Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC
|
|
|
- Teresa Franklin
- 5 years ago
- Views:
Transcription






1 Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC Record the frequency that the resident was restrained by any of the listed devices at any time during the day/ night over the lookback period 1


2 Use not prohibited in nursing homes. o Cannot be imposed for discipline or convenience o Must be required to treat resident s medical symptoms Must assess resident needs and medical symptoms before using physical restraints Use of physical restraints should be the exception, not the rule. Play a limited role in medical care. Physical restraints limit mobility. Physical restraints increase risk of adverse outcomes. o Functional decline o Agitation o Diminished sense of dignity o Depressed mood o Pressure ulcers 2


3 Cognitively-impaired residents at higher risk due to physical restraints: o Entrapment o Injury o Death Significant risk of restraint-related injury or death Manual method or physical or mechanical device, material, or equipment Attached or adjacent to the resident s body that the individual cannot remove easily Which restricts freedom of movement or normal access to one s body 3


4 Removes easily o Can be removed intentionally by the resident in the same manner as it was applied by the staff o Consider the resident s physical condition and ability to accomplish his or her objective. Freedom of movement o Any change in place or position for the body, or any part of the body, that the person is physically able to control or access Leg restraints Arm restraints Hand mitts Soft ties/vests Lap cushions Lap trays Position change alarms Facility practices o Side rails o Velcro on sheets o Devices used with chairs (tray, table, bar, or belt) o Placement of chair or bed 4


5 Review resident s medical record. o Physician s orders o Nurses notes o Nursing assistant documentation Consult the nursing staff across all shifts. o Resident s cognitive status and limitations o Physical status and limitations Observe the resident. o Determine the effect on the resident s normal function. o Do not focus on type, intent, or reason for use. Evaluate whether the resident can easily and voluntarily remove the device. Determine if the device restricts freedom of movement or access to the body. Determine if device meets criteria of the definition of a physical restraint for purpose of MDS

6 Do not focus on the intent or reason for using the device, material, or equipment. Focus only on the effect of the device on the resident. Assess each resident individually. Exclude devices typically used for provision of care. The complete definition of a restraint must be met. Any device that meets the definition of a physical restraint must have: o Physician documentation of a medical symptom that supports the use of the restraint o Physician s order for the type of physical restraint and parameters of use o Care plan and a process in place for systematic and gradual physical restraint reduction (and/ or elimination, if possible), as appropriate 6

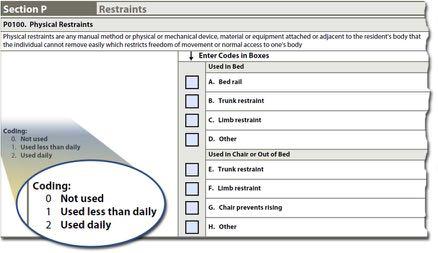
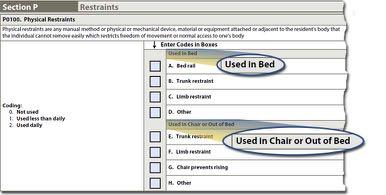
7 When coding this section, do not consider as a restraint a locked/secured unit or building in which the resident has the freedom to move about the locked/secured unit or building. Additional guidance regarding locked/secured units is provided in the section Considerations Involving Secured/Locked Areas of F603 in Appendix PP of the State Operations Manual. How often the physical restraint was used Location of the physical restraint o In bed o In a chair or out of bed Category of the physical restraint o Bed rails or chairs that prevent rising o Trunk or limb restraint Code all physical restraints used in the look-back period. 7
8 8


9 Bed rails Trunk restraints Limb restraints Chair that prevents rising Other o Any device that does not fit listed categories o Meets the criteria of physical restraints o Should be care-planned and monitored Include any type of chair with a locked lap board, that places the resident in a recumbent position that restricts rising, or a chairs that are soft and low to the floor, chairs that have a cushion placed in the seat that prohibit the resident from rising, geriatric chairs, and enclosed-frame wheeled walkers. 9

10 Health-related Quality of Life An alarm is any physical or electronic device that monitors resident movement and alerts the staff, by either audible or inaudible means, when movement is detected, and may include bed, chair and floor sensor pads, cords that clip to the resident s clothing, motion sensors, door alarms, or elopement/wandering devices. While often used as an intervention in a resident s fall prevention strategy, the efficacy of alarms to prevent falls has not been proven; therefore, alarm use must not be the primary or sole intervention in the plan. 19 The use of an alarm as part of the resident s plan of care does not eliminate the need for adequate supervision, nor does the alarm replace individualized, person-centered care planning. Adverse consequences of alarm use include, but are not limited to, fear, anxiety, or agitation related to the alarm sound; decreased mobility; sleep disturbances; and infringement on freedom of movement, dignity, and privacy

11 Individualized, person-centered care planning surrounding the resident s use of an alarm is important to the resident s overall well-being. When the use of an alarm is considered as an intervention in the resident s safety strategy, use must be based on the assessment of the resident and monitored for efficacy on an ongoing basis, including the assessment of unintended consequences of the alarm use and alternative interventions. There are times when the use of an alarm may meet the definition of a restraint, as the alarm may restrict the resident s freedom of movement and may not be easily removed by the resident. 21 When an alarm is used as an intervention in the resident s safety strategy, the effect the alarm has on the resident must be evaluated individually for that resident. 11

12 1. Review the resident s medical record (e.g., physician orders, nurses notes, nursing assistant documentation) to determine if alarms were used during the 7-day look-back period. 2. Consult the nursing staff to determine the resident s cognitive and physical status/limitations. 3. Evaluate whether the alarm affects the resident s freedom of movement when the alarm/device is in place. For example, does the resident avoid standing up or repositioning himself/herself due to fear of setting off the alarm? 23 Identify all alarms that were used at any time (day or night) during the 7-day look-back period. After determining whether or not an item listed in P0200 was used during the 7-day look-back period, code the frequency of use: Code 0. Not used: if the device was not used during the 7- day look-back period. Code 1. Used less than daily: if the device was used less than daily. Code 2. Used daily: if the device was used on a daily basis during the look-back period

13 Bed alarm includes devices such as a sensor pad placed on the bed or a device that clips to the resident s clothing. Chair alarm includes devices such as a sensor pad placed on the chair or wheelchair or a device that clips to the resident s clothing. Floor mat alarm includes devices such as a sensor pad placed on the floor beside the bed. Motion sensor alarm includes infrared beam motion detectors. 25 Wander/elopement alarm includes devices such as bracelets, pins/buttons worn on the resident s clothing, sensors in shoes, or building/unit exit sensors worn/attached to the resident that alert the staff when the resident nears or exits an area or building. This includes devices that are attached to the resident s assistive device (e.g., walker, wheelchair, cane) or other belongings. Other alarm includes devices such as alarms on the resident s bathroom and/or bedroom door, toilet seat alarms, or seatbelt alarms

14 Code any type of alarm, audible or inaudible, used during the look-back period in this section. If an alarm meets the criteria as a restraint, code the alarm use in both P0100. Physical Restraints, and P0200. Alarms. Motion sensors and wrist sensors worn by the resident to track the resident s sleep patterns should not be coded in this section. Wandering is random or repetitive locomotion. This movement may be goal-directed (e.g., the resident appears to be searching for something such as an exit) or may be non-goal directed or aimless. Nongoal directed wandering requires a response in a manner that addresses both safety issues and an evaluation to identify root causes to the degree possible. 27 While wander, door, or building alarms can help monitor a resident s activities, staff must be vigilant in order to respond to them in a timely manner. Alarms do not replace necessary supervision Wander/elopement alarm includes devices such as bracelets, pins/buttons worn on the resident s clothing, sensors in shoes, or building/unit exit sensors worn by/attached to the resident that activate an alarm and/or alert the staff when the resident nears or exits a specific area or the building. This includes devices that are attached to the resident s assistive device (e.g., walker, wheelchair, cane) or other belongings

15 Do not code a universal building exit alarm applied to an exit door that is intended to alert staff when anyone (including visitors or staff members) exits the door. When determining whether the use of an alarm also meets the criteria of a restraint, refer to the section Determination of the Use of Position Change Alarms as Restraints of F604 in Appendix PP of the State Operations Manual. Using bed rails that keep a resident from voluntarily getting out of bed; Placing a chair or bed close enough to a wall that the resident is prevented from rising out of the chair or voluntarily getting out of bed; Placing a resident on a concave mattress so that the resident cannot independently get out of bed; Tucking in a sheet tightly so that the resident cannot get out of bed, or fastening fabric or clothing so that a resident s freedom of movement is restricted; Placing a resident in a chair, such as a beanbag or recliner, that prevents a resident from rising independently; jb
16 Slide 30 jb1 made into 2 slides so that could be more legible - we tend not to use a font less than 22 Jane Belt, 7/17/2017

17 Using devices in conjunction with a chair, such as trays, tables, cushions, bars or belts, that the resident cannot remove and prevents the resident from rising; Applying leg or arm restraints, hand mitts, soft ties or vests that the resident cannot remove; Holding down a resident in response to a behavioral symptom or during the provision of care if the resident is resistive or refusing the care; Placing a resident in an enclosed framed wheeled walker, in which the resident cannot open the front gate or if the device has been altered to prevent the resident from exiting the device; and Using a position change alarm to monitor resident movement, and the resident is afraid to move to avoid setting off the alarm 31 Position change alarms are any physical or electronic device that monitors resident movement and alerts the staff when movement is detected. Types of position change alarms include chair and bed sensor pads, bedside alarmed mats, alarms clipped to a resident s clothing, seatbelt alarms, and infrared beam motion detectors. Position change alarms do not include alarms intended to monitor for unsafe wandering such as door or elevator alarms


18 While position change alarms may be implemented to monitor a resident s movements, for some residents, the use of position change alarms that are audible to the resident(s) may have the unintended consequence of inhibiting freedom of movement. For example, a resident may be afraid to move to avoid setting off the alarm and creating noise that is a nuisance to the resident(s) and staff, or is embarrassing to the resident. For this resident, a position change alarm may have the potential effect of a physical restraint. 33 Examples of negative potential or actual outcomes which may result from the use of position change alarms as a physical restraint, include: Loss of dignity; Decreased mobility; Bowel and bladder incontinence; Sleep disturbances due to the sound of the alarm or because the resident is afraid to move in bed thereby setting off the alarm; and Confusion, fear, agitation, anxiety, or irritation in response to the sound of the alarm as residents may mistake the alarm as a warning or as something they need to get away from

19 The regulation limits the use of any physical restraint to circumstances in which the resident has medical symptoms that warrant the use of restraints. There must be documentation identifying the medical symptom being treated and an order for the use of the specific type of restraint. However, the practitioner s order alone (without supporting clinical documentation) is not sufficient to warrant the use of the restraint. The facility is accountable for the process to meet the minimum requirements of the regulation including appropriate assessment, care planning by the interdisciplinary team, and documentation of the medical symptoms and use of the physical restraint for the least amount of time possible and provide ongoing re-evaluation. The resident or resident representative may request the use of a physical restraint; however, the nursing home is responsible for evaluating the appropriateness of the request, and must determine if the resident has a medical symptom that must be treated and must include the practitioner in the review and discussion. If there are no medical symptoms identified that require treatment, the use of the restraint is prohibited. Also, a resident, or the resident representative, has the right to refuse treatment; however, he/she does not have the right to demand a restraint be used when it is not necessary to treat a medical symptom. 18


20 Facilities are responsible for knowing the effects devices have on its residents. If a device has a restraining effect on a resident, and is not administered to treat a medical symptom, the device is acting as a physical restraint. The restraining effects to the resident may have been caused intentionally or unintentionally by staff, and would indicate an action of discipline or convenience. In the case of an unintentional physical restraint, the facility did not intend to restrain a resident, but a device is being used that has that same effect, and is not being used to treat a medical symptom. These effects may result in convenience for the staff, as the resident may require less effort than previously required. If a resident is identified with a physical restraint, the facility must be able to provide evidence that ensures: The resident's medical symptom that requires the use of a physical restraint has been identified; A practitioner s order is in place for the use of the specific physical restraint based upon the identified medical symptom; 19


21 Interventions, including less restrictive alternatives were attempted to treat the medical symptom but were ineffective; The resident/representative was informed of potential risks and benefits of all options under consideration including using a restraint, not using a restraint, and alternatives to restraint use; The length of time the restraint is anticipated to be used to treat the medical symptom, the identification of who may apply the restraint, where and how the restraint is to be applied and used, the time and frequency the restraint should be released, and who may determine when the medical symptom has resolved in order to discontinue use of the restraint; The type of specific direct monitoring and supervision provided during the use of the restraint, including documentation of the monitoring; The identification of how the resident may request staff assistance and how needs will be met during use of the restraint, such as for re-positioning, hydration, meals, using the bathroom and hygiene; 20

![0, Chapter 3, Section P-Restraints for further guidance and 42 CFR 483.25(d) [F689] for concerns related to ensuring the resident receives adequate supervision to prevent accidents).](/docs-images/90/102020450/images/22-1.jpg "NOTE: If a resident is recently admitted to the facility and a restraint was used in a previous health care setting, the facility must still conduct an assessment to determine the existence of")
22 The resident s record includes ongoing reevaluation for the need for a restraint and is effective in treating the medical symptom; and The development and implementation of interventions to prevent and address any risks related to the use of the restraint (See also the Long-Term Care Facility Resident Assessment Instrument User s Manual, Version 3.0, Chapter 3, Section P-Restraints for further guidance and 42 CFR (d) [F689] for concerns related to ensuring the resident receives adequate supervision to prevent accidents). NOTE: If a resident is recently admitted to the facility and a restraint was used in a previous health care setting, the facility must still conduct an assessment to determine the existence of medical symptoms that warrant the continued use of the restraint. NOTE: The resident, or resident representative (if applicable), has the right to refuse the use of a restraint and may withdraw consent to use of the restraint at any time. If so, the refusal must be documented in the resident s record. The facility is expected to assess the resident and determine how resident s needs will be met if the resident refuses/declines treatment. NOTE: Falls do not constitute self-injurious behavior or a medical symptom that warrants the use of a physical restraint. Although restraints have been traditionally used as a falls prevention 21

.")
23 NOTE: Falls do not constitute self-injurious behavior or a medical symptom that warrants the use of a physical restraint. Although restraints have been traditionally used as a falls prevention approach, they have major, serious drawbacks and can contribute to serious injuries. There is no evidence that the use of physical restraints, including, but not limited to, bed rails and position change alarms, will prevent or reduce falls. Additionally, falls that occur while a person is physically restrained often result in more severe injuries (e.g., strangulation, entrapment). A facility must not impose physical restraints for purposes of discipline or convenience. The facility is prohibited from obtaining permission from the resident, or resident representative, for the use of restraints when the restraint is not necessary to treat the resident s medical symptoms. Anecdotally, it has been reported that staff will inform a resident, or the resident representative, that a restraint will be beneficial to the resident to prevent a fall or to safeguard the resident who may be wandering into other resident s rooms. However, in these instances, the surveyor should consider whether the restraint was used for the sake of staff convenience. 22


24 Staff state that a resident was placed in a restraint because staff are too busy to monitor the resident, and their workload includes too many residents to provide monitoring; Staff believe that the resident does not exercise good judgment, including that he/she forgets about his/her physical limitations in standing, walking, or using the bathroom alone and will not wait for staff assistance; Staff state that family have requested that the resident be restrained, as they are concerned about the resident falling especially during high activity times, such as during meals, when the staff are busy with other residents; When a resident is confused and becomes combative when care is provided and staff hold the resident s arms and legs down to complete the care (NOTE: This example differs from an emergency situation where staff briefly hold a resident for the sole purpose of providing necessary immediate medical care ordered by a practitioner). Some facilities have identified that a situation occurred in which the resident(s) is in imminent danger and there was fear for the safety and wellbeing of the resident(s) due to violent behavior, such as physically attacking others. In these situations, the order from the practitioner and supporting documentation for the use of a restraint must be obtained either during the application of the restraint, or immediately after the restraint has been applied. The failure to immediately obtain an order is viewed as the application of restraint without an order and supporting documentation. 23


25 Determine that a physical restraint is a measure of last resort to protect the safety of the resident or others; Provide ongoing direct monitoring and assessment of the resident s condition during use of the restraint; Provide assessment by the staff and practitioner to address other interventions that may address the symptoms or cause of the situation (e.g., identification of an infection process or delirium, presence of pain); Ensure that the resident and other residents are protected until the resident s behavioral symptoms have subsided, or until the resident is transferred to another setting; Discontinue the use of the restraint as soon as the imminent danger ends; and Immediately notify the resident representative of the symptoms and temporary intervention implemented. Documentation must reflect what the resident was doing and what happened that presented the imminent danger, interventions that were attempted, response to those interventions, whether the resident was transferred to another setting for evaluation, whether the use of a physical restraint was ordered by the practitioner, and the medical symptom(s) and cause(s) that were identified. 24

26 Facilities must use a person-centered approach when determining the use of bed rails, which would include conducting a comprehensive assessment, and identifying the medical symptom being treated by using bed rails. Bed rails may have the effect of restraining one individual but not another, depending on the individual resident s conditions and circumstances. To determine if a bed rail is being used as a restraint, the resident must be able to easily and voluntarily get in and out of bed when the equipment is in use. If the resident cannot easily and voluntarily release the bed rails, the use of the bed rails may be considered a restraint. 25

27 26
SECTION P: RESTRAINTS
 SECTION P: RESTRAINTS Intent: The intent of this section is to record the frequency over the 7-day look-back period that the resident was restrained by any of the listed devices at any time during the
SECTION P: RESTRAINTS Intent: The intent of this section is to record the frequency over the 7-day look-back period that the resident was restrained by any of the listed devices at any time during the
CMS RAI MANUAL ERRATA DOCUMENT
 CMS RAI MANUAL ERRATA DOCUMENT SECTION I UTI S In Chapter 3, page I-9, under Coding Tips in I: Active Diagnoses in the Last 7 Days, a third bullet has been added: If the diagnosis of UTI was made prior
CMS RAI MANUAL ERRATA DOCUMENT SECTION I UTI S In Chapter 3, page I-9, under Coding Tips in I: Active Diagnoses in the Last 7 Days, a third bullet has been added: If the diagnosis of UTI was made prior
The New Survey Process for the NAC. Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC
 The New Survey Process for the NAC Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC Faculty Disclosure I have no financial relationships to disclose I have no conflicts of interests to disclose I will not promote
The New Survey Process for the NAC Carol Maher, RN-BC, RAC-CT, RAC-MT, CPC Faculty Disclosure I have no financial relationships to disclose I have no conflicts of interests to disclose I will not promote
Center for Clinical Standards and Quality/Survey & Certification Group
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop C2-21-16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop C2-21-16 Baltimore, Maryland 21244-1850 Center for Clinical Standards and Quality/Survey
We use many of them. The devices are part of our restraint policy. See below
 Do you utilize body pillow, beveled mattresses, moxi mattresses, rolled blankets, swim noodles for positioning or bed demarcation? Do you have a comprehensive device assessment? If so, would you please
Do you utilize body pillow, beveled mattresses, moxi mattresses, rolled blankets, swim noodles for positioning or bed demarcation? Do you have a comprehensive device assessment? If so, would you please
Restraint Update 2016
 Restraint Update 2016 For questions contact: Weddy Balmaceda, MSN, RN-BC, CCRN, CCDS Professional Development Ext. 5241 Source: RBMC policy and procedures Objectives Review types of restraints Review RBMC
Restraint Update 2016 For questions contact: Weddy Balmaceda, MSN, RN-BC, CCRN, CCDS Professional Development Ext. 5241 Source: RBMC policy and procedures Objectives Review types of restraints Review RBMC
RESIDENT CARE AND SERVICES MANUAL SECTION: RESIDENT SAFETY INDEX I.D.: E-25. APPROVED BY: REVISED DATE: April 30, 2010
 SUBJECT: RESTRAINTS PAGE: 1 OF 6 STANDARD: 1. The decision to use restraints is based on the principle that least restraint can only be considered after the interdisciplinary team had tried alternatives
SUBJECT: RESTRAINTS PAGE: 1 OF 6 STANDARD: 1. The decision to use restraints is based on the principle that least restraint can only be considered after the interdisciplinary team had tried alternatives
The policy applies to all SHS employees involved in direct patient care and medical staff.
 Restraints Use of Violent - System Introduction Restraints, Use of Violent System Introduction SCOPE The policy applies to all SHS employees involved in direct patient care and medical staff. Implementation
Restraints Use of Violent - System Introduction Restraints, Use of Violent System Introduction SCOPE The policy applies to all SHS employees involved in direct patient care and medical staff. Implementation
Resident Rights in Nursing Facilities
 Your Guide to Resident Rights in Nursing Facilities 1-800-499-0229 1 Table of Contents The Ombudsman Advocate...3 You Take Your Rights with You...4 Federal Regulations Protect You...5 Medical Assessment
Your Guide to Resident Rights in Nursing Facilities 1-800-499-0229 1 Table of Contents The Ombudsman Advocate...3 You Take Your Rights with You...4 Federal Regulations Protect You...5 Medical Assessment
Requirements for Successful Completion
 Faculty Disclosure I have no financial relationships to disclose I have no conflicts of interests to disclose I will not promote any commercial products or services 2 Requirements for Successful Completion
Faculty Disclosure I have no financial relationships to disclose I have no conflicts of interests to disclose I will not promote any commercial products or services 2 Requirements for Successful Completion
Appendix E: Minimizing Restraining Staff Training Presentation. Least Restraint, Last Resort
 Appendix E: Minimizing Restraining Staff Training Presentation Least Restraint, Last Resort Audience: Registered Staff Release Date: December 3, 2010 Adapted from educational materials provided by Belmont
Appendix E: Minimizing Restraining Staff Training Presentation Least Restraint, Last Resort Audience: Registered Staff Release Date: December 3, 2010 Adapted from educational materials provided by Belmont
Site: Lovelace Health System Title: PATIENT CARE - Restraints Approved Date: 08/28/2015 Effective Date: TBD
 Approved Date: 08/28/2015 Effective Date: TBD 08/01/2018 Document Number P-NS-1063.6 Document Type: Policy Page 1 of 11 1. Policy: All patients have the right to be free from physical or mental abuse,
Approved Date: 08/28/2015 Effective Date: TBD 08/01/2018 Document Number P-NS-1063.6 Document Type: Policy Page 1 of 11 1. Policy: All patients have the right to be free from physical or mental abuse,
Restraints and Seclusion Use Training
 Restraints and Seclusion Use Training Table of Content TOPIC PAGE NUMBER OBJECTIVES 2 WHAT ARE RESTRAINTS? 3 INTRODUCTION 4 WHAT IS A RESTRAINT? 6 A RESTRAINT FREE ENVIRONMENT 8 THE MOST COMMON REASONS
Restraints and Seclusion Use Training Table of Content TOPIC PAGE NUMBER OBJECTIVES 2 WHAT ARE RESTRAINTS? 3 INTRODUCTION 4 WHAT IS A RESTRAINT? 6 A RESTRAINT FREE ENVIRONMENT 8 THE MOST COMMON REASONS
Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care
 Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care Page 594 Prepared by Cathy Lieblich, Director of Network Relations, Pioneer Network G. Benefits of Final Rule: This
Notes from CMS Final Rule Document Pertinent to Culture Change and Person-directed Care Page 594 Prepared by Cathy Lieblich, Director of Network Relations, Pioneer Network G. Benefits of Final Rule: This
Restraint Use, Regulations and Safe Practice Script
 Restraint Use, Regulations and Safe Practice Script Note: this script may vary slightly from the recording Segment 1 Slide 2 In this segment, we will discuss: Definition of Restraint Other Important Terms
Restraint Use, Regulations and Safe Practice Script Note: this script may vary slightly from the recording Segment 1 Slide 2 In this segment, we will discuss: Definition of Restraint Other Important Terms
VETERANS HEALTH ADMINISTRATION Use of Physical Restraint for the Veteran at Risk of Falling/Fall-Related Injury Policy and Procedure Template
 VETERANS HEALTH ADMINISTRATION Use of Physical Restraint for the Veteran at Risk of Falling/Fall-Related Injury Policy and Procedure Template PURPOSE: The Veterans Health Administration (VHA) provides
VETERANS HEALTH ADMINISTRATION Use of Physical Restraint for the Veteran at Risk of Falling/Fall-Related Injury Policy and Procedure Template PURPOSE: The Veterans Health Administration (VHA) provides
Implementing a Restraint Free Policy. Esther Vance NSW Falls Injury Prevention Network Prince of Wales Medical Research Institute March 2008
 Implementing a Restraint Free Policy Esther Vance NSW Falls Injury Prevention Network Prince of Wales Medical Research Institute March 2008 Restraint Definition anything that limits an individual s voluntary
Implementing a Restraint Free Policy Esther Vance NSW Falls Injury Prevention Network Prince of Wales Medical Research Institute March 2008 Restraint Definition anything that limits an individual s voluntary
Observations for all areas: What type of supervision is provided to the resident and by whom? How are care-planned interventions implemented?
 Use this pathway for a resident who requires supervision and/or assistive devices to prevent accidents and to ensure the environment is free from accident hazards as is possible. Review the Following in
Use this pathway for a resident who requires supervision and/or assistive devices to prevent accidents and to ensure the environment is free from accident hazards as is possible. Review the Following in
Chapter 11. Preventing Falls. Copyright 2019 by Elsevier, Inc. All rights reserved.
 Chapter 11 Preventing Falls Copyright 2019 by Elsevier, Inc. All rights reserved. Lesson 11.1 Define the key terms and key abbreviations in this chapter. Identify the causes and risk factors for falls.
Chapter 11 Preventing Falls Copyright 2019 by Elsevier, Inc. All rights reserved. Lesson 11.1 Define the key terms and key abbreviations in this chapter. Identify the causes and risk factors for falls.
9/17/2015. Bed Rail Safety A Clinical Process Guideline. Background. Federal Nursing Home Reform Act
 Bed Rail Safety A Clinical Process Guideline Laura Funsch, RN, BSN, MS, Director of Regulatory Strategy Background Safety hazards related to bed rail use have been realized since 1990. Michigan s initial
Bed Rail Safety A Clinical Process Guideline Laura Funsch, RN, BSN, MS, Director of Regulatory Strategy Background Safety hazards related to bed rail use have been realized since 1990. Michigan s initial
Bed Rail Safety A Clinical Process Guideline. Laura Funsch, RN, BSN, MS, Director of Regulatory Strategy
 Bed Rail Safety A Clinical Process Guideline Laura Funsch, RN, BSN, MS, Director of Regulatory Strategy Background Safety hazards related to bed rail use have been realized since 1990. Michigan s initial
Bed Rail Safety A Clinical Process Guideline Laura Funsch, RN, BSN, MS, Director of Regulatory Strategy Background Safety hazards related to bed rail use have been realized since 1990. Michigan s initial
BED RAIL SAFETY 9/15/2015. A Clinical Process Guideline. Background. Federal Nursing Home Reform Act
 BED RAIL SAFETY A Clinical Process Guideline Laura Funsch, RN, BSN, MS Director of Regulatory Strategy, LeadingAge Michigan Background Safety hazards related to bed rail use have been realized since 1990.
BED RAIL SAFETY A Clinical Process Guideline Laura Funsch, RN, BSN, MS Director of Regulatory Strategy, LeadingAge Michigan Background Safety hazards related to bed rail use have been realized since 1990.
How To Resolve Common Nursing Home Problems
 August 4, 2015 How To Resolve Common Nursing Home Problems Eric Carlson Webinar Logistics Everyone is on mute. Use Question function to submit questions. You will be sent slides, which also will be available
August 4, 2015 How To Resolve Common Nursing Home Problems Eric Carlson Webinar Logistics Everyone is on mute. Use Question function to submit questions. You will be sent slides, which also will be available
RALF Behavior Management Rules IDAPA
 RALF Behavior Management Rules IDAPA 16.03.22 DEFINITIONS: 010.10. Assessment. The conclusion reached using uniform criteria which identifies resident strengths, weaknesses, risks and needs, to include
RALF Behavior Management Rules IDAPA 16.03.22 DEFINITIONS: 010.10. Assessment. The conclusion reached using uniform criteria which identifies resident strengths, weaknesses, risks and needs, to include
Institutional Handbook of Operating Procedures Policy Responsible Vice President: Executive Vice President and CEO, Health System
 Section: Clinical Subject: General Policies Institutional Handbook of Operating Procedures Policy 09.13.06 Responsible Vice President: Executive Vice President and CEO, Health System Responsible Entity:
Section: Clinical Subject: General Policies Institutional Handbook of Operating Procedures Policy 09.13.06 Responsible Vice President: Executive Vice President and CEO, Health System Responsible Entity:
Common Nursing Home Problems, and How to Resolve Them
 June 23, 2016 Common Nursing Home Problems, and How to Resolve Them Eric Carlson Publication Available On-Line 20 Common Nursing Home Problems and How to Resolve Them Newly updated; available at justiceinaging.org
June 23, 2016 Common Nursing Home Problems, and How to Resolve Them Eric Carlson Publication Available On-Line 20 Common Nursing Home Problems and How to Resolve Them Newly updated; available at justiceinaging.org
Bed Rail Entrapment Risk Notification Guide
 Bed Rail Entrapment Risk Notification Guide EN NOTICE TO EQUIPMENT PROVIDER: These instructions, in their entirety, must be provided to the patient, the patient s family and/or the patient s primary day-to-day
Bed Rail Entrapment Risk Notification Guide EN NOTICE TO EQUIPMENT PROVIDER: These instructions, in their entirety, must be provided to the patient, the patient s family and/or the patient s primary day-to-day
Physical Restraints. Purpose Policy Statement. Applicability
 Approved by: Physical Restraints Senior Vice President, Medicine Vice President, Covenant Health Rural Health Services & Executive Lead for Professional Practice and Research Corporate Policy & Procedures
Approved by: Physical Restraints Senior Vice President, Medicine Vice President, Covenant Health Rural Health Services & Executive Lead for Professional Practice and Research Corporate Policy & Procedures
Adaptation, Equipment and Safety Equipment Assessment. REVISED July 2016
 Adaptation, Equipment and Safety Equipment Assessment REVISED July 2016 Page 1 of 5 Adaptations and Equipment Policy Statement The Wellbeing Residential Group believes that its service users should expect
Adaptation, Equipment and Safety Equipment Assessment REVISED July 2016 Page 1 of 5 Adaptations and Equipment Policy Statement The Wellbeing Residential Group believes that its service users should expect
Make observations of the resident for at least a two- to eight-hour period. Record observation details in Comments for each section.
 Resident Room Observer Observation Date Make observations of the resident for at least a two- to eight-hour period. Record observation details in Comments for each section. Screening 1. Is the resident
Resident Room Observer Observation Date Make observations of the resident for at least a two- to eight-hour period. Record observation details in Comments for each section. Screening 1. Is the resident
Session #8. The Key to Preventing Immediate Jeopardies. Speaker: Janine Lehman 4/17/2013 KBN:
 2013 KAHCF Spring Education Conference Session #8 The Key to Preventing Immediate Jeopardies Speaker: Janine Lehman 4/17/2013 KBN: 5-0002-707-041-1217 The Key to Preventing Immediate Jeopardies Janine
2013 KAHCF Spring Education Conference Session #8 The Key to Preventing Immediate Jeopardies Speaker: Janine Lehman 4/17/2013 KBN: 5-0002-707-041-1217 The Key to Preventing Immediate Jeopardies Janine
POLICY AND PROCEDURE RESTRAINT/SECLUSION, MEDICAL CENTER PATIENT CARE Effective Date: March 2010
 Number: MS 08:03:05 Submitted by: BEHAVIORAL HEALTH CLINICAL PRACTICE TEAM Issuing Department: PATIENT CARE SERVICES Approved By: Reviewed by: Date: Patient Care Practice & 12/09 Outcomes David W. Cress,
Number: MS 08:03:05 Submitted by: BEHAVIORAL HEALTH CLINICAL PRACTICE TEAM Issuing Department: PATIENT CARE SERVICES Approved By: Reviewed by: Date: Patient Care Practice & 12/09 Outcomes David W. Cress,
Hospice and End of Life Care and Services Critical Element Pathway
 Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
PRACTICE STANDARD. Restraints. Table of Contents. Introduction 3. What are Restraints? 3. Assumptions 4. Policy Direction: Least Restraint 4
 PRACTICE STANDARD Restraints Table of Contents Introduction 3 What are Restraints? 3 Assumptions 4 Policy Direction: Least Restraint 4 Quality Practice Settings 4 Nursing Responsibilities 5 Case Studies
PRACTICE STANDARD Restraints Table of Contents Introduction 3 What are Restraints? 3 Assumptions 4 Policy Direction: Least Restraint 4 Quality Practice Settings 4 Nursing Responsibilities 5 Case Studies
Restraint Reduction. Moving Towards Restraint Free Care
 Restraint Reduction Moving Towards Restraint Free Care Revised: BW/January 2016 RESTRAINTS: Defined Any manual method, physical or mechanical device, material or equipment, that immobilizes or reduces
Restraint Reduction Moving Towards Restraint Free Care Revised: BW/January 2016 RESTRAINTS: Defined Any manual method, physical or mechanical device, material or equipment, that immobilizes or reduces
ATTENTION ALL C.N.A S
 ATTENTION ALL C.N.A S October s monthly Education Manual will not be the usual booklet. You will find a different handout with required reading and a post test. This handout will meet your required units
ATTENTION ALL C.N.A S October s monthly Education Manual will not be the usual booklet. You will find a different handout with required reading and a post test. This handout will meet your required units
LESSON ASSIGNMENT. Environmental Health and the Practical Nurse. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 6 Environmental Health and the Practical Nurse. LESSON ASSIGNMENT Paragraphs 6-1 through 6-5. LESSON OBJECTIVES After completing this lesson, you should be able to: 6-1. Select
LESSON ASSIGNMENT LESSON 6 Environmental Health and the Practical Nurse. LESSON ASSIGNMENT Paragraphs 6-1 through 6-5. LESSON OBJECTIVES After completing this lesson, you should be able to: 6-1. Select
PATIENT RESTRAINT-MINIMISATION POLICY Page 1 of 7 Reviewed: June 2017
 Page 1 of 7 Policy Applies to All Mercy Hospital clinical staff. Compliance will be facilitated for Credentialed Specialists and Allied Health personnel involved in patient care. Exclusions: This policy
Page 1 of 7 Policy Applies to All Mercy Hospital clinical staff. Compliance will be facilitated for Credentialed Specialists and Allied Health personnel involved in patient care. Exclusions: This policy
MDS Essentials. MDS Essentials: Content. Faculty Disclosures 5/22/2017. Educational Activity Completion
 MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
MDS Essentials MDS Essentials: Introduction to Care Area Assessments and Care Plans 4 Faculty Disclosures I have no financial relationships to disclose I have no conflicts of interests to disclose I will
ADULT LONG-TERM CARE SERVICES
 ADULT LONG-TERM CARE SERVICES Long-term care is a broad range of supportive medical, personal, and social services needed by people who are unable to meet their basic living needs for an extended period
ADULT LONG-TERM CARE SERVICES Long-term care is a broad range of supportive medical, personal, and social services needed by people who are unable to meet their basic living needs for an extended period
a guide to Oregon Adult Foster Homes for potential residents, family members and friends
 a guide to Oregon Adult Foster Homes for potential residents, family members and friends Table of contents Overview of adult foster homes...1 The consumer s choice...1 When adult foster care should be
a guide to Oregon Adult Foster Homes for potential residents, family members and friends Table of contents Overview of adult foster homes...1 The consumer s choice...1 When adult foster care should be
OAR Changes. Presented by APD Medicaid LTC Policy
 OAR 411-015 Changes 1 Presented by APD Medicaid LTC Policy Table of Contents 2 Service Priority OAR 411-015 Project Overview Why Are We Making These Changes Overarching Changes Changes to ADLS (each ADL
OAR 411-015 Changes 1 Presented by APD Medicaid LTC Policy Table of Contents 2 Service Priority OAR 411-015 Project Overview Why Are We Making These Changes Overarching Changes Changes to ADLS (each ADL
Preventing Falls in the Home
 ~ VOLUME I ISSUE V LESSON PLAN ~ OBJECTIVES Upon completion of this program, the home health aide will be able to:» Identify four variables that increase the likelihood of falls» List three common hazards
~ VOLUME I ISSUE V LESSON PLAN ~ OBJECTIVES Upon completion of this program, the home health aide will be able to:» Identify four variables that increase the likelihood of falls» List three common hazards
Chapter 14. Body Mechanics and Safe Resident Handling, Positioning, and Transfers
 Chapter 14 Body Mechanics and Safe Resident Handling, Positioning, and Transfers Body Mechanics Body mechanics means using the body in an efficient and careful way. It involves: Good posture Balance Using
Chapter 14 Body Mechanics and Safe Resident Handling, Positioning, and Transfers Body Mechanics Body mechanics means using the body in an efficient and careful way. It involves: Good posture Balance Using
REHABILITATION AND RESTORATIVE CARE UPDATE APRIL 2013
 REHABILITATION AND RESTORATIVE CARE UPDATE APRIL 2013 Rehabilitation Helping patients attain the highest possible level of functional ability Focusing on physical ability Restorative care Helping attain
REHABILITATION AND RESTORATIVE CARE UPDATE APRIL 2013 Rehabilitation Helping patients attain the highest possible level of functional ability Focusing on physical ability Restorative care Helping attain
Mental Health Commission Rules
 Mental Health Commission Rules Reference Number: R-S69(2)/02/2006 RULES GOVERNING THE USE OF SECLUSION AND MECHANICAL MEANS OF BODILY RESTRAINT 1 st November 2006 PREAMBLE Section 69(2) of the Mental Health
Mental Health Commission Rules Reference Number: R-S69(2)/02/2006 RULES GOVERNING THE USE OF SECLUSION AND MECHANICAL MEANS OF BODILY RESTRAINT 1 st November 2006 PREAMBLE Section 69(2) of the Mental Health
Tip Sheet Promoting Mobility, Reducing Falls and Alarms
 Tip Sheet Promoting Mobility, Reducing Falls and Alarms WHAT IT IS: Promoting mobility means building and maintaining core strength, endurance and balance, and providing supports to enable residents to
Tip Sheet Promoting Mobility, Reducing Falls and Alarms WHAT IT IS: Promoting mobility means building and maintaining core strength, endurance and balance, and providing supports to enable residents to
Restraint Education Program JHS Annual Mandatory Clinical Education
 Restraint Education Program 2017 JHS Annual Mandatory Clinical Education Program Goals Prevent, reduce and eliminate use of restraints Initiate restraint only when other less restrictive measures have
Restraint Education Program 2017 JHS Annual Mandatory Clinical Education Program Goals Prevent, reduce and eliminate use of restraints Initiate restraint only when other less restrictive measures have
Listed below are additional coding tips: you think the patient can do or what the patient s potential is. your shift, even if it only occurs once.
 1 It is important to always accurately code how much assistance your patients require to perform their activities of daily living and provide assistance in the safest manner possible for you and the patient.
1 It is important to always accurately code how much assistance your patients require to perform their activities of daily living and provide assistance in the safest manner possible for you and the patient.
Pharmacy Services. Division of Nursing Homes
 Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
PRINTED: 01/25/2008 FORM APPROVED CENTERS FOR MEDICARE & MEDICAID SERVICES 2567-L (X2) MULTIPLE CONSTRUCTION STREET ADDRESS, CITY, STATE, ZIP CODE
 MULTIPLE CONSTRUCTION STREET ADDRESS, CITY, STATE, ZIP CODE") S FOR MEDICARE & MEDICA SERVICES 2567-L NAME OF PROVER OR SUPPLIER (X1) PROVER/SUPPLIER/CLIA ENTIFICATION NUMBER: (X3) SURVEY D (X4) PROVER'S PLAN OF CORRECTION F 000 INITIAL COMMENTS F 000 No Plan of
S FOR MEDICARE & MEDICA SERVICES 2567-L NAME OF PROVER OR SUPPLIER (X1) PROVER/SUPPLIER/CLIA ENTIFICATION NUMBER: (X3) SURVEY D (X4) PROVER'S PLAN OF CORRECTION F 000 INITIAL COMMENTS F 000 No Plan of
RULES OF DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES DIVISION OF MENTAL HEALTH SERVICES
 RULES OF DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES DIVISION OF MENTAL HEALTH SERVICES CHAPTER 0940-3-9 USE OF ISOLATION, MECHANICAL RESTRAINT, AND PHYSICAL HOLDING RESTRAINT TABLE OF CONTENTS
RULES OF DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES DIVISION OF MENTAL HEALTH SERVICES CHAPTER 0940-3-9 USE OF ISOLATION, MECHANICAL RESTRAINT, AND PHYSICAL HOLDING RESTRAINT TABLE OF CONTENTS
Center for Medicaid and State Operations/Survey and Certification Group
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2-12-25 Baltimore, Maryland 21244-1850 Center for Medicaid and State Operations/Survey
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2-12-25 Baltimore, Maryland 21244-1850 Center for Medicaid and State Operations/Survey
2017 MDS Update. Start time: 3:30 p.m. EDT
 2017 MDS Update Start time: 3:30 p.m. EDT Find audio connection information under the Quick Start tab near the top left corner of your screen. Connect to audio using your computer s microphone and speakers,
2017 MDS Update Start time: 3:30 p.m. EDT Find audio connection information under the Quick Start tab near the top left corner of your screen. Connect to audio using your computer s microphone and speakers,
MDS 3.0/RUG IV OVERVIEW
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
Restraint Reduction. Moving Towards Restraint Free Care
 Restraint Reduction Moving Towards Restraint Free Care Revised: BW/September 2010 RESTRAINTS: Defined Any manual method, physical or mechanical device, material or equipment, that immobilizes or reduces
Restraint Reduction Moving Towards Restraint Free Care Revised: BW/September 2010 RESTRAINTS: Defined Any manual method, physical or mechanical device, material or equipment, that immobilizes or reduces
Documenting and Reporting
 Duty: Communicate Client Information to Authorized Persons Task : E.01 Report abuse of client E.02 Report client s unusual behavior E.03 Complete incident report E.05 Respond to authorized persons request
Duty: Communicate Client Information to Authorized Persons Task : E.01 Report abuse of client E.02 Report client s unusual behavior E.03 Complete incident report E.05 Respond to authorized persons request
Fall Prevention Protocol
 Fall Prevention Protocol I. Assessment Each patient should be assessed for fall risk: On admission to the facility On any transfer from one unit to another within the facility Following any change of status
Fall Prevention Protocol I. Assessment Each patient should be assessed for fall risk: On admission to the facility On any transfer from one unit to another within the facility Following any change of status
Rules of Participation, Phase 1 Review
 1 Rules of Participation, Phase 1 Review A Foundation check to launch Phase 2 from Presented by: Anabelle Locsin, RN, Ed.D., RAC-CT, LNC Quality Improvement Consultant PROGRAM OVERVIEW 2 This program was
1 Rules of Participation, Phase 1 Review A Foundation check to launch Phase 2 from Presented by: Anabelle Locsin, RN, Ed.D., RAC-CT, LNC Quality Improvement Consultant PROGRAM OVERVIEW 2 This program was
Preventing In-Facility Falls
 Preventing In-Facility Falls Presented by Paul Shekelle, M.D., Ph.D. RAND Corporation Evidence-based Practice Center Introduction: Making Health Care Safer II: An Updated Critical Analysis of the Evidence
Preventing In-Facility Falls Presented by Paul Shekelle, M.D., Ph.D. RAND Corporation Evidence-based Practice Center Introduction: Making Health Care Safer II: An Updated Critical Analysis of the Evidence
Iowa. Phone. Web Site. https://dia-hfd.iowa.gov/dia_hfd/home.do. Licensure Term
 Iowa Phone Agency Department of Inspections and Appeals, Health Facilities Division (515) 281-6325 Contact Linda Kellen (515) 281-7624 E-mail Linda.Kellen@dia.iowa.gov. Web Site https://dia-hfd.iowa.gov/dia_hfd/home.do
Iowa Phone Agency Department of Inspections and Appeals, Health Facilities Division (515) 281-6325 Contact Linda Kellen (515) 281-7624 E-mail Linda.Kellen@dia.iowa.gov. Web Site https://dia-hfd.iowa.gov/dia_hfd/home.do
Position Statement. Position Statement on the Use of Restraints in Client Care Settings
 Position Statement Position Statement on the Use of Restraints in Client Care Settings June 1 Approved by the College and Association of Registered Nurses of Alberta () Provincial Council, June. Permission
Position Statement Position Statement on the Use of Restraints in Client Care Settings June 1 Approved by the College and Association of Registered Nurses of Alberta () Provincial Council, June. Permission
OCTOBER 2017 RAI MANUAL UPDATES
 OCTOBER 2017 RAI MANUAL UPDATES CMS released the updated RAI Manual on August 31, 2017 for use with Assessment Reference Dates (ARD) on or after Oct 1, 2017. There are two sections that are completely
OCTOBER 2017 RAI MANUAL UPDATES CMS released the updated RAI Manual on August 31, 2017 for use with Assessment Reference Dates (ARD) on or after Oct 1, 2017. There are two sections that are completely
Reducing and Discontinuing Resident Alarms. The False Reassurance of Personal Alarms
 Across the country, state health organizations, nursing homes, private and government quality improvement organizations have all been studying the impact of personal alarms on the lives of residents in
Across the country, state health organizations, nursing homes, private and government quality improvement organizations have all been studying the impact of personal alarms on the lives of residents in
Safe Patient Handling:
 Safe Patient Handling: The Hazards of Immobility Prepared by : Learning Objectives Discuss the opportunity for quality improvement using SPHM practices Discuss expected positive patient outcomes using
Safe Patient Handling: The Hazards of Immobility Prepared by : Learning Objectives Discuss the opportunity for quality improvement using SPHM practices Discuss expected positive patient outcomes using
Resident Rights Bingo Activity Long-Term Care Learning Activity
 Item Objective: Materials Needed: Total Time for Activity: Prior to Class: Description Surveyor will identify the resident right used in the scenario, as identified in the Long-Term Care (LTC) requirements.
Item Objective: Materials Needed: Total Time for Activity: Prior to Class: Description Surveyor will identify the resident right used in the scenario, as identified in the Long-Term Care (LTC) requirements.
C: Safety. Alberta Licensed Practical Nurses Competency Profile 23
 C: Alberta Licensed Practical Nurses Competency Profile 23 Competency: C-1 Fire Emergency C-1-1 C-1-2 C-1-3 C-1-4 C-1-5 C-1-6 Demonstrate ability to apply critical thinking and clinical judgment in response
C: Alberta Licensed Practical Nurses Competency Profile 23 Competency: C-1 Fire Emergency C-1-1 C-1-2 C-1-3 C-1-4 C-1-5 C-1-6 Demonstrate ability to apply critical thinking and clinical judgment in response
Disclaimer. Objectives: !"#$"%&' ! The learner will be able to:
 Best Practices: How Enclosure Beds Can Be An Effective Intervention In The Clinical Setting. Presented by Sue Pugh, RN, MSN, CRRN, CNRN, CNS-BC, CBIS, FAHA Clinical Nurse Specialist Sinai Hospital of Baltimore
Best Practices: How Enclosure Beds Can Be An Effective Intervention In The Clinical Setting. Presented by Sue Pugh, RN, MSN, CRRN, CNRN, CNS-BC, CBIS, FAHA Clinical Nurse Specialist Sinai Hospital of Baltimore
RULES OF TENNESSEE DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES OFFICE OF LICENSURE
 RULES OF TENNESSEE DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES OFFICE OF LICENSURE CHAPTER 0940-5-24 MINIMUM PROGRAM REQUIREMENTS FOR MENTAL RETARDATION TABLE OF CONTENTS 0940-5-24-.01 Health,
RULES OF TENNESSEE DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES OFFICE OF LICENSURE CHAPTER 0940-5-24 MINIMUM PROGRAM REQUIREMENTS FOR MENTAL RETARDATION TABLE OF CONTENTS 0940-5-24-.01 Health,
Attachment A - Comparison of OASIS-C (Current Version) to OASIS-C1 (Proposed Data Collection)
 to OASIS-C1 (Proposed Data Collection)") Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
F-TAG 675 QUALITY OF LIFE
 F-TAG 675 QUALITY OF LIFE Quality of life is a fundamental principle that applies to all care and services provided to facility residents. Each resident must receive and the facility must provide the necessary
F-TAG 675 QUALITY OF LIFE Quality of life is a fundamental principle that applies to all care and services provided to facility residents. Each resident must receive and the facility must provide the necessary
Patient Safety: Fall Prevention. Unlicensed Assistive Personnel
 Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
[ ] POSITIVE SUPPORT STRATEGIES AND EMERGENCY MANUAL RESTRAINT; LICENSED FACILITIES AND PROGRAMS.
![[ ] POSITIVE SUPPORT STRATEGIES AND EMERGENCY MANUAL RESTRAINT; LICENSED FACILITIES AND PROGRAMS.](/thumbs/78/78464102.jpg "[ ] POSITIVE SUPPORT STRATEGIES AND EMERGENCY MANUAL RESTRAINT; LICENSED FACILITIES AND PROGRAMS.") Sec. 4. [245.8251] POSITIVE SUPPORT STRATEGIES AND EMERGENCY MANUAL RESTRAINT; LICENSED FACILITIES AND PROGRAMS. Subdivision 1. Rules. The commissioner of human services shall, within 24 months of enactment
Sec. 4. [245.8251] POSITIVE SUPPORT STRATEGIES AND EMERGENCY MANUAL RESTRAINT; LICENSED FACILITIES AND PROGRAMS. Subdivision 1. Rules. The commissioner of human services shall, within 24 months of enactment
Falls Prevention In Rehabilitation
 Falls Prevention In Rehabilitation Robyn Walker Rankin Park Centre Greater Newcastle Cluster March 2008 1 Frequency of Falls A total of 157 patients fell in Rankin Park Centre during the 12 months from
Falls Prevention In Rehabilitation Robyn Walker Rankin Park Centre Greater Newcastle Cluster March 2008 1 Frequency of Falls A total of 157 patients fell in Rankin Park Centre during the 12 months from
Patient Rights. Dianne McKissack Senior Program Director Johnson Regional Medical Center Clarksville, AR
 CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2014 Patient Rights Dianne McKissack Senior Program Director Johnson Regional Medical Center Clarksville, AR Objectives: Patients will be able to understand
CMS HOSPITAL CONDITIONS OF PARTICIPATION (COPS) 2014 Patient Rights Dianne McKissack Senior Program Director Johnson Regional Medical Center Clarksville, AR Objectives: Patients will be able to understand
Comparison of Violent or Self Destructive vs. Non-Violent Restraints
 Description Restraints can be initiated when unanticipated outbursts of severely aggressive or destructive behavior poses an imminent danger to the patient or others due to an underlying behavioral diagnosis
Description Restraints can be initiated when unanticipated outbursts of severely aggressive or destructive behavior poses an imminent danger to the patient or others due to an underlying behavioral diagnosis
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE RESTRAINT AS A LAST RESORT - ACUTE CARE INPATIENT - PEDIATRIC SCOPE Provincial: Acute Care Inpatient Pediatric APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Senior Operating
TITLE RESTRAINT AS A LAST RESORT - ACUTE CARE INPATIENT - PEDIATRIC SCOPE Provincial: Acute Care Inpatient Pediatric APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Senior Operating
Evaluating Needs* ADAPTED from Seniorhousingnet.com
 DIRECTIONS: Evaluating Needs is an assessment tool that can be used as a guideline to determine which type of housing or care best meets needs for support services (e.g. meals, housekeeping) or assistance
DIRECTIONS: Evaluating Needs is an assessment tool that can be used as a guideline to determine which type of housing or care best meets needs for support services (e.g. meals, housekeeping) or assistance
Survey Protocol for Long Term Care Facilities
 Attachment B Survey Protocol for Long Term Care Facilities The provision of home dialysis treatments in a Long Term Care (LTC) facility place an increased burden on the LTC facility staff and may place
Attachment B Survey Protocol for Long Term Care Facilities The provision of home dialysis treatments in a Long Term Care (LTC) facility place an increased burden on the LTC facility staff and may place
Nursing Assistant
 Western Technical College 30543300 Nursing Assistant Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 3.00 The course prepares individuals for employment
Western Technical College 30543300 Nursing Assistant Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 3.00 The course prepares individuals for employment
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress
 Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
Minimizing Fall Risk in the Nursing Home: What Residents Need to Know
 Minimizing Fall Risk in the Nursing Home: What Residents Need to Know Objectives: 1. Review environmental and internal risk factors that contribute to an increased risk for falls. 2. Identify interventions
Minimizing Fall Risk in the Nursing Home: What Residents Need to Know Objectives: 1. Review environmental and internal risk factors that contribute to an increased risk for falls. 2. Identify interventions
3/12/2015. Session Objectives. RAI User s Manual. Polling Question
 Session Objectives MDS 3.0 Coding Challenges: Questions, Answers, and Explanations Jen Pettis, BS, RN, WCC Associate March 19, 2015 Upon completion of the program, the participate will: Describe the four
Session Objectives MDS 3.0 Coding Challenges: Questions, Answers, and Explanations Jen Pettis, BS, RN, WCC Associate March 19, 2015 Upon completion of the program, the participate will: Describe the four
ALTERNATIVES TO RESTRAINTS
 ALTERNATIVES TO RESTRAINTS PROGRAM GUIDE FOR HEALTH CARE PROFESSIONALS National Educational Video, Inc. TM is an approved provider of continuing education. State Board provider numbers: Florida NCE2896,
ALTERNATIVES TO RESTRAINTS PROGRAM GUIDE FOR HEALTH CARE PROFESSIONALS National Educational Video, Inc. TM is an approved provider of continuing education. State Board provider numbers: Florida NCE2896,
Appendix: Behavioural Management of Agitation following Brain Injury
 If Agitation is present: 1. Refer to Management of Post Traumatic Agitation Following Brain Injury Algorithm 2. Complete the Agitated Behaviour Scale (ABS). If score is > 21, initiate ABS q hourly for
If Agitation is present: 1. Refer to Management of Post Traumatic Agitation Following Brain Injury Algorithm 2. Complete the Agitated Behaviour Scale (ABS). If score is > 21, initiate ABS q hourly for
POSITION SUMMARY. 2. Communicates: Reads, writes and speaks in English as required for taking direction and performing job-related activities.
 Department/s: Nursing Approved By: Senior Management Committee Date Approved: Mar 20 1992 Date Revised: Feb 16 2010 Page 1 of 6 POSITION SUMMARY The Personal Support Worker (PSW) at Fairhaven is responsible
Department/s: Nursing Approved By: Senior Management Committee Date Approved: Mar 20 1992 Date Revised: Feb 16 2010 Page 1 of 6 POSITION SUMMARY The Personal Support Worker (PSW) at Fairhaven is responsible
Review of F323 Related to Falls. Marilyn Hirsch Region V December 16, 2015
 Review of F323 Related to Falls Marilyn Hirsch Region V December 16, 2015 Objectives Describe Region V F323 Project Review F323 Regulation Review and discuss citations History At our meeting two years
Review of F323 Related to Falls Marilyn Hirsch Region V December 16, 2015 Objectives Describe Region V F323 Project Review F323 Regulation Review and discuss citations History At our meeting two years
Page Introduction 1. Factors to Consider When Evaluating Whether an Individual Needs to be Screened 1. Pre-Admission Screening Criteria 2
 Revision Date APPENDIX B PRE-ADMISSION SCREENING CRITERIA Revision Date i TABLE OF CONTENTS APPENDIX B Introduction 1 Factors to Consider When Evaluating Whether an Individual Needs to be Screened 1 2
Revision Date APPENDIX B PRE-ADMISSION SCREENING CRITERIA Revision Date i TABLE OF CONTENTS APPENDIX B Introduction 1 Factors to Consider When Evaluating Whether an Individual Needs to be Screened 1 2
G0110: Activities of Daily Living (ADL) Assistance
 Assistance") SECTION G: FUNCTIONAL STATUS Intent: Items in this section assess the need for assistance with activities of daily living (ADLs), altered gait and balance, and decreased range of motion. In addition, on
SECTION G: FUNCTIONAL STATUS Intent: Items in this section assess the need for assistance with activities of daily living (ADLs), altered gait and balance, and decreased range of motion. In addition, on
GUIDELINES FOR THE USE OF ASSISTIVE TECHNOLOGY EQUIPMENT IN COMMUNITY INPATIENT UNITS
 GUIDELINES FOR THE USE OF ASSISTIVE TECHNOLOGY EQUIPMENT IN COMMUNITY INPATIENT UNITS Guideline Reference: 1666 Version: 2.1 Status: Adopted Type: Clinical Guideline Guideline applies to (Staff Group)
GUIDELINES FOR THE USE OF ASSISTIVE TECHNOLOGY EQUIPMENT IN COMMUNITY INPATIENT UNITS Guideline Reference: 1666 Version: 2.1 Status: Adopted Type: Clinical Guideline Guideline applies to (Staff Group)
11/23/2011. Identify Residents risks for decline to establish programs to stave off decline unless it is clinically unavoidable.
 Robin A. Bleier, RN, HCRM-FACDONA Clinical Risk & Operations Consultant R B Health Partners, Inc. 210 So. Pinellas Ave. Suite 260 Tarpon Springs, FL 34689 robin@rbhealthpartners.com 727-744-2021 Restorative
Robin A. Bleier, RN, HCRM-FACDONA Clinical Risk & Operations Consultant R B Health Partners, Inc. 210 So. Pinellas Ave. Suite 260 Tarpon Springs, FL 34689 robin@rbhealthpartners.com 727-744-2021 Restorative
SECTION IV INTERPRETATIONS OF THE ADULT CARE HOME RESIDENTS' BILL OF RIGHTS
 SECTION IV INTERPRETATIONS OF THE ADULT CARE HOME RESIDENTS' BILL OF RIGHTS INTERPRETATIONS OF THE ADULT CARE HOME RESIDENTS' BILL OF RIGHTS Below are some interpretations of the Adult Care Home Residents'
SECTION IV INTERPRETATIONS OF THE ADULT CARE HOME RESIDENTS' BILL OF RIGHTS INTERPRETATIONS OF THE ADULT CARE HOME RESIDENTS' BILL OF RIGHTS Below are some interpretations of the Adult Care Home Residents'
Activities of Daily Living (ADL) Critical Element Pathway
 Critical Element Pathway") Use this pathway for a resident who requires assistance with or is unable to perform ADLs (Hygiene bathing, dressing, grooming, and oral care; Elimination toileting; Dining eating, including meals and
Use this pathway for a resident who requires assistance with or is unable to perform ADLs (Hygiene bathing, dressing, grooming, and oral care; Elimination toileting; Dining eating, including meals and
PHYSICAL RESTRAINTS. Guidelines & Federal Regulations
 PHYSICAL RESTRAINTS Awareness regarding physical restraint use in nursing homes has increased since the federal government enacted the Omnibus Budget Reconciliation Act (OBRA) of 1987. Among its provisions
PHYSICAL RESTRAINTS Awareness regarding physical restraint use in nursing homes has increased since the federal government enacted the Omnibus Budget Reconciliation Act (OBRA) of 1987. Among its provisions
Announced Inspection Report care for older people in acute hospitals
 Announced Inspection Report care for older people in acute hospitals Hairmyres Hospital NHS Lanarkshire Healthcare Improvement Scotland is committed to equality. We have assessed the inspection function
Announced Inspection Report care for older people in acute hospitals Hairmyres Hospital NHS Lanarkshire Healthcare Improvement Scotland is committed to equality. We have assessed the inspection function
Definition of a Restraint
 Definition of a Restraint Person-directed care: the road to restraint-free care and quality of life Joanne Rader, RN,MN, PMNNP any manual method or physical or mechanical device, material, or equipment
Definition of a Restraint Person-directed care: the road to restraint-free care and quality of life Joanne Rader, RN,MN, PMNNP any manual method or physical or mechanical device, material, or equipment
Fall Prevention. Falls 1
 Falls 1 Fall Prevention A fall is defined as an unplanned descent to the floor with or without injury. Patient falls contribute to mortality and increased morbidity in the general patient population. Implementation
Falls 1 Fall Prevention A fall is defined as an unplanned descent to the floor with or without injury. Patient falls contribute to mortality and increased morbidity in the general patient population. Implementation
Christian Brothers Risk Management Services. Nursing Home & Health Care Ministry Documentation: Are you open for a lawsuit?
 2013 Spring Webinar Series 2013 Christian Brothers Services, Romeoville, IL. All Rights Reserved. No part of this presentation may be reproduced, stored in a retrieval system, or transmitted by any means
2013 Spring Webinar Series 2013 Christian Brothers Services, Romeoville, IL. All Rights Reserved. No part of this presentation may be reproduced, stored in a retrieval system, or transmitted by any means
MEDICAL UNIVERSITY OF SOUTH CAROLINA DEPARTMENT OF PUBLIC SAFETY. EFFECTIVE DATE: 1 January 1999 PAGE 1 OF 10
 MEDICAL UNIVERSITY OF SOUTH CAROLINA DEPARTMENT OF PUBLIC SAFETY POLICY AND PROCEDURE # 70 SUBJECT: Searching and Transportation of Prisoners EFFECTIVE DATE: 1 January 1999 PAGE 1 OF 10 REVIEW DATE: 30
MEDICAL UNIVERSITY OF SOUTH CAROLINA DEPARTMENT OF PUBLIC SAFETY POLICY AND PROCEDURE # 70 SUBJECT: Searching and Transportation of Prisoners EFFECTIVE DATE: 1 January 1999 PAGE 1 OF 10 REVIEW DATE: 30
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to