Longitudinal Coordination of Care Overview to HL7 Patient Care WG. Wednesday, March 27 th, 2013
|
|
|
- Tobias Marsh
- 5 years ago
- Views:
Transcription


1 Longitudinal Coordination of Care Overview to HL7 Patient Care WG Wednesday, March 27 th, 2013





.")
2 Meeting Etiquette Remember: If you are not speaking, please keep your phone on mute Do not put your phone on hold. If you need to take a call, hang up and dial in again when finished with your other call o Hold = Elevator Music = frustrated speakers and participants This meeting is being recorded o Another reason to keep your phone on mute when not speaking Use the Chat feature for questions, comments and items you would like the moderator or other participants to know. o Send comments to All Participants so they can be addressed publically in the chat, or discussed in the meeting (as appropriate). From S&I Framework to Participants: Hi everyone: remember to keep your phone on mute All Participants
3 Agenda Topic LCC Background and Overview Care Plan and Care Planning Alignment to HL7 PC Care Plan DAM Presenter Evelyn Gallego Larry Garber Russ Leftwich + LCC Leads
4 Longitudinal Coordination of Care Workgroup Overview This is Part 1 of a two-part slide deck 4
5 S&I Longitudinal Coordination of Care (LCC) Workgroup Initiated in October 2011 as a community-led initiative with multiple public and private sector partners, each committed to overcoming interoperability challenges in long-term, post-acute care (LTPAC) transitions Supports and advances interoperable health information exchange (HIE) on behalf of LTPAC stakeholders and promotes LCC on behalf of medically-complex and/or functionally impaired persons Goal is to identify standards that support LCC of medically-complex and/or functionally impaired persons that are aligned with and could be included in the EHR Meaningful Use Programs Seeks to influence Meaningful Use Stage 3 Consists of three sub-workgroups (SWGs): Longitudinal Care Plan (LCP) LTPAC Care Transition Patient Assessment Summary (PAS)* 5 * The work of the PAS SWG completed in JAN13
 G O A")
 information exchange using a single standard for LTPAC transfer")
6 LCC Sub Workgroups (SWG) COMMUNITY-LED INITIATIVE Longitudinal Coordination of Care Workgroup Providing subject matter expertise and coordination of SWGs Developing systems view to identify interoperability gaps and prioritize activities, and align identified standards with the EHR MU Program Longitudinal Care Plan SWG LTPAC Care Transition SWG Patient Assessment Summary (PAS SWG) G O A L S Identify standards for an interoperable, longitudinal care plan* which aligns, supports and informs person-centric care delivery regardless of setting or service provider Identify the key business and technical challenges that inhibit LTC data exchanges Define data elements for long-term and post-acute care (LTPAC) information exchange using a single standard for LTPAC transfer summaries Established the standards for the exchange of Patient Assessment Summary (PAS) documents Provided consultation to the transformation tool being developed by Geisinger to transform the noninteroperable MDSv3 and OASIS-C into an interoperable clinical HL7 CDA document *Care Plan standards will enable providers to create, transmit and incorporate care plans and needed content for the benefit of medically complex and/or functionally impaired individuals, their families and caregivers. 6
7 LCC Initiative: Resources & Questions LCC Leads Dr. Larry Garber Dr. Terry O Malley (tomalley@partners.org) Dr. Bill Russell (drbruss@gmail.com) Sue Mitchell (suemitchell@hotmail.com) LCC/HL7 Coordination Lead Dr. Russ Leftwich (Russell.Leftwich@tn.gov) Federal Partner Lead Jennie Harvell (jennie.harvell@hhs.gov) Initiative Coordinator Evelyn Gallego (evelyn.gallego@siframework.org) Project Management Becky Angeles (becky.angeles@esacinc.com) Sweta Ladwa (sweta.ladwa@esacinc.com) LCC Wiki Site: 7
8 LCC WG Key Successes to meet MU3 needs (JUNE 12) LCC Use Case 1.0: Expanded from S&I ToC Use Case; identified 360+ additional data elements (AUG 12) Care Plan Whitepaper Meaningful Use Requirements For: Transitions of Care & Care Plans (OCT 12) IMPACT Dataset: Consensus built Transitions of Care and Care Plan/HHPoC dataset (483 data elements). Deep dive of LCC Use Case 1.0 (MAY- SEPT 12) Balloted 3 standards through HL7: C-CDA Refinements interoperable exchange of Functional Status, Cognitive Status, & Pressure Ulcer; and LTPAC Summary IG. Also balloted through HL7 standards for Questionnaire Assessment. Stage 2 MU incorporated requirements for functional and cognitive status. (OCT 12) Stage 3 MU Care Plan Questions for HITPC MU WG (DEC 12) Care Plan Glossary (JAN 13) Community Led submission to HITPC RFC Stage 3 MU (MAR 13) IMPACT ToC High-level IG 8


9 9 Lantana has been contracted to work with LCC to make and ballot HL7 CDA IGs Shared Care Encounter Summary: Office Visit to PHR Consultant to PCP ED to PCP, SNF, etc Home Health Plan of Care Care Plan Consultation Request: PCP to Consultant PCP, SNF, etc to ED Transfer of Care: Hospital to SNF, PCP, HHA, etc SNF, PCP, etc to HHA PCP to new PCP



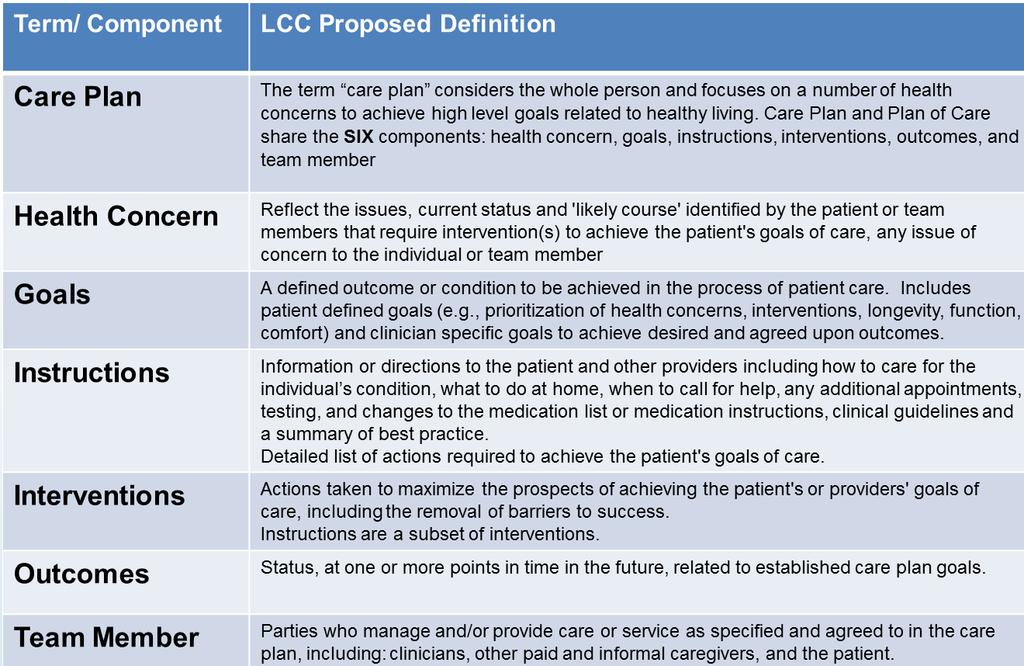
10 LCC WG Care Plan Artifacts: Glossary and Use Case 10
11 Care Plan & Care Planning 11
12 Key Discussion Points The HL7 Care Model is great! Let s work together to ensure our clinical speak aligns with your modeling speak Barriers and Risks Goals (patient and provider / computable vs. behavior vs. patientspecified) Team Members (include patient and family)
 to determine their status")
13 Patient Status Functional Cognitive Physical Environmental Assessments Patients are evaluated with assessments (history, symptoms, physical exam, testing, etc ) to determine their status 13
14 Disease Progression Health Conditions/ Concerns Active Problems Risks/Concerns: Wellness Barriers Injury (e.g. falls) Illness (e.g. ulcers, cancer, stroke, hypoglycemia, hepatitis, diarrhea, depression, etc ) Risks Risk Factors Age, gender Significant Past Medical/Surgical Hx Family Hx, Race/Ethnicity, Genetics Historical exposures/lifestyle (e.g. alcohol, smoke, radiation, diet, exercise, workplace, sexual ) Patient Status Functional Cognitive Physical Environmental Treatment Assessments Side effects Patient Status helps define the patient s current conditions, concerns, and risks for conditions Risks/concerns come from many sources 14
15 Disease Progression Care Plan Decision Modifiers Patient/family preferences (values, priorities, wishes, adv directives, expectations, etc ) Patient situation (access to care, support, resources, setting, transportation, etc ) Health Conditions/ Concerns Active Problems Risks/Concerns: Wellness Barriers Injury (e.g. falls) Illness (e.g. ulcers, cancer, stroke, hypoglycemia, hepatitis, diarrhea, depression, etc ) Risks Risk Factors Age, gender Significant Past Medical/Surgical Hx Family Hx, Race/Ethnicity, Genetics Historical exposures/lifestyle (e.g. alcohol, smoke, radiation, diet, exercise, workplace, sexual ) Prioritize Goals Desired outcomes and milestones Readiness Prognosis Related Interventions Progress Patient Status Functional Cognitive Physical Environmental Treatment Assessments Side effects Goals for treatment of health conditions and prevention of concerns are created collaboratively with patient taking into account their statuses and Care Plan 15 Decision Modifiers
16 Disease Progression Care Plan Decision Modifiers Patient/family preferences (values, priorities, wishes, adv directives, expectations, etc ) Patient situation (access to care, support, resources, setting, transportation, etc ) Health Conditions/ Concerns Active Problems Risks/Concerns: Wellness Barriers Injury (e.g. falls) Illness (e.g. ulcers, cancer, stroke, hypoglycemia, hepatitis, diarrhea, depression, etc ) Risks Risk Factors Age, gender Significant Past Medical/Surgical Hx Family Hx, Race/Ethnicity, Genetics Historical exposures/lifestyle (e.g. alcohol, smoke, radiation, diet, exercise, workplace, sexual ) Prioritize Decision Support Goals Desired outcomes and milestones Readiness Prognosis Related Interventions Progress Patient Status Functional Cognitive Physical Environmental Treatment Assessments Side effects Decision making is enhanced with evidence based medicine, clinical practice guidelines, and other medical knowledge 16
17 Disease Progression Health Conditions/ Concerns Active Problems Risks/Concerns: Wellness Barriers Injury (e.g. falls) Illness (e.g. ulcers, cancer, stroke, hypoglycemia, hepatitis, diarrhea, depression, etc ) Risks Risk Factors Age, gender Significant Past Medical/Surgical Hx Family Hx, Race/Ethnicity, Genetics Historical exposures/lifestyle (e.g. alcohol, smoke, radiation, diet, exercise, workplace, sexual ) Care Plan Decision Modifiers Patient/family preferences (values, priorities, wishes, adv directives, expectations, etc ) Patient situation (access to care, support, resources, setting, transportation, etc ) Patient allergies/intolerances Prioritize Decision Support Goals Desired outcomes and milestones Readiness Prognosis Related Interventions Progress Patient Status Functional Cognitive Physical Environmental Treatment Orders, etc.. Decision Support Assessments Interventions/Actions (e.g. medications, wound care, procedures, tests, diet, behavior changes, exercise, consults, rehab, calling MD for symptoms, education, anticipatory guidance, services, support, etc ) Start/stop date, interval Authorizing/responsible parties/roles/contact info Setting of care Instructions/parameters Supplies/Vendors Planned assessments Expected outcomes Status of intervention Side effects Interventions and actions to achieve goals are identified collaboratively with patient taking into account their values, situation, statuses, risks & benefits, etc 17
18 Disease Progression Care Plan Health Conditions/ Concerns Active Problems Risks/Concerns: Wellness Barriers Injury (e.g. falls) Illness (e.g. ulcers, cancer, stroke, hypoglycemia, hepatitis, diarrhea, depression, etc ) Risks Risk Factors Age, gender Significant Past Medical/Surgical Hx Family Hx, Race/Ethnicity, Genetics Historical exposures/lifestyle (e.g. alcohol, smoke, radiation, diet, exercise, workplace, sexual ) Care Plan Decision Modifiers Patient/family preferences (values, priorities, wishes, adv directives, expectations, etc ) Patient situation (access to care, support, resources, setting, transportation, etc ) Patient allergies/intolerances Prioritize Decision Support Goals Desired outcomes and milestones Readiness Prognosis Related Interventions Progress Patient Status Functional Cognitive Physical Environmental Orders, etc.. Decision Support Assessments Interventions/Actions (e.g. medications, wound care, procedures, tests, diet, behavior changes, exercise, consults, rehab, calling MD for symptoms, education, anticipatory guidance, services, support, etc ) Start/stop date, interval Authorizing/responsible parties/roles/contact info Setting of care Instructions/parameters Supplies/Vendors Planned assessments Expected outcomes Status of intervention Side effects The Care Plan is comprised of Modifiers, Conditions/Concerns, their Goals, Interventions/Actions/Instructions, Assessments and the Care Team members that actualize it 18
19 Disease Progression Care Plan Health Conditions/ Concerns Active Problems Risks/Concerns: Wellness Barriers Injury (e.g. falls) Illness (e.g. ulcers, cancer, stroke, hypoglycemia, hepatitis, diarrhea, depression, etc ) Risks Risk Factors Age, gender Significant Past Medical/Surgical Hx Family Hx, Race/Ethnicity, Genetics Historical exposures/lifestyle (e.g. alcohol, smoke, radiation, diet, exercise, workplace, sexual ) Care Plan Decision Modifiers Patient/family preferences (values, priorities, wishes, adv directives, expectations, etc ) Patient situation (access to care, support, resources, setting, transportation, etc ) Patient allergies/intolerances Prioritize Decision Support Goals Desired outcomes and milestones Readiness Prognosis Related Interventions Progress Patient Status Functional Cognitive Physical Environmental Orders, etc.. Decision Support Assessments Outcomes Interventions/Actions (e.g. medications, wound care, procedures, tests, diet, behavior changes, exercise, consults, rehab, calling MD for symptoms, education, anticipatory guidance, services, support, etc ) Start/stop date, interval Authorizing/responsible parties/roles/contact info Setting of care Instructions/parameters Supplies/Vendors Planned assessments Expected outcomes Status of intervention Side effects Interventions and actions achieve outcomes that make progress towards goals, cause interventions to be modified, and change health conditions 19
20 Disease Progression Care Plan Health Conditions/ Concerns Active Problems Risks/Concerns: Wellness Barriers Injury (e.g. falls) Illness (e.g. ulcers, cancer, stroke, hypoglycemia, hepatitis, diarrhea, depression, etc ) Risks Risk Factors Age, gender Significant Past Medical/Surgical Hx Family Hx, Race/Ethnicity, Genetics Historical exposures/lifestyle (e.g. alcohol, smoke, radiation, diet, exercise, workplace, sexual ) Care Plan Decision Modifiers Patient/family preferences (values, priorities, wishes, adv directives, expectations, etc ) Patient situation (access to care, support, resources, setting, transportation, etc ) Patient allergies/intolerances Prioritize Decision Support Goals Desired outcomes and milestones Readiness Prognosis Related Interventions Progress Patient Status Functional Cognitive Physical Environmental Orders, etc.. Decision Support Assessments Outcomes Interventions/Actions (e.g. medications, wound care, procedures, tests, diet, behavior changes, exercise, consults, rehab, calling MD for symptoms, education, anticipatory guidance, services, support, etc ) Start/stop date, interval Authorizing/responsible parties/roles/contact info Setting of care Instructions/parameters Supplies/Vendors Planned assessments Expected outcomes Status of intervention Side effects The Care Plan (Concerns, Goals, Interventions, and Care Team), along with Risk Factors and Decision Modifiers, iteratively evolve over time 20
21 Care Plan Decision Modifiers Patient/family preferences (values, priorities, wishes, adv directives, expectations, etc ) Patient situation (access to care, support, resources, setting, transportation, etc ) Patient allergies/intolerances Health Conditions/ Concerns Active Problems Risks/Concerns: Wellness Barriers Injury (e.g. falls) Illness (e.g. ulcers, cancer, stroke, hypoglycemia, hepatitis, diarrhea, depression, etc ) 0 Goals Desired outcomes and milestones Readiness Prognosis Related Interventions Progress Interventions/Actions (e.g. medications, wound care, procedures, tests, diet, behavior changes, exercise, consults, rehab, calling MD for symptoms, education, anticipatory guidance, services, support, etc ) Start/stop date, interval Authorizing/responsible parties/roles/contact info Setting of care Instructions/parameters Supplies/Vendors Planned assessments Expected outcomes Status of intervention A many-to-many-to-many relationship exists between Health Conditions/Concerns, Goals and Interventions/Actions 21
22 Care Team Members each have their own responsibilities Health Conditions/ Concerns Active Problems Risks/Concerns: Wellness Barriers Injury (e.g. falls) Illness (e.g. ulcers, cancer, stroke, hypoglycemia, hepatitis, diarrhea, depression, etc ) Care Plan Decision Modifiers Patient/family preferences (values, priorities, wishes, adv directives, expectations, etc ) Patient situation (access to care, support, resources, setting, transportation, etc ) Patient allergies/intolerances Goals Desired outcomes and milestones Readiness Prognosis Related Interventions Progress Patient Status Functional Cognitive Physical Environmental Interventions/Actions (e.g. medications, wound care, procedures, tests, diet, behavior changes, exercise, consults, rehab, calling MD for symptoms, education, anticipatory guidance, services, support, etc ) Start/stop date, interval Authorizing/responsible parties/roles/contact info Setting of care Instructions/parameters Supplies/Vendors Planned assessments Expected outcomes Status of intervention 22
23 How to represent many-to-many-tomany-to-many??? Health Conditions/ Concerns Active Problems Risks/Concerns: Wellness Barriers Injury (e.g. falls) Illness (e.g. ulcers, cancer, stroke, hypoglycemia, hepatitis, diarrhea, depression, etc ) Care Plan Decision Modifiers Patient/family preferences (values, priorities, wishes, adv directives, expectations, etc ) Patient situation (access to care, support, resources, setting, transportation, etc ) Patient allergies/intolerances 0 Goals Desired outcomes and milestones Readiness Prognosis Related Interventions Progress 0 0 Patient Status Functional Cognitive Physical Environmental 0 Interventions/Actions (e.g. medications, wound care, procedures, tests, diet, behavior changes, exercise, consults, rehab, calling MD for symptoms, education, anticipatory guidance, services, support, etc ) Start/stop date, interval Authorizing/responsible parties/roles/contact info Setting of care Instructions/parameters Supplies/Vendors Planned assessments Expected outcomes Status of intervention 23
24 The MAP Master All-care Plan Care Plan Decision Modifiers Patient/family preferences (values, priorities, wishes, adv directives, expectations, etc ) Patient situation (access to care, support, resources, setting, transportation, etc ) Patient allergies/intolerances Health Conditions/ Concerns Active Problems Risks/Concerns: Wellness Barriers Injury (e.g. falls) Illness (e.g. ulcers, cancer, stroke, hypoglycemia, hepatitis, diarrhea, depression, etc ) Item #1 Goals Desired outcomes and milestones Readiness Prognosis Related Interventions Progress 0 0 Patient Status 0 Functional Master Cognitive All-care Plan 0 Physical Item #2 Environmental Relationship (e.g. Goal-for-Problem, Intervention-for- Problem, Goal-for-Intervention, Performing Team Memberfor-Intervention, Performing Team Member-for-Assessment, Team Member Responsible-for-Problem, Team Member Following-Problem, Problem-Problem Causality, etc ) Interventions/Actions (e.g. medications, wound care, procedures, tests, diet, behavior changes, exercise, consults, rehab, calling MD for symptoms, education, anticipatory guidance, services, support, etc ) Start/stop date, interval Authorizing/responsible parties/roles/contact info Setting of care Instructions/parameters Supplies/Vendors Planned assessments Expected outcomes Status of intervention 24
 Illness (e.g. ulcers, cancer, stroke, hypoglycemia, hepatitis, diarrhea, Who on my Care Team is taking care of my wound?")
25 The MAP Master All-care Plan enables many views Health Conditions/ Concerns Active Problems Risks/Concerns: Wellness Barriers Injury (e.g. falls) Illness (e.g. ulcers, cancer, stroke, hypoglycemia, hepatitis, diarrhea, Who on my Care Team is taking care of my wound? depression, etc ) Item #1 Item #2 Care Plan Decision Modifiers Patient/family preferences (values, priorities, wishes, adv directives, expectations, etc ) Patient situation (access to care, support, resources, setting, transportation, etc ) Patient allergies/intolerances 0 Which problems 0 am I responsible for? Goals Desired outcomes and milestones Readiness Prognosis Related Interventions Progress What problems 0 are treated by this intervention and what 0 are the goals of treatment? Patient Status Functional Master Cognitive All-care Plan Physical Environmental Relationship (e.g. Goal-for-Problem, Intervention-for- Problem, Goal-for-Intervention, Performing Team Memberfor-Intervention, Performing Team Member-for-Assessment, Team Member Responsible-for-Problem, Team Member Following-Problem, Problem-Problem Causality, etc ) Interventions/Actions (e.g. medications, wound care, procedures, tests, diet, behavior changes, exercise, consults, rehab, calling MD for symptoms, education, anticipatory guidance, services, support, etc ) Start/stop date, interval Authorizing/responsible parties/roles/contact info Setting of care Instructions/parameters Supplies/Vendors Planned assessments What Expected interventions outcomes are in place for this health concern? Status of intervention Patient Family Physicians Non-physician Nursing Coordinators Providers 25
26 Disease Progression Care Plan Decision Modifiers Patient/family preferences (values, priorities, wishes, adv directives, expectations, etc ) Patient situation (access to care, support, resources, setting, transportation, etc ) Patient allergies/intolerances Care Plan Health Conditions/ Concerns Active Problems Risks/Concerns: Wellness Barriers Injury (e.g. falls) Illness (e.g. ulcers, cancer, stroke, hypoglycemia, hepatitis, diarrhea, depression, etc ) Risks Risk Factors Age, gender Significant Past Medical/Surgical Hx Family Hx, Race/Ethnicity, Genetics Historical exposures/lifestyle (e.g. alcohol, smoke, radiation, diet, exercise, workplace, sexual ) Prioritize Decision Support Goals Desired outcomes and milestones Readiness Prognosis Related Interventions Progress Patient Status Functional Cognitive Physical Environmental Side effects Orders, etc.. Decision Support Assessments Outcomes Questions? Interventions/Actions (e.g. medications, wound care, procedures, tests, diet, behavior changes, exercise, consults, rehab, calling MD for symptoms, education, anticipatory guidance, services, support, etc ) Start/stop date, interval Authorizing/responsible parties/roles/contact info Setting of care Instructions/parameters Supplies/Vendors Planned assessments Expected outcomes Status of intervention 26
27 Part 2: Alignment to HL7 Domain Analysis Model (DAM) To be continued
Interoperability and Patient Centred Care Coordination. Russell Leftwich, MD
 Interoperability and Patient Centred Care Coordination Russell Leftwich, MD Agenda The data of care coordination Interoperability Clinical information models and FHIR profiles The path ahead Coordination
Interoperability and Patient Centred Care Coordination Russell Leftwich, MD Agenda The data of care coordination Interoperability Clinical information models and FHIR profiles The path ahead Coordination
Taking Lessons on Care Coordination from Professional Sports
 Taking Lessons on Care Coordination from Professional Sports PANELISTS Dr. Russell Leftwich - Chief Medical Informatics Officer, Tennessee Office of ehealth Initiatives MODERATOR Kate Berry Chief Executive
Taking Lessons on Care Coordination from Professional Sports PANELISTS Dr. Russell Leftwich - Chief Medical Informatics Officer, Tennessee Office of ehealth Initiatives MODERATOR Kate Berry Chief Executive
IMPACT - Connecting Nursing Facilities and Home Care to the Healthcare System of the Future
 IMPACT - Connecting Nursing Facilities and Home Care to the Healthcare System of the Future MA Health Data Consortium CIO Forum January 17 th, 2013 Drs. Larry Garber and Terry O Malley Agenda IMPACT addressing
IMPACT - Connecting Nursing Facilities and Home Care to the Healthcare System of the Future MA Health Data Consortium CIO Forum January 17 th, 2013 Drs. Larry Garber and Terry O Malley Agenda IMPACT addressing
NQF HIT Critical Paths: Care Coordination. Webinar October 15, 2012
 NQF HIT Critical Paths: Care Coordination Webinar 1 Speakers Rita M. Mangione Smith, MD MPH Professor of Pediatrics and Adjunct Professor of Health Services, Seattle Children's Research Institute, Seattle,
NQF HIT Critical Paths: Care Coordination Webinar 1 Speakers Rita M. Mangione Smith, MD MPH Professor of Pediatrics and Adjunct Professor of Health Services, Seattle Children's Research Institute, Seattle,
and the Movement Towards Acute Care Data Transfer June 5 th, 2013 Larry Garber, M.D. Reliant Medical Group George Richardson CIO, VNA Care Network
 The Federal IMPACT Project and the Movement Towards Uniform Electronic Post- Acute Care Data Transfer New England Home Care Conference June 5 th, 2013 Larry Garber, M.D. Reliant Medical Group George Richardson
The Federal IMPACT Project and the Movement Towards Uniform Electronic Post- Acute Care Data Transfer New England Home Care Conference June 5 th, 2013 Larry Garber, M.D. Reliant Medical Group George Richardson
12/7/2014 L25. These presenters have nothing to disclose
 L25 These presenters have nothing to disclose Accountable Care Communities for Frail Elders Joanne Lynn, MD, Altarum Institute Brenda Schmitthenner, San Diego County Aging and Independence Services Mimi
L25 These presenters have nothing to disclose Accountable Care Communities for Frail Elders Joanne Lynn, MD, Altarum Institute Brenda Schmitthenner, San Diego County Aging and Independence Services Mimi
Town Hall Meeting on Health
 10/7/2013 Town Hall Meeting on Health IT Interoperability, Standards & Certification Alisa Ray, Executive Director and CEO, CCHIT aray@cchit.org National Association for Home Care & Hospice Annual Meeting
10/7/2013 Town Hall Meeting on Health IT Interoperability, Standards & Certification Alisa Ray, Executive Director and CEO, CCHIT aray@cchit.org National Association for Home Care & Hospice Annual Meeting
11/25/2014. Session: L25. These presenters have nothing to disclose
 Session: L25 These presenters have nothing to disclose Accountable Care Communities for Frail Elders Joanne Lynn, MD, Altarum Institute Brenda Schmitthenner, San Diego County Aging and Independence Services
Session: L25 These presenters have nothing to disclose Accountable Care Communities for Frail Elders Joanne Lynn, MD, Altarum Institute Brenda Schmitthenner, San Diego County Aging and Independence Services
Using Data to Promote Continuity of Care and Increase Accountability
 Using Data to Promote Continuity of Care and Increase Accountability USING DATA TO PROMOTE CONTINUITY OF CARE AND INCREASE ACCOUNTABILITY KAREN WOLK FEINSTEIN, PHD PRESIDENT AND CHIEF EXECUTIVE OFFICER
Using Data to Promote Continuity of Care and Increase Accountability USING DATA TO PROMOTE CONTINUITY OF CARE AND INCREASE ACCOUNTABILITY KAREN WOLK FEINSTEIN, PHD PRESIDENT AND CHIEF EXECUTIVE OFFICER
Implementing Health Information Exchange in the Long-term and Post Acute Care Community
 Implementing Health Information Exchange in the Long-term and Post Acute Care Community Perspectives for LTPAC Providers and their Affiliated Organizations Webinar December 12, 2012 To ask a question during
Implementing Health Information Exchange in the Long-term and Post Acute Care Community Perspectives for LTPAC Providers and their Affiliated Organizations Webinar December 12, 2012 To ask a question during
IT Enabled Quality Measurement IOM Dec 2012
 IT Enabled Quality Measurement IOM Dec 2012 Kevin Larsen MD, FACP Medical Director of Meaningful Use, ONC December 6, 2012 Our National Quality Strategy Aims Better Health for the Population Better Care
IT Enabled Quality Measurement IOM Dec 2012 Kevin Larsen MD, FACP Medical Director of Meaningful Use, ONC December 6, 2012 Our National Quality Strategy Aims Better Health for the Population Better Care
Health IT Council and Advisory Committee Meeting. June 18, 2012 One Ashburton Place, 21 st Floor Boston, MA
 Health IT Council and Advisory Committee Meeting June 18, 2012 One Ashburton Place, 21 st Floor Boston, MA Agenda I. Approval of April 30, 2011 minutes (HIT Council Motion) II. Introduction of Laurance
Health IT Council and Advisory Committee Meeting June 18, 2012 One Ashburton Place, 21 st Floor Boston, MA Agenda I. Approval of April 30, 2011 minutes (HIT Council Motion) II. Introduction of Laurance
Thinking Ahead in Post Acute Care
 Thinking Ahead in Post Acute Care Stella Mandl, RN Technical Advisor Division of Chronic and Post Acute Care Center for Clinical Standards and Quality Center for Medicare & Medicaid Services Stella.mandl@cms.hhs.gov
Thinking Ahead in Post Acute Care Stella Mandl, RN Technical Advisor Division of Chronic and Post Acute Care Center for Clinical Standards and Quality Center for Medicare & Medicaid Services Stella.mandl@cms.hhs.gov
Responsible Entity The owner of the project HealthShare Exchange of Southeastern Pennsylvania
 HealthShare Exchange of Southeastern Pennsylvania -- Examples of Successful Interoperability Automated Care Team Finder Profile Element Description Responsible Entity The owner of the project HealthShare
HealthShare Exchange of Southeastern Pennsylvania -- Examples of Successful Interoperability Automated Care Team Finder Profile Element Description Responsible Entity The owner of the project HealthShare
Medicare & Medicaid EHR Incentive Programs
 Medicare & Medicaid EHR Incentive Programs Puerto Rico Health & Insurance Conference 2012 Economic Transformation in Health Thomas Novak Health Information Technology for Economic & Clinical Health Centers
Medicare & Medicaid EHR Incentive Programs Puerto Rico Health & Insurance Conference 2012 Economic Transformation in Health Thomas Novak Health Information Technology for Economic & Clinical Health Centers
Winning at Care Coordination Using Data-Driven Partnerships
 Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
Idriz Limaj, LNHA, RN Chief Operating Officer Winning at Care Coordination Using Data-Driven Partnerships Session #166, February 22, 2017 1 Steven Littlehale, MS, GCNS-BC EVP & Chief Clinical Officer Speaker
January 04, Submitted Electronically
 January 04, 2016 Submitted Electronically Mr. Andy Slavitt Acting Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
January 04, 2016 Submitted Electronically Mr. Andy Slavitt Acting Administrator Centers for Medicare & Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
Transforming Health Care with Health IT
 Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
ARRA New Opportunities for Community Mental Health
 ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
Blending Behavioral Health and Primary Care. Applying the Model. Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist
 Blending Behavioral Health and Primary Care Applying the Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Overview Introducing the Model to Patients Key Components
Blending Behavioral Health and Primary Care Applying the Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Overview Introducing the Model to Patients Key Components
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
HSX Meaningful Use Support of Transitions of Care
 HSX Meaningful Use Support of Transitions of Care Pam Clarke, Senior Director of Engagement and Adoption Daniel Wilt, Senior Director of Information Technology HSX: Making connections for a collaborative,
HSX Meaningful Use Support of Transitions of Care Pam Clarke, Senior Director of Engagement and Adoption Daniel Wilt, Senior Director of Information Technology HSX: Making connections for a collaborative,
COMPETITION #SON-CLIN-2017 Clinical Instructor Positions - Anticipatory Pool
 COMPETITION #SON-CLIN- Positions - Anticipatory Pool - Applications are invited for an anticipatory staffing process for an indeterminate number of clinical instructor positions in the fall term, winter
COMPETITION #SON-CLIN- Positions - Anticipatory Pool - Applications are invited for an anticipatory staffing process for an indeterminate number of clinical instructor positions in the fall term, winter
IMPROVING MEDICATION RECONCILIATION WITH STANDARDS
 Presented by NCPDP and HIMSS for the Pharmacy Informatics Community IMPROVING MEDICATION RECONCILIATION WITH STANDARDS December 13, 2012 Keith Shuster, Manager, Acute Pharmacy Services, Norwalk Hospital
Presented by NCPDP and HIMSS for the Pharmacy Informatics Community IMPROVING MEDICATION RECONCILIATION WITH STANDARDS December 13, 2012 Keith Shuster, Manager, Acute Pharmacy Services, Norwalk Hospital
Health Information Exchange Activities for LTPAC and Behavioral Health Communities
 Health Information Exchange Activities for LTPAC and Behavioral Health Communities ASPE Sponsored Webinar December 4, 2012 To ask a question during the live webinar 1) Post a question at any time in the
Health Information Exchange Activities for LTPAC and Behavioral Health Communities ASPE Sponsored Webinar December 4, 2012 To ask a question during the live webinar 1) Post a question at any time in the
Activity Based Cost Accounting and Payment Bundling
 Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Activity Based Cost Accounting and Payment Bundling 1 Agenda Introduction of Speakers Fast Facts about Jewish Senior Life/Jewish Home of Rochester Determining the need and uses for an Activity Based Cost
Project Narrative Improving Massachusetts Post Acute Care Transfers (IMPACT)
") Project Narrative Improving Massachusetts Post Acute Care Transfers (IMPACT) Section 1: Understanding of Project Purpose The healthcare system in the United States reflects significant patient safety and
Project Narrative Improving Massachusetts Post Acute Care Transfers (IMPACT) Section 1: Understanding of Project Purpose The healthcare system in the United States reflects significant patient safety and
LET S SEE HOW IT MIGHT HAVE GONE..
 Would watching the Jetson s have given you any prediction on the future for OASIS? Presented by: Fern Dewert, R.N., O.E.C., C.O.S.C, & Joyce Rackers, R.N., B.S.N, C.O.S.C Bureau of Home Care & Rehabilitative
Would watching the Jetson s have given you any prediction on the future for OASIS? Presented by: Fern Dewert, R.N., O.E.C., C.O.S.C, & Joyce Rackers, R.N., B.S.N, C.O.S.C Bureau of Home Care & Rehabilitative
HIT Glossary and Acronym List
 HIT Glossary and Acronym List November 2011 FACT SHEET ACA Patient Protection and Affordable Care Act (see PPACA). ACO Accountable Care Organization: A group of health care providers (e.g. primary care,
HIT Glossary and Acronym List November 2011 FACT SHEET ACA Patient Protection and Affordable Care Act (see PPACA). ACO Accountable Care Organization: A group of health care providers (e.g. primary care,
Emerging Issues in Post Acute Care Trends
 Emerging Issues in Post Acute Care Trends Lavonne Elston, PT Senior Director of Operations & Strategic Initiatives Skilled Nursing & Rehabilitation Kingston HealthCare Company April 28, 2016 Disclosures
Emerging Issues in Post Acute Care Trends Lavonne Elston, PT Senior Director of Operations & Strategic Initiatives Skilled Nursing & Rehabilitation Kingston HealthCare Company April 28, 2016 Disclosures
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
RE: Request for Comments Regarding Meaningful Use Stage 2
 February 25, 2011 Department of Health and Human Services Office of the National Coordinator for Health Information Technology Attention: Joshua Seidman Mary Switzer Building 3330 C Street SW, Suite 1200
February 25, 2011 Department of Health and Human Services Office of the National Coordinator for Health Information Technology Attention: Joshua Seidman Mary Switzer Building 3330 C Street SW, Suite 1200
Preparing Your Infrastructure for New Payment Models
 Preparing Your Infrastructure for New Payment Models For more information about WEDI webinars or if you are interested in speaking, please contact Samantha Holvey sholvey@wedi.org JANUARY 29: Assessing
Preparing Your Infrastructure for New Payment Models For more information about WEDI webinars or if you are interested in speaking, please contact Samantha Holvey sholvey@wedi.org JANUARY 29: Assessing
Patient-Centered Specialty Practice: Building the Medical Neighborhood
 Patient-Centered Specialty Practice: Building the Medical Neighborhood Margaret E. O Kane President, National Committee for Quality Assurance June 6, 2014 1 Overview Central challenge: Creating systems
Patient-Centered Specialty Practice: Building the Medical Neighborhood Margaret E. O Kane President, National Committee for Quality Assurance June 6, 2014 1 Overview Central challenge: Creating systems
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Via Electronic Submission to:
 Via Electronic Submission to: https://www.healthit.gov/isa/iii-j-consumer-accessexchangehealth-information November 20, 2017 Office of the National Coordinator Department of Health and Human Services Hubert
Via Electronic Submission to: https://www.healthit.gov/isa/iii-j-consumer-accessexchangehealth-information November 20, 2017 Office of the National Coordinator Department of Health and Human Services Hubert
Meaningful Use Stage 2
 Meaningful Use Stage 2 Objectives Gain understanding of the changes Focus on Transitions in Care and Patient Engagement Recognize the increasing HIE role Who Are You? What is YOUR Need Today? A. Office
Meaningful Use Stage 2 Objectives Gain understanding of the changes Focus on Transitions in Care and Patient Engagement Recognize the increasing HIE role Who Are You? What is YOUR Need Today? A. Office
Stage 2 Meaningful Use Final Rule CPeH Advocacy Opportunities
 Stage 2 Meaningful Use Final Rule CPeH Advocacy Opportunities August 29, 2012 Agenda Review EHR Incentive Program and Intended Purpose Walk through Stage 2 Final Rule Changes to Stage 1 Stage 2 Criteria
Stage 2 Meaningful Use Final Rule CPeH Advocacy Opportunities August 29, 2012 Agenda Review EHR Incentive Program and Intended Purpose Walk through Stage 2 Final Rule Changes to Stage 1 Stage 2 Criteria
Readmission Reduction: Patient Interviews. KHA Quality Conference March, 2018
 Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
Readmission Reduction: Patient Interviews KHA Quality Conference March, 2018 Initial Driver Diagram Use Data and Root Cause Analysis to drive Continuous Improvement Analyze data to inform targeting approach
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT
 Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
Rick Bikowski MD Chief Quality Officer, EVMS Medical Group CARE MANAGEMENT Medicare Wellness Visit: Background Until recently, Medicare did not pay for preventive services Welcome to Medicare visit initiated
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
EHR Data Integration and Seamless Exchange of Clinical Information to Enable Next-Generation Pharmacy Services
 EHR Data Integration and Seamless Exchange of Clinical Information to Enable Next-Generation Pharmacy Services Presenter: Shelly Spiro RPh, FASCP Pharmacy HIT, Executive Director Objectives 1. Explain
EHR Data Integration and Seamless Exchange of Clinical Information to Enable Next-Generation Pharmacy Services Presenter: Shelly Spiro RPh, FASCP Pharmacy HIT, Executive Director Objectives 1. Explain
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
Conversation Starters: Research Insights from Clinicians and Patients on Conversations About End-of-Life Care and Wishes
 Conversation Starters: Research Insights from Clinicians and Patients on Conversations About End-of-Life Care and Wishes Webinar December 1, 2016 Logistics Audio: Streaming audio is available through your
Conversation Starters: Research Insights from Clinicians and Patients on Conversations About End-of-Life Care and Wishes Webinar December 1, 2016 Logistics Audio: Streaming audio is available through your
Enhancing Patient Care through Effective and Efficient Nursing Documentation
 Enhancing Patient Care through Effective and Efficient Nursing Documentation Session NI1, March 5, 2018 Jane Englebright, PhD, RN, CENP, FAAN HCA Senior Vice President & Chief Nurse Executive 1 Conflict
Enhancing Patient Care through Effective and Efficient Nursing Documentation Session NI1, March 5, 2018 Jane Englebright, PhD, RN, CENP, FAAN HCA Senior Vice President & Chief Nurse Executive 1 Conflict
Nutrition Informatics: Dietitians improving practice through technology
 Nutrition Informatics: Dietitians improving practice through technology Ben Atkinson, MS RDN April 17, 2018 4/4/2018 Speaker Disclosure Receives travel reimbursement from the AND ISC. 2 1 Speaker Ben Atkinson
Nutrition Informatics: Dietitians improving practice through technology Ben Atkinson, MS RDN April 17, 2018 4/4/2018 Speaker Disclosure Receives travel reimbursement from the AND ISC. 2 1 Speaker Ben Atkinson
HIE & Interoperability: Roadmap to Continuum of Care Michael McPherson MU Coordinator KDHE
 HIE & Interoperability: Roadmap to Continuum of Care Michael McPherson MU Coordinator KDHE DISCLAIMER: The views and opinions expressed in this presentation are those of the author and do not necessarily
HIE & Interoperability: Roadmap to Continuum of Care Michael McPherson MU Coordinator KDHE DISCLAIMER: The views and opinions expressed in this presentation are those of the author and do not necessarily
2015 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 EHR Documentation and CDI: What to Expect and How to Successfully Handle the Transition Sam Antonios, MD, FACP, FHM, CCDS CDI and ICD 10 Physician Advisor Hospital CMIO Via Christi Health Wichita, Kansas
EHR Documentation and CDI: What to Expect and How to Successfully Handle the Transition Sam Antonios, MD, FACP, FHM, CCDS CDI and ICD 10 Physician Advisor Hospital CMIO Via Christi Health Wichita, Kansas
Reducing Medicaid Readmissions
 Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Reducing Medicaid Readmissions Webinar 1: Medicaid Readmissions 101 Amy E. Boutwell, MD MPP Co-Principal Investigator AHRQ Reducing Medicaid Readmissions Project February 25 2015 Agenda Introduction to
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Breaking HIE Barriers
 Breaking HIE Barriers Session #20, February 20, 2017 Robert M. Cothren, PhD, Executive Director California Association of Health Information Exchanges 1 Speaker Introduction Robert M. Cothren, PhD Executive
Breaking HIE Barriers Session #20, February 20, 2017 Robert M. Cothren, PhD, Executive Director California Association of Health Information Exchanges 1 Speaker Introduction Robert M. Cothren, PhD Executive
Elmhurst Memorial Healthcare Successfully Attests to Stage 1 Meaningful Use
 Welcome! Elmhurst Memorial Healthcare Successfully Attests to Stage 1 Meaningful Use Presented by: Larry Katzovitz & Judy Triano Elmhurst Memorial Healthcare Kay Jackson (978) 805-3104 Kay.Jackson@iatric.com
Welcome! Elmhurst Memorial Healthcare Successfully Attests to Stage 1 Meaningful Use Presented by: Larry Katzovitz & Judy Triano Elmhurst Memorial Healthcare Kay Jackson (978) 805-3104 Kay.Jackson@iatric.com
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
Kentucky HIE Examples of Successful Interoperability Description Template
 Kentucky HIE Examples of Successful Interoperability Description Template Profile Element Description Responsible Entity The owner of the project The responsible entities or owners of the project are the
Kentucky HIE Examples of Successful Interoperability Description Template Profile Element Description Responsible Entity The owner of the project The responsible entities or owners of the project are the
Copyright All Rights Reserved.
 Copyright 2012. All Rights Reserved. No part of this document may be reproduced or shared with anyone outside of your organization without prior written consent from the author(s). You may contact us at
Copyright 2012. All Rights Reserved. No part of this document may be reproduced or shared with anyone outside of your organization without prior written consent from the author(s). You may contact us at
1 - ICU EVALUATION. inconsistently synthesizes accurate, thorough histories, exams, and data to diagnose critically ill patients
 - ICU EVALUATION NOTE: LEVEL behaviors constitute critical deficiencies. Most beginning R's will be at level. Most R' will be at LEVELS -4. Graduating R's should be at LEVEL 4 across most subcompetencies.
- ICU EVALUATION NOTE: LEVEL behaviors constitute critical deficiencies. Most beginning R's will be at level. Most R' will be at LEVELS -4. Graduating R's should be at LEVEL 4 across most subcompetencies.
INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014
 INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014 Intergy Meaningful Use 2014 User Guide 2 Copyright 2014 Greenway Health, LLC. All rights reserved. This document and the information it contains
INTERGY MEANINGFUL USE 2014 STAGE 1 USER GUIDE Spring 2014 Intergy Meaningful Use 2014 User Guide 2 Copyright 2014 Greenway Health, LLC. All rights reserved. This document and the information it contains
Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12
 New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
Building Coordinated, Patient Centered Care Management Teams
 Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
What is Value-Based Care
 Genesis HealthCare Value-Based Care Initiatives and BPCI Model 3 Aug 4, 2017 Copyright 2017 by Genesis HealthCare LLC. All Rights Reserved. What is Value-Based Care 2 Value-based care delivery is an approach
Genesis HealthCare Value-Based Care Initiatives and BPCI Model 3 Aug 4, 2017 Copyright 2017 by Genesis HealthCare LLC. All Rights Reserved. What is Value-Based Care 2 Value-based care delivery is an approach
Developing Primary Care Measures that Matter: Creating a CHC Primary Care Dashboard. Clinical Team Advisory Group
 Developing Primary Care Measures that Matter: Creating a CHC Primary Care Dashboard Clinical Team Advisory Group CHC and AHAC ED Network Committee Structure Board ED Network (CHC and AHAC) Association
Developing Primary Care Measures that Matter: Creating a CHC Primary Care Dashboard Clinical Team Advisory Group CHC and AHAC ED Network Committee Structure Board ED Network (CHC and AHAC) Association
CMS EHR Incentive Programs Overview
 CMS EHR Incentive Programs Overview Elizabeth Holland and Robert Anthony Session 20, Room 320 Monday, February 24 at 11:30 AM DISCLAIMER: The views and opinions expressed in this presentation are those
CMS EHR Incentive Programs Overview Elizabeth Holland and Robert Anthony Session 20, Room 320 Monday, February 24 at 11:30 AM DISCLAIMER: The views and opinions expressed in this presentation are those
Overcome Challenges/Obstacles to Achieving Interoperability
 Overcome Challenges/Obstacles to Achieving Interoperability Session #86 Tuesday, February 21, 2017 Kathleen Sheehan, Program Director, Universal Health Services, Inc. Sindhu R. Kammath, MD, Clinical Informaticist,
Overcome Challenges/Obstacles to Achieving Interoperability Session #86 Tuesday, February 21, 2017 Kathleen Sheehan, Program Director, Universal Health Services, Inc. Sindhu R. Kammath, MD, Clinical Informaticist,
Provider Perspectives on Patient Information: Results of 2017 Survey. October 19, 2017
 Provider Perspectives on Patient Information: Results of 2017 Survey October 19, 2017 1 Agenda Welcome and Introductions Jennifer Covich Bordenick, CEO, ehealth Initiative Comments from National Coordinator
Provider Perspectives on Patient Information: Results of 2017 Survey October 19, 2017 1 Agenda Welcome and Introductions Jennifer Covich Bordenick, CEO, ehealth Initiative Comments from National Coordinator
Meaningful Use Stages 1 & 2
 Meaningful Use Stages 1 & 2 Making Sure You Get the Most Out of Your EHR Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Meaningful Use Stages & Incentive Program Timing 2014 Changes to
Meaningful Use Stages 1 & 2 Making Sure You Get the Most Out of Your EHR Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Meaningful Use Stages & Incentive Program Timing 2014 Changes to
Merit-Based Incentive Payment System (MIPS) Promoting Interoperability Performance Category Transition Measure 2018 Performance Period
 Promoting Interoperability Performance Category Transition Measure 2018 Performance Period") Merit-Based Incentive Payment System (MIPS) Promoting Interoperability Performance Category Transition Measure 2018 Performance Period Objective: Measure: Measure ID: Patient Electronic Access View, Download
Merit-Based Incentive Payment System (MIPS) Promoting Interoperability Performance Category Transition Measure 2018 Performance Period Objective: Measure: Measure ID: Patient Electronic Access View, Download
CY 2018 Home Health PPS Proposed Rule
 CY 2018 Home Health PPS Proposed Rule Rochelle Archuleta & Caitlin Gillooley AHA Policy August 24, 2017 CY 2018 Proposed Rule Published in July 28 Federal Register Net Reduction: 0.4%, -$80m Same for facility-based
CY 2018 Home Health PPS Proposed Rule Rochelle Archuleta & Caitlin Gillooley AHA Policy August 24, 2017 CY 2018 Proposed Rule Published in July 28 Federal Register Net Reduction: 0.4%, -$80m Same for facility-based
Community-based Care Coordination (CCC) Maturity Assessment RidgePointe Healthcare District
 Maturity Assessment RidgePointe Healthcare District") Who/What Program Elements Level 1. Beginning Level 2. Progressing Level 3. Intermediate Level 4. Advanced Organization(s) sponsoring CCC Providers Community services Patients (pts) Payers A. LEADERSHIP
Who/What Program Elements Level 1. Beginning Level 2. Progressing Level 3. Intermediate Level 4. Advanced Organization(s) sponsoring CCC Providers Community services Patients (pts) Payers A. LEADERSHIP
CMS-0044-P; Proposed Rule: Medicare and Medicaid Programs; Electronic Health Record Incentive Program Stage 2
 May 7, 2012 Submitted Electronically Ms. Marilyn Tavenner Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
May 7, 2012 Submitted Electronically Ms. Marilyn Tavenner Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Room 445-G, Hubert H. Humphrey Building
The Key Principles And Characteristics Of An Effective Hospital Medicine Group
 The Key Principles And Characteristics Of An Effective Hospital Medicine Group Management Infra. Adequate Resources Effective Leadership Engaged Hospitalists Quality, Safety, & Efficiency Satisfaction
The Key Principles And Characteristics Of An Effective Hospital Medicine Group Management Infra. Adequate Resources Effective Leadership Engaged Hospitalists Quality, Safety, & Efficiency Satisfaction
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM. November 20, 2015
 THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
THE REIMBURSEMENT SHIFT: PREPARING YOUR PRACTICE FOR PATIENT-CENTERED PAYMENT REFORM November 20, 2015 TODAYS PRESENTERS Kavon Kaboli Consultant Galen Healthcare Solutions Cece Teague Consultant Galen
OASIS-B1 and OASIS-C Items Unchanged, Items Modified, Items Dropped, and New Items Added.
 Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
2015 MU Reporting Overview of Requirements/Tasks
 2015 MU Reporting Overview of Requirements/Tasks Presented by: Patty Kosednar, HTS MU Consultant Co-Hosted by Sarah Leake, HTS Quality Reporting and Payment Reform Specialist 11/04/2015 1-2 PM MST HTS,
2015 MU Reporting Overview of Requirements/Tasks Presented by: Patty Kosednar, HTS MU Consultant Co-Hosted by Sarah Leake, HTS Quality Reporting and Payment Reform Specialist 11/04/2015 1-2 PM MST HTS,
2018 Conditions of Participation. OASIS-D in 2019
 The IMPACAT Act of 2014 & Progressing from the 2018 Conditions of Participation to the Next Big Change: OASIS-D in 2019 Sharon Hamilton MS, RN, NLCP-C, CFDS OBJECTIVES Briefly explain the requirements
The IMPACAT Act of 2014 & Progressing from the 2018 Conditions of Participation to the Next Big Change: OASIS-D in 2019 Sharon Hamilton MS, RN, NLCP-C, CFDS OBJECTIVES Briefly explain the requirements
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention
 Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Stroke Patients: Transition From Hospital to Home
 Stroke Patients: Transition From Hospital to Home Lauren Pond RN CCM Administrative Director, Case Management Jennifer Thiesen RNP CCRN Director, Care Transitions Presenter Disclosure Information Lauren
Stroke Patients: Transition From Hospital to Home Lauren Pond RN CCM Administrative Director, Case Management Jennifer Thiesen RNP CCRN Director, Care Transitions Presenter Disclosure Information Lauren
UHF Quality Institute. Patient-Reported Outcomes in Primary Care New York PROPC-NY. Module 2 Webinar
 UHF Quality Institute Patient-Reported Outcomes in Primary Care New York PROPC-NY Module 2 Webinar Lucy Savitz, Assistant Vice President for Delivery System Science, Intermountain Healthcare January 24,
UHF Quality Institute Patient-Reported Outcomes in Primary Care New York PROPC-NY Module 2 Webinar Lucy Savitz, Assistant Vice President for Delivery System Science, Intermountain Healthcare January 24,
Medicare: This subset aligns with the requirements defined by CMS and is for the review of Medicare and Medicare Advantage beneficiaries
 InterQual Level of Care Criteria Subacute & SNF Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
InterQual Level of Care Criteria Subacute & SNF Criteria Review Process Introduction InterQual Level of Care Criteria support determining the appropriateness of admission, continued stay, and discharge
What Have we Learned from the Pioneer ACO Model?
 What Have we Learned from the Pioneer ACO Model? Sherly Binu, CMMI December 7, 2016 Disclaimers 2 This presentation was prepared as a tool to assist providers and is not intended to grant rights or impose
What Have we Learned from the Pioneer ACO Model? Sherly Binu, CMMI December 7, 2016 Disclaimers 2 This presentation was prepared as a tool to assist providers and is not intended to grant rights or impose
Meaningful Use - Modified Stage 2. Brett Paepke, OD David Wolfson Marni Anderson
 Meaningful Use - Modified Stage 2 Brett Paepke, OD David Wolfson Marni Anderson Wait! Where did Stage 1 and Stage 2 go? Traditional stages eliminated in late 2015 in order to: 1. reduce reporting requirements
Meaningful Use - Modified Stage 2 Brett Paepke, OD David Wolfson Marni Anderson Wait! Where did Stage 1 and Stage 2 go? Traditional stages eliminated in late 2015 in order to: 1. reduce reporting requirements
CMS Modifications to Meaningful Use in Final Rule. Slide materials and recording will be available after the webinar
 CMS Modifications to Meaningful Use in 2015-2017 Final Rule Denise Satterfield Practice Solutions Advisor December 2015 Welcome Slide materials and recording will be available after the webinar Submit
CMS Modifications to Meaningful Use in 2015-2017 Final Rule Denise Satterfield Practice Solutions Advisor December 2015 Welcome Slide materials and recording will be available after the webinar Submit
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver JULY 18, 2016
 Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
Post-Acute Care Networks: How to Succeed and Why Many Fail to Deliver HEALTH FORUM AND AHA LEADERSHIP SUMMIT JULY 18, 2016 SAN DIEGO, CALIFORNIA Please note that the views expressed are those of the conference
The Role of the Pharmacist in Value Based Health Care Systems. Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine
 The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
Clinical Summary. Empowering Extraordinary Patient Care
 Clinical Summary Empowering Extraordinary Patient Care All phone lines have been placed on mute To ask Questions during the Webcast Please enter them in the Questions section of your Webcast Control box
Clinical Summary Empowering Extraordinary Patient Care All phone lines have been placed on mute To ask Questions during the Webcast Please enter them in the Questions section of your Webcast Control box
TIPS FROM OUR CONSULTANT By: Joy Newby, LPN, CPC, PCS Newby Consulting
 TIPS FROM OUR CONSULTANT By: Joy Newby, LPN, CPC, PCS Newby Consulting CONFUSED ABOUT MEDICARE PREVENTATIVE VISITS? SO ARE YOUR PATIENTS! Congress legislated coverage for two preventive visits for Medicare
TIPS FROM OUR CONSULTANT By: Joy Newby, LPN, CPC, PCS Newby Consulting CONFUSED ABOUT MEDICARE PREVENTATIVE VISITS? SO ARE YOUR PATIENTS! Congress legislated coverage for two preventive visits for Medicare
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Data Segmentation for Privacy (DS4P)
") Data Segmentation for Privacy (DS4P) Where It s Been and Where It s Going Jeremy Maxwell, PhD Office of the Chief Privacy Officer Office of the National Coordinator for Health IT US Department of Health
Data Segmentation for Privacy (DS4P) Where It s Been and Where It s Going Jeremy Maxwell, PhD Office of the Chief Privacy Officer Office of the National Coordinator for Health IT US Department of Health
Medicare and Medicaid Programs: Electronic Health Record Incentive Program -- Stage 3 and Modifications to Meaningful Use in 2015 through 2017
 Medicare and Medicaid Programs: Electronic Health Record Incentive Program -- Stage 3 and Modifications to Meaningful Use in 2015 through 2017 and 2015 Edition Health Information Technology Certification
Medicare and Medicaid Programs: Electronic Health Record Incentive Program -- Stage 3 and Modifications to Meaningful Use in 2015 through 2017 and 2015 Edition Health Information Technology Certification
Under the MACRAscope:
 Under the MACRAscope: G08: Under the MACRAscope: MIPS and EHRs Robert Tennant, MA Director, HIT Policy, MGMA Government Affairs rtennant@mgma.org Learning Objectives This session will provide you with
Under the MACRAscope: G08: Under the MACRAscope: MIPS and EHRs Robert Tennant, MA Director, HIT Policy, MGMA Government Affairs rtennant@mgma.org Learning Objectives This session will provide you with
Meaningful Use Participation Basics for the Small Provider
 Meaningful Use Participation Basics for the Small Provider Vidya Sellappan Centers for Medicare & Medicaid Services Office of E-Health Standards and Services HIT Initiatives Group July 30, 2014 EHR INCENTIVE
Meaningful Use Participation Basics for the Small Provider Vidya Sellappan Centers for Medicare & Medicaid Services Office of E-Health Standards and Services HIT Initiatives Group July 30, 2014 EHR INCENTIVE
Outcomes Measurement in Long-Term Care (LTC)
") ASHA Short Course Outcomes Measurement in Long-Term Care (LTC) Bill Goulding, MS/CCC-SLP November 19, 2012 How Do We Show Value? Easy to measure! Not so easy! V $$$ A L Impact? Cost U Benefit E What do
ASHA Short Course Outcomes Measurement in Long-Term Care (LTC) Bill Goulding, MS/CCC-SLP November 19, 2012 How Do We Show Value? Easy to measure! Not so easy! V $$$ A L Impact? Cost U Benefit E What do
MEASURING POST ACUTE CARE OUTCOMES IN SNFS. David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015
 MEASURING POST ACUTE CARE OUTCOMES IN SNFS David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015 Principles Guiding Measure Selection PAC quality measures need to Reflect
MEASURING POST ACUTE CARE OUTCOMES IN SNFS David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015 Principles Guiding Measure Selection PAC quality measures need to Reflect
CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW
 Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Presented by AIRA June 21 st, 2011
 Presented by AIRA June 21 st, 2011 Rob Savage Northrop Grumman contractor supporting IISSB interoperability efforts V 2.5.1 Implementation Guide Support vocabulary needs for Immunization messaging Co-chair
Presented by AIRA June 21 st, 2011 Rob Savage Northrop Grumman contractor supporting IISSB interoperability efforts V 2.5.1 Implementation Guide Support vocabulary needs for Immunization messaging Co-chair
Mass HIway Use Case Workshop. Sean Kennedy Mass ehealth Institute Director, Health Information Exchange
 Mass HIway Use Case Workshop Sean Kennedy Mass ehealth Institute Director, Health Information Exchange Learning Objectives Communicate the benefits of a use case Identify a use case scenario / user story
Mass HIway Use Case Workshop Sean Kennedy Mass ehealth Institute Director, Health Information Exchange Learning Objectives Communicate the benefits of a use case Identify a use case scenario / user story
Improving the Quality of Care Coordination Across Settings
 Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Improving the Quality of Care Coordination Across Settings Eric A. Coleman, MD, MPH Associate Professor Divisions of Geriatric Medicine and Health Care Policy and Research University of Colorado Health
Rapid-Learning Healthcare Systems
 Rapid-Learning Healthcare Systems in silico Research and Best Practice Adoption in Promoting Rapid Learning Sharon Levine MD July 11, 2012 NIH Training Institute for Dissemination and Implementation Rapid-Learning
Rapid-Learning Healthcare Systems in silico Research and Best Practice Adoption in Promoting Rapid Learning Sharon Levine MD July 11, 2012 NIH Training Institute for Dissemination and Implementation Rapid-Learning
WPCC Workgroup. 2/20/2018 Meeting
 WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep