Managing Acute Care for People across the Health Care System - Is more capacity the answer?
|
|
|
- Shona Melton
- 5 years ago
- Views:
Transcription
1 Managing Acute Care for People across the Health Care System - Is more capacity the answer? Dr Ian Sturgess Partner, NHS Interim Management and Support National Clinical Lead for Urgent and Emergency Care, Intensive Support Team
2 What are we trying to achieve? Getting patients better faster and safer through better integration and alignment. Pursuing Perfection Safety Ideal Care No avoidable deaths No harm No unnecessary pain No waste No delays No feelings of helplessness No inequality Flow Reliability
3 "Hospital beds by country", OECD. Retrieved fromhttp://
4 Emergency Care Improvement Understanding demand : capacity : activity : queue Setting Intent Data vs Intelligence Leadership Executive and Clinical Governance Bottlenecks in the System Silos vs Integration Rework and unnecessary steps Sharing and Trust Does the system say YES or NO
5 Defining demand, capacity activity and queue Demand on the services is all the requests or referrals into the service from all sources Capacity is all of the resources required to do the work and includes staff and equipment Activity is the work done, it is the throughput of the system Backlog is the demand which has not been dealt with the queue or waiting list
6 Demand and capacity definitions: Demand = All requests for a service = what we should do Waiting list, queue = what we should have done Capacity = what we could do Activity = what we did
7 Measuring demand, capacity activity and queue Why is it important to understand the four measures of demand, capacity, activity and queue? To identify the bottleneck or constraint in the care process To increase capacity at the stage of the process where it will create the greatest outcome To reduce inappropriate demand to the constraint To redesign services or plan services
8 Setting Intent Achieving the target without missing the point What does good look like? Reduced LTC progression Reduced institutionalisation Increased independence Reduced ED attendances and emergency admissions Reduced occupancy of baseline adult non-elective beds Institute of Medicine - Quality Chasm 1. Safety avoid injuries 2. Effectiveness evidence based care 3. Patient centeredness 4. Timeliness avoid harmful delays 5. Efficiency avoid waste 6. Equity prevent quality differences
9 Data vs Intelligence Activity vs Demand : capacity analysis Predictive modelling Averages vs variance Point prevalence vs run charts/spc Response to variance Special cause vs Common cause Capability assessment For strategic planning, monitoring impact of projects, and operational management.
10 A whole system perspective Focus on CDM and more effective responses to urgent care needs ACS condition management General Practice & GP OOH Clear operational performance framework and integrated in to primary care Community Support Improved integration with primary care responders Ambulance Service & GP OOH Front load senior decision process incl primary care A+E MAU/SAU/ Short Stay Inpatient Wards Health Promotion Discharge Process Optimise ambulatory emergency care Information flow converting the unheralded to the heralded Redesign to left shift LOS Preventative/ Predictive care Disease management Managed populations Alternatives to acute admission settings Alternative access for diagnosis Alternative settings for therapy Alternative sites for discharge Alternative sites for readmission
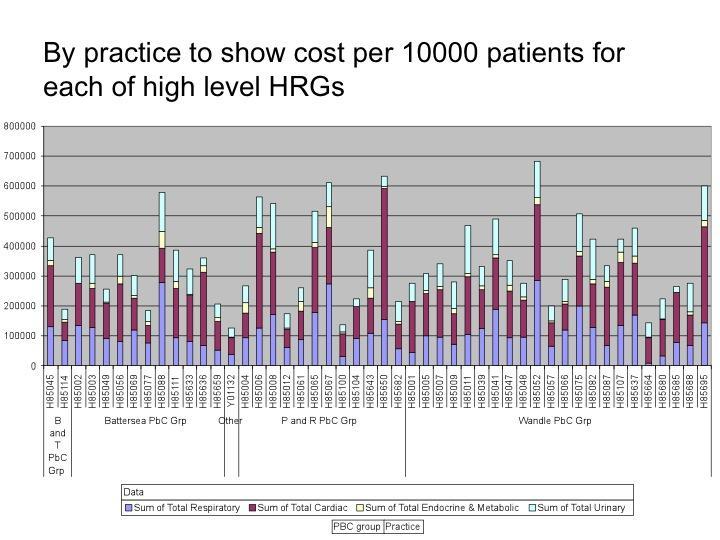
11 Engaging GPs Sensible data in graphical form Enable practices to rank themselves Non-elective cost by HRG chapter Use of OOH Predictive modelling PARR ++, Combined Predictive Model, HUM, EARLI Focus for PBC Same day care in general practice increasing focus

12 Urgent Care in Primary Care 12 Recommendations Access and responsiveness Understanding capacity and demand Assessment and response Standards and quality Integration Information systems eg OOH With community services
13

14 Roland M BMJ Preventing Emergency Admissions excessive focus on frequent flyers? Does current GP consultation model and QOF allow comprehensive assessment/anticipatory care etc in older people with complex needs?
15 Admitted Acute Care - Required Actions Identify the drivers Quality IOM 6 domains Create the tension for change Governance and leadership Structure and Behaviours Create the vision Identify added value Alignment for delivery Understand the flow streams Demand, Capacity and Variability Standardise the processes Measure for success - publish Outcome, process and balancing
16 Reasons/Excuses for not changing Our LOS is OK Flaw of averages How are average LOS calculated? Our patients are different Not believing the data Simple solution just compare yourself with yourself are we improving enough outliers and extra beds? We re a Teaching Hospital So what! The problem is with someone else: Social services Care Homes Diagnostics The patients ie complex elderly - is blaming the patients a good idea? Result = Safer patient care is compromised
17 Using Data to Drive Improvement If you cannot measure it, you cannot improve it Lord Kelvin, Stages of facing reality: The data are wrong The data are right, but it s not a problem The data are right; it is a problem; but it is not my problem I accept the burden of improvement Berwick D. Qual Saf Health Care 2003;12(S1):2-6

18 Risks of Hospital Over-crowding Patient flow is not just about productivity and efficiency its about patient safety. 90%+ of in-hospital deaths occur in the nonelective pathway. The majority of avoidable deaths occur in this pathway. Sprivulis PC, Da Silva JA, Jacobs IG, Frazer AR, Jelinek GA. The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments. Med J Aust. 2006; 184:208 12
19 Beds occupied = The Queue of unfinished work! A bed is where a patient waits for the next useful thing to happen The importance of the hard red line Aim Reduce Acute beds occupied to SPC mean of 600 or less + reduce crude in-hospital mortality rate by 10% + a fall in SCHMI by 31 st March 2012 Process measure The whole system action plan etc etc ie holding the system to account not just the acute sector. Balancing Deliver a decrease in Long term care ie more patients returning to live at home. No increase in 30 day re-admission rate
20 Care Coordination The health system delivered the required care, but was it in a time frame that suited the patient, carer or staff? Wait Care Wait Care Wait Care Wait By reducing the waiting time overall LOS is reduced without changing the clinical care received by the patient
21 Adding value for emergency admissions 1. Timely senior assessment 2. Timely case management plan What, where, when, and communication 3. Timely delivery of inputs Diagnostics Interventions 4. Maintaining the tempo Daily review against plan
22 Balancing Measures Unintended consequences Building a Cascade of Measures L 1 Board & CEO L 2 Service Line Outcome High level eg death, harm etc Process + Outcome L 3 Microsystems: Units, Depts L 4/ 5 Physician & Patient Process (+ Outcome) Individual Process Metrics Adapted from Lloyd & Caldwell
23 Delivering the Added Value The Process Internal professional standards Standardised documentation Timeliness of assessments, decisions and treatment Timeliness of diagnostics Definition of responsibilities Senior clinical team Managerial team Support services Measurement for improvement Outcome, process and balancing Make visible share and publish Improve design, peer support, escalation

24 Understanding Demand ED Attendance Admitted and Not Admitted Aim reduce emergency admission from ED to an SPC mean of < 40 per day Process Deliver S+T, RAT, + Intermediate care + Mental Health improvements Balancing 7 day re-attendance and 30 day re-admission

25 Understanding Demand ED arrival times by day of the week For ease I have used the average, for planning strategic, tactical and operational you would use the 85 th centile of the variance Erlang s Rule


26 Flow within the ED Where is the problem non-admitted patients?


27 Flow within the ED Where is the problem admitted patients?
28 Emergency Department Setting the Standards Internal clock setting, floor management + visual display Time to stream/triage Time to medical assess Time to Clinical Decision Time to dispersal admitting team responsibility Stream management See and Treat - minors RAT/STARR with SIFT Observation/CDU/SSA protocol driven Aiming for single piece flow Treatment unit vs Triage unit Referral protocols + Direct admissions Inward vs outward looking integration with community
29 EKHUFT NEL In-Day Bed Swing

30 Trust NEL Admissions and Discharges Demand and surrogate for capacity Aim Reduce emergency admissions by 20 by 31 st March 2012 Processes RAT in A+E, 1 0 Care improvements, improved EoL care etc Balancing - prevent any increase in institutional care
31 Consequences of admissions & discharges variation mismatch Backlog guaranteed: Patients stored in Assessment Units A&E flow compromised Patients to the wrong wards Outliers Quality Mortality and harm events Patient and staff experience Additional Cost: Overtime, locum, agency and opening wards
32 Traditional Model for Acute Care GP referrals Handover Short Stay Unit Social care A+E Referrals MAU - Decision to admit Handover Handover Specialist units Home D+T - OPA IC Handover Churn Handover
33 Assessment Units/ Admitting Specialty Team Setting the Standards Internal clock setting, floor management + visual display Time to stream +/_rapid senior assess and treatment STAT/RAT Process Southampton/Nottingham Time to medical assess and decision support diagnostics Time to Senior Clinical Decision (Consultant) 80% of admissions < 3 hrs, last 20% < 12 hrs Use of evidence based algorithms timelines to treatment Standardising the clinical decision Single piece flow vs batch processing Virtual/real Merger with ED Team
34 What Constitutes a Senior Clinical Decision Effective senior clinical decision at point of entry being there!: 1 o Diagnosis (or differential) Co-morbidity diagnoses + functional/social problems Case management plan: ZLOS - 1 o care/ic/sc/opa/joint care (Teams walls) Non ZLOS: Why admission required monitoring/interventions Investigations/interventions not just what but when and make it happen! Clinical criteria for discharge + Expected discharge date Stream by LOS see later What to expect post-discharge recovery + follow up
35 Expected Date of Discharge and Clinical Criteria for Discharge Using EDD and clinical criteria for discharge to support Care Coordination. When setting an EDD do not build in the delays that exist within the system (clinical length of stay only) EDD can be changed for (real) clinical reasons only EDD is a coordination target Set the clinical (incl functional) criteria for discharge Communicate Plan, EDD and Criteria for discharge Creating the expectation Clinical Team Patient and family
36 Improving Flow in In-patients Remove redundant steps Point of entry decision making team at front of house Handover = delayed decisions = increased LOS Reduce variation in emergency discharges Reduce internal batching and carve-out Reduce impact of intake and twice weekly ward round processes Visual work space management + Daily Consultant review daily drum beat! Standardisation of processes Segmentation of patient by LOS Principle of lanes on a motorway Different process speed and variation Standardise case management processes where possible
37 In-Patient Units/Specialty Team Setting the Standards Internal clock setting, floor management + visual display Ownership of the case management plan Flow streams Alignment to the EDD (date and time) Control of who can change the EDD Visual display to facilitate daily board review Planning today + tomorrow Expected discharge rates One stop ward rounds Service response time to ED/Assessment Unit request Role of the Senior Clinician (Consultant) Review of entire bed base daily Managing variance from case management plan Re-enforcing the clinical criteria for discharge A specialty can only be considered a specialty if it can deliver specialty care to all inpatients referred to it on a daily basis.
38 Discharge Planning Standards To commence on day of admission Aligned to EDD and re-enforce clinical criteria Parallel planning no waiting until medically fit MDT role solutions not just identify the problem Balanced risk No discharge is unsafe statements from MDT Process for changing EDD Can only be changed with direct consultation with the Consultant
39 Pareto Analysis Complex Cumulative Demand 100% 20 Short Stay 30% 15% 5% of demand: Red stream: Rare Strangers 50% of demand = 7% of types: Green stream: Runners \ 80 0 Sick Specialty Sick General LOS Glenday Sieve

40 LOS Cumulative Profile Excl Paeds, Obstetrics, Midwifery, Zero LOS Colchester %OBD <50% = 3 midnights 10.1% <80% = 11 midnights 36.6% <95% = 28 midnights 70.9% >95% 29.1%
41 Number of patients Managing the Streams Identify the stream Short stay Sick specialty Sick Frail Complex Allocate early to teams skilled in that stream Short stay manage to the hour Maximise ambulatory care Clarity of specialty criteria Specialty case management plan at Handover no delays Green bed days vs red bed days Minimise handover Decompensation risk Early assertive management Green bed days vs red bed days Complex needs how much is decompensation? Detect early and design simple rules for discharge Length of stay (days)
42

43 Zero LOS Discharges - Trust Excl paediatrics, midwifery and obstetrics Aim Increase zero LOS Process deliver AEC Balancing Reduce overall NEL admissions

44 2 midnights or less LOS Discharges - Trust Aim Increase short stay discharges Process deliver AEC + short stay review process Balancing Reduce overall NEL admissions
45 In-Patients with LOS 14 days or more Aim Reduce I/P with LOS 14 + to 75 or less by 31 st March 2012 Process Early identification of at risk group, CGA, early supported discharge schemes Balancing no increase in institutional care aim for a reduction in over 75s in Long term Care
46 Integrated Emergency Needs Assessment Service RAT/STAT Model Of Acute Care Handover = Handoff = Increased LOS Sick General/ Complex discharges detect early Social care Stabilisation unit = AMU Ambulatory and Short Stay Unit Home D+T - OPA Small Specialist units IC Discharge plan and case management Measuring Standards Publicise Performance
Targets, flow, exit block, stranded patients, red2green. What s any of this got to do with good patient care?
 Targets, flow, exit block, stranded patients, red2green. What s any of this got to do with good patient care? Lee Dowson Divisional Director of Medicine Royal Wolverhampton NHS Trust Clinical Associate
Targets, flow, exit block, stranded patients, red2green. What s any of this got to do with good patient care? Lee Dowson Divisional Director of Medicine Royal Wolverhampton NHS Trust Clinical Associate
What good looks like in the emergency pathway
 What good looks like in the emergency pathway @ECISTNetwork @PeteGordon68 I m going to cover Safer Faster Better The evidence Myths What we ve found over 150 engagements Why we need simple rules We recommend
What good looks like in the emergency pathway @ECISTNetwork @PeteGordon68 I m going to cover Safer Faster Better The evidence Myths What we ve found over 150 engagements Why we need simple rules We recommend
A Step-by-Step Guide to Tackling your Challenges
 Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
BOARD OF DIRECTORS. Sue Watkinson Chief Operating Officer
 Affiliated Teaching Hospital BOARD OF DIRECTORS 28 TH SEPTEMBER 2012 AGENDA ITEM: 11.1 TITLE: INTENSIVE SUPPORT TEAM REPORT PURPOSE: The Board of Directors is presented with the report from the Intensive
Affiliated Teaching Hospital BOARD OF DIRECTORS 28 TH SEPTEMBER 2012 AGENDA ITEM: 11.1 TITLE: INTENSIVE SUPPORT TEAM REPORT PURPOSE: The Board of Directors is presented with the report from the Intensive
Unscheduled care Urgent and Emergency Care
 Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Redesign of Front Door
 Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Online library of Quality, Service Improvement and Redesign tools. Discharge planning. collaboration trust respect innovation courage compassion
 Online library of Quality, Service Improvement and Redesign tools Discharge planning collaboration trust respect innovation courage compassion Discharge planning What is it? A specific targeted discharge
Online library of Quality, Service Improvement and Redesign tools Discharge planning collaboration trust respect innovation courage compassion Discharge planning What is it? A specific targeted discharge
Boarding Impact on patients, hospitals and healthcare systems
 Boarding Impact on patients, hospitals and healthcare systems Dan Beckett Consultant Acute Physician NHSFV National Clinical Lead Whole System Patient Flow Project Scottish Government May 2014 Important
Boarding Impact on patients, hospitals and healthcare systems Dan Beckett Consultant Acute Physician NHSFV National Clinical Lead Whole System Patient Flow Project Scottish Government May 2014 Important
Final Version Simple Guide to the Care Act and Delayed Transfers of Care (DTOC) SIMPLE GUIDE TO THE CARE ACT AND DELAYED TRANSFERS OF CARE (DTOC)
 SIMPLE GUIDE TO THE CARE ACT AND DELAYED TRANSFERS OF CARE (DTOC)") SIMPLE GUIDE TO THE CARE ACT AND DELAYED TRANSFERS OF CARE (DTOC) 1. UNDERPINNING PRINCIPLES Across the whole system, our common aims are to: Improve services for patients by avoiding situations where,
SIMPLE GUIDE TO THE CARE ACT AND DELAYED TRANSFERS OF CARE (DTOC) 1. UNDERPINNING PRINCIPLES Across the whole system, our common aims are to: Improve services for patients by avoiding situations where,
Urgent & Emergency Care Strategy Update
 RCCG/GB/17/144 Urgent & Emergency Care Strategy Update 1. Introduction The purpose of this paper is to provide assurance on the effective delivery to date of our urgent and emergency care strategy within
RCCG/GB/17/144 Urgent & Emergency Care Strategy Update 1. Introduction The purpose of this paper is to provide assurance on the effective delivery to date of our urgent and emergency care strategy within
South Warwickshire s Whole System Approach Transforms Emergency Care. South Warwickshire NHS Foundation Trust
 South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS Foundation Trust South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS
South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS Foundation Trust South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Same day emergency care: clinical definition, patient selection and metrics
 Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust Tel
 Lean Thinking Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust neil.westwood@institute.nhs.uk Tel 07747794976 NHS Institute for Innovation and Improvement Plan for today
Lean Thinking Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust neil.westwood@institute.nhs.uk Tel 07747794976 NHS Institute for Innovation and Improvement Plan for today
Mental Health Short Stay
 Mental Health Directorate Central Adelaide Local Health Network Mental Health Short Stay Model of Care January 2016 Extracted from Improving Unplanned Emergency Access pathways (IUEAP) Model of Care: Mental
Mental Health Directorate Central Adelaide Local Health Network Mental Health Short Stay Model of Care January 2016 Extracted from Improving Unplanned Emergency Access pathways (IUEAP) Model of Care: Mental
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Addressing ambulance handover delays: actions for local accident and emergency delivery boards
 Addressing ambulance handover delays: actions for local accident and emergency delivery boards Published by NHS England and NHS Improvement November 2017 Contents Foreword... 2 Actions to be taken now,
Addressing ambulance handover delays: actions for local accident and emergency delivery boards Published by NHS England and NHS Improvement November 2017 Contents Foreword... 2 Actions to be taken now,
NHS. Top tips to overcome the challenge of commissioning diagnostic services. NHS Improvement - Diagnostics. NHS Improvement Diagnostics CANCER
 CANCER NHS NHS Improvement Diagnostics DIAGNOSTICS HEART LUNG STROKE NHS Improvement - Diagnostics Top tips to overcome the challenge of commissioning diagnostic services Top tips to overcome the challenge
CANCER NHS NHS Improvement Diagnostics DIAGNOSTICS HEART LUNG STROKE NHS Improvement - Diagnostics Top tips to overcome the challenge of commissioning diagnostic services Top tips to overcome the challenge
Seven day hospital services: case study. South Warwickshire NHS Foundation Trust
 Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
North West London Accident and Emergency Performance Report for the winter of 2016/17. North West London Joint Health Overview and Scrutiny Committee
 North West London Accident and Emergency Performance Report for the winter of 2016/17 North West London Joint Health Overview and Scrutiny Committee 20 April 2017 1 This paper will summarise the performance
North West London Accident and Emergency Performance Report for the winter of 2016/17 North West London Joint Health Overview and Scrutiny Committee 20 April 2017 1 This paper will summarise the performance
Putting It All Together: Strategies to Achieve System-Wide Results
 1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
RBCH Actions to meet CQC Essential Standards
 RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
A new integrated model for Care Homes from Walsall CCG/Healthcare NHS Trust
 A new integrated model for Care Homes from Walsall CCG/Healthcare NHS Trust Sally Roberts - Director of Governance, Quality & Safety. Walsall CCG Katie Welborn Advanced Nurse Practitioner- Walsall Healthcare
A new integrated model for Care Homes from Walsall CCG/Healthcare NHS Trust Sally Roberts - Director of Governance, Quality & Safety. Walsall CCG Katie Welborn Advanced Nurse Practitioner- Walsall Healthcare
Winter/Surge Capacity Plan 1 st December 2013 to 31 st March Position as at September 2013
 Winter/Surge Capacity Plan 1 st December 2013 to 31 st March 2014 Position as at September 2013 Contents 1. Introduction and background... 3 2. Demand and capacity... 4 2.1. Anticipated bed demand... 4
Winter/Surge Capacity Plan 1 st December 2013 to 31 st March 2014 Position as at September 2013 Contents 1. Introduction and background... 3 2. Demand and capacity... 4 2.1. Anticipated bed demand... 4
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Urgent Care Short Term Actions to Improve Performance
 To: Trust Board From: Chief Operating Officer Date: March 2017 Healthcare standard Title: Urgent Care Short Term Actions to Improve Performance Author/Responsible Director: Michael Woods / Andrew Prydderch
To: Trust Board From: Chief Operating Officer Date: March 2017 Healthcare standard Title: Urgent Care Short Term Actions to Improve Performance Author/Responsible Director: Michael Woods / Andrew Prydderch
Report to the Board of Directors 2016/17
 Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
Integrated heart failure service working across the hospital and the community
 Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
2018 Optional Special Interest Groups
 2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve
2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve
Ambulatory emergency care Reimbursement under the national tariff
 HFMA briefing Ambulatory emergency care Reimbursement under the national tariff Introduction Ambulatory emergency care is defined as a service that allows a patient to be seen, diagnosed and treated and
HFMA briefing Ambulatory emergency care Reimbursement under the national tariff Introduction Ambulatory emergency care is defined as a service that allows a patient to be seen, diagnosed and treated and
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Kingston Hospital NHS Foundation Trust Length of stay case study. October 2014
 Kingston Hospital NHS Foundation Trust Length of stay case study October 2014 The hospital has around 520 beds and provides acute medical services for a population of around 320,000 in Kingston, Richmond,
Kingston Hospital NHS Foundation Trust Length of stay case study October 2014 The hospital has around 520 beds and provides acute medical services for a population of around 320,000 in Kingston, Richmond,
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
PHFT Building Voluntary working with the Voluntary Sector. Val Horn :Discharge Services Manager Carol Smith: RC Service Manager Dorset
 PHFT Building Voluntary working with the Voluntary Sector Val Horn :Discharge Services Manager Carol Smith: RC Service Manager Dorset WE ARE ALL BUSY! Emergency Attendances Emergency Admissions GP Admissions
PHFT Building Voluntary working with the Voluntary Sector Val Horn :Discharge Services Manager Carol Smith: RC Service Manager Dorset WE ARE ALL BUSY! Emergency Attendances Emergency Admissions GP Admissions
AMP Health and Social Care Professional Implementation Group Update
 AMP Health and Social Care Professional Implementation Group Update November 2016 Welcome to another update from the National Acute Medicine Programme s Health and Social Care Professionals Implementation
AMP Health and Social Care Professional Implementation Group Update November 2016 Welcome to another update from the National Acute Medicine Programme s Health and Social Care Professionals Implementation
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
Plan for investment of retained marginal rate payment for emergency admissions in Gloucestershire
 Plan for investment of retained marginal rate payment for emergency admissions in Gloucestershire 1. Purpose of document This document summarises and explains how Gloucestershire CCG has used the funds
Plan for investment of retained marginal rate payment for emergency admissions in Gloucestershire 1. Purpose of document This document summarises and explains how Gloucestershire CCG has used the funds
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Leicester, Leicestershire and Rutland s Sustainability & Transformation Plan (STP)
") Leicester, Leicestershire and Rutland s Sustainability & Transformation Plan (STP) UPDATE Toby Sanders, STP Lead 13 September, 2016 What is the STP? Health and care place based plan for Leicester, Leicestershire
Leicester, Leicestershire and Rutland s Sustainability & Transformation Plan (STP) UPDATE Toby Sanders, STP Lead 13 September, 2016 What is the STP? Health and care place based plan for Leicester, Leicestershire
ANEURIN BEVAN HEALTH BOARD Stroke Delivery Plan Template for 2009/2010
 ANEURIN BEVAN HEALTH BOARD Stroke Delivery Plan Template for 2009/2010 Objective Action Desired Output / Monitor and manage all those at risk of stroke and, refer as appropriate to smoking cessation services,
ANEURIN BEVAN HEALTH BOARD Stroke Delivery Plan Template for 2009/2010 Objective Action Desired Output / Monitor and manage all those at risk of stroke and, refer as appropriate to smoking cessation services,
The Community Based Target Model
 1 The Community Based Target Model Integrated Single System Leadership and Management The Core (as a minimum all LCNs should encompass) Working with High Impact Changes Lambeth Serving geographically coherent
1 The Community Based Target Model Integrated Single System Leadership and Management The Core (as a minimum all LCNs should encompass) Working with High Impact Changes Lambeth Serving geographically coherent
Acceleration for ACS. NSTEMI Event 09 November. Outputs from Table Discussions
 Acceleration for ACS NSTEMI Event 09 November Outputs from Table Discussions 1 1. What mechanism do we need to have to identify patients early (within 6 hours of admission to hospital)? Have identification
Acceleration for ACS NSTEMI Event 09 November Outputs from Table Discussions 1 1. What mechanism do we need to have to identify patients early (within 6 hours of admission to hospital)? Have identification
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
DRAFT. Rehabilitation and Enablement Services Redesign
 DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
Urgent and Emergency Care Review update: from design to delivery
 The Kings Fund September 2015 Keith Willett Director of Acute Care Urgent and Emergency Care Review update: from design to delivery What does the experience and data from recent winters tell us? Surge
The Kings Fund September 2015 Keith Willett Director of Acute Care Urgent and Emergency Care Review update: from design to delivery What does the experience and data from recent winters tell us? Surge
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16
 Schemes for 2015/16") Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Strategies to Achieve System-Wide Hospital Flow
 M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
M15 This presenter has nothing to disclose Strategies to Achieve System-Wide Hospital Flow Katharine Luther and Pat Rutherford IHI s 26th Annual National Forum on Quality Improvement in Health Care December
Mid Powys Cluster Plan
 Mid Powys Cluster Plan 2016-17 The Cluster Network Development Domain with the Quality & Outcomes Framework supports medical practices to work collaboratively to: Understand local health needs and priorities
Mid Powys Cluster Plan 2016-17 The Cluster Network Development Domain with the Quality & Outcomes Framework supports medical practices to work collaboratively to: Understand local health needs and priorities
Our Journey to Discharge to Assess (D2A)
") Our Journey to Discharge to Assess (D2A) Jane Ives Director of Operations South Warwickshire NHS Foundation Trust Wendy Lane Senior Partner Transformation & Innovation Arden Commissioning Support Zoe Bogg
Our Journey to Discharge to Assess (D2A) Jane Ives Director of Operations South Warwickshire NHS Foundation Trust Wendy Lane Senior Partner Transformation & Innovation Arden Commissioning Support Zoe Bogg
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
2. This year the LDP has three elements, which are underpinned by finance and workforce planning.
 Directorate for Health Performance and Delivery NHSScotland Chief Operating Officer John Connaghan T: 0131-244 3480 E: john.connaghan@scotland.gsi.gov.uk John Burns Chief Executive NHS Ayrshire and Arran
Directorate for Health Performance and Delivery NHSScotland Chief Operating Officer John Connaghan T: 0131-244 3480 E: john.connaghan@scotland.gsi.gov.uk John Burns Chief Executive NHS Ayrshire and Arran
Self-assessment surveys details & definitions
 Self-assessment surveys details & definitions Completing the Paradigm self assessment surveys is the very first step in achieving the Paradigm Award. Only organizations who complete the self assessment
Self-assessment surveys details & definitions Completing the Paradigm self assessment surveys is the very first step in achieving the Paradigm Award. Only organizations who complete the self assessment
UEC system outcomes and measures. Ciaran Sundstrem Senior Programme Lead: Urgent and Emergency Care Review NHS England
 UEC system outcomes and measures Ciaran Sundstrem Senior Programme Lead: Urgent and Emergency Care Review NHS England NHS Confederation: UEC Review update Ciaran Sundstrem 25 March 2015 Urgent and Emergency
UEC system outcomes and measures Ciaran Sundstrem Senior Programme Lead: Urgent and Emergency Care Review NHS England NHS Confederation: UEC Review update Ciaran Sundstrem 25 March 2015 Urgent and Emergency
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
NHS Greater Glasgow and Clyde Alison Noonan
 NHS Board Contact Email NHS Greater Glasgow and Clyde Alison Noonan alison.noonan@ggc.scot.nhs.uk Title Category Background/ context Problem Effective Discharge Planning and the Introduction of Delegated
NHS Board Contact Email NHS Greater Glasgow and Clyde Alison Noonan alison.noonan@ggc.scot.nhs.uk Title Category Background/ context Problem Effective Discharge Planning and the Introduction of Delegated
18 Weeks Referral to Treatment (RTT) Standard Recovery Planning and Assurance Framework
 Standard Recovery Planning and Assurance Framework") 18 Weeks Referral to Treatment (RTT) Standard Recovery Planning and Assurance Framework Vicky Scott Head of Delivery & Development (North West London) NHS Trust Development Authority Lyndsay Pendegrass
18 Weeks Referral to Treatment (RTT) Standard Recovery Planning and Assurance Framework Vicky Scott Head of Delivery & Development (North West London) NHS Trust Development Authority Lyndsay Pendegrass
CUH Looking beyond the hospital for solutions
 CUH Looking beyond the hospital for solutions ED More than a hospital department Room with a view. Avilene Casey Executive Performance Improvement Lead (USC) HSE. Length of stay reduction equates to extra
CUH Looking beyond the hospital for solutions ED More than a hospital department Room with a view. Avilene Casey Executive Performance Improvement Lead (USC) HSE. Length of stay reduction equates to extra
EQuIPNational Survey Planning Tool NSQHSS and EQuIP Actions 4.
 Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement
Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement
WAITING TIMES AND ACCESS TARGETS
 NHS Board Meeting Tuesday 17 December 2013 Lead Director (Acute Services Division) Board Paper No 13/60 Recommendation: WAITING TIMES AND ACCESS TARGETS The NHS Board is asked to note progress against
NHS Board Meeting Tuesday 17 December 2013 Lead Director (Acute Services Division) Board Paper No 13/60 Recommendation: WAITING TIMES AND ACCESS TARGETS The NHS Board is asked to note progress against
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, Mike Williams, MPH/HSA The Abaris Group
 NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
Future Hospital Programme: - a Partner perspective
 Future Hospital Programme: - a Partner perspective Dr Roger Duckitt Royal College of Physicians Loughborough February 2017 Future hospital timeline Launch of Future Hospital Commission March 2012 Sept
Future Hospital Programme: - a Partner perspective Dr Roger Duckitt Royal College of Physicians Loughborough February 2017 Future hospital timeline Launch of Future Hospital Commission March 2012 Sept
Fixing Unscheduled Care in the Republic of Ireland. Prof. Garry Courtney Lead, National Acute Medicine Programme
 Fixing Unscheduled Care in the Republic of Ireland Prof. Garry Courtney Lead, National Acute Medicine Programme CCPs arose from HSE/RCPI/RCSI collaboration 2010 Or to put it another way Our Health Service
Fixing Unscheduled Care in the Republic of Ireland Prof. Garry Courtney Lead, National Acute Medicine Programme CCPs arose from HSE/RCPI/RCSI collaboration 2010 Or to put it another way Our Health Service
Northumbria Whole System Review 22 nd to 25 th November 2016
 Northumbria Whole System Review 22 nd to 25 th November 2016 Introduction The Emergency Care Improvement Team would like to thank the leaders of the health system and network for inviting us to review
Northumbria Whole System Review 22 nd to 25 th November 2016 Introduction The Emergency Care Improvement Team would like to thank the leaders of the health system and network for inviting us to review
SAFE STAFFING GUIDELINE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health
 REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
London CCG Neurology Profile
 CCG Neurology Profile November 214 Summary NHS Hammersmith And Fulham CCG Difference from Details Comments Admissions Neurology admissions per 1, 2,13 1,94 227 p.1 Emergency admissions per 1, 1,661 1,258
CCG Neurology Profile November 214 Summary NHS Hammersmith And Fulham CCG Difference from Details Comments Admissions Neurology admissions per 1, 2,13 1,94 227 p.1 Emergency admissions per 1, 1,661 1,258
DIVISION OF EMERGENCY MEDICINE DEPARTMENT OF ACUTE MEDICINE
 DIVISION OF EMERGENCY MEDICINE DEPARTMENT OF ACUTE MEDICINE Ambulatory Care Unit Standard Operational Policy Document Control Reference No: First published: November 2014 Version: 004 Current Version Published:
DIVISION OF EMERGENCY MEDICINE DEPARTMENT OF ACUTE MEDICINE Ambulatory Care Unit Standard Operational Policy Document Control Reference No: First published: November 2014 Version: 004 Current Version Published:
Tackling Emergency Department Crowding
 The Royal College of Emergency Medicine Tackling Emergency Department Crowding Safe Efficient Effective Care Service Design and Delivery Introduction I welcome the publication of this toolkit and strongly
The Royal College of Emergency Medicine Tackling Emergency Department Crowding Safe Efficient Effective Care Service Design and Delivery Introduction I welcome the publication of this toolkit and strongly
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators April Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Indicators April 2011 Report to: Trust Board 24 May 2011 Report from: Sponsoring Executive: Aim of Report / Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Indicators April 2011 Report to: Trust Board 24 May 2011 Report from: Sponsoring Executive: Aim of Report / Principle Topic: Review History to date:
Can physicians do as well as orthopaedic surgeons: letting go of the discharge decision.
 Can physicians do as well as orthopaedic surgeons: letting go of the discharge decision. Dr. Simon Watkin Consultant physician NHS Borders Simon.watkin@borders.scot.nhs.uk What does it mean The establishment
Can physicians do as well as orthopaedic surgeons: letting go of the discharge decision. Dr. Simon Watkin Consultant physician NHS Borders Simon.watkin@borders.scot.nhs.uk What does it mean The establishment
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Ambulatory Emergency Care The role of the ED - a journey travelled!
 Ambulatory Emergency Care The role of the ED - a journey travelled! Dr Taj Hassan President RCEM Twitter : @RCEMpresident WHERE? WHAT? HOW? Drivers for change Demand Value for money Patient centred care
Ambulatory Emergency Care The role of the ED - a journey travelled! Dr Taj Hassan President RCEM Twitter : @RCEMpresident WHERE? WHAT? HOW? Drivers for change Demand Value for money Patient centred care
BOARD CLINICAL GOVERNANCE AND QUALITY UPDATE FEBRUARY 2016
 Borders NHS Board BOARD CLINICAL GOVERNANCE AND QUALITY UPDATE FEBRUARY 2016 Aim This report aims to provide the Board with an overview of progress in the areas of: Patient Safety Clinical Effectiveness
Borders NHS Board BOARD CLINICAL GOVERNANCE AND QUALITY UPDATE FEBRUARY 2016 Aim This report aims to provide the Board with an overview of progress in the areas of: Patient Safety Clinical Effectiveness
Building Partnerships and Reducing Demand through Telemedicine
 Building Partnerships and Reducing Demand through Telemedicine Alex Blake TANP Digital Care Airedale NHS Foundation Trust Telemedicine Right care, right place, right time What is telemedicine? How does
Building Partnerships and Reducing Demand through Telemedicine Alex Blake TANP Digital Care Airedale NHS Foundation Trust Telemedicine Right care, right place, right time What is telemedicine? How does
WEST HAMPSHIRE PERFORMANCE REPORT. Based on performance data available as at 11 th January 2018
 WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
Quick guide: planning for increased seasonal demand in respiratory illness
 Quick guide: planning for increased seasonal demand in respiratory illness Published by NHS England and NHS Improvement December 2017 The British Thoracic Society is pleased to endorse this quick guide,
Quick guide: planning for increased seasonal demand in respiratory illness Published by NHS England and NHS Improvement December 2017 The British Thoracic Society is pleased to endorse this quick guide,
Strategic KPI Report Performance to December 2017
 Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
Reducing emergency admissions
 A picture of the National Audit Office logo Report by the Comptroller and Auditor General Department of Health & Social Care NHS England Reducing emergency admissions HC 833 SESSION 2017 2019 2 MARCH 2018
A picture of the National Audit Office logo Report by the Comptroller and Auditor General Department of Health & Social Care NHS England Reducing emergency admissions HC 833 SESSION 2017 2019 2 MARCH 2018
Personalised Health and Care 2020: Next steps
 Personalised Health and Care 2020: Next steps Paul Rice PhD Head of Technology Strategy NHS England www.england.nhs.uk Better use of data and technology has the power to improve health, transforming
Personalised Health and Care 2020: Next steps Paul Rice PhD Head of Technology Strategy NHS England www.england.nhs.uk Better use of data and technology has the power to improve health, transforming
Modelling patient flow in ED to better understand demand management strategies.
 Modelling patient flow in ED to better understand demand management strategies. Elizabeth Allkins Sponsor Supervisor Danny Antebi University Supervisors Dr Julie Vile and Dr Janet Williams Contents Background
Modelling patient flow in ED to better understand demand management strategies. Elizabeth Allkins Sponsor Supervisor Danny Antebi University Supervisors Dr Julie Vile and Dr Janet Williams Contents Background
Discharge to Assess Warwickshire Model
 Discharge to Assess Warwickshire Model Bie Grobet General Manager Warwickshire Community Services South Warwickshire NHS Foundation Trust Wendy Lane Consultancy Services Director Arden and Greater East
Discharge to Assess Warwickshire Model Bie Grobet General Manager Warwickshire Community Services South Warwickshire NHS Foundation Trust Wendy Lane Consultancy Services Director Arden and Greater East
Chapter 39 Bed occupancy
 National Institute for Health and Care Excellence Final Chapter 39 Bed occupancy Emergency and acute medical care in over 16s: service delivery and organisation NICE guideline 94 March 218 Developed by
National Institute for Health and Care Excellence Final Chapter 39 Bed occupancy Emergency and acute medical care in over 16s: service delivery and organisation NICE guideline 94 March 218 Developed by
Commissioning Intentions 2019 / 20
 Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report
 Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Australasian Health Facility Guidelines. Part B - Health Facility Briefing and Planning Medical Assessment Unit - Addendum to 0340 IPU
 Australasian Health Facility Guidelines Part B - Health Facility Briefing and Planning 0330 - Medical Assessment Unit - Addendum to 0340 IPU Revision 2.0 01 March 2016 COPYRIGHT AND DISCLAIMER Copyright
Australasian Health Facility Guidelines Part B - Health Facility Briefing and Planning 0330 - Medical Assessment Unit - Addendum to 0340 IPU Revision 2.0 01 March 2016 COPYRIGHT AND DISCLAIMER Copyright
Change in the Acute Setting. Dr Veronica Devlin Lean Leader NHS Lanarkshire
 Change in the Acute Setting Dr Veronica Devlin Lean Leader NHS Lanarkshire 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 World class facilities World class staff
Change in the Acute Setting Dr Veronica Devlin Lean Leader NHS Lanarkshire 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 World class facilities World class staff
SCHEDULE 2 THE SERVICES Service Specifications
 SCHEDULE 2 THE SERVICES Service Specifications Service Specification No Service ParaDoc Commissioner City and Hackney CCG Commissioner Lead Leah Herridge Provider CHUHSE Provider Lead Date of Review September
SCHEDULE 2 THE SERVICES Service Specifications Service Specification No Service ParaDoc Commissioner City and Hackney CCG Commissioner Lead Leah Herridge Provider CHUHSE Provider Lead Date of Review September
This SLA covers an enhanced service for care homes for older people and not any other care category of home.
 Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Rapid improvement guide to appointment slot issues
 Rapid improvement guide to appointment slot issues October 2017 This guidance provides information to help providers maintain high standards of clinical care by minimising and managing the number of patients
Rapid improvement guide to appointment slot issues October 2017 This guidance provides information to help providers maintain high standards of clinical care by minimising and managing the number of patients
Portsmouth Hospitals NHS Trust Winter/Surg Plan 2013/14. pg. 1
 Portsmouth Hospitals NHS Trust Winter/Surg Plan 2013/14 pg. 1 Introduction The purpose of this winter/surg plan is to ensure that Portsmouth Hospitals NHS Trust (PHT) is prepared and co-ordinated to respond
Portsmouth Hospitals NHS Trust Winter/Surg Plan 2013/14 pg. 1 Introduction The purpose of this winter/surg plan is to ensure that Portsmouth Hospitals NHS Trust (PHT) is prepared and co-ordinated to respond
Emergency Medicine Programme
 Emergency Medicine Programme Implementation Guide 8: Matching Demand and Capacity in the ED January 2013 Introduction This is a guide for Emergency Department (ED) and hospital operational management teams
Emergency Medicine Programme Implementation Guide 8: Matching Demand and Capacity in the ED January 2013 Introduction This is a guide for Emergency Department (ED) and hospital operational management teams
BGS Spring Conference 2015
 Advanced Clinical Practitioner working with older patients with Sarah Goldberg Associate Professor in Older Persons Care University of Nottingham School of Health Sciences frailty Caroline Barclay Consultant
Advanced Clinical Practitioner working with older patients with Sarah Goldberg Associate Professor in Older Persons Care University of Nottingham School of Health Sciences frailty Caroline Barclay Consultant
Neurosurgery. Themes. Referral
 06 04 Neurosurgery The following recommendations were produced by the British Society of Neurological Surgeons to highlight where resources could be released in NHS neurological services, while maintaining
06 04 Neurosurgery The following recommendations were produced by the British Society of Neurological Surgeons to highlight where resources could be released in NHS neurological services, while maintaining
AMBULATORY CARE OUTLINE BUSINESS CASE
 AMBULATORY CARE OUTLINE BUSINESS CASE Abstract This business case describes changes to the management of people with ambulatory illnesses and conditions within the Emergency Department (ED) that will be
AMBULATORY CARE OUTLINE BUSINESS CASE Abstract This business case describes changes to the management of people with ambulatory illnesses and conditions within the Emergency Department (ED) that will be
The new CQC approach to hospital inspection. Ann Ford Head of Hospital Inspection (North West) June 2014
 June 2014") The new CQC approach to hospital inspection Ann Ford Head of Hospital Inspection (North West) June 2014 1 Our purpose and role Our purpose We make sure health and social care services provide people with
The new CQC approach to hospital inspection Ann Ford Head of Hospital Inspection (North West) June 2014 1 Our purpose and role Our purpose We make sure health and social care services provide people with
Performance. Improvement in Scheduled Care Waiting List Management TOOLKIT. An Roinn Sláinte DEPARTMENT OF HEALTH. January 2013
 Performance TOOLKIT in Scheduled Care January 2013 Patient Toolkit Pathways Performance in Scheduled Care Setting the context and initiating whole systems change for the delivery of scheduled care and
Performance TOOLKIT in Scheduled Care January 2013 Patient Toolkit Pathways Performance in Scheduled Care Setting the context and initiating whole systems change for the delivery of scheduled care and
Introduction to Population Health Healthcare Public Health
 Introduction to Population Health Healthcare Public Health Dr Jason Horsley Senior Clinical Lecturer in Public Health, ScHARR Consultant in Public Health, Sheffield City Council j.horsley@sheffield.ac.uk
Introduction to Population Health Healthcare Public Health Dr Jason Horsley Senior Clinical Lecturer in Public Health, ScHARR Consultant in Public Health, Sheffield City Council j.horsley@sheffield.ac.uk