Dudley Clinical Commissioning Group Long Term Strategic Plan From: Dependency, Hierarchy and Modernism To: Autonomy, Networks and Mutualism
|
|
|
- Alvin Ward
- 5 years ago
- Views:
Transcription


1 Dudley Clinical Commissioning Group Long Term Strategic Plan From: Dependency, Hierarchy and Modernism To: Autonomy, Networks and Mutualism CCG Strategic Commissioning Plan 1 P a g e
2
3 Contents Page Item 2 Background 3 Re-Imagining Healthcare 5 Arriving at and Agreeing our Vision 9 Achieving Sustainable Care In A Reductionist Economy 11 Our Underlying Principles 15 Our Key Outcome Objectives 19 A Re-Imagined Health and Care System 29 System Initiatives Impact on Providers and Partners 35 Managing Relationships and the Market 36 Next Steps Implementing the Vision 1 P a g e
4 Dudley Clinical Commissioning Group Long Term Strategic Plan From: Dependency, hierarchy and modernism To: Autonomy, Networks and Mutualism 1. Background This plan sets out where we expect the Dudley health and care system to be in five years time, the objectives we wish to fulfil and the characteristics it will display. It reflects our vision to promote health and wellbeing and to ensure high quality services for the people of Dudley. It is designed to support our overarching objective to improve the healthy life expectancy of the population. To achieve this we must:- promote good health and wellbeing; reduce inequalities in health; and commission services and interventions that help us all achieve those goals; privilege services which operate on a population basis and which are designed to support health and wellbeing particularly primary prevention services; recognise the key role of the individual person, in contributing to their personal health and wellbeing and the collective engagement of the local population in contributing to their collective health and wellbeing; so promoting recognition of autonomy for the individual alongside mutual roles and responsibilities. Overall our key aims are to improve: healthy life expectancy; health outcomes; quality and safety; and system effectiveness. We must allow variations in the delivery of services to reflect different needs and inequalities in health in our local communities. However, we must remove variations in the delivery of services to reflect different needs and inequalities in health in our local communities and we must remove variations in performance and clinical practice which adversely affect the delivery of health outcomes. In so doing, our system will be built in a way which reflects the 5 domains of: - preventing premature deaths; best quality of life for people with long term conditions; quick and successful recovery following ill health; great care experience; keeping patients safe and protected from harm. 2 P a g e
5 2. Re-Imagining Healthcare We have re-imagined healthcare in terms of:- a mutualist culture the structure of the system population health and wellbeing services health and wellbeing centres for the 21 st Century Innovation and learning and in a way which reflects the 6 key system characteristics necessary for a sustainable health and care system set out in Everyone Counts: Planning for Patients 2014/15 to 2018/19. 3 P a g e
6 Five-year Strategy Plan on a Page To promote good health and wellbeing; and ensure high quality health services for the people of Dudley From: Dependency, Hierarchy and Modernism To: Autonomy, Networks and Mutualism Objective: Effective and Efficient Care Clinicians have more time to spend with those who need it most Pathways of care (both urgent and planned) are as efficient as possible 20% efficiency gain for planned care 15% reduction in urgent care Avoidable emergency admissions reduced to 2332 per 100,000 by 2018/19 Objective: Healthy Life Expectancy Premature mortality is reduced Inequalities in Health between all population groups are reduced Health and wellbeing services are at the heart of healthcare delivery 3.5% reduction in potential years of life lost per annum to 1685/100,000 by 2018/19 Objective: Mutual approach to achieving best possible outcomes Patients can quantify the real value of the services that they receive Individuals achieve greater autonomy from healthcare All service providers network better around the needs of patients EQ 5D Score 74% of people reporting health has improved by 2018/19 Objective: High Quality Care for all Services are safe and unwarranted variations are minimal Patients are treated with care and dignity and not over-treated Our system is transparent and learns and improves with the public Eliminating avoidable hospital deaths MRSA zero tolerance Grade 4 pressure ulcers zero tolerance Reimagining: A MUTUALIST CULTURE. Creating opportunities for active citizenship in vibrant communities and a participative mechanism of engagement for all registered members. Changing the way we evaluate healthcare so that the patient can articulate the value of the services they are receiving. Promoting mutual responsibility between patient and professional to manage risk and personalise healthcare planning. Reimagining: A NEW STRUCTURE OF DELIVERY Changing the definitions of services from primary, community, mental health, social care and acute to: planned care, urgent care, reablement care and proactive care. Removing the boundaries between different professions to privilege population-based healthcare in the community with a networked primary care and registered population at the centre. Reimagining: POPULATION HEALTH AND WELLBEING. Enabling a step change in how our GPs coordinate the systematic management of long term conditions to achieve healthy life expectancy. Differentiating between: population health and wellbeing services - where continuity is key; from urgent care - where responsive access is the priority. st Reimagining: HEALTH & WELLBEING CENTRES FOR THE 21 CENTURY. Supporting the development of new centres of care across the borough to provide modern facilities in our communities. Investing in front-line staff so they have the best possible training, support and satisfaction from a job well done and by extension providing best possible care to our population. Reimagining: INNOVATION AND LEARNING. Using research to test and evaluate the key components of this strategy. Making it our business to focus on achieving efficiency and best practice in front-line care. Working better with technology: both within the health and social care eco-system as well as with individual patients. Supported by: Our 2-year Organisational Development Plan and our 2-Year Operating Plan Enabler: A mutualist based relationship with member practices and responsible local citizens developing PPGs and an autonomous registered membership. Enabler: Development of person-centred information: PSIAMS personalised patient-driven reporting on the value of care ; Risk stratification to target resources based upon individual patient risk profiling. Enabler: Commissioning for value: removing unwarranted variation in care and evaluating individual clinical performance to inform patient choice Enabler: Commissioning-led populationbased information systems and integrated IT that enable health and wellbeing services; mobilise front-line staff; support market shaping and market entry; and reduced cost to providers Enabler: Our Primary Care Strategy and Estates Strategy with Co-Commissioning of Primary Care with NHS England. Enabler: Joint governance, performance and commissioning frameworks with all partners. Better Care Fund with Dudley MBC. Memorandum of Understanding with the Office of Public Health. Enabler: Network leadership, training, evaluation and research programmes 4 P a g e
7 3. Arriving At and Agreeing Our Vision a) Agreement and Governance Our re-imagined system has been designed and based upon our analysis of the challenges our system faces. These are described further below. This is a Dudley system plan arrived at by working with our partners. Our 2 year operational plan, our Better Care Fund Plan, the associated metrics and outcome targets were approved by the Dudley Health and Wellbeing Board, in the context of Dudley s Joint Strategic Needs Assessment (JSNA) and Joint Health and Wellbeing Strategy (JHWS), on 26 th March This strategic plan was subsequently approved by the Health and Wellbeing Board on 17 th June The Health and Wellbeing Board has ultimate responsibility for holding the system to account for the delivery of this plan. The plan complements and is consistent with the Joint Health and Wellbeing Strategy, the CCG s Operational Plan, the Better Care Fund Plan and the Operational Capacity and Resilience Plan all of which have been reported to the Health and Wellbeing Board. The Board will be responsible for overseeing a series of performance metrics which underpin these complementary plans from a system perspective. In this context, there are two key issues which partners face across the NHS and local government delivering an effective urgent care system and integrating services in such a way as to deliver the objectives of the Better Care Fund. Our system wide governance arrangements reflect this. Our Urgent Care Working Group and our Integrated Services Working Group both report to the Health and Social Care Leadership Group/System Resilience Group which consists of chief executive/director representatives from the NHS, local government and the voluntary sector. This in turn reports to the Health and Wellbeing Board on key aspects of system wide performance which includes delivery of:- Joint Health and Wellbeing Strategy priorities; this plan; the Better Care Fund plan; urgent care system performance. We anticipate receiving refreshed planning guidance from NHS England in late 2014 and we will refresh all our plans for approval by the Health and Wellbeing Board as necessary, including this Strategic Plan. H AND WELLBEING BOARD HEALTH AND SOCIAL CARE 5 P a g e
8 Health and Wellbeing Board Health and Social Care LEADERSHIP GROUP INTEGRATED SERVICES WORKING GROUP URGENT CARE WORKING GROUP 6 P a g e
9 Our Strategy reflects our system values and principles:- aiming for the provision of innovative, integrated, localised and personalised services that give excellent value for money; focusing services on prevention and early detection and recognising the need for people to take responsibility for their own health and wellbeing; recognising the potential for individuals and communities to maintain and sustain health and wellbeing and the contribution they can make to shaping services; tackling health inequalities through the concept of proportionate universalism ; working in partnership to improve health and wellbeing; continued improvement in the quality and safety of our services; safeguarding children, young people and adults. The analysis set out below provides the basis for our re-imagined system. Much of the detail is contained within our operational and organisational development plans. b) Challenges There are a number of significant challenges in terms of the system, the financial environment, performance and health status. These are described in our operational plan (pp. 8 13). i) The system The key system challenges are:- growing demand from an ageing population; sustainability of our main provider Dudley Group NHS FT and our local authority; inflexibility of local organisations and unresponsive service provision; cultural changes required to secure the engagement of clinicians and deliver our integrated service model. ii) Financial The key financial challenges are:- delivering a redesigned urgent care system and an integrated service delivery model capable of reducing demand on hospital services; delivering the efficiencies required to achieve a balanced Better Care Fund Plan; the long term sustainability of the health and social care economy. In terms of long term sustainability, our analysis of all existing financial plans indicates that, to varying degrees, all our NHS partners face significant challenges in delivering a sustainable long term financial plan. Continuing with a situation where one, or all, of our 7 P a g e
10 main providers cannot demonstrate that they have a sustainable solution puts services and patient outcomes at risk. Given this set of circumstances, we assume it will be necessary to restructure our providers to contribute significant efficiency improvements to the local system, unless alternative solutions are available. We have asked all our main NHS providers to enter into an open and transparent process to assess their long term financial plans. WE have requested sight of these plans and the expected impact that any further improvements or collaboration might deliver. These submissions will be evaluated and a specific meeting convened to discuss the options for the future. iii) Provider Performance Specific performance challenges remain in relation to:- ED 4 hour wait; referral to treatment times for elective care; waiting times for some community services Our operational plan sets out the specific initiatives we will put in place to address these challenges. iv) Health Status and Health Inequalities We have examined the JSNA, Commissioning for Prevention, CSU QIPP Opportunities Pack, the Commissioning for Value Pack and the CCG Outcome Indicators Framework. These show that:- we have specific health inequalities for the male population both in terms of mortality rates in the year age band and alcohol specific problems for the year age band; this is contributing to a widening of the life expectancy gap between the most and least deprived parts of our population; we need to ensure our locality based service delivery model (see below) provides an appropriate, differential intervention at neighbourhood level to respond to local health inequalities; interventions in relation to cancer, heart disease, stroke, liver disease and stroke are required. We must ensure that our practices perform well in delivering smoking cessation services; the systematic management of patients with long term conditions in primary care and community health services will be a major contributor to our success, including the management of diabetes; we need to make every contact count in primary care and other settings; we have a growing frail elderly population, we need to improve the care pathway to prevent unnecessary admissions and create the conditions to enable people to be re-abled and retain their independence in their 8 P a g e
11 communities; we require a continued focus on mental health, in the context of achieving parity of esteem, as well as the relationship between mental health, physical health and the management of long term conditions; we need to ensure that our approach to prescribing and the input of our practice based pharmacists continues to improve our performance in relation to the use of drugs to reduce cholesterol, reduce blood pressure and manage atrial fibrillation; we need to ensure that our work on the systematic management of long term conditions, redesigning urgent and planned care pathways and integrating services in our localities is sensitive to the needs of our child population; as part of our approach to the Equality Delivery Scheme, we need to facilitate work with those groups protected by legislation where the difference in health outcome and need is greatest, as well as analyse the barriers to improved patient access and experience for these groups. This will be reflected in our Equality Objectives; we need to use an asset based approach to our work with partners in addressing the wider determinants of health. c) Community and Clinician Engagement Our re-imagined system has been formed by engaging with:- our healthcare forum our network of patient participation groups the Health and Wellbeing Board and our JHWS our GP membership stakeholders through the Call to Action process This engagement has informed, in particular, our plans for:- a simplified emergency and urgent care system improved access to primary care integrated community health and social care services more support to enable patients to manage health problems, including long term conditions 4. Achieving Sustainable Care in a Reductionist Economy Our NHS is at a tipping point. The NHS cannot continue to deliver healthcare using the same organising principles as it has done in the past. Rising demands from the growing elderly population, patients with increased co-morbidities, an increased range of therapies, rising costs of all treatment modalities, and limited economic resources create big challenges we must address. However, these challenges are not insurmountable. The greater challenge is whether we can re-imagine how we work and adapt to delivering healthcare in a networked society. 9 P a g e
12 Our NHS organisations have been established within a modernist paradigm, working with imposed reductionist efficiency, performance targets and operating in organisational and professional silos which are insufficient to respond to these big challenges. This undermines the ability to deliver better outcomes for our population and contributes to risk averse practices, creating dependency and overmedicalisation of care. Our structures, business models, service provision and organisational cultures need to be radically re-assessed in light of the social, technological, environmental and economic challenges we face. In current thinking, hospitals are conceptualized and invested in as the central delivery point of healthcare; healthcare is delivered as a supply-led process: patients fit into the system - it is not demand-led, i.e. designed around individual patient contexts and needs. Healthcare economics attempt to measure and cost episodes of care, thereby turning patients into diagnostic categories and numbers. This is false accounting as it doesn t account for externalities, i.e. the unseen costs of the holistic social and health care required by a patient who increasingly presents with complex healthcare needs. In addition, there is a dependency and conformist mindset which risks diminishing human compassion, creativity and innovation. Instead we conceptualize Community Hubs (10 15 locations across 5 localities) of healthcare as the central delivery point of health and well-being; GPs as generalists are highly regarded within the healthcare system, and hold commissioning power; registered members of GP practices (their patients) are members of the mutualist healthcare community and as members contribute fully to healthcare decisions within their locality. Autonomy is a principle that ensures registered members have maximum control over their lives; and healthcare economics are holistic and systemic, accounting for real costs of care, including external costs and taking longer-term perspectives. Finally our workforce is encouraged to be collaborative, transparent and develop an adaptive culture, that is more human in its response, and always thinks about patients in their context. We will mitigate the risks associated with this approach in a number of ways:- reviewing, as part of our proposed co-commissioning arrangements, all contracts for primary medical services and moving our practices onto a single contract negotiated locally; resources released as a result of this process being reinvested to support our community hubs; ensuring we exploit the opportunities generated by a single IT system across primary care in terms of protocol development and payment systems to build primary care at scale. So our strategy endeavours to reassess these factors, proposing a new vision for health and wellbeing services. This strategy starts with the patient perspective, in the context of a networked community. It will recognise the importance of clinical leadership and the pivotal role of general practice. Reimagining the organisation and 10 P a g e
13 culture of services to enable sustained health and wellbeing for everyone is our challenge. 5. Our Underlying Principles We operate to six key principles: a) Patient and Public Involvement The meaningful involvement of patients and public is of paramount importance. Throughout the NHS the patient is usually the coordinator of their care. It is key to our approach that contact with healthcare professionals adds clinical value. We believe this contact must be re-aligned, from a hierarchical dialogue expert to receptive patient, to a horizontal dialogue expert to expert. Patients/families are most knowledgeable about their symptoms, bodies and psychological and social state. This self- expertise remains an under-tapped resource that if accessed will transform healthcare and well-being. Supporting autonomous living is of paramount importance. However when people do use healthcare we want them to have clearer information about the quality of services in order to inform their choices; and we want them to be better able to share whether services are working for them. We have a number of engagement channels which encourage patients and the public to be actively involved in the decision making process on how their health care services are planned, developed and delivered, these include:- a thriving network of Patient Participation Groups. These groups provide a patient voice on the provision of primary care but also a resource which we use to shape wider discussions on commissioning intentions and other health and social care related issues. Our aim is to develop a locality and borough wide structure, mirroring our GP membership structure, which enables our PPGs to network and share best practice, communicate with each other more effectively and have a stronger voice at board level; our Patient Opportunities Panel (POP) membership is drawn from PPGs across the borough. The purpose of the POP is to give patient representatives a direct influence on the strategic commissioning process; our Health Care Forum (HCF) a less formal public meeting held quarterly with an emphasis on information sharing about health care developments and appropriate access to healthcare services. Our vision to develop more integrated services is also reflected in the joint work on involvement we carry out with our local authority and other partner organisations, which includes:- Building Healthy Partnerships a funded piece of work bringing together the NHS, local authority and voluntary sector to promote joined up working to empower local people to make healthy lifestyle choices, support them in making informed choices about health and social care. Specific projects 11 P a g e
14 include the development of a Community Information Directory, which will provide a single point of access for information on a wide range of health and social care services; in partnership with the local authority, public health and third sector we also hold quarterly Community Engagement Network (CEN) events focusing on engagement techniques and approaches. We will continue to gather, and act on, patient feedback from a wide variety of sources. This includes data collected from online feedback channels, social media and provider complaints, as well as our own channels including:- service specific consultations; specific pieces of work such as our vox pop Feet on the Street videos which are screened to public Board meetings and other committees; our Patient Participation Groups, Patient Opportunities Panel and Health Care Forum; announced and unannounced visits to providers by the patient experience team; feedback from GP forums including locality and borough wide members meetings. We will use the PSIAMS system of personal and social impact action measurement to understand the impact of our commissioning interventions as part of our approach to commission for value. b) Clinically Led The public register with their GP and through the coordination that their GP provides, that they are able to best access the healthcare they need. So our future health system will be organised around this key relationship between patient and their GP; providing a personalised service. Similarly, all population-based healthcare will be commissioned on a registered-population basis and will be organised in accordance with our GP and CCG structures (so around practices, localities and borough-wide) in order to enable a clear clinically-led approach to healthcare delivery. c) Primary care at our heart The vast majority of care is either delivered by General Practice or is accessed through it. The success of primary care is therefore central to the future success of our health services locally. We have already developed a primary care strategy, in conjunction with the Health and Wellbeing Board and NHS England. There are significant recruitment and retention challenges for our primary care services so development of primary care infrastructure and workforce will be central components 12 P a g e
15 to our on-going work we want Dudley to have a national reputation as the best place to work for GPs along with their extended primary care and community staff. We will further enhance our shared commissioning of primary care with NHS England in order to ensure that this can be achieved. d) Working with Partners in our Communities Our locality-based approach to the Better Care Fund initiative recognises the need to network our GPs, patients and associated primary care/community services, social care and the voluntary sector in order to respond to the variable needs of different communities across our population. Health inequalities can only be addressed through a jointly targeted community-based approach. We will build our partnership relationships through the organisation of all of our services for all of our populations based on clinical need. e) Focus on Quality and Continuous Improvement We will take a predominantly developmental approach to quality improvement that encourages transparency by all our service providers to reduce variations in care and outcomes; and to aim for best practice performance. We will expect every service to be able to demonstrate the value and quality that it provides to patients. We will utilise a continuous evaluation process that will ultimately ensure that we do not commission any service that cannot demonstrate value; and will actively promote those that can demonstrate best outcomes for patients. f) Live Within Available Resources Dudley CCG will meet its financial responsibilities to address the reasonable needs of our population within available resources. This necessitates a drive for continuous efficiency and improvement given the economic constraints we face. Our emphasis will always be to maximise the effectiveness and availability of front-line services. It is against these principles that we test out each commissioning initiative. Our analysis of two key initiatives urgent care and services integration is set out below:- 13 P a g e
16 Principle Urgent Care Model Service Integration Patient and Public Involvement Clinically Led Primary Care at Our Heart Working with Partners in Our Communities Focus on Quality and Continuous Improvement Informed by patient and public engagement via Healthcare Forum and other mechanisms The prime point of contact for registered patients, in the first instance, should be their general practice. Through our cocommissioning arrangements we will work with our membership to increase access to primary care for registered patients and ensure that unregistered patients are given the opportunity to register. A better service model, enabling GPs and other clinicians to use their skills to manage urgent care better within a supportive system will enhance the workforce and attract staff to Dudley. Being able to access care appropriately is a key mechanism for responding to health need. Variability of access leads to health inequality. Our urgent care model is designed to facilitate access, whilst ensuring that other community based responses to urgent care situations are available. We will develop clear clinical protocols that provide a consistent response to those patients accessing the system Informed by patient and public engagement via Healthcare Forum and other mechanisms A common population base is the pre-requisite for this model. Services will be organised at practice, locality and borough levels led by clinicians. Enhancing clinical leadership and giving clear responsibility to deliver effective services for their registered patients will be a key factor in building an enhanced workforce and attracting staff to Dudley. Our service model will provide a targeted response to health need and health inequality. A voluntary sector link worker in each locality will ensure that services are connected to voluntary and community sector services and opportunities to enhance capacity identified for action. We will have clear indicators in place for all our integrated teams at each population level, linked to the Better Care Fund metrics. These will 14 P a g e
17 Live Within Available Resources Our urgent care service will ensure appropriate access to urgent care, avoid unnecessary use of ED and deliver an economic benefit. be used to drive up performance and reduce unnecessary variation. Our integrated services model is designed to remove unnecessary admissions to secondary care and nursing/residential care, as well as facilitating early discharge and reducing the dependency of individuals. This will deliver a clear economic benefit to the system. 6. Our Key Outcome Objectives Our key outcome objectives are derived from the findings in our Joint Strategic Needs Assessment and designed to meet the needs of our population. These objectives include parameters that we can currently measure; however we will also be designing new measures which in the future will more accurately reflect the new structure and design of services that we are trying to create. Our operational plan (pp14 18) and Appendix 1 to this plan sets out our outcome ambitions, their relationship to the JSNA and our initiatives to respond to them. a) Effective and Efficient Care Our health and social care system must be as efficient, effective and adaptive as possible in order to meet the rising needs of our population within our more challenging economic constraints. Therefore our emphasis will be to maximise the benefit and potential of front-line interactions by our clinicians with our patients; and to avoid unnecessary interventions wherever possible. Existing measures in place include:- 15 P a g e
18 reducing time spent avoidably in hospital - 2,322 avoidable admissions per 100,000 by 2018/ Emergency admissions composite indicator Emergency admissions composite indicator 2250 Baseline 2014/ / / / /19 increasing proportion of older people living at home: People still at home 91 days after discharge 230 as at 2018/19 We will identify the most efficient pathway for each intervention and de-commission pathways that do not meet this standard Future measures will evaluate:- ensuring clinicians have more time to spend with those who need it most pathways of care (both urgent and planned care services) are as efficient as possible with minimal variations in performance between clinicians b) Healthy Life Expectancy Our overarching objective is to improve the healthy life expectancy of the population we serve. Existing measures that we use to evaluate this include:- securing a 3.5% reduction per annum in avoidable years of life lost for people with treatable conditions to 1685/100,000 in 2018/19 16 P a g e
19 improving quality of life for people with Long-term conditions - 74% of people report their health status has improved in 2018/19 to bring the CCG up to the performance of comparator CCGs Future measures will include:- delivering improvement to reduce the inequalities in health between different groups thus ensuring parity of esteem for all vulnerable groups; ensuring Health and wellbeing services are at the heart of healthcare delivery. c) Mutual Approach to Achieving Best Possible Outcomes Improvements needs to be measured and understood both from a clinical outcome perspective but also from the value that is derived and perceived by the patients receiving care. Also outcome objectives need to be shared in advance between the individual and the service. 17 P a g e
20 Existing measures in place include a variety of patient related outcome measures for certain treatments and somewhat limited patient experience measures:- increasing people's positive experience of hospital care: average number of negative responses per 100 patients reduced to 145 by 2018/19 to bring the CCG up to the performance of comparator CCGs increasing number of people with positive experience of care in general practice and the community: Average number of negative responses reduced to 5/100 patients by 2018/19 to bring the CCG up to the performance of comparator CCGs However in the future we will develop measures which place the emphasis on patient-led outcome objectives to:- enable patients to quantify the real value of the services that they receive; ensure our PSIAMs system of personalised patient driven reporting is in place for all commissioned services. demonstrate how individuals achieve greater autonomy from healthcare; demonstrate how all service providers network better around the needs of patients. 18 P a g e
21 d) High Quality Care For All The public expect the NHS to deliver safe and effective services. We already have a wide range of quality improvement measures and CQUIN arrangements which cover mortality indices, reducing rates of infection, safeguarding children and adults from harm, and evaluating and learning from serious incidents. As we progress with the delivery of this strategy we will develop measures to ensure that:- services are safe and unwarranted variations are minimal patients are treated with care and dignity and not over-treated our system is transparent and learns and improves with the public 7. A Re-Imagined Health and Care System a) Re-Imagining Healthcare a Mutualist Culture (Citizen participation and empowerment) The NHS constitution sets out rights for the individual in respect of healthcare which Dudley CCG supports and we will ensure these are delivered for our population. However, rights alone are insufficient. They promote a consumerist attitude to healthcare and also a top-down culture whereby those in power give rights to the recipients of care. This is unsustainable and undesirable in an economically constrained system. It fails to recognise the importance of mutual engagement which balances rights alongside responsibilities. Individuals are then expected to use resources responsibly and to recognise that they are part of a community, and the community is part of them. Individuals must take responsibility, as much as is possible, for managing their own health and wellbeing. Our philosophy is to support individuals to do this and so reduce their demands on healthcare. We will therefore invest in activities that encourage adoption to this way of thinking and which provide proactive intervention and advice to the population. We will also foster health as a community responsibility by supporting integration with the voluntary sector; facilitating active community engagement between NHS services, public health and voluntary/community sector services. In addition, we will change the basis of future engagement from the representative mechanism of the willing, to a participative mechanism for all. This will involve the development of information tools that enable every person receiving healthcare to articulate the benefits (or otherwise) of the care that they receive and the personal impact that it has had for them (One such mechanism currently being piloted through 19 P a g e
22 our Building Healthy Partnerships Programme is the PSIAMS tool (see Operational Plan pp. 25 and 26). We will then be able to use actual patient feedback to evaluate the effectiveness of services as determined by the patients themselves. Ensuring that every person is an engaged and registered member of our CCG is also an important way in which we will address inequalities in health and parity of esteem for all vulnerable groups including the homeless, ethnic groups, disabled people, new migrants and arrivals to the borough - and is central to our approach to equality, diversity and inclusion. Priority of action will be given to ensuring reliable data in primary care to identify groups with worse outcomes; and we will design new services to ensure improved access (so for example our new urgent care centre will include mechanisms for registering anyone who attends, who is not already registered with a GP). Our CCG is a membership organisation and is ultimately funded to support those people who register with our GPs. We have started our membership engagement through the development of our patient participation groups linked to each of our practices; and we will continue to strengthen this as a key means of engagement. However in five years we will have developed an active membership programme for all those people registered with our GPs. This will incorporate a patient portal providing health and wellbeing advice enabling access to their records; and clear mechanisms for support and access to healthcare through their GP. Opportunities for giving feedback and participating in shaping and informing the development of their local healthcare services will be integral. We currently have a way of working where increasingly components of our healthcare service work on a protocol driven model of care. This is positive in creating minimum and consistent standards but it also leads to reduced individual clinical judgement and a risk averse approach which ultimately results in too many people being referred on to more intensive services and contributes to rising patient dependency. Instead we will actively promote a new way of working which encourages mutual responsibility between patient and professional; and supports increased personalised care which enables individuals to have a greater say in managing risk and the outcomes that they want to achieve. This approach will reduce dependency and over-medicalisation of patients. This mutualist approach will create a more engaged relationship with our registered population where they have a clear share in how services are shaped and developed; as well as a more personalised service which encourages more autonomous self-management. Most importantly our members will know, value and understand the benefits of being a member of our CCG. 20 P a g e
23 b) Re-Imagining Healthcare the Structure of the System (Access to highest quality urgent and emergency care) (A step change in productivity of elective care) The traditional organisational structures of healthcare are inadequate to meet the conflicting challenge of rising demand versus reducing resources. The existing separation of services into primary care, community services, mental health services and acute services is artificial, contributes to silo working and doesn t reflect the needs of the modern population. We have already started to rethink the organisation of care into four different groupings: - planned care: value-added treatment interventions with defined outcomes; - urgent care: short-term interventions to help and treat you in a crisis; - reablement care: services designed to help reduce your dependency; - proactive care: population-based care to help you manage your health needs. Commissioning healthcare on this basis enables us to set common performance improvement requirements for each of these groups of services and brings consistency for mental health patients as well as other vulnerable groups. Parity of esteem for all groups is a theme throughout our organisation and our providers. In planned care we will be commissioning based on measureable value-based outcomes of the services provided. We will have systems in place to monitor and report on variations in individual clinical performance with the aim of improving both the whole pathway efficiency of services (left-shifting the distribution curve), as well as the outcomes of treatment. Ultimately, we will set prices for planned care on the basis of best practice performance (on effectiveness of outcomes and total pathway efficiency) and will expect providers to adhere to those performance standards. We will expect our service providers to have dedicated facilities and capacity for planned care, without risk of significant interruption from urgent care, so that both clinicians and patients can provide and experience a high quality, efficient and effective service. 21 P a g e

24 With urgent care we will have established our new urgent care centre at Russell s Hall Hospital and we will implement new pathways of care for both our frail elderly population and also for mental health care, so that A&E is not part of the pathway, but instead enables patients to go direct to the most appropriate service. We will commission emergency medical care as an extension and integral part of population-based health and wellbeing services. This will then create a paradigm- shift in the organisation of care for our frail elderly population: instead of urgent treatment being managed within the confines of the hospital; services will instead be managed between the home and the hospital. This will both enable more patients to stay at home as well as enable clinicians to better co-ordinate capacity between community and hospital care. Similarly A&E will therefore be available solely to provide genuine accident and emergency care particularly trauma and emergency surgery. Our reablement services will form part of our extended partnership with social services and the voluntary sector. We will be commissioning services specifically to reduce dependency and enable individuals to return or stay at home wherever possible. This directly correlates to the national Better Care Fund objectives of reducing the future need for residential and nursing care. Also, we will engage with the public about expectations on healthcare to ensure that patients, carers and families support the need for people to move quickly to as low a dependency setting as possible, recognising that hospitals should only be used for short-term treatment interventions that make a difference. Our integration model works on five local communities and is designed to deliver our approach to proactive care. This organises services based around the needs of the person and integrates community services, mental health services and social services around our general practices so that all services are working with the same groups of patients. This enables both personalised care, as well as firmly basing the team that supports them within the local community of healthcare. This emphasises a network approach to health and social care delivery. Our partnership with Dudley MBC and with the local VCSE through our Building Healthy Partnerships programme is essential to securing a sustainable and integrated service. 22 P a g e
25 We will commission services that are available 7 days per week. The developments we are already implementing in relation to our integrated service delivery model will be available on this basis. Over the next five years we will develop our integration model into comprehensive, population based, health and well-being services. This will include the management of all long-term conditions and emergency medical care for the frail elderly. c) Re-Imagining Healthcare Population Health and Wellbeing Services (A modern model of integrated care) Within the next five years will re-commission pro-active population-based healthcare services via a different model. We need a step change in how primary care systematically manages long term conditions to deliver healthy life expectancy: so we will bring together all populationbased care into one set of integrated services based upon the populations registered with general practice. GPs are at the heart of this model, as the key co-ordinators of care; and this recognises the dual roles of providing: on-going health and wellbeing care support which can be planned over time; as well as the need for more urgent access in times of illness or crisis. We will therefore commission these two types of activity separately:- - for health and wellbeing care patients prefer continuity of clinician/professional; - for urgent care, speed and ease of access is important. In addition we will differentiate between different levels of intensity of service. For example:- - proactive care is about supporting people to remain healthy and is linked to the Dudley Office of Public Health and Dudley MBC programmes for prevention; - long-term care support to those living with long-term conditions would include a mix of longer, pre-bookable appointments with GPs and/or specialists; - enhanced and end of life care (including community care in the home, or nursing / residential care) will be improved through the use of risk stratification, partnership with social care and the voluntary sector; - we will engage in a broader discussion with the public about how best to support people at home near the end of their lives. Should so many treatments that overmedicalise care be carried out? We will be having discussions with our population, our patients and their families to ensure they have the support they need to manage their circumstances, whatever they may be, with dignity and compassion 23 P a g e
 and support Long-term Care Helping individuals to manage living with their long-term condition(s)")
26 level of intensity of support high low Population Health and Wellbeing Services Health and Wellbeing Care Urgent Care Starts with universal Advice on how to services for children. Proactive Care Self-management manage minor Includes wellbeing advice ailments (NHS 111) and support Long-term Care Helping individuals to manage living with their long-term condition(s) Pharmaceutical support Medication and advice from your pharmacist Enhanced Care End of Life Care Care and support when you need it most. Community Rapid Response to the home For the frail elderly and those with complex conditions Note: there is an assumption in this table that end of life demands high support- whereas our aim is to return the care to the community- diminishing professional support 24 P a g e
27 Health and Wellbeing Care will be personalised to the individual. For many individuals they are the main co-ordinator of their care for 99% of the time so the level of intervention and NHS support will be minimal; will be designed to enhance the individual s self-management; and can be provided on a planned basis particularly proactive care and long-term care. Enhanced Care will include some enhanced support that would be provided on an on-going 7-day basis depending on the needs of the individual (eg: community nursing support into the home; or 7-day nursing or residential care). Similarly End of Life Care will include access to significant support on a 7-day basis if and when it is necessary. Urgent Care within this model will be provided on a 7-day basis. In these circumstances, expediency of access to an appropriately qualified individual, based on an assessment of your need, is more important than continuity of care. Therefore GP services in particular can only be provided once primary care is organised at scale across localities. However the lack of continuity of individual clinician can be mitigated through continuity of information by our establishment of a single GP IT system which allows access to complete medical records. These plans can be achieved through commissioning the services at scale; and by improved integrated commissioning with NHS England (as the organisation that procures GP services) - so we will pilot this approach with NHS England for co- commissioning this model of service. This will bring together their contracting of primary care with our contracting of community care. This will enable an integrated model of delivery, supporting the national Better Care Fund initiative; will remove traditional boundaries between services by bringing together all population-based care into one set of integrated services based upon the general practice registered patients; and will establish shared outcome measures for improved population health and wellbeing. Our shared intention with NHS England will be to achieve a stepped change in how primary care systematically manages long-term conditions to deliver healthy life expectancy. This will enable us to significantly refocus large proportions of care and support into the community, based around general practice; and will enable us to establish more comprehensive and fully integrated outcome objectives to understand the needs of those living with long-term conditions and reflect them in our priorities. 25 P a g e
28 d) Re-Imagining Healthcare Health and Wellbeing Centres for the 21st Century (Wider primary care, provided at scale) In Dudley we are fortunate to have modern hospital facilities that can provide excellent care for our population when they need it. However, the quality of primary and community care facilities is much more variable and much of it does not meet the needs of our population. High quality facilities are key to allow us to make the quantum leap in terms of care for our communities. In addition we have a workforce that is often under pressure and there are increasingly shortages (nationally) of staff in key groups. For example, a significant proportion of our GPs are expected to retire in the next 5 years so we need to recruit new GPs in to work in Dudley. During the next five years we will put in place an innovative development programme for the healthcare estate in Dudley. We will encourage existing practices to come together to both make full use of the existing high quality facilities as well as develop new larger centres. These new centres will provide the focal point for our approach to delivering health and wellbeing services and so will have the capacity to provided specialist clinics (eg: for long-term conditions) as well as extended general practice. This will bring longer-term population-based healthcare out into the community as part of our locally integrated services. We will be actively encouraging independent developers to work with us to access the capital required for this development programme; and we will be working with NHS England to put in place the necessary agreements on pooling CCG and NHS England resources in order to develop the financial arrangements to provide the revenue support needed. We want Dudley to be the place where people want to come and work because they will get the best possible training, support and satisfaction from a job well done; by extension, our population will get the best possible care. So investing in our workforce is mission critical. We will therefore expand our current education and training programme to put in place comprehensive training and support for all the staff groups that are part of these new health and wellbeing services. We have inherited a system from our predecessor organisations which has allowed significant variation (over 100% variation) in the levels of investment in primary care between practices; and in the organisation of community services across the borough. We will implement a new quality performance framework that correlates financial investment with outcome performance in order to incentivise high performance - but paid for at the right price. In addition, we intend to free-up our front-line staff across primary and community services, to both maximise their opportunities for work with patients and achieve 26 P a g e
29 better outcomes. To achieve this we will invest in systems design and integrated services at scale, to both centralise support functions and improve technological support to maximise front-line capacity and efficiency. e) Re-Imagining Healthcare Innovation and Learning We are a learning organisation and as such we highly value, and are investing in, research and organisational development. We have established links with the HSMC at Birmingham University to develop our evaluation and review of services; and we have developed a substantial organisational development programme for both the CCG and our healthcare system. We will also use research to explore and evaluate some of the key concepts and ideas in our strategic plan to ensure that we accelerate our progress - so developing the best possible services for our population. Funding will be made available to support innovation at both practice and locality level. This resource, a total of 200,000 on a non-recurrent basis, will be allocated to our five localities and they will determine how it is used. In conjunction with the HSMC, we will develop a consistent mechanism for the evaluation of our development programme and use this to inform future commissioning decisions. This will be complemented by a new research assistant post to enhance our research and development capacity and capability. We will seek to embed the principles of invention, adoption and diffusion. Innovation, in terms of:- the development of our community rapid response service; measuring individual consultant performance; having one IT system for all 49 GP practices; using the PSIAMS system to understand commissioning impact; providing practices with the opportunity to innovate with our innovation fund. lies at the heart of our plan In our first year we will make significant steps to improved working with technology as all our GPs will be using the same clinical IT system. This will not only enable integrated working between practices but will also enable access to other services (such as A&E) and so significantly improve the quality and safety of care to all of our population. Subsequently, we will commission for a comprehensive information system, which incorporates GP IT, to provide the infrastructure and system support for all services that are part of our integration model. We will then require all providers that 27 P a g e
30 contribute to the integrated model, to use this information system thus establishing a comprehensive population-based information database which underpins our population-based health and wellbeing services. We will only commission from service providers who commit to using this system and database and this system will very clearly incorporate rules on data sharing so that only the right people have the right access at the right time. This approach to commissioning-led information will also significantly improve provider efficiency and effectiveness; reduce barriers to market entry; and improve contractual efficiency with our CCG. So for example: all the required performance reporting, invoicing and validation processes will be co-ordinated centrally and derived from the directly inputted patient/clinician activity. Payments will be automatically made by the CCG to providers in accordance with the agreed contract so all associated back-office functions for both primary and community providers will no longer be necessary. Smaller organisations, including new social enterprises and VCSE organisations will more easily be able to participate in our health and social care economy because they will not need to invest in these costs, which can often be prohibitively expensive for smaller organisations. A key strategic objective is to improve system effectiveness. This means making it our business to focus on achieving efficiency and best practice in front-line care: Firstly, enabling providers to improve back-office efficiency and reduce overheads in order to focus on front-line care. The development of commissioning-led information systems is a key component of this approach. Secondly, ensuring that we maximise the efficiency and opportunity of our front-line staff. We will invest in IT designed for a specific purpose: to develop systems to benefit clinical effectiveness efficiency and safety. We will also invest in mobile technology for all primary and community services Thirdly, reducing variations in practice in order to eradicate inefficiencies. We will benchmark variation by individual clinician and clinical team. We will use centralised risk stratification and population utilisation analytics to identify vulnerable patients and at risk groups who aren t receiving the care they need and would benefit from targeted support. Fourthly, supporting patients in maximising their autonomy. We will empower our population by investing in publicity and advice; recognise that the individual s identification with community is manifest through a multitude of different networks; we will invest in voluntary sector support and learn from their connections and identity with communities; and we will embrace new technologies which enable remote or self-monitoring of health conditions. 28 P a g e
31 Our population-based design to future healthcare delivery will make it easier for other GPs to join our CCG in the future. We will develop an induction process to support new practices to join our CCG which will include GP IT integration: a practice development and mentorship programme: our approach to mutualist healthcare and registered membership; and the integration of community and social care services around the practice. We also believe that we have a responsibility with the wider NHS to share our good practice and also learn from others. So we will work with other CCGs to establish an Organisational Development and Learning network to exchange ideas and learning. We will also develop a franchise approach to our population health and wellbeing model of delivery, linked to registered membership. This will enable other CCGs, with endorsement from NHS England to utilise and apply our new model of care with their groups of practices. This will therefore enable a rapid roll-out of our model to other areas of the NHS, should they want our help and support. 8. System Initiatives Our operational plan (pp.24 45) sets out the key initiatives we will implement during in relation to the 6 key system characteristics of:- citizen participation and empowerment wider primary care, provided at scale a modern model of integrated care access to highest quality urgent and emergency care a step change in the productivity of elective care specialised services concentrated in centres of excellence The next step is to build on these initiatives to create our re-imagined system that is consistent with these 6 characteristics. This requires the implementation of some key system enablers:- a) Co - Commissioning Primary Care We will review existing contractual arrangements with our member practices, establishing a clear set of financial rules. As a result of this we will work with practices to reconfigure the primary care landscape, create more efficient provider models and release revenue streams for reinvestment in our system of primary care at scale. b) Developing the Estate We will review our existing infrastructure and agree a development plan that will support our vision of modern health and wellbeing centres. We will support the revenue consequences of the development programme through reinvesting resources released from our reconfiguration of primary care. 29 P a g e
32 c) Exploiting Information Technology The implementation of a single IT system for primary care and the development of a commissioner led information system to be used consistently by our commissioned providers will provide the basis for delivering service efficiencies by:- removing unnecessary transaction costs systematising the way in which care is delivered, removing unnecessary variation delivering better quality emergency and urgent care through the use of a single IT platform improving productivity d) Encouraging Market Entry We will create more responsive community health services geared towards our view of population health and wellbeing. These services will be consistent with our model of integrated delivery at borough, locality and practice level. We will extend our existing delivery model through the further transfer of services from secondary care into the community such that the prime point of access to consultant level services takes place outside the hospital setting. These actions will support:- wider primary care provided at scale through revitalised general practice, delivered from first class premises using modern technology, integrated with other services around the patient and delivering consistent services. a modern model of integrated care with the patient and primary care at its heart as part of a mutual culture. Where services operate at practice, locality and borough level, using the hospital as the delivery point of last resort and enhance the health and wellbeing of the population served. access to the highest quality urgent and emergency care through integrated community services and a modern urgent care centre. 9. Impact on Providers and Partners Our plan impacts on providers in two ways:- in terms of the assumptions we have made about commissioned levels of activity and the associated impact on income; our view of the shape of future health and care delivery. 30 P a g e
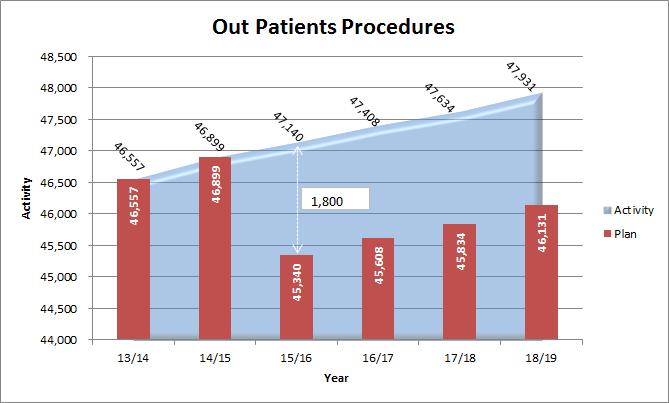
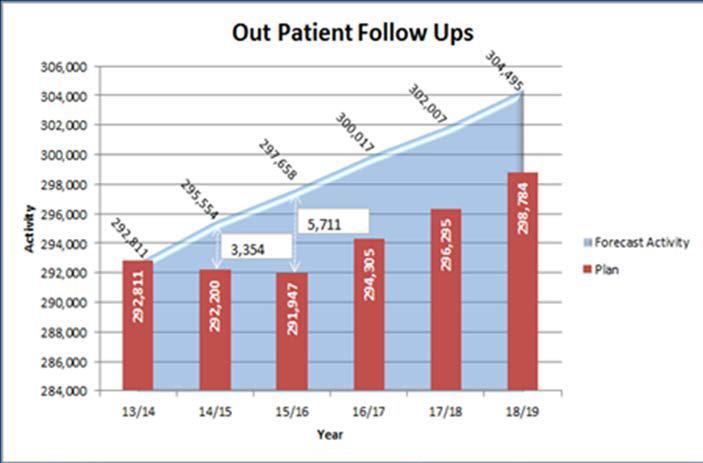
33 a) Future commissioned activity Our operational plan (pp.36 42) and the graphs below show that by 2018/19 activity levels, having accounted for demographic growth, will have reduced as follows:- emergency admissions 1574 admissions ED 24,145 attendances elective inpatients 800 cases day cases 3,665 cases out - patient first appointments 1,686 attendances 31 P a g e

34 32 P a g e

35 33 P a g e
36 These changes will have a prime impact on our main provider of acute and community health services Dudley Group NHS FT. To be sustainable this requires the implementation of a significant cost reduction programme to bring income and expenditure into balance by 2015/16 in the first instance and through to 2018/19. b) Future shape of health and care delivery Our re-imagined health and care system is based upon:- a renewed role for general practice at its heart; the integration of community health, mental health and social care services led by general practice; the market entry of new providers of community health, including mental health services; the movement of more services from hospital settings into the community supported by a refreshed 21 st Century infrastructure; professionals organising themselves differently in teams around the patient with a distributed system of leadership. This will have an impact upon:- Dudley Group NHS FT as our provider of hospital and community health services; Dudley and Walsall Mental Health Partnership NHS Trust as our provider of acute and community mental health services; Dudley MBC as the provider of adult social care services. The scenarios they face are:- i) Do nothing activity levels in relation to emergency admissions to hospital and residential/nursing care will increase. Discharges from care will be delayed. Dependency levels will increase. Better Care Fund financial planning assumptions will not be delivered. Additional costs will be incurred by the CCG, Dudley Group NHS FT and Dudley MBC placing further strain on the system, requiring health and social care services to be de-commissioned. ii) Base Case all partners and providers implement the integrated care model. Unnecessary admissions to hospital and residential/nursing care will be prevented. Discharges will take place in a timely manner to the most appropriate setting, reducing levels of dependency. Appropriate community infrastructure will be available to support people living in supportive settings. Better Care Fund financial planning assumptions will be met. The health and care system will be in equilibrium. iii) Best case all partners and providers recognise the need to secure significant organisational change and create a more responsive and appropriate service model. A community health, mental health and social care 34 P a g e
37 provider/s is/are established integrating services around the patient and led by general practice; utilising a modern estate and IT infrastructure, delivering population based health and wellbeing. There is a clear bias towards delivering more services out of acute settings and in the community. In patient services are of a specialist nature only. Better Care Fund financial planning assumptions are met. Change is continuous. Service efficiencies are driven out to maintain performance. The best case is reflected in our activity assumptions that have been agreed with providers and reflected in our contracts. The table below illustrates the potential impact of these changes on existing providers: - Provider 14/15 Contract value 15% NEL Reduction Potential Loss of Income due to Strategic Plan 20% Electives Services potentially CQUIN Efficiency reprocured as part of Impact new community model Total Value at Risk Dudley Group of Hospitals 184,648,535 6,221,850 6,635,764 44,226,619 1,427,106 58,511,340 Dudley & Walsall Mental Health 26,193, ,209, ,244 17,640,021 Black Country Partnerships 11,209, ,574, ,363 4,688,889 West Midlands Ambulance 8,405, , ,100 15, , ,825,851 6,635,764 66,010,922 1,986,813 80,855,350 The financial impact on the 15% non-elective and 20% elective efficiency targets are built into our contracts with the key providers as well as being agreed with the Health and Wellbeing Board. Further discussions will take place regarding our community services model. 10. Managing Relationships and the Market The CCG and the system have a multi-faceted approach to relationship and market management. This is delivered through:- a) our formal contractual relationships - holding our providers to account for performance and using contractual levers such as the application of penalties, to deliver service change; b) testing the market - using appropriate procurement mechanisms such as AQP, where value and outcomes are not being delivered; c) monthly strategic partnership meetings with our main providers designed to oversee major strategic change; d) joint appointments to manage interface issues; e) clinical engagement between CCG clinical leaders and clinicians in our providers; f) system wide groups ( see above) dealing with key strategic issues service integration and urgent care; 35 P a g e


38 36 P a g e g) an organisational development programme across the CCG, Dudley Group NHS FT, Dudley and Walsall Mental Health Partnership NHS Trust and Dudley MBC to deliver the system s distributed leadership model. The significant steps required to deliver this are already being implemented: - activity levels agreed in contracts; acute capacity reduction plan agreed; procurement process for new urgent care centre commenced; community rapid response service commissioned and implementation commenced; supporting organisational development programme commenced across health and social care. The governance process described at page 5 will continue to provide oversight of this. 11. Next Steps Implementing This Vision As the local leaders of the healthcare system, our OD programme for the system is one of the most important aspects of what we do. So our organisational development plan realises our strategic vision by setting out the development programme and operational objectives for all of the components of this strategy over the first two years. This takes account of the external environment, constraints and challenges within which we are working and maps out our programme for development against the six components of our OD model:- - Purpose - Structure - Rewards - Mechanisms - Relationships - Leadership 36 Page

39 Then the first operational stages of this five-year strategy are set out in our two-year operating plan. The following diagram provides an illustration of how the main operational plan initiatives provide the start point to subsequently enable our reimagined health and social care system as set out in this strategy. This is then fully realised with the addition of the key enablers that are explained in both the operational plan and this strategy. These plans together therefore lay the foundations for all of the key components for achieving this longer-term vision. 37 P a g e
Expression of Interest for the Co-commissioning of Primary Care Services STATEMENT FROM OUR CHAIRMAN AND CHIEF ACCOUNTABLE OFFICER
 Brierley Hill Health and Social Care Centre Venture Way Brierley Hill West Midlands DY5 1RU Tel: 01384 321763 Fax: 01384 322414 20 June 2014 Dudley Clinical Commissioning Group Expression of Interest for
Brierley Hill Health and Social Care Centre Venture Way Brierley Hill West Midlands DY5 1RU Tel: 01384 321763 Fax: 01384 322414 20 June 2014 Dudley Clinical Commissioning Group Expression of Interest for
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Reducing Variation in Primary Care Strategy
 Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Birmingham Solihull and the Black Country Area Team
 Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Healthy London Partnership. Transforming London s health and care together
 Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Quality Strategy. CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July Head of Clinical Quality & Patient Safety
 Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Longer, healthier lives for all the people in Croydon
 D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Dudley Clinical Commissioning Group. Commissioning Intentions Black Country Partnerships NHS Foundation Trust
 Appendix 3 Dudley Clinical Commissioning Group Commissioning Intentions Black Country Partnerships NHS Foundation Trust 2013/2014 1 Strategy and Context Our Commissioning Intentions indicate to our current
Appendix 3 Dudley Clinical Commissioning Group Commissioning Intentions Black Country Partnerships NHS Foundation Trust 2013/2014 1 Strategy and Context Our Commissioning Intentions indicate to our current
Our Health & Care Strategy
 MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
Cranbrook a healthy new town: health and wellbeing strategy
 Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Chapter 2. At a glance. What is health coaching? How is health coaching defined?
 Chapter 2 What is health coaching? This chapter describes: What health coaching is and it s applications How health coaching relates to wider systems and programmes of care How health coaching relates
Chapter 2 What is health coaching? This chapter describes: What health coaching is and it s applications How health coaching relates to wider systems and programmes of care How health coaching relates
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
Quality and Leadership: Improving outcomes
 Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
Quality Framework Supplemental
 Quality Framework 2013-2018 Supplemental Staffordshire and Stoke on Trent Partnership Trust Quality Framework 2013-2018 Supplemental Robin Sasaru, Quality Team Manager Simon Kent, Quality Team Manager
Quality Framework 2013-2018 Supplemental Staffordshire and Stoke on Trent Partnership Trust Quality Framework 2013-2018 Supplemental Robin Sasaru, Quality Team Manager Simon Kent, Quality Team Manager
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme. Frequently Asked Questions Second Edition
 Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Aneurin Bevan Health Board. Neighbourhood Care Network. Strategic Plan
 Agenda Item: 3.8 Appendix Two Aneurin Bevan Health Board Neighbourhood Care Network Strategic Plan 2013-2018 1 CONTENTS 1 Purpose & Scope 3 2 National and Local Context 6 3 The Vision 10 4 Strategic Themes
Agenda Item: 3.8 Appendix Two Aneurin Bevan Health Board Neighbourhood Care Network Strategic Plan 2013-2018 1 CONTENTS 1 Purpose & Scope 3 2 National and Local Context 6 3 The Vision 10 4 Strategic Themes
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS
 CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
Strategic Plan for Fife ( )
") www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
In this edition we will showcase the work of the development of a model for GP- Paediatric Hubs
 Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
End of Life Care Strategy
 End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS...
 CONTENTS EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS... 6 WHAT WE WILL CONTINUE TO ACHIEVE THROUGH THE HEALTH
CONTENTS EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS... 6 WHAT WE WILL CONTINUE TO ACHIEVE THROUGH THE HEALTH
Sunderland Health & Care System Strategic Plan Version 1.0 Working Draft
 Sunderland Health & Care System Strategic Plan 2014-2019 Version 1.0 Working Draft 1 Contents 1.0 Sunderland Health & Care System... 3 2.0 Our Vision and Strategic Objectives... 5 2.1 Our Vision for 2018/19...
Sunderland Health & Care System Strategic Plan 2014-2019 Version 1.0 Working Draft 1 Contents 1.0 Sunderland Health & Care System... 3 2.0 Our Vision and Strategic Objectives... 5 2.1 Our Vision for 2018/19...
Greenwich Clinical Commissioning Group. Patient and Public Engagement Strategy ( )
") Greenwich Clinical Commissioning Group Patient and Public Engagement Strategy (2017 2020) Page 1 of 22 Contents Page Executive Summary 3 Background 4 Statutory Duties, Guidance and Good Practice Local
Greenwich Clinical Commissioning Group Patient and Public Engagement Strategy (2017 2020) Page 1 of 22 Contents Page Executive Summary 3 Background 4 Statutory Duties, Guidance and Good Practice Local
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
A consultation on the Government's mandate to NHS England to 2020
 A consultation on the Government's mandate to NHS England to 2020 October 2015 You may re-use the text of this document (not including logos) free of charge in any format or medium, under the terms of
A consultation on the Government's mandate to NHS England to 2020 October 2015 You may re-use the text of this document (not including logos) free of charge in any format or medium, under the terms of
Our next phase of regulation A more targeted, responsive and collaborative approach
 Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
General Practice Commissioning Strategy Development
 General Practice Commissioning Strategy Development Katharine Denton (Wandsworth CCG) 3 December 2014 Version 5. 03.12.2014 1 1. Introduction Strong General Practice is at the heart of any high quality
General Practice Commissioning Strategy Development Katharine Denton (Wandsworth CCG) 3 December 2014 Version 5. 03.12.2014 1 1. Introduction Strong General Practice is at the heart of any high quality
NHS West Cheshire Clinical Commissioning Group
 NHS West Cheshire Clinical Commissioning Group Five Year Strategy: 2014/15-2018/19 1 Our Planning Footprint In developing our system vision for 2018/2019 NHS West Cheshire Clinical Commissioning Group
NHS West Cheshire Clinical Commissioning Group Five Year Strategy: 2014/15-2018/19 1 Our Planning Footprint In developing our system vision for 2018/2019 NHS West Cheshire Clinical Commissioning Group
Five year strategy for Leeds A view from the Leeds Unit of Planning June submission.
 Five year strategy for Leeds A view from the Leeds Unit of Planning June submission. Background - Leeds Leeds has an ambition to be internationally renowned for its excellent health and social care economy
Five year strategy for Leeds A view from the Leeds Unit of Planning June submission. Background - Leeds Leeds has an ambition to be internationally renowned for its excellent health and social care economy
Our NHS, our future. This Briefing outlines the main points of the report. Introduction
 the voice of NHS leadership briefing OCTOBER 2007 ISSUE 150 Our NHS, our future Lord Darzi s NHS next stage review, interim report Key points The interim report sets out a vision of an NHS that is fair,
the voice of NHS leadership briefing OCTOBER 2007 ISSUE 150 Our NHS, our future Lord Darzi s NHS next stage review, interim report Key points The interim report sets out a vision of an NHS that is fair,
INTEGRATION TRANSFORMATION FUND
 MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
Suffolk Health and Care Review
 Suffolk Health and Care Review Update on Health and Social Care System Redesign and Re-commissioning of GP Out of Hours, 111 and Community Healthcare services An Insight into the Health and Social Care
Suffolk Health and Care Review Update on Health and Social Care System Redesign and Re-commissioning of GP Out of Hours, 111 and Community Healthcare services An Insight into the Health and Social Care
Marginal Rate Emergency Threshold. Executive Summary
 Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
2020 Objectives July 2016
 ... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
04c. Clinical Standards included in the Strategic Outline Care part 1, published in December 216
 0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
The Bedfordshire CCG and Bedford Borough Council Better Care Plan Executive Summary: Our approach to Better Care planning
 DRAFT Version 16 19 March 2014 The Bedfordshire CCG and Bedford Borough Council Better Care Plan Executive Summary: Our approach to Better Care planning Bedford Borough and Bedfordshire CCG s Better Care
DRAFT Version 16 19 March 2014 The Bedfordshire CCG and Bedford Borough Council Better Care Plan Executive Summary: Our approach to Better Care planning Bedford Borough and Bedfordshire CCG s Better Care
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
WELCOME. To our first Annual General Meeting (AGM) Local clinicians working with local people for a healthier future
 Local clinicians working with local people for a healthier future") WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan. October 2016 submission to NHS England Public summary
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS. September 2014
 OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS September 2014 1 SUMMARY Our vision for the City and Hackney health economy is: Patients in control of their health and wellbeing; A joined-up system which is safe,
OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS September 2014 1 SUMMARY Our vision for the City and Hackney health economy is: Patients in control of their health and wellbeing; A joined-up system which is safe,
Primary Care Strategy. Draft for Consultation November 2016
 Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
JOB DESCRIPTION. Joint Commissioning Manager for Older People s Residential Care and Nursing Homes
 JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
Improving General Practice for the People of West Cheshire
 Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY
 Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Norfolk and Waveney STP - summary of key elements
 Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
grampian clinical strategy
 healthfit caring listening improving grampian clinical strategy 2016 to 2021 1 summary version For full version of the Grampian Clinical Strategy, please go to www.nhsgrampian.org/clinicalstrategy Document
healthfit caring listening improving grampian clinical strategy 2016 to 2021 1 summary version For full version of the Grampian Clinical Strategy, please go to www.nhsgrampian.org/clinicalstrategy Document
Prospectus for the Procurement and. Commissioning of a Multi-Specialty. Community Provider (MCP) 1 P age
 1 P age") Prospectus for the Procurement and Commissioning of a Multi-Specialty Community Provider (MCP) 1 P age Dudley Clinical Commissioning Group Prospectus for the Procurement and Commissioning of a Multi-Specialty
Prospectus for the Procurement and Commissioning of a Multi-Specialty Community Provider (MCP) 1 P age Dudley Clinical Commissioning Group Prospectus for the Procurement and Commissioning of a Multi-Specialty
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION THE BUDGET NUMBERS
 BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL
 DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
4 Year Patient and Public Involvement Strategy
 4 Year Patient and Public Involvement Strategy 2015-18 Contents Page(s) 1. Introduction - 2. Summary of the patient and public involvement strategy 2015-18 - 3. Definitions of involvement and best practice
4 Year Patient and Public Involvement Strategy 2015-18 Contents Page(s) 1. Introduction - 2. Summary of the patient and public involvement strategy 2015-18 - 3. Definitions of involvement and best practice
High level guidance to support a shared view of quality in general practice
 Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Core Domain You will be able to: You will know and understand: Leadership, Management and Team Working
 DEGREE APPRENTICESHIP - REGISTERED NURSE 1 ST0293/01 Occupational Profile: A career in nursing is dynamic and exciting with opportunities to work in a range of different roles as a Registered Nurse. Your
DEGREE APPRENTICESHIP - REGISTERED NURSE 1 ST0293/01 Occupational Profile: A career in nursing is dynamic and exciting with opportunities to work in a range of different roles as a Registered Nurse. Your
Primary Care. Strategy. April 2016
 Primary Care Strategy 1 April 2016 TABLE OF CONTENTS 1. Executive summary 5-8 2. Delivering the strategy and next steps 8-10 3. Vision for the future: 24 hour integrated community care that s 11-12 easy
Primary Care Strategy 1 April 2016 TABLE OF CONTENTS 1. Executive summary 5-8 2. Delivering the strategy and next steps 8-10 3. Vision for the future: 24 hour integrated community care that s 11-12 easy
grampian clinical strategy
 healthfit caring listening improving consultation grampian clinical strategy 2016 to 2021 1 summary version NHS Grampian Clinical Strategy 2016 to 2021 Purpose and aims 5 Partnership working and the changing
healthfit caring listening improving consultation grampian clinical strategy 2016 to 2021 1 summary version NHS Grampian Clinical Strategy 2016 to 2021 Purpose and aims 5 Partnership working and the changing
Welcome. PPG Conference North and South Norfolk CCGs June 14 th 2018
 Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
Living With Long Term Conditions A Policy Framework
 April 2012 Living With Long Term Conditions A Policy Framework Living with Long Term Conditions Contents Page Number Minister s Foreword 3 Introduction 4 Principles 13 Chapter 1 Working in partnership
April 2012 Living With Long Term Conditions A Policy Framework Living with Long Term Conditions Contents Page Number Minister s Foreword 3 Introduction 4 Principles 13 Chapter 1 Working in partnership
DRAFT. Primary Care Networks Reference Guide: Draft pre-release
 Primary Care Networks Reference Guide: Draft pre-release This draft reference guide has been developed with input from a range of stakeholders to provide further information and guidance on what we mean
Primary Care Networks Reference Guide: Draft pre-release This draft reference guide has been developed with input from a range of stakeholders to provide further information and guidance on what we mean
NHS Ambulance Services
 Report by the Comptroller and Auditor General NHS England NHS Ambulance Services HC 972 SESSION 2016-17 26 JANUARY 2017 4 Key facts NHS Ambulance Services Key facts 1.78bn the cost of urgent and emergency
Report by the Comptroller and Auditor General NHS England NHS Ambulance Services HC 972 SESSION 2016-17 26 JANUARY 2017 4 Key facts NHS Ambulance Services Key facts 1.78bn the cost of urgent and emergency
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
Approve Ratify For Discussion For Information
 NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
Bury Health and Wellbeing Board. Annual Report for 2016/17
 Bury Health and Wellbeing Board Annual Report for 2016/17 Bury Health and Wellbeing Board Annual Report for 2016-17 Contents 1. Introduction... 3 2. Background to the Health and Wellbeing Board... 5 3.
Bury Health and Wellbeing Board Annual Report for 2016/17 Bury Health and Wellbeing Board Annual Report for 2016-17 Contents 1. Introduction... 3 2. Background to the Health and Wellbeing Board... 5 3.
TAMESIDE & GLOSSOP SYSTEM WIDE SELF CARE PROGRAMME
 Report to: HEALTH AND WELLBEING BOARD Date: 8 March 2018 Executive Member / Reporting Officer: Subject: Report Summary: Recommendations: Links to Health and Wellbeing Strategy: Policy Implications: Chris
Report to: HEALTH AND WELLBEING BOARD Date: 8 March 2018 Executive Member / Reporting Officer: Subject: Report Summary: Recommendations: Links to Health and Wellbeing Strategy: Policy Implications: Chris
NHS GRAMPIAN. Clinical Strategy
 NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
Suffolk & North East Essex STP Implementation Plan. 20 th October Draft
 Suffolk & North East Essex STP Implementation Plan 20 th October 2016 Draft 1 Executive Summary In Suffolk and North East Essex, the NHS, general practice and local government have come together to develop
Suffolk & North East Essex STP Implementation Plan 20 th October 2016 Draft 1 Executive Summary In Suffolk and North East Essex, the NHS, general practice and local government have come together to develop
Figure 1: Domains of the Three Adult Outcomes Frameworks
 Outcomes Frameworks across Public Health, Social Care and NHS Relevance to Ealing Health & Wellbeing Strategy 1. Overview For adults there are three outcomes frameworks, one each for public health, NHS
Outcomes Frameworks across Public Health, Social Care and NHS Relevance to Ealing Health & Wellbeing Strategy 1. Overview For adults there are three outcomes frameworks, one each for public health, NHS
Quality Strategy and Improvement Plan
 Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
Solent. NHS Trust. Allied Health Professionals (AHPs) Strategic Framework
 Strategic Framework") Solent NHS Trust Allied Health Professionals (AHPs) Strategic Framework 2016-2019 Introduction from Chief Nurse, Mandy Rayani As the executive responsible for providing professional leadership for the
Solent NHS Trust Allied Health Professionals (AHPs) Strategic Framework 2016-2019 Introduction from Chief Nurse, Mandy Rayani As the executive responsible for providing professional leadership for the
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
Cheshire & Merseyside Sustainability and Transformation Plan. People and Services Fit for the Future
 Cheshire & Merseyside Sustainability and Transformation Plan People and Services Fit for the Future 2 The Challenge for the NHS As a nation we are fortunate to have a National Health Service that is free
Cheshire & Merseyside Sustainability and Transformation Plan People and Services Fit for the Future 2 The Challenge for the NHS As a nation we are fortunate to have a National Health Service that is free
STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby
 STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby http://nhsbetterhealth.org.uk/wp-content/uploads/2016/11/stp-draft-plan-on-page- Final-1.pdf The STP Process Q1. Version Control:
STP analysis Durham, Darlington, Teesside, Hambleton, Richmondshire and Whitby http://nhsbetterhealth.org.uk/wp-content/uploads/2016/11/stp-draft-plan-on-page- Final-1.pdf The STP Process Q1. Version Control:
North West London Sustainability and Transformation Plan Summary
 North West London Sustainability and Transformation Plan Summary Being well, living well: a sustainability and transformation plan for North West London November 2016 Have your say We want to hear your
North West London Sustainability and Transformation Plan Summary Being well, living well: a sustainability and transformation plan for North West London November 2016 Have your say We want to hear your
DRAFT. Rehabilitation and Enablement Services Redesign
 DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
NHS Providers Strategy Directors Network meeting Five Year Forward View and Vanguards - Birmingham Community Healthcare NHS Trust our story
 NHS Providers Strategy Directors Network meeting Five Year Forward View and Vanguards - Birmingham Community Healthcare NHS Trust our story Lorraine Thomas Director of Business and Organisational Development
NHS Providers Strategy Directors Network meeting Five Year Forward View and Vanguards - Birmingham Community Healthcare NHS Trust our story Lorraine Thomas Director of Business and Organisational Development
Direct Commissioning Assurance Framework. England
 Direct Commissioning Assurance Framework England NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning Development Finance Human Resources
Direct Commissioning Assurance Framework England NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning Development Finance Human Resources
CLINICAL AND CARE GOVERNANCE STRATEGY
 CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
Best Care Clinical Strategy Principles for the next 10 years of Best Care. Dr Caroline Allum, Executive Medical Director
 Best Care Clinical Strategy 2017 2027 Principles for the next 10 years of Best Care Produced By: Produced For: Dr Caroline Allum, Executive Medical Director NELFT Board Date Produced: 17 th July 2017 Version:
Best Care Clinical Strategy 2017 2027 Principles for the next 10 years of Best Care Produced By: Produced For: Dr Caroline Allum, Executive Medical Director NELFT Board Date Produced: 17 th July 2017 Version:
The state of care in general practice 2014 to Findings from CQC s programme of comprehensive inspections of GP practices
 The state of care in general practice 2014 to 2017 Findings from CQC s programme of comprehensive inspections of GP practices Our purpose The Care Quality Commission is the independent regulator of health
The state of care in general practice 2014 to 2017 Findings from CQC s programme of comprehensive inspections of GP practices Our purpose The Care Quality Commission is the independent regulator of health
The Cumbria Local Health Economy Strategic Plan
 The Cumbria Local Health Economy Strategic Plan 2014-2019 Executive Summary Executive Summary 1 Status of this Document This document sets out the collective five year plan for the Cumbria Local Health
The Cumbria Local Health Economy Strategic Plan 2014-2019 Executive Summary Executive Summary 1 Status of this Document This document sets out the collective five year plan for the Cumbria Local Health
Guideline scope Intermediate care - including reablement
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
Page1. NL CCG strategic plan 2014/15-18/19. V3.3.final
 Page1 North Lincolnshire Clinical Commissioning Group Unit of Planning Plan for the Commissioning of High Quality Services for North Lincolnshire; 2014/15-2018/19 Page2 Contents Section Page 1.0 Foreword
Page1 North Lincolnshire Clinical Commissioning Group Unit of Planning Plan for the Commissioning of High Quality Services for North Lincolnshire; 2014/15-2018/19 Page2 Contents Section Page 1.0 Foreword