IOM REPORT: GOVERNANCE AND FINANCING OF GRADUATE MEDICAL EDUCATION
|
|
|
- Hannah Wood
- 5 years ago
- Views:
Transcription
1 IOM REPORT: GOVERNANCE AND FINANCING OF GRADUATE MEDICAL EDUCATION Barbara Ross-Lee, D.O., FACOFP Vice President Health Sciences & Medical Affairs New York Institute of Technology
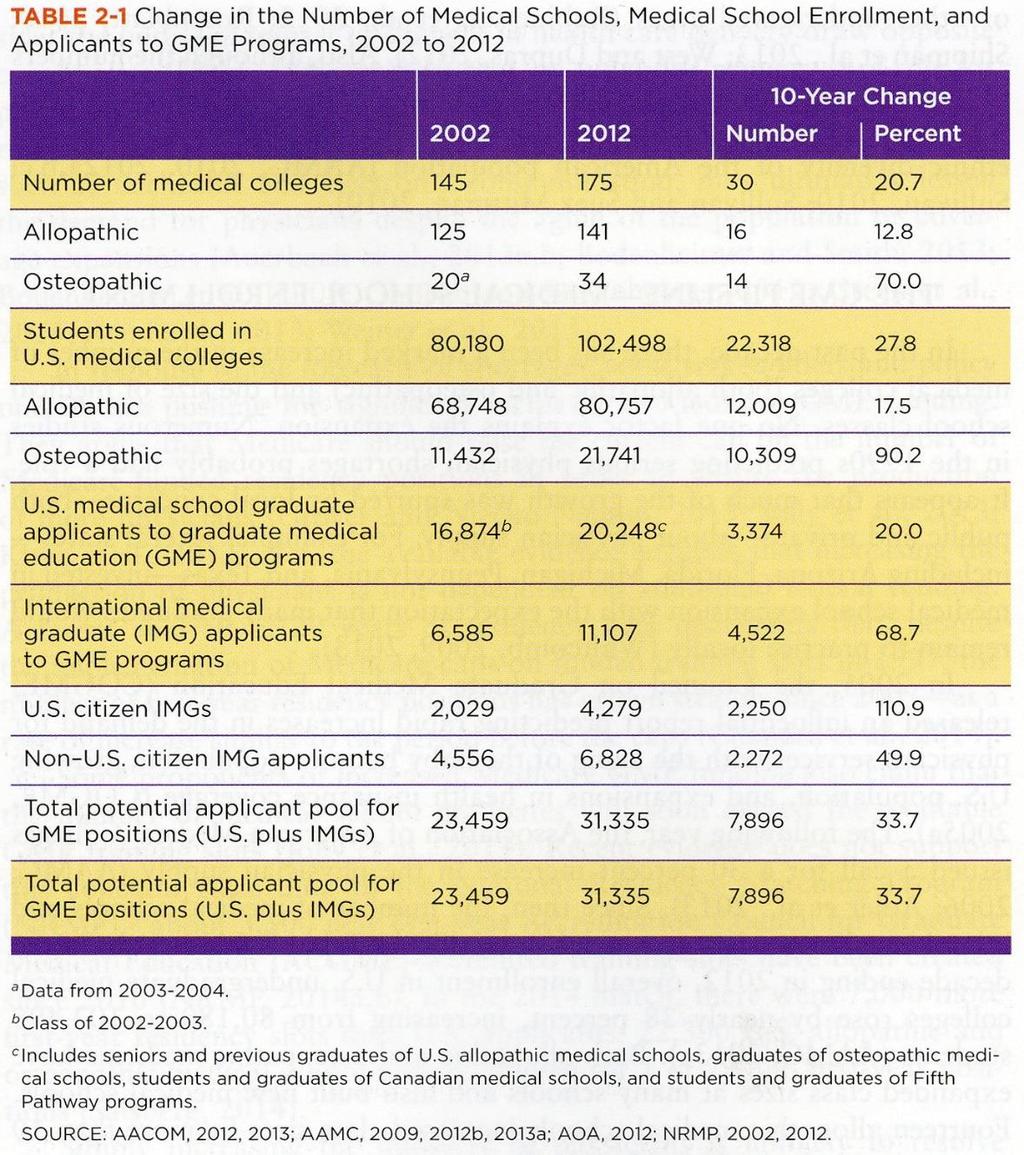
2 CONTEXT COGME prediction of oversupply of physicians Rapidly increasing IMG recruitment into US GME (without a ceiling) Growth of Osteopathic Medical Schools (parallel GME pathway-opti) Concensus statement limit GME slots to current level of US Graduates; restrain growth in UGME 1995
3 CONTEXT Cap on Medicare funded GME positions BBA 1997 Buz Cooper:Economic Model projects physician shortage Chronic and persistent geographic maldistribution Progressive specialty shortages reported Federal deficit reduction strategies by Congress
4 DEFICIT REDUCTION EFFORTS Simpson/Bowles (2010) Domenici-Rivlin (2010) Cut GME funding $10-20B Potentially eliminate GME BCA -sequestration (2010) Cut GME 2% Biden Negotiations (2010) Cut GME 15%
5 DEFICIT REDUCTION EFFORTS Super Committee (2011) Cut GME 15-60% Obama Budget (2012, 2013) Cut GME 10% Sen. Corker R-Tn (2012) CAP (2012) Cut GME by $50B/10yrs Cut GME by $28B/10yrs
6 DEFICIT REDUCTION EFFORTS CBO Deficit reduction (2012) Cut $20B/annual by 2020 Obama fiscal cliff (11/29/12) Republican fiscal cliff (12/3/12) Domenici/Rivkin task force Cut $400B care payments Cut $600B in health spending Cut $65B in health spending Bipartisaon Policy Center (2013) Cut IME % (5.5 to 3.5)
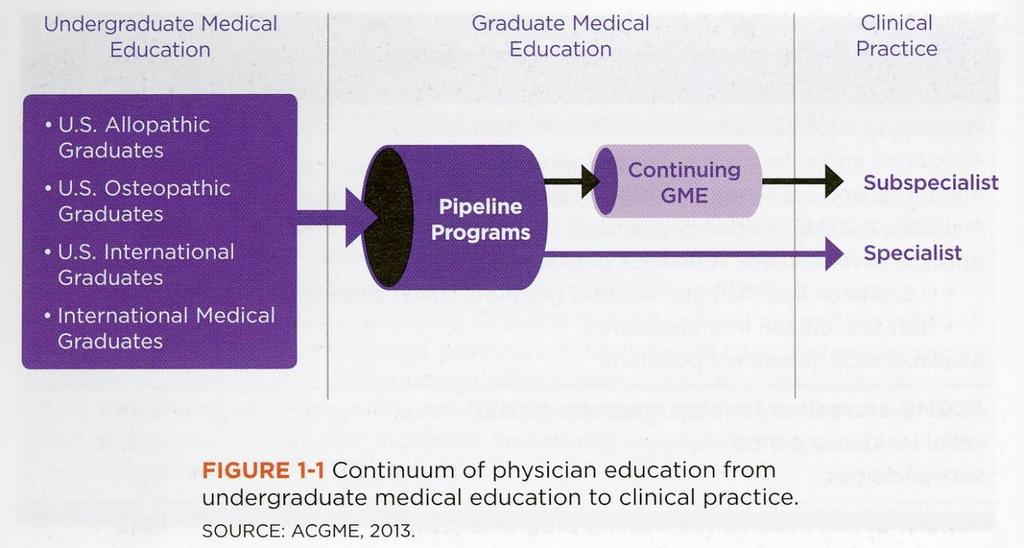
7 CHARGE TO THE COMMITTEE The IOM will develop a report with recommendations for policies to improve GME, with an emphasis on the training of physicians. Specific attention will be given to increasing the capacity of the nation s clinical workforce that can deliver efficient and high-quality health care that will meet the needs of our diverse population.
8 CHARGE TO THE COMMITTEE In developing its recommendations, the committee will consider: the current GME financing and governance structure the residency pipeline geographic distribution of generalist and specialist clinicians types of training sites relevant federal statutes and regulations respective roles of safety net providers, community health/teaching health centers, and academic health centers
9 GUIDING PRINCIPLES: TRIPLE AIM Improving the patient experience of care (including quality and satisfaction) Improving the health of populations Reducing the per capita cost of
10
11
12 FUNDAMENTAL CONCEPTS Alignment with needs/responsive Transparency Accountability Modernize/diminish complexity Transformation/innovation Flexibility Link GME Policy with GME funding Endorsement of Medicare funding for GME Establish a pathway to lift the cap on GME slots
13 PERSISTENT CONCERNS Mismatch between health needs and the specialty make up of the physician workforce Geographic maldistribution Insufficient diversity of the physician trainee pool
14 PERSISTENT CONCERNS Gap between physicians knowledge and skills and the competencies required for current medical practice Cultural competence Quality improvement, patient satisfaction, cost Health information technology Team-based care
15 Key Findings:PHYSICIAN WORKFORCE The number of GME positions offered is not connected to local, regional, or national workforce needs; neither is their distribution across specialties or geographic locations GME programs are producing an increasingly specialized workforce GME graduates preparation for practice-and their choices of practice type and location-are likely influenced by the predominance of training occurring in hospital settings More information about how to effectively influence trainee s career choices is needed.
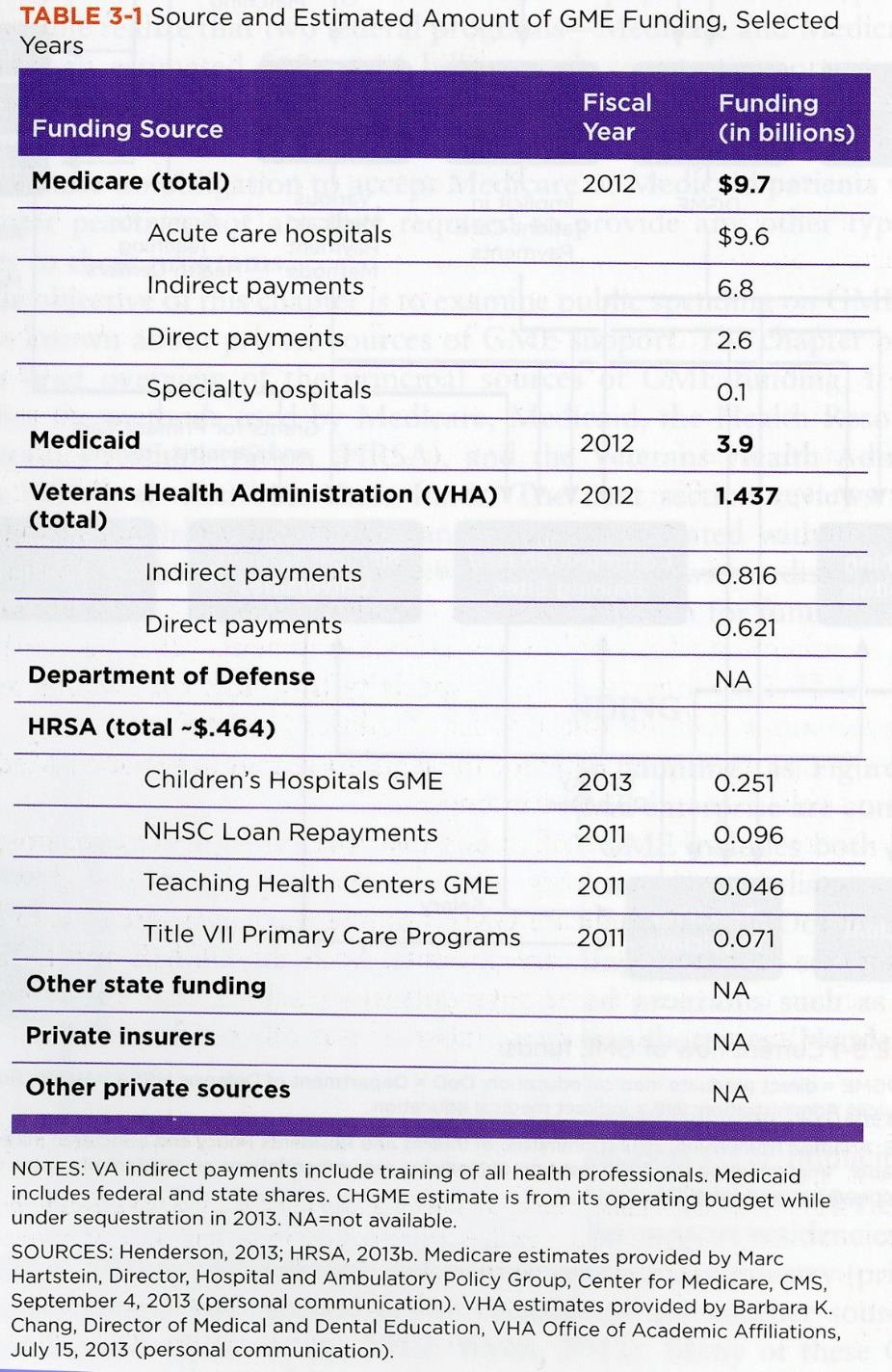
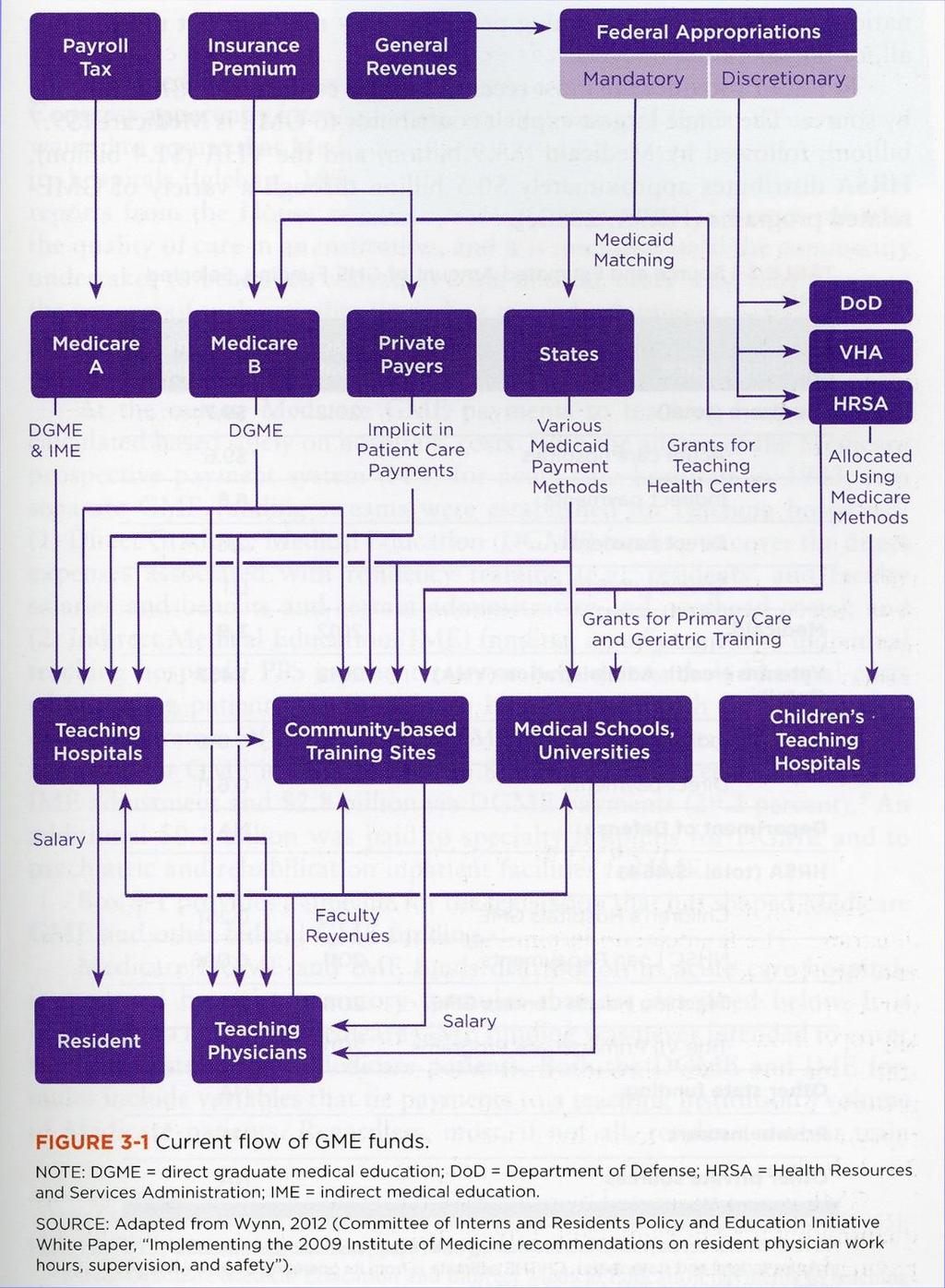
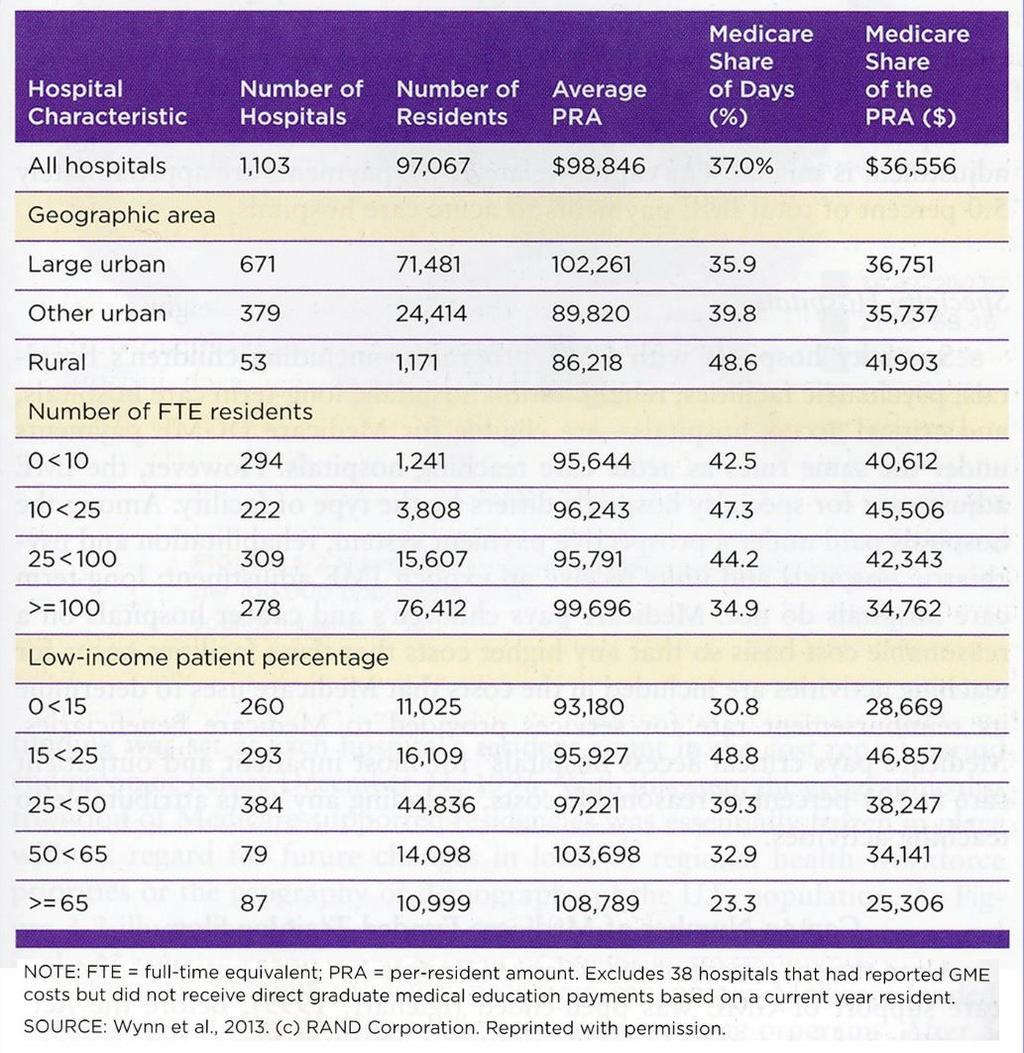
16 Key Findings: FINANCE I. Payments flow directly to teaching hospitals: UNINTENDED CONSEQUENCES Payments are not tied to outcomes; no financial incentive to improve the quality or efficiency of physician training Physician training in community based settings is discouraged Specialty mix of trainees is largely determined by teaching hospitals not local, regional, or national workforce priorities. UNINTENDED CONSEQUENCES:
17
18 Key Findings: FINANCE III. IME adjustment to DRG rates UNINTENDED CONSEQUENCES Inhibits the development and financial stability of training programs in non-hospital settings.
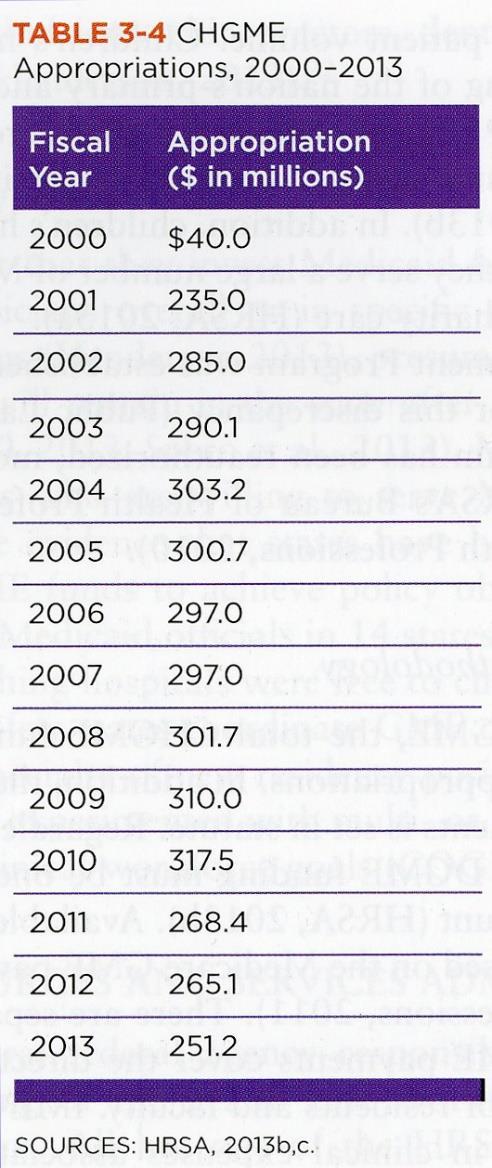
19 Key Findings: FINANCE II. Payments directly linked with Medicare patient volume UNINTENDED CONSEQUENCES Children s and other hospitals with small Medicare caseloads receive minimal support Creates a disincentive to providing services outside hospitals
20
21 Key Findings: FINANCE III. IME adjustment to DRG rates UNINTENDED CONSEQUENCES Inhibits the development and financial stability of training programs in non-hospital settings.
22 Key Findings: FINANCE III. IME adjustment to DRG rates UNINTENDED CONSEQUENCES Inhibits the development and financialstability of training programs in non-hospital settings.
23 Key Findings: FINANCE III. IME adjustment to DRG rates UNINTENDED CONSEQUENCES Inhibits the development and financialstability of training programs in non-hospital settings.
24 Key Findings: FINANCE IV. Per-resident payments are based on decades-old historical costs UNINTENDED CONSEQUENCES (Sub)specialties in short supply are funded at the same level as specialties with excess supply (Sub)specialties that boost revenues/productivity receive same support as specialties that need financial support.
25
26 Key Findings: FINANCE V. Cap on Medicare funded slots is based on training arrangement in 1996 UNINTENDED CONSEQUENCES Contributes to substantial geographic imbalance of GME payments and training slots Favors Northeastern states despite considerable movement of the U.S. population growth toward other regions of the country
27
28 Recommendation 1: INVEST STRATEGICALLY Maintain Medicare GME support at the current aggregate amount (in an agreed-on base year, adjusted annually for inflation) while taking essential steps to modernize GME payment methods based on performance, to ensure program oversight and accountability, and to incentivize innovation in the content and financing of GME. The current Medicare GME payment system should be phased out.
29 Recommendation 2: BUILD A GME POLICY AND FINANCING INFRASTRUTURE 2a. Create a GME Policy Council in the Office of the Secretary of the U.S. Department of Health and Human Services. Council members should be appointed by the Secretary and provided with sufficient funding, staff, and technical resources to fulfill the responsibilities listed below.
30 Recommendation 2a (continued): Development and oversight of a strategic plan for Medicare GME financing Research and policy development regarding the sufficiency, geographic distribution, and specialty configuration of the physician workforce; Development of future federal policies concerning the distribution and use of Medicare GME funds; Convening, coordinating, and promoting collaboration between and among federal agencies and private accreditation and certification organizations; and Provision of progress reports to Congress and the Executive Branch on the state of GME
31
32 Recommendation 2 continued: 2b. Establish a GME Center within the Centers for Medicare & Medicaid Services with the following responsibilities in accordance with and fully responsive to the ongoing guidance of the GME Council Management of the operational aspects of GME Medicare funding; Management of the GME Transformation Fund including solicitation and oversight of demonstrations; and Data collection and detailed reporting to ensure transparency in the distribution and use of Medicare GME funds.
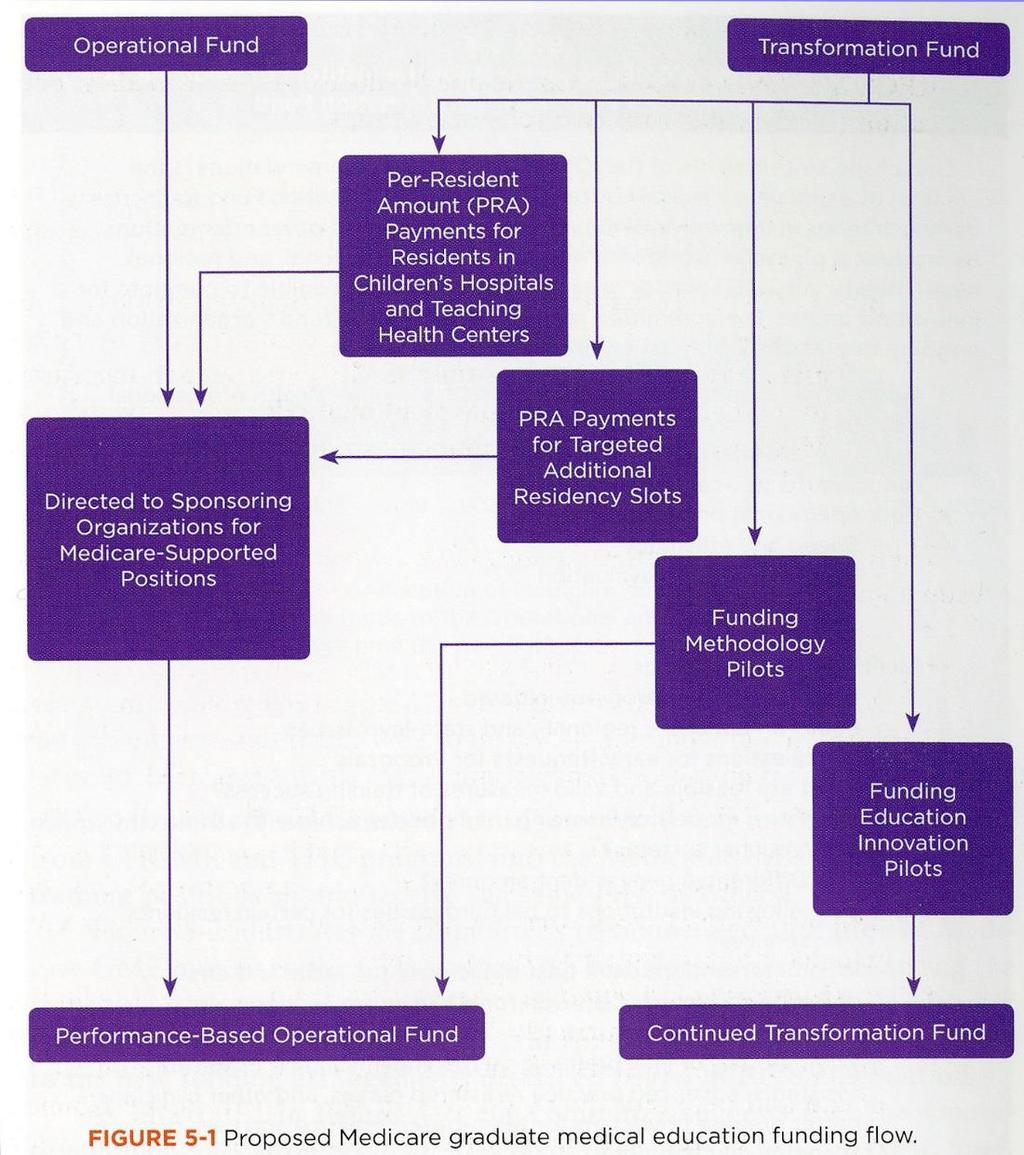
33 Recommendation 3 CREATE ONE MEDICARE GME FUND WITH TWO SUBSIDIARY FUNDS 3a. A GME Operational Fund to distribute ongoing support for residency training positions that are currently approved and funded. 3b. A GME Transformation Fund to finance initiatives to develop and evaluate innovative GME programs, to determine and validate appropriate GME performance measures, to pilot alternative GME payment methods, and to award new Medicare-funded GME training positions in priority disciplines and geographic areas.
34
35 Recommendation 4: MODERNIZE MEDICARE GME PAYMENT METHODOLOGY 4a. Replace the separate indirect medical education and direct GME funding streams with one payment to organizations sponsoring GME programs, based on a national per-resident amount (PRA) with a geographic adjustment. 4b. Set the PRA to equal the total value of the GME Operational Fund divided by the current number of Medicare-funded training slots.
36 Recommendation 4 continued: MODERNIZE MEDICARE GME PAYMENT METHODOLOGY 4c. Redirect the funding stream so that GME operational funds are distributed directly to GME sponsoring organizations. 4d. Implement performance-based payments using information from Transformation Fund pilots.
37 Recommendation 5: MEDICAID GME Medicaid GME funding should remain at the state s discretion. However, Congress should mandate the same level of transparency and accountability in Medicaid GME as it will require under the changes in Medicare GME herein proposed.
Comparison of ACP Policy and IOM Report Graduate Medical Education That Meets the Nation's Health Needs
 IOM Recommendation Recommendation 1: Maintain Medicare graduate medical education (GME) support at the current aggregate amount (i.e., the total of indirect medical education and direct graduate medical
IOM Recommendation Recommendation 1: Maintain Medicare graduate medical education (GME) support at the current aggregate amount (i.e., the total of indirect medical education and direct graduate medical
Graduate Medical Education Payments. Mark Miller, PhD Executive Director February 20, 2015
 Graduate Medical Education Payments Mark Miller, PhD Executive Director February 20, 2015 About MedPAC Independent, nonpartisan Congressional support agency 17 national experts selected for expertise Appointed
Graduate Medical Education Payments Mark Miller, PhD Executive Director February 20, 2015 About MedPAC Independent, nonpartisan Congressional support agency 17 national experts selected for expertise Appointed
Re: Rewarding Provider Performance: Aligning Incentives in Medicare
 September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
GME FINANCING AND REIMBURSEMENT: NATIONAL POLICY ISSUES
 GME FINANCING AND REIMBURSEMENT: NATIONAL POLICY ISSUES Tim Johnson, Senior Vice President Association of Hospital Medical Education (AHME) Institute May 18, 2016 2 About GNYHA Greater New York Hospital
GME FINANCING AND REIMBURSEMENT: NATIONAL POLICY ISSUES Tim Johnson, Senior Vice President Association of Hospital Medical Education (AHME) Institute May 18, 2016 2 About GNYHA Greater New York Hospital
Medicare GME Payment - A Review AODME-AACOM Annual Conference Baltimore, MD
 Medicare GME Payment - A Review 2013 AODME-AACOM Annual Conference Baltimore, MD Dominant GME Funder In Federal fiscal year 2011, Medicare paid teaching hospitals Approximately $3.2 billion in DGME payments
Medicare GME Payment - A Review 2013 AODME-AACOM Annual Conference Baltimore, MD Dominant GME Funder In Federal fiscal year 2011, Medicare paid teaching hospitals Approximately $3.2 billion in DGME payments
Complexities & Progress in Graduate Medical Education
 Complexities & Progress in Graduate Medical Education NHPF Meeting on GME Atul Grover, M.D., Ph.D., FACP, FCCP Chief Public Policy Officer, AAMC September 6, 2013 Key Principles of Accountability Measures
Complexities & Progress in Graduate Medical Education NHPF Meeting on GME Atul Grover, M.D., Ph.D., FACP, FCCP Chief Public Policy Officer, AAMC September 6, 2013 Key Principles of Accountability Measures
Ensuring an Effective Physician Workforce for America: Recommendations for an Accountable Graduate Medical Education System
 CONFERENCE SUMMARY October 2010 Atlanta, Georgia Ensuring an Effective Physician Workforce for America: Recommendations for an Accountable Graduate Medical Education System The graduate medical education
CONFERENCE SUMMARY October 2010 Atlanta, Georgia Ensuring an Effective Physician Workforce for America: Recommendations for an Accountable Graduate Medical Education System The graduate medical education
How Many Doctors, Nurses, and Other Health Professionals Do You Need?
 How Many Doctors, Nurses, and Other Health Professionals Do You Need? The Impact of New Delivery System Models on Your State s Workforce Needs? Barbara F. Brandt, PhD, Director Associate Vice President
How Many Doctors, Nurses, and Other Health Professionals Do You Need? The Impact of New Delivery System Models on Your State s Workforce Needs? Barbara F. Brandt, PhD, Director Associate Vice President
Alternative Managed Care Reimbursement Models
 Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
Geographic Adjustment Factors in Medicare
 Institute of Medicine Geographic Adjustment Factors in Medicare Roland Goertz, MD, MBA President January 20, 2011 Issues Addressed Family physician demographics Practice descriptions AAFP policy Potential
Institute of Medicine Geographic Adjustment Factors in Medicare Roland Goertz, MD, MBA President January 20, 2011 Issues Addressed Family physician demographics Practice descriptions AAFP policy Potential
Policies for Controlling Volume January 9, 2014
 Policies for Controlling Volume January 9, 2014 The Maryland Hospital Association Policies for controlling volume Introduction Under the proposed demonstration model, the HSCRC will move from a regulatory
Policies for Controlling Volume January 9, 2014 The Maryland Hospital Association Policies for controlling volume Introduction Under the proposed demonstration model, the HSCRC will move from a regulatory
The Basics of GME Finance for Program Directors February 26, 2015
 Accreditation Council for Graduate Medical Education The Basics of GME Finance for Program Directors February 26, 2015 Louis Ling, MD Senior VP for Hospital-based Accreditation lling@acgme.org mliehlai@acgme.org
Accreditation Council for Graduate Medical Education The Basics of GME Finance for Program Directors February 26, 2015 Louis Ling, MD Senior VP for Hospital-based Accreditation lling@acgme.org mliehlai@acgme.org
Statement for the Record. American College of Physicians. Hearing before the House Energy & Commerce Subcommittee on Health
 Statement for the Record American College of Physicians Hearing before the House Energy & Commerce Subcommittee on Health A Permanent Solution to the SGR: The Time Is Now January 21-22, 2015 The American
Statement for the Record American College of Physicians Hearing before the House Energy & Commerce Subcommittee on Health A Permanent Solution to the SGR: The Time Is Now January 21-22, 2015 The American
The Health System is Transforming: Now What?
 The Health System is Transforming: Now What? Katie Gaul, MA and Erin Fraher, PhD MPP Program on Health Workforce Research & Policy Cecil G. Sheps Center for Health Services Research, UNC-CH; and the Health
The Health System is Transforming: Now What? Katie Gaul, MA and Erin Fraher, PhD MPP Program on Health Workforce Research & Policy Cecil G. Sheps Center for Health Services Research, UNC-CH; and the Health
Addressing VA Physician Shortages: The Link between VA and Medicare GME
 Addressing VA Physician Shortages: The Link between VA and Medicare GME Congressional Staff Briefing Atul Grover, M.D., Ph.D. July 17, 2014 What we want to tell you today Medical schools, teaching hospitals
Addressing VA Physician Shortages: The Link between VA and Medicare GME Congressional Staff Briefing Atul Grover, M.D., Ph.D. July 17, 2014 What we want to tell you today Medical schools, teaching hospitals
Long term commitment to a new vision. Medical Director February 9, 2011
 ACCOUNTABLE CARE ORGANIZATION (ACO): Long term commitment to a new vision Michael Belman MD Michael Belman MD Medical Director February 9, 2011 Physician Reimbursement There are three ways to pay a physician,
ACCOUNTABLE CARE ORGANIZATION (ACO): Long term commitment to a new vision Michael Belman MD Michael Belman MD Medical Director February 9, 2011 Physician Reimbursement There are three ways to pay a physician,
Policy Analysis. Matching Supply to Demand: Addressing the U.S. Primary Care Workforce Shortage
 Policy Analysis NO. 7 DECEMBER 2011 CONTENT Increasing Primary Care Capacity Other Policy Options Expanding Scope of Practice Payment Policies for Team-Based Care Looking Ahead About the Institute. The
Policy Analysis NO. 7 DECEMBER 2011 CONTENT Increasing Primary Care Capacity Other Policy Options Expanding Scope of Practice Payment Policies for Team-Based Care Looking Ahead About the Institute. The
Rural Health Disparities 5/22/2012. Rural is often defined by what it is not urban. May 3, The Rural Health Landscape
 5/22/2012 May 3, 2012 The Rural Health Landscape Alan Morgan Chief Executive Officer National Rural Health Association National Rural Health Association Membership 2012 NRHA Mission The National Rural
5/22/2012 May 3, 2012 The Rural Health Landscape Alan Morgan Chief Executive Officer National Rural Health Association National Rural Health Association Membership 2012 NRHA Mission The National Rural
Joint Medicaid Oversight Committee Medicaid Behavioral Health Re-Design Panel Testimony
 Joint Medicaid Oversight Committee Medicaid Behavioral Health Re-Design Panel Testimony Jennifer Riha, BAS, MAC, Vice President of Operations A Renewed Mind Behavioral Health September 22, 2016 Senator
Joint Medicaid Oversight Committee Medicaid Behavioral Health Re-Design Panel Testimony Jennifer Riha, BAS, MAC, Vice President of Operations A Renewed Mind Behavioral Health September 22, 2016 Senator
Medicare Fee-For Service Provider Utilization & Payment Data Inpatient Public Use File: A Methodological Overview
 Medicare Fee-For Service Provider Utilization & Payment Data Inpatient Public Use File: A Methodological Overview May 30, 2014 Prepared by: The Centers for Medicare and Medicaid Services, Office of Information
Medicare Fee-For Service Provider Utilization & Payment Data Inpatient Public Use File: A Methodological Overview May 30, 2014 Prepared by: The Centers for Medicare and Medicaid Services, Office of Information
HEALTH PROFESSIONAL WORKFORCE
 HEALTH PROFESSIONAL WORKFORCE (SECTION-BY-SECTION ANALYSIS) (Information compiled from the Democratic Policy Committee (DPC) Report on The Patient Protection and Affordable Care Act and the Health Care
HEALTH PROFESSIONAL WORKFORCE (SECTION-BY-SECTION ANALYSIS) (Information compiled from the Democratic Policy Committee (DPC) Report on The Patient Protection and Affordable Care Act and the Health Care
Rural Health Clinics
 Rural Health Clinics * An Issue Paper of the National Rural Health Association originally issued in February 1997 This paper summarizes the history of the development and current status of Rural Health
Rural Health Clinics * An Issue Paper of the National Rural Health Association originally issued in February 1997 This paper summarizes the history of the development and current status of Rural Health
Health Workforce 2025
 Health Workforce 2025 Workforce projections for Australia Mr Mark Cormack Chief Executive Officer, HWA Organisation for Economic Co-operation and Development Expert Group on Health Workforce Planning and
Health Workforce 2025 Workforce projections for Australia Mr Mark Cormack Chief Executive Officer, HWA Organisation for Economic Co-operation and Development Expert Group on Health Workforce Planning and
The Law and EHRs in Medical Education: The ARRA World. Overview
 The Law and EHRs in Medical Education: The ARRA World David Donnersberger MD, JD Clinical Assistant Professor of Medicine MS3 Site Director University of Chicago Pritzker School of Medicine Overview American
The Law and EHRs in Medical Education: The ARRA World David Donnersberger MD, JD Clinical Assistant Professor of Medicine MS3 Site Director University of Chicago Pritzker School of Medicine Overview American
Healthcare Reimbursement Change VBP -The Future is Now
 Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
Healthcare Reimbursement Change VBP -The Future is Now 1 On the Move Volume/ Fee-for-Service Fee-for-service reimbursement High quality not rewarded No shared financial risk Stand-alone systems can thrive
Training Physicians for Careers in Public Health
 Training Physicians for Careers in Public Health Michael Parkinson, MD, MPH, FACPM Presented to the IOM Committee on Training Physicians for Careers in Public Health October 5, 2006 About ACPM l National
Training Physicians for Careers in Public Health Michael Parkinson, MD, MPH, FACPM Presented to the IOM Committee on Training Physicians for Careers in Public Health October 5, 2006 About ACPM l National
Hospital Rate Setting
 Hospital Rate Setting Calendar Year 2014 Wisconsin Department of Health Services Division of Health Care Access and Accountability Bureau of Fiscal Management September 6, 2013 1 Agenda 1. Introduction
Hospital Rate Setting Calendar Year 2014 Wisconsin Department of Health Services Division of Health Care Access and Accountability Bureau of Fiscal Management September 6, 2013 1 Agenda 1. Introduction
Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction
 Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction Background Beginning in June 2016, the Alcohol and Drug Abuse Division (ADAD) of the Minnesota Department of Human Services convened
Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction Background Beginning in June 2016, the Alcohol and Drug Abuse Division (ADAD) of the Minnesota Department of Human Services convened
The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform. Summary
 Reform. Summary") Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Doctor Shortage: CONDITION CRITICAL RESULTS OF HANYS 2012 PHYSICIAN ADVOCACY SURVEY
 Doctor Shortage: CONDITION CRITICAL RESULTS OF HANYS 2012 PHYSICIAN ADVOCACY SURVEY Primary care physicians are at the forefront of a physician shortage that continues to worsen in New York State, according
Doctor Shortage: CONDITION CRITICAL RESULTS OF HANYS 2012 PHYSICIAN ADVOCACY SURVEY Primary care physicians are at the forefront of a physician shortage that continues to worsen in New York State, according
Summary of U.S. Senate Finance Committee Health Reform Bill
 Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
PROPOSED POLICY AND PAYMENT CHANGES FOR INPATIENT STAYS IN ACUTE-CARE HOSPITALS AND LONG-TERM CARE HOSPITALS IN FY 2014
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
Health Care Reform Provisions Affecting Older Adults and Persons with Special Needs 3/30/10
 Health Care Reform Provisions Affecting Older Adults and Persons with Special Needs 3/30/10 On March 23, 2010, President Obama signed a comprehensive health care reform bill (H.R. 3590) into law. On March
Health Care Reform Provisions Affecting Older Adults and Persons with Special Needs 3/30/10 On March 23, 2010, President Obama signed a comprehensive health care reform bill (H.R. 3590) into law. On March
Rodney M. Wiseman, DO, FACOFP dist. ACOFP President
 November 20, 2017 VIA ELECTRONIC SUBMISSION (CMMI_NewDirection@cms.hhs.gov) Seema Verma, Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMMI Request
November 20, 2017 VIA ELECTRONIC SUBMISSION (CMMI_NewDirection@cms.hhs.gov) Seema Verma, Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Attention: CMMI Request
The Workforce Needed to Staff Value-Based Models of Care
 The Workforce Needed to Staff Value-Based Models of Care Erin Fraher, PhD, MPP Assistant Professor Departments of Family Medicine and Surgery, UNC Chapel Hill Director, Program on Health Workforce Research
The Workforce Needed to Staff Value-Based Models of Care Erin Fraher, PhD, MPP Assistant Professor Departments of Family Medicine and Surgery, UNC Chapel Hill Director, Program on Health Workforce Research
Expanding Nursing's Influence in 21st Century Health Care
 Expanding Nursing's Influence in 21st Century Health Care Title text here Brenda L. Cleary, PhD, RN, FAAN Director, Center to Champion Nursing in America Objectives - In the context of the current era
Expanding Nursing's Influence in 21st Century Health Care Title text here Brenda L. Cleary, PhD, RN, FAAN Director, Center to Champion Nursing in America Objectives - In the context of the current era
THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM
 THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM THE REASON FOR CHANGE VOLUME TO VALUE Fee-for-service PAYMENT Bundled, Shared Patient FOCUS
THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM THE REASON FOR CHANGE VOLUME TO VALUE Fee-for-service PAYMENT Bundled, Shared Patient FOCUS
HRSA Administrator Describes Role of Family Physicians, PCMH in Health Care System
 Return to Previous Page HRSA Administrator Describes Role of Family Physicians, PCMH in Health Care System By James Arvantes Posted: 10/20/2010, 4:45 p.m. -- The Health Resources and Services Administration,
Return to Previous Page HRSA Administrator Describes Role of Family Physicians, PCMH in Health Care System By James Arvantes Posted: 10/20/2010, 4:45 p.m. -- The Health Resources and Services Administration,
Request for Information Regarding Accountable Care Organizations (ACOs) and Medicare Shared Savings Programs (CMS-1345-NC)
 and Medicare Shared Savings Programs (CMS-1345-NC)") Via Electronic Submission Donald Berwick, MD, MPP Administrator Centers for Medicare & Medicaid Services ATTN: CMS-1345-NC 7500 Security Blvd. Baltimore, MD 21244-8013 Re: Request for Information Regarding
Via Electronic Submission Donald Berwick, MD, MPP Administrator Centers for Medicare & Medicaid Services ATTN: CMS-1345-NC 7500 Security Blvd. Baltimore, MD 21244-8013 Re: Request for Information Regarding
Draft for the Medicare Performance Adjustment (MPA) Policy for Rate Year 2021
 Policy for Rate Year 2021") Draft for the Medicare Performance Adjustment (MPA) Policy for Rate Year 2021 October 2018 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764-2605 FAX: (410)
Draft for the Medicare Performance Adjustment (MPA) Policy for Rate Year 2021 October 2018 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764-2605 FAX: (410)
Texas Health Care Transformation and Quality Improvement Program - FAQ
 Texas Health Care Transformation and Quality Improvement Program - FAQ http://www.hhsc.state.tx.us/1115-faq.shtml 1115 Waiver Approval and Effective Date Why is HHSC seeking an 1115 waiver under the Social
Texas Health Care Transformation and Quality Improvement Program - FAQ http://www.hhsc.state.tx.us/1115-faq.shtml 1115 Waiver Approval and Effective Date Why is HHSC seeking an 1115 waiver under the Social
Workforce Issues & Solutions for Emergency Medical Services
 Workforce Issues & Solutions for Emergency Medical Services Institute of Medicine Dissemination Workshop October 27, 2006 -- Chicago, Illinois Steven E. Krug, MD Head, Division of Emergency Medicine Children
Workforce Issues & Solutions for Emergency Medical Services Institute of Medicine Dissemination Workshop October 27, 2006 -- Chicago, Illinois Steven E. Krug, MD Head, Division of Emergency Medicine Children
Evaluation & Management ( E/M ) Payment and Documentation Requirements
 Payment and Documentation Requirements") National Partnership for Hospice Innovation 1299 Pennsylvania Ave., Suite 1175 Washington DC, 20004 September 10, 2017 Seema Verma Administrator Centers for Medicare & Medicaid Services, Department of
National Partnership for Hospice Innovation 1299 Pennsylvania Ave., Suite 1175 Washington DC, 20004 September 10, 2017 Seema Verma Administrator Centers for Medicare & Medicaid Services, Department of
LESSONS LEARNED IN LENGTH OF STAY (LOS)
") FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
Transforming Louisiana s Long Term Care Supports and Services System. Initial Program Concept
 Transforming Louisiana s Long Term Care Supports and Services System Initial Program Concept August 30, 2013 Transforming Louisiana s Long Term Care Supports and Services System Our Vision Introduction
Transforming Louisiana s Long Term Care Supports and Services System Initial Program Concept August 30, 2013 Transforming Louisiana s Long Term Care Supports and Services System Our Vision Introduction
Statement for the Record. American College of Physicians. U.S. House Committee on Ways and Means Subcommittee on Health
 Statement for the Record American College of Physicians U.S. House Committee on Ways and Means Subcommittee on Health Hearing on Implementation of MACRA s Physician Payment Policies March 21, 2018 The
Statement for the Record American College of Physicians U.S. House Committee on Ways and Means Subcommittee on Health Hearing on Implementation of MACRA s Physician Payment Policies March 21, 2018 The
FEDERAL FUNDS ARE FLOWING: WHO'S GETTING WHAT, WHERE AND WHY?
 Not Peer Reviewed FEDERAL FUNDS ARE FLOWING: WHO'S GETTING WHAT, WHERE AND WHY? Dianne Heffron Principal 1050 Connecticut Ave., NW Suite 700 Washington, DC National Governor s Association Learning From
Not Peer Reviewed FEDERAL FUNDS ARE FLOWING: WHO'S GETTING WHAT, WHERE AND WHY? Dianne Heffron Principal 1050 Connecticut Ave., NW Suite 700 Washington, DC National Governor s Association Learning From
Vision to Action Prof. Robert Harris Director of Strategy - NHS England
 Vision without action is a daydream; Action without vision is a nightmare Vision to Action Prof. Robert Harris Director of Strategy - NHS England 65 years ago, the NHS began Founding Context Founded in
Vision without action is a daydream; Action without vision is a nightmare Vision to Action Prof. Robert Harris Director of Strategy - NHS England 65 years ago, the NHS began Founding Context Founded in
Medicaid Managed Long Term Care in Florida Issue Brief December 2017 by LuMarie Polivka-West, Sr. Research Associate Volunteer
 Medicaid Managed Long Term Care in Florida Issue Brief December 2017 by LuMarie Polivka-West, Sr. Research Associate Volunteer Henry is a 76 year old, previously self-employed, very frail man with advanced
Medicaid Managed Long Term Care in Florida Issue Brief December 2017 by LuMarie Polivka-West, Sr. Research Associate Volunteer Henry is a 76 year old, previously self-employed, very frail man with advanced
2017/2018. KPN Health, Inc. Quality Payment Program Solutions Guide. KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc.
 KPN Health, Inc.") 2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
2017/2018 KPN Health, Inc. Quality Payment Program Solutions Guide KPN Health, Inc. A CMS Qualified Clinical Data Registry (QCDR) KPN Health, Inc. 214-591-6990 info@kpnhealth.com www.kpnhealth.com 2017/2018
1 MINNESOTA STATUTES J.692
 1 MINNESOTA STATUTES 2015 62J.692 62J.692 MEDICAL EDUCATION. Subdivision 1. Definitions. For purposes of this section, the following definitions apply: (a) "Accredited clinical training" means the clinical
1 MINNESOTA STATUTES 2015 62J.692 62J.692 MEDICAL EDUCATION. Subdivision 1. Definitions. For purposes of this section, the following definitions apply: (a) "Accredited clinical training" means the clinical
Integrated Leadership for Hospitals and Health Systems: Principles for Success
 Integrated Leadership for Hospitals and Health Systems: Principles for Success In the current healthcare environment, there are many forces, both internal and external, that require some physicians and
Integrated Leadership for Hospitals and Health Systems: Principles for Success In the current healthcare environment, there are many forces, both internal and external, that require some physicians and
Medicaid Supplemental Hospital Funding Programs Fiscal Year
 Fiscal Year 2014-2015 General Revenue Grants and Donations Trust Fund Medical Care Trust Fund Total Rural Proportional Primary Care Hospitals Trauma Level I Trauma Level II or Pediatric Trauma Trauma Level
Fiscal Year 2014-2015 General Revenue Grants and Donations Trust Fund Medical Care Trust Fund Total Rural Proportional Primary Care Hospitals Trauma Level I Trauma Level II or Pediatric Trauma Trauma Level
The President s Fiscal Year 2014 Budget Overview
 The President s Fiscal Year 2014 Budget Overview The President s Fiscal Year 2014 Budget demonstrates that we can make critical investments to strengthen the middle class, create jobs, and grow the economy
The President s Fiscal Year 2014 Budget Overview The President s Fiscal Year 2014 Budget demonstrates that we can make critical investments to strengthen the middle class, create jobs, and grow the economy
Place Based Placement Funding Models 2018 to Frequently Asked Questions
 Place Based Placement Funding Models 2018 to 2021 Frequently Asked Questions Version Author Date 1.0 HEE Policy & Regulation Team 23 July 2018 RATIONALE FOR PILOTING Why is HEE piloting a new model for
Place Based Placement Funding Models 2018 to 2021 Frequently Asked Questions Version Author Date 1.0 HEE Policy & Regulation Team 23 July 2018 RATIONALE FOR PILOTING Why is HEE piloting a new model for
Health Center Program Update
 Health Center Program Update NACHC Policy & Issues Forum March 14, 2018 Jim Macrae Associate Administrator, Bureau of Primary Health Care (BPHC) Health Resources and Services Administration (HRSA) 3/22/2018
Health Center Program Update NACHC Policy & Issues Forum March 14, 2018 Jim Macrae Associate Administrator, Bureau of Primary Health Care (BPHC) Health Resources and Services Administration (HRSA) 3/22/2018
Health Workforce Australia. Health Workforce 2025 Volume 3 Medical specialties. Adelaide: HWA,
 Fostering generalism in the medical workforce 2012 This document outlines the AMA position on the broad measures that should be in place to promote generalist medical practice as a desirable career option
Fostering generalism in the medical workforce 2012 This document outlines the AMA position on the broad measures that should be in place to promote generalist medical practice as a desirable career option
Good afternoon. My name is Deborah Franklin and I am the Chairperson of the Florida Health Care Association Prospective Payment Task Force.
 Florida Health Care Association Testimony before the Agency for Health Care Administration Meeting Regarding Nursing Home Prospective Payment Reimbursement Methodology August 18, 2016 Good afternoon. My
Florida Health Care Association Testimony before the Agency for Health Care Administration Meeting Regarding Nursing Home Prospective Payment Reimbursement Methodology August 18, 2016 Good afternoon. My
2018 CALL FOR IDEAS AlohaCare Community Innovation Investment Program
 2018 CALL FOR IDEAS AlohaCare Community Innovation Investment Program Waiwai Ola AlohaCare is seeking to identify opportunities to partner with, and fund, primary care innovation in the communities we
2018 CALL FOR IDEAS AlohaCare Community Innovation Investment Program Waiwai Ola AlohaCare is seeking to identify opportunities to partner with, and fund, primary care innovation in the communities we
The Health Services Workers. Chapter 8
 The Health Services Workers Chapter 8 Objectives Provided an overview of the health services workforce in the United States. Introduction From its beginning as a cottage industry at the turn of the century
The Health Services Workers Chapter 8 Objectives Provided an overview of the health services workforce in the United States. Introduction From its beginning as a cottage industry at the turn of the century
June 18, 2009 Page 1
 Base Year Current LOC base rates calculated using: Wyoming Medicaid inpatient hospital claims data from July 1, 1994 through December 31, 1996 Most recently audited Medicare cost report with provider fiscal
Base Year Current LOC base rates calculated using: Wyoming Medicaid inpatient hospital claims data from July 1, 1994 through December 31, 1996 Most recently audited Medicare cost report with provider fiscal
Primary Care Capacity Assessment
 Better Information for Better Outcomes Primary Care Capacity Assessment The 22nd Annual Symposium on Health Care Services in New York: Research and Practice Wednesday October 12, 2011 Jean Moore, Director
Better Information for Better Outcomes Primary Care Capacity Assessment The 22nd Annual Symposium on Health Care Services in New York: Research and Practice Wednesday October 12, 2011 Jean Moore, Director
FEDERAL FUNDING OUTLOOK. Caps, Cuts, Squeezes and Sequesters. Joel Packer, Executive Director The Committee for Education Funding
 FEDERAL FUNDING OUTLOOK Caps, Cuts, Squeezes and Sequesters Joel Packer, Executive Director The Committee for Education Funding Jpacker@cef.org Committee For Education Funding The Committee for Education
FEDERAL FUNDING OUTLOOK Caps, Cuts, Squeezes and Sequesters Joel Packer, Executive Director The Committee for Education Funding Jpacker@cef.org Committee For Education Funding The Committee for Education
Briefing. NHS Next Stage Review: workforce issues
 Briefing NHS Next Stage Review: workforce issues Workforce issues, and particularly the importance of engaging and involving staff, are a central theme of the NHS Next Stage Review (NSR). It is the focus
Briefing NHS Next Stage Review: workforce issues Workforce issues, and particularly the importance of engaging and involving staff, are a central theme of the NHS Next Stage Review (NSR). It is the focus
National League for Nursing February 5, 2016 Interprofessional Education and Collaborative Practice: The New Forty-Year-Old Field
 National League for Nursing February 5, 2016 Interprofessional Education and Collaborative Practice: The New Forty-Year-Old Field Barbara F. Brandt, PhD, Director Associate Vice President for Education
National League for Nursing February 5, 2016 Interprofessional Education and Collaborative Practice: The New Forty-Year-Old Field Barbara F. Brandt, PhD, Director Associate Vice President for Education
August 31, Missouri State Board of Registration for the Healing Arts PO Box 4 Jefferson City, MO RE: Proposed Assistant Physician Rules
 August 31, 2016 Missouri State Board of Registration for the Healing Arts PO Box 4 Jefferson City, MO 65102 RE: Proposed Assistant Physician Rules Dear Missouri State Board of Registration for the Healing
August 31, 2016 Missouri State Board of Registration for the Healing Arts PO Box 4 Jefferson City, MO 65102 RE: Proposed Assistant Physician Rules Dear Missouri State Board of Registration for the Healing
State Medicaid Directors Driving Innovation: Continuous Quality Improvement February 25, 2013
 State Medicaid Directors Driving Innovation: Continuous Quality Improvement February 25, 2013 The National Association of Medicaid Directors (NAMD) is engaging states in shared learning on how Medicaid
State Medicaid Directors Driving Innovation: Continuous Quality Improvement February 25, 2013 The National Association of Medicaid Directors (NAMD) is engaging states in shared learning on how Medicaid
INTEGRATED DELIVERY SYSTEM PLANNING PROJECT
 INTEGRATED DELIVERY SYSTEM PLANNING PROJECT San Francisco Department of Public Health May 15, 2012 2 IDS Planning and Other Long-Range Planning Efforts Citywide Strategic Efforts Community Health Improvement
INTEGRATED DELIVERY SYSTEM PLANNING PROJECT San Francisco Department of Public Health May 15, 2012 2 IDS Planning and Other Long-Range Planning Efforts Citywide Strategic Efforts Community Health Improvement
Osteopathic Advocacy: Partnering to Advance Sound Health Policy. Nicholas Schilligo, MS Associate Vice President, State Government Affairs
 Osteopathic Advocacy: Partnering to Advance Sound Health Policy Nicholas Schilligo, MS Associate Vice President, State Government Affairs Our Work Work with a variety of stakeholders to promote AOA policies
Osteopathic Advocacy: Partnering to Advance Sound Health Policy Nicholas Schilligo, MS Associate Vice President, State Government Affairs Our Work Work with a variety of stakeholders to promote AOA policies
Healthcare Workforce to Promote
 Accreditation, Certification, and Credentialing: Levers for Training the Healthcare Workforce to Promote Children s Behavioral Health Marci Nielsen, PhD, MPH President & CEO Patient-Centered Primary Care
Accreditation, Certification, and Credentialing: Levers for Training the Healthcare Workforce to Promote Children s Behavioral Health Marci Nielsen, PhD, MPH President & CEO Patient-Centered Primary Care
Technical Overview of HCIP/CCIP
 Technical Overview of HCIP/CCIP Using Care Redesign to Align Provider Incentives Presentation to HFMA, Maryland Chapter HSCRC Care Redesign Summit August 18, 2017 Facilitators Nicole Stallings Vice President,
Technical Overview of HCIP/CCIP Using Care Redesign to Align Provider Incentives Presentation to HFMA, Maryland Chapter HSCRC Care Redesign Summit August 18, 2017 Facilitators Nicole Stallings Vice President,
PATIENT ATTRIBUTION WHITE PAPER
 PATIENT ATTRIBUTION WHITE PAPER Comment Response Document Written by: Population-Based Payment Work Group Version Date: 05/13/2016 Contents Introduction... 2 Patient Engagement... 2 Incentives for Using
PATIENT ATTRIBUTION WHITE PAPER Comment Response Document Written by: Population-Based Payment Work Group Version Date: 05/13/2016 Contents Introduction... 2 Patient Engagement... 2 Incentives for Using
Critical Revenue Growth Strategies for Home Health Agencies. NAHC Annual Conference Nashville, TN October 28, 2015 Session 102
 Critical Revenue Growth Strategies for Home Health Agencies NAHC Annual Conference Nashville, TN October 28, 2015 Session 102 Jeff Aspacher, VP Finance and CFO Community Health System Nick Seabrook, Managing
Critical Revenue Growth Strategies for Home Health Agencies NAHC Annual Conference Nashville, TN October 28, 2015 Session 102 Jeff Aspacher, VP Finance and CFO Community Health System Nick Seabrook, Managing
Driving Out Clinical Variation to Drive Up Your Bottom Line
 In Cooperation With: Executive White Paper Series, October 2017 Driving Out Clinical Variation to Drive Up Your Bottom Line Hospitals have always worked to be efficient. Now more than ever, it is increasingly
In Cooperation With: Executive White Paper Series, October 2017 Driving Out Clinical Variation to Drive Up Your Bottom Line Hospitals have always worked to be efficient. Now more than ever, it is increasingly
Payment Rule Summary. Medicare Inpatient Psychiatric Facility Prospective Payment System: Update Notice for Federal Fiscal Year 2013
 Payment Rule Summary Medicare Inpatient Psychiatric Facility Prospective Payment System: Update Notice for Federal Fiscal Year 2013 August 2012 Table of Contents Overview and Resources... 2 Inpatient Psychiatric
Payment Rule Summary Medicare Inpatient Psychiatric Facility Prospective Payment System: Update Notice for Federal Fiscal Year 2013 August 2012 Table of Contents Overview and Resources... 2 Inpatient Psychiatric
Overview and History of the Community Mental Health Authority of Clinton, Eaton, and Ingham Counties 2012
 Overview and History of the Community Mental Health Authority of Clinton, Eaton, and Ingham Counties 2012 I. Overview of CMH The Community Mental Health Authority of Clinton, Eaton, and Ingham Counties
Overview and History of the Community Mental Health Authority of Clinton, Eaton, and Ingham Counties 2012 I. Overview of CMH The Community Mental Health Authority of Clinton, Eaton, and Ingham Counties
Medicaid Update Special Edition Budget Highlights New York State Budget: Health Reform Highlights
 Page 1 of 6 New York State April 2009 Volume 25, Number 4 Medicaid Update Special Edition 2009-10 Budget Highlights David A. Paterson, Governor State of New York Richard F. Daines, M.D. Commissioner New
Page 1 of 6 New York State April 2009 Volume 25, Number 4 Medicaid Update Special Edition 2009-10 Budget Highlights David A. Paterson, Governor State of New York Richard F. Daines, M.D. Commissioner New
Improve the geographic distribution of health professionals; Increase access to health care for underserved populations; and
 The members of the Health Professions and Nursing Education Coalition (HPNEC) are pleased to submit this statement for the record in support of the health professions education programs authorized under
The members of the Health Professions and Nursing Education Coalition (HPNEC) are pleased to submit this statement for the record in support of the health professions education programs authorized under
11/10/2015. Workforce Shortages and Maldistribution. Health Care Workforce Shortages/Maldistribution: Why? Access to Health Care Services
 Workforce Shortages and Maldistribution DEVELOPING NEW STATE LEGISLATIVE HEALTH LEADERS Access to Health Care Services Health Professional Shortage Areas (HPSAs) are geographic areas, or populations within
Workforce Shortages and Maldistribution DEVELOPING NEW STATE LEGISLATIVE HEALTH LEADERS Access to Health Care Services Health Professional Shortage Areas (HPSAs) are geographic areas, or populations within
A Primer on Activity-Based Funding
 A Primer on Activity-Based Funding Introduction and Background Canada is ranked sixth among the richest countries in the world in terms of the proportion of gross domestic product (GDP) spent on health
A Primer on Activity-Based Funding Introduction and Background Canada is ranked sixth among the richest countries in the world in terms of the proportion of gross domestic product (GDP) spent on health
Chapter 14. Conclusions: The Availability of Health Personnel in Rural Areas
 Chapter 14 Conclusions: The Availability of Health Personnel in Rural Areas r SUPPLY OF HEALTH PERSONNEL....................................... ~ IDENTIFYING SHORTAGE AREAS: FEDERAL AND STATE EFFORTS............
Chapter 14 Conclusions: The Availability of Health Personnel in Rural Areas r SUPPLY OF HEALTH PERSONNEL....................................... ~ IDENTIFYING SHORTAGE AREAS: FEDERAL AND STATE EFFORTS............
UnitedHealth Center for Health Reform & Modernization September 2014
 Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?
Health Reform & Modernization September 2014 2014 UnitedHealth Group. Any use, copying or distribution without written permission from UnitedHealth Group is prohibited. Overview Why Focus on Primary Care?
Minnesota Statewide Quality Reporting and Measurement System: Quality Incentive Payment System Framework
 Minnesota Statewide Quality Reporting and Measurement System: Quality Incentive Payment System Framework AUGUST 2017 Minnesota Statewide Quality Reporting and Measurement System: Quality Incentive Payment
Minnesota Statewide Quality Reporting and Measurement System: Quality Incentive Payment System Framework AUGUST 2017 Minnesota Statewide Quality Reporting and Measurement System: Quality Incentive Payment
Hospice Program Integrity Recommendations
 Hospice Program Integrity Recommendations Projected increases in the elderly population and the number of Medicare beneficiaries will likely result in continued growth in utilization of hospice services.
Hospice Program Integrity Recommendations Projected increases in the elderly population and the number of Medicare beneficiaries will likely result in continued growth in utilization of hospice services.
The Patient Protection and Affordable Care Act Summary of Key Health Information Technology Provisions June 1, 2010
 The Patient Protection and Affordable Care Act Summary of Key Health Information Technology Provisions June 1, 2010 This document is a summary of the key health information technology (IT) related provisions
The Patient Protection and Affordable Care Act Summary of Key Health Information Technology Provisions June 1, 2010 This document is a summary of the key health information technology (IT) related provisions
Accountable Care Organizations. What the Nurse Executive Needs to Know. Rebecca F. Cady, Esq., RNC, BSN, JD, CPHRM
 JONA S Healthcare Law, Ethics, and Regulation / Volume 13, Number 2 / Copyright B 2011 Wolters Kluwer Health Lippincott Williams & Wilkins Accountable Care Organizations What the Nurse Executive Needs
JONA S Healthcare Law, Ethics, and Regulation / Volume 13, Number 2 / Copyright B 2011 Wolters Kluwer Health Lippincott Williams & Wilkins Accountable Care Organizations What the Nurse Executive Needs
Physician Workforce Fact Sheet 2016
 Introduction It is important to fully understand the characteristics of the physician workforce as they serve as the backbone of the system. Supply data on the physician workforce are routinely collected
Introduction It is important to fully understand the characteristics of the physician workforce as they serve as the backbone of the system. Supply data on the physician workforce are routinely collected
Primary Health Care Access Reform: Community Health Centers and the National Health Service Corps
 Testimony before the U.S. SENATE COMMITTEE ON HEALTH, EDUCATION, LABOR, AND PENSIONS On Primary Health Care Access Reform: Community Health Centers and the National Health Service Corps Fitzhugh Mullan,
Testimony before the U.S. SENATE COMMITTEE ON HEALTH, EDUCATION, LABOR, AND PENSIONS On Primary Health Care Access Reform: Community Health Centers and the National Health Service Corps Fitzhugh Mullan,
Beyond RVUs: Changing Your Primary Care Compensation Plan from Volume to Value
 Beyond RVUs: Changing Your Primary Care Compensation Plan from Volume to Value Objectives Compare different primary care compensation models Identify keys to success and best methods for transitioning
Beyond RVUs: Changing Your Primary Care Compensation Plan from Volume to Value Objectives Compare different primary care compensation models Identify keys to success and best methods for transitioning
on how to complete this line if you have a new program for which the period of years is less than Rev. 7
 4034 FORM CMS-2552-10 09-15 4034. WORKSHEET E-4 - DIRECT GRADUATE MEDICAL EDUCATION (GME) AND ESRD OUTPATIENT DIRECT MEDICAL EDUCATION COSTS Use this worksheet to calculate each program s payment (i.e.,
4034 FORM CMS-2552-10 09-15 4034. WORKSHEET E-4 - DIRECT GRADUATE MEDICAL EDUCATION (GME) AND ESRD OUTPATIENT DIRECT MEDICAL EDUCATION COSTS Use this worksheet to calculate each program s payment (i.e.,
Comparison of Health IT Provisions in H.R. 6 (21 st Century Cures Act) and S (Improving Health Information Technology Act)
 and S (Improving Health Information Technology Act)") Comparison of Health IT Provisions in H.R. 6 (21 st Century Cures Act) and S. 2511 (Improving Health Information Technology Act) Policy Proposal Health Software Regulation Senate Innovations Initiative
Comparison of Health IT Provisions in H.R. 6 (21 st Century Cures Act) and S. 2511 (Improving Health Information Technology Act) Policy Proposal Health Software Regulation Senate Innovations Initiative
A Tale of Three Regions: Texas 1115 Waiver Journey Regional Healthcare Partnership 3 Shannon Evans, MBA, LSSGB Regional Healthcare Partnership 6
 A Tale of Three Regions: Texas 1115 Waiver Journey Regional Healthcare Partnership 3 Shannon Evans, MBA, LSSGB Regional Healthcare Partnership 6 Carol Huber, MBA Regional Healthcare Partnership 1 Daniel
A Tale of Three Regions: Texas 1115 Waiver Journey Regional Healthcare Partnership 3 Shannon Evans, MBA, LSSGB Regional Healthcare Partnership 6 Carol Huber, MBA Regional Healthcare Partnership 1 Daniel
Institute of Medicine. Committee on Public Health Strategies to Improve Health
 Institute of Medicine Committee on Public Health Strategies to Improve Health About the Institute of Medicine (IOM) The Institute of Medicine is part of the National Academies and was founded in 1970.
Institute of Medicine Committee on Public Health Strategies to Improve Health About the Institute of Medicine (IOM) The Institute of Medicine is part of the National Academies and was founded in 1970.
Before The Senate Finance Committee Regarding Lessons Learned From A Year Of Implementation Of The Affordable Care Act
 Before The Senate Finance Committee Regarding Lessons Learned From A Year Of Implementation Of The Affordable Care Act March 16, 2011 The American Academy of Family Physicians (AAFP), representing 97,600
Before The Senate Finance Committee Regarding Lessons Learned From A Year Of Implementation Of The Affordable Care Act March 16, 2011 The American Academy of Family Physicians (AAFP), representing 97,600
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Richard Mollot, Esq. Executive Director Cynthia Rudder, PhD, Director of Special Projects Long Term Care Community Coalition
 Richard Mollot, Esq. Executive Director Cynthia Rudder, PhD, Director of Special Projects Long Term Care Community Coalition www.nursinghome411.org www.ltccc.org www.assistedliving411.org Presented at
Richard Mollot, Esq. Executive Director Cynthia Rudder, PhD, Director of Special Projects Long Term Care Community Coalition www.nursinghome411.org www.ltccc.org www.assistedliving411.org Presented at
hfma Maryland Chapter New All-Payer Model for Maryland Maryland Health Services Cost Review Commission
 hfma Maryland Chapter New All-Payer Model for Maryland Maryland Health Services Cost Review Commission October 2013 1 HSCRC Preparation for New All Payer Hospital Model Maryland prepared updated application
hfma Maryland Chapter New All-Payer Model for Maryland Maryland Health Services Cost Review Commission October 2013 1 HSCRC Preparation for New All Payer Hospital Model Maryland prepared updated application
Overview of Select Health Provisions FY 2015 Administration Budget Proposal
 Overview of Select Health Provisions FY 2015 Administration Budget Proposal On March 4, 2014, President Obama released his Administration s FY 2015 budget proposal to Congress. The budget contains a number
Overview of Select Health Provisions FY 2015 Administration Budget Proposal On March 4, 2014, President Obama released his Administration s FY 2015 budget proposal to Congress. The budget contains a number
STATEMENT. of the. American Medical Association. for the Record. United States Senate Committee on Veterans Affairs.
 STATEMENT of the American Medical Association for the Record United States Senate Committee on Veterans Affairs Re: Pending Legislation: Improving the Veterans Choice Program S. 2646, Veterans Choice Improvement
STATEMENT of the American Medical Association for the Record United States Senate Committee on Veterans Affairs Re: Pending Legislation: Improving the Veterans Choice Program S. 2646, Veterans Choice Improvement
Origins of Medicare Physician Fee Schedule. Paul B. Ginsburg, Ph.D. Director, USC-Brookings Schaeffer Initiative for Health Policy
 Origins of Medicare Physician Fee Schedule Paul B. Ginsburg, Ph.D. Director, USC-Brookings Schaeffer Initiative for Health Policy Context for Reform Initiative came from the Congress Engaged Administration
Origins of Medicare Physician Fee Schedule Paul B. Ginsburg, Ph.D. Director, USC-Brookings Schaeffer Initiative for Health Policy Context for Reform Initiative came from the Congress Engaged Administration