State of Rural Healthcare In US
|
|
|
- Linda Campbell
- 5 years ago
- Views:
Transcription


1
: There")

2 State of Rural Healthcare In US According to the American Hospital Association (AHA): There are 5564 registered hospital in US 4862 are considered community hospitals 1829 are rural hospitals

3 Aging Population in Rural Geographies According to the US Census Bureau, adults in rural areas are older than those living in nonrural areas, with a median age of 51, compared to age 45 in non-rural areas Hospitalization rates and lengths of stay increase with age among adults, peaking for those over 65 This creates increased demand for healthcare in rural areas As a result, the majority of rural providers serve a greater proportion of patients over the age of 65 than two-thirds of all U.S. acute care hospitals

4 State of Rural Healthcare In US According to a report from ivantage Health Analytics, a firm that compiles a hospital strength index based on data about financial stability, patients and quality indicators: 80 rural hospitals have closed since 2010 Across the US 673 rural hospitals are vulnerable to closure Although nearly all rural hospitals are feeling the squeeze, facilities in states that have not expanded Medicaid are under more financial pressure CLOSED % of hospitals vulnerable to closure are in states that have not expanded Medicaid.


5 State of Rural Healthcare In US Rural America includes approximately 57 million people, about 18% of the population and 84% of the geographic area of the USA There are 1,855 rural hospitals that support nearly 2 million jobs Every dollar spent by a rural hospital produces another $2.29 of economic activity A typical critical access hospital employs 141 community members Rural hospitals handle more than 21.5 million emergency visits



6 State of Rural Healthcare In US According to the ivantage Study: Across the U.S., 673 rural hospitals are vulnerable to closure Of the 673 hospitals, 355 are in markets with great health disparities If the 673 vulnerable hospitals were to close, 99,000 healthcare jobs in rural communities across the nation would be lost Closure of the at-risk hospitals would result in an estimated $277 billion loss to the gross domestic product

7 State of Rural Healthcare In US Diabetes Rural hospitals serve communities with greater rates of diabetes Diabetes is the seventh-leading cause of death in the nation The American Diabetes Association estimates the total cost of diabetes has risen 41 percent from $174 billion in 2007 to $245 billion in 2012 Particularly prevalent in rural America, rural hospitals are on the frontline in providing diabetic screening and care for populations which may not have access to primary or specialty care

8 State of Rural Healthcare In US Opioid Epidemic According to the CDC, the death rate from opioid-related overdoses is 45 percent higher in nonmetropolitan counties Distances in rural geographies mean longer wait times for critical interventions and antidotes like Naloxone Rural communities are isolated from treatment facilities and addiction counseling Nationwide, only 11 percent of patients seeking addiction treatment receive care
9 Maryland Hospitals Maryland hospitals are protected with the all payer waiver with CMS GRMC was first hospital in US with global budget revenue reimbursement GBR created by the Maryland Health Services Cost Review Commission (HSCRC) to give hospitals a financial incentive to change the way they manage their resources With the ultimate goal of slowing down cost increases while preserving the quality of care Maryland already regulated charges in all the state s acute care hospitals, but GBR takes it a step farther
10 Maryland Hospitals focus: Value, not Volume HSCRC sets rates annually based on patient mix and services Revenue becomes predictable Revenue is adjusted population, service levels or shifting services to other settings Focus is shifted from volume to improving care and managing health at the community level Hospitals are financially motivated to control lengths of stay, reduce unnecessary testing, prevent inappropriate admissions, and generally operate in a more efficient manner Hospitals are incentivized to reduce readmissions, a motivator for careful patient education and postdischarge follow-up
11
12 Hospital Reimbursement Maryland vs. Rest of Nation Nation $2.50 Charge to Cost Ratio (Illus.) $2.00 $ % 250% 200% 150% 100% 50% 0% 1.2 to 1 Maryland 2.5 to 1 Nation $1.00 $0.50 $0.00 $2.50 $2.00 Medicare/Mcaid Comm. SelfPay Avg. Cost Payments Maryland Cost Mark-up $1.50 $1.00 $0.50 $0.00 Medicare/Mcaid Comm. SelfPay Avg. 12 Cost Payments
13 Hospital Reimbursement Maryland vs. Rest of Nation The Statewide UCC % is built into all hospitals rates; the UCC Pool acts as a settlement methodology to account for hospitals that experience more or less UCC than the State Low UCC Funding Hospital pays into UCC Pool Statewid e UCC Included in all hospital rates High UCC Funding Hospital receives payments from UCC Pool The Statewide UCC pool fund 13
14 HSCRC s Mandate Ensure Equity / Fairness / Stability Maximize Access to Care Contain Hospital Costs Reduce the Total Cost of Care per Medicare Beneficiary Provide Accountability 14
15 CMS Demonstration Model Effective January 1, Year Pilot Project Annual all-payer, per capita, total hospital cost growth limited to 3.58% Maryland s Medicare per beneficiary total hospital cost growth rate must be below the national Medicare per beneficiary average, resulting in $330m of Medicare savings over five years Maryland s Medicare per beneficiary total cost growth rate cannot exceed the national average by more than 1 percentage point, and must be break even with the national average by year 4. Maryland will reduce its 30-day Medicare readmission rate to the national average in five years Annual Potentially Preventable Complication (PPC) reduction of 6.89%, for a cumulative 5 year reduction of 30% 15
16 Global Budget Revenue (GBR) Inpatient and outpatient revenue is constrained by the GBR System GBR provides hospitals with a global revenue base that is 100% fixed Approved revenue amount in a given year is fixed cap No adjustment for changes in volume or service mix No adjustment for changes in Case Mix Index (CMI) Overall incentive to reduce service utilization and encourage improvements in population health If hospitals are successful in reducing utilization, AND, associated variable costs, profitability should increase Changes to hospital s rate order are made annually 16
17 Rate Order Revenue Center: Hospitals have different revenue centers depending on the services they provide Service Unit: The service unit is the same for all hospitals (i.e. every hospital charges for Operating Room services by the minute) Unit Rates: Unit rates (prices) vary by hospital These rates must be charged to all payers - no contract negotiations Service Unit Revenue Center Unit Rates Med./Surg. Acute Patient Days $1, Obstetric Acute Patient Days $ Med./Surg. I.C.U. Patient Days $2, New Born Nursery Patient Days $ Admissions Admission $ Emergency Services MD RVU'S $ Clinic Services RVU'S $ Operating Room Minutes $ Laboratory MD RVU'S $ Radiology-Diagnostic HSCRC RVU'S $ Physical Therapy MD RVU'S $ Observation RVU'S $
18 Rate Center Corridors +10 % +5 % Rate Center - 5 % - 10 % Total GBR charged at the end of each 6 month increment Must be with 0.5% of the Total Budget 18
19 Updates to Rate Orders Hospitals generally receive an updated rate order once per year - effective July 1 Unit rates are updated for: Inflation (Update Factor) Change in Markup (Payer Mix and UCC) Population Infrastructure Investments Price Variances and Penalties NSP I and NSP II Assessments and Fees Quality Measures (MHAC, QBR) Other Adjustments (RRR, Market Share) 19
20 Maryland s System Spurs Innovation: GRMC s Well Patient Program GRMC developed an innovative approach to Care Coordination called the Well-patient Program Patients are identified as high utilizers of hospital care via data analytics (CRISP) integrated to hospital IT system (Care Alerts) Patients Enrolled into Well-patient Program: Assigned Nurse Navigator Social Worker Psychiatrist or psychologist PCP s partner to manage chronic conditions
21 Maryland s System Spurs Innovation: GRMC s Well Patient Program Hospital Services Supporting Wellness: Cardiopulmonary Rehabilitation Obesity Management and Education Smoking Cessation Classes Chronic Kidney Disease (CKD) Clinic CHF Clinic Health Education and literacy programs Community Health Workers Home Health Telemedicine

22 Maryland s system allowed GRMC to be the first hospital in the US to implement a Global Budget RESULTS: According to CRISP data, GRMC has an extremely low cost per Medicare beneficiary Below state average Below national average
23 Percentage Garrett Regional Medical Center Potentially Avoidable Utilization Revenue PAU Rate for CY15 and CY16 Compared to the State PAU Rate GRMC PAU Rate CY 15 CY 16 Jan-April CY 16 Jan-Jun I M P R O V E M E N T
24 GRMC Surgical Site Infection Rate (Drives Readmission Rates and indicator for quality and safety) One of the drivers of GRMC s low readmission rate is surgical site infection rate Percent 0.26% 0.22% 0.16% GRMC Self Directed Goal was for SSI to be < 0.6% Garrett Nation I M P R O V E M E N T Very Low in 2014, still made improvement in 2015 CDC January 2015 SSI event Module- reports NHSN data for (16,147 SSI s following 849,659 operative procedure) showed an overall SSI rate of 1.9%
25 Garrett Regional Medical Center HSCRC reported Risk Adjusted 30 Day Inpatient All Payer Readmission Rate Comparative for All Maryland Hospitals for Jan-April % 14% 12% 10% 8% 6% 4% 2% 0% 5.9% 7.3% 9.1% 9.3% 9.5% 9.5% 9.5% 9.7% 9.7% 9.9% 10.0% 10.1% 10.1% 10.1% 10.3% 10.4% 10.5% 10.5% 10.6% 10.7% 10.7% 10.8% 10.8% 10.8% 11.0% 11.1% 11.3% 11.4% 11.4% 11.6% 11.8% 11.8% 11.9% 11.9% 11.9% 12.1% 12.1% 12.3% 12.5% 12.6% 12.7% 12.9% 13.9% 13.9% 14.3% 14.6% 14.8% GRMC 5.9% Statewide Average 11.4% GARRETT COUNTY MEMORIAL UM-REHABILITATION & ATLANTIC GENERAL HOSPITAL UM-CHARLES REGIONAL CALVERT MEMORIAL HOSPITAL FREDERICK MEMORIAL PENINSULA REGIONAL PRINCE GEORGES HOSPITAL UM-SHORE REGIONAL HEALTH SHADY GROVE ADVENTIST WASHINGTON ADVENTIST GREATER BALTIMORE MEDSTAR MONTGOMERY FORT WASHINGTON MEDICAL ANNE ARUNDEL MEDICAL MEDSTAR ST. MARY'S UM-ST. JOSEPH MEDICAL HOWARD COUNTY GENERAL WESTERN MARYLAND MEDSTAR SOUTHERN UM-SHORE REGIONAL HEALTH SUBURBAN HOSPITAL MERITUS MEDICAL CENTER UNION HOSPITAL OF CECIL LEVINDALE CARROLL HOSPITAL CENTER DOCTORS COMMUNITY UM-UPPER CHESAPEAKE LAUREL REGIONAL HOSPITAL MEDSTAR HARBOR HOSPITAL MEDSTAR FRANKLIN SQUARE HOLY CROSS HOSPITAL MEDSTAR UNION MEMORIAL UM-HARFORD MEMORIAL MEDSTAR GOOD SAMARITAN SINAI HOSPITAL MERCY MEDICAL CENTER ST. AGNES HOSPITAL NORTHWEST HOSPITAL CENTER UM-BALTIMORE WASHINGTON UNIVERSITY OF MARYLAND JOHNS HOPKINS HOSPITAL UM-SHORE REGIONAL HEALTH BON SECOURS HOSPITAL JOHNS HOPKINS BAYVIEW MCCREADY MEMORIAL UMMC MIDTOWN CAMPUS P O S I T I V E
26 Survival Rate in Percent Garrett Regional Medical Center Risk Adjusted Survival Rate Trend Mortality Rate Rapid Improvement Final Jan- Sep Final Sep- Dec 2014 GRMC State Final Jan- Jun 2015 Time Frame Final Jan- Dec I M P R O V E M E N T Prelim Jan- Jun 2016 Source: CRISP Data Report
27 Garrett Regional Medical Center Maryland Hospital Acquired Conditions (MHAC) Scores rd best performance in Maryland! Improvement GRMC Maryland Hospital Acquired Conditions 0.3 Jan- June Prelim CY14 Jan- June CY14 n= 43 Jan- Sept CY14 n= 56 Jan- Dec CY14 n=71 Jan-Mar CY15 Final n= 5 Jan-June CY15 Final n= 11 Jan- SeptJan- Dec CY15 Final CY15 Final n= 25 n=25 Jan-Feb CY16 n=4

28 According to Senator Ben Cardin GRMC is the role model for rural healthcare in the US today According to GRMC CEO: It s Because of the Maryland System

29
STATE OF MARYLAND DEPARTMENT OF HEALTH AND MENTAL HYGIENE
 STATE OF MARYLAND DEPARTMENT OF HEALTH AND MENTAL HYGIENE John M. Colmers Chairman Herbert S. Wong, Ph.D. Vice-Chairman George H. Bone, M.D. Stephen F. Jencks, M. D., M.P.H. Jack C. Keane Bernadette C.
STATE OF MARYLAND DEPARTMENT OF HEALTH AND MENTAL HYGIENE John M. Colmers Chairman Herbert S. Wong, Ph.D. Vice-Chairman George H. Bone, M.D. Stephen F. Jencks, M. D., M.P.H. Jack C. Keane Bernadette C.
Final Recommendation for the Potentially Avoidable Utilization Savings Policy for Rate Year 2018
 Final Recommendations for the Potentially Avoidable Utilization Policy Final Recommendation for the Potentially Avoidable Utilization Policy for Rate Year 2018 June 14, 2017 Health Services Cost Review
Final Recommendations for the Potentially Avoidable Utilization Policy Final Recommendation for the Potentially Avoidable Utilization Policy for Rate Year 2018 June 14, 2017 Health Services Cost Review
MHA S 2018 VALUE REPORT TO MEMBERS
 FOR Patients FOR Communities FORward $30 million reduction in Medicaid sick tax $75 million avoidance of hospital assessment to stabilize insurance markets $36 million full funding for Institutions for
FOR Patients FOR Communities FORward $30 million reduction in Medicaid sick tax $75 million avoidance of hospital assessment to stabilize insurance markets $36 million full funding for Institutions for
Maryland s Public Behavioral Health System (PBHS) Emergency Petition Billing Manual
 Emergency Petition Billing Manual") Maryland s Public Behavioral Health System (PBHS) Emergency Petition Billing Manual TABLE OF CONTENTS Introduction... 1 Claims from a Facility for Emergency Room Services... 1 Claims from a Physician for
Maryland s Public Behavioral Health System (PBHS) Emergency Petition Billing Manual TABLE OF CONTENTS Introduction... 1 Claims from a Facility for Emergency Room Services... 1 Claims from a Physician for
Technical Overview of HCIP/CCIP
 Technical Overview of HCIP/CCIP Using Care Redesign to Align Provider Incentives Presentation to HFMA, Maryland Chapter HSCRC Care Redesign Summit August 18, 2017 Facilitators Nicole Stallings Vice President,
Technical Overview of HCIP/CCIP Using Care Redesign to Align Provider Incentives Presentation to HFMA, Maryland Chapter HSCRC Care Redesign Summit August 18, 2017 Facilitators Nicole Stallings Vice President,
Performance Measurement Work Group Meeting 10/18/2017
 Performance Measurement Work Group Meeting 10/18/2017 Welcome to New Members QBR RY 2020 DRAFT QBR Policy Components QBR Program RY 2020 Snapshot QBR Consists of 3 Domains: Person and Community Engagement
Performance Measurement Work Group Meeting 10/18/2017 Welcome to New Members QBR RY 2020 DRAFT QBR Policy Components QBR Program RY 2020 Snapshot QBR Consists of 3 Domains: Person and Community Engagement
Final Recommendation for the Potentially Avoidable Utilization Savings Policy for Rate Year 2019
 Final Recommendation for the Potentially Avoidable Utilization Savings Policy for Rate Year 2019 June 9, 2018 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410)
Final Recommendation for the Potentially Avoidable Utilization Savings Policy for Rate Year 2019 June 9, 2018 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410)
Policies for Controlling Volume January 9, 2014
 Policies for Controlling Volume January 9, 2014 The Maryland Hospital Association Policies for controlling volume Introduction Under the proposed demonstration model, the HSCRC will move from a regulatory
Policies for Controlling Volume January 9, 2014 The Maryland Hospital Association Policies for controlling volume Introduction Under the proposed demonstration model, the HSCRC will move from a regulatory
ESRD Network Council Meeting
 Mid-Atlantic Renal Coalition ESRD Network 5 NHSN Data Quality QIA 2016 Pilot - Fresenius 2016 Council Meeting 1 ESRD AIM Network 3 5 Reduce Costs of ESRD Care by Improving 2016 Council Meeting Care 2 NHSN
Mid-Atlantic Renal Coalition ESRD Network 5 NHSN Data Quality QIA 2016 Pilot - Fresenius 2016 Council Meeting 1 ESRD AIM Network 3 5 Reduce Costs of ESRD Care by Improving 2016 Council Meeting Care 2 NHSN
Overview of the HSCRC
 Overview of the HSCRC William J. Mooney, Jr. Memorial Education Series December 4, 2014 Arin Foreman Manager KPMG LLP What is the HSCRC? Health Services Cost Review Commission State regulatory commission
Overview of the HSCRC William J. Mooney, Jr. Memorial Education Series December 4, 2014 Arin Foreman Manager KPMG LLP What is the HSCRC? Health Services Cost Review Commission State regulatory commission
Progress on the MPSC s Incident Reporting System
 Progress on the MPSC s Incident Reporting System Third Annual Maryland Patient Safety Center Conference March 23, 2007 Vahé A. Kazandjian, PhD, MPH President, LogicQual Research Institute Co-Chair, MPSC
Progress on the MPSC s Incident Reporting System Third Annual Maryland Patient Safety Center Conference March 23, 2007 Vahé A. Kazandjian, PhD, MPH President, LogicQual Research Institute Co-Chair, MPSC
Understanding HSCRC Quality Programs and Methodology Updates
 Understanding HSCRC Quality Programs and Methodology Updates Kristen Geissler, MS, PT, CPHQ, MBA Managing Director Beth Greskovich - Director Berkeley Research Group August 19, 2016 Maryland Waiver and
Understanding HSCRC Quality Programs and Methodology Updates Kristen Geissler, MS, PT, CPHQ, MBA Managing Director Beth Greskovich - Director Berkeley Research Group August 19, 2016 Maryland Waiver and
Region III STEMI Plan
 Region III STEMI Plan I. Plan Goals A. To develop a Region III STEMI System that when implemented, will result in decreased mortality and morbidity in the MIEMSS Region III. In order to accomplish this,
Region III STEMI Plan I. Plan Goals A. To develop a Region III STEMI System that when implemented, will result in decreased mortality and morbidity in the MIEMSS Region III. In order to accomplish this,
Planning a Course to Population Health Management
 Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
hfma Maryland Chapter New All-Payer Model for Maryland Maryland Health Services Cost Review Commission
 hfma Maryland Chapter New All-Payer Model for Maryland Maryland Health Services Cost Review Commission October 2013 1 HSCRC Preparation for New All Payer Hospital Model Maryland prepared updated application
hfma Maryland Chapter New All-Payer Model for Maryland Maryland Health Services Cost Review Commission October 2013 1 HSCRC Preparation for New All Payer Hospital Model Maryland prepared updated application
Final Recommendations on the Update Factors for FY 2017
 Final Recommendations on the Update Factors for FY 2017 June 8, 2016 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764-2605 FAX: (410) 358-6217 This document
Final Recommendations on the Update Factors for FY 2017 June 8, 2016 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764-2605 FAX: (410) 358-6217 This document
The Nexus of Quality and Finance
 The Nexus of Quality and Finance Kristen Geissler Pat Ercolano March 4, 2014 Transition from Volume to Value: IHI Triple Aim IHI Triple Aim Improve patient experience of care (quality & satisfaction) Improve
The Nexus of Quality and Finance Kristen Geissler Pat Ercolano March 4, 2014 Transition from Volume to Value: IHI Triple Aim IHI Triple Aim Improve patient experience of care (quality & satisfaction) Improve
The MARYLAND HEALTH CARE COMMISSION
 The MARYLAND HEALTH CARE COMMISSION Our Role The MHCC is responsible to advance a strong, flexible health IT ecosystem that can appropriately support clinical decision-making, reduce redundancy, enable
The MARYLAND HEALTH CARE COMMISSION Our Role The MHCC is responsible to advance a strong, flexible health IT ecosystem that can appropriately support clinical decision-making, reduce redundancy, enable
Rural Relevance in Oklahoma
 Rural Relevance in Oklahoma OHA Annual Conference 2017 November 1, 2017 Agenda Introductions The Rural Relevance Study Impact of Current and Proposed Health Policies on Rural Providers Oklahoma Rural Hospitals:
Rural Relevance in Oklahoma OHA Annual Conference 2017 November 1, 2017 Agenda Introductions The Rural Relevance Study Impact of Current and Proposed Health Policies on Rural Providers Oklahoma Rural Hospitals:
Report to the Governor
 Report to the Governor Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764-2605 October 2016 Table of Contents Introduction... 1 The New All-Payer Model with
Report to the Governor Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764-2605 October 2016 Table of Contents Introduction... 1 The New All-Payer Model with
The Health Services Cost Review Commission s (HSCRC) global budget revenue contracts state:
 global budget revenue contracts state:") Global Budget Revenue (GBR) Reporting on Investment in Infrastructure Background The Health Services Cost Review Commission s (HSCRC) global budget revenue contracts state: The Hospital shall provide an
Global Budget Revenue (GBR) Reporting on Investment in Infrastructure Background The Health Services Cost Review Commission s (HSCRC) global budget revenue contracts state: The Hospital shall provide an
Staff Draft Recommendations for Updating the Quality-Based Reimbursement Program for Rate Year 2020
 RY 2020 Draft Recommendation for QBR Policy Staff Draft Recommendations for Updating the Quality-Based Reimbursement Program for Rate Year 2020 November 13, 2017 Health Services Cost Review Commission
RY 2020 Draft Recommendation for QBR Policy Staff Draft Recommendations for Updating the Quality-Based Reimbursement Program for Rate Year 2020 November 13, 2017 Health Services Cost Review Commission
The Maryland All Payer Hospital Rate Setting System Experience
 The Maryland All Payer Hospital Rate Setting System Experience Presentation for Legislative Joint Interim Task Force on Health Care Cost Review Robert B Murray Global Health Payment LLP Former Executive
The Maryland All Payer Hospital Rate Setting System Experience Presentation for Legislative Joint Interim Task Force on Health Care Cost Review Robert B Murray Global Health Payment LLP Former Executive
Global Budget Revenue. October 8, 2015
 Global Budget Revenue October 8, 2015 Goals Understand GBR s connection to the goals of Maryland s Demonstration Understand impact on budgeting and planning for RFP and future phases Answer questions that
Global Budget Revenue October 8, 2015 Goals Understand GBR s connection to the goals of Maryland s Demonstration Understand impact on budgeting and planning for RFP and future phases Answer questions that
Maryland Association of Healthcare Executives presents:
 Maryland Association of Healthcare Executives presents: 1 Today s Expert Panel Moderator: Michael Cetta, MD FACEP, Chief Strategy Officer US Acute Care Solutions Charles W. Callahan, DO, Vice President
Maryland Association of Healthcare Executives presents: 1 Today s Expert Panel Moderator: Michael Cetta, MD FACEP, Chief Strategy Officer US Acute Care Solutions Charles W. Callahan, DO, Vice President
Solution Title Reducing Patient Harm: Multidisciplinary Teamwork leads to Hospital -wide Success
 Organization Frederick Memorial Hospital Solution Title Reducing Patient Harm: Multidisciplinary Teamwork leads to Hospital -wide Success Program / Project Description, including Goals: Statistics regarding
Organization Frederick Memorial Hospital Solution Title Reducing Patient Harm: Multidisciplinary Teamwork leads to Hospital -wide Success Program / Project Description, including Goals: Statistics regarding
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES
 EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
EMERGENCY DEPARTMENT DIVERSIONS, WAIT TIMES: UNDERSTANDING THE CAUSES Introduction In 2016, the Maryland Hospital Association began to examine a recent upward trend in the number of emergency department
Clinical Quality Payment Policies Impact to Finance and Operations
 Clinical Quality Payment Policies Impact to Finance and Operations Kristen Geissler, MS, PT, MBA, CPHQ Director Berkeley Research Group December 4, 2014 What s the Buzz? Cost Efficient VALUE Effective
Clinical Quality Payment Policies Impact to Finance and Operations Kristen Geissler, MS, PT, MBA, CPHQ Director Berkeley Research Group December 4, 2014 What s the Buzz? Cost Efficient VALUE Effective
Rural Health Disparities 5/22/2012. Rural is often defined by what it is not urban. May 3, The Rural Health Landscape
 5/22/2012 May 3, 2012 The Rural Health Landscape Alan Morgan Chief Executive Officer National Rural Health Association National Rural Health Association Membership 2012 NRHA Mission The National Rural
5/22/2012 May 3, 2012 The Rural Health Landscape Alan Morgan Chief Executive Officer National Rural Health Association National Rural Health Association Membership 2012 NRHA Mission The National Rural
Transforming the Future Nursing Workforce: Innovative Statewide Opportunities
 Transforming the Future Nursing Workforce: Innovative Statewide Opportunities Peg Daw, DNP, RN-BC, CNE Nurse Support Program II, MHEC Joan Warren, PhD, RN-BC, NEA-BC, FAAN Associate Professor, University
Transforming the Future Nursing Workforce: Innovative Statewide Opportunities Peg Daw, DNP, RN-BC, CNE Nurse Support Program II, MHEC Joan Warren, PhD, RN-BC, NEA-BC, FAAN Associate Professor, University
ACCESS TO MENTAL HEALTH CARE IN RURAL AMERICA: A CRISIS IN THE MAKING FOR SENIORS AND PEOPLE WITH DISABILITIES
 ACCESS TO MENTAL HEALTH CARE IN RURAL AMERICA: A CRISIS IN THE MAKING FOR SENIORS AND PEOPLE WITH DISABILITIES A Capitol Hill Briefing Sponsored by the: AMERICAN MENTAL HEALTH COUNSELORS ASSOCIATION (AMHCA)
ACCESS TO MENTAL HEALTH CARE IN RURAL AMERICA: A CRISIS IN THE MAKING FOR SENIORS AND PEOPLE WITH DISABILITIES A Capitol Hill Briefing Sponsored by the: AMERICAN MENTAL HEALTH COUNSELORS ASSOCIATION (AMHCA)
Public Policy Forum Impact of Emergency Department Use on the Health Care System in Maryland
 Public Policy Forum Impact of Emergency Department Use on the Health Care System in Maryland Pamela W. Barclay Director, Center for Hospital Services Maryland Health Care Commission University of Maryland
Public Policy Forum Impact of Emergency Department Use on the Health Care System in Maryland Pamela W. Barclay Director, Center for Hospital Services Maryland Health Care Commission University of Maryland
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS)
") The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
Appendix B: Formulae Used for Calculation of Hospital Performance Measures
 Appendix B: Formulae Used for Calculation of Hospital Performance Measures ADJUSTMENTS Adjustment Factor Case Mix Adjustment Wage Index Adjustment Gross Patient Revenue / Gross Inpatient Acute Care Revenue
Appendix B: Formulae Used for Calculation of Hospital Performance Measures ADJUSTMENTS Adjustment Factor Case Mix Adjustment Wage Index Adjustment Gross Patient Revenue / Gross Inpatient Acute Care Revenue
HOME DIALYSIS REIMBURSEMENT AND POLICY. Tonya L. Saffer, MPH Senior Health Policy Director National Kidney Foundation
 HOME DIALYSIS REIMBURSEMENT AND POLICY Tonya L. Saffer, MPH Senior Health Policy Director National Kidney Foundation Objectives Understand the changing dynamics of use of home dialysis Know the different
HOME DIALYSIS REIMBURSEMENT AND POLICY Tonya L. Saffer, MPH Senior Health Policy Director National Kidney Foundation Objectives Understand the changing dynamics of use of home dialysis Know the different
paymentbasics The IPPS payment rates are intended to cover the costs that reasonably efficient providers would incur in furnishing highquality
 Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
Hospital ACUTE inpatient services system basics Revised: October 2015 This document does not reflect proposed legislation or regulatory actions. 425 I Street, NW Suite 701 Washington, DC 20001 ph: 202-220-3700
NOTICE OF WRITTEN COMMENT PERIOD
 NOTICE OF WRITTEN COMMENT PERIOD Notice is hereby given that the public and interested parties are invited to submit written comments to the Commission on any or all of the following staff draft recommendations
NOTICE OF WRITTEN COMMENT PERIOD Notice is hereby given that the public and interested parties are invited to submit written comments to the Commission on any or all of the following staff draft recommendations
Quality Based Impacts to Medicare Inpatient Payments
 Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
Quality Based Impacts to Medicare Inpatient Payments Overview New Developments in Quality Based Reimbursement Recap of programs Hospital acquired conditions Readmission reduction program Value based purchasing
LESSONS LEARNED IN LENGTH OF STAY (LOS)
") FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
FEBRUARY 2014 LESSONS LEARNED IN LENGTH OF STAY (LOS) USING ANALYTICS & KEY BEST PRACTICES TO DRIVE IMPROVEMENT Overview Healthcare systems will greatly enhance their financial status with a renewed focus
I. General Description
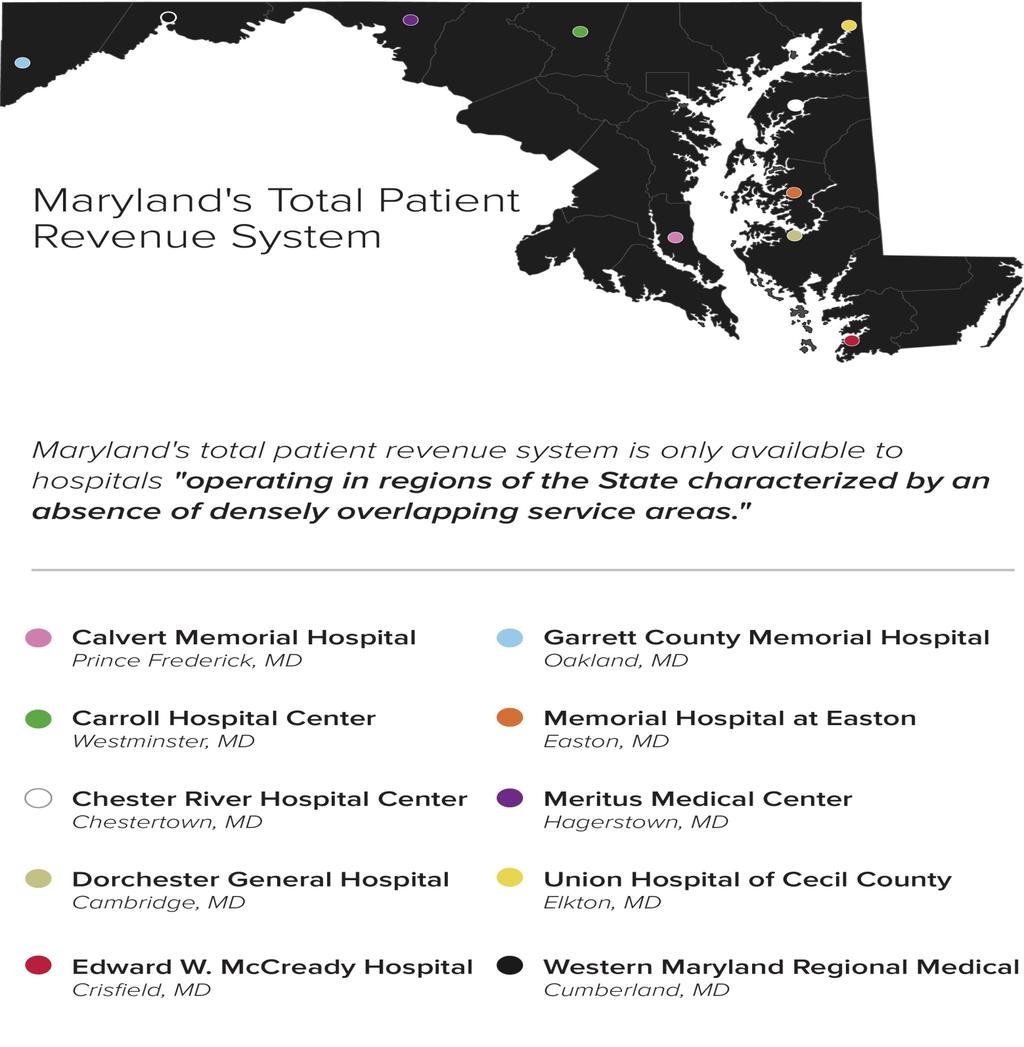
 SUCCESSOR AGREEMENT BETWEEN THE HEALTH SERVICES COST REVIEW COMMISSION AND CARROLL HOSPITAL CENTER REGARDING THE APPLICATION OF THE TOTAL PATIENT REVENUE SYSTEM This Agreement made this 31 st day of December,
SUCCESSOR AGREEMENT BETWEEN THE HEALTH SERVICES COST REVIEW COMMISSION AND CARROLL HOSPITAL CENTER REGARDING THE APPLICATION OF THE TOTAL PATIENT REVENUE SYSTEM This Agreement made this 31 st day of December,
Maryland Medicaid Program. Aaron Larrimore Medicaid Department of Health and Mental Hygiene May 31, 2012
 Maryland Medicaid Program Aaron Larrimore Medicaid Department of Health and Mental Hygiene May 31, 2012 1 Maryland Medicaid In Maryland, Medicaid is also called Medical Assistance or MA. MA is a joint
Maryland Medicaid Program Aaron Larrimore Medicaid Department of Health and Mental Hygiene May 31, 2012 1 Maryland Medicaid In Maryland, Medicaid is also called Medical Assistance or MA. MA is a joint
Summary of U.S. Senate Finance Committee Health Reform Bill
 Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
Summary of U.S. Senate Finance Committee Health Reform Bill September 2009 The following is a summary of the major hospital and health system provisions included in the Finance Committee bill, the America
A Tale of Three Regions: Texas 1115 Waiver Journey Regional Healthcare Partnership 3 Shannon Evans, MBA, LSSGB Regional Healthcare Partnership 6
 A Tale of Three Regions: Texas 1115 Waiver Journey Regional Healthcare Partnership 3 Shannon Evans, MBA, LSSGB Regional Healthcare Partnership 6 Carol Huber, MBA Regional Healthcare Partnership 1 Daniel
A Tale of Three Regions: Texas 1115 Waiver Journey Regional Healthcare Partnership 3 Shannon Evans, MBA, LSSGB Regional Healthcare Partnership 6 Carol Huber, MBA Regional Healthcare Partnership 1 Daniel
Report to the MSFA Executive Committee. R Adams Cowley Shock Trauma Center December 6, 2014 Tara Reed Carlson, MS, RN Business Development
 Report to the MSFA Executive Committee R Adams Cowley Shock Trauma Center December 6, 2014 Tara Reed Carlson, MS, RN Business Development Total Patient Admissions Lost Interhospital Transfers 1000 900
Report to the MSFA Executive Committee R Adams Cowley Shock Trauma Center December 6, 2014 Tara Reed Carlson, MS, RN Business Development Total Patient Admissions Lost Interhospital Transfers 1000 900
HEALTH CARE REFORM IN THE U.S.
 HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
Home Health Agency Partnership Development Guide Overview
 Home Health Agency Partnership Development Guide Overview This Home Health Agency (HHA) Partnership Development Guide aims to help s hospitals identify, develop, and strengthen formal and informal partnerships
Home Health Agency Partnership Development Guide Overview This Home Health Agency (HHA) Partnership Development Guide aims to help s hospitals identify, develop, and strengthen formal and informal partnerships
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Value Based Purchasing
 Value Based Purchasing Baylor Health Care System Leadership Summit October 26, 2011 Sheri Winsper, RN, MSN, MSHA Vice President for Performance Measurement & Reporting Institute for Health Care Research
Value Based Purchasing Baylor Health Care System Leadership Summit October 26, 2011 Sheri Winsper, RN, MSN, MSHA Vice President for Performance Measurement & Reporting Institute for Health Care Research
The Essential Care, Everywhere study provides new insight into Washington s rural communities, and their 42 hospitals.
 Transforming the Delivery of Essential Care in Rural Communities Medical Design Forum AIA Seattle/AHP Medical Forum February 7, 2013 The Essential Care, Everywhere study provides new insight into Washington
Transforming the Delivery of Essential Care in Rural Communities Medical Design Forum AIA Seattle/AHP Medical Forum February 7, 2013 The Essential Care, Everywhere study provides new insight into Washington
Figure 1. Massachusetts Statewide Aggregate Hospital Acquired Infection Data Summary. Infection Rate* Denominator Count*
 Massachusetts Hospitals Statewide Performance Improvement Agenda Final Report MHA Board-approved Quality & Safety Goal January 2013 Reduce preventable CAUTI, CLABSI and SSI by 40% by 2015 Figure 1. Massachusetts
Massachusetts Hospitals Statewide Performance Improvement Agenda Final Report MHA Board-approved Quality & Safety Goal January 2013 Reduce preventable CAUTI, CLABSI and SSI by 40% by 2015 Figure 1. Massachusetts
June 25, Shamis Mohamoud, David Idala, Parker James, Laura Humber. AcademyHealth Annual Research Meeting
 Evaluation of the Maryland Health Home Program for Medicaid Enrollees with Severe Mental Illnesses or Opioid Substance Use Disorder and Risk of Additional Chronic Conditions June 25, 2018 Shamis Mohamoud,
Evaluation of the Maryland Health Home Program for Medicaid Enrollees with Severe Mental Illnesses or Opioid Substance Use Disorder and Risk of Additional Chronic Conditions June 25, 2018 Shamis Mohamoud,
Improving Patient Safety Across Michigan and Illinois
 Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
Improving Patient Safety Across Michigan and Illinois Readmissions Collaborative Kickoff January 20, 2016 1 Agenda Readmissions Collaborative Structure and Overview Business case for readmissions Using
University of Iowa Health Care
 University of Iowa Health Care Presentation to The Board of Regents, State of Iowa April 11-12, 2018 1 Agenda Today s Presentation Opening Remarks Operating and Financial Performance Preliminary FY19 Operating
University of Iowa Health Care Presentation to The Board of Regents, State of Iowa April 11-12, 2018 1 Agenda Today s Presentation Opening Remarks Operating and Financial Performance Preliminary FY19 Operating
Prepared for North Gunther Hospital Medicare ID August 06, 2012
 Prepared for North Gunther Hospital Medicare ID 000001 August 06, 2012 TABLE OF CONTENTS Introduction: Benchmarking Your Hospital 3 Section 1: Hospital Operating Costs 5 Section 2: Margins 10 Section 3:
Prepared for North Gunther Hospital Medicare ID 000001 August 06, 2012 TABLE OF CONTENTS Introduction: Benchmarking Your Hospital 3 Section 1: Hospital Operating Costs 5 Section 2: Margins 10 Section 3:
Medicare Value Based Purchasing Overview
 Medicare Value Based Purchasing Overview Washington State Hospital Association Apprise Health Insights / Oregon Association of Hospitals and Health Systems DataGen Susan McDonough Lauren Davis Bill Shyne
Medicare Value Based Purchasing Overview Washington State Hospital Association Apprise Health Insights / Oregon Association of Hospitals and Health Systems DataGen Susan McDonough Lauren Davis Bill Shyne
Involuntary Discharges and Transfers from
 Nursing Home Residents Involuntary Discharges and Transfers from Nursing Homes: Know Your Rights Equal Access to Justice: Legal Aid Equal Justice for Maryland Since 1911 Your Rights as a Nursing Home Resident
Nursing Home Residents Involuntary Discharges and Transfers from Nursing Homes: Know Your Rights Equal Access to Justice: Legal Aid Equal Justice for Maryland Since 1911 Your Rights as a Nursing Home Resident
Final Recommendation for the Medicare Performance Adjustment (MPA) for Rate Year 2020
 for Rate Year 2020") Final Recommendation for the Medicare Performance Adjustment (MPA) for Rate Year 2020 November 13, 2017 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764-2605
Final Recommendation for the Medicare Performance Adjustment (MPA) for Rate Year 2020 November 13, 2017 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764-2605
Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital
 Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital November 5, 2013 Martin Luther King, Jr. Community Hospital Page 1 11/05/2013 Agenda
Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital November 5, 2013 Martin Luther King, Jr. Community Hospital Page 1 11/05/2013 Agenda
Using the BaldrigeCriteria to Achieve High Reliability
 Using the BaldrigeCriteria to Achieve High Reliability John Chessare MD, MPH President and CEO Carolyn Candiello Vice President for Quality and Patient Safety GBMC HealthCare System Organizational Profile:
Using the BaldrigeCriteria to Achieve High Reliability John Chessare MD, MPH President and CEO Carolyn Candiello Vice President for Quality and Patient Safety GBMC HealthCare System Organizational Profile:
Preventable Readmissions Payment Strategies
 Preventable Readmissions Payment Strategies 3M 2007. All rights reserved. Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions
Preventable Readmissions Payment Strategies 3M 2007. All rights reserved. Strategy to reduce readmissions and increase quality needs to have the following elements A tool to identify preventable readmissions
Managing Healthcare Payment Opportunity Fundamentals CENTER FOR INDUSTRY TRANSFORMATION
 Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
Managing Healthcare Payment Opportunity Fundamentals dhgllp.com/healthcare 4510 Cox Road, Suite 200 Glen Allen, VA 23060 Melinda Hancock PARTNER Melinda.Hancock@dhgllp.com 804.474.1249 Michael Strilesky
4160 Patterson Avenue, Baltimore, Maryland Phone: Fax: Toll Free: hscrc.maryland.
 4160 Patterson Avenue, Baltimore, Maryland 21215 Phone: 410-764-2605 Fax: 410-358-6217 Toll Free: 1-888-287-3229 hscrc.maryland.gov 536th MEETING OF THE HEALTH SERVICES COST REVIEW COMMISSION December
4160 Patterson Avenue, Baltimore, Maryland 21215 Phone: 410-764-2605 Fax: 410-358-6217 Toll Free: 1-888-287-3229 hscrc.maryland.gov 536th MEETING OF THE HEALTH SERVICES COST REVIEW COMMISSION December
Developing a Unique Patient ID: Proposed Data Submission Fields. March 24, 2011 MARYLAND HEALTH SERVICES COST REVIEW COMMISSION
 Developing a Unique Patient ID: Proposed Data Submission Fields March 24, 2011 MARYLAND HEALTH SERVICES COST REVIEW COMMISSION Agenda 1. Background: Incentive programs and readmissions 2. Proposed additional
Developing a Unique Patient ID: Proposed Data Submission Fields March 24, 2011 MARYLAND HEALTH SERVICES COST REVIEW COMMISSION Agenda 1. Background: Incentive programs and readmissions 2. Proposed additional
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Navigating an Enhanced Rural Health Model for Maryland
 Executive Summary HEALTH MATTERS: Navigating an Enhanced Rural Health Model for Maryland LESSONS LEARNED FROM THE MID-SHORE COUNTIES To access the Report and Accompanied Technical Reports go to: go.umd.edu/ruralhealth
Executive Summary HEALTH MATTERS: Navigating an Enhanced Rural Health Model for Maryland LESSONS LEARNED FROM THE MID-SHORE COUNTIES To access the Report and Accompanied Technical Reports go to: go.umd.edu/ruralhealth
Healing America s Communities: Best Practices in Mental Health. Kevin Young, FACHE President
 Healing America s Communities: Best Practices in Mental Health Kevin Young, FACHE President Why is Behavioral Health Treatment Important? In the treatment of the sick the effect of mental influence should
Healing America s Communities: Best Practices in Mental Health Kevin Young, FACHE President Why is Behavioral Health Treatment Important? In the treatment of the sick the effect of mental influence should
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
For further information call: Robert B. Murray * For release 1:30 p.m. EST * Wednesday, July 6, 2005
 For further information call: Robert B. Murray * For release 1:30 p.m. EST 410-764-2605 * Wednesday, July 6, 2005 Average Amount Paid For A Hospital Stay in Maryland The rate of increase in charges for
For further information call: Robert B. Murray * For release 1:30 p.m. EST 410-764-2605 * Wednesday, July 6, 2005 Average Amount Paid For A Hospital Stay in Maryland The rate of increase in charges for
Draft for the Medicare Performance Adjustment (MPA) Policy for Rate Year 2021
 Policy for Rate Year 2021") Draft for the Medicare Performance Adjustment (MPA) Policy for Rate Year 2021 October 2018 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764-2605 FAX: (410)
Draft for the Medicare Performance Adjustment (MPA) Policy for Rate Year 2021 October 2018 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764-2605 FAX: (410)
State of Maryland Department of Health and Mental Hygiene
 John M. Colmers Chairman Herbert S. Wong, Ph.D. Vice-Chairman George H. Bone, M.D. Stephen F. Jencks, M.D., M.P.H. Jack C. Keane Bernadette C. Loftus, M.D. Thomas R. Mullen State of Maryland Department
John M. Colmers Chairman Herbert S. Wong, Ph.D. Vice-Chairman George H. Bone, M.D. Stephen F. Jencks, M.D., M.P.H. Jack C. Keane Bernadette C. Loftus, M.D. Thomas R. Mullen State of Maryland Department
Neighborhoods, resources and capacity to improve
 Neighborhoods, resources and capacity to improve Jane Brock, MD, MSPH Telligen QIN QIO National Coordinating Center This material was prepared by Telligen, the Quality Innovation Network National Coordinating
Neighborhoods, resources and capacity to improve Jane Brock, MD, MSPH Telligen QIN QIO National Coordinating Center This material was prepared by Telligen, the Quality Innovation Network National Coordinating
network news Exciting updates to kp.org coming soon! FOR NETWORK PROVIDERS OF KAISER PERMANENTE
 network Produced by Kaiser Foundation Health Plan of the Mid-Atlantic States, Inc., with the Mid-Atlantic Permanente Medical Group, P.C. Web site: www.providers.kp.org/mas news MARCH 2011 FOR NETWORK PROVIDERS
network Produced by Kaiser Foundation Health Plan of the Mid-Atlantic States, Inc., with the Mid-Atlantic Permanente Medical Group, P.C. Web site: www.providers.kp.org/mas news MARCH 2011 FOR NETWORK PROVIDERS
Moving the Dial on Quality
 Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
Moving the Dial on Quality Washington State Medical Oncology Society November 1, 2013 Nancy L. Fisher, MD, MPH CMO, Region X Centers for Medicare and Medicaid Serving Alaska, Idaho, Oregon, Washington
Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks
 Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks Agenda Define ACO, CIN, and Coordinated Care Review ACO/CIN
Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks Agenda Define ACO, CIN, and Coordinated Care Review ACO/CIN
American Health Lawyers Association Institute on Medicare and Medicaid Payment Issues. History of the Physician Fee Schedule
 American Health Lawyers Association Institute on Medicare and Medicaid Payment Issues March 20-22, 2013 Baltimore, Maryland Sidney S. Welch, Esq. 1 History of the Physician Fee Schedule Prior to 1992,
American Health Lawyers Association Institute on Medicare and Medicaid Payment Issues March 20-22, 2013 Baltimore, Maryland Sidney S. Welch, Esq. 1 History of the Physician Fee Schedule Prior to 1992,
Overview of Alaska s Hospitals and Nursing Homes. House HSS Committee March 1, 2012
 Overview of Alaska s Hospitals and Nursing Homes House HSS Committee March 1, 2012 Alaska Hospital and Nursing Homes Testifying Today Fairbanks Memorial Hospital Mike Powers Central Peninsula Hospital
Overview of Alaska s Hospitals and Nursing Homes House HSS Committee March 1, 2012 Alaska Hospital and Nursing Homes Testifying Today Fairbanks Memorial Hospital Mike Powers Central Peninsula Hospital
UTILIZING TELEHEALTH SERVICES TO IMPROVE ACCESS TO QUALITY CARE IN RURAL SETTINGS
 UTILIZING TELEHEALTH SERVICES TO IMPROVE ACCESS TO QUALITY CARE IN RURAL SETTINGS Charles Gizara, MS, BSN, RN, CCM Director Integrated Care Management Jennifer Light, RN Telehealth Coordinator Goals /
UTILIZING TELEHEALTH SERVICES TO IMPROVE ACCESS TO QUALITY CARE IN RURAL SETTINGS Charles Gizara, MS, BSN, RN, CCM Director Integrated Care Management Jennifer Light, RN Telehealth Coordinator Goals /
Patient Navigator Program
 Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
Using Patient Navigators and Education to Improve Post-Acute Transitions Emerging innovators in post-acute care delivery models are finding ways to provide patient-centered, quality care to integrate today
Reforming Health Care with Savings to Pay for Better Health
 Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
Medicaid Update Special Edition Budget Highlights New York State Budget: Health Reform Highlights
 Page 1 of 6 New York State April 2009 Volume 25, Number 4 Medicaid Update Special Edition 2009-10 Budget Highlights David A. Paterson, Governor State of New York Richard F. Daines, M.D. Commissioner New
Page 1 of 6 New York State April 2009 Volume 25, Number 4 Medicaid Update Special Edition 2009-10 Budget Highlights David A. Paterson, Governor State of New York Richard F. Daines, M.D. Commissioner New
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
Ohio Medicaid Overview
 Ohio Medicaid Overview May 2014 John McCarthy Ohio Medicaid Director Medicaid Overview Medicaid is Ohio s largest health payer 83,000 active providers, hospitals, nursing homes and other providers care
Ohio Medicaid Overview May 2014 John McCarthy Ohio Medicaid Director Medicaid Overview Medicaid is Ohio s largest health payer 83,000 active providers, hospitals, nursing homes and other providers care
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Rural and Independent Primary Care.
 Rural and Independent Primary Care www.caravanhealth.com Agenda 2015 Results from Rural ACO Participants Fundamental population health programs. Overview of additional rural value-based payments Opportunities
Rural and Independent Primary Care www.caravanhealth.com Agenda 2015 Results from Rural ACO Participants Fundamental population health programs. Overview of additional rural value-based payments Opportunities
Estimated Decrease in Expenditure by Service Category
 Public Notice for June 2009 Release PUBLIC NOTICE COLORADO MEDICAID Department of Health Care Policy and Financing Fee-for-Service Provider Payments Effective July 1, 2009, in an effort to reduce expenditures
Public Notice for June 2009 Release PUBLIC NOTICE COLORADO MEDICAID Department of Health Care Policy and Financing Fee-for-Service Provider Payments Effective July 1, 2009, in an effort to reduce expenditures
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Grants and Per Capita Funding
 HHS Joint Appropriations Subcommittee Implications of Possible Medicaid Block Grants and Per Capita Funding Steve Owen, Fiscal Research Division March 15, 2017 Presentation Objectives Federal Legislation
HHS Joint Appropriations Subcommittee Implications of Possible Medicaid Block Grants and Per Capita Funding Steve Owen, Fiscal Research Division March 15, 2017 Presentation Objectives Federal Legislation
First Look: Plan Benefit Filings
 July 30, 2014 First Look: Plan Filings Maryland and Washington, D.C. 1 Disclaimers MedStar does not currently have a contract with CMS for the State of MD nor any special needs plans in Washington, D.C.
July 30, 2014 First Look: Plan Filings Maryland and Washington, D.C. 1 Disclaimers MedStar does not currently have a contract with CMS for the State of MD nor any special needs plans in Washington, D.C.
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW OHA Finance/PFS Webinar Series. May 10, 2016
 MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
MEDICARE FFY 2017 PPS PROPOSED RULES OVERVIEW 2016 OHA Finance/PFS Webinar Series May 10, 2016 Spring is Medicare PPS Proposed Rules Season Inpatient Hospital Long-Term Acute Care Hospital Inpatient Rehabilitation
HSCRC Update on Maryland's Health Care Transformation. March 2017
 HSCRC Update on Maryland's Health Care Transformation March 2017 Background: Maryland s All-Payer Model Since 1977, Maryland has had an all-payer hospital ratesetting system In 2014, Maryland updated its
HSCRC Update on Maryland's Health Care Transformation March 2017 Background: Maryland s All-Payer Model Since 1977, Maryland has had an all-payer hospital ratesetting system In 2014, Maryland updated its
Eliminating Excessive, Unnecessary, and Wasteful Expenditures: Getting to a High Performance U.S. Health System
 Eliminating Excessive, Unnecessary, and Wasteful Expenditures: Getting to a High Performance U.S. Health System Karen Davis President, The Commonwealth Fund IOM Workshop Series: The Policy Agenda September
Eliminating Excessive, Unnecessary, and Wasteful Expenditures: Getting to a High Performance U.S. Health System Karen Davis President, The Commonwealth Fund IOM Workshop Series: The Policy Agenda September
How to Win Under Bundled Payments
 How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
How to Win Under Bundled Payments Donald E. Fry, M.D., F.A.C.S. Executive Vice-President, Clinical Outcomes MPA Healthcare Solutions Chicago, Illinois Adjunct Professor of Surgery Northwestern University
Medicare Value Based Purchasing Overview
 Medicare Value Based Purchasing Overview South Carolina Hospital Association DataGen Susan McDonough Bill Shyne October 29, 2015 Today s Objectives Overview of Medicare Value Based Purchasing Program Review
Medicare Value Based Purchasing Overview South Carolina Hospital Association DataGen Susan McDonough Bill Shyne October 29, 2015 Today s Objectives Overview of Medicare Value Based Purchasing Program Review
Evidence of Coverage
 January 1 December 31, 2017 Evidence of Coverage Your Medicare Health Benefits and Services as a Member of Kaiser Permanente Medicare Plus (Cost) This booklet gives you the details about your Medicare
January 1 December 31, 2017 Evidence of Coverage Your Medicare Health Benefits and Services as a Member of Kaiser Permanente Medicare Plus (Cost) This booklet gives you the details about your Medicare
2018 DOM HealthCare Quality Symposium Poster Session
 Winner - Outstanding Faculty Project Author Hillary Lum, MD, Faculty Division/Department Geriatric Medicine / Department of Medicine UCHealth Patient use of a Medical Power of Attorney via My Health Connection
Winner - Outstanding Faculty Project Author Hillary Lum, MD, Faculty Division/Department Geriatric Medicine / Department of Medicine UCHealth Patient use of a Medical Power of Attorney via My Health Connection
Understanding the Implications of Total Cost of Care in the Maryland Market
 Understanding the Implications of Total Cost of Care in the Maryland Market January 29, 2016 Joshua Campbell Director KPMG LLP Matthew Beitman Sr. Associate KPMG LLP The concept of total cost of care is
Understanding the Implications of Total Cost of Care in the Maryland Market January 29, 2016 Joshua Campbell Director KPMG LLP Matthew Beitman Sr. Associate KPMG LLP The concept of total cost of care is
UI Health Hospital Dashboard September 7, 2017
 UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
Incentives and Penalties
 Incentives and Penalties CAUTI & Value Based Purchasing and Hospital Associated Conditions Penalties: How Your Hospital s CAUTI Rate Affects Payment Linda R. Greene, RN, MPS,CIC UR Highland Hospital Rochester,
Incentives and Penalties CAUTI & Value Based Purchasing and Hospital Associated Conditions Penalties: How Your Hospital s CAUTI Rate Affects Payment Linda R. Greene, RN, MPS,CIC UR Highland Hospital Rochester,
Reinventing Health Care: Health System Transformation
 Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
Reinventing Health Care: Health System Transformation Aspen Institute Patrick Conway, M.D., MSc CMS Chief Medical Officer Director, Center for Clinical Standards and Quality Acting Director, Center for
The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform. Summary
 Reform. Summary") Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to
Current Law The President s and Other Bipartisan Proposals to Reform Medicare: Post-Acute Care (PAC) Reform Summary Home Health Agencies Under current law, beneficiaries who are generally restricted to