at with. (Date) (Time) (Physician)
|
|
|
- Jemima Newton
- 5 years ago
- Views:
Transcription
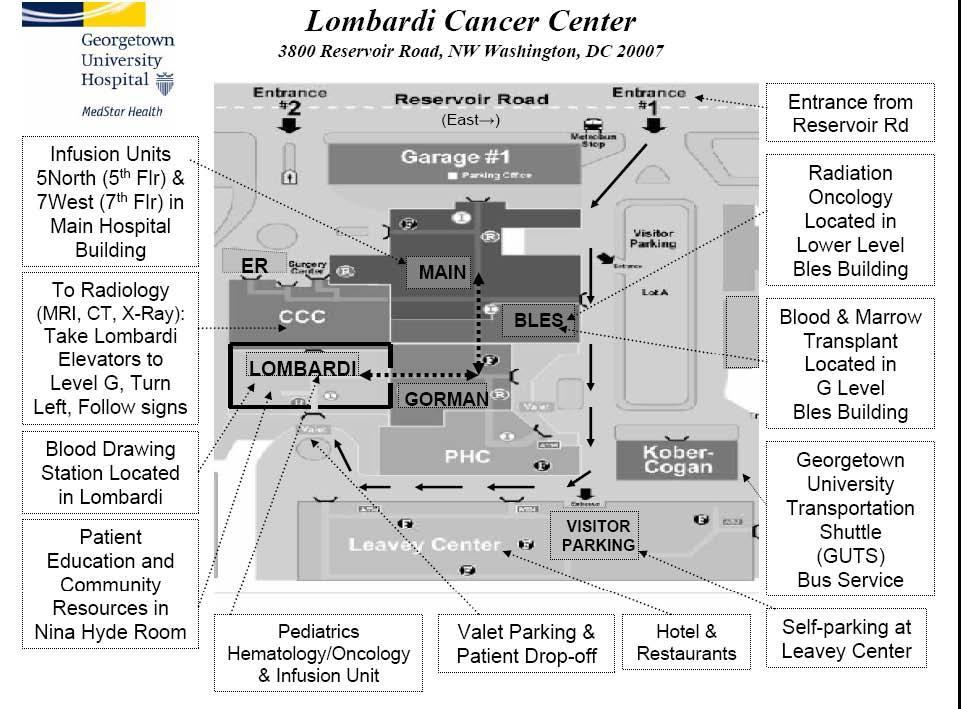
1 Dear Lombardi Patient: Georgetown University Hospital s physicians and staff would like to welcome you and thank you for choosing the Lombardi Comprehensive Cancer Center for your care. Our goal is to make your experience here at Lombardi as comfortable and smooth as possible. This letter is to confirm that an appointment was scheduled for you on: at with. (Date) (Time) (Physician) Please plan to arrive at least minutes prior to your visit in order to complete our registration process. Let us know if you are running late for your appointment by calling the front desk at (202) For your first visit here, we ask that you bring the following information with you to your appointment: A Photo ID Your Insurance Card(s) Your Referral Form if required by your health plan Documentation from the referring physician with diagnosis Your current list of medications All x-rays, scans (CT/MRI/PET), lab work, pathology reports, and supporting medical records pertaining to your diagnosis The completed health history form (attached) In order for our physicians to treat you appropriately, we may have already informed you that we needed to receive your medical records prior to your appointment. Please fax records at least 48 hours in advance to (202) Someone from our office will contact you if we have any questions or concerns regarding receipt of your records. If you need to get in touch with our office, please call the appointment scheduling desk at (202) Use this number for appointment verification, changes, or cancellations. Feel free to leave a message and someone from our office will call you back within 24 hours. The Lombardi Comprehensive Cancer Center is an outpatient clinic in the hospital. Therefore your insurance will receive a minimum of 2 bills one for the professional fee for the provider, and one for the facility. If x-rays or labs are done, those will be billed to your insurance company separately. On behalf of our physicians and staff, thank you for choosing the Lombardi Comprehensive Cancer Center.
2 Lombardi Comprehensive Cancer Center New Patient Health History Form Name Age Birth date Occupation Birthplace Marital Status: Single Married Widowed Divorced Separated Phone number to use for appointments, lab results, etc.: Home: Work: Cell: Whom should we contact in case of emergency? Relationship: Phone: Do you have: An Advanced Directive Yes No A Living Will.. Yes A Durable or Medical Power Of Attorney.. Yes No No Would you like information on advance directives?. Yes Do you reside alone?...yes If No, Who do you reside with? No No Please briefly explain why you are coming to the Lombardi Comprehensive Cancer Center.
3 Please provide the names of the other Health Care Providers involved in your care. Referring Physician Primary Care Physician Surgeon Radiation Oncologist Other Physician Other Physician FAMILY MEDICAL HISTORY Mother Maternal Grandmother Maternal Grandfather Maternal Aunts Maternal Uncles Maternal Cousins(M/F) Father Paternal Grandmother Paternal Grandfather Paternal Aunts Paternal Uncles Paternal Cousins Siblings(M/F) Members Living/Deceased Health Issues Children(M/F) PERSONAL MEDICAL HISTORY SURGERY ADULT ILLNESSES TONSILLECTOMY.YES DIABETES.YES APPENDECTOMY.. YES HIGH BLOOD PRESSURE YES
4 PERSONAL MEDICAL HISTORY CONT. HYSTERECTOMY..YES HEART PROBLEMS..YES Including the ovaries...yes RESPIRATORY PROBLEMS YES HERNIA REPAIR....YES BLEEDING PROBLEMS...YES GALLBLADDER SURGERY.YES MENTAL ILLNESS YES OTHER (explain)..yes DEPRESSION.YES OTHER(explain)..YES INJURIES SIGNIFICANT ACCIDENTS..YES BROKEN BONES... YES GENERAL MEDICAL INFORMATION HEIGHT WEIGHT Current One year ago Maximum EXPOSURES MEASLES.. YES MUMPS.. YES CHICKEN POX.. YES TUBERCULOSIS... YES OTHER (explain)... YES PNEUMOVAX... YES TETANUS... YES HEPATITIS B VACCINE YES FLU VACCINE.... YES OTHER (explain)... YES WOMEN S HEALTH MENSES: age of onset cycle duration last menstrual cycle ESTROGENS: oral contraceptives.. YES hormone replacement YES PAP SMEAR: last examination abnormal YES MAMMOGRAM: last study abnormal...yes IMMUNIZATIONS PREGNANCIES: total number live births miscarriages complications....yes AGE AT 1st FULL TERM PREGNANCY MEN S HEALTH PROSTATE: last examination abnormal YES PSA: last test abnormal YES TESTICULAR SELF EXAMS YES
5 SOCIAL HISTORY FAT INTAKE TOBACCO USE CAFFEINE INTAKE CAFFEINATED DRINKS PER DAY: EXERCISE ALCOHOL USE PRESCRIPTION MEDICATIONS MEDICATION DOSE FREQUENCY REASON
6 N-PRESCRIPTION MEDICATIONS (PLEASE INCLUDE OVER THE COUNTER MEDICATIONS, VITAMINS, SUPPLEMENTS, ETC) MEDICATION DOSE FREQUENCY REASON MEDICATION ALLERGIES MEDICATION REACTION
7 General Medical Records release and Authorization for Use or Disclosure of Protected health Information Please complete the following information: Patient Name: Address: Phone: SSN: Date of Birth: / / I authorize the custodian of records of: or other person/entity (specifically describe) to disclose/release the following information (check all that apply): All records Laboratory/pathology records Billing records X-ray/radiology records Pharmacy/prescription records Abstract/Summary Other (please describe) These records are for services provided on the following date(s): Please send the records listed above to (use additional sheets if necessary): Name: Address: Phone: Fax: The information may be used/disclosed for each of the following purposes: At my request (only the patient can check this box) For employment purposes For my health care For payment/insurance Other (please describe) This authorization shall expire no later than: / / or upon the following event (whichever is sooner), except this authorization shall automatically expire upon a minor s 18th birthday and may not be valid for greater than one year from the date of the signature for Maryland medical records. I understand that after the custodian of records discloses my health information, it may no longer be protected by federal privacy laws. I further understand that this authorization is voluntary and that I may refuse to sign this authorization. My refusal to sign will not affect my ability to obtain treatment; receive payment; or eligibility for benefits unless allowed by law. By signing below, I represent and warrant that I have authority to sign this document and authorize the use or disclosure of protected health information and that there are no claims or orders pending or in effect that would prohibit, limit, or otherwise restrict my ability to authorize the use or disclosure of this protected health information. Signature of patient or patient s legal representative Date Printed name of patient representative Representative s authority to sign for the patient, (parent, guardian, power of attorney for healthcare, executor, etc.) You have the right to revoke this authorization, except to the extent the custodian of records has relied on it, by sending your written request to Privacy Liaison, 3800 Reservoir Road NW, Washington, DC
8
Patient Name:,, Address: Phones:,, Home Work Cell. Primary Physician: Emergency Contact: Phone#:
 Patient Information Patient Name:,, Last First middle initial Address: Phones:,, Home Work Cell Sex: Female Male E-Mail: Date of Birth: / / Mo. Day Year Primary Physician: Marital Status: Single Married
Patient Information Patient Name:,, Last First middle initial Address: Phones:,, Home Work Cell Sex: Female Male E-Mail: Date of Birth: / / Mo. Day Year Primary Physician: Marital Status: Single Married
Sage Medical Center New Patient Forms
 Sage Medical Center New Patient Forms Patient Name: DOB: Providers and Suppliers of Your Medical Care: Please list all providers and suppliers of your medical care such as primary care physicians, specialty
Sage Medical Center New Patient Forms Patient Name: DOB: Providers and Suppliers of Your Medical Care: Please list all providers and suppliers of your medical care such as primary care physicians, specialty
MAIN STREET MEDICAL NEW PATIENT QUESTIONNAIRE
 NEW PATIENT QUESTIONNAIRE Patient Name: Date: Date of Birth: SSN: Male Female Guarantor Name: SSN: DOB: Home Phone: Cell Phone: Street Address: Apt#: City: State: Zip: Billing Address (if different): Email
NEW PATIENT QUESTIONNAIRE Patient Name: Date: Date of Birth: SSN: Male Female Guarantor Name: SSN: DOB: Home Phone: Cell Phone: Street Address: Apt#: City: State: Zip: Billing Address (if different): Email
LAST NAME: FIRST NAME: MI: STREET ADDRESS: CITY: STATE: ZIP CODE: DOB: AGE: SEX: M F: TELEPHONE#: ( ) CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W
 CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W") PATIENT REGISTRATION LAST NAME: FIRST NAME: MI: STREET ADDRESS: CITY: STATE: ZIP CODE: DOB: AGE: SEX: M F: TELEPHONE#: ( ) CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W D OTHER: SPOUSE S NAME: EMAIL ADDRESS:
PATIENT REGISTRATION LAST NAME: FIRST NAME: MI: STREET ADDRESS: CITY: STATE: ZIP CODE: DOB: AGE: SEX: M F: TELEPHONE#: ( ) CELL PHONE#: ( ) SSN#: MARITAL STATUS: S M W D OTHER: SPOUSE S NAME: EMAIL ADDRESS:
WILMINGTON HEALTH Patient Information
 WILMINGTON HEALTH Patient Information Account No. Doctor s No. PLEASE ANSWER ALL QUESTIONS PATIENT INFORMATION NAME: LAST BIRTHDATE SS# HOME PHONE CELL PHONE EMAIL ADDRESS FIRST MIDDLE SEX M F RACE White/Caucasian
WILMINGTON HEALTH Patient Information Account No. Doctor s No. PLEASE ANSWER ALL QUESTIONS PATIENT INFORMATION NAME: LAST BIRTHDATE SS# HOME PHONE CELL PHONE EMAIL ADDRESS FIRST MIDDLE SEX M F RACE White/Caucasian
Please complete all pages of this form. Your physician will review the form with you during your appointment. Last Name: First Name: Middle Initial:
 Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
Please complete all pages of this form. Your physician will review the form with you during your appointment. Last Name: First Name: Middle Initial:
 Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
Please complete all pages of this form. Your physician will review the form with you during your appointment. Patient Information Last Name: First Name: Middle Initial: Date of Birth: / / Age: SSN: - -
Page 1 of 5 1/4/17. Print Guardian Name (If not patient) DOB: Circle One: - - Patients Name: (Last, First, MI):
 DOB: Circle One: - - Patients Name: (Last, First, MI):") Patients Name: (Last, First, MI): SSN: DOB: Circle One: Male Mailing Address: Apt. #: City: State: Zip Code: Female Race: Ethnicity Primary Language: Home Phone: Preferred? Cell Phone: Preferred? Employer:
Patients Name: (Last, First, MI): SSN: DOB: Circle One: Male Mailing Address: Apt. #: City: State: Zip Code: Female Race: Ethnicity Primary Language: Home Phone: Preferred? Cell Phone: Preferred? Employer:
PATIENT'S NAME DATE OF BIRTH SOCIAL SECURITY # HOME PHONE # CELL PHONE # WORK PHONE #
 PATIENT INFORMATION PATIENT'S NAME DATE OF BIRTH SOCIAL SECURITY # STREET ADDRESS CITY, STATE, ZIP HOME PHONE # CELL PHONE # WORK PHONE # Emergency Contact & relationship: Phone #: Pharmacies local and
PATIENT INFORMATION PATIENT'S NAME DATE OF BIRTH SOCIAL SECURITY # STREET ADDRESS CITY, STATE, ZIP HOME PHONE # CELL PHONE # WORK PHONE # Emergency Contact & relationship: Phone #: Pharmacies local and
NAME SS# ADDRESS CITY STATE ZIP. TELEPHONE (home) (business) Cell SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE
 (business) Cell SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE") REGISTRATION (please print) PATIENT INFORMATION DATE: NAME SS# ADDRESS CITY STATE ZIP TELEPHONE (home) (business) Cell Email SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE MOTHER'S FIRST NAME
REGISTRATION (please print) PATIENT INFORMATION DATE: NAME SS# ADDRESS CITY STATE ZIP TELEPHONE (home) (business) Cell Email SEX M F BIRTH DATE PLACE OFBIRTH RACE ETHNICITY LANGUAGE MOTHER'S FIRST NAME
PATIENT INFORMATION When registering please provide proof of insurance and Picture ID Payment is expected at time of service.
 KENTUCKY FERTILITY, GYNECOLOGY AND OBSTETRICS PRIMARY HEALTH CARE 170 North Eagle Creek DR Suite 101 Lexington KY 40509 Phone 859-277-5736 Fax 859-276-2236 PATIENT INFORMATION When registering please provide
KENTUCKY FERTILITY, GYNECOLOGY AND OBSTETRICS PRIMARY HEALTH CARE 170 North Eagle Creek DR Suite 101 Lexington KY 40509 Phone 859-277-5736 Fax 859-276-2236 PATIENT INFORMATION When registering please provide
ADULT PATIENT INFORMATION. Patient Name: Last Name First Name Address: City: State: Zip Code: Phone #: Cell Phone #: Social Security:
 716 S. Goldenrod Road n 3315 Orange Blossom Trail Fax (407) 658-2536 Fax (407) 343-1907 ADULT PATIENT INFORMATION Patient Name: Last Name First Name MI Address: City: State: Zip Code: Phone #: Cell Phone
716 S. Goldenrod Road n 3315 Orange Blossom Trail Fax (407) 658-2536 Fax (407) 343-1907 ADULT PATIENT INFORMATION Patient Name: Last Name First Name MI Address: City: State: Zip Code: Phone #: Cell Phone
Responsible Party (Guarantor) Info. Insurance Information
 Info. Insurance Information") Associates in Women s Health, P.C. 2801 YOUNGFIELD STREET, SUITE 200 GOLDEN, CO 80401 P: 303-940-1867 F: 303-940-1894 Please Circle Your Doctor: ELLIS GANTER PYTHON SCHOEN WESSELL, WHNP PATIENT INFORMATION
Associates in Women s Health, P.C. 2801 YOUNGFIELD STREET, SUITE 200 GOLDEN, CO 80401 P: 303-940-1867 F: 303-940-1894 Please Circle Your Doctor: ELLIS GANTER PYTHON SCHOEN WESSELL, WHNP PATIENT INFORMATION
Karen Lopez - Bartlett, FNP-C 2400 Augusta Suite 210 Houston, Texas Phone: Fax:
 Karen Lopez - Bartlett, FNP-C 2400 Augusta Suite 210 Houston, Texas 77057 Phone: 832.970.0228 Fax: 713.278-7885 Welcome! We are honored that you have chosen us to help in your search for optimum health.
Karen Lopez - Bartlett, FNP-C 2400 Augusta Suite 210 Houston, Texas 77057 Phone: 832.970.0228 Fax: 713.278-7885 Welcome! We are honored that you have chosen us to help in your search for optimum health.
PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D KLONDIKE RD SW SUITE 205 CONYERS, GA TELEPHONE FAX
 PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D. 1506 KLONDIKE RD SW SUITE 205 CONYERS, GA 30094 678-750-4000 TELEPHONE 678-750-4005 FAX www.pcfwellness.com Dear Family, We are excited to welcome
PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D. 1506 KLONDIKE RD SW SUITE 205 CONYERS, GA 30094 678-750-4000 TELEPHONE 678-750-4005 FAX www.pcfwellness.com Dear Family, We are excited to welcome
Date: Name: Date of birth: Reason for today s visit: If yes, what are you allergic to and what type of reaction/symptoms did you have?
 Date: Name: Date of birth: Nickname/prefer to be called: Date that your last menstrual period began: Reason for today s visit: Allergies to medications/foods/substances? Yes No If yes, what are you allergic
Date: Name: Date of birth: Nickname/prefer to be called: Date that your last menstrual period began: Reason for today s visit: Allergies to medications/foods/substances? Yes No If yes, what are you allergic
Welcome to the Southeastern Urology Associates meridianemr Patient Portal
 New Patients: Please register for our Portal following the instructions below and send us a Message though the New Message Message for Office Section to let us know you received this packet and are confirming
New Patients: Please register for our Portal following the instructions below and send us a Message though the New Message Message for Office Section to let us know you received this packet and are confirming
From: AR Center (Arkansas Center for the Study of Integrative Medicine)! PLEASE READ FIRST!!
! PLEASE READ FIRST!!") From: AR Center (Arkansas Center for the Study of Integrative Medicine) PLEASE READ FIRST Please be sure that you have a QUALIFYING MEDICAL CONDITION for Medical Marijuana in Arkansas. If you do not have
From: AR Center (Arkansas Center for the Study of Integrative Medicine) PLEASE READ FIRST Please be sure that you have a QUALIFYING MEDICAL CONDITION for Medical Marijuana in Arkansas. If you do not have
PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip
 PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip Primary Phone ( ) Secondary Phone ( ) Other Phone ( ) SS# - - Race Ethnicity Email address Preferred language Marital Status Minor Single
PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip Primary Phone ( ) Secondary Phone ( ) Other Phone ( ) SS# - - Race Ethnicity Email address Preferred language Marital Status Minor Single
Augmentative-Alternative Communication Adult Intake Form
 College of Health and Public Affairs Department of Communication Sciences and Disorders and Communication Disorders Clinic FAAST Atlantic Region Assistive Technology Demonstration Center Augmentative-Alternative
College of Health and Public Affairs Department of Communication Sciences and Disorders and Communication Disorders Clinic FAAST Atlantic Region Assistive Technology Demonstration Center Augmentative-Alternative
Augmentative-Alternative Communication Adult Intake Form
 College of Health and Public Affairs Department of Communication Sciences and Disorders and Communication Disorders Clinic FAAST Atlantic Region Assistive Technology Demonstration Center Augmentative-Alternative
College of Health and Public Affairs Department of Communication Sciences and Disorders and Communication Disorders Clinic FAAST Atlantic Region Assistive Technology Demonstration Center Augmentative-Alternative
Welcome Letter- Orchard School Clinic
 Welcome Letter- Orchard School Clinic Dear Parent or Guardian: Orchard School Clinic is a school-based location of RiverStone Health Clinic. This is a collaborative effort between RiverStone Health, Billings
Welcome Letter- Orchard School Clinic Dear Parent or Guardian: Orchard School Clinic is a school-based location of RiverStone Health Clinic. This is a collaborative effort between RiverStone Health, Billings
ALFRED ALINGU, MD INTERNAL MEDICINE
 Name Date of Birth Social Security Number Marital Status Address City State Zip Code Home Phone Cell Phone E-mail Address Pharmacy Name Pharmacy Phone Number Emergency Contact Phone Number Relationship
Name Date of Birth Social Security Number Marital Status Address City State Zip Code Home Phone Cell Phone E-mail Address Pharmacy Name Pharmacy Phone Number Emergency Contact Phone Number Relationship
INSURANCE INFORMATION
 2014 575 Hill Country Dr. Ste 202 Kerrville, TX 78028 (830)258-6237 Office (830)315-1366 Fax Patient Name (last, first, MI) of Birth Social Security Number Mailing Address Home Telephone Work Telephone
2014 575 Hill Country Dr. Ste 202 Kerrville, TX 78028 (830)258-6237 Office (830)315-1366 Fax Patient Name (last, first, MI) of Birth Social Security Number Mailing Address Home Telephone Work Telephone
Print Guardian Name (If not patient) DOB: Patients Name: (Last, First, MI): Circle One: - - / / Mailing Address: Apt. #: City: State: Zip Code:
 DOB: Patients Name: (Last, First, MI): Circle One: - - / / Mailing Address: Apt. #: City: State: Zip Code:") Patients Name: (Last, First, MI): SSN: DOB: Circle One: Male Mailing Address: Apt. #: City: State: Zip Code: Female Race: Ethnicity Primary Language: Home Phone: Preferred? Cell Phone: Preferred? Employer:
Patients Name: (Last, First, MI): SSN: DOB: Circle One: Male Mailing Address: Apt. #: City: State: Zip Code: Female Race: Ethnicity Primary Language: Home Phone: Preferred? Cell Phone: Preferred? Employer:
(Please Print) PATIENT INFORMATION. Sex: Male Female Home phone no: ( ) City: State: Zip: Cell phone no: ( ) Occupation: Employer: Work phone no: ( )
 PATIENT INFORMATION. Sex: Male Female Home phone no: ( ) City: State: Zip: Cell phone no: ( ) Occupation: Employer: Work phone no: ( )") (Please Print) Today s date: Primary Care Physician: PATIENT INFORMATION First name: Middle: Last: Former name: Marital Status: Single Married Divorced Widowed Street address: Birthdate: SSN: Email Address:
(Please Print) Today s date: Primary Care Physician: PATIENT INFORMATION First name: Middle: Last: Former name: Marital Status: Single Married Divorced Widowed Street address: Birthdate: SSN: Email Address:
PATIENT INSTRUCTIONS FOR PAPERWORK
 330 Mallory Sta-on Rd., Suite B3 Franklin, TN 37067 Ph. 615-944-3530 Fax. 615-550.2641 PATIENT INSTRUCTIONS FOR PAPERWORK Thank you so much for trus0ng your care to Integra0ve Family Medicine. A
330 Mallory Sta-on Rd., Suite B3 Franklin, TN 37067 Ph. 615-944-3530 Fax. 615-550.2641 PATIENT INSTRUCTIONS FOR PAPERWORK Thank you so much for trus0ng your care to Integra0ve Family Medicine. A
DECLARATION AND CONSENT TO TREATMENT
 3160 Steeles Avenue East, Suite 204 Markham, ON L3R 4G9 T. 905.477.0200 F. 905.477.0028 E. info@mnhc.ca W. www.mnhc.ca DECLARATION AND CONSENT TO TREATMENT Patients Name _ Date City Province Postal Code
3160 Steeles Avenue East, Suite 204 Markham, ON L3R 4G9 T. 905.477.0200 F. 905.477.0028 E. info@mnhc.ca W. www.mnhc.ca DECLARATION AND CONSENT TO TREATMENT Patients Name _ Date City Province Postal Code
Please allow us hours to refill the medication; approval from your medical provider is required on all refills.
 Thank you for choosing Rex Primary Care of Holly Springs for your primary care needs. To keep our patients better informed we have created a list of our office policies to make your visit and continuation
Thank you for choosing Rex Primary Care of Holly Springs for your primary care needs. To keep our patients better informed we have created a list of our office policies to make your visit and continuation
2017 Medi-Slim Weight Loss Patient Information Form
 Medi-Slim Weight Loss Patient Information Form Patient Name (Last) (First) (MI) Name you prefer to be called: Patient Address: City:_ State Zip Phone number you would prefer us to use: May we email you?
Medi-Slim Weight Loss Patient Information Form Patient Name (Last) (First) (MI) Name you prefer to be called: Patient Address: City:_ State Zip Phone number you would prefer us to use: May we email you?
PATIENT INFORMATION. Patient s Name: Birthdate: ( ) F ( ) M LAST FIRST MI. ( ) Married ( ) Single ( ) Divorced ( ) Separated ( ) Widowed Occupation:
 F ( ) M LAST FIRST MI. ( ) Married ( ) Single ( ) Divorced ( ) Separated ( ) Widowed Occupation:") UPON COMPLETION OF PATIENT REGISTRATION PACKET, PLEASE BRING ALL FORMS TO YOUR APPOINTMENT. YOU MAY ALSO FAX COMPLETED FORMS TO THE OFFICE AT 910-575- 9103. THANK YOU. PATIENT INFORMATION Patient s Name:
UPON COMPLETION OF PATIENT REGISTRATION PACKET, PLEASE BRING ALL FORMS TO YOUR APPOINTMENT. YOU MAY ALSO FAX COMPLETED FORMS TO THE OFFICE AT 910-575- 9103. THANK YOU. PATIENT INFORMATION Patient s Name:
Patient: Gender: Male Female. Mailing Address: Ethnicity: Not Hispanic or Latin Hispanic/Latin Home Phone #:
 5002 Highway 39 N Bldg. A Meridian, MS 39301 Phone: 601-512-0500 Fax: 601-512-0505 Patient Information Patient: Gender: Male Female First Middle Last Primary Language: English Spanish Other Mailing Address:
5002 Highway 39 N Bldg. A Meridian, MS 39301 Phone: 601-512-0500 Fax: 601-512-0505 Patient Information Patient: Gender: Male Female First Middle Last Primary Language: English Spanish Other Mailing Address:
Women s Specialty Care, P.C 682 Hemlock Street Suite 300 Macon GA WELCOME
 Women s Specialty Care, P.C 682 Hemlock Street Suite 3 Macon GA 3121 478-744-9683 WELCOME Thank you for choosing Women s Specialty Care, P.C. for your OB/GYN needs. We ask that you complete all of the
Women s Specialty Care, P.C 682 Hemlock Street Suite 3 Macon GA 3121 478-744-9683 WELCOME Thank you for choosing Women s Specialty Care, P.C. for your OB/GYN needs. We ask that you complete all of the
Social Security Number: Employment Status: Employed Unemployed Address: Student Retired
 Please complete all forms fully and to the best of your ability. If something does not apply to you please write N/A in the field. Patient Demographics: Name: Sex: Male Female Address: Apt: City: Marital
Please complete all forms fully and to the best of your ability. If something does not apply to you please write N/A in the field. Patient Demographics: Name: Sex: Male Female Address: Apt: City: Marital
SPOUSE/GUARDIAN (If patient is married, give spouse information. If patient is a child, give parent information.)
") Please Fill Out Completely: St. Mary s Women s Center 1000 Cowles Clinic Way, Suite D-300 Greensboro, GA 30642 762-243-3860 phone 762-243-3879 fax Patient s Last Name First Name MI Social Security Number
Please Fill Out Completely: St. Mary s Women s Center 1000 Cowles Clinic Way, Suite D-300 Greensboro, GA 30642 762-243-3860 phone 762-243-3879 fax Patient s Last Name First Name MI Social Security Number
HEALTH HISTORY QUESTIONNAIRE
 Patient Name: of Birth: HEALTH HISTORY QUESTIONNAIRE Primary Care Physician: Other physicians you currently see: Emergency Phone #: Contact Person/Relationship: Reason for the Visit: Please list your medications
Patient Name: of Birth: HEALTH HISTORY QUESTIONNAIRE Primary Care Physician: Other physicians you currently see: Emergency Phone #: Contact Person/Relationship: Reason for the Visit: Please list your medications
The Providers and Staff of Baptist Medical Group Primary Care- LiveOak BAPTISTMEDICALGROUP.ORG. Primary Care - Live Oak.
 BAPTISTMEDICALGROUP.ORG Primary Care - Live Oak Dear Patient, Thank you for choosing Baptist Medical Group Primary Care - Live Oak to provide you with compassionate care for your health care needs. We
BAPTISTMEDICALGROUP.ORG Primary Care - Live Oak Dear Patient, Thank you for choosing Baptist Medical Group Primary Care - Live Oak to provide you with compassionate care for your health care needs. We
Date: Name: Date of birth: Reason for today s visit: If yes, what are you allergic to and what type of reaction/symptoms did you have?
 Date: Name: Date of birth: Nickname/prefer to be called: Date that your last menstrual period began: Reason for today s visit: Allergies to medications/foods/substances? Yes No If yes, what are you allergic
Date: Name: Date of birth: Nickname/prefer to be called: Date that your last menstrual period began: Reason for today s visit: Allergies to medications/foods/substances? Yes No If yes, what are you allergic
Adult Health History
 Adult Health History Name: DOB: Please list medications, including: vitamins, herbs, homeopathic remedies, and nonprescription medicines on the attached medication sheet. Medical History: High blood pressure
Adult Health History Name: DOB: Please list medications, including: vitamins, herbs, homeopathic remedies, and nonprescription medicines on the attached medication sheet. Medical History: High blood pressure
Office Hours Our office hours are Monday through Friday 7:30 am to 5:30pm. Our office is closed on all major Holidays.
 Dear New Patient: We would like to welcome you to our practice. Our goal is to make your experience with us as pleasant as possible. In order to help us meet this goal we have listed some helpful hints
Dear New Patient: We would like to welcome you to our practice. Our goal is to make your experience with us as pleasant as possible. In order to help us meet this goal we have listed some helpful hints
GRAHAM CHIROPRACTIC CENTER, INC. BRYAN GRAHAM, DC, CCSP
 New Patient Intake Form Patient Information Thank you for choosing our practice for your chiropractic needs. Please fill out this form as completely as possible. If you have any questions or concerns,
New Patient Intake Form Patient Information Thank you for choosing our practice for your chiropractic needs. Please fill out this form as completely as possible. If you have any questions or concerns,
Patient Name: Date: RETURNING THIS CASE HISTORY DOES NOT GUARANTEE THAT YOUR HEALTH CARE CAN BE ACCOMPLISHED OVER THE PHONE.
 6839 Fort Dent Way, Suite 134 Tukwila, Washington 98188 Phone (206) 812-9988 Fax (206) 812-9989 Medical Director Jonathan V. Wright, MD Patient Name: Date: Thank You for your interest in Tahoma Clinic
6839 Fort Dent Way, Suite 134 Tukwila, Washington 98188 Phone (206) 812-9988 Fax (206) 812-9989 Medical Director Jonathan V. Wright, MD Patient Name: Date: Thank You for your interest in Tahoma Clinic
ObGyne Consultants ObGyne After Hours Middle Georgia Immediate Care Center
 1 ObGyne Consultants ObGyne After Hours Middle Georgia Immediate Care Center http://obgyneconsultants.com http://obgynepatientnews.com Macon 639 Hemlock St. Macon, GA 31201 P: (478) 745-3014 F: (478) 745-9887
1 ObGyne Consultants ObGyne After Hours Middle Georgia Immediate Care Center http://obgyneconsultants.com http://obgynepatientnews.com Macon 639 Hemlock St. Macon, GA 31201 P: (478) 745-3014 F: (478) 745-9887
Welcome to Hawaii Women s Healthcare
 Cheryl Lynn T. Rudy, M.D. Cheryl L. Leialoha, M.D. Erin C. Gertz, M.D. Laura A. Spector, D.O. Andrea Wieland, APRN Welcome to Hawaii Women s Healthcare Hawaii Women s Healthcare strives to provide you
Cheryl Lynn T. Rudy, M.D. Cheryl L. Leialoha, M.D. Erin C. Gertz, M.D. Laura A. Spector, D.O. Andrea Wieland, APRN Welcome to Hawaii Women s Healthcare Hawaii Women s Healthcare strives to provide you
Welcome to University Family Healthcare, PA.
 Welcome to University Family Healthcare, PA. We re delighted that you have chosen us as your primary care providers. We work hard to earn your trust and to see that you have the best healthcare possible.
Welcome to University Family Healthcare, PA. We re delighted that you have chosen us as your primary care providers. We work hard to earn your trust and to see that you have the best healthcare possible.
The process has been designed to be user friendly and involves a few simple steps.
 HOW DO I ENROLL A PATIENT WITH HOUSECALL MD? The process has been designed to be user friendly and involves a few simple steps. It is the patient s/family s/dpoa s/guardian s decision, if they want to
HOW DO I ENROLL A PATIENT WITH HOUSECALL MD? The process has been designed to be user friendly and involves a few simple steps. It is the patient s/family s/dpoa s/guardian s decision, if they want to
NURSING STUDENT HEALTH & IMMUNIZATION RECORDS
 NURSING STUDENT HEALTH & IMMUNIZATION RECORDS *********************************** COMPLETE THE ATTACHED HEALTH PACKET AND SUBMIT TO THE NURSING DEPARTMENT NO LATER THAN THE ASN ORIENTATION. **************************************
NURSING STUDENT HEALTH & IMMUNIZATION RECORDS *********************************** COMPLETE THE ATTACHED HEALTH PACKET AND SUBMIT TO THE NURSING DEPARTMENT NO LATER THAN THE ASN ORIENTATION. **************************************
The Home Doctor. Registration Checklist
 The Home Doctor Registration Checklist All enrollees: ( ) Enrollment Form ( ) Copy of Insurance card(s) ( ) Medication List ( ) POA/Guardianship documents NOTICE Please allow two weeks for processing this
The Home Doctor Registration Checklist All enrollees: ( ) Enrollment Form ( ) Copy of Insurance card(s) ( ) Medication List ( ) POA/Guardianship documents NOTICE Please allow two weeks for processing this
R. B. KO L A C H A L A M M. D. GENERAL SURGERY
 GENERAL SURGERY Patient Information (Please Print and Circle or check the appropriate response) Patient s Name: DOB: _ Address: City: _ Zip: Home Phone: Cell: Work:_ Email Address: Patient s SSN: Male
GENERAL SURGERY Patient Information (Please Print and Circle or check the appropriate response) Patient s Name: DOB: _ Address: City: _ Zip: Home Phone: Cell: Work:_ Email Address: Patient s SSN: Male
HARBOR CARE HEALTH & WELLNESS CENTER Patient Intake Form Please print clearly. Please ask for assistance in completing this form if needed.
 Today date: HARBOR CARE HEALTH & WELLNESS CENTER Patient Intake Form Please print clearly. Please ask for assistance in completing this form if needed. Patient Full Name: Of Birth: Street: City: Zip Code:
Today date: HARBOR CARE HEALTH & WELLNESS CENTER Patient Intake Form Please print clearly. Please ask for assistance in completing this form if needed. Patient Full Name: Of Birth: Street: City: Zip Code:
The Priority Care Center
 The Priority Care Center Care Coordination Services The Priority Care Center offers Care Coordination services to individuals needing extra support in meeting their health related goals. Services include:
The Priority Care Center Care Coordination Services The Priority Care Center offers Care Coordination services to individuals needing extra support in meeting their health related goals. Services include:
NEW PATIENT INFORMATION
 NEW PATIENT INFORMATION Welcome to Nephrology Hypertension Specialists! In order to make your first visit with us as smooth as possible, we have put together a new patient package. It includes the following
NEW PATIENT INFORMATION Welcome to Nephrology Hypertension Specialists! In order to make your first visit with us as smooth as possible, we have put together a new patient package. It includes the following
PAYMENT IS REQUIRED AT THE TIME SERVICES ARE RENDERED. THANK YOU!
 PATIENT INFORMATION FORM PATIENT DATA: - - PATIENT NAME (LAST, FIRST, MIDDLE) SOCIAL SECURITY # SEX ( ) - ( ) - ADDRESS HOME PHONE NUMBER MOBILE PHONE NUMBER CITY STATE ZIP CODE OCCUPATION / / DATE OF
PATIENT INFORMATION FORM PATIENT DATA: - - PATIENT NAME (LAST, FIRST, MIDDLE) SOCIAL SECURITY # SEX ( ) - ( ) - ADDRESS HOME PHONE NUMBER MOBILE PHONE NUMBER CITY STATE ZIP CODE OCCUPATION / / DATE OF
! Thank you for including Lane Community College Health Clinic as part of your
 Welcome to the Lane Community College Health Clinic!! Thank you for including Lane Community College Health Clinic as part of your healthcare team. We provide accessible, high-quality medical treatment
Welcome to the Lane Community College Health Clinic!! Thank you for including Lane Community College Health Clinic as part of your healthcare team. We provide accessible, high-quality medical treatment
New Patient Medical Form (Please use BLACK ink)
") New Patient Medical Form (Please use BLACK ink) Patient Name: First Middle Initial Last Address: Street City State Zip Code Home Phone: ( ) - - Work Phone: ( ) - - Cell Phone: ( ) - - Gender: [] Female
New Patient Medical Form (Please use BLACK ink) Patient Name: First Middle Initial Last Address: Street City State Zip Code Home Phone: ( ) - - Work Phone: ( ) - - Cell Phone: ( ) - - Gender: [] Female
Name DOB / / SS# / / Street Address City/State/Zip. Home ( ) - Cell( ) - Work( ) - Emergency Contact Day Phone( ) -
 - Cell( ) - Work( ) - Emergency Contact Day Phone( ) -") Wellesley Women s Care, P.C. PPG Thank you for taking the time to complete this form. We ask that you complete this entire form once a year or when you have any NEW information. PATIENT INFORMATION (Please
Wellesley Women s Care, P.C. PPG Thank you for taking the time to complete this form. We ask that you complete this entire form once a year or when you have any NEW information. PATIENT INFORMATION (Please
1301 W. 38th St. Medical Park Tower, Suite 113 Austin, TX Dear Patient:
 1301 W. 38th St. Medical Park Tower, Suite 113 Austin, TX 78705 Dear Patient: Welcome to Seton Healthcare Family s Cancer Care Collaborative. We are honored you chose Seton to assist you in your medical
1301 W. 38th St. Medical Park Tower, Suite 113 Austin, TX 78705 Dear Patient: Welcome to Seton Healthcare Family s Cancer Care Collaborative. We are honored you chose Seton to assist you in your medical
WELCOME TO THE UPMC LIVER CANCER CENTER PLEASE FILL OUT AND BRING WITH YOU TO YOUR APPOINTMENT
 WELCOME TO THE UPMC LIVER CANCER CENTER PLEASE FILL OUT AND BRING WITH YOU TO YOUR APPOINTMENT You are scheduled to have an appointment at the UPMC Liver Cancer Center which is located in the UPMC Montefiore
WELCOME TO THE UPMC LIVER CANCER CENTER PLEASE FILL OUT AND BRING WITH YOU TO YOUR APPOINTMENT You are scheduled to have an appointment at the UPMC Liver Cancer Center which is located in the UPMC Montefiore
This is to confirm my appointment on at with Dr..
 TAHOMA CLINIC Clinic & Dispensary Jonathan V. Wright, MD 801 Southwest 16 th, Suite 121 Medical Director Renton, Washington 98057 Office (425) 264-0059 Fax (425) 264-0071 Patient Name: Date: This is to
TAHOMA CLINIC Clinic & Dispensary Jonathan V. Wright, MD 801 Southwest 16 th, Suite 121 Medical Director Renton, Washington 98057 Office (425) 264-0059 Fax (425) 264-0071 Patient Name: Date: This is to
Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR fax Physician
 Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR 97031 541-387-6125 fax 541-387-6315 Physician Welcome to the Columbia Gorge Heart Clinic. We welcome you as a patient and
Columbia Gorge Heart Clinic 1108 June St. Appointment date/time Hood River, OR 97031 541-387-6125 fax 541-387-6315 Physician Welcome to the Columbia Gorge Heart Clinic. We welcome you as a patient and
Entrance Case History (Please write or print clearly)
") Stony Brook Medical Park 2500 Nesconset Highway Suite 4-A Stony Brook, NY 11790 (631) 675-9000 Fax (631) 675-9002 www.naturalapproach.us Entrance Case History (Please write or print clearly) Today s Date
Stony Brook Medical Park 2500 Nesconset Highway Suite 4-A Stony Brook, NY 11790 (631) 675-9000 Fax (631) 675-9002 www.naturalapproach.us Entrance Case History (Please write or print clearly) Today s Date
714 Beacon Street, Newton Centre, MA,
 Nancy Cooper, MD Kari Emsbo, MD Yana Urman, MD 714 Beacon Street Newton Centre, MA 02459 617-332-1001 Phone 617-332-5154 Fax Dear Patient: On behalf of all of us at Beth Israel Deaconess HealthCare-Newton
Nancy Cooper, MD Kari Emsbo, MD Yana Urman, MD 714 Beacon Street Newton Centre, MA 02459 617-332-1001 Phone 617-332-5154 Fax Dear Patient: On behalf of all of us at Beth Israel Deaconess HealthCare-Newton
Seasons Women s Care Patient Registration Form
 Seasons Women s Care Patient Registration Form Name: of Birth: Address: City: St: Zip Home Phone: Cell: Best Number: Email: Race or Ethnicity: Marital Status: SS# Drivers Lic#: Employer: Work# Occupation:
Seasons Women s Care Patient Registration Form Name: of Birth: Address: City: St: Zip Home Phone: Cell: Best Number: Email: Race or Ethnicity: Marital Status: SS# Drivers Lic#: Employer: Work# Occupation:
Renée Rinaldi, MD Dahlia Carr, MD Ami Ben-Artzi, MD
 Renée Rinaldi, MD Dahlia Carr, MD Ami Ben-Artzi, MD RHEUMATOLOGY CONSUTLATION ARTHRITIC CONDITIONS AUTOIMMUNE DISEASES MUSCULOSKELETAL ULTRASOUND Name: First Name Last Name Social Security Number: Sex:
Renée Rinaldi, MD Dahlia Carr, MD Ami Ben-Artzi, MD RHEUMATOLOGY CONSUTLATION ARTHRITIC CONDITIONS AUTOIMMUNE DISEASES MUSCULOSKELETAL ULTRASOUND Name: First Name Last Name Social Security Number: Sex:
ST. LAWRENCE REHABILITATION CENTER OUTPATIENT POLICIES AND REGISTRATION INFORMATION
 Outpatient Services 2381 Lawrenceville Road 609-896-9500 voice Patient Name: Account #: ST. LAWRENCE REHABILITATION CENTER OUTPATIENT POLICIES AND REGISTRATION INFORMATION Your first day of outpatient
Outpatient Services 2381 Lawrenceville Road 609-896-9500 voice Patient Name: Account #: ST. LAWRENCE REHABILITATION CENTER OUTPATIENT POLICIES AND REGISTRATION INFORMATION Your first day of outpatient
Beck & Blackley Chiropractic Clinic
 Address City State Zip Code Home Phone Cell Phone Work Phone Email Address Sex: M F Marital Status: M S D W Date of Birth SS# Spouse Name How did you hear about our office? Employer Name/Occupation Emergency
Address City State Zip Code Home Phone Cell Phone Work Phone Email Address Sex: M F Marital Status: M S D W Date of Birth SS# Spouse Name How did you hear about our office? Employer Name/Occupation Emergency
MR #: Patient Name: Page: 1 of 4 PROGRESSIVE PHYSICAL THERAPY PATIENT DATA SHEET. May we send you text messages relating to your care with us?
 MR #: Patient Name: Page: 1 of 4 PROGRESSIVE PHYSICAL THERAPY PATIENT DATA SHEET First: MI: Last: of Birth: Age: Gender: Male Female Mailing Address: Physical Address: May we send you text messages relating
MR #: Patient Name: Page: 1 of 4 PROGRESSIVE PHYSICAL THERAPY PATIENT DATA SHEET First: MI: Last: of Birth: Age: Gender: Male Female Mailing Address: Physical Address: May we send you text messages relating
Patient Registration Form
 Padma Sripada MD, Columbia Internal Medicine 2500 Pond View, Suite 202 Castleton on Hudson, NY 12033 Phone: 518-391-2889 Date: Patient Registration Form First Name Middle Last Name... Sex: M F Preferred
Padma Sripada MD, Columbia Internal Medicine 2500 Pond View, Suite 202 Castleton on Hudson, NY 12033 Phone: 518-391-2889 Date: Patient Registration Form First Name Middle Last Name... Sex: M F Preferred
Patient Name Date of Birth / / We need the following information in order to comply with federal regulatory standards, thank you.
 The Women s Clinic of Northern Colorado New Patient Exam Intake History (970) 493-7442 1107 S Lemay Ave, Ste 300, Fort Collins ~ 2500 Rocky Mountain Ave, North MOB, Ste 150, Loveland Patient Name Date
The Women s Clinic of Northern Colorado New Patient Exam Intake History (970) 493-7442 1107 S Lemay Ave, Ste 300, Fort Collins ~ 2500 Rocky Mountain Ave, North MOB, Ste 150, Loveland Patient Name Date
Date: PATIENT REGISTRATION Chart # PLEASE PRINT FILL OUT ALL AREAS PATIENT INFORMATION CHILD S NAME BIRTHDATE SSN SEX CELL PHONE# (14 YRS & OLDER)
") PEDIATRIC ASSOCIATES OF MADISON 21 Hughes Rd., Suite 2 Madison, Alabama 35758 256-772-2037 Fax 256-772-9523 www.pedsofmadison.com Tonya T. Zbell, M.D. Robbie F. Dudley, M.D. Charlotte M. Meadows, M.D.
PEDIATRIC ASSOCIATES OF MADISON 21 Hughes Rd., Suite 2 Madison, Alabama 35758 256-772-2037 Fax 256-772-9523 www.pedsofmadison.com Tonya T. Zbell, M.D. Robbie F. Dudley, M.D. Charlotte M. Meadows, M.D.
Authorization, Fees, and Office Policy
 a Authorization, Fees, and Office Policy Authorization for Treatment I hereby authorize the staff of Compassionate Care Clinics of Pinellas to render medical services as deemed necessary. I also certify
a Authorization, Fees, and Office Policy Authorization for Treatment I hereby authorize the staff of Compassionate Care Clinics of Pinellas to render medical services as deemed necessary. I also certify
ADMISSION FORM. Employment Status: Retired Unemployed Employed Full Time Employed Part Time
 Patient ID Number A. PATIENT INFORMATION: First Name & Middle Initial: Home Address: ADMISSION FORM Last Name: Apartment Number: City: State: Zip: Phone: Home Cell Second Phone: Work Cell Email Address:
Patient ID Number A. PATIENT INFORMATION: First Name & Middle Initial: Home Address: ADMISSION FORM Last Name: Apartment Number: City: State: Zip: Phone: Home Cell Second Phone: Work Cell Email Address:
Medications List. Allergies. Drug Name Dosage Directions Reason Taking
 Patient Name: DOB: Medications List Allergies Please list any medications you are currently taking Drug Name Dosage Directions Reason Taking Preferred Pharmacy: Date: Location/Number: New Patient Background
Patient Name: DOB: Medications List Allergies Please list any medications you are currently taking Drug Name Dosage Directions Reason Taking Preferred Pharmacy: Date: Location/Number: New Patient Background
Patient Name Age Date of Birth. Patient Address. City State Zip Code. Home Phone Cell Phone Work Phone
 Patient Registration Date Patient Information Patient Name Age Date of Birth Patient Address City State Zip Code Home Phone Cell Phone Work Phone Last 4 Digits of Your Social Security Number Email Marital
Patient Registration Date Patient Information Patient Name Age Date of Birth Patient Address City State Zip Code Home Phone Cell Phone Work Phone Last 4 Digits of Your Social Security Number Email Marital
Welcome to the Office of Dr. Sam Van Kirk!
 Welcome to the Office of Dr. Sam Van Kirk! We understand that you have a choice in selecting your healthcare provider and we are pleased that you picked our practice. Our goal is to provide respectful,
Welcome to the Office of Dr. Sam Van Kirk! We understand that you have a choice in selecting your healthcare provider and we are pleased that you picked our practice. Our goal is to provide respectful,
New Patient Intake Form
 Phone: (336) 538-0089 Fax: (336) 538-0097 Burlington, NC 27253 New Patient Intake Form Provider: Dr. Martin DeFrancesco Melody Burr Lindsey Overton Patient Name: DOB: Marital Status: Single Married Divorced
Phone: (336) 538-0089 Fax: (336) 538-0097 Burlington, NC 27253 New Patient Intake Form Provider: Dr. Martin DeFrancesco Melody Burr Lindsey Overton Patient Name: DOB: Marital Status: Single Married Divorced
Developmental Pediatrics of Central Jersey
 PATIENT INFORMATION: CLIENT INFORMATION Date: Name: (Last) (First) (M.I.) Birthdate: Sex: Race: Address: City: State: Zip: Phone: (Home) (Work) (Cell) Email Address: Regarding the office staff or physician
PATIENT INFORMATION: CLIENT INFORMATION Date: Name: (Last) (First) (M.I.) Birthdate: Sex: Race: Address: City: State: Zip: Phone: (Home) (Work) (Cell) Email Address: Regarding the office staff or physician
Patient Registration Form
 908 South 10 th Street Office: 337.392.2330 Fax: 337.392.2580 West State Orthopedics and Sports Medicine Clinic, LLC Patient Registration Form Date: / / Patient Name: Birth Date: / / (last) (first) (mi)
908 South 10 th Street Office: 337.392.2330 Fax: 337.392.2580 West State Orthopedics and Sports Medicine Clinic, LLC Patient Registration Form Date: / / Patient Name: Birth Date: / / (last) (first) (mi)
Pediatric Patient History
 Pediatric Patient History Childs Name: Today s Date: Primary Doctor: Date of Birth: Age: Reason for visit: List all chronic medical problems: List all medication dosages and frequency taken (including
Pediatric Patient History Childs Name: Today s Date: Primary Doctor: Date of Birth: Age: Reason for visit: List all chronic medical problems: List all medication dosages and frequency taken (including
Patient Registration Form
 Date: Padma Sripada MD, Columbia Internal Medicine 2500 Pond View, Suite 202 Castleton on Hudson, NY 12033 Phone: 518-391-2889 Patient Registration Form First Name Middle Last Name... Sex: M F Date of
Date: Padma Sripada MD, Columbia Internal Medicine 2500 Pond View, Suite 202 Castleton on Hudson, NY 12033 Phone: 518-391-2889 Patient Registration Form First Name Middle Last Name... Sex: M F Date of
Patient Information: Last Name First Name MI. Address Apt/Room # City Zip. Community name (if not at home) Martial Status: S M W D
 Martial Status: S M W D") HouseCalls-MD 2998 W. Montague Ave. Suite 117 N. Charleston, SC 29418 Info@housecalls-md.com Office 843-501-2031 www.housecalls-md.com Fax 888-453-0810 Patient Information: Last Name First Name MI Gender
HouseCalls-MD 2998 W. Montague Ave. Suite 117 N. Charleston, SC 29418 Info@housecalls-md.com Office 843-501-2031 www.housecalls-md.com Fax 888-453-0810 Patient Information: Last Name First Name MI Gender
NORTH COUNTY PHYSICAL THERAPY, INC. DBA MISSION PHYSICAL THERAPY GROUP
 NORTH COUNTY PHYSICAL THERAPY, INC. DBA MISSION PHYSICAL THERAPY GROUP Last Name First Name MI Mailing Address City State Zip Date of Birth Age SSN: - - Gender: M or F Home Phone Cell Phone Email: Patient
NORTH COUNTY PHYSICAL THERAPY, INC. DBA MISSION PHYSICAL THERAPY GROUP Last Name First Name MI Mailing Address City State Zip Date of Birth Age SSN: - - Gender: M or F Home Phone Cell Phone Email: Patient
ADMISSION INFORMATION CHECKLIST
 APPLICANT: ADMISSION INFORMATION CHECKLIST Below is a listing of information needed before scheduling the Pre-Admission Interdisciplinary meeting. NEED: 1. Release of Information 2. Fully Completed Application
APPLICANT: ADMISSION INFORMATION CHECKLIST Below is a listing of information needed before scheduling the Pre-Admission Interdisciplinary meeting. NEED: 1. Release of Information 2. Fully Completed Application
South Shore Counseling & Psychological Services, P.C.
 South Shore Counseling & Psychological Services, P.C. 3340 Manchester Road, Wantagh, New York 11793 Phone: 516-785-0323 Fax: 516-785-6026 Child/Adolescent Registration Form EVERYTHING MUST BE FILLED OUT
South Shore Counseling & Psychological Services, P.C. 3340 Manchester Road, Wantagh, New York 11793 Phone: 516-785-0323 Fax: 516-785-6026 Child/Adolescent Registration Form EVERYTHING MUST BE FILLED OUT
M or F Patient s Date of Birth Patient s Social Security Number Sex. Secondary Address: (if have, Northern) Street City State Zip Code
 Street City State Zip Code") PATIENT REGISTRATION PLEASE PRINT Today's Date: Referred by: Patient s Name: Last First M.I. M or F Patient s Date of Birth Patient s Social Security Number Sex Primary Address: Street Apt/Unit # City
PATIENT REGISTRATION PLEASE PRINT Today's Date: Referred by: Patient s Name: Last First M.I. M or F Patient s Date of Birth Patient s Social Security Number Sex Primary Address: Street Apt/Unit # City
2201 Murphy Avenue, Suite 307 Nashville, TN Phone Fax Date. Patient s Full Name
 Patient Information 2201 Murphy Avenue, Suite 307 Nashville, TN 37203 Phone 615-401- 9454 Fax 615-873- 1934 www.robbinsplasticsurgery.com Date Patient s Full Name Last First M.I. Preferred Name (if different
Patient Information 2201 Murphy Avenue, Suite 307 Nashville, TN 37203 Phone 615-401- 9454 Fax 615-873- 1934 www.robbinsplasticsurgery.com Date Patient s Full Name Last First M.I. Preferred Name (if different
W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c
 W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c N E W P A T I E N T I N T A K E F O R M Print Name Today s Date Address City State Zip Email Address Date of Birth Male Female Social Security
W e l c o m e t o B i l l e r i c a C h i r o p r a c t i c N E W P A T I E N T I N T A K E F O R M Print Name Today s Date Address City State Zip Email Address Date of Birth Male Female Social Security
Outpatient Wellness Clinic
 Outpatient Wellness Clinic Patient Name: Date of Birth: Address: Phone: Email: Emergency Contact: Relationship: Phone: What is the reason for the appointment? Who were you referred by? (Physician, agency/
Outpatient Wellness Clinic Patient Name: Date of Birth: Address: Phone: Email: Emergency Contact: Relationship: Phone: What is the reason for the appointment? Who were you referred by? (Physician, agency/
MonaLisa Touch Patient Questionnaire & Health History
 MonaLisa Touch Patient Questionnaire & Health History Name: (Last) (First) (Middle) Date of Birth: Age: Occupation: Home Address: City: State: Zip: Home Phone: Cell Phone: Work: E-Mail Address: May we
MonaLisa Touch Patient Questionnaire & Health History Name: (Last) (First) (Middle) Date of Birth: Age: Occupation: Home Address: City: State: Zip: Home Phone: Cell Phone: Work: E-Mail Address: May we
Does My Child Have a Speech Problem? A Case History Form
 Does My Child Have a Speech Problem? A Case History Form Martine Vanryckeghem, Ph.D. University of Central Florida Speech and Hearing Clinic 3280 Progress Dr, Suite 500, Orlando, Fl 32826 (407)882-0468
Does My Child Have a Speech Problem? A Case History Form Martine Vanryckeghem, Ph.D. University of Central Florida Speech and Hearing Clinic 3280 Progress Dr, Suite 500, Orlando, Fl 32826 (407)882-0468
Dodge. County. Schools
 Welcome to the Dodge School Based Health Clinic. Dodge Board of Education and Dodge Connection-Communities In of Dodge, Inc. are continuing to move forward with our goal of serving the children and families
Welcome to the Dodge School Based Health Clinic. Dodge Board of Education and Dodge Connection-Communities In of Dodge, Inc. are continuing to move forward with our goal of serving the children and families
Nurse Aide. We reserve the right to cancel any class due to insufficient enrollment.
 Nurse Aide We reserve the right to cancel any class due to insufficient enrollment. **All clinical dates may vary according to site and instructor availability ABOUT THE NURSE AIDE PROGRAM The Nurse Aide
Nurse Aide We reserve the right to cancel any class due to insufficient enrollment. **All clinical dates may vary according to site and instructor availability ABOUT THE NURSE AIDE PROGRAM The Nurse Aide
PATIENT INTAKE PACKET
 PATIENT INTAKE PACKET Welcome to the CannaMD family - you're in great hands! To reduce your visit and wait time, we ask that you please complete and submit this intake packet at least 24 hours prior to
PATIENT INTAKE PACKET Welcome to the CannaMD family - you're in great hands! To reduce your visit and wait time, we ask that you please complete and submit this intake packet at least 24 hours prior to
PATIENT REGISTRATION FORM
 Natalie A. Nealeigh, PA-C PATIENT REGISTRATION FORM PATIENT INFORMATION (PLEASE PRINT) Last Name: First Name: MI: Street Address: City: State: Zip: Home #: Cell #: Work #: DOB: Age: Sex (M/F): Marital
Natalie A. Nealeigh, PA-C PATIENT REGISTRATION FORM PATIENT INFORMATION (PLEASE PRINT) Last Name: First Name: MI: Street Address: City: State: Zip: Home #: Cell #: Work #: DOB: Age: Sex (M/F): Marital
Male Female Mailing Address: Apt. #: City: State: Zip Code:
 Patients ame: (Last, First, MI): DOB: SS: Circle One: / / Male Female Mailing Address: Apt. #: City: State: Zip Code: Driver s Lic or ID #: How would you like to be contacted for appointment reminders?
Patients ame: (Last, First, MI): DOB: SS: Circle One: / / Male Female Mailing Address: Apt. #: City: State: Zip Code: Driver s Lic or ID #: How would you like to be contacted for appointment reminders?
Welcome to Mid-State Health Center. Our Promise to You. Locations and Hours. After-Hours Access
 101 Boulder Point Drive, Suite 1 Plymouth, NH 03264 603-536-4000 www.midstatehealth.org Welcome to Mid-State Health Center Mid-State Health Center looks forward to working with you and your family. Your
101 Boulder Point Drive, Suite 1 Plymouth, NH 03264 603-536-4000 www.midstatehealth.org Welcome to Mid-State Health Center Mid-State Health Center looks forward to working with you and your family. Your
PATIENT S NAME: LAST NAME: FIRST NAME: MI: DOB: MARRIED: SINGLE: SOCIAL SECURITY: HOME ADDRESS: APT# CITY: STATE: ZIP: CELLULAR PHONE:
 5056 THOROUGHBRED LANE BRENTWOOD, TN 37027 TODAY S DATE: PHONE: 615-373-3337 FAX: 615-373-3782 PATIENT S NAME: DATE OF BIRTH: M F RESPONSIBLE PARTY/GUARANTOR INFORMATION LAST NAME: FIRST NAME: MI: DOB:
5056 THOROUGHBRED LANE BRENTWOOD, TN 37027 TODAY S DATE: PHONE: 615-373-3337 FAX: 615-373-3782 PATIENT S NAME: DATE OF BIRTH: M F RESPONSIBLE PARTY/GUARANTOR INFORMATION LAST NAME: FIRST NAME: MI: DOB:
Responsible Party Information (Information used for patient balance statements) Responsible Party Another Patient Guarantor Self
 Responsible Party Another Patient Guarantor Self") Patient Information (Please Print) Dr. Miss Mr. Mrs. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Home Phone Cell No. Work Phone Ext. Primary Care Provider (PCP)
Patient Information (Please Print) Dr. Miss Mr. Mrs. Sir Patient s Name (Last) (First) (MI) Previous Name Address Line 1 City, State ZIP Home Phone Cell No. Work Phone Ext. Primary Care Provider (PCP)
COLON & RECTAL SURGERY, INC.
 COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
COLON & RECTAL SURGERY, INC. Please complete attached paperwork and bring to your appointment with your insurance card, co-pay and photo ID. If a referral is required, please be sure to contact your insurance
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice