Primary Care. Strategy. April 2016
|
|
|
- Solomon O’Connor’
- 5 years ago
- Views:
Transcription










1 Primary Care Strategy 1 April 2016
2 TABLE OF CONTENTS 1. Executive summary Delivering the strategy and next steps Vision for the future: 24 hour integrated community care that s easy to access Supplementary information: Chapter 1 Demographics Chapter 2 - Quality and reduction in inequalities Chapter 3 - Premises and investment Chapter 4 - Workforce: recruitment, retention, training and education Chapter 5 - Technology and information sharing 28 Chapter 6 - Co-commissioning of primary care services Chapter 7 - Detection and prevention of disease 32 Chapter 8 - Collaborative working 33 Chapter 9 - Research 34 Chapter 10 - Patient and carer support Chapter 11 - Consolidated Fund Framework (CFF) 37 Appendices Appendix 1 Our stakeholders views Appendix 2 Cancer metrics Appendix 3 Locality roadmaps Glossary 51 2

3 Why have we developed a primary care strategy? Our Vision To deliver integrated physical, mental health and social care in the community, which meets patients needs in the most appropriate setting. Primary Care and its component parts are pivotal to sustaining the health economy and must be at the centre of the development of local services. Together with our partners, our strategy will create a patient-centred, sustainable primary care system which addresses east and north Hertfordshire s challenges. We recognise that each of our six localities faces different challenges and will sometimes need to achieve the same goals in different ways. Irrespective of how healthcare is delivered, we will ensure that all patients living in east and north Hertfordshire receive the highest quality care which is easy to access and have the best possible outcomes. 3
4 What is Primary Care? This strategy looks at Primary Care as all healthcare delivered outside of the acute hospital setting and within this context we particularly focus on general practice improvement for East and North Hertfordshire. The CCG commissions community services, community mental health services and through co-commissioning, general practice services. A small number of services are commissioned from Community Pharmacy contractors. The strategy focuses predominantly on these services for which the CCG has planning responsibility. Commissioning responsibility for the standard community pharmacy, dentistry and optometry services currently rest with NHS England and are not included in co-commissioning arrangements. It is recognised however that these providers play a very important role in the primary care system and will be included in future healthcare planning through working with NHS England as part of the evolving co-commissioning developments. Ambitions and outcomes We have two key ambitions - high quality primary care and resilient primary care. 1. High quality primary care provision: Increase the number of patients dying in their preferred location from the current rate of 66%. Reduce 0-2 day emergency admissions to hospital for over 75s Earlier diagnosis of cancer to improve survival rates Better cancer screening rates Good dementia diagnosis to achieve 67% in east and north Hertfordshire Ensure patients requiring IAPT are referred achieving a 15% referral rate. 2. Resilient primary care: Practices will meet - or exceed - the NHS England Central Midlands GP patient survey average for: ease of telephone access; overall experience of making an appointment; overall experience of GP surgery; whether patients would recommend the GP surgery to someone who has just moved to the local area Reduction in primary care workforce vacancy rates New ways of working integration and primary care at scale Fit for purpose health and social care premises. 4
5 1. Executive Summary General practice is the foundation of the National Health Service. Around 90% of all patients contacts with the NHS take place in GP surgeries, pharmacies dental practices, and in opticians. However the main focus of this strategy relates to GP services. At present, general practice receives around 9% of the total NHS budget. Getting primary healthcare right in our local communities should prevent ill health occurring, ensure long-term conditions are managed effectively and improve the health and wellbeing of the population. Our strengths We are proud of our general practice services, which are recognised as being of a high standard. Since April 2013, we have commissioned a range of innovative new primary care services. The hospital-at-home scheme HomeFirst, the acute in-hours GP home visiting service and support for patients in nursing and care homes all focus on enhancing the quality of patient care and improving recovery rates. Results from early evaluation of these new care models are very encouraging. In some areas, these initiatives are already delivering better experiences for patients, improving patients health and making the most effective use of the resources available. Our challenges Despite these early successes, there are still some areas where we need to do even better in order to ensure that primary care services consistently meet the needs and expectations of our local population. There are some limitations to the current model of primary care being able to deliver these improvements and so we need to make changes to the way we provide services. The following challenges have been identified in east and north Hertfordshire: The population is a growing and ageing one. More people are living with multiple long-term physical and mental health conditions which place increasing demands on general practice and community services. There are also ever-increasing demands on hospital emergency departments and unscheduled admissions There has been an increase in the 0-17 age group becoming significant service users 5
6 One in four of the population will need treatment for mental health problems at some point in their lifetime and the majority of these will be managed in general practice A variety of information and technology systems used across health and social care services do not connect with each other meaning delivery of care is not as efficient, effective and safe as it could be Some premises are not fit for purpose and do not meet the minimum standards that all patients should expect in Patients are frequently left frustrated as it is often difficult to get appointments when needed There is a shortage of staff in general practice and recruitment is difficult. This affects the ability to provide consistently high quality care and access to services There are variations across east and north Hertfordshire in areas such as access to general practice services, A&E attendances, hospital admissions, outpatients appointments, long-term conditions management and cancer screening and outcomes. These issues are not unique to east and north Hertfordshire. Publications such as NHS England s A Call to Action, the Kings Fund s Commissioning & Funding General Practice and Department of Health s Transforming Primary Care have all outlined aspects of the challenges that general practice is facing at a national level. Our strategy supports the objectives of our five-year strategic commissioning plan and the NHS Five Year Forward View which stresses the importance of a radical upgrade in prevention and public health. Our primary care strategy describes how we will work with school children and new parents to stay well and safely self-care. It also talks about giving patients greater control of their own care, and sets out a commitment to supporting carers and making best use of voluntary organisations. Removing barriers in how care is provided by different health and social care professionals is important and this is echoed in our strategy. We will consider new options for healthcare delivery including models where GPs combine with nurses, hospital and mental health specialists, and other primary care providers. The redesign of urgent and emergency care services to create integration between A&E departments, GP out-of-hours services, urgent care centres, NHS 111 and ambulance services is a fundamental change for the NHS. Our ambition locally is aligned with these plans, having one point of access for all healthcare needs and to consider integration of the Acute In-Hours Visiting Service (AIHVS) with other urgent care services. 6
7 In developing our primary care strategy, we have worked with stakeholders and patients to understand their views on existing services, the problems they encounter and the changes necessary to make things better. General practice and primary care that is fit for the future Our vision and priorities support five key functions of integrated primary care services working in partnership to deliver: Improved population health, particularly among those at greatest risk of illness or injury Managing short-term non-urgent episodes of minor illness or injury Managing and co-ordinating the health and care of those with long-term conditions Managing urgent episodes of illness or injury Managing and co-ordinating care for those who are nearing the end of their lives. How we will deliver our vision We have identified a range of enablers available to localities; An interoperable new electronic patient record a single system wherever possible, which supports safe, effective, joined-up patient care across health and social care organisations New access models, for example, a single point of access to better integrated primary care services, signposting patients to the most appropriate service to meet their needs Primary care premises fit for purpose as our population increases and ages, and open and accessible to patients when they are needed A well-trained, supported and motivated workforce of employees and volunteers who pull together to provide high quality patient care Consistently good practice across general practice, with providers learning from each other. Involving patients in their own care, improving cancer screening and treatment, managing long-term health conditions, reducing A&E attendances and hospital admissions and offering timely outpatients appointments A robust, flexible marketplace of provider organisations that can meet the needs of our patients 7
8 Promotion of seamless co-ordinated care across primary/secondary care; working constructively with secondary care colleagues to provide integrated care Modern general practice services that retain the original qualities that are so important to people. We understand that changes to the way primary care is delivered will at times create anxiety. We will only make changes that deliver better quality care and are in the best interests of our local population. We will continue to be open and transparent at all times in our planning of new services and ways of working. Everyone who is affected by our strategy will have the opportunity to contribute to its development and implementation. 2. Delivering the strategy and next steps A key role for the East and North Hertfordshire CCG is to enable practices and their localities to fully understand and address local issues and concerns in primary care. This strategy identifies a range of potential enablers which are expected to help deliver the necessary transformational change. This is not a one size fits all solution as each locality will develop its own priorities under the overarching CCG primary care strategy. This will be achieved through the further development of locality road maps (appendix 3) and locality commissioning plans and form part of the CCG s operational and Five Year 2016/ /21 Sustainability and Transformation Plans. It is important that the CCG s future Strategic Estates Plan and Digital Road Map support and drive the necessary changes required in estates and technology. GPs and their teams are innovative and resilient and they understand that standing still is not an option. We know that we need to work differently, but we also want to retain the social heritage and unique qualities of general practice. We know that patients and GPs value the trusting relationship and role of general practice in the community. The health service will continue to see many challenges in the next five years. Delivery of this strategy provides a great opportunity to improve services for patients and ensure primary care is well-resourced, sustainable, a good place to work and fit for the demographic changes ahead. We will ensure that all key stakeholders including service users and the local representative committees are fully engaged in the development and delivery of the locality operational plans. These plans will translate strategic ambition into tangible changes to service delivery. 8

9 This vision is aligned with the nine CCG ambitions 9
10 Primary Care Strategy enablers 10
11 3. Vision for the future: 24 hour integrated community care that s easy to access Integration of primary, community and social care, wrapped around the patient We will build a system to deliver 8am 8pm, 7-day services that are clinically appropriate to local health and care needs in line with the Five Year Forward View. In addition to being more joined up, we will also ensure new services have fewer entry points and are much easier for patients to access. This new model of care will require collaborative working between GP practices and other providers, including the voluntary sector, to deliver locality based healthcare at greater scale. Acute In-Hours Visiting Service (AIHVS) provides additional home-visit support during normal GP practice hours, allowing practice staff to focus on more complex patients, such as those with long-term conditions. Following a successful pilot, this is now a permanent service, with scope to become part of the new integrated community care models. East and North Hertfordshire Integrated Care Programme Board is a collaboration of health and care providers working together to improve delivery of integrated, person centred and co-ordinated care. The aim is to improve the care and independence of over 65-year-olds with complex needs and long-term chronic physical and mental health conditions. The programme is focused on three areas and is closely aligned with the Vanguard care home programme. Improving access to simplify how services are delivered through an improvement in the coordination and quality of access and assessment. Ensuring seamless transitions of care to improve quality and minimise numbers of care transfers between providers Integrating care in the community - to improve the number of people having care closer to home through a focus on transforming the approach to proactive care planning by integrated teams The HomeFirst service is an example of an integrated service in two localities. An integrated health and social care team delivers care for vulnerable patients at home, preventing avoidable hospital admission. It is achieved by providing a rapid response service in the community and a case management service to plan patients care and is proving both successful and popular with patients. The Rapid Response component of the scheme is now being rolled out more widely across east and north Hertfordshire led by the Integrated Care Programme Board. 11
12 Future adaptations of the model in localities will be further developed and could involve greater integration of additional services, to meet local needs, and systems to ensure enhanced discharge pathways from hospitals. Children and families are another important sector of the community that require seamless holistic care from a range of agencies. We will work to strengthen frameworks to support children and young families. 12

13 SUPPLEMENTARY INFORMATION Chapter 1 Demographics People are living longer with multiple health issues. Lifestyle factors including obesity, alcohol consumption and smoking - and the diseases they contribute to - all place a significant burden on the health economy, and there are improvements in detection and management of long-term conditions. Over the coming 10 years the demand for appointments with general practitioners is forecast to possibly double. In east and north Hertfordshire there is substantial planned housing growth with 38,100 new dwellings expected by The impact of this is of concern particularly considering it is already an area with a slightly higher than average number of patients per square metre per general practice. East and north Hertfordshire is one of the least deprived areas in England based on the Index of Multiple Deprivation (IMD) report for The seven domains were combined using the following weights to produce the overall score. Despite being one of the least deprived areas in England, there are still challenges. 13

14 Several areas have higher than average deprivation scores (outlined in the diagram) including wards in Stevenage, Hatfield, Broxbourne, Sawbridgeworth, Letchworth Garden City and Hitchin: People in more socio-economically deprived situations tend to have greater health needs and worse health outcomes than the general population. This involves a number of factors including lifestyle or health behaviour risk factors such as smoking and poor diet. Poorer health, access to services, unemployment, lower levels of educational attainment and poor housing conditions are also prevalent. Patterns and overall levels of deprivation in east and north Hertfordshire are not expected to change in the next five years. Mortality A Hertfordshire woman can expect to live 84 years (compared to 83.1 years for England) and a Hertfordshire man 80.6 years (compared to 79.4 years for England). 14

15 In East and North Hertfordshire CCG, for both men and women, there is an association between higher levels of deprivation (IMD score) and higher premature mortality rates from: All causes of premature mortality combined Cancer Heart disease and stroke Lung disease Liver disease. While the number of people overall who have unhealthy lifestyles such as smoking, excessive drinking, or poor diet has reduced, those from poorer backgrounds, and the most vulnerable, are more likely to have three or more behaviours which in turn can lead to an earlier onset of some of the major causes of early death. Ethnicity In 2011 approximately 89.8% of residents of East and North Hertfordshire CCG were White, 2.3% Mixed, 4.6% Asian or Asian British, 2.8% Black or Black British and 0.6% Other (Table 1.2). 15

16 East and North Hertfordshire CCG has a higher proportion of white residents than England generally, but a slightly lower proportion than the East of England. Approximately 200 different languages are spoken by pupils living in the county of Hertfordshire. Table 1.2: Population estimates, persons, number* and percentage by ethnicity, NHS East & North Herts CCG, 2011 *figures in this table may not add exactly because they have been rounded to the nearest 100 Source: 2011 Census, ONS, July 2012 Quality in primary care can be defined as: Reducing avoidable mortality Improving quality of life for people with long-term conditions Providing swift and effective responses to acute illness or injury Patient experience, including experience of access Patient safety. These significant areas will be reviewed on a regular basis by the quality and safety committee. We will support those practices which deviate most greatly from the benchmark (known as an outlier) and share best practice through regular education and training events, networking and practice nurse workshops. We will also support initiatives to drive up patient experience and overall quality within general practice. This underpins our ambition to achieve consistency in the quality of care across our patient population. 16
17 Chapter 2 - Quality and reduction in inequalities Underpinning outcomes will drive up the quality of primary care to meet the health needs of the population. Quality should include: In addition we must achieve value for money while still delivering good quality care for patients. To do this we must measure services against standards set either nationally or locally and compare them. Clinical effectiveness An essential component of clinical governance is to improve and assure quality. As with all aspects of clinical governance, clinical effectiveness is about improving patients' total experience of their healthcare. Priorities include: 17

18 This is achieved by: Timely access to healthcare services Use of data intelligence i.e. Commissioning for Value and Locality Information Packs Locality board assessment and agreement of local priorities Effective use of GP leadership, to deliver through Long-term Conditions group, Mental Health Leaders Group, End of Life Forum, Respiratory network and Diabetes Management GP educational events Enhanced Commissioning Framework/ Consolidated Funding Framework. Patient experience It is important that we listen, understand and respond to our patients over their experiences of care. Good patient experience is essential to support improved outcomes and maintain effective doctor-patient relationships. Our practices understand the importance of continuity of care, although this has to be balanced against growing local and national workforce pressures. Stresses on the system are seasonal so we plan to continue to invest in our Winter Pressures Schemes. 18
19 Patient experience will be positively influenced by: Practices signing up to extended opening hours throughout the year Admin and reception staff development in the interest of customer service IT investment into practices for self-check-in and improved telephony Practice and locality PPGs network Patient network for quality Reduction in referral variation to ensure timely, quality referral letters to the right destination, supported by the use of Choose & Book with patient involvement in decision making. In order to hear our patients we are supported by our local patient engagement network based around practice PPGs and locality groups, as well as patients providing direct feedback into our quality teams via the Patient Network for Quality. Patient safety Most work around ensuring patient safety is covered by the requirements of the GMS contract and clinical appraisal process. There is an expectation that practices have robust complaints procedures and that clinicians share and learn from regular discussions of complaints and significant event analysis. Issues around prescribing variation will be tackled through local prescribing forums where we will support both local and national initiatives. Safeguarding of adults and children remains a high priority locally with clinical updates and rapid advice available through our locally commissioned safeguarding teams. We plan to work closely with regulatory bodies to support visits and their outcomes, along with proactive work in supporting practices identified as needing change or improvement. NHS England has developed the Primary Care Web Tool which highlights practice outliers from a variety of indicators. This information is fed into Locality Information Packs circulated to all practices to promote cross-challenge, support and ultimately improve services. Quality visits to those practices which are outliers in certain areas currently take place between NHSE and the CCG and will continue to wherever concerns about quality provision of general practice arise. Cancer profiles While these are nationally co-ordinated programmes, GPs have the potential to influence uptake and we are testing new ideas to help with this. These include making patients aware of the importance of screening during appointments and flu clinics, offering extended hours for cervical screening and writing to patients who have not responded to screening invites. The recent NICE guidance on the two week wait cancer pathway is a national driver for improving early diagnosis and screening. The map of medicine guidelines will also aid this process. 19


20 This Public Health England table summarises key cancer performance covering 2014/15 across the main clinical outcomes. The key below shows where our CCG is lower, similar or higher than the national average. Further information on the cancer metrics can be found in Appendix 2. 20
21 Chapter 3 - Premises and investment Across East and North Hertfordshire CCG there is variation in the standard of general practice premises. Some practices have insufficient space to deliver care that consistently improves outcomes for patients, including meeting regulatory core standards. Premises are also a limiting factor in plans to enable collaborative working, including extended hours and reducing reliance on secondary care services. NHS England Central Midlands Region premises team has worked consistently to identify those premises that are a priority for improvement. Localities have also been developing Locality Commissioning Plans which include the availability of suitable premises to accommodate integrated primary and community services. Limited capital was available from NHS England to make improvements to the general practice estate until January Practices were invited to submit bids for funding from a 1billion non-recurring Primary Care Infrastructure Fund (PCIF) in February In March 2015 a number of improvement grants were supported. Four premises schemes were approved in principal to go ahead and further develop business cases and enabling funding to support the work. The enabling funding was confirmed at the end of October 2015 and one improvement grant scheme has gone ahead. New bids were invited to be submitted to the Primary Care Transformation Fund (PCTF) (previously the PCIF) via the CCG in April It is essential for longer term sustainability that best use is made of existing available buildings. This needs to include consolidation of premises to improve service delivery and patient care whilst enabling them to be delivered more economically. Currently premises are used for approximately 30% of the week so there is potential to further utilise existing premises. Priorities for funding to underpin new ways of working must demonstrate that they meet one or more of the following criteria: Improved access to meet the national mandate and constitution standards particularly with increased capacity for integrated primary care services out of hospital Improved responsiveness to urgent care needs, with a commitment to a wider range of relevant services in line with commissioning intentions to reduce unplanned clinically inappropriate admissions to hospital Improved seven day access to effective care within extended hours particularly for general practice at scale Improved recruitment and retention and increased training capacity at CCG and locality level. Locality commissioning plans will consider primary care premises in the context of local population health needs, with premises being a key enabler to delivery. This will include 21
22 working with local health and social care providers to identify opportunities to make better use of all existing public sector estate and to co-locate and integrate care. Locality estates plans should also take into account: Creation of locality health and social care hubs Consolidation of general practice functions and co-operative working Delivery of general practice at scale Co-location and integration with other out-of-hospital services Better use of technology including near patient testing, telehealth, self-monitoring and reporting, especially for patients with long-term care conditions and co-morbidity. Funding from PCTF will be prioritised for schemes which deliver new models of working across more than one practice. The expectation is that all providers in a locality will talk to each other to remodel the total local estate to maximise capacity and share costs and risks, providing value for money for the public sector. East and North Hertfordshire has been asked to develop a local estates strategy which includes primary care premises priorities. Work on the strategy will be complete by the end of March 2016 and the data collected in each locality will inform locality estate plans. 22
23 Chapter 4 - Workforce: recruitment, retention, training and education Recruitment of general practitioners and practice nurses in East and North Hertfordshire CCG is reported via local GPs and the Local Medical Committee to be significantly challenging. This reflects what is now recognised as a national crisis. Some practices report that they are simply unable to recruit following months of advertising, and retention of newly appointed staff is also a problem. Recruitment into the traditional partnership model of general practice is becoming less attractive to newly qualified GPs. Reasons include ever-increasing workload, poor morale, financial commitment and risk, lack of career development and lack of flexibility in working patterns. We know the concept of a portfolio career is becoming more popular and there are examples of GPs working within east and north Hertfordshire pursuing this career structure. Retention of staff at other levels is a problem for both health and social care providers. General up-skilling in reception duties, would enable me to offer a service I feel I am more than capable of providing. But restrictions on who can do what means staff capability is under used - receptionist Welwyn Hatfield The market for home care is starting to be developed, but additional capacity and attractive career opportunities in caring roles needs to be supported. Providers are currently employing health and social care staff from the same pool. Career opportunities need to be better developed to avoid staff being lost to the health and care sector Poor development opportunities/lack of prospects of increased earning/decrease in job satisfaction/high stress levels - practice manager, Upper Lea Valley The current retirement bulge looming in general practice and practice nursing makes addressing the existing recruitment, retention and growth issues an urgent priority. Without action, the situation will deteriorate further. Some member practices have described the current situation as critical and the perfect storm. To build capacity and enhance patient care we will continue to commission different models of primary care from external providers, such as Acute In-Hours Visiting Service (AIHVS). This will likely require up-skilling of the primary care workforce and adaption of the skill mix. These new services provide flexibility for health professionals and offer a variety of roles for younger GPs who may not find traditional general practice attractive. We are mindful that providers of these new services are currently seeking employees from a diminishing pool and are competing with practices for staff. 23
24 Capacity around home care and community nursing needs to be expanded if we are to meet likely future needs of keeping people independent and in their own home for as long as possible. NHS England Primary Care Public Health Profile for NHS England Central Midlands (previously Herts and South Midlands Area Team) Sept 2013 stated a national average rate of one GP per 1,351 registered population. The rate in East and North Hertfordshire CCG is significantly lower at one GP per 1,538 patients). East and North Hertfordshire CCG is also significantly lower than NHS England Midlands & East (Central Midlands) rate of one GP per 1,434 registered population. Based on these figures, we would need approximately 50 more GPs in east and north Hertfordshire to meet the national average of GPs per 1,000 patients. There is also considerable variation between practices with some significantly below the CCG rate. There may be a range of reasons for the variation. A strong commitment to providing training and education for primary care staff helps recruit and retain a highly skilled workforce and we have developed a new network to support and oversee this important programme. 24
25 Primary care workforce, planning and education network Development of primary care is underpinned by the need for a comprehensive framework for education, training and research and we are establishing a targeted network to achieve this. The network covers all staff working in primary care including all aspects of general practice and the objectives will be to: develop an education and training strategy to include consistent use of TARGET (Time for Audit, Research, Guidelines, Education and Training) events and supporting education for the whole practice team critically assess the value and outcomes of TARGET and other educational meetings across all four participant groups and to share outcomes across localities and member practices ensure future general practice staffing needs are fed into the work of the LETB (Beds and Herts Workforce Partnership) work with other stakeholders such as community and acute trusts work with other primary care providers work with the University of Hertfordshire and other educational institutions (HEIs) ensure all general practice staff have the necessary training and education to be competent in delivering high quality healthcare, including mental health develop and establish innovative posts in general practice increase student nurse pre-registration placements in general practice introduce a practice nurse and HCA development programme develop integrated practice/community nursing increase practice awareness and engagement in research introduce a dedicated sustainable budget for education and training encourage employers to ensure that all general practice staff have an annual good quality appraisal and a PDP, and to share information to help shape locality, federation and CCG development plans ensure co-ordination of multi-professional educational work streams, especially across CCG priority clinical pathways. The network will also be involved in workforce planning. Due to increasing workload driven by demographic changes, complexity of long-term conditions and increasing community care, workforce development is essential. This does not just mean more GPs, but requires reviewing the skill mix of primary care as part of a more flexible integrated team. This is essential as we introduce new ways of working in line with the Five Year Forward View. At present there is no clear career framework for practice nurses, there is a lack of preregistration placements in general practice and no clear career path after registration. Practice nursing has a poor image and so we must highlight the appeal of a nursing career in general practice. We will re-establish the role of primary care nurse tutors, and develop primary care nurse training. 25
26 An East and North Hertfordshire CCG-wide practice nurse network is being established as a sub-group of the Long-terms Conditions Group. This will help to meet training and education needs of local practice nurses and provide peer support. We have a thriving GP training scheme but must create a general practice environment where they want to stay and develop their careers. This will involve the introduction of post specialist training GP fellowship schemes. A practice staff survey asked all staff to identify their top three training needs and this information will be used to help develop training plans. We will work vigorously to strengthen our relationship with the Beds and Herts Workforce Partnership/LETB ensuring the CCG is clearly linked into the LETB with clinical input. We will encourage the rapid collection of enhanced workforce data for analysis. The initial focus will be on general practice, but with the intention of extending this to primary care more broadly. We will take forward our concerns, which will include lobbying for increased resources to improve capacity, career progression and professional fulfilment. Developing the workforce within community pharmacy Strategy for Pharmacy Services 2016: Mission statement We would like to see recognition and integration of community pharmacy services into care pathways and service redesign. We support pharmacists working more clinically to improve patient outcomes and it is key that we do all we can to develop a culture of prevention and self-reliance through public health, health promotion and self-care. It is vital that we increase the capacity and capability of primary care to manage patients with complex health needs and long-term conditions. We need to deliver medicines optimisation priorities so patients gain optimal benefits from medicines. We need to improve the transition of medicines use across care boundaries by improving links between community pharmacies and hospital pharmacy services as well as GP practices Patient benefits will include improved medicines safety, better patient experience, improved transfer of care and reduced reliance on GP services and more support to be cared for at home. We would like community pharmacy to be the first port of call for self-care in the community; to be a first line option from NHS 111 to avoid inappropriate use of A&E and out of hours services. (e.g. Community Pharmacy Emergency Supply Service CPESS). 26
27 Pharmacists roles in NHS 111 can also be developed. We will support the establishment of clinical pharmacists working in GP practices who are able to prescribe and work alongside GPs. We will continue to develop the benefits of clinical pharmacists in care homes and multidisciplinary teams by exploring independent prescribing roles. We will establish a team of in practice pharmacists to support medicines optimisation at practice level, as well as developing pharmacist support to the expanding HomeFirst service. We will further promote better use of established services e.g MURs and NMS. We will also explore how pharmacists can support those with minor illness and injuries. We want pharmacists to support patients to make the most of their medicines, promote health and provide advice on how to live better, harnessing the skills of the wider pharmacy team to support and deliver high quality patient centred health and care. Key priority areas: To support any skill mix reviews across the workforce To support the roll out of SCR to community pharmacies To review and evaluate CPESS To support development of the pharmacy workforce to meet future challenges potentially including pharmacists as prescribers within care pathways, where appropriate. To explore how to make best use of the community pharmacy network Enablers: These include good engagement with the LPC, pharmacy contractors, LPN, and local authority; collaborative working with local schools of pharmacy, LETBs, AHSNs and workforce development teams; a robust and comprehensive Pharmaceutical Needs Assessment (PNA) to inform local commissioning, and an integrated programme board pharmacy work stream. Challenges: Lack of understanding by commissioners of the opportunities and potential of the existing community pharmacy workforce Insufficient pharmacists with advanced clinical expertise Lack of evidence to demonstrate effectiveness/efficiency of new services provided by pharmacies Potential upheaval within the community pharmacy infrastructure as DH proposals are negotiated and implemented. 27
28 Chapter 5 - Technology and information sharing Current information sharing across health and social care services is suboptimal. This leads to inefficiencies, wasted resources and increased clinical risk. The diverse numbers of clinical systems in use do not integrate effectively, adding risk and frustration for all concerned. Patients in particular, often have to repeat their story unnecessarily and experience fragmented care. The government has made a commitment that all patient and care records will be digitally interoperable and paperless by 2020 and CCGs are required to have a digital road map by the summer of A number of key technological enablers have been identified. Greater sharing of the electronic patient record across health and social care, is considered to be one of the most important, starting with GP practices and out of hospital services and then extending to acute hospital services, GP out-of-hours and social care. There is significant technology available to help make clinical care safer, easier to access more joined up, and efficient, thereby providing a better patient experience. Initiatives include the introduction of Map of Medicine (MoM) and utilising pseudoanonymised GP data extraction (where a patient s NHS Number is scrambled so that it is not identifiable but it still allows records for the same patient to be linked across multiple data sources) to enhance risk stratification. A single electronic patient record system is the intention for general practice across east and north Hertfordshire, and support will be given to practices in the process of migration, as it can be time consuming and disruptive. Technology facilitating shared record access between different systems already exists and is constantly being developed. A single system may not be preferable or realistic in all cases, but interoperability gateway solutions, which allow clinicians to securely share up-to-date patient data across systems, where appropriate, will be considered and investigated. To date, existing technology has not enabled the creation of a truly shared record that can be viewed and edited by multiple healthcare providers. 28
29 Chapter 6 - Co-commissioning of primary care services Background Co-commissioning is the formal involvement of CCGs in the planning and purchasing of primary healthcare services previously solely undertaken by NHS England. East and North Hertfordshire CCG first started co-commissioning in the first year the initiative was launched. Co-commissioning presents an important opportunity to break down some of the barriers to significant future transformational change - change that will ultimately deliver higher quality more sustainable services for the local population. We see co-commissioning as an enabler to: Reduce variation and improve quality and clinical outcomes in general practice Explore the potential for wider co-commissioning with local authorities, including public health Commission enhanced pharmacy services Promote the need for premises improvements both at local and national level. Cocommissioning is the mechanism for the CCG to invest in on-going revenue funding for general practice premises development Align enhanced funding to the CCG s key strategic objectives of better patient outcomes Achieving a well-trained and fully staffed primary care workforce that benefits from new clinical roles and integrated service models. East and North Hertfordshire CCG selected a joint co-commissioning model for and opted to remain in a joint co-commissioning model for Member practices and service users were effectively engaged in the planning and decision-making process. The benefits to patient care were recognised through this consultation. Concerns were raised by governing body GPs and member practices about the increased conflict of interest that cocommissioning creates. To help ensure that such conflicts are effectively managed the CCG lay membership has been increased from two to three roles and the CCG s conflict of interest management policy has been updated. Co-commissioning of primary care - design principles for clinical care A senior clinician capable of making decisions about the correct course of action is available to patients as early as possible in the process especially using telephone advice where appropriate 29
30 Patients have the minimum number of separate visits and consultations that are necessary, with access to the quickest advice in appropriate locations underpinned by systematic use of latest secure electronic communications technology Patients are offered continuity of relationship where this is important and access at the best times to support anticipated care management especially for those with longterm conditions Care is pro-active and population based where possible across practices and localities Care for frail people with multi-morbidities is tailored to individual needs and shaped with them and their carers particularly in residential and nursing home settings Where possible patients are supported to identify their own goals and take responsibility for self-care in managing their own condition and care. Work plan Co-commissioning will strengthen the development and delivery of CCG operational and five-year sustainability and transformation plans (STP) 2016/ /21. This is directly linked to the CCG locality commissioning plans and estates and technology strategies. As part of delivering strategic plans the CCG will, through co-commissioning arrangements, also need to have appropriate input and oversight of key contractual functions such as primary medical services procurement. Clarity on responsibilities and professional boundaries is important to ensure the benefits of co-commissioning are realised, and this is an area for further development. Future developments It is expected that during CCGs will have the opportunity to reconsider and alter their level of involvement in co-commissioning for Thorough preparation for any future transition to delegated co-commissioning (which is the likely direction of travel although no formal decisions have been made at this stage) is very important. This will help ensure the CCG is adequately resourced to discharge its new responsibilities. Finance East and North Hertfordshire CCG s allocation of funding in 2016/17, for the services it commissions is million. This does not include the cost of GPs, other practice staff or GP premises, which are commissioned by NHS England. This represents an increase of approximately 6% over the 2015/16 allocation - a higher increase than the national average. It is higher because the CCG s funding is deemed to be below its target fair share based on population weighted for age and need. NHS England has also published allocations for the following four years, 2017/18 to 2020/21, when growth reduces to 2.7%, 2.8%, 2.9%, 4.6% respectively, with the latter two years being indicative only. 30
31 Each year the CCG governing body agrees a balanced financial plan taking account of changes to tariff prices paid to NHS Trusts, other inflation, efficiency savings, investments, population growth and other growth. In 2016/17 the CCG is also required to deliver a 1% cumulative underspend, to set aside 1% of its allocation to be spent non-recurrently, and to set aside a contingency reserve of a minimum 0.5%. In 2015/16 the CCG s spend is forecast as shown in the chart below: Acute services Mental health/ld services Community services Continuing healthcare Prescribing Other Primary Care services Running Costs The total spend identified in the chart for Other Primary Care Services is 17.9m relates to services commissioned by the CCG only, (i.e. excludes services commissioned by NHS England). Further detail is given in the table below: Primary Care Services '000 Out of hours services 4,553 Acute in hours visiting service 1,567 Primary care IT 1,495 Enhanced services* 5,716 Over 75s enhanced service 2,936 Quality premium 849 Home oxygen 754 Total 17,870 * Enhanced services includes funding of the consolidated fund framework, enhanced services provided to care homes, and a number of other services provided in GP practices. 31
32 Chapter 7 - Detection and prevention of disease We would like to put prevention of disease at the heart of our work streams. We will ensure that diseases and risk factors are identified early. This will help prevent the development of complications and therefore reduce A&E attendance and unplanned admissions. We will work to support public health teams in commissioning NHS health checks and also continue to develop new schemes such as the nursing home Vanguard project, where we are providing additional clinical support to care home staff and residents. We will continue to work with Public Health England to try and increase the uptake of seasonal flu vaccines amongst those vulnerable and most at risk. All primary care services and healthcare workers have an important role to play in the prevention of disease and prevention of complications of disease. We will work with NHS England to develop and align prevention strategy and interventions for community pharmacists, dentists and optometrists. 32
33 Chapter 8 - Collaborative working Experiences in other parts of England suggest there are patient experience, quality improvement outcomes and financial gains to be had from GP practices working together as either federations or collaborations. It is widely believed that new ways of working across general practice will be a key factor in ensuring a resilient service in the future. We firmly believe the development of collaborative working is essential. This will be of mutual benefit to our member practices and the CCG, as a commissioning organisation, because it will enable general practice to develop at scale around a registered population. A collaborative working model will also help general practice engage with the local integrated provider group to deliver true patient centred integrated care. Collaborative models of working either exist or are forming in all six localities. All areas will be offered support for transformational change, with the goal of delivering higher quality general practice services which meets the commissioning requirements of the CCG. This will be in collaboration with the LMC. We will also support the exploration of general practice and federations working more closely with other providers. 33
34 Chapter 9 Research We want to encourage and promote research within general practice (as well as supporting opportunities in primary care more broadly) and will provide support for practices to develop their research expertise and workforce. There are two research related national funding streams which can help general practice to participate in research: Research Site Initiative scheme (RSI) financial support provided to practices that meet defined governance and quality standards for research. National Institute for Health Research (NIHR) Research Capability Funding (RCF) is a recurrent funding stream designed to support research-active NHS organisations. Our priority will be for RCF to be reinvested in general practice in order to develop and promote the research portfolio. We will work in partnership with other organisations such as the University of Hertfordshire to ensure funding delivers the best developments in medicines and technology for patients. 34
35 Chapter 10 Patient and carer support There is currently a culture of reliance by local people on GPs and general practice as the principal contact for healthcare needs. If general practice is to remain sustainable we must work in partnership with patients, their carers and relatives, our partners and stakeholders to make good health everyone s responsibility. To ensure our local communities are engaged we will establish locality based patient and carer reference groups to contribute to and review development of our primary care development plans. In addition, working in partnership with patient participation groups, public health, social care and local authorities we will look to: - Utilise and develop our existing patient participation network to engage and communicate with the wider population on the appropriate use of healthcare services and self-care tools - Target appropriate identified representatives of community groups whose voice is less heard in healthcare, ensuring their needs are recognised and considered - Work proactively with new parents, children s centres, nurseries and schools to provide information and raise confidence in undertaking appropriate self-care, and use of local services for children and young people - Use all appropriate communications channels to promote key health and wellbeing messages and appropriate services particularly digital and social media, as well as local media. - Ensure all GP practices across east and north Hertfordshire have an up-to-date website containing relevant information that is easily accessible for their population - Work towards each practice having a lead for patient self-management, and motivational consultation techniques - Ensure patients have knowledge of, and can easily access, public health initiatives, e.g. health walks - Ensure linkage to Better Care Fund plans. Supporting the role of the carer There are about 56,000 family carers in east and north Hertfordshire, which is around 10 per cent of our population, although this could be an underestimate. Supporting and identifying carers is a topic of particular importance to our patient and carer network. It currently contributes to a number of initiatives in partnership with GP practices and voluntary sector organisations, to help identify and provide support to carers in east and north Hertfordshire. 35
36 We are committed to; Identifying carers of all ages and ensuring they have sufficient support to stay well and healthy Working with the voluntary sector to ensure best use of available services Continuing to consult and work in partnership with our patient and carer member network on carer support, and identifying initiatives Commissioning services that ensure no carer goes unidentified through lack of awareness. 36
37 Chapter 11 Consolidated Fund Framework (CFF) proposals The governing body of the CCG has agreed to consolidate existing funding streams and add a small new resource from PMS review. This is to create financial stability for general practice to invest in the workforce and achieve our strategic ambitions. The two existing streams are for the enhanced care of over 75s, and the current commissioning framework focused on long term care conditions. The key change is that this money will be recurring for four years with being a shadow year to get systems, processes and incentives right. The following three years will see recruitment and retention of staff to support care management across general practice. In line with the priorities in this strategy, the overall objective is to allow general practice to lead and develop care management and care co-ordination for those with cancer and longterm conditions. These patients are growing in numbers and are 60% of the urgent care system users. The aim is to increase the focus on prevention, anticipating care, and creating measurable improvements in outcomes for patients and population. Details of how the CFF will operate are being finalised for April The key headlines based on registered patient numbers would be a CFF of approximately 5.8m split 20% across enabling funds and addressing financial balance and 80% for cancer and care management. This is against an agreed list of patients, some from risk stratification and some from local discretion, of those at risk of emergency admission. The CFF will enable GPs and practice staff to work with self-care patients and carers and shared-care patients with secondary care consultants. 37
38 APPENDICES 38
39 Appendix 1: Our stakeholders views A joint approach between the CCG and patient participation groups at all levels is essential if the current challenges are to be addressed and new ways of delivering services with good outcomes are to be implemented. Since the inception of the health service the GP has been the first point of contact and in order to deliver the transforming agenda required to meet the increasing demand on services and finite financial resources this will need to change. Patients in general will find this a difficult step to take and patient participation groups are in an ideal position to take forward the positive aspects of the change agenda and reassure other patients that this does not mean a decline in the services which they receive but an enhanced service, delivered in a different way, with patients being able to take a positive approach to influencing their own healthcare within a sustainable economy. Patients will need to understand the totality of primary care and not see this just as their GP being available on demand. Patient participation groups (both actual and virtual) are within the community, able to take forward these messages to friends and neighbours along with the local and national publicity. Carol Taylor PPG Church Street Surgery, Ware, PCG Upper Lea Valley Primary Care Strategy Service User Reference Group Herts LMC is pleased that East & North Herts CCG recognises the importance of strong and stable general practice to their whole commissioning strategy, while at the same time recognising the unprecedented challenges GPs are facing. We look forward to working with the CCG to ensure the sustainability and development of general practice which will result in continued improvements in quality, safety and diversity of services provided in the community for all of the population of East and North Hertfordshire. Peter Graves Chief Executive Herts Local Medical Committee (LMC) East and North Herts CCG is consulting with Hertfordshire Local Pharmaceutical Committee (LPC) on primary care development recognising community pharmacy as an integral part of primary care by investigating innovative ways to support general practice and others in providing coordinated care to patients. We hope that community pharmacy will continue to be involved and consulted at the beginning of new developments by the CCG to ensure that there is a coordinated and a whole system approach to patient care. We look forward to building on collaborative relationships with commissioners and other healthcare professions to ensure patients get the right care at the right place at the right time whilst helping them to be as healthy as they can throughout their life. Helen Musson Executive Officer Herts Local Pharmaceutical Committee (LPC) 39
40 Although public health and primary care are often conceptualised, organised, and funded as two separate entities, strengthening primary care can support some public health functions and public health can in return enhance the provision of population-wide primary care. Therefore a well-developed primary care system creates benefits in terms of population health, with the reduction of avoidable morbidities and mortality, and hospitalisations as recognised in the Hertfordshire Public Health Strategy We look forward to working with the CCG and general practices of east and north Hertfordshire to ensure the sustainability and development of primary care which will result in continued improvements in the population health of east and north Hertfordshire. Dr V K Nagaraj, Consultant Public Health 40

41 Appendix 2 Emergency admissions with cancer (per 100,000 population) 41


42 Females, 25-64, attending cervical screening within target period (3.5 or 5.5 years) 42


43 Persons, 60-69, screened for bowel cancer in last 30 months (2.5 year coverage) 43


44 New cancer cases treated (Detection rate: % of which resulted from a two week wait referral) 44

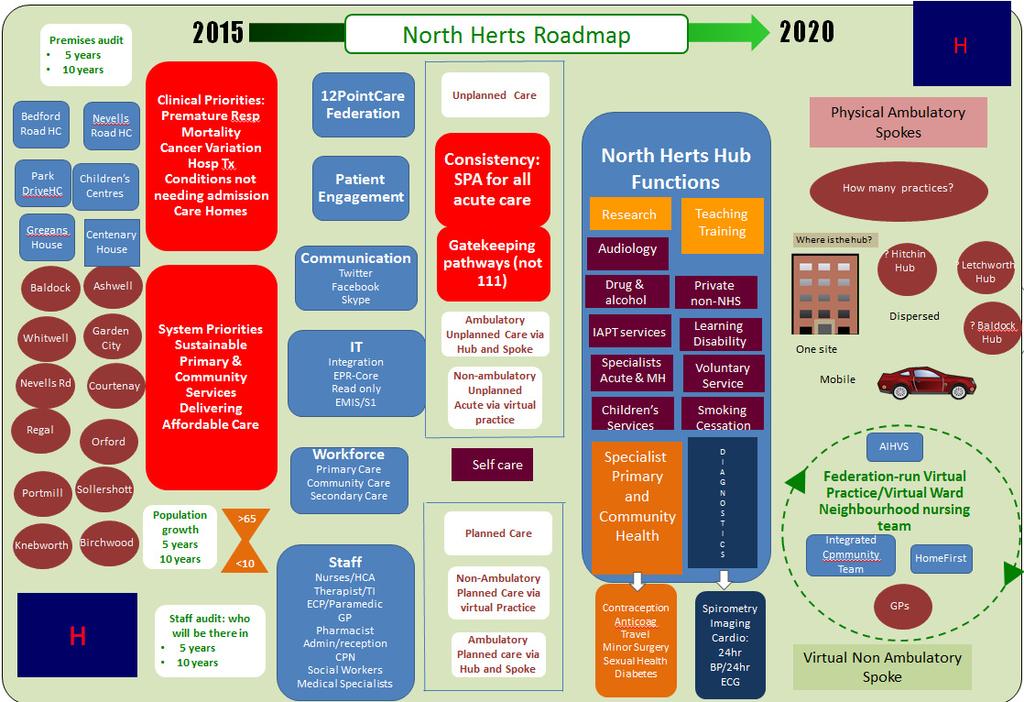
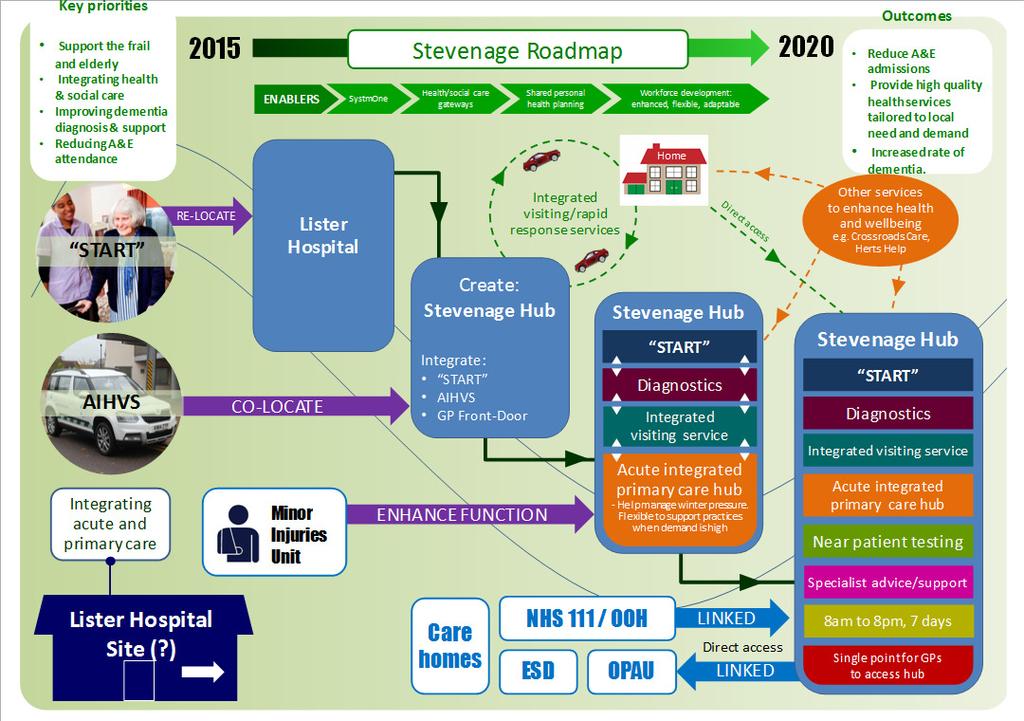
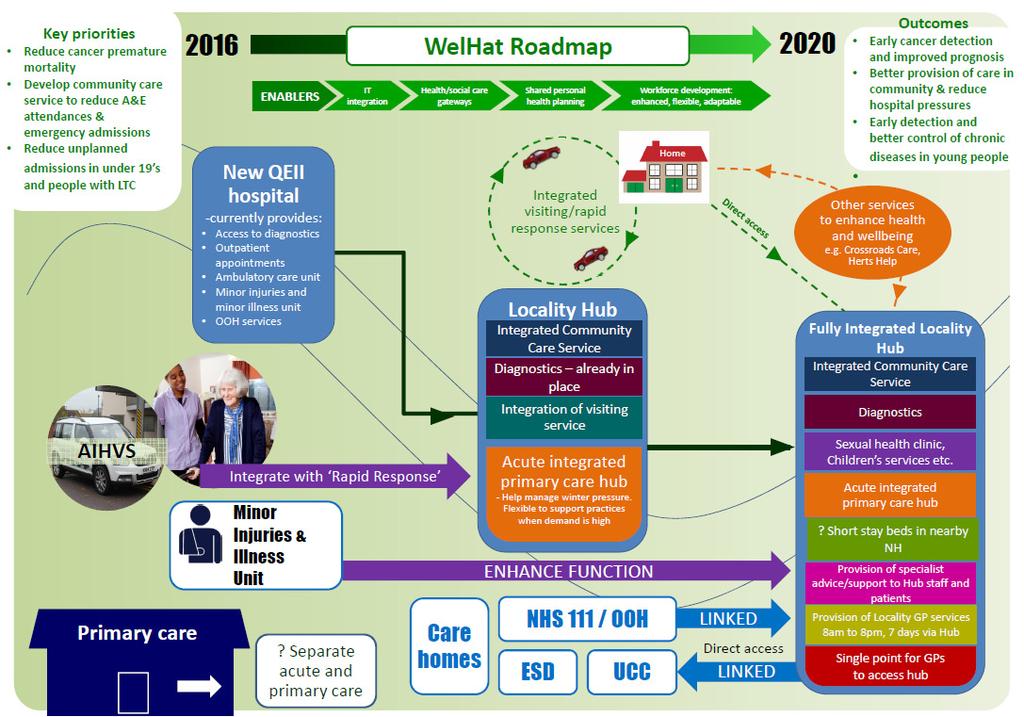
45 Appendix 3: Locality roadmaps 45
46 46
47 47
48 48
49 49
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Cranbrook a healthy new town: health and wellbeing strategy
 Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Birmingham Solihull and the Black Country Area Team
 Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
Birmingham Solihull and the Black Country Area Team A summary of the Five Year Primary Care Strategy: High quality care for all now and for future generations 1 NHS England The Birmingham, Solihull and
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Trust Board Meeting 05 May 2016
 Trust Board Meeting 05 May 2016 Title of the paper: Sustainability and Transformation Plan (STP) Update Agenda item: 15/37 Lead Executive: Trust objective: Purpose: Link to Board Assurance Framework (BAF)
Trust Board Meeting 05 May 2016 Title of the paper: Sustainability and Transformation Plan (STP) Update Agenda item: 15/37 Lead Executive: Trust objective: Purpose: Link to Board Assurance Framework (BAF)
Commissioning Strategy for General Practice
 Commissioning Strategy for General Practice 2016-2021 Section Contents Page Foreword 3 1 Executive Summary 4 2 Introduction 7 3 Setting the scene 10 4 The case for change 23 5 Developing our strategy 25
Commissioning Strategy for General Practice 2016-2021 Section Contents Page Foreword 3 1 Executive Summary 4 2 Introduction 7 3 Setting the scene 10 4 The case for change 23 5 Developing our strategy 25
Healthy London Partnership. Transforming London s health and care together
 Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Primary Care Strategy. Draft for Consultation November 2016
 Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
Quality Strategy. CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July Head of Clinical Quality & Patient Safety
 Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE. Purpose of Report: For Note
 Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
North School of Pharmacy and Medicines Optimisation Strategic Plan
 North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
Our Health & Care Strategy
 MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL
 DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
CCG authorisation: the role of medicines management
 May 2012 The NHS medicines bill for 2010 was 12.9 billion, of which secondary care costs accounted for 32%. Prescribing inflation in 2010 ran at 4.8% and it is estimated that around 14% of total CCG budgets
May 2012 The NHS medicines bill for 2010 was 12.9 billion, of which secondary care costs accounted for 32%. Prescribing inflation in 2010 ran at 4.8% and it is estimated that around 14% of total CCG budgets
Norfolk and Waveney STP - summary of key elements
 Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
Welcome. PPG Conference North and South Norfolk CCGs June 14 th 2018
 Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
In this edition we will showcase the work of the development of a model for GP- Paediatric Hubs
 Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Delivering the Five Year Forward View Personalised Health and Care 2020
 Paper Ref: NIB 0607-006 Delivering the Five Year Forward View Personalised Health and Care 2020 INTRODUCTION The Five Year Forward View set out a clear direction for the NHS showing why change is needed
Paper Ref: NIB 0607-006 Delivering the Five Year Forward View Personalised Health and Care 2020 INTRODUCTION The Five Year Forward View set out a clear direction for the NHS showing why change is needed
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
NHS ENGLAND BOARD PAPER
 NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
Reducing Variation in Primary Care Strategy
 Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
Reducing Variation in Primary Care Strategy September 2014 Page 1 of 14 REDUCING VARIATION IN PRIMARY CARE STRATEGY 1. Introduction The Reducing Variation in Primary Care Strategy should be seen as one
CLINICAL AND CARE GOVERNANCE STRATEGY
 CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
A consultation on the Government's mandate to NHS England to 2020
 A consultation on the Government's mandate to NHS England to 2020 October 2015 You may re-use the text of this document (not including logos) free of charge in any format or medium, under the terms of
A consultation on the Government's mandate to NHS England to 2020 October 2015 You may re-use the text of this document (not including logos) free of charge in any format or medium, under the terms of
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan. October 2016 submission to NHS England Public summary
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Agenda Item No. 9. Key Information
 Key Information Name of footprint and no: Sussex and East Surrey (33) Region: NHSE South Nominated lead of the footprint including organisation/function: Michael Wilson, Chief Executive, Surrey and Sussex
Key Information Name of footprint and no: Sussex and East Surrey (33) Region: NHSE South Nominated lead of the footprint including organisation/function: Michael Wilson, Chief Executive, Surrey and Sussex
The incentives framework for ACOs
 New care models The incentives framework for ACOs Accountable Care Organisation (ACO) Contract package - supporting document Our values: clinical engagement, patient involvement, local ownership, national
New care models The incentives framework for ACOs Accountable Care Organisation (ACO) Contract package - supporting document Our values: clinical engagement, patient involvement, local ownership, national
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary
 Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
NHS West Cheshire Clinical Commissioning Group
 NHS West Cheshire Clinical Commissioning Group Five Year Strategy: 2014/15-2018/19 1 Our Planning Footprint In developing our system vision for 2018/2019 NHS West Cheshire Clinical Commissioning Group
NHS West Cheshire Clinical Commissioning Group Five Year Strategy: 2014/15-2018/19 1 Our Planning Footprint In developing our system vision for 2018/2019 NHS West Cheshire Clinical Commissioning Group
Welcome to. Northern England and the Five Year Forward View for Mental Health. Thursday 2 February 2017 at the Radisson Blu, Durham
 Welcome to. Northern England and the Five Year Forward View for Mental Health Thursday 2 February 2017 at the Radisson Blu, Durham Introductions Chairs: Catherine Haigh, Chair of North East together and
Welcome to. Northern England and the Five Year Forward View for Mental Health Thursday 2 February 2017 at the Radisson Blu, Durham Introductions Chairs: Catherine Haigh, Chair of North East together and
Southwark s Primary and Community Care Strategy
 Southwark s Primary and Community Care Strategy 2013/2014 2017/2018 Southwark Primary and Community Care Strategy 2013/2014 2017/2018 Table of Contents Section Page Number Executive Summary 3 1. Introduction,
Southwark s Primary and Community Care Strategy 2013/2014 2017/2018 Southwark Primary and Community Care Strategy 2013/2014 2017/2018 Table of Contents Section Page Number Executive Summary 3 1. Introduction,
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST CHIEF EXECUTIVE S BRIEFING BOARD OF DIRECTORS 16 NOVEMBER 2016
 B SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST CHIEF EXECUTIVE S BRIEFING BOARD OF DIRECTORS 16 NOVEMBER 2016 1. Integrated Performance Report The Integrated Performance Report is attached at Appendix
B SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST CHIEF EXECUTIVE S BRIEFING BOARD OF DIRECTORS 16 NOVEMBER 2016 1. Integrated Performance Report The Integrated Performance Report is attached at Appendix
Strategic overview: NHS system
 Strategic overview: NHS system Dr Keith Ridge, Chief Pharmaceutical Officer 1 November 2016 A collaborative approach Five Year Forward View Oct 2014 NHS planning guidance, Dec 2015: Every health and care
Strategic overview: NHS system Dr Keith Ridge, Chief Pharmaceutical Officer 1 November 2016 A collaborative approach Five Year Forward View Oct 2014 NHS planning guidance, Dec 2015: Every health and care
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
DRAFT. Rehabilitation and Enablement Services Redesign
 DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Planning for. Patients. Our Strategic Plan. Published July 2014
 Planning for Patients Our Strategic Plan 2014 2019 Published July 2014 CHAPTER 1 System Vision The CCG aims to make a positive contribution to the people of East and North Hertfordshire by empowering
Planning for Patients Our Strategic Plan 2014 2019 Published July 2014 CHAPTER 1 System Vision The CCG aims to make a positive contribution to the people of East and North Hertfordshire by empowering
Longer, healthier lives for all the people in Croydon
 D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
NHS Norwich CCG Operational Plan and
 NHS Norwich CCG Operational Plan 2017-18 and 2018-19 Commissioning NHS care for the people of Norwich 1 Release: V17 Final Date: 2016.01.11 Table of Contents Page 1 Introduction 4 2 National Background
NHS Norwich CCG Operational Plan 2017-18 and 2018-19 Commissioning NHS care for the people of Norwich 1 Release: V17 Final Date: 2016.01.11 Table of Contents Page 1 Introduction 4 2 National Background
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
Appendix 1: Integrated Urgent Care Service Update. 1. Purpose
 Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Our next phase of regulation A more targeted, responsive and collaborative approach
 Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Kingston Primary Care commissioning strategy Kingston Medical Services
 Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
NHS Providers Strategy Directors Network meeting Five Year Forward View and Vanguards - Birmingham Community Healthcare NHS Trust our story
 NHS Providers Strategy Directors Network meeting Five Year Forward View and Vanguards - Birmingham Community Healthcare NHS Trust our story Lorraine Thomas Director of Business and Organisational Development
NHS Providers Strategy Directors Network meeting Five Year Forward View and Vanguards - Birmingham Community Healthcare NHS Trust our story Lorraine Thomas Director of Business and Organisational Development
Prospectus for the Procurement and. Commissioning of a Multi-Specialty. Community Provider (MCP) 1 P age
 1 P age") Prospectus for the Procurement and Commissioning of a Multi-Specialty Community Provider (MCP) 1 P age Dudley Clinical Commissioning Group Prospectus for the Procurement and Commissioning of a Multi-Specialty
Prospectus for the Procurement and Commissioning of a Multi-Specialty Community Provider (MCP) 1 P age Dudley Clinical Commissioning Group Prospectus for the Procurement and Commissioning of a Multi-Specialty
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
IUC and Vanguard. Greater Nottingham Integrated Urgent Care 1
 IUC and Vanguard The 2016/17 Vanguard funding has been confirmed at 1.3M This funding is to deliver the 8 elements of Integrated Urgent Care by March 2017 With careful management of funds we will be able
IUC and Vanguard The 2016/17 Vanguard funding has been confirmed at 1.3M This funding is to deliver the 8 elements of Integrated Urgent Care by March 2017 With careful management of funds we will be able
EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS...
 CONTENTS EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS... 6 WHAT WE WILL CONTINUE TO ACHIEVE THROUGH THE HEALTH
CONTENTS EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS... 6 WHAT WE WILL CONTINUE TO ACHIEVE THROUGH THE HEALTH
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Council of Members. 20 January 2016
 Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
NHS Kingston Clinical Commissioning Group. Primary Care Strategy Achieving excellence in primary care
 NHS Kingston Clinical Commissioning Group Primary Care Strategy Achieving excellence in primary care Version control Version 1 020615 Version 2 100815 Shared with PM Version 3 170815 Shared with PM, RB,
NHS Kingston Clinical Commissioning Group Primary Care Strategy Achieving excellence in primary care Version control Version 1 020615 Version 2 100815 Shared with PM Version 3 170815 Shared with PM, RB,
South Yorkshire & Bassetlaw Health and Care Working Together Partnership
 South Yorkshire & Bassetlaw Health and Care Working Together Partnership Memorandum of Understanding Agreement Final Draft June 2017 1 Title Drafting coordinator Target Audience Version V 0.3 Memorandum
South Yorkshire & Bassetlaw Health and Care Working Together Partnership Memorandum of Understanding Agreement Final Draft June 2017 1 Title Drafting coordinator Target Audience Version V 0.3 Memorandum
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Our vision. Ambition for Health Transforming health and social care services in Scarborough, Ryedale, Bridlington and Filey
 Ambition for Health Transforming health and social care services in Scarborough, Ryedale, Bridlington and Filey Our vision www.ambitionforhealth.co.uk Contents 1.0 Introduction: A shared ambition for health
Ambition for Health Transforming health and social care services in Scarborough, Ryedale, Bridlington and Filey Our vision www.ambitionforhealth.co.uk Contents 1.0 Introduction: A shared ambition for health
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
Summary annual report 2014/15
 1 Summary annual report 2014/15 2 Annual Report Summary 2014/15 3 St Thomas Hospital Guy s Hospital CATHEDRAL CHAUCER GRANGE RIVERSIDE ROTHERHITHE SURREY DOCKS Key facts about Southwark GP practices in
1 Summary annual report 2014/15 2 Annual Report Summary 2014/15 3 St Thomas Hospital Guy s Hospital CATHEDRAL CHAUCER GRANGE RIVERSIDE ROTHERHITHE SURREY DOCKS Key facts about Southwark GP practices in
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT
 NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
South East Essex. Discharge to Assess Strategy
 South East Essex Discharge to Assess Strategy 2018-2020 Version 3.5 27 th March 2018 Document Control: Revision: Name Date: Version 2.0 Shirley Regan 12 December 2017 Version 2.1 Amendments-Paul 19 December
South East Essex Discharge to Assess Strategy 2018-2020 Version 3.5 27 th March 2018 Document Control: Revision: Name Date: Version 2.0 Shirley Regan 12 December 2017 Version 2.1 Amendments-Paul 19 December
Strategic Commissioning Plan for Primary Care: Hull Primary Care Blueprint
 APPENDIX 1: 1. Vision and context The vision for the Blueprint being proposed is consistent with the CCG s Hull 2020 Transformation Programme and the direction of travel and new models of care outlined
APPENDIX 1: 1. Vision and context The vision for the Blueprint being proposed is consistent with the CCG s Hull 2020 Transformation Programme and the direction of travel and new models of care outlined
OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS. September 2014
 OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS September 2014 1 SUMMARY Our vision for the City and Hackney health economy is: Patients in control of their health and wellbeing; A joined-up system which is safe,
OUTLOOK FOR THE NEXT 5 YEARS OUR PLANS September 2014 1 SUMMARY Our vision for the City and Hackney health economy is: Patients in control of their health and wellbeing; A joined-up system which is safe,
Urgent and Emergency Care - the new offer
 Urgent and Emergency Care - the new offer If it s really serious I want specialist care Help me to help myself and not bother the NHS If only they could talk to my GP? London Clinical Senate Keith Willett
Urgent and Emergency Care - the new offer If it s really serious I want specialist care Help me to help myself and not bother the NHS If only they could talk to my GP? London Clinical Senate Keith Willett
WELCOME. To our first Annual General Meeting (AGM) Local clinicians working with local people for a healthier future
 Local clinicians working with local people for a healthier future") WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
Wolverhampton Clinical Commissioning Group 1
 Wolverhampton Clinical Commissioning Group 1 Introduction and Context In 2014, along with our partners, the CCG established our five year strategy for the Wolverhampton Health Economy. This set out our
Wolverhampton Clinical Commissioning Group 1 Introduction and Context In 2014, along with our partners, the CCG established our five year strategy for the Wolverhampton Health Economy. This set out our
Approve Ratify For Discussion For Information
 NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
2015/16 Annual General Meeting
 2015/16 Annual General Meeting Welcome Dr Hari Pathmanathan tweet #ENHCCGAGM follow us @enhertsccg Financially Healthy? 2015/16 Finance Report Alan Pond Chief Finance Officer Statutory financial duties
2015/16 Annual General Meeting Welcome Dr Hari Pathmanathan tweet #ENHCCGAGM follow us @enhertsccg Financially Healthy? 2015/16 Finance Report Alan Pond Chief Finance Officer Statutory financial duties
Driving and Supporting Improvement in Primary Care
 Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
Driving and Supporting Improvement in Primary Care 2016 2020 www.healthcareimprovementscotland.org Healthcare Improvement Scotland 2016 First published December 2016 The publication is copyright to Healthcare
Bedfordshire, Luton and Milton Keynes. Sustainability and Transformation Plan. Central Brief: February 2018
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan Central Brief: February 2018 Issue date: February 2018 News Transforming care closer to home Our ambition is to build high quality,
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan Central Brief: February 2018 Issue date: February 2018 News Transforming care closer to home Our ambition is to build high quality,
Sussex and East Surrey STP narrative
 Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
17. Updates on Progress from Last Year s JSNA
 17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
Vanguard Programme: Acute Care Collaboration Value Proposition
 Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Improving General Practice for the People of West Cheshire
 Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
FIVE TESTS FOR THE NHS LONG-TERM PLAN
 Briefing 10 September 2018 FIVE TESTS FOR THE NHS LONG-TERM PLAN The new NHS long-term plan is a significant opportunity for the health service. It can set out a clear and achievable path for sustaining
Briefing 10 September 2018 FIVE TESTS FOR THE NHS LONG-TERM PLAN The new NHS long-term plan is a significant opportunity for the health service. It can set out a clear and achievable path for sustaining
The operating framework for. the NHS in England 2009/10. Background
 the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
Summary two year operating plan 2017/18
 One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report
 Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Urgent and Emergency Care Review update: from design to delivery
 The Kings Fund September 2015 Keith Willett Director of Acute Care Urgent and Emergency Care Review update: from design to delivery What does the experience and data from recent winters tell us? Surge
The Kings Fund September 2015 Keith Willett Director of Acute Care Urgent and Emergency Care Review update: from design to delivery What does the experience and data from recent winters tell us? Surge
National Primary Care Cluster Event ABMU Health Board 13 th October 2016
 National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
Joint framework: Commissioning and regulating together
 With support from NHS Clinical Commissioners Regulation of General Practice Programme Board Joint framework: Commissioning and regulating together A practical guide for staff January 2018 Publications
With support from NHS Clinical Commissioners Regulation of General Practice Programme Board Joint framework: Commissioning and regulating together A practical guide for staff January 2018 Publications
Suffolk & North East Essex STP Implementation Plan. 20 th October Draft
 Suffolk & North East Essex STP Implementation Plan 20 th October 2016 Draft 1 Executive Summary In Suffolk and North East Essex, the NHS, general practice and local government have come together to develop
Suffolk & North East Essex STP Implementation Plan 20 th October 2016 Draft 1 Executive Summary In Suffolk and North East Essex, the NHS, general practice and local government have come together to develop
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Particulars Version 22. NHS Standard Contract 2018/19. Particulars Enhanced Homeless Health
 NHS Standard Contract 2018/19 Particulars Enhanced Homeless Health 1 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service OOHS_011 Enhanced Homeless Health Commissioner Lead
NHS Standard Contract 2018/19 Particulars Enhanced Homeless Health 1 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service OOHS_011 Enhanced Homeless Health Commissioner Lead
COMMON GROUND EAST REGION. DEVELOPING A HEALTH AND SOCIAL CARE PLAN FOR THE EAST OF SCOTLAND Staff Briefing
 COMMON GROUND EAST REGION DEVELOPING A HEALTH AND SOCIAL CARE PLAN FOR THE EAST OF SCOTLAND Staff Briefing SEPTEMBER 2018 1 COMMON GROUND It is fitting that in the 70th anniversary year of our National
COMMON GROUND EAST REGION DEVELOPING A HEALTH AND SOCIAL CARE PLAN FOR THE EAST OF SCOTLAND Staff Briefing SEPTEMBER 2018 1 COMMON GROUND It is fitting that in the 70th anniversary year of our National
GP Cover of Nursing, Residential, Extra Care and Intermediate Care Homes. Camden Clinical Commissioning Group. Care Home LES Spec v1
 Local Enhanced Service Clinical Lead Commissioner Reporting Mechanism/Frequency Payment Frequency Payment Contact This Version GP Cover of Nursing, Residential, Extra Care and Intermediate Care Homes Dr
Local Enhanced Service Clinical Lead Commissioner Reporting Mechanism/Frequency Payment Frequency Payment Contact This Version GP Cover of Nursing, Residential, Extra Care and Intermediate Care Homes Dr
The Bedfordshire CCG and Bedford Borough Council Better Care Plan Executive Summary: Our approach to Better Care planning
 DRAFT Version 16 19 March 2014 The Bedfordshire CCG and Bedford Borough Council Better Care Plan Executive Summary: Our approach to Better Care planning Bedford Borough and Bedfordshire CCG s Better Care
DRAFT Version 16 19 March 2014 The Bedfordshire CCG and Bedford Borough Council Better Care Plan Executive Summary: Our approach to Better Care planning Bedford Borough and Bedfordshire CCG s Better Care
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme. Frequently Asked Questions Second Edition
 Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
South Yorkshire and Bassetlaw Accountable Care System Chief Executives
 South Yorkshire and Bassetlaw Accountable Care System PMO Office: 722 Prince of Wales Road Sheffield S9 4EU 0114 305 4487 23 June 2017 Letter to: South Yorkshire and Bassetlaw Accountable Care System Chief
South Yorkshire and Bassetlaw Accountable Care System PMO Office: 722 Prince of Wales Road Sheffield S9 4EU 0114 305 4487 23 June 2017 Letter to: South Yorkshire and Bassetlaw Accountable Care System Chief
Expression of Interest for the Co-commissioning of Primary Care Services STATEMENT FROM OUR CHAIRMAN AND CHIEF ACCOUNTABLE OFFICER
 Brierley Hill Health and Social Care Centre Venture Way Brierley Hill West Midlands DY5 1RU Tel: 01384 321763 Fax: 01384 322414 20 June 2014 Dudley Clinical Commissioning Group Expression of Interest for
Brierley Hill Health and Social Care Centre Venture Way Brierley Hill West Midlands DY5 1RU Tel: 01384 321763 Fax: 01384 322414 20 June 2014 Dudley Clinical Commissioning Group Expression of Interest for