Information Needed for Registration
|
|
|
- Peter Dean
- 5 years ago
- Views:
Transcription
1 Information Needed for Registration Prospective Kindergarten students must be five years old by September 30, Prospective Pre-Kindergarten students must be four years old by September 30, All students must have the following documentation to submit a completed registration packet. Completed Registration form with: The (Yellow) ZELC Pre-K Tuition Eligibility Form A Non-Refundable Registration Fee of $50 (Made Payable to ZELC). Please put your child s name in the memo section of your check or money order. Birth Certificate Social Security card Current immunization record Four current proofs of Zachary residence in the parent or legal guardian s name/address. * Provisional custody or custody by mandate is not accepted. Documents must include: Mortgage or Lease agreement/rental contract on company letterhead with the landlord s name and phone number Utility bill (City of Zachary gas/water bill, showing name and address) And at least 2 of the following: Entergy or DEMCO bill and Cable TV / Satellite bill or Telephone bill Current Medical/Medicare or social security insurance card or Tax Assessor s bill Homestead Exemption Both tuition and non-tuition Pre-Kindergarten spaces are limited and applications will be processed on a first come, first served basis. Zachary Early Learning Center s monthly tuition from August through May is $ Families who wish to apply for non-tuition Pre-Kindergarten must provide proof of family income for an application to be considered. *Proof of income may include one of the following: Two current consecutive check stubs for EACH PARENT or CAREGIVER in the household. An official letter from your employer stating all of the following o Where parent/guardian is employed o Hourly rate of pay o The average number of hour(s) parent/guardian works per week. SNAP Card/Food Stamps and Case Detail Sheet: must include the child's name and valid effective dates. A statement from the Social Security Administration verifying that the child listed on the application is a recipient of SSI benefits, which must be accompanied by two current check stubs. Current foster care placement agreement from DCFS. Parents who are unemployed must submit a letter of support and income documentation from support source. Further questions can be answered at for Pre-K students and for Kindergarten students.
2 Zachary Community Schools School Registration School Date SID# Teacher Method of Transportation Bus # Student Information Social Security or ID assigned by previous LA District Birth Certificate # Last Name First Name Middle Name Sex Primary Ethnic: (choose one) Grade Generation (Jr., III, etc) 0 White 1 Black 2 Hispanic 3 Asian 4 Native American/Alaskan Native 5 Hawaiian/Pacific Islander Secondary Ethnic: (if applicable) 0 White 1 Black 2 Hispanic 3 Asian 4 Native American/Alaskan Native 5 Hawaiian/Pacific Islander Language spoken at home Language first acquired by student Language most often spoken by student Birth Date Place of Birth Month Day Year Date of Entry to U.S. (if not a natural born citizen) Address Information Physical Address Apt.# Apt. Complex House# City Zip Code Mailing Address City Zip Code Home Telephone (225) Names of Other ZCSB Students living at the student s primary residence
3 Guardian Information Father or Legal Guardian 1 Relationship to Student Title Last Name First Name Apt.# Apt. Complex House# Street City Zip Code Phone Home # Work # Cell # Mother or Legal Guardian 2 Relationship to Student Title Last Name First Name Apt.# Apt. Complex House# Street City Zip Code Phone Home # Work # Cell # Emergency Contact 1 Last Name Phone Medical Information Relationship to Student First Name Address Emergency Contact 2 Relationship to Student Last Name First Name Phone Address Preferred Hospital Physician Telephone Allergies Physical Handicaps Additional Information Please check any special education services your child has ever received Speech Special Education 504 Gifted Talented Other, please list Has this student ever attended school in Zachary Community School System? If yes, where? Elementary aged students: Check all programs attended: Play School Nursery School Pre Kindergarten Kindergarten Headstart Incoming Kindergarteners: Check all programs attended: Home (no Pre-K) Tribal Schools Public School PreK NonPublic PreK Licensed Childcare Head Start Programs Please list the schools with the grades the student has attended School Grade School Grade School Grade School Grade School Grade School Grade My signature attests to the accuracy of the information given on this form under penalty of law.
4
5 OFFICE USE ONLY: RETURNING STUDENT NEW ENROLLEE CHANGE OF ADDRESS REQUESTED ZACHARY COMMUNITY SCHOOLS Complete One Per Student School Year Zachary Community School Bus Service Request Form Please NEATLY PRINT or Type All Information Student s Name:. I, (parent/guardian s name), DO ( ) ** DO NOT( ) want bus service for my child for the school year. If you DO NOT want bus service for your child, please enter your name and your child s name on the lines above, sign on the signature line below*, and return this form to your child s school. If you DO WANT bus service for your child, please enter ALL requested information on this form and return to your child s school immediately. If a child does not need transportation in the morning or evening because of car pooling or other arrangements, please indicate so by writing no ride in the morning or evening box. Parent/Guardian Signature* Sign Here Today s Date Student s School for : Student s Grade for : Parent/Guardian s Name: Physical Home Address (No P.O. Boxes): Town/City, Zip Code: ENTIRE PHYSICAL ADDRESS WHERE CHILD WILL BE PICKED UP IN THE MORNING (NO P.O BOXES): ENTIRE PHYSICAL ADDRESS WHERE CHILD WILL BE DROPPED OFF IN THE EVENING (NO P.O. BOXES): If No Ride in AM or PM please place No Ride on appropriate Line. No response means student will be dropped at same location as picked up. Home Phone Number: Work Phone Number of Mother: Cell #: Work Phone Number of Father: Cell#: Other Emergency Names and Phone Numbers: If your child receives Special Education services, does your child s I.E.P. indicate special transportation services be provided? Yes NO Thanks in Advance for Your Assistance Please Allow 2-3 Business Days
6 ZACHARY COMMUNITY SCHOOL BOARD Parental Authorization to Publish Student Names, Videos, Photos, or Work Dear Parent, Your child's art, writing, video or picture may be considered for publication on the Zachary Community School Board website or other media outlets. The website is located on the Internet at Please complete and return the following consent form. Forms will be filed at the school location. The following information is considered private and will not be placed in any publication, except where described below. Today's Date School Year Student's Name Mailing Address City, State, and Zipcode Home Phone Age Grade Teacher's Name School I give permission for my child's writing, picture, video or art, first name and last name initial, age, grade, and school's name to be published on the Zachary Community School Board website at or in other media outlets. Parent's Signature Teacher's Signature I have written this composition myself. This work of art is my own original work. Student's Signature

7 ZACHARY COMMUNITY SCHOOLS SCHOOL NURSE DEPARTMENT Welcome to Zachary Community Schools. We are excited that you have chosen our school system, which is one of the fastest growing, top-rated districts in the state, to educate your child. In order to provide the best care possible for your child while at school, it is important for us to be aware of any medical conditions that might affect them during school hours or any condition that requires medication or possible nursing assistance (e.g. asthma, seizure disorder, diabetes, severe allergies, etc.). If your child does not have any medical issues or does not require any medication at school, we only need your signature on the HIPAA Policy form to be returned to school. If your child has special medical needs, please complete and sign the enclosed forms. In addition, if your child requires medication at school, you may pick up the state mandated medication packet at your child s school or you may download these forms from website ( and complete and return them to school. A parent will have to bring the medication to school to be checked and logged in. Please note that medication of any kind, including over-the-counter medication, may NEVER be sent to school with your child, and MUST be checked in by a parent along with the medication packet completed. Also, please ensure that your child s immunizations are up-to-date and that his/her school has an updated copy. This is required by Louisiana Department of Health and Hospitals and must be on file for your child to attend school. Thank you in advance for your cooperation. We look forward to caring for your child. Zachary Community School Nurses
8 HIPAA POLICY NOTICE OF USE OF PERSONAL HEALTH INFORMATION This notice describes how medical information about your child may be used and disclosed and how you can get access to this information. Please review it carefully: We understand that any information we collect about your child and their health is personal. Keeping your child s health information private is one our most important responsibilities. We are committed to protecting their health information and following all laws about its use. You have the right to discuss your concerns with the system s Privacy Officer about how their health information is shared. The law says: 1. We must keep student s health information from others who do not need it. 2. You may ask us not to share certain health services information with others. However, occasionally certain situations prohibit us from complying with a request as such. Your child may receive certain services from nurses, therapists, social workers, doctors, or other healthcare related individuals. They may see, use, and share your child s health or medical information to determine any plan of treatment, diagnosis, or outcome of the said information as described in an Individualized Education Program (IEP) or other plan document. This use may cover such health services your child had before now or may have later. We review such health services information and claims to make sure that you get quality services and that all laws regarding providing and paying for such health services are followed. We may also use the information to remind you about services or to inform you about treatment alternatives. In addition, we may also use the information to obtain payments for such services as a result of the Medicaid program. We must submit information that identifies you and your child, your child s diagnosis, and the type of services provided to your child for reimbursement by Medicaid. We may share your health care information with teachers through health plans, with insurance companies and/or government programs in order for our school system to be reimbursed for such health care or medical services rendered during the school day. As a general rule, you may request to see your child s health information. However, the request may not include psychotherapy notes or information being gathered for judicial proceedings. There may be legal reasons or safety concerns that would limit the amount of information that you may see. You may ask in writing to receive a copy of your child s health information. We may ask for payment for copying costs. If you suspect some of your child s health information is wrong, you may ask in writing that we correct or amend it and you must provide the appropriate documentation, if applicable, from your child s physician in order to verify it. You may request in the form of a signed Authorization of Release of Information that any health information be sent to others who have received your child s health information previously from us. In addition, you may also request a comprehensive list of any recipients of such information. At any time, you may stop or limit the amount of information being shared by informing us in writing.
9 Note: A child 18-years old or older can give consent for his or her health information to be shared by signing an Authorization of Release of Information. In certain situations, we are mandated to abide by laws pertaining to sharing particular health information regarding your child, even if an Authorization of Release of Information is not signed. We always report: 1. Contagious diseases, birth defects, and cancer; 2. Firearm injuries and other trauma events; 3. Reactions to problems with medicines or defective medical equipment; 4. To the police or other governmental agencies when required by law; 5. When a court orders us; 6. To the government to review how our programs are working; 7. To Worker s Compensation for work related injuries; 8. Date of birth and immunization information; 9. Abuse, neglect, and domestic violence, if related to child protection or vulnerable adults; or 10. To parents and other designated by law. We may also share health care information for permitted research purposes and for matters concerning serious threats to public health or safety. Furthermore, if the health information falls within the FERPA definition of education record, it will not be considered private health information under HIPAA, and therefore, will not be regulated by HIPAA. If you have any questions about this notice of privacy rights or feel that such rights have been violated, you may contact: Zachary Community School Board Office (225) telephone 3755 Church Street, Zachary, LA You can also complain to the federal government Secretary of Health and Human Services (HHS) or to the HHS Office of Civil Rights. Your health care services will not be affected by any complaint made to the Zachary Community School Board, Secretary of Health and Human Services, or Office of Civil Rights. You may ask for additional copies of our HIPAA policy at any time. The following link provides additional information regarding HIPAA and FERPA relevant to student health records.
10 ZACHARY COMMUNITY SCHOOL BOARD Dear Parent, Attached you will find the Zachary Community School Board HIPAA policy Notice of Use of Personal Health Information. Please sign and return this form, so that we may maintain a record of your having received the information. Failure to return the signed form may result in a delay in servicing your child. Thank you, Zachary Community School Nurses This is to certify that I have received and read a copy of the Notice of Use of Personal Health Information. Parent s Signature Names of children attending Zachary Community Schools and grades/homeroom teachers of each: Name Grade Homeroom Teacher Name Grade Homeroom Teacher Name Grade Homeroom Teacher Name Grade Homeroom Teacher Name Grade Homeroom Teacher If you have any questions, please feel free to contact your child s school Church Street Zachary, LA Fax:
11 STATE OF LOUISIANA HEALTH INFORMATION TO BE COMPLETED BY PARENT/LEGAL GUARDIAN PART 1: PARENT OR LEGAL GUARDIAN TO COMPLETE. Parent/Legal Guardian is encouraged to participate in the development of an Individual Health Care Plan if needed. Use additional sheets, if necessary, for further explanation. Student Name: Last First M.I. Sex: M F DOB: Grade: School: Student s Mailing Address: City: State: Zip: Student s Physical Address: City: State: Zip: Name of Mother/Legal Guardian Home Phone Work Phone Cell Phone Employer Name of Father/Legal Guardian Home Phone Work Phone Cell Phone Employer Name of pediatrician/primary care provider Phone No Name of medical specialists/clinics Phone No. Parents: Please notify the school nurse of any changes in the student s medical condition. Parent/Legal Guardian Signature Date Please check the type of health insurance your child has: Private Medicaid/LaCHIP None If your child does not have health insurance, would you like information on no-cost health insurance? In case of emergency, if parent or legal guardian cannot be reached, contact the following: Yes No Name Phone Number Cell Phone Number My child has a medical, mental, or behavioral condition that may affect his/her school day: No Yes (If yes, please complete Part 2) PART 2: COMPLETE ALL BOXES THAT APPLY TO YOUR CHILD. Parent/Legal Guardian is responsible for providing the school with any medication and may be responsible for providing the school with any special food or equipment that the student will require during the school day. Check with the school nurse to obtain correct medication and procedure forms. Parents are responsible to keep the school nurse informed regarding their child s health status. ALLERGIES Allergy Type: Food (list food(s) Insect sting (list insect(s) Other (list) Reactions- Date of last occurrence: Coughing Date: Difficulty breathing Date:_ Hives Date: Swelling Date: Nausea Date: Wheezing Date: Medication (list medication(s) Rash Date: Other
12 Health Information Page 2 of 3 Currently prescribed medications and treatments: Oral antihistamine (Benadryl, etc.) Epi-pen Other ASTHMA Triggers (i.e., tobacco,dust, pets, pollen, etc.) (list) Does your child experience asthma symptoms with exercise? No Yes Symptoms: Chest tightness, discomfort, or pain Difficulty breathing Coughing Wheezing Other Currently prescribed medications and treatments: Date of last hospitalization related to asthma Date of last ER visit related to asthma Does your child have a written asthma management plan? No Yes Is peak flow monitoring used? No Yes DIABETES Currently prescribed medications and treatments: Insulin Syringe Pen Pump Blood sugar testing Glucagon Oral medication(s) List medication(s) Is special scheduling of lunch or Physical Education required? No Yes: SEIZURE DISORDER Type of seizure: Absence (staring, unresponsive) Generalized Tonic-Clonic (Grand Mal/Convulsive) Complex Partial Other (explain) Physical Education Restrictions: No Yes Medication(s): No Yes List medication(s) Date of last seizure Length of seizure OTHER HEALTH CONDITIONS Chicken Pox: Date of disease: Anemia Digestive disorders Sickle Cell Disease ADD/ADHD Psychological Skin disorders Cancer Juvenile Rheumatoid Arthritis Speech problems Cerebral Palsy Hemophilia Other (explain) Cystic Fibrosis Depression Heart condition Physical disability Physical Education Restrictions: No Yes (explain): Medication(s): No Yes List medication(s) Special procedures required (i.e., catheterization, oxygen, gastrostomy care, tracheostomy care, suctioning): No Yes (explain): VISION CONDITIONS Contacts/glasses Other HEARING CONDITIONS Hearing aid(s) Other:
13 Health Information Page 3 of 3 ENVIRONMENTAL ADJUSTMENTS DUE TO A HEALTH CONDITION Special adjustments of the school environment or schedule needed? No Yes (explain): (i.e., seizures, limitations in physical activity, periodic breaks for endurance, part-time schedule, building modifications for access) Special adjustments to classroom or school facilities needed? No Yes (explain) (i.e., temperature control, refrigeration/medication storage, availability of running water) Special safety considerations required: No Yes (explain): (i.e., precautions in lifting or positioning, transportation emergency plan, safety equipment, techniques for positioning or feeding) Special assistance with activities of daily living needed: No Yes (explain): (i.e., eating, toileting,walking) Special diet required? No Yes (explain) (i.e., blended, soft, low salt, low fat, liquid supplement): Are there anticipated frequent absences or hospitalizations? No Yes (explain): PART 3: SCHOOL NURSE TO REVIEW if parent/legal guardian indicates medical condition. Nurse Notes: School Nurse Signature Date
14 MEDICAL HISTORY FORM ZACHARY COMMUNITY SCHOOLS Medical information is needed for the following student in order to determine if there are health impairments sufficient to warrant special education services. This information will also be utilized by the school nurse to provide health services. This form is to be completed by the Doctor. Please check appropriate behaviors and provide a simple explanation when indicated. Name: DOB: Name of Parent(s)/Guardian: Current Diagnosis, Medical Status, and Current Medication: Date Last Seen: Return to Clinic Date: Severity of Illness: Mild Moderate Severe Condition Causes: temporary or chronic lack of strength temporary or chronic lack of vitality temporary lack of alertness reduced efficiency in school work because of Student is substantially limited in the following major life activity/activities: caring for one s self seeing working hearing walking performing manual tasks breathing speaking learning other major life activity (describe): Recommendations For Student Integration Into The School Setting Activity Restrictions/Limitations Accommodations Nutritional/Dietary Special Procedures Speech Therapy Physical Therapy/ Occupational Therapy/ Adaptive Physical Education Please check if you agree to your patient receiving OT/PT (will be considered orders for service for one year from date doctor signed) Occupational Therapy Physical Therapy Physician s Signature: Date: Print Physician s Name: Physician s Address: Office #: Fax #: 7/2016
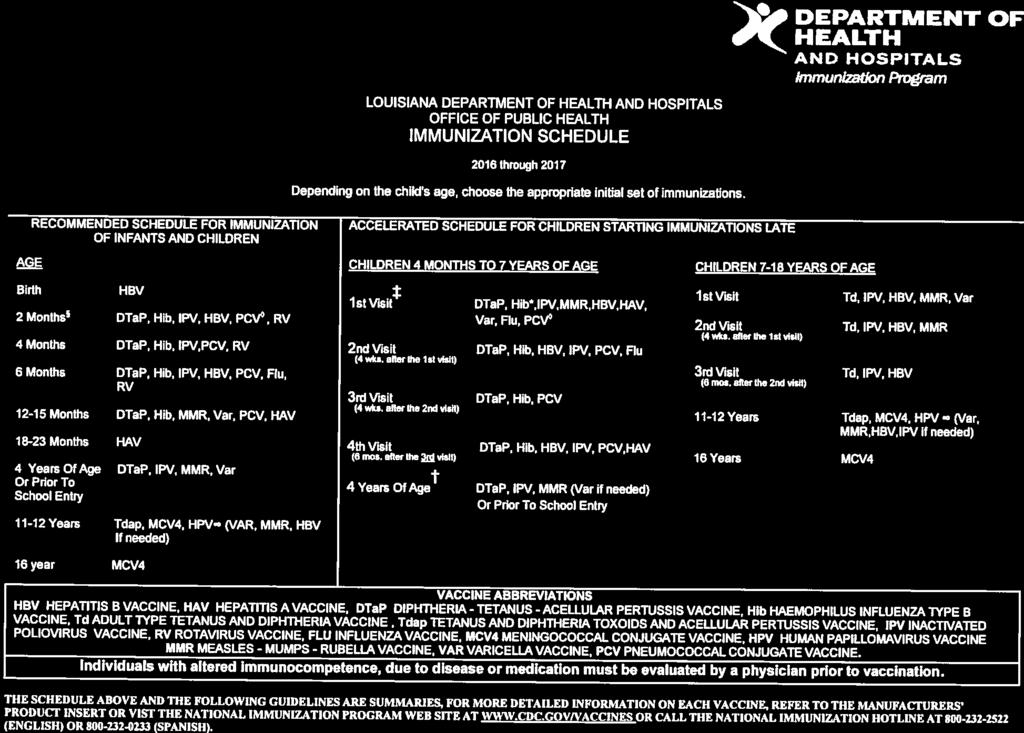
15 PRE-KINDERGARTEN IMMUNIZATION Under Louisiana Revised Statue 17:170, each student entering school within the state, "shall present satisfactory evidence of immunity to or immunization against vaccinepreventable diseases according to a schedule approved by the office of public health, Department of Health and Hospitals, or shall present evidence of an immunization program in progress." Please submit an up-to date- copy of your child's immunization before school starts: DTaP 5 Doses IPV - 4 Doses MMR - 2 Doses VAR 2 Doses or history of having chicken pox HBV- 3 Doses HIB 4 Doses If you have any questions or concerns, please feel free to contact your child s school nurse. For More Information: Louisiana Department of Health and Hospitals: Thank you, Zachary Community Schools Nursing Department

16
Information Needed for Registration
 Information Needed for Registration Prospective Kindergarten students must be five years old by September 30, 2017. Prospective Pre-Kindergarten students must be four years old by September 30, 2017. All
Information Needed for Registration Prospective Kindergarten students must be five years old by September 30, 2017. Prospective Pre-Kindergarten students must be four years old by September 30, 2017. All
Zachary Early Learning Center 4400 Rollins Place Zachary, Louisiana 70791
 Zachary Early Learning Center 4400 Rollins Place Zachary, Louisiana 70791 Pre-Kindergarten Registration Packet Prospective Pre-Kindergarten Students must be 4 years old by September 30, 2012 Requirements
Zachary Early Learning Center 4400 Rollins Place Zachary, Louisiana 70791 Pre-Kindergarten Registration Packet Prospective Pre-Kindergarten Students must be 4 years old by September 30, 2012 Requirements
School Based Oral Health Services
 Seal a Smile Oral Health Program A project of Whitney M. Young Jr. Health Services and the Healthy Capital District Initiative School Based Oral Health Services Oral health classroom education Dental screenings
Seal a Smile Oral Health Program A project of Whitney M. Young Jr. Health Services and the Healthy Capital District Initiative School Based Oral Health Services Oral health classroom education Dental screenings
To be completed by healthcare provider
 Allergy and Anaphylaxis Action Plan and Medication Orders Student s Name: D.O.B. Grade: School: Teacher: ALLERGY TO: Place child s photo here To be completed by healthcare provider History: Asthma: YES
Allergy and Anaphylaxis Action Plan and Medication Orders Student s Name: D.O.B. Grade: School: Teacher: ALLERGY TO: Place child s photo here To be completed by healthcare provider History: Asthma: YES
RETURNING Student Information Update
 Today s Date: RETURNING Student Information Update OFFICE USE ONLY School # Student # Grade Level Teacher Student Legal Name (first, middle, last) Suffix (Jr., Sr., II, lii, IV, V) Student Date of Birth
Today s Date: RETURNING Student Information Update OFFICE USE ONLY School # Student # Grade Level Teacher Student Legal Name (first, middle, last) Suffix (Jr., Sr., II, lii, IV, V) Student Date of Birth
School-Based Health Center William Penn High School 713 E. Basin Road New Castle, DE Phone: Fax:
 School-Based Health Center William Penn High School 713 E. Basin Road New Castle, DE 19720 Phone: 324 5740 Fax: 324 5745 Dear Parents/Guardians: The William Penn School Based Health Center (SBHC) is a
School-Based Health Center William Penn High School 713 E. Basin Road New Castle, DE 19720 Phone: 324 5740 Fax: 324 5745 Dear Parents/Guardians: The William Penn School Based Health Center (SBHC) is a
A copy of the birth certificate or proof of birth letter from the hospital. Your support in this matter is greatly appreciated.
 Attention Parents We are required by the Commonwealth of Virginia to secure, before the child may attend, and maintain, while in our care, a current file containing specific information regarding the health
Attention Parents We are required by the Commonwealth of Virginia to secure, before the child may attend, and maintain, while in our care, a current file containing specific information regarding the health
School Based Health Consent for Services Grace Community Health Center, Inc.
 School Based Health Consent for Services Grace Community Health Center, Inc. Please read carefully: In order for us to see your child in school based clinics, all pages of this form must be completed by
School Based Health Consent for Services Grace Community Health Center, Inc. Please read carefully: In order for us to see your child in school based clinics, all pages of this form must be completed by
12 King Philip Rd. Sudbury, MA (585)
") Dear Parents, In order to get started with speech therapy services including screening, evaluation, and treatment, we ask that you submit the following registration paperwork to Sudbury Speech and Language
Dear Parents, In order to get started with speech therapy services including screening, evaluation, and treatment, we ask that you submit the following registration paperwork to Sudbury Speech and Language
Hampton Roads Regional Schools Life-Threatening Allergy Management Protocol Forms
 Newport News Public Schools Hampton Roads Regional Schools Life-Threatening Allergy Management Protocol Forms Developed by the Hampton Roads School Nurse Managers Parents/Guardians: Please complete Life
Newport News Public Schools Hampton Roads Regional Schools Life-Threatening Allergy Management Protocol Forms Developed by the Hampton Roads School Nurse Managers Parents/Guardians: Please complete Life
(PLEASE PRINT) Sex M F Age Birthdate Single Married Widowed Separated Divorced. Business Address Business Phone Cell Phone
 Sex M F Age Birthdate Single Married Widowed Separated Divorced. Business Address Business Phone Cell Phone") (PLEASE PRINT) Emma Warner, MSW, LCSW, ACSW Tulsa, OK 74105 (918) 749-6935 Personal Information Name Address Last Name First Name Initial Home Phone Soc. Sec. # City State Zip Sex M F Age Birthdate Single
(PLEASE PRINT) Emma Warner, MSW, LCSW, ACSW Tulsa, OK 74105 (918) 749-6935 Personal Information Name Address Last Name First Name Initial Home Phone Soc. Sec. # City State Zip Sex M F Age Birthdate Single
Total Grace Achievers Academy Summer Camp Enrollment Application. Where kids can experience Life and Learn to Achieve
 Total Grace Achievers Academy Summer Camp Enrollment Application Where kids can experience Life and Learn to Achieve Student Information Child s Name DOB Age Grade School: Street Address City State Zip
Total Grace Achievers Academy Summer Camp Enrollment Application Where kids can experience Life and Learn to Achieve Student Information Child s Name DOB Age Grade School: Street Address City State Zip
Broomall Patients ONLY may send forms via to:
 Thank you for choosing Children s Dentistry! To expedite your check in, please complete the forms in this packet and bring with you to your appointment. You may also FAX these forms to the office where
Thank you for choosing Children s Dentistry! To expedite your check in, please complete the forms in this packet and bring with you to your appointment. You may also FAX these forms to the office where
Additionally, the parent or legal guardian must provide the following documents upon registration of a new student:
 Montgomery County Public Schools requires several documents upon registration of a new student. Below is a list of documents which may be downloaded and reviewed and/or completed by the parent or legal
Montgomery County Public Schools requires several documents upon registration of a new student. Below is a list of documents which may be downloaded and reviewed and/or completed by the parent or legal
Columbia Medical Practice- Pediatrics Ken Klebanow M.D. and Associates
 HOWARD COUNTY HEALTH DEPARTMENT SCHOOL-BASED WELLNESS CENTERS PROGRAM TELEMEDICINE SERVICES A partnership between the Howard County Health Department and the Howard County Public School System What is
HOWARD COUNTY HEALTH DEPARTMENT SCHOOL-BASED WELLNESS CENTERS PROGRAM TELEMEDICINE SERVICES A partnership between the Howard County Health Department and the Howard County Public School System What is
Practice Limited to Infants, Children, & Adolescents
 Practice Limited to Infants, Children, & Adolescents 9290 SE Sunnybrook Blvd., #200, Clackamas, OR 97015 (503) 659-1694 5050 NE Hoyt St., #B55, Portland, Oregon 97213 (503) 233-5393 16144 SE Happy Valley
Practice Limited to Infants, Children, & Adolescents 9290 SE Sunnybrook Blvd., #200, Clackamas, OR 97015 (503) 659-1694 5050 NE Hoyt St., #B55, Portland, Oregon 97213 (503) 233-5393 16144 SE Happy Valley
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Ivis M. Getz, D.M.D. Caring For Kids Pediatric Dentistry, P.C. 140 Lockwood Avenue, Suite 315, New Rochelle, NY 10801
 How did you hear of our office? New Patient Registration SECTION 1: PATIENT INFORMATION Patient Name: M / F Date of Birth: Address: City: State: Zip Code: SECTION 2: PARENT / GUARDIAN / INSURANCE Name:
How did you hear of our office? New Patient Registration SECTION 1: PATIENT INFORMATION Patient Name: M / F Date of Birth: Address: City: State: Zip Code: SECTION 2: PARENT / GUARDIAN / INSURANCE Name:
FROM THE DESK OF THE SCHOOL NURSE School Year
 FROM THE DESK OF THE SCHOOL NURSE School Year 2016-2107 Dear Parents, Our goal is to provide for the health and well being of your child while s/he is attending school. Please read this letter carefully,
FROM THE DESK OF THE SCHOOL NURSE School Year 2016-2107 Dear Parents, Our goal is to provide for the health and well being of your child while s/he is attending school. Please read this letter carefully,
2017 Medi-Slim Weight Loss Patient Information Form
 Medi-Slim Weight Loss Patient Information Form Patient Name (Last) (First) (MI) Name you prefer to be called: Patient Address: City:_ State Zip Phone number you would prefer us to use: May we email you?
Medi-Slim Weight Loss Patient Information Form Patient Name (Last) (First) (MI) Name you prefer to be called: Patient Address: City:_ State Zip Phone number you would prefer us to use: May we email you?
Food / Insect Allergy Action Plan
 Food / Insect Allergy Action Plan 2017-2018 Student s Name: of Birth: Teacher Allergy to: Asthmatic: Yes* No Grade *Higher risk for severe reaction Step 1: Treatment Symptoms Give Checked Medication**
Food / Insect Allergy Action Plan 2017-2018 Student s Name: of Birth: Teacher Allergy to: Asthmatic: Yes* No Grade *Higher risk for severe reaction Step 1: Treatment Symptoms Give Checked Medication**
Pediatric New Patient Form
 Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
School Based Health Services Consent Form
 MRN: PCP: Teacher: Grade: School Based Health Services Consent Form Before your child sees a provider, we are asking you to authorize medical and/ or dental treatment. We will work with you to improve
MRN: PCP: Teacher: Grade: School Based Health Services Consent Form Before your child sees a provider, we are asking you to authorize medical and/ or dental treatment. We will work with you to improve
Do You Qualify? Please Read Carefully:
 Do You Qualify? Please Read Carefully: You are NOT eligible if any of these apply: I am pregnant I am under the age of 18 I have more than two children in my custody My child(ren) is(are) three years old
Do You Qualify? Please Read Carefully: You are NOT eligible if any of these apply: I am pregnant I am under the age of 18 I have more than two children in my custody My child(ren) is(are) three years old
2201 Murphy Avenue, Suite 307 Nashville, TN Phone Fax Date. Patient s Full Name
 Patient Information 2201 Murphy Avenue, Suite 307 Nashville, TN 37203 Phone 615-401- 9454 Fax 615-873- 1934 www.robbinsplasticsurgery.com Date Patient s Full Name Last First M.I. Preferred Name (if different
Patient Information 2201 Murphy Avenue, Suite 307 Nashville, TN 37203 Phone 615-401- 9454 Fax 615-873- 1934 www.robbinsplasticsurgery.com Date Patient s Full Name Last First M.I. Preferred Name (if different
Surgical Associates of Central FL, PA 1181 Orange Avenue Winter Park, FL
 Surgical Associates of Central FL, PA 1181 Orange Avenue Winter Park, FL 32789 407-647-1331 Name Date Email @ Please Circle One: Ethnicity: Hispanic or Latino American/White Not Hispanic or Latino Unknown
Surgical Associates of Central FL, PA 1181 Orange Avenue Winter Park, FL 32789 407-647-1331 Name Date Email @ Please Circle One: Ethnicity: Hispanic or Latino American/White Not Hispanic or Latino Unknown
2.. The two persons trained shall be regular members of the school staff, which ensures at least one of the two being present during school hours.
 STUDENTS August 30, 2012 STUDENTS Health Services Allergic Reactions When a student s physician prescribes emergency allergy injections and related medication (Epinephrine, EpiPen, EpiPen Jr.), and there
STUDENTS August 30, 2012 STUDENTS Health Services Allergic Reactions When a student s physician prescribes emergency allergy injections and related medication (Epinephrine, EpiPen, EpiPen Jr.), and there
PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D KLONDIKE RD SW SUITE 205 CONYERS, GA TELEPHONE FAX
 PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D. 1506 KLONDIKE RD SW SUITE 205 CONYERS, GA 30094 678-750-4000 TELEPHONE 678-750-4005 FAX www.pcfwellness.com Dear Family, We are excited to welcome
PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D. 1506 KLONDIKE RD SW SUITE 205 CONYERS, GA 30094 678-750-4000 TELEPHONE 678-750-4005 FAX www.pcfwellness.com Dear Family, We are excited to welcome
Allergy Consultants, P.A. Visit Date: Specialist in Pediatric and Adult Allergy, Asthma, and Sinus Disease
 Allergy Consultants, P.A. Visit Date: Specialist in Pediatric and Adult Allergy, Asthma, and Sinus Disease Arthur Fost, M.D. David Fost, M.D. Satya Narisety, M.D. Anthony J. Piccolo, PA-C Patient s Name
Allergy Consultants, P.A. Visit Date: Specialist in Pediatric and Adult Allergy, Asthma, and Sinus Disease Arthur Fost, M.D. David Fost, M.D. Satya Narisety, M.D. Anthony J. Piccolo, PA-C Patient s Name
HARRISON COUNTY SCHOOLS OFFICE OF HEALTH SERVICES
 HARRISON COUNTY SCHOOLS OFFICE OF HEALTH SERVICES 445 W. Main Street Clarksburg, WV 26301 (304) 326-7690 FAX (304) 326-7691 Dear Parent, Date Please complete the enclosed forms and return them to your
HARRISON COUNTY SCHOOLS OFFICE OF HEALTH SERVICES 445 W. Main Street Clarksburg, WV 26301 (304) 326-7690 FAX (304) 326-7691 Dear Parent, Date Please complete the enclosed forms and return them to your
Pediatric Patient History
 Pediatric Patient History Childs Name: Today s Date: Primary Doctor: Date of Birth: Age: Reason for visit: List all chronic medical problems: List all medication dosages and frequency taken (including
Pediatric Patient History Childs Name: Today s Date: Primary Doctor: Date of Birth: Age: Reason for visit: List all chronic medical problems: List all medication dosages and frequency taken (including
Adventure Club. Before and After School Care Enrollment Packet. Before and After School Care Mission:
 Adventure Club Before and After School Care Enrollment Packet Before and After School Care Mission: Our before and after school care is designed to provide children with a safe, loving and exciting environment
Adventure Club Before and After School Care Enrollment Packet Before and After School Care Mission: Our before and after school care is designed to provide children with a safe, loving and exciting environment
POTS Treatment Center 7515 Greenville Avenue, Suite 1005 Dallas, TX
 Patient Registration: POTS Treatment Center 7515 Greenville Avenue, Suite 1005 Dallas, TX 75231 214-369-8717 Date: Briefly state the medical problem for which you made this appointment today : Name : Address:
Patient Registration: POTS Treatment Center 7515 Greenville Avenue, Suite 1005 Dallas, TX 75231 214-369-8717 Date: Briefly state the medical problem for which you made this appointment today : Name : Address:
Patient s Full Name DOB Age. Patient s SSN Sex: Male Female Preferred Language. Place of Birth: City State Country
 Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
Back-Up Care Advantage Program Registration Materials
 Registration Materials Dear Parent, Welcome to the Back-Up Care Advantage Program! An important part of preparing for a day of back-up care is ensuring that your care provider will have the information
Registration Materials Dear Parent, Welcome to the Back-Up Care Advantage Program! An important part of preparing for a day of back-up care is ensuring that your care provider will have the information
Welcome Letter- Orchard School Clinic
 Welcome Letter- Orchard School Clinic Dear Parent or Guardian: Orchard School Clinic is a school-based location of RiverStone Health Clinic. This is a collaborative effort between RiverStone Health, Billings
Welcome Letter- Orchard School Clinic Dear Parent or Guardian: Orchard School Clinic is a school-based location of RiverStone Health Clinic. This is a collaborative effort between RiverStone Health, Billings
MONTGOMERY COUNTY SCHOOLS STUDENT INFORMATION FORM
 Entry : Homeroom Teacher: NEW STUDENT ENROLLMENT ONLY MONTGOMERY COUNTY SCHOOLS STUDENT INFORMATION FORM Student s Legal Name: Last First Middle Suffix Social Security Number: / / of Birth: Birthplace:
Entry : Homeroom Teacher: NEW STUDENT ENROLLMENT ONLY MONTGOMERY COUNTY SCHOOLS STUDENT INFORMATION FORM Student s Legal Name: Last First Middle Suffix Social Security Number: / / of Birth: Birthplace:
SEVERE ALLERGIC REACTION MANAGEMENT PROCEDURE QUESTIONAIRE. Student Name: Current Date: Date of Birth: Grade:
 SEVERE ALLERGIC REACTION MANAGEMENT PROCEDURE QUESTIONAIRE Student Name: Current Date: Date of Birth: Grade: 1. Describe in detail what your child is allergic to: 2. How often does your child have a severe
SEVERE ALLERGIC REACTION MANAGEMENT PROCEDURE QUESTIONAIRE Student Name: Current Date: Date of Birth: Grade: 1. Describe in detail what your child is allergic to: 2. How often does your child have a severe
TOPS Piano and Creative Writing Camp Registration Form Summer 2018
 TOPS Piano and Creative Writing Camp Registration Form Summer 2018 Returning Camper New Camper Camper s Name Email(s) Address City Zip code Home phone Work phone(s) Cell phone(s) Parent/Guardian name Please
TOPS Piano and Creative Writing Camp Registration Form Summer 2018 Returning Camper New Camper Camper s Name Email(s) Address City Zip code Home phone Work phone(s) Cell phone(s) Parent/Guardian name Please
CENTRAL JERSEY COLLEGE PREP
 CENTRAL JERSEY COLLEGE PREP CHARTER SCHOOL Dear Parents/Guardians, Congratulations and welcome to the Central Jersey College Prep Charter School. We will do our best to help you with the enrollment process.
CENTRAL JERSEY COLLEGE PREP CHARTER SCHOOL Dear Parents/Guardians, Congratulations and welcome to the Central Jersey College Prep Charter School. We will do our best to help you with the enrollment process.
New Patient Information
 New Patient Information PATIENT INFORMATION M / F Last Name First Name Middle Name Suffix- Jr, Sr, etc. Mr, Mrs, Ms, Dr Sex Date of Birth Social Security Number Alias- Nickname (Last, First, Middle) Permanent
New Patient Information PATIENT INFORMATION M / F Last Name First Name Middle Name Suffix- Jr, Sr, etc. Mr, Mrs, Ms, Dr Sex Date of Birth Social Security Number Alias- Nickname (Last, First, Middle) Permanent
Dodge. County. Schools
 Welcome to the Dodge School Based Health Clinic. Dodge Board of Education and Dodge Connection-Communities In of Dodge, Inc. are continuing to move forward with our goal of serving the children and families
Welcome to the Dodge School Based Health Clinic. Dodge Board of Education and Dodge Connection-Communities In of Dodge, Inc. are continuing to move forward with our goal of serving the children and families
Request for Severe Allergy Information
 Request for Severe Allergy Information Dear Parent, You have disclosed that your child has a severe allergy. Wylie ISD requires additional information in order to take necessary precautions for your Child
Request for Severe Allergy Information Dear Parent, You have disclosed that your child has a severe allergy. Wylie ISD requires additional information in order to take necessary precautions for your Child
MAIN STREET RADIOLOGY
 MAIN STREET RADIOLOGY PATIENT REGISTRATION FORM **OFFICE USE ONLY** TODAY S DATE: MR#: LAST NAME: FIRST NAME: ADDRESS: APT: CITY: STATE: ZIP CODE: HOME PHONE #: ( ) - CELL PHONE#: ( ) - DATE OF BIRTH:
MAIN STREET RADIOLOGY PATIENT REGISTRATION FORM **OFFICE USE ONLY** TODAY S DATE: MR#: LAST NAME: FIRST NAME: ADDRESS: APT: CITY: STATE: ZIP CODE: HOME PHONE #: ( ) - CELL PHONE#: ( ) - DATE OF BIRTH:
Reminders for you as you come in for your first appointment
 Reminders for you as you come in for your first appointment * Please complete this paperwork and bring it to your first appointment If you are unable to complete this paperwork prior to your appointment,
Reminders for you as you come in for your first appointment * Please complete this paperwork and bring it to your first appointment If you are unable to complete this paperwork prior to your appointment,
Extended Day Registration Packet
 St. Benedicts School Extended Day Registration Packet 2014 2015 School Year 4811 Wallingford Avenue North Seattle, Washington 98103 206-518.6009 l.wescott@stbens.net A Registration Packet Contents The
St. Benedicts School Extended Day Registration Packet 2014 2015 School Year 4811 Wallingford Avenue North Seattle, Washington 98103 206-518.6009 l.wescott@stbens.net A Registration Packet Contents The
Patient Information. Date of Birth Sex Marital Status / / Male Female Single Married Other. Address
 Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
NEW PATIENT INFORMATION: ADULT
 NEW PATIENT INFORMATION: ADULT Patient Last Name: Patient First Name: Patient Middle Name: DOB: Sex: M F SSN: Address: City: Zip: Home Phone: Cell Phone: Email: EMERGENCY CONTACT INFORMATION Last Name:
NEW PATIENT INFORMATION: ADULT Patient Last Name: Patient First Name: Patient Middle Name: DOB: Sex: M F SSN: Address: City: Zip: Home Phone: Cell Phone: Email: EMERGENCY CONTACT INFORMATION Last Name:
RIVER CITY ADVOCACY COUNSELING SERVICES 145 Landa Street New Braunfels, TX (830)
") Date / / Client information: First name Middle initial Last name Parent/Legal Guardian (for 17 and under) Address Phone number Home Wk Cell Date of birth / / Sex Marital Status Ethnicity Employment status:
Date / / Client information: First name Middle initial Last name Parent/Legal Guardian (for 17 and under) Address Phone number Home Wk Cell Date of birth / / Sex Marital Status Ethnicity Employment status:
PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip
 PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip Primary Phone ( ) Secondary Phone ( ) Other Phone ( ) SS# - - Race Ethnicity Email address Preferred language Marital Status Minor Single
PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip Primary Phone ( ) Secondary Phone ( ) Other Phone ( ) SS# - - Race Ethnicity Email address Preferred language Marital Status Minor Single
Kenilworth Public Schools Harding Elementary School 426 Boulevard Kenilworth, New Jersey
 Assistant Dear Parent/Guardian: Harding Elementary School Kathleen Murphy Principal Ronald Bubnowski Assistant Principal Attached, please find the Kindergarten registration packet for the Kenilworth School
Assistant Dear Parent/Guardian: Harding Elementary School Kathleen Murphy Principal Ronald Bubnowski Assistant Principal Attached, please find the Kindergarten registration packet for the Kenilworth School
PATIENT INFORMATION Indiana Plastic Surgery Center, PC
 PATIENT INFORMATION DATE: / / PHYSICIAN REFERAL: FAMILY/FRIEND REFERAL: PRIMARY CARE PHYSICIAN: LAST NAME FIRST M.I. HOME ( ) - CELL( ) - WORK( ) - EMAIL MAY WE CONTACT YOU: BY CELL PHONE / TEXTING?: YES
PATIENT INFORMATION DATE: / / PHYSICIAN REFERAL: FAMILY/FRIEND REFERAL: PRIMARY CARE PHYSICIAN: LAST NAME FIRST M.I. HOME ( ) - CELL( ) - WORK( ) - EMAIL MAY WE CONTACT YOU: BY CELL PHONE / TEXTING?: YES
Pediatric New Patient Intake Form
 Name: DOB: Page 1 of 5 Pediatric New Patient Intake Form Patient Information Last Name: First Name: DOB: Home Mobile Preferred (circle) : Home / Cell Email: Gender: Primary Pediatrician: Pediatrician Address:
Name: DOB: Page 1 of 5 Pediatric New Patient Intake Form Patient Information Last Name: First Name: DOB: Home Mobile Preferred (circle) : Home / Cell Email: Gender: Primary Pediatrician: Pediatrician Address:
School-Based Health Center Wilmington Charter/Cab Calloway High Schools 100 N. Dupont Road Wilmington, DE Phone: Fax:
 Dear Parents/Guardians: School-Based Health Center Wilmington Charter/Cab Calloway High Schools 100 N. Dupont Road Wilmington, DE 19807 Phone: 651-2100 Fax: 651-2111 The Wilmington Charter/Cab Calloway
Dear Parents/Guardians: School-Based Health Center Wilmington Charter/Cab Calloway High Schools 100 N. Dupont Road Wilmington, DE 19807 Phone: 651-2100 Fax: 651-2111 The Wilmington Charter/Cab Calloway
Hope Academy of Public Service GENERAL STUDENT INFORMATION
 Hope Academy of Public Service GENERAL STUDENT INFORMATION First Name: Middle Name: Last Name: SSN: Current Grade: Birth date: Age: Gender: M or F Ethnicity (check one): Primary Race (check only one):
Hope Academy of Public Service GENERAL STUDENT INFORMATION First Name: Middle Name: Last Name: SSN: Current Grade: Birth date: Age: Gender: M or F Ethnicity (check one): Primary Race (check only one):
Patient: Gender: Male Female. Mailing Address: Ethnicity: Not Hispanic or Latin Hispanic/Latin Home Phone #:
 5002 Highway 39 N Bldg. A Meridian, MS 39301 Phone: 601-512-0500 Fax: 601-512-0505 Patient Information Patient: Gender: Male Female First Middle Last Primary Language: English Spanish Other Mailing Address:
5002 Highway 39 N Bldg. A Meridian, MS 39301 Phone: 601-512-0500 Fax: 601-512-0505 Patient Information Patient: Gender: Male Female First Middle Last Primary Language: English Spanish Other Mailing Address:
INFORMED CONSENT FOR TREATMENT
 INFORMED CONSENT FOR TREATMENT I (name of patient), agree and consent to participate in behavioral health care services offered and provided at/by Children s Respite Care Center, a behavioral health care
INFORMED CONSENT FOR TREATMENT I (name of patient), agree and consent to participate in behavioral health care services offered and provided at/by Children s Respite Care Center, a behavioral health care
ST. LAWRENCE REHABILITATION CENTER OUTPATIENT POLICIES AND REGISTRATION INFORMATION
 Outpatient Services 2381 Lawrenceville Road 609-896-9500 voice Patient Name: Account #: ST. LAWRENCE REHABILITATION CENTER OUTPATIENT POLICIES AND REGISTRATION INFORMATION Your first day of outpatient
Outpatient Services 2381 Lawrenceville Road 609-896-9500 voice Patient Name: Account #: ST. LAWRENCE REHABILITATION CENTER OUTPATIENT POLICIES AND REGISTRATION INFORMATION Your first day of outpatient
2018 SUMMER CAMP NANSEMA REGISTRATION NORTH SUBURBAN YMCA
 2018 SUMMER CAMP NANSEMA REGISTRATION NORTH SUBURBAN YMCA CONTACT INFORMATION Camper s Name: Grade entering Fall 2018: Gender: Female Male Not specified DOB: Age as of 1st day of camp: Address: City: Zip
2018 SUMMER CAMP NANSEMA REGISTRATION NORTH SUBURBAN YMCA CONTACT INFORMATION Camper s Name: Grade entering Fall 2018: Gender: Female Male Not specified DOB: Age as of 1st day of camp: Address: City: Zip
Client Information Form
 Client Information Form Please read and complete all information requested. Date: Name: Address: City, State and Zip: Social Security Number: Home Phone: Work Phone: Cell Phone: E-mail: If client is a
Client Information Form Please read and complete all information requested. Date: Name: Address: City, State and Zip: Social Security Number: Home Phone: Work Phone: Cell Phone: E-mail: If client is a
APPLICATION. Name (Last, First, MI): Address: City, State, & Zip Code: Home Telephone: Cell Telephone: Date of Birth: / /
: Address: City, State, & Zip Code: Home Telephone: Cell Telephone: Date of Birth: / /") Girls in Engineering Academy (GEA) July 10 August 4, 2017 APPLICATION A Summer Pre-Engineering Program for Middle School Girls Please print or type all information. Additional sheets may be attached if
Girls in Engineering Academy (GEA) July 10 August 4, 2017 APPLICATION A Summer Pre-Engineering Program for Middle School Girls Please print or type all information. Additional sheets may be attached if
MONTGOMERY COUNTY SCHOOLS STUDENT INFORMATION FORM
 NEW STUDENT ENROLLMENT ONLY Entry : Homeroom Teacher: MONTGOMERY COUNTY SCHOOLS STUDENT INFORMATION FORM Student s Legal Name: Last First Middle Suffix Social Security Number: / / of Birth: Birthplace:
NEW STUDENT ENROLLMENT ONLY Entry : Homeroom Teacher: MONTGOMERY COUNTY SCHOOLS STUDENT INFORMATION FORM Student s Legal Name: Last First Middle Suffix Social Security Number: / / of Birth: Birthplace:
ALFRED ALINGU, MD INTERNAL MEDICINE
 Name Date of Birth Social Security Number Marital Status Address City State Zip Code Home Phone Cell Phone E-mail Address Pharmacy Name Pharmacy Phone Number Emergency Contact Phone Number Relationship
Name Date of Birth Social Security Number Marital Status Address City State Zip Code Home Phone Cell Phone E-mail Address Pharmacy Name Pharmacy Phone Number Emergency Contact Phone Number Relationship
TOS Health Questionnaire
 Name Referring Physician Main Reason for Medical Evaluation of Injury/Length of symptoms: Is this a work related problem? Y N Are you right or left handed? Occupation What treatment have you received for
Name Referring Physician Main Reason for Medical Evaluation of Injury/Length of symptoms: Is this a work related problem? Y N Are you right or left handed? Occupation What treatment have you received for
VETERINARY & BIOMEDICAL SCIENCES SUMMER CAMP-2018 REGISTRATION FORM
 1 VETERINARY & BIOMEDICAL SCIENCES SUMMER CAMP-2018 REGISTRATION FORM When: Residential camp: June 24 (Sunday)-June 29 (Friday), 2018 Commuters: June 25 (Monday)-June 29, 2018 In order to get personal
1 VETERINARY & BIOMEDICAL SCIENCES SUMMER CAMP-2018 REGISTRATION FORM When: Residential camp: June 24 (Sunday)-June 29 (Friday), 2018 Commuters: June 25 (Monday)-June 29, 2018 In order to get personal
Thank you for choosing Oakland Medical Center as your Patient-Centered Medical Home
 Thank you for choosing Oakland Medical Center as your Patient-Centered Medical Home We ask that you complete the enclosed paperwork and bring it with you at the time of your appointment. We also ask that
Thank you for choosing Oakland Medical Center as your Patient-Centered Medical Home We ask that you complete the enclosed paperwork and bring it with you at the time of your appointment. We also ask that
EMERGENCY CONTACT INFORMATION LIST ALL OTHER ADULTS YOU AUTHORIZE CONNECT STAFF TO RELEASE YOUR CHILD TO:
 AFTER SCHOOL PROGRAM Fall Spring CHILD PERSONAL DATA SHEET Child s DOB Home Address City State Zip Gender School Enrolled in: : Employer Email : Employer Email Work APP Requested Work APP Requested EMERGENCY
AFTER SCHOOL PROGRAM Fall Spring CHILD PERSONAL DATA SHEET Child s DOB Home Address City State Zip Gender School Enrolled in: : Employer Email : Employer Email Work APP Requested Work APP Requested EMERGENCY
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 9 Consent for Use and Disclosure of Information 10 Authorization for Use and Disclosure of Protected Health Information 11 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 9 Consent for Use and Disclosure of Information 10 Authorization for Use and Disclosure of Protected Health Information 11 Notice
Counseling Center of Montgomery County
 Counseling Center of Montgomery County 212 Conroe Drive (936) 760-1880 Office Conroe, TX 77301 (936) 760-2915 Office CCMC@CounselingCenterMoCo.com (936) 760-9101 Fax CHILD/ADOLESCENT PSYCHOSOCIAL HISTORY
Counseling Center of Montgomery County 212 Conroe Drive (936) 760-1880 Office Conroe, TX 77301 (936) 760-2915 Office CCMC@CounselingCenterMoCo.com (936) 760-9101 Fax CHILD/ADOLESCENT PSYCHOSOCIAL HISTORY
RETURNING STUDENT INFORMATION UPDATE
 ST. FRANCIS CATHOLIC SCHOOL Student Information Date: RETURNING STUDENT INFORMATION UPDATE Student Name Last First Middle I Nickname Birth Date Gender Grade Entering Birth Country Birth City Birth State
ST. FRANCIS CATHOLIC SCHOOL Student Information Date: RETURNING STUDENT INFORMATION UPDATE Student Name Last First Middle I Nickname Birth Date Gender Grade Entering Birth Country Birth City Birth State
1.1 To provide guidelines for medication administration to students while at school.
 Windsor-Essex Catholic District School Board NUMBER: Pr ST: 11 Section: Students PROCEDURE Pr ST: 11 Student Health Support (Including Medication Administration at School) EFFECTIVE: Oct. 26, 1999 AMENDED:
Windsor-Essex Catholic District School Board NUMBER: Pr ST: 11 Section: Students PROCEDURE Pr ST: 11 Student Health Support (Including Medication Administration at School) EFFECTIVE: Oct. 26, 1999 AMENDED:
Dear New Patient, Once again, we would like to thank you for choosing us as your primary health care provider. We look forward to working with you.
 307 West Central Street Wendy J. Parker, M.D. Natick, MA 01760 Deborah J. Riester, M.D. Telephone: 508-820-8383 Jo-Ann Suna,M.D. Fax: 508-820-0250 Hadia F. Tirmizi, M.D. Natalia Sedo, N.P. Christine Chang,
307 West Central Street Wendy J. Parker, M.D. Natick, MA 01760 Deborah J. Riester, M.D. Telephone: 508-820-8383 Jo-Ann Suna,M.D. Fax: 508-820-0250 Hadia F. Tirmizi, M.D. Natalia Sedo, N.P. Christine Chang,
CORAZON PANES SANCHEZ., M.D., L.L.C.
 PERRYVILLE, MD 21903 Rising sun, MD 21911 BALTIMORE, MD 21221 PATIENT REGISTRATION NAME: DOB: SEX: ( ) MALE ( ) FEMALE SOCIAL SECURITY #: - - ADDRESS: CITY/STATE: ZIP:_ TELEPHONE #: MOTHER S NAME: FATHER
PERRYVILLE, MD 21903 Rising sun, MD 21911 BALTIMORE, MD 21221 PATIENT REGISTRATION NAME: DOB: SEX: ( ) MALE ( ) FEMALE SOCIAL SECURITY #: - - ADDRESS: CITY/STATE: ZIP:_ TELEPHONE #: MOTHER S NAME: FATHER
Please review the following list of medications and mark the ones for which you consent:
 MONTGOMERY COUNTY SCHOOL HEALTH UNIT CONSENT FOR SERVICES 20 Student Name: Grade: School: The School Health Unit will provide care for all students. This includes, but is not limited to, illness/injury
MONTGOMERY COUNTY SCHOOL HEALTH UNIT CONSENT FOR SERVICES 20 Student Name: Grade: School: The School Health Unit will provide care for all students. This includes, but is not limited to, illness/injury
Wynne Public Schools P.O. Box 69 Wynne, Arkansas Seizure Care In The School
 Date_ Student_ Dear Parent/Guardian, Wynne Public Schools P.O. Box 69 Wynne, Arkansas 72396 Seizure Care In The School Grade Our records indicate that your child has a seizure disorder; good management
Date_ Student_ Dear Parent/Guardian, Wynne Public Schools P.O. Box 69 Wynne, Arkansas 72396 Seizure Care In The School Grade Our records indicate that your child has a seizure disorder; good management
From: AR Center (Arkansas Center for the Study of Integrative Medicine)! PLEASE READ FIRST!!
! PLEASE READ FIRST!!") From: AR Center (Arkansas Center for the Study of Integrative Medicine) PLEASE READ FIRST Please be sure that you have a QUALIFYING MEDICAL CONDITION for Medical Marijuana in Arkansas. If you do not have
From: AR Center (Arkansas Center for the Study of Integrative Medicine) PLEASE READ FIRST Please be sure that you have a QUALIFYING MEDICAL CONDITION for Medical Marijuana in Arkansas. If you do not have
THE COUNSELING PLACE ADULT INTAKE FORM Yearly Family Income:
 Person to Contact in Case of Emergency Name Relationship Best Contact Number Alternative Contact Number Office Use Only Intake Date Reason for referral Counselor THE COUNSELING PLACE ADULT INTAKE FORM
Person to Contact in Case of Emergency Name Relationship Best Contact Number Alternative Contact Number Office Use Only Intake Date Reason for referral Counselor THE COUNSELING PLACE ADULT INTAKE FORM
Directions to our office are included in this mailing.
 Welcome to University Audiology Associates. We appreciate the opportunity to provide you with comprehensive hearing services. are services. Please complete the enclosed forms and bring these completed
Welcome to University Audiology Associates. We appreciate the opportunity to provide you with comprehensive hearing services. are services. Please complete the enclosed forms and bring these completed
Diane Kulas, LSW. Dear Parent/Guardian,
 Dear Parent/Guardian, Thank you for your interest in Camp Chimaqua, an overnight bereavement camp, through Hospice & Community Care s Pathways Center for Grief & Loss. The camp will be held on June 9-11,
Dear Parent/Guardian, Thank you for your interest in Camp Chimaqua, an overnight bereavement camp, through Hospice & Community Care s Pathways Center for Grief & Loss. The camp will be held on June 9-11,
*Family Chiropractic Care* New Patient Information Worksheet*
 *Family Chiropractic Care* New Patient Information Worksheet* Name: SSN: Age: Address: City: State: Zip: Phone Hm: Wk: Date of Birth: E-Mail Employer: Insurance: Policy/I.D. # : Spouses Name: Marital Status:
*Family Chiropractic Care* New Patient Information Worksheet* Name: SSN: Age: Address: City: State: Zip: Phone Hm: Wk: Date of Birth: E-Mail Employer: Insurance: Policy/I.D. # : Spouses Name: Marital Status:
MEDICAL HISTORY QUESTIONNAIRE Last name First Name MI DOB. Please answer the following questions about your current eye problems and medical history:
 MEDICAL HISTORY QUESTIONNAIRE Last name First Name MI DOB Please answer the following questions about your current eye problems and medical history: 1. What problems are you CURRENTLY having with your
MEDICAL HISTORY QUESTIONNAIRE Last name First Name MI DOB Please answer the following questions about your current eye problems and medical history: 1. What problems are you CURRENTLY having with your
Parental Consent For Minors to Receive Services
 Parental Consent For Minors to Receive Services Welcome to the University of San Diego s Wellness Area! We appreciate your coming our way, and look forward to working with you. The following provides important
Parental Consent For Minors to Receive Services Welcome to the University of San Diego s Wellness Area! We appreciate your coming our way, and look forward to working with you. The following provides important
The process has been designed to be user friendly and involves a few simple steps.
 HOW DO I ENROLL A PATIENT WITH HOUSECALL MD? The process has been designed to be user friendly and involves a few simple steps. It is the patient s/family s/dpoa s/guardian s decision, if they want to
HOW DO I ENROLL A PATIENT WITH HOUSECALL MD? The process has been designed to be user friendly and involves a few simple steps. It is the patient s/family s/dpoa s/guardian s decision, if they want to
CAMP CO-OP 2018 Registration Packet
 CAMP CO-OP 2018 Registration Packet Registration Begins February 15, 2018 This summer day camp is designed for Charles County Public School students with significant cognitive delay who are receiving special
CAMP CO-OP 2018 Registration Packet Registration Begins February 15, 2018 This summer day camp is designed for Charles County Public School students with significant cognitive delay who are receiving special
Welcome to Optimum Chiropractic & Wellness Center To The NEW PATIENT Outline of Procedures for Care And Consent to Initiate Care
 Welcome to Optimum Chiropractic & Wellness Center To The NEW PATIENT Outline of Procedures for Care And Consent to Initiate Care We are dedicated to providing the highest quality chiropractic health care
Welcome to Optimum Chiropractic & Wellness Center To The NEW PATIENT Outline of Procedures for Care And Consent to Initiate Care We are dedicated to providing the highest quality chiropractic health care
New Patient Paperwork
 Your Vision Is Our Focus New Patient Paperwork Dear Patient, Please fill out all of the following pages, and bring them with you to your scheduled appointment time. If you have questions regarding your
Your Vision Is Our Focus New Patient Paperwork Dear Patient, Please fill out all of the following pages, and bring them with you to your scheduled appointment time. If you have questions regarding your
1.2 ADULT CLIENT INTAKE FORM: Client Information
 1.2 ADULT CLIENT INTAKE FORM: Client Information FOR OFFICIAL USE ONLY: Client Number Effective Insurance No OH No CLIENT INFORMATION Client name of significant other CHILDREN INFORMATION of birth of birth
1.2 ADULT CLIENT INTAKE FORM: Client Information FOR OFFICIAL USE ONLY: Client Number Effective Insurance No OH No CLIENT INFORMATION Client name of significant other CHILDREN INFORMATION of birth of birth
Patient Name: Last First Middle
 Wilmington Ear Nose & Throat Associates, PA Patient Information Form Patient Name: Last First Middle Mailing Address: Street Address (if different from above): City: State: Zip Code: Social Security #:
Wilmington Ear Nose & Throat Associates, PA Patient Information Form Patient Name: Last First Middle Mailing Address: Street Address (if different from above): City: State: Zip Code: Social Security #:
CURE CARDIOVASCULAR CONSULTANTS
 NEW PATIENT PACKET There are six pages in this packet that will help us get a clearer picture of your medical history and physical health. Please note: SIGNATURES are required on pages 2, 4, and 6. Please
NEW PATIENT PACKET There are six pages in this packet that will help us get a clearer picture of your medical history and physical health. Please note: SIGNATURES are required on pages 2, 4, and 6. Please
PATIENT INFORMATION. In Case of Emergency Notification
 PATIENT INFORMATION Patient Name Date Nickname DOB Age Sex Race/Ethnicity Language(s) spoken at home Person completing form Relation to Patient Patient Address City State Zip Phone # Other Phone Medical
PATIENT INFORMATION Patient Name Date Nickname DOB Age Sex Race/Ethnicity Language(s) spoken at home Person completing form Relation to Patient Patient Address City State Zip Phone # Other Phone Medical
Stepping Stones Early Intervention Program 19 Harrison Avenue Roseland, NJ Phone: x1223
 Stepping Stones Early Intervention Program 19 Harrison Avenue Roseland, NJ 07068 Phone: 973-535-1181 x1223 Dear Parents/Guardians: Welcome to the 2018-2019 Stepping Stones Early Intervention Program. Each
Stepping Stones Early Intervention Program 19 Harrison Avenue Roseland, NJ 07068 Phone: 973-535-1181 x1223 Dear Parents/Guardians: Welcome to the 2018-2019 Stepping Stones Early Intervention Program. Each
Pediatric Psychology
 Pediatric Psychology Welcome to Pediatric Psychology at CHOC Children's. Please read this information carefully and write down any questions that you might have, so that we can discuss them. PSYCHOLOGICAL
Pediatric Psychology Welcome to Pediatric Psychology at CHOC Children's. Please read this information carefully and write down any questions that you might have, so that we can discuss them. PSYCHOLOGICAL
If you would like your child to participate in the Life Health Center School Wellness Program, please complete pages 1-5.
 If you would like your child to participate in the Life Health Center School Wellness Program, please complete pages 1-5. Student Name of Birth Sex: Male Female Address Street City State Zip Grade Room
If you would like your child to participate in the Life Health Center School Wellness Program, please complete pages 1-5. Student Name of Birth Sex: Male Female Address Street City State Zip Grade Room
Welcome to St. Bonaventure University. We are glad you re here!
 Welcome to. We are glad you re here! The staff of the Center for Student Wellness in Doyle Hall welcomes you to the next step of your life: COLLEGE! We want to make sure you have the best experience possible
Welcome to. We are glad you re here! The staff of the Center for Student Wellness in Doyle Hall welcomes you to the next step of your life: COLLEGE! We want to make sure you have the best experience possible
WELCOME TO OUR OFFICE!
 WELCOME TO OUR OFFICE! Name Date: / / Address City State Zip Home Phone Cell Phone E-Mail Birthdate Age SS# Race: Marital Status: M W D S Employer Work Phone Occupation Name & Birthdate of Primary Insured
WELCOME TO OUR OFFICE! Name Date: / / Address City State Zip Home Phone Cell Phone E-Mail Birthdate Age SS# Race: Marital Status: M W D S Employer Work Phone Occupation Name & Birthdate of Primary Insured
Welcome to the YMCA Great Escape Before & After School Program
 Welcome to the YMCA Great Escape Before & After School Program 2016-2017 The YMCA Great Escape Program is designed to offer well-supervised, safe, quality care for school age children. Our program is set
Welcome to the YMCA Great Escape Before & After School Program 2016-2017 The YMCA Great Escape Program is designed to offer well-supervised, safe, quality care for school age children. Our program is set
MONTAGUE RESIDENTS MONTAGUE NEW STUDENT REGISTRATION
 Patricia Romyns Assistant to the Chief School Administrator MONTAGUE RESIDENTS John W. Waycie Business Administrator/Bd. Secretary Christopher Gregory Assistant Principal MONTAGUE NEW STUDENT REGISTRATION
Patricia Romyns Assistant to the Chief School Administrator MONTAGUE RESIDENTS John W. Waycie Business Administrator/Bd. Secretary Christopher Gregory Assistant Principal MONTAGUE NEW STUDENT REGISTRATION
Also, you must acknowledge that you understand the following by signing and dating this sheet:
 To the parents of You have registered a child for one of our programs and indicated that he or she has a documented life threatening food or insect allergy or other severe allergic reaction that requires
To the parents of You have registered a child for one of our programs and indicated that he or she has a documented life threatening food or insect allergy or other severe allergic reaction that requires
RESPITE CARE VOUCHER PROGRAM
 HELPING HANDS of VEGAS VALLEY 2320 Paseo Del Prado B-204, Las Vegas, NV 89102 (702) 507-1848 or Fax (702) 728-2963 cory.lutz@hhovv.org RESPITE CARE VOUCHER PROGRAM Dear Applicant: Thank you for your interest
HELPING HANDS of VEGAS VALLEY 2320 Paseo Del Prado B-204, Las Vegas, NV 89102 (702) 507-1848 or Fax (702) 728-2963 cory.lutz@hhovv.org RESPITE CARE VOUCHER PROGRAM Dear Applicant: Thank you for your interest
Medication Administration Skill Checklist (to be accompanied by daily medication log for applicable students) 1 page
 1 page") See the following pages for exhibits relating to medical treatment: Exhibit A: Exhibit B: Exhibit C: Exhibit D: Exhibit E: Medication Administration Request Form and Guidelines for Administration of Medication
See the following pages for exhibits relating to medical treatment: Exhibit A: Exhibit B: Exhibit C: Exhibit D: Exhibit E: Medication Administration Request Form and Guidelines for Administration of Medication