A Plan for General Practice in Cornwall and the Isles of Scilly
|
|
|
- Iris Gray
- 5 years ago
- Views:
Transcription
1 A Plan for General Practice in Cornwall and the Isles of Scilly Purpose It is a requirement of the NHS Operational and Planning and Contracting Guidance issued by NHS England and NHS Improvement. The guidance sets out what should be included in the Plan as a minimum requirement. It is an opportunity to establish a shared plan as a health and social care system for the implementation of the General Practice Forward View, to strengthen general practice in the short term and support sustainable transformation of primary and community care for the future. This plan is consistent with the Primary Care strand of the Cornwall and Isles of Scilly Sustainability and Transformation Plan, such that it represents the detailed plans supporting the STP aims. The leadership, governance and objectives are one and the same as the STP. Version: working draft v7 This is a working draft for input and comment from everyone with an interest in how we can collectively address the current issues facing GP Services. Priorities for the development of GP Services will be the subject of conversations with local communities and providers during December and January as part of the wider engagement programme for the Sustainability Transformation Plan and the results of those conversations discussed with representatives of local GP Practices will shape a further iteration of this Plan. Please send information/comments to janet.popham@nhs.net
2 Contents Introduction 1 Page Stabilising the current situation, building resilience and releasing capacity for change General Practice today in Cornwall and the Isles of Scilly Workload Workforce Preparing the infrastructure for change Information technology Estates Delivering change Drivers for change Redesigning the delivery model Investments Annex 1-10 High Impact Changes
3 Introduction GP Practices are at the heart of healthcare in Cornwall and the Isles of Scilly (CIOS). They are the foundation on which an effective local health service is built. GPs across CIOS are members of NHS Kernow CCG, with each Practice having a Mandated GP working together in localities to drive the work of CCG. A renewed focus for the CCG is now required to strengthen the resources and support we can offer General Practice teams, to ensure GPs and their teams are front and centre of our commissioning strategy, and the delivery of a more integrated health and care system. Working with our Locality Lead GPs, individual Practices, the Local Medical Committee and NHS England, we intend to support Practices to capitalise upon the increased focus NHS England is now placing upon Primary Care, with the development of community based teams working together, across organisational boundaries, to deliver the aims of this plan and the wider Sustainability and Transformation Plan. As individual small businesses, based on the partnership model, General Practice is very different from other NHS organisations. GPs have a level of personal financial liability that is not experienced in other parts of the healthcare system, and changed cannot be directed top-down by NHS and Social Care bodies; instead, it requires GPs together with their community colleagues, to lead bottom up the changes they believe are in the best interests of the populations they serve. The role of the CCG is to facilitate and support local clinical and managerial leaders to deliver this plan. However, Practices are currently facing issues around workload and workforce that require immediate action to stabilise the situation and build resilience to meet the increasing demands being placed on them. At the same time the rest of the healthcare community have significant financial and performance issues. Our population is increasing and ageing with more people with complex needs. We have an increasing demand for help, inefficiencies created by fragmented services, variations in practice, a heavy reliance on expensive bed-based care and significant overlap and duplication. NHS England has set out in the Five Year Forward View and the Urgent and Emergency Care Review, a framework for transformation, which places increased emphasis on out of hospital services. It includes several initiatives such as making greater use of the skills and availability of clinical pharmacists, the voluntary sector and social prescribing in support of General Practice. In addition, in its General Practice Forward View NHS England commits to reducing bureaucracy, increasing the available workforce, improving the interface between primary and secondary care including better GP access to consultant advice, and improved automation of tasks. We all need to take action: NHS England, local commissioners, providers and system partners as well as GP Practices. Our Plan must (a) Stabilise the current situation (b) Provide a framework for the future development of General Practice services 1
4 As set out in the GP Forward View, the four key elements, which are supported by targeted investment nationally and locally, are:- 1. Workload 2. Workforce 3. Practice infrastructure (information technology and accommodation) 4. Care redesign Delivering this ambitious and necessary plan will require strong clinical leadership and on-going engagement with staff and the public. We cannot sort General Practice in isolation of the rest of the system, and neither should we be supporting change in our large NHS institutions without involving General Practice and Primary Care colleagues. There are things we need to do immediately to stabilise the current situation around workload and workforce. Care redesign and changing patient behaviour must ensure a manageable workload in the future and will have implications for developing the workforce. Practices are at differing levels of vulnerability and at differing stages in exploring new models of care. It means some of the work to stabilise the current situation will run in parallel with redesigning care. 2
5 3

6 General Practice today in Cornwall and the Isles of Scilly We have 63 GP Practices with 54 branch surgeries on the mainland. There is one Practice on St Mary s with 4 branch surgeries on the smaller islands for the Isles of Scilly. The location of the surgeries reflects our geography and settlement pattern of a dispersed rural population living in small towns and villages. It hasn t always reflected need, or been efficient with more than one branch surgery serving a village or town. Each Practice is an autonomous business but all GPs in Cornwall are represented by the Local Medical Committee and Practices have also collectively established a single federation to act strategically on their behalf (Kernow Health CIC). Each Practice is based on the partnership model and has a registered practice population. Practice populations range in size from 2,363 people to 31,362 with 40 having less than 9,000 people. The current model of service delivery is based around the 10 minute face to face consultation followed by advice, treatment or referral. Community health services, which include district nurses and community matrons, are commissioned from a different provider, and are not as well developed as other parts of the county, e.g. no 24/7 District Nursing cover, require GP Out of Hours to cover this need. GP Practice services are commissioned by NHS England, whilst the local clinical commissioning group (NHS Kernow) is responsible for the development of General Practice locally and can commission some enhanced services from Practices. We have a relatively high number of Practices dispensing medicines compared to most other parts of the country 1 : 51% of the Practices and 42% of the branch surgeries. This again reflects our settlement pattern. Other areas with a high proportion also have 1 NHS Business Services Authority apps.nhsbsa.nhs.uk/infosystems/report PCO List Size and GP Count (April 2016) 4

7 dispersed rural populations e.g. Norfolk and Suffolk. We are towards the top of the best performing quartile nationally for people s experience of GP services, although there is variation in this at Practice level. We are also in the best performing quartile nationally for the proportion of people with a learning disability on the GP register receiving an annual health check (60.4%). However, we have less awareness of online appointment booking than the national average. Almost all practices have had a Care Quality Commission inspection. Overall 56 Practices have been inspected so far, 6 Practices were rated as outstanding, 47 as good and only 2 required improvement and only 1 was found to be inadequate. There is a significant risk, however, that this could rapidly worsen if current pressures are not urgently addressed. Workload Issues GP Practices are unique in the NHS family of organisations. At the moment hospitals and other health service providers are contracted to provide a certain level of activity. Figure 1 GPs are contracted to support a local population, however much activity that population generates. It means they have an open ended workload and some local GPs are describing demand as insatiable. Local experience is supported by the national 2015 BMA survey results that workload was the single biggest issue of concern to GPs and their staff. Over the next 5 years we will not have enough Practice nurses or GPs to meet the current demand for services, based upon the current service delivery model, and the Partnership model is no longer attractive to many young doctors. 5
8 We are also struggling to fill recruitment places for nurses and doctors which places us in vicious cycle. Moreover, the Cornish population also continues to grow year on year with net inward migration reflected in significant new housing development, as well as significant influx during the summer period from tourism. Some Practices are supporting people living in areas recognised nationally as areas of deprivation where people are at greater risk of long-term conditions. Other Practices have a very high proportion of the very elderly, some living in remote areas who are at risk from rural isolation. Pressures on social care budgets means social care services are only available to support those with greatest need. GPs are advising that some people are seeking help from them when the underlying issue is some form of life event with which they need help to cope rather than a clinical need. GPs also talk of spending time chasing care packages. The Primary Care Foundation and the NHS Alliance in their report Making Time in General Practice found that the top three sources of bureaucracy were as follows: processes used to make and claim payments, keeping up to date with information from commissioners and national bodies, and reporting for contract monitoring or regulation. The report also estimated that around 27% of appointments could potentially be avoided if there was more coordinated working between GPs and hospitals, wider use of primary care staff, better use of technology to streamline administrative burdens and wider system changes. Research undertaken nationally in May 2016 by the Kings Fund found that GP workload has grown significantly in both volume and complexity The research sample shows a 15 per cent overall increase in contacts: a 13 per cent increase in face-to-face contacts and a 63 per cent increase in telephone contacts over 5 years. Population changes account for some of this increase, but changes in medical technology and new ways of treating patients also play a role. Wider system factors have compounded the situation. For example, changes in other services such as community nursing, mental health and care homes are putting additional pressure on General Practice. Communication issues with secondary care colleagues and with community hospitals have exacerbated GP workload. The Kings Fund s Fund also found that the increase in workload has not been matched by a transfer in the proportion of funding or staff. Local experience is that improving discharge summaries from acute and community hospitals should be a priority to reduce time spent in checking action required and updating care records. There is also feedback from local Practices that significant time is spent chasing information. The pressures GPs are under are not as well documented and not as visible as in other parts of the healthcare system. Results in the GP Survey show an increasing public dissatisfaction around difficulties in getting appointments. 6
9 What we need to achieve In the short term we need to immediately release capacity among GPs from nonclinical activity, or from activity that other professionals could do, to provide additional clinical time to meet existing demand. In the longer term we need to reconfigure services to cope with the predicted ongoing increase in demand. How we will do it Releasing capacity in GP Practices Building on evidence gathered through the Making Time report and the Prime Minister s GP Access Fund, ten high impact actions have been identified that could release capacity in GP Practices. These are all ways of working that have been found to simultaneously release clinician time and improve care for patients. NHS England is supporting this with a General Practice Development Programme plus investment in training reception and clerical staff in handling clinical paperwork and helping patients navigate the system; in practice manager development; and to support development of on-line consultation. NHS England has a number of investment initiatives to support General Practice and it will be important to coordinate them locally to ensure Practices derive maximum value in stabilisation, sustainability and transformation. Eleven of our Practices have already completed the Productive General Practice training and under our Community Education Provider Network (CEPN) seventeen others have enrolled on the NHS England Productive General Practice Fast Start targeted / Productive General Practice Light. Practices have selected from a range of Productive General Practice modules that will add most value, most quickly to them. The Community Education Provider Network is also working with NHS England to launch in Spring 2017 the local Time for Care programme, whereby practices will elect to work in local groups selfselecting up to 3 appropriate ten high impact actions. Learning from all of these Programmes is being coordinated and shared through the Community Education Provider Network and will be published on the Kernow Health CIC website for the Network for everyone to access. The full list of ten high impact actions is in annex 1 with links to national case studies/examples which also appear on the Kernow Health CIC website We will encourage all Practices to continue to participate and share learning through the local Community Education Provider Network. In addition to this, NHS Kernow has worked with NHS England to produce a Memorandum of Understanding for the drawdown of appropriate interventions aligned with either the resilience or transformation agendas. Money allocated to this will be split between ensuring vulnerable practices are supported and transformation is enabled. Kernow Health CIC have worked with a range of partners to create a local offer of support across a range of disciplines 7


10 including finance, mergers, closer working and working at scale. Practices will be able to access this support. A number of specific schemes are being managed directly by the Community Education Provider Network, hosted by Kernow Health CIC, and these include care navigation / reception training, Practice Manager Training and improving the take up of apprenticeships in General Practice. The CEPN is also delivering a local nursing workforce strategy for Cornwall and the Isles if Scilly, working with the Workforce Development workstream of the CIOS Sustainability and Transformation Plan. Active signposting Funding has been received for training receptionists and clerical staff within Practices. Training needs are being reviewed and a training programme established. Signposting links to our development of optimal pathways i.e. people do not always need to see a GP and some could be signposted to pharmacy or physiotherapy services or to local services/ groups in the community or to local peer groups. New consultation types Many Practices are already exploring alternatives to traditional appointment booking for face-toface appointments. For example, some have implemented a telephone triage service where a GP will ring the person back to discuss the condition and often avoid a face to face appointment. As well as being more convenient for the person seeking advice, the system is more efficient for the surgery and one Practice reports that they have found that they need fewer GPs to their registered patient list as a result. Over the past 12 months the Kernow Health CIC Community Education Provider Network has also undertake a full trial of an e-consulting system across a practice population of 100,000. The results of the trial will be published in January with lessons learned which will help inform local commissioning decisions about the wider roll-out of e- consultation systems. It will be used to determine how the national funding available for online consultations should Figure 2 best be used to support patient care. It needs a careful assessment to ensure that by creating an additional channel we do not add to demand. Through the Estates and Technology Transformation Fund, we have secured funding to allow other technology to be implemented across Cornwall and the Isles 8
11 of Scilly, including cloud-based telephony and video conferencing. Improving interfaces GP Practices interface with a range of other services (figure 2). With acute care Improvements to the interface with acute care have been built into the NHS standard contract. The GP Forward View 2 describes the legal requirements in the NHS Standard Contract for hospitals that should relieve some of the administrative burden on practices These include: local access policies where hospitals will not be able to automatically discharge people who do not attend back to their GP for re-referral; consultant to consultant referrals for a non-urgent condition related to the original referral ; electronic discharge summaries within 24 hours; outpatient clinic letters and management plans within 14 days (aiming for 24 hours in 2017/18); hospitals to organise the different steps in a care pathway promptly including hospitals notifying; patients of the results of clinical investigations e.g. by telephone; supplying patients with medication following discharge for a minimum of 7 days (unless clinically indicated to be shorter). These are part of a service development and improvement plan with providers in contracts for 2017/18 and 2018/19. NHS Kernow will monitor compliance through the contractual process and through specific audits during 2017/18. However, critical to success is the CCG and our Acute partners supporting our primary and secondary care clinicians to work together to develop the interfaces and build the pathways of care which transcend organisational and contractual boundaries. With community and mental health services One of the major obstacles to better delivery of integrated care has been the fragmentation of care in the community. There is still some duplication of effort in recording patient information such as care plans, by more than one provider. For example, care homes may hold a paper care plan and there is not a copy of this in the GP surgery nor is it accessible remotely by the out of hours GP service. Through the Estates and Technology Transformation Fund NHS Kernow has secured monies to implement an electronic end of life care plan that can be shared across organisations. This will be implemented in 2017/18 and we see it as the first step towards a fully integrated care record. With NHS 111 / OOH 2 pp
12 During the out of hours period, from 18:30 until 08:00 weekdays, and at weekends and bank holidays, urgent access to GP services is provided by the Out of Hours service. NHS Kernow, as part of the STP, is procuring integrated NHS 111 / OOH services, with the aim of improving the decision-making processes within NHS 111 and strengthening the interface between in-hours primary care and out of hours primary care. Local GPs have been shaping the service specification to ensure the service can be relied upon and trusted by patients, GPs and the wider system. We will be piloting this across two areas (South Kerrier and North Kerrier) within Cornwall and the Isles of Scilly, with a view to further roll out in line with the national programme. The pilot has been chosen to support the wave 1 GP Access Fund scheme running from Camborne Redruth Community Hospital and Helston Medical Centre. Further information on our longer-term plan for interoperability is in the Information and Management Technology section of this plan. Interoperability across all interfaces As an interim solution GURU and MIG GP system interoperability solutions have been deployed to enable the GP Out of Hours service and acute hospitals to view at the point of care patient information held by GP Practices. NHS Kernow has successfully bid to become a first of type pilot site for the national solution to systems interoperability GP Connect. 10

13 Improving business intelligence There is limited reporting of current practice activity in the same way that activity in acute hospitals is monitored against standards in the NHS constitution. This means that pressure on General Practice is less visible and less well understood. e) Watch for trends in the health and well-being of their population The impact of these pressures in General Practice on other providers is not visible and cannot be monitored. Similarly, the reverse is true where the impact of wider system pressure on General Practice is also not understood Figure 3 sets out the various streams of business intelligence that we are supporting Practices to develop further to a) support resilience b) understand demand for services c) check the quality of people s experience of their services d) understand their registered population s use of health services to identify opportunities for quality improvements and financial savings. Figure 3 11
14 Workforce Issues Nationally the King s Fund research into understanding pressures in General Practice found that The number of GPs has grown more quickly than the population but has not kept pace with groups most likely to use primary care (over 65s and over 85s). GPs are increasingly opting for portfolio careers or part-time work. Only 11 per cent of GP trainees surveyed intend to do full-time clinical work five years after qualification. Locally, Practices have reported difficulties in both recruiting new GPs and retaining existing ones. Some of our more remote rural practices also have difficulties in finding locums. Practices are finding that the existing partnership model is no longer attractive to younger GPs, particularly where it involves buying of the premises. Our workforce is aging as well as the population they support. In September 2015 Health Education England recorded 357 GPs (excluding locums) practising in Cornwall and the Isles of Scilly and 20% were aged over 54. There were 250 nurses in the General Practice workforce, of whom 31% were aged over 54. We currently have an imminent crisis in recruitment and retention of our nursing workforce. Looking at the whole population we have slightly fewer people per GP (fte) than the England average (1,772 compared to 1,977) but a higher proportion of patients over the age of 74 i.e % compared to 7.91%. The report of The Primary Care Workforce Commission highlights the need nationally to also improve recruitment and retention in primary care nursing in order to address current shortfalls and the number of nurses due to retire in the next 5-10 years. It also recommends greater involvement of clinical pharmacists, including prescribing pharmacists, in the management of people on long-term medication and people in care homes. Indicating that this role is best carried out in the GP practice in order to allow full access to the patient record and to maximise interaction between the pharmacist and other clinical staff in the practice. What we need to achieve A resilient General Practice workforce and sufficient clinical and administrative capacity to meet current and future needs, bringing together primary care and community teams. How we will do it Improving career opportunities As a system, we will develop the offer of a portfolio of work for GPs, which could be across practices in a cluster or working in acute and other community settings as an acute physician, for example. As it develops as an approach a wider range of options may be identified allowing further flexibility in how people build their own 12
15 portfolios. This work is being led by our Community Education Provider Network. Our aim will be to develop a career path for all clinical and non-clinical staff. Alongside the portfolio approach is the option of offering a salary to GPs instead of a partnership. We need to develop a way in which a GP can work across a number of practices and points of delivery. NHS Kernow, the Local Medical Committee and Kernow Health CIC will work together to develop this approach. We also need to make the role of a partner attractive again by trying to address property issues. We will explore opportunities to attract former GPs back to Practices to undertake a clinical support role to release time for GPs to focus their expertise where it is most needed. We will also look for opportunities to increase skills and competencies of the non-clinical workforce. Creating overspill provision Local GPs have suggested what they called overspill provision to help with immediate capacity issues i.e. an additional resource to call on when a Practice reaches full capacity or has an unexpected shortfall in capacity. Kernow Health CIC has established a locum chamber to help with capacity issues and we are looking to develop an urgent home visiting service. As part of a re-procured integrated 111/OOH service, we are also looking to develop a single point of access that brings together various clinical staff who are currently employed disparately. Acute GPs and GPs with special interests There are a number of GPs carrying out various roles at the moment beyond the traditional in and out of hours services. These include those working in the Acute GP Service, the GP Access site at Camborne/Redruth Community Hospital, working in community hospitals providing medical cover and as GPs with a special interest. There are particular areas where we are looking to recruit GPs with special interests as there are issues with consultant capacity the medical cover at Liskeard hospital is an immediate example. We will continue to encourage the diversity of roles and look at other areas of the country to wee what portfolio careers are being offered to attract more GPs into the area. Developing a Community Education Provider Network Kernow Health CIC is the host of the Community Education Provider Network in Cornwall and the Isles of Scilly. A project manager has been appointed and a programme of work is being drawn up. The Network has a Steering Group which met for the first time in December 2016 to review a number of work streams and funding streams 13
16 14
 platform to enable greater collaboration and integration of Primary Care services.")
17 Infrastructure enabling change Information technology Our unified communications platform We made a successful application to the Estates and Technology Transformation Fund (ETTF) for a 2.6m programme to deploy a Unified Communications (UC) platform to enable greater collaboration and integration of Primary Care services. The scheme will provide the flexible, efficient and effective communications capabilities required to deliver the Target Operating Model (TOM) outlined in our Sustainability and Transformation Plan, and transform the provision of place-based integrated care communities. Services on the platform include:- Voice (including IP telephony), mobility features Convergence of fixed line and mobile device to provide single number reach Dynamic call routing, including extension mobility both within and between sites Instant messaging (chat), Presence information, Virtual Consultation through the use of audio, web and video conferencing capabilities, Desktop sharing, data sharing (including web connected electronic interactive whiteboards), Call control and management Speech recognition with non-real-time communication services such as unified messaging (integrated voic , , SMS and fax) Co-ordination of communications across multiple channels enabling an individual to send a message on one medium, and receive the same communication on another medium. For example, one can receive a voic message and choose to access it through or a mobile phone. If the sender is online according to the presence information and currently accepts calls, the response can be sent immediately through text, chat or video call. The scheme supports the vision in the Local Digital Roadmap of One Person, One Digital Record and will play a key role in improving digital maturity for all our health and social care organisations during 2017/18 and 2018/19. It creates the capability for us to capture information digitally at the point of care and then share it across care settings. It will provide the communications platform to underpin primary care working at scale and the creation of Integrated Care Teams. It will enable a cluster of GP Practices to share calls from patients, which will underpin working at scale to deliver extended access in 15

18 the evenings and at weekends and sharing workload if a Practice has peaks in demand or has an unexpected shortage of clinicians. It can support pop up surgeries giving GPs the full capability to handle calls as though they were in their main surgery, providing an option for coping with increases in demand, such as created by tourism, or sudden loss in capacity, when for example a GP Partner becomes ill. Based on the release of funding from the Estates and Technology Transformation Fund, the design phase of this project will commence in January 2017 with the target to deliver pathfinder projects at two significant but manageable primary care localities. It will enable a blueprint for Cornwall and the Isles of Scilly to be established providing: A scalable design template A robust deployment approach that will significantly reduce implementation risk; A robust baseline view of costs, potential benefits and return on investment Examples of creating new ways of working such as virtual consultations, case based conferences with multi-agency care specialists and greater federation of services between Practices, administration hubs and primary care hubs. The delivery phase of the project will run through to the second quarter of 2018 by which time all 64 GP Practices will have been provided with a modern and cost effective unified communications solution. 16

 Critical to UP1 is updating the Information Sharing Agreement that all GP Practices have signed up to. The illustration below highlights progress.")

: ED; Pharmacy; Pre-Op Assessment; Diabetes. CFT: Mental Health and Adult Community Services.")

 is available to secondary care clinicians at the point of care.")
19 Universal priorities Delivering NHS England s universal priorities is the first phase of our digital roadmap to be completed in 2017/18. Several of the universal priorities are a key part of developing the infrastructure that will underpin how we provide services in the future. Universal priority 1: Professionals across settings can access GP held information (medications etc.) Critical to UP1 is updating the Information Sharing Agreement that all GP Practices have signed up to. The illustration below highlights progress. Version 2 of the Information Sharing Agreement to support the sharing of patient records between Primary Care and Secondary Care has been signed by 67% of GP Practices with full compliance expected by 31 January GURU is the current primary method for sharing and viewing the primary care patient record across care settings. GURU provides the full patient record from Microtest practices accesses key information from EMIS Web and TPP SystmOne Practices via the MIG. Cornwall Health Out of Hours clinicians; GURU has been deployed: RCHT (Acute): ED; Pharmacy; Pre-Op Assessment; Diabetes. CFT: Mental Health and Adult Community Services. RCHT Outpatient clinics (May 2017) GURU will be rolled out to: Cornwall Council Social Care teams (April 2017) Community Pharmacists (May 2017) Ongoing discussions with PHNT and NEW Devon CCG to deploy in ED; elective care and Outpatient clinics. SCR AI (Additional Information) has been deployed across all EMIS Web and TPP SystmOne Practices and will be rolled out to all Microtest Practices from January 2017 Impact on GP workload/capacity Ensures key information (e.g. recent treatment, allergies and medication) is available to secondary care clinicians at the point of care. More efficient patient management - one setting understands how a patient is being managed in another and does not inadvertently disrupt that management causing additional work e.g. by changing the medicines Impact on the organisation of primary care Guru can enable sharing of patient records between GP Practices Guru could enable an overspill home visiting service by a central pool of GPs supporting Practices 17
. Ambulance crews use the SCR to access patient information.")



20 Universal priority 2: Clinicians in urgent & emergency care settings can access key GP held information GURU is the current primary method for sharing and viewing the primary care patient record with clinicians in urgent and emergency care settings including RCHT ED and Cornwall Health (OOH). Ambulance crews use the SCR to access patient information. Currently this is restricted to patients at EMIS Web and TPP SystmOne Practices with Microtest rolling out SCR in January 2017 to provide full County-wide compliance. It is an enabler for closer working between in-hours and out of hours GP services. Universal priority 3: Patients can access their GP record and universal priority 10: patients can book appointments and order repeat prescriptions from their GP practice Patient online services need to be deployed across all Practices the illustration below highlights progress to date. Patient online services have been deployed at all 64 GP Practices in Cornwall 43 have achieved the NHSE target of 10% of patients enabled for on-line appointments. There is a significant range of achievement with our best performing Practices achieving 30% or more of their patients enabled for patient online services and the worst performing Practices with none. We will aim to bring the remaining 21 GP Practices (with 10 showing reporting zero patients enabled at the moment) up to the 10% threshold by June 2017 It will enable patients to choose self-service options for routine appointments and tasks (e.g. renewing repeat prescriptions); Promotes greater patient choice in the range of contact channels offered encouraging selfservice and selffulfilment Supports the adoption of low cost on-line methods of contacting and transacting with Primary Care. Workload for GP Practice will increase during the initial set-up and adoption phase GP Practices achieving or exceeding the 10% target will benefit from reduced workloads and increased capacity. Driving greater utilisation of patient online services across Primary Care in Cornwall and the Isles of Scilly 18
21 Universal priority 4: GPs can refer electronically to secondary care This has been implemented with use of ers to reduce the workload associated with referrals into secondary care. From April 2017 the use of ers will be mandatory and from October 2018 payments for referrals that are non-ers will be withheld and acute providers will be able to return them to GPs. Universal priority 5: GPs receive timely discharge summaries from secondary care This is partially implemented First phase complete against the NHS England Level 1 requirement with discharge summaries attached as a PDF document via NHSmail All Secondary Care providers (RCHT and CFT) are contracted to achieve Level 2 compliance during 2017 (Level 2 is a basic structured message) By 1 April 2018 all providers will be expected to meet full level 3 compliance to provide a more structured information set This has been flagged up by local GPs as a key issue impacting on their workload. By 2018, ALL future Transfer of Care document types including Outpatient Letters, Referrals and information from Ambulance crews will be transferred electronic using the CDA / FHIR electronic messages. Overall there will be faster and more accurate sharing of information for patients moving between care settings, reducing delays for patients. All providers should benefit from a more efficient work flow. Universal priority 9: GPs and community pharmacists can utilise electronic prescriptions This is partially implemented 35 out of 64 Practices are already live We have a high proportion of dispensing pharmacies in our rural Practices and the national solution does not yet support them, but this is expected to be resolved in 2017 Our aim is to have it deployed to all 64 GP Practices during 2017/18 OptimiseRx (medicines optimisation software) has been deployed to all EMIS and TPP SystmOne sites and c60% of Microtest site. Full deployment expected by March


22 Shaping the estate for the future What it is like today A recent review of our primary care estate emphasised the very limited investment over the last 18 years and the lack of a strategic plan. In the past there has been very limited working with partners in other fields of health and social care, surgeries have been considered in isolation. Today, population growth and substantial new housing developments are increasing pressure on time, skills and space. The recently adopted Local Plan for Cornwall has a policy target of a minimum of 52,500 homes between 2010 and 2030 at an average rate of about 2,625 per year to Our Practices submitted 26 projects to a recent national initiative inviting bids for funding for infrastructure development. It is an indication of the scale of development needed. Unfortunately only two were successful. Work underway We are now working collectively as a system (NHS Kernow, Kernow Health CIC, Cornwall Council, and the Community Health Partnerships) to look at the opportunities for different models of ownership for GP surgeries and with the Royal Cornwall Hospitals Trust and Cornwall Partnership Foundation Trust to look at rationalisation of the overall estate. 20

23 This work is not only looking at opportunities to develop the buildings clinicians need to work from but also making certain the links within them work, the local estate is rationalised and it makes sense to local people. This sense of change has started to lead towards innovative ideas. In Bodmin, for example two GP Practices are already moving onto the same clinical system so that they can share patients. They have recently secured funding for a feasibility study to see if they can replace their two separate surgeries in the town and move together onto a site near the local community hospital where they currently provide medical cover. The study will include the Royal Cornwall Hospital and the Cornwall Partnership Foundation Trust to look at opportunities to bring together a number of different service elements that would make more sense for both people using the services and service providers. In Camelford a partnership of the GPs, Cornwall Council, Camelford Town Council and NHS Kernow has secured national capital funding of 750,000 to build a health and well-being centre. The aim is to develop a suitable base for community nurses plus other facilities that suit local needs and that also enable the centre to generate a sustainable income to meet running costs. Learning from this as it develops will be shared with other 21
24 localities to see if it could provide a model for other areas. Joint work in underway with Cornwall Council, Community Health Partnerships, GPs and other providers to start to look in details at localities and particular areas within them to understand the detail because without that understanding of the local detail the plans will not make sense. Location Our dispersed rural population is a significant factor. Approximately 42% of our population live in towns and villages of less than 3,000 people. The average number of people in a Practice population per GP is 1,772 (1,977 for England). The population in our smaller towns and villages is not large enough to support a Practice as it needs more than one GP to be resilient. Accommodation There needs to be accommodation of sufficient size (clinical and administrative space) within a cluster of Practices to support a multi-disciplinary team either an extended primary care team or a larger multidisciplinary team including community matrons and community nurses. If we are to be successful in recruiting younger doctors it needs to be an attractive working environment with space within a cluster of Practice for training facilities. A significant number of people already have to travel to larger centres of population to access GP Services face to face and that is likely to continue. The alternative will be online consultations. 22

25 23
 4 Health Education England report for Cornwall and the Isles of Scilly (2015) 5 Analyse for the STP by Cornwall Council Public Health (2016) 6. General Practice Resilience Programme 7.")
26 Drivers for change 1The Kings Fund: Understanding pressures in General Practice (2016) 2 Local GPs description of workload 3 Primary Care Foundation & NHS Alliance: Making time in General Practice (2015) 4 Health Education England report for Cornwall and the Isles of Scilly (2015) 5 Analyse for the STP by Cornwall Council Public Health (2016) 6. General Practice Resilience Programme 7. General Practice Development Programme 8. Estates and Technology Transformation Fund 9. General Practice Forward View 24
27 Design principles and objectives Design principles The role of Practices and GPs GP Practices retain their unique relationship with patients it is a personal response to a dedicated patient list GPs are the expert generalist with a specialist knowledge of their local population and care system. Deliver the triple aim Simultaneously improve health and wellbeing, improve people s experience of care, and reduce the cost of care per capita Our approach to care and support Encourage people to take responsibility and enable self-care Maximise prevention and early detection Tailor care and support to individual needs Support people with long term conditions to define and achieve personal goals Continuity of care for those who need it Access at the right time and in the right way Make the most effective use of digital and assistive technologies A flexible workforce providing integrated care Provide a muti-disciplainary workfoce so that the patient will see the most appropriate person, who may not be a GP Impact Enable people to live independently and remain socially active A reduction in avoidable demand on health and social care Changes will not knowingly destabilise other providers of care and support Reduced demand on GPs General Practice in Cornwall and the Isles of Scilly is an attractive place to work Objectives a) Further improve resilience Further improve the resilience of General Practice at the heart of a coordinated system of care and support b) Improve population health and well-being Enable local Practices to increase their contribution to managing and improving the health and well-being of their local population c) Improve people s experience of care and support Enable General Practice to offer continuity of care, enhanced access and services, and support people to take greater responsibility themselves for managing long-term conditions d) Reduce cost per capita Increase the capability and capacity of General Practice to detect and manage (or resolve) health issues in primary care preventing future avoidable demand for expensive acute hospital services 25

28 A framework for redesigning care to meet local needs Understanding local demand Our population has been growing since 1961 when it was 342,301. It is now 560,593 and is expected to increase to 604,591 by We have a higher proportion of older people than nationally i.e. 10.3% are aged 75+, compared with 7.8% for England. Over the next five years the age group (22.3%) and 85+ age group (17.6%) will have the highest rates of growth. The change over the next 10 years is an increase of 50.6% in the group and 41.8% in the 85+ group. Statistics from our acute hospital show that the number of co-morbidities recorded increases significantly from age 60 and from age 70 onwards, 60%-70% of all patients admitted have co-morbidities. The average cost of an emergency admission is 20% higher when co-morbidities are present. We have nearly 70,000 people living in areas of deprivation classified as being among the worst 20% nationally. The Marmot Review found that people living at higher levels of deprivation are more likely to live with a debilitating condition, more likely to live with more than one condition, and for more of their lives. More of our households (35,000) live in fuel poverty than regional and national averages. Cold weather experienced in the winter months can affect or exacerbate a range of health problems, including respiratory and circulatory conditions, cardio vascular disease, mental health and accidental injury. Nearly 16% of our children live in low income families with an increased risk of experiencing a start to life that can affect their emotional as well as their physical well-being and affect their ability to do well at school. Map of deprivation darker areas are the more deprived Figure 4 35 miles 75 miles The prevalence of cardiovascular disease, diabetes and osteoarthritis is high. We have higher rates of obesity than comparable areas. In designing our new model of care we need to work with partners to target prevention at people at risk of long-term conditions so that they are able to live longer healthily. We also 3 Source Cornwall Council, Public Health service 26


29 needs to increase detection and early intervention for cardiovascular disease. We need to ensure that our new model of care includes starting well in life and ageing well. We will need to build capacity to meet the needs of our growing and ageing population. Designing a model of care around populations at risk Better population health management to suit different groups of the population..a stronger focus on population health, prevention, and supporting and mobilising patients and communities Integrated community based teams Co-ordinated care GP Forward View We are currently designing intelligence for each of our six localities that will enable Practices to target the most appropriate cohorts within their local population. 27


30 Shaping delivery around populations with differing needs One size does not fit all, it does not give patients the optimum service and it prevents services from being delivered with optimum efficiency. For example, people at risk from chronic conditions or who are frail will benefit from longer consultations and need home visits. A strong relationship with care providers will be important to them. Another group could be the working well who experience a minor ailment and need a quick, convenient solution who could be sign posted to online advice or to a community pharmacist. It would be a more efficient and cost effective way of providing a service for that group of people. 28
31 29


32 An example of how care could be shaped 30
33 according to particular population cohorts 31

34 Understanding local constraints The capability we need to build Cornwall and the Isles of Scilly comprises a large rural peninsula and islands (figure 4). It has a dispersed population in many small villages and market towns. It is not feasible to provide urgent care in one central location for the whole of Cornwall and the Isles of Scilly. Equity in access to services is a challenge. Our geography affects people s experience of care and the cost of providing it. It also constrains market development. We need to carefully locate services to minimise travel for users and providers and take advantage of information technology so that face to face contact is only used when essential. Location of services needs to be balanced with affordability. 32

35 Moving towards place-based 33
36 commissioning We have recognised the importance of commissioning a new model of care that preserves and enhances the relationship GPs have with their Practice population. We are asking GPs to enhance that by seeing their Practice population in the context of the local geographic communities where they live and where there are community groups, volunteers and physical assets to help improve health or help with recovery from an illness. The table shows the differing scales at which services can be provided and the outcomes to be achieved at that scale. For example, most individual GP Practices working alone would struggle to have the capacity to provide extended access to services at weekends. However, a cluster of Practices working together could create that capacity if the local population needs it. 34
37 Initial focus If we can resolve current workload and workforce issues, GP Practices with registered populations and existing on-going relationships with groups of people within those populations are the foundation stone for building a stronger focus on population health. We need to focus initially on (a) shaping care and support for our ageing population (b) earlier detection and management in primary care of our most prevalent long-term conditions (c) targeting obesity to prevent a further escalation in the numbers of people with long term conditions (d) targeting families and young children in areas of deprivation and troubled families to give everyone the opportunity to start life well and live well Better access By 2020 everyone has access to GP services, including sufficient appointments at evenings and weekends to meet locally determined demand, alongside effective access to out of hours and urgent care services GP Forward View Working at scale across Practices to provide extended access collectively Phase 1 is being implemented in 2016/17 in North and South Kerrier as part of the national pilot for the GP Access Fund. Practices in North Kerrier are working together to provide extended access utilising the local Camborne/Redruth community hospital as the location for the service. Practices in South Kerrier are working together to provided extended access utilising the local community hospital as the location in Helston. A minimum level of bookable appointments has already been introduced on both sites and is being scaled up further during the last quarter of 2016/17. Learning from both sites will be applied to the further roll out of extended access across Cornwall, which will take place when the additional investment becomes available from NHS England in 2018/19. Better use of a wider workforce Initiatives are being tested by clusters of Practices working with community nursing staff. Once evaluated by one cluster learning can be shared with other clusters to implement if they have the same issues in their area. This includes, for example, a cluster of Practices working with the community nursing service provider to establish a leg ulcer club in Penwith. Integrated care Primary Care Home sites St Austell Healthcare (formed in 2015 from the merger of three Practices) have been one of the 15 rapid test sites nationally for the primary care home. Other GP Practices have recently been accepted as Primary Care Home sites and 35
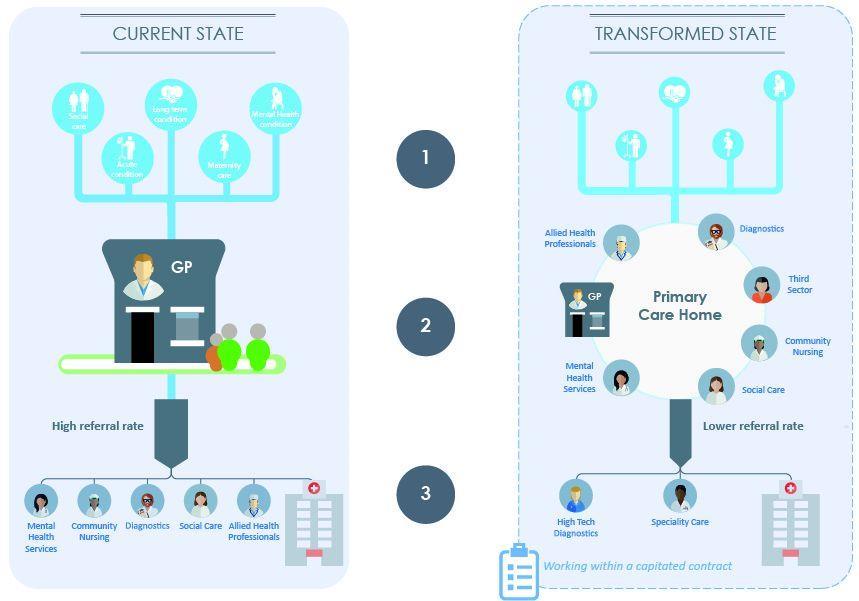
38 2/3rds of our population are now within a Primary Care Home site. The Practices that have been accepted have come together in the following clusters for the purpose:- Penwith North Cornwall East Cornwall South Kerrier Lostwithiel, St Blazey and Fowey Truro Penryn and Perranporth Further information on the Primary Care Home can be found at The Primary Care Home is a form of multispecialty community provider model. At its most mature its key features are:- Provision of care to a defined, registered population of between 30,000 and 50,000 Aligned clinical financial drivers through a unified, capitated budget with appropriate shared risks and rewards An integrated workforce, with a strong focus on partnerships spanning primary, secondary and social care, an A combined focus on personalisation of care with improvements in population health outcomes. The key benefits for patients are a single integrated and multi-disciplinary team, working to provide comprehensive and personalised care to individuals. Working at this scale ensures everyone within the team knows everyone else and the patient has a more consistent experience of care. It provides our clusters of practices with a framework to develop a number of areas that they have been working on. At the moment the clusters of practices just setting out on the journey are viewing it as a way of Our clusters of practices just starting out on the journey are using it initially as a way of creating an environment that allows practitioners to work in a more collaborative way as a single team, introducing a set of behaviours and values that they can all adhere to and then explore the efficiencies of working for a single goal to support an individual to the best of their ability. The diagram overleaf shows how the Primary Care Home works compared to the traditional approach, illustrating the team approach to supporting patients, whereby a range of clinical, non-clinical, employed and volunteers work as part of the primary care home, to reduce the need to refer on to secondary care. 36
39 37
Primary Care Strategy. Draft for Consultation November 2016
 Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Briefing on Shaping Our Future urgent care work stream progress
 Briefing on Shaping Our Future urgent care work stream progress 1. Purpose The purpose of this paper is to describe, update and clarify on the Cornwall and the Isles of Scilly s Shaping Our Future urgent
Briefing on Shaping Our Future urgent care work stream progress 1. Purpose The purpose of this paper is to describe, update and clarify on the Cornwall and the Isles of Scilly s Shaping Our Future urgent
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Bedfordshire, Luton and Milton Keynes. Sustainability and Transformation Plan. Central Brief: February 2018
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan Central Brief: February 2018 Issue date: February 2018 News Transforming care closer to home Our ambition is to build high quality,
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan Central Brief: February 2018 Issue date: February 2018 News Transforming care closer to home Our ambition is to build high quality,
Welcome. PPG Conference North and South Norfolk CCGs June 14 th 2018
 Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
Approve Ratify For Discussion For Information
 NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
Approve Ratify For Discussion For Information
 NHS North Cumbria CCG Governing Body Agenda Item 4 October 2017 11 Implementation of Digital road Map Update Purpose of the Report To update the Governing Body as to progress in meeting national targets
NHS North Cumbria CCG Governing Body Agenda Item 4 October 2017 11 Implementation of Digital road Map Update Purpose of the Report To update the Governing Body as to progress in meeting national targets
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan. October 2016 submission to NHS England Public summary
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE. Purpose of Report: For Note
 Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
General Practice Forward View Mark Sanderson Deputy Regional Medical Director NHS England - Midlands and East
 General Practice Forward View Mark Sanderson Deputy Regional Medical Director NHS England - Midlands and East Overview of GPFV What's happening across Midlands and East The picture in the East of England
General Practice Forward View Mark Sanderson Deputy Regional Medical Director NHS England - Midlands and East Overview of GPFV What's happening across Midlands and East The picture in the East of England
Improving General Practice for the People of West Cheshire
 Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL
 DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
North School of Pharmacy and Medicines Optimisation Strategic Plan
 North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report
 Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
National Primary Care Cluster Event ABMU Health Board 13 th October 2016
 National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
NHS Somerset CCG OFFICIAL. Overview of site and work
 NHS Somerset CCG Overview of site and work NHS Somerset CCG comprises 400 GPs (310 whole time equivalents) based in 72 practices and has responsibility for commissioning services for a dispersed rural
NHS Somerset CCG Overview of site and work NHS Somerset CCG comprises 400 GPs (310 whole time equivalents) based in 72 practices and has responsibility for commissioning services for a dispersed rural
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Meeting in Common of the Boards of NHS England and NHS Improvement. 1. This paper updates the NHS England and NHS Improvement Boards on:
 NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
NHS GRAMPIAN. Grampian Clinical Strategy - Planned Care
 NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
PRIMARY CARE GP FORWARD VIEW PLAN 2017/ /19
 PRIMARY CARE GP FORWARD VIEW PLAN 2017/18 2018/19 1 Primary Care: GP Forward View Plan Contents 1. Introduction 3 2. The Buckinghamshire Primary Care Strategy 4 3. Workforce 7 4. Workload 10 5. Infrastructure
PRIMARY CARE GP FORWARD VIEW PLAN 2017/18 2018/19 1 Primary Care: GP Forward View Plan Contents 1. Introduction 3 2. The Buckinghamshire Primary Care Strategy 4 3. Workforce 7 4. Workload 10 5. Infrastructure
Vanguard Programme: Acute Care Collaboration Value Proposition
 Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
GP Forward View Operational Plan Draft Narrative December 2016 Subject to final approvals
 GP Forward View Operational Plan 2017-2019 Draft Narrative December 2016 Subject to final approvals Chairman s Foreword In March 2015 we published our Primary Care Strategy, which alongside its accompanying
GP Forward View Operational Plan 2017-2019 Draft Narrative December 2016 Subject to final approvals Chairman s Foreword In March 2015 we published our Primary Care Strategy, which alongside its accompanying
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CASE FOR CHANGE - CLINICAL SERVICES REVIEW
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CASE FOR CHANGE - CLINICAL SERVICES REVIEW Date of the meeting 19/03/2014 Author Sponsoring Board Member Purpose of Report Recommendation
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CASE FOR CHANGE - CLINICAL SERVICES REVIEW Date of the meeting 19/03/2014 Author Sponsoring Board Member Purpose of Report Recommendation
NHS North Norfolk and NHS South Norfolk General Practice Forward View Operational Plan
 NHS North Norfolk and NHS South Norfolk General Practice Forward View Operational Plan Ensuring high quality healthcare services for the people of North and South Norfolk 1 VERSION CONTROL Document Purpose:
NHS North Norfolk and NHS South Norfolk General Practice Forward View Operational Plan Ensuring high quality healthcare services for the people of North and South Norfolk 1 VERSION CONTROL Document Purpose:
04c. Clinical Standards included in the Strategic Outline Care part 1, published in December 216
 0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
Melanie Craig NHS Great Yarmouth and Waveney CCG Chief Officer. Rebecca Driver, STP Communications and Jane Harper-Smith, STP Programme Director
 Agenda Item: 9 Governing Body Thursday 25 January 2018 Subject: Presented By: Prepared By: Submitted To: Purpose of Paper: Norfolk and Waveney Sustainability and Transformation Partnership Update Melanie
Agenda Item: 9 Governing Body Thursday 25 January 2018 Subject: Presented By: Prepared By: Submitted To: Purpose of Paper: Norfolk and Waveney Sustainability and Transformation Partnership Update Melanie
DRAFT. Primary Care Networks Reference Guide: Draft pre-release
 Primary Care Networks Reference Guide: Draft pre-release This draft reference guide has been developed with input from a range of stakeholders to provide further information and guidance on what we mean
Primary Care Networks Reference Guide: Draft pre-release This draft reference guide has been developed with input from a range of stakeholders to provide further information and guidance on what we mean
Norfolk and Waveney STP - summary of key elements
 Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
IUC and Vanguard. Greater Nottingham Integrated Urgent Care 1
 IUC and Vanguard The 2016/17 Vanguard funding has been confirmed at 1.3M This funding is to deliver the 8 elements of Integrated Urgent Care by March 2017 With careful management of funds we will be able
IUC and Vanguard The 2016/17 Vanguard funding has been confirmed at 1.3M This funding is to deliver the 8 elements of Integrated Urgent Care by March 2017 With careful management of funds we will be able
Driving and Supporting Improvement in Primary Care
 Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
Improving Healthcare Together : NHS Surrey Downs, Sutton and Merton clinical commissioning groups Issues Paper
 Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Guy s and St. Thomas Healthcare Alliance. Five-year strategy
 Guy s and St. Thomas Healthcare Alliance Five-year strategy 2018-2023 Contents Contents... 2 Strategic context... 3 The current environment... 3 National response... 3 The Guy s and St Thomas Healthcare
Guy s and St. Thomas Healthcare Alliance Five-year strategy 2018-2023 Contents Contents... 2 Strategic context... 3 The current environment... 3 National response... 3 The Guy s and St Thomas Healthcare
North West London Sustainability and Transformation Plan Summary
 North West London Sustainability and Transformation Plan Summary Being well, living well: a sustainability and transformation plan for North West London November 2016 Have your say We want to hear your
North West London Sustainability and Transformation Plan Summary Being well, living well: a sustainability and transformation plan for North West London November 2016 Have your say We want to hear your
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms
 Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
workshops and care; feedback from HealthWatch, participating in
 SUMMARY REPORT Transformation Board Meeting In Public 8 August 2018 Item: 06 Title of report Senior Responsible Officer (SRO) Author(s) Purpose of report Recommendation Engagement and Consultation Undertaken
SUMMARY REPORT Transformation Board Meeting In Public 8 August 2018 Item: 06 Title of report Senior Responsible Officer (SRO) Author(s) Purpose of report Recommendation Engagement and Consultation Undertaken
Delivering the Five Year Forward View Personalised Health and Care 2020
 Paper Ref: NIB 0607-006 Delivering the Five Year Forward View Personalised Health and Care 2020 INTRODUCTION The Five Year Forward View set out a clear direction for the NHS showing why change is needed
Paper Ref: NIB 0607-006 Delivering the Five Year Forward View Personalised Health and Care 2020 INTRODUCTION The Five Year Forward View set out a clear direction for the NHS showing why change is needed
Our aims Working together to achieve better health and wellbeing
 Our aims 2017-2018 Working together to achieve better health and wellbeing Welcome The South West Academic Health Science Network (SW AHSN) is one of 15 AHSNs set up by NHS England to spread health and
Our aims 2017-2018 Working together to achieve better health and wellbeing Welcome The South West Academic Health Science Network (SW AHSN) is one of 15 AHSNs set up by NHS England to spread health and
Appendix 1: Integrated Urgent Care Service Update. 1. Purpose
 Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Papers for the. West Kent Primary Care Commissioning Committee (Improving Access) Tuesday 21 st August at 4 4:30 pm
 Tuesday 21 st August at 4 4:30 pm") Papers for the West Kent Primary Care Commissioning Committee (Improving Access) on Tuesday 21 st August at 4 4:30 pm at Hadlow Suite, Hadlow Manor Hotel Hadlow, TN11 0JH 1 of 23 Primary Care Commissioning
Papers for the West Kent Primary Care Commissioning Committee (Improving Access) on Tuesday 21 st August at 4 4:30 pm at Hadlow Suite, Hadlow Manor Hotel Hadlow, TN11 0JH 1 of 23 Primary Care Commissioning
Clinical Pharmacists in General Practice March 2018
 Clinical Pharmacists in General Practice March 2018 1. Background Following a successful national pilot programme, the General Practice Forward View committed over 100million to support an extra 1,500
Clinical Pharmacists in General Practice March 2018 1. Background Following a successful national pilot programme, the General Practice Forward View committed over 100million to support an extra 1,500
Using information and technology to transform health and care
 Using information and technology to transform health and care Welcome to NHS Digital We are the national information and technology partner to the health and social care system. We re at the forefront
Using information and technology to transform health and care Welcome to NHS Digital We are the national information and technology partner to the health and social care system. We re at the forefront
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
Urgent and Emergency Care - the new offer
 Urgent and Emergency Care - the new offer If it s really serious I want specialist care Help me to help myself and not bother the NHS If only they could talk to my GP? London Clinical Senate Keith Willett
Urgent and Emergency Care - the new offer If it s really serious I want specialist care Help me to help myself and not bother the NHS If only they could talk to my GP? London Clinical Senate Keith Willett
Urgent and Emergency Care Review update: from design to delivery
 The Kings Fund September 2015 Keith Willett Director of Acute Care Urgent and Emergency Care Review update: from design to delivery What does the experience and data from recent winters tell us? Surge
The Kings Fund September 2015 Keith Willett Director of Acute Care Urgent and Emergency Care Review update: from design to delivery What does the experience and data from recent winters tell us? Surge
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary
 Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
Trust Board Meeting 05 May 2016
 Trust Board Meeting 05 May 2016 Title of the paper: Sustainability and Transformation Plan (STP) Update Agenda item: 15/37 Lead Executive: Trust objective: Purpose: Link to Board Assurance Framework (BAF)
Trust Board Meeting 05 May 2016 Title of the paper: Sustainability and Transformation Plan (STP) Update Agenda item: 15/37 Lead Executive: Trust objective: Purpose: Link to Board Assurance Framework (BAF)
Greater Manchester Health and Social Care Strategic Partnership Board
 Greater Manchester Health and Social Care Strategic Partnership Board 7 Date: 13 October 2017 Subject: Report of: Greater Manchester Model for Urgent Primary Care Dr Tracey Vell, Associate Lead for Primary
Greater Manchester Health and Social Care Strategic Partnership Board 7 Date: 13 October 2017 Subject: Report of: Greater Manchester Model for Urgent Primary Care Dr Tracey Vell, Associate Lead for Primary
INTEGRATION TRANSFORMATION FUND
 MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
CONSULTATION ON THE RE-PROCUREMENT OF THE NHS DIABETES PREVENTION PROGRAMME - FOR PRIMARY CARE AND LOCAL HEALTH ECONOMIES
 CONSULTATION ON THE RE-PROCUREMENT OF THE NHS DIABETES PREVENTION PROGRAMME - FOR PRIMARY CARE AND LOCAL HEALTH ECONOMIES Background: 5 million people in England are at high risk of developing Type 2 diabetes,
CONSULTATION ON THE RE-PROCUREMENT OF THE NHS DIABETES PREVENTION PROGRAMME - FOR PRIMARY CARE AND LOCAL HEALTH ECONOMIES Background: 5 million people in England are at high risk of developing Type 2 diabetes,
20 February 2018 Paper No: 18/04 DELIVERING THE NEW 2018 GENERAL MEDICAL SERVICES CONTRACT IN SCOTLAND
 NHS Greater Glasgow & Clyde NHS Board Meeting David Leese, Chief Officer Renfrewshire HSCP and Lead Chief Officer Primary Care Support 20 February 2018 Paper No: 18/04 DELIVERING THE NEW 2018 GENERAL MEDICAL
NHS Greater Glasgow & Clyde NHS Board Meeting David Leese, Chief Officer Renfrewshire HSCP and Lead Chief Officer Primary Care Support 20 February 2018 Paper No: 18/04 DELIVERING THE NEW 2018 GENERAL MEDICAL
Cranbrook a healthy new town: health and wellbeing strategy
 Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Strategic overview: NHS system
 Strategic overview: NHS system Dr Keith Ridge, Chief Pharmaceutical Officer 1 November 2016 A collaborative approach Five Year Forward View Oct 2014 NHS planning guidance, Dec 2015: Every health and care
Strategic overview: NHS system Dr Keith Ridge, Chief Pharmaceutical Officer 1 November 2016 A collaborative approach Five Year Forward View Oct 2014 NHS planning guidance, Dec 2015: Every health and care
Cornwall Community Education Provider Projects March 2018
 Cornwall Community Education Provider Projects March 2018 NATIONAL FUNCTION NUMBER (NF No): 1: SUPPORT FOR WORKFORCE PLANNING AND DEVELOPMENT to respond to local needs and enable the redesign of services
Cornwall Community Education Provider Projects March 2018 NATIONAL FUNCTION NUMBER (NF No): 1: SUPPORT FOR WORKFORCE PLANNING AND DEVELOPMENT to respond to local needs and enable the redesign of services
DRAFT. Rehabilitation and Enablement Services Redesign
 DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
Healthy London Partnership. Transforming London s health and care together
 Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
OFFICIAL. Commissioning a Functionally Integrated Urgent Care Access, Treatment and Clinical Advice Service
 Our Ref: BH/2015/253 Publications Gateway Ref. No. 03568 NHS England Quarry House Quarry Hill Leeds LS2 7UE Email : england.nhs111@nhs.net To: CCG Accountable Officers CCG Clinical Leaders Cc: Regional
Our Ref: BH/2015/253 Publications Gateway Ref. No. 03568 NHS England Quarry House Quarry Hill Leeds LS2 7UE Email : england.nhs111@nhs.net To: CCG Accountable Officers CCG Clinical Leaders Cc: Regional
Committee of Public Accounts
 Written evidence from the NHS Confederation AMBULANCE SERVICE NETWORK/NATIONAL AMBULANCE COMMISSIONING GROUP KEY LINES ON FUTURE MODELS FOR AMBULANCE SERVICE COMMISSIONING Executive Summary Equity and
Written evidence from the NHS Confederation AMBULANCE SERVICE NETWORK/NATIONAL AMBULANCE COMMISSIONING GROUP KEY LINES ON FUTURE MODELS FOR AMBULANCE SERVICE COMMISSIONING Executive Summary Equity and
Urgent Treatment Centres Principles and Standards
 Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Knowledge for healthcare: A briefing on the development framework
 Developing people for health and healthcare Knowledge for healthcare: A briefing on the development framework for NHS library and knowledge services in England 2015-2020 Library and Knowledge Services
Developing people for health and healthcare Knowledge for healthcare: A briefing on the development framework for NHS library and knowledge services in England 2015-2020 Library and Knowledge Services
Board Meeting. Date of Meeting: 30 November 2017 Paper No: 17/78
 Board Meeting Date of Meeting: 30 November 2017 Paper No: 17/78 Title of Paper: Primary Care locality place based plans Paper is for: (please delete tick as appropriate) Discussion Decision Information
Board Meeting Date of Meeting: 30 November 2017 Paper No: 17/78 Title of Paper: Primary Care locality place based plans Paper is for: (please delete tick as appropriate) Discussion Decision Information
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
 Cornwall and Isles of Scilly draft pending formal approval master 301015 Source documents: http://www.cornwall.gov.uk/health-and-social-care/cornwall-and-isles-of-scilly-drug-and-alcohol-action-team-(cios-daat)/about-cornwalland-isles-of-scilly-drug-and-alcohol-action-team-(cios-daat)/?alttemplate=_standard
Cornwall and Isles of Scilly draft pending formal approval master 301015 Source documents: http://www.cornwall.gov.uk/health-and-social-care/cornwall-and-isles-of-scilly-drug-and-alcohol-action-team-(cios-daat)/about-cornwalland-isles-of-scilly-drug-and-alcohol-action-team-(cios-daat)/?alttemplate=_standard
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
Developing primary care in Barnet
 Developing primary care in Barnet Introduction In January 2012, the Joint Boards of NHS North Central London (NCL) approved a NCL Primary Care Strategy, which describes development of the primary care
Developing primary care in Barnet Introduction In January 2012, the Joint Boards of NHS North Central London (NCL) approved a NCL Primary Care Strategy, which describes development of the primary care
 Changing Structure of Scottish Economy More Drivers for Change Economic Growth Disjoint Services Legislation Big Data Analytics Digital Policy Life Science Advances Technology Advances Cultural Public
Changing Structure of Scottish Economy More Drivers for Change Economic Growth Disjoint Services Legislation Big Data Analytics Digital Policy Life Science Advances Technology Advances Cultural Public
This will activate and empower people to become more confident to manage their own health.
 Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
Quarterly Reporting Template - Guidance
 Quarterly Reporting Template - Guidance Notes for Completion The data collection template requires the Health & Wellbeing Board to track through the high level metrics and deliverables from the Health
Quarterly Reporting Template - Guidance Notes for Completion The data collection template requires the Health & Wellbeing Board to track through the high level metrics and deliverables from the Health
1. EXECUTIVE SUMMARY Plan on a page CONTEXT... 7
 November 2016 NHS South West London Local Digital Roadmap 2 1. EXECUTIVE SUMMARY... 4 1.1 Plan on a page... 6 2. CONTEXT... 7 2.1 The National Context... 7 2.2 The London Context... 8 2.2.1 London Digital
November 2016 NHS South West London Local Digital Roadmap 2 1. EXECUTIVE SUMMARY... 4 1.1 Plan on a page... 6 2. CONTEXT... 7 2.1 The National Context... 7 2.2 The London Context... 8 2.2.1 London Digital
Update Report to Clinical Members. Quarter 3; what have we done so far
 Update Report to Clinical Members Quarter 3; what have we done so far Introduction: Dr Charlotte Canniff, Clinical Chair Following our Council of Members meeting in October we heard and recognised a clear
Update Report to Clinical Members Quarter 3; what have we done so far Introduction: Dr Charlotte Canniff, Clinical Chair Following our Council of Members meeting in October we heard and recognised a clear
Cheshire & Merseyside Sustainability and Transformation Plan. People and Services Fit for the Future
 Cheshire & Merseyside Sustainability and Transformation Plan People and Services Fit for the Future 2 The Challenge for the NHS As a nation we are fortunate to have a National Health Service that is free
Cheshire & Merseyside Sustainability and Transformation Plan People and Services Fit for the Future 2 The Challenge for the NHS As a nation we are fortunate to have a National Health Service that is free
NORTH WALES CLINICAL STRATEGY. PRIMARY CARE & COMMUNITY SERVICES SBAR REPORT February 2010
 NORTH WALES CLINICAL STRATEGY PRIMARY CARE & COMMUNITY SERVICES SBAR REPORT February 2010 Situation The Primary Care & Community Services workstream had been tasked with answering the following question:
NORTH WALES CLINICAL STRATEGY PRIMARY CARE & COMMUNITY SERVICES SBAR REPORT February 2010 Situation The Primary Care & Community Services workstream had been tasked with answering the following question:
Purpose Approval Discussion Information Assurance X. Louise Sturgess, Commissioning Manager for Urgent Care Appendices None
 Report Summary Sheet Title Urgent Care Procurements Agenda Item 4.1 Purpose Approval Discussion Information Assurance X Meeting Board Date 29.3.18 Title of Paper Urgent Care Procurements Executive Lead
Report Summary Sheet Title Urgent Care Procurements Agenda Item 4.1 Purpose Approval Discussion Information Assurance X Meeting Board Date 29.3.18 Title of Paper Urgent Care Procurements Executive Lead
Kingston Primary Care commissioning strategy Kingston Medical Services
 Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Our Health & Care Strategy
 MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
NHS ENGLAND BOARD PAPER
 NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
In this edition we will showcase the work of the development of a model for GP- Paediatric Hubs
 Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Personalised Health and Care 2020: Next steps
 Personalised Health and Care 2020: Next steps Paul Rice PhD Head of Technology Strategy NHS England www.england.nhs.uk Better use of data and technology has the power to improve health, transforming
Personalised Health and Care 2020: Next steps Paul Rice PhD Head of Technology Strategy NHS England www.england.nhs.uk Better use of data and technology has the power to improve health, transforming
LymeForward Health and Wellbeing Group
 LymeForward Health and Wellbeing Group Proposals for improvement in provision of local health, care and support services January 2018 Life is really simple, but we insist on making it complicated. Confucius
LymeForward Health and Wellbeing Group Proposals for improvement in provision of local health, care and support services January 2018 Life is really simple, but we insist on making it complicated. Confucius
about urgent healthcare
 The NHS your views about urgent healthcare The NHS Helping you get the most out of local services Tuesday 22 November to Friday 23 December 2016 The NHS Better health for Sunderland 1 1 Your views about
The NHS your views about urgent healthcare The NHS Helping you get the most out of local services Tuesday 22 November to Friday 23 December 2016 The NHS Better health for Sunderland 1 1 Your views about
Developing Plans for the Better Care Fund
 Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Dalton Review RCR Clinical Radiology Proposal Radiology in the UK the case for a new service model July 2014
 Dalton Review RCR Clinical Radiology Proposal Radiology in the UK the case for a new service model July 2014 Radiology services in the UK are in crisis. The ever-increasing role of imaging in modern clinical
Dalton Review RCR Clinical Radiology Proposal Radiology in the UK the case for a new service model July 2014 Radiology services in the UK are in crisis. The ever-increasing role of imaging in modern clinical
S.U.C.C.E.S.S. Project Overview. Project Initiation Document (PID) (Part 1)
 (Part 1)") S.U.C.C.E.S.S. Project Overview Project Initiation Document (PID) (Part 1) June Governing Body 2014 SUCCESS Project Project Initiation Document (PID) Part 1 Project Name Project Description The SUCCESS
S.U.C.C.E.S.S. Project Overview Project Initiation Document (PID) (Part 1) June Governing Body 2014 SUCCESS Project Project Initiation Document (PID) Part 1 Project Name Project Description The SUCCESS
The number of people aged 70 and over stood at 324,530 in This is projected to increase to 363,000 by 2011 and to 433,000 by 2016.
 Community health service provision in Ireland Jimmy Duggan Department of Health and Children Brian Murphy Health Service Executive Profile of Ireland By April 2008, the population in Ireland reached 4.42
Community health service provision in Ireland Jimmy Duggan Department of Health and Children Brian Murphy Health Service Executive Profile of Ireland By April 2008, the population in Ireland reached 4.42
Prime Minister s Challenge Fund (PMCF): Improving Access to General Practice. Innovation Showcase Series Effective Leadership
: Improving Access to General Practice. Innovation Showcase Series Effective Leadership") Prime Minister s Challenge Fund (PMCF): Improving Access to General Practice Innovation Showcase Series Effective Leadership July 2015: Showcase Seven About PMCF In October 2013, the Prime Minister announced
Prime Minister s Challenge Fund (PMCF): Improving Access to General Practice Innovation Showcase Series Effective Leadership July 2015: Showcase Seven About PMCF In October 2013, the Prime Minister announced
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
LOCAL DELIVERY PLAN PRIMARY CARE STRATEGIC AIMS
 LOCAL DELIVERY PLAN PRIMARY CARE STRATEGIC AIMS LEADERSHIP & WORKFORCE The key focus for 2015-16 is the development of a clinical strategy for NHS Fife which has a major strand of work in relation to primary
LOCAL DELIVERY PLAN PRIMARY CARE STRATEGIC AIMS LEADERSHIP & WORKFORCE The key focus for 2015-16 is the development of a clinical strategy for NHS Fife which has a major strand of work in relation to primary
Training Hubs - Funding Allocation Paper
 Training Hubs - Funding Allocation Paper Background Health Education England (HEE), NHS England, the Royal College of General Practitioners (RCGP) and the BMA GPs Committee (GPC) are working together to
Training Hubs - Funding Allocation Paper Background Health Education England (HEE), NHS England, the Royal College of General Practitioners (RCGP) and the BMA GPs Committee (GPC) are working together to
STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby
 STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby http://nhsbetterhealth.org.uk/wp-content/uploads/2016/11/stp-draft-plan-on-page- Final-1.pdf The STP Process Q1. Version Control:
STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby http://nhsbetterhealth.org.uk/wp-content/uploads/2016/11/stp-draft-plan-on-page- Final-1.pdf The STP Process Q1. Version Control:
Longer, healthier lives for all the people in Croydon
 D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
Dispensing doctors and the NHS Five Year Forward View. Deborah Jaines, Head of Primary Care Policy and Contracts, NHS England
 Dispensing doctors and the NHS Five Year Forward View Deborah Jaines, Head of Primary Care Policy and Contracts, NHS England Dispensing Doctors and the NHS Five Year Forward View Deborah Jaines Head of
Dispensing doctors and the NHS Five Year Forward View Deborah Jaines, Head of Primary Care Policy and Contracts, NHS England Dispensing Doctors and the NHS Five Year Forward View Deborah Jaines Head of