EMERGENCY MEDICINE PHYSICIAN E & M, CRITICAL CARE AND OBSERVATION & PROCEDURE CODING. Medical Account Services, Inc.
|
|
|
- Jocelyn Lamb
- 5 years ago
- Views:
Transcription


1 EMERGENCY MEDICINE PHYSICIAN E & M, CRITICAL CARE AND OBSERVATION & PROCEDURE CODING Medical Account Services, Inc. Presented By: Lynne Severn MBA, CPC, CPMA 351 Ballenger Center Drive, Ste. 250 Frederick, MD severnl@masbilling.com All rights reserved g T B THE BASICS 2 1
2 CHECK YOUR RECORDS FOR THE FOLLOWING: The medical record should be complete and legible The patient s name and the date of service should appear on every page of the record Date of Service on the record should match the date of service on the claim The medical record should clearly indicate the identity and professional credentials of all the people who contributed to the service Information in the record should support all diagnosis reported on the claim All procedures should be clearly documented E & M Documentation should include HPI, ROS, PFSH, Exam and MDM Health risk factors should be identified Patient s progress, response to and changes in treatment, and diagnosis revisions should be documented Any condition that prevents you from collecting basic information should be noted 3 PROVIDER SIGNATURES Documents must have a legible full signature Legible first initial & last name If the signature is not legible then over or under the illegible signature you must : Type or print the provider s name Requirements are not considered to be met if: Initials only There is an unsigned typed note with providers typed name There is an unsigned handwritten note Statement - signature on file Illegible full or partial signature Stamp signatures CMS Signature Requirements -CMS MLN MM March 16,
3 ICD-9 SIGNS AND SYMPTOMS VS. FINAL DIAGNOSIS ICD-9s are reported on all bills. The ICD-9 rules were not designed for billing purposes. Unfortunately, payers are now using the ICD-9s to establish medical necessity for claims. Payers can use the diagnosis to deny line items/claims. Claims processing problems arise when the services provided are not supported by the primary diagnosis. Conclusion Be aware of the need to establish medical necessity Use pain and injury codes where appropriate Incorporate signs and symptoms as appropriate ICD-9 codes should explain the reason for the visit in the medical record and support the necessity for the treatment of an illness and are important in submitting a claim cleanly the first time. 5 6 SHARED VISITRULESR 3
4 SPLIT/SHAREDVISIT RULES Qualified Non Physician Providers (NPPs) who are permitted to assist a physician during a shared visit are: Nurse practitioners Physician assistants Clinical nurse specialists Certified nurse midwife Medicare reimburses services provided by an NPP alone at 85% of the rate it reimburses physicians. However, CMS reimburses visits shared between the physician and the NPP at 100% of the allowed amount to the physician. To obtain the full reimbursement allowed, the physician must document his or her participation in the care of the patient along with the NPP s documentation of his or her portion of the care. If the documentation does not support the physician s presence and the portion of work the physician performed, the NPP should report the care alone. 7 REPORTINGSPLIT/SHARED VISITS TO MEDICARE The split/shared visit rules state that both the NPP and the physician must have a face-to-face encounter with the patient on the day the facility or practice reports the service. (The Handshake Rule) Both the physician and the NPP should document their own participation in the medical record. The physician practice employs the NPP. Warning - do not report a shared visit when a hospital facility or other entity employs the NPP. The physician cannot simply co-sign the chart and state reviewed and agree in the record without seeing the patient personally. The physician must perform and document at least some of the three key components of E/M services (i.e., the history, the exam, and the medical decision-making) 8 4

5 9 TEACHING PHYSICIAN RULES 10 5
6 Why Do We Need to Know the Teaching Physician Rules? The PATH audits led to the creation of compliance programs at major teaching institutions across the United States, often because those institutions were forced to pay settlements to the federal government due to abuses found when teaching physicians either did not meet the physical presence requirements when residents or fellows performed services or did not properly document their role in the billing of those services. HIM professionals must understand the guidelines to accurately code and bill medical services properly and handle PATH audits. 11 BECAUSE. Resident services are paid directly to hospitals via the Accreditation Council for Graduate Medical Education (ACGME). Teaching physicians are paid for their hi involvement in the care of patients, not for time spent teaching. According to the Medicare Part B Reference Manual: In the teaching setting, physician services provided to individual patients are considered to be the payment responsibility of the Part B carrier. Conversely, physician services that are furnished for the general benefit of patients (i.e., supervising and teaching of residents) are considered to be services to the hospital and are therefore the payment responsibility of the Part A intermediary. 4 In other words, teaching physicians who intend to bill for their services must document their involvement in the specific care of the patient. 12 6

7 TP RULES The TP must demonstrate in the documentation their personal involvement in the care of the patient. The TP must briefly describe his/her presence and participation in the service. The TP must see the patient and personally write or dictate a note in order to bill for the services. The TP must Tie-In to the resident note to be able to use their documentation to support the code selected for payment purposes. 13 TEACHING PHYSICIAN TIE IN STATEMENT The attending physician always needs to write a linking statement in order for us to be able to use any of the resident s documentation 14 7





8 WE CANNOT USE ANY OF THE RESIDENT S DOCUMENTATION TO SUPPORT THE LEVEL OF SERVICE BILLED WITHOUT THE TEACHING PHYSICIAN LINKING STATEMENT. THE TP DOCUMENTATION DO S ANDDON'TS It has been clearly established that the following statements by the teaching physician, appended to the resident/fellow s note, are not sufficient i to support a billable service. 16 8


9 TEACHING PHYSICIAN REQUIREMENTS FOR PROCEDURE NOTES Use the GC modifier to indicate that the Teaching Physician (TP) was present during the key portion and immediately available during other parts of the service 5 minutes or Less Resident must document that the TP was present for the entire procedure or surgery and both must sign the note Endoscopy procedures - the TP must be present for the entire viewing Longer than 5 minutes TP must be present during key portion(s) of the procedure Resident must document the TP s presence during the key portions of the procedure in the note and both must sign GOODPROCEDURENOTE BY ATTENDING & RESIDENT Detailed notes from senior resident As well as the Teaching Physician 18 9



10 Students can only document History Never the exam or MDM Recommend students not document on any of the documentation used for billing E&MC CODING 10








11 EM/LEVEL WORKSHEET 1. History 2. Physical Examination 3. Medical Decision Making 21 HIGHMARK AUDIT SHEET 22 11









12 HIGHMARK INTERPRETATION NEGATIVELY IMPACTS MDM IN THE ED SETTING EKGs Pulse Oxygen Minimal Low Moderate & High NEED 4 (coders often can only find 2 or 3 data points) 23 PLEASE NOTE IN ED NOT THE SAME AS OFFICE 24 12
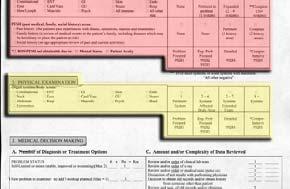
13 EMERGENCY & OBSERVATION DOCUMENTATION REQUIREMENTS Service CPT History Physical Exam MDM EMS Level Problem Focused Problem Focused Straightforward EMS Level Expanded Problem Focused EMS Level Expanded Problem Focused Expanded Problem Focused Expanded Problem Focused Low Moderate EMS Level Detailed Detailed Moderate EMS Level Comprehensive Comprehensive High Observation Level 1 Mult. Calendar Days Observation Level 2 Mult. Calendar Days Observation Level 3 Mult. Calendar Days Detailed or Comprehensive Detailed or Comprehensive Straightforward to Low Comprehensive Comprehensive Moderate Comprehensive Comprehensive High Observation D/C Day Same Day OBS & D/C Level 1 Same Day OBS & D/C Level 2 Same Day OBS & D/C Level Detailed or Comprehensive Detailed or Comprehensive Straightforward or Low Comprehensive Comprehensive Moderate Comprehensive Comprehensive High 25 THE FINAL LEVEL CODED IS ONLY AS STRONG AS THE WEAKEST COMPONENT If one key component falls short of a given E/M level, the final code level l falls as well. Three Documentation Sections: History Physical Exam Medical Decision Making 26 13
14 CHIEF COMPLAINT Required for all visit and levels of service. This must be noted for every patient seen in the Emergency Department 27 HPI ALWAYS TRY TO LIST FOUR OF THE FOLLOWING ELEMENTS THIS ALLOWS THE CODERS TO POTENTIALLY MEET A LEVEL Modifying Factors Quality Severity Timing Context Location Duration Associated Signs & Symptoms 28 14
 elements - Patient complains of dull ache in left ear over the past 24 hours Extended at least 4 HPI elements (99284 99285) Patient complains of dull ache in")
15 EXAMPLE OF AN EXTENDED HPI CONTEXT, QUALITY, LOCATION AND ASSOCIATED SIGNS AND SYMPTOMS 29 HPI Levels 99281, & Need 1 to 3 elements Levels & Need 4 or more elements Two HPI Types: Brief 1 to 3 HPI ( ) elements - Patient complains of dull ache in left ear over the past 24 hours Extended at least 4 HPI elements ( ) Patient complains of dull ache in left ear over the past 24 hours. Patient states he went swimming two days ago. Symptoms somewhat relieved by warm compress and ibuprofen 30 15
16 REVIEW OF SYSTEMS Levels 99281, and require one system Level requires 2 to 9 systems Level requires 10 systems or more unless you note that all systems were negative except as marked or you note that the history collection was limited due to the patient s altered mental status or patient acuity 31 THIRD DOCUMENTATION REQUIREMENT REVIEW OF SYSTEMS Constitutional Eyes Ears, Nose, Mouth, Throat Cardiovascular Respiratory Gastrointestinal Genitourinary Musculoskeletal Integumentary Neurological l Psychiatric Endocrine Hematologic/Lymphatic Allergic/immunologic 1. Complete ROS consists of at least 10 organ systems 2. The ROS can be documented by listing the system followed by negative or normal 3. The ROS can also be documented by listing the signs or symptoms that the patient has denied 4. Documenting review of systems negative or normal does not meet any numerical requirement and is not considered a ROS. Always indicate a negative or positive statement for each system 5. Documenting any pertinent positives and negative combined with the statement all other systems negative will be considered a complete ROS. However, all other systems negative indicates that the physician has reviewed all 14 systems 32 16



17 JUST NOTING ALL OTHER SYSTEMS NEGATIVE IS NOT ENOUGH DOCUMENTATION TO SCORE A COMPLETE ROS. YOU MUST HAVE SOME PERTINENT POSITIVES OR NEGATIVES 33 ROS ITEMS CAN BE FROM TAKEN FROM THE HPI SECTION BUT YOU CANNOT USE THE SAME DOCUMENTED ELEMENT AS AN ROS ELEMENT IF YOU HAVE ALREADY USED IT AS AN HPI ELEMENT. HPI Elements Location GI Duration 2 days Quality Like no Pain she has ever had Associated Signs and Symptoms diarrhea with some blood tinged to it ROS Elements GI Cardiovascular Respiratory GU 34 17


 cases Review 2 of the")


18 PFSH TWO TYPES PERTINENT & COMPLETE 1. Pertinent (1 area) 2. Complete - In-patient & Observation Complete (2 areas) cases Review 2 of the history areas: Medical Family Social Review all 3 history areas: Medical Family Social 35 NO PAST, FAMILY OR SOCIAL HISTORY COLLECTED =
 care; domiciliary care; home care b) Consultations c) Initial hospital care d) Hospital Observation e) Comprehensive nursing facility assessments 37 THE EMERGENCY MEDICINE CAVEAT If")
19 E/M DOCUMENTATION INSTRUCTIONS *Complete PFSH: 2 hx areas: a) Estab pts, office (outpt) care; domiciliary care; home care b) Emergency Dept c) Subseq nursing facility care 3 hx areas: a) New pts, office (outpt) care; domiciliary care; home care b) Consultations c) Initial hospital care d) Hospital Observation e) Comprehensive nursing facility assessments 37 THE EMERGENCY MEDICINE CAVEAT If the physician is unable to obtain history from the patient or other source, the record should describe the patient s medical condition/other circumstance, which precludes obtaining a history. CMS 1995 Guidelines Urgent/emergency conditions Patient s inability to communicate Patient at a very high level of risk Immediate action necessary 38 19
20 THE EMERGENCY MEDICINE CAVEAT You must state the reason the history is not obtained and documented on the record. Must act quickly to prevent deterioration of patient statuss Patient too ill to speak, uncooperative, unconscious 39 EXAM EXAMINATION GUIDELINES Problem Focused 1 Body Area or Organ System Expanded dproblem Focused 2-7Body Areas or Organ Systems; with ihlimited i dexam of Affected Body Area/System. Detailed Comprehensive 2-7 Body Areas or Organ Systems; with Extended Exam of Affected Body Area/System. 8 or More Organ Systems; or a Complete Single System Exam Body Areas Head (including face); Neck; Chest (including breast/axillae); Abdomen; Genatalia; Groin; Buttocks; Back (including spine); Each Extremity Organ Systems Constitutional (vital signs, general appearance); Eyes; ENT; Cardiovascular; Respiratory; Gastrointestinal; Genitourinary; Musculoskeletal; Skin; Neurologic; Psychiatric; Hematologic/Lymphatic/Immunologic



21 DOCUMENTING A SYSTEM = COMPLETING AT LEAST TWO BULLET ITEMS 41 Medical Necessity MEDICAL NECESSITY IS THE OVERRIDING FACTOR IN DETERMINING WHETHER A SERVICE IS A COVERED BENEFIT. YOU CAN PERFORM A COMPLETE HISTORY AND EXAM BUT WITHOUT DOCUMENTING THAT IT IS MEDICALLY NECESSARY THE OIG WOULD SAY THE CASE WAS OVER-CODED IF THE LEVEL OF SERVICE PROVIDED WAS MORE THAN WHAT IS NECESSARY TO EVALUATE AND MANAGE THE PATIENT S CONDITION THAT PROMPTED THE VISIT
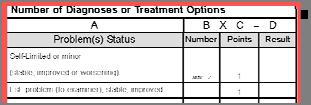
22 MEDICALDECISION MAKING Number of Dx or Treatment Options Almost all ED patients qualify as a new problem to the examiner. They only differ based on whether or not any additional workup is planned. 43 NUMBER OF DIAGNOSIS OR TREATMENT OPTIONS -CONTROVERSY Method 1 - Counting any diagnostic work-up that occurs in the ED as additional work-up planned tends to cause many encounters to score to a higher MDM and E&M level than what may be warranted dbased on the nature of presenting problem. From a clinical i l perspective it is hard to make the argument that a patient that presents with a sore throat and has a strep test done should be scored as Extensive with regards to the number of diagnoses or management options. This can lead to scoring low risk cases as 99284s simply because of the MDM scoring system. Method 2 - For ED E&M services reserve the additional work-up planned for those patients who will receive additional work-up after the ED encounter. This will help your coders more clearly differentiate between 99283, and within your practice. The 2 common interpretations are described above, however, Medicare carrier Highmark s interpretation is an extension of #2. The state that the additional work-up must be after the current encounter and has to be performed by the same MD. Their position is that the ED MD would never be given credit for additional work-up planned

 Minimal/No ne Limited (2) Limited (2)")

23 AMOUNT/COMPLEXITY OF DATA REVIEWED Points Type of Data 1 Review/Order Clinical Lab Tests 1 Review/Order Tests in 7XXXX of CPT 1 Review/Order Tests in 9XXXX of CPT 1 Discuss Test Results with Performing MD 2 Independent Visualization of Image, Trace, Specimen 1 Decision to Obtain Old Records/ HX from others 2 Review/Summarize Old Records and/or Obtain HX from Others, and/or Discuss with other Provider SF Low Moderate High Number of Diagnostic and Management Options Amount and/or Complexity of Data Reviewed Minimal (1) Minimal/No ne Limited (2) Limited (2) Multiple (3) Moderate (3) Extensive (4) Extensive (4) Risk (refer to table of risk) Minimal Low Moderate High 45 WEAK MDM BECAUSEWECAN T SCOREDATA REVIEWED POINTS OR DOCUMENT RISK = EKG BOX NOT CHECKED FOR INTERP. BY ME, NO TREATMENT NOTED, NO RXS, NO CONSULTS = WEAK MDM 46 23


24 Speaking with another health care provider from another practice or service = 2 MDM points you must be specific and identify who you spoke with. 47 Deciding to collect the history from the parents or others = 1 point Summarizing and collecting the history from the parents = 2 points 48 24



25 Ordering an EKG = 1 MDM point Doing the interpretation = 2 MDM points but you must indicate it was my interpretation 49 NO EXTRA MDM DATA POINTS SCORED 50 25

26 EXAMPLES OF T-SYSTEM BOXES THAT SCORE MDM DATA POINTS 1. Hx Exam Limited 3. X-Rays 2. ROS Box 4. Wound Description / Repair 51 MORE MDM DOCUMENTATION BOXES 5. Prior Records Reviewed & Counseled Patient etc. 6. Treatment / Intubated 7. EKG, Lab, X-Rays 8. Procedures 52 26
 Minimal /None Limited (2) Limited (2) Multiple (3) Moderate (3) Extensive (4) Extensive (4) Minimal Low Moderate High 53 FOR A LEVEL 99285: Points Type of Data 1 Review/Order Clinical Lab")

27 MEDICAL DECISION MAKING Risk of complications and/or morbidity SF Low Moderate High Number of Diagnostic and Management Options Amount and/or Complexity of Data Reviewed Risk (refer to table of risk) Minimal (1) Minimal /None Limited (2) Limited (2) Multiple (3) Moderate (3) Extensive (4) Extensive (4) Minimal Low Moderate High 53 FOR A LEVEL 99285: Points Type of Data 1 Review/Order Clinical Lab Tests 1 Review/Order Tests in 7XXXX of CPT 1 Review/Order Tests in 9XXXX of CPT 1 Discuss ss Test Results with Performing MD 2 Independent Visualization of Image, Trace, Specimen 1 Decision to Obtain Old Records/ HX from others 2 Review/Summarize Old Records and/or Obtain HX from Others, and/or Discuss with other Provider HISTORY: 04 HPI PHYSICAL EXAM: 10 ROS 8 Organ Systems with 02 PFSH two bullets each MDM: High Risk and 4 Data Points See chart above 54 27
28 55 CRITICALCAREC CODING DEFINITION OF CRITICAL CARE Critical care is the direct delivery by a physician(s) of medical care for a critically ill or critically injured patient. A critical illness or injury acutely impairs one or more vital organ systems such that there is a high probability of imminent or life threatening deterioration in the patient's condition. Critical care involves high complexity decision making to assess, manipulate, and support vital system function(s) to treat single or multiple vital organ system failure and/or to prevent further life threatening deterioration of the patient's condition. Examples of vital organ system failure include, but are not limited to; central nervous system failure, circulatory failure, shock, renal, hepatic, metabolic, and/or respiratory failure
29 MEDICARE POLICY FOR CRITICAL CARE Before coding critical care ask and answer the following questions: 1. Does the record demonstrate work preformed during the encounter is more intensive than the work of other E/M codes of the same time duration? 2. Does the record demonstrate the patient has acute impairment of one or more vital organ systems and has a high probability of imminent or life-threatening deterioration? 3. Does your documentation demonstrate; direct personal involvement, frequent assessments, a high-complexity of MDM and urgent interventions? 4. Is the time spent specifically recorded? 57 ACTIVITIES QUALIFYING FOR CRITICAL CARE Time spent w/patient Reviewing test results Discussing patient s care w/medical staff Documenting critical care services in medical services record Discussing patient s condition with family (but only questions regarding treatment) 58 29
30 OTHER CODING REQUIREMENTS Only one physician may bill for critical care services during any one single period of time even if more than one physician is providing care to a critically ill/injured patient. Both of the following medical review criteria must be met in addition to the CPT definitions: Clinical Condition Criterion There is a high probability of sudden, clinically significant, or life threatening deterioration in the patient s condition which requires the highest level of physician preparedness to intervene urgently. Treatment Criterion Critical care services require direct personal management by the physician. They are life and organ supporting interventions that require frequent, personal assessment and manipulation by the physician. Withdrawal of, or failure to initiate these interventions on an urgent basis would likely result in sudden, clinically significant or life threatening deterioration in the patient s condition. Providing medical care to a critically ill patient should not be automatically determined to be a critical care service for the sole reason that the patient is critically ill. The physician service must be medically necessary and meet the definition of critical care services as described previously in order to be considered covered. 59 No Shared Visits When Billing for Critical Care A split/shared E/M service performed by a physician and a qualified NPP of the same group practice (or employed by the same employer) cannot be reported as a critical care service. Critical care services are reflective of the care and management of a critically ill or critically injured patient by an individual physician or qualified NPP for the specified reportable period of time and shall not be representative ti of a combined service between a physician and a qualified NPP
31 TP CRITICAL CARE RULES Time spent teaching may not be counted towards critical care time. Time spent by the resident in the absence of the Teaching Physician is not counted toward critical care time. The Teaching Physician must be present for all critical care time billed. Only time spent by the resident and Teaching Physician together with the patient, or time spent by the Teaching Physician alone with the patient, may be counted towards critical care time. The TP must document their PERSONAL time involved. 61 Medical Review Guidelines regarding Full Attention Since critical care is a time-based code, the physician s progress note must contain documentation of the total time involved providing critical care services. Time involved performing procedures that are not bundled into critical care (i.e., billed separately) may not be included ddand counted toward critical care time. The physician s py progress note must document that time involved vdin the performance of separately billable procedures was not counted toward critical care time. Time involved with family members or other surrogate decision makers, whether to obtain a history or to discuss treatment options may be counted toward critical care time only when the patient is unable or incompetent to participate in giving a history and/or making treatment decisions and the discussion is absolutely necessary for treatment decisions under consideration that day, and all of the following are documented in the physician s progress note for that day: the reason the patient was unable or incompetent to participate in giving history and/or making treatment decisions the necessity of the discussion (e.g., no other source was available to obtain a history or because the patient was deteriorating so rapidly needed to discuss treatment options with family immediately ) the treatment decisions for which the discussion was needed a summary of the discussion as related to the treatment decision. The physician s progress note must link the family discussion to a specific treatment issue and explain why the discussion was necessary on that day. All other family discussions, no matter how lengthy, may not be counted towards critical care time
32 CRITICAL CARE 99291: Code used to report the 1 st hour ( up to 74 minutes) on a given date of service : Code used for each 30 minutes beyond the 1 st hour. Critical care of less than 30 minutes may not be reported separately 63 BUNDLED SERVICES Interpretation of cardiac output measurements Chest x-rays Blood gases Blood draw from specimen Analysis of information data stored in computers Gastric intubation Pulse oximetry Temporary transcutaneous pacing Ventilator Management Vascular access procedures Family psychotherapy 64 32
33 65 O C OBSERVATION CODING OBSERVATION CARE DEFINED Observation care is a well-defined set of specific, clinically appropriate services, which include ongoing short term treatment, assessment, and reassessment, that are furnished while a decision is being made regarding whether patients will require further treatment as hospital inpatients or if they are able to be discharged from the hospital. Highmark/CMS 66 33
34 IT ISIMPORTANT TO DOCUMENT OBSERVATION CORRECTLY BECAUSE: OIG CERT findings of inappropriate admits RAC findings lack of medical necessity for short stays Coding and Billing rules are confusing Hospital and Physician billing both depend on time line being established 67 OBSERVATION REQUIREMENTS Intended for short stays of hours Out-patient locations 22 or 23 A written order to begin observation services is required Start time must be documented End time must be documented Services provided must be consistent with the order 68 34
35 OBSERVATION DOCUMENTATION Medical record must demonstrate: Consistency between the practitioner intent and services provided Medical necessity of services Medical appropriateness of the observation stay **Include a dated and timed order for observation, interval progress notes and a discharge note** 69 OBSERVATION SERVICES Observation care discharge Initial Observation care Subsequent Observation care Observation or Inpatient Care Services (Including Admission and Discharge Services) 70 35
 New patients, office, out-patient care; domiciliary care; home")
 YOU CANNOT BILL ABOVE OBSERVATION CODES")
36 E/M DOCUMENTATION INSTR. *Complete PFSH: 3 hx areas: a) New patients, office, out-patient care; domiciliary care; home care b) Consultations c) Initial hospital care d) Hospital Observation e) Comprehensive nursing facility assessments 71 WITHOUT ALL 3 HISTORIES (PFSH) YOU CANNOT BILL ABOVE OBSERVATION CODES OR NO MATTER WHAT THE PATIENT S ACUITY AND MDM INDICATE 72 36
37 73 P N PROCEDURE NOTES INTUBATION- NEED TO KNOW; SIZE OF THE TUBE, HOW IT WAS PLACED, CONFIRM CORRECT PLACEMENT, POST PROCEDURE PATIENT STATUS The patient was positioned appropriately and a # 4 endotracheal tube was placed under direct laryngoscopy. Correct placement was confirmed by presence of bilateral breath sounds without air sounds in the abdomen on auscultation. A CO 2 monitor was also used to confirm tracheal placement of the ET tube. A chest x-ray was ordered to assess for pneumothorax and verify endotracheal tube placement. The patient tolerated the procedure well and there were no complications
38 LUMBAR PUNCTURE NEED TO KNOW; ANESTHESIA TYPE, PREPPED AND DRAPED, SIZE OF NEEDLE, WHERE IT WAS INSERTED, HOW MUCH FLUID WAS REMOVED, TESTS ORDERED, AND PATIENT S POST PROCEDURE STATUS Procedure - Lumbar Puncture Indication meningitis Anesthesia - local 1% lidocaine w/ epi. Informed consent was obtained from the patient's mother. The area was prepped and draped in the usual sterile fashion. Using landmarks, a 22 gauge spinal needle was inserted in the L4-L5 space. The stylet t was removed and the opening pressure was measured at 18 cm of water. 4cc of clear fluid was collected and sent for routine studies. CSF was also sent for HSV and EBV PCR. The patient tolerated the procedure well. There 75 was no blood loss or hematoma. DOCUMENTING THE INTERPRETATION OF A 12 LEAD EKG Document at least 3 of the following 6 elements: Rhythm h and rate Axis Intervals ST segment change Comparison to prior EKG Diagnosis (i.e. acute inferior MI ) Use personal pronouns to indicate that the interpretation i was done by the ED physician My interpretation follows 76 38

39 BILLABLE EKG NOTE CPT CODE INTERPRETATION AND REPORT ONLY 77 SUTURING May bill in addition to E&M code (use modifier 25 on the E&M level as appropriate) Use total length of all wounds of the same type in same area Describe the complexity of the repair. Is there: Extensive contamination, i Foreign body removal Defect creation or margin revision for proper closure 78 39
40 FAST EXAMS (FOCUSED ASSESSMENT BY SONOGRAPHY FOR TRAUMA) Clinical approach- There is no fast exam specific code a. First look for fluid around the heart by performing a limited trans thoracic echocardiography. b. Then look for free fluid in the abdomen by performing a limited abdominal ultrasound. Dual Service 2 separate CPT codes Eh rdi rph r ltim Echocardiography real time Ultrasound abdominal real time *Remember you are required to retain the actual image in your documentation as well as your separately identifiable interpretive report. 79 FAST EXAM DOCUMENTATION Looks for heart activity & pericardial fluid. It is directed to a single diagnostic problem. NOTE: Identify the presence or absence of pericardial fluid Looks for free fluid in the abdomen or hemoperitoneum. NOTE: Identify the presence or absence of pericardial or intraperitoneal fluid
41 OTHER BILLABLE ULTRASOUNDS Abdominal Aortic Aneurysm Echography, abdominal, B-scan and/or real time with image documentation limited (single organ, quadrant, follow-up) Pericardial Fluid Echocardiography, transthoracic, real-time with image documentation; limited 81 BILLABLE NOTE FOR
42 OTHER COMMON ULTRASOUNDS DONE IN THE EMERGENCY DEPARTMENT Pregnancy state is known prior to the study Use CPT code Pregnancy state not known prior to the study Use CPT code Echography, pregnant uterus, realtime with image; limited Echography Pelvic (non-obstetric), real-time with image; limited Is used to determine the status of the pregnancy or to evaluate a pregnancy-related condition Is used to assess a non-pregnancyrelated pelvic condition 83 ULTRASOUND GUIDANCE FOR NEEDLE PLACEMENT CPT CODE Ultrasound guidance is sometimes used for needle placement when performing a biopsy, aspiration, injection or starting an IV. Use still must retain an image Also used when performing the following procedures; paracentesis, thoracentesis, suprapubic aspiration, foreign body localization, or locating an abscess for drainage
43 CONSCIOUS SEDATION = MODERATE SEDATION Documentation Rules Tell us who performs the procedure requiring sedation Tell us who provides the moderate sedation services Tell us the patient s age Tell us who is helping you to monitor the patient if you are also performing the procedure Tell us about monitoring the patient s cardiorespiratory functions (pulse-oximetry, cardiorespiratory monitor, and blood pressure) for the duration of the procedure Tell us when you start and stop the procedure If the same person is performing the procedure and providing the moderate sedation then we need you to note that there was an independent trained observer assisting in the monitoring of the patients level of consciousness and physiological status if the answer is yes we can bill for the procedure and the conscious sedation This is good news! 85 REMEMBER Moderate Sedation begins with the administration of the sedating agent, requires continuous face-to-face attendance, and ends at the conclusion of personal contact by the physician providing the sedation under 5 years - same physician performing the procedure under 5 years - different physician performing the procedure over 5 years - same physician performing the procedure over 5 years different physician performing the procedure In addition to & you can report for each additional 15 minutes beyond the first 30 minutes In addition to & you can report for each additional 15 minutes beyond the first 30 minutes 86 43
44 CORRECT ORTHO CODES FOR FRACTURE/DISLOCATION CARE DEPEND ON EXTENT OF TREATMENT Coders apply orthopedic codes for the treatment of fractures, sprains and other orthopedic injuries only when the ED delivers definitive care, sometimes also called restorative care. Definitive care aims to repair, rather than simply stabilize the injury. Along with casting, definitive care may also include splinting, strapping and/or pain management. 87 FRACTURE VS. SPLINTING/STABILIZATION CARE CHART Scenario: The emergency department physician s role in fracture care. He or She Report Code For: Fracture and/or Dislocation Care ( ) Stabilization Care ( ) Assumes fracture care responsibility Yes No Applies cast/splint for stability; refers patient to specialist for fracture care No Yes Replaces damaged or inadequate cast during or after the global follow up No Yes 88 44

45 BILLABLE NOTE FOR FRACTURE CARE 89 DEFINITIVE FRACTURE CARE IN THE ED Many ED physicians provide definitive fracture care for fractures such as: Finger Fractures 26720, Toes Fractures 28490, Clavicle Fractures Rib Fractures Nasal Fractures These are high RVU procedures and should not be overlooked
46 SPLINTS If a splint is applied and checked by the ED physician this level of care usually does not meet the requirement for definitive or restorative care but a splinting code can be billed for stabilizing the fracture. Common splinting CPT codes include: Finger Short Arm Long Arm Short Leg Long Leg PQRS MEASURES IN THE ED 46
47 Suggested PQRS Measures in the ED Number Measure ICD-9 Codes CPT II Code Lead Electrocardiogram 413.0, 413.1, 413.9, 3120F (ECG) Performed for Non , , , Traumatic Chest Pain - Age > 40 yrs. Reporting Modifier 1P Reporting Modifier 2P Reporting Modifier 3P Reporting Modifier 8P Documentation of medical Documentation of Patient 12-Lead ECG Not performed, reason(s) for not performing reason(s) for not reason not otherwise specified a 12-Lead ECG performing a 12-Lead ECG Lead Electrocardiogram G8704 Documentation of medical Documentation of Patient 12-Lead ECG Not performed, (ECG) Performed for reason(s) for not performing reason(s) for not reason not otherwise specified Syncope - Age > 60 yrs. a 12-Lead ECG performing a 12-Lead ECG 56 Community-Acquired 481, 482.0, 482.1, 2010F Pneumonia (CAP): Vital 482.2, , , Signs - Age > 18 yrs , , , G8546 or G8550 if all four , , , Community Acquired , , , Pneumonia (CAP) Measures , , , have been performed 482.9, 483.0, 483.1, 483.8, 485, 486, Community-Acquired 481, 482.0, 482.1, 3028F Pneumonia 482.2, , , (CAP):Assessment of Oxygen , , , Saturation - Age > 18 yrs , , , G8546 or G8550 if all four , , , CAP Measures have been , , , performed 482.9, 483.0, 483.1, 483.8, 485, 486, Documentation of medical reason(s) for not documenting and reviewing oxygen saturation Vital signs (temperature, pulse, respiratory rate, and blood pressure) not documented and reviewed Documentation of Patient Documentation of system Oxygen Saturation not reason(s) for not reason(s) for not Documented and Reviewed, documenting and documenting and Reason no Specified reviewing oxygen reviewing oxygen saturation saturation 58 Community-Acquired 481, 482.0, 482.1, 2014F Mental Status no Assessed, Pneumonia (CAP): , , , Reason not Specified Assessment of Mental Status , , , - Age > 18 yrs. G8546 or , , , G8550 if all four CAP , , , Measures have been , , , performed 482.9, 483.0, 483.1, 483.8, 485, 486, Community-Acquired Pneumonia (CAP): Empiric Antibiotic - Age >18 yrs. G8546 or G8550 if all four CAP Measures have been performed 481, 482.0, 482.1, 4045F 482.2, , , , , , , , , , , , , , , 482.9, 483.0, 483.1, 483.8, 485, 486, Documentation of medical Documentation of patient Documentation of system Appropriate empiric antibiotic reason(s) for not prescribing reason(s) for not reason(s) for not not prescribed, reason not appropriate empiric prescribing appropriate prescribing appropriate otherwise specified antibiotic empiric antibiotic empiric antibiotic 93 PQRS PNEUMONIA MEASURES Community Acquired Pneumonia PQR's measures 56, 57, 58, 59 Medicare Patients ONLY 18 or older CAP if all 4 measures are done (VS, PO, Mental status. ABX) - G8550 CAP if all 4 measures are not done G8546 VS done 2010F PO Done 3028F Mental Status done 2014F ABX NOT given 4045F Modifier indicating why (1P, 2P, 3P, 8P) CAP if all 4 measures are not done G8546 VS done 2010F PO Done 3028F Mental Status NOT done 2014F Modifier indicating why (1P, 2P, 3P, 8P) ABX given 4045F CAP if all 4 measures are not done G8546 VS done 2010F PO NOT Done 3028F Modifier indicating why (1P, 2P, 3P, 8P) Mental Status done 2014F ABX given 4045F CAP if all 4 measures are not done G8546 VS NOT done 2010F Modifier indicating why (1P, 2P, 3P, 8P) PO Done 3028F Mental Status done 2014F ABX given 4045F 94 47
48 REFERENCES 95 REFERENCES AMA CPT Professional Edition ICD-9-CM For Physicians df M5993.pdf Management/Ultrasound/
Evaluation and Management Auditing Back to the Basics. Objectives. Audit Start with the benchmarks CMS MEDPAR by specialty 4/22/2013
 Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Documenting & Coding for Compliance
 Documenting & Coding for Compliance Department of Family and Community Medicine October 17, 2012 UNMMG Compliance Documentation Documentation Why is it important? Enables the physician and other health
Documenting & Coding for Compliance Department of Family and Community Medicine October 17, 2012 UNMMG Compliance Documentation Documentation Why is it important? Enables the physician and other health
Presented for the AAPC National Conference April 4, 2011
 Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
The World of Evaluation and Management Services and Supporting Documentation
 The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
The World of Evaluation and Management Services and Supporting Documentation Presented by Cahaba Government Benefit Administrators, LLC Provider Outreach and Education May 14, 2009 Disclaimers Disclaimer
Critical Care, Evaluation and Management Services (99291, 99292)
") Manual: Policy Title: Reimbursement Policy Critical Care, Evaluation and Management Services (99291, 99292) Section: Evaluation & Management Services Subsection: None Date of Origin: 10/28/2014 Policy
Manual: Policy Title: Reimbursement Policy Critical Care, Evaluation and Management Services (99291, 99292) Section: Evaluation & Management Services Subsection: None Date of Origin: 10/28/2014 Policy
Evaluation and Management
 Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
E/M: Coding Opportunities- Documentation is key
 E/M: Coding Opportunities- Documentation is key Compiled and Presented by: Suzan Berman CPC, CEMC, CEDC The duplication of this presentation, all or in part, without the expression permission of the presenter,
E/M: Coding Opportunities- Documentation is key Compiled and Presented by: Suzan Berman CPC, CEMC, CEDC The duplication of this presentation, all or in part, without the expression permission of the presenter,
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
E & M Coding. Welcome To The Digital Learning Center. Today s Presentation. Course Faculty. Beyond the Basics. Presented by
 Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
Welcome To The Digital Learning Center Presented by Your Partner In Building High Performance Practices Today s Presentation E & M Coding Beyond the Basics Course Faculty R. Thomas (Tom) Loughrey, MBA,
Coding Complexities of Critical Care
 Coding Complexities of Critical Care Jill Young, CPC, CEDC, CIMC Young Medical Consulting, LLC East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing.
Coding Complexities of Critical Care Jill Young, CPC, CEDC, CIMC Young Medical Consulting, LLC East Lansing, Michigan 1 Disclaimer This material is designed to offer basic information for coding and billing.
Critical Care What Makes this so Difficult
 Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC
 Service in RHC") How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
How To Document and Select Outpatient Levels of Evaluation and Management (E&M) Service in RHC John F. Burns, CPC, CPC-I, CPMA, CEMC Vice President, Audit and Compliance Services jburns@ruralhealthcoding.com
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation
 A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
A Guide to Compliance at New York City s Health and Hospitals Corporation Resident Orientation 1 General Principles of Documentation 2 7 General Principles of Documentation 1. Medical record should be
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule. Grace Wilson, RHIA
 Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Start with the Problem
 Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
Start with the Problem Jen Godreau, BA, CPC, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com December 2011 Phone: (866)-228-9252 E-Mail: customerservice@supercoder.com
EMERGENCY MEDICINE CLINICAL ROTATION COMPETENCY BASED CURRICULUM
 CLINICAL ROTATION COMPETENCY BASED CURRICULUM EMERGENCY MEDICINE During the third year of the curriculum, students expand their knowledge of emergent conditions and gain the ability to apply the knowledge
CLINICAL ROTATION COMPETENCY BASED CURRICULUM EMERGENCY MEDICINE During the third year of the curriculum, students expand their knowledge of emergent conditions and gain the ability to apply the knowledge
9/17/2018. Place of Service Type of Service Patient Status
 Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Urgent Care Coding. Webinar Subscription Access Expires December 31.
 Urgent Care Coding Questions Answers Webinar Subscription Access Expires December 31. How long can I access the on demand version? You will find that in the same instructions box you utilized to access
Urgent Care Coding Questions Answers Webinar Subscription Access Expires December 31. How long can I access the on demand version? You will find that in the same instructions box you utilized to access
EM Coding Newsletter & Advisory Critical Care Update
 EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
Medical Necessity verses Medical Decision Making. Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC
 Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Advanced Evaluation and. AAPC Regional Conference Chicago 10/27/12
 Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
Evaluation & Management
 Evaluation & Management Shannon O. DeConda CPC, CPC-I, CPMA, CEMC, CEMA, CRTT President, NAMAS Partner, DoctorsManagement Evaluation and Management Components We will now look at the each of the components
Evaluation & Management Shannon O. DeConda CPC, CPC-I, CPMA, CEMC, CEMA, CRTT President, NAMAS Partner, DoctorsManagement Evaluation and Management Components We will now look at the each of the components
6/14/2017. Evaluation and Management Coding. Jeffrey D. Lehrman, DPM, FASPS, MAPWCA
 Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
PRIVILEGE APPLICATION FORM - [Mercy Medical Center]
![PRIVILEGE APPLICATION FORM - [Mercy Medical Center]](/thumbs/85/91362180.jpg "PRIVILEGE APPLICATION FORM - [Mercy Medical Center]") Current Privilege Status Key Practitioner's Current Privilege status is signified in ( ) preceding each privilege. G = W = Withdrawn T = Temporary P = With Proctor A = Assist with C = With Consult E =
Current Privilege Status Key Practitioner's Current Privilege status is signified in ( ) preceding each privilege. G = W = Withdrawn T = Temporary P = With Proctor A = Assist with C = With Consult E =
Clinical Privileges Profile Family Medicine. Kettering Medical Center System
 Clinical Privileges Profile Kettering Medical Center Sycamore Medical Center Kettering Medical Center System Applicant: Check off the Requested box for each privilege requested. Applicants have the burden
Clinical Privileges Profile Kettering Medical Center Sycamore Medical Center Kettering Medical Center System Applicant: Check off the Requested box for each privilege requested. Applicants have the burden
Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC Disclaimer
 Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
2/28/2017 NO DISCLOSURES. K 1/Partner
 NO DISCLOSURES LaMon Norton NP Participant will recognize origin & role of Relative Value Unit (RVU) in coding and reimbursement. Participant will be able to link documentation points to coding and RVU
NO DISCLOSURES LaMon Norton NP Participant will recognize origin & role of Relative Value Unit (RVU) in coding and reimbursement. Participant will be able to link documentation points to coding and RVU
Medical Decision Making
 Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
Medical Decision Making Jen Godreau, BA, CPC, CPMA, CPEDC Director of Development & Operations Supercoder.com jenniferg@supercoder.com February 2012 What s he thinking? What Is the Table of Risk? 1 of
Evaluation & Management Documentation Training Tool
 Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest to the RIGHT in the table, which
Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest to the RIGHT in the table, which
Evaluation and Management Services
 Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Anthem Blue Cross and Blue Shield Commercial Professional Reimbursement Policy
 Subject: Documentation and Reporting Guidelines for Evaluation and Management Services IN, KY, MO, OH, WI Policy: 0024 Effective: 10/01/2016 Coverage is subject to the terms, conditions, and limitations
Subject: Documentation and Reporting Guidelines for Evaluation and Management Services IN, KY, MO, OH, WI Policy: 0024 Effective: 10/01/2016 Coverage is subject to the terms, conditions, and limitations
RVU KILLERS The Most Common Reimbursement Documentation Errors. Michael Granovsky MD CPC CEDC FACEP President LogixHealth
 RVU KILLERS The Most Common Reimbursement Documentation Errors Michael Granovsky MD CPC CEDC FACEP President LogixHealth Documentation-Why Does It Matter? Must communicate to the payer your concerns and
RVU KILLERS The Most Common Reimbursement Documentation Errors Michael Granovsky MD CPC CEDC FACEP President LogixHealth Documentation-Why Does It Matter? Must communicate to the payer your concerns and
See the Time chapter for complete instructions regarding how to code using time as the controlling E/M factor.
 2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
Basic Teaching Physician Presence and Documentation
 Basic Teaching Physician Presence and Documentation Welcome to the Children s University Medical Group (CUMG) training on the Teaching Physician Presence and Documentation. The goal of this module is to
Basic Teaching Physician Presence and Documentation Welcome to the Children s University Medical Group (CUMG) training on the Teaching Physician Presence and Documentation. The goal of this module is to
Evaluation and Management Services Guide
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Evaluation and Management Services Guide November 2014 / ICN: 006764 PREFACE This guide is offered as a reference tool
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services R Evaluation and Management Services Guide November 2014 / ICN: 006764 PREFACE This guide is offered as a reference tool
Privilege Request Form Emergency Medicine
 Privilege Request Form SECTION I GENERAL REQUIREMENTS EMERGENCY MEDICINE Requested Staff Category Active Courtesy Consulting Affiliate Basic Education: MD or DO INITIAL APPOINTMENT Minimal formal training
Privilege Request Form SECTION I GENERAL REQUIREMENTS EMERGENCY MEDICINE Requested Staff Category Active Courtesy Consulting Affiliate Basic Education: MD or DO INITIAL APPOINTMENT Minimal formal training
Evaluation & Management Documentation Training Tool
 A MS Medicare Administrative ontractor Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest
A MS Medicare Administrative ontractor Evaluation & Management Documentation Training Tool 1 History Refer to the data section (below) in order to quantify. After referring to data, circle the entry farthest
8/19/2017. The OIG Report
 This presentation was created by me with the best intentions and believable resources. I however am not a lawyer, doctor or self-proclaimed expert, but I have watched plenty on TV. The information and
This presentation was created by me with the best intentions and believable resources. I however am not a lawyer, doctor or self-proclaimed expert, but I have watched plenty on TV. The information and
Emergency Department Student Elective Goals and Objectives
 Emergency Department Student Elective Goals and Objectives Goals: During the Emergency Department (ED) rotation, the student will develop his/her knowledge and skills associated with the evaluation, treatment
Emergency Department Student Elective Goals and Objectives Goals: During the Emergency Department (ED) rotation, the student will develop his/her knowledge and skills associated with the evaluation, treatment
MEDICARE RULE FOR TEACHING PHYSICIANS Effective July 1, 1996.
 MEDICARE RULE F TEACHING PHYSICIANS Effective July 1, 1996. 1.0 GENERAL RULE: If a resident participates in a service provided in a teaching setting, the teaching physician may not bill Medicare for such
MEDICARE RULE F TEACHING PHYSICIANS Effective July 1, 1996. 1.0 GENERAL RULE: If a resident participates in a service provided in a teaching setting, the teaching physician may not bill Medicare for such
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION ------------------------------------------------------------------------------------------ 2 STATE DEPARTMENT
Hospitalist Coding Compliance sponsored by CHMB
 Hospitalist Coding Compliance sponsored by CHMB CHMB Corporate Overview Founded in 1995 o Privately Held, Profitable and P.E. Funded for Rapid Growth o Inc. 5000 Fastest Growing Private Companies 2008-2012
Hospitalist Coding Compliance sponsored by CHMB CHMB Corporate Overview Founded in 1995 o Privately Held, Profitable and P.E. Funded for Rapid Growth o Inc. 5000 Fastest Growing Private Companies 2008-2012
E/M Auditing: History is the Key
 E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
Are they coming to get you! Todd Thomas, CCS-P
 Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 4 MMIS MODIFIERS... 4 MEDICINE SECTION... 7 GENERAL INFORMATION
NEW YORK STATE MEDICAID PROGRAM MIDWIFE PROCEDURE CODES Table of Contents GENERAL INFORMATION... 3 SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 4 MMIS MODIFIERS... 4 MEDICINE SECTION... 7 GENERAL INFORMATION
SPECIALTY TIP #13 Evaluation and Management (E&M)
") ICD- 10 SPECIALTY TIPS SPECIALTY TIP #13 Evaluation and Management (E&M) This topic is being addressed in our Specialty Tips series as most providers rate Evaluation and Management as one of the more challenging
ICD- 10 SPECIALTY TIPS SPECIALTY TIP #13 Evaluation and Management (E&M) This topic is being addressed in our Specialty Tips series as most providers rate Evaluation and Management as one of the more challenging
Programming a Spinal Cord Neurostimulator
 Programming a Spinal Cord Neurostimulator August 10, 2017 My surgeon wants to bill 95972 for programming along with placement of a spinal neurostimulator. Isn t the programming inclusive to the surgical
Programming a Spinal Cord Neurostimulator August 10, 2017 My surgeon wants to bill 95972 for programming along with placement of a spinal neurostimulator. Isn t the programming inclusive to the surgical
NEXTGEN E&M CODING DEMONSTRATION
 NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
EVALUATION & MANAGEMENT SERVICES CODING. Part I: What is an E&M? Where do you start? Jennifer Jones, CPC, CPC-I
 DOTHAN AL CHAPTER AAPC FALL WORKSHOP Friday November 17, 2017 REGISTRATION BEGINS AT 7:15 am PROGRAM TIME IS 8:00 am 12:30 pm Earn 4 CEU s for a Fee of only $50.00 per attendee (Snacks will be provided
DOTHAN AL CHAPTER AAPC FALL WORKSHOP Friday November 17, 2017 REGISTRATION BEGINS AT 7:15 am PROGRAM TIME IS 8:00 am 12:30 pm Earn 4 CEU s for a Fee of only $50.00 per attendee (Snacks will be provided
N: Emergency Nursing. Alberta Licensed Practical Nurses Competency Profile 135
 N: Emergency Nursing Alberta Licensed Practical Nurses Competency Profile 135 Competency: N-1 Multi-Systems Assessment N-1-1 N-1-2 N-1-3 N-1-4 Demonstrate knowledge and ability to apply critical thinking
N: Emergency Nursing Alberta Licensed Practical Nurses Competency Profile 135 Competency: N-1 Multi-Systems Assessment N-1-1 N-1-2 N-1-3 N-1-4 Demonstrate knowledge and ability to apply critical thinking
CODING vs AUDITING Does it all boil down to Medical Necessity?
 PERFORM REGULAR AUDITS You provide routine maintenance for your car- but what about your documentation? CODING vs AUDITING Does it all boil down to Medical Necessity? EDUCATE WISELY Be sure and discern
PERFORM REGULAR AUDITS You provide routine maintenance for your car- but what about your documentation? CODING vs AUDITING Does it all boil down to Medical Necessity? EDUCATE WISELY Be sure and discern
Transition Care Management Update: Practical Applications for 2016
 60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
NEXTGEN E&M CODING DEMONSTRATION
 NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
NEXTGEN E&M CODING DEMONSTRATION This demonstration reviews usage of the E&M Coding template. Details of the workflow will likely vary somewhat among departments, though this should give you a good idea
E/M Fast Finder. CPT only 2012 American Medical Association. 1 All Rights Reserved.
 E/M Fast Finder The E/M Fast Finder is a carry-along reference to assist in assigning the Evaluation and Management (E/M) codes that are part of the 99000 series of Current Procedural Terminology (CPT
E/M Fast Finder The E/M Fast Finder is a carry-along reference to assist in assigning the Evaluation and Management (E/M) codes that are part of the 99000 series of Current Procedural Terminology (CPT
Evaluation & Management 101 for Clinicians
 Evaluation & Management 101 for Clinicians Kerin Draak, MSN, WHNP BC, CPC, CEMC, COBGC, CPC I System Director of Clinical & Financial Integration Hospital Sisters Health System This is the Full Title of
Evaluation & Management 101 for Clinicians Kerin Draak, MSN, WHNP BC, CPC, CEMC, COBGC, CPC I System Director of Clinical & Financial Integration Hospital Sisters Health System This is the Full Title of
HC 1930 HC 1930 ICD-9-CM III/CPT Coding II
 South Central College HC 1930 HC 1930 ICD-9-CM III/CPT Coding II Course Information Description Total Credits 4.00 Total Hours 80.00 Types of Instruction This course is a continuation of HC 1920, 1925,
South Central College HC 1930 HC 1930 ICD-9-CM III/CPT Coding II Course Information Description Total Credits 4.00 Total Hours 80.00 Types of Instruction This course is a continuation of HC 1920, 1925,
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents GENERAL INFORMATION 2 STATE DEPARTMENT OF HEALTH CONDITIONS FOR PAYMENT 3 PRACTITIONER SERVICES PROVIDED IN HOSPITALS
Office of Compliance. Complete & Accurate Documentation Core Curriculum for GWU Residents
 Office of Compliance Complete & Accurate Documentation Core Curriculum for GWU Residents December 3, 2014 Medical Record The medical record tells the story of the patient from start to finish. If the story
Office of Compliance Complete & Accurate Documentation Core Curriculum for GWU Residents December 3, 2014 Medical Record The medical record tells the story of the patient from start to finish. If the story
2019 Evaluation and Management Coding Advisor. Advanced guidance on E/M code selection for traditional documentation systems
 2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
2019 Evaluation and Management Coding Advisor Advanced guidance on E/M code selection for traditional documentation systems POWER UP YOUR CODING with Optum360, your trusted coding partner for 32 years.
Critical Care Services
 Critical Care Services MEHIMA Spring Meeting March 17, 2016 Dianne Rodrigue, PA, MHP, CCDS, CPC Disclaimer This presentation is for general education purposes only. The information contained in these materials
Critical Care Services MEHIMA Spring Meeting March 17, 2016 Dianne Rodrigue, PA, MHP, CCDS, CPC Disclaimer This presentation is for general education purposes only. The information contained in these materials
Care Transition Strategies: The 2013 Transition Care Management Codes
 Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
History of CPT. History of CPT. History of CPT. History of CPT. History of E&M. Workshop Evaluation and Management Coding on the River 2010
 Workshop Evaluation and Management Coding on the River 2010 Presented By: Freda Brinson, CPC, CPC-H, CEMC Freda.brinson@aapcca.org or brinsonfr@sjchs.org Faye Grile, CPC, CPMA, CEMC grilefa1@memorialhealth.com
Workshop Evaluation and Management Coding on the River 2010 Presented By: Freda Brinson, CPC, CPC-H, CEMC Freda.brinson@aapcca.org or brinsonfr@sjchs.org Faye Grile, CPC, CPMA, CEMC grilefa1@memorialhealth.com
How does one report the performance of both a screening mammogram on the right breast and a diagnostic on the left breast at the same encounter?
 1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
Focus On Observation
 Focus On Observation Introduction CPT and CMS Requirements CPT Codes Documentation Requirements Observation Coding: Facility Considerations 2 LogixHealth s unsurpassed service stems from the fact that
Focus On Observation Introduction CPT and CMS Requirements CPT Codes Documentation Requirements Observation Coding: Facility Considerations 2 LogixHealth s unsurpassed service stems from the fact that
NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES. SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION
 NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION Table of Contents GENERAL RULES AND INFORMATION... 3 MMIS MODIFIERS... 13 EVALUATION AND MANAGEMENT
NEW YORK STATE MEDICAID PROGRAM PHYSICIAN PROCEDURE CODES SECTION 2 MEDICINE, DRUGS and DRUG ADMINISTRATION Table of Contents GENERAL RULES AND INFORMATION... 3 MMIS MODIFIERS... 13 EVALUATION AND MANAGEMENT
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES
 NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents Contents GENERAL INFORMATION... 3 PRACTITIONER SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 5 MMIS MODIFIERS... 5 MEDICINE
NEW YORK STATE MEDICAID PROGRAM NURSE PRACTITIONER PROCEDURE CODES Table of Contents Contents GENERAL INFORMATION... 3 PRACTITIONER SERVICES PROVIDED IN ARTICLE 28 FACILITIES... 5 MMIS MODIFIERS... 5 MEDICINE
Message Response Message
 Message If established pt wouldn't 2 out of 3 still require the level for slide 5? Response Message Can you re-state your question? I am unclear on what you are asking. Thanks You stated that even when
Message If established pt wouldn't 2 out of 3 still require the level for slide 5? Response Message Can you re-state your question? I am unclear on what you are asking. Thanks You stated that even when
Electronic Health Records - Advantages and Pitfalls of Documentation
 Electronic Health Records - Advantages and Pitfalls of Documentation Kansas City, KS HCCA Regional Conference September 25, 2015 1:00 P.M. 2:00 P.M. Presented by: Cynthia A. Swanson, RN, CPC, CEMC, CHC,
Electronic Health Records - Advantages and Pitfalls of Documentation Kansas City, KS HCCA Regional Conference September 25, 2015 1:00 P.M. 2:00 P.M. Presented by: Cynthia A. Swanson, RN, CPC, CEMC, CHC,
Emergency Department Update 2010 Outpatient Payment System
 Emergency Department Update 2010 Outpatient Payment System ED Facility Level Guidelines: Still No National Guidelines Triage Only Services Critical Care Requires CMS Documentation E/M Physician of Payment
Emergency Department Update 2010 Outpatient Payment System ED Facility Level Guidelines: Still No National Guidelines Triage Only Services Critical Care Requires CMS Documentation E/M Physician of Payment
Preventive and Sick Visits Same Day. Objectives
 Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
During the hospital medicine rotation, residents will focus on the following procedures as permitted by case mix:
 Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Charting for Midwives. Getting Credit For the Work You Do
 Charting for Midwives Getting Credit For the Work You Do Moving Beyond S.O.A.P. The U.S. health care system is moving past fee-for-service billing. In the future, the providers will be reimbursed based
Charting for Midwives Getting Credit For the Work You Do Moving Beyond S.O.A.P. The U.S. health care system is moving past fee-for-service billing. In the future, the providers will be reimbursed based
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL
 Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
News SEPTEMBER. Hospital Outpatient Quality Reporting Program. Support Contractor
 Volume 1, Issue 4 Hospital Outpatient Quality Reporting Program Support Contractor News SEPTEMBER 2011 In This Issue... Emergency Department Arrival and Departure Times Page 2 Hospital OQR Benchmarks Page
Volume 1, Issue 4 Hospital Outpatient Quality Reporting Program Support Contractor News SEPTEMBER 2011 In This Issue... Emergency Department Arrival and Departure Times Page 2 Hospital OQR Benchmarks Page
Coding and Billing for Lifestyle Medicine
 Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
NEONATAL-PERINATAL MEDICINE CLINICAL PRIVILEGES
 Name: Page 1 Initial Appointment Reappointment All new applicants must meet the following requirements as approved by the governing body effective: 8/5/2015. Applicant: Check off the Requested box for
Name: Page 1 Initial Appointment Reappointment All new applicants must meet the following requirements as approved by the governing body effective: 8/5/2015. Applicant: Check off the Requested box for
Documentation for ED Visits with "Additional Work-Up" Planned. Presented by Rae Jimenez, CPC, CDEO, CPB, CPMA, CPPM, CPC-I, CCS
 Documentation for ED Visits with "Additional Work-Up" Planned Presented by Rae Jimenez, CPC, CDEO, CPB, CPMA, CPPM, CPC-I, CCS Course Objectives Discuss gray areas for E/M selection for the professional
Documentation for ED Visits with "Additional Work-Up" Planned Presented by Rae Jimenez, CPC, CDEO, CPB, CPMA, CPPM, CPC-I, CCS Course Objectives Discuss gray areas for E/M selection for the professional
UNIVERSAL PROTOCOL POLICY FOR CORRECT SITE IDENTIFICATION (VERIFICATION OF CORRECT SITE FOR INVASIVE, HIGHRISK, OR SURGICAL PROCEDURES)
") UNIVERSAL PROTOCOL POLICY FOR CORRECT SITE IDENTIFICATION (VERIFICATION OF CORRECT SITE FOR INVASIVE, HIGHRISK, OR SURGICAL PROCEDURES) PURPOSE: To promote patient safety by providing guidelines for verification
UNIVERSAL PROTOCOL POLICY FOR CORRECT SITE IDENTIFICATION (VERIFICATION OF CORRECT SITE FOR INVASIVE, HIGHRISK, OR SURGICAL PROCEDURES) PURPOSE: To promote patient safety by providing guidelines for verification
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
General Internal Medicine Clinical Privileges REAPPOINTMENT Effective from July 1, 2015 to June 30, 2016
 Name: Initial privileges (initial appointment) Renewal of privileges (reappointment) All new applicants must meet the following requirements as approved by the governing body, effective: 04/Jun/2013. Applicant:
Name: Initial privileges (initial appointment) Renewal of privileges (reappointment) All new applicants must meet the following requirements as approved by the governing body, effective: 04/Jun/2013. Applicant:
Procedure Codes Assigned to Surgical Benefit Categories
 Manual: Policy Title: Reimbursement Policy Procedure Codes Assigned to Surgical Benefit Categories Section: Surgery Subsection: None Date of Origin: 1/1/2000 Policy Number: RPM023 Last Updated: 4/5/2017
Manual: Policy Title: Reimbursement Policy Procedure Codes Assigned to Surgical Benefit Categories Section: Surgery Subsection: None Date of Origin: 1/1/2000 Policy Number: RPM023 Last Updated: 4/5/2017
UNMH Family Medicine Clinical Privileges
 All new applicants must meet the following requirements as approved by the UNMH Board of Trustees effective: 07/31/2015 INSTRUCTIONS Applicant: Check off the "Requested" box for each privilege requested.
All new applicants must meet the following requirements as approved by the UNMH Board of Trustees effective: 07/31/2015 INSTRUCTIONS Applicant: Check off the "Requested" box for each privilege requested.
SCOPE OF PRACTICE. Internal Medicine Residency USF Health Morsani College of Medicine University of South Florida
 SCOPE OF PRACTICE Internal Medicine Residency USF Health Morsani College of Medicine University of South Florida Background Internal Medicine Residency is clinical training in a supervised environment
SCOPE OF PRACTICE Internal Medicine Residency USF Health Morsani College of Medicine University of South Florida Background Internal Medicine Residency is clinical training in a supervised environment
Basics of Coding for Compliance. Health Systems Compliance Presented by JoAnn Martinez, CPC Compliance Educator
 Basics of Coding for Compliance Health Systems Compliance Presented by JoAnn Martinez, CPC Compliance Educator Documentation Best Practice Common Themes ICD-10 that support E/M & Procedure Coding Type
Basics of Coding for Compliance Health Systems Compliance Presented by JoAnn Martinez, CPC Compliance Educator Documentation Best Practice Common Themes ICD-10 that support E/M & Procedure Coding Type
Learning Objectives. Denver Health Medical Center. Complex Coding Scenarios and Resolution
 Complex Coding Scenarios and Resolution Eric Ryland, MS, RHIA, CCDS, CHDA, CCS, CPC Manager of Coding Denver Health Medical Center Denver, Colo. 2 Learning Objectives Denver Health Medical Center Evaluate
Complex Coding Scenarios and Resolution Eric Ryland, MS, RHIA, CCDS, CHDA, CCS, CPC Manager of Coding Denver Health Medical Center Denver, Colo. 2 Learning Objectives Denver Health Medical Center Evaluate
Corporate Medical Policy Bundling Guidelines
 Corporate Medical Policy Bundling Guidelines File Name: bundling_guidelines Policy Number: ADM9020 Origination: 1/2000 Last Review: 03/2006 Next Review: 03/2007 Discussion Related to Blue Care, Blue Choice,
Corporate Medical Policy Bundling Guidelines File Name: bundling_guidelines Policy Number: ADM9020 Origination: 1/2000 Last Review: 03/2006 Next Review: 03/2007 Discussion Related to Blue Care, Blue Choice,
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO
 EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
EVALUATION AND MANAGEMENT: GETTING PAID FOR WHAT YOU DO Kim Huey, MJ, CHC, CPC, CCS-P, PCS, CPCO Sandy Giangreco, RHIT, CCS, CCS-P, CHC, CPC, COC, CPC-I, COBGC Agenda 2014 OIG Report CMS Documentation
DELINEATION OF PRIVILEGES - ANESTHESIOLOGY
 KALEIDA HEALTH Name Date DELINEATION OF PRIVILEGES - ANESTHESIOLOGY PLEASE NOTE: Please check the box for each privilege requested. Do not use an arrow or line to make selections. We will return applications
KALEIDA HEALTH Name Date DELINEATION OF PRIVILEGES - ANESTHESIOLOGY PLEASE NOTE: Please check the box for each privilege requested. Do not use an arrow or line to make selections. We will return applications
FAMILY MEDICINE CLINICAL PRIVILEGES
 Name: Page 1 Initial Appointment Reappointment All new applicants must meet the following requirements as approved by the governing body effective: 4/3/2013. Applicant: Check off the Requested box for
Name: Page 1 Initial Appointment Reappointment All new applicants must meet the following requirements as approved by the governing body effective: 4/3/2013. Applicant: Check off the Requested box for
STANDARDIZED PROCEDURE LUMBAR DRAIN INSERTION (Adults, Peds)
") I. Definition The purpose of this standardized procedure is for the Advanced Health Practitioner to safely place a lumbar drain. II. Background Information A. Setting: The setting (inpatient vs outpatient)
I. Definition The purpose of this standardized procedure is for the Advanced Health Practitioner to safely place a lumbar drain. II. Background Information A. Setting: The setting (inpatient vs outpatient)
DIAGNOSTIC AND THERAPEUTIC PROCEDURES
 LIFE THREATENING CRITICAL CARE The service rendered when a physician provides critical care to a critically ill or critically injured patient. For the purpose of this service, a critical illness or critical
LIFE THREATENING CRITICAL CARE The service rendered when a physician provides critical care to a critically ill or critically injured patient. For the purpose of this service, a critical illness or critical
Regions Hospital Delineation of Privileges Physician Assistant Emergency Medicine
 Regions Hospital Delineation of Privileges Physician Assistant Emergency Medicine Applicant s Name: Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting.
Regions Hospital Delineation of Privileges Physician Assistant Emergency Medicine Applicant s Name: Last First M. Instructions: Place a check-mark where indicated for each core group you are requesting.
See the Time chapter for complete instructions on how to code using time as the controlling factor when selecting an E/M code.
 2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
UNMH Family Medicine Clinical Privileges. Name: Effective Dates: From To
 All new applicants must meet the following requirements as approved by the UNMH Board of Trustees, effective April 28, 2017: Initial Privileges (initial appointment) Renewal of Privileges (reappointment)
All new applicants must meet the following requirements as approved by the UNMH Board of Trustees, effective April 28, 2017: Initial Privileges (initial appointment) Renewal of Privileges (reappointment)
To teach residents the fundamentals of patient triage and prioritization of medical care.
 EMERGENCY MEDICINE Overview Most of the Emergency Medicine Experience occurs predominantly during PGY-1 or PGY-2 Emergency Blocks. In addition, all inpatient rotations provide residents varying degrees
EMERGENCY MEDICINE Overview Most of the Emergency Medicine Experience occurs predominantly during PGY-1 or PGY-2 Emergency Blocks. In addition, all inpatient rotations provide residents varying degrees
follow-up for pneumonia
 Questions How long can I access the on demand version. Where can I ask questions after the webinar? Can the CC be used as an element of HPI? I have a co-worker who believes it cannot be used at all towards
Questions How long can I access the on demand version. Where can I ask questions after the webinar? Can the CC be used as an element of HPI? I have a co-worker who believes it cannot be used at all towards
COBAFOLIO: DOCUMENTING THE EVIDENCE OF COMPETENCE
 COBAFOLIO: DOCUMENTING THE EVIDENCE OF COMPETENCE (2006) The CoBaTrICE Collaboration: 1 st September 2006. European Society of Intensive Care Medicine (ESICM) Avenue Joseph Wybran 40, B-1070,Brussels.
COBAFOLIO: DOCUMENTING THE EVIDENCE OF COMPETENCE (2006) The CoBaTrICE Collaboration: 1 st September 2006. European Society of Intensive Care Medicine (ESICM) Avenue Joseph Wybran 40, B-1070,Brussels.
Empire BlueCross BlueShield Professional Reimbursement Policy
 Subject: Global Surgery NY Policy: 0012 Effective: 02/01/2014 05/31/2014 Coverage is subject to the terms, conditions, and limitations of an individual member s programs or products and policy criteria
Subject: Global Surgery NY Policy: 0012 Effective: 02/01/2014 05/31/2014 Coverage is subject to the terms, conditions, and limitations of an individual member s programs or products and policy criteria