PEARLS OF THE ACC CV SUMMIT: THOUGHTS FROM THE OYSTER BED OF CLINICAL PRACTICE
|
|
|
- Leonard Edmund Woods
- 5 years ago
- Views:
Transcription

1 PEARLS OF THE ACC CV SUMMIT: THOUGHTS FROM THE OYSTER BED OF CLINICAL PRACTICE IN-ACC October 13, 2018 Linda Gates-Striby CCS-P, ACS-CA St. Vincent Medical Group Director Quality Assurance
2 Nothing to Disclose DISCLOSURES
3 2019 PFS PEARLS TO WATCH E/M Changes - 4 options for documenting, flat rate, PCP complex add on, Specialty complex add on, new prolonged service code, minimize redocumenting, 50% reduction in E/M plus procedure Communication Technology - adding coverage for a provider checking on a patient to determine if they need to be seen, remote eval of recorded video or image to determine if they need to be seen Professional Internet Consultation pay for physician to physician consult Medicare Telehealth add preventative services to covered list AUC On Track for 2020, Provider designee could use the AUC tool, report info on global, professional, or technical Price Transparency - Hospitals must publish cost data
4 E/M PROPOSAL FINANCIAL IMPACT New Pt CPT $45 $ $ $110 $ $ $211 Est Pt CPT $22 $ $ $74 $ $ $148 CMS is also proposing 2 new codes to capture increased complexity One code unique to PCP - $5 increase requirements to be determined The second code unique to certain specialties - $14 requirements to be determined CMS Proposed Specialties For Add On Code Include: Allergy/Immunology, Cardiology, Endocrinology, Hematology/Oncology, Interventional Pain Management- Centered Care, Neurology, Obstetrics/Gynecology, Otolaryngology,Rheumatology, Urology
5 NEW CODE FOR PROLONGED SERVICE ADD ON TO E/M Proposing A new code to add-on to any office visit lasting more than 30 minutes beyond the office visit (i.e., hour long visits in total). GPRO1 Prolonged evaluation and management or psychotherapy services(s) (List separately in addition to code for office or other outpatient Evaluation and Management or psychotherapy service) Will have a payment rate of $67. Example: A cardiologist currently reporting a and spending more than 60 minutes with a patient would be paid $211. Under the proposed new method, the cardiologist would report: , depending on their documentation selection, - $135 GCG0X specialty add on - $14 GPRO1 prolonged service $67 Total combined payment of $215.
6 MISCELLANEOUS E/M RELATED Reduce E/M by 50% when billing with modifier 25 Intended to be when used in conjunction with another procedure. In order for this to work CMS needs to first establish a base line with all MACS on how and when this is to be used. Some MACs such as ours require it with services such as an EKG, Immunization administration, etc. Eliminate duplicate requirements for Teaching Provider Documentation - Basically have an option very similar to what was just implemented for students, the residents could document the TP services. Teaching providers would not have to redocument their services. Other Entries -Allowing practitioners to review and verify certain information in the medical record that is entered by ancillary staff or the beneficiary rather than re-entering it Providers choose from one of 4 documentation options Use Medical Decision Making Use Time Continue using 1995 Guidelines Continue using 1997 Guidelines Minimum base documentation would be that of the current level 2
7 COMMUNICATION TECHNOLOGY BASED SERVICES Technology-Based services CMS Proposing: Separate payment for Technology-Based services such as Checking in with patients via phone or other devices to determine if a visit or other service is required. Remote evaluation of recorded video and/or images submitted by the patient to determine if a visit or other service is needed. Chronic Care Proposal: Separately paying for new coding described as Chronic Care Remote Physiologic Monitoring 3 codes proposed Inter-Professional Internet Consultations Proposal: Separately paying for Inter-Professional Internet Consultations 6 codes proposed Telehealth Add 2 new codes for preventative services via telehealth


8 DIAGNOSIS CODING: SHARPENING OUR FOCUS Clinicians have focused on patient care CQI for years but what are we doing about CQI of diagnosis coding? Coding specificity, accuracy, and compliance NOW is having an increasing impact on Medicare reimbursement in the years to come. Coders and Clinicians need to understand and work together to sharpen the focus on coding in our new world of value.
9 RAF - RISK ADJUSTMENT FACTOR WHAT DO WE MEAN BY RAF? Used to access the clinical complexity of a patient and predict the burden of illness for individuals and populations Acts as a multiplier when calculating CMS payments in a year Factors into bidding and payment of MA plans Focuses on identification, management, and treatment of chronic conditions Additional Resources Better Analytics Encourages Regular Management Provides a payer with additional resources to manage the health of a riskier population More accurate coding leads to improved practice modeling and stratification of a population Encourages regular outreach to patients who aren t coming to the practice but may need follow-up
10 HCC HIERARCHICAL CONDITION CATEGORY 101 The Least You Need To Know Model Is Here To Stay In One Form Or Another Goes To A Blank Slate Every Calendar Year Subject To Data Validation Sampling The HCC & RAF Connection 79 to 3,000 The HCC model has been the basis for reimbursement to MAO plans since Due to it s proven success in predicting resource use it is now being used to determine much more and by more payors. The CMS model is accumulative a patient can have more than one HCC category assigned to them. Some categories override others and there is a hierarchy of categories. The HCC must be captured using claims data every 12 months. The HCC must be documented and supported in the medical record and this can be subject to a data validation review The plan must submit the one best medical record that supports the patient s HCC scoring if identified for validation. Patients with multiple HCCs in a single category will be scored at the highest level *Add l risk is scored when certain conditions coexist If multiple conditions are present, a higher score will be used. i.e. CHF & COPD or CHF and CRF

11 DOCUMENTATION & CODING = RAF/HCC SCORE
12 DOCUMENTATION & CODING GUIDELINES Per ICD-10 Official Guidelines for coding and reporting Code all documented conditions that coexist at the time of the encounter/visit, and require or affect patient care treatment or management. Access all conditions that coexist that day are treated, managed, & affect patient care Consider, document and report the disease as accurately as possible use specificity codes Ensure you are addressing and reporting/coding these conditions at least once per calendar year


13 CAPTURING COMORBIDITIES IS ESSENTIAL In our Fee-for-Service model we have gotten used to making sure a diagnosis justifies medical necessity for the CPT codes on a claim. Many practices stop short of documenting and capturing comorbidities that show complicated medical decision making, treatment plans, and more accurately reflect the condition of the patient. In contrast the majority of practices indicate that their physicians do a good job of documenting these comorbidities in the note. The change may not be one of documentation, but more of a coding change that is needed. Practices who want to more accurately reflect patient acuity need to do a good job of coding comorbidities
14 DON T MISS CHRONIC CONDITIONS DM & complications CHF COPD A Fib Morbid Obesity HTN & complications (HTN alone does not have a RAF score) Major Depression PVD Malnutrition Use ICD-10 Appropriately I.E. as specific as possible Provider s role is to accurately capture the conditions that are treated, managed, or impact care Coded conditions must be documented i.e. MEAT manage, evaluate, assessment, treatment plan Accurate coding and documentation is critical to risk scoring and our future

15 MEAT THE CONDITION(S) Conditions billed Subject to random sampling to review documentation Documentation contains MEAT Monitor Evaluate Signs, symptoms, disease progression, disease regression Test results, medication effectiveness, results to treatment Multiple condition s Assess Address Ordering tests, discussion, review of records RAF score at year end Treat Medication, therapy, other modalities Example: CHF symptoms well controlled with Lasix and ACE continue current doses
16 WHAT DOES AND DOES NOT RISK ADJUST DOES CKD stage IV & V Morbid Severe Obesity Angina, Unstable Angina Complete AV Block ASCVD with intermittent claudication DOES NOT CKD Stage I, II, and III Obesity Unspecified Chest Pain AV Block 1 st or 2 nd degree ASCVD unspecified Seeing a pattern? Don t code to a greater degree than you document!
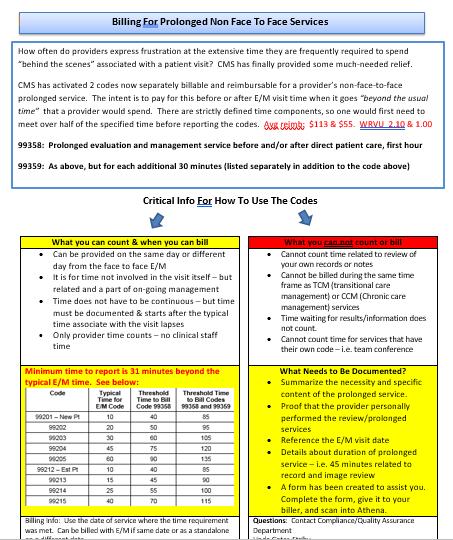
17 PROLONGED NFTF- NEW REVENUE? CMS has activated 2 codes now separately billable and reimbursable for a provider s non-face-to-face prolonged service. The intent is to pay for this before or after E/M visit time when it goes beyond the usual time that a provider would spend. There are strictly defined time components, so one would first need to meet over half of the specified time before reporting the codes. Avg reimb: $113 & $55. WRVU 2.10 & : Prolonged evaluation and management service before and/or after direct patient care, first hour 99359: As above, but for each additional 30 minutes (listed separately in addition to the code above)
18 IN A NUT SHELL WHAT YOU CAN COUNT Can be provided on the same day or different day from the face to face E/M It is for time not involved in the visit itself but related and a part of on-going management Time does not have to be continuous but time must be documented & starts after the typical time associate with the visit lapses Only provider time counts no clinical staff time WHAT YOU CAN NOT COUNT Can not count time related to review of your own records or notes Can not be billed during the same time frame as TCM (transitional care management) or CCM (Chronic care management) services Time waiting for results/information does not count. Can not count time for services that have their own code i.e. team conference

19 ADDITIONAL INFO CONTINUED TYPICAL TIME WHAT NEEDS TO BE DOCUMENTED? Summarize the necessity and specific content of the prolonged service. Proof that the provider personally performed the review/prolonged services Reference the E/M visit date Details about duration of prolonged service i.e. 45 minutes related to record and image review
20 TOOLS TO ASSIST DOCUMENTATION/BILLING FORM
21 POTENTIAL USE CASES? Modified Form for CTO By Dr. Jarrod Fizzell Congenital Disease CHF Patients Device Implant Patients The possibilities are numerous!

22 ALL THESE QUALITY METRICS TAKE LONGER! I can only see so many patients in my clinic each day and I am under pressure to increase my wrvu/production I am so tired of clicking on my computer We have had to or need to hire more people to meet all these quality goals What if you are already doing things you aren t being paid for, but if you tweak them a bit you could be billing them?
23 SMOKING AND TOBACCO USE CESSATION Limited to face-to-face services (also telehealth) This a distinct from an E/M service and may be reported separately the 25 modifier would be attached to the E/M to signify a significant and separate service. These are time based services and time spent must be documented Can be reported in office and or hospital sites of service Medicare, Medicaid, and most commercial payors cover Build a simple template to assist with documentation Smoking and tobacco use cessation counseling visit; intermediate, greater than 3 minutes up to 10 minutes intensive, greater than 10 minutes
24 NEW CODE IN 2017 CCM INITIATING VISIT How often do you see a patient that is fragile/unstable and you know you are going to ask the nurse to call and or follow-up with them? Would you like to be able to bill for some of your phone care? G Comprehensive assessment of and care planning by the physician or other qualified health care professional for patients requiring chronic care management services billed separately from monthly care management services This is a code providers are eligible to bill to account for the additional work that they may personally do. CMS states Practitioners who furnish a CCM initiating visit and personally perform extensive assessment and CCM care planning outside of the usual effort described by the initiating visit code may also bill HCPCS code G0506

25 CCM: WHAT ARE THE CODES
26
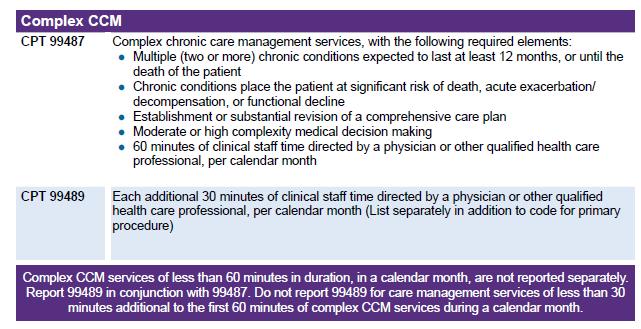
27 CHRONIC & COMPLEX CHRONIC CARE MANAGEMENT COMMON TO BOTH Many of the guidelines are common to both categories of codes. Common elements include: Pt at home, domiciliary, rest home or assisted living Care management services available 24/7 2 or more chronic conditions place pt at significant risk of death, acute exacerbation/decomp or functional decline A comprehensive care plan established, implemented, revised or monitored COMPLEX ONLY 60 MINUTES In order to qualify for complex, one or more of the following must apply: Requires Moderate or High complexity MDM (defers to E/M definitions) Need for coordination of a number of specialties or services Inability to perform activities of daily living and/or cognitive impairment resulting in poor adherence to the tx plan w/o substantial assistance from a caregiver Psych and or other co-morbidities (i.e. dementia, COPD, DM) that complicate their care and/or Social support requirements or difficulty with access to care

28

29 THERE S MORE Don t forget these other services you are likely providing and not billing for: But I am out of time Advanced Care Planning Counseling on the need for LDCT scans With some operational modifications: Transitional Care Management
30 QUESTIONS? Thank-you! Linda Gates-Striby
Impact of Risk Scoring And Attribution October 2017 Linda Gates-Striby
 STRATEGIC CODING IN THE ERA OF MACRA: Impact of Risk Scoring And Attribution October 2017 Linda Gates-Striby Lggates@ascension.org Disclosures Linda Gates-Striby Nothing To Disclose Increasing Our Focus
STRATEGIC CODING IN THE ERA OF MACRA: Impact of Risk Scoring And Attribution October 2017 Linda Gates-Striby Lggates@ascension.org Disclosures Linda Gates-Striby Nothing To Disclose Increasing Our Focus
Chronic Care Management Coding Guidelines Effective January 1, 2017
 Capture Billing & Consulting, Inc. 25055 Riding Plaza, Suite 160 South Riding, VA 20152 (703) 327-1800 Chronic Care Management Coding Guidelines Effective January 1, 2017 The Centers for Medicare and Medicaid
Capture Billing & Consulting, Inc. 25055 Riding Plaza, Suite 160 South Riding, VA 20152 (703) 327-1800 Chronic Care Management Coding Guidelines Effective January 1, 2017 The Centers for Medicare and Medicaid
Risk Adjusted Diagnosis Coding:
 Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare
Risk Adjusted Diagnosis Coding: Reporting ChronicDisease for Population Health Management Jeri Leong, R.N., CPC, CPC-H, CPMA, CPC-I Executive Director 1 Learning Objectives Explain the concept Medicare
Deleted Codes. Agenda 1/31/ E/M Codes Deleted Codes New Codes Changed Codes
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February Jean C. Russell, MS, RHIT Richard Cooley, BA, CCS
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
Medical Practice Executive Insights
 Proposed 2019 Medicare Physician Payment and Quality Reporting Changes MGMA MEMBER-EXCLUSIVE ANALYSIS The Centers for Medicare & Medicaid Services (CMS) recently proposed changes to both Medicare physician
Proposed 2019 Medicare Physician Payment and Quality Reporting Changes MGMA MEMBER-EXCLUSIVE ANALYSIS The Centers for Medicare & Medicaid Services (CMS) recently proposed changes to both Medicare physician
Telehealth. Administrative Process. Coverage. Indications that are covered
 Telehealth These services may or may not be covered by your HealthPartners plan. Please see your plan documents for your specific coverage information. If there is a difference between this general information
Telehealth These services may or may not be covered by your HealthPartners plan. Please see your plan documents for your specific coverage information. If there is a difference between this general information
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO
 EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care
 P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
P R A C T I C E R E S O U R C E A P R I L 2015 NO.2 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care By Margaret McManus, MHS The National Alliance to Advance Adolescent
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Describe the process for implementing an OP CDI program
 1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
Emerging Outpatient CDI Drivers and Technologies
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE
 CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
CHRONIC CARE MANAGEMENT IMPLEMENTATION GUIDE TABLE OF CONTENTS What is Chronic Care Management (CCM)?... 2 Why CCM?... 2 Clinician/Practice Benefits... 3 Patient Benefits... 4 What is Included in CCM?...
Coding Guidance for HIV Clinical Practices: Care Management Services
 Coding Guidance for HIV Clinical Practices: Care Management Services HIV medical practices and clinicians provide many services outside of a face-to-face encounter with a patient. Some of these services
Coding Guidance for HIV Clinical Practices: Care Management Services HIV medical practices and clinicians provide many services outside of a face-to-face encounter with a patient. Some of these services
MEDICAL POLICY No R2 TELEMEDICINE
 Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
MEDICAL POLICY No R1 TELEMEDICINE
 Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
Summary of Changes MEDICAL POLICY TELEMEDICINE Effective Date: March 1, 2016 Review Dates: 12/12, 12/13, 11/14, 11/15 Date Of Origin: December 12, 2012 Status: Current Clarifications: Deletions: Pg. 4,
February Jean C. Russell, MS, RHIT Richard Cooley, BA, CCS
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims
 March 8, 2018 Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims By Kristi Pollard, RHIT, CCS, CPC, CIRCC, AHIMA-approved ICD-10- CM/PCS trainer There is
March 8, 2018 Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims By Kristi Pollard, RHIT, CCS, CPC, CIRCC, AHIMA-approved ICD-10- CM/PCS trainer There is
the role of HCCs in a value-based payment system
 REPRINT October 2017 Donna M. Smith L. Gordon Moore healthcare financial management association hfma.org the role of HCCs in a value-based payment system Appropriate documentation and coding of hierarchical
REPRINT October 2017 Donna M. Smith L. Gordon Moore healthcare financial management association hfma.org the role of HCCs in a value-based payment system Appropriate documentation and coding of hierarchical
"Strategies for Enhancing Reimbursement " September 16, 2015
 "Strategies for Enhancing Reimbursement- 99080" September 16, 2015 Chat box feature Chat Box is available to you to ask questions or make comments anytime throughout today s webinar. Submit to Host and
"Strategies for Enhancing Reimbursement- 99080" September 16, 2015 Chat box feature Chat Box is available to you to ask questions or make comments anytime throughout today s webinar. Submit to Host and
Today s Presenters. Paula Murray Educator, Provider Services. Lara Adelberger STARS Clinical Coordinator 5/12/2017 5
 Today s Presenters Paula Murray Educator, Provider Services Lara Adelberger STARS Clinical Coordinator 5/12/2017 5 Risk Adjustment, Quality Measures, and Care of Older Adults April 27, 2017 Agenda Risk
Today s Presenters Paula Murray Educator, Provider Services Lara Adelberger STARS Clinical Coordinator 5/12/2017 5 Risk Adjustment, Quality Measures, and Care of Older Adults April 27, 2017 Agenda Risk
Medical Appropriateness and Risk Adjustment
 Medical Appropriateness and Risk Adjustment Medical Appropriateness David Rzeszutko, MD Medical Director November 10, 2017 Objectives Medical necessity Value equation Medical appropriateness Why? To improve
Medical Appropriateness and Risk Adjustment Medical Appropriateness David Rzeszutko, MD Medical Director November 10, 2017 Objectives Medical necessity Value equation Medical appropriateness Why? To improve
Care Transition Strategies: The 2013 Transition Care Management Codes
 Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
CY 2019 Physician Fee Schedule Proposed Rule Summary
 CY 2019 Physician Fee Schedule Proposed Rule Summary On July 11, 2018, the Center for Medicare and Medicaid Services (CMS) released the proposed Medicare Physician Fee Schedule (MPFS) for 2019, which for
CY 2019 Physician Fee Schedule Proposed Rule Summary On July 11, 2018, the Center for Medicare and Medicaid Services (CMS) released the proposed Medicare Physician Fee Schedule (MPFS) for 2019, which for
Primary Care Setting Behavioral Health Billing Codes
 Primary Care Setting s Medicaid Medicare Third Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though
Primary Care Setting s Medicaid Medicare Third Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
JOHNS HOPKINS HEALTHCARE
 Page 1 of 16 ACTION: New Policy Effective Date: 10/01/2013 Revising : Review Dates: 03/29/16, 06/29/17, Superseding 09/01/17, 12/01/17 Archiving Retiring Johns Hopkins HealthCare LLC (JHHC) provides a
Page 1 of 16 ACTION: New Policy Effective Date: 10/01/2013 Revising : Review Dates: 03/29/16, 06/29/17, Superseding 09/01/17, 12/01/17 Archiving Retiring Johns Hopkins HealthCare LLC (JHHC) provides a
PREVENTIVE MEDICINE AND SCREENING POLICY
 UnitedHealthcare Oxford Reimbursement Policy PREVENTIVE MEDICINE AND SCREENING POLICY Policy Number: ADMINISTRATIVE 238.19 T0 Effective Date: July 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...
UnitedHealthcare Oxford Reimbursement Policy PREVENTIVE MEDICINE AND SCREENING POLICY Policy Number: ADMINISTRATIVE 238.19 T0 Effective Date: July 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...
Reimbursement Environment
 Reimbursement Environment 1 2017 Medicare Physician Fee Schedule Enhancing Integrative Medicine: CMS adopting additional care management codes in 2017 MPFS. Support patient centered and collaborative strategies.
Reimbursement Environment 1 2017 Medicare Physician Fee Schedule Enhancing Integrative Medicine: CMS adopting additional care management codes in 2017 MPFS. Support patient centered and collaborative strategies.
JOHNS HOPKINS HEALTHCARE
 Page 1 of 19 ACTION: New Policy Effective Date: 10/01/2013 Revising : Review Dates: 03/29/16, 06/29/17, Superseding 09/01/17, 12/01/17, 05/15/18 Archiving Retiring Johns Hopkins HealthCare LLC (JHHC) provides
Page 1 of 19 ACTION: New Policy Effective Date: 10/01/2013 Revising : Review Dates: 03/29/16, 06/29/17, Superseding 09/01/17, 12/01/17, 05/15/18 Archiving Retiring Johns Hopkins HealthCare LLC (JHHC) provides
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
Updates in Coding & Billing Strategies.
 Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Updates in Coding & Billing Strategies. Drew Keister MD, FAAFP Lehigh Valley Health Network, Drew_M.Keister@lvhn.org Follow
Lehigh Valley Health Network LVHN Scholarly Works Department of Family Medicine Updates in Coding & Billing Strategies. Drew Keister MD, FAAFP Lehigh Valley Health Network, Drew_M.Keister@lvhn.org Follow
Transitional Care Management (TCM) and Chronic Care Management (CCM) Overview and Billing Process. April 19, :00 PM
 and Chronic Care Management (CCM) Overview and Billing Process. April 19, :00 PM") Transitional Care Management (TCM) and Chronic Care Management (CCM) Overview and Billing Process April 19, 2016 2:00 PM 2 Discussion Topics TCM Requirements TCM Services and C247 Process Medical Decision
Transitional Care Management (TCM) and Chronic Care Management (CCM) Overview and Billing Process April 19, 2016 2:00 PM 2 Discussion Topics TCM Requirements TCM Services and C247 Process Medical Decision
Behavioral Health Billing and Coding Guide for Montana FQHCs & Primary Care Providers. Virna Little, PsyD, LCSW-R, SAP, CCM Laura Leone, MSSW, LMSW
 Behavioral Health Billing and Coding Guide for Montana FQHCs & Primary Care Providers Virna Little, PsyD, LCSW-R, SAP, CCM Laura Leone, MSSW, LMSW Objectives Answer questions specific to FQHC and Primary
Behavioral Health Billing and Coding Guide for Montana FQHCs & Primary Care Providers Virna Little, PsyD, LCSW-R, SAP, CCM Laura Leone, MSSW, LMSW Objectives Answer questions specific to FQHC and Primary
Risk Adjustment Medicare and Commercial
 Risk Adjustment Medicare and Commercial 900 1671 0416 Transform your thinking about Introduction In a time of continual regulatory reform and the evolution of payer/provider reimbursement models, are you
Risk Adjustment Medicare and Commercial 900 1671 0416 Transform your thinking about Introduction In a time of continual regulatory reform and the evolution of payer/provider reimbursement models, are you
FQHC Behavioral Health Billing Codes
 FQHC s Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though process clearly reflected in assessment
FQHC s Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though process clearly reflected in assessment
E. Improving Payment Accuracy for Primary Care, Care Management and Patient-Centered
 CMS-1654-F 212 E. Improving Payment Accuracy for Primary Care, Care Management and Patient-Centered Services 1. Overview In recent years, we have undertaken ongoing efforts to support primary care and
CMS-1654-F 212 E. Improving Payment Accuracy for Primary Care, Care Management and Patient-Centered Services 1. Overview In recent years, we have undertaken ongoing efforts to support primary care and
MLN Matters Number: MM6740 Revised Related Change Request (CR) #: Related CR Transmittal #: R1875CP Implementation Date: January 4, 2010
 #: Related CR Transmittal #: R1875CP Implementation Date: January 4, 2010") News Flash Flu Season is upon us! CMS encourages providers to begin taking advantage of each office visit to encourage your patients with Medicare to get a seasonal flu shot; it s their best defense against
News Flash Flu Season is upon us! CMS encourages providers to begin taking advantage of each office visit to encourage your patients with Medicare to get a seasonal flu shot; it s their best defense against
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) Updated March 2018 No portion of this white paper may be used or duplicated
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) Updated March 2018 No portion of this white paper may be used or duplicated
Telemedicine Guidance
 Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Telemedicine Guidance GEORGIA DEPARTMENT OF COMMUNITY HEALTH DIVISION OF MEDICAID Revised: October 1, 2017 Policy Revisions Record Telemedicine Guidance 2017 REVISION DATE Oct. 1, 2017 SECTION REVISION
Coding and Billing for Lifestyle Medicine
 Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Regulatory Compliance Risks. September 2009
 Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Strategies for Coding, Billing and Getting Paid Appropriately
 Strategies for Coding, Billing and Getting Paid Appropriately 2015 Monograph Update California Academy of Family Physicians Another new year and time to make sure your practice is doing everything possible
Strategies for Coding, Billing and Getting Paid Appropriately 2015 Monograph Update California Academy of Family Physicians Another new year and time to make sure your practice is doing everything possible
Clinic Specific Coding and Reporting Changes for 2017
 January 2017 Jean C. Russell, MS, RHIT jrussell@epochhealth.com 518-369-4986 Richard Cooley, BS, CCS, rcooley@epochhealth.com 518-430-1144 Matthew H. Lawney, MSPT, MBA, CHC mlawney@epochhealth.com 845-642-6462
January 2017 Jean C. Russell, MS, RHIT jrussell@epochhealth.com 518-369-4986 Richard Cooley, BS, CCS, rcooley@epochhealth.com 518-430-1144 Matthew H. Lawney, MSPT, MBA, CHC mlawney@epochhealth.com 845-642-6462
Third Party Payer Days. IMGMA February 25, 2015
 Third Party Payer Days IMGMA February 25, 2015 Agenda 2015 Medicare Physician Fee Schedule Medicare Physician Fee Schedule Database Transitional Care Management - Reminder Medicare - Coverage Guidelines
Third Party Payer Days IMGMA February 25, 2015 Agenda 2015 Medicare Physician Fee Schedule Medicare Physician Fee Schedule Database Transitional Care Management - Reminder Medicare - Coverage Guidelines
3/28/2016. Evaluation and Management. Evaluation and Management Emerging Trends. Disclosures. Evaluation and Management The History
 Evaluation and Management Emerging Trends Peter Hollmann MD Past CPT Panel Chair Disclosures Ambassador for AMA CPT Member RBRVS Update Committee 2 Evaluation and Management The History Evaluation and
Evaluation and Management Emerging Trends Peter Hollmann MD Past CPT Panel Chair Disclosures Ambassador for AMA CPT Member RBRVS Update Committee 2 Evaluation and Management The History Evaluation and
Core Services Provided in Federally Clinical Coverage Policy No: 1D-4 Qualified Health Centers and Amended Date: October 1, 2015 Rural Health Clinics
 Qualified Health Centers and Amended Date: October 1, 2015 Rural Health Clinics Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Federally Qualified Health Centers... 1
Qualified Health Centers and Amended Date: October 1, 2015 Rural Health Clinics Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Federally Qualified Health Centers... 1
Highlights of the 2018 Medicare Physician Fee Schedule (MPFS) Final Rule
 Final Rule") Highlights of the 2018 Medicare Physician Fee Schedule (MPFS) Final Rule Physician Payment Update & Misvalued Codes Target The update to payments under the PFS in 2018 will be +0.31 percent. This reflects
Highlights of the 2018 Medicare Physician Fee Schedule (MPFS) Final Rule Physician Payment Update & Misvalued Codes Target The update to payments under the PFS in 2018 will be +0.31 percent. This reflects
Evaluation & Management ( E/M ) Payment and Documentation Requirements
 Payment and Documentation Requirements") National Partnership for Hospice Innovation 1299 Pennsylvania Ave., Suite 1175 Washington DC, 20004 September 10, 2017 Seema Verma Administrator Centers for Medicare & Medicaid Services, Department of
National Partnership for Hospice Innovation 1299 Pennsylvania Ave., Suite 1175 Washington DC, 20004 September 10, 2017 Seema Verma Administrator Centers for Medicare & Medicaid Services, Department of
Provider-Based RHC Billing June 8, 2018
 Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
OBSERVATION CARE EVALUATION AND MANAGEMENT CODES POLICY
 OBSERVATION CARE EVALUATION AND MANAGEMENT CODES POLICY UnitedHealthcare Oxford Reimbursement Policy Policy Number: ADMINISTRATIVE 232.10 T0 Effective Date: March 1, 2017 Table of Contents Page INSTRUCTIONS
OBSERVATION CARE EVALUATION AND MANAGEMENT CODES POLICY UnitedHealthcare Oxford Reimbursement Policy Policy Number: ADMINISTRATIVE 232.10 T0 Effective Date: March 1, 2017 Table of Contents Page INSTRUCTIONS
Chronic Care Management (CCM): An Overview for Pharmacists. March Developed Through a Collaboration Among:
: An Overview for Pharmacists. March Developed Through a Collaboration Among:") Chronic Care Management (CCM): An Overview for Pharmacists March 2017 Developed Through a Collaboration Among: Overview of CCM and Complex CCM Beginning January 1, 2015, the Medicare Physician Fee Schedule
Chronic Care Management (CCM): An Overview for Pharmacists March 2017 Developed Through a Collaboration Among: Overview of CCM and Complex CCM Beginning January 1, 2015, the Medicare Physician Fee Schedule
Risk Adjustment and Hierarchial Condition Category Coding and Auditing
 December 2, 2016 Risk Adjustment and Hierarchial Condition Category Coding and Auditing Risk Adjustment (RA) and Hierarchical Condition Category (HCC) coding is a payment model mandated by CMS in 1997,
December 2, 2016 Risk Adjustment and Hierarchial Condition Category Coding and Auditing Risk Adjustment (RA) and Hierarchical Condition Category (HCC) coding is a payment model mandated by CMS in 1997,
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
Children s Hospital Association Summary of Final Regulation. November 9, 2012
 Medicaid Program; Payment for Services Furnished by Certain Primary Care Physicians and Charges for Vaccine Administration under the Vaccine for Children Program Children s Hospital Association Summary
Medicaid Program; Payment for Services Furnished by Certain Primary Care Physicians and Charges for Vaccine Administration under the Vaccine for Children Program Children s Hospital Association Summary
Transition Care Management Update: Practical Applications for 2016
 60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI)
") October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
October 27, 2016 To: Subject: National Institutes of Health, National Heart, Lung and Blood Institute (NHLBI) COPD National Action Plan As the national professional organization with a membership of over
Initial Summary of the 2019 Medicare Physician Fee Schedule (PFS) and Quality Payment Program (QPP) Proposed Rule
 and Quality Payment Program (QPP) Proposed Rule") Initial Summary of the 2019 Medicare Physician Fee Schedule (PFS) and Quality Payment Program (QPP) Proposed Rule On July 12, 2018, the Centers for Medicare and Medicaid Services (CMS) released the Revisions
Initial Summary of the 2019 Medicare Physician Fee Schedule (PFS) and Quality Payment Program (QPP) Proposed Rule On July 12, 2018, the Centers for Medicare and Medicaid Services (CMS) released the Revisions
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid s MLN Matters Number: MM9269 Revised Related CR Release : January 26, 2016 Related Transmittal #: R1596OTN Change Request (CR) #:
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid s MLN Matters Number: MM9269 Revised Related CR Release : January 26, 2016 Related Transmittal #: R1596OTN Change Request (CR) #:
Chronic Care Management Services: Advantages for Your Practices
 Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
2019 Evaluation and Management Coding Advisor. Advanced guidance on E/M code selection for traditional documentation systems
 2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
Cognitive Emotional Social Behavioral functioning
 TIP SHEET Health and Behavior Assessment and Intervention (HBAI) Services Coverage of Chronic Disease Self-Management Education Medicare and Medicare Advantage Purpose: The HBAI services are used to identify
TIP SHEET Health and Behavior Assessment and Intervention (HBAI) Services Coverage of Chronic Disease Self-Management Education Medicare and Medicare Advantage Purpose: The HBAI services are used to identify
Via electronic submission (
 Via electronic submission (www.regulations.gov) The Honorable Seema Verma Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Hubert H. Humphrey Building 200
Via electronic submission (www.regulations.gov) The Honorable Seema Verma Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Hubert H. Humphrey Building 200
Annual Wellness Visit (AWV) Delivery Business Case
 Delivery Business Case") Annual Wellness Visit (AWV) Delivery Business Case The implications of the adopting and/or actively promoting AWV services for the practice s bottom line are dependent on a number of factors, including:
Annual Wellness Visit (AWV) Delivery Business Case The implications of the adopting and/or actively promoting AWV services for the practice s bottom line are dependent on a number of factors, including:
Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT
 1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
1 Transitional Care Management JANET BEASY, CPC, CPCO, CMC, CMOM PRACTICE EDUCATION CONSULTANT Initial Requirements 2 Services required when patient returns to community after discharge from specified
Improve Your Revenue for the Services Your Provide with Proper Coding and Documentation. by Christina Rock, BSN, RN Supervisor, Clinical Education
 Improve Your Revenue for the Services Your Provide with Proper Coding and Documentation by Christina Rock, BSN, RN Supervisor, Clinical Education Objectives Awareness of resources and reference materials
Improve Your Revenue for the Services Your Provide with Proper Coding and Documentation by Christina Rock, BSN, RN Supervisor, Clinical Education Objectives Awareness of resources and reference materials
2017 Proposed Rule Physician Fee Schedule in the Federal Register
 2017 Proposed Rule Physician Fee Schedule in the Federal Register Thursday, December 15, 2016 Noon 1:00 Pacific / 1:00 2:00 Mountain / 2:00 3:00 Central / 3:00-4:00 PM Eastern Lucy Zielinski, Vice President
2017 Proposed Rule Physician Fee Schedule in the Federal Register Thursday, December 15, 2016 Noon 1:00 Pacific / 1:00 2:00 Mountain / 2:00 3:00 Central / 3:00-4:00 PM Eastern Lucy Zielinski, Vice President
2017 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care
 P R A C T I C E R E S O U R C E NO.2 M A R C H 2 0 1 7 U P D A T E 2017 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care Margaret McManus, MHS Patience White, MD, MA
P R A C T I C E R E S O U R C E NO.2 M A R C H 2 0 1 7 U P D A T E 2017 Coding and Reimbursement Tip Sheet for Transition from Pediatric to Adult Health Care Margaret McManus, MHS Patience White, MD, MA
DIVISION OF HEALTHCARE FINANCING CMS 1500 ICD-10. October 1, 2017
 DIVISION OF HEALTHCARE FINANCING CMS 1500 ICD-10 October 1, 2017 General Information Overview Thank you for your willingness to serve clients of the Medicaid Program and other medical assistance programs
DIVISION OF HEALTHCARE FINANCING CMS 1500 ICD-10 October 1, 2017 General Information Overview Thank you for your willingness to serve clients of the Medicaid Program and other medical assistance programs
Multi-payer G and CPT Care Management Code Summary v7
 Purpose This document is a guide to help care management team members quickly understand the requirements and documentation fields required for billing care management-related G and CPT codes. Please note
Purpose This document is a guide to help care management team members quickly understand the requirements and documentation fields required for billing care management-related G and CPT codes. Please note
Time-Based Coding. Agenda. AMA Time Rule Physical Medicine Services Anesthesia Evaluation and Management Services Mental Health Services 2016 Changes
 Time-Based Coding Presented by: Mike Strong, SFM The Work Comp Experts Agenda AMA Time Rule Physical Medicine Services Anesthesia Evaluation and Management Services Mental Health Services 2016 Changes
Time-Based Coding Presented by: Mike Strong, SFM The Work Comp Experts Agenda AMA Time Rule Physical Medicine Services Anesthesia Evaluation and Management Services Mental Health Services 2016 Changes
Long Term Care Hospital Clinical Coverage Policy No: 2A-2 Services (LTCH) Amended Date: October 1, Table of Contents
 Amended Date: October 1, Table of Contents") Long Term Care Hospital Clinical Coverage Policy No: 2A-2 Services (LTCH) Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 2.0 Eligibility Requirements...
Long Term Care Hospital Clinical Coverage Policy No: 2A-2 Services (LTCH) Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 2.0 Eligibility Requirements...
Risk Adjustment. Here s What You ll Learn:
 Risk Adjustment Chandra Stephenson, CPC, CIC, COC, CPB, CDEO, CPCO, CPMA, CRC, CCS, CPC-I, CANPC, CCC, CEMC, CFPC, CGSC, CIMC, COBGC, COSC Program Director- Certification Coaching Organization Here s What
Risk Adjustment Chandra Stephenson, CPC, CIC, COC, CPB, CDEO, CPCO, CPMA, CRC, CCS, CPC-I, CANPC, CCC, CEMC, CFPC, CGSC, CIMC, COBGC, COSC Program Director- Certification Coaching Organization Here s What
Clinically Focused. Outcomes Oriented. Technology Driven. Chronic Care Management. eqguide. (CPT Codes 99490, 99487, 99489)
") Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
Clinically Focused. Outcomes Oriented. Technology Driven. 2017 Chronic Care Management eqguide (CPT Codes 99490, 99487, 99489) www.eqhs.org Table of Contents 01 State of Population Health and Chronic Care
Corporate Reimbursement Policy
 Corporate Reimbursement Policy Code Bundling Rules Not Addressed in ClaimCheck or Correct File Name: code_bundling_rules_not_addressed_in_claim_check Origination: 6/2004 Last Review: 12/2017 Next Review:
Corporate Reimbursement Policy Code Bundling Rules Not Addressed in ClaimCheck or Correct File Name: code_bundling_rules_not_addressed_in_claim_check Origination: 6/2004 Last Review: 12/2017 Next Review:
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement. Craig J. Wilson
 Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
HFMA - Northern California. Otani Consulting Group Inc, Hawthorne Blvd, #216, Torrance, CA 90503
 1 HFMA - Northern California 2 Module 2: Departments that Impact Accounts Receivables Clinical and Technical Departments that impact Account Receivables Financial Clearance (FC) Centralized Units Case
1 HFMA - Northern California 2 Module 2: Departments that Impact Accounts Receivables Clinical and Technical Departments that impact Account Receivables Financial Clearance (FC) Centralized Units Case
Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM
 The Harvard Pilgrim Independence Plan SM") Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM Plan Year: July 2010 June 2011 Background The Harvard Pilgrim Independence Plan was developed in 2006 for the Commonwealth of Massachusetts
Frequently Asked Questions (FAQ) The Harvard Pilgrim Independence Plan SM Plan Year: July 2010 June 2011 Background The Harvard Pilgrim Independence Plan was developed in 2006 for the Commonwealth of Massachusetts
9/17/2018. Critical to Practices
 Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule. Grace Wilson, RHIA
 Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes
 CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
CHRONIC CARE MANAGEMENT TOOL KIT What Practices Need to Do to Implement and Bill CCM Codes Understanding CCM Chronic Care Management (CCM) is defined as the non-face-to-face services provided to Medicare
How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21.
 How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21. If only some of the charges are noncovered, per CMS Internet-Only Manual,
How do you bill noncovered charges? If all charges are noncovered, send 710 TOB with all charges as noncovered and condition code 21. If only some of the charges are noncovered, per CMS Internet-Only Manual,
Cigna Medical Coverage Policy
 Cigna Medical Coverage Policy Subject Observation Care Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 4 References... 5 Effective Date... 10/15/2014 Next Review
Cigna Medical Coverage Policy Subject Observation Care Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 4 References... 5 Effective Date... 10/15/2014 Next Review
Chronic Care Management INFORMATION RESOURCE
 Contents Chronic Care Management INFORMATION RESOURCE Purpose... 1 What Is CCM?... 1 Background... 1 Initiating Visit and Person-Centered Plan... 2 Clinical Supervision... 2 Qualifications for Personnel
Contents Chronic Care Management INFORMATION RESOURCE Purpose... 1 What Is CCM?... 1 Background... 1 Initiating Visit and Person-Centered Plan... 2 Clinical Supervision... 2 Qualifications for Personnel
Fee-For-Service Population Health Management Services: Getting Paid Now to Prepare for the Future
 Fee-For-Service Population Health Management Services: Getting Paid Now to Prepare for the Future No portion of this white paper may be used or duplicated by any person or entity for any purpose without
Fee-For-Service Population Health Management Services: Getting Paid Now to Prepare for the Future No portion of this white paper may be used or duplicated by any person or entity for any purpose without
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Disclosure Statement
 2017 Coding and Medicare Changes for Physician Fee Schedule Billing Presented by Jean Acevedo, CHC CPC CENTC LHRM Disclosure Statement No financial relationships to disclose. 1 Disclaimer The information
2017 Coding and Medicare Changes for Physician Fee Schedule Billing Presented by Jean Acevedo, CHC CPC CENTC LHRM Disclosure Statement No financial relationships to disclose. 1 Disclaimer The information
CY 2018 Medicare Physician Fee Schedule Proposed Rule Summary
 CY 2018 Medicare Physician Fee Schedule Proposed Rule Summary On July 13, 2017, the Center for Medicare and Medicaid Services (CMS) released the proposed Medicare Physician Fee Schedule (MPFS) for 2018.
CY 2018 Medicare Physician Fee Schedule Proposed Rule Summary On July 13, 2017, the Center for Medicare and Medicaid Services (CMS) released the proposed Medicare Physician Fee Schedule (MPFS) for 2018.
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
E/M Auditing: History is the Key
 E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
Coding Guidelines for Certain Respiratory Care Services January 2018 (updates in red)
") Coding Guidelines for Certain Respiratory Care Services (updates in red) Overview From time to time the AARC receives inquiries about respiratory-related coding and coverage issues through its Help Line
Coding Guidelines for Certain Respiratory Care Services (updates in red) Overview From time to time the AARC receives inquiries about respiratory-related coding and coverage issues through its Help Line
Evaluation and Management Auditing Back to the Basics. Objectives. Audit Start with the benchmarks CMS MEDPAR by specialty 4/22/2013
 Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
2017 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Focus On Observation
 Focus On Observation Introduction CPT and CMS Requirements CPT Codes Documentation Requirements Observation Coding: Facility Considerations 2 LogixHealth s unsurpassed service stems from the fact that
Focus On Observation Introduction CPT and CMS Requirements CPT Codes Documentation Requirements Observation Coding: Facility Considerations 2 LogixHealth s unsurpassed service stems from the fact that