Continuous Safety Improvement Through Incident Learning. Lulu Jordan B.S. R.T.(T) & Josh Carlson B.S.
|
|
|
- Kerry Wilkerson
- 5 years ago
- Views:
Transcription

1 Continuous Safety Improvement Through Incident Learning Lulu Jordan B.S. R.T.(T) & Josh Carlson B.S.
2 No Disclosure Statement AAMD Annual Meeting Disclosure: Lulu Jordan B.S. R.T.(T) & Josh Carlson B.S. With respect to the following presentation, there has been no relevant (direct or indirect) financial relationship between the party listed above (and/or spouse/partner) and any for profit company in the past 24 months which could be considered a conflict of interest.
3 Why study near misses? 1. Improve patient care 2. Improve operations 3. Provides an administrative metric 4. Recommended at the society-level
4 Patient Care Nitin et al, 5, JNCI 2012 Noncompliance with radiotherapy (RT) protocol guidelines has been linked to inferior clinical outcomes. We per formed a meta analysis of cooperative group trials to examine the association between RT quality assurance (QA) deviations and disease control and overall survival (OS).
5 Patient Care Seriously non compliant (12% of plans) Peters et al. JCO, 28(18), 2996, 2010
6 Patient Care Mardon et al. AHRQ, J Patient Saf, 6, , 2010 NUMBER OF REPORTS vs. NUMER of patient safety incidents R 2 = 0.33 p<0.001
7 Improved Operations CONSULT SIMULATION TREATMENT PLANNING Complex technology Complex process TREATMENT Ford et al. Int J Radiat Oncol Biol Phys, 74(3), ,





8 Improved Operations


9 Administrative Metrics Near Miss Reports Physicist 23% Dosimetri st 46% Therapist 24% Attending Physician 6% Other* 1%
10 Societal Recommendations AAMD Ethical Standards A CMD shall always promote the safety and welfare of his or her patients by performing medical dosimetry procedures safely and with reasonable skill... ASTRO report 2012 Safety is No Accident: A Framework for Quality Radiation Oncology and Care. Zeitman A, Palta J, Steinberg M. ASTRO; 2012 AAPM white paper 2012 Consensus recommendations for incident learning database structures in radiation oncology. Ford EC, Fong de Los Santos L, Pawlicki T, Sutlief S, Dunscombe P. Med Phys. 2012;39(12): ASRT safety white paper Radiation Therapy Safety: The Critical Role of the Radiation Therapist. Odle, T, Rosier, N. ASRT Education and Research Fnd




11 Societal examples Aviation Nuclear power Manufacturing Healthcare Climbing

12 Why track near misses and incidents?

13 Each department should have a department wide review committee which monitors quality problems, near misses and errors. Employees should be encouraged to report both errors and near misses. Near misses should be addressed with a similar vigor as that applied to errors, and reported through the Quality Assurance Committee. Zietman et al. 2012

14 Quality/Safety Improvement ACT PLAN STUDY DO W. Edwards Deming
15 Active incident learning improves the culture of safety
16 Why study near misses at the University of Washington? Why are we depending on the Radiation Therapists to be the gatekeepers? Do we really want to wait that late in the process to keep the patient safe? Why isn t staff getting feedback when near misses happen?
17 RT Process Map CONSULT SIMULATION Complex process Complex technology TREATMENT PLANNING TREATMENT Ford et al. Int J Radiat Oncol Biol Phys, 74(3), ,

18 Swiss Cheese model of accidents
19 University of Washington Near Miss program Establish leadership support Assess your Safety Culture What should be reported? How will you collect the Data? How will you review incidents? How will you give feedback? How are we doing after 2 years
20 University of Washington Near Miss program Establish leadership support Assess your Safety Culture What should be reported? How will you collect the Data? How will you review incidents? How will you give feedback? How are we doing after 2 year
21 University of Washington Near Miss program Hospital Leadership Physician Leadership CSI Seattle Multidisciplinary team Medical Director Physicist Technical Manager IT Manager Nursing Manager Resident
22 University of Washington Near Miss program Establish leadership support Assess your Safety Culture What should be reported? How will you collect the Data? How will you review incidents? How will you give feedback? How are we doing after 2 year
23 Tools for measuring your safety culture Agency for Healthcare Research and Quality patientsafety/patientsafetyculture/ Hospital Survey on Patient Safety Culture. Medical Office Survey on Patient Safety Culture AAPM Task Group on Prevention of Errors Safety Profile Assessment
24 Department Safety Survey Combined AHRQ and Johns Hopkins questions. Conducted: February 1 to March 1, 2012 Encouraged all staff to participate through s, meetings and 1/1 rounding. 78% response rate
25 CSI Meeting 2012 Total responses (N): 68 Did not respond: 0 Numeric value Answer Frequency Percentage 1 Administrative Assistant/Fiscal Specialist % 2 Administration/Management % 3 Attending/Staff Physician % 4 Dietician / Social worker % 5 Dosimetrist % 6 MA % 7 Physician Assistant/Nurse Practitioner % 8 PSS/PCC % 9 Physicist % 10 Radiation therapist % 11 Registered Nurse % 12 Resident Physician/Physician in Training % 13 Other: %














26 Self Assessed Patient Safety Grade Overall Patient Safety Grade A=EXCELLENT B=VERY GOOD C=ACCEPTABLE D=POOR E=FAILING AHRQ (%) UWMC (2012)
 EFFECT ON DEPARTMENT REPUTATION 31")


27 Barriers to Reporting Error Reporting Concerns (2012) EFFECT ON DEPARTMENT REPUTATION 31 PROVOKING RETRIBUTION FROM COLLEAGUES 35 EMBARASSMENT IN FRONT OF COLLEAGUES 37 ADMITTING LIABILITY 25 GETTING MY COLLEAGUES IN TROUBLE 49 DEPARTMENTAL OR PROFESSIONAL SANCTIONS Percentage (%)









28 Similar Results to AHRQ WHEN AN EVENT IS REPORTED, IT FEELS LIKE THE PERSON IS BEING WRITTEN UP, NOT THE PROBLEM PATIENT SAFETY IS NEVER SACRIFICED TO GET MORE WORK DONE WHEN A LOT OF WORK NEEDS TO GET DONE QUICKLY, WE WORK TOGETHER AS A TEAM TO GET WORK DONE UWMC 2012 (%) AHRQ (%)
 TOO")




29 Sources of Error Percentage (%) TOO HIGH A WORKLOAD 19 INSUFFICIENT TRAINING 12 TECHNICAL FAILURES (HARDWARE AND SOFTWARE) 12 FAILURE TO FOLLOW STANDARD OPERATING PROCEDURES 16 COMMUNICATION FAILURE

30
31 University of Washington Near Miss program Establish leadership support Assess your Safety Culture What should be reported? How will you collect the Data? How will you review incidents? How will you give feedback? How are we doing after 2 year
32 University of Washington Near Miss program What should be reported? Everything Near miss data is important for patient safety Employees should be encouraged to report both errors and near misses. CONSULT SIMULATION TREATMENT PLANNING TREATMENT
33 Who should use the system? Everyone in the department Why put in a near miss report? Why NOT CONSULT SIMULATION TREATMENT PLANNING TREATMENT

34 GPS made me do it KOMO4 news, June 15 th, 2011

35 GPS made me do it KOMO4 news, June 15 th, 2011
36 What should I report? A few examples: Contrast not ordered. Patient not given proper prep information for simulation. Set up instructions from simulation not complete. Nursing handoff to floors. Medication documentation. Use of wrong CT data set in Pinnacle (e.g. multiple scans). Wrong trial transferred from Pinnacle to Mosaiq. Wrong shift at machine. Setup to wrong marks.
37 University of Washington Near Miss program Establish leadership support Assess your Safety Culture What should be reported? How will you collect the Data? How will you review incidents? How will you give feedback? How are we doing after 2 years
38

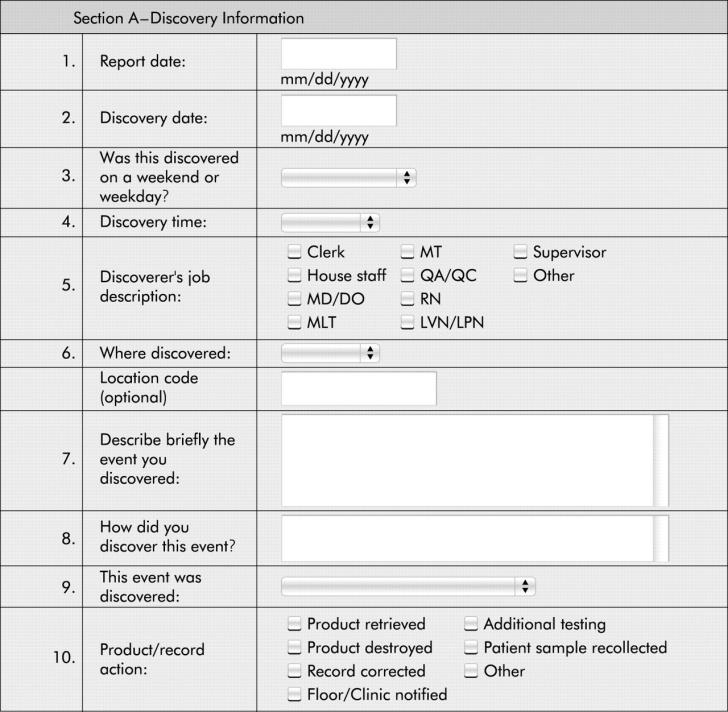
39 Electronic CSI report system Rolled out Feb 16 th 2012
40 CSI=Near Miss
41 University of Washington Near Miss program Establish leadership support Assess your Safety Culture What should be reported? How will you collect the Data? How will you review incidents? How will you give feedback? How are we doing after 2 years



42
43 Safety Committee Weekly CSI Review Medical director Nurse Manager Physicist Resident Technical Manager Dosimetrist IT Manager Chief Therapist CSI submissions range from items. Tag, set severity level Triage for root cause analysis.
44 Pathway of a Report Report Submitted <1 min Supervisor Review ~15 min Safety Committee Review 1 hour / week Apparent cause and track Root-cause Analysis ~5 hours Implement Corrective Actions CSI meeting

45
46
47 Safety Principles Automate when appropriate include use of forcing functions Standardize reduce reliance on memory Use checklists Reduce the number of steps and handoffs Add redundancy (double checks) for high risk processes Institute for safe medical practices
48 RCA Overview Identify teams Gather data and formulate a chronology. Investigate the timeline of the incident Interview involved staff recording all relevant information.. Pull data as needed from Mosaiq, Pinnacle, and other clinical computer systems. Do not troubleshoot at this point. Just the facts, Ma am. Identify Care Delivery Problems (what went wrong) Identify contributory factors Develop action plan
49
50

51 Poor human factors engineering Relevant policy on verifying pinnacle images with in room therapist for iso marking nonexistent Poor communication Physical environments
52 University of Washington Near Miss program Establish leadership support Assess your Safety Culture What should be reported? How will you collect the Data? How will you review incidents? How will you give feedback? How are we doing after 2 years
53 Feedback Staff meetings/process improvement meetings Reminders Policies Procedures Task forces Monthly Continuous Safety Improvement meeting Topics/trends RCAs Successes

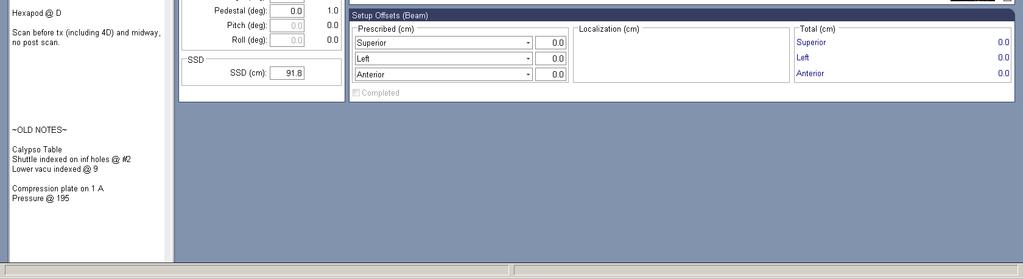
54 CSI 1018 Compression plate to limit breathing motion Used for SBRT Important settings: size of plate, number on compression screw
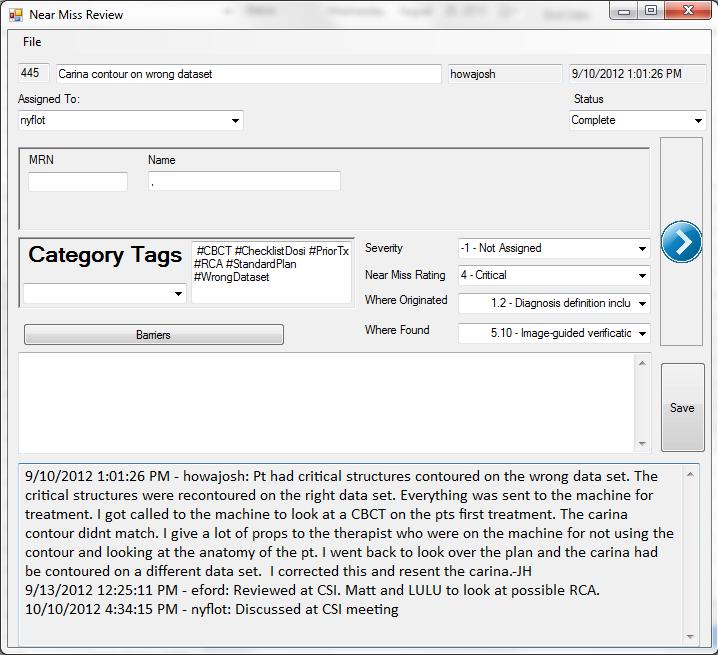
55 CSI 1018 Issue: SBRT patient had 4 different compression plate numbers documented. 1. The patient was simulated on February 13, Dry run scheduled for March 13, During the patient set up there was conflicting documentation of the compression plate numbers. SBRT set up page read 181 SBRT immobilization Photo shows 181. Site set up said 195 The attending physician s notes said 198
56 CSI 1018
57 CSI 1018 Issue: SBRT patient had 4 different compression plate numbers. 1. The patient was simulated on February 13, Dry run scheduled for March 13, During the patient set up there was conflicting documentation of the compression plate numbers. SBRT set up page read 181 SBRT immobilization Photo shows 181. Site set up said 195 The attending physician s notes said 198

58 CSI 1018
59 CSI 1018 Issue: SBRT patient had 4 different compression plate numbers. 1. The patient was simulated on February 13, Dry run scheduled for March 13, During the patient set up there was conflicting documentation of the compression plate numbers. SBRT set up page read 181 SBRT immobilization Photo shows 181. Site set up said 195 The attending physician s notes said 198

60 CSI 1018
61 CSI 1018 Issue: SBRT patient had 4 different compression plate numbers. 1. The patient was simulated on February 13, Dry run scheduled for March 13, During the patient set up there was conflicting documentation of the compression plate numbers. SBRT set up page read 181 SBRT immobilization Photo shows 181. Site set up said 195 The attending physician s notes said 198
62 CSI Sim was called to consult on the patient set up and said it was 181 due to the compression the patient was able to handle during the simulation. 195 and 198 too tight 5. The team decided to go with the 198 from the attending physician notes. 6. The CBCT showed a drastic difference between the simulation scans and dry run scans. 7. The team decided to use 185.
63 Process Improvement Documentation merged the SBRT set up sheet with the site setup. Standardization developed a standardized way to document in site set up for all patients. Education Lock site set up in simulation after documentation. Reminders Trust your photos from sim. Do not use physician notes!
64
65 CSI 1018
66 University of Washington Near Miss program Establish leadership support Assess your Safety Culture What should be reported? How will you collect the Data? How will you review incidents? How will you give feedback? How are we doing after 2 years?


67 Number of Near Miss Reports 160 Near Miss Reports

68 Reporter by Role
69 University of Washington Near Miss program Safety Culture Survey 2012 Response Rate: 78% 2013 Response Rate: 80% 2014 Response Rate: 87%
70 80 Overall Patient Safety Grade A=Excellent B=Very Good C=Acceptable D=Poor E=Failing 2012% 2013% 2014%
71 Barriers to Reporting The effect it may have on our departments reputation Provoking retrobution from colleagues Embarrassement in front of colleagues* P=0.02 Admitting Liability Getting my colleagues in trouble * P=0.01 Departmental or Professional Sanctions
72 Number of reports respodents said they filed in past 12 months 21 or more to to to to None
73 Survey Results: UWMC In this unit, we discuss ways to prevent errors from happening again % 81% * 85% p< 0.01 After we make changes to improve patient safety we evaluate their effectiveness. I have confidence that my error/near miss reports get used to improve our system. 46% 66% * 66% 53% 74% * 78%
74 CSI Successes Pediatric TBI program technical revamp Transfer patients from outside facilities Contrast issues and patient prep Isocenter placement process change Procedures for ABC Treatment plan sign off and MOSAIQ lock Diode sign off and RadCalc IQ scripting purchased for improved communication
75 University of Washington Near Miss program Establish leadership support Assess your Safety Culture What should be reported? How will you collect the Data? How will you review incidents? How will you give feedback? How are we doing after 1 year
76 Identifying Areas Of Improvement by analyzing CSI Reports
77 The Management Tool Capable of organizing and managing large number of reports. Database structures based on consensus recommendations Non discoverable Customizable Secure Tracks changes
78 NMSI How bad would it be if the near miss were not caught? Useful indicator of problem areas Scale from 0 4: None, Mild, Moderate, Severe, Critical Reports scored at weekly meeting at least one representative from physician, physics, and dosimetry/therapy group Reports tagged with categories
79 The Tags
80 UW incident review Keyword tagging Freeform categorization No limits on # of tags Searchable in DB Near Miss Severity Index 4: Critical 3: Severe 2: Moderate 1: Mild 0: None Categorization and scoring Track and correlate uncommon incidents Prioritize most serious interventions Measure improvement Input into national system

81 Reports with highest average NMSI Tag n average Wrong Dataset Isocenter Concerns Patient Setup Prior Radiation Treatment Standardizing Plans Standardizing Sim Unnecessary Dose Electrons Resim/Replan Clinical Set Collision ChecklistSim ChangeToPlan Pediatrics
82 Iso center concerns Improved access to schedule simulations. We eliminated an appointment for the patient. Improved communication. Improved team time utilization

83 ISOcenter Concerns IsoCenter Concerns

84 Prior RTResults 662 incidents submitted from Feb. Dec. 2012
85 Results 19 near miss incidents related to repeat irradiation 11 (59%) due to incorrect information in patient chart due to old treatment plan 4 (21%) isocenter concerns 4 (21%) related to wrong image set 10/11 caught at pre treatment imaging (last check before beamon) 5 (26%) related to difficulty obtaining prior radiation records 3 others: naming confusion, prior tattoo, photon/electron issues

86 2.5 Average Severity Score by Origination Patient Assesment/Orders Simulation Treatment Planning/ Contouring Pre Treatment Plan Checks Treatment Machine/ Therapist Chart Check Equipment Issues Other
 Patient Assesment/ Orders Treatment Machine/ Therapist Chart Check 10.")

87 Origination of Reports (n=1377) Post Treatment Check 0.07% Equipment Issues 13.36% Other (including 1.21) 7.99% Other (including 1.21) Patient Assesment/ Orders Treatment Machine/ Therapist Chart Check 10.75% Pre Treatment Plan Checks 5.52% Patient Assesment/ Orders 15.69% Simulation 12.06% Simulation Treatment Planning/ Contouring Pre Treatment Plan Checks Treatment Machine/ Therapist Chart Check Post Treatment Check Treatment Planning/ Contouring 34.57% Equipment Issues

88 Origination of Errors within Treatment Planning (n=476) 3.36% 1.26% 3.1 Registration of image sets 3.2 Delineation of Target(s) 34.87% 3.16 Plan information transfer 16.60% 3.2 Delineation of Targets 4.20% 2.73% 0.21% 3.99% 3.3 Delineation of organs at risk 3.4 Preliminary prescription parameters, constraints & 3.5 Selection of applicator 3.7 Selection of template or other auxiliary instruments 3.9 Physics consult 3.10 Dose distribution optimization 11.55% 0.63% 3.11 Dose Distribution Calculation 0.21% 14.50% 4.20% 1.68% 3.11 Dose distribution calculation 3.13 Preliminary evaluation of treatment plan by physician 3.14 Iteration of treatment plan 3.15 Final plan approval and prescription by physician 3.16 Plan information transfer to radiation oncology information system 3.17 Other *3.11: Dose Distribution Calculation had higher severity score of 1.78 versus 1.52 (p=.05)
89 Analysis: automated DosiCheck Have identified 308 incidents as candidates for automated end of planning checks Category Problem Automated Check Bolus Bolus improperly specified in Tx field Check Field:Bolus against known entries CBCT Patient Setup Tx Plan Rx CBCT not exported to MQ or planned for machine without CBCT Field specified as prone instead of supine Planned for incorrect fractions or dose Check Orders:CBCT and D&I:CBCT, Field:Machine Check Field:Orientation and SiteSetup:Orientation Check Rx:Fractions, Rx:Dose and TxCalendar:Sessions, D&I:Dosimetry Nyflot et al, ASTRO 2013


90 Post Treatment Check 2.03% Equipment Issues 0.29% Detection Point of Errors (n=1377) Other (including 1.21) 1.67% Patient Assesment/ Orders 1.09% Simulation 6.54% Other (including 1.21) Patient Assesment/ Orders TreatmentMachine/ Therapist Chart Check 50.18% Treatment Planning/ Contouring 17.43% Pre Treatment Plan Checks 20.77% Simulation Treatment Planning/ Contouring Pre Treatment Plan Checks TreatmentMachine/ Therapist Chart Check Post Treatment Check Equipment Issues
91 Projects Developed from CSI Automation Projects Dosimetry Plan Check Clinical planning constraints Patient check in Standardization Projects Simulation Treatment Calendar Nurse Handoff Outside records Scheduling Plan/Image Archive Site setup Patient ID Photos


92 Process Improvement
93 Conclusions Implementation of safety processes is coming Society recommendations National reporting systems Billing pressures Near miss incident review is extremely high yield for our institution Improved care Improved safety culture Quantitative metrics for evaluation and correlation

94 RO-ILS Mission Facilitate safer and higher quality care in radiation oncology by providing a mechanism for shared learning in a secure and non-punitive environment.
95 Acknowledgments University of Washington, Seattle Eric Ford, PhD Aaron Kusano, MD Jing Zeng, MD Gabrielle Kane, MD Patty Sponseller CMD Matthew Nyflot PhD Lora Holland B.S.RTT Avery Novak B.S.
96
8/2/2017. Strategies for Quality Improvement based on RO-ILS
 Strategies for Quality Improvement based on RO-ILS Lakshmi Santanam Ph.D We cannot Change Human condition, but we can change the conditions under which humans work Active failures- Swat one by one Still
Strategies for Quality Improvement based on RO-ILS Lakshmi Santanam Ph.D We cannot Change Human condition, but we can change the conditions under which humans work Active failures- Swat one by one Still
VA Radiotherapy Incident Reporting and Analysis System (RIRAS)
") VA Radiotherapy Incident Reporting and Analysis System (RIRAS) Jatinder R Palta PhD Rishabh Kapoor MS Michael Hagan, MD National Radiation Oncology Program(10P11H) Veterans Health Administration Disclosure
VA Radiotherapy Incident Reporting and Analysis System (RIRAS) Jatinder R Palta PhD Rishabh Kapoor MS Michael Hagan, MD National Radiation Oncology Program(10P11H) Veterans Health Administration Disclosure
Clinical Implementation of Electronic Charting
 Clinical Implementation of Electronic Charting Lisa Benedetti, M.S. Beaumont Health System 2013 AAPM Spring Clinical Meeting Outline I. Implementation Team II. III. IV. Process Mapping External Beam Radiation
Clinical Implementation of Electronic Charting Lisa Benedetti, M.S. Beaumont Health System 2013 AAPM Spring Clinical Meeting Outline I. Implementation Team II. III. IV. Process Mapping External Beam Radiation
Overview of TG262 on Electronic Record Keeping & Clinical Experience with ARIA. March 7, 2016 James Mechalakos Chair, TG-262
 Overview of TG262 on Electronic Record Keeping & Clinical Experience with ARIA March 7, 2016 James Mechalakos Chair, TG-262 Overview TG262 overview ARIA as an information repository ARIA as a workflow
Overview of TG262 on Electronic Record Keeping & Clinical Experience with ARIA March 7, 2016 James Mechalakos Chair, TG-262 Overview TG262 overview ARIA as an information repository ARIA as a workflow
An Update of Radiation Oncology Quality and Safety Initiatives
 An Update of Radiation Oncology Quality and Safety Initiatives Amy Heath, MS, RT(T) University of Wisconsin Hospital and Clinics Objectives Review importance of quality and safety in radiation oncology.
An Update of Radiation Oncology Quality and Safety Initiatives Amy Heath, MS, RT(T) University of Wisconsin Hospital and Clinics Objectives Review importance of quality and safety in radiation oncology.
Overview of TG262 on Electronic Record Keeping & Clinical Experience with ARIA. March 7, 2016 James Mechalakos Chair, TG-262
 Overview of TG262 on Electronic Record Keeping & Clinical Experience with ARIA March 7, 2016 James Mechalakos Chair, TG-262 Overview TG262 overview ARIA as an information repository ARIA as a workflow
Overview of TG262 on Electronic Record Keeping & Clinical Experience with ARIA March 7, 2016 James Mechalakos Chair, TG-262 Overview TG262 overview ARIA as an information repository ARIA as a workflow
AAPM TG-100 : A new paradigm for quality management in radiation therapy
 AAPM TG-100 : A new paradigm for quality management in radiation therapy M. Saiful Huq, PhD, FAAPM, FInstP Professor and Director of Medical Physics University of Pittsburgh Cancer Institute and UPMC CancerCenter
AAPM TG-100 : A new paradigm for quality management in radiation therapy M. Saiful Huq, PhD, FAAPM, FInstP Professor and Director of Medical Physics University of Pittsburgh Cancer Institute and UPMC CancerCenter
Year in Review ro ils RO ILS
 RO ILS RADIATION ONCOLOGY INCIDENT LEARNING SYSTEM Sponsored by ASTRO and AAPM Year in Review 2015 1 ro ils noun \ˈro i(-ə)ls\ Radiation Oncology Incident Learning System; a system to facilitate safer
RO ILS RADIATION ONCOLOGY INCIDENT LEARNING SYSTEM Sponsored by ASTRO and AAPM Year in Review 2015 1 ro ils noun \ˈro i(-ə)ls\ Radiation Oncology Incident Learning System; a system to facilitate safer
Introduction. Human Factors Engineering and Safety in Radiation Oncology
 Human Factors Engineering and Safety in Radiation Oncology Introduction Jim Schewe Philips Radiation Oncology Systems North Central Chapter, AAPM Fall 2015 1 Overview Human Factors in Software: General
Human Factors Engineering and Safety in Radiation Oncology Introduction Jim Schewe Philips Radiation Oncology Systems North Central Chapter, AAPM Fall 2015 1 Overview Human Factors in Software: General
Fundamental Aspects of SBRT
 What Are Fundamental Aspects? Fundamental Aspects of SBRT Fang-Fang Yin, PhD Duke University SBRT and its workflow Resources Staff Equipment Training Processes Safety Acceptance Commissioning Quality assurance
What Are Fundamental Aspects? Fundamental Aspects of SBRT Fang-Fang Yin, PhD Duke University SBRT and its workflow Resources Staff Equipment Training Processes Safety Acceptance Commissioning Quality assurance
Conflict of Interest. Patient Safety and the Training of the Medical Physicist. Training in Patient Safety
 Patient Safety and the Training of the Medical Physicist Peter Dunscombe, Ph.D. Derek Brown, Ph.D. University of Calgary/ Tom Baker Cancer Centre Conflict of Interest Peter Dunscombe and Derek Brown are
Patient Safety and the Training of the Medical Physicist Peter Dunscombe, Ph.D. Derek Brown, Ph.D. University of Calgary/ Tom Baker Cancer Centre Conflict of Interest Peter Dunscombe and Derek Brown are
The Practice Standards for Medical Imaging and Radiation Therapy. Medical Dosimetry Practice Standards
 The Practice Standards for Medical Imaging and Radiation Therapy Medical Dosimetry Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of this
The Practice Standards for Medical Imaging and Radiation Therapy Medical Dosimetry Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of this
APEx Program Standards
 APEx Program Standards The following standards are the basis of the APEx program. Level 1 standards are indicated in bold. Standard 1: Patient Evaluation, Care Coordination and Follow-up The radiation
APEx Program Standards The following standards are the basis of the APEx program. Level 1 standards are indicated in bold. Standard 1: Patient Evaluation, Care Coordination and Follow-up The radiation
The ASRT is seeking public comment on proposed revisions to the Practice Standards for Medical Imaging and Radiation Therapy titled Medical Dosimetry.
 The ASRT is seeking public comment on proposed revisions to the Practice Standards for Medical Imaging and Radiation Therapy titled Medical Dosimetry. To submit comments please access the public comment
The ASRT is seeking public comment on proposed revisions to the Practice Standards for Medical Imaging and Radiation Therapy titled Medical Dosimetry. To submit comments please access the public comment
Steven Sutlief, PhD UC San Diego February 13 th, 2015
 Corrective Actions Steven Sutlief, PhD UC San Diego February 13 th, 2015 Objectives By the end of this presentation, the listener should gain A vocabulary to discussing and thinking about corrective actions,
Corrective Actions Steven Sutlief, PhD UC San Diego February 13 th, 2015 Objectives By the end of this presentation, the listener should gain A vocabulary to discussing and thinking about corrective actions,
Patient Risk (Safety) in Radiation Therapy
 in Radiation Therapy") Patient Risk (Safety) in Radiation Therapy Michael G. Herman, Ph.D. Professor and Chair, Medical Physics Mayo Clinic Patient Safety 10/18/11 Herman # 1 Outline Radiation Therapy What Can/Did Happen? Is
Patient Risk (Safety) in Radiation Therapy Michael G. Herman, Ph.D. Professor and Chair, Medical Physics Mayo Clinic Patient Safety 10/18/11 Herman # 1 Outline Radiation Therapy What Can/Did Happen? Is
3/20/2012. Presentation Outline. Objectives Abt Associates Model (2008) Abt-III? What (who) is that?
 Abt-III? What (who) is that?") Presentation Outline Michael D. Mills, Ph.D., Ph.D.(c) Chair, AAPM Workforce Assessment Committee Current Manpower Resources and Models Abt Model Battista Model Mills Model (work in progress) Current Manpower
Presentation Outline Michael D. Mills, Ph.D., Ph.D.(c) Chair, AAPM Workforce Assessment Committee Current Manpower Resources and Models Abt Model Battista Model Mills Model (work in progress) Current Manpower
UWDRO RESIDENT SUPERVISION POLICY
 Roles, Responsibilities and Patient Care Activities of Residents UNIVERSITY OF WASHINGTON RADIATION ONCOLOGY RESIDENT EDUCATION PROGRAM UNIVERSITY OF WASHINGTON MEDICAL CENTER HARBORVIEW MEDICAL CENTER
Roles, Responsibilities and Patient Care Activities of Residents UNIVERSITY OF WASHINGTON RADIATION ONCOLOGY RESIDENT EDUCATION PROGRAM UNIVERSITY OF WASHINGTON MEDICAL CENTER HARBORVIEW MEDICAL CENTER
Medical Error Prevention
 Medical Error Prevention Matthew Studenski, PhD September 9, 2016 Disclosures Nothing to disclose. 1 Medical Error Prevention Definition of a medical event Look back on human error assessment Current recommendations
Medical Error Prevention Matthew Studenski, PhD September 9, 2016 Disclosures Nothing to disclose. 1 Medical Error Prevention Definition of a medical event Look back on human error assessment Current recommendations
Medical Errors in Radiation Therapy
 Medical Errors in Radiation Therapy 2014-2015 T. Yvette Forrest Division of Emergency Preparedness and Community Support Bureau of Radiation Control Florida Department of Health 1 Reportable Medical Events
Medical Errors in Radiation Therapy 2014-2015 T. Yvette Forrest Division of Emergency Preparedness and Community Support Bureau of Radiation Control Florida Department of Health 1 Reportable Medical Events
RADIATION ONCOLOGY RESIDENCY SUPERVISION POLICY
 RADIATION ONCOLOGY RESIDENCY SUPERVISION POLICY This policy is intended to guide the activities of radiation oncology residents in insuring that patient care activities in which residents participate are
RADIATION ONCOLOGY RESIDENCY SUPERVISION POLICY This policy is intended to guide the activities of radiation oncology residents in insuring that patient care activities in which residents participate are
SUPPLEMENTAL MATERIAL
 Practical Radiation Oncology (2011) SUPPLEMENTAL MATERIAL Safety Considerations for IMRT Jean M. Moran, Ph.D.,* Melanie Dempsey, M.S., Avraham Eisbruch, M.D.,* Benedick A. Fraass, Ph.D.*, James M. Galvin,
Practical Radiation Oncology (2011) SUPPLEMENTAL MATERIAL Safety Considerations for IMRT Jean M. Moran, Ph.D.,* Melanie Dempsey, M.S., Avraham Eisbruch, M.D.,* Benedick A. Fraass, Ph.D.*, James M. Galvin,
Establishing a Radiation Safety Culture in Health Care
 2 nd WHO Global Forum on Medical Devices Geneva 22-24 November 2013 Establishing a Radiation Safety Culture in Health Care Kin Yin Cheung, Ph.D. President, IOMP Hong Kong Sanatorium & Hospital, Hong Kong
2 nd WHO Global Forum on Medical Devices Geneva 22-24 November 2013 Establishing a Radiation Safety Culture in Health Care Kin Yin Cheung, Ph.D. President, IOMP Hong Kong Sanatorium & Hospital, Hong Kong
Incident Learning Systems in Radiation Therapy: Role of Culture and Potential Benefits
 Incident Learning Systems in Radiation Therapy: Role of Culture and Potential Benefits Sasa Mutic Mallinckrodt Institute of Radiology Washington University St. Louis, MO Conflict of Interest Director TreatSafely.org
Incident Learning Systems in Radiation Therapy: Role of Culture and Potential Benefits Sasa Mutic Mallinckrodt Institute of Radiology Washington University St. Louis, MO Conflict of Interest Director TreatSafely.org
Application of systems and control theory-based hazard analysis to radiation oncology
 Application of systems and control theory-based hazard analysis to radiation oncology Todd Pawlicki 1, Aubrey Samost 2, Derek Brown 1, Ryan Manger 1, Gwe-Ya Kim 1 and Nancy Leveson 3 1 UC San Diego, Department
Application of systems and control theory-based hazard analysis to radiation oncology Todd Pawlicki 1, Aubrey Samost 2, Derek Brown 1, Ryan Manger 1, Gwe-Ya Kim 1 and Nancy Leveson 3 1 UC San Diego, Department
Clinical Implementation of a High Dose Rate Brachytherapy Program. Hania Al Hallaq, Ph.D. Jacqueline Esthappan, Ph.D. Joann Prisciandaro, Ph.D.
 Clinical Implementation of a High Dose Rate Brachytherapy Program Hania Al Hallaq, Ph.D. Jacqueline Esthappan, Ph.D. Joann Prisciandaro, Ph.D. Learning Objectives Summarize national and international safety
Clinical Implementation of a High Dose Rate Brachytherapy Program Hania Al Hallaq, Ph.D. Jacqueline Esthappan, Ph.D. Joann Prisciandaro, Ph.D. Learning Objectives Summarize national and international safety
The Practice Standards for Medical Imaging and Radiation Therapy. Radiation Therapy Practice Standards
 The Practice Standards for Medical Imaging and Radiation Therapy Radiation Therapy Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of this
The Practice Standards for Medical Imaging and Radiation Therapy Radiation Therapy Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of this
Toward Minimum Practice Standards in Clinical Medical Physics:
 Toward Minimum Practice Standards in Clinical Medical Physics: Response to an increasing focus on reducing medical errors and validating professional competence Per Halvorsen, MS, DABR, FACR, FAAPM October
Toward Minimum Practice Standards in Clinical Medical Physics: Response to an increasing focus on reducing medical errors and validating professional competence Per Halvorsen, MS, DABR, FACR, FAAPM October
Hands-on SBRT Workshop
 Hands-on SBRT Workshop October 14-16, 2016 in partnership with ~ AAPM endorses the educational component of this program. ~ It does not however, endorse any product used or referred to in the program.
Hands-on SBRT Workshop October 14-16, 2016 in partnership with ~ AAPM endorses the educational component of this program. ~ It does not however, endorse any product used or referred to in the program.
Monaco treatment planning enhances departmental efficiencies
 Customer Perspective Monaco treatment planning enhances departmental efficiencies The time savings and workflow efficiencies introduced with Monaco version 5.11, including the use of Monaco templates for
Customer Perspective Monaco treatment planning enhances departmental efficiencies The time savings and workflow efficiencies introduced with Monaco version 5.11, including the use of Monaco templates for
Practical Considerations for Aria and Epic EMR Integration. Murat Surucu, PhD, John Roeske, PhD, William Small Jr., MD, Abhishek Solanki, MD
 Practical Considerations for Aria and Epic EMR Integration Murat Surucu, PhD, John Roeske, PhD, William Small Jr., MD, Abhishek Solanki, MD Introduction Radiation Therapy (RT)-specific aspects of a patient
Practical Considerations for Aria and Epic EMR Integration Murat Surucu, PhD, John Roeske, PhD, William Small Jr., MD, Abhishek Solanki, MD Introduction Radiation Therapy (RT)-specific aspects of a patient
NOVALIS STANDARD V 1.1
 NOVALIS STANDARD V 1.1 Quality and safety requirements in Stereotactic Radiosurgery (SRS) and Stereotactic Body Radiation Therapy (SBRT) Programs DEVELOPED AND ENDORSED BY: Timothy D. Solberg, PHD, UT
NOVALIS STANDARD V 1.1 Quality and safety requirements in Stereotactic Radiosurgery (SRS) and Stereotactic Body Radiation Therapy (SBRT) Programs DEVELOPED AND ENDORSED BY: Timothy D. Solberg, PHD, UT
Incident learning in radiation oncology: A review
 Incident learning in radiation oncology: A review Eric C. Ford a) Department of Radiation Oncology, University of Washington, Seattle, WA 98195, USA Suzanne B. Evans Department of Radiation Oncology, Yale
Incident learning in radiation oncology: A review Eric C. Ford a) Department of Radiation Oncology, University of Washington, Seattle, WA 98195, USA Suzanne B. Evans Department of Radiation Oncology, Yale
Department of Radiation Oncology University of Michigan Health Systems 1
 Initiative for Medical Physics Practice Guidelines Joann I. Prisciandaro, Ph.D. The Department of Radiation Oncology University of Michigan Every patient with cancer deserves to receive the best possible
Initiative for Medical Physics Practice Guidelines Joann I. Prisciandaro, Ph.D. The Department of Radiation Oncology University of Michigan Every patient with cancer deserves to receive the best possible
Medical Errors and Medical Physics
 Medical Errors and Medical Physics Michael Herman Ph.D. Peter Dunscombe, Ph.D. Bruce Thomadsen, Ph.D. Outline Introduction Are Errors A Problem? Are Medical Physicists Part of it? Quantitative Assessment
Medical Errors and Medical Physics Michael Herman Ph.D. Peter Dunscombe, Ph.D. Bruce Thomadsen, Ph.D. Outline Introduction Are Errors A Problem? Are Medical Physicists Part of it? Quantitative Assessment
Operator Training in HDR Brachytherapy: Preventing Treatment Errors. Disclosure
 Operator Training in HDR Brachytherapy: Preventing Treatment Errors Zoubir Ouhib, MS, DABR The Lynn Cancer Institute at Boca Raton Regional Hospital Boca Raton, FL Disclosure Zoubir Ouhib, MS, DABR, is
Operator Training in HDR Brachytherapy: Preventing Treatment Errors Zoubir Ouhib, MS, DABR The Lynn Cancer Institute at Boca Raton Regional Hospital Boca Raton, FL Disclosure Zoubir Ouhib, MS, DABR, is
8/2/2012. ACR-ASTRO Radiation Oncology Practice Accreditation Program. Accreditation Program Goals
 ACR-ASTRO Radiation Oncology Practice Accreditation Program Tariq M Patrick Conway, MD FACR Tariq Mian, Ph.D. FACR Accreditation Program Goals Provide impartial, third party peer review Evaluate and promote
ACR-ASTRO Radiation Oncology Practice Accreditation Program Tariq M Patrick Conway, MD FACR Tariq Mian, Ph.D. FACR Accreditation Program Goals Provide impartial, third party peer review Evaluate and promote
Medical Event Reporting
 Medical Event Reporting Scott Dube, MS DABR Morton Plant Hospital Clearwater, FL New Voluntary Reporting System For some, reporting is mandatory Radioactive materials are regulated by either the NRC or
Medical Event Reporting Scott Dube, MS DABR Morton Plant Hospital Clearwater, FL New Voluntary Reporting System For some, reporting is mandatory Radioactive materials are regulated by either the NRC or
YEAR IN REVIEW. ro ils RO-ILS INCIDENT LEARNING SYSTEM
 RO ILS R A D I AT I O N O N C O L O G Y INCIDENT LEARNING SYSTEM Sponsored by ASTRO and AAPM 2017 YEAR IN REVIEW ro ils 1 noun \ˈro i(-ə)ls\ Radiation Oncology Incident Learning System; a system to facilitate
RO ILS R A D I AT I O N O N C O L O G Y INCIDENT LEARNING SYSTEM Sponsored by ASTRO and AAPM 2017 YEAR IN REVIEW ro ils 1 noun \ˈro i(-ə)ls\ Radiation Oncology Incident Learning System; a system to facilitate
Louisville, Kentucky! MEDICAL PHYSICS WORKFORCE ASSESSMENT 2012 AAPM SPRING CLINICAL MEETING. List of Topics. Complexity, Safety and Quality Assurance
 Louisville, Kentucky! Michael D. Mills MEDICAL PHYSICS WORKFORCE ASSESSMENT 2012 AAPM SPRING CLINICAL MEETING List of Topics Complexity, Safety and Quality Assurance Where is the QA Knowledge? Staffing
Louisville, Kentucky! Michael D. Mills MEDICAL PHYSICS WORKFORCE ASSESSMENT 2012 AAPM SPRING CLINICAL MEETING List of Topics Complexity, Safety and Quality Assurance Where is the QA Knowledge? Staffing
7/31/2017. SPG: A Practical Subcommittee of the AAPM Professional Council. Origins. Origins
 SPG: A Practical Subcommittee of the AAPM Professional Council Brent C. Parker, PhD Director, Division of Physics and Engineering The University of Texas Medical Branch Galveston, TX Origins Subcommittee
SPG: A Practical Subcommittee of the AAPM Professional Council Brent C. Parker, PhD Director, Division of Physics and Engineering The University of Texas Medical Branch Galveston, TX Origins Subcommittee
Quality Products & Physics Services for Radiation Oncology. 1. Radiation Oncology Performance Enhancement (ROPE) Database. 2. TMA Web Portal Content
 Database. 2. TMA Web Portal Content") TMA Technology, Ltd. Quality Products & Physics Services for Radiation Oncology Content: 1. Radiation Oncology Performance Enhancement (ROPE) Database 2. TMA Web Portal Content 3. Physics Services 4. Pricing
TMA Technology, Ltd. Quality Products & Physics Services for Radiation Oncology Content: 1. Radiation Oncology Performance Enhancement (ROPE) Database 2. TMA Web Portal Content 3. Physics Services 4. Pricing
Radiation Therapy. 1. Introduction. 2. Documentation of Compliance. 3. Didactic Competency Requirements. 4. Clinical Competency Requirements
 PRIMARY CERTIFICATION AND REGISTRATION Radiation Therapy 1. Introduction Candidates for certification and registration are required to meet the Professional Education Requirements specified in the ARRT
PRIMARY CERTIFICATION AND REGISTRATION Radiation Therapy 1. Introduction Candidates for certification and registration are required to meet the Professional Education Requirements specified in the ARRT
AAPM Responds to Follow up Questions from Congress after Hearing on Radiation in Medicine
 AAPM Responds to Follow up Questions from Congress after Hearing on Radiation in Medicine Table of Contents Letter from the Congressman Henry A. Waxman, Chairman of the House of Representatives Committee
AAPM Responds to Follow up Questions from Congress after Hearing on Radiation in Medicine Table of Contents Letter from the Congressman Henry A. Waxman, Chairman of the House of Representatives Committee
Radiation Oncology Practice Accreditation Program Requirements
 Radiation Oncology Practice Accreditation Program Requirements Contents Introduction... 4 Application for Accreditation... 4 Preliminary Self-Assessment (ROPA Website Toolkit)... 4 Checklist for Site Survey...
Radiation Oncology Practice Accreditation Program Requirements Contents Introduction... 4 Application for Accreditation... 4 Preliminary Self-Assessment (ROPA Website Toolkit)... 4 Checklist for Site Survey...
Jean St. Germain, CHP, DABMP, RMP Attending Physicist Radiation Safety Officer Memorial Sloan-Kettering Cancer Center
 Jean St. Germain, CHP, DABMP, RMP Attending Physicist Radiation Safety Officer Memorial Sloan-Kettering Cancer Center Public Concern About Radiation Articles in Philadelphia Inquirer about prostate treatments
Jean St. Germain, CHP, DABMP, RMP Attending Physicist Radiation Safety Officer Memorial Sloan-Kettering Cancer Center Public Concern About Radiation Articles in Philadelphia Inquirer about prostate treatments
QUARTERLY REPORT PATIENT SAFETY WORK PRODUCT Q APRIL 1, 2017 JUNE 30, 2017
 QUARTERLY REPORT PATIENT SAFETY WORK PRODUCT Q2 2017 APRIL 1, 2017 JUNE 30, 2017 CLARITY PSO, a Division of Clarity Group, Inc. 8725 West Higgins Road Suite 810 Chicago, IL 60631 T: 773.864.8280 F: 773.864.8281
QUARTERLY REPORT PATIENT SAFETY WORK PRODUCT Q2 2017 APRIL 1, 2017 JUNE 30, 2017 CLARITY PSO, a Division of Clarity Group, Inc. 8725 West Higgins Road Suite 810 Chicago, IL 60631 T: 773.864.8280 F: 773.864.8281
10/8/12. Radiation Reduction and Monitoring Program: What the FDA and Other Regulatory Agencies Want. Disclosures. Two Principles of Radiation Safety
 NASCI October 16, 2012 Radiation Reduction and Monitoring Program: What the FDA and Other Regulatory Agencies Want Tessa S. Cook, MD PhD Hospital of the University of Pennsylvania Philadelphia, PA, USA
NASCI October 16, 2012 Radiation Reduction and Monitoring Program: What the FDA and Other Regulatory Agencies Want Tessa S. Cook, MD PhD Hospital of the University of Pennsylvania Philadelphia, PA, USA
Improving Patient Safety and Quality in Radiation Oncology
 Improving Patient Safety and Quality in Radiation Oncology Bhisham Chera, MD Assistant Professor Director of Patient Safety and Quality Dept. of Radiation Oncology October 25 th, 2013 Primum non nocere
Improving Patient Safety and Quality in Radiation Oncology Bhisham Chera, MD Assistant Professor Director of Patient Safety and Quality Dept. of Radiation Oncology October 25 th, 2013 Primum non nocere
Electronic Prescribing of Chemotherapy-It s Not a Video Game!
 Faculty Disclosures Electronic Prescribing of Chemotherapy-It s Not a Video Game! Mary Mably has no disclosures Mary S. Mably, RPh, BCOP Pharmacy Oncology Coordinator, University of Wisconsin Hospital
Faculty Disclosures Electronic Prescribing of Chemotherapy-It s Not a Video Game! Mary Mably has no disclosures Mary S. Mably, RPh, BCOP Pharmacy Oncology Coordinator, University of Wisconsin Hospital
3D surface image guided based DIBH clinical implementation
 3D surface image guided based DIBH clinical implementation Lily Tang, Ph.D. Memorial Sloan Kettering Cancer Center tangx@mskcc.org Outline System overview AlignRT we focus on this system C-rad Clinical
3D surface image guided based DIBH clinical implementation Lily Tang, Ph.D. Memorial Sloan Kettering Cancer Center tangx@mskcc.org Outline System overview AlignRT we focus on this system C-rad Clinical
Advance Radiation Therapy Practice:
 Advance Radiation Therapy Practice: A view from 30000ft and the front lines Nicole Harnett, MRT(T), AC(T), BSc, MEd Grace Lee, MRT(T), BSc, CMD, MHSc. 2016 CAMRT Annual General Conference June 9 12, 2016,
Advance Radiation Therapy Practice: A view from 30000ft and the front lines Nicole Harnett, MRT(T), AC(T), BSc, MEd Grace Lee, MRT(T), BSc, CMD, MHSc. 2016 CAMRT Annual General Conference June 9 12, 2016,
Tools & Resources for QI Success
 Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
Tools & Resources for QI Success Pediatric Hospital Medicine National Conference Kiran Kulkarni, MD Cynthia Castiglioni, MD, MS (HQPS) Sangeeta Schroeder, MD, MS (HQPS) Anu Subramony, MD MBA July 22, 2017
RADIATION THERAPY STAFFING SURVEY 2007
 RADIATION THERAPY STAFFING SURVEY 2007 A Nationwide Survey of Radiation Therapy Facility Managers and Directors Conducted by The American Society of Radiologic Technologists Reported October 2007 Copyright
RADIATION THERAPY STAFFING SURVEY 2007 A Nationwide Survey of Radiation Therapy Facility Managers and Directors Conducted by The American Society of Radiologic Technologists Reported October 2007 Copyright
Types of Errors 3/29/12. Approaches of other industries: To err is human, to forgive is divine... Human errors vs. Medical errors vs.
 Medical Errors Management and Early Warning for the Medical Physicist David Hintenlang, Types of Errors Human errors vs. Medical errors vs. Medical events To err is human, to forgive is divine... Approaches
Medical Errors Management and Early Warning for the Medical Physicist David Hintenlang, Types of Errors Human errors vs. Medical errors vs. Medical events To err is human, to forgive is divine... Approaches
ACR Radiation Oncology Practice Accreditation Program (ROPA)
") ACR Radiation Oncology Practice Accreditation Program (ROPA) ACR Radiation Oncology Practice Accreditation Program Everything You Need to Know Brian T. Monzon MBA RT(R)(T) Program Manager Quality and Safety
ACR Radiation Oncology Practice Accreditation Program (ROPA) ACR Radiation Oncology Practice Accreditation Program Everything You Need to Know Brian T. Monzon MBA RT(R)(T) Program Manager Quality and Safety
Compliance with IR(ME)R in radiotherapy departments across England
R in radiotherapy departments across England") C Compliance with IR(ME)R in radiotherapy departments across England A summary of our programme of inspections during 2007 to 2009 January 2011 Introduction During 2007 to 2009, we carried out a programme
C Compliance with IR(ME)R in radiotherapy departments across England A summary of our programme of inspections during 2007 to 2009 January 2011 Introduction During 2007 to 2009, we carried out a programme
Incidents reported to MERU, HSE in Diagnostic Radiology (including Nuclear Medicine) and in Radiotherapy The MERU, HSE (2013)
 and in Radiotherapy The MERU, HSE (2013)") Incidents reported to MERU, HSE in Diagnostic Radiology (including Nuclear Medicine) and in Radiotherapy 2010-2012 The MERU, HSE (2013) CONTENT Executive summary.. 2 Introduction 3 Incidents reported in
Incidents reported to MERU, HSE in Diagnostic Radiology (including Nuclear Medicine) and in Radiotherapy 2010-2012 The MERU, HSE (2013) CONTENT Executive summary.. 2 Introduction 3 Incidents reported in
Practice Analysis and Content Specifications. for Radiation Therapy
 Practice Analysis and Content Specifications for Radiation Therapy Final Report For New Documents Implemented January 2017 The American Registry of Radiologic Technologists 1255 Northland Drive St. Paul,
Practice Analysis and Content Specifications for Radiation Therapy Final Report For New Documents Implemented January 2017 The American Registry of Radiologic Technologists 1255 Northland Drive St. Paul,
Tools for risk assessment in radiation therapy
 Tools for risk assessment in radiation therapy ICRP Symposium on the International System of Radiological Protection October 24-26, 2011 Bethesda, MD, USA Dr. Pedro Ortiz López ICRP Committee 3 Task
Tools for risk assessment in radiation therapy ICRP Symposium on the International System of Radiological Protection October 24-26, 2011 Bethesda, MD, USA Dr. Pedro Ortiz López ICRP Committee 3 Task
Radiation Dose Management Requirements from MACRA and Joint Commission, Potential Effects on Reimbursement
 Radiation Dose Management Requirements from MACRA and Joint Commission, Potential Effects on Reimbursement Radiation dose requirements are being slowly integrated into key performance indicators and metrics
Radiation Dose Management Requirements from MACRA and Joint Commission, Potential Effects on Reimbursement Radiation dose requirements are being slowly integrated into key performance indicators and metrics
Failure mode and effects analysis: A community practice perspective
 Received: 16 February 2017 Revised: 27 July 2017 Accepted: 1 August 2017 DOI: 10.1002/acm2.12190 MANAGEMENT AND PROFESSION Failure mode and effects analysis: A community practice perspective Bradley W.
Received: 16 February 2017 Revised: 27 July 2017 Accepted: 1 August 2017 DOI: 10.1002/acm2.12190 MANAGEMENT AND PROFESSION Failure mode and effects analysis: A community practice perspective Bradley W.
Research in Simulation: Research and Grant Writing 101
 Research in Simulation: Research and Grant Writing 101 Valerie J. De Maio, MD, MSc, FACEP Director, Clinical Research Unit WakeMed Health & Hospitals Gina Della Porta, MHS Grants Specialist WakeMed Foundation
Research in Simulation: Research and Grant Writing 101 Valerie J. De Maio, MD, MSc, FACEP Director, Clinical Research Unit WakeMed Health & Hospitals Gina Della Porta, MHS Grants Specialist WakeMed Foundation
Analyzing Physician Task Allocation and Patient Flow at the Radiation Oncology Clinic. Final Report
 Analyzing Physician Task Allocation and Patient Flow at the Radiation Oncology Clinic Final Report Prepared for: Kathy Lash, Director of Operations University of Michigan Health System Radiation Oncology
Analyzing Physician Task Allocation and Patient Flow at the Radiation Oncology Clinic Final Report Prepared for: Kathy Lash, Director of Operations University of Michigan Health System Radiation Oncology
The Practice Standards for Medical Imaging and Radiation Therapy. Limited X-Ray Machine Operator Practice Standards
 The Practice Standards for Medical Imaging and Radiation Therapy Limited X-Ray Machine Operator Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all
The Practice Standards for Medical Imaging and Radiation Therapy Limited X-Ray Machine Operator Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all
QAPI Making An Improvement
 Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
The Practice Standards for Medical Imaging and Radiation Therapy. Quality Management Practice Standards
 The Practice Standards for Medical Imaging and Radiation Therapy Quality Management Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of
The Practice Standards for Medical Imaging and Radiation Therapy Quality Management Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of
University of Michigan Health System
 University of Michigan Health System Program and Operations Analysis Utilization Study of Linear Accelerators in the Radiation Oncology Department Project Report To: Kathy Lash: Director of Operations
University of Michigan Health System Program and Operations Analysis Utilization Study of Linear Accelerators in the Radiation Oncology Department Project Report To: Kathy Lash: Director of Operations
Medication Safety Technology The Good, the Bad and the Unintended Consequences
 Medication Safety Technology The Good, the Bad and the Unintended Consequences Michelle Mandrack RN, MSN Director of Consulting Services Matthew Fricker, RPh, MS Program Director 1 Objectives Consider
Medication Safety Technology The Good, the Bad and the Unintended Consequences Michelle Mandrack RN, MSN Director of Consulting Services Matthew Fricker, RPh, MS Program Director 1 Objectives Consider
A Resident-led PICU Morbidity and Mortality Conference
 A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
Incident Reporting Systems
 Patient Safety in Radiation Oncology, Melbourne 4-54 5 October 2012 Incident Reporting Systems Ola Holmberg, PhD Head, Radiation Protection of Patients Unit Radiation Safety and Monitoring Section NSRW
Patient Safety in Radiation Oncology, Melbourne 4-54 5 October 2012 Incident Reporting Systems Ola Holmberg, PhD Head, Radiation Protection of Patients Unit Radiation Safety and Monitoring Section NSRW
Quality and Safety Considerations You Haven t Thought About
 Quality and Safety Considerations You Haven t Thought About Learning Objectives Understand safety from a systems view. Understand & give examples of safety barriers. Be able to take actions to improve
Quality and Safety Considerations You Haven t Thought About Learning Objectives Understand safety from a systems view. Understand & give examples of safety barriers. Be able to take actions to improve
Introduction of EPMA in paediatric practice in UK:
 Introduction of EPMA in paediatric practice in UK: REALISING THE CLINICAL BENEFITS AND ENGAGING CLINICAL STAFF Stephen Marks Consultant Paediatric Nephrologist and EPMA lead Great Ormond Street Hospital
Introduction of EPMA in paediatric practice in UK: REALISING THE CLINICAL BENEFITS AND ENGAGING CLINICAL STAFF Stephen Marks Consultant Paediatric Nephrologist and EPMA lead Great Ormond Street Hospital
Compounded Sterile Preparations Pharmacy Content Outline May 2018
 Compounded Sterile Preparations Pharmacy Content Outline May 2018 The following domains, tasks, and knowledge statements were identified and validated through a role delineation study. The proportion of
Compounded Sterile Preparations Pharmacy Content Outline May 2018 The following domains, tasks, and knowledge statements were identified and validated through a role delineation study. The proportion of
The Alphabet Soup of Regulatory Compliance: Being Prepared for Inspections. Objectives. Inspections are often unannounced, so DOCUMENTATION
 The Alphabet Soup of Regulatory Compliance: Being Prepared for Inspections Linda Kroger, MS UC Davis Health System Objectives Recognize the various regulatory bodies and organizations with oversight or
The Alphabet Soup of Regulatory Compliance: Being Prepared for Inspections Linda Kroger, MS UC Davis Health System Objectives Recognize the various regulatory bodies and organizations with oversight or
Proceedings of the 2014 Winter Simulation Conference A. Tolk, S. Y. Diallo, I. O. Ryzhov, L. Yilmaz, S. Buckley, and J. A. Miller, eds.
 Proceedings of the 2014 Winter Simulation Conference A. Tolk, S. Y. Diallo, I. O. Ryzhov, L. Yilmaz, S. Buckley, and J. A. Miller, eds. ASSESSING THE RELIABILITY OF THE RADIATION THERAPY CARE DELIVERY
Proceedings of the 2014 Winter Simulation Conference A. Tolk, S. Y. Diallo, I. O. Ryzhov, L. Yilmaz, S. Buckley, and J. A. Miller, eds. ASSESSING THE RELIABILITY OF THE RADIATION THERAPY CARE DELIVERY
20 STEPS FROM STUDY IDEA INCEPTION TO PUBLISHING RESEARCH/ Evidence-Based Practice
 20 STEPS FROM STUDY IDEA INCEPTION TO PUBLISHING RESEARCH/ Evidence-Based Practice Nursing Research/ Evidence-Based Practice Checklist (Version 31 January 2012) Specify the date in the left column when
20 STEPS FROM STUDY IDEA INCEPTION TO PUBLISHING RESEARCH/ Evidence-Based Practice Nursing Research/ Evidence-Based Practice Checklist (Version 31 January 2012) Specify the date in the left column when
What is Medical Physics 3.0?
 Weds: 10:15 MP3.0 in Design Weds: 1:45 MP3.0 in Practice 8/2/2017 What is Medical Physics 3.0? Ehsan Samei Ehsan Samei: What is Medical Physics 3.0 Robin Miller: Leadership in decision-making Mary Fox:
Weds: 10:15 MP3.0 in Design Weds: 1:45 MP3.0 in Practice 8/2/2017 What is Medical Physics 3.0? Ehsan Samei Ehsan Samei: What is Medical Physics 3.0 Robin Miller: Leadership in decision-making Mary Fox:
University of Washington School of Nursing - Continuing Nursing Education 1
 A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
A Team Approach to Patient Safety: TeamSTEPPS University of Washington Medical Center Kat Comstock, Associate Director Center for Clinical Excellence/Patient Safety Officer Describe TEAMSTEPPS using the
MOSAIQ Evaluate. Integrated plan management and dose review. A new paradigm of treatment planning management
 MOSAIQ Evaluate Integrated plan management and dose review A new paradigm of treatment planning management MOSAIQ Evaluate Integrated plan management and dose review MOSAIQ Evaluate delivers a truly integrated
MOSAIQ Evaluate Integrated plan management and dose review A new paradigm of treatment planning management MOSAIQ Evaluate Integrated plan management and dose review MOSAIQ Evaluate delivers a truly integrated
LEAN Transformation Storyboard 2015 to present
 LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
OHTAC Recommendation. Implementation and Use of Smart Medication Delivery Systems
 OHTAC Recommendation Implementation and Use of Smart Medication Delivery Systems July 2009 Background The Ontario Health Technology Advisory Committee (OHTAC) engaged the University Health Network s (UHN)
OHTAC Recommendation Implementation and Use of Smart Medication Delivery Systems July 2009 Background The Ontario Health Technology Advisory Committee (OHTAC) engaged the University Health Network s (UHN)
Sunnybrook Health Sciences Centre Fully Affiliated with the University of Toronto
 Appendix2 Sunnybrook Health Sciences Centre Fully Affiliated with the University of Toronto Vacancy Exists For: Advanced Practice Radiation Therapist (APRT) SBRT Program Competition # Location: Odette
Appendix2 Sunnybrook Health Sciences Centre Fully Affiliated with the University of Toronto Vacancy Exists For: Advanced Practice Radiation Therapist (APRT) SBRT Program Competition # Location: Odette
Objectives. Key Elements. ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management 5/20/2014
 ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management Matthew Fricker, RPh, MS, FASHP Program Director, ISMP Rebecca Lamis, PharmD, FISMP Medication Safety Analyst,
ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management Matthew Fricker, RPh, MS, FASHP Program Director, ISMP Rebecca Lamis, PharmD, FISMP Medication Safety Analyst,
HOWARD UNIVERSITY Position Description. POSITION TITLE: Radiation Safety Officer SALARY GRADE: HU-13. DATE REVISED: December 01, 2014 EEO CODE: 02
 DEPARTMENT: POSITION NO: REPORTS TO: GRANT: No Yes BASIC FUNCTION: SUPERVISORY ACCOUNTABILITY: NATURE AND SCOPE: PRINCIPAL ACCOUNTABILITIES: Directs, develops and maintains a comprehensive radiological
DEPARTMENT: POSITION NO: REPORTS TO: GRANT: No Yes BASIC FUNCTION: SUPERVISORY ACCOUNTABILITY: NATURE AND SCOPE: PRINCIPAL ACCOUNTABILITIES: Directs, develops and maintains a comprehensive radiological
The Practice Standards for Medical Imaging and Radiation Therapy. Radiography Practice Standards
 The Practice Standards for Medical Imaging and Radiation Therapy Radiography Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of this document
The Practice Standards for Medical Imaging and Radiation Therapy Radiography Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of this document
The Practice Standards for Medical Imaging and Radiation Therapy. Computed Tomography Practice Standards
 The Practice Standards for Medical Imaging and Radiation Therapy Computed Tomography Practice Standards 2011 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of
The Practice Standards for Medical Imaging and Radiation Therapy Computed Tomography Practice Standards 2011 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of
Continuous Quality Improvement Made Possible
 Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1)
 Medication Chart implementation and training guide (version 1.1)") Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
Profiles in CSP Insourcing: Tufts Medical Center
 Profiles in CSP Insourcing: Tufts Medical Center Melissa A. Ortega, Pharm.D., M.S. Director, Pediatrics and Inpatient Pharmacy Operations Tufts Medical Center Hospital Profile Tufts Medical Center (TMC)
Profiles in CSP Insourcing: Tufts Medical Center Melissa A. Ortega, Pharm.D., M.S. Director, Pediatrics and Inpatient Pharmacy Operations Tufts Medical Center Hospital Profile Tufts Medical Center (TMC)
Implementation Assessment: Quantitative Interview
 CUSP 4 MVP VAP Improving Care for Mechancially Ventilated Patients Implementation Assessment: Quantitative Interview ICU Unit Type: Hospital Name: Interview Date: Interviewer Name: Section 1: Staff Safety
CUSP 4 MVP VAP Improving Care for Mechancially Ventilated Patients Implementation Assessment: Quantitative Interview ICU Unit Type: Hospital Name: Interview Date: Interviewer Name: Section 1: Staff Safety
The Patient Safety Act Reporting and RCA Requirements
 The Patient Safety Act Reporting and RCA Requirements Patient Safety Initiative Health Care Quality Assessment NJ Department of Health and Senior Services 1 Goals for Workshop Today Review legislation
The Patient Safety Act Reporting and RCA Requirements Patient Safety Initiative Health Care Quality Assessment NJ Department of Health and Senior Services 1 Goals for Workshop Today Review legislation
Error and Near-Miss Reporting in Radiotherapy
 Error and Near-Miss Reporting in Radiotherapy Sasa Mutic Department of Radiation Oncology Mallinckrodt Institute of Radiology Washington University St. Louis, MO Outline Introduction Reporting infrastructure
Error and Near-Miss Reporting in Radiotherapy Sasa Mutic Department of Radiation Oncology Mallinckrodt Institute of Radiology Washington University St. Louis, MO Outline Introduction Reporting infrastructure
Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02
 Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02 V02 issued Issue 1 May 11 Issue 2 Dec 11 Planned review May
Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02 V02 issued Issue 1 May 11 Issue 2 Dec 11 Planned review May
How to Build a Quality Infrastructure
 1 Imaging Performance Partnership How to Build a Quality Infrastructure Research Brief October 2013 Ben Lauing, Analyst lauingb@advisory.com 2 Building a Solid Foundation Three Imperatives to Create a
1 Imaging Performance Partnership How to Build a Quality Infrastructure Research Brief October 2013 Ben Lauing, Analyst lauingb@advisory.com 2 Building a Solid Foundation Three Imperatives to Create a
MARYLAND RADIATION CONTROL ADVISORY BOARD MINUTES December 4, 2017
 MARYLAND RADIATION CONTROL ADVISORY BOARD MINUTES December 4, 2017 Maryland Department of the Environment Air and Radiation Administration Radiological Health Program MEMBERS PRESENT Richard Hudes, M.D.
MARYLAND RADIATION CONTROL ADVISORY BOARD MINUTES December 4, 2017 Maryland Department of the Environment Air and Radiation Administration Radiological Health Program MEMBERS PRESENT Richard Hudes, M.D.
Guidance for Medication Reconciliation and System Integration Process
 Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
The Practice Standards for Medical Imaging and Radiation Therapy. Radiologist Assistant Practice Standards
 The Practice Standards for Medical Imaging and Radiation Therapy Radiologist Assistant Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part
The Practice Standards for Medical Imaging and Radiation Therapy Radiologist Assistant Practice Standards 2017 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part
- Questioned about whether patients discontinue treatment and stop showing up when the side effects kick in. Surprisingly this is extremely rare.
 RADAID Report for visit to Kenyatta Hospital in Nairobi, Kenya Submitted by Kim Rans, Regina Ley, and Shilpen Patel for a visit from August 6 th -August 14th Background: The Kenyatta National Hospital
RADAID Report for visit to Kenyatta Hospital in Nairobi, Kenya Submitted by Kim Rans, Regina Ley, and Shilpen Patel for a visit from August 6 th -August 14th Background: The Kenyatta National Hospital
Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program. Radiation Oncology
 Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program Radiation Oncology Prepared by: Medical Compliance Services, Miller School of Medicine/University of Miami and Compliance
Office of Billing Compliance 2014 Professional Coding, Billing and Documentation Program Radiation Oncology Prepared by: Medical Compliance Services, Miller School of Medicine/University of Miami and Compliance