Detailed business case proposal: A single integrated Triborough Community Independence Service (CIS)
|
|
|
- Wesley Anderson
- 5 years ago
- Views:
Transcription
1 Detailed business case proposal: A single integrated Triborough Community Independence Service (CIS) September 2014 Version 4.5 1
2 Amendment History Version Date Author Reason August 2014 Deborah Jenkins & PPL / PA Team Detailed Business case developed August 2014 PPL/ PA Team Updates and revisions following feedback and review August 2014 PPL / PA Team Final revisions prior to SRO update August 2014 PPL / PA Team Significant redraft following SRO feedback September 2014 PPL / PA Team Revisions following CCG executive feedback September 2014 PPL / PA Team Final revisions ahead of publication September 2014 PPL/ PA Team Minor edits September 2014 PPL/PA Team Updates following discussions with Liz Bruce and Daniel Elkeles and Senior teams September 2014 PPL/PA Team Minor edits Draft distribution list Name PPL / PA team Elizabeth Youard Robert Sainsbury James Cuthbert Daniel Elkeles Liz Bruce Clare Parker Jenny Platt Adele Yemm Rachel Wigley Louise Proctor Philippa Jones Matthew Bazeley Liz Bailey Role in BC production Co-producers / reviewers Circulation for first draft SRO for Group A Triborough BCF projects SRO for Group A Triborough BCF projects SRO for Group A Triborough BCF projects Chief Officer; CWHHE ASC Executive Director; Triborough ASC Chief Financial Officer and Deputy Chief Officer; CWHHE Deputy Out of Hospital Delivery Manager; HFCCG Project Manager, Out of Hospital Care; WLCCG Director of Finance; Triborough ASC Managing Director; WLCCG Managing Director; HFCCG Managing Director; CLCCG External reviewer 2
3 Contents Foreword...4 Executive Summary Introduction High level CIS outcomes Population needs Whole Systems context Opportunities for strategic alignment The Current Position Attributes of existing CIS services - Triborough Baseline spend Baseline current contractual arrangements with CIS providers Proposed Integrated CIS Service specification Gap analysis Activity Modelling and Financial Implications Introduction to the CIS financial and activity model The conceptual model Key findings Funding the new service Risk / reward proposed principles Conclusions from the financial and activity modelling Options Appraisal Discussion of options Recommended option Transition and implementation planning Next steps for commissioners Proposed governance and management arrangements Principles of engagement for commissioners Developing the CIS through incremental change Transition plans Risk management Conclusions and next steps Next steps Appendices Appendix A. Index of figures and tables Appendix B: List of key stakeholders Appendix C: Enablers for the core CIS components Appendix D: IT/ IG considerations Appendix E: Detailed gap analysis Appendix F: LOS reduction by CCG Appendix G: List of acronyms
4 Foreword The purpose of this document is to set out the proposed way forward for commissioners to jointly develop a single Community Independence Service (CIS) across the Triborough and to gain agreement to this from all 6 sovereign bodies. The CIS will deliver more rapid and responsive out of hospital care for people with acute needs which will be provided by health and social care teams working together in a coordinated way. This business case demonstrates the anticipated costs and benefits, phased over time, of the proposed CIS and outlines its implications, in particular, the further work required to make these new ways of working a reality in 2014/15 and in the next financial year 2015/16. The programme to develop a standardised CIS care pathway lies at the core of the Triborough Better Care Fund (BCF) plan. This plan was collaboratively developed across all 6 partner organisations in the Triborough at the beginning of The BCF is a national policy directive which seeks to create a pooled, multi-year fund to catalyse investment into integrated services across health and social care. The CIS initiative is the critical piece of whole system change which will enable and support the shift of activity from expensive acute settings into the community and is a tangible example of bringing better organised care and services as close as possible to people s homes. Following combined work between health and social care commissioners and wider system leaders, the Triborough BCF Plan achieved approval from all sovereign bodies and the 3 Health and Wellbeing boards in April 2014 and is currently ranked second nationally following an external assurance process in July As such, this gives us a strong platform from which to press ahead with the commissioning direction set out in this business case. This business case will be scrutinised and signed off by the following governance bodies, and hence these are the main audience for this business case: Health and Wellbeing Boards: Hammersmith and Fulham, Kensington and Chelsea and Westminster Clinical Commissioning Group Governing Bodies: Hammersmith and Fulham, West London and Central London CCGs Cabinets: London Borough of Hammersmith and Fulham, Royal Borough Kensington and Chelsea and Westminster City Council London Borough of Hammersmith and Fulham Policy and Accountability Committee and London Borough of Hammersmith and Fulham Business Board This business case is being recommended for agreement at this time because findings will be translated into commissioning and contracting intentions for 2015/16 which are published at the end of September Agreement to the recommendations within, will enable immediate consultation with existing health and social care providers on the most 4
5 effective way of bringing about the necessary operational and service transformation. This will also allow a period of 6 months during October 2014 to March 2015 for providers to prepare the workforce for new ways of working. These timescales will ensure that in April 2015 we start to reap the benefits of the new service, improving people s experiences of care and delivering system wide savings. Approval is sought for the direction of travel proposed; a single, integrated and standardised care pathway developed with providers over time. Sign off of the financial and costs and benefits approved will be through CCG Finance and Performance Committees and Local Authority Cabinets. Daniel Elkeles Chief Officer Central London, West London and Hammersmith & Fulham CCGs Liz Bruce Executive Director of Adult Social Care Triborough Local Authorities 5
6 [IMPORTANT: Please note that the financials presented in this document are near final and subject to a final Quality Assurance of the financial model v6.0 and subsequent scrutiny and review through the CCG Finance and Performance Committees and Local Authority Finance Committees. Please also note that in text and the financial tables, benefits are expressed as -, to denote a saving] Executive Summary This business case proposes the way forward to develop a Triborough Integrated Community Independence Service (CIS) which will integrate and enhance existing local models and delivery frameworks to achieve common and improved outcomes for the local population. The Community Independence Service (CIS) The Community Independence Service provides a range of functions including rapid response services to prevent people going into hospital and rehabilitation and reablement which enables people to regain their independence and remain in their own homes. The service is currently delivered by a multidisciplinary team of community nurses, social workers, occupational therapists, GPs, geriatricians, mental health workers, reablement officers and others. What is in scope? Figure A provides a simple visual of the proposed CIS model from the perspective of a person using the service. Summary descriptions of each of the core services can be found in Figure B. Figure A: Overview of CIS 6

7 Figure B: Descriptions of core services It is important to note that CIS is only one part of the intermediate care pathway. Intermediate care is a range of integrated services to promote faster recovery from illness, prevent unnecessary acute hospital and premature admission to long-term residential care, support timely discharge from hospital and maximise independent living. 1 What is out of scope? There are a number of other services and parts of the intermediate care pathway with key interfaces to the CIS to which this service will need access. These services may move into scope in a later phase of development if considered appropriate. Many of these form separate projects within the Group A (Integrated Services) and Group C (Integrated Commissioning) workstreams of the Better Care Fund (BCF) programme for Triborough. The services / functions which are out of scope are: All bedded care (including community neuro rehabilitation beds) Homecare Nursing Home and Residential Home care 7 day social work hospital discharge team 1 Source: DH; Intermediate Care Halfway Home,
8 Whilst the above services are out of the scope of this business case, all are being developed in detail elsewhere, and the ways in which CIS will work across the boundaries of each out of scope area has been taken into account. Relationship to wider services The design of the single integrated model for the CIS aims to achieve simplification in delivery and ensure that a person s journey is integrated with smooth and rapid flow of knowledge and safe clinical transfer between interfacing services. For example, professionals working in the homecare service could refer a person into the CIS if a potential crisis or reablement need is identified. Likewise, following an assessment of needs, the CIS may request equipment/ adaptations in a person s home to help keep their independence or refer them to bedded care for a short period of time. Homecare is the service that cares for people with less complex needs in their own home on a long-term basis, before, during and after any crisis that may see them undergo a period of reablement with CIS. It is expected that the combined effect of a single integrated CIS and a refreshed homecare provision with a reablement focus, hybrid health and social care working and smoother transition pathways, will reduce the use of residential and nursing home placements, as community services become better equipped to handle more complex cases in people s homes. The same design principles will equally apply across all the areas identified above as out of scope : inpatient bedded care, nursing and residential home care, 7 day social work hospital discharge team and homecare. There will be future opportunities for providers to discuss organisational development and where local roles such as care co-ordination and care navigation resources fit in. There is wide recognition of the importance of the GP in this model of care although this is not addressed directly in this case for change. Why is a single integrated CIS so important? There are a number of key strategic drivers in both the internal and external environment. Together these create a compelling case for change and present a unique opportunity to deliver a core component of out of hospital care in an innovative and integrated way. a) Population need The demographic pressures of an ageing population with increasingly longer term, complex care needs and the downward pressure on public finances have compounded and require urgent and innovative responses from the health and social care sector. There is a clear need for integration to support the shift in the centre of gravity away from treating people in expensive and often inappropriate acute settings and a move towards treatment and support for people in their own homes. A Needs Assessment analysis conducted by Triborough Public Health leads in July 2014 focused on intermediate care and identified that demographic change is likely to increase intermediate care need by around 40% over the next 20 years, as the number of older people and the number of people with long-term conditions (LTCs) increases. 8
9 b) Whole Systems context The Triborough Councils and CCGs are uniquely placed to be in the vanguard of health and social care integration nationally, not only due to the partnership amongst the Local Authorities and combined approach to commissioning, but also due to the multiple change programmes already in progress across North West London which are transforming and reshaping the local health and social care economy. The landscape is ripe for implementing initiatives such as the CIS. The sophistication and maturity with which commissioners and system leaders already work together under Whole Systems Integrated Care (WSIC) and the Health and Wellbeing Boards creates a powerful springboard for change. Across the Triborough health and social care environment, there is already a shared commitment that: people are enabled and supported to stay as healthy and as independent as possible for as long as possible people are supported to live in the most appropriate place according to their choice and needs and are able to maintain maximum control over their lives All of the major change programmes have consistent and complementary visions and are discussed in more detail in Section 1.3. Over the next 5 years their planned impacts include: improving access to primary care, joining up, standardising and improving processes for delivery of social care across Triborough, the reconfiguration of the acute sector and a combined and holistic approach to mental health commissioning. The BCF, which creates a pooled fund to catalyse integrated working, is entirely compatible with whole systems integrated care programme, both of which deliver tangible multidisciplinary and integrated services and teams focused on delivering benefits to distinct cohorts of the population. Current position and gap analysis Across the 3 Triborough areas the total current cost of those services defined as belonging to the CIS is 16.8 million. There are approximately 5000 referrals per year and there is a multidisciplinary workforce in place of c186 WTE. A strategic review of the 3 Triborough areas community independence services highlighted various inconsistencies in service management and delivery. Each borough has a very different starting point from which to change. 9

10 Figure C: CIS starting positions Further breakdown of service differentiation by Triborough area can be found in Section 2.1. In order to achieve the ambition of a single integrated CIS, these gaps must be closed and the journey for each borough will be different. We have assessed each borough in terms of how far existing services have to go to reach the parameters outlined in the single standardised and integrated service specification and provide a summary below. 2 Proposed solutions and a more detailed breakdown can be found in Section 6.2 and Appendix E. Triborough area HFCCG/ LBHF WLCCG/ RBKC Distance to travel Low Medium Explanation HFCCG/LBHF have the shortest distance to travel to meet requirements for 2015/16 delivery. The model in place broadly aligns to the proposed 2015/16 CIS specification, and plans are already in place for further development in line with the requirements set out in this business case. WLCCG/RBKC intermediate care model meets some of the requirements set out in the CIS specification, but still has distance to travel to meet all 2015/16 intentions. WLCCG/RBKC are listed as medium rather than low due to the current level of investment and contractual position in comparison to CLCCG/WCC which must overcome more complex contractual arrangements stated below. 2 It is important to highlight that the boundaries for CLCCG/WCC and WLCCG/ RBKC are not co-terminus. Analysis has found that 23% of the WCC activity sits within the WLCCG/ RBKC boundary. Therefore in Figure C below and throughout the document; when referencing WLCCG/ RBKC this also includes a proportion of the WCC population. This assumption has also been applied to the financial model and is reflected in the detailed assumptions log in Appendix D. 10
11 Triborough area CLCCG/ WCC Distance to travel High Explanation CLCCG/WCC has the furthest to travel to align their service model with that proposed for 2015/16. This is primarily because reablement care delivery is outsourced to Allied Healthcare and other spot purchased providers, which adds additional complexity to funding, contracting and delivery arrangements. It also means a significant volume of work is delivered by staff not directly part of and managed by the core CIS team. Figure D: Distance to travel by borough Specification for future CIS A single integrated service specification for the CIS starting in 2015/16 has been drawn up. This specification is for health and social care providers to work to one standard. The specification proposes an integrated, multidisciplinary model of care that includes: A Single Point of Referral (SPoR) and referral (triage) A rapid response multidisciplinary team (MDT) providing community care within 2 hours and for up to 5 days Non-bedded community rehabilitation, treating non-complex conditions in a community setting Integrated reablement with access to short term community beds between 6 and 12 weeks 7 day support to help people leave hospital This improved, integrated and standardised service aims to address an anticipated increase in demand for intermediate care services. It will create demand for care and support services in the community, especially home care and, for people with acute and complex needs. As a consequence, demand for residential care might increase where suitable alternative housing cannot be found. The lack of availability of appropriate housing for older people across the Triborough may therefore influence the delivery of intermediate care services in the home. This is being looked at more widely in Triborough through extra care housing provision and the SHSOP programme. The integrated CIS will improve the person s and practitioner s experience of communitybased care and drive improved quality and savings by treating people outside of the acute hospital setting. The services within scope are selected on the basis of evidence including needs analysis, local best practice and learning from innovation. More information on how best practice has been incorporated is available in the stakeholder summary report in Appendix B. Incorporated findings are consistent with the feedback from local end users and clinical and social care practitioners. This all points to the need to enhance these in scope areas, especially out of hours and over seven days. 11
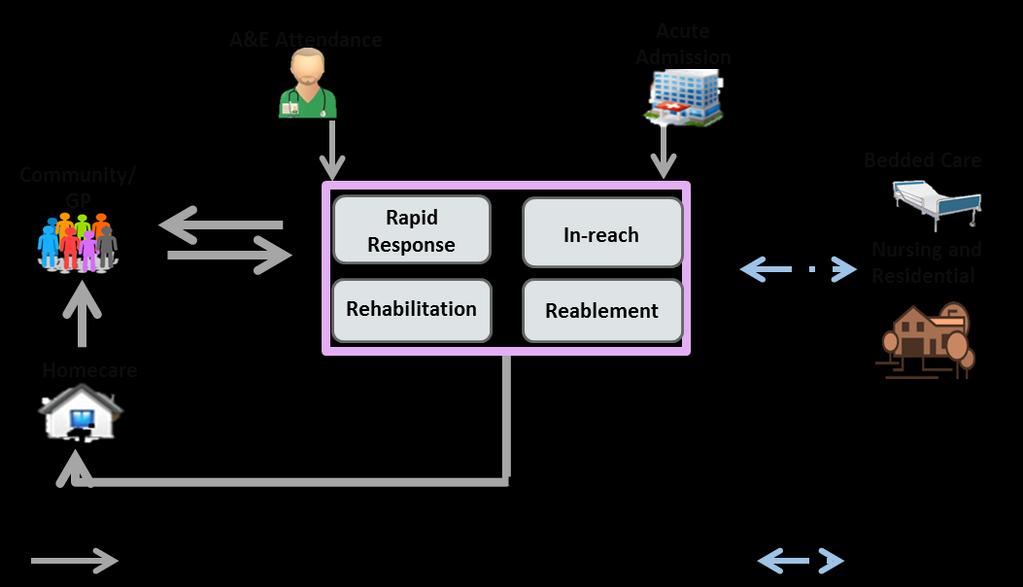
12 Significantly, this will mean the following differences from April 2015 onwards: Single entry point into the service which is clinically led Rapid access to reablement, including 2 hour rapid response Single assessment process Integrated multidisciplinary team working to a common set of standards Medical input across all three services Standardised hours for all functions 7 day working Single set of KPIs and outcomes monitoring framework Joint workforce and competency framework agreements established across each of the Triborough areas and providers Model and findings A financial model has been developed through engagement with CCG and LA leads working with key provider partners through existing consultation and engagement mechanisms such as the CCG / Local Authority centred whole systems integrated care (WSIC) consultation process and Triborough Urgent Care Board. It is built from evidence of what currently exists using data sources identified in Section 2. A detailed financial appraisal of the costs and benefits will be carried out by relevant leads from the CCGs and LAs immediately. The evidence base upon which this business case has been developed and the baseline based. It builds upon local clinical and social care practitioner experience and ambition. It creates a tool for a system which can be adapted for the future and form the basis for benefits tracking. Figure E1 below shows a simplified conceptual model for the person flows within different parts of the system. The core CIS service is shown in the purple box in the middle. The black arrows are the current people and financial flows which the model seeks to reduce. The grey arrows are those which the model seeks to increase, redirecting flows of both people and money away from expensive and inappropriate hospital and care homes and into the CIS to be supported and reabled in their own homes. The first pathway gives an example of a pathway without the CIS intervention and the second pathway gives an alternative flow. These pathway are described in more detail in Figure

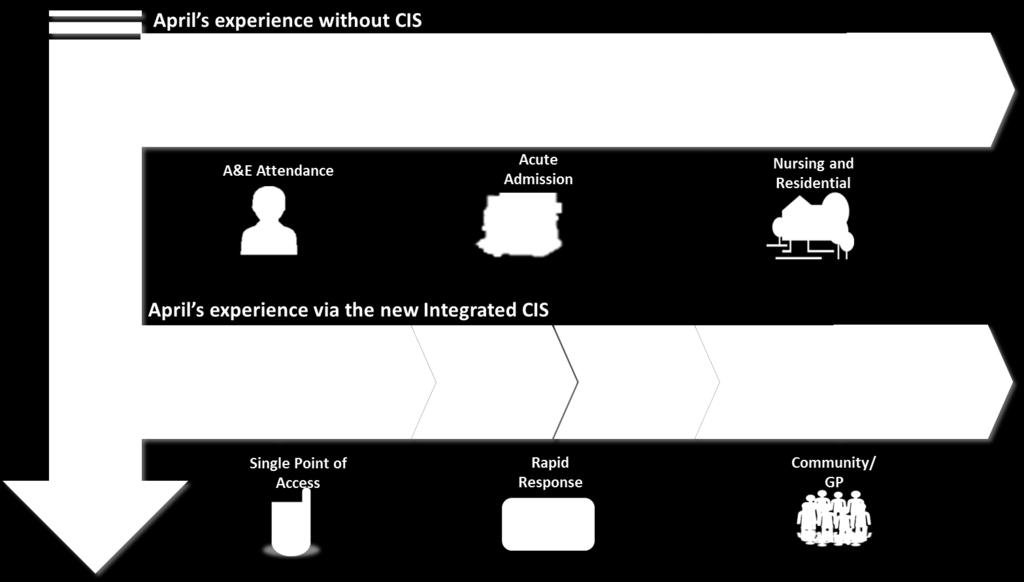
13 Figure E1: Simplified conceptual model Figure E2: The benefit of the new CIS 13
14 Financial results The current level of investment ( 16.8m p.a.) is not sufficient to maintain a stable service and meet the need of the local population as evidenced by the repeated bids for winter pressure funds each year to supplement the existing service. Undue reliance upon nonrecurrent funding is not sustainable and limits the ability of the providers to establish a stable workforce plan. Financial modelling of the new integrated service shows that new investment costs in 2015/16 year 1 of 7.4m and that benefits achieved are in the range of -9.8m. This gives us high level net benefits of -2.4m in 2015/16. The detail is to be scrutinised within existing LA and CCG process, for example the CCG Finance and Performance Committees. Triborough Net Benefit Projections NET Benefits Year 1 Year 2 Year 3 Year / / / /19 Total Increase in Expenditure 7,463,015 12,661,367 16,067,751 17,540,517 Total Gross Benefits - 9,867,043-16,452,201-21,156,668-23,935,077 NET Benefits - 2,404,028-3,790,834-5,088,918-6,394,559 Figure F: Triborough Net Benefits The proposed funding arrangements are still to be determined. There are two possible options (or variations on the two) one in which there is a realistic sharing of the costs and benefits or alternatively, it is proposed that NHS commissioners fund all the incremental costs in getting CIS up to a consistent standard in 2015/16 and that this then forms part of wider considerations as part of BCF risk and reward discussions. In addition to commissioner net benefits of 17.7m in the first four years, hospital length of stay (LOS) reductions as a result of the CIS Inreach service are calculated to be 1.09m over the first 4 year period. These are excluded from the overall model as these benefits mostly accrue to the provider however, this clearly forms part of case that investment in CIS provides benefits to the wider health and social care economy and helps acute providers to achieve efficiencies. Triborough Inreach LOS Reduction FY15/16 FY16/17 FY17/18 FY18/19 Projected in reach Referrals Total Days Saved Total Saving ( ) 168, , , ,495 Total Saving (FY15/16 to FY19/19) 1,092,173 Figure G: Triborough Inreach LOS reduction Options analysis 3 main options were considered for the delivery of the new CIS model from April 2015/16. Option 2 has two distinct variations 14
15 1) Do nothing: Continue with existing fragmented services 2) Single co-ordinated approach with existing providers: Continue with existing multiple providers, however standardise provision under one single specification and focus on integration & interoperability improvement initiatives. Package up the new investment in the service ( 7.4m) to use as a financial incentive to appoint a lead provider or, 2 lead providers. a. Single lead provider from within existing providers b. Alliance of two lead providers (one from health and one from social care) from within existing providers 3) Prime Contractor: Single provider working under a single service specification (potentially including TUPE d workforce) via a full procurement to the market These options are considered in detail in Section 5. For 2015/16, to ensure stability, it is proposed that the service continues to be delivered with multiple existing providers but through a single co-ordinated approach and specification. The recommended option is Option 2b: Single co-ordinated approach with existing providers, led by an alliance of two lead providers (one from health and one from social care). To enable transformational change without creating instability, the recommended approach for 2015/16 is to enter a year of transition during which a phased approach can be taken and incremental improvement brought about. The provider community is best placed to advise commissioners on the most effective way of bringing about operational and service transformation. It is planned that subject to agreement of this business case, that necessary 6 months of transition will start from end September Section 6 gives further details including high level risks. Implementation and transition There needs to be one clear framework upon which to build. It will be necessary to establish formal agreements between all commissioners and similarly, should Option 2b be approved a formal agreement between the two lead providers. There will need to be clear management and governance arrangements between all Local Authorities, CCGs and all existing health and social care providers contributing CIS services within Triborough in 2015/16. This arrangement needs to enable commissioners and providers to work together under a common framework. See section 6 for more details of the set of principles for engagement to which all commissioners must agree to work together. The way in which the investment offer is packaged up for existing health providers must be linked to an agreement which allows providers and commissioners to track impact and benefits. For the immediate future, the conclusions and recommendations from this business case will be translated into commissioning and contracting intentions for 2015/16. 15

16 The work over the next 6 months will prepare the ground, to allow providers the time to prepare for change, and commissioners time to translate the investment case into new contract agreements A high level transition plan and summary of required changes can be found in Section 6. Figure H: Transition Plan Summary The new CIS service will be integrated and multidisciplinary, provide proactive and reactive care and support to people at risk of admission to hospital and enable recovery. Through detailed and robust modelling, using an approach agreed across health and social care commissioners, we envisage that implementation can achieve gross financial benefits totalling - 9.8m 3 in 2015/16. Taking into account the investment costs of 7.4m, this delivers net benefits of - 2.4m in year 1. The new approach has been developed from existing ways of working and has system-wide consequences. That is why it is better to achieve simplification and standardisation, on a coordinated basis. If there is a particular reason or local condition to be met, the model can be used as the basis for adaptation to the local situation. A standardised service better meets the operational needs of acute providers who discharge people across all 3 Triborough areas and is a better experience for the individual people and carers. The new enhanced and integrated service will be much more empowering for people using services; bringing better organised care and services as close as possible to people s homes. That is why it is so important to achieve a co-ordinated agreement across 6 sovereign bodies to move forwards. 3 Note: Financial savings are represented as a negative number. Costs are represented as benefits. 16
17 We recommend the endorsement of this business case and Single co-ordinated approach with existing providers, led by an alliance of two lead providers (one from health and one from social care) to take forward this new CIS in 2015/16. 17
18 1. Introduction The purpose of this business case is to set out the case for the development of a Community Independence Service (CIS) across the Triborough. This document outlines the preferred commissioning approach for 2015/16 and makes the case for an expansion of CIS activity in subsequent years. The proposed CIS lies at the core of the Triborough Better Care Fund proposals which were developed in context of wider strategic plans agreed in and across each of the CCGs and the Local Authorities that constitute the Triborough. These 6 partner organisations agree that an integrated CIS will underpin the realisation of a number of strategic and operational goals, and provides an opportunity to: reduce the number of unnecessary admissions to hospital and residential and nursing care improve people s journey across secondary, primary and community services by offering integrated care in the community move care closer to home and ensure high quality care that is co-ordinated across the region and between providers and delivered in a range of community settings keep people independent and supported in their own homes for as long as possible As the work undertaken to develop this business case demonstrates, it is preferable that the single specification is delivered, at least initially, by existing delivery partners, who are able to develop their services during 2015/16, which will act as a transition year. This transition year will ensure that the development of an integrated CIS across the Triborough is well managed and reviewed regularly to ensure it achieves intended objectives and outcomes. Subject to the approval of this business case, commissioners will move forward with the proposals and will work with providers from September 2014 to March 2015 to implement service change. The CIS is at the heart of joined up working between health and social care and dealing with increasing volumes of people who have complex health and social care needs. Challenging financial and non-financial targets have been set for 2015/16 and beyond, emphasising the need for a swift and effective development of community services. This business case considers the development of 4 core CIS functions (i.e. Rapid Response, In Reach, Non-Bedded Rehabilitation and Reablement) and tests the following 4 hypotheses that CIS functions work more effectively within and across Triborough areas when it is: coordinated: the health and adult social care components are better co-ordinated integrated: the health and adult social care components are better integrated delivered over 7 days: available 7 days a week delivered at scale: services will work more effectively when both volume and activity and the breadth of service available are increased 18
19 This business case presents detailed activity and cost modelling and analysis of the trajectory for change within each authority and across the Triborough for 2015/16 and beyond. 1.1 High level CIS outcomes The service specification is being commissioned with the intention of improving the outcomes of people with above moderate levels of need. At a national level, the direction of travel is towards an outcomes based service. The shift to commissioning for outcomes recognises the need to move away from simply commissioning quantities of activity and to shift towards measuring desired outcomes, as defined by the people using the services. Regardless of whether a formal outcomes-based contract is designed, clear outcomes should form the basis for commissioning decisions in order to meet the needs of the local population. The NHS Outcomes Framework 4 contains a number of indicators, selected to provide a balanced coverage of NHS activity. The Adult Social Care Outcomes Framework 5 has a clear focus on promoting people s quality of life and experience of care, and on the provision of care and support that is both personalised and preventative. Following stakeholder engagement at a workshop of senior health and social care commissioners and providers in October 2013, a set of high level outcomes for the Triborough CIS model have been identified, as shown in Figure 1.1 below. Please see Appendix B for more information on stakeholder engagement. a) To enable people to be as healthy and independent as possible maintaining / or regaining / or improving their quality of life and well being. b) To support people choice to live in the most appropriate place for them, according to their needs and to have control over their lives. c) To ensure that people s experiences are positive by ensuring the service is personalised and seamless within the system. d) To ensure that the treatment, care and support that is provided is right for the person s needs, in the right setting and respects their individuality and dignity. e) To increase integration and efficiencies across health and social care to ensure strategic investment of funds and resources to maximise value for money. Figure 1.1: Agreed high level outcomes for the Triborough CIS 4 Department of Health, 2013; 5 Department of Health, 2013; 19

20 These outcomes will produce benefits across the entire breadth of stakeholders including commissioners, providers, the people using services and the future CIS workforce. Work is in progress to create a set of KPIs to measure these outcomes and monitor performance of the CIS service across Triborough. Achievement of these outcomes will represent a positive change for the residents of Triborough and significant step along the path outlined by the strategic programmes in wider North West London. There is also a need to ensure that the proposed change is viable and sustainable for commissioners within Triborough. 1.2 Population needs National drivers The demographic pressures of an ageing population combined with budgetary pressures and increasing costs exacerbates an already challenging environment. At present, care is fragmented across the health and social care provision and the approach to managing longterm conditions is outdated. 6 Local population need for intermediate care Figure 1.2 illustrates that the pressures are faced not only the health and social care economy in Triborough, but also nationally. The intention for community care, of which the proposals for CIS form a part, is that resources will be made available to support the delivery of high quality care, with people in control of their care, within a viable and sustainable health and social care economy. Figure 1.2: Pressures and potential solutions for the local health and social care economy 7 6 Source: NHS England; A Call to Action, Source: Triborough ASC vision 20
21 In July 2014, an assessment of the population need for Intermediate Care in the Triborough was completed. It considered: What is the need for intermediate care services in the local population? Do existing services meet this need? How will need change over the next 20 years? The aims of intermediate care are to: help people avoid going into hospital unnecessarily help people be as independent as possible after a stay in hospital prevent people from having to move into a residential home until they really need to The report identified the following key findings: Intermediate care services are mainly (but not exclusively) used by older people. Based on data from Hammersmith & Fulham, three-quarters are 71+ and 92% are 56+. Demographic change is likely to mean that need for intermediate care will increase by around 40% over the next 20 years, as the number of older people and the number of people with long-term conditions increases. 1.3 Whole Systems context The proposed changes to CIS are not being developed in isolation. Rather, they are part of a radical overhaul to the way in which health and social care services are delivered in the Triborough and more widely in North West London. This section provides a brief overview of the national and local context of the transformation that is occurring across the entire health and social care economy, of which the proposed changes to the Triborough CIS is just a part. Across North West London, the removal of acute beds from the system is being offset by investment and new capacity in out of hospital care. There are a number of key transformational programmes in the Triborough (and wider North West London) which aim to improve the future health and wellbeing of c.600,000 people who live in Hammersmith & Fulham, Kensington & Chelsea and the City of Westminster including: Out of Hospital Strategies Adult Social Care Transformation (ASC Transformation) Whole Systems Integrated Care (WSIC) The Better Care Fund (BCF) Primary Care Transformation (PC Transformation) Mental Health Programme (MHP) There is strong alignment between the visions of all 6 programmes and all these initiatives focus on strengthening out of hospital care through bringing care closer to home. The overall objective is to work as a single team across health, adult social care, public health, housing, mental health, primary care, community care, hospital care and other allied services. 21
22 The existence of cross-cutting interlinked strategies means that: all stakeholders are already used to working together in partnership end users and providers have been working together through whole systems integrated care (WSIC) co-production by CCG / LA partnership through 2014 this approach together with the LA customer journey programme has informed the rationale and proposals for moving forward Strategic programmes in Triborough Triborough Adult Social Care Transformation Programme Whole Systems Integrated Care Vision and impacts Tri-borough Adult Social Care transformation programme is an overarching 3- year change programme that will: Help achieve savings of 45m over three years, Meet the increased demand for care services from an aging population and new Care Act Improve the experience of people by making services clearer and easier to use and more joined up. The programme focuses on aligning assessment and care management services within ASC to create a consistent core service offer and operating model; building more personalised community delivered care services that help people to be more independent; integrating social services with health, focusing on intermediate short-term care and care for people with disabilities and long-term health conditions. NW London WSIC programme aims to redesign models of care to make better use of the total available resource within the system to achieve effective and cost effective outcomes through implementation of integrated care models codesigned through multi-stakeholder collaboration. It involves 31 collaborating organisations across 8 boroughs and has been selected as one of 14 national pioneer networks. The programme stratifies the total NW London population into cohorts based on care need and service utilisation. Initial cohorts of particular interest are the over 75s and adults with long-term conditions (LTC). Better Care Fund 8 There are 10 early adopter sites in NW London; 4 within the Triborough area. National Policy initiative to create a pooled fund to develop integrated services across health and social care. 8 A proportion of the performance allocation (the local share of the national 1bn performance element of the 3.8bn fund) will be payable for delivery of a locally set target for reducing emergency admissions (they suggested at least 3.5% reduction). The balance of the allocation will be available upfront to spend on out of hospital NHS commissioned services, as agreed by the Health and Wellbeing Board. This provides greater assurance to the NHS and mitigates the risk of unplanned acute activity. If the target for reducing admissions is not met, a proportion of the 1bn funding will remain with the NHS and not transfer to the BCF for joint use. The reduction in unplanned admissions indicator will be the only indicator underpinning the pay for performance element of the BCF. Hospital providers are being asked to confirm agreement with the proposed reduction in non-elective activity. 22
23 15 constituent programmes of which this CIS is a core part in supporting and enabling the shift of activity to out of hospital settings Primary Care Transformation Mental Health Programme The recent national changes to BCF have clarified that the pay for performance element is linked to successful reduction of Non-elective admissions. PMCF is a national scheme set up to test access to primary care; NW London is one of the largest of 20 pilot PMCF sites. The programme includes work to: (i) Extend access and continuity in the short term (by end of 2014/15) (ii) Support the development, and grow, GP networks that can hold contracts (in 2014/15 onwards) (iii) Put in place IT infrastructure, streamline appointment booking, broaden access and networked working. (iv) Provide the NWL workforce with training and education to deliver the new model of care. NWL recognises the importance of parity of esteem that is looking at people s wellbeing as a whole. This recognition of emotional and physical health needs is also recognised in the CIS planning. Figure 1.3: Strategic programmes in Triborough 1.4 Opportunities for strategic alignment There are a number of opportunities created by the above described strategic environment: To focus on a co-ordinated approach across health and social care that maximises the benefits of the single integrated care pathway from the point of view of those using services. This is entirely compatible with the whole systems approach to care planning for people with long-term conditions and complex needs To continue to ensure this work is fully embedded in whole systems design, owned and sighted by whole systems design clinical / social care leads that has been worked up with each area s key stakeholders. To make the most of working together to standardise through one single specification across Triborough where standardisation creates the best solution at scale, e.g. for mapping across acute sites such as Imperial or Chelsea and Westminster To design the best workforce solution that identifies the most confident clinical / social care leadership and care response possible to drive integrated multidisciplinary team working forward. This needs to focus on a co-ordinated, integrated competency framework for out of hospital care To incorporate best practice and learning into our work, and to make sure we re clear where and how this works. The process to date has referred to innovations in and outside London. Wherever relevant it has built on existing experience and depth of learning within Triborough of developing a Virtual Ward within HF. Lessons have been learnt from local best practice in Greenwich, Brent STARRS (Short-Term Assessment, Rehabilitation and Reablement Service model, Camden and the Local Government Association value cases as noted in Appendix B. 9 9 Sources for additional information:
24 2. The Current Position We are building upon a system and process already in development Commissioners across health and social care are building upon system wide learning from 2014/15 winter initiatives. This learning and associated planning has been extended to the CIS business case. This business case takes that knowledge and projects that forward into 2015/16. There is a natural stakeholder group and process already in place Triborough Urgent Care Board (UCB) and its local UCB subgroups working together on system capacity and pressures. This has created an identified need for a better process and standardisation through collective effort of commissioners and providers, health and social care, assessing what works and what is required. UCB system leads have followed an agreed system-wide process for selecting and prioritising initiatives which will improve capacity and ways of working. These initiatives are compatible with the long-term proposals for integration and standardisation through the application of the Triborough BCF and proposed integration and co-ordination of functions under the CIS. Providers have highlighted the need for better feedback across commissioners and providers about what capacity is available, what is working, and what needs improvement, for system-wide gain. This insight, together with the need for all parties to find ways of tracking and evaluating system changes, impact, and areas for development, create an opportunity for enhancing the 2015/16 CIS model should it be taken forward in transition planning. In summary, there is a great opportunity within whole system change for this initiative, which also works at scale. This is supported by the learnings derived from assessing the current position which are described in the following sections. Assessment of the baseline. What is in existence already? Significant work has been undertaken to understand the attributes of existing CIS services in each Triborough area. In developing this business case, we have worked with commissioning managers from each CCG and social care leads to answer a number of key questions about existing CIS services in the Triborough area. Key information presented in the rest of this chapter is divided into 2 sections: Attributes of existing CIS services: this summarises the key features of existing CIS models, captured for each Tri-borough CIS service Baseline data: data on current activity and spend which acts as a baseline for the activity and cost modelling presented in Section 4 24


25 2.1 Attributes of existing CIS services - Triborough The 4 service components core to each CIS model are: Rapid Response In Reach/ Supported discharge Non-bedded intermediate care (Rehabilitation) Reablement Analysis There is significant variation in management structures, operational process, care delivery and staff roles and ways of working across the three existing CIS services. Figure 2.1 below highlights the key areas. Figure 2.1: CIS starting positions The extent to which CIS teams are already co-ordinated and integrated varies. At present, the Virtual Ward model in Hammersmith and Fulham is the most integrated with joint management posts and a S113 agreement 10 in place. In all models, providers currently have their own referral routes and undertake their own assessment; again there is collaboration between staff but further work would be required to streamline processes and integrate these functions. 10 Section 113 of the Local Government Act 1972 allows a local authority to enter into an agreement with another authority to place its officers at the disposal of the other authority, subject to consultation with the staff concerned and negotiation 25
26 The following diagrams (Figures 2.2, 2.3 and 2.4) set out the parameters of each Triborough areas service model to outline the different starting points for the journey of change to a single standardised service. Figure 2.5 draws on the data captured in the detailed baseline mapping and summarises the key features of each existing CIS service (as at July 2014). 26
27 Figure 2.2: RBKC/WLCCG as-is depiction 27
28 Figure 2.3: LBHF/HFCCG as-is depiction 28


29 Figure 2.4: WCC/CLCCG as-is depiction 29
30 As-is key attributes of existing Triborough CIS models RBKC/ WLCCG WCC/ CLCCG LBHF/ HFCCG Commissioning arrangement Core CIS services are commissioned separately by CCG and LA CIS services are commissioned separately by CCG and LA The CIS/Virtual Ward service is jointly commissioned by CCG and LA Core components Rapid Response, In Reach, Non-bedded Intermediate Care/Rehabilitation and Reablement Teams RBKC: Reablement: Advice, Information and Assessment (AIA) service; reablement care delivery teams CLCH: Rapid Response; In Reach; Nonbedded Intermediate Care/Rehabilitation. Additionality: GP Community Psychiatric Nurse WCC: Reablement: Access, Assessment; Care management CLCH: Rapid Response; In Reach; Non-bedded Intermediate Care/Rehabilitation Allied Healthcare/ spot purchased providers: Reablement Care delivery contracts with Allied Healthcare and spot purchased providers Additionality: Intermediate Mental Health and Physical Care team (IMPs) LBHF/ HFCCG: All core components now form part of the Virtual Ward. This is operationally managed as a single service under a jointly (CCG & LA) funded Head of CIS The Service Manager s team includes both health and social care staff as well as hybrid roles Additionality -Virtual Ward: Social Workers Health and Social Care Case Managers GP and Geriatrician Mental Health worker Referral routes Referrals come into the CIS from GPs, hospitals, social workers and other community-based staff, nursing and residential homes and through self-referral or referral by family, friends or carers. People using services are also identified by the In Reach team Referrals to Rapid Response come only from health and social care professionals who contact the RR Nurses directly on their mobile phones. 30
31 As-is key attributes of existing Triborough CIS models RBKC/ WLCCG WCC/ CLCCG LBHF/ HFCCG Access and triage RBKC Council Advice Line RBKC AIA team CLCH SPoR desk WCC Council Advice Line WCC Reablement access service WCC CIS OT care managers (assessment) CLCH SPoR CIS duty desk (all providers) Single team CLCH SPoR and LBHF CIS assessment LBHF Council Advice Line LBHF Community and hospital assessment service Assessment CLCH SPoR initial assessment and RBKC AIA initial assessment. Staff confer, most appropriate professional dispatched. RBKC AIA will undertake comprehensive assessment (as required) at the outset. This produces a holistic assessment and may result in referrals to services outside the core CIS (for example the Memory Clinic, Podiatry, Carers Assessments, Age UK) during the initial 6-week period. CLCH SPoR initial assessment and WCC initial assessment. Staff confer, most appropriate professional dispatched. Frameworki provides the WCC team with a structured process and CLCH have tried to align their initial assessment forms with this process.(see Appendix D for more information) Single team assessment (CLCH and LBHF staff). People are assigned to a virtual bed. This categorisation also reflects the services required. Red bed users are those at high risk of immediate (re)admission to hospital or those in need of rapid access nursing or rapid access therapy. Amber bed users are those requiring 6-12 weeks of support from the CIS/VW rehabilitation and reablement teams. Green bed users are those who can (re)enter core services. Duration of CIS service Standard service: 0 6 weeks People will exit the service before the end of the 6 week period if they have reached their goals. Standard service: 0 6 weeks People will exit the service before the end of the 6 week period if they have reached their goals. The CIS/VW is piloting a 12 week standard duration time in 14/15. 31
32 As-is key attributes of existing Triborough CIS models RBKC/ WLCCG WCC/ CLCCG LBHF/ HFCCG CLCH and RBKC use the 6 week period flexibly and if it is clear someone will achieve their goals in week 7 or 8, will work with them beyond the 6 week period. CLCH and WCC use the 6 week period flexibly and if it is clear someone will achieve their goals in week 7 or 8, will work with them beyond the 6 week period. Joint working Joint visits by health and social care staff are often undertaken. CLCH and RBKC use a common screening tool for first visits. Internal multidisciplinary meeting once a week to discuss people s care plans and goals. Delivery teams tend to deliver care separately, although CLCH staff will feed information back to the WCC Assessment and Care Management team. Co-location and joint management supports integrated working and the team work together to identify both health and social care needs. Figure 2.5: As-is key attributes of existing Triborough CIS models 32
33 2.2 Baseline spend The total baseline spend for the current CIS services across the Triborough is 16.8m. Commissioner Core CIS service line(s) Total spend core CIS service line HFCCG WLCCG CLCCG Rapid Response, In Reach, Rehabilitation 3,033,651 Contributions from reablement grant 571,000 Rapid Response, In Reach, Rehabilitation 3,736,668 Contributions from reablement grant 570,048 Rapid Response, In Reach, Rehabilitation 3,594,220 Contributions from reablement grant 667,254 LBHF Reablement 1,335,000 RBKC Reablement 1,691,000 WCC Reablement 1,644,022 TOTAL COST 16,842,863 Figure 2.6: Summary of CCG and Local Authority spend on CIS services (2013/14) 2.3 Baseline current contractual arrangements with CIS providers The baseline mapping captured information about current contractual arrangements for CIS services across the Triborough area. It is proposed that contract agreements are coordinated in the future, to simplify process and facilitate better tracking of cost and impact of investment. The information gathered to date is summarised in Figure 2.7. Commissioner Providers Service type Contract type Contract end date CLCH In Reach Block contract March 2015 Rapid Response Block contract March 2015 Nursing IC Therapy - (nonbed) Block contract March 2015 based LCW Rapid Response Fixed term contract Extension of contract to April 2015 CNWL Intermediate MH Fixed term contract Not known 33
34 Commissioner Providers Service type Contract type Contract end date WLCCG-RBKC RBKC Adult Social Care Reablement In-house RBKC staff Grant to March 2015 CLCH In Reach Block contract March 2015 HFCCG-LBHF Rapid Response Nursing IC Therapy - (nonbed) based S113 between community provider and LA social care Block contract S113 between community provider and LA social care Block contract S113 between community provider and LA social care WLMHT Intermediate MH Fixed term contract LBHF Reablement Adult Social Care In-house LBHF staff S113 between community provider and LA social care March 2015 March 2015 Pilot end date not known Grant to March 2015 CLCH In Reach Block contract March 2015 CLCCG-WCC WCC Adult Social Care Allied Health and spot purchased providers Rapid Response Nursing IC Therapy - (nonbed) based Reablement (assessment and care planning/ care management only) Reablement and reablement spot contracted care delivery Block contract March 2015 Block contract March 2015 In-house WCC staff Allied Healthcare 3 year contract, no automatic renewal, no contractual provision for Grant to March 15 Allied Healthcare expires May
35 Commissioner Providers Service type Contract type Contract end date extension beyond that date. Contract isn t exclusive. Spot purchasing of care when Allied Healthcare do not have resources to address need CNWL Intermediate MH Intermediate Mental and Physical Health team (IMPs) Not known Figure 2.7: Baseline mapping of contractual arrangements 2014/15 (captured July 14) 35
36 3. Proposed Integrated CIS Figure 3.1 shows a simple overview of the core CIS functions from the perspective of people who are using the services. Figure 3.1: Overview of CIS Relationship to wider services The specification for a single integrated model for CIS aims to achieve simplification in delivery and ensure that a person s journey is integrated with smooth and rapid flow of knowledge and safe clinical transfer between interfacing services. For example, professionals working in the homecare service could refer a person into the CIS if a potential crisis or reablement need is identified. Likewise, following an assessment of needs, the CIS may request equipment/ adaptations in a person s home to help keep their independence or refer them to bedded care for a short period of time. Homecare is the service that cares for people with less complex needs in their own home on a long-term basis, before, during and after any crisis that may see them undergo a period of reablement with CIS. It is expected that the combined effect of a single integrated CIS and a refreshed homecare provision with a reablement focus, hybrid health and social care working and smoother transition pathways will reduce the use of residential and nursing home placements, as community services become better equipped to handle more complex cases in people s homes. 36
37 The same design principles will equally apply across all the areas identified above as out of scope : inpatient bedded care, nursing and residential home care, 7 day social work hospital discharge team and homecare. There will be future opportunities for providers to discuss organisational development and where local roles such as care co-ordination and care navigation resources fit in. There is wide recognition of the importance of the GP in this model of care although this is not addressed directly in this case for change. What will be different in 2015/16? The following attributes will be different in 2015/16: Single entry point into the service which is clinically led Rapid access to reablement, including 2 hour rapid response Single assessment process Single, integrated multidisciplinary team working to a common set of standards Medical input across all three services Standardised hours for all functions 7 day working Single set of KPIs and outcomes monitoring framework Joint workforce and competency framework agreements established across each of the Triborough areas and providers Overall statement of vision and model of care The proposed integrated service will be delivered by single multidisciplinary team who will work together in a collaborative approach to ensure each person s pathway is seamless, reduces duplication of assessment and ensures the correct outcomes are achieved. Efforts and resources will be directed towards enabling services to work together, aligning incentives and measuring performance in ways that reward early intervention and prevention and in the long-term promoting sustained wellbeing for local people. There are 4 overall features to this model of care: 1. Intensive support to deliver care at home a service which provides immediate intensive support in a co-ordinated and comprehensive health and social care package, with the flexibility to enable people to move across service interfaces according to people s individual needs 2. Collaborative multidisciplinary working professionals will work in integrated multidisciplinary teams across health and social care with a case management function that closely involves GPs 3. Effective information sharing - promote collaborative working to reduce duplication, improve care coordination, planning and management. 4. Best use of workforce skills integrated team with a balanced and appropriate mix of medical, nursing, social care, therapy, mental health reablement workers and non-clinical members of the team to deliver intensive support at home provided 7 days a week 37

38 Who is the CIS for? Based on CWHH risk stratification data, it has been assumed that all of the moderate and high and approximately 30% of the very high risk cohorts would be eligible for care and support from the service. On this basis, the proposed Triborough CIS is aimed at a section of the population equating to approximately 70,000 people or 11.5% of the Triborough population however, only a small proportion of this population will need to use it within any given year and some may never use it. The positive impact and benefits of a Triborough service will however extend much wider than the immediate circle of people receiving care and support, to those people s carers, family, friends and the local community. The CIS will provide support and care for: Figure 3.2: CWHH risk stratification diagram a) People with long-term care requirements who need support to prevent crises or deterioration b) People who require support following discharge from hospital/ care homes c) People who need support to prevent (or delay) admission into hospital. d) People who want to regain their independence at home or in another community setting. e) People who require urgent care 38


39 The long-term vision for the service (as developed to date) includes the alignment of the 4 core CIS service components and the potential inclusion of local additionality. Homecare Equipment Core CIS Friends Step-up/ step-down Intermediate Care Carers Religious community Family Neighbours Rapid Response Neuro beds Reablement In-reach Care coordination Inner Core: Individual s informal network Outer Core: CIS network of services Supporting services: Coordinated to CIS Key interfaces: with wider health/ social care sector Other interfaces: with wider statutory services Figure 3.3: Picture of the integrated Triborough CIS Primary care services will be instrumental to ensuring that the CIS is a success. GPs will play a key role in case management and care planning alongside care co-ordinators in the CIS. This will deliver a number of benefits to both GPs and people using the service by providing a single point of contact to ensure consistency throughout the care pathway. 39
40 3.1 Service specification A high level summary of the service specification is given below in Figure 3.4 Specifications of the CIS core components Rapid Response In Reach Nonbedded IC/Rehab Reablement A multi-professional (medical, nursing and social care) Rapid Response service, operating 8am to 8pm; 7 days a week), that can provide face to face assessment at home within 2 hours of referral, support up to 5 days following referral and provide referrals to ongoing support. An integrated case finding and in reach service, operating 8am to 8pm; 7 days a week, with a presence in A&E. The Inreach service links to the wider urgent care system, community beds, care homes urgent care and out of hours services (including NHS 111). Provides proportionate assessment and referrals to ongoing support A delivery team, working as part of an integrated CIS (medical and social care), operating 8am to 8pm; 7 days a week, that provides time-bound rehabilitation (therapies) for referrals via the SPoR service by treating people with non-complex conditions in a community setting with the aim of goal attainment. Responds to all referrals within 24 hours and commencement of care within 72 hours A delivery team, working as part of an integrated CIS (medical and social care), that provides reablement services for referrals via the SPoR for people for up to 12 weeks (as required). Responds to all referrals within 24 hours and commencement of care within 72 hours. Includes specialist falls input within CIS timeframe (6-12 weeks over time). Where longer term care is required, includes links to additional reablement services including assistive technology provision such as telecare Figure 3.4: Specification of core CIS components 11 The transition year of 2015/16 will also ensure that 11 enablers for the service meet the requisite standards to support the 4 core areas (see Appendix C). 3.2 Gap analysis Using the current baseline in each Triborough area (as at July 2014) and understanding the proposed future model, it is possible to assess the quantum shift required in each Triborough area to reach a single standard specification. Figure 3.4 compares the current position of the CIS services with the position specified for the 2015/16 transition year. It is not reflective of the effectiveness of existing services in each area, but rather indicates the distance to travel to meet the service model outlined in the specification. 11 Note: This figure has been translated from the draft service specification as of August
41 Tri-borough area HFCCG/LBHF Distance to travel Low Explanation HFCCG/LBHF have the shortest distance to travel to meet requirements for 2015/16 delivery. The model in place broadly aligns to the proposed 2015/16 CIS specification, and plans are already in place for further development in line with the requirements set out in this business case. Proposed solutions/next steps HFCCG/LBHF will continue resourcing the Virtual Ward model recruitment of additional medical cover is underway. Work is underway to streamline and integrate the referral, triage and assessment process. Hybrid health and social care delivery roles are being developed. Work is underway to develop core and specialist CIS skills amongst team members. Joint management posts underpin the development of an integrated team. WLCCG/RBKC Medium WLCCG/RBKC intermediate care model meets some of the requirements set out in the CIS specification, but still has distance to travel to meet all 2015/16 intentions. WLCCG/RBKC are listed as medium rather than high due to their funding and contractual position in comparison to WCC/CLCCG as described below. WLCCG/RBKC will continue work to date to develop integrated ways of working within CIS. More work is required to align referral, triage and assessment processes to the requirements of the new specification. More work is needed to develop integrated working amongst delivery teams and to develop hybrid roles. Additional resource may be required to meet proposals for 2 hour response with multidisciplinary input. CLCCG/WCC High CLCCG/WCC has the furthest to travel to align their service model with that proposed for 2015/16. This is primarily because reablement care delivery is outsourced to Allied Health and other spot purchased providers, which adds additional complexity to funding, contracting and delivery arrangements. It also means a significant volume of work is delivered by staff not directly part of and managed by the core CIS team. Older Adults Support Team being recruited during 2014/15 which will provide 2.5 WTE consultants (1 WTE psycho-geriatrician) during 2014/15 and 3 WTE consultants by April 2015/16 to support the reactive and proactive care pathways as a core element of CIS service. CLCCG/WCC will prioritise the recruitment of medical cover and the integration of health and social care CIS team members. The development of a CIS Duty Desk for referral and triage led by a jointly funded CIS Lead will help facilitate change. The immediate focus for WCC/CLCCG will be the development of future plans for the outsourced reablement care delivery contract, which expires April Figure 3.5: High level gap analysis and transition plan 41
42 4. Activity Modelling and Financial Implications 4.1 Introduction to the CIS financial and activity model An initial review in September/October 2013 examined national and international best practice including strong evidence from other areas such as Greenwich, Northamptonshire and Greater Manchester. 12 During 2014, significant resource and effort has been spent developing a financial and activity model to inform decision making and support the case for new investment in the CIS in 2015/16 and beyond. The model estimates the financial costs and benefits of the new CIS service, incorporating links to and impacts on associated services (e.g. homecare, nursing and residential care home placements). It has been developed with significant involvement from CCGs and LAs. As activity shifts from a hospital setting into the community it is logical that extra pressures and costs will be created for those organisations who deliver care in the community setting including but not limited to; primary care, community health services, voluntary and third sector organisations and the local authority providing social care. Evidence from London Borough of Greenwich who implemented their integrated care team with similar service functions showed a saving of 900k on residential and nursing home placements and the number of people entering long-term social care reduced by 50% in the first year in addition to delivering significant non-elective admissions (NEL) to hospital. Inevitably, however there is likely to be an increased need for homecare packages over time and it is likely that as the model evolves and grows the level of complexity of people s care needs at home will increase. The balance of activities, costs and related risk share across health and social care commissioners will be the subject of a negotiation process as part of the BCF planning process and the financial model will inform the decision making process. The model has been co-designed with senior managers and built with the best possible available and most recent data sources from across health and social care. It has been developed through a structured process involving technical specialists and clinical input to verify the data and assumptions. However, it is a representation of reality and as with any model it has certain limitations and detailed assumptions are being recorded. There are 3 key things to understand about the model: The model adapted the approach and assumptions used in the HF Virtual Ward modelling. Drawing upon data provided by CCGs, the Local Authorities and providers working across Triborough and utilising a range of assumptions developed with senior managers, service leads and health and social care professionals we have developed a robust financial model. The savings in CIS are delivered by supporting people in the community rather than in hospital or in care homes. The financial assumption underpinning the CIS is that it is less expensive to support someone in the community and in their home and therefore, savings can be made by shifting activity from (more expensive) hospital and care homes to (less expensive) community-based settings. 12 Source: LGA Integrated Care Value cases; 42
43 The model is predicated on a NEL savings cap of 5% this is to ensure a challenging but realistic target for reduction of admissions but ensures that the provider is not destabilised in the process. There are 2 key parts to the model: 1) Conceptual model showing the flow of people (reference section below) 2) Detailed Excel spreadsheet (summary of findings provided in Section 4.3) The objective of the model is to provide more robust evidence for the BCF business case, and a more detailed platform to build upon for ongoing work (e.g. transition plans, cost and benefit monitoring / reporting). The financial model has confirmed that the new CIS service will deliver savings through shifting activity from (more expensive) hospital and care homes to (less expensive) community-based settings. The financial benefits are derived from the reduction in activity of the following: Non elective admissions (CCG benefit) ASC residential and nursing care home placements and LOS (LA benefit) A&E attendances (CCG benefit) Homecare hours for new clients with reablement support (LA benefit) LOS and DTOC (Acute providers benefit) Length of stay (LOS) savings and Delayed Transfers of Care (DTOCs) will accrue as benefits to the providers and will support the ability of the acute providers to deliver efficiency savings. We estimate these to be - 168k in year /16. Over the next four years the model estimates a total cumulative gain of 1.09m. Appendix F provides a breakdown of these figures by CCG. Estimated Triborough Inreach LOS Reduction 2015/ / / /19 Projected in reach Referrals Total Days Saved Total Saving ( ) - 168, , , ,495 Total Saving (FY15/16 to FY19/19) - 1,092,173 Figure 4.1: Estimated Triborough in reach LOS reduction The main drivers of expenditure are: Investment in workforce and skills (cost to CCGs and LA) Investment e.g. IT/IG and PMO change management (CCG cost) Ongoing delivery costs e.g. growth in homecare hours through avoiding care home demand through the CIS service (LA cost) CR/ CIS resource costs (CCG and LA cost) Intermediate care equipment (LA cost) 43

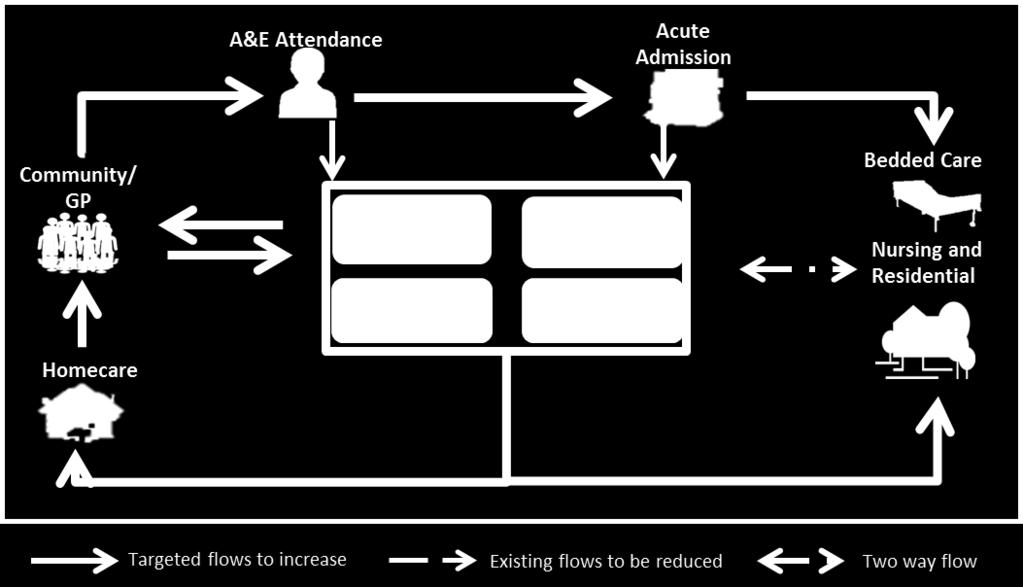
44 4.2 The conceptual model The Community Independence Service (CIS) lies at the heart of integrating care across health and social care. It is critical to enable the shift in the care of people requiring services from acute to community settings. It is both the largest source of investment and benefits (financial and non-financial) in the Triborough Better Care Fund (BCF) plan. We outline below the overall model for financial costs and benefits in the BCF plan. The conceptual model The conceptual model explains, visually, how the savings and costs will be generated based on the future flow of people across a number of interlinked services. It shows how benefits may be realised in acute and care home provision through crisis prevention, discharge support, homecare and reablement. Figure 4.2: Conceptual Model flow of people within the CIS system Within the conceptual model, the services within the purple box represent the core components of the CIS service: In reach/ supported discharge (through hospital discharge team) Rapid Response (RR) Intermediate care rehabilitation Intermediate care reablement The conceptual model also shows the services that will directly be impacted as a result of the new service, e.g. nursing care, residential care, acute admissions and homecare. These services will be included within the financial modelling to ensure all costs and benefits directly associated with CIS model are captured appropriately. 44

45 It highlights the existing flows of people that are to be reduced by the CIS service, represented by the black arrows. At a high level, the model shows that the CIS service will result in a reduction in care home placements and acute admissions, which in turn will increase the flow of people into the CIS and homecare as more people are treated in the community. The grey arrows indicate the targeted flows that will result in an increase in activity and costs. Working assumptions of conceptual model The following diagram shows the projected flows of people (based on the conceptual model) and the core assumptions underpinning this: Figure 4.3: Working assumptions of conceptual model Key assumptions The development of key assumptions is critical to the approach and methods underpinning the financial model. Activity was modelled through understanding the impact the CIS will have on the flow of people. The total number of projected referrals were modelled through drawing upon the HFCCG/LBHF Virtual Ward assumptions. Figure 4.4 identifies the high level assumptions. 45

46 Figure 4.4: High level assumptions The assumptions underpinning the financial model have been developed in line with the CCGs QIPP as their long-term financial plans and for LAs the mid-year financial planning process. 4.3 Key findings Financial modelling of the new integrated service shows that new investment costs in 2015/16 year 1 of 7.4m and that benefits achieved are - 9.8m. This gives us high level net benefits of - 2.4m in 2015/16. Triborough Net Benefit Projections NET Benefits Year 1 Year 2 Year 3 Year / / / /19 Total Increase in Expenditure 7,463,015 12,661,367 16,067,751 17,540,517 Total Gross Benefits - 9,867,043-16,452,201-21,156,668-23,935,077 NET Benefits - 2,404,028-3,790,834-5,088,918-6,394,559 Figure 4.5: Triborough Net Benefits A breakdown by Borough and CCG will be provided once the v6.0 of the financial model has been quality assured and signed off. 46
47 4.4 Funding the new service There are a range of scenarios under which the costs and benefits may be shared across health and social care commissioners. The options below represent the upper and lower ranges for subsequent discussion and agreement to fund the new service. One scenario is based upon a realistic sharing of both the costs and benefits and the second scenario is that NHS commissioners fund all the incremental costs in getting CIS up to a consistent standard in 2015/16. There are also a range of possibilities between these upper and lower ranges. Depending on what is subsequently agreed and negotiated the associated risk and reward solutions will be different. This also then forms part of wider considerations as part of BCF risk and reward discussions. Once the business case has been approved, as part of the immediate next steps, risk and reward discussions will be held between all associated commissioners. Year 1 Year 2 Year 3 Year 4 Option 1 - realistic sharing Gross CCG cost (+) CCG 4,909,835 8,733,956 11,079,012 11,468,781 Gross CCG benefit (-) CCGB -6,219,878-10,963,903-14,394,481-15,773,106 Net cost / benefit -1,310,043-2,229,947-3,315,469-4,304,325 Gross LA cost (+) LA 2,553,179 3,927,411 4,988,738 6,071,736 Gross CCG benefit (-) LAB -3,647,165-5,488,298-6,762,187-8,161,970 Net cost / benefit -1,093,985-1,560,887-1,773,449-2,090,234 Option 2 - health funds service costs Gross CCG cost (+) CCG 7,463,015 12,661,367 16,067,751 17,540,517 Gross CCG benefit (-) CCGB -6,219,878-10,963,903-14,394,481-15,773,106 Net cost / benefit 1,243,136 1,697,464 1,673,270 1,767,411 Gross LA cost (+) LA Gross CCG benefit (-) LAB -3,647,165-5,488,298-6,762,187-8,161,970 Net cost / benefit -3,647,165-5,488,298-6,762,187-8,161,970 TOTAL INCREASE IN EXPENDITURE 7,463,015 12,661,367 16,067,751 17,540,517 TOTAL INCREASE IN BENEFITS -9,867,043-16,452,201-21,156,668-23,935,077 NET BENEFITS -2,404,028-3,790,834-5,088,918-6,394,559 Figure 4.6 Funding Options 47
48 4.5 Risk / reward proposed principles Depending upon the funding option chosen the risk /reward principles will differ. If option 1 realistic sharing is chosen then the starting point for further discussions as proposed by Adult Social Care Commissioners are the following: Beyond the principles of fairness and transparency that should accompany any risk-sharing arrangement, the agreement should: 1) Compensate a commissioner that does not get intrinsic benefit from their investment in CIS (In this case, intrinsic benefit means "a saving from their own budget" in ASC's case, the budgets for long-term care services) 2) Provide an incentive not just reimbursement. (Compensation must pay for more than the difference between investment and return. i.e. the payment must cover the risk and the opportunity-cost of undertaking this initiative in favour of other alternatives) 3) Pay for all work that reduces activity, whether or not the activity is taken as cash savings 4) Commit to a monitoring framework that can spot problems with costs and returns quickly and reliably 5) Give clear conditions for withdrawal if losses are unacceptable (The agreement should be clear how and when withdrawal is possible if the services is not achieving its stated aims) These will be discussed and finalised as part of wider considerations as part of BCF risk and reward discussions and form a key part of transition planning activity. 4.6 Conclusions from the financial and activity modelling The savings in CIS are delivered by supporting people in the community rather than in hospital or in care homes. The financial assumption underpinning the CIS is that it is less expensive to support someone in the community and in their home. Savings can be made by shifting activity from (more expensive) hospital and care homes to (less expensive) community-based settings. The evidence from the financial modelling supports this premise. The CIS is forecast to deliver net benefits of - 2.4m in 2015/16 and rising to - 6.4m in 2018/19 and confirms that the implementation of the CIS service is financially beneficial across Triborough. In addition, there are also LoS benefits of -1.09m to the acute sector over the first four years. 48
49 5. Options Appraisal Section 3 outlined the current baseline of activity across the three boroughs. Subsequently, Section 4 presented a summary of the single specification for the future state of CIS which is fully integrated and standardised across the Triborough. The gap analysis to compare current models against the future state then demonstrated the distance to travel for each of the services in the Triborough areas (please note that this is not an assessment of the effectiveness of the current service but a measure of maturity of the service against the desired future state). The journey to integrate and achieve the significant benefits of a single model will be different for each borough. Consequently, the challenge for commissioners is to establish the best available route to deliver the required service transformation and consider the contractual mechanisms available to drive this forward. Three options for change were assessed and Option 2b was selected as the preferred option, on the grounds that it would achieve the most integrated care pathway as early as possible and was judged to give the greatest likelihood of releasing the opportunities and benefits modelled. The three options are described below and Figure 5.1 provides a summary description of each option considered. Option # Option Description 1 Do nothing Continue with existing fragmented services. No investment in to enhance or integrate existing models of the CIS. 2a Single coordinated approach with existing providers Led by a single lead provider Continue with existing multiple providers, however standardise provision under one single specification through appropriate contract amendment to existing health and social care contracts. This would involve implementation of commissioner principles of engagement translated into provider collaboration agreements. Potentially this could be achieved through development of a formal agreement between providers. To underpin this, there will be a need to build strong levels of trust and good relationships across organisation al boundaries in order for step change to be delivered. A programme of change across the provider landscape will be required to focus on integration to work as a single team. Financial incentives in the form of the proposed new investment in 2015/16 would be used to incentivize integrated working. This will be discussed with providers throughout the transition period. Option 2a: To ensure integration of the service, the new investment of 7.4m would be packaged up and offered out to the existing set of providers, in order to appoint a single lead provider to manage the delivery of the new service. Appointment of the lead provider would be made jointly by health and adult social care commissioners. 49
50 2b Single coordinated approach with existing providers Led by an alliance of two lead providers As above in 2a, with the exception that a competition is run between existing providers in order to appoint 2 lead providers, (1 in social care and 1 in health) who would then work together in partnership to ensure delivery of a single integrated CIS. A formal alliance would be formed between the two lead providers via the establishment of a formal agreement. Appointment of the two lead providers would be made jointly by health and adult social care commissioners. 3 Prime Contractor Single provider organisation following a competitive procurement process working under a single service specification which may include a TUPE d workforce. This is a contracting model which enables commissioners to transfer the responsibility and risk for the delivery of specific services to a single provider. The commissioning organisation holds the commissioning contract with the Prime Contractor who may subcontract some of the services to Third Party Provider(s). The Commissioners can protect personal choice through careful management of Prime (in the way it uses its supply chain and refers activity to them). 5.1 Discussion of options Figure 5.1: Options descriptions 13 Figure 5.2 shows a detailed consideration of the advantages, disadvantages, risks / issues and timescales associated with each option. Consideration was also given to the complexity of solution and whether benefits would be achieved in 2015/16. OPTION 1: Do nothing: Continue with existing fragmented services While good models of care already exist across the three boroughs the strategic review in September / October 2013 showed that there are a number of known and acknowledged issues: Inconsistent opening hours Different ways of referring people into the system (multiple points of contact) Inconsistency in what care is offered, when and for how long Inconsistency in people-centred outcomes The same or similar services are called different things which can cause confusion amongst both health and social care professionals and people Varying costs for similar services Duplication in assessments and delivery of services 13 Note: The above three options are not exclusive and do not rule out the consideration of other contracting mechanisms in the future. 50
51 Patchy knowledge and understanding of the service by both people and professionals referring into the service In addition, the services are not sustainable financially as evidenced by repeated bids for winter pressures funding to support the services. The option to Do nothing is considered incompatible with the opportunities created by the BCF and whole systems integrated design. It would not deliver better co-ordinated integrated care out of hospital nor customer journey transformational benefits. This option was ruled out as the preferred option. OPTION 2: Single co-ordinated approach with existing providers: Continue with existing multiple providers, however standardise provision under one single specification and focus on integration and improvement initiatives. By working with existing health and social care providers on a system-wide basis, commissioners will enable delivery partners to build upon the body of expertise already built up around addressing capacity gaps in resilience and winter pressures planning. Working on a co-ordinated basis with existing teams preserves existing focus on improving the single integrated care pathway that is at the centre of the customer journey and whole systems integrated care vision. Expertise can be channelled on creating a single competency framework for workforce planning, organisational development, and making the most of the opportunities to improve efficiency and productivity created by standardisation. Focus and momentum around transformation initiatives already underway and pilots already in place can be sustained without diversion. By avoiding the disruption created by uncertainty, existing commitments to working collaboratively in local areas can be applied at scale. Selecting this option is most compatible with the implementation of whole systems integrated care and achieving the intent of the BCF at any earlier stage, without ruling out future developmental change. This option offers the greatest opportunity and preserves the benefits of continuity for 2015/16. Option 2a: gives the simplicity of a single lead provider, however runs the risk of conflict of interest due to the joint role of adult social care as commissioner and provider. Option 2b: ensures a financial incentive for providers to work towards integration, simplifies the provider accountability down to two and ensures that the health and social care lead providers work together in partnership without any conflict of interest to the local authority due to the provider commissioner split. Following discussion between Senior Officers about the pros and cons of the different options, Option 2b was selected as the preferred option. OPTION 3: Prime Contractor: Single provider organisation following a competitive procurement process Because of the lead-in time (12-18 months) associated with a procurement exercise there is greater potential to disrupt or defer integrated care pathway planning and this is associated 51
52 with greater likelihood of creating instability. This was assessed as more likely to disrupt engagement and create an uncertain timeline for the release of opportunities and benefits. In addition, the diversity of employment arrangements assessed in the 2014/15 baseline points to the likelihood that a major consultation and consolidation exercise would have to take place before significant progress around the integrated care pathway could happen. This creates greater likelihood of creating instability. This option was assessed as having greater potential to disrupt or defer integrated care and was not selected as the preferred option for 2015/16 because of its potential to delay release of Better Care Fund and whole systems integrated care benefits. Option 3 was not selected as the preferred option due to its complexity and potential for disruption to service delivery, which was considered was too great to be delivered within the timescales available (i.e. for service go-live date of April 2015). This option was discarded for 2015/16 because of its potential to delay to release of BCF and whole systems integrated care benefits. 5.2 Recommended option The recommended option is Option 2b: Single co-ordinated approach with existing providers, Led by an alliance of two lead providers For 2015/16, to ensure stability, it is proposed that the service continues to be delivered with multiple existing providers but through a single co-ordinated approach /specification. New investment into the service 7.4m in 2015/16 would be packaged up and a competition would be run to appoint 2 lead providers (1 in health and one in social care) to ensure integration across the provider landscape. To enable transformational change without creating instability, the recommended approach for 2015/16 is to enter a year of transition during which a phased approach can be taken and incremental improvement brought about. The provider community is best placed to advise commissioners on the most effective way of bringing about operational and service transformation, and as soon as this case is agreed, that necessary 6 months of transition will be brought about. These options are considered in more detail in Figure 5.1. Section 6.4 contains a summary of risks and mitigations of implementing the new service. Formal agreements between commissioners and between commissioners and providers The challenge remains of what tools to use in order to transform the service delivered by existing providers in the year of transition 2015/16 and how to ensure they work collaboratively as one single team and effectively manage incentive and risk. The Lead Provider mechanism proposed in Option 2 is a way of packaging up new investment into the service to provide a financial incentive for change however there will need to be collaborative agreements in place for all providers to implement the necessary changes. These arrangements need to enable commissioners and providers to work together under a common framework. The development of a formal agreements between commissioners will be necessary to cover all boroughs and all CCGs. 52
53 Option Advantages Disadvantages Risks/Issues Timescale required Complexity Benefits 2015/16 Option 1 Do Nothing Least effort and cost Does not address the increased requirement for intermediate care services in the Triborough nor inconsistencies in the current service models nor deliver further integration services. No delivery of benefits or impact on NELs and length of stay in nursing home and residential home care, no additional impact on health and wellbeing outcomes. Failure to simplify and standardise and to improve people s journeys drives up health and social care cost, impacting on CCG and LA long-term financial plans. Unsustainable financial model currently, supported by winter pressures funding. Immediate Low X Misses key opportunities to deliver improved care and integrated services offered by the Better Care Fund. Also impacts negatively on the ability of other inter-related schemes (such as 7 day hospital discharge) to deliver benefits. 53
54 Option Advantages Disadvantages Risks/Issues Timescale required Comple xity Benefits 2015/16 Option 2 Single coordinated approach with existing providers 2a single lead provider 2b Alliance of 2 lead providers (1 from Health and 1 from Adult social care) Minimal impact on providers and hence minimum disruption in care delivery and people s experiences. Maintains focus on improving people s experiences through progressing ASC customer journey and WSIC focus on single front door. Continued focus on improving existing care pathways, referral routes, functions and teams and integration initiatives still under development. Sustains focus and momentum around integration through emerging GP networks and whole system provider network initiatives. Transitional change can be implemented for 2014/15 and 2015/16 with earlier delivery of specified benefits. Leaves options open for future models of contracting. Option 2a provides simplicity of accountability with one lead provider. Option 2b offers an alliance of two lead providers simplifying and aligning the health providers and the social care providers Insufficient assurance of step change to deliver single front door, improved customer journey and experience. Relies on trust and good relationships between commissioners and providers. Relies upon collective approach to culture change to underpin delivery, as well as contractual or workforce changes. This will rely on successful engagement process over 6 months transition period and into the long-term to deliver MOU. Relies on transparency and close co-operation from all parties to address specific local areas of improvement. For example, if workforce skill set needs enhancement in one area or recruitment needs to be tackled in another area, relies on a mature approach to prioritization. Fragmentation across boroughs / CCGs could continue unless collaborative working and partnership agreements are put in place. May not deliver sufficiently robust step change to deliver consistent benefits including contract efficiencies. Continued overhead from duplication if partners fail agree single tracking of productivity gain. Accountability and clinical responsibility may be unclear because of different starting points across the CCGs and boroughs. To mitigate this risk, close monitoring and feedback on progress must flow across all strategic and operational levels of commissioner and provider partnerships. Risk and reward agreements i.e. contract incentives or penalties fail to deliver accountability for performance and outcomes. Option 2a. presents a conflict of interest for the local authority in terms of the providers commissioner split 6 months Medium 54
55 Option Advantages Disadvantages Risks/Issues Timescale required Complexity Benefits 2015/16 Option 3 Prime Contractor Potentially opens up market place to new entrants. Opportunity for competition to test for innovation and new ways of working. Opportunities to access a wider pool of talent and wider track record. Clear governance and simplicity of contracts. Steps up the focus on improving people s experiences through progressing ASC customer journey & WSIC focus on single front door. Provider lead acceptance and support across all providers untested; possible disengagement of some providers; willingness of single provider to take on risk uncertain. Provider impact would be high. Step change in keeping with LA customer journey transformational change and WSIC transitional change. No benefits delivered in 205/16 Non delivery of key BCF benefits in 15/16 would results in payment for performance element of plan being restricted. Uncertainty could be very disruptive for staff morale and hence delivery of services may suffer. Destabilisation existing providers. of 18 months High X Drives on integration step-change to enhance focus on improving existing care pathways, referral routes, functions and teams and integration initiatives still under development. Opportunity to redesign key points to support acuity out of hospital i.e. supported care at home to avert crisis / admission. Could simplify care pathway wrapped around WS GP & GP-focused MDT. Accommodates transition and incremental improvement alongside phased benefits release. Figure 5.2: Detailed options appraisal 55
56 6. Transition and implementation planning 6.1 Next steps for commissioners Following agreement of the recommendations, it is timely and right to move on to work with providers on translating the implications into practical and implementable steps. As a first step, there will be immediate consultation with existing health and social care providers on the use of the proposed 2015/16 investment in a way that works best for the system, as a whole systems approach. In return, there must be a set of principles for engagement to which all commissioners sign up to. The way in which the investment offer is packaged up for existing health and social care providers must be linked to an agreement which allows providers and commissioners to track impact and benefits and holds providers to account. For the immediate future, findings will be translated into commissioning and contracting intentions for 2015/16. The work over the next 6 months will prepare the ground, to allow providers the time to prepare for change, and commissioners to make translate the investment case into new contract agreements 6.2 Proposed governance and management arrangements New governance and management arrangements will need to be established to effectively manage the new Triborough CIS from April 2015 onwards. It is proposed that an operational management committee is established with representation from across the 6 commissioning organisations and that it will also include provider representation. If option 2b is approved this will include but will not be limited to the two lead providers. The Committee will meet monthly to review performance and take key decisions in the ongoing delivery and development of the CIS. A single framework of Key Performance Indicators (KPIs) will be developed with associated dashboard reports to enable transparency of service delivery performance and enable the tracking of both costs and benefits. The Committee will also track the development of the provider programme of integration and interoperability initiatives across the multiple providers to ensure that the transition year achieves the target of delivering a single service. The purpose of the Committee is to hold providers to account but it will also act in a spirit of partnership to resolve issues swiftly and enable the single service to develop. The upwards governance of the CIS then falls under the established governance mechanisms for the Better Care Fund which reports up through JET (the Joint Executive Team across Health and Adult Social Care) through the Health and Wellbeing boards and to the 6 sovereign bodies (CCG Governing bodies and Local Authority Cabinets). It is proposed that the operational management committee for CIS is established immediately after approval and sign off of this business case in order to govern the preparatory arrangements leading to service go live in April 2015 and in particular, the appointment of lead providers (option 2b) which will need to happen by end of December 56
57 2014. It will then evolve into the management of the actual integrated service from April 2015 onwards. 6.3 Principles of engagement for commissioners The overall Better Care Fund Plan submissions supported by CCGs and LAs reflect overarching principles for the joint approach under the Better Care Fund by CCG/LA area within Triborough. In the next steps, these will be discussed with health commissioners as part of the wider discussions around Better Care Fund. The integrated approach to crisis response / community independence service through a year of change in 2015/16 necessitates a particular need for commissioners to sign up to set of consistent commissioning principles across all 6 authorities, CCGs and LAs. To minimise bureaucracy and maximise partnership benefits, commissioning partners across the Triborough will agree and sign up to the principles and rules of engagement with respect to the CIS. A joint commissioning approach should therefore apply the following proposed principles: One approach to planning and building upon demonstrable achievement joint commissioning intentions in 2015/16 and beyond Transparency, consistency and accountability taking an open book approach Taking and applying one approach to measuring progress Assessing the achievements of the integrated CIS Tracking through one consistent methodological approach actual benefits and savings by LA / CCG Testing on one single basis overall value for money from the pooled Better Care Fund budget 6.4 Developing the CIS through incremental change There are 4 key stages to delivering this programme. The 4 phases are: Design confirming the need for change and agreeing the future service model (April to September 2014) Preparation planning for changes required and building shadow capability Transitional improvement making interim changes to how services are delivered Single service running sustainable and cost effective service as envisioned Figure 6.1 provides a pictorial overview of these different stages and the key objectives and deliverables for each stage. This section also considers the key risks to the successful delivery of the CIS. 57


58 Figure 6.1: Overview of incremental change to CIS 58
59 6.5 Transition plans There are 2 main factors impacting the resource each CIS service will require to deliver services as planned from 2015 onwards: the single specification (operational requirements) activity (the volume of referrals coming into the service) Subject to the approval of this business case, further work will be required in each authority to refine these plans. The initial descriptions of the transition requirements and trajectory for change identify: gaps and development requirements suggested solutions (e.g. ways to bridge the gap) resource implications (financial) phasing Transition arrangements in Figure 6.2 Immediate Next Steps are summarised. Design and preparation September 2014 to March 2015 The core aim of the period between September 2014 and March 2015 is to ensure alignment by both commissioners and providers across the Triborough to commence delivery of the single service specification from April At the heart of this will be the need for commissioners and providers to work together to undertake more detailed design work and operational development work to set up systems, processes and ways of working to achieve the deliverables as set out in the service specification. 6.6 Risk management An initial view of the key risks that may occur during the preparation and transition stages of the programme has been captured. Following the assessment of all identified risks, those scoring the highest for impact and/or likelihood have been further evaluated and are highlighted in Figure 6.3. They focus on the central areas of needing to shift activity, ensuring alignment with other programmes, developing the necessary contractual arrangements and issues around workforce and systems that are most likely to limit the ability of the CIS to fully meet the requirements of the single specification. 59

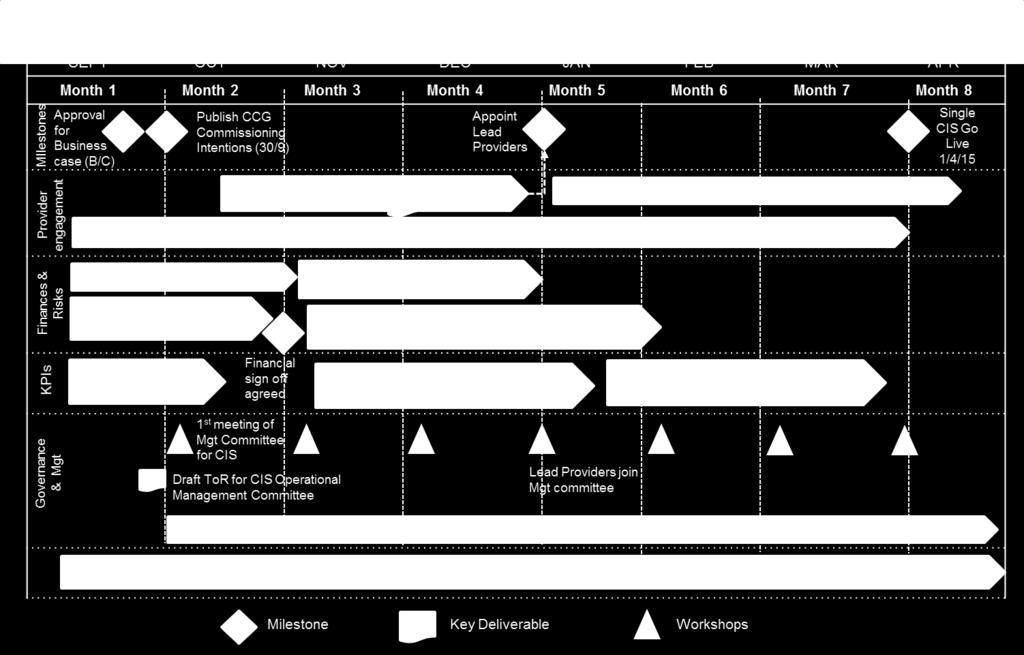
60 Figure 6.2 CIS high level implementation plan 60
Integrating Health And Social Care Community Services. Richard Milner and Stella Baillie
 Integrating Health And Social Care Community Services Richard Milner and Stella Baillie AGENDA 1. Why we are doing this 2. Our plans for integrating Adult Social Care Assessment and Care Management with
Integrating Health And Social Care Community Services Richard Milner and Stella Baillie AGENDA 1. Why we are doing this 2. Our plans for integrating Adult Social Care Assessment and Care Management with
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Westminster Partnership Board for Health and Care. 21 February pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Guideline scope Intermediate care - including reablement
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
North West London Draft Sustainability and Transformation Plan Review
 North West London Draft Sustainability and Transformation Plan Review In carrying out our work and preparing our report, we have worked solely on the instructions of the West London Alliance (specifically
North West London Draft Sustainability and Transformation Plan Review In carrying out our work and preparing our report, we have worked solely on the instructions of the West London Alliance (specifically
Mental Health URGENT CARE AND ASSESSMENT Business Case. CCG Summary paper
 1. Purpose of this paper Mental Health URGENT CARE AND ASSESSMENT Business Case. CCG Summary paper This paper sets out the rationale for investment in new more effective urgent care pathways for people
1. Purpose of this paper Mental Health URGENT CARE AND ASSESSMENT Business Case. CCG Summary paper This paper sets out the rationale for investment in new more effective urgent care pathways for people
Westminster Partnership Board for Health and Care. 17 January pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Central London Clinical Commissioning Group Governing Body Meeting 13 August 2014
 Central London Clinical Commissioning Group Governing Body Meeting 13 August 2014 CONTRACT AWARD - CARE PROVIDER PROCUREMENT OF SPECIALIST HOUSING FOR OLDER PEOPLE IN WESTMINSTER (SHSOP) 1. Executive Summary
Central London Clinical Commissioning Group Governing Body Meeting 13 August 2014 CONTRACT AWARD - CARE PROVIDER PROCUREMENT OF SPECIALIST HOUSING FOR OLDER PEOPLE IN WESTMINSTER (SHSOP) 1. Executive Summary
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
PARTNERSHIP AGREEMENTS FOR THE COMMISSIONING OF HEALTH, WELLBEING AND SOCIAL CARE SERVICES
 PARTNERSHIP AGREEMENTS FOR THE COMMISSIONING OF HEALTH, WELLBEING AND SOCIAL CARE SERVICES 1. EXECUTIVE SUMMARY Commissioning is the process used by local authorities and NHS bodies to arrange services
PARTNERSHIP AGREEMENTS FOR THE COMMISSIONING OF HEALTH, WELLBEING AND SOCIAL CARE SERVICES 1. EXECUTIVE SUMMARY Commissioning is the process used by local authorities and NHS bodies to arrange services
South East Essex. Discharge to Assess Strategy
 South East Essex Discharge to Assess Strategy 2018-2020 Version 3.5 27 th March 2018 Document Control: Revision: Name Date: Version 2.0 Shirley Regan 12 December 2017 Version 2.1 Amendments-Paul 19 December
South East Essex Discharge to Assess Strategy 2018-2020 Version 3.5 27 th March 2018 Document Control: Revision: Name Date: Version 2.0 Shirley Regan 12 December 2017 Version 2.1 Amendments-Paul 19 December
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
NHS North West London
 NHS North West London Shaping a Healthier Future Pre-Consultation Business Case Volume 6 Appendices A1 & A2 Edition: 1 20 June 2012 Page 1 of 29 APPENDIX A1 Programme Governance A.1.1 Key governance principles
NHS North West London Shaping a Healthier Future Pre-Consultation Business Case Volume 6 Appendices A1 & A2 Edition: 1 20 June 2012 Page 1 of 29 APPENDIX A1 Programme Governance A.1.1 Key governance principles
INTEGRATION TRANSFORMATION FUND
 MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
REABLEMENT SERVICE FOR NORTHERN IRELAND REGIONAL REABLEMENT PATHWAY. (for use by Health and Social Care Trusts)
") REABLEMENT SERVICE FOR NORTHERN IRELAND REGIONAL REABLEMENT PATHWAY (for use by Health and Social Care Trusts) July 2016 INDEX Section 1: Introduction - Regional Definition for Reablement - Regional Reablement
REABLEMENT SERVICE FOR NORTHERN IRELAND REGIONAL REABLEMENT PATHWAY (for use by Health and Social Care Trusts) July 2016 INDEX Section 1: Introduction - Regional Definition for Reablement - Regional Reablement
Mental Health Social Work: Community Support. Summary
 Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Developing Plans for the Better Care Fund
 Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Sustainability and Transformation Plan (STP)
") Trust board public: 25 May 2016 Agenda item: 4.1 Paper number: 13 Report to: Date of meeting Trust board - public 25 May 2016 Sustainability and Transformation Plan (STP) Executive summary: STPs are place
Trust board public: 25 May 2016 Agenda item: 4.1 Paper number: 13 Report to: Date of meeting Trust board - public 25 May 2016 Sustainability and Transformation Plan (STP) Executive summary: STPs are place
My Discharge a proactive case management for discharging patients with dementia
 Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
NICE guideline Published: 22 September 2017 nice.org.uk/guidance/ng74
 Intermediate care including reablement NICE guideline Published: 22 September 2017 nice.org.uk/guidance/ng74 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Intermediate care including reablement NICE guideline Published: 22 September 2017 nice.org.uk/guidance/ng74 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Merton Integration & Better Care Fund Plan 2017/19
 Merton Better Care Fund Programme Merton Clinical Commissioning Group Merton Integration & Better Care Fund Plan 2017/19 Area London Constituent Health and Wellbeing Boards Merton Constituent CCGs Merton
Merton Better Care Fund Programme Merton Clinical Commissioning Group Merton Integration & Better Care Fund Plan 2017/19 Area London Constituent Health and Wellbeing Boards Merton Constituent CCGs Merton
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Review of Local Enhanced Services
 Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Adult Social Care Assessment & care management In-house care services
 Adult Social Care Assessment & care management In-house care services Service Plan 2015/16 Date 19/03/15 Final Directorate: Education Health and Social Care 1. Introduction Policy Context The Adult Social
Adult Social Care Assessment & care management In-house care services Service Plan 2015/16 Date 19/03/15 Final Directorate: Education Health and Social Care 1. Introduction Policy Context The Adult Social
Brent Better Care Fund Plan BRENT COUNCIL AND NHS BRENT CCG (V1.0 FINAL)
") Brent Better Care Fund Plan 2017-2019 BRENT COUNCIL AND NHS BRENT CCG (V1.0 FINAL) 0 Contents 1. Introduction... 2 2. Case for Change... 2 3. Brent s vision for health and care... 5 4. Better Care Fund
Brent Better Care Fund Plan 2017-2019 BRENT COUNCIL AND NHS BRENT CCG (V1.0 FINAL) 0 Contents 1. Introduction... 2 2. Case for Change... 2 3. Brent s vision for health and care... 5 4. Better Care Fund
Investment Committee: Extended Hours Business Case (Revised)
") PAPER 06 Investment Committee: Extended Hours Business Case (Revised) OVERALL STRATEGY 1. SaHF Care Closer to Home This Extended Hours Business Case is developed within the context of Shaping a Healthier
PAPER 06 Investment Committee: Extended Hours Business Case (Revised) OVERALL STRATEGY 1. SaHF Care Closer to Home This Extended Hours Business Case is developed within the context of Shaping a Healthier
Islington Integrated Networks
 Islington Integrated Networks Inner London borough: Islington Population 249,000 registered population/33 GP practices Most densely populated borough in England 24 th most deprived borough in England (down
Islington Integrated Networks Inner London borough: Islington Population 249,000 registered population/33 GP practices Most densely populated borough in England 24 th most deprived borough in England (down
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
BETTER CARE FUND 2016/17
 BETTER CARE FUND 2016/17 NHS Dorset CCG Dorset County Council Bournemouth Borough Council Borough of Poole Final 03 05 16 The Systems Leadership Team (SLT) in Dorset is working towards integrating health
BETTER CARE FUND 2016/17 NHS Dorset CCG Dorset County Council Bournemouth Borough Council Borough of Poole Final 03 05 16 The Systems Leadership Team (SLT) in Dorset is working towards integrating health
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering the Five Year Forward View Personalised Health and Care 2020
 Paper Ref: NIB 0607-006 Delivering the Five Year Forward View Personalised Health and Care 2020 INTRODUCTION The Five Year Forward View set out a clear direction for the NHS showing why change is needed
Paper Ref: NIB 0607-006 Delivering the Five Year Forward View Personalised Health and Care 2020 INTRODUCTION The Five Year Forward View set out a clear direction for the NHS showing why change is needed
Appendix 5.5. AUTHOR & POSITION: Jill Shattock, Director of Commissioning CONTACT DETAILS:
 Appendix 5.5 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE Wednesday, 30 July 2014 TITLE: North Central London (NCL) NHS 111 and GP Out of Hours LEAD GOVERNING Jill Shattock,
Appendix 5.5 MEETING: Haringey Clinical Commissioning Group Governing Body Meeting DATE Wednesday, 30 July 2014 TITLE: North Central London (NCL) NHS 111 and GP Out of Hours LEAD GOVERNING Jill Shattock,
Transforming the NHS in North West London
 Transforming the NHS in North West London Integrating health and social care with the leadership of local GPs and working in partnership with NHS England North West London - Five Year Strategic Plan 2014/15-2018/19
Transforming the NHS in North West London Integrating health and social care with the leadership of local GPs and working in partnership with NHS England North West London - Five Year Strategic Plan 2014/15-2018/19
Metrics for integrated care: What should we measure to know that care is improving?
 Metrics for integrated care: What should we measure to know that care is improving? Better Care Support Team Webinar Deborah Rozansky, SCIE Associate 27 June 2018 Webinar learning objectives To understand
Metrics for integrated care: What should we measure to know that care is improving? Better Care Support Team Webinar Deborah Rozansky, SCIE Associate 27 June 2018 Webinar learning objectives To understand
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Westminster Health and Wellbeing Board
 Westminster Health and Wellbeing Board Date: 13 July 2017 Classification: Title: Report of: Cabinet Member Portfolio: Wards Involved: Policy Context: Report Author and Contact Details: General Release
Westminster Health and Wellbeing Board Date: 13 July 2017 Classification: Title: Report of: Cabinet Member Portfolio: Wards Involved: Policy Context: Report Author and Contact Details: General Release
Growth in older people
 Agenda 1. Why create an Integrated Care Organisation (ICO)? 2. NHS vs Local Authority 3. Salford Together 4. Integrated Care Organisation 5. The Financial Negotiation 2 Why integration? -Number of people
Agenda 1. Why create an Integrated Care Organisation (ICO)? 2. NHS vs Local Authority 3. Salford Together 4. Integrated Care Organisation 5. The Financial Negotiation 2 Why integration? -Number of people
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CASE FOR CHANGE - CLINICAL SERVICES REVIEW
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CASE FOR CHANGE - CLINICAL SERVICES REVIEW Date of the meeting 19/03/2014 Author Sponsoring Board Member Purpose of Report Recommendation
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CASE FOR CHANGE - CLINICAL SERVICES REVIEW Date of the meeting 19/03/2014 Author Sponsoring Board Member Purpose of Report Recommendation
BETTER CARE FUND UPDATE
 MEETING DATE: 13 February 2014 AGENDA ITEM NUMBER: Item 6.2 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire CCG REPORT TO THE CLINICAL COMMISSIONING GROUP
MEETING DATE: 13 February 2014 AGENDA ITEM NUMBER: Item 6.2 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire CCG REPORT TO THE CLINICAL COMMISSIONING GROUP
North West London Accident and Emergency Performance Report for the winter of 2016/17. North West London Joint Health Overview and Scrutiny Committee
 North West London Accident and Emergency Performance Report for the winter of 2016/17 North West London Joint Health Overview and Scrutiny Committee 20 April 2017 1 This paper will summarise the performance
North West London Accident and Emergency Performance Report for the winter of 2016/17 North West London Joint Health Overview and Scrutiny Committee 20 April 2017 1 This paper will summarise the performance
IUC and Vanguard. Greater Nottingham Integrated Urgent Care 1
 IUC and Vanguard The 2016/17 Vanguard funding has been confirmed at 1.3M This funding is to deliver the 8 elements of Integrated Urgent Care by March 2017 With careful management of funds we will be able
IUC and Vanguard The 2016/17 Vanguard funding has been confirmed at 1.3M This funding is to deliver the 8 elements of Integrated Urgent Care by March 2017 With careful management of funds we will be able
Dudley Clinical Commissioning Group. Commissioning Intentions Black Country Partnerships NHS Foundation Trust
 Appendix 3 Dudley Clinical Commissioning Group Commissioning Intentions Black Country Partnerships NHS Foundation Trust 2013/2014 1 Strategy and Context Our Commissioning Intentions indicate to our current
Appendix 3 Dudley Clinical Commissioning Group Commissioning Intentions Black Country Partnerships NHS Foundation Trust 2013/2014 1 Strategy and Context Our Commissioning Intentions indicate to our current
CASE STUDY: THE ADULT MENTAL HEALTH (AMH) MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS.
 MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS.") CASE STUDY: THE ADULT MENTAL HEALTH (AMH) MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS. Summary The Adult Mental Health (AMH) model is a new initiative which
CASE STUDY: THE ADULT MENTAL HEALTH (AMH) MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS. Summary The Adult Mental Health (AMH) model is a new initiative which
Hospital discharge: working for everyone I was helped to regain my independence when I thought I would have to go into care
 Hospital discharge: working for everyone I was helped to regain my independence when I thought I would have to go into care Introduction Every council and hospital aim to deliver a smooth and timely hospital
Hospital discharge: working for everyone I was helped to regain my independence when I thought I would have to go into care Introduction Every council and hospital aim to deliver a smooth and timely hospital
Chief Officer s Report December 2013/January 2014
 Chief Officer s Report December 2013/January 2014 Purpose This paper provides a summary of the key areas of business as led by the Chief Officer for this and the other four Clinical Commissioning Groups
Chief Officer s Report December 2013/January 2014 Purpose This paper provides a summary of the key areas of business as led by the Chief Officer for this and the other four Clinical Commissioning Groups
Chief Officer s Report March and April 2018
 Purpose This paper provides a summary of the key areas of business led by the Chief Officer in the CWHHE Clinical Commissioning Groups. CWHHE comprises NHS Central London, NHS West London, NHS Hammersmith
Purpose This paper provides a summary of the key areas of business led by the Chief Officer in the CWHHE Clinical Commissioning Groups. CWHHE comprises NHS Central London, NHS West London, NHS Hammersmith
Director of Adult Social Care and Health, East Sussex County Council
 Report to: East Sussex Health and Wellbeing Board Agenda Item 9 Date: 13 February 2014 By: Title of Report: Purpose of Report: Director of Adult Social Care and Health, East Sussex County Council Joint
Report to: East Sussex Health and Wellbeing Board Agenda Item 9 Date: 13 February 2014 By: Title of Report: Purpose of Report: Director of Adult Social Care and Health, East Sussex County Council Joint
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Marginal Rate Emergency Threshold. Executive Summary
 Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Healthy Wirral Vanguard New Care Model Value Proposition th February 2016
 Healthy Wirral Vanguard New Care Model Value Proposition 2016-17 8 th February 2016 1 Contents Section Page(s) Introduction and Strategic context Page 3 High level Programme Overview Page 4 Enablers: Cross
Healthy Wirral Vanguard New Care Model Value Proposition 2016-17 8 th February 2016 1 Contents Section Page(s) Introduction and Strategic context Page 3 High level Programme Overview Page 4 Enablers: Cross
Memorandum of understanding for shadow Accountable Care Systems
 Since Previously Discussed by BLMK CEOs: Memorandum of understanding for shadow Accountable Care Systems Dear Richard, As described in Next Steps on the NHS Five Year Forward View, we intend to name a
Since Previously Discussed by BLMK CEOs: Memorandum of understanding for shadow Accountable Care Systems Dear Richard, As described in Next Steps on the NHS Five Year Forward View, we intend to name a
What matters to Me Supporting the health and wellbeing of our older population
 What matters to Me Supporting the health and wellbeing of our older population The new way of working for health and social care across the Western bay region What we will do 1. We will focus on the needs
What matters to Me Supporting the health and wellbeing of our older population The new way of working for health and social care across the Western bay region What we will do 1. We will focus on the needs
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
Shakeel Sabir Head of MERIT Vanguard
 MERIT Excellence, Resilience Innovation & Training Jointly developing Mental Health Service in the West Midlands Shakeel Sabir Head of MERIT Vanguard Background - New care models Multispecialty community
MERIT Excellence, Resilience Innovation & Training Jointly developing Mental Health Service in the West Midlands Shakeel Sabir Head of MERIT Vanguard Background - New care models Multispecialty community
BUSINESS CASE FOR LEVEL 2 SPECIALIST NEURO-REHABILITATION BEDS : SLIDE PACK & FINANCIAL MODEL
 BUSINESS CASE FOR LEVEL 2 SPECIALIST NEURO-REHABILITATION BEDS : SLIDE PACK & FINANCIAL MODEL V8 June 2015 1 Index Executive summary Slides 3-5 Business Case on a Page Slide 6 Model methodology Index/
BUSINESS CASE FOR LEVEL 2 SPECIALIST NEURO-REHABILITATION BEDS : SLIDE PACK & FINANCIAL MODEL V8 June 2015 1 Index Executive summary Slides 3-5 Business Case on a Page Slide 6 Model methodology Index/
Mental Health Crisis Care: The Five Year Forward View. Steven Reid Consultant Psychiatrist, Psychological Medicine CNWL NHS Foundation Trust
 Mental Health Crisis Care: The Five Year Forward View Steven Reid Consultant Psychiatrist, Psychological Medicine CNWL NHS Foundation Trust Overview Parity of esteem What are the challenges for people
Mental Health Crisis Care: The Five Year Forward View Steven Reid Consultant Psychiatrist, Psychological Medicine CNWL NHS Foundation Trust Overview Parity of esteem What are the challenges for people
North West London Sustainability and Transformation Plan Summary
 North West London Sustainability and Transformation Plan Summary Being well, living well: a sustainability and transformation plan for North West London November 2016 Have your say We want to hear your
North West London Sustainability and Transformation Plan Summary Being well, living well: a sustainability and transformation plan for North West London November 2016 Have your say We want to hear your
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS
 CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
Vanguard Programme: Acute Care Collaboration Value Proposition
 Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
FIVE TESTS FOR THE NHS LONG-TERM PLAN
 Briefing 10 September 2018 FIVE TESTS FOR THE NHS LONG-TERM PLAN The new NHS long-term plan is a significant opportunity for the health service. It can set out a clear and achievable path for sustaining
Briefing 10 September 2018 FIVE TESTS FOR THE NHS LONG-TERM PLAN The new NHS long-term plan is a significant opportunity for the health service. It can set out a clear and achievable path for sustaining
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION THE BUDGET NUMBERS
 BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Hammersmith and Fulham CCG Governing Body Meeting Minutes
 Tuesday 10 th September 2013 1.30pm-3.00pm Part 2 St Pauls Church, Hammersmith Elected and co-opted Members present: Tim Spicer H & F Clinical Commissioning Group GP (Chair) TS Susan McGoldrick H & F Clinical
Tuesday 10 th September 2013 1.30pm-3.00pm Part 2 St Pauls Church, Hammersmith Elected and co-opted Members present: Tim Spicer H & F Clinical Commissioning Group GP (Chair) TS Susan McGoldrick H & F Clinical
This paper explains the way in which part of the system is changing to become clearer and more accessible, beginning with NHS 111.
 Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
Meeting in Common of the Boards of NHS England and NHS Improvement. 1. This paper updates the NHS England and NHS Improvement Boards on:
 NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
Sussex and East Surrey STP narrative
 Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
The Bedfordshire CCG and Bedford Borough Council Better Care Plan Executive Summary: Our approach to Better Care planning
 DRAFT Version 16 19 March 2014 The Bedfordshire CCG and Bedford Borough Council Better Care Plan Executive Summary: Our approach to Better Care planning Bedford Borough and Bedfordshire CCG s Better Care
DRAFT Version 16 19 March 2014 The Bedfordshire CCG and Bedford Borough Council Better Care Plan Executive Summary: Our approach to Better Care planning Bedford Borough and Bedfordshire CCG s Better Care
The Integrated Support and Assurance Process (ISAP): guidance on assuring novel and complex contracts
: guidance on assuring novel and complex contracts") The Integrated Support and Assurance Process (ISAP): guidance on assuring novel and complex contracts Part A: Introduction Published by NHS England and NHS Improvement August 2017 First published: Friday
The Integrated Support and Assurance Process (ISAP): guidance on assuring novel and complex contracts Part A: Introduction Published by NHS England and NHS Improvement August 2017 First published: Friday
Integrated Care Co-Ordination Model. Healthier Together. Project Initiation Document
 Appendix A Integrated Care Co-Ordination Model Healthier Together Project Initiation Document Contents 1. Purpose... 2 1.1 Key Deliverable... 2 1.2 Approach... 2 2. Introduction... 3 3. Programme Vision...
Appendix A Integrated Care Co-Ordination Model Healthier Together Project Initiation Document Contents 1. Purpose... 2 1.1 Key Deliverable... 2 1.2 Approach... 2 2. Introduction... 3 3. Programme Vision...
London s Mental Health Discharge Top Tips. LONDON Urgent and Emergency Care Improvement Collaborative
 London s Mental Health Discharge Top Tips LONDON Urgent and Emergency Care Improvement Collaborative November 2017 1 Introduction These Top Tips commenced their journey at the Pan London Reducing delays
London s Mental Health Discharge Top Tips LONDON Urgent and Emergency Care Improvement Collaborative November 2017 1 Introduction These Top Tips commenced their journey at the Pan London Reducing delays
04c. Clinical Standards included in the Strategic Outline Care part 1, published in December 216
 0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
GE1 Clinical Utilisation Review
 GE1 Clinical Utilisation Review Scheme Name QIPP Reference Eligible Providers GE1 Clinical Utilisation Review QIPP 16-17 S40-Commercial 17/18 QIPP reference to be added locally. This CQUIN is supported
GE1 Clinical Utilisation Review Scheme Name QIPP Reference Eligible Providers GE1 Clinical Utilisation Review QIPP 16-17 S40-Commercial 17/18 QIPP reference to be added locally. This CQUIN is supported
GOVERNING BODY MEETING in Public 29 November 2017 Agenda Item 5.4
 GOVERNING BODY MEETING in Public 29 November 2017 Paper Title Paper Author Jacki Wilkes Associate Director of Commissioning Redesign of adult and older peoples specialist mental health services pre-consultation
GOVERNING BODY MEETING in Public 29 November 2017 Paper Title Paper Author Jacki Wilkes Associate Director of Commissioning Redesign of adult and older peoples specialist mental health services pre-consultation
England. Questions and Answers. Draft Integrated Care Provider (ICP) Contract - consultation package
 Contract - consultation package") England Questions and Answers Draft Integrated Care Provider (ICP) Contract - consultation package August 2018 Questions and Answers Draft Integrated Care Provider (ICP) Contract - consultation package
England Questions and Answers Draft Integrated Care Provider (ICP) Contract - consultation package August 2018 Questions and Answers Draft Integrated Care Provider (ICP) Contract - consultation package
Imperial College Health Partners - at a glance
 Imperial College Health Partners - at a glance Imperial College Health Partners - at a glance Our vision and purpose This document is intended to provide an introduction to Imperial College Health Partners
Imperial College Health Partners - at a glance Imperial College Health Partners - at a glance Our vision and purpose This document is intended to provide an introduction to Imperial College Health Partners
Delivering the Five Year Forward View. through Business Intelligence
 Delivering the Five Year Forward View through Business Intelligence Introduction The market for analytics has matured significantly in the past five years and, although the health sector in the UK has
Delivering the Five Year Forward View through Business Intelligence Introduction The market for analytics has matured significantly in the past five years and, although the health sector in the UK has
REPORT 1 FRAIL OLDER PEOPLE
 REPORT 1 FRAIL OLDER PEOPLE Contents Vision f-3 Principles / Parameters f-4 Objectives f-6 Current Frail Older People Model f-8 ABMU Model for Frail and Older People f-11 Universal / Enabling f-12 Specialist
REPORT 1 FRAIL OLDER PEOPLE Contents Vision f-3 Principles / Parameters f-4 Objectives f-6 Current Frail Older People Model f-8 ABMU Model for Frail and Older People f-11 Universal / Enabling f-12 Specialist
service users greater clarity on what to expect from services
 briefing November 2011 Issue 227 Payment by Results in mental health A challenging journey worth taking Key points Commissioners and providers support the introduction of Payment by Results for adult mental
briefing November 2011 Issue 227 Payment by Results in mental health A challenging journey worth taking Key points Commissioners and providers support the introduction of Payment by Results for adult mental
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD
 BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD") INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
Mick Hancock, Assistant Director Joint Commissioning
 Subject: Meeting: Better Care Fund NHS Milton Keynes CCG Board Date of Meeting: 25 th March 2014 Report of: Mick Hancock, Assistant Director Joint Commissioning Is this document: Commercially Sensitive
Subject: Meeting: Better Care Fund NHS Milton Keynes CCG Board Date of Meeting: 25 th March 2014 Report of: Mick Hancock, Assistant Director Joint Commissioning Is this document: Commercially Sensitive
Report by the Local Government and Social Care Ombudsman. Investigation into a complaint against North Somerset Council (reference number: )
") Report by the Local Government and Social Care Ombudsman Investigation into a complaint against North Somerset Council (reference number: 16 018 163) 16 March 2018 Local Government and Social Care Ombudsman
Report by the Local Government and Social Care Ombudsman Investigation into a complaint against North Somerset Council (reference number: 16 018 163) 16 March 2018 Local Government and Social Care Ombudsman
Healthy London Partnership. Transforming London s health and care together
 Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Update on NHS Central London CCG QIPP schemes
 Update on NHS Central London CCG QIPP schemes NHS Central London CCG has identified circa 11m for QIPP during 2013/14. Commissioning Intentions approved by the governing body included transformational
Update on NHS Central London CCG QIPP schemes NHS Central London CCG has identified circa 11m for QIPP during 2013/14. Commissioning Intentions approved by the governing body included transformational
South West London Commissioning Intentions 2015/16
 Attach 5 NHS SOUTH WEST LONDON COMMISSIONING COLLABORATIVE South West London Commissioning Intentions 2015/16 Draft v0.7 8/21/2014 Document version Date of revision Document Iterations made Status v0.1
Attach 5 NHS SOUTH WEST LONDON COMMISSIONING COLLABORATIVE South West London Commissioning Intentions 2015/16 Draft v0.7 8/21/2014 Document version Date of revision Document Iterations made Status v0.1
16 May Elizabeth James Director of Clinical Commissioning, Barnet CCG
 Barnet Health Overview and Scrutiny Committee 16 May 2016 Title North West London, Barnet & Brent Wheelchairs Service Redesign Report of Elizabeth James Director of Clinical Commissioning, Barnet CCG Wards
Barnet Health Overview and Scrutiny Committee 16 May 2016 Title North West London, Barnet & Brent Wheelchairs Service Redesign Report of Elizabeth James Director of Clinical Commissioning, Barnet CCG Wards
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme. Frequently Asked Questions Second Edition
 Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Quarterly Reporting Template - Guidance
 Quarterly Reporting Template - Guidance Notes for Completion The data collection template requires the Health & Wellbeing Board to track through the high level metrics and deliverables from the Health
Quarterly Reporting Template - Guidance Notes for Completion The data collection template requires the Health & Wellbeing Board to track through the high level metrics and deliverables from the Health
Council of Members. 20 January 2016
 Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Islington Practice Based Mental Health Care: Roll-out plans and progress
 Report to: Board of Directors (Public) Paper number: 3.2 Report for: Information Date: 26 th October 2017 Report author/s: Emily van de Pol, Divisional Director, Community Mental Health and Primary Care
Report to: Board of Directors (Public) Paper number: 3.2 Report for: Information Date: 26 th October 2017 Report author/s: Emily van de Pol, Divisional Director, Community Mental Health and Primary Care
South Yorkshire & Bassetlaw Health and Care Working Together Partnership
 South Yorkshire & Bassetlaw Health and Care Working Together Partnership Memorandum of Understanding Agreement Final Draft June 2017 1 Title Drafting coordinator Target Audience Version V 0.3 Memorandum
South Yorkshire & Bassetlaw Health and Care Working Together Partnership Memorandum of Understanding Agreement Final Draft June 2017 1 Title Drafting coordinator Target Audience Version V 0.3 Memorandum