TRUST BOARD EXCELLENCE IN SAFETY, QUALITY AND PATIENT EXPERIENCE REPORT JUNE 2013
|
|
|
- Lynette Day
- 5 years ago
- Views:
Transcription
1 TRUST BOARD EXCELLENCE IN SAFETY, QUALITY AND PATIENT EXPERIENCE REPORT JUNE 2013 TO WHAT EXTENT ARE WE DELIVERING THE SAFEST CARE? 1. IMPROVING OUR MORTALITY RATE AND REDUCING HARM Understanding the causes of our mortality, our mortality rate and how we benchmark against peers is important in order to ensure we have robust and proactive systems in place to continuously improve, reduce patient harm and save more lives. The Institute for Healthcare Improvement states best practice in measuring and understanding causes of mortality is to report (i) the crude death rate (ii) the risk adjusted mortality rate; and (iii) the mortality 30 days after discharge. During the last three months the reports to the Board have been developed to provide this information which is now included in this report. 1.1 Weekly Monitoring of Patient Deaths In accordance with the Trust s mortality framework all deaths that have been identified within the SPC monitoring process have been reviewed by the Medical Director and Director of Nursing. There have been 16 weekly triggers reviewed since the Board report in April This report includes the accumulative results of the review of 143 case notes to date within the medical and surgical business units. Any deaths which are highlighted by the weekly trigger tool are reviewed and added to the report on a monthly basis. The Medical Director confirms that the clinical teams have reviewed 52 sets of case notes and has found no issue within 47 sets of notes. 4 cases were reported as issue but not material and 1 reported as an issue that needs addressing. In hospital deaths: outcome of casenote review following implementation of trigger tool A - No Issue B - Issue but not material C - Issue and needs addressing D - Catastrophic, immediate action
2 Individual clinical areas are beginning to undertake monthly reviews of deaths within their respective areas in addition to the SPC trigger process. The results will be reported within the relevant Business Unit Boards. 1.2 What is our mortality rate after discharge from hospital (SHMI)? The latest update of the national mortality indicator, the SHMI (Summary Hospital-Level Mortality Indicator) was published by the NHS Information Centre in January, and covers the period October 2011 to September This indicator includes all deaths in hospital plus those occurring within 30 days of discharge. The Trust s value of 110 was categorised as as expected. Although the observed number of deaths is greater than expected, this is not statistically significant using 95% confidence intervals. It is important to highlight that the SHMI is being re-based nationally; therefore this may impact on the Trust s position in comparison to the rest of the Country. From time to time Dr Foster rebase the HSMR data (altering the expected deaths), we understand from the Keogh Review team, this process is due and whilst our mortality has fallen rebasing seems likely to make NCUH an outlier on the rebased funnel plot. The funnel plot below shows how the Trust compares to the rest of the trusts in England: Analysis by diagnostic group, using the CCS (Clinical Classification System) methodology, shows that for 3 diagnostic groups, the number of observed deaths was significantly greater than the expected number produced by the model (using 95% confidence intervals) :- The following care groups have been identified to the Keogh Review team and it has been agreed with the TDA to identify external support to increase NCUH capacity to undertake these reviews, as concern was expressed as to our ability to cope with this internally. Pneumonia; care bundle and AQUA programme in place. 2
3 RAMI 13 Congestive heart failure, non-hypertensive; an audit of this group of patients with the support of the cardiology team to investigate why this group of patients remain an outlier is being planned. This will provide us with the information to better understand the reason why this HRG group is an outlier and will enable us to develop an action plan to address care issues that are identified. We will report this audit back to board in June CD for cardiology has already identified that there is poor co-morbidity coding in the group of patients that affect their HSMR and is awaiting the notes of one years worth of patients to audit with his team, clearly the June deadline was overly ambitious. Gastrointestinal haemorrhage (this will be managed by the transfer of high risk pathways from WCH to CI and a 24-hour on-call emergency service, 7 days a week will be provided). Neck of femur transfer of trauma on 10 June will enhance our outcomes and investment in an orthogeriatric service and will increase our outcomes.. Bundle rate is 12% and we aim to achieve 80% by March What is the real-time trend in our risk-adjusted within-hospital mortality level? Risk Adjusted Mortality Index 2012 The Risk Adjusted Mortality Index has recently been rebased to recalibrate it and bring it back to 100. The chart below shows that our risk-adjusted index is 99 (May12-Apr13) NCUH Crude Death Rate and Risk Adjusted Mortality Index (RAMI 2013) All Admissions TRUST Crude Death Rate Crude Death Rate Crude Death Rate Over the last 3 years, the Trust s Crude Death Rate peaked in January 2011 at 1.53%. During the following year, the rate declined steadily and reached a low of 1.38% in January More recently, having plateaued at 1.43% from November 2012 to February 2013, the latest figures show a rise to 1.46% in April
4 RAMI How does our hospital mortality level compare with that of our peer group of Trusts? 180 Risk Adjusted Mortality Index 2013: Trust v Peer Group All Admissions TRUST Peer Average HES Peer Average Northumbria's Peer Group The chart above shows how the Trust s mortality index (standardised to the CHKS RAMI 2013 model) has changed during the period Apr 2008 to April 2013, compared to the mortality index of the peer group of Trusts, and also HES peers. Prior to Oct 2010, the Trust s Index was lower than that of its peer group. From Nov 2010 however, the Trust s index rose above its peers, although still showing a steady decline. Since then, the rate has continued to decline and the latest position (May12-April13) shows that the Trust s index is almost in line with that of the peer group at 99. The index has been consistently above HES peers since 2008/09, although the gap has been seen to be narrowing throughout the last 12 months. The North East Safer Care Observatory team will present their opinion about the trend at the next Board meeting. 1.5 Low Risk Group Mortality We have commenced the review into low risk group mortality and identified that there are 39 patients who have died over the past year (Feb 12- Jan 13) who fall into the low risk group of HRG s using the methodology as described by Dr Foster. Included in this group is a wide variety of different conditions. Of this group 27 were admitted under the Medical Business Unit while 8 were attributed to the Surgical Business unit. 33 patients were admitted as emergencies and 31 were described with 5 or more secondary diagnosis suggesting significant co-existing co-morbidities. The measure of the Charleson index (measure of existing co-morbidities) shows 12 patients as scoring 0 ie low risk with the other 27 scoring an average of 12.7 ie significant co-morbidities with a range of Each of these cases needs to be subjected to the mortality framework process to identify whether the death is of concern or otherwise. This has commenced and will be reported to the Board in July

5 1.6 Hospital Standardised Mortality Rate The Hospital Standardised Mortality Ratio (HSMR) is a measure published by Dr Foster Health which compares the expected rate of death with the actual rate of death. The chart below summarises the Trust s Hospital Standardised Mortality Ratio since 2001 Higher than expected mortality rate for two consecutive years: 5

6 The chart below summarises the HSMR trend for the most recent 12 months 1.7 Trust wide Framework for Reviewing Mortality and Reducing Harm As reported to the Board last month, the revised Trust wide framework for mortality has been implemented and the first meeting of the Mortality Review Group took place on 12 June This group will initially focus: Review the implementation and outputs from the weekly trigger process Review the progress and outputs from the specialty M&M meetings to ensure they are functioning well Ensure that the mortality framework is being embedded in all of the Clinical Business Units. The Mortality Review Group will form a core part of the work of the new Safety Panel. 6
7 2. MORTALITY FRAMEWORK STAGE ONE REPORTABLE DEATHS 2013/14 Following the updating of the mortality framework described in section 1.6, the monthly reporting to the Board will now include all deaths which are categorised as stage one reportable deaths. Type April-March 2012/13 Reviewed April-May 2013/14 Maternal deaths 0 0 Neonatal deaths 0 0 Planned procedures 0 0 During elective admissions (within 30 days) 18 See below 0 The Trust identified 18 elective deaths within 30 days of admission from April 2012 to February However two of these cases have been found to be non-elective admissions. All 18 deaths have been reviewed by the clinical teams, Medical Director and Director of Nursing. The Medical Director has asked the relevant clinical teams to provide a more detailed report on the two cases identified within the issues that need addressing category. The outcomes from these two cases involved identification and management of Sepsis and escalation of the Early Warning Score. Both of these cases have been reported back to the Clinical Business Units for discussion at the Mortality and Morbidity meetings in order to determine any lessons to be learned across the clinical teams. This will be completed by the end of June Outcome of elective casenote review A - No Issue B - Issue but not material C - Issue and needs addressing D - Catastrophic, immediate action
8 3. IMPROVEMENT THEMES FROM MORTALITY AND HARM REVIEW 2012/13 Theme One: Clinical Care Themes Action To ensure a robust system of monitoring and escalation to cover all specialties. Increased senior presence for Acute Admissions - A dedicated Acute Care Physician (ACP) system (seven days 8am-8pm) was introduced to CIC in August 2012 and this system was further enhanced in March 2013 by a minimum of 3 ACPs working the rota (seven days 8am-8pm). At West Cumberland Hospital the ACP system was introduced in November 2012 (Monday to Friday 8am-6pm) and this is being enhanced from 3 June Out of Hours Surgery Since November, surgery Out of Hours is led by a Consultant Surgeon and Consultant Anaesthetist. Management of the Deteriorating Patient Group - The management of the deteriorating patient group meetings started in March. The key areas of focus from the May meeting included: Completed Partial Completed Established Embed the NEWS audit results Pneumonia care bundles Sepsis 6 audit Implementing National Early Warning Score (NEWS) System. The launch of the NEWS system took effect on Monday, 4 th March at both the Cumberland Infirmary and West Cumberland Infirmary site. Summary of audit results are: Partial Audit results on next page chart accuracy is usually greater than 90%. What we need to improve on algorithm escalation, documentation (nursing & medical), correct grade of medical review. There are similar results across both sites for NEWS accuracy but a huge disparity in the figures between CIC and WCH on the algorithm escalation section of the audit, which will be discussed at the next management of deteriorating patient group meeting. Implementing Pneumonia care bundle (including AQuA). The Trust already participates in the AQUA improvement project for pneumonia. This is being reviewed with the aim of improving the timeliness and validity of the data by making the collection more real time/ contemporaneous. Implementing Sepsis Care Bundle. The sepsis 6 bundle boxes are in place at the Cumberland Infirmary and West Cumberland Hospital. The sepsis guidelines are being updated and refresher training will be supported by the lead nursing team and the clinical business unit directors. Modified Early Obstetric Warning System (MEOWS) Paediatric Early Warning Score System (PEWS) Transfer of high risk pathways from WCH to CIC. The key priority from the review was the establishment of an OOH service for Emergency GI. The Business unit are currently out to advert for 4 gastroenterologists to support the OOH GI bleeding rota for North Cumbria with an interview date of 22/8/13. The implementation date will depend on the recruitment of additional resource. Finalise in July Implemented Audit results in September Audit results in July Planned for late
9 The audit tool for sepsis is being developed which is up and running at the Cumberland Infirmary and will commence in West Cumberland Hospital from May The sepsis audits have not commenced yet but are in progress. Improving the Trust s mechanisms for identifying patients with potential Acute Kidney Injury. Alerts to possible Acute Kidney Injury (AKI) have been added to Biochemistry reports to enable the early identification of patients suffering from changes in their kidney function and prompt more urgent review and potential treatment of this condition. This has been in place at the Cumberland Infirmary since October 2012 and has been rolled out to West Cumberland Hospital since March Pilot and assess the benefits of a Medical Emergency Team to support escalation. This is a longer term development and is subject to a pilot. This pilot started in January and Dr Sturman will provide an update to CPG in June Audit results in July Completed Long term development Theme Two: Leadership and Reporting Culture To encourage all staff to take responsibility for patient safety and the delivery of harm free care by implementing best practice from teams that have locally embedded reporting and responding systems to all locations in the Trust. To promote Patient Safety and local innovative safety improvements by running hospital wide Patient Safety Days from March To improve communication and learning from safety incidents by using new methods of communication and reporting. Development of Business Unit Clinical Governance A half-day session was held with the Business Units in March to review the local arrangements for clinical governance at ward/speciality and business unit level. A key focus of this was reviewing the systems in place to review incidents and complaints. Fully compliant in March 2014 The first clinical governance business unit meetings have now taken place in all of the Clinical Business Units. The Trust Board and Executive Management Team will be reviewing the evidence of identifying the top three areas of improvement arising from incidents reported on the individual clinical areas and how this is being shared with all staff working in that clinical area. The Business Units will be presenting to the Board in June 2013 on the progress on developing their local clinical governance arrangements to demonstrate the focus on improving quality and safety. Patient Safety Days - The first patient safety day for the Trust was held on Friday 14 June and was attended by over 120 members of staff from the Cumberland Infirmary. The day was a huge success and involved a range of key patient safety workshops, a safety culture survey, patient stories and team work from the individual wards on service improvement. The West Cumberland Hospital Patient Safety Day will be held on 12 July Process for investigating and learning from SUIs -Significant progress has been made on implementing the revised SUI process, which will be fully operational from July Training has been organised for all senior clinical and operational managers in SUI investigation, which will take place in June and July Partial July 9
10 Theme Three: Improved Use of Clinical Information To promote safe discharge by ensuring all inpatients and day cases have an acceptable discharge summary at the time of discharge. To develop and strategic plan for clinical records and improved case note availability, tracking and better structured content. Patient discharge - A revised discharge process was established in March 2013, which focuses on three core stages of improving patient discharge: Implemented % of discharges had a letter in the case notes November 2012 % of discharges had a letter in the case notes March 2013 % of discharges had a letter in the case notes May 2013 % of discharges had a letter in the case notes September 2013 CIC 30% 70% 84.77% 90% WCH 30% 70% 83.06% 90% Improving Clinical Records - A records user group has been established with the focus on right note, right place, right time. Incident reporting for regarding clinical records will be introduced as a defined reporting field on Ulysses from 1 April Business cases for a central contact centre and a centralised store for medical records has been approved and plans are currently progressing on the project management arrangements which need to be implemented. Implemented and ongoing development 10
11 Cumberland Infirmary NEWS Audit Results April - NEWS correctly calculated May - NEWS correctly calculated April - Algorithm activated correctly May - Algorithm activated correctly
12 Cumberland Infirmary NEWS Audit Results April - Medical response documented May - Medical response documented April - Review by correct grade of medic May - Review by correct grade of medic 12
13 West Cumberland Hospital NEWS Audit Results 10 April - NEWS correctly calculated May - NEWS correctly calculated April - Algorithm activated correctly May - Algorithm activated correctly
14 West Cumberland Hospital NEWS Audit Results April - Medical response documented May - Medical response documented April - Review by correct grade of medic May - Review by correct grade of medic

 Upper Quartile")
15 The top quartile and the national average are based on patient safety incidents reported between 1 April 2012 and 30 September Incidents Reported to NPSA (Per 100 Admissions) Upper Quartile National Median 15

16 Harm Group Reducing harm group to enhance trust wide systems of care The reducing harm group, led by the Business Unit Director of Clinical Support, is now scheduled to meet on a monthly basis to review 40 sets of case notes for patients with a length of stay greater than 24hrs. Trigger Total E F G H I G1 General Care Module Lack of EWS or EWS requiring response G2 Any Patient Fall G4 Readmission to hospital within 30 days G5 Shock or Cardiac Arrest G6 DVT/PE following admission evidenced by imaging +/or D dimmers G7 Complication of procedure or treatment G8 Transfer of higher level of care S2 Surgical Care Module Change in planned procedure S3 Removal/Injury or repair of organ I2 Intensive Care Module Unplanned transfer to ICU or HDU Lab Test Module L2 Transfusion L3 Abrupt drop in Hb or Hct (>25%) L4 Rising urea or creatinine (>2x baseline) L8 Raised Troponin (>1.5ng/ml) L10 C.Difficile


17 2013/ / /12 3 LEARNING FROM PATIENT INCIDENTS Learning from patient incidents, including serious untoward incidents is a core part of reducing harm and improving the safety of care given to patients. The Trust reports incidents in accordance with the NPSA 5 categories of harm. The table below summarises the reported incidents for the last three years. All Patient Safety Incidents No Harm Minor Moderate Major Catas Near Miss The chart below summarises the top five incidents reported: Top Five Cause Groups for Patient Safety Incidents Medication Error/Problems Lack Of Resources Maternal Incidents Pressure Ulcer Slips,Trips & Falls Medication Error/Problems Maternal Incidents Staffing Levels Lack Of Resources Slips,Trips & Falls Documentation Pressure Ulcer Medication Error/Problems Lack Of Resources Slips,Trips & Falls Our priorities for improvement are: (i) Enhanced nurse staffing on shift each day to match patient needs (ii) Enhanced reconciliations of medicines (iii) Reduction in Slips, trips and falls particularly fractured neck of femurs 17
18 4.1 Meeting the Contractual Duty of Candour The standard NHS contract requires all NHS organisations to ensure that patients/their families are informed about any patient safety incident that has affected them during their care. How are we implementing this contractual duty? The following steps have been put in place to ensure this duty is met: Guidance issues to Business Unit Management Teams, Senior Nurses, Ward Sisters and Consultants. Patient leaflet and guidance on reports developed and will be approved at Clinical Policy group in June The Ulysses reporting system has been updated to make the field of patient informed mandatory. Weekly incident review meetings are in place across the Business Units to ensure the incidents of severe/catastrophic and moderate harm are being reviewed in relation to the Duty of Candour. Trust performance Incidents April May June July August September Serious 3 5 Met 100% 100% Moderate Met 26% 13% 4.2 Serious Untoward Incidents (SUIs) From the SUIs declared in 2012/13 our priorities for improvement are: (i) Escalation of the deteriorating patients (ii) Reduced neck of femur following in hospital falls (iii) Reduced HAI (iv) Enhance discharge communications (v) Human factors training in response to the five never events in 2012/13 18
19 4.2.1 SUIs declared in May 2013 Five Serious Untoward Incidents were declared during May 2013: INCIDENT DESCRIPTION SITE CLINICAL AREA IMMEDIATE ACTION TAKEN Patient Suicide WCH Patterdale Ward Joint review arranged with Cumbria Partnership NHS Foundation Trust regarding mental health assessment of patient. System (A&E/Mental Assessment) Failure Health Never Event retained guidewire Theatre ventilation / potential surgical infections CIC A&E Joint meeting with Cumbria Partnership NHS Foundation Trust arranged to review delay in obtaining mental health assessment. WCH Intensive Care Independent review of this case and a previous Never Event in January 2013 has been commissioned and is in progress. WCH Theatres Independent review of surgical site infections following ventilation concerns commissioned. Initial findings are that there are no issues regarding increased infection due to the failings in theatre plant. Fracture from a fall WCH Gable Ward Review of patients care in accordance with slips, trips and falls policy. Confirmation that policy was followed. Delay in obtaining X- ray has been highlighted and fed back to the clinical teams in relation to post falls care. Embedding Learning from previous Serious Incidents The Trust is committed to ensuring learning from SUIs is embedded particularly where there are trends in incident causes or in a particular clinical area. From the serious incidents declared in May, two of the incidents relate to ensuring patients in our care have the correct escalation and assessment in place for their mental health needs as well as treating their medical conditions. Previous SUIs in the Trust has involved patients who have absconded and subsequently died. The respective Medical Directors (NCUH and CPFT) will ensure that the outputs of these investigations also review learning and recommendations from previous incidents. The never event declared in May 2013 is the second never event relating to a retained guidewire in the same clinical area, therefore an independent review has been commissioned. The learning from the fracture following a fall relates to post falls care, which the Trust already has improvement plans in place. 19


20 The graph below shows the SUI incidents declared in 2013/14 to date: Serious Untoward Incidents 2013/14 Suicide by Inpatient Health & Safety Unexpected Death System Failure Drug Incident Surgical Error Fall No. Incidents 4.3 Never Events 2012/13 There was one Never Event declared in May 2013 relating to a retained guide wire at West Cumberland Hospital. This incident was reviewed at the Clinical Policy Group in May This is the second never event relating to a retained guide wire and the Trust has commissioned an independent review of both events. 20

21 No. Complaints 5 LEARNING FROM COMPLAINTS The NHS Complaints Regulations 2009 specifically require Trusts to conform to a number of key performance indicators which have been developed during the last month in order to regularly report this item to the Board. This information also supports the Trust s compliance with the CQC outcome for complaints. Complaints Performance Indicators Complaints Received (Total) Complaints Received (Initially Graded as Serious) Acknowledged within 3 days Complaints Closed Type of Complaint April 2013 May 2013 New Complaint 28 * 27 FLR 2 4 New Complaint 5 11 FLR 0 0 New Complaint 29 (100%) 25 (93%) FLR 2 (100%) 3 (75%) New Complaint FLR 3 4 Complaints Closed New Complaint 0 (of 1 initially serious) 0 (of 4 initially serious) (Upheld as Serious) FLR 0 (of 0 initially serious) 0 (of 1 initially serious) * N.B.1 complaint withdrawn from April 13 total A complaints development workshop was held with over 60 senior nurses and managers on 18 June The workshop looked at the external environment in terms of the national review of the NHS complaints process, our current process and what we needed to improve, good and poor examples of how we have investigated and responded to complaints and how patient complaints form a core part of clinical governance in the organisation. The session resulted in a revised complaints process being agreed by all the staff who attended which is being written into a revised complaints policy and procedure. 5.1 Performance on responding to complaints The graph below highlights the key challenge we have regarding improving our performance in closing/responding to complainants: 12 Complaints Closed in May New Complaints FLR Time+10 Days Time+30 Days Time+Over 30 Days 21
 requires organisations to agree with the complainant a timeframe for seeking resolution, if this is not possible then the Trust should default to a minimum standard for")


22 Improving our performance on responding to complainants in a timelier manner is a key priority for the Trust. The complaints guidance (2009) requires organisations to agree with the complainant a timeframe for seeking resolution, if this is not possible then the Trust should default to a minimum standard for responding to the complaint. The Trust s default is the previous 25 working days which is used in a number of Trusts as a default. The percentage of complaints responded to within 25 days remains low, however it is important to highlight that the agreed date with the complainant is not always recorded resulting in this performance figure sometimes being inaccurate. This will be resolved through the new process which will be introduced. The weekly complaints monitoring charts have been developed to show the outstanding complaints and their grading in terms of seriousness. Monthly performance reports against individual complaint investigators is now published and discussed at SMT and business unit performance reviews. An improvement plan has been agreed with the Chief Executive to target complaints over 100 days, 50 days and 30 days. This includes new complaints and those complaints which have come back for further local resolution. 5.2 Serious Complaints Closed During the Reporting Period No serious complaints were closed during May The year to date position on upheld serious complaints is zero. 5.3 What are the themes/trends from our complaints? The graphs below shows the themes of the complaints received for the new financial period 2013/14.The graph below illustrates the key themes from complaints received in April Complaints Received By Subject April & May 2013 Treatment Discharges Diagnosis Attitude Of Staff Medical Communication Appt Admin OPD Appt Delay OPD Attitude Of Staff (Nurse) Appt OPD Wait In Clinic Records Appt Delay IP Appt Cancelled OPD New Complaint FLR



23 Communication Attitude Of Staff Medical Discharges Treatment Attitud e Of Staff Medical Diagnos is Discharges Treatment Complaints Received by Detail for Top 4 subjects April 2013: Complaints Received By Detail Of Top 4 Subjects April & May 2013 Treatment Delay In Treatment Outcome Of Treatment Anaesthetic Not Worked Inappropriate Discharge New Compliant FLR Discharge Process Delay In Diagnosis Attitude Of Medical Staff The graphs below identified the top subjects regarding complaints in April 2013 which is also split per hospital site: Complaints Received By Detail Of Top 4 Subjects - CIC April & May 2013 Treatment Delay In Treatment Outcome Of Treatment Inappropriate Discharge Discharge Process New Complaint FLR Attitude Of Medical Staff Communication - Medical Communication - Nursing


24 Attitude Of Staff Discharges Diagno sis Treatment Complaints Received By Detail Of Top 4 Subjects - WCH April & May 2013 Outcome Of Treatment Delay In Treatment Treatment Anaesthetic Not Worked Delay In Diagnosis Inappropriate Discharge New Complaint FLR Discharge Process Attitude Of Nursing Staff Attitude Of Medical Staff Following the last Trust Board meeting, a review of complaints regarding treatment, outcome of treatment and delay in diagnosis/treatment has commenced. This review will focus on reviewing the complaint to identify whether this complaint is serious and whether we have upehld the complaint. The outputs from this review were scheduled to be reported in May, however this will now be reported to the Board in June Complaints Received by Site for Primary subject for April 2013 (including reopened cases): Complaints Received For Site By Subject April & May 2013 Appt Cancelled OPD Appt Delay IP West Cumberland Hospital Cumberland Infirmary Records Appt OPD Wait In Clinic Attitude Of Staff (Nurse) Appt Delay OPD Appt Admin OPD Communication No. Complaints Attitude Of Staff Medical 24
25 5.4 Are complainants satisfied with our complaints process? We reported last month that understanding the themes from complaints from patients, their families and carers is important in order to learn lessons and change practice where necessary. It is equally important for the Trust to obtain feedback from complainants as to how they feel we have investigated and responded to their complaint. Satisfaction surveys are now issued to all complainants, which commenced in March questionnaires were sent out at the beginning of March to people who received a complaint response in January and February The response rate (2 months of Quarter 4) was 44% - a higher return than expected. Of the 14 questionnaires returned In total the results from Q4 2012/2013 confirm that: 57% of those who responded felt that their questions were addressed 42% felt the Trust had taken their concerns seriously 50% received a response between 1 4weeks 36% taking longer than 3 months to respond 43% felt that the Trust had taken action regarding their complaint 42% feeling that we had learned from their complaint 64% were satisfied overall with the process and response. This information will now be updated on a quarterly basis and will be reported to Trust Board again in July

 / Number applicable Compliance % with NICE policy = (Not applicable")
26 6 CLINICAL AUDIT AND EFFECTIVENESS The Clinical Audit Plan for 2013/14 has been approved by the Trust Board and is being implemented across the Clinical Business Units. A report on the delivery and monitoring of the plan is currently being developed to ensure the frequency and monitoring of the outcomes from clinical audit can be evidence and tracked through the organisation. Work has commenced on updating the Trust s NICE Register in order to improve the Trust s compliance position against NICE guidance. The table below summarises the position for the last three years: Compliance % of applicable Guidelines - = (Not audited + Audited) / Number applicable Compliance % with NICE policy = (Not applicable + Number applicable) / Number published At Clinical Policy Group in April the revised policy and process for implementing NICE was discussed which is now being implemented. A plan has been agreed to start work on reviewing the 208 guidelines which are awaiting response during quarter 1, which will start with reviewing those guidelines which pose the greatest clinical risk. This table will be updated each quarter to provide the Board with assurance on the implementation of NICE Guidelines across the organisation. 26

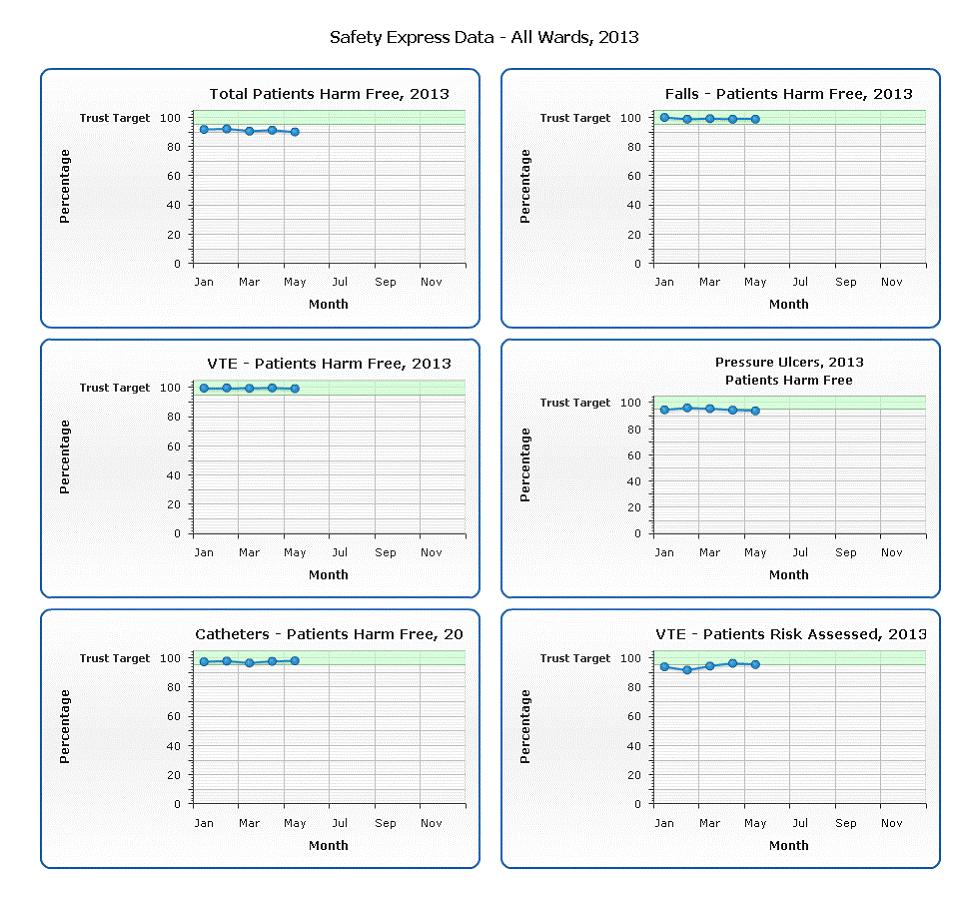
27 7. SAFETY THERMOMETER 503 patient s audits were completed in May 2013 and the graph below shows the percentage of patients who are receiving new harm free care is 94% this equates to 51 new harms within our organisation. The graphs below show a combination of harm free and new harm free care for each of the four harms from an organisational perspective which identifies that we had 51 Harms across the Trust for May The individual graphs show the percentage of harm free care relating to: Pressure Ulcers: 32 harms, Catheters: 10 harms, VTE: 4 harms, Falls: 7 harms VTE assessment: 95%. 27
28 28
29 Patients per 1,000 with harm free care Patients per 1,000 with harm free care Acute organisations: Harm free care 1020 Select view: Select organisation to highlight: Number of patients surveyed *NHS Organisations harm free care May 2013 Acute organisations: Harm free care 40 Select view: Select organisation to highlight: Number of patients surveyed *NHS Organisations New Pressure Areas May
30 7.2 Pressure Ulcers on admission and following admission Admitted with pressure ulcers Grade 1 Grade 2 Grade 3 Grade 4 Total no. ulcers Total no. pts. April May Pressure ulcers developed following admission Grade 1 Grade 2 Grade 3 Grade 4 Total no. ulcers Total no. pts. April May The first meeting of the new tissue viability group took place on 17 June This meeting will be held every two weeks and will review all grade 3 and 4 pressure ulcers acquired in our care. Month Grade Ward Immediate Actions May 4 Willow A Unavoidable May 3 Elm A Unavoidable May 3 Gable Unavoidable May 3 Larch A/B Avoidable. Catheter management discussed with the team. 30
31 8. IMPROVING PATIENT EXPERIENCE 8.1 Strategic Aim: To provide excellent patient-centric customer care This report outlines our local approach to improving patient experience and our position at the end of March The Trust is now in a position to carry out surveys on a scale that will allow for reliable results to be available at a Trust, Site, Department, Speciality, Ward and individual consultant level. The surveys have been designed to include all of the key questions from the questionnaire used in the CQC national patient survey programme but also include locally important priorities. 8.2 Key strategic question: To what extent are we meeting our patients expectations? Patient Perspective Data: Inpatients and Day Cases this is based on 391 patients (172 inpatients and 219 day cases) Likelihood of recommending the service to family and friends Overall satisfaction, (rating the inpatient service as excellent, very good or good) May-13 Inpatient 72.2% Day Case 86.4% May-13 Inpatient 89.8% Day Case 96.7% Patient Perspective Data: Outpatients this is based on 1798 patients Likelihood of recommending the service to family and friends May-13 Outpatient 79.5% Overall satisfaction, (rating the outpatient service as excellent, very good or good) May-13 Outpatient 95.1% 31

32 8.3 Key strategic question: Do we know what is important to our patients? The real time face to face programme is built around the things that really matter to patients. The Summary below provides a breakdown by ward of the 127 people interviewed in May. Real time Ward and site summary May 2013 Carlisle No of Patients Surveye d Coordination Respec t and dignity Involvemen t Doctor s Domains Nurse s Cleanlines s Pain Contro l Medicine s Domain Average Key Promote r Score No of Patients Surveye d Coordination Respec t and dignity Involvemen t Doctor s Nurse s Cleanlines s Pain Contro l Medicine s Domain Average Larch A Larch B Maple B Maple D Whitehaven Key Promote r Score No of Patients Surveye d Coordination Respec t and dignity Involvemen t Doctor s Nurse s Cleanlines s Pain Contro l Medicine s Domain Average Overwater Overwater Key Promote r Score Patterdale Pillar The Trust wide improvements on baseline are encouraging and should be celebrated at team level. Month on month ward teams will be encouraged to improve on their baseline performance by responding to the needs and feedback of patients in their care. 32
33 8.4 Friends and Family Test Inpatient Service Cumulative May 2013 FFT 2mins Extremely likely Likely Neither likely nor unlikely Unlikely Extremely Unlikely Don't Know Total Net Promoter Score % April % May % Total % Accident & Emergency Services May 2013 Cumulative DH Returns Extremely likely Likely Neither likely nor unlikely Unlikely Extremely Unlikely Don't Know Total Net Promot er Score % Respon se rate for each A&E Carlisle % 31.11% Whitehaven % 49.40% Total % 40.54% 9. RECOMMENDATION The Board are asked to approve the report. 33
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013
 TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
Mortality Report Learning from Deaths. Quarter
 Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Quality Improvement Scorecard December 2017
 Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
Quality Improvement Scorecard March 2018
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Quality Improvement Scorecard November 2017
 Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Quality Improvement Scorecard December 2016
 Mortality: HSMR Nat The improvement in performance has been maintained in year. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
Mortality: HSMR Nat The improvement in performance has been maintained in year. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
Sue Brown Clinical Audit and Effectiveness Manager. Safety and Quality Committee
 Report to Trust Board of Directors Date of Meeting: 24 June 2014 Enclosure Number: 11 Title of Report: Clinical Audit Plan for 2014/15 Author: Executive Lead: Responsible Sub- Committee (if appropriate):
Report to Trust Board of Directors Date of Meeting: 24 June 2014 Enclosure Number: 11 Title of Report: Clinical Audit Plan for 2014/15 Author: Executive Lead: Responsible Sub- Committee (if appropriate):
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Quality Improvement Scorecard June 2017
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES
 Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Quality Improvement Scorecard February 2017
 Mortality: HSMR Nat Performance continued to improve into Q3 2016/17. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
Mortality: HSMR Nat Performance continued to improve into Q3 2016/17. NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday)
TRUST CORPORATE POLICY RESPONDING TO DEATHS
 SCOPE OF APPLICATION AND EXEMPTIONS CONSULT ATION COR/POL/224/2017-001 TRUST CORPORATE POLICY RESPONDING TO DEATHS APPROVING COMMITTEE(S) EFFECTIVE FROM DISTRIBUTION RELATED DOCUMENTS STANDARDS OWNER AUTHOR/FURTHER
SCOPE OF APPLICATION AND EXEMPTIONS CONSULT ATION COR/POL/224/2017-001 TRUST CORPORATE POLICY RESPONDING TO DEATHS APPROVING COMMITTEE(S) EFFECTIVE FROM DISTRIBUTION RELATED DOCUMENTS STANDARDS OWNER AUTHOR/FURTHER
Board of Director s Meeting
 Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Richard Wilson, Quality Insight and Intelligence Director
 To: Board For meeting: 24 May 2018 Agenda item: 8 Report by: Richard Wilson, Quality Insight and Intelligence Director Report on: Quality Dashboard Purpose 1. This paper highlights the key observations
To: Board For meeting: 24 May 2018 Agenda item: 8 Report by: Richard Wilson, Quality Insight and Intelligence Director Report on: Quality Dashboard Purpose 1. This paper highlights the key observations
BSUH INTEGRATED PERFORMANCE REPORT. 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain
 Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain") BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
Together for Health A Delivery Plan for the Critically Ill
 Together for Health A Delivery Plan for the Critically Ill 2013-2016 March 2015 Approved at CPG Board 25 th March 2015 1. BACKGROUND AND CONTEXT Together for Health a Delivery Plan for the Critically Ill
Together for Health A Delivery Plan for the Critically Ill 2013-2016 March 2015 Approved at CPG Board 25 th March 2015 1. BACKGROUND AND CONTEXT Together for Health a Delivery Plan for the Critically Ill
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
QUALITY REPORT. Part A Patient Experience
 QUALITY REPORT Part A Patient Experience 1 Number of complaints Complaints and Patient Advice and Liaison Report 40 Total number of complaints received 30 20 10 Number of complaints received Trendline
QUALITY REPORT Part A Patient Experience 1 Number of complaints Complaints and Patient Advice and Liaison Report 40 Total number of complaints received 30 20 10 Number of complaints received Trendline
Integrated Quality Report
 Integrated Quality Report Data provided by Patient Services and the Clinical Governance and Risk Department June 2018 Included this month: Health-care Associated Infections Patient Falls Pressure Ulcers
Integrated Quality Report Data provided by Patient Services and the Clinical Governance and Risk Department June 2018 Included this month: Health-care Associated Infections Patient Falls Pressure Ulcers
Recognise and Rescue: A hospital wide collaboration to improve response to the deteriorating patient at Nottingham University Hospitals NHS Trust
 Recognise and Rescue: A hospital wide collaboration to improve response to the deteriorating patient at Nottingham University Hospitals NHS Trust Mark Simmonds (Acute and Critical Care Medicine Consultant,
Recognise and Rescue: A hospital wide collaboration to improve response to the deteriorating patient at Nottingham University Hospitals NHS Trust Mark Simmonds (Acute and Critical Care Medicine Consultant,
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 2018
 Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Policy on Learning from Deaths
 Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Quality & Performance Report. Public Board
 Agenda Item 12.1 Quality & Performance Report Public Board 27 th November 2014 Presented for: Presented by: Author: Previous Committees: Governance Professor Suzanne Hinchliffe CBE Chief Nurse / Interim
Agenda Item 12.1 Quality & Performance Report Public Board 27 th November 2014 Presented for: Presented by: Author: Previous Committees: Governance Professor Suzanne Hinchliffe CBE Chief Nurse / Interim
Appendix 1 MORTALITY GOVERNANCE POLICY
 Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
The Royal Wolverhampton Hospitals NHS Trust
 The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
MATERNITY SERVICES RISK MANAGEMENT STRATEGY
 Trust Board Agenda Item 8.3 Enc 10 Appendix 1 January 2012 MATERNITY SERVICES NORTH CUMBRIA MATERNITY SERVICES RISK MANAGEMENT STRATEGY 2011-13 DOCUMENT CONTROL Author/Contact Head Of Midwifery / Clinical
Trust Board Agenda Item 8.3 Enc 10 Appendix 1 January 2012 MATERNITY SERVICES NORTH CUMBRIA MATERNITY SERVICES RISK MANAGEMENT STRATEGY 2011-13 DOCUMENT CONTROL Author/Contact Head Of Midwifery / Clinical
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Gatwick Park Hospital Povey Cross Road, Horley, RH6 0BB
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Gatwick Park Hospital Povey Cross Road, Horley, RH6 0BB
This paper provides an update on the the recent national SPSP conference the programme of work for Tissue Viability Acute Adult Care SPSP
 Greater Glasgow and Clyde NHS Board Board Meeting December 2016 Board Paper No. 16/81 Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP) is one of the family
Greater Glasgow and Clyde NHS Board Board Meeting December 2016 Board Paper No. 16/81 Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP) is one of the family
Learning from Deaths; Mortality Review Policy
 Learning from Deaths; Mortality Review Policy Version: 4.0 New or Replacement: Replacement Policy number: CESC/2012/066 (Version 4) Document author(s): Executive Sponsor: Non-Executive Sponsor: Title of
Learning from Deaths; Mortality Review Policy Version: 4.0 New or Replacement: Replacement Policy number: CESC/2012/066 (Version 4) Document author(s): Executive Sponsor: Non-Executive Sponsor: Title of
Delivering Improvement in Practice
 v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST NHS SAFETY THERMOMETER
 Agenda item A5(vi) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST NHS SAFETY THERMOMETER EXECUTIVE SUMMARY The NHS Safety Thermometer is a point of care survey, which is a local improvement tool
Agenda item A5(vi) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST NHS SAFETY THERMOMETER EXECUTIVE SUMMARY The NHS Safety Thermometer is a point of care survey, which is a local improvement tool
April Clinical Governance Corporate Report Narrative
 April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
April 14 - Clinical Governance Corporate Report Narrative ITEM 7B Narrative has been provided where there is something of note in relation to a specific metric; this could be positive improvement, decline
Item E1 - Bart s Health Quality Indicators
 Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Nottingham University Hospitals Emergency Department Quality Issues Related to Performance
 RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Quality Improvement Strategy
 / Colchester Hospital University NHS Foundation Trust Quality Improvement Strategy 2015-2018 Including our four Quality goals Strategy Author Angela Tillett, Medical Director Version 1 Date of Issue -
/ Colchester Hospital University NHS Foundation Trust Quality Improvement Strategy 2015-2018 Including our four Quality goals Strategy Author Angela Tillett, Medical Director Version 1 Date of Issue -
Integrated Performance Report December 2015
 Portsmouth Hospitals NHS Trust QAH Hospital Page 1 Integrated Performance Report December 2015 Portsmouth Hospitals NHS Trust QAH Hospital Page 2 Contents Section Page 1 Performance Outcomes 3 2 Quality
Portsmouth Hospitals NHS Trust QAH Hospital Page 1 Integrated Performance Report December 2015 Portsmouth Hospitals NHS Trust QAH Hospital Page 2 Contents Section Page 1 Performance Outcomes 3 2 Quality
NHS TAYSIDE MORTALITY REVIEW PROGRAMME
 NHS TAYSIDE MORTALITY REVIEW PROGRAMME Aim Primary Drivers Processes, Rules of Conduct, Structure MEASUREMENT Secondary Drivers Components, Activities Understand how mortality rates/ratios are measured
NHS TAYSIDE MORTALITY REVIEW PROGRAMME Aim Primary Drivers Processes, Rules of Conduct, Structure MEASUREMENT Secondary Drivers Components, Activities Understand how mortality rates/ratios are measured
SUMMARY OF INDICATOR CHANGES FOR VERSION 3 INTELLIGENT MONITORING REPORTS Acute and Specialist NHS Trusts 23 June Final Draft, Subject to Change
 Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
This is a high level overview report to update the Board on the Acute Adult Safety Programme consisting of the following sections:
 Greater Glasgow and Clyde NHS Board Board Meeting June 2014 Board Paper No. 14/34 Board Medical Director Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP)
Greater Glasgow and Clyde NHS Board Board Meeting June 2014 Board Paper No. 14/34 Board Medical Director Scottish Patient Safety Programme Update 1. Background The Scottish Patient Safety Programme (SPSP)
Integrated Performance Report
 Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Measuring for improvement The new CQC hospital programme. Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013
 Measuring for improvement The new CQC hospital programme Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013 1 Our purpose and role Our purpose We make sure health and
Measuring for improvement The new CQC hospital programme Professor Sir Mike Richards Chief Inspector of Hospitals King s Fund 6 th November 2013 1 Our purpose and role Our purpose We make sure health and
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Early Warning Score Procedure
 Procedure Contents Purpose... 2 Scope/Audience... 2 Associated documents... 3 Definitions... 4 Adult patients... 4 Maternity patients... 4 Paediatric patients... 4 Equipment... 5 Education and training
Procedure Contents Purpose... 2 Scope/Audience... 2 Associated documents... 3 Definitions... 4 Adult patients... 4 Maternity patients... 4 Paediatric patients... 4 Equipment... 5 Education and training
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE
 Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Complaints, Litigation, Incident & PALS (CLIP) Summary Report Q2 July September 2009
 Summary Report Q2 July September 2009") Agenda 24/1 Public Board Meeting, 28 JAN 21 Complaints, Litigation, Incident & PALS (CLIP) Summary Report Q2 July September Presented by: Colin Johnston, Medical Director 1. Purpose The following CLIP
Agenda 24/1 Public Board Meeting, 28 JAN 21 Complaints, Litigation, Incident & PALS (CLIP) Summary Report Q2 July September Presented by: Colin Johnston, Medical Director 1. Purpose The following CLIP
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support The Open and Honest Care: Driving Improvement organisations to become more transparent
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support The Open and Honest Care: Driving Improvement organisations to become more transparent
Quarter /13 Quality Account (Quality and Safety)
") Airedale NHS Foundation Trust Board of Directors:23 rd January 213 Title: Quarter 2 212/13 Quality Account (Quality and Safety) Author: Alison Fuller, Assistant Director Healthcare Quarter 2 212/13 Quality
Airedale NHS Foundation Trust Board of Directors:23 rd January 213 Title: Quarter 2 212/13 Quality Account (Quality and Safety) Author: Alison Fuller, Assistant Director Healthcare Quarter 2 212/13 Quality
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Fitzwilliam Hospital Milton Way, South Bretton, Peterborough,
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Fitzwilliam Hospital Milton Way, South Bretton, Peterborough,
FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 HOW WE MEASURE QUALITY 16
 Contents FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 - Our achievements so far - Our aims for quality 2017 2020 AIM 1: AIM 2: AIM 3: AIM 4: Reducing
Contents FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 - Our achievements so far - Our aims for quality 2017 2020 AIM 1: AIM 2: AIM 3: AIM 4: Reducing
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Overview. Dr Stephen Gulliford & AKI Specialist Nurse Suzanne Wilson Page 1
 Improving Patient Safety and Reducing Harm through the Development of an Acute Kidney Injury Specialist Service at Wrightington, Wigan and Leigh NHS Foundation Trust Overview Acute Kidney Injury (AKI)
Improving Patient Safety and Reducing Harm through the Development of an Acute Kidney Injury Specialist Service at Wrightington, Wigan and Leigh NHS Foundation Trust Overview Acute Kidney Injury (AKI)
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Authors: Head of Outcomes & Effectiveness, Quality Project Manager and Deputy MD, Sponsor: Medical Director
 UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST MORTALITY REVIEW COMMITTEE 7 TH NOVEMBER 2017 EXECUTIVE QUALITY BOARD 7 TH NOVEMBER 2017 QUALITY ASSURANCE COMMITTEE 30 TH NOVEMBER 2017 TRUST BOARD 7 TH DECEMBER
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST MORTALITY REVIEW COMMITTEE 7 TH NOVEMBER 2017 EXECUTIVE QUALITY BOARD 7 TH NOVEMBER 2017 QUALITY ASSURANCE COMMITTEE 30 TH NOVEMBER 2017 TRUST BOARD 7 TH DECEMBER
MORTALITY REVIEW POLICY
 MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Paper 8 DECISION NOTE. Recommendation
 Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to: Discuss the current performance in relation to key quality indicators as at the end of August 20 Consider the actions being
Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to: Discuss the current performance in relation to key quality indicators as at the end of August 20 Consider the actions being
Learning from Deaths Framework Policy
 Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Care of Critically Ill & Critically Injured Children in the West Midlands
 Care of Critically Ill & Critically Injured Children in the West Midlands University Hospitals Coventry & Warwickshire NHS Trust Visit Date: 4 th December 2013 Report Date: April 2014 Images courtesy of
Care of Critically Ill & Critically Injured Children in the West Midlands University Hospitals Coventry & Warwickshire NHS Trust Visit Date: 4 th December 2013 Report Date: April 2014 Images courtesy of
Serious Incident Report Public Board Meeting 28 July 2016
 Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
Serious Incident Report Public Board Meeting 28 July 2016 Presented for: Presented by: Author Previous Committees Governance Dr Yvette Oade, Chief Medical Officer Louise Povey, Serious Incidents Investigations
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015 Subject: Supporting TEG Member: Authors: Status 1 Data Quality Baseline Assessment
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY REPORT TO THE TRUST BOARD HELD ON 18 NOVEMBER 2015 Subject: Supporting TEG Member: Authors: Status 1 Data Quality Baseline Assessment
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Clinical Governance report prepared for NHS Lanarkshire Board Report title Clinical Governance Corporate Report - October 2015
 Page 1 of 22 Print :15/1/215 Page 2 of 22 Print :15/1/215 Quality Ambition: Safe NHS Lanarkshire aims to be the safest health and care system in Scotland with no avoidable deaths, reduction in avoidable
Page 1 of 22 Print :15/1/215 Page 2 of 22 Print :15/1/215 Quality Ambition: Safe NHS Lanarkshire aims to be the safest health and care system in Scotland with no avoidable deaths, reduction in avoidable
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP
 COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
Strategic KPI Report Performance to December 2017
 Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
 Patient experience Litigation/Inquests April 216 The receipt of a formal letter of claim is the trigger for both clinical and non-clinical negligence claims against the Trust. The litigation team also
Patient experience Litigation/Inquests April 216 The receipt of a formal letter of claim is the trigger for both clinical and non-clinical negligence claims against the Trust. The litigation team also
Recognising a Deteriorating Patient. Study guide
 Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Recognising a Deteriorating Patient Study guide Recognising a deteriorating patient Recognising and responding to clinical deterioration Background Clinical deterioration can occur at any time in a patient
Care Quality Commission (CQC) Inspection Briefing
 Inspection Briefing") Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
Learning from the Deaths of Patients in our Care Policy
 Learning from the Deaths of Patients in our Care Policy Approved By: Date of Original Approval: UHL Mortality Review Committee UHL Policies & Guidelines Committee September 2017 Trust Reference: B31/2017
Learning from the Deaths of Patients in our Care Policy Approved By: Date of Original Approval: UHL Mortality Review Committee UHL Policies & Guidelines Committee September 2017 Trust Reference: B31/2017
Integrated Performance Report
 Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Percent Unadjusted Inpatient Mortality (NHSL Acute Hospitals) Numerator: Total number of in-hospital deaths
 Numerator: Total number of in-hospital deaths") Page 1 of 23 Quality Ambition: Safe NHS Lanarkshire aims to be the safest health and care system in Scotland with no avoidable deaths, reduction in avoidable harm, a sustainable infrastructure for patient
Page 1 of 23 Quality Ambition: Safe NHS Lanarkshire aims to be the safest health and care system in Scotland with no avoidable deaths, reduction in avoidable harm, a sustainable infrastructure for patient
Moving to 7 Day Services. Kerry Gant, Head of Finance Change Team/Debbie Freake, Executive Director of Strategy
 Report to Trust Board of Directors Date of Meeting: 24 March 2015 Enclosure Number: 12 Title of Report: Author: Executive Lead: Responsible Sub- Committee (if appropriate): Executive Summary: Moving to
Report to Trust Board of Directors Date of Meeting: 24 March 2015 Enclosure Number: 12 Title of Report: Author: Executive Lead: Responsible Sub- Committee (if appropriate): Executive Summary: Moving to
BOARD CLINICAL GOVERNANCE AND QUALITY UPDATE FEBRUARY 2016
 Borders NHS Board BOARD CLINICAL GOVERNANCE AND QUALITY UPDATE FEBRUARY 2016 Aim This report aims to provide the Board with an overview of progress in the areas of: Patient Safety Clinical Effectiveness
Borders NHS Board BOARD CLINICAL GOVERNANCE AND QUALITY UPDATE FEBRUARY 2016 Aim This report aims to provide the Board with an overview of progress in the areas of: Patient Safety Clinical Effectiveness
Inpatient, Day case and Outpatient Stage of Treatment Waiting Times
 Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 30 June 2016 Publication date 30 August 2016 A National Statistics Publication for Scotland
Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 30 June 2016 Publication date 30 August 2016 A National Statistics Publication for Scotland
Integrated Performance Report
 Integrated Performance Report M04 July 2016 Presented by: Angela Stevenson (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M04 July 2016 Presented by: Angela Stevenson (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Quality Strategy: Liverpool Women s NHS Foundation Trust
 Quality Strategy: 2017-2020 Liverpool Women s NHS Foundation Trust Contents Foreword... 3 Our Trust... 4 Trust Board... 4 What is our Vision and what are our Aims and Values?... 5 The drivers in developing
Quality Strategy: 2017-2020 Liverpool Women s NHS Foundation Trust Contents Foreword... 3 Our Trust... 4 Trust Board... 4 What is our Vision and what are our Aims and Values?... 5 The drivers in developing
NHS Borders Feedback and Complaints Annual Report
 NHS Borders Feedback and Complaints Annual Report 2016-17 1 Introduction NHS Borders Feedback and Complaints Annual Report 2016-17 is a summary of the feedback provided by the complaints, comments, concerns
NHS Borders Feedback and Complaints Annual Report 2016-17 1 Introduction NHS Borders Feedback and Complaints Annual Report 2016-17 is a summary of the feedback provided by the complaints, comments, concerns
CRAB : Big Scale Routine Data as First Alert
 Workshop 3: Patient safety and mhealth/big data/hand held services CRAB : Big Scale Routine Data as First Alert Ingo Gurcke, Dipl. Kaufmann (FH), Marsh Medical Consulting GmbH, Managing Director, Germany
Workshop 3: Patient safety and mhealth/big data/hand held services CRAB : Big Scale Routine Data as First Alert Ingo Gurcke, Dipl. Kaufmann (FH), Marsh Medical Consulting GmbH, Managing Director, Germany
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST. Quarterly Clinical Effectiveness and Outcomes Report:
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Quarterly Clinical Effectiveness and Outcomes Report: Report to Trust Board 27 th September 2011 Report from Sponsoring Executive Aim of Report Jane Druce, Quality
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Quarterly Clinical Effectiveness and Outcomes Report: Report to Trust Board 27 th September 2011 Report from Sponsoring Executive Aim of Report Jane Druce, Quality
TRUST BOARD. Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director. Jo Hunter, Deputy Chief Nurse. Mary Heritage, Assistant Director of Quality
 TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
Our Achievements. CQC Inspection 2016
 Our Achievements CQC Inspection 2016 Issued February 2017 HOW FAR WE VE COME SAFE Last year, we set out our achievements in a document for staff and patients. It was extremely well received, and as a result,
Our Achievements CQC Inspection 2016 Issued February 2017 HOW FAR WE VE COME SAFE Last year, we set out our achievements in a document for staff and patients. It was extremely well received, and as a result,
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support The Open and Honest Care: Driving Improvement organisations to become more transparent
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support The Open and Honest Care: Driving Improvement organisations to become more transparent
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital Report for: Royal Wolverhampton NHS Trust January 2016 The Open and Honest Care: Driving Improvement Programme aims to support organisations to become more transparent
Open and Honest Care in your Local Hospital Report for: Royal Wolverhampton NHS Trust January 2016 The Open and Honest Care: Driving Improvement Programme aims to support organisations to become more transparent
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Warrington and Halton Hospitals NHS Foundation Trust Quality Report
 Warrington and Halton Hospitals NHS Foundation Trust Quality Report 2016-2017 Contents Part 1 Statement of Quality from the Chief Executive 7 Part 2 Improvement Priorities & Statement of Assurance from
Warrington and Halton Hospitals NHS Foundation Trust Quality Report 2016-2017 Contents Part 1 Statement of Quality from the Chief Executive 7 Part 2 Improvement Priorities & Statement of Assurance from
SAFE CARE. Scottish Patient Safety Programme. SPSP Adult Acute
 SAFE CARE NHS Greater Glasgow and Clyde (NHS GGC) is committed to providing safe high quality care that our staff and patients can be proud of. Over recent years the Scottish Patient Safety Programme has
SAFE CARE NHS Greater Glasgow and Clyde (NHS GGC) is committed to providing safe high quality care that our staff and patients can be proud of. Over recent years the Scottish Patient Safety Programme has
Assessing Quality of Hospital Services - the importance of national clinical audits
 Assessing Quality of Hospital Services - the importance of national clinical audits Professor Sir Mike Richards Chief Inspector of Hospitals November 2015 1 Overview CQC s role and purpose Our approach
Assessing Quality of Hospital Services - the importance of national clinical audits Professor Sir Mike Richards Chief Inspector of Hospitals November 2015 1 Overview CQC s role and purpose Our approach
SUBJECT: CLINICAL GOVERNANCE
 Meeting of Lanarkshire NHS Board Lanarkshire NHS Board Kirklands 25 September 2013 Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk 1. PURPOSE SUBJECT: CLINICAL GOVERNANCE
Meeting of Lanarkshire NHS Board Lanarkshire NHS Board Kirklands 25 September 2013 Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk 1. PURPOSE SUBJECT: CLINICAL GOVERNANCE
PERFORMANCE IMPROVEMENT REPORT
 PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
Quality and Safety Strategy
 Quality and Safety Strategy 2017-2020 Vision statement ESHT combines community and hospital services to provide safe, compassionate, and high quality care to improve the health and wellbeing of the people
Quality and Safety Strategy 2017-2020 Vision statement ESHT combines community and hospital services to provide safe, compassionate, and high quality care to improve the health and wellbeing of the people
System enablers practical aspects Chair Lesley Anne Smith
 System enablers practical aspects Chair Lesley Anne Smith Time Topic Room Optional lunchtime sessions, numbers limited to 50 per room, catering provided in the room 13.15 QI Harris Level 1 Service Users
System enablers practical aspects Chair Lesley Anne Smith Time Topic Room Optional lunchtime sessions, numbers limited to 50 per room, catering provided in the room 13.15 QI Harris Level 1 Service Users
Ayrshire and Arran NHS Board
 Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz