Nature of Risk Exec Lead(s) Current Risk Score
|
|
|
- Sherman Allison
- 5 years ago
- Views:
Transcription
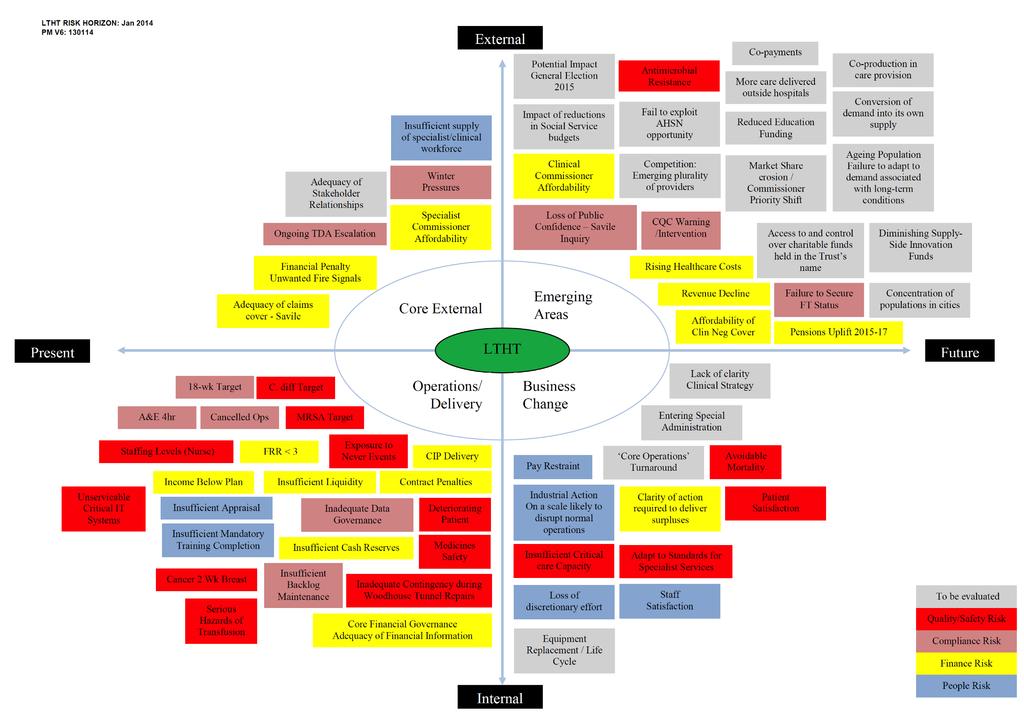
1 Corporate Register 1. LTHT has identified a range of material risks, which are currently being mitigated, whose impact could have a direct bearing on requirements within the NTDA s Accountability Framework, CQC registration or the achievement of corporate objectives should the mitigation plans be ineffective. 2. All corporate risks are co- owned by each member of the Board of Directors and each risk has an executive director lead identified for oversight, leadership and monitoring purposes. Currently, the material risks identified relate to the following areas: Nature of Current Score Within Tolerance? Safety & Quality CRR1 Inadequate Nurse Staffing Levels Chief Nurse 20 No 3 CRR2 Exposure to Healthcare Associated Infection - Clostridium difficile & MRSA Chief Medical Officer 25 No 4 D129 Impact of undertaking repairs to Woodhouse Tunnel Director of Estates & Facilities 15 No 5 Financial CRR9 Failure to ensure a minimum FRR of level 3 Director of Finance 25 No 6 People CRR10 Inadequate employee appraisal or supervision Director of Human Resources 16 No 7 CRR11 Inadequate completion of mandatory training Director of Human Resources 16 No 8 CRR Day Cancer Target Chief Operating Officer 15 No 11 CRR18 Reducing supply of doctors in training Chief Medical Officer 16 No 13 Compliance CRR12 A&E Target non- compliance Chief Operating Officer 15 Yes 9 CRR week RTT target non- compliance Chief Operating Officer 20 No 10 CRR17 Inadequate data quality and data governance Director of Informatics 15 No 12 Symbols used in this report Inherent and Unmitigated Score Residual Score (Current Exposure)! Target / Appetite Threshold " Page
2
3 APPENDIX 1: LTHT MATERIAL RISK ANALYSIS January 2014 LTHT CORPORATE RISK REGISTER V13 04/03/2014 CRR1: Inadequate Nurse Staffing Levels L=4 "! Safety & Quality CORPORATE OBJECTIVE 1: Drive quality improvement for patients to become among the safest organisations in the country Potential Insufficient nurse staffing levels. Caused by high levels of sickness/absence; insufficient investment in nurse staffing; high vacancy factor; insufficient workforce planning or adjustment for case-mix; or insufficient supply qualified staff. May result in an inadequate patient experience; a failure to protect patients or staff from serious harm; loss of stakeholder confidence; and/or a material breach of CQC conditions of registration. Suzanne Hinchliffe Treatment Duty Rotas prepared and communicated in advance Agreed minimum staffing thresholds (numbers and skill mix) in all clinical areas - blue print for the Trust (informed by AUKUH Safe Staffing Tool, with 1:8 roster tool undertaken from October 2013) All annual, special or study leave is booked and agreed at least 6 weeks in advance to allow sufficient planning to take place (except where required in an emergency) Flu Jab uptake for front line colleagues Proposal for 30 month transitional investment plan identified Review of commissions undertaken Regular discussions held with LETB and HEI Expansion of Band 4 Assistant Practitioners - cohorts have commenced Non-attendance is notified to direct line manager as per sickness procedures Duty Managers report 4 times per day identifying staff gaps and planned actions Direct observation - Patient Safety Walkrounds Adverse event reports - incidents or complaints Responsive visits where concerns have been identified Monthly Workforce Health Check Bed numbers within wards are reduced to reflect nurse staffing levels in association with redirecting activity to private sector in light of staffing levels Operating Procedure: Actions to be taken when the numbers of nurses or midwives per shift falls short of the agreed roster template(currently being updated) Discretionary use of bank or agency cover in the event of an identified shortfall Redeployment of colleagues on duty where staffing levels permit Contract with NHSP who also are the agent for agency progression Block booking of flexible labour is supported in required circumstances Specialist and corporate nursing colleagues are required to work clinical shifts where required Further Actions Planned Investment options to be presented to and supported in principle by Finance & Investment Committee (Chief Nurse 09/01/2014) Shorter term supply management - recruitment process over next 12 months commenced (Chief Nurse - In Progress) Agree recruitment and retention premia where appropriate (Chief Nurse - expected to be agreed by 31st march 2014) Deliver agreed priority investments in staffing as per acuity tool (see investment plan - Chief Nurse - In Progress) ANTICIPATED EFFECT ON CONTROL / COMMENT Clinical Practice Recommendation/Decision Required: to acknowledge the level of risk exposure remains unacceptable and continue reducing exposure by improving control effectiveness and delivering the action plan. Board of Directors 27/03/2014 3
4 CRR2: Exposure to Healthcare Associated Infection - Clostridium difficile & MRSA Board of Directors 27/03/ LTHT CORPORATE RISK REGISTER V13 04/03/ L=5 "! Compliance National Target CORPORATE OBJECTIVE 1: Drive quality improvement for patients to become among the safest organisations in the country Potential Effective management systems are not in place or sufficient to protect people from the risk of hospital acquired Clostridium difficile or MRSA. Caused by insufficient compliance with infection prevention procedures, including hand hygiene, decontamination, environmental cleaning and others; and insufficient training May result in serious harm or death to a patient, prolonged LOS, unsatisfactory patient experience; significant financial loss; loss of stakeholder confidence; and/or a material breach of CQC conditions of registration. Yvette Oade Treatment Patient level assessment of risk on admission/arrival (filed in patient care record) Use of Standard Precautions Specific measures to reduce contamination (environmental cleaning, decontamination of equipment, single use items, rolling programme of HPV Fogging, segregation and safe disposal of contaminated waste) Environmental cleaning in accordance with National Specification Antimicrobial Prescribing Policy and Standards Antimicrobial Stewardship Rounds led by Microbiologist Mandatory Infection Prevention & Control Training to all staff Overarching Infection Prevention Policy and suite of Guidelines and SOPs MRSA decolonisation for specific patients Provision and use of hand hygiene materials and washing facilities Provision and use of Personal Protective Clothing (gloves, aprons, masks, eye protection etc) Side room facilities MRSA Screening Procedure Surgical site infection surveillance Catheter-related blood stream infection surveillance in critical care Safety thermometer - catheter-relates UTI Alert organism surveillance Ward-based surveillance (viral gastroenteritis) Protocol for [C. difficile] Cell Cytotoxin Assay testing Daily IPC Team Review of cases with Microbiological support Root Cause Analysis of identified cases Hand hygiene and source isolation audits Audit of compliance with High Impact Interventions at Ward level Ward Health Check - Monthly Management of Outbreak Guideline Enhanced IPC Team intervention & support Cohort isolation practices (ring-fenced CDI cohort facility) Closure of Ward(s) to new admissions (where necessary) Increase the number of hand hygiene basins (at strategic locations within or adjacent to specified clinical areas) (Chief Medical Officer - In Progress) Ensure all staff undertake and complete mandatory training (Director of HR - see CRR11) Accelerate planned programme of whole ward decant HPV fogging (Director of Estates & Facilities - TBC) Review the need for cohort isolation facilities for CDI at LGI (Chief Medical Officer - 31st March 2014) Improve reliability of senior review of antimicrobial prescriptions (Chief Medical Officer - TBC) Explain to commissioners the increased sensitivity of the Cell Cytotoxin Assay test and it s the impact on the number of cases identified at LTHT, and reach agreement in advance with commissioners which CDI cases will count towards the Trust s trajectory for financial penalties in future (Chief Medical Officer - date TBC) Clinical Practice The 2013/14 year-end outturn will be above trajectory for Clostridium difficile, although the Trust remains on course to achieve an overall reduction in the number of cases by approximately 10% compared to 2012/13. The 2013/14 year-end outturn will be above target for MRSA. Recommendation/Decision Required: to acknowledge the level of risk exposure remains unacceptable and continue reducing exposure by improving control effectiveness and delivering the action plan.
5 D129: Impact of undertaking repairs to Woodhouse Tunnel LTHT CORPORATE RISK REGISTER V13 04/03/ L=3 "! Safety & Quality CORPORATE OBJECTIVE 1: Drive quality improvement for patients to become among the safest organisations in the country Potential Potential disruption to the provision of paediatric and trauma/orthopaedic services at LGI on a scale likely to have significant impact across the Leeds health economy Caused by excessive vibration and noise arising from drilling deep within Woodhouse Tunnel May result in a higher frequency of inter-hospital transfers overnight during the period of repairs; increased cancellations for non-clinical reasons; loss of activity; increased operational pressure across the health economy should it not be possible to operate a full service in floors A and B of Clarendon Wing. Darryn Kerr Not applicable. Treatment Civil Engineer s / Surveyor s Reports Briefings from Directors of Estates & Facilities Minimise impact by undertaking work at night (this will help keep the MR scanner operational during periods of peak activity) The works directly beneath Clarendon Wing to be active during the month of August 2014 when demand is expected to be less intensive for Paediatrics and Orthopaedics. Develop and agree with contractors procedures to halt drilling should vibration compromise image quality of scans and it be necessary to undertake an emergency MR scan during the night (Director of Estates 28th Feb 2014) Undertake and review a formal Health & Safety Assessment, taking whatever steps are necessary to protect staff and patients from the effects of excessive noise and vibration (Director of Estates 28th Feb 2014) Develop, approve and test a contingency plan for use in the event of a significant deterioration in the condition of the tunnel, or should it become necessary to temporarily close floors A and B of Clarendon Wing during the period of repairs (Director of Estates & Chief Operating Officer 28th Feb 2014) Assessment Recommendation/Decision Required: accept the level of risk exposure subject to satisfactory confirmation of further actions outlined above. Board of Directors 27/03/2014 5
6 CRR9: Failure to ensure a minimum FRR of level ! L=5 " Financial CORPORATE OBJECTIVE 6: Improve financial margins to support the delivery of high quality care Potential Effective management systems are not in place or sufficient to ensure a minimum FRR of level 3. Caused by the aggregate effect of insufficient income, inadequate financial control/information, insufficient liquidity, contract penalties, insufficient CIP delivery and SC affordability. May result in the Trust entering special administration. Tony Whitfield Treatment Board owned recovery and financial plans. Establishment of realistic CSU budgets and plans. Finance supports the process and works with budget holders to ensure ownership. Close working between Finance and CSUs to identify threats to plan delivery and formulate mitigations 13-Week rolling cash forecast anchored to long term plans Weekly review of cash position and payables due Weekly payment values determined by Senior Finance staff s Monthly board/budget reporting and outturn forecasts Liquidity score calculated and reported monthly Performance Review Meetings with Finance/COO Corporate approach to problem resolution Negotiation with TDA on surplus or deficit Application to TDA for borrowing or, in extremis, distress funding In-year review and revision of capital commitments Renegotiation with Commissioners to minimise threat of penalties Appointment of Financial Turnaround Director - commenced 2nd Jan 2014 Develop Financial Turnaround Plan and agree with TDA/Commissioners (Director of Finance 31/03/14) Delivery of identified CIP in 2012/13 and 2013/14 (All Directors plus CSU ownership of delivery with Finance support) Redevelop LTFM In line with Board strategy (Director of Finance 31/03/14) Agree realistic thresholds and deliver all CQUINs in 2013/14 (Delivered via CSUs supported by Finance) Modify Scheme of Delegation to reduce authorisation limits (Director of Finance 31/03/14) Establish Working Capital Loan Facility (Director of Finance 31/03/14) Establish I&E/P&L accounts for service lines (Director of Finance 31/03/14) Develop and improve capacity planning to enhance income position (Director of Finance, Director of Strategy & COO 31/03/14) Robustly verify data completeness, accuracy and income coding to enhance income position (Director of Finance 31/03/14) Review SFI s taking whatever action is necessary to strengthen core financial governance (Director of Finance 31/03/14) Deliver training on MyFIT to all budget holders(director of Finance 31/03/14) Consider options for Pay restraint (Director of HR/Finance) Review staff benefits - CEA s, subsidies (Director of HR & Director of Finance 31/01/14) Review stock control/review/run down where appropriate (Director of Finance & COO 31/03/14) Attempt to reduce/influence prices - procurement opportunities (Director of Finance 31/03/14) MARS/PAUL (Planned Additional Unpaid Leave) Schemes (Director of HR & Director of Finance 31/03/14) Board of Directors 27/03/ Assessment 31/03/2014 Recommendation/Decision Required: to acknowledge the level of risk exposure remains unacceptable and continue reducing exposure by improving control effectiveness and delivering the action plan.
7 CRR10: Inadequate employee appraisal or supervision S= L=4 "! People CORPORATE OBJECTIVE 2: Develop a highly engaged, high performing workforce and positive patient centred culture delivering great care to patients Potential Effective management systems are not in place or sufficient to ensure all employees receive an appraisal or the level of supervision required. Caused by lack of time, inefficient processes or insufficient priority assigned by management. May result in a failure to remedy personal development needs, insufficient service improvement and/or breach of CQC conditions of registration. Jackie Green Treatment Appraisal policy, paperwork and system for recording are in place for medical and non-medical staff Consultant appraisal linked to revalidation User guides available for managers and employees Training programme available for managers Monthly reporting at department / CSU / organisation-wide level Assurance reported to Workforce Committee CSU performance reports include appraisal compliance Updates reported to COO and utive Team Targeted intervention for worst performing departments Revised policies for appraisal and pay progression (Director of HR - 31st March 2014) Refreshed paperwork incorporating Leeds Way (Director of HR - 31st March 2014) Communication / training plan (Director of HR - 31st March 2014) Pay progression dependent on satisfactory appraisal for non-medical staff (to be agreed) (Director of HR - 31st March 2014) Successful appraisal for line managers will include appraisal compliance for staff they manage (to be agreed) (Director of HR - 31st March 2014) Performance Management Recommendation/Decision Required: to acknowledge the level of risk exposure remains unacceptable and continue reducing exposure by improving control effectiveness and delivering the action plan. Board of Directors 27/03/2014 7
8 S=4 CRR11: Inadequate completion of mandatory training L=4 "! People CORPORATE OBJECTIVE 2: Develop a highly engaged, high performing workforce and positive patient centred culture delivering great care to patients Potential Effective management systems are not in place or sufficient to ensure all employees complete and keep up to date with their mandatory training requirements. Caused by lack of time, inefficient processes or insufficient priority assigned by management or employees. May result in a failure to remedy personal development needs, unsafe care, insufficient service improvement and/or breach of CQC conditions of registration. Jackie Green Treatment Systems and procedures in place for delivering and recording mandatory training Consultant revalidation requires mandatory training compliance Training interface available for managers and employees to view their personal mandatory training record, requirements and advice on accessing training Extensive mandatory training programme available including open days and on-line resources Monthly reporting at department / CSU / organisation-wide level Monitored at Workforce Committee Assurance reported to Workforce Committee CSU performance reports include mandatory training compliance Mandatory Training leads meet every month to address areas of poor performance Revise training policies incorporating mandatory and priority training (Director of HR - 31st March 2014) Satisfactory appraisal dependent on individuals mandatory training being up-todate (to be agreed) (Director of HR - 31st March 2014) Review capacity to deliver required mandatory training and develop proposals for improvement (Director of HR - 31st March 2014) Optimise use of electronic learning opportunities. E-learning available on interface from February (Director of HR - 28th Feb 2014) Review all options to widen access to training materials in order to increase uptake and improve completion rates (Director of HR - 31st March 2014) Performance Management Recommendation/Decision Required: to acknowledge the level of risk exposure remains unacceptable and continue reducing exposure by improving control effectiveness and delivering the action plan. Board of Directors 27/03/2014 8
9 CRR12: A&E target non-compliance L=3 "! Compliance National Target CORPORATE OBJECTIVE 4: Deliver all mandatory standards in line with NHS Constitution and all regulatory requirements including improvement of care, capacity and demand management Potential Failure to achieve the maximum waiting time of four hours from arrival to admission, transfer or discharge (95% threshold). Caused by an increase in demand and/ or failure to discharge patients to manage demand and may, when aggregated with other potential factors, contribute to an inadequate patient experience and/or deterioration in LTHT s governance rating. Mark Smith Treatment Capacity and demand modelling refreshed every 6 weeks within the Emergency Department Agreed staffing levels with rotas aligned to seasonal variation and anticipated peaks in demand Rapid Assessment - Consultant led in place Triage protocols developed and in use Pathways for rapid specialty referral and response Admission avoidance schemes articulated cross organisation Direct Admission to Medicine and Elderly Services (DAMES) in place to accelerate flow and reduce duplication Early Senior Review Availability of prescribing pharmacist Access to Allied Health Professionals within ED and medical assessment 7/7 Consultant presence within the ED 24 hours 24 hour assessment facility in operation within surgery and medicine at SJUH and Children s at LGI Early Discharge Assessment Team (during core hours) comprising Occupational Therapist, Physiotherapist, Discharge Nurse, Social Worker and Geriatrician, working across primary, secondary and social care sectors s Performance monitored hour by hour, every day NHSBAR iphone App - real-time remote access to performance monitoring operational issues Weekly performance sent to CSU senior leadership and relevant corporate leads Weekly Trigger Meeting Root Cause Analysis for breaches Monitored via Integrated Quality & Performance Report Daily Operational Performance Meeting chaired by ADOP to ensure balance of activity aligned to ensure delivery Discretionary use of Bank/Agency/Locum to address shortfalls in staffing levels Escalation routines including procedures to apply depending on the level of performance (refreshed hourly) Specific plan for handling an unexpected surge in demand Board of Directors 27/03/ Length of Stay reduction - trust-wide adoption and use of Expected Discharge Dates for all inpatient admissions - implemented by local CSU management teams by end of QTR /15 (Chief Operating Officer) Develop capacity to report live bed state - real-time Admission, Discharge or Transfer (ADT) information (Chief Operating Officer - date TBC) Through the work of the Strategic Urgent Care Board, actively engage to develop proposals to reconfigure urgent care models across Leeds (Chief Operating Officer - In Progress) Performance Management LTHT has met this standard consistently since June There remains some uncertainty regarding the demand for urgent care during the remainder of the winter period and the potential impact on year end outturn; thus, whilst the current risk is tolerable, the residual risk remains significant at 15 reflecting a cautious approach. Recommendation/Decision Required: accept the level of risk exposure subject to satisfactory confirmation of further actions outlined above.
10 CRR13: 18-week RTT target non-compliance L=4 "! Compliance National Target CORPORATE OBJECTIVE 4: Deliver all mandatory standards in line with NHS Constitution and all regulatory requirements including improvement of care, capacity and demand management Potential Failure to achieve the maximum waiting time of 18-weks from referral to treatment (90% for admitted pathway, 95% for non-admitted pathway). Caused by ineffective waiting list management, insufficient capacity at specialty level, insufficient control over pathways of care, demand exceeding planned levels of activity. May result in poor quality care, unacceptable delays for patients, and/or deterioration in LTHT s governance rating Mark Smith Treatment Capacity and demand modelling is in place for priority RTT specialties All CSUs have established targets for 1st and 2nd OP waits and are provided with data to monitor this as part of their weekly access meetings Access Policy and Procedures Waiting List management and referral procedures Bed management and discretionary (limited) use of ring-fencing Theatre utilisation Restrict the use of medical outlying Pathways of care s Weekly performance sent to CSU senior leadership and relevant corporate leads Weekly Trigger Meeting Performance reviewed by each CSU as part of their weekly access meeting (supported by a member of the performance team) Root Cause Analysis for breaches Monitored via Integrated Quality & Performance Report Contingency Discretionary use of Bank/Agency/Locum to address shortfalls in staffing levels Escalation routine to Medical Director for Operations, Associate Directors of Operations and Director of Planned Care Escalation to Chief Operating Officer Enactment of Special Measures - intensive monitoring and support in the event of significant performance dip Length of Stay reduction - trust-wide adoption and use of Expected Discharge Dates for all inpatient admissions - to be implemented by local CSU management teams by QTR /15 Complete capacity & demand modelling and roll out to all specialties with quarterly refresh (Chief Operating Officer - date TBC) Extend pathways of care to cover full range of elective services provided (Chief Operating Officer - date TBC) Optimise theatre utilisation (Chief Operating Officer - date TBC) Roll out and extend use of Clinical Portal (Chief Operating Officer - date TBC) Roll out Order Comms (Chief Operating Officer - date TBC) Performance Management Recommendation/Decision Required: to acknowledge the level of risk exposure remains unacceptable and continue reducing exposure by improving control effectiveness and delivering the action plan. Board of Directors 27/03/
11 CRR15: 62-Day Cancer Target L=3 "! Compliance National Target CORPORATE OBJECTIVE 4: Deliver all mandatory standards in line with NHS Constitution and all regulatory requirements including improvement of care, capacity and demand management Potential Effective management systems are not in place or sufficiently resilient to ensure treatment within 62 days following receipt of urgent referral by a GP for suspected cancer. Caused by late referral from other providers, ineffective access policies or waiting list management, insufficient critical care capacity, insufficient control over pathways of care, higher than expected urgent care demand, or insufficient theatre utilisation. May result in poor quality care, unsatisfactory patient experience, unacceptable delays for patients, and/or deterioration in LTHT s governance rating. Mark Smith Treatment Access policy and procedures Waiting list management and referral procedures on Patient Pathway Manager Efficient use of critical care beds Procedure to govern cancellations Application of cancer waiting time guidance Yorkshire Cancer Network guidelines for each tumour group 54-day pathway mapped out for each tumour group MDT Meetings s Weekly performance sent to CSU senior leadership and relevant corporate leads Weekly Trigger Meeting Performance reviewed by each CSU as part of their weekly access meeting (supported by a member of the performance team) Root Cause Analysis for breaches Monitored via Integrated Quality & Performance Report Contingency Discretionary use of Bank/Agency/Locum to address shortfalls in staffing levels Escalation routine to Medical Director for Operations, Associate Directors of Operations and Director of Planning Escalation to Chief Operating Officer Enactment of Special Measures intensive monitoring and support in the event of significant performance dip Length of Stay reduction - trust-wide adoption and use of Expected Discharge Dates for all inpatient admissions - to be implemented by local CSU management teams by QTR /15 Complete capacity & demand modelling and roll out to all specialties with quarterly refresh (Chief Operating Officer - date TBC) Extend pathways of care to cover full range of elective services provided (Chief Operating Officer - date TBC) Optimise theatre utilisation (Chief Operating Officer - date TBC) Roll out and extend use of Clinical Portal (Chief Operating Officer - date TBC) Roll out Order Comms (Chief Operating Officer - date TBC) Performance Management 31/03/2014 Recommendation/Decision Required: to acknowledge the level of risk exposure remains unacceptable and continue reducing exposure by improving control effectiveness and delivering the action plan. Board of Directors 27/03/
12 CRR17: Inadequate Data Quality or Data Governance LTHT CORPORATE RISK REGISTER V13 04/03/ L=3 "! Compliance National Target CORPORATE OBJECTIVE 4: Deliver all mandatory standards in line with NHS Constitution and all regulatory requirements including improvement of care, capacity and demand management Potential Effective management systems are not in place or sufficient to ensure data completion, data quality or data governance. Caused by a large volume of local systems lacking administration and local control. May result in erroneous reporting; inadequate board assurance; loss of stakeholder confidence; financial or regulatory penalty. Alison Dailly Treatment All staff are made aware of their specific duties in respect of data governance via Information Governance training provided on induction and annual updates thereafter All new database or software systems require prior approval of Informatics Board before installation (this control has been in operation for 4 years) Approval is verified before system is procured or purchased Access to install any database or software without authorisation is denied and can only be installed by authorised informatics staff Technical controls exist to minimise risk of inadvertent, accidental or malicious installation of software onto trust systems Access to system is restricted to those with authorised log in Responsibilities are reinforced at each log in Use of portable devices is restricted to trust standard encrypted devices Clinical coding undertaken by trained coding practitioners in association with clinical teams Verification via order/supplies route Formal business case gateway Back office checking reporting reviewed by Systems Administrators and Data Quality Team with KPIs for Trustwide systems and a subset of local systems Data Quality Audits undertaken for core data sets undertaken as part of a rolling programme Any violation of technical controls is subject to disciplinary action Continue to deliver Informatics Strategy - Director of Informatics and reduce volume of small/bespoke clinical systems (Director of Informatics - In Progress) Conclude baseline audit of data governance in all clinical systems (Director of Informatics - 31 st March 2014) Identify and plan data governance requirements for each clinical system (Director of Informatics - ongoing throughout 2014/15) Reach agreement on extending the provision for data quality audits to cover non-core data sets that may be subject to external reporting requirements (Director of Informatics - 31st March 2014) Assessment There is a particular vulnerability in respect of the volume of databases/systems not under sufficient control within clinical areas. Recommendation/Decision Required: to acknowledge the level of risk exposure remains unacceptable and continue reducing exposure by improving control effectiveness and delivering the action plan. Board of Directors 27/03/
13 S=4 CRR18: Reducing supply of doctors in training L=4 "! Compliance National Target CORPORATE OBJECTIVE 4: Deliver all mandatory standards in line with NHS Constitution and all regulatory requirements including improvement of care, capacity and demand management Potential Insufficient numbers of trainee medical staff on a scale likely to disrupt normal operations Caused by reductions in trainee placements and funding which lead to non complaint or non feasible rotas and a failure to ameliorate the reduction in junior doctors entering the workforce May result in severe pressure to deliver safe and effective clinical services; delays in responding to the deteriorating patient; and/or poor experience in training for junior doctors resulting in a further reduction in posts. Yvette Oade Treatment Workforce planning The Trust lobbies the Deanery and Health Education England to secure sufficient trainee placements to meet expected service demands Compliant duty rotas and shift patterns Extending and developing roles of Nursing and AHP practitioners Improving the trainee experience DatixWeb Attendance Management Use of locum doctors Merging of rotas leading to less specialist input Use of consultants in place of trainees Review and develop workforce plans alongside activity forecasts in order to anticipate future workforce requirements and any adjustments required to adapt to reducing numbers of junior doctors and/or retirements (Chief Medical Officer & Director of Human Resources date TBC) Assessment Recommendation/Decision Required: to acknowledge the level of risk exposure remains unacceptable and continue reducing exposure by improving control effectiveness and delivering the action plan. Board of Directors 27/03/
Public Board 28 July 2016 Corporate Risk Register
 Agenda Item 11 Public Board 28 July 2016 Corporate Register Presented for: Presented by: Author Previous Committees Assurance Julian Hartley, Chief utive Suzanne Hinchliffe, Chief Nurse and Deputy Chief
Agenda Item 11 Public Board 28 July 2016 Corporate Register Presented for: Presented by: Author Previous Committees Assurance Julian Hartley, Chief utive Suzanne Hinchliffe, Chief Nurse and Deputy Chief
CORPORATE RISK REGISTER JANUARY2017
 Agenda Item 11.1 CORPORATE RISK REGISTER JANUARY2017 G:\s_Support_Team\General\Trust Board\2016-17\BoD\Formal Board Meetings\05 26 January 2017\Public\Final\11.1 Corporate Register January 2017.docx Summary
Agenda Item 11.1 CORPORATE RISK REGISTER JANUARY2017 G:\s_Support_Team\General\Trust Board\2016-17\BoD\Formal Board Meetings\05 26 January 2017\Public\Final\11.1 Corporate Register January 2017.docx Summary
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
Portsmouth Hospitals NHS Trust Winter/Surg Plan 2013/14. pg. 1
 Portsmouth Hospitals NHS Trust Winter/Surg Plan 2013/14 pg. 1 Introduction The purpose of this winter/surg plan is to ensure that Portsmouth Hospitals NHS Trust (PHT) is prepared and co-ordinated to respond
Portsmouth Hospitals NHS Trust Winter/Surg Plan 2013/14 pg. 1 Introduction The purpose of this winter/surg plan is to ensure that Portsmouth Hospitals NHS Trust (PHT) is prepared and co-ordinated to respond
BSUH INTEGRATED PERFORMANCE REPORT. 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain
 Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain") BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
PUBLIC BOARD - 25 JANUARY 2018 Corporate Risk Register
 Agenda Item 11 PUBLIC BOARD - 25 JANUARY 2018 Corporate Register Presented for: Presented by: Author Previous Committees Assurance Julian Hartley, Chief utive Suzanne Hinchliffe, Chief Nurse and Deputy
Agenda Item 11 PUBLIC BOARD - 25 JANUARY 2018 Corporate Register Presented for: Presented by: Author Previous Committees Assurance Julian Hartley, Chief utive Suzanne Hinchliffe, Chief Nurse and Deputy
NHSi June 2016)and integrated business plan completed (submitted to TDA in February 2014) NHSi Plan submitted 2016.
and integrated business plan completed (submitted to TDA in February 2014) NHSi Plan submitted 2016.") 1604 Executive 18/06/2014 1603 Executive 18/06/2014 Finance - Fin. Management 1491 Responsiveness 29/08/2013 ED - Adult Involvement of Service Users 11//2017 Failure to maintain Emergency Department performance
1604 Executive 18/06/2014 1603 Executive 18/06/2014 Finance - Fin. Management 1491 Responsiveness 29/08/2013 ED - Adult Involvement of Service Users 11//2017 Failure to maintain Emergency Department performance
Prevention and control of healthcare-associated infections
 Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Integrated Performance Report
 Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
HEI self-assessment. Completing the self-assessment - Guidance to NHS boards
 HEI self-assessment Completing the self-assessment - Guidance to NHS boards INTRODUCTION This document should be read in conjunction Healthcare Improvement Scotland healthcare associated infection (HAI)
HEI self-assessment Completing the self-assessment - Guidance to NHS boards INTRODUCTION This document should be read in conjunction Healthcare Improvement Scotland healthcare associated infection (HAI)
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY: BOARD OF DIRECTORS 22 FEBRUARY 2012
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY: BOARD OF DIRECTORS C 22 FEBRUARY 2012 Subject: Supporting : Author: Status (see footnote): Update on the Clostridium difficile (C.diff)
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY: BOARD OF DIRECTORS C 22 FEBRUARY 2012 Subject: Supporting : Author: Status (see footnote): Update on the Clostridium difficile (C.diff)
Author: Kelvin Grabham, Associate Director of Performance & Information
 Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Trust Policy Title: Access Policy Author: Kelvin Grabham, Associate Director of Performance & Information Document Lead: Kelvin Grabham, Associate Director of Performance & Information Accepted by: RTT
Board of Directors. Approval Discussion Information Assurance
 Report Title: Executive/NED Lead: Report author(s): Previously considered by: Board of Directors Tuesday, 31 October 17 Board Assurance Framework & Corporate Risk Register Ann Alderton, Company Secretary
Report Title: Executive/NED Lead: Report author(s): Previously considered by: Board of Directors Tuesday, 31 October 17 Board Assurance Framework & Corporate Risk Register Ann Alderton, Company Secretary
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Integrated Performance Report
 Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Strategic Risk Report 12 September 2016
 Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
CCDM Programme Standards
 CCDM Programme Standards Standard 1.0 CCDM Governance Standard 1.0 The CCDM governance councils (organisation and ward/unit) ensure that care capacity demand management is planned, coordinated and appropriate
CCDM Programme Standards Standard 1.0 CCDM Governance Standard 1.0 The CCDM governance councils (organisation and ward/unit) ensure that care capacity demand management is planned, coordinated and appropriate
Key Objectives To communicate business continuity planning over this period that is in line with Board continuity plans and enables the Board:
 Golden Jubilee Foundation Winter Plan 2016/2017 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This plan
Golden Jubilee Foundation Winter Plan 2016/2017 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This plan
NHS England (South) Surge Management Framework
 Surge Management Framework") NHS England (South) Surge Management Framework THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK 2 NHS England (South) Surge Management Framework Version number: 1.0 First published: August 2015 Prepared by:
NHS England (South) Surge Management Framework THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK 2 NHS England (South) Surge Management Framework Version number: 1.0 First published: August 2015 Prepared by:
Strategic Risk Report 4 July 2016
 Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
NHS England (London) Assurance of the BEH Clinical Strategy
 Assurance of the BEH Clinical Strategy") NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
Emergency Care Network Capacity Management and Escalation Plan Action Cards December 2009 December 2010
 Coventry and Warwickshire Emergency Care Network Emergency Care Network Capacity Management and Escalation Plan Action Cards December 2009 December 2010 This aim of this plan is to provide a high level
Coventry and Warwickshire Emergency Care Network Emergency Care Network Capacity Management and Escalation Plan Action Cards December 2009 December 2010 This aim of this plan is to provide a high level
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
Strategic Risk Report 1 March 2018
 Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report 1 March 2018 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
The safety of every patient we care for is our number one priority
 HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
Infection Prevention. & Control. Report
 Infection Prevention & Control Report April 2012 March 2013 Author Joanne Raper, Infection Prevention & Control Nurse Manager Page 1 of 10 1.0 Purpose of the Paper The purpose of this report is to provide
Infection Prevention & Control Report April 2012 March 2013 Author Joanne Raper, Infection Prevention & Control Nurse Manager Page 1 of 10 1.0 Purpose of the Paper The purpose of this report is to provide
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April Ipswich Hospital NHS Trust NHS East of England Department of Health
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
Public health guideline Published: 11 November 2011 nice.org.uk/guidance/ph36
 Healthcare-associated infections: prevention ention and control Public health guideline Published: 11 November 2011 nice.org.uk/guidance/ph36 NICE 2017. All rights reserved. Subject to Notice of rights
Healthcare-associated infections: prevention ention and control Public health guideline Published: 11 November 2011 nice.org.uk/guidance/ph36 NICE 2017. All rights reserved. Subject to Notice of rights
Appendix 1: Croydon Clinical Commissioning Group Risk Register and Board Assurance Framework - 9th April 2013
 Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
The prevention, management and control of Healthcare Associated Infections (HCAI) in hospitals (ROCR-LITE/08/014/FT6)
 in hospitals (ROCR-LITE/08/014/FT6)") NATIONAL AUDIT OFFICE STUDY The prevention, management and control of Healthcare Associated Infections (HCAI) in hospitals (ROCR-LITE/08/014/FT6) National Audit Office study The prevention, management
NATIONAL AUDIT OFFICE STUDY The prevention, management and control of Healthcare Associated Infections (HCAI) in hospitals (ROCR-LITE/08/014/FT6) National Audit Office study The prevention, management
Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations
 No. Domain CQC Recommendation Lead Operational Lead Current Status 1 Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations Wording in long
No. Domain CQC Recommendation Lead Operational Lead Current Status 1 Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations Wording in long
Taranaki District Health Board
 Taranaki District Health Board Current Status: 15 October 2013 The following summary has been accepted by the Ministry of Health as being an accurate reflection of the Certification Audit conducted against
Taranaki District Health Board Current Status: 15 October 2013 The following summary has been accepted by the Ministry of Health as being an accurate reflection of the Certification Audit conducted against
2017/18 Trust Balanced Scorecard
 ITEM 8b ENC 9 2017/18 Trust Balanced Scorecard Author: Performance Management Team March 2017 The purpose of this paper is to provide an update on the development of the 2017/18 Balanced Scorecard for
ITEM 8b ENC 9 2017/18 Trust Balanced Scorecard Author: Performance Management Team March 2017 The purpose of this paper is to provide an update on the development of the 2017/18 Balanced Scorecard for
FT Keogh Plans. Medway NHS Foundation Trust
 FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
Quality Assurance Framework
 Quality Assurance Framework NHS Bromley Clinical Commissioning Group Quality Assurance Framework was developed to support the commissioning, contract monitoring and procurement processes. NAME OF ORGANISATION/SERVICE
Quality Assurance Framework NHS Bromley Clinical Commissioning Group Quality Assurance Framework was developed to support the commissioning, contract monitoring and procurement processes. NAME OF ORGANISATION/SERVICE
EQuIPNational Survey Planning Tool NSQHSS and EQuIP Actions 4.
 Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement
Standard 1: Governance for safety and Quality and Standard 2: Partnering with Consumers Section 1 Governance, Policies, Business decision making, Organisational / Strategic planning, Consumer involvement
Summary two year operating plan 2017/18
 One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
Clostridium difficile Infection (CDI) Trigger Tool
 Trigger Tool") Hospital ward/clinical Area Date Trigger Tool Commenced Date Trigger Tool Closed Person closing the CDI Trigger Health Protection Scotland March 2014 Version 3.0 A CDI trigger is the number of new CDI
Hospital ward/clinical Area Date Trigger Tool Commenced Date Trigger Tool Closed Person closing the CDI Trigger Health Protection Scotland March 2014 Version 3.0 A CDI trigger is the number of new CDI
Purpose of the Report: Update to the Trust Board on the clinically-led Trauma and Orthopaedic GIRFT review. Information Assurance X
 Item 9.4 To: Trust Board From: Mark Brassington Date: 18 th May 2018 Healthcare Standard Title: Trauma and Orthopaedic GIRFT Author: Richard James, General Manager Responsible Director/s: Mark Brassington
Item 9.4 To: Trust Board From: Mark Brassington Date: 18 th May 2018 Healthcare Standard Title: Trauma and Orthopaedic GIRFT Author: Richard James, General Manager Responsible Director/s: Mark Brassington
Seven day hospital services: case study. South Warwickshire NHS Foundation Trust
 Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Report of the Care Quality Commission. May 2017
 Report of the Care Quality Commission May 2017 1. Purpose 1.1 The purpose of this report is to formally confirm the findings of the Care Quality Commission (CQC) following its inspection in October 2016;
Report of the Care Quality Commission May 2017 1. Purpose 1.1 The purpose of this report is to formally confirm the findings of the Care Quality Commission (CQC) following its inspection in October 2016;
Report to the Board of Directors 2016/17
 Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
Job Description. CNS Clinical Lead
 Job Description CNS Clinical Lead POST: BASE: ACCOUNTABLE TO: REPORTS TO: RESPONSIBLE FOR: CNS Clinical Lead St John s Hospice Head of Nursing and Quality Head of Nursing and Quality Community Clinical
Job Description CNS Clinical Lead POST: BASE: ACCOUNTABLE TO: REPORTS TO: RESPONSIBLE FOR: CNS Clinical Lead St John s Hospice Head of Nursing and Quality Head of Nursing and Quality Community Clinical
APPENDIX 7C BENEFITS REALISATION PLAN
 APPENDIX 7C BENEFITS REALISATION PLAN 150804 Shropshire Future Fit SOC v2.2 Appendices APPENDICES Draft Benefits Realisation Plan V0.9 150415 FutureFit Benefits Realisation Plan V0.9 Page 1 The purpose
APPENDIX 7C BENEFITS REALISATION PLAN 150804 Shropshire Future Fit SOC v2.2 Appendices APPENDICES Draft Benefits Realisation Plan V0.9 150415 FutureFit Benefits Realisation Plan V0.9 Page 1 The purpose
Standard of Care for MTC inpatients
 Standard of Care for MTC inpatients The following document is intended to summarise the model of care for patients admitted under the care of the Leeds Major Trauma System. It will outline expected duties
Standard of Care for MTC inpatients The following document is intended to summarise the model of care for patients admitted under the care of the Leeds Major Trauma System. It will outline expected duties
Inspecting Informing Improving. Hygiene code inspection report: West Hertfordshire Hospitals NHS Trust
 Inspecting Informing Improving Hygiene code inspection report: West Hertfordshire Hospitals NHS Trust December 2008 Outcome of inspection for: Hospital(s) visited: West Hertfordshire Hospitals NHS Trust
Inspecting Informing Improving Hygiene code inspection report: West Hertfordshire Hospitals NHS Trust December 2008 Outcome of inspection for: Hospital(s) visited: West Hertfordshire Hospitals NHS Trust
Shetland NHS Board. Board Paper 2017/28
 Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
SAFE STAFFING GUIDELINE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
Risk Register Summary Analysis Report
 1. Corporate Risk Register High risks There are 11 risks currently categorised as High, i.e. scoring 15 or more using the risk grading matrix set out in appendix 1. 1. 1819 Risk of poor patient experience
1. Corporate Risk Register High risks There are 11 risks currently categorised as High, i.e. scoring 15 or more using the risk grading matrix set out in appendix 1. 1. 1819 Risk of poor patient experience
RTT Recovery Planning and Trajectory Development: A Cambridge Tale
 RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
YORKSHIRE AMBULANCE SERVICE NHS TRUST Quality Improvement Action Plan 23/05/1017 FINAL. Deputy/ Associate Director. Executive Director TRUST WIDE
 YORKSHIRE AMBULANCE SERVICE NHS TRUST Quality Improvement Action Plan 23/05/1017 FINAL CQC findings TRUST WIDE 1.1 1.2 Ensure that at all times there are qualified experienced staff (including Staff communication
YORKSHIRE AMBULANCE SERVICE NHS TRUST Quality Improvement Action Plan 23/05/1017 FINAL CQC findings TRUST WIDE 1.1 1.2 Ensure that at all times there are qualified experienced staff (including Staff communication
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
Operational Plan 2018/19
 Operational Plan 2018/19 Contents 1. Introduction... 4 2. Overview... 4 3. Strategic Context... 5 Strategic Vision... 5 National Context... 5 Local Context... 5 West Yorkshire and Harrogate Health and
Operational Plan 2018/19 Contents 1. Introduction... 4 2. Overview... 4 3. Strategic Context... 5 Strategic Vision... 5 National Context... 5 Local Context... 5 West Yorkshire and Harrogate Health and
Ayrshire and Arran NHS Board
 Paper 12 Ayrshire and Arran NHS Board Monday 30 January 2017 Medical Education and Training: Update on Enhanced monitoring status of University Hospital Ayr Medical Department Author: Hugh Neill, Director
Paper 12 Ayrshire and Arran NHS Board Monday 30 January 2017 Medical Education and Training: Update on Enhanced monitoring status of University Hospital Ayr Medical Department Author: Hugh Neill, Director
Update on NHS Central London CCG QIPP schemes
 Update on NHS Central London CCG QIPP schemes NHS Central London CCG has identified circa 11m for QIPP during 2013/14. Commissioning Intentions approved by the governing body included transformational
Update on NHS Central London CCG QIPP schemes NHS Central London CCG has identified circa 11m for QIPP during 2013/14. Commissioning Intentions approved by the governing body included transformational
Title Open and Honest Staffing Report April 2016
 Title Open and Honest Staffing Report April 2016 File location WILJ2102 Meeting Board of Directors Date 25 th May 2016 Executive Summary This paper provides a stocktake on the position of South Tyneside
Title Open and Honest Staffing Report April 2016 File location WILJ2102 Meeting Board of Directors Date 25 th May 2016 Executive Summary This paper provides a stocktake on the position of South Tyneside
Checklists for Preventing and Controlling
 Checklists for Preventing and Controlling Clostridium difficile Infection (CDI) This document has been developed to specifically assist senior management and all ward staff to take appropriate actions,
Checklists for Preventing and Controlling Clostridium difficile Infection (CDI) This document has been developed to specifically assist senior management and all ward staff to take appropriate actions,
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators April Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Indicators April 2011 Report to: Trust Board 24 May 2011 Report from: Sponsoring Executive: Aim of Report / Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Indicators April 2011 Report to: Trust Board 24 May 2011 Report from: Sponsoring Executive: Aim of Report / Principle Topic: Review History to date:
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Hard Truths Public Board 29th September, 2016
 Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
REFERRAL TO TREATMENT ACCESS POLICY
 Directorate of Strategy & Planning REFERRAL TO TREATMENT ACCESS POLICY Reference: DCP175 Version: 7.0 This version issued: 17/12/15 Result of last review: Major changes Date approved by owner (if applicable):
Directorate of Strategy & Planning REFERRAL TO TREATMENT ACCESS POLICY Reference: DCP175 Version: 7.0 This version issued: 17/12/15 Result of last review: Major changes Date approved by owner (if applicable):
Nottingham University Hospitals Emergency Department Quality Issues Related to Performance
 RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
July (Month 4) Integrated Performance Report. John Grinnell, Director of Finance. Executive Directors. For Information For Discussion For Approval
 Integrated Performance Report. John Grinnell, Director of Finance. Executive Directors. For Information For Discussion For Approval") BOARD OF DIRECTORS Subject/Title July (Month 4) Integrated Performance Report Executive Responsible Paper prepared by (if different from above) John Grinnell, Director of Finance Executive Directors Nature
BOARD OF DIRECTORS Subject/Title July (Month 4) Integrated Performance Report Executive Responsible Paper prepared by (if different from above) John Grinnell, Director of Finance Executive Directors Nature
Trust Board Meeting : Wednesday 11 March 2015 TB
 Trust Board Meeting : Wednesday 11 March 2015 Title Business Case for the Refurbishment and Reconfiguration of the bed based areas of the Emergency Assessment Unit at the John Radcliffe Hospital, to deliver
Trust Board Meeting : Wednesday 11 March 2015 Title Business Case for the Refurbishment and Reconfiguration of the bed based areas of the Emergency Assessment Unit at the John Radcliffe Hospital, to deliver
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST
 EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS MEETING DATE: 29 JANUARY 2015 SUBJECT: REPORT FROM: PURPOSE: CQC ACTION PLAN CHAIR OF IMPROVEMENT PLAN DELIVERY BOARD Discussion
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS MEETING DATE: 29 JANUARY 2015 SUBJECT: REPORT FROM: PURPOSE: CQC ACTION PLAN CHAIR OF IMPROVEMENT PLAN DELIVERY BOARD Discussion
NHS England South Escalation Framework
 NHS England South Escalation Framework Escalation Framework NHS England South First published: April 2013: Version 1.0 Updated: May 2013: Version 2.0 Prepared by Gail King, Head of EPRR, Thames Valley
NHS England South Escalation Framework Escalation Framework NHS England South First published: April 2013: Version 1.0 Updated: May 2013: Version 2.0 Prepared by Gail King, Head of EPRR, Thames Valley
Dudley & Walsall Mental Health Partnership NHS Trust Board
 Dudley & Walsall Mental Health Partnership NHS Trust Board Date of Board Meeting: 29 th July 2 Subject: Performance Corporate Dashboard Month 3 Trust Board Lead: Jacky O Sullivan, Director of Performance
Dudley & Walsall Mental Health Partnership NHS Trust Board Date of Board Meeting: 29 th July 2 Subject: Performance Corporate Dashboard Month 3 Trust Board Lead: Jacky O Sullivan, Director of Performance
is asked to NOTE the update provided on fragile services.
 Recommendation DECISION NOTE (select) Reporting to: The Trust Board is asked to NOTE the update provided on fragile services. Trust Board Date Thursday 27 th July 2017 Paper Title Brief Description Services
Recommendation DECISION NOTE (select) Reporting to: The Trust Board is asked to NOTE the update provided on fragile services. Trust Board Date Thursday 27 th July 2017 Paper Title Brief Description Services
Clostridium difficile Infection (CDI) Trigger Tool
 Trigger Tool") Hospital ward/clinical Area Date Trigger Tool Commenced Date Trigger Tool Closed Person closing the CDI Trigger Health Protection Scotland V2.0 November 2011 A CDI Trigger is the point at which the Infection
Hospital ward/clinical Area Date Trigger Tool Commenced Date Trigger Tool Closed Person closing the CDI Trigger Health Protection Scotland V2.0 November 2011 A CDI Trigger is the point at which the Infection
Standard 1: Governance for Safety and Quality in Health Service Organisations
 Standard 1: Governance for Safety and Quality in Health Service Organisations riterion: Governance and quality improvement system There are integrated systems of governance to actively manage patient safety
Standard 1: Governance for Safety and Quality in Health Service Organisations riterion: Governance and quality improvement system There are integrated systems of governance to actively manage patient safety
The impact of a flu or norovirus outbreak could have a significant impact on health and social services and could involve:
 NHS National Waiting Times Centre Winter Plan 2010/11 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This
NHS National Waiting Times Centre Winter Plan 2010/11 Introduction This plan outlines the proposed action that would be taken to deliver our key business objectives supported by contingency planning. This
An Overview for F2 Doctors of Foundation Programme attachments to General Practice
 An Overview for F2 Doctors of Foundation Programme attachments to General Practice July 2011 Contents Page GP Placements 2 Guidance on Educational Agreements 4 Key facts about F2 Placements 6 The Foundation
An Overview for F2 Doctors of Foundation Programme attachments to General Practice July 2011 Contents Page GP Placements 2 Guidance on Educational Agreements 4 Key facts about F2 Placements 6 The Foundation
SUPPORT FOR VULNERABLE GP PRACTICES: PILOT PROGRAMME
 Publications Gateway Reference 04476 For the attention of: NHS England Directors of Commissioning Operations Clinical Leaders and Accountable Officers, NHS Clinical Commissioning Groups Copy: NHS England
Publications Gateway Reference 04476 For the attention of: NHS England Directors of Commissioning Operations Clinical Leaders and Accountable Officers, NHS Clinical Commissioning Groups Copy: NHS England
Debbie Vogler, Director of Business & Enterprise. Kate Shaw, Associate Director of Service Transformation
 Reporting to: Trust Board 24 September 2015 Paper 5 Title Sponsoring Director Author(s) Future Configuration of Hospital Services - Post-Project Evaluation Debbie Vogler, Director of Business & Enterprise
Reporting to: Trust Board 24 September 2015 Paper 5 Title Sponsoring Director Author(s) Future Configuration of Hospital Services - Post-Project Evaluation Debbie Vogler, Director of Business & Enterprise
Diabetes Eye Screener / Photographer Job Description
 Diabetes Eye Screener / Photographer Job Description Post Title: Band: Directorate: Base: Managerially accountable to: Professional Accountable to: Diabetes Eye Screener / Photographer 4 (Subject to AFC)
Diabetes Eye Screener / Photographer Job Description Post Title: Band: Directorate: Base: Managerially accountable to: Professional Accountable to: Diabetes Eye Screener / Photographer 4 (Subject to AFC)
Winter/Surge Capacity Plan 1 st December 2013 to 31 st March Position as at September 2013
 Winter/Surge Capacity Plan 1 st December 2013 to 31 st March 2014 Position as at September 2013 Contents 1. Introduction and background... 3 2. Demand and capacity... 4 2.1. Anticipated bed demand... 4
Winter/Surge Capacity Plan 1 st December 2013 to 31 st March 2014 Position as at September 2013 Contents 1. Introduction and background... 3 2. Demand and capacity... 4 2.1. Anticipated bed demand... 4
CT Scanner Replacement Nevill Hall Hospital Abergavenny. Business Justification
 CT Scanner Replacement Nevill Hall Hospital Abergavenny Business Justification Version No: 3 Issue Date: 9 July 2012 VERSION HISTORY Version Date Brief Summary of Change Owner s Name Issued Draft 21/06/12
CT Scanner Replacement Nevill Hall Hospital Abergavenny Business Justification Version No: 3 Issue Date: 9 July 2012 VERSION HISTORY Version Date Brief Summary of Change Owner s Name Issued Draft 21/06/12
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015 Subject: Supporting TEG Member: Authors: Status 1 Data Quality Baseline Assessment
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015 Subject: Supporting TEG Member: Authors: Status 1 Data Quality Baseline Assessment
Review of Nurse Staffing - Six Month Update Public Board 25 th September 2014
 Review of Nurse Staffing - Six Month Update Public Board 25 th September 2014 Presented for: Presented by: Author Previous Committees Information Professor Suzanne Hinchliffe CBE, Chief Nurse / Interim
Review of Nurse Staffing - Six Month Update Public Board 25 th September 2014 Presented for: Presented by: Author Previous Committees Information Professor Suzanne Hinchliffe CBE, Chief Nurse / Interim
Kingston Hospital NHS Foundation Trust Length of stay case study. October 2014
 Kingston Hospital NHS Foundation Trust Length of stay case study October 2014 The hospital has around 520 beds and provides acute medical services for a population of around 320,000 in Kingston, Richmond,
Kingston Hospital NHS Foundation Trust Length of stay case study October 2014 The hospital has around 520 beds and provides acute medical services for a population of around 320,000 in Kingston, Richmond,
SURGE PLAN (A&E Sustainability Plan) for Wolverhampton Health Economy 2013/14
 for Wolverhampton Health Economy 2013/14") SURGE PLAN (A&E Sustainability Plan) for Wolverhampton Health Economy 2013/14 Acute Trust: CCG: Local Authority: Mental Health: Community WiC: OOH provider: Ambulance Svs: CCG Partners: Royal Wolverhampton
SURGE PLAN (A&E Sustainability Plan) for Wolverhampton Health Economy 2013/14 Acute Trust: CCG: Local Authority: Mental Health: Community WiC: OOH provider: Ambulance Svs: CCG Partners: Royal Wolverhampton
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome:
 TRUST BOARD Date of Meeting: Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome: For noting For information For decision Title of Report: Update on Clinical Strategy Aims: To brief Trust Board
TRUST BOARD Date of Meeting: Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome: For noting For information For decision Title of Report: Update on Clinical Strategy Aims: To brief Trust Board
Infection Prevention and Control Strategy (NHSCT/11/379)
") Infection Prevention and Control Strategy (NHSCT/11/379) September 2010 September 2010 Contents Page No. 1. Foreword 1 2. Introduction 2-3 3. Key Principles 4-5 4. Objectives 6-13 5. Organisational Arrangements
Infection Prevention and Control Strategy (NHSCT/11/379) September 2010 September 2010 Contents Page No. 1. Foreword 1 2. Introduction 2-3 3. Key Principles 4-5 4. Objectives 6-13 5. Organisational Arrangements
Integrated Performance Report
 Integrated Performance Report M04 July 2016 Presented by: Angela Stevenson (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M04 July 2016 Presented by: Angela Stevenson (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Job Description and Person Specification
 Job Description and Person Specification Chief Nursing Officer / Director of Infection Prevention and Control RESPONSIBLE TO: ACCOUNTABLE TO: LIAISES WITH: Chief Executive Chief Executive Executive and
Job Description and Person Specification Chief Nursing Officer / Director of Infection Prevention and Control RESPONSIBLE TO: ACCOUNTABLE TO: LIAISES WITH: Chief Executive Chief Executive Executive and
Business Case Authorisation Cover Sheet
 Business Case Authorisation Cover Sheet Section A Business Case Details Business Case Title: Directorate: Division: Sponsor Name Consultant in Anaesthesia and Pain Medicine Medicine and Rehabilitation
Business Case Authorisation Cover Sheet Section A Business Case Details Business Case Title: Directorate: Division: Sponsor Name Consultant in Anaesthesia and Pain Medicine Medicine and Rehabilitation
OPERATIONAL PERFORMANCE REPORT: March Swindon Community Health Services Overview
 OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
Item E1 - Bart s Health Quality Indicators
 Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
South Canterbury District Health Board
 South Canterbury District Health Board - Timaru Hospital Introduction This report records the results of a Surveillance Audit of a provider of hospital services against the Health and Disability Services
South Canterbury District Health Board - Timaru Hospital Introduction This report records the results of a Surveillance Audit of a provider of hospital services against the Health and Disability Services
COUNCIL OF GOVERNORS MEETING. Thursday, 20 April 2017 PERFORMANCE ASSURANCE REPORT. Non-Executive Directors
 3.5 COUNCIL OF GOVERNORS MEETING Thursday, 20 April 2017 PERFORMANCE ASSURANCE REPORT Non-Executive Directors PURPOSE OF THE PAPER: The National Health Service Act 2006 (as amended) places a general duty
3.5 COUNCIL OF GOVERNORS MEETING Thursday, 20 April 2017 PERFORMANCE ASSURANCE REPORT Non-Executive Directors PURPOSE OF THE PAPER: The National Health Service Act 2006 (as amended) places a general duty
WRIGHTINGTON, WIGAN AND LEIGH HEALTH SERVICES NHS TRUST DIRECTOR OF INFECTION PREVENTION AND CONTROL ANNUAL REPORT
 WRIGHTINGTON, WIGAN AND LEIGH HEALTH SERVICES NHS TRUST DIRECTOR OF INFECTION PREVENTION AND CONTROL ANNUAL REPORT 2006-2007 Author(s) Gill Harris, Director of Infection Prevention and Control EXECUTIVE
WRIGHTINGTON, WIGAN AND LEIGH HEALTH SERVICES NHS TRUST DIRECTOR OF INFECTION PREVENTION AND CONTROL ANNUAL REPORT 2006-2007 Author(s) Gill Harris, Director of Infection Prevention and Control EXECUTIVE
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP
 COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
Strategic KPI Report Performance to December 2017
 Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A