Quantitative Analysis of Nonvisit Care Activities Performed by Ambulatory Care. Kimberly A. Kosloski Tarpenning, Pharm.D. 1
|
|
|
- Jasper Potter
- 5 years ago
- Views:
Transcription

1 -- Quantitative Analysis of Nonvisit Care Activities Performed by Ambulatory Care Pharmacists in the Outpatient Primary Care Clinic Setting Running title: Ambulatory Pharmacist Nonvisit Care Kimberly A. Kosloski Tarpenning, Pharm.D. 1 Sarah A. McGill, Pharm.D. 2 Jessica A. Peterson, Pharm.D. 3 Kaitlin J. Yost, Pharm.D. 4 Marc D. Tumerman, M.D. 5 Author Affiliations: 1 Pharmacy Services, Mayo Clinic Health System in Owatonna, Owatonna, Minnesota; 2 Pharmacy Services, Mayo Clinic Health System-Franciscan Healthcare in Sparta, Sparta, Wisconsin; 3 Pharmacy Services, Mayo Clinic, Jacksonville, Florida; 4 Pharmacy Services, Mayo Clinic Health System in Eau Claire, Eau Claire, Wisconsin, and Mayo Clinic Health System Chippewa Valley in Chippewa Falls, Chippewa Falls, Wisconsin; 5 Department of Family Medicine, Mayo Clinic Health System-Franciscan Healthcare in Sparta, Sparta, Wisconsin. Corresponding Author: Marc D. Tumerman, M.D., Department of Family Medicine, Mayo Clinic Health System-Franciscan Healthcare in Sparta, 310 W Main St, Sparta, WI 54656; tumerman.marc@mayo.edu. This article has been accepted for publication and undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process which may lead to differences between this version and the Version of Record. Please cite this article as doi: /jac5.1094
2 Acknowledgment: We thank Gabrielle Thompson for her contribution to data compilation, as well as Jordan Haag, Pharm.D. and Audrey Umbreit, Pharm.D. for their assistance in project design, technical editing, and language editing and for comments that greatly improved the manuscript. Conflict of interest: The authors have no conflicts of interest to declare.
3 Abstract Introduction: The value of pharmacists as direct patient care providers in integrated ambulatory care teams has been demonstrated. As the reimbursement landscape changes, patient care outside of office visits is increasing through nonvisit care. Objective: We aimed to quantify the time spent by ambulatory care pharmacists on nonvisit care activities in the outpatient primary care clinic setting. Methods: Data were collected from four outpatient ambulatory care practices in our institution over 12 weeks. The primary objective was to quantify the time spent performing nonvisit care activities. Secondary objectives were to quantify the number of patients affected, the number of nonvisit care activities, the types of medication therapy problems (MTPs) encountered during nonvisit care activities, and the resulting medication therapy interventions. Results: A total of 1311 patients were affected during the study, and pharmacists spent a daily average of 1.6 hours performing nonvisit patient care. Among 1548 nonvisit care activities, staff face-to-face curbside consult was the most frequent (41%). Among 1866 MTPs identified (1.4 MTP per patient), the most common problems identified were need for education (31%), adverse medication events (21%), need for an additional medication (20%), and nonadherence (12%). The most common interventions were health care team education (28%), recommendation to switch medication (18%), patient education (17%), and start a new medication (14%). Conclusion: Ambulatory care pharmacists spent considerable time performing nonvisit care, with multiple MTPs identified during these encounters. Health care teams
4 frequently used pharmacists for nonvisit patient care. Further research is needed to determine the best utilization of pharmacist resources allocated to nonvisit care in an integrated ambulatory care practice. Keywords: ambulatory care; pharmacy; population health; practice management
5 Pharmacists roles within the health care team have expanded from medication dispensing to include new roles as patient care providers. In our institution, as well as many other organizations, pharmacists serve as advanced practice providers delivering comprehensive medication management (CMM) in the outpatient primary care setting. According to the American College of Clinical Pharmacy, CMM is defined as the standard of care that ensures each patient s medications (ie, prescription, nonprescription, alternative, traditional, vitamins, or nutritional supplements) are individually assessed to determine that each medication is appropriate for the patient, effective for the medical condition, safe given the patient s comorbidities and other medications being taken, and able to be taken by the patient as intended. 1 CMM is a formal, collaborative approach in which clinical pharmacists work together with members of the health care team to optimize therapeutic outcomes for patients. 1 Through CMM, clinical pharmacists actively manage medication therapies; identify, prevent, and resolve medication therapy problems (MTPs); and formulate follow-up and monitoring plans to assess patients progress toward therapeutic goals. 2,3 With this innovative pharmacist role, several studies have established that pharmacist-provided CMM services can improve patient outcomes while simultaneously decreasing overall health care spending. 4,5 Specifically, pharmacist-provided CMM has led to significant clinical improvements in diabetes mellitus and hypertension management. 6 Other studies have shown that pharmacist-provided CMM services have had a positive return on investment, with $1.29 to $12 savings in overall health care costs
6 for every $1 spent on CMM services. 5,7 CMM services provided by pharmacists integrated within the health system have been shown to produce high rates of patient satisfaction. In one study of patient surveys completed over 10 years, 95.3% of respondents agreed or strongly agreed that their overall health and well-being had improved because of CMM, and 98.1% agreed or strongly agreed that they would recommend this service to family and friends. 5 The value of pharmacists in the interdisciplinary patient care team has been recognized and in the primary care setting, more pharmacists are serving as advanced practice providers focusing not only on CMM but also on other direct patient care activities including comprehensive disease state management, disease prevention, care coordination, and follow-up care. 3,8 Previous studies have focused on the clinical, financial, and humanistic impact of pharmacist integration relating to direct patient care, but there are few data on the effects of integrated pharmacists on indirect patient care. Pharmacists embedded in a primary care practice frequently perform a combination of indirect and direct patient care duties in addition to administrative functions and provision of formalized staff education. Indirect care, hereafter termed nonvisit care, includes individualized patient care activities outside of scheduled face-to-face or telehealth appointments. Examples of nonvisit care include informal curbside consults with other health care providers regarding a patient-specific medication question, electronic communication with health care staff providing education about a patient s new medication, or a patient telephone call to discuss adverse effect management.
7 With the changing reimbursement landscape, from a fee-for-service to a value-based payment model, our organization and others have recognized the importance of effectively managing nonvisit care activities by using the knowledge and expertise of advanced practice pharmacists. Despite these additional responsibilities being assumed by integrated pharmacists, data specifically quantifying the amount of time they spend on nonvisit care activities are lacking. Quantifying pharmacist time spent and describing the types of nonvisit care activities is an initial step toward evaluating the role and effects of integrated pharmacists on nonvisit care. Several organizations have published minimum standards of care for CMM pharmacists These expectations encompass patient assessment and collaboration with the health care team, but another key component of CMM services is the identification and resolution of MTPs (also known as drug therapy problems). In past studies, 4,5,7 MTPs have been used to classify types of pharmacist interventions regarding direct patient care but could also be used for analyzing the influence of pharmacists on nonvisit care. Typically, MTPs are classified into several categories and subcategories: indication (unnecessary medication, need for additional medication), effectiveness (ineffective medication, dosage too low), safety (dosage too high, adverse medication event), and convenience/compliance (nonadherence). 5,12,13 In one study from a large, multicenter integrated health system with data from 10 years of pharmacist-provided CMM services, the MTPs most commonly identified were needs additional therapy (indication), dosage too low (effectiveness), and nonadherence (convenience/compliance). 5 In
8 addition to identifying and resolving MTPs, CMM pharmacists often provide nonvisit care in the form of medication education for patients and providers. 9,10 As the primary care environment continues to transition from volume-based to value-based care, the optimized utilization of advanced practice pharmacists may substantially affect health care outcomes and costs. One critical factor in optimizing utilization of advanced practice pharmacists is discovering the proper balance between the time spent on direct patient care versus nonvisit care. Because of the lack of research regarding how pharmacists nonvisit care activities affect the health care team and their patients, we aimed to describe and quantify nonvisit care activities provided by four advance practice pharmacists, or ambulatory care pharmacists, at four different outpatient primary care practices at our institution. The primary objective was to quantify the time outpatient ambulatory care pharmacists spent completing nonvisit care activities over a 12-week period in primary care clinics. Secondary objectives were to quantify the number of patients affected, determine the types of nonvisit care activities completed, and classify the types of MTPs and medication therapy interventions most frequently addressed during nonvisit care activities. Methods Project Design, Setting, and Participants This quantitative evaluation study included information gathered between February and September 2017 at four ambulatory care practices within Mayo Clinic Enterprise. The collection window was established to ensure that data were collected
9 before workflow changes occurred in the department. Data were obtained during a 12- week period to account for the variability in practice changes across the different sites during data collection. Because of the differences in practices and schedules, each investigative pharmacist chose a predetermined 12-week period within the collection window to gather data for the study. The ambulatory care practices, located in three states (Minnesota, Wisconsin, and Florida), support clinics that consist of primary care providers in family medicine, internal medicine, or both services, along with a varying number of specialty providers. The number of paneled patients in the clinics ranged from 7300 to more than 37,000 (Table 1). Each ambulatory care practice schedule had 2 hours of each 8-hour clinic day set aside for responsibilities outside of patient appointments, including administrative work, nonvisit care activities, patient appointment preparation, and documentation. Nonvisit care activities in this study were defined as patient-specific clinical problems or questions that occur outside of formal health care team education and patient care appointments conducted either in the clinic, electronically, or by telephone. These nonvisit care activities are communications initiated by either the patient or a member of the health care team to the ambulatory care pharmacist for the purpose of patient care. This study was reviewed by our institutional review board and considered exempt from further review, with categorization as a quality assurance project. Data Collection Data were collected through two different methods: an internally developed software program, PhARMS (Pharmacist Ambulatory Resource Management System),
10 and a spreadsheet created to collect data. PhARMS is a software program used by pharmacists to manually record daily activities as part of a departmental data collection workflow. Investigative pharmacists, all of whom are authors, each collected data during a predetermined 12-week period completed between February and September Primary outcome data were manually recorded and collected using PhARMS through normal workflow, which allowed for classification of nonvisit care activities into specific subcategories to determine type of nonvisit care activities used (Table 2). In this study, information entered in the PhARMS nonvisit care activities work category during the study period was obtained through generated reports for each ambulatory care practice. Each report contained the following information for each entry: unique patient identifier, nonvisit care activity subcategory, time spent, and date of service. Secondary outcome data were collected using a spreadsheet generated for this study to capture data not gathered by PhARMS, such as MTP and medication therapy intervention for each nonvisit care activity, in addition to a unique patient identifier for each entry. Each investigator used a separate identical spreadsheet to collect appropriate data for nonvisit care activities completed at their respective practice. To comprehensively study the resources pharmacists dedicate to nonvisit care, it is imperative to find a way to capture this educational role that pharmacists provide when a traditional MTP may not be an appropriate choice. For this purpose, we elected to include education as an additional MTP category, which allowed us to capture all pharmacist interventions while continuing to use the traditional MTP identification classification.
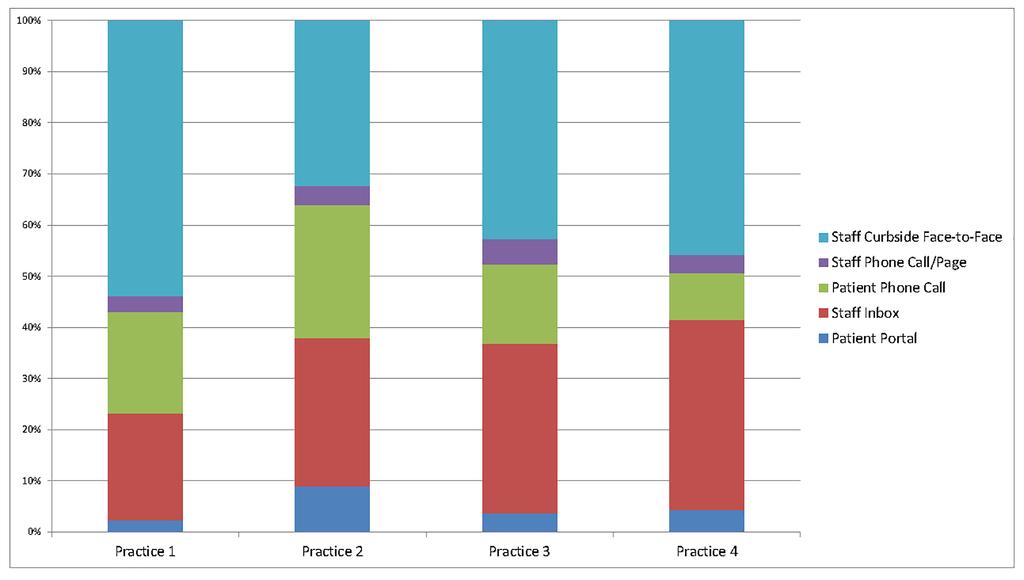
11 Pharmacists from each ambulatory care practice reviewed multiple different scenarios for each nonvisit care activity type before data collection to establish consistent categorization. Quality assurance discussions occurred consistently throughout the data collection periods to maintain nonvisit care activity categorization. Descriptive Statistics Raw data were analyzed using means and ranges. Before beginning data collection, an internal statistician was consulted about the study to ensure that proper statistics were used. Results Primary Outcome: Time Spent This study was conducted by four ambulatory care pharmacists with a total of 3.6 full-time equivalents, spread out between four ambulatory care practices in one health system. During the 12-week period, 346 total hours were spent on nonvisit care activities, out of 1728 total clinic hours scheduled, on the basis of pharmacist full-time equivalents. The mean time spent per day on nonvisit care activities was 1.6 hours per practice (range, hours). The time spent per activity varied by activity type. Patient telephone call and patient portal message took the most time per activity, both averaging 17 minutes per activity. Staff inbox message averaged 15 minutes per activity, and staff telephone call averaged 14 minutes per activity. Staff face-to-face curbside consult was the least timeconsuming, averaging 10 minutes per activity.
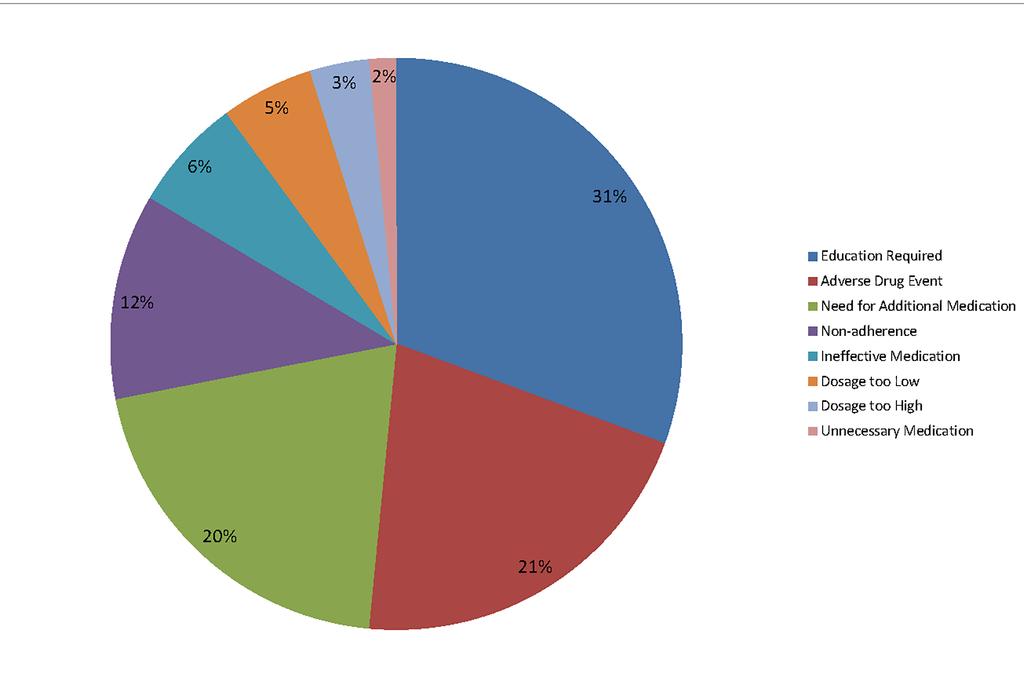
12 Secondary Outcomes Patients Affected A total of 1311 patients were affected by nonvisit care activities during the study, with a mean (range) of 327 patients ( patients) per pharmacist. The mean number of patients affected each day by an ambulatory care pharmacist was 6. Number and Type of Nonvisit Care Activities A total of 1548 nonvisit care activities were completed during the study period, with a mean of 7.2 activities per day. The most frequent type of nonvisit care activity was staff face-to-face curbside consult, which accounted for 41% (638 activities). Staff inbox message accounted for 30% (466 activities), and patient telephone call accounted for 19% (297 activities). The remaining activity types, patient portal message and staff telephone call/page, accounted for 6% (86 activities) and 4% (61 activities), respectively. The most commonly used nonvisit care activity types were similar across each ambulatory care practice (Figure 1). MTPs and Medication Therapy Interventions Of 1866 total MTPs identified during the study (mean, 1.4 MTPs per patient), the most common type was education required (31%, n=572). Adverse medication events (21%, n=390) and need for additional medication (20%, n=380) were also frequently identified (Figure 2). Nonadherence represented 12% (n=217) of MTPs, and the remaining 16% (n=307) comprised a combination of ineffective medication, dosage too low, dosage too high, and unnecessary medication. Each ambulatory care practice identified a different primary MTP, but the top four MTPs education required,
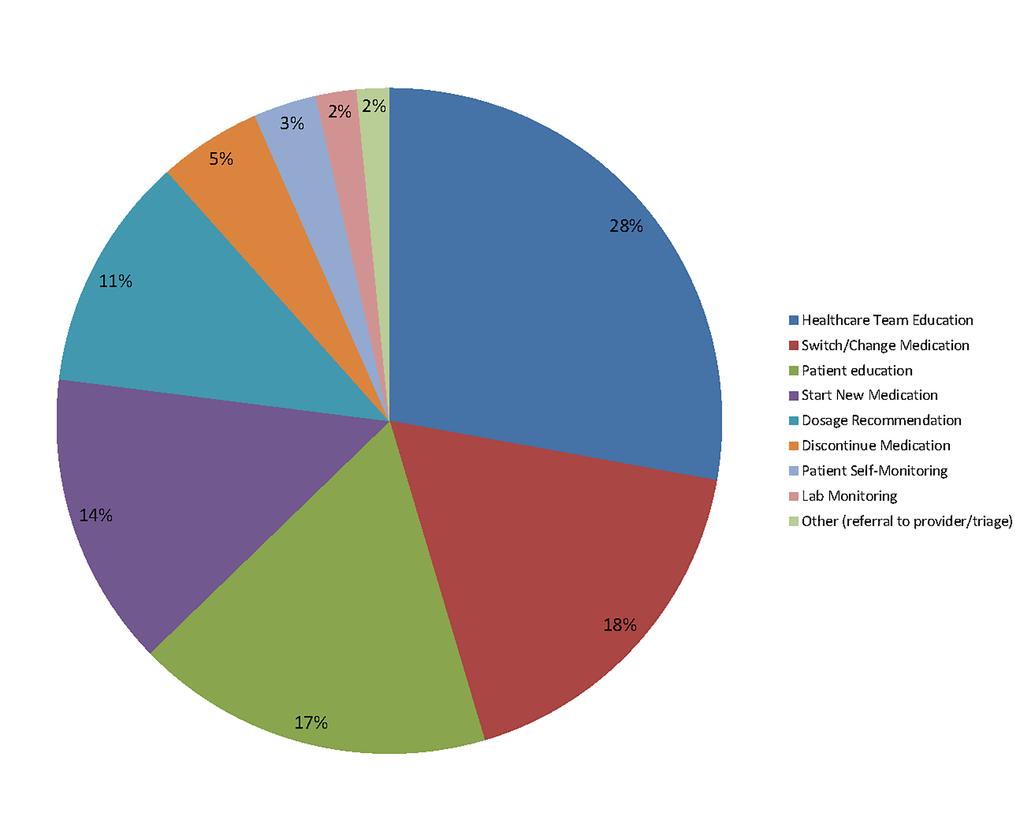
13 nonadherence, adverse medication event, and need for additional medication were consistent between all of the practices. The most frequent medication therapy intervention was health care team education, which accounted for 28% (n=520) (Figure 3). Eighteen percent (n=327) of the medication therapy interventions were attributed to switch/change medication, and 17% (n=324) to patient education. Start new medication or dosage recommendation was the recommended medication therapy intervention for 14% (n=266) and 11% (n=213), respectively. The remaining 12% of medication therapy interventions consisted of medication discontinuation, patient self-monitoring, laboratory monitoring, or other (referrals to providers or triage). Discussion For each 8-hour day, ambulatory care pharmacists dedicated, on average, 20% of their time (96 minutes) to nonvisit care activities. Not only is this a substantial component of an ambulatory care pharmacist s time, this assistance with nonvisit care activities may increase the capacity of other health care team members. Using the ambulatory care pharmacist for medication-related nonvisit care activities leverages the distinctive knowledge of the pharmacist as the medication expert. Time spent on nonvisit care activities varied considerably among pharmacists, with several contributing factors considered. Each ambulatory care practice varied substantially in provider composition, availability of specialty services, responsibilities associated with inpatient services, and pharmacist full-time equivalent
14 support (Table 1). The tenure of each pharmacist in each practice and the ambulatory services offered were different between sites and may have affected staff familiarity with pharmacist services and their subsequent utilization for nonvisit care activities. Furthermore, some ambulatory care practices were involved in preparation for and implementation of electronic health record vendor change during data collection, which most likely affected practice through all disciplines. These practice-specific factors, in addition to pharmacist-specific factors, may help explain the noticeable variability in total time spent on nonvisit care (range, hours per day) among individual pharmacists. Although staff face-to-face curbside consults were the most frequent type of nonvisit care activity, they also required the least time per activity (mean, 10 minutes per activity). Other nonvisit care types took substantially longer, averaging 14 to 17 minutes per activity. This could provide some further direction with regard to the most efficient use of ambulatory care pharmacist time for nonvisit care activities. This finding also indicates that ambulatory care pharmacists are often used for nonvisit care activities conducted in person, which may imply that pharmacist visibility and availability encourage staff engagement for a brief consult or question. Individual ambulatory care pharmacists responded to between 5 and 10 nonvisit care activities on average daily, with more nonvisit care activities correlating to more time spent per day on nonvisit care. Variability is expected because of unique ambulatory care practice and team factors including, but not limited to, patient population and number and type of providers. Also, a temporal increase in education-based nonvisit care activities seemed to occur when practices added new providers, particularly those
15 early in their practice career. In ambulatory care practices where the pharmacist was a highly visible physical presence in the health care team, overall utilization may have been higher. This may have affected the nonvisit care activity type, thus further contributing to variability in overall time spent on nonvisit care activities between practices. Ambulatory care pharmacists with a heavier direct patient care volume and administrative workload would most likely be less visible to clinic staff, which may have deterred providers from engaging the pharmacist in nonvisit care activities. Education, adverse medication event, need for additional medication, and nonadherence were the four most frequent MTPs identified in the study and were similar in all ambulatory care practices. This correlated to a previous study of pharmacistprovided direct patient care, which identified the top three MTPs of needing additional medication, dose change, and nonadherence. 5 Although pharmacist-provided education to patients and the health care team is not a traditional MTP category, it was included in this study in an attempt to fully capture how ambulatory care pharmacist time was spent on nonvisit care activities. 5,12,13 Education accounted for approximately 30% of total MTPs, with health care team education occurring at nearly twice the frequency of patient education. This extent of pharmacologic education to patients and staff further illustrates the need to use ambulatory care pharmacists unique knowledge base and skill set in the primary care setting. Applicability of billing for nonvisit care activities, such as chronic care management billing, would most likely be limited in the sense that nonvisit care activities, such as those captured in this study, seem to occur at unique time points for
16 patients with limited follow-up. Because pharmacists spent substantial time each day on nonvisit care activities, reviewing the billing opportunities available could be considered a priority in the ambulatory care practice. This study focused exclusively on nonvisit care activities that directly affected individual patient care. Pharmacists are also involved in population-based activities, such as provider in-service education, quality assurance programs, or other clinic-based initiatives. Because these activities have limited effects on individual patient care, they were excluded from this study. Further research should evaluate the effects of pharmacist involvement with population-based activities in a clinic setting. Limitations This description of outpatient ambulatory care pharmacist involvement in nonvisit care is limited in scope and by the lack of comparative published literature for external validation of findings. Also, because of the unique structure of outpatient ambulatory care pharmacist utilization in our institution, the applicability of this study to other practices may be limited. One way to further describe practices and evaluate consistency between sites would be to capture nonvisit care activities in conjunction with scheduled pharmacist appointment volume and time spent. The 12-week time frame was believed to be adequate for both collecting data and minimizing variability in day-to-day practice. Although this time frame was limited it provides a basis for further research opportunities in the future to support these findings. Classification of education required as an MTP has not previously been included by other known studies. Arguably, this may not represent an MTP itself but may
17 be considered as a separate classification of nonvisit care activity. This decision to include education required as an MTP influences the overall description and quantification of nonvisit care activities, and further consideration may be needed to determine how to best capture this pharmacist-provided service. Another limitation of the study are the major variabilities between the ambulatory care practices included. In addition to number and type of primary care providers, availability of specialty services, and populations served, pharmacist-specific factors including use of collaborative practice agreements and length of time in an established role contributed to variation in study sites. Although this variability helps diversify the study, the heterogeneity may have skewed the data. Conclusion This study demonstrated that an ambulatory care pharmacist embedded in a primary care team offers additional resources that health care organizations can leverage to assist with nonvisit care activities. Although consistencies were identified in the type of nonvisit care activities performed by each ambulatory care pharmacist, practicespecific factors most likely affected the extent of individual pharmacist utilization. The study results were similar to those of previous work in direct patient care in the type of MTPs identified, with an additional category of pharmacist-provided education captured to more fully quantify ambulatory care pharmacist contributions through nonvisit care. Providers have voiced that, in a busy practice, it is often difficult to do timely research on the best treatment options for complex medical conditions while ensuring safe prescribing. Having an ambulatory care pharmacist readily available for curbside
18 consults to assist in these decisions enhances provider satisfaction through better efficiency and increases quality and safety of patient care. Team-based care is emphasized to the patient when they are part of shared decision-making that occurs in real time with multiple medical disciplines. In the midst of health care practices so highly dependent on electronic data processing, curbside consults with an ambulatory care pharmacist also facilitate a richness of professional interaction among members of the health care team that enhances provider satisfaction and thus favors reduced burnout. The findings of this study and providers viewpoints should lead future research to quantify the decrease in workload burden for consulting providers and care team members, determine the best utilization strategy for ambulatory care pharmacists for nonvisit care activities, determine billing opportunities for nonvisit care activities, and evaluate patient and provider satisfaction with pharmacist involvement.
19 References 1. American College of Clinical Pharmacy. Comprehensive medication management in team-based care. Available from Accessed January 24, American College of Clinical Pharmacy, McBane SE, Dopp AL, et al. Collaborative drug therapy management and comprehensive medication management Pharmacotherapy 2015;35(4):e Giberson S, Yoder S, Lee M. Improving patient and health system outcomes through advanced pharmacy practice. A report to the U.S. Surgeon General [2011]. Available from Accessed January 24, Isetts BJ, Schondelmeyer SW, Artz MB, et al. Clinical and economic outcomes of medication therapy management services: the Minnesota experience. J Am Pharm Assoc (2003) 2008;48(2): Ramalho de Oliveira D, Brummel AR, Miller DB. Medication therapy management: 10 years of experience in a large integrated health care system. J Manag Care Pharm 2010;16(3): Brummel AR, Soliman AM, Carlson AM, de Oliveira DR. Optimal diabetes care outcomes following face-to-face medication therapy management services. Popul Health Manag 2013;16(1):28-34.
20 7. Brummel A, Lustig A, Westrich K, et al. Best practices: improving patient outcomes and costs in an ACO through comprehensive medication therapy management. J Manag Care Spec Pharm 2014;20(12): Alkhateeb FM, Clauson KA, McCafferty R, Latif DA. Physician attitudes toward pharmacist provision of medication therapy management services. Pharm World Sci 2009;31(4): American College of Clinical Pharmacy, Burke JM, Miller WA, et al. Clinical pharmacist competencies. Pharmacotherapy 2008;28(6): American College of Clinical Pharmacy. Standards of practice for clinical pharmacists. Pharmacotherapy 2014;34(8): Buxton JA, Babbitt R, Clegg CA, et al. ASHP guidelines: Minimum standard for ambulatory care pharmacy practice. Am J Health Syst Pharm 2015;72(14): Kaur S, Roberts JA, Roberts MS. Evaluation of medication-related problems in medication reviews: a comparative perspective. Ann Pharmacother 2012;46(7-8): Cipolle RJ, Strand LM, Morley PC. Pharmaceutical care practice: the clinician's guide. 2nd ed. New York: McGraw-Hill Medical Pub. Division, 2004.
21 Table 1. Ambulatory Care Practice Characteristics During Data Collection Characteristic Practice 1 Practice 2 Practice 3 Practice 4 Pharmacist FTE allotment Clinic primary care Family Family Family Family practice description Medicine Medicine Medicine Medicine Internal Internal Medicine Medicine No. of paneled patients ,035 17,523 37,588 No. of primary care physicians No. of primary care advanced practice providers Duration pharmacist was established in practice at time of data collection, months FTE = full-time equivalent. Including residents.
22 Table 2. Nonvisit Care Subcategory Descriptions Nonvisit Care Subcategory Patient portal message Description Secure electronic communication initiated by a patient to the health care team via electronic health record Staff inbox message Electronic communication initiated by a health care team member to the ambulatory care pharmacist via electronic health record or secure messaging Patient telephone call Communication via telephone initiated by a patient to the ambulatory care pharmacist excluding scheduled appointments Staff telephone call/page Internal communication via telephone initiated by a health care team member to the ambulatory care pharmacist Staff face-to-face curbside consult Face-to-face communication initiated by a health care team member to the ambulatory care pharmacist
23 Figure Legends Figure 1. Nonvisit care activity types by practice. Figure 2. Medication therapy problems identified. Figure 3. Medication therapy interventions identified.
24 JAC5_1094_ File002.tif
25 JAC5_1094_ File003.tif
26 JAC5_1094_ File004.tif
Student Project PRACTICE-BASED RESEARCH
 A Description of Medication Therapy Management Services in Minnesota Amie Jo Digatono, Pharm.D. Candidate, College of Pharmacy, University of Minnesota Key words: medication therapy management, Minnesota,
A Description of Medication Therapy Management Services in Minnesota Amie Jo Digatono, Pharm.D. Candidate, College of Pharmacy, University of Minnesota Key words: medication therapy management, Minnesota,
Performance Measurement of a Pharmacist-Directed Anticoagulation Management Service
 Hospital Pharmacy Volume 36, Number 11, pp 1164 1169 2001 Facts and Comparisons PEER-REVIEWED ARTICLE Performance Measurement of a Pharmacist-Directed Anticoagulation Management Service Jon C. Schommer,
Hospital Pharmacy Volume 36, Number 11, pp 1164 1169 2001 Facts and Comparisons PEER-REVIEWED ARTICLE Performance Measurement of a Pharmacist-Directed Anticoagulation Management Service Jon C. Schommer,
Pharmacists Providing Comprehensive Medication Management
 Pharmacists Providing Comprehensive Medication Management Welcome We will begin shortly. Please ensure your computer speakers are turned on. Before we begin Welcome! Housekeeping Notes Polls Speaker Introduction
Pharmacists Providing Comprehensive Medication Management Welcome We will begin shortly. Please ensure your computer speakers are turned on. Before we begin Welcome! Housekeeping Notes Polls Speaker Introduction
The Patient Care Process for Delivering Comprehensive Medication Management (CMM)
") The Patient Care Process for Delivering Comprehensive Medication Management (CMM) Optimizing Medication Use in Patient-Centered, Team-Based Care Settings Acknowledgements Funding for this research was
The Patient Care Process for Delivering Comprehensive Medication Management (CMM) Optimizing Medication Use in Patient-Centered, Team-Based Care Settings Acknowledgements Funding for this research was
The Pharmacist Patient Care Process: Implications for Preceptors And Student- Interns
 Objectives The Pharmacist Patient Care Process: Implications for Preceptors And Student- Interns Define the Joint Commission of Pharmacy Practitioners (JCPP) Pharmacist Patient Care Process (PPCP) and
Objectives The Pharmacist Patient Care Process: Implications for Preceptors And Student- Interns Define the Joint Commission of Pharmacy Practitioners (JCPP) Pharmacist Patient Care Process (PPCP) and
Analysis of Nursing Workload in Primary Care
 Analysis of Nursing Workload in Primary Care University of Michigan Health System Final Report Client: Candia B. Laughlin, MS, RN Director of Nursing Ambulatory Care Coordinator: Laura Mittendorf Management
Analysis of Nursing Workload in Primary Care University of Michigan Health System Final Report Client: Candia B. Laughlin, MS, RN Director of Nursing Ambulatory Care Coordinator: Laura Mittendorf Management
Bringing the Clinical Mindset to the Retail Pharmacist
 Bringing the Clinical Mindset to the Retail Pharmacist Sarah Griffin, Pharm.D. Harding University College of Pharmacy White County Medical Center Objectives Describe challenging situations faced by pharmacists
Bringing the Clinical Mindset to the Retail Pharmacist Sarah Griffin, Pharm.D. Harding University College of Pharmacy White County Medical Center Objectives Describe challenging situations faced by pharmacists
Practice Tools for Safe Drug Therapy
 Practice Tools for Safe Drug Therapy Practice Tools for Safe Drug Therapy Pharmacists and pharmacy technicians make sure the right person gets the right dose of the right drug at the right time and takes
Practice Tools for Safe Drug Therapy Practice Tools for Safe Drug Therapy Pharmacists and pharmacy technicians make sure the right person gets the right dose of the right drug at the right time and takes
Original Research PRACTICE-BASED RESEARCH
 Patient-perceived value of Medication Therapy Management (MTM) services: a series of focus groups Heidi Schultz, PharmD 1 ; Sarah M. Westberg, PharmD, BCPS 2 ; Djenane Ramalho de Oliveira, PhD 1 ; and
Patient-perceived value of Medication Therapy Management (MTM) services: a series of focus groups Heidi Schultz, PharmD 1 ; Sarah M. Westberg, PharmD, BCPS 2 ; Djenane Ramalho de Oliveira, PhD 1 ; and
Medication Therapy Management
 Medication Therapy Management Presented by Sylvia Saade, PharmD Ghada Khoury, Pharm D, BCACP Objectives Describe the components of medication therapy management (MTM) programs Discuss the needs of MTM
Medication Therapy Management Presented by Sylvia Saade, PharmD Ghada Khoury, Pharm D, BCACP Objectives Describe the components of medication therapy management (MTM) programs Discuss the needs of MTM
T O G E T H E R W E M A K E A G R E A T T E A M. January 6, 2014
 7272 Wisconsin Avenue Bethesda, Maryland 20814 301-657-3000 Fax: 301-664-8877 www.ashp.org Richard Kronick, Ph.D. Director, Agency for Healthcare Research and Quality Agency for Healthcare Research and
7272 Wisconsin Avenue Bethesda, Maryland 20814 301-657-3000 Fax: 301-664-8877 www.ashp.org Richard Kronick, Ph.D. Director, Agency for Healthcare Research and Quality Agency for Healthcare Research and
Educating Payers on the Pharmacist Medication Therapy Management (MTM) Billing Codes
 Billing Codes") Educating Payers on the Pharmacist Medication Therapy Management (MTM) Billing Codes REQUEST FOR PROPOSALS The instructions in this Request for Proposals should be followed carefully. Only after all the
Educating Payers on the Pharmacist Medication Therapy Management (MTM) Billing Codes REQUEST FOR PROPOSALS The instructions in this Request for Proposals should be followed carefully. Only after all the
Experiential Education
 Experiential Education Experiential Education Page 1 Experiential Education Contents Introduction to Experiential Education... 3 Experiential Education Calendar... 4 Selected ACPE Standards 2007... 5 Standard
Experiential Education Experiential Education Page 1 Experiential Education Contents Introduction to Experiential Education... 3 Experiential Education Calendar... 4 Selected ACPE Standards 2007... 5 Standard
Course Descriptions for PharmD Classes of 2021 and Beyond updated November 2017
 Course Descriptions for PharmD Classes of 2021 and Beyond updated November 2017 PHRD 510 - Pharmacy Seminar I Credit: 0.0 hours PHRD 511 Biomedical Foundations Credit: 4.0 hours This course is designed
Course Descriptions for PharmD Classes of 2021 and Beyond updated November 2017 PHRD 510 - Pharmacy Seminar I Credit: 0.0 hours PHRD 511 Biomedical Foundations Credit: 4.0 hours This course is designed
9/20/16. MTM Roundtable: Pharmacist Workload Metric. Objectives. Pretest Question #1
 MTM Roundtable: Pharmacist Workload Metric Audrey Umbreit, PharmD, BCACP Senior Manager Clinical Pharmacy, Primary Care Mayo Clinic Health System MPhA Annual Learning Networking Event Friday, September
MTM Roundtable: Pharmacist Workload Metric Audrey Umbreit, PharmD, BCACP Senior Manager Clinical Pharmacy, Primary Care Mayo Clinic Health System MPhA Annual Learning Networking Event Friday, September
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016
 UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
UNIVERSITY OF WISCONSIN HOSPITAL AND CLINICS DEPARTMENT OF PHARMACY SCOPE OF PATIENT CARE SERVICES FY 2017 October 1 st, 2016 Department Name: Department of Pharmacy Department Director: Steve Rough, MS,
Improving Access in Infusion Therapy
 Improving Access in Infusion Therapy Timmi Anne Boesken, MHA, CPhT Medication Access Services Coordinator Kathryn Clark McKinney, PharmD, MS, BCPS, FACHE Director of Pharmacy Services Michelle Dusing Wiest,
Improving Access in Infusion Therapy Timmi Anne Boesken, MHA, CPhT Medication Access Services Coordinator Kathryn Clark McKinney, PharmD, MS, BCPS, FACHE Director of Pharmacy Services Michelle Dusing Wiest,
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE
 COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
Integrated Clinical Pharmacy Services
 Integrated Clinical Pharmacy Services Best Practices Toolkit This toolkit was developed by RiverStone Health through the generous support of a grant from the Montana Healthcare Foundation What is a Clinical
Integrated Clinical Pharmacy Services Best Practices Toolkit This toolkit was developed by RiverStone Health through the generous support of a grant from the Montana Healthcare Foundation What is a Clinical
Professional Student Outcomes (PSOs) - the academic knowledge, skills, and attitudes that a pharmacy graduate should possess.
 - the academic knowledge, skills, and attitudes that a pharmacy graduate should possess.") Professional Student Outcomes (PSOs) - the academic knowledge, skills, and attitudes that a pharmacy graduate should possess. Number Outcome SBA SBA-1 SBA-1.1 SBA-1.2 SBA-1.3 SBA-1.4 SBA-1.5 SBA-1.6 SBA-1.7
Professional Student Outcomes (PSOs) - the academic knowledge, skills, and attitudes that a pharmacy graduate should possess. Number Outcome SBA SBA-1 SBA-1.1 SBA-1.2 SBA-1.3 SBA-1.4 SBA-1.5 SBA-1.6 SBA-1.7
Community Pharmacy Advanced Pharmacy Practice Experience SPPS 402
 Community Pharmacy Advanced Pharmacy Practice Experience SPPS 402 Office of Experiential Education James Colbert, Pharm.D. Sarah Lorentz, Pharm.D. Associate Dean of Experiential Education Clinical Professor
Community Pharmacy Advanced Pharmacy Practice Experience SPPS 402 Office of Experiential Education James Colbert, Pharm.D. Sarah Lorentz, Pharm.D. Associate Dean of Experiential Education Clinical Professor
Medication Adherence
 Medication Adherence Robert DiGregorio, PharmD, FNAP, BCACP Professor (Long Island University) Sr. Director, Pharmacy & Pharmacotherapy Services (TBHC) Chief, Pharmacotherapy Department of Internal Medicine
Medication Adherence Robert DiGregorio, PharmD, FNAP, BCACP Professor (Long Island University) Sr. Director, Pharmacy & Pharmacotherapy Services (TBHC) Chief, Pharmacotherapy Department of Internal Medicine
Hospitals organize medications according to a formulary
 INNOVATIONS IN PHARMACY PRACTICE: CLINICAL PRACTICE Going through the Motions: A Time-and- Motion Study of Workload Associated with Nonformulary Medication Orders Elaine Chang, Angus Kinkade, Anthony C
INNOVATIONS IN PHARMACY PRACTICE: CLINICAL PRACTICE Going through the Motions: A Time-and- Motion Study of Workload Associated with Nonformulary Medication Orders Elaine Chang, Angus Kinkade, Anthony C
Chapter 13. Documenting Clinical Activities
 Chapter 13. Documenting Clinical Activities INTRODUCTION Documenting clinical activities is required for one or more of the following: clinical care of individual patients -sharing information with other
Chapter 13. Documenting Clinical Activities INTRODUCTION Documenting clinical activities is required for one or more of the following: clinical care of individual patients -sharing information with other
Prior to implementation of the episode groups for use in resource measurement under MACRA, CMS should:
 Via Electronic Submission (www.regulations.gov) March 1, 2016 Andrew M. Slavitt Acting Administrator Centers for Medicare and Medicaid Services 7500 Security Boulevard Baltimore, MD episodegroups@cms.hhs.gov
Via Electronic Submission (www.regulations.gov) March 1, 2016 Andrew M. Slavitt Acting Administrator Centers for Medicare and Medicaid Services 7500 Security Boulevard Baltimore, MD episodegroups@cms.hhs.gov
EXPERIENTIAL EDUCATION Medication Therapy Management Services Provided by Student Pharmacists
 EXPERIENTIAL EDUCATION Medication Therapy Management Services Provided by Student Pharmacists Micah Hata, PharmD, a Roger Klotz, BSPharm, a Rick Sylvies, PharmD, b Karl Hess, PharmD, a Emmanuelle Schwartzman,
EXPERIENTIAL EDUCATION Medication Therapy Management Services Provided by Student Pharmacists Micah Hata, PharmD, a Roger Klotz, BSPharm, a Rick Sylvies, PharmD, b Karl Hess, PharmD, a Emmanuelle Schwartzman,
Journal of Pharmacy Practice and Community Medicine.2017, 3(4s):S61-S66
:S61-S66") Journal of Pharmacy Practice and Community Medicine.2017, 3(4s):S61-S66 http://dx.doi.org/10.5530/jppcm.2017.4s.50 RESEARCH ARTICLE OPEN ACCESS Pharmacy Workload and Workforce Requirements at MOH Primary
Journal of Pharmacy Practice and Community Medicine.2017, 3(4s):S61-S66 http://dx.doi.org/10.5530/jppcm.2017.4s.50 RESEARCH ARTICLE OPEN ACCESS Pharmacy Workload and Workforce Requirements at MOH Primary
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report
 Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
Team 10 Med-List University of Michigan Health System Program and Operations Analysis Cost-Benefit Analysis of Medication Reconciliation Pharmacy Technician Pilot Final Report To: John Clark, PharmD, MS,
Clinical Management of patients: The case for Comprehensive Medication Therapy Management Services
 Clinical Management of patients: The case for Comprehensive Medication Therapy Management Services Professor Djenane Ramalho de Oliveira, PhD Director, Centro de Estudos em Atenção Farmacêutica (CEAF)
Clinical Management of patients: The case for Comprehensive Medication Therapy Management Services Professor Djenane Ramalho de Oliveira, PhD Director, Centro de Estudos em Atenção Farmacêutica (CEAF)
Medido, a smart medication dispensing solution, shows high rates of medication adherence and potential to reduce cost of care.
 White Paper Medido, a smart medication dispensing solution, shows high rates of medication adherence and potential to reduce cost of care. A Philips Lifeline White Paper Tine Smits, Research Scientist,
White Paper Medido, a smart medication dispensing solution, shows high rates of medication adherence and potential to reduce cost of care. A Philips Lifeline White Paper Tine Smits, Research Scientist,
Original Research PRACTICE-BASED RESEARCH. University Wexner Medical Center
 Evaluation of provider documentation of medication management in a Patient-Centered Medical Home (PCMH) Trang T. Nguyen, PharmD 1 ; Bella H Mehta, PharmD, FAPhA 2 ; Jennifer L. Rodis, PharmD, BCPS 2 ;
Evaluation of provider documentation of medication management in a Patient-Centered Medical Home (PCMH) Trang T. Nguyen, PharmD 1 ; Bella H Mehta, PharmD, FAPhA 2 ; Jennifer L. Rodis, PharmD, BCPS 2 ;
Background and Methodology
 Study Sites and Investigators Emergency Department Pharmacists Improve Patient Safety: Results of a Multicenter Study Supported by the ASHP Foundation Jeffrey Rothschild, MD, MPH-Principal Investigator
Study Sites and Investigators Emergency Department Pharmacists Improve Patient Safety: Results of a Multicenter Study Supported by the ASHP Foundation Jeffrey Rothschild, MD, MPH-Principal Investigator
Medicare Part D Member Satisfaction of the Comprehensive Medication Review. Katie Neff-Golub, PharmD, CGP, CPh WellCare Health Plans
 Medicare Part D Member Satisfaction of the Comprehensive Medication Review Katie Neff-Golub, PharmD, CGP, CPh WellCare Health Plans 1 Disclosure Statement Disclosure Statement: These individuals have the
Medicare Part D Member Satisfaction of the Comprehensive Medication Review Katie Neff-Golub, PharmD, CGP, CPh WellCare Health Plans 1 Disclosure Statement Disclosure Statement: These individuals have the
Learning Experiences Descriptions
 Anticoagulation Management Clinic Learning Experiences Descriptions The Anticoagulation Management rotation is an elective learning experience that focuses on the outpatient management of anticoagulation.
Anticoagulation Management Clinic Learning Experiences Descriptions The Anticoagulation Management rotation is an elective learning experience that focuses on the outpatient management of anticoagulation.
Specialty Pharmacy: The Evolution of the Comprehensive Pharmaceutical Care Model. Arash Dabestani, PharmD, MHA, FASHP, FABC
 Specialty Pharmacy: The Evolution of the Comprehensive Pharmaceutical Care Model Arash Dabestani, PharmD, MHA, FASHP, FABC OBJECTIVES Discuss the history of clinical pharmacy relative to specialty pharmacy
Specialty Pharmacy: The Evolution of the Comprehensive Pharmaceutical Care Model Arash Dabestani, PharmD, MHA, FASHP, FABC OBJECTIVES Discuss the history of clinical pharmacy relative to specialty pharmacy
Note EDUCATION. Keywords: Pharmacists Patient Care Process, faculty development, video
 Use of a Video Module to Improve Faculty Understanding of the Pharmacists Patient Care Process Crystal M. Deas, PharmD, BCPS; Angela R. Thomason, PharmD, BCPS; Robert M. Riggs, PhD, RPh; Michael C. Thomas,
Use of a Video Module to Improve Faculty Understanding of the Pharmacists Patient Care Process Crystal M. Deas, PharmD, BCPS; Angela R. Thomason, PharmD, BCPS; Robert M. Riggs, PhD, RPh; Michael C. Thomas,
Clinical Pharmacy Practice Models
 Disclosure Clinical Pharmacy Practice Models in Oncology Patient Care Rachel Matthews, PharmD, BCOP I have no actual or potential conflict of interest in relation to this program/presentation. Objectives
Disclosure Clinical Pharmacy Practice Models in Oncology Patient Care Rachel Matthews, PharmD, BCOP I have no actual or potential conflict of interest in relation to this program/presentation. Objectives
Literature review: pharmaceutical services for prisoners
 Author: Rosemary Allgeier, Principal Pharmacist in Public Health. Date: 08 October 2012 Version: 1a Publication and distribution: NHS Wales (intranet and internet) Public Health Wales (intranet and internet)
Author: Rosemary Allgeier, Principal Pharmacist in Public Health. Date: 08 October 2012 Version: 1a Publication and distribution: NHS Wales (intranet and internet) Public Health Wales (intranet and internet)
Evolving to a Clinical Practice: New Paradigm, New Thinking
 : New Paradigm, New Thinking Henri R. Manasse Jr., Ph.D., Sc.D. (Hon.), FFIP Professor and Dean Emeritus University of Illinois at Chicago Chair, FIPEd Steering Committee Outline 1. WHO Consultations on
: New Paradigm, New Thinking Henri R. Manasse Jr., Ph.D., Sc.D. (Hon.), FFIP Professor and Dean Emeritus University of Illinois at Chicago Chair, FIPEd Steering Committee Outline 1. WHO Consultations on
Medication Adherence. Pharmacy and Pharmaceutical Sciences
 Pharmacy and Pharmaceutical Sciences Medication Adherence Sabrina Anne Jacob B.Pharm(Hons.), MPharm, PhD(Clinical Pharmacy) Lecturer School of Pharmacy Monash University Malaysia Adherence is the extent
Pharmacy and Pharmaceutical Sciences Medication Adherence Sabrina Anne Jacob B.Pharm(Hons.), MPharm, PhD(Clinical Pharmacy) Lecturer School of Pharmacy Monash University Malaysia Adherence is the extent
Coastal Medical, Inc.
 A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
Understanding Antimicrobial Stewardship: Is Your Organization Ready? A S H LEIGH MOUSER, PHARM D, BCPS
 Understanding Antimicrobial Stewardship: Is Your Organization Ready? A S H LEIGH MOUSER, PHARM D, BCPS Objectives Discuss the need for antimicrobial stewardship programs Explain the components of an effective
Understanding Antimicrobial Stewardship: Is Your Organization Ready? A S H LEIGH MOUSER, PHARM D, BCPS Objectives Discuss the need for antimicrobial stewardship programs Explain the components of an effective
Bob Davis, PharmD, FAPhA Professor and Chair, KPIC
 Bob Davis, PharmD, FAPhA Professor and Chair, KPIC davisb@kennedycenter.sc.edusc edu South Carolina Primary Health Care Association September 19, 2015 Myrtle Beach, SC Disclosures Robert E. Davis declare(s)
Bob Davis, PharmD, FAPhA Professor and Chair, KPIC davisb@kennedycenter.sc.edusc edu South Carolina Primary Health Care Association September 19, 2015 Myrtle Beach, SC Disclosures Robert E. Davis declare(s)
Optimizing pharmaceutical care via Health Information Technology:
 Optimizing pharmaceutical care via Health Information Technology: The Epic Challenge Rilwan Badamas, PharmD, CAHIMS Pharmacy Grand Rounds 01/03/2017 2011 MFMER slide-1 The medication management team requests
Optimizing pharmaceutical care via Health Information Technology: The Epic Challenge Rilwan Badamas, PharmD, CAHIMS Pharmacy Grand Rounds 01/03/2017 2011 MFMER slide-1 The medication management team requests
Fundamentals of Medication Therapy Management (MTM) Services By Bruce R. Siecker, Ph.D., R.Ph.
 Services By Bruce R. Siecker, Ph.D., R.Ph.") Fundamentals of Medication Therapy Management (MTM) Services By Bruce R. Siecker, Ph.D., R.Ph. Bruce Siecker is president of Paradigm Research & Advisory Services, Inc. based in Stone Ridge, Virginia.
Fundamentals of Medication Therapy Management (MTM) Services By Bruce R. Siecker, Ph.D., R.Ph. Bruce Siecker is president of Paradigm Research & Advisory Services, Inc. based in Stone Ridge, Virginia.
Block Title: Patient Care Experience Block #: PHRM 701, 702, 703, 704 and PHRM 705, 706, and 707 (if patient care)
") Block Coordinator & Contact Information: Credit(s) & format: Section I. Block Description & Goals Jeremy Hughes, PharmD Director for Experiential Education & Assistant Professor Office: Creighton Hall
Block Coordinator & Contact Information: Credit(s) & format: Section I. Block Description & Goals Jeremy Hughes, PharmD Director for Experiential Education & Assistant Professor Office: Creighton Hall
Community Pharmacists Attitudes Toward an Expanded Class of Nonprescription Drugs
 Community Pharmacists Attitudes Toward an Expanded Class of Nonprescription Drugs Ruchit Shah 1 Erin Holmes 1 Donna West-Strum 1 Amit Patel 1,2 1 Department of Pharmacy Administration, The University of
Community Pharmacists Attitudes Toward an Expanded Class of Nonprescription Drugs Ruchit Shah 1 Erin Holmes 1 Donna West-Strum 1 Amit Patel 1,2 1 Department of Pharmacy Administration, The University of
Pharmacy Leadership and Administration Learning Experience Rev 12/16/16
 Pharmacy Leadership and Administration Learning Activities (Longitudinal): Preceptors: Jordan Dow, PharmD MS FACHE (Regional Pharmacy Director); Michele Richmond, RPh (Outpatient Pharmacy Director); Maggie
Pharmacy Leadership and Administration Learning Activities (Longitudinal): Preceptors: Jordan Dow, PharmD MS FACHE (Regional Pharmacy Director); Michele Richmond, RPh (Outpatient Pharmacy Director); Maggie
Pharmacist prescribing within an integrated health system in Washington
 Pharmacist prescribing within an integrated health system in Washington Roger Woolf, Pharm.D., Virginia Mason Medical Center, Seattle, WA. Amanda Locke, Pharm.D., BCACP, Virginia Mason Medical Center,
Pharmacist prescribing within an integrated health system in Washington Roger Woolf, Pharm.D., Virginia Mason Medical Center, Seattle, WA. Amanda Locke, Pharm.D., BCACP, Virginia Mason Medical Center,
Integrating Components of Medication Therapy Management Services into Community Pharmacy Workflow
 Volume 5 Number 2 Article 158 2014 Integrating Components of Medication Therapy Management Services into Community Pharmacy Workflow Corey A. Lester Jennifer L. Helmke Tana N. Kaefer Leticia R. Moczygemba
Volume 5 Number 2 Article 158 2014 Integrating Components of Medication Therapy Management Services into Community Pharmacy Workflow Corey A. Lester Jennifer L. Helmke Tana N. Kaefer Leticia R. Moczygemba
ROTATION DESCRIPTION
 ROTATION DESCRIPTION ROTATION TITLE: PGY1 - Outpatient Transplant Ambulatory Care PURPOSE The Medical Center performed over 200 abdominal organ transplants annually. This clinical practice site will provide
ROTATION DESCRIPTION ROTATION TITLE: PGY1 - Outpatient Transplant Ambulatory Care PURPOSE The Medical Center performed over 200 abdominal organ transplants annually. This clinical practice site will provide
Evidence-based guidelines support integrated disease management as the optimal model of hemophilia care
 Evidence-based guidelines support integrated disease management as the optimal model of hemophilia care S. W. Pipe 1 and C. M. Kessler 2 1 Departments of Pediatrics and Pathology, University of Michigan,
Evidence-based guidelines support integrated disease management as the optimal model of hemophilia care S. W. Pipe 1 and C. M. Kessler 2 1 Departments of Pediatrics and Pathology, University of Michigan,
Hospital Self Assessment Worksheet
 DESCRIPTION AND INSTRUCTIONS This worksheet consists of 106 questions assessing adoption of the Hospital Self- Assessment recommendations at the hospital level. These recommendations were based on the
DESCRIPTION AND INSTRUCTIONS This worksheet consists of 106 questions assessing adoption of the Hospital Self- Assessment recommendations at the hospital level. These recommendations were based on the
Educational. PPCP Foundations 3/5/17. Integrating the LLM / JCPP-PPCP in Experiential Education. Session Objectives
 Integrating the LLM / JCPP-PPCP in Experiential Education Seena Haines, PharmD, BCACP, FASHP, FAPhA, BC-ADM, CDE Chair and Professor of Pharmacy Practice Jenny A. Van Amburgh, PharmD, RPh, FAPhA, BCACP,
Integrating the LLM / JCPP-PPCP in Experiential Education Seena Haines, PharmD, BCACP, FASHP, FAPhA, BC-ADM, CDE Chair and Professor of Pharmacy Practice Jenny A. Van Amburgh, PharmD, RPh, FAPhA, BCACP,
ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610-X-5 ADVANCED PRACTICE NURSING COLLABORATIVE PRACTICE TABLE OF CONTENTS
 Nursing Chapter 610-X-5 ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610-X-5 ADVANCED PRACTICE NURSING COLLABORATIVE PRACTICE TABLE OF CONTENTS 610-X-5-.01 610-X-5-.02 610-X-5-.03 610-X-5-.04 610-X-5-.05
Nursing Chapter 610-X-5 ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610-X-5 ADVANCED PRACTICE NURSING COLLABORATIVE PRACTICE TABLE OF CONTENTS 610-X-5-.01 610-X-5-.02 610-X-5-.03 610-X-5-.04 610-X-5-.05
MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS
 MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS Implementation Toolkit Last Updated: 02/2018 OneCity Health Services 199 Water Street, 31st Floor, New
MEDS TO BEDS AND CARE MANAGEMENT MEDICATION ASSESSMENT TOOLKIT: FOR HOSPITAL TEAM AND PHARMACISTS Implementation Toolkit Last Updated: 02/2018 OneCity Health Services 199 Water Street, 31st Floor, New
Ambulatory Care Advanced Pharmacy Practice Experience SPPS 401A SPPS 401B
 Ambulatory Care Advanced Pharmacy Practice Experience SPPS 401A SPPS 401B Office of Experiential Education James Colbert, Pharm.D. Sarah Lorentz, Pharm.D. Associate Dean of Experiential Education Clinical
Ambulatory Care Advanced Pharmacy Practice Experience SPPS 401A SPPS 401B Office of Experiential Education James Colbert, Pharm.D. Sarah Lorentz, Pharm.D. Associate Dean of Experiential Education Clinical
EVALUATION OF THE FINANCIAL IMPACT OF MEDICATION BACKORDERS IN A TERTIARY CARE HOSPITAL. Kalyn Marie Acker
 EVALUATION OF THE FINANCIAL IMPACT OF MEDICATION BACKORDERS IN A TERTIARY CARE HOSPITAL by Kalyn Marie Acker PharmD, University of Texas at Austin, 2015 BS in Biochemistry, Texas Tech University, 2011
EVALUATION OF THE FINANCIAL IMPACT OF MEDICATION BACKORDERS IN A TERTIARY CARE HOSPITAL by Kalyn Marie Acker PharmD, University of Texas at Austin, 2015 BS in Biochemistry, Texas Tech University, 2011
Medication Therapy Management in Pharmacy Practice. Core Elements of an MTM Service Model
 Medication Therapy Management in Pharmacy Practice Core Elements of an MTM Service Model Version 2.0 March 2008 Medication Therapy Management in Pharmacy Practice: Core Elements of an MTM Service Model
Medication Therapy Management in Pharmacy Practice Core Elements of an MTM Service Model Version 2.0 March 2008 Medication Therapy Management in Pharmacy Practice: Core Elements of an MTM Service Model
Partnering with Pharmacists to Enhance Medication Management
 Partnering with Pharmacists to Enhance Medication Management Tamara Ravn PharmD BCACP Staff Pharmacist Clinical Cancer Pharmacy Froedtert & The Medical College of Wisconsin April 6, 2016 Objectives Describe
Partnering with Pharmacists to Enhance Medication Management Tamara Ravn PharmD BCACP Staff Pharmacist Clinical Cancer Pharmacy Froedtert & The Medical College of Wisconsin April 6, 2016 Objectives Describe
Transition of Care Practices. Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI
 Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI Objectives Pharmacist 1. Describe transition of care opportunities 2. Explain ways to use pharmacist extenders
Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI Objectives Pharmacist 1. Describe transition of care opportunities 2. Explain ways to use pharmacist extenders
IMPROVING CARE TRANSITIONS: Optimizing Medication Reconciliation
 IMPROVING CARE TRANSITIONS: Optimizing Medication Reconciliation MARCH 2012 Improving Care Transitions: Optimizing Medication Reconciliation Developed by: American Pharmacists Association American Society
IMPROVING CARE TRANSITIONS: Optimizing Medication Reconciliation MARCH 2012 Improving Care Transitions: Optimizing Medication Reconciliation Developed by: American Pharmacists Association American Society
PHARMACEUTICAL CARE PRACTICE
 third PHARMACEUTICAL CARE PRACTICE THE PATIENT-CENTERED APPROACH TO MEDICATION MANAGEMENT SERVICES Robert J. Cipolle, PharmD Professor Emeritus Linda M. Strand, PharmD, PhD, DSc (Hon) Professor Peter C.
third PHARMACEUTICAL CARE PRACTICE THE PATIENT-CENTERED APPROACH TO MEDICATION MANAGEMENT SERVICES Robert J. Cipolle, PharmD Professor Emeritus Linda M. Strand, PharmD, PhD, DSc (Hon) Professor Peter C.
Pharmacist Services Framework Within Saskatchewan Primary Health Care
 Pharmacist Services Framework Within Saskatchewan Primary Health Care The following report was written by Dr. Victoria Losinski and sponsored by the Pharmacists Association of Saskatchewan (now the Pharmacy
Pharmacist Services Framework Within Saskatchewan Primary Health Care The following report was written by Dr. Victoria Losinski and sponsored by the Pharmacists Association of Saskatchewan (now the Pharmacy
Pharm2Pharm Standard Operating Procedures. University of Hawai i at Hilo The Daniel K. Inouye College of Pharmacy Center for Rural Health Science
 Pharm2Pharm Standard Operating Procedures University of Hawai i at Hilo The Center for Rural Health Science INTRODUCTION PURPOSE: The purpose of the Pharm2Pharm Standard Operating Procedures (SOPs) is:
Pharm2Pharm Standard Operating Procedures University of Hawai i at Hilo The Center for Rural Health Science INTRODUCTION PURPOSE: The purpose of the Pharm2Pharm Standard Operating Procedures (SOPs) is:
Key Words: Transitions of care, care coordination, medication management, drug therapy problem
 Implementing a Pharmacist-Led Medication Management Pilot to Improve Care Transitions Rachel Root, PharmD, MS* 1, Pamela Phelps, PharmD, FASHP 2, Amanda Brummel, PharmD 2, and Craig Else, PharmD, MBA 3
Implementing a Pharmacist-Led Medication Management Pilot to Improve Care Transitions Rachel Root, PharmD, MS* 1, Pamela Phelps, PharmD, FASHP 2, Amanda Brummel, PharmD 2, and Craig Else, PharmD, MBA 3
Disclosures. Objectives. Leveraging and Developing Your Team for Optimal Outcomes. None
 Leveraging and Developing Your Team for Optimal Outcomes Michelle W. McCarthy, PharmD, FASHP Coordinator, Pharmacy Education and Graduate Programs Charlottesville, VA November 6, 2017 Disclosures None
Leveraging and Developing Your Team for Optimal Outcomes Michelle W. McCarthy, PharmD, FASHP Coordinator, Pharmacy Education and Graduate Programs Charlottesville, VA November 6, 2017 Disclosures None
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Improvement Activities for ACI Bonus Measures
 Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
PHCY 471 Community IPPE. Student Name. Supervising Preceptor Name(s)
") PRECEPTOR CHECKLIST /SIGN-OFF PHCY 471 Community IPPE Student Name Supervising Name(s) INSTRUCTIONS The following table outlines the primary learning goals and activities for the Community IPPE. Each student
PRECEPTOR CHECKLIST /SIGN-OFF PHCY 471 Community IPPE Student Name Supervising Name(s) INSTRUCTIONS The following table outlines the primary learning goals and activities for the Community IPPE. Each student
Ambulatory Care Advanced Pharmacy Practice Experience Course Title: PHAR 9981
 Ambulatory Care Advanced Pharmacy Practice Experience Course Title: PHAR 9981 Preceptor: Office: Office Phone: Cell Phone: Email: Current Semester/Year: Office Hours: By arrangement with preceptor Credit
Ambulatory Care Advanced Pharmacy Practice Experience Course Title: PHAR 9981 Preceptor: Office: Office Phone: Cell Phone: Email: Current Semester/Year: Office Hours: By arrangement with preceptor Credit
Board of Pharmacy Specialties Portfolio Requirements for Added Qualifications in Infectious Diseases Pharmacotherapy
 Effective 2016-2017 Application cycle Board of Pharmacy Specialties Portfolio Requirements for Added Qualifications in Infectious Diseases Pharmacotherapy Board Certified Pharmacotherapy Specialists (BCPS)
Effective 2016-2017 Application cycle Board of Pharmacy Specialties Portfolio Requirements for Added Qualifications in Infectious Diseases Pharmacotherapy Board Certified Pharmacotherapy Specialists (BCPS)
Request for Proposal: Primary Medication Non-Adherence
 Request for Proposal: Primary Medication Non-Adherence Release date: January 4, 2011 Due date: March 15, 2011 Interested stakeholders are encouraged to participate in the NACDS Foundation conference call
Request for Proposal: Primary Medication Non-Adherence Release date: January 4, 2011 Due date: March 15, 2011 Interested stakeholders are encouraged to participate in the NACDS Foundation conference call
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
Acute Crisis Units. Shelly Rhodes, Provider Relations Manager
 Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
PROMISe Phase Two Final Report to the Pharmacy Guild of Australia (RFT , Evaluation of Clinical Interventions in Community Pharmacies)
") PROMISe Phase Two Final Report to the Pharmacy Guild of Australia (RFT 2003-2, Evaluation of Clinical Interventions in Community Pharmacies) This research was funded by the Australian Government Department
PROMISe Phase Two Final Report to the Pharmacy Guild of Australia (RFT 2003-2, Evaluation of Clinical Interventions in Community Pharmacies) This research was funded by the Australian Government Department
Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System
 Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System Designed Specifically for International Quality and Performance Use A white paper by: Marc Berlinguet, MD, MPH
Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System Designed Specifically for International Quality and Performance Use A white paper by: Marc Berlinguet, MD, MPH
Antithrombotic Traineeship
 ASHP Foundation Antithrombotic Traineeship Application Policies and Guidelines The distance education and experiential program components of the traineeship offers continuing pharmacy education hours for
ASHP Foundation Antithrombotic Traineeship Application Policies and Guidelines The distance education and experiential program components of the traineeship offers continuing pharmacy education hours for
LESSON ASSIGNMENT. Professional References in Pharmacy.
 LESSON ASSIGNMENT LESSON 1 Professional References in Pharmacy. TEXT ASSIGNMENT Paragraphs 1-1 through 1-8. LESSON OBJECTIVES 1-1. Given a description of a reference used in pharmacy and a list of pharmacy
LESSON ASSIGNMENT LESSON 1 Professional References in Pharmacy. TEXT ASSIGNMENT Paragraphs 1-1 through 1-8. LESSON OBJECTIVES 1-1. Given a description of a reference used in pharmacy and a list of pharmacy
UC San Diego Policy & Procedure Manual
 UC San Diego Policy & Procedure Manual Search A Z Index Numerical Index Classification Guide What s New PERSONNEL-ACADEMIC Section: 230-275 Effective: 07/01/2017 Supersedes: New Review Date: 07/01/2020
UC San Diego Policy & Procedure Manual Search A Z Index Numerical Index Classification Guide What s New PERSONNEL-ACADEMIC Section: 230-275 Effective: 07/01/2017 Supersedes: New Review Date: 07/01/2020
Who Cares About Medication Reconciliation? American Pharmacists Association American Society of Health-system Pharmacists The Joint Commission Agency
 The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
Original Research PRACTICE-BASED RESEARCH
 Primary Care Providers experiences with Pharmaceutical Care-based Medication Therapy Management Services Heather L. Maracle, Pharm.D. 1 ; Djenane Ramalho de Oliveira, Ph.D. 2 ; and Amanda Brummel, Pharm.D.
Primary Care Providers experiences with Pharmaceutical Care-based Medication Therapy Management Services Heather L. Maracle, Pharm.D. 1 ; Djenane Ramalho de Oliveira, Ph.D. 2 ; and Amanda Brummel, Pharm.D.
Disclosure. SwedishAmerican Hospital A Division of UW Health. Learning Objectives. Medication History. Medication History 2/2/2017
 Disclosure Pharmacy Technician- Acquired Medication Histories in the ED: A Path to Higher Quality of Care David Huhtelin, PharmD Emergency Medicine Clinical Pharmacist SwedishAmerican Hospital A Division
Disclosure Pharmacy Technician- Acquired Medication Histories in the ED: A Path to Higher Quality of Care David Huhtelin, PharmD Emergency Medicine Clinical Pharmacist SwedishAmerican Hospital A Division
What is MTM? Objectives. MTM: Successfully Engaging Eligible Patients. What is MTM? MTM Background. MTM Examples 09/11/2012
 MTM: Successfully Engaging Eligible Patients Objectives Explain What MTM is as defined by the Medicare Modernization Act Describe examples of MTM services Recognize the various entities who pay for MTM
MTM: Successfully Engaging Eligible Patients Objectives Explain What MTM is as defined by the Medicare Modernization Act Describe examples of MTM services Recognize the various entities who pay for MTM
3. Does the institution have a dedicated hospital-wide committee geared towards the improvement of laboratory test stewardship? a. Yes b.
 Laboratory Stewardship Checklist: Governance Leadership Commitment It is extremely important that the Laboratory Stewardship Committee is sanctioned by the hospital leadership. This may be recognized by
Laboratory Stewardship Checklist: Governance Leadership Commitment It is extremely important that the Laboratory Stewardship Committee is sanctioned by the hospital leadership. This may be recognized by
Quality Data Model (QDM) Style Guide. QDM (version MAT) for Meaningful Use Stage 2
 Style Guide. QDM (version MAT) for Meaningful Use Stage 2") Quality Data Model (QDM) Style Guide QDM (version MAT) for Meaningful Use Stage 2 Introduction to the QDM Style Guide The QDM Style Guide provides guidance as to which QDM categories, datatypes, and attributes
Quality Data Model (QDM) Style Guide QDM (version MAT) for Meaningful Use Stage 2 Introduction to the QDM Style Guide The QDM Style Guide provides guidance as to which QDM categories, datatypes, and attributes
Benefits of National Provider Identifier
 Florida Pharmacy Association Professional Affairs Council Benefits of National Provider Identifier Written by: Kayla Mackanin, USF PharmD Candidate 2015, Professional Affairs Council Member Created on:
Florida Pharmacy Association Professional Affairs Council Benefits of National Provider Identifier Written by: Kayla Mackanin, USF PharmD Candidate 2015, Professional Affairs Council Member Created on:
Preceptor Development: Patient Care Process. The Pharmacy Care Plan
 Preceptor Development: Patient Care Process The Pharmacy Care Plan Outline Setting the stage for precepting the pharmacy care plan Elements of the pharmacy care plan Feedback and evaluation of your student
Preceptor Development: Patient Care Process The Pharmacy Care Plan Outline Setting the stage for precepting the pharmacy care plan Elements of the pharmacy care plan Feedback and evaluation of your student
Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B for CY 2013 [File Code CMS 1590 P]
![Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B for CY 2013 [File Code CMS 1590 P]](/thumbs/79/80256172.jpg "Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B for CY 2013 [File Code CMS 1590 P]") Centers for Medicare & Medicaid Services Attention: CMS 1590 P Mail Stop C4 26 05 7500 Security Boulevard Baltimore, MD 21244 1850 [Submitted online at: http://www.regulations.gov] Re: Medicare Program;
Centers for Medicare & Medicaid Services Attention: CMS 1590 P Mail Stop C4 26 05 7500 Security Boulevard Baltimore, MD 21244 1850 [Submitted online at: http://www.regulations.gov] Re: Medicare Program;
Profiles in CSP Insourcing: Tufts Medical Center
 Profiles in CSP Insourcing: Tufts Medical Center Melissa A. Ortega, Pharm.D., M.S. Director, Pediatrics and Inpatient Pharmacy Operations Tufts Medical Center Hospital Profile Tufts Medical Center (TMC)
Profiles in CSP Insourcing: Tufts Medical Center Melissa A. Ortega, Pharm.D., M.S. Director, Pediatrics and Inpatient Pharmacy Operations Tufts Medical Center Hospital Profile Tufts Medical Center (TMC)
ELECTIVE COMPETENCY AREAS, GOALS, AND OBJECTIVES FOR POSTGRADUATE YEAR ONE (PGY1) PHARMACY RESIDENCIES
 PHARMACY RESIDENCIES") ELECTIVE COMPETENCY AREAS, GOALS, AND OBJECTIVES FOR POSTGRADUATE YEAR ONE (PGY1) PHARMACY RESIDENCIES Introduction The competency areas, goals, and objectives are for use with the ASHP Accreditation Standard
ELECTIVE COMPETENCY AREAS, GOALS, AND OBJECTIVES FOR POSTGRADUATE YEAR ONE (PGY1) PHARMACY RESIDENCIES Introduction The competency areas, goals, and objectives are for use with the ASHP Accreditation Standard
Fundamentals of Self-Limiting Conditions Prescribing for Manitoba Pharmacists. Ronald F. Guse Registrar College of Pharmacists of Manitoba (CPhM)
") Fundamentals of Self-Limiting Conditions Prescribing for Manitoba Pharmacists Ronald F. Guse Registrar College of Pharmacists of Manitoba (CPhM) 1 Learning Objectives Upon successful completion of this
Fundamentals of Self-Limiting Conditions Prescribing for Manitoba Pharmacists Ronald F. Guse Registrar College of Pharmacists of Manitoba (CPhM) 1 Learning Objectives Upon successful completion of this
Practice Advancement Initiative (PAI) Using the ASHP PAI Ambulatory Care Self-Assessment Survey
 Using the ASHP PAI Ambulatory Care Self-Assessment Survey") Practice Advancement Initiative (PAI) Using the ASHP PAI Ambulatory Care Self-Assessment Survey Jodie Elder, PharmD, BCPS September 14, 2017 Objectives List the key components of the Practice Advancement
Practice Advancement Initiative (PAI) Using the ASHP PAI Ambulatory Care Self-Assessment Survey Jodie Elder, PharmD, BCPS September 14, 2017 Objectives List the key components of the Practice Advancement
UW HEALTH JOB DESCRIPTION
 NURSE CASE MANAGER - ED Job Code: 801009 FLSA Status: Mgt. Approval: B Liegel Date: 6-18 Department: Coordinated Care Department 93070 HR Approval: M Buenger Date: 6-18 JOB SUMMARY The Nurse Case Manager,
NURSE CASE MANAGER - ED Job Code: 801009 FLSA Status: Mgt. Approval: B Liegel Date: 6-18 Department: Coordinated Care Department 93070 HR Approval: M Buenger Date: 6-18 JOB SUMMARY The Nurse Case Manager,
Documentation Guidelines. Medication Therapy Management (MTM)
") Documentation Guidelines Medication Therapy Management (MTM) Effective Date Revision Letter Applies To: FINAL A UNMMG 1.0 Purpose This document provides guidelines for Pharmacist Clinicians (PhC) and other
Documentation Guidelines Medication Therapy Management (MTM) Effective Date Revision Letter Applies To: FINAL A UNMMG 1.0 Purpose This document provides guidelines for Pharmacist Clinicians (PhC) and other
Outpatient Hospital Facilities
 Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Acute Care Cardiology Learning Description at Emory University Hospital Midtown (EUHM)
") Acute Care Cardiology Learning Description at Emory University Hospital Midtown (EUHM) Preceptor: Candace R. Stearns, PharmD, BCPS Office: EUHM, Peachtree Building, 2 nd floor, room 2182 Hours: ~ 7:30
Acute Care Cardiology Learning Description at Emory University Hospital Midtown (EUHM) Preceptor: Candace R. Stearns, PharmD, BCPS Office: EUHM, Peachtree Building, 2 nd floor, room 2182 Hours: ~ 7:30
Building Ambulatory Clinical Pharmacy Services: Demonstrating Value. Amy L Stump, PharmD, BCPS October 17, 2012
 Building Ambulatory Clinical Pharmacy Services: Demonstrating Value Amy L Stump, PharmD, BCPS October 17, 2012 1 Objectives Develop a list of outcomes that could be used to determine the benefit of a pharmacist
Building Ambulatory Clinical Pharmacy Services: Demonstrating Value Amy L Stump, PharmD, BCPS October 17, 2012 1 Objectives Develop a list of outcomes that could be used to determine the benefit of a pharmacist
By Marie Smith, Margherita R. Giuliano, and Michael P. Starkowski
 doi: 10.1377/hlthaff.2011.0002 HEALTH AFFAIRS 30, NO. 4 (2011): 646 654 2011 Project HOPE The People-to-People Health Foundation, Inc. By Marie Smith, Margherita R. Giuliano, and Michael P. Starkowski
doi: 10.1377/hlthaff.2011.0002 HEALTH AFFAIRS 30, NO. 4 (2011): 646 654 2011 Project HOPE The People-to-People Health Foundation, Inc. By Marie Smith, Margherita R. Giuliano, and Michael P. Starkowski