Health Board 27 th March Purpose This report provides the Board with the Risk Management Strategy and Corporate Risk Register.
|
|
|
- Victoria Simmons
- 5 years ago
- Views:
Transcription
1 SUMMARY REPORT ABM University Health Board Health Board 27 th March 2014 Agenda item 2(vii) Subject Risk Management Strategy Prepared by Hazel Lloyd, Head of Quality Assurance Approved by Christine Williams, Acting Director of Nursing Presented by Christine Williams, Acting Director of Nursing Purpose This report provides the Board with the Risk Management Strategy and Corporate Risk Register. Decision Approval Information Other Corporate Objectives Safety Quality Efficiency Workforce Health Governance X X X Executive Summary The report provides the Board with the Risk Management Strategy, reviewed by the Risk Management Review Group and Audit Committee. The Corporate Risk Register is also provided following a review by the Executive Directors and Quality & Safety and Audit committees. X Key Recommendations The Board is asked to consider and approve, subject to final amendments, the Risk Management Strategy and note the contents of the Corporate Risk Register. Assurance Framework These documents are a key part of the internal control in operation within the Health Board and support the Assurance Framework. Next Steps The Risk Management Strategy, once approved, will be published via the internet and will be subject of regular review through the Quality & Safety and Audit Committees to ensure they are up to date and take account of changes within the Health Board and NHS Wales. 1
2 Corporate Impact Assessment Quality and Safety The documents relate to a number of Standards, although the main standards covered include: 1 - Governance & Accountability 6 - Participating in Quality Improvement initiatives 22 - Risk Management and Health & Safety 23 - Managing Concerns Financial Implications Legal Implications N/A Equality & Diversity There are no specific resource impacts in preparing this report. There are no specific issues related to Equality and Diversity within this report 2
3 Main Report Subject Quality & Safety Prepared by Hazel Lloyd, Head of Quality Assurance Approved by Christine Williams, Acting Director of Nursing Presented by Christine Williams, Acting Director of Nursing Health Board Meeting On 27 TH MARCH 2014 Agenda item 2(vii) 1 PURPOSE To provide the Board with key documents, for approval, they will support the internal control assurance framework within the Health Board. 2 INTRODUCTION Risk Management, is a shared responsibility between the Medical Director and Director of Nursing. The Risk Management Strategy has been in use within the Health Board since its inception although has been updated to take account of organisational changes and reviewed as a minimum on an annual basis. The Strategy will need to be kept under regular review in 2014/15 to ensure it is updated to reflect changes in the Health Board. The key objectives of the document is to ensure: consistency in approach to the overall management of risks; and clear organisational arrangements to enable the Health Board to meet its strategic aims within a framework of strong, effective governance and risk management. 3 Risk Management Risk Management is an increasingly important driver in terms of strategic risks and decision making as well as operational management of risks. A process is required to ensure a consistent approach is applied to the management of risks once identified to ensure: Risks are understood in terms of achieving objectives; Overall level of risk is understood within processes and objectives; There is a mechanism to prioritise significant risks and; Identify weak controls. The aim is ensure compliance with regulations and legislation, assurance and enhance decision making. 3.1 Risk Management Strategy The revised Risk Management Strategy, attached as Appendix 1, was subject of review by the Risk Management Review Group and discussed at a Risk Management Workshop held in January The document has also been 3
4 circulated to Executive Directors, members of the Quality & Safety Committee and reviewed by the Audit Committee in March Corporate Risk Register The Corporate Risk Register is attached as Appendix 2 and contains risks linked to the objectives (aims and priorities) of the Health Board and is underpinned by high operational risks considered through the Risk Management Review Group. There are a number of risks which are of concern which are highlighted below: Unscheduled Care (Risk Ref 1) Effectiveness of Care (Risk Ref 3) Service Delivery (Risk Ref 5) Service Change (Risk Ref 19) The controls in place and actions being taken to decrease the risk are provided within the relevant entry on the Corporate Risk Register. The top three risks for the Health Board relate to: Unscheduled Care (Risk Ref 1) The performance and improvement actions identified have previously been submitted to the Quality & Safety Committee and are summarised in the Register. An update against the unscheduled care action plan is provided in Agenda Item 4.2. Effectiveness of Care (Risk Ref 3) The controls in place and actions being taken to decrease the risk are provided within the relevant entry on the Corporate Risk Register for the risk identified. There are 21 operational risks relating to workforce issues which may impact on effectiveness of care. Cardiac Services (Risk Ref 32) Cardiac Action Plan is in place and monitored through the Cardiac Thoracic Directorate Board and reported through to the Quality & Safety Committee to every other meeting. A risk register workshop for the Cardiac Thoracic Directorate was held on 5 th February to support the development and integration of their risk register within their core business. 4. RECOMMENDATION The Board is asked to note the contents of the report and approve the Risk Management Strategy. 4
5 APPENIDX 1 Risk Management Strategy & Policy This document may be made available in alternative formats and other languages, on request, as is reasonably practicable to do so. Policy Owner: Approved by: Quality Assurance Department Risk Management Review Group Issue Date: Review Date: Policy ID: 1
6 Contents Section Page 1. Risk Management Policy Statement 3 2. Introduction 4 3. Strategy Objectives 5 4. Significant Risks 6 5. Roles and Responsibility 6 6. Risk Management Reporting Structure 8 7. Risk Management Process Risk Register Risk Management Training Glossary References Appendices Appendix 1 Key Policies 21 Appendix 2 Standards for Health Services in Wales 22 Appendix 3 Scheme of Delegation 23 Appendix 4 Executive Lead Groups 24 Appendix 5 Risk Management Reporting Structure 25 Appendix 6 Specialist Groups/Committees Reporting to the Quality & Safety Forum 26 Appendix 7 Terms of Reference Risk Management Review Group 27 Appendix 8 Risk Matrix 29 Appendix 9 Risk Register Template 31 Appendix 10 Population of Risk Register Flowchart 32 Appendix 11 Process to Request Transfer of a Risk from a Directorate Risk 33 Register to the Corporate Risk Register Flowchart 2
7 1. Risk Management Policy Statement Abertawe Bro Morgannwg University Health Board (ABMU) is committed to providing safe and effective, high quality healthcare. We mandate a culture and environment, which minimises and actively seeks to reduce risk and promotes the health, safety and well-being of patients, staff, visitors and the general public. ABMU recognises that all health service activity carries risks including harm to patients which need to be managed through a systematic framework. This will ensure that risks to patient safety and the organisations objectives are identified, assessed, eliminated or minimised so far as is reasonably practicable. The aim being to minimise the chance of the risk being realised, although where this has not been possible then we will review, learn and share the learning to minimise the likelihood of reoccurrences in an open and fair culture. All staff have a responsibility for promoting risk management, adhering to ABMU policies and have a personal responsibility for patients safety as well as their own and colleagues health and safety. ABMU encourages staff to take ownership of their responsibilities through a twoway communication process, with appropriate training and support, to identify and manage risk. To support the development of good risk management practice in the organisation ABMU aims to ensure: the risk management process is robust, integral to the day to day operation of the organisation, consistent and supports the achievements of ABMU s objectives; the level of risk tolerance is defined and the appetite for risk is clear to support taking calculated risks to encourage innovation; a safe, high quality service is provided to patients and continuous improvement is promoted; we have a safe environment for patients, staff and visitors through the identification of hazards and the management of risks; awareness of risk management is raised through education/training and guidance to ensure they are aware of potential hazards/risks and how they can be minimised; there is a culture of learning from everything we do to improve safety in ABMU, compliance with legislation and continuous improvement by using the Doing Well, Doing Better Standards for Health Services in Wales as a framework; risk management is linked to clinical audit to prioritise risk based audits and risks identified following audit are risk assessed and added to the appropriate risk register; roles, responsibility and accountability for risk management is clear and well documented within policies, procedures and Job Descriptions; regular review of policies and procedures; there is an open and fair culture in which staff can highlight and discuss risks openly. Ensuring robust risk management systems are in place will enable the organisation to: - be proactive rather than reactive; - identify and treat risks within the organisation; - improve identification of opportunities and threats; - comply with legislation and regulations. Signed: Chief Executive Date 3
8 2. Introduction The foundation of Risk Management in the NHS is set out in HSC 1999/123 which details the requirements for Controls Assurance which were incorporated into the Welsh Risk Management Standards and are now detailed in the technical guides for the Healthcare Standards. Risk Management is therefore a holistic approach to identify and effectively manage clinical, health & safety, financial and organisational risks based on best governance practice which conforms with the Doing Well, Doing Better Standards for Health Services in Wales and the guidance produced by HM Treasury. ABMU recognises that effective Risk Management plays a pivotal role in ensuring high quality services are provided to its patients from an environment that is safe for patients, staff and visitors within the hospital and the community. This document sets out the Board s strategy and policy regarding Risk Management confirming the accountability and structural arrangements, resources available and guidance on risk management and levels of risk. Risk Management underpins the governance arrangements for the System of Internal Control. Ensuring risk management systems and processes are in place, which are subject to regular review through internal and external assessment, with evidence that Internal Control is in place and that ABMU is committed to manage itself so as to meet its objectives, identify principal risks and manage them. The Chief Executive carries ultimate responsibility, delegated by the ABMU Health Board, for assuring the quality of the services provided and for ensuring the implementation of effective Governance arrangements. Good risk management awareness and practice at all levels is considered a critical success factor for ABMU as managing risk is inherent in everything that we do: treating patients, determining service priorities, managing projects, purchasing new medical equipment, taking decisions about future strategies, or even deciding where it is appropriate not to take any action at all. This document identifies where accountability and responsibility lie and sets out the framework to follow for the reduction of risks to a minimum. There are a number of policies and procedures which support risk management. These are listed in Appendix 1. For Risk Management to be truly effective, ABMU recognises that it must have a safety culture embedded within the organisation. To support this, the HB promotes an open and fair culture where safety is paramount, encourages feedback to staff and to learn lessons from incidents, complaints and risk identification. A patient safety programme is being developed to Strategy Objectives The objectives of this Risk Management Strategy are: To ensure risk management becomes an integral part of the organisation s culture and is used to identify and manage significant risks to the Health Board s objectives and operational risks; 4
9 All aspects of risk management are approached in a consistent and structured manner and Risk Registers are used as the tool to manage risk within ABMU; Objectives, responsibilities and accountabilities for risk management are clearly defined at every level of the organisation; Staff are aware of their responsibility to minimise and manage clinical, financial and organisational risks and to discuss risks as part of the individual performance review process; Staff are empowered to prioritise patient safety, report hazards, incidents and identify risks; Ensure the Doing Well, Doing Better Standards for Health Services in Wales are implemented across ABMU, within Directorates/Localities/Sites undertaking self assessments against the Standards ensuring benchmarking takes place and action plans are completed to improve quality and safety of services; Strategies, policies, structures and processes are constantly reviewed and evaluated to ensure that patient safety and service quality is continuously improved and that ABMU objectives are being achieved; Risk Management process will underpin the Health Boards Quality and Safety agenda. 4. Significant Risks The significant risks facing ABMU are the risks linked to achieving ABMU s objectives and the operational risks which have been escalated, in line with the risk management process, by Directorates/Localities/Sites mechanisms. The organisational objectives are referred to in the Health Board s 3 Year Plan referred to as the Integrated Medium Term Plan for (IMTP). The priorities are: Public Health Excellent outcomes Excellent people Excellent governance Sustainable services The organisational priorities are monitored by the Board and Board Committees through assurance and exception reports. The Executive Team will use the IMTP as the basis for performance monitoring of Directorates/Localities/Sites and Corporate Directorate priorities. Monthly Performance meetings, aligned to the IMTP with the Directorates/Localities/Sites to monitor performance against the priorities and other Key indicators. Details of the Doing Well, Doing Better Standards for Health Services in Wales are provided in Appendix 2. Following the Annual self assessments an Improvement Plan is developed which is reviewed by the Health Boards Standards for Health Services in Wales Scrutiny Panel and a report submitted on key issues to the Quality & Safety Committee, as 5
10 a minimum, on a quarterly basis. The Improvement Plan identifies actions to develop the Standards and ensure they are all scored, as a minimum, Level 3 - DEVELOPING. 5. Risk Management Roles and Responsibility 5.1 Chief Executive As Accountable Officer the Chief Executive has responsibility for ensuring that the Health Board meets all its statutory and legal requirements and adheres to guidance issued by the Welsh Government in respect of governance. This responsibility encompasses the elements of financial control, organisational control, quality, Health & Safety and risk management. Each year the Chief Executive sets out the risk management arrangements and issues within the Health Board within the Annual Governance Statement which forms part of the Annual Accounts and is scrutinised by the Audit Committee. The Medical Director and Director of Nursing are responsible for Quality and Safety, ensuring robust systems are in place. They are supported to drive forward the patient safety agenda through their Assistant Directors who have roles in quality and safety, safeguarding, Infection Control and education, all supporting patient safety. 5.2 Director of Nursing and Medical Director The Director of Nursing and Medical Director have specific responsibilities for Risk Management and will support the Chief Executive by providing competent advice and support in the development of effective systems and arrangements to help facilitate the management of risk, this will include arranging to: Produce and regularly review the Risk Management Strategy; Draft the Risk Management section of the Corporate Plan; Ensure key risks are co-ordinated and reported to the Executive Board, Board Committees and Health Board; Draft the Annual Governance Statement. In undertaking this role the Director of Nursing and Medical Director are supported by the Head of Quality Assurance. 5.3 Executive Directors Each Executive Director is responsible for managing risk within their area of responsibility. This means they will: Ensure staff are appropriately trained in risk assessment and management. Ensure there are mechanisms in place for identifying, managing and alerting the Board to significant risks within their areas of responsibility through regular, timely and accurate reports to the Executive Board, relevant Board Committees and the Health Board. Ensure there are mechanisms in place to learn lessons from any incidents or untoward occurrences and that corrective action is taken where required. 6
11 Provide details of the key risks within their area of responsibility to the Board Secretary every 6 months to coincide with the IMTP development and review process. Ensure compliance with Health Board policies, legislation and regulations and professional standards for their functions. A schedule setting out key areas of responsibility of individual Directors are set out in detail in the Scheme of Delegation appended to Standing Orders and are supplemented by individual job descriptions. A summary of each Executive areas of responsibility are summarised in Appendix 3 and Appendix 4 identifies the main Executive Lead Groups in the Health Board. 5.4 Head of Quality Assurance The Head of Quality Assurance acts on behalf of the Directors of Nursing and Medical Director to achieve high standards of risk management for the Health Board, including the ongoing review and development of the Health Boards Risk Management Strategy. Responsibilities include continuing development of a proactive risk management culture and practice throughout the organisation; actively promoting and ensuring good risk management practices, an open, just and fair culture and the achievement of national risk management standards and continual improvement through the framework or Standards for Health Services in Wales. 5.5 Head of Health & Safety The Head of Health and Safety, supported by the Health & Safety Department, are responsible for policy development and implementation. Providing professional advice in respect of health and safety management. Ensuring the Health Boards risk management methodology is applied to Health and Safety issues. 5.6 Specialist Advisors There are a number of specialist advisers within the Health Board who provide advice on specific areas of risk management. These include: Safeguarding, Fire; Health & Safety; Infection Prevention & Control; Information Governance; Medical Devices; Radiation Protection; Resuscitation and Security Management etc. 5.7 Operational Risk Management Arrangements Clinical Directors/Locality Directors/Directorate Managers/Site Executive Director, Heads of Nurses and senior managers who have devolved responsibilities for risk are responsible for ensuring that: Staff are aware of the Risk Management Strategy, are aware of their responsibilities, understands the extent to which they are empowered to take risk, and are appropriately trained in risk assessment and risk management; The Directorate/Locality/Sites adopts an open and fair culture; 7
12 Hazards, incidents and risk are identified using a consistent approach in the Directorate/Locality to ensure that a learning approach results in continuous improvement; Risks are managed within the Directorate/Locality and significant unresolved risks reported to the appropriate Director; Appropriate governance arrangements are established to manage risks, ensure action is taken and lessons learned; Staff are released to attend mandatory/statutory training; Staff receive regular PDR s/appraisals; They have effective arrangements in place to identify and manage risk; Risks identified outside their control, must be communicated effectively through to the Chief Operating Officer; Clearly defined structure to ensure the appropriate management of risk and this should be communicated to all staff within the Directorate/Locality; Up to date Risk Register and log of risks they have mitigated to a risk tolerated level, and together with risks that have been treated; Staff are aware of the Risk Management Strategy; Risks are managed and minimised within the Directorate/Locality/Site and significant unresolved risks reported to the Chief Operating Officer/Site Executive and the Risk Management Review Group; Governance forum is established to consider all types of risks, ensure action is taken and lessons learned and review the Directorate/Locality Risk Register; Staff are released to attend mandatory/statutory training. 5.5 Ward / Departmental Managers promotes an open and fair culture for staff to report incidents; promptly investigates incidents and supports staff through the process; completes or ensures risk assessments are completed and, as a minimum, reviewed on an annual basis; reports risks identified from risk assessments into the Directorate/Locality/Site Risk Register; monitor staff attendance at mandatory/statutory training. 5.6 Independent Contractors The Localities are responsible for working with independent contractors and ensuring appropriate risk management arrangements and systems are in place. 5.7 All Employees Everyone working in ABMU has a responsibility to continuously improve patient safety, minimise risk and to ensure that they: - comply with policies, procedures, protocols and guidelines; complete risk assessment and report hazards and incidents; inform their manager of risks which they have identified; ensure that there is an open and fair culture in their work place. 8
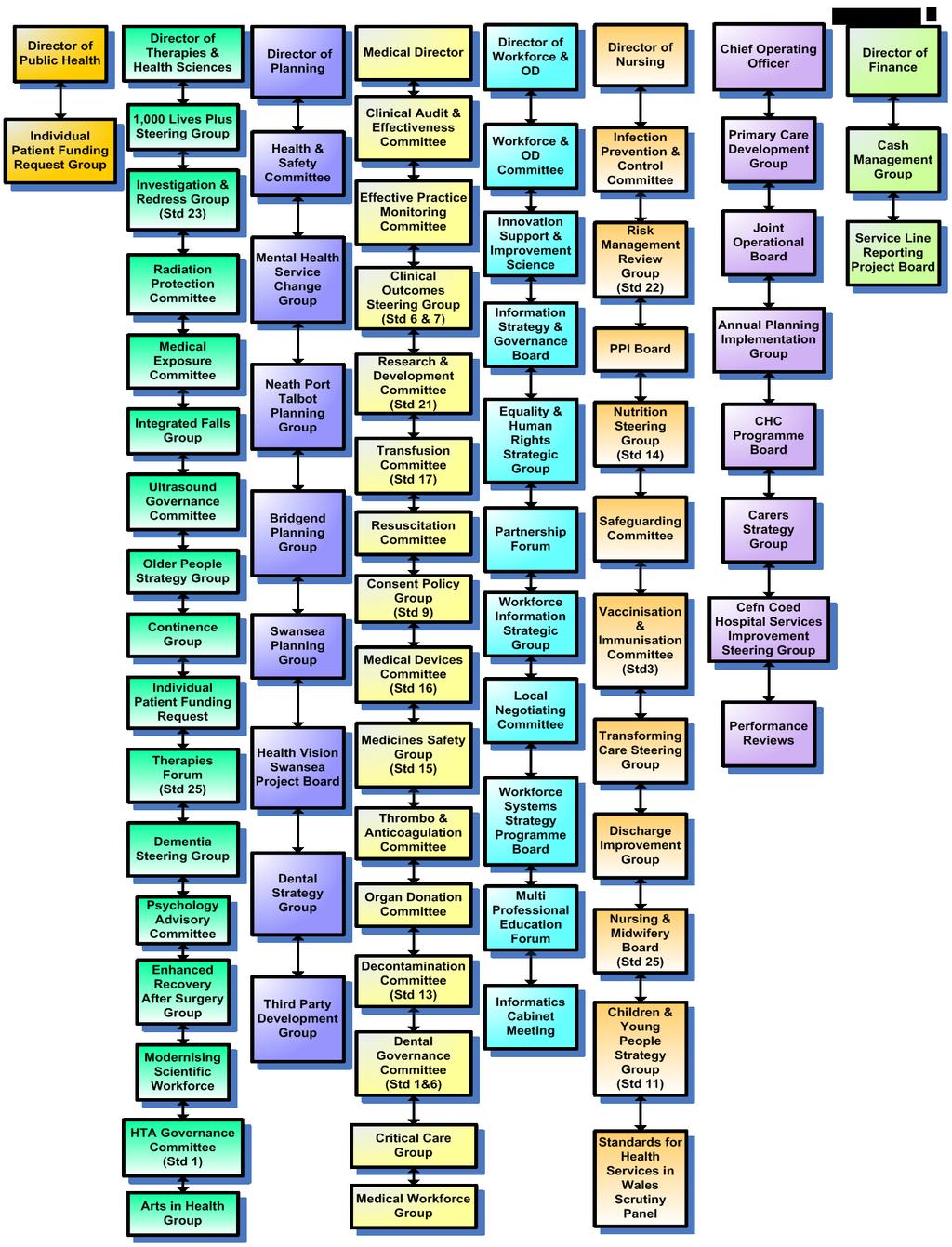
13 6. Risk Management Reporting Structure Attached as Appendix 5 is the reporting arrangements and Committee Structure, that details ABMU s structural arrangements for the risk management process. The remainder of this section sets out the roles and responsibilities of the component parts of this structure and its relationship to the risk management process. Each of the summaries regarding the specific areas of risk management is supported by detailed Terms of Reference. 6.1 Health Board The ABMU Board shall, in relation to risk management: - Critically review and, when content, endorse the Risk Management Strategy and associated Policies/procedures/methodologies; Deliberate annual reports and annual assurance statements; Consider where lessons may be learnt from clinical/non-clinical incidents to foster continuous improvement; Consider any legal claims in accordance with the HB s Standing Orders and Financial Instructions; Consider where lessons may be learnt from significant complaints, "no harm incidents" and other incidents to foster continuous improvement; The ABMU Board will receive regular progress reports on the implementation of Risk Management and Standards for Health Services in Wales Implementation Plan through the Quality & Safety Committee. Each Executive Director will produce a high level risk schedule, which is then used to formulate the IMTP and appended to the Plan as a Risk Register. The Plan would then be approved by the Executive Board, Audit Committee and Board. The Plan will be reviewed on a 6 monthly review following the same process. Alongside this key risks will be highlighted through all main plans e.g. for service change proposals and in key reports to the Board, its Committees and the Executive Board as a key element to decision making. The ABMU Board will appropriately delegate its responsibilities and functions in accordance with the arrangements set out in this document and Standing Orders. The ABMU Board is responsible for the system of internal control, including risk management. The Quality & Safety Committee will provide assurance that risk management systems are in place and functioning properly to assure patient safety through the minimisation of risk. 6.2 Audit Committee The Audit Committee provides assurance that adequate systems are in place to ensure that Action Plans produced and agreed through the delivery of Annual Audit Operational Plans are implemented, reporting mechanisms deliver regular reports to the Board and independent verification is in place. Internal Audit 9
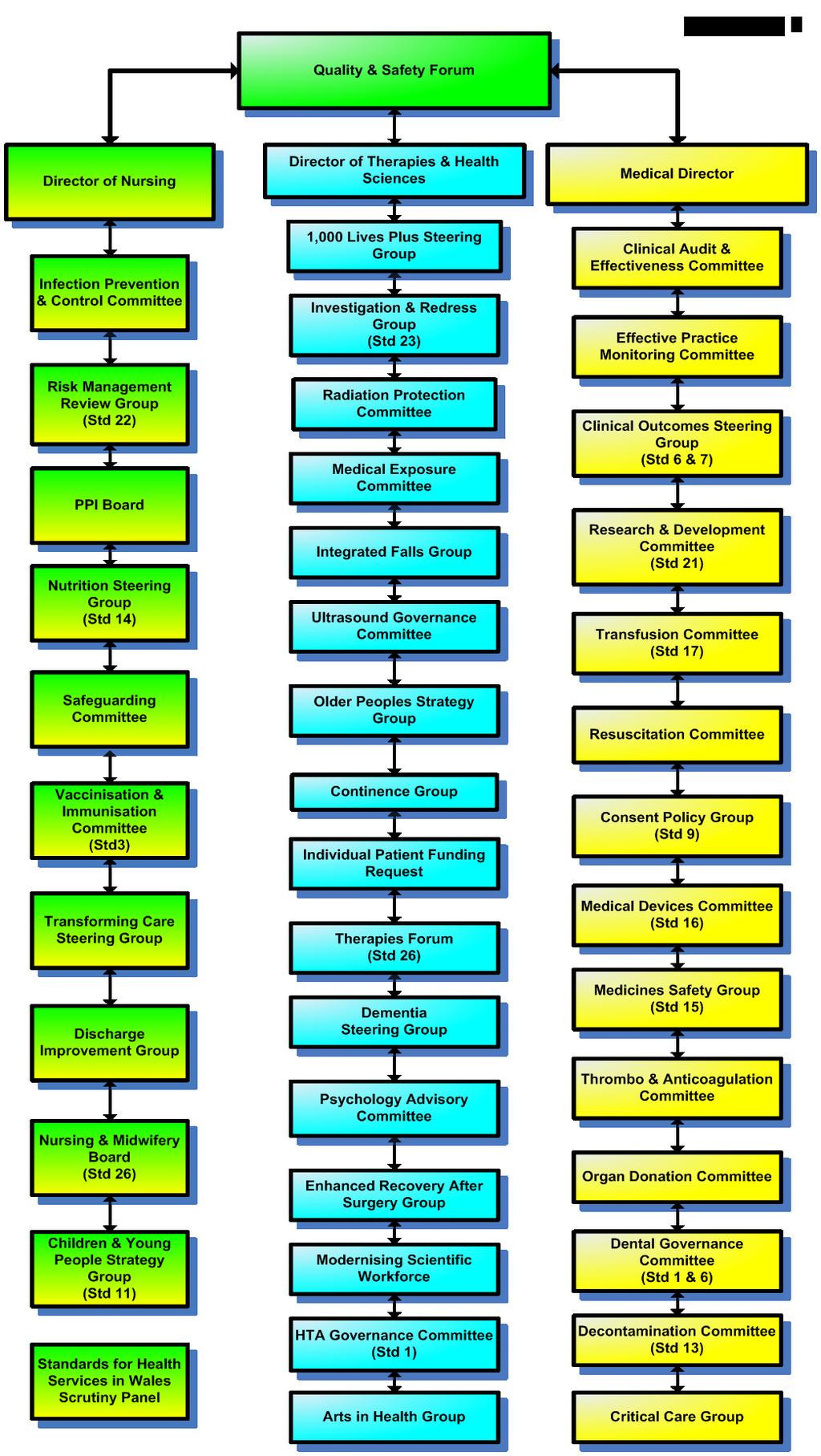
14 Internal Audit will, through a programme of work based on risk, provide ABMU Board with independent assurance of the adequacy of the systems of internal control across a range of financial and business areas in accordance with the Wales Internal Audit Standard. 6.4 Quality & Safety Committee The Quality & Safety Committee is responsible for monitoring the implementation of Quality and Safety across the organisation including the integration of quality activities. The Terms of Reference of this Committee are set out in the Standing Orders approved by the Health Board and available on the Intranet. The Quality and Safety Committee will be supported in its role by a number of key specialty Groups/Committees which are overseen by the Quality & Safety Forum which is an Executive Management Group and Appendix 6 sets out the main specialty groups/committees reporting to the Forum. The Standards for Health Services in Wales Scrutiny Panel is a formal sub Committee of the Quality & Safety committee chaired by a Non Officer member Standards for Health Service in Wales Scrutiny Panel The Scrutiny Panel oversees the implementation of the self assessments against the Standards for Health Services in Wales and scrutinises the core Standards and the performance of: Corporate leads; Directorates/Localities self assessment submissions and The annual corporate quality improvement plan Quality and Safety Forum The Forum is an Executive Lead Group Chaired by the Medical Director established to support the Quality & Safety Committee and oversee the work of the specialist quality and safety groups and committees Risk Management Review Group This Group will review the Risk Management Strategy and highlight significant risks to the organisation. This is a Management Group, Terms of Reference attached as Appendix 7, which reports to the Committees of the Board which is tasked with the overall responsibility to ensure: Continuous improvement in patient safety and service quality The Risk Management Strategy aims and objectives are delivered; There is effective co-ordination and prioritisation of financial, business, and organisational risk management issues across the organisation; There is appropriate awareness of risk management at all levels of the organisation; Welsh Government requirements are met for the monitoring of progress on the Standards for Health Services in Wales Improvement Plan; Overall responsibility for the Risk Management methodology and the integration of risk management processes across the organisation; 10
15 Identifying learning through risk management processes and reporting them to the Effective Practice Monitoring Group for consideration in the Clinical Audit Plan Investigations & Redress Group The NHS Redress legislation received Royal Assent in July 2008 and came into force in NHS Wales in April The Measure is intended to ensure that patients can seek Redress by means of treatment, support and compensation, if appropriate, for lower-value clinical negligence claims without the need to instigate legal action through the Courts. Regulations setting out the detail of the new arrangements have been developed in close consultation with the NHS, patient groups and Community Health Councils and the Putting Things Right Project. The previous Incident, Complaints and Claims policies and procedures have been reviewed in line with the Regulations and changes made to produce an integrated Putting Things Right Policy and Procedure. Incidents Incidents will be managed and reported in accordance with the ABMU s Putting Things right Policy & Procedure. Incidents are analysed for trends and to ensure action is taken and a Root Cause Analysis Investigation of serious incidents. Guidance on Root Cause Analysis is contained within the Putting Things Right Policy as an appendix document. Incident Reporting is not part of the ABMU s disciplinary process. However, examples of situations where disciplinary action may be necessary are as follows: Criminal Activity (eg theft, assault and fraud) Professional misconduct Acts of gross misconduct (eg treating patients under the influence of alcohol) Malicious activity (eg malicious reporting of untrue allegations against a colleague) Repeated unreported errors or violations of procedures Complaints Complaints are managed in accordance with ABMU Putting Things Right Policy and procedure. Each complaint received is risk assessed in terms of the severity of the complaint and likelihood of the circumstances re occurring. The Department of Investigation and Redress grade complaints and ensure that appropriate investigations are instigated. In addition, analyses of serious complaints are presented to the Risk Management Group for inclusion in the relevant Risk Register as appropriate. Action plans produced to reduce the risk of the complaint reoccurring are reviewed and monitored by the Investigation and Redress Group, with lessons learned from investigations shared throughout ABMU via this Group. Claims Claims are managed in accordance with ABMU s Claims Policy & Procedure. Claims management and trend analysis are reviewed by the Claims Management Sub Committee. Lessons learned, where identified, are disseminated throughout ABMU via the 11
16 Investigations and Redress Group, with high risk issues going to the Risk Management Review Group and signposted within the Risk Management Quarterly Reports Effective Practice Monitoring Group It is essential that clinical audit and effectiveness and risk are linked to ensure that issues identified are considered for inclusion with the Clinical Audit Plan. A member of the Clinical Audit & Effectiveness Team is a member of the Investigations and Redress Group and the Assistant Medical Director for Patient Safety is both as a member of the Investigations and Redress Group and the Effective Practice Monitoring Group. Issues identified for action, following a clinical audit, will be reviewed in line with the Risk Management Strategy and managed through Directorate/Locality Risk Registers Patient Safety Work Programme This work programme is committed to reducing harm, variation and waste and thereby reducing harm to patients. Key priorities have been identified, based on high risk areas, and included within the IMTP and excellent patient outcomes Health & Safety Committee The Health & Safety Committee is chaired by the Director of Planning and is supported by the Head of Health & Safety. The Head of Health & Safety is a member of the Risk Management Review Group and Quality & Safety Forum to ensure there are strong links between the risk management and health & safety agendas within the Health Board. The Health and Safety Committee oversees the development of policy, risk control systems and reviews health & Safety arrangements in the Health Board. The Committee monitors and advises on all health and safety risks detailed on the Corporate Risk Register and operational risks escalated to the Head of Health & Safety to consider whether any further control measures can be implemented to mitigate the risk. The Committee reports quarterly to the Quality & Safety Committee and produce an annual report also reported to the Quality & Safety Committee Directorate/Locality/Site Governance Forums The Chief Operating Officer reports directly to the Chief Executive and is responsible for the following Directorates/Localities: Clinical Support Services Neath Port Talbot Locality Swansea Locality Mental Health Directorate Musculo-Skeletal Learning Disabilities Directorate Regional Services Surgical Services Women & Child Health 12
17 The Executive Director of Princess of Wales Hospital is responsible for all services within the Hospital. Each Locality/Clinical Directorate/Site Executive has a Locality/Directorate Board, which is ultimately responsible for Risk Management, specifically operational risks within the Locality/Directorate. The Locality/Directorate/Site Boards will ensure that risk management issues, which can not be managed at Locality/Directorate/Site level or high level risks, which may impact on strategic objectives, are reported, to the Health Board Governance Group and linked into the performance, planning process and capital planning programme. There are nine Corporate Directorates: Medical Director s Directorate Nursing Directorate Directorate of Therapies & Health Sciences Finance Workforce and Organisational Development Planning Chief Operating Officer Public Health Directorate Each Corporate Directorate has a Risk Register and any risk management issue identified as a high risk is reported to the Health Board s Risk Management Review Group/Executive Board and linked into the planning process, capital planning programme and Corporate Plan by identifying risks against the Board Objectives with the IMTP and against the Five Year Strategy. 7. Risk Management Process This section of the document sets out an approach to the assessment of risk and the development of an integrated framework for risk management for the HB. It is a summary of the detailed risk management tools adopted by the HB and should be read in conjunction with the Risk Assessment Management Guidance document. When considering risk management it is important to understand the Health Board s risk appetite and risk tolerance to specific risks as these will change, as they are not single fixed concepts, and will vary over time, and current influential factors at a strategic, tactical and operational level. Risk appetite is about the pursuit of risk and risk tolerance is about what the Health Board will allow management levels within the organisation to deal with. Both risk appetite and risk tolerance are inextricably linked to performance over time. The Health Board s Board is explicitly responsible for determining the nature and extent of the significant risks the organisation is willing to take to achieve strategic objectives risk appetite and tolerance Methodology 13
18 The methodology for identifying risk used within HB is the Australian/New Zealand model AS/NZ; Guidance upon acceptable risk is addressed within this methodology to assist managers to make informed decisions as to the extent of the risk and the application of appropriate action thereafter. For each issue/risk identified the LIKELIHOOD & CONSEQUENCE mechanism will be utilised. Essentially this examines each of the issues and attempts to assess the likelihood of the event occurring (PROBABILITY) and the effect it could have on the HB (IMPACT). This process ensures that the HB will be focusing on those risks which require immediate attention, rather than spending time on areas which are, relatively, a lower priority. The prioritising of risk using this mechanism is detailed in Appendix 8 The Heath Board uses the risk module of Datix to record and monitor all risks with a rating of 16, as a minimum, from an operational perspective and all risks considered to be risks to achieving the organisations objectives/aims referred to as the Corporate Risk Register. The Corporate Risk Register can be accessed through the Health Boards intranet and internet and is updated on a quarterly basis. 7.2 Establish the context Establish the strategic, organisational and risk management context in which the rest of the process will take place. Criteria against which risk will be evaluated should be established and the structure of the analysis defined. The context can include the financial, operational, competitive, political (public perceptions/image), social, client, cultural and legal aspects of the HB s functions. Within these areas it is critical to identify the internal and external stakeholders/partners which may include any of the following: Welsh Assembly Government, patients, staff and contractors. Once the stakeholders/partners have been identified it is important to consider their objectives, take into account their perceptions, and establish communication policies with these parties. It is also important to consider these issues when considering relationships inside and outside the NHS the behaviour of the partners and the organisation and how this will affect any risks identified Risk Identification Risk identification can be undertaken on an individual basis or as part of a multidisciplinary team and can be reactive or proactive and linked to strategic objectives, underpinning the assurance framework, or operational services we provide. Details of how to identify risks are provided within the Risk Management Guidance document which supports the implementation of the Risk Management Strategy Strategic Risk and IMTP Plan (associated with the achievement of aims and objectives of the HB). The IMTP Plan sets out the organisational objectives for 2014/17 the achievement of these objectives will ensure the Health Board effectively manages key organisational risks. This 14
19 will be a "top down" approach, undertaken collectively by the members of the Executive Board. The risk of not achieving the objective and the risks to that objective will be highlighted, as appropriate, to the Health Board, Stakeholders and partners Operational Risk (associated with the direct delivery of services by the organisation area i.e. risks arising from operational activities). This will be a "bottom up" approach undertaken by the staff within individual Directorates/Localities/Sites overseen by the Management Boards. Where "operational" issues raise questions over the strategic objectives of the HB, these will be considered in detail by the Governance Group Patient/Health & Safety Management Patient and Health & Safety assessment involves identifying the significant risk areas in Directorates/Localities/Sites, prioritising them and deciding what action to take. Significant patient/health & Safety risks are classified as those: that could lead to death, disability or severe distress to patients/staff/visitors; that are less serious but could occur more frequently or affect large numbers of patients/staff/visitors should also be included that could impact on the finances or reputation of the HB Analyse/Evaluate risks Determine the existing controls and analyse risks in terms of consequence and likelihood in the context of those controls. The analysis should consider the range of potential consequences and how likely those consequences are to occur. This enables risk to be ranked so as to identify management priorities. If the levels of risk established are low, then risks may fall into an acceptable category and treatment may not be required. Consideration should be given to the balance between potential benefits and adverse outcomes of managing these risks. The risk mapping exercise will be based around an analysis of the likelihood of the risk materialising and its impact should it materialise. Whilst there are quite complex models available, a simple model has been adopted and it is important to recognise that discussion of the risks is essential to determine within the risk description what the actual risk level is at the time of identification and review. In addition the description should set out the consequences of not taking the actions identified to support and inform management decisions and the IMTP process Acceptable Risk: Risk Score of 1 4 (Green) Realistically it is never possible to eliminate all risks, and there will be a range of risks identified within the HB that would require us to go beyond reasonable action, if any, required to eliminate or reduce them, i.e. the cost in time or resources required to reduce the risks would outweigh the potential for harm. These risks would be considered acceptable by the HB. Examples are frequent, low consequence events such as minor property loss or damage, injuries requiring first aid only, or potentially serious events that are unlikely to occur and for which reasonable preventative measures are already in place. 15
20 Manageable Risk: Risk Score of 5 9 (Yellow) The risk can be realistically reduced, within a reasonable time scale, through cost effective measures through the purchase of new equipment and or training. Examples are manual handling injury, malicious damage, and injury to staff or patients. Action would normally be the responsibility of the department or directorate Moderate Risk: Risk Score (Amber) The risk will need to be reduced within 6 months, given that it is a moderate risk, action would normally be the responsibility of the Directorate. The Directorate should notify these risks to the HB Risk Management Group with details of the actions planned High Risk: Risk Score of (Red) Significant risks are where the consequences of the event could seriously impact on the organisation and threaten its objectives. As examples accidental death, major fire, and major disruption of services. This category might include risks that are individually manageable but cumulatively serious, such as a series of similar injuries. Risks identified as being serious should be reported to the HB Board via the organisation s Risk Management Group Risk Management and Control For identified risks, the organisation will agree a programme of actions to manage and control the risks. This will take into account value of money, quality of service delivery, quality and reliability of the evidence to support the identified risk and the impact upon the organisation, stakeholders and partners. Consideration will be given to how to develop and implement specific cost-effective strategies to increase benefits and reduce potential costs. The HB will use the following approaches to risk control: Risk Appetite and Tolerance The Chief Executive and the Board encourage the taking of controlled risks, the grasping of new opportunities and the use of innovative approaches to further the interests of the organisation and achieve its objectives, provided the resultant exposures are understood and acceptable. When deciding if a risk should be tolerated it is necessary to consider a number of factors, e.g. legislation, clinical governance, patient experience, requirements of commissioners and the appetite for these risks. Risk appetite and tolerance considers what risks the Health Board is prepared to take in pursuit of achieving its objectives. This document sets out levels of risks and within these levels there is a management structure which supports decision making in terms of risk appetite and tolerance. Risks rated up to 15 can be managed including determining the risk appetite and tolerance within Directorates/Localities/Sites. Risks rated 16 and above will need to be considered at Executive level in terms of the risk appetite and tolerance levels. Each risk must be considered individually to determine the level of risk appetite and tolerance. 16
21 Organisational policies and written control documents define where there are mandatory processes and procedures, e.g. the Equality and Human Rights Policy etc. Noncompliance with prescribed policies and procedures constitutes an unacceptable risk and possibly a contravention of legislation. Some risks are tolerable provided the prescribed organisational process is followed, e.g. expenditure proposals, staff recruitment, and designated responsibilities/ authorities are adhered to. Managers may take risk management decisions on the basis of their delegated financial authority and the devolved responsibilities set out in the Scheme Delegation within the Standing Orders Treat the Risk Treat by taking action to contain the risk to an acceptable level using internal controls which include: Reactive controls these controls are designed to identify occasions of undesirable outcomes having been achieved after the event so only appropriate when it is possible to accept the loss or damage incurred e.g. post implementation reviews to detect lessons to be learnt from projects for application in future work. Proactive controls designed to ensure a particular outcome is achieved or to ensure an undesirable event is avoided e.g. health and safety guidelines etc. Preventative controls limit the possibility of an undesirable event being realised e.g. separation of duties etc Corrective controls to correct undesirable outcomes which have been realised provide a route of recourse to achieve some recovery against loss or damage e.g. design contract terms to allow recovery of overpayment Terminate the Risk Terminate decision not to take the risk. This might be where the level of risk outweighs the possible benefits, and the risk is terminated by not doing something or doing something differently thereby removing the risk (where it is feasible to do so) Transfer the Risk Transfer decision is made to transfer the risk to others, e.g., through insurance, contracting out the provision of service or paying a third party to take it on. Overall accountability for the risk may still remain with the HB and therefore assurance would still need to be gained in this area. In addition, many areas of business and reputational risk cannot be transferred at all. Action plans will be developed to set out the steps required to manage each risk and will include the approach chosen to control the risk as detailed above. Where additional resources are required to effectively manage a risk, this will be linked into the HB s business planning process. 7.6 Communicate and Consult 17
22 Communicate and consult with internal and external stakeholders and partners as appropriate at each stage of the risk management process and concerning the process as a whole. The frequency of the communication will vary depending upon the severity of the risk and should be discussed and agreed with the stakeholders and partners. This process will be led by the person nominated as the lead to manage the risk and for communication with external stakeholders this will be the appointed Executive Director lead for the risk. Effective internal and external communication is important to ensure that those responsible for implementing risk management, and those with a vested interest understand the basis on which decisions are made and why particular actions are required. Internal stakeholders can include any managers which the risk identified may impact on their service or staff. External stakeholders will vary depending on the type of risk and the risk lead for the Directorate/Locality HB will need to consider which external stakeholders will need to be notified. All significant risks will be reported to the Welsh Assembly Government through the weekly brief from organisations and quarterly performance review meetings. 8. Risk Register Once the risk has been identified and analysed the next stage is to ensure the risk is recorded on the Directorate/Locality Risk Register. The principal tool that the organisation will use for managing the risk assessment systems and processes will be the HB Risk Register, template attached as Appendix 9. The HB Risk Register can be described as a log of all the risks that may threaten the success of the HB in achieving its declared aims and objectives. Identifying and logging the risk will ensure that the Department/Directorate/Locality are aware of the risk and, following consideration of any existing controls in place, whether other options exist to further reduce or eliminate the risk. Appendix 10. An Action Plan will be approved and monitored by the Directorate/Locality/Site Board setting out action to be taken and priorities within their Directorate/Locality. The Head of Quality Assurance will coordinate the Corporate Risk Register and produce a HB Risk Register Report and action plan, for risks with a risk rating of 16 and above. The HB Risk Management Review Group will oversee and approve the Corporate Risk Register. The HB Risk Management Review Group will also agree the significant risks to be submitted to the Executive Board, and Quality & Safety Committee and HB Board for review and approval of the proposed action and risk treatments recommended Appendix 11. The Departments, Directorates/Localities/Sites and HB Wide Risk Registers will be analysed by the Clinical Director, General Manager/Executive Director and Governance Lead for the directorate/locality/site respectively. Risk profiling will be undertaken to ensure that trends, where appropriate, are identified from a review of information from the risk register, risk assessments, incidents, claims and complaints. The link with the requirements of the core Standards for Health Services in Wales which require the organisation to have a risk register that is populated by data representing all 18
23 known risks". In order to understand an organisation s comprehensive risk profile, there must be a repository for all risk information, the risk register. Risk Registers will continue to be developed to include risks identified from: Deficiencies with various Standards for Health Services in Wales; findings from department specific and organisational wide hazard reports and risk assessments; underlying "root" causes of incidents complaints and claims; underlying causes related to poor trends identified from key performance indicators; actions to reduce risks which could not be or were not implemented for various reasons, such as resource limitations; and any other source of information that could be considered to be threat to patient, staff, visitors, environmental safety or the organisations well being. 9. Risk Management Training The successful establishment of a risk management culture will require a varying level of training across the HB. Ward/Department Managers will be primarily responsible for implementing process and a minimum of 2 members of staff, including the Manager, will be trained to carry out risk assessments. These staff will be expected to oversee the risk assessments carried out in their area of work and be responsible to cascade this training to their staff with particular reference to: the general principles and objectives of risk management; the role of staff in the risk management process; reporting systems and the importance of following them; risk register and; risk assessment. Training will be reinforced by references in the Staff Handbook, posters, etc. Refresher training will be provided at appropriate intervals. All training provided to staff (of whatever grade) is to be recorded centrally and in personnel records with the signature of the recipient. 19
24 10. Glossary Risk Appetite The amount of risk that an organisation is willing to seek or accept in the pursuit of its long term objectives. Risk Tolerance The boundaries of risk taking outside of which the organisation is not prepared to venture in the pursuit of its long term objectives. Risk Universe The full range of risks which could impact, either positively or negatively, on the ability of the organisation to achieve its long term objectives. Risk analysis Systematic use of information to identify opportunities and threats and to estimate the likelihood of occurrence and severity of the impact Risk assessment The approach and process used to prioritise and determine the likelihood of risks occurring and their potential impact on the achievement of objectives. Risk identification Determination of what could pose a risk; the process to describe and list sources of risks (opportunities and threats). Risk Management The process of identifying and assessing risks, assigning ownership, taking actions to mitigate or anticipate them, and monitoring and reviewing progress. This provides a disciplined environment for proactive decision making. Risk & assurance framework As an integral aspect of planning and performance management, sets the context within which risks are managed in terms of how they will be identified, analysed, controlled, monitored and reviewed. Risk management matrix Tool to assess the overall risk rating using a 5x5 matrix based on the impact of the risk and the likelihood of the risk being realised. Risk owner An individual who is in a position to ensure a risk is managed and controlled. Risk rating The overall score given to a risk based on an assessment of both its likelihood of being realised and its potential impact, measured on a scale of 1 (lowest) to 25 (highest). Significant risk Those risks assessed to have an overall rating of 16 or above (using risk management matrix). 20
25 Strategic risk Risk concerned with where the organisation wants to go, how it plans to get there and how it can ensure success. Terminate Remove the risk by termination or doing things differently. Tolerate Continue with a risk as it is at a reasonable level but monitor regularly. Transfer Transfer the risk to a third party such as insurance. Treat Control the risk by taking contingent or containment action e.g. security checks etc. 11. References 1. Building the Assurance Framework: A Practical Guide for NHS Boards (Department of Health, Gatelog Ref 1054, March 2003) 2. Doing Well, Doing Better Standards for Health Services in Wales (Welsh Assembly Government, April 2010) 3. Draft BS ISO Risk management Principles and guidelines on implementation (British Standards Institute, DPC/ DC, May 2008) 4. Getting the Assurance you need:a guide to Boards Draft (Welsh Assembly Government, November 2009) 5. Identifying risk, taking action: Monitor s approach to service performance in NHS foundation trusts (Monitor, IRREP 02/03,) 6. Audit Committee Handbook June Leading health and safety at work Leadership actions for Directors and Board Members (Institute of Directors and Health and Safety Executive, INDG417, 09/09) 8. Risk Assessment Framework: a tool for departments (HM Treasury, ISBN , July 2009) 9. Risk Essentials A Risk Management Framework (Welsh Government, Version 2, October 2006) 10. Risk Management in the NHS (NHS Management Executive, December 1993) 11. The Orange Book: Management of Risk Principles and Concepts ( HM Treasury, ISBN , October 2004) 12. Your Risk & Assurance Framework: A structured approach (Welsh Government, December 2009) 21
26 Appendix 1 Policies available to assist with Risk Management Business Continuity Strategy & Policy Consent Policy Communications Policy Drug Administration Policy Fire Policy Health and Safety Policy Risk Assessment Policy & Procedure Health Surveillance Policy Immunisation of Employees Policy Infection Control Policy Putting Things Right Policy Counter Fraud Policy and Response Plan Intravenous Drug Supply and Administration Policy Latex Allergy Policy Manual Handling Policy Medical Use of Ionising Radiation Policy Records Management Strategy Policy and Guidelines on Dealing with Violence and Aggression Policy & Procedure for the Management of Asbestos Policy for Policies Policy on the Segregation and Safe Disposal of Waste Pre Employment Screening Policy Records Management Resuscitation Policy Risk Register Guidance Standing Orders Standing Financial Instructions Violence & Aggression Policy Whistleblowing Policy 22
27 Doing Well, Doing Better: Standards for Health Services in Wales* Appendix 2 Standard Executive Lead Group/Committee Overseeing the Standard 1. Governance & Accountability Board Secretary Quality & Safety Forum Framework 2. Equality, Diversity and Human Rights Director of Workforce and Organisational Equality & Diversity Group Development 3. Health Promotion, Protection & Director of Public Health ABM Public Health Team Meetings Improvement 4. Civil Contingency & Emergency Director of Planning Emergency Planning Group Planning Arrangements 5. Citizen Engagement and Feedback Director of Nursing and Director of Planning Patient Experience Board 6. Participating in Quality Improvement Medical, Nursing and Therapies & Health Science Quality & Safety Forum and ISIS Activities Directors 7. Safe and Clinically Effective Care Medical, Nursing and Therapies & Health Science Effective Practice Monitoring Group Directors 8. Care Planning and Provision Director of Planning Executive Board 9. Patient Information and Consent Medical Director Consent Group 10. Dignity and Respect Medical, Nursing and Therapies & Health Science Directors Nursing & Midwifery Board Older Peoples Strategy Group Younger Persons Strategy Group 11. Safeguarding Children and Director of Nursing Safeguarding Committee Safeguarding Vulnerable Adults 12. Environment Director of Planning Executive Board 13. Infection Prevention and Control (IPC) and Decontamination Director of Nursing Infection, Prevention and Control Committee 14. Nutrition Directors of Nursing and Therapies & Health Nutrition Steering Group Science 15. Medicines Management Medical Director Medicines Management Safety Group 16. Medical Devices, Equipment and Medical Director Medical Devices Committee Diagnostic Systems 17. Blood Management Medical Director Transfusion Committee 18. Communicating Effectively Board Secretary Patient Experience Board Director of Nursing 19. Information Management & Director of Workforce and Organisational Information Governance Board Communications Technology Development 20. Records Management Director of Workforce and Organisational Information Governance Board Development 21. Research, Development and Innovation Medical Director Research & Development Committee 22. Managing Risk and Health and Safety Director of Planning and Director of Nursing Risk Management Review Group Health & Safety Committee 23. Dealing with concerns and managing Director of Therapies & Health Science Investigations & Redress Group incidents 24. Workforce Planning Director of Workforce and Organisational Workforce & OD Committee Development 25. Workforce Recruitment and Director of Workforce and Organisational Workforce & OD Committee Employment Practices Development 26. Workforce Training and Organisational Development Director of Workforce and Organisational Development Workforce & OD Committee * Standards in Full are available on the Health Boards Intranet on the Risk Management site or by contacting the Head of Quality Assurance 23
28 Appendix 3 Scheme of Delegation 24
29 25
30 Appendix 5 BOARD Strategic Assurance Remuneration Committee Audit Committee Quality & Safety Committee Workforce & OD Committee Pharmaceutical Charitable Funds Mental Health Act Monitoring Committee Mental Health Managers Committee SHSIW Srutiny Panel Executive Team Health & Safety Committee Quality & Safety Forum Innovation, Support & Improvement Science Core Group Executive Board Joint Operational Board Tactical Operational Specialist Quality & Safety Management Committee/ Groups Directorate Quality Forums Locality Quality Forums Service Operational 26
31 27
CLINICAL AND CARE GOVERNANCE STRATEGY
 CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
Date 4 th September 2015 Dr Ruth Charlton, Joint Medical Director / Jill Down, Associate Director of Quality Laura Rowe, Compliance Manager
 TB 099/15 Meeting title Report title Trust Board Risk Management Strategy Date 4 th September 2015 Lead director Report author FOI status Dr Ruth Charlton, Joint Medical Director / Jill Down, Associate
TB 099/15 Meeting title Report title Trust Board Risk Management Strategy Date 4 th September 2015 Lead director Report author FOI status Dr Ruth Charlton, Joint Medical Director / Jill Down, Associate
Internal Audit. Health and Safety Governance. November Report Assessment
 November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
HEALTH AND SAFETY POLICY
 NHS GREATER GLASGOW AND CLYDE HEALTH AND SAFETY POLICY November 2015 Lead Manager: K. Fleming Head of Health and Safety Responsible Director A. MacPherson Director of Human Resources and Organisational
NHS GREATER GLASGOW AND CLYDE HEALTH AND SAFETY POLICY November 2015 Lead Manager: K. Fleming Head of Health and Safety Responsible Director A. MacPherson Director of Human Resources and Organisational
Health and Safety Policy
 Health and Safety Policy 2015 Statement of Health and Safety Policy The University recognises its obligations to properly control the risks to the health of its staff, students and visitors. Strong strategic
Health and Safety Policy 2015 Statement of Health and Safety Policy The University recognises its obligations to properly control the risks to the health of its staff, students and visitors. Strong strategic
Document Details Clinical Audit Policy
 Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
POLICY ON THE IMPLEMENTATION OF NICE GUID ANCE
 POLICY ON THE IMPLEMENTATION OF NICE GUID ANCE Document Type Corporate Policy Unique Identifier CO-019 Document Purpose To outline the process for the implementation and compliance with NICE guidance and
POLICY ON THE IMPLEMENTATION OF NICE GUID ANCE Document Type Corporate Policy Unique Identifier CO-019 Document Purpose To outline the process for the implementation and compliance with NICE guidance and
RISK MANAGEMENT STRATEGY
 RISK MANAGEMENT STRATEGY Version Number 6.1 Version Date February 2018 Policy Owner Chief Executive Author Trust Risk and Patient Safety Manager First approval or date last reviewed The Risk Management
RISK MANAGEMENT STRATEGY Version Number 6.1 Version Date February 2018 Policy Owner Chief Executive Author Trust Risk and Patient Safety Manager First approval or date last reviewed The Risk Management
MATERNITY SERVICES RISK MANAGEMENT STRATEGY
 Trust Board Agenda Item 8.3 Enc 10 Appendix 1 January 2012 MATERNITY SERVICES NORTH CUMBRIA MATERNITY SERVICES RISK MANAGEMENT STRATEGY 2011-13 DOCUMENT CONTROL Author/Contact Head Of Midwifery / Clinical
Trust Board Agenda Item 8.3 Enc 10 Appendix 1 January 2012 MATERNITY SERVICES NORTH CUMBRIA MATERNITY SERVICES RISK MANAGEMENT STRATEGY 2011-13 DOCUMENT CONTROL Author/Contact Head Of Midwifery / Clinical
Health and Safety Strategy
 NHS Newcastle Gateshead Clinical Commissioning Group Health and Safety Strategy Document Status Equality Impact Assessment Document Ratified/Approved By Final No impact Quality, Safety and Risk Committee
NHS Newcastle Gateshead Clinical Commissioning Group Health and Safety Strategy Document Status Equality Impact Assessment Document Ratified/Approved By Final No impact Quality, Safety and Risk Committee
Visiting Celebrities, VIPs and other Official Visitors
 Visiting Celebrities, VIPs and other Official Visitors Who Should Read This Policy Target Audience Healthcare Professionals Executive Team Version 1.0 May 2016 Ref. Contents Page 1.0 Introduction 4 2.0
Visiting Celebrities, VIPs and other Official Visitors Who Should Read This Policy Target Audience Healthcare Professionals Executive Team Version 1.0 May 2016 Ref. Contents Page 1.0 Introduction 4 2.0
Management of Violence and Aggression Policy
 Management of Violence and Aggression Policy Approved by: Trust Health and Safety Committee Date First Issued: August 2000 Reviewed July 2006 TABLE OF CONTENTS Section Page No 1 STATEMENT OF POLICY 2 SCOPE
Management of Violence and Aggression Policy Approved by: Trust Health and Safety Committee Date First Issued: August 2000 Reviewed July 2006 TABLE OF CONTENTS Section Page No 1 STATEMENT OF POLICY 2 SCOPE
cc: Emergency Ambulance Services Committee Members EMERGENCY AMBULANCE SERVICES COMMITTEE ANNUAL GOVERNANCE STATEMENT 2015/16
 EASC Agenda Item 4.5 Appendix 1 To: Mrs Allison Williams, Chief Executive, Cwm Taf University Health Board cc: Emergency Ambulance Services Committee Members EMERGENCY AMBULANCE SERVICES COMMITTEE ANNUAL
EASC Agenda Item 4.5 Appendix 1 To: Mrs Allison Williams, Chief Executive, Cwm Taf University Health Board cc: Emergency Ambulance Services Committee Members EMERGENCY AMBULANCE SERVICES COMMITTEE ANNUAL
Central Alerting System (CAS) Policy
 Policy") Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
SAFEGUARDING CHILDREN SUPERVISION POLICY
 SAFEGUARDING CHILDREN SUPERVISION POLICY Approved by Safeguarding Committee Submitted by: Head of Safeguarding Children Approved on: 6 th December 2010 Review Date: December 2013 Version: 2.0 Index Page
SAFEGUARDING CHILDREN SUPERVISION POLICY Approved by Safeguarding Committee Submitted by: Head of Safeguarding Children Approved on: 6 th December 2010 Review Date: December 2013 Version: 2.0 Index Page
EXECUTIVE MEDICAL DIRECTOR JOB DESCRIPTION. Medical Education Leads Clinical Directors (professional leadership) Director of Clinical Audit
 Director of Clinical Audit") EXECUTIVE MEDICAL DIRECTOR JOB DESCRIPTION Job Title: Accountable to: Responsible for: Executive Medical Director Chief Executive Director of Research & Development Medical Education Leads Clinical Directors
EXECUTIVE MEDICAL DIRECTOR JOB DESCRIPTION Job Title: Accountable to: Responsible for: Executive Medical Director Chief Executive Director of Research & Development Medical Education Leads Clinical Directors
QUALITY STRATEGY
 QUALITY STRATEGY 2012-2016 SPONSOR: Sue Hardy Director of Nursing Signature: AUTHORS: Sue Hardy Director of Nursing Denise Flowers Associate Director Clinical Effectiveness APPROVED BY: Southend University
QUALITY STRATEGY 2012-2016 SPONSOR: Sue Hardy Director of Nursing Signature: AUTHORS: Sue Hardy Director of Nursing Denise Flowers Associate Director Clinical Effectiveness APPROVED BY: Southend University
DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY
 DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY (To be read in conjunction with Diagnostic Imaging Requesting and Interpreting Radiographs by Non Medical Practitioners Policy, Consent
DIAGNOSTIC CLINICAL TESTS AND SCREENING PROCEDURES MANAGEMENT POLICY (To be read in conjunction with Diagnostic Imaging Requesting and Interpreting Radiographs by Non Medical Practitioners Policy, Consent
POLICY & PROCEDURE FOR INCIDENT REPORTING
 POLICY & PROCEDURE FOR INCIDENT REPORTING APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE February 2015 Date of Issue: 25 February 2015 Version No:
POLICY & PROCEDURE FOR INCIDENT REPORTING APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE February 2015 Date of Issue: 25 February 2015 Version No:
SAFEGUARDING ADULTS POLICY
 SAFEGUARDING ADULTS POLICY This document may be made available in alternative formats and other languages, on request, as is reasonably practicable to do so. Policy Owner: Approved by: POVA Operational
SAFEGUARDING ADULTS POLICY This document may be made available in alternative formats and other languages, on request, as is reasonably practicable to do so. Policy Owner: Approved by: POVA Operational
Appendix 1 MORTALITY GOVERNANCE POLICY
 Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Integration Scheme. Between. Glasgow City Council. and. NHS Greater Glasgow and Clyde
 Integration Scheme Between Glasgow City Council and NHS Greater Glasgow and Clyde December 2015 Page 1 of 60 1. Introduction 1.1 The Public Bodies (Joint Working) (Scotland) Act 2014 (the Act) requires
Integration Scheme Between Glasgow City Council and NHS Greater Glasgow and Clyde December 2015 Page 1 of 60 1. Introduction 1.1 The Public Bodies (Joint Working) (Scotland) Act 2014 (the Act) requires
Quality Impact Assessment Policy
 Quality Impact Assessment Policy Date: February 2016 Version: 2.1 Review Due: February 2018 Reader information Reference Directorate Document purpose Q005 Quality The purpose of this policy is to set out
Quality Impact Assessment Policy Date: February 2016 Version: 2.1 Review Due: February 2018 Reader information Reference Directorate Document purpose Q005 Quality The purpose of this policy is to set out
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
JOB DESCRIPTION. Specialist Practitioner of Transfusion for Shrewsbury, Telford and surrounding community hospitals. Grade:- Band 7 Line Manager:-
 JOB DESCRIPTION Job Title:- Specialist Practitioner of for Shrewsbury, Telford and surrounding community hospitals. Grade:- Band 7 Line Manager:- Associate Director of Patient Safety Professionally Accountability
JOB DESCRIPTION Job Title:- Specialist Practitioner of for Shrewsbury, Telford and surrounding community hospitals. Grade:- Band 7 Line Manager:- Associate Director of Patient Safety Professionally Accountability
Policy for the Reporting and Management of Incidents Including Serious Incidents. Version Number: 006
 CONTROLLED DOCUMENT Policy for the Reporting and Management of Incidents Including Serious Incidents CATEGORY: CLASSIFICATION: PURPOSE Controlled Number: Document Policy Governance To set out the principles
CONTROLLED DOCUMENT Policy for the Reporting and Management of Incidents Including Serious Incidents CATEGORY: CLASSIFICATION: PURPOSE Controlled Number: Document Policy Governance To set out the principles
Health Board Report SOCIAL SERVICES AND WELL-BEING ACT (WALES) 2014: REVISED REGIONAL IMPLEMENTATION PLAN
 2014: REVISED REGIONAL IMPLEMENTATION PLAN") Agenda Item 3.3 27 JANUARY 2016 Health Board Report SOCIAL SERVICES AND WELL-BEING ACT (WALES) 2014: REVISED REGIONAL IMPLEMENTATION PLAN Executive Lead: Director of Planning & Performance Author: Assistant
Agenda Item 3.3 27 JANUARY 2016 Health Board Report SOCIAL SERVICES AND WELL-BEING ACT (WALES) 2014: REVISED REGIONAL IMPLEMENTATION PLAN Executive Lead: Director of Planning & Performance Author: Assistant
SAFETY, HEALTH AND WELLBEING POLICY
 LEEDS BECKETT UNIVERSITY SAFETY, HEALTH AND WELLBEING POLICY www.leedsbeckett.ac.uk/staff Policy Statement The University is committed to provide a safe and healthy environment for work and study in support
LEEDS BECKETT UNIVERSITY SAFETY, HEALTH AND WELLBEING POLICY www.leedsbeckett.ac.uk/staff Policy Statement The University is committed to provide a safe and healthy environment for work and study in support
Meeting of Governing Body
 Meeting of Governing Body Date: 7 August 2018 Time: 1.30pm Location: Clevedon Hall, Elton Rd, Clevedon, North Somerset, BS21 7RQ Agenda number: 10.3 Report title: Business Continuity Policy Report Author:
Meeting of Governing Body Date: 7 August 2018 Time: 1.30pm Location: Clevedon Hall, Elton Rd, Clevedon, North Somerset, BS21 7RQ Agenda number: 10.3 Report title: Business Continuity Policy Report Author:
Health and Safety Policy
 Document reference: 210A2015 Date: March 2015 Health and Safety Policy Index 1.0 Introduction 2 2.0 Health and safety policy statement 2 3.0 Health and safety responsibilities 3 4.0 Health and safety risks
Document reference: 210A2015 Date: March 2015 Health and Safety Policy Index 1.0 Introduction 2 2.0 Health and safety policy statement 2 3.0 Health and safety responsibilities 3 4.0 Health and safety risks
Health and Safety Policy and Managerial Responsibilities
 Health and Safety Policy and Managerial Responsibilities 1.0 Purpose This document outlines the policies, procedures and practices governing the manner in which the Royal Conservatoire of Scotland manages
Health and Safety Policy and Managerial Responsibilities 1.0 Purpose This document outlines the policies, procedures and practices governing the manner in which the Royal Conservatoire of Scotland manages
FORTH VALLEY CLINICAL AND CARE GOVERNANCE FRAMEWORK
 HEALTH AND SOCIAL CARE INTEGRATION: FORTH VALLEY CLINICAL AND CARE GOVERNANCE FRAMEWORK The Scottish Government, National Health and Wellbeing Outcomes: A framework for improving the planning and delivery
HEALTH AND SOCIAL CARE INTEGRATION: FORTH VALLEY CLINICAL AND CARE GOVERNANCE FRAMEWORK The Scottish Government, National Health and Wellbeing Outcomes: A framework for improving the planning and delivery
The Mid Yorkshire Hospitals NHS Trust. Risk Management Strategy
 The Mid Yorkshire Hospitals NHS Trust Risk Management Strategy Document control Author Assistant director governance and patient safety Director sponsor Medical Director Date August 2011 Version 6 Draft
The Mid Yorkshire Hospitals NHS Trust Risk Management Strategy Document control Author Assistant director governance and patient safety Director sponsor Medical Director Date August 2011 Version 6 Draft
Version: 3.0. Effective from: 29/08/2012
 Policy No: RM51 Version: 3.0 Name of policy: Learning from Experience Policy A systematic approach to incident, complaint and clai management, analysis and sharing safety lessons Effective from: 29/08/2012
Policy No: RM51 Version: 3.0 Name of policy: Learning from Experience Policy A systematic approach to incident, complaint and clai management, analysis and sharing safety lessons Effective from: 29/08/2012
Section 10: Guidance on risk assessment and risk management within the Adult Safeguarding process
 Section 10: Guidance on risk assessment and risk management within the Adult Safeguarding process 10.1 Definition Risk is the likelihood that a person may be harmed or suffers adverse effects if exposed
Section 10: Guidance on risk assessment and risk management within the Adult Safeguarding process 10.1 Definition Risk is the likelihood that a person may be harmed or suffers adverse effects if exposed
Implementation of Quality Framework Update
 Joint Committee Meeting 26 January 2016 Title of the Committee Paper Framework Update Executive Lead: Director of Nursing & Quality Assurance Author: Director of Nursing & Quality Assurance Contact Details
Joint Committee Meeting 26 January 2016 Title of the Committee Paper Framework Update Executive Lead: Director of Nursing & Quality Assurance Author: Director of Nursing & Quality Assurance Contact Details
QUALITY COMMITTEE. Terms of Reference
 QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
Agenda item 3.3 Appendix 4 MANDATORY TRAINING POLICY
 Agenda item 3.3 Appendix 4 MANDATORY TRAINING POLICY Reference No: Issued by Policy Manager Version No: 1 Previous Trust / LHB Ref No: n/a Documents to read alongside this Policy Study Leave Guidelines
Agenda item 3.3 Appendix 4 MANDATORY TRAINING POLICY Reference No: Issued by Policy Manager Version No: 1 Previous Trust / LHB Ref No: n/a Documents to read alongside this Policy Study Leave Guidelines
Governance and Quality Committee Review. Wendy Pugh Director of Operations and Nursing. Innovation Tom Jinks - Governance Manager.
 Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
Board meeting date: 29 th May 2013 Agenda Item number:10.1 Enclosure:5 Title and Quality Committee Review Accountable Director: Author (name & title): Wendy Pugh Director of Operations and Nursing Rosie
Corporate. Health and Safety Policy. Document Control Summary. Contents
 Corporate Health and Safety Policy Document Control Summary Status: Version: Author/Title: Owner/Title: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation Date: Review Date:
Corporate Health and Safety Policy Document Control Summary Status: Version: Author/Title: Owner/Title: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation Date: Review Date:
EMERGENCY PRESSURES ESCALATION PROCEDURES
 OP48 EMERGENCY PRESSURES ESCALATION PROCEDURES INITIATED BY: Director of Therapies & Health Sciences / Chief Operating Officer APPROVED BY: Executive Board DATE APPROVED: 21 September 2016 VERSION: 3 OPERATIONAL
OP48 EMERGENCY PRESSURES ESCALATION PROCEDURES INITIATED BY: Director of Therapies & Health Sciences / Chief Operating Officer APPROVED BY: Executive Board DATE APPROVED: 21 September 2016 VERSION: 3 OPERATIONAL
GOVERNANCE REVIEW. Contact Details for further information: Pam Wenger, Committee Secretary.
 Joint Committee Meeting 26 January 2016 Title of the Committee Paper GOVERNANCE REVIEW Executive Lead: Chair Author: Committee Secretary Contact Details for further information: Pam Wenger, Committee Secretary.
Joint Committee Meeting 26 January 2016 Title of the Committee Paper GOVERNANCE REVIEW Executive Lead: Chair Author: Committee Secretary Contact Details for further information: Pam Wenger, Committee Secretary.
HEALTH AND SAFETY POLICY
 HEALTH AND SAFETY POLICY Version: 4 Ratified by: Trust Board (Required) Date ratified: January 2016 Title of originator/author: Title of responsible committee/group: Head of Corporate Business Date issued:
HEALTH AND SAFETY POLICY Version: 4 Ratified by: Trust Board (Required) Date ratified: January 2016 Title of originator/author: Title of responsible committee/group: Head of Corporate Business Date issued:
HEALTH AND SAFETY POLICY
 HEALTH AND SAFETY POLICY Category: Health and Safety Date Created: July 2016 Responsibility: Chief Executive Date Last Reviewed: October 2017 Approval: UCOL Council Version: 17.1 UCOL Health and Safety
HEALTH AND SAFETY POLICY Category: Health and Safety Date Created: July 2016 Responsibility: Chief Executive Date Last Reviewed: October 2017 Approval: UCOL Council Version: 17.1 UCOL Health and Safety
Methods: Commissioning through Evaluation
 Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
NHS SHETLAND CLINICAL GOVERNANCE STRATEGY
 NHS SHETLAND CLINICAL GOVERNANCE STRATEGY 2010-13 Clinical governance is the defining heart and inspiration of quality in the NHS Aidan Halligan 2006 Last version date: March 2007 Next Formal Review January
NHS SHETLAND CLINICAL GOVERNANCE STRATEGY 2010-13 Clinical governance is the defining heart and inspiration of quality in the NHS Aidan Halligan 2006 Last version date: March 2007 Next Formal Review January
Work Health and Safety Committee Terms of Reference
 Work Health and Safety Committee Terms of Reference Related Policy Work Health and Safety Policy Responsible Officer Executive Director Human Resources Approved by Executive Director Human Resources Approved
Work Health and Safety Committee Terms of Reference Related Policy Work Health and Safety Policy Responsible Officer Executive Director Human Resources Approved by Executive Director Human Resources Approved
IMPROVING QUALITY. Clinical Governance Strategy & Framework
 IMPROVING QUALITY Clinical Governance Strategy & Framework NHS GREATER GLASGOW & CLYDE Approval: Quality & Performance Committee Responsible Director: Medical Director Custodian: Head of Clinical Governance
IMPROVING QUALITY Clinical Governance Strategy & Framework NHS GREATER GLASGOW & CLYDE Approval: Quality & Performance Committee Responsible Director: Medical Director Custodian: Head of Clinical Governance
SUBJECT: NHSL CORPORATE RISK REGISTER. For approval For endorsement X To note. Prepared Reviewed X Endorsed
 Meeting of Lanarkshire NHS Board 31st August 2016 Lanarkshire NHS Board Kirklands Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk 1. PURPOSE SUBJECT: NHSL CORPORATE RISK
Meeting of Lanarkshire NHS Board 31st August 2016 Lanarkshire NHS Board Kirklands Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk 1. PURPOSE SUBJECT: NHSL CORPORATE RISK
Mortality Policy. Learning from Deaths
 Mortality Policy Learning from Deaths Name of Author and Job Title: Frank Jacobs, Datix project manager Ian Brandon, Head of governance and risk Name of Review/ Development Body: Ratification Body: Mortality
Mortality Policy Learning from Deaths Name of Author and Job Title: Frank Jacobs, Datix project manager Ian Brandon, Head of governance and risk Name of Review/ Development Body: Ratification Body: Mortality
EQuIPNational Survey Planning Tool NSQHSS and EQuIP Actions 4.
 Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement
Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement
Learning from Deaths Framework Policy
 Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
VIP Visitors Policy. Purpose of Agreement. Document Type. Policy SOP Guideline. Version Version 1. Operational Date July 2015
 VIP Visitors Policy Please be aware that this printed version of the Policy may NOT be the latest version. Staff are reminded that they should always refer to the Intranet for the latest version. Purpose
VIP Visitors Policy Please be aware that this printed version of the Policy may NOT be the latest version. Staff are reminded that they should always refer to the Intranet for the latest version. Purpose
CLINICAL GOVERNANCE STRATEGY. For West Sussex PCT
 CLINICAL GOVERNANCE STRATEGY For West Sussex PCT 2006 2009 Agreed by the Clinical Governance Committee: 31/01/07 Effective from: 31/01/07 Review: 31/07/07 Page 1 of 8 Contents Page Introduction 3 Principles
CLINICAL GOVERNANCE STRATEGY For West Sussex PCT 2006 2009 Agreed by the Clinical Governance Committee: 31/01/07 Effective from: 31/01/07 Review: 31/07/07 Page 1 of 8 Contents Page Introduction 3 Principles
Corporate. Visitors & VIP s Standard Operating Procedure. Document Control Summary. Contents
 Corporate Visitors & VIP s Standard Operating Procedure Document Control Summary Status: Version: Author/Owner: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation Date:
Corporate Visitors & VIP s Standard Operating Procedure Document Control Summary Status: Version: Author/Owner: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation Date:
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
DOH Policy on Healthcare Emergency & Disaster Management for the Emirate of Abu Dhabi
 DOH Policy on Healthcare Emergency & Disaster Management for the Emirate of Abu Dhabi Department of Health, October 2017 Page 1 of 22 Document Title: Document Number: Ref. Publication Date: 24 October
DOH Policy on Healthcare Emergency & Disaster Management for the Emirate of Abu Dhabi Department of Health, October 2017 Page 1 of 22 Document Title: Document Number: Ref. Publication Date: 24 October
HEALTH AND SAFETY POLICY
 Reference Number: UHB 021 Version Number: 4 Date of Next Review: 24 Nov 2019 Previous Trust/LHB Reference Number: T29 HEALTH AND SAFETY POLICY Statement On behalf of Cardiff and Vale University Local Health,
Reference Number: UHB 021 Version Number: 4 Date of Next Review: 24 Nov 2019 Previous Trust/LHB Reference Number: T29 HEALTH AND SAFETY POLICY Statement On behalf of Cardiff and Vale University Local Health,
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS
 ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version
A concern means any complaint, claim or reported patient safety incident.
 PUTTING THINGS RIGHT ANNUAL REPORT -2017 Introduction The Putting Things Right Annual Report provides information on the progress and performance of Powys Teaching Local Health Board (hereafter, the health
PUTTING THINGS RIGHT ANNUAL REPORT -2017 Introduction The Putting Things Right Annual Report provides information on the progress and performance of Powys Teaching Local Health Board (hereafter, the health
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine
 Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
INTRODUCTION TO THE UK PUBLIC HEALTH REGISTER ROUTE TO REGISTRATION FOR PUBLIC HEALTH PRACTITIONERS
 INTRODUCTION TO THE UK PUBLIC HEALTH REGISTER ROUTE TO REGISTRATION FOR PUBLIC HEALTH PRACTITIONERS This introduction consists of: 1. Introduction to the UK Public Health Register 2. Process and Structures
INTRODUCTION TO THE UK PUBLIC HEALTH REGISTER ROUTE TO REGISTRATION FOR PUBLIC HEALTH PRACTITIONERS This introduction consists of: 1. Introduction to the UK Public Health Register 2. Process and Structures
Emergency Ambulance Services Committee Report CHIEF AMBULANCE SERVICES COMMISSIONER S UPDATE REPORT
 AGENDA ITEM 3.2 22 MARCH 2016 Emergency Ambulance Services Committee Report CHIEF AMBULANCE SERVICES COMMISSIONER S UPDATE REPORT Executive Lead: Chief Ambulance Services Commissioner Author: Chief Ambulance
AGENDA ITEM 3.2 22 MARCH 2016 Emergency Ambulance Services Committee Report CHIEF AMBULANCE SERVICES COMMISSIONER S UPDATE REPORT Executive Lead: Chief Ambulance Services Commissioner Author: Chief Ambulance
BRIEFING REPORT ON VERBAL FEEDBACK FROM HEALTH & SAFETY MANAGEMENT AUDIT 2012/13
 AGENDA ITEM 4.1 BRIEFING REPORT ON VERBAL FEEDBACK FROM HEALTH & SAFETY MANAGEMENT AUDIT 2012/13 Executive Lead: Deputy Chief Executive Author: Head of Health and Safety Contact Details for further information:
AGENDA ITEM 4.1 BRIEFING REPORT ON VERBAL FEEDBACK FROM HEALTH & SAFETY MANAGEMENT AUDIT 2012/13 Executive Lead: Deputy Chief Executive Author: Head of Health and Safety Contact Details for further information:
Children Education & Families Health and Safety Arrangements Part 3
 Version 2 Children Education & Families Health and Safety Arrangements Part 3 Education & Learning Statement of Intent I, the undersigned, fully endorse Oxfordshire County Council s Part 1 Health and Safety
Version 2 Children Education & Families Health and Safety Arrangements Part 3 Education & Learning Statement of Intent I, the undersigned, fully endorse Oxfordshire County Council s Part 1 Health and Safety
National Waiting Times Centre Board. Clinical Governance Committee
 Board Strategy National Waiting Times Centre Board Name Q-Pulse No Summary Associated documents Target audience Board-Strategy-3 Outlines the Board s approach to delivery of safe and effective care through
Board Strategy National Waiting Times Centre Board Name Q-Pulse No Summary Associated documents Target audience Board-Strategy-3 Outlines the Board s approach to delivery of safe and effective care through
Slips Trips and Falls Policy (Staff and Others)
") Title Reference Slips Trips and Falls Policy (Staff and Others) HS/POL/076 Description of document The purpose of this policy is to ensure all Norfolk Community Health & Care NHS Trust staff are aware
Title Reference Slips Trips and Falls Policy (Staff and Others) HS/POL/076 Description of document The purpose of this policy is to ensure all Norfolk Community Health & Care NHS Trust staff are aware
Moving and Handling Policy
 Moving and Handling Policy Ratified Quality, Patient Safety and Risk / 16/04/2014 / 2014-40 Status Ratified Issued April 2014 Approved By Quality, Patient Safety and Risk Committee Consultation Quality,
Moving and Handling Policy Ratified Quality, Patient Safety and Risk / 16/04/2014 / 2014-40 Status Ratified Issued April 2014 Approved By Quality, Patient Safety and Risk Committee Consultation Quality,
MINIMUM CRITERIA FOR REACH AND CLP INSPECTIONS 1
 FORUM FOR EXCHANGE OF INFORMATION ON ENFORCEMENT Adopted at the 9 th meeting of the Forum on 1-3 March 2011 MINIMUM CRITERIA FOR REACH AND CLP INSPECTIONS 1 MARCH 2011 1 First edition adopted at the 6
FORUM FOR EXCHANGE OF INFORMATION ON ENFORCEMENT Adopted at the 9 th meeting of the Forum on 1-3 March 2011 MINIMUM CRITERIA FOR REACH AND CLP INSPECTIONS 1 MARCH 2011 1 First edition adopted at the 6
Title of the Health Board Report
 AGENDA ITEM 3.2 Title of the Health Board Report IMPLEMENTING THE OUTCOME OF THE SOUTH WALES PROGRAMME THROUGH ACUTE CARE ALLIANCES AND DEVELOPMENT OF THE SOUTH WALES HEALTH COLLABORATIVE Executive Lead:
AGENDA ITEM 3.2 Title of the Health Board Report IMPLEMENTING THE OUTCOME OF THE SOUTH WALES PROGRAMME THROUGH ACUTE CARE ALLIANCES AND DEVELOPMENT OF THE SOUTH WALES HEALTH COLLABORATIVE Executive Lead:
Health & Safety Policy Statement
 Health & Safety Policy Statement DOCUMENT CONTROL POLICY NO. H&S 01 Policy Group Health & Safety Author Andy Howat Version no. 6.0 Reviewer Andy Howat Implementation date 1 st April 2011 Status FINAL Next
Health & Safety Policy Statement DOCUMENT CONTROL POLICY NO. H&S 01 Policy Group Health & Safety Author Andy Howat Version no. 6.0 Reviewer Andy Howat Implementation date 1 st April 2011 Status FINAL Next
JOB DESCRIPTION. The hospital has been consistently growing over the past few years, almost doubling since 2008.
 JOB DESCRIPTION JOB TITLE: Modern Matron CLINICAL UNIT: Paediatrics BASE: The Portland Hospital for Women and Children MANAGED BY: Children s Services Manager ACCOUNTABLE TO: Chief Nursing Officer HOSPITAL
JOB DESCRIPTION JOB TITLE: Modern Matron CLINICAL UNIT: Paediatrics BASE: The Portland Hospital for Women and Children MANAGED BY: Children s Services Manager ACCOUNTABLE TO: Chief Nursing Officer HOSPITAL
Workforce Planning. Internal Audit Report 2017/18. Powys Teaching Health Board. NHS Wales Shared Services Partnership. Audit and Assurance Service
 Workforce Planning Internal Audit Report 2017/18 Powys Teaching Health Board NHS Wales Shared Services Partnership Audit and Assurance Service Workforce Planning Powys Teaching Health Board Report Contents
Workforce Planning Internal Audit Report 2017/18 Powys Teaching Health Board NHS Wales Shared Services Partnership Audit and Assurance Service Workforce Planning Powys Teaching Health Board Report Contents
HEALTH AND SAFETY MANAGEMENT AT UWE
 HEALTH AND SAFETY MANAGEMENT AT UWE Introduction This document sets out the University s strategic approach to health and safety management. It contains the Statement of Intent that outlines the University
HEALTH AND SAFETY MANAGEMENT AT UWE Introduction This document sets out the University s strategic approach to health and safety management. It contains the Statement of Intent that outlines the University
The safety of every patient we care for is our number one priority
 HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
Moving and Handling Policy
 Moving and Handling Policy Ratified Status Approved Final Issued 28 April 2016 Approved By Quality, Patient Safety and Risk Committee Consultation Executive Committee Equality Impact Assessment Embedded
Moving and Handling Policy Ratified Status Approved Final Issued 28 April 2016 Approved By Quality, Patient Safety and Risk Committee Consultation Executive Committee Equality Impact Assessment Embedded
Public Health Skills and Career Framework Multidisciplinary/multi-agency/multi-professional. April 2008 (updated March 2009)
") Public Health Skills and Multidisciplinary/multi-agency/multi-professional April 2008 (updated March 2009) Welcome to the Public Health Skills and I am delighted to launch the UK-wide Public Health Skills
Public Health Skills and Multidisciplinary/multi-agency/multi-professional April 2008 (updated March 2009) Welcome to the Public Health Skills and I am delighted to launch the UK-wide Public Health Skills
Learning from Deaths Policy. This policy applies Trust wide
 Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
specialising in maths and computing Health, Safety and Environmental Policy Date March 2012 Review Date March 2014 Governor Committee Health & Safety
 specialising in maths and computing Health, Safety and Environmental Policy Date March 2012 Review Date March 2014 Governor Committee Health & Safety HEALTH, SAFETY AND ENVIRONMENTAL POLICY HEALTH AND
specialising in maths and computing Health, Safety and Environmental Policy Date March 2012 Review Date March 2014 Governor Committee Health & Safety HEALTH, SAFETY AND ENVIRONMENTAL POLICY HEALTH AND
SAFEGUARDING ADULTS STRATEGY
 SAFEGUARDING ADULTS STRATEGY Originator: Corporate Nursing Date Approved: May 2009 Approved by: Safeguarding Committee Date for Review: May 2011 Contents Page 1. Introduction 3 1.1 Vision 3 1.2 Scope 3
SAFEGUARDING ADULTS STRATEGY Originator: Corporate Nursing Date Approved: May 2009 Approved by: Safeguarding Committee Date for Review: May 2011 Contents Page 1. Introduction 3 1.1 Vision 3 1.2 Scope 3
Job Description. Ensure that patients are offered appropriate creative and diverse activities within a therapeutic environment.
 Job Description POST: HOURS: ACCOUNTABLE TO: REPORTS TO: RESPONSIBLE FOR: Complementary Therapy Coordinator 30 37.5 hours Head of Nursing & Quality Day Therapy Clinical Lead Volunteer Complementary Therapists
Job Description POST: HOURS: ACCOUNTABLE TO: REPORTS TO: RESPONSIBLE FOR: Complementary Therapy Coordinator 30 37.5 hours Head of Nursing & Quality Day Therapy Clinical Lead Volunteer Complementary Therapists
Children and Families Service Quality Assurance Framework
 Children and Families Service Quality Assurance Framework 2016-2018 [IL0: UNCLASSIFIED] Document Control Version Date Summary of Changes Changes Made by Draft / V001 28 July 2016 First draft of the Quality
Children and Families Service Quality Assurance Framework 2016-2018 [IL0: UNCLASSIFIED] Document Control Version Date Summary of Changes Changes Made by Draft / V001 28 July 2016 First draft of the Quality
POLICY FOR INCIDENT AND SERIOUS INCIDENT REPORTING
 POLICY FOR INCIDENT AND SERIOUS INCIDENT REPORTING Policy Acceptance Applies to: All staff, patients, & carers Date Issued: 7 th March 2016 Status Ratified Version 4 Date for Review March 2018 Responsible
POLICY FOR INCIDENT AND SERIOUS INCIDENT REPORTING Policy Acceptance Applies to: All staff, patients, & carers Date Issued: 7 th March 2016 Status Ratified Version 4 Date for Review March 2018 Responsible
Date ratified November Review Date November This Policy supersedes the following document which must now be destroyed:
 Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Cleaning Policy NTW(O)71 James Duncan Deputy Chief Executive / Executive Director of Finance Steve Blackburn Deputy
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Cleaning Policy NTW(O)71 James Duncan Deputy Chief Executive / Executive Director of Finance Steve Blackburn Deputy
EAST & NORTH HERTS, HERTS VALLEYS CCGS SAFEGUARDING CHILDREN & LOOKED AFTER CHILDREN TRAINING STRATEGY
 EAST & NORTH HERTS, HERTS VALLEYS CCGS Page 1 of 16 DOCUMENT CONTROL SHEET Document Owner: Directors of Nursing and Quality Document Author(s): Beverly Mukandi - Deputy Designated Nurse Safeguarding Children,
EAST & NORTH HERTS, HERTS VALLEYS CCGS Page 1 of 16 DOCUMENT CONTROL SHEET Document Owner: Directors of Nursing and Quality Document Author(s): Beverly Mukandi - Deputy Designated Nurse Safeguarding Children,
Supporting information for appraisal and revalidation: guidance for Supporting information for appraisal and revalidation: guidance for ophthalmology
 FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
CHWARAEON CYMRU SPORT WALES
 CHWARAEON CYMRU SPORT WALES INTERNAL AUDIT REPORT Review of National Governing Body Grants /Local Authority Partnership Agreements REPORT STATUS: FINAL DISTRIBUTED TO: Director of Corporate Services: Chris
CHWARAEON CYMRU SPORT WALES INTERNAL AUDIT REPORT Review of National Governing Body Grants /Local Authority Partnership Agreements REPORT STATUS: FINAL DISTRIBUTED TO: Director of Corporate Services: Chris
Quality and Safety Committee Date of Meeting: 23 rd February 2017 Agenda item : 4.5
 SUMMARY REPORT ABM University Health Board Quality and Safety Committee Date of Meeting: 23 rd February 2017 Agenda item : 4.5 Report Title Prepared, Approved and Presented by Review of the Blood Glucometry
SUMMARY REPORT ABM University Health Board Quality and Safety Committee Date of Meeting: 23 rd February 2017 Agenda item : 4.5 Report Title Prepared, Approved and Presented by Review of the Blood Glucometry
POLICY ON LONE WORKING JANUARY 2012
 POLICY ON LONE WORKING JANUARY 2012 Author: Sheena Gordon V&A Co-ordinator Responsible Director: Ian Reid Director of HR Approved by: Health and Safety Forum Date for Review: January 2014 Version: 2.0
POLICY ON LONE WORKING JANUARY 2012 Author: Sheena Gordon V&A Co-ordinator Responsible Director: Ian Reid Director of HR Approved by: Health and Safety Forum Date for Review: January 2014 Version: 2.0
Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse
 TRUST BOARD IN PUBLIC REPORT TITLE: Date: 28 March 2013 Agenda Item: 2.4 Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse EXECUTIVE SPONSOR: Dr. Des Holden, Medical Director
TRUST BOARD IN PUBLIC REPORT TITLE: Date: 28 March 2013 Agenda Item: 2.4 Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse EXECUTIVE SPONSOR: Dr. Des Holden, Medical Director
NON-MEDICAL PRESCRIBING POLICY
 NON-MEDICAL PRESCRIBING POLICY To be read in conjunction with the Medicines Policy, Controlled Drug Policy and the FP10 Prescribing Forms Policy Version: 5 Date of issue: August 2017 Review date: August
NON-MEDICAL PRESCRIBING POLICY To be read in conjunction with the Medicines Policy, Controlled Drug Policy and the FP10 Prescribing Forms Policy Version: 5 Date of issue: August 2017 Review date: August
SAFEGUARDING CHILDREN POLICY
 SAFEGUARDING CHILDREN POLICY The child s needs are paramount, and the needs and wishes of each child, be they a baby or infant, or an older child, should be put first Working Together 2015 p 8 Keeping
SAFEGUARDING CHILDREN POLICY The child s needs are paramount, and the needs and wishes of each child, be they a baby or infant, or an older child, should be put first Working Together 2015 p 8 Keeping
NHS England (Wessex) Clinical Senate and Strategic Networks. Accountability and Governance Arrangements
 Clinical Senate and Strategic Networks. Accountability and Governance Arrangements") NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
Quality and Safety Committees
 Quality and Safety Committees Guidance and Resources This document replaces the previously published Quality and Safety Committee(s) Guidance and Sample Terms of Reference Document (May 2013). It forms
Quality and Safety Committees Guidance and Resources This document replaces the previously published Quality and Safety Committee(s) Guidance and Sample Terms of Reference Document (May 2013). It forms
Sample CHO Primary Care Division Quality and Safety Committee. Terms of Reference
 DRAFT TITLE: Sample CHO Primary Care Division Quality and Safety Committee Terms of Reference AUTHOR: [insert details] APPROVED BY: [insert details] REFERENCE NO: [insert details] REVISION NO: [insert
DRAFT TITLE: Sample CHO Primary Care Division Quality and Safety Committee Terms of Reference AUTHOR: [insert details] APPROVED BY: [insert details] REFERENCE NO: [insert details] REVISION NO: [insert
Document Details Title
 Document Details Title Quality and Equalities Impact Assessment (QEIA) Process Guidance Trust Ref No 2046-45852 Local Ref (optional) Main points the document This document explains the process for QEIA,
Document Details Title Quality and Equalities Impact Assessment (QEIA) Process Guidance Trust Ref No 2046-45852 Local Ref (optional) Main points the document This document explains the process for QEIA,
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Indicators for the Delivery of Safe, Effective and Compassionate Person Centred Service
 Inspections of Mental Health Hospitals and Mental Health Hospitals for People with a Learning Disability Indicators for the Delivery of Safe, Effective and Compassionate Person Centred Service 1 Our Vision,
Inspections of Mental Health Hospitals and Mental Health Hospitals for People with a Learning Disability Indicators for the Delivery of Safe, Effective and Compassionate Person Centred Service 1 Our Vision,
Agenda item 8.5. Meeting date: Meeting / committee: Board of Directors. 24 th June Title: Emergency Preparedness Annual Report 2013/14.
 Agenda item 8.5 Meeting / committee: Board of Directors Meeting date: 24 th June 2014 Title: Preparedness Annual Report 2013/14 Purpose: This report outlines and summarises the activities and actions undertaken
Agenda item 8.5 Meeting / committee: Board of Directors Meeting date: 24 th June 2014 Title: Preparedness Annual Report 2013/14 Purpose: This report outlines and summarises the activities and actions undertaken
ABMU R&D Operational Framework
 ABMU R&D Operational Framework 2017 ABMU R&D Operational Framework 1 R&D Operational Arrangements University Partnership As a University Health Board, ABMU has signed a Memorandum of Understanding (MOU)
ABMU R&D Operational Framework 2017 ABMU R&D Operational Framework 1 R&D Operational Arrangements University Partnership As a University Health Board, ABMU has signed a Memorandum of Understanding (MOU)