Buckinghamshire Health & Social Care. Operational Resilience & Capacity Plan
|
|
|
- Megan Strickland
- 5 years ago
- Views:
Transcription
1 Operational Resilience & Capacity Plan 1
2 DOCUMENT CONTROL Title Operational Resilience and Capacity Plan Author Bernadette Devine Urgent Care Commissioning Lead Owner Approval Routes Robert Majilton Buckinghamshire Urgent Care Working Group (Systems Resilience Group) V4.3 Resubmission Systems Resilience Task & Finish Group Internal approval by organisations in line with their internal governance processes DOCUMENT HISTORY Version Date Comment V Internal draft V Internal Draft V Draft For Provider Input - Circulated V Final Submitted to Area Team V BHT amends (SC) V Internal draft following NHSE feedback (Ian Cave) V Internal Draft BD V Internal Draft Updates from KH V RM In Put BD FINAL Submission V Submission to NHSE V Resubmission incorporating feedback from NHSE 2
3 CONTENTS Executive Summary... Section 1 Overview Executive Summary 1.1 Introduction 1.2 Context and Overview 1.3 System Risks 1.3c Mitigating actions 1.3b Risk management 1.4 Urgent care national and local 1.5 Performance Intelligence and System Resilience Plans 2014/ Urgent care current performance Sustaining Resilience in Urgent Care (criteria 1-13) Sustaining Resilience in Elective Care (criteria 1-13) 2.0 BHT Acute Site Partner 2.1 Winter 2013/14 2.2a ECIST 2.2b Care Quality Commission (CQC) 2.3 RUC Work Programme Plans & Impact 3.0 SCAS & Resilience Planning for Buckinghamshire 4.0 System Resilience Planning 2014/ National Timeline 4.2 ORCP Assurance Process 4.3 Continued Governance & Oversight 4.4 High Risk Reporting Requirements 4.5 SRG Task & Finish Group 4.6 Daily Resilience Calls 4.7 Patient Centred Service 4.8 Ambulatory Care Pathways 5.0 Stakeholder Engagement and Empowerment 5.1 System Winter Communications and Engagement 6.0 Primary Care: Planning and Whole System Capability 6.1 Flu Planning 7.0 Mental Health Services 8.0 Evidence Based and Research Reviews 8.1 Winter Review and Lessons Learned 8.2 Resilience Bids 2014/ Whole System Review: SRG Task & Finish Process 9.0 Winter Bids 9.1 SRG ORCP Template Collation 3
4 Appendices Appendix I 2013/2014 Winter Schemes Appendix II Gap Analysis Appendix III- 2014/15 Winter Schemes Prioritisation Framework & Bid Template Appendix IV SRG Templates Appendix V - NHS England Meeting the Standards for Urgent Care: A minimum standards checklist. 4
5 Performance Overview 1.0 Executive Summary Buckinghamshire Operational Resilience & Capacity Plan (ORCP) has a vision for unscheduled care to ensure that people receive good access to high quality services according to their clinical needs, and that these services are delivered coherently and at best value for money. The overarching aim is to commission an integrated urgent care system that seeks to reduce demand for hospital based services by commissioning responsive, accessible and integrated services outside of hospital that offer choice, meet local need and are value for money and produce a sustainable and measureable return on investment. Our vision for the future is one of increasingly integrated services that meet patient needs, delivers better outcomes and makes efficient use of available resources. A greater proportion will be provided outside hospital settings whether for acute, community, mental health or other needs. Patients will be active participants in maintaining their own health as well as exercising choice in relation to care. Where it is appropriate for care to be based in hospitals, this will be delivered to higher standards and in line with agreed pathways. This document sets out the plans of health and social care partners to support the unscheduled care patient pathway and is informed by national frameworks of both description and delivery of service provision 1. 1 Transforming urgent and emergency care services in England Phase 1 Report 5
6 1.1 Introduction This plan has been developed in response to the Operational Resilience and Capacity Planning guidance for published on 13 June 2014 and prepared by NHS England, the NHS Trust Development Authority, Monitor and the Association of Directors of Adult Social Services. It describes the Buckinghamshire health and social care approach to operational resilience and capacity planning for The work described in this plan will set the ground work for longer term outputs from the National Urgent and Emergency Care Review. The plan will be subject to further development during August and posted on the websites of the Buckinghamshire (CCGs) in September The plan will be refreshed in October prior to winter This ORCP complements both the Whole Systems Resilience Escalation Framework for Berkshire & Buckinghamshire , and the Major Incident Plan. The former describes how to manage surges in demand and lack of capacity on a daily basis within existing resources. The latter describes how to respond to extraordinary events. The ORCP describes how additional resources will be utilised to improve patient flow and reduce delays. 1.2 Context and Overview The Buckinghamshire health and social care economy is comprised of the following key organisations: Aylesbury Vale CCG, with a population of 200,000 Chiltern CCG with a population of 320,000 Buckinghamshire County Council Buckinghamshire Healthcare NHS Trust Oxford Health NHS Foundation Trust Bucks Urgent Care South Central Ambulance Service NHS Foundation Trust Heatherwood and Wexham Park Hospital NHS Foundation Trust Buckinghamshire Healthcare is co-terminous with Buckinghamshire County Council, covering a population of over 500,000. This affords excellent partnership and joint planning 2 Whole Systems Resilience Escalation Framework for Berkshire & Buckinghamshire v 2.0 March



7 opportunities and provides sufficient critical mass for our specialist services. As expected from this geographical co-terminosity, our main commissioners are Aylesbury Vale and Chiltern Clinical commissioning Groups, which account for over 86% of our local income. This is set out in the diagram below: Figure 1: Clinical Commissioning Groups 7


8 Fig 2 Population Heat map and Acute Care Settings AVCCG Settings Local intelligence and analysis demonstrates that population growth and demographics will be a major factor in understanding the future baseline demand levels and service provision required. Over 17% of Buckinghamshire s population is over 65 with the proportion predicted to increase to 21% by It is this section of the community who are major users of health services with 40% of people over 65 years reporting a limiting long-term illness. Within Buckinghamshire, there are two main areas of deprivation, Aylesbury and High Wycombe, accounting for 2.5% of the local population living in the most disadvantaged 30% of the population as a whole. Such populations have high levels of morbidity and in Buckinghamshire, cardiovascular disease, cancer, diabetes and COPD are long term conditions of high prevalence locally. The health impact and disease burden is as follows: Circulatory Disease 35% Cancers 28% 8
9 Respiratory Disease 14% The local health economy is facing a significant financial challenge. To address this the local health and social care community have been working together to outline a strategy to reduce the reliance on acute care through increasing the range and availability of services in community/primary care and develop more integrated services across health and social care. This is explicit in the commissioning intentions for both Chiltern and Aylesbury Vale CCGs. BHT has sought to ensure its strategy is aligned to that of its commissioners. In order to deliver their commissioning intentions the two CCGs will work together to jointly commission through matrix working. Five Programme Boards have been established to implement change across the area and support the QIPP agenda. These intentions are reflected in our strategy to further develop our integrated services, provide more comprehensive out of hospital alternatives and develop a more planned approach to managing those with long-term conditions a System Risks The Urgent Care pathway and the Planned Care pathway are both central to the system resilience delivery 2014/15 and are acknowledged as part of the overall strategic risk for BHT. Key risks for include: BHT expanded bed capacity not being in place until January 2015 Social care Primary care capacity Lead in time for recruitment of new staff. There is a financial risk of slippage. This is low risk as it involves specific funding for teams, risk of higher agency costs if recruitment slips. But there are opportunities from slippage on other schemes to mitigate this if it occurs. 1.3b Risk management Management of resilience risks are an integral part of the existing risk management processes for urgent care which form part of the CCGs corporate risk management framework. Urgent Care risk registers are reviewed by SRG / UCWG monthly. High risks are escalated to CCGs Executive Teams and Governing Bodies. 3 BHT Integrated Business Plan 2014/ /19 V1.0 9
10 There are twice daily resilience teleconferences which are part of the system escalation framework and organisations have business continuity plans (BCP) in place. The BHT BCP has recently been recognised by the Thames Valley NHSE Emergency Planning lead as being of a high standard. Operationally many key performance indicators for monitoring resilience are already in place and reviewed by the BHT Reforming Urgent Care (RUC) Programme Board every two weeks and by SRG / UCWG each month. These will be supplemented by additional measures for new services funded over winter. Every week the System Resilience Programme Manager employed by the CCG will meet with the Urgent Care Programme Manager from BHT and other key Providers to review these KPIs during the weekly SRG sub group meetings. This will facilitate early issues identification and early escalation. This will create the ability to utilise funding from slippage to effectively respond to events as they unfold on the ground e.g. by implementing bids which have been kept in reserve. 1.3c Mitigating actions Actions to mitigate key risks included: a) BHT expanded bed capacity not being in place until January 2015 Mitigation: BHT reconfiguring existing bed use to reduce safari ward rounds and so improve Estimated Date of Discharge (EDD) planning and reduce length of stay (LOS) so reducing the bed capacity required. Implementation of ambulatory care Flexible use of escalation beds Predictive modelling of demand to inform staff rotas so that there is adequate staff capacity b) Social care : Quantification of the impact of same day and 7-day s256 initiatives Mitigation: Utilise BCF mechanisms to implement changes Working in partnership with Bucks CC through Adult Joint Executive Team meetings to maximise use of s256 funding. These schemes will be in place during Q3 so SRG can assess impact early 10
11 c) Primary care capacity Mitigation: Use of Over 75s funding ( 1m AVCCG + 1.6m Chiltern) e.g. Care Home Matron; Vulnerable Older Persons Peripatetic Nursing; Primary Care Early Intervention team. Piloting and evaluating Doctor first approach to GP triage Implementing an acute visiting service in Chiltern and exploring extending this. d) Lead in time for recruitment of new staff. Mitigation: Using a range of existing staff more flexibly Funding Psychiatric In-Reach Liaison Service (PIRLS) to older people wards to reduce LOS and increase capacity in A&E to reduce 4hr breaches. Funding 7/7 support services; phlebotomy and a team of pharmacists to cover A&E CDU seven days a week 7am-8pm and at weekends. Funding increased radiology resource to increase the urgent care capacity. 1.4 Urgent Care National and Local Urgent care describes medical conditions which do not require hospital admission and can be managed without a trip to an emergency department. Instead the patient could be treated using local community services or out-of-hospital facilities. This is distinct from 999 life threatening emergencies and those major traumas that must be dealt with in Accident & Emergency Departments, and regional centers such as the specialised stroke unit and cardiology unit. Over recent years, NHSE and stakeholder partners have been developing Urgent Care pathways to provide the best care in the most appropriate care setting. A variety of facilities and pathways have been developed, including Walk in Centers, Minor Injury and Illness Units and Urgent Care facilities. The initial provision and development was to reduce pressure on A&E as understood in the formal definition of such facilities (Tier 1-3). However, A&E has continued to see a sustained growth in both demand and activity and locally, has struggled to reach the 95% performance target levels on a consistent basis in the first quarter of 2014/15. 11
12 Nationally the directive is now to call any facility and pathway that does not require advanced clinical life support and trauma input a Urgent Care Centre, this, it is hoped will reduce any confusion in communication that the public may be have in relation as to where to go for the best and most appropriate level of care. In turn, this will reduce the pressure in Emergency Departments and will ensure patients get the best care possible in the best place for both their immediate needs and longer term health outcomes. The development of Urgent Care Networks will also facilitate the development of comprehensive urgent care pathways, including that of Ambulatory Emergency Care, which has the potential to develop Cardiology, Respiratory, Neurology, Rheumatology pathways along with medical HOT clinics. Locally across Buckinghamshire there are a suite of Urgent care provision centers, including a minor illnesses and injuries unit at High Wycombe. MuDAS is a service also based at High Wycombe which provides direct GP access for elderly patient assessment which is widely recognised as an excellent contribution to patient experience and outcomes, along with admission avoidance. The current challenge with MuDAS is increasing its use and there are plans to expand the service to the Stoke Mandeville site to spread the learning and incorporate MuDAS at the front door provision of Stoke Mandeville hospital. Currently patients that arrive at Stoke Mandeville Hospital are transported to the High Wycombe site, and both the challenge and opportunity of the current provision is being picked up as resilience bid initiatives. 1.5 Performance Intelligence and System Resilience Plans 2014/15 Buckinghamshire s plans to develop a system-wide dashboard will enable the system to see it performance in a targeted way, enabling better use of resources going forwards. Along with plans to standardize the reporting templates, including that used on the daily resilience call. This will allow clear views of current performance and will result in faster decision making. Linking performance and activity to clinical outcomes will support future commissioning decisions which reflect the development of the new system-wide pathways, such as frail elderly care, which further reflects the population health and social care needs of Buckinghamshire. 1.6 Urgent Care Current Performance 12

13 A&E 4 Hour target The Buckinghamshire urgent and emergency care system performed relatively well during 2013/14 achieving 94.9% overall for the year (compared to the target of 95%). However Quarter 1 of 2014/15 has been a challenge to consistently hit the 95%. A number of local acute providers are also struggling to consistently deliver the 4 hour standard Urgent Care Information 13
14 The Urgent Care Working Group has been reviewing the Management Information pack and this is being co-ordinated through Central Southern CSU and provider information teams to develop a richer source of information (part of developing the Urgent Care dashboard) from which to drive actions to improve performance across the urgent care system and support monitoring impact of resilience plans. Some initial analysis of available commissioner information is provided below while that work continues. The examples below are surrounding A&E. The data is largely comparing April and May 2013 with the equivalent in Accident and Emergency Who attends A&E? Table 1 A&E attendances by age group and arrival method
15 The largest groups are over 75 (who largely arrive by ambulance) and 0 4 (who arrive by another means). How do they get there? Table 2 Source of Referral for A&E attendances
16 Table 2 shows that of the 3 top categories general increases of 3 5% have been seen in self referrals and emergency services with a 3 10% increase in GP referrals. When do they get there? Table 3 A&E attendances by Age and day of week
.")
17 This chart shows the largest groups of attendances are Over 75 and 0 4. For over 75 the busiest days are Monday and Friday and the busiest day (Friday is 19% higher than Sunday). For 0 4 the busiest day is Sunday which is 18% higher than Wednesday. TABLE 4 Hour of arrival by age group

18 The table above shows a heat map of hour of arrival by age group showing the spread of attendances. What happens to them? Table 5 Discharge Destination

19 The majority are discharged either with our without follow up from their GP with the next largest group being admitted
20 Figure 11: Our emergency activity by division and specialty 2013/14 Emergency Admissions by Division Surgery & Critical Care 20% Integrated Medicine 39% Urology 2% Stroke Medicine 3% Midwife Episode 6% Trauma & Orthopaedics 6% Emergency Admissions by Specialty Respiratory Medicine 2% Other 9% General Medicine 22% Paediatrics 20% Specialist Services 41% Cardiology 8% General Surgery 8% Obstetrics 14% Figure 12: Our elective activity by division and specialty 2013/14 Surgery & Critical Care 48% Elective & Daycase Admissions by Division Integrated Medicine 27% Specialist Services 25% Gynaecology 4% Urology 5% Elective & Daycase Admissions by Specialty Other 24% Plastic Surgery 6% General Surgery 7% Gastroenterol ogy 18% Clinical Clinical Oncology Haematology 9% 7% Ophthalmolo gy 10% Trauma & Orthopaedics 10% Elective Care Graph 1 Reduction Trajectory 18 Weeks / Plastic Surgery 20
21 1.6.8 Graph 2 Reduction Trajectory 18 Weeks / Trauma & Orthopaedics Sustaining Resilience in Urgent Care 21
22 1 Enabling better and more accurate capacity modelling and scenario planning across the system SCAS already use historical information to model and predict the staff capacity required on a daily basis across the eastern node area, and the number of patients who will be conveyed to hospital. Commissioners are working with SCAS to identify whether this data can be used to assist BHT and HWWP to proactively plan for admissions. BHT A&E department also use historical data to predict daily A&E attendances and plan staff capacity so they have sufficient staff to manage the majority of patients who are discharged from A&E. UCWG have already undertaken modelling of urgent care flow across the pre-hospital system comparing activity and flow on bank holiday Monday with a normal Monday to identify bottlenecks in the pathway. This demonstrated the ability of providers to reduce variation in demand for A&E
23 BHT have followed best practice to implement a Rapid Access Team (RAT known locally as IAT) at the front door and segmentation of patients requiring more than 4 hours for treatment into CDU, AMU and SAU. But this has not been sufficient to improve patient flow through the entire hospital. As a result Capita has undertaken bed modelling within BHT and highlighted SMH is 20 medical beds short which is preventing patients being admitted to a specialty ward and gaining fast access to the relevant clinicians. The resilience plan, supported by a bid against strategic capital (pending), consolidates escalation capacity within the main Stoke Mandeville Hospital site, by providing 20 bed capacity. SCAS recognise periods of high activity (using our predicative capability) and are proposing to deploy system capacity vehicles to mitigate the possibility of patient risk, as part of bids for resilience funding Central Southern CSU has Simul8 software which we are exploring for use in capacity modelling. It can be used to compare the effectiveness of existing BHT systems (A&E; CDU; AMU; SAU) with IMAS experience and recommendations 23
24 and_and_delivering_quality.pdf The Thames Valley Area Team is identifying potential capacity modelling tools to be adopted across Thames Valley, and Buckinghamshire CCGs are keen to participate fully in the use of any tools adopted. The CCG led Long Term Conditions programme are implementing initiatives to reduce variation in demand for urgent care. These include rollout of Adastra electronic template for Advanced Care Plans, which are shared with other urgent care providers. This will be incentivised by the Admissions Avoidance DES and improve the quality of patents experience by increasing the number of people who die in their preferred place. It will also reduce admissions to hospital in the last 72 hours of life. 2 Working with NHS 111 providers to identify the service that is best able to meet patients urgent care needs Within the ORCP NHS 111 provision is central to current delivery of patient pathways and vital for future resilience and capacity planning. NHS 111 is a non-emergency number for accessing local health services. The service acts as a single point of access for urgent care, providing triage and assessment for callers to ensure they access the best care by simplifying access to urgent care and emergency care where necessary. NHS 111 pathways and Directory of Service development (DOS) are part of a continual process of national development for local delivery and in Buckinghamshire, NHS 111 have developed a recover plan to ensure resilience and performance monitoring and service delivery. Buckinghamshire CCGs directly commissions the Central Southern Commissioning Support Unit (CSCSU) to maintain, expand and update the Directory of Services (DoS) supporting NHS 111. The NHS 111 team performs multiple functions, including Forward-planning and transformative management and the operational maintenance of the DOS Including: 24
25 3 Taking part in the Thames Valley dental Out of Hours Review, ensuring that improvements to community services directly enhance the ability of NHS 111 to refer effectively into urgent dental care. 4 Reviewing access criteria for walk-in services (Walk-in-Clinics, Minor Illness/Injury Units, Urgent Care Centres etc), to signpost away from Emergency Departments and into local community services that provide efficiencies for the health economy as well as a better pathway for the caller 5 In-depth analysis of call-data from the NHS 111 provider leading to improvements to NHS 111 referrals, from minor service entry edits for clarity, to re-prioritisation of services and re-modelling of how the patient can receive the care they require in the best timeframe 6 Plans to expand DoS capabilities, 7 Having mobile device access for community health professionals to be able to look up services anywhere at any time 8 DoS rollout to healthcare colleagues in practice settings for information on 3 rd sector, charity and other support networks where they overlap health and social care. In a single package, the system can support NHS 111 Pathways in the call centre and also health colleagues across the economy. 9 Ensuring Protected Learning Time cover is seamless when callers are re-directed from 111 to the covering organisation; that Bank Holiday extended opening times for pharmacies are always accurate so a patient is never incorrectly signposted; changing details when service demographics change. 10 Clinical leads are always consulted by DoS management upon a change to an entry, be it the introduction of a new service or pathway, or due to an upgrade to the Pathways triage tool meaning DoS must be edited. This process is proven to be robust and has been in-place since go-live. 3 Additional Capacity for Primary Care Primary care provision and capability is central to the overall delivery of the resilience and capacity planning currently underway in Buckinghamshire. Patients interface with primary care 95% of the time in all health profiles, and as such primary care becomes increasingly central to health and social care delivery. Practices across Buckinghamshire are facing high urgent care needs demands and a number of schemes are underway, supported by the current resilience bids submitted. 25
26 Seven day working and greater access to multiple primary care sites and care /social needs provision will also provide patients with responsive and flexible care which will also prevent patients going to A&E as a default position, thereby reducing A&E minor attendances. Research has shown that busy and clogged A&E departments place patients at greater risk. As part of planning for 2014/2015, the system has looked back on winter 2013/2014, and has reflected that it was mild overall with minimal disruptive weather, and few cases of noro virus outbreak. This will also facilitate a more targeting approach to seasonal surge and resilience planning across the winter months of 2014/15. It is anticipated that primary care will play a pivotal role in delivering our vision to meet people s needs in the community wherever possible and the CCGs will look to facilitate this through the development and implementation of a Primary Care Strategy, including well developed primary care co-commissioning arrangements with NHS England which will enable us to improve quality in primary care and to employ new contracting mechanisms as appropriate. Improving Access to Primary Care initiatives: Doctor first type telephone triage has been piloted in Chiltern CCG and has been found to improve patient access and GP capacity. The CCG is engaged with five more Practices to extend this further during In AVCCG two Practices are exploring the use of Web GP. This will be evaluated as part of increasing Primary Care resilience. Further use of technology to improve capacity and resilience in primary care is being explored. The following approaches are being considered by practices to improve capacity. e.g. patients questions to GPs via secure Texts for appointment reminders and possibly for sharing test results Online viewing of patient records by patients (including results) Online repeat prescription requests Online appointment booking 26
27 Over 75s funding and Admissions avoidance DES ( 1m AVCCG + 1.6m Chiltern) 4 Improve services to provide more responsive and patient-centred delivery seven days a week & 6 Seven Day working arrangements Actions taken within Buckinghamshire Whole System: A seven day working gap analysis was undertaken with BHT to review provision, gaps to inform the internal BHT Reforming Urgent Care Board, (Se Appendix II). Funding extending Psychiatric In-Reach Liaison Service (PIRLS) to older people wards to reduce LOS and increase capacity in A&E to reduce 4hr breaches. KPI: Time of referral request to being seen. Funding 7/7 support services; phlebotomy and a team of pharmacists to cover A&E CDU seven days a week 7am-8pm and 7-8 at weekends. Funding increased radiology resource to increase the urgent care capacity. Recruited for 7/7 social care staff at SMH to increase weekend discharge. Investing in additional ACHT cover out of hours. Implemented ambulance referral to ACHT, MuDAS and Falls service. Utilising Red Cross services following discharge to reduce readmissions. ASC are developing 7 day capacity for social care due to begin in September 5 SRGs should serve to link Better Care Fund (BCF) principles in with the wider planning agenda Rolling out 2 hours crisis response to provide carers at home to prevent admissions. This is jointly supported by ACHT and BCC commissioned Buckinghamshire Care staff. 27
28 Buckinghamshire has aspirations to create a large BCF that covers the commissioning of all out of hospital services for older people (up to 100m). An Outline Business Case has been approved and further work will be undertaken to develop the model and align existing services to it in the interim. For example the development of 7 day services for social care, funded from s256 monies will be in line with the model described in the OBC 6- See Point 4 7 Expand, adapt and improve established pathways for highest intensity users within emergency departments. Within BHT and Heatherwood & Wexham Park Hospitals, work has been undertaken to review and streamline pathways. At BHT the Reforming Urgent Care Programme Board (RUC) has clearly defined work streams to look at identified pathways and the patients therein, to ensure patient needs are met. The frail elderly pathway has also been reviewed as a whole system improvement process by the August Urgent Care Working Group, see page 24, whereby gaps and recommendations have been identified. The frail elderly, due to their complexity require multi-disciplinary input and continued assessment across multiple agencies and in all settings of care, including their own home, and by the whole system mapping exercise, the system know better understands the need beyond bed based care and location specific provision. The requirement for better social care involvement is understood and is a focus of current work stream developments. The mental health pathway has also been a focus of reform, and locally, services are in place in the Accident & Emergency setting to ensure patients receive assessment and care early on in their presentation. The PIRLS service and the extension of the PRILS service via current winter funding bids 2014/15, will continue to support mental health crisis patients who present to the acute sector. The minors pathway is clearly established in all acute trust sites with the MIIU based at High Wycombe providing further access for the treatment of minor injuries and illnesses, ensuring robust streaming of care pathways and increasing access by 24/7 provision. 28


29 AVCCG has returned the table below to the Area team as part of a recent audit request to underpin local system resilience, and has undertaken a system-wide Frail Elderly Pathway review as part of the local Urgent Care Working Group and SRG work programme. Table AVCCG Area Team Return Local Resilience Best Practice Diagram Frail Elderly Flow Diagram Worked up by AVCCG & CCCG August
30 8 Have Consultant-led rapid assessment and treatment systems (or similar models) within emergency departments and acute medical units during hours of peak demand The PIRLS service has been commissioned to provide rapid assessment within the ED service. As of the 18th August the service will be present within the department from 07:30-21:00 7 days per week. The service is seeking to enhance its activity and output via winter bids submission and hopes to be able to provide at 24/7 service. Nationally there is a shortage of inpatient mental health beds and this does impact on the A&E department and 4 hour times as patients experience delays in accessing care in the appropriate setting. This is borne out by local resilience call information. BHT have: Extended the physician of the day (POD) provision at weekends. The Trust now have a second Physician of the Day present on site on Saturdays and Sundays. This ensures that patients have access to senior decisions makers. POD hours have also been extended to later in the evening (20.00) 7 days per week. This accelerates response times for access to a senior decision maker early into the evening. Invested in ED nursing and medical workforce alongside on-going workforce redesign and development. Redesigned the pathway in ED to enable rapid assessment of arrivals and early redirection to appropriate services. Reconfigured the bed base to open an Acute Medical Unit and Surgical Assessment Unit and developed short stay ward pathways including specialist in-reach. Introduced a multi-disciplinary and multi-agency review team across A&E and Acute Medicine to review frail older people on arrival at hospital to support discharge decision making. Increased ACHT transfer of care lead presence on the Acute site and this is now the case 7 days a week. 30
31 Introduced Geriatric Liaison Services and multi-agency review teams to offer early specialist assessment and planning. Appointed more senior consultants to provide a 7 day a week service and Community geriatrician to develop an emphasis on admission avoidance/discharge to assess. Introduced multi agency groups at practice level to support patients to access care in advance of a crisis and support prevention. 9 All parts of the system should work towards ensuring patients medicines are optimised prior to discharge BHT as the acute provider have undertaken the following actions to improve patient medicine optimisation: There are clinical pharmacists at ward level who reconcile patient medicines on admission and discharge and throughout the patient s stay, to optimise medicines for patients and support patient outcomes - Reconciliation includes medication interaction of newly prescribed medicines Urgent Care Pathway focus incudes oversight and intervention via the pharmacists on the wards who are close to the very sick and or deteriorating patients TTOs are prepared in timely manner. In 2014 satellite pharmacy has been introduced in cardiology, acute medicine and surgery. This reduces dispensing time, which at ward level =is minutes turnaround time and in main pharmacy it would be 90 minutes electronic discharge summaries are being developed and this will include medicines as part of the summary with a copy for the patient and an copy to the GP, this begins in November/December as a pilot. 10 Processes to minimise delayed discharge and good practice on discharge BHT continues with its RUC programmes chaired by the COO to ensure delivery of the determined change programme. The RUC s five work streams are looking at the internal flow system of BHT and redesigning flows, pathways, roles and settings of care as part of its 31
32 portfolio to begin to free up the internal flow. The front door aspects of BHT are also dependent to an extent on the backdoor discharge flow being available and the RUC also focuses on the entire pathway. New models include, Discharge to Assess / Assess to Admit, and the integration of Health and Social Care Funds, providing an opportunity to link up the system for the best outcomes for patients, carers, and families. Which simplified, illustrates the expectation and outcome of right care right place right patient ethos, alongside three sections of pathway: A) flow prior to hospital admission, B) flow through hospital admission C) discharge and discharge / community interfaces. Current actions and progress includes: Recruiting for 7/7 social care staff at SMH to increase weekend discharges Investing in additional ACHT cover out of hours Funding additional spot purchase of beds Implementing discharge to assess models of care Funding increased BHT Rehabilitation and Reablement Service Funding extra step down community rehab bed capacity for Bucks patients in Wexham Park A&E and PACE service Funding a vulnerable care home nurse facing WPH Fund a Carer's Hub from Mon-Fri at SMH Implemented ambulance referral to ACHT, MuDAS and Falls service Within BHT current actions include: Daily Operational (site management) meeting attended by multi-disciplinary teams to enable identification and owner of the actions needed to ensure the most efficient use of bed capacity within BHT whilst ensuring that patients are placed appropriately according to their clinical needs. Attended by ward sisters at 08:30 daily to identify 32
33 patients ready for discharge and any issues that need addressing to enable progression along the discharge pathway. Daily Facilitated meetings Monday Friday- These involve a multidisciplinary, including ASC, review of patients daily on wards to gather intelligence of systematic delays and an action plan to resolve. Going forward these are further enhanced by the consultant based on the ward to support and lead discharge planning Daily Integrated Discharge meetings (IDM) with Adult Social Care to identify patient needs and agree actions in order that patients are transferred safely and timely to appropriate care settings for their needs. The forum is a platform for raising awareness of patient s individual needs and where a whole system approach works for the patient and their carers needs to minimise constraints and resolve issues using a collaborative approach. Delayed discharges are identified and plans agreed to progress discharge. Daily teleconference call with CHC to discuss patients who meet Continuing Healthcare eligibility and agree the Lead responsible for co-ordinating care. Information is fed into Daily IDM. Daily teleconference call with Herts to discuss patients who are eligible for Hertfordshire social care support. Information is fed into the daily IDM Teleconference call with Hertfordshire CHC as needed to discuss patients who meet Continuing Healthcare eligibility and agree the Lead responsible for coordinating care. Information is fed into Daily IDM. Call with other OOA authorities as needed to discuss patients who meet CHC/ASC eligibility and agree the lead responsible for co-ordinating care. Information is fed into Daily IDM. Escalation pathways for OOA are in place and utilised as required. 11 Plans should aim to deliver a considerable reduction in permanent admissions of older people to residential and nursing care homes 33
34 Bucks has a low rate of hospital admissions from Care Homes compared to many other areas which are cited as good practice e.g. Bath & NE Somerset and Derbyshire. This position has been achieved following HIEC work in AVCCG and Milton Keynes in 2012 and taken forward through a local enhanced service which ensures residents of care homes receive weekly access to GPs in the Care Homes to provide long term conditions management, medicines optimisation and advanced care planning. This service is supported by a community geriatrician who has been appointed in the last year by BHT. She is able to bridge secondary and community care and target her input to those care homes with high NHS use which have not benefited fully from the GP LES. This NHS work is in partnership with the local authority Care in Quality Team (QiCT), which work closely with Bucks care homes to ensure they achieve the required standards expected by CQC. In 2013/14 BHT led on a winter bid scheme for spot purchasing of beds. The extra capacity was seen as providing useful system capacity and has been repeated for 2014/15 as a winter bid led by both CCGs. There is also a Medicines Management Pharmacist supporting QiCT and reviewing medication in care homes. This complementary and co-ordinated approach enables care homes in apparently high use of NHS services to receive input which assists them in being as efficiently organised as possible and for their residents to benefit from optimisation of their medical conditions. The CCGs regularly evaluate which care homes are having high SCAS; A&E and admissions, and reprioritise these services to support where there is greatest need. In the south of the county we plan to fund a vulnerable care home nurse facing WPH In AVCCG one locality is also piloting a Care Home Matron approach to identify added value to the existing services. In addition the CCG s are investing under the Over 75 Fund in Primary care capacity to support older people where they reside. 12 SRG plans should utilise patient risk stratification tools with an aim of gaining a better understanding of the needs of the 2-5% percent of highest risk patients 34
35 Buckinghamshire resilience planning incorporates the Unplanned admissions DES and locally, 100% of GP practices have signed up to deliver, participate in and work through MAGs to ensure best practice for patients for their care needs. This includes the use of the ACG clinical risk stratification tool, and completion of the Bucks Coordinated Care Record which is supported via the Adastra platform. This care record enables out of hours care providers to access patient level data which in turn provides immediate access to clinical information on which to make well informed decisions. Again, supporting unplanned admission avoidance, keeping the patient close to their home and relatives and ensuring the right health and social care input is given first time right place. Having successfully implemented practice-based risk stratification and multi-agency care planning (MAGs) for high risk patients, our GPs are well placed to take on the role of Accountable clinician for patients who may be at risk of admission; co-ordinating care provided by a range of professionals to enable patients to remain in the community and are starting to do so through the Admissions Avoidance Directly Enhanced Service and other arrangements being put in place to support the care of the over 75s and high risk patients. The interface between general practice, community services and social care is likely to change, as new integrated models emerge. The SUS+ Urgent Care View online system provides primary care with information about their patients who are starting to use. 13 Use of Real-time System-wide Data SCAS ED Interface: SCAS ED IM&T interface allows real time review of current A&E department activity and waiting times. Alongside this, SCAS also has a whole system overview due to the geographical basis of the SCAS footprint. This allows contemporaneous overview of both ambulance pick and arrival activity and also sight of the ambulance handover times and clear times. To implement a live EPR system in ophthalmology which supports the merging of clinical management systems with patient pathway tracking, providing real time scheduling. 35
36 TVEA maintain information about capacity across Thames Valley and this will be extended by use of CMS for all areas. Sustaining Resilience in Elective Care Context Pressure within referral to treatment pathways at BHT began to build in the summer of 2013, particularly in the specialities of T&O and plastics. Initial action was taken to secure additional external capacity which came on-line later that summer. However the backlog continued to grow, along with overall waiting list numbers throughout the rest of the year, with a number of other surgical pathways including some diagnostics starting to show significant backlogs. Senior leadership at the Trust sought support of the Intensive Support Team (IST) in November and immediate validation and reanalysis of all referral to treatment pathways was undertaken. Detailed backlog recovery trajectories were produced for all breaching RTT pathways showing clearance rates by week running from December 2013 to the end of September. One example, orthopaedics had a backlog of 680 patients which is due to be reduced to 66 cases by the end of August. Similarly average waiting times are being lowered in all supporting diagnostic specialities, for example radiology MRI is reducing by half the number of patients currently being booked in at over 4 weeks. Delivery of consistent 18-week RTT performance In line with the Driver Tree from the national elective care guidance, the system will work together to assure delivery of consistent 18-week performance through the following steps: Maintain capacity and demand balance The Trust completed capacity plans in July for all specialities, with the support of IMAS. Output of this work was then shared across the system, including executives at the Trust and local CCGs. Additional external capacity has been sourced from three independent providers which have been used initially to help in reducing the backlog. This external capacity will also be used in the medium term to address the system capacity gap in Orthopaedics. Pathway Management The Initial work on capacity has identified a clear ongoing gap in orthopaedics and key pressure areas on diagnostic pathways. The 36
37 orthopaedic pressure requires the development of a sustainable new pathway to right size capacity to demand. The commissioner and provider are working together to develop a plan to support the delivery of sustainable orthopaedic services (including pain services and imaging within this). A first design workshop is being held in August to agree the patient outcome measures expected and possible options for how to deliver these. The Trust is leading, under the chairmanship of the Chief Operating Officer and Medical Director, a Reforming Elective Care programme to transform planned care pathways with the aim of improving the quality of care for patients and maintaining sustainable access times for the first time in several years. The core work streams of this programme are: Quality in Outpatients Theatre productivity Rapid diagnostics Data quality Whole pathway capacity and transformation Tracking and validation Weekly tracking information is available across the system from Bucks Healthcare Trust. It shows the patient tracking lists (PTL) for all stages of the pathway IP, OP and diagnostic. The commissioner makes weekly outpatient referral information available to GP practices. The system is able to see the stage of treatment summary for first appointment, follow up appointment, diagnostic admission and admission combined along with the target levels. The ambition for the system will be to add the referral information to this to complete a full picture. The Trust and the Commissioner have agreed to a process in which weekly data packs reflect real time information at the point of submission. Patient Tracking Lists are cleansed and signed off prior to submission to the Commissioner. In addition, a forecast is included that shows: Numbers of patients breaching without a date; Estimated backlog at the end of month vs plan; and Forecast booking profile for the following month to give assessment of breach profile. External activity and capacity are also factored into the forecast. Regular cleansing and validation of data is necessary as uncleansed data may reflect bits of dirty data: patients treated who haven t yet been removed, or patients who have joined the 37
38 list as data errors and need correcting, or patients who have been treated by external capacity and not yet removed. Performance management All waiting time information and backlog trajectories are published on a weekly basis and made available across the system. The Trust meets internally on a weekly basis through an access and performance management group to review this information and delivery progress. The commissioner meets informally with the Trust on a two weekly basis and formally on a monthly basis with clinical leaders from both organisations to review performance. Leadership and focus Both commissioner and Trust provider boards receive a monthly performance report of elective pathway performance. Each CCG has a GP clinical lead for elective care who meets regularly with clinical colleagues at the provider trust. The Trust has asked the IST to review operational reports and working arrangements of their internal performance group. 1 Review and revise patient access policy, and supporting operating procedures The Trust's Access Policy was significantly revised in January 2014 and signed off by the Trust executive in April Alongside this a revised set of Standard Operating Procedures has been published. The implementation of these operating procedures is clearly visible to the commissioner in the weekly information set. For example the information set shows by speciality the admitted clock stop patient numbers including total activity, breaches and previous week comparison. The commissioner has revised all policies on procedures of limited clinical value and put these updates into the local contract schedules. SRG will review the Access Policy against national rules and guidance in September. 2 Develop and implement a Referral to Treatment (RTT) training programme for all appropriate staff The Trust is implementing training for over 150 administrative staff by the end of August 2014 against the revised standards. This is followed by full competency assessment, a 38
39 training programme for new starters, and an onward monitoring and SOP adherence programme. There is also development of an e-learning module to ensure all clinical and booking staff are aware of the rules around RTT, and embed a forward monitoring programme and module for all new starters upon induction. Assurance will be provided by monitoring numbers of clinical teams completing the training package. 3 Carry out an annual analysis of capacity and demand for elective services at sub specialty level, keeping under regular review and updating when necessary With IMAS support, an annual programme of capacity and demand management was completed in July 2014 for the majority of core specialties. The outputs from this were shared with members of the executive and colleagues from CCGs. The outputs from this will feed into capacity and operating plans for 2015/16, and a programme of annual refresh is timetabled. Further work is required to do a deeper review of key pressured specialties (orthopaedics) and to pick up key pressure areas on diagnostic pathways. Further IST support is proposed to further complete this work. The aim is to complete this by the end of September. 4 Build upon any capacity mapping that is currently already underway, and use the outputs from mapping exercises as an annex to resilience and capacity plans. This will avoid duplication and integrate capacity mapping into 'business as usual' arrangements The capacity and demand planning piece completed in (3) above will be used as an annex to operational resilience and capacity plans. 5 Ensure that all specialties understand the elective pathways for common referral reason/treatment plans, and have an expected RTT timeline for each All specialty areas have identified 'timed pathways' for all stages of treatment: these are identified and monitored through the Trust's Access and Performance Group. 39
40 6 Right size outpatient, diagnostic and admitted waiting lists, in line with demand profile and pathway timelines The sub-specialty capacity gaps demonstrated in the work above (3), are proposed to be managed through a transformational cross organisational programme board; 'Reforming Elective Care'. This is a system wide service improvement forum to track key pathway changes from referral, through outpatients, diagnostics, theatres and discharge. This group will track the capacity gaps identified through the IMAS supported analysis completed and ensure a programme of work to cost effectively 'right size' the gaps. All specialty areas that had identified gaps in their capacity plans are the subject of individual action plans to ensure that the appropriate staffing, facility and pathway efficiency measures are in place to meet the future demands for 14/15 and onwards. These are being completed across the healthcare system and are accompanied by appropriate contracting and cross organisational pathway improvement discussions. The major area of focus for the system is a network wide review of MSK, including pain, orthopaedics and rheumatology (including imaging). This will be a joint provider and commissioner led review with recommendations around the future make up of regional MSK services to ensure appropriate pathways, capacity, cost effectiveness and outcomes. This will be accompanied by a specific provider led programme looking at internal orthopaedic culture, ways of working and processes, building on work scoped through a series of learning events at other providers in the UK and abroad. This will focus on removing all waste from the MSK provider pathway, focusing especially on outpatients /diagnostics, and theatres. 7 With immediate effect, review local application of RTT rules against the national guidance, paying particular attention to new clock starts and patient pauses As part of the Reforming Elective Care board, there is a specific data quality work stream that completes the following: Ensuring all staff appropriately trained in RTT rules and data validation. Completing an audit programme - 'validating the validation'. 40
41 Establishing clinical sign off of timed pathways and agreed clock stop 'rules'. Use of system reporting to flag areas of concern and deviations from agreed standards. Review of RTT outcome form - design and clinician accuracy. 8 Pay attention to RTT data quality. Carry out an urgent one off validation if necessary and instigate a programme of regular audits Strengthen the internal data validation team, moving towards a 'semi-permanent' team (6 months) with both a specific training and audit programme. Complete full PTL validation as a first priority as a one off exercise and then establish targeted rolling programme 9 Put in place clear and robust performance management arrangements, founded on use of an accurate RTT patient tracker list (PTL) and use this is discussion across the local system The Trust runs a weekly Access and Performance Management Group (APMG) that is accountable for reviewing all Trust PTLs and timed pathways. This group is accountable to the COO / Deputy CEO and monitors any deviation from agreed pathways. The operational reports and working arrangements for the group are currently being reviewed by the IST. A summary position of the overall system compliance is monitored through the Right Care Steering Group. 10 Ensure that supporting KPIs are well established (size of waiting list, clearance time, weekly activity to meet demand, RoTT rate etc) and are actively monitored All supporting KPIs are reported at a sub-specialty level through APMG. IST are providing active support in reviewing these and also making recommendations as to how these should be reflected in subsequent board reporting. 41
42 11 Demonstrate how good practice in referral management is being followed All referrals into the organisation are visible and managed to strict standards (reported through APMG) of time taken to upload onto the system, make visible and appointments being booked. In addition the Trust has undertaken 3 audits in the last 6 months of referrals from intermediate services to ensure correct clock information is available to the Trust when the referral is received (MSK and gynaecology). Onward audits are programmed for these areas for November 2014 to check ongoing compliance and implementation of suggested improvements. 12 Demonstrate that patients receiving NHS funded elective care are made aware of and are supported to exercise choice of provider Choice of provider embedded at the point of referral. 13 Provide assurance during Q2 2014/15 at Board level on implementation of the above BHT - sign off by board in Q2 CCG - assurance through the Right Care Group up then to board Innovation Remove diagnostic delays for vascular imaging Pilot through the use of additional ultra-sonographer support a one stop imaging service for all new and follow up vascular appointments. KPI: reduction in diagnostic referrals (Target: Reduce by 75% by 01/02/15) and removal of unnecessary follow ups (Target: Reduce by 15% by 01/02/15). 42
43 Reduce orthopaedic follow up appointments (elective) and fracture clinic appointments, increasing new appointments in a cost effective way Establishment of virtual clinic model: use of technology to screen and remotely manage both elective and acute orthopaedic referrals - free up consultant time for elective new work. KPI: New appointment times for orthopaedics (Target: 4 week maximum wait by 28/2/15) Reduce follow up appointments Digitalisation programme to facilitate the establishment across all relevant specialties of nonface to face contacts where possible. KPI: Reduction follow up appointments (Target: 0.2 ratio change 31/3/15) Robust PTL and RTT tracking of all patients in a 'live' EPR pilot To use a bespoke IT solution in ophthalmology (largest elective specialty) to merge the clinical management system with patient pathway tracking, removing RTT paper forms and providing real time scheduling. KPI: RTT performance (Target: Specialty specific compliance 2% + above baseline) A range of further innovations are being progressed across the system to support changes to the current treatment pathways with the aim of improving quality and increasing efficiency. Some examples would be: Introduction of an advice and guidance service by the provider Trust to support GPs and offer a choice in not necessarily moving straight to making a referral. The establishment of a virtual clinic model through the use of technology to screen and remotely manage both elective and acute orthopaedic referrals. To implement a live EPR system in ophthalmology which supports the merging of clinical management systems with patient pathway tracking, providing real time scheduling. App development and use service finder Synergistic cross professional posts 2.0 BHT Acute Site Partner Urgent Care Pathway Within Buckinghamshire there are three acute hospital trusts, BHT, Heatherwood and Wexham Park and Milton Keynes. The acute pathway for BHT is provided across two sites, 43
44 Stoke Mandeville and High Wycombe, with the former dealing with Type 1 A&E flow and the latter taking acute stroke and cardiac flows and the non- elective provision. There are some patient flows into Heatherwood and Wexham Park, along with some to Oxfordshire and Bedfordshire due to the logistical nature of population based care provision by CCGs. At the BHT site, there are urgent care pathways for A& E, acute medical and surgical patients (CDU, AMU, and SAU ) allowing patients to be seen and treated in a safe environment. 2.1 Winter2013/14 Over winter 2013/14 and continuing into this financial year, 2014, BHT has struggled to meet its AE 95% performance target. This figure is closely monitored by the local CCG and is taken as a system indicator along with the other acute trusts in Buckinghamshire as a sense check for system pressure and patient experience. The visibility of reporting enables the system to work together with the acute trusts, BHT in this instance to look at capacity and demand, flow, innovation and ambulatory care pathway development. BHT has submitted 17 briefings to the Trust Development Authority (TDA) in which they have reported 15 occasions of not meeting the 4hr wait and 2 where they have achieved the target. 2.2a ECIST BHT have worked with ECIST to review its Emergency flow and ECIST have revisited the Trust to review its progress twice over the past 12 months. The most recent ECIST visit was March 2014 and recommendations included: Develop a new clinical model for the front door ED/CDU/AMU/SSU and ambulatory care including frailty pathways that is deliverable with your current workforce Undertake a review of workforce and develop a deliverable workforce plan in the light of the constraints in employing the medical workforce originally desired Develop ambulatory care as a process rather than individual pathways this can be done quickly and from experience elsewhere has a significant impact on flow Work with commissioners and social care to develop a robust intermediate tier of services with a single point of access that ensures more patients go home to be assessed rather than waiting in hospital to have assessments completed. Link to work streams overseen by the Urgent Care Working Group Make greater use of MUDAS on the Wycombe site 44
45 ECIST diagnostic also identified Workforce constraints are confounding new pathways Ambulatory care required further development Intermediate tier services in the community are not rapidly pulling medically fit patients out of hospital Managerial processes to manage patient flow are complex and reactive and could be streamlined and more proactive Alternatives to hospital are not being fully utilised Deeper investigation of the urgent care pathway illustrated that peak flow times that put any extra demand in the system, noted as between 7pm and 2 am began to tip the system flow balance into the negative, causing further back log into the ED department itself. 2.2b Care Quality Commission (CQC) In June 2014 the Care Quality Commission published the Chief Inspector of Hospitals report on BHT. This made recommendations for improvement in the following areas: 1. Reduce mortality 2. Reduce harm 3. Improve patient experience 4. Goals for organisational safety culture 5. Goals for Improvement Methodology Lessons learnt from these sources in addition to local analytics of activity and finance across the system and lessons learnt from last winter, are fundamental drivers underpinning development of the ORCP plan 2.3 RUC Work Programme Plans & Impact Within BHT the Reforming Urgent Care board has a clear work programme, clinically led and locally delivered. Initiatives include: Expansion of the Frail Elderly assessment services: Ensuring fewer frail elderly patients are admitted to an Acute bed following an attendance to A&E for a fall Introduction of Ambulatory Care Services : Implement new AEC to reduce the length of time that patients are waiting in A&E and to improve the number that are admitted to a ward or discharged within 4 hours of arrival at A&E 45
46 Review and redesign of our Acute Medical Model and ward based working: To ensure that patients are admitted to a speciality ward with fat access to the relevant clinicians and reducing the number of moves some patients experience Surgical reviews within 2 hours of arrival: To aid patient flow and reduce the length of time that patients are waiting for a surgical review Discharge to assess: To reduce the LOS of patients requiring care in their usual place of residence. BHT will be delivering the Perfect Week as outlined in the ECIST recommendations. A project team, led by Clinicians and with CCG involvement has been formed with the aim to set up the Perfect Week in October There has been an expansion of the POD role to facilitate patient assessment, discharge and flow. The Acute Care Hub Model was scoped as part of the RUC last year and as a result the AMU and short stay model was implemented 3.0 SCAS & Resilience Planning for Buckinghamshire SCAS is the provider of both emergency 999 and 111 dispositions cross Buckinghamshire and is central to the whole systems resilience plan. SCAS is also part of the major incident response for Buckinghamshire and has robust internal business continuity plans. Links to the local council(s) for logistical operational planning and incident management, such as large public gatherings also fall under this arena. Emergency Preparedness, Resilience and Response (EPRR), Business continuity and Daily Resilience To comply with the requirements of a category 2 responder (Civil Contingency Act 2004) and the NHS Standard Contract section 30, Aylesbury Vale CCG and Chiltern CCG have a Major Incident Framework 2014, Incident Response Plan 2014, Business Continuity Plans 2014 and CCG escalation Framework 2014 in place. This is supported by the 24/7 on call director arrangements. All the on call directors have been trained to the required Skills for Justice National Occupational Standards. As part of the national 2013/14 Emergency Preparedness, Resilience and Response (EPRR) assurance process Aylesbury Vale CCG and Chiltern CCG provided assurance to NHS England and the CCGs Governing Body that they were fully compliant with the NHS core standards for Emergency Preparedness, Resilience and Response This was 46
47 completed in March These EPRR core standards are the minimum standards which NHS organisations and providers of NHS funded care must meet in order to ensure that they have appropriate plans in place for responding to a wide range of incidents such as flooding, extreme weather, surge in demand and incidents effecting business continuity. As part of the annual EPRR assurance process for 2013/14 Buckinghamshire Healthcare NHS Trust was required to assess itself against the NHS core standards for EPRR. In the main BHT was compliant and developed an improvement plan for outstanding actions. BHT has a Resilience Committee chaired by the Accountable Emergency Officer. The Resilience Committee has clear roles and responsibilities with designated working groups to complete the action plan. The Resilience Committee has been cited as an example of good practice by NHS England Thames Valley. The new assurance framework was published in July 2014 and Aylesbury Vale CCG and Chiltern CCG are in the process of repeating the self-assessment. This will be undertaken before winter. The CCG is currently reviewing the 2014/15 submission from BHT. All organisations have robust business continuity plans in place which detail individual service line responses to service interruption, including management of services during inclement weather. Currently, the overarching CSU plan is currently expected by the National Business Continuity team. Daily Whole System Resilience. Buckinghamshire and Berkshire CCGs Escalation Framework 2014 was updated after the Buckinghamshire whole systems winter exercise 2013 and the updated NHS England Thames Valley Framework The framework sets out the procedures to manage day to day variations in demand across health and social care systems as well as the procedures for managing significant surges in demand. The purpose is to ensure that all partners, health and social care have a mechanism to access additional capacity in the right part of the system when demand peaks. The CCG has responsibility, working with partners, to manage resilience within the system. On a daily basis Thames Valley Emergency Access coordinates the system supported by the CCG which provides in hours operational manager and 24/7 coverage at Director level as required. 4.0 System Resilience Planning 2014/15 47
48 The ORCP and vision is to ensure robust resilience and capacity planning going forwards into Nationally this has been driven by the recognition of the pressure A&E s continue to be under and in a local context it offers a system-wide approach to cross-provider planning and joined up care. This in turn benefits patients, carers and families, and also allows for better staff planning and provision. Completing the national template has provided a system-wide opportunity to undertake a gap analysis around services currently in place, and this has begun to highlight what needs to be developed next. Within the resilience portfolio, the ORCP also includes working relationships with the Bucks County Council and the Thames Valley Area Team for areas such as flu planning and Primary Care capacity. The ORCP is currently in the process of setting local service provision within the national strategic direction by: Reviewing the terms of reference of the Urgent Care Working Group to take into account local delivery of system resilience across urgent and planned care Setting up an operational System Resilience Task & Finish Group to develop the plan. The ongoing requirement for this group is being reviewed as it has been considered a useful operational forum. Acknowledging and utilising opportunities for provider cross-working and coterminus service and personnel / staff funding. Planning based on business intelligence to produce evidence based outcomes of care which benefits patients by intelligent dashboard development. Supporting an overall system performance within the UCWG/ SRG and by linking to internal provider programmes to broker service development interfaces. Coordinating and planning with provider partner stakeholders to ensure system-wide cohesion, performance and service delivery. 4.1 National Timeline 48
49 As a High Risk system, Buckinghamshire will receive support and input into the resilience and capacity planning feedback and will work with NHSE and the TDA to ensure recovery and service improvement plans are put in place. The subsequent plans will be signed off by the SRG and internal stakeholder boards, with the final plans being signed off by all partner organisations and published on CCG websites during September. Plans will be revisited in October, and it is noted that the public visibility of the plans will require communication strategies to be put in place. Risk assessment processes have been put in place as part of general controls assurance for Buckinghamshire and the SRG has oversight and ownership of the plans. Risk areas are noted as primary care and pace of change within social care requirements. 4.2 ORCP Assurance Process The process for system resilience plan sign off for Buckinghamshire will follow the national timetable and the internal agreed oversight procedure defined in the CCG s Urgent Care Working Group /SRG Terms of Reference. 4 The Executive Board will be sighted on the contents of the capacity and resilience plan, and the SRG will be the oversight, scrutiny, and decision making body, supported by the SRG Task and Finish Group. External review and ratification will be undertaken in line with the Area Teams (NHSE) process which is as follows: a. Elective ECIST Workshop: b. Collective Assurance of ORCP Plans TOR awaited from the Area Team. 49
50 c. Area Team, and TDA attendance at the September SRG The on-going developmental assurance and oversight within the template has been iterative in nature and this has ensured whole system input and agreement. The template itself has been fully reviewed and correlated with the Winter Bids allocations 2014/15 to deliver cross provider pathway working, inter provider operability and innovation. The System Resilience Group discussed the initial bids from organisations for the available funding at the meeting on 29 th July. The group prioritised those bids which would add greatest value to the system resilience and agreed the initial submission to NHSE. The meeting also included confirmation from all organisations that their submissions which formed the plan had been approved by their Chief Executive and Finances by the Director of Finance. On the 9 th September the revised plan was approved by SRG for submission to NHSE for the assurance meeting on the 16th September. The SRG included Director level representatives who were able to agree this system wide approach on behalf of their organisations. Once the plan has been agreed by NHSE the plan will be taken to organisations Boards. The system maturity is reflected in the overall decision making process and progress as detailed in the return. The exercise itself has been transparent and focused on on-going resilience rather than short term fixes. Financial governance and guidance is awaited from the Area Team as Buckinghamshire has been determined as a High Risk system, and as such, monies have not been released to local finance officers. SCAS national allocation is being hosted by one nominated CCG West Berkshire, and this allocation utilisation is still in discussion. 4.3 Continued Governance & Oversight The delivery mechanism is governed monthly by the System Resilience Group (SRG) and the Urgent Care Working Group (UCWG). These meet on alternate months. SRG membership includes Director level representatives from NHS and Bucks County Council commissioners, Health Watch and all urgent care Provider stakeholders. While the UCWG has a smaller membership including CCGs, Bucks CC, SCAS, BHT, HWWP and focuses on specific topics for more in depth analysis. Both groups routinely review activity, performance, 50
51 service improvement project delivery including from the BHT Reforming Urgent Care programme (RUC) and the urgent care risk register and agree system wide actions to mitigate risks. These metrics will be supplemented by additional KPIs to ensure the ORCP is effectively governed. These groups report to the Urgent Care Joint Executive Team (UC JET), which consists of health and social care commissioners only, and review finances and performance of individual providers against their contracts. This joint approach is adopted across Buckinghamshire and also delivers efficient and integrated working across both CCGs for several other programmes of work including elective care (Right Care Group), long term conditions (Medicines Management JET), children (Children s JET) and services jointly commissioned with Bucks CC (Adult JET). JETs report to individual CCG Executive teams and through these to individual CCG Governing Bodies. 51
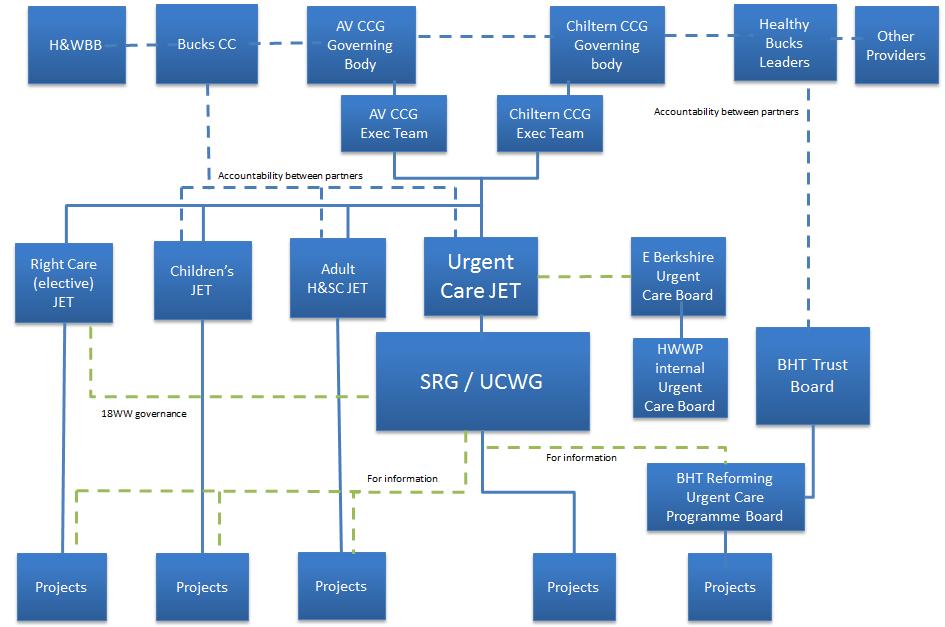
52 52
53 4.4 High Risk Reporting Requirements As a high risk system (influenced by the RTT 18 week target) TDA and Area team oversight and scrutiny will form part of the governance and reporting requirements. The SRG will be supported by a programme approach ensuring that delivery is both efficient and effective and remains focused on the desired outcomes, this will be a joint role with supporting the Reforming Urgent Care programme at BHT improvement alignment of programme reporting and delivery and reducing duplication in the system. This PMO approach brings a number of benefits to the system around the area of Resilience and capacity planning, which is both the business development driver : Provides a rapid response approach to projects and work streams Encourages a culture of empowerment and ownership by providing fit for purpose support where needed Aligns with the organisational development plan in developing and up skilling staff Provides specific support to the ORCP and RUC This approach was used successfully during the Better Healthcare in Buckinghamshire programme. The daily monitoring of demand and capacity by the winter pressure team also ensures relevant information especially during rising pressures to both the duty manager and the oncall executive. This is through a series of updates outlining any key issues, action taken or required. This is especially pertinent during times of rising pressures in preparation for the weekend should demand exceed capacity and commissioner support be required. 4.5 SRG Task & Finish Group 53
54 The SRG Task & finish Group held weekly meetings commencing the week of the 25 th June 2014, which described the process initially and oversaw the return process of both the resilience bids and the provider stakeholder templates, This was also in conjunction with the Urgent Care Working group. On 15 th July the Urgent care Working Group agreed the process setting the following timeline; SRG T&F weekly meetings Resilience Bid process deadline 22 nd July SRG T&F Template oversight and gap analysis meeting: 22 nd July UCWG sign off process 29 th July The meeting continues to run supporting the operational delivery of the wider Urgent Care Working Group / Systems Resilience group. 4.6 Daily Resilience Calls The daily resilience call also underpins system real-time analysis and immediate opportunity to make decisions and broker partner stakeholder actions. The ORCP has provided have instigated a more robust presence on the call to support providers to understand and manage bottlenecks and capacity surge; escalating within organisations and between organisations where appropriate to facilitate improved provider intra-operability. Within all of the above and particularly as part of the daily resilience call process, the ORCP process will be part of the Buckinghamshire Escalation Framework, allowing timely responses to emerging service surges or risks. Involvement of commissioners in the daily system resilience teleconferences when the system is under pressure, is key to ensuring escalation occurs based on the objective criteria within the Thames Valley escalation framework. The framework includes the requirement for Providers to not declare black status until they have discussed all options with the CCG duty director on call and agreed that this is the only option. When the system is at red escalation or higher, there is an afternoon follow up call to ensure actions decided in the morning have been completed and to decide next steps. This provides commissioners with the opportunity to deescalate quickly when circumstances have improved. The Escalation Framework This follows the NHS England alert levels, comprising 4 distinct alert levels. 54
55 Table 2: Definition of Escalation Statuses GREEN AMBER Level 1: patient flow management - The Local Health and Social Care System capacity is such that organisations are able to maintain patient flow and are able to meet anticipated demand within available resources. Commissioned levels of service will be decided locally. Level 2: mitigation of escalation The Local Health and Social Care System starting to show signs of pressure. Focused actions are required in organisations showing pressure to mitigate further escalation. Enhanced co-ordination will alert the whole system to take action to return to green status as quickly as possible. RED Level 3: whole system compromised Actions taken in Level 2 have failed to return the system to Level 1 and pressure is BLACK worsening. The Local Health and Social Care System is experiencing major pressures compromising patient flow, Further urgent actions are required across the system by all partners. Level 4: severe pressure and failure of actions All actions have failed to contain service pressures and the local Health and Social Care system is unable to deliver comprehensive emergency care. There is potential for patient care to be compromised and a serious untoward incident is reported by the system. Decisive action must be taken to recover capacity. 4.7 Patient Centred Services With the patient at the heart of all service planning and delivery both for health and episodes of care need, understanding our resilience and current capacity allows for proactive forecasting and planning. Getting it right first time in terms of care requirement, level of intervention and care provision is key to the Urgent Care work stream within the overall ORCP. The demographics of Buckinghamshire includes a recognition of the significant impact of an ageing population as part of its growth in demand. 4.8 Ambulatory Care Pathways Ambulatory care pathways will be supported by the Unplanned Admissions DES and the development of MAGS which identify, stratify and assess patient need to ensure their clinical 55
56 and social needs to not escalate and result in an unplanned and unnecessary admission. This will be dependent upon the cohesion of the ORCP along with 7/7 working. This approach will also support patients to received timely intervention, prevention and care closer to their own homes, preventing condition deterioration and promoting admission avoidance. Supporting vulnerable patients within their own local home and or / care environments is accepted as both best practice and best for patient outcomes. This does require close joint working with social care services as patients often have multiple health co-morbidities along with complex social care requirements. As part of the overall development of Unplanned Care a number of supportive programmes of work have been and continue to be underway across all partner stakeholders underpinning the planning and delivery of the ORCP. Within the ORCP planning process, three key flows are identified as follows, and planning and bid review and allocation undertaken accordingly. They are: Admission Avoidance Prior to Admission Assessment Services ED Front Door and in Hospital Flow Supported Discharge See fig 1.0 Pre- Hospital Community Ed front Door & In Hospital Flow Supported Discharge Which may be understood as a non-linear whole system of health and social care provision which maximises patient experiences and outcomes along with ensuring best value for 56
57 money and return on an investment that includes health outcomes, staff performance and asset utilization. 5.0 Stakeholder Engagement and Empowerment Across the Buckinghamshire system, patient engagement, involvement and empowerment is seen as central to delivery of service provision. Patient behaviour, footfall and health and social care access is recognised as key to new pathway redesign, new ways of working and as such, produces a strong Compaq between services and outcomes. Engaging patients, carers, their families and friends is understood to build a capability that will help whole system sustainability and balance. Using the communication strategy to sign post patients to the most appropriate care setting during the winter months will help Buckinghamshire deliver the right care in the right place at the right level of intervention. Using an effective communication for the winter, which has been put forward as a winter bid, Buckinghamshire will communicate using new methods of technology, including an via an app for phones, which hosts a service finder. Further, by using intelligence to target HRGs by practice. Flu planning is also central to patient and public engagement, and again this unifies aspects of both winter bids and system resilience planning. The allocation of funding for the carer s hub based at Stoke Mandeville Hospital will enable carers of in patients to visit a one stop shop to get advice, support and sign posting to support themselves and the person the care for. Carers and their position are statutorily recognised, however, it is envisaged that the carers hub will also provide invaluable informal support, and its success has been demonstrated elsewhere. Plans to expand the carers hub to include the High Wycombe site have been discussed and will form part of the ongoing capacity & resilience programme to ensure equality of access to such support on both BHT sites. For High Wycombe this will be important due to the presence of the cardiac and stroke pathways for Buckinghamshire. 5.1 System Winter Communications and Engagement: Over the Winter months there will be an integrated communication and engagement winter pressures campaign designed to reduce inappropriate A&E attendances from Bucks residents whilst providing an instant online signposting and self-care information source. The campaign will utilise both traditional and modern communication channels and 57
58 materials, including media, social medial, leaflets and posters. There has been much liaison with communication staff in neighbouring CCG areas, to identify their needs as well as those of Bucks, so that we can achieve joined up messaging around the CCG borders and avoid confusion of patients in those areas e.g. South Bucks/East Berkshire Communications though all relevant channels are designed to:- Clearly signpost Bucks residents to appropriate health services for their needs Provide health instant self-care/health advice Encourage appropriate use of NHS 111, pharmacies and MIIU services Encourage appropriate use of health services by parents of under-fives Encourage earlier take up of pharmacy services by the elderly Promote uptake of flu vaccination Provide reassurance and increase confidence in resilience of services Action Description Audience Implementation System Confidence Letters to local MPs, HASC and other key influencing stakeholders to share resilience plans Key influencing stakeholders 1st October2014 Media release, website and newsletter content outlining actions being taken to increase resilience and to launch campaigns Staff in health and social care organisations, General public October Flu Vaccination Treat Yourself Better Talk Before You Walk The Earlier The Better Health Help Now Just Because Reminder public messaging around key dates holiday pharmacy opening times Working jointly with PH and NSHE to amplify campaign through all channels Roll out of Pharmacy Voice campaign in Bucks All Better Now campaign targeting parents of underfives using social media, shopping centre road shows materials widely distributed. Campaign to encourage frail elderly and their carers to seek pharmacy help Self-care portal to go live with promotional campaign Campaign to provide appropriate services information Vulnerable target groups as per PH plan People of working age. Parents of Under- Fives specifically fever / bronchiolitis prevention Elderly and carers All general public Students As required September/October September through to end Feb. October through to end Feb End October through to end Feb November launch. December pre- Christmas and January after Christmas. 58
59 6.0 Primary Care: Planning and Whole System Capability 6.1 Flu Planning The ORCP includes input locally on flu planning mechanisms for 2014/15. This will include both flu vaccination and prevention and NHS Pandemic flu resilience preparation. The former will focus on both at risk groups and staff groups via individual providers. Pregnant women will also be able to access flu vaccine at their booking antenatal appointments led by BHT. The communications strategy will include both the general public, patients and hard to reach groups. Taking advantage of pharmacy capability and capacity the 2014/15 ORCP will utilise pharmacists to administer the flu vaccine At Risk category patients, again providing innovation and better health outcomes for the local population Mental Health Services Mental health provision remains a priority for both local CCG pathway development and also as part of overall resilience and capacity planning for winter planning 2014/15. In up to 5% of visits made to emergency departments, the patient has a primary diagnosis of mental ill health problem. The interface between BHFT and RBH has improved in recent years and there is better joint working between these two organisations. SCAS have a CQUIN in their contract to incentivise improved management of patients with a mental health need. The PIRLS service in BHT is also an example of mental health patient pathway improvement, providing early assessment for patients who present at A&E. A previously mentioned in section 8 Rapid Assessment in Accident & Emergency Departments PIRLS is also seeking to expand its service both in terms of access service provision and as inpatient ward in-reach to improve the experience and outcomes of mental health patients. 8.0 Evidence Base and Research Review As part of overall resilience planning, AVCCG requested local public health leads to identify evidence-based interventions for reducing demand for urgent care in Bucks. The meta analysis report produced summarised the evidence from the published literature on the topic of urgent care, broken down into the areas of:
60 Section A: Section B: demand? Section C: Section D: What do we know about why Urgent and Emergency Care demand has increased generally? What does the evidence say about effective interventions for reducing What are the findings from other places? Urgent and emergency care: a prescription for the future (Recommendations from the Think-Tanks). 6 A summary of the analysis is as follows: Reasons for increased demand: A recent King s Fund report i found that age is the strongest driver for the use of hospital emergency beds with very young children and older people being at risk of higher admissions. Social deprivation and higher levels of morbidity are strongly correlated with higher rates of admissions Geographic location those who live nearer an A&E are more likely to access it whereas rural communities have lower hospital usage There is also longstanding evidence of supply induced demand suggesting that health care is more closely correlated with supply rather than need. Evidence of effective interventions: Despite considerable efforts by the health community and numerous examples of innovative programmes across England, emergency admissions have continued to rise ii. 6 Dr Shakiba Habibula Public Health team, Buckinghamshire County Council; , ref also to the RAND StudyPurdy. S Avoiding hospital Admissions. What does the evidence say? [Internet. London: The King s Fund;
61 There is very little evidence on what can be put into place to reduce non- elective admissions. The evidence that exists demonstrates that it is very hard to reduce nonelective admissions but reducing length of stay is easier. Reducing non-elective admissions is extremely challenging. The challenge is demonstrated clearly in a recent study by the King s Fund, which showed that the best performing areas in the country for reducing length of stay for over 65s (some by as much as 23%), were unable to reduce their rates of admission at all between 2006 and 2010 (Imison, 2012). The Nuffield Trust has recently considered (June 2013) thirty different service models, finding it hard to uncover those which were successful in reducing emergency admissions something that a recent review by the Kings Fund and others have also iii iv noted There is some consensus in both the published and the unpublished literature that senior decision making at the earliest possible stage will reduce attendance at A&E conversion to admission. This also seems true of reducing length of stay in elderly patients it is vital to get them on the right care plan, as defined by a senior clinician, as soon as possible. Evidence so far from numerous studies have not been able to demonstrate a reduction in A & E admissions or attendances due to generic case management of high risk patients, in fact, the evaluation of the recent English integrated care pilots found a significant increase in emergency admissions (Roland et al, 2012) and these were most marked in case management sites. (See Appendix IV) /14 Winter Review and Lessons Learned In January 2014 the Bucks Urgent Care Working Group (UCWG) undertook a hot debrief to identify lessons learnt that would assist in planning for This involved stakeholders 61

62 from Health and Social Care commissioners and Providers including BHT, HWWP, SCAS, Bucs CC and Oxford Health. Key learning points were: There are reduced discharges at week-ends due to lack of ASC staff to organise care packages Spot purchasing is useful in transferring people out of hospital HALO in A&E reduces handover delays Patients requiring admission are arriving late in the day Variation between demand for admission and discharges leading to acute capacity problems and 100% bed capacity, which exacerbates efforts to reduce LOS These have informed these plans for In 2013/14, the schemes were mainly targeted at the acute flow sector as that was highlighted as the greatest performance risk area. Going forwards, 2014/15 will see a system-wide approach with clearly determined KPIs and performance monitoring. 2013/14 performance data review illustrates the necessity to establish a known baseline, whilst setting aspirational improvement measures for 2014/15, during the winter months and through steady sate behaviours throughout the financial year. In terms of staff post implementations, lessons learned also include the need to understand the lead in time for posts to become live from bid allocation stage to on site working, this has to be taken in to account for new posts requested in 2014/15. Some staff groups are a scare resource nationally, and so as part of whole systems thinking new ways of working, professional accountability and resourceful job planning with extended roles into areas such as nurse led discharge have to be part of the forward ORCP. 62

63 8.2 Resilience Bids 2014/15 The Resilience bids process for 2014/15 has been undertaken as part of the overall Resilience and Capacity Planning process as stipulated by NHSE and Monitor 7, with a funding potential of 2.7 million. The aim of the planning guidance is to ensure resilient plans that support delivery across Buckinghamshire and stakeholder providers in times of surge demand, such as winter. The process itself has provided the opportunity for a gap analysis which has allowed Buckinghamshire health and social care providers to see where steady state operational planning is not yet providing fully assured capability and, and such poses a risk to increased seasonal surge demand. Using the funds to support seasonal surge predicted demand in winter 2014/15 the SRG reviewed 27 bids in total. The SRG took the decision to allocate funds across the provider stakeholder organisations based on system capacity and resilience requirements going forwards. A summary of current funding proposals are included in Appendix III, key elements include: Remodelling of pathways and service provision Supporting ECIST recommendations Ambulatory Care Development 7 silience_and_capacity_planning_for_ pdf 63
64 Discharge to Access Bed capacity Admissions Avoidance Ambulance Capacity & Turnaround Extension to Mental Health In-reach Carers Hub Development Communications Support South Bucks Flows Around Heatherwood & Wexham park This will ensure that the rising demand for services is managed across a broader portfolio of provision and intervention which will ensure return on investment, best value for money and improved patient outcomes. Underpinning this will be the management of the Urgent care pathway in a broader framework which will reduce A&E demand and see an increase in services being provided differently at a variety of stratified care needs locations. The resilience plan and bid allocation has been taken with due consideration from all partner stakeholders via the SRG and has taken into account system-wide challenges. The SRG have also attempted to look longer term within this planning process whilst accepting winter non-recurrent funding is time limited. A fully transparent process has been undertaken and some challenging choices made within the financial envelope available. The SRG group has made financial allocation decision based on the best fit and best system return in line with the strategic direction of travel. The ORCP resilience bid submission for 2014/15 clearly describes a portfolio of provision ranging from staff, to transport, to increased clinical and social care capacity, alongside innovation. These bids must be seen in the wider context of other investments such as through the Section 256 in Social Care Services with a health benefit and in Primary Care through the Unplanned Admissions DES and Over 75 fund. A financial summary is included below: Within the resilience bids for 2014/15, and as a prerequisite from NHSE and Monitor to release the funding to local CCGs, Buckinghamshire bids all have pre-determined KPIs which detail per scheme their predicted outcome. This will be monitored weekly and published monthly on a public facing website having been locally agreed and signed off through the SRG and the accountable officer. Buckinghamshire as a High Risk system will 64
65 now also work with closely with all parties, including the TDA and NHSE to ensure delivery across the provider network. 8.3 Whole System Review: SRG Task & Finish Process The bids and the KPIs have been agreed through the SRG process and represent whole systems resilience thinking. The SRG Task and Finish meeting held on 22 nd July reviewed all SRG plans to date and undertook a matrix mapping exercise of the bid requirements per provider. This provided a gap analysis of what areas require development for ORCP going forwards. A key component of managing winter pressures includes the flexibility to commission additional short-term health and social care capacity, such as spot purchasing beds, and light building alterations to facilitate timely discharge. This acknowledges that despite robust escalation plans, winter places on the system additional surges in demand and pressures on capacity. This can be multifactorial and includes infectious disease outbreaks.e.g. norovirus or reduced capacity as part of planned strategic changes. For winter 2014/2015, the CCGs have the ability to fund additional capacity across primary, secondary, community health and social care with an investment of 2.7 million across both AVCCG and CCCG locally. A cost-benefits analysis is currently underway of all schemes to inform what the priorities should be to support the system in winter 2014/2015. There has been some success using the Winter Monies during 2013/14, however the system is still not achieving all key performance measures, and further improvement is needed. We have reflected upon the lessons learnt from last winter. Key themes have emerged which have been shared at the Thames Valley Area Team: 1. The outcomes to be delivered must be determined at the outset with clarity on the Whole System impact. System wide improvement to drive use of resources. 2. Each project scope, interfaces, interdependencies should be clearly determined. 65
66 3. Clear KPI s and milestones to be set with all interested parties and actively used to ensure the project is delivering each month. 4. Risks to delivery should be identified early such as hard to recruit staff or complex IT requirements. 5. Need to establish an overarching programme approach with proportionate individual project reporting. Reporting mechanisms to be agreed for each organisation and across organisations. 6. Minimum performance standards should be used to indicate where a scheme is failing and should be halted. 7. Value for money criteria should agreed at the outset. 8. Evaluation methodology of each scheme needs to be built into original proposal. Alongside this work sits escalation planning which forms an integral part of system resilience and winter planning within the Local Health & Social Care Community, throughout all community and hospital care settings. The integrated framework will aim to provide a consistent and co-ordinated approach to the management of pressures across the CCGs acute and emergency care systems. The 2013/2014 escalation plan review commenced at the end of March and includes key pieces of work being taken forward: These themes have been shared with the SRG and have been incorporated into the planning, allocation and oversight of the 2014/15 resilience bids. 9.0 Winter Bids 2013/14 During 2013/2014 all bids were assessed against the following principles and criteria and these will be utilised again during 2014/2015: (See table 2.0). 66

67 The winter bid offers escalation capacity that is above core contract provision and supports resilience at times of system surge. The winter bid ensures that patient safety and quality are maintained or improved. Primary care options deflecting ED attendance and admission (where clinically appropriate) Providing a cohort of escalation beds to support extremis pressures e.g. times of demand surge or noro-virus outbreaks etc Supports 7/7 working Supports delivery of targets, Handover times, ED & DToCs Alongside a further set of questions which focus on whole system fit: Table SRG ORCP Template Collation 67
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
NHS ENGLAND BOARD PAPER
 NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
Developing out of hospital care: Update on community hubs pilot April 2017 August 2017
 Developing out of hospital care: Update on community hubs pilot April 2017 August 2017 Contents Heading 1 Executive summary 3 2 Developing out of hospital care: what we have done 5 3 How have we improved
Developing out of hospital care: Update on community hubs pilot April 2017 August 2017 Contents Heading 1 Executive summary 3 2 Developing out of hospital care: what we have done 5 3 How have we improved
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Seven day hospital services: case study. South Warwickshire NHS Foundation Trust
 Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
RTT Recovery Planning and Trajectory Development: A Cambridge Tale
 RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
North West London Accident and Emergency Performance Report for the winter of 2016/17. North West London Joint Health Overview and Scrutiny Committee
 North West London Accident and Emergency Performance Report for the winter of 2016/17 North West London Joint Health Overview and Scrutiny Committee 20 April 2017 1 This paper will summarise the performance
North West London Accident and Emergency Performance Report for the winter of 2016/17 North West London Joint Health Overview and Scrutiny Committee 20 April 2017 1 This paper will summarise the performance
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Kingston Hospital NHS Foundation Trust Length of stay case study. October 2014
 Kingston Hospital NHS Foundation Trust Length of stay case study October 2014 The hospital has around 520 beds and provides acute medical services for a population of around 320,000 in Kingston, Richmond,
Kingston Hospital NHS Foundation Trust Length of stay case study October 2014 The hospital has around 520 beds and provides acute medical services for a population of around 320,000 in Kingston, Richmond,
Aylesbury Vale Clinical Commissioning Group Innovation & QIPP Report, September 2013
 Aylesbury Vale Clinical Commissioning Group Innovation & QIPP Report, September 2013 1. Introduction Programme Activity Finance Milestones InPACT (Urgent Care) Chronic diseases (LTCs) Early Years (Children
Aylesbury Vale Clinical Commissioning Group Innovation & QIPP Report, September 2013 1. Introduction Programme Activity Finance Milestones InPACT (Urgent Care) Chronic diseases (LTCs) Early Years (Children
Redesign of Front Door
 Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
BOARD OF DIRECTORS. Sue Watkinson Chief Operating Officer
 Affiliated Teaching Hospital BOARD OF DIRECTORS 28 TH SEPTEMBER 2012 AGENDA ITEM: 11.1 TITLE: INTENSIVE SUPPORT TEAM REPORT PURPOSE: The Board of Directors is presented with the report from the Intensive
Affiliated Teaching Hospital BOARD OF DIRECTORS 28 TH SEPTEMBER 2012 AGENDA ITEM: 11.1 TITLE: INTENSIVE SUPPORT TEAM REPORT PURPOSE: The Board of Directors is presented with the report from the Intensive
Report to the Board of Directors 2016/17
 Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
This SLA covers an enhanced service for care homes for older people and not any other care category of home.
 Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
NHS England (South) Surge Management Framework
 Surge Management Framework") NHS England (South) Surge Management Framework THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK 2 NHS England (South) Surge Management Framework Version number: 1.0 First published: August 2015 Prepared by:
NHS England (South) Surge Management Framework THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK 2 NHS England (South) Surge Management Framework Version number: 1.0 First published: August 2015 Prepared by:
Key Objectives To communicate business continuity planning over this period that is in line with Board continuity plans and enables the Board:
 Golden Jubilee Foundation Winter Plan 2016/2017 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This plan
Golden Jubilee Foundation Winter Plan 2016/2017 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This plan
NHS Electronic Referrals Service. Paper Switch Off an update Digital Health Webinar 4 May 2018
 NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
Summary two year operating plan 2017/18
 One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
Buckinghamshire Integrated Care System. Integrated Operations Plan
 Buckinghamshire Integrated Care System Integrated Operations Plan 2018-19 Integrated Operational System Plan 2018-19 01 Executive Summary 02 Introduction 03 Our Emerging Care Models 04 Our Transformation
Buckinghamshire Integrated Care System Integrated Operations Plan 2018-19 Integrated Operational System Plan 2018-19 01 Executive Summary 02 Introduction 03 Our Emerging Care Models 04 Our Transformation
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Greater Manchester Health and Social Care Strategic Partnership Board
 Greater Manchester Health and Social Care Strategic Partnership Board 7 Date: 13 October 2017 Subject: Report of: Greater Manchester Model for Urgent Primary Care Dr Tracey Vell, Associate Lead for Primary
Greater Manchester Health and Social Care Strategic Partnership Board 7 Date: 13 October 2017 Subject: Report of: Greater Manchester Model for Urgent Primary Care Dr Tracey Vell, Associate Lead for Primary
Strategic Risk Report 12 September 2016
 Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
DRAFT. Rehabilitation and Enablement Services Redesign
 DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Strategic Risk Report 4 July 2016
 Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
This will activate and empower people to become more confident to manage their own health.
 Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
Meeting in Common of the Boards of NHS England and NHS Improvement. 1. This paper updates the NHS England and NHS Improvement Boards on:
 NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
Better Healthcare in Bucks Reconfiguring acute services
 service redesign case study March 2013 No. 3 Reconfiguring acute services Key points Reach a shared understanding of the case for change across the local health economy. Start public engagement as early
service redesign case study March 2013 No. 3 Reconfiguring acute services Key points Reach a shared understanding of the case for change across the local health economy. Start public engagement as early
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL
 DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
18 Weeks Referral to Treatment (RTT) Standard Recovery Planning and Assurance Framework
 Standard Recovery Planning and Assurance Framework") 18 Weeks Referral to Treatment (RTT) Standard Recovery Planning and Assurance Framework Vicky Scott Head of Delivery & Development (North West London) NHS Trust Development Authority Lyndsay Pendegrass
18 Weeks Referral to Treatment (RTT) Standard Recovery Planning and Assurance Framework Vicky Scott Head of Delivery & Development (North West London) NHS Trust Development Authority Lyndsay Pendegrass
NHS 111 Clinical Governance Information Pack
 NHS 111 Clinical Governance Information Pack This pack is designed to help you develop your local NHS 111 clinical governance framework and explain how it fits in to the wider context. It takes you through
NHS 111 Clinical Governance Information Pack This pack is designed to help you develop your local NHS 111 clinical governance framework and explain how it fits in to the wider context. It takes you through
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
5. Does this paper provide evidence of assurance against the Governing Body Assurance Framework?
 Item Number: 6.3 Governing Body Meeting: 4 February 2016 Report Sponsor Anthony Fitzgerald Director of Strategy and Delivery Report Author Anthony Fitzgerald Director of Strategy and Delivery 1. Title
Item Number: 6.3 Governing Body Meeting: 4 February 2016 Report Sponsor Anthony Fitzgerald Director of Strategy and Delivery Report Author Anthony Fitzgerald Director of Strategy and Delivery 1. Title
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report
 Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
Winter/Surge Capacity Plan 1 st December 2013 to 31 st March Position as at September 2013
 Winter/Surge Capacity Plan 1 st December 2013 to 31 st March 2014 Position as at September 2013 Contents 1. Introduction and background... 3 2. Demand and capacity... 4 2.1. Anticipated bed demand... 4
Winter/Surge Capacity Plan 1 st December 2013 to 31 st March 2014 Position as at September 2013 Contents 1. Introduction and background... 3 2. Demand and capacity... 4 2.1. Anticipated bed demand... 4
MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE. Purpose of Report: For Note
 Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
Report to the Board of Directors 2015/16
 Attachment 9 Report to the Board of Directors 2015/16 Date of meeting 18 Subject Report of Prepared by Seven Day Services Medical Director Ashling Rivá, Project Manager Previously considered by Transformation
Attachment 9 Report to the Board of Directors 2015/16 Date of meeting 18 Subject Report of Prepared by Seven Day Services Medical Director Ashling Rivá, Project Manager Previously considered by Transformation
A meeting of NHS Bromley CCG Governing Body 25 May 2017
 South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST BOARD OF DIRECTORS. Emergency Department Progress Report
 UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST Date of meeting: 27 June Title / Subject: Status Purpose: Report of: Prepared by: BOARD OF DIRECTORS Public To update the Board of actions being
UNIVERSITY HOSPITALS OF MORECAMBE BAY NHS FOUNDATION TRUST Date of meeting: 27 June Title / Subject: Status Purpose: Report of: Prepared by: BOARD OF DIRECTORS Public To update the Board of actions being
OFFICIAL. Commissioning a Functionally Integrated Urgent Care Access, Treatment and Clinical Advice Service
 Our Ref: BH/2015/253 Publications Gateway Ref. No. 03568 NHS England Quarry House Quarry Hill Leeds LS2 7UE Email : england.nhs111@nhs.net To: CCG Accountable Officers CCG Clinical Leaders Cc: Regional
Our Ref: BH/2015/253 Publications Gateway Ref. No. 03568 NHS England Quarry House Quarry Hill Leeds LS2 7UE Email : england.nhs111@nhs.net To: CCG Accountable Officers CCG Clinical Leaders Cc: Regional
Approve Ratify For Discussion For Information
 NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
The Five Year Forward View and Commissioning Mental Health Services in 2015 and Beyond
 The Five Year Forward View and Commissioning Mental Health Services in 2015 and Beyond Thames Valley Strategic Clinical Networks February 2015 Table of Contents Introduction & Context pp 3-11 SCN recommendations
The Five Year Forward View and Commissioning Mental Health Services in 2015 and Beyond Thames Valley Strategic Clinical Networks February 2015 Table of Contents Introduction & Context pp 3-11 SCN recommendations
Strategic Risk Report 1 March 2018
 Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
Primary Care Strategy. Draft for Consultation November 2016
 Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
The Bedfordshire CCG and Bedford Borough Council Better Care Plan Executive Summary: Our approach to Better Care planning
 DRAFT Version 16 19 March 2014 The Bedfordshire CCG and Bedford Borough Council Better Care Plan Executive Summary: Our approach to Better Care planning Bedford Borough and Bedfordshire CCG s Better Care
DRAFT Version 16 19 March 2014 The Bedfordshire CCG and Bedford Borough Council Better Care Plan Executive Summary: Our approach to Better Care planning Bedford Borough and Bedfordshire CCG s Better Care
Marginal Rate Emergency Threshold. Executive Summary
 Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Urgent & Emergency Care Strategy Update
 RCCG/GB/17/144 Urgent & Emergency Care Strategy Update 1. Introduction The purpose of this paper is to provide assurance on the effective delivery to date of our urgent and emergency care strategy within
RCCG/GB/17/144 Urgent & Emergency Care Strategy Update 1. Introduction The purpose of this paper is to provide assurance on the effective delivery to date of our urgent and emergency care strategy within
Portsmouth Hospitals NHS Trust Winter/Surg Plan 2013/14. pg. 1
 Portsmouth Hospitals NHS Trust Winter/Surg Plan 2013/14 pg. 1 Introduction The purpose of this winter/surg plan is to ensure that Portsmouth Hospitals NHS Trust (PHT) is prepared and co-ordinated to respond
Portsmouth Hospitals NHS Trust Winter/Surg Plan 2013/14 pg. 1 Introduction The purpose of this winter/surg plan is to ensure that Portsmouth Hospitals NHS Trust (PHT) is prepared and co-ordinated to respond
Agenda Item 3.3 IMPLEMENTATION OF SETTING THE DIRECTION - WHOLE SYSTEMS CHANGE PROGRESS UPDATE
 FOR INFORMATION UHB Board Meeting: 17 January 2012 IMPLEMENTATION OF SETTING THE DIRECTION - WHOLE SYSTEMS CHANGE PROGRESS UPDATE Report of Paper prepared by Executive Summary Director of Public Health
FOR INFORMATION UHB Board Meeting: 17 January 2012 IMPLEMENTATION OF SETTING THE DIRECTION - WHOLE SYSTEMS CHANGE PROGRESS UPDATE Report of Paper prepared by Executive Summary Director of Public Health
Aylesbury Vale Clinical Commissioning Group Innovation & QIPP Report, October 2013
 Aylesbury Vale Clinical Commissioning Group Innovation & QIPP Report, October 2013 1. Introduction Programme Activity Finance Milestones InPACT (Urgent Care) Chronic diseases (LTCs) Early Years (Children
Aylesbury Vale Clinical Commissioning Group Innovation & QIPP Report, October 2013 1. Introduction Programme Activity Finance Milestones InPACT (Urgent Care) Chronic diseases (LTCs) Early Years (Children
NHS GRAMPIAN. Grampian Clinical Strategy - Planned Care
 NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
The Welsh NHS Confederation response to the Health, Social Care and Sport Committee Inquiry into winter preparedness 2016/17.
 Contact: The Welsh NHS Confederation response to the Health, Social Care and Sport Committee Inquiry into winter preparedness 2016/17. Date: 8 September 2016 Nesta Lloyd Jones, Policy and Public Affairs
Contact: The Welsh NHS Confederation response to the Health, Social Care and Sport Committee Inquiry into winter preparedness 2016/17. Date: 8 September 2016 Nesta Lloyd Jones, Policy and Public Affairs
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
This paper explains the way in which part of the system is changing to become clearer and more accessible, beginning with NHS 111.
 Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
Urgent Treatment Centres Principles and Standards
 Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Driving and Supporting Improvement in Primary Care
 Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER C Hickson, Head of Management Accounts
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
NHS England (London) Assurance of the BEH Clinical Strategy
 Assurance of the BEH Clinical Strategy") NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
Integrated Care in North Central London
 Integrated Care in North Central London 5 th July 2012 Sylvia Kennedy AD Strategy & Planning Strategic context Many of our frailest and sickest groups receive care in a fragmented and disorganised way
Integrated Care in North Central London 5 th July 2012 Sylvia Kennedy AD Strategy & Planning Strategic context Many of our frailest and sickest groups receive care in a fragmented and disorganised way
Clinical Pharmacists in General Practice March 2018
 Clinical Pharmacists in General Practice March 2018 1. Background Following a successful national pilot programme, the General Practice Forward View committed over 100million to support an extra 1,500
Clinical Pharmacists in General Practice March 2018 1. Background Following a successful national pilot programme, the General Practice Forward View committed over 100million to support an extra 1,500
Halton. Local system review report Health and Wellbeing Board. Background and scope of the local system review. The review team
 Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
Urgent and Emergency Care Review and a commissioning perspective
 Urgent and Emergency Care Review and a commissioning perspective Anne Joshua NHS 111 Pharmacy Lead, NHS England 26 th March 2015 National vision for urgent and emergency care: Whole system transformation
Urgent and Emergency Care Review and a commissioning perspective Anne Joshua NHS 111 Pharmacy Lead, NHS England 26 th March 2015 National vision for urgent and emergency care: Whole system transformation
15. UNPLANNED CARE PLANNING FRAMEWORK Analysis of Local Position
 15. UNPLANNED CARE PLANNING FRAMEWORK 15.1 Analysis of Local Position 15.1.1 Within Renfrewshire unplanned care spans the organisational boundaries of acute and primary care services and social work services
15. UNPLANNED CARE PLANNING FRAMEWORK 15.1 Analysis of Local Position 15.1.1 Within Renfrewshire unplanned care spans the organisational boundaries of acute and primary care services and social work services
Author: Kelvin Grabham, Associate Director of Performance & Information
 Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
2020 Objectives July 2016
 ... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
NHS Portsmouth CCG 2013/14 Contract Agreements Summary. Michelle Spandley Deputy Chief Finance Officer May Improving health services
 NHS Portsmouth CCG 2013/14 Contract Agreements Summary Michelle Spandley Deputy Chief Finance Officer May 2013 Contents Contracts Summary Portsmouth Hospitals NHS Trust Solent NHS Trust South Central Ambulance
NHS Portsmouth CCG 2013/14 Contract Agreements Summary Michelle Spandley Deputy Chief Finance Officer May 2013 Contents Contracts Summary Portsmouth Hospitals NHS Trust Solent NHS Trust South Central Ambulance
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board. Audit year: Issued: October 2015 Document reference: 491A2015
 Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
The Board is asked to note the report and to support the delivery of the Operational Plan and associated work programmes during 2017/18 and 2018/19.
 Subject: Reason for briefing note: Responsible officer(s): Senior leader sponsor: Windsor, Ascot & Maidenhead CCG Operating Plan 2017-19 Refresh To present the WAM CCG Operating Plan Refresh information
Subject: Reason for briefing note: Responsible officer(s): Senior leader sponsor: Windsor, Ascot & Maidenhead CCG Operating Plan 2017-19 Refresh To present the WAM CCG Operating Plan Refresh information
04c. Clinical Standards included in the Strategic Outline Care part 1, published in December 216
 0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
Westminster Partnership Board for Health and Care. 17 January pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Trust Board Meeting 05 May 2016
 Trust Board Meeting 05 May 2016 Title of the paper: Sustainability and Transformation Plan (STP) Update Agenda item: 15/37 Lead Executive: Trust objective: Purpose: Link to Board Assurance Framework (BAF)
Trust Board Meeting 05 May 2016 Title of the paper: Sustainability and Transformation Plan (STP) Update Agenda item: 15/37 Lead Executive: Trust objective: Purpose: Link to Board Assurance Framework (BAF)
Improving Healthcare Together : NHS Surrey Downs, Sutton and Merton clinical commissioning groups Issues Paper
 Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Moving to 7 Day Services. Kerry Gant, Head of Finance Change Team/Debbie Freake, Executive Director of Strategy
 Report to Trust Board of Directors Date of Meeting: 24 March 2015 Enclosure Number: 12 Title of Report: Author: Executive Lead: Responsible Sub- Committee (if appropriate): Executive Summary: Moving to
Report to Trust Board of Directors Date of Meeting: 24 March 2015 Enclosure Number: 12 Title of Report: Author: Executive Lead: Responsible Sub- Committee (if appropriate): Executive Summary: Moving to
Review of Local Enhanced Services
 Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
South East Essex. Discharge to Assess Strategy
 South East Essex Discharge to Assess Strategy 2018-2020 Version 3.5 27 th March 2018 Document Control: Revision: Name Date: Version 2.0 Shirley Regan 12 December 2017 Version 2.1 Amendments-Paul 19 December
South East Essex Discharge to Assess Strategy 2018-2020 Version 3.5 27 th March 2018 Document Control: Revision: Name Date: Version 2.0 Shirley Regan 12 December 2017 Version 2.1 Amendments-Paul 19 December
DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES
 Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Improving General Practice for the People of West Cheshire
 Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Unscheduled care Urgent and Emergency Care
 Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
OFFICIAL. Integrated Urgent Care Key Performance Indicators and Quality Standards Page 1 of 20
 Integrated Urgent Care Key Performance Indicators and Quality Standards 2018 Page 1 of 20 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing
Integrated Urgent Care Key Performance Indicators and Quality Standards 2018 Page 1 of 20 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing
WELCOME. To our first Annual General Meeting (AGM) Local clinicians working with local people for a healthier future
 Local clinicians working with local people for a healthier future") WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual