The Shrewsbury and Telford Hospital NHS Trust
|
|
|
- Allen Woods
- 5 years ago
- Views:
Transcription
1 The Shrewsbury and Telford Hospital NHS Trust Paper 2 TRUST BOARD MEETING Held on Thursday 1 May 2014 at 9.30 am Lecture Theatre, Education Centre, Princess Royal Hospital PUBLIC SESSION MINUTES Present: In attendance Mr P Latchford Mr H Darbhanga Dr R Hooper Mr D Jones Mrs D Leeding Mr B Newman Dr S Walford Mr P Herring Mrs S Bloomfield Dr E Borman Mrs D Kadum Mr N Nisbet Mrs J Clarke Miss V Maher Mrs D Vogler Chair Non Executive Director (NED) Non Executive Director (NED) Non Executive Director (NED) Non Executive Director (NED) Non Executive Director (NED) Non Executive Director (NED) Chief Executive (CEO) Director of Nursing and Quality (DNQ) Medical Director (MD) Chief Operating Officer (COO) Finance Director (FD) Director of Corporate Governance/Company Secretary (DCG) Workforce Director (WD) Director of Business & Enterprise (DBE) Meeting Secretary Mrs B Graham Committee Secretary Apologies: / /058.1 None WELCOME: The Chair welcomed everyone to the meeting. The Chair also welcomed Mr Brian Newman to his first Board meeting and congratulated him on his appointment on 1 April as a Non Executive Director. The Chair also congratulated Sarah Bloomfield on her substantive appointment to the role of Director of Nursing & Quality. CHAIR S AWARD This month s Chair s Award went to Sister Nicky Brierley who had been nominated by her colleagues in the Coronary Care Unit at the Princess Royal Hospital for several reasons. Her fundraising efforts included her most recent run at the London Marathon, raising over 1,000 for Sense which supports the blind and deaf people. This run is one of eight long distance runs she is taking part in this year; others include A Good Day to Tri Hard on 14 June for the Lingen Davies Cancer Fund, as well as completing the Ironbridge Half Marathon for a friend and colleague who was diagnosed with an aggressive form of breast cancer /058.2 RETIREMENT The Director of Corporate Governance (DCG) wished to put on record her thanks to Barbara Graham, Committee Secretary, for her contribution to the Trust Board as it was her last meeting before retiring after nearly 34 years in the NHS. The Board presented Barbara with a retirement gift and card and made tribute to the many years of support and diligence to the Board and the organisation. 1 Chair 29 May 2014
2 2014.1/059 PATIENT STORY The Director of Nursing & Quality (DNQ) introduced Mrs Julie Locke who briefed the Board on the importance of communication, particularly in relation to end of life care. Mrs Locke took the opportunity to thank the many doctors and nurses who had previously cared for her husband David when he had a renal transplant 23 years ago and also had major surgery for bowel cancer. She said unfortunately the last few weeks of his life did not reflect that care. Mrs Locke said there was a lack of information in the last week of David s life and no one mentioned end stage renal failure to them. She found out later that low blood pressure which he had had prior to admission was a clear indicator of this condition. She felt patients families need to know the facts because if she had known the true position she would never have gone home on the Saturday and her son would have been by his father s bedside when David died. Mrs Locke said the response to her initial letter was very positive and she had met with the Consultant Oncologist and agreed on key points around communication. Also the Renal Unit had secured funding for a Renal Psychologist to support end stage failure; also comments from the Renal Consultants were taken back to the Renal Unit after David s death to make sure this experience did not happen to others. Mrs Locke thanked the Board for listening to her story and said that David s death had left a huge void in their lives, he loved his cricket and they would always be grateful to the doctors that gave him a chance of life following his transplant 23 years ago. She reminded the Board that knowledge is powerful so not talking is not an option. The Director of Nursing & Quality (DNQ) said she had met with Mrs Locke, followed up issues from the nursing perspective and acknowledged that there were huge learning points to come out of this story, and from the medical point of view. The DNQ said that when objective setting for the year ahead, end of life care should be included, particularly around having timely and informed conversations with patients and their families. The Medical Director (MD) added that end of life is a subject our society in the 20 th century finds difficult to discuss and this includes senior clinicians who view death as failure because they are trained to look for success and ensure people survive. Mrs Leeding (NED) said after listening to a number of patient stories over the last few months she saw a trend around communication and she felt there needed to be a plan drawn up on how to more effectively communicate with patients as the Trust appears to have a basic problem to address on every level. Dr Walford (NED) said from his experience the more people that are involved in a patient s care the less likely it is that anyone takes responsibility for communications, however, he said that the DNQ is working on a strategy that will include more emphasis on this for the future. The Chair said there were three main themes taken from this patient story to ensure SaTH becomes an excellent organisation, these included : Integrated support and lead clinicians; Improving communications End of life care and choices The Board thanked Mrs Locke for sharing her experience and agreed that it would regularly review main themes arising from patient stories to ensure actions were being progressed. Action : DNQ /060 DECLARATION OF INTEREST An up-to-date list of interests was presented of members declarations and this included Mr Newman s (NED) declarations. There were no interests declared in relation to any matters on the agenda. 2 Chair 29 May 2014
3 2014.1/061 MINUTES OF THE MEETING HELD IN PUBLIC on 27 March 2014 were APPROVED subject to the following amendments : Page 5, Financial Strategy 2014/15, last bullet point to be deleted and replaced with the following : The TDA are expecting a five year plan from the Trust by July Page 12, Trust Committee Meetings Update, Finance Committee meeting 25 Mar 2014, last bullet point should have read Losses/Special Payment the Committee received and reviewed these items. Page 13, Stakeholder Communications, last paragraph, 2 nd line, 3 rd sentence should have commenced In relation to performance MATTERS ARISING FROM THE FORMAL BOARD MEETING HELD ON 27 MARCH /024 Winter Planning for Emergency Services This item is on the agenda but the formal assessment will be presented to Board on 26 June Action : COO /028 IPR Workforce The WD said this is included in the Workforce Committee summary later. Item complete /031 HR Policies Guidance on NEDs expenses to be brought back to the Board. Action: WD - 29 May /040 CEOs Briefing Impact of key staffing shortages to be discussed under CEO s Update. Item complete /041 Future Fit Programme Mr Walford (NED) said the Board did not want the plan to contradict guidance e.g. day case surgery. Discussion concluded that it is not a point in time but confirmed that the Q&S Committee will follow this up. Item complete /042 Financial Strategy 2014/15 The Finance Committee received the CIPs by Centre. Item complete. Outcome of arbitration and budget to be discussed later. Item complete /045 IPR Self Certification a qualifying note was sent. Item complete /048 Board Assurance Framework Clinical Service Vision to be presented to the Board in Five Year plan. Action: CEO 26 June /049 Healthcare Economy-wide flow improvements progress is included in the report. Item complete /051 Trust Committee Meetings Update Finance Committee - Booking & Scheduling full report due to Fin. Committee in Jun. Action: COO Learning from RCA - General Summary in IPR, more information will follow. Action: DNQ 26 Jun /053 People Strategy : WD and Head OD to present on workforce transformation. Action: WD 26 Jun /062 FORWARD PLAN for the period May to June 2014 was RECEIVED. It was noted that the Strategic Planning item had been included on the Forward Plan for the Board Development agenda in September It was suggested that a pre meeting for the Non Executive Directors (NEDs) would be arranged prior to the next Board meeting. It was therefore agreed that the next Board meeting should commence at 10 am instead of 9.30 am. Action: Secretary /063 CHIEF EXECUTIVE S OVERVIEW: Future Fit Programme The CEO said discussion with the Project Team suggested that the modelling required will be extensive and will push the public consultation back until at least June 2015, after the general election. However it is expected that in January 2015 clarity about the options and the preferred service model with some indication of the estate options may be agreed and available to the public. Outcome of formal arbitration with Telford & Wrekin CCG At the last Board meeting the prospect of arbitration regarding the 2014/15 contract with Telford & Wrekin CCG was identified. Further discussions with the CCG failed to reach agreement and a formal arbitration panel considered the CCG s case and the Trust s counter-arguments on 1 April There were four items disputed by the CCG: Changes to the coding and counting of patient activity initiated by the Trust in 2013/14 equivalent to 0.8 million. The Panel found in favour of the Trust. 3 Chair 29 May 2014
4 The CCG disputed a number of issues relating to Rehabilitation Services at PRH. The Panel found in favour of the Trust but suggested that the nature of the rehabilitation service required by the Commissioners should be resolved as soon as possible. Discussions are on-going. The CCG disputed the coding of Stroke services but as the financial value was 140,000, the Panel did not consider this item, due to the low materiality of the issue. The CCG wished to reduce the contract value by 2.6 million to reflect the impact of their QIPP (Quality, Innovation, Productivity & Prevention) savings schemes. The Panel reinforced the national guidance that QIPP schemes must be underpinned by robust plans that are properly formed and evidenced. Therefore the Trust has not yet finalised the contract with Telford & Wrekin CCG. Assessment of workforce risks associated with dual site services The CEO said the review of the level of risk associated with the limited medical workforce availability in the Emergency Departments and in Acute and General Medicine, and to a lesser extent ITU, is in progress with a view to this being submitted to the May Board meeting. Action: CEO - 29 May National Sustainability Award The Trust participated in the National Sustainability Award in London and the CEO was delighted to announce that SaTH was a runner up for its work with volunteers and community engagement. We now have over 400 Trust volunteers and the Trust was commended in the way we engage with staff, working with young people, and over 600 partner volunteers from Leagues of Friends and Royal Voluntary Service. The CEO congratulated the DCG and her team on this achievement. Members NOTED the CEO s report / CLINICAL SERVICE STRATEGY UPDATES : Unscheduled Care Presentation from Dr Kevin Eardley, Care Group Medical Director for Unscheduled Care. A copy of the PowerPoint slide is attached to the minutes. Dr Eardley described the challenges and opportunities for unscheduled care in our hospitals. He outlined several drivers for change including the importance of meeting and maintaining national standards and guidance, the Keogh review, making sure that services are clinically and financially sustainable, having the workforce to deliver safe care, meeting changing patient needs and expectations. In particular delivering excellence that the Trust needs to attract, support and retain excellent staff. It also needs to deliver quality first, in a way that best delivers access for patients, with a trained and supported workforce, within the resources available. Dr Eardley described a focus on three particular areas of length of stay - 0 day, 3 day and 7 day. Focusing on each of these stages helps to ensure that people stay in hospital no longer than they need to in order to receive the care and treatment that only hospitals can provide. At the shorter end this includes early consultant assessment, ambulatory care and short stay (e.g. 23 hour); middle range includes early specialist opinion and pull/push to the appropriate ward; at the longer end this includes focusing on issues such as frailty and early planning for safe and timely discharge. Underpinning all of this is the need and desire for more integrated working with health and care partners, and moving towards seven-day working etc. Priorities for the coming years include: Embedding a patient safety focused culture Developing the transition plan to keep services safe during the NHS Future Fit review Developing and implementing the workforce strategy that supports the above In partnership with commissioners, focus on service redesign for cardiology, urgent care centres and care of the older patient. Engaging staff in service redesign, reform and reconfiguration Potential actions in the coming years include: 4 Chair 29 May 2014
5 Opening Ward 17 short stay ward this opened earlier in April Further development of ambulatory care Implementing an Urgent Care Centre model alongside ED A particular challenge is the wider unscheduled care team and in particular the dwindling availability of specialist geriatricians (in common with other hospitals across the country) there is a need to think very differently about the workforce model for providing care for the elderly. Alongside these challenges there are some workforce opportunities as we could bring more cardiology care back into the county so that fewer patients need to transfer out of county to specialist heart centres but achieving this would mean consolidating some of our specialist expertise onto one of our two sites so that services can be kept safe in the county with senior clinicians available or accessible 24hrs 7 days a week. Dr Eardley said that these steps are likely to only mitigate the risks we face in the short and medium term, and on behalf of our patients we need the NHS Future Fit Programme to develop a compelling and safe vision for the future. Dr Walford (NED) speaking from a clinical background complimented Dr Eardley on his presentation. He said there was outstanding clarity and understanding in this group and he would be confident to endorse what had been said. Mr Newman (NED) referred to the difficulties in recruiting to key posts and asked if it was a reflection of national or local issues. Dr Eardley said it was both: there are national shortages in key skills, and in this market we are not a competitive employer given the duplication of services across two small sites, the challenges of split-site working and the onerous on-call responsibilities. Doctors are much more attracted to bigger, specialist centres elsewhere. Dr Eardley said if the Trust was able to develop a compelling clinical vision for the future then it will be better able to retain our current staff and attract new ones, and this will keep services safe and keep them in the county Scheduled Care Presentation from Mr Mark Cheetham, Care Group Medical Director for Scheduled Care and Consultant Colorectal Surgeon. A copy of the PowerPoint slide is attached to the minutes. Mr Cheetham highlighted some of the key successes over the last few years e.g. establishing RSH as the county's main centre for acute surgery giving patients early and regular access to consultant opinion; establishing the Trust as a Centre for Abdominal Aortic Aneurysm screening which is helping to keep vascular surgery in our hospitals, and opening the new Lingen Davies Cancer Centre. The surgical developments have also helped to establish RSH as a Trauma Unit as part of region-wide Major Trauma Networks. Some of the big drivers for change in scheduled care includes seeking to separate Emergency and Elective surgery wherever possible (e.g. so that demands for emergency care do not put pressure on beds and resources leading to frustration and inconvenience of cancellations; there is better senior supervision of major/complex cases, and quality of care is improved) and finding ways to bring more planned care closer to home. Key design principles include making sure that the way we provide care is wrapped around the patient, and designing pathways of care that provide as much as possible as close to home and/or at the convenience of the patient. The Trust has not consistently met 18-week referral to treatment time (RTT) standards and improvements needs to be relentless in looking at every step in the journey for the patient. In cancer standards we need to launch a review; and there are also reviews required in Ophthalmology and Musculoskeletal (MSK). There is a health community-wide review underway in MSK to make sure that we have the right pathways in place for the future. There is an important link to NHS Future Fit as with a single Major Emergency Centre we would be able to benefit from bringing specialist expertise together into a single Major Orthopaedic Trauma service. There is a need to develop robust plans to achieve the Critical Care quality standards, a need to continue to improve Patient Access and Outpatient Services and review performance of all financially challenged specialties. 5 Chair 29 May 2014
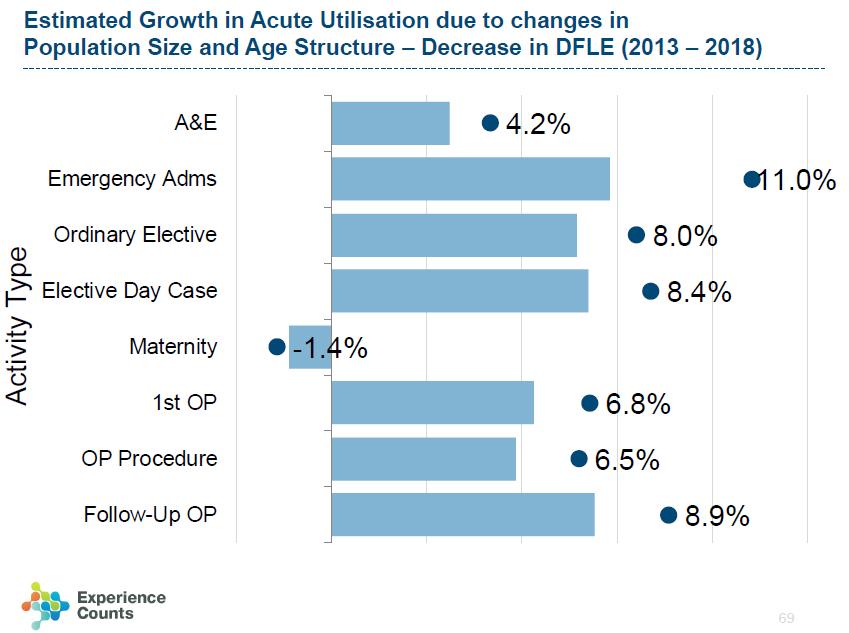
6 Another driver relates to the Trust facing growing demands i.e. the population is growing and this includes an ageing population with multiple co morbidities. The Board was updated on the current stage of development of the model for Planned Care that is emerging from the NHS Future Fit work. The vision has been developed with staff and patients focusing on (a) what specialties and services need to be available alongside Major Emergency Centres and (b) what specialties and services can be at a Planned Care Treatment Centre with separate resources and capacity from the main Emergency Centres. Some surgical specialties must be located alongside the emergency front door so that critically ill patients have early access to specialist clinical opinion; others can be located away from this site as the majority of activity is planned and/or routine. It was also acknowledged that the experience of Booking & Scheduling for our patients is not always up to the high standards they deserve. Improvements are underway including the recent establishment of a dedicated Booking Office which helps to extend opening hours and improve response times for calls and queries. This Office does not yet cover all types of bookings, and we are looking at ways to bring more of our booking processes into a one-stop-shop for patients. The focus of the Scheduled Care Group strategy over the next few years will be to improve the efficiency of pathways and service lines, by reviewing systems and processes whilst aiming to improve clinical standards, clinical outcomes and the patient experience to ensure that services are clinical and financial sustainable as the FutureFit solution becomes a reality. The Chairman said he found both presentations helpful in considering the Trust s 5-year plan and they made absolutely clear the need for review and reconfiguration of hospital services, in order to keep these services safe and in the county. He said we need clear plans for managing the transition until there is a clear vision for the future. However it is clear that: 1. There is a need for clinical reconfiguration in short/medium term. 2. We need to ensure any future design attracts medical staff needed to deliver the services. 3. The current duplication of services is placing increasing pressure and risk on services 4. Clinical Leads will need to shape decisions and take responsibility for the governance journey. The Board thanked Dr Eardley and Mr Cheetham for their presentations and looked forward to receiving the presentation on Women s & Children at the next meeting. Action: DBE 29 May /065.1 STRATEGIC PRIORITIES YEAR END REPORT 2013/14 The Board RECEIVED and NOTED progress against delivery of our 2013/14 Strategic Priorities. The report was submitted for information and had been discussed last month /065.2 FINAL TWO YEAR OPERATING PLAN 2014/15 AND 2015/16 The Director of Business & Enterprise (DBE) introduced the Two Year Operating Plan which set out how the Trust intends to deliver appropriate, high quality and cost effective services for patients over the next two years in light of the challenges facing the NHS. The Trust submitted its initial Draft Two Year Operating Plan to the Trust Development Authority (TDA) on 5 March Following the submission, the Trust received feedback from the TDA including challenges with regard to its Long Term Financial Plan (LTFP). The plan was subsequently reviewed to reflect feedback from both the TDA and comments from the March Trust Board. During March, contract discussions progressed and the financial implications have been reflected in changes to the final financial plan which was submitted to the TDA on 4 April The Board s attention was drawn to the following material changes to the Operating Plan in sections: s8.3 Operating surplus/deficits: The forecast operating deficit for 2014/15 has moved from a deficit of 6.2 million to a deficit of 8.2 million based on the final level of transitional support agreed by the CCGs. 6 Chair 29 May 2014
7 s8.4 Transition support: The Trust assumes that transitional support will be provided over the years 2014/15 to 2017/18 in recognition that costs of duplication will remain unavoidable until service reconfiguration has been completed. The level of transitional support assumed is as follows: 2014/ million and from 2015/ million each year thereafter. s8.6 QIPP assumptions: Local QIPP schemes for the 2014/15 require a greater level of development by both Clinical Commissioning Groups, and hence do not feature within the 2014/15 contract. This position was accepted by Shropshire County CCG as part of contract negotiations. The arbitration held on the 1 April 2014 adopted this position in respect of Telford and Wrekin CCG. The Trust, in setting its financial plan for the period 2014/ /19, has recognised that QIPP savings will be required to support financial sustainability within the health economy; as such progressive levels of QIPP savings ( 3 million per year) have been introduced from 2015/16. The DBE said that the Trust has further meetings with the Trust Development Authority (TDA) in May 2014 to discuss further our financial position therefore this may be brought back to the Board at a future date. The Board APPROVED the Two Year Operating Plan subject to any further proposed changes to the plan being reported back to the Board /066 CARE QUALITY COMMISSION (CQC) INPATIENT SURVEY The Director of Nursing & Quality (DNQ) introduced the results of the annual national inpatient survey conducted by the Picker Institute on behalf of the Care Quality Commission (CQC) across all acute and specialist NHS hospitals. Data was collected in September 2013 from patients admitted during the month of August 2013, with the results released in April The results are used by the CQC to inform their quarterly Intelligent Monitoring Report (IMR) and by other organisations such as NHS England and NTDA. The DNQ said the most recent survey was generally positive and demonstrated that the Trust had made significant improvements in a number of areas. There were no areas which showed a statistically significant decrease in performance. Compared to the 2012 survey, 10 areas had moved from the "worse" to the "about the same" bracket. More focused work is required in order to build on and deliver further improvements. An action plan to focus on all areas including those seen to be worse than other Trusts will be reviewed quarterly by the Clinical Quality & Safety Committee and much of this work will be incorporated into the Patient Experience Strategy which is currently being developed. The DNQ expressed thanks to the people of Shropshire for responding to the survey and the positive messages would be used to encourage staff to make the necessary improvements. The Board RECEIVED and NOTED the Inpatient Survey /067 INTEGRATED PERFORMANCE REPORT (IPR), BOARD GOVERNANCE AND MONITOR LICENCE CONDITIONS SELF-CERTIFICATIONS The Board RECEIVED the Integrated Performance Report (IPR) in respect of the month of March 2014 which summarised the Trust s performance against all the key quality, finance, compliance and workforce targets and indicators for 2013/14. The report confirmed that SaTH is currently at Escalation Level 4 (of 5) in the NHS Trust Development Authority s Accountability Framework. This is classified as a material issue requiring interaction led by the Director of Delivery & Development. Regular meetings are being held with the TDA to update them on SaTH s improvement trajectories. Key areas have been highlighted in the report. QUALITY (Patient Safety, Effectiveness and Patient Experience) The Director of Nursing & Quality (DNQ) provided an overview of the activity in March 2014 when a number of improvements within quality and safety were noted including eliminating Grade 4 pressure ulcers and further work is being conducted to make improvements with Grade 2 and 3 pressure ulcers. The following points were noted: WHO checklist (safer surgery) some external scrutiny is being undertaken on this issue at present relating to performance and methodology of measurement. Infection Prevention & Control showed 3 cases of C difficile in March, a year-end performance of 31 cases against a target of 27; and an improved performance of 31% reduction compared to last year. 7 Chair 29 May 2014
8 The target set for is generously set at 38 whereas the previous year was 27 cases. An internal target will also be set. The Chair said the Board needs to know how targets are set for and asked for more information at the next meeting. Action: DNQ 29 May Risk Adjusted Mortality Index (RAMI) The Medical Director (MD) said that the Trust is tracking the national peer average and this showed sustained improvement over the last 3 years. Systems are being put in place that leap frog to achieve much better performance. From the beginning of April 2014 completed consultant-related outcome performance will be available relating to individuals and teams. The Chair said that national benchmarking data was often complex and it was important for the Board to be aware of where the Trust sits in relative terms in relation to clinical outcomes. Reference was made to the action in June 2014 when the Board would receive performance, quality, finance and workforce issues in a more integrated approach and the Board supported the move for consultant performance to be included in this. Action: MD 26 Jun There were 12 Serious Incidents reported in March, 11 related to clinical effectiveness. OPERATIONAL PERFORMANCE The Chief Operating Officer (COO) gave an overview of the operational performance for March RED RAG : Overview of Performance Standards by Exception was included in the report. Board members were briefed on the following : A&E 4 Hour Access Standard : The year-end position was 93.4%, and 10,000 more patients were treated within the four hour target. March s performance saw the highest Emergency Department attendance over the year by 10%. Referral to Treatment (RTT) : Admitted - All specialties are on track to achieve 18 weeks in accordance with the Remedial Action Plan (RAP) but, the Trust failed the national RTT target in March. The COO advised that she had received a call from NTDA for SaTH to develop a plan to bring our target forward and to do this the Trust will look at providing an extra Day Surgery Theatre at PRH. Referral to Treatment (RTT) : Non admitted - The Trust failed to deliver the overall performance of the nonadmitted standard, which was predicted, as it is now reducing the Ophthalmology backlog (those waiting over 18 weeks). This work will continue for a few months. The CCGs have commissioned additional activity from The Practice (an independent provider) to cope with the level of demand within this service. SaTH needs to have a sustainable 18-week trajectory to be able to tender, therefore the glaucoma service will close to all routine referrals (to enable the backlog of patients to be cleared as quickly as possible) and they will go through triage as part of a new service model. NHS England had re-commissioned the Oral surgery service at Stirchley Dental Practice (a primary care service) with effect from 1 May 2014 and this will support the delivery of the Oral Surgery non-admitted performance within SaTH. This service was closed in December and subsequently SaTH has been receiving in excess of 50 additional referrals per week. These referrals are being clinically reviewed and where appropriate will be seen in the primary care service. Cancer Performance : The unvalidated position for March indicates that the Trust had only failed the 62-day target, which is a significant improvement on previous performance. Further details of the reasons for nonachievement of the 62-day standard were detailed in the exception report. A Remedial Action Plan [RAP] is in place for cancer and details the actions to be taken in the four challenged tumour sites: Colorectal, Lung, Upper GI and Urology. The Intensive Support Team (IST) will be working with the clinical centres to review patient pathways so that SaTH delivers all of the cancer standards from Quarter 2 in 2014/15. They are also working with Radiology to assess the gaps in capacity in relation to demand through the Cancer pathways. Winter the Trust has delivered higher activity levels than ever before. Cancelled operations have reduced as well as ambulance delays. The COO paid tribute to the staff for their hard work as whilst we are not where we want to be the improvement is significant. In answer to questions, the COO confirmed the following : In terms of harm to patients, it was pointed out that a process is in place to identify long waiters. Over the last year there had been 15 patients. 8 Chair 29 May 2014
9 The Trust has not damaged its customer based market in Ophthalmology as the current alternative provider is a temporary situation. Our strategy is to get our own house in order to enable pathway change. Mr Newman (NED) said that in terms of market research we have been consistently losing market share and asked whether a reduction in waiting times could help the position. The FD said that this would not be possible because our contract is based on delivering a specified amount of activity and Commissioners would not be able to fund any increase. The CEO added that once the backlog is cleared it will provide the opportunity to regain our market share. The Board AGREED that the direction of travel is very positive. FINANCIAL PERFORMANCE The Finance Director (FD) introduced the item and advised that at year-end (31 March 2014) the Trust recorded a surplus amounting to 65k, but he said it is worth reflecting at half-year we had a 6.2 million deficit and a programme was put in to accelerate cost savings. In the month of March there was a surplus of 1.2 million; pay costs increased in the month to 17.7 million due in part to staff delaying annual leave to deliver operational goals. It was noted that overall, pay costs have been around 17.4 million which is consistent with our budget. A cash balance of 2.2 million was held on the Balance Sheet at the end of March The Trust repaid all temporary borrowing as required on 24 March 2014 following receipt for support of 4 million from NHS England. The Trust overall achieved the three statutory targets i.e. the breakeven target by delivering a surplus of 65k; achieved the External Financing Limit of 21.3 million and achieved the Capital Resource Limit of 29.7 million.. Mr Jones (NED) said that whilst this is a positive picture there is a need to monitor Pay and Non Pay budgets for the year and to operate within them. The CEO said the whole issue of annual leave is being discussed at the Hospital Executive Committee on 27 May 2014 WORKFORCE The Workforce Director (WD) introduced this section of the paper, the following points were NOTED : Sickness Absence - the year end position was 4.12% against an annual target of below 4%. Whilst the target had not been met it showed an improvement which equated to 3,326 calendar days being saved compared to last year. Appraisal rate had improved during March when 80% of staff had received an appraisal also a significant increase was seen in the number of doctor appraisals. Apprenticeship Framework over the last 12 months the Trust had supported 166 individuals through an apprenticeship framework, this is the highest in the West Midlands region. People Strategy Implementation of the strategy commenced in April. Key activities were to begin to embed the values, roll out the Leadership Development Programme, draft a 5 year Workforce Plan and introduce a values-based recruitment for consultant appointments. On concern from Dr Hooper (NED) in relation to the appraisal rate, Mrs Leeding (NED) said that she had met with the Workforce Director and the biggest issue is quality of the appraisals. This will be the next stage and then to start implementing improvement plans to take this forward. The Medical Director added that the appraisal rate for medical staff had improved to 83% from 70%. MONITOR LICENCE CONDITIONS SELF-CERTIFICATIONS Appendix 1 & 2 - Monthly Self Certifications NHS Trust Development Authority (NTDA) Requirement 9 Chair 29 May 2014
10 The Trust followed the formal process and will submit the monthly self-certification templates for March 2014 : Monitor Licensing Requirements summary of each relevant licence condition. A summary of the submission was included at Appendix 1 of the report. All conditions were marked compliant. Trust Board Self Certification Board Statements covering clinical quality, finance and governance was included in the report at Appendix 2. The Trust is reporting a Financial Risk Rating of 3 for the month of March 2014 and 2 for the year. Non-compliance around performance issues. Action plans are in place to recover all the targets. The Board NOTED the Integrated Performance Report for March 2014 and APPROVED the self-certification submissions to the NTDA. It was noted that this is for March 2014 and whilst there are risks going on next year SaTH is still a going concern. The Board AGREED that a qualifying note should continue to accompany the Self Certification to the NTDA approving finance but on the understanding that NTDA is underwriting a known deficit. Action: FD /068 SATH 2013/14 WINTER PLAN REVIEW The Chief Operating Officer (COO) presented a brief summary of the review of the Trust s Winter Plan for 2013/14 and some of the recommendations for the 2014/15 Winter Plan. The COO said whilst this report looks at SaTH s actions and its continued ongoing programmes all year round, emergency pressures do not switch off at the end of April. Feedback from staff across the Trust indicated that this winter felt much better. No patients waited over 12 hours and the number of cancelled operations had also reduced from 100 the previous year to 14 in 2013/14. Discussions are already underway internally and with our local health economy in preparation for Winter 2014/15. Feedback had been given to the TDA and NHS England regarding the need to release Winter funding earlier to enable the recruitment of staff on short-term contracts rather than having to rely on expensive agency staff. As a health and social economy the initial discussions have been centred around ensuring that planning for winter is a whole year event. The Trust is also in discussion with smaller local providers who are now in the process of closing down their additional winter facilities. Also for 2014/15 planning we are in discussions with Healthcare at Home a private company - about a proposed recovery at home initiative to manage patients with special acute medical needs. They are currently contracted with many Trusts (e.g. Heart of England, Coventry & Warwick and others) and are carrying out a scoping exercise to look at releasing hospital capacity for the coming winter. There is also a need to look at ways to improve discharge rates for the weekends. The Board NOTED that the report concluded with some recommendations to be taken into consideration in the development of the 2014/15 Winter Plan as follows : A focus on continuous improvement across urgent care pathways all year round must continue; Lessons learnt from Winter 2013/14 will be used to inform both our own internal plan and the whole health and social care economy plan for Winter 2014/15; Baseline reports to be in place prior to the winter to better monitor the impact of winter funding and return on investment; Recruitment to winter funded posts to commence in June 2014 with staff in post by October 2014; Integrated working to be developed with Shropshire Community Trust to maximise the benefit to patients both as business as usual. The need to make improvements in performance against the A&E 4 hour standard, across the whole year, but in particular over the Winter period. The Formal Review of the Health Economy report will be reported to the Urgent Care Working Board this month and then to the Board. Action: COO 26 Jun Chair 29 May 2014
11 Dr Hooper (NED) expressed significant thanks for this report. He said that Executive Directors had put forward plans for the winter, the plans had been delivered and this delivery has had the intended outcome. He said it was a credit to the frontline staff and clinical/operational teams who have made this happen /069 SYSTEM STRATEGY UPDATE The Chief Executive gave a verbal report. He said last month this item was introduced with the aim of trying to improve our systems as an organisation. Four important areas were laid out to try to leap frog ahead i.e. Develop an appropriate strategy for investment because we have a reactive approach; Develop a coherent strategy around Information Technology because we have out of date equipment (e.g. Radiology) Develop a comprehensive strategy for re-design Use market analysis and business intelligence to improve and develop the business. The CEO said this is work in progress and gave the following update : The CEO and DBE met with BT Healthcare to see how they can help SaTH improve technology; Wider system strategy - a team from University Hospital of North Staff (UHNS) met EDs and discussed what could be done in partnership. It was agreed in principle to engage in discussions about mutually advantageous network arrangements with UHNS going forward. The Board NOTED the update /070 INFORMATION GOVERNANCE REPORT 2013/14 The Finance Director provided the report which demonstrated SaTH's 2014 Annual Assessment scores and included relevant updates in the IG Framework. Information Governance is now included in the Trust Development Authority (TDA) Accountability Framework. The Board RECEIVED and REVIEWED the Information Governance Toolkit update /071 TRUST COMMITTEE MEETINGS UPDATE The Chair advised that he had proposed to establish a new Committee of the Board called Business Development and Engagement Committee as it was felt there was a gap in that area. If approved this Committee would be Chaired by the Director of Business & Engagement The Board also NOTED that : the Financial Recovery Board is to be dis-established as it was agreed that the current structure was not adding value to the process. To gain greater ownership throughout the organisation there will now be a regular update on progress every two weeks to the Executive Directors and a monthly update to the Finance Committee through the Finance Director. Following the appointment of Mr Newman (NED) from 1 April 2014, the Chair had refreshed NED Committee membership and responsibilities along with the current Committee structure at Attachment 2. The COO s name was omitted from the Workforce Committee membership. Action: DCG to amend. Mr Jones (NED) / Chair of Finance Committee pointed out that the current quoracy required and Executive Director in addition to the FD s deputy, when the FD was unable to attend and it was proposed to change this. The Board AGREED to this change. Action: Finance Committee to amend ToR. Dr Walford (NED) / Chair of Q&S Committee also referred to a quoracy and the deputy issue and said this would need to come back to the Board in June. Action: Q&S Committee to consider ToR. NED Leads now included Mr B Newman overseeing Procurement. 11 Chair 29 May 2014
12 o o o o Finance Committee meeting 29 April 2014: The summary was TABLED and NOTED. Mr Jones (NED) Chair of the Committee confirmed that two monthly reviews of the Future Configuration of Hospital Services (FCHS) indicated that the project is on track for completion in September 2014 and is on budget. Clinical Quality & Safety (Q&S) Committee meeting 23 April 2014: The summary was NOTED. Dr Walford (NED) Chair of the Committee briefed the Board on the Adult Safeguarding section of the summary. It was noted that this is a relatively new procedure where other organisations can raise concerns and he was assured that SaTH s data is completely transparent. The Q&S Committee supported the view of the DNQ that the Adult Safeguarding Board would benefit from the appointment of a suitable independent Chair. The Board also SUPPORTED and ENDORSED this view. Hospital Executive Committee meeting 29 April 2014: The summary was TABLED and NOTED. Workforce Committee meeting 11 April 2014: The summary was NOTED. The Workforce Director (WD) referred to the second summary point relating to Improving People Management in the organisation, where the Committee received a proposal relating to two key issues (i) for all managers to attend a briefing session led by the CEO; the session will ensure a shared understanding of the role of a manager and will cover regular communications. It will also be an opportunity to talk about our values and the importance of managers living the values. (ii) a Management Development Programme is being proposed which should improve managers skills. The Board RECEIVED and REVIEWED Committee Updates. The Board NOTED the NED membership, role responsibilities and the Committee structure and the new reporting arrangements for financial recovery schemes. The Board APPROVED the establishment of the Business Development and Engagement Committee as a formal Sub-Committee of the Board /072 REPORT ON THE USE OF THE CORPORATE SEAL The Director of Corporate Governance (DCG) introduced the report which updated on the use of the Trust s Common Seal since the last update in April 2013, pursuant to Section 9 Standing Orders Custody of Seal and Sealing of Documents. The Board NOTED the Sealings as detailed in the Register for the period 9 March 2013 to 31 March /073 ANNUAL LOSSES AND COMPENSATIONS AND WRITE OFFS The Finance Director (FD) introduced the report and advised that the report summarised the losses and special payments during 2013/14 that required Trust Board approval. The Board NOTED and APPROVED the annual losses, compensation and write-offs of bad debts /074 STAKEHOLDER ENGAGEMENT The Communications Director provided an update when the Board NOTED the following : The Trust Charity Development Lead had been successful in recent grant applications for the Women & Children s Unit; and held a Charity Team Party earlier in the month. Over Easter a young child called Luke, from Sir Alexander Fleming School in Telford, organised a competition at his school and all the proceeds raised paid for Easter eggs for the Children s Ward. The two Leagues of Friends and Lingen Davies Fundraisers are working together on shared goals. Funding had been received from the Arts Council to improve photography throughout RSH. The Communications Team is sadly losing two of its members - Chris Hudson has already left and Andy Rogers will be leaving shortly. Recruitment has commenced. Dr Walford (NED) asked whether there was more that can be done to engage our shadow members who had been recruited in anticipation of our FT Board of Governors. The DCG said there are almost 10,000 members and there were a number of mechanisms in place to engage with them, but that previous advice had not supported forming a shadow Council of Governors. 12 Chair 29 May 2014
13 2014.1/075 QUESTIONS/COMMENTS FROM THE FLOOR 1) A member of the public was very impressed with the level of enthusiasm in the Trust to make real changes quickly to improve services. He urged more engagement in this work to design services that patients need. The Chair thanked him and said this would feature in Board meetings. 2) The following questions related to the Two Year Operating Plan and the NHS Future Fit Review : (a) Would one of the existing two sites be substantially downgraded if there is a new Major Emergency Centre on a new site? The CEO said it needs to be clear that there is a service vision i.e. specialist emergency hospital and another diagnostic centre for planned work. The options to have this configuration have been modelled and during the course of the next 12 months that modelling around different site options should proceed so there is no pre-conceived view on what the solutions would be. (b) Reference to Value for Money (VFM), the Emergency Care Centre could cost 200 million but there is no indication in the plan where this money is coming from. The CEO said in relation to VFM, it is important in this evaluation to particularly note that RSH site is much older, the backlog is significant and development is more complex. That will be a factor to be taken into account however there are no conclusions drawn from this. (c) Has the Trust has considered the potential impact if Commissioners take a more competitive approach by putting more services out to tender? The Medical Director said he was aware of the potential impact and there is a risk. He said the need for co-operation is absolutely paramount. (d) The change of direction by the new Chief Executive of NHS England had been noted and will this mean that there is a different direction going forward for local hospitals? The Medical Director said he has regular discussions with the CEO of NHS England and there is potential for a different model. There is a need to demonstrate to NHS England how to make substantive improvements in care. 3) Mr Sandbach handed over a letter to the Chair which suggested that SaTH make immediate temporary changes to clinical services in the interest of improving patient safety. He said he was very worried that the Trust is at major risk in recruiting key staff and having reliance on locums. He believed this could lead to catastrophic failure leading to avoidable injury and death. Dr Walford (NED) said the Board had heard a range of views today and it demonstrated the difficulties the Board is trying to deal with. The Chair said there was a lot of detail covered in this item and he would be willing to meet with Mr Sandbach outside the meeting. 4) Mr Jones, PALS Volunteer, personally thanked Barbara Graham for providing him with Board information over the years and said she will be missed. The PALS service has been very busy. Mr Jones also referred to his treatment of glaucoma five years ago and said he had recently received "brilliant" treatment again from Mr Ewan Craig and he would like his comments passed on to Mr Craig. Action: MD /076 REVIEW OF MEETING Observational Review 1. A member of the public referred to the CQC inpatient survey and spoke personally about his experience at the beginning of January 2014 when he was an inpatient for 10 days. He said he received high quality care on the Respiratory Ward. His experience of the care from staff and information shared was very positive. 2. Mr Sandbach also said a member of his family received services and although staff are dedicated one of the flaws in the system was discharge processes and he suggested that members of the Board sit in the discharge area and listen to what patients are saying. Delay in receiving medication is an issue. Members Review : The CEO said that the meeting had lasted four hours which was considered too long. The CEO noted the comment from the floor that if items are removed from the meeting then the information must remain available to the public by other means. 13 Chair 29 May 2014
14 2014.1/077 DATE OF NEXT MEETING Formal Board Meeting Thursday 29 May 2014 at am in Seminar Rooms 1 & 2, Shropshire Education & Conference Centre, Royal Shrewsbury Hospital. Special Board Meeting Thursday 5 June 2014 at 5 pm in Seminar Room 1, Shropshire Education & Conference Centre, Royal Shrewsbury Hospital (to Adopt the Annual Accounts). The meeting then closed. 14 Chair 29 May 2014
15 MATTERS ARISING FROM THE PUBLIC TRUST BOARD MEETING ON 1 MAY 2014 ACTION DUE DATE Item Issue OWNER 2014/010 Integrated Performance Report To develop Board reporting so all papers include performance, quality, finance and workforce issues in a more integrated approach and to routinely include Centre-specific performance against all these measures in IPR. CEO 26 Jun /024 Winter Planning for Emergency Services Formal Review of Health Economy report not due until April. COO 26 Jun /031 HR13 Reimbursement of Travel, Accommodation & Subsistence Expenses - Guidance for NEDs expenses from TDA around change of the scope. WD 29 May /040 CEO s Briefing Impact of key staffing shortages NEDs attendance at CCG Boards/vice versa. Chair to discuss representation at respective Boards. Chair /048 Board Assurance Framework Clinical Service Vision to be presented to the Board. CEO 29 May /051 Trust Committee Meetings Update Finance Committee : Booking & Scheduling source of leadership be agreed to ensure SOP compliance. Full report due in June Learning from RCA - Summary of changes to operational systems and clinical care derived from learning to be summarized at public Boards. COO ADNQ 26 Jun Jun /053 People Strategy WD and Head of OD to present on workforce transformation. WD 26 Jun /059 Patient Stories DNQ to regularly review main themes arising from patient stories to ensure actions are progressed. DNQ On-going /063 CEO s Overview Assessment of Workforce Risks Review of the level of risk to be submitted in May. CEO 29 May /067 IPR Quality : Target setting for 2014/15 - The Board requested more information on how targets are set; Risk Adjusted Mortality Index (RAMI) Consultant related outcome performance to be included in new integrated approach IPR report /067 IPR Finance : Issue of annual leave will be discussed at next HEC meeting on 27 May and outcome will be reported to the Board /071 Trust Committee Meetings Update Q&S Committee Quoracy and the deputy issue to be brought back to the Board in June /075 Questions/Comments from the floor Appreciation to be passed to Mr E Craig. If Board meeting is made shorter; it was requested that some items should remain available to the public by other means. DNQ MD 29 May Jun 2014 CEO 29 May 2014 Q&S Chr 26 Jun 2014 MD CEO May 2014 Monthly 15 Chair 29 May 2014
16 The Shrewsbury and Telford Hospital NHS Trust Scheduled Care Clinical Service Strategy
17 Drivers for Change Design Principles Separation of Emergency and Elective Surgery Delivering Core Standards Growing Demand Financial Sustainability Future Fit

18 Drivers for Change Design Principles
19 Drivers for Change Separation of Emergency and Elective Surgery Separating elective care from emergency pressures through the use of dedicated beds, theatres and staff can if well planned, resourced and managed reduce cancellations, achieve a more predictable workflow, provide excellent training opportunities, increase senior supervision of complex/emergency cases, and therefore improve the quality of care delivered to patients. Recommendations for practice, published by the Royal College of Surgeons of England (2007)

20 Drivers for Change Delivering Core Standards

21 Drivers for Change FutureFit
22 Our Vision for Surgery Services in Major Emergency Centre Critical Care Services Orthopaedic Trauma Major Vascular surgery Major colorectal surgery Bariatric surgery Major urology Head & Neck Cancer surgery Maxillofacial trauma Ophthalmology emergencies Diagnostic including cross sectional imaging Services in Planned Care Treatment Centre Facility to initiate organ support and safe transfer Elective orthopaedics Breast surgery Venous surgery Hernia and laparoscopic cholecystectomy ENT, Max Facs & oral Cataract surgery & occuloplastics Medical retina treatment Outpatients and Diagnostics
23 Scheduled Care Group - Priorities The Scheduled Care Group has mapped its priorities against the Trust wide objectives: Address the existing capacity shortfall and process issues to consistently deliver national healthcare standards: - Deliver RTT consistently and sustainably - Complete a root and branch review of our cancer services - Detailed service reviews for ophthalmology and musculoskeletal services Develop robust plans to achieve Critical Care quality standards Continue improvements in Patient Access and Outpatients Services Review performance of all financially challenged specialties through SLR

24 Our Priorities Improving Productivity Enhanced Recovery Programme
25 Our Priorities -Sustainable RTT Performance Specialty RTT Admitted performance delivery date RTT Non Admitted performance delivery date Admitted Sustainable Non Admitted Sustainable Colorectal surgery 01/03/ /05/2014 Upper GI 01/04/ /04/2014 Vascular 01/02/ /02/2014 Breast Urology 01/04/ /04/2014 ENT 01/07/ /07/2014 Max fax and oral surgery No date Ophthalmology 01/03/2014 TBC 01/07/2014 Gynaecology T&O upper limb 01/10/ /10/2014 T&O lower limb 01/10/ /10/2014 Spinal Gastroenterology 01/07/ /07/2014 Cardiology 01/05/2014 Dermatology NA NA Neurology NA NA Respiratory NA NA 01/03/2014 General Medicine NA NA Cardiothoracic surgery NA NA Neuro surgery NA NA Other (inc Pain) 01/05/ /05/2014
26 Our Priorities -Patient Access and Outpatients Centre Roll out Netcall remind + outpatient reminder service to all OPD clinics Trial and finalise the Friends and family test to OPD clinics Work with centres to improve planning processes and embed the notion of the reasonable offer of appointment timing of no less than 3 weeks notice Improving communication within teams and centres Work in partnership with clinical centres and CCG colleagues to maximise Choose and Book usage Develop Standard Operating Procedures for nursing teams Develop options appraisal for evening and weekend working session Develop board metrics and dashboards on performance and quality metrics Work toward centralising admissions teams, booking teams and reception function throughout the Trust
27 Cancer Services SWOT ANALYSIS STRENGTHS Robust Peer Review schedule delivered within National deadlines MDT metrics for each MDT team established Auditable mechanism for 2WW referrals Macmillan Cancer Information & Support Centre Manager in post for patient support Cancer Service Improvement Facilitator in post Cancer Survivorship Service Improvement Facilitator recruited to commence April 2014 Secured funding for Macmillan therapy team OPPORTUNITIES First appointments within 7 days (not 14 days) Diagnostic investigations within 7 days Histopathology reporting within 7 days Appointments with Oncologists within 7 days Service improvements based on cancer patient feedback (National and local MDT Cancer Patient Experience survey results WEAKNESSES Insufficient operational capacity within some specialties and departments No dedicated Teenage & Young Adults (TYA) lead for the Trust Poor compliance with Peer Review measures in some areas Skin cancer patients outsourced to third party private provider without a robust SLA and penalty system in place Reliance on tertiary referral providers for some specialities (e.g. Upper GI, Gynae) THREATS Lack of Clinical Nurse Specialist for some areas including TYA services Patients choosing to have treatment elsewhere
28 Our Priorities - Cancer Services Service Improvement Establish a Cancer Programme Board and develop a Cancer Strategy Ensure delivery of the Cancer waiting time standards consistently across all MDTs Enhance patient experience through engaging with patient representatives for pathway mapping within MDT teams Collaborate with all MDTs to develop a Cancer Strategy and ensure robust service model for all areas especially where current gaps exist Standardise operating procedures, data reporting and escalation processes to improve MDT working & patient tracking. Develop Health & Well Being services for cancer survivors
29 Our Priorities - Cancer Services Service Developments Improve pathways in Lung, Upper GI, Colorectal and Urology Investment in Radiotherapy Service 3 rd Linear Accelerator Cancer Screening Programmes for Bowel Scoping and Breast age extention Macmillam Integrated Therapy Service
30 Our Priorities - Critical Care Strategy Clinical Standards Current Service on 2 sites Dedicated on call rota Performance against national standards Recruitment Plan (next 12 months) Critical Care Nursing Standards Development of a workforce plan Growth in Demand Bed Occupancy Additional Capacity Business Case FutureFit Solution
31 Other Priorities - Musculoskeletal Challenged Speciality Health Economy Review Provider of Choice Service Model Issues (RSH, PRH, RJ&AH) RTT Challenge Largest Income Generator but negative contribution Health Economy Review Best Practice Tariff opportunities for fractured neck of femur Single Orthopaedic Trauma Site FutureFit

32 Summary The focus of the scheduled care group strategy over the next few years will be to improve the efficiency of pathways and service lines, by reviewing systems and processes, while aiming to improving clinical standards, clinical outcomes and the patient experience to ensure that services are clinically and financial sustainable as the FutureFit solution becomes the reality.
33 The Shrewsbury and Telford Hospital NHS Trust Unscheduled Care Clinical Service Strategy
34 Drivers for Change Provision of a high quality safe emergency services Clinically and financially sustainable Workforce 7 days a week Changing Demographic and Patient Needs New model required in the delivery of Emergency and Urgent Care services





35 Drivers for Change
36 Unscheduled Care Aims & Objectives Right place, Right person Valued & skilled teams Quality, safety, flow in ways that are clinically and financially sustainable
37 Unscheduled Care Operational concepts Operational concepts: Four themes of operational working that underpin the methods by which we will achieve our aims. These are: 1. Supporting service improvements led by the specialist multidisciplinary team 2. Building resilience into processes that deliver high quality care 3. Optimally use bed base in support of patients going to the correct specialist ward 4. Engaging staff to share our values, standards and aims.
38 Service Improvement ANATOMY + PHYSIOLOGY
39 Excellence Excellent People Motivated and well managed workforce with sufficient capacity to deliver quality, safety and flow seven days a week in a way that is clinically and financially sustainable Appropriate environment that supports continual improvement
40 Quality Cost CLINICALLY & FINANCIALLY SUSTAINABLE Access Workforce
41 Unscheduled Care making it happen Early Consultant Assessment Ambulatory Care Short Stay Ward/Unit Early specialist opinion Pull/push onto appropriate specialist ward Number of admissions 3 days Length of Stay Planning management and discharge Board Round Frailty Project Integrated working with health and social care service partners Cross site working; RSH bed reconfiguration; Site management Stroke service; 7 Day Working; workforce review

42 Emergency admissions where the length of stay is zero 10


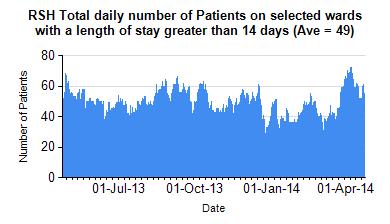
43 Average length of stay of an episode (excludes zero LOS) (medical only) Royal Shrewsbury Hospital 11
44 Unscheduled Care Priorities 1. Embed a patient focussed safety culture to ensure that services are safe and key quality standards are achieved 2. Develop a transition plan that maintains the safety and short term sustainability of our services pending the outcome of the FutureFit 3. Develop and implement a Workforce Strategy in support of Point In partnership with commissioners progress service reconfiguration and service transformation priorities being Cardiology, Urgent Care Centres & Care of the Older patient. 5. Staff Engagement Plan to motivate and involve staff in service redesign, reform and reconfiguration to reduce existing recruitment issues and increase capacity 6. Identify efficiencies through service redesign and effective data capture to ensure the long term financial sustainability of services
45 Unscheduled Care making it happen Year 1 2 PRH Continuing Improvements in delivery of care to the elderly Further Development of Ambulatory Care Mitigating the risks associated with Emergency Department Implementation of a number of workforce initiatives Implement UCC Model alongside ED Examining Options for establishing a CDU facility within A&E Developing the Cardiac Centre model, in support of a Cardiac Centre for the Trust Open the new short stay ward (Ward 17) Maintain and improving the single site hyper acute, acute Stroke unit
46 Unscheduled Care making it happen Year 1 2 RSH Continuing Improvements in delivery of care to the elderly Further Development of Ambulatory Care Mitigating the risks associated with Emergency Department (ED) Implementation of a number of workforce initiatives Implement Urgent Care Centre Model alongside ED Establish the RSH Children s Assessment Unit alongside ED Medical bed reconfiguration
47 Unscheduled Care making it happen Whole system approach Innovative workforce
48 Unscheduled Care making it happen Improving care for those attending our Emergency Departments with Minor Illness and Minor Injury Whole system approach Innovative workforce
49 Urgent Care Centre Primary Care clinicians delivering a new stream for patients whoattend our Emergecy departments with minor illness and minor injuries: UCC Walk Ins Minors Majors Walk Ins Minors Majors
50 Unscheduled Care making it happen Improving care of the elderly in our hospitals Whole system approach Innovative workforce
51
52

53 Number of A&E attendances where disposal is admitted to hospital by site Winter 10/11 Winter 11/12 Winter 12/13 21

54 UCGE Activity January 2014 Winter 10/11 Winter 11/12 Winter 12/13 22
55
56 Model of Excellent Care for the Elderly Excellence is more a model of care than a physical location The absolute key to this model is the need to recognize the speed that decompensation can take hold in elderly patients. The benefit therefore starts with a model that focuses on optimizing individual patient potential and mobilisation from the start. The full benefit of this model can only be realised through whole health economy change. What we have learnt from other health economies which are move evolved is the benefit of being able to offer a range of options so that care can be stepped up or down according to the needs of an individual patient. This is more easily achieved in a vertically integrated model that has overcome the handicaps of organizational boundaries, competitive behaviours and separate funding streams
57 Care of the Elderly Centre of Excellence This Care of the Elderly Service could be provide using a Hub and Spoke Methodology Service which could be delivered in the Acute (Hub) Urgent care centre, ED, CCC or direct referral from GP Frailty team (Geriatrician, nurse, therapists placed in AMU and available at each stage) Integrated social worker Elderly Care Assessment Acute beds (aim for +/- 72 hour LOS and AVLOS 6 days) Acute rehab beds (stage 1 step down) Service which could be delivered in the Community (Spoke) Community hospital beds Community rehab service ( integrated) Virtual Ward (manage patients with comprehensive advice and care package in own home) Future potential for GP Virtual Ward hub (admission avoidance)
58 Unscheduled Care making it happen Improving care for those Cardiac Disease requiring interventional Treatment/diagnostics Our anatomy and physiology

59 Development on Cardiology The Model below summarises how services could further develop across community, acute and tertiary care over the next 2 years subject to the necessary business case approvals.
60 Development on Cardiology The Model below summarises how services could further develop across community, acute and tertiary care over the next 2 years subject to the necessary business case approvals. Anatomy PRH create an Ambulatory Care and Cardiac Transfer Unit Physiology Daily Coronary angio/intervention list Daily AMU in reach
61 Unscheduled Care making it happen Yes, but
62 Unscheduled Care making it happen Futurefit Shaping healthcare together

63 One Major Emergency Centre Our clinicians are unanimous in their view that the only clinically sustainable solution to the configuration of our EDs is a single site. Future Fit:Acute and Episodic Care Model
is asked to NOTE the update provided on fragile services.
 Recommendation DECISION NOTE (select) Reporting to: The Trust Board is asked to NOTE the update provided on fragile services. Trust Board Date Thursday 27 th July 2017 Paper Title Brief Description Services
Recommendation DECISION NOTE (select) Reporting to: The Trust Board is asked to NOTE the update provided on fragile services. Trust Board Date Thursday 27 th July 2017 Paper Title Brief Description Services
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
Service Transformation Report. Resource and Performance
 SUMMARY REPORT Meeting Date: 31 May 2018 Agenda Item: 9.1 Enclosure Number: 9 Meeting: Trust Board (Part 1) Title: Author: Accountable Director: Other meetings presented to or previously agreed at: Service
SUMMARY REPORT Meeting Date: 31 May 2018 Agenda Item: 9.1 Enclosure Number: 9 Meeting: Trust Board (Part 1) Title: Author: Accountable Director: Other meetings presented to or previously agreed at: Service
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Debbie Vogler, Director of Business & Enterprise. Kate Shaw, Associate Director of Service Transformation
 Reporting to: Trust Board 24 September 2015 Paper 5 Title Sponsoring Director Author(s) Future Configuration of Hospital Services - Post-Project Evaluation Debbie Vogler, Director of Business & Enterprise
Reporting to: Trust Board 24 September 2015 Paper 5 Title Sponsoring Director Author(s) Future Configuration of Hospital Services - Post-Project Evaluation Debbie Vogler, Director of Business & Enterprise
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
Summarise the Impact of the Health Board Report Equality and diversity
 AGENDA ITEM 4.1 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact Details for further
AGENDA ITEM 4.1 Health Board Report INTEGRATED PERFORMANCE DASHBOARD Executive Lead: Director of Planning and Performance Author: Assistant Director of Performance and Information Contact Details for further
PUBLIC SESSION MINUTES. Chair
 1 The Shrewsbury and Telford Hospital NHS Trust TRUST BOARD MEETING Held on Thursday 3 December 2015 Seminar Rooms 1&2, Shropshire Education & Conference Centre, RSH Paper 2 Present: In attendance Meeting
1 The Shrewsbury and Telford Hospital NHS Trust TRUST BOARD MEETING Held on Thursday 3 December 2015 Seminar Rooms 1&2, Shropshire Education & Conference Centre, RSH Paper 2 Present: In attendance Meeting
THE FUTURE OF YOUR HOSPITALS: Planned Care site
 THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
Strategic Risk Report 12 September 2016
 Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Strategic Risk Report 4 July 2016
 Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April Ipswich Hospital NHS Trust NHS East of England Department of Health
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Hertfordshire Community NHS Trust NHS East of England Department of Health
Strategic Risk Report 1 March 2018
 Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018
 Produced in February 2018") 6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
Agenda Item number: 9.1. Maggie Bayley, Director of Nursing and Quality
 Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL
 DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
RBCH Actions to meet CQC Essential Standards
 RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
APPENDIX 7C BENEFITS REALISATION PLAN
 APPENDIX 7C BENEFITS REALISATION PLAN 150804 Shropshire Future Fit SOC v2.2 Appendices APPENDICES Draft Benefits Realisation Plan V0.9 150415 FutureFit Benefits Realisation Plan V0.9 Page 1 The purpose
APPENDIX 7C BENEFITS REALISATION PLAN 150804 Shropshire Future Fit SOC v2.2 Appendices APPENDICES Draft Benefits Realisation Plan V0.9 150415 FutureFit Benefits Realisation Plan V0.9 Page 1 The purpose
Title Open and Honest Staffing Report April 2016
 Title Open and Honest Staffing Report April 2016 File location WILJ2102 Meeting Board of Directors Date 25 th May 2016 Executive Summary This paper provides a stocktake on the position of South Tyneside
Title Open and Honest Staffing Report April 2016 File location WILJ2102 Meeting Board of Directors Date 25 th May 2016 Executive Summary This paper provides a stocktake on the position of South Tyneside
Vanguard Programme: Acute Care Collaboration Value Proposition
 Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
The Shrewsbury and Telford Hospital NHS Trust. Trust Board 24 th February The Future Configuration of Hospital Services Programme
 Enclosure 2 The Shrewsbury and Telford Hospital NHS Trust Trust Board 24 th February 2011 The Future Configuration of Hospital Services Programme Executive Lead Adam Cairns, Chief Executive Authors Kate
Enclosure 2 The Shrewsbury and Telford Hospital NHS Trust Trust Board 24 th February 2011 The Future Configuration of Hospital Services Programme Executive Lead Adam Cairns, Chief Executive Authors Kate
Stewart Mason, Emergency Planning and Resilience Officer Tom Jones, Clinical Programme Manager
 Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to RECEIVE and APPROVE the Emergency Department Service Continuity Plan (Princess Royal Hospital site). Trust Board Date Thursday
Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to RECEIVE and APPROVE the Emergency Department Service Continuity Plan (Princess Royal Hospital site). Trust Board Date Thursday
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
RTT Recovery Planning and Trajectory Development: A Cambridge Tale
 RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust
 Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
WEST HAMPSHIRE PERFORMANCE REPORT. Based on performance data available as at 11 th January 2018
 WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
 APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
Reporting to: Trust Board Meeting - 26 th June Title Integrated Performance Report - May 2014/15. Previously considered by Not Applicable
 Reporting to: Trust Board Meeting - 26 th June 2014 Paper 6 Title Integrated Performance Report - May 2014/15 Sponsoring Director Author(s) Peter Herring - Chief Executive Directors Previously considered
Reporting to: Trust Board Meeting - 26 th June 2014 Paper 6 Title Integrated Performance Report - May 2014/15 Sponsoring Director Author(s) Peter Herring - Chief Executive Directors Previously considered
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
Author: Kelvin Grabham, Associate Director of Performance & Information
 Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Improving Healthcare Together : NHS Surrey Downs, Sutton and Merton clinical commissioning groups Issues Paper
 Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
NHS GRAMPIAN. Grampian Clinical Strategy - Planned Care
 NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
FT Keogh Plans. Medway NHS Foundation Trust
 FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
2. This year the LDP has three elements, which are underpinned by finance and workforce planning.
 Directorate for Health Performance and Delivery NHSScotland Chief Operating Officer John Connaghan T: 0131-244 3480 E: john.connaghan@scotland.gsi.gov.uk John Burns Chief Executive NHS Ayrshire and Arran
Directorate for Health Performance and Delivery NHSScotland Chief Operating Officer John Connaghan T: 0131-244 3480 E: john.connaghan@scotland.gsi.gov.uk John Burns Chief Executive NHS Ayrshire and Arran
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Ayrshire and Arran NHS Board
 Paper 12 Ayrshire and Arran NHS Board Monday 9 October 2017 Planned Care Performance Report Author: Fraser Doris, Performance Information Analyst Sponsoring Director: Liz Moore, Director for Acute Services
Paper 12 Ayrshire and Arran NHS Board Monday 9 October 2017 Planned Care Performance Report Author: Fraser Doris, Performance Information Analyst Sponsoring Director: Liz Moore, Director for Acute Services
Performance and Quality Report Sean Morgan Director of Performance and Delivery Mary Hopper Director of Quality Dino Pardhanani, Clinical Director
 Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Patient Experience Strategy
 Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
Report to the Board of Directors 2016/17
 Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013
 TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
Care Quality Commission (CQC) Inspection Briefing
 Inspection Briefing") Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST
 EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS DATE: 7 AUGUST 2015 SUBJECT: REPORT FROM: PURPOSE: CHIEF EXECUTIVE S REPORT CHIEF EXECUTIVE Decision CONTEXT / REVIEW HISTORY
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS DATE: 7 AUGUST 2015 SUBJECT: REPORT FROM: PURPOSE: CHIEF EXECUTIVE S REPORT CHIEF EXECUTIVE Decision CONTEXT / REVIEW HISTORY
GUIDANCE NOTES FOR THE EMPLOYMENT OF SENIOR ACADEMIC GPs (ENGLAND) August 2005
 August 2005") GUIDANCE NOTES FOR THE EMPLOYMENT OF SENIOR ACADEMIC GPs (ENGLAND) August 2005 Guidance Notes for the Employment of Senior Academic GPs (England) Preamble i) A senior academic GP is defined as a clinical
GUIDANCE NOTES FOR THE EMPLOYMENT OF SENIOR ACADEMIC GPs (ENGLAND) August 2005 Guidance Notes for the Employment of Senior Academic GPs (England) Preamble i) A senior academic GP is defined as a clinical
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Governance and Quality Committee Review. Wendy Pugh Director of Operations and Nursing. Innovation Tom Jinks - Governance Manager.
 Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
The Yorkshire & Humber Improvement Academy Clinical Leadership Training Programme
 The Yorkshire & Humber Improvement Academy Clinical Leadership Training Programme The Improvement Academy (IA) is one of the leading quality and safety improvement networks in the UK. The IA works across
The Yorkshire & Humber Improvement Academy Clinical Leadership Training Programme The Improvement Academy (IA) is one of the leading quality and safety improvement networks in the UK. The IA works across
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS
 CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
NHS GRAMPIAN. Local Delivery Plan - Section 2 Elective Care
 NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Measuring for improvement The new CQC hospital programme. Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013
 Measuring for improvement The new CQC hospital programme Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013 1 Our purpose and role Our purpose We make sure health and
Measuring for improvement The new CQC hospital programme Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013 1 Our purpose and role Our purpose We make sure health and
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
We plan. We achieve.
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
Newham Borough Summary report
 Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Care of Critically Ill & Critically Injured Children in the West Midlands
 Care of Critically Ill & Critically Injured Children in the West Midlands Heart of England NHS Foundation Trust Visit Date: 3 rd and 4 th October 2013 Report Date: December 2013 Images courtesy of NHS
Care of Critically Ill & Critically Injured Children in the West Midlands Heart of England NHS Foundation Trust Visit Date: 3 rd and 4 th October 2013 Report Date: December 2013 Images courtesy of NHS
PUBLIC SESSION MINUTES. Chair. Director of Corporate Governance / Company Secretary
 1 Present: Mr P Latchford Mr H Darbhanga Mr C Deadman Dr D Lee Mrs T Mingay Mr B Newman Dr C Weiner Mr S Wright Dr E Borman Mrs D Kadum Mr N Nisbet Mrs D Fowler Mrs J Clarke The Shrewsbury and Telford
1 Present: Mr P Latchford Mr H Darbhanga Mr C Deadman Dr D Lee Mrs T Mingay Mr B Newman Dr C Weiner Mr S Wright Dr E Borman Mrs D Kadum Mr N Nisbet Mrs D Fowler Mrs J Clarke The Shrewsbury and Telford
Implementation of the right to access services within maximum waiting times
 Implementation of the right to access services within maximum waiting times Guidance for strategic health authorities, primary care trusts and providers DH INFORMATION READER BOX Policy HR / Workforce
Implementation of the right to access services within maximum waiting times Guidance for strategic health authorities, primary care trusts and providers DH INFORMATION READER BOX Policy HR / Workforce
James Blythe, Director of Commissioning and Strategy. Agenda item: 09 Attachment: 04
 Title of paper: Author: Exec Lead: Community Hospital Services Review Tom Elrick, Urgent Care Programme Lead James Blythe, Director of Commissioning and Strategy Date: 23 rd February 2015 Meeting: Executive
Title of paper: Author: Exec Lead: Community Hospital Services Review Tom Elrick, Urgent Care Programme Lead James Blythe, Director of Commissioning and Strategy Date: 23 rd February 2015 Meeting: Executive
Welcome, Apologies for Absence and Declaration of Board Members Interest
 DRAFT Minutes of the of the Royal Cornwall Hospitals NHS Trust held on Thursday 30 March 2017 11.00 13.00 in the Knowledge Spa, Royal Cornwall Hospital Present: Mr Jim McKenna Ms Kathy Byrne Ms Catrin
DRAFT Minutes of the of the Royal Cornwall Hospitals NHS Trust held on Thursday 30 March 2017 11.00 13.00 in the Knowledge Spa, Royal Cornwall Hospital Present: Mr Jim McKenna Ms Kathy Byrne Ms Catrin
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
Summary two year operating plan 2017/18
 One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
Presentation to the Care Quality Commission. Dr. Lucy Moore, CEO 15 September 2015
 Presentation to the Care Quality Commission Dr. Lucy Moore, CEO 15 September 2015 Our Improvement Journey- Key Messages We have Board, Executive and Divisional leadership teams now in place with serious
Presentation to the Care Quality Commission Dr. Lucy Moore, CEO 15 September 2015 Our Improvement Journey- Key Messages We have Board, Executive and Divisional leadership teams now in place with serious
Appendix 1: Integrated Urgent Care Service Update. 1. Purpose
 Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Sarah Bloomfield, Director of Nursing and Quality
 Reporting to: Trust Board - 25 June 2015 Paper 8 Title CQC Inpatient Survey 2014 Published May 2015 Sponsoring Director Author(s) Sarah Bloomfield, Director of Nursing and Quality Graeme Mitchell, Associate
Reporting to: Trust Board - 25 June 2015 Paper 8 Title CQC Inpatient Survey 2014 Published May 2015 Sponsoring Director Author(s) Sarah Bloomfield, Director of Nursing and Quality Graeme Mitchell, Associate
1. This letter summarises the mairi points discussed and actions arising from the Annual Review and associated meetings in Glasgow on 20 August.
 Cabinet Secretary for Health, Wellbeing and Sport ShonaRobisonMSP T: 0300 244 4000 E:scottish.ministers@gov.scot Andrew Robertson OBE Chairman NHS Greater Glasgow and Clyde JB Russell House Gartnavel Royal
Cabinet Secretary for Health, Wellbeing and Sport ShonaRobisonMSP T: 0300 244 4000 E:scottish.ministers@gov.scot Andrew Robertson OBE Chairman NHS Greater Glasgow and Clyde JB Russell House Gartnavel Royal
Annual Complaints Report 2017/2018
 . Annual Complaints Report 2017/2018 CCG Information Reader Box Document Purpose CCG Website Link Title Author For information www.easterncheshireccg.nhs.uk NHS Eastern Cheshire Clinical Commissioning
. Annual Complaints Report 2017/2018 CCG Information Reader Box Document Purpose CCG Website Link Title Author For information www.easterncheshireccg.nhs.uk NHS Eastern Cheshire Clinical Commissioning
BIRMINGHAM CITY COUNCIL
 BIRMINGHAM CITY COUNCIL PUBLIC REPORT Report to: CABINET Report of: Strategic Director for People Date of Decision: 28 th June 2016 SUBJECT: STRATEGY AND PROCUREMENT PROCESS FOR THE PROVISION OF EARLY
BIRMINGHAM CITY COUNCIL PUBLIC REPORT Report to: CABINET Report of: Strategic Director for People Date of Decision: 28 th June 2016 SUBJECT: STRATEGY AND PROCUREMENT PROCESS FOR THE PROVISION OF EARLY
REFERRAL TO TREATMENT ACCESS POLICY
 Directorate of Strategy & Planning REFERRAL TO TREATMENT ACCESS POLICY Reference: DCP175 Version: 7.0 This version issued: 17/12/15 Result of last review: Major changes Date approved by owner (if applicable):
Directorate of Strategy & Planning REFERRAL TO TREATMENT ACCESS POLICY Reference: DCP175 Version: 7.0 This version issued: 17/12/15 Result of last review: Major changes Date approved by owner (if applicable):
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
BOARD OF DIRECTORS. Sue Watkinson Chief Operating Officer
 Affiliated Teaching Hospital BOARD OF DIRECTORS 28 TH SEPTEMBER 2012 AGENDA ITEM: 11.1 TITLE: INTENSIVE SUPPORT TEAM REPORT PURPOSE: The Board of Directors is presented with the report from the Intensive
Affiliated Teaching Hospital BOARD OF DIRECTORS 28 TH SEPTEMBER 2012 AGENDA ITEM: 11.1 TITLE: INTENSIVE SUPPORT TEAM REPORT PURPOSE: The Board of Directors is presented with the report from the Intensive
Report of the Care Quality Commission. May 2017
 Report of the Care Quality Commission May 2017 1. Purpose 1.1 The purpose of this report is to formally confirm the findings of the Care Quality Commission (CQC) following its inspection in October 2016;
Report of the Care Quality Commission May 2017 1. Purpose 1.1 The purpose of this report is to formally confirm the findings of the Care Quality Commission (CQC) following its inspection in October 2016;
NHS England (London) Assurance of the BEH Clinical Strategy
 Assurance of the BEH Clinical Strategy") NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY
 Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
ANSWERS TO QUESTIONS YOU MAY HAVE
 ANSWERS TO QUESTIONS YOU MAY HAVE What is Better Care Together really all about? Better Care Together is about ensuring that health and social care services in Leicester, Leicestershire and Rutland are
ANSWERS TO QUESTIONS YOU MAY HAVE What is Better Care Together really all about? Better Care Together is about ensuring that health and social care services in Leicester, Leicestershire and Rutland are
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY PART 1
 REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY PART 1 Date of Meeting: 24 September 2015 Agenda No: 8.2 Attachment: 14 Title of Document: South West London Collaborative Commissioning programme
REPORT TO MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY PART 1 Date of Meeting: 24 September 2015 Agenda No: 8.2 Attachment: 14 Title of Document: South West London Collaborative Commissioning programme
Reducing Elective Waits: Delivering 18 week pathways for patients. Programme Director NHS Elect Caroline Dove.
 Reducing Elective Waits: Delivering 18 week pathways for patients Programme Director NHS Elect Caroline Dove What I will cover 1. Why 18 Weeks is different 2. Where are we now 3. New models of delivery
Reducing Elective Waits: Delivering 18 week pathways for patients Programme Director NHS Elect Caroline Dove What I will cover 1. Why 18 Weeks is different 2. Where are we now 3. New models of delivery
Summary Annual Report 2017/18
 Summary Annual Report 2017/18 Reporting back Guy s and St Thomas has, once again, performed well both operationally and financially, despite a challenging year which has seen unprecedented demand on our
Summary Annual Report 2017/18 Reporting back Guy s and St Thomas has, once again, performed well both operationally and financially, despite a challenging year which has seen unprecedented demand on our
STATEMENT OF PURPOSE August Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008)
") 1. Trust Profile STATEMENT OF PURPOSE August 2015 Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008) 1.1 Worcestershire Acute Hospitals NHS Trust was formed on 1
1. Trust Profile STATEMENT OF PURPOSE August 2015 Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008) 1.1 Worcestershire Acute Hospitals NHS Trust was formed on 1
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017
 Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST. PATIENT ACCESS MANAGEMENT POLICY (Previously known as Waiting List Management Policy) Documentation Control
 Documentation Control") NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST PATIENT ACCESS MANAGEMENT POLICY (Previously known as Waiting List Management Policy) Documentation Control Reference CL/CGP/026 Approving Body Senior Management
NOTTINGHAM UNIVERSITY HOSPITAL NHS TRUST PATIENT ACCESS MANAGEMENT POLICY (Previously known as Waiting List Management Policy) Documentation Control Reference CL/CGP/026 Approving Body Senior Management
Patient Experience Strategy. Director of Nursing & Quality
 Reporting to: Trust Board 2 February 2017 Paper 8 Title Sponsoring Director Author(s) Patient Experience Strategy Director of Nursing & Quality Graeme Mitchell Previously considered by Executive Summary
Reporting to: Trust Board 2 February 2017 Paper 8 Title Sponsoring Director Author(s) Patient Experience Strategy Director of Nursing & Quality Graeme Mitchell Previously considered by Executive Summary