdon Hospitals NHS Foundation Trust (THH)
CLINICAL AND CARE GOVERNANCE STRATEGY
 CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
Visit to Hull & East Yorkshire Hospitals NHS Trust
 Yorkshire and the Humber regional review 2014 15 Visit to Hull & East Yorkshire Hospitals NHS Trust This visit is part of a regional review and uses a risk-based approach. For more information on this
Yorkshire and the Humber regional review 2014 15 Visit to Hull & East Yorkshire Hospitals NHS Trust This visit is part of a regional review and uses a risk-based approach. For more information on this
SPECIALTY TRAINING PROGRAMME IN OPHTHALMOLOGY IN WESSEX DEANERY
 SPECIALTY TRAINING PROGRAMME IN OPHTHALMOLOGY IN WESSEX DEANERY This is a 7 year training programme in Ophthalmology for which 4 posts are available at ST1 level, starting August 2014. The programme is
SPECIALTY TRAINING PROGRAMME IN OPHTHALMOLOGY IN WESSEX DEANERY This is a 7 year training programme in Ophthalmology for which 4 posts are available at ST1 level, starting August 2014. The programme is
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014
 Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
SPONSORSHIP AND JOINT WORKING WITH THE PHARMACEUTICAL INDUSTRY
 SPONSORSHIP AND JOINT WORKING WITH THE PHARMACEUTICAL INDUSTRY 1 SUMMARY This document sets out Haringey Clinical Commissioning Group policy and advice to employees on sponsorship and joint working with
SPONSORSHIP AND JOINT WORKING WITH THE PHARMACEUTICAL INDUSTRY 1 SUMMARY This document sets out Haringey Clinical Commissioning Group policy and advice to employees on sponsorship and joint working with
Quality Assurance of Specialty Education and Training 2016 Pilot Activity Report
 December 2016 Executive Summary Quality Assurance of Specialty Education and Training 2016 Pilot Activity Report 1. Further to the publication of the Standards for Specialty Education 1 and Council agreement
December 2016 Executive Summary Quality Assurance of Specialty Education and Training 2016 Pilot Activity Report 1. Further to the publication of the Standards for Specialty Education 1 and Council agreement
Validation Date: 19/11/2015. Ratified Date: 22/02/2016
 Document Type: POLICY Title: Supervision of Junior Doctors Target Audience: Trust Wide Author / Originator and Job Title: Dr Linda Hacking, Director of Medical Education and Kate Stannard, Head of Medical
Document Type: POLICY Title: Supervision of Junior Doctors Target Audience: Trust Wide Author / Originator and Job Title: Dr Linda Hacking, Director of Medical Education and Kate Stannard, Head of Medical
Ensuring our safeguarding arrangements act to help and protect adults TERMS OF REFERENCE AND GOVERNANCE ARRANGEMENTS
 Ensuring our safeguarding arrangements act to help and protect adults TERMS OF REFERENCE AND GOVERNANCE ARRANGEMENTS April 2017 Contents Page 1. Purpose 2 2. Key Functions 2 3. Governance and Administrative
Ensuring our safeguarding arrangements act to help and protect adults TERMS OF REFERENCE AND GOVERNANCE ARRANGEMENTS April 2017 Contents Page 1. Purpose 2 2. Key Functions 2 3. Governance and Administrative
Directorate/Department: Relevant Trust care group e.g. cancer care Faculty of Health Sciences, University of Southampton Grade: AfC Band 5
 Post Title: Agenda for Change: Job Description Staff Nurse & Clinical Doctoral Fellow Directorate/Department: Relevant Trust care group e.g. cancer care Faculty of Health Sciences, University of Southampton
Post Title: Agenda for Change: Job Description Staff Nurse & Clinical Doctoral Fellow Directorate/Department: Relevant Trust care group e.g. cancer care Faculty of Health Sciences, University of Southampton
Regional Medicines Optimisation Committees
 Regional Medicines Optimisation Committees Operating Model First Edition, April 2017 NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations Patients and Information Nursing Trans.
Regional Medicines Optimisation Committees Operating Model First Edition, April 2017 NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations Patients and Information Nursing Trans.
Consultant psychiatrist job description and person specification
 Consultant psychiatrist job description and person specification The following job description is provided as a resource to the recruiting trust and may be used as a template. It is not designed to be
Consultant psychiatrist job description and person specification The following job description is provided as a resource to the recruiting trust and may be used as a template. It is not designed to be
Briefing. NHS Next Stage Review: workforce issues
 Briefing NHS Next Stage Review: workforce issues Workforce issues, and particularly the importance of engaging and involving staff, are a central theme of the NHS Next Stage Review (NSR). It is the focus
Briefing NHS Next Stage Review: workforce issues Workforce issues, and particularly the importance of engaging and involving staff, are a central theme of the NHS Next Stage Review (NSR). It is the focus
Salford Integrated Care System Governance Framework: Adult Health and Care Services FINAL
 Salford Integrated Care System Governance Framework: Adult Health and Care Services FINAL 1 Background and Scope Salford is a forward thinking health and social care economy and as such has established
Salford Integrated Care System Governance Framework: Adult Health and Care Services FINAL 1 Background and Scope Salford is a forward thinking health and social care economy and as such has established
CPD profile. 1.1 Full name: Manager 1.2 Profession: Occupational Therapist 1.3 Registration number: OT Summary of recent work/practice
 CPD profile 1.1 Full name: Manager 1.2 Profession: Occupational Therapist 1.3 Registration number: OT1234 2. Summary of recent work/practice I work as an occupational therapy service manager within a primary
CPD profile 1.1 Full name: Manager 1.2 Profession: Occupational Therapist 1.3 Registration number: OT1234 2. Summary of recent work/practice I work as an occupational therapy service manager within a primary
ADVISORY COMMITTEE ON CLINICAL EXCELLENCE AWARDS NHS CONSULTANTS CLINICAL EXCELLENCE AWARDS SCHEME (WALES) 2008 AWARDS ROUND
 2008 AWARDS ROUND") ADVISORY COMMITTEE ON CLINICAL EXCELLENCE AWARDS NHS CONSULTANTS CLINICAL EXCELLENCE AWARDS SCHEME (WALES) 2008 AWARDS ROUND Guide for applicants employed by NHS organisations in Wales This guide is available
ADVISORY COMMITTEE ON CLINICAL EXCELLENCE AWARDS NHS CONSULTANTS CLINICAL EXCELLENCE AWARDS SCHEME (WALES) 2008 AWARDS ROUND Guide for applicants employed by NHS organisations in Wales This guide is available
WELSH RENAL CLINICAL NETWORK TERMS OF REFERENCE
 INTRODUCTION WELSH RENAL CLINICAL NETWORK TERMS OF REFERENCE In accordance with WHSSC Standing Order 3, the Joint Committee may and, where directed by the LHBs jointly or the Welsh Government must, appoint
INTRODUCTION WELSH RENAL CLINICAL NETWORK TERMS OF REFERENCE In accordance with WHSSC Standing Order 3, the Joint Committee may and, where directed by the LHBs jointly or the Welsh Government must, appoint
Medical Revalidation Responsible Officer Report¹
 Medical Revalidation Responsible Officer Report¹ 1. EXECUTIVE SUMMARY LTHT is a designated body with 1247 doctors assigned to it for the 2016-17 appraisal year, of whom 96% completed their yearly appraisal
Medical Revalidation Responsible Officer Report¹ 1. EXECUTIVE SUMMARY LTHT is a designated body with 1247 doctors assigned to it for the 2016-17 appraisal year, of whom 96% completed their yearly appraisal
SPECIALTY TRAINING PROGRAMME IN PALLIATIVE MEDICINE IN WESSEX DEANERY
 SPECIALTY TRAINING PROGRAMME IN PALLIATIVE MEDICINE IN WESSEX DEANERY This is a 4 year training programme in Palliative Medicine at ST3 level aimed at doctors who can demonstrate the essential competencies
SPECIALTY TRAINING PROGRAMME IN PALLIATIVE MEDICINE IN WESSEX DEANERY This is a 4 year training programme in Palliative Medicine at ST3 level aimed at doctors who can demonstrate the essential competencies
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust
 Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Removal of Annual Declaration and new Triennial Review Form. Originated / Modified By: Professional Development and Education Team
 Review Circulation Application Ratificatio n Author Minor Amendment Supersedes Title DOCUMENT CONTROL PAGE Title: Mentorship in Nursing and Midwifery Policy Version: 14.1 Reference Number: Supersedes:.14.0
Review Circulation Application Ratificatio n Author Minor Amendment Supersedes Title DOCUMENT CONTROL PAGE Title: Mentorship in Nursing and Midwifery Policy Version: 14.1 Reference Number: Supersedes:.14.0
Primary Care Commissioning Next Steps to Delegated Commissioning September Board Paper. 2.0 Delegated Opportunities, Benefits and Risks
 Primary Care Commissioning Next Steps to Delegated Commissioning September Board Paper 1.0 Introduction This paper provides a briefing to the Wandsworth CCG Board on our progress in developing a Primary
Primary Care Commissioning Next Steps to Delegated Commissioning September Board Paper 1.0 Introduction This paper provides a briefing to the Wandsworth CCG Board on our progress in developing a Primary
Information for Doctors in Training (including LATs) about the Local Revalidation Process
 about the Local Revalidation Process") Information for Doctors in Training (including LATs) about the Local Revalidation Process 1. What is Revalidation? Medical revalidation is the process by which the General Medical Council (GMC) confirms
Information for Doctors in Training (including LATs) about the Local Revalidation Process 1. What is Revalidation? Medical revalidation is the process by which the General Medical Council (GMC) confirms
ROTATIONS & ALLOCATIONS FAQS FOR DOCTORS IN TRAINING
 ROTATIONS & ALLOCATIONS FAQS FOR DOCTORS IN TRAINING I have not received formal notification of my placement, when will this be available? You should receive formal notification of your placement from
ROTATIONS & ALLOCATIONS FAQS FOR DOCTORS IN TRAINING I have not received formal notification of my placement, when will this be available? You should receive formal notification of your placement from
Next steps towards primary care cocommissioning
 Next steps towards primary care cocommissioning November 2014 1 NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations Patients and Information Nursing Trans. & Corp. Ops. Commissioning
Next steps towards primary care cocommissioning November 2014 1 NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations Patients and Information Nursing Trans. & Corp. Ops. Commissioning
Final Accreditation Report
 Guidance producer: Healthcare Infection Society Guidance product: Clinical Guidelines Date: 23 March 2015 Version: 1.6 Final Accreditation Report Page 1 of 19 Contents Introduction... 3 Accreditation recommendation...
Guidance producer: Healthcare Infection Society Guidance product: Clinical Guidelines Date: 23 March 2015 Version: 1.6 Final Accreditation Report Page 1 of 19 Contents Introduction... 3 Accreditation recommendation...
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
Governance and Quality Committee Review. Wendy Pugh Director of Operations and Nursing. Innovation Tom Jinks - Governance Manager.
 Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
Sample CHO Primary Care Division Quality and Safety Committee. Terms of Reference
 DRAFT TITLE: Sample CHO Primary Care Division Quality and Safety Committee Terms of Reference AUTHOR: [insert details] APPROVED BY: [insert details] REFERENCE NO: [insert details] REVISION NO: [insert
DRAFT TITLE: Sample CHO Primary Care Division Quality and Safety Committee Terms of Reference AUTHOR: [insert details] APPROVED BY: [insert details] REFERENCE NO: [insert details] REVISION NO: [insert
Royal College of Surgeons Review Action Plan
 Department and team working in the context of the strategic aims of the Trust 1. Strategic aims and strategic plan Alder Hey and the University of Liverpool (UoL) are already in an active process of reviewing
Department and team working in the context of the strategic aims of the Trust 1. Strategic aims and strategic plan Alder Hey and the University of Liverpool (UoL) are already in an active process of reviewing
Public Health Skills and Career Framework Multidisciplinary/multi-agency/multi-professional. April 2008 (updated March 2009)
") Public Health Skills and Multidisciplinary/multi-agency/multi-professional April 2008 (updated March 2009) Welcome to the Public Health Skills and I am delighted to launch the UK-wide Public Health Skills
Public Health Skills and Multidisciplinary/multi-agency/multi-professional April 2008 (updated March 2009) Welcome to the Public Health Skills and I am delighted to launch the UK-wide Public Health Skills
Delegated Commissioning Updated following latest NHS England Guidance
 Delegated Commissioning Updated following latest NHS England Guidance 13th August 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England (Direct
Delegated Commissioning Updated following latest NHS England Guidance 13th August 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England (Direct
NES General Practice Nursing Education Supervisor (General Practice, Medical Directorate)
") NES General Practice Nursing Education Supervisor (General Practice, Medical Directorate) APPLICANT GUIDE BACKGROUND INFORMATION ON GENERAL PRACTICE NURSING (GPN) EDUCATION SUPERVISOR ROLE In March 2011
NES General Practice Nursing Education Supervisor (General Practice, Medical Directorate) APPLICANT GUIDE BACKGROUND INFORMATION ON GENERAL PRACTICE NURSING (GPN) EDUCATION SUPERVISOR ROLE In March 2011
This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version
 This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version NHS Continuing Healthcare Policy for the provision of NHS Continuing Healthcare: Choice,
This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version NHS Continuing Healthcare Policy for the provision of NHS Continuing Healthcare: Choice,
Australian Medical Council Limited
 Australian Medical Council Limited Procedures for Assessment and Accreditation of Specialist Medical Programs and Professional Development Programs by the Australian Medical Council 2017 Specialist Education
Australian Medical Council Limited Procedures for Assessment and Accreditation of Specialist Medical Programs and Professional Development Programs by the Australian Medical Council 2017 Specialist Education
Terms of Reference Executive Research Education & Training Committee
 Terms of Reference Executive Research Education & Training Committee 1. Main Authority / Limitations 1.1 The Board hereby resolves to establish a management committee to be known as the Research and Education
Terms of Reference Executive Research Education & Training Committee 1. Main Authority / Limitations 1.1 The Board hereby resolves to establish a management committee to be known as the Research and Education
MSc Public Health Application Handbook
 MSc Public Health Application Handbook 2018-2019 Masters Public Health Postgraduate Diploma Public Health Postgraduate Certificate Public Health Course Leader: Course Administrator: Dr Priya Paudyal Charlotte
MSc Public Health Application Handbook 2018-2019 Masters Public Health Postgraduate Diploma Public Health Postgraduate Certificate Public Health Course Leader: Course Administrator: Dr Priya Paudyal Charlotte
British Cardiovascular Society. Revalidation of cardiologists: Standards and Content of a portfolio for revalidation
 Page 1 of 8 British Cardiovascular Society Revalidation of cardiologists: Standards and Content of a portfolio for revalidation David Hackett Vice-President, Clinical Standards Division August 2009 Introduction:
Page 1 of 8 British Cardiovascular Society Revalidation of cardiologists: Standards and Content of a portfolio for revalidation David Hackett Vice-President, Clinical Standards Division August 2009 Introduction:
Clinical Supervision Policy
 Clinical Supervision Policy Version: 3.2 Bodies consulted: Professional Advisory Committee Approved by: PASC Date Approved: 13.8.15 Lead Manager: Jessica Yakeley Responsible Director: Medical Director
Clinical Supervision Policy Version: 3.2 Bodies consulted: Professional Advisory Committee Approved by: PASC Date Approved: 13.8.15 Lead Manager: Jessica Yakeley Responsible Director: Medical Director
Guidance on supporting information for revalidation
 Guidance on supporting information for revalidation Including specialty-specific information for medical examiners (of the cause of death) General introduction The purpose of revalidation is to assure
Guidance on supporting information for revalidation Including specialty-specific information for medical examiners (of the cause of death) General introduction The purpose of revalidation is to assure
CONTINUING PROFESSIONAL DEVELOPMENT (CPD)
") CONTINUING PROFESSIONAL DEVELOPMENT (CPD) www.fph.org.uk CPD POLICIES, PROCESSES AND STRATEGIC DIRECTION CPD Policy 01 CONTENTS Prelude CPD in 2007 and beyond 02 1. Context, definitions and aim of continuing
CONTINUING PROFESSIONAL DEVELOPMENT (CPD) www.fph.org.uk CPD POLICIES, PROCESSES AND STRATEGIC DIRECTION CPD Policy 01 CONTENTS Prelude CPD in 2007 and beyond 02 1. Context, definitions and aim of continuing
QUALITY COMMITTEE. Terms of Reference
 QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
Apprenticeship Standard for Nursing Associate at Level 5. Assessment Plan
 Apprenticeship Standard for Nursing Associate at Level 5 Assessment Plan Summary of Assessment On completion of this apprenticeship, the individual will be a competent and job-ready Nursing Associate.
Apprenticeship Standard for Nursing Associate at Level 5 Assessment Plan Summary of Assessment On completion of this apprenticeship, the individual will be a competent and job-ready Nursing Associate.
DOCTORS HOSPITAL, INC. Medical Staff Bylaws
 3.1.11 FINAL VERSION; AS AMENDED 7.22.13; 10.20.16; 12.15.16 DOCTORS HOSPITAL, INC. Medical Staff Bylaws DMLEGALP-#47924-v4 Table of Contents Article I. MEDICAL STAFF MEMBERSHIP... 4 Section 1. Purpose...
3.1.11 FINAL VERSION; AS AMENDED 7.22.13; 10.20.16; 12.15.16 DOCTORS HOSPITAL, INC. Medical Staff Bylaws DMLEGALP-#47924-v4 Table of Contents Article I. MEDICAL STAFF MEMBERSHIP... 4 Section 1. Purpose...
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS
 ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version