Making Compliance Gains Through Technology:
|
|
|
- Moris Allison
- 5 years ago
- Views:
Transcription
1 Making Compliance Gains Through Technology: Lessons from Eight Years at the Point of Care Cynthia Trapp, CHFP, CMPE, CPC, CPC-I, CCS-P, CHC, PCA Sherry Weisse, CPC, PCA Health Care Compliance Association s 13 th Annual Compliance Institute Sunday April 26, Presenters: Cynthia Trapp CHFP, CMPE, CPC, CPC-I, CCS-P, CHC, PCA Director, Professional Coding Lahey Clinic, Inc. 41 Mall Road Burlington, MA cynthia.a.trapp@lahey.org Sherry Weisse, CPC, PCA Professional Coding Systems Project Manager Lahey Clinic, Inc. 41 Mall Road Burlington, MA sherry.weisse@lahey.org 2 1
2 Objectives Identify components of charge capture technology that directly impacts the day-to-day needs of professional compliance programs Discuss the limitations of EMR technology on the charge capture process as the central focus point in a compliance program Understand the key players in a roll-out of charge capture and identify their institution s own readiness for undertaking such an initiative 3 Outline Compliance and it s challenges Compliance, Coding, and Charge Capture Charge Capture then and now Charge Capture Technology Implementation of a Technological Solution A case study Charge Capture, Compliance, and the EMR Overall Considerations Conclusion 4 2
3 Compliance - History 1860 FCA False Claims Act 1978 Inspector General Act (Public Law ) 1992 Presidential Campaign 1993 OBRA Omnibus Budget Reconciliation Act 1996 OIG Audits began 1996 HIPAA authorized Medicare Integrity Program 1996 Health Care Fraud and Abuse Control Panel More OIG Audits 1998 ORT Operation Restore Trust 1998 Balanced Budget Act 1999 Balanced Budget Relief Act 5 Medicare Integrity Program Congress allocated $100 Million to begin crackdown on Medicare fraud Further funded by: Proceeds from fraud and abuse investigations Annual allocations from Congress But why??? 6 3
4 Why the crackdown? Public demand for better healthcare services Increased cost to deliver healthcare Evidence of deliberate acts of fraud and abuse Public awareness with the 1992 Presidential Campaign And now.an even greater need to ensure compliance in healthcare with the new plans by the new administration. 7 Medicare Trust Fund Million beneficiaries $309 Billion in expenditures Projection to solvency 2020 Limited solutions to prevent solvency 8 4
5 Projections of Medicare Trust Fund Year of Report Years to Insolvency Year of Insolvency *The Compliance Officer s Handbook, 2006 HCPro, Inc. 9 Office of Inspector General Issued Program Guidance Issues annual OIG Work Plan Investigates healthcare fraud and abuse Recommends further investigations by Department of Justice 10 5
6 Seven Elements of OIG Program Guidance 1. Standards and Procedures 2. Compliance Officer 3. Training and Education 4. Communication 5. Response to detected problems 6. Internal auditing and monitoring 7. Enforcement of disciplinary standards 11 Fraud and Abuse Fraud deliberate act intended to obtain improper payments Abuse repeated act that may not be deliberate but results in improper payment 12 6
7 Compliance Enforcement Office of Inspector General (OIG) Centers for Medicare & Medicaid Services (CMS) Department of Justice (DOJ) U. S. Attorney s Office Federal Bureau of Investigation (FBI) State Medicaid Fraud Control Units Office for Civil Rights (OCR) Private Payers 13 Enforcement Results Millions / Billions returned to Medicare Trust Fund 1998 $271M 2000 $577M 2002 $1.4B 2004 $1.5B 2006 $1.5B Fed Share of Medicaid 1998 $9M 2000 $27M 2002 $59M 2004 $99M 2006 $177M 14 7
8 Enforcement Results Since 1998 Over $11.2 Billion returned to the Medicare Trust Fund Over $900 Million recovered as the Federal share of Medicaid restitution 15 Enforcement Results returned to the Medicare Trust Fund Millions Returned to Medicare Trust Fund 2,000 Millions of Dollars 1,500 1, ,000 1, ,510 1,550 1, Year 16 8
9 Enforcement Results Recovered as the Federal share of Medicaid Restitution Millions Recovered as Federal Share of Medicaid Restitution Millions of Dollars Year 17 OIG Compliance Risk Areas Billing for services not performed Billing for services not medically necessary Billing higher levels of services through upcoding or DRG s Billing for duplicate services Unbundling 18 9
10 OIG Compliance Risk Areas Teaching physician guidelines Billing for outpatient services for inpatient stays False Cost Reports Billing for discharge in lieu of transfer Patient s freedom of choice Failure to refund credit balances 19 OIG Compliance Risk Areas Financial arrangements between hospitals and physicians Kickbacks Joint ventures Stark physician self-referral law Failure to provide services to patient s of an HMO Patient dumping 20 10
11 2009 OIG Work Plan Medicare and Medicaid Services Hospitals and Physician Services Nursing Homes Home Health Services Hospice Services Medical Equipment and Supplies Medicare Part A and Part B Contractor Medicare Part B Prescription Drugs Medicare Part C Program Medicare Part D Program OIG Work Plan Medicare and Medicaid Services Medicaid Hospitals Medicaid Home, Community, Nursing Home Care Medicaid Prescription Drugs Medicaid Administration Medicare and Medicaid IS and Data Security State Children s Health Insurance Program Legal Activities 22 11
12 2009 OIG Work Plan Public Health and Human Service Programs Centers for Disease Control and Prevention Food and Drug Administration Health Resources and Services Administration Indian Health Service National Institutes of Health Substance Abuse and Mental Health Services Administration Crosscutting Public Health Activities OIG Work Plan Human Service Programs Administration on Aging Administration on Children and Families 24 12
13 2009 OIG Work Plan Department Wide Audits Financial Statement Audits Other financial Accounting Reviews Automated Information Systems Other Issues OIG Focus on Physicians Place of Service Errors E/M Services in Global Periods Medicare Expenses by Specialties Clinical Social Worker Services Outpatient Physical Therapy Payments for Colonoscopy Incident to Services Polysomnography 26 13
14 2009 OIG Focus on Physicians Long distance physician claims requiring face-to-face visit Ultrasound Services Independent Diagnostic Testing Facilities High Frequency Chiropractic Treatment Physician Reassignment of Benefits Unlisted Procedure Codes Unbundling In Clinical Labs Laboratory Pricing Clotting Factor Furnishing Fee Medicare Billing with GY Modifier 27 Past OIG Plans have included Welcome to Medicare Visits Wound Care E/M during global surgical period Psychiatric Services Eye Surgeries Cardiography, Echocardiography Services Consult billing Teaching Physician Guidelines 28 14
15 Coding for Compliance Follow CPT/AMA coding guidelines Follow all CCI Guidelines Follow LCD s, (LMRP s) and NCD s Follow Official ICD-9-CM guidelines Follow Medical Necessity Rules Follow all CMS and Payer Billing Guidelines Educate physicians on rules Be aware of OIG Work Plan Review documentation and advise physicians 29 Risk areas for Coding Compliance Consults Teaching physician guidelines Place of service errors Global surgery rules High Utilization Diagnostic Testing High Utilization Chiropractic Services Medical Necessity Services Incident To services Evaluation and Management documentation 30 15

 (ICD-10 will have up to 7 digits of specificity) Over")

16 Complexities of Coding ICD-9 Documentation Medical Necessity Charge CPT-4 /HCPCS Edits 31 Complexity of Professional Coding and Billing Over 15,000 ICD-9-CM Diagnosis codes With 5 digits of specificity (ICD-10 will have over 155,000 codes) (ICD-10 will have up to 7 digits of specificity) Over 8,000 CPT Procedure codes Over 50 possible Medicare edits per CPT Over 150 Level I and Level II modifiers Complicated E/M coding guidelines 32 16
17 Complexity of Coding Compliance CCI Edits (Correct Coding Initiative) Flags for unbundling comprehensive, component, and mutually exclusive codes. Over 193,000 unique CCI edit combinations LCD Edits (Local Coverage Determination) Formerly called LMRP s Local Medicare Review Policies Flags when diagnosis code does not support medical necessity to support the procedure code. Average 500,000 edits per carrier CPT to ICD All FI s and Carriers maintain their own 33 Coding Compliance cont Additional concerns for: General and Relational Medicare Edits Flags when sex or age does not match procedure Over 50,000 Medicare edits 34 17
18 How can an electronic solution help with compliance? 35 Charge Capture Coding Documentation Compliance By utilizing technology to put the pieces together! 36 18
19 Elements of an electronic addition to a compliance program A system that can handle complex regulatory requirements A software that can assist the clinician to code accurately A software that provides a mechanism to open lines of communication between the language of the coder and the language of the physician/clinician. A software that is updated to meet regulatory requirements on time. 37 A technological solution to a charge capture challenge!!! Enormous administrative overhead Significant loss from missing charges Lost $$ due to missed filing limits Lost $$ due to missing information Lost $$ due to manual data entry error Lost $$ due to lost paper encounters 6-7 people handle paper claim 38 19

20 What is charge capture technology? A major leap above 39.the encounter form
21 It s a technological solution to a coding and compliance challenge!!! Encounter form updates burdensome Compliance risk for coding inaccuracy Revenue risk for coding inaccuracy CCI edits, LCD s (LMRP s), payer edits Gender edits ICD-9 coding rules CPT coding guidelines Enormous administrative overhead 41 It s a solution HELP!! 42 21


22 To an outdated paper process! 43 Paper Charge Entry Process 44 22




23 Challenges to the paper process Often there are. Lost charges Poor handwriting Communication issues 45 Coding Then 46 23


24 And Now 47 Charge Entry Then 48 24

25 And Now 49 Charge entry: electronic vs. paper 50 25


26 Reconciling charges then 51 And Now 52 26

27 Technological Charge Entry Process 53 How does an electronic charge capture solution help to meet the day-to-day needs of an effective compliance program? This is what we will explore 54 27
28 The purpose of an electronic solution To provide an automated solution to ensure compliant capture of all professional/facility charges that would: Provide coding assistance for the physician/clinician Include all elements required for the claim Streamline the amount of hands touching the claim Assist the physician/clinician in daily workflow of administrative functions Pay for itself 55 The purpose cont that would: Eliminate use of unspecific diagnosis codes Reduce the number of claims edits/rejections Reduce the risk of audits Reduce the risk of fines, penalties, and unwelcome publicity Improve revenue capture/cash flow Assist in compliance efforts 56 28

29 So, how does a charge capture solution help with compliance? Electronic solution for physician edits Improve accuracy from physician Eliminate manual paper review of encounters Eliminate missing/illegible information Eliminate chasing after the physician Eliminate lost/missing charges Improve MD communication/interaction 57 It starts with the appointment and follows to the charge The physician enters his codes electronically Through Handheld Tablet PC 58 29




30 MD chooses the E/M level and procedures Unlike paper encounters, all CPT-4 codes are available 59 Review of Systems and E/M Components E/M Wizard assists MD to choose most accurate E/M Code! 60 30


31 MD is warned for Modifiers Modifiers are available and flagged if required 61 MD is warned for CCI edits CCI Edit LCD Edit 62 31


32 MD is warned for Medical Necessity All ICD-9-CM Codes are available and edit for medical necessity. 63 And diagnosis linkage 64 Linking Diagnoses to Procedures is imperative to proper billing. 32


33 Unlinked code warnings 65 Linking Diagnoses to Procedures is imperative to proper billing. Rounding list so all patient charges are accounted for 66 33

34 Alerts for better communication 67 Coders communicate with MD s 68 34



35 MD s can view patient history 69 And can be prompted for quality measures such as PQRI 70 35


36 We can manage and create rules 71 Such as ICD-9 rules 72 36

37 that warn us for missing underlying diseases for manifestations codes. 73 or that warn us for using well visit codes for sick E/M visits


38 Coders and physicians can be warned for medical necessity on the web version. 75 or of course on the handheld 76 38


39 We can manage global windows 77 Warnings on the web 78 39



40 or on the physician s handheld 79 We can manage surgical rules 80 40

41 and LCD s or NCD s! 81 We can manage Place of Service for outpatient and 82 41

42 Inpatient locations 83 We can view number of inpatient days charged at a glance 84 42


43 We can also manage POS for centers. 85 We can manage requesting provider for consults through edits


44 Reconciliation: Electronic vs. paper 87 Outpatient Charge Reconciliation 88 44

45 and inpatient 89 We can reconcile by provider 90 45
46 or location 91 We can reconcile professional (physician) charges
 charges 93")

47 and technical (facility) charges 93 We can create rules for crossreconciliation 94 47


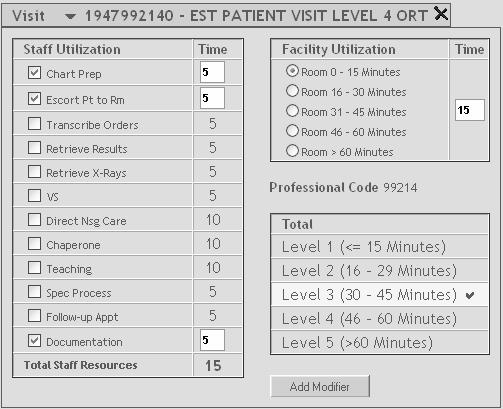
48 The Power of Cross Reconciliation Compliance and Charge Capture Bridging the gap between physician and hospital charges! Hospital Coding Physician Coding 95 Time auto calculates and pulls in the visit category provided by the physician 96 48


49 Drug and supply charges are easily monitored for missing or duplicates 97 Charge master for drugs and supplies are centrally managed to avoid incorrect or duplicate charging 98 49


50 Rules managed centrally for missing information for facility and professional 99 And of course, electronically, there is a permanent audit trail
51 Electronic charge reconciliation allows us the ability to Recover missing / avoid duplicate charges Cross reconcile professional (physician) and technical (facility) charges Manage drugs and supply charges centrally to avoid errors Manage accuracy of charges and edits Manage compliance efforts through edits Manage training and education through technology 101 We asked ourselves
52 What else can an electronic tool help us with??? Can we really replace the paper? 103 We couldn t afford not to Paper processes have Costly overhead, enormous waste Enormous risk for error Charge entry errors Numbers of people touching the claim Money left on the table Missing charges Late charges Inability to match hospital to pro charges Risk for error and non-compliance
53 The Big Picture... Appointment Reconciliation LMRP s Coding Dictation Problem List Documentation Patient Visit Edits ABN s Billing Medical Necessity Reference Tools Order Entry Prescription 105 How we got started Team development Vendor selection Partnership decision Planning the project Product development Timeline Pilot Implementation
54 What we looked for... The best software products The best vendors willing to partner to provide an integrated solution Hardware able to handle multiple integrated solutions on one medium Options for use with PC, handheld, tablet, or a physician workstation A device for use at any point of service 107 What we looked for continued... Real-time interface capability from Registration/Scheduling Interface capability with other systems Adaptability to the clinical workflow Adaptability to the business practices Data integrity Quality control Reconciliation
55 Other factors we considered Physician Acceptance/Ownership Culture Change Training Deployment of the Hardware Network Capabilities Enterprise-Wide Integration Testing Ongoing support Qualitative/Quantitative Measurements 109 Team development Admissions /Registration Scheduling Vendor Project Management Professional Coding Team Physician Workflow F Billing Charge Entry IT Application Hardware Network Support Administrative Champion/Support Metrics/ Measurements Finance Compliance Audit Clinical Management Staff Business Process
56 Core Implementation Team Project Manager Coder Clinical Manager Surgical/Medicine Professional Billing Technical Billing Charge entry Registration/Scheduling Admissions VP Champion MD Champion Non-physician practitioner Software Applications Hardware Applications Applications Integration Network Compliance/Internal Audit 111 The planning phase Roadmap Development Requirements Gathering Spec Development Interface Development Design Unit Testing Integrated Testing Issues list/resolutions Timeline Pilot Feedback
57 Sample Issues/Enhancement List 113 The implementation Developed roll-out plan Conducted extensive rigorous testing Unit testing / integrated testing See Test Script Scenarios All codes / all physicians / all departments Conducted pre- and post- coding audits to provide education to physicians Held group and individual training sessions Provided Go-live and ongoing support Continued interactive coder/physician communication/education
58 The roll-out plan Timeline Six weeks per group Training One-hour presentation Scope/purpose of project 5 minutes Software presentation 20 minutes Hardware/Network overview 15 minutes Hand out IPAQ s and practice 20 minutes One-week practice time/non-live environment Additional one-on-one session if needed Onsite support on Go-live day 115 Sample Roll-out Checklist
59 Sample Roll-out Checklist continued 117 The Testing Test ADT interface feed to build shell to ensure HL7 messages were coming across correctly Run initial short one-day test for locations Run small test file with one MD for each specialty currently live to ensure header hierarchy Add special cases such as WC, MVA, other accident Run full integrated test files for all scenarios through entire cycle (Sched to BAR) If fail, analyze data, keep running until perfect Final run with errors to test our TES edits
60 The Testing cont Some things we specifically tested No-name patients Trauma patients into the ER Transfer of patient from ER to bed Transfer of patient from bed to bed, room to room, location to location, facility to facility Transfer of patient from Dr. to Dr., specialty to specialty Flips of observation to inpatient and vice versa Code combinations within each specialty Consults, inpatient/outpatient visits, procedures, admits, discharges, transfers, etc 119 Sample Test Case Scenarios
61 Lahey Clinic Case Study 121 Started with a pilot group. Four Departments GIM, Neurosurgery, General Surgery, Gastroenterology Outpatient visits only / one location 15 physicians 30 Day dual process 90 Day Nov. Dec. Jan. ( ) 30 Day Evaluation ROI Success and decision to move forward!
62 The return on investment (ROI) Pre-Implementation Measurements June, July, August 2001 Post-Implementation Measurements Dec 2001, Jan, Feb 2002 Data IDX BAR missing charge report (standard) Custom extraction of data from IDX BAR By department / by physician / by payer Over 22,000 encounters monitored 123 The case study What was studied Over 22,000 encounters Recovery of lost/missing charges Change in distribution and intensity of codes Time to charge entry Time to claim submission Time of claim submission to payment What was not studied Change in collection performance due to change in claim denial/rejections. Decrease in costs of follow-up activities for claim denial/rejections
63 Deciding factors to move forward Significant positive ROI Results Capture of missing revenue Cost savings Positive Physician feedback from pilot User friendliness Adaptability to daily work-flow Team acceptance 125 The case study results Pre 1.1% lost charges 48 missing charges 2.29 average days to charge entry 35.3 average days from claim to payment Post 0% lost charges Zero missing charges.46 average days to charge entry 31.1 average days from claim to payment *22,000 claims studied
64 The case study results 79% improvement in average time from patient visit to billing system entry. 11.9% improvement in average days from claim to payment 1.1% recovery of missing charges Recovery of over 11,000 claims yearly for Lahey or over $1,000,000. Hold encounters not studied 127 Coding study results New Patient Visits Coding intensity 7.59% Gross charges per visit 7.04% Established Patient Visits Coding Intensity.91% Gross charges per visit 1.04% Consult Visits (outpatient office) Coding Intensity.8% Gross charges 1.03%
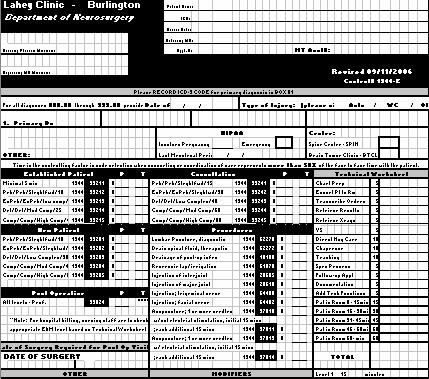
65 LAHEY CLINIC FINANCIAL BENEFIT REVIEW Summary Charge Data 1 Department-Level Summary Prior to MedAptus - 3 Month Period 2 After MedAptus Implementation 3 Average Arrived Encounters Missing Total Charge Per Arrived Encounters Missing Total Department/Physician Patients With Charges Encounters Charges Encounter Patients With Charges Encounters Charges General Internal Medicine 1,615 1, $ 163,337 $ 102 1,672 1,672 - $ 175,578 Gastroenterology 1,092 1, , ,476 Neurosurgery 1,292 1, , ,190 1,190-77,362 General Surgery , ,660 Total - All Departments 4,309 4, $ 372,344 $ 87 3,992 3,992 - $ 344,076 LAHEY CLINIC FINANCIAL BENEFIT REVIEW Comparison of Coding Levels & Distribution 1 E&M Coding Levels - All Departments Prior to MedAptus After MedAptus Implementation Variance 3 Gross Code Gross Code Gross Code E&M Category/Code Volume Charges Distribution Volume Charges Distribution Volume Charges Distribution Office New Patient Visits Level 1 25 $ 1, % 21 $ % % Level , % 32 2, % % Level , % 48 4, % % Level , % 25 3, % % Level 5 8 1, % 11 1, % % New Patient Visit Total 152 $ 12, $ 12,522 Average Code Level/Charges $ $ $ % 7.04% Office Established Patient Visits Level 1 92 $ 2, % 37 $ % % Level , % , % % Level 3 1,312 73, % 1,147 64, % % Level , % , % % Level , % 75 9, % % Established Patient Visit Total 2,585 $ 144,530 2,475 $ 139,823 Average Code Level/Charges $ $ $ % 1.04% Office Consultation Visits Level 1 52 $ 3, % 20 $ 1, % % Level , % , % % Level , % , % % Level , % , % % Level , % 29 7, % % Consultation Visit Total 863 $ 122, $ 93, Average Code Level/Charges $ $ (0.02) $ (1.45) -0.80% -1.03% Based on a custom extraction of data from IDX BAR provided by Lahey Clinic staff. Represents the weighted average level of coding (i.e., ranging from level 1 to level 5) and gross charges per visit within each visit category. Variance presents the change in average coding level and gross charges per visit represented as a both numeric and percentage change. 65
66 A few interesting findings Opened lines of communication between MD and coder that we didn t expect! Some surgeons were using level ones! MD s not charging for inpt subsequent care visits. MD s weren t charging because they send the residents to visit the patient Encounters show revenue, but were not going out the door on-hold OVNC 131 Benefits to our clinic Eliminated missing charges Developed sound reconciliation process Reduced Lag days to charge entry Charges processed in one day Instant documentation of patient visit Wireless access to patient history Wireless access to patient demographics Improved quality of coding
67 Benefits to our clinic Reduced denials due to inaccurate codes Provided educational/collaborative tool for coding support Improved quality of information available Coding, Edits, Reference tools Improved quality of information flow Registration, appointments, patient demographics Improved operational efficiencies 133 Benefits to our clinic Reduced overhead costs Created paperless environment Provided universal access platform for other functionalities such as dictation, e-prescription, medical reference information, lab ordering Improved organizational compliance

68 A Useful Tool For Internal Audits Education through Internal Audits Perform random internal audits Two reviews of 20 visits per MD per year Review results with MD and provide feedback and education Review risk areas Review documentation Review claim from schedule to payment for proper coding Provide ongoing education to MD s
69 Coding Documentation Audits Review CPT, ICD-9, HCPCS Review modifiers Review place of service Review billing guidelines Review E/M levels Review codes for unbundling Review documentation requirements Legibility Time documented when appropriate 137 The pre/post coding audits Conduct pre/post clinician coding audits to show benefits and educational needs Followed standard CMS 1995 or 1997 guidelines Document results for compliance plan Used results to provide education pre and post Charge Capture system implementation

70 Sample Coding audit report 139 Sample high level audit report
71 When asked how the electronic solution helps them, some coders commented it has given us the opportunity to interact more often with the physician with regard to overall coding issues the reality is they (MD s) now have the coding tools resulting in more coding inquiries and opportunities for education and awareness. 141 Others commented it has given me the ability to see each code that each physician has reported via the web and alerts us to any problems that may need to be addressed as opposed to looking at each and every paper encounter. It saves time. There is no paperwork so there is no running around the hospital no problems with legibility
72 Current State of Electronic Coding and Charge Capture Professional (Physician) Charges 32 Specialty Departments Live 533 MD s and NPP s live 51 Centers live 10 Outpatient Locations 54 Inpatient Locations Inpatient Outpatient Surgical 53% of all professional revenue through this electronic solution 24% comes through ancillary hospital interfaces 143 Current State of Electronic Facility Charge Capture Hospital (Facility) Charges 24 Groups live 204 Users 2 Locations 27 Nursing Stations Outpatient Clinics 6.35% Revenue comes through this software 56% comes through ancillary hospital interfaces


73 What about the EMR? How does that fit with our current charge capture solution? 145 What about the EMR? Best of Breed Approach Recognized need for EMR Vendor Evaluation - Outpatient Charge Capture Deep Dive Evaluation for Compliance Analysis of Results Lessons Learned from Evaluation Current approach to integration with EMR
74 Need for an EMR Internal and external clinicians and staff Communication with patients Secure and auditable interaction Single sign-on Access to all clinical information Ability to view all patient history Ability to place orders Ability to complete documentation 147 Best of Breed Approach Lab System Radiology System Order Entry System OR System Registration and Scheduling System Dictation System Billing System Charge Capture System E-Prescribing System
75 Clinical Systems Map 149 Vendor Selection Formed Steering and Advisory Committees Inventoried Clinical Application Systems Constructed Architectural Diagrams Developed Strategy for Vendor Assessment Developed Vendor Requirements Developed Vendor Evaluation Tools Developed Use Case Scenarios Held Vendor Demos with Scenarios Performed Deep-Dives with chosen vendors
76 Vendor Evaluation For Coding, Charge Capture, Compliance Through individual deep dives Evaluated all scenarios using our developed test case scenarios Asked ourselves the tough question. What systems can be eliminated? Goal Documentation, electronically Not to lose any benefit we currently have today! 151 Evaluated all vendors on All Charge processes, current and future state Outpatient and Inpatient Professional and Hospital Charges Consults, Office Visits, ED visits Surgical Multiple Locations and sites Multiple clinicians/centers Coding, charging Capable of charging for professional and technical Edits, rejections, and scrubbers
77 Evaluated all vendors on All functionality (current and future state) Rounding list Schedule (arrivals, no shows, cancellations) Audit trail on changed E/M levels PQRI Shortcut structures Eligibility Checks Compliance Frequency Limitations Global Windows Capability 153 Example of Test Case Scenario
78 Example of Test Case Scenario 155 Example of Test Case Scenario
79 Deep Dive of Vendor Products 157 Deep Dive of Vendor Products
80 Deep Dive of Vendor Products 159 Deep Dive of Vendor Products
81 Deep Dive of Vendor Products 161 Deep Dive of Vendor Products
82 Deep Dive of Vendor Products 163 Deep Dive of Vendor Products

83 Deep Dive of Vendor Products 165 Deep Dive of Vendor Products
84 Objectives Identify components of charge capture technology that directly impacts the day-to-day needs of professional compliance programs Discuss the limitations of EMR technology on the charge capture process as the central focus point in a compliance program Understand the key players in a roll-out of charge capture and identify their institution s own readiness for undertaking such an initiative 167 In Conclusion Compliance and it s challenges Compliance, Coding, and Charge Capture Charge Capture then and now Charge Capture Technology Implementation of a Technological Solution A case study Charge Capture, Compliance, and the EMR
85 Thank you Contact information: Cynthia Trapp CHFP, CMPE, CPC, CPC-I, CCS-P, CHC, PCA Director, Professional Coding Lahey Clinic, Inc. 41 Mall Road Burlington, MA Sherry Weisse, CPC, PCA Professional Coding Systems Project Manager Lahey Clinic, Inc. 41 Mall Road Burlington, MA
The Business of Medicine
 The Business of Medicine Coding as a profession Objectives How the coder fits in Hospital vs. physician services Hierarchy of providers Reimbursement aspects Payers Medical necessity ABN 1 Regulations
The Business of Medicine Coding as a profession Objectives How the coder fits in Hospital vs. physician services Hierarchy of providers Reimbursement aspects Payers Medical necessity ABN 1 Regulations
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
2014 CODING & DOCUMENTATION UPDATE. Healthcare Services Group November 2013
 2014 CODING & DOCUMENTATION UPDATE Healthcare Services Group November 2013 Overview of Topics ICD-10 Implementation 2013 OIG Work Plan Physician, ASC and Hospital 2014 CPT Code Changes 2 ICD-10-CM & ICD-10-PCS
2014 CODING & DOCUMENTATION UPDATE Healthcare Services Group November 2013 Overview of Topics ICD-10 Implementation 2013 OIG Work Plan Physician, ASC and Hospital 2014 CPT Code Changes 2 ICD-10-CM & ICD-10-PCS
9/25/2012 AGENDA. Set the Stage Monitoring versus Audit Identifying Risk Strategies related to an audit plan Corrective Action Plans Examples
 The Art and Science of Designing a Physician Practice Audit : Unique Techniques Lori Laubach, Partner MOSS ADAMS LLP 1 AGENDA Set the Stage Monitoring versus Audit Identifying Risk Strategies related to
The Art and Science of Designing a Physician Practice Audit : Unique Techniques Lori Laubach, Partner MOSS ADAMS LLP 1 AGENDA Set the Stage Monitoring versus Audit Identifying Risk Strategies related to
Compliance Workplan for Physician Practices
 Compliance Workplan for Physician Practices Ronda Tews, CPC, CHC, CCP-P St. John s Health System Springfield, MO www.hcca-info.org 888-580-8373 Put together a practical plan for your physician s practice
Compliance Workplan for Physician Practices Ronda Tews, CPC, CHC, CCP-P St. John s Health System Springfield, MO www.hcca-info.org 888-580-8373 Put together a practical plan for your physician s practice
Froedtert Health Billing Compliance Policy. description. Policy Number. Supersedes. Purpose. Definitions
 Froedtert Health Billing Compliance Policy description Hospital and Professional Billing Compliance Policy, Provider Billing, Provider Coding, Billable Providers, Billing Compliance, Compliance, Revenue
Froedtert Health Billing Compliance Policy description Hospital and Professional Billing Compliance Policy, Provider Billing, Provider Coding, Billable Providers, Billing Compliance, Compliance, Revenue
Responding to Today s Health Care Regulatory Environment
 Responding to Today s Health Care Regulatory Environment St. Joseph s Health Michael R. Holper SVP, Compliance and Audit Services October 26, 2016 2014 Trinity Health. All Rights Reserved. 1 We operate
Responding to Today s Health Care Regulatory Environment St. Joseph s Health Michael R. Holper SVP, Compliance and Audit Services October 26, 2016 2014 Trinity Health. All Rights Reserved. 1 We operate
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL
 Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Achieving Operational Excellence with an EHR a CIO s Perspective
 Achieving Operational Excellence with an EHR a CIO s Perspective Phyllis Schuck, SPHR CIO of Pinehurst Surgical HIT Session 6.02 Thursday, March 29, 2007 Pinehurst Surgical Organization Overview Founded
Achieving Operational Excellence with an EHR a CIO s Perspective Phyllis Schuck, SPHR CIO of Pinehurst Surgical HIT Session 6.02 Thursday, March 29, 2007 Pinehurst Surgical Organization Overview Founded
A McKesson Perspective: ICD-10-CM/PCS
 A McKesson Perspective: ICD-10-CM/PCS Its Far-Reaching Effect on the Healthcare Industry Executive Overview While many healthcare organizations are focused on qualifying for American Recovery & Reinvestment
A McKesson Perspective: ICD-10-CM/PCS Its Far-Reaching Effect on the Healthcare Industry Executive Overview While many healthcare organizations are focused on qualifying for American Recovery & Reinvestment
CURRENT OIG ENFORCEMENT INITIATIVES: A ROAD MAP FOR HIGH RISK COMPLIANCE AREAS
 10 th Annual HCCA Compliance Institute Session Las Vegas, NV April 25, 2006 CURRENT OIG ENFORCEMENT INITIATIVES: A ROAD MAP FOR HIGH RISK COMPLIANCE AREAS MARK HARDIMAN HOOPER, LUNDY & BOOKMAN, INC. 1875
10 th Annual HCCA Compliance Institute Session Las Vegas, NV April 25, 2006 CURRENT OIG ENFORCEMENT INITIATIVES: A ROAD MAP FOR HIGH RISK COMPLIANCE AREAS MARK HARDIMAN HOOPER, LUNDY & BOOKMAN, INC. 1875
Cloning and Other Compliance Risks in Electronic Medical Records
 Cloning and Other Compliance Risks in Electronic Medical Records Lori Laubach, Partner, Moss Adams LLP Catherine Wakefield, Vice President, Corporate Compliance and Internal Audit, MultiCare 1 AGENDA Basic
Cloning and Other Compliance Risks in Electronic Medical Records Lori Laubach, Partner, Moss Adams LLP Catherine Wakefield, Vice President, Corporate Compliance and Internal Audit, MultiCare 1 AGENDA Basic
Emerging Outpatient CDI Drivers and Technologies
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
Stark, False Claims and Anti- Kickback Laws: Easy Ways to Stay Compliant with the Big Three in Healthcare
 Stark, False Claims and Anti- Kickback Laws: Easy Ways to Stay Compliant with the Big Three in Healthcare In health care, we are blessed with an abundance of rules, policies, standards and laws. In Health
Stark, False Claims and Anti- Kickback Laws: Easy Ways to Stay Compliant with the Big Three in Healthcare In health care, we are blessed with an abundance of rules, policies, standards and laws. In Health
ICD-10: It s Really Coming. Are You Ready? John Behn May 14, 2013 Small Rural Hospital Improvement Grant Program (SHIP)
") ICD-10: It s Really Coming. Are You Ready? John Behn May 14, 2013 Small Rural Hospital Improvement Grant Program (SHIP) Background ICD = International Statistical Classifications of Diseases and Related
ICD-10: It s Really Coming. Are You Ready? John Behn May 14, 2013 Small Rural Hospital Improvement Grant Program (SHIP) Background ICD = International Statistical Classifications of Diseases and Related
Sharpen coding skills and reimbursement strategies during ICD-10 delay The Centers for Medicare & Medicaid Services (CMS) once again has extended the
 once again has extended the") Ambulatory Surgery Centers Sharpen coding skills and reimbursement strategies during ICD-10 delay The Centers for Medicare & Medicaid Services (CMS) once again has extended the deadline to begin using
Ambulatory Surgery Centers Sharpen coding skills and reimbursement strategies during ICD-10 delay The Centers for Medicare & Medicaid Services (CMS) once again has extended the deadline to begin using
Coding, Corroboration, and Compliance How to assure the 3 C s are met
 Coding, Corroboration, and Compliance How to assure the 3 C s are met Sue Roehl, RHIT, CCS sroehl@eidebailly.com 701-476-8770 OIG 1996 - $23.2 Billion errors Figure 1 Insufficient/No documentation 46.76%
Coding, Corroboration, and Compliance How to assure the 3 C s are met Sue Roehl, RHIT, CCS sroehl@eidebailly.com 701-476-8770 OIG 1996 - $23.2 Billion errors Figure 1 Insufficient/No documentation 46.76%
Success with ICD-10: Streamlining Clinical Workflow. November 8, 2013
 Success with ICD-10: Streamlining Clinical Workflow November 8, 2013 Culbert Healthcare Solutions Angela Hickman CPC, CEDC, AHIMA-approved ICD-10- CM/PCS Trainer, AHIMA Ambassador Senior Consultant Angela
Success with ICD-10: Streamlining Clinical Workflow November 8, 2013 Culbert Healthcare Solutions Angela Hickman CPC, CEDC, AHIMA-approved ICD-10- CM/PCS Trainer, AHIMA Ambassador Senior Consultant Angela
Certified Ophthalmic Executive (COE) Review Day
 Review Day") Certified Ophthalmic Executive (COE) Review Day Compliance Plan & Chart Audits Financial Disclosure The instructor acknowledges a financial interest in the subject matter of this presentation. Presented
Certified Ophthalmic Executive (COE) Review Day Compliance Plan & Chart Audits Financial Disclosure The instructor acknowledges a financial interest in the subject matter of this presentation. Presented
CDx ANNUAL PHYSICIAN CLIENT NOTICE
 CDx ANNUAL PHYSICIAN CLIENT NOTICE - 2018 CDX Diagnostics is providing this annual notice in accordance with the recommendations made by the Office of Inspector General (OIG) as part of our CDx Compliance
CDx ANNUAL PHYSICIAN CLIENT NOTICE - 2018 CDX Diagnostics is providing this annual notice in accordance with the recommendations made by the Office of Inspector General (OIG) as part of our CDx Compliance
ICD-10 Frequently Asked Questions - SurgiSource
 ICD-10 Frequently Asked Questions - SurgiSource What Version of SurgiSource is ICD-10 Compliant? Version 6.0 Where can I find ICD-10 Training Materials for SurgiSource? 1. Visit our Client Portal (portal.sourcemed.net)
ICD-10 Frequently Asked Questions - SurgiSource What Version of SurgiSource is ICD-10 Compliant? Version 6.0 Where can I find ICD-10 Training Materials for SurgiSource? 1. Visit our Client Portal (portal.sourcemed.net)
3M Health Information Systems. A case study in coding compliance: Achieving accuracy and consistency
 3M Health Information Systems A case study in coding compliance: Achieving accuracy and consistency A case study in coding compliance: Achieving accuracy and consistency The challenge Coding compliance
3M Health Information Systems A case study in coding compliance: Achieving accuracy and consistency A case study in coding compliance: Achieving accuracy and consistency The challenge Coding compliance
Meaningful Use Modified Stage 2 Roadmap Eligible Hospitals
 Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Meaningful Use requirements,
Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Meaningful Use requirements,
Alabama Primary Health Care Association October 4, Separating Clinical Documentation, Professional Coding, and Billing: A Workflow Analysis
 Alabama Primary Health Care Association October 4, 2017 Separating Clinical Documentation, Professional Coding, and Billing: A Workflow Analysis Presented by: Gary Lucas, M.Sc., CPC, CPC-I, AHIMA ICD-10
Alabama Primary Health Care Association October 4, 2017 Separating Clinical Documentation, Professional Coding, and Billing: A Workflow Analysis Presented by: Gary Lucas, M.Sc., CPC, CPC-I, AHIMA ICD-10
YOUR HEALTH INFORMATION EXCHANGE
 YOUR HEALTH INFORMATION EXCHANGE Introduction to Health Information Exchange Healthcare organizations are experiencing substantial pressures from initiatives and reforms such as new payment models, care
YOUR HEALTH INFORMATION EXCHANGE Introduction to Health Information Exchange Healthcare organizations are experiencing substantial pressures from initiatives and reforms such as new payment models, care
A Day in the Life of a Compliance Officer
 A Day in the Life of a Compliance Officer (for small physician practices) Mina Sellami, MBA, PMP, JD MedProv, LLC Julia Konovalov Medical Business Partners September 29, 2016 Agenda Government Regulations
A Day in the Life of a Compliance Officer (for small physician practices) Mina Sellami, MBA, PMP, JD MedProv, LLC Julia Konovalov Medical Business Partners September 29, 2016 Agenda Government Regulations
Outpatient Hospital Facilities
 Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
PEACE, LOVE & ICD10. Kimberly Barca, RHIA HIM Regulatory & Project Manager Princeton Healthcare System 6/10/2014
 PEACE, LOVE & ICD10 Kimberly Barca, RHIA HIM Regulatory & Project Manager Princeton Healthcare System 6/10/2014 AGENDA Brief History of ICD-10 Why ICD-10? Implementation News What Does ICD-10 Mean To My
PEACE, LOVE & ICD10 Kimberly Barca, RHIA HIM Regulatory & Project Manager Princeton Healthcare System 6/10/2014 AGENDA Brief History of ICD-10 Why ICD-10? Implementation News What Does ICD-10 Mean To My
Regulatory Compliance Risks. September 2009
 Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Getting Started with OIG Compliance
 Getting Started with OIG Compliance Kathy Mills Chang, MCS-P CCPC Do You Feel Like This? Or This? Does Your Business Deserve the Same Focus Your Patients Do? How This Training Will Protect You! Stay within
Getting Started with OIG Compliance Kathy Mills Chang, MCS-P CCPC Do You Feel Like This? Or This? Does Your Business Deserve the Same Focus Your Patients Do? How This Training Will Protect You! Stay within
Chapter 02 Hospital Based Care
 Chapter 02 Hospital Based Care MULTICHOICE 1. The physician sends the patient to the hospital for a radiological examination. The patient returns to the physician's office for follow-up of test results.
Chapter 02 Hospital Based Care MULTICHOICE 1. The physician sends the patient to the hospital for a radiological examination. The patient returns to the physician's office for follow-up of test results.
Describe the process for implementing an OP CDI program
 1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
Auditing and Monitoring in Clinics and Physician Practices
 Auditing and Monitoring in Clinics and Physician Practices Dawnese Kindelt, CPC System Compliance Director Clinics Catholic Healthcare West Health Care Compliance Association 6500 Barrie Road, Suite 250,
Auditing and Monitoring in Clinics and Physician Practices Dawnese Kindelt, CPC System Compliance Director Clinics Catholic Healthcare West Health Care Compliance Association 6500 Barrie Road, Suite 250,
Compliance Program Updated August 2017
 Compliance Program Updated August 2017 Table of Contents Section I. Purpose of the Compliance Program... 3 Section II. Elements of an Effective Compliance Program... 4 A. Written Policies and Procedures...
Compliance Program Updated August 2017 Table of Contents Section I. Purpose of the Compliance Program... 3 Section II. Elements of an Effective Compliance Program... 4 A. Written Policies and Procedures...
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability
 Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
The Transition to Version 5010 and ICD-10
 The Transition to Version 5010 and ICD-10 An Overview Denise M. Buenning, MsM Director, Administrative Simplification Group Office of E-Health Standards and Services Centers for Medicare & Medicaid Services
The Transition to Version 5010 and ICD-10 An Overview Denise M. Buenning, MsM Director, Administrative Simplification Group Office of E-Health Standards and Services Centers for Medicare & Medicaid Services
ICD-10 Frequently Asked Questions - AdvantX
 ICD-10 Frequently Asked Questions - AdvantX What Version of AdvantX is ICD-10 Compliant? Version 5.0.01 Where can I find ICD-10 Training Materials for AdvantX? 1. Visit our Client Portal (portal.sourcemed.net)
ICD-10 Frequently Asked Questions - AdvantX What Version of AdvantX is ICD-10 Compliant? Version 5.0.01 Where can I find ICD-10 Training Materials for AdvantX? 1. Visit our Client Portal (portal.sourcemed.net)
8/28/2014. Compliance and Practical Challenges When Using Scribes: Just What the Doctor Ordered? Objectives of the Presentation
 Compliance and Practical Challenges When Using Scribes: Just What the Doctor Ordered? Jerry Williamson MD. MJ. CHC. LHRM Objectives of the Presentation Definition of a Scribe Duties of a Scribe Regulatory
Compliance and Practical Challenges When Using Scribes: Just What the Doctor Ordered? Jerry Williamson MD. MJ. CHC. LHRM Objectives of the Presentation Definition of a Scribe Duties of a Scribe Regulatory
Electronic Medical Record (EMR) How to Audit the Risks. Schawn Pedersen, CPC, CPC-E/M Manager Moss Adams LLP
 How to Audit the Risks. Schawn Pedersen, CPC, CPC-E/M Manager Moss Adams LLP") Electronic Medical Record (EMR) How to Audit the Risks Schawn Pedersen, CPC, CPC-E/M Manager Moss Adams LLP Health Care Compliance Association 6500 Barrie Road, Suite 250, Minneapolis, MN 55435 888-580-8373
Electronic Medical Record (EMR) How to Audit the Risks Schawn Pedersen, CPC, CPC-E/M Manager Moss Adams LLP Health Care Compliance Association 6500 Barrie Road, Suite 250, Minneapolis, MN 55435 888-580-8373
5/30/2012. ICD 10 Implementation HCCA. Agenda. Understanding ICD 10. June 8, ICD 10 Overview Planning Communication Education Physician Training
 ICD 10 Implementation HCCA June 8, 2012 1 Agenda ICD 10 Overview Planning Communication Education Physician Training 2 Understanding ICD 10 The key to accepting any change is understanding Why is this
ICD 10 Implementation HCCA June 8, 2012 1 Agenda ICD 10 Overview Planning Communication Education Physician Training 2 Understanding ICD 10 The key to accepting any change is understanding Why is this
Examining Compliance from an Internal Audit Perspective
 Examining Compliance from an Internal Audit Perspective Beth A. Schindler, CPA, CIA, CISA, CHC April 19, 2016 0 Houston Methodist Who We Are About Houston Methodist A leading Academic Medical Center 7
Examining Compliance from an Internal Audit Perspective Beth A. Schindler, CPA, CIA, CISA, CHC April 19, 2016 0 Houston Methodist Who We Are About Houston Methodist A leading Academic Medical Center 7
AVOIDING HEALTHCARE FRAUD AND ABUSE; Responsibility, Protection, Prevention
 AVOIDING HEALTHCARE FRAUD AND ABUSE; Responsibility, Protection, Prevention Presented by: www.thehealthlawfirm.com Copyright 2017. George F. Indest III. All rights reserved. George F. Indest III, J.D.,
AVOIDING HEALTHCARE FRAUD AND ABUSE; Responsibility, Protection, Prevention Presented by: www.thehealthlawfirm.com Copyright 2017. George F. Indest III. All rights reserved. George F. Indest III, J.D.,
Procedural andpr Diagnostic Coding. Copyright 2012 Delmar, Cengage Learning. All rights reserved.
 Procedural andpr Diagnostic Coding What is Coding? Converting descriptions of disease, injury, procedures, and services into numeric or alphanumeric descriptors Accurate coding maximizes reimbursement
Procedural andpr Diagnostic Coding What is Coding? Converting descriptions of disease, injury, procedures, and services into numeric or alphanumeric descriptors Accurate coding maximizes reimbursement
MDCH Office of Health Services Inspector General
 MDCH Office of Health Services Inspector General Recovery Audit Contract (RAC) Provider Outreach & Education Spring 2014 Background Recovery Audit Contractor Medicare Modernization Act of 2003 created
MDCH Office of Health Services Inspector General Recovery Audit Contract (RAC) Provider Outreach & Education Spring 2014 Background Recovery Audit Contractor Medicare Modernization Act of 2003 created
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011
 PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
Payment Policy: Visits On Same Day As Surgery Reference Number: CC.PP.040 Product Types: ALL Effective Date: 03/01/2018
 Payment Policy: Visits On Same Day As Surgery Reference Number: CC.PP.040 Product Types: ALL Effective Date: 03/01/2018 Revision Log See Important Reminder at the end of this policy for important regulatory
Payment Policy: Visits On Same Day As Surgery Reference Number: CC.PP.040 Product Types: ALL Effective Date: 03/01/2018 Revision Log See Important Reminder at the end of this policy for important regulatory
General Documentation Compliance. Review for Provider Reappointment
 U N C U H N E C A L H T E H A L C T A H R E C A S R Y E S T E M General Documentation Compliance Review for Provider Reappointment May 2018 Objectives 1 2 Review the principles of compliant billing and
U N C U H N E C A L H T E H A L C T A H R E C A S R Y E S T E M General Documentation Compliance Review for Provider Reappointment May 2018 Objectives 1 2 Review the principles of compliant billing and
LIFE SCIENCES CONTENT
 Model Coding Curriculum Checklist Approved Coding Certificate Programs must be based on content appropriate to prepare students to perform the role and functions associated with clinical coders in healthcare
Model Coding Curriculum Checklist Approved Coding Certificate Programs must be based on content appropriate to prepare students to perform the role and functions associated with clinical coders in healthcare
Doris V. Branker, CPC, CPC-I, CEMC
 Doris V. Branker, CPC, CPC-I, CEMC 1 Identify the common sources for missed reimbursement in the specialty practice Identify the common sources for reduced reimbursement in the specialty practice Identify
Doris V. Branker, CPC, CPC-I, CEMC 1 Identify the common sources for missed reimbursement in the specialty practice Identify the common sources for reduced reimbursement in the specialty practice Identify
Implementation Issues of the Physician Practice. for ICD-10-CM
 Implementation Issues of the Physician Practice for ICD-10-CM What are ICD-10-CM and the Version 5010? The Centers for Medicare & Medicaid Services (CMS) is driving the industry to upgrade core HIPAA transactions
Implementation Issues of the Physician Practice for ICD-10-CM What are ICD-10-CM and the Version 5010? The Centers for Medicare & Medicaid Services (CMS) is driving the industry to upgrade core HIPAA transactions
CAC: Understanding the Technology and Lessons Learned from Early Adopters and The Next Big Thing : Core Measures and Quality Reporting
 CAC: Understanding the Technology and Lessons Learned from Early Adopters and The Next Big Thing : Core Measures and Quality Reporting Matt Turner, Regional Manager, Dolbey mturner@dolbey.com What is Computer-Assisted
CAC: Understanding the Technology and Lessons Learned from Early Adopters and The Next Big Thing : Core Measures and Quality Reporting Matt Turner, Regional Manager, Dolbey mturner@dolbey.com What is Computer-Assisted
Advanced Evaluation and. AAPC Regional Conference Chicago 10/27/12
 Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
San Francisco Department of Public Health
 San Francisco Department of Public Health Barbara A. Garcia, MPA Director of Health City and County of San Francisco Edwin M. Lee, Mayor San Francisco Department of Public Health Policy & Procedure Detail*
San Francisco Department of Public Health Barbara A. Garcia, MPA Director of Health City and County of San Francisco Edwin M. Lee, Mayor San Francisco Department of Public Health Policy & Procedure Detail*
2. What is the main similarity between quality assurance and quality improvement?
 Chapter 6 Review Questions 1. Quality improvement focuses on: a. Individual clinicians or system users b. Routine measurement of performance c. Information technology issues d. Constant training 2. What
Chapter 6 Review Questions 1. Quality improvement focuses on: a. Individual clinicians or system users b. Routine measurement of performance c. Information technology issues d. Constant training 2. What
Grow Your Own Coders: Training Options for the Modern HIM World
 Grow Your Own Coders: Training Options for the Modern HIM World Healthcon 2016 April Date 13, 2016 Presentation by Pamela Haney, MS, RHIA, CCS, CIC, COC Director of Presentation Training and byeducation
Grow Your Own Coders: Training Options for the Modern HIM World Healthcon 2016 April Date 13, 2016 Presentation by Pamela Haney, MS, RHIA, CCS, CIC, COC Director of Presentation Training and byeducation
Two birds with one stone Financially Clearing a Patient & and Improving Patient satisfaction at the same time
 Two birds with one stone Financially Clearing a Patient & and Improving Patient satisfaction at the same time Manoj Chhabra DCS Global Systems, Inc. Presentation Agenda Objectives Problem Defined Patient
Two birds with one stone Financially Clearing a Patient & and Improving Patient satisfaction at the same time Manoj Chhabra DCS Global Systems, Inc. Presentation Agenda Objectives Problem Defined Patient
Care360 EHR Frequently Asked Questions
 Care360 EHR Frequently Asked Questions Table of Contents Care360 EHR... 4 What is Care360 EHR?... 4 What are the current capabilities of Care 360 EHR?... 4 Is Care 360 EHR an EMR?... 5 Can I have Care360
Care360 EHR Frequently Asked Questions Table of Contents Care360 EHR... 4 What is Care360 EHR?... 4 What are the current capabilities of Care 360 EHR?... 4 Is Care 360 EHR an EMR?... 5 Can I have Care360
Bad Data s Effect on Population Health Performance
 Session #180: Bad Data s Effect on Population Health Performance Wednesday April 15, 2015 1-2pm Bill Gillis Chief Information Officer DISCLAIMER: The views and opinions expressed in this presentation are
Session #180: Bad Data s Effect on Population Health Performance Wednesday April 15, 2015 1-2pm Bill Gillis Chief Information Officer DISCLAIMER: The views and opinions expressed in this presentation are
MLN Matters Number: MM6740 Revised Related Change Request (CR) #: Related CR Transmittal #: R1875CP Implementation Date: January 4, 2010
 #: Related CR Transmittal #: R1875CP Implementation Date: January 4, 2010") News Flash Flu Season is upon us! CMS encourages providers to begin taking advantage of each office visit to encourage your patients with Medicare to get a seasonal flu shot; it s their best defense against
News Flash Flu Season is upon us! CMS encourages providers to begin taking advantage of each office visit to encourage your patients with Medicare to get a seasonal flu shot; it s their best defense against
The Intersection of Health Care Fraud and Patient Safety
 The Intersection of Health Care Fraud and Patient Safety Anthony Baize, Inspector General January 16, 2018 Wisconsin Department of Health Services Office of the Inspector General Overview The Wisconsin
The Intersection of Health Care Fraud and Patient Safety Anthony Baize, Inspector General January 16, 2018 Wisconsin Department of Health Services Office of the Inspector General Overview The Wisconsin
HealthStream Regulatory Script. Corporate Compliance: A Proactive Stance. Version: [February 2007]
![HealthStream Regulatory Script. Corporate Compliance: A Proactive Stance. Version: [February 2007]](/thumbs/80/80691517.jpg "HealthStream Regulatory Script. Corporate Compliance: A Proactive Stance. Version: [February 2007]") HealthStream Regulatory Script Corporate Compliance: A Proactive Stance Version: [February 2007] Lesson 1: Introduction Lesson 2: Importance of Compliance & Compliance Programs Lesson 3: Laws and Regulations
HealthStream Regulatory Script Corporate Compliance: A Proactive Stance Version: [February 2007] Lesson 1: Introduction Lesson 2: Importance of Compliance & Compliance Programs Lesson 3: Laws and Regulations
Roll Out of the HIT Meaningful Use Standards and Certification Criteria
 Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
How can oncology practices deliver better care? It starts with staying connected.
 How can oncology practices deliver better care? It starts with staying connected. A system rooted in oncology Compared to other EHRs that I ve used, iknowmed is the best EHR for medical oncology. Physician
How can oncology practices deliver better care? It starts with staying connected. A system rooted in oncology Compared to other EHRs that I ve used, iknowmed is the best EHR for medical oncology. Physician
OPNS Suite of Products Opportunities Contact OPNS Informatics Department
 EMR/e-Rx Practice Fusion EMR/e-Rx Advanced MD Health Connect Health Connect OPNS Preferred Suite of Products OPNS Suite of Products Opportunities Contact OPNS Informatics Department OPNS Middle Range Suite
EMR/e-Rx Practice Fusion EMR/e-Rx Advanced MD Health Connect Health Connect OPNS Preferred Suite of Products OPNS Suite of Products Opportunities Contact OPNS Informatics Department OPNS Middle Range Suite
CDERC, CCS-P Vice President Strategic Development American Academy of Professional Coders
 ICD-10-CM Implementation Part 3 Deborah Grider, CPC, CPC-I, CPC-H, CPC-P, P COBGC, CEMC, CDERC, CCS-P Vice President Strategic Development American Academy of Professional Coders Goal This Webinar conference
ICD-10-CM Implementation Part 3 Deborah Grider, CPC, CPC-I, CPC-H, CPC-P, P COBGC, CEMC, CDERC, CCS-P Vice President Strategic Development American Academy of Professional Coders Goal This Webinar conference
A Lawyer s Take on Meaningful Use. By Steven J. Fox & Vadim Schick
 A Lawyer s Take on Meaningful Use By Steven J. Fox & Vadim Schick Overview American Reinvestment & Recovery Act (ARRA) February 2009 HITECH Act provides incentives for EHR adoption EHR Incentive NPRM issued
A Lawyer s Take on Meaningful Use By Steven J. Fox & Vadim Schick Overview American Reinvestment & Recovery Act (ARRA) February 2009 HITECH Act provides incentives for EHR adoption EHR Incentive NPRM issued
A Revenue Cycle Process Approach
 A Revenue Cycle Process Approach VALERIUS BAYES NEWBY Education BLOCHOWIAK Preface x Parti Chapter1 WORKING WITH MEDICAL INSURANCE AND BILLING Chapter 3 Introduction to the Revenue Cycle 2 1.1 Working
A Revenue Cycle Process Approach VALERIUS BAYES NEWBY Education BLOCHOWIAK Preface x Parti Chapter1 WORKING WITH MEDICAL INSURANCE AND BILLING Chapter 3 Introduction to the Revenue Cycle 2 1.1 Working
Medicare Recovery Audit Contractors. Chicago, IL August 1, 2008
 Medicare Recovery Audit Contractors Chicago, IL August 1, 2008 1 Recovery Audit Contractors Demo Summary National Rollout AHA Strategy AHA RACTrac Overview 2 Recovery Audit Contractors Medicare Modernization
Medicare Recovery Audit Contractors Chicago, IL August 1, 2008 1 Recovery Audit Contractors Demo Summary National Rollout AHA Strategy AHA RACTrac Overview 2 Recovery Audit Contractors Medicare Modernization
ICD-10 Transition Provider Roadshow. October 2012
 ICD-10 Transition Provider Roadshow October 2012 About ICD-10 ICD-10 CM for diagnosis coding For use in all US healthcare settings Uses 3 to 7 digits instead of the 3 to 5 digits ICD-10-PCS for inpatient
ICD-10 Transition Provider Roadshow October 2012 About ICD-10 ICD-10 CM for diagnosis coding For use in all US healthcare settings Uses 3 to 7 digits instead of the 3 to 5 digits ICD-10-PCS for inpatient
A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012
 A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012 Introduction The Computer-Based Record Institute (CPRI) established the
A Framework for Evaluating Electronic Health Records Overview - Applying to the Davies Ambulatory Awards Program Revised May 2012 Introduction The Computer-Based Record Institute (CPRI) established the
Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC Disclaimer
 Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
How to Overhaul your Internal Structure to be Prepared for the New Home Health CoPs. Program Objectives
 How to Overhaul your Internal Structure to be Prepared for the New Home Health CoPs 2015 NAHC Annual Meeting 106 October 28, 4:30 5:30 p.m. Nashville, Tennessee Kathleen Spooner, RN, CMC Kathleen A. Hessler,
How to Overhaul your Internal Structure to be Prepared for the New Home Health CoPs 2015 NAHC Annual Meeting 106 October 28, 4:30 5:30 p.m. Nashville, Tennessee Kathleen Spooner, RN, CMC Kathleen A. Hessler,
11/3/2014. September 20, Initiatives of ICD 10 the American Update Medical. Medicine is in Your Hands!! ICD-10 Timeline - 1
 Initiatives of ICD 10 the American Update Medical Association W. Jeff -- Terry, The MD Future of Medicine is in Your Hands!! September 20, 2014 ICD-10 Timeline - 1 * ICD is the acronym for International
Initiatives of ICD 10 the American Update Medical Association W. Jeff -- Terry, The MD Future of Medicine is in Your Hands!! September 20, 2014 ICD-10 Timeline - 1 * ICD is the acronym for International
9/11/15. Reimbursement for Non- Physician Providers Real Life Practice Objectives
 Reimbursement for Non- Physician Providers Real Life Practice 2015 John F. Bishop, PA, CPC, CPMA, CGSC, CPRC AAPA National Chair Reimbursement and ICD-10 Work Groups Principle, John Bishop and Associates,
Reimbursement for Non- Physician Providers Real Life Practice 2015 John F. Bishop, PA, CPC, CPMA, CGSC, CPRC AAPA National Chair Reimbursement and ICD-10 Work Groups Principle, John Bishop and Associates,
2013 OIG Work Plan. Scott McBride Baker & Hostetler LLP 1000 Louisiana, Suite 2000 Houston, Texas
 2013 OIG Work Plan Scott McBride Baker & Hostetler LLP 1000 Louisiana, Suite 2000 Houston, Texas 77002 713.646.1390 smcbride@bakerlaw.com Webinar Essentials * Session is currently being recorded, and will
2013 OIG Work Plan Scott McBride Baker & Hostetler LLP 1000 Louisiana, Suite 2000 Houston, Texas 77002 713.646.1390 smcbride@bakerlaw.com Webinar Essentials * Session is currently being recorded, and will
Excellence in Patient Care & High Performance Revenue Optimization
 HALO TM Health Information Management Services Leading Provider of End-to-End HIM Services Excellence in Patient Care & High Performance Revenue Optimization End-to-End Health Information Management Services
HALO TM Health Information Management Services Leading Provider of End-to-End HIM Services Excellence in Patient Care & High Performance Revenue Optimization End-to-End Health Information Management Services
ICD-10 Frequently Asked Questions
 ICD-10 Frequently Asked Questions September 2015 pulseinc.com + 1.800.444.0882 We care for your practice, as if it were our own. Acknowledgments Document Number: 01 Date: September 7, 2015 Pulse Systems
ICD-10 Frequently Asked Questions September 2015 pulseinc.com + 1.800.444.0882 We care for your practice, as if it were our own. Acknowledgments Document Number: 01 Date: September 7, 2015 Pulse Systems
The presenter has owns Kelly Willenberg, LLC in relation to this educational activity.
 Kelly M Willenberg, MBA, BSN, CCRP, CHC, CHRC 1 The presenter has owns Kelly Willenberg, LLC in relation to this educational activity. 2 1 Medical Necessity when you submit claims Coding for qualifying
Kelly M Willenberg, MBA, BSN, CCRP, CHC, CHRC 1 The presenter has owns Kelly Willenberg, LLC in relation to this educational activity. 2 1 Medical Necessity when you submit claims Coding for qualifying
UW MEDICINE ICD-10 Program UW MEDICINE ICD-10
 UW MEDICINE ICD-10 Program UW MEDICINE ICD-10 There and back again INTEGRATION OF MANDATES ACO Quality Based Reimbursement Meaningful Use, P4P, etc. ICD-10 HIPAA, 5010 2 STRATEGIC OPPORTUNITIES Significant
UW MEDICINE ICD-10 Program UW MEDICINE ICD-10 There and back again INTEGRATION OF MANDATES ACO Quality Based Reimbursement Meaningful Use, P4P, etc. ICD-10 HIPAA, 5010 2 STRATEGIC OPPORTUNITIES Significant
Providing and Billing Medicare for Chronic Care Management Services
 Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Providing and Billing Medicare for Chronic Care Management Services (and Other Fee-For-Service Population Health Management Services) No portion of this white paper may be used or duplicated by any person
Diane Meyer, CHC (650) Agenda
 Agenda") The Road Ahead and How to Navigate It Kevin D. Lyles, Esq. kdlyles@jonesday.com (614) 281-3821 Diane Meyer, CHC DMeyer@stanfordmed.org (650) 724-2572 Frank E. Sheeder, Esq. fesheeder@jonesday.com (214)
The Road Ahead and How to Navigate It Kevin D. Lyles, Esq. kdlyles@jonesday.com (614) 281-3821 Diane Meyer, CHC DMeyer@stanfordmed.org (650) 724-2572 Frank E. Sheeder, Esq. fesheeder@jonesday.com (214)
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Toward the Electronic Patient Record:
 June 2007 Toward the Electronic Denise Henderson Director, Consulting Services MedSynergies, Inc. Toward the Electronic The TEPR (Toward the Electronic Patient Record) conference held by the Medical Records
June 2007 Toward the Electronic Denise Henderson Director, Consulting Services MedSynergies, Inc. Toward the Electronic The TEPR (Toward the Electronic Patient Record) conference held by the Medical Records
Compliance Considerations for Clinical Laboratories
 Compliance Considerations for Clinical Laboratories Elizabeth Sullivan, Esq. McDonald Hopkins, LLC 600 Superior Ave., E, Suite 2100 Cleveland, Ohio 44114 P: 216.348.5401 / F: 216.348.5474 esullivan@mcdonaldhopkins.com
Compliance Considerations for Clinical Laboratories Elizabeth Sullivan, Esq. McDonald Hopkins, LLC 600 Superior Ave., E, Suite 2100 Cleveland, Ohio 44114 P: 216.348.5401 / F: 216.348.5474 esullivan@mcdonaldhopkins.com
Electronic Health Records - Advantages and Pitfalls of Documentation
 Electronic Health Records - Advantages and Pitfalls of Documentation Kansas City, KS HCCA Regional Conference September 25, 2015 1:00 P.M. 2:00 P.M. Presented by: Cynthia A. Swanson, RN, CPC, CEMC, CHC,
Electronic Health Records - Advantages and Pitfalls of Documentation Kansas City, KS HCCA Regional Conference September 25, 2015 1:00 P.M. 2:00 P.M. Presented by: Cynthia A. Swanson, RN, CPC, CEMC, CHC,
Presented to you by The Cooperative of American Physicians, Inc.
 ICD-10 Action Guide for Medical Practices PAGE 1 Presented to you by The Cooperative of American Physicians, Inc. Table of Contents Introduction... 3 What Is Changing and Why?... 4 What Are the Main Provisions
ICD-10 Action Guide for Medical Practices PAGE 1 Presented to you by The Cooperative of American Physicians, Inc. Table of Contents Introduction... 3 What Is Changing and Why?... 4 What Are the Main Provisions
OUTPATIENT DOCUMENTATION IMPROVEMENT
 OUTPATIENT DOCUMENTATION IMPROVEMENT Pam Brooks, MHA, COC, PCS, CPC Coding Manager Wentworth-Douglass Hospital Dover NH Disclaimer This presentation is for general education purposes only. The information
OUTPATIENT DOCUMENTATION IMPROVEMENT Pam Brooks, MHA, COC, PCS, CPC Coding Manager Wentworth-Douglass Hospital Dover NH Disclaimer This presentation is for general education purposes only. The information
Assessment. SMP Foundations Training Kit. Table of Contents
 SMP Foundations Training Kit Assessment Table of Contents Participant Assessment Questions and Answer Form Assessment Questions... 10 Pages Answer Form... 2 Pages Trainer s Resources Answer Key... 2 Pages
SMP Foundations Training Kit Assessment Table of Contents Participant Assessment Questions and Answer Form Assessment Questions... 10 Pages Answer Form... 2 Pages Trainer s Resources Answer Key... 2 Pages
PHILADELPHIA COLLEGE OF OSTEOPATHIC MEDICINE COMPLIANCE AND ETHICS PROGRAM MANUAL
 PHILADELPHIA COLLEGE OF OSTEOPATHIC MEDICINE COMPLIANCE AND ETHICS PROGRAM MANUAL I. COMPLIANCE AND ETHICS PROGRAM BACKGROUND Philadelphia College of Osteopathic Medicine (PCOM) is committed to upholding
PHILADELPHIA COLLEGE OF OSTEOPATHIC MEDICINE COMPLIANCE AND ETHICS PROGRAM MANUAL I. COMPLIANCE AND ETHICS PROGRAM BACKGROUND Philadelphia College of Osteopathic Medicine (PCOM) is committed to upholding
Auditing and Monitoring in Smallville, U.S.A.
 Auditing and Monitoring in Smallville, U.S.A. Able to Leap Short Buildings in a Single Bound... Or Maybe Two! Kirk Ruddell, CHC HCCA Compliance Institute April 23-26, 2006 Las Vegas, Nevada Background
Auditing and Monitoring in Smallville, U.S.A. Able to Leap Short Buildings in a Single Bound... Or Maybe Two! Kirk Ruddell, CHC HCCA Compliance Institute April 23-26, 2006 Las Vegas, Nevada Background
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play?
 Programs: What Role Should Compliance Play?") Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Clinical Documentation Improvement (CDI) Programs: What Role Should Compliance Play? June 17, 2016 Agenda Clinical Documentation Improvement (CDI) Perspective An Effective CDI Program Core Focus: Compliance
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model
 Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
A Million Little Pieces: Developing a Controlled Substance Diversion Program. Tanya Y. Barnhart, PharmD, BCPS
 A Million Little Pieces: Developing a Controlled Substance Diversion Program Tanya Y. Barnhart, PharmD, BCPS I have no conflicts of interest to disclose Objectives Explain the importance of building a
A Million Little Pieces: Developing a Controlled Substance Diversion Program Tanya Y. Barnhart, PharmD, BCPS I have no conflicts of interest to disclose Objectives Explain the importance of building a
EHR Enablement for Data Capture
 EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
Reimbursement Environment
 Reimbursement Environment 1 2017 Medicare Physician Fee Schedule Enhancing Integrative Medicine: CMS adopting additional care management codes in 2017 MPFS. Support patient centered and collaborative strategies.
Reimbursement Environment 1 2017 Medicare Physician Fee Schedule Enhancing Integrative Medicine: CMS adopting additional care management codes in 2017 MPFS. Support patient centered and collaborative strategies.
The Impact of Physician Quality Measures on the Coding Process
 The Impact of Physician Quality Measures on the Coding Process The Impact of Physician Quality Measures on the Coding Process by Mark Morsch, MS; Ronald Sheffer, Jr., MA; Susan Glass, RHIT, CCS-P; Carol
The Impact of Physician Quality Measures on the Coding Process The Impact of Physician Quality Measures on the Coding Process by Mark Morsch, MS; Ronald Sheffer, Jr., MA; Susan Glass, RHIT, CCS-P; Carol
Mental Health Care and OpenVista
 Medsphere Systems Corporation Mental and OpenVista Version 2.0 The OpenVista Platform: Integrated Support for Mental Designed by clinicians from all healthcare disciplines, OpenVista is guided by the principle
Medsphere Systems Corporation Mental and OpenVista Version 2.0 The OpenVista Platform: Integrated Support for Mental Designed by clinicians from all healthcare disciplines, OpenVista is guided by the principle
Mental Health Care and OpenVista
 Medsphere Systems Corporation Mental and OpenVista Version 2.0 The OpenVista Platform: Integrated Support for Mental Designed by clinicians from all healthcare disciplines, OpenVista is guided by the principle
Medsphere Systems Corporation Mental and OpenVista Version 2.0 The OpenVista Platform: Integrated Support for Mental Designed by clinicians from all healthcare disciplines, OpenVista is guided by the principle
601-Audit Plan for Medicare s Shared Visit Rule
 601-Audit Plan for Medicare s Shared Visit Rule Elin Baklid-Kunz, MBA, CPC, CCS Health Care Compliance Association 6500 Barrie Road, Suite 250, Minneapolis, MN 55435 888-580-8373 www.hcca-info.org Presentation
601-Audit Plan for Medicare s Shared Visit Rule Elin Baklid-Kunz, MBA, CPC, CCS Health Care Compliance Association 6500 Barrie Road, Suite 250, Minneapolis, MN 55435 888-580-8373 www.hcca-info.org Presentation
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual