Meeting Report: Newborn Health Indicators Working Group Meeting March 18-19, Saving Newborn Lives Save the Children Washington, DC
|
|
|
- Emery Daniel
- 5 years ago
- Views:
Transcription
1 Meeting Report: Newborn Health Indicators Working Group Meeting March 18-19, 2015 Saving Newborn Lives Save the Children Washington, DC APRIL 8,
2 The Newborn Health Indicators Technical Working Group (TWG) met March 18-19, 2015 at the Save the Children office in Washington, DC. The agenda is given in Appendix 1; participants are listed in Appendix 2; presentations in Appendix 3. Day 1: March 18 th 1. Welcome and introductions Lara Vaz gave welcoming remarks and an overview of the meeting objectives. During the first half day of the meeting, updates were shared from the subgroups formed in March of last year as well as other newborn health measurement issues. The rest of the 1.5 day meeting focused on working in 3 subgroups on KMC indicators, HMIS, and Health Facility Assessments to move work forward in each of these areas. The meeting was attended by approximately 45 people, participating both in-person and over the phone. 2. ENAP Measurement Plan & Bringing together Maternal & Newborn Metrics Agendas Joy Lawn presented an update on the work being led by the ENAP Metrics group. The presentation complements the webinar held the previous week providing an overview of the work being done through the aegis of ENAP. Joy provided an overview of indicators, plans for improvement of measurement, and how individuals could get involved. Joy explained how ENAP came to be launched and its scope of work. The action plan was launched last July; during the World Health Assembly (WHA) meeting in May 2015, a resolution was passed that within a year, there would be a plan to improve data what s to be tracked, and a plan for improvement. ENAP, co-chaired by WHO and UNICEF, has since structured its work into three streams (country implementation, metrics, advocacy), with a fourth group, research, crosscutting the others. The ENAP metrics group is led by WHO and the London School of Tropical Medicine and Hygiene (LSHTM) it encourages and advocates for validity, rigor, and strengthened technical capacity in measurement. There is a Core Group with representation from various groups including the Newborn Indicators TWG, as well as specific task teams for care specific newborn interventions. A meeting was held in December with over 60 participants from the task teams and others to provide inputs on the core coverage indicators for 5 specific newborn care interventions. ENAP is working within the larger context of Sustainable Development Goal (SDG) target setting. ENAP set NMR and stillbirths targets of 12 or less (per 1000 live births and per 1000 total births, respectively) by 2030, after lots of discussion of the merits of relative versus absolute targets. The SDGs as yet do not have any mention of stillbirths; there is still a chance to get it in, and a petition is being organized to go on change.org. ENAP metrics has three streams of work: technical mapping and planning indicators, tools, and other work in progress; institutionalization of metrics in national platforms and in global metrics architecture with accountability; and leadership development to improve & use the data for action. There is an intentional plan to transfer the testing and research on measurement work to Africa and Asia three academic institutions have been identified (in Ghana, Tanzania, Bangladesh) along with two networks INDEPTH and Beyond Survival. The rest of the presentation focused on the development of the ENAP core indicators, which can be lumped into impact, process and coverage for key interventions (for all babies as well as interventions addressing complications), counting, and quality of care indicators. The immediate focus has been on 2
3 process and coverage indicators for complications because that is where the biggest gap lies, in both definitions as well as tools for capture. For interventions for all newborns, work is needed on content/quality of care, strongly tied to maternal metrics communities. For the impact indicators, the focus will have to be on better tools and improved quantity and quality of data. The latest version of indicators was shared and reviewed (See Annex 1). These indicators are a starting point; the coverage indicators need to be tested to assess both feasibility and utility. But to move the agenda forward, a list of proposed indicators and measurement questions that need answering will be published at the time of the WHA as part of a special supplement on the ENAP process. Inputs are welcome on core definitions and should be forwarded to Hattie (harriet.rees-forman@lshtm.ac.uk). Testing will involve the academic institutions in the three countries working on quality of care initiatives (Bangladesh, Ghana and Tanzania), as well as the two networks of INDEPTH (Peter Waiswa, lead, Makerere, Uganda) and Beyond Survival (Ashok Deorari, lead, AIIMS, India). There was a specific call for additional partners to engage in the testing, as a coordinated approach will yield the fastest collective progress. Allisyn Moran presented on plans to bring the maternal and newborn metrics communities together at global level. The rationale behind the creation of a reference group is to ensure convergence of global efforts to end preventable mortality maternal, newborn, and child; the need for better indicators to report on progress towards targets set within SDG and ENAP; and the need to take advantage the opportunities to collaborate and harmonize efforts across different groups working independently on metrics for maternal and newborn health. The scope of the group is being defined, but could include to improve guidance on data collection and use for monitoring progress towards improved maternal and newborn health at global, national, and sub-national levels. Pieces under consideration for the group s mandate include development of consensus on a monitoring framework, being a forum for sharing, identifying gaps and facilitating the prioritization and commission of work to address those gaps, and to provide overall guidance for improving metrics. WHO, along with UNICEF and UNFPA, are identifying the experts that would be part of this group. The current plan is for this group to be announced at a side event at the World Health Assembly at the end of May. Allisyn also reported that the Ending Preventable Maternal Mortality (EPMM) coordinating group hopes to collaborate with us on newborn measurement the group would be developing core indicators for maternal health and similarly achieve consensus. The first meeting is potentially in April. This new group would also would feed into the proposed reference group. Discussion points: - Should ENAP process indicators be more of a composite, similar to KMC, which would be a closer proxy to coverage than others? Thoughts are welcome something that can be used now if preferable (collected now); should there be one for chlorhexidine - There is interest from groups working on quality to link to Every Mother Every Newborn (EMEN) UNICEF is developing 10 standards, similar to Mother-Baby Friendly initiative. Joy will approach WHO/UNICEF to request a webinar to discuss those efforts. 3. Updates from TWG Subgroups KMC Tanya Guenther gave an overview of what the KMC indicators working group has done, beginning in March 2014 with indicator scoping to come up with a list of over 55 KMC indicators. After developing an indicator framework and a series of small group consultations, the group was able to come up with 10 core KMC indicators ready for testing. The group wants to be clear that these indicators are for measurement, and are not implementation standards. There are 4 service readiness indicators, 2 on 3
4 identification, 2 on services initiated and provided, 1 on discharge and 1 on follow up. The full list can be found in the slides in Appendix 3. Next steps were identified at the November 2014 KMC meeting and include: disseminate indicators and prepare supporting materials, identify opportunities for country-level use and documentation, and gather resources and tools. See Annex 2 for the KMC indicator framework. Household Surveys Deborah Sitrin gave an update from the household survey subgroup. This group has a history of making significant contributions to global newborn measurement. In 2008, this group began working on questions on postnatal care contacts, which were revised and standardized in both DHS and MICS surveys. In 2010, the group began focusing on questions on newborn care practices and content of PNC; in 2014, the group submitted joint comments/recommendations for changes to the DHS. The new and revised questions to the DHS core questionnaire include: facility births are now asked about the first pre-discharge AND first post-discharge postnatal check; PNC content within 2 days after birth (cord examined, temperature assessed, counseling on danger signs for newborns, and counseling on and observing breastfeeding); and immediate skin to skin. Countries will start implementing these questions this year; data will be available in An optional newborn module is also under development, which will include more questions not found in the core questionnaire. DHS is developing a module this year and MICS-6 will do an assessment of the current PNC indicators to inform changes. Members of this group can advocate for countries to use the newborn modules. Deborah also discussed ongoing and proposed analyses. UNICEF is leading an analysis of PNC contacts and SNL is leading an analysis of newborn care practices. A third proposed analysis, on factors associated with coverage of PNC contact, was proposed to the Countdown Coverage WG but has not been taken up due to time and manpower constraints. Discussion points: - The revised DHS core module is now online - The content of PNC can be disaggregated by weight, but birthweight is often not recorded, so take caution if attempting to disaggregate this way. - Is there anything from MICS or DHS to guide how to interpret trends over time for PNC contacts as questions have changed? Part of the assessment that MICS will do will explore the quality of the questions and responses from PNC contacts. One objective is to see if the information make senses & trends can be identified. 4. Harmonization of Facility Assessment Efforts Nancy Fronczak, a consultant for WHO, provided an overview of ongoing efforts to harmonize health facility assessment surveys. The aim is to so this in the same way that household surveys like DHS and MICS have been harmonized. Harmonization is needed to reduce duplication, improve data quality, and ensure comparability across time and geography in terms of indicators and data collection methodology. Compromise is needed for harmonization in terms of timing of data collection, selection of indicators, indicator definitions, and agreement on minimum methodological standards to ensure minimum standard for data quality. This effort also includes a vision for periodic coordination within countries to meet the needs of various stakeholders (similar to a DHS planning and coordination process). 4
5 Facility surveys do not replace routine supervision and program monitoring, and should not be the primary source for information on basic program functionality. Instead, surveys focus on key, standardized indicators and help validate data reported through routine systems. Core facility audit indicators are being defined, as well as additional indicators that countries can opt to include. Quality of care indicators take more time and resources to collect because they are often based on observation or detailed record reviews, and so countries will need to prioritize which QoC indicators they chose to gather. Ideally, countries would be able to have availability and readiness assessments annually and quality of care periodically, depending upon need and resources. The WHO convened a meeting in November 2014 to get buy-in and review a list of 100+ indicators and draft definitions; early draft data collection tools and sampling methods have since been prepared. Data collection tools would offer a question bank to measure different indicators to allow easy integration into various data collection activities, but still maintain standard definition and methodology. Various technical groups will be asked to review indicators and prioritize which should be core versus optional; map indicators to data collection tools to ensure essential information is collected; and pre-test the feasibility of record reviews (to see if information is available and the time and level of knowledge required). Discussion points: A question was asked whether this harmonization will permit for newborn content, since facility assessments have often collected little data for newborns, Nancy assured the group that it is certainly feasible to include more newborn content, particularly around readiness. But it is harder to collect indicators for services that are usually not documented and may require observation (e.g. immediate drying of newborns) Ideally this process will replace existing tools with a question bank that focusses on specific indicators rather than having separate ways to collect similar information. WHO is leading the harmonization process, and Global Fund and World Bank are also heavily invested because they do a lot of facility surveys as well as USAID, other donors, UNFPA WHO recently reached consensus on a core list of 100 indicators, but they are mostly household survey indicators, and there are gaps for what is collected at health facilities. This process will help fill in the gaps. 5. Global Stillbirth Estimates LSHTM and a wide group of investigators (stillbirth investigator group and Lancet stillbirth series 2015 team) are working on stillbirth rate estimates for 196 countries, funded by SNL. The last estimates (2.6 million stillbirths) were published in 2009 in the Lancet Stillbirth series. These estimates showed massive regional variation with a large proportion of stillbirths occurring in rural Africa and Asia, however, the data had major gaps and there was wide uncertainty in the estimates. Stillbirth rate is a core ENAP impact indicator, and the target is for countries to reach stillbirth rate of 12 or less by The current effort to update estimates will provide data to inform and accelerate progress for reaching the 2030 target: Stillbirth rates estimates for 196 countries to 2015 Stillbirth rate projections to 2030, which countries need most change to meeting ENAP target to end preventable stillbirths and meet ENAP target Data on timing of stillbirths to focus action in order to accelerate progress 5
6 However, there is need to improve measurement and recording to be able to monitor progress towards the target. The differences in stillbirth definitions across and within countries has hampered ability to collect stillbirth data. This work will strengthen estimates for low and middle income countries, but will still rely on modelling for 31 countries (reduced from 68 countries in 2011). Intrapartum stillbirth rate data is especially problematic and is relying on perinatal epidemiology from HIC because there are still 120 countries with no data on intrapartum stillbirths at all. Preliminary results will be ready by end of April 2015, with a peer review publication by October There will be ongoing dissemination work throughout the process. Discussion points: Most data from LMIC currently uses fresh versus macerated stillbirth as a proxy for intrapartum stillbirths. However, many settings aren t collecting any data at all currently on timing of stillbirth. The UN is not collating stillbirth data regularly. Lack of accountability mechanism is major issue hampering progress. ENAP work aims to change this. Looking for this to be taken up as part of the SDGs and UN organization to have regular stillbirth estimates. Countries are collecting it but difficult to get to this data (frequently not in the public domain or difficult to locate within national statistical offices or ministry of health reports and websites). Needs to be incorporated in global accountability mechanisms or else the problem of stillbirths will not have visibility. Major impact on families. Neonatal deaths and stillbirths need to be very closely linked. 6. HMIS Review & Day of Birth Initiative Overview: Vikas presented results from MCHIP s review of facility registers and reporting forms to see what information related to newborn care is collected and reported. In general, critical life-saving interventions for newborns are rarely collected. MCSP is now looking at what additional data elements are available through surveillance systems in Bangladesh (91 sites) and Malawi and whether there is plan to integrate surveillance into routine system for the whole county. Moving forward, MCSP will expand the HMIS review to all 24 MCSP priority countries and expand the scope of the review to include all services in the RMNCH continuum of care. MCSP will also be facilitating a process for testing the quality of care indicators recently recommended by WHO (coming from the December 2013 meeting). The ultimate goal is recommendation for countries on what to include in HMIS and strengthening data use. Discussion points: Countries need guidance on minimum number of indicators. There is need to prioritize indicators and we should consider not prioritizing actions health workers know they are supposed to do and may not provide very accurate information (eg, breastfeeding within 1 hour, immediate drying, etc). Though Dominican Republic collects information on breastfeeding within 1 hour routinely and finds about 30% are breastfed, which is close to what is expected and presumed to be reality. An immediate next step could be to review data from countries that collect such practices to see if data appear to be reasonably accurate and complete. MCSP found some surprising results, especially notable are some countries that are not collecting or reporting many interventions for newborns (Nepal, Bangladesh). It shows that countries may be implementing, but not recording or reporting. In LAC region, a similar review 6
7 found similar results - newborn complications are not captured. A review of the quality of sepsis management in Dominican Republic found that recording was a big issue. MCHIP review looked at what data are collected in standardized patient charts or partographs, but did not review completed charts/partographs. Since few countries had standardized patient charts, there was not much information definitively recorded in these tools. Every Preemie is doing a survey with key informant interviews in 24 countries and can look at what data are collected, to build on the MCHIP review. 7. Newborn in Emergencies Preetha Iyengar, the newborn health in Emergencies advisor for Save the Children, presented an update on work being done in emergency settings for maternal and newborn health. Ebola heavily impacted Guinea, Liberia and Sierra Leone, all countries with a significant neonatal mortality rate. Prior to the outbreak, Liberia was reporting strong data that showed they were on track to achieve MDG 4. In the months where the disease was most active, August- October, health facilities closed and the largest numbers of healthcare workers had died. A paper on what happened to mothers and newborns during this time is forthcoming. Save the Children has been working on a field guide for newborn health in emergencies that is set to pilot (Spring 2015). The field guide is designed for health staff and focuses on three main causes of death with a quick reference for solutions and priority on highest-impact interventions. The team is looking for ways to accurately measure newborn health in emergencies and has identified some primary outcome measures around infection prevention, thermal protection, breastfeeding, asphyxia prevention, assessment, and others (See slides for a full list). 8. Sub-Group Work KMC See Annex 3 HF Assessments N/A HMIS See Annex 4 7
8 Day 2: March 19 th 1. Report out from Sub-groups KMC The group revisited indicators along the KMC action sequence (presented yesterday) and looked at what is already collected in major tools. The group then discussed how to define the ENAP process indicator facilities with KMC operational and identified 3 tracer indicators already collected in facility assessment tools designated or integrated space for KMC, trained staff, and weighing scale. Using these 3 tracers means there is a KMC process indicator can be collected now with existing sources, while work is ongoing to improve this indicator. The KMC group also discussed other components to add to facility based surveys if an extra newborn module added. The group now wants to work together with the facility assessment subgroup to understand what facility surveys could include in the future. The group ended with a discussion on how to test indicators. Path is working in 4 regions of Ghana and will be conducting facility based surveys soon, giving an opportunity to test indicators. To test coverage indicators, the group discussed using data sets from Columbia, which has more complex data, and other settings including Rwanda, Mali, Malawi, etc. The KMC group also intends to collect example tools for sharing and will update the repository on HNN. Items to discuss with other small groups: How much can be including in facility based surveys Talk to HMIS group about KMC coverage indicator With all, discuss how to ensure KMC indicators are part of broader care of small and sick newborns. Discussion points: - There is an upcoming Training in Asia on Essential care for every baby and small babies. Will focus on training and capacity building, but there is a small amount of time to focus on system blocks and there will be a session on ENAP metrics and WHO s new guidelines. Could be an opportunity to share the work from this group. These trainings have often been missed opportunities to discuss indicators and measurement. 8
9 HF Assessments Building on Nancy s presentation in the morning on the WHO-led process to harmonize facility surveys, the HF group discussed indicators that should be included in this harmonized list and tools to assess readiness to deliver interventions for newborns. The group focused on indicators that could be collected via facility audit (easiest to start with; observation, record reviews, client interviews were not discussed) and reviewed the list of indicators this group developed years ago and shared with SPA and SARA. The group first discussed indicators of services availability, which have been based on self-report and used to determine if follow up questions on readiness should be asked. The group decided indicators should be kept for key life-saving interventions for newborns (with addition of those currently missing from existing tools), but these should not be used as the denominator for subsequent readiness indicators since facilities may not report providing a service but do have some elements of readiness. Therefore, the denominator for readiness indicators would be facilities with delivery services (all facilities for availability of sepsis treatment). Since there has not been a question on availability for newborn sepsis management, the group discussed whether it should focus on sepsis management (which could include facilities that identify and refer only) or antibiotic treatment. This group ultimately recommended to focus on collecting the number of facilities that actually offer antibiotic treatment (may be first dose and referral or full treatment). The group then discussed indicators of service readiness for key life-saving interventions, focusing on 4 sub-areas used by SPA and SARA staff and guidelines, equipment, diagnostics, medicines & commodities. For staffing, SPA uses staff interviews but it is easier to use an interview of one knowledgeable person and is less dependent on who is available day of survey. However, one person will not be fully aware of all training received, so there is need to test and compare these methods. SPA and SARA already ask about many of the necessary equipment, diagnostics, medicines & commodities, though the KMC group has already suggested a few additional ones. HF group wants to develop short lists of tracer items for key interventions, with supplemental longer lists of other items that may be required or helpful to provide the intervention. The group then discussed indicators of service provision. Existing tools typically use self-report for provision of services, as is done for BEmONC signal functions. (Has x service been provided in the past 3 months?). The group discussed whether it would be better to measure documentation of cases (eg At least x recorded cases treated in the past x months) or actual quality, recognizing that documentation can be difficult to find and often poor quality. There is need to test indicators for feasibility and accuracy. However, the group agreed that it is very important to attempt to measure that services are actually provided, not just readiness. Lastly, the group discussed a few indicators on documentation (if there is space to document interventions) and evidence of data use. Though there was not time in this meeting, this group also wants to review indicators under ANC, birth preparedness, care of newborns that are not the life-saving interventions we discussed today. 9
10 Items to discuss with other small groups: With HMIS group, discuss what will be recorded, and thereby extracted during record review. How to recommend key readiness ingredients (ie tracers) when there are often long list of things needs for a given intervention (SPA already collects a lot) Discussion points: - There was a question on whether to weight components in a composite indicator, but the group decided it was too complicated and not useful for the intended purpose of these indicators. The lists would be short, ideally just about 3 components. - Members of KMC group expressed preference for measuring service provision by looking for documentation of cases. There was most discussion and warning from some not to underestimate how hard it is to find the documentation. - There was discussion of measuring the process and the gap when services are not provided even if the facility is ready. There could be an opportunity to test questions perhaps on working conditions. HMIS The HMIS made a list of indicators for collection and use at facility level, with a focus on ENAP interventions. The group presented an overview of the recommended indicators for each intervention (see Annex 4) and discussed many issues with accuracy of numerators and denominators. Discussion points: - The KMC group gave feedback on the proposed denominator for KMC since the KMC group has already spent a lot of time discussing denominators. - There is need for a broader set of perinatal indicators, beyond the ENAP interventions. Decision-makers at facility level need indicators to take action. While ENAP is more focused on national/global tracking. - Discussion touched on whether some indicators (such as drying and immediate breastfeeding) would be ticked for all babies since providers know it should be done. If information is not contributing to improvement of quality, then should not be collecting because takes away time from patient care. But there was an example from the Dominican Republic BF within first hour was collected on registers and found to be 33%, which is probably close to reality. Yet in South Africa, early and exclusive BF were found to be 60%, but reality is probably <10% breastfeed. In areas where doing quality improvement, need that data. But at national level, need to just cut data and can t collect everything. Need to compare to observation data. Part of HMIS review where know collected can so data quality and use. - There is need to review existing data and see if results are meaningful. During MCHIP quality of care survey, most births were dried immediately after birth (collected via observation) except Zanzibar, so this indicator may be too universal to be useful. - Routine monitoring is dynamic. Once everyone knows something should be done, then we need to rethink if that information needs to collect. The ultimate question should be whether data leads to action. - The next phase of the HMIS review (presented by Vikas in the morning), will try to look at use of data and perhaps even review the data available for some of the proposed indicators that are already collected through HMIS in some countries - Cannot just recommend indicators, and there are already a lot of efforts out there to recommend indicators (by WHO, ENAP). MCSP Day of birth initiative is intended to not only support data collection but also the process of data use; make sure data are aggregated and analyzed. 10
11 2. Cross-group discussion Following the report-outs, the subgroups reconvened to reflect on the discussion and plan their next steps. The subgroups then shared their next steps with the full group (see slides). The KMC subgroup identified these next steps: Develop specific questions for HF assessments for KMC based on small group discussion and engage with HF assessment group on next steps Develop two brief concept notes for testing KMC indicators Explore opportunities to test in other settings: Develop brief on KMC indicators for dissemination Prepare peer-reviewed paper on the KMC indicators Engage with HMIS sub-group to understand how to contribute Engage with HNN and communications department to design webpage for sharing KMC resources (review existing materials, collect and organize tools, etc) The Health Facility Assessment subgroup identified these next steps: Send existing list and tools for review within smaller group, focusing on Facility Audit methodology for now (not looking at Records Reviews and Observation at present) within overarching packages of Antenatal Care, Safe Delivery/ BEmONC, and Newborn/Postnatal care Draft potential questions and definitions to measure service provision/experience for newborn interventions, which would be reviewed with wider group that includes ENAP metrics task teams Share proposed service readiness indicators with ENAP metrics teams for feedback; this would include additional inventory from delivery room and relevant pharmacy The HMIS/routine systems subgroup reflected on the need to keep abreast of the work of the KMC acceleration group, including plans examining the extent to which low birthweight can be captured; the need to test/assess an immediate drying indicator before advocating for its use (either through MCSP s HMIS review or through other means); and the need to test/review the appropriate denominator for a neonatal resuscitation coverage indicator at facility level. The group nominated Vikas and Yordi to serve as co-chairs. Next steps include: Finalize review of indicators and provide inputs to ENAP metrics from HMIS perspective Assess incorporation of core supplies into LMIS (sepsis, CHX) through existing groups Move ahead with testing (coordinate) -- MCSP Tanzania, Bangladesh Work closely with topical groups (KMC, CHX, sepsis, neonatal resuscitation) in seeking inputs. The HMIS group seeks to provide perspective on information systems to inform the finalization and operationalization of proposed indicators for routine information systems. 3. Next Steps for NITWG The NITWG will continue to meet once per year for information sharing, technical inputs on partner work, and to identify areas of collaboration in newborn health metrics. Small groups will continue to move forward with their specific workplans and remain flexible to convene a small working meeting if needs arise. Feedback requested on initiatives, tools, and documents will continue to be sought from group members and shared as one common voice. 11
12 The work of the NITWG will continue to play an important role in the agenda for advancing newborn health measurement and working towards the milestones set forward in the Every Newborn Action Plan. The NITWG will endeavor to seek wider involvement from other partners, particularly UN agencies and academic institutions actively engaged in newborn health measurement work. Hosting meetings outside of Washington (e.g. London or Geneva) will be considered to facilitate participation. 12
13 Annex 1: ENAP Core indicators 13
14 Every Newborn Action Plan (ENAP) Core and some of the additional indicators: Definitions and data sources (DRAFT) FOR DETAILS RE TESTING SEE EXCEL ON ENAP METRICS IMPROVEMENT PLAN: COMMENTS ON THIS PLS JOY LAWN& MATTHEWS MATTHAI c/o Source: Core metrics table as published in Every Newborn Action Plan and Lancet Every Newborn series 2014, with some further refinements and showing the definitions and data sources. Selected additional indicators included notably immediate breastfeeding (as tracer indicator for essential newborn care) and chlorhexidine cord cleansing and C-section. See table footnotes re key for shaded cells, red text, italics etc. Numerator Denominator DATA SOURCE DEFINITION SOURCE Maternal mortality ratio Number of maternal deaths per year during pregnancy and childbirth or within 42 days of termination of pregnancy, irrespective of the duration and site of the pregnancy. Defined as a death from any cause related to or aggravated by pregnancy or its management (excluding accidental or incidental causes) Per 100,000 live births per year ICD10. For more details see WHO/UNFPA/UNICEF estimates 2014 IMPACT Stillbirth rate Number of babies with no signs of life born at or after 28 weeks' gestation per year (ICD officially lists birth weight >1000 gm with 28 weeks gestation as next option but in practice Per 1,000 total (live and stillborn) births per year GA is almost always used rather than birth weight surrogate. Note BWT and GA cut off differ and result in some difference in SBR) CVRS and registries (when high coverage and quality) or Surveys or facility/hmis and/or estimation modelling ICD10. See Lancet Stillbirth series 2011 Lawn et al for details of variations Neonatal mortality rate Number of live born infants per year dying before reaching 28 days of age Per 1,000 live births per year ICD10. See Lancet Every newborn for discussion of reporting of defns Intrapartum care tracked by the contact point of skilled attendant at birth Number of women ages with a live birth X years prior to survey who were delivered by skilled health personnel (doctor, nurse, midwife or auxiliary midwife) (Countdown, 2015) Number of women aged years with a live birth who were attended by skilled health personnel during their most recent live birth (MICS - 2 years preceding the survey) Number of live births assisted by a skilled provider (doctor, nurse midwife, and auxiliary nurse/midwife) (DHS - five years preceding the survey ) Total number of last-born babies in X years in the survey (Countdown, 2015) Total number of live births to women aged years with a live birth in the last 2 years (MICS) WHO Skilled attendant case defn. Countdown to 2015 defn list. DHS and MICS modules, COVERAGE: Care for all mothers and newborns Early postnatal care contact for mothers and babies Essential Newborn Care with Early Initiation of breastfeeding as Tracer indicator Mother: Number of women ages who received postnatal care within two days of childbirth (regardless of place of delivery), (Countdown, 2015) Number of women years who received a health check while in a facility or at home following delivery or a postnatal care visit within 2 days after delivery other most recent live birth (MICS - 2 years preceding the survey) Number of women year giving birth in the two years preceding the survey with a postnatal check up in the first 2 days after birth (DHS - 2 years preceding the survey) Newborn: Number of babies who received postnatal care within two days of birth (regardless of place of delivery) (Countdown, 2015) Number of last live births who received a health check while in a facility or at home following delivery or a postnatal care visit within 2 days after delivery (MICS - 2 years preceding the survey) Number of last birth preceding the survey with a postnatal check up in the first 2 days after birth (DHS- 2 years preceding the survey) Number of live born infants who are breastfed within first hour after birth Number of women with a live birth in the X years prior to survey who put the newborn infant to the breast within 1 hour of birth (countdown, 2015) Mother: Total number of women with a last live births in X years in the survey (Countdown, 2015) Total number of live births in last 2 years (DHS & MICS ) Newborn: Total number of women with a last live births in last X years in the survey (Countdown, 2015) Total number of live births in the last 2 years (DHS & MICS) Total number of women with a live birth in X years in the survey (Countdown) Total number of live born infants (DHS & MICS) Household surveys (e.g. DHS, MICS) or National facility data/hmis or DHIS Countdown, MICS, DHS, Exclusive breastfeeding to 6 months Number of infants aged 0-5 months who are exclusively breastfed (Countdown, 2015) Number of live born infants under 6 months of age who are exclusively breastfed (MICS) (MICS allows ORS, vitamins, mineral supplements and medicines) Number of babies 0-6 months who are exclusively breastfed (DHS) Total number of infants 0-5 months surveyed (Countdown, 2015) Total number of infants under 6 months of age (DHS & MICS)
15 COVERAGE: Complications and Extra Care (specific treatment interventions) Antenatal corticosteroid use Newborn Resuscitation Treatment of neonatal sepsis Kangaroo mother care Chlorhexidine cord cleansing Caesarean Section Rate Process Indicator: In line with UN commodities report: The number countries with ACS on the essential drug list for the purpose of fetal lung maturation Coverage indicator (needs validation work): All women giving birth in facility who are <34 completed weeks and received one dose of ACS for being at risk of preterm birth Process indicator: Number of facilities with a neonatal mask and bag in the labour and delivery ward (as defined in WHO QoC report and collected in many Health Facility Assessment tools) Coverage indicator (needs validation work): Number of newborns who were not breathing spontaneously/crying at birth for whom resuscitation (actions) WITH BAG AND MASK were initiated immediately Process Indicator: Proportion of assessed facilities with uninterrupted stock of injectable gentamicin in the past 3 months Coverage indicator (needs validation work): Number of newborns that received at least one dose of antibiotic injection in a facility for PSBI Process indicator: Number of facilities offering KMC to minimum standard (as defined in WHO QoC report and collected in some Health Facility Assessment tools) Coverage indicator (needs validation work): Number of newborns admitted to inpatient KMC Coverage indicator (needs validation work): Number of newborns that received at least one dose of CHX (7.1%) to the cord on the first day after birth Number of women ages with a live birth in the X years preceding survey delivered by caesarean section (Countdown, 2015) Options to be tested: Per 100 live births (or estimated) Per total number of live births in facility per year Per gestational age grouping (in weeks). (Note initial focus on counting all whilst testing ways to split by GA at birth to identify women treated who did not deliver preterm) Total number of facilities with inpatient maternity services Options to be tested: Per 100 live births (or estimated) Per total number of live births in facility per year Total number of live births in facility per year who are not breathing spontaneously/crying after immediate drying (if can be validated and routinely collected) Number of assessed facilities with no reported stock out of injectable gentamicin in the past 3 months. Options to be tested: Per 100 live births (or estimated) Per total number of live births in facility (or catchment area) per year Number of newborns with any illness presenting to facilities Number of newborns diagnosed with PSBI Total number of facilities with inpatient maternity services Options to be tested: Per 100 live births (or estimated) Per total number of live births in facility per year Total number of births <2000g (if can be validated and routinely collected) Total number of live births in surveyed population (or total number of live births at home depending on national policy/data available) Number of women ages with a live birth in the X years preceding survey (Countdown, 2015) Facility based: National facility based data or facility survey (SARA, SPA etc), potential in HMIS (initial focus of data collection in facilities WHO guidelines for these are mainly for facility treatment but for countries with major national scale up of community provision eg of sepsis case management, additional community tracking will be required). Household surveys :These treatment interventions are unlikely to be measureable in Household surveys based on sample size, and challenges with defining denominators especially for parental recognition and also in knowing or recalling details of numerator (eg ACS injection vs. Oxytocin inj). National facility based data or facility survey, potential in HMIS National facility based data or facility survey, potential in HMIS, and to be tested in household surveys Potential to collect in household surveys (e.g. DHS, MICS) but needs sample size calculations and validation study National facility based data, or facility survey, HMIS, or household surveys WHO QoC meeting report for process indicators. For coverage indicators, work in progress by ENAP Metrics groups and Coverage task teams Countdown, 2015 QUALITY INDICATORS: Every Mother Every Newborn service delivery packages for quality care at birth and care of small and sick newborns Emergency Obstetric care (EmOC) Care of small and sick newborns Number of facilities in area providing basic or comprehensive EmOC Population of area divided by Other norms and standards to be defined as part of work for EMEN and ENAP metrics Definitions and measurement approach to be defined Facility based survey, or potentially from national facility based data / HMIS Facility based survey, or potentially from national facility based data / HMIS UNFPA/WHO/UNICF EmOC care indicators (Monitoring Obstetric Care, 2009) Counting Birth registration Number of children under age of 5 who had a birth certificate (DHS question allows split by age in years) Number of children under age of five years in survey Household surveys (e.g. DHS, MICS) or National facility data/hmis. RVS systems UNICEF Blue coloured cells= not currently routinely tracked and collated by UN Bold italics = indicator needing further work to ensure availability of consistent data in routine information systems. Red= service delivery package for which norms and standards will be defined and tracked. All coverage indicators to be tracked in such a way that they can be broken down to assess equity-e.g., urban or rural, regional, wealth quintile.
16 Annex 2: KMC indicator framework Figure 1. Framework for Kangaroo Mother Care Indicator Development 14
17 Figure 2. Summary of core KMC indicators according to framework 15
18 Table 1. KMC indicator definitions and data sources Indicator Metric Data source(s) and methods of collection Frequency KMC in national policy: National policy recommends KMC for lowbirthweight newborns Yes = national policy recommends KMC for LBW newborns; No = national policy does not recommend KMC for National policy documents - record review; Key informants through interview Annually or less KMC indicator in HMIS: National HMIS includes the number of newborns who received facility-based KMC care Costed plan includes KMC: Costed national implementation plans for maternal newborn health include KMC KMC service availability: Percentage of facilities with in-patient maternity services with operational KMC Weighed at birth: Percentage of newborns weighed at birth Identification of newborns <2000g: Percentage of live births identified as <2000g KMC coverage: Percentage of newborns initiated on facility-based KMC 2 LBW newborns Yes = national HMIS includes the number of newborns who received facility-based KMC No = national HMIS does not include the number of newborns who received facility-based KMC Yes = costed plan or plans to scale up maternal, newborn and child health intervention includes KMC components No = no costed implementation plan OR costed implementation plan does not include KMC components Numerator: Number of health facilities in which KMC is operational 1 Denominator: Number of health facilities with inpatient maternity services Numerator: Number of newborns weighed at birth Denominator: Number of live births Numerator: Number of newborns identified as <2000g Denominator: Number of live births Numerator: Number of newborns initiated on facility-based KMC Denominator: Expected number of live births OR expected number of LBW babies HMIS documents - record review; Key informants through interview Costed plans - record review; Key informants through interview Facility assessments and MOH records (collected through supervision or periodic audits) Interviews with mothers + child health card review - collected through household surveys; L&D registers - collected through record review as part of facility assessment or supervision L&D registers - collected through HMIS (see notes) or through register review as part of supervision or facility assessment KMC registers - reported through HMIS or collected through register review as part of facility assessment; Denominator available through national and global estimates updated annually Annually or less Annually or less Annually or less Periodic for household surveys; routinely (monthly/quarterly) depending on need Routinely (monthly/quarterly) Annually 1 KMC elements already collected through Service Provision Assessments (SPA) include: staff receiving in-service training on KMC; identified space for KMC; and availability of functional infant scale. Additional components are being proposed and tested for inclusion in future harmonized facility assessments and could be integrated into supervision checklists and MOH audits. 2 This may include facility-initiated ambulatory KMC as in Latin America (e.g. Colombia); this indicator has been prioritized for further testing by the KMC Acceleration and ENAP metrics group, with particular focus on establishing the most feasible, valid, and reliable denominator. 16
19 Indicator Metric Data source(s) and methods of collection Frequency KMC monitoring: Percentage of KMC newborns who are monitored by HF staff according to protocol KMC patient charts - collected through record review as part of facility assessment/supervision visits Status at KMC discharge: Percentage of facility KMC newborns: discharged according to criteria; left against medical advice; referred out; or died before discharge Numerator: Number of newborns admitted to KMC who are monitored by HF staff according to protocol* *includes at minimum: assessing feeding, STS duration, weight, temperature, breathing, heart rate, urine/ stools) Denominator: Number of newborns initiated on facility-based KMC Numerator: Number of newborns admitted to facility KMC: 1) discharged alive per protocol; 2) leave against medical advice; 3) referred out; 4) died before discharge Denominator: Number of newborns discharged from facility-based KMC KMC registers - reported through HMIS or collected through register review as part of facility assessment Quarterly or less; to be determined at country level Routinely (monthly/quarterly) KMC follow-up: Percentage of newborns discharged from facilitybased KMC that received follow-up per protocol Numerator: Number of newborns discharged from facility-based KMC that received follow-up per protocol Denominator: Number of newborns discharged alive from facility-based KMC KMC registers/records reported through HMIS or collected through register review as part of facility assessment and/or ) Interviews with caregivers/mothers of newborns discharged from KMC Routinely (monthly/quarterly) 17
20 Annex 3: KMC facility indicator input & indicator testing opportunities Services for Newborns - Availability, Readiness, and Capacity Service Availabili ty (reporte Service Readiness Staff and guidelines Equipment Diagnos tics KMC Proportion of facilities with delivery services that provide kangaroo mother care 1 (KMC) for preterm/lbw babies Proportion of facilities providing KMC with at least one provider of delivery/newborn services trained in the past 12 months on KMC for low birth weight babies Proportion of facilities providing KMC with national guidelines for KMC Possible items: defined space, designated beds, NG feeding tubes for newborns, cups and spoons for infant feeding Proportion of facilities providing KMC with infant scale available and functioning in delivery area (observed) Recommendations to HF group and areas for testing Change to maternity services: Proportion of facilities with maternity services that report providing kangaroo mother care (KMC) for preterm/lbw babies Trained staff: for now, can use what is there for SPA (captures in-service training on KMC within the last 24 months or more than 24 months ago or none) ; but for indicator, it shouldn t be based on 12 month time period; just use any in-service training (can disaggregate by time period) OR any pre-service training Proportion of facilities with maternity services that have staff providing newborn care who have received training in KMC Guidelines for KMC: guidelines should be up-to-date (most recent) and accessible Proportion of facilities with maternity services that have up-to-date KMC guidelines available Agreed important to collect data on 3 key equipment items: space, feeding utensils and NG feeding tubes for newborns Space: need to do more research to identify the best way to ask about space. Could test asking: Is there a space for KMC (whether a separate room or integrated into the post-natal ward)? OR integrated into the care of small and sick newborn; For now, can use SPA question since its already there. Could also ask: Is there a way for mothers to room-in with small or premature babies? OR is there a policy where the place where small babies are cared for that mothers/fathers can access 24 hours? Infant scale: functional and available Thermometer: functional and available Medicin es & Commo Possible items: caps/hats for newborns Acceptable head covering for newborns: (give guidance for what acceptable in the data collector notessince sometime facilities make their own coverings (from gauze or other materials) Documentation Agreed documentation was important, and identified 3 types of documentation that are important for KMC. Documentation: 1. Service statistics: Space where KMC services are recorded (register) and aggregated for monthly reporting 2. Clinical management: individual patient charts to record vital signs, feeding, weight and danger signs) 3. Follow-up: System in place for documenting follow-up of babies discharged from KMC (could be part of the register or a separate system) 18
21 OVERALL L READINESS Service Experience (or Services Documented?) Proportion of facilities providing KMC with trained staff and a functional scale available. Proportion of facilities providing KMC with at least 1 documented baby initiated in KMC in the past 3 months As part of the assessment whether KMC is operations, the HF tool could include questions about whether there is documentation of KMC service delivery (through register or through individual patient charts) in the previous 3 months; would not recommend counting the number of cases, just determining whether KMC services were provided and documented More testing needed; for now, SPA collects information on in-service training, space, and scale. Indicator could be: Proportion of facilities with maternity services with staff trained in KMC, space for KMC and a functional infant scale. In future, would want to test looking at other components as well: KMC guidelines, feeding utensils (cup and spoon), infant scale, NG feeding tubes, appropriate head covering for small newborns Note that also need to explore what items may not be necessary to provide KMC (for example, while infant scale may be highly desirable, we can explore whether we find instances of KMC services provided without, same with the other supplies) See notes under documentation above - wouldn t want to state specific number of cases (just keep it as documentation of KMC services provided in the next 3 months) Indicator should be reworded: Proportion of facilities with maternity services with documentation of KMC services provided in the last 3 months (report using 2 denominators: all facilities with maternity services and facilities with maternity services that report offering KMC) CAPACITY TO PROVIDE SERVICES Proportion of facilities providing KMC with overall readiness and service experience in KMC. Indicator should be reworded: Proportion of facilities with maternity services with operational KMC Proposed criteria for operational: 1) Operational - basic (already collected in SPA): staff receiving in-service training in KMC; space and infant scale 2) Operational: (proposed components need to be tested and could be part of newborn module if not able to include in core tools): Trained staff (pre or in-service), KMC guidelines, space, feeding utensils (cup and spoon), infant scale, NG feeding tubes, head covering for small newborns, clinical charts, documentation of KMC services provided in the last 3 months 19
22 Country opportunities for testing and documenting use of KMC core indicators: # Country Specific opportunity Anticipated outputs Organization(s) Timelines Comments People responsible A. KMC Acceleration Priority Countries 1 Bangladesh 2 Indonesia 3 India 4 Ethiopia 5 Malawi 6 Nigeria 7 Rwanda Partners in Health (Hema) Potential setting for testings? B. Non-Acceleration Countries 1 Ghana 32 facilities in the northern part of Ghana being supported to scale up KMC - UNICEF supported implementation. Two main teaching hospitals are Kumasi hospital (Priscilla Wobell) and Korle bu hospital (teaching hospital in Accra). PATH project, making every baby count, is implementing KMC in 4 regions (CIFF supported project) and there are 4 regional hospital involved. North Carolina Chapel Hill (Kybele project) are subcontractors of PATH Making Every baby count. PATH belongs to subcommittee for newborn health in Ghana. Timing for testing and validating of indicators, facility based working towards definition of operational PATH is working in 4 regions. Ashanti next year and Volta regions in April/May. Testing of facility/process indicators Potential testing of HMIS eg coverage indicators with different denominators. AND record review for status at discharge and follow up. (potential consultancy funded by SNL- KMC research acceleration). Neena Khadka Save the Children - MCSP PATH INDEPTH also working in Ghana. Survey planned in April/May in Volta region Survey planned in Ashanti for 2016 Goldy Mazia and Magdalena Serpa to make contacts. Bina Valsangkar, Tanya Guenther to make concept notes. Need to enquire on what KMC work is being carried out by INDEPTH what are they testing and where? 20
23 Annex 4: HMIS subgroup notes Newborn Indicators Technical Working Group HMIS subgroup session Routine monitoring service delivery at what level of health system (facility, district, etc): focus on facility and district Did not consider: o Care of small and sick newborn o PNC o General outcome measures Measure skin-to-skin and breastfeeding separately, based Intervention Area: KMC (reviewed KMC Acceleration group recommendations and ENAP) Indicator Numerator Denominator Source Comments KMC Proportion of babies weighed at birth Number of babies weighed at birth Number of live births register Percent of newborns who received facility-based KMC Number of babies who are < 2000 g and initiated KMC that included: skin-to-skin and feeding Number of live births weighing less than <2000 g (would be hard to get estimated births at facility level) Registers from facility, compiled into monthly report forms This indicator tells you whether service is being provided with some level of quality of care coverage, implementation at health facility with a minimum of quality of care) Quality of care provided should be assessed during supervision visits, facility 21
24 Indicator Numerator Denominator Source Comments assessments or other special studies May want to report or review the two data elements numerator and denominator because some facilities may have small numbers and so a percentage may be harder to interpret Ratio of newborns discharged from facilitybased KMC that received follow-up per protocol Number of newborns discharged alive from KMC that received at least one follow-up at facility Number of newborns discharged alive from facility-based KMC Registers from facility compiled into monthly report forms (implication that there may need to be longitudinal registers for KMC) This indicator would tell us something about the quality of care If a patient tracking system can be put in for newborns with KMC (or other d Special studies would be more feasible 22
25 Indicator Numerator Denominator Source Comments Could test out mobile systems for data capture for newborns (Rwanda) and other sites In higher volume sites, this ratio would be somewhat stable and be interpretable; probably not review the data more than quarterly 23
26 Newborn Indicators Technical Working Group HMIS subgroup session Routine monitoring service delivery at what level of health system (facility, district, etc) Next steps: to review what data exists in the system as part of HMIS review to look at the reliability of the reporting Intervention Area: Essential newborn care and birth asphyxia Indicator Numerator Denominator Source Comments reviewed ENAP recommendations ENC ENC BA Proportion of babies dried immediately after birth Proportion of babies put to breast within one hour of delivery Number of newborns for whom resuscitation actions with bag and mask were initiated Number of babies dried immediately after birth Number of babies put to breast within one hour of delivery Total number of newborns where resuscitation with bag and mask was initiated Total number of births register Facility supervisor would use this information to assess how well essential newborn care is being implemented. We know that this is self-report by and may be subject to bias. Special studies or quality assessments may be needed to assess the validity. Total number of live births Total of live births plus fresh stillbirths register register We know that this is self-report by and may be subject to bias. Special studies or quality assessments may be needed to assess the validity. Would look at this indicator to assess how well resuscitation efforts are being implemented; need to look at trends, along with the survival rates, to see whether overall efforts are successful. May actually see declines in resuscitation with bag and mask over time if other resuscitation measures are successful 24
27 Indicator Numerator Denominator Source Comments Would also want to triangulate this information from perinatal death reviews. Would need to look at literature for what used for denominators have been to determine what proportion of births would need bag and mask resuscitation, and whether or not you would test a denominator that includes macerated stillbirths. 25
28 Newborn Indicators Technical Working Group HMIS subgroup session Routine monitoring service delivery at what level of health system (facility, district, etc) Quality of antibiotics needs to be examined in care quality there is a mobile check application. Indicator Numerator Denominator Source Comments Intervention Area: CHX and sepsis reviewed ENAP recommendations sepsis Proportion of newborns initiating treatment for sepsis Number of newborns with suspected PSBI that received at least one dose of antibiotic injections Number of newborns with suspected PSBI seen at the facility Register Used to assess whether services for newborn sepsis are being provided at the facility Need to assess what denominator would be best per 100 live births, per babies presenting with illness to facility, with diagnosis of PSBI One injection would not be sufficient, but it is an indication of availability of care and care begun, quality of care would need to look at treatment completion with appropriate regimens Need to test feasibility of data capture multiple points of care with difficult consolidation of information. May want to get number of babies coming in with possible severe bacterial infection Special studies could provide additional information on quality of care, including delays in care seeking and provision Gets more complicated once you get into inborn versus outborn cases 26
29 Indicator Numerator Denominator Source Comments Sepsis Number of newborns presenting with illness No denominator Outpatient registers Would be important to track to see whether identification is occurring and patients are coming into the facility Do we want to capture some commodities incorporated into LMIS gentamicin and chlorhexidine for cord care, maybe also bag and mask recommendation that yes, but additional discussion needed Would have to determine period of time for stockout --- within last 30 days, within last 90 days 27
30 Appendix 1: Agenda AGENDA Newborn Health Indicator Technical Working Group Meeting Save the Children Offices, Washington DC 2000 L St NW Suite 500, Conference Room ABC March 2015 Meeting Objectives 1. Provide updates since January 2013 meeting 2. To advance subgroup work and outputs through small-group discussions 3. Provide updates on other newborn health and associated measurement issues Day 1 Wednesday March 18, 2015 Time Session/Activity Presenter / Facilitator 8:30-9:00 am Breakfast 9:00-9:15 am Welcome and Introductions Lara Vaz, Save/SNL Objectives of Meeting 9:15-10:30 am ENAP Metrics Update and Bringing together Joy Lawn, LSHTM Maternal and Newborn metrics agenda 10:30-11:00 am Updates from TWG Subgroups - KMC - Household Surveys Allisyn Moran, USAID Sarah Moxon, LSHTM & Tanya Guenther, Save Deborah Sitrin, Save/SNL 11:00-11:15 am Harmonization of Facility Assessment Efforts Nancy Fronczak, consultant 11:15-11:30 am Discussion Kate Kerber 11:30-11:45 am Global Stillbirth Estimates Hannah Blencowe, LSHTM 11:45 am-12:00 pm Newborn in Emergencies Preetha Iyengar, Save 12:00 pm-12:15 pm HMIS Review and Day of Birth Initiative Vikas Dwivedi, MCSP 12:15pm 12:45 pm Discussion & Overview of Afternoon Lara Vaz, Save/SNL 12:45-1:15 pm Lunch 1:15-4:30 pm Small group work (with working break) 1. KMC 2. HF Assessments 3. HMIS Day 2 Thursday March 19, :30-9:00am Breakfast 9:00-9:10 am Overview of Day 2 Greta Wetzel 9:10-10:15 am Report out from sub-groups -KMC -HF Assessments -HMIS/routine TBD 10:15-10:30 am Break 10:30 am 1:00 pm Cross - group discussions (small group) Summary & Next Steps for NITWG 1:00 Lunch Tanya Guenther/Sarah Moxon Deborah Sitrin/Nancy Fronczak Vikas Dwivedi/Lara Vaz Lara Vaz 28
31 Sub-Group Agendas KMC Health Facility Assessments 1. Agree on immediate and longer-term dissemination plan for KMC indicators and what supporting materials should be prepared (by who, when, etc) 2. Identify specific opportunities for testing and documenting use of the KMC indicators, with special focus on KMC Acceleration priority countries 3. Map out KMC M&E resources and identify plan to review and share 4. Discuss input for KMC questions to include in health facility assessments (link to harmonization exercise and HF sub-group) 1. Review indicators recommended by this Newborn Indicators TWG years ago for facility assessments (most now in SPA and SARA) 2. Use SARA domains (components of readiness) to organize indicators, identify gaps, and prioritize core facility audit indicators 3. Agree on definition for overall readiness to deliver key newborn interventions 4. Plan to develop indicators of quality of care to collect when possible through facility assessment (record reviews, observation, etc) HMIS The purpose of this session is to have a focused discussion on the DOB initiative and its packages. The subgroup will focus on three topical areas: ENC & Birth Asphyxia; Preterm / LBW and KMC and Sepsis and CHX. For each topic, the group will work on 1. What are the ideal DOB indicators that can be included in the HMIS? a. How would the indicators be used at facility, district level 2. What should be the numerator and denominator for the selected indicators? How should they be collected? 3. Which of the indicators selected can be tested in country programs partners are supporting? 29
32 Appendix 2: Meeting Participants Name Greta Wetzel Tanya Guenther Preetha Iyengar Bina Valsangkar Magdalena Serpa Nancy Fronczak Sarah Moxon Joseph de Graft-Johnson Stella Abwao Yordi Molla Molly Strachan Deborah Sitrin Agbessi Amouzou Linda Wright Joy Fishel LaRue Seims Donna Vivio Neena Khadaka Karen Kirk Anne Palaia Goldy Mazia Vikas Dwivedi Steve Wall Lara Vaz Auditayo Omoni Kate Kerber Allisyn Moran Heather Rosen Indira Naratanan Jim Litch Joy Lawn Hannah Blencow Hattie Rees-Forman Juan Dwez Barbara Madaj Luigi D Aquino Kate Somers Lyn Nguyen Patsy Bailey Suzanne Fournier Uzma Syed Erica Corbett Lily Kak Organization Save the Children Save the Children Save the Children Save the Children PATH Consultant (WHO) LSHTM Save the Children Save the Children/MSCP Save the Children Jhpiego/MCSP Save the Children/SNL UNICEF NICHD DHS PCI USAID Save the Children/MCSP Population Council USAID PATH/MCSP JSI/MCSP Save the Children Save the Children Save the Children Save the Children USAID Consultant Consultant PATH/Gapps LSHTM LSHTM LSHTM Center for MNH, Liverpool Center for MNH, Liverpool Center for MNH, Liverpool BMGF CIFF Save the Children Rwanda Midwives USAID 30
33 Appendix 3: Presentations 31
34 Welcome & Introductions 1
35 Meeting Objectives 1. To provide updates of work since January 2013 meeting 2. To advance subgroup work and outputs through small-group discussions 3. To provide updates on other newborn health and associated measurement issues
36 Agenda: Wednesday, 18 March Time Session/Activity 8:30 9:00 am Breakfast 9:00 9:15 am Welcome and Introductions Objectives of Meeting 9:15 10:30 am ENAP Metrics Update and Bringing together Maternal and Newborn metrics agenda 10:30 11:00 am Updates from TWG Subgroups - KMC - Household Surveys 11:00 11:15 am Harmonization of Facility Assessment Efforts 11:15 11:30 am Discussion 11:30 11:45 am Global Stillbirth Estimates 11:45 am 12:00 pm Newborn in Emergencies 12:00 pm 12:15 pm HMIS Review and Day of Birth Initiative 12:15pm 12:45 pm Discussion & Overview of Afternoon 12:45 1:15 pm Lunch 1:15 4:30 pm Small group work (with working break) 1. KMC 2. HF Assessments 3. HMIS
37 Agenda: Thursday, 19 March Time Session/Activity 8:30 9:00am Breakfast 9:00 9:10 am Overview of Day 2 9:10 10:15 am Report out from sub-groups -KMC -HF Assessments -HMIS/routine 10:15 10:30 am Break 10:30 am 1:00 pm Cross - group discussions (small group) Summary & Next Steps for NITWG 1:00 Lunch
38 ENAP Metrics Update 5

39 EVERY NEWBORN An Action Plan To End Preventable Deaths Measurement Improvement Plan NBITWG 17 March 2015 #EveryNewborn
40 Overview 1. Overview ENAP core indicators and improvement Joy Lawn, LSHTM (on behalf of Matthews Mathai, WHO and the ENAP metrics gp) 2. Discussion ENAP measurement improvement plan 3. Integrating Maternal and newborn health metrics Allisyn Moran 4. Next steps #EveryNewborn




41 Every Newborn Series 5 papers 6 comments 55 authors from 18+ countries 60+ partner organisations Main funders: Bill & Melinda Gates Foundation, USAID, Children s Investment Fund Foundation Every Newborn Action Plan Based on the evidence from the Series Co-led by UNICEF & WHO, Consultation >60 country governments >80 organisations, >1000 individuals World Health Assembly 2014 resolution Launched June 2014 Now to action in many countries #EveryNewborn

42 Every Newborn action now: Three main streams of activities are ensuring the action plan leads to real change in countries: 1. Country implementation: identifying and responding to technical support needs, supporting translation of evidence into action, including Every Mother Every Newborn quality improvement initiative. 2. Metrics: improving and institutionalizing metrics to track coverage and impact based on the goals and targets of the ENAP and five strategic objectives. 3. Advocacy: strengthening maternal and newborn health advocacy efforts globally and in countries, building a movement for change. Research as cross cutting #EveryNewborn

43 CO CHAIRS COORDINATION GROUP (to link to existing metrics work, and institutionalize) TASK TEAMS ACADEMIC PARTNERS to promote leadership especially Africa & Asia WIDER INTEREST GROUP wide and inclusive ENAP Metrics work and who is involved WHO: Matthews Mathai LSHTM: Joy Lawn UNICEF: Agbessi Amouzou, Holly Newby UNFPA: Sennen Hounton SNL/NBITWG: Lara Vaz CIFF: Suzanne Fournier Gates: John Grove USAID: Allisyn Moran MHTF: linked via by ENAP management team Task teams with initial focus on specific newborn care interventions linked with existing initiatives especially UNCoLSC and others Three countries with EMEN project sites (Ghana, Tanzania, Bangladesh) Two networks: 1. Mortality focus: led by INDEPTH Maternal and Newborn Group (Peter Waiswa et al) 2. Beyond Survival /follow up of at risk newborns: led by All India Institute of Medical Sciences (Ashok Deorari et al) Also welcoming inputs from other institutions, partners and countries >50 at ENAP metrics improvement planning meeting by WHO Dec 2014 >100 people drawn from wider metrics community including Newborn Indicators Technical Working Group #EveryNewborn
")
44 Three tracks of work linked with ENAP metrics - overview 1 Technical mapping & planning of indicators, tools & work in progress 2 Institutionalise in national collection platforms and in global metrics architecture, with accountability Indicators for impact, coverage, process of maternal & newborn care Initial focus on the treatment interventions KMC (led by KMC acceleration group) Resuscitation (UNCoLSC, USAID, SNL Bangladesh, WHO, HBB etc) Antenatal Corticosteroids (WHO and UNCoLSC TRT etc) Sepsis case mx (WHO, UNCoLSC etc) CHX cord cleansing (UNCoLSC, SNL etc) Priority research to improve the metrics for use Birth and perinatal death certificates, coverage & quality Develop and test Minimum Perinatal Dataset Perinatal Mortality audit tool, linked to Maternal Mortality audit Inputs to facility HMIS, Health Facility Assessments such as SARA, and to household surveys 3 Leadership development to improve & use the data for action Testing in countries also linked to EMEN work Southern institutions as centres of excellence Integrated technical oversight especially with maternal health User friendly formats eg score cards, links to accountability and parent voices (eg partnerships with E4A and WRA) #EveryNewborn

. WHO Meeting Report in process Measurement of care for small and sick newborns is a total GAP!")
45 WHO ENAP Metrics meeting December 2014 Selected quotes... Who? >60 technical experts from Africa, Asia, North and South America and Europe including UN, academics, clinicians, programme experts, DHS, MICS, SARA, SPA, DHIS, CVRS & many others What? Two days of hard work! Emphasis on harmonisation with related metrics work eg WHO QoC metrics,100 core indicator list Results? Advances for core indicators, accelerating change (ENAP measurement Improvement Plan). WHO Meeting Report in process Measurement of care for small and sick newborns is a total GAP! Could be tackled like EmOC core competencies Important to remember essential newborn care in our metrics Treatment indicators stink and the worst part is the denominator! Prioritization is key as ambitious timeline for collecting data at-scale! #EveryNewborn
46 ENDING PREVENTABLE CHILD AND MATERNAL DEATHS #EveryNewborn
47 Ending preventable maternal deaths Maternal mortality target also included in Every Newborn Action Plan Lancet GH Sept 2013 : The Lancet Global Health 2013; 1:e176-e177 (DOI: /S X(13) ) Global average MMR of 70 per 100,000 with different targets for different countries Also need clear target for sexual and reproductive health (MDG 5 b) #EveryNewborn

48 Ending preventable child and newborn deaths Mortality targets in Every Newborn Action Plan and A Promise Renewed Every Newborn target by 2030: National NMR of 12 or less From 2.8 to 0.8 million neonatal deaths ~100 countries have already met the target focus on equity gaps About 29 countries will have to more than double their rates of progress Source: Lancet Every Newborn series, paper 2 #EveryNewborn
49 Also ending preventable stillbirths Every Newborn target by 2030: National SBR of 12 or less Source: Lancet Every Newborn series, paper 2 From 2.6 to 1.1 million stillbirths Aligned with NMR target but more ambitious change needed Stillbirths still NOT MENTIONED in any SDG document few weeks left to change this please sign the petition on Everynewborn.org #EveryNewborn
50 ACTING ON THE ACTION PLAN 17 #EveryNewborn


51 #EveryNewborn


52 5 things to do differently Intentional leadership development Especially in countries with highest burden Integrated Plans Integrated service delivery, continuum of care, coordination Investment for impact Governance, community participation, partner alignment Implementation & Innovation Address health system bottlenecks, Every Mother Every Newborn initiative Indicators & metrics Targets in post 2015 Measurement of progress and impact AMBITIOUS MEASUREMENT CHANGE IS CRITICAL TO EVERY STEP Eg for HIV/AIDS, malaria and EPI #EveryNewborn
53 Improving, institutionalising & using ENAP metrics for action ENAP Milestones by 2020 Count births and deaths in CVRS (women, newborns and stillbirths) Minimum perinatal dataset & perinatal mortality audit being widely used in countries ENAP core indicators to be defined, incorporated in national metrics platforms and widely used 2020 World Health Assembly May/June 2014 Dec 2014 Meeting To scope ENAP Metrics improvement plan Jan- May 2015 Refining and consulting on metrics plan & ENAP monitoring FW June May 2018 Testing indicators and tools in limited number of countries x June May 2020 Wide use in many countries CVRS, facility HMIS, surveys linked to health systems scale up #EveryNewborn
54 Core indicators selection during ENAP development Step 1: Developed matrix of relevant indicators Organised according to ENAP Framework from impact (mortality) down to inputs including financial (>120 rows in the Excel!) Step 2: Graded each indicator as follows: Direct relevance to the 5 ENAP objectives and focus (from A to C) Current availability of the data (from 1 to 3) Step 3: Ranked indicators By A to C, with A being closest match to ENAP focus. By 1 to 3 where 1 is most currently available Ref: Every Newborn: From evidence to action to deliver a healthy start for the next generation. Mason et al for the Lancet Every Newborn Study Group. Lancet Ambition to count what matters Indicators prioritised by importance (category A) Urgent work to improve the input data, specific milestones in ENAP for this #EveryNewborn
55 Impact Coverage: Care for all mothers and newborns Coverage: Complications & extra care Every Newborn action plan included core indicators Core ENAP Indicators 1. Maternal Mortality Ratio Additional Indicators 2. Stillbirth Rate Intrapartum Stillbirth Rate 3. Neonatal Mortality Rate Low birth weight rate Preterm birth rate Small for gestational age Neonatal morbidity rates Disability after neonatal conditions 4. Skilled attendant at birth 5. Early postnatal care for mothers and babies 6. Essential newborn care (tracer of immediate breastfeeding) 7. Antenatal corticosteroid use Caesarean section rate 8. Newborn resuscitation 9. Kangaroo mother care, feeding support 10. Treatment of neonatal sepsis Chlorhexidine cord cleansing Counting Birth registration Death registration, cause of death ENAP service delivery packages (process) Every Mother Every Newborn quality initiative Care of small and sick newborn Shaded = not currently routinely tracked. Bold = indicator requiring additional evaluation for consistent measurement Ref: Every Newborn: From evidence to action to deliver a healthy start for the next generation. Mason et al for the Lancet Every Newborn Study Group. Lancet #EveryNewborn
 www.everynewborn.org Core ENAP Indicators 1.")
 7. Antenatal corticosteroid use 8.")


56 Impact Every Newborn action plan core indicators New work needed on content Coverage: of care critical to Care for all mothers and link with maternal metrics newborns communities Coverage: Complications & extra care Counting ENAP service delivery packages (quality of care) Core ENAP Indicators 1. Maternal Mortality Ratio Definitions clear but need 2. Stillbirth Rate better tools, improved 3. Neonatal Mortality Rate quantity and quality of data 4. Skilled attendant at birth 5. Early postnatal care for mothers and babies 6. Essential newborn care (tracer of immediate breastfeeding) 7. Antenatal corticosteroid use 8. Newborn resuscitation 9. Kangaroo mother care, feeding support 10. Treatment of neonatal sepsis Chlorhexidine cord cleansing C-Section rate Birth registration Every Mother Every Newborn quality initiative Care of small and sick newborn Shaded = not currently routinely tracked. Bold = indicator requiring additional evaluation for consistent measurement Task Teams working. Significant progress Ref: Every Newborn: From evidence to action to deliver a healthy start for the next generation. Mason et al for the Lancet Every Newborn Study Group. Lancet Excel sheet has details of definitions and testing questions Please send questions or ideas to Harriet Rees-Forman harriet.rees-forman@lshtm.ac.uk #EveryNewborn
57 Please see excel of core definitions Note that we have received great feedback from many over the last week since the ENAP metrics webinar. We are taking every single input seriously but have not yet managed to address and reply to all. Also welcome more inputs by end of March #EveryNewborn
58 Measurement tools to be improved/developed and linked Civil Registration and Vital Statistics Birth certificates (improved weight, possibly gestational age) Perinatal Death certificates and ICD codes (linked to new WHO ICD-perinatal mortality classification) Facility and HMIS Perinatal mortality audit (linked to maternal audit) Minimum perinatal dataset DHIS2 and other HMIS collation for highly prioritised data points Health facility assessment tools (treatment indicators, process) Population based surveillance and surveys (DHS/MICS) Mortality capture including recall, misclassification of stillbirth/neonatal death and pregnancy vs live birth Verbal autopsy for stillbirths and neonatal deaths Social autopsy Birth weight, birth size and gestational age Core perinatal dataset Facility based More complex facility setting Research studies Eg as per data on ICD perinatal death certificate Eg South Africa PPIP Eg Vermont Oxford neonatal network Potentially with biodata #EveryNewborn

59 Networks to ensure testing and use in many contexts Mortality data etc Beyond newborn survival data INDEPTH Maternal & Newborn Interest Group 20+ sites in Africa and Asia Population-based pregnancy surveillance of births, stillbirths, neonatal deaths. Opportunities to advance validation of pregnancy history modules, verbal autopsy, improved LBW assessment etc. With UNICEF and others partners in India and beyond Follow up at risk newborns by varying levels of health care Opportunities to validate and test feasibility of follow up, screening for disability, ROP and models to improve care #EveryNewborn
60 Building on 3 countries working on quality initiatives including Every Mother Every Newborn Ghana Tanzania Bangladesh Validation and feasibility testing for facility-based coverage data Also tools such as audit, min perinatal dataset, simplified gest age assessment etc Also opportunities to test similar questions in other countries and with other organisations. Coordinated approach will yield the fastest collective progress #EveryNewborn
61 1 Which indicators to use now for what and more detail on ENAP metrics definitions Review excel, welcome to send questions or ideas to Harriet Rees-Forman (on behalf of Matthews Mathai & Joy Lawn) Discussion opportunities at Newborn indicators Technical Working Group in DC next week (18 th ) if you will be there Upcoming WHO ENAP meeting report and BMC paper Metrics Improvement Plan 2 More technical information Ideas for improvement or other inputs please contact Harriet Rees-Forman We have the potential to transform survival and health for EVERY newborn EVERY mother including for the world s poorest families Acting on the plan depends on better data #EveryNewborn
62 ENAP measurement plan discussion 1. Overall concept for coverage data improvement (focus on facility data, validating, testing feasibility)? 2. Impact data improvement, tools for CRVS, facility, pop-based (eg surveys, VA) 3. Quality data linked to EMEN, esp testing facility readiness for care of small and sick newborns 4. Leadership development with 3 country hubs and 2 networks #EveryNewborn

63 Every day. In times of crisis. For our future. TWG Subgroup Updates Kangaroo Mother Care Household Surveys Health Facility Assessments
64 KMC Acceleration 31
65 KMC indicators Aim: to reach consensus on a common set of indicators to track facility-based KMC implementation and progress Process: Consultation 1 Small Group, Consultation 2 KMC indicators meeting, DC, Oct 2014 Consultation 3 KMC Acceleration Mtg, Kigali, Nov 2014 Dissemination & Testing Phase Indicator Scoping Sept 2014 Mar indicators 18 indicators + draft framewok 12 indicators; revised framework 10 Core indicators + Final framework 32
66 KMC indicator framework 33

67 Summary of core KMC indicators according to framework 34
68 KMC: next steps Disseminate indicators and prepare supporting materials Identify opportunities for country-level use and documentation Gather resources and tools Small group work: 1. Discuss input for KMC questions to include in health facility assessments (link to HF sub-group and the ENAP indicator) 2. Agree on immediate and longer-term dissemination plan for KMC indicators and what supporting materials should be prepared 3. Identify specific opportunities for testing and documenting use of the KMC indicators, with special focus on KMC Acceleration priority countries 4. Map out KMC M&E resources and identify plan to review and share 35
69 Household Surveys 36
70 Revisions to DHS core questionnaire NEW Facility births asked about pre-discharge AND first post-discharge postnatal check ( & ) PNC content (457) During the first two days after (NAME) s birth, did any health care provider do the following: Examine the cord? Measure (NAME) s temperature? Counsel you on danger signs for newborns? Counsel you on breastfeeding? Observe (NAME) breastfeeding? Immediate skin to skin (434) Immediately after the birth, was (NAME) put directly on the bare skin of your chest? 37
71 Revisions to DHS core questionnaire NEW Emergency vs planned c-section (433) When was the decision made to have the caesarean section? Was it before or after your labor pains started? Record miscarriages, abortions, stillbirths in preceding 5 years (237) Did you have any miscarriages, abortions or stillbirths that ended before 2010? REVISED Questions on postnatal checks (#438, 453) includes explanation of what is meant by a check on the newborn s health. Now I would like to talk to you about checks on (NAME) s health after delivery for example, someone examining (NAME), checking the cord, or seeing if (NAME) is OK. Did anyone check on (NAME) s health while you were still in the facility? 38
72 Optional newborn modules DHS Will start developing modules later this year To be finished by September MICS Comprehensive tool revision early next year with testing of specific questions/modules including the newborn module. Learn from DHS experience Final questionnaires for next MICS must be informed by final SDG indicators. 39
73 Proposed analyses Newborn care practices SNL leading Data from 7 countries, 9 surveys Paper outline drafted Need to re-analyze data for cross-country comparison Levels and patterns of PNC contacts, with trends over time UNICEF leading Waiting for more MICS 5 data (with pre and post-discharge checks) Factors associated with coverage of PNC contacts Proposed to Countdown Coverage working group, but did not have bandwidth to take on another analysis. 40
74 Harmonization of Facility Assessments 41
75 UPDATE ON HARMONIZATION OF HEALTH FACILITY BASED INDICATORS AND METHODS N F R O N C Z A K ( W H O C O N S U L T A N T ) M A R C H 1 8, W A S H I N G T O N D C
76 WHY HARMONIZE? Cost-effectiveness Current situation: Multiple facility surveys in same countries for different objectives Duplication: Personnel/perdiems and travel logistics same expenses multiple times Wide variation in quality of survey implementation
77 WHY HARMONIZE? (2) Comparability across time and geography Currently different definitions (e.g., time for stockouts, items required for safe delivery) Different methods (items observed vs reported available)
78 ADVANTAGES OF HARMONIZATION Reduce costs, interruptions to facility services and MOH staff time. Use the opportunity to collect key information for multiple programs With uniform definitions and methods, can monitor change over time and between geographic areas
79 UNDERLYING PREMISES ABOUT FACILITY SURVEY Not replacement for routine supervision and program monitoring Should not be the primary source for information on basic program functionality Routine systems look at all details of program; survey looks at KEY INDICATORS from among all the details Can be primary source for information not yet routinely monitored but where information is needed
80 UNDERLYING PREMISES ABOUT FACILITY SURVEY (2) Provides external validation for self reported information routine supervision and program monitoring results HMIS reports Should provide uniformly defined and collected indicators that can be monitored across time and geography
81 WHAT IS NEEDED FOR HARMONIZATION? COMPROMISE Timing for data collection Definitions Agreement on minimum methodology standards to ensure minimum standard for data quality
82 WHAT IS NEEDED FOR HARMONIZATION (2) COMPROMISE IN SELECTING Critical indicators Additional indicators Quality of patient care indicators
83 PLAN FOR IMPLEMENTING HARMONIZED HFS Periodic coordination within country to meet needs of various stakeholders during the survey Similar to DHS process Core facility audit indicators always collected, then allow additional countryspecific needs Country selection among core patient QOC indicators depending on need which service and which method
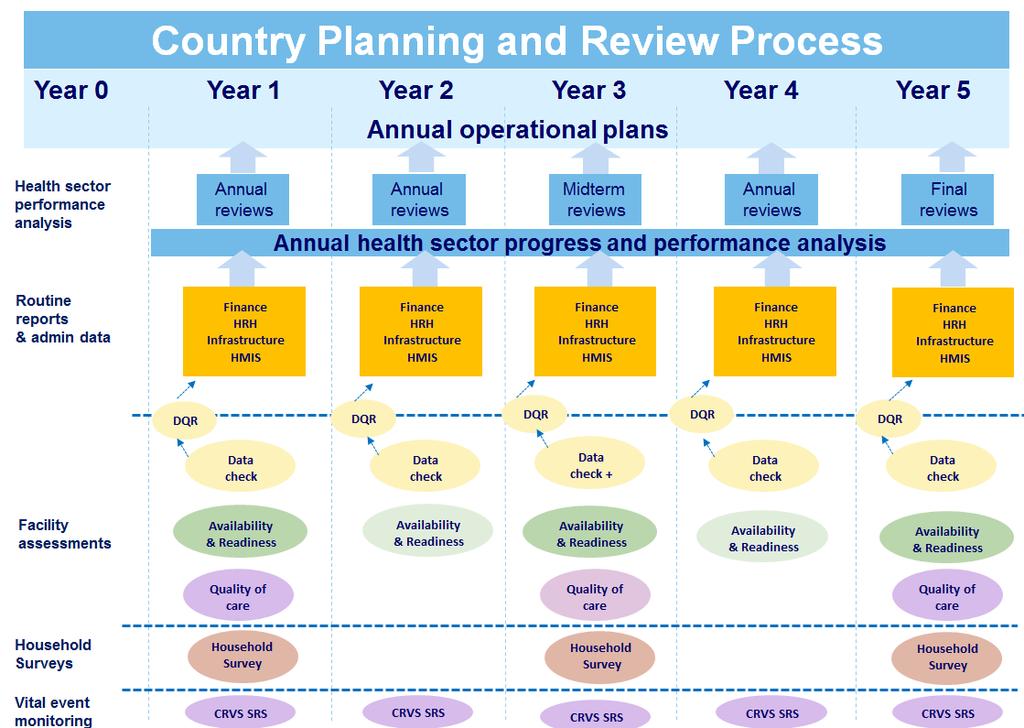
84
85 HARMONIZATION STATUS Meeting November 2014 List of core indicators (Global WHO 100 plus additions from various programs) Draft definitions, data collection tools with specific questions mapped to indicators. Draft sampling methods Draft recommendations for record review tools, methods, what is feasible during any given survey Tools comprise question bank for how to measure different indicators
86 FIGURE 1 ILLUSTRATIVE TOOLKIT OF HEALTH FACILITY ASSESSMENT MODULES AND INDICATOR DOMAINS SERVICE AVAILABILITY MANAGEMENT & FINANCE SERVICE READINESS CLIENT CARE DATA VERIFICATION Facility Infrastructure, amenities Management practices General readiness Client Care process Crosscutting Staff and beds Finance Servicespecific Readiness Client outcomes Programme specific Services offered Utilisation & efficiency Provider knowledge Client perspective Community linkages Health worker absentism perspective Systems for quality & safetey
87 DATA COLLECTION TOOLS Facility audit(service availability and readiness) Provider interview training, education, experience, duties Provider knowledge (proxy indicator of QOC in practice) response to case study/vignette response to questions on guidelines and standard practices Quality of patient care [All methods for all services not feasible in same facility during same survey) Observation patient/provider interaction using checklists Client exit interview (feedback plus service specific questions) Record reviews Provider knowledge
88 ISSUES FOR QOC INDICATORS Identify what requires special study because of time and level of expertise required for collecting information in each facility (e.g., Observation of deliveries and newborn care Record reviews when information is not in register columns or reports or requires linking information in multiple registers (e.g., postpartum sepsis) Infrequent events making case identification for record review time consuming (how newborn with sepsis is treated)
89 WHERE ARE WE? Technical groups to: Review indicators, definitions, map to data collection tools to see if essential information for indicator calculation is being collected. Consensus needed among different players for each technical group Recommend additions/deletions/changes Prioritize core (more frequent) indicators, additional (less frequent) indicators Pretest needed for feasibility of record reviews (availability of information, time and Level of knowledge required)
90 FACILITY ASSESSMENT SUBGROUP: WHAT WE AIM TO ACCOMPLISH TODAY Review indicators recommended by this Newborn Indicators TWG years ago for facility assessments (most now in SPA and SARA) Use SARA domains (components of readiness) to organize indicators, identify gaps, and prioritize core facility audit indicators Agree on definition for overall readiness to deliver key newborn interventions Plan to develop indicators of quality of care to collect when possible through facility assessment (record reviews, observation, etc)
91 Discussion 58
92 Global Stillbirth Estimates 59


93 Update on stillbirth rate estimates for 196 countries Dr Hannah Blencowe Professor Joy Lawn On behalf of the stillbirth investigator group For the Lancet Stillbirth Series 2015 team Work funded by Saving Newborn Lives:
62187-3.")
94 Source: Lawn JE, Blencowe H, Pattinson R, et al, for The Lancet s Stillbirths Series steering committee. Stillbirths: Where? When? Why? How to make the data count? Lancet 2011; published online April 14. DOI: /S (10) Large impact on women and families Last estimates for 2009 Regional variation for Stillbirth rate (SBR) and intrapartum SBR, showing uncertainty ranges An estimated 2.6 million stillbirths 98% in lowincome & middleincome countries 55% for rural African & Asian families
95 For women, stillbirths, newborns, the time of highest risk is the same Birth day 1.2 million intrapartum stillbirths >1 million neonatal deaths ~113,000 maternal deaths Source: Lancet Every Newborn series, paper 2 Over half of the 2.2 million deaths around the time of birth are stillbirths #EveryNewborn
96 ENAP target for ending preventable stillbirths Target requested by countries and set with multi-county consultation re various options 2030 Every Newborn target National stillbirth rate of 10 or less Source: Lancet Every Newborn series, paper 2 From 2.6 to 1.1 million stillbirths Aligned with NMR target but more ambitious change needed than for NMR 58 countries need to more than double their current progress Sub national equity goals also to be set #EveryNewborn
97 Impact Coverage: Care for all mothers and newborns Coverage: Complications & extra care Every Newborn action plan core indicators Core ENAP Indicators 1. Maternal Mortality Ratio Additional Indicators 2. Stillbirth Rate Intrapartum Stillbirth Rate 3. Neonatal Mortality Rate Low birth weight rate Preterm birth rate Small for gestational age Neonatal morbidity rates Disability after neonatal conditions 4. Skilled attendant at birth 5. Early postnatal care for mothers and babies 6. Essential newborn care (tracer of immediate breastfeeding) 7. Antenatal corticosteroid use Caesarean section rate 8. Newborn resuscitation 9. Kangaroo mother care, feeding support 10. Treatment of neonatal sepsis Chlorhexidine cord cleansing Counting Birth registration Death registration, cause of death ENAP service delivery packages (process) Every Mother Every Newborn quality initiative Care of small and sick newborn Shaded = not currently routinely tracked. Bold = indicator requiring additional evaluation for consistent measurement Ref: Every Newborn: From evidence to action to deliver a healthy start for the next generation. Mason et al for the Lancet Every Newborn Study Group. Lancet #EveryNewborn
98 Overview of stillbirth rate estimation work Overall aim: To provide data to inform accelerated progress for reaching 2030 targets A. Progress in reducing stillbirths Stillbirth Rate estimates for 196 countries to 2015, uncertainty and trends (aim ). Stillbirth Rate projections to 2030, which countries need most change to meet ENAP target to end preventable stillbirths (all countries to achieve stillbirth rate of 12 or less by 2030.) B. Data on timing of stillbirths to focus action in order to accelerate progress IP SBRs for 195 countries for 2014/5 (insufficient data for trends). [Note aiming for estimates to 2015 since UN report in Sept 2015 will be for 2015]
99 Definition of stillbirth WHO definition is late fetal death with birthweight of 1000g or gestational age of 28 weeks (3rd trimester). Definitions variability especially in high income countries. Many countries use gestational age in preference to birthweight: 24 weeks (UK), 22 weeks (many HIC countries), 20 weeks (USA, Australia and New Zealand) Definition used has a large effect on stillbirth rate e.g. USA 2012: Definition used 20 weeks 24 weeks 28 weeks 500g 1000g Number of stillbirths 23,886 15,692 11,648 13,711 9,466 Stillbirth Rate Source: Updated from Lawn J, Blencowe H et al,. Stillbirths: Where? When? Why? How to make the data count Lancet 2011;
100 Every Newborn Action Plan metrics group data status report cards Report card: Stillbirth rate data Number of countries with stillbirth rate by data source High quality Civil /Vital Registration Used as reported Household Surveys as input Other country data as input As input CVRS HMIS Facility Studies Population based studies No country data (Model alone) Total countries Stillbirth Rate 2011 Estimates Cousens et al Lancet New estimates for 2015 (provisional) To be finalised countries 17 min bias 46 with bias Model ESTIMATION DATASET FOR countries, 2810 data points 37 more countries with data, double the number of datapoints,
101 For 2015: Will refit with updated input data, then run for with updated covariate time series to 2015 and add uncertainty estimates using bootstrapping Key issue for time trends are the covariate predictors especially LBW rate and we have been working with UNICEF and WHO on these time series to improve the data Modeling approach for stillbirth rates Modeling in 2011 (Cousens et al): Restricted max likelihood estimation with country-level random effect Outcome: Natural log stillbirth rate Predictors in model for 2011: NMR, LBW, GNI, and region Type of data source, definition of stillbirth
102 Report card: Intrapartum stillbirth rate data Number of countries with intrapartum stillbirth rate by data source Intrapartum stillbirth rate 2011 estimates Lawn et al Lancet 2011 High quality Civil /Vital Registration Used as As input reported Household Surveys as input Other country data as input No country data (Model alone) Regional median Total countries 0 9 NA New estimates for 2015 (provisional) To be finalised 17 NA ESTIMATION DATASET FOR countries, 453 data points (plus further awaited) Four fold more data, but still 122 countries without data Every Newborn Action Plan metrics group data status report cards
103 Timeline Stillbirth rate estimates timeline March Finalising dataset Modelling & time trends April Finalise SBR model and results Present at WHO 22 nd /23 rd April May Anticipated WHO country review SBRs Submit Lancet Stillbirth Series Epi paper June October Oct - Dec Submit SBR/ IPSBR methods paper Anticipated launch of new SBR estimates and Lancet stillbirth series 2015 at FIGO in Vancouver Ongoing dissemination including Maternal Newborn Meeting in Mexico

104 Discussion and Questions 1. Intrapartum stillbirth data gaps Offers of data or suggestions 2. Other questions? Thank you


105 N E W B O R N H E A LT H I N E M E R G E N C I E S
106 Why is it Important? Over 40% of all deaths among children under 5 are neonatal deaths (0 28 days) Many of the countries with the highest neonatal mortality rates currently or have recently been affected by complex humanitarian emergencies Little is known about the epidemiology or best practices for neonatal survival in these settings Need to better understand the magnitude of the disease burden and interventions to improve neonatal health in complex humanitarian emergencies Morof et al.: Neonatal survival in complex humanitarian emergencies: setting an evidence-based research agenda. Conflict and Health :8.
107 N E W B O R N H E A LT H I N E B O L A A F F E C T E D C O U N T R I E S
108 Newborn Health during Ebola Outbreak Liberia, Sierra Leone, and Guinea First reported in Guinea in December 2014, then Liberia and Sierra Leone in March 2014 >22,000 people affected and >8500 deaths All are in the bottom ten countries in the Human Development Index Sierra Leone and Guinea remain in the list of top 10 countries with highest neonatal mortality rate, but Liberia had recently made substantial gains Prior to the outbreak, in Liberia 96% of women had at least one antenatal care visit, and 61% were delivered by a skilled provider (DHS 2013) Declared on track for MDG4 (IGME 2014) 62% of health facilities were closed by September due to the outbreak

109 Methodology Reviewed HMIS data from 2014 Well-known indicators with impact on maternal deaths, stillbirths and neonatal deaths were evaluated Total antenatal care visits Total pregnant women receiving intermittent preventive treatment for malaria Total number of facility deliveries
110 Pregnant Women Receiving IPTp Margibi County, March December Total Antenatal Care Visits Margibi County, March December Total Health Facility Deliveries Margibi County, March December
111 P I L OT S T U DY : N E W B O R N H E A LT H I N E M E R G E N C I E S F I E L D G U I D E
112 Field Guide Inter-agency collaboration Complements Inter-agency Field Manual on Reproductive Health in Humanitarian Settings Focuses on 3 main causes of death with quick reference solutions and priority on highest-impact interventions Aimed at health staff involved in designing, initiating, managing, monitoring and evaluating newborn health services within humanitarian settings Program and surge staff Technical, planning, and programmatic aspects

113 Newborn Health Kits Provision of supplies by level of facility Education materials Medicines Medical devices Lab supplies Newborn care supplies Raj Yagnik/Save the Children
114 Overall Design South Sudan, In internally displaced persons (IDP) camps and refugee camp health centers Obtain baseline data from hospital settings on newborn and maternal health indicators Train healthcare staff on use of field guide and newborn health practices Provide monitoring and supervision Monitor indicators for improvement of newborn health outcomes in the facility-setting
115 Study Aims Specific Aim 1: To qualitatively explore factors that facilitate or hinder adherence to implementation of the Newborn Health in Humanitarian Settings Field Guide among program implementers in South Sudan displaced person camps. Specific Aim 2: To qualitatively assess attitudes toward adoption of a newborn package of interventions among community and facility health workers in South Sudan displaced person camps. Specific Aim 3: To determine the effect of a newborn care package on the quality of newborn care practices among newborns delivered in South Sudanese, camp-based health facilities during the delivery and postnatal period.
116 Primary Outcome Measures: Draft Infection prevention Proportion of newborns with cord cut using new blade or boiled instrument Proportion of newborns with nothing (harmful) applied to cord Proportion of newborns with chlorhexidine applied on the cord on day of birth Proportion of newborns given first dose of Hepatitis B vaccine Proportion of newborns given a birth dose of oral polio vaccine (OPV) Thermal protection Proportion of newborns dried immediately after birth Proportion of newborns wrapped in a towel Proportion of newborns placed on the mother s bare chest after delivery Breastfeeding Proportion of newborns put to the breast within one hour of birth
117 Primary Outcome Measures Cntd. Asphyxia prevention Proportion of deliveries with suction device prepared Proportion of deliveries with neonatal ambu bag and mask prepared Proportion of deliveries with neonatal emergency tray prepared Proportion of newborns that had their breathing checked Proportion of newborns having trouble breathing at birth (or was not breathing at birth) where resuscitation techniques were used Assessment Proportion of newborns with a recorded birth weight Other Proportion of newborns given 1 mg of vitamin K intramuscularly (IM) after the first hour of birth
118 Desired Outcomes Feedback on the practicalities of implementation of field guide recommendation Finalization of supplementary tools for implementation to make it useful and ready for use Wide endorsement for adoption in emergency settings to catalyze improved outcomes for newborns

119 Projects in Development Retrospective survey of healthcare practices and behaviors by pregnant mothers during the outbreak and MNH programming in Liberia Study of effects of flooding on KMC programming in Malawi Newborn health in emergencies field guide pilot and mortality survey in Somalia
120 C U R R E N T P RO J E C T S

121 62% of health facilities were closed by September, leaving minimal primary health care services for communities, and virtually no treatment for non- Ebola related disease. Survival gains that were made in maternal and newborn health are at risk of being lost: Existing information can be used to focus attention on this issue and advocate for improved data collection in emergency settings 88 Alberto Rojas/Save the Children
122 General Areas of Focus Advocacy Newborns in emergencies are valuable to families and society and deserve to survive and thrive We know what works in development settings. Newborn deaths are not inevitable, even in a crisis. There are things that can be done within existing services to prevent stillbirths and save newborn lives. Many of these things also benefit the mother and prevent child deaths and disability as well. Develop evidence-base We need more information about the number and causes of death, and the specific challenges of implementing these interventions in emergency settings in order to make sure we are continuing to deliver results. Develop evidence-based guidelines to catalyze action by other humanitarian actors
123 HMIS Review and Day of Birth Initiative 90

124 A review of MNH-related data elements collected through national health management information systems Vikas Dwivedi, Mary Drake, Molly Strachan, Barbara Rawlins, Tanvi Monga, Kirsten Unfried
125 Overview of the presentation Purpose & Scope Method and countries Results Next steps 92
126 MNH HMIS Review Purpose of this Review To better understand what information on MNH service content, quality and health outcomes is currently included in national HMIS for 13 select priority countries. Specific objectives include Document current MNH (ANC/L&D) indicators included in the HMIS Document current MIP indicators in 6 PMI focus countries Identify gaps and advocate at the national level for incorporation of new indicators on content and quality of MNH services Provide recommendations to WHO on MIP-related indicators and data collection formats
127 Countries Included in the HMIS Review 6 MIP Focus countries - Malawi, Mali, Uganda, Mozambique, Tanzania, Kenya Other 7 countries India, Nigeria (Sokoto state), Bangladesh, Nepal, Ethiopia, Rwanda, Zimbabwe Nepal Mali India Bangladesh Nigeria Ethiopia Rwanda Malawi Uganda Kenya Tanzania PMI focus countries Zimbabwe Mozambique Other countries
128 Methods Review of HMIS data collection and reporting formats Identified focus on ANC, delivery and immediate post-natal care and developed list of indicators of interest (modified later) Collected HMIS forms from 13 countries Reviewed ANC client card, maternity charts/partographs, ANC and labor and delivery registers, facility monthly/quarterly summary forms Used standardized data abstraction template to conduct review Overall synthesis report on MNH produced for all countries 95




129 Identification of priority indicators for review 96

130 RESULTS In monthly facility summary form and in register In registers but not in monthly summary form Not captured in register or monthly summary form Client Card (CC) 97
131 Newborn Care Ethiopia Kenya Malawi Mali FORM Mozambique LIVE BIRTHS IMMEDIATE DRYING IMMEDIATE SKIN TO SKIN CARE BREASTFEEDING WITHIN ONE HOUR Nigeria CC CC CC Rwanda Tanzania Uganda Zimbabwe Bangladesh India Nepal In monthly facility summary form and in register In registers but not in monthly summary form Not captured in register or monthly summary form
132 Incidence & management of Newborn Complications during labor and Delivery F ORM ANY COMPLI CATI ON LOW BIRTH WEI GHT SEPSI S PRETERM ASPHY X I A TETANU S OTHER SKIN-TO- SKIN / KMC NEWBORN RESU SCI TATED Ethiopia Kenya CC Malawi Mali Mozambique Nigeria Rwanda Tanzania Uganda Zimbabwe Bangladesh India Nepal In monthly facility summary form and in register In registers but not in monthly summary form Not captured in register or monthly summary form 99
133 Maternal and Newborn Mortality COUNTRIES Ethiopia Kenya Malawi Mali Mozambique MATERNAL DEATHS MATERNAL DEATHS BY CAUSE STILLBIRTHS STILLBIRTHS FRESH Nigeria CC * Rwanda Tanzania Uganda Zimbabwe Bangladesh India Nepal STILLBIRTHS MACERATED VERY EARLY NEWBORN DEATHS (WITHIN 24 HOURS OR BEFORE DISCHARGE) * In both the register and the monthly summary form, there is a field for stillbirth with positive heart tones on admission (fresh stillbirth). VERY EARLY NEWBORN DEATHS BY CAUSE In monthly facility summary form and in register In registers but not in monthly summary form Not captured in register or monthly summary form 100
134 General Observations (Cont.) Labor and Delivery Interventions Critical life-saving interventions, such as Newborn Resuscitation, are not being measured across countries. Lack of information on quality and content services around birth. A little more information available for ANC. Limited indicators on routine newborn care in L&D Complications Recording for Maternal and newborn complications in L&D not standardized 101
135 Next steps 102
136 Bangladesh: Newborn Care Surveillance In 91 representative surveillance sites from 8 districts both community and facility data sources Number of deliveries Number of live births Number of fresh still birth Number of macerated still birth Number of babies not breathing at birth Number of babies dried Number of babies suctioned Number of babies stimulated Number of babies ventilated using bag and mask Number of babies that were referred
137 Expand review of HMIS Expand the HMIS review to all 24 priority countries Expand review to include RMNCH continuum of care

138 Indicator testing Testing indicators for improving quality of care
139 Newborn Health - 1 Core Indicators Numerator Denominator Proportion of health facilities with maternity services that have functional bag & masks (2 neonatal mask sizes) in the delivery areas Proportion of newborns who received all four elements of essential newborn care immediate and thorough drying immediate skin-to-skin contact delayed cord clamping initiation of breastfeeding in the first hour # of health facilities with maternity services that have functional bag & masks (2 neonatal mask sizes) in the delivery areas # of newborns who received all four elements of essential newborn care Total # of health facilities with maternity services Total # of live births in the health facility *Consultation on Improving measurement of the quality of maternal, newborn and child care in health facilities, World Health Organization and Partnership for Maternal, Newborn and Child Health
140 Newborn Health - 2 Core Indicators Numerator Denominator Proportion of health facilities where Kangaroo Mother Care is operational, by level of facility # of health facilities where Kangaroo Mother Care is operational, by level of facility Total # of health facilities with maternity services Facility neonatal mortality rate disaggregated by birth weight: >4000 g, g, g, g, < 1500 g # of neonatal deaths by categories of birth weight: >4000 g, g, g, g, < 1500 g Total # of live births in the health facility segregated by birth weight Proportion of health facilities offering maternity services that have BFHI certification and recertification not older than two years # of health facilities offering maternity services that have BFHI certification and recertification not older than two years Total # of health facilities with maternity services *Consultation on Improving measurement of the quality of maternal, newborn and child care in health facilities, World Health Organization and Partnership for Maternal, Newborn and Child Health

141 MCSP: Continuum of care & MCSP big ideas
Quality, Equity, Dignity: A WHO Network for Improving Quality of Care for Maternal, Newborn and Child Health
 Monitoring Framework Quality, Equity, Dignity: A WHO Network for Improving Quality of Care for Maternal, Newborn and Child Health Contents Quality of Care Network Goals... 2 Purpose of the Monitoring Framework...
Monitoring Framework Quality, Equity, Dignity: A WHO Network for Improving Quality of Care for Maternal, Newborn and Child Health Contents Quality of Care Network Goals... 2 Purpose of the Monitoring Framework...
Saving Every Woman, Every Newborn and Every Child
 Saving Every Woman, Every Newborn and Every Child World Vision s role World Vision is a global Christian relief, development and advocacy organization dedicated to improving the health, education and protection
Saving Every Woman, Every Newborn and Every Child World Vision s role World Vision is a global Christian relief, development and advocacy organization dedicated to improving the health, education and protection
MEETING THE NEONATAL CHALLENGE. Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009
, GoI New Delhi November 14, 2009") MEETING THE NEONATAL CHALLENGE Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009 Presentation Outline 1. Background 2. Key Initiatives of GoI 3. Progress 4. Major challenges & way
MEETING THE NEONATAL CHALLENGE Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009 Presentation Outline 1. Background 2. Key Initiatives of GoI 3. Progress 4. Major challenges & way
A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH
 EXECUTIVE SUMMARY THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL Executive Summary The State of the World s Midwifery
EXECUTIVE SUMMARY THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL Executive Summary The State of the World s Midwifery
GOVERNMENT OF MALAWI EVERY NEWBORN ACTION PLAN: AN ACTION PLAN TO END PREVENTABLE NEONATAL DEATHS IN MALAWI
 GOVERNMENT OF MALAWI EVERY NEWBORN ACTION PLAN: AN ACTION PLAN TO END PREVENTABLE NEONATAL DEATHS IN MALAWI ACKNOWLEDGEMENTS We would like to express our sincere gratitude to all the partners, institutions
GOVERNMENT OF MALAWI EVERY NEWBORN ACTION PLAN: AN ACTION PLAN TO END PREVENTABLE NEONATAL DEATHS IN MALAWI ACKNOWLEDGEMENTS We would like to express our sincere gratitude to all the partners, institutions
World Breastfeeding Week (WBW) 1-7 August 2017
 1-7 August 2017") World Breastfeeding Week (WBW) 1-7 August 2017 Sustaining Breastfeeding - Together! WBW Annual Survey Summary Survey Content Baby Friendly Hospital Initiative Hong Kong Association (BFHIHKA) was incorporated
World Breastfeeding Week (WBW) 1-7 August 2017 Sustaining Breastfeeding - Together! WBW Annual Survey Summary Survey Content Baby Friendly Hospital Initiative Hong Kong Association (BFHIHKA) was incorporated
Evidence Based Comprehensive Continuum of Care Package for Maternal & Newborn
 Evidence Based Comprehensive Continuum of Care Package for Maternal & Newborn Dr. M L Jain Director State Institute of Healthand and Family Welfare, Rajasthan Jaipur SIHFW: an ISO 9001: 2008 certified
Evidence Based Comprehensive Continuum of Care Package for Maternal & Newborn Dr. M L Jain Director State Institute of Healthand and Family Welfare, Rajasthan Jaipur SIHFW: an ISO 9001: 2008 certified
A Concept note and Terms of Reference on Assessment of Community-Based Integrated Management of Neonatal and Childhood Illness (CB-IMNCI) Program
 Program") A Concept note and Terms of Reference on Assessment of Community-Based Integrated Management of Neonatal and Childhood Illness (CB-IMNCI) Program Background Nepal has a long history of implementation of
A Concept note and Terms of Reference on Assessment of Community-Based Integrated Management of Neonatal and Childhood Illness (CB-IMNCI) Program Background Nepal has a long history of implementation of
(4-years project - funded by a grant from EU FP7 ) 10/11/2017 2
 10/11/2017 2") 10/11/2017 1 Linking communities and facilities to improve maternal and newborn health: Lessons from the Expanded Quality Management Using Information Power trial in Uganda and Tanzania (4-years project
10/11/2017 1 Linking communities and facilities to improve maternal and newborn health: Lessons from the Expanded Quality Management Using Information Power trial in Uganda and Tanzania (4-years project
ESSENTIAL NEWBORN CARE: INTRODUCTION
 ESSENTIAL NEWBORN CARE: INTRODUCTION Essential Newborn Care Implementation Toolkit 2013 The Introduction defines Essential Newborn Care and provides an overview of Newborn Care in South Africa and how
ESSENTIAL NEWBORN CARE: INTRODUCTION Essential Newborn Care Implementation Toolkit 2013 The Introduction defines Essential Newborn Care and provides an overview of Newborn Care in South Africa and how
Managing Programmes to Improve Child Health Overview. Department of Child and Adolescent Health and Development
 Managing Programmes to Improve Child Health Overview Department of Child and Adolescent Health and Development 1 Outline of this presentation Current global child health situation Effective interventions
Managing Programmes to Improve Child Health Overview Department of Child and Adolescent Health and Development 1 Outline of this presentation Current global child health situation Effective interventions
2018 PROGRESS REPORT: REACHING EVERY NEWBORN NATIONAL 2020 MILESTONES
 2018 PROGRESS REPORT: REACHING EVERY NEWBORN NATIONAL 2020 MILESTONES MARCH 2018 2018 PROGRESS REPORT: REACHING EVERY NEWBORN NATIONAL 2020 MILESTONES MARCH 2018 About the Every Newborn Action Plan In
2018 PROGRESS REPORT: REACHING EVERY NEWBORN NATIONAL 2020 MILESTONES MARCH 2018 2018 PROGRESS REPORT: REACHING EVERY NEWBORN NATIONAL 2020 MILESTONES MARCH 2018 About the Every Newborn Action Plan In
Improving PE/E and PPH care and using routine information sources to inform and track progress
 Improving PE/E and PPH care and using routine information sources to inform and track progress An Unfinished Agenda in Maternal Health: Meeting the Needs of Women with PE/E and PPH Washington, DC June
Improving PE/E and PPH care and using routine information sources to inform and track progress An Unfinished Agenda in Maternal Health: Meeting the Needs of Women with PE/E and PPH Washington, DC June
Integrated Management of Childhood Illness (IMCI)
") CHAPTER 5 III Integrated Management of Childhood Illness (IMCI) Tigest Ketsela, Phanuel Habimana, Jose Martines, Andrew Mbewe, Abimbola Williams, Jesca Nsungwa Sabiiti,Aboubacry Thiam, Indira Narayanan,
CHAPTER 5 III Integrated Management of Childhood Illness (IMCI) Tigest Ketsela, Phanuel Habimana, Jose Martines, Andrew Mbewe, Abimbola Williams, Jesca Nsungwa Sabiiti,Aboubacry Thiam, Indira Narayanan,
Maternal Health: Delivery and Newborn Care Tanzania Service Provision Assessment (TSPA)
") Maternal Health: Delivery and Newborn Care 2014-15 Tanzania Service Provision Assessment (TSPA) Background of Delivery Care Services Availability of Services Service Readiness Management Practices and
Maternal Health: Delivery and Newborn Care 2014-15 Tanzania Service Provision Assessment (TSPA) Background of Delivery Care Services Availability of Services Service Readiness Management Practices and
MEASURE DHS SERVICE PROVISION ASSESSMENT SURVEY HEALTH WORKER INTERVIEW
 06/01/01 MEASURE DHS SERVICE PROVISION ASSESSMENT SURVEY HEALTH WORKER INTERVIEW Facility Number: Interviewer Code: Provider SERIAL Number: [FROM STAFF LISTING FORM] Provider Sex: (1=MALE; =FEMALE) Provider
06/01/01 MEASURE DHS SERVICE PROVISION ASSESSMENT SURVEY HEALTH WORKER INTERVIEW Facility Number: Interviewer Code: Provider SERIAL Number: [FROM STAFF LISTING FORM] Provider Sex: (1=MALE; =FEMALE) Provider
Informal Meeting on provision of home-based care to mother and child in the first week after birth
 Informal Meeting on provision of home-based care to mother and child in the first week after birth Follow-up to the Joint WHO/UNICEF Statement on home visits for the newborn child MEETING REPORT 8 10 FEBRUARY
Informal Meeting on provision of home-based care to mother and child in the first week after birth Follow-up to the Joint WHO/UNICEF Statement on home visits for the newborn child MEETING REPORT 8 10 FEBRUARY
An Update Technical brief: Saving Low Birth Weight Newborn Lives through Kangaroo Mother Care (KMC) PRRINN-MNCH Experience
 PRRINN-MNCH Experience") An Update Technical brief: Saving Low Birth Weight Newborn Lives through Kangaroo Mother Care (KMC) PRRINN-MNCH Experience I. Background Introduction of Kangaroo Mother Care in Nigeria KMC was first introduced
An Update Technical brief: Saving Low Birth Weight Newborn Lives through Kangaroo Mother Care (KMC) PRRINN-MNCH Experience I. Background Introduction of Kangaroo Mother Care in Nigeria KMC was first introduced
DHS COMPARATIVE REPORTS 41
 LEVELS AND TRENDS IN NEWBORN CARE SERVICE AVAILABILITY AND READINESS IN BANGLADESH, HAITI, MALAWI, SENEGAL, AND TANZANIA DHS COMPARATIVE REPORTS 41 August 2016 This publication was produced for review
LEVELS AND TRENDS IN NEWBORN CARE SERVICE AVAILABILITY AND READINESS IN BANGLADESH, HAITI, MALAWI, SENEGAL, AND TANZANIA DHS COMPARATIVE REPORTS 41 August 2016 This publication was produced for review
STATUS OF MATERNAL, INFANT, AND YOUNG CHILD NUTRITION (MIYCN) IN MEDICAL COLLEGES & HOSPITALS
 IN MEDICAL COLLEGES & HOSPITALS") STATUS OF MATERNAL, INFANT, AND YOUNG CHILD NUTRITION (MIYCN) IN MEDICAL COLLEGES & HOSPITALS KEY FINDINGS BASELINE ASSESSMENT 2017 UTTAR PRADESH & BIHAR Image: Velocity Creative Introduction Despite a
STATUS OF MATERNAL, INFANT, AND YOUNG CHILD NUTRITION (MIYCN) IN MEDICAL COLLEGES & HOSPITALS KEY FINDINGS BASELINE ASSESSMENT 2017 UTTAR PRADESH & BIHAR Image: Velocity Creative Introduction Despite a
Improving Quality of Care during Childbirth: Learnings & Next Steps from the BetterBirth Trial
 Improving Quality of Care during Childbirth: Learnings & Next Steps from the BetterBirth Trial 24 April 2018 Katherine Semrau, PhD, MPH Health Systems Global Webinar Introductions Bejoy Nambiar Chair,
Improving Quality of Care during Childbirth: Learnings & Next Steps from the BetterBirth Trial 24 April 2018 Katherine Semrau, PhD, MPH Health Systems Global Webinar Introductions Bejoy Nambiar Chair,
The USAID portfolio in Health, Population and Nutrition (HPN)
") The USAID portfolio in Health, Population and Nutrition (HPN) Goal: Promote and improve health and well-being of Malawians through investing in sustainable, high-impact health initiatives in line with
The USAID portfolio in Health, Population and Nutrition (HPN) Goal: Promote and improve health and well-being of Malawians through investing in sustainable, high-impact health initiatives in line with
Indian Council of Medical Research
 Indian Council of Medical Research Call for Letters of Intent Grants Programme for Implementation Research on Maternal and Child Health Deadline: 31 May 2017 India has made significant progress in reducing
Indian Council of Medical Research Call for Letters of Intent Grants Programme for Implementation Research on Maternal and Child Health Deadline: 31 May 2017 India has made significant progress in reducing
UNICEF Baby Friendly Hospital Initiative Hong Kong Association. Baby-Friendly Hospital Designation. Hong Kong
 UNICEF Baby Friendly Hospital Initiative Hong Kong Association Baby-Friendly Hospital Designation In Hong Kong Revised June 2018 www.babyfriendly.org.hk Content Page Introduction to Baby-Friendly Hospital
UNICEF Baby Friendly Hospital Initiative Hong Kong Association Baby-Friendly Hospital Designation In Hong Kong Revised June 2018 www.babyfriendly.org.hk Content Page Introduction to Baby-Friendly Hospital
KANGAROO MOTHER CARE PROGRESS MONITORING TOOL (Version 4)
") MRC Research Unit for Maternal and Infant Health Care Strategies, 2002, 2004, 2007, 2009 University of Pretoria and Kalafong Hospital PO Box 667, Pretoria 0001, South Africa KANGAROO MOTHER CARE PROGRESS
MRC Research Unit for Maternal and Infant Health Care Strategies, 2002, 2004, 2007, 2009 University of Pretoria and Kalafong Hospital PO Box 667, Pretoria 0001, South Africa KANGAROO MOTHER CARE PROGRESS
Mother Baby Friendly Health Facility Initiative (MBFHI): Linking BFHI and MNH QI in Ghana Dr. Priscilla Wobil (Health Specialist-UNICEF)
: Linking BFHI and MNH QI in Ghana Dr. Priscilla Wobil (Health Specialist-UNICEF)") Mother Baby Friendly Health Facility Initiative (MBFHI): Linking BFHI and MNH QI in Ghana Dr. Priscilla Wobil (Health Specialist-UNICEF) Background Outline Country profile MNCH coverage and Quality gaps
Mother Baby Friendly Health Facility Initiative (MBFHI): Linking BFHI and MNH QI in Ghana Dr. Priscilla Wobil (Health Specialist-UNICEF) Background Outline Country profile MNCH coverage and Quality gaps
Mongolia. Situation Analysis. Policy Context Global strategy on women and children/ commitment. National Health Sector Plan and M&E Plan
 COUNTRY ACCOUNTABILITY FRAMEWORK: Assessment* Manila, Philippines Accountability Workshop, March 19-20, 2012 Information updated: April 19, 2012 Policy Context Global strategy on women and children/ commitment
COUNTRY ACCOUNTABILITY FRAMEWORK: Assessment* Manila, Philippines Accountability Workshop, March 19-20, 2012 Information updated: April 19, 2012 Policy Context Global strategy on women and children/ commitment
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region. Community IMCI. Community IMCI
 Implementation in the Western Pacific Region. Community IMCI. Community IMCI") Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region 5 What is community IMCI? is one of three elements of the IMCI strategy. Action at the level of the home and
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region 5 What is community IMCI? is one of three elements of the IMCI strategy. Action at the level of the home and
Newborn Health in Humanitarian Settings CORE Group Webinar 16 February 2017 Elaine Scudder
 Newborn Health in Humanitarian Settings CORE Group Webinar 16 February 2017 Elaine Scudder Newborn Health in Humanitarian Settings: Background Newborn Health in Humanitarian Settings 16 February 2017 An
Newborn Health in Humanitarian Settings CORE Group Webinar 16 February 2017 Elaine Scudder Newborn Health in Humanitarian Settings: Background Newborn Health in Humanitarian Settings 16 February 2017 An
IMPROVING QUALITY OF NEWBORN CARE IN HOIMA REGION THROUGH A REGIONAL LEARNING NETWORK
 University Research Co., LLC IMPROVING QUALITY OF NEWBORN CARE IN HOIMA REGION THROUGH A REGIONAL LEARNING NETWORK A collaborative effort of Uganda ministry of Health, Save the Children and University
University Research Co., LLC IMPROVING QUALITY OF NEWBORN CARE IN HOIMA REGION THROUGH A REGIONAL LEARNING NETWORK A collaborative effort of Uganda ministry of Health, Save the Children and University
Defining competent maternal and newborn health professionals
 Prepared for WHO Executive Board, January 2018. This is a pre-publication version and not intended for quotation or citation. Please contact the Secretariat with any queries, by email to: reproductivehealth@who.int
Prepared for WHO Executive Board, January 2018. This is a pre-publication version and not intended for quotation or citation. Please contact the Secretariat with any queries, by email to: reproductivehealth@who.int
Assignment 2: KMC Global: Ghana
 Assignment 2: KMC Global: Ghana Ghana o Household About 1/3 are women 40% of Ghanaian population is under age 15 Families often live with extended family members Tradition of either move in to live with
Assignment 2: KMC Global: Ghana Ghana o Household About 1/3 are women 40% of Ghanaian population is under age 15 Families often live with extended family members Tradition of either move in to live with
A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH
 EXECUTIVE SUMMARY THE STATE OF THE WORLD S MIDWIFERY 214 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL Executive Summary The State of the World s Midwifery
EXECUTIVE SUMMARY THE STATE OF THE WORLD S MIDWIFERY 214 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL Executive Summary The State of the World s Midwifery
A survey of the views of civil society
 Transforming and scaling up health professional education and training: A survey of the views of civil society Contents Executive summary...3 Introduction...5 Methodology...6 Key findings from the CS survey...8
Transforming and scaling up health professional education and training: A survey of the views of civil society Contents Executive summary...3 Introduction...5 Methodology...6 Key findings from the CS survey...8
Acronyms and Abbreviations
 Redacted Acronyms and Abbreviations CES CIP FP ISDP MCHIP MOH NGO OFDA PHC PHCC PITC PPH USAID WES Central Equatoria State County Implementing Partner Family Planning Integrated Service Delivery Project
Redacted Acronyms and Abbreviations CES CIP FP ISDP MCHIP MOH NGO OFDA PHC PHCC PITC PPH USAID WES Central Equatoria State County Implementing Partner Family Planning Integrated Service Delivery Project
Review of Neonatal Resuscitation Service Measurements
 Review of Neonatal Resuscitation Service Measurements www.mcsprogram.org November 2015 Contributors Yordanos B Molla, MCSP/Save the Children, USA Neena Khadka, MCSP/Save the Children, USA Barbara Rawlins,
Review of Neonatal Resuscitation Service Measurements www.mcsprogram.org November 2015 Contributors Yordanos B Molla, MCSP/Save the Children, USA Neena Khadka, MCSP/Save the Children, USA Barbara Rawlins,
Essential Newborn Care Corps. Evaluation of program to rebrand traditional birth attendants as health promoters in Sierra Leone
 Essential Newborn Care Corps Evaluation of program to rebrand traditional birth attendants as health promoters in Sierra Leone Challenge Sierra Leone is estimated to have the world s highest maternal mortality
Essential Newborn Care Corps Evaluation of program to rebrand traditional birth attendants as health promoters in Sierra Leone Challenge Sierra Leone is estimated to have the world s highest maternal mortality
Experts consultation on growth monitoring and promotion strategies: Program guidance for a way forward
 Experts consultation on growth monitoring and promotion strategies: Program guidance for a way forward Recommendations from a Technical Consultation UNICEF Headquarters New York, USA June 16-18, 2008-1
Experts consultation on growth monitoring and promotion strategies: Program guidance for a way forward Recommendations from a Technical Consultation UNICEF Headquarters New York, USA June 16-18, 2008-1
A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH
 FAST FACTS THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL STATE OF THE WORLD S MIDWIFERY CHALLENGES The 73 countries
FAST FACTS THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL STATE OF THE WORLD S MIDWIFERY CHALLENGES The 73 countries
The World Breastfeeding Trends Initiative (WBTi)
") The World Breastfeeding Trends Initiative (WBTi) MALAWI ASSESSMENT REPORT MINISTRY OF HEALTH NUTRITION UNIT 1 Acronyms: AIDS BFHI GIMS HIV HTC IBFAN IEC ILO IYCF MDHS M & E MOH MPC MTCT NGO PMTCT UNICEF
The World Breastfeeding Trends Initiative (WBTi) MALAWI ASSESSMENT REPORT MINISTRY OF HEALTH NUTRITION UNIT 1 Acronyms: AIDS BFHI GIMS HIV HTC IBFAN IEC ILO IYCF MDHS M & E MOH MPC MTCT NGO PMTCT UNICEF
Photo: Dr. Karima Noori (centre) conducts a midwifery training course at Faizabad Hospital in Badakshan Province. UNICEF/Khemka
 conducts a midwifery training course at Faizabad Hospital in Badakshan Province. UNICEF/Khemka") Quality, Equity, Dignity A Network for Improving Quality of Care for Maternal, Newborn and Child Health MONITORING FRAMEWORK Working document Quality of Care Network Goals Reduce maternal and newborn mortality
Quality, Equity, Dignity A Network for Improving Quality of Care for Maternal, Newborn and Child Health MONITORING FRAMEWORK Working document Quality of Care Network Goals Reduce maternal and newborn mortality
8 November, RMNCAH Country Case-Studies: Summary of Findings from Six Countries
 8 November, 2012 RMNCAH Country Case-Studies: Summary of Findings from Six Countries Country Case-Studies: September October 2012 6 countries Bangladesh, India, Indonesia, Nepal, Papua New Guinea and Solomon
8 November, 2012 RMNCAH Country Case-Studies: Summary of Findings from Six Countries Country Case-Studies: September October 2012 6 countries Bangladesh, India, Indonesia, Nepal, Papua New Guinea and Solomon
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region. IMCI Monitoring and Evaluation
 Implementation in the Western Pacific Region. IMCI Monitoring and Evaluation") Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI Monitoring and Evaluation 8 IMCI Monitoring and Evaluation Why is monitoring and evaluation of IMCI important?
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI Monitoring and Evaluation 8 IMCI Monitoring and Evaluation Why is monitoring and evaluation of IMCI important?
IMCI at the Referral Level: Hospital IMCI
 Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI at the Referral Level: Hospital IMCI 6 IMCI at the Referral Level: Hospital IMCI Hospital referral care:
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI at the Referral Level: Hospital IMCI 6 IMCI at the Referral Level: Hospital IMCI Hospital referral care:
Rwanda EPCMD Country Summary, March 2017
 Rwanda EPCMD Country Summary, March 2017 Community Health Workers dance during a fistula awareness campaign organized by MCSP. Photo by Mamy Ingabire Selected Demographic and Health Indicators for Rwanda
Rwanda EPCMD Country Summary, March 2017 Community Health Workers dance during a fistula awareness campaign organized by MCSP. Photo by Mamy Ingabire Selected Demographic and Health Indicators for Rwanda
RWANDA. COUNTRY ACCOUNTABILITY FRAMEWORK: Assessment*, Dar-es-Salaam, Tanzania, February 13-15, 2012
 COUNTRY ACCOUNTABILITY FRAMEWORK: Assessment*, Dar-es-Salaam, Tanzania, February 13-15, 2012 Policy Context Global strategy on women and children/ commitment National Health policy/national Health Plan/Strategies
COUNTRY ACCOUNTABILITY FRAMEWORK: Assessment*, Dar-es-Salaam, Tanzania, February 13-15, 2012 Policy Context Global strategy on women and children/ commitment National Health policy/national Health Plan/Strategies
REQUEST FOR PROPOSALS
 REQUEST FOR PROPOSALS REQUEST FOR PROPOSALS (RFP) FOR THE PROVISION OF CONSULTANCY SERVICES TO SUPPORT IMPROVEMENT OF MATERNAL AND NEW BORN CARE IN THE 16 RHITES SW DISTRICTS In support of ELIZABETH GLASER
REQUEST FOR PROPOSALS REQUEST FOR PROPOSALS (RFP) FOR THE PROVISION OF CONSULTANCY SERVICES TO SUPPORT IMPROVEMENT OF MATERNAL AND NEW BORN CARE IN THE 16 RHITES SW DISTRICTS In support of ELIZABETH GLASER
Ruth Patterson, RNC, BSN, MHSA, Integrated Quality Services
 Improving Your Joint Commission Perinatal Care Core Measure of Exclusive Breast Milk Feeding Through Baby Friendly Implementation of Evidence Based Maternity Practices Ruth Patterson, RNC, BSN, MHSA, Integrated
Improving Your Joint Commission Perinatal Care Core Measure of Exclusive Breast Milk Feeding Through Baby Friendly Implementation of Evidence Based Maternity Practices Ruth Patterson, RNC, BSN, MHSA, Integrated
Managing possible serious bacterial infection in young infants 0 59 days old when referral is not feasible
 WHO/UNICEF Joint Statement Managing possible serious bacterial infection in young infants 0 59 days old when referral is not feasible Key points in this Joint Statement n Infections are currently responsible
WHO/UNICEF Joint Statement Managing possible serious bacterial infection in young infants 0 59 days old when referral is not feasible Key points in this Joint Statement n Infections are currently responsible
Pre-Eclampsia/Eclampsia: Prevention, Detection and Management
 PROGRAM IMPLEMENTATION GUIDANCE Pre-Eclampsia/Eclampsia: Prevention, Detection and Management DECEMBER As maternal mortality ratios have declined globally, there have been accompanying shifts in the leading
PROGRAM IMPLEMENTATION GUIDANCE Pre-Eclampsia/Eclampsia: Prevention, Detection and Management DECEMBER As maternal mortality ratios have declined globally, there have been accompanying shifts in the leading
Indicator. unit. raw # rank. HP2010 Goal
 Kentucky Perinatal Systems Perinatal Regionalization Meeting October 28, 2009 KY Indicators of Perinatal Health Infant mortality in Kentucky has been decreasing and is currently equal to the national average
Kentucky Perinatal Systems Perinatal Regionalization Meeting October 28, 2009 KY Indicators of Perinatal Health Infant mortality in Kentucky has been decreasing and is currently equal to the national average
WORLD BREASTFEEDING TRENDS INITIATIVE (WBTi) DATABASE QUESTIONNAIRE
 DATABASE QUESTIONNAIRE") WORLD BREASTFEEDING TRENDS INITIATIVE (WBTi) DATABASE QUESTIONNAIRE Part I (1) Percentage of babies breastfed within one hour of birth (26.3%) (2) Percentage of babies 0
WORLD BREASTFEEDING TRENDS INITIATIVE (WBTi) DATABASE QUESTIONNAIRE Part I (1) Percentage of babies breastfed within one hour of birth (26.3%) (2) Percentage of babies 0
NIGERIA EVERY NEWBORN ACTION PLAN
 Federal Ministry of Health NIGERIA EVERY NEWBORN ACTION PLAN A Plan To End Preventable Newborn Deaths in Nigeria a Caborro blatur mi, quidelliqui consequ amusdant, ulparum facessi optates ducienem dolenimus
Federal Ministry of Health NIGERIA EVERY NEWBORN ACTION PLAN A Plan To End Preventable Newborn Deaths in Nigeria a Caborro blatur mi, quidelliqui consequ amusdant, ulparum facessi optates ducienem dolenimus
Basic newborn care and neonatal resuscitation: a multi-country analysis of health system bottlenecks and potential solutions
 RESEARCH Open Access Basic newborn care and neonatal resuscitation: a multi-country analysis of health system bottlenecks and potential solutions Christabel Enweronu-Laryea 1*, Kim E Dickson 2, Sarah G
RESEARCH Open Access Basic newborn care and neonatal resuscitation: a multi-country analysis of health system bottlenecks and potential solutions Christabel Enweronu-Laryea 1*, Kim E Dickson 2, Sarah G
Water, sanitation and hygiene in health care facilities in Asia and the Pacific
 Water, sanitation and hygiene in health care facilities in Asia and the Pacific A necessary step to achieving universal health coverage and improving health outcomes This note sets out the crucial role
Water, sanitation and hygiene in health care facilities in Asia and the Pacific A necessary step to achieving universal health coverage and improving health outcomes This note sets out the crucial role
Quality, Humanized & Respectful Care for Mothers and Newborns. The Model Maternity Initiative
 Quality, Humanized & Respectful Care for Mothers and Newborns The Model Maternity Initiative Field Office: Mozambique Presenter: Maria da Luz Vaz Presentation Outline Country: Main Demographic and Health
Quality, Humanized & Respectful Care for Mothers and Newborns The Model Maternity Initiative Field Office: Mozambique Presenter: Maria da Luz Vaz Presentation Outline Country: Main Demographic and Health
National Newborn. Health Bulletin
 National Newborn April-June 2017 Issue - 3 Photo : Save the Children/ GMB Akash Health Bulletin Editorial note It is my great pleasure to share the 3rd issue of the National Newborn Health Bulletin from
National Newborn April-June 2017 Issue - 3 Photo : Save the Children/ GMB Akash Health Bulletin Editorial note It is my great pleasure to share the 3rd issue of the National Newborn Health Bulletin from
JOINT STATEMENT International Policy Statement for Universal Use of Kangaroo Mother Care for Preterm and Low Birthweight Infants
 JOINT STATEMENT International Policy Statement for Universal Use of Kangaroo Mother Care for Preterm and Low Birthweight Infants Commitment to Action from Professional Health Associations A This International
JOINT STATEMENT International Policy Statement for Universal Use of Kangaroo Mother Care for Preterm and Low Birthweight Infants Commitment to Action from Professional Health Associations A This International
Standards for competence for registered midwives
 Standards for competence for registered midwives The Nursing and Midwifery Council (NMC) is the nursing and midwifery regulator for England, Wales, Scotland and Northern Ireland. We exist to protect the
Standards for competence for registered midwives The Nursing and Midwifery Council (NMC) is the nursing and midwifery regulator for England, Wales, Scotland and Northern Ireland. We exist to protect the
Baby Friendly Hospital Initiative Hong Kong Association. Baby-Friendly Maternal and Child Health Centres. Hong Kong
 Baby Friendly Hospital Initiative Hong Kong Association Baby-Friendly Maternal and Child Health Centres In Hong Kong March 2016 www.babyfriendly.org.hk Content Introduction to Baby-Friendly Hospital Initiative
Baby Friendly Hospital Initiative Hong Kong Association Baby-Friendly Maternal and Child Health Centres In Hong Kong March 2016 www.babyfriendly.org.hk Content Introduction to Baby-Friendly Hospital Initiative
Economic and Social Council
 United Nations E/CN.3/2015/20 Economic and Social Council Distr.: General 8 December 2014 Original: English Statistical Commission Forty-sixth session 3-6 March 2015 Item 4 (a) of the provisional agenda*
United Nations E/CN.3/2015/20 Economic and Social Council Distr.: General 8 December 2014 Original: English Statistical Commission Forty-sixth session 3-6 March 2015 Item 4 (a) of the provisional agenda*
Using lay health workers to improve access to key maternal and newborn health interventions in sexual and reproductive health
 Using lay health workers to improve access to key maternal and newborn health interventions in sexual and reproductive health improve access to key maternal and newborn health interventions A lay health
Using lay health workers to improve access to key maternal and newborn health interventions in sexual and reproductive health improve access to key maternal and newborn health interventions A lay health
Acronyms and Abbreviations
 Redacted Acronyms and Abbreviations AA Associate Award ANC Antenatal Care BCC Behavior Change Communication CBT Competency-based Training cpqi Community Performance and Quality Improvement CSO Civil Society
Redacted Acronyms and Abbreviations AA Associate Award ANC Antenatal Care BCC Behavior Change Communication CBT Competency-based Training cpqi Community Performance and Quality Improvement CSO Civil Society
Bright Futures: An Essential Resource for Advancing the Title V National Performance Measures
 A S S O C I A T I O N O F M A T E R N A L & C H I L D H E A L T H P R O G R A MS April 2018 Issue Brief An Essential Resource for Advancing the Title V National Performance Measures Background Children
A S S O C I A T I O N O F M A T E R N A L & C H I L D H E A L T H P R O G R A MS April 2018 Issue Brief An Essential Resource for Advancing the Title V National Performance Measures Background Children
Health Management Information Systems (HMIS) Review
 Review") Health Management Information Systems (HMIS) Review Survey on Data Availability in Electronic Systems for Maternal and Newborn Health Indicators in 24 USAID Priority Countries www.mcsprogram.org This report
Health Management Information Systems (HMIS) Review Survey on Data Availability in Electronic Systems for Maternal and Newborn Health Indicators in 24 USAID Priority Countries www.mcsprogram.org This report
MINISTRY OF HEALTH ON INFANT AND YOUNG CHILD FEEDING
 MINISTRY OF HEALTH CONTINUOUS TRAINING PROGRAM ON INFANT AND YOUNG CHILD FEEDING Manuals for Health Workers on maternal and child health care at all levels Hanoi, January 2015 INTRODUCTION The United
MINISTRY OF HEALTH CONTINUOUS TRAINING PROGRAM ON INFANT AND YOUNG CHILD FEEDING Manuals for Health Workers on maternal and child health care at all levels Hanoi, January 2015 INTRODUCTION The United
Quality Surveillance Team. Neonatal Critical Care (NCC) Quality Indicators
 Quality Indicators") Quality Surveillance Team Neonatal Critical Care (NCC) Quality Indicators Neonatal Critical Care Quality Indicators Introduction These neonatal critical care quality indicators have been developed using
Quality Surveillance Team Neonatal Critical Care (NCC) Quality Indicators Neonatal Critical Care Quality Indicators Introduction These neonatal critical care quality indicators have been developed using
EMERGENCY CARE SYSTEMS
 OVERVIEW Emergency and Trauma Care Systems The DCP emergency components of essential packages WHO Emergency Care System Framework Emergency Care System Assessment Tool PREVENTION PREHOSPITAL & TRANSPORT
OVERVIEW Emergency and Trauma Care Systems The DCP emergency components of essential packages WHO Emergency Care System Framework Emergency Care System Assessment Tool PREVENTION PREHOSPITAL & TRANSPORT
REPORT WHO/UNICEF WORKSHOP TO REVIEW PROGRESS AND ACTIONS TO IMPROVE CHILD SURVIVAL. Convened by:
 WPR/DHP/04/CHD(1)/2009 Report series number: RS/2009/GE/55(CHN) English only REPORT WHO/UNICEF WORKSHOP TO REVIEW PROGRESS AND ACTIONS TO IMPROVE CHILD SURVIVAL Convened by: WORLD HEALTH ORGANIZATION REGIONAL
WPR/DHP/04/CHD(1)/2009 Report series number: RS/2009/GE/55(CHN) English only REPORT WHO/UNICEF WORKSHOP TO REVIEW PROGRESS AND ACTIONS TO IMPROVE CHILD SURVIVAL Convened by: WORLD HEALTH ORGANIZATION REGIONAL
Service Provision Assessment (SPA) Surveys
 Surveys") Service Provision Assessment (SPA) Surveys Overview of Methodology, Key MNH Indicators and Service Readiness Indicators Paul Ametepi, MEASURE DHS 01/14/2013 Outline of presentation Overview of SPA methodology
Service Provision Assessment (SPA) Surveys Overview of Methodology, Key MNH Indicators and Service Readiness Indicators Paul Ametepi, MEASURE DHS 01/14/2013 Outline of presentation Overview of SPA methodology
Nepal - Health Facility Survey 2015
 Microdata Library Nepal - Health Facility Survey 2015 Ministry of Health (MoH) - Government of Nepal, Health Development Partners (HDPs) - Government of Nepal Report generated on: February 24, 2017 Visit
Microdata Library Nepal - Health Facility Survey 2015 Ministry of Health (MoH) - Government of Nepal, Health Development Partners (HDPs) - Government of Nepal Report generated on: February 24, 2017 Visit
COLLEGE OF MIDWIVES OF BRITISH COLUMBIA
 COLLEGE OF MIDWIVES OF BRITISH COLUMBIA DEFINITION OF A MIDWIFE MIDWIFERY MODEL OF PRACTICE A midwife is a person who, having been regularly admitted to a midwifery educational programme duly recognised
COLLEGE OF MIDWIVES OF BRITISH COLUMBIA DEFINITION OF A MIDWIFE MIDWIFERY MODEL OF PRACTICE A midwife is a person who, having been regularly admitted to a midwifery educational programme duly recognised
An investigation of breastfeeding support in Coventry November 2012
 An investigation of breastfeeding support in Coventry November 2012 Responses received 1 LINk s Recommendations 1. Commissioners ensure adequate provision of antenatal support for women in pregnancy regarding
An investigation of breastfeeding support in Coventry November 2012 Responses received 1 LINk s Recommendations 1. Commissioners ensure adequate provision of antenatal support for women in pregnancy regarding
Every Woman, Every Newborn: BMC Pregnancy and Childbirth September, 2015
 Every Woman, Every Newborn: BMC Pregnancy and Childbirth September, 2015 Edited by Joy Lawn, Kim Dickson, Matthews Matthai and Sarah Moxon Weblink: http://www.biomedcentral.com/bmcpregnancychildbirth/supplements/15/s2
Every Woman, Every Newborn: BMC Pregnancy and Childbirth September, 2015 Edited by Joy Lawn, Kim Dickson, Matthews Matthai and Sarah Moxon Weblink: http://www.biomedcentral.com/bmcpregnancychildbirth/supplements/15/s2
TERMS OF REFERENCE: PRIMARY HEALTH CARE
 TERMS OF REFERENCE: PRIMARY HEALTH CARE A. BACKGROUND Health Status. The health status of the approximately 21 million Citizens of Country Y is among the worst in the world. The infant mortality rate is
TERMS OF REFERENCE: PRIMARY HEALTH CARE A. BACKGROUND Health Status. The health status of the approximately 21 million Citizens of Country Y is among the worst in the world. The infant mortality rate is
Improving Quality of Maternal, Newborn, and Child Care in Uganda. Dr. Jesca Nsungwa Sabiiti, Uganda MOH September 2018
 Improving Quality of Maternal, Newborn, and Child Care in Uganda Dr. Jesca Nsungwa Sabiiti, Uganda MOH September 2018 RMNCAH in Uganda: Selected Indicators 600 500 400 300 200 100 0 UGANDA TRENDS IN MATERNAL,
Improving Quality of Maternal, Newborn, and Child Care in Uganda Dr. Jesca Nsungwa Sabiiti, Uganda MOH September 2018 RMNCAH in Uganda: Selected Indicators 600 500 400 300 200 100 0 UGANDA TRENDS IN MATERNAL,
Improving Quality of Maternal and Newborn Health in India
 Improving Quality of Maternal and Newborn Health in India Fact Sheet: January 2017 Partners: Government of India (GoI), State Governments of Rajasthan, Maharashtra, Uttar Pradesh, Jharkhand, Andhra Pradesh
Improving Quality of Maternal and Newborn Health in India Fact Sheet: January 2017 Partners: Government of India (GoI), State Governments of Rajasthan, Maharashtra, Uttar Pradesh, Jharkhand, Andhra Pradesh
CLINICAL GOVERNANCE Fostering a culture of learning,
 CLINICAL GOVERNANCE Fostering a culture of learning, quality, and accountability within hospitals and health centers to ensure maternal and newborn survival TECHNICAL REPORT SEPTEMBER 2015 TABLE OF CONTENTS
CLINICAL GOVERNANCE Fostering a culture of learning, quality, and accountability within hospitals and health centers to ensure maternal and newborn survival TECHNICAL REPORT SEPTEMBER 2015 TABLE OF CONTENTS
Improving Maternal Health in Low-resource settings: Niger Case Study, Part 1
 Improving Maternal Health in Low-resource settings: Niger Case Study, Part 1 Kathleen Hill, M.D. M.P.H. MCSP Maternal Health Team Lead February 2016 Annual Meeting American College of Preventive Medicine
Improving Maternal Health in Low-resource settings: Niger Case Study, Part 1 Kathleen Hill, M.D. M.P.H. MCSP Maternal Health Team Lead February 2016 Annual Meeting American College of Preventive Medicine
These slides are to explain why the Trust is adopting the National Early Warning Score which is being adopted across all sectors of health care in
 These slides are to explain why the Trust is adopting the National Early Warning Score which is being adopted across all sectors of health care in the UK and beyond. 1 The first EWS was devised in 1997
These slides are to explain why the Trust is adopting the National Early Warning Score which is being adopted across all sectors of health care in the UK and beyond. 1 The first EWS was devised in 1997
Population Council, Bangladesh INTRODUCTION
 Performance-based Incentive for Improving Quality Maternal Health Care Services in Bangladesh Mohammad Masudul Alam 1, Ubaidur Rob 1, Md. Noorunnabi Talukder 1, Farhana Akter 1 1 Population Council, Bangladesh
Performance-based Incentive for Improving Quality Maternal Health Care Services in Bangladesh Mohammad Masudul Alam 1, Ubaidur Rob 1, Md. Noorunnabi Talukder 1, Farhana Akter 1 1 Population Council, Bangladesh
Improving Access to and Quality of Essential Obstetric and Newborn Care in the Lowest Coverage Districts of Cotopaxi Province, Ecuador
 URC Improving Access to and Quality of Essential Obstetric and Newborn Care in the Lowest Coverage Districts of Cotopaxi Province, Ecuador Dr. Jorge Hermida Regional Director, LAC Programs University Research
URC Improving Access to and Quality of Essential Obstetric and Newborn Care in the Lowest Coverage Districts of Cotopaxi Province, Ecuador Dr. Jorge Hermida Regional Director, LAC Programs University Research
FANTA III. Improving Pre-Service Nutrition Education and Training of Frontline Health Care Providers TECHNICAL BRIEF
 TECHNICAL BRIEF Food and Nutrition Technical Assistance III Project June 2018 Improving Pre-Service Nutrition Education and Training of Frontline Health Care Providers Introduction The purpose of this
TECHNICAL BRIEF Food and Nutrition Technical Assistance III Project June 2018 Improving Pre-Service Nutrition Education and Training of Frontline Health Care Providers Introduction The purpose of this
Quality of Medicines for Non-Communicable Diseases (NCD): opportunities to improve the evidence
: opportunities to improve the evidence") Quality of Medicines for Non-Communicable Diseases (NCD): opportunities to improve the evidence Veronika J. Wirtz & Richard Laing Quality of Medical Products and Public Health Boston July 14 2017 Contents
Quality of Medicines for Non-Communicable Diseases (NCD): opportunities to improve the evidence Veronika J. Wirtz & Richard Laing Quality of Medical Products and Public Health Boston July 14 2017 Contents
Setting Up a Self-Sustaining Quality Improvement Network in India
 CASE STUDY Setting Up a Self-Sustaining Quality Improvement Network in India Summary In May 206, Kalawati Saran Children s Hospital (KSCH) began using QI approaches to improve maternal and newborn care
CASE STUDY Setting Up a Self-Sustaining Quality Improvement Network in India Summary In May 206, Kalawati Saran Children s Hospital (KSCH) began using QI approaches to improve maternal and newborn care
James Meloche, Executive Director. Healthy Human Development Table Meeting January 14, 2015
 James Meloche, Executive Director Healthy Human Development Table Meeting January 14, 2015 2 1. Introduction to PCMCH 2. Overview of Perinatal Mental Health 3. Perinatal Mental Health Initiatives at PCMCH
James Meloche, Executive Director Healthy Human Development Table Meeting January 14, 2015 2 1. Introduction to PCMCH 2. Overview of Perinatal Mental Health 3. Perinatal Mental Health Initiatives at PCMCH
Tanzania Country Summary, March 2017
 Tanzania Country Summary, March 2017 Charles Wanga/ MCSP Tanzania Tanzania Selected Demographic and Health Indicators Indicator Data Indicator Data Indicator Data Population (3) 44,928,923 Live births/year
Tanzania Country Summary, March 2017 Charles Wanga/ MCSP Tanzania Tanzania Selected Demographic and Health Indicators Indicator Data Indicator Data Indicator Data Population (3) 44,928,923 Live births/year
Maternal and neonatal health skills of nurses working in primary health care centre of Eastern Nepal
 Original Article Chaudhary et.al. working in primary health care centre of Eastern Nepal RN Chaudhary, BK Karn Department of Child Health Nursing, College of Nursing B.P. Koirala Institute of Health Sciences
Original Article Chaudhary et.al. working in primary health care centre of Eastern Nepal RN Chaudhary, BK Karn Department of Child Health Nursing, College of Nursing B.P. Koirala Institute of Health Sciences
TECHNICAL ASSISTANCE GUIDE
 TECHNICAL ASSISTANCE GUIDE COE DEVELOPED CSBG ORGANIZATIONAL STANDARDS Category 3 Community Assessment Community Action Partnership 1140 Connecticut Avenue, NW, Suite 1210 Washington, DC 20036 202.265.7546
TECHNICAL ASSISTANCE GUIDE COE DEVELOPED CSBG ORGANIZATIONAL STANDARDS Category 3 Community Assessment Community Action Partnership 1140 Connecticut Avenue, NW, Suite 1210 Washington, DC 20036 202.265.7546
IMCI and Health Systems Strengthening
 Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI and Health Systems Strengthening 7 IMCI and Health Systems Strengthening What components of the health
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI and Health Systems Strengthening 7 IMCI and Health Systems Strengthening What components of the health
Pfizer Foundation Global Health Innovation Grants Program: How flexible funding can drive social enterprise and improved health outcomes
 INNOVATIONS IN HEALTHCARE Pfizer Foundation Global Health Innovation Grants Program: How flexible funding can drive social enterprise and improved health outcomes ERIN ESCOBAR, ANNA DE LA CRUZ, AND ANDREA
INNOVATIONS IN HEALTHCARE Pfizer Foundation Global Health Innovation Grants Program: How flexible funding can drive social enterprise and improved health outcomes ERIN ESCOBAR, ANNA DE LA CRUZ, AND ANDREA
Virtual Meeting Track 2: Setting the Patient Population Maternity Multi-Stakeholder Action Collaborative. May 4, :00-2:00pm ET
 Virtual Meeting Track 2: Setting the Patient Population Maternity Multi-Stakeholder Action Collaborative May 4, 2017 1:00-2:00pm ET Highlights and Key Takeaways MAC members participated in the virtual
Virtual Meeting Track 2: Setting the Patient Population Maternity Multi-Stakeholder Action Collaborative May 4, 2017 1:00-2:00pm ET Highlights and Key Takeaways MAC members participated in the virtual
The Bihar, India Experience
 The Bihar, India Experience A CARE India - PRONTO International partnership Mobile Nurse Mentoring Programme Date: 16- th part September, of the Bihar 2015 Technical Support Programme Supported by the
The Bihar, India Experience A CARE India - PRONTO International partnership Mobile Nurse Mentoring Programme Date: 16- th part September, of the Bihar 2015 Technical Support Programme Supported by the
Community-Based Intervention to Reduce Neonatal Mortality in Bangladesh. Projahnmo - I Project for Advancing the Health of Newborns and Mothers
 Community-Based Intervention to Reduce Neonatal Mortality in Bangladesh Projahnmo - I Project for Advancing the Health of Newborns and Mothers Sylhet District, Bangladesh Final Report January 17, 2007
Community-Based Intervention to Reduce Neonatal Mortality in Bangladesh Projahnmo - I Project for Advancing the Health of Newborns and Mothers Sylhet District, Bangladesh Final Report January 17, 2007
INTRODUCTION. 76 MCHIP End-of-Project Report. (accessed May 8, 2014).
.") Redacted INTRODUCTION Between 1990 and 2012, India s mortality rate in children less than five years of age declined by more than half (from 126 to 56/1,000 live births). The infant mortality rate also
Redacted INTRODUCTION Between 1990 and 2012, India s mortality rate in children less than five years of age declined by more than half (from 126 to 56/1,000 live births). The infant mortality rate also
4/27/2011. Kim Wilson, MD MPH Boston Children s Hospital
 Providing Care to Dominican Transnational Families Is Global Health Linked to Local Public Health? Kim Wilson, MD MPH Boston Children s Hospital Overview Providing care to Dominican transnational families
Providing Care to Dominican Transnational Families Is Global Health Linked to Local Public Health? Kim Wilson, MD MPH Boston Children s Hospital Overview Providing care to Dominican transnational families
The World Breastfeeding Trends Initiative (WBTi)
") The World Breastfeeding Trends Initiative (WBTi) Name of the Country: Swaziland Year: 2009 MINISTRY OF HEALTH KINGDOM OF SWAZILAND 1 Acronyms AIDS ART CBO DHS EGPAF FBO MICS NGO AFASS ANC CHS CSO EPI HIV
The World Breastfeeding Trends Initiative (WBTi) Name of the Country: Swaziland Year: 2009 MINISTRY OF HEALTH KINGDOM OF SWAZILAND 1 Acronyms AIDS ART CBO DHS EGPAF FBO MICS NGO AFASS ANC CHS CSO EPI HIV
Information for Midwives in relation to the Midwifery Scope of Practice Further interpretation, March 2005
 Information for Midwives in relation to the Midwifery Scope of Practice Further interpretation, March 2005 March 2005 Although the Midwifery Council provided information in October 2004 about midwives
Information for Midwives in relation to the Midwifery Scope of Practice Further interpretation, March 2005 March 2005 Although the Midwifery Council provided information in October 2004 about midwives
Contents: Introduction -- Planning Implementation -- Managing Implementation -- Workbook -- Facilitator Guide.
 WHO Library Cataloguing-in-Publication Data Managing Programmes to Improve Child Health Contents: Introduction -- Planning Implementation -- Managing Implementation -- Workbook -- Facilitator Guide. Child
WHO Library Cataloguing-in-Publication Data Managing Programmes to Improve Child Health Contents: Introduction -- Planning Implementation -- Managing Implementation -- Workbook -- Facilitator Guide. Child
WHO STANDARDS OF CARE TO IMPROVE MATERNAL AND NEWBORN QUALITY OF CARE IN FACILITIES
 Quality, Equity, Dignity A Network for Improving Quality of Care for Maternal, Newborn and Child Health WHO STANDARDS OF CARE TO IMPROVE MATERNAL AND NEWBORN QUALITY OF CARE IN FACILITIES Background The
Quality, Equity, Dignity A Network for Improving Quality of Care for Maternal, Newborn and Child Health WHO STANDARDS OF CARE TO IMPROVE MATERNAL AND NEWBORN QUALITY OF CARE IN FACILITIES Background The