SHIFTS IN PUBLIC POLICY: THE AGS GUIDE FOR GERIATRICS HEALTH CARE PROFESSIONALS
|
|
|
- Evan Summers
- 5 years ago
- Views:
Transcription

1 SHIFTS IN PUBLIC POLICY: THE AGS GUIDE FOR GERIATRICS HEALTH CARE PROFESSIONALS Michael Malone, MD, Kathleen Unroe, MD Peter Hollmann, MD Paul Rudolf, MD, JD May 20, 2016
2 Conflict of Interest Statement There is no conflict of interest to report
3 Overview of Presentation Quick Overview of 2016 Policy Highlights Policy Implications for Post-Acute and Long-Term Care New Payment Codes Medicare Access and CHIP Reauthorization Act (MACRA) MIPS APMS Implications for Geriatrics and Next Steps
4 AGS Policy Work in 2016 Key Successes Older Americans Act reauthorized Advance Care Planning codes paid by Medicare Passage of the IMPACT Act What we continue to work on: Implementation of MACRA Legislation to create clinician educator awards Payment for new and innovative codes Increased funding for key workforce and research programs
5 A Briefing on Post-Acute and Long-Term Care Kathleen Unroe, MD
6 Post-Acute Care/ Long-Term Care Policy Considerations Protecting Access to Medicare ACT (PAMA) IMPACT Act Quality Measures
7 Protecting Access to Medicare Act PAMA passed in 2014 (included doc fix ) Included provisions to promote reduction of avoidable hospital transfers from SNFs through financial incentives and penalties
8 Protecting Access to Medicare Act All SNFs will experience a 2% reduction in their reimbursement from the CMS starting in SNFs will be able to recoup a portion of this by demonstrating an acceptable risk-adjusted readmission ratio and nationally benchmarked rate as calculated by CMS.
9 Protecting Access to Medicare Act October 2016 CMS will provide SNFs with feedback on their readmission rates. October 2017 these rates will be publicly reported on the Nursing Home Compare website. By October 1, 2018 application of this measure and associated penalties for SNFs will start.
10 The IMPACT Act What is the goal? - develop one common data reporting structure across home care, subacute facilities, rehab facilities. each site uses redundant but different tools (such as OASIS, MDS) that are not directly comparable for research or utilization management purposes.
11 The IMPACT Act Requires standardized patient data: Functional status, such as mobility and self care at admission and discharge Cognitive function Special services and treatments Conditions and co-morbidities Impairments, e.g. incontinence, hearing loss
12 Quality Measures April 27, 2016 CMS added 6 new quality measures to Nursing Home Compare. The new measures will be incorporated into nursing home star ratings in July 2016.
13 Quality Measures % of short-stay residents successfully discharged to the community % of short-stay residents with ED visit % of short-stay residents re-hospitalized % of short-stay residents with improvements in function % of long-stay residents whose ability to move independently worsened % of long-stay residents who received an antianxiety or hypnotic medication
14 Key Takeaways Financial penalties will continue to keep focus on developing and implementing best practices to reduce readmissions from SNFs. Lots of important detail to watch for in quality metric development measures need appropriate adjustment for socioeconomic status, morbidity.
15 Coding and Background on MACRA Peter Hollmann, MD
16 New Payment Codes AGS working to improve reimbursement for key services not adequately recognized or valued. CMS expressed interest in payment for new codes for collaborative care, intense complexity and other undervalued professional work. Our work is two-fold Working directly with CMS Working through the AMA CPT and RUC processes Successes to date: TCM, CCM, Advanced Care Plan and for CPT 2018 Cognitive Assessment and Care Plan. AGS plays a lead role in multi-specialty work (geriatric and other chronic illness specialties)
17 New Codes We d Like to See Codes not presently reimbursed by Medicare that we are currently working towards: Complex chronic care management (99487) Acute episode non face-to-face care management (2 codes: home, SNF/NF) Pharmacist services incident to E/M professional (physician, NP, CNS, PA) Falls evaluation and care plan
18 What is MACRA? Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), repealed and replaced Medicare s Sustainable Growth Rate (SGR) formula. MACRA changes the way Medicare incorporates quality and cost efficiency measures into physician/ clinician payments. MACRA incentivizes physicians to participate in alternative payment models.
19 The Background Which Led to MACRA The year to year SGR approach to review and address the rates for Medicare payments to physicians was not working. The anticipated 25% payment cut for physician services was not acceptable. The payment to physicians (SGR fix) was an opportunity to link payment to improved quality of care. MACRA shifted the focus from volume to value, heightening physician incentives to make treatment decisions considering quality and resource use. Congressional Budget Office. March 15, 2015: Cost Estimate and Supplemental Analyses for H.R. 2, the Medicare Access and CHIP Reauthorization Act of Accessed April 20, 2016.
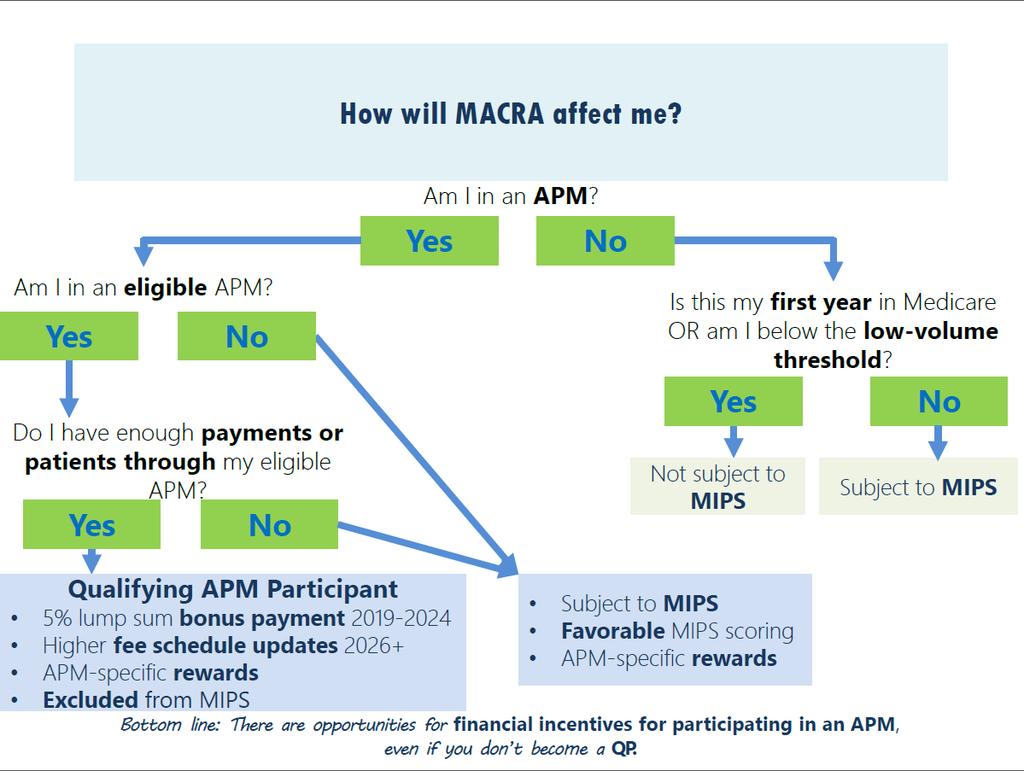
20 The Basics of MACRA and the Key Concepts of Alternate Physician Payment MACRA provides two paths in 2019 both focus on paying for value instead of volume: 1. Incentive payments and higher rate payments for clinicians who participate in eligible Alternative Payment Models (APM s) than for others. 2. Merit-Based Incentive Payment System (MIPS) for clinicians not meeting APM criteria. Better care. Smarter spending. Healthier people. 5% bonus each year if physicians derive a specified minimum amount of income from services furnished in APM entities Scoring system based on quality measures and utilization measures Bonus or Penalty will be based on 2017 performance. We are six months away from this.
21 MACRA Alternative Payment Pathway Paul Rudolf, MD, JD

22 Physicians Face a Dilemma: Will I be Assigned to MIPS or APMs? Merit-based Incentive Payment System Alternative Payment Model While payments affected beginning in 2019, decisions start even earlier initial performance period is 2017 for assignment to MIPS or advanced APMS Participation in APMs not available to all docs CMS estimates only between 31,000 90,000 doctors will be assigned to advanced APMs in 2019 which means 90 percent or more of doctors will be in MIPS 22
23 Long-Term Advantage of APMs ( ) Annual Medicare Income $620,000 $600,000 $580,000 $560,000 $540,000 $520,000 $500, $500K 2035 $513K / $539K 2045 $526K / $581K APM MIPS Year
24 Proposed Advanced APM Requirements Demonstration required by law Thesis being tested Entities must have agreement with CMS Require clinicians to use certified EHR Use quality measures comparable to those in MIPS Bear more than nominal risk or be a medical home CMS proposes that whether an APM is an Advanced APM depends solely upon how the APM is designed Performance within the APM does not affect bonus
25 Financial Risk Requirement If actual expenditures > expected expenditures, one of the following mechanisms is used to recoup the excess: Withhold payment for services to the APM or the APM entity s eligible clinicians; Reduce payments rates to the APM or the APM entity s eligible clinicians; or Require the APM entity to owe payments to CMS.
26 Financial Risk Criterion APM entity can be allowed small excess in actual expenditures (up to 4%) before recoupment mechanism kicks in Called the minimum loss ratio (MLR) Above MLR, APM entity must be at risk for at least 30% of excess expenditures Referred to as the marginal risk Maximum losses for APM entity can be capped but must be at least 4% of expected expenditures Financial risk requirements for Medical Homes are different
27 Financial Risk Example
28 APMs for the First Performance Year (2017) CMS identified 5 current APMs that will be advanced APMs in 2017 Tracks 2 and 3 of Medicare Shared Savings Program Next Generation ACO Model Comprehensive ESRD Care Comprehensive Primary Care Plus Oncology Care Model (2018) Any additional advanced APMs will be identified when announced
29 Medical Home Features Primary care practices or multispecialty practices which include PCPs Geriatric medicine is one of the specialties identified as primary care Empanelment of each patient to a primary clinician At least four of the following: Planned coordination of chronic and preventive care Patient access and continuity of care Risk-stratified care management Coordination of care across the medical neighborhood Patient and caregiver engagement Shared decision-making Payment arrangements in addition to, or substituting for, FFS payments After 2017, medical homes subject to size limit (<50 eligible clinicians) and must have increasing amount of revenue at risk
30 Status of Advanced APMs Advanced APM Model Start Date Notice/ Letter of Intent (LOI) Due Application Due Additional Application Cycles Expected? Medicare Shared Savings Program Next Generation ACO Comprehensive ESRD Care Comprehensive Primary Care + 1/1/17 5/31/16 7/29/16 1/1/17 5/20/16 5/25/16 10/1/ /1/17 N/A 9/1/16 (Participation is limited to practices in up to 20 geographic regions selected based on reach of participating payers) Yes No No Unclear Oncology Care Model 1/1/18 (two-sided risk track) No

31 Where s the Action? * Under MIPS, APM participants guaranteed to receive at least a half credit score for Clinical Practice Improvement Activity Category * Qualifying Participant (QPs)
32 APM Qualified Participants Must be listed as an Advanced APM participant by the Advanced APM in its participation agreement with CMS Advanced APMs must list all participating TINs The TINs include all eligible QPs as identified by their NPIs Listed by December 31 of the QP performance period by the Advanced APM entity Advanced APM entity, through collective calculation of all its eligible clinicians, meets the QP payment amount threshold or the QP patient count threshold All eligible QPs in the Advanced APM receive QP status QPs with multiple TINs receive QP status across all TINs Bonus applies to all payments from all TINs
33 Threshold Changes Over Time Percent of $$$ paid through Advanced APM or # of patients seen by Advanced APM increases over time Harder to reach threshold especially if multiple Advanced APMs in one region CMS proposes steps to mitigate this problem However, no guarantee of assignment to APM pathway
34 APM Bonus Bonus is based on estimated aggregate payments for professional services furnished year prior to the payment year (i.e., 2018 for 2019 bonus) processed through first three months of the bonus year Proposal is to pay lump sum bonus to the TIN not the QP If QP participates in multiple qualifying APMs then bonus is paid to each TIN proportionately If QP participates in multiple APMs but no individual APM meets threshold for that clinician then QP gets bonus
35 Non-Advanced APMs Clinicians in non-advanced APMs are in MIPs CMS calculates performance score differently in order to be consistent with mission of APM Quality measures and advancing care information given weight of 0 Entire score based on clinical practice improvement activities and cost Scored in the aggregate not individually

36 Advanced APM Caveat: In a given year, one has to be ready to be in MIPS, in case a threshold of $$ volume is missed. Medicare Payment Systems for Physician Services
37 MACRA MIPS Michael Malone, MD
 and Alternative Payment Model (APM) Incentive under the Physician Fee Schedule, and Criteria for Physician-Focused Payment")
38 Generally, all physicians will be eligible to join MIPS. Physicians who do not report MIPS measures will receive low performance scores and negative payment updates. Reference: Medicare Program; Merit-Based Incentive Payment System (MIPS) and Alternative Payment Model (APM) Incentive under the Physician Fee Schedule, and Criteria for Physician-Focused Payment Models Medicare Payment Systems for Physician Services
39 What is the Merit- Based Incentive Payment System (MIPS)? This is a new program in the Medicare fee- for- service payment system. This program consolidates 3 existing programs into a single program, and adds a 4th: Meaningful Use. The Physician Quality Reporting System. The Value- Based Payment Modifier Merit- Based Incentive Payment System (MIPS) 2017 performance data will be used for 2019 payment adjustment. CMS proposes to use claims processed up to 90 days after the end of the performance period. Physicians can participate as individuals or as a group: defined by Taxpayer ID number.


40 Who is eligible for the Merit- Based Payment System (MIPS)? MIPS eligible clinicians: All physicians. Physician assistants. Nurse practitioners. Clinical nurse specialists. Certified registered nurse anesthetists. Groups that include such clinicians. Practitioners excluded from MIPS: Newly Medicareenrolled eligible clinicians. Certain participants in Advanced APMs. Low- volume threshold clinicians*. *Less than $10,000 in Medicare charges and 100 or less Medicare patients in one year.
41 What is the Merit- Based Incentive Payment System (MIPS)? The MIPS will assess individual physician performance in 4 categories and generate a composite score. Clinical Quality: 50%* Resource Use/ Cost: 10%** Meaningful use of certified electronic health record technology: 25% Clinical practice improvement activities: 15% *year 1 proposed. ** Over time, MIPS has an escalating focus on cost.
42 The Four Components of MIPS (10 percent of total score in year 1; replaces the cost component of the Value Modifier Program, also known as Resource Use) (50 percent of total score in year 1; replaces the Physician Quality Reporting System and the quality component of the Value Modifier Program) (15 percent of total score in year 1) Quality Payment Program - Centers for Medicare & Medicaid Services, April 27,2016. Accessed May 15,2016. (25 percent of total score in year 1; replaces the Medicare EHR Incentive Program for physicians, also known as Meaningful Use )

43 What is the Merit- Based Incentive Payment System (MIPS)? Beginning in 2019, clinicians participating in the MIPS will be eligible for positive or negative Medicare payments. Start at 4% and gradually increase to 9% for The threshold for these payment adjustments will be the mean composite score for all MIPS- eligible professionals during the previous year. The distribution of payments will follow a bell- shaped curve is proposed as the performance period for 2019 payment adjustments.
44 The Impact of the Proposed Rule CMS estimates that overall, most MIPS physicians (54%) will have positive adjustment. Hardest hit specialties include chiropractors, dentistry, podiatry, psychiatry, and plastic surgeons. Likelihood of positive adjustment increases with practice size: Practice Size Eligible Clinicians (ECs) Percent with Negative Impact Solo 102,788 87% 2-9 ECs 123,695 70% ECs 81,207 59% ECs 147,976 45% 100+ ECs 305,676 18% 44
45 The Key Themes of How MIPS Works MIPS Information Publicly Reported On Physician Compare Web site Individual physician composite score of Clinical Quality: 50% Resource use: 10% Meaningful use of certified electronic health record technology: 25% Clinical practice improvement activities: 15% Physicians whose score is >=above the threshold will receive a maximum positive payment adjustment of +4% on each claim for the following year. Additional bonus is possible for exceptional performance. Physicians who score at the threshold composite score will receive no payment adjustment. Physicians whose composite score is below the threshold will receive a maximum negative adjustment of -4% on each claim for the following year.
46 1 Components of MIPS Quality Key Points: Clinicians would choose to report six measures. This category gives clinicians reporting options to choose from to accommodate differences in specialty and practices. (50 percent of total score in year 1; replaces the Physician Quality Reporting System and the quality component of the Value Modifier Program)
47 Quality Measure Category (50%) Eligible Clinician selects 6 measures From individual measures or from specialty measure set Must include 1 cross-cutting measure AND 1 outcome measure (or another high priority measure if outcome is unavailable) Bonus points available for reporting high priority measures High Priority Measures Outcome (including intermediate outcome) Appropriate use Patient Safety Efficiency Patient Experience Care coordination
48 Cross-Cutting Quality Measures Title Description Title Description Care Plan Documentation of Current Medications in the Medical Record % of patients aged 65+ with an advance care plan or surrogate decision maker documented in the medical record or documentation in the medical record that an advance care plan was discussed but the patient did not wish or was not able to name a surrogate decision maker or provide an advance care plan. % of visits for patients aged 18+ for which the eligible clinician attests to documenting a list of current medications using all immediate resources available on the date of the encounter. List must include ALL known prescriptions, over-the-counters, herbals, and vitamin/mineral/dietary (nutritional) supplements AND must contain the medications name, dosage, frequency and route of administration. Screening for High Blood Pressure and Follow-Up Documented Receipt of Specialist Report Tobacco Use and Help with Quitting Among Adolescents Unhealthy Alcohol Use: Screening & Brief Counseling % of patients aged 18 + seen during the reporting period who were screened for high blood pressure AND a recommended follow-up plan is documented based on the current blood pressure reading as indicated. % of patients with referrals, regardless of age, for which the referring provider receives a report from the provider referred to % of adolescents aged with a primary care visit during the measurement year for whom tobacco use status was documented and received help with quitting if identified as a tobacco user % of patients aged 18 + screened at least once within the last 24 months for unhealthy alcohol use using a systematic screening method AND who received brief counseling if identified as an unhealthy alcohol user Tobacco Use: Screening and Cessation Intervention Controlling High Blood Pressure % of patients aged 18+ screened for tobacco use one or more times within 24 months AND who received cessation counseling intervention if identified as a tobacco user. % of patients aged with a diagnosis of hypertension whose blood pressure was adequately controlled (<140/90 mmhg) during the measurement period. Body Mass Index (BMI) Screening and Follow-Up Plan CAHPS for MIPS Clinician/Group Survey % of patients aged 18+ with a BMI documented during the current encounter or during the previous six months AND with a BMI outside of normal parameters, a follow-up plan is documented during the encounter or during the previous six months of the current encounter. Summary Survey Measures
49 Requirements for MIPS Quality Measures Must be established through notice-and-comment rulemaking. Prior to inclusion in final rule, must be submitted for publication in applicable specialty-appropriate, peerreviewed journals with the method for developing and selecting such measure, including clinical and other data supporting such measure. Be endorsed by a consensus-based entity or have a focus that is evidence-based. Measures used by a qualified clinical data registry are not subject to these requirements.
50 2 Components of MIPS Cost (10 percent of total score in year 1; replaces the cost component of the Value Modifier Program, also known as Resource Use) Key Points: Score would be based on Medicare claims. No reporting requirements for clinicians. More than 40 episode-specific measures to account for differences among specialties.
51 Components of MIPS Cost (10 percent of total score in year 1; replaces the cost component of the Value Modifier Program, also known as Resource Use) CMS calculates from claim data. No reporting requirement. Key Points: The law requires CMS to measure resources used to treat similar cases across practices: Episode groups - based on care provided. Condition groups - based on patient s clinical condition. CMS must also create patient relationship codes to allow physicians to classify themselves in relation to the patient: Primary responsibility for general and ongoing care, Continuing basis during an acute episode, but in a supportive role, etc.
52 3 Components of MIPS Clinical Practice Improvement Activities (15 percent of total score in year 1) Key Points: Clinicians would be rewarded for clinical practice improvement activities such as activities focused on care coordination, beneficiary engagement, and patient safety. Clinicians may select activities that match their practices goals from a list of more than 90 options.

53 Components of MIPS Clinical Practice Improvement Activities (15 percent of total score in year 1) Maximum of 60 points from >90 activities. The physician must select at least one and can get additional credit for more activities. Key Points: Highly weighted activities: Patient Centered Medical Home. Activities that support the transformation of clinical practice, or public health priorities. Activities addressing patient experience. Activities to improve timely access.
54 4 Components of MIPS Advancing Care Information Key Points: Clinicians would choose to report customizable measures that reflect how they use EHR technology in their day-to-day practice. A particular emphasis is on interoperability and information exchange. This category would not require an all-or-nothing EHR measurement or quarterly reporting. (25 percent of total score in year 1)
55 Components of MIPS Advancing Care Information

56 Components of MIPS Advancing Care Information Six Measures for Base Score:

57 Components of MIPS Advancing Care Information Public Health Registry* *Beyond an immunization registry.
58 The Four Components of MIPS (10 percent of total score in year 1; replaces the cost component of the Value Modifier Program, also known as Resource Use) (50 percent of total score in year 1; replaces the Physician Quality Reporting System and the quality component of the Value Modifier Program) (15 percent of total score in year 1) Quality Payment Program - Centers for Medicare & Medicaid Services, April 27,2016. Accessed May 15,2016. (25 percent of total score in year 1; replaces the Medicare EHR Incentive Program for physicians, also known as Meaningful Use )
59 Source:
60 *Exceptional performance adjustment for those with the highest composite scores, limited to additional adjustment of 10% per year. **HHS can increase the maximum MIPS positive adjustment (not counting the exceptional performance adjustment) to no more than 3x maximum MIPS incentive adjustment for that calendar year, if there are sufficient funds available. HHS cannot increase the maximum negative MIPS adjustment by more than the amount specified. Prepared by the American College of Physicians, Division of Governmental Affairs and Public Policy Under MACRA, what s the range of possible FFS updates and incentive payments per year? (Physicians can participate in either MIPS or APM, not both) Date Baseline MIPS (incentive adjustments), without exceptional performance adjustment* Baseline, plus/minus MIPS, without exceptional performance adjustment* MIPS maximum, with exceptional performance adjustment* APM (FFS bonus only, does not include incentives from own APM pay structure) % instead of 21% SGR cut N/A N/A N/A N/A thru % Per year N/A N/A N/A N/A % +/- 4.0%** = -3.5% to +4.5%** 14.5% FFS bonus: +5% % +/- 5.0%** = -5.0% to +5.0%** 15% FFS bonus: +5% % +/- 7.0%** = -7.0% to +7.0%** 17% FFS bonus: +5% 2022, 2023 and % +/- 9.0%** = -9.0% to + 9.0%** 19% FFS bonus +5% % +/- 9.0%** = -9.0-% to plus 9.0%** N/A 0% 2026 and subsequent years 0.25% (for non-apm physicians only) +/- 9.0%** = -8.75% to plus 9.25% ** N/A 0.75%
61 The Economics of Medicare s Quality Payment Program Most Medicare clinicians will initially participate in the Quality Payment Program through MIPS. Advanced Alternative Payment Models in 2019 will have 31,000 to 90,000 qualified providers. $146 to $429 million in incentive payments. MIPS will distribute payment adjustments to 687,000 to 746,000 eligible clinicians in $833 million in positive and negative payment adjustments. $500 million in exceptional performance payments. Financial incentives in both programs are proposed to drive quality improvement for Medicare beneficiaries.
62 Projected Timeline of CMS Activity and Opportunities for AGS to Comment 1Q16 2Q16 3Q16 4Q16 1Q17 2Q17 3Q17 4Q17 Episode Groups Initial Comment Period (3/1/16) Comments due 8/25/16 on final set of 57 episode groups CMS releases draft groups (11/16) Public comment (3/17) CMS releases operational groups (12/17) Patient Relationship Codes CMS releases categories and codes (4/16) Comments due 8/15/16 CMS releases operational list (4/17) MIPS/APM Proposed Rule Comments due 6/27/16 MIPS Performance Period
63 How will Medicare beneficiaries see the changes in the delivery system? Their providers are using an EHR during each interaction. Their provider is working on strategies to improve care coordination. Their providers are reviewing more outcomes measures during their clinical interactions. Their practice site is working on more practice improvement efforts: Expanded access/ Portals/ After hours urgent care. Practice sites will develop into Patient Centered Medical Homes. Efforts to control the costs of care.
64 What are the key questions geriatricians need to be asking of their group? Which direction will we take for our Medicare FFS payments in 2017 and beyond: APM or MIPS? What information do we need in order to inform that decision? Are you in a group? Do we have the infrastructure in place to manage these changes? How will these decisions affect my income?
65 What can you do to prepare for MIPS? 1. Understand how clinical quality will be measured at your site. 2. Define which measures will best meet your patients needs. 3. Learn more about episode groups and condition groups. 4. Become involved in qualified: Clinical practice improvement activities. Care delivery improvement activities. Patient- centered medical homes.
66 The Optimal Role of the AGS Prepare and educate our members. Continue to monitor and comment on all the rules and regulations. Continued guidance from our regulatory experts. Comment on how each activity affects our pathways: Making practice desirable. Building our workforce. Improving care. Building the value proposition for geriatrics. Advocating for the vulnerable population: Those with multiple co- morbid conditions. Those with cognitive impairment. The frail.
67 Themes The current system of physician payment does not work well for geriatricians. We (the AGS) bring(s) a lot of value to the table in the care of older individuals. There is a lot we still don t know, but we are committed to getting this right. Our patients need and deserve this type of transformation of care.
Kate Goodrich, MD MHS. Director, Center for Clinical Standards & Quality. Center for Medicare and Medicaid Services (CMS) May 6, 2016
 May 6, 2016") Kate Goodrich, MD MHS Director, Center for Clinical Standards & Quality Center for Medicare and Medicaid Services (CMS) May 6, 2016 THE MEDICARE ACCESS & CHIP REAUTHORIZATION ACT OF 2015 Quality Payment
Kate Goodrich, MD MHS Director, Center for Clinical Standards & Quality Center for Medicare and Medicaid Services (CMS) May 6, 2016 THE MEDICARE ACCESS & CHIP REAUTHORIZATION ACT OF 2015 Quality Payment
QUALITY PAYMENT PROGRAM
 NOTICE OF PROPOSED RULE MAKING Medicare Access and CHIP Reauthorization Act of 2015 QUALITY PAYMENT PROGRAM Executive Summary On April 27, 2016, the Department of Health and Human Services issued a Notice
NOTICE OF PROPOSED RULE MAKING Medicare Access and CHIP Reauthorization Act of 2015 QUALITY PAYMENT PROGRAM Executive Summary On April 27, 2016, the Department of Health and Human Services issued a Notice
CMS Quality Payment Program: Performance and Reporting Requirements
 CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
WELCOME. Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association
 WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
MACRA Implementation: A Review of the Quality Payment Program
 MACRA Implementation: A Review of the Quality Payment Program Neal Logue, Kirk Sadur Centers for Medicare and Medicaid Services, Region IX, September 15, 2017 Disclaimer This presentation was prepared
MACRA Implementation: A Review of the Quality Payment Program Neal Logue, Kirk Sadur Centers for Medicare and Medicaid Services, Region IX, September 15, 2017 Disclaimer This presentation was prepared
Here is what we know. Here is what you can do. Here is what we are doing.
 With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
2017/2018. KPN Health, Inc. Quality Payment Program Solutions Guide. KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc.
 KPN Health, Inc.") 2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
2017 Transition Into Value Based Care
 2017 Transition Into Value Based Care Provider Meeting August 3 rd, 2017 Objectives Define MACRA, MIPS, and APM Overview of MIPS Performance Categories within the Quality Payment Program (QPP) Provide
2017 Transition Into Value Based Care Provider Meeting August 3 rd, 2017 Objectives Define MACRA, MIPS, and APM Overview of MIPS Performance Categories within the Quality Payment Program (QPP) Provide
SVS QUALITY AND PERFORMANCE MEASURES COMMITTEE (QPMC) New Member Orientation
 New Member Orientation") SVS QUALITY AND PERFORMANCE MEASURES COMMITTEE (QPMC) New Member Orientation 2017-2018 SVS QPMC Quality and Performance Measures Committee Policy and Advocacy Council (Chair Sean Roddy) Chair: Brad Johnson,
SVS QUALITY AND PERFORMANCE MEASURES COMMITTEE (QPMC) New Member Orientation 2017-2018 SVS QPMC Quality and Performance Measures Committee Policy and Advocacy Council (Chair Sean Roddy) Chair: Brad Johnson,
MACRA for Critical Access Hospitals. Tuesday, July 26, 2016 Webinar
 MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
Medicare Physician Payment Reform:
 Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
MACRA & Implications for Telemedicine. June 20, 2016
 MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
MACRA, MIPS, and APMs What to Expect from all these Acronyms?!
 MACRA, MIPS, and APMs What to Expect from all these Acronyms?! ACP Pennsylvania Council Meeting Saturday, December 5, 2015 Shari M. Erickson, MPH Vice President, Governmental Affairs & Medical Practice
MACRA, MIPS, and APMs What to Expect from all these Acronyms?! ACP Pennsylvania Council Meeting Saturday, December 5, 2015 Shari M. Erickson, MPH Vice President, Governmental Affairs & Medical Practice
Strategic Implications & Conclusion
 Kelly Court Chief Quality Officer Wisconsin Hospital Association Brian Vamstad Government Relations Consultant Gundersen Health System Overview and Key Takeaways of the Medicare Quality Payment Program
Kelly Court Chief Quality Officer Wisconsin Hospital Association Brian Vamstad Government Relations Consultant Gundersen Health System Overview and Key Takeaways of the Medicare Quality Payment Program
MACRA MACRA MACRA 9/30/2015. From the Congress: A New Medicare Payment System. The Future of Medicare: A Move Toward Value Driven Healthcare W20.
 W20.8XXA The Future of Medicare: A Move Toward Value Driven Healthcare Emily L. Graham, RHIA, CCS-P VP, Regulatory Affairs, Hart Health Strategies Consultant, Coalition of State Rheumatology Organizations
W20.8XXA The Future of Medicare: A Move Toward Value Driven Healthcare Emily L. Graham, RHIA, CCS-P VP, Regulatory Affairs, Hart Health Strategies Consultant, Coalition of State Rheumatology Organizations
Quality Payment Program MIPS. Advanced APMs. Quality Payment Program
 Proposed Rule: Merit-Based Incentive Payment System (MIPS) and Alternative Payment Model (APM) Incentive under the Physician Fee Schedule, and Criteria for Physician-Focused Payment Models The Department
Proposed Rule: Merit-Based Incentive Payment System (MIPS) and Alternative Payment Model (APM) Incentive under the Physician Fee Schedule, and Criteria for Physician-Focused Payment Models The Department
MACRA Fall into Place. By Stephanie Cecchini, CPC, CEMC, CHISP, AAPC Fellow, AAPC MACRA Prof
 MACRA Fall into Place By Stephanie Cecchini, CPC, CEMC, CHISP, AAPC Fellow, AAPC MACRA Prof About the Presenter https://www.linkedin.com/in/stephaniececchini 2 Introduction Love it Hate it Don t know a
MACRA Fall into Place By Stephanie Cecchini, CPC, CEMC, CHISP, AAPC Fellow, AAPC MACRA Prof About the Presenter https://www.linkedin.com/in/stephaniececchini 2 Introduction Love it Hate it Don t know a
The Quality Payment Program Overview Fact Sheet
 Quality Payment Program The Quality Payment Program Overview Background On October 14, 2016, the Department of Health and Human Services (HHS) issued its final rule with comment period implementing the
Quality Payment Program The Quality Payment Program Overview Background On October 14, 2016, the Department of Health and Human Services (HHS) issued its final rule with comment period implementing the
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program
 March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
Alternative Payment Models and Health IT
 Alternative Payment Models and Health IT Health DataPalooza Preconference May 8, 2016 Kelly Cronin, MS, MPH, Director, Office of Care Transformation, ONC/HHS HHS Goals for Medicare Payment Reform In January
Alternative Payment Models and Health IT Health DataPalooza Preconference May 8, 2016 Kelly Cronin, MS, MPH, Director, Office of Care Transformation, ONC/HHS HHS Goals for Medicare Payment Reform In January
Health System Transformation, CMS Priorities, and the Medicare Access and CHIP Reauthorization Act
 Health System Transformation, CMS Priorities, and the Medicare Access and CHIP Reauthorization Act Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services
Health System Transformation, CMS Priorities, and the Medicare Access and CHIP Reauthorization Act Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services
Here is what we know. Here is what you can do. Here is what we are doing.
 With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
MACRA Quality Payment Program
 The American College of Surgeons Resources for the New Medicare Physician System Table of Contents Understanding the... 3 Navigating MIPS in 2017... 4 MIPS Reporting: Individuals or Groups... 6 2017: The
The American College of Surgeons Resources for the New Medicare Physician System Table of Contents Understanding the... 3 Navigating MIPS in 2017... 4 MIPS Reporting: Individuals or Groups... 6 2017: The
ACCOUNTABLE CARE ORGANIZATION & ALTERNATIVE PAYMENT MODEL SUMMIT
 ACCOUNTABLE CARE ORGANIZATION & ALTERNATIVE PAYMENT MODEL SUMMIT The Centers for Medicare and Medicaid Services Kate Goodrich, MD MHS Director, Clinical Standards & Quality Chief Medical Officer 1 DISCLAIMERS
ACCOUNTABLE CARE ORGANIZATION & ALTERNATIVE PAYMENT MODEL SUMMIT The Centers for Medicare and Medicaid Services Kate Goodrich, MD MHS Director, Clinical Standards & Quality Chief Medical Officer 1 DISCLAIMERS
Understanding Medicare s New Quality Payment Program
 Understanding Medicare s New Quality Payment Program Your introduction to MACRA and getting started with MIPS 1 Understanding Medicare s New Quality Payment Program 2016 Mingle Analytics. All Rights Reserved.
Understanding Medicare s New Quality Payment Program Your introduction to MACRA and getting started with MIPS 1 Understanding Medicare s New Quality Payment Program 2016 Mingle Analytics. All Rights Reserved.
MACRA: Disrupting the health care system at every level
 Health Policy Brief MACRA: Disrupting the health care system at every level Produced by the Deloitte Center for Health Solutions and the Deloitte Center for Regulatory Strategies Executive summary The
Health Policy Brief MACRA: Disrupting the health care system at every level Produced by the Deloitte Center for Health Solutions and the Deloitte Center for Regulatory Strategies Executive summary The
Passage of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): The Doc Fix
: The Doc Fix") April, 2015 Passage of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): The Doc Fix Author: Annemarie Wouters, Senior Advisor The President has signed into law the bipartisan bill H.R. 2,
April, 2015 Passage of Medicare Access and CHIP Reauthorization Act of 2015 (MACRA): The Doc Fix Author: Annemarie Wouters, Senior Advisor The President has signed into law the bipartisan bill H.R. 2,
CMS Priorities, MACRA and The Quality Payment Program
 CMS Priorities, MACRA and The Quality Payment Program Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services Presentation on behalf of HSAG November 16, 2016
CMS Priorities, MACRA and The Quality Payment Program Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services Presentation on behalf of HSAG November 16, 2016
MACRA and the Quality Payment Program. Frequently Asked Questions Edition
 MACRA and the Quality Payment Program Frequently Asked Questions 2018 Edition What is MACRA?...3 What is the Quality Payment Program?...3 How do payments work under the QPP?...3 What is at risk under
MACRA and the Quality Payment Program Frequently Asked Questions 2018 Edition What is MACRA?...3 What is the Quality Payment Program?...3 How do payments work under the QPP?...3 What is at risk under
MIPS/APM Proposed Rule Summary On Monday, May 9, 2016 the Centers for Medicare and Medicaid Services (CMS) published in the Federal Register the
 published in the Federal Register the") MIPS/APM Proposed Rule Summary On Monday, May 9, 2016 the Centers for Medicare and Medicaid Services (CMS) published in the Federal Register the proposed criteria for the Quality Payment Program as prescribed
MIPS/APM Proposed Rule Summary On Monday, May 9, 2016 the Centers for Medicare and Medicaid Services (CMS) published in the Federal Register the proposed criteria for the Quality Payment Program as prescribed
MIPS, MACRA, & CJR: Medicare Payment Transformation. Presenter: Thomas Barber, M.D. May 31, 2016
 MIPS, MACRA, & CJR: Medicare Payment Transformation Presenter: Thomas Barber, M.D. May 31, 2016 Michael Porter- Value Based Care Delivery, Annals of Surgery 2008 Principals: Define Value as a Goal Care
MIPS, MACRA, & CJR: Medicare Payment Transformation Presenter: Thomas Barber, M.D. May 31, 2016 Michael Porter- Value Based Care Delivery, Annals of Surgery 2008 Principals: Define Value as a Goal Care
The Merit-Based Incentive Payment System (MIPS) Survival Guide. August 11, 2016
 Survival Guide. August 11, 2016") The Merit-Based Incentive Payment System (MIPS) Survival Guide August 11, 2016 Speakers Nina Marshall, MSW, Senior Director, Policy and Practice Improvement, National Council for Behavioral Health Elizabeth
The Merit-Based Incentive Payment System (MIPS) Survival Guide August 11, 2016 Speakers Nina Marshall, MSW, Senior Director, Policy and Practice Improvement, National Council for Behavioral Health Elizabeth
Advancing Care Information- The New Meaningful Use September 2017
 Advancing Care Information- The New Meaningful Use September 2017 ACO Announcements Reminders: ACO Notifications PECOS-Maintain active enrollment 2017 Patient Prospective Lists Upcoming provider/office
Advancing Care Information- The New Meaningful Use September 2017 ACO Announcements Reminders: ACO Notifications PECOS-Maintain active enrollment 2017 Patient Prospective Lists Upcoming provider/office
Meaningful Use 2016 and beyond
 Meaningful Use 2016 and beyond Main Street Medical Consulting May 12, 2016 Meaningful use, MACRA, MIPS? Whaaaaat? 1 Reporting Period and Timeline In 2016 all providers are required to use CEHRT versions
Meaningful Use 2016 and beyond Main Street Medical Consulting May 12, 2016 Meaningful use, MACRA, MIPS? Whaaaaat? 1 Reporting Period and Timeline In 2016 all providers are required to use CEHRT versions
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement. Craig J. Wilson
 Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
Thank You to Our Sponsor!
 AMCP Webinar Emerging Physician Payment Models: What Does it Mean for AMCP Members and Medication Management? April 19, 2017 Thank You to Our Sponsor! 1 Disclaimer Organizations may not re use material
AMCP Webinar Emerging Physician Payment Models: What Does it Mean for AMCP Members and Medication Management? April 19, 2017 Thank You to Our Sponsor! 1 Disclaimer Organizations may not re use material
Overview of Quality Payment Program
 Overview of Quality Payment Program Policies for 2017 & 2018 Performance Years The Medicare program has transformed how it reimburses psychiatrists and other clinicians for providing services, under the
Overview of Quality Payment Program Policies for 2017 & 2018 Performance Years The Medicare program has transformed how it reimburses psychiatrists and other clinicians for providing services, under the
MACRA-Impacts on Primary
 MACRA-Impacts on Primary Care Providers and Practices Jennifer Bell, MS, Chamber Hill Strategies Mara McDermott, JD, CAPG Shari Erickson, MPH (Moderator), American College of Physicians Macaran Baird,
MACRA-Impacts on Primary Care Providers and Practices Jennifer Bell, MS, Chamber Hill Strategies Mara McDermott, JD, CAPG Shari Erickson, MPH (Moderator), American College of Physicians Macaran Baird,
The Influence of Health Policy on Clinical Practice. Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center
 The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
Submitted electronically:
 Mr. Andy Slavitt Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS-5517-FC P.O. Box 8013 7500 Security Boulevard Baltimore, MD 21244-8013
Mr. Andy Slavitt Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS-5517-FC P.O. Box 8013 7500 Security Boulevard Baltimore, MD 21244-8013
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization. Quality Forum August 19, 2015
 The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
The Evolving Landscape of Healthcare Payment: Incentive Programs and ACO Model Optimization Quality Forum August 19, 2015 Ross Manson rmanson@eidebailly.com 701.239.8634 Barb Pritchard bpritchard@eidebailly.com
Quality Payment Program Year 2: 2018 MIPS Participation. An Introductory Guide for CRNAs in 2018
 Quality Payment Program Year 2: 2018 MIPS Participation An Introductory Guide for CRNAs in 2018 Quality Payment Program (QPP) The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) established
Quality Payment Program Year 2: 2018 MIPS Participation An Introductory Guide for CRNAs in 2018 Quality Payment Program (QPP) The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) established
Glossary of Acronyms for the Quality Payment Program
 The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative Glossary of Acronyms for the Quality Payment Program 1 P a g e MEDICARE QPP PHYSICIAN EDUCATION
The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative Glossary of Acronyms for the Quality Payment Program 1 P a g e MEDICARE QPP PHYSICIAN EDUCATION
MACRA is Coming: Reimbursement for Quality and the Shift to Population-Based Care
 MACRA is Coming: Reimbursement for Quality and the Shift to Population-Based Care AMERICAN NEUROLOGICAL ASSOCIATION October 17, 2017 Marc R. Nuwer, MD PhD Professor and Vice Chair UCLA Lyell K. Jones,
MACRA is Coming: Reimbursement for Quality and the Shift to Population-Based Care AMERICAN NEUROLOGICAL ASSOCIATION October 17, 2017 Marc R. Nuwer, MD PhD Professor and Vice Chair UCLA Lyell K. Jones,
Agenda. Surviving the New Program Requirements and the Financial Penalties Under MIPS 9/9/2016. Steps to take to prepare for MIPS
 Surviving the New Program Requirements and the Financial Penalties Under MIPS September 2016 Selena Hood Agenda Steps to take to prepare for MIPS Introduction and Evaluation of the Merit-Based Incentive
Surviving the New Program Requirements and the Financial Penalties Under MIPS September 2016 Selena Hood Agenda Steps to take to prepare for MIPS Introduction and Evaluation of the Merit-Based Incentive
The Healthcare Roundtable
 The Healthcare Roundtable MACRA Update Jayme R. Matchinski Greensfelder, Hemker & Gale, P.C. April 7, 2017 New Orleans, Louisiana This presentation and outline are limited to a discussion of general principles
The Healthcare Roundtable MACRA Update Jayme R. Matchinski Greensfelder, Hemker & Gale, P.C. April 7, 2017 New Orleans, Louisiana This presentation and outline are limited to a discussion of general principles
Steps toward Sustainability with the second year of the Quality Payment Program
 Steps toward Sustainability with the second year of the Quality Payment Program Deanna Graham, QI Consultant, Qualis Health March 27, 2018 Speaker Deanna Graham QI Principal Qualis Health 2 Qualis Health
Steps toward Sustainability with the second year of the Quality Payment Program Deanna Graham, QI Consultant, Qualis Health March 27, 2018 Speaker Deanna Graham QI Principal Qualis Health 2 Qualis Health
MIPS Program: 2018 Advancing Care Information Category
 MIPS Program: 2018 Advancing Care Category The 2018 Quality Payment Program (QPP) Year Two final rule continues to implement the programs authorized under the Medicare and CHIP Reauthorization Act of 2015
MIPS Program: 2018 Advancing Care Category The 2018 Quality Payment Program (QPP) Year Two final rule continues to implement the programs authorized under the Medicare and CHIP Reauthorization Act of 2015
Are physicians ready for macra/qpp?
 Are physicians ready for macra/qpp? Results from a KPMG-AMA Survey kpmg.com ama-assn.org Contents Summary Executive Summary 2 Background and Survey Objectives 5 What is MACRA? 5 AMA and KPMG collaboration
Are physicians ready for macra/qpp? Results from a KPMG-AMA Survey kpmg.com ama-assn.org Contents Summary Executive Summary 2 Background and Survey Objectives 5 What is MACRA? 5 AMA and KPMG collaboration
Navicent Health Physician Group Risk-Based Payments: Assessment of Readiness and Performance for Multiple Reporting Requirements
 Creating Clinically Integrated Health System-Based Medical Groups Collaborative Case Study Navicent Health Physician Group Risk-Based Payments: Assessment of Readiness and Performance for Multiple Reporting
Creating Clinically Integrated Health System-Based Medical Groups Collaborative Case Study Navicent Health Physician Group Risk-Based Payments: Assessment of Readiness and Performance for Multiple Reporting
MACRA Frequently Asked Questions
 Following the release of the Quality Payment Program Interim Final Rule, the American Medical Association (AMA) conducted numerous informational and training sessions for physicians and medical societies.
Following the release of the Quality Payment Program Interim Final Rule, the American Medical Association (AMA) conducted numerous informational and training sessions for physicians and medical societies.
Quality Measurement and Reporting Kickoff
 Quality Measurement and Reporting Kickoff All Shared Savings Program ACOs April 11, 2017 Sandra Adams, RN; Rabia Khan, MPH Division of Shared Savings Program Medicare Shared Savings Program DISCLAIMER
Quality Measurement and Reporting Kickoff All Shared Savings Program ACOs April 11, 2017 Sandra Adams, RN; Rabia Khan, MPH Division of Shared Savings Program Medicare Shared Savings Program DISCLAIMER
The Quality Payment Program: Overview & Roles and Responsibilities
 The Quality Payment Program: Overview & Roles and Responsibilities National Tribal Health Conference Susy Postal DNP, RN-BC Chief Health Informatics Officer September 27, 2017 INDIAN HEALTH SERVICE / OFFICE
The Quality Payment Program: Overview & Roles and Responsibilities National Tribal Health Conference Susy Postal DNP, RN-BC Chief Health Informatics Officer September 27, 2017 INDIAN HEALTH SERVICE / OFFICE
MACRA Quality Payment Program
 The American College of Surgeons Resources for the New Medicare Physician System Table of Contents Simple Steps to Determine If MIPS Applies to Your Practice Situation... 3 5 Understanding the... 6 7 Big
The American College of Surgeons Resources for the New Medicare Physician System Table of Contents Simple Steps to Determine If MIPS Applies to Your Practice Situation... 3 5 Understanding the... 6 7 Big
The MIPS Survival Guide
 The MIPS Survival Guide The Definitive Guide for Surviving the Merit-Based Incentive Payment System TABLE OF CONTENTS 1 An Introduction to the Merit-Based Incentive Payment System (MIPS) 2 Survival Tip
The MIPS Survival Guide The Definitive Guide for Surviving the Merit-Based Incentive Payment System TABLE OF CONTENTS 1 An Introduction to the Merit-Based Incentive Payment System (MIPS) 2 Survival Tip
From Surviving to Thriving in the QPP World
 From Surviving to Thriving in the QPP World Today s Objectives Brief MACRA Overview Where are we going?: Advanced Alternative Payment Models (APMs) Where are we now? Merit Incentive-Based Payment System
From Surviving to Thriving in the QPP World Today s Objectives Brief MACRA Overview Where are we going?: Advanced Alternative Payment Models (APMs) Where are we now? Merit Incentive-Based Payment System
2017 Transition Year Flexibility Improvement Activities Category Options
 The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative 2017 Transition Year Flexibility Improvement Activities Category Options 1 P a g e Ad MEDICARE
The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative 2017 Transition Year Flexibility Improvement Activities Category Options 1 P a g e Ad MEDICARE
MACRA WHAT DOES IT MEAN FOR YOUR PRACTICE?
 MACRA WHAT DOES IT MEAN FOR YOUR PRACTICE? A Presentation for ASMA and MIEC Members & Guests Copyrighted 2017, The Sage Associates, Pismo Beach, California All rights reserved. All material contained in
MACRA WHAT DOES IT MEAN FOR YOUR PRACTICE? A Presentation for ASMA and MIEC Members & Guests Copyrighted 2017, The Sage Associates, Pismo Beach, California All rights reserved. All material contained in
Getting Ready for the Post-SGR World. Presented by: Sybil R. Green, JD, RPh, MHA. West Virginia Oncology Society Spring Meeting May 5, 2016
 Getting Ready for the Post-SGR World Presented by: Sybil R. Green, JD, RPh, MHA West Virginia Oncology Society Spring Meeting May 5, 2016 CME/CE Information For Physicians: This activity has been planned
Getting Ready for the Post-SGR World Presented by: Sybil R. Green, JD, RPh, MHA West Virginia Oncology Society Spring Meeting May 5, 2016 CME/CE Information For Physicians: This activity has been planned
Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians
 Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians This document supplements the AMA s MIPS Action Plan 10 Key Steps for 2017 and provides additional
Medicare Quality Payment Program: Deep Dive FAQs for 2017 Performance Year Hospital-Employed Physicians This document supplements the AMA s MIPS Action Plan 10 Key Steps for 2017 and provides additional
Statement for the Record. American College of Physicians. Hearing before the House Energy & Commerce Subcommittee on Health
 Statement for the Record American College of Physicians Hearing before the House Energy & Commerce Subcommittee on Health A Permanent Solution to the SGR: The Time Is Now January 21-22, 2015 The American
Statement for the Record American College of Physicians Hearing before the House Energy & Commerce Subcommittee on Health A Permanent Solution to the SGR: The Time Is Now January 21-22, 2015 The American
Centers for Medicare & Medicaid Services: Innovation Center New Direction
 Centers for Medicare & Medicaid Services: Innovation Center New Direction I. Background One of the most important goals at CMS is fostering an affordable, accessible healthcare system that puts patients
Centers for Medicare & Medicaid Services: Innovation Center New Direction I. Background One of the most important goals at CMS is fostering an affordable, accessible healthcare system that puts patients
Quality Payment Program: The future of reimbursement
 Quality Payment Program: The future of reimbursement Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC NCICS CCCPC CPC-I MCS-P CPMA CMQP Executive Vice President 1 Dr. Evan Gwilliam Education Bachelor
Quality Payment Program: The future of reimbursement Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC NCICS CCCPC CPC-I MCS-P CPMA CMQP Executive Vice President 1 Dr. Evan Gwilliam Education Bachelor
Quality Payment Program October 14, 2016
 Executive Summary Department of Health and Human Services Centers for Medicare & Medicaid Services 42 CFR Parts 414 and 495 [CMS-5517-FC] RIN 0938-AS69 Medicare Program; Merit-based Incentive Payment System
Executive Summary Department of Health and Human Services Centers for Medicare & Medicaid Services 42 CFR Parts 414 and 495 [CMS-5517-FC] RIN 0938-AS69 Medicare Program; Merit-based Incentive Payment System
MACRA, Implications for Physician Agreements
 MACRA, Implications for Physician Agreements Mark C Herbers, Director, AlixPartners, LLP Chicago, IL The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) creates powerful incentives for all
MACRA, Implications for Physician Agreements Mark C Herbers, Director, AlixPartners, LLP Chicago, IL The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) creates powerful incentives for all
Maximizing Your Potential Under MIPS Oregon MACRA Playbook Conference
 Maximizing Your Potential Under MIPS Oregon MACRA Playbook Conference June 22, 2017 Michael J. Sexton, MD Catherine I. Hanson, JD COI Disclosure To assure the highest quality of CME programming, the OMA
Maximizing Your Potential Under MIPS Oregon MACRA Playbook Conference June 22, 2017 Michael J. Sexton, MD Catherine I. Hanson, JD COI Disclosure To assure the highest quality of CME programming, the OMA
Under the MACRAscope:
 Under the MACRAscope: G08: Under the MACRAscope: MIPS and EHRs Robert Tennant, MA Director, HIT Policy, MGMA Government Affairs rtennant@mgma.org Learning Objectives This session will provide you with
Under the MACRAscope: G08: Under the MACRAscope: MIPS and EHRs Robert Tennant, MA Director, HIT Policy, MGMA Government Affairs rtennant@mgma.org Learning Objectives This session will provide you with
Physician Quality Reporting System & VBPM, 2015
 Physician Quality Reporting System & VBPM, 2015 Andrew Bienstock Transformation Support Services Manager 1 Agenda 1. PQRS Penalty 2. PQRS Eligibility 3. PQRS Reporting Options 4. Value Based Payment Modifier
Physician Quality Reporting System & VBPM, 2015 Andrew Bienstock Transformation Support Services Manager 1 Agenda 1. PQRS Penalty 2. PQRS Eligibility 3. PQRS Reporting Options 4. Value Based Payment Modifier
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Objectives. Preparing for Value-Based Reimbursement 3/28/2016
 Preparing for Value-Based Reimbursement Tracy Bird, FACMPE, CPC, CPMA, CPC-I, CEMC Sr. Advisor Education and Consulting KaMMCO April 12, 2016 1 2 Objectives A look back - how did we get here Existing and
Preparing for Value-Based Reimbursement Tracy Bird, FACMPE, CPC, CPMA, CPC-I, CEMC Sr. Advisor Education and Consulting KaMMCO April 12, 2016 1 2 Objectives A look back - how did we get here Existing and
MACRA The shift to Value Based Care and Payment. Michael Munger, M.D., FAAFP
 MACRA The shift to Value Based Care and Payment Michael Munger, M.D., FAAFP Current State Silos of Care Over Utilization Volume over Value Push Towards Value and Quality 85% Medicare Payments tied to quality
MACRA The shift to Value Based Care and Payment Michael Munger, M.D., FAAFP Current State Silos of Care Over Utilization Volume over Value Push Towards Value and Quality 85% Medicare Payments tied to quality
Understanding PQRS and the Value-Based Modifier: CMS Plan to Achieve High Value Care through Transforming Payment Systems
 Understanding PQRS and the Value-Based Modifier: CMS Plan to Achieve High Value Care through Transforming Payment Systems Dr. Ashby Wolfe, Chief Medical Officer Centers for Medicare and Medicaid Services,
Understanding PQRS and the Value-Based Modifier: CMS Plan to Achieve High Value Care through Transforming Payment Systems Dr. Ashby Wolfe, Chief Medical Officer Centers for Medicare and Medicaid Services,
Alternative Payment Model Environment Implications for Specialty Providers and their Partners
 Alternative Payment Model Environment Implications for Specialty Providers and their Partners Bob Dowling MD Vice President Medical Affairs and Policy ION Solutions/IntrinsiQ Specialty Solutions June 20,
Alternative Payment Model Environment Implications for Specialty Providers and their Partners Bob Dowling MD Vice President Medical Affairs and Policy ION Solutions/IntrinsiQ Specialty Solutions June 20,
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Legislative Update Wipfli CAH/RHC Conference
 Legislative Update Wipfli CAH/RHC Conference Nathan Baugh Director, Government Relations (202) 543-0348 Baughn@capitolassociates.org www.narhc.org Overview NARHC Washington Update MACRA Overview and Update
Legislative Update Wipfli CAH/RHC Conference Nathan Baugh Director, Government Relations (202) 543-0348 Baughn@capitolassociates.org www.narhc.org Overview NARHC Washington Update MACRA Overview and Update
Statement for the Record. American College of Physicians. U.S. House Committee on Ways and Means Subcommittee on Health
 Statement for the Record American College of Physicians U.S. House Committee on Ways and Means Subcommittee on Health Hearing on Implementation of MACRA s Physician Payment Policies March 21, 2018 The
Statement for the Record American College of Physicians U.S. House Committee on Ways and Means Subcommittee on Health Hearing on Implementation of MACRA s Physician Payment Policies March 21, 2018 The
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM. Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017
 ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
INTRODUCTION TO POPULATION HEALTH. Kathy Whitmire, Vice President
 INTRODUCTION TO POPULATION HEALTH Kathy Whitmire, Vice President 1 Learning Objectives 1. Provide an overall framework for population health 2. Allow clinics to understand why population health is important
INTRODUCTION TO POPULATION HEALTH Kathy Whitmire, Vice President 1 Learning Objectives 1. Provide an overall framework for population health 2. Allow clinics to understand why population health is important
Medicare Part B Updates and Changes 2016/2017. Presented by Tammy Ewers, CPC Education and Outreach Representative
 Medicare Part B Updates and Changes 2016/2017 Presented by Tammy Ewers, CPC Education and Outreach Representative DISCLAIMER This information release is the property of Noridian Healthcare Solutions, LLC.
Medicare Part B Updates and Changes 2016/2017 Presented by Tammy Ewers, CPC Education and Outreach Representative DISCLAIMER This information release is the property of Noridian Healthcare Solutions, LLC.
June 27, Dear Secretary Burwell and Acting Administrator Slavitt,
 June 27, 2016 The Honorable Sylvia Matthews Burwell Secretary, U.S. Department of Health and Human Services 200 Independence Avenue, SW Washington, D.C. 20201 Mr. Andy Slavitt Acting Administrator, Centers
June 27, 2016 The Honorable Sylvia Matthews Burwell Secretary, U.S. Department of Health and Human Services 200 Independence Avenue, SW Washington, D.C. 20201 Mr. Andy Slavitt Acting Administrator, Centers
MIPS Program: 2017 Advancing Care Information Category (formerly known as Meaningful Use) Proposed Rule Guide
 Proposed Rule Guide") MIPS Program: 2017 Advancing Care Information Category (formerly known as Meaningful Use) Proposed Rule Guide On April 27, 2016, CMS released a proposed rule on the Quality Payment Program, which includes
MIPS Program: 2017 Advancing Care Information Category (formerly known as Meaningful Use) Proposed Rule Guide On April 27, 2016, CMS released a proposed rule on the Quality Payment Program, which includes
MACRA FLEXIBILITY & THE MACRA FINAL RULE. Compliance & Opportunity for Your Practice
 MACRA FLEXIBILITY & THE MACRA FINAL RULE Compliance & Opportunity for Your Practice CONTENTS Overview... 5 What s new... 5 Advancing Care Information... 8 Major changes... 9 Proposed rule vs. final rule
MACRA FLEXIBILITY & THE MACRA FINAL RULE Compliance & Opportunity for Your Practice CONTENTS Overview... 5 What s new... 5 Advancing Care Information... 8 Major changes... 9 Proposed rule vs. final rule
VALUE BASED ORTHOPEDIC CARE
 VALUE BASED ORTHOPEDIC CARE Becker's 14th Annual Spine, Orthopedic and Pain Management- Driven ASC Conference + The Future of Spine June 9-11, 2016 Swissotel, Chicago, IL LES JEBSON Administrator, Adjunct
VALUE BASED ORTHOPEDIC CARE Becker's 14th Annual Spine, Orthopedic and Pain Management- Driven ASC Conference + The Future of Spine June 9-11, 2016 Swissotel, Chicago, IL LES JEBSON Administrator, Adjunct
2016 MEANINGFUL USE AND 2017 CHANGES to the Medicare EHR Incentive Program for EPs. September 27, 2016 Kathy Wild, Lisa Sagwitz, and Joe Pinto
 2016 MEANINGFUL USE AND 2017 CHANGES to the Medicare EHR Incentive Program for EPs September 27, 2016 Kathy Wild, Lisa Sagwitz, and Joe Pinto Agenda Meaningful Use (MU) in 2016 MACRA and MIPS (high level
2016 MEANINGFUL USE AND 2017 CHANGES to the Medicare EHR Incentive Program for EPs September 27, 2016 Kathy Wild, Lisa Sagwitz, and Joe Pinto Agenda Meaningful Use (MU) in 2016 MACRA and MIPS (high level
Virtual Group Participation Overview Fact Sheet
 Virtual Group Participation Overview Fact Sheet Starting on January 1, 2017, eligible clinicians began participation in the Quality Payment Program in one of two ways: Merit-based Incentive Payment System
Virtual Group Participation Overview Fact Sheet Starting on January 1, 2017, eligible clinicians began participation in the Quality Payment Program in one of two ways: Merit-based Incentive Payment System
VALUE PAYMENT: A NEW REIMBURSEMENT SYSTEM USING QUALITY AS CURRENCY
 VALUE PAYMENT: A NEW REIMBURSEMENT SYSTEM USING QUALITY AS CURRENCY Danielle Hansen, DO, MS (Med Ed), MHSA Healthcare Quality/ Value Challenge 1 Value-Based Programs Supports the IHI Triple Aim: 1. Better
VALUE PAYMENT: A NEW REIMBURSEMENT SYSTEM USING QUALITY AS CURRENCY Danielle Hansen, DO, MS (Med Ed), MHSA Healthcare Quality/ Value Challenge 1 Value-Based Programs Supports the IHI Triple Aim: 1. Better
MACRA Open Call December 5 th, 2016
 MACRA Open Call December 5 th, 2016 Leila Volinsky, MHA, MSN, RN Quality Reporting Program Administrator This material was prepared by the New England QIN-QIO, the Medicare Quality Innovation Network-Quality
MACRA Open Call December 5 th, 2016 Leila Volinsky, MHA, MSN, RN Quality Reporting Program Administrator This material was prepared by the New England QIN-QIO, the Medicare Quality Innovation Network-Quality
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
UPDATED WITH FINAL RULE NOVEMBER 11, Preparing for Success With MACRA
 UPDATED WITH FINAL RULE NOVEMBER 11, 2016 G A M E C H A N G E R : Preparing for Success With MACRA Overview The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) dramatically impacts the way
UPDATED WITH FINAL RULE NOVEMBER 11, 2016 G A M E C H A N G E R : Preparing for Success With MACRA Overview The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) dramatically impacts the way
MACRA and MIPS. How Medicare Meaningful Use and PQRS are Changing
 MACRA and MIPS How Medicare Meaningful Use and PQRS are Changing Link to recorded session: https://attendee.gotowebinar.com/recording/1305549490878052097 Presenting Today: Molly Goodhart Joined Quatris
MACRA and MIPS How Medicare Meaningful Use and PQRS are Changing Link to recorded session: https://attendee.gotowebinar.com/recording/1305549490878052097 Presenting Today: Molly Goodhart Joined Quatris
MIPS (Merit-based Incentive Payment System) Clinical Practice Improvement Activities
 Clinical Practice Improvement Activities") MIPS (Merit-based Incentive Payment System) Clinical Practice Improvement Activities Today we will cover: 2 General review of the Quality Payment Programs as per the final rule. Who is Eligible/Exceptions
MIPS (Merit-based Incentive Payment System) Clinical Practice Improvement Activities Today we will cover: 2 General review of the Quality Payment Programs as per the final rule. Who is Eligible/Exceptions
Describe the process for implementing an OP CDI program
 1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
Highlights of the 2018 Medicare Physician Fee Schedule (MPFS) Final Rule
 Final Rule") Highlights of the 2018 Medicare Physician Fee Schedule (MPFS) Final Rule Physician Payment Update & Misvalued Codes Target The update to payments under the PFS in 2018 will be +0.31 percent. This reflects
Highlights of the 2018 Medicare Physician Fee Schedule (MPFS) Final Rule Physician Payment Update & Misvalued Codes Target The update to payments under the PFS in 2018 will be +0.31 percent. This reflects
Stage 3 and ACI s Relationship to Medicaid MU Massachusetts Medicaid EHR Incentive Program
 Stage 3 and ACI s Relationship to Medicaid MU Massachusetts Medicaid EHR Incentive Program September 19 & 20, 2017 Today s presenters: Brendan Gallagher Thomas Bennett Agenda Stage 3 Meaningful Use (MU)
Stage 3 and ACI s Relationship to Medicaid MU Massachusetts Medicaid EHR Incentive Program September 19 & 20, 2017 Today s presenters: Brendan Gallagher Thomas Bennett Agenda Stage 3 Meaningful Use (MU)
Surviving and thriving in the time of MACRA: What you need to know now to optimize your future.
 Surviving and thriving in the time of MACRA: What you need to know now to optimize your future. Risk Adjustment in the Resource Use Performance Measures 2017 SGIM Annual Meeting Thursday, April 20, 2017
Surviving and thriving in the time of MACRA: What you need to know now to optimize your future. Risk Adjustment in the Resource Use Performance Measures 2017 SGIM Annual Meeting Thursday, April 20, 2017
CHIA PRESENTATION HANDOUT
 5055 E. McKinley Ave, Fresno CA 95407 Tel: (559) 251 5038 Info@ CHIA PRESENTATION HANDOUT 2018 CHIA CONVENTION & EXHIBIT SAN DIEGO, CA MACRA and HIM Doing the Impossible Presented by: Moshe Starkman Presented
5055 E. McKinley Ave, Fresno CA 95407 Tel: (559) 251 5038 Info@ CHIA PRESENTATION HANDOUT 2018 CHIA CONVENTION & EXHIBIT SAN DIEGO, CA MACRA and HIM Doing the Impossible Presented by: Moshe Starkman Presented
2017 Physician Fee Schedule Impact on Medicare ACOs REGULATORY UPDATES
 2017 Physician Fee Schedule Impact on Medicare ACOs REGULATORY UPDATES 2017 Physician Fee Schedule Impact on Medicare ACOs 1. Allowing ACO Participants to report PQRS separately from ACO 2. ACO Quality
2017 Physician Fee Schedule Impact on Medicare ACOs REGULATORY UPDATES 2017 Physician Fee Schedule Impact on Medicare ACOs 1. Allowing ACO Participants to report PQRS separately from ACO 2. ACO Quality
Value-Based Reimbursements are Here: Are you Ready?
 Value-Based Reimbursements are Here: Are you Ready? White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO Published by Becker s Hospital Review April 2016 White Paper Value-Based Reimbursements are
Value-Based Reimbursements are Here: Are you Ready? White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO Published by Becker s Hospital Review April 2016 White Paper Value-Based Reimbursements are
March 28, Dear Dr. Yong:
 March 28, 2018 Pierre Yong, MD Director Quality Measurement and Value-Based Incentives Group Centers for Medicare and Medicaid Services 7500 Security Boulevard Baltimore, MD 21244 Dear Dr. Yong: The American
March 28, 2018 Pierre Yong, MD Director Quality Measurement and Value-Based Incentives Group Centers for Medicare and Medicaid Services 7500 Security Boulevard Baltimore, MD 21244 Dear Dr. Yong: The American