Toronto s Mental Health and Addictions Emergency Department Alliance
|
|
|
- Georgiana McKinney
- 5 years ago
- Views:
Transcription



")





1 Toronto s Mental Health and Addictions Emergency Department Alliance Ian Dawe, MHSc, MD, FRCP(C) Physician-in-Chief Ontario Shores Centre for Mental Health Sciences Head, Division of General Psychiatry Associate Professor, Department of Psychiatry University of Toronto 6/22/2011
2 Learning objectives To enhance knowledge of: The City of Toronto s Mental Health and Addictions Emergency Department Alliance (Alliance) Answers to important questions such as : What resources exist within Toronto (Ontario, Canada) Emergency Departments to serve people with mental health and addiction needs? How much are these resources being used? Who is using Toronto Emergency Departments for mental health and addiction needs? How are people moving into, through and out of Toronto Emergency Departments? How were the Health Leaders and MDs engaged? 2
3 The Mental Health and Addictions Emergency Department Alliance Alliance Steering Committee Medical Director Manager and Flow Coordinator Alliance Partner Hospital IP Medical Directors Alliance Partner Hospital PES Medical Directors Alliance Frequent Users Work Group Seniors Mental Health Working Group Common Assessment Working Group Inter-Hospital Bed Access Model Working Group Indicators of Alliance Impact Working Group
4 4
5 Toronto s MH&A Emergency Department opportunity Issues Consumer and family dissatisfaction Variable priority given within each organization Inter-organizational silos; limited coordination Resource limitations Stigma and discrimination System Transformation Opportunity Collaborate to improve how MH&A services are delivered in downtown Toronto Emergency Departments Supporting enablers Opportunity for improvement long identified Toronto Central LHIN focus on mental health and addictions Government priority to reduce Emergency Dep t wait times Interest across organizations to work together 5
6 The Flow Map current state Success/leading/ evidence-based practice Issue/ challenge How people enter EDs Once in a TC LHIN ED** coordination across How people leave EDs SJHC CAMH MSH UHN SMH SHSC MH&A EDA Ad hoc vs. systemic collaboration/ organizations TEGH Hard to transfer people across organizations Disposition often determined by resource availability, not the person s needs MCITs Walks-in alone Comes with/brought by family, friend or neighbour Sent by primary care provider or community psychiatrist Sent by community worker/organization* Accompanied by community worker/ organization* Transferred by acute care/psychiatric hospital Brought by crisis team (community; MCITs) Brought in by police Brought in by EMS Sent/transferred by criminal justice system (corrections facilities/courts) Limited capacity of/ insufficient communication about the existing available alternatives to the ED Voluntary Bribed/coerced Involuntary First-time visit Repeat visit Multiple visits to multiple sites Chose site Did not choose site Ill physical health Physically healthy Safety concerns (for self and/or others) No safety concerns Connected to supports Unconnected TC LHIN resident City of Toronto GTA and beyond People brought to ED with shortest wait vs. one with most appropriate services Variety of fast forward processes Insufficient ability to respond competently to the needs of Toronto s diverse populations (e.g., ethnocultural groups, transitionalaged youth, etc.) Triage (nurse) Registration (worker/nurse) ED team; can include: Nurse Social worker Students Resident(s) (if on) MD Other staff (e.g., security) Large number of people involved in care Psychiatric Emergency Services team (n/a for MSH; if needed, refer to CAMH); can include: Nurse Social worker Psychiatric assistant Resident(s) (if on) MD Other staff (e.g., security) Little/no consistent information collected and reviewed across the system Variation in practice at the individual level Short-stay/ assessment beds Little infrastructure for research Insufficient ability to identify subacute addiction needs Addictions specialist in the ED Environment not typically conducive for people with mental health and addiction needs Lengthy waits often experienced through all parts of the process Psychogeriatric specialist in the ED Admitted Varying models of service delivery Insufficient capacity and flow through some communitybased services Transition between hospital and community services not always well managed No bed; wait in ED until bed available or admission no longer needed Few complex care community services Leave under own volition Without being seen by a physician Against medical advice Discharged Without referral or follow-up appointment Discharged With follow-up appointment within same organization With referral to hospital service provider With referral to community service provider Partnerships with selected community services Inpatient beds not available when needed Admitted No partnerships with community providers at the system level Day/outpatient services for follow-up Management of inpatient flows Transferred to bed in same organization Psychiatric Medical Transferred to bed at different organization * For example: social service agency; community mental health agency; addiction treatment organization; long-term care home; school/college/university; community service organization; other organizations ** Excludes The Hospital for Sick Children Source: Team analysis 6
7
8 Partners, purpose and projects Partners Purpose Projects SHSC SJHC MSH CAMH Provide the right care, in the right place, at the right time in a respectful, client-centred manner through a collaborative process of reforming existing emergency mental health & addictions services MH&A ED Alliance Project Team Standardized assessment form Inter-hospital bed access model Psychogeriatric popl n demo n SMH TEGH UHN Reduce Emerg y Dep t wait times Ensure delivery of consistently high quality care Improve consumer and family satisfaction Increase capacity to serve specific populations Indicators of Alliance impact Frequent user popl n demo n Community partnership devel t Consultation with consumers, family members and community-based service providers * CAMH = Centre for Addiction and Mental Health; MSH = Mount Sinai Hospital; SHSC = Sunnybrook Health Sciences Centre; SJHC = St. Joseph s Health Centre; SMH = St. Michael s Hospital; TEGH = Toronto East General Hospital; UHN = University Health Network 8
9 4. Our projects and anticipated outcomes Projects, purposes and anticipated outcomes Project Purpose Anticipated outcomes Standardized assessment form project Inter-hospital bed access model Improve the consistency of approach to assessment and data collection across Toronto Central LHIN EDs Increase people s access to the services they need when they need them More consistent interdisciplinary approach to assessment and its documentation across the MH&A EDA sites More consistent approach to data collection across Toronto Central LHIN Emergency Departments Increased amount of, easier and more effective inter-organization communication and decisionmaking in patient transfer situations Increased consumer and family satisfaction with their ED experience Implementation of a protocol to facilitate and track MH&A patient transfers among MH&A EDA hospitals Reduced number of people waiting in admit-no-bed status for reduced lengths of time Improved quality of care Increased consumer and family satisfaction with their experience 9
10 Projects, purposes and anticipated outcomes (cont d) Project Purpose Anticipated outcomes Seniors MH&A project Frequent user project Improve the quality, consistency, and seamlessness of MH&A ED services to seniors Improve the quality of care provided to frequent users of Toronto Central LHIN Emergency Departments Set of best practice clinical guidelines and hospitalcommunity communication and linkage protocols Improved consistency and quality of care across MH&A EDA sites Reduced wait times in EDs More seamless transitions for seniors moving between community (e.g., CCAC services, Long-Term Care Homes, Outreach Teams) and ED services Increased consumer and family satisfaction with their ED experience Set of best practice clinical guidelines and hospitalcommunity communication and linkage protocols Improved consistency and quality of care across MH&A EDA sites Reduced use of and wait times in EDs for frequent users of MH&A ED services Increased connection and more seamless transitions for frequent users of MH&A EDA services with hospital outpatient and community-based services Increased consumer and family satisfaction with their ED experience 10
11 Projects, purposes and anticipated outcomes (cont d) Project Purpose Anticipated outcomes Indicators of Alliance impact Accurately track and report on the volumes and flow of people with MH&A needs through Toronto Central LHIN EDs Set of standardized utilization and outcome indicators and related data collection, reporting and continuous improvement processes/ infrastructure Increased ability to identify, capitalize and evaluate the impact of continuous improvement initiatives both at the individual hospital and system level 11

12 The Process of Change
13 Engaging MDs as EHLs in a Change Process Key Strategies Recognize strong orientation towards achievement Recognize pride in achievement and opportunities to disseminate results Hold responsible and accountable Provide recognition early and often 13
14 Ladder of Engagement Level Positioning Examples 8 Engagement 7 Management 6 Collaborative 5 Consultative 4 Supportive 3 Tokenism 2 Decoration 1 Manipulation MDs have ideas, set up project, and invite others to join in decision making. MDs have initial idea and decide how project is carried out; MDs take charge. Others have idea and MDs are involved in each step of project planning and implementation. Project designed/managed by others but MDs are consulted. Their views and input are valued. Others decide on project. MDs volunteer their support and others respect their views. MDs are asked for their opinions and have little to no control over how views are expressed. MDs take part in a project/initiative. MDs do or say what others instruct them to. Adapted from: Hunt, JC et al. Engaging the next generation of health leaders: Perspectives of emerging health leaders Healthcare Management Forum Spring

15 Data Collection
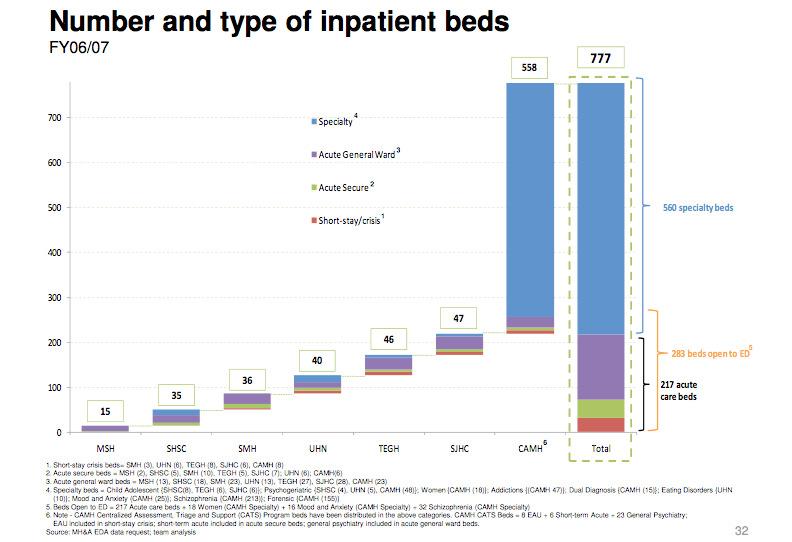
16 Summary snapshot monthly indicators Indicator July 10 August 10 September 10 July-Sept. 10 Avg. number of MHA visits per day to Alliance hospitals Total 3,057 2,935 2,777 8,769 Total number of MHA visits Period low per day Period high per day Avg. number of MHA visits per day by hospital Low High Proportion of time EDA system in surge 19% 36% 10% 20% Proportion of time EDA system in contraction 16% 32% 13% 23% Proportion of time EDA system not surging/contracting simultaneously 65% 32% 77% 57% % of MHA visits referred to PES (general hospitals) Low 19% 17% 21% 19% High 54% 51% 56% 53% Avg. psychiatric inpatient bed occupancy rate (all hospitals)* 93% 88% 91% 90% Avg. number of psychiatric inpatient beds available per day at 12am census (all hospitals) Avg. psychiatric inpatient bed occupancy rate (gen l hospitals) 91% 88% 90% 90% Avg. number of psychiatric inpatient beds available per day at 12am census (general hospitals) As of January, 10 Occupancy rate is calculated based on Acute Service beds, General Ward beds, and CAMH Schizophrenia beds, but not Short Stay beds As of April, 10 the SHSC Geriatric beds are included in the calculation. ** July-September, 09 information is not available.
17 Summary snapshot monthly indicators Indicator July 10 August 10 September 10 July-Sept. 10 Avg. occupancy rates by hospital (All hospitals) Low 79% 61% 71% 70% High 97% 96% 97% 97% Number (%) admitted to inpatient bed <3 hrs (from time of Disposition) Number (%) admitted to inpatient bed 3 hrs to 8 hrs (from time of Disposition) Number (%) admitted to inpatient bed >=8 hrs (from time of Disposition) Number (%) admitted to inpatient bed <3 hrs (from time of Patient Initial Triage)* Number (%) admitted to inpatient bed 3 hrs to 8 hrs (from time of Patient Initial Triage)* Number (%) admitted to inpatient bed >=8 hrs (from time of Patient Initial Triage)* 410 (71%) 413 (75%) 414 (72%) 1237 (73% ) 58 (10%) 73 (13%) 67 (12%) 198 (12%) 108 (19%) 63 (11%0 97 (17%) 268 (16%) 88 (15%) 59 (11%) 74 (13%) 221 (13%) 213 (37%) 222 (40%) 235 (41%) 670 (39%) 275 (48%) 268 (49%) 269 (47%) 812 (48%) Avg. wait time from the admission disposition to physical admission to an inpatient bed (general hospitals) Total average 7:40 hrs 4:07 hrs 6:44 hrs 6:11 hrs 95% CI Information is not reported Longest duration waited by a patient (general hospitals) 95:35 hrs 48:55 hrs 72:31 hrs 84:03 hrs Shortest avg. wait time (general hospitals) 3:08 hrs 2:39 hrs 3:17 hrs 3:12 hrs Data is reported as of April, 2010 ** July-September, 09 information is not available.
18 Mental Health and Addictions Emergency Department (ED)visits percent daily difference from 3 month daily average 150.0% Percent, by hospital and total system, July September, 2010 July August September 100.0% 50.0% % difference 0.0% All hospitals -50.0% % % CAMH MSH SHSC SJHC SMH TEGH UHN All hospitals No. of days the system surged* 18 No. of days the system contracted** 21 No. of days the system did not surge/contract 53 *Surge: when mental health and addictions Emergency Department visit volumes per organization are above each organization s monthly average for 5 or more hospitals ** Contraction: when mental health and addictions Emergency Department volumes per organization are less than each organization's monthly average for 5 or more hospitals Source: Decision Support Services; team analysis
19 Mental Health and Addictions Emergency Department (ED) visits total number of visits per day All Alliance hospitals, July September, July August Period high September 100 Period average 95 Number of visits 75 Period low Jul Jul Jul Jul Aug Aug Aug Sep Sep Sep-10 July 26 August 24 September23 Source: Decision Support Services; team analysis July-September, 2010 Total number of MH&A visits to the ED 8,769 Total number of ED visits 107,417 % of MH&A visits of total ED visits 8.2%
20 20
21 The Flow Map future state vision Future state vision How people enter EDs Once in a TC LHIN ED** How people leave EDs People diverted from EDs through the creation of alternatives in the community in collaboration with community network partners Walks-in alone Comes with/brought by family, friend or neighbour Sent by primary care provider or community psychiatrist Sent by community worker/organization* Accompanied by community worker/ organization* Transferred by acute care/psychiatric hospital Brought by crisis team (community; MCITs) Brought in by police Brought in by EMS Sent/transferred by criminal justice system (corrections facilities/courts) Voluntary Bribed/coerced Involuntary First-time visit Repeat visit Multiple visits to multiple sites SJHC Chose site Did not choose site Ill physical health Physically healthy Safety concerns (for self and/or others) No safety concerns Connected to supports Unconnected TC LHIN resident City of Toronto GTA and beyond CAMH People with mental health and addiction needs feel welcome and well-treated in TC LHIN EDs Reduced wait times and eradication of process- or nonvolume-related delays Consistent quality of service provided no matter who, where or how people access the system MSH Triage (nurse) Registration (worker/nurse) ED team; can include: Nurse Social worker Students Resident(s) (if on) MD Other staff (e.g., security) UHN SMH SHSC Psychiatric Emergency Services team (n/a for MSH; if needed, refer to CAMH); can include: Nurse Social worker Psychiatric assistant Resident(s) (if on) MD Other staff (e.g., security) Consistent, accurate data collection and analysis; on-going system monitoring and improvement action and implementation planning More coordinated approach to training, research and knowledge transfer within and across EDs Replication of leading and evidence-based practices across TC LHIN EDs Replication of leading and evidence-based practices across TC LHIN EDs Enhancement of general ED staff ability to serve people with mental health and addiction needs well Minimization of retelling of story through better information capture/ access and a primary focus on the person s felt need at the given time Variety of mechanisms in place to secure ongoing consumer, family and service provider input Admitted TEGH Legislationadherent sharing of information (subject to consumer consent) Community provider and ED collaboration at the system, organization and individual levels Consistent, reliable, timely connection and supported transition of people from ED to community and vice-versa No bed; wait in ED until bed available or admission no longer needed Right person is admitted to the right bed in a timely manner; eradication of admit-no-bed situations Leave under own volition Without being seen by a physician Against medical advice Discharged Without referral or follow-up appointment Discharged With follow-up appointment within same organization With referral to hospital service provider With referral to community service provider Enhanced capacity to serve people with complex but not acute needs in the community Admitted Minimization of people leaving without being seen Length of inpatient stays based on need rather than resource availability Transferred to bed in same organization Psychiatric Medical Transferred to bed at different organization * For example: social service agency; community mental health agency; addiction treatment organization; long-term care home; school/college/university; community service organization; other organizations ** Excludes The Hospital for Sick Children Source: Team analysis 21
22 Conclusions 22
23 COMPLETED OBJECTIVES Now, you have enhanced knowledge of: The City of Toronto s Mental Health and Addictions Emergency Department Alliance (Alliance) Answers to important questions such as : What resources exist within Toronto (Ontario, Canada) Emergency Departments to serve people with mental health and addiction needs? How much are these resources being used? Who is using Toronto Emergency Departments for mental health and addiction needs? How are people moving into, through and out of Toronto Emergency Departments? How were the Health Leaders and MDs engaged? 23
24 Questions? 24
Improving Flow in the Emergency Department for Mental Health and Addiction Services. Session Summary
 60 Renfrew Drive, Suite 300 Markham, ON L3R 0E1 Tel: 905 948-1872 Fax: 905 948-8011 Toll Free: 1 866 392-5446 www.centrallhin.on.ca Improving Flow in the Emergency Department for Mental Health and Addiction
60 Renfrew Drive, Suite 300 Markham, ON L3R 0E1 Tel: 905 948-1872 Fax: 905 948-8011 Toll Free: 1 866 392-5446 www.centrallhin.on.ca Improving Flow in the Emergency Department for Mental Health and Addiction
Elaine Burr - TC-CCAC Sandra Dickau - Michael Garron Hospital
 Leading Practices in Alternative Levels of Care (ALC Avoidance): Creating a Standard Framework to Support Improvement Elaine Burr - TC-CCAC Sandra Dickau - Michael Garron Hospital June 6 th 2016 OACCAC
Leading Practices in Alternative Levels of Care (ALC Avoidance): Creating a Standard Framework to Support Improvement Elaine Burr - TC-CCAC Sandra Dickau - Michael Garron Hospital June 6 th 2016 OACCAC
TC LHIN Quality Indicators: Big Dot (System) and Small Dot (Sector Specific) Indicators. November 29, 2013
 and Small Dot (Sector Specific) Indicators. November 29, 2013") TC LHIN Quality Indicators: Big Dot (System) and Small Dot (Sector Specific) Indicators November 29, 2013 1 Contents 1. TC LHIN Quality Framework, Themes and Focus Areas 2. Big Dot System Indicators 3.
TC LHIN Quality Indicators: Big Dot (System) and Small Dot (Sector Specific) Indicators November 29, 2013 1 Contents 1. TC LHIN Quality Framework, Themes and Focus Areas 2. Big Dot System Indicators 3.
IMPROVING TRANSITIONS FROM ACUTE CARE TO REHAB: SPREADING CHANGE ACROSS GTA HOSPITAL SITES FOR PATIENTS POST-HIP FRACTURE
 IMPROVING TRANSITIONS FROM ACUTE CARE TO REHAB: SPREADING CHANGE ACROSS GTA HOSPITAL SITES FOR PATIENTS POST-HIP FRACTURE GTA Rehab Network Charissa Levy, Sharon Ocampo-Chan, Donna Renzetti October 2016
IMPROVING TRANSITIONS FROM ACUTE CARE TO REHAB: SPREADING CHANGE ACROSS GTA HOSPITAL SITES FOR PATIENTS POST-HIP FRACTURE GTA Rehab Network Charissa Levy, Sharon Ocampo-Chan, Donna Renzetti October 2016
TCLHIN Standardized Discharge Summary
 TCLHIN Standardized Discharge Summary ehealth Conference June 4, 2014 Kara Kitts Quality Improvement Manager St. Michael s Hospital Ontario Healthcare System 14 Local Health Integration Networks (LHINs)
TCLHIN Standardized Discharge Summary ehealth Conference June 4, 2014 Kara Kitts Quality Improvement Manager St. Michael s Hospital Ontario Healthcare System 14 Local Health Integration Networks (LHINs)
PSYCHIATRY SERVICES UPDATE
 PSYCHIATRY SERVICES UPDATE Mark Leary MD, Interim Chief Kathy Ballou RN, Director of Nursing Anton Nigusse Bland MD, PES Medical Director Emily Lee MD, Inpatient Psychiatry Medical Director TRUE NORTH
PSYCHIATRY SERVICES UPDATE Mark Leary MD, Interim Chief Kathy Ballou RN, Director of Nursing Anton Nigusse Bland MD, PES Medical Director Emily Lee MD, Inpatient Psychiatry Medical Director TRUE NORTH
CE LHIN Board Ontario Shores Update January 19, Glenna Raymond, President and CEO
 CE LHIN Board Ontario Shores Update January 19, 2010 Glenna Raymond, President and CEO Ontario Shores: The Journey Begins 2 Divestment from Government March 27, 2006 a standalone public hospital Creation
CE LHIN Board Ontario Shores Update January 19, 2010 Glenna Raymond, President and CEO Ontario Shores: The Journey Begins 2 Divestment from Government March 27, 2006 a standalone public hospital Creation
Toronto Central LHIN 2016/2017 QIP Snapshot Report. Health Quality Ontario The provincial advisor on the quality of health care in Ontario
 Toronto Central LHIN 2016/2017 QIP Snapshot Report Health Quality Ontario The provincial advisor on the quality of health care in Ontario INTRODUCTION Purpose To give each Local Health Integration Network
Toronto Central LHIN 2016/2017 QIP Snapshot Report Health Quality Ontario The provincial advisor on the quality of health care in Ontario INTRODUCTION Purpose To give each Local Health Integration Network
FY 2016 PERFORMANCE PLAN
 Program Purpose Program Information PM1: How much did we do? FY 2016 PERFORMANCE PLAN BHD/CSE Alexis Mapes, x4889 Leslie Weisman, x4888 Maintain safety of individuals experiencing mental health crises
Program Purpose Program Information PM1: How much did we do? FY 2016 PERFORMANCE PLAN BHD/CSE Alexis Mapes, x4889 Leslie Weisman, x4888 Maintain safety of individuals experiencing mental health crises
(please print) Date of Referral: Name of referring psychiatrist / therapist / case manager: Primary Referring hospital / agency:
 Date of Referral: Name of referring psychiatrist / therapist / case manager: Primary Referring hospital / agency:") ACTT Program Referral Form Mount Sinai Hospital Community Mental Health Program Assertive Community Treatment Team (ACTT) In joint venture with Hong Fook Mental Health Association Suite 204, 260 Spadina
ACTT Program Referral Form Mount Sinai Hospital Community Mental Health Program Assertive Community Treatment Team (ACTT) In joint venture with Hong Fook Mental Health Association Suite 204, 260 Spadina
Central LHIN Community Governance Council Meeting. May 23 & 30, 2012
 Central LHIN Community Governance Council Meeting May 23 & 30, 2012 Agenda Wl Welcome and dit Introductions ti Central LHIN Overview Draft ftstrategic t Vision i and dprinciples i Community Sector Optimization
Central LHIN Community Governance Council Meeting May 23 & 30, 2012 Agenda Wl Welcome and dit Introductions ti Central LHIN Overview Draft ftstrategic t Vision i and dprinciples i Community Sector Optimization
Champlain LHIN Mental Health and Addictions Value Stream Mapping Summit February 12, 2013 Overview. Event
 1 Champlain LHIN Mental Health and Addictions Value Stream Mapping Summit February 12, 2013 Overview Event Morning Afternoon Current State Mapping Identifying opportunities Developing Action Plans 2 Participation
1 Champlain LHIN Mental Health and Addictions Value Stream Mapping Summit February 12, 2013 Overview Event Morning Afternoon Current State Mapping Identifying opportunities Developing Action Plans 2 Participation
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2014 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November 2017
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
ABC s of PES. Greg Miller, MD MBA CMO Unity Center for Behavioral Health
 ABC s of PES Greg Miller, MD MBA CMO Unity Center for Behavioral Health Content Outline Overview of Unity Services Emergency Psychiatry: Historical Perspective Emergency Psychiatry: Current Service Delivery
ABC s of PES Greg Miller, MD MBA CMO Unity Center for Behavioral Health Content Outline Overview of Unity Services Emergency Psychiatry: Historical Perspective Emergency Psychiatry: Current Service Delivery
Transforming Health Care For Seniors in the Mississauga Halton LHIN Right care, right time, right setting, right cost
 Transforming Health Care For Seniors in the Mississauga Halton LHIN Right care, right time, right setting, right cost Narendra Shah COO MH LHIN September 29, 2010 1 Implications of Alternate Level of Care
Transforming Health Care For Seniors in the Mississauga Halton LHIN Right care, right time, right setting, right cost Narendra Shah COO MH LHIN September 29, 2010 1 Implications of Alternate Level of Care
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 03/15/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 03/15/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Stronger Connections. Better Health. Primary Care Strategy Update
 Stronger Connections Better Health Primary Care Strategy Update Summer 2017 Get Involved: Connecting Primary Care through Networks Primary Care Providers have an important and unique perspective on the
Stronger Connections Better Health Primary Care Strategy Update Summer 2017 Get Involved: Connecting Primary Care through Networks Primary Care Providers have an important and unique perspective on the
2017/18 Quality Improvement Plan
 2017/18 Improvement Plan Aim Change Enough information at discharge. Readmissio ns CHF Readmissio ns COPD Did you receive enough information from hospital staff about what to do if you were worried about
2017/18 Improvement Plan Aim Change Enough information at discharge. Readmissio ns CHF Readmissio ns COPD Did you receive enough information from hospital staff about what to do if you were worried about
Improving Quality at Toronto Central LHIN. 2012/13 Year in Review
 Improving Quality at Toronto Central LHIN 2012/13 Year in Review Quality is an integral part of Toronto Central (TC) LHIN s Integrated Health Services Plan 2013-16, reflected in the goal, Better Health
Improving Quality at Toronto Central LHIN 2012/13 Year in Review Quality is an integral part of Toronto Central (TC) LHIN s Integrated Health Services Plan 2013-16, reflected in the goal, Better Health
A Model for Psychiatric Emergency Services
 A Model for Psychiatric Emergency Services Improving Access and Quality Reducing Boarding, Re-Hospitalizations and Costs Scott Zeller, MD Chief, Psychiatric Emergency Services Alameda Health System, Oakland,
A Model for Psychiatric Emergency Services Improving Access and Quality Reducing Boarding, Re-Hospitalizations and Costs Scott Zeller, MD Chief, Psychiatric Emergency Services Alameda Health System, Oakland,
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 4/1/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Behavioural Supports System Action Plan
 Behavioural Supports System Action Plan December 2012 December 2011 i Contents Background... 1 Introduction... 2 Target Population... 3 BSO Framework for Care Pillar # 1: System Coordination... 4 Current
Behavioural Supports System Action Plan December 2012 December 2011 i Contents Background... 1 Introduction... 2 Target Population... 3 BSO Framework for Care Pillar # 1: System Coordination... 4 Current
ConnectingGTA Overview. April 29, 2014
 ConnectingGTA Overview April 29, 2014 ConnectingGTA will improve the patient and clinician experience by delivering a regional electronic health record for 6.75M individuals 6 Local Health Integration
ConnectingGTA Overview April 29, 2014 ConnectingGTA will improve the patient and clinician experience by delivering a regional electronic health record for 6.75M individuals 6 Local Health Integration
Julie Kelley, MSW, MPH Program Chief, Mental Heath/Psychiatry Contra Costa Regional Medical Center Martinez, CA
 Julie Kelley, MSW, MPH Program Chief, Mental Heath/Psychiatry Contra Costa Regional Medical Center Martinez, CA Patients and Families as Care Partners April 20, 2011 Little about us Contra Costa Regional
Julie Kelley, MSW, MPH Program Chief, Mental Heath/Psychiatry Contra Costa Regional Medical Center Martinez, CA Patients and Families as Care Partners April 20, 2011 Little about us Contra Costa Regional
Psychiatric Patient Boarding Problems in the Emergency Department
 Psychiatric Patient Boarding Problems in the Emergency Department IMPROVING TIMELINESS, ACCESS, AND QUALITY LOWERING COSTS AND RE-HOSPITALIZATIONS Scott Zeller, MD Chief, Psychiatric Emergency Services
Psychiatric Patient Boarding Problems in the Emergency Department IMPROVING TIMELINESS, ACCESS, AND QUALITY LOWERING COSTS AND RE-HOSPITALIZATIONS Scott Zeller, MD Chief, Psychiatric Emergency Services
Rouge Valley Health System and Durham Mental Health Services Integration Presentation. CE LHIN Board Meeting: December 22, 2010
 Rouge Valley Health System and Durham Mental Health Services Integration Presentation CE LHIN Board Meeting: December 22, 2010 Background Mental Health Service Providers, Consumers and Family Members observed
Rouge Valley Health System and Durham Mental Health Services Integration Presentation CE LHIN Board Meeting: December 22, 2010 Background Mental Health Service Providers, Consumers and Family Members observed
Transitions in Care. Discharge Planning Pathway & Dashboard
 Transitions in Care Discharge Planning Pathway & Dashboard Scott Jarrett Executive Vice President and Chief of Clinical Programs Humber River Hospital Carol Hatcher Vice President Clinical Programs Humber
Transitions in Care Discharge Planning Pathway & Dashboard Scott Jarrett Executive Vice President and Chief of Clinical Programs Humber River Hospital Carol Hatcher Vice President Clinical Programs Humber
Community Health and Hospital Services Integration Planning Process DRAFT Integrated Service Delivery Model for Northumberland County December 2013
 Overview The Central East Local Health Integration Network is one of 14 Local Health Integration Networks (LHINs) established by the Government of Ontario in 2006. LHINs are community-based organizations
Overview The Central East Local Health Integration Network is one of 14 Local Health Integration Networks (LHINs) established by the Government of Ontario in 2006. LHINs are community-based organizations
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL
 HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
Agenda Item 9 Integration Strategy. Presentation to the Board of Directors
 Agenda Item 9 Integration Strategy Presentation to the Board of Directors What is Integration? Our integration lens reflects a continuum of approaches from Informal Relationships to Structured Collaboration
Agenda Item 9 Integration Strategy Presentation to the Board of Directors What is Integration? Our integration lens reflects a continuum of approaches from Informal Relationships to Structured Collaboration
Emergency Department Clinical Pathways
 The Emergency Department (ED) Clinical Pathways is an intervention that uses evidence -informed resources and decision-support tools. Its aim is to improve the quality of response to children and youth
The Emergency Department (ED) Clinical Pathways is an intervention that uses evidence -informed resources and decision-support tools. Its aim is to improve the quality of response to children and youth
Implementation and Outcomes from Connecticut s Mobile Crisis Intervention Service
 Implementation and Outcomes from Connecticut s Mobile Crisis Intervention Service Jeffrey J. Vanderploeg, Ph.D. Vice President for Mental Health Child Health & Development Institute of Connecticut Tim
Implementation and Outcomes from Connecticut s Mobile Crisis Intervention Service Jeffrey J. Vanderploeg, Ph.D. Vice President for Mental Health Child Health & Development Institute of Connecticut Tim
3.12. Specialty Psychiatric Hospital Services. Chapter 3 Section. 1.0 Summary. Ministry of Health and Long-Term Care
 Chapter 3 Section 3.12 Ministry of Health and Long-Term Care Specialty Psychiatric Hospital Services 1.0 Summary There are about 2,760 long-term psychiatric beds in 35 facilities (primarily hospitals)
Chapter 3 Section 3.12 Ministry of Health and Long-Term Care Specialty Psychiatric Hospital Services 1.0 Summary There are about 2,760 long-term psychiatric beds in 35 facilities (primarily hospitals)
NC Division of Mental Health, Developmental Disabilities, and Substance Abuse Services (DMH/DD/SAS)
") NC Division of Mental Health, Developmental Disabilities, and Substance Abuse Services (DMH/DD/SAS) Perception of Care Survey of Alliance Consumers Fiscal Year 2014 Background Information The Division
NC Division of Mental Health, Developmental Disabilities, and Substance Abuse Services (DMH/DD/SAS) Perception of Care Survey of Alliance Consumers Fiscal Year 2014 Background Information The Division
REDEFINING ACCESS BY CONNECTING THE DOTS BUILDING AN INTEGRATED ACCESS TO CARE MODEL
 REDEFINING ACCESS BY CONNECTING THE DOTS BUILDING AN INTEGRATED ACCESS TO CARE MODEL Toronto Central LHIN Discussion Paper July 2014 Intent of the Discussion Paper This discussion paper has been drafted
REDEFINING ACCESS BY CONNECTING THE DOTS BUILDING AN INTEGRATED ACCESS TO CARE MODEL Toronto Central LHIN Discussion Paper July 2014 Intent of the Discussion Paper This discussion paper has been drafted
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August 2016
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August By: Terry Dentoni, MSN, RN, CNL, SFGH Chief Nursing Officer 1. Professional Nursing..1 2. Emergency Department
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, August By: Terry Dentoni, MSN, RN, CNL, SFGH Chief Nursing Officer 1. Professional Nursing..1 2. Emergency Department
Common ACTT Referral Form
 Common ACTT Referral Form WELCOME! Please ensure that you have completed the accompanying screening tool to ensure that the applicant qualifies for this service. We want to process this application as
Common ACTT Referral Form WELCOME! Please ensure that you have completed the accompanying screening tool to ensure that the applicant qualifies for this service. We want to process this application as
Brief Overview: Mental Health Urgent Care
 Brief Overview: Mental Health Urgent Care John Boyd, Psy.D, MHA, FACHE Sutter s System Chief Mental Health Officer Email: boydj@sutterhealth.org Phone: (916) 208-0267 johnboydpsyd Historical Context Insufficient
Brief Overview: Mental Health Urgent Care John Boyd, Psy.D, MHA, FACHE Sutter s System Chief Mental Health Officer Email: boydj@sutterhealth.org Phone: (916) 208-0267 johnboydpsyd Historical Context Insufficient
The Scarborough Hospital - Alliance Discussions. Presented to the Central East LHIN Board of Directors February 22, 2012
 The Scarborough Hospital - Alliance Discussions Presented to the Central East LHIN Board of Directors February 22, 2012 Objective To respond and provide direction to Integration discussions between The
The Scarborough Hospital - Alliance Discussions Presented to the Central East LHIN Board of Directors February 22, 2012 Objective To respond and provide direction to Integration discussions between The
Recommendation 1: All patients brought into St.
 Recommendation Accountability Response and Action Leads: Regional Emergency Department Head (Dr. Eric Grafstein) and Mental Health Physician Program Director/Department Head Psychiatry, Providence Health
Recommendation Accountability Response and Action Leads: Regional Emergency Department Head (Dr. Eric Grafstein) and Mental Health Physician Program Director/Department Head Psychiatry, Providence Health
North East Behavioural Supports Ontario Sustainability Plan
 North East Behavioural Supports Ontario Sustainability Plan - 2 - NORTH EAST LHIN BSO SUSTAINABILITY PLAN The development of the North East BSO sustainability plan has provided the North East LHIN with
North East Behavioural Supports Ontario Sustainability Plan - 2 - NORTH EAST LHIN BSO SUSTAINABILITY PLAN The development of the North East BSO sustainability plan has provided the North East LHIN with
Behavioral Health Services. San Francisco Department of Public Health
 Behavioral Health Services San Francisco Department of Public Health Slide 2 Agenda Behavioral Health Services in San Francisco Mental Health Services Substance Use Disorder Services Levels of Care Behavioral
Behavioral Health Services San Francisco Department of Public Health Slide 2 Agenda Behavioral Health Services in San Francisco Mental Health Services Substance Use Disorder Services Levels of Care Behavioral
How can we provide the same world class care to patients with psychiatric disorders? 11/27/2016. Dec 2016 Orlando, FL
 The presenters have nothing to disclose Transforming Emergency Psychiatry Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Hospital
The presenters have nothing to disclose Transforming Emergency Psychiatry Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Hospital
Optimizing Patient Care Transitions
 Optimizing Patient Care Transitions Leveraging ereferral Technology in a Time of System Change In this time of unprecedented change, health care leaders are challenged to improve the quality, access and
Optimizing Patient Care Transitions Leveraging ereferral Technology in a Time of System Change In this time of unprecedented change, health care leaders are challenged to improve the quality, access and
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Mental Health Care In Elgin. Celebrating the future, honouring the past. Introducing the new. Southwest Centre for Forensic Mental Health Care
 Mental Health Care In Elgin Celebrating the future, honouring the past Introducing the new Southwest Centre for Forensic Mental Health Care Congratulations... There s a strong history of excellence in
Mental Health Care In Elgin Celebrating the future, honouring the past Introducing the new Southwest Centre for Forensic Mental Health Care Congratulations... There s a strong history of excellence in
Mental Health Accountability Framework
 Mental Health Accountability Framework 2002 Chief Medical Officer of Health Report Injury: Predictable and Preventable Contents 3 Executive Summary 4 I Introduction 6 1) Why is accountability necessary?
Mental Health Accountability Framework 2002 Chief Medical Officer of Health Report Injury: Predictable and Preventable Contents 3 Executive Summary 4 I Introduction 6 1) Why is accountability necessary?
Central East LHIN Strategic Aims
 Central East LHIN Strategic Aims Mental Health and Addictions Strategic Aim Update December 16, 2015 Presented By: Dr. Ian Dawe, Jai Mills and Marilee Suter Agenda Background and Overview Aim Metrics Update
Central East LHIN Strategic Aims Mental Health and Addictions Strategic Aim Update December 16, 2015 Presented By: Dr. Ian Dawe, Jai Mills and Marilee Suter Agenda Background and Overview Aim Metrics Update
Building Bridges to Improve Care in First Nations Communities
 Building Bridges to Improve Care in First Nations Communities Contact: M. Janet Kasperski RN, MHSc, CHE The Ontario College of Family Physicians 340 Richmond St. W., Toronto, Ontario M5V 1X2 Telephone
Building Bridges to Improve Care in First Nations Communities Contact: M. Janet Kasperski RN, MHSc, CHE The Ontario College of Family Physicians 340 Richmond St. W., Toronto, Ontario M5V 1X2 Telephone
South East Toronto Improving Transitions in Care. Family Health Team VIRTUAL WARD PROGRAM
 VIRTUAL WARD PROGRAM South East Toronto Improving Transitions in Care Family Health Team In partnership with: Toronto East General Hospital (TEGH) TC-LHIN Community Care Access Centre (CCAC) Ontario Telemedicine
VIRTUAL WARD PROGRAM South East Toronto Improving Transitions in Care Family Health Team In partnership with: Toronto East General Hospital (TEGH) TC-LHIN Community Care Access Centre (CCAC) Ontario Telemedicine
Community and. Patti-Ann Allen Manager of Community & Population Health Services
 Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Developing ABF in mental health services: time is running out!
 Developing ABF in mental health services: time is running out! Joe Scuteri (Managing Director) Health Informatics Conference 2012 Tuesday 31 st July, 2012 The ABF Health Reform From 2014/15 the Commonwealth
Developing ABF in mental health services: time is running out! Joe Scuteri (Managing Director) Health Informatics Conference 2012 Tuesday 31 st July, 2012 The ABF Health Reform From 2014/15 the Commonwealth
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/24/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/24/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plans (QIP): Progress Report for the 2016/17 QIP
: Progress Report for the 2016/17 QIP") Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
Quality Improvement Plans (QIP): Progress Report for the QIP Medication Reconciliation ID Measure/Indicator from as stated on QIP 2017 1 Best possible medication history(bpmh) completion: The total number
GOB Project 193 Mental Health Diversion Facility Service Capacity and Fiscal Impact Estimates June 9, 2016
 GOB Project 193 Mental Health Diversion Facility Service Capacity and Fiscal Impact Estimates June 9, 2016 I. SUMMARY The purpose of the Mental Health Diversion Facility (Facility) is to create a comprehensive
GOB Project 193 Mental Health Diversion Facility Service Capacity and Fiscal Impact Estimates June 9, 2016 I. SUMMARY The purpose of the Mental Health Diversion Facility (Facility) is to create a comprehensive
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives"
 2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
2016/17 Quality Improvement Plan "Improvement Targets and Initiatives" Queensway-Carleton Hospital 3045 Baseline Road AIM Measure Quality dimension Objective Measure/Indicator Unit / Population Source
Identifying Gaps in Data Collection Practices of Health, Justice and Social Service Agencies Serving Survivors of Interpersonal Violence in Peel.
 Identifying Gaps in Data Collection Practices of Health, Justice and Social Service Agencies Serving Survivors of Interpersonal Violence in Peel. A Pilot Study Preliminary Analysis May 2015 1 Overview
Identifying Gaps in Data Collection Practices of Health, Justice and Social Service Agencies Serving Survivors of Interpersonal Violence in Peel. A Pilot Study Preliminary Analysis May 2015 1 Overview
Sub-Acute Care Capacity Plan
 Sub-Acute Care Capacity Plan Final Report Submitted to: Champlain LHIN Sub-Acute Capacity Planning Steering Committee Hay Group Health Care Consulting 121 King Street West Suite 700 Toronto, Ontario M5H
Sub-Acute Care Capacity Plan Final Report Submitted to: Champlain LHIN Sub-Acute Capacity Planning Steering Committee Hay Group Health Care Consulting 121 King Street West Suite 700 Toronto, Ontario M5H
Mississauga Halton Local Health Integration Network (LHIN) Francophone Community Consultation - May 9, 2009
 Francophone Community Consultation - May 9, 2009") Mississauga Halton Local Health Integration Network (LHIN) Francophone Community Consultation - May 9, 2009 The LHIN invited representatives of the francophone community in the LHIN area to discuss the
Mississauga Halton Local Health Integration Network (LHIN) Francophone Community Consultation - May 9, 2009 The LHIN invited representatives of the francophone community in the LHIN area to discuss the
Behavioral Wellness. Garden Fountain by Bridget Hochman RECOMMENDED BUDGET & STAFFING SUMMARY & BUDGET PROGRAMS CHART
 Garden Fountain by Bridget Hochman RECOMMENDED BUDGET & STAFFING SUMMARY & BUDGET PROGRAMS CHART Operating $ 133,861,700 Capital $ 0 FTEs 384.4 Alice Gleghorn, PhD Director Administration & Support Mental
Garden Fountain by Bridget Hochman RECOMMENDED BUDGET & STAFFING SUMMARY & BUDGET PROGRAMS CHART Operating $ 133,861,700 Capital $ 0 FTEs 384.4 Alice Gleghorn, PhD Director Administration & Support Mental
Unscheduled care Urgent and Emergency Care
 Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
SFGH Dept of Psychiatry August 14, 2012
 SFGH Dept of Psychiatry August 14, 2012 James W. Dilley, MD Professor of Clinical Psychiatry Chief, SFGH Department of Psychiatry Vice Chair UCSF Dept of Psychiatry Executive Director UCSF Alliance Health
SFGH Dept of Psychiatry August 14, 2012 James W. Dilley, MD Professor of Clinical Psychiatry Chief, SFGH Department of Psychiatry Vice Chair UCSF Dept of Psychiatry Executive Director UCSF Alliance Health
Behavioral Wellness. Garden Fountain by Bridget Hochman BUDGET & FULL-TIME EQUIVALENTS SUMMARY & BUDGET PROGRAMS CHART
 Garden Fountain by Bridget Hochman BUDGET & FULL-TIME EQUIVALENTS SUMMARY & BUDGET PROGRAMS CHART Operating $ 109,040,762 Capital $ 46,000 FTEs 432.10 Alice Gleghorn, PhD Director Administration & Support
Garden Fountain by Bridget Hochman BUDGET & FULL-TIME EQUIVALENTS SUMMARY & BUDGET PROGRAMS CHART Operating $ 109,040,762 Capital $ 46,000 FTEs 432.10 Alice Gleghorn, PhD Director Administration & Support
Healing America s Communities: Best Practices in Mental Health. Kevin Young, FACHE President
 Healing America s Communities: Best Practices in Mental Health Kevin Young, FACHE President Why is Behavioral Health Treatment Important? In the treatment of the sick the effect of mental influence should
Healing America s Communities: Best Practices in Mental Health Kevin Young, FACHE President Why is Behavioral Health Treatment Important? In the treatment of the sick the effect of mental influence should
The Scope and Impact of the Metropolitan St. Louis Psychiatric Center (MPC) Emergency Department (ED)/Acute Care Closure
 Emergency Department (ED)/Acute Care Closure") The Scope and Impact of the Metropolitan St. Louis Psychiatric Center (MPC) Emergency Department (ED)/Acute Care Closure Draft Prepared by the Short-Term Crisis Management Team June 23, 2010 Background
The Scope and Impact of the Metropolitan St. Louis Psychiatric Center (MPC) Emergency Department (ED)/Acute Care Closure Draft Prepared by the Short-Term Crisis Management Team June 23, 2010 Background
Mental Health Liaison Workshop
 Mental Health Liaison Workshop UEC Improvement Collaborative Event The Kia Oval, 07 December 2017 Neil Brimblecombe - Chair (co MH Clinical Lead UECC) Barbara Cleaver - Consultant in Emergency Medicine
Mental Health Liaison Workshop UEC Improvement Collaborative Event The Kia Oval, 07 December 2017 Neil Brimblecombe - Chair (co MH Clinical Lead UECC) Barbara Cleaver - Consultant in Emergency Medicine
Central East Health Links. Supporting the Spread of Health Links and Coordinated Care Planning in the Central East LHIN
 Central East Health Links Supporting the Spread of Health Links and Coordinated Care Planning in the Central East LHIN Presenters Mandy Lee Quality Improvement Facilitator Central East Health Links Andrea
Central East Health Links Supporting the Spread of Health Links and Coordinated Care Planning in the Central East LHIN Presenters Mandy Lee Quality Improvement Facilitator Central East Health Links Andrea
Rapid Recovery Therapy Program. GTA Rehab Network Best Practices Day 2017 Joan DeBruyn & Helen Janzen
 Rapid Recovery Therapy Program GTA Rehab Network Best Practices Day 2017 Joan DeBruyn & Helen Janzen $1 Million Photo credit: Physi-med.org Agenda About the Program Description of the Rapid Recovery Therapy
Rapid Recovery Therapy Program GTA Rehab Network Best Practices Day 2017 Joan DeBruyn & Helen Janzen $1 Million Photo credit: Physi-med.org Agenda About the Program Description of the Rapid Recovery Therapy
Mental Health Services 2010 Mental Health Catchment Area Report
 Mental Health Services 2010 Mental Health Catchment Area Report MENTAL HEALTH CATCHMENT AREA (SUPER CATCHMENT AREA) HSE AREA MENTAL HEALTH SERVICES Limerick, North Tipperary, Clare West Limerick, Clare,
Mental Health Services 2010 Mental Health Catchment Area Report MENTAL HEALTH CATCHMENT AREA (SUPER CATCHMENT AREA) HSE AREA MENTAL HEALTH SERVICES Limerick, North Tipperary, Clare West Limerick, Clare,
A new integrated model for Care Homes from Walsall CCG/Healthcare NHS Trust
 A new integrated model for Care Homes from Walsall CCG/Healthcare NHS Trust Sally Roberts - Director of Governance, Quality & Safety. Walsall CCG Katie Welborn Advanced Nurse Practitioner- Walsall Healthcare
A new integrated model for Care Homes from Walsall CCG/Healthcare NHS Trust Sally Roberts - Director of Governance, Quality & Safety. Walsall CCG Katie Welborn Advanced Nurse Practitioner- Walsall Healthcare
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE
 EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
Border Region Mental Health & Mental Retardation Community Center Adult Jail Diversion Action Plan FY
 ATTACHMENT 3 b Border Region Mental Health & Mental Retardation Community Center Adult Jail Diversion Action Plan FY 2010086 The Border Region MHMR Community Center developed a Jail Diversion Plan for
ATTACHMENT 3 b Border Region Mental Health & Mental Retardation Community Center Adult Jail Diversion Action Plan FY 2010086 The Border Region MHMR Community Center developed a Jail Diversion Plan for
TOOLKIT COORDINATED CARE PLANNING. London Middlesex Health Link
 TOOLKIT COORDINATED CARE PLANNING The toolkit is for any individual/organization who will be participating in the Health Link approach to coordinated care planning September 2016 London Middlesex Health
TOOLKIT COORDINATED CARE PLANNING The toolkit is for any individual/organization who will be participating in the Health Link approach to coordinated care planning September 2016 London Middlesex Health
Ontario Systems Projects
 Drug Treatment Funding Program () Delivered by Project Leads at the Launch Event October 13 th and 14 th, 2011, Toronto Investment areas The supports sustainable improvement in the quality and organization
Drug Treatment Funding Program () Delivered by Project Leads at the Launch Event October 13 th and 14 th, 2011, Toronto Investment areas The supports sustainable improvement in the quality and organization
The LHIN s role in creating integrated health service delivery systems
 PATIENTS FIRST UPDATE The LHIN s role in creating integrated health service delivery systems February 7, 2018 Overview 1. Review of five goals of Patients First 2. South West LHIN committees, alliances
PATIENTS FIRST UPDATE The LHIN s role in creating integrated health service delivery systems February 7, 2018 Overview 1. Review of five goals of Patients First 2. South West LHIN committees, alliances
Diversion and Forensic Capacity: Presentation to the Senate Committee on Health and Human Services
 Diversion and Forensic Capacity: Presentation to the Senate Committee on Health and Human Services Mike Maples, Deputy Commissioner Lauren Lacefield Lewis, Assistant Commissioner Department of State Health
Diversion and Forensic Capacity: Presentation to the Senate Committee on Health and Human Services Mike Maples, Deputy Commissioner Lauren Lacefield Lewis, Assistant Commissioner Department of State Health
Quality on the Frontlines: Coordinating Care Across Sectors and Achieving Better Outcomes
 Quality on the Frontlines: Coordinating Care Across Sectors and Achieving Better Outcomes Presenter Disclosures Moderator: Dr. Walter Wodchis Presenters: o Jocelyn Bennett o Mark Fam, Tory Merritt o Dr.
Quality on the Frontlines: Coordinating Care Across Sectors and Achieving Better Outcomes Presenter Disclosures Moderator: Dr. Walter Wodchis Presenters: o Jocelyn Bennett o Mark Fam, Tory Merritt o Dr.
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, March 2018
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, March By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing......1-2 2. Emergency
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, March By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing......1-2 2. Emergency
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/31/2016 Holland Bloorview Kids Rehabilitation Hospital 1 Overview Holland Bloorview continues to lead pediatric rehabilitation
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/31/2016 Holland Bloorview Kids Rehabilitation Hospital 1 Overview Holland Bloorview continues to lead pediatric rehabilitation
Ministère de la Santé et des Soins de longue durée Bureau du ministre
 Ministry of Health and Long-Term Care Office of the Minister 10 th Floor, Hepburn Block 80 Grosvenor Street Toronto ON M7A 2C4 Tel 416-327-4300 Fax 416-326-1571 www.ontario.ca/health May 1, 2017 Ministère
Ministry of Health and Long-Term Care Office of the Minister 10 th Floor, Hepburn Block 80 Grosvenor Street Toronto ON M7A 2C4 Tel 416-327-4300 Fax 416-326-1571 www.ontario.ca/health May 1, 2017 Ministère
Caregiver Respite Program: An Organizational strategy to support Caregivers' Unique Needs
 Caregiver Respite Program: An Organizational strategy to support Caregivers' Unique Needs Gayle Seddon, RN BScN MSH CHE VP, Home and Community Care Toronto Central LHIN HSSO Achieving Excellence Conference
Caregiver Respite Program: An Organizational strategy to support Caregivers' Unique Needs Gayle Seddon, RN BScN MSH CHE VP, Home and Community Care Toronto Central LHIN HSSO Achieving Excellence Conference
WAY BEHIND: Report on the State of Mental Health in 2014 DMH Budget: Last in Growth in New England since 2009
 WAY BEHIND: Report on the State of Mental Health in 2014 Authored by Caity Stuhan, Intern, Graduate Student at Harvard School of Public Health Revised Edition: May 27, 2014 In 2009, the National Alliance
WAY BEHIND: Report on the State of Mental Health in 2014 Authored by Caity Stuhan, Intern, Graduate Student at Harvard School of Public Health Revised Edition: May 27, 2014 In 2009, the National Alliance
PRHC Strategic Plan Guided by you Doing it right Depend on us
 PRHC Strategic Plan 2017-2020 Guided by you Doing it right Depend on us www.prhc.on.ca TABLE OF CONTENTS A Message from the Board of Directors Who We Are Who We Serve Building On our Achievements to Date
PRHC Strategic Plan 2017-2020 Guided by you Doing it right Depend on us www.prhc.on.ca TABLE OF CONTENTS A Message from the Board of Directors Who We Are Who We Serve Building On our Achievements to Date
Background on Outpatient/Ambulatory Minimum Data Set Initiative and Provincial Validation Survey FAQ
 Background on Outpatient/Ambulatory Minimum Data Set Initiative and Provincial Validation Survey FAQ Mandate of the Outpatient/Ambulatory Task Group Develop a comprehensive and standardized minimum dataset
Background on Outpatient/Ambulatory Minimum Data Set Initiative and Provincial Validation Survey FAQ Mandate of the Outpatient/Ambulatory Task Group Develop a comprehensive and standardized minimum dataset
Flexible Assertive Community Treatment (FACT)
") Flexible Assertive Community Treatment (FACT) Dutch model for recovery oriented cure & care for people with severe mental illness Dan Cohen Consensus Development Conference Edmonton 2014 Statement of Potential
Flexible Assertive Community Treatment (FACT) Dutch model for recovery oriented cure & care for people with severe mental illness Dan Cohen Consensus Development Conference Edmonton 2014 Statement of Potential
Summary Report. Outpatient Rehabilitation Access & Transition Indicators FY
 Summary Report Outpatient Rehabilitation Access & Transition Indicators 2015-16 FY Table of Contents 1. Background... 3 1.1. Current outpatient rehabilitation data reporting initiatives... 3 1.2. Objective
Summary Report Outpatient Rehabilitation Access & Transition Indicators 2015-16 FY Table of Contents 1. Background... 3 1.1. Current outpatient rehabilitation data reporting initiatives... 3 1.2. Objective
Assertive Community Treatment (ACT)
") Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
Program of Assertive Community Treatment (PACT) BHD/MH
 BHD/MH") Program of Assertive Community Treatment () BHD/MH Luis Marcano, x5343 Alan Orenstein, x0927 Program Purpose Help individuals with serious mental illness achieve and maintain community integration through
Program of Assertive Community Treatment () BHD/MH Luis Marcano, x5343 Alan Orenstein, x0927 Program Purpose Help individuals with serious mental illness achieve and maintain community integration through
The Movement Towards Integrated Funding Models
 The Movement Towards Integrated Funding Models Financial Models and Fiscal Incentives in Health Conference Board of Canada Toronto, December 1, 2015 Jason M. Sutherland Associate Prof, Centre for Health
The Movement Towards Integrated Funding Models Financial Models and Fiscal Incentives in Health Conference Board of Canada Toronto, December 1, 2015 Jason M. Sutherland Associate Prof, Centre for Health
Sunnybrook Health Sciences Centre Quality Improvement Plans (QIP): Progress Report for 2016/17 QIP. Target as stated on QIP 2016/
: Progress Report for 2016/17 QIP. Target as stated on QIP 2016/") Sunnybrook Health Sciences Centre Quality Improvement Plans (QIP): Progress Report for 2016/17 QIP ID Measure/Indicator from 2016/17 1 % of patients who have delirium recorded in their health record (
Sunnybrook Health Sciences Centre Quality Improvement Plans (QIP): Progress Report for 2016/17 QIP ID Measure/Indicator from 2016/17 1 % of patients who have delirium recorded in their health record (
Balanced Scorecard Highlights
 Balanced Scorecard Highlights Highlights from 2011-12 fourth quarter (January to March) Sick Time The average sick hours per employee remains above target this quarter at 58. Human Resources has formed
Balanced Scorecard Highlights Highlights from 2011-12 fourth quarter (January to March) Sick Time The average sick hours per employee remains above target this quarter at 58. Human Resources has formed
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016
 Narrative for Health Care Organizations in Ontario 3/15/2016") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/15/2016 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
2018/19 QUALITY IMPROVEMENT PLAN. Markham Stouffville Hospital Indicators Posted: April 1 st, 2018
 2018/19 QUALITY IMPROVEMENT PLAN Markham Stouffville Hospital Indicators Posted: April 1 st, 2018 Overview of Markham Stouffville s - Quality Improvement Plan 2018/19 2018/19 Quality Improvement Plan Quality
2018/19 QUALITY IMPROVEMENT PLAN Markham Stouffville Hospital Indicators Posted: April 1 st, 2018 Overview of Markham Stouffville s - Quality Improvement Plan 2018/19 2018/19 Quality Improvement Plan Quality
Dear Ms. McCulloch, I am pleased to present you with the Toronto Central LHIN s (TC LHIN) Annual Business Plan (ABP) for 2014/2015.
 Annual Business Plan (ABP) for 2014/2015.") 425 Bloor Street East, Suite 201 Toronto, ON M4W 3R4 Tel: 416 921-7453 Fax: 416 921-0117 Toll Free: 1 866 383-5446 www.torontocentrallhin.on.ca October 10, 2014 Ms. Kathryn McCulloch Director LHIN Liaison
425 Bloor Street East, Suite 201 Toronto, ON M4W 3R4 Tel: 416 921-7453 Fax: 416 921-0117 Toll Free: 1 866 383-5446 www.torontocentrallhin.on.ca October 10, 2014 Ms. Kathryn McCulloch Director LHIN Liaison
Minutes. Board of Directors Meeting Toronto Central Local Health Integration Network. Wednesday, April 27, 2016, 4:00 7:00 p.m.
 Minutes Board of Directors Meeting Toronto Central Local Health Integration Network Wednesday, April 27, 2016, 4:00 7:00 p.m. Boardroom, Toronto Central LHIN 425 Bloor Street East, Suite 201, Toronto,
Minutes Board of Directors Meeting Toronto Central Local Health Integration Network Wednesday, April 27, 2016, 4:00 7:00 p.m. Boardroom, Toronto Central LHIN 425 Bloor Street East, Suite 201, Toronto,
The Community Crisis House model
 An evaluation of Wales first crisis house If it had not been for the Crisis House staff I honestly don t think I would still be here. I can t thank you enough for all your help. I now feel that I actually
An evaluation of Wales first crisis house If it had not been for the Crisis House staff I honestly don t think I would still be here. I can t thank you enough for all your help. I now feel that I actually
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/22/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/22/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
The number of patients admitted to acute care hospitals
 Hospitalist Organizational Structures in the Baltimore-Washington Area and Outcomes: A Descriptive Study Christine Soong, MD, James A. Welker, DO, and Scott M. Wright, MD Abstract Background: Hospitalist
Hospitalist Organizational Structures in the Baltimore-Washington Area and Outcomes: A Descriptive Study Christine Soong, MD, James A. Welker, DO, and Scott M. Wright, MD Abstract Background: Hospitalist
NHS Grampian. Intensive Psychiatric Care Units
 NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance