About the Center. Goal: Purpose: For information, resources and technical assistance contact the CIHS team at:
|
|
|
- Philip Arnold
- 5 years ago
- Views:
Transcription
1 About the Center In partnership with Health & Human Services (HHS)/Substance Abuse and Mental Health Services Administration (SAMHSA), Health Resources and Services Administration (HRSA). Goal: To promote the planning, and development and of integration of primary and behavioral health care for those with serious mental illness and/or substance use disorders and physical health conditions, whether seen in specialty mental health or primary care safety net provider settings across the country. Purpose: To serve as a national training and technical assistance center on the bidirectional integration of primary and behavioral health care and related workforce development To provide technical assistance to PBHCI grantees and entities funded through HRSA to address the health care needs of individuals with mental illnesses, substance use and co-occurring disorders For information, resources and technical assistance contact the CIHS team at: Online: integration.samhsa.gov Phone: Integration@thenationalcouncil.org


2 A (Health) Home Run: Operationalizing Behavioral Health Homes Friday, January 18 th

3 Join audio: Choose Mic & Speakers to use VoIP Choose Telephone and dial using the information provided Submit questions and comments via the Questions panel or raise your hand to speak over the phone. Today s webinar is being recorded and will be available within 48 hours.
4 What we ll cover today Overview of the Medicaid health home option Core clinical features of a behavioral health home Structuring the behavioral health home Action steps for stakeholders Operationalizing the core clinical features lessons from the field Q & A session
5 The Clinical Work of Effective Behavioral Health Homes Laurie Alexander, PhD, Alexander BH Consulting Benjamin G. Druss, MD, MPH, Emory University
6 OVERVIEW OF THE MEDICAID HEALTH HOME OPTION
7 Context The ACA created a new option for state Medicaid programs to provide health homes for enrollees with chronic conditions, including MH & SU conditions Became effective 1/1/2011 Subject to CMS approval of state plan amendment Program provides financial incentives for states 90% FMAP for health home-related services for 1 st 8 quarters Alternative payment models Incentive grants
8 Required services Each patient must have a comprehensive care plan; Services must be quality-driven, cost effective, culturally appropriate, person-/family-centered, and evidence-based; Services must include prevention and health promotion, healthcare, mental health and substance use disorder, long-term care services, as well as linkages to community supports and resources;
9 Required services (continued) Service delivery must involve continuing care strategies, including care management, care coordination, and transitional care from the hospital to the community; Health home providers do not need to provide all the required services themselves, but must ensure the full array of services is available and coordinated; and Providers must be able to use health information technology (HIT) to facilitate the work of the health home and establish quality improvement efforts
10 Target populations Two or more chronic health conditions i.e., MH or SU condition, asthma, diabetes, heart disease, or overweight; OR One chronic condition and at risk for another; OR One serious and persistent mental health condition Note: Regardless of which condition(s) are selected, states must address MH and SU conditions and consult with SAMHSA on their treatment and prevention
11 The opportunity MH and SU treatment providers can become a health home for the people they serve A behavioral health-based health home
12 Current Status of Medicaid State Health Home Amendments Eight states have received federal approval for their programs under Section 2703 of the ACA, and six more states have amendments under review. All of the approved states include people with serious mental illnesses as a target population, and use financing methods such as per-member-per-month (PMPM) payments to Health Home providers
13 The challenge To create a behavioral health home capable of functioning effectively at both the administrative and clinical levels Focus of this webinar (& paper): The clinical piece How to improve outcomes for people with MH and SU conditions in a behavioral health-based health home
14 CORE CLINICAL FEATURES OF A BEHAVIORAL HEALTH HOME
15 Redesigning care to serve as health home Core elements of the Chronic Care Model: Self-management support Delivery system design Decision support Clinical information systems Community linkages
16 Self-management support Activated consumers have skills to: self-manage their care collaborate with providers maintain their health
17 Delivery system design Care system is redesigned in key ways, including: Formation of multidisciplinary practice teams Clear roles Single care plan Effective communication Mechanisms for coordinating care between team members Provision of care management Client activation and education Care coordination Monitoring consumers participation in and response to treatment (when treating provider is part of team)
18 Decision support Ensure clinical care is provided in line with best practices by: Involving specialists Embedding evidence-based guidelines in routine care provision
19 Clinical information systems Support organization of data At the population level helps maximize outcomes for defined groups of consumers At the individual level helps maximize consumer s outcomes Regardless of format, necessary functions include: Organizing data at population and individual level Delivering reminders to providers (and consumers) Providing feedback to clinicians (and consumers)
20 Community linkages Develop an understanding of the contextual factors (e.g., poverty) that may underpin consumers poor health Support consumers connections to care and resources in the community Become familiar with the area s community resources Link consumers to them Track referrals
21 STRUCTURING THE BEHAVIORAL HEALTH HOME
22 Structuring the behavioral health home Several options depending on the behavioral health provider s resources: In-house model Co-located partnership model Facilitated referral model
23 In-house model The behavioral health agency provides and owns the complete array of primary care and specialty behavioral health services. The agency ensures communication across providers and coordination of services that allow it to deliver care that is integrated from the consumer s perspective
24 Co-located partnership model The behavioral health agency arranges for healthcare providers to provide primary care services onsite Processes must be in place beyond simple colocation to ensure that effective communication and coordination between providers happens routinely
25 Facilitated referral model Most primary care services are not provided onsite, but the agency ensures coordination of care provided offsite. The agency conducts health screenings, links clients to PCPs in the community, and facilitates communication and coordination with health providers typically with the support of a medical care manager.
26 Action steps to consider Reach out to the relevant state agencies Master the health home s key clinical features and the system-level strategies that support them; Create a strategic plan, including the clinical model, budget, and implementation plan; Start the change management process;
27 Action steps (continued) Formalize partnerships with community partners; Regularly update state agencies on progress; Identify and include relevant stakeholders in the decision-making and strategizing process; and Seek support and guidance/training from colleagues, experts, and leaders of relevant efforts.
28 Missouri CMHC Health Homes Joe Parks, MD Medical Director Missouri Department of Mental Health
29 My Background Missouri DMH Medical Director Consultant to Mo HealthNet (Missouri Medicaid) Director and Distinguished Professor of Science Missouri Institute of Mental Health University of Missouri St. Louis President NASMHPD Medical Director s Council Practicing FQHC Psychiatrist
30 DMH NET Strategy Health technology is utilized to support the service system. Care Coordination is best provided by a local community-based provider. MH Community Support Workers who are most familiar with the consumer provide care coordination at the local level. Primary Care Nurse Care Managers working within each CMHC provide system support. Statewide coordination and training support the network of CMHC Health Homes.
31 CMHC Healthcare Homes State Plan Amendment approved 10/20/11 Effective 1/1/12 27 CMHC Healthcare Homes 17,882 individuals auto-enrolled CMHC consumers with at least $10,000 Medicaid costs PMPM Staffing: $78.74 Health Home Director 1 per 500 enrollees Primary Care Physician Consultant 1hr per enrollee Nurse Care Managers 1 per 250 enrollees Care Coordinator 1 per 500 enrollees
32 CMHC as Health Care Home Case management coordination and facilitation of healthcare Primary Care Nurse Care Managers Medical disease management for persons with SMI Preventive healthcare screening and monitoring by MH providers Integrated/consolidated CMHC/CHC Services
33 Medical Needs Have Same Priority as MH Needs Obtaining a medical home a primary care provider responsible for overall coordination Medication adherence just as important for non-mh meds Assisting in scheduling and keeping medical care appointments
34 Comprehensive Care Management Identification and targeting of high-risk individuals Monitoring of health status and adherence Development of treatment guidelines Individualized planning with the consumer
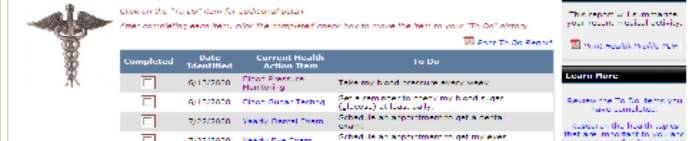
35 Step 1 Create Disease Registry Get Historic Diagnosis from Admin Claims Get Clinical Values from Metabolic Screening Combine into EHR Disease Registry Online Access available to all Providers
36 Metabolic Syndrome Disease Registry Metabolic Syndrome Obesity - weight height Cholesterol Triglycerides Blood pressure Blood sugar Screening Required Annually since 2010 Disease registry with results maintained on PROACT Billing Code under Rehab Option
37 Step 2 Identify Care Gaps and ACT! Compare Combined Disease Registry Data to accepted Clinical Quality Indicators Identify Care Gaps Sort patients with care gaps into agency specific To-Do lists Send to CMHC nurse care manager Set up PCP visit and pass on info with request to treat
38 DMHNET HEIDIS Indicators DM1: Use of inhaled corticosteroid medications by persons with a history of COPD (chronic obstructive pulmonary disease) or Asthma. DM2: Use of ARB (angiotensin II receptor blockers) or ACEI (angiotensin converting enzyme inhibitors) medications by persons with a history of CHF (congestive heart failure). DM3: Use of beta-blocker medications by persons with a history of CHF (congestive heart failure). DM4: Use of statin medications by persons with a history of CAD (coronary artery disease).
39 Initial Results Provide specific lists of CMHC clients with care gaps as identified by HEIDIS indicators to CMHC primary care nurse liaisons quarterly Provide HEIDIS indicator/disease state training on standard of care to CMHC MH case managers First quarter focus on indicator one-asthma substantially reduced percentage with care gap Range 22% - 62% reduction Median 45% reduction
40 Care Coordination Coordinating with the patients, caregivers and providers Implementing plan of care with treatment team Planning hospital discharge Scheduling Communicating with collaterals
41 Provide Information to Other Healthcare Providers HIPAA permits sharing information for coordination of care Nationally consent not necessary Exceptions: HIV Substance abuse treatment not abuse itself Stricter local laws
42 CyberAccess TM Patient demographics Electronic Health Record Record all of participant prescriptions All procedures codes All diagnosis codes E prescribing Preferred Drug List support Access to preferred medication list Precertification of medications via clinical algorithms Prior authorization of medications Medication possession ratio
43 CyberAccess - Log-In Screen
44 CyberAccess HIPAA Attestation
45 CyberAccess - Home Page
46 Demographics

47 Paid Drug Claims



48 Paid Drug Claims/MPR An MPR between % will display in green text. An MPR between 60-79% will display in yellow text. An MPR of less than 60% will display in red text. If an MPR does not exist for type of drug or the drug is not for maintenance the column will display a dash.
49 Medical Procedures

50 Diagnosis Codes
51 Comprehensive Transitional Care Medicaid requires hospitals to notify MHN within 24 hours of a new admission of any Medicaid enrollee and provide information about diagnosis, condition and treatment for authorization of an inpatient stay using a web based tool. A daily data transfer listing all new hospital admissions discharges is transferred to the HH data analytic staff New admits are matched to the list of all persons assigned and/or enrolled in a healthcare home. An Automated notifies the healthcare home provider of the admission. Patients are seen within 72 hours of discharge for medication reconciliation, health status check and planning for follow-up care
52 Support Patient Wellness through Self Management using Peer Specialists Implement a physical health/wellness approach that is consistent with recovery principles, including supports for smoking cessation, good nutrition, physical activity and healthy weight. Educate patient on implications of psychotropic drugs Teach/support wellness self-management skills Teach/support decision making skills using Direct Inform Use motivational interviewing techniques New psychosocial rehab focus Smoking cessation Enhancing Activity Obesity Reduction/Prevention


53 DirectInform An EHR for Patients 53

54 What is a CMHC Healthcare Home? Not just a Medicaid Benefit Not just a Program or a Team A System and Organizational Transformation

55 Practice Transformations Focus on overall health More medically oriented team members Open access scheduling No-show/cancellation policies Increased patient input processes Significant increase in data reporting and outcomes Treatment planning tools supported by treatment guidelines
56
57 WebSites ehome.htm

58 For more information Download the paper today Executive summary and full report are available to at: Integrated Care Models
59 Any Questions?

60 For information, resources and technical assistance contact the CIHS team at: Online: integration.samhsa.gov Phone:
CMHC Healthcare Homes. The Natural Next Step
 CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
Paving the Way for. Health Homes
 Paving the Way for Health Homes Paving the Way for Healthcare Homes Affordable Care Act The Affordable Care Act passed by Congress and signed into law by the president in March 2010, provides a variety
Paving the Way for Health Homes Paving the Way for Healthcare Homes Affordable Care Act The Affordable Care Act passed by Congress and signed into law by the president in March 2010, provides a variety
Section 2703: State Option to Provide Health Homes for Enrollees with Chronic Conditions
 Section 2703: State Option to Provide Health Homes for Enrollees with Chronic Conditions Center for Medicaid, CHIP, and Survey & Certification Centers for Medicare & Medicaid Services Background. A goal
Section 2703: State Option to Provide Health Homes for Enrollees with Chronic Conditions Center for Medicaid, CHIP, and Survey & Certification Centers for Medicare & Medicaid Services Background. A goal
SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2
 Program Grantees: Part 2") SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2 Ken Bachrach, Ph.D., Clinical Director Jim Sorg, Ph.D., Director of Care Integration and IT Tarzana Treatment Centers
SAMHSA Primary and Behavioral Health Care Integration (PBHCI) Program Grantees: Part 2 Ken Bachrach, Ph.D., Clinical Director Jim Sorg, Ph.D., Director of Care Integration and IT Tarzana Treatment Centers
2015 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
SHOW-ME INNOVATION: Missouri s Health Care Homes Integrate Behavioral Health and Primary Care Jaron Asher, MD February 28, 2014
 SHOW-ME INNOVATION: Missouri s Health Care Homes Integrate Behavioral Health and Primary Care Jaron Asher, MD February 28, 2014 Jaron Asher, MD Medical Director at Places for People in St. Louis, MO Chief
SHOW-ME INNOVATION: Missouri s Health Care Homes Integrate Behavioral Health and Primary Care Jaron Asher, MD February 28, 2014 Jaron Asher, MD Medical Director at Places for People in St. Louis, MO Chief
60 Minutes for Docs: Preparing Psychiatrists for Health Reform
 60 Minutes for Docs: Preparing Psychiatrists for Health Reform John S. Kern MD Senior Medical Consultant, MTM Services Chief Medical Officer Regional Mental Health Center Merrillville, IN June 19, 2013
60 Minutes for Docs: Preparing Psychiatrists for Health Reform John S. Kern MD Senior Medical Consultant, MTM Services Chief Medical Officer Regional Mental Health Center Merrillville, IN June 19, 2013
Health Home Flow Hypothetical Patient Scenario
 Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
NGA and Center for Health Care Strategies Summit: High Utilizers
 Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015
 Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
South Dakota Health Homes Care Coordination Innovation
 South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
2017 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
HEALTH HOME INTEGRATED PRIMARY AND BEHAVIORAL HEALTH CARE SERVICES
 COMPARISON OF EXISTING SERVICES AND DELIVERY MODELS WITH DEFINITIONS PRIMARY CARE CASE MANAGEMENT (PCCM) Oklahoma s PCCM program is called SoonerCare Choice (SCC), in which each enrollee is linked to a
COMPARISON OF EXISTING SERVICES AND DELIVERY MODELS WITH DEFINITIONS PRIMARY CARE CASE MANAGEMENT (PCCM) Oklahoma s PCCM program is called SoonerCare Choice (SCC), in which each enrollee is linked to a
Grant Writing: SAMHSA and Beyond
 Grant Writing: SAMHSA and Beyond Steve Estrine, CEO Heidi Arthur, VP SAE and Associates SAE Who We Are > Behavioral health program specialists Populations with Serious Mental Illness and Co-Occurring Disorders
Grant Writing: SAMHSA and Beyond Steve Estrine, CEO Heidi Arthur, VP SAE and Associates SAE Who We Are > Behavioral health program specialists Populations with Serious Mental Illness and Co-Occurring Disorders
Specialty Behavioral Health and Integrated Services
 Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
California s Health Homes Program
 California s Health Homes Program HPSM Network Webinar 9/05/18 Goals for Today: Health Homes Program overview CB-CME requirements Program readiness and implementation timeline Gather take-away questions
California s Health Homes Program HPSM Network Webinar 9/05/18 Goals for Today: Health Homes Program overview CB-CME requirements Program readiness and implementation timeline Gather take-away questions
Physical Health Integration Within Behavioral Healthcare: Promising Practices
 Physical Health Integration Within Behavioral Healthcare: Promising Practices 9:45 AM 10:45 AM Steering Toward Success: Achieving Value in Whole Person Care September 25 and October 26, 2017 The Healthier
Physical Health Integration Within Behavioral Healthcare: Promising Practices 9:45 AM 10:45 AM Steering Toward Success: Achieving Value in Whole Person Care September 25 and October 26, 2017 The Healthier
Welcome to the Agency for Health Care Administration (AHCA) Training Presentation for Managed Medical Assistance Specialty Plans
 Training Presentation for Managed Medical Assistance Specialty Plans") Welcome to the Agency for Health Care Administration (AHCA) Training Presentation for Managed Medical Assistance Specialty Plans The presentation will begin momentarily. Please dial in to hear audio: 1-888-670-3525
Welcome to the Agency for Health Care Administration (AHCA) Training Presentation for Managed Medical Assistance Specialty Plans The presentation will begin momentarily. Please dial in to hear audio: 1-888-670-3525
Articles of Importance to Read: UnitedHealthcare Goes Live With 13th Edition of Milliman Care Guidelines. Summer 2009
 Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Summer 2009 UnitedHealthcare Goes Live With 13th Edition of Milliman Care
Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Summer 2009 UnitedHealthcare Goes Live With 13th Edition of Milliman Care
Accountable Care and the Laboratory Value Proposition. Les Duncan Director of Operations Highmark Health - Home and Community Services
 Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Provider Guide. Medi-Cal Health Homes Program
 Medi-Cal Health Provider Guide This provider guide provides information on the California Medi-Cal Health (HHP) for Community-Based Care Management Entities (CB-CMEs), providers, community-based organizations,
Medi-Cal Health Provider Guide This provider guide provides information on the California Medi-Cal Health (HHP) for Community-Based Care Management Entities (CB-CMEs), providers, community-based organizations,
Computer Provider Order Entry (CPOE)
") Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Integrated Care: Considerations for Quality. May 13, 2015 Megan Marx MPA Associate Director
 Integrated Care: Considerations for Quality May 13, 2015 Megan Marx MPA Associate Director GoToWebinar Housekeeping: Attendee participation Your Participation Join audio: Choose Mic & Speakers to use VoIP
Integrated Care: Considerations for Quality May 13, 2015 Megan Marx MPA Associate Director GoToWebinar Housekeeping: Attendee participation Your Participation Join audio: Choose Mic & Speakers to use VoIP
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Checklist for Ocean County Community Health Improvement Plan Implementation of Strategies- Activities for Ocean County Health Centers: CHEMED & OHI
 Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
MEDICAID MODEL DATA LAB
 MEDICAID MODEL DATA LAB Id: OHIO State: Ohio Health Home Services Forms (ACA 2703) Page: 1-10 TN#: OH-12-0013 Superseeds TN#: OH-00-0000 Effective Date: 10/01/2012 Approved Date: 09/17/2012 Transmital
MEDICAID MODEL DATA LAB Id: OHIO State: Ohio Health Home Services Forms (ACA 2703) Page: 1-10 TN#: OH-12-0013 Superseeds TN#: OH-00-0000 Effective Date: 10/01/2012 Approved Date: 09/17/2012 Transmital
ACO Information Required to be Published on ACO Website per CMS Regulations
 ACO Name and Location SJFI, LLC dba Oklahoma Health Initiatives St. John Administration 1923 S. Utica Ave Tulsa, OK 74104 ACO Primary Contact Ann Paul, MPH ACO President OKHI@sjmc.org 918.744.2180 Organizational
ACO Name and Location SJFI, LLC dba Oklahoma Health Initiatives St. John Administration 1923 S. Utica Ave Tulsa, OK 74104 ACO Primary Contact Ann Paul, MPH ACO President OKHI@sjmc.org 918.744.2180 Organizational
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE. Tennessee Primary Care Association Annual Conference October 25 26, 2012.
 IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2012 DATA PUBLISHED 2015 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY HOSPITAL PERFORMANCE REPORT 2012 DATA PUBLISHED 2015 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2012 DATA PUBLISHED 2015 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
Exhibit A.11.DY3. DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements
 Requirements") Exhibit A.11.DY3 DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements 1. Generally. This Exhibit contains the requirements and substantiations associated with each of the metrics required
Exhibit A.11.DY3 DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements 1. Generally. This Exhibit contains the requirements and substantiations associated with each of the metrics required
Integrated Behavioral Health Project Phase III Project Description
 Integrated Behavioral Health Project Phase III Project For Phase III, the Integrated Behavioral Health Project has selected seven grantees to advance the base of knowledge concerning integrated care in
Integrated Behavioral Health Project Phase III Project For Phase III, the Integrated Behavioral Health Project has selected seven grantees to advance the base of knowledge concerning integrated care in
Benchmark Data Sources
 Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond)
") Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Measures Reporting for Eligible Hospitals
 Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Health Homes in KanCare
 Health Homes in KanCare INTRODUCTION The term health home is unique to Medicaid Health homes are an option which states can choose to provide within their Medicaid programs A health home is not a building,
Health Homes in KanCare INTRODUCTION The term health home is unique to Medicaid Health homes are an option which states can choose to provide within their Medicaid programs A health home is not a building,
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule
 Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP)
 & Chronic Care Improvement Program (CCIP)") Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP) Medicare Drug and Health Plan Contract Administration Group Donna Williamson & Brandy Alston December 6, 2016
Medicare Advantage Quality Improvement Project (QIP) & Chronic Care Improvement Program (CCIP) Medicare Drug and Health Plan Contract Administration Group Donna Williamson & Brandy Alston December 6, 2016
Recovery Homes: Recovery and Health Homes under Health Care Reform
 Recovery Homes: Recovery and Health Homes under Health Care Reform 4/27/11 Richard H. Dougherty, Ph.D. DMA Health Strategies Challenges of health reform Increasing coverage Reducing costs of coverage Reducing
Recovery Homes: Recovery and Health Homes under Health Care Reform 4/27/11 Richard H. Dougherty, Ph.D. DMA Health Strategies Challenges of health reform Increasing coverage Reducing costs of coverage Reducing
Building Connective Tissue for Integrated Care The Unfolding NH Medicaid Story. April 17, 2018
 Building Connective Tissue for Integrated Care The Unfolding NH Medicaid Story April 17, 2018 Who Are We Supporting In IDN-1? Source: MAeHC Analysis, NH Medicaid IDN Region 1 Data Book Release 1 Findings:
Building Connective Tissue for Integrated Care The Unfolding NH Medicaid Story April 17, 2018 Who Are We Supporting In IDN-1? Source: MAeHC Analysis, NH Medicaid IDN Region 1 Data Book Release 1 Findings:
New York State s Ambitious DSRIP Program
 New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program
 March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
Hot Spotter Report User Guide
 PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
PATIENT-CENTERED CARE Hot Spotter Report User Guide Overview The Hot Spotter Report is designed to give providers and care team members a heads up when their attributed patients appear to be at risk for
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Community Mental Health and Care integration. Zandrea Ware and Ricardo Fraga
 Community Mental Health and Care integration Zandrea Ware and Ricardo Fraga One in Five Approximately 1 in 5 adults in the U.S. 43.8 million, or 18.5% experiences mental illness in their lifetime. Community
Community Mental Health and Care integration Zandrea Ware and Ricardo Fraga One in Five Approximately 1 in 5 adults in the U.S. 43.8 million, or 18.5% experiences mental illness in their lifetime. Community
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals
 Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
Health Home State Plan Amendment
 Health Home State Plan Amendment OMB Control Number: 0938-1148 Expiration date: 10/31/2014 Transmittal Number: OK-14-0011 Supersedes Transmittal Number: Proposed Effective Date: Jan 1, 2015 Approval Date:
Health Home State Plan Amendment OMB Control Number: 0938-1148 Expiration date: 10/31/2014 Transmittal Number: OK-14-0011 Supersedes Transmittal Number: Proposed Effective Date: Jan 1, 2015 Approval Date:
CONNECTED SM. Blue Care Connection SIMPLY AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT
 SIMPLY CONNECTED SM Blue Care Connection AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT Jeanine Patterson, MS, RN, HSMI Clinical Account Consultant July 23, 2013 Blue Cross and Blue Shield of Illinois,
SIMPLY CONNECTED SM Blue Care Connection AN ACTIVE APPROACH TO INTEGRATED HEALTH MANAGEMENT Jeanine Patterson, MS, RN, HSMI Clinical Account Consultant July 23, 2013 Blue Cross and Blue Shield of Illinois,
CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW
 Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM. Bluebonnet Trails Community Services
 TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
Dual-eligible SNPs should complete and submit Attachment A and, if serving beneficiaries with end-stage renal disease (ESRD), Attachment D.
, Attachment D.") Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Health Homes (Section 2703) Frequently Asked Questions
 Frequently Asked Questions") Health Homes (Section 2703) Frequently Asked Questions Following are Frequently Asked Questions regarding opportunities made possible through Section 2703 of the Affordable Care Act to develop health home
Health Homes (Section 2703) Frequently Asked Questions Following are Frequently Asked Questions regarding opportunities made possible through Section 2703 of the Affordable Care Act to develop health home
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
The CCBHC: An Innovative Model of Care for Behavioral Health
 The CCBHC: An Innovative Model of Care for Behavioral Health B R E N D A G O G G I N S, J D V I C E P R E S I D E N T O A K S I N T E G R A T E D C A R E M I C H A E L D A M I C O, L C S W D I R E C T
The CCBHC: An Innovative Model of Care for Behavioral Health B R E N D A G O G G I N S, J D V I C E P R E S I D E N T O A K S I N T E G R A T E D C A R E M I C H A E L D A M I C O, L C S W D I R E C T
Provider Information Guide Complex Care and Condition Care Overview
 Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
Certified Community Behavioral Health Centers and New York State s Healthcare Reform: Considerations for Providers
 Certified Community Behavioral Health Centers and New York State s Healthcare Reform: Considerations for Providers November 30, 2015 Joshua Rubin HealthManagement.com Plan CCBHC basics NYS Health Reform
Certified Community Behavioral Health Centers and New York State s Healthcare Reform: Considerations for Providers November 30, 2015 Joshua Rubin HealthManagement.com Plan CCBHC basics NYS Health Reform
CCBHCs 101: Opportunities and Strategic Decisions Ahead
 CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
Measures Reporting for Eligible Providers
 Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
Transitioning to Community Services: HARPS, Health Homes and SPOA
 Transitioning to Community Services: HARPS, Health Homes and SPOA P R E S E N T E R : G L E N N L I E B M A N, C EO Mental Health Association in New York State, Inc. Brief History of Health and Recovery
Transitioning to Community Services: HARPS, Health Homes and SPOA P R E S E N T E R : G L E N N L I E B M A N, C EO Mental Health Association in New York State, Inc. Brief History of Health and Recovery
Meaningful Use Final Rule:
 Meaningful Use Final Rule: Safety and Quality of Care Jonathan Teich, FACMI, FHIMSS, MD, PhD CMIO, Elsevier Health Sciences August 4, 2010 Today s webinar is sponsored by History HITECH Feb. 2009 Initial
Meaningful Use Final Rule: Safety and Quality of Care Jonathan Teich, FACMI, FHIMSS, MD, PhD CMIO, Elsevier Health Sciences August 4, 2010 Today s webinar is sponsored by History HITECH Feb. 2009 Initial
SECTION 3. Behavioral Health Core Program Standards. Z. Health Home
 SECTION 3 Behavioral Health Core Program Standards Z. Health Home Description Health home is a healthcare delivery approach that focuses on the whole person and provides integrated healthcare coordination
SECTION 3 Behavioral Health Core Program Standards Z. Health Home Description Health home is a healthcare delivery approach that focuses on the whole person and provides integrated healthcare coordination
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses
Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses
HITECH Act American Recovery and Reinvestment Act (ARRA) Stimulus Package. HITECH Act Meaningful Use (MU)
 Stimulus Package. HITECH Act Meaningful Use (MU)") Presents Presents: Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com HITECH Act Meaningful Use (MU) Definition
Presents Presents: Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com HITECH Act Meaningful Use (MU) Definition
Overview of New Nursing Roles in Whole Person Care. Session 1
 Overview of New Nursing Roles in Whole Person Care Session 1 1 Introductions Anne Shields, MHA, RN Associate Director, UW AIMS Center 2 Learning Objectives RN Primary Care Managers Focus Patient Population:
Overview of New Nursing Roles in Whole Person Care Session 1 1 Introductions Anne Shields, MHA, RN Associate Director, UW AIMS Center 2 Learning Objectives RN Primary Care Managers Focus Patient Population:
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Joseph W. Thompson, MD, MPH Arkansas Surgeon General Director, Arkansas Center for Health Improvement
 Joseph W. Thompson, MD, MPH Arkansas Surgeon General Director, Arkansas Center for Health Improvement Arkansas Health System Improvement Workforce Payment System Health Information Technology Insurance
Joseph W. Thompson, MD, MPH Arkansas Surgeon General Director, Arkansas Center for Health Improvement Arkansas Health System Improvement Workforce Payment System Health Information Technology Insurance
Special Needs Plan Model of Care Chinese Community Health Plan
 Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
Special Needs Plan Model of Care 2017 2017 Chinese Community Health Plan Elements of CCHP SNP Model of Care Special Needs Plan (SNP) Goals CCHP Dual Eligible SNP Enrollment & Eligibility Vulnerable Beneficiaries
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
ALL MENTAL HEALTH AND SUBSTANCE USE DISORDER PROGRAMS MUST INCLUDE PSYCHOSOCIAL AND PSYCHIATRIC EVALUATIONS
 COUNTY of NASSAU DEPARTMENT OF HUMAN SERVICES Office of Mental Health, Chemical Dependency and Developmental Disabilities Services 60 Charles Lindbergh Boulevard, Suite 200, Uniondale, New York 11553-3687
COUNTY of NASSAU DEPARTMENT OF HUMAN SERVICES Office of Mental Health, Chemical Dependency and Developmental Disabilities Services 60 Charles Lindbergh Boulevard, Suite 200, Uniondale, New York 11553-3687
Integrated Mental Health Care. Questions
 Integrated Mental Health Care Closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Questions Due to the large number of participants, it is not practical to take questions over
Integrated Mental Health Care Closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Questions Due to the large number of participants, it is not practical to take questions over
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines Specialist Edition 2016-2017 Blue Cross Blue Shield of Michigan
BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines Specialist Edition 2016-2017 Blue Cross Blue Shield of Michigan
Practice Implications for Accountable Care Organizations
 Practice Implications for Accountable Care Organizations An Overview following the Final Rule Gregory M. Marsh, MPH, PMP December 14, 2011 Why CCME? Effective EHR/HIE Implementation will: Improve patient
Practice Implications for Accountable Care Organizations An Overview following the Final Rule Gregory M. Marsh, MPH, PMP December 14, 2011 Why CCME? Effective EHR/HIE Implementation will: Improve patient
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Harnessing the Power of MHS Information Systems to Achieve Meaningful Use of Health Information
 2011 Military Health System Conference Harnessing the Power of MHS Information Systems to Achieve Meaningful Use of Health Information The Quadruple Aim: Working Together, Achieving Success Forum Moderator:
2011 Military Health System Conference Harnessing the Power of MHS Information Systems to Achieve Meaningful Use of Health Information The Quadruple Aim: Working Together, Achieving Success Forum Moderator:
Shared Savings Program ACO Public Reporting Instructions. with Pre-Populated Template
 Shared Savings Program ACO Public Reporting Instructions Introduction with Pre-Populated Template The purpose of this document is to provide ACOs participating in the Shared Savings Program with a public
Shared Savings Program ACO Public Reporting Instructions Introduction with Pre-Populated Template The purpose of this document is to provide ACOs participating in the Shared Savings Program with a public
PROVIDER. Newsletter BETTER QUALITY IS OUR GOAL IN THIS ISSUE MEDICARE 2015 ISSUE II
 MEDICARE 2015 ISSUE II PROVIDER Newsletter BETTER QUALITY IS OUR GOAL Our Quality Improvement (QI) program is dedicated to finding ways to help deliver better care and service to our members, in collaboration
MEDICARE 2015 ISSUE II PROVIDER Newsletter BETTER QUALITY IS OUR GOAL Our Quality Improvement (QI) program is dedicated to finding ways to help deliver better care and service to our members, in collaboration
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Organized, Evidence-based Care
 Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Organized, Evidence-based Care Planning Care for Individual Patients and Whole Populations MODERATOR: Nicole Van Borkulo, MEd, Practice Improvement Specialist, SNMHI, Qualis Health SPEAKERS: Ed Wagner,
Eligible Professionals (EP) Meaningful Use Final Objectives and Measures for Stage 1, 2011
 Meaningful Use Final Objectives and Measures for Stage 1, 2011") Eligible Professionals (EP) Meaningful Use Final Objectives and Measures for Stage 1, 2011 1 On demand webinars are best heard through a headset or earphones (ipod for example) that can be plugged into
Eligible Professionals (EP) Meaningful Use Final Objectives and Measures for Stage 1, 2011 1 On demand webinars are best heard through a headset or earphones (ipod for example) that can be plugged into
Financing the Integration of Behavioral Health: Three Cases Studies: Texas, Oklahoma and Georgia
 National Association of State Mental Health Program Directors 66 Canal Center Plaza, Suite 302 Alexandria, Virginia 22314 Assessment #8 Financing the Integration of Behavioral Health: Three Cases Studies:
National Association of State Mental Health Program Directors 66 Canal Center Plaza, Suite 302 Alexandria, Virginia 22314 Assessment #8 Financing the Integration of Behavioral Health: Three Cases Studies:
BCBSM Physician Group Incentive Program. Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor
 BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
BCBSM Physician Group Incentive Program Patient-Centered Medical Home and Patient-Centered Medical Home-Neighbor Interpretive Guidelines 2016-2017 V11.0 Blue Cross Blue Shield of Michigan is a nonprofit
Coastal Medical, Inc.
 A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
Stage 1 Meaningful Use Objectives and Measures
 Stage 1 Meaningful Use Objectives and Measures Author: Mia Evans About Technosoft Solutions: Technosoft Solutions is a healthcare technology consulting, dedicated to providing software development services
Stage 1 Meaningful Use Objectives and Measures Author: Mia Evans About Technosoft Solutions: Technosoft Solutions is a healthcare technology consulting, dedicated to providing software development services
Provide an understanding of what comprises "meaningful use" of EHR technology
 1 Provide background on federal electronic health record (EHR) incentives Overview of Health IT Incentives Medicare/Medicaid EHR incentives Provide an understanding of what comprises "meaningful use" of
1 Provide background on federal electronic health record (EHR) incentives Overview of Health IT Incentives Medicare/Medicaid EHR incentives Provide an understanding of what comprises "meaningful use" of
Medicare & Medicaid EHR Incentive Program Final Rule. Implementing the American Recovery & Reinvestment Act of 2009
 Medicare & Medicaid EHR Incentive Program Final Rule Implementing the American Recovery & Reinvestment Act of 2009 Conceptual Approach to Meaningful Use Improved Data capture and sharing Advanced Clinical
Medicare & Medicaid EHR Incentive Program Final Rule Implementing the American Recovery & Reinvestment Act of 2009 Conceptual Approach to Meaningful Use Improved Data capture and sharing Advanced Clinical
Falcon Quality Payment Program Checklist- 2017
 Falcon Quality Payment Program Checklist- 2017 DISCLAIMER: This material is provided for informational purposes only and should not be relied upon as legal or compliance advice. If legal advice or other
Falcon Quality Payment Program Checklist- 2017 DISCLAIMER: This material is provided for informational purposes only and should not be relied upon as legal or compliance advice. If legal advice or other
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Full speech capability, allowing you to speak your information and inquiries or use your touchtone
 NEW YORK 2015 ISSUE IV PROVIDER Newsletter NEW PROVIDER SERVICES TECHNOLOGY WellCare is excited to announce some major technology improvements within our call centers, making it easier for providers to
NEW YORK 2015 ISSUE IV PROVIDER Newsletter NEW PROVIDER SERVICES TECHNOLOGY WellCare is excited to announce some major technology improvements within our call centers, making it easier for providers to
Integration Forum Workforce Committee
 Integration Forum Workforce Committee May 27, 2016 Phone: 866-740-1260 Access Code: 3185489 Chairs: Yumi Jarris (Georgetown University School of Medicine) Randy Wykoff (East Tennessee State University)
Integration Forum Workforce Committee May 27, 2016 Phone: 866-740-1260 Access Code: 3185489 Chairs: Yumi Jarris (Georgetown University School of Medicine) Randy Wykoff (East Tennessee State University)