Essex Primary Care Workforce Strategy
|
|
|
- Nickolas Tyler
- 5 years ago
- Views:
Transcription
1 Essex Primary Care Workforce Strategy
2 CONTENTS Page Introduction 4 Executive Summary 5 Aim 6 National Context for Primary Care 6 Future Access to Services in Essex 7 Local Workforce Context for Primary Care 8 Workforce Strategy 10 Workforce Challenges for Essex 11 The Current Workforce in Essex 12 MAINTAIN AND DEVELOP THE CURRENT PRIMARY CARE BASE Medical Workforce 14 General Practitioners 14 GP trainees 15 Salaried GPs 15 GP Flexible Roles 15 EU GP recruitment 15 Nursing Workforce 16 Clinical leadership/lead Nurse 16 Advanced Nurse Practitioners 17 General Practice Nurses 17 Health Care Assistants 18 Community Pharmacy 18 Mental Health Therapists 18 Non-clinical Workforce 18 Operations Practice Manager 18 Practice Manager 20 Care Co-ordination service 21 GP Care Advisors 21 Clinical & Non-clinical Apprenticeships 22 SCALING UP SERVICES AND THE NEW ROLES REQUIRED IN A SUPER PRACTICE/GP ALLIANCE General Practitioners 23 CQC Inspection/Visit Preparation Support 24 Lead Nurse Revalidation Support and Development 24 Specialist Nurses 24 General Practice Nurses 25 Student nurses 25 Health Care Assistants 25 Associate Practitioner 25 Nurse Associate 26 Physicians Associates 26 Community Pharmacy 26 Physiotherapists 27 Paramedics 27 WORK ACROSS BOUNDARIES TO DELIVER STPs
3 Virtual Surgery 28 Social Workers 29 UNDERPINNING THE WORKFORCE STRATEGY Patient Participation Groups (PPG) 29 Voluntary Sector 29 Recruiting and Retaining Staff 29 Promoting General Practice as a Career 30 Training and Development 30 Technology 30 Workforce planning 30 Agile Working 31 Conclusion 32 Summary 33 Next Steps 33 Appendices 1. Primary Care Foundation with the NHS Alliance (2015) Making 34 time in general practice. 2. GP workforce '10 point' plan Health Education England GP Workforce Survey Health Education England Nursing Education Framework (2016) Projected Placement of Split of Full Time Nursing Students Intake The 15 standards in the Care Certificate CCG Key Deliverables High Level Overview GPFV Schemes 41 Glossary 43 References 44
4 Primary Care Workforce Strategy Introduction Primary Care is the shop window of healthcare services, prevention and management and offers exciting career opportunities. The huge variety of roles and scope for innovation is vast and is due to the fact that over 80% of healthcare is delivered outside of the Acute Hospital sector. The steady stream of patients with varying needs makes the most of the skills and front line engagement across all roles - GP, Nurse, Physiotherapist, Apprentice, Care Navigator, Pharmacist in fact the entire Primary Care Team. To create a healthier and more sustainable future for the people of Essex, Clinical Commissioning Groups (CCGs) need to develop and manage services to meet the increasingly complex care needs of patients, through commissioning high quality care in the most appropriate place, at the optimal time, within the resources available. GP consultation rates have continued to increase by 40% between 2005 and 2008 and are predicted to rise by a further 35% by But in a recent survey conducted by HEE, 27% of GPs were thinking of retiring within the next five years, 11% were thinking of leaving clinical practice for other reasons and 3% were moving to another speciality. When asked what factors would influence them to remain in general practice, 29% said salary, 25% said flexible working hours with the most commonly occurring theme in the other responses was workload. Primary Care in Essex is central to the future delivery of health care and promotion to the people of Essex. In order to do this we need to: build on the best of what is already in place develop new ways of working work with other organizations In order to achieve this we will: extend current roles develop new roles work across organizational boundaries Therefore new models of care are being planned for Primary Care. Many existing healthcare professionals will be able to expand and develop their roles, and roles will evolve meaning patients will be seen by the most appropriate healthcare professional. Clinical staff will have better administrative support and, when needed, healthcare professionals will be able to spend more time with their patients to discuss and plan their care. They will also be able to use a variety of ways to communicate with patients and colleagues using telephone, , electronic messaging and videoconferencing as appropriate. Strategies need to be put into place which help change public perception that they always need to see a GP or if they need to visit a GP. Practices and all services need to promote the appropriate use of other health practitioners and give guidance as to with whom, when and where they can access such services. Primary Care will still be based around the GP practice holding responsibility for the care of its registered patients, but they will have a stronger population focus and an expanded workforce through the collaborations of the Super practice/gp Alliances. These will have a variety of roles and
5 services embedded to enable the service to run as a One Stop Shop. This means it must have near to patient diagnostics, nurse led services, midwifery/health Visitor services, MSK and Social Services along with Specialist GP sessions. This will enable MDT formation and collaboration at a muchenhanced level. The old boundaries of working practices will need to be changed in line with new professional ways of working. New services require new ways of working and structure such changes are challenging but are required given that current demand and services are no longer sustainable with existing models. This strategy paper outlines the workforce roles and actions for Essex to develop and deliver an innovative, integrated care workforce model to deliver services effectively. It will be a challenge to overcome deep rooted cultural and established practices to move to new roles, new practices and joint working not only individually but across individual organisations and care providers. However, with the right support, collaborative working and combined leadership it should be achievable. Executive Summary An overarching sustainable primary care workforce planning strategy is critical to ensure that there is a skilled workforce to deliver current and future services with new ways of working. Workforce models should aim to deliver a capable, coordinated, sustainable and resilient workforce to meet the needs of patients. This strategy recognises that a change in basic assumptions is required from many people being acutely unwell and requiring complex care in hospital settings, to more people taking responsibility for their own health and wellbeing, with more care being delivered in the community and closer to patients homes. The primary care workforce strategy has a comprehensive, collaborative approach towards commissioning the future workforce training and development. This includes planning the change management required to deliver services as envisioned by the General Practice 5 Year Forward View (GPFV) and Shape of Caring Review policies alongside the Sustainability and Transformation Plans (STP) now under consideration. The Community Education Provider Network (CEPN) has developed strong partnerships working with stakeholders including GPs, Essex County Council, and others, to input into the recently published STP now in consultation. The first stage of assessing the development of an integrated health and social care workforce has been undertaken and the primary care GPFV operational plans were submitted to NHSE in February These give a high-level outline of how the activity is planned to be delivered across the CCGs and STP areas. A detailed analysis and research has been undertaken by CEPN, and the CCGs with input from a variety of stakeholders and resources including Health Education England (HEE), Education & Quality in Primary Care (EQUIP) and Essex Primary Care Inter-professionals Centre for Workforce Development (EPIC). The remit is to develop existing roles and to expand these roles. A focus on creating and developing new roles and competencies, new ways of working to deliver services across historic boundaries. This will build upon the Primary Care Foundation report recommendations Making time in general practice (PCF 2015). This paper seeks to collate the combined strategies that seek to continue the Essex-wide primary care workforce transformation journey to address current key workforce issues. The work considers what needs to be addressed, highlights the developments achieved to date, and identifies what new roles may be required. It also highlights potential solutions and the key deliverables to be considered as part of a comprehensive implementation plan.

6 Aim The aim of this workforce strategy is to highlight potential ways to develop and recruit a primary care workforce to deliver current and future developments in services on a sustainable basis. This will be achieved with a strategic focus on recruitment and attraction alongside retention of the highly skilled staff currently in the workforce. A key aim will be to develop and educate the workforce, across the Essex STP footprints enabling staff to be confident and competent to deliver services to patients. All services will include a care focus that enhances and encourages patient self-management enabling as well as being supportive across their care pathway and the STP area. National Context for Primary Care Investment in primary care has fallen well behind investment in hospitals, despite increasing expectations of the work that could be done in primary care. Between 2003 and 2013, the number of hospital consultants increased by 48 percent while GP numbers increased by only 14 percent. Indeed, the number of GPs per head of population has declined since 2009, with major recruitment and retention problems. The latest data from the General Medical Council (GMC) Register shows an increase in overall numbers to 67,772 GPs on the Register by the end of 2016 (Graph1). However only 61,137 were licenced to practise. At this stage, there is no clear evidence as to why this is the case. Graph 1: Doctors on the GP Register each year from Source: GMC Register of GPs 2016 In comparison, GP consultation rates have continued to increase by 40% between 2005 and 2008 and are predicted to rise by a further 35% by Therefore, strategies need to be put into place which help change public perception that they always need to see a GP or if they need to visit a GP. Practices and all services need to promote the appropriate use of other health practitioners and give guidance as to with whom, when and where they can access such services. NHSE and Public Health have used this strategy of multi-professional team working across primary and secondary care during the winter to reduce inappropriate attendance at A&E s and General Practice although the impact of these messages is not yet known. However, the Vanguards have recently evaluated the impact of their pilots to reduce the pressure on A&E and hospitals. One such example is the Better Care Together vanguard in Morecambe in the rural area of Millom where GPs have been supported by a community paramedic with the use of video links to A&E. This
7 remote specialist triage in the community has avoided unnecessary attendance at A&E with a reduction of 29% in A&E attendances from in this area (Jones, 2017). Another area of focus in the GPFV is how to better provide services for patients with long term conditions (LTC) which currently takes up around 50% of all GP appointments. The PCF suggested 10 high impact actions that could help manage the workload (Appendix 3). NHSE, HEE, RCGP and BMA have produced a joint paper Building the Workforce the new deal for general practice which highlights a 10-point plan for the recruitment, retention and return of GPs (Appendix 2) (NHSE 2015). Nursing is another area of serious concern, with an ageing workforce in General Practice Nursing (GPN) and similar problems of recruitment and retention. Between 2001 and 2011 the number of community nurses fell by 38 per cent and there is a growing dependency on agency staff. Only in pharmacy does there appear to be a potentially adequate supply of newly trained graduates (Primary Care Workforce Commission, 2015). There is a growing gap between patients needs and the skills and knowledge of the workforce. The current workforce was trained for acute, episodic, single disease based models of care. Those now placing the greatest demands on the health service are LTCs and multiple illnesses. Therefore, the GPFV strategy looks to change models and care pathways by integrating care services to streamline care across traditional boundaries towards providing seamless care. Patients and their carers require services that meet those needs and these may not necessarily be from just one organisation. Therefore, commissioning must be on a needs basis built on integrated pathways and services with a multi-functional workforce in place to deliver those services. With these challenges, there are also opportunities to redesign services and to access resources available through the GPFV, new GP contract agreements and with NHSE funding allocations. This strategy will support Essex CCGs to take advantage of such opportunities identifying areas for focus. Future Access to Services in Essex Essex CCGs have a vision of how people in the catchment area are able to access services now and in the future. The development of several Super partnerships/gp Alliances outlined in the STPs and the GPFV will bring together the primary care, secondary care and third sector services across the county. The aim of these is to provide a positive experience with ease of access to all the information they may require a shop window to the locality with clear signposting to meet their needs. For ease of reference, the term Super practices/gp Alliance has been used throughout this document in referring to this model of services. It is important to recognise that whilst this term is used it is not envisaged that this will necessarily be a physical place; rather it is a virtual Super practice/gp Alliance describing a way of working and as such may be configured very differently according to local need. There are a variety of visual graphics across the CCGs describing a Super practice/gp Alliance and all are very similar to the Canterbury (New Zealand) Health System model shown in Diagram 1. The focus of this, and the proposed model, is for the patient to be at the centre of care for all services working together with a Care Coordinator helping the patient by navigating the services throughout. The GPFV actions in regards to access and services have been summarised into a deliverables plan taken from each CCGs GPFV plans (Appendix 7).
. Within the Essex population there is a very mixed age and social demographic (Graph 2).")
8 Diagram 1: Vision for patient/family access to services Local Workforce Context for Primary Care Canterbury New Zealand Health System (2016) Essex currently has 1,214* GPs active across the CCGs with a population of 1,860,696** registered with all GP practices in the area (*EPIC 2017, **HISIC 2017). Within the Essex population there is a very mixed age and social demographic (Graph 2). Therefore, it will be important to have a whole population approach with Public Health for targeting the differing groups to meet their healthcare and lifestyle needs of the future. This includes health education information, what services are appropriate, how these can be accessed and who can deliver them. The GPFV and Making Time in General Practice papers indicate that, to prepare for the reduction in workforce, a growing population and the elderly living longer with complex co-morbidities, Primary Care needs to find alternative and innovative ways to reduce pressure on the GPs, provide additional access for patients and increase promotion of self-care. Navigating through a complex health and social care system is challenging for patients and their carers. Therefore, an effective marketing and communication strategy to educate and promote self-care and its benefits is required. This would help to change patient expectations and behaviours. Upskilling the receptionist to a Care Navigator will help to safely signpost patients to appropriate services including those provided by the voluntary and community sectors. It would be a process designed to educate, empower and provide advocacy for patients and carers to ensure they have the best possible experience of prevention, intervention, support and care and that their intended health outcomes are met, whilst maximising the use of limited resources and reducing costs where possible.

9 For patients to make informed choices about the most appropriate person to see they will need clear information that sets out what that person does and why they are being seen by that professional rather than a GP. A joint communication strategy on public information media that can be tailored also to locality to provide consistent messaging is required. Also, ensuring that staff are given training on services and signposting patients as a joint initiative with other stakeholders would ensure consistency. This training initiative should be led by the CEPNs /LWABs with HEE. Graph 2: Age Demographics of GP Practice Registered Patients across Essex CCGs Age Demographics Essex 300, , , , ,000 50, , , , , , , , , , ,709 23,360 18,007 Source: HISIC Data: accessed January 2017 In line with the national picture, Essex is anticipating a highly significant change in the county s older demographics. The current age demographics for over 65 s can be seen in Graph 3 which identifies a significant difference between male: female ratios especially noticeable in the 95+ age group. This shows that the male: female ratio is 30%/70%. For the age group, there is a smaller gap with male: female ratios of 39%/61%. Graph 3: No. Essex GP Practice Patients by Age Group Essex Age Demographics Male:Female 175, , , , , , , ,283 91,375 Male Female 109,124 75,000 50,000 25,000 52,429 55,582 62,693 65,992 18,981 12,664 - Source: HISIC Data accessed January 2017 Research in the medical data would assist in highlighting the reasons for such a disparity and help towards health intervention targeting which may need to be gender specific. People with LTCs, such as diabetes, chronic obstructive pulmonary disease, arthritis and hypertension, account for around 50% of all GP appointments. Those with LTCs also fill 64% of hospital outpatient appointments and 70% of inpatient bed days. Approximately 7 of every 10 spent on health and social care is spent on LTCs (Department of Health, 2012). The number of people with three or more LTCs is rising, and it is expected there will be over 45,000 in North East Essex, West and East Sussex by 2018.
10 The new GP Contract will benefit from the transfer of funds to help GP practices to implement care measures for frail and elderly patients as 157 million from a previous earmarked scheme will be transferred into core GP funding so that family doctors can be more flexible in how they care for the frailest. Therefore, the practices may be able to access this funding to help identify service development that could support the aged workforce shown in the demographics (Thomas 2017). This service development will include more direct access for patients from the multi-professional team and care-navigator support as described elsewhere in this document. Therefore, delivering services differently must be a key part of managing the demographic change as the current models are not sustainable for such increased need. Not changing the way services are delivered is no longer an option Workforce Strategy To aid this process, in September 2016 CEPN invited NHSP Workforce Insight (NHSP) to assist in the development of a document which sets out a shared understanding of the vision for: The future internal workforce needs for Essex across the boundaries, especially for medicine and nursing A recruitment & retention strategy for the primary care workforce Potential of new worker roles and how these could be used across differing organisations Development and implementation of new ways of working based on best practice models In order to achieve this vision we (Essex CCGs and our constituent practices) will need to undertake the actions set out in this document. Several CCGS have taken significant steps to move forward with the creation and development of new roles to support GPs and nursing. Medical forums are well embedded but nursing ones less so. However, where CCGs and EPIC have created informal forums this does help bring professional leadership into the teams. Castle Point & Rochford have developed a practice nurse forum over the last 12 months as part of their Time To Learn development sessions. This has helped those involved consider issues such as professional development and Revalidation requirements as well as share good practice. However, such forums across other areas are patchy and there is a need to ensure good practice and success is replicated across all the CCGs, in line with the aims and objectives of both STPs for the area. There is also a need to develop the workforces knowledge with updates on services available to be able to be consistent in the approach to guiding and educating patients towards self-care safely and effectively. Regular sharing or access to the outcomes and work of the primary care vanguards would be an advantage so that the whole team can look to see what service development could prove advantageous to their localities. There are five ways of supporting the workforce to meet the changes:

11 The importance of staff development and support is an investment that will benefit both staff and the public. Therefore, this strategy seeks to outline the type of workforce and skills required in the future. New ways of working are always a challenge to put into place and the following are key elements to delivering a supported, successful partnership process to take forward such a strategy: Leadership Workforce Intelligence Job/role design Training Capacity Skills Organisational structure design Culture change Table 1: Key Characteristics to Success Change Process Strong leadership structure across all sectors to create an environment of collaboration, monitoring and continuous improvement for an integrated workforce Accurate up to date workforce database in place to inform future workforce strategy and planning Determine responsibilities and accountabilities of roles for effective workflow which are competency based with clear role expectations Training practices that currently facilitates and supports the training of staff to be fully quantified and objectively evaluated to show attraction, retention, development, and investment return. Develop training to support changing practices, clinical and service development that supports new roles Ensuring sufficient resources in place for effective delivery and performance for service needs with clear, co-joined strategies across all staff groups/providers Ensuring the right skills are available/developed to meet the changing needs of services Development and implementation of organisational structures that support cost effective business processes, effective governance, and workforce development To support the workforce in adopting new working roles, practices with collaborative working and desired behaviours Workforce Challenges for Essex The challenge to provide and deliver high quality, seamless integrated care services by skilled staff is huge and there are significant barriers to overcome. These include skill shortages, attrition from nursing and medical courses, lack of career and development opportunities and the requirements for flexible working arrangements. Current demands are unsustainable within existing resources and this is resulting in staff leaving, retiring as soon as possible, or the continued risk of experiencing burn out.
12 With potential new care models needing integration between sectors, staff may require additional training, development, and support to adapt and be confident. Alongside this there may well be a need for a change in mind-set to be able to align with new culture and strategic direction. There will be a need to commission training and support to help staff meet these new challenges and feel confident in new ways of working. The Vanguard pilots have demonstrated a number of ways of working differently and effectively and that experience will be utilised as part of the ongoing workforce strategy programme ( In any collaborative, joint workforce initiatives, it is important that consideration is given to designing arrangements that can ensure employees can work in a variety of suitable locations with appropriate indemnity and accountability. As well as these roles, which encompass the need for greater geographical mobility (multi-site working), there is a need to have acknowledgement of this in the terms and conditions to cover mileage/travel costs. It would be beneficial to commence pooling and sharing of these policies and agreements at an early stage to develop joint agreements and terms. A detailed gap analysis should be undertaken of the education, training needs and future regulatory requirements for all groups building on the work undertaken by EQUIP and HEE to date. The considerable work undertaken by EPIC already on behalf of the CCGs needs to be objectively evaluated to learn what has proved to be most beneficial from both a service and individual aspect. Any future evaluation should include a focus on any new roles and those currently still in development (Nursing Associate, Apprentice, new AHP roles) and new models of care not basing assumptions on the status quo as this is not sustainable. The Super partnerships/gp Alliances will need to ensure that their model encompasses the needs of the rural practices and their needs also based on this hub and spoke approach to services. To do this, then partnership initiatives require collaboration on standardising care models and ways of working so that one care model or stakeholder does not dominate but instead creates an environment for creative, innovative staff who are well motivated and engaged. Junior staff roles clinical or administrative can also play a valuable part in development of services. It is important that the geographical location variances are acknowledged and taken into consideration - rural communities are not well served by public transport and this is something that needs to be considered for access to training and when developing/relocating services. Regardless of the models and workforce distribution, what is clear is there is a need to strengthen and support strong, visible and dynamic clinical leadership, as well as general organisational leaders which has started through the EPIC model. Clinical leadership gives confidence to clinical staff and patients that services/changes are developed with the patient at the centre of care, are based on best clinical practice with a sound evidence-base. The Current Workforce in Essex Health Education East of England (HEE) have been developing a detailed 5-year workforce strategy in conjunction with stakeholders. Their aim is to describe the workforce educational needs, staff mixture and educational levels for future provision setting out the transformation programme required for developing the future workforce in conjunction with the CCGs. Such a strategy needs to be owned and shared with all stakeholders when available to ensure comprehensive, practical and positive engagement. Therefore, Essex CCGs are engaging with HEE to undertake this work and are encouraging providers to fully participate with different workgroups across the County exploring their locality needs.
13 However, there is still some way to go to achieve comprehensive detail on the workforce numbers and structures across the STP footprints which cross the boundaries. The basic aims and objectives are relevant to all the CCGs and adaptable to be sustainable and meet the varying local needs. The current workforce issues are detailed in Table 2 although it is accepted that there are significant variances between practices which are impacted by locality - urban and rural practices. ISSUE FOUND National levels of GP Trainee Applications have reduced Capacity for GP Supervisor/ Trainer to increase GP trainee numbers Recruitment of GP Trainee on qualification Poor recruitment levels for Nursing staff HCA role, skills and competencies variable RISK STATUS/IMPACT ASSESSMENT Currently places filled to capacity but at risk of reducing due to: increased competition from London & Cambridge limited availability of GP Supervisor time in the Practices Constraints due to the current number of Supervisor & Trainers funded and in place Inability to recruit into vacant posts, salaried or partnership Inability to provide qualified nursing services; Inability to provide mentorship to student nurses; inability to supervise and mentor the HCA workforce; patient care will be compromised Standards of skills, competencies and access to training is inconsistent ACTION REQUIRED Rotational trainee programme to give variety of experience; Improved presence on all websites; Recruitment campaign offering flexible portfolio packages Utilize findings from EPICT Trainee GP survey findings Increase trainer time provision by use of retired/flexi time GPs on a flexible basis: To demonstrate the benefit of retention of skills /experience To provide mentoring support to trainees/newly qualified GPs To Provide supervision/support for potential nurse prescribers. Recruitment strategy to offer flexible, salaried contracts across the whole CCG area: Super practice/gp Alliance posts used to highlight the flexibility, professional satisfaction, quality services values of the roles and career potential The advantages of working in Essex to be given a higher profile on EPIC website to engage prospective applicant when landing on home page CCG/EQUIP website linked to facilitate advertising all local vacancies - all stakeholders linked The role of nurses NP and ANP to be standardised Terms & Conditions of employment need to be standardised Support to evidence professional development, skills enhancement with role development opportunities Rotational opportunities with secondary care especially for specialist nurses i.e. Diabetes, Tissue Viability, COPD The role and scope of HCA s to be standardised Terms & Conditions of employment need to be standardised Table 2: Issue/RAG status IDEAL OUTCOME/RAG STATUS All places fully subscribed Increased GP trainee places available Increased attraction & recruitment of GP trainees & newly qualified Increased applications for GP roles Super partnerships/gp Alliances become beacon site for trainees All posts filled Recruitment robust ANP roles developed to lead in specialties GP workload reduced Increased job satisfaction Enhanced patient satisfaction Roles are standardised and recruitment is robust to meet
14 ISSUE FOUND GPs not fully engaged in services for Care Homes RISK STATUS/IMPACT ASSESSMENT Current workload constrains access and access to other HCP needs to be enhanced to provide a more effective service to these patients ACTION REQUIRED Care Certificate to be implemented: For HCAs to achieve this minimum standard by providing access point and support For HCAs employed in social care sector/social services to have access and support to achieve this standard Personal development, skills enhancement, role development, career opportunities all to be evident Develop ANPs and community pharmacists to take on this role Triaging by ANP s avoiding unnecessary admission to A&E New role development opportunities such as paramedics IDEAL OUTCOME/RAG STATUS standards Recruitment is robust Role and career development opportunities Medication costs reduce Care is provided in the community Avoids admission to acute sector MAINTAIN AND DEVELOP THE CURRENT PRIMARY CARE BASE Clinical leadership is needed across all the different clinical professional workforce as there are varied professional needs and strategies therefore leadership needs are to be a part of any transformation strategy. Medical Workforce General Practitioners: Investment in Primary Care has fallen behind that of Secondary Care. Between 2003 and 2013 the number of GPs increased by only 14% and the number of GPs per head of population has fallen since 2009 with major issues around recruitment and retention with GPs happy to train in Essex but having no plans to remain after training. The North & South Essex GP Workforce Survey 2014, showed that Essex already has one of the lowest concentrations of GPs per 1,000 patients in England with a 27% vacancy rate. Essex needs to recruit an additional 143 GPs just to reach the national average. A staggering 46% of GPs are due to retire in the next 15 years (NHSE & LM 201). There is a belief that there are female GPs to recruit if there are suitable, flexible posts on offer. However, there is no information on actual numbers in Essex to use as a reference point. The strategy actions are based on the National and the Essex specific GP workforce information (Appendix 3). GP trainees:
15 In Essex, there is full recruitment to GP training but this is because of London circuits being oversubscribed. This turns what could be an advantage into a disadvantage with trainees coming to Essex to train and then returning to London. Although there are a high number of training practices in most CCGs, and support already in place in some areas, this is variable across the County. However, any increase in the number of training places would give more opportunity to recruit. It is recognised that training places attract income but they also have a cost impact which may not be fully recovered with the current model. However, if these could be further expanded, consideration of the logistical support required needs to be considered to prevent overloading the current level of trainers available. If trainees have a good experience and some flexibility of funding across a Super practice/gp Alliance patch could be created, or new roles being available even for a short period, it may be possible to encourage them to stay in the area Salaried GPs: To increase the use of salaried GPs, a new model of employment could be considered for these posts to be employed by a host organisation or by one of the CCGs rather than an individual practice as an approach to service provision county-wide. This would be a new approach but worth considering as there is evidence from the national picture that stability and certainty is becoming a more attractive proposition (BMA 2016; NSE 2015). All the reports suggest that there is a need to develop different and more flexible working arrangements that allow health care professionals to use their specialist skills. This is also noted in the North & South Essex GP Workforce Survey as an option that could encourage recruitment and retention (Appendix 3). Therefore, there is a need to collate information county-wide that shows all the current service models in operation i.e. evening surgeries, telephone triage, nurse led clinics, weekend options. The information is needed as to how these services are accessed, utilised and evaluated by patients to assess if these are options that should be offered in key practices around the county or Super partnerships/gp Alliances. The National data shows that the number of GPs over 55 years old leaving the profession, has risen over the last 10 years. To mitigate against this, HEE are launching a GP Career Plus scheme pilot in 2017/18 to test ways of offering flexibility and support for experienced GPs at risk of leaving general practice. This is recommended in the GPFV and the high impact actions as research suggests that experienced GPs may remain practicing if there is an opportunity to work more flexibly. This also mirrors the GP Workforce survey findings that GPs desire more flexible contract options that allow for the development of special interests and an improved work/life balance. These opportunities could help develop the infrastructure more to include opportunities for specialists to work within the Super partnerships/gp Alliances such as Gynaecology, Paediatrics, etc. to avoid referral to hospital. There could also be opportunities for secondary care specialists to gain experience in general practice. GP Flexible Roles: An option to consider is to have a placement for GPs to go into while they wait for a post to become available - such as a research role or community liaison role. GPs could be offered development opportunities in the CCG to better understand commissioning. Roving GP and Virtual GP roles trialled in other CCG Super practice/gp Alliance services (West Heath, Birmingham, and
16 Bradford) could be a flexible holding post potentially. The return and retention scheme could be utilised to support these roles. EU GP recruitment: The GPFV outlined NHS England s plan to attract 500 GPs of its 5,000 GP target from overseas; the pilot currently underway in Lincolnshire offers a six to 12 month supported training programme, followed by two years of support and mentoring. At this stage, there is limited information about the scheme and planned outputs (NHSE 2016; Matthews-King 2016). Six CCGs in Essex (West Essex CCG is not involved) came together with Health Education England and NHS England to bid for funds for an initiative to recruit GPs from overseas. The bid was successful and they plan to recruit 20 GPs in 2017 and 30 in The doctors recruited will: have GMC registration have IELTS 7.5 be eligible to work in UK be capable of joining Performers List They will have a practice-based induction programme with HEE that lasts approximately nine months. Most of the cost of the induction programme is met by NHSE but the employing practice contributes. CCGs will ensure that the overseas GP is placed in an appropriate learning environment and they offer a two-day course for GPs who are not trainers, or associate trainers, to prepare them to provide supervision of an overseas GP on the induction programme. Nursing Workforce Nationally the picture of the GPN workforce is one of an ageing workforce of whom 33.4% are due to retire by This demographic is this is also reflective of the local GPN workforce in that there are significant numbers eligible for retirement within the next 5 years. It is proving difficult to attract recruits (QNI 2016). With limited opportunities for career development, variable salary progression and terms and conditions of employment, it does not appear an attractive proposition. Nationally almost 90% of GPNs do not hold an NMC recordable specialist practice qualification in General Practice Nursing (QNI 2016) and member practices have widely varied approaches to GPN development. Unfortunately, the impression that this role could be career limiting is likely to be the overall impression with student nurses and experienced nurses who therefore opt for other more dynamic pathways. However, the autonomy and 1:1 patient contact that GPNs have is something that should be used as a recruitment attraction initiative. Several case studies, profiles and stories about the exciting role of the GPN need to be highlighted to both nursing and the public. This can be done by using nurses currently in role, newly appointed nurses, to write short pieces for the practice website, poster and as part of any recruitment campaign. Showcasing work at the local universities as part of the student nurse course and HCA courses would help encourage potential applicants and give a better insight into this role and what it can achieve. Further promotion by the CCG Nurse Directors and input into the student nursing courses could also prove to be an excellent way of encouraging nurses into primary care. It also needs to be acknowledged that some of the skills that nurses need for general practice are not obtained elsewhere in nursing. Practices tend to advertise for experienced practice nurses which may deter nurses from making the transition into general practice nursing. There is a need to
17 help the practices change their approach towards nurse recruitment and development. Clinical leadership/lead Nurse: The national shortage of nurses means they can be selective about where they choose to work. A visible, respected nurse leader is attractive to new recruits and will help motivate and inspire nurses to innovate, develop and deliver the changing service required for a very different demographic of patients in the future. They will also enable good governance and ensure alignment of nursing standards across CCGs. They have an important role to play in ensuring nurses are developed and revalidated and so able to support the training of other nursing staff. To recruit and retain the best possible nursing workforce, it is necessary to demonstrate high levels of access for a nurse career pathway from apprenticeship to advanced practice and leadership roles Although there is evidence from the local HEE that Student Nurse Attrition has reduced considerably, commissioning numbers are still insufficient and this is likely to become more of an issue with the removal of the bursary. Advanced Nurse Practitioners: There is evidence that Advanced Nurse (ANP) reduce admissions, waiting times are shorter, patients have better access to services and care can be provided in the community. ANPs score highly in patient satisfaction surveys and are shown to reduce GP workload (Pierce & Belling, 2011). This is part of Raising the bar: Shape of Caring review in assessing specialist skills (Appendix 4; HEE 2014). The potential of specialising and leading in several long-term conditions, and enhanced roles such as the ANP, could be attractive if managed differently. They may also be of more benefit if their base is the Super practice/gp Alliance as this would help provide a higher profile clinical leadership model. Also, this could utilise their skills and expertise to greater benefit. General Practice Nurses: According to EPIC s 2016 review there are currently 18 practices in Essex which undertake Practice Nurse audits for placement. Included in this list are practices which have only signed up to short term placement where students are there for 4 weeks but not assessed (5 of the 18). This leaves 13 practices set up for core placements where the nurses are assessed and will have mentors. Below are the numbers of projected placement of split of Full Time nursing students intake 2016 further details can be found in Appendix 5. Table 3: Projected Placement Split of Full-time Nursing Students September 2016 intake Primary Adult Mental Adult Mental Health Placement Child ARU Health ARU U of E Area U of E ARU Totals BSc BSc MSc BSc BSc BSc MSc Pathway Totals Course Totals Projected Placement of Full-time Nursing Students for March 2016 intake Primary Care Placement Numbers Adult Nursing ARU Child Nursing ARU Source: EPIC Workforce Development 2016
18 In North Wales, a new practice nurse trainee role is being introduced to encourage new nurses to move into primary care. This innovative unique new role will offer a 12-month clinical placement within local GP practices. It will enable junior nurses to learn the fundamentals of practice nursing in a safe managed structure. A programme of learning is being provided and this will be university accredited, with mentorship, peer support and clinical supervision. For Essex, the development of the Super practice/gp Alliance gives an ideal opportunity to commission such roles with HEE and across CCGs to help recruit and retain nurses, giving the skill base required for the dynamic changes planned. This will require working closely with HEIs to develop programmes that ensure nurses receive the development they need to be able to fulfil the new roles and ways of working in primary care. Current programmes can also be reviewed so that any opportunities to promote primary care as a workplace are fully utilised. NB: All of the above nursing roles should be available and in line with HEE (2015) standards as shown in Appendix 6. It should be noted that there are significant number of GPNs who are in Level 6 in the county. Health Care Assistants: The Practices and CCGs have embraced the HCA role and the development opportunities. The key now is to set the standards and competencies to ensure clarity about the role and its responsibilities, as well as provide professional support and development opportunities. Following the report of the Francis Inquiry in 2013 which identified serious failures in healthcare provision, the Secretary of State asked Camilla Cavendish to review and make recommendations on the recruitment, learning and development, management and support of healthcare assistants and social care support workers, to help ensure that this workforce provided compassionate care (HMSO 2013; Cavendish 2013). As a result, the Care Certificate was developed jointly by Skills for Care, Health Education England and Skills for Health. Designed with non-regulated workers in mind, the Care Certificate is a set of standards that social care and health workers stick to in their daily working life and sets out the minimum standards that should be covered as part of induction training of new care workers (see Appendix 6). The Care Certificate was launched on April 1st 2015, with organisations having until September 2015 to implement it. Whilst the Care Certificate is not mandatory, providers regulated by the CQC are expected to ensure that the standards of the Care Certificate are covered in their induction of new staff. Community Pharmacy: NHSE has launched a scheme to get 1,500 more clinical pharmacists working in GP Surgeries. By taking responsibility for patients with chronic diseases, clinical pharmacists can free up GPs for other appointments and so reducing the numbers of people presenting at A&E departments. They will work closely with community and hospital pharmacists to provide joined-up NHS pharmacy services for patients and so ease pressures on other parts of the health service. Within Essex, there have been pilots for the employment of pharmacists within practices. Due to the positive work undertaken and the potential for further funding, the development and potential of these roles is covered in the Section on scaling up services and new roles. Mental Health Therapists
19 The GPFV sets a goal of 3,000 new mental health therapists located in GP practices, this will mean an average of a full-time therapist for every 2-3 typically sized practices. The rationale for this is to help relieve the pressure on general practice resulting from unmet mental health needs. It is also likely to result in greater job satisfaction for GPs. Non-clinical Workforce Operations Practice Manager: There needs to be consideration of the general management of the Super practice/gp Alliance and this will need to include new combined roles, as well as potentially centralized employment of some staffing groups. An Operations Practice Manager is an example of a senior management role which oversees the general operational management of the Super practice/gp Alliance to enable it to run effectively, and generate cost efficiencies due to the level of increased buying/negotiation power. An example of the role descriptor is below: Operations Practice Manager Neighbourhood Team/Super practice/gp Alliance Coordinate use of Super practice/gp IT systems Alliance Coordinate GP training programme Procurement for Super practice/gp Alliance and practices Coordinate Virtual GP/roving GP/GP Participate in contract management Locums Coordinate other practice staff Leadership locality GP practice managers Manage use of premises by others Participate in commissioning for practice services This is just a sample role outline of a management model and there are others available. However, it is important that there is some standardisation so that staff training can be developed that will also give a clear career pathway for staff to aspire to. This would be best achieved by moving line management/employer to a host organisation to enable a move to team working within the Super practice/gp Alliance. Examples from elsewhere: Vanguard Dudley CCG has formed a Multi-Specialty Community Provider (MSCP) clinical team structure Teams without Walls. This structure uses a collaborative partner approach for care pathways and deploys the multi-disciplinary team across partner organisations. It has an outcomes framework which services are measured against and the core of the service is the patient/family. Diagram 2: Maximising potential to work efficiently and effectively together

20 Stephanie Carter (Dudley CCG) 2016 This is an approach that Essex could use across the CCGs and with individual GP practices which would fit with the Vanguard and STP approach nationally. This model is also noted in the STPs for West Essex and Mid-South Essex. Practice Manager: Practice Managers have a key role to play in educating GPs about the roles of others and have a pivotal role in the management and development of services. The Practice Manager role plays a critical part in co-ordination of services and the general operation of individual practices and the responsibilities vary dependent on the size of the practice. Development of this role needs to also have a clear career pathway and senior professional leadership could help highlight the opportunities the role brings. The Operations Manager role outlined could fulfil this function and would mean that for each locality there would be a senior manager giving support, leadership and mentorship. All of which would be attractive for building a career pathway for Practice Managers. EPIC Workforce Development recently undertook a survey of practice managers in Essex. The participating practices represented approximately 1,585,470 patients which equates to 87% of the patient population registered in Essex. They achieved a very strong response rate to the survey of 71% from the total survey base of 276 practices (184 responses). The data from this survey gives some valuable insight on the role, the current workforce demographic, and the workforce challenges they face. The key findings of the survey were: 75% of PMs that took part in the survey were over 50 The average estimated age of PMs participating in the survey was 53 60% of PMs plan to retire within the next 10 years 40% of PMs said they had current staff vacancies within their practice 62% of GP vacancies take over 2 months to fill The survey highlights that this important role needs more focus to promote it and encourage development of current staff who could see this as a great career move and attract new recruits. NB: EQUIP currently have a pool in place, however, the deployment and management of this could potentially be managed better by centralising either in each Super practice/gp Alliance or one Super practice/gp Alliance taking overall charge. It would also be possible to consider a standardised rate
21 scale based on skills and experience. This would avoid wide variations in rates and would link into the NHSE s agency capping policy for which further expansion and restrictions are likely to be applied in The current ad hoc arrangements could be more efficient and target resources better. This set up would enable staff to work across practices. Negotiate with the GP Federation to increase cross cover and reduce reliance on locums Super practices/gp Alliances to explore how they source and manage locums to help reduce the use of Locums. To note: From April 2017, there are changes to the way the current intermediary s legislation (known as IR35) is applied to off-payroll working in the public sector. Where the rules apply, people who work in the public sector through an intermediary will pay employment taxes in a similar way to employees. Locum doctors frequently work through their own Personal Service Company (PSC) or another intermediary Therefore, they will need to: provide the fee-payer (public sector client, or agency, or other third party) with the information they need to help determine whether the off-payroll rules should apply where the off-payroll working, rules apply, provide the fee-payer with the information required to allow them to deduct tax and NICs from the payment they make to the intermediary reporting to HMRC on own, and company s tax affairs Care Co-ordination service: SOURCE: HMRC website There are different models across Essex for example the CP&R one which was launched in September 2015 providing a 7-day service across the localities which offers support to those identified as complex/at risk. Named coordinators are allocated to patients, undertaking regular reviews to ensure outcomes are achieved and patients are managed within their own home, supporting them to stay healthy and independent for as long as possible. Alongside this new role and an integral part of the pathway is the establishment of the locality based MDT meetings which case manage patients and develop a single multi-agency care plan. These developments are still at an early stage but are critical factors in enablement of joint working and cohesive patient care management from both a health and social care perspective. Signposting to the Care Navigator role and managing patient expectations of that role will become an important message to patients going forward. GP Care Advisors GP Care Advisors are practice based and have direct access to the primary care team. They use a person-centred approach to make a holistic assessment of a patient s needs. They consider all aspects of a patient s health, financial and social situation and work with patients in order to minimise their need to use primary and secondary care services. Due to the complexity of the assessments and needs of the patients/carers, time spent with each person can vary greatly in order to achieve a positive outcome. GP Care Advisors also provide essential support and reassurance to carers who may feel isolated and unable to manage. Referrals are made to statutory services for assessment of a carer s needs. This assessment could result in respite care, direct payments or a sitting service. Referrals are also made to Third Sector organisations. GP Care Advisors also assist surgeries in identifying carers and maintaining their register of carers. Clinical & Non-clinical Apprenticeships:
22 A number of CCGs are keen to participate in the scheme and/or have started progress on this journey. Some have already had one or two placements and these are proving particularly successful in the GP practices. This success has helped to engage partners and it is an expectation that by offering a variety of experiences, this will be an attractive career option to take out to schools and colleges in the locality as well as continue to develop the course proposition with HEE (see Diagram 5 for the career pathway envisaged). This is an opportunity to be creative in developing interest in a career in health and social care. Examples have been givens to cadetship, apprentice and work experience models. Cadetship/Apprentice schemes can work in many ways with introductory placements in the CCG, GP practices, working alongside nursing, pharmacy as well as in the social care environment. A scheme covering a 2-year programme would not be unreasonable as it would give a decent amount of placement time in a number of areas to gain a realistic insight and determine next career steps. An example of a pathway is shown in Diagram 3. As stated previously, a number of CCGs have already taken great strides forward in this area with apprentices for general roles and have planned to promote the extension of the number and variety of placements including CCGs themselves. Diagram 3 - Introduction into Health & Social Care Apprentice Model Introductory module CCG GP Practice Admin GP Nursing Social Care Pharmacy Acute Placement Selective Placement Assessment Career choice However, there is concern at the costs to the GP practices and perhaps more would be able to participate if there was some funding available. Although these schemes are acknowledged to be successful and an excellent opportunity, funding is an inhibiting factor. The apprentice levy will apply to all healthcare organisations and is payable from 1 st April 2017 details of the levy are shown in diagram 4 below: Diagram 4 Changes to Apprenticeship Funding
23 Source: Health Education England There are concerns that funding is insufficient with the financial envelope currently being squeezed across the health economy with many CCGs and GP Practices facing difficult choices on services now. CEPNs and CCGs could with HEE, strategically co-ordinate apprentice models across primary care and ensure a consistent approach and build upon the experience gained by the EPIC pilot. Funding could potentially be gained by accessing the Digital Vouchers scheme and working collaboratively with neighbouring practices and/or utilising the Super partnerships/gp Alliances to be the core employer to achieve economies of scale and co-investing. Examples of how to do this: Web advertisement of all apprentice and training opportunities - both clinical and nonclinical including basic information on how to apply for apprenticeships Create a central Super practice/gp Alliance for information (web link) building on EPIC work Branded for Essex with consistent marketing material, messaging, style and approach; Data collection of all apprentice schemes currently in place, all training available, evaluation of training outcomes to ensure ongoing training needs analysis can be translated into action Build the base for and launch a formal Apprentice Network across Essex Aims will be to ensure all stakeholders and STP s have access to consistent good quality information on the benefit of apprentices; including case studies and learning opportunities to share across all stakeholders Expansion of training capacity, standards and quality assessment, with HEE by working together to ensure economies of scale and develop local learning support e.g. mentors, role models (current and past apprentices could take on part of these roles) Lead and facilitate local health system discussions on apprenticeships including direct engagement of schools through opportunities like the Careers Enterprise Company SCALING UP SERVICES AND THE NEW ROLES REQUIRED IN A SUPER PRACTICE/GP ALLIANCE To deliver services optimally in this format requires a workforce strategy that covers all services including social care; however, the scope of this strategy is limited to Primary Care.
24 There needs to be some consistency in recruitment practices which are currently variable perhaps due to a lack of Human Resource expertise and input available to them. Therefore, it is important to build a joint workforce strategy that is agreed across stakeholders with robust HR process in place. Diagram 2 indicates the complexity of the workforce roles for a Super practice/gp Alliance model which crosses several traditional professional boundaries. General Practitioners: Anglia Ruskin University (ARU) has been making plans to establish an undergraduate medical school in Essex for approximately two years and the University is responding to the Government s consultation on the additional 1500 medical students across England, and it is our intention to bid for places for 2018 subject to the necessary approval of the GMC. The University is currently on course with the General Medical Council to commence teaching the first Essex trained medical students next Autumn. Essex has a population of 1.8 million citizens and is one of only a few large English Counties without a medical school. It is known that graduates often remain in the area in which they were trained and Essex has a strong reputation for training students from other universities, but they tend to return to their teaching bases and this undoubtedly contributes to our recruitment problems. ARU has an excellent reputation as an innovative and dynamic centre of learning and already trains a wide range of health professionals and scientists. The ARU School of Medicine will be closely integrated with other University departments and will develop doctors in a multi-professional modern environment. The School will also aim to train a significant number of Essex based students who will then become Essex doctors treating Essex patients. The course will include clinical attachments from year one and strong links to primary care have already been established. Eighteen months prior to enrolling the first students the University has 124 confirmed placements across 41 general practices. The enthusiasm from clinicians across all healthcare establishments in the County for this new development has been universal and a new medical school will do a great deal to drive other recruitment and retention initiatives. CQC Inspection/Visit Preparation Support: This innovative role has been created to support GP Practices to be better prepared for CQC visits and helping the practice meet its CQC obligations and inspections. A stretched clinical workforce has welcomed this support mechanism. Thurrock CCG were successful in a bid fund a small Primary Care team who work very closely with the Nursing and Quality team. As well as relationship building and other areas of support, they have developed a CQC template that the locality managers use with the practices in advance of any CQC visit. Work is done with the practices to ensure they are well prepared and a mock inspection is carried out with the Nursing and Quality team before the actual CQC visit. NP and ANP Support Network Each CCG/CEPN/LWAB area should establish a nurse forum to facilitate professional networking, networking and sharing of ideas/practice. This could include support for nurses working in care homes. The forum would be a place to consider development needs and help support ways of meeting those needs with HEE, ECC and other stakeholders.
25 This gives the CCGs/CEPNs/LWABs a number of opportunities to ensure that the primary care nurse workforce is supported to achieve their maximum potential a benefit to patients, employers and the nurses themselves. This is a good benchmark for other CCGs, therefore, this is recommended. Specialist Nurses: Specialist Nurses are nurses who have been educated to degree level or above and hold specialist knowledge, skills, competencies and experience. Practising at an advanced level, they often have sole responsibility for a care episode or defined client/group. These are primarily clinical roles and provide education and support for patients to manage their symptoms, particularly patients with long term conditions and multiple morbidities. The Super practice/gp Alliance model offers an opportunity for the development of specialist nurse roles. This is also an opportunity to work with secondary care and the third sector. Depending on the local priorities these roles could include: COPD Dementia Multiple Sclerosis Parkinson s Cancer Dermatology Sexual health Rheumatology Diabetes Heart failure Stroke Tissue viability General Practice Nurses: We will work with the Super partnerships/gp Alliances to develop core standards for GPNs: Terms and conditions, this would include titles, job description, competencies, salary scales Indemnity would be covered as standard employer responsibility Access to development and training formalized and linked with appraisal Support with revalidation Career pathway opportunities Student nurses: It is important to continue to work closely with HEE to help influence and increase the numbers commissioned with the variety of placements and rotational programs offered to improve quality and placement experience. The detail of the practices participating in the student placement programme can be seen in Appendix 5. Nurse mentors need to be developed to support student nurses across member practices. This may encourage students to consider GPN roles when newly qualified or might be a role for newly retired GPNs. There is interest in supporting student nurses as indicated by the number of nurses willing to train or update their mentorship qualification. However, there appears to be a lack of courses and access to funding to maximize this opportunity. This is something that needs to be addressed and coordinated to ensure these are available across the geographic region. Practices interested Nurses interested Refresher required Training required
26 Source: EPIC Workforce Development 2016 Health Care Assistants: Liaise with Local Authorities to work in collaboration to influence the quality agenda for Care Homes provide assurance that staff have or are working towards the Care Certificate to meet the obligations outlined. This is an important quality and governance aspiration that supports our commissioning agenda on quality, safe services for those using these services Associate Practitioner: This is a relatively new role which would give a development programme for the current HCA workforce. It gives an opportunity for HCA s to be recognised for their advanced skills therefore there is a need to work with HEE to enable a conversion-style programme which will recognise current skills, competencies and experience. The role has potential to attract new applicants to work in the community due to the career pathway it offers. It is within this role that there is potential to consider different ways of working by these being joint roles with Social Care. The Associate Practitioner role could certainly be a role that could be utilised for domiciliary care; it could be a gateway to a social work career pathway as well as into nursing. Nurse Associate: Nurse Associates will undertake a two-year training and on completion of are employed at Band 4. These courses started in January 2017 and so it will be some time before their impact can be evaluated. The Nurse Associate role offers opportunity to develop the current workforce as well as being used to recruit. They will require practice assessment and this needs to be factored in to any work done on student nurse and other placements. Physicians Associates: Physicians Associates are trained on a 2 year post graduate degree programme. They are taught following the medical model and experience a 50:50 split between knowledge based and clinical teaching. There is an issue around the supervision of this role and the need to backfill clinical sessions whilst a GP is training and mentoring the PA. The PA role is to take on tasks traditionally performed by a GP and includes such things as: - taking medical histories performing examinations diagnosing illnesses analysing test results developing management plans As Essex has a shortage of GPs this may be a useful role to develop. However, Nurse Practitioners, physiotherapists and pharmacists can work more independently and as such are likely to be a more useful solution to filling the gap. Community Pharmacy/Clinical Pharmacists: Care Home Medicine Management & Expanded Roles
27 During 2016, NHSE launched a 3-year part funded pilot scheme for the employment of clinical pharmacists in Primary Care. As a result, 36 clinical pharmacists have been employed in a number of locations around the country of which 13 are situated within the Essex region. Funding has been extended into 2017 and the CCG s will continue to encourage General Practice to employ pharmacists to boost the workforce in Primary Care Two areas in Essex won bids to pilot a 3-year scheme for pharmacists to be employed in practices. The intention is to use the pharmacists to re-authorise and manage prescriptions as studies show that a large portion of the GP s time is taken up on meds management. They also have a large role to play in prescribing budgets and dealing with regulatory issues. It is envisaged that, over time, they will also be able to see and assess patients with minor illnesses and long term conditions once mentoring and training has been undertaken. Applications for this next phase, worth over 100m, opened in January 2017 as NHS England and its partners target a further 1,500 clinical pharmacists working in general practice by 2020/21, a commitment set out in the General Practice Forward View. It is possible that funding could be sourced from current research funding, social care partners or if available redirect funding from any vacant community pharmacy post. The alternative is to source research funding from relevant organisations or consider the potential return on investment from prescribing savings as being sufficient to fund the post. Flexible working could be an attractive option for these roles. Individual general practices and community pharmacies will work more closely together via networks and the federations providing a wider range of services. Integrated IT systems will be a key requirement across providers of primary care to facilitate comprehensive patient care information is accessible as appropriate. Primary and community care staff will also work closely with other stakeholders utilising the models outlined in the NHS Five Year Forward View. Physiotherapists: A greater role for physiotherapy in primary care offers an immediate solution to the GP shortage. They are autonomous practitioners able to assess, diagnose manage and discharge patients. They are trained to identify possible serious pathology in the same way as GPs and many are also qualified to administer injections or prescribe drugs without medical approval. The benefits of employing a Physio to work across a number of practices would be to keep care closer to patients homes and avoid referrals into the hospitals. A recent study shows that MSK conditions make up to 30% of a GPs caseload which rises to 50% for demographics of patients 75 and over. 80% of these patients did not need to see a GP and could have seen a physio as a first contact with only a small number of patients then having to make an appointment with the GP. Early appointments with a physio could prevent a short-term issue becoming a LTC. Physios could play a big part in Care Homes to prevent falls (Cameron et al 2012). Paramedics: By recruiting paramedics into the Primary Care workforce and becoming paramedic practitioners they could be the frontline resources for home visits and care homes. With additional training, they could be utilised to assess and treat patients with chronic illness, minor injuries, refer patients to specialists or hospital if needed and respond to emergency calls from patients or care homes without advising them to ring 999 or go to A&E. They could also be utilised to triage calls.
28 An example of this can be seen in the Specialist Paramedic Practitioner (SPP) role developed by Health Education Kent, Surrey & Sussex. St George s University of London offer a 15 month CPD Diploma which includes a two month GP placement. SPPs work to Evidence Based Clinical Management Plans developed and approved by the GP and Paramedic as shown in Table 4. Table 4: Evidence Based Clinical Management Plans Respiratory Asthma LRTI Shortness of breath Neurological Headaches Care of epileptic patients Febrile convulsions Head injury TIA/CVA pathway Integumentary and Wound Care Minor burns and scalds Pre-tibial lacerations Wound assessment and care Wound closure with glue and sutures Bites Rashes Skin infections inc cellulitis Men s Health Scrotal swelling Dysuria/Discharge Sexual health Cardiovascular and Endocrine Heart Failure Chest Pain (non cardiac) Palpitations, syncope and presyncope Diabetes Eyes Foreign body including abrasions Arc eye Chemicals Pain, loss of vision, red eye Blephritis Meibomian/Chalazion Women s Health Pelvis pain Dysuria/Discharge/bleeding PV Pregnancy and obstetric complications Sexual health Mental Health Panic/anxiety attack Depression Deliberate self harm/neglect Overdose Abdominal and Genito Urinary Gastro-eneritis UTI Haematuria Pain Catheter problems Retention of urine Constipation/impaction Ear Nose and Throat URTI/Tonsilitis Otitis media Otitis externa Epistaxis Dental problems Orthopaedic and Trauma Non traumatic MSK back pain Hip pain Knee, shoulder, wrist, hand, finger, ankle pain/injuries Olecranon bursitis Radial Hed subluxation in children C-spine clearance following RTC/whiplash Gout Miscellaneous, Palliative and Social Palliative care Pyrexia of unknown origin Acopia Frequent fallers Multi casualty RTC Non accidental injuries WORK ACROSS BOUNDARIES TO DELIVER STPs The Virtual Surgery:
29 The virtual surgery could take on the care of those in care homes as they do not need a physical surgery to attend given that they will be receiving home visits. It also enables patients to access guidance and advice quickly from the most appropriate specialist which should reduce A&E attendance and the need for a GP appointment. The team would consist of: Pharmacist who would proactively support practice based pharmacists and pharmacy technicians integrated within primary care to continue to improve quality and patient safety with respect to medicines optimisation ANP who would see patients with undiagnosed, undifferentiated medical conditions and make treatment decisions, including ordering necessary investigations and prescribe any medicine for any condition within their competence Physiotherapists who would triage all MSK patients with early access and advice giving appointments. This would reduce referrals to secondary care as evidence indicates early intervention and guidance is successful Paramedics could be used to triage calls, assess and treat minor injuries in the care home and refer on as appropriate Care Homes are often dealt with by more than one practice and this can result in a GP for 2 to 3 practices being called out for a home visit and all being at the care home at the same time. A professional from the virtual team could be assigned to the care home and deal with all patients regardless of where they are registered and have access to be able to update the patients records remotely. By working with the LWAB and other partners, including the Ambulance Trust, there would be the possibility to develop a pilot in one of the STP areas to assess the model, impacts and quality outcomes Social Workers: Two social worker appointments working as part of the MDT have already had some success by working closely with the nursing team helping remove some of the role barriers to deliver the right service and facilities the patients and carers need with joint working. These roles focus on a user/patient enablement model and will provide a valuable opportunity to be a part of a signposting function to other services. Planned evaluation of these roles will cover both the patient and carers experience and include assessing any improved quality of life criteria. Patient Participation Groups (PPG): UNDERPINNING THE WORKFORCE STRATEGY Primary care practices all work in partnership with their Patient Participation Groups (PPG) to implement a continuous improvement of services and offer high quality and responsive care. Each PPG s membership is expected to reflect the diversity of individual practice populations across Essex to ensure the views of local populations are heard. The aim will be that greater integration between health and social care organisations will improve patient experience, delivering equitable provision of effective, efficient and quality services in the optimum way. In order to evaluate the effect of any changes made in Primary Care and to change the public perception of the current culture, we will need to build on relationships with service users, patients and carers, engaging and informing them of how patients can influence and shape the future of their own healthcare.
30 Voluntary sector: There are many public and voluntary support services offering practical help and advice in our local communities such as Age UK and many others. By working closely with the voluntary sector, we can signpost those most in need of additional support, including carers, those with long-term conditions and people with mental health needs, to the most appropriate help they need in the locality. Recruiting and Retaining staff: Many of the GP practices and CCGs in Essex are seen as good places to work and this is demonstrated with high retention across most staff groups. It is also reflected in the staff surveys which show low attrition and recruitment levels for these organisations. This good news message needs to have a higher profile perhaps on individual websites and on a more centralised website also covering the whole of Essex this perhaps could be a page(s) hosted on Essex County Council website. It would be worth exploring if HEE or local university websites could be used to explore this as an opportunity for the future and guiding students towards employment within Essex. All the individual websites could be better utilised to showcase Essex overall as an attractive place to work and live. By aligning this the Essex Council and Social Care website with joint messaging there would be a shop window to help patients and service users navigate services available and are a useful signposting mechanism. Consistency in messaging is a key component in the care navigator role and this may be a requirement for future training in guiding communications for the future. One opportunity has been utilised more is referring any interested applicant direct to the NHS vacancy website on some of the individual CCG websites. Member practices could also benefit from having their vacancies also advertised on their own websites as well as on other stakeholders in Social Care. EQUIP has a facility which is used to advertise roles this is free to members of EQUIP with a small charge to non-members. The RCGP also has this facility and this should be utilised given that it is likely that medical staff would look on this website first for any vacancies for regions they are considering. In addition, a new dedicated webpage has been developed for general practice (GP) NHS England on their website. The GP microsite has been developed for those working in general practice to make it easier to navigate and find content specific to this area (Appendix 1; PCWC 2015). Development opportunities for health and social care staff are not easily found in a central point currently therefore making these more prominent both for current staff and prospective employees would be advantageous. New emerging roles will be attractive but need to be known about therefore improved use of websites and their management will be a key element for the recruitment and workforce strategy. Promoting General Practice as a Career: Through collaboration with County Councils, schools, local colleges and Universities we can highlight the varying roles and the benefits of working within Primary Care. It will give opportunities to share successes and generally encourage interest of a career in the Primary Care sector. It would provide an opportunity to gain interest in apprenticeships. A further opportunity would be to develop Open Days for those interested with role models providing information on their roles as part of the attraction process. Training and Development:

31 All future training should be provided in a consistent manner across the county and centrally commissioned. There should be a robust, monthly evaluation of outcomes gained from outsourced training to ensure it remains relevant and achieves the aims commissioned. All information from the courses types, dates, venues should be accessed via a hyperlink to where such information will be maintained for CEPN i.e. HEE or one CCG so that there is consistent messaging and access for all staff. Outcomes and successes should be published on CCG websites to celebrate and encourage staff and potential new recruits. When looking at pooling funds in future this workforce strategy should be used as the basis for funding and bid making decisions. CEPN could be tasked with developing a map of funding streams. This would include working with Finance Directors to unpick where training funding is in budgets so they can be used collectively. Technology Workforce planning: Across Essex within the STP Footprint, several ICT sub groups (including from other stakeholders) have been created. These are to support the planning and delivery of services to the people of Essex by working together to co-ordinate and implement fit for purpose; and interoperable infrastructure. Through the shared values of information sharing, innovation, collaboration by using informatics that have demonstrable value across the health and care system to benefit patients and partners. Good examples of using IT in workforce planning are available which can help in this challenging area, especially when there is a need to consider new services or reconfiguration of services. WRaPT is one such workforce tool developed by HEE and it is available free of charge to NHS organisations. Examples from organisations which have used this tool can be seen below: Stockport CCG is committed to being an intelligence-led organisation. The WRaPT tool allows us to apply the same rigour we use in quality assurance and contracting to our workforce planning so that our new models of care are backed up by the right skills and capacity within our collective workforce across health and social care in Stockport. Angela Dawber, Head of Strategic Development, NHS Stockport WRaPT has proven to be an excellent tool in supporting clinicians design the appropriate workforce for our redesigned model of care. We have been able to integrate and analyse data across organisations and build scenarios to test the proposed changes in care. We now have an effective tool to safely model our new workforce and have committed to use WRaPT for all workforce changes within the ICNT project. Kristina Wright, Elective Services Clinical Lead, Adults Services Directorate, Bridgewater Community Healthcare NHS Foundation Trust The WRaPT tool has been instrumental in supporting the Cumbria Success Regime produce high quality workforce modelling to support transformational change across organisations. We are in the process of training our in-house analysts to ensure we embed the tool and its associated processes within our business / workforce planning methodology across the STP. Lynn Marsland, Director of Workforce & OD, Cumbria Partnership NHS Trust Source: GE Healthcare/Health Education England 2016 Healthcare and social services need to be dynamic and responsive to the changes that can already be foreseen in the patient demographic so having an e-tool to cost and try variations of staffing requirements will save costly errors.
32 Agile Working For agile working, there is a need to ensure that there is good use of technology which enables the capture and transfer of information. This can save time in administration for clinicians (Total mobile case study reference); This is only one example but such systems can be adapted for all clinical specialties including GP s, community pharmacists and other AHPs. The CCGs need to collaborate and invest in systems that would benefits all practices. Such tools that can centralise claims and reporting, is part of a decision support tool, assisting with medicines management and other functions which would reduce workload. One system that is under consideration is Care IS which provides an interface technology with the ability to link to any record system that has structured coded data and that has an API. The prime links are with the four GPSOC approved primary care EHRs. Working with a well-established partner with a substantial presence in secondary care and an integration layer, the DS can be linked into all secondary care systems whether new or departmental legacy systems. Two-way information flows into and from: Patients and carers General practice Community providers Secondary care Social care Implementation of a real-time, in-consultation clinical decision support (CDS) platform integrated into primary care patient electronic health records (EHRs). The CDS will be provided with a suite of associated reporting tools to assess financial, quality and outcome information at a healthcare professional, practice and aggregated at a federation and CCG level. All functionality is based on commissioner clinical lead approved, local adaptions of NICE guidance. Moving to a Super practice/gp Alliance model means that the workforce for these needs significant co-ordination across all the staff groups involved. This gives a layer of rota management complexity that is not usually encountered in even the larger GP practices which tend to be manual systems. Therefore, there may be a need to consider and explore the benefits of a simple erostering system that could be web-based to enable staff and managers to access remotely. There are several systems on the market that may be suitable for consideration. Conclusion Primary Care offers a vast choice in careers with several employment models to choose from including return to work schemes and options for part-time schedules. There are more options for flexibility and balance than in many specialties which should help with workforce recruitment and development strategy aims. Health care is not just about dealing with the presenting issue; it includes preventative medicine and self-care. It can be anything from health decision-making, health screening, monitoring medications and treatments, counseling on healthy eating, smoking cessation, and family planning to name just a few. Primary Care is the shop window of healthcare services, prevention and management and so is an exciting career opportunity and should be promoted as such. With so much talk about the financial struggles and day-to-day hassles of practicing in Primary Care it is easy to lose sight of the very positive side of working in Primary Care. The huge variety of roles and scope for innovation is vast in this area and is due to the fact that over 80% of healthcare is delivered outside of the Acute Hospital sector. The steady stream of patients with varying needs
33 make the most of the skills and front line engagement across all roles - GP, Nurse, Physiotherapist, Apprentice, Care Navigator, Pharmacist in fact the entire Primary Care Team. As this Strategy describes the future will also require change. Primary Care will still be based around the GP practice holding responsibility for the care of its registered patients, but they will have a stronger population focus and an expanded workforce through the collaborations of the Super practice/gp Alliances. These will have a variety of roles and services embedded to enable the service to run as a One Stop Shop. This means it must have near to patient diagnostics, nurse led services, midwifery/health Visitor services, MSK and Social Services along with Specialist GP sessions. This will enable MDT formation and collaboration at a much-enhanced level. The old boundaries of working practices will need to be changed in line with new professional ways of working. New services require new ways of working and structure such changes are challenging but are required given that current demand and services are no longer sustainable with existing models. Many existing healthcare professionals are able to expand and develop their roles, and roles will evolve meaning patients will be seen by the most appropriate healthcare professional. Clinical staff will have better administrative support and, when needed, healthcare professionals will be able to spend more time with their patients to discuss and plan their care. They will also be able to use a variety of ways to communicate with patients and colleagues using telephone, , electronic messaging and video-conferencing as appropriate. Senior leadership and clinical ownership to engage with all stakeholders are essential to deliver complex change on such a scale. The Essex partnership has worked hard to provide support and development for leaders across all areas, and will continue to develop and build relationships across all stakeholder groups county wide. This makes it well placed to lead this strategy. For the future service and workforce models to work, there is a need for a comprehensive Estate and IT strategy to complement the strategy. This strategy paper outlines the workforce roles and actions for Essex to develop and deliver an innovative, integrated care workforce model to deliver services effectively. It will be a challenge to overcome deep rooted cultural and established practices to move to new roles, new practices and joint working not only individually but across individual organisations and care providers. However, with the right support, collaborative working and combined leadership it should be achievable. All the action points raised in the sections will assist in the recruitment, retention, development elements of the Workforce Strategy. These are all documented in the more detailed action plan for the CCGs to assess which are applicable to their localities and STP area and commit to the actions that are required in taking this agenda forward. However, it is by working collectively and collaboratively across the boundaries of CCGs and STPs that they will successfully achieve the results which will benefit patients, families and the staff of the future. Summary Primary Care in Essex is central to the future delivery of health care and promotion to the people of Essex. In order to do this we will need to build on the best of what is already in place develop new ways of working work with other organizations In order to achieve this we will:
34 extend current roles develop new roles work across organizational boundaries Next Steps The actions points set out in this strategy have been used to develop an action plan in an excel format that CEPN can use to monitor progress across the CCGs. Action Points/Aims Primary Care Workforce Strategy Ta
35 APPENDIX 1 Primary Care Foundation with the NHS Alliance (2015) Making time in general practice. 10 high impact actions to release time for care 1. Active signposting: Provides patients with a first point of contact which directs them to the most appropriate source of help. Web and app-based portals can provide self-help and selfmanagement resources as well as signposting to the most appropriate professional. 2. New consultation types: Introduce new communication methods for some consultations, such as phone and , improving continuity and convenience for the patient, and reducing clinical contact time 3. Reduce Did Not Attend (DNAs): Maximise the use of appointment slots and improve continuity by reducing DNAs. Changes may include redesigning the appointment system, encouraging patients to write appointment cards themselves, issuing appointment reminders by text message, and making it quick for patients to cancel or rearrange an appointment. 4. Develop the team: Broaden the workforce in order to reduce demand for GP time and connect the patient directly with the most appropriate professional. 5. Productive work flows: Introduce new ways of working which enable staff to work smarter, not harder. 6. Personal productivity: Support staff to develop their personal resilience and learn specific skills that enable them to work in the most efficient way possible. 7. Partnership working: Create partnerships and collaborations with other practices and providers in the local health and social care system. 8. Social prescribing: Use referral and signposting to non-medical services in the community that increase wellbeing and independence. 9. Support self care: Take every opportunity to support people to play a greater role in their own health and care with methods of signposting patients to sources of information, advice and support in the community. 10. Develop QI expertise: Develop a specialist team of facilitators to support service redesign and continuous quality improvement.
36 APPENDIX 2 RCGP, BMA, NHS England & Health Education England Building the Workforce the New Deal for General practice Aims of the 10 point plan GP workforce '10 point' plan The 10 point plan aims to target the following problem areas within general practice. Click on the relevant links to access helpful guidance and practical support and advice. Recruit 1. Promoting general practice 2. Improving the breadth of training 3. Training Hub/Super practice/gp Alliance 4. Targeted support Retain 5. Investment in retainer schemes 6. Improving the training capacity in general practice 7. Incentives to remain in practice 8. New ways of working Return 9. Easy return to practice 10. Targeted investment in returners
37 APPENDIX 3 HEE GP Workforce Survey A recent survey conducted by HEE shows that a greater proportion of those qualifying prior to 1995 went straight into GP Partnerships but from 2000 onwards more were a salaried GP. The proportion as a Locum GP has remained relatively consistent over time. Figures also show that around 64% of respondents had a first post within the same region as they trained. Nationally GP consultation rates increased by 40% in the period and are predicted to continue to rise by a further 35% by The average member of the public now sees a GP almost six times a year, twice as often as a decade ago and the average time a GP spends with each patient is now just under 12 minutes, compared with just over eight minutes in Demand on GPs in the county will only increase as the number of patients with long term conditions increases. This patient group currently makes up around 50% of all GP appointments (Source: North & South Essex LMS GP Workforce Survey, 2014). The GPs surveyed were asked about their plans over the next 5 years: - 27% considered retiring (13% were between 46 to 50 years old & 27% aged 51 to 55) 11% thinking of leaving clinical practice for other reasons 3% moving to another to another specialty When asked what factors would influence them to remain in general practice, 29% said salary, 25% said flexible working hours with the most commonly occurring theme in the other responses was workload. Factors that contribute to job satisfaction Factors that distract from job satisfaction 80% professional satisfaction 86.5% workload 77% additional roles (includes teaching, 72% re-organisation of Primary Care research, etc.) Varity of work 23.4% salary 46% Other includes location, colleagues, 23% Other includes media comments, QOF, getting to know patients CQC, interference from Government, recruitment constant change, undervalued Spiralling MDO fees and pension contributions Source: North & South Essex LMS GP Workforce Survey, 2014 When asked for other comments about careers in General Practice to help with future workforce planning the following statements were made: - Workload too high Not enough time with patients Loser older GPs not enough is being done to retain them Low morale, undervalued by government, negative press Increasingly demanding patients and unrealistic expectations New GP do not want to be partners, work full time Lack of support, nothing being done to reduce patients demand Better promotion of opportunities and variety of work, improve image of General Practice Government interference, concern about future changes and plans i.e. 7-day working
38 One of the main points to come out of the survey was that inadequate coverage of GP Practices and Primary Care is given in medical school, lack of mentors and trainers leaving students to only know what they hear and read in the press about the long hours, too much admin and not enough time with patients. It is no wonder that newly qualified students do not want a career in General Practice. The Essex Area Team s Primary Care Strategy recognised that the county already has one of the lowest concentrations of GPs per 1,000 patients in England and needed to recruit an additional 143 WTE GPs just to reach the English average. 46% of GPs in Essex are due to retire in the next 15 years. The GP Workforce survey confirmed from responders that 50+ GPs and approximately 25 nurses across the county were planning to leave within the next twelve months. The demographics of the workforce would suggest that this was a reasonable reflection (N&E SE LMS GP Workforce Survey, 2014). Pension arrangements mean that early retirement is financially viable especially with the amount of locum work available Essex currently has 1,214* GPs active across the CCGs with a population of 1,860,696** registered with all GP practices in the area (*EPIC 2017, **HISIC 2017).
39 APPENDIX 4 Health Education England Nursing Education Framework (2016) Developing People for Healthcare - General Practice Education and Career Framework Advanced Community Nurse Practitioner Level 8 Senior General Practice Nurse Level 7 General Practice Nurse Level 6 General Practice Nurse Level 5 Assistant Practitioner Level 4 Health Care Assistant Level 3 Health Care Assistant Level 2 Pre- employment level Minimum Professional and Educational Requirements for the role Registered with the Nursing and Midwifery Council Post graduate diploma meeting ANP requirements and to include level 8 high intensity interventions (see NICE guidelines for descriptors of behaviour change interventions) Masters degree Independent and supplementary prescribing Registered with the Nursing and Midwifery Council First degree and working towards postgraduate level qualification NMC mentorship qualification Independent and supplementary prescribing V300 Registered on Part 1 of the Nursing and Midwifery Council register Degree level qualification/equivalent experience NMC Specialist Community Practitioner Qualification Practice nurse/relevant experience NMC mentorship qualification Registered on Part 1 of the Nursing and Midwifery Council register Higher Care Certificate (currently under development) Hold or working towards Foundation degree at level 5 Care Certificate (highly recommended) to include, or have as an addition, training for working alone in community settings and specific skills needed for the role Level 2 brief intervention training (see NICE guidelines) Level 3 apprenticeship or QCF level 3 Diploma in Clinical Healthcare Support or the equivalent Math s and English functional skills qualification Care Certificate (highly recommended to include, or to have as an addition, training for working alone in community settings and specific skills needed for the role Hold or working towards Level 2 QCF Diploma in Clinical Healthcare Support or equivalent Math s and English functional skills qualification some of the requirements may change when new NOS are published Examples: work experience, traineeship, pre-employment programme, cadetship
40 APPENDIX 5 Projected Placement of Split of Full Time Nursing Students Intake 2016 Primary Placement Area Projected Placement Split of Full-time Nursing Students September 2016 intake. Adult ARU Adult UofE Child ARU Mental Health ARU Projected Placement Split of Full-time Nursing Students March 2016 intake. Mental Health UofE Totals BSc BSc MSc BSc BSc BSc MSc NEPFT (C) SEPT (S) North Essex (C) Mid Essex (C) West Essex 35 PAH (S) South West 44 Essex (S) South East 42 Essex (S) Pathway Totals Course Totals Source Epic Primary Placement Child Adult ARU Area ARU North Essex 13 5 Mid Essex 16 5 West Essex 14 5 South West Essex 16 5 South East Essex 13 5 total 72 25
41 APPENDIX 6 The 15 standards in the Care Certificate are: Care Certificate 1 Understand your role 2 Your personal development 3 Duty of care 4 Equality and diversity 5 Work in a person-centred way 6 Communication 7 Privacy and dignity 8 Fluids and nutrition 9 Awareness of mental health, dementia & learning disability 10 Safeguarding adults 11 Safeguarding Children 12 Basic Life Support 13 Health and Safety 14 Handling information 15 Infection prevention and control 70% of assessment is knowledge based, 30% is to be assessed in practice.

42 CCG Key Deliverables High Level Overview GPFV Schemes APPENDIX 7
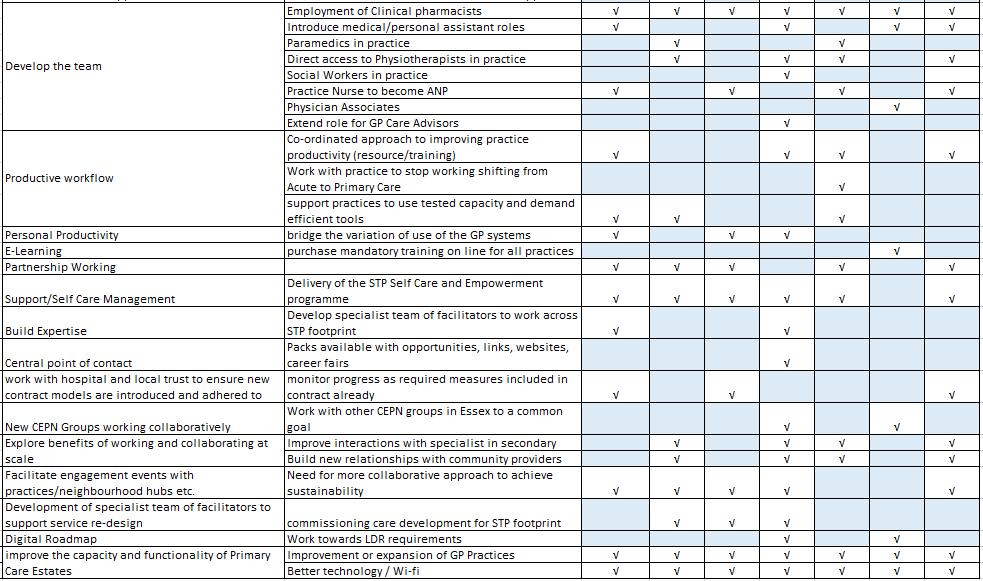
43
Approve Ratify For Discussion For Information
 NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
Training Hubs - Funding Allocation Paper
 Training Hubs - Funding Allocation Paper Background Health Education England (HEE), NHS England, the Royal College of General Practitioners (RCGP) and the BMA GPs Committee (GPC) are working together to
Training Hubs - Funding Allocation Paper Background Health Education England (HEE), NHS England, the Royal College of General Practitioners (RCGP) and the BMA GPs Committee (GPC) are working together to
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
GP Forward View Operational Plan Draft Narrative December 2016 Subject to final approvals
 GP Forward View Operational Plan 2017-2019 Draft Narrative December 2016 Subject to final approvals Chairman s Foreword In March 2015 we published our Primary Care Strategy, which alongside its accompanying
GP Forward View Operational Plan 2017-2019 Draft Narrative December 2016 Subject to final approvals Chairman s Foreword In March 2015 we published our Primary Care Strategy, which alongside its accompanying
DRAFT. Rehabilitation and Enablement Services Redesign
 DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
North School of Pharmacy and Medicines Optimisation Strategic Plan
 North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
General Practice Nurse (GPN) Ready Scheme. Information Pack for Primary Care
 Ready Scheme. Information Pack for Primary Care") General Practice Nurse (GPN) Ready Scheme Information Pack for Primary Care What is GPN Ready? General Practice Nurses (GPNs) need support and development when they first work in a primary care environment.
General Practice Nurse (GPN) Ready Scheme Information Pack for Primary Care What is GPN Ready? General Practice Nurses (GPNs) need support and development when they first work in a primary care environment.
Primary Care Strategy. Draft for Consultation November 2016
 Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
General Practice Forward View Mark Sanderson Deputy Regional Medical Director NHS England - Midlands and East
 General Practice Forward View Mark Sanderson Deputy Regional Medical Director NHS England - Midlands and East Overview of GPFV What's happening across Midlands and East The picture in the East of England
General Practice Forward View Mark Sanderson Deputy Regional Medical Director NHS England - Midlands and East Overview of GPFV What's happening across Midlands and East The picture in the East of England
North West London Workforce Transformation Strategic Plan
 North West London Workforce Transformation Strategic Plan 2016 2021 Health Education England North West London & Strategy and Transformation, Workforce Transformation Team Contents Executive summary...
North West London Workforce Transformation Strategic Plan 2016 2021 Health Education England North West London & Strategy and Transformation, Workforce Transformation Team Contents Executive summary...
Cambridgeshire and Peterborough s General Practice Forward View Strategy DRAFT February 2017
 Cambridgeshire and Peterborough s General Practice Forward View Strategy 2017-2020 DRAFT February 2017 Table of Contents i Foreword 1. Introduction...5 2. Model of Care...8 3. Improving Access... 14 4.
Cambridgeshire and Peterborough s General Practice Forward View Strategy 2017-2020 DRAFT February 2017 Table of Contents i Foreword 1. Introduction...5 2. Model of Care...8 3. Improving Access... 14 4.
Report on District Nurse Education in England, Wales and Northern Ireland 2012/13
 Report on District Nurse Education in England, Wales and Northern Ireland 2012/13 Introduction The QNI has become concerned at recent reports of a fall in the number of District Nurses currently in training
Report on District Nurse Education in England, Wales and Northern Ireland 2012/13 Introduction The QNI has become concerned at recent reports of a fall in the number of District Nurses currently in training
Cornwall Community Education Provider Projects March 2018
 Cornwall Community Education Provider Projects March 2018 NATIONAL FUNCTION NUMBER (NF No): 1: SUPPORT FOR WORKFORCE PLANNING AND DEVELOPMENT to respond to local needs and enable the redesign of services
Cornwall Community Education Provider Projects March 2018 NATIONAL FUNCTION NUMBER (NF No): 1: SUPPORT FOR WORKFORCE PLANNING AND DEVELOPMENT to respond to local needs and enable the redesign of services
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms
 Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Welcome. PPG Conference North and South Norfolk CCGs June 14 th 2018
 Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
INFORMATION REGARDING ADVANCED PRACTICE & ADVANCED CLINICAL PRACTITIONERS (ACPs) IN GENERAL PRACTICE (DERBYSHIRE)
 IN GENERAL PRACTICE (DERBYSHIRE)") INFORMATION REGARDING ADVANCED PRACTICE & ADVANCED CLINICAL PRACTITIONERS (ACPs) IN GENERAL PRACTICE (DERBYSHIRE) INTRODUCTION Derbyshire Advanced Practice Strategy Group are seeking to address some of
INFORMATION REGARDING ADVANCED PRACTICE & ADVANCED CLINICAL PRACTITIONERS (ACPs) IN GENERAL PRACTICE (DERBYSHIRE) INTRODUCTION Derbyshire Advanced Practice Strategy Group are seeking to address some of
MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE. Purpose of Report: For Note
 Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Business Case Advanced Physiotherapy Practitioners in Primary Care
 1 Business Case Advanced Physiotherapy Practitioners in Primary Care 1.0 Introduction This scheme supports the sustainability of primary care and the move towards a first line prudent multi-professional
1 Business Case Advanced Physiotherapy Practitioners in Primary Care 1.0 Introduction This scheme supports the sustainability of primary care and the move towards a first line prudent multi-professional
Consultation on draft health and care workforce strategy for England to 2027
 13 December 2017 Consultation on draft health and care workforce strategy for England to 2027 Health Education England () has published Facing the facts, shaping the future, a draft health and care workforce
13 December 2017 Consultation on draft health and care workforce strategy for England to 2027 Health Education England () has published Facing the facts, shaping the future, a draft health and care workforce
JOB DESCRIPTION AND PERSON SPECIFICATION JOB DESCRIPTION
 JOB DESCRIPTION AND PERSON SPECIFICATION JOB DESCRIPTION Job Title Directorate Nurse Clinical Champion Health and Wellbeing Pay Band 74.88 PAYE or 82.88 umbrella per 4 hour half day. Hours/Sessions per
JOB DESCRIPTION AND PERSON SPECIFICATION JOB DESCRIPTION Job Title Directorate Nurse Clinical Champion Health and Wellbeing Pay Band 74.88 PAYE or 82.88 umbrella per 4 hour half day. Hours/Sessions per
Guy s and St. Thomas Healthcare Alliance. Five-year strategy
 Guy s and St. Thomas Healthcare Alliance Five-year strategy 2018-2023 Contents Contents... 2 Strategic context... 3 The current environment... 3 National response... 3 The Guy s and St Thomas Healthcare
Guy s and St. Thomas Healthcare Alliance Five-year strategy 2018-2023 Contents Contents... 2 Strategic context... 3 The current environment... 3 National response... 3 The Guy s and St Thomas Healthcare
Shakeel Sabir Head of MERIT Vanguard
 MERIT Excellence, Resilience Innovation & Training Jointly developing Mental Health Service in the West Midlands Shakeel Sabir Head of MERIT Vanguard Background - New care models Multispecialty community
MERIT Excellence, Resilience Innovation & Training Jointly developing Mental Health Service in the West Midlands Shakeel Sabir Head of MERIT Vanguard Background - New care models Multispecialty community
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS
 CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Supporting the acute medical take: advice for NHS trusts and local health boards
 Supporting the acute medical take: advice for NHS trusts and local health boards Purpose of the statement The acute medical take has proven to be a challenge across acute hospital trusts and health boards
Supporting the acute medical take: advice for NHS trusts and local health boards Purpose of the statement The acute medical take has proven to be a challenge across acute hospital trusts and health boards
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL
 DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
Our community nursing roles
 Our community nursing roles Community Nursing Services provide nursing care to house-bound patients within the community. Our aim is to help patients to remain healthy and independent for as long as possible,
Our community nursing roles Community Nursing Services provide nursing care to house-bound patients within the community. Our aim is to help patients to remain healthy and independent for as long as possible,
Consultant Radiographers Education and CPD 2013
 Consultant Radiographers Education and CPD 2013 Consultant Radiographers Education and Continuing Professional Development Background Although consultant radiographer posts are relatively new to the National
Consultant Radiographers Education and CPD 2013 Consultant Radiographers Education and Continuing Professional Development Background Although consultant radiographer posts are relatively new to the National
Summary and Highlights
 Meeting: Trust Board Date: 23 November 2017 Agenda Item: TB/17-18/114 Boardpad ref:14 Agenda item Nursing Strategy Item from Attachments Summary and Highlights Mary Mumvuri Nursing Strategy This agenda
Meeting: Trust Board Date: 23 November 2017 Agenda Item: TB/17-18/114 Boardpad ref:14 Agenda item Nursing Strategy Item from Attachments Summary and Highlights Mary Mumvuri Nursing Strategy This agenda
This will activate and empower people to become more confident to manage their own health.
 Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
NHS GRAMPIAN. Grampian Clinical Strategy - Planned Care
 NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
Association of Pharmacy Technicians United Kingdom
 Please find below APTUKs views to the proposals for change in Community Pharmacy as discussed at the Community Pharmacy in 2016/2017 and beyond stakeholder meeting on the 4 th February 2016 Introduction
Please find below APTUKs views to the proposals for change in Community Pharmacy as discussed at the Community Pharmacy in 2016/2017 and beyond stakeholder meeting on the 4 th February 2016 Introduction
Responding to a risk or priority in an area 1. London Borough of Sutton
 Responding to a risk or priority in an area 1 London Borough of Sutton October 2017 Contents Contents... 2 Introduction... 3 Scope and activity... 4 What did we do?... 5 Framework... 6 Key findings...
Responding to a risk or priority in an area 1 London Borough of Sutton October 2017 Contents Contents... 2 Introduction... 3 Scope and activity... 4 What did we do?... 5 Framework... 6 Key findings...
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
The Symphony Programme an example from the UK of integrated working between primary and secondary care. Jeremy Martin, Symphony Programme Director
 The Symphony Programme an example from the UK of integrated working between primary and secondary care Jeremy Martin, Symphony Programme Director About South Somerset 135,000 population, older age profile
The Symphony Programme an example from the UK of integrated working between primary and secondary care Jeremy Martin, Symphony Programme Director About South Somerset 135,000 population, older age profile
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Report on District Nurse Education in the United Kingdom
 Report on District Nurse Education in the United Kingdom 2015-16 1 District Nurse Education 2015-16 Contents Key points 3 Findings Universities running the programme 3 Applicants who did not enter the
Report on District Nurse Education in the United Kingdom 2015-16 1 District Nurse Education 2015-16 Contents Key points 3 Findings Universities running the programme 3 Applicants who did not enter the
Our Health & Care Strategy
 MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
National Primary Care Cluster Event ABMU Health Board 13 th October 2016
 National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
Transforming General Practice in Greater Nottingham
 Transforming General Practice in Greater Nottingham 2017/18-2018/19 Version 1.0 February 2017 NHS Nottingham City Clinical Commissioning Group NHS Nottingham North and East Clinical Commissioning Group
Transforming General Practice in Greater Nottingham 2017/18-2018/19 Version 1.0 February 2017 NHS Nottingham City Clinical Commissioning Group NHS Nottingham North and East Clinical Commissioning Group
Briefing 73. Preparing for change: implementing the new pre-registration nursing standards
 September 2010 Briefing 73 The new standards for education from the Nursing and Midwifery Council provide the framework for pre-registration nurse education programmes and will determine how we train our
September 2010 Briefing 73 The new standards for education from the Nursing and Midwifery Council provide the framework for pre-registration nurse education programmes and will determine how we train our
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
Mid and South Essex Success Regime Overview and next steps. Andy Vowles, Programme Director. 18 April 2016
 Mid and South Essex Success Regime Overview and next steps Andy Vowles, Programme Director 18 April 2016 What s in this briefing Part 1 overview Background to the Success Regime Action to date The challenge
Mid and South Essex Success Regime Overview and next steps Andy Vowles, Programme Director 18 April 2016 What s in this briefing Part 1 overview Background to the Success Regime Action to date The challenge
Higher Education Funding Reforms. Clinical Placements
 Higher Education Funding Reforms Clinical Placements Background The reforms announced in the Comprehensive Spending Review (CSR) in 2015 will lead to significant changes in the way health education funding
Higher Education Funding Reforms Clinical Placements Background The reforms announced in the Comprehensive Spending Review (CSR) in 2015 will lead to significant changes in the way health education funding
Appendix 1: Integrated Urgent Care Service Update. 1. Purpose
 Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Joint framework: Commissioning and regulating together
 With support from NHS Clinical Commissioners Regulation of General Practice Programme Board Joint framework: Commissioning and regulating together A practical guide for staff January 2018 Publications
With support from NHS Clinical Commissioners Regulation of General Practice Programme Board Joint framework: Commissioning and regulating together A practical guide for staff January 2018 Publications
The Future Primary Care Workforce: Martin Roland, Chair, Primary Care Workforce Commission
 The Future Primary Care Workforce: Martin Roland, Chair, Primary Care Workforce Commission Primary Care Workforce Commission Aim: to identify models of primary care to meet the future needs of the NHS
The Future Primary Care Workforce: Martin Roland, Chair, Primary Care Workforce Commission Primary Care Workforce Commission Aim: to identify models of primary care to meet the future needs of the NHS
James Blythe, Director of Commissioning and Strategy. Agenda item: 09 Attachment: 04
 Title of paper: Author: Exec Lead: Community Hospital Services Review Tom Elrick, Urgent Care Programme Lead James Blythe, Director of Commissioning and Strategy Date: 23 rd February 2015 Meeting: Executive
Title of paper: Author: Exec Lead: Community Hospital Services Review Tom Elrick, Urgent Care Programme Lead James Blythe, Director of Commissioning and Strategy Date: 23 rd February 2015 Meeting: Executive
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
NHS Somerset CCG OFFICIAL. Overview of site and work
 NHS Somerset CCG Overview of site and work NHS Somerset CCG comprises 400 GPs (310 whole time equivalents) based in 72 practices and has responsibility for commissioning services for a dispersed rural
NHS Somerset CCG Overview of site and work NHS Somerset CCG comprises 400 GPs (310 whole time equivalents) based in 72 practices and has responsibility for commissioning services for a dispersed rural
Job Description. CNS Clinical Lead
 Job Description CNS Clinical Lead POST: BASE: ACCOUNTABLE TO: REPORTS TO: RESPONSIBLE FOR: CNS Clinical Lead St John s Hospice Head of Nursing and Quality Head of Nursing and Quality Community Clinical
Job Description CNS Clinical Lead POST: BASE: ACCOUNTABLE TO: REPORTS TO: RESPONSIBLE FOR: CNS Clinical Lead St John s Hospice Head of Nursing and Quality Head of Nursing and Quality Community Clinical
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme. Frequently Asked Questions Second Edition
 Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Intensive Psychiatric Care Units
 NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan. October 2016 submission to NHS England Public summary
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Bexley Whole Health System Fellows. Development opportunities for recently qualified GPs. December 2017
 Bexley Whole Health System Fellows Development opportunities for recently qualified GPs December 2017 Would you like to be part of a unique fellowship giving participants the opportunity to work in General
Bexley Whole Health System Fellows Development opportunities for recently qualified GPs December 2017 Would you like to be part of a unique fellowship giving participants the opportunity to work in General
LEARNING FROM THE VANGUARDS:
 LEARNING FROM THE VANGUARDS: STAFF AT THE HEART OF NEW CARE MODELS This briefing looks at what the vanguards set out to achieve when it comes to involving and engaging staff in the new care models. It
LEARNING FROM THE VANGUARDS: STAFF AT THE HEART OF NEW CARE MODELS This briefing looks at what the vanguards set out to achieve when it comes to involving and engaging staff in the new care models. It
Commissioning Strategy for General Practice
 Commissioning Strategy for General Practice 2016-2021 Section Contents Page Foreword 3 1 Executive Summary 4 2 Introduction 7 3 Setting the scene 10 4 The case for change 23 5 Developing our strategy 25
Commissioning Strategy for General Practice 2016-2021 Section Contents Page Foreword 3 1 Executive Summary 4 2 Introduction 7 3 Setting the scene 10 4 The case for change 23 5 Developing our strategy 25
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary
 Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
Meeting the Needs of a 21st Century Society. Care England Manifesto for the Independent Care Sector (ICS)
") Meeting the Needs of a 21st Century Society Manifesto for the Independent Care Sector (ICS) Introduction Expectations from citizens have risen. They experience social and health care as a continuum and
Meeting the Needs of a 21st Century Society Manifesto for the Independent Care Sector (ICS) Introduction Expectations from citizens have risen. They experience social and health care as a continuum and
Healthcare Apprentice Scheme Information pack for practices
 Healthcare Apprentice Scheme 2017-18 Information pack for practices Document Title: HCA Apprentice Scheme 2017-18 First Published: May 2017 Due for review: Last quarter of the financial year 2017-18 Contents
Healthcare Apprentice Scheme 2017-18 Information pack for practices Document Title: HCA Apprentice Scheme 2017-18 First Published: May 2017 Due for review: Last quarter of the financial year 2017-18 Contents
1. Roles & Responsibilities of the LMC and 2. Current Political Scene. Dr Peter Graves Chief Executive Beds & Herts LMC Ltd
 1. Roles & Responsibilities of the LMC and 2. Current Political Scene Dr Peter Graves Chief Executive Beds & Herts LMC Ltd Learning objectives The LMC who we are and what we do The current political scene
1. Roles & Responsibilities of the LMC and 2. Current Political Scene Dr Peter Graves Chief Executive Beds & Herts LMC Ltd Learning objectives The LMC who we are and what we do The current political scene
Health & Care Partnership for Cheshire & Merseyside PRIMARY CARE NETWORK DEVELOPMENT FUND APPLICATION PACK
 Health & Care Partnership for Cheshire & Merseyside PRIMARY CARE NETWORK DEVELOPMENT FUND APPLICATION PACK Electronic copies of this application form are available from: England.PCN-Development@nhs.net
Health & Care Partnership for Cheshire & Merseyside PRIMARY CARE NETWORK DEVELOPMENT FUND APPLICATION PACK Electronic copies of this application form are available from: England.PCN-Development@nhs.net
Shetland NHS Board. Board Paper 2017/28
 Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Buckinghamshire, Oxfordshire and Berkshire West Sustainability and Transformation Plan (BOB STP)
") Buckinghamshire, Oxfordshire and Berkshire West Sustainability and Transformation Plan (BOB STP) Q. What is a Sustainability and Transformation Plan? A. The NHS and local authorities across Buckinghamshire,
Buckinghamshire, Oxfordshire and Berkshire West Sustainability and Transformation Plan (BOB STP) Q. What is a Sustainability and Transformation Plan? A. The NHS and local authorities across Buckinghamshire,
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Our next phase of regulation A more targeted, responsive and collaborative approach
 Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Vanguard Programme: Acute Care Collaboration Value Proposition
 Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
The NHS Employers submission to the Migration Advisory Committee (MAC) call for evidence
 call for evidence") The NHS Employers submission to the Migration Advisory Committee (MAC) call for evidence Our organisation represents the whole range of views from across employing organisations in the NHS in England on
The NHS Employers submission to the Migration Advisory Committee (MAC) call for evidence Our organisation represents the whole range of views from across employing organisations in the NHS in England on
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report
 Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Pharmacy Workforce Summit Report: right place, right time, right number positioning the workforce for patients
 Pharmacy Workforce Summit Report: right place, right time, right number positioning the workforce for patients March 2017 Contents 1. Introduction.2 2. Background..2 3. Emerging themes and considerations..3
Pharmacy Workforce Summit Report: right place, right time, right number positioning the workforce for patients March 2017 Contents 1. Introduction.2 2. Background..2 3. Emerging themes and considerations..3
Clinical Pharmacists in General Practice March 2018
 Clinical Pharmacists in General Practice March 2018 1. Background Following a successful national pilot programme, the General Practice Forward View committed over 100million to support an extra 1,500
Clinical Pharmacists in General Practice March 2018 1. Background Following a successful national pilot programme, the General Practice Forward View committed over 100million to support an extra 1,500
THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS
 THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS ICCHNR SYMPOSIUM University of Kent at Canterbury 15 th -16 th September 2016 Dr John M Ribchester GP Chair and Clinical Lead for Encompass MCP
THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS ICCHNR SYMPOSIUM University of Kent at Canterbury 15 th -16 th September 2016 Dr John M Ribchester GP Chair and Clinical Lead for Encompass MCP
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Improving General Practice for the People of West Cheshire
 Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Healthcare. Higher Apprenticeship. Assistant Practitioner. shu.ac.uk/apprenticeships
 Healthcare Assistant Practitioner Higher Apprenticeship shu.ac.uk/apprenticeships Healthcare Assistant Practitioner Higher Apprenticeship Programme Outline Overview The Healthcare Assistant Practitioner
Healthcare Assistant Practitioner Higher Apprenticeship shu.ac.uk/apprenticeships Healthcare Assistant Practitioner Higher Apprenticeship Programme Outline Overview The Healthcare Assistant Practitioner
DEEP END MANIFESTO 2017
 DEEP END MANIFESTO 2017 In March 2013 Deep End Report 20 (Annex A) took the form of a manifesto entitled:- What can NHS Scotland do to prevent and reduce health inequalities? The report and recommendations
DEEP END MANIFESTO 2017 In March 2013 Deep End Report 20 (Annex A) took the form of a manifesto entitled:- What can NHS Scotland do to prevent and reduce health inequalities? The report and recommendations
Mental Health Crisis Care: Essex Summary Report
 Mental Health Crisis Care: Essex Summary Report Date of local area review: Onsite 16-17 December 2014 Date of publication: June 2015 This inspection was carried out under section 48 of the Health and Social
Mental Health Crisis Care: Essex Summary Report Date of local area review: Onsite 16-17 December 2014 Date of publication: June 2015 This inspection was carried out under section 48 of the Health and Social
Improving Access to Psychological Therapies. Guidance for Commissioning IAPT Training 2012/13. Revised July 2012
 Improving Access to Psychological Therapies Guidance for Commissioning IAPT Training 2012/13 Revised July 2012 IAPT Programme Department of Health Wellington House 133-155 Waterloo Road London SE1 8UG
Improving Access to Psychological Therapies Guidance for Commissioning IAPT Training 2012/13 Revised July 2012 IAPT Programme Department of Health Wellington House 133-155 Waterloo Road London SE1 8UG
UKMi and Medicines Optimisation in England A Consultation
 UKMi and Medicines Optimisation in England A Consultation Executive Summary Medicines optimisation is an approach that seeks to maximise the beneficial clinical outcomes for patients from medicines with
UKMi and Medicines Optimisation in England A Consultation Executive Summary Medicines optimisation is an approach that seeks to maximise the beneficial clinical outcomes for patients from medicines with
Meeting in Common of the Boards of NHS England and NHS Improvement. 1. This paper updates the NHS England and NHS Improvement Boards on:
 NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
Medical and Clinical Services Directorate Clinical Strategy
 www.ambulance.wales.nhs.uk Medical and Clinical Services Clinical Strategy Unique reference No: Version: 1.4 Title of author: Medical and Clinical Services No of Pages: 11 Implementation date: Next review
www.ambulance.wales.nhs.uk Medical and Clinical Services Clinical Strategy Unique reference No: Version: 1.4 Title of author: Medical and Clinical Services No of Pages: 11 Implementation date: Next review
Newham Community Education Provider Network Annual Report April 2015 March 2016
 1 Newham Community Education Provider Network Annual Report April 2015 March 2016 EXECUTIVE SUMMARY 2015/16 marks the second year of operation for Newham Together, the Newham Community Education Provider
1 Newham Community Education Provider Network Annual Report April 2015 March 2016 EXECUTIVE SUMMARY 2015/16 marks the second year of operation for Newham Together, the Newham Community Education Provider
Solent. NHS Trust. Allied Health Professionals (AHPs) Strategic Framework
 Strategic Framework") Solent NHS Trust Allied Health Professionals (AHPs) Strategic Framework 2016-2019 Introduction from Chief Nurse, Mandy Rayani As the executive responsible for providing professional leadership for the
Solent NHS Trust Allied Health Professionals (AHPs) Strategic Framework 2016-2019 Introduction from Chief Nurse, Mandy Rayani As the executive responsible for providing professional leadership for the
In this edition we will showcase the work of the development of a model for GP- Paediatric Hubs
 Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
High level guidance to support a shared view of quality in general practice
 Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Primary Care in Scotland Looking to the future. Fiona Duff Senior Advisor, Primary Care Division, Scottish Government
 Primary Care in Scotland Looking to the future Fiona Duff Senior Advisor, Primary Care Division, Scottish Government TRANSFORMING PRIMARY CARE: WHY? National Clinical Strategy: a business case for
Primary Care in Scotland Looking to the future Fiona Duff Senior Advisor, Primary Care Division, Scottish Government TRANSFORMING PRIMARY CARE: WHY? National Clinical Strategy: a business case for
NHS ENGLAND BOARD PAPER
 NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
Developing primary care in Barnet
 Developing primary care in Barnet Introduction In January 2012, the Joint Boards of NHS North Central London (NCL) approved a NCL Primary Care Strategy, which describes development of the primary care
Developing primary care in Barnet Introduction In January 2012, the Joint Boards of NHS North Central London (NCL) approved a NCL Primary Care Strategy, which describes development of the primary care
LymeForward Health and Wellbeing Group
 LymeForward Health and Wellbeing Group Proposals for improvement in provision of local health, care and support services January 2018 Life is really simple, but we insist on making it complicated. Confucius
LymeForward Health and Wellbeing Group Proposals for improvement in provision of local health, care and support services January 2018 Life is really simple, but we insist on making it complicated. Confucius
Guidelines for the appointment of. General Practitioners with Special Interests in the Delivery of Clinical Services. Respiratory Medicine
 Guidelines for the appointment of General Practitioners with Special Interests in the Delivery of Clinical Services Respiratory Medicine April 2003 Respiratory Medicine This General Practitioner with a
Guidelines for the appointment of General Practitioners with Special Interests in the Delivery of Clinical Services Respiratory Medicine April 2003 Respiratory Medicine This General Practitioner with a
Library and Knowledge Services Annual Report
 Library and Knowledge Services Annual Report 2016-2017 West Hertfordshire Hospitals NHS Trust Katherine Teal Annual Report 2016-2017 Foreword This year has seen significant changes in the Library and Knowledge
Library and Knowledge Services Annual Report 2016-2017 West Hertfordshire Hospitals NHS Trust Katherine Teal Annual Report 2016-2017 Foreword This year has seen significant changes in the Library and Knowledge
Registered nurses in adult social care, Skills for Care, Registered nurses in adult social care
 Registered nurses in adult social care, Skills for Care, 2015 1 Registered nurses in adult social care 2015 Registered nurses in adult social care, Skills for Care, 2015 2 Contents 1. Introduction... 3
Registered nurses in adult social care, Skills for Care, 2015 1 Registered nurses in adult social care 2015 Registered nurses in adult social care, Skills for Care, 2015 2 Contents 1. Introduction... 3
Mental Health Social Work: Community Support. Summary
 Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine
 Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Mental Health Crisis Pathway Analysis
 Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
York Teaching Hospital NHS Foundation Trust. Caring with pride. The Nursing and Midwifery Strategy
 York Teaching Hospital NHS Foundation Trust Caring with pride The Nursing and Midwifery Strategy 2017-2020 1 To be a nurse, a midwife or member of care staff is an extraordinary role. What we do every
York Teaching Hospital NHS Foundation Trust Caring with pride The Nursing and Midwifery Strategy 2017-2020 1 To be a nurse, a midwife or member of care staff is an extraordinary role. What we do every