Positive Practice in Mental Health Collaborative Event In Partnership with
|
|
|
- Adela Burke
- 5 years ago
- Views:
Transcription
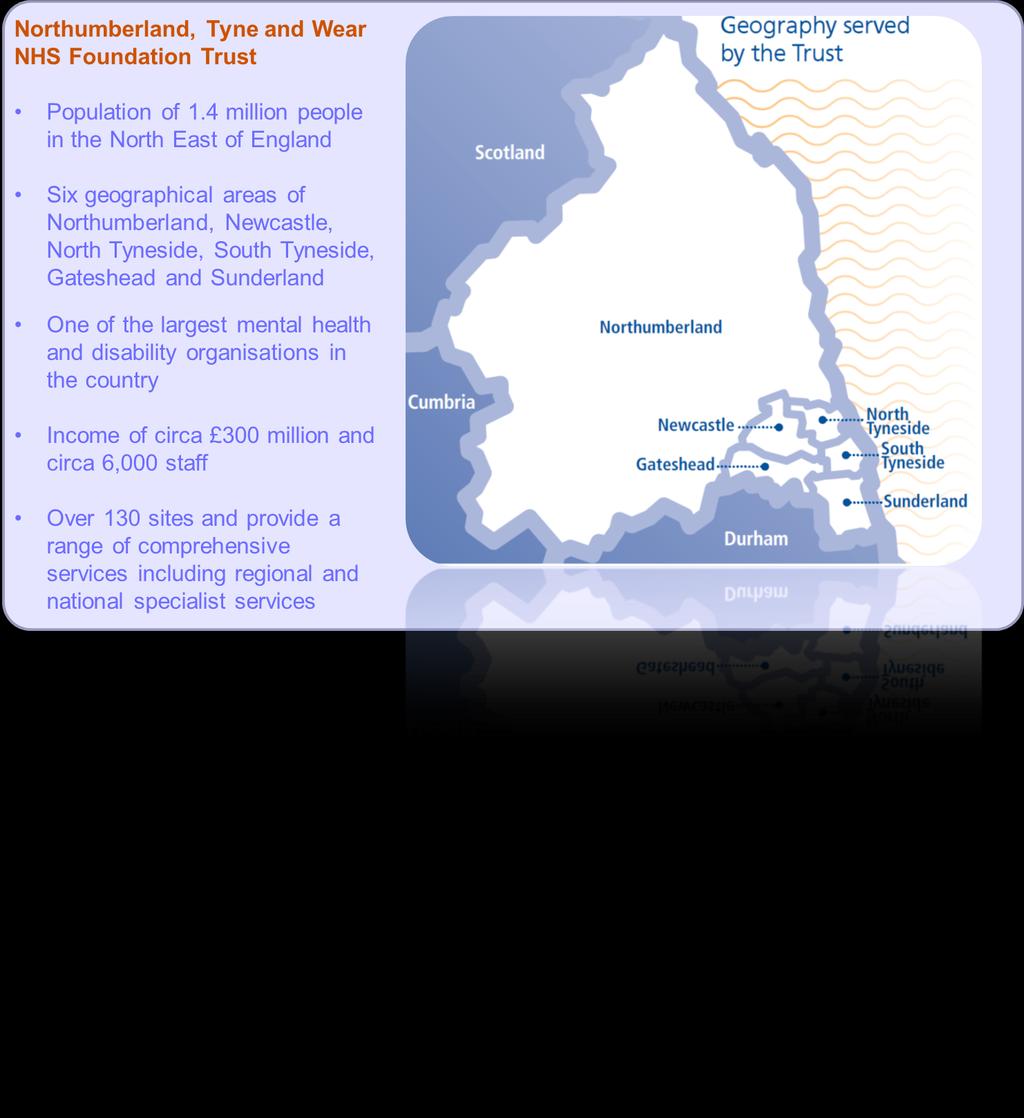
1 Positive Practice in Mental Health Collaborative Event In Partnership with Northumberland, Tyne and Wear NHS Foundation Trust Hertfordshire Partnership Foundation Trust Supported by Breakthrough
2 Introductions and setting the scene Tony Russell - Director of Breakthrough and Founder of Collaborative Gary O Hare - Executive Director of Nursing and Operations
3
4 Strategic Direction The environment in which we work: Quality -20% Cost Sustainability We have to improve quality for the patient We have to reduce our overall cost of doing so by 20% We aim to improve clinical effectiveness thus reducing reliance on inpatient beds We have to create sustainable services, delivered by sustainable organisations, operating in a sustainable system
5 What our partners have told us: We have to get much better at what we do and how we do it We have to get better at listening and acting on what people are telling us We have to be consistently good across all our services We need to get the patient quickly into the right services and then deliver the best outcome possible
6 What patients and carers have told us: Patient They want high-quality, safe care close to home They want inpatient services to be of a high standard They want services designed and operated around the needs of patients They want the patient to be truly at the centre They want to gain and re-gain independence, as far as possible


7 The need to realign and balance resources: At any time, 3% of patients are consuming 52% of resources Inpatient Services 92.2M NTW Whole costs Community Services 84.8M NTW Whole costs We spend in inpatient areas to the detriment of community services A few patients consume much of the resource Many in-patients perhaps don t need to be, but we lack the necessary community services to support them out of hospital We need to balance resources to maximise quality over cost
8 The Access Model Dr Carole Kaplan Transformation Programme Director
9 The Service Model Request for Help More Intensive Packages of Care Initial Response Initial evaluation regarding nature, risk, complexity and urgency of the problem Information & Advice Hospital Home Treatment Intensity Medium Security Psychiatric Intensive Care Low Security Specialist Ward Environment PICU Crisis Beds Acute Ward Low Security Intermediate In the Community beds Intermediate Facility Acute Ward Crisis Bed Challenging Behaviour Assessment Intensive Home At Home Treatment Intensive Challenging Home Behaviour Etc. Treatment Assessment Formulation & Treatment Planning Mild - severe non - psychotic Signposting to principal service pathway for assessment and formulation Very severe & complex nonpsychotic Psychosis Dementia Neuro - disability Learning Disability Children & Young People Substance Misuse Scaffolding Crisis Assessment Discharge
10 Principal Community Pathways A programme to design and implement new, evidence-based community pathways for adults and older people. Our ambition is high and is matched by the expectations of service users and carers. The new pathways will: Significantly improve quality for the patient Double current productive time of community services by redesigning current systems Enhance the skills of our workforce Improve ways of working and interfaces with partners Reduce reliance on inpatient beds and enable cost savings This is not achievable in isolation and to be successful we need it to be part of integrated work with partners
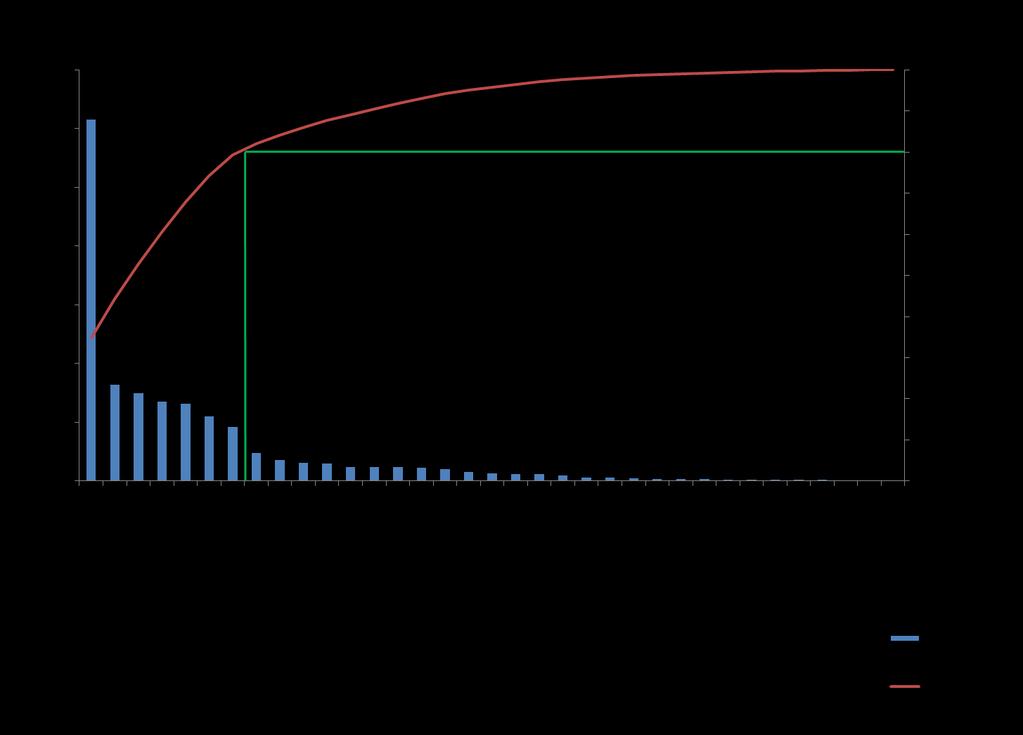
11 Phase 1: The case for change Sunderland was chosen as the location for the development of a new access model following discussions with service users, carers, GPs and commissioners. A key issue was that the Crisis team, commissioned to deliver assessment and support for serious mental health problems, was not responsive as it was saturated with responding to a wide variety of requests. A scoping exercise identified that only 35% of all contacts needed the response of the Crisis Team. 43% of the inappropriate contacts were for advice or help and often these were people clearly in need of support and signposting, but considered to be at low risk of requiring hospital admission.






12 Initial Response Team South of Tyne and Wear Information Collection & Routing Gateshead Rapid Response 11 Nurses Triage & Action GH UCT Home Based Treatment Assessment Gatekeeping ICTS OPS LD REQUEST FOR HELP South Tyneside Rapid Response 11 Nurses Triage & Action ST UCT Home Based Treatment Assessment Gatekeeping ICTS OPS LD ROUTING Sunderland Rapid Response 11 Nurses Triage & Action SL UCT Home Based Treatment Assessment Gatekeeping ICTS OPS LD

13 Phase 2 Model Urgent IRT Rapid Response 11 Nurses Triage & Action UCT Home Based Treatment Assessment Gatekeeping ICTS OPS LD Single Point of Referral Triage Team Noncomplex Clinical Diary Routine Complex Huddle Clinical Diary
14 Phase 1: The Model IRT to offer 24/7 Universal telephone access for requests for urgent help. No restrictions on who could refer Triage and Routing over the phone- (Mental Health and other local Services) Face to Face Triage (Rapid Response) if clear plan cannot be determined over the phone Seven Band 6 Nurses for Telephone and Rapid Response Five Band 3 Nurses for call handling and Rapid Response Use of digital dictation and 3G laptops for clinical documentation Flexible interchangeable roles and rotation between Crisis Team and IRT roles dependant on demand.
15 Phase 1: Benefits of IRT Quick and efficient responses to requests for help Effective routing to the correct services in and out of NTW Flexible and collaborative working with newly configured UCT which will focus on the work for which it is commissioned Reduction of clinician administration burden, and freeing time to care (mainly through adoption of digital dictation) Improving personal and clinical outcomes for people in crisis with mental ill health by reducing harm and premature mortality, improving patient safety and patient experience
16 Typical weekly activity Evaluation-IRT in numbers Incoming telephone calls 1000 Total Contacts 400 Home-based Treatment contacts 50 Crisis Assessments 100 Rapid Responses and growing 90% calls answered within 15 seconds >98% within 3 minutes (Average=9 Seconds) >80% rapid responses achieved in under one hour




17 Service User Experience Service Feedback Carer Feedback The Team were excellent Wonderful support! keep this very valuable service going Brilliant team! More manageable Staff Feedback Skills are valued GP Feedback Did the Initial Response Team meet your needs? A lot happier Spend more time Yes Fantastic a huge improvement!! No You should have done it before
18 Recovery through care coordination research Nicola Armstrong PCP Facilitator Lisa Matthews WRAP educator / volunteer
19 A 28 month project. The Research Working with NTW NHS Trust, local service user and carer organisations/network and Northumbria University. The views and experiences of service users and carers have driven this project right from the beginning. They have been researchers, collecting and analysing the data and are now sharing the findings. Training programme and accreditation Originally 85 postal questionnaires, leading to 52 service user, 30 carer and 18 professional interviews. Recovery and Care Coordination
20 The Data (Action Research) Collection of Qualitative and Quantitative Analysis Coding - Themes (Generate Questions) Confirmation of Themes Delphi Service User, Carer and Professional Interviews Service User, Carer and Professional Events Other Dissemination Toolkit IMPACT Co production Recovery and Care Coordination
21 Emancipatory Research Research Ethics Organic Tight structure Challenges hierarchies Free flowing Power sharing Political Culture Cash Regimented Bureaucratic Risk averse Traditionalist Recovery and Care Coordination

22 My Ethics Experience Recovery and Care Coordination
23 Delphi Data DELPHI STATEMENTS SERVICE USERS CARERS PROFESSIONALS Recovery is self-defined hope and personal meaning Strong agreement Strong agreement Weak agreement Strong support networks including family and friends increases recovery Moderate agreement Strong agreement Moderate agreement Recovery is a return to functioning at a level experienced before the disorder Disagreement Strong agreement Disagreement Service users should be active participants in care coordination Strong agreement Weak agreement Strong agreement Promoting recovery / mutually agreed goals is central to care coordination Strong agreement Strong agreement Weak agreement Lack of time care coordinators are able to spend in face to face contact inhibits good care coordination Strong agreement Strong agreement Disagreement Recovery and Care Coordination
24 Recovery Themes Services for life versus getting on with life Reactive versus proactive Involvement versus non involvement Keeping people safe versus positive opportunities Personal responsibility versus being cared for Hope versus hopelessness Recovery and Care Coordination
25 Recovery Quotes I think I m always going to be in the mental health system (Service User) I don t think there s such a thing (as recovery) in mental health...there is going from what the person was through the mental issues to being something different at the end (Carer) Its not a recovery focused plan and they re not recovering and both parties are stuck. The service user is stuck But actually the professional is stuck (Professional) Recovery and Care Coordination
26 Recovery Quotes I came into the service with the wrong idea. I came in looking for a fix... and slowly but surely discovered that there is no fix. I m going to have this for the rest of my entire life. I m managing it with medication and a different way of thinking (Service User) Recovery to me is a continuum it s affected so many different things. So wellness, recovery is a line people go up and down you have to take responsibility for yourself you have to trial it on your own and apply it in terms of your own recovery (Carer) so no matter what s wrong with you whether that includes the diagnosis or not the goal is for you to recover. Or, the goal might be for you to leave the service and the rest of your recovery might be done elsewhere (Professional) Recovery and Care Coordination
27 Care Coordination Themes What it is - confusion? Ticking boxes and/or face to face support The value of good care coordination The impact of poor care coordination The barriers of confidentiality Recovery and Care Coordination
28 Care Coordination Quote You know it just feels like I am accessing three separate services within one service that is meant to be working as part of a team (Service user) Care coordination isn't about the carer. cos there s been a lot of times where (the service user) has gone into different kinds of services; CBT, CPN, whatever else and they don t seem to communicate a lot with each other, so there s a lot of things get missed out (Carer) care coordination is not for care and treatment of the patient. Care coordination is the administrative process that is used to capture the care and treatment to patients (Professional) Recovery and Care Coordination
29 Care Coordination Quote I ve always been listened to and I felt they ve worked with me, they ve valued what my opinions are, I ve not been pushed into anything. I've not been treated as someone who hasn t got anything to give in my recovery or anything like that. (Service user) Well I think it was good because it was informative, you know, for me and also felt as though somebody else was keeping an eye on him (workers name) (Carer) Good care coordination is being able to negotiate a relationship where the person can say what they think and you can, as a worker, you can make mistakes, and get it wrong, because there is that trust and respect... (Professional) Recovery and Care Coordination



30 Recovery through Quality Care Coordination! Change in Culture Moving Forward Learning Together
31 Professional Professional Learning opportunities I think there needs to be investment in not just helping teams to be really robust and creative but a bit same approach for the team in the broader sense including service users and carers. Which is, for example, why this research project is so good, because it s an example of it. So it s not research by the professionals its research by a team. A whole team of service users, professionals, carers. PR17 I think that the times when it s gone really wrong for me is where the MDT haven t been aware of what each other are doing and certainly, the service user in the middle of that hasn t been aware of, you know, all of the different things that are or aren t happening, cos sometimes, its about, things I think people think are happening, but actually, they re not happening. PR16 Information to support We should all know who s involved in the care: what the care is and when it s next planned to be reviewed. Now that s not rocket science: we seem to have wrapped an awful lot of complexity around it, but at the heart of it for me, that s what CPA is and I think that the issue is that organisationally, it s one of the few universal tangible things we ve got in the system. PR15 I think there is a lot of information we can give to people up front, which will I guess, help manage their expectations, the patients and carers about what care coordination is, how long someone is likely to be care coordinated for, what goals will be identified and aimed for. I think there is a lot of information that we can give that we are not giving now. PR04 I think service user involvement is absolutely key, because it communicates that sense that we re all in it together and some are service users some of the time and some aren t, but actually that s a flow and there are times in all our lives when we can be fragile and needy and I think that has to be part of day to day life. PR06 It s not the entire remit of mental health services and that s about signposting and enabling people to use other things that are going on in their lives to build up their wellbeing and I think making connections between people is something we could do better... PR06 Service User I did a WRAP plan. Wellness Recovery Action Plan, which really helped and because the team are aware of it they could, when things were bad, they could actually encourage us to use little bits of my WRAP plan. SU146 I had a WRAP plan. A wellness, recovery action plan. Which highlights my triggers, early warning signs. It tells you what steps I need to take to hopefully prevent things breaking down. It has a crisis plan section. And I would hope that that would be used. And that I would use that in planning for my future care. SU125 So the whole point of you working with someone, you know, it s identifying what recovery journey they re working on and we re agreeing together, collaboratively I suppose, what we re aiming for. PR01 Carer I feel as though I m pushed out, but then when anything goes wrong, I mean, they re saying to me Oh well, she could do this, she could do that I think: Aye, she could do a lot of things, but you haven t got her 24/7. C14 We worked as a team; she valued me as a carer. She has not seen me as interfering she knows I have good experience. C43 Service User Yeah. [CPN] has always been really good with me anyway. Like, he hasn t done anything without my consent. Like, if he s going to make a decision, he always comes to me first and asks about things. I was told when I was diagnosed that it was very, very important that my close friends and family were very boned up about [mental illness] and how they should support me in times of mania and depression I and was also told times when of I was being diagnosed well but that not too it was well very, that very I tip important into mania. that my SU104 close friends and family were very boned up about [mental illness] and how they should support me in times of mania and depression and also times of being well but not too well that I tip into mania. Care coordination is where one person ultimately has responsibility to ensure that everybody s working in the same way and that everybody s aware of what s happening within your care and that information is a two-way process between you and them. SU146 Carer Something that is important to me is to talk about how somebody becoming unwell affects the family C44 There didn t seem to be anything where there was, like, a flow diagram or Or a tree or like a where it said These do this, these do that, and that s where these go into that. C03 A huge thing would have been education and understanding around supporting the crisis, supporting recovery, understanding my partner s diagnosis through crisis, you end up back there again but with no tools to kind of, cope or deal with it I didn't know how to best handle it. C44 Once I reached a point of being physically and mentally well enough to start thinking about what I want I wanted to do next, you know, it was me that went out and looked at what training was on offer, looked at what other organisations were out there that I could become members of, or you know, access their services and it was mostly around like the voluntary and community sector where I got that support. SU126 I think it s just committing and having respect for the triangle of care, because carers should be equal partners. C35 I do feel that I ve moved on from somebody who got distressed and panicked by crisis to someone who has some understanding and education. And I feel empowered and more in control because of that. So I think I m in a better place than I was. C44 LEARNING TOGETHER I want information because I want to know how he s going to recover and if there s a chance that he will be back to the way he was and what the process is, cos they just try every kind of medication under the sun. Maybe if I had information on them, I would know what they re trying now. C07 Challenges around sharing information Professional carers wanting information or wanting to tell you something saying I can t talk to you cos so and so won t talk to you Well, you can always listen as long as you don t give any confidential information away, you can listen. It s very frustrating to be a carer and people say I knew this was going to happen and I told you this was going to happen and nobody listened to me. Some of that will be retrospective I know and maybe not accurate but it s really important. PR02 I mean we are often in a position where we need to consider issues of confidentiality around carers when the patient doesn t want the relative to know, or the next of kin to know about their diagnosis or what kind of treatment they are receiving and yet the family are very concerned about the individual. I think we take the view which is sort of National Guidelines that we need to give carers the information or enough information for them to be able to support that individual like how they can access services in a crisis and who to go to PR04 I ve said about them hiding behind the confidentiality card I guess there is complications in that, but it s certainly been dramatically overplayed. PR08 Carer *Carers+ have a right to know, because sometimes when they discharge people, they just discharge them back home and to say to a family Well, you re not entitled to any information about your loved one. Oh, P.S. We re discharging him on Friday back into your care, that s setting the carer up to fail and the service user up to fail This is what that service user needs. Now, carer, what do you need? Because you have rights in your own right.. C35 I had never dealt with someone with a mental health problem. I was looking online and ringing loads of services and trying to ask them what to do I was ringing and nobody would help us and everything was anonymous and they couldn t disclose anything to us. C07 If you ve got a service user who just goes on his own to his appointments and doesn t ask the carer to come along, the carer just won t come along on their own without that service user asking them. In which case, the professionals should be saying Now, next time you come, you might want to bring along a family member or a friend or something and yes, I ll see you on your own, but we need to have at least ten minutes with them or something, you know? So it should be introduced into the conversation. C35 Service User Yeah. *CPN+ has always been really good with me anyway. Like, he hasn t done anything without my consent. Like, if he s going to make a decision, he always comes to me first and asks about things. Yeah. *CPN+ has always been really good with me anyway. Like, he hasn t done anything without my consent. Like, if he s going to make a decision, he always comes to me first and asks about things. SU133 Care coordination is where one person ultimately has responsibility to ensure that everybody s working in the same way and that everybody s aware of what s happening within your care and that information is a two-way process between you and them. SU146 if I was to become unwell I would want to be receiving home treatment, medication I wouldn t want Haloperidol or Amisulpride or Risperidone. I would want probably Olanzapine I would want me friends and family to be more informed as to what s going on because they have always been victims of patient confidentiality a lot of the time. SU131 Recovery and Care Coordination
32 Professional Professional Support I would also like to develop some kind of peer support for those patients so that they are actually meeting other patients that might live in their local community there might be patients that have recovered which will give them more hope. I think there s a lot more interest in the peer support workers that we are starting to use in other services and people are beginning to think how we could use peer support workers in our service. PR12 guess your service users that you ve interviewed will be telling us whether it s changed or not...i think it has changed but I don t think it s quite as clear cut I think more and more people are talking about enabling, about people recovering, about people having more independence, and having more control over their care plan, their journey of recovery. I don t think we re there yet within services. I think the organisation conflicts with that sometimes because to enable someone to have more control over their recovery, we also have to get into some positive risk taking and that means that professionals have to be able to have that conversation. PR01 Stepping outside the comfort zone What I do now, if I meet somebody for the first time I will always say look I won t be with you forever this piece of work that I m going to do with you is going to be time limited. I m not going to come next week and say right. you ve got four weeks and that will be it bye bye, I m not going to change your life, I m not going to change your diagnosis I can t do that but I m going to help you cope with it PR11 If we started to talk about safety planning or planning safety, as opposed to risk management and changing what the concept is through using different words...finding out from people What do you need in order for you to feel safe? to support recovery more as opposed to it just being that process that is just there. If we are putting risk management and support processes in place that s really just preventing people from having the opportunities to try things in life and I think that s the way we currently set things up. I think that happens an awful lot. What we haven t done is assess the risk, but what s the risk of that person not having that opportunity. PR16 Service User when I became well enough I did start getting involved in some local services where they deliver support and education for service users so I have started like doing a bit of peer support. SU126 They do see me they won t go to the care team, they feel they can come and talk to me because I am a service user as they are and I'm on their level. SU101 But if I got to the stage of recovery where I was well enough to go to work or well enough to socialise with other people more than I do now, erm, than I would consider I had been through enough to be supportive enough to somebody else. SU141 I think we have got to recognise the value of people having time, to consider and reflect and think carefully about how we are supporting people with their recovery. I think the less we do that and the more we move towards the treadmill experience, were we just kind of take people through, then the more we are as services at risk of not being able to do kind of what we wanted to do. There is something for me about teams feeling safe to work in that way as well. PR16 You have to allow people to develop, you have to allow people to take risks but it can feel pretty scary if somebody s vulnerable and certainly the clinicians feel they ll get hung, drawn and quartered if something goes wrong. PR08 Carer that would be brilliant if you could get a database of people who are interested in talking to each other about their stresses in their life to do with, and whether they have had success, that s the most important thing. C33 I used to go to meetings and all that and they were very good, oh they were all carers themselves, you know, but erm, I found after a while I got tired of talking about mental health. C12 Service User Yeah. [CPN] has always been really good with me anyway. Like, he hasn t done anything without my consent. Like, if he s going to make a decision, he always comes to me first and asks about things. I just wanted to go and start applying for jobs. But we have now talked about instead of the next stage being going back to work, maybe the next stage is like a short college course or something. I Something was told when with I deadlines was diagnosed and a that wee it bit was of pressure very, very that important I had to that my attend. close But friends again and something family were that s very not boned going up to about totally [mental set illness] back. and SU134 how they should support me in times of mania and depression and also times of being well but not too well that I tip into mania. Erm, it s about for me, it s about the positive risk taking and about allowing us to take some risks in that just because it s a risk doesn t mean that the outcome is a good or a bad thing. SU140 I think that s what my care coordinators do with me. Put me at risk. Because I said, like, I didn't want to travel on public transport. But now I ve got a concessionary travel pass and I do that. It s fine. SU145 Carer I am being that careful but I mean now she says that she needs some of her independence back, which is understandable, I understand, so we are sort of experimenting a little bit where she has got her own little bit of bank account and we pay a little bit of money into that and she has got to use it sensibly because she could just go mad. C10 I think there has been a lot of cossetting in mental health and I think you know, we should be working on people s confidence; we should be working on people s self-belief; we should be helping them to identify their strengths, so we can build on them, because how do you build confidence if you keep on doing the things that s within your comfort zone? C35 a lot more people could be helped if there was more what s the word? Just people who know what they re talking about. You know? CPNs to me, it s just they learn from university; they read from a book I mean, some of them will have experiences of people with mental health problems in their own lives. C06 MOVING FORWARD Responsibility and dependency Professional Your responsible for yourself and were responsible for helping you to make the best of your life and overcome your problems. I think we are far too quick to take responsibility away from service users. I can t see how recovery can happen without them taking it back... PR08 I don t think recovery equals cure in mental health. I think it s about a person... If their symptom free great, if they've got residual symptoms its about that person feeling confident to manage those symptoms when they experience them whilst they are fulfilling the roles they need to fulfil, like parenting, picking the kids up from school, driving, working, whatever. PR04 I think sometimes we sort of engender a sort of dependence which makes us feel wanted. It s not very healthy. PR02 I guess the overall aim is to get people out of services as quickly as possible because I think we have recognised over the years is unintentionally mental health services have often promoted a dependency on services. If you think pre the; last guidance which is 2008 it was severe and enduring mental health issues and it was almost like, enduring means it never goes away and I know it doesn t go away, but it s almost like You ve got an enduring mental health problem, your always going to be with mental health services, which is obviously anti recovery and actually anti being sensible. I think we ve moved towards recognising that it is about supporting people to leave but I don t think the word recovery is used a lot PR14 Carer they are not overprotective and I think they get fed up with me taking things on board they would want her to take more responsibility, which I agree with but I know she's not going to do it C43 to make sure the person that I care for has got all the help that she needs and that she is organised with the proper medical support and erm, that she has everything that she needs and that she s content You want to do the best you can for that person, but it can be very difficult. C01 I think, in the past, I ve taken too much responsibility. You know, tried to do too many things for him and I m really trying to step back and... You know, let him do as much, be as independent as he can be. That is a difficult one at times I think. But, yeah, trying... Definitely trying to do that. C04 I can t get him... It doesn t matter what it is, I can t get him motivated in anything. Everything is such hard work. You ve got to keep pushing, pushing. You know, you feel actually a little bit like a nagger. And I hate that blinking label. C05 Service User Yeah. *CPN+ has always been really good with me anyway. Like, he hasn t done anything without my consent. Like, if he s going to make a decision, he always comes to me first and asks about things. I think that I am lucky in the fact that I have a good team, but also because of how forward thinking I am, I think that also helps, because obviously taking personal responsibility the majority of the time helps to be able to focus the recovery better, but when I lose sight of that, then it s much harder for other people to see it, cos they know that I can take personal responsibility. SU140 But I just need the services to be able to listen to my dad more than anything, because I m a... I mean, I'm just not with it at all. I mean... I can t... I m not in a position to be able to be given the responsibility to help myself. SU119 Well, I have been discharged now so I am kind of responsible, I am making sure I take me *medication+ every night and that s about it, and sort of if I am, I ve kind of, me best friend encouraged us last year when I was going through a particularly difficult patch to like go and get some anxiety management so I had some IAPT intervention two years ago. SU131 Recovery and Care Coordination
33 Process and system versus relationship Professional Oh, they go to ASDA and have a cup of coffee with their service users. That s the culture that goes before us and that s the culture that we re still up against. PR05 If you feel personally responsible for every single decision you make around risk and then it goes wrong, it s going to be your fault, then you start acting in a different way. Whereas if you ve established that on an equal footing with the service user, and that if something goes wrong, then it s going to be a joint responsibility, that would be different. Now I m not sure the services are really set up for that. PR02 And there is no evidence basis for many of the interventions that people like to have. It doesn t mean they don t work. There s part of me thinks if something works, does it really matter if there is an evidence base? Some of my colleagues would be horrified if they heard me saying that you know. Some of the homeopathic things and counselling, not a lot of evidence, but people like it. So it s tricky isn t it. It s an NHS where we are strapped for cash, so what do we provide I think...tends towards the more probably medical focused interventions. PR02 Getting on with life Professional Everybody is capable of improving and it ll depend on what they call recovery, I think. There will be some people who will remain very unwell, I imagine, and end up for example, in rehabilitation services but even within that, I think there has to be hope of, you know, some improvement in quality of life. PR02 But, there s also a significant number of people who feel very anxious about I guess recovery. You know, what happens again, in case they want to remain involved with services, just in case they become unwell and I think for a lot of people that s understandable. PR04 People are often suffering a great deal, but I wonder if we underestimate people s strengths, and what they can build on and work with and so obviously that then affects how hopeful or positive you are and the direction you take, but it s really really important that you do maintain that energy and focus. I think the notion of resilience is really helpful, cos I think that s something we can build up and something that s generalised to all of us and all of us at times may experience depletions in that for good reason. PR06 Service User And the whole health team were sitting there and my wife and I were outside but by this time the health team had already had time to sit down, must have spent 20 minutes, I don t know, 20 minutes, half an hour, all discussing and when I went into the room with my wife, you felt as though you were being put on the spot and then they started discussing things and you'd have the psychiatrist sitting there and he s looking at maybe *name of member of staff+ or he s got somebody sitting there and he s looking at a social worker or you've got somebody there and he s looking at an occupational therapist and they're all jumping in but the carers and the service user or me as an identity in myself didn t get the chance to say what I wanted to say and just felt as though I was answering questions to tick their boxes and I actually did leave the room and I refused to go back in. SU101 Carer if she *CPN+ could see a problem with my wife she would there and then phone the doctors; I want an appointment or am I going to do this or that. That was great but now people just seem to be - if you don t mind me saying - ticking boxes. C09 the risk assessment was just a piece of paper that I got a copy of, and I put in the drawer. Because I knew in reality, as I said earlier, when it went wrong there wasn t anybody there. To risk plan meant nothing. C03 Service User Yeah. [CPN] has always been really good with me anyway. Like, he hasn t done anything without my consent. Like, if he s going to make a decision, he always comes to me first and asks about things. I think I'm always going to be in the mental health system. SU110 I was told when I was diagnosed that it was very, very important that my I just close feel friends as if, like, and everybody family were is very just wanting boned up the about best [mental for me, illness] you and know. how And they that... should they re support all working me times for me of mania and... and And depression trying to... and Trying also to times make of me being to the well best but I not can too be, well you know. that I tip So into it s... mania. It s working well, like. It s champion. SU148 Recovery doesn t mean cure, it s just getting to a stage where you can still live a decent quality of life that you want to live. It might be different to what you originally thought it was going to be, but then again it can be really better. SU124 Carer the last two years, he s actually turned around. He s now on a treatment order, community treatment order, has been for the last two years and he s actually turning his life around he s well on the way to recovery He s actually got a part time job now as well, so so he s doing really well. C16 I think he has just sort of settled in a nice comfortable rut and he is quite happy to stay there whether he thinks he s recovering or not I don t know. C22 Because they actually listen. They don t listen to the degree of you either.. they actually look at you and listen and make you feel like they're listening and care. That s what it is. They know how important it is to get it right. SU106 No, I find that they would be more able to help if they weren t under so much stress themselves. You know the time would be the same with them but it would be of a better quality. SU120 CULTURE CHANGE Times of crisis Professional I think maybe there is the potential to try and look past the kind of crisis, to look at objectives and goals, but it s difficult, because if crises are kind of persistent and frequently you do get into responding to those. PR06 God, this sounds awful I think if staff tick too many of the boxes on the first risk assessment, then they ve got to do a crisis contingency plan and I think they avoid it. PR12 Yes we do a care plan, a risk management plan? How often do we say and if in crisis, ring the crisis team. PR03 Carer it was actually getting professionals to listen. Erm, realise that we weren t crying wolf; that he needed help. You know, he never ever rang up unless there was a problem. You know, we supported him, did whatever chivvied him along and it was only when an acute episode occurred that the help wasn t around. C16 *The policewoman+ said: Why did you ring the police? and I went Because I was told. The crisis team couldn t help us and I was led to believe that I would ring the police and the crisis team would follow on and they didn t. There was nobody. Nobody came after that. C39 Service User Yeah. *CPN+ has always been really good with me anyway. Like, he hasn t done anything without my consent. Like, if he s going to make a decision, he always comes to me first and asks about things. I ve always been listened to and I felt they ve worked with me, they ve valued what, you know, what my opinions are, I've not been pushed into anything. I've not been treated as someone who hasn t got anything to give in my recovery or anything like that. No, I just sort of feel I've been involved in every step of the way with them all. SU113 Crisis services, cos they don t treat you they say that they look at you as an individual there and then, but actually, they don t; they ll say we know this person and this is how this person behaves in this situation, rather than looking at the here and now and why am I presenting at that time. SU140 Recovery and Care Coordination
34 What Next? We are designing a Toolkit to support recovery focused care coordination. We need a commitment to change research steering group Trust training and PCP... Potential Future Experience/Impact film PCP Evaluation PCP? and Clinical Research Group Recovery and Care Coordination
35 The project received the Best Service User Involvement Plan Award at the National Institute for Health Research, Mental Health Research Network, Scientific Research Conference on the 21st April Contact s: Steering/Research Group: Nicola Armstrong, Helen Atkin, Deb Helme, Alison Flaherty, Caroline Kemp, Lisa Matthews, Stephanie Morley, Louise Thomson, Mick Hill, Oliver Wood, Liz Bowman, Alasdair Cameron, Paula Edwards, Shula Ramon, Jan Wallcraft and Simon Douglas Recovery and Care Coordination
36 This work presents independent research funded by the National Institute for Health Research (NIHR) under its Research for Patient Benefit Programme (Grant Reference Number RfPB PB-PG ). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. The research team are grateful for the on-going support of the NIHR Recovery and Care Coordination
37 The Design Phase Stewart Gee PCP Programme Manager

38 A? B SMR
39 GP / Other CPN B6 physio 1.24 hrs Medic OP Service 0.64 hrs B6 Discharge Understanding our current state Explored 720 patient journeys, by cluster and locality, looking at patient clinical contact and bed usage Created current Value Stream Maps (VSMs) and do analysis of what happens now? NTW NC Total Total Number of Clients ,490 1, ,334 1, ,764 1, ,293 20,745 Female , ,101 1, ,361 11,466 Male , ,932 9,279 Percentage Split 1.8% 1.1% 3.0% 9.1% 9.3% 3.4% 3.3% 4.5% 4.5% 3.7% 14.2% 8.2% 3.0% 0.8% 0.3% 1.4% 1.2% 10.7% 11.0% 4.7% 1.1% 100.3% Percentage Split 0-17 only 2.5% 1.5% 4.1% 12.5% 12.8% 4.6% 4.5% 6.1% 6.3% 5.0% 19.6% 11.3% 4.2% 1.1% 0.4% 1.9% 1.6% Total Number of InPatients ADULT CONTINUING CARE ADULT MH ACUTE ASSESSMENT & TREATMENT ADULT MH PSYCHIATRIC INTENSIVE CARE ADULT MH REHABILITATION OPS ACUTE ASSESSMENT FUNCTIONAL OPS ACUTE ASSESSMENT ORGANIC OPS CHALLENGING BEHAVIOUR OPS LONG TERM CARE Total Number of Community Clients ,623 1, ,674 1, ,879 1, ,293 22,231 ADULT ASSERTIVE OUTREACH ADULT CMHT ADULT COMMUNITY MENTAL HEALTH , ,387 8,743 ADULT COMMUNITY NURSING ,731 Care Pathway - CURRENT ADULT COMMUNITY PERI-NATAL ADULT COMMUNITY REHABILITATION Locality Population: Newcastle ADULT CRISIS RESPONSE & HOME TREATMENT Cluster: 18 ADULT DAY SERVICES ADULT DRUG & ALCOHOL ADULT PSYCHOTHERAPY % Patients by % Patients by Population Data 14% Primary Care Entry Point Entry Point COGNITIVE ANALYTICAL THERAPY % Hospitalised COGNITIVE BEHAVIOURAL THERAPY 76% GP/Other Discharged1 69% % Treatment completed / discharge EARLY INTERVENTION PSYCHOSIS Treatment % Deceased OPS CHALLENGING BEHAVIOUR1% Cluster Cluster % % DNA / Withdrew OP CMHT OP Medic 1% Inappropriate referral Expected prevalence OPS of COMMUNITY MENTAL HEALTH 1% Cluster hrs ,131 1, Cluster % 1,047 4,884 16% Internal transfer Cluster 18 patients in OPS DAY SERVICES Newcastle Actual FLOW IN Assessment / Review Assessment / Review Actual FLOW OUT OPS MEMORY One ASSESSMENT patient every SERVICE 5% Cluster 3 14 Patient assigned 3 Cluster Patient 1 discharged from Cluster % 473 One 1,980 patient every Number days Cluster 18 OPS PSYCHOLOGY days 3% Cluster 4 Medic Medic Cluster 4 1% 142 OPS YOUNGER PEOPLE WITH DEMENTIA 7 Physio1 Dementia hrs SELF HARM LIAISON SERVICES 9% Cluster hrs Cluster 3 3 1% B Mean Days in Cluster 5% Other Other 160 1% Mean Days Open to NTW 1,996 1,240 1,260 1,208 1,026 1,135 1,357 1,815 1, ,692 2,845 2,897 1,813 1,493 2,154 3, ,085 1,378 Inpatient Service Users with IP stays in last 12 Months Intensity: mins days ,054 0 per month % SU with IP stays in last 12 months 4.3% 7.5% 7.6% 6.5% 9.3% 12.7% 9.0% 11.1% 22.4% 22.8% 10.3% 22.4% 31.3% 63.4% 25.6% 36.7% 40.7% 2.0% 5.9% 12.0% 30.5% Mean OBD for Service Users with InPatient Stays Mean Frequency of Contacts within Cluster (days) mins 261 days 30 mins Locality: Newcastle 0 0 Pathway: Cognitive Cluster 18 Resources Defect List Clinical Resource required = Sum of cycles / Flow in = 6.62 / (5.34*1.14) % Appointments DNA / Cancelled 11.5% = 1.09 wte 0.2 Medic Inappropriate referrals during LOS Physio 0.78 Band 6 Required Beds 0 beds Work In Progress (WIP) Cluster 19 Actual WIP 400 Patient FLOW Standard WIP 223 Flow In one patient every 1.14 days = LOS / Flow In Flow Out one patient every 1.44 days Net change in number of patients per year 67 patients / year Cluster 20 Explored flow and interfaces High-level Summation (Direct contact for Clusters: 3,4,6,8,10-14, 18-20) Output of data analysis and VSMs: North South This is the sum of the community clinical WTE Newcastle Sunderland Gateshead TOTAL Tyneside Tyneside data in the resource box of the current state value stream maps. It suggests thewte required Community WTE to deliver the clinical contact derived from Number of beds Cluster 21 Non-Psychosis Possible Assumptions for worst case scenario: Impact on above figures Calculated resources required to deliver the current state (25% contact, 75% bed usage) Northumberland has bed need and WTE need equal to mean Factor in Northumberland average of all other clusters data The 8 clusters not examined have bed need equal to 1/7th of the clusters that were examined (1/7th reflects snapshot bed usage of Increase Beds by 14.3% those clusters) The 8 clusters not examined have WTE need equal to 25% of the average of the clusters that were examined (25% represents Increase WTE by 25% snapshot patient population by cluster) Possible worst case scenario North South Newcastle Sunderland Gateshead North'l'd TOTAL Tyneside Tyneside Community WTE Number of beds Actual position of WTE and beds North South Newcastle Sunderland Gateshead North'l'd TOTAL Tyneside Tyneside in Newc/Nty Community WTE figure Number of beds 753 Acute OP Stepped PICU OP Organic TOTAL Bed Type Assessment Functional care Number of beds This increases the community clinical WTE and bed numbers derived from the sampling of patient journeys, to take into account that not all clusters and localities were considered. This is the result of applying the assumptions above to the data table at the top of the page This is the actual community clinical WTE and Bed numbers by locality, taken from dashboard and staff numbers (from finance) Psychosis Community WTE Efficiency (contact resource/total clinical resource) Assuming contact activity is fully recorded Bed Efficiency (Bed need / Beds available) Efficiency 25% 72% From the sampling of patient journeys, aggregated with assumptions above, this is the overall % WTE in direct contact with patients and bed utlisation / efficiency. Actual bed utilisation from the dashboard is 78%. The 25% direct contact correlates with figures produced in the Transforming Community Services project having observed teams at work
40 What we learned about our current community pathways Not always obvious that the patient was on a pathway Patients were often with us for a long time, during which they seemed to have relatively little direct clinical contact Where patients came from (cluster-wise) and where they went to (cluster-wise) did not always make sense some pathways looked almost random Concern that we may be making some patients worse Flow was variable, yet resources were not, causing peaks and troughs right across the pathway and the inevitable blockages and waits that ensue

41 How CPN s spend their time
42 Need to capture patient experience at every point of the pathway Not all assessments in clinic - travel time may be required to patient home Standard work required to reduce variability in which assessments are sought Non-med prescriber or pharmacy role possible? Should we keep in contact with these people, say with a support worker every 3/6 months in a phonecall or visit? The approach we took We held a series of clinically-led workshops Pathway: Cognitive Future State Value Stream Map Date: Cluster: 18 Version: 0.1 Drafter: P Ian Railton Patient/Family/carer present Process box 25 September 2012 Which explored the current state VSMs Effect Care Coordination Undertake Care Coordination throughout Face to face Telephone call resource Ideas for further development task time 9.5% Number of patients in queue Overall % patients that flow this way 1 30% 1 Efficacy Review Review treatment; instigate psychological step 1 and offer step 2/3 as appropriate, Occ/Soc & Fam/carer interventions instigated 1% 1 1% 1 Specialist Occ/Soc From OT Spec Assesssment P? 600 mins Step 3 Psychological Structured Psychotherapy sessions month Review Undertake review; agree discharge / further treatment / involvement of others Repeat 1 Discharge Complete discharge tasks P Clinical Psychologist (6-8) Initial Assessment & Access Phase Assessment & Formulation 720 mins Formulation 3 days max 28 days max within 1 month of results - FP10 FP10 Further Consider Assess current Diagnosis & Involvement of Risk Contact with MHCT scored & Care Coord Consider further Review assessments Initial diagnosis & Step 2 Step 2 Receive referral information Initial triage detailed care working Check meds others Assessment family / friends clustered identified assessments / investigations formulation sought assessment arrangements formulation 50% 62% Psychological Psychological Log on Rio from other captured and Assessment Holistic re: capacity, assess level of including inform initial following MDT and investigations in MDT Discuss with pt / fam Confirm medication Education Coping with 1 referrers re: 1 logged 1 appointment 1 assessment of 1 MH status, 1 carer need; 1 safeguarding 1 management 1 1 discussion and confirm 1 tolerance. Issue risk, needs, offered risks and how services plan clustering. Meds FP10 higher dose Group - 8 per forgetting 6-8 wk 1 physical programme urgency 90% needs health, Cog work for patient 80% prescribed group complete function, etc P P P P P P P P P P % total wait?? days days 2 clinicians (L8 & 6) days days admin CPN 6 CPN 6 CPN 6 CPN Band 6 MDT: Level 8; CPN Band 6; AHP/Psy (3 professionals) MDT + spec ass Level 8 CPN 6 CPN 6 CPN 6 CPN 6 mins 10 mins 15 mins 5 mins 90 minutes 15 minutes 15 mins 45 mins 15 mins 60 mins 60 mins 480 mins 60 mins 10% 10% 2% 1 FP10 Consider Assess current Diagnosis & Risk Contact with MHCT scored & Care Coord Consider further Further Further Further 2.5% detailed care working Review medication Review medication Assessment family / friends clustered identified assessments Assessments Assessments Assessments assessment arrangements formulation 2.5% Holistic re: capacity, assess level of including inform initial following MDT and investigations and investigations and investigations and investigations Patient not tolerant Patient not tolerant 1 assessment of MH status, carer need; safeguarding management discussion risks and physical how services plan EG Neuropsychiatry Assessment EG OT EG? 1 10% needs health, Cog work for patient complex needs complete function, etc P P P P P P P P P Patient Contact Resource Time per patient per task Access 30 mins 30 mins Initial Assess Level 8 90 mins 9 mins 90 minutes 180 mins 120 mins mins 30 mins 30 mins Initial Assess CPN 90 mins 81 mins Average clinical time per patient journey minutes Average clinical contact time per patient journey 369 minutes Resources per locality (WTE) Resources per locality (WTE) MDT 45 mins 40.5 mins to compare with baseline data 38% Further Assessments 300 mins 54 mins Northumberland 1.09 Northumberland 0.84 Assessment & Formulation (MDT) 45 mins 40.5 mins Newcast 1.33 Newcastle 1.02 Assessment & Formulation 45 mins 45 mins Sunderland 3.19 Sunderland 2.45 Sucessful meds 15 mins 7.5 mins South Tyneside 1.48 South Tyneside 1.14 Med resistant 60 mins 1.5 mins Total 7.09 Total 5.45 Step 2 psychological 135 mins 83.7 mins Flow rate in Q1&Q2 2012) Step 3 psychological 720 mins 7.2 mins Northumberland 1.38 Specialist occ/social 600 mins 6 mins Newcastle 1.13 Efficacy and periodic review 120 mins 74.4 mins Sunderland 0.47 Discharge 0 mins 0 mins South Tyneside 1.01 Assumed LOS in cluster Assumed review period 12 months 12 months Average patient journey and designed a future state VSM based on the CPP specifications 40-50% contact 50-60% bed usage? mins


43 The design workshop process Invite people Gather data Design and Standard Work #1 Refine Reasonable adjustment for pathway Design and Standard Work #2 Scope Boundaries Principles Benefits People Constraints Workshop Product Specification Design Workshop Check Does this meet the Product Specification? Check Does this reflect previous discussion and principles? Sign off Ready to test Week 0 Week 6 Week 7 Week 8

44 Our Clinical Workshops Access Assessment & Formulation Treatment Discharge Transitions Advice and Information Urgent Referral Non-urgent referrals Marketing Information and Preparation Assessment and Formulation Cluster and Book Meet and agree Treatment Treatment Optimising resources Develop discharge plan Implement discharge plan Augmenting Transitions
45 Other Workshops Non Clinical Activity CPA Scaffolding Estates Admin I.T
46 Treatment Patient pathway Planned Access Assessment Formulation Treatment Review Discharge = time per patient X number of patients = Total Time By skill level, cluster, pathway and sub-pathway CPP Specifications SMR Patient Need Evidence Base Treatment options per Cluster For each Treatment Type(200+): Length of one treatment session Number of sessions (range) Preparation time per session Number of staff required to deliver treatment session Skill level of staff delivering treatment Expected % patients by cluster having treatment Group size (1:1 or group treatment) Treatment venue (home, clinic, community) X the number of patients = Total Time required for Treatment ----> WTE (by skill level, cluster and pathway) Clinical Judgement
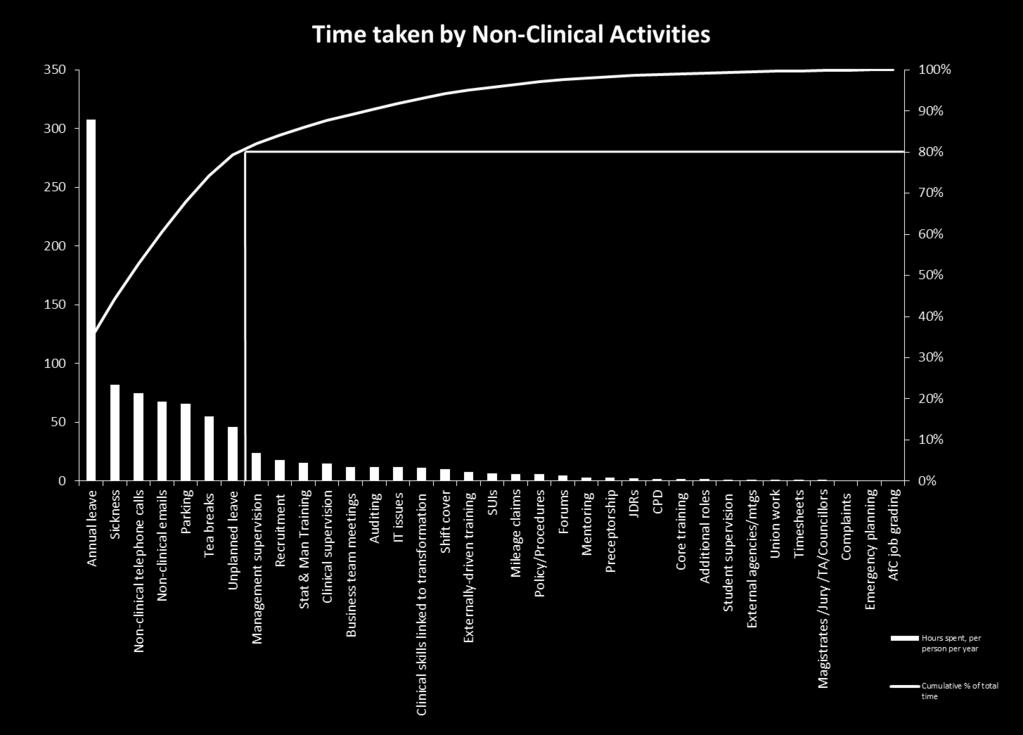
47 Non-clinical activity workshop
48 Principles for the Estate Workshop Service User + Carer first Right location and facilities for staff Community IN the community - make it accessible 24/7 IT support Seniority doesn t have priority for space inside + out No auto entitlement to own space No exclusivity for service re a building/space (hot desking areas) Remain open minded re use of open spaces High quality patient areas All trust areas equal importance/status Standardisation across areas Maintain social elements/ team aspects of work
49 Where are the patients?

50 Psychosis & Non-psychosis 3 Sunderland 1 South Tyneside

51 Cognitive and Learning Disabilities Cognitive LD


52 Principal Community Pathways Detailed Design So far 362 people have attended the 27 clinical and supporting systems workshops, these have included: GPs, Local Authority staff, Acute Trust staff, Community and voluntary sector staff, CCG staff, NTW staff and most importantly our service users and carers. Our Trust-wide Service User and Carer Reference Group has been involved throughout We have presented our plans to various groups including HealthNet and South Tyneside GP Education Forum We ve been walking the wall with all of our stakeholders and have so far run sessions for over 1200 people
A New Model of Urgent and Emergency Mental Health Care
 A New Model of Urgent and Emergency Mental Health Care Transforming Urgent Access to Mental Health Services across 7 days & Interfacing with the wider system Dr Paul Brown- Consultant Psychiatrist, Sunderland
A New Model of Urgent and Emergency Mental Health Care Transforming Urgent Access to Mental Health Services across 7 days & Interfacing with the wider system Dr Paul Brown- Consultant Psychiatrist, Sunderland
A Model of Urgent and Emergency Mental Health Care
 A Model of Urgent and Emergency Mental Health Care Transforming Urgent Access to Mental Health Services across 7 days & Interfacing with the wider system Kate Chartres, Nurse Consultant, Psychiatric Liaison,
A Model of Urgent and Emergency Mental Health Care Transforming Urgent Access to Mental Health Services across 7 days & Interfacing with the wider system Kate Chartres, Nurse Consultant, Psychiatric Liaison,
Improving Mental Health Services in Bath & North East Somerset
 Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
Tatton Unit at a glance:
 Tatton Unit Staff are helpful, you can talk to them anytime. Tatton Unit at a glance: 16 - bed Low Secure Unit 18-65 For men aged between 18 and 65 years - admissions can be accepted for those older than
Tatton Unit Staff are helpful, you can talk to them anytime. Tatton Unit at a glance: 16 - bed Low Secure Unit 18-65 For men aged between 18 and 65 years - admissions can be accepted for those older than
POLICE Seeking help for a mental health problem. Blue Light Programme
 POLICE Seeking help for a mental health problem Blue Light Programme Seeking help for a mental health problem This is a guide for police service staff and volunteers on how to seek professional help for
POLICE Seeking help for a mental health problem Blue Light Programme Seeking help for a mental health problem This is a guide for police service staff and volunteers on how to seek professional help for
OPEN BOARD OF DIRECTORS 8 June 2016
 OPEN BOARD OF DIRECTORS 8 June 2016 Open BoD: 08.06.16 Item: 5 TITLE OF PAPER Community Enhanced Recovery Team (CERT) Progress on Development, and the partnership between the Trust and South Yorkshire
OPEN BOARD OF DIRECTORS 8 June 2016 Open BoD: 08.06.16 Item: 5 TITLE OF PAPER Community Enhanced Recovery Team (CERT) Progress on Development, and the partnership between the Trust and South Yorkshire
Re-designing Adult Mental Health Secondary Care Services through co-production and consultation. 1 Adult Mental Health Secondary Care Services
 2016 Re-designing Adult Mental Health Secondary Care Services through co-production and consultation 1 Adult Mental Health Secondary Care Services Contents Forward Vision & Values Introduction Adult Mental
2016 Re-designing Adult Mental Health Secondary Care Services through co-production and consultation 1 Adult Mental Health Secondary Care Services Contents Forward Vision & Values Introduction Adult Mental
Strong Medicine Interview with Cheryl Webber, 20 June ILACQUA: This is Joan Ilacqua and today is June 20th, 2014.
 Strong Medicine Interview with Cheryl Webber, 20 June 2014 ILACQUA: This is Joan Ilacqua and today is June 20th, 2014. I m here with Cheryl Weber at Tufts Medical Center. We re going to record an interview
Strong Medicine Interview with Cheryl Webber, 20 June 2014 ILACQUA: This is Joan Ilacqua and today is June 20th, 2014. I m here with Cheryl Weber at Tufts Medical Center. We re going to record an interview
OUTLINE PROPOSAL BUSINESS CASE
 OUTLINE PROPOSAL BUSINESS CASE Name of proposer: Dr. David Keith Murray, General Practitioner, Leeds Student Medical Practice, 4, Blenheim Court, Blenheim Walk, LEEDS LS2 9AE Date: 20 Aug 2014 Title of
OUTLINE PROPOSAL BUSINESS CASE Name of proposer: Dr. David Keith Murray, General Practitioner, Leeds Student Medical Practice, 4, Blenheim Court, Blenheim Walk, LEEDS LS2 9AE Date: 20 Aug 2014 Title of
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL
 HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
HOME TREATMENT SERVICE OPERATIONAL PROTOCOL Document Type Unique Identifier To be set by Web and Systems Development Team Document Purpose This protocol sets out how Home Treatment is provided by Worcestershire
National Patient Experience Survey Mater Misericordiae University Hospital.
 National Patient Experience Survey 2017 Mater Misericordiae University Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017,
National Patient Experience Survey 2017 Mater Misericordiae University Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017,
Daily Summary from Workshop 1 Day 3 (Wednesday 2 May 2018) Access to Community Mental Health Services
 Access to Community Mental Health Services") Daily Summary from Workshop 1 Day 3 (Wednesday 2 May 2018) Access to Community Mental Health Services Context The group summarised the work carried out throughout the last couple of days and reflected
Daily Summary from Workshop 1 Day 3 (Wednesday 2 May 2018) Access to Community Mental Health Services Context The group summarised the work carried out throughout the last couple of days and reflected
Monitoring the Mental Health Act 2015/16 SUMMARY
 Monitoring the Mental Health Act 2015/16 SUMMARY Foreword The work of monitoring the Mental Health Act 1983 (MHA) is a distinct but supportive role to CQC s wider regulatory task. It is distinct, in part,
Monitoring the Mental Health Act 2015/16 SUMMARY Foreword The work of monitoring the Mental Health Act 1983 (MHA) is a distinct but supportive role to CQC s wider regulatory task. It is distinct, in part,
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms
 Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Community Mental Health Teams (CMHTs)
") Community Mental Health Teams (CMHTs) Community Mental Health Teams (CMHTs) support people living in the community who have complex or serious mental health problems. Different mental health professionals
Community Mental Health Teams (CMHTs) Community Mental Health Teams (CMHTs) support people living in the community who have complex or serious mental health problems. Different mental health professionals
Health and care services in Herefordshire & Worcestershire are changing
 Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Working for adult mental health services
 Oxford Health NHS Foundation Trust Recruitment Working for adult mental health services Switchboard: 01865 902288 Website: www.oxfordhealth.nhs.uk Recruitment About us We provide specialist mental health
Oxford Health NHS Foundation Trust Recruitment Working for adult mental health services Switchboard: 01865 902288 Website: www.oxfordhealth.nhs.uk Recruitment About us We provide specialist mental health
Improving Mental Health Services in South Gloucestershire
 Improving Mental Health Services in South Gloucestershire Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers Information
Improving Mental Health Services in South Gloucestershire Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers Information
Care Programme Approach (CPA)
") Care Programme Approach (CPA) The Care Programme Approach (CPA) is a package of care that may be used to plan your mental health care. This factsheet explains what CPA is, when you should get and when
Care Programme Approach (CPA) The Care Programme Approach (CPA) is a package of care that may be used to plan your mental health care. This factsheet explains what CPA is, when you should get and when
Mental Health Crisis Care: The Five Year Forward View. Steven Reid Consultant Psychiatrist, Psychological Medicine CNWL NHS Foundation Trust
 Mental Health Crisis Care: The Five Year Forward View Steven Reid Consultant Psychiatrist, Psychological Medicine CNWL NHS Foundation Trust Overview Parity of esteem What are the challenges for people
Mental Health Crisis Care: The Five Year Forward View Steven Reid Consultant Psychiatrist, Psychological Medicine CNWL NHS Foundation Trust Overview Parity of esteem What are the challenges for people
Best-practice examples of chronic disease management in Australia
 Best-practice examples of chronic disease management in Australia With the introduction of Health Care Homes, practices will have greater flexibility to provide comprehensive, coordinated, patient-centred
Best-practice examples of chronic disease management in Australia With the introduction of Health Care Homes, practices will have greater flexibility to provide comprehensive, coordinated, patient-centred
Martin Nesbitt Tape 36. Q: You ve been NCNA s legislator of the year 3 times?
 Martin Nesbitt Tape 36 Q: You ve been NCNA s legislator of the year 3 times? A: Well, it kinda fell upon me. I was named the chair of the study commission back in the 80s when we had the first nursing
Martin Nesbitt Tape 36 Q: You ve been NCNA s legislator of the year 3 times? A: Well, it kinda fell upon me. I was named the chair of the study commission back in the 80s when we had the first nursing
Young Peoples Transition project: Focus Group Summary
 Young Peoples Transition project: Focus Group Summary The Queen s Nursing Institute (QNI) is funded by the Burdett Trust for Nursing to deliver a programme of work to improve the experience of a young
Young Peoples Transition project: Focus Group Summary The Queen s Nursing Institute (QNI) is funded by the Burdett Trust for Nursing to deliver a programme of work to improve the experience of a young
PRISM: GPs - your questions answered
 PRISM: GPs - your questions answered 1. What is Prism? Prism is our new primary care service for mental health and run by Cambridgeshire and Peterborough NHS Foundation Trust (CPFT). The service puts specialist
PRISM: GPs - your questions answered 1. What is Prism? Prism is our new primary care service for mental health and run by Cambridgeshire and Peterborough NHS Foundation Trust (CPFT). The service puts specialist
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
My Discharge a proactive case management for discharging patients with dementia
 Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Care Coordination and Care Programme Approach Practice Guidance Note Learning Disability Admissions Urgent Care Only V02
 Care Coordination and Care Programme Approach Practice Guidance Note Learning Disability Admissions Urgent Care Only V02 Date issued Issue 2 Dec 15 Issue 3 Dec 17 Author/Designation Responsible Officer
Care Coordination and Care Programme Approach Practice Guidance Note Learning Disability Admissions Urgent Care Only V02 Date issued Issue 2 Dec 15 Issue 3 Dec 17 Author/Designation Responsible Officer
Islington Practice Based Mental Health Care: Roll-out plans and progress
 Report to: Board of Directors (Public) Paper number: 3.2 Report for: Information Date: 26 th October 2017 Report author/s: Emily van de Pol, Divisional Director, Community Mental Health and Primary Care
Report to: Board of Directors (Public) Paper number: 3.2 Report for: Information Date: 26 th October 2017 Report author/s: Emily van de Pol, Divisional Director, Community Mental Health and Primary Care
Modernising Mental Health Service User and Carer GP Feedback Event
 Modernising Mental Health Service User and Carer GP Feedback Event 1. Introduction Bristol Clinical Commissioning Group (CCG) is in the process of re-commissioning Mental Health services for the Bristol
Modernising Mental Health Service User and Carer GP Feedback Event 1. Introduction Bristol Clinical Commissioning Group (CCG) is in the process of re-commissioning Mental Health services for the Bristol
Orchard Home Care Services Limited
 Orchard Home Care Services Limited Orchard Home Care Inspection report 2 Ashfield Terrace Chester-le-street County Durham DH3 3PD Tel: 0191 389 0072 Website: www.cqc.org.uk Date of inspection visit: 12
Orchard Home Care Services Limited Orchard Home Care Inspection report 2 Ashfield Terrace Chester-le-street County Durham DH3 3PD Tel: 0191 389 0072 Website: www.cqc.org.uk Date of inspection visit: 12
Medical Home Phone Conference November 27, 2007 "Transitioning Young Adults With Congenital Heart Defects" Dr. Angela Yetman, MD
 Medical Home Phone Conference November 27, 2007 "Transitioning Young Adults With Congenital Heart Defects" Dr. Angela Yetman, MD Dr Samson-Fang: Today we are joined by Dr. Yetman from Pediatric Cardiology
Medical Home Phone Conference November 27, 2007 "Transitioning Young Adults With Congenital Heart Defects" Dr. Angela Yetman, MD Dr Samson-Fang: Today we are joined by Dr. Yetman from Pediatric Cardiology
Avon and Wiltshire Mental Health Partnership NHS Trust
 Avon and Wiltshire Mental Health Partnership NHS Trust Community-based mental health services for adults of working age Quality Report Head Office, Jenner House Langley Park Chippenham Wiltshire SN15 1GG
Avon and Wiltshire Mental Health Partnership NHS Trust Community-based mental health services for adults of working age Quality Report Head Office, Jenner House Langley Park Chippenham Wiltshire SN15 1GG
End of Life Care Strategy
 End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
A new mindset: the Five Year Forward View for mental health
 A new mindset: the Five Year Forward View for mental health Paul Farmer Chief Executive mind.org.uk Five Year Forward View for Mental Health Simon Stevens: Putting mental and physical health on an equal
A new mindset: the Five Year Forward View for mental health Paul Farmer Chief Executive mind.org.uk Five Year Forward View for Mental Health Simon Stevens: Putting mental and physical health on an equal
A thematic review of six independent investigations. A report for NHS England, North Region
 A thematic review of six independent investigations A report for NHS England, North Region November 2014 Authors: Chris Brougham Liz Howes Verita 2014 Verita is a management consultancy that works with
A thematic review of six independent investigations A report for NHS England, North Region November 2014 Authors: Chris Brougham Liz Howes Verita 2014 Verita is a management consultancy that works with
Welcome to. Northern England and the Five Year Forward View for Mental Health. Thursday 2 February 2017 at the Radisson Blu, Durham
 Welcome to. Northern England and the Five Year Forward View for Mental Health Thursday 2 February 2017 at the Radisson Blu, Durham Introductions Chairs: Catherine Haigh, Chair of North East together and
Welcome to. Northern England and the Five Year Forward View for Mental Health Thursday 2 February 2017 at the Radisson Blu, Durham Introductions Chairs: Catherine Haigh, Chair of North East together and
Three steps to success
 Inpatient care for people with diabetes at Russells Hall Hospital (The Dudley Group NHS Foundation Trust) Three steps to success The ThinkGlucose team at Russells Hall Hospital developed a three-stage
Inpatient care for people with diabetes at Russells Hall Hospital (The Dudley Group NHS Foundation Trust) Three steps to success The ThinkGlucose team at Russells Hall Hospital developed a three-stage
Somerset Care Community (Taunton Deane)
") Somerset Care Limited Somerset Care Community (Taunton Deane) Inspection report Huish House Huish Close Taunton Somerset TA1 2EP Tel: 01823447120 Date of inspection visit: 11 January 2016 12 January 2016
Somerset Care Limited Somerset Care Community (Taunton Deane) Inspection report Huish House Huish Close Taunton Somerset TA1 2EP Tel: 01823447120 Date of inspection visit: 11 January 2016 12 January 2016
South Of Tyne, Older Persons Occupational Therapy Service POLO Occupational Therapy Placement Information
 A Complete South Of Tyne, Older Persons Occupational Therapy Service POLO Occupational Therapy Placement Information 1 Placement Information Clinical Area: Older Persons Mental health. Northumberland,
A Complete South Of Tyne, Older Persons Occupational Therapy Service POLO Occupational Therapy Placement Information 1 Placement Information Clinical Area: Older Persons Mental health. Northumberland,
EVALUATION OF PILGRIMS HOSPICES RAPID RESPONSE HOSPICE AT HOME SERVICE
 EVALUATION OF PILGRIMS HOSPICES RAPID RESPONSE HOSPICE AT HOME SERVICE Summary of findings March 2015 Laura Holdsworth Research Fellow, Centre for Health Services Studies, University of Kent Annette King
EVALUATION OF PILGRIMS HOSPICES RAPID RESPONSE HOSPICE AT HOME SERVICE Summary of findings March 2015 Laura Holdsworth Research Fellow, Centre for Health Services Studies, University of Kent Annette King
TEES, ESK & WEAR VALLEYS NHS FOUNDATION TRUST: DEVELOPING A MODEL LINE FOR RECOVERY- FOCUSED CARE
 TEES, ESK & WEAR VALLEYS NHS FOUNDATION TRUST: DEVELOPING A MODEL LINE FOR RECOVERY- FOCUSED CARE Summary Tees, Esk and Wear Valleys NHS Foundation Trust (TEWV) adapted the model line concept from industry
TEES, ESK & WEAR VALLEYS NHS FOUNDATION TRUST: DEVELOPING A MODEL LINE FOR RECOVERY- FOCUSED CARE Summary Tees, Esk and Wear Valleys NHS Foundation Trust (TEWV) adapted the model line concept from industry
Cimla Health and Social Care Centre
 Cimla Health and Social Care Centre 26 th November 2015 Presented by: Louise Barry Head of Integrated Community Services Andrew Griffiths - Integrated Community Services Manager Sarah Waite Community Resource
Cimla Health and Social Care Centre 26 th November 2015 Presented by: Louise Barry Head of Integrated Community Services Andrew Griffiths - Integrated Community Services Manager Sarah Waite Community Resource
Angel Care Tamworth Limited
 Angel Care Tamworth Limited Angel Care Tamworth Limited Inspection report Unit 4, Anker Court Bonehill Road Tamworth Staffordshire B78 3HP Date of inspection visit: 14 August 2017 Date of publication:
Angel Care Tamworth Limited Angel Care Tamworth Limited Inspection report Unit 4, Anker Court Bonehill Road Tamworth Staffordshire B78 3HP Date of inspection visit: 14 August 2017 Date of publication:
Ambulatory Emergency Care A Flexible Approach to Ambulatory Care at Pennine Acute Hospitals. The Pennine Acute Hospitals NHS Trust
 Ambulatory Emergency Care A Flexible Approach to Ambulatory Care at Pennine Acute Hospitals The Pennine Acute Hospitals NHS Trust A Flexible Approach to Ambulatory Care at Pennine Acute Hospitals The Pennine
Ambulatory Emergency Care A Flexible Approach to Ambulatory Care at Pennine Acute Hospitals The Pennine Acute Hospitals NHS Trust A Flexible Approach to Ambulatory Care at Pennine Acute Hospitals The Pennine
Worcestershire Early Intervention Service. Operational Policy
 Worcestershire Early Intervention Service Operational Policy Document Type Service Operational Unique Identifier CL-158 Document Purpose To Outline The Operation Of The Early Intervention Service Document
Worcestershire Early Intervention Service Operational Policy Document Type Service Operational Unique Identifier CL-158 Document Purpose To Outline The Operation Of The Early Intervention Service Document
The Community Crisis House model
 An evaluation of Wales first crisis house If it had not been for the Crisis House staff I honestly don t think I would still be here. I can t thank you enough for all your help. I now feel that I actually
An evaluation of Wales first crisis house If it had not been for the Crisis House staff I honestly don t think I would still be here. I can t thank you enough for all your help. I now feel that I actually
Strategic Plan for Fife ( )
") www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
LEARNING FROM THE VANGUARDS:
 LEARNING FROM THE VANGUARDS: STAFF AT THE HEART OF NEW CARE MODELS This briefing looks at what the vanguards set out to achieve when it comes to involving and engaging staff in the new care models. It
LEARNING FROM THE VANGUARDS: STAFF AT THE HEART OF NEW CARE MODELS This briefing looks at what the vanguards set out to achieve when it comes to involving and engaging staff in the new care models. It
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
FREQUENTLY ASKED QUESTIONS / KEY ISSUES RAISED DURING THE CONSULTATION PERIOD (updated 7 September 2017)
") TRANSFORMING MENTAL HEALTH SERVICES Consultation 22 June 15 September 2017 FREQUENTLY ASKED QUESTIONS / KEY ISSUES RAISED DURING THE CONSULTATION PERIOD (updated 7 September 2017) Q1. Why has some documentation
TRANSFORMING MENTAL HEALTH SERVICES Consultation 22 June 15 September 2017 FREQUENTLY ASKED QUESTIONS / KEY ISSUES RAISED DURING THE CONSULTATION PERIOD (updated 7 September 2017) Q1. Why has some documentation
A STRATEGY FOR SURVIVAL At Wishaw General Hospital there is growing awareness that advanced nurse practitioners are the way ahead. Without them local
 A STRATEGY FOR SURVIVAL At Wishaw General Hospital there is growing awareness that advanced nurse practitioners are the way ahead. Without them local services are not sustainable, but urgent investment
A STRATEGY FOR SURVIVAL At Wishaw General Hospital there is growing awareness that advanced nurse practitioners are the way ahead. Without them local services are not sustainable, but urgent investment
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary
 Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
EXECUTIVE SUMMARY OF THE INDEPENDENT INVESTIGATION INTO THE MENTAL HEALTH CARE AND TREATMENT OF PATIENT E COMMISSIONED BY THE FORMER NORTH EAST
 EXECUTIVE SUMMARY OF THE INDEPENDENT INVESTIGATION INTO THE MENTAL HEALTH CARE AND TREATMENT OF PATIENT E COMMISSIONED BY THE FORMER NORTH EAST STRATEGIC HEALTH AUTHORITY 1 Contents Page The Panel 3 1
EXECUTIVE SUMMARY OF THE INDEPENDENT INVESTIGATION INTO THE MENTAL HEALTH CARE AND TREATMENT OF PATIENT E COMMISSIONED BY THE FORMER NORTH EAST STRATEGIC HEALTH AUTHORITY 1 Contents Page The Panel 3 1
Inpatient and Community Mental Health Patient Surveys Report written by:
 2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
National Patient Experience Survey South Tipperary General Hospital.
 National Patient Experience Survey 2017 South Tipperary General Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to
National Patient Experience Survey 2017 South Tipperary General Hospital /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Job Description. Job title: Uro-Oncology Clinical Nurse Specialist Band: 7
 Job Description Job title: Uro-Oncology Clinical Nurse Specialist Band: 7 Department: Cancer Services Hours: 37.5 (min 22.5 hrs) Reports to: Lead Nurse for Cancer We are a pioneering research active organisation
Job Description Job title: Uro-Oncology Clinical Nurse Specialist Band: 7 Department: Cancer Services Hours: 37.5 (min 22.5 hrs) Reports to: Lead Nurse for Cancer We are a pioneering research active organisation
Care and Treatment Review: Policy and Guidance
 Care and Treatment Review: Policy and Guidance With policy and guidance on Care, Education and Treatment Reviews for children and young people Easy Read Version 2017 1 Contents Foreword from Gavin Harding...
Care and Treatment Review: Policy and Guidance With policy and guidance on Care, Education and Treatment Reviews for children and young people Easy Read Version 2017 1 Contents Foreword from Gavin Harding...
Urgent and emergency mental health care pathways
 Urgent and emergency mental health care pathways Initial guidance for improving data quality in the Mental Health Services Dataset (MHSDS) Published August 2018 Copyright 2018 NHS Digital Contents Who
Urgent and emergency mental health care pathways Initial guidance for improving data quality in the Mental Health Services Dataset (MHSDS) Published August 2018 Copyright 2018 NHS Digital Contents Who
Report on Call for Evidence: Elderly Hospital Care, Hospital Discharge & Dementia Identification
 Report on Call for Evidence: Elderly Hospital Care, Hospital Discharge & Dementia Identification Healthwatch Sunderland October 2014 Elderly People are not always thoroughly assessed in hospital. This
Report on Call for Evidence: Elderly Hospital Care, Hospital Discharge & Dementia Identification Healthwatch Sunderland October 2014 Elderly People are not always thoroughly assessed in hospital. This
NELFT Integrated Adult Care Pathway - Acute and Crisis Care. Asif Bachlani Wellington Makala
 NELFT Integrated Adult Care Pathway - Acute and Crisis Care Asif Bachlani Wellington Makala Introductions Dr Asif Bachlani Consultant Psychiatrist B&D Access, Assessment and Brief Intervention Team Associate
NELFT Integrated Adult Care Pathway - Acute and Crisis Care Asif Bachlani Wellington Makala Introductions Dr Asif Bachlani Consultant Psychiatrist B&D Access, Assessment and Brief Intervention Team Associate
We had 7 folk on the phones (who took these calls on phones away from the public sales desk) and 3 with face to face customers.
 and 3 with face to face customers.") APPENDIX F Difficulty Getting a Same Day Appointment (copied and pasted from our website) The problem with this type of appointment system seems to be that when attempting to make an appointment for not
APPENDIX F Difficulty Getting a Same Day Appointment (copied and pasted from our website) The problem with this type of appointment system seems to be that when attempting to make an appointment for not
Improvement Happens: An Interview with Deeb Salem, MD and Brian Cohen, MD
 INNOVATION AND IMPROVEMENT Improvement Happens: An Interview with Deeb Salem, MD and Brian Cohen, MD Matthew J. Press, MD, MSc Departments of Public Health and Medicine, Weill Cornell Medical College,
INNOVATION AND IMPROVEMENT Improvement Happens: An Interview with Deeb Salem, MD and Brian Cohen, MD Matthew J. Press, MD, MSc Departments of Public Health and Medicine, Weill Cornell Medical College,
BIRMINGHAM COMMUNITY HEALTHCARE NHS TRUST: HEALTHY VILLAGES AND THE COMPLETE CARE MODEL
 BIRMINGHAM COMMUNITY HEALTHCARE NHS TRUST: HEALTHY VILLAGES AND THE COMPLETE CARE MODEL Summary Healthy Villages is a partnership between Birmingham Community Healthcare (BCH) and other NHS providers and
BIRMINGHAM COMMUNITY HEALTHCARE NHS TRUST: HEALTHY VILLAGES AND THE COMPLETE CARE MODEL Summary Healthy Villages is a partnership between Birmingham Community Healthcare (BCH) and other NHS providers and
HIGHLAND USERS GROUP (HUG) WARD ROUNDS
 WARD ROUNDS") HIGHLAND USERS GROUP (HUG) WARD ROUNDS A Report on the views of Highland Users Group on what Ward Rounds are like and how they can be made more user friendly June 1997 Highland Users Group can be contacted
HIGHLAND USERS GROUP (HUG) WARD ROUNDS A Report on the views of Highland Users Group on what Ward Rounds are like and how they can be made more user friendly June 1997 Highland Users Group can be contacted
Analysis of Continence Service In Teesside
 Analysis of Continence Service In Teesside Feedback September 2017 Introduction Local Healthwatches have been set up across England to create a strong, independent consumer champion with the aim to: Strengthen
Analysis of Continence Service In Teesside Feedback September 2017 Introduction Local Healthwatches have been set up across England to create a strong, independent consumer champion with the aim to: Strengthen
THE ROLE OF COMMUNITY MENTAL HEALTH TEAMS IN DELIVERING COMMUNITY MENTAL HEALTH SERVICES
 THE ROLE OF COMMUNITY MENTAL HEALTH TEAMS IN DELIVERING COMMUNITY MENTAL HEALTH SERVICES Interim Policy Implementation Guidance and Standards [July 2010] - 1 - CONTENTS 1. Introduction... 3 2. The guiding
THE ROLE OF COMMUNITY MENTAL HEALTH TEAMS IN DELIVERING COMMUNITY MENTAL HEALTH SERVICES Interim Policy Implementation Guidance and Standards [July 2010] - 1 - CONTENTS 1. Introduction... 3 2. The guiding
Annual Report Summary 2016/17
 Annual Report Summary 2016/17 Making sure you get the healthcare you need Annual Report summary 2016/17 Introduction by our Clinical Chair and Chief Executive Officer Dr Chris Ritchieson Clinical Chair
Annual Report Summary 2016/17 Making sure you get the healthcare you need Annual Report summary 2016/17 Introduction by our Clinical Chair and Chief Executive Officer Dr Chris Ritchieson Clinical Chair
Patient Experience Strategy
 Patient Experience Strategy Published: June 2017 Find us online at cornwallft 1.Introduction At Cornwall Partnership NHS Foundation Trust (CFT) we believe in delivering high quality care. We care deeply
Patient Experience Strategy Published: June 2017 Find us online at cornwallft 1.Introduction At Cornwall Partnership NHS Foundation Trust (CFT) we believe in delivering high quality care. We care deeply
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Precious Homes Hertfordshire and Bedfordshire Oster House, Flat1,
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Precious Homes Hertfordshire and Bedfordshire Oster House, Flat1,
Report by the Local Government and Social Care Ombudsman. Investigation into a complaint against North Somerset Council (reference number: )
") Report by the Local Government and Social Care Ombudsman Investigation into a complaint against North Somerset Council (reference number: 16 018 163) 16 March 2018 Local Government and Social Care Ombudsman
Report by the Local Government and Social Care Ombudsman Investigation into a complaint against North Somerset Council (reference number: 16 018 163) 16 March 2018 Local Government and Social Care Ombudsman
Caremark Watford & Hertsmere
 S V Care Limited Caremark Watford & Hertsmere Inspection report 95 St Albans Road Watford Hertfordshire WD17 1SJ Tel: 01923729898 Date of inspection visit: 17 October 2017 30 October 2017 31 October 2017
S V Care Limited Caremark Watford & Hertsmere Inspection report 95 St Albans Road Watford Hertfordshire WD17 1SJ Tel: 01923729898 Date of inspection visit: 17 October 2017 30 October 2017 31 October 2017
SAFE Standard of Care
 SAFE Standard of Care THE NEW UK STANDARD OF CARE BANISH MEDICATION ERRORS We all know that when medication is prescribed, dispensed and administered correctly it can dramatically improve the quality of
SAFE Standard of Care THE NEW UK STANDARD OF CARE BANISH MEDICATION ERRORS We all know that when medication is prescribed, dispensed and administered correctly it can dramatically improve the quality of
Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan
 Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan 2015-2020 1 Introduction 1.1 Welcome to the update on Warrington s Local Transformation Plan for Children and
Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan 2015-2020 1 Introduction 1.1 Welcome to the update on Warrington s Local Transformation Plan for Children and
NHS Grampian. Intensive Psychiatric Care Units
 NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
Shaping the best mental health care in Manchester
 Clinical Transformation Plans Manchester Shaping the best mental health care in Manchester Meeting the needs of our communities Improving Lives OUR SHARED WAY AHEAD... Clinical Service Transformation in
Clinical Transformation Plans Manchester Shaping the best mental health care in Manchester Meeting the needs of our communities Improving Lives OUR SHARED WAY AHEAD... Clinical Service Transformation in
Clinical Strategy
 Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
CASE STUDY: THE ADULT MENTAL HEALTH (AMH) MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS.
 MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS.") CASE STUDY: THE ADULT MENTAL HEALTH (AMH) MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS. Summary The Adult Mental Health (AMH) model is a new initiative which
CASE STUDY: THE ADULT MENTAL HEALTH (AMH) MODEL-REDESIGN OF INTEGRATED SERVICES FOR WORKING AGE ADULTS WITH SEVERE MENTAL ILLNESS. Summary The Adult Mental Health (AMH) model is a new initiative which
NURS 6051: Transforming Nursing and Healthcare through Information Technology Electronic Health Records Program Transcript
 NURS 6051: Transforming Nursing and Healthcare through Information Technology Electronic Health Records Program Transcript [MUSIC PLAYING] NARRATOR: Because patient data, research evidence, and best practices
NURS 6051: Transforming Nursing and Healthcare through Information Technology Electronic Health Records Program Transcript [MUSIC PLAYING] NARRATOR: Because patient data, research evidence, and best practices
Health and Social Care Alliance Scotland Carer Responses Analysis: Summary of Findings
 Health and Social Care Alliance Scotland Carer Responses Analysis: Summary of Findings 1. Introduction Professors Jane Joy, University Teacher, Nursing and Health Care and her colleague Diane Willis, University
Health and Social Care Alliance Scotland Carer Responses Analysis: Summary of Findings 1. Introduction Professors Jane Joy, University Teacher, Nursing and Health Care and her colleague Diane Willis, University
Rapid Response. Crisis Team. Anne Williams Alison Dalley
 Rapid Response Health and Social Care Health and Social Care Crisis Team Anne Williams Alison Dalley Salford the context Population 220,000 Long history of joint working across Council/PCT Provide range
Rapid Response Health and Social Care Health and Social Care Crisis Team Anne Williams Alison Dalley Salford the context Population 220,000 Long history of joint working across Council/PCT Provide range
September Workforce pressures in the NHS
 September 2017 Workforce pressures in the NHS 2 Contents Foreword 3 Introduction and methodology 5 What professionals told us 6 The biggest workforce issues 7 The impact on professionals and people with
September 2017 Workforce pressures in the NHS 2 Contents Foreword 3 Introduction and methodology 5 What professionals told us 6 The biggest workforce issues 7 The impact on professionals and people with
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS
 CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
Gerry Bennett Ward (Mile End Hospital) - Enter and View Report
 - Enter and View Report") Gerry Bennett Ward (Mile End Hospital) - Enter and View Report Service: Gerry Bennett Ward (Mile End Hospital) Provider: Barts Health - CHS Date / Time: 24 th February 2015 / 10.00am -13.00pm Healthwatch
Gerry Bennett Ward (Mile End Hospital) - Enter and View Report Service: Gerry Bennett Ward (Mile End Hospital) Provider: Barts Health - CHS Date / Time: 24 th February 2015 / 10.00am -13.00pm Healthwatch
Key findings from the Healthwatch Southwark report Appointment systems at GP practices are they working?
 About this event Key findings from the Healthwatch Southwark report Appointment systems at GP practices are they working? What the NHS Southwark CCG is doing to support general practice services and how
About this event Key findings from the Healthwatch Southwark report Appointment systems at GP practices are they working? What the NHS Southwark CCG is doing to support general practice services and how
Adult Mental Health Team AMHT Standard Operating Procedure
 SH CP 198 Adult Mental Health Team AMHT Standard Operating Procedure Summary: Keywords: Target Audience: This Standard Operating Procedure describes the roles and functions of The Acute Mental Health Teams
SH CP 198 Adult Mental Health Team AMHT Standard Operating Procedure Summary: Keywords: Target Audience: This Standard Operating Procedure describes the roles and functions of The Acute Mental Health Teams
Connected Palliative Care Partnership End of Year Report
 where everyone matters Sandwell and West Birmingham Hospitals NHS Trust Connected Palliative Care Partnership End of Year Report 2016 2017 Sandwell and West Birmingham Clinical Commissioning Group Contents
where everyone matters Sandwell and West Birmingham Hospitals NHS Trust Connected Palliative Care Partnership End of Year Report 2016 2017 Sandwell and West Birmingham Clinical Commissioning Group Contents
Improving General Practice for the People of West Cheshire
 Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
List of Electronic Areas where patient information is held within the patient s folders on RiO / IAPTus. RiO CHECKLIST
 Appendix 7 List of Electronic Areas where patient information is held within the patient s folders on RiO / IAPTus. RiO CHECKLIST NTW SOT Initial response team folder NTW IRT Telephone triage NTW IRT Rapid
Appendix 7 List of Electronic Areas where patient information is held within the patient s folders on RiO / IAPTus. RiO CHECKLIST NTW SOT Initial response team folder NTW IRT Telephone triage NTW IRT Rapid
Issue No. 5, May 2014
 Issue No. 5, May 2014 OPAC on TRACK We wanted to update you as to the huge amount of work ongoing in regards to OPAC in Raigmore. We realise it has been a while since we last issued this newsletter, however,
Issue No. 5, May 2014 OPAC on TRACK We wanted to update you as to the huge amount of work ongoing in regards to OPAC in Raigmore. We realise it has been a while since we last issued this newsletter, however,
Bowel Independence Day A survey on bowel management in multiple sclerosis. Supported by
 Bowel Independence Day 2014 A survey on bowel management in multiple sclerosis Supported by July 2014 1 Contents Introduction... 3 Overview of views from people with MS... 5 Overview of views from specialist
Bowel Independence Day 2014 A survey on bowel management in multiple sclerosis Supported by July 2014 1 Contents Introduction... 3 Overview of views from people with MS... 5 Overview of views from specialist
NHS Continuing Healthcare Funded Care Report Frequently Asked Questions 2017/18
 NHS Continuing Healthcare Funded Care Report Frequently Asked Questions 2017/18 Version: 3.1 NHS Continuing Healthcare Funded Care Report Frequently Asked Questions 2017/18 Version number: 3.1 First released:
NHS Continuing Healthcare Funded Care Report Frequently Asked Questions 2017/18 Version: 3.1 NHS Continuing Healthcare Funded Care Report Frequently Asked Questions 2017/18 Version number: 3.1 First released:
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST EXECUTIVE REPORT - CURRENT ISSUES
 THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST EXECUTIVE REPORT - CURRENT ISSUES Agenda item A4(i) 1. Executive Team Particular attention is drawn to: i) Executive arrangements during the period
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST EXECUTIVE REPORT - CURRENT ISSUES Agenda item A4(i) 1. Executive Team Particular attention is drawn to: i) Executive arrangements during the period
Homecare Support Support Service Care at Home 152a Lower Granton Road Edinburgh EH5 1EY
 Homecare Support Support Service Care at Home 152a Lower Granton Road Edinburgh EH5 1EY Type of inspection: Unannounced Inspection completed on: 19 December 2014 Contents Page No Summary 3 1 About the
Homecare Support Support Service Care at Home 152a Lower Granton Road Edinburgh EH5 1EY Type of inspection: Unannounced Inspection completed on: 19 December 2014 Contents Page No Summary 3 1 About the
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
North Gwent Crisis Resolution & Home Treatment Team Operational Policy
 North Gwent Crisis Resolution & Home Treatment Team Operational Policy Mission Statement The purpose of the Crisis Resolution & Home Treatment Team (CRHTT) is to provide emergency assessment and intervention
North Gwent Crisis Resolution & Home Treatment Team Operational Policy Mission Statement The purpose of the Crisis Resolution & Home Treatment Team (CRHTT) is to provide emergency assessment and intervention
Referral Received. Triage. Non-Urgent Referral. MDT Meeting. Complete Core Information (Protocol for Completion) Complete Risk Assessment.
 Complete Risk Assessment.") I want to go straight to Forms and Templates I want to go back to Care Pathways Website Use Core Pathway checklist Referral Received Admin Tasks Triage ONE WEEK Urgent Referral (Triggers) Non-Urgent Referral
I want to go straight to Forms and Templates I want to go back to Care Pathways Website Use Core Pathway checklist Referral Received Admin Tasks Triage ONE WEEK Urgent Referral (Triggers) Non-Urgent Referral
Mental Health Services 2011
 Mental Health Services 2011 Inspection of Mental Health Services Resource Centre Day Hospital Inspected Executive Catchment Area HSE Area Droumleigh Resource Centre, Bantry South Lee, West Cork, South
Mental Health Services 2011 Inspection of Mental Health Services Resource Centre Day Hospital Inspected Executive Catchment Area HSE Area Droumleigh Resource Centre, Bantry South Lee, West Cork, South
Mental Health Crisis Pathway Analysis
 Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking