Solution Title: Multidisciplinary Approach to Reduce Delirium in the ICU
|
|
|
- Darrell Lawrence
- 5 years ago
- Views:
Transcription
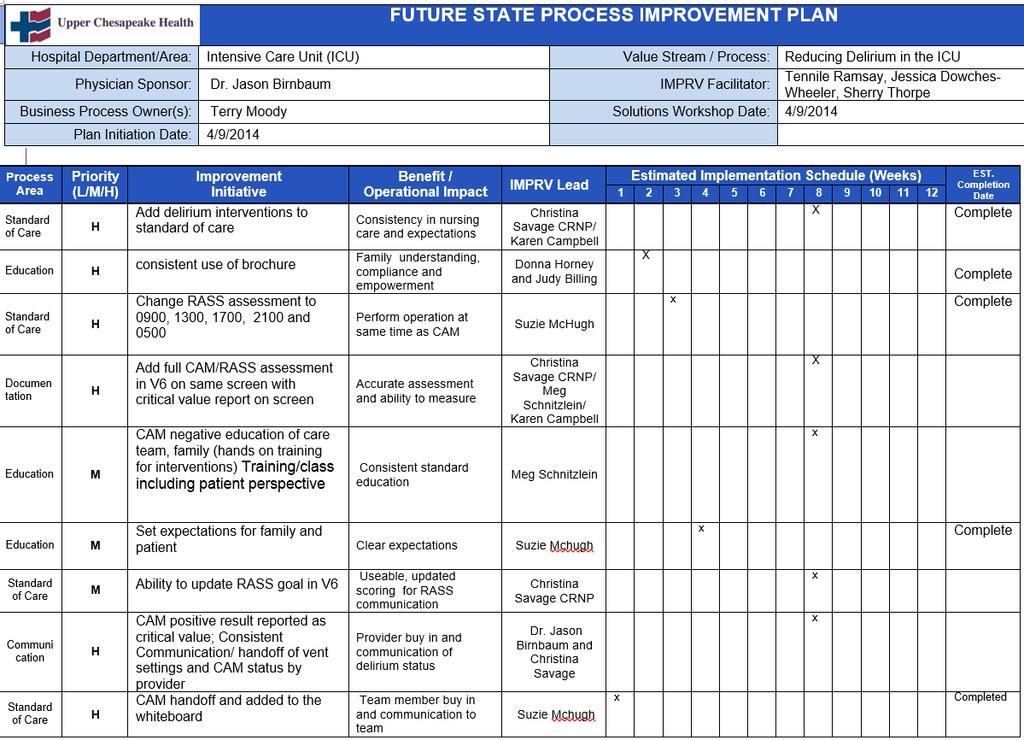
1 Solution Title: Multidisciplinary Approach to Reduce Delirium in the ICU Program/Project Description, including Goals What was the problem to be solved? How was it identified? Delirium leads to a three-fold increase of death in ICU patients and predisposes ICU survivors to prolonged neuropsychological deficits and/or long-term cognitive impairment. Assessing for delirium on admission and throughout a patient s stay in the ICU, along with establishing standard interventions to reduce and/or eliminate delirium, greatly improves patient safety by reducing ICU and total hospital length stay, decreasing time on ventilator support and reducing the incidence of delirium diagnoses overall. Prior to July 2014, delirium was inconsistently recognized and assessed in the ICU at Upper Chesapeake Medical Center and the importance in the utilization of the Confusion Assessment Method for the ICU (CAM-ICU) by team members was poorly understood. Thereby, concern was present that delirium may be affecting our patients length of stays (LOS) and therefore be at an increased risk of developing the above mentioned deficits as well as other medical complications such as hospital acquired infections, pneumonia, and deep vein thromboses. What baseline data existed? In the baseline year of FY 2014 the UCMC saw 779 total ICU cases with an average length of stay of 68 hours. Of the total cases, 7% (n=52) of patients had a recorded delirium diagnosis. Patients with a delirium diagnosis had an average LOS of 146 hours. What were the goals how would you know if you were successful? To determine if the workgroup was successful with the development and implementation of a program to reduce delirium the following goals were established: 1. Have an increase in the team member buy-in to the process of reducing delirium. 2. Have an increase in the team member understanding of the importance of the CAM-ICU. 3. Have consistent documentation of CAM-ICU scores/presence of delirium. 4. Have a decrease in delirium diagnoses. 5. Have a decrease in patient mortality, adverse outcomes, length of hospital stay, cost, falls and self-extubation. Process & Solution What methodology or process was used to develop the solution? The Delirium workgroup leveraged an in-house performance improvement strategy called IMPRV Methodology. IMPRV (Identify, Measure, Process, Re-Think and Validate) is a best-in- 1
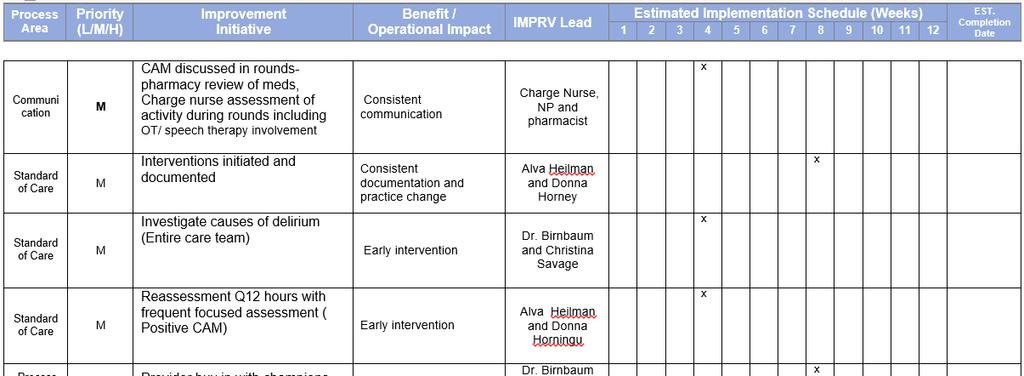
2 class methodology founded upon the key tenets of Lean, Six Sigma, project management and change leadership theories. IMPRV provides a structured way for UM UCH teams to develop new processes and programs or re-design existing processes. The workgroup began in February 2014 and leveraged IMPRV Methodology as follows: Identify: The team first met with the Process Owner to completely understand the problem at hand. Following the meeting, the workgroup met to develop the Project Charter and a high-level process map called SIPOC (Supplier, Input, Process, Output, Customer). The key objective of the Identify Phase is to clearly define the problem state and develop a solid business justification for executive and organizational sponsorship. Once the team felt that they had a keen understanding of the problem to be solved, they moved on to Measure Phase. Measure: The key objective in Measure Phase is to thoroughly understand the current state of the process and collect sound data on process performance. In this phase, the IMPRV Facilitator led the workgroup through development of a process flowchart. The team used swim lanes on the flowcharts to designate tasks completed by various members of the care team. Data was collected on all delirium cases to identify trends. Process: After collecting all pertinent data, the workgroup moved into the Process Phase. In this phase, the key objective is to assess and analyze process data for root cause identification of waste and inefficiency. During the flowchart session, the team identified potential problems using a red dot sticker. These red dot problems were then analyzed using a tool called the 5 Whys Analysis. Some of the problems identified were: lack of provider support, nurses oversedating patients, no interventions for negative CAM, and CAM missing from plan of care. Re-Think: The key objective of the Re-Think Phase is to architect a more efficient process and draft a full-scale implementation plan of improvement solutions. In this phase, warmly referred to as solution mode, the workgroup started to develop solutions to solve the root causes of the afore mentioned issues. The team developed a future state value stream map to incorporate solutions including adding delirium interventions to plan of care, consistent use of patient/family brochure, changing RASS (Richmond Agitation Assessment Scale) assessment time, adding RASS and full CAM assessment to the same screen in Meditech V6, and CAM score added to patient communication board. Prevention and early detection of ICU delirium by addressing physical, emotional, and cognitive needs are vital components of the solution. Modifiable factors contributing to delirium were identified and include disruption in sleep patterns, immobility, unfamiliar environment, sensory deprivation, stress, pain management, and pharmacological regimens. The team focused on implementation of multifaceted interventions aimed directly at these factors to decrease the occurrence of delirium. Patients are reoriented to person, time, place, and situation during each face to face interaction with the multidisciplinary team. Assistive devices such as glasses, hearing aids, and writing boards are employed to facilitate communication. Family interaction is greatly encouraged with open visiting hours and participation in daily Interdisciplinary ICU Rounds. Family members are provided education about delirium by nursing staff so they will be able to assist in preventing delirium or detect it through subtle changes that they notice in their family member. Staff members question family members about patients preferences regarding television programs, music, reading materials, or other activities such as working on cross word puzzles to guide the care team in keeping the patient stimulated 2
3 during daytime hours. Shades are open during the day and lights are dimmed at night in an effort to maintain normal sleep cycles. Uninterrupted sleep is encouraged and patients are not disturbed from 12 a.m. to 5 a.m. as their condition warrants. Routine tests, treatments, and baths are avoided during those hours to facilitate restful sleep. A calm and quiet environment is maintained. Patients reliant on ventilator support have daily sedation weaning and a spontaneous breathing trial in an effort to extubate them as soon as safely possible. Shift to shift and provider to provider results of trials are conveyed frequently to the health care team, patient, and family members. Early mobility decreases the development of delirium. Daily activity goals are determined by the patient, their family, and the care team. Charge nurses round on patients to ensure activity goals are met. Use of restraints and other restrictive medical devices is evaluated hourly and discontinued as soon as feasible. The ICU point-of-care pharmacist reviews medication lists each day. Early detection is achieved as CAM status is relayed via various tools. CAM was integrated into the ICU Standard of Care in Meditech V6 as were RASS assessments to be performed every 4 hours. These additions made for uniform documentation by the nursing staff. Goals of care were expanded to include achieving the provider prescribed goal for the individual s target RASS (Richmond Agitation Sedation Scale). CAM results are documented at 0500 and 1700 in the electronic health record. A white board located in the patient s room readily alerts anyone who comes into contact with the patient of their current CAM status. CAM status is noted during Interdisciplinary rounds and during nurse to nurse bedside report. The nursing staff is held accountable for reporting CAM positive status as a critical value to the Physician, PA, or CRNP. Compliance reports are generated and reviewed. Interventions to prevent or combat delirium are documented at least every 12 hours in the nursing computerized flowsheet. Validate: In the final phase of IMPRV methodology, the workgroup will start to transfer ownership from the lead facilitators to the process owners and team members. The key objective is to complete solution implementation, ensure process accuracy and provide comprehensive training for improvement, sustainment and ownership. At 30, 60 and 90 days, the IMPRV Facilitator will follow-up with an internal process audit to measure compliance. Some of the actions implemented and monitored for sustainability include: Assessment screen built into Meditech V6 Added new delirium interventions to RN worklist to address and document CAM+ is now a critical value reported to provider Nursing education module in HealthStream Patient & family education brochure Verbal education and support in morning briefs by Clinical Nurse Manager Leadership rounding by Clinical Nurse Manager Provider champion (Medical Director of ICU) Measurable Outcomes After the implementation of the above standardized solutions, the number of delirium cases dropped to 5% (n=40) and the LOS for delirium patients dropped to 80 hours (55% reduction in LOS). Another noteworthy outcome is a 50% reduction in self-extubations (n=18 in first 6 3
4 months of 2014; n=17 in 12 months post implementation). It is noteworthy to mention that although the delirium population saw a reduction in LOS, there was no change in the remaining ICU population s LOS. The decrease in LOS also decreases the risk for other adverse outcomes, including pneumonia, clots, and other hospital acquired infections. On average, the approximate cost per day at UM UCH for an ICU patient is $1,000 per day. The decrease in LOS of 2.75 days for the delirium population achieves a cost savings of $2,750 per patient, or $110,000 for the year (n=40, ICU only). Sustainability What measures are being taken to ensure that results can be sustained and spread? Using IMPRV Methodology, the team developed standard interventions and protocols. This initiative was a top priority for the ICU team, which resulted in increased awareness and buy-in from the entire multidisciplinary care team. Standard interventions include: CAM-ICU and RASS scores documented both within hospital documentation system as well as on patient communication boards, a unit-based pharmacist who reviews medications and participates in ICU Rounds, a unit-based physical therapist who assesses functional limitations and participates in ICU Rounds to advocate for patient mobility and other rehabilitation needs including ambulation on the ventilator when deemed appropriate, a designated quiet time to allow for patients to rest, and inclusion of family in all interventions. All interventions were added to the nursing worklist to ensure review and action. The ICU care team has fully adopted the standard interventions and protocols and taken ownership in reducing delirium. In addition, they create solutions to improve patient experiences such as taking patients to the healing garden and orienting patients to time of day. Delirium continues to be monitored through the ICU s IMPRV DASHboard for daily review. Not only have these solutions proven to be sustainable over the last year, they are replicable for the HMH ICU. Role of Collaboration and Leadership Upper Chesapeake Medical Center s leadership was and remains engaged in making patient safety a priority. This has been clearly demonstrated through the restructured Performance Improvement Department and intense training of leaders on the IMPRV methodology as a standardized project management tool using principles from Lean Six Sigma and this department s partnership with Nursing and other clinical departments establishing patient safety as a priority. There was Executive and physician support from Dr. Jason Birnbaum, Medical Director of the Intensive Care Unit and Chairman of the Department of Medicine and Terrence Moody, MS, RN, Director of Acute Care. Progress on the project was reported monthly at the ICU Operations Committee meeting. The vision for success in decreasing the number of patients who test positive for delirium in the ICU was shared by the multidisciplinary Kaizen team that was established to quickly address the issue, produce solutions and develop strategies for gathering data to measure progress. The team consisted of bedside critical care nurses, critical care techs, providers (MD, CRNP), ancillary team members from Respiratory Therapy, Rehabilitation, and Pharmacy, the Clinical Nurse 4
5 Manager, Director of Nursing and project facilitators from the Performance Improvement Department. All members have been and remain engaged from the redesign of the process, to implementation of solutions, to sustainability. Senior leadership demonstrates support of this project as evidenced by funding the application for the American Association of Critical Care Nurses Beacon Award for Excellence which was awarded to the ICU in 2013 and the reapplication process has begun for Outcome measurement, one of five categories scored, is worth 450 out of 1000 points. This category focuses on results achieved from objective evaluation and measuring progress so you can assess and improve processes related to patient outcomes. Innovation University of Maryland, Upper Chesapeake Medical Center (UM UCMC) is the first hospital in the University of Maryland Medical System to embark upon the issue of delirium, and the importance of delirium reduction in the Intensive Care Unit. Understanding the importance of early detection, and implementation of evidence-based treatments, has been at the forefront of the unit s awareness. Research has consistently supported the multiple adverse outcomes of delirium in critically ill patients, including those creating both clinical and fiscal consequences. Daily interdisciplinary rounds in the unit are innovative, including a unit-based physical therapist and pharmacist. The unit-based physical therapist has been invaluable to patient care. The nonpharmacological intervention of early mobilization has been shown to be a consistent approach to decrease delirium in critically ill patients. Upper Chesapeake Medical Center s family presence policy, of 24 hour visiting, is beneficial to the patient and the health care team. Families are invited to attend daily rounds. Family presence can be a tremendous comfort to the patient, and also be invaluable to the health care team. The family has the opportunity to share awareness of any behaviors or cultures related to the patient that may impede success. The unit is committed to a period of uninterrupted rest for patients (if their condition allows) from 12 AM to 5 AM. Lights are dimmed, noise kept to a minimum, overhead pages are rare. Staff has been educated on the effects of a continuous rest period for patients, as well as numerous additional interventions. In the morning, lights are turned on, shades are raised, and glasses and hearing aids are given to the patient if applicable. Patients are also mobilized, whether it is ambulating, assisting the patient out of bed to a chair, or range of motion. Each patient has a large white board, which aids in patient orientation. The board is updated twice a day and includes the name of staff, day of the week, date, and daily patient goals. Finally, the unit s providers, both physicians and nurse practitioners have been committed to the project s workgroup with invaluable support and contributions for solutions. 5

6 Addendums Identify: Project Charter Identify: SIPOC SIPOC DIAGRAM (PROCESS MAP) Process Name: Reducing Delirium in the ICU S Suppliers I Inputs P Process O Outputs C Customer Patien information/ Sending Unit Verbal/ written report 1 Obtain report from ED, PACU, or Unit ICU Knowledge/ Room Prep Sending Unit RN RN/ PCT Provider Respiratory Therapist Provider Care Team Care Team Care Team RN Care Team Care Team Patient Admission/ Assessment, screen & CAM tool sheet/ Packet with delirium brochure, Admission Chart and EMR Respiratory Assessment/ Intervention screens Test Plan of Care Ongoing assessments, interdisciplinary rounds Ongoing assessments, interdisciplinary rounds Patient, RASS & CAM tools Ongoing assessments, interdisciplinary rounds report/ Discharge process, screen and information Ancillary testing for patient 8 11 CAM Positive Information Pt admitted Care plan implementation Initial Assessment( CAM included) 4 Invite Family back to unit 5 Patient Orders 6 Respiratory assessment 12 re evaluation of medications/ Interventions? Interventions/ Plan of Care Patient Information Information Information/Plan of care Information/Plan of care results Interventions 9 Patient monitoring Plan of Care 10 Patient reassessed Plan of Care Care team & Patient / Family Care team & Patient / Family Care team & Patient / Family 13 Transfer/ Discharge Patient leaves Patient/ Family ICU Care Team, Patient, family Patient/Family RN, Pharmacy, ancillary Care team & Patient Care team & Patient Patient/ Family Care team & Patient / Family 6
7 Measure: Process Flowchart Decreasing Delirium in the ICU Call from OR, ED or Provider/ RRT call Patient Assessment Notified of Admission Room Preparation Admission treatment orders Review H&P, labs& prior hospitalization Transfer/ admit to ICU Vitals, height/weight and check orders Respiratory notified of admission OT consulted as needed Speech Therapy Consult Initiate Standard of care Assessment PT consulted as needed Speaking valve Swallowing studies, and other Start Procedures Admission Assessment Assist with procedures Assist with Procedures Order Sets & Vent management, intubations, Pt assessment and determines interventions Orders to correspond with plan of care Rounding every 12 hours Review Plan of care RASS Begin Patient/ Family education Patient vitals, weight, glucose, labs, other duties as Write on white board; assist with mobility Weaning protocol Daily round with Care team CAM Assessment Negative Investigate causes of patient delirium Positive Discuss in rounds CAM assessment at 0500 & 1700 Initiate interventions Address interventions Update White board Q12 hour assessments and frequent focused SLP Rehab Respiratory PCT Nursing Provider 7
: N/A Cycle Time(mins): N/A Cycle Time(mins): N/A Cycle Time(mins): N/A Cycle Time(mins): N/A Cycle")
8 Process: 5 Whys Analysis Re-Think: Future State Value Stream Map Patient VALUE STREAM MAP (Future State) Reducing Delirium in the ICU Admission Admission CAM/RASS CAM positive CAM interventions Provider Communication Provider Nursing Nursing Care Team Nursing Provider Cycle Time(mins): N/A Cycle Time(mins): N/A Cycle Time(mins): N/A Cycle Time(mins): N/A Cycle Time(mins): N/A Cycle Time(mins): N/A P/T: mins 0 P/T: mins 0 P/T: mins 0 P/T: mins 0 P/T: mins 0 P/T: mins 0 D/Ts: mins D/Ts: mins D/Ts: mins D/Ts: mins D/Ts: mins D/Ts: mins D/Ti: mins 0 D/Ti: mins 0 D/Ti: mins 0 D/Ti: mins 0 D/Ti: mins 0 D/Ti: mins Touches mins Touches mins Touches mins Touches mins Touches mins Touches Patient assessement Notified of admission RN completes RASS Q4H CAM positive result reported as critical value Revise intervention list by cognitive, physical and emotional needs Consistent Communication/ handoff of vent settings and CAM status by provider Admission orders Room Preparation Change RASS assessment to 9,1 and 5, and both CAM and RASS on same screen CAM handoff and added to the whiteboard Create daily schedule (timeframe) Admit to ICU Review labs and H&P CAM assessment at 0500 and Start Procedures Vitals, Height, weight, etc Add full CAM assessment in Initiate standard of care Add delirium interventions to standard of care Admission assessment Begin family/ Patient education consistent use of brocure CAM negative education of care team, family (hands on training for interventions) Set expectations for family an Unable to update RASS goal CAM discussed in roundspharmcay review of meds Interventions initiated and documented Provider buy in with champions Investigate causes Reassessment Q12 hours with frequent focused assessment Charge nurse aeessment of activity during rounds AM care huddle including PT to discuss ambulation/mobility and place on whiteboard OT/ speech therapy involvement Training/class including patient perspective Nursing to assess and mobilze patient on both shifts 8
9 Re-Think: Implementation Plan 9
10 Validate: Process Assessment (Internal Audit) IMPRV Internal Audit Checklist Process: Department: Delirium ICU Patient Care Services ICU Date: Reviewer: 8/12/2014 Tennile Ramsay 30 Days 60 Days 90 Days 6 Months 1 Year Audit Technique Auditable Item, Observation, Procedure, etc. Status Status Status Status Status Electronic Data Have all RNs been trained? In Progress Complete Electronic Data Is training documentation available? In Progress Complete Electronic Data Is training documentation current? In Progress Complete Observation Is the visual storyboard visible on the unit? In Progress Verbal Inquiry Is there buy in from all stakeholders? Incomplete Incomplete Observation Is RASS and CAM scheduled for same time? Complete Complete Electronic Data Is the CAM assessment completed per protocol? Incomplete Complete Electronic Data are positive CAM assessments called as Critical Value Incomplete Incomplete Number of Incomplete Observations Total Observations Corrective Actions Required Reviewer Comments The CAM ICU screen went live on 6/25/2014. All assigned RNs completed Healthstream education by 6/30/2014. Currently one third of CAM positive assessments reported as critical value. 10
Collaboration and Coordination in the MRICU: An Interprofessional Approach to Implementation of a Daily Review of Sedation Strategy, Liberation
 Collaboration and Coordination in the MRICU: An Interprofessional Approach to Implementation of a Daily Review of Sedation Strategy, Liberation Potential and Mobility Plan Amy Dean, MS, RN, CCRN Kristin
Collaboration and Coordination in the MRICU: An Interprofessional Approach to Implementation of a Daily Review of Sedation Strategy, Liberation Potential and Mobility Plan Amy Dean, MS, RN, CCRN Kristin
VAE PROJECT MASTER ACTION PLAN. Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies
 VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
Building a Lean Team. Using Lean Methodology to Develop a Collaborative Rounding Model. April 28 th, 2010
 Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Policies and Procedures. I.D. Number: 1145
 Policies and Procedures Title: VENTILATION CHRONIC- CARE OF MECHANICALLY VENTILATED ADULT PERSON RNSP: RN Clinical Protocol: Advanced RN Intervention LPN Additional Competency: Care of Chronically Mechanically
Policies and Procedures Title: VENTILATION CHRONIC- CARE OF MECHANICALLY VENTILATED ADULT PERSON RNSP: RN Clinical Protocol: Advanced RN Intervention LPN Additional Competency: Care of Chronically Mechanically
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
ABCDEF Bundle Implementation
 ABCDEF Bundle Implementation Anne Putzer, MS, RN, ACNS-BC, CCRN Cat Zyniecki, BSN, RN, CCRN Columbia St. Mary s Wisconsin Association of Clinical Nurse Specialists CNO/CNS/Shared Governance Breakfast September
ABCDEF Bundle Implementation Anne Putzer, MS, RN, ACNS-BC, CCRN Cat Zyniecki, BSN, RN, CCRN Columbia St. Mary s Wisconsin Association of Clinical Nurse Specialists CNO/CNS/Shared Governance Breakfast September
In a common ICU situation like this, there are two main questions we have to answer daily:
 MICU ROUNDING PLAN // 12.3.2014 This document contains 4 sections: 1. Rationale 2. Assumptions and ground rules 3. Detailed plan for rounding structure 4. 1-page outline of rounding structure 1. Rationale
MICU ROUNDING PLAN // 12.3.2014 This document contains 4 sections: 1. Rationale 2. Assumptions and ground rules 3. Detailed plan for rounding structure 4. 1-page outline of rounding structure 1. Rationale
SOLUTION TITLE: Can Critical Care Become A Restraint Free Environment?
 ORGANIZATION: ST AGNES MEDICAL CENTER SOLUTION TITLE: Can Critical Care Become A Restraint Free Environment? PROGRAM/PROJECT DESCRIPTION INCLUDING GOALS: The critical care environment is perhaps the last
ORGANIZATION: ST AGNES MEDICAL CENTER SOLUTION TITLE: Can Critical Care Become A Restraint Free Environment? PROGRAM/PROJECT DESCRIPTION INCLUDING GOALS: The critical care environment is perhaps the last
Policies and Procedures. ID Number: 1138
 Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Unplanned Extubation In Intensive Care Units (ICU) CMC Experience. Presented by: Fadwa Jabboury, RN, MSN
 CMC Experience. Presented by: Fadwa Jabboury, RN, MSN") Unplanned Extubation In Intensive Care Units (ICU) CMC Experience Presented by: Fadwa Jabboury, RN, MSN Introduction Basic Definitions: 1. Endotracheal intubation: A life saving procedure for critically
Unplanned Extubation In Intensive Care Units (ICU) CMC Experience Presented by: Fadwa Jabboury, RN, MSN Introduction Basic Definitions: 1. Endotracheal intubation: A life saving procedure for critically
Transformational Patient Care Redesign Project
 Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Transformational Patient Care Redesign Project Kaveh Houshmand Azad 1 Summary In 2008 2009, Providence Holy Cross Medical Center, a 340- bed hospital located in Mission Hills, California embarked upon
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress
 Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
Exemplary Professional Practice: Patient Care Delivery Model(s)
") Exemplary Professional Practice: Patient Care Delivery Model(s) EP7EO Nurses systematically evaluate professional organizations standards of practice, incorporating them into the organization s professional
Exemplary Professional Practice: Patient Care Delivery Model(s) EP7EO Nurses systematically evaluate professional organizations standards of practice, incorporating them into the organization s professional
Improving Outcomes for High Risk and Critically Ill Patients
 Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
Improving Outcomes for High Risk and Critically Ill Patients KP Woodland Hills Medical Center Presented by: Sharon M. Kent RN BSN, CCRN Lynne M. Agocs-Scott RN MN, CCRN CCNS Introduction of the IHI The
19th Annual. Challenges. in Critical Care
 19th Annual Challenges in Critical Care A Multidisciplinary Approach Friday August 22, 2014 The Hotel Hershey 100 Hotel Road Hershey, Pennsylvania 17033 A continuing education service of Penn State College
19th Annual Challenges in Critical Care A Multidisciplinary Approach Friday August 22, 2014 The Hotel Hershey 100 Hotel Road Hershey, Pennsylvania 17033 A continuing education service of Penn State College
Tools & Resources for QI Success
 Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
Contents. Introduction 3. Required knowledge and skills 4. Section One: Knowledge and skills for all nurses and care staff 6
 Decision-making frameworks in advanced dementia: Links to improved care project. Page 2 of 17 Contents Introduction 3 Required knowledge and skills 4 Section One: Knowledge and skills for all nurses and
Decision-making frameworks in advanced dementia: Links to improved care project. Page 2 of 17 Contents Introduction 3 Required knowledge and skills 4 Section One: Knowledge and skills for all nurses and
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Delirium management initiative: Guarding the minds of our patients
 Delirium management initiative: Guarding the minds of our patients Introduction This past January (2014), in response to requests from a number of our physicians, a new effort began at Baptist Health,
Delirium management initiative: Guarding the minds of our patients Introduction This past January (2014), in response to requests from a number of our physicians, a new effort began at Baptist Health,
Beyond the Bundle. Improving Ventilator Related Outcomes through Multidisciplinary Collaboration
 Beyond the Bundle Improving Ventilator Related Outcomes through Multidisciplinary Collaboration Definitions VAE Ventilator associated event global term for NHSN reporting criteria VAC: Ventilator Associated
Beyond the Bundle Improving Ventilator Related Outcomes through Multidisciplinary Collaboration Definitions VAE Ventilator associated event global term for NHSN reporting criteria VAC: Ventilator Associated
Discharge Before Noon DH32
 Discharge Before Noon DH32 Green Belts: Champion: Susan Christensen, RN Eric Belen Hai Tran Alice Issai Date: March 21, 2012 1 DEFINE Problem Statement 1. Baseline data shows only 18% of patient discharges*
Discharge Before Noon DH32 Green Belts: Champion: Susan Christensen, RN Eric Belen Hai Tran Alice Issai Date: March 21, 2012 1 DEFINE Problem Statement 1. Baseline data shows only 18% of patient discharges*
Eliminating Common PACU Delays
 Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
TITLE: Processing Provider Orders: Inpatient and Outpatient
 POLICY and PROCEDURE TITLE: Processing Provider Orders: Inpatient and Outpatient Number: 13211 Version: 13211.10 Type: Patient Care Author: Carol Vanetti; Provider Order Policy Committee Effective Date:
POLICY and PROCEDURE TITLE: Processing Provider Orders: Inpatient and Outpatient Number: 13211 Version: 13211.10 Type: Patient Care Author: Carol Vanetti; Provider Order Policy Committee Effective Date:
Code Sepsis: Wake Forest Baptist Medical Center Experience
 Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Regenstrief Center for Healthcare Engineering
 Purdue University Purdue e-pubs RCHE Publications Regenstrief Center for Healthcare Engineering 3-31-2007 All Bundled Out - Application of Lean Six Sigma techniques to reduce workload impact during implementation
Purdue University Purdue e-pubs RCHE Publications Regenstrief Center for Healthcare Engineering 3-31-2007 All Bundled Out - Application of Lean Six Sigma techniques to reduce workload impact during implementation
Implementation Guide Version 4.0 Tools
 Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Implementation Guide Version 4.0 Tools Program Overview Purpose of the Guide This Guide is intended primarily for INTERACT champions and trained educators who are responsible for implementing and sustaining
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Welcome to the Rehabilitation (Rehab) Unit
 Unit") Welcome to the Rehabilitation (Rehab) Unit How to contact the Rehab Unit Page 2 What to expect with your child s care Page 3 Daily rounds Page 5 Staying overnight and visiting hours Page 8 Keeping your
Welcome to the Rehabilitation (Rehab) Unit How to contact the Rehab Unit Page 2 What to expect with your child s care Page 3 Daily rounds Page 5 Staying overnight and visiting hours Page 8 Keeping your
Guidelines for Physiatric Practice and Inpatient Review Criteria
 Guidelines for Physiatric Practice and Inpatient Review Criteria Table of Contents PART I: GUIDELINES Guidelines for Physiatric Practice PART II: INPATIENT REVIEW Instructions: Pre-admission or Admission
Guidelines for Physiatric Practice and Inpatient Review Criteria Table of Contents PART I: GUIDELINES Guidelines for Physiatric Practice PART II: INPATIENT REVIEW Instructions: Pre-admission or Admission
Raise your game: The UP Campaign. Bruce Spurlock, M.D. Cynosure Health
 Raise your game: The UP Campaign Bruce Spurlock, M.D. Cynosure Health 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Can we streamline & simplify making it easier for front-line staff and still improve safety? 16
Raise your game: The UP Campaign Bruce Spurlock, M.D. Cynosure Health 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Can we streamline & simplify making it easier for front-line staff and still improve safety? 16
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Hardwiring Processes to Improve Patient Outcomes
 Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Hardwiring Processes to Improve Patient Outcomes Barbara Adcock Mohr, Administrative Director, Rehabilitation Services Mark Prochazka, Assistant Director, Rehabilitation Services UNC Hospitals FIM, UDSMR,
Bethesda Hospital PGY1 Residency Program Learning Experiences
 Bethesda Hospital PGY1 Residency Program Learning Experiences Required rotations Orientation This rotation will orient the resident to hospital pharmacy and the responsibilities of a staff pharmacist.
Bethesda Hospital PGY1 Residency Program Learning Experiences Required rotations Orientation This rotation will orient the resident to hospital pharmacy and the responsibilities of a staff pharmacist.
Form CMS (5/2017) Page 1
 Page 1") Use this pathway for a resident who has pain symptoms or can reasonably be expected to experience pain (i.e., during therapy) to determine whether the facility has provided and the resident has received
Use this pathway for a resident who has pain symptoms or can reasonably be expected to experience pain (i.e., during therapy) to determine whether the facility has provided and the resident has received
QUALIS HEALTH HONORS WASHINGTON HEALTHCARE PROVIDERS
 LEADERSHIP IN IMPROVING HEALTHCARE Harborview Medical Center Code Sepsis: Improving Survival in Sepsis with Early Identification and Activation of a Critical Care Team Sepsis, one of the highest causes
LEADERSHIP IN IMPROVING HEALTHCARE Harborview Medical Center Code Sepsis: Improving Survival in Sepsis with Early Identification and Activation of a Critical Care Team Sepsis, one of the highest causes
Physicians Who Care for People with MS
 Physicians Who Care for People with MS Neurologists: Specialize in the diagnosis and treatment of conditions related to the nervous system including the brain, spinal cord, and nerves. Many neurologists
Physicians Who Care for People with MS Neurologists: Specialize in the diagnosis and treatment of conditions related to the nervous system including the brain, spinal cord, and nerves. Many neurologists
Patient Safety: Fall Prevention. Unlicensed Assistive Personnel
 Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
Patient Safety: Fall Prevention Unlicensed Assistive Personnel Purpose and Objectives Purpose: Review the UCH Fall Prevention Program Objectives: 1. Present evidence about patient safety and falls. 2.
We use many of them. The devices are part of our restraint policy. See below
 Do you utilize body pillow, beveled mattresses, moxi mattresses, rolled blankets, swim noodles for positioning or bed demarcation? Do you have a comprehensive device assessment? If so, would you please
Do you utilize body pillow, beveled mattresses, moxi mattresses, rolled blankets, swim noodles for positioning or bed demarcation? Do you have a comprehensive device assessment? If so, would you please
THE DOWNFALL TEAM PRESENTS BE ON THE BALL PREVENT A FALL!
 THE DOWNFALL TEAM PRESENTS BE ON THE BALL PREVENT A FALL! Multi-Disciplinary Team Peggy Benenati Risk Management Beverly Campbell Nursing Kim Cerri Quality Roberta Farley Physical Therapy Kelli Farnell
THE DOWNFALL TEAM PRESENTS BE ON THE BALL PREVENT A FALL! Multi-Disciplinary Team Peggy Benenati Risk Management Beverly Campbell Nursing Kim Cerri Quality Roberta Farley Physical Therapy Kelli Farnell
Organization: Meritus Medical Center, Hagerstown, Maryland. Solution Title: Routine Vital Sign Protocols: Putting Evidence-Based Practice into Motion
 Organization: Meritus Medical Center, Hagerstown, Maryland Solution Title: Routine Vital Sign Protocols: Putting Evidence-Based Practice into Motion Problem/Goal: The problem is the risk to quality patient
Organization: Meritus Medical Center, Hagerstown, Maryland Solution Title: Routine Vital Sign Protocols: Putting Evidence-Based Practice into Motion Problem/Goal: The problem is the risk to quality patient
Acute Care to Rehab & Complex Continuing Care (CCC) Referral
 Referral") o General Rehabilitation Low Intensity Rehabilitation (GRH, SJHCG) o (CMH, GRH, SJHCG) o Chronic Assisted Ventilator (GRH only) o o Ischemic o Hemorrhagic Stroke Rehab: Program Readiness Date: Complex
o General Rehabilitation Low Intensity Rehabilitation (GRH, SJHCG) o (CMH, GRH, SJHCG) o Chronic Assisted Ventilator (GRH only) o o Ischemic o Hemorrhagic Stroke Rehab: Program Readiness Date: Complex
Clinical and Financial Successes at Advocate Health Care Utilizing our
 Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
AARC Clinical Practice Guideline
 AARC Clinical Practice Guideline Discharge Planning for the Respiratory Care Patient DPRP 1.0 PROCEDURE: Development and implementation of a comprehensive plan for the safe discharge of the respiratory
AARC Clinical Practice Guideline Discharge Planning for the Respiratory Care Patient DPRP 1.0 PROCEDURE: Development and implementation of a comprehensive plan for the safe discharge of the respiratory
PREVENTION OF POSTOPERATIVE PULMONARY COMPLICATIONS: Reducing Postoperative Mechanical Ventilation
 PREVENTION OF POSTOPERATIVE PULMONARY COMPLICATIONS: Reducing Postoperative Mechanical Ventilation Rowena Chona O. Sano, MSN, RN, CNL, CPHQ Memorial Hermann Greater Heights Hospital Houston, TX Nothing
PREVENTION OF POSTOPERATIVE PULMONARY COMPLICATIONS: Reducing Postoperative Mechanical Ventilation Rowena Chona O. Sano, MSN, RN, CNL, CPHQ Memorial Hermann Greater Heights Hospital Houston, TX Nothing
ROTATION DESCRIPTION FORM PGY1
 ROTATION DESCRIPTION FORM PGY1 Rotation Title Medicine Intensive Care Unit (MICU) Level of Learner PY4 PGY1 PGY2 Preceptor(s) Stacy Campbell-Bright, Brian Murray Preceptor Contact Stacy.Campbell-Bright@unchealth.unc.edu;
ROTATION DESCRIPTION FORM PGY1 Rotation Title Medicine Intensive Care Unit (MICU) Level of Learner PY4 PGY1 PGY2 Preceptor(s) Stacy Campbell-Bright, Brian Murray Preceptor Contact Stacy.Campbell-Bright@unchealth.unc.edu;
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program
 Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program April 30, 2016 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate Health
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program April 30, 2016 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate Health
Critical Thinking Steps
 CAA s = Critical Thinking CAROL SIEM, MSN, RN, BC, GNP Clinical Educator/Team Leader for QIPMO Critical Thinking Steps Recognition/Assessment Gather essential information about the individual Problem definition
CAA s = Critical Thinking CAROL SIEM, MSN, RN, BC, GNP Clinical Educator/Team Leader for QIPMO Critical Thinking Steps Recognition/Assessment Gather essential information about the individual Problem definition
Meeting Joint Commission Standards for Health Literacy. Communication and Health Care. Multiple Players in Communication
 Meeting Joint Commission Standards for Health Literacy Christina L. Cordero, PhD, MPH Project Manager Division of Standards and Survey Methods The Joint Commission Wisconsin Literacy SW/SC Regional Health
Meeting Joint Commission Standards for Health Literacy Christina L. Cordero, PhD, MPH Project Manager Division of Standards and Survey Methods The Joint Commission Wisconsin Literacy SW/SC Regional Health
Get UP to Drive Harm Down. ND Webinar March 29, 2018 Maryanne Whitney RN CNS MSN Cynosure Health
 Get UP to Drive Harm Down ND Webinar March 29, 2018 Maryanne Whitney RN CNS MSN Cynosure Health What is your role in your organization? Quality Leader RN MD Rehab specialist RT Other- please chat in your
Get UP to Drive Harm Down ND Webinar March 29, 2018 Maryanne Whitney RN CNS MSN Cynosure Health What is your role in your organization? Quality Leader RN MD Rehab specialist RT Other- please chat in your
Patient Safety. If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator Updated:
 Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Documentation & Communication in Adult/Medical Settings. Devina Acharya, MA, CCC/SLP, CSUSM
 Documentation & Communication in Adult/Medical Settings Devina Acharya, MA, CCC/SLP, CSUSM When in Rome. do as your facility does 2 Who s the Boss? Doctor makes decisions and bears ultimate responsibility
Documentation & Communication in Adult/Medical Settings Devina Acharya, MA, CCC/SLP, CSUSM When in Rome. do as your facility does 2 Who s the Boss? Doctor makes decisions and bears ultimate responsibility
CLINICAL CRITERIA FOR UM DECISIONS Skilled Nursing Facilities
 COMMERCIAL CLINICAL CRITERIA FOR UM DECISIONS Skilled Nursing Facilities Capital Health Plan (CHP) will provide coverage for care in a skilled nursing facility, subject to the benefit limitations of the
COMMERCIAL CLINICAL CRITERIA FOR UM DECISIONS Skilled Nursing Facilities Capital Health Plan (CHP) will provide coverage for care in a skilled nursing facility, subject to the benefit limitations of the
How Allina Saved $13 Million By Optimizing Length of Stay
 Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Success Story How Allina Saved $13 Million By Optimizing Length of Stay EXECUTIVE SUMMARY Like most large healthcare systems throughout the country, Allina Health s financial health improves dramatically
Rapid Response Team Building
 Nicole Sardinas BSN, RN, CCRN Clinical Educator- Critical Care Ext.2703 Mabel LaForgia MSN, RN, CCRN, CNL Clinical Nurse Leader- Critical Care Ext.4149 201-978- 6423 355 Grand Street «AddressBlock», NJ
Nicole Sardinas BSN, RN, CCRN Clinical Educator- Critical Care Ext.2703 Mabel LaForgia MSN, RN, CCRN, CNL Clinical Nurse Leader- Critical Care Ext.4149 201-978- 6423 355 Grand Street «AddressBlock», NJ
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE RESTRAINT AS A LAST RESORT - CRITICAL CARE SCOPE Provincial: Critical Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Senior Operating Officer, Glenrose Rehabilitation Hospital
TITLE RESTRAINT AS A LAST RESORT - CRITICAL CARE SCOPE Provincial: Critical Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Senior Operating Officer, Glenrose Rehabilitation Hospital
Patients Being Weaned From the Ventilator: Positive Effects of Guided Imagery. Authors McVay, Frank; Spiva, Elizabeth; Hart, Patricia L.
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Solution Title: Sustaining Fall Prevention Over Time, Is It Possible?
 Organization: Sinai Hospital of Maryland Solution Title: Sustaining Fall Prevention Over Time, Is It Possible? Focus rea: Preventing Falls with Injury Program/Project Description, Including Goals: In 2010,
Organization: Sinai Hospital of Maryland Solution Title: Sustaining Fall Prevention Over Time, Is It Possible? Focus rea: Preventing Falls with Injury Program/Project Description, Including Goals: In 2010,
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
The STAAR Initiative
 The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
Early Mobility in the Intensive Care Unit
 Early Mobility in the Intensive Care Unit Marianne Munson, PT, DPT University of Rochester Strong Memorial Hospital Physical Medicine and Rehabilitation Objectives Summarize the benefits of early mobility
Early Mobility in the Intensive Care Unit Marianne Munson, PT, DPT University of Rochester Strong Memorial Hospital Physical Medicine and Rehabilitation Objectives Summarize the benefits of early mobility
Louise Rose RN, BN, ICU Cert, Adult Ed Cert, MN, PhD
 Louise Rose RN, BN, ICU Cert, Adult Ed Cert, MN, PhD TD Nursing Professor in Critical Care Research, Sunnybrook Health Sciences Centre Associate Professor, LSBFON, University of Toronto CIHR New Investigator
Louise Rose RN, BN, ICU Cert, Adult Ed Cert, MN, PhD TD Nursing Professor in Critical Care Research, Sunnybrook Health Sciences Centre Associate Professor, LSBFON, University of Toronto CIHR New Investigator
A Resident-led PICU Morbidity and Mortality Conference
 A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
Interim Final Interpretive Guidelines Version 1.1
 Interim Final Interpretive Guidelines Version 1.1 Big Changes from November 2008 to January 2009 418.54 Condition of participation: Initial and Comprehensive assessment of the patient L522 418.54(a) Standard:
Interim Final Interpretive Guidelines Version 1.1 Big Changes from November 2008 to January 2009 418.54 Condition of participation: Initial and Comprehensive assessment of the patient L522 418.54(a) Standard:
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018
 FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
Determining the Appropriate Inpatient Rehabilitation Candidate
 Determining the Appropriate Inpatient Rehabilitation Candidate Brandi Damron, OTR/L, MBA Program Director Norton Community Hospital Inpatient Rehab Unit Objectives Discuss the preadmission process limitations
Determining the Appropriate Inpatient Rehabilitation Candidate Brandi Damron, OTR/L, MBA Program Director Norton Community Hospital Inpatient Rehab Unit Objectives Discuss the preadmission process limitations
Partnerships- Cooperation with other care providers that is guided by open communication, trust, and shared decision-making.
 1 E P 7: Describe and demonstrate the structure(s) and process(es) used to engage internal experts and external consultants to improve care in the practice setting. When Riverside nurses from any level
1 E P 7: Describe and demonstrate the structure(s) and process(es) used to engage internal experts and external consultants to improve care in the practice setting. When Riverside nurses from any level
Adherence to the ICU Liberation ABCDEF Bundle Improves Patient Outcomes in the ICU
 Walden University ScholarWorks Walden Dissertations and Doctoral Studies Walden Dissertations and Doctoral Studies Collection 2018 Adherence to the ICU Liberation ABCDEF Bundle Improves Patient Outcomes
Walden University ScholarWorks Walden Dissertations and Doctoral Studies Walden Dissertations and Doctoral Studies Collection 2018 Adherence to the ICU Liberation ABCDEF Bundle Improves Patient Outcomes
REDUCING READMISSIONS FOR SNF PATIENTS
 REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
REDUCING READMISSIONS FOR SNF PATIENTS Amy E. Boutwell, MD, MPP President, Collaborative Healthcare Strategies New York State Partnership for Patients HIIN September 28, 2017 Objective Identify 3 practical
Ayrshire and Arran NHS Board
 Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Exhibit A. Part 1 Statement of Work
 Exhibit A Part 1 Statement of Work Contractor shall provide Basic Neurological services as described herein to Medicaid eligible Clients who are authorized to receive services at the Contractor s owned
Exhibit A Part 1 Statement of Work Contractor shall provide Basic Neurological services as described herein to Medicaid eligible Clients who are authorized to receive services at the Contractor s owned
Safeguarding life, property and the environment
 A New Choice for Hospitals: Achieving Both Medicare Accreditation and ISO 9001 Certification At The Same Time Introduction to DNV Healthcare and NIAHO Lab Quality Confab DNV Established in 1864 Third Party
A New Choice for Hospitals: Achieving Both Medicare Accreditation and ISO 9001 Certification At The Same Time Introduction to DNV Healthcare and NIAHO Lab Quality Confab DNV Established in 1864 Third Party
Communication Challenges Overcoming the Barriers to Improve Quality. Presented by: Christy Brinkman LNHA Laura Seleen RN
 Communication Challenges Overcoming the Barriers to Improve Quality Presented by: Christy Brinkman LNHA Laura Seleen RN 6-16-16 Objectives The participant will be able to identify a process to follow to
Communication Challenges Overcoming the Barriers to Improve Quality Presented by: Christy Brinkman LNHA Laura Seleen RN 6-16-16 Objectives The participant will be able to identify a process to follow to
Stroke Coordinator Boot Camp
 Stroke Coordinator Boot Camp Gena Kreiner RN BSN FHS Stroke Coordinator Karen C. Kiesz MN RN CNRN SCRN MHS Stroke Program Manager Lisa Shumaker, BSN, RN, CMSRN (Moderator) PRMC- Everett Stroke Program
Stroke Coordinator Boot Camp Gena Kreiner RN BSN FHS Stroke Coordinator Karen C. Kiesz MN RN CNRN SCRN MHS Stroke Program Manager Lisa Shumaker, BSN, RN, CMSRN (Moderator) PRMC- Everett Stroke Program
Learning Experiences Descriptions
 Anticoagulation Management Clinic Learning Experiences Descriptions The Anticoagulation Management rotation is an elective learning experience that focuses on the outpatient management of anticoagulation.
Anticoagulation Management Clinic Learning Experiences Descriptions The Anticoagulation Management rotation is an elective learning experience that focuses on the outpatient management of anticoagulation.
Rita Hunsucker, DNP, Nicole Cornell, MS, Gerald Hobbs, PhD, Jorge Con, MD & Alison Wilson, MD WVU Medicine, J.W. Ruby Memorial Hospital
 Rita Hunsucker, DNP, Nicole Cornell, MS, Gerald Hobbs, PhD, Jorge Con, MD & Alison Wilson, MD WVU Medicine, J.W. Ruby Memorial Hospital The authors have nothing to disclose. Post extubation dysphagia (PED)
Rita Hunsucker, DNP, Nicole Cornell, MS, Gerald Hobbs, PhD, Jorge Con, MD & Alison Wilson, MD WVU Medicine, J.W. Ruby Memorial Hospital The authors have nothing to disclose. Post extubation dysphagia (PED)
Psychotropic Drug Use To Medicate or Not to Medicate?
 Psychotropic Drug Use To Medicate or Not to Medicate? Presented by: Lydia Restivo, RN CDONA Regulatory Compliance Consultant West & Restivo Quality Consulting Cell: 516 318-9088 Email: lydrestivo@verizon.net
Psychotropic Drug Use To Medicate or Not to Medicate? Presented by: Lydia Restivo, RN CDONA Regulatory Compliance Consultant West & Restivo Quality Consulting Cell: 516 318-9088 Email: lydrestivo@verizon.net
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Sustaining Improvements in Pediatric Critical Care Outcomes: Toolkit for a Structured Approach
 Sustaining Improvements in Pediatric Critical Care Outcomes: Toolkit for a Structured Approach INTRODUCTION Target Audience This toolkit is geared toward health care teams who have a basis of quality improvement
Sustaining Improvements in Pediatric Critical Care Outcomes: Toolkit for a Structured Approach INTRODUCTION Target Audience This toolkit is geared toward health care teams who have a basis of quality improvement
The Health Care Improvement Foundation 2015 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Magee Rehabilitation
 The Health Care Improvement Foundation 2015 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Magee Rehabilitation 2. Title Of Initiative Innovations to Stop Pressure Ulcers
The Health Care Improvement Foundation 2015 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Magee Rehabilitation 2. Title Of Initiative Innovations to Stop Pressure Ulcers
LEAN Transformation Storyboard 2015 to present
 LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
Activities of Daily Living (ADL) Critical Element Pathway
 Critical Element Pathway") Use this pathway for a resident who requires assistance with or is unable to perform ADLs (Hygiene bathing, dressing, grooming, and oral care; Elimination toileting; Dining eating, including meals and
Use this pathway for a resident who requires assistance with or is unable to perform ADLs (Hygiene bathing, dressing, grooming, and oral care; Elimination toileting; Dining eating, including meals and
SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY
 PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
Progressive Mobility in the ICU: Improving the Patient Experience. Rachel Lewis-Bayliss BSN, RN Theresa M. Davis PhD, RN, NE-BC
 Progressive Mobility in the ICU: Improving the Patient Experience Rachel Lewis-Bayliss BSN, RN Theresa M. Davis PhD, RN, NE-BC Early Progressive Mobility Team Jason Vourlekis MD, MBA: Medical Director
Progressive Mobility in the ICU: Improving the Patient Experience Rachel Lewis-Bayliss BSN, RN Theresa M. Davis PhD, RN, NE-BC Early Progressive Mobility Team Jason Vourlekis MD, MBA: Medical Director
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
Mohamad Fakih, MD, MPH
 Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
ADMISSION CARE PLAN. Orient PRN to person, place, & time
 ADMISSION DATE: CODE STATUS: ADMISSION CARE PLAN ADMISSION DIAGNOSIS: 1. DELIRIUM 2. COGNITIVE LOSS Resident will be as alert and oriented as possible Resident will be as alert and oriented as comfortable
ADMISSION DATE: CODE STATUS: ADMISSION CARE PLAN ADMISSION DIAGNOSIS: 1. DELIRIUM 2. COGNITIVE LOSS Resident will be as alert and oriented as possible Resident will be as alert and oriented as comfortable
Stellar Hospital PGY-1 Pharmacy Residency
 (Required Rotation) Learning Experience Description Xxxx xxxx, Pharm.D., BCPS xxxx.xxxx@xxxx.org xxxxx xxxxx, Pharm.D., BCPS xxxxx.xxxxxxxx@xxxxx.org xxxx xxxxx, PharmD, BCPS xxxx.xxxxx@xxxx.org I. General
(Required Rotation) Learning Experience Description Xxxx xxxx, Pharm.D., BCPS xxxx.xxxx@xxxx.org xxxxx xxxxx, Pharm.D., BCPS xxxxx.xxxxxxxx@xxxxx.org xxxx xxxxx, PharmD, BCPS xxxx.xxxxx@xxxx.org I. General
Running head: LEADERSHIP ANALYSIS: ROUNDING 1
 Running head: LEADERSHIP ANALYSIS: ROUNDING 1 Leadership Analysis: Rounding Jerrene Bramble, Tara Braun, Pamela Dusseau, Angelique Kinyon, William McKinley, Noranne Morin, Nicky Reed, and Ashleigh Wash
Running head: LEADERSHIP ANALYSIS: ROUNDING 1 Leadership Analysis: Rounding Jerrene Bramble, Tara Braun, Pamela Dusseau, Angelique Kinyon, William McKinley, Noranne Morin, Nicky Reed, and Ashleigh Wash
Child and Family Development and Support Services
 Child and Services DEFINITION Child and Services address the needs of the family as a whole and are based in the homes, neighbourhoods, and communities of families who need help promoting positive development,
Child and Services DEFINITION Child and Services address the needs of the family as a whole and are based in the homes, neighbourhoods, and communities of families who need help promoting positive development,
Restraint Reduction. Moving Towards Restraint Free Care
 Restraint Reduction Moving Towards Restraint Free Care Revised: BW/September 2010 RESTRAINTS: Defined Any manual method, physical or mechanical device, material or equipment, that immobilizes or reduces
Restraint Reduction Moving Towards Restraint Free Care Revised: BW/September 2010 RESTRAINTS: Defined Any manual method, physical or mechanical device, material or equipment, that immobilizes or reduces
Falls Prevention: Engaging Volunteers That CARE Upper Chesapeake Medical Center
 Falls Prevention: Engaging Volunteers That CARE Upper Chesapeake Medical Center Program/Project Description The 3E - Oncology Unit at Upper Chesapeake Medical Center (UCMC) is a 30 bed unit that specializes
Falls Prevention: Engaging Volunteers That CARE Upper Chesapeake Medical Center Program/Project Description The 3E - Oncology Unit at Upper Chesapeake Medical Center (UCMC) is a 30 bed unit that specializes
NURSING HOME MODULE THE ABACUS NURSING HOME MODULE IS CAPABLE OF PERFORMING MANY FUNCTIONS PERTINENT TO NURSING HOME APPLICATIONS.
 NURSING HOME MODULE THE ABACUS NURSING HOME MODULE IS CAPABLE OF PERFORMING MANY FUNCTIONS PERTINENT TO NURSING HOME APPLICATIONS. For instance, you have the ability to produce a forwarded physician s
NURSING HOME MODULE THE ABACUS NURSING HOME MODULE IS CAPABLE OF PERFORMING MANY FUNCTIONS PERTINENT TO NURSING HOME APPLICATIONS. For instance, you have the ability to produce a forwarded physician s
2013 Falls Action Plan Updated 5/29/13. Action Initiatives Responsible Person
 2013 Falls Action Plan Updated 5/29/13 Action Initiatives Responsible Establishment of a Review data relevant P. Petrucelli and Falls Task Force to falls(assessment, falls team hourly rounds and white
2013 Falls Action Plan Updated 5/29/13 Action Initiatives Responsible Establishment of a Review data relevant P. Petrucelli and Falls Task Force to falls(assessment, falls team hourly rounds and white
Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers
 Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers Melissa A. Fitzpatrick, RN, MSN, FAAN VP & Chief Clinical Officer, Hill-Rom Trends Driving Our Industry Aging
Using People, Process and Technology to Enhance Outcomes for Patients and Their Caregivers Melissa A. Fitzpatrick, RN, MSN, FAAN VP & Chief Clinical Officer, Hill-Rom Trends Driving Our Industry Aging
Reducing the Risk of Wrong Site Surgery
 Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Seattle Nursing Research Consortium Abstract Style and Reference Guide
 Seattle Nursing Research Consortium Abstract Style and Reference Guide Page 1 SNRC Revised 7/2015 Table of Contents Content Page How to classify your Project. 3 Research Abstract Guidelines 4 Research
Seattle Nursing Research Consortium Abstract Style and Reference Guide Page 1 SNRC Revised 7/2015 Table of Contents Content Page How to classify your Project. 3 Research Abstract Guidelines 4 Research
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition
 Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
Procedure. Applies To: UNM Hospitals Responsible Department: Quality Revised: 03/2014
 Procedure Patient Age Group: ( ) N/A ( ) All Ages ( ) Newborns (X) Pediatric (x ) Adult DESCRIPTION/OVERVIEW UNM Hospitals (UNMH) is recognized as a large academic health care system providing services
Procedure Patient Age Group: ( ) N/A ( ) All Ages ( ) Newborns (X) Pediatric (x ) Adult DESCRIPTION/OVERVIEW UNM Hospitals (UNMH) is recognized as a large academic health care system providing services
Getting a zero deficiency rating on a recent Joint Commission survey and bringing
 Leadership Perioperative services overhaul proves effort is worth the time Getting a zero deficiency rating on a recent Joint Commission survey and bringing sterile processing in house are 2 of many improvements
Leadership Perioperative services overhaul proves effort is worth the time Getting a zero deficiency rating on a recent Joint Commission survey and bringing sterile processing in house are 2 of many improvements
Occupation: Other Professional Occupations in Therapy and Assessment
 NOC: 3144 Occupation: Other Professional Occupations in Therapy and Assessment Occupation Description: Responsibilities include using techniques such as art, athletics, dance, music or recreational therapy
NOC: 3144 Occupation: Other Professional Occupations in Therapy and Assessment Occupation Description: Responsibilities include using techniques such as art, athletics, dance, music or recreational therapy