IAPT Service Review Norfolk and Waveney STP
|
|
|
- Jewel Stafford
- 5 years ago
- Views:
Transcription


1 IAPT Service Review Norfolk and Waveney STP Intensive Support Team Mental Health 20 th April 2017
2 Context The Mental Health Intensive Support Team (IST) Part of the NHS Improvement A free resource to NHS organisations Work with local health communities that are facing particular challenges in delivery of the Access, Recovery and Waiting Times KPIs, as well as delivering the IAPT Quality Standards IST Approach Diagnostic Review Agree scope and expectations with the provider and commissioner Obtain information from provider and commissioner to facilitate diagnostic Additional data collection and telephone conference calls to seek clarification as required Feedback and recommendations NHS England IAPT Website including: IAPT Quality Standards Link to national archives Three year Report Link to National Archives IAPT annual report 2
3 Scope Reasons for Engagement Understand the reason for low outcomes Help to strengthen existing recovery plans Identify good practice from high-performing services Limitations: Despite several attempts, NSFT have not been able to produce reliable data relating to sessional dose, outcomes, scores and clusters. This report is provided in order to maintain momentum from the visit but this should be borne in mind when viewing some of the slides where data is questioned this is clearly flagged. This summary report is provided to facilitate discussion but it should be noted that a diagnostic review is inherently high level. The interpretation of IST findings should be followed up with more detailed local discussion. This summary covers: Value for Money Referrals, Access and Waits Severity and Complexity Staffing, Leadership and Management Recovery and reliable improvement Data Quality and Reporting 3
4 Good Practice Patient engagement, navigators and ambassadors Plans for moving to national tariff are well advanced and most patients are clustered Systems and processes for front end (first and second) appointments seem effective Good self-referrals and options for walk in access Focus on social component and peer support Clinical/managerial alignment at senior level Low overheads with over 80% of funding spent on staff and direct costs 4
5 Executive Summary Service user involvement in the service is strong and an area of good practice Many patients currently do not receive an assessment and this is contrary to NICE guidelines Over-reliance on groups and lack of assessment have created a complex, inefficient pathway delivering poor outcomes Local contractual incentives for short waits to first and second appointment have hidden waits of up to one year between second and third appointment Productivity amongst clinical staff is low and is not effectively managed by the provider A significant number of counselling staff do not have an IAPT qualification Investment is high, particularly considering the levels of activity and outcomes delivered Analytical support is under-resourced and accurate data is not available to either provider or commissioners Patients are limited to their home GP practice at the expense of waiting times and appropriateness of treatment In the context of current productivity, pathway and allocative efficiency, capacity is inadequate to deliver timely treatment 5
6 The Model Systems and Processes, Waits, Staffing and Supervision
7 Patient Pathway: Challenges The front end of the patient s pathway and entry to treatment is complex and lacks consistency. Patients can enter the service and receive treatment in the workshop element of the service without assessment. They can remain there for long periods without being evaluated staff gave examples of up to a year. This is not consistent with NICE guidelines 1 The decision to treat is reported by clinical staff to be based on several non-clinical factors including Pressure in the service (e.g. waiting times) A perception that clinicians should place patients in a workshop rather than individual therapy Patients are experiencing long waits for treatment in some areas (up to one year was reported in Norwich CCG). Staff are recording treatment as having started at assessment/review appointments even when patients are being placed on waiting lists and not receiving treatment. Although a high number of sessions are being offered to some patients elsewhere in the service, counsellors are not offering full dosage as prescribed by NICE. Some counsellors are not trained or qualified in an IAPT modality. Clinical staff referred to a perceived gap between the offer made in primary care and what is available in secondary care. Staff reported a lack of psychological therapy resource within secondary care mental health services. 7 1 Quality standard 1: People who may have depression receive an assessment that identifies the severity of symptoms, the degree of associated functional impairment and the duration of the episode
8 Clinical Leadership The service has appointed leads in all areas of the service and this is good practice. Leaders have an awareness of the challenges due to frequent and often rushed change and the impact this has on the workforce. Morale is low within the staff groups and this is a challenge to leadership in continuing to implement service improvement. There is an over-reliance on the patient to indicate that they require a different intervention. This is problematic given the nature of anxiety and depression. Whilst it is recognised that it is good practice to use a holistic model of patient care, the service is in danger of encouraging a reductionist view if it continues to see the social element of the model in isolation. 8
9 Staffing and Training High-Intensity Therapist Type Current Ratio NICE-Suggested Ratio 1,2 CBT 61.3% 68% - 73% Counselling for Depression 1.1% 3% - 5% IPT 0.2% 11% - 17% Couples Therapy 1.2% 3% - 5% Psychodynamic 0.0% 5% EMDR 4.9% 2% Not IAPT Qualified 30.1% 0% Step 2 to Step 3 Staff Ratio 41:59 Admin to Therapy Staff Ratio 1:6.9 1 Suggested ratios derived from (a) NHS England Action for Choice of Therapies (ACT) working assumptions, based on NICE Guidance and relative prevalence of conditions (Prof David Clarke) (b) NICE National Collaborating Centre for Mental Health Estimates (Prof Steve Pilling) 2 Assumes patients with a particular condition would choose equally between the NICErecommended options for that condition. A significant number of counsellors are employed by the service who do not have any IAPT qualification IAPT funding should not be used to fund non-evidence-based interventions e.g. person-centred counselling The trust appears to have significant gaps, particularly relating to IPT and DIT Peer Support Workers appear to be providing some IAPT interventions e.g. Behavioural Activation which may be appropriate to be included in the IAPT dataset as part of an evidence-based pathway led by IAPT-qualified staff 9 Data source: Staffing Information Provided by the Trust
10 Investment The IAPT Model As a guide, the investment in step 2/3 psychological therapies needs to equate to around per head of prevalence. In most cases this should be sufficient to deliver 16.8% Access and 50% Recovery based on a set of modelling assumptions. Those assumptions are: positive clinical contact hours are delivered per WTE therapist per week 2. An overall average of around 6 sessions per patient entering treatment. This comprises of courses of treatment (two or more sessions) averaging 9 sessions (combined Step 2&3). In addition there will be a number of patients who drop out after a single session, giving an overall average of around 6 sessions 3. 75% - 80% of investment converts to a Clinical Staff budget and approximately 20% to overheads/indirect cost. The following slides describe where the service currently sits against these criteria. N.B. The model described here should be a starting point for discussion. As soon as the locally agreed pathways change from the above assumptions (and there may be good reasons for doing so), the level of investment required to achieve 16.8% Access and 50% recovery will change. 10
11 Investment Actual Planned investment by the CCGs for 17/18 is 10,179,759 and the estimated prevalence is 112,291. Investment assumptions Per Head of Prevalence Value: staff percentage % Staff/Direc t Cost Prevalence Investment in MH Dashboard Trust IAPT Spend Dashboard Trust Spend Staff and Direct Costs West Norfolk 18,500 1,750,000 1,609, ,379,267 86% South Norfolk 25,565 2,019,000 1,932, ,591,279 82% Norwich 22,457 2,317,000 2,296, ,826,149 80% North Norfolk 18,567 1,868,000 1,733, ,472,269 85% Great Yarmouth and Waveney 27,202 2,674,000 2,608, ,107,519 81% Norfolk & Waveney STP 112,291 10,628,000 10,179, ,376,482 82% On this basis spending on IAPT in Norfolk is around 91 per head of prevalence. The expected investment level to deliver 16.8% prevalence is per head. Given the ambition of the CCG to deliver 16% in 17/18 this is substantially above normal expectations subject to the three assumptions listed on the previous slide, which are explored in more detail on the following slides. 11
12 Assumption 1 Productivity Assumption: positive clinical contact hours are delivered per WTE therapist per week WTE Step 2 Step 3 Total Unadjusted 26,506 31,780 58,285 Vacancy/Absence 4,652 1,344 5,996 After Overtime 31,157 33,124 64,281 Net Total 26,506 31,780 58,285 Patient Hours/WTE Step 2 Step 3 Total Annual Week Year Week Year The trust has not been able to provide reliable information about productivity It is not, therefore, possible to ensure that therapists are productive and the service delivering value for money Based on data provided by the Trust, productivity is extremely low This may not reflect that staff are not working hard, but that the activity undertaken is not always value-adding This is also likely reflective of the degree of complexity in the current treatment pathways and size of waiting lists for subsequent treatments 12 Data source: 1/3/16-28/2/17 Data Provided by the Trust
13 Assumption 2 Average Sessions Assumption: An overall average of 6-7 sessions per patient entering treatment. Including Single Sessions Excluding Single Sessions Summary Data Step Two Step Three Total Step Two Step Three Total Mean Sessions Median Sessions This is likely to be inaccurate but is based on current data as provided The trust are not able to provide accurate information about sessions attended Without accurate information there is no way for the trust to be able to monitor or demonstrate adherence to NICErecommended dosage 13 Data source: 1/3/16-28/2/17 Data Provided by the Trust
14 Assumption 3 Clinical Staff Spend Assumption: 75% - 80% of investment converts to a Clinical Staff budget and approximately 20% to overheads/ indirect costs Around 82% of the overall budget YTD has been spent on direct costs for clinical staff. Based on this figure the service has low overheads compared to spending on staff, and NSFT have confirmed that there are no indirect costs allocated to the IAPT service. Staffing levels sense check Based on high-level guideline of WTE therapy staff per 1,000 prevalence: CCG prevalence suggests around WTE clinical staff to deliver 16.8% access and 50% recovery rates, depending on the model commissioned. The current therapist establishment is around 142WTE in budget. Current staffing levels are at the higher end of expectations based on the current level of access in terms of WTE, but may be in line with the expected numbers needed to deliver the 16.8% access planned for a clinically-appropriate number of sessions. 14
15 Commissioning CCGs have committed funding to IAPT expansion to 16.8% for 17/18 Commissioners are well-prepared for the move to National Tariff although further work is needed at pace Commissioners have decided to reduce funding for IAPT to provide a non-iapt Enhanced Care Pathway Commissioning is clinically-led with a strong GP voice but it is important that this is heard within the context of delivering clinically-appropriate treatments, reasonable waiting times and value for money Contacts, KPIs and monitoring information is not aligned to national CCG performance standards Performance currently provided to CCG Boards does not match actual reported performance The IST heard that CCGs were offered the alternative of more accurate NHS Digital data but declined CCGs are committed to the development of LTC pathways but have not yet developed a plan or engaged with either NSFT or acute providers to discuss 15
16 Referrals and Access
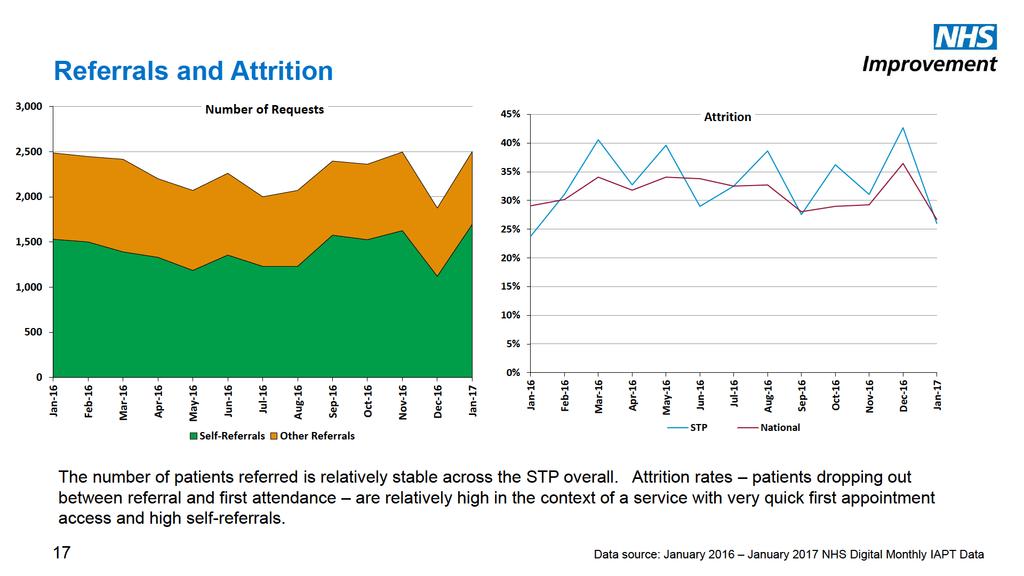
17
18 Completion/Drop Outs Invalid/No Reason/Unknown, 0.00% Not IAPT, 1.83% Pathway End Reasons In addition to patients dropping out prior to first appointment, it appears that more patients drop out than complete treatment. Stepped Down, 0.00% Stepped Up, 0.00% Assessed Only, 0.00% Completed, 27.23% Dropped Out, 37.30% In light of the general level of data quality in NSFT IAPT data, it is recommended that the trust assess the accuracy with which this data item is completed by staff before drawing firm conclusions from this information. Deceased, 0.00% Referred Elsewhere, 0.23% Mutual Agreement, 7.09% Signposted, 6.86% Declined, 17.39% It is recommended that the trust audit attrition reasons, first using data (discharge/end reasons) then patient notes in order to understand why patients are not engaging with the service and then develop action plans accordingly. Not Suitable, 1.14% 0% 5% 10% 15% 20% 25% 30% 35% 40% 18 Data source: January 2017 NHS Digital Monthly IAPT Data
19
20 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Equity of Access Older Adults Services need to provide prompt access and equity of access ensuring inclusion of marginalised groups such as older people, the long term unemployed, BME groups and under-represented clinical conditions. 16% 14% 12% Proportion of Patients Referred Over 65 Norwich CCG National evidence is that older people do well in IAPT services. The national recovery rate for people aged over 65 in was 57%. 10% 8% The percentage of older people referred in Norfolk is less than might be expected. 6% South, West and North Norfolk CCGs have chosen not to use the 17/18 Quality Premium to prioritise equity of access to IAPT ( Reasons to be explored include: Lack of awareness amongst health professionals, including GPs Marketing not targeted sufficiently to reach older people and/or the offer does not meet their need 20 4% 2% 0% Actual Prevalence Data source: Q Q NHS Digital Quarterly IAPT Data
21 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Equity of Access Older Adults 25% Proportion of Patients Referred Over 65 South Norfolk 25% Proportion of Patients Referred Over 65 North Norfolk 20% 20% 15% 15% 10% 10% 5% 5% 0% 0% Actual Prevalence Actual Prevalence 21 Data source: Q Q NHS Digital Quarterly IAPT Data
22 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Equity of Access Older Adults 25% Proportion of Patients Referred Over 65 GY&W 25% Proportion of Patients Referred Over 65 West Norfolk 20% 20% 15% 15% 10% 10% 5% 5% 0% 0% Actual Prevalence Actual Prevalence 22 Data source: Q Q NHS Digital Quarterly IAPT Data
23
24 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 25% Norwich CCG 20% GY&W CCG 18% 20% 16% 14% 15% 12% 10% 10% 8% 6% 5% 4% 2% 0% 0% CCG Standard National CCG Standard National 24
25 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Stable Access 20% South Norfolk CCG 25% North Norfolk CCG 18% 16% 20% 14% 12% 15% 10% 8% 10% 6% 4% 5% 2% 0% 0% CCG Standard National CCG Standard National 25
26 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Declining Access and Referrals 25% 20% West Norfolk CCG In West Norfolk in particular it appears that both access (blue line) and referrals (puce line) are declining, in the context of a requirement to increase both. 15% 10% Across all areas it is important to understand the reasons behind any decline by engaging with GPs and other referrers; it is also important to identify gaps in referrals along lines of gender, ethnicity, locality, age etc. 5% The extent of first treatment activity variation across different services underscores the important of ensuring that NSFT is able to manage capacity flexibly across different teams. 0% 0 Access Rate Standard Referrals 26
27 Severity and Complexity Severity PHQ, GAD7 Complexity WSAS and Clustering
28
29 Enhanced Care Pathway (ECP) The IST heard that the ECP is intended to provide holistic support to patients who are deemed to be not ready for an IAPT intervention The data in regard to severity and complexity suggest that, prior to the implementation of the ECP, the complexity/severity patient profile matched the national picture Use of ECP could be expected to reflect in the service seeing/treating patients that are less complex/severe than the average IAPT service. If this is the case the recovery rate can be expected to be well in excess of the 50% target, and NSFT and commissioners would not have outcomes information to monitor the effectiveness of the ECP IST expressed concern in regard to patients on the ECP. During the visit it was suggested, and accepted, that once an ECP patient is ready for psychological therapy intervention, their data will be included in the IAPT dataset Extra funding is to be provided for the ECP outwith the IAPT investment detailed earlier The primary care mental health resources to deliver the ECP could alternatively be used to support core IAPT, in the context of a requirement for IAPT expansion 29
30
31
32 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 DNAs Low DNA rates are correlated to high recovery and reliable improvement rates as they evidence high patient engagement. 25% 20% DNA Rate DNA rates in the Trust are extremely high. It is felt that this is disproportionately due to DNAs in groups. Even excluding groups, the trust has higher DNA rates than the national average. It is also likely the case that long waiting times are suppressing DNA rates and that as waits come down there may be a rise in DNAs. The trust does not have visibility of therapist/modality DNA rates which is likely to give rise to considerable variation. 15% 10% 5% 0% STP National 32 Data source: January 2016 January 2017 NHS Digital Monthly IAPT Data
33 Outcomes Recovery and Reliable Improvement Factors Affecting Recovery Rates
34
35 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Outcomes In addition the following factors contribute to those primary factors explored in other slides: 1) High DNA rate 2) High drop out rates, due to poor processes 70% 60% 50% 40% Three-Month Rolling Reliable Improvement Rate 3) Long waits 4) Poor recording of outcomes scores (all ADSMs) and presenting problem codes. 5) Stepped Care not used appropriately 6) Low self-referrals 7) Clinical Leadership and Supervision; Audit 30% 20% 10% 0% STP National 35 Data source: November 2015 January 2017 NHS Digital Monthly IAPT Data
36
37 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Reliable Deterioration 10% Three-Month Rolling Reliable Deterioration Rate People who have not benefited from treatment in IAPT would be expected to show some reliable deterioration as natural fluctuations in their condition would persist. There is, however, a growing body of evidence 1 which indicates that some psychological therapies when delivered in certain ways, can cause harm. It is recommended that the Trust ask the following: Are the people who show reliable deterioration predominantly people who start below caseness or are they people who already have symptoms of clinical severity? Do some therapists who have seen a reasonable number of cases have particularly high reliable deterioration rates? 9% 8% 7% 6% 5% 4% 3% 2% 1% 0% Do some therapies or staff groups have particularly high reliable deterioration rates as currently implemented in the service? Do patients with some particular problems (ICD-10 codes) or particular backgrounds (age, gender, sexual orientation, ethnicity etc.) have particularly high reliable deterioration rates. 1 Barlow, D.H. (2010). Negative effects from psychological treatments. American Psychologist, 65, Data source: November 2015 January 2017 NHS Digital Monthly IAPT Data STP National
38 Data Completeness Problem Descriptor NHS Digital data for Q3 shows that around 97% of patients had a problem descriptor (ICD10) code recorded at the start or during treatment as Other which is the default value added by admin staff on referral. Problem Descriptor at Treatment Other, 96.94% Many patients are not currently assessed, and problem descriptors are not used even where assessments do take place. Problem definition should be used to ensure that the treatment chosen is NICE-recommended for the presenting condition during treatment (assuming appropriate treatment choices are available), to maximise recovery potential. Mixed Anxiety/Depressive, 0.49% Generalised Anxiety, 0.37% Mixed anxiety and depression should only be used for people with milder symptoms of depression and anxiety that are insufficiently severe or extensive to warrant any other (depression or anxiety) problem descriptor. Services that incorrectly use the mixed anxiety and depression code for people with a depressive episode AND an anxiety disorder run the risk that they will miss the key features of the latter and hence give sub-optimal treatment. 38 Depression, 1.71% 0% 20% 40% 60% 80% 100% 120% Data source: Q3 2016/17 NHS Digital Quarterly IAPT Data
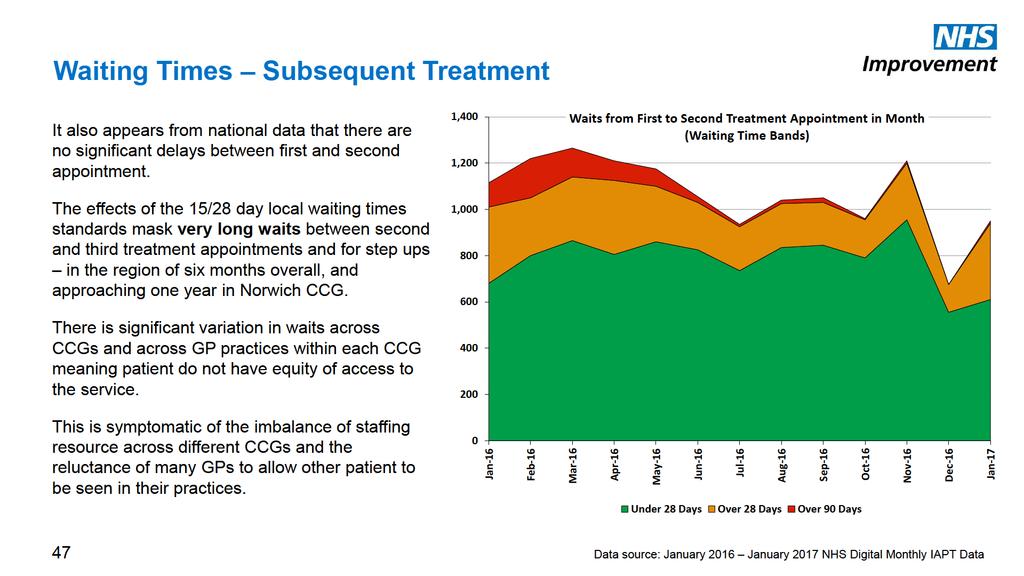
39 Administrative Processes and Waits Waiting Times and Waiting List Management Information and Reports
40 Administration and Pathway Patients who are referred through the SPOA (GP and health professional referrals) are triaged twice, mainly to identify if a patient is suitable for groups Booking processes are generally slick and patients are contacted an booked quickly for first and second appointments Only one attempt is made to contact patients by phone before they are sent a booking letter There is no guarantee that this attempt will be made out of hours Dedicated new slots are made available by all therapists. Where insufficient new slots are available (Norwich), this capacity is not flexed and patients wait longer. Many GP surgeries will not permit other surgeries patients to be seen, increasing waiting times and reducing access to the full range of IAPT modalities There is an inconsistent approach to charging for GP premises 45
41
42
43 Information and Reports Data is not signed off prior to or after upload and there are no related governance processes in NSFT There is a redundant system to reconcile two local datasets, but no reconciliation of local to NHS Digital data Both provider and commissioner boards receive inaccurate local data There is regular data quality monitoring from a dedicated staff member, and issues are addressed with staff who make repeated errors Data quality checks are not currently aligned to data items which are key to supporting the service and reporting accurately e.g. paired scores, problem descriptors, ADSM use Data is not stored on the trust data warehouse making reporting time-consuming and inaccurate NHS Digital data is not checked and reconciled with local reports, and the NHS Digital PAVE and data quality reports are not used Regular waiting lists reports are produced to support first and second appointment processes No waiting list reports are produced to summarise and monitor third treatment waits Therapist dashboards are not currently in use and outcomes and productivity are not monitored at therapist level 48
44 Conclusions and Recommendations
45 Clinical and Pathway Recommendations Revise the patient pathway to ensure it is simplified, clear and more linear for the patient Ensure that all patients are assessed on entering the service Ensure that all patients are clustered at assessment Problem descriptors should be recorded at assessment and decision to treat should be based on the problem descriptor and NICE guidance. Patients on the enhanced care pathway who receive an IAPT psychological therapy should be included in IAPT data. Some of the social care pathway could be considered for inclusion in IAPT data set e.g. groups/interventions that are behavioural activation and supervised by a qualified member of staff. Address long waits and consider an interim pathway for longest waits. Ensure all interventions/treatments are evidence-based and the full dosage available to patients, Counsellors should be required to train in an IAPT modality and a training plan put in place. 50
46 Admin and Management Recommendations Examine reasons behind high attrition rates and declining referrals, as well as underprovision to older adults and BME communities Revisit demand and capacity planning to address root cause of long waits Allocate increased analytical resource to IAPT within NSFT, ensure that IAPT data is easily accessible and, where possible, automated through trust data warehouse Use NHS Digital data in internal reports within both NSFT and CCGs, with local data only used for most recent months where NHS Digital data is not yet available Carry out monthly reconciliation of NHS Digital and local data using the PAVE report Align data quality measures to priorities such as problem descriptor, cluster and scores Develop more sophisticated waiting list management processes and reports for all waits Strengthen case management to include monitoring of delivered and forthcoming sessions, outcomes and DNA rates Develop therapist dashboards to support case management Regularly analyse outcomes by team/modality/therapist in order to focus service improvement 51
47 Contact Follow us on Michael Watson Intensive Support Manager Intensive Support Team (Mental Health) M E M.Watson@nhs.net W improvement.nhs.uk Follow NHS Improvement on: Twitter LinkedIn 52
Evaluation of NHS111 pilot sites. Second Interim Report
 Evaluation of NHS111 pilot sites Second Interim Report Janette Turner Claire Ginn Emma Knowles Alicia O Cathain Craig Irwin Lindsey Blank Joanne Coster October 2011 This is an independent report commissioned
Evaluation of NHS111 pilot sites Second Interim Report Janette Turner Claire Ginn Emma Knowles Alicia O Cathain Craig Irwin Lindsey Blank Joanne Coster October 2011 This is an independent report commissioned
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Improving Access to Psychological Therapies. Guidance for Commissioning IAPT Training 2012/13. Revised July 2012
 Improving Access to Psychological Therapies Guidance for Commissioning IAPT Training 2012/13 Revised July 2012 IAPT Programme Department of Health Wellington House 133-155 Waterloo Road London SE1 8UG
Improving Access to Psychological Therapies Guidance for Commissioning IAPT Training 2012/13 Revised July 2012 IAPT Programme Department of Health Wellington House 133-155 Waterloo Road London SE1 8UG
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
PRIMARY CARE COMMISSIONING COMMITTEE
 PRIMARY CARE COMMISSIONING COMMITTEE 1. Date of Meeting: 2. Title of Report: Western Avenue Medical Centre Personal Medical Services (PMS) Reinvestment Report 3. Key Messages: The Personal Medical Services
PRIMARY CARE COMMISSIONING COMMITTEE 1. Date of Meeting: 2. Title of Report: Western Avenue Medical Centre Personal Medical Services (PMS) Reinvestment Report 3. Key Messages: The Personal Medical Services
Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk
 Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
OUTLINE PROPOSAL BUSINESS CASE
 OUTLINE PROPOSAL BUSINESS CASE Name of proposer: Dr. David Keith Murray, General Practitioner, Leeds Student Medical Practice, 4, Blenheim Court, Blenheim Walk, LEEDS LS2 9AE Date: 20 Aug 2014 Title of
OUTLINE PROPOSAL BUSINESS CASE Name of proposer: Dr. David Keith Murray, General Practitioner, Leeds Student Medical Practice, 4, Blenheim Court, Blenheim Walk, LEEDS LS2 9AE Date: 20 Aug 2014 Title of
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING ADULT AND CHILDREN CONTINUING HEALTHCARE ANNUAL REPORT
 9.6 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING ADULT AND CHILDREN CONTINUING HEALTHCARE ANNUAL REPORT Date of the meeting 18/07/2018 Author Sponsoring Board member Purpose of Report
9.6 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING ADULT AND CHILDREN CONTINUING HEALTHCARE ANNUAL REPORT Date of the meeting 18/07/2018 Author Sponsoring Board member Purpose of Report
Waiting Times Report Strategic. Thematic Goals
 Strategic Improved Quality of Care Transformation - Prevention & Wellbeing Thematic Goals Waiting Times Report 2016-17 Transformation through Integration Improved Access to Services Improved Value This
Strategic Improved Quality of Care Transformation - Prevention & Wellbeing Thematic Goals Waiting Times Report 2016-17 Transformation through Integration Improved Access to Services Improved Value This
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms
 Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
2. The mental health workforce
 2. The mental health workforce Psychiatry Data provided by NHS Digital demonstrates that in September 2016 there were 8,819 psychiatrists (total number across all grades). This is 6.3% more psychiatrists
2. The mental health workforce Psychiatry Data provided by NHS Digital demonstrates that in September 2016 there were 8,819 psychiatrists (total number across all grades). This is 6.3% more psychiatrists
Child and Adolescent Mental Health Services Waiting Times in NHSScotland
 Publication Report Child and Adolescent Mental Health Services Waiting Times in NHSScotland Quarter ending 30 September 2016 Publication date 6 December 2016 An Official Statistics Publication for Scotland
Publication Report Child and Adolescent Mental Health Services Waiting Times in NHSScotland Quarter ending 30 September 2016 Publication date 6 December 2016 An Official Statistics Publication for Scotland
Community Pharmacy in 2016/17 and beyond
 Community Pharmacy in 2016/17 and beyond Stakeholder briefing sessions 1 CONTENTS Contents This presentation describes our vision for community pharmacy, and outlines proposals for achieving that vision,
Community Pharmacy in 2016/17 and beyond Stakeholder briefing sessions 1 CONTENTS Contents This presentation describes our vision for community pharmacy, and outlines proposals for achieving that vision,
WEST HAMPSHIRE PERFORMANCE REPORT. Based on performance data available as at 11 th January 2018
 WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014
 Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
Board Briefing. Board Briefing of Nursing and Midwifery Staffing Levels. Date of Briefing January 2018 (December 2017 data)
") Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing January 2018 (December 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author:
Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing January 2018 (December 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author:
Monthly and Quarterly Activity Returns Statistics Consultation
 Monthly and Quarterly Activity Returns Statistics Consultation Monthly and Quarterly Activity Returns Statistics Consultation Version number: 1 First published: 08/02/2018 Prepared by: Classification:
Monthly and Quarterly Activity Returns Statistics Consultation Monthly and Quarterly Activity Returns Statistics Consultation Version number: 1 First published: 08/02/2018 Prepared by: Classification:
Child and Adolescent Mental Health Services Waiting Times in NHSScotland
 Publication Report Child and Adolescent Mental Health Services Waiting Times in NHSScotland Quarter ending 30 September 2017 Publication date 12 December 2017 A National Statistics Publication for Scotland
Publication Report Child and Adolescent Mental Health Services Waiting Times in NHSScotland Quarter ending 30 September 2017 Publication date 12 December 2017 A National Statistics Publication for Scotland
New Savoy Conference Psychological Therapies in the NHS
 New Savoy Conference Psychological Therapies in the NHS Claire Murdoch CEO, Central and North West London NHS FT & National Mental Health Director, NHS England 21 March 2018 Mental Health Five Year Forward
New Savoy Conference Psychological Therapies in the NHS Claire Murdoch CEO, Central and North West London NHS FT & National Mental Health Director, NHS England 21 March 2018 Mental Health Five Year Forward
Overview of a new study to assess the impact of hospice led interventions on acute use. Jonathan Ellis, Director of Policy & Advocacy
 Overview of a new study to assess the impact of hospice led interventions on acute use Jonathan Ellis, Director of Policy & Advocacy The problem Almost 600,000 people die each year Half will die in a hospital
Overview of a new study to assess the impact of hospice led interventions on acute use Jonathan Ellis, Director of Policy & Advocacy The problem Almost 600,000 people die each year Half will die in a hospital
NHS Electronic Referrals Service. Paper Switch Off an update Digital Health Webinar 4 May 2018
 NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
NHS Electronic Referrals Service Paper Switch Off an update Digital Health Webinar 4 May 2018 Aims of Session Introductions and refresh of Paper Switch Off Sharon Wilson Implementation manager NHS Digital
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
Child and Adolescent Mental Health Services Waiting Times in NHSScotland
 Publication Report Child and Adolescent Mental Health Services Waiting Times in NHSScotland Quarter ending 30 June 2017 Publication date 5 September 2017 A National Statistics Publication for Scotland
Publication Report Child and Adolescent Mental Health Services Waiting Times in NHSScotland Quarter ending 30 June 2017 Publication date 5 September 2017 A National Statistics Publication for Scotland
EDS 2. Making sure that everyone counts Initial Self-Assessment
 EDS 2 Making sure that everyone counts Initial Self-Assessment Equality Delivery System for the NHS EDS2 Summary Report Implementation of the Equality Delivery System EDS2 is a requirement on both NHS
EDS 2 Making sure that everyone counts Initial Self-Assessment Equality Delivery System for the NHS EDS2 Summary Report Implementation of the Equality Delivery System EDS2 is a requirement on both NHS
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
Norfolk Island Central and Eastern Sydney PHN
 Norfolk Island Central and Eastern Sydney PHN Activity Work Plan 2016-2018: Norfolk Island Coordinated and Integrated Primary Health Care Services Mental Health and Suicide Prevention Drug and Alcohol
Norfolk Island Central and Eastern Sydney PHN Activity Work Plan 2016-2018: Norfolk Island Coordinated and Integrated Primary Health Care Services Mental Health and Suicide Prevention Drug and Alcohol
Performance and Quality Report Sean Morgan Director of Performance and Delivery Mary Hopper Director of Quality Dino Pardhanani, Clinical Director
 Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Preparing to implement mental health access and waiting time standards
 Preparing to implement mental health access and waiting time standards Becki Hemming MH Access & Waits Programme Lead, NHS England Presentation summary 1. Context 2. The standards to be introduced from
Preparing to implement mental health access and waiting time standards Becki Hemming MH Access & Waits Programme Lead, NHS England Presentation summary 1. Context 2. The standards to be introduced from
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
RTT Recovery Planning and Trajectory Development: A Cambridge Tale
 RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan
 Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan 2015-2020 1 Introduction 1.1 Welcome to the update on Warrington s Local Transformation Plan for Children and
Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan 2015-2020 1 Introduction 1.1 Welcome to the update on Warrington s Local Transformation Plan for Children and
Any Qualified Provider: your questions answered
 Any Qualified Provider: your questions answered September 8, 2011 These answers cover a range of questions about the detail of Any Qualified Provider on integrated care, competition and procurement, liability
Any Qualified Provider: your questions answered September 8, 2011 These answers cover a range of questions about the detail of Any Qualified Provider on integrated care, competition and procurement, liability
Mental Health Crisis Pathway Analysis
 Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
NHS Rushcliffe CCG Governing Body Meeting. CCG Improvement and Assurance Framework. 15 March 2018
 RCCG/GB/18/039 NHS Rushcliffe CCG Governing Body Meeting 15 March 2018 Introduction 1. This paper provides the Governing Body with an update on the progress being made by the Greater Nottingham CCGs in
RCCG/GB/18/039 NHS Rushcliffe CCG Governing Body Meeting 15 March 2018 Introduction 1. This paper provides the Governing Body with an update on the progress being made by the Greater Nottingham CCGs in
A Successful Health Visitor Retention Strategy - Walsall Healthcare NHS Trust
 A Successful Health Visitor Retention Strategy - Walsall Healthcare NHS Trust Health Visiting Local Picture Population of approx 21,000 under 5s 10 Health Visitor Teams across the borough New model of
A Successful Health Visitor Retention Strategy - Walsall Healthcare NHS Trust Health Visiting Local Picture Population of approx 21,000 under 5s 10 Health Visitor Teams across the borough New model of
Hard Truths Public Board 29th September, 2016
 Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
NHS GRAMPIAN. Local Delivery Plan - Mental Health and Learning Disability Services
 NHS GRAMPIAN Board Meeting 01.06.17 Open Session Item 8 Local Delivery Plan - Mental Health and Learning Disability Services 1. Actions Recommended The Board is asked to: Note the context regarding the
NHS GRAMPIAN Board Meeting 01.06.17 Open Session Item 8 Local Delivery Plan - Mental Health and Learning Disability Services 1. Actions Recommended The Board is asked to: Note the context regarding the
Mental Health Services - Delayed Discharges: Update
 NHS Greater Glasgow & Clyde NHS Board Meeting Chief Officer, Glasgow City HSCP and Nurse Director October 20 Paper No: /56 Mental Health Services - Delayed Discharges: Update Recommendation:- The NHS Board
NHS Greater Glasgow & Clyde NHS Board Meeting Chief Officer, Glasgow City HSCP and Nurse Director October 20 Paper No: /56 Mental Health Services - Delayed Discharges: Update Recommendation:- The NHS Board
Delivering the transformation of children and young people s mental health services
 Delivering the transformation of children and young people s mental health services Simon Medcalf Head of Mental Health, NHS England 4 October 2016 1 Context: Implementing the Five Year Forward View for
Delivering the transformation of children and young people s mental health services Simon Medcalf Head of Mental Health, NHS England 4 October 2016 1 Context: Implementing the Five Year Forward View for
Improvement and Assessment Framework Q1 performance and six clinical priority areas
 Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
Developing an outcomes-based approach in mental health. The policy context
 briefing December 2011 Issue 231 Developing an outcomes-based approach in mental health Key points A new Mental Health Network report explores the issue of outcome measurement in mental health. The report
briefing December 2011 Issue 231 Developing an outcomes-based approach in mental health Key points A new Mental Health Network report explores the issue of outcome measurement in mental health. The report
Safety in Mental Health Collaborative
 NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
Developing Plans for the Better Care Fund
 Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Submitted to: NHS West Norfolk CCG Governing Body, 24 September 2015
 Agenda Item: 12.2 Subject: Presented by: Continuing Health Care Pathway Proposal Dr Sue Crossman, Chief Officer Submitted to: NHS West Norfolk CCG Governing Body, 24 September 2015 Purpose of Paper: Decision
Agenda Item: 12.2 Subject: Presented by: Continuing Health Care Pathway Proposal Dr Sue Crossman, Chief Officer Submitted to: NHS West Norfolk CCG Governing Body, 24 September 2015 Purpose of Paper: Decision
Improving Access to Psychological Therapies, Key Performance Indicators (IAPT KPIs) Q4 2011/12 final and Q1 2012/13 provisional
 Q4 2011/12 final and Q1 2012/13 provisional") Improving Access to Psychological Therapies, Key Performance Indicators (IAPT KPIs) Q4 2011/12 final and Q1 2012/13 provisional Copyright 2012, Health and Social Care Information Centre. All Rights Reserved.
Improving Access to Psychological Therapies, Key Performance Indicators (IAPT KPIs) Q4 2011/12 final and Q1 2012/13 provisional Copyright 2012, Health and Social Care Information Centre. All Rights Reserved.
SPSP Medicines. Prepared by: NHS Ayrshire and Arran
 SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
Nottingham University Hospitals Emergency Department Quality Issues Related to Performance
 RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
Workflow. Optimisation. hereweare.org.uk. hereweare.org.uk
 Workflow Optimisation Dr. Paul Deffley & Jaivir Pall Clinical Lead & Commercial Lead About Here Not-for-profit social enterprise Membership organisation (our members are local GPs, Practice Managers, Practice
Workflow Optimisation Dr. Paul Deffley & Jaivir Pall Clinical Lead & Commercial Lead About Here Not-for-profit social enterprise Membership organisation (our members are local GPs, Practice Managers, Practice
EQUALITY AND DIVERSITY DATA ANALYSIS WORKFORCE INFORMATION SUMMARY REPORT
 EQUALITY AND DIVERSITY DATA ANALYSIS WORKFORCE INFORMATION SUMMARY REPORT 2014-15 1. Introduction 1.1 Yeovil District Hospital (The Trust) is committed to engaging a diverse workforce that meets the requirements
EQUALITY AND DIVERSITY DATA ANALYSIS WORKFORCE INFORMATION SUMMARY REPORT 2014-15 1. Introduction 1.1 Yeovil District Hospital (The Trust) is committed to engaging a diverse workforce that meets the requirements
ASPIRE. Allied Health Professions Supporting and Promoting Improvement, Rehabilitation and Enabling Others ADVANCED PRACTICE SPECIALIST GENERALIST
 ASPIRE Allied Health Professions Supporting and Promoting Improvement, Rehabilitation and Enabling Others ADVANCED PRACTICE SPECIALIST GENERALIST ENABLING OTHERS AHP Strategy 2017 2021 CONTENTS Introduction
ASPIRE Allied Health Professions Supporting and Promoting Improvement, Rehabilitation and Enabling Others ADVANCED PRACTICE SPECIALIST GENERALIST ENABLING OTHERS AHP Strategy 2017 2021 CONTENTS Introduction
Healthy lives, healthy people: consultation on the funding and commissioning routes for public health
 Healthy lives, healthy people: consultation on the funding and commissioning routes for public health December 2010 The coalition Government published Healthy Lives, Health people: consultation on the
Healthy lives, healthy people: consultation on the funding and commissioning routes for public health December 2010 The coalition Government published Healthy Lives, Health people: consultation on the
Allied Health Review Background Paper 19 June 2014
 Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
Birmingham Solihull and the Black Country Area Team
 Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Inpatient, Day case and Outpatient Stage of Treatment Waiting Times
 Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 30 June 2016 Publication date 30 August 2016 A National Statistics Publication for Scotland
Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 30 June 2016 Publication date 30 August 2016 A National Statistics Publication for Scotland
National Trends Winter 2016
 National Trends Winter 216 About the National Trends data This report presents a unique and real-time view of trends within temporary nursing including bank and agency usage. The data used has been drawn
National Trends Winter 216 About the National Trends data This report presents a unique and real-time view of trends within temporary nursing including bank and agency usage. The data used has been drawn
Policy for Patient Access
 Policy for Patient Access DOCUMENT CONTROL Revision Date Old Version 10/12/2014 1.0 01/07/2016 1.1 30/04/17 1.2 Amendment General Management Review General Management Review General Management Review Authored
Policy for Patient Access DOCUMENT CONTROL Revision Date Old Version 10/12/2014 1.0 01/07/2016 1.1 30/04/17 1.2 Amendment General Management Review General Management Review General Management Review Authored
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
Board Briefing. Board Briefing of Nursing and Midwifery Staffing Levels. Date of Briefing August 2017 (July 2017 data)
") Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing August 2017 (July 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author: Workforce
Board Briefing Board Briefing of Nursing and Midwifery Staffing Levels Date of Briefing August 2017 (July 2017 data) This paper is for: Sponsor: Chief Nurse- Dame Eileen Sills (DBE) Decision Author: Workforce
2016 Safeguarding Data Report THE NATIONAL SAFEGUARDING OFFICE
 2016 Safeguarding Data Report THE NATIONAL SAFEGUARDING OFFICE 1 Contents Overview... 2 2016 Safeguarding Returns... 4 Safeguarding Concerns by Age Category... 7 Safeguarding concerns by Gender/Age...
2016 Safeguarding Data Report THE NATIONAL SAFEGUARDING OFFICE 1 Contents Overview... 2 2016 Safeguarding Returns... 4 Safeguarding Concerns by Age Category... 7 Safeguarding concerns by Gender/Age...
Inpatient and Community Mental Health Patient Surveys Report written by:
 2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
A must have for any GP surgery. It is like having our own Social Worker, CAB, Mental Health Worker all rolled into one who will chase up patients on
 A must have for any GP surgery. It is like having our own Social Worker, CAB, Mental Health Worker all rolled into one who will chase up patients on the phone and even go out to their houses if needed
A must have for any GP surgery. It is like having our own Social Worker, CAB, Mental Health Worker all rolled into one who will chase up patients on the phone and even go out to their houses if needed
The Long Path to Primary Care Mental Health. Dr David Smart GP NHS Northamptonshire
 The Long Path to Primary Care Mental Health : Dr David Smart GP NHS Northamptonshire Common Mental Health Common 2007 Prevalence 16.2% > Elderly / Deprivation > South Asian women Life time 25% 8% pop warrant
The Long Path to Primary Care Mental Health : Dr David Smart GP NHS Northamptonshire Common Mental Health Common 2007 Prevalence 16.2% > Elderly / Deprivation > South Asian women Life time 25% 8% pop warrant
Welcome. PPG Conference North and South Norfolk CCGs June 14 th 2018
 Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
COUNCIL OF GOVERNORS MEETING. Thursday, 20 April 2017 PERFORMANCE ASSURANCE REPORT. Non-Executive Directors
 3.5 COUNCIL OF GOVERNORS MEETING Thursday, 20 April 2017 PERFORMANCE ASSURANCE REPORT Non-Executive Directors PURPOSE OF THE PAPER: The National Health Service Act 2006 (as amended) places a general duty
3.5 COUNCIL OF GOVERNORS MEETING Thursday, 20 April 2017 PERFORMANCE ASSURANCE REPORT Non-Executive Directors PURPOSE OF THE PAPER: The National Health Service Act 2006 (as amended) places a general duty
Safer Nursing and Midwifery Staffing Recommendation The Board is asked to: NOTE the report
 To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
To: Board of Directors Date of Meeting: 26 th July 20 Title Safer Nursing and Midwifery Staffing Responsible Executive Director Nicola Ranger, Chief Nurse Prepared by Helen O Dell, Deputy Chief Nurse Workforce
Managing Elective Waiting Times A checklist for NHS health boards
 12 March 2015 Archwilydd Cyffredinol Cymru Auditor General for Wales Managing Elective Waiting Times A checklist for NHS health boards Introduction 1 The Auditor General published his report on NHS Waiting
12 March 2015 Archwilydd Cyffredinol Cymru Auditor General for Wales Managing Elective Waiting Times A checklist for NHS health boards Introduction 1 The Auditor General published his report on NHS Waiting
service users greater clarity on what to expect from services
 briefing November 2011 Issue 227 Payment by Results in mental health A challenging journey worth taking Key points Commissioners and providers support the introduction of Payment by Results for adult mental
briefing November 2011 Issue 227 Payment by Results in mental health A challenging journey worth taking Key points Commissioners and providers support the introduction of Payment by Results for adult mental
Nurse Led End of Life Care. Catherine Malia- St Gemma s Hospice, Leeds Lynne Symonds- St Catherine s Hospice, Scarborough
 Nurse Led End of Life Care Catherine Malia- St Gemma s Hospice, Leeds Lynne Symonds- St Catherine s Hospice, Scarborough SETTING THE SCENE Preferences for Place of Death 2014 Home 72% Hospice 10% Care
Nurse Led End of Life Care Catherine Malia- St Gemma s Hospice, Leeds Lynne Symonds- St Catherine s Hospice, Scarborough SETTING THE SCENE Preferences for Place of Death 2014 Home 72% Hospice 10% Care
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Mental Health Social Work: Community Support. Summary
 Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
A new mindset: the Five Year Forward View for mental health
 A new mindset: the Five Year Forward View for mental health Paul Farmer Chief Executive mind.org.uk Five Year Forward View for Mental Health Simon Stevens: Putting mental and physical health on an equal
A new mindset: the Five Year Forward View for mental health Paul Farmer Chief Executive mind.org.uk Five Year Forward View for Mental Health Simon Stevens: Putting mental and physical health on an equal
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4. Mandatory but detail for local determination and agreement Optional headings 5-7. Optional to use, detail for local determination
SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4. Mandatory but detail for local determination and agreement Optional headings 5-7. Optional to use, detail for local determination
Urgent Care Short Term Actions to Improve Performance
 To: Trust Board From: Chief Operating Officer Date: March 2017 Healthcare standard Title: Urgent Care Short Term Actions to Improve Performance Author/Responsible Director: Michael Woods / Andrew Prydderch
To: Trust Board From: Chief Operating Officer Date: March 2017 Healthcare standard Title: Urgent Care Short Term Actions to Improve Performance Author/Responsible Director: Michael Woods / Andrew Prydderch
National Homecare KPI performance March 2017
 National Homecare KPI performance March 2017 Foreword We are pleased to publish our latest KPI report, continuing our commitment to the transparency of the service we provide to our patients and customers,
National Homecare KPI performance March 2017 Foreword We are pleased to publish our latest KPI report, continuing our commitment to the transparency of the service we provide to our patients and customers,
Update Report to Clinical Members. Quarter 3; what have we done so far
 Update Report to Clinical Members Quarter 3; what have we done so far Introduction: Dr Charlotte Canniff, Clinical Chair Following our Council of Members meeting in October we heard and recognised a clear
Update Report to Clinical Members Quarter 3; what have we done so far Introduction: Dr Charlotte Canniff, Clinical Chair Following our Council of Members meeting in October we heard and recognised a clear
Integrating Telemedicine into mental Health Care
 Integrating Telemedicine into mental Health Care learning from a Care Homes Vanguard Rachel Binks Nurse Consultant Digital & Acute Care Airedale NHS Foundation Trust Chris North Care Home Liaison Team
Integrating Telemedicine into mental Health Care learning from a Care Homes Vanguard Rachel Binks Nurse Consultant Digital & Acute Care Airedale NHS Foundation Trust Chris North Care Home Liaison Team
Sheffield Teaching Hospitals NHS Foundation Trust
 Sheffield Teaching Hospitals NHS Foundation Trust @seamlesssurgery Seamless Surgery Team Sheffield Teaching Hospitals NHS Foundation Trust July 2017 PROUD TO MAKE A DIFFERENCE PROUD TO MAKE A DIFFERENCE
Sheffield Teaching Hospitals NHS Foundation Trust @seamlesssurgery Seamless Surgery Team Sheffield Teaching Hospitals NHS Foundation Trust July 2017 PROUD TO MAKE A DIFFERENCE PROUD TO MAKE A DIFFERENCE
PRISM: GPs - your questions answered
 PRISM: GPs - your questions answered 1. What is Prism? Prism is our new primary care service for mental health and run by Cambridgeshire and Peterborough NHS Foundation Trust (CPFT). The service puts specialist
PRISM: GPs - your questions answered 1. What is Prism? Prism is our new primary care service for mental health and run by Cambridgeshire and Peterborough NHS Foundation Trust (CPFT). The service puts specialist
DRAFT. Primary Care Networks Reference Guide: Draft pre-release
 Primary Care Networks Reference Guide: Draft pre-release This draft reference guide has been developed with input from a range of stakeholders to provide further information and guidance on what we mean
Primary Care Networks Reference Guide: Draft pre-release This draft reference guide has been developed with input from a range of stakeholders to provide further information and guidance on what we mean
Improving Mental Health Services in Bath & North East Somerset
 Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
JOB DESCRIPTION. Pharmacy Technician
 JOB DESCRIPTION Pharmacy Technician Issued by AT Medics Primary Care Pharmacy Technician Job Description Job Title: Reporting to: Location: Salary: Job status: Contract: Notice Period: Primary care pharmacy
JOB DESCRIPTION Pharmacy Technician Issued by AT Medics Primary Care Pharmacy Technician Job Description Job Title: Reporting to: Location: Salary: Job status: Contract: Notice Period: Primary care pharmacy
Review of Local Enhanced Services
 Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
STATISTICAL PRESS NOTICE MONTHLY CRITICAL CARE BEDS AND CANCELLED URGENT OPERATIONS DATA, ENGLAND March 2018
 STATISTICAL PRESS NOTICE MONTHLY CRITICAL CARE BEDS AND CANCELLED URGENT OPERATIONS DATA, ENGLAND March 2018 Main Findings March 2018: Critical Care Beds There were 4,064 adult critical care beds available
STATISTICAL PRESS NOTICE MONTHLY CRITICAL CARE BEDS AND CANCELLED URGENT OPERATIONS DATA, ENGLAND March 2018 Main Findings March 2018: Critical Care Beds There were 4,064 adult critical care beds available
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
ENCLOSURE: J. Date of Trust Board 29 February Pressure Ulcer Clinical Improvement Programme. Purpose of Report
 ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Mental Health (Wales) Measure Implementing the Mental Health (Wales) Measure Guidance for Local Health Boards and Local Authorities
 Measure Implementing the Mental Health (Wales) Measure Guidance for Local Health Boards and Local Authorities") Mental Health (Wales) Measure 2010 Implementing the Mental Health (Wales) Measure 2010 Guidance for Local Health Boards and Local Authorities Januar y 2011 Crown copyright 2011 WAG 10-11316 F6651011 Implementing
Mental Health (Wales) Measure 2010 Implementing the Mental Health (Wales) Measure 2010 Guidance for Local Health Boards and Local Authorities Januar y 2011 Crown copyright 2011 WAG 10-11316 F6651011 Implementing
Within both PCTs, smokers were referred directly to the local stop smoking service at the time of the health check.
 Improving Healthy Lifestyles Pilot Site Evaluation Report Key findings The health check is a good opportunity to deliver brief lifestyle behaviour advice to patients, most of which is recalled three months
Improving Healthy Lifestyles Pilot Site Evaluation Report Key findings The health check is a good opportunity to deliver brief lifestyle behaviour advice to patients, most of which is recalled three months
Influence of Patient Flow on Quality Care
 Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Influence of Patient Flow on Quality Care Patients Waiting on Trolleys for an Inpatient Bed Patients who are Medically Fit to be discharged and cared for at Home with Support or in a Nursing Home or District
Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance
 Directorate for Health Workforce and Performance") Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance A Whole System Approach to Patient Flow for Scotland Our Quality Improvement Approach Jane Murkin Programme
Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance A Whole System Approach to Patient Flow for Scotland Our Quality Improvement Approach Jane Murkin Programme
Inpatient, Day case and Outpatient Stage of Treatment Waiting Times
 Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 31 December 2016 Publication date 28 February 2017 A National Statistics Publication
Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 31 December 2016 Publication date 28 February 2017 A National Statistics Publication
Psychological therapies for common mental illness: who s talking to whom?
 Primary Care Mental Health 2005;3:00 00 # 2005 Radcliffe Publishing Research papers Psychological therapies for common mental illness: who s talking to whom? Ruth Lawson Specialist Registrar in Public
Primary Care Mental Health 2005;3:00 00 # 2005 Radcliffe Publishing Research papers Psychological therapies for common mental illness: who s talking to whom? Ruth Lawson Specialist Registrar in Public
NHS Awards 2013 Endoscopy Unit
 NHS Awards 201 Endoscopy Unit 1. Storyboard Title Improving the quality of the patients experience of the endoscopy service: achieving full JAG accreditation in Bronglais District General Hospital utilising
NHS Awards 201 Endoscopy Unit 1. Storyboard Title Improving the quality of the patients experience of the endoscopy service: achieving full JAG accreditation in Bronglais District General Hospital utilising
Appendix 1: Croydon Clinical Commissioning Group Risk Register and Board Assurance Framework - 9th April 2013
 Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
Appendix 1: Croydon Clinical Register and Board Assurance Framework - 9th April 2013 Principal to Delivery Key Assurance on we have in in our are 1. To achieve financial sustainability in three years (2013-2014
Agenda Item: 10.1 (3) HR & OD Monthly Trust Report (September 2016)
 HR & OD Monthly Trust Report (September 2016)") Agenda Item: 10.1 (3) HR & OD Monthly Trust Report (September 2016) Prepared by: Karen Taylor, Assistant Director of HR & Kyriacos Kyriacou, Interim Deputy Director of HR & OD Presented by: Louise Ludgrove,
Agenda Item: 10.1 (3) HR & OD Monthly Trust Report (September 2016) Prepared by: Karen Taylor, Assistant Director of HR & Kyriacos Kyriacou, Interim Deputy Director of HR & OD Presented by: Louise Ludgrove,
OPERATIONAL PERFORMANCE REPORT: March Swindon Community Health Services Overview
 OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
Council of Members. 20 January 2016
 Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,