Urgent Care Strategy
|
|
|
- Cory Allan Griffin
- 5 years ago
- Views:
Transcription

1 Urgent Care Strategy Page 1
2 Urgent Care Strategy Please complete the table below: Strategy ref no: BCCG Urgent Care 2016 Author (inc job title) Graham Wilson, Urgent Care Transformation Manager Lesley Ward Urgent Care Clinical Lead Date Approved 15 th July 2016 Approved by Bristol Clinical Commissioning Group Governing Body Date of next Annual Review - June 2017 review Page 2
3 Bristol Urgent Care Strategy The delivery of high quality and accessible urgent care services is an important priority for the Bristol Health and Social Care Economy. Our aim as both commissioners and providers of care is to ensure that urgent care services in the future are delivered in a seamless integrated way to best meet the needs of our local population. This strategy covers all age groups who require urgent care from children to the elderly population. There are many challenges ahead, but by working as a whole community we can achieve the ambitions outlined in this document. We believe that, by working together, we will be able to deliver benefits for the patients we serve and to improve the working environment of our staff, despite the challenging financial climate in which we are trying to transform services. Over the coming years, we will see through successful implementation of this strategy:- An overall reduction in the number of o Ambulance call outs o Avoidable emergency hospital attendances, particularly in primary care conditions related presentations. o Shortened Lengths of Stay and Exceed Bed Days An increase in the use of services such as o Pharmacies o Urgent Care Centres who will treat patients with a higher level of medical complexity. A clinically supported NHS 111 that will link people directly into the service that they need. Patients waiting no longer than 4 hours in an Emergency Department (ED) Higher level of patient satisfaction with access to General Practice (GPs), with improved evening and weekend capability through an integrated out of hours service Fewer emergency admissions Shorter lengths of stay following an emergency admission Patients discharged from hospital when they are medically fit with community teams assessing their care needs at their residential setting No person admitted to acute hospital where their primary need is for care Improved out of hours community provision which provide effective response to crisis and delayed transfers of care (DToC) are kept to a minimum More patients treated in their own home or closer to home in existing community or general practice facilities Higher number of patients with more complex needs treated in community beds. No difference in the level of provision or the clinical outcomes delivered regardless of the day of the week Overall mortality rates across the health and social care economy will be at or below average and there is no excess mortality for patients admitted at weekends All professionals will be able to access, view and contribute to care plans for people with existing conditions in which emergency care is a predictable need, subject to proper information governance, data protection and patient agreement Page 3
4 This strategy for Bristol has been developed through an inclusive partnership between commissioners and providers of health and social care across Bristol. A key strength is that this is not just a commissioning strategy, but also a strategy that supports our priorities for shaping future service development and transformation through 2014/15 and beyond. Organisations working together on the development and delivery of this strategy Bristol Clinical Commissioning Group (CCG) NHS England (NHSE) Bristol City Council (BCC) University Hospital Bristol NHS Foundation Trust (UHBristol) North Bristol NHS Trust (NBT) Bristol Community Health (BCH) Avon & Wiltshire Mental Health Partnership (AWP) BrisDoc South West Ambulance Service Trust (SWASFT) NHS 111 Page 4
5 Contents Page(s) Introduction 3-4 Executive Summary 7-8 Chapter 1 Purpose of the Document What is Urgent Care? 9 Our Vision for Urgent Care 10 Principles of Working Together 10 Strategic Aims Chapter 2 Current Urgent Care System Urgent Care In Bristol Service Provision Challenges 25 Bristol Urgent Care System Diagram 25 Urgent Care Funding 26 Our Local Population 27 Non-Elective Admissions Primary Care 28 Out of Hours 28 Ambulance Service 28 Urgent Care Centres 28 Emergency Attendances 29 Length of Stay Comparisons 29 Emergency Admissions 30 Community Services What does this mean for Bristol Chapter 3 The Case for Change National Context KEOGH Review 35 Our local Context 37 Financial Challenge for Bristol 37 Future of Acute Hospital Services in 37 Bristol Social Care Transformation 38 Page 5
6 What will the Future look like? Local Context 38 Bristol Population 39 Public Health Outcome Framework 39 Life Expectancy 39 Wider Determinants of Health 40 Health Improvement 40 Health Protection 40 Healthcare and Premature Mortality 40 Public Health England Profile Chapter 4 Managing the Transition Governance Arrangements 44 Programme Management 44 Monitor and Measuring Impact Appendix 1 Service Provision Map - In Hours 47 Appendix 2 Service Provision Map - Out of Hours 48 Bibliography 49 Page 6
7 Executive Summary This document sets out our vision and details our strategy for the future of urgent care in Bristol. Underpinning the strategy will be a programme for implementation, in order to make the strategy a reality for the local population, and to deliver the required changes. The strategy will run from 2015 until 2020, by which time we will have made a radical difference to the way in which urgent care services are delivered and accessed in Bristol. In order to deliver our strategy we have agreed three strategic underpinning principles, which align with our ambitions under Better Care Bristol; a programme to deliver improvement in and integration of services across the whole system of adult health and social care, to make a real difference to service users, and to reduce costs to enable more investment in community services. These principles are:- Admission prevention and avoidance Enhance out of hospital urgent care services and focus on routine care so unnecessary emergency admissions can be avoided wherever possible Provide the right care, at the right time, in the right place Give people the best care in the appropriate place within the fastest time possible Effective patient flows Promote rapid discharge to the most appropriate place for recovery in a planned manner, to reduce length of stay and excess bed days We recognise that the urgent care system in Bristol is complex and the number of different entry points can be confusing to people, at a time when they need it to be simple. We recognise that our role as system leaders and providers is to remove this confusion and present the community with a straightforward set of options that are easy to navigate. This will require us to make changes to the structure of the existing services, including enhancing some services and reducing or stopping others when they are no longer appropriate. We have finite resources available with which to deliver sustainable services. We believe that by delivery of our strategy we will improve services, deliver a more effective system and reduce the current cost. Bristol, in recent years has seen a pattern of increasing ED attendances, 999 calls, GP appointments and emergency admissions. We have seen some reductions in GP referred emergency admissions delivered by the GP Support Unit service that is located in the Bristol Royal Infirmary; a service that further supports community GPs and their patients to access treatment and diagnostics in the acute hospital without the need for emergency admission, where the patient's condition permits. This service has been in place under different guises for the last 6 years, but a procurement undertaken in 2013 saw the service integrated with Bristol Royal Infirmary Ambulatory Care Unit with dedicated nursing and hospital consultant Page 7
8 support. We need to make changes for our system to be sustainable and to manage the demographic changes, which show that over the life of this strategy the population aged over 65 is expected to grow by 8%, an additional 4,500 people. [1]. If we don t change the way we provide services and work in a more integrated way, the number of emergency admissions for those aged 75 and over, is likely to increase to more than 11,400 a year by (Page shows population growth statistics). Page 8
9 Chapter 1 Introduction Purpose of the Document 1. This strategy sets out in a single document, our future plans for the urgent care system in Bristol. Whatever the urgent or emergency need is and in whatever location, our aim is to ensure that our community has access to the best care from the right person, in the right place, and at the right time. 2. Quality and safety are at the heart of what we are aiming to deliver. The strategy sets out and defines our shared vision, strategic principles and ambitions for future urgent care in Bristol. The strategy identifies how we will work together across the local health and social economy and respond to the changing needs of our population. 3. Given the complexity of patient flows across different services, this strategy will reflect a whole system approach across the acute, primary and community care and social services, recognising the need to develop a truly integrated health and care system to achieve this. In Bristol we have established the Better Care Bristol programme as a collaboration of all the main providers and commissioners across health and social care to work together to deliver integrated and seamless services. 4. Our strategy provides a framework for developing our partnership approach and providing excellent urgent care practices to ensure services are relevant and responsive for those people with urgent needs. What is Urgent Care? We have defined urgent care in this strategy in the following way:- 1. Urgent and emergency care is a range of health services available to people who need medical advice, diagnosis and / or treatment quickly and unexpectedly. 2. People using services and their carers should expect to be able to access essential, high quality, consistent advice, review and treatment 24 hours a day, seven days a week 24/7. 3. An effective urgent and emergency care system should be:- patient / user focused delivering good clinical outcomes delivering good patient experience timely right the first time Page 9
10 available 24/7 at a consistent standard Our Vision for Urgent Care 1. All partners in the Bristol health and social care economy have agreed our vision. It has informed all our work recently, including our Better Care Bristol, Organisational Resilience and Capacity Planning and Organisational Operational Plans. 2. The Bristol Urgent Care vision is:- Patients can expect high quality care based out of hospital with support from the right people for example GPs, nurses, therapists, social workers, volunteers, and paramedics. When required these staff will have access to specialist advice, investigations and treatment. Where the patient s care is best supported by treatment in hospital this will be consultant led with a clear plan of care. Discharge planning will commence at the time of admission to support safe and timely return to the patient s normal place of residence and if further care is required this will be provided out of hospital. All individuals providing care will have access to the relevant patient information to deliver the most appropriate care. 3. Delivery of our vision will require integration across our urgent care system to transform traditional pathways of care, reduce duplication and improve sharing of relevant information and be cost effective and sustainable. Principles of working together:- 1. As a health and social care economy, we have established three principles that all partners have signed up to as our guide for service development and transformation across urgent care pathways. Admission prevention and avoidance: Enhance out of hospital urgent care services including primary care to avoid emergency admissions wherever possible. To achieve this we will develop effective and simplified alternatives to hospital admission, which will be available seven days a week. This is especially important for patients and their carers with complex needs and those with chronic illness. Right care, right time, right place: Treat people with the best care in the right place, as quickly as possible. To achieve this we will simplify our urgent care system to enable patients to access expert diagnosis and assessment in the setting that is most appropriate to their clinical Page 10
11 needs. Senior clinical decision making will take place as early in the patient journey as possible, seven days a week. This will include effective sharing of information and high quality communication. Effective patient flow: Promote rapid discharge to the most appropriate place for recovery in a planned manner. To achieve this we will focus on planning discharge and supporting patients to leave hospital seven days a week. Effective discharge planning can reduce length of stay and readmission and is therefore a vital element of emergency care. A safe supported discharge relies on the effective integration of primary, community, secondary and social care services, which should be available seven days a week including out of hours periods. Strategic Aims Whilst the principles outline how we will work together, the strategic aims will identify what we intend to do. These have been identified and agreed by all partners and endorsed by the Health and Wellbeing Board for Bristol. 1. Aim: To create a system which is straightforward for patients to know which option is the right one to choose in an urgent care situation. What does this mean: We will ensure patients and their carers know which option is the right one for their condition and that they are then able to access that option easily to help reduce pressure on our emergency departments. Recent national studies have suggested that between 15-40% of patients who attend A&E departments were discharged requiring no treatment and could have been treated in the community rather than as an emergency case in hospital [2]. Despite the inconsistency in the findings, these results are useful as an opportunity to design services fit for the future. Of the 15%, the largest subgroup was young children presenting with symptoms of minor illness. Also, the A&E brand is so strong that it is seen by many as the first port of call before an out of hours GP service, urgent care centre or a minor injury unit outside general practice opening hours. 40% of attendances by children in A&E in resulted in no treatment or dispensing of medicine [3]. What we will do: Design a simplified system with fewer access points, greater coordination across pathways and between providers supported by more effective information sharing Empower and facilitate patients and their carers to self-care and to take control of their own healthcare management by improved access to information and relevant services Page 11
12 Work with appropriate support groups, target community wide education and information campaigns to raise awareness Obtain feedback following inappropriate use of services to share learning and inform changes. This will include enabling individuals to understand the choices they made and the alternative options available to them What will success look like: An overall reduction in the number of unnecessary ambulance call outs and ED attendances, particularly those that are considered inappropriate or from people presenting with primary care manageable conditions An increase in the use of services such as pharmacies and walk-in centres and urgent care centres which will treat patients with a higher level of medical complexity. A clinically supported NHS 111 service will link people directly into the service/care that they need. 2. Aim: To put primary care at the heart of urgent care provision What does this mean: General practice, supported by effective community services, provides the majority of urgent care. General practice will lead the coordination of care for the majority of patients. Small changes to improve access to primary care supplemented by an investment in integrated community services will have a significant effect on ED attendances, hospital admissions, length of stay, discharge and readmission rates. Access to primary care, particularly GP services, will need to be improved through a more integrated approach with out of hours services. What we will do: Provide more primary and community care closer to home Have integrated service models to provide seamless care for patients and their carers that are led by primary care and supported by hospital based specialists What will success look like: Joined up care for patients Reduction in unnecessary hospital admissions Page 12
13 3. Aim: To ensure that patients are only admitted to hospital when necessary and only stay in hospital as long as is clinically appropriate What does this mean: Providing appropriate access to admission avoidance support for ambulance paramedics, emergency department doctors and general practitioners will help to ensure that patients and their carers can be directed to the right treatment or support immediately, rather than travelling through the whole urgent care pathway before ending up in the correct place. What we will do: Expand provision of telephone specialist advice for GPs and other healthcare professionals through a single point of access supported by shared understanding and risk sharing Invest in community services such as rehabilitation, enhanced care teams, and other community based admission avoidance schemes Ensure early consultant assessment and interventions take place to ensure that patients start on the right pathway of care as soon as possible Ensure there are 7 day consultant reviews to support rapid discharge Implement effective discharge planning at the point of admission Improve automation of discharge processes including pharmacy, patient transport bookings and communication Ensure effective sharing of information and improved communication What will success look like: Fewer emergency admissions, more emergency adult patients on planned ambulatory care pathways being managed safely and efficiently on the same day avoiding admission to a hospital bed, shorter lengths of stay following an emergency admission and fewer patients waiting to be discharged when their medical care is complete More appropriate community service in place during out of hours, providing an effective response to a crisis in health or provision of care Delayed transfers of care kept to a minimum Page 13
14 4. Aim: Enhance and transform urgent care pathways, including better use of the full range of community and social care services. What does this mean: Effective community and social care services working with primary care and the ambulance service will ensure that patients and their carers are supported in their own home, or as close to home as possible. What we will do: - As a system, support the ambulance service to deliver their vision to be an emergency healthcare provider, supporting increased use of hear and treat and see and treat options as an alternative to taking a patient to hospital Improve access to information and care plans and improve communication between the professionals involved in care Improve access to diagnostics and specialist advice to support an appropriate decision to admit to hospital rather than admit to investigate Implement discharge to assess through ensuring that patients who are unable to readily return to their normal place of residence and who require an ongoing assessment and rehabilitation are transferred to an appropriate community setting for their assessment rather than receiving that assessment whilst in an acute hospital bed Develop community medical leadership that supports delivery of a sub-acute model and safely enables patients with a higher level of clinical risk to be managed in a community setting As part of the Better Care Bristol programme we will work to deliver real whole system change for our health and social care economy to provide an appropriate level of care in community settings, enabling us to keep people in their own homes for as long as possible. This means, for example, focussing on avoiding inappropriate admissions or long term placements, minimising length of stay and providing effective care co-ordination What will success look like: All complex or frail patients will have a care plan that is easily accessible to the patients themselves and all those involved in their care More patients treated in their own home or closer to home in community facilities Higher numbers of patients with more complex needs will be managed in community beds Community teams are enabled to assess patients further needs in Page 14
15 the most appropriate place for recovery following an admission to hospital to support timely discharge 5. Aim: Ensure seven day service provision with equitable outcomes What does this mean: Nationally, it is recognised that we need to improve equitable outcomes and delivery. To support this, the NHS needs to move towards a system of seven day services and the priority should be improving diagnostics (e.g. X-rays and blood tests) and securing robust, high quality urgent and emergency care. What we will do: - Implement a whole system approach to ensure access to all essential services consistently over the course of a week Enhance seven day provision in primary care and improve access to urgent primary care appointments including improved integration with out of hours primary care Consultant and middle grade doctor cover in key hospital speciality areas over the seven-day week Ensure that there are daily medical ward rounds as standard across all bedded units and, where appropriate, multiple day ward rounds to facilitate timely discharges Provide seven day access to health and social care assessments Ensure that access to care homes and transitional care is available seven days per week What will success look like: No difference in the clinical outcomes for patients delivered in emergency and urgent care, regardless of the day of the week Overall trust mortality rates at or below the national average No excess mortality for patients admitted at weekends 6. Aim: Share information more effectively to support improved patient care What does this mean: Ensuring that relevant information is shared by all professionals involved in the care of a patient is critical to effective and safe service delivery. This is reliant on consistent electronic clinical data recording and better integrated IT systems so that patients are not repeatedly being asked for the same information by different organisations. What we will do: - Introduce a system to integrate existing emergency care records and ensure that all relevant professionals can see all necessary Page 15
16 records when emergency care is required Implement a consistent IT strategy across all GP practices in Bristol and ensure that appropriate access to the records held in primary care is available to other practitioners who will legitimately require access to provide high quality safe care Build on opportunities created to join up information through the Connecting Care Programme, to deliver a detailed, local shared patient record that pulls together health and social care information providing a holistic view to facilitate improved care provision and clinical decision-making Ensure that care plans can be accessed by all appropriate practitioners so all can see what actions should be implemented during predictable urgent care episodes Ensure that discharge summaries following an emergency episode are accurate, timely and relevant from hospitals to the patient s own GP What will success look like: Where necessary ED, ambulance and enhanced care team staff can view essential records on GP systems as part of their routine treatment. All professionals will be able to access and view care plans for people with existing conditions in which emergency care is a predictable need. Successful Delivery of these aims 1. Successful delivery of these aims will underpin the three steps to better urgent care, and in turn deliver the agreed vision for the health and social care economy. The table below maps out the link between our aims and three principles. Mapping of strategic aims to three principles Avoid Admission Right Place, Right Time Improved Patient Flow Create a system which is simple for patients and their carers to know which option is the right one to choose in an urgent care situation Design simplified systems with fewer access points, greater co-ordination across pathways and between providers supported by more effective information sharing Page 16
17 Improve awareness and access to preventative and self-care services in the community, particularly for the elderly and people with mental health needs Work with appropriate support groups, target community wide education and information campaigns to raise awareness Obtain feedback following inappropriate use of services to share learning and inform changes Put primary care at the heart of urgent care provision Provide more primary and community care closer to home Have integrated service models to provide seamless care for patients and their carers that are led by primary care and supported by hospital based specialists Ensure that patients are only admitted when necessary and only stay as long as is clinically appropriate Expand provision of telephone specialist advice for GPs and other health care professionals through a single point of access Invest in community services such as rehabilitation, enhanced care teams, step up facilities and other admission avoidance schemes Ensure early consultant assessment and interventions to ensure that patients start on the right pathway of care as soon as possible Ensure seven day consultant reviews to support rapid discharge Implement effective discharge planning in advance Improve automation of discharge processes including pharmacy; patient transport bookings and communication Enhance and transform urgent care pathways, including better use of the full range of community and social care services As a system, support the ambulance service to deliver their vision to be an emergency healthcare provider, supporting Page 17
18 increased use of hear and treat and see and treat options as an alternative to taking the patient to hospital Improve access to diagnostics and specialist advice to support an appropriate decision to admit rather than admit to investigate Implement discharge to assess through ensuring that patients who are unable to readily return to their normal place of residence and who require an ongoing assessment and rehabilitation are transferred to an appropriate community setting for their assessment rather than receiving that assessment whilst in an acute hospital bed Develop community medical leadership that supports delivery of a sub-acute model and safely enables patients with a higher level of clinical risk to be managed in a community setting Working jointly to review and redesign adult health and social care to more effectively support the urgent care system Seven day service provision with equitable outcomes Implement a whole system approach to access all essential services consistently over the course of a week Enhance seven day provision in primary care and extend access to urgent primary care appointments Deliver consultant and middle grade doctor cover over a seven day period in key speciality areas Ensure that there are daily medical ward rounds as standard across all bedded units and where appropriate multiple day ward rounds are undertaken to facilitate timely discharges Provide seven day access to health and social care assessments Ensure that access to care homes and transitional care is available 7 days per week Page 18
19 Share information more effectively to support improved patient care Introduce a system to integrate existing emergency care records and ensure that all relevant professionals can see all necessary records when emergency care is administered Implement a consistent IT strategy across all GP practices in Bristol and ensure that appropriate access to the records held in primary care is available to other practitioners who will legitimately require access to provide high quality safe care Build on opportunities created to join up information through Connecting Care Programme Ensure that care plans can be accessed by all appropriate practitioners so all can see what actions should be implemented during predictable emergency Ensure that discharge summaries following an emergency episode are accurate, timely and relevant from hospitals to the patient s own GP Page 19
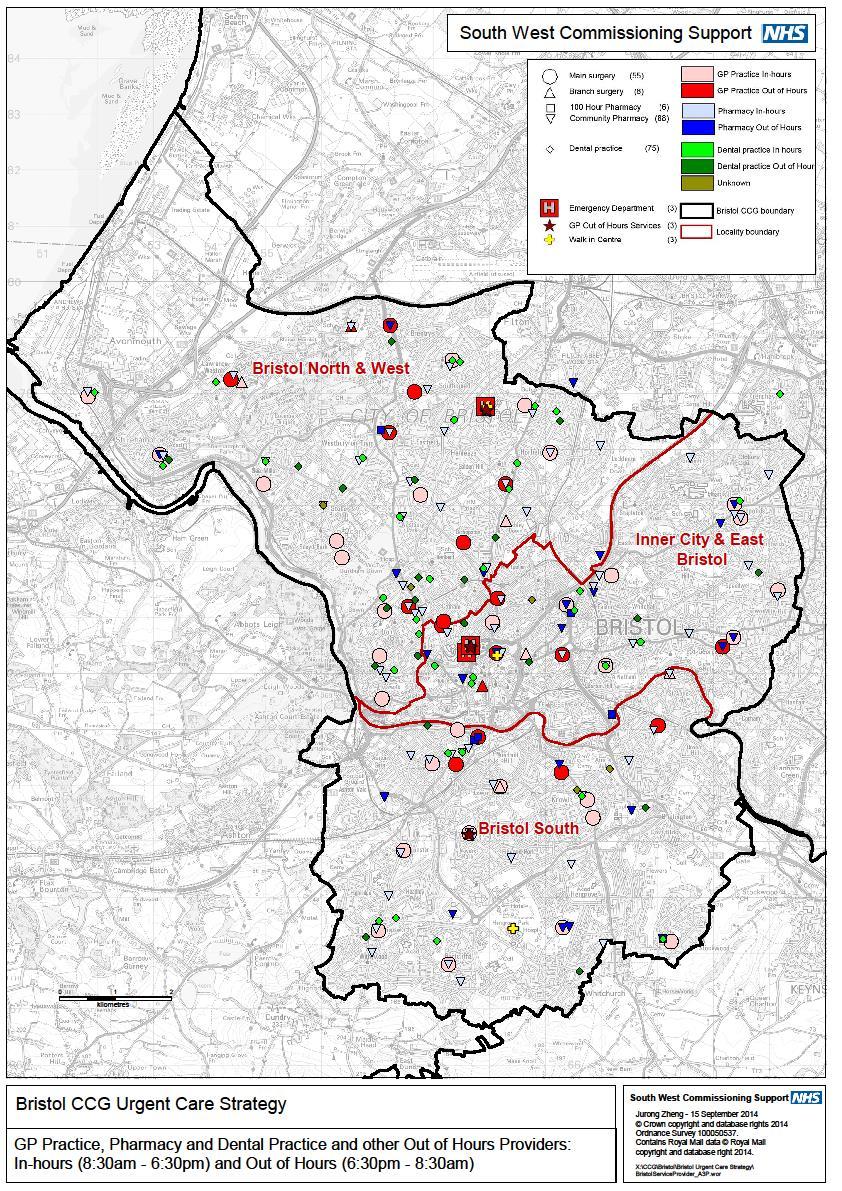
20 Chapter 2 Current Urgent Care System Urgent care in Bristol 1. The Bristol urgent care system is complex and contains a number of different services, which operate at different times. We recognise that this needs to be simplified to ensure that users can make an informed choice regarding the best service for them or their families. A key component of our strategy is to help ensure that this is delivered. Please see attached maps (Appendix 1 & 2) 2. We have a wealth of services available to the people of Bristol and these services support the current urgent and emergency care system across the city. These are summarised below:- Pharmacies - 98 General Practices 55 Walk In Centre GP Out of hours service - accessed through NHS 111 NHS 111 non-emergency medical advice service Minor Injury Unit South Bristol Community Hospital Urgent Care Centre Social care services Ambulance service Bristol Royal Infirmary, Bristol Royal Hospital for Children (children only) and Southmead (over 16 only) Accident and Emergency Departments (A&E) and MIU for Children Service What it does Ambulance Based Service 999 Ambulance Service Right Care phases 1 & 2 Care for people with serious, life threatening injury or illness at the place of illness or injury. Urgent transportation to hospital ED and other departments The Right Care Phase 1 initiative focussed on ensuring that patients receive the best possible care, in the right place, at the right time, delivered through a wide range of developments all aimed at improving the appropriateness of care given to patients. Right Care Phase 2 is based on the Ambulance Trust continuing to deliver an outcome of a reduction in the percentage of patients conveyed to Emergency Departments Page 20
21 across the South West. The key elements of the Right Care 2 initiative are the following interventions that will be delivered after an appropriate assessment to preserve life, and support a person s clinical condition. Hear and Treat patient is provided suitable self-care advice and support to manage their needs in the home over telephone advice and appropriate signposting to alternative services to ambulance transport and emergency department See and Treat On scene treatment with no onward transport (but with advice and if necessary, appropriate signposting to alternative services) Treatment and transfer onwards to; o Primary Care Intervention (e.g. GP, Walk in Centre) o Other community service as defined as appropriate by the CMS Directory of Services o Non-Acute facility (e.g. Urgent Care Centres) o Acute facility (e.g. Emergency Department) Patient Transport Service (PTS) The PTS service is for non-emergency patients and their escorts who meet the eligibility criteria. These are journeys between their place of residence and healthcare facilities, and between hospitals. The place of residence is defined as any address specified at the time of booking, e.g. home, nursing home, hospice, hospital or treatment centre. PTS is only available for patients with a clear and genuine medical need. Primary Care Based Services GP practices / Pharmacies / Dentists Walk In Centre (based in Boots the Chemist at Broadmead) GP Support Unit for Primary health care provides the first point of contact in the health care system. In the NHS, the main source of primary health care is general practice. The aim is to provide an easily accessible route to care, whatever the patient s problem. Primary health care is based on caring for people rather than specific diseases. The walk in centre provides treatment for a range of illnesses and injuries by a team of experienced nurses. The service is available 7 days a week and you can walk in or book appointments. Opening hours vary Monday to Saturday 8am to 8pm and Sundays 11:00-15:30. The GP Support Unit (GPSU) is based in the Bristol Royal Page 21
22 healthcare professionals 24/7 medical support and advice line for healthcare professionals Out of hours NHS 111 Infirmary (BRI). This service is run by GPs and manages patient admissions into the hospital by taking telephone referrals from GPs, ambulance crews and Emergency Department within local Bristol GP Practices who are seeking to admit a medical patient. The team of GPs organise investigations and seek alternative care pathways to provide the best possible patient care. This service is available twelve hours per day five days per week and limited hours during the weekend. BrisDoc Professional Line - GP Support to healthcare professionals with advanced decision making skills to avoid unnecessary conveyance to hospitals. Urgent primary care outside normal practice hours is accessible through NHS 111. GPs and nurses, who can offer telephone advice, face-to-face consultations, or home visits for patients who are housebound, provide this service. This service is available for treating conditions that cannot wait until your GP surgery reopens. These services are available from weekdays, 24 hours a day over the weekends and Bank Holidays. NHS 111 is a telephone triage service that makes it easier for the public to access local NHS healthcare services for medical help not a 999 emergency. NHS 111 is available 24 hours a day, 365 days a year. Acute Hospital Based Services ED/A&E departments Assess and treat people requiring immediate medical attention for serious illness or injury. Medical Assessment The medical assessment unit is the first point of entry for Unit patients referred to hospital as emergencies by their GP and Older Person Assessment Unit Surgical & Trauma Assessment Unit Eye Hospital Emergency Department GP Support Unit those requiring admission from the Emergency Department. This unit is set up to care for frail elderly patients who have specific care needs. It is managed by a multi organisational/multi-disciplinary team approach and aims to deliver high quality medical care and effective early discharge from Hospital. This receives direct GP referrals as well as patients transferred from the Emergency Department. Assess and treat people requiring immediate medical attention for serious injuries or conditions that are specific to eyes. The GP Support Unit (GPSU) is based in the Bristol Royal Infirmary (BRI). This service manages patient admissions into the hospital by taking telephone referrals from Page 22
23 Ambulatory Care Unit Primary Percutaneous Coronary Intervention Unit Community Based Services South Bristol Community Hospital GPs within local Bristol GP practices who are seeking to admit a medical patient. The team of GPs organise investigations and seek alternative care pathways to provide the best possible patient care. This service is available twelve hours per day five days per week. Ambulatory emergency care services provided in the Bristol Royal Infirmary based ACU, and in Southmead A&E This is a centre based in the Heart Institute at University Hospitals Bristol where procedures for the treatment of myocardial infarctions (heart attack) take place. South Bristol Community Hospital has taken on many of the services provided by the old Bristol General Hospital, which closed on 4 April University Hospitals Bristol is providing a number of services at South Bristol, listed below Day assessment Day surgery Homeopathic medicine Outpatients clinics Radiology Rehabilitation Stroke service Urgent care services Dental community based teaching Urgent Care Centre (based at South Bristol Community hospital) Equipment Service Early supported discharge team Mental Health Crisis Service Crisis Sanctuary Care Home Liaison Team The urgent care centre deals with minor injuries and illnesses and is staffed by experienced nurses who can treat both adults and children. X-Ray facilities are available. Patients can visit the urgent care centre without an appointment and it is open 8am-8pm every day of the week. This service provides equipment for patients at home or going home and needs to be ordered by qualified staff. This team works from the stroke wards at both the acute trusts to support early discharge. This service is available 24 hours a day 7 days a week and can be accessed by anyone via a single telephone number. This service is available from Thursday to Monday 7pm till 2am and provides a safe space out of hours for those who are experiencing high levels of emotional distress or precrisis. Accessed by self-referral. Group of professionals who work with the care home staff to support them to manage individuals with dementia/functional illness to enable them to stay in their usual place of Page 23
24 Assertive Engagement Service Intermediate Care Rapid Response Admission Avoidance Beds residence. Professional referral. This service is provided by AWP and works with individuals on an outpatient basis. This service aims to support individuals who have chaotic and complex issues including drugs, alcohol and homelessness. Rapid response responds within 30 minutes onwards for individuals over the age of 16 years to support them to remain at home. This is for people who have an acute health crisis that does not required hospital treatment. The rapid response team accesses these beds to offer alternative support to individuals who require temporary additional support. 3 admission avoidance beds at St Monicas 4 admission avoidance beds at South Bristol Community Hospital Intra Venous(IV) Therapy Service Falls Service Night sitting service Social Care Based Services Approved Mental Health Professional Service. Reablement and Out of Hours Home care Immediate Response Team The IV Service supports patients to receive medication via an IV route up to three times per day for a time limited period. The team will initiate treatment in conjunction with GPs and other medical staff and start treatment. They also support other health professionals to undertake the intervention as prescribed. A service which will respond to individuals who have fallen and not sustained an injury to help them off the floor. This service can be accessed by the community team and ambulance service. Rapid response can access this service to sit with individuals at home. Provides urgent mental health assessments during office hours by relevant professional. Direct referral. Out of Hours through Emergency Duty Team (SGCC). This service provides a 24/7 response to alarm calls generally for individuals who have fallen. It also responds to carers card requests where capacity allows and this may include night sits or scheduled visits to replace carer input if the carer has gone into hospital, for example. This team provides urgent social care assessments and support planning including day and night support via Care Direct during office hours. Page 24
25 It is clear that there are a number of challenges, which are highlighted in the table of service provision below: Service Provision Challenges Multiple and often confusing access points in an urgent or emergency situation Potential for multiple transfers and ineffective use of some key community facilities Poor integration in some areas across, primary, community and acute services, particularly during times of care transition Little focus on prevention and self-care alternatives Lack of consistent clinical accountability for care on transfer between organisations The need for improved pathways of care, not more services Figure 1: Bristol urgent care system NHS 111 Primary Care BrisDoc 24/7 professional line MIU SWASFT GP Out of hours Accident and Emergency - UHB 7 Day BRI GPSU Emergency Admissions UHB Page 25
26 Urgent Care Funding 1. With the development of Better Care Bristol and the drive towards integration, our ambition is to drive a significant shift in the focus of resources on urgent care away from acute hospital based care towards care based in people s home or their local community where it is safe to do so. 2. Acute hospital care will only be used for patients it would not be possible to care for safely and appropriately in a community setting or other environments. Whilst this type of transformation will take many years to achieve, over the life of this strategy we would like to make a significant shift towards this. Page 26
27 Central Manchester Newcastle West Nottingham City Birmingham Crosscity Newcastle North & East Leeds South and East Leeds West Bristol Leeds North Non elective admissions per 100,000 Our Local Population and Activity Trends 1. Overall Bristol has a low level of emergency admissions compared to other parts of the country and the overall number of emergency admissions has not increased as fast as in many other parts of the United Kingdom. Figure 1: Non-elective admissions for people aged 65+ per 100,000, Source: (Dr Foster Intelligence) 2. However, we have identified particular groups of people that our future model of delivery will need to specifically focus on. These are:- Younger Age Groups - 11% (4,343) of emergency admissions for people in Bristol were for patients aged under 16 [1]. Frail and Complex Demographic changes will place enormous pressure on the urgent care system in future. Forecasts suggest that there will be a 60% increase in emergency admissions among in the 75+ age group in the next 11 years. Whilst this age group only accounts for 13 % of our population, they account for 37% of our emergency admissions [5]. Page 27
28 Preventable Admissions Almost 20% of emergency admissions are classified as ambulatory care sensitive conditions, which should be treatable without the need for an admission. Bristol has a significantly lower rate of admissions for ambulatory care sensitive conditions compared with the rest of England in [NHS England]. Primary Care 1. Nationally, the overall primary care consultation rate increased from 3.9 consultations per person per year in 1995/6 to 5.5 in 2008/9. This is projected to hit 6.4 during 2015/16. For a population of 437,000 people this is equivalent to a rise from 1.1m to 2.8m over 20 years an increase of 156% over 20 years [4]. 2. The GP patient survey has indicated a positive association between high satisfaction with practices and lower ED attendance rates and conversely a strong correlation between poor access to general practice and high ED use. Out of Hours 1. BrisDoc responds to around an average of 10,222 out of hours calls from patients per month. Around 10% of those calls result in a GP visit, 27% advice and guidance and the rest are offered appointments at a primary and community care centre. 2. Improving integration and handover between in-hours, out of hours and other local urgent care services will be a key priority, in particular with regard to the focus on sharing critical information more effectively across the system. Ambulance Service 1. There was a steady increase in the number of incidents reported to the ambulance service, rising from 60,642 in 2010/2011 to 67,889 in 2013/14, an increase of 6%. This trend has continued in 2014/2015 [5]. 2. The proportion of incidents resulting in an emergency response has also risen by 6.38% between 2010/2011 and 2013/2014 [5]. Urgent Care Centre 1. Bristol has an urgent care centre operated by Bristol Community Health at the South Bristol Community Hospital. At present it sees an average of 1153 Page 28
29 Length of Stary (Days) more or less than the expected rate Length of Stary (Days) more or less than the expected rate attendances every week 1. The trend is remaining relatively steady in the past two years. Emergency Attendances 1. A&E attendances for patients from the Bristol CCG area have continued to rise in numerical terms, but the rate within the population has declined. In the period between April and October 2014 there were 78,697 attendances for Bristol patients at A&E [5]. 2. The figure above is 3.6% higher than the same period in However this is an increase of only 0.02% as a directly standardised rate for the same period. Comparison of lengths of stay for emergency admissions. 2.5 Emergency admissions to medical specialties Length of stay vs expected, Emergency admissions to surgical specialties Length of stay vs expected, Bradford Southend Barts Leicester James Paget Colchester Norfolk & Norwich Derby South Tees Oxford Radcliffe North Cumbria Devon & Exeter Nottingham UCL Brighton North Staffs Wirral Royal Free South Mancester Imperial Barking Aintree North Middlesex Plymouth St George's Epsom King's Birmingham Leeds Addenbrookes Cambridge UHB West Middlesex Sheffield Newcastle Royal Liverpool Basildon & Thurrock Guys and St Thomas Southampton North Bristol NHS Trust Central Manchester -3.5 West Middlesex Southend North Staffs Epsom North Middlesex East Kent Brighton Guy's and St Thomas' Cambridge Addenbrookes Devon & Exeter Barts North Cumbria Homerton Pxfprd Radcliffe UHB Colchester Imperial Coventry Liverpool King's NBT UCL Chelsea Royal Free St George's Norfolk & Norwich Plymouth Barking Aintree Nottingham Derby Bradford James Paget Southampton Leicester Wirral Hull Sheffield Basildon Birmingham Children's Leeds South Mancester Central Manchester Morecombe Bay South Tees Newcastle Birmingham These graphs show the difference between expected and actual length of stay for emergency admissions to medical and surgical specialties in university hospitals (i.e. large acute hospitals) between January and December 2014, sourced from the Dr Foster benchmarking tool. This tool calculates the expected length of stay adjusted for case mix if the rate was the same as it was for all hospitals in England. If a hospital has a length of stay above the axis then the average length of stay is higher than expected. From the data above it can be seen that both of Bristol s large hospitals (highlighted in yellow) have higher than expected lengths of stay for medical admissions quite different to other similar hospitals in England. The picture is much better for emergency admissions to surgical specialities with lower than expected lengths of stay in line with most similar hospitals in England. (Dr Foster Intelligence). 1 Weekly Sitrep data, HSCIC. Page 29
30 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Percentage change since Q Emergency Admissions 1. According to NHS comparators, the NHS Bristol standardised emergency admission rate is amongst the lowest compared to the NHS core cities in (NHS England) 2. However there will be key challenges in the future as a result of the changing demography and population growth across the two ED sites (University Hospitals Bristol and Southmead Hospital) where we see around 39,251 emergency admissions per year. (South Central and West CSU) 3. Emergency admissions have increased year on year from 19,680 in the first six months of 2010/2011 to 20,186 in the same period in 2014/15. (South Central and West CSU) Figure 2: Emergency admissions for NHS Core cities compared with Q1 2009/ % Trend compared with Q1 2009/ Present 20% 15% 10% 5% 0% -5% -10% -15% -20% -25% Nhs Bristol Ccg Source: (Dr Foster Intelligence) 4. In the period between April and October 2014 there has been an increase of 1500 additional emergency admissions via A&E [5]. Page 30
31 5. While there has been relative stability in emergency admissions for some years, the increasing numbers of older people within Bristol may present a longer term challenge to maintaining Bristol s current low rates. Page 31
32 Community Services 1. There are 195 community beds across Bristol. University Hospitals Bristol manages 53 of these beds at South Bristol Community Hospital. 131 beds in the community (not including 8 social care interim beds) admitted 651 patients between January and November These beds are used flexibly especially at times of pressure to support the flow of patients through the whole health and social care system. Beds NHS funded out of hospital (OOH) beds Residential Rehab Centre beds Nursing Home Rehab beds End of Life Care community beds Admission Avoidance beds Services 52 NHS funded out of hospital beds. These are for patients who are medically fit for discharge but require continuing discharge planning assessments. There were 171 admissions from January to November 2014 with an average length of stay of 35 days. 40 rehab beds managed by Bristol City Council and assessed via the Community Discharge Co-ordination Centre. These are for patients who have rehab needs, which can be met in a non-acute setting. There were 182 admissions with an average length of stay of 36 days from January to November rehab beds overseen by the Community Discharge Co-ordination Centre. There were 62 admissions with an average length of stay of 57 days from January to November End of Life care beds managed by Palliative Care Home Support. These beds are used for patients in receipt of Continuing Healthcare Fast Track funding. There were 85 admissions with an average length of stay of 36 days from January to November beds managed by the Rapid Response team. These are for people in the community who cannot remain at home and require urgent care but Page 32
33 Social Care Resource beds Social Care Interim beds not in an acute setting. There were 85 admissions with an average length of stay of days from January to November beds managed by Social Care. This is a council run reablement centre. There were 66 admissions with an average length of stay of 41 days from January to November There will be an additional 5 beds from January beds managed by Bristol City Council. What does it mean for Bristol? 1. Bristol CCG is committed to providing high quality and fit for purpose services for its population at all times. To achieve this requires examining our approaches to accommodate a number of key challenges. These include: Attracting and retaining a qualified and sustainable healthcare workforce in all staff groups. Creating and supporting the workforce required to delivery future demands will be top of the list of priorities. Ensuring high quality, safe and clinically sustainable services, which meet required standards of care and are safe 24/7. This means having the appropriate infrastructure to support our new ways of working. Dealing with demography: While at present Bristol has a relatively young population, compared with local health geographies, the increasing numbers of older people may present a challenge to sustainability in the longer term. In addition, proactive approaches to prevent risk behaviours amongst the large proportion of younger people will be required. Achieving greater integration of care: We need this to remove the fragmentation of services across primary, community, social and acute care that leads to patients being forced to move between beds, teams and care settings with inadequate communication and information. Page 33
34 Developing Transformation Capacity: Creating the conditions to deliver large-scale system organisational change whilst engaging staff that provide services on a day-to-day basis will be a significant challenge. Page 34
35 Chapter 3 The Case for Change National Context The Keogh Review The inability of emergency departments nationally to meet the 4-hour waiting time target in the early months of 2013 reflected the ever-greater demands that are being placed on the emergency care system. The problems that have manifested themselves within emergency care cannot be attributed to any one factor within the system and most certainly cannot be attributed to inefficiencies in the emergency departments. Emergency departments are a barometer of the efficient operation of the whole local health and social care economy and are the place where failings in the efficient operations of the whole system materialise very quickly. What has been identified is the broader challenge resulting from the fragmented provision of emergency and urgent care and a structure that is confusing to patients. Emergency Departments remain the default option for many patients. The rise of 40% in emergency admissions, between 2003/4 and 2010/11 has been attributed to a number of factors including a rise in the number of frail elderly people, increasing morbidities, more treatable illnesses and increased public expectation of healthcare. All of these contribute to ever-greater pressure on health and social care services, an increase in short stay admissions and an increase in emergency re admissions. Nationally, there is high demand in the system, for example last year there were: 5.2 million emergency admissions 21.7 million attendances at ED departments, MIUs and UCCs 6.7 million emergency ambulance journeys 24 million calls to NHS urgent and emergency care telephone services The evidence base from the Urgent and Emergency Care Review June 13 sets out to review the urgent and emergency system in England and draws out evidence to illustrate the main challenges it currently faces. Starting with overall patient experience it highlights issues within each part of the urgent and emergency care system in the order of the perceived levels of patient need that it addresses: Self-care and self-management Telephone care Face to face care 999 emergency services Emergency Departments Page 35
36 The review has identified 12 system design objectives. These are set out below: Make it simpler for my family and me / carer to access and navigate urgent and emergency care services and advice Increase my or my family / carer s awareness of early detection and options for self-care and support me to manage my acute or long term physical mental condition Increase my or my family/carer s awareness of and publicise the benefits of phone before you go If my need is urgent, provide me with guaranteed same day access to a primary care team that is integrated with my GP practice and my hospital specialist team Improve my care, experience and outcome by ensuring early senior clinical input in the urgent and emergency care pathway Wherever appropriate manage me where I present (including at home and over the telephone) If it is not appropriate to manage me where I present (including at home and over the phone) take or direct me to a place of definitive treatment within a safe amount of time; ensure I have rapid access to a highly specialist centre if needed Ensure all urgent and emergency care facilities are capable of transferring me urgently and that the mode of transport is capable, appropriate and authorised Information, critical for my care is available to all those treating me Where I need wider support for my mental, physical and social needs ensure it is available Each of my clinical experiences should be part of programmes to develop and train the clinical staff and ensure their competence and the future quality of the service is constantly developed The quality of my care should be measured in a way that reflects the urgency and complexity of my illness These are suggested outcomes, which should be delivered in any future urgent, and emergency care system taking a patient- centred focus, which we are fully committed to addressing. Page 36
37 Our Local Context We are developing our urgent care strategy in an economically challenging environment in which service delivery will significantly change over the next few years. There are a number of external and internal factors, which we explicitly need to take account of, some of which we recognise as risks or threats to our success. These include: Financial Challenge for Bristol The financial challenge facing the Bristol health and social care economy is significant. Over the next few years, health and social care commissioners need to release savings from the existing health system to reinvest into more services closer to home and in the community working together. Bristol CCG s draft financial plan shows that in order to meet our financial targets we need to make efficiency savings of circa 20m during 2015/16. In 2015/16 this equates to circa 6m in urgent care, which will be achieved in the main by renegotiating some elements of our contracts and reducing emergency admissions, lengths of stay, excess bed days and overall unplanned activity within our hospitals to enable us to invest in more self-care and preventative care in the community. Future of Acute Hospital Services in Bristol Commissioning high quality and accessible urgent care services is an important priority for Bristol CCG. Our urgent care focus aims to have the patient seen by the right clinician, at the right time in the right place. This includes providing more services in the community, with appropriate use of secondary care, maximising primary care access and managing patients in the most clinically appropriate costeffective setting for their urgent care needs. The NHS England Emergency Care Intensive Support Team (ECIST), invited by University Hospitals Bristol NHS Foundation Trust, undertook a system diagnostic of our urgent care system in the summer of The key recommendations from this review have been included within this strategy. The Urgent Care strategy will continue to be informed by the outcomes of this review and any other reviews undertaken for urgent care and revised accordingly. The Care Quality Commission's 2014 inspection identified the need for all parts of the system to work together to improve patient care. This strategy builds on those recommendations. Page 37
38 Social Care Transformation The changing landscape of social care presents a number of significant threats for delivery of our Urgent Care Strategy in Bristol. The Council has faced real term cuts in social care budgets at a time when demographics suggest that increased funding and access to services is required. To support the efficiency challenge for the Council, the whole system is working jointly as part of our Better Care Bristol programme to ensure that we explore opportunities for more integration, joining up services and to remove duplication in the system and improve joint assessments. We will look to develop more integration of health and social care where appropriate to support the delivery of an integrated system approach to urgent care. The exact model will be developed as part of the delivery of this strategy and our Better Care Bristol vision and ambitions. The new Care Act consolidates all existing legislation under which adult social care is delivered and introduces reforms in funding and charging for care and support. The Care Act is to be implemented into two stages. In April 2015 changes in overall duties for wellbeing, assessment and eligibility come into effect. In April 2016 reforms of funding and charging for care will come into effect. Adult social care will need to transform in order to meet these new statutory duties. Bristol has embarked on a new programme of work to transform social care. This is a major change programme over the next 2/3 years to ensure that the Council continues to offer high quality services that meet the requirement of the Care Bill and other national legislation, and contribute to resolving the Council s financial challenges. The programme will review and reform all aspects of adult social care. It will result in new models of care that promote health and independence, increase choice and control and reduce the need for long term services by maximising the impact of investment in prevention and recover. This forms part of Better Care Bristol, which is a system wide programme focused around prevention, self-care, supporting people more effectively in the community, improved rehabilitation and reablement to support efficient discharge from hospital and enable people to go home as soon as they are medically fit to do so. What will the future look like? Local Context Bristol is the largest city in the South West and the seventh largest in the country. The resident population of Bristol CCG is 432,500 and is considerably larger than the average national CCG footprint of 261,000. This population is served by a total of 56 GP practices. These practices are grouped into localities Page 38

39 with distinct local needs and ambitions. Bristol Population In general, Bristol has worse health outcomes than England overall and much worse outcomes than neighbouring local authorities. Deprivation is higher than the national average. 60,665 people in Bristol live in areas that are amongst the most deprived 10% in England and 1,630 people live in the most deprived 1% of areas in England. 19,700 children live in poverty. Life expectancy at birth for females is similar to the national average but for males it is significantly worse. Bristol has a resident population of 432,500 (mid 2012 ONS estimate), with 80,700 children under 16 (18.6% of the population), a working age (16-64 year olds) population of 294,600 people (68.1%), and 57,200 older people over 65 (13.2%). This is a significantly younger age profile than the national average. 16% of the Bristol population (68,640) describe their ethnicity as black or minority ethnic (BME), higher than the 14% average for England & Wales, and increased significantly from 8.2% in Across the city, by Bristol CCG locality, the BME population ranges from 7.4% in South Bristol and 12.1% in North & West to 30.6% in Inner City & Bristol East locality (shown separately as 21% East & 40% in the Inner City). Within Bristol s over 65 year old population, only 5.2% (2,930 people) are from BME groups, compared to the all-age average of 16%, and for children (0-15), the Bristol average is 27.8% BME. Public Health Outcomes Framework 2013 ( Life Expectancy Life expectancy at birth in Bristol is similar to national levels for females, but significantly worse for males (78.3 years v years). However, both male and female life expectancy does continue to Page 39
40 rise. For healthy life expectancy at birth Bristol s figures are lower than the England average but are not significantly different. There is an 8.4-year gap for males between the most deprived and most affluent areas in Bristol, for females it is 4.9 years. Wider determinants of health Compared to England, Bristol does not perform particularly well on these outcomes; in particular many related to childhood children in poverty, pupil absence, first time entrants to the justice system and year olds not in education, employment or training. Health Improvement Bristol s outcomes are mainly similar to England, however a number of outcomes are significantly worse: breast and cervical cancer screening rates are worse than the England average and are showing no sign of either improving. Bristol performs significantly worse than England for hospital admissions for injuries due to falls both for people aged and people aged over 80. Although hospital admissions for falls are high, hip fractures for the same age groups are lower in Bristol than in England as a whole. Health Protection Bristol is significantly worse than England for uptake of a number of key vaccinations Hib/Men C booster in 2 and 5 year olds, MMR, HPV and flu vaccination for at risk individuals. Flu vaccinations for people aged 65yrs+ are significantly better than England. Healthcare and premature mortality Bristol s premature mortality (under 75s) is worse than England for some causes, although overall premature mortality is falling. Premature cancer mortality, in particular for males, is significantly worse than England and shows no sign of catching up with the national average. Also premature mortality due to liver disease, in particular in males, is significantly worse than England. Page 40
41 Public Health England Health Profile 2013 ( All age all-cause mortality is falling, however, the gap between Bristol and England has not narrowed. Premature mortality for CVD has fallen and the gap between Bristol and England has almost closed. Premature cancer mortality has fallen slightly over the last ten years but the gap has not narrowed and Bristol is significantly worse than England. Of the 32 indicators in the 2013 PHE Health Profile, Bristol is significantly worse than England on 13 of them (41%). Bristol is significantly better on 7 indicators (22%). The main areas of poor performance are hospital stays for self-harm, hospital stays for alcohol related harm (still rising), drug misuse, male life expectancy, smoking related mortality and premature cancer mortality (the main causes are lung cancer, breast, pancreas and oesophageal). Page 41
42 We know the current system is fragmented and difficult to navigate. The public s perception is that the Accident & Emergency Department can do everything and is the easiest way to access care. There is poor understanding of urgent care centres, out of hospital services and walk-in-centres, and this has led the public to feel confused about where to access the right services in a time of urgent need. It is our intention in Bristol to rationalise the myriad of options down to a lower number of easy to understand, and more importantly easy to navigate emergency care access points. We know that sharing of patient information is poor as they move between different providers and this creates a significant challenge in providing care in an emergency resulting in patients often waiting longer, having repeated assessments and diagnostics and unnecessary duplication of care. Sometimes important information such as drug histories are simply not accessible at the time of urgent treatment. As well as creating delays and inefficiencies it also has a significant impact on the quality of care. It is our intention to ensure that all professionals that have a role to play in someone s care, can easily access all of the relevant information and medical history to enable effective provision of that care. After several years of above inflation growth, supplemented with historically high levels of year on year growth, the NHS is now in its third year of limited growth. The Comprehensive Spending Review for 2015/ /18 has confirmed that this funding freeze will continue into the medium term and that the level of challenge involved will be proportionally bigger. This is particularly relevant for urgent care, which not only consumes a large proportion of health care sources, but because of the rapid increase in demand and expenditure. It is our intention in this strategy to maximise value for money within a high quality care system by reducing, changing or even closing and re-providing services in a different way to ensure sustainability for those services that are considered core to the delivery of urgent care. Quality of patient care and experience is often influenced by the number and seniority of the clinical staff available, which can often depend on the time of day or day of the week. This prompts patients to avoid these services and go directly to hospital A&E, where the workforce is often influenced by these working practices. This has resulted in difficulty filling key positions across the system to manage demand effectively and recruit and retain staff in key services. It is our intention to ensure that we deploy staffing resources across the urgent care system as effectively as possible and to ensure that all partners play an active role in changing the way they plan services and roster staff in order to achieve this. The current system is not joined up or co-ordinated to support many frail and complex patients, especially those with long term conditions with urgent and emergency care needs so the default solution is an ambulance journey, attendance at A&E and possible hospital admission. With an expected growth in the number of people over 75years old by 2021, our challenge is embedding more self- Page 42
43 Population management and out of hospital care alternatives to support people alongside our health and social care partners. It is our intention, through the development of the Better Care Bristol programme and through the Social Care Transformation programme to radically transform the way in which urgent care services for the frail and elderly are designed and provided in Bristol. These trends, projects and challenges are complex and as a health and social care economy we have not yet defined the true impact of these factors and how we will respond to them across the whole system. We will develop a demand and capacity model, which is system wide and supported by all partners to inform future decisions that we need to take around urgent care. Figure 3: Projected population growth in the City of Bristol, ,000 60,000 50,000 40,000 30,000 20,000 10, People aged People aged People aged People aged People aged People aged 90 and over Source: Poppi Page 43
44 Chapter 4 Managing the transition Governance Arrangements The Urgent Care Steering Group will take ultimate responsibility for the development of our strategy and will hold partners accountable for delivering the actions outlined in this strategy. The CCG Clinical Lead chairs the Urgent Care Steering Group for Urgent Care with senior managers across all commissioning partner organisations represented. A System Resilience Group has been established, which covers Bristol, North Somerset and South Gloucestershire area (BNSSG) and they will work with partners to agree intentions where these are wider than Bristol CCG & Bristol City Council boundaries. Bristol CCG and Bristol City Council are responsible to the Health & Wellbeing Board which will hold the commissioners and providers accountable for delivery. Programme Management The foundations for effective delivery of our urgent care strategy are grounded in principles we have established as partners and set out clearly in the Better Care Fund Guidance, where commissioners and providers will work together to achieve whole system change and are jointly responsible. We have set up an Urgent Care Transformation Programme Board and will develop together a joint programme of work, setting out the key projects to be delivered and their timescales. These will be reviewed regularly in terms of focus, scope, pace and outcome delivery against our intentions set out in this document. We will use a programme management approach for delivery of all projects across the system. Page 44
45 Monitor and Measuring Impact The measure of success that we will use to monitor the successful implementation of our strategy is: Impact Areas Aligned to Strategic Principles Measures Avoid Acute Hospital Emergency Admissions 1. Reduced number of 999 Calls 2. Reduced number of Emergency Department attendances 3. Reduced number of emergency admissions overall 4. Reduce / prevent number of unnecessary or avoidable emergency admissions from care homes 5. Increased number of acute ambulatory care sensitive treatments without admission 6. Reduced number of inpatient hospital infections Treat with the Best care in the Best Place in the Fastest Time 1. Consistent delivery of improved performance against the 95% standard 2. Increased number of Minor Injury Units and Urgent Care Centres 3. Improved performance on ambulance response times 4. Increased number of admissions to virtual wards or referrals to community teams 5. Reduced ambulance conveyance rate 6. Increased number of urgent care centre attendances 7. Reduced number of cancelled elective admissions 8. Reduced number of readmissions < 30 days of discharge 9. Achievement of 100% stroke Page 45
46 performance 10. Reduced number of ambulance turnaround breaches 11. Reduced trolley waits over 8 hours in ED Discharge from Acute Settings As Soon As Possible- Improved Patient Flow 1. Reduced number of patients in acute hospitals that no longer require acute hospital care 2. Reduced average length of stay following an emergency admission 3. Reduced average patient time in ED 4. Reduced delayed discharges from secondary care 5. Increase timeliness of discharge to other care settings 6. Increased proportion of discharges directly back to normal place of residence Page 46
47 Page 47
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Seven day hospital services: case study. South Warwickshire NHS Foundation Trust
 Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Discharge to Assess Standards for Greater Manchester
 Discharge to Assess Standards for Greater Manchester 1 Contents 1. Introduction... 3 2. Definition of Discharge to Assess... 3 3. Discharge to Assess Pathways... 4 4. Greater Manchester Standards for Discharge
Discharge to Assess Standards for Greater Manchester 1 Contents 1. Introduction... 3 2. Definition of Discharge to Assess... 3 3. Discharge to Assess Pathways... 4 4. Greater Manchester Standards for Discharge
Developing an urgent care strategy for South Tees how you can have your say July/August 2015
 Developing an urgent care strategy for South Tees how you can have your say July/August 2015 Foreword Commissioning high quality, accessible urgent care services is a high priority for South Tees Clinical
Developing an urgent care strategy for South Tees how you can have your say July/August 2015 Foreword Commissioning high quality, accessible urgent care services is a high priority for South Tees Clinical
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
DRAFT Service Specification GP-led Urgent Treatment Centre (UTC) Service
 Service") DRAFT Service Specification GP-led Urgent Treatment Centre (UTC) Service Executive summary: The Cornwall Sustainability and Transformation Plan known as Shaping our Future will describe a new model of
DRAFT Service Specification GP-led Urgent Treatment Centre (UTC) Service Executive summary: The Cornwall Sustainability and Transformation Plan known as Shaping our Future will describe a new model of
This paper explains the way in which part of the system is changing to become clearer and more accessible, beginning with NHS 111.
 Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
Shetland NHS Board. Board Paper 2017/28
 Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Local system reviews. Interim report
 Local system reviews Interim report December 2017 The Care Quality Commission (CQC) is the independent regulator of health and adult social care in England. We make sure that health and social care services
Local system reviews Interim report December 2017 The Care Quality Commission (CQC) is the independent regulator of health and adult social care in England. We make sure that health and social care services
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Final Version Simple Guide to the Care Act and Delayed Transfers of Care (DTOC) SIMPLE GUIDE TO THE CARE ACT AND DELAYED TRANSFERS OF CARE (DTOC)
 SIMPLE GUIDE TO THE CARE ACT AND DELAYED TRANSFERS OF CARE (DTOC)") SIMPLE GUIDE TO THE CARE ACT AND DELAYED TRANSFERS OF CARE (DTOC) 1. UNDERPINNING PRINCIPLES Across the whole system, our common aims are to: Improve services for patients by avoiding situations where,
SIMPLE GUIDE TO THE CARE ACT AND DELAYED TRANSFERS OF CARE (DTOC) 1. UNDERPINNING PRINCIPLES Across the whole system, our common aims are to: Improve services for patients by avoiding situations where,
Briefing on Shaping Our Future urgent care work stream progress
 Briefing on Shaping Our Future urgent care work stream progress 1. Purpose The purpose of this paper is to describe, update and clarify on the Cornwall and the Isles of Scilly s Shaping Our Future urgent
Briefing on Shaping Our Future urgent care work stream progress 1. Purpose The purpose of this paper is to describe, update and clarify on the Cornwall and the Isles of Scilly s Shaping Our Future urgent
South East Essex. Discharge to Assess Strategy
 South East Essex Discharge to Assess Strategy 2018-2020 Version 3.5 27 th March 2018 Document Control: Revision: Name Date: Version 2.0 Shirley Regan 12 December 2017 Version 2.1 Amendments-Paul 19 December
South East Essex Discharge to Assess Strategy 2018-2020 Version 3.5 27 th March 2018 Document Control: Revision: Name Date: Version 2.0 Shirley Regan 12 December 2017 Version 2.1 Amendments-Paul 19 December
Listening to and collecting your views and experiences about urgent care in Newcastle
 Listening to and collecting your views and experiences about urgent care in Newcastle 20 November 2017 to 10 January 2018 Right care, time and place Welcome NHS Newcastle Gateshead Clinical Commissioning
Listening to and collecting your views and experiences about urgent care in Newcastle 20 November 2017 to 10 January 2018 Right care, time and place Welcome NHS Newcastle Gateshead Clinical Commissioning
Shaping the best mental health care in Manchester
 Clinical Transformation Plans Manchester Shaping the best mental health care in Manchester Meeting the needs of our communities Improving Lives OUR SHARED WAY AHEAD... Clinical Service Transformation in
Clinical Transformation Plans Manchester Shaping the best mental health care in Manchester Meeting the needs of our communities Improving Lives OUR SHARED WAY AHEAD... Clinical Service Transformation in
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
What will the NHS be like in 5 years, 20 years time?
 What will the NHS be like in 5 years, 20 years time? NHS Castle Point and Rochford Clinical Commissioning Group (CCG) and NHS Southend CCG are groups of local doctors and other health professionals who
What will the NHS be like in 5 years, 20 years time? NHS Castle Point and Rochford Clinical Commissioning Group (CCG) and NHS Southend CCG are groups of local doctors and other health professionals who
The Emergency Care Intensive Support Team (ECIST) Driving Improvement along Emergency Care Pathways: A Master Class
 Driving Improvement along Emergency Care Pathways: A Master Class") The Emergency Care Intensive Support Team (ECIST) Driving Improvement along Emergency Care Pathways: A Master Class WORKSHOP INFORMATION Morning Workshops (Workshops 1-4) Delegates have a choice of two
The Emergency Care Intensive Support Team (ECIST) Driving Improvement along Emergency Care Pathways: A Master Class WORKSHOP INFORMATION Morning Workshops (Workshops 1-4) Delegates have a choice of two
Greater Manchester Health and Social Care Strategic Partnership Board
 Greater Manchester Health and Social Care Strategic Partnership Board 7 Date: 13 October 2017 Subject: Report of: Greater Manchester Model for Urgent Primary Care Dr Tracey Vell, Associate Lead for Primary
Greater Manchester Health and Social Care Strategic Partnership Board 7 Date: 13 October 2017 Subject: Report of: Greater Manchester Model for Urgent Primary Care Dr Tracey Vell, Associate Lead for Primary
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Seven Day Services Clinical Standards September 2017
 Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Seven Day Services Clinical Standards September 2017 11 September 2017 Gateway reference: 06408 Patient Experience 1. Patients, and where appropriate families and carers, must be actively involved in shared
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report
 Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Plan for investment of retained marginal rate payment for emergency admissions in Gloucestershire
 Plan for investment of retained marginal rate payment for emergency admissions in Gloucestershire 1. Purpose of document This document summarises and explains how Gloucestershire CCG has used the funds
Plan for investment of retained marginal rate payment for emergency admissions in Gloucestershire 1. Purpose of document This document summarises and explains how Gloucestershire CCG has used the funds
NHS ENGLAND BOARD PAPER
 NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
Recommendations of the NH Strategy
 Urgent care Newark Hospital should continue to provide sub-acute care1, based on the existing ambulance diversion protocol. Refine the ambulance protocol to include additional sub-acute presentations that
Urgent care Newark Hospital should continue to provide sub-acute care1, based on the existing ambulance diversion protocol. Refine the ambulance protocol to include additional sub-acute presentations that
Wolverhampton CCG Commissioning Intentions
 Wolverhampton CCG Commissioning Intentions 2015-16 * Areas of particular focus and priority CI Ref Contract Provider Brief CI001 CI002 CI003 Child Protection Information Sharing Implement the new Child
Wolverhampton CCG Commissioning Intentions 2015-16 * Areas of particular focus and priority CI Ref Contract Provider Brief CI001 CI002 CI003 Child Protection Information Sharing Implement the new Child
YOUR MORTALITY RATE IS YOUR PULSE
 4 YOUR MORTALITY RATE IS YOUR PULSE (KEEP YOUR FINGER ON IT) MEASURING MORTALITY IN THE NHS MEASURING DEATHS IS A GOOD WAY OF CHECKING HOW WELL HOSPITALS ARE CARING FOR PATIENTS FIND MORE INFORMATION ABOUT
4 YOUR MORTALITY RATE IS YOUR PULSE (KEEP YOUR FINGER ON IT) MEASURING MORTALITY IN THE NHS MEASURING DEATHS IS A GOOD WAY OF CHECKING HOW WELL HOSPITALS ARE CARING FOR PATIENTS FIND MORE INFORMATION ABOUT
Guideline scope Intermediate care - including reablement
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
Report to the Board of Directors 2016/17
 Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
Attachment 8 Report to the Board of Directors 2016/17 Date of meeting 30 September 2016 Subject Report of Prepared by Purpose of report Previously considered by (Committee/Date) Local A&E Delivery Board
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Health and Care Framework
 Annex 1 Health and Care Framework The NHS Grampian 2020 A Possible Future 1. NHS Grampian has agreed its Health Plan and has embarked on its Health and Care Framework (H&CF) process to determine in detail
Annex 1 Health and Care Framework The NHS Grampian 2020 A Possible Future 1. NHS Grampian has agreed its Health Plan and has embarked on its Health and Care Framework (H&CF) process to determine in detail
OFFICIAL. Integrated Urgent Care Key Performance Indicators and Quality Standards Page 1 of 20
 Integrated Urgent Care Key Performance Indicators and Quality Standards 2018 Page 1 of 20 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing
Integrated Urgent Care Key Performance Indicators and Quality Standards 2018 Page 1 of 20 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing
Urgent Treatment Centres Principles and Standards
 Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Improving General Practice for the People of West Cheshire
 Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Marginal Rate Emergency Threshold. Executive Summary
 Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
NHS Provider Trust CEOs CCG Accountable Officers CCG Clinical Leads Local Authority Chief Executives and Directors of Adult Social Care
 12 October 2017 Pauline Philip National Urgent and Emergency Care Director Wellington House 133-155 Waterloo Road London, SE1 8UG To: Cc: NHS Provider Trust CEOs CCG Accountable Officers CCG Clinical Leads
12 October 2017 Pauline Philip National Urgent and Emergency Care Director Wellington House 133-155 Waterloo Road London, SE1 8UG To: Cc: NHS Provider Trust CEOs CCG Accountable Officers CCG Clinical Leads
about urgent healthcare
 The NHS your views about urgent healthcare The NHS Helping you get the most out of local services Tuesday 22 November to Friday 23 December 2016 The NHS Better health for Sunderland 1 1 Your views about
The NHS your views about urgent healthcare The NHS Helping you get the most out of local services Tuesday 22 November to Friday 23 December 2016 The NHS Better health for Sunderland 1 1 Your views about
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Norfolk and Waveney STP - summary of key elements
 Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Our community nursing roles
 Our community nursing roles Community Nursing Services provide nursing care to house-bound patients within the community. Our aim is to help patients to remain healthy and independent for as long as possible,
Our community nursing roles Community Nursing Services provide nursing care to house-bound patients within the community. Our aim is to help patients to remain healthy and independent for as long as possible,
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Welcome. PPG Conference North and South Norfolk CCGs June 14 th 2018
 Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
IUC and Vanguard. Greater Nottingham Integrated Urgent Care 1
 IUC and Vanguard The 2016/17 Vanguard funding has been confirmed at 1.3M This funding is to deliver the 8 elements of Integrated Urgent Care by March 2017 With careful management of funds we will be able
IUC and Vanguard The 2016/17 Vanguard funding has been confirmed at 1.3M This funding is to deliver the 8 elements of Integrated Urgent Care by March 2017 With careful management of funds we will be able
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Integrated heart failure service working across the hospital and the community
 Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
DRAFT. Rehabilitation and Enablement Services Redesign
 DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
Urgent care strategy: 2014/ /20
 Urgent care strategy: 2014/15 2019/20 1 Version control Date Version Discussed at 11 th November 2014 1.0 Urgent care strategy task and finish group: sections 1, 2 and 3. Urgent care board: sections 1,
Urgent care strategy: 2014/15 2019/20 1 Version control Date Version Discussed at 11 th November 2014 1.0 Urgent care strategy task and finish group: sections 1, 2 and 3. Urgent care board: sections 1,
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Implementing NHS Services Seven Days a Week
 Implementing NHS Services Seven Days a Week Deborah Williams 7 Day Services Programme Manager NHS England November 2015 NHS Five Year Forward View To reduce variations in when patients receive care, we
Implementing NHS Services Seven Days a Week Deborah Williams 7 Day Services Programme Manager NHS England November 2015 NHS Five Year Forward View To reduce variations in when patients receive care, we
04c. Clinical Standards included in the Strategic Outline Care part 1, published in December 216
 0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
Report to the Board of Directors 2015/16
 Attachment 9 Report to the Board of Directors 2015/16 Date of meeting 18 Subject Report of Prepared by Seven Day Services Medical Director Ashling Rivá, Project Manager Previously considered by Transformation
Attachment 9 Report to the Board of Directors 2015/16 Date of meeting 18 Subject Report of Prepared by Seven Day Services Medical Director Ashling Rivá, Project Manager Previously considered by Transformation
Unscheduled care Urgent and Emergency Care
 Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
Unscheduled care Urgent and Emergency Care Professor Derek Bell Acute Medicine Director NIHR CLAHRC for NW London Imperial College London Chelsea and Westminster Hospital Value as the overarching, unifying
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Quality and Leadership: Improving outcomes
 Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
This SLA covers an enhanced service for care homes for older people and not any other care category of home.
 Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Committee of Public Accounts
 Written evidence from the NHS Confederation AMBULANCE SERVICE NETWORK/NATIONAL AMBULANCE COMMISSIONING GROUP KEY LINES ON FUTURE MODELS FOR AMBULANCE SERVICE COMMISSIONING Executive Summary Equity and
Written evidence from the NHS Confederation AMBULANCE SERVICE NETWORK/NATIONAL AMBULANCE COMMISSIONING GROUP KEY LINES ON FUTURE MODELS FOR AMBULANCE SERVICE COMMISSIONING Executive Summary Equity and
Online library of Quality, Service Improvement and Redesign tools. Discharge planning. collaboration trust respect innovation courage compassion
 Online library of Quality, Service Improvement and Redesign tools Discharge planning collaboration trust respect innovation courage compassion Discharge planning What is it? A specific targeted discharge
Online library of Quality, Service Improvement and Redesign tools Discharge planning collaboration trust respect innovation courage compassion Discharge planning What is it? A specific targeted discharge
Improving Mental Health Services in Bath & North East Somerset
 Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Urgent & Emergency Care Strategy Update
 RCCG/GB/17/144 Urgent & Emergency Care Strategy Update 1. Introduction The purpose of this paper is to provide assurance on the effective delivery to date of our urgent and emergency care strategy within
RCCG/GB/17/144 Urgent & Emergency Care Strategy Update 1. Introduction The purpose of this paper is to provide assurance on the effective delivery to date of our urgent and emergency care strategy within
Mental Health Crisis Pathway Analysis
 Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
SAFE STAFFING GUIDELINE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
MKCCG Estates Statement January 2015
 MKCCG Estates Statement January 2015 This statement should be read in conjunction with the Milton Keynes CCG Primary Care Strategy and Care Closer to Home Strategy. Background Milton Keynes CCG (MKCCG)
MKCCG Estates Statement January 2015 This statement should be read in conjunction with the Milton Keynes CCG Primary Care Strategy and Care Closer to Home Strategy. Background Milton Keynes CCG (MKCCG)
Health and care services in Herefordshire & Worcestershire are changing
 Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Seven day hospital services: case study. University Hospital Southampton NHS Foundation Trust
 Seven day hospital services: case study University Hospital Southampton NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health
Seven day hospital services: case study University Hospital Southampton NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health
Calderdale and Huddersfield NHS Foundation Trust End of Life Care Strategy
 Calderdale and Huddersfield NHS Foundation Trust End of Life Care Strategy 2016-2017 Contents Acknowledgements Subject Page Number 1. Introduction 4 2. Vision 5 3. National policy Context 5-6 4. Local
Calderdale and Huddersfield NHS Foundation Trust End of Life Care Strategy 2016-2017 Contents Acknowledgements Subject Page Number 1. Introduction 4 2. Vision 5 3. National policy Context 5-6 4. Local
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
Strategic Plan for Fife ( )
") www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
OFFICIAL. Commissioning a Functionally Integrated Urgent Care Access, Treatment and Clinical Advice Service
 Our Ref: BH/2015/253 Publications Gateway Ref. No. 03568 NHS England Quarry House Quarry Hill Leeds LS2 7UE Email : england.nhs111@nhs.net To: CCG Accountable Officers CCG Clinical Leaders Cc: Regional
Our Ref: BH/2015/253 Publications Gateway Ref. No. 03568 NHS England Quarry House Quarry Hill Leeds LS2 7UE Email : england.nhs111@nhs.net To: CCG Accountable Officers CCG Clinical Leaders Cc: Regional
Cheshire & Merseyside Sustainability and Transformation Plan. People and Services Fit for the Future
 Cheshire & Merseyside Sustainability and Transformation Plan People and Services Fit for the Future 2 The Challenge for the NHS As a nation we are fortunate to have a National Health Service that is free
Cheshire & Merseyside Sustainability and Transformation Plan People and Services Fit for the Future 2 The Challenge for the NHS As a nation we are fortunate to have a National Health Service that is free
What matters to Me Supporting the health and wellbeing of our older population
 What matters to Me Supporting the health and wellbeing of our older population The new way of working for health and social care across the Western bay region What we will do 1. We will focus on the needs
What matters to Me Supporting the health and wellbeing of our older population The new way of working for health and social care across the Western bay region What we will do 1. We will focus on the needs
Rapid Response. Crisis Team. Anne Williams Alison Dalley
 Rapid Response Health and Social Care Health and Social Care Crisis Team Anne Williams Alison Dalley Salford the context Population 220,000 Long history of joint working across Council/PCT Provide range
Rapid Response Health and Social Care Health and Social Care Crisis Team Anne Williams Alison Dalley Salford the context Population 220,000 Long history of joint working across Council/PCT Provide range
Job Description. Job title: Uro-Oncology Clinical Nurse Specialist Band: 7
 Job Description Job title: Uro-Oncology Clinical Nurse Specialist Band: 7 Department: Cancer Services Hours: 37.5 (min 22.5 hrs) Reports to: Lead Nurse for Cancer We are a pioneering research active organisation
Job Description Job title: Uro-Oncology Clinical Nurse Specialist Band: 7 Department: Cancer Services Hours: 37.5 (min 22.5 hrs) Reports to: Lead Nurse for Cancer We are a pioneering research active organisation
A&E Attendances and Emergency Admissions
 A&E Attendances and Emergency Admissions A&E Attendances and Emergency Admissions May 2016 Monthly Report Version number: 1 First published: 14 th July 2016 Prepared by: NHS England, Operational Information
A&E Attendances and Emergency Admissions A&E Attendances and Emergency Admissions May 2016 Monthly Report Version number: 1 First published: 14 th July 2016 Prepared by: NHS England, Operational Information
Effective discharge from hospital: the role of communication of home circumstances February 2017
 Effective discharge from hospital: the role of communication of home circumstances February 2017 Page 1 of 10 1. Introduction 1.1 Healthwatch Coventry is the independent champion for health and social
Effective discharge from hospital: the role of communication of home circumstances February 2017 Page 1 of 10 1. Introduction 1.1 Healthwatch Coventry is the independent champion for health and social
Requesting Ambulance Transport (999 or Urgent) A Guide for Healthcare Professionals
 A Guide for Healthcare Professionals") Requesting Ambulance Transport (999 or Urgent) A Guide for Healthcare Professionals Contents Page No. Introduction... 3 Glossary of terms... 4 Which patients should have 999 or urgent ambulance transport
Requesting Ambulance Transport (999 or Urgent) A Guide for Healthcare Professionals Contents Page No. Introduction... 3 Glossary of terms... 4 Which patients should have 999 or urgent ambulance transport
Winter Planning 2017/18. Marc Hopkinson - NGCCG Barbara Goodfellow - NuTH Nichola Fairless GHFT Simon Swallow - NEAS
 Winter Planning 2017/18 Marc Hopkinson - NGCCG Barbara Goodfellow - NuTH Nichola Fairless GHFT Simon Swallow - NEAS Context Newcastle and Gateshead services have a history of consistently delivering high
Winter Planning 2017/18 Marc Hopkinson - NGCCG Barbara Goodfellow - NuTH Nichola Fairless GHFT Simon Swallow - NEAS Context Newcastle and Gateshead services have a history of consistently delivering high
Mental Health Crisis Care Programme Update: Clinical Senate Council 24 th May 2016
 Mental Health Crisis Care Programme Update: Clinical Senate Council 24 th May 2016 1 Mental Health Crisis Care Programme: Summary The state of mental health crisis care needs to improve across London.
Mental Health Crisis Care Programme Update: Clinical Senate Council 24 th May 2016 1 Mental Health Crisis Care Programme: Summary The state of mental health crisis care needs to improve across London.
Review of Local Enhanced Services
 Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
Primary Care Strategy. Draft for Consultation November 2016
 Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
Addressing ambulance handover delays: actions for local accident and emergency delivery boards
 Addressing ambulance handover delays: actions for local accident and emergency delivery boards Published by NHS England and NHS Improvement November 2017 Contents Foreword... 2 Actions to be taken now,
Addressing ambulance handover delays: actions for local accident and emergency delivery boards Published by NHS England and NHS Improvement November 2017 Contents Foreword... 2 Actions to be taken now,
The future of healthcare in Dorset
 The future of healthcare in Dorset Are you entitled to a FREE flu jab? Every year the NHS offers a free vaccination against flu to people who are considered to be at risk. Visit www.dorsetccg.nhs.uk/staywell
The future of healthcare in Dorset Are you entitled to a FREE flu jab? Every year the NHS offers a free vaccination against flu to people who are considered to be at risk. Visit www.dorsetccg.nhs.uk/staywell
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan. October 2016 submission to NHS England Public summary
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Kingston Hospital NHS Foundation Trust Length of stay case study. October 2014
 Kingston Hospital NHS Foundation Trust Length of stay case study October 2014 The hospital has around 520 beds and provides acute medical services for a population of around 320,000 in Kingston, Richmond,
Kingston Hospital NHS Foundation Trust Length of stay case study October 2014 The hospital has around 520 beds and provides acute medical services for a population of around 320,000 in Kingston, Richmond,
Economic Evaluation of the Implementation of an Electronic Palliative Care Coordination System (EPaCCS) in Lincolnshire using My RightCare
 in Lincolnshire using My RightCare") Economic Evaluation of the Implementation of an Electronic Palliative Care Coordination System (EPaCCS) in Lincolnshire using My RightCare This paper will provide an economic assessment of utilising the
Economic Evaluation of the Implementation of an Electronic Palliative Care Coordination System (EPaCCS) in Lincolnshire using My RightCare This paper will provide an economic assessment of utilising the
Our Journey to Discharge to Assess (D2A)
") Our Journey to Discharge to Assess (D2A) Jane Ives Director of Operations South Warwickshire NHS Foundation Trust Wendy Lane Senior Partner Transformation & Innovation Arden Commissioning Support Zoe Bogg
Our Journey to Discharge to Assess (D2A) Jane Ives Director of Operations South Warwickshire NHS Foundation Trust Wendy Lane Senior Partner Transformation & Innovation Arden Commissioning Support Zoe Bogg