Commissioning Intentions 2016/17 and 2017/18
|
|
|
- Gwen Marsh
- 5 years ago
- Views:
Transcription


1 Commissioning Intentions 2016/17 and 2017/18 1 P a g e
2 1.0 Background 1.1 These commissioning intentions are designed to build upon and implement the strategic objectives set out in our 5 year strategic plan for 2014/19 and reflected in our Operational Plan for 2015/16:- Efficient and Effective Care Healthy Life Expectancy Mutual Approach to Achieving the Best Possible Outcomes High Quality Care for All 1.2 Since the development of these strategic objectives, our participation in the Five Year Forward View New Models of Care Programme, as a national Vanguard site, provides an added impetus and opportunity to secure their delivery. 1.3 Our New Model of Care for the population is based on the principles of shared ownership, shared responsibility and shared benefits, maximising the potential of:- individual patients and citizens; our staff in supporting those individuals; our staff working effectively with each other. 1.4 Our ambition is enabled by:- better communication with patients and between staff; improved access to different types of consultation and diagnostics in the community; continuity of care in supporting the management of peoples long term conditions; effective coordination of care for the frail elderly and those with the most complex conditions. 1.5 To respond to this, the focus of our model of care builds on a joined up network of GP-led, community-based Multi-Disciplinary Teams (MDTs) which enable staff from health, social care and the voluntary sector to work better together, as part of a Multi-Specialty Community Provider (MCP). This is also underpinned by a complementary process of developing standardised best practice pathways of care. Through this we will ensure that all services provided outside of the MCP are commissioned in a way which incentivises optimum outcomes for the patient, maximises efficiency and enables effective communication back with the GP. 2 P a g e
 will be familiar with the model and we have come together under our Partnership Board arrangements to implement it.")
3 1.6 Our main partners The Dudley Group NHS FT (DGFT), Dudley and W alsall NHS Partnership Trust (DW MPT), Black Country Partnership NHS FT (BCPFT), Dudley Metropolitan Borough Council (DMBC) and Dudley Council for Voluntary Services (DCVS) will be familiar with the model and we have come together under our Partnership Board arrangements to implement it. Through this arrangement we have agreed to manage the risks together and find new ways of thinking and doing to make the difference that we have not been able to make to date. 1.7 There are three elements to the model based upon the fundamental principle of supporting population-based health and wellbeing. This starts with the patient registered with their GP - the main co-ordinator of their care. This is delivered through a mutual network of care, best exemplified by the work of a practice based Multi-Disciplinary Team (MDT), linked to a series of other community-based services. This, in effect, is the MCP based on the principles of shared ownership, shared responsibility & shared benefits. 1.8 The mutual network of care, to be delivered by the MCP, will be commissioned around the following themes and outcomes:- better communication with patients and between staff; improved access to different types of consultation and diagnostics in the community; continuity of care in supporting the management of peoples long term conditions; effective coordination of care for the frail elderly and those with the 3 P a g e
4 most complex conditions. 1.9 W e will support people to remain at home wherever possible by developing evidence based best practice pathways of care. This is the second element of the model. W e will reduce variation, so that all services are commissioned and delivered in a way which incentivises optimum outcomes for the patient, shares risk, makes the best of the resources we have available; and enables effective communication between all stakeholders. To enable the delivery of pathways for value-added treatments in relation to both planned and urgent care, we intend to move away from Payment by Results (PbR) tariffs to a payment that reflects best practice The final element is a re-commissioned primary medical services system. This will be commissioned through a refreshed outcomes based contractual framework, again reflecting the themes of access, continuity and co-ordination Our objective has always been to achieve progress wherever possible through collaboration with our providers and significant progress has already been made in implementing elements of the new care model as a result of this collaboration, regardless of how services have been contracted for previously Our intention is to now build on this development and to fully contract for the model of care. The challenges are significant and changes are vital if we are to continue with sustainable health and social care in Dudley, that meets the needs of our population. Therefore, the contract changes that will be necessary are also correspondingly significant W e hope that we will be able to achieve these changes through continued collaboration and these intentions set out some of the collaborative processes we will follow to enable this. However, we also recognise that the need to do what is right for our population may have consequential and possibly unforeseen impacts on existing providers in their current form. This is one key reason why we are adopting an 18 month process essentially the first six months will be used to fully scope, quantify and map out how existing services translate to the new model of care; thus giving a further 12 months to both implement the new contractual arrangements, as well as allow time for existing providers to adjust how they provide services W e intend to have a single contract framework to deliver the MCP component of the model and our commissioning intentions are designed to have this fully in place by 1 April W e expect certain elements of the model to be in place with effect from 1 April 4 P a g e
5 2016, with full implementation from 1 April That s why this year we are publishing commissioning intentions to cover both 2016/17 and 2017/18. W e intend to exploit whatever freedoms are available to us as a Vanguard site to make our new model of care a reality. 2.0 Context and Environment 2.1 As a health and social care economy, the financial environment in which we operate in Dudley is reflective of the position nationally. W e are facing, however, the most significant financial challenge we have experienced for a number of years. 2.2 The CCG can expect a minimal increase in resource from NHS England, which will be utilised by demographic growth, increased demand and increasing acuity of patients. Our main provider of acute care, Dudley Group NHS FT, is in breach of its Monitor license on financial grounds; our provider of children s and learning disability services, Black Country Partnership NHS FT, is currently being investigated by Monitor to see if its license has been breached on financial grounds; our provider of mental health services Dudley and W alsall Mental Health Partnership NHS Trust has not been approved for FT status; and our local authority, Dudley MBC, is predicting a significant reduction in its operating budget for social care services. 2.3 The value proposition submitted to NHS England as part of the Vanguard initiative indicated the requirement to achieve 32m of cash releasing and productivity savings from the CCG s budgets for the next 3 years. The cash releasing element, approximately 21m, is 10m higher than current CCG financial plans, and is required to invest in the new model of care. 2.4 We believe the new care model will provide the opportunity for care to be delivered to the population of Dudley in a more efficient manner, by reducing variation, eliminating waste, and providing care in the most appropriate setting. In conjunction with providers we will model the potential financial impact on all aspects of the health and social care economy. However, organisational sustainability cannot take precedence over the delivery of good quality health and social care. 3.0 Key Enabling Partnerships and Programmes of work 3.1 W e have established some key partnerships and ways of working to enable us to implement the model of care. W e will expect full cooperation from our providers in each of these areas of work. 5 P a g e
6 Integration of health and social care 3.2 The heart of our model of care aligns social care and health together with the voluntary sector. Firstly, this is right for our population because very often they will present with both health and social care needs, so to separate services artificially ignores the needs of our population. Secondly, the challenges faced by social care are such that we believe the only long-term solution for sustainable delivery is to fully integrate health and social care so that the challenges are fully shared. 3.3 Consequently, to match integrated delivery of services, we are working with Dudley MBC to appropriately integrate the commissioning of services so that there will ultimately be an integrated contractual process for all of the services that form part of the MCP. W e expect to have this fully in place for April Empowering teams without walls 3.4 Central to our way of working is an empowerment methodology which creates the right framework and tools for teams (initially our community MDTs) to work together to solve the problems and challenges in meeting the needs of their population. This builds capability in teams and gives flexibility to different teams to respond to different needs and challenges with their specific population. 3.5 Part of our empowerment methodology includes the implementation of a crosssystem organisational development programme which utilises staff from within our existing providers to support the development of the teams. Therefore, we will expect full collaboration from all providers to contribute their staff time to participate in this OD programme. Creating a self-improving system 3.6 A key aspect to Dudley CCG s plans for the MCP is the commitment to a robust evaluation of impact. The CCG has commissioned the CSU Strategy Unit to assist in devising this evaluation. Evaluation is an active component of change management, ideally achieving a balance of meaningful practical application and methodological rigour. For the Vanguards, dealing with high levels of complexity and uncertainty, theory-based evaluation offers a robust approach to measuring impact. The logic model is a key tool to support this approach. The logic model will be a graphic representation of the relationship between programme assets, activities and intended outcomes. Currently the required outcomes are being assessed along with the degree of change and impact for service users. Thereafter, the evaluation development will be focused on working backwards from these outcomes through to the connected activities and resources required. Appendix 1 shows the preliminary set of outcomes. These may be modified or 6 P a g e
7 expanded during the development of the Logic Model. W e will expect full collaboration from all providers in prioritising this work. 3.7 The starting point for our approach to evaluation is to see it as a fundamental part of a self-improving system. One of the characteristics of such a system is that it seeks and acts upon evidence; that it adopts a reflexive and healthily selfcritical approach; and that there is a feedback loop of producing, interpreting and acting upon information. This understanding runs throughout the proposed design of our evaluation and our entire way of working with the Strategy Unit. The evaluation will therefore be:- highly formative - we will use the evaluation on an ongoing basis; there will be short feedback loops between evidence gathering and reporting; and we will base the design and ongoing operation of our model upon the best available and most current evidence; here we will benefit from the Strategy Unit s evidence review capability to create a living review, which would be updated frequently and used by us as a key design input; facilitative and empowering - in order for evaluation to act as one of the feedback loops in our system, several conditions must be present. On the supply side, evaluative evidence must be available at the right time and be of the right type; and, on the demand side, there must be sufficient capability within the system to interpret and act upon it. Therefore, our evaluation would work closely with MDTs to help define, capture and report metrics that are of use to these teams; MDTs will also be given training in the use / interpretation of evidence as part of our empowerment methodology. 3.8 The evaluation will also examine different levels of the system, gathering evidence and feeding back insights:- at the micro level looking at interactions between clinician and patient. For example, this might mean asking more questions about the causes of attendance at primary care such as social isolation driven by the knowledge that there are now services to help address such causes. The focus here would be on outcomes for patients and individual staff members; at the meso level looking at the operation of the MDTs. This would entail examining the operation of the MDT model across l ocalities, tracing their development from representatives of individual organisations to genuine whole team working. The focus here would be on more efficient and effective ways of working and the evaluation would play a highly developmental role - extracting and transferring elements of effective practice across localities; at the macro level looking at the Dudley health and social care economy. 7 P a g e
8 Here the evaluation would examine the role of the Vanguard in creating a sustainable and self-improving system. This would entail gathering evidence and insights from different partner agencies the local authority, the voluntary and community sector, the acute and mental health providers to trace changes at this level. One of the key aspects of change tested at this level would be the increasing adoption of a system perspective, as opposed to an individual organisational perspective. Effective IT systems and support 3.9 IT is an essential component and enabling factor in the delivery of our care model. So we have commissioned Alscient Ltd to provide us with external expertise to oversee improvements in our IT infrastructure. There are two main components to this work:- a) Ensuring future-fit-for-purpose IT support. W e will shortly commence a tender process to secure the necessary managed IT support services that will be needed to first-and-foremost provide an effective and efficient service to General Practice. W e have the option of extending that tender process to incorporate IT support to other providers that have a predominant interest particularly in the MCP component of the model of care. Expressions of interest in joining the CCG in this tender would need to be made to us by 16 October b) Developing an integrated IT solution. An essential component of empowering staff to work effectively together is to ensure that they are working together accessing a single consistent patient view. It is therefore our intention to ensure that all services that form part of the MCP are working in this way. This will also facilitate the ability to meet the new national requirements on providing patients with access to their records. Dudley Partnership Board and external expertise through the national New Care Models Programme Our main providers, together with Dudley MBC and Dudley CVS are working with us, through the newly formed Partnership Board, to collaborate on the development of the new model of care. W e will continue to use the Partnership Board as the main forum for this collaboration throughout the next 18 month period Through the national New Care Models Programme we will be accessing external support to assist in the implementation and contracting for our new model of care. This will include legal and procurement advice on the process for implementing the new contracts to enable the new model of care; 8 P a g e
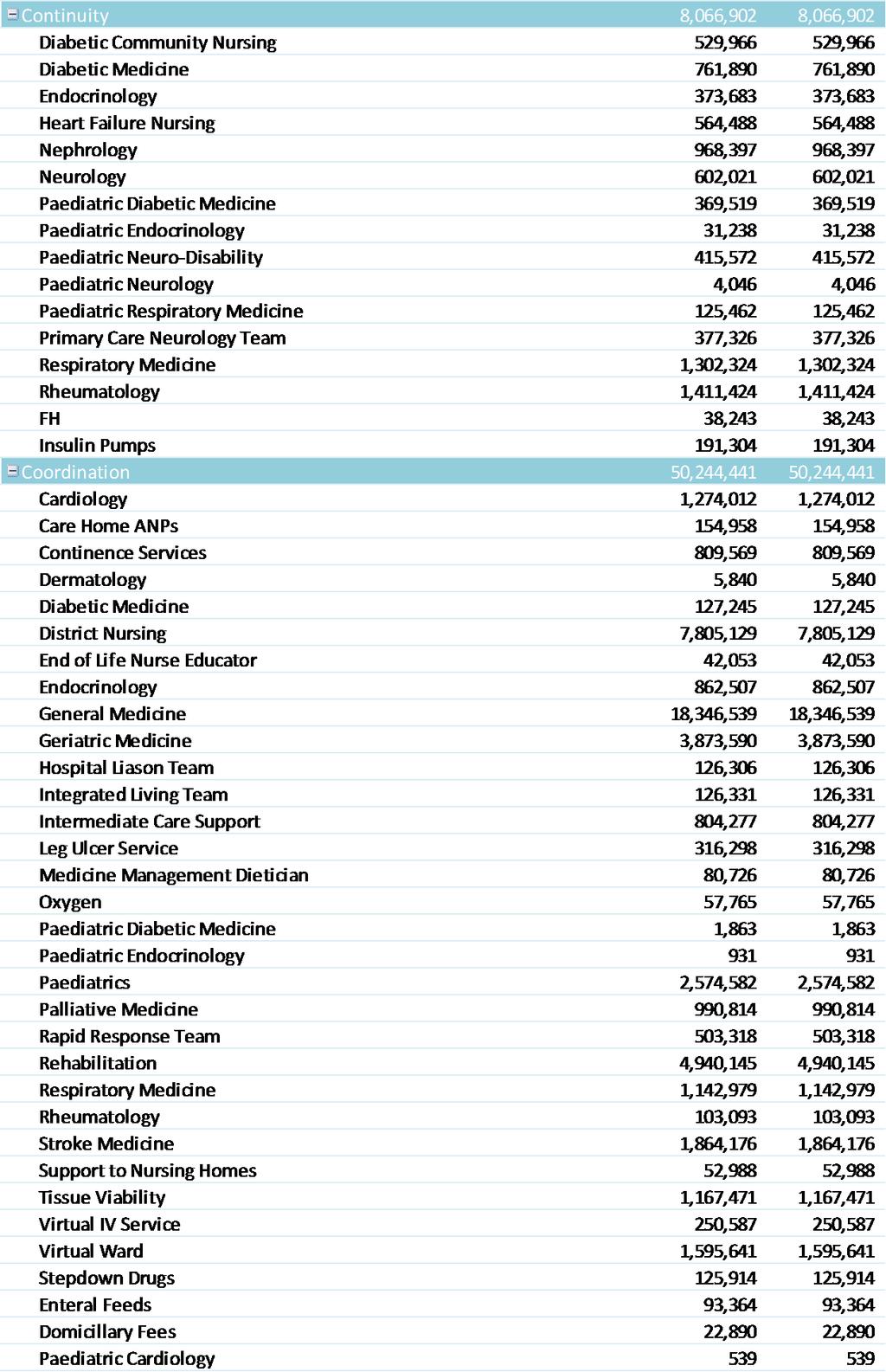
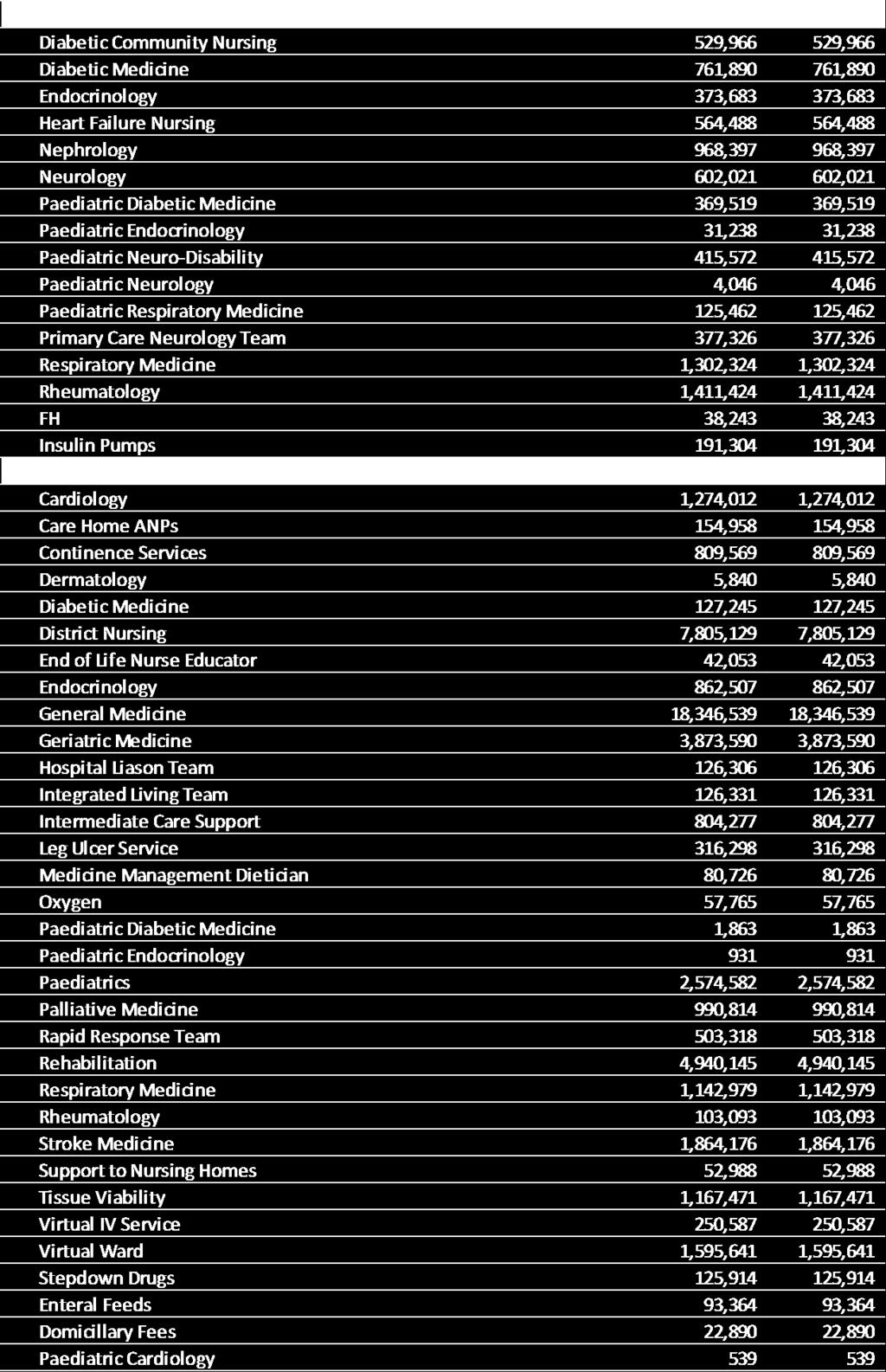
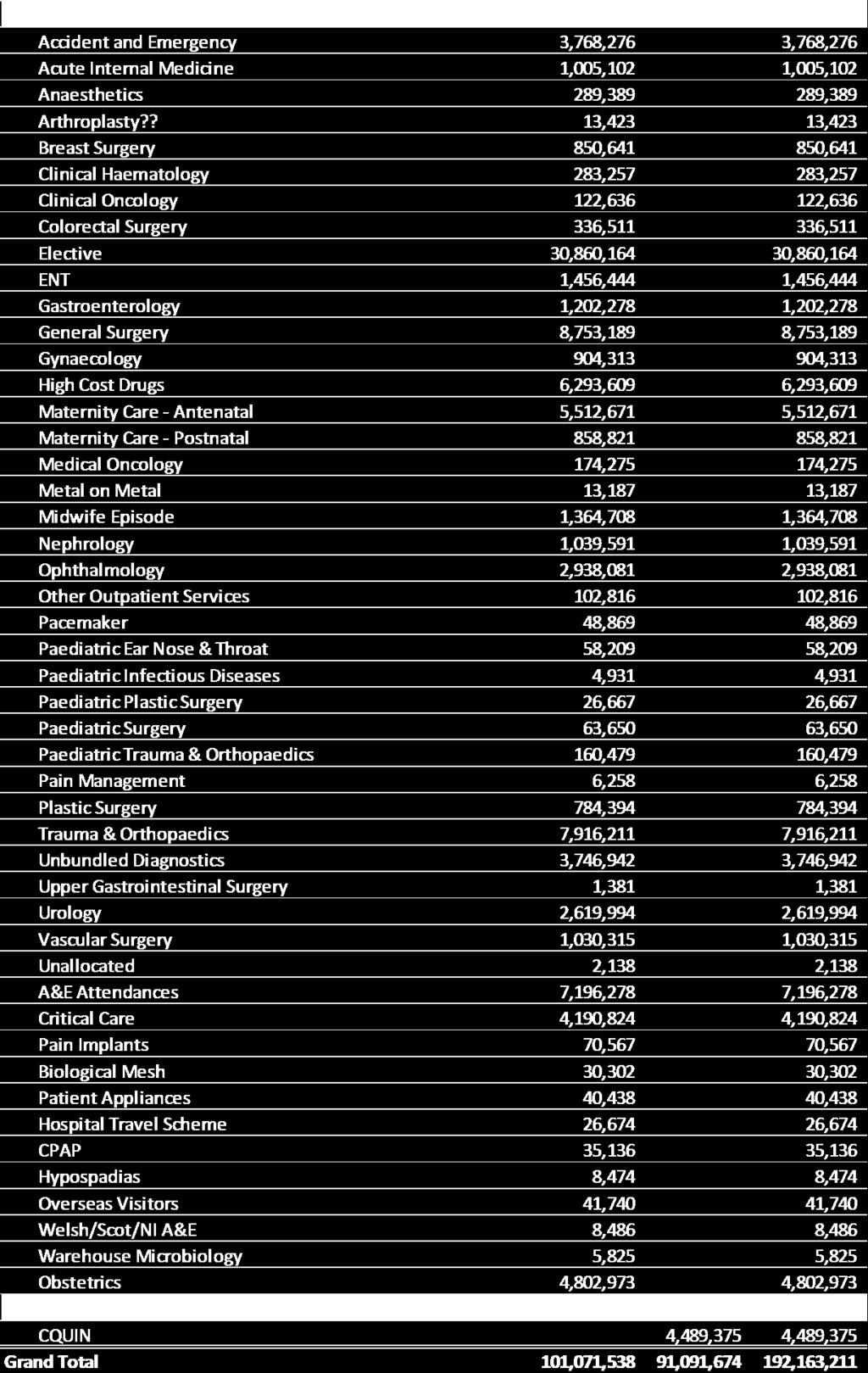
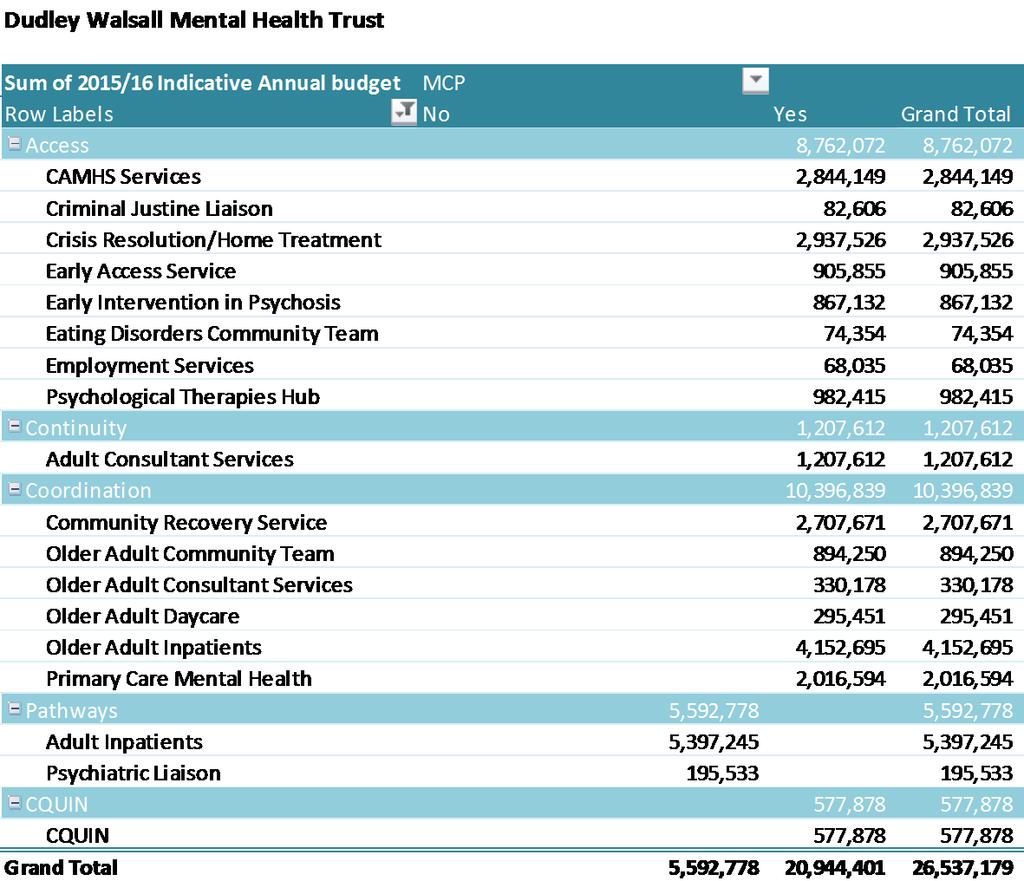
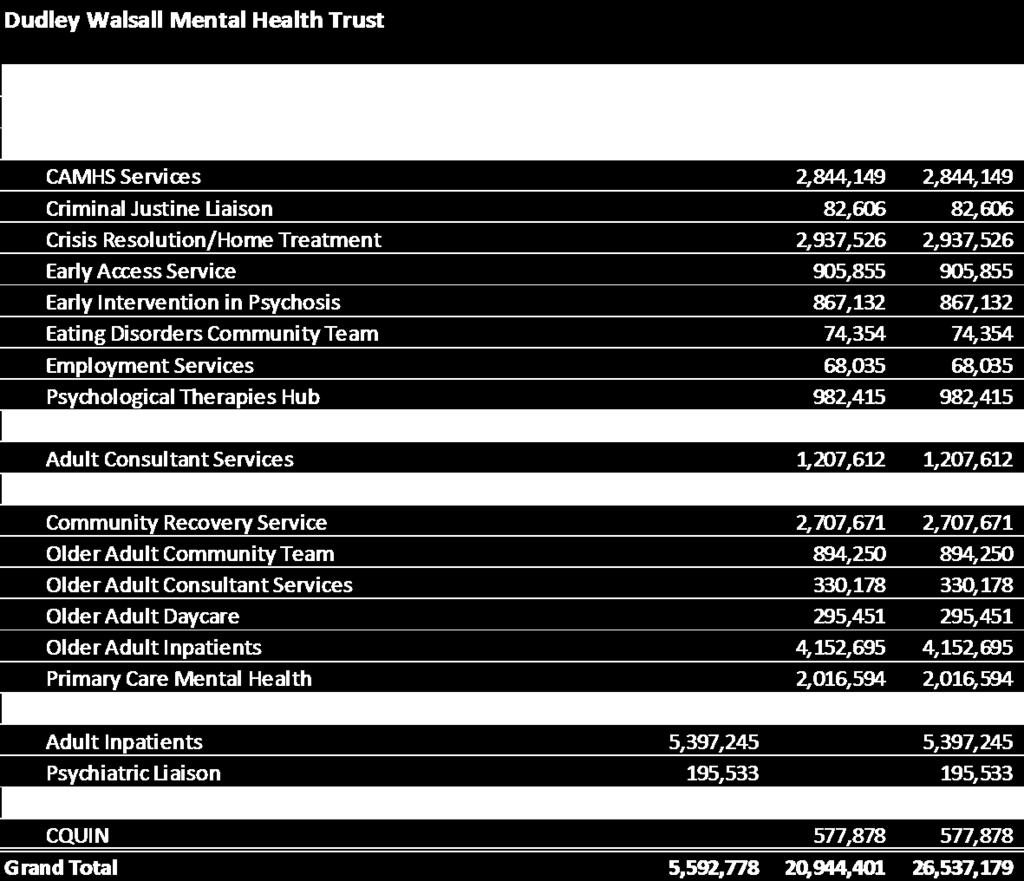
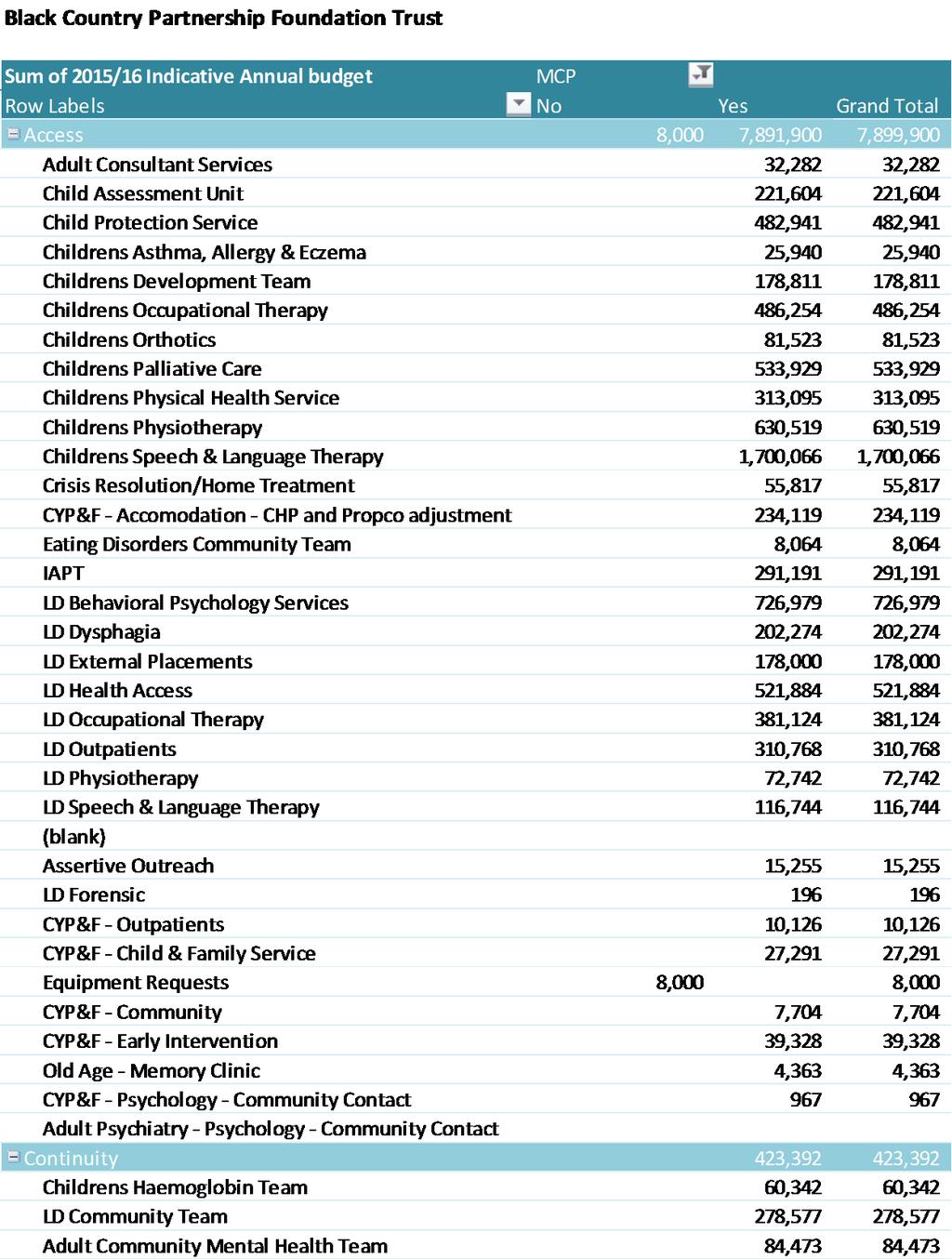
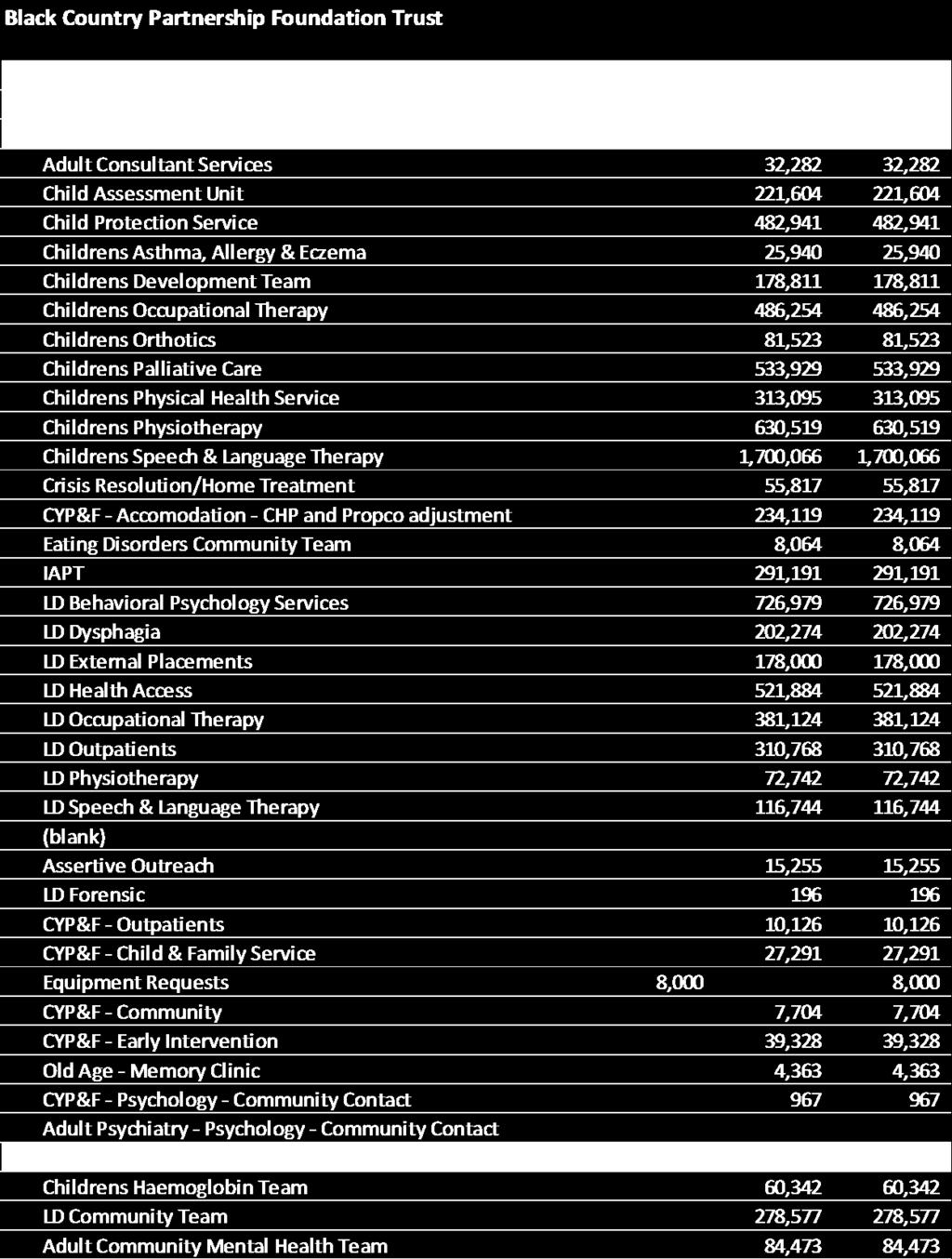
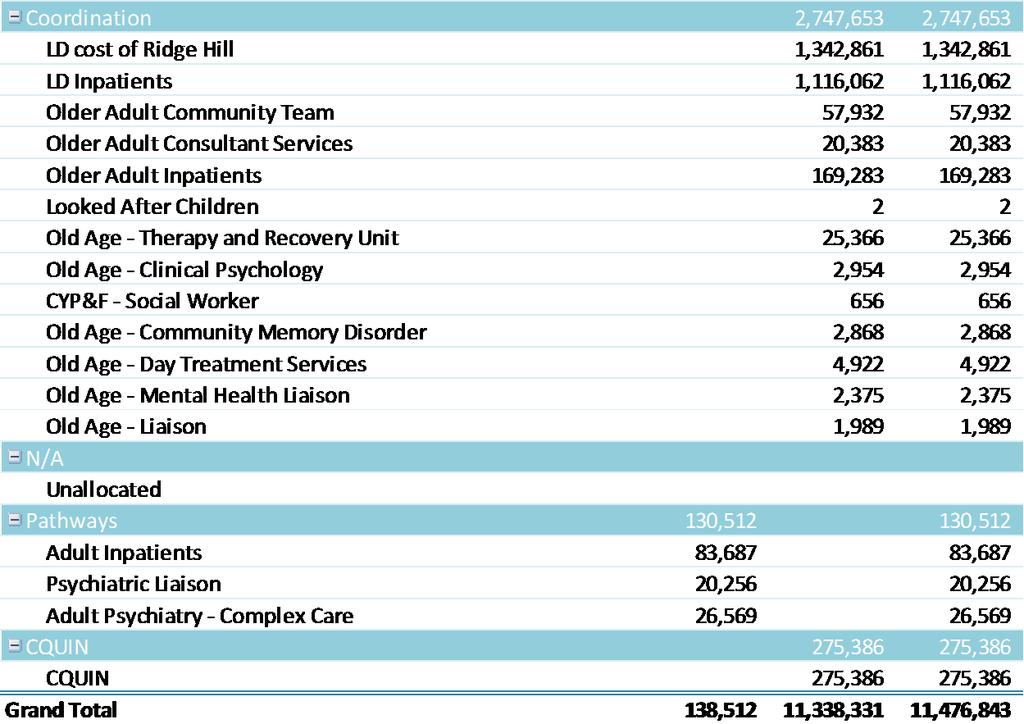
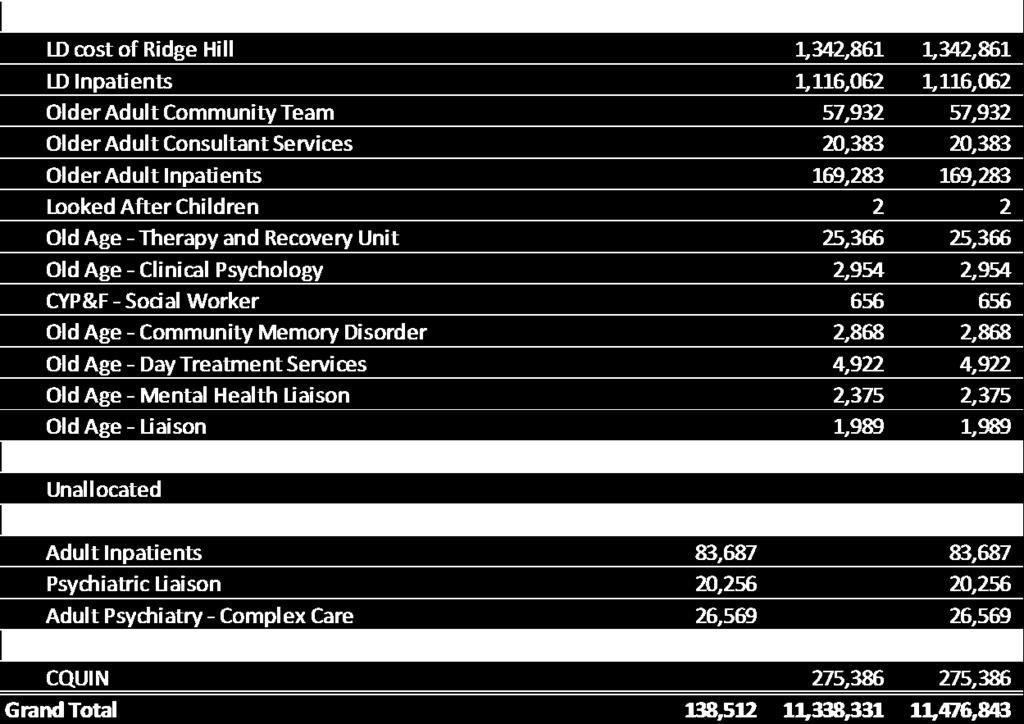
9 engagement with regulators on new contractual types and pricing methodology; sharing and learning of best practice for rapid adoption within our system where appropriate; workforce development to enable the new care model. 4.0 Changes in the distribution of resources and the value of services 4.1 W e identified in 1.13 above that there will be consequences for our providers in implementing the new model of care. One of those consequences will be the financial impact arising from the redistribution of resources across the system. 4.2 Our initial analysis of current services that can be mapped against the MCP model services (see Appendix 3) shows the impact for our three NHS providers as follows: 2015/16 Annual Budget Provider Access Continuity Coordination Total MCP Pathways CQUIN Grand Total Dudley Group NHS FT 28,290,955 8,066,902 50,244,441 86,602, ,071,538 4,489, ,163,211 Dudley Walsall Mental Health Partnership NHST 8,762,072 1,207,612 10,396,839 20,366,523 5,592, ,878 26,537,179 Black Country Partnership NHSFT 7,899, ,392 2,747,653 11,070, , ,386 11,476,843 Grand Total 44,952,927 9,697,906 63,388, ,039, ,794,828 5,342, ,177, On the basis of the intentions described we anticipate the balance of investment at a time of reducing resources to be:- planned care reduction as waste and variation are eliminated; urgent care reduction due to impact of specific measures; continuity and co-ordination elements increased on the basis of the use of new technology and enhanced team working to contain demand for other services including urgent care; primary care increased to create the scale the model of care requires. 4.4 Assumptions at the time of publishing these intentions are set out below. Further 9 P a g e
10 cash releasing efficiency savings will be required by the system as a whole, not least to manage the financial challenge facing adult social care. These will be set prior to the Dudley Summit for our main partners, referred to below. Cash releasing Productivity Total Likely provider to be impacted Elective Dudley Group Urgent Care/Non Elective Dudley Group Primary Care Community Prescribing n/a Other TBC It is vitally important that we have a shared understanding with our providers on the likely end point regarding the distribution of resources so that we can understand the potential consequences as soon as possible and build any mitigating actions into the 2016/17 contract in preparation for full implementation by April The steps that we intend to go through to get to this understanding will be as follows:- first: map every existing contract line to their future expected component of the model of care (MCP Access, MCP Continuity, MCP Coordination, Urgent pathways, Elective pathways). A first draft has been produced by our CCG and is included with these commissioning intentions. This should be reviewed by providers by 15 October 2015; second: identify likely changes in demand based on population requirements for each contract line / service. First draft will be produced by the CCG by 13 November 2015 and then confirmed by the provider by 18 December 2015; third: confirm expected efficiency or decommissioning requirement for each contract line / service. First draft will be produced by the CCG and then confirmed by the provider, no later than Dudley Summit provisional date 30 November 2015; fourth: identify consequential impact and mitigating action for each contract line/service. First draft will be produced by the provider by 31 December 2015 and then confirmed by the CCG by 31 December 2015 and 31 January W e recognise that this is a challenging timescale, however, this is necessary to ensure contracts are signed. 4.6 The process that we undertake in the next six months will be designed to achieve as much collaboration as possible on understanding the scale of change required. 10 P a g e
11 However, whilst we will engage providers in a shared discussion on the scale of change, in order to determine the level of efficiency needed from each service, the focus will be on delivering that scale of change and level of efficiency itself. The level of efficiency required will be a given and not negotiable. This is essential to ensure the stability of the health and social care system. 4.7 W e will assume that participation in this process includes acceptance that services will need to change and therefore efficiencies and improvements will have to be delivered which will necessarily result in the need to change how care is provided and what activity levels are appropriate. W e will expect collaboration from providers on proactively identifying the opportunities for implementing improvements and achieving best practice. Therefore, we expect the emphasis of our negotiations will be on determining what actions and mitigations are needed to achieve the scale of change required (not whether the change should happen). If any provider believes that the expected scale of change required for any given service is not achievable, then we expect this to be identified by the provider early in this process, i.e. by 31 December 2015, so that the issue can be escalated for review as soon as possible. Determining the value of services and efficiency requirements 4.8 In previous years commissioning intentions we invited providers to identify their view of the value of the services that they provide (for example - what outcomes is a service designed to achieve, how is this measured, and is it value for money). The response to this invitation was disappointingly very limited and the reporting on the value of services is very variable (so for example we have a clear record on longterm conditions management in primary care through the QOF but no comparable measures for equivalent secondary care services). However, it is essential that we have a shared view with our providers about the contribution that each service makes to the new model of care. 4.9 Therefore, for inclusion within the 2016/17 contracts we expect to have agreed with each provider, for each individual contract line / service, the following schedule of information:- agreed referral route(s) into the service open access, GP, etc.; which component of the model of care the service is part of (MCP Access, MCP Continuity, MCP Coordination, Urgent pathways, Elective pathways); the key outcome measure for the service; the location(s) of service delivery across the borough; if the service cannot identify clear outcome measures, or those measures suggest that the service is not delivering, the service should be flagged for review and possible decommissioning (including public consultation). Possible mitigating actions in the 2016/17 contracts 4.10 W e will be open to views from providers about the range of mitigating actions that 11 P a g e
12 might be taken in 2016/17 to support moving fully to the new model of care from April This might include:- fixing contract values (or a significant proportion thereof) in order to give security whilst the provider implements the required changes, or tries new ways of working; risk pooling resources between services, across providers, where this might enable joint working to address key challenges; project management or equivalent support to give providers enhanced capacity to make the improvements required; targeted use of CQUINS to facilitate key changes; changing contract terms to support the new ways of working W e will expect all mitigating actions to be built into the 2016/17 contract against a clear set of expectations about how this enables the new contracts to be established from April First Component of the Model of Care : Primary Care at the heart of the MCP 5.1 General Practice is at the heart of the model it starts with the patient registered with the practice. A New Contractual Framework 5.2 W e intend to use our delegated responsibilities for commissioning primary medical services to full effect. W e will suspend the QOF element of the existing GMS contract with effect from 1st October 2015 and we expect practices to take the necessary steps to prepare for the implementation of a new contract from 1st April This contract will reflect the three themes of access, continuity and coordination. This is now the subject of consultation with local practices and will include:- a) Access enabling resilience in primary care is critical through the CCG s primary care strategy and development programme; supporting practices to work in partnership together where appropriate (for example: in providing urgent advice and guidance to local paramedic teams see section 7); working with practices to meet the requirements to enable full access to records for all patients across the system; creating a new back office function and eliminating unnecessary transaction costs to support efficiency improvement in primary care; standardising referral protocols, triage and discharge information to improve efficiency of communication (both ways) between primary and secondary care; ensuring all practices can utilise the full range of options for providing access to 12 P a g e
13 their patients (eg: online, telephone appointments, etc ); implementation of our estate strategy to support enhanced primary and community care capacity and capability; b) Continuity an annual assessment of all patients with long term conditions; a named care co-ordinator; joint development of care plans with the patient; condition specific outcome targets - many shared with secondary care; the use of consistent templates through the EMIS system to support this. c) Coordination an annual enhanced assessment of the frail elderly; monthly MDT meetings carried out to a consistent format; providing professional advice and guidance to the MDTs; unplanned admissions replication of the existing Directed Enhanced Service; support for patients with dementia and palliative/ end of life needs; systematic management of patients in care homes; systematic management of repeat prescribing. 5.3 Systematic actions in primary care and the rest of the system will place an emphasis on upstream preventative interventions. Shared Responsibility for Shared Outcomes 5.4 W e will reflect this principle in the way this contract and that for services within the rest of the care model are framed. There will be explicit agreements between the GPs and clinicians elsewhere in the system about their respective responsibilities for managing practices patient population in relation to specific service areas. For example:- each MDT will share responsibility for the outcomes for their population of patients; for each long-term condition, where continuity of care may take place across more than one service provider, there will be a shared objective between that provider and general practice. 5.5 W e expect to begin this process with key services from 1 April 2016 with full roll-out to all relevant services by 1 April The initial services we expect this to cover from April 2016 are:- core services to the MDTs, including mental health; the following long-term conditions diabetes and respiratory. 13 P a g e
14 Attached as Appendix 2 are our expected outcome objectives for each continuity service. 6.0 The Multi-Specialty Community Provider (MCP) 6.1 As stated above we intend to commission certain aspects of the model of care from 1 April 2016, in such a way as to facilitate the commissioning of services as an MCP with effect from 1 April As well as ensuring that primary care is delivered as described above, we will commission those services that form the wider mutual network of care and so come together to form the MCP. Those services we envisage being delivered by the MCP with effect from 1 April 2017 are:- all existing community based physical and mental health services for all ages; the majority of medical specialty outpatient services, both as part of the MCP and in a community based setting; the full frail elderly pathway of care including relevant physical and mental health inpatient services; the vast majority of children s health services. learning disability assessment and treatment services consistent with the requirements of Transforming Care. 6.2 The starting point for this is the Multi-Disciplinary Team (MDT) to deliver on the co- ordination of care. Care co-ordination will then be further enhanced at scale by the delivery of a new frail elderly pathway. In addition there are a range of condition- specific services which will link to GPs to provide continuity of care; and a range of services which will be on a community access basis. A first draft detailed breakdown is available for each of our three main providers attached as Appendix 3. Commissioning the practice MDT 6.3 The existing essential elements of the MDT are:- GP primarily commissioned as described earlier; community nurse; mental health professional; social care professional; access to a practice pharmacist; voluntary sector link worker. 6.4 W e will enhance the capabilities of the existing roles by requiring from 1 April 2016 that all of the above elements are organised so that the person participating in the MDT is also the person that has responsibility in their service 14 P a g e
15 for the MDT patients i.e. we will move away from link-workers (with the exception of the voluntary sector posts) to dedicated resources to the MDT in this way the staff will be better empowered to take together a shared responsibility for the outcomes for their patients and for working more effectively. 6.5 W e will extend the capabilities of the MDTs from April 2016 to include:- links to other public sector agencies such as the fire service; the introduction of generic workers (both through the voluntary sector and in assistance to the MDT as a whole); the introduction of specialised palliative care HCAs provided by and linked into hospice provision in order to enhance our ability to address end-of-life concerns and fully support patients with comprehensive advanced care plans accordingly; the introduction of linked paramedic teams (as part of the existing W MAS emergency ambulance service) who will work with a locality of MDTs see urgent care pathway below; other service groups/professions where it can be demonstrated that they will enhance the capabilities of the MDT. 6.6 Our empowerment methodology will give scope to the MDTs to determine for themselves how they meet the required objectives for their population. This needs to include the capability for teams to flex or change the balance of skills within their teams, to reflect the particular needs of their population. Therefore, to facilitate this we will introduce to the contract from April 2017 the capitation resource for each MDT and the flexibility for the team to modify the use of that resource (within definable parameters) accordingly. 6.7 W e will introduce a tiered approach on how we will measure populations and outcomes that is consistent with the principle of shared responsibility for shared outcomes. This starts with the individual person; the collective outcomes for these individuals then form the population objectives for the GP/MDT; the collective outcomes for the GP/MDTs then form the population objectives for services operating at scale across the borough. 6.8 The initial set of shared outcome objectives for each MDT will be established from April 2016 and service specifications for each one of the services that form the core of the MDT in 2016/17 will reflect this approach. W e then intend to convert this into a set of outcome objectives and a single contractual framework for each MDT and the MCP overall with a view to reflecting this in a capitation based contract from 1 April Whilst much of the focus of our work will be on using the care model to manage the needs of an increasingly frail elderly population, we recognise, in conjunction 15 P a g e
16 with our partners, the opportunities that exist to use this model to deliver more integrated children s services, particularly for those children with more complex needs. This will include the commissioning of a children s community nursing team to manage this population and coordinate their care. In addition, we will develop a more integrated response to children with emotional health and wellbeing needs W hilst for adults, the practice is a key locus of activity, for children with both complex and less complex needs the school has a significant role as well. The intention will be to replicate integrated working across physical health, mental health, children s social care and education services all on the basis of a team with shared responsibility, for a shared population and shared objectives. Discussions are progressing with DMBC and BCP NHS FT W e will work with our partners, including Dudley MBC, to commission the Multi Agency Safeguarding Hub (MASH). Commissioning the mutual network of care - access 6.12 A number of services that are part of the wider mutual network of care within the MCP are predominantly value-added treatments. As part of the mapping process we will confirm this list of services and the expected outcomes for each one W e will be giving consideration as to whether some of these services should be opened up to the public so that they can access the service directly without having to be referred by their GP and therefore reduce the burden of activity on general practice. Initially we will review the potential risks and benefits in doing this for primary mental health care, counselling, orthopaedics and physiotherapy; Commissioning the mutual network of care - continuity 6.14 W e intend to extend the team without walls concept that has been developed with the MDTs, to incorporate a similar team approach across primary and secondary care, taking shared responsibility for shared objectives on specific long-term conditions and mental illness Our intention is to transform the services so that:- the majority of care is delivered in the community; each patient is clear who is leading on the continuity of their care (through, where required, shared care arrangements and clear records linked back to the GP practice); 16 P a g e
17 there are clear outcome objectives for each service and those objectives are shared across all the contributors to that service; 6.16 For 1 April 2016 we will prioritise the full implementation of the new models of care for diabetes and respiratory services and if necessary we will recommission these services through a competitive process. All other relevant services will be incorporated into the care model from April Service specifications will support the alignment of teams within the network, removing artificial barriers by ensuring all parts of the system are working to the objectives defined in Appendix 2. Commissioning the mutual network of care - coordination 6.17 W e have described above how we will commission primary care to be at the heart of the model with the GP as the overall co-ordinator of care. In addition, we have described how we will commission the MDT W e will extend further the concept of care-coordination to include all services delivered at scale in support of the objectives for the MDTs. This will include all components of the frail elderly pathway such as:- geriatricians and medical care for the elderly; the further alignment of social care services; intermediate care services and discharge support services; assessment services; continuing healthcare and nursing home care; prevention services such as falls prevention The frail elderly pathway will start and finish with the MDT as the locus of control for complex care management with shared outcomes relating to:- secondary care admission avoidance; care home admission avoidance; supporting reablement; enabling improved end-of-life planning and compliance; Reducing social isolation These other, at scale, services will be contracted to achieve the same outcome objectives as the MDTs and will work in support of the MDTs. Our intention will be to commission these services together from April 2017 so that care across the pathway is fully integrated, removing delayed transfers of care by virtue of the fact that it is the same service providing the care across the whole system so no transfers take place From 1 April 2017, the frail elderly pathway will be commissioned as a single service that supports the MDT. The MDT will control access to intermediate care 17 P a g e
18 in conjunction with the intermediate care assessors and be responsible for ensuring assessments for NHS Continuing Healthcare take place. W e will review the intermediate care pathway and associated re-ablement services with a view to ensuring appropriate investment across the health and care system The role of care homes in the system is crucial. W e intend, in conjunction with our local authority partners, to ensure that appropriate contractual incentives are in place and supporting services are available to support best practice in relation to:- avoiding unnecessary 999 calls and emergency admissions; managing patients appropriately at the end of life; facilitating effective discharges from secondary care The timetable for the development of this work is as set out below:- all MDT staff to have responsibility for their MDT patients by 1 April 2016; MDT extended to include other agencies e.g. fire, generic workers, palliative care workers and linked paramedic teams by 1 April 2016; establish MDT outcomes by 1 April 2016; assess open access option for Primary Mental Health care, orthopedics and physiotherapy by 1 December 2016; contract for open access where appropriate by April 2016; new service models for Diabetes and Respiratory in place by 1 April 2016; new contract for care homes in place by 1 April 2016; all MCP services commissioned by 1 April 2017, including frail elderly pathway; capitation based contract for MDT/MCP by 1 April Single patient portal 6.24 W e want to create a local public service for Dudley people that improves their ease of access and enables appropriate advice and guidance to connect up with the ability to book appointments. From 1 April 2017, we intend to bring together a range of services into a single integrated approach across health and social care which will give the public just one point of contact to access relevant and inter-connected services. This builds on some existing arrangements and will include:- NHS 111; telehealth and telecare; online services; social care emergency duty services; those access services within the MCP which are bookable; community mental health hub; GP out-of-hours. 18 P a g e
19 6.25 Patients and professionals will use a single number to use the centre. The centre will also actively manage call flow and use down time to make proactive calls to cohorts of patients e.g. reminding them about appointments, medicine reviews, vaccinations or alerts from their telecare/health devices. The option for any primary medical service provider to use this resource for appointments and telephone advice will also be incorporated This will be a complex project to bring together all of these services so we are inviting existing providers and partners to the MCP to express an interest in taking a lead role. W e will provide initial funding for a project director and for resources to scope and produce the business case for implementation. Expressions of interest from providers should be submitted by 16 October 2015 to the CCG This process is aimed at bringing services together. Any associated procurements where contracts do not currently exist will be conducted in accordance with the timetable below. W ithin this we will incorporate our tender process for NHS 111 with Sandwell and W est Birmingham CCG. The timetable is as set out below:- commence consultations and service specification work (includes mapping as is/to be processes and requirements) October 2015; full time Programme Director appointed and commences work 2 January 2016; market testing day - March 2016; advert issued 1 April 2016; PQQ issued April 2016; PQQ Deadline May 2016; PQQ results and recommendations June 2016; ITT Issued 1 July 2015; ITT provider response deadline August 2016; ITT marking and Results signed off by CCG Boards September 2016; announcement to successful provider September 2016; contract Award 1st October 2016; contract mobilisation October 2016 March 2017; service go-live 1st April Effective Care Pathways 7.1 W e intend to commission effective and efficient care pathways that enable 19 P a g e
20 practices to manage their patients appropriately. This will be based upon:- Introducing appropriate triage to streamline processes and improve efficiency; Implementing best practice pathways to reduce the total number of pathways and eliminate unwarranted variation within pathways; locating out-patient services, where appropriate, in more local community settings. 7.2 For all patients referrals from general practice will initially be for advice and guidance only. Each Provider who delivers services under an NHS Standard Contract must offer clinical advice and guidance to GPs on potential referrals through the NHS E-Referral Service, whether this leads to a referral being made or not. 7.3 GPs should use all reasonable endeavours to ensure that all referrals are made through the NHS E-Referral Service. NHS E-Referral Service replaced Choose and Book in June Providers therefore have a contractual obligation to include Advice and Guidance for all services and specialties on the NHS E-Referral Service. 7.4 Furthermore each provider must make the e-referral information available to prospective, patients through the NHS Choices W ebsite. It must also use NHS Choices to promote awareness of the services among the communities it serves, ensuring the information provided is accurate, up-to-date, and complies with the provider profile policy set out at Advice, guidance and triage 7.5 The current system of referral is hugely problematic and can often create extra work for both GPs and secondary care. W e will therefore work with GPs and consultants to develop an effective triage arrangement for all elective services. This will be designed to streamline working practices and ensure consistency and efficiency of referral; as well as consistency and efficiency of guidance or discharge information back to practices. W e expect to trial this approach from April 2016 in those specialties which currently have the most significant accessibility problems; with a view to full roll-out from April Best practice pathways 7.6 W ork has already commenced, under the oversight of the Clinical Strategy Board, to develop a series of efficient elective pathways focusing on the following specialities:- Ophthalmology MSK Urology ENT 20 P a g e
21 More recently IAPT and EIS 7.7 A key aspect of the unwarranted variation is the significant difference in levels of follow-up activity. Our initial analysis indicates the potential to reduce numbers of follow-ups in elective specialties as follows:- Ophthalmology 12% Rheumatology - 12% Urology 10% ENT 6% 7.8 W e expect to agree a significant reduction in the levels of follow-up activity for the April 2016/17 contract; followed by a move away from PbR tariffs with contracts set on the basis of the optimum pathway. 7.9 Planned care interventions will be supported by appropriate diagnostic services in the community wherever possible Outcome objectives for these and other access services will be based upon both timeliness of response and upon the expected value-added outcome improvements that the service is designed to achieve. If value-added outcome measures cannot be demonstrated for any service(s) then we will establish a review process with a view to decommissioning the service(s) by April 2017 following public consultation. Urgent and Crisis Care 7.11 W e want to make the process of care as simple to navigate as possible. Therefore, we will work with providers to reduce the number of portals of entry to the urgent and crisis care pathways. This will include a rationalisation across physical and mental health and the incorporation of the ambulance service into the system with the same shared outcome objectives W e have already brought physical health services together with the new Urgent Care Centre. W e will establish a similar process to create a single point of access for mental health services operating 7 days per week The emergency ambulance service provided by W MAS is an integral part of our urgent care pathway but the service currently operates remotely from the new model of care. W e intend to change this by two means:- creating a locality focus for paramedic ambulances so that at least one ambulance is linked to a locality and can build relationships with the MDTs in that locality; 21 P a g e
22 specialist accessible advice and guidance for these paramedics, to be immediately available on the phone, to enhance their decision-making when attending a patient in a home or nursing home, so that they are better enabled to reduce the number of conveyances to hospital Key milestones are:- urgent and crisis care pathways rationalised and in contracts by 1 April 2016; ambulances linked to localities by 1 April 2016; accessible advice and guidance available to paramedics by 1 September Patient Experience 8.1 W e expect providers to be responsive to complaints and patient feedback, dealing with them in an open, rapid and fair manner. W e will roll out the patient experience app Mi Experience - to all commissioned services across Dudley to enable people to give real time feedback. 8.2 W e expect there to be a culture of information sharing about the experience of patients in order that patients, carers and the public can have confidence in the services that we commission. 8.3 It is our intention to encourage the development of mature relationships between partners and providers based on integrity, openness and transparency. W e therefore expect there to be an open culture of information sharing which uses patient experience to build a more detailed picture of an individual s experience at varying points of their care. This will see us moving from the comprehensive and rich picture we have of all services to focus on a select number of pathways to track an individual s experience. This change will enable us to measure individuals experiences and link them back to their own journey. 8.4 Throughout 2016/17 we will explore ways of measuring experience along a whole pathway, regardless of organisational boundary and linked back to the individual and their expected outcomes. 8.5 W e will build a network of Young Health Champions who will play a pivotal role in bridging the gap between organisations and the needs of young people accessing services in the borough. 9.0 Commissioning for Quality and Innovation (CQUIN) 9.1 As stated, in 2016/17 and beyond we intend to focus efforts not just on 22 P a g e
23 national goals but on delivery of our care model. 9.2 The Five Year Forward View and our participation in the Vanguard Programme, sets out the vision for transformational change to improve outcomes, eliminate waste and reduce cost. A key element of our work will be to align incentives with the reform of payment approaches and contracts. W e will work with partners and the system to ensure that future incentive schemes are designed to help drive the changes required. 9.3 This will include incentives in relation to readmissions. Any taking place within 14 days of discharge will be reviewed in terms of their appropriateness and any inappropriate admissions will be penalised Communications 10.1 All patient level clinical communications from providers (excluding discharge and transfer from care correspondence which shall remain in accordance with the requirements of the NHS Standard Contract Service Condition 11) shall be accurate and be delivered to the registered General Practice by the 2nd operational day post patient contact date. It is the CCG s intention to audit the threshold of achievement at each provider through entry to a quality requirement threshold within the local quality requirement section of the particulars for 2016/17 NHS Standard Contracts 11.0 Contract Type and Tariff 11.1 It is our intention to review the different contractual methodologies available to deliver our objectives with a view to implementing these from April At this stage it appears that the main options are:- lead provider (the MCP) with sub contracts; an alliance contract. However alternative options may arise as part of our discussions with the New Care Models Team and our external legal and procurement advice. There is strong international evidence to suggest that there are economic benefits to be gained from bringing together service commissioning and provision in one organisation an Accountable Care Organisation (ACO). Our analysis of options will be mindful of this. Lead Provider 11.2 Under this model, the CCG would enter into a contract with a provider (the prime contractor or lead provider). That contract allocates risk and reward as between 23 P a g e
24 the commissioner and the prime contractor. The prime contractor then subcontracts specific roles and responsibilities (and allocates risk associated with their performance) to other providers. The prime contractor remains responsible to the CCG for the delivery of the entire service and for the coordination of its supply chain (i.e. its sub-contracted providers), in order to ensure that it can and does deliver that entire service. The prime contractor is likely to be a provider of clinical services itself, however, it could sub-contract all but the co-ordination role. Alliance 11.3 The key characteristics of alliance contracting are alignment of objectives and incentives amongst providers; sharing of risks; success being judged on the performance of all with collective accountability; contracting for outcomes; and an expectation of innovation. A model alliance contract is being developed by NHS England. The process of determination 11.4 W e will consult the system on the methodology to be adopted, with a view to reaching a conclusion by 31 March Tariffs 11.5 By April 2017 we will move away from PbR tariffs to:- MCP capitation methodology and shared outcomes linked to incentives; Care Pathways a tariff per defined pathway, linked to outcomes W e will identify those areas where we wish to do this in shadow format for 2016/17, with full implementation for 2017/18. Price/activity matrices in contracts will reflect the transition in the contractual process between 2015/16 and 2016/ W here services that are part of the care model serve patients registered with practices who are not part of the CCG, we will discuss with the relevant CCG the tariff arrangements we expect to apply Given the proposed move away from PbR, where any refinement of coding by providers leads to different pricing that has a negative impact on the system, this will need to be offset by efficiency savings by that provider so that the final impact is neutral Contract Timetable and Process 12.1 Attached as Appendix 4 is the timetable we will work to in term of finalising 24 P a g e
25 contracts by 31 st March Summary Timetable of Commissioning Intentions 1 April April 2017 Trial of triage for elective pathways Full roll out of triage for elective pathways Reduced levels of outpatient follow up activity commissioned Urgent and crisis care pathways rationalised Paramedics attached to localities Individual patient experience tracking to begin Penalties in place for inappropriate readmissions Consultation on new contract methodology completed Services that do not demonstrate value added outcome improvements decommissioned New contract methodology in place, dependent upon ACO development New tariffs in place All proposed MCP services identified MCP commissioned to include services shown in Appendix 3 New service specifications in place for these services. New primary medical services contract in place Mitigations built into 2016/17 contracts Shared outcome objectives for core MDT services, diabetes and respiratory in place Renewal of MDT link workers all MDT staff to be responsible for same population MDT extended Potential open access to some services New care home contract in place Capitation based contract at MDT/MCP levels with associated objectives End to end frail elderly pathway commissioned as part of MCP Shared outcome objectives for all MCP services Single patient portal operational 14.0 Provider Event 14.1 We will be holding an event for all providers to discuss the implications of these intentions in more detail on Thursday 19 th November, in Brierley Hill Civic Hall, commencing at 12.30p.m. You can register your interest by ing Fiona.jolly@dudleyccg.nhs.uk 14.2 A separate summit for our main providers and partners will take place, subject to final confirmation, on 30 November P a g e

26 Appendix 1 1 P a g e
27 2 P a g e
28 3 P a g e
29 4 P a g e
30 5 P a g e
31 Appendix 2 Shared Outcome Objectives for Continuity Services Generic Prevention Indicators G1 G2 Indicator Target Primary care Specialities to be Threshold aligned All people coded with a LTC to receive a holistic N/A 85-95% Diabetes / Stroke / comprehensive assessment on at least an annual basis Respiratory / Renal including medication review using the recommended / Cardiology/ CCG template (bi-annual if patient has diabetes or Mental Health / COPD) Neurology / Rheumatology / All people coded with a LTC to have a named clinician N/A 85 95% N/A who is the main key co-ordinator responsible for their care related to their condition/s Secondary care Threshold Care plan to be undertaken and shared with GP 85-95% G3 All people coded with a LTC to receive an care plan which has been co-developed with the patient and details individual personal goals which are reviewed on an at least an annual basis N/A 85 95% See G1 G4 All people coded with a LTC to have a physical activity assessment in the last 12 months and if appropriate are referred to a physical activity support programme N/A 70 90% Diabetes / Stroke / Respiratory / Cardiology/ Mental Health / Neurology / Rheumatology / 70 90% Information to be shared with GP G5 All people coded with a LTC to have a blood pressure 140/ % Diabetes / stroke / 50 70% taken at least 2 readings 6 months apart within the last /80 (diabetes 40 55% Respiratory / Renal 40 55% months and CKD) / Cardiology/ Mental Health / Neurology / Rheumatology / G6 All people coded with a LTC to have screen for depression on an annual basis using the 2Q depression score N/A 85 95% Diabetes / stroke / Respiratory / Renal / Cardiology/ Mental Health / 85 95%
32 G7 All people coded with a LTC to receive the appropriate vaccinations in the last 12 months (influenza, pneumococcal, shingles ) Rheumatology / Gastroentology N/A 70 95% N/A G8 G9 G10 All people coded with a LTC to have a documented assessment of smoking status in the last 12 months and if appropriate referral to smoking cessation services All people coded with a LTC to have a documented BMI at the time of annual review and if >30 (>28 in ethnic minority patients) to receive appropriate referral to weight management services All people coded with a LTC to have a fasting cholesterol taken in the last 12 months and treated to target G11 All people coded with a LTC will have an alcohol / substance misuse screen using AUDIT C at their annual review G12 All people coded with a LTC are offered referral to the self-management programme and/or structured education programmes where appropriate at their annual review N/A 60-90% Diabetes / stroke / Respiratory / Renal / Cardiology/ Mental Health / Neurology / Rheumatology / N/A 70-90% Diabetes / stroke / Respiratory / Renal / Cardiology/ Mental Health / Neurology / Rheumatology / <4 mmol/l 40 60% Diabetes / stroke / Respiratory / Renal / Cardiology/ Mental Health / Neurology / Rheumatology / N/A 85 95% Diabetes / stroke / Respiratory / Renal / Cardiology/ Mental Health / Neurology / Rheumatology / N/A 85 95% 60-90% Information to be shared with GP 70-90% Information to be shared with GP 40 60% Information to be shared with GP 85 95% Information to be shared with GP
33 Atrial Fibrillation AF1 Indicator Target Primary Care Specialities to be Secondary Care Threshold aligned Threshold The percentage of patients with atrial fibrillation in whom N/A 60-80% Cardiology / stroke 60-80% stroke risk has been assessed using the CHA2DS2- VASc score risk stratification scoring system and bleeding risk assessed using the HASBLED risk assessment in the last 12 months AF2 In those patients with atrial fibrillation with a record of a CHA2DS2-VASc score of 2 or more, the percentage of patients who are currently treated with anticoagulation drug therapy N/A 60 80% Cardiology / stroke 60 80% Vascular Conditions (to include Coronary heart disease, Stroke/TIA and Peripheral artery disease) VAS1 Indicator Target Primary Care Specialities to be Threshold aligned The percentage of patients record with Vascular disease N/A 50-95% Cardiology / stroke (CHD/Stroke(non-haemorrhagic)/TIA/ PAD) with a record in / vascular the previous 12 months that either an antiplatelet agent (PAD) or an anticoagulant has been taken Secondary Care Threshold 50-95% VAS2 In those patients with Vascular disease the percentage who have been offered and referred to a Cardiovascular rehabilitation programme N/A 40 60% Cardiology / stroke / vascular 50-95%
34 Heart Failure HF1 Indicator Target Primary Care Specialities to be Secondary Care Threshold aligned Threshold In those patients with a current diagnosis of heart failure N/A 45-70% Cardiology 45-70% due to left ventricular systolic dysfunction who are currently treated with an ACE-I or ARB, the percentage of patients who are additionally currently treated with a beta-blocker licensed for heart failure and whose medication is optimised Diabetes DM1 Indicator Target Threshold Specialities to be aligned The percentage of patients with a diagnosis of 75mmol/mol or less 60-92% Diabetes diabetes in whom the last IFCC-HbA1c is 64 mmol/mol has been measured and recorded in the 64mmol/mol or less 50 83% preceding 12 months 59mmol/mol or less 45 75% Secondary Care Threshold 60-80% achievement 40 60% achievement Service Users without complications expected 90% discharge rate DM2 DM3 The percentage of patients with a diagnosis of diabetes with a record of a foot examination and risk classification documented and an assessment for neuropathy in the last 12 months The percentage of patients with a diagnosis of diabetes with a record of recieving advice for attendance for retinopathy screening and urinary albumin creatine ratio testing N/A 55 90% N/A N/A 50 90% N/A
35 Asthma AST1 Indicator Target Primary Care Specialities to be Secondary Care Threshold The percentage of patients with a diagnosis of asthma N/A 50 75% aligned Respiratory Threshold 50 75% who have had an asthma review in the preceding 12 months that includes an assessment of asthma control using the 3 RCP and has documented asthma control targets Chronic obstructive pulmonary disease (COPD) Indicator Target Primary Care Specialities to be Secondary Care Threshold aligned Threshold COPD1 The percentage of patients with COPD in whom the N/A 50 85% Respiratory 50 85% diagnosis has been confirmed by post bronchodilator assessment COPD2 The percentage of patients with COPD who have had a breathlessness assessment and documented score using MRC / CAT in the last 12 months COPD3 The percentage of patients with COPD with a record of FEV1 and oxygen saturation in the last 12 months COPD4 The percentage of patients with COPD who are offered and referred to pulmonary rehabilitation services N/A 50 90% Respiratory 50 90% N/A 40 90% Respiratory 40 90% N/A 40 90% Respiratory 40 90% Depression DEP1 Indicator Target Primary Care Specialities to be Threshold aligned The percentage of patients with a 2Q depression N/A 85 95% N/A score 3 or more who have an assessment for depression using the PHQ-9 and anxiety using GAD-7
36 DEP2 DEP3 The percentage of patients with a diagnosis of depression who have received a risk assessment and appropriate treatment in accordance with steppedcare model The percentage of patients with a diagnosis of depression who have received the appropriate evidence based interventions N/A 85 95% Mental Health 85 95% N/A 85-95% Mental Health 85 95% Mental Health MH1 Indicator Target Primary Care Threshold Specialities to be aligned Secondary Care Threshold The percentage of patients with a diagnosis of mental N/A 85 95% Mental Health The percentage of health (schizophrenia, bipolar affective disorder and patients with a other psychoses) who have a Cardiovascular disease diagnosis of risk assessment mental health (schizophrenia, bipolar affective disorder and other psychoses) who are under inpatient care who have a Cardiovascular disease risk assessment Cancer CAN1 Indicator Target Primary Care Threshold Specialities to be aligned The percentage of patients with a lifetime diagnosis N/A 50 80% N/A cancer who have been offered and received a comprehensive cancer care plan review in the last 12 months Secondary Care Threshold
37 Chronic Kidney Disease / Acute Kidney Injury CKD1 Indicator Target Primary Care Threshold Specialities to be aligned Secondary Care Threshold The percentage of patients on the CKD whose have a N/A 50 80% Renal 50 80% record of a urine albumin:creatinie ratio (or protein:creatinine ratio) test in the preceding 12 months and who are appropriately treated with and ACE-1 or ARB CKD2 Refer a patient for a specialist assessment with a sustained decrease in egfr of 25% or more, and a change in egfr category or sustained decrease in agfr of 15 ml/min/1.73 m 2 or more within 12 months N/A % Urology / cardiology / Diabetes / stroke / elderly care % AKI 1 Regular review of egfr and creatinine as clinically appropriate, and refer urgently when a rise in serum creatinine of 26 micromol/l or greater within 48 hours or a 50% or greater rise in serum creatinine known or presumed to have occurred within the past 7 days N/A 50 80% Urology / cardiology / diabetes/ stroke / elderly care 50 80%

38 Appendix 3
39
40
41
42
43
Service Scope and Service Model. for Multi-Specialty Community. Provider. Document 12
 Service Scope and Service Model for Multi-Specialty Community Provider Document 12 A. Introduction... 3 B. Process... 3 C. Engagement... 3 D. Service Scope Summary... 4 E. How the Scope of Services Comes
Service Scope and Service Model for Multi-Specialty Community Provider Document 12 A. Introduction... 3 B. Process... 3 C. Engagement... 3 D. Service Scope Summary... 4 E. How the Scope of Services Comes
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
England. Questions and Answers. Draft Integrated Care Provider (ICP) Contract - consultation package
 Contract - consultation package") England Questions and Answers Draft Integrated Care Provider (ICP) Contract - consultation package August 2018 Questions and Answers Draft Integrated Care Provider (ICP) Contract - consultation package
England Questions and Answers Draft Integrated Care Provider (ICP) Contract - consultation package August 2018 Questions and Answers Draft Integrated Care Provider (ICP) Contract - consultation package
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Dudley Clinical Commissioning Group. Commissioning Intentions Black Country Partnerships NHS Foundation Trust
 Appendix 3 Dudley Clinical Commissioning Group Commissioning Intentions Black Country Partnerships NHS Foundation Trust 2013/2014 1 Strategy and Context Our Commissioning Intentions indicate to our current
Appendix 3 Dudley Clinical Commissioning Group Commissioning Intentions Black Country Partnerships NHS Foundation Trust 2013/2014 1 Strategy and Context Our Commissioning Intentions indicate to our current
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby
 STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby http://nhsbetterhealth.org.uk/wp-content/uploads/2016/11/stp-draft-plan-on-page- Final-1.pdf The STP Process Q1. Version Control:
STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby http://nhsbetterhealth.org.uk/wp-content/uploads/2016/11/stp-draft-plan-on-page- Final-1.pdf The STP Process Q1. Version Control:
Any Qualified Provider: your questions answered
 Any Qualified Provider: your questions answered September 8, 2011 These answers cover a range of questions about the detail of Any Qualified Provider on integrated care, competition and procurement, liability
Any Qualified Provider: your questions answered September 8, 2011 These answers cover a range of questions about the detail of Any Qualified Provider on integrated care, competition and procurement, liability
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
Westminster Partnership Board for Health and Care. 17 January pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Dudley Multi-specialty Community Provider Delivering a whole population budget via a single provider
 Dudley Multi-specialty Community Provider Delivering a whole population budget via a single provider Mr Paul Maubach Chief Executive Officer Dudley Clinical Commissioning Group Timeline for MCP procurement
Dudley Multi-specialty Community Provider Delivering a whole population budget via a single provider Mr Paul Maubach Chief Executive Officer Dudley Clinical Commissioning Group Timeline for MCP procurement
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
NHS Providers Strategy Directors Network meeting Five Year Forward View and Vanguards - Birmingham Community Healthcare NHS Trust our story
 NHS Providers Strategy Directors Network meeting Five Year Forward View and Vanguards - Birmingham Community Healthcare NHS Trust our story Lorraine Thomas Director of Business and Organisational Development
NHS Providers Strategy Directors Network meeting Five Year Forward View and Vanguards - Birmingham Community Healthcare NHS Trust our story Lorraine Thomas Director of Business and Organisational Development
Update on NHS Central London CCG QIPP schemes
 Update on NHS Central London CCG QIPP schemes NHS Central London CCG has identified circa 11m for QIPP during 2013/14. Commissioning Intentions approved by the governing body included transformational
Update on NHS Central London CCG QIPP schemes NHS Central London CCG has identified circa 11m for QIPP during 2013/14. Commissioning Intentions approved by the governing body included transformational
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014
 Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
Healthy Wirral Vanguard New Care Model Value Proposition th February 2016
 Healthy Wirral Vanguard New Care Model Value Proposition 2016-17 8 th February 2016 1 Contents Section Page(s) Introduction and Strategic context Page 3 High level Programme Overview Page 4 Enablers: Cross
Healthy Wirral Vanguard New Care Model Value Proposition 2016-17 8 th February 2016 1 Contents Section Page(s) Introduction and Strategic context Page 3 High level Programme Overview Page 4 Enablers: Cross
THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS
 THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS ICCHNR SYMPOSIUM University of Kent at Canterbury 15 th -16 th September 2016 Dr John M Ribchester GP Chair and Clinical Lead for Encompass MCP
THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS ICCHNR SYMPOSIUM University of Kent at Canterbury 15 th -16 th September 2016 Dr John M Ribchester GP Chair and Clinical Lead for Encompass MCP
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme. Frequently Asked Questions Second Edition
 Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Integrating care: contracting for accountable models NHS England
 New care models Integrating care: contracting for accountable models NHS England Accountable Care Organisation (ACO) Contract package - supporting document Our values: clinical engagement, patient involvement,
New care models Integrating care: contracting for accountable models NHS England Accountable Care Organisation (ACO) Contract package - supporting document Our values: clinical engagement, patient involvement,
Prospectus for the Procurement and. Commissioning of a Multi-Specialty. Community Provider (MCP) Document P a g e
 Document P a g e") Prospectus for the Procurement and Commissioning of a Multi-Specialty Community Provider (MCP) Document 11 1 P a g e Dudley Clinical Commissioning Group Prospectus for the Procurement and Commissioning
Prospectus for the Procurement and Commissioning of a Multi-Specialty Community Provider (MCP) Document 11 1 P a g e Dudley Clinical Commissioning Group Prospectus for the Procurement and Commissioning
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL
 DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
5. Integrated Care Research and Learning
 5. Integrated Care Research and Learning 5.1 Introduction In outlining the overall policy underpinning the reform programme, Future Health emphasises important research and learning from the international
5. Integrated Care Research and Learning 5.1 Introduction In outlining the overall policy underpinning the reform programme, Future Health emphasises important research and learning from the international
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
BETTER CARE FUND UPDATE
 MEETING DATE: 13 February 2014 AGENDA ITEM NUMBER: Item 6.2 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire CCG REPORT TO THE CLINICAL COMMISSIONING GROUP
MEETING DATE: 13 February 2014 AGENDA ITEM NUMBER: Item 6.2 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire CCG REPORT TO THE CLINICAL COMMISSIONING GROUP
Halton. Local system review report Health and Wellbeing Board. Background and scope of the local system review. The review team
 Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
Mental Health Social Work: Community Support. Summary
 Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
Vanguard Programme: Acute Care Collaboration Value Proposition
 Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
IT Driving Efficiency or Efficiency Driving IT?
 IT Driving Efficiency or Efficiency Driving IT? Dr. Naresh Rati CEO, Modality Partnership Mr. Paul Kemp Head of IT, Modality Partnership Case for Change The current health and social care economy is facing
IT Driving Efficiency or Efficiency Driving IT? Dr. Naresh Rati CEO, Modality Partnership Mr. Paul Kemp Head of IT, Modality Partnership Case for Change The current health and social care economy is facing
Urgent Treatment Centres Principles and Standards
 Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
General Practice Commissioning Strategy Development
 General Practice Commissioning Strategy Development Katharine Denton (Wandsworth CCG) 3 December 2014 Version 5. 03.12.2014 1 1. Introduction Strong General Practice is at the heart of any high quality
General Practice Commissioning Strategy Development Katharine Denton (Wandsworth CCG) 3 December 2014 Version 5. 03.12.2014 1 1. Introduction Strong General Practice is at the heart of any high quality
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Meeting in Common of the Boards of NHS England and NHS Improvement. 1. This paper updates the NHS England and NHS Improvement Boards on:
 NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
The Integrated Support and Assurance Process (ISAP): guidance on assuring novel and complex contracts
: guidance on assuring novel and complex contracts") The Integrated Support and Assurance Process (ISAP): guidance on assuring novel and complex contracts Part A: Introduction Published by NHS England and NHS Improvement August 2017 First published: Friday
The Integrated Support and Assurance Process (ISAP): guidance on assuring novel and complex contracts Part A: Introduction Published by NHS England and NHS Improvement August 2017 First published: Friday
Draft Briefing Document. Procurement of a Partial Multi-specialty Community Provider Contract. What does it mean for GPs and Practices?
 Draft Briefing Document Procurement of a Partial Multi-specialty Community Provider Contract What does it mean for GPs and Practices? April 2017 Contents 1. Procuring a provider for community services
Draft Briefing Document Procurement of a Partial Multi-specialty Community Provider Contract What does it mean for GPs and Practices? April 2017 Contents 1. Procuring a provider for community services
This will activate and empower people to become more confident to manage their own health.
 Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
Memorandum of understanding for shadow Accountable Care Systems
 Since Previously Discussed by BLMK CEOs: Memorandum of understanding for shadow Accountable Care Systems Dear Richard, As described in Next Steps on the NHS Five Year Forward View, we intend to name a
Since Previously Discussed by BLMK CEOs: Memorandum of understanding for shadow Accountable Care Systems Dear Richard, As described in Next Steps on the NHS Five Year Forward View, we intend to name a
IOW Integrated Commissioning Intentions
 Introduction IOW Integrated Commissioning Intentions 2017-19 This year as part of the Sustainability and Transformation Plan (STP) development, commissioners and providers have been working collectively
Introduction IOW Integrated Commissioning Intentions 2017-19 This year as part of the Sustainability and Transformation Plan (STP) development, commissioners and providers have been working collectively
Prospectus for the Procurement and. Commissioning of a Multi-Specialty. Community Provider (MCP) 1 P age
 1 P age") Prospectus for the Procurement and Commissioning of a Multi-Specialty Community Provider (MCP) 1 P age Dudley Clinical Commissioning Group Prospectus for the Procurement and Commissioning of a Multi-Specialty
Prospectus for the Procurement and Commissioning of a Multi-Specialty Community Provider (MCP) 1 P age Dudley Clinical Commissioning Group Prospectus for the Procurement and Commissioning of a Multi-Specialty
Briefing: NIB Priority Domains
 Briefing: NIB Priority Domains Update on the Roadmaps June 2015 Following the publication of the Five Year Forward View and the Framework Personalised Health and Care 2020, the National Information Board
Briefing: NIB Priority Domains Update on the Roadmaps June 2015 Following the publication of the Five Year Forward View and the Framework Personalised Health and Care 2020, the National Information Board
DRAFT. Primary Care Networks Reference Guide: Draft pre-release
 Primary Care Networks Reference Guide: Draft pre-release This draft reference guide has been developed with input from a range of stakeholders to provide further information and guidance on what we mean
Primary Care Networks Reference Guide: Draft pre-release This draft reference guide has been developed with input from a range of stakeholders to provide further information and guidance on what we mean
TAMESIDE & GLOSSOP SYSTEM WIDE SELF CARE PROGRAMME
 Report to: HEALTH AND WELLBEING BOARD Date: 8 March 2018 Executive Member / Reporting Officer: Subject: Report Summary: Recommendations: Links to Health and Wellbeing Strategy: Policy Implications: Chris
Report to: HEALTH AND WELLBEING BOARD Date: 8 March 2018 Executive Member / Reporting Officer: Subject: Report Summary: Recommendations: Links to Health and Wellbeing Strategy: Policy Implications: Chris
Birmingham Solihull and the Black Country Area Team
 Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Guy s and St. Thomas Healthcare Alliance. Five-year strategy
 Guy s and St. Thomas Healthcare Alliance Five-year strategy 2018-2023 Contents Contents... 2 Strategic context... 3 The current environment... 3 National response... 3 The Guy s and St Thomas Healthcare
Guy s and St. Thomas Healthcare Alliance Five-year strategy 2018-2023 Contents Contents... 2 Strategic context... 3 The current environment... 3 National response... 3 The Guy s and St Thomas Healthcare
Greater Manchester Health and Social Care Strategic Partnership Board
 Greater Manchester Health and Social Care Strategic Partnership Board 7 Date: 13 October 2017 Subject: Report of: Greater Manchester Model for Urgent Primary Care Dr Tracey Vell, Associate Lead for Primary
Greater Manchester Health and Social Care Strategic Partnership Board 7 Date: 13 October 2017 Subject: Report of: Greater Manchester Model for Urgent Primary Care Dr Tracey Vell, Associate Lead for Primary
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Appendix 1: Integrated Urgent Care Service Update. 1. Purpose
 Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST EXECUTIVE REPORT - CURRENT ISSUES
 THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST EXECUTIVE REPORT - CURRENT ISSUES Agenda item A4(i) 1. Executive Team Particular attention is drawn to: i) Executive arrangements during the period
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST EXECUTIVE REPORT - CURRENT ISSUES Agenda item A4(i) 1. Executive Team Particular attention is drawn to: i) Executive arrangements during the period
A meeting of NHS Bromley CCG Governing Body 25 May 2017
 South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
London s Mental Health Discharge Top Tips. LONDON Urgent and Emergency Care Improvement Collaborative
 London s Mental Health Discharge Top Tips LONDON Urgent and Emergency Care Improvement Collaborative November 2017 1 Introduction These Top Tips commenced their journey at the Pan London Reducing delays
London s Mental Health Discharge Top Tips LONDON Urgent and Emergency Care Improvement Collaborative November 2017 1 Introduction These Top Tips commenced their journey at the Pan London Reducing delays
The Symphony Programme an example from the UK of integrated working between primary and secondary care. Jeremy Martin, Symphony Programme Director
 The Symphony Programme an example from the UK of integrated working between primary and secondary care Jeremy Martin, Symphony Programme Director About South Somerset 135,000 population, older age profile
The Symphony Programme an example from the UK of integrated working between primary and secondary care Jeremy Martin, Symphony Programme Director About South Somerset 135,000 population, older age profile
Report to the Board of Directors 2016/17
 Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Westminster Partnership Board for Health and Care. 21 February pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
NHS ENGLAND BOARD PAPER
 NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
NHS GRAMPIAN. Local Delivery Plan - Section 2 Elective Care
 NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD
 BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD") INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
Developing Plans for the Better Care Fund
 Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Dudley Clinical Commissioning Group Long Term Strategic Plan From: Dependency, Hierarchy and Modernism To: Autonomy, Networks and Mutualism
 Dudley Clinical Commissioning Group Long Term Strategic Plan 2014-2019 From: Dependency, Hierarchy and Modernism To: Autonomy, Networks and Mutualism CCG Strategic Commissioning Plan 1 P a g e Contents
Dudley Clinical Commissioning Group Long Term Strategic Plan 2014-2019 From: Dependency, Hierarchy and Modernism To: Autonomy, Networks and Mutualism CCG Strategic Commissioning Plan 1 P a g e Contents
The operating framework for. the NHS in England 2009/10. Background
 the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
Improving General Practice for the People of West Cheshire
 Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
The incentives framework for ACOs
 New care models The incentives framework for ACOs Accountable Care Organisation (ACO) Contract package - supporting document Our values: clinical engagement, patient involvement, local ownership, national
New care models The incentives framework for ACOs Accountable Care Organisation (ACO) Contract package - supporting document Our values: clinical engagement, patient involvement, local ownership, national
INCENTIVE SCHEMES & SERVICE LEVEL AGREEMENTS
 MAY 2007 INCENTIVE SCHEMES & SERVICE LEVEL AGREEMENTS Practice Based Commissioning North and South Essex Local Medical Committees CLARIFYING THE RELATIONSHIP BETWEEN PBC GROUPS AND PCTS AIMS The aim of
MAY 2007 INCENTIVE SCHEMES & SERVICE LEVEL AGREEMENTS Practice Based Commissioning North and South Essex Local Medical Committees CLARIFYING THE RELATIONSHIP BETWEEN PBC GROUPS AND PCTS AIMS The aim of
In this edition we will showcase the work of the development of a model for GP- Paediatric Hubs
 Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Information and technology for better care. Health and Social Care Information Centre Strategy
 Information and technology for better care Health and Social Care Information Centre Strategy 2015 2020 Information and technology for better care Information and technology for better care Health and
Information and technology for better care Health and Social Care Information Centre Strategy 2015 2020 Information and technology for better care Information and technology for better care Health and
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
04c. Clinical Standards included in the Strategic Outline Care part 1, published in December 216
 0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
GE1 Clinical Utilisation Review
 GE1 Clinical Utilisation Review Scheme Name QIPP Reference Eligible Providers GE1 Clinical Utilisation Review QIPP 16-17 S40-Commercial 17/18 QIPP reference to be added locally. This CQUIN is supported
GE1 Clinical Utilisation Review Scheme Name QIPP Reference Eligible Providers GE1 Clinical Utilisation Review QIPP 16-17 S40-Commercial 17/18 QIPP reference to be added locally. This CQUIN is supported
Shakeel Sabir Head of MERIT Vanguard
 MERIT Excellence, Resilience Innovation & Training Jointly developing Mental Health Service in the West Midlands Shakeel Sabir Head of MERIT Vanguard Background - New care models Multispecialty community
MERIT Excellence, Resilience Innovation & Training Jointly developing Mental Health Service in the West Midlands Shakeel Sabir Head of MERIT Vanguard Background - New care models Multispecialty community
Integrated Care in North Central London
 Integrated Care in North Central London 5 th July 2012 Sylvia Kennedy AD Strategy & Planning Strategic context Many of our frailest and sickest groups receive care in a fragmented and disorganised way
Integrated Care in North Central London 5 th July 2012 Sylvia Kennedy AD Strategy & Planning Strategic context Many of our frailest and sickest groups receive care in a fragmented and disorganised way
Council of Members. 20 January 2016
 Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
IUC and Vanguard. Greater Nottingham Integrated Urgent Care 1
 IUC and Vanguard The 2016/17 Vanguard funding has been confirmed at 1.3M This funding is to deliver the 8 elements of Integrated Urgent Care by March 2017 With careful management of funds we will be able
IUC and Vanguard The 2016/17 Vanguard funding has been confirmed at 1.3M This funding is to deliver the 8 elements of Integrated Urgent Care by March 2017 With careful management of funds we will be able
South Yorkshire & Bassetlaw Health and Care Working Together Partnership
 South Yorkshire & Bassetlaw Health and Care Working Together Partnership Memorandum of Understanding Agreement Final Draft June 2017 1 Title Drafting coordinator Target Audience Version V 0.3 Memorandum
South Yorkshire & Bassetlaw Health and Care Working Together Partnership Memorandum of Understanding Agreement Final Draft June 2017 1 Title Drafting coordinator Target Audience Version V 0.3 Memorandum
Marginal Rate Emergency Threshold. Executive Summary
 Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Kingston Primary Care commissioning strategy Kingston Medical Services
 Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Strategic Commissioning Plan for Primary Care: Hull Primary Care Blueprint
 APPENDIX 1: 1. Vision and context The vision for the Blueprint being proposed is consistent with the CCG s Hull 2020 Transformation Programme and the direction of travel and new models of care outlined
APPENDIX 1: 1. Vision and context The vision for the Blueprint being proposed is consistent with the CCG s Hull 2020 Transformation Programme and the direction of travel and new models of care outlined
Principles for Integrated Care
 Page 1 Principles for Integrated Care The lack of joined-up care is the biggest frustration for patients, service users and carers. Conversely, achieving integrated care would be the biggest contribution
Page 1 Principles for Integrated Care The lack of joined-up care is the biggest frustration for patients, service users and carers. Conversely, achieving integrated care would be the biggest contribution
Approve Ratify For Discussion For Information
 NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
Expression of Interest for the Co-commissioning of Primary Care Services STATEMENT FROM OUR CHAIRMAN AND CHIEF ACCOUNTABLE OFFICER
 Brierley Hill Health and Social Care Centre Venture Way Brierley Hill West Midlands DY5 1RU Tel: 01384 321763 Fax: 01384 322414 20 June 2014 Dudley Clinical Commissioning Group Expression of Interest for
Brierley Hill Health and Social Care Centre Venture Way Brierley Hill West Midlands DY5 1RU Tel: 01384 321763 Fax: 01384 322414 20 June 2014 Dudley Clinical Commissioning Group Expression of Interest for
The Board is asked to note the report and to support the delivery of the Operational Plan and associated work programmes during 2017/18 and 2018/19.
 Subject: Reason for briefing note: Responsible officer(s): Senior leader sponsor: Windsor, Ascot & Maidenhead CCG Operating Plan 2017-19 Refresh To present the WAM CCG Operating Plan Refresh information
Subject: Reason for briefing note: Responsible officer(s): Senior leader sponsor: Windsor, Ascot & Maidenhead CCG Operating Plan 2017-19 Refresh To present the WAM CCG Operating Plan Refresh information
Norfolk and Waveney STP. Meeting with East Suffolk Partnership 27 September 2017
 Norfolk and Waveney STP Meeting with East Suffolk Partnership 27 September 2017 2 The Norfolk and Waveney STP Members Waveney District Council Focus of Norfolk and Waveney STP Our plan is in line with
Norfolk and Waveney STP Meeting with East Suffolk Partnership 27 September 2017 2 The Norfolk and Waveney STP Members Waveney District Council Focus of Norfolk and Waveney STP Our plan is in line with
OPERATIONAL PLANNING & CONTRACTING PLANNING GUIDANCE ON THE DAY BRIEFING
 22 September Month 2016 2017-2019 OPERATIONAL PLANNING & CONTRACTING PLANNING GUIDANCE ON THE DAY BRIEFING Today the national bodies NHS England (NHSE) and NHS Improvement (NHSI) have published their planning
22 September Month 2016 2017-2019 OPERATIONAL PLANNING & CONTRACTING PLANNING GUIDANCE ON THE DAY BRIEFING Today the national bodies NHS England (NHSE) and NHS Improvement (NHSI) have published their planning
Haringey and Islington
 Haringey and Islington Wellbeing Partnership Who we are Thoughts on system leadership and on leading within complex systems Observations from our experience Recognising where we are seeing and showing
Haringey and Islington Wellbeing Partnership Who we are Thoughts on system leadership and on leading within complex systems Observations from our experience Recognising where we are seeing and showing
Delivering the Five Year Forward View Personalised Health and Care 2020
 Paper Ref: NIB 0607-006 Delivering the Five Year Forward View Personalised Health and Care 2020 INTRODUCTION The Five Year Forward View set out a clear direction for the NHS showing why change is needed
Paper Ref: NIB 0607-006 Delivering the Five Year Forward View Personalised Health and Care 2020 INTRODUCTION The Five Year Forward View set out a clear direction for the NHS showing why change is needed
Leicester, Leicestershire and Rutland s Sustainability & Transformation Plan (STP)
") Leicester, Leicestershire and Rutland s Sustainability & Transformation Plan (STP) UPDATE Toby Sanders, STP Lead 13 September, 2016 What is the STP? Health and care place based plan for Leicester, Leicestershire
Leicester, Leicestershire and Rutland s Sustainability & Transformation Plan (STP) UPDATE Toby Sanders, STP Lead 13 September, 2016 What is the STP? Health and care place based plan for Leicester, Leicestershire
INTEGRATION TRANSFORMATION FUND
 MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
Wolverhampton Clinical Commissioning Group 1
 Wolverhampton Clinical Commissioning Group 1 Introduction and Context In 2014, along with our partners, the CCG established our five year strategy for the Wolverhampton Health Economy. This set out our
Wolverhampton Clinical Commissioning Group 1 Introduction and Context In 2014, along with our partners, the CCG established our five year strategy for the Wolverhampton Health Economy. This set out our