AGENDA. Part I. Start of NHS Salford Clinical Commissioning Group Primary Care Commissioning Committee
|
|
|
- Austen Foster
- 5 years ago
- Views:
Transcription

1 NHS Salford Clinical Commissioning Group Primary Care Commissioning Committee Tuesday, 28 th November :30-12:00Hrs The Salford Room, St. James s House AGENDA Part I Start of NHS Salford Clinical Commissioning Group Primary Care Commissioning Committee 10:30 Public Meeting Open Agenda for Members of the Public to raise items previously mentioned to the Senior Committee Support Officer 10:35 Start of NHS Salford Clinical Commissioning Group Primary Care Commissioning Committee Item Time Description Lead 1 10:35 Apologies for absence Chair 2 Declaration of Interest in items on this Meeting s Agenda 3 Minutes of the meeting held on 26 th September a) Action Log from the meeting held on 26 th September 2017 b) Matters Arising from the meeting held on 26 th September 2017 Chair Chair Chair Chair For Assurance/Decision 5 10:45 Community Based Care a) Salford Wide Extended Access Pilot Update Report (paper) b) Salford Standard Proposal for 2018/19 c) Ellenbrook Medical Practice Application to close the patient list Head of Service Improvement (Integrated Care System) Head of Service Improvement (Primary Care) Head of Service Improvement (Primary Care) 6 11:00 Performance a) Financial Performance (paper) Chief Finance Officer
2 b) Primary Care Commissioning Committee Work Plan Review (paper) Head of Service Improvement (Primary Care) For Information 7 11:30 Minutes/Reports of Partnership Boards/Sub Committees a) Primary Care Operational Group Report (paper) b) Primary Care Quality Group Report (paper) 8 11:55 Reflection a) Key Decisions b) Key Messages c) Benefits to the Population of Salford 9 12:00 Meeting to close Head of Service Improvement Director of Quality and Innovation Chair Date and Time of Next Meeting: Tuesday, 30 th January 2018, 10:30-12:30, Salford Suite, St. James s House
3 Minutes of NHS Salford Clinical Commissioning Group Primary Care Commissioning Committee (PCCC) 26 th September 2017, 10:30-12:00Hrs in the Salford Room St James s House, Salford Present: Mr Brian Wroe (BW) Mr Paul Newman (PN) Mr Steve Dixon (SD) Mrs Karen Proctor (KP) Mr Ben Squires (BS) In Attendance: Mrs Francine Thorpe (FT) Dr Jenny Walton (JW) Miss Siobhan Farmer (SF) Mr Harry Golby (HG) Mrs Anna Ganotis (AG) Mr David Dobson (DD) Mrs Natalie McInerney (NM) Apologies: Mr Anthony Hassall (AH) Mrs Delana Lawson (DL) Mrs Sara Roscoe (SR) Dr Jeremy Tankel (JW) Part I Lay Member for Engagement, Salford CCG (Chair) Lay Member for Commercial, Salford CCG Chief Finance Officer, Salford CCG Director of Commissioning, Salford CCG Head of Primary Care Operations, Greater Manchester Health and Social Care Partnership (GMHSCP) NHS England Director of Quality and Innovation, Salford CCG Representative Salford and Trafford LMC Consultant in Public Health (representative for the Health and Wellbeing Board), attending on behalf of Mr David Herne Salford City Council Head of Service Improvement, Salford CCG Head of Service Improvement, Salford CCG Senior Committee Support Officer, Salford CCG Service Improvement Manager, Salford CCG Chief Accountable Officer, Salford CCG Chief Officer, Healthwatch Salford Head of Primary Care Transformation Greater Manchester Health and Social Care Partnership (GMHSCP) NHS England Medical Director, Salford CCG 1. Welcome and Introductions 1.1 BW formally opened the meeting with introductions made by those present. There were no questions raised by members of the public which had been submitted in advance of the meeting. 2. Declarations of Interest 2.1 No declarations of interests were declared. 3. Minutes of the last Meeting of 18 th July The minutes were approved as a true and accurate reflection. Primary Care Joint Commissioning Meeting 26 th September 2017 Part 1 Page 1 of 8
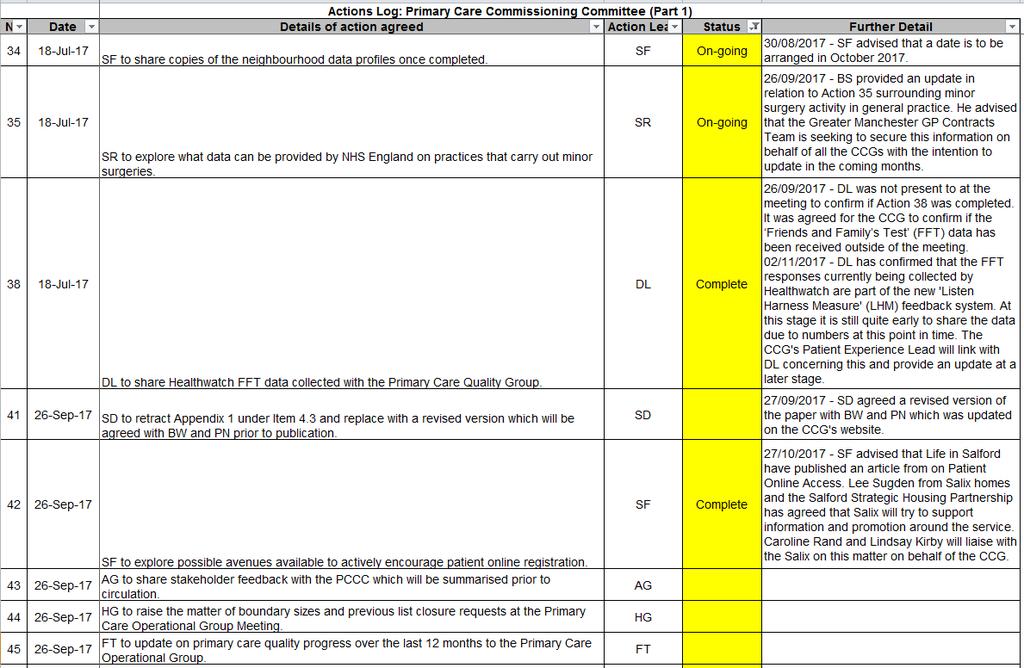
4 4. Action Log and Matters Arising from 18 th July Action Log Action 30 was agreed to be closed, HG confirmed that the Primary Care Operational Group now receives a regular report on patient online access. SF advised that in relation to Action 32 she and BS met last week. She added that an update will be provided to the PCCC in due course regarding the additional capacity and provision required for other primary care services across the locality. BS provided an update in relation to Action 35 surrounding minor surgery activity in general practice. He advised that the Greater Manchester GP Contracts Team is seeking to secure this information on behalf of all the CCGs with the intention to update in the coming months. BS advised that in respect of national contracting negotiations for GPs, the GMHSCP have no formal inclusion in this role, however feedback and shared learning has been escalated within NHS England following the previous discussions under Action 37. DL was not present at the meeting to confirm if Action 38 was completed. It was agreed for the CCG to confirm if the Friends and Family s Test (FFT) data has been received outside of the meeting. HG advised that Action 40 was discussed at Primary Care Operational Group regarding managing conflicts of interests. 4.2 Matters Arising PCCC Risk Register AG provided an update against the PCCC Risk Register which it had been agreed to schedule for 6 monthly updates. She advised that there were no increases in any risk scores, noting some decreasing as well as one additional risk being added. It was reported that there is a robust process in place for managing and monitoring the risks. The PCCC recognised the current issues which are included in the risk register, in addition to the work being carried out to mitigate and manage these areas with the CCG. 4.3 Primary Care Estates Update SD updated the PCCC on actions being taken to implement the CCG s estates strategy, with specific reference to primary care. He reported that updates are provided to the CCG s Executive Team with oversight by the Salford Locality Estates Group that includes representation from providers, commissioners and estates organisations which is chaired by Charlotte Ramsden from Salford City Council. It was noted that the CCG has a strategic estates strategy, following formally taking responsibility for this area in August SD reported that the previous arrangements had meant that NHS England were responsible before delegating this function to CCGs It was noted that the CCG are exploring estates challenges, with reference made to the new provision such as the Gateway facilities across the City. SD reported that the Group were currently exploring the possibility of new hubs or Gateway facilities in the remaining neighbourhoods across Salford. Reference was made to the Group exploring utilisation of the current provision in health centres and what availability can be offered for the delivery from out of hospital care. The second strand of the estates strategy is to explore the increased utilisation in out of hospital care facilities as well as delivering value for money from publicly owned buildings. Salford Primary Care Together Primary Care Joint Commissioning Meeting 26 th September 2017 Part 1 Page 2 of 8
5 (SPCT) is now working with GP practices to explore the provision of privately owned practice buildings. The plan from this work is to analyse the estates survey results from the work being carried out by SPCT to provide a full picture of premise capacity in primary care facilities. SD highlighted that the detailed appendix refers to a new build in Little Hulton. He reported that at least three practices will co-locate into this new practice, with the outline business case having been approved by the CCG s Executive Team SD reported that in relation to the Lower Broughton neighbourhood a new site has been identified. The CCG are now working with practices to consider proposals going forward. It was noted that for the Irlam and Cadishead neighbourhood, the CCG is working with practices, but no site has currently been identified. AG highlighted the six facet survey results will be good data to analyse in the CCG, as well as being able to work with CCG colleagues and with the Local Authority A discussion took place as to the estates group needing to communicate decisions being made in a timely and effective manner once reached. It was recognised that the estates group should also be taking into consideration the information being provided to GPs and making this more accessible. SF advised that it was agreed at the Health and Wellbeing Board for a small working group including Dr Tom Tasker, Chair of the CCG, to explore pharmacy provision across the City. The level of detail was highlighted in appendix 1. It was agreed to retract the published document due to the level of detail not being necessary and publish a revised version once agreed with BW and PN. Action: SD to retract Appendix 1 under Item 4.3 and replace with a revised version which will be agreed with BW and PN prior to publication The PCCC noted the contents of the report and the progress made on the schemes to date. 4.4 Patient Online Update SD advised that this subject is to be a regular reporting item to the PCCC. He advised that when the CCG originally explored the data, it was noted that there was a difference in level of success. The CCG have been proactive with the Head of Business Intelligence and Information Technology visiting neighbourhoods. The PCCC noted that the 10% target has now increased to 20%, but is based on per practice compliance and not an entire population. Some practices have been very successful and have already exceeded the 20% target. The remaining practices are being supported with data shared from other practices, all of which is nationally available data. A discussion took place as to the changes being made within primary care over time, such as the implementation of the Salford Standard, with further plans to consider including patient online compliance as a domain of the Salford Standard SF requested clarification as to whether the 20% target is for all patients registered at a practice, not just over 16? SD confirmed that the target for practices relate to their whole registered population. It was noted that anyone aged 14 and over can register themselves. BS advised that anyone aged 11 Primary Care Joint Commissioning Meeting 26 th September 2017 Part 1 Page 3 of 8
6 or under can be registered by their parents. PN enquired as to what the comparable data reports about Salford against other localities in Greater Manchester. SD reported that when originally benchmarked, Salford was second from bottom across the North West of England. A discussion took place as to demographical indicators for areas which are more affluent than others. It was recognised that some practices in Salford have been very successful compared to others. SF offered initiatives for supporting older people, as well as the My City Help link. It was agreed for SF to explore possible avenues available to actively encourage patient online registration. Action: SF to explore possible avenues available to actively encourage patient online registration The PCCC noted the contents of the report. 5. Community Based Care 5.1 Primary Care Investment Agreement AG advised that the Primary Care Investment Agreement has already been approved by PCCC members outside of committee meetings, with the version provided for noting following submission to the GMHSCP. She added that comments and feedback were noted and incorporated, including information provided by the LMC. It was noted that a decision has not yet been communicated to the CCG, however the GMHSCP have reported that the letter is due imminently. AG made reference to the recommendation, in which the paper requests what members would prefer for the reporting frequency.sd advised that the document and appendix mainly referred to 7 day access, which is now up and running and is being rolled a neighbourhood at a time The PCCC noted the contents of the report and attached investment agreement. The frequency of update reports was agreed for 6 monthly and report by exception to the PCCC when required. 5.2 Newbury Green Medical Practice and Limefield Medical Practice Merger AG advised of the importance of this paper, as it is the first time the PCCC will need to consider a practice merger, following the co-commissioning and delegated arrangements. The CCG were already aware of the challenges in capacity at Limefield Medical Practice. It was agreed that the consultation feedback will be shared with the PCCC. A discussion took place as to the need for being mindful of quality improvements required. HG advised that the report reflects the need to merge and the challenges at Limefield Medical Practice should be supported and alleviated. The comments regarding quality issues are being monitored by the CCG which will continue should the merger take place. AG advised that the practices had discussed not having a merger take place until April 2018, using the time between now and then for both practices to work together to improve the standards and quality of care. HG advised that from a quality perspective, the data will merge if completed. Action: AG to share stakeholder feedback with the PCCC which will be summarised prior to circulation. Primary Care Joint Commissioning Meeting 26 th September 2017 Part 1 Page 4 of 8
7 5.2.2 SF enquired as to how does a practice list work post-merger? BS reported that there will only be one practice list once the merger has taken place. He added that there will be one contract, with one contract becoming obsolete and the practice would have all patients coded for the contract which remains. JW enquired as to whether both practices are on GMS contracts. BS confirmed that this was the case for both practices A discussion took place as to the current large boundary size of the Newbury Green Medical Practice, noting that this is down to the practice to decide. It was recognised that patients can move address and therefore retain their current GP. SD reported that the challenge is that there is no national limit on a boundary size, however, in the past the CCG have considered list closures for other practices across the City. HG agreed to raise this matter at the Primary Care Operational Group Meeting. Action: HG to raise the matter of boundary sizes and previous list closure requests at the Primary Care Operational Group Meeting Based upon the outcome of the options appraisal and some of the considerations regarding the impact upon quality of care, the Primary Care Commissioning Committee supported Option 1 and approved the application to merge the two practices (subject to appropriate patient and stakeholder consultation, equality impact assessment outcomes and agreed merger date). The CCG will work with the two practices and the GMHSCP in developing a project plan to support a smooth transition to the new arrangements within the agreed timescales. Updates will be provided via the Primary Care Operational Group. 6 Performance 6.1 Primary Care Finance Report SD reported that in respect of primary care finances, the CCG are on track to break even and are projected to achieve a slight under spend on primary care medical services. This is due to the re-procurement of the Height Medical Contract which was an AMPS contract, rather than a core GMS contract. The new contract is now in line with other GP practices on a GMS contract. It was noted that dialogue continues between the CCG and NHS Property Services regarding premises costs. NHS Property Services are now recalculating invoices based all their market rent which has resulted in a significant difference in costs. This has been implemented mid-year and being back dated onto CCG s as of 1 st April The PCCC recognised the interpretation costs which are a continued pressure with progress acknowledged towards improving the situation The PCCC noted the contents of the report. 6.2 Salford Standard AG provided an overview of the paper which detailed the 2016/17 performance of the Salford Standard. She advised that this was the first year s data and welcomed feedback on the format and inclusion of information within the report. It was recognised that there is variance in data of practices across the City. Evidence shows that following the investment and incentivised Primary Care Joint Commissioning Meeting 26 th September 2017 Part 1 Page 5 of 8
8 approach of the Salford Standard, there has been an increase in staffing in practices across the city. The CCG are already considering what next year s Salford Standard will look like, with internal discussions taking place by a Design Group. Next year s review will be a more fundamental approach as the funding was initially agreed for a 3 year period KP made reference to Section 3.4 of the report, quoting the areas of good progress. She enquired as to whether there was any benchmarking data to measure the improved position since the implementation of the Salford Standard. AG reported that the CCG were not able to quantify any data prior to the implementation of the Standard to be able to carry out comparisons against. She added that now the CCG have benchmarking in place, this can be evidenced and compared going forward. JW enquired as to whether the LMC can be involved in discussions to review data on practice s performance against the Salford Standard. NM advised that she will explore representatives and key stakeholders to be required in the review process. SD reported that there is a need to demonstrate the wider value and improvements which the Salford Standard can make. A discussion took place which considered the need to review the workforce impact and benefits of this BW highlighted that any review would need to include the learning points, recognising that an organisation may not always achieve the desired outcome at the first attempt. He added that the review should consider what has been done right and what the CCG could have done better. He also challenged the independence of the forthcoming review with those invited to take part. HG reported that the Design Group will include CCG members of staff and GPs in their commissioning capacity, as well as other clinical members of staff. This group will consider any changes required for next year s standard. It was noted that for the full review next year, the same group will be used; however the PCCC were made aware of the significant conflict of interest due to member practices being the beneficiaries of the outcome. The review will aim to separate the conversations between clinical decision making and the financial benefits. It was agreed that the review will require independent input and require strong challenge. HG advised that he will need to set out what the options are to be considered as part of the review in readiness for 2019/20. This recommendation will then be for consideration and require formal approval by the Governing Body The PCCC noted the contents of the report and the progress made in the development and performance against the Salford Standard in 2016/17. 7 Minutes/Reports of Partnership Boards/Sub Committees 7.1 Primary Care Operational Group Report HG explained that the report provides an update from the most recent meetings of the Primary Care Operational Group for consideration by the PCCC. A correction was noted in Section 7.1, being Prince s Park, not Princess Park. SD advised that Section 3.7 detailed the CQC re-inspection of Manchester Road East Medical Practice being positive news. He added that the CCG has already contacted the Practice to formally acknowledge the Primary Care Joint Commissioning Meeting 26 th September 2017 Part 1 Page 6 of 8
9 CCG s appreciation for the hard work and effort. The report noted that the Sorrel Group Practice has now become a single-handed contract holder. The practice has a large list size and it was suggested that this poses a considerable risk. AG advised that the practice is currently going through the process to add new partners to the contractual arrangements The PCCC noted the contents of the report. 7.2 Primary Care Quality Group Review Report FT joined the meeting FT reported that to date 44 out of our 45 GP Practices have been inspected by CQC. Of these 2 have been rated as Outstanding, 39 rated as Good and 2 as Requires Improvement. The PCCC were informed that no practice in the City is currently rated as Inadequate. The CCG are awaiting a report for one practice following their recent inspection. It was noted that several inspection reports were published in July and August 2017 with key areas identified in the report being highlighted FT reported that Dearden Avenue Medical Practice is now rated as Good in all categories, which is an improvement from their previously rating of Requires Improvement in the Safe category. Dr Davis Medical Practice was noted as being Good with Requires Improvement in the Safe category, which is an improvement from their previous inspection of Requires Improvement overall. Springfield Medical Practice was noted as being Good in all categories, with FT reporting this was a previously uninspected practice. In relation to Dr Khan s Practice at Manchester Road East, the inspection outcome was Good, with the PCCC noting this a significant achievement as they were previously rated as Inadequate and have worked hard to achieve this grading. A congratulations letter has been sent on behalf of the CCG from Dr Jeremy Tankel. It was reported that the LMC had supported Dr Khan s practice prior to their latest inspection. The Height Medical Practice has been inspected at the end of August, however no outcome has been conveyed as the report s publication hasn t yet taken place FT reported that Irlam Group Practice is due for re-inspection following their Requires Improvement rating. It is anticipated that their re-inspection will take place in either September or October. The practice is currently receiving support from another Practice Manager from Royton Medical Practice who is working part-time at the practice to make the required improvements. FT added that she has met with the Practice Manager and is confident that the next inspection will have a more positive outcome. She also reported that a recurrent theme in recent inspection reports was around practices failing to have sufficient risk assessments in relation to Legionella. The Infection Control Team has since published guidance in the GP newsletter for practices. It was noted that this is a positive picture which has been achieved over the last months for CQC reports in general practice BW noted the positive impact by the CCG and partner organisations in addressing the CCG s quality concerns. He added that there is a need to acknowledge and recognise the work of practices post their respective Primary Care Joint Commissioning Meeting 26 th September 2017 Part 1 Page 7 of 8
10 inspections. KP suggested using the member s event to provide practices with an update on the improved position over the last 12 months. FT advised on the CQC National State of Primary Care provision which will allow the CCG to carry out an analysis of the progress made and present to the Primary Care Operational Group. Action: FT to update on primary care quality progress over the last 12 months to the Primary Care Operational Group The PCCC noted the verbal update provided by FT. 8 Reflection 8.1 BW reflected on the progress made in the merger proposals at Newbury Green and Limefield Medical Practices, which will in turn deliver efficiencies. He reflected on the information provided in the Primary Care Investment Agreement which was seen as good news, with the CCG awaiting the outcome of the funding agreement. The PCCC recognised the finance report which explained how the CCG is managing to ensure an efficient delivery of services within budget. The Salford Standard annual report highlighted the positive news, as well as identifying lessons learnt in the future. The verbal update provided by FT regarding the CQC inspection reports provided the PCCC with an overview of performance being largely successful. 9 The meeting closed at 11:55Hrs. Primary Care Joint Commissioning Meeting 26 th September 2017 Part 1 Page 8 of 8
11
12 28 th November 2017 Item 5 (a) NHS SALFORD CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE PART 1 AGENDA ITEM NO 5 (A) Item for Decision/Assurance/Information Date of Committee: November 2017 REPORT OF: Neil Cudby Head of Service Improvement ICS DATE OF PAPER: 20 th November 2017 SUBJECT: Salford Wide Extended Access Pilot IN CASE OF QUERY PLEASE CONTACT: STRATEGIC PRIORITIES: Quality Community Based Care Integrated Care In Hospital Care Long Term Conditions and Mental Health Effective Organisation Neil Cudby Service Improvement Team Please tick which strategic priorities the paper relates to: PURPOSE OF PAPER: This report gives an update on the mobilisation of the Salford Wide Extended Access Pilot; Salford Primary Care Together remains on track to deliver extended access Salford wide by March RECOMMENDATIONS OF THIS PAPER: Primary Care Commissioning Committee is asked to note the content of the report and accept it as assurance of progress made and the mechanisms in place to oversee mobilisation, delivery and performance of SWEAP. Page 1 of 7
13 28 th November 2017 Item 5 (a) HOW WILL THIS BENEFIT THE HEALTH AND WELL BEING OF SALFORD RESIDENTS OR THE CLINICAL COMMISSIONING GROUP? Patients will benefit from additional access to primary care services in Salford. WHAT RISKS MAY ARISE AS A RESULT OF THIS PAPER? HOW CAN THEY BE MITIGATED? IT Interoperability to share patient records is a key risk; risk owned by IM&T Group and solutions being developed/tested. WHAT EQUALITY-RELATED RISKS MAY ARISE AS A RESULT OF THIS PAPER? HOW WILL THESE BE MITIGATED? None. Equality Analysis completed as part of business case no issues identified. DOES THIS PAPER HELP ADDRESS ANY EXISTING HIGH OR EXTREME RISKS FACING THE ORGANISATION? IF SO WHAT ARE THEY AND HOW DOES THIS PAPER REDUCE THEM? Yes. It is intended that this service will prevent pressures on the delivery of core general practice, as reported by members practices. PLEASE DESCRIBE ANY POSSIBLE CONFLICTS OF INTEREST ASSOCIATED WITH THIS PAPER. GP members have a conflict of interest. These have been managed via the CCG s Conflicts of Interest policy. PLEASE IDENTIFY ANY CURRENT SERVICES OR ROLES THAT MAY BE AFFECTED BY ISSUES WITHIN THIS PAPER: Primary Care (Medical Services) Footnote: Members of NHS Salford Clinical Commissioning Group Governing Body will read all papers thoroughly. Once papers are distributed no amendments are possible. Page 2 of 7
14 28 th November 2017 Item 5 (a) Document Development Process Yes No Public Engagement (Please detail the method ie survey, event, consultation) Clinical Engagement (Please detail the method ie survey, event, consultation) Has due regard been given to Equality Analysis (EA) of any adverse impacts? (Please detail outcomes, including risks and how these will be managed) Legal Advice Sought Not Applicable Comments and Date (i.e. presentation, verbal, actual report) Outcome Presented to any other groups or committees, including Partnership Groups Page 3 of 7
15 28 th November 2017 Item 5 (a) 1 Executive Summary Salford Wide Extended Access Pilot (SWEAP) This report provides an update on the mobilisation of the Salford Wide Extended Access Pilot (SWEAP); Salford Primary Care Together (SPCT) to date have mobilised this service in 2 out of 5 Neighbourhoods and have plans to mobilise the remaining 3 Neighbourhoods by March The SWEAP activity and performance dashboard is still in development; however, early headline data and feedback relating to the service has been positive. Progress against mobilisation, associated risks/issues and service activity performance are monitored as part of the monthly contract meeting between Salford CCG and SPCT. The Greater Manchester (GM) Primary Care Reform Investment Agreement provides supporting funding (c 970kpa) for delivery of 7 day access provision; as this is dependent on provision being across 100% of the Salford population the CCG will only receive a proportion of this for 17/18 (c 826k). Primary Care Commissioning Committee is asked to note the content of the report and accept it as assurance of progress made and the mechanisms in place to oversee mobilisation, delivery and performance of SWEAP. 2 Introduction and Background 2.1 The CCG has committed to the development of primary and community care at scale, with greater scope, to reshape service delivery and standards in Salford; improving access to primary care services, including improved opening at weekends and the evening is a key priority. The vision is to provide 7 day access to high quality primary care services that addresses the needs of patients, is sustainable and provides a complimentary and seamless service to current in-hours primary care. 2.2 To support this transformation Primary Care Commissioning Committee approved a business case on the 11 th July 2016 to commission a Salford Wide Extended Access Pilot for Primary Care. The business case was for a two year pilot with phased implementation in year one across the five neighbourhoods; the financial envelope for year 1 was 845,892 and year 2 was 1,296, The procurement process began on the 28 th October 2016 and, after some slippage in the timeline in order to enable the evaluation panel to seek the necessary clarification and assurances in relation to the bid, was completed on the 14 th February The Salford Wide Extended Access Pilot contract was awarded to Salford Primary Care Together (SPCT). Page 4 of 7
16 28 th November 2017 Item 5 (a) 3 Mobilisation Update 3.1 The anticipated timeline for mobilisation across the five Neighbourhoods in Salford at the time of going out to procurement was: Swinton - April 2017 Eccles & Irlam - July 2017 Little Hulton & Walkden - September 2017 Ordsall & Claremont - December 2017 Broughton - March With the procurement process being extended by 6 weeks SPCT initially requested that the service commencement date be moved from the 1 st April to the 8 th May The CCG agreed to this; however, advised SPCT that the service must still mobilise in each of the five Neighbourhoods providing cover to 100% of the Salford population by March Due to a combination of IT issues (relating to the implementation of the service and utilisation of Vison 360) and estates issues (relating to opening of buildings and provision of security at weekends) the initial mobilisation has seen further delays. 3.4 The service successfully mobilised in the Swinton Neighbourhood (Swinton Gateway) on the 14th August 2017 providing bookable appointments to patients Monday to Friday evenings and Saturday, Sunday mornings. 3.5 The service subsequently mobilised in the Eccles & Irlam Neighbourhood (Eccles Gateway) on the 9th October. This didn t initially include Sunday appointments due to issues in relation to opening the building and provision of security on a Sunday. These issues were resolved to enable Sunday opening from the 12 th November. 3.6 SPCT are implementing a communication plan to support the mobilisation in each Neighbourhood; activities include briefings to key stakeholders, posters in practices and community venues, social media campaigns and information on practice websites. 3.7 SPCT has confirmed that they remain on track to deliver extended access city wide by March 2018; Broughton (Newbury Place) will be the 3 rd Neighbourhood to mobilise with an expected go live date of the 12 th December. 3.8 Early headlines from the service provision in Swinton over August and September are positive: 570 extended access appointments have been offered 85% utilisation rate 94% of those surveyed rate the service as Excellent or Very Good 98% of those surveyed would use again 100% of those surveyed either Extremely Likely or Likely to recommend the service 3.9 The breakdown of number of days from booking to appointment in Swinton over August and September has been: Page 5 of 7
17 28 th November 2017 Item 5 (a) 0-1 day 15% 2-3 days 55% 4-5 days 22% 6+ days 8% 3.10 For those surveyed the main reasons for attending the service have been reported as (respondents can choose more than one option): GP practice unable to offer an appointment in normal working hours 54% I work during normal GP hours 48% Appointment available sooner under extended access service 19% 3.11 Patients surveyed have been asked who they would have sought help from if the extended access service was not available; their responses were: NHS 111 8% Internet 4% Pharmacy 6% A&E 12% Wait for GP appointment 70% 4 Governance 4.1 A monthly SPCT contract performance meeting has been established at which progress against mobilisation of SWEAP and associated risks/issues is a regular agenda item. SPCT are developing an activity and performance dashboard for SWEAP and as mobilisation progresses the focus of attention will shift to reviewing service performance. 4.2 Options for the evaluation of the impact of SWEAP are currently being explored; an outline scope for the evaluation has been drafted with the following key measures identified: Number of minute s appointment time per 1000 population offered and utilisation rates. Demographic of patients accessing the service, assess equality of access. Outcomes of consultation i.e. advice, treatment, prescribing, referral. Number of patients returning to see GP in the 7 days following attending extended access service. Impact on continuity of care for patient groups i.e. patients with long term conditions (measure for continuity of care being considered). Patient experience, satisfaction, feedback; assess patient view of whether the service is equivalent to going to their own practice Core GP experience and satisfaction; assess quality of handover from extended access service including accuracy, quality of documentation and quality / timeliness of communication. Impact on the urgent care system i.e. A&E attendances, GP Out of Hours activity, NHS 111 activity etc. Page 6 of 7
 5")

 under the Greater Manchester (GM) Primary Care Reform Investment Agreement. 5.")
18 28 th November 2017 Item 5 (a) 5 Financial Position 5.1 The CCG receives 891,430 in its recurrent allocation to support extended access in Primary Care. 5.2 In addition, from 17/18 to 19/20 the CCG will receive funding up to an amount of 950,722 per year for delivery of 7 day access provision (Provision of neighbourhood based primary care hubs offering access to general practice in evenings and weekends) under the Greater Manchester (GM) Primary Care Reform Investment Agreement. 5.3 The Greater Manchester Health & Social Care Partnership (GMHSCP) have informed that CCG s are only able to access the entirety of this extended access funding when they are delivering this extended access to 100% of their population. In Salford, with SWEAP not planned to achieve 100% coverage until early 2018, the CCG will only receive a proportion of the 950k under the investment agreement in 17/ The CCG has submitted the revised investment profile below to the GMHSCP in which 826,083 is being requested for 17/18 with the full 950,722 funding per year expected in 18/19 and 19/20. GM Primary Care Investment Agreement Investment Profile 6 Recommendations 6.1 Primary Care Commissioning Committee is asked to note the content of the report and accept it as assurance of progress made and the mechanisms in place to oversee mobilisation, delivery and performance of SWEAP Neil Cudby Head of Service Improvement ICS Salford CCG Page 7 of 7
19 Agenda Item No 5 (b) NHS SALFORD CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE AGENDA ITEM NO 5 (B) Item for Information Date of Meeting REPORT OF: Natalie McInerney Service Improvement Manager Dr Tom Regan Clinical Director for Transformation DATE OF PAPER: November 2017 SUBJECT: Salford Standard 2018/19 Proposal IN CASE OF QUERY PLEASE CONTACT: STRATEGIC PRIORITIES: Quality Community Based Care Natalie McInerney Service Improvement Manager Please tick which strategic priorities the paper relates to: Integrated Care In Hospital Care Long Term Conditions and Mental Health Effective Organisation Page 1 of 46
20 Agenda Item No 5 (b) PURPOSE OF THIS PAPER: This paper provides the Primary Care Commissioning Committee (PCCC) with a summary of the proposed amendment, addition and deletion of KPIs for the 2018/19 contract. This paper also provides the PCCC with a summary of the KPIs within the 2017/18 Salford Standard that require amendment in-year and also the proposal in regards to the 2018/19 contractual sign-up requirements. RECOMMENDATION OF THIS PAPER: The PCCC is asked to discuss and approve in principle, subject to the recommendation of the Integrated Community Based Care Commissioning Group (ICBCCG), the proposed changes to the Salford Standard: a. Amendments to a number of KPIs in-year (2017/18) as outlined in Appendix 1 and section 3 of the report; b. Amendments to a number of KPIs for the 2018/19 contract as outlined in Appendix 2 and 3 and section 4 of the report; c. 2018/19 contract sign up requirements as outlined in Appendix 4 and section 5 of the report. (Please see further explanatory requirements overleaf) Page 2 of 46
21 Agenda Item No 5 (b) Further explanatory information required HOW WILL THIS BENEFIT THE HEALTH AND WELL BEING OF SALFORD RESIDENTS OR THE CLINICAL COMMISSIONING GROUP? The Salford Standard is working to improve the quality of care in primary care across Salford. WHAT RISKS MAY ARISE AS A RESULT OF THIS PAPER? HOW CAN THEY BE MITIGATED? Challenges from practices. Amendments have arisen as a result of feedback from practices. WHAT EQUALITY-RELATED RISKS MAY ARISE AS A RESULT OF THIS PAPER? HOW WILL THESE BE MITIGATED? None. DOES THIS PAPER HELP ADDRESS ANY EXISTING HIGH OR EXTREME RISKS FACING THE ORGANISATION? IF SO WHAT ARE THEY AND HOW DOES THIS PAPER REDUCE THEM? None. PLEASE DESCRIBE ANY POSSIBLE CONFLICTS OF INTEREST ASSOCIATED WITH THIS PAPER Domain clinical leads and members of the Salford Standard design group are also CCG GP Members and practice staff. PLEASE IDENTIFY ANY CURRENT SERVICES OR ROLES THAT MAY BE AFFECTED BY ISSUES WITHIN THIS PAPER: Salford GP practices. Page 3 of 46
22 Agenda Item No 5 (b) Primary Medical Care Commissioning Principles 1. Investment in general practice will continue to, as a minimum, be in line with the recommendations of the General Practice Forward View in order to strengthen resilience and sustainability of general practice by building capacity and capability. 2. The CCG will seek to maximise opportunities to commission primary medical services at scale (for example through a GP provider organisation) where this is expected to improve patient experience or be more efficient. 3. When commissioning decisions need to be made regarding primary medical service contracts, an options appraisal will be undertaken in order to determine the option that is most likely to meet the needs of the population group and most likely to deliver the CCG s strategic ambitions. This may not always be re-procuring a like for like service. 4. The CCG will commission general practice services from providers that are able to demonstrate good outcomes, value for money and care for patients that is holistic and provided to consistently high standards of quality and safety. 5. The CCG will seek to engage with the local population and acknowledge patient views when making primary medical services commissioning decisions. 6. The CCG will ensure that the primary medical services in Salford continue to meet the needs of a growing and increasingly diverse population. This will include promoting patient choice and equality and seeking to ensure that commissioning decisions improve the economic, social and environmental wellbeing of Salford. 7. The CCG will encourage and support general practice to play a pivotal role within the emerging accountable care system, with leadership through federated arrangements. 8. The CCG will embrace opportunities to commission primary medical services in an integrated way where this has benefits for patient care, e.g. through pooling budgets for health and social care services, or commissioning community services to be Addressed in this paper? The Salford Standard increases the investment into general practice. N/A N/A The Salford Standard will be commissioned from Salford practices that are able to demonstrate compliance to a number of contractual sign-up requirements and progression against the key performance indicators. As part of the 2019/20 fundamental contract review. An aim of the Salford Standard is to meet the primary medical care needs of the Salford population. No No Page 4 of 46
23 Agenda Item No 5 (b) delivered on a neighbourhood basis from multidisciplinary integrated teams. 9. The CCG will embrace new contracting mechanisms where they support the viability, sustainability and resilience of general practice, including practices working collaboratively in neighbourhood groups to deliver agreed outcomes and to share resources such as staff and back office services. 10. The CCG will support making general practice in Salford becoming an attractive place to work. This will include encouraging and supporting general practice to: embrace innovation and new ways of working; adapt and skill-up the workforce to meet patient need; make greater use of technology; and work from modern and fit for purpose premises. 11. The CCG, as a commissioner of primary medical services, cannot assume responsibility for, or become involved in, matters relating to the management of GP practices, including practice disputes and legal matters. 12. The CCG will proactively work with partners, including Salford Primary Care Together (as Salford s GP provider organisation) and the Salford and Trafford Local Medical Committee, in a transparent and supportive manner. No Practices have invested the funding received from the Salford Standard in a number of ways, for example, recruitment and up-skilling of workforce and investing in technology and new ways of working. Footnote: Members of NHS Salford Clinical Commissioning Group Primary Care Commissioning Committee will read all papers thoroughly. Once papers are distributed no amendments are possible. No No Page 5 of 46
24 Agenda Item No 5 (b) Document Development Public Engagement Process Yes No (Please detail the method ie survey, event, consultation) Clinical Engagement (Please detail the method ie survey, event, consultation) Has due regard been given to Equality Analysis (EA) of any adverse impacts? (Please detail outcomes, including risks and how these will be managed) Legal Advice Sought Presented to the Commissioning Committee Presented to the Health and Wellbeing Board Presented to the Integrated Joint Commissioning Board Presented to any other groups or committees, including Partnership Groups (Please specify in comments) X Not Applicable X X X X X X X Integrated Community Based Care Commissioning Group Comments and Date (i.e. presentation, verbal, actual report) Reviewed by Salford Standard Implementation Group and Salford Standard Design Group. Will be presented to Integrated Community Based Care Commissioning Group on Outcome Note: Please ensure that it is clear in the comments and date column how and when particular stakeholders were involved in this work and ensure there is clarity in the outcome column showing what the key message or decision was from that group and whether amendments were requested about a particular part of the work. Page 6 of 46
25 Agenda Item No 5 (b) 1 Executive Summary Salford Standard 2018/19 Review This report highlights recommendations for amendments to the Salford Standard domains and KPIs which would be implemented in the 2018/19 contract. The paper also discusses options regarding sign-up to the Salford Standard in 2018/19. The paper also provides a summary of proposed amendments to some 2017/18 KPIs. These proposals require implementing in-year as a result of ongoing monitoring and feedback from clinical leads and member practices. 2 Introduction 2.1 The Salford Standard business case highlighted that following the launch of the locally commissioned service, the CCG would need to maintain its programme of stakeholder engagement in order to learn lessons and adjust plans. This engagement has been ongoing and the CCG s Service Improvement Team has established a mechanism to manage changes and a log of suggestions has been created. 2.2 This paper provides the Primary Care Commissioning Committee (PCCC) with a summary of the KPIs within the 2017/18 Salford Standard that require amendment in-year. The paper also summarises the proposed amendment, addition and deletion of KPIs for the 2018/19 contract and the proposals in regards to contractual sign-up requirements. 2.3 The proposed amendments have been discussed and agreed with each relevant clinical lead and are supported by the Salford Standard Design Group, with conflicts of interest managed appropriately. If the Primary Care Commissioning Committee (PCCC) Integrated Community Based Care Commissioning Group agree the proposed changes, the amendments will be presented to the Integrated Community Based Care Commissioning Group (ICBCCG) for their support. The financial model associated with the proposed changes will not be considered via PCCC but will be worked up by CCG officers with a decision made by the CCG s Executive Team. 2.4 The original Salford Standard business case outlined the agreement that the initial contract term would be for three years, the decision to invest in year three has therefore already been made. The CCG is not planning to conduct any external consultation in regards to these proposals as there are no significant changes to the 2017/18 contract. The Salford Standard Design Group has representation from CCG clinical leads, GPs, a practice manager and a practice nurse in order to act as the voice of general practice. The CCG is planning a fundamental review of the Salford Standard for the 2019/20 contract, which will include full consultation with all member practices. Page 7 of 46
26 Agenda Item No 5 (b) 3 Proposed Changes In-Year 3.1 Changes to some of the 2017/18 Salford Standard KPIs are proposed as a result of feedback from practices and domain leads on the issue of capturing and reporting the data. The proposed changes and rationale are detailed in Appendix The Salford Standard Design Group does not recommend that any changes are made to the funding associated with the amended public health KPI thresholds. 3.3 Should the removal of the MDG KPI be approved, the proposal is that the funding will be redistributed across the remaining KPI within that domain. This decision will be referred to the CCG s Executive Team for their approval. 4 Proposed changes for 2018/ A Salford Standard Design Group was established in June 2017 to review the contract for 2018/19 and propose any amendments. The Design Group included representation from a practice manager; a practice nurse; GPs; and CCG contracting, finance, business intelligence and data quality. The group sought input from all clinical and CCG domain leads 4.2 It was stressed to leads that in order to provide continuity to practices, the assumption was that there would not be any significant changes in year three. Any wholescale changes suggested will be considered as part of a fundamental review for the 2019/20 contract. Therefore, the proposed changes have been kept to a minimum. 4.3 The Design Group s approach was to consider domains and/or KPIs where the CCG was aware of any particular issues; for example, difficulties associated with measuring KPIs or feedback suggesting that the KPI was not incentivising good clinical practice. 4.4 Currently, there are 61 KPIs within the Salford Standard. The proposal for the 2018/19 contract is as follows: o Remove seven KPIs and include these as part of the contract sign up requirement (this will be discussed further in section 5) (Appendix 2) o A further two KPIs are recommended to be removed (Appendix 2) o Four KPIs to be merged into two KPIs o Nine new KPIs to be added o 27 contract sign-up requirements 4.5 There are therefore a proposed 58 KPIs remaining within the Salford Standard in 2018/19. These proposed changes are detailed in Appendix Should the KPIs for 2018/19 be agreed, the changes to the monitoring of the KPIs are reflected below. Page 8 of 46
27 Agenda Item No 5 (b) Current Arrangements Proposed Arrangements Quarterly 7 Quarterly 14 Bi-annual 13 Bi-annual 3 Annual 41 Annual Within the current 2017/18 contract, the funding for each of the KPIs has been weighted evenly within each domain (with the exception of two KPIs within the Safeguarding domain). The proposal for 2018/19 is to weight the KPIs within each domain dependent upon the amount of effort required. Should the amendments outlined in this report be approved, the Salford Standard Design Group will begin to review this and present a number of options to the CCG s Executive Team for their approval /19 Contract Sign Up 5.1 In 2017/18, practices received 50% of the available funding for signing up to the Salford Standard and 50% upon achievement of KPIs. At this stage the assumption for 2018/19 is that this funding split remains the same, however this is a decision that will need to be made as part of the financial modelling. 5.2 The proposal for the initial 50% in 2018/19 is similar to that in 2017/18 and will require practices to submit a portfolio of evidence against the contractual requirements by March (Appendix 4). The proposal is that practices will receive the full 50% upon submission of the contractual sign-up requirements. The CCG has introduced a small number of additional contract sign-up requirements for 2018/19. Some of these were previously KPIs in 2017/18 but are felt to be more of a one-off response than a KPI. 5.3 As part of the 2017/18 contract sign-up, practices were asked to submit an implementation plan outlining how they had utilised the Salford Standard funding against a number of elements; workforce, estates, technology, processes and training. A summary of the additional workforce employed across Salford since the introduction of the Salford Standard in April 2016 shows that there has been an increase in the number of clinical and non-clinical staff. This includes staff who were originally employed on a fixed-term contract who were then recruited into permanent positions due to the Salford Standard funding and requirement for additional workforce. However, whilst all practices have recruited new staff, not all practices have invested in recruiting additional clinical staff. 5.4 Analysis on the 2017/18 implementation plans also highlighted a number of initiatives and investments that have enabled practices to achieve the requirements of the Salford Standard in 2016/17. Examples of these include: Employment of a full-time member of staff who has the primary role of coordinating the practice in the delivery of the Salford Standard; Upgraded digital information system in the waiting room enabling patient engagement and education; Text message bundles for long-term condition reviews, on-line patient health promotion information, on-line questionnaires such as audit-c and smoking; Page 9 of 46
28 Agenda Item No 5 (b) Purchase of name calling equipment in the reception to reduce reception workload; Installing short cut keys and macros to support accurate coding; Intallation of Iplato software allowing two way communication with patients on a number of campaigns (smoking, BP, Carers, flu). The clinical system is automatically updated with the appropriate response READ codes. This system cuts down on the expense of postal correspondence, man power involved, increases uptake (more people respond to text) and reduces coding errors; Purchase of Jayex self-check in boards which will also ask patients health information when they check in for their appointments. 5.5 The intention for 2018/19 is that practices will be asked to provide greater clarity in regards to the workforce element. The CCG is particularly interested in understanding the additional investment that practices have been able to make as a result of the Salford Standard. 5.6 Practices will be required to submit their workforce plan as part of an intended CCG questionnaire during 2018/19. It is proposed that failure to submit this will result in 25% of the initial 50% contract sign-up funding being clawed back. 6 Recommendations 6.1 The PCCC is asked to discuss and approve in principle, subject to the recommendation of the Integrated Community Based Care Commissioning Group (ICBCCG), the proposed changes to the Salford Standard: a. Amendments to a number of KPIs in-year (2017/18) as outlined in Appendix 1 and section 3 of the report; b. Amendments to a number of KPIs for the 2018/19 contract as outlined in Appendix 2 and 3 and section 4 of the report; c. 2018/19 contract sign up requirements as outlined in Appendix 4 and section 5 of the report. Natalie McInerney Service Improvement Manager (Primary Care) Page 10 of 46
29 Agenda Item No 5b Appendix 1 Proposed amendments 2017/18 KPIs Standard Public Health Screening (national) KPI Practices to read code DNAs and f/u with advice and support to promote the uptake of cervical screening: (25-49 yrs = 3-yearly, 50-64yrs = 5-yearly); this will demonstrate a reduction in DNAs Practices to promote the uptake of bowel screening every 2 years to all patients aged 60-74yrs by follow up of no response according Measure Code 2017/18 PH13 PH17 Measure No. of Women aged 25-49yrs recorded as DNA cervical screening given advice re screening or coded as declined screening following recording of DNA in the last 3 yrs and No. of Women aged 50-64yrs recorded as DNA cervical screening given advice re screening or coded as declined screening following recording of DNA in the last 5 years. Total no. of Women aged 25-49yrs recorded as DNA cervical screening in last 3 yrs and total no. of Women aged 50-64yrs recorded as DNA cervical screening in the last 5 years No. of patients aged yrs recorded as no response to bowel screening in the last 2 years according to the national programme given advice 2017/18 Threshold 1% above 2016/17 practice baseline = Green - Achieved; payment made 1% above 2016/17 practice baseline = Green - Achieved; payment Business Rules Females Aged > 25-49y WITH 9NiT. Did not attend cervical smear (DENOMINATOR) cervical smear non-responder AND Health ed. - cervical cytology OR Ca cervix screen - not wanted 685L. Cervical smear refused 9O8Q. Cerv.smear disclaimer received (IF IN LAST 3 YEARS) (NUMERATOR) > 01/04/2015 OR 67DA Provision of information about cervical screening programme OR 4K22. Cervical smear: negative 4K23. Cerv.smear: mild dyskaryosis 4K24. Cerv.smear: severe dyskaryosis 4K25. Cerv.smear:severe dysk.?inv.ca 4K26. Cervical smear:? gland neopl. 4K27. Cervical smear:atrophic change 4K28. Cerv.smear: mod.dyskaryosis 4K29% Cerv.smear: borderline changes 4K2C. Smear NAD - no endocervical cells 4K2H. Cervical smear epithelial cells absent 4K2F. Cervical smear pus cells present 4K2G. Cervical smear red blood cells present 4KA1. Vaginal vault smear negative Aged > 60-74y WITH 9Ow2. No response to bowel cancer screening programme invitation (DENOMINATOR) AND 8CAy. Advice given about bowel cancer Monitoring and implementation timescales Annual Annual Proposal AMEND Amend threshold in year to 75% AMEND Amend threshold in year to 75% Rationale The 2016/17 data is not robust enough in order to set a 1% improvement target for 2017/18. Practices are aware of the patients who make up the denominator so should be able to follow up those who do not respond or DNA to a high number. The 2016/17 data is not robust enough in order to set a 1% improvement target for 2017/18. Page 1 of 32
30 Agenda Item No 5b MDGs to the national screening programme Practice to demonstrate an improvement on the offer and uptake of Chlamydia screening with 15 to 25 year olds when compared to the baseline set in 2016/17 Care Coordination & Informing the Patient PH12 PORT5 No. of patients aged 60-74yrs who have been offered bowel screening in the last 2 years (excluding declined in last 2 years) according to the national programme Improvement on the offer and uptake of Chlamydia screening with 15 to 25 year olds when compared to the baseline set in 2016/17 1. The name of the care coordinator in the individual s shared care record 2. Number of Shared Care Plans handed back to the individual 3. patient awareness of the care co-ordinator through the annual patient satisfaction survey made 1% above 2016/17 practice baseline = Green - Achieved; payment made 75% compliance = Green - Achieved: payment made screening programme OR 8IA3. Bowel cancer screening declined > 01/04/2016 (NUMERATOR) n/a Annual AMEND n/a Annual Remove in year Practices are aware of the patients who make up the denominator so should be able to follow up those who do not respond or DNA to a high number. Propose to amend threshold in year to count the number of offers, not a 1% improvement. Target - increase from 17/18 figures Points two and three are not underway and point one is carried out by SRFT administrators - not general practice Page 2 of 32
31 Agenda Item No 5b Appendix /18 KPIs to be removed in 2018/19 Domain Ref Standard KPI Measure Code 2017/18 Measure 2017/18 Threshold Business Rules Monitoring Monitoring and implementation timescales Proposal Rationale 2 Meds Optimisation 2.1 Medicine Safety - PINCER II Patients prescribed aspirin or clopidogrel, or prasugrel or ticagrelor who have a history of peptic ulceration or gastrointestinal bleed and are not prescribed a gastro-protective medicine Prescription of warfarin and aspirin in combination (without co-prescription of an ulcer-healing drug) Prescription of warfarin or NOAC (rivaroxaban, apixaban, dabigatran) in combination with an oral NSAID In a patient aged 65 years prescription of an oral NSAID without co-prescription of an ulcer-healing drug (n.b. aim is to focus particularly on patients with additional risk factors for GI bleed) MS01 MS02 MS03 MS04 Patients prescribed aspirin or clopidogrel, or prasugrel or ticagrelor who have a history of peptic ulceration or gastro-intestinal bleed and are not prescribed a gastro-protective medicine Prescription of warfarin and aspirin in combination (without coprescription of an ulcerhealing drug) Prescription of warfarin or NOAC (rivaroxaban, apixaban, dabigatran) in combination with an oral NSAID In a patient aged 65 years prescription of an oral NSAID without coprescription of an ulcerhealing drug (n.b. aim is to focus particularly on patients with additional risk factors for GI bleed) <=10% = Green - Achieved: <=10% = Green - Achieved: <=10% = Green - Achieved: <=20% = Green - Achieved: Measured through SMASH Measured through SMASH Measured through SMASH Measured through SMASH 6 monthly review using dashboard 6 monthly review using dashboard 6 monthly review using dashboard 6 monthly review using dashboard Bi-annual Bi-annual Bi-annual Bi-annual Remove Remove Remove Remove Move to being a contract sign-up KPI to be audited twice a year Move to being a contract sign-up KPI to be audited twice a year Move to being a contract sign-up KPI to be audited twice a year Move to being a contract sign-up KPI to be audited twice a year Page 3 of 32
32 Agenda Item No 5b 4 Safeguarding 4.1 Safeguarding Part 2 - Embedding Safeguarding within all GP Practices Reduce the number of patients diagnosed with chronic kidney disease (CKD) stage 3B, 4 or 5 or with a latest egfr of <45mL/min who are prescribed a NSAID Reduce the number of patients with CKD stage 3B, 4 or 5 or with a latest egfr of <45 ml/min who have been prescribed an ACE inhibitor, loop diuretic and a NSAID (the triple whammy 80% Clinical and nonclinical practice staff to attend the domestic abuse training. MS05 MS06 SG07_P Reduce the number of patients diagnosed with chronic kidney disease (CKD) stage 3B, 4 or 5 or with a latest egfr of <45mL/min who are prescribed a NSAID Reduce the number of patients with CKD stage 3B, 4 or 5 or with a latest egfr of <45 ml/min who have been prescribed an ACE inhibitor, loop diuretic and a NSAID (the triple whammy Practice staff (Clinical and non-clinical) to attend training and complete attendance sheet <=20% = Green - Achieved: <=10% = Green - Achieved: >=80% = Green - Achieved; Measured through SMASH Measured through SMASH n/a 6 monthly review using dashboard 6 monthly review using dashboard Annual review of completion of training via Safeguarding Team Database Bi-annual Bi-annual Annual Remove Remove Remove Move to being a contract sign-up KPI to be audited twice a year Move to being a contract sign-up KPI to be audited twice a year Replaced with New KPI on IRIS training - dependent on funding. Should the funding not be approved, this original domestic abuse KPI will remain Page 4 of 32
33 Agenda Item No 5b QOF LD Register AND 918e. On LD register 5 Vulnerable Groups 5.4 Learning Difficulties and ASC Practice to have an LD Register and cross reference this with the councils (CTLD) and share their autism numbers and Downs Syndrome register. PORT6 Practice to maintain record of contact made with CTLD to cross reference LD register and share autism numbers and Downs Syndrome register Practices to maintain a record of contact made with LD team to cross reference LD register and share their autism numbers and downs syndrome register (not including patient identifiable information) to srhtr.ldhealthfacili tator@nhs.net E140% Infantile autism Eu840% Childhood autism Eu841% Atypical autism Eu845 Asperger's syndrome Eu84z11 Autistic spectrum disorder PJ0% Down's syndrome - trisomy 21 Not measured through Informatica - codes above are for practice use only Audit of contact made with CTLD Annual Remove Move to being a contract sign-up requirement Page 5 of 32
34 Agenda Item No 5b Patients aged 14yrs+ on LD register to have an LD Health check and provide a Health Action Plan (HAP) where appropriate LD5.4 Numerator: Number of patients aged 14yrs+ on LD register who have an LD health check Denominator: Number of patients aged 14yrs+ on LD register 75% = Green - Achieved: QOF LD Register Aged > 14y (DENOMIN ATOR) WITH 9HB5. Learning disabilities annual health assessmen t OR 9HB6. Learning disabilities annual health assessmen t declined > 01/04/2017 (NUMERA TOR) Read coding via clinical system Annual Remove Practices already get paid for this through the LD DES Page 6 of 32
35 Agenda Item No 5b Appendix 3 Proposed 2018/19 KPIs Domain Standard KPI Measure 2017/18 Threshold Exclusions Monitoring Monitoring and implementation timescales Proposal Rationale 1 Long Term Conditions Holistic Care CVD Ensure systems are in place to provide a clinically comprehensive holistic annual review for all patients with a LTC (including patients diagnosed with either breast or prostate cancer in the last 5 years). Patients may require a 6 monthly review where necessary but this is not a key performance indicator. To reduce the incidence of ischaemic stroke across the city by: Appropriate primary prevention Atrial fibrillation case finding Effective anticoagulation Secondary prevention of transient ischaemic attacks (TIAs) and stroke No. of LTC patients with a LTC Annual Review Total no. of Patients with a LTC Completion of an annual review 2017/18 review for patients with a LTC The number of hospital admissions with ischaemic stroke Q1-3, 2018/19 75% = Green - Achieved: Practices that follow the processes identified to reduce the incidence of ischaemic stroke. High incidence of stroke does not automatically mean the KPI is not achieved, it acts as an indicator for the CCG to investigate the practices' systems QOF palliative care patients Read coded data will inform the number of patients with a LTC and an annual review Monitored PINGR via Annual Annual Remain Remain Page 7 of 32
36 Agenda Item No 5b further Respiratory Disease - COPD All eligible MRC 3 or 4 patients to be offered Pulmonary Rehabilitation in the last 12m All eligible patients to be referred to Pulmonary Rehabilitation Number of patients identified as MRC 3 or 4 offered Pulmonary Rehabilitation recorded in last 12m Number of eligible patients with COPD MRC3 or MRC4 referred for Pulmonary Rehabilitation since April 1 =75% = Green - Achieved; 20% = Green Achieved; 9kf0. Chronic obstructive pulmonary disease patient unsuitable for pulmonary rehabilitation - enhanced services administration QOF care palliative patients 13CA. Housebound 13C6. Bed-ridden Read coding via clinical system Annual AMEND Combine LCT19 and LTC20 into one KPI: Number of eligible patients with COPD who have had an exacerbation and been referred for Pulmonary Rehabilitation Target: 20% Page 8 of 32
37 Agenda Item No 5b All eligible MRC 2 patients to be offered Pulmonary Rehabilitation within 2 months of exacerbation All eligible MRC 2 patients to be referred for Pulmonary Rehabilitation Number of patients identified as MRC 2 with an exacerbation recorded after 31/03/2017 who have been offered Pulmonary Rehabilitation within 2 months of exacerbation Number of eligible patients with COPD MRC2 who have had an exacerbation and been referred for Pulmonary Rehabilitation within 2 months following exacerbation. =75% = Green - Achieved: 20% =Green Achieved; 9kf0. Chronic obstructive pulmonary disease patient unsuitable for pulmonary rehabilitation - enhanced services administration QOF care palliative patients 13CA. Housebound 13C6. Bed-ridden Read coding via clinical system Annual Page 9 of 32
38 Agenda Item No 5b Review patients with COPD to be prescribed home rescue packs Diabetes - Identification Clinically appropriate patients with COPD should be prescribed home rescue packs (steroids and/or antibiotics) to treat exacerbations only as part of a management plan and supporting information to use correctly this has been shown to help prevent hospital admissions and is recommended in the NICE clinical guideline on COPD as part of selfmanagement of exacerbations. The standard seeks to ensure all patients being issued with rescue packs receive appropriate clinical reviews and not excessive rescue packs. Patients on the NDH register will have a follow up, including HbA1c, within the preceding 12 months to monitor status and identify development of Diabetes Numerator: Number of patients receiving rescue packs with a COPD review, read coded as 66YM. Denominator: Number of patients receiving rescue packs, read coded as 8BMW Issue of COPD Rescue Pack. Numerator: No of patients with NDH with a HbA1c blood test in the preceding 12 months Denominator: No of patients with NDH 85% = Green - Achieved; <85% - 60% = Amber; payment not made <60% - 50% = Red; payment not made 75% = Green - Achieved: Please note that there is no exclusion code for COPD review declined QOF Diabetes register QOF palliative care patients Read coding via clinical system Read coding via clinical system Annual Annual Remain Remain Page 10 of 32
39 Agenda Item No 5b Diabetes - NDH - identification and onward referral The percentage of patients identified as having NDH, who have been given lifestyle advice/ information about the risk of developing Diabetes. Numerator: Number of patients coded as having NDH who have been given lifestyle advice/ information re risk of developing diabetes Denominator: Number of patients coded as having NDH 75% = Green - Achieved: QOF Diabetes register QOF palliative care patients Read coding via clinical system Annual Remain Diabetes - Treatment The percentage of patients on the Diabetes register who have achieved the three NICE recommended diabetes treatment targets: 1. HbA1C less than or equal to 58mmol/mol 2. BP less than or equal to 140/80 3. Cholesterol less than or equal to 5mmol/L Numerator: Number of patients on the Diabetes register achieving the NICE recommended 3 treatment targets Denominator: Number of patients on diabetes register 44% = Green - Achieved: 8BL0. Patient on maximal tolerated antihypertensive therapy (FOR BP TARGET ONLY) 8BL1. Patient on maximal tolerated lipid lowering therapy (FOR CHOLESTEROL TARGET ONLY) 8BL2. Patient on maximal tolerated therapy for diabetes QOF palliative care patients Read codes through Informatica and National Diabetes Audit Annual Remain Page 11 of 32
40 Agenda Item No 5b Chronic Kidney Disease - Treatment 1. The percentage of patients on the CKD Register with a BP recorded in the last 12 months, who have a BP of <=140/ The percentage of patients on the CKD Register with Diabetes with a BP recorded in the last 12 months who have a BP recorded of <=130/80 3. The percentage of patients on the CKD Register with ACR 70mg/mmol or more with a BP recorded in the last 12 months, who have a BP recorded of <=130/80 Numerator: No. of pts on CKD Register latest BP recorded <=140/90 (Numerator) Denominator: Total no. of patients on CKD Register with a BP recorded in the last 12 months (Denominator) Numerator: No. of pts on CKD Register with Diabetes latest BP recorded <=130/80 (Numerator) Denominator: Total no. of patients on CKD Register with diabetes with a BP recorded in the last 12 months (Denominator) Numerator: No. of pts on CKD Register with ACR 70mg/mmol or more and latest recorded BP <= 130/80 in the last 12 months Denominator: Total no. of patients on CKD Register with ACR 70mg/mmol or more with a BP recorded in the last 12 months 70% = Green - Achieved: 50% = Green - Achieved: 50% = Green - Achieved: 8BL0. Patient on maximal tolerated antihypertensive therapy QOF palliative care patients 8BL0. Patient on maximal tolerated antihypertensive therapy QOF palliative care patients 8BL0. Patient on maximal tolerated antihypertensive therapy (FOR BP TARGET ONLY) QOF palliative care patients Read coding via clinical system Read coding via clinical system Read coding via clinical system Annual Annual Annual Remain Remain Remain Page 12 of 32
41 Agenda Item No 5b 2 Meds Optimisation EOL Drug Monitoring Antimicrobial stewardship Practices to provide evidence of an 'after death analysis' (mortality review) at four GSF meetings throughout 2017/18. Drugs to be monitored in line with shared care protocol monitoring guidance for each drug To reduce the prescribing of antibiotics based on prescription numbers by practice Submission of one anonymised after death analysis (mortality review) template per quarter to the portal (four in total per practice per year). Drugs to be monitored in line with shared care protocol monitoring guidance for each drug Numerator: Number of prescriptions for antibiotics in 2017/18 Denominator: Number of prescriptions for antibiotics in 2018/19 Quarterly submission of template = Green - Achieved; 95% = Green - Achieved: Red 10% reduction = Achieved; Amber 7.5% reduction = Achieved; Light green 5% reduction = Achieved; Dark green 2.5% reduction = Achieved; (maintenance of performance of practices at dark green status will not be marked as 'not achieved' but will not receive payment n/a n/a Quarterly submission of template through the portal Quarterly audit by pharmacists Monitoring via epact2 Quarterly Quarterly Bi-annual Annual Remain Remain New To remain as a KPI in 2018/19. Pay on a sliding scale similar to the Safeguarding KPIs Bi-annual return to be completed by practices and NIPs Page 13 of 32
42 Agenda Item No 5b 3 Children & Young People 4 Safeguarding Childhood Asthma Safeguarding Part 1 - Developing the GP Safeguarding Lead Role All 0-17(inc.) yr olds with asthma to receive an annual structured review All 0-17(inc.) yr olds with asthma to receive a medication review All 0-17(inc.) yr olds with asthma to receive an age appropriate personalised asthma action plan All 0-17(inc.) yr olds with asthma to receive specific training and/or assessment of inhaler technique (if patient has inhaler) GP Safeguarding Lead Forum Meetings: 1. Attendance by the GP Safeguarding Lead (minimum of 4 of 6 meeting in 2017/18) 2. Dissemination of information from all GP Safeguarding Leads meetings % that received an annual structured review % that received medication review % that received an age appropriate personalised asthma action plan % that received specific training and assessment of inhaler technique Each practice GP Safeguarding Lead to sign attendance record at each meeting they attend Each GP Safeguarding Lead to disseminate information to their practice from their attendance at the meeting and / or minutes of the meeting and record signature on the action log from the GP Safeguarding Leads meeting. 60%= Green - Achieved: 60%= Green - Achieved: 60%= Green - Achieved: 60%= Green - Achieved: 1. Attendance at bimonthly meetings 4/6 per year = Green - Achieved; 2. 6/6 meetings (even if nonattendance) = Green - Achieved; QOF palliative care patients QOF palliative care patients QOF palliative care patients QOF palliative care patients Read coding via clinical system Read coding via clinical system Read coding via clinical system Read coding via clinical system Annual review of individual practice attendance by the Safeguarding Team Recorded submission of evidence - GP Safeguarding Leads signature sheet submitted quarterly to the Safeguarding Team Annual Annual Annual Annual Annual Remain Remain Remain Remain Remain Page 14 of 32
43 Agenda Item No 5b Safeguarding Part 2 - Embedding Safeguarding within all GP Practices GP Safeguarding Lead monthly meeting with Practice Health Visitor GP Safeguarding Lead attendance at and completion of training: Adult Safeguarding, Children's Safeguarding Level 2 & 3, CSE, LAC, FGM Domestic Abuse, Prevent and MCA/ DoLs (as minimum) 80% of all staff (clinical and nonclinical) to complete mandatory Adult Safeguarding Training every 3 years 80% of all staff (clinical and nonclinical) to complete mandatory Level 2 Safeguarding Children Training every 3 years excluding GPs See Each GP and HV to record signatures at their monthly meeting Each GP Safeguarding Lead to disseminate information to their practice from their attendance at the meeting and / or minutes of the meeting facilitating practice discussion on cases as required Each GP Safeguarding Lead to attend required training and complete attendance sheet Practice staff (Clinical and nonclinical) to attend training and complete attendance sheet Practice staff (Clinical and nonclinical) to attend training and complete attendance sheet Attendance at monthly meetings (10/12) = Green - Achieved; 100% = Green - Achieved; >=80% = Green - Achieved; >=80% = Green - Achieved; Recorded submission of evidence - GP Safeguarding Leads and HV signature sheet quarterly to the Safeguarding Team Annual review of completion of training via Safeguarding Team Database Annual review of completion of training via Safeguarding Team Database Annual review of completion of training via Safeguarding Team Database Quarterly Annual Annual Annual Remain with slight amendment as to how measured Remain Remain Remain Remain but with new training added (FGM and LAC. CSE training has been removed) If the new IRIS KPI is approved, the domestic abuse element on this KPI will be removed Page 15 of 32
44 Agenda Item No 5b Safeguarding Part 3 - Patient Standard SG06_P 80% of all GPs and other relevant clinical staff (e.g. ANPs) to complete mandatory Level 3 Safeguarding Children training every 3 years 50% Clinical staff (GP s and Practice Nurses) are expected to undertake MCA/ DoLs training 50% Clinical staff (GP s and Practice Nurses) are expected to undertake Prevent Training All General Practices to engage with and implement the IRIS project to support Domestic Abuse Identification Application of domestic abuse Read codes of GPs to attend training and complete attendance sheet Practice clinical staff to attend training and complete attendance sheet Practice clinical staff to attend training and complete attendance sheet Practice to: Become an IRIS Practice 80% of staff (all clinical and nonclinical) to complete training (refresher training every 3 years) To engage with the project and submit IRIS referrals as appropriate To display IRIS posters and leaflets for patients to access - To implement HARKs on Vision / EMIS Practice to apply read codes to identified patient >=80% = Green - Achieved; >=50% = Green - Achieved; >=50% = Green - Achieved; 80% of staff trained Implementation of HARKS on Vision / EMIS and referrals where appropriate 100% = Green - Achieved; n/a Annual review of completion of training via Safeguarding Team Database Annual review of completion of training via Safeguarding Team Database Annual review of completion of training via Safeguarding Team Database Annual review of completion of training and referrals via Safeguarding Team Database Submission of Read coded audit returned to Annual Annual Annual Annual Quarterly Remain Remain Remain New Remain Agreed subject to funding being agreed for additional staff member Should the funding not be approved, the original domestic abuse KPI will remain Page 16 of 32
45 Agenda Item No 5b Records and Safeguarding Reports patient records for: Notified cases heard at MARAC Patients subject to DOLS Children placed on Child Protection Plan Looked After Children 90% Completion of MARAC requests 100% Completion of requested case conference reports, submitted within the requested timescale on the GP initial case conference report proforma records as informed by the Safeguarding Team. Audit run of Read coded records to be undertaken quarterly Reports to be submitted by the practice following the request from the Safeguarding Team Reports completed and submitted by the practice following the request from the Safeguarding Team within timescale and practices should use the current report proforma and guidance developed by the Safeguarding Team for undertaking the report. >=90% = Green - Achieved; 100% = Green - Achieved; Safeguarding Team. Quarterly review of practice submissions of MARAC reports via Safeguarding Team Database Completion & submission of requested conference reports in the required timescale monitored by the Safeguarding Team and recorded via database - Quarterly review Quality assurance of reports and completion of the correct proforma monitored by the safeguarding Team and recorded on the database Quarterly payment weighted dependent on the number of reports submitted Quarterly payment weighted dependent on the number of reports submitted Remain Remain Page 17 of 32
46 Agenda Item No 5b Assess the effectiveness of the practice to refer patients for diagnosis Dementia diagnosis rate (number of patients with a dementia diagnosis as a percentage of the expected prevalence for the practice) for the preceding 12 months Numerator: QoF dementia register 80%* = Green - Achieved: Dementia Register and CFAS II methodology in Dementia UK report Annual Remain 5 Vulnerable Groups Dementia & MCI Serious Mental Illness Improve the care plans for dementia patients Improve provision of giving appropriate information to patients Ensure patients on the SMI register Denominator: GP list size with CFAS II methodology applied as outlined in the Dementia UK report No. of patients with dementia whose care plan has been reviewed with a face-to-face review within the preceding 12 months No. of patients with newly diagnosed dementia being given information about local services within 6 months of the diagnosis date No. of patients on the SMI register 80% = Green - Achieved: <80% - 70% =Amber; payment not made < 70% = Red; payment not made 90% = Green - Achieved: <90% - 80% =Amber; payment not made < 80% - 60% = Red; payment not made 75% = Green - Achieved: QOF palliative care patients QOF palliative care patients QOF palliative care patients Read coding via clinical system clinical system Read coding via clinical system Annual AMEND Combine D4 & D5 into one KPI to include the following: No. of patients with dementia whose care plan has been reviewed with a face-to-face review AND given information about local services since April 1 80% target to remain Annual Remain Greater weighting Page 18 of 32
47 Agenda Item No 5b Learning Difficulties and ASC Asylum Seekers Carers attend for their annual physical health check As per the shared care protocol, patients commenced on atypical antipsychotics will, for the first 6 weeks of treatment, have their physical health monitoring addressed by secondary care mental health services. Thereafter this responsibility transfers to primary care Promote the uptake of cancer screening for patients with LD Practices must record country of origin, first language, ethnicity and whether the asylum seeking patients need an interpreter or not Increase the number of carers over the age of 18 registered who have attended for their annual physical health review No. of patients commenced on an atypical antipsychotic who have been monitored as per the standard for their physical health monitoring No. of eligible patients with LD to be up to date with cancer screening (presently 33% breast, 24% cervical % 50% bowel) Record country of origin, first language, ethnicity and if an interpreter is required Number of registered patients aged 18 and over <75%* 60% = Amber; payment not made < 60% - 50% = Red; payment not made 75% = Green - Achieved: <75%* 60% = Amber; payment not made < 60% - 50% = Red; payment not made 70% = Green - Achieved: 80% = Green - Achieved: <80% - 50% = Amber; payment not made <50% = Red; payment not made 2% of list size = Green - Achieved: QOF palliative care patients if no longer a carer code 918f Read coding via clinical system Annual submission of template through the portal Read coding via clinical system Read coding via clinical system Annual Remain Lower weighting Annual Bi-annual Annual Annual Remain Remain Remain Now includes the option for patients to decline and practices not to offer where appropriate. Practices with high opt-out rates will be audited Page 19 of 32
48 Agenda Item No 5b within practices Increase the number of carers aged 17and under registered within practices Offer annual health checks to adult carers and to all the young carers on the carers register in 2017/18 read coded as a carer in the last 12 months Number of registered patients aged 17 and under read coded as a carer in the last 12 months Offer to 70% of carers on register At least 3 per practice = Green - Achieved; 70% offered = Green - Achieved: if no longer a carer code 918f QOF palliative care patients Read coding via clinical system Read coding via clinical system Annual Annual Remain Remain AMEND Threshold for 2018/19 will be determined once Q4 data has been validated 6 Public Health Health improvement All patients aged to be offered and complete a health Check No. of initial NHS Health Checks offered and completed (aged years) Total no. of health checks offered to yr olds No. of NHS Health Checks completed (aged years) in 2018/19 on eligible high risk patients No. of eligible high risk patients 1233% uptake = Green - Achieved: Read coding via clinical system Annual Practices to invite 100% of eligible high risk patients AND complete a health check on 33% Options for consideration as part of the funding review: Option 1: weight funding equally across remaining public health KPs Option 2: review the funding attached to each domain Salford is on track to achieve around 3800 health checks carried out in 2017/18. Numbers are expected to stay the same in 2018/19 and for GPs to ensure those at highest risk (from the total 5 year cohort) are prioritised for checks in 2018/19. Achieving 3800 checks per year would equate to 33.33% uptake from the eligible in year cohort (total of 11,400 in 2017/18). Page 20 of 32
49 Agenda Item No 5b QOF palliative care patients and weighting for each KPI to reflect amount of work required All patients over 16 years to have had an AUDIT C or FAST within the last 2 years All patients over 16 years to have their smoking status recorded within the last 2 years All patients over 30 to have their BP recorded in the last 5 yrs No. of patients 16yrs+ who have had an audit C or FAST within the last 2 yrs Total no. of patients 16 yrs and offered an audit C check within the last 2 yrs No. of patients who have had their smoking status recorded within the last 2 yrs Total no. of registered patients 16yrs+ No. of patients over 30 who have had their BP recorded in the last 5yrs Total no. of patients % = Green - Achieved: <50% - 30% = Amber; payment not made <30% = Red; payment not made 50% uptake = Green - Achieved: 75% uptake = Green - Achieved: Teetotaller Stopped drinking alcohol 136e. Declines to state current alcohol consumption 8IH4. Alcohol Use Disorders Identification Test declined QOF palliative care patients QOF Hypertension Register QOF palliative care patients Read coding via clinical system Read coding via clinical system Read coding via clinical system Annual Annual Annual AMEND Remain Remain Threshold changed to 20% over 5 years Page 21 of 32
50 Agenda Item No 5b Screening (national) Practices to read code DNAs and f/u with advice and support to promote the uptake of cervical screening: (25-49 yrs = 3-yearly, 50-64yrs = 5-yearly); this will demonstrate a reduction in DNAs Practices to promote the uptake of bowel screening every 2 years to all patients aged 60-74yrs by follow up of no response according to the national screening programme No. of Women aged 25-49yrs recorded as DNA cervical screening given advice re screening or coded as declined screening following recording of DNA in the last 3 yrs and No. of Women aged 50-64yrs recorded as DNA cervical screening given advice re screening or coded as declined screening following recording of DNA in the last 5 years. Total no. of Women aged 25-49yrs recorded as DNA cervical screening in last 3 yrs and total no. of Women aged 50-64yrs recorded as DNA cervical screening in the last 5 years No. of patients aged yrs recorded as no response to bowel screening in the last 2 years according to the national programme given advice No. of patients 1% above 2016/17 practice baseline = Green - Achieved; 1% above 2016/17 practice baseline = Green - Achieved; QOF palliative care patients QOF palliative care patients Read coding via clinical system Read coding via clinical system Annual Annual AMEND AMEND Propose to amend threshold in year to 75% Propose to amend threshold in year to 75% Page 22 of 32
51 Agenda Item No 5b 7 Proactive Care 8 Access Sexual Health MDGs Access Practice to demonstrate an improvement on the offer and uptake of Chlamydia screening with 15 to 25 year olds when compared to the baseline set in 2016/17 Practice attendance at MDG meetings in 2017/18 Provide appointments for 9% of the registered practice list size per week aged 60-74yrs who have been offered bowel screening in the last 2 years (excluding declined in last 2 years) according to the national programme Improvement on the offer and uptake of Chlamydia screening with 15 to 25 year olds when compared to the baseline set in 2016/17 Evidenced through the sign in sheets at meetings Does your practice provide appointments for 9% of the registered practice list size per week? Clinical staff categories included in the count are: GPs Nurse Practitioners (for Acute conditions only) Pharmacists (for Acute conditions only) 1% above 2016/17 practice baseline = Green - Achieved; 75% compliance = Green - Achieved: 9% = Green - Achieved: QOF palliative care patients RU Clear and READ coding via clinical system Annual audit of the signing in sheets Quarterly submission through the portal CCG will communicate, before the quarter end, the two particular weeks that we wish to count. Practices may choose which week (of the two) to submit Annual Annual Quarterly AMEND KPI on hold until review has been completed Remain Propose to amend threshold in year to count the number of offers, not a 1% improvement. Target - increase from 17/18 figures Page 23 of 32
52 Agenda Item No 5b Time to Third Next Routine Available Appointment (TNAA) for a routine appointment with any GP within the practice Practices to evidence that they offer a range of GP appointments every day (that the practice is open) TNRAA to be measured in hours for routine appointments only Practices to evidence that they offer a range of the following categories of GP appointments every day (that the practice is open): Emergency or Urgent same day Routine prebookable 6 weeks in advance Telephone consultations Online prebookable X hours or less = Achieved: payment made X hours or more = Not achieved; payment not made TARGET TO BE AGREED All listed GP appointment categories are offered every day that the practice is open = Achieved; Any listed GP appointment categories not offered every day that the practice is open = Not achieved; payment not made Any practitioner other than a GP Any practitioner other than a GP CCG will do a quarterly ring round of all practices on a particular day and time and will collate the data CCG will communicate, before the quarter end, the particular week (which will be in the future to avoid having patient names visible) and practices to submit an unpopulated screenshot of the clinical system to demonstrate the different categories of appointment available for patients (usually colour coded) Quarterly Quarterly New New Practices operating a long wait time for routine appointments risk the patient s condition being more serious than recognised by the patient, and therefore prevents early diagnosis for serious conditions. This component aims to cut the waiting time for the next routine appointment. Patients can be frustrated at the lack of ability to access the type of appointment that they need when they call the practice. Page 24 of 32
53 Agenda Item No 5b Practices to demonstrate that they offer a minimum of 10% Patient Online slots for every GP each day Practices to demonstrate that they offer a minimum of 10% Patient Online slots for every GP each day NB MORNING SLOTS NOT BOOKED BY 9AM CAN BE RELEASED TO USE AS ON THE DAY APPOINTMENTS AFTERNOON SLOTS NOT BOOKED BY 2PM CAN BE RELEASED TO USE AS ON THE DAY APPOINTMENTS Minimum of 10% of slots per GP per day = Achieved; Payment made Less than 10% of slots per day per GP = Not achieved; payment not made Any practitioner other than a GP Quarterly portal submission - CCG will communicate, before the quarter end, the particular week that we wish to see evidenced. The CCG wish to collect information about the uptake of online appointments. This is not a target, as it is recognised that patients choose how they wish to make a booking Practices to submit: the number of appointments offered online the number of appointments booked online Quarterly New Practices are contractually required as part of GMS/PMS/APMS to achieve 20% (for 2017/18) of their registered patient list signed up to Patient Online. This highlights the importance placed on implementing this method of patient access, by the NHSE central team. It is anticipated that a greater usage of this functionality has the potential to free up Receptionist time, which could be used for other tasks, therefore this is considered a stretch target. This component seeks assurances that practices are using this functionality in a meaningful way and specifically around the availability of appointments for those patients choosing to use Patient Online. Page 25 of 32
54 Agenda Item No 5b Patient Access Survey Practices to use their PPG members to facilitate a patient survey for 50 patients every quarter with collation and analysis to be carried out and submitted to the CCG, using the following questions which relate to Access Practices to attain a higher percentage than the 16/17 Salford average for the quarterly Patient Survey % of patients who find it easy to get through to the practice on the phone % of patients able to get an appointment to see or speak to someone the last time they tried % of patient patients who say the last appointment they got was convenient 50 surveys per quarter submitted and > the Salford average for 16/17 = Achieved; Payment made Less than 50 surveys submitted and/or < the Salford average for 16/17 = Not achieved; Payment not made 50 surveys per quarter submitted and > the Salford average for 16/17 = Achieved; Payment made Less than 50 surveys submitted and/or < the Salford average for 16/17 = Not achieved; Payment not made 50 surveys per quarter submitted and > the Salford average for 16/17 = Achieved; Payment made Less than 50 surveys submitted and/or < the Salford average for 16/17 = Not achieved; Payment not made n/a n/a n/a Quarterly submission of survey results Quarterly submission of survey results Quarterly submission of survey results Quarterly Quarterly Quarterly New New New Patient experience is valued by the CCG Patient experience is valued by the CCG Patient experience is valued by the CCG Page 26 of 32
55 Agenda Item No 5b 9 Safety & experience Patient Safety - learning from events / incidents / Patient Experience GP practices to report, investigate and manage incidents, including identifying lessons learnt, using the Insight (datix) system. Demonstrate learning from own practice incidents which have been discussed at practice and neighbourhood level; the changes which have occurred as a result of incidents; how the changes have been embedded within practice; and what impact these changes have had on the quality, safety or experience of patients, carers or staff % of patients who describe their experience of making an appointment as good Bi-annual Annual report submitted by each GP practice cross referenced with information on the Insight (datix) system 50 surveys per quarter submitted and > the Salford average for 16/17 = Achieved; Payment made Less than 50 surveys submitted and/or < the Salford average for 16/17 = Not achieved; Payment not made 100% = Green - Achieved; n/a Quarterly submission of survey results Quarter 2 & Quarter 4 Annual submissions through the portal Quarterly Annual Bi-annual New Slight amendment Patient experience is valued by the CCG Demonstrate how information from Page 27 of 32
56 Agenda Item No 5b 10 Business Management Membership Engagement reported own practice incidents and near misses, have been linked to patient experience data (e.g. FFT, GP survey, complaints, compliments) to identify any themes and trends; how learning from these have been used to improve quality, safety and patient experience; how the changes made have been embedded within the practice; how learning has been shared within the practice and across the neighbourhood. Practices will ensure they are represented at Neighbourhood CCG meetings Practices will ensure that they are represented at practice managers meetings Practice representation documented at NCCG meetings (1x clinical and 1 x non-clinical staff member) Practice representation documented at Practice Managers meetings 100% representation = Green - Achieved: % = Amber; payment not made <75% = Red: payment not made Attendance at a minimum of 5 out of 6 meetings = Green - Achieved; Quarterly audit of the signing in sheets Annual audit of the signing in sheets Quarterly Annual Remain Remain Reduce funding as length of meetings has reduced Page 28 of 32
57 Agenda Item No 5b Practices will be expected to attend two annual members events meetings Practice representation documented at two annual members events meetings (at least 1x clinical and 1 x non-clinical staff member) 100% representation = Green - Achieved: % = Amber; payment not made <75% = Red; payment not made Bi-annual audit of the signing in sheets Bi-annual Remain Page 29 of 32
58 Agenda Item No 5b Appendix 4 Proposed 2018/19 contract sign-up requirements Domain Standard Requirement Measure Code Portal Question 1 Long Term Conditions Medicines Optimisation 3 Children 5 Vulnerable Groups Holistic Care Support the raising of awareness of the prevention, screening and management of LTCs by utilising local and national campaigns materials i.e. displaying posters and making leaflets available Ensure the appropriate clinician/s attend mandated education sessions as well as the required number of optional education sessions. Clinician must have signed register of attendance and remain for the full education session. Sepsis Practices to work in partnership across the healthcare system to tackle the threat of sepsis NEW Cancer Diabetes Medicine Safety Childhood Asthma Dementia & MCI Each practice to have a practice cancer champion and for them to attend the training (1 hour) and disseminate this learning within the practice Practices to engage in the production of an improvement plan where the practice is identified as requiring support Practices to apply the principles of the PINCER intervention to reduce the number of medicines-related patient safety incidents Prescriber (medical and non-medical) housekeeping Each practice to have a named asthma clinical lead All 0-19 yr olds with asthma to be entered onto the paediatric asthma register Have a Dementia register in place Have a MCI register in place CSR_1a CSR_1b NEW CSR_1c NEW NEW CSR_1d CSR_1e CSR_1f CSR_1g Has your practice developed a communication engagement strategy? Does your practice agree to meet the educational requirements of the Salford Standard as outlined in the guidance? Has your practice discussed recognition, diagnosis and early management of sepsis in a practice meeting as per the NICE guidance? Does your practice have a cancer champion who has attended the Salford Cancer Champion training and disseminated this learning within the practice Does your practice agree to engage in the production and implementation of a diabetes improvement plan if you are identified as requiring support? Does your practice agree to apply the principles of the PINCER intervention to reduce the number of medicines-related patient safety incidents? Does your practice agree to maintain an accurate prescriber list? Does your practice have a named childhood asthma clinical lead? Please provide their name in the comments box. Does your practice have a paediatric asthma register in place? Please include the register size in the comments box. Does your practice have a dementia register in place? Please include the register size in the comments box. Does your practice have an MCI register in place? Please include the register size in the comments box. Page 30 of 32
59 Agenda Item No 5b 6 Public Health 8 Access Military Veterans Learning Difficulties and ASC Sign up online to the Dementia Action Alliance Sign up to the Salford Way app Work with Alzheimer s Society so patients and staff gain up to date information; Contact Marion Coleman Marion.Coleman@alzheimers.org.uk from Alzheimer s Society to come and talk to the Dementia Champion in Practice after training to discuss: > Dementia Friendly Toolkit making the surgery dementia friendly > Information for surgery The CCG will develop an information pack for all surgeries once they have signed up to the Dementia Action Alliance and the Salford way app. Practices to record the status of Military Veterans and Reservists Sign up to the LD DES and deliver requirements Practice to have an LD Register and cross reference this with the councils (CTLD) and share their autism numbers and Downs Syndrome register CSR_1h Asylum Seekers Practice to develop an Asylum Seeker Register CSR_1k Pride in Practice All practices to complete the Pride in Practice award NEW Suicide Prevention Health Protection Practice to update their suicide prevention awareness and knowledge All practices to Sign up to the Influenza DES and deliver requirements Sexual Health All practices to register as a chlamydia screening centre RU Clear CSR_1m Access Practice Access Plan CSR_1n CSR_1i CSR_1j NEW NEW CSR_1l 1. Has your practice signed up online to the Dementia Action Alliance? 2. Has your practice signed up to the Salford Way app? 3. Has your practice worked with the Alzheimer's Society so patients and staff gain up-to-date information? 4. Has your practice contacted and had a visit from Marion Coleman from the Alzheimer's Society? Does your practice record the status of Military Veterans and Reservists using the Read Code 13Ji% or 13JY. Please include the register size in the comments box. Does your practice agree to sign-up to the LD DES in 2018/19 and commit to delivering the requirements of the specification? Does your practice maintain a record of contact made with Community Team Learning Difficulties (CTLD) to cross reference LD register and share Autism numbers and Downs Syndrome register? Does your practice have an Asylum Seeker Register? Please include the register size in the comments box. Does your practice commit to completing the Pride in Practice award? Does your practice agree to use the Salford Suicide Awareness Pack and share learning and knowledge with all staff members? Does your practice agree to sign-up to the Influenza DES in 2017/18 and commit to delivering the requirements of the specification? Is your practice registered as a RU Clear chlamydia screening centre? Does your practice have an access plan that includes all of the elements set out in the guidance? Page 31 of 32
60 Agenda Item No 5b 9 Safety & Experience 10 Business Management Patient experience Demand management Business Continuity / resilience plans Accessible Information Declarations of Conflicts of Interest GP practices will be required to provide evidence to demonstrate that their patient participation group is active, and that specific improvements, feedback and learning is being acted upon within the practice, and where appropriate Neighbourhood wide. CSR_1o Does your practice have an active PPG? Upload your Improvement Action Plan to demonstrate your PPG is active, i.e. minutes, feedback and learning is being acted upon within the practice and where appropriate neighbourhood wide. This should include specific improvements made as a result of FFT and GP survey results Practices to ensure use of NHS e-referrals system (NHS e-referrals booking reports) CSR_1p Does your practice use the NHS e-referral system? Does your practice ensure that EUR policies are easily Practices to ensure that EUR policies are easily accessible for all referrers within practices and that they are CSR_1q accessible for all referrers within your practice and that discussed with staff they are discussed with staff? Practices to have an adequate and up to date Business Continuity Plan Comply with the Accessible Information Standard SCCI All members and staff of the CCG to complete declarations of interest forms by all groups covered by the scope of this standard CSR_1r CSR_1s CSR_1t Does your practice commit to submitting an updated Business Continuity Plan? Does your practice comply with the accessible information standard SCCI-1605? Have all members and staff of the CCG completed declaration of interest forms? This includes GP partners (or where the practice is a company, each director).; and any individual directly involved with the business or decision-making of the CCG. Page 32 of 32
61 NHS SALFORD CLINICAL COMMISSIONING GROUP Primary Care Commissioning Committee AGENDA ITEM NO 5 (c) Item for Decision/Assurance/Information 28 November 2017 REPORT OF: Karen Proctor Director of Commissioning DATE OF PAPER: 22 November 2017 SUBJECT: Ellenbrook Medical Practice Application to close the patient list IN CASE OF QUERY PLEASE CONTACT: STRATEGIC PRIORITIES: Quality Community Based Care Sam Glynn-Atkins Service Improvement Manager samantha.glynn-atkins@nhs.net Please tick which strategic priorities the paper relates to: Integrated Care In Hospital Care Long Term Conditions and Mental Health Effective Organisation PURPOSE OF THIS PAPER: This paper is supplied to the Primary Care Commissioning Committee, to request a decision on the list closure application from Ellenbrook Medical Practice, which proposes to close the patient list to new patients for a period of 4 months. RECOMMENDATION OF THIS PAPER: To reject the application to close the patient list to new registrations.
62 Further explanatory information required HOW WILL THIS BENEFIT THE HEALTH AND WELL BEING OF SALFORD RESIDENTS OR THE CLINICAL COMMISSIONING GROUP? Not applicable WHAT RISKS MAY ARISE AS A RESULT OF THIS PAPER? HOW CAN THEY BE MITIGATED? Not applicable WHAT EQUALITY-RELATED RISKS MAY ARISE AS A RESULT OF THIS PAPER? HOW WILL THESE BE MITIGATED? Not applicable DOES THIS PAPER HELP ADDRESS ANY EXISTING HIGH OR EXTREME RISKS FACING THE ORGANISATION? IF SO WHAT ARE THEY AND HOW DOES THIS PAPER REDUCE THEM? Not applicable to organisational red risks PLEASE DESCRIBE ANY POSSIBLE CONFLICTS OF INTEREST ASSOCIATED WITH THIS PAPER. Not applicable PLEASE IDENTIFY ANY CURRENT SERVICES OR ROLES THAT MAY BE AFFECTED BY ISSUES WITHIN THIS PAPER: Salford GP practices Wigan GP practices
63 Primary Medical Care Commissioning Principles 1. Investment in general practice will continue to, as a minimum, be in line with the recommendations of the General Practice Forward View in order to strengthen resilience and sustainability of general practice by building capacity and capability. 2. The CCG will seek to maximise opportunities to commission primary medical services at scale (for example through a GP provider organisation) where this is expected to improve patient experience or be more efficient. 3. When commissioning decisions need to be made regarding primary medical service contracts, an options appraisal will be undertaken in order to determine the option that is most likely to meet the needs of the population group and most likely to deliver the CCG s strategic ambitions. This may not always be re-procuring a like for like service. 4. The CCG will commission general practice services from providers that are able to demonstrate good outcomes, value for money and care for patients that is holistic and provided to consistently high standards of quality and safety. 5. The CCG will seek to engage with the local population and acknowledge patient views when making primary medical services commissioning decisions. 6. The CCG will ensure that the primary medical services in Salford continue to meet the needs of a growing and increasingly diverse population. This will include promoting patient choice and equality and seeking to ensure that commissioning decisions improve the economic, social and environmental wellbeing of Salford. 7. The CCG will encourage and support general practice to play a pivotal role within the emerging accountable care system, with leadership through federated arrangements. 8. The CCG will embrace opportunities to commission primary medical services in an integrated way where this has benefits for patient care, e.g. through pooling budgets for health and social care services, or commissioning community services to be delivered on a neighbourhood basis from multidisciplinary integrated teams. 9. The CCG will embrace new contracting mechanisms where they support the viability, sustainability and resilience of general practice, including practices working collaboratively in Addressed in this paper? No No. Yes contained within the paper No Yes via Healthwatch Yes considered within the paper No No No
64 neighbourhood groups to deliver agreed outcomes and to share resources such as staff and back office services. 10. The CCG will support making general practice in Salford becoming an attractive place to work. This will include encouraging and supporting general practice to: embrace innovation and new ways of working; adapt and skill-up the workforce to meet patient need; make greater use of technology; and work from modern and fit for purpose premises. 11. The CCG, as a commissioner of primary medical services, cannot assume responsibility for, or become involved in, matters relating to the management of GP practices, including practice disputes and legal matters. 12. The CCG will proactively work with partners, including Salford Primary Care Together (as Salford s GP provider organisation) and the Salford and Trafford Local Medical Committee, in a transparent and supportive manner. No No The LMC and other key partners have been consulted on the proposal Footnote: Members of NHS Salford Clinical Commissioning Group Primary Care Commissioning Committee will read all papers thoroughly. Once papers are distributed no amendments are possible.
65 28 November 2017 Agenda item 5 (c) Document Development Process Yes No Not Applicable Comments and Date (i.e. presentation, verbal, actual report) Outcome Public Engagement (Please detail the method ie survey, event, consultation) Stakeholder letters sent including to Healthwatch (see Section 5 for details) Responses due to be returned by 27 November 2017 Clinical Engagement (Please detail the method ie survey, event, consultation) Has due regard been given to Equality Analysis (EA) of any adverse impacts? (Please detail outcomes, including risks and how these will be managed) Stakeholder letters sent to neighbouring practices (see Section 5 for details) EA considered within the body of this paper Responses due to be returned by 27 November 2017 To be reviewed once a decision is made Legal Advice Sought Presented to the Commissioning Committee Presented to the Health and Wellbeing Board Presented to the Integrated Commissioning Board Presented to any other groups or committees, including Partnership Groups Shared virtually the Primary Care Operational Group Note: Please ensure that it is clear in the comments and date column how and when particular stakeholders were involved in this work and ensure there is clarity in the outcome column showing what the key message or decision was from that group and whether amendments were requested about a particular part of the work.
66 28 November 2017 Agenda item 5 (c) List closure application P87624 Ellenbrook Medical Practice 1 Executive Summary This paper outlines an application that has been submitted by Ellenbrook Medical Practice, which proposes that the patient list be closed to new applications for a period of 4 months. This paper summarises the history of the practice in terms of historical requests to close the patient list and review the practice border, and outlines other local issues which may impact on patient care within the local area. It is recommended that the Primary Care Commissioning Committee is asked to approve Option 2 to reject the application to close the patient list on the basis that the application will be reconsidered in conjunction with the application from the Walkden Medical Centre in order to enable the CCG to take a wider perspective on capacity issues within the Walkden and Little Hulton Neighbourhood and to ensure that the needs of patients residing in this area are fully considered. 2 Introduction 2.1 NHS Salford Clinical Commissioning Group (CCG) received an application on 16 November 2017 from Ellenbrook Medical Practice to close the practice s patient list to new registrations, for a period of 4 months. The application can be viewed in Appendix The CCG has followed the guidance for dealing with a practice list closure application, as laid out in the Primary Medical Care Policy and Guidance Manual (PGM). 2.3 Sections and of the PGM set out the timescales in which the decision must be made: The Commissioner must make a decision, within a period of 21 days starting on the date of receipt of the Application (or within a longer period as the parties may agree): to approve the Application and determine the date the closure is to take effect and the date the list of patients is to reopen; or to reject the Application The Commissioner must notify the contractor of its decision in writing as soon as possible after the 21 day period. 2.4 Section of the PGM requires Commissioners and contractors to keep an open dialogue in order to prevent list closure where possible. With a view to possibly enabling the contractor to keep its list of patients open, the Commissioner and the contractor must talk openly to establish: what support the Commissioner may give the contractor; or changes the Commissioner or contractor may make 2.5 When making the decision regarding the list closure application, the PCCC have the following options available to them:
67 28 November 2017 Agenda item 5 (c) Option 1 Approve the list closure for 4 months Option 2 Reject the application to close the patient list 3 Background 3.1 Ellenbrook Medical Practice holds a GMS contract and is situated in Ellenbrook, Worsley which borders both Wigan and Bolton. 3.2 The practice currently has 2 GP partners, plus a salaried GP, equating to a total of 2.0 WTE for GP cover, according to the practice. Two practice partners retired from the practice in May 2017 and July 2017 respectively. The practice also has an Advanced Nurse Practitioner and a full time Practice Nurse. The practice GP WTE has been benchmarked by GMHSCP against local practices. This is included as Appendix 5 and specifies a 1.73 WTE for GPs. 3.3 The practice list size was 4,982 as at 30 September Appendix 4 shows the list size fluctuation since April According to data provided by GMHSCP, the practice have registered an additional 1,004 patients in the last 12 months, and deducted 406, giving a net increase of 598 patients. 3.4 The practice has made regular contract variation requests to GMHSCP, as detailed in the table below: Date Request Outcome 20 November 2013 List closure Granted for 12 months from to March 2015 List closure Rejected 31 March 2015 List closure - appeal to decision Rejected 11 December 2015 List closure Rejected 15.February 2016 List closure Rejected March 2016 Boundary change request Not progressed 10 January 2017 Change to inner and outer Rejected boundary 16 November 2017 List closure Pending decision Current Quality of Services Quality Assurance Dashboard 3.5 Practice performance against the Salford Quality Assurance Dashboard, which has been developed by the Primary Care Quality Group, has been assessed. Ellenbrook Medical Practice achieves highly on this dashboard and is currently ranked 3 rd out of 45 Salford practices.
68 28 November 2017 Agenda item 5 (c) 3.6 In summary, the practice have a total of 12 indicators that are green or dark green, 0 amber and 3 red indicators. The 3 red indicators relate to: - Electronic Prescribing Service - Trimethoprim and Nitrofurantoin prescribing - GP Safeguarding Forum Leads attendance (the practice are working through an issue with the CCG s Safeguarding Team, who will not permit a deputy to attend, despite the practice Safeguarding Lead being unable to attend the dates that have been scheduled) 3.7 The GP survey results indicate that 95.5% of patients would recommend the practice to someone who has just moved to the local area. A comparison of the survey results for 2016 against 2017 is included as Appendix 6. Care Quality Commission Inspection 3.8 The practice rating from the Care Quality Commission (CQC) is as follows: Practice Overall rating Date of inspection Ellenbrook Medical Practice Good 11 May 2016 Quality and Outcomes Framework Breakdown Safe Effective Caring Responsive Well led Rating Good Good Good Good Good 3.9 The practice s performance on the Quality Outcomes Framework (QOF) for 2016/17 is as follows: Quality Outcome Framework Maximum points possible Ellenbrook Medical Practice Clinical Public Health all Total % 97.8% Salford Standard 3.10 The table below shows that in 2016/17, Ellenbrook Medical Practice were ranked 11/45 against the Salford Standard key performance indicators. The Red RAG rating for 2017/18 is to be expected at the end of Quarter 2, as the majority of indicators are annual indicators and performance against these increases throughout the year. The practice has moved from 34/45 in Quarter 1, to 22/45 at the end of Quarter 2.
69 28 November 2017 Agenda item 5 (c) Salford Standard Performance Practice Overall rating* Rank** Payment received 2016/17 Green 75% 11th 118,938 Qtr 2-17/18 Red 35% 22 nd (34 th in Q1) *Green = >75% Amber = 50%- 74% (2016/17) 60% 75% (2017/18) Red = <50% (2016/17) <60% (2017/18) ** out of 45 practices 77,374 KPI status Red 29 Amber 3 Green 96 Red 24 Amber 1 Green 21 Number of KPIs*** 4 Current position 4.1 The practice has submitted an application to close the patient list to new registrations, included as Appendix In accordance with of the PGM, following the receipt of the application, the practice was offered a meeting with representatives from the Greater Manchester Health & Social Care Partnership (GMHSCP) and the CCG, to discuss the application and to look at whether any support could be provided. This offer was declined, as the practice had already highlighted a number of issues directly with the CCG, which extend beyond the list closure application. As a result, a meeting had been scheduled at the practice on 22 November 2017, to be attended by both the Chief Accountable Officer and Chair of the CCG. 4.3 GMHSCP colleagues provided several maps to support the decision making process for the January 2017 boundary change request. Appendix 2 shows the practice boundaries of both Ellenbrook Medical Practice and the neighbouring Salford GP practices, for reference within this application. 4.4 Various support measures have been made available to the Ellenbrook Medical Practice and other practices in the Walkden and Little Hulton Neighbourhood over the past couple of years: Productive General Practice Programme The CCG made funding available for all Salford practices to participate in the Productive General Practice Programme which supports practices to streamline processes and make efficiencies. Ellenbrook Medical Practice started the programme but did not complete, expressing concerns about how useful the programme was for them and indicating that it may not have fallen at the right time, due to volume of work at the practice Neighbourhood Integrated Practice Pharmacists A service to provide Pharmacists in all Salford GP practices has been commissioned and mobilised. The number of sessions per week has been allocated to practices based on list size. Ellenbrook Medical Practice therefore receive 4 sessions per week, however this is currently 3 sessions due to sickness within the service.
70 28 November 2017 Agenda item 5 (c) Little Hulton & Walkden Virtual Ward (Innovation Fund Bid) - This service provides a multidisciplinary specialist team working alongside the practices aimed at the top 2% of frail elderly who need high volume care Acute Home Visiting Service (Innovation Fund Bid) a bid to provide an Acute Home Visiting Service using Advanced Practitioner Paramedics, for all practices in Walkden was approved, with Salford Primary Care Together taking the lead for project management on behalf of the neighbourhood. The service is not yet live due to difficulties in recruitment. 4.5 Within the application, the practice acknowledges that they have not taken part in initiatives previously offered by the CCG, but now express a willingness to engage. 5 Patient and stakeholder engagement 5.1 In line with the Primary Medical Care Policy and Guidance Manual, a consultation letter has been circulated to potentially affected parties as follows: Healthwatch Salford the Salford and Trafford Local Medical Committee (LMC) the Wigan Local Medical Committee (LMC) Neighbouring Salford GP practices (Dr Loomba, Salford Health Matters, Cherry Medical Practice, Orchard Medical Centre, The Gill Medical Centre, The Limes, Walkden Medical Centre) Neighbouring Wigan practice (Dr Anderson) 5.2 A summary of the responses received will be included as Appendix 3, once available. 6 Options 6.1 There are 3 options available to the CCG: 1. Approve the list closure for 4 months 2. Reject the application to close the patient list The implications of these options are discussed in the next section. 7 Considerations 7.1 There are a number of factors that should be considered in relation to this application, and these are articulated below Existing list closure application from a neighbouring practice Walkden Medical Centre submitted an application to close the practice list to new registrations on 25 October 2017, however the practice agreed to pause the 21 day timescales allowed for a decision, in order to take up the offer of a meeting with the CCG and with representatives from the Greater Manchester Health & Social Care Partnership (GMHSCP), to discuss the application and to look at whether any support could be provided. This meeting will take place on 30 November The Primary Care
71 28 November 2017 Agenda item 5 (c) Commissioning Committee will need to ensure that there is equity in decision making across the two applications Impact on service users A decision to approve the application would reduce the choice available to patients. This would need to be considered in conjunction with as a decision to approve two practice list closures in the area would impact significantly on the remaining choice for patients Consultation Stakeholder consultation has been undertaken by the CCG as described in section 5 of this paper, with the responses received forming Appendix Local housing developments A number of new housing developments are either planned or in progress, and an agreement to close the list would make Ellenbrook Medical Practice unable to accept residents who move into these properties, thus potentially increasing the pressure on neighbouring practices. The locations of the new developments particularly relevant to this application, shown on Appendix 7, are as follows: Bourke Gardens (housing for Independent Living), Walkden Town Centre Burgess Farm, Hilton Lane (north of the practice) These sites make up around 480 households, with an expected 1,300 people becoming resident in them over the next few years Equality Assessment (EA) No specific equality concerns have been identified at this stage, however it is acknowledged that there is a risk that the wider effect of reduced access/limited choice would likely be felt by all patients, including those with protected characteristics Impact on and risks for other primary care providers It should be noted that a Walkden practice has recently requested a list closure, and the decision is pending. Additionally there are significant service needs for residents of forthcoming developments and the impact of this would be shared with one, or two, less GP practices if the proposed list closures were granted, leaving other primary care providers potentially under increased pressure List size and GP Whole Time Equivalents (WTE) - Upon receipt of the application, information was gathered in relation to list size and the number of GP WTE at the practice. The list size was reviewed over a period of months, and is displayed under Appendix 4. There has been steady increase in list size over the past 12 months. The practice GP WTE has been benchmarked by GMHSCP against local practices. This is included as Appendix Core hours opening The CCG are seeking to harmonise the practice physical opening times across Salford. In doing this, it should be noted that Ellenbrook Medical Practice close the practice doors during lunchtimes, resulting in a total of 7 hours of closure during core opening times (8.00am 6.30pm). Should the CCG pursue a full opening from all practices, as is likely to be the case within the 18/19 Salford Standard, the practice may consider that this puts additional pressure on the practice. 8 Conclusion and Next Steps 8.1 The Ellenbrook has long reported struggling with capacity and this is demonstrated with a succession of list closure / boundary change applications over the last 4 years.
72 28 November 2017 Agenda item 5 (c) 8.2 The practice achieves high level of quality performance. 8.3 The CCG has commissioned a range of support measures for the Walkden and Little Hulton Neighbourhood. 8.4 The proposed list closure will reduce patient choice, and potentially increase pressure on neighbouring practices. 8.5 Another list closure application has been received for a practice within the Walkden and Little Hulton neighbourhood and this application will need to be considered in that light. Next steps 8.6 The Primary Medical Care Policy and Guidance Manual (PGM) details the next steps in responding to an application for a list closure, as follows: The Commissioner must make a decision, within a period of 21 days starting on the date of receipt of the Application (or within a longer period as the parties may agree): to approve the Application and determine the date the closure is to take effect and the date the list of patients is to reopen; or to reject the Application. The Commissioner must notify the contractor of its decision in writing as soon as possible after the 21 day period. 8.7 In the circumstances of a decision to decline the request to close the practice list, the practice are entitled to appeal the decision within 28 days and the CCG would need to follow the process set out in the PGM Managing Disputes. If local resolution cannot be reached, the NHS dispute resolution procedure must be followed. The practice can make a further application after 3 months, starting on the date of the PCCC s decision to reject the application, or the final determination following dispute resolution. 9 Recommendation 9.1 The Primary Care Commissioning Committee is asked to: approve Option 2 to reject the application to close the patient list on the basis that the application will be reconsidered in conjunction with the application from the Walkden Medical Centre in order to enable the CCG to take a wider perspective on capacity issues within the Walkden and Little Hulton Neighbourhood and to ensure that the needs of patients residing in this area are fully considered. Sam Glynn-Atkins Service Improvement Manager 22 November 2017 Acknowledgements
73 28 November 2017 Agenda item 5 (c) Lisa Best Chris Tyson Lauren Smith Gail Henshaw Quality Assurance Manager Business Intelligence Manager Salford CCG Senior Service Improvement Officer Salford CCG Greater Manchester Health & Social Care Partnership
74 28 November 2017 Agenda item 5 (c) Appendix 1 List closure application Application to close patient list Practice stamp Please complete the following: Briefly describe your main reasons for applying to close your practice s register to new registrations: We have again seen a significant increase in the practice list size. We ve attached a built in search from Emis Web that outlines the year on year differences in list size. You ll see that it has been rising and falling over the years but the list had remained steady at around We had the opportunity to close the list in December 2013 for 12 months, this saw the list stabilise to 4,574. After an increase in the list, and an unsuccessful application to close the list 2015, we were advised to remove patients from outside the boundary. This is evident in the change in list size from 2 years ago to 1 year ago. However, you ll see in the last year we ve taken on at least another 400 patients. Our current list size stands at The figures on Open Exeter show the count of patients registered in past 12 months as 691. We feel this is posing a significant risk to both patients and staff. Clinically we cannot keep on top of all the work associated with the increasing number of patients. There can be 100+ prescriptions to complete and 100+ post and Docman. Our clinics are running in the morning up until lunchtime (often running late due to numerous/complicated issues patients attend) with hardly any time to complete the listed admin duties/visits before the surgeries start in the afternoon. We are dealing with above issues in order of urgency but eventually the routine ones become the urgent ones. We currently have approx. 301 face to face or telephone appointments each week with a GP/ANP and then a minimum of 15 per day clinical queries which result in some form of action from the GP, on many occasions a phone call to the patient. This equates to a minimum of 75 queries with access to a clinician on a weekly basis. Staff morale is low, and we ve always prided ourselves on a very happy team. Staff are receiving negative comments on a near daily basis about the decline in service, lack of appointments and delay in routine requests such as prescriptions. We re extremely concerned this is going to have an impact on sick leave and staff turnover. We have computers at any spare station available and now have no space left. We
75 28 November 2017 Agenda item 5 (c) Appendix 1 List closure application feel that we are staffed to the relevant level but they are also having difficulties in coping with the large volume of foot and telephone traffic. The cost associated with the extra patients is now proving to be a problem. In order to achieve targets such as Salford Standard and QoF we are having to contact many more patients and have seen a massive increase in telephone/stationary costs compared to previous years. This was highlighted by our accountant. As we are an area of low deprivation, our payment per patient is not high enough to make significant impact on improving our financial situation. Thus, as our list size increase our workload increases but our payments do not seem to adequately reflect this. What options have you considered, rejected or implemented to relieve the difficulties you have encountered about your open list and, if any were implemented, what was your success in reducing or erasing such difficulties? We altered our appointments to 15 minutes in order to ensure the clinicians had more time to fully consult with patients. We realise now that even 15 minutes is not enough time to complete the consultation and all the extra work associated with QoF and Salford Standard. Following advice from CCG and NHSE we removed patients outside of our practice boundary and though this gave relief for a short period the list has again increased significantly with no indication of slowing down. We ve had 2 partners leave within the last 6 months. Both have been replaced with extra sessions. We have one salaried GP and one advanced nurse practitioner. Both highly experienced and fitted into our team well. Yet we are also concerned that the volume of work may become too much for them. We ve employed a full time practice nurse who has been trained to complete routine Docman/post for us. Our other practice nurse is now trained to view and action blood results. Whilst this has alleviated some of the work it hasn t relieved the time pressures as much as we had hoped. The CCG practice pharmacist has been more than invaluable in supporting with medication reviews, discharge summaries and hypertension clinics. The fact that she is able to prescribe is an excellent asset to us. We feel we adhere to and follow the prescribing policies of NHSE and CCG and this is reflected in our excellent prescribing position within the CCG. We do not close half a day a week and have never done this. We continue to offer telephone consultations in conjunction with face to face appointments, though this inevitable uses up the time we have for administrative purposes. We are currently looking at setting up Mjog to create a more efficient and cost effective communication system with patients. However, this is again more money that requires investment which the practice does not have.
76 28 November 2017 Agenda item 5 (c) Appendix 1 List closure application We have promoted and encouraged the use of the online service so much so we have already exceed the 20% target set by NHSE before the deadline of March Figures show our level at 28%. We trialled a pilot with Alere late 2016/early 2017 which saw patients attend the local pharmacy to have CRP testing to determine whether they had an infection and therefore antibiotics could be prescribed. This proved successful in both educating patients and reducing unnecessary antibiotic prescribing. Have you had any discussions with your registered patients about your difficulties maintaining an open list and if so, please summarise them, including whether registered patients thought the list of patients should or should not be closed? This has been discussed at most meetings with our PPG group. The following comments have been made by 2 of our reps 1. If the list carries on growing I am certain it will be detrimental to the existing and new patients. Appointments would be much harder to be given, time with the doctor reduced. I also believe it would put tremendous strain on the doctors and staff. 2. As you know my views are very strong with regard to the size of the list, our practice has continually had good comments re service, appointment times etc however it is obvious that pressure is building and appointment times are becoming lengthier, to say nothing about the pressure on all the staff.. If the list continues to grow then all of the above will only become worse and all the hard work the doctors, you, and the team have put in will be lost, therefore you have my 100% support in your submission to close the list. Have you spoken with other contractors in the practice area about your difficulties maintaining an open list and if so, please summarise your discussions including whether other contractors thought the list of patients should or should not be closed? We have discussed with a number of different practices and we are aware that one other practice is also experiencing similar difficulties to what we are. Whilst we appreciate that other contractors may be affected by our request to close the list our paramount priorities must be the patients and staff at our practice and we feel this overrides any objections from other contractors. How long do you wish your list of patients to be closed? (This period must be more than three months and less than 12 months) Currently we feel that 4 months list closure is required until the end of the financial year.
77 28 November 2017 Agenda item 5 (c) Appendix 1 List closure application What reasonable support do you consider the AT would be able to offer, which would enable your list of patients to remain open or the period of proposed closure to be minimised? We are aware, in the past, we have decided against programmes such as Productive General Practice. If the CCG feels that this programme would be of benefit to the practice we are willing to engage, however we don t feel that this will support stability of the practice in the short term. We are also aware of other programmes of work such as the Care Navigator programme which we are willing to work with the CCG on developing should this enable our organisation to run more efficiently. Do you have any plans to alleviate the difficulties you are experiencing in maintaining an open list, which you could implement when the list of patients is closed, so that list could reopen at the end of the proposed closure period? Should the list closure be successful we would hope in this period that working with the CCG and NHSE we could highlight the affect the proposed and current building works in our vicinity are having on practices, including working with the council in Wigan as many of the works are being undertaken on that side of the boundary. We will increase the practice nurse training to enable them to further aid with GP workload. Engage with productive general practice to ensure back office running as efficiently as possible and increased training to sign post patients to relevant/appropriate services. Review appointment system, through productive general practice, to ensure maximising appropriate contact with clinicians. This will include running audits to determine the needs of the patients and whether these needs could have been dealt with in a more efficient way. We are also considering an effective way to triage patients to reduce inappropriate attendances. We are hoping to receive the maximum number of sessions available to us from the practice pharmacist, we will meet with her to discuss how best to make use of her time. The landlord will be consulted to determine whether further space could be made available. We will also review the use of clinical rooms to ensure utilised to maximum potential. We are also keen to work with other practices, other agencies such as SPCT and LMC to improve the service provided to Salford patients and ensure a good and happy work-life balance for all staff. We already have meetings arranged with another local practice and have spoken to the LMC to discuss ways of working more effectively and efficiently. We are confident that all of the above will place us in a better position to provide the high level of care we have always prided ourselves on providing but are currently struggling to maintain.
78 28 November 2017 Agenda item 5 (c) Appendix 1 List closure application Do you have any other information to bring to the attention of the AT about this application? We feel our concerns are real. Though we have highlighted that the practice cannot afford to support the rising costs of running the practice with an increasing list, we d like to make it clear our priority is the safety and wellbeing of the patients and staff. Clinical Workforce Details No. of General Practitioners 3 Total GP WTE* 2 No. of Nurse Practitioners 1 Total Nurse Practitioner WTE* 0.7 No. of Practice Nurses 2 Total Practice Nurse WTE* 1.7 *WTE = whole time equivalent based on full time or 1.0 WTE being 9 sessions per week Please note that this application does not concert any obligation on the NHS CB to agree to this request To be signed by all parties to the contract (where this is reasonably achievable): Signed:.. Print:.. Date:.. Signed:.. Print:.. Date:.. Signed:.. Print:.. Date:.. Signed:.. Print:.. Date:..

79 28 November 2017 Agenda item 5 (c) Appendix 2 Map detailing boundaries of neighbouring Salford GP practices
80 28 November 2017 Agenda item 5 (c) Appendix 3 Stakeholder comments The following responses were received from stakeholders: Salford & Trafford LMC No response yet received - Deadline for response is Monday 27 November 2017 Wigan CCG on behalf of Wigan practices No response yet received - Deadline for response is Monday 27 November 2017 Healthwatch Wigan LMC Salford GP Walkden Gateway Medical Practice Salford GP Salford Health Matters Salford GP Cherry Medical Practice Salford GP Orchard Medical Practice Salford GP The Gill Medical Practice Salford GP The Limes Medical Practice Salford GP Walkden Medical Centre No response yet received - Deadline for response is Monday 27 November 2017 No response yet received - Deadline for response is Monday 27 November 2017 No response yet received - Deadline for response is Monday 27 November 2017 No response yet received - Deadline for response is Monday 27 November 2017 No response yet received - Deadline for response is Monday 27 November 2017 No response yet received - Deadline for response is Monday 27 November 2017 No response yet received - Deadline for response is Monday 27 November 2017 No response yet received - Deadline for response is Monday 27 November 2017 No response yet received - Deadline for response is Monday 27 November 2017
81 28 November 2017 Agenda item 5 (c) Appendix 4 List size fluctuation
82 28 November 2017 Agenda item 5 (c) Appendix 5 GP Whole Time Equivalent (WTE) GP FTE List Oct 17 List/FTE P87624 Ellenbrook Medical Centre P87627 Orchard Medical Centre P87008 Walkden Medical Centre P87017 The Limes Medical Centre P87028 The Gill Medical Centre P87618 Walkden Gateway P87661 The Surgery

83 28 November 2017 Agenda item 5 (c) Appendix 6 Patient Survey results 2016 & 2017

84 28 November 2017 Agenda item 5 (c) Appendix 7 Developments in the Walkden area
85 Date of Meeting 28 th November 2017 Agenda Item No 6(a) NHS SALFORD CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE AGENDA ITEM NO 6 (A) Item for Information Date of Meeting 28 th November 2017 REPORT OF: Chief Finance Officer DATE OF PAPER: 13 November 2017 SUBJECT: Primary Care Finance Report Month 7 IN CASE OF QUERY PLEASE CONTACT: Elaine Vermeulen STRATEGIC PRIORITIES: Please tick which strategic priorities the paper relates to: Quality Community Based Care Integrated Care In Hospital Care Long Term Conditions and Mental Health Effective Organisation PURPOSE OF THIS PAPER: The purpose of this paper is to provide the Primary Care Commissioning Committee with information on the primary care budgets and finances. The report is based on information that was available at the end of October RECOMMENDATION OF THIS PAPER: The Committee is asked to note the report. (Please see further explanatory requirements overleaf) Page 1 of 8
86 Date of Meeting 28 th November 2017 Agenda Item No 6(a) Further explanatory information required HOW WILL THIS BENEFIT THE HEALTH AND WELL BEING OF SALFORD RESIDENTS OR THE CLINICAL COMMISSIONING GROUP? None. WHAT RISKS MAY ARISE AS A RESULT OF THIS PAPER? HOW CAN THEY BE MITIGATED? None. WHAT EQUALITY-RELATED RISKS MAY ARISE AS A RESULT OF THIS PAPER? HOW WILL THESE BE MITIGATED? None. DOES THIS PAPER HELP ADDRESS ANY EXISTING HIGH OR EXTREME RISKS FACING THE ORGANISATION? IF SO WHAT ARE THEY AND HOW DOES THIS PAPER REDUCE THEM? None. PLEASE DESCRIBE ANY POSSIBLE CONFLICTS OF INTEREST ASSOCIATED WITH THIS PAPER. None. PLEASE IDENTIFY ANY CURRENT SERVICES OR ROLES THAT MAY BE AFFECTED BY ISSUES WITHIN THIS PAPER: None. Footnote: Members of NHS Salford Clinical Commissioning Group Primary Care Commissioning Committee will read all papers thoroughly. Once papers are distributed no amendments are possible. Page 2 of 8
87 Date of Meeting 28 th November 2017 Agenda Item No 6(a) Document Development Public Engagement Process Yes No (Please detail the method ie survey, event, consultation) Clinical Engagement (Please detail the method ie survey, event, consultation) Has due regard been given to Equality Analysis (EA) of any adverse impacts? (Please detail outcomes, including risks and how these will be managed) Legal Advice Sought Presented to the Commissioning Committee Presented to the Health and Wellbeing Board Presented to the Integrated Joint Commissioning Board Presented to any other groups or committees, including Partnership Groups (Please specify in comments) Not Applicable X X X X X X X X Comments and Date (i.e. presentation, verbal, actual report) Outcome Note: Please ensure that it is clear in the comments and date column how and when particular stakeholders were involved in this work and ensure there is clarity in the outcome column showing what the key message or decision was from that group and whether amendments were requested about a particular part of the work. Page 3 of 8
88 Date of Meeting 28 th November 2017 Agenda Item No 6(a) 1 Executive Summary Primary Care Finance Report This paper provides the Primary Care Commissioning Committee (PCCC) with a view of the primary care budgets and finances. This includes budgets for locally commissioned services and prescribing which have historically been managed by the CCG, and delegated cocommissioning budgets for primary medical services. The paper provides PCCC members with information on: GP services (including Primary Care contracts - GMS PMS and APMS) Locally Commissioned Services, including the Salford Standard contracts Prescribing and other budgets 2 Primary Medical Services Forecast YTD YTD YTD Financial Summary Table Annual budget Forecast Variance Budget Actual Variance '000 '000 '000 '000 '000 '000 GP Services General Practice - GMS 16,665 16, ,721 9, General Practice - PMS 6,809 6, ,972 3, General Practice - APMS 1,962 1, ,145 1, QOF 2,878 3, ,678 1, Enhanced services - DESs Enhanced services - Other 1, Premises Cost Reimbursement 4,388 4, ,559 2, Dispensing/Prescribing Drs (PA Drugs) Other GP Services 1,189 1, Void & Subsidy 1,446 1, Total PRC Cost Centre 37,401 36, ,596 21, Financial Summary The table details the CCG allocation, 2017/18 GP services budgets and the total forecast operating costs for 2017/18 as at month 7. The overall reported year to date position for primary care services at month 7 is an underspend of 316k year-to-date ( 60k overspend at month 5) and a forecast underspend of 414k ( 179k underspend at month 5). The main reason for the favourable movement is the finalisation of the cost for the 2016/17 Directed Enhanced Services, which was 239k less than estimated and additional rates refunds of 211k. These have been partly offset by additional charges from Community Health Partnerships of 155k. Page 4 of 8
89 Date of Meeting 28 th November 2017 Agenda Item No 6(a) 2.2 Primary Care Contracts (GMS, PMS and APMS) GMS: The annual budget for GMS is 16.7m and comprises of the global sum payment, Minimum Practice Income Guarantee (MPIG) payment and also includes deductions for opt outs. The current budget is based on the revised GMS rate for 2017/18 of per weighted patient, and including all the associated opt out rates and MPIG rate for 2017/18. The current forecast is based on the revised GMS rate for 2017/18 and the weighted list size for quarter three. This area is reporting a year to date underspend of 87k and the forecast underspend is 96k. PMS: The annual budget for PMS is 6.8m. PMS contract budgets have been set in line with the current contract status as at 1st April 2017, with applied uplifts as per national guidance and local demographic growth. PMS is showing a year-to-date underspend of 5k and a year-end forecast underspend position of 34k. APMS: The annual budget for APMS is 2m and is showing a year-to-date underspend of 61k and forecast underspend is 264k, which reflects the savings generated as a result of the reprocurement of The Heights practice. This revised contract for the Heights will be reimbursed at the same rate per patient as the GMS contracts ( per weighted patient), commencing in October QOF The budgets were based on the achievement for 2015/16 in the absence of 2016/17 achievement data, amended for an expected reduction in 2016/17 achievement. The QOF sign-off process for 2016/17 is almost complete with just one practice outstanding. This area is reporting a year-to-date overspend of 196k and the forecasted overspend is 334k, as the expected reduction will not materialise. 2.4 Enhanced Services The annual budget for enhanced services totals 1.9m and comprises 0.8m for directed enhanced services (DESs) for minor surgery, learning disabilities, extended hours and violent patients and 1.1m for workforce and practice development. All practices have signed up to the DESs and the forecasts reflect this. At the end of each year, an estimate is included in the accounts for anticipated achievement against the enhanced services. The actual achievement is not known at the time of completed the accounts, therefore an estimate is used. Final achievement against the 2016/17 enhanced services has been calculated which has resulted in actual costs being lower than the estimated costs. This has resulted in a financial benefit in the 2017/18 financial position. The actual costs of the DESs for 2016/17 are 239k less than previously estimated, mainly in respect of the avoiding unplanned admissions and extended hours DESs. 2.5 Premises Costs reimbursement The annual budget for premises cost reimbursement is 4.4m. Premises costs comprise of rent, rates, water and clinical waste costs. The forecast outturn has been amended to a forecast underspend of 288k (breakeven at month 5). The main reason for this is the outcome of the national exercise regarding the refund of rates and water rates. Although this was expected and factored into the budget setting process for 2017/18, refunds received for prior years have exceeded the estimate. Whilst this is a non recurrent benefit for 2017/18, there will be an element of recurrent savings to be released from 2018/19 onwards. Page 5 of 8
90 Date of Meeting 28 th November 2017 Agenda Item No 6(a) 2.6 Premises Costs Building Void, Subsidy and Bookable costs The combined budget for building void, subsidy and bookable costs for Community Health Partnerships (CHP) and NHS Property Services (NHSPS) is 1.4m. The budget has been set on 2016/17 outturn which included the market rent increases, current occupancy rates and further information received on the billing models. Revised billing schedules for 2017/18 have been produced and shared by CHP, and these indicate a cost pressure of 155k compared to budget. Revised schedules are yet to be received from NHSPS. 2.7 Other GP Services The annual budget for other GP Services is 1.2m and includes seniority payments, costs for suspended GPs, CQC fees, indemnity fees, interpretation costs and locum costs in relation to maternity, paternity and sickness. There have been significant changes in the Statement of Financial Entitlements (SFE) from the 1st April 2017 which were outlined in the previous finance report to Primary Care Commissioning Committee. To date the only material cost pressures are in relation to interpretation costs, and the cost of a suspended GP locum; all other elements are broadly in line with the new estimated budgets. Budgets for interpretation costs have been maintained at the 2016/17 level for 2017/18, although this was an area of overspend in 2016/17. Detailed discussions are ongoing with the service providers to ensure that the CCG is only being invoiced for Salford primary care patients, and only for services requested by practices. The year to date position is 95k overspent with a forecast overspend of 177k ( 164k forecast overspend at month 5). The CCG has undertaken a significant amount of work in analysing and challenging the charges from these providers to ensure accuracy, and booking procedures have been amended and clarified. A paper outlining the commissioning options for this service will be presented to a future meeting of the Primary Care Commissioning Committee. 3 Locally Commissioned Services Annual Forecast YTD YTD YTD Forecast Financial Summary Table budget Variance Budget Actual Variance '000 '000 '000 '000 '000 '000 Locally Commissioned Services: Salford Standard 6,223 6, ,635 4,635 0 Extended Access 1,345 1, Cataract Referrals Low Vision Aids Intraocular Hypertension Homeless service palliative care Minor Ailments Scheme ,808 7, ,477 5,482 5 Page 6 of 8
91 Date of Meeting 28 th November 2017 Agenda Item No 6(a) 3.1 Salford Standard The recurrent annual budget requirement for the Salford Standard is 7.3m but this has been reduced to 6.2m in 2017/18 to reflect the anticipated performance in this second year of operation. The budget comprises a fixed payment amount of 25% for signing the contract and 25% for submission of an acceptable implementation plan. The remaining 50% is available for achievement of the KPIs associated with the standards. The upfront payment for signing the contract has been released for all practices with one exception. The 25% payment for the approved implementation plans has also been made. In relation to KPI achievement, it was agreed to pay GP practices up front, on an assumed level of achievement against KPIs, in order to ensure a regular cash flow to GP practices. Two quarterly payments have been made in June and September with quarter three due for payment in December. These payments assumed that the practice will achieve 60% of the KPIs. If the practice achieves higher than this threshold, then a final payment will be made when the quarter four information has been validated. Conversely, if a practice s achievement is below this 60% threshold, then there will be a clawback of monies already paid. Practices are being monitored on their achievement of the KPIs and average overall achievement to date is 36%, however one practice has already exceeded the expected 60% mark. Although the final achievement for 2017/18 will only be known in the first quarter of 2018/19, a more informed assessment of the likelihood of an under or overspend against this budget will be made following quarter three. 3.2 Extended Access An amount of 0.8m has been set aside in 2017/18 for the Salford Wide Extended Access scheme, and this will increase to 1.3m recurrently for 2018/19. The remaining 0.5m for extended access relates to the three non-recurrent pilots which will cease during 2017/18 as the Salford Wide scheme is rolled out. To date, one of the pilots has been subsumed into the Salford wide scheme and this is the reason for the forecast underspend of 146k. 4 Prescribing and Other Financial Summary Table Annual budget Forecast Forecast Variance YTD YTD YTD Budget Actual Variance '000 '000 '000 '000 '000 '000 Prescribing: Main line 41,194 42,694 1,500 24,030 23, Optum Health Solutions Licence Total Prescribing 41,278 42,776 1,498 24,079 23, Out of Hours 1,669 1, Home Oxygen Central Drugs 1,214 1, Total Other 3,219 3, ,878 1, Page 7 of 8
92 Date of Meeting 28 th November 2017 Agenda Item No 6(a) 4.1 Prescribing The forecasting tool for the primary care prescribing budget provided by the Business Services authority (BSA) has this month predicted a 0.7m underspend on the annual primary care prescribing budget. This is based on actual spend up to August However, the CCG does not think that the BSA forecast includes the impact of the ongoing instability in the pricing of generic drugs listed in Category M of the Drug Tariff and the increase in pressure for NCSO (no cheaper stock obtainable) drugs. The CCG s Head of Medicine Optimisation has worked with finance department and calculated the underlying forecast position will be an overspend of 1.5m. 4.2 Other The out of hours service is provided by Salford Royal and is part of the Integrated Care budget. Home Oxygen and central drugs expenditure is received from the NHS Business Services Authority and forecasts are calculated based on 2016/17 average and actuals to date in 2017/18. 5 Recommendation 5.1 The Committee is asked to note the report. Steve Dixon Chief Finance Officer Page 8 of 8
93 Agenda Item No 6 (b) Primary Care Commissioning Committee Work Plan 2017/18 According to the terms of reference, the role of the Primary Care Commissioning Committee is to carry out the functions relating to the commissioning of primary medical services. Committee Function Current CCG Work Plan Nov 17 Update GMS, PMS and APMS contracts (including the design of PMS and APMS contracts, monitoring of contracts, taking contractual action such as issuing branch/remedial notices, and removing a contract) - Re-procurement of The Heights Medical Practice - Commissioning of a new practice in Ordsall Complete In progress Newly designed enhanced services ( Local Enhanced Services and Directed Enhanced Services ) - Update reports from the Primary Care Operational Group - Update reports from the Primary Care Quality Group - Monitoring of the Care Homes Medical Practice Key Performance Indicators - Contractual actions will be taken as necessary - Contract Transfers to Salford Primary Care Together - Increasing patient uptake of Patient Online across Salford - Monitoring and reviewing the implementation of the Salford Standard via the Primary Care Quality Group Reports Ongoing Ongoing In progress As required In progress In progress Ongoing 1
94 Agenda Item No 6 (b) - Implement the recommendations of the Violent Patient Enhanced Service review Review pending Design of local incentive schemes as an alternative to the Quality Outcomes Framework (QOF) Decision making on whether to establish new GP practices in an area - Implement the recommendations of the Care of Review in progress the Homeless Local Commissioned Service review Nothing currently planned although the Salford NA Standard does incentivise quality over and above the requirements of QOF - Review of GP capacity in Ordsall September 2018 Approving practice mergers Making decisions on discretionary payment (e.g., returner/retainer schemes) To plan, including needs assessment, primary medical care services in Salford To undertake reviews of primary medical care services in Salford This will be undertaken as necessary along with decisions regarding other contract variations, e.g. practice boundary changes and list closures. - Decisions to be made by PCCC on a case by case basis - A business case for the re-current funding of the Salford Standard - Undertake an assessment of primary care capacity by neighbourhood and use this to prioritise future capacity expansion plans - As required dependent upon the outcome of the monitoring and review of primary medical services. - Review the Care of the Homeless Local Commissioned Service Merger decision made at September 2017 meeting As required November 2018 In progress As required In progress 2

95 Agenda Item No 6 (b) - Review the Violent Patient Enhanced Service 2018 To co-ordinate a common approach to the commissioning of primary care services generally - Review and update of the Salford Standard for 2018/19 - Annual review report for the Salford Standard - Monitoring and reviewing the Care of the Homeless Local Commissioned Service via the Primary Care Operational Group Reports - Monitoring and reviewing the Directed Enhanced Services - Keep abreast of local and national strategy and consider the implications for the CCG and the commissioning of primary medical services November 2017 Complete for 2016/17 Complete for 2016/17 Complete for 2016/17 As required To manage the budget for commissioning of primary medical care services in Salford - Oversee the delivery of the projects receiving funding via the GM Primary Care Investment agreement - Monthly budget monitoring reports Ongoing 6mthly reports from March 2018 onwards 3
96 Agenda Item No 7(a) NHS SALFORD CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE AGENDA ITEM NO 7 (A) Item for Information 28 November 2017 REPORT OF: Harry Golby, Head of Service Improvement DATE OF PAPER: November 2017 SUBJECT: IN CASE OF QUERY PLEASE CONTACT: STRATEGIC PRIORITIES: Quality Community Based Care Primary Care Operational Group Report Anna Ganotis, Head of Service Improvement (Primary Care) Anna.ganotis@nhs.net Please tick which strategic priorities the paper relates to: Integrated Care In Hospital Care Long Term Conditions and Mental Health Effective Organisation PURPOSE OF THIS PAPER: The Primary Care Operational Group (PCOG) is responsible for overseeing and managing the delivery of the Medical and Task Functions as specified by NHS England. The group is required to submit recommendations for decision making / ratification to the Primary Care Commissioning Committee (PCCC). Therefore, this paper provides an update on the work that is overseen by the PCOG. RECOMMENDATION OF THIS PAPER: The PCCC is asked to: - Note the contents of this report (Please see further explanatory requirements overleaf) Page 1 of 10
97 Agenda Item No 7(a) Further explanatory information required HOW WILL THIS BENEFIT THE HEALTH AND WELL BEING OF SALFORD RESIDENTS OR THE CLINICAL COMMISSIONING GROUP? WHAT RISKS MAY ARISE AS A RESULT OF THIS PAPER? HOW CAN THEY BE MITIGATED? WHAT EQUALITY-RELATED RISKS MAY ARISE AS A RESULT OF THIS PAPER? HOW WILL THESE BE MITIGATED? DOES THIS PAPER HELP ADDRESS ANY EXISTING HIGH OR EXTREME RISKS FACING THE ORGANISATION? IF SO WHAT ARE THEY AND HOW DOES THIS PAPER REDUCE THEM? PLEASE DESCRIBE ANY POSSIBLE CONFLICTS OF INTEREST ASSOCIATED WITH THIS PAPER. PLEASE IDENTIFY ANY CURRENT SERVICES OR ROLES THAT MAY BE AFFECTED BY ISSUES WITHIN THIS PAPER: The Primary Care Operational Group is working to improve the quality of care in primary care across Salford. NA update paper. Risks will be managed within each individual programme of work. NA update paper. Risks will be managed within each individual programme of work. NA As a GP-led organisation, conflicts of interest are not entirely avoidable. This report concerns recommendations and decisions made regarding individual GP practices, so there is a potential conflict of interest associated with each decision. These are managed via the CCG s policy. No GP practices are represented on the PCOG. NA Footnote: Members of NHS Salford Clinical Commissioning Group Primary Care Commissioning Committee will read all papers thoroughly. Once papers are distributed no amendments are possible. Page 2 of 10
98 Agenda Item No 7(a) Primary Medical Care Commissioning Principles 1. Investment in general practice will continue to, as a minimum, be in line with the recommendations of the General Practice Forward View in order to strengthen resilience and sustainability of general practice by building capacity and capability. 2. The CCG will seek to maximise opportunities to commission primary medical services at scale (for example through a GP provider organisation) where this is expected to improve patient experience or be more efficient. 3. When commissioning decisions need to be made regarding primary medical service contracts, an options appraisal will be undertaken in order to determine the option that is most likely to meet the needs of the population group and most likely to deliver the CCG s strategic ambitions. This may not always be re-procuring a like for like service. 4. The CCG will commission general practice services from providers that are able to demonstrate good outcomes, value for money and care for patients that is holistic and provided to consistently high standards of quality and safety. 5. The CCG will seek to engage with the local population and acknowledge patient views when making primary medical services commissioning decisions. 6. The CCG will ensure that the primary medical services in Salford continue to meet the needs of a growing and increasingly diverse population. This will include promoting patient choice and equality and seeking to ensure that commissioning decisions improve the economic, social and environmental wellbeing of Salford. 7. The CCG will encourage and support general practice to play a pivotal role within the emerging accountable care system, with leadership through federated arrangements. 8. The CCG will embrace opportunities to commission primary medical services in an integrated way where this has benefits for patient care, e.g. through pooling budgets for health and social care services, or commissioning community services to be delivered on a neighbourhood basis from multidisciplinary integrated teams. Addressed in this paper? Yes Ordsall Pilot Project and estates projects Yes Salford Health Matters Contract Transfer and Ordsall Pilot Project Yes Limefield / Newbury Green contract merger Yes Care of the Homeless Review Yes Ordsall Pilot Project / Newbury Green contract merger / Care of the Homeless review Yes Ordsall Pilot Project / 7-day Access / General Practice Capacity Benchmarking / Care of the Homeless review No No Page 3 of 10
99 Agenda Item No 7(a) 9. The CCG will embrace new contracting mechanisms where they support the viability, sustainability and resilience of general practice, including practices working collaboratively in neighbourhood groups to deliver agreed outcomes and to share resources such as staff and back office services. 10. The CCG will support making general practice in Salford becoming an attractive place to work. This will include encouraging and supporting general practice to: embrace innovation and new ways of working; adapt and skill-up the workforce to meet patient need; make greater use of technology; and work from modern and fit for purpose premises. 11. The CCG, as a commissioner of primary medical services, cannot assume responsibility for, or become involved in, matters relating to the management of GP practices, including practice disputes and legal matters. 12. The CCG will proactively work with partners, including Salford Primary Care Together (as Salford s GP provider organisation) and the Salford and Trafford Local Medical Committee, in a transparent and supportive manner. Yes Ordsall Pilot Project / Salford Health Matters Contract Transfer Yes Ordsall Pilot Project / General Practice Capacity Benchmarking / Estates Update / Patient Online Yes Leaving the Eccles Gateway Medical Practice to resolve their managerial issues, although continuing to provide support as necessary Yes The LMC attend PCOG meetings and we are working with SPCT on a number of projects, including the Ordsall Pilot Project Footnote: Members of NHS Salford Clinical Commissioning Group Primary Care Commissioning Committee will read all papers thoroughly. Once papers are distributed no amendments are possible. Page 4 of 10
100 Agenda Item No 7(a) Document Development Public Engagement Process Yes No (Please detail the method ie survey, event, consultation) Clinical Engagement (Please detail the method ie survey, event, consultation) Has due regard been given to Equality Analysis (EA) of any adverse impacts? (Please detail outcomes, including risks and how these will be managed) Legal Advice Sought Presented to the Commissioning Committee Presented to the Health and Wellbeing Board Presented to the Integrated Joint Commissioning Board Presented to any other groups or committees, including Partnership Groups (Please specify in comments) Not Applicable Comments and Date (i.e. presentation, verbal, actual report) Outcome Note: Please ensure that it is clear in the comments and date column how and when particular stakeholders were involved in this work and ensure there is clarity in the outcome column showing what the key message or decision was from that group and whether amendments were requested about a particular part of the work. Page 5 of 10
101 Agenda Item No 7(a) 1 Executive Summary Primary Care Operational Group Report This paper provides an update on the work that is overseen by the Primary Care Operational Group (PCOG). This includes updates on: practice specific contractual issues; core contractual requirements; enhanced services; general practice capacity; and estates projects. The Primary Care Commissioning Committee is asked to note the content of this report. 2 Introduction and Background 2.1 The Primary Care Operational Group (PCOG) provides an update report to every Primary Care Commissioning Committee (PCCC) meeting. 2.2 This report covers the PCOG meetings held in October and November Practice Contractual Issues Broughton Neighbourhood 3.1 Limefield Medical Practice Merger with Newbury Green Medical Practice The PCCC made the decision to approve the merger of the Limefield Medical Practice and the Newbury Green Medical Practice in September A provisional merger date of 30 April 2018 has been identified. It was noted that there has been some difficulty in arranging a meeting between the two practices, the CCG and the Greater Manchester Health and Social Care Partnership (GMHSCP). The importance of securing engagement from both practices was discussed. 3.2 Dr Davis Medical Practice Dr Davis s Medical Practice recently underwent a CQC inspection. The overall outcome was Good, however, the inspection highlighted some areas where the practice was not compliant in respect of the GMS contractual requirements. The practice was asked to submit the necessary assurances which have now been submitted and approved. Therefore, no further contractual action will be taken. Eccles and Irlam Neighbourhood 3.3 Dr Singh & Partners PCOG received an update regarding some ongoing organisational issues at the practice. 3.4 Irlam Group Practice It was noted that following their Requires Improvement inspection in March 2017, the CQC undertook a focused inspection at the Irlam Group Practice in September 2017 to check that the practice had met the requirements of the Warning Notices. Some improvements were noted, but further improvements were still required to ensure that safety is maintained. It was noted that a temporary practice Page 6 of 10
102 Agenda Item No 7(a) manager has been working at the practice, but concerns were raised regarding sustainability once she leaves. There are plans for the practice to recruit a senior administrator. 3.5 Salford Health Matters It was reported that following an article in the CCG s member newsletter regarding contractual requirements in relation to the subcontracting of clinical services, Salford Health Matters have reported (as previously communicated to the CCG) that they subcontract some telephone consultations to Care UK. Any necessary actions will be picked up via the Salford Health Matters Contract Meeting. Ordsall and Claremont Neighbourhood 3.6 Sorrel Group Practice A member of the CCG s Service Improvement Team has now visited the Sorrel Group Practice to discuss the practice plan that was submitted with the paperwork for the practice to become a single-handed contract holder. There are plans for new partners to join the contract and the PCOG were re-assured regarding practice capacity. However, it was agreed that progress against the plan would be reviewed in March The results of an infection control audit at the Sorrel Group Practice were also discussed. 3.7 The Height Medical Practice It was reported that although the report had not yet been published, the outcome from the recent CQC inspection at The Height Medical Practice was an Outstanding rating. This achievement was noted by the group and it was agreed that once the report was been published, the practice should be congratulated. Walkden and Little Hulton Neighbourhood 3.8 Walkden Medical Centre The CCG has received a formal application from the Walkden Medical Centre to close their patient list. The practice have agreed to pause the allotted time that the CCG has to consider the application in order to allow opportunity for the CCG and the GMHSCP to meet with the practice to discuss any support that the practice might require in order to maintain an open list. A visit is scheduled for 30 November Ellenbrook Medical Practice It was noted that the CCG had received an MP letter regarding a constituent s concerns regarding appointment availability at the Ellenbrook Medical Practice. There was also an update on some analysis that the Service Improvement Team had undertaken to look at the ratio of GPs to patient list size following the retirement of two GP partners at the practice. Initial indications were that this was not a concern, but some further analysis is to be undertaken. The PCOG also noted that the Ellenbrook Medical Practice had informally approached the CCG regarding a potential list closure application. Page 7 of 10
103 Agenda Item No 7(a) 4 Core Contractual Issues The Height Medical Practice 4.1 The new contract for The Height Medical Practice came in to force on 1 October Salford Health Matters Contract Transfer 4.2 PCOG members were informed that the application for Salford Health Matters to transfer their contract to Salford Primary Care Together was considered in Part 2 of the September 2017 PCCC meeting and the application was approved in principle, with some caveats / recommendations. The CCG s Chief Accountable Officer has formally written to Salford Primary Care Together to communicate the decision. 7-Day Access / Practice Closures 4.3 Following some work that had been undertaken by PCOG members to review practices who still had half-day closures, some analysis was undertaken to assess where Salford practices are not open for their full core contractual hours (8am 6:30pm Monday Friday). A number of practices, whilst not closing for a half day, are routinely shut at either end of the working day or over lunchtime. Therefore, it was agreed that some additional work would be undertaken to audit the opening times data against practice Salford Standard submissions so that the CCG can take steps to ensure that all practices are fulfilling their contractual responsibilities. Cost Rent 4.4 PCOG members were told the cost rent for GP practices has not been reviewed since the transfer from PCTs in April The GMHSCP will be writing to practices to review whether or not they are still eligible for cost rent / notional rent. 2016/17 QOF Performance 4.5 A report compiled by the GMHSCP which breaks down 2016/17 QOF performance was shared with group members. It was agreed that this information would be used to feed in to the CCG practice quality assurance visits. Patient Online 4.6 At the November PCOG meeting, the CCG s Head of Business Intelligence & Information Technology attended to give an update on Patient Online. She will return on a quarterly basis to provide updates. It was explained that there has been a delay in obtaining the August 2017 data, so the latest data that the CCG holds on performance against the 20% target is the July 2017 data that was shared with the PCCC in September Up until now, the CCG has taken a supportive approach to helping practices to achieve the 20% target, however, it has been agreed that for those practices still not achieving, a more formal approach now needs to be taken. Therefore, there is a plan to write to all practices not achieving the target, asking them to submit an action plan, Page 8 of 10
104 Agenda Item No 7(a) with a view to more formal contractual action being taken for those practices who do not achieve at the end of the financial year. Some additional support mechanisms were also discussed, including a joint LMC / CCG workshop and some additional support materials for practices. 5 Enhanced Services Care of the Homeless Locally Commissioned Service Review 5.1 Work has begun to undertake a review of the Care of the Homeless Locally Commissioned Service which is delivered by Salford Health Matters. The intention is for a report to come to PCCC in early Avoiding Unplanned Admissions Clawbacks 5.2 The GMHSCP have been facilitating a process to clawback funding from those practices who did not achieve all components of the Avoiding Unplanned Admissions Enhanced Service in 2016/17. The relevant practices have been written to and any appeals will need to be considered by the CCG. 6 General Practice Capacity Ordsall Commissioning Project 6.1 Progress on implementing the Ordsall Pilot Project has slowed whilst Salford Primary Care Together (SPCT) have been focusing upon securing innovation monies to support the elements of the business case which focused upon neighbourhood working. The CCG has communicated to SPCT that these will be treated as two separate projects, with different reporting and governance routes. General Practice Capacity Benchmarking 6.2 A meeting was held between the CCG, Salford City Council and Salford Primary Care Together in order to move forward work on the general practice capacity benchmarking exercise. The aim is to produce something to share with the neighbourhoods by the end of the year. 7 Estates and Facilities Update 7.1 At the October 2017 meeting, an update was given regarding the CCG s three major primary care estates projects: - Progress is being made in relation to the Little Hulton development - A stakeholder workshop is to be held in order to move forward the Lower Broughton project. - Some progress has been made regarding the Irlam development. Page 9 of 10
105 Agenda Item No 7(a) 7.2 PCOG noted that due to population growth in the Ordsall area, there is a need to reconsider the CCG s Strategic Estates Strategy as there may be a gap. 7.3 PCOG members were informed that an improvement grant has been approved which will increase clinical space at the Cleggs Lane Medical Practice. 8 Recommendations 8.1 The PCCC is asked to: - Note the contents of this report Anna Ganotis Head of Service Improvement Page 10 of 10
106 Agenda Item No 7(b) NHS SALFORD CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE AGENDA ITEM NO 7(b) Item for Information 28 November 2017 REPORT OF: Francine Thorpe Director of Quality & Innovation DATE OF PAPER: 17/11/2017 SUBJECT: Primary Care Quality Group Review Paper IN CASE OF QUERY PLEASE CONTACT: STRATEGIC PRIORITIES: Quality Community Based Care Lisa Best Quality Assurance Manager Please tick which strategic priorities the paper relates to: Integrated Care In Hospital Care Long Term Conditions and Mental Health Effective Organisation Page 1 of 11
107 Agenda Item No 7(b) PURPOSE OF THIS PAPER: This paper provides an update on actions taken to improve the quality of primary care. The Primary Care Quality Group (PCQG) is required to submit recommendations for decision making / ratification to the Primary Care Commissioning Committee (PCCC). Therefore, this paper provides an update on the work that is overseen by the PCQG. RECOMMENDATION OF THIS PAPER: Insert the recommendations for this paper, such as decisions, approvals or importance information to note 1. Note the contents of this report and the progress made in developing the quality and safety agenda within primary care. (Please see further explanatory requirements overleaf) Page 2 of 11
108 Agenda Item No 7(b) Further explanatory information required HOW WILL THIS BENEFIT THE HEALTH AND WELL BEING OF SALFORD RESIDENTS OR THE CLINICAL COMMISSIONING GROUP? The Primary Care Quality Group is working to improve the quality of care in primary care across Salford. WHAT RISKS MAY ARISE AS A RESULT OF THIS PAPER? HOW CAN THEY BE MITIGATED? NA update paper. Risks will be managed within each individual programme of work. WHAT EQUALITY-RELATED RISKS MAY ARISE AS A RESULT OF THIS PAPER? HOW WILL THESE BE MITIGATED? NA update paper. Risks will be managed within each individual programme of work. DOES THIS PAPER HELP ADDRESS ANY EXISTING HIGH OR EXTREME RISKS FACING THE ORGANISATION? IF SO WHAT ARE THEY AND HOW DOES THIS PAPER REDUCE THEM? None. PLEASE DESCRIBE ANY POSSIBLE CONFLICTS OF INTEREST ASSOCIATED WITH THIS PAPER. None. PLEASE IDENTIFY ANY CURRENT SERVICES OR ROLES THAT MAY BE AFFECTED BY ISSUES WITHIN THIS PAPER: Quality by its very nature is everyone s business therefore it will impact across all areas of care planning and delivery. Footnote: Members of NHS Salford Clinical Commissioning Group Primary Care Commissioning Committee will read all papers thoroughly. Once papers are distributed no amendments are possible. Page 3 of 11
109 Agenda Item No 7(b) Document Development Public Engagement (Please detail the method i.e. survey, event, consultation) Clinical Engagement (Please detail the method i.e. survey, event, consultation) Process Yes No Has due regard been given to Equality Analysis (EA) of any adverse impacts? (Please detail outcomes, including risks and how these will be managed) Legal Advice Sought Presented to the Commissioning Committee Presented to the Health and Wellbeing Board Presented to the Integrated Joint Commissioning Board Presented to any other groups or committees, including Partnership Groups (Please specify in comments) Not Applicable X X X X X X X X Comments and Date (i.e. presentation, verbal, actual report) Outcome Note: Please ensure that it is clear in the comments and date column how and when particular stakeholders were involved in this work and ensure there is clarity in the outcome column showing what the key message or decision was from that group and whether amendments were requested about a particular part of the work. Page 4 of 11
110 Agenda Item No 7(b) 1 Executive Summary Primary Care Quality Group Review Paper This paper provides an overview on a number of areas that are used to measure the quality and safety of patient care within the primary care services commissioned by NHS Salford CCG. An update is provided on issues that have been discussed at the regular Primary care Quality Group meetings along with information on how any themes or trends that have been identified and associated actions taken. Key issues discussed with individual practices are also outlined along with information on how any concerns are being addressed. The Primary Care Commissioning Committee is asked to note the content of this report. 2 Introduction and Background 2.1 The Primary Care Quality Group (PCQG) provides an update report to every Primary Care Commissioning Committee (PCCC) meeting to ensure that members of PCCC are sighted on the quality of GP practices in Salford. 2.2 This paper provides an overview of issues that have been discussed at the regular Primary Care Quality Group meetings, along with quality and safety information gained from other sources, including CQC, the quality assurance dashboard and CCG quality assurance visits. 2.3 This report covers the PCQG meeting held in September 2017 and any verbal updates provided ahead of the November 2017 meeting. 3 Patient Safety 3.1 Medicines Optimisation Patient Safety Alert In April 2017 the MHRA released a Patient Safety Alert asking all organisations providing NHS funded care where valproate is prescribed or dispensed to undertake systematic identification of girls and women who are taking valproate, and ensure the MHRA resources are used to support them to make informed choices. This work had a deadline of the 6th October 2017 to be implemented. 3.2 The CCG medicines optimisation team pharmacists have led a piece of work to ensure compliance with this alert in Salford within the time frames requested. This work identified 124 women registered with GP practices that are currently prescribed this medication and required a specialist review to discuss their ongoing treatment options. 3.3 Members of the Medicines Optimisation team have worked closely with GP practices and the practice pharmacists to ensure that these patients have been reviewed and enabled to make an informed choice about their ongoing management. All practices Page 5 of 11
111 Agenda Item No 7(b) 4 CQC engaged with this process, recognising the safety issues that required a timely response. 4.1 To date, 44 of our 45 GP Practices have been inspected by CQC. Of these, 3 have now been rated Outstanding, 39 rated Good and 2 Requires Improvement. No practices are currently rated Inadequate. 4.2 Care Homes Practice was inspected as part of Salford Royal s overall inspection in There are currently no plans for the CQC to perform a full inspection at this practice. The CCG have expressed concern to CQC around the limitations this provides in terms of assurance and are currently in discussions with CQC about this matter. In the absence of a full CQC inspection the CCG will be undertaking a quality assurance visit at the Care Homes Practice on 29th November. 4.3 The following inspection reports were published between June 2017 and October 2017: Dearden Avenue Medical Practice (Overall rating: Good ) Dr Davis Medical Practice (Overall rating: Good ) Springfield Medical Practice (Overall rating: Good ) Manchester Road East Medical Practice (Overall rating: Good ) The Sides Medical Practice follow-up (now rated Good in all categories) 4.4 Manchester Road East Medical Practice has been commended by the CCG in their recent inspection report for improving in their overall rating from Inadequate. The CCG, LMC and GMHSCP have all worked closely with the Practice to support the staff in meeting the required standards and the Practice itself has worked hard to make all necessary improvements to increase their overall rating to Good. The CCG is now assured that the Practice is operating safely and providing good quality care for patients and a letter of congratulations has been issued on behalf of the CCG. 4.5 Following recent inspection, Dr Davis Medical Practice has also improved its overall rating from Requires Improvement to Good. The Practice continues to be rated as Requires Improvement in the Safe domain, with improvements still to be made around monitoring of blank prescriptions and calibration of medical equipment. CQC will now schedule a follow-up visit within the next 6 months to ensure all agreed actions have been met. 4.6 CQC has recently performed a follow-up visit at Dearden Avenue Medical Practice and issued the Practice with an overall rating of Good. The CQC confirmed that the improvements required under the Safe domain had been implemented. 4.7 On initial inspection in August 2017, The Sides Medical Practice were awarded a rating of Good overall, but requiring improvement in the Safe domain. Following a follow-up visit, the Practice has now been awarded a rating of Good in all domains. 4.8 Following inspection in March 2017, the CQC rated Irlam Group Pratice as Requires Improvement and issued the Practice with a legal warning notice in relation to Page 6 of 11
112 Agenda Item No 7(b) Regulation 12 Safe care and treatment and Regulation 13 Safeguarding service users from abuse and improper treatment. The main areas for concern were that: The Practice did not have a robust system in place for audit or safeguarding, There was no regular communication between partners and staff There were no clear methods to discuss performance. Clinical staff were not always aware of relevant clinical guidelines There was no system in place to receive and disseminate patient safety and medicine alerts There was no robust system in place for investigating complaints The Practice did not have a Legionella risk assessment. 4.9 Irlam Group Practice has since engaged with the CCG and partners to receive support in addressing the areas requiring improvement. With the additional support of temporary management from a practice from a neighbouring CCG, the Practice is now working towards making the necessary improvements. Having met with the temporary Practice Manager, the CCG is assured that the correct changes are being made, but have expressed some concern to the Practice around the long-term limitations of the new temporary staffing measures. The CQC performed a focussed visit in September 2017 to ensure the improvements around the legal notices had been implemented. Although satisfied that legal requirements have now been met and that some improvement has been made, the CQC noted that further requirements were still required to ensure safety was maintained. In particular, there were still some improvements to be made to the safety and medicines alert system to ensure alerts were dealt with in a timely manner. A full re-inspection will take place on 1 st December The CQC has confirmed that rating of Outstanding for The Heights Medical Practice has been approved by the CQC Board and the full report has been published on the CQC website The issue of practices failing to have sufficient Legionella risk assessments has been highlighted in a number of CQC reports and has subsequently been addressed with the Infection Control Team, who have published additional guidance in the members newsletter Limefield Medical Practice has recently re-registered with CQC, following the change of premises, which means they are likely to be inspected in the coming months. The Practice has now been granted approval to merge with Newbury Green, therefore the new practice will also be inspected, following the merger CQC has announced that, as part of on-going improvement work, it will be reinspecting up to 10% of Salford practices currently rated as Good in the coming months. The names of the practices are yet to be announced. 5 Salford Standard 5.1 The average year-to-date (YTD) practice performance at the end of Q1 is 25.4%. Using the early warning system from the escalation policy and the YTD performance Page 7 of 11
113 Agenda Item No 7(b) at the end of Q1, all practices are at red status, <60%. This is to be expected at this early stage in monitoring performance, with practices expected to demonstrate gradual progression towards these throughout the year. Q2 data has now been submitted and will be detailed in the next report. 5.2 In accordance with the Salford Standard Escalation Policy, the six practices who are at the bottom of the dashboard have been contacted and advised that should they remain within the bottom five and at red status once quarter two data has been validated, they will enter the support and escalation process. These practices have been offered additional support and training. Should they remain in the same position at the end of Q2, they will enter into the formal escalation process and be asked to provide action plans. 5.3 A Salford Standard Design Group has been established with the responsibility of reviewing and recommending amendments to the domains and KPIs for the 2018/19 Salford Standard contract. This will be undertaken in conjunction with clinical leads and member practices to ensure that the updated contract for 2018/19 is in place by April As reported previously, the CCG has made the decision not to commission the Salford Standard from one of the practices within the Eccles & Irlam neighbourhood in 2017/18 (as a result of internal issues within the practice) and to seek an alternative provider. Four expressions of interest in the opportunity from other practices within the same neighbourhood were received, but unfortunately, the practice advised that they do not want to co-operate with this process and that although they will not submit evidence to the CCG, they will complete the work agreed for Salford Standard. This means that another provider will not be able to deliver any of the Salford Standard on their behalf. The CCG is therefore, at present, not proposing to progress the expressions of interest any further and will continue to monitor the practice s performance through the Informatica data retrievals at the end of each quarter. 6 Quality Assurance Dashboard 6.1 Final amendments have now been made and the dashboard has been fully automated, as shown in the extract in appendix The dashboard consists of a quality assurance summary sheet, quality assurance ranking sheet (ranking of each practice according to performance on indicators) and an indicator definitions sheet, which explains the detail around each indicator. 6.3 The dashboard will now be used as a quality assurance tool, with key intelligence derived from it being presented at the Primary Care Quality Group. It has already been used in order to inform decision around the quality assurance visits for 2017/18. 7 Quality Assurance Visits 7.1 Following feedback from the Executive Team, it was agreed that the original schedule of vising all 45 practices per year would prove too labour intensive. Page 8 of 11
114 Agenda Item No 7(b) Subsequently, the Terms of Reference for the Primary Care Quality Assurance Visits have now been revised. 7.2 It has now been agreed by the group that there will be 8 visits per year based upon which practices are flagging concerns but with the option for the CCG to call for additional visits where required. 7.3 The schedule of visits for 17/18 has now been drafted. Visits have been planned in collaboration with the Safeguarding, Service Improvement and Infection Control teams to ensure that they are not completed in isolation and that there is no duplication of dates. 7.4 Practices have been chosen based on assessment against the quality assurance dashboard, CQC rating and soft intelligence and those displaying the highest levels of risk in terms of quality will be visited first, followed by a selection of practices that are performing well and where best practice can be identified and shared. 7.5 Each practice will be contacted by the Quality Assurance Team prior to each visit and provided with pre-visit information. 7.6 The first of the 8 visits took place on Friday 10 th November at Sorrell Group Practice. The visit was welcomed by the Practice and enabled CCG representatives to gain assurance around the quality of the service being provided, as well as offer advice on further improvement. 8 Patient Experience 8.1 Patient Experience is a key component of quality and there are a number of mechanisms in place to ensure it remains an area of focus for practices. In addition to the national GP Survey results being published every July, practices are also required to submit an annual patient experience improvement plan in March each year. Comparison of both sets of data enables both the practice and the CCG to identify areas of best practice and areas requiring further improvement. 8.2 The Patient Experience Team has analysed July 2016 GP survey data against July 2017 data and cross-referenced this with information submitted in the 2017 patient experience improvement plans. 8.3 Findings revealed several areas of improvement being considered by practices that directly relate to GP survey results. Ease of getting through to someone at GP surgery on the telephone was the main area practices chose to focus on, and may also have a knock on effect on other questions such as Impression of Waiting Time because if a patient cannot get through on the telephone then impressions of the waiting times for that practice may also be adversely affected. 10 Practices chose to focus upon this area in their improvement plans with 17/18 data showing that 29 practices have improved their figures on this particular survey question since 16/ Performance at Leicester Road Medical Practice has decreased by 13% since 16/17, but they have implemented a number of actions to address this issue. These actions include: Page 9 of 11
115 Agenda Item No 7(b) Practice employed 2 extra staff members to answer phones - extra desks, telephones and handsets Welcome message on phone shortened and provided options menu 8.5 St Andrew s Medical Practice was one of the practices who chose to focus on the area of getting through on the telephone and the Practice has seen initially very positive results. Actions taken to address this area included: Increased the number of staff answering calls (particularly at peak times) Undertaken staff training so that the average call length is reduced New headsets so calls are automatically put through as one call ends Auditing of call length, time taken to answer 8.6 Pendleton have also seen an increase in their figures of 12% and focused upon this area. Pendleton has implanted the following actions: From 8am-9:30am the telephones are redirected to the back reception staff, freeing up patient facing receptionists Work is ongoing to look at changing telephone system to have dedicated numbers for patients to press for appointments and queries. 8.7 The Heights has achieved an annual 35% increase in their performance for getting through on the telephone. Actions taken by the Heights include: Promotion of online service through PPG, newsletter and website to free up phones Ensuring practice has adequate staff to deal with all telephone lines coming into the practice - 3 rings policy 9 Summary 9.1 Improvement in the quality and safety of primary medical services remains a key priority for NHS Salford CCG. Progress continues to be made on a range of projects to support this aim. 10 Recommendations 10.1 PCCC is asked to note the contents of this report and the progress made in developing the quality and safety agenda within primary care. Lisa Best Quality Assurance Manager (Primary Care) Page 10 of 11


116 Agenda Item No 7(b) Appendix 1 Quality Assurance Dashboard Extract Page 11 of 11
NHS Salford Clinical Commissioning Group Governing Body Meeting Wednesday, 30 th November :00 17:00Hrs Salford Suite, St. James s House AGENDA
 NHS Salford Clinical Commissioning Group Governing Body Meeting Wednesday, 30 th November 2016 14:00 17:00Hrs Salford Suite, St. James s House AGENDA Part I Start of NHS Salford Clinical Commissioning
NHS Salford Clinical Commissioning Group Governing Body Meeting Wednesday, 30 th November 2016 14:00 17:00Hrs Salford Suite, St. James s House AGENDA Part I Start of NHS Salford Clinical Commissioning
Primary Care Quality Assurance Framework (Medical Services)
") PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
Salford Integrated Care System Governance Framework: Adult Health and Care Services FINAL
 Salford Integrated Care System Governance Framework: Adult Health and Care Services FINAL 1 Background and Scope Salford is a forward thinking health and social care economy and as such has established
Salford Integrated Care System Governance Framework: Adult Health and Care Services FINAL 1 Background and Scope Salford is a forward thinking health and social care economy and as such has established
Joint framework: Commissioning and regulating together
 With support from NHS Clinical Commissioners Regulation of General Practice Programme Board Joint framework: Commissioning and regulating together A practical guide for staff January 2018 Publications
With support from NHS Clinical Commissioners Regulation of General Practice Programme Board Joint framework: Commissioning and regulating together A practical guide for staff January 2018 Publications
Papers for the. West Kent Primary Care Commissioning Committee (Improving Access) Tuesday 21 st August at 4 4:30 pm
 Tuesday 21 st August at 4 4:30 pm") Papers for the West Kent Primary Care Commissioning Committee (Improving Access) on Tuesday 21 st August at 4 4:30 pm at Hadlow Suite, Hadlow Manor Hotel Hadlow, TN11 0JH 1 of 23 Primary Care Commissioning
Papers for the West Kent Primary Care Commissioning Committee (Improving Access) on Tuesday 21 st August at 4 4:30 pm at Hadlow Suite, Hadlow Manor Hotel Hadlow, TN11 0JH 1 of 23 Primary Care Commissioning
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 12. Date of Meeting: 23 rd March 2018 TITLE OF REPORT:
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 12 Date of Meeting: 23 rd March 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 12 Date of Meeting: 23 rd March 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
Salford Standard Support & Escalation Process
 Salford Standard Support & Escalation Process Job title of lead contact: Service Improvement Manager Version number: Version 2.2 Group responsible for Primary Care Quality Group approving the document:
Salford Standard Support & Escalation Process Job title of lead contact: Service Improvement Manager Version number: Version 2.2 Group responsible for Primary Care Quality Group approving the document:
MEMORANDUM OF UNDERSTANDING
 MEMORANDUM OF UNDERSTANDING Memorandum of Understanding Co-Commissioning Between NHS England Lancashire And South Cumbria And Clinical Commissioning Groups 1 Memorandum of Understanding (MoU) for Primary
MEMORANDUM OF UNDERSTANDING Memorandum of Understanding Co-Commissioning Between NHS England Lancashire And South Cumbria And Clinical Commissioning Groups 1 Memorandum of Understanding (MoU) for Primary
Clinical Commissioning Group Governing Body Paper Summary Sheet For: PUBLIC session PRIVATE session. Date of Meeting: 24 March 2015
 Clinical Commissioning Group Governing Body Paper Summary Sheet For: PUBLIC session PRIVATE session Date of Meeting: 24 March 205 For: Decision Discussion Noting Agenda Item and title: Author: GOV/5/03/20
Clinical Commissioning Group Governing Body Paper Summary Sheet For: PUBLIC session PRIVATE session Date of Meeting: 24 March 205 For: Decision Discussion Noting Agenda Item and title: Author: GOV/5/03/20
Appendix 1: Integrated Urgent Care Service Update. 1. Purpose
 Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Delegated Commissioning of Primary Medical Services Briefing Paper
 Appendix One Delegated Commissioning of Primary Medical Services Briefing Paper 1.0 Introduction Swindon CCG has been jointly commissioning Primary Medical Services with NHS England under co-commissioning
Appendix One Delegated Commissioning of Primary Medical Services Briefing Paper 1.0 Introduction Swindon CCG has been jointly commissioning Primary Medical Services with NHS England under co-commissioning
Oxfordshire Primary Care Commissioning Committee
 Oxfordshire Clinical Commissioning Group Oxfordshire Primary Care Commissioning Committee Date of Meeting: 2 May 2017 Paper No: 15 Title of Paper: Memorandum of Understanding (MOU) for Primary Medical
Oxfordshire Clinical Commissioning Group Oxfordshire Primary Care Commissioning Committee Date of Meeting: 2 May 2017 Paper No: 15 Title of Paper: Memorandum of Understanding (MOU) for Primary Medical
Safeguarding Children and Vulnerable Adults Update
 Appendix 3 Safeguarding Children and Vulnerable Adults Update Executive Summary This paper provides the Salford CCG Governing Body with an update report in relation to the work undertaken by the CCG Safeguarding
Appendix 3 Safeguarding Children and Vulnerable Adults Update Executive Summary This paper provides the Salford CCG Governing Body with an update report in relation to the work undertaken by the CCG Safeguarding
Delegated Commissioning Updated following latest NHS England Guidance
 Delegated Commissioning Updated following latest NHS England Guidance 13th August 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England (Direct
Delegated Commissioning Updated following latest NHS England Guidance 13th August 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England (Direct
QUALITY COMMITTEE. Terms of Reference
 QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
Title of meeting: Primary Care Joint Commissioning Committee (JCC) Committees in Common (CIC). Date of Meeting 12 th April 2016 Paper Number 7
 Committees in Common (CIC). Date of Meeting 12 th April 2016 Paper Number 7") Title of meeting: Primary Care Joint Commissioning Committee (JCC) Committees in Common (CIC). Date of Meeting 12 th April 2016 Paper Number 7 Title Sponsoring Director (name and job title) Sponsoring
Title of meeting: Primary Care Joint Commissioning Committee (JCC) Committees in Common (CIC). Date of Meeting 12 th April 2016 Paper Number 7 Title Sponsoring Director (name and job title) Sponsoring
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
TITLE OF REPORT: Looked After Children Annual Report
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 13 Date of Meeting:..27 th October 2017.. TITLE OF REPORT: Looked After Children Annual Report 2016-2017 AUTHOR: Christine Dixon,
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 13 Date of Meeting:..27 th October 2017.. TITLE OF REPORT: Looked After Children Annual Report 2016-2017 AUTHOR: Christine Dixon,
Internal Audit. Health and Safety Governance. November Report Assessment
 November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
Please indicate: For Decision For Information For Discussion X Executive Summary Summary
 Governing Body 22 March 2017 Details Part 1 X Part 2 Agenda Item No. 10 Title of Paper: Board Member: Author: Presenter: PAHT Quality Improvement Plan Catherine Jackson, Executive Nurse Catherine Jackson,
Governing Body 22 March 2017 Details Part 1 X Part 2 Agenda Item No. 10 Title of Paper: Board Member: Author: Presenter: PAHT Quality Improvement Plan Catherine Jackson, Executive Nurse Catherine Jackson,
The safety of every patient we care for is our number one priority
 HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
JOB DESCRIPTION. Joint Commissioning Manager for Older People s Residential Care and Nursing Homes
 JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
Leeds West CCG Governing Body Meeting
 Agenda Item: LW2015/115 FOI Exempt: N Leeds West CCG Governing Body Meeting Date of meeting: 4 vember 2015 Title: Delegated Commissioning of Primary Medical Services Lead Governing Body Member: Dr Simon
Agenda Item: LW2015/115 FOI Exempt: N Leeds West CCG Governing Body Meeting Date of meeting: 4 vember 2015 Title: Delegated Commissioning of Primary Medical Services Lead Governing Body Member: Dr Simon
NHS 111 Clinical Governance Information Pack
 NHS 111 Clinical Governance Information Pack This pack is designed to help you develop your local NHS 111 clinical governance framework and explain how it fits in to the wider context. It takes you through
NHS 111 Clinical Governance Information Pack This pack is designed to help you develop your local NHS 111 clinical governance framework and explain how it fits in to the wider context. It takes you through
Chief Accountable Officer Director Transformation and Quality. Director Transformation and Quality Chief Accountable Officer
 Governing Body Assurance Framework (July/August 2016) Introduction The Governing Body Assurance Framework identifies the CCG s principal, strategic objectives and the principal risks to their delivery.
Governing Body Assurance Framework (July/August 2016) Introduction The Governing Body Assurance Framework identifies the CCG s principal, strategic objectives and the principal risks to their delivery.
A meeting of NHS Bromley CCG Governing Body 25 May 2017
 South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
James Blythe, Director of Commissioning and Strategy. Agenda item: 09 Attachment: 04
 Title of paper: Author: Exec Lead: Community Hospital Services Review Tom Elrick, Urgent Care Programme Lead James Blythe, Director of Commissioning and Strategy Date: 23 rd February 2015 Meeting: Executive
Title of paper: Author: Exec Lead: Community Hospital Services Review Tom Elrick, Urgent Care Programme Lead James Blythe, Director of Commissioning and Strategy Date: 23 rd February 2015 Meeting: Executive
Co-Commissioning Arrangements in Primary Care (GP practices) - Principles and Process for managing Quality and Contracting
 - Principles and Process for managing Quality and Contracting") Co-Commissioning Arrangements in Primary Care (GP practices) - Principles and Process for managing and Contracting 1. Purpose The CCG will have delegated authority to commission primary care (For clarity,
Co-Commissioning Arrangements in Primary Care (GP practices) - Principles and Process for managing and Contracting 1. Purpose The CCG will have delegated authority to commission primary care (For clarity,
QUALITY IMPROVEMENT COMMITTEE
 : 2016-002.a QUALITY IMPROVEMENT COMMITTEE Minutes of the meeting held on 11 th February 2016, Conference Room D, 1829 Building Present: Faulkner, Sarah (SF) (Chair) Lay Member, NHS West Cheshire CCG Cavanagh,
: 2016-002.a QUALITY IMPROVEMENT COMMITTEE Minutes of the meeting held on 11 th February 2016, Conference Room D, 1829 Building Present: Faulkner, Sarah (SF) (Chair) Lay Member, NHS West Cheshire CCG Cavanagh,
Urgent Primary Care Update Paper
 Urgent Primary Care Update Paper Primary Care Commissioning Committee meeting D 17 May 2018 Author(s) Sponsor Director Purpose of Paper Kate Gleave Brian Hughes, Director of Commissioning The purpose of
Urgent Primary Care Update Paper Primary Care Commissioning Committee meeting D 17 May 2018 Author(s) Sponsor Director Purpose of Paper Kate Gleave Brian Hughes, Director of Commissioning The purpose of
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10. Date of Meeting: 31 st August 2018 TITLE OF REPORT:
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10 Date of Meeting: 31 st August 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 10 Date of Meeting: 31 st August 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
Quality Strategy. CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July Head of Clinical Quality & Patient Safety
 Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Primary Care Commissioning Committee. Phil Davis, Head of Primary Care, NHS Hull CCG. Hayley Patterson, Assistant Primary Care Contracts Manager,
 Item: 7.2 Report to: Date of Meeting: Subject: Presented by: Author: Primary Care Commissioning Committee 27 th April 2018 Primary Care Update Hayley Patterson, Assistant Primary Care Contracts Manager,
Item: 7.2 Report to: Date of Meeting: Subject: Presented by: Author: Primary Care Commissioning Committee 27 th April 2018 Primary Care Update Hayley Patterson, Assistant Primary Care Contracts Manager,
Agenda Item. 12 July NHS North Cumbria CCG Primary Care Committee. Approval of ICC Primary Care Investment Proposals. Purpose of the Report
 NHS North Cumbria CCG Primary Care Committee Agenda Item 12 July 2018 6 Approval of ICC Primary Care Investment Proposals Purpose of the Report The purpose of this report is: - To formally ratify the decision
NHS North Cumbria CCG Primary Care Committee Agenda Item 12 July 2018 6 Approval of ICC Primary Care Investment Proposals Purpose of the Report The purpose of this report is: - To formally ratify the decision
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
TERMS OF REFERENCE. Transformation and Sustainability Committee. One per month (Second Thursday) GP Board Member (Quality) Director of Commissioning
 GP Board Member (Quality) Director of Commissioning") TERMS OF REFERENCE Committee: Frequency Of Meetings: Committee Chair: Membership: Attendance: Lead Officer: Secretary: Transformation and Sustainability Committee One per month (Second Thursday) GP Board
TERMS OF REFERENCE Committee: Frequency Of Meetings: Committee Chair: Membership: Attendance: Lead Officer: Secretary: Transformation and Sustainability Committee One per month (Second Thursday) GP Board
Primary Care Commissioning Next Steps to Delegated Commissioning September Board Paper. 2.0 Delegated Opportunities, Benefits and Risks
 Primary Care Commissioning Next Steps to Delegated Commissioning September Board Paper 1.0 Introduction This paper provides a briefing to the Wandsworth CCG Board on our progress in developing a Primary
Primary Care Commissioning Next Steps to Delegated Commissioning September Board Paper 1.0 Introduction This paper provides a briefing to the Wandsworth CCG Board on our progress in developing a Primary
The Integrated Support and Assurance Process (ISAP): guidance on assuring novel and complex contracts
: guidance on assuring novel and complex contracts") The Integrated Support and Assurance Process (ISAP): guidance on assuring novel and complex contracts Part A: Introduction Published by NHS England and NHS Improvement August 2017 First published: Friday
The Integrated Support and Assurance Process (ISAP): guidance on assuring novel and complex contracts Part A: Introduction Published by NHS England and NHS Improvement August 2017 First published: Friday
PRIMARY CARE COMMISSIONING COMMITTEE MEETING
 PRIMARY CARE COMMISSIONING COMMITTEE MEETING Date of meeting Title of report 20 th June 2017 Agenda item number Unscheduled Primary Care Services for the Fylde Coast 7 Paper Presented by: Alison Kerfoot,
PRIMARY CARE COMMISSIONING COMMITTEE MEETING Date of meeting Title of report 20 th June 2017 Agenda item number Unscheduled Primary Care Services for the Fylde Coast 7 Paper Presented by: Alison Kerfoot,
South Central. Operationalisation of NHS England Framework for Responding to Care Quality Commission (CQC) Inspections of GP Practices
 Inspections of GP Practices") South Central Operationalisation of NHS England Framework for Responding to Care Quality Commission (CQC) Inspections of GP Practices NHS England, South Central Operationalisation of NHS England Framework
South Central Operationalisation of NHS England Framework for Responding to Care Quality Commission (CQC) Inspections of GP Practices NHS England, South Central Operationalisation of NHS England Framework
Enhanced service specification. Avoiding unplanned admissions: proactive case finding and patient review for vulnerable people
 Enhanced service specification Avoiding unplanned admissions: proactive case finding and patient review for vulnerable people 1 Enhanced service specification Avoiding unplanned admissions: proactive case
Enhanced service specification Avoiding unplanned admissions: proactive case finding and patient review for vulnerable people 1 Enhanced service specification Avoiding unplanned admissions: proactive case
SUPPORT FOR VULNERABLE GP PRACTICES: PILOT PROGRAMME
 Publications Gateway Reference 04476 For the attention of: NHS England Directors of Commissioning Operations Clinical Leaders and Accountable Officers, NHS Clinical Commissioning Groups Copy: NHS England
Publications Gateway Reference 04476 For the attention of: NHS England Directors of Commissioning Operations Clinical Leaders and Accountable Officers, NHS Clinical Commissioning Groups Copy: NHS England
Investment Committee: Extended Hours Business Case (Revised)
") PAPER 06 Investment Committee: Extended Hours Business Case (Revised) OVERALL STRATEGY 1. SaHF Care Closer to Home This Extended Hours Business Case is developed within the context of Shaping a Healthier
PAPER 06 Investment Committee: Extended Hours Business Case (Revised) OVERALL STRATEGY 1. SaHF Care Closer to Home This Extended Hours Business Case is developed within the context of Shaping a Healthier
Update on co-commissioning of primary care: guidance for CCG member practices and LMCs
 Update on co-commissioning of primary care: guidance for CCG member practices and LMCs British Medical Association bma.org.uk This paper is an update of previous GPC (general practitioners committee) guidance
Update on co-commissioning of primary care: guidance for CCG member practices and LMCs British Medical Association bma.org.uk This paper is an update of previous GPC (general practitioners committee) guidance
TRUST BOARD. Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director. Jo Hunter, Deputy Chief Nurse. Mary Heritage, Assistant Director of Quality
 TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
Quality Strategy and Improvement Plan
 Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Quality and Governance Committee. Terms of Reference
 Quality and Governance Committee Terms of Reference 1. Constitution 1.1 The Clinical Commissioning Group s Governing Body hereby resolves to establish a Committee of the Governing Body known as the Quality
Quality and Governance Committee Terms of Reference 1. Constitution 1.1 The Clinical Commissioning Group s Governing Body hereby resolves to establish a Committee of the Governing Body known as the Quality
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
GREATER MANCHESTER HEALTH AND SOCIAL CARE STRATEGIC PARTNERSHIP BOARD
 GREATER MANCHESTER HEALTH AND SOCIAL CARE STRATEGIC PARTNERSHIP BOARD 6 Date: 16 December 2016 Subject: Report of: Transformation Fund Update Steve Wilson PURPOSE OF REPORT: The purpose of the report is
GREATER MANCHESTER HEALTH AND SOCIAL CARE STRATEGIC PARTNERSHIP BOARD 6 Date: 16 December 2016 Subject: Report of: Transformation Fund Update Steve Wilson PURPOSE OF REPORT: The purpose of the report is
Primary Care Strategy. Draft for Consultation November 2016
 Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
Welcome. PPG Conference North and South Norfolk CCGs June 14 th 2018
 Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
INTEGRATION TRANSFORMATION FUND
 MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
Director of Acute & Primary Care Commissioning, BaNES CCG. Assistant Director of Nursing and Quality, BaNES CCG
 Primary Care Commissioning Committee Held in Public Meeting Thursday 6 July 2017 2pm-4pm Boardroom, Kempthorne House, St Martins Hopsital, Bath, BA2 5RP Minutes Members of the Committee Suzannah Power
Primary Care Commissioning Committee Held in Public Meeting Thursday 6 July 2017 2pm-4pm Boardroom, Kempthorne House, St Martins Hopsital, Bath, BA2 5RP Minutes Members of the Committee Suzannah Power
Greater Manchester Health and Social Care Strategic Partnership Board
 Greater Manchester Health and Social Care Strategic Partnership Board 7 Date: 13 October 2017 Subject: Report of: Greater Manchester Model for Urgent Primary Care Dr Tracey Vell, Associate Lead for Primary
Greater Manchester Health and Social Care Strategic Partnership Board 7 Date: 13 October 2017 Subject: Report of: Greater Manchester Model for Urgent Primary Care Dr Tracey Vell, Associate Lead for Primary
Urgent Primary Care Consultation Report
 Urgent Primary Care Consultation Report Primary Care Commissioning Committee meeting 22 March 2018 1. Introduction 1.1 Sheffield CCG ran a formal public consultation between 26 th September 2017 and 31
Urgent Primary Care Consultation Report Primary Care Commissioning Committee meeting 22 March 2018 1. Introduction 1.1 Sheffield CCG ran a formal public consultation between 26 th September 2017 and 31
Looked After Children Annual Report
 Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
Extended access to general practice. A guide to completing the extended access survey
 Extended access to general practice A guide to completing the extended access survey NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing
Extended access to general practice A guide to completing the extended access survey NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
OFFICIAL. Integrated Urgent Care Key Performance Indicators and Quality Standards Page 1 of 20
 Integrated Urgent Care Key Performance Indicators and Quality Standards 2018 Page 1 of 20 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing
Integrated Urgent Care Key Performance Indicators and Quality Standards 2018 Page 1 of 20 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing
NHS TRAFFORD CLINICAL COMMISSIONING GROUP GOVERNING BODY 19 DECEMBER 2017
 Part 1 X Part 2 NHS TRAFFORD CLINICAL COMMISSIONING GROUP GOVERNING BODY 19 DECEMBER 2017 Title of report Purpose of the report and key highlights Directorate Update - Nursing The report updates the Governing
Part 1 X Part 2 NHS TRAFFORD CLINICAL COMMISSIONING GROUP GOVERNING BODY 19 DECEMBER 2017 Title of report Purpose of the report and key highlights Directorate Update - Nursing The report updates the Governing
Westminster Health and Wellbeing Board
 Westminster Health and Wellbeing Board Date: 13 July 2017 Classification: Title: Report of: Cabinet Member Portfolio: Wards Involved: Policy Context: Report Author and Contact Details: General Release
Westminster Health and Wellbeing Board Date: 13 July 2017 Classification: Title: Report of: Cabinet Member Portfolio: Wards Involved: Policy Context: Report Author and Contact Details: General Release
In Attendance: Arlene Sheppard (AMS) Note Taker WNCCG Sarah Haverson (SHv) Commissioning Support Officer WNCCG
 Note Taker WNCCG Sarah Haverson (SHv) Commissioning Support Officer WNCCG") Agenda Item: 17.62 DRAFT Minutes of West Norfolk Primary Care Commissioning Committee Part One (Quorate) Held on 26th May 2017 2pm Education Room, Town Hall, Saturday Market Place, Kings Lynn PE30 5DQ
Agenda Item: 17.62 DRAFT Minutes of West Norfolk Primary Care Commissioning Committee Part One (Quorate) Held on 26th May 2017 2pm Education Room, Town Hall, Saturday Market Place, Kings Lynn PE30 5DQ
Next steps towards primary care cocommissioning
 Next steps towards primary care cocommissioning November 2014 1 NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations Patients and Information Nursing Trans. & Corp. Ops. Commissioning
Next steps towards primary care cocommissioning November 2014 1 NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations Patients and Information Nursing Trans. & Corp. Ops. Commissioning
Kingston Clinical Commissioning Group Report Summary
 Kingston Clinical Commissioning Group Report Summary Meeting Title Governing Body in public Date 7 th November 2017 Report Title Health & Well Being Board Minutes 14 th September 2017 Agenda Item 15 Attachment
Kingston Clinical Commissioning Group Report Summary Meeting Title Governing Body in public Date 7 th November 2017 Report Title Health & Well Being Board Minutes 14 th September 2017 Agenda Item 15 Attachment
General Practice Extended Access: September 2017
 General Practice Extended Access: September 2017 General Practice Extended Access September 2017 Version number: 1.0 First published: 31 October 2017 Prepared by: Hassan Ismail, NHS England Analytical
General Practice Extended Access: September 2017 General Practice Extended Access September 2017 Version number: 1.0 First published: 31 October 2017 Prepared by: Hassan Ismail, NHS England Analytical
Manchester Health and Care Commissioning Board. A partnership between Manchester. City Council and NHS Manchester Clinical Commissioning Group
 Manchester Health and Care Commissioning Board A partnership between Manchester City Council and NHS Manchester Clinical Commissioning Group Agenda Item: Report Title: Date: Strategic Commissioning Prepared
Manchester Health and Care Commissioning Board A partnership between Manchester City Council and NHS Manchester Clinical Commissioning Group Agenda Item: Report Title: Date: Strategic Commissioning Prepared
WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE
 Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
Wolverhampton Clinical Commissioning Group WOLVERHAMPTON CLINICAL COMMISSIONING GROUP QUALITY & SAFETY COMMITTEE Minutes of the Quality and Safety Committee Meeting held on Tuesday 12 th May 2015 Commencing
With these corrections made, it was agreed that the Minutes be approved as a correct record.
 Agenda item 14 CCG Operational Leadership Team 18 July 2013, 8.30 11.30am Board Room, Trust HQ, St Martin s Hospital In Attendance: Simon Douglass (Chair) (SD) Hester McLain (For Item 10) Tracey Cox (Chair)
Agenda item 14 CCG Operational Leadership Team 18 July 2013, 8.30 11.30am Board Room, Trust HQ, St Martin s Hospital In Attendance: Simon Douglass (Chair) (SD) Hester McLain (For Item 10) Tracey Cox (Chair)
Serious Incident Management Policy
 Serious Incident Management Policy Standard Operating Procedure Version Version 2 Implementation Date 01 November 2017 Review Date 31 October 2019 St Helens CCG Serious Incident Management Policy Approved
Serious Incident Management Policy Standard Operating Procedure Version Version 2 Implementation Date 01 November 2017 Review Date 31 October 2019 St Helens CCG Serious Incident Management Policy Approved
NHS DORSET CLINICAL COMMISSIONING GROUP JOINT PRIMARY CARE COMMISSIONING COMMITTEE. 3 February 2016 PART ONE PUBLIC MINUTES
 NHS DORSET CLINICAL COMMISSIONING GROUP JOINT PRIMARY CARE COMMISSIONING COMMITTEE 3 February 2016 PART ONE PUBLIC MINUTES Part 1 of the Joint Primary Care Commissioning Committee of NHS Dorset Clinical
NHS DORSET CLINICAL COMMISSIONING GROUP JOINT PRIMARY CARE COMMISSIONING COMMITTEE 3 February 2016 PART ONE PUBLIC MINUTES Part 1 of the Joint Primary Care Commissioning Committee of NHS Dorset Clinical
Commissioner Guidelines for Responding to Requests from Practices to Temporarily Suspend Patient Registration
 Commissioner Guidelines for Responding to Requests from Practices to Temporarily Suspend Patient Registration NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised
Commissioner Guidelines for Responding to Requests from Practices to Temporarily Suspend Patient Registration NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised
COMMUNITY AND OLDER PEOPLE S MENTAL HEALTH SERVICE FRAMEWORK FOR:
 MINDING THE GAP COMMUNITY AND OLDER PEOPLE S MENTAL HEALTH SERVICE FRAMEWORK FOR: GOVERNANCE ASSURANCE AND PERFORMANCE. 1. INTRODUCTION AND CONTEXT Providing, delivering and developing the highest standards
MINDING THE GAP COMMUNITY AND OLDER PEOPLE S MENTAL HEALTH SERVICE FRAMEWORK FOR: GOVERNANCE ASSURANCE AND PERFORMANCE. 1. INTRODUCTION AND CONTEXT Providing, delivering and developing the highest standards
Music Education Hubs External Investment Process Guidance
 Music Education Hubs 2018 20 External Investment Process Guidance Contents Introduction... 2 1 Stage one: Summer progress meetings (May July 2017)... 2 1.1 Ensuring Quality... 2 1.2 Core and extension
Music Education Hubs 2018 20 External Investment Process Guidance Contents Introduction... 2 1 Stage one: Summer progress meetings (May July 2017)... 2 1.1 Ensuring Quality... 2 1.2 Core and extension
Agenda Item number: 9.1. Maggie Bayley, Director of Nursing and Quality
 Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
CCG Finance and Performance Committee Minutes of Meeting held on Tuesday 17 th March 2015, 9:00-10:30am Sovereign Court, Hounslow
 CCG Finance and Performance Committee Minutes of Meeting held on Tuesday 17 th March 2015, 9:00-10:30am Sovereign Court, Hounslow Present In Attendance Prash Gupta (PG) HCCG (Chair) Natasha Malhotra (NM)
CCG Finance and Performance Committee Minutes of Meeting held on Tuesday 17 th March 2015, 9:00-10:30am Sovereign Court, Hounslow Present In Attendance Prash Gupta (PG) HCCG (Chair) Natasha Malhotra (NM)
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Methods: Commissioning through Evaluation
 Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Report. Report Author Presented By Responsible Director Susi Clarke, Primary Care Strategic Development Lead
 Governing Body Meeting Held in Public Report Date of Meeting: 5.7.18 Agenda Item: 11.0 Report Title Extended Access Update Report Author Presented By Responsible Director Susi Clarke, Primary Care Strategic
Governing Body Meeting Held in Public Report Date of Meeting: 5.7.18 Agenda Item: 11.0 Report Title Extended Access Update Report Author Presented By Responsible Director Susi Clarke, Primary Care Strategic
DRAFT - NHS CHC and Complex Care Commissioning Policy.
 DRAFT - NHS CHC and Complex Care Commissioning Policy. 1. Introduction 1.1 This policy describes the way the following Clinical Commissioning Groups (CCGs) NHS Wirral Clinical Commissioning Group, NHS
DRAFT - NHS CHC and Complex Care Commissioning Policy. 1. Introduction 1.1 This policy describes the way the following Clinical Commissioning Groups (CCGs) NHS Wirral Clinical Commissioning Group, NHS
NHS ENGLAND BOARD PAPER
 NHS ENGLAND BOARD PAPER Paper: PB.04.07.2018/05 Title: Developing the NHS long term plan: primary care reform Lead National Director: Ian Dodge, National Director, Strategy and Innovation Purpose of Paper:
NHS ENGLAND BOARD PAPER Paper: PB.04.07.2018/05 Title: Developing the NHS long term plan: primary care reform Lead National Director: Ian Dodge, National Director, Strategy and Innovation Purpose of Paper:
NHS England (South) Surge Management Framework
 Surge Management Framework") NHS England (South) Surge Management Framework THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK 2 NHS England (South) Surge Management Framework Version number: 1.0 First published: August 2015 Prepared by:
NHS England (South) Surge Management Framework THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK 2 NHS England (South) Surge Management Framework Version number: 1.0 First published: August 2015 Prepared by:
INCENTIVE SCHEMES & SERVICE LEVEL AGREEMENTS
 MAY 2007 INCENTIVE SCHEMES & SERVICE LEVEL AGREEMENTS Practice Based Commissioning North and South Essex Local Medical Committees CLARIFYING THE RELATIONSHIP BETWEEN PBC GROUPS AND PCTS AIMS The aim of
MAY 2007 INCENTIVE SCHEMES & SERVICE LEVEL AGREEMENTS Practice Based Commissioning North and South Essex Local Medical Committees CLARIFYING THE RELATIONSHIP BETWEEN PBC GROUPS AND PCTS AIMS The aim of
Yorkshire and Humber Integrated Urgent Care: Service Development and Procurement
 Yorkshire and Humber Integrated Urgent Care: Service Development and Procurement NHS Hull Clinical Commissioning Group Governing Body Meeting 23 rd March 2018 1. Purpose Integrated Urgent Care (IUC) is
Yorkshire and Humber Integrated Urgent Care: Service Development and Procurement NHS Hull Clinical Commissioning Group Governing Body Meeting 23 rd March 2018 1. Purpose Integrated Urgent Care (IUC) is
Responding to a risk or priority in an area 1. London Borough of Sutton
 Responding to a risk or priority in an area 1 London Borough of Sutton October 2017 Contents Contents... 2 Introduction... 3 Scope and activity... 4 What did we do?... 5 Framework... 6 Key findings...
Responding to a risk or priority in an area 1 London Borough of Sutton October 2017 Contents Contents... 2 Introduction... 3 Scope and activity... 4 What did we do?... 5 Framework... 6 Key findings...
COMMISSIONING FOR QUALITY FRAMEWORK
 This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version COMMISSIONING FOR QUALITY FRAMEWORK Document Title: Commissioning for Quality Framework
This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version COMMISSIONING FOR QUALITY FRAMEWORK Document Title: Commissioning for Quality Framework
NHS GRAMPIAN. Grampian Clinical Strategy - Planned Care
 NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
This paper explains the way in which part of the system is changing to become clearer and more accessible, beginning with NHS 111.
 Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April The Broadway, Wimbledon, SW19 1RH
 MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April 2018 120 The Broadway, Wimbledon, SW19 1RH Chair: Dr Andrew Murray In attendance: Members SB Sarah Blow Accountable Officer
MINUTES MERTON CLINICAL COMMISIONING GROUP GOVERNING BODY PART 1 18 th April 2018 120 The Broadway, Wimbledon, SW19 1RH Chair: Dr Andrew Murray In attendance: Members SB Sarah Blow Accountable Officer
A concern means any complaint, claim or reported patient safety incident.
 PUTTING THINGS RIGHT ANNUAL REPORT -2017 Introduction The Putting Things Right Annual Report provides information on the progress and performance of Powys Teaching Local Health Board (hereafter, the health
PUTTING THINGS RIGHT ANNUAL REPORT -2017 Introduction The Putting Things Right Annual Report provides information on the progress and performance of Powys Teaching Local Health Board (hereafter, the health
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER C Hickson, Head of Management Accounts
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
General Practice Extended Access: March 2018
 General Practice Extended Access: March 2018 General Practice Extended Access March 2018 Version number: 1.0 First published: 3 May 2017 Prepared by: Hassan Ismail, Data Analysis and Insight Group, NHS
General Practice Extended Access: March 2018 General Practice Extended Access March 2018 Version number: 1.0 First published: 3 May 2017 Prepared by: Hassan Ismail, Data Analysis and Insight Group, NHS
Mental Health Social Work: Community Support. Summary
 Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix