PATIENT CONTROLLED ANALGESIA THERAPY
|
|
|
- Gervais Phelps
- 5 years ago
- Views:
Transcription
1 KINGSTON GENERAL HOSPITAL NURSING SERVICE PATIENT CONTROLLED ANALGESIA THERAPY LEARNING GUIDE Prepared by: Date: Revised: Revised: Revised: Nursing Education 1992 September 1997 August 2000 June 2010 January
2 Page 2 TABLE OF CONTENTS Page 1.0 Introduction Learning Objectives Concepts of Pain Concepts of Post-Operative Pain Principles of Patient Controlled Analgesia What is PCA? Who Decides Who Goes on the PCA Pump? Can Other Sedatives, Narcotics or Antiemetics be Given While on the PCA 07 Pump? How Does the PCA Pump Work? Alaris PCA Parameters Priming the Line Manual Method Required Tubing for Use with Alaris PCA Alaris PCA Module Inserting / Changing the PCA Syringe Verifying the PCA Program Settings Obtaining the Patient History Making a Demand for Analgesia Stopping the PCA Pump Patient Education Pharmacological Aspects of Morphine Classification Mode of Action Side Effects of Morphine Drug Compatibility Pharmacological Aspects of Fentanyl Classification Mode of Action Side Effects Patient Assessment Pain Scale Level of Sedation (LOS) Respiratory Status PCA Flow Sheet Analgesia Flow Sheet Reporting to the Anesthesiologist Case History... 23
3 Page 3 Page 10.0 PCA-IV Order Transcription References Evaluation of Learning Activity NOTE: This learning guide contains information current at the time of distribution. Policies and procedures are frequently revised. Please refer to related policies and procedures (P-300) contained in the Nursing Policy and Procedure Manual for ongoing current information.
4 Page INTRODUCTION Patient Controlled Analgesia (PCA) is a method of pain management that allows for the self-administration of intravenous analgesics, within the limits of safety. This learning guide is designed to provide nurses with information about the principles of pain assessment and management using PCA therapy. It is hoped that this information will facilitate safe and effective usage of the PCA system. 1.1 Learning Objectives The purpose of this learning guide is to provide the nurse with an understanding of PCA therapy. Upon completion of the manual, the nurse will be able to: 1) Define patient controlled analgesia. 2) Explain the purpose of PCA. 3) Become familiar with the Alaris PCA 4) Describe the principles and practices of narcotic administration. 5) Instruct the patient and family about the purpose, use and possible side effects of PCA therapy. 6) Document patient assessment using the PCA flow sheet.
5 Page CONCEPTS OF PAIN Nurses play an integral role in the management of pain. Pain is a subjective phenomenon that is complex and often variable. The nursing profession has universally accepted the following definition: "Pain is whatever the experiencing person says it is, existing whenever it does and not what others think it ought to be " (McCaffery, 1989, p7). Many times patients have more fears about the prospect of pain than the risks associated with the procedure itself. Several factors make up a patient's perception of pain and the need for narcotic analgesia, including: 1) The patient's previous experience with pain. 2) The ethnic, cultural and religious background. 3) The myths about narcotic use such as dependence and addiction. 4) The patient's age. 5) The type of surgery. 6) The site of the surgical incision. Traditional methods of pain control depend upon the intramuscular administration of narcotics on a PRN basis. However, the unpredictable blood concentration of narcotics following injection and the substantial delays between the time pain is perceived and relief is obtained, interfere with adequate analgesia. Sedation Patient need PAIN Call Nurse Relief Absorption from Site Administer Injection Nurse Response Screening Obtain Narcotic Keys Prepare Injection Sign out Medication Figure 1: Conventional Analgesic Therapy (Adapted from Graves, D., Foster, T.S., Batenhorst, R.L.., et al: Patient controlled analgesia, Ann Intern Medicine 99: 361)
6 Page 6 To eliminate the peaks and valleys caused by intermittent drug administration, different analgesic therapies have been developed. Patient Controlled Analgesia (PCA) is one method of pain management that allows for self-administration of intravenous analgesics. 3.0 CONCEPTS OF POST-OPERATIVE PAIN Pain is a common occurrence after nearly every type of surgical procedure. It may be caused by the stimulation of nerve endings by chemical substances released during surgery or from tissue ischemia caused by the interruption of blood supply to a particular body part. Following surgery, other factors can enhance the pain that a patient experiences. They include pressure from issue edema, abdominal distention and muscle spasms surrounding the incision. Poor management of post-operative pain can interfere with early ambulation, deep breathing and coughing, and other patient activities that promote early recovery. Post-operative complications such as atelectasis and deep vein thrombosis may develop when post-operative pain is poorly controlled. It is impossible to prevent the occurrence of post-operative pain, but it can be minimized so that the patient is comfortable. PCA therapy provides a consistent pattern of pain relief. In addition, patients have a much greater sense of control over their pain. 4.0 PRINCIPLES OF PATIENT CONTROLLED ANALGESIA 4.1 What is PCA? Patient Controlled Analgesia (PCA) is a method of pain management that allows for the self-administration of intravenous analgesics. This form of therapy may be used in the management of acute and chronic pain situations such as postoperative pain, trauma, acute or chronic low back pain, migraine headaches and pain in terminal illness. PCA therapy provides the patient with a sense of control over his/her pain within the limits of safety. PCA can potentially bypass the delays and deficiencies of the traditional methods of pain control. PCA therapy maintains analgesic blood levels within therapeutic range. PCA therapy may be used at any given time and as long as necessary to alleviate pain. 4.2 Who Decides Who Goes on the PCA Pump? The staff of the Acute Pain Service, which is comprised of anesthesiologists and an APN, decides who is a candidate for the PCA pump. Generally, patients are excluded from patient controlled analgesia in the following situations: extremes of age, for example, less than five years; drug addiction;
7 Page 7 allergy to analgesia; unconscious, confused, or requiring restraint; brain injury; pulmonary disease with carbon dioxide retention; hepatic, renal or cardiac disease; absence of nurses or physicians qualified to manage PCA. The Acute Pain Service is consulted by other services for pain management. The staff of Acute Pain Service are the only physicians who can write programming orders for the PCA pump. 4.3 Can Other Sedatives, Narcotics or Antiemetics be Given While on the PCA Pump? Because of the potential cumulative effects of combining other medications with the analgesic the patient receives while on PCA, no other narcotics, sedatives, or antiemetics are administered unless ordered by the anesthesiologist from the Acute Pain Services.
8 Page 8 When the PCA pump is discontinued all orders written by the Acute Pain Service are also discontinued. Pain management then becomes the responsibility of the attending service. 4.4 How Does the PCA Pump Work? The Alaris PCA module is attached to an Alaris brain. At the base of the module a handset is connected. When the patient feels pain the handset button can be pressed which triggers the pump to deliver a fixed bolus of drug. Immediately after this a lockout period starts. During this time the pump will ignore any further requests for analgesia. This safety feature allows the drug to exert its maximum effect and prevent an overdose. Alaris Brain

9 r Page 9

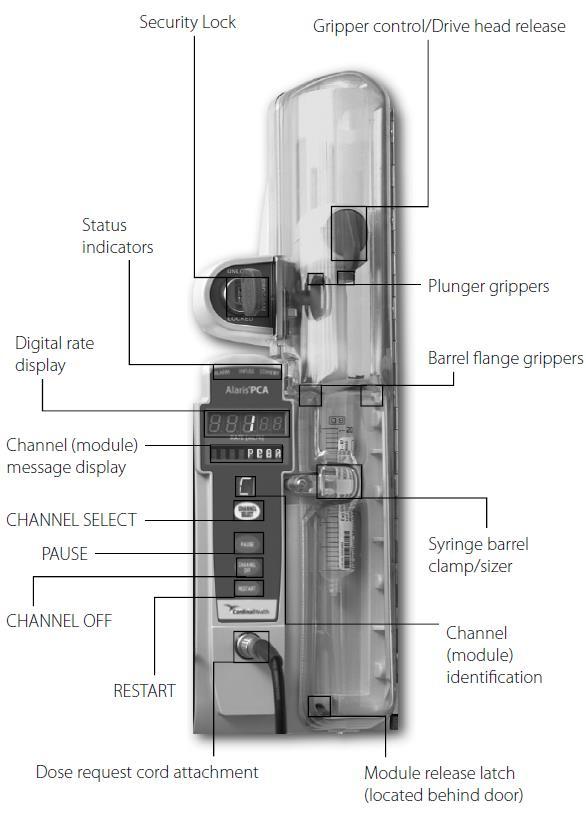
10 Page 10 PCA Module The patient cord leads to the hand set and should never be removed Hand set cord PROGRAMMING OF THE ALARIS PCA, BOLUS DOSING OR ANY CHANGE IN PROGRAMING IS COMPLETED BY ANESTHESIOLOGY OR THE ACUTE PAIN SERVICE Alaris PCA Parameters PRESS CHANNEL SELECT TO VERIFY SETTINGS PCA Dose The amount of drug programmed to be delivered upon patient demand Lockout Interval This is the length of time after receiving a PCA dose, when another dose cannot be administered.
11 Page 11 Continuous Dose PCA pump can infuse a small dose of analgesia continuously. This parameter only appears if a continuous infusion set Concentration (Conc) The strength of the analgesic solution programmed in the pump. The Pharmacy Department at the Kingston General Hospital supplies each unit with pre-mixed syringes of morphine 2.5mg/ml; however, HYDROmorphone or fentanyl may be used. NOTE: Nurses never mix syringes for the PCA pumps. Only pharmacy or anesthesia may mix the syringes. Press Channel Select, Options and Patient History Last Cleared Time displayed when pump last cleared. NOTE: pump is cleared every 4 hours with vital signs and documentation Total Drug This is the total amount (in milligrams) of analgesia infused since the PCA was initiated and/or cleared. Total Demands This is the number of times the patient has demanded a bolus of drug. Delivered This is the number of times that the patient received a bolus of the drug 4.5 Priming the Line Manual Method Attach the minibore to the narcotic syringe and manually prime with a very small amount of narcotic solution. Connect the luer end of the minibore tubing to one end of the Y-connector and manually prime with a small amount of narcotic solution. Prime the mainline tubing with the IV solution and attach the adapter to the second end of the Y-connector. Prime the remainder of the tubing with IV solution ensuring that all air is expelled. The PCA system is now ready to be connected to the patient. A second infusion is attached to the PCA tubing only when using a Y-connector with a non-return valve.

12 Page Required Tubing for use with Alaris PCA Minibore tubing for PCA Syringe PCA-IV anti-reflux Y-connector To assemble these tubings, see picture below connect PCA syringe here connect IV tubing here (Minimum rate = 30mL/h) Minibore extension set connect to patient IV
13 Page Alaris PCA Module The Alaris PCA module should be attached to the right to maintain a secured locked position The Security Lock is key operated and has three positions 1. Unlock position unlocks the security door to load or change the syringe 2. Program allows for changes in the device programming without unlocking the security door or interrupting the current infusion. This feature would only be used when the syringe is changed for the nurse to restore the infusion. 3. Lock locks the security door. The key must turn to this position to start an infusion. The PCA keys are kept on the narcotic key ring on most of the nursing units. Check with charge nurse or educator as some are kept on a separate ring locked in the narcotic cupboard. 4.7 Inserting / Changing the Alaris PCA Syringe 1. Press pause on the Alaris PCA. Always clamp administration set and disconnect from patient before changing the syringe. 2. Use PCA key and Unlock to remove syringe. Press silence. 3. To remove open door, pull syringe barrel clamp out and hold it, rotate clamp to left until it clears the syringe chamber then gently release. 4. Turn gripper control to the right until in open position then raise the drive head to full extension, release gripper control and remove old syringe. 5. Attach new syringe to tubing and load new syringe into PCA 6. Insert new syringe by sliding flat edge of syringe between the barrel flange grippers 7. Open the gripper control and lower the drive head gently to secure the new syringe 8. Rotate syringe barrel clamp back to the right over the syringe 9. Close door and turn key back to program 10. Reestablish PCA administration set to patient 11. Press channel select and press syringe choice then confirm by pressing the soft key 12. Restore will be the next prompt, at the bottom left corner of the Alaris brain press soft key. 13. Next prompt is to confirm PCA bolus and lockout, press soft key 14. Final prompt will be to lock door and press Start.
14 Page 14
15 Page Verifying the PCA Program Settings The PCA program settings are checked with the physician's orders. In PACU with anesthesiologist or against APMS orders With changes in nursing responsibility (e.g. at the start of the shift, unit to unit transfer) Following a syringe change When change in dose or rate has been made by APMS See policy P-300 in Nursing policy and procedure manual Press Channel Select Alaris PCA module and check PCA-IV bolus Lock out interval Continuous infusion if any Press start once confirmed If any discrepancy between patient orders and parameters in the pump call APMS 4.9 Obtaining the Patient History Every 24 hours the Alaris PCA-IV clears the patient history therefore the pump is cleared every 4 hours with vital signs and documentation to ensure a record of ongoing data Press channel select then: Options soft key Patient history soft key Document on the PCA-IV analgesia flow sheet the total demands/delivered and the total drug Press clear history, pump will ask if you want to clear patient history, press yes Press exit at the bottom of the Alaris brain then start 4.10 Making a Demand for Analgesia A demand for analgesia may be made by the patient by pressing the demand button on the handset once. One of two responses occurs: 1. The PCA pump beeps (indicating that it has received the message), and the patient receives a bolus dose. A green light flashes and the display indicates delivering PCA or 2. The patient does not receive a bolus because the demand was made during the lockout.
16 Page Stopping the PCA Pump Stop the PCA pump at any time by pressing 'Pause or Channel off '. This can be done without unlocking the syringe cover. If the pump is discontinued, send pump brain with attached PCA module to central processing. If an ongoing infusion is required use a new (non-pca) Alaris pump brain and module Never detach the hand-set from the PCA-IV module Once PCA therapy is discontinued, discard the analgesic remaining in the syringe. A second nurse must co-sign this wastage on the narcotic sheet
17 Page PATIENT EDUCATION The objective of patient education is to instruct the patient to effectively operate the PCA pump in order to decrease the intensity of the pain to a level that is tolerable to the patient. 1. While teaching the patient how to use the PCA pump during the preoperative period is preferable it is not essential. Due to the limited number of PCA pumps, it is not always possible for the anesthesiologist to pre-determine who will receive PCA therapy. Patients who receive PCA therapy but have not received preoperative education in its use require simple, repeated instructions during the postoperative period. 2. Patient education should include: expectations of the quality, location, severity and duration of the pain normally associated with the procedure; use of the PCA device, background infusion, bolus dose, frequency of assessment, duration of PCA therapy; coping strategies to mobilize the patient's defences, decrease anxiety and give the patient a sense of control; realistic expectations of pain, pain relief, narcotic analgesics, and nonpharmacological pain relief measures, e.g., deep breathing, muscle relaxation and distraction; review of concerns related to safety issues and fear of addiction. 3. PCA therapy instruction provided while the patient is receiving PCA may include: reinforcement of instruction previously received; encouragement to use the device frequently to achieve comfort; 6.0 PHARMACOLOGICAL ASPECTS OF MORPHINE 6.1 Classification Different narcotic analgesics may be administered via the PCA system, such as fentanyl, hydromorphone and morphine. At Kingston General Hospital, the drug of choice is morphine. 6.2 Mode of Action
18 Page 18 Narcotics relieve pain at the level of the central nervous system (CNS) by binding to opioid receptor sites at the brain and spinal levels. Narcotics produce an alteration of the pain perception, interfere with pain conduction or CNS response to pain, and/or elevate the pain threshold. When administered intravenously, morphine has a: rapid onset peak effect duration of action a few minutes 6-8 minutes 2-3 hours 6.3 Side Effects of Morphine 1. Respiratory Depression All narcotics, including morphine, are capable of having an effect on the respiratory cycle and thus producing respiratory depression. Naloxone is the narcotic antagonist of choice. It must be available at all times. In the event of respiratory depression, the anesthesiologist orders the administration of naloxone ( mg IV doses at 2-3 minute intervals up to 2.0mg). This is an added nursing skill for which the nurse must be authorized. 2. Nausea and Vomiting Approximately 20-30% of patients feel nauseated while receiving morphine. Prochlorperazine (Stemetil) and dimenhydrinate (Gravol) are the antiemetics of choice. The nurse may administer the antiemetic prescribed by the anesthesiologist on the pre-printed order form. 3. Sedation The patient receiving morphine may develop somnolence because of the direct depressant effect of narcotics on the CNS. The goal in pain management is that the patient be pain free and be alert enough to perform activities that promote early recovery. The nurse assesses the level of sedation using the scale provided. This is discussed in the patient assessment section of the learning guide. 4. Other Patients receiving morphine may develop urinary retention, headache, pruritus and dizziness. Narcotics may cause some dilation of blood vessels. This does not present a problem in the well-hydrated patient. However, in the hypovolemic patient, there is an increased risk of hypotension. If this occurs, notify the anesthesiologist. 6.4 Drug Compatibility With the PCA system, an intravenous infusion is administered concurrently with the morphine solution. All of the medications listed below are compatible with morphine.
19 Page 19 ancef cimetidine clindamycin cloxacillin erythromycin gentamycin heparin metronidazole penicillin G solucortef tobramycin vancomycin Insulin preparations are NOT compatible with morphine. Should questions arise, verify with the pharmacist. NOTE: If the patient has limited venous access, blood may be administered through the second end of the Y-connector while the patient is receiving PCA therapy. 7.0 PHARMACOLOGICAL ASPECTS OF FENTANYL 7.1 Classification When a patient has a known allergy to morphine, fentanyl may be substituted. Fentanyl is absorbed into the plastic of the syringe and is therefore only stable for 7 days. An anesthesiologist must prepare the syringe as necessary. 7.2 Mode of Action Fentanyl is chemically unrelated to morphine. It does have similar pharmacological effects. Fentanyl acts as an analgesic and a sedative agent. When administered intravenously, Fentanyl has a: rapid onset duration of action 3-5 minutes minutes 7.3 Side Effects The side effects exhibited by Fentanyl are similar to those of morphine. Side effects include: respiratory depression, apnea, muscle rigidity, bradycardia, hypotension, nausea and vomiting and urinary retention. Naloxone is the narcotic antagonist of choice. It must be kept available at all times. In the event of respiratory depression, the anesthesiologist will order the administration of naloxone ( mg IV doses at 2-3 minute intervals up to 2.0mg). This is an added nursing skill for which the nurse must be authorized.
20 Page PATIENT ASSESSMENT This section of the learning guide includes guidelines for monitoring the patient receiving PCA therapy. The nurse is responsible for ensuring that the patient is provided adequate analgesia with minimal side effects. The nurse must assess (a minimum of q4h) the level of pain, the level of sedation, the respiratory rate and the PCA therapy administered to the patient. 8.1 Pain Scale Nursing assessment is a key factor in the success of PCA. A pain rating scale is attached to each PCA pump to assist the nurses when assessing the patient's pain level No pain Severe pain Patients have different ways of expressing pain. Using the slide ruler, the nurse may ask, "How bad is your pain on a scale of 0 to 5, 0 being no pain at all, 5 being the worst pain imaginable?" Physical signs of pain include: facial grimacing; increased systolic pressure; increased heart rate; agitation; and muscle spasms. 8.2 Level of Sedation (LOS) The level of sedation (LOS) provides information about how sensitive the patient is to morphine. The nurse may use the following scale to determine the patient's LOS: 1. Wide awake: The patient is alert and oriented. 2. Drowsy: The patient falls asleep when you are talking to him/her. 3. Dozing intermittently: The patient sleeps but frequently awakens. 4. Mostly sleeping: The patient appears to sleep deeply without interruption. He/she is easily aroused at the time of assessment and responds appropriately. 5. Only awakens when stimulated: When the sternum is rubbed, the patient only moans and moves his/her limbs weakly.
21 Page 21 Notify the anesthesiologist STAT if the patient scores a 5 on the LOS scale. Stop the PCA pump immediately. 8.3 Respiratory Status Narcotic analgesics may cause respiratory depression. It is therefore essential that the nurse assess the respiratory rate and depth for a minimum of 30 seconds if no pulmonary dysfunction is suspected or for a full minute otherwise. If the respiratory rate is less than the rate specified by Anesthesia, stop the pump and notify the anesthesiologist. The anesthesiologist may instruct the nurse (who has been authorized for this added nursing skill) to administer naloxone (Narcan) below the drip chamber. 8.4 PCA Flow Sheet Note there are now two separate analgesia flow sheets in use at KGH, one PCA-IV and PCA-SC Analgesia Flowsheet and one Regional Analgesia Flowsheet. The flow sheets will provide both the nurse and the anesthesiologist with information about the amount of narcotic the patient is receiving while on PCA therapy. The PCA orders must be checked with the PCA pump parameters at the beginning of each shift and documented on the PCA-IV and PCA-SC Analgesia Flow Sheet. This includes the current lock out period, bolus dose, drug concentration, analgesic ordered, and continuous infusion rate. This is done by pressing the "Channel select" button. Once confirmed the pump will alarm unless Start is pressed. Patient assessment must be performed a minimum of q4h. See P-300 nursing policy for details. The pain assessment scale and the level of sedation scale have been included as a quick reference for the nurse when observing the patient. As well, the nurse must clearly indicate the drug name, concentration, and if appropriate, the loading dose at the top of the flow sheet. Each flow sheet must be stamped with the addressograph, as it is a permanent record for the patient.
22 8.4.1 Analgesia Flowsheet Page 22
23 Page 23
24 Page Reporting to the Anesthesiologist The anesthesiologist from the Acute Pain Service should be notified if any of the following occur: the patient has many unsuccessful attempts to receive a bolus dose and continues to rate the pain as extreme; hypotension after starting PCA; nausea and vomiting unresponsive to antiemetics; respiratory depression; level of somnolence of 5; urinary retention; and pruritus. 9.0 CASE HISTORY Mr. Key is a 58 year old who has arrived to the unit from PACU following a right hemicolectomy for colon cancer. At 1500h, the nurse verifies the PCA-IV settings by pressing the channel select and documenting the PCA dose and lockout interval. The nurse verifies that the concentration is the same as what is ordered. Next, the nurse will perform an assessment including vitals and pain assessment. Channel select will be pressed then options and then patient history soft key: The nurse will document as shown below and then clear history, exit and press start. At 2000 the nurse reassesses Mr. Key who states his pain is 3/10 at rest and 5/10 with deep breathing. The nurse provides health teaching regarding the use of the PCA-IV hand set especially prior to deep breathing or movement that may increase pain. The nurse presses channel select, options and the patient history soft key. The total demands/delivered and total drug is documented and the pump is cleared.
25 Page 25
26 Page 26
27 Page PCA-IV ORDER TRANSCRIPTION Important Points The anesthesiologist writes the orders on pre-printed order forms entitled "Acute Pain Service (APMS): Intravenous Patient Controlled Analgesia (PCA-IV) orders (see copy next page). There are adult and pediatric versions of these pre-printed orders. These orders come with the patient from the operating room. When transcribing the orders, the following information must be written on the Patient Profile (Kardex): patient on PCA pump; if respirations fall below (specified by the anesthesiologist) stop pump, notify Anesthesia STAT. When transcribing the orders, the following information must be written on the patient's Medication Administration Record (MAR): the analgesic ordered; the loading dose (if given); the PCA dose; the continuous rate, if applicable; the lockout interval; the antiemetic and co-analgesics prescribed; and changes in the continuous rate.
28 Page 28
29 Page REFERENCES Canadian Pharmaceutical Association (1991). Compendium of pharmaceuticals and specialties 91. Author. Collier, M. (1990). Controlling postoperative pain with patient-controlled analgesia. Journal of Professional Nursing, 6(2) Cardinal Health. (2008). Alaris System Implementation. Learner s Workbook, Kingston General Hospital, Kingston, ON Gagnon,M. (1990). Patient controlled analgesia learning manual. Nursing Department, Jewish General Hospital. Montreal, PQ. Goremi, L.E., & Hayes, J.W. (1982). Drugs and nursing implications. Connecticut: Appleton-Century-Crofts. Graves, D., Foster, T.S., Batenhorst, R.L., et al. (1983). Patient controlled analgesia. Ann Intern Medicine, Johnson, L.R., Magnani, B., Chan, V., & Ferrante, F.M. (1989). Modifiers of patient controlled analgesia efficacy: Locus of control. Pain, McCaffery, M., & Beebe, A. (1989). Pain: Clinical manual for nursing practice. St. Louis: The C.V. Mosby Company. Springhouse Corporation. (1987). Nursing '87 drug handbook Springhouse, Pennsylvania. Author. Smythe, M. (1992). Patient controlled analgesia: A review. Pharmacotherapy, 12(2)
30 Page EVALUATION OF LEARNING ACTIVITY TOPIC: Patient Controlled Analgesia (PCA) Therapy PRESENTER/TEACHER: LEARNING ACTIVITY/METHOD: Please check ( ) one or more of the following: 1. lecture 2. demonstration 3. video 4. other Please evaluate the learning activity in which you participated. Your comments and suggestions are valuable as a basis for improving future educational activities. Check ( ) the most appropriate response for each item below. 1. I feel that my learning needs were met. Strongly Disagree Strongly Agree The overall quality of the learning guide was excellent. 3. The content was clear and understandable. 4. The method(s) used enhanced my learning. 5. This will help me meet the knowledge/skill requirements of my job. Comment briefly: One way that I could use the information in this session is: Please give the completed evaluation to your Clinical Instructor. Thank you.
Policies and Procedures. Title:
 Policies and Procedures Title: PATIENT CONTROLLED ANALGESIA (PCA) LPN Additional Competency: Patient Controlled Analgesia with an Established Plan of Care RN Entry-Level Competency Authorization: [X] Former
Policies and Procedures Title: PATIENT CONTROLLED ANALGESIA (PCA) LPN Additional Competency: Patient Controlled Analgesia with an Established Plan of Care RN Entry-Level Competency Authorization: [X] Former
MEDICATION ADMINISTRATION: BELOW THE DRIP CHAMBER
 KINGSTON GENERAL HOSPITAL MEDICATION ADMINISTRATION: BELOW THE DRIP CHAMBER LEARNING GUIDE FOR REGISTERED NURSES AND REGISTERED PRACTICAL NURSES Prepared by: Nursing Education Date: 2001 November Revised:
KINGSTON GENERAL HOSPITAL MEDICATION ADMINISTRATION: BELOW THE DRIP CHAMBER LEARNING GUIDE FOR REGISTERED NURSES AND REGISTERED PRACTICAL NURSES Prepared by: Nursing Education Date: 2001 November Revised:
Staff Responsible Procedure Rationale/Reason
 Subject: Patient Controlled Analgesia Date: October 2011 UPMC St. Margaret UPMC St. Margaret Harmar Outpatient Center Clinical Practice Council Policy #2005 Overview: To promote appropriate PCA use and
Subject: Patient Controlled Analgesia Date: October 2011 UPMC St. Margaret UPMC St. Margaret Harmar Outpatient Center Clinical Practice Council Policy #2005 Overview: To promote appropriate PCA use and
PATIENT CARE MANUAL PROCEDURE
 PATIENT CARE MANUAL PROCEDURE NUMBER III-130 PAGE 1 OF 5 APPROVED BY: CATEGORY: Vice President and Senior Operating Officer, Rural Health Services & Professional Practice Lead Medication Administration
PATIENT CARE MANUAL PROCEDURE NUMBER III-130 PAGE 1 OF 5 APPROVED BY: CATEGORY: Vice President and Senior Operating Officer, Rural Health Services & Professional Practice Lead Medication Administration
Patient Controlled Analgesia Guidelines
 Patient Controlled Analgesia Guidelines Date: August 2005 Ref : PCD005 Vers : 2 Policy Profile Policy Reference Number PCD005 Version 2 Status Approved Trust Lead Director of Nursing/Acute Pain Team Implementation
Patient Controlled Analgesia Guidelines Date: August 2005 Ref : PCD005 Vers : 2 Policy Profile Policy Reference Number PCD005 Version 2 Status Approved Trust Lead Director of Nursing/Acute Pain Team Implementation
Unless this copy has been taken directly from the Trust intranet site (Pandora) there is no assurance that this is the most up to date version
 there is no assurance that this is the most up to date version") Policy No: OP49 Version: 4.0 Name of Policy: Patient Controlled Analgesia in Adult Patients Effective From: 28/11/2017 Date Ratified 21/09/2017 Ratified Medicines Group Review Date 01/09/2019 Sponsor Director
Policy No: OP49 Version: 4.0 Name of Policy: Patient Controlled Analgesia in Adult Patients Effective From: 28/11/2017 Date Ratified 21/09/2017 Ratified Medicines Group Review Date 01/09/2019 Sponsor Director
If viewing a printed copy of this policy, please note it could be expired. Got to to view current policies.
 If viewing a printed copy of this policy, please note it could be expired. Got to www.fairview.org/fhipolicies to view current policies. Department Policy Entity: Fairview Pharmacy Services Department:
If viewing a printed copy of this policy, please note it could be expired. Got to www.fairview.org/fhipolicies to view current policies. Department Policy Entity: Fairview Pharmacy Services Department:
Protocol for patient controlled analgesia (PCA) with morphine in obstetrics (CG567)
 with morphine in obstetrics (CG567)") Protocol for patient controlled analgesia (PCA) with morphine in obstetrics (CG567) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical Governance Committee
Protocol for patient controlled analgesia (PCA) with morphine in obstetrics (CG567) Approval Approval Group Job Title, Chair of Committee Date Maternity & Children s Services Clinical Governance Committee
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
VAN WERT COUNTY HOSPITAL. Policy/Procedure: Interdepartmental No.: N Issue Date: 6-90 By: Nursing No. of Pages: 9
 VAN WERT COUNTY HOSPITAL Policy/Procedure: Interdepartmental No.: N 7-14 Issue Date: 6-90 By: Nursing No. of Pages: 9 Reviewed: 6-14, 12-13, 5-11 Revised: 6-14 Distribution List: All Nursing Departments,
VAN WERT COUNTY HOSPITAL Policy/Procedure: Interdepartmental No.: N 7-14 Issue Date: 6-90 By: Nursing No. of Pages: 9 Reviewed: 6-14, 12-13, 5-11 Revised: 6-14 Distribution List: All Nursing Departments,
Adult Patient Controlled Analgesia (PCA)
") Contents... 1 Policy... 1 Scope/Audience... 1 Associated Documents... 1 Statement... 2 Criteria... 2 Patient and Whanau Education... 2 Procedural Considerations... 3 Pre Administration... 3 Patient Monitoring...
Contents... 1 Policy... 1 Scope/Audience... 1 Associated Documents... 1 Statement... 2 Criteria... 2 Patient and Whanau Education... 2 Procedural Considerations... 3 Pre Administration... 3 Patient Monitoring...
Your Anesthesiologist, Anesthesia and Pain Control
 You should avoid having pain after surgery by planning ahead. For example, if you know that you are going to be getting up to do your exercises with the therapist, ask for pain control medication in advance.
You should avoid having pain after surgery by planning ahead. For example, if you know that you are going to be getting up to do your exercises with the therapist, ask for pain control medication in advance.
MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY
 POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
POLICY MONITORING AND SUPPORT OF PATIENTS RECEIVING MODERATE SEDATION AND ANALGESIA DURING DIAGNOSTIC AND THERAPUTIC PROCEDURES POLICY A policy sets forth the guiding principles for a specified targeted
Your Anesthesiologist, Anesthesia and Pain Control
 You can reduce your pain level after surgery by planning ahead. For example, if you know that you are going to be getting up to do your exercises with the therapist, ask for pain control medication in
You can reduce your pain level after surgery by planning ahead. For example, if you know that you are going to be getting up to do your exercises with the therapist, ask for pain control medication in
SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY
 PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
PS1070 SARASOTA MEMORIAL HOSPITAL PERIOPERATIVE DEPARTMENT POLICY TITLE: ADMISSION/DISCHARGE CRITERIA: POST ANESTHESIA CARE UNITS (PACU) EFFECTIVE DATE: REVIEWED/REVISED DATE: POLICY TYPE: Job Title of
Session 2 Improving Narcotics and Opiate Management
 Session 2 Improving Narcotics and Opiate Management Frank Federico, RPh, IHI Executive Director Steve Meisel, Pharm.D., IHI Faculty January 31,2012 12:00-1:00pm ET Beth O Donnell, MPH Beth O Donnell, MPH,
Session 2 Improving Narcotics and Opiate Management Frank Federico, RPh, IHI Executive Director Steve Meisel, Pharm.D., IHI Faculty January 31,2012 12:00-1:00pm ET Beth O Donnell, MPH Beth O Donnell, MPH,
Clinical Skills Validation: Alaris Pump System
 Clinical Skills Validation: Alaris Pump System These documents are intended for use by CW Nurse Clinical Leadership Team. The method used to implement the validation of the Alaris Pump System is unit specific.
Clinical Skills Validation: Alaris Pump System These documents are intended for use by CW Nurse Clinical Leadership Team. The method used to implement the validation of the Alaris Pump System is unit specific.
Patient controlled analgesia for pain relief after surgery
 Information for patients and carers Patient controlled analgesia for pain relief after surgery Diagnostics and Clinical Services Anaesthetics and Acute Pain Team This leaflet is for anyone who may benefit
Information for patients and carers Patient controlled analgesia for pain relief after surgery Diagnostics and Clinical Services Anaesthetics and Acute Pain Team This leaflet is for anyone who may benefit
PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS)
") PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS) REQUIRES SAFETY IMPROVEMENTS From the July 16, 2009 issue Problem: In our May 21, 2009, newsletter we noted an association
PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS) REQUIRES SAFETY IMPROVEMENTS From the July 16, 2009 issue Problem: In our May 21, 2009, newsletter we noted an association
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV TREPROSTINIL (REMODULIN ) Job Title of Reviewer: Director, Pharmacy POLICY
PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV TREPROSTINIL (REMODULIN ) Job Title of Reviewer: Director, Pharmacy POLICY
By Yvonne D Arcy, CRNP, CNS, MS
 2.0 ANCC/AACN CONTACT HOURS Keep your patient By Yvonne D Arcy, CRNP, CNS, MS PATIENT-CONTROLLED ANALGESIA (PCA), an attractive short-term option for managing acute postoperative pain, puts the patient
2.0 ANCC/AACN CONTACT HOURS Keep your patient By Yvonne D Arcy, CRNP, CNS, MS PATIENT-CONTROLLED ANALGESIA (PCA), an attractive short-term option for managing acute postoperative pain, puts the patient
Statement on Safe Use of Propofol (Approved by ASA House of Delegates on October 27, 2004);
;") CREDENTIALING GUIDELINES FOR PRACTITIONERS WHO ARE NOT ANESTHESIA PROFESSIONALS TO ADMINISTER ANESTHETIC DRUGS TO ESTABLISH A LEVEL OF MODERATE SEDATION (Approved by the House of Delegates on October 25,
CREDENTIALING GUIDELINES FOR PRACTITIONERS WHO ARE NOT ANESTHESIA PROFESSIONALS TO ADMINISTER ANESTHETIC DRUGS TO ESTABLISH A LEVEL OF MODERATE SEDATION (Approved by the House of Delegates on October 25,
201 KAR 20:490. Licensed practical nurse intravenous therapy scope of practice.
 201 KAR 20:490. Licensed practical nurse intravenous therapy scope of practice. RELATES TO: KRS 314.011(10)(a), (c) STATUTORY AUTHORITY: KRS 314.011(10)(c), 314.131(1), 314.011(10)(c) NECESSITY, FUNCTION,
201 KAR 20:490. Licensed practical nurse intravenous therapy scope of practice. RELATES TO: KRS 314.011(10)(a), (c) STATUTORY AUTHORITY: KRS 314.011(10)(c), 314.131(1), 314.011(10)(c) NECESSITY, FUNCTION,
Surgical Weight Loss at Eastern Maine Medical Center Your Inpatient Nursing Stay
 Surgical Weight Loss at Eastern Maine Medical Center Your Inpatient Nursing Stay Dear Prospective Patient: I have recently been informed that you are considering weight loss surgery at EMMC. As you know
Surgical Weight Loss at Eastern Maine Medical Center Your Inpatient Nursing Stay Dear Prospective Patient: I have recently been informed that you are considering weight loss surgery at EMMC. As you know
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
CONSENT FOR SURGERY OR SPECIAL PROCEDURES
 Admission Date THE VALLEY HOSPITAL CONSENT FOR SURGERY OR SPECIAL PROCEDURES - Colonoscopy 1. Authorization. I hereby authorize Dr. (" my Doctor") and any such assistants or designees as may be selected
Admission Date THE VALLEY HOSPITAL CONSENT FOR SURGERY OR SPECIAL PROCEDURES - Colonoscopy 1. Authorization. I hereby authorize Dr. (" my Doctor") and any such assistants or designees as may be selected
Abdominal Surgery. Beyond Medicine. What to Expect While You Are in the Hospital. ilearning about your health
 ilearning about your health Abdominal Surgery What to Expect While You Are in the Hospital www.cpmc.org/learning Beyond Medicine. Table of Contents On the Day of Your Surgery...3 Your Nursing Care...3
ilearning about your health Abdominal Surgery What to Expect While You Are in the Hospital www.cpmc.org/learning Beyond Medicine. Table of Contents On the Day of Your Surgery...3 Your Nursing Care...3
Raise your game: The UP Campaign. Bruce Spurlock, M.D. Cynosure Health
 Raise your game: The UP Campaign Bruce Spurlock, M.D. Cynosure Health 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Can we streamline & simplify making it easier for front-line staff and still improve safety? 16
Raise your game: The UP Campaign Bruce Spurlock, M.D. Cynosure Health 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Can we streamline & simplify making it easier for front-line staff and still improve safety? 16
The ASA defines anesthesiology as the practice of medicine dealing with but not limited to:
 1570 Midway Pl. Menasha, WI 54952 920-720-1300 Procedure 1205- Anesthesia Lines of Business: All Purpose: This guideline describes Network Health s reimbursement of anesthesia services. Procedure: Anesthesia
1570 Midway Pl. Menasha, WI 54952 920-720-1300 Procedure 1205- Anesthesia Lines of Business: All Purpose: This guideline describes Network Health s reimbursement of anesthesia services. Procedure: Anesthesia
Institutional Handbook of Operating Procedures Policy
 Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Alaris Guardrails Quick Overview for Staff Pharmacists
 Alaris Guardrails Quick Overview for Staff Pharmacists Ruth LaCasse Kalish, RPh 3-16-2016 Objectives Provide information to pharmacists that may assist when a nurse calls with an issue with the guardrails.
Alaris Guardrails Quick Overview for Staff Pharmacists Ruth LaCasse Kalish, RPh 3-16-2016 Objectives Provide information to pharmacists that may assist when a nurse calls with an issue with the guardrails.
Opioid Sedation Comparison Study
 Opioid Sedation Comparison Study Barbara U. Ochampaugh, RN, BSN, CPAN Level IV; Sandra Lowery, RN, CPAN Level III; Deborah J. Marra, RN, BS, CPAN Level III; and Nancy Salerno RN, MSN Respiratory depression
Opioid Sedation Comparison Study Barbara U. Ochampaugh, RN, BSN, CPAN Level IV; Sandra Lowery, RN, CPAN Level III; Deborah J. Marra, RN, BS, CPAN Level III; and Nancy Salerno RN, MSN Respiratory depression
WYOMING STATE BOARD OF NURSING ADVISORY OPINION
 WYOMING STATE BOARD OF NURSING ADVISORY OPINION INTRAVENOUS THERAPY BY LICENSED PRACTICAL NURSES Advisory Opinion Number: 03-123 Board Meeting Date: April 28-May 1, 2003 January 7-10, 2008 Introduction:
WYOMING STATE BOARD OF NURSING ADVISORY OPINION INTRAVENOUS THERAPY BY LICENSED PRACTICAL NURSES Advisory Opinion Number: 03-123 Board Meeting Date: April 28-May 1, 2003 January 7-10, 2008 Introduction:
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: ACUTE AND POST OPERATIVE EPIDURAL/INTRATHECAL PAIN Job Title of Responsible Owner: Acute Pain Coordinator EFFECTIVE DATE: REVISED DATE:
PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: ACUTE AND POST OPERATIVE EPIDURAL/INTRATHECAL PAIN Job Title of Responsible Owner: Acute Pain Coordinator EFFECTIVE DATE: REVISED DATE:
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 +PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: INTRAVENOUS PATIENT CONTROLLED ANALGESIA AND NARCOTIC INFUSIONS Job Title of Reviewer: Acute Pain Coordinator EFFECTIVE DATE: REVISED
+PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: INTRAVENOUS PATIENT CONTROLLED ANALGESIA AND NARCOTIC INFUSIONS Job Title of Reviewer: Acute Pain Coordinator EFFECTIVE DATE: REVISED
U: Medication Administration
 U: Medication Administration Alberta Licensed Practical Nurses Competency Profile 199 Competency: U-1 Pharmacology and Principles of Administration of Medications U-1-1 U-1-2 U-1-3 U-1-4 Demonstrate knowledge
U: Medication Administration Alberta Licensed Practical Nurses Competency Profile 199 Competency: U-1 Pharmacology and Principles of Administration of Medications U-1-1 U-1-2 U-1-3 U-1-4 Demonstrate knowledge
ASSESSMENT OF COMPETENCE FOR: Management of Patient Controlled Analgesia (PCA) used for adults and/or children, excluding obstetrics
 used for adults and/or children, excluding obstetrics") ASSESSMENT OF COMPETENCE FOR: Management of Patient Controlled Analgesia (PCA) used for adults and/or children, excluding obstetrics Practitioner s name: Department/Ward: Assessors Name: Training period:
ASSESSMENT OF COMPETENCE FOR: Management of Patient Controlled Analgesia (PCA) used for adults and/or children, excluding obstetrics Practitioner s name: Department/Ward: Assessors Name: Training period:
Pharmacy Services. Division of Nursing Homes
 Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
Pharmacy Services Division of Nursing Homes 1 483.45 Pharmacy Services Overview The Pharmacy Services section of Appendix PP contains all Pharmacy Services requirements and interpretive guidelines (IG)
ENVIRONMENT Preoperative evaluation clinic. Preoperative evaluation clinic. Preoperative evaluation clinic. clinic. clinic. Preoperative evaluation
 Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
Required Organizational Practices Resources for 2016
 Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
Required Organizational Practices Resources for 2016 ROPs Tests for Compliance Things to Consider Available Resources CLIENT IDENTIFICATION Working in partnership with clients and families, at least two
Peri-operative Pain Management - a multi-disciplinary team-based approach
 Peri-operative Pain Management - a multi-disciplinary team-based approach Dr Steven Wong Chief of Service Department of Anaesthesiology & OT Services Queen Elizabeth Hospital Outline Development of postoperative
Peri-operative Pain Management - a multi-disciplinary team-based approach Dr Steven Wong Chief of Service Department of Anaesthesiology & OT Services Queen Elizabeth Hospital Outline Development of postoperative
Continuous Monitoring of Patients on Opioids: Capnography Initiative at BJC Healthcare. Friday October 14, 2016
 Continuous Monitoring of Patients on Opioids: Capnography Initiative at BJC Healthcare Friday October 14, 2016 AAMI Foundation Vision: To drive the safe adoption and safe use of healthcare technology National
Continuous Monitoring of Patients on Opioids: Capnography Initiative at BJC Healthcare Friday October 14, 2016 AAMI Foundation Vision: To drive the safe adoption and safe use of healthcare technology National
GENERAL PROGRAM GOALS AND OBJECTIVES
 BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
Benefits of a pathway: The experience of utilizing a NOF pathway. Megan Yeomans Clinical Nurse Consultant Pain Team, Austin Health
 Benefits of a pathway: The experience of utilizing a NOF pathway Megan Yeomans Clinical Nurse Consultant Pain Team, Austin Health Our health service # NOF Presentations 2010-2011: 262 2011-2012: 246 Management
Benefits of a pathway: The experience of utilizing a NOF pathway Megan Yeomans Clinical Nurse Consultant Pain Team, Austin Health Our health service # NOF Presentations 2010-2011: 262 2011-2012: 246 Management
WYOMING STATE BOARD OF NURSING ADVISORY OPINION INTRAVENOUS THERAPY BY LICENSED PRACTICAL NURSES
 WYOMING STATE BOARD OF NURSING ADVISORY OPINION INTRAVENOUS THERAPY BY LICENSED PRACTICAL NURSES Advisory Opinion Number: 03-123 Board Meeting Date: April 28-May 1, 2003 January 7-10, 2008 February 18,
WYOMING STATE BOARD OF NURSING ADVISORY OPINION INTRAVENOUS THERAPY BY LICENSED PRACTICAL NURSES Advisory Opinion Number: 03-123 Board Meeting Date: April 28-May 1, 2003 January 7-10, 2008 February 18,
SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV EPOPROSTENOL (FLOLAN, VELETRI ) POLICY #: EFFECTIVE DATE: REVISED DATE: POLICY
PS1006 SARASOTA MEMORIAL HOSPITAL NURSING DEPARTMENT POLICY TITLE: NURSING AND PHARMACY GUIDELINES FOR THE ADMINISTRATION OF IV EPOPROSTENOL (FLOLAN, VELETRI ) POLICY #: EFFECTIVE DATE: REVISED DATE: POLICY
Just Culture Toolkit Scenarios
 Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Enhanced Recovery Programme
 Enhanced Recovery Programme Page 14 Contact details South Tyneside NHS Foundation Trust Harton Lane South Shields Tyne and Wear NE34 0PL For advice please contact ward 1 on 4041001 Or ward 3 on 0191 4041003.
Enhanced Recovery Programme Page 14 Contact details South Tyneside NHS Foundation Trust Harton Lane South Shields Tyne and Wear NE34 0PL For advice please contact ward 1 on 4041001 Or ward 3 on 0191 4041003.
STATEMENT ON GRANTING PRIVILEGES FOR ADMINISTRATION OF MODERATE SEDATION TO PRACTITIONERS WHO ARE NOT ANESTHESIA PROFESSIONALS
 NOT ANESTHESIA PROFESSIONALS (Approved by the ASA House of Delegates on October 25, 2005, and amended on October 18, 2006) Outcome Indicators for Office-Based and Ambulatory Surgery (ASA Committee on Ambulatory
NOT ANESTHESIA PROFESSIONALS (Approved by the ASA House of Delegates on October 25, 2005, and amended on October 18, 2006) Outcome Indicators for Office-Based and Ambulatory Surgery (ASA Committee on Ambulatory
Care of Patients Receiving Analgesia by Catheter Techniques Position Statement and Policy Considerations
 Care of Patients Receiving Analgesia by Catheter Techniques Position Statement and Policy Considerations Position Statement Registered nurses (RNs) are valuable members of the patient care team who are
Care of Patients Receiving Analgesia by Catheter Techniques Position Statement and Policy Considerations Position Statement Registered nurses (RNs) are valuable members of the patient care team who are
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Poon EG, Keohane CA, Yoon CS, et al. Effect of bar-code technology
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Poon EG, Keohane CA, Yoon CS, et al. Effect of bar-code technology
SCIP-Inf-2, SCIP-Inf-3, SCIP-Inf-4, SCIP-Inf- 9, SCIP-Inf-10, SCIP-VTE-1, SCIP-VTE-2 Anesthesia End Time 5
 Release Notes: Alphabetical Data Dictionary Version 3.3 Surgical Care Improvement Project (SCIP) - Data Dictionary The General Abstraction Guidelines explain the different sections of the data element
Release Notes: Alphabetical Data Dictionary Version 3.3 Surgical Care Improvement Project (SCIP) - Data Dictionary The General Abstraction Guidelines explain the different sections of the data element
Administration of Medications A Self-Assessment Guide for Licensed Practical Nurses
 Administration of Medications A Self-Assessment Guide for Licensed Practical Nurses March 2018 College of Licensed Practical Nurses of Nova Scotia http://clpnns.ca Starlite Gallery, 302-7071 Bayers Road,
Administration of Medications A Self-Assessment Guide for Licensed Practical Nurses March 2018 College of Licensed Practical Nurses of Nova Scotia http://clpnns.ca Starlite Gallery, 302-7071 Bayers Road,
UNIVERSITY OF MASSACHUSETTS MEDICAL SCHOOL ANESTHESIOLOGY RESIDENCY PROGRAM GOALS AND OBJECTIVES
 UNIVERSITY OF MASSACHUSETTS MEDICAL SCHOOL ANESTHESIOLOGY RESIDENCY PROGRAM GOALS AND OBJECTIVES CA-2/CA-3 REQUIRED ROTATIONS IN PEDIATRIC ANESTHESIOLOGY The Department of Anesthesiology has established
UNIVERSITY OF MASSACHUSETTS MEDICAL SCHOOL ANESTHESIOLOGY RESIDENCY PROGRAM GOALS AND OBJECTIVES CA-2/CA-3 REQUIRED ROTATIONS IN PEDIATRIC ANESTHESIOLOGY The Department of Anesthesiology has established
Acknowledgement. Speaker Disclosure Statement. ASPMN 21 st National Conference Tucson, AZ September 9,
 Monitoring Over Sedation in Adult and Pediatric Patients Receiving Opioids for Michele Farrington, BSN, RN, CPHON michele farrington@uiowa.edu Staff Nurse Anne Smith, MSN, RN BC anne m smith@uiowa.edu
Monitoring Over Sedation in Adult and Pediatric Patients Receiving Opioids for Michele Farrington, BSN, RN, CPHON michele farrington@uiowa.edu Staff Nurse Anne Smith, MSN, RN BC anne m smith@uiowa.edu
1. Introduction. 1 CMS section
 1. Introduction Anesthesiology is the practice of medicine including, but not limited to, preoperative patient evaluation, anesthetic planning, intraoperative and postoperative care and the management
1. Introduction Anesthesiology is the practice of medicine including, but not limited to, preoperative patient evaluation, anesthetic planning, intraoperative and postoperative care and the management
Principles In developing these recommendations the Consensus Panel first established the following principles for anesthesia outcomes capture:
 Outcomes of Anesthesia: Core Measures The following Core Measures are the consensus recommendations of the Anesthesia Quality Institute (AQI) and the Multicenter Perioperative Outcomes Group (MPOG). They
Outcomes of Anesthesia: Core Measures The following Core Measures are the consensus recommendations of the Anesthesia Quality Institute (AQI) and the Multicenter Perioperative Outcomes Group (MPOG). They
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
 Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
Use for a resident who has potentially unnecessary medications, is prescribed psychotropic medications or has the potential for an adverse outcome to determine whether facility practices are in place to
G: Surgical. College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 67
 G: Surgical College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 67 Major Competency Area: G Surgical Competency: G-1 Surgical Nursing Date: June 1, 2015 G-1-1 G-1-2 G-1-3
G: Surgical College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 67 Major Competency Area: G Surgical Competency: G-1 Surgical Nursing Date: June 1, 2015 G-1-1 G-1-2 G-1-3
The University of Arizona Pediatric Residency Program. Primary Goals for Rotation. Anesthesia
 The University of Arizona Pediatric Residency Program Primary Goals for Rotation Anesthesia 1. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation.
The University of Arizona Pediatric Residency Program Primary Goals for Rotation Anesthesia 1. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation.
(b) Is administered via a transdermal route; or
 Is administered via a transdermal route; or") ACTION: To Be Refiled DATE: 10/10/2018 2:31 PM 4723-9-10 Formulary; standards of prescribing for advanced practice registered nurses designated as clinical nurse specialists, certified nurse-midwives,
ACTION: To Be Refiled DATE: 10/10/2018 2:31 PM 4723-9-10 Formulary; standards of prescribing for advanced practice registered nurses designated as clinical nurse specialists, certified nurse-midwives,
Administration of Medication IV Push to Neonatal/Paediatric & Adult Patients Self-Learning Package
 Administration of Medication IV Push to Neonatal/Paediatric & Adult Patients Self-Learning Package Prepared by Cheryl Owen, CPL Medicine, Rose Owen CPL NICU/SCN; Jan. 2008 Revised by Rose Owen CPL NICU/SCN;
Administration of Medication IV Push to Neonatal/Paediatric & Adult Patients Self-Learning Package Prepared by Cheryl Owen, CPL Medicine, Rose Owen CPL NICU/SCN; Jan. 2008 Revised by Rose Owen CPL NICU/SCN;
Improving the Safe Use of Multiple IV Infusions
 QUICK GUIDE Improving the Safe Use of Multiple IV Infusions The AAMI Foundation is grateful to its collaborating partners in the National Coalition for Infusion Therapy Safety: Acknowledgements The AAMI
QUICK GUIDE Improving the Safe Use of Multiple IV Infusions The AAMI Foundation is grateful to its collaborating partners in the National Coalition for Infusion Therapy Safety: Acknowledgements The AAMI
The Ohio State University Department of Orthopaedics. Residency Curriculum. PGY1 Rotations
 The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
The Ohio State University Department of Orthopaedics Residency Curriculum PGY1 Rotations Goals and Objectives Anesthesiology Rotation PGY1 Level I. Core Competency Areas By the end of the PGY1 rotation
KINGSTON GENERAL HOSPITAL NURSING POLICY & PROCEDURE
 KINGSTON GENERAL HOSPITAL NURSING POLICY & PROCEDURE SUBJECT Documentation - Medication NUMBER PAGE 1 of 7 ORIGINAL ISSUE 1985 April REVIEW REVISION 2014 May Policy: 1. A standardized documentation process
KINGSTON GENERAL HOSPITAL NURSING POLICY & PROCEDURE SUBJECT Documentation - Medication NUMBER PAGE 1 of 7 ORIGINAL ISSUE 1985 April REVIEW REVISION 2014 May Policy: 1. A standardized documentation process
Anaesthesia. Patient-controlled Analgesia (PCA)
") Anaesthesia Patient-controlled Analgesia (PCA) The Anaesthesia department comprises doctors and nurses, whose primary role is to ensure a safe and pain-free journey for patients undergoing surgery. An
Anaesthesia Patient-controlled Analgesia (PCA) The Anaesthesia department comprises doctors and nurses, whose primary role is to ensure a safe and pain-free journey for patients undergoing surgery. An
Plum 360 TM Infusion System with Full IV-EHR Interoperability
 Plum 360 TM Infusion System with Full IV-EHR Interoperability Your Direct Connection To Clinical Excellence > Air management that doesn t require disconnecting from the patient > A secondary line that
Plum 360 TM Infusion System with Full IV-EHR Interoperability Your Direct Connection To Clinical Excellence > Air management that doesn t require disconnecting from the patient > A secondary line that
Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN
 Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN Fairview Health Services 6 hospitals, ranging from rural
Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN Fairview Health Services 6 hospitals, ranging from rural
PROCEDURAL SEDATION AND ANALGESIA: HOSPITAL-WIDE POLICY
 CLINICAL PRACTICE POLICY PAGE: 1 OF 6 PURPOSE: These policies will allow clinicians to provide their patients with the benefits of procedural sedation and analgesia while minimizing the associated risks.
CLINICAL PRACTICE POLICY PAGE: 1 OF 6 PURPOSE: These policies will allow clinicians to provide their patients with the benefits of procedural sedation and analgesia while minimizing the associated risks.
Alaris System. Medication safety system focused at the point of care
 Alaris System Medication safety system focused at the point of care A safety platform you can build on TM Different care areas have different needs. That s why the Alaris System* gives you a platform you
Alaris System Medication safety system focused at the point of care A safety platform you can build on TM Different care areas have different needs. That s why the Alaris System* gives you a platform you
Client Alert. CMS Clarifies Interpretive Guidelines for Hospitals Providing Anesthesia Services
 Contact Attorneys Regarding This Matter: Mark A. Guza 404.873.8796 - direct 404.873.8797 - fax mark.guza@agg.com Diana Rusk Cohen 404.873.8108 - direct 404.873.8109 - fax diana.cohen@agg.com Client Alert
Contact Attorneys Regarding This Matter: Mark A. Guza 404.873.8796 - direct 404.873.8797 - fax mark.guza@agg.com Diana Rusk Cohen 404.873.8108 - direct 404.873.8109 - fax diana.cohen@agg.com Client Alert
CA-1 Curriculum Acute Pain Service and Regional Anesthesia West Virginia University Department of Anesthesiology
 CA-1 Curriculum Acute Pain Service and Regional Anesthesia West Virginia University Department of Anesthesiology Description of Rotation or Educational Experience The Regional/Acute Pain Services occurs
CA-1 Curriculum Acute Pain Service and Regional Anesthesia West Virginia University Department of Anesthesiology Description of Rotation or Educational Experience The Regional/Acute Pain Services occurs
Your Results for: "NCLEX Review"
 Your Results for: "NCLEX Review" Site Title: Medical-Surgical Nursing Book Title: Medical-Surgical Nursing Location on Site: PART 1: MEDICAL-SURGICAL NURSING PRACTICE > Chapter 5: Nursing Care of Clients
Your Results for: "NCLEX Review" Site Title: Medical-Surgical Nursing Book Title: Medical-Surgical Nursing Location on Site: PART 1: MEDICAL-SURGICAL NURSING PRACTICE > Chapter 5: Nursing Care of Clients
Post-operative "Fast-Track" pathways for lung resection. Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic
 Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic
Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE RESTRAINT AS A LAST RESORT - CRITICAL CARE SCOPE Provincial: Critical Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Senior Operating Officer, Glenrose Rehabilitation Hospital
TITLE RESTRAINT AS A LAST RESORT - CRITICAL CARE SCOPE Provincial: Critical Care APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Senior Operating Officer, Glenrose Rehabilitation Hospital
Alaris Products. Protecting patients at the point of care
 Alaris Products Protecting patients at the point of care Overview The medication process is the largest source of medical errors 1 with medication errors costing an estimated $3.5 billion yearly in hospitals.
Alaris Products Protecting patients at the point of care Overview The medication process is the largest source of medical errors 1 with medication errors costing an estimated $3.5 billion yearly in hospitals.
Ans: A) Chemoreceptor trigger zone (CTZ) Ans: C) 100 mg rectally. Ans: D) Photosensitivity. Ans: D) Alcohol
 Chemoreceptor trigger zone (CTZ) Ans: C) 100 mg rectally. Ans: D) Photosensitivity. Ans: D) Alcohol") A high school student starts vomiting and goes to see the school nurse. The student asks the nurse what part of his brain makes him vomit. What area of the brain will the nurse tell the student must be
A high school student starts vomiting and goes to see the school nurse. The student asks the nurse what part of his brain makes him vomit. What area of the brain will the nurse tell the student must be
Hospira Sapphire PCA/Epidural Pump Handout
 Important Information You Need to Know 1. Order Sets Have been updated to reflect the new device terminology 2. Terminology: Crosswalk Current (Gemstar) New (Sapphire) Continuous Dose Continuous Rate Bolus
Important Information You Need to Know 1. Order Sets Have been updated to reflect the new device terminology 2. Terminology: Crosswalk Current (Gemstar) New (Sapphire) Continuous Dose Continuous Rate Bolus
CRAIG HOSPITAL POLICY/PROCEDURE
 CRAIG HOSPITAL POLICY/PROCEDURE Approved: P&T, MEC, NPC, P&P 03/09 Effective Date: 02/95 P&T, MEC, P&P 08/09; P&P 08/10; P&T, MEC 10/10, P&T, P&P 12/10 ; MEC 01/11; P&T, MEC 02/11, 04/11 ; P&T, P&P 12/11
CRAIG HOSPITAL POLICY/PROCEDURE Approved: P&T, MEC, NPC, P&P 03/09 Effective Date: 02/95 P&T, MEC, P&P 08/09; P&P 08/10; P&T, MEC 10/10, P&T, P&P 12/10 ; MEC 01/11; P&T, MEC 02/11, 04/11 ; P&T, P&P 12/11
TheValues History: A Worksheet for Advance Directives Courtesy of Somerset Hospital s Ethics Committee
 TheValues History: A Worksheet for Advance Directives Courtesy of Somerset Hospital s Ethics Committee Advance Directives Living Wills Power of Attorney The Values History: A Worksheet for Advanced Directives
TheValues History: A Worksheet for Advance Directives Courtesy of Somerset Hospital s Ethics Committee Advance Directives Living Wills Power of Attorney The Values History: A Worksheet for Advanced Directives
Sedation/Analgesia by Non-Anesthesiologists. THE UNIVERSITY OF TOLEDO Approving Officer:
 Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
Name of Policy: Policy Number: 3364-100-53-11 Department: Hospital Administration Medical Staff ^HEALTH THE UNIVERSITY OF TOLEDO Approving Officer: Chief Executive Officer - UTMC Responsible Agent: -Chief
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Wyoming STATE BOARD OF NURSING
 David D. Freudenthal Governor Wyoming STATE BOARD OF NURSING Mary Kay Goetter, PhD, RNC, NEA-BC Executive Director 1810 Pioneer Avenue Cheyenne, Wyoming 82002 Phone: 307-777-7601 FAX: 307-777-3519 http://nursing.state.wy.us
David D. Freudenthal Governor Wyoming STATE BOARD OF NURSING Mary Kay Goetter, PhD, RNC, NEA-BC Executive Director 1810 Pioneer Avenue Cheyenne, Wyoming 82002 Phone: 307-777-7601 FAX: 307-777-3519 http://nursing.state.wy.us
APC 20 Procedural Sedation Analgesia by Non-Anesthesia Provider. Assessment & Provision of Care
 APC 20 Procedural Sedation Analgesia by Non-Anesthesia Provider Policy Executive: VP Medical Affairs/CMO Patient Care Policy Assessment & Provision of Care Policy Owner: Director Nursing ATTACHMENTS: 1.
APC 20 Procedural Sedation Analgesia by Non-Anesthesia Provider Policy Executive: VP Medical Affairs/CMO Patient Care Policy Assessment & Provision of Care Policy Owner: Director Nursing ATTACHMENTS: 1.
Hip Replacement Surgery
 Hip Replacement Surgery Preparation and Healing Introduction Congratulations. By considering hip replacement surgery, you re taking a giant step toward improving your mobility and relieving your pain.
Hip Replacement Surgery Preparation and Healing Introduction Congratulations. By considering hip replacement surgery, you re taking a giant step toward improving your mobility and relieving your pain.
UNMH Anesthesiology Clinical Privileges
 For eligibility to request privileges in Anesthesiology, applicants must have appointment as a Faculty member of the UNM Department of Anesthesiology & Critical Care Medicine. All new applicants must meet
For eligibility to request privileges in Anesthesiology, applicants must have appointment as a Faculty member of the UNM Department of Anesthesiology & Critical Care Medicine. All new applicants must meet
Laparoscopic partial nephrectomy
 Laparoscopic partial nephrectomy This leaflet is written to give you information and answer questions you may have about your surgery. If you have any further questions, please speak to your doctor or
Laparoscopic partial nephrectomy This leaflet is written to give you information and answer questions you may have about your surgery. If you have any further questions, please speak to your doctor or
UCSD DEPARTMENT OF ANESTHESIOLOGY
 UCSD DEPARTMENT OF ANESTHESIOLOGY LEARNING OBJECTIVES FOR POSTANESTHESIA CARE ROTATION, UCSD MEDICAL CENTER I. PATIENT CARE Residents will demonstrate competence in: 1. Placement/Removal of central and
UCSD DEPARTMENT OF ANESTHESIOLOGY LEARNING OBJECTIVES FOR POSTANESTHESIA CARE ROTATION, UCSD MEDICAL CENTER I. PATIENT CARE Residents will demonstrate competence in: 1. Placement/Removal of central and
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE PROCEDURAL SEDATION SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Health Professions Strategy & Practice PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
TITLE PROCEDURAL SEDATION SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Health Professions Strategy & Practice PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
Policies and Procedures. ID Number: 1138
 Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
Policies and Procedures Title: VENTILATION Acute-Care of Mechanically Ventilated Patient - Adult RN Specialty Practice: RN Clinical Protocol: Advanced RN Intervention ID Number: 1138 Authorization: [X]
What to Expect on. Your Surgery Day. at Seattle Children s Bellevue Clinic and Surgery Center
 What to Expect on Your Surgery Day at Seattle Children s Bellevue Clinic and Surgery Center A note for parents/caregivers: This book was written for patients of different ages. Patients also have different
What to Expect on Your Surgery Day at Seattle Children s Bellevue Clinic and Surgery Center A note for parents/caregivers: This book was written for patients of different ages. Patients also have different
PREPARATION AND ADMINISTRATION
 LESSON PLAN: 12 COURSE TITLE: UNIT: IV MEDICATION TECHNICIAN PREPARATION AND ADMINISTRATION SCOPE OF UNIT: Guidelines and procedures for preparation, administration, reporting, and recording of oral, ophthalmic,
LESSON PLAN: 12 COURSE TITLE: UNIT: IV MEDICATION TECHNICIAN PREPARATION AND ADMINISTRATION SCOPE OF UNIT: Guidelines and procedures for preparation, administration, reporting, and recording of oral, ophthalmic,
Louise Rose RN, BN, ICU Cert, Adult Ed Cert, MN, PhD
 Louise Rose RN, BN, ICU Cert, Adult Ed Cert, MN, PhD TD Nursing Professor in Critical Care Research, Sunnybrook Health Sciences Centre Associate Professor, LSBFON, University of Toronto CIHR New Investigator
Louise Rose RN, BN, ICU Cert, Adult Ed Cert, MN, PhD TD Nursing Professor in Critical Care Research, Sunnybrook Health Sciences Centre Associate Professor, LSBFON, University of Toronto CIHR New Investigator
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
CarePartners Nursing Care Plan Anticoagulant Therapy
 CarePartners Nursing Care Plan Anticoagulant Therapy ** If a CarePartners wound pathway, palliative care plan or oncology care plan is being used to guide the patient s care, this Nursing Care Plan may
CarePartners Nursing Care Plan Anticoagulant Therapy ** If a CarePartners wound pathway, palliative care plan or oncology care plan is being used to guide the patient s care, this Nursing Care Plan may
St. Vincent s Health System Page 1 of 8. Nursing Administration HOSPITAL SHARED POLICY?
 St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
A PARENT S GUIDE TO PEDIATRIC DAY SURGERY PROVIDENCE MEDICAL CENTER ALASKA PEDIATRIC SURGERY 4100 LAKE OTIS PARKWAY SUITE
 ALASKA PEDIATRIC SURGERY 4100 LAKE OTIS PARKWAY SUITE 206 929-7337 A PARENT S GUIDE TO PEDIATRIC DAY SURGERY AT PROVIDENCE MEDICAL CENTER Pre- Admission Appointment, Tours and Pre- Registration If pre-
ALASKA PEDIATRIC SURGERY 4100 LAKE OTIS PARKWAY SUITE 206 929-7337 A PARENT S GUIDE TO PEDIATRIC DAY SURGERY AT PROVIDENCE MEDICAL CENTER Pre- Admission Appointment, Tours and Pre- Registration If pre-
University of Virginia Medical Center Clinical Protocol for Moderate or Deep Sedation/Analgesia in Adult Patients
 A. PURPOSE University of Virginia Medical Center Clinical Protocol for Moderate or Deep Sedation/Analgesia in Adult Patients Sedation and analgesia are used alone or in combination to facilitate the performance
A. PURPOSE University of Virginia Medical Center Clinical Protocol for Moderate or Deep Sedation/Analgesia in Adult Patients Sedation and analgesia are used alone or in combination to facilitate the performance
Proposed Standards Revisions Related to Pain Assessment and Management
 Leadership (LD) Chapter LD.0001 Proposed Standards Revisions Related to Pain Assessment and Management 1 2 Leaders establish priorities for performance improvement. (Refer to the "Performance Improvement"
Leadership (LD) Chapter LD.0001 Proposed Standards Revisions Related to Pain Assessment and Management 1 2 Leaders establish priorities for performance improvement. (Refer to the "Performance Improvement"
Sharp HealthCare Safety Training 2015 Module 3, Lesson 2 Always Events: Line and Tube Reconciliation and Guardrails Use
 Sharp HealthCare Safety Training 2015 Module 3, Lesson 2 Always Events: Line and Tube Reconciliation and Guardrails Use Our vision is to create a culture where patients and those who care for them are
Sharp HealthCare Safety Training 2015 Module 3, Lesson 2 Always Events: Line and Tube Reconciliation and Guardrails Use Our vision is to create a culture where patients and those who care for them are