Connecticut interchange MMIS
|
|
|
- Roger Ferguson
- 5 years ago
- Views:
Transcription
 55 Farmington Avenue Hartford, CT 06105 HP Enterprise Services 195 Scott Swamp Road Farmington, CT")
1 Connecticut interchange MMIS Provider Manual Chapter 8 Hospital Claim Submission Instructions Connecticut Department of Social Services (DSS) 55 Farmington Avenue Hartford, CT HP Enterprise Services 195 Scott Swamp Road Farmington, CT 06032
2 Amendment History Version Version Date Reason for Revision Section Page(s) /01/2008 Initial Release. All All /17/2008 Updates made to reflect NDC requirements; added CT BHP claim submission address; incorporated changes as a result of the Charter Oak Health Plan Program, clarified Medicare billing instructions , , 19-21, 23, 25-30, /30/2008 Updates made to billing instructions for field /10/2008 Updates made to billing instructions for field 50, Figure 1 replaced so that it is more easily viewable , /23/2009 Added patient status code 70 to field /05/2009 Added Hospice claim submission information, updated other insurance/medicare billing requirements , 26 28, 30 32, /26/2009 Updated Hospice effective date /05/2010 Updated all EDS references to HP, added present on admission and birth weight information /16/2010 Updated billing instructions for fields 4 and 67A Q with erroneous surgery information , , /22/2010 Updated to reflect discontinuation of SAGA program and the implementation of the Medicaid Low Income Adults program; replaced references to OI/Medicare Billing Guide links with Chapter , 21, 27, II
3 29-31, /11/2011 Updated as a result of PPACA Hospice clarifications for children under the age of /20/2011 Updated as a result of the Behavioral Health Expansion Project /21/2011 Removed present on admission indicator value of 1, removed references to SAGA program, updated mailing address /05/2012 Updates made as a result of TB Waiver and ASO transition, as well as new radiology requirements , , , 19-20, All /12/2012 Added link to RCC Request Form in field 42, added modifier billing instructions to field 44, added billing instructions for Birth Centers , 20, /26/2012 Revised address for the submission of out-ofstate claims /19/2013 Revised claim billing instructions /02/2013 Added OPR edits , , /30/2013 Updates made to reflect the shutdown of the Charter Oak Health Plan Program , & 21 III
4 2.9 01/27/ /19/ /05/2014 Eliminated the language that indicates the providers must contact CHN if the admission is to a medical bed with a Primary Diagnosis of 291.0, Outpatient RCC Requiring CPT or HCPCS Code as of May 1, 2014 and Attachment B All Revenue Center Codes Requiring CPT/HCPCS Codes. Updated billing instructions to indicate ICD-10 diagnosis and surgical codes effective 10/1/2014. Updated billing instructions to indicate procedure code and date not required for outpatient claims. Updates also made to Attachment B. Updated to reflect delay in ICD-10 implementation , 28, 29, , 33, 34, 35, & IV
5 Table of Contents 8.1 Overview Prior Authorization Forms EPSDT Information Behavioral Health Claims Claim Submission Instructions for the UB-04 Claim Form V
6 8.1 Overview 1
7 Chapter 8 contains the claim submission information and procedures for inpatient, outpatient, and laboratory services provided by acute care and psychiatric hospitals, as well as information and procedures for birth centers. It also includes claim submission instructions (paper claims only) for acute care and psychiatric hospitals participating in the Connecticut Medical Assistance Program. For timely filing guidelines, providers should refer to Chapter 5, Section 6, Claim Submission Information. Hospital dental clinics should refer to the provider specific claim submission instructions in Chapter 8, Dental Services Claim Submission Instructions. Providers interested in electronic claim submission should refer to Chapter 6, Electronic Data Interchange Options. Providers interested in submitting claims through the internet should refer to Chapter 10 for internet claim submission instructions. Claim Submission Help Text for the internet claim submission feature is also located on the claim submission panel by clicking on the Quick Links in the upper left corner of the Web page, and/or by clicking on HELP in the upper right corner of the Web page. However, the information in Chapter 8 is important for all hospital providers. The Department of Social Services (DSS) and CHNCT have prepared benefit coverage grids that outline covered services for clients in the HUSKY Health Program and Charter Oak*. Benefit information is broken down by provider type and benefit plan. The contents provide a general summary of HUSKY Health and Charter Oak* benefits. Providers can access the benefit coverage grids from the Providers page of the CHNCT website under Benefits and Authorization. The link to the benefit coverage grids is listed below. Please Note: The benefit plan coverage grids provide a high level summary of covered services and exceptions. For more detailed information on coverage policy, providers should refer to the policy chapter, Chapter 7, of their Provider Manual. Providers should review these grids to determine the services covered for a client s benefit plan. The benefit coverage grids will be updated periodically. * Please note that the Charter Oak Health Plan Program was terminated as of January 1, Providers may continue to submit claims for Charter Oak Health Plan Program clients with dates of service prior to January 1, 2014, following timely filing guidelines. Connecticut Behavioral Health Partnership The Connecticut Behavioral Health Partnership (CT BHP), a joint initiative between the Department of Social Services, the Department of Children and Families (DCF), and the Department of Mental Health and Addiction Services (DMHAS), provides utilization management of behavioral health services for HUSKY A, HUSKY B, HUSKY C previously referred to as Medicaid, HUSKY D previously referred to as Medicaid LIA, Charter Oak health plan (for dates of service prior to January 1, 2014), and DCF funded clients. Providers must submit behavioral health claims for services covered by these programs directly to HP for processing. Hospice A Hospice benefit is available for all HUSKY C clients. Any outpatient hospital service related to the client s terminal illness is the responsibility of the hospice. Outpatient claims unrelated to the terminal illness must be billed with a specific condition code to indicate that the service is not related to the hospice patient s terminal illness, as referenced in Section 8.6, Claim Submission Instructions for the UB- 04 Claim Form. Effective March 23, 2010, the Patient Protection and Affordable Care Act (PPACA) amended the definition of hospice and provides that election of hospice by a child under the age of 21 shall not constitute a waiver of payment for treatment of the condition for which the terminal diagnosis has been made. This same change was made to the Children s Health Insurance Program and allows children to receive hospice services concurrently with treatment of the child s condition. Note that these changes 2
8 apply only to children defined as those under the age of 21 for HUSKY A, HUSKY C, and HUSKY D clients, and under the age of 19 for HUSKY B clients. Although outpatient claims for Hospice clients must use the condition code 07 - Treatment of Nonterminal Condition for Hospice to indicate that the hospitalization is not related to the client s terminal illness, this condition code is not required for children under the age of 21 for HUSKY A, HUSKY C, and HUSKY D clients, and under the age of 19 for HUSKY B clients. For specific information about the Hospice benefit, providers can access the Chapter 8 Hospice Services Manual located at by selecting Information, Publications and Hospice from the Chapter 8 drop down box. For information on obtaining Hospice client eligibility information, refer to Chapter 4, also located at by selecting Information, Publications. Providers should review the client s eligibility information to determine under which Hospice Agency care is being provided. Tuberculosis (TB) Covered Services Current HUSKY Health Plan clients and those with a Tuberculosis Covered Services Only benefit are eligible for TB-related services only. Outpatient hospitals may bill for procedures on their individual fee schedules that are related to a TB diagnosis. The Department has identified the following ICD-9 diagnoses as TB related: , , , 771.2, and NOTE: For additional information, hospital providers can refer to the Connecticut Uniform Billing Committee (CUBC) Manual. 3
9 8.2 Prior Authorization 4
10 Prior authorization (PA) is required for most acute, psychiatric, out-patient behavioral health procedures. Information concerning which behavioral health services require authorization and the processes for obtaining authorizations can be found on the CT BHP website at or by contacting the CT BHP by telephone at For hospice clients, if the hospice agency believes the hospitalization is unrelated to the terminal illness, PA may be requested. Please follow the normal PA process to request an authorization when necessary. The Department approves only those requests that are clearly not related to the client s terminal condition. The HUSKY Health Program and Charter Oak Health Plan s* radiology management program includes the requirement of authorization for advanced imaging CT, CTA, MRI, MRA, PET, PET/CT and nuclear cardiology studies. For dates of service June 1, 2012 and forward, non-emergent advanced imaging and nuclear cardiology services require prior authorization when performed in an outpatient setting. Please refer to Section 8.6 for revenue center codes (RCCs) and corresponding CPT codes. * Please note that the Charter Oak Health Plan Program was terminated as of January 1, Providers may continue to submit prior authorization requests for Charter Oak Health Plan Program clients for dates of service prior to January 1, Please refer to Chapter 9 of the Provider Manual for full Prior Authorization requirements, contact information and related forms. 5
11 8.3 Forms 6
12 Forms used by the hospital provider community can be found in Chapter 5, Claim Submission Information. 7
13 8.4 EPSDT Information 8
14 Information regarding the State of Connecticut s Federal Early and Periodic Screening, Diagnosis and Treatment (EPSDT) program is located in Chapter 5, Claim Submission Information. 9
15 8.5 Behavioral Health Claims 10
16 Overview The following section provides information on behavioral health claim submission. Refer to Chapter 5, Claim Submission Information, Section 8, for additional information regarding behavioral health services claim submission. Connecticut Behavioral Behavioral health claims for HUSKY A, HUSKY B, HUSKY C, Health Partnership (CT BHP) HUSKY D, Charter Oak (for dates of service prior to January 1, 2014), and DCF funded clients are sent to HP at the following address: HP P.O. Box 2961 Hartford, CT CT BHP claims with attachments to support requests for timely filing overrides including other insurance are sent to HP at the following address: HP P.O. Box 2971 Hartford, CT Pediatric Inpatient Admissions When the hospital has an inpatient claim with both acute care days that Contain Medically and discharge delay days, the hospital will need to submit two claims Necessary Discharge Delay to HP. One claim should be billed for the acute care days as a Type of Days Bill (TOB) 112 with a patient status 30. The second claim for the discharge delay days (RCC 224) should be billed as a TOB 114 with patient status 01. Intermediate Duration Acute Psychiatric Care Hospital Claims Hospitals enrolled as an Intermediate Duration Acute Psychiatric Care Hospital (IDAPC) are required to request PA through CT BHP and must submit claims using Revenue Center Code 124 and taxonomy 283Q00000X. 11
17 8.6 Claim Submission Instructions for the UB-04 Claim Form 12
18 Instructions for Completion of UB-04 Required Fields for Claim Submission This section includes complete claim submission instructions for the UB-04 claim form for HUSKY C/HUSKY D Inpatient (IP), HUSKY C/ HUSKY D Outpatient (OP), Connecticut Behavioral Health Partnership (CT BHP) services, and the Charter Oak Heath Plan Program (for dates of service prior to January 1, 2014). Black ink only should be used when completing the claim form. Do not use highlighter on claims or attachments. Hospitals interested in electronic claim submission should refer to Chapter 6, Electronic Data Interchange Options or Chapter 10 for Internet Claim Submission instructions. Some of the required fields on the UB-04 claim form vary based on the type of claim being submitted, for example, inpatient versus outpatient. For ease of understanding the following instructions, the required fields are designated with codes. The codes indicate whether the field is required for specific program claim submission. The codes are described below: IP refers to those fields required for inpatient claims submitted to HP. OP refers to those fields required for outpatient claims submitted to HP. A copy of the UB-04 claim form and instructions follows this section. How to Obtain the Claim Form Providers must submit paper claims using original red UB-04 claim forms, as these claims will be electronically scanned. Providers may obtain UB-04 forms through private printing vendors. Where to Send the Completed Claim Form Border Hospital Mail the completed UB-04 claim forms to the following address: HP P.O. Box 2961 Hartford, CT A border hospital is an out-of-state hospital which has a common medical delivery area with the State of Connecticut, provides services to Connecticut Department of Social Services clients, and is deemed a border hospital by the Connecticut Department of Claims submitted by border hospitals must follow the same UB-04 claim submission guidelines as established by the Connecticut Medical Assistance Program for in-state hospitals. Border hospitals will submit claims using three (3) digit standard Revenue Center Codes for appropriate accommodation and ancillary services provided. 13
19 Border hospitals should mail completed UB-04 claim forms to the following address: HP P.O. Box 2961 Hartford CT Out-of-State Inpatient Hospitals Claims submitted by hospitals located outside of the State of Connecticut for services provided to Connecticut Department of Social Services clients must follow the same UB-04 claim submission guidelines as established by the Connecticut Medical Assistance Program for in-state hospitals. All out-of-state, non-emergency hospital services require prior authorization. Refer to Chapter 9 of this manual for prior authorization guidelines and requirements. Out-of-state providers should mail completed UB-04 claim forms to the following address: HP Written Correspondence P.O. Box 2991 Hartford CT Birth Centers Hospitals enrolled as a Birth Center are required to submit claims using Revenue Center Code (RCC) 724 (birthing center) when the labor and delivery are completed at the birth center or RCC 729 (other labor room/delivery) when a woman begins labor at the birth center but is transferred to a hospital for delivery or post-delivery care. The claim type is inpatient and the Type of bill is 841. Inpatient hospitals that bill for Revenue Center Code (RCC) 724 or 729 as ancillary codes for inpatient claims will be required to bill these services under RCC 720. National Drug Codes (NDCs) for Outpatient Hospital Claims The Connecticut Medical Assistance Program requires the submission of the National Drug Code (NDC) qualifier, the NDC, NDC units of measure, and NDC quantity on all claims with procedure codes for physician administered drugs. This is to support the Federal Deficit Reduction Act of 2005, which mandates the submission of NDCs. The purpose of this requirement is to assure that the State Medicaid Agencies obtain a rebate from those manufacturers who have signed a rebate agreement with the Centers for Medicare and Medicaid Services (CMS). Claims for services provided to HUSKY D clients are included in this requirement. This mandate affects all providers who submit electronically or by paper for procedure-coded drugs, with the exception of those providers identified as 340B providers by the Office of Pharmacy Affairs (OPA). A 14
20 list of 340B providers is located at by clicking on the covered entity tab. Hospital providers can find more information about becoming a 340B provider in provider bulletin PB-41, located at under Information/Publications. Because the State may pay up to the 20% Medicare B co-payment for dual eligible individuals, the NDC qualifier, NDC, NDC units of measure, and NDC quantity will also be required on Medicare crossover claims for all applicable procedure codes. Outpatient and Outpatient Medicare crossover claims for Revenue Center Codes (RCC) , 258, 259, will require a Healthcare Common Procedure Coding (HCPC) code and the corresponding NDC information. The RCC listed above are billable as outpatient services if the RCC is specified on your Connecticut Medical Assistance Program provider contract letter. NDC Requirements for Claims Processing Claims that do not comply with the mandate will be denied. Claims will be denied if the NDC is missing, invalid, terminated, not rebateable, DESI, institutional, repackage, inner package, or the NDC qualifier is missing or invalid. A list of DESI drugs is maintained at by selecting Pharmacy Information, then Pharmacy Program Publications, and locating the DESI List. Claims for services provided to HUSKY D clients are included in this requirement. Participating labelers Connecticut Medicaid, by statute, will only pay for a drug procedure billed with an NDC when the pharmaceutical manufacturer of that drug is a participating labeler with the Centers for Medicare and Medicaid Services (CMS). Claims for services provided to HUSKY D clients are included in this requirement. A participating labeler is a pharmaceutical manufacturer that has entered into a federal rebate agreement with CMS to provide each State a rebate for products reimbursed by Medicaid Programs. A labeler is identified by the first 5 digits of the NDC. To assure a product is payable for administration to a Medicaid beneficiary, compare the labeler code (the first 5 digits of the NDC) to the list of participating labelers which is maintained on the Connecticut Medical Assistance Program Web site at Providers may access this list by clicking on the Pharmacy Information page, then on the client s benefit plan under the Drug Manufacturer Rebate Lists posted in the Pharmacy Program Publications panel. Providers can determine whether an NDC is rebateable or not by utilizing the Drug Search functionality under Provider from the Web site. NDC Formatting When completing a claim for administering a drug, providers must submit the HIPAA standard 11-digit NDC without dashes or spaces. The 11-15

21 digit NDC is comprised of three segments or codes: a 5-digit labeler code, a 4-digit product code and a 2-digit package code. If the NDC does not contain 11 digits, it must be changed to comply with the HIPAA format. The 10-digit NDC assigned by the FDA printed on the drug package must be changed to the 11-digit format by inserting a leading zero in one of the three segments. Below is an example of a FDA assigned NDC on a package and how it should be changed to the appropriate 11-digit HIPAA standard format. Example 1 displays a 10-digit NDC with a labeler code as five digits; the product code as three digits and the package code as two digits. Since the NDC on the label is not configured in the format, a zero should be placed at the beginning of the second segment of the NDC. Therefore the correct configuration is This change is also reflected in the first row of Table 1. Example 1: Table 1 NDC Configuration NDC From Label HIPAA Format NOTE: Because the vial from which the drug is administered is frequently not in the accepted 11-digit format, please refer to Table 1 above for examples on how to format and bill the NDC correctly. NDCs billed to the Connecticut Medical Assistance Program for payment must use the 11-digit format without dashes or spaces between the numbers. NDCs submitted in any configuration other than the 11-digit format will be denied. 16
22 Radiology Services Corresponding CPT codes For hospitals billing in an institutional claim format, revenue center codes 35X, 404, 61X and 34X must be billed with the following corresponding CPT codes grid. RCC 34X can be billed with a different CPT code then what is on the grid but it still must be a valid CPT code. Computed Tomography (CT) - Computed Tomographic Angiography (CTA) Revenue Code Series: 35X Magnetic Resonance Imaging (MRI) Magnetic Resonance Angiography (MRA) Revenue Code Series: 61X Positron Emission Tomography (PET) Revenue Code:
23 Nuclear Cardiology Revenue Code Series: 34X
24 19
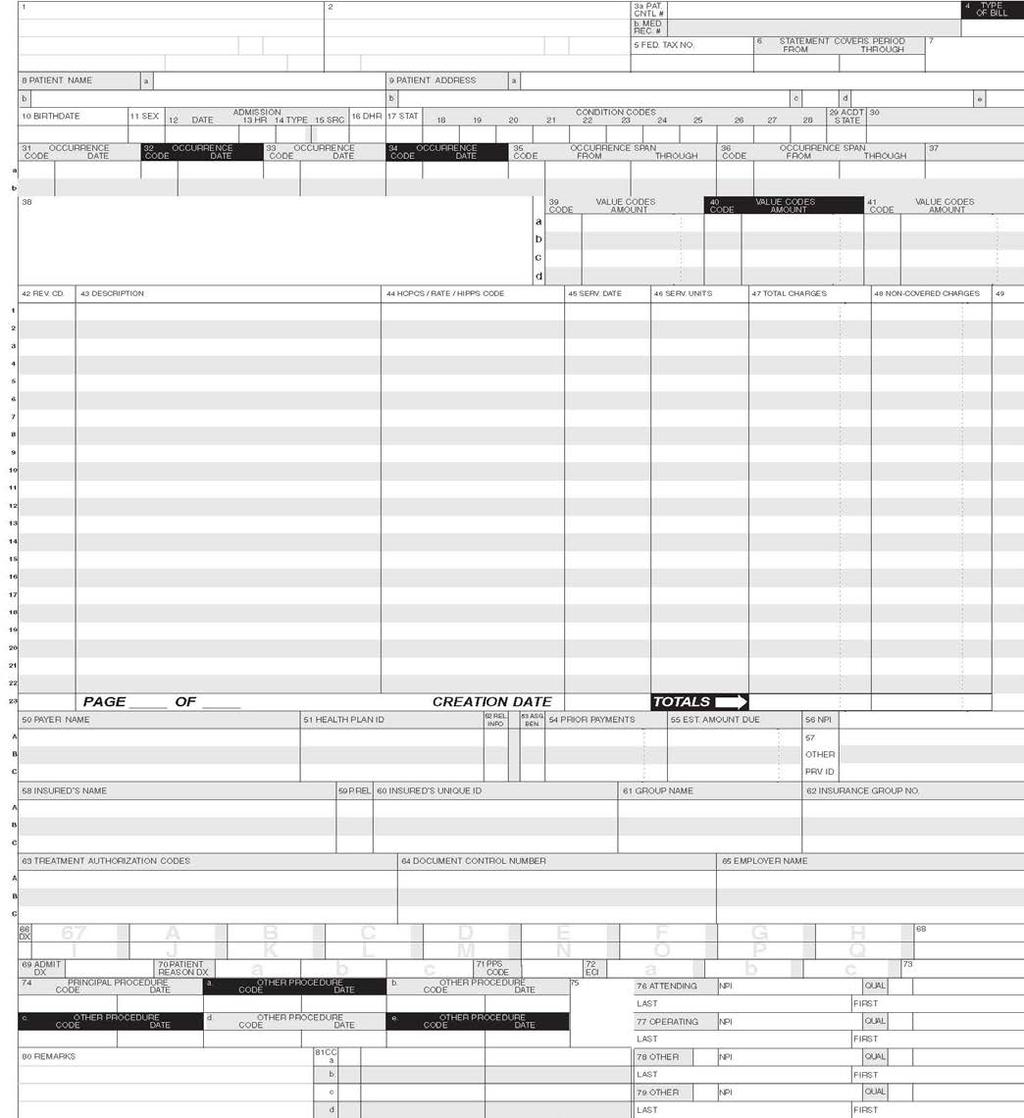
25 How to Fill Out the UB-04 Form Paper Claim Field No. and Name 1. UNLABELED FIELD 2. UNLABELED FIELD 3a. PATIENT CONTROL NO. (IP, OP) Enter the provider s name, address and zip + 4. This address must be the address provided upon enrollment in the Medical Assistance Program. Enter the patient s account number. Providers have the option of submitting up to 12 alphanumeric characters for their own accounting purposes. 3b. MEDICAL RECORD NO. 4. TYPE OF BILL (IP, OP) Enter the 3 or 4-digit code that identifies the type of bill. The code identifies the type of facility and the bill classification. First digit indicates claim classification Code 1 Hospital 8 Special facility (Birth Centers) Second digit indicates claim classification Code 1 Inpatient (including Medicare Part A) 2 Inpatient (Medicare Part B only) 3 Outpatient 4 Outpatient (non-patient Clinical Laboratory only) Third digit indicates frequency Code 0 No-pay claim 1 Admit through discharge date (one claim covers entire stay) 2 Interim first claim 3 Interim continuing claim 4 Interim last claim 7 Replacement 8 Void NOTE: The third digit of 7 or 8 can only be used for electronic claims submitted through Provider Electronic Solutions or vendor software. These are not valid values for paper claims and should not be used. 5. FEDERAL TAX ID NUMBER 20
26 Paper Claim Field No. and Name 6. STATEMENT COVERS PERIOD FROM/THROUGH (IP, OP) Enter the beginning and ending dates of service for the period covered on the claim in MM/DD/YY format for paper claims. Include the discharge date or date of death, if applicable. For an inpatient admission, all UB-04 claim form required fields must be completed. Inpatient Admit Change from Medical to Psychiatric Inpatient Admit Change from Psychiatric to Medical If the HUSKY or Charter Oak client is admitted with a primary medical diagnosis and then is subsequently admitted to a psychiatric unit, the initial authorization from CHN CT will cover the entire inpatient admission. If the Hospital splits the claim for processing, the admit date on both claims must reflect the first date of the inpatient admission. If the HUSKY or Charter Oak client is admitted with a primary behavioral health diagnosis and then is subsequently admitted to a medical unit, the provider will need to contact CT BHP to handle the authorization for the entire stay and claims are to be submitted to HP for processing. 7. UNLABELED FIELD 8a. PATIENT NAME - ID 8b. PATIENT NAME The client s Medicaid ID is required in field 60. Enter the client s name (last name, first name, middle initial) 9a- 9e. (IP, OP) PATIENT ADDRESS NOTE: The client s name should be spelled as it is in the Automated Eligibility Verification System or as indicated on the client s Connect card. 10. BIRTHDATE 11. SEX 12. ADMISSION DATE (IP) Enter the admission date in MM/DD/YY format associated with the period being submitted. This date cannot be greater than the from date in Field ADMISSION HOUR (IP) Enter the hour that the client entered the facility. Use the corresponding 2-digit codes below: Code Time a.m :00-12:59 (Midnight) 21
27 Paper Claim Field No. and Name 01 01:00-01: :00-02: :00-03: :00-04: :00-05: :00-06: :00-07: :00-08: :00-09: :00-10: :00-11: ADMISSION TYPE (IP) Code Time p.m :00-12:59 (Noon) 13 01:00-01: :00-02: :00-03: :00-04: :00-05: :00-06: :00-07: :00-08: :00-09: :00-10: :00-11:59 Enter the corresponding code from the primary admission reason list below: Code 1 Emergency 2 Urgent 3 Elective 4 Newborn 5 Trauma 15. ADMISSION SOURCE (IP, OP) Enter the corresponding source of admission code from the list below: Code 1 Non-health Care Facility Point of Origin 2 Clinic or Physician s Office 4 Transfer from a Hospital (different facility) 5 Transfer from a SNF, ICF, or ALF 6 Transfer from Another Health Care Facility 8 Court/Law Enforcement 9 Information Not Available B Transfer from Another Home Health Agency D Transfer from One Distinct Unit of the Hospital to another Distinct Unit of the Same Hospital Resulting in 22
28 Paper Claim Field No. and Name E F a Separate Claim to the Payer Transfer from Ambulatory Surgery Center Transfer from a Hospice Facility When the Admission Type in field 14 is 4, enter the appropriate Admission Source from the list below: Code 5 Born Inside this Hospital 6 Born Outside of this Hospital 16. DISCHARGE HOUR (IP) 17. DISCHARGE STATUS (IP) Indicate the hour that the client was discharged from the facility. Use the 2-digit codes listed below. Code Time a.m :00-12:59 (Midnight) 01 01:00-01: :00-02: :00-03: :00-04: :00-05: :00-06: :00-07: :00-08: :00-09: :00-10: :00-11:59 Code Time p.m :00-12:59 (Noon) 13 01:00-01: :00-02: :00-03: :00-04: :00-05: :00-06: :00-07: :00-08: :00-09: :00-10: :00-11:59 Enter the code indicating the patient s status at the time of discharge, as of the Through Date in Field 6; choose from table below: Code 01 Discharged to home or self care (routine discharge) 23
29 Paper Claim Field No. and Name 02 Discharged/transferred to a short term, general hospital for inpatient care 03 Discharged/transferred to a skilled nursing facility (SNF) with Medicare Certification in anticipation of covered skilled care 04 Discharged/transferred to an intermediate care facility (ICF) 05 Discharged/transferred to another type of institution not defined elsewhere in this code list 06 Discharged/transferred to home under care of an organized home health service organization in anticipation of covered skilled care 07 Left against medical advice or discontinued care DISCHARGE STATUS (IP) (cont) CONDITION CODES (IP, OP) Code 08 Discharged/transferred to home under care of home IV provider 09 Admitted as an inpatient to this hospital 20 Expired 30 Still a patient 40 Expired at home 41 Expired in a medical facility (e.g. hospital, ICF, SNF, or free standing hospice) 42 Expired place unknown 43 Discharged/transferred to a federal health care facility 50 Hospice home 51 Hospice medical facility 61 Discharged/transferred to hospital-based Medicare approved swing bed 62 Discharged/transferred to an inpatient rehabilitation facility (IRF) including rehabilitation distinct part units of a hospital 63 Discharged/transferred to a Medicare certified long term care hospital (LTCH) 64 Discharged/transferred to a nursing facility certified under Medicaid but not certified under Medicare 65 Discharged/transferred to a psychiatric hospital or psychiatric distinct part unit of a hospital 66 Discharged/transferred to a Critical Access Hospital (CAH) 70 Discharges or transfers to other types of health care institutions not defined Enter the appropriate condition codes to identify conditions that determine eligibility for EPSDT Related services and establish primary and/or secondary responsibility. Up to eleven (11) may be submitted on a paper claim. The following codes are the subset used for the Connecticut Medical Assistance Program: EPSDT RELATED SERVICES: For EPSDT, always enter condition code A1 in this field. 24
30 Paper Claim Field No. and Name Code A1 A4 G0 ESPDT Family planning related Distinct medical visit 01 Military service related 02 Employment related 03 Covered by insurance not reflected here 05 Lien has been filed NOTE: The condition codes listed below should only be used if an abortion was performed due to rape, incest, or life endangerment. CONDITION CODES (IP, OP) (cont) Code AA AB AD A7 A8 Abortion performed due to rape Abortion performed due to incest Abortion performed due to a life endangering physical condition caused by or arising from pregnancy itself Induced abortion endangerment to life Induced abortion victim of rape/incest HOSPICE: Outpatient claims for Hospice clients must use the condition code below to indicate that the hospitalization is not related to the client s terminal illness. This condition code is not required for children under the age of 21 for fee for service and HUSKY A clients, and under the age of 19 for HUSKY B clients. Code 07 Treatment of Non-terminal Condition for Hospice 29. ACCIDENT STATE 30. UNLABELED FIELD OCCURRENCE CODE/DATE (IP, OP) Enter the applicable code and date, in MM/DD/YY format for paper claims that define a significant event relating to this stay. The following codes are the subset used for the Connecticut Medical Assistance Program: Code 01 Accident/Medical Coverage 02 No fault insurance 03 Accident/tort liability 04 Accident/employment-related 05 Accident/No Medical or Liability Coverage 06 Crime victim 11 Onset of symptoms/illness 21 UR notice received 24 Date Insurance Denied 25
31 Paper Claim Field No. and Name OCCURRENCE SPAN CODE/FROM/ THROUGH (IP, OP) 37. UNLABELED FIELD 38. UNLABELED FIELD 39a. - 41d. VALUE CODES CODE/AMOUNT (IP, OP) Enter the occurrence span code and date in MM/DD/YY, if applicable. Responsible Party Name and Address. Enter the appropriate value code and then dollar amount(s) for Medicare coinsurance and deductible only. The value codes should be selected from the list below and be consistent with the Medicare indicator on Line A, B or C in Field 50 (Payer Name). MEDICARE PART A DEDUCTIBLE, PART B CO-INSURANCE AND OUTPATIENT CO-INSURANCE MEDICARE HMO: If the client has Medicare coverage, the provider must bill Medicare first. If a deductible or co-insurance amount is due after Medicare payments have been issued to the provider, indicate the value code in Box 39 followed by the amount of Medicare deductible or co-insurance. This amount should be the amount that is indicated on the provider s Explanation of Medicare Benefits (EOMB). Medicare payments should not appear on the claim. The provider must submit a duplicate of the claim processed for Medicare payment, indicating the client s nine (9) digit Connecticut Medical Assistance Program ID number in Field 60. Institutional Part A Deductible Code A1 B1 C1 Deductible payer A Deductible payer B Deductible payer C Institutional Part A Coinsurance Code A2 Coinsurance payer A B2 Coinsurance payer B C2 Coinsurance payer C 08 Medicare lifetime reserve coinsurance amount in first calendar year 09 Medicare coinsurance amount in first calendar year 10 Medicare lifetime reserve coinsurance amount in second calendar year 11 Medicare coinsurance amount in second calendar year Professional Part B Deductible 26
32 Paper Claim Field No. and Name Code A1 B1 C1 Deductible payer A Deductible payer B Deductible payer C Professional Part B Coinsurance Code A2 Coinsurance payer A B2 Coinsurance payer B C2 Coinsurance payer C VALUE CODES CODE/AMOUNT (IP, OP) (cont) Code A7 Co-Payment payer A B7 Co-Payment payer B Covered Days Code 80 Covered Days Newborn Birth Weight Code 54 Newborn Birth Weight in Grams 42. REVENUE CODE (IP, OP) For additional detailed information on other insurance and Medicare billing, providers should refer to Chapter 11 of the Provider Manual. This chapter is available at by selecting Information, then Publications, and scrolling down to Provider Manuals Chapter 11. From the drop down box, select the Institutional claim type. Enter the Revenue Center Code (RCC) applicable to the service rendered. To request that a RCC be added for use by your facility, please complete the Revenue Center Code (RCC) Request Form for Hospitals, W This form is available at by selecting Information, then Publications, and scrolling down to the Provider Enrollment/Maintenance Forms section. 43. DESCRIPTION For claims with dates of service on or after July 1, 2008 and procedure codes for physician administered drugs: 1. Enter the NDC Qualifier of N4 in the first 2 positions on the left side of the field. 2. Enter the NDC 11-digit numeric code in the format. Do not use hyphens. 3. Enter the NDC Units of Measurements Qualifier. F2 - International Unit GR - Gram ML - Milliliter UN - Unit 27
33 Paper Claim Field No. and Name 4. Enter the NDC Quantity (administered amount) with up to three decimal places such as The information in the Revenue field is entered without delimiters, such as commas or hyphens. Line 23 PAGE OF 44. HCPCS/RATE/ HIPPS CODE (OP) NOTE: When administering multiple NDCs within a single HCPC, each NDC must be identified at the time of billing. For additional information on billing multiple NDCs per RCC/HCPCs, refer to the section at the end of the Claim Submission Instructions. Enter page number and the total number of pages of the claim. Enter the procedure code applicable to the service rendered. OUTPATIENT LABORATORY: When submitting for outpatient laboratory services with revenue center codes (RCC) in Field 42, indicate the HealthCare Common Procedure Coding System (HCPCS) in Field 44. Effective November 1, 2013, RCCs will require the hospital to indicate the HCPCS code in Field 44. RADIOLOGY SERVICES: When submitting for outpatient radiology services with revenue center codes 34X, 35X, 404 and 61X in field 42, you are required to indicate the HealthCare Common Procedure Coding System (HCPCS) in Field 44. If the radiology service was approved with a modifier, you are required to enter that modifier after the HCPCS code. If submitting an NDC in field 43, enter the corresponding HCPCS associated with the NDC. For those drug products without an associated HCPC code, one of the following HCPC codes should be used: J3490 Unclassified Drugs, J3590 Unclassified Biologics, J8999 Prescription Drug, Oral, Chemotherapeutic, NOS or J9999 Not Otherwise Classified, Antineoplastic Drugs. Effective May 1, 2014, the Department will require that most outpatient RCCs be submitted with a CPT or HCPCS code. Please refer to Attachment B List of All Revenue Center Codes Requiring CPT/HCPCS Codes for the complete list of RCCs that require CPT/HCPCS. The following provides a quick link to that attachment in this chapter: Attachment B All Revenue Center Codes Requiring CPT/HCPCS Codes 45. SERVICE DATE (OP) Line 23 CREATION DATE 46. SERVICE UNITS (IP, OP) Enter the single date of service in MM/DD/YY format. NOTE: Only one (1) date is allowed per line item. Enter date claim was created. Enter the number of units of service provided. 28
34 Paper Claim Field No. and Name 47. TOTALCHARGES (IP, OP) Line 23 TOTALS 48. NON-COVERED CHARGES Line 23 TOTALS 49. UNLABELED FIELD If submitting an NDC in field 43, enter the number of HCPCS units provided. Enter the hospital s usual and customary charge for the corresponding services indicated in Field 42. Enter the sum of all detail charges at the bottom of the Total Charges column, designated for Total Charges. 29
35 Paper Claim Field No. and Name 50. PAYER NAME A,B, C (IP, OP) Enter the primary payer on line A and subsequent payer on lines B (secondary) and C (tertiary), as instructed below. Medicaid is always the payer of last resort. Medicare Insurance When Medicare is the primary payer and makes a payment, indicate the specific coverage (i.e., Medicare Part A (or MPA), Medicare Part B (or MPB), or Medicare HMO). If a denial is received from Medicare, indicate Medicare N/A, MPA N/A, MPB N/A, or Medicare HMO N/A, and the date of Medicare s denial. Refer to Chapter 5, Section 3, Instructions and Forms for Third Party Liability, for more information on third party billing requirements. The Explanation of Medicare Benefits (EOMB), indicating a denial from Medicare, should not be attached to the paper claim. The Explanation of Medicare Benefits (EOMB), indicating a payment from Medicare, is always required to be attached to the paper claim. The date of service, billed amount, and coinsurance/deductible amount must match between the EOMB and the claim. For coinsurance and/or deductible claims that are submitted on paper, providers must submit one paper claim attached to one EOMB. When submitting a paper coinsurance and/or deductible claim for Connecticut Medical Assistance Program payment, providers must submit the claim information on an original (red) paper claim form. Claims with multiple EOMBs attached to one claim or multiple claims attached to one EOMB will not be processed and will be returned to the provider. Non Medicare Other Insurance Enter the 3-digit carrier code(s) if the client has other insurance coverage or Medicare. A response from each and every other insurance policy the client has must be indicated in this field. A complete listing of insurance carrier codes can be accessed/downloaded from the Web site by selecting Information, then Publications. The 3-digit insurance code(s) may also be obtained through client eligibility verification on the Provider secure Web site at and through the AEVS. If the 3-digit code for a specific insurance carrier does not appear on the list, the provider should enter "999", along with the name of the insurance carrier in Field 50. Refer to Chapter 4, Section 3 for information on accessing the AEVS and Section 4 for information on client eligibility verification through the Provider secure site. If a payment is received, the amount paid by the other insurer must be indicated in Field 54 of the claim form. The other insurance paid date must be entered in Field 80. If a denial is received from the other insurance carrier, indicate Not Applicable or N/A after the carrier code. Indicate occurrence code 24 and the date of insurance denial(s) in fields as applicable. 30
36 Paper Claim Field No. and Name 50. PAYER NAME A, B, C (Cont d) The other insurance Explanation of Benefits (EOB), indicating a payment or denial, should not be attached to the claim, unless required to override timely filing. Refer to Section 5.6 for additional information on timely filing. For subrogation procedures, refer to Chapter 5, Section 3, Instructions and Forms for Third Party Liability. INPATIENT ADMINISTRATIVELY NECESSARY DAYS: Administratively Necessary Days (AND) are inpatient hospital days reimbursed by Medicaid for services to eligible patients who no longer require an acute level-of-care and are awaiting placement at a skilled or intermediate level-of-care facility. Administratively necessary days are submitted as follows: 077 for the first seven days 078 for the next seven days 079 for all remaining days Providers must attach a copy of the Medicare Determination Letter indicating no further payment will be made by Medicare and indicate Medicare n/a in Field 50. INPATIENT ADMINISTRATIVELY NECESSARY DAYS: Providers must indicate that Medicare Part B is applicable to the ancillary charges on this claim for Administratively Necessary Days in Field 50. The total Medicare allowed amount should be indicated in Field 54 by adding the Medicare payment amount, the coinsurance amount and the deductible amount. If the Medicare Part B allowed amount is equal to or greater than the Medicaid allowed amount, no payment will be made by Medicaid. Providers must attach the corresponding Explanation of Medicare Benefits (EOMB) to the claim form. Inpatient with Spenddown: When Spenddown exists for a client, the provider must indicate this by the 3-digit carrier code 800 followed by the word Spenddown. 51. HEALTH PLAN ID. A, B, C 52. RELEASE OF INFORMATION A, B, C 53. ASSIGNMENT OF BENEFITS A, B, C For additional detailed information on other insurance and Medicare billing, providers should refer to Chapter 11 of the Provider Manual. This chapter is available at by selecting Information, then Publications, and scrolling down to Provider Manuals Chapter 11. From the drop down box, select the Institutional claim type. 31
37 Paper Claim Field No. and Name 54. PRIOR PAYMENTS A, B, C (IP, OP) Enter the amount paid by the corresponding insurance payer(s) as indicated in Field 50, if applicable. If code in Field 50 is 800, Spenddown, enter the amount Due from Patient in field 54. SPENDDOWN: The amount of the payment should be indicated in Field 54 so that the amount can be deducted from the total allowed amount of the claim. If the Spenddown payment amount is equal to or greater than the Medicaid allowed amount, no payment will be made by Medicaid. The provider must obtain this information from the client. DSS does not provide this information via EMS verification. This field is also used to indicate the Medicare Part B allowed amount when Medicare Part A coverage is exhausted or not applicable. Enter the sum of the Medicare paid amount, the coinsurance amount and the deductible amount located on the Medicare Explanation of Benefits. In this case, no coinsurance amount or deductible amount is entered in fields 39a 41d. 55. EST. AMOUNT DUE A, B, C 56. NPI (IP, OP) 57a.-c. OTHER PRV ID. A, B, C (IP, OP) 58. INSURED S NAME A, B, C 59. P. REL A, B, C 60. INSURED S UNIQUE ID A, B, C (IP, OP) 61. GROUP NAME A, B, C For additional detailed information on other insurance and Medicare billing, providers should refer to Chapter 11 of the Provider Manual. This chapter is available at by selecting Information, then Publications, and scrolling down to Provider Manuals Chapter 11. From the drop down box, select the Institutional claim type. Enter the 10 digit National Provider Identifier of the billing provider. Enter the client s 9-digit Connecticut Medical Assistance Program ID number exactly as it appears on the CONNECT Card, or as it was obtained through the Automated Eligibility Verification System (AEVS). 32
38 Paper Claim Field No. and Name 62. INSURANCE GROUP NO. A, B, C 63. TREATMENT AUTHORIZA- TION CODES A, B, C NOTE: The system matches the services billed against authorizations data by using information related to the provider, client, dates of service and services rendered. 64. DOCUMENT CONTROL NUMBER A, B, C 65. EMPLOYER NAME A, B, C 66. DX Enter the applicable ICD indicator to identify which version of ICD codes is being reported. 9 for ICD-9-CM (Please note that this is currently the only valid indicator for this field and will continue to be used for dates of service through 9/30/2015.) 0 for ICD-10-CM Please note that this indicator will become valid in the future for dates of service on or after 10/1/2015.) NOTE: Claims for dates of service 10/1/2015 forward will require the ICD-10- CM indicator. 33
39 Paper Claim Field No. and Name 67. UNLABELED FIELD (IP, OP) For dates of service prior to 10/01/2015, enter the primary diagnosis code from the International Classification of Diseases, 9 th Revision, Clinical Modification (ICD-9-CM) Manual. For dates of service 10/1/2015 forward, enter the ICD-10-CM diagnosis code. Enter Present on Admission Indicator in shaded area. Present on Admission Indicator Code Y Diagnosis was present at time of inpatient admission. N Diagnosis was not present at time of inpatient admission. U Documentation insufficient to determine if the condition was present at the time of inpatient admission. W Clinically undetermined. Provider unable to clinically determine whether the condition was present at the time of inpatient admission. Blank As long as the corresponding diagnosis is on the POA exempt list. For a complete list of codes on the POA exempt list, see the Official Coding Guidelines for ICD- 9-CM located at: Exempt_Diagnosis_Codes.zip 34
40 Paper Claim Field No. and Name 67A.- 67Q. UNLABELED FIELD (IP, OP) Enter any additional diagnosis codes. For dates of service prior to 10/1/2015, enter the additional diagnosis code from the International Classification of Diseases, 9 th Revision, Clinical Modification (ICD-9-CM) Manual. For dates of service 10/1/2015 forward, enter the ICD-10-CM diagnosis code, if applicable. For erroneous surgeries on an inpatient claim or For other provider preventable conditions (OPPCs) provided by a hospital outpatient department, enter one of the following ICD-9-CM diagnosis codes: E876.5 Performance of wrong operation (procedure) on correct patient (existing code). E876.6 Performance of operation (procedure) on patient not scheduled for surgery. E876.7 Performance of correct operation (procedure) on wrong side/body part. The diagnosis code listed above should be reported in the diagnosis position 2 9, not in the External Cause of Injury (E-code) field. Enter Present on Admission Indicator in shaded area. 68. UNLABELED FIELD 69. ADMIT. DX. (IP) 70a.-c. PATIENT S REASON DX Present on Admission Indicator Code Y Diagnosis was present at time of inpatient admission. N Diagnosis was not present at time of inpatient admission. U Documentation insufficient to determine if the condition was present at the time of inpatient admission. W Clinically undetermined. Provider unable to clinically determine whether the condition was present at the time of inpatient admission. For dates of service prior to 10/1/2015, enter the ICD-9-CM diagnosis code provided at the time of admission. For dates of service 10/1/2015 forward, enter the ICD-10-CM diagnosis code. 71. PPS CODE 72a.-c. ECI 35
41 Paper Claim Field No. and Name 73. UNLABELED FIELD 74. PRINCIPAL PROCEDURE CODE/ DATE (IP) For dates of service prior to 10/1/2015, enter the appropriate ICD-9-CM procedure code and the date, in MM/DD/YY format, for the procedure that was performed, if applicable. ICD-9-CM surgical procedure codes are the only values to be used here prior to 10/1/2015. For dates of service 10/1/2015 forward, enter the ICD-10- CM surgical procedure codes. 74 a.-e. OTHER PROCEDURE CODE/DATE (IP) For dates of service prior to 10/1/2015, enter the appropriate ICD-9-CM other procedure code(s) and the date(s), in MM/DD/YY format, for the other procedure(s) performed, if applicable. ICD-9-CM surgical procedure codes are the only values to be used here for dates of service prior to 10/1/2015. For dates of service 10/1/2015 forward, enter the ICD-10-CM surgical procedure codes. 75. UNLABELED FIELD 76. ATTENDING NPI/QUAL/LAST /FIRST (IP, OP) 77. OPERATING NPI/QUAL/LAST/ FIRST (IP, OP) 78. OTHER NPI/QUAL/LAST/ FIRST (IP, OP) 79. OTHER NPI/QUAL/LAST/ FIRST Enter the 10 digit National Provider Identifier, qualifier (71), and the last and first name of the attending physician or the physician who had primary responsibility for the client s care and treatment. Enter the 10 digit National Provider Identifier, Qualifier (82), and the Last and First Name of the operating physician if applicable. Enter the 10 digit National Provider Identifier, Qualifier, and the Last and First Name of the referring, rendering or other operating physician if applicable. Hospitals are required to submit the referring provider if the referring provider is different than the attending provider. Qualifier 82 Rendering Provider DN Referring Provider Enter the 10 digit National Provider Identifier, Qualifier, and the Last and First Name of the referring, rendering or other operating physician if applicable. Hospitals are required to submit the referring provider if the referring provider is different than the attending provider. Qualifier 82 DN Rendering Provider Referring Provider 36
42 Paper Claim Field No. and Name 80. REMARKS Enter the other insurance or spenddown paid date if applicable. This would include entering the Medicare Part B paid date when Medicare Part B makes a payment on an inpatient claim after Medicare Part A denies the claim as benefits exhausted. 81a.-d. CC For additional detailed information on other insurance and Medicare billing, providers should refer to Chapter 11 of the Provider Manual. This chapter is available at by selecting Information, then Publications, and scrolling down to Provider Manuals Chapter 11. From the drop down box, select the Institutional claim type. Enter the NUBC qualifier B3 in the Qualifier field, followed by the billing provider s taxonomy code. 37
 to make up the total dose.")
43 Multiple NDCs per RCC/HCPCs When administering multiple NDCs within a single HCPC, each NDC must be identified at the time of billing. This scenario may occur if the physician needs to administer a specific dose of a drug that requires the use of two different vials of a drug (two different NDCs) to make up the total dose. This is accomplished by adding sequence details for each NDC. Figure 1 below illustrates how this should be accomplished. Figure 1 In Figure 1, a detail signifies the RCC (and HCPCS) code, whereas a sequence signifies the corresponding additional NDC. If the RCC code and the HCPCS code had multiple NDCs, there would be one detail with multiple sequences. In this example above: Detail 1 for RCC code 636 is being submitted with 2 sequences, which indicates it is comprised of a detail with the same RCC, same HCPCS, and 2 different NDCs. Field 43 indicated the qualifier N4, NDC, units of measure, and the NDC quantity. Field 44 indicated the HCPCS. Field 46 indicates the HCPCS quantity for all associated sequences Note sequence 2 does not show a value. The total units for a detail that has more than one sequence should be the sum of all the units at the sequence level, but included only on detail 1 and sequence 1. In this example, 2 units is the sum of the units from sequence 1 and 2. Field 47 indicates the total cost for all associated sequences - Note sequence 2 shows a value of Zero. The total charges for sequence 1 and 2 must be included in only detail 1, sequence 1. In this example Detail 2 for RCC 305 is not for a physician administered drug, therefore, no sequence or NDC is needed. Detail 3 for RCC 636 is displaying 1 sequence to indicate the 1 NDC administered. 38
Subject: Updated UB-04 Paper Claim Form Requirements
 INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 7 0 2 J A N U A R Y 3 0, 2 0 0 7 To: All Providers Subject: Updated UB-04 Paper Claim Form Requirements Overview The following
INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 7 0 2 J A N U A R Y 3 0, 2 0 0 7 To: All Providers Subject: Updated UB-04 Paper Claim Form Requirements Overview The following
Hospital Refresher Workshop. Presented by The Department of Social Services & HP Enterprise Services
 Hospital Refresher Workshop Presented by The Department of Social Services & HP Enterprise Services 1 Training Topics Provider Bulletins Outpatient Claim Billing Changes Explanation of Benefit Codes Web
Hospital Refresher Workshop Presented by The Department of Social Services & HP Enterprise Services 1 Training Topics Provider Bulletins Outpatient Claim Billing Changes Explanation of Benefit Codes Web
Tips for Completing the UB04 (CMS-1450) Claim Form
 Claim Form") Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
Tips for Completing the UB04 (CMS-1450) Claim Form As a Beacon facility partner, we value the services you provide and it is important to us that you are reimbursed for the work you do. To assure your
UB-04, Inpatient / Outpatient
 UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
UB-04, Inpatient / Outpatient
 UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
UB-04, Inpatient / Outpatient Hospital (Inpatient and Outpatient), Hospice (Nursing Home and Home Services), Home Health, Rural Health linic, Federally Qualified Health enter, IF/MR, Birthing enter, and
UB-92 Billing Instructions
 August 26, 2005 UB-92 Billing Instructions 2005 Hospital Provider Workshop Conduent MS Medicaid Project Government Healthcare Solutions Objective & Definition To explain how to complete a UB-92 claim form
August 26, 2005 UB-92 Billing Instructions 2005 Hospital Provider Workshop Conduent MS Medicaid Project Government Healthcare Solutions Objective & Definition To explain how to complete a UB-92 claim form
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL. Hospital
 KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim................
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim................
Information for Skilled Nursing Facilities, Hospice R&B Providers & Supportive Living Programs: Authorizations, Billing and Claims
 Information for Skilled Nursing Facilities, Hospice R&B Providers & Supportive Living Programs: Authorizations, Billing and Claims Skilled Nursing Facility Services Custodial Care, SLP and Hospice R&B
Information for Skilled Nursing Facilities, Hospice R&B Providers & Supportive Living Programs: Authorizations, Billing and Claims Skilled Nursing Facility Services Custodial Care, SLP and Hospice R&B
Archived 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION BILLING PROCEDURES FOR MEDICARE/MO HEALTHNET...5
 SECTION 15 - BILLING INSTRUCTIONS Contents 15.1 ELECTRONIC DATA INTERCHANGE...4 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION...4 15.3 UB-04 (CMS-1450) CLAIM FORM...5 15.4 PROVIDER COMMUNICATION UNIT...5 15.5
SECTION 15 - BILLING INSTRUCTIONS Contents 15.1 ELECTRONIC DATA INTERCHANGE...4 15.2 INTERNET ELECTRONIC CLAIM SUBMISSION...4 15.3 UB-04 (CMS-1450) CLAIM FORM...5 15.4 PROVIDER COMMUNICATION UNIT...5 15.5
HOW TO SUBMIT OWCP-04 BILLS TO ACS
 HOW TO SUBMIT OWCP-04 BILLS TO ACS The following services should be billed on the OWCP-04 Form: General Hospital Hospice Nursing Home Rehabilitation Centers As a provider you have the option of sending
HOW TO SUBMIT OWCP-04 BILLS TO ACS The following services should be billed on the OWCP-04 Form: General Hospital Hospice Nursing Home Rehabilitation Centers As a provider you have the option of sending
Nursing Facility UB-04 Paper Billing Guide
 Nursing Facility UB-04 Paper Billing Guide Oregon Medicaid Nursing Facilities November 2008 1 Effective 11/17/08 TABLE OF CONTENTS Introduction... 3 Claims Processing General Information... 4 Required
Nursing Facility UB-04 Paper Billing Guide Oregon Medicaid Nursing Facilities November 2008 1 Effective 11/17/08 TABLE OF CONTENTS Introduction... 3 Claims Processing General Information... 4 Required
Connecticut Medical Assistance Program Refresher for Hospice Providers. Presented by The Department of Social Services & HP for Billing Providers
 Connecticut Medical Assistance Program Refresher for Hospice Providers Presented by The Department of Social Services & HP for Billing Providers 1 Training Topics Hospice Agenda HIPAA 5010 Hospice Form
Connecticut Medical Assistance Program Refresher for Hospice Providers Presented by The Department of Social Services & HP for Billing Providers 1 Training Topics Hospice Agenda HIPAA 5010 Hospice Form
UB-04 Claim Form Instructions
 UB-04 Claim Form This document explains the UB-04 claim form, which is used for submitting claims for reimbursement for specially designated facilities. The instructions included in this section are excerpts
UB-04 Claim Form This document explains the UB-04 claim form, which is used for submitting claims for reimbursement for specially designated facilities. The instructions included in this section are excerpts
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL. Hospital
 KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim................
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim................
CMS-1500 Billing and Reimbursement. HP Provider Relations/October 2013
 CMS-1500 Billing and Reimbursement HP Provider Relations/October 2013 Agenda Common Denials for CMS-1500 CMS-1500 Claims Billing Types of CMS-1500 Claims Paper Claim Billing Fee Schedule Crossover Claims
CMS-1500 Billing and Reimbursement HP Provider Relations/October 2013 Agenda Common Denials for CMS-1500 CMS-1500 Claims Billing Types of CMS-1500 Claims Paper Claim Billing Fee Schedule Crossover Claims
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL. Hospital
 KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim..................
KANSAS MEDICAL ASSISTANCE PROGRAM PROVIDER MANUAL Hospital PART II Introduction Section BILLING INSTRUCTIONS Page 7000 UB-04 Billing Instructions.................. 7-1 Submission of Claim..................
FHCA 2014 Annual Conference & Trade Show
 FHCA 2014 Annual Conference & Trade Show CE Session #49 Medicaid Managed Care Billing: Purely A Provider s Perspective Thursday, July 10 4:00 to 6:00 p.m. Crystal N/J2 Finance/Development Upon completion
FHCA 2014 Annual Conference & Trade Show CE Session #49 Medicaid Managed Care Billing: Purely A Provider s Perspective Thursday, July 10 4:00 to 6:00 p.m. Crystal N/J2 Finance/Development Upon completion
Format Specifications For the MHA DMS Publish Date: 11/20/2017
 Specifications For the MHA DMS 10 1.00.10 Publish Date: 11/20/2017 This document is updated periodically. If you are not reading this on the web but are instead reading a printed copy, please check our
Specifications For the MHA DMS 10 1.00.10 Publish Date: 11/20/2017 This document is updated periodically. If you are not reading this on the web but are instead reading a printed copy, please check our
Connecticut Medical Assistance Program Refresher for Hospice Providers. Presented by The Department of Social Services & HP for Billing Providers
 Connecticut Medical Assistance Program Refresher for Hospice Providers Presented by The Department of Social Services & HP for Billing Providers 1 Hospice Agenda Overview Forms Fee Schedule/Reimbursement
Connecticut Medical Assistance Program Refresher for Hospice Providers Presented by The Department of Social Services & HP for Billing Providers 1 Hospice Agenda Overview Forms Fee Schedule/Reimbursement
Connecticut Medical Assistance Program. Hospice Refresher Workshop
 Connecticut Medical Assistance Program Hospice Refresher Workshop Training Topics What s New in 2015? Electronic Messaging Claim Adjustments Messages Archived Proposed Changes in Hospice Rates Fiscal Year
Connecticut Medical Assistance Program Hospice Refresher Workshop Training Topics What s New in 2015? Electronic Messaging Claim Adjustments Messages Archived Proposed Changes in Hospice Rates Fiscal Year
WV Medical CAQH Phase 3 CARC-RARC Modifications.xlsx
 1 SNF-No Authorization CO B5 CO 15 N517 SNF-Member Share of Cost Reduced From Contracted 2 Amount CO 142 CO 142 3 Benefit Exhaustion Period Reported CO 119 CO 119 Medicare Crossover QMB 7 processing rules
1 SNF-No Authorization CO B5 CO 15 N517 SNF-Member Share of Cost Reduced From Contracted 2 Amount CO 142 CO 142 3 Benefit Exhaustion Period Reported CO 119 CO 119 Medicare Crossover QMB 7 processing rules
North Carolina Emergency Department Visit Data - Data Dictionary FY2012 Alphabetic List of Variables and Attributes Standard Research File
 North Carolina Emergency Department Visit Data - Data Dictionary FY2012 Alphabetic List of Variables and Attributes Standard Research File One of these three variables must be suppressed (diag1, fac, or
North Carolina Emergency Department Visit Data - Data Dictionary FY2012 Alphabetic List of Variables and Attributes Standard Research File One of these three variables must be suppressed (diag1, fac, or
North Carolina Ambulatory Surgery Visit Data - Data Dictionary FY2011 Alphabetic List of Variables and Attributes Standard Research File
 North Carolina Ambulatory Surgery Visit Data - Data Dictionary FY2011 Alphabetic List of Variables and Attributes Standard Research File One of these three variables must be suppressed (Diag1, fac, ptzip)
North Carolina Ambulatory Surgery Visit Data - Data Dictionary FY2011 Alphabetic List of Variables and Attributes Standard Research File One of these three variables must be suppressed (Diag1, fac, ptzip)
PARTNERSHIP HEALTHPLAN OF CALIFORNIA MEDI-CAL PROVIDER MANUAL CLAIMS DEPARTMENT
 III.A. CMS 1500 Billing Form Effective April 1, 2014, the information listed below are the CMS 1500 fields that must be completed accurately and completely in order to avoid claim suspense or denial. A
III.A. CMS 1500 Billing Form Effective April 1, 2014, the information listed below are the CMS 1500 fields that must be completed accurately and completely in order to avoid claim suspense or denial. A
Dana Bernier Provider Education MO HealthNet Division (MHD)
") Dana Bernier Provider Education MO HealthNet Division (MHD) 1 MO HealthNet policy updates Resources available to providers Navigating Provider Participation webpage Spenddown & Eligibility Electronic Claim
Dana Bernier Provider Education MO HealthNet Division (MHD) 1 MO HealthNet policy updates Resources available to providers Navigating Provider Participation webpage Spenddown & Eligibility Electronic Claim
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
BCBSNC Best Practices
 BCBSNC Best Practices Thank you for attending today! We value your commitment of caring for our members your patients and our shared goals for their improved health An independent licensee of the Blue
BCBSNC Best Practices Thank you for attending today! We value your commitment of caring for our members your patients and our shared goals for their improved health An independent licensee of the Blue
Medicare Hospice Billing 2015 & Beyond!
 Medicare Hospice Billing 2015 & Beyond! Presented By: Melinda A. Gaboury, CEO Healthcare Provider Solutions, Inc. Sequential Claim Billing The NOE must be in S/LOC P B9997 prior to submitting the first
Medicare Hospice Billing 2015 & Beyond! Presented By: Melinda A. Gaboury, CEO Healthcare Provider Solutions, Inc. Sequential Claim Billing The NOE must be in S/LOC P B9997 prior to submitting the first
Tips for Completing the CMS-1500 Version 02/12 Claim Form
 Tips for Completing the CMS-1500 Version 02/12 Claim Form NOTE: FAILURE TO PROVIDE VALID INFORMATION MATCHING THE INSURED S ID CARD COULD RESULT IN A REJECTION OF YOUR CLAIM. Enter in the white, open carrier
Tips for Completing the CMS-1500 Version 02/12 Claim Form NOTE: FAILURE TO PROVIDE VALID INFORMATION MATCHING THE INSURED S ID CARD COULD RESULT IN A REJECTION OF YOUR CLAIM. Enter in the white, open carrier
AMBULATORY SURGICAL CENTERS PROVIDER MANUAL Chapter Twenty-nine of the Medicaid Services Manual
 AMBULATORY SURGICAL CENTERS PROVIDER MANUAL Chapter Twenty-nine of the Medicaid Services Manual Issued November 1, 2010 Claims/authorizations for dates of service on or after October 1, 2015 must use the
AMBULATORY SURGICAL CENTERS PROVIDER MANUAL Chapter Twenty-nine of the Medicaid Services Manual Issued November 1, 2010 Claims/authorizations for dates of service on or after October 1, 2015 must use the
Rural Health Clinic Overview
 TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
TrailBlazer Health Enterprises Rural Health Clinic Overview Steven W. Mildward Published March 2012 108724 2012 TrailBlazer Health Enterprises /TrailBlazer. All rights reserved. Important The information
Important Billing Guidelines
 Important Billing Guidelines The guidelines contained herein are meant to assist GHP Family Participating Providers in billing appropriately for medically necessary services rendered to GHP Family Members.
Important Billing Guidelines The guidelines contained herein are meant to assist GHP Family Participating Providers in billing appropriately for medically necessary services rendered to GHP Family Members.
Required Data for Claim Forms (CMS-1500 & UB-04) Claim Submission Instructions (MLTC) Care Healthcare and VNSNY CHOICE Transition
 Claim Submission Instructions (MLTC) Care Healthcare and VNSNY CHOICE Transition") 2018 Provider Manual VNSNY CHOICE Appendix V Claims CMS-1500 Form (Sample) UB-04 Form (Sample) Required Data for Claim Forms (CMS-1500 & UB-04) Claim Submission Instructions (MLTC) ICD-10 FAQ Care Healthcare
2018 Provider Manual VNSNY CHOICE Appendix V Claims CMS-1500 Form (Sample) UB-04 Form (Sample) Required Data for Claim Forms (CMS-1500 & UB-04) Claim Submission Instructions (MLTC) ICD-10 FAQ Care Healthcare
Home and Community- Based Services Waiver Program. HP Provider Relations/October 2014
 Home and Community- Based Services Waiver Program HP Provider Relations/October 2014 Agenda Objectives Overview of the Home and Community- Based Services (HCBS) Waiver Program Member eligibility Billing
Home and Community- Based Services Waiver Program HP Provider Relations/October 2014 Agenda Objectives Overview of the Home and Community- Based Services (HCBS) Waiver Program Member eligibility Billing
Policies Regarding Network Provider Payment
 CLAIMS PAYMENT (NOTE: Below please find guidelines ValueOptions follows when processing claims for most accounts. If you believe there may be a specific set of guidelines that need to be followed for your
CLAIMS PAYMENT (NOTE: Below please find guidelines ValueOptions follows when processing claims for most accounts. If you believe there may be a specific set of guidelines that need to be followed for your
INPATIENT/COMPREHENSIVE REHAB AUDIT DICTIONARY
 Revised 11/04/2016 Audit # Location Audit Message Audit Description Audit Severity 784 DATE Audits are current as of 11/04/2016 The date of the last audit update Information 1 COUNTS Total Records Submitted
Revised 11/04/2016 Audit # Location Audit Message Audit Description Audit Severity 784 DATE Audits are current as of 11/04/2016 The date of the last audit update Information 1 COUNTS Total Records Submitted
Version 5010 Errata Provider Handout
 Version 5010 Errata Provider Handout 5010 Bringing Clarity & Consistency To Your Electronic Transactions Benefits Transactions Impacted Changes Impacting Providers While we have highlighted the HIPAA Version
Version 5010 Errata Provider Handout 5010 Bringing Clarity & Consistency To Your Electronic Transactions Benefits Transactions Impacted Changes Impacting Providers While we have highlighted the HIPAA Version
NJDDCS VERSION 2 DATA DICTIONARY And DATA EXTRACT FILE LAYOUT Version 17.2
 NJDDCS VERSION 2 DATA DICTIONARY And DATA EXTRACT FILE LAYOUT Version 17.2 Table of Contents Introduction... 5 Accident State... 6 Acute Days... 7 Admission Hour... 8 Admission/Start of Care Date (Admission
NJDDCS VERSION 2 DATA DICTIONARY And DATA EXTRACT FILE LAYOUT Version 17.2 Table of Contents Introduction... 5 Accident State... 6 Acute Days... 7 Admission Hour... 8 Admission/Start of Care Date (Admission
5010 Changes. CHAMPS Changes 01/01/12 4/4/12. Copyright Kearney & Associates, Inc 1. 01/01/2012 Change From 4010 to 5010
 Flowing Change Julie Kearney Kearney & Associates, Inc. 5010 Changes 01/01/2012 Change From 4010 to 5010 Went From Allowing 8 Diagnosis to 12 Diagnosis Postponed fines, and compliance until 04/01/2012
Flowing Change Julie Kearney Kearney & Associates, Inc. 5010 Changes 01/01/2012 Change From 4010 to 5010 Went From Allowing 8 Diagnosis to 12 Diagnosis Postponed fines, and compliance until 04/01/2012
Presented by: Jodie Edmonds VP Medicaid Revenue Consultant Passport Health Communications
 Presented by: Jodie Edmonds VP Medicaid Revenue Consultant Passport Health Communications Complete and correct coding of claims will become more important, and will have an effect on claim payment. The
Presented by: Jodie Edmonds VP Medicaid Revenue Consultant Passport Health Communications Complete and correct coding of claims will become more important, and will have an effect on claim payment. The
DC Medicaid EAPG Training
 DC Medicaid EAPG Training Provider Training 2013 Xerox Corporation. All rights reserved. Xerox and Xerox Design are trademarks of Xerox Corporation in the United States and/or other countries. Agenda Project
DC Medicaid EAPG Training Provider Training 2013 Xerox Corporation. All rights reserved. Xerox and Xerox Design are trademarks of Xerox Corporation in the United States and/or other countries. Agenda Project
Outpatient Hospital Facilities
 Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Chapter 12 Section 6
 Home Health Care (HHC) Chapter 12 Section 6 Home Health Benefit Coverage And Reimbursement - Claims And Billing Submission Under Home Health Agency Prospective Payment System (HHA PPS) Issue Date: Authority:
Home Health Care (HHC) Chapter 12 Section 6 Home Health Benefit Coverage And Reimbursement - Claims And Billing Submission Under Home Health Agency Prospective Payment System (HHA PPS) Issue Date: Authority:
ICD-10/APR-DRG. HP Provider Relations/September 2015
 ICD-10/APR-DRG HP Provider Relations/September 2015 Agenda ICD-10 ICD-10 General Overview Who is affected Preparation Testing Prior Authorization APR-DRG Inpatient hospital rates Crosswalks Questions 2
ICD-10/APR-DRG HP Provider Relations/September 2015 Agenda ICD-10 ICD-10 General Overview Who is affected Preparation Testing Prior Authorization APR-DRG Inpatient hospital rates Crosswalks Questions 2
1. Section Modifications
 Table of Contents 1. Section Modifications... 1 2. UB04 Claim Form... 5 3. Completing the UB04... 6 3.1. Helpful Tips for Filling out a Paper Claim... 6 3.2. Claim Form Field s... 6 4. Billing Information...
Table of Contents 1. Section Modifications... 1 2. UB04 Claim Form... 5 3. Completing the UB04... 6 3.1. Helpful Tips for Filling out a Paper Claim... 6 3.2. Claim Form Field s... 6 4. Billing Information...
EFFECTIVE 4/1/ Texas Administrative Code Chapter GENERAL MEDICAL PROVISIONS
 28 Texas Administrative Code Chapter 133 - GENERAL MEDICAL PROVISIONS Subchapter B - HEALTH CARE PROVIDER BILLING PROCEDURES AMENDED: 133.10 Adopted: 12/16/2013 Effective: 4/1/2014 Adoption: http://texashistory.unt.edu/ark:/67531/metapth379970/m1/186/?q=133.10
28 Texas Administrative Code Chapter 133 - GENERAL MEDICAL PROVISIONS Subchapter B - HEALTH CARE PROVIDER BILLING PROCEDURES AMENDED: 133.10 Adopted: 12/16/2013 Effective: 4/1/2014 Adoption: http://texashistory.unt.edu/ark:/67531/metapth379970/m1/186/?q=133.10
HCPCS - C9716* SI - S APC Short Descriptor - Radiofrequency Energy to Anus
 HMI Corporation Second Quarter 2004 June 21, 2004 C ODING & B ILLING F OR P ROSPECTIVE P AYMENT S YSTEMS JULY 2004 UPDATE OF THE HOSPITAL OUTPATIENT Inside this Issue: July 2004 Update of the Hospital
HMI Corporation Second Quarter 2004 June 21, 2004 C ODING & B ILLING F OR P ROSPECTIVE P AYMENT S YSTEMS JULY 2004 UPDATE OF THE HOSPITAL OUTPATIENT Inside this Issue: July 2004 Update of the Hospital
Home Health & HP Provider Relations
 Home Health & Hospice HP Provider Relations October 2010 Agenda Session Objectives Home Health Benefit Coverage Billing Overhead Multiple Visits Most Common Denials Hospice Benefit Coverage Election/Revocation/Discharge
Home Health & Hospice HP Provider Relations October 2010 Agenda Session Objectives Home Health Benefit Coverage Billing Overhead Multiple Visits Most Common Denials Hospice Benefit Coverage Election/Revocation/Discharge
District of Columbia Medicaid Specialty Hospital Project Frequently Asked Questions
 District of Columbia Medicaid Specialty Hospital Project Frequently Asked Questions Version Date: September 22, 2014 UPDATE: The District of Columbia Department of Health Care Finance (DHCF) is submitting
District of Columbia Medicaid Specialty Hospital Project Frequently Asked Questions Version Date: September 22, 2014 UPDATE: The District of Columbia Department of Health Care Finance (DHCF) is submitting
Screening, Brief Intervention and Referral to Treatment (SBIRT) Program
 Program") Screening, Brief Intervention and Referral to Treatment (SBIRT) Program (SBIRT) Services... 1 Program Overview... 1 Billing Information... 1 National Provider Identifier (NPI)... 1 Paper Claims... 1 Electronic
Screening, Brief Intervention and Referral to Treatment (SBIRT) Program (SBIRT) Services... 1 Program Overview... 1 Billing Information... 1 National Provider Identifier (NPI)... 1 Paper Claims... 1 Electronic
Medicare Advantage Outreach and Education Bulletin
 Medicare Advantage Outreach and Education Bulletin December 2010 To: All Medicare Advantage (MA) Physicians & Practitioners, Hospitals & Facilities* *Contracting physicians & practitioners, hospitals &
Medicare Advantage Outreach and Education Bulletin December 2010 To: All Medicare Advantage (MA) Physicians & Practitioners, Hospitals & Facilities* *Contracting physicians & practitioners, hospitals &
ICD-10 Frequently Asked Questions - SurgiSource
 ICD-10 Frequently Asked Questions - SurgiSource What Version of SurgiSource is ICD-10 Compliant? Version 6.0 Where can I find ICD-10 Training Materials for SurgiSource? 1. Visit our Client Portal (portal.sourcemed.net)
ICD-10 Frequently Asked Questions - SurgiSource What Version of SurgiSource is ICD-10 Compliant? Version 6.0 Where can I find ICD-10 Training Materials for SurgiSource? 1. Visit our Client Portal (portal.sourcemed.net)
CHAPTER 59B-9 PATIENT DATA COLLECTION, AMBULATORY SURGERY AND EMERGENCY DEPARTMENT
 CHAPTER 59B-9 PATIENT DATA COLLECTION, AMBULATORY SURGERY AND EMERGENCY DEPARTMENT 59B-9.030 59B-9.031 59B-9.032 59B-9.033 59B-9.034 59B-9.035 59B-9.036 59B-9.037 59B-9.038 59B-9.039 Purpose of Ambulatory
CHAPTER 59B-9 PATIENT DATA COLLECTION, AMBULATORY SURGERY AND EMERGENCY DEPARTMENT 59B-9.030 59B-9.031 59B-9.032 59B-9.033 59B-9.034 59B-9.035 59B-9.036 59B-9.037 59B-9.038 59B-9.039 Purpose of Ambulatory
CHAPTER 3: EXECUTIVE SUMMARY
 INDIANA PROVIDER MANUAL EXECUTIVE SUMMARY Indiana Family and Social Services Administration (FSSA) contracts with Anthem Insurance Companies, Inc. (dba Anthem Blue Cross and Blue Shield) for the provision
INDIANA PROVIDER MANUAL EXECUTIVE SUMMARY Indiana Family and Social Services Administration (FSSA) contracts with Anthem Insurance Companies, Inc. (dba Anthem Blue Cross and Blue Shield) for the provision
WYOMING MEDICAID PROVIDER MANUAL. Medical Services HCFA-1500
 WYOMING MEDICAID PROVIDER MANUAL Medical Services HCFA-1500 Medical Services March 01,1999 Table of Contents AUTHORITY... 1-1 Chapter One... 1-1 General Information... 1-1 How the Billing Manual is organized...
WYOMING MEDICAID PROVIDER MANUAL Medical Services HCFA-1500 Medical Services March 01,1999 Table of Contents AUTHORITY... 1-1 Chapter One... 1-1 General Information... 1-1 How the Billing Manual is organized...
Ch. 912 DATA REPORTING REQUIREMENTS CHAPTER 912. DATA REPORTING REQUIREMENTS
 Ch. 912 DATA REPORTING REQUIREMENTS 28 912.1 CHAPTER 912. DATA REPORTING REQUIREMENTS Subchap. Sec. A. GENERAL PROVISIONS... 912.1 B. PENNSYLVANIA UNIFORM CLAIMS AND BILLING FORM SUBMISSION SCHEDULES...
Ch. 912 DATA REPORTING REQUIREMENTS 28 912.1 CHAPTER 912. DATA REPORTING REQUIREMENTS Subchap. Sec. A. GENERAL PROVISIONS... 912.1 B. PENNSYLVANIA UNIFORM CLAIMS AND BILLING FORM SUBMISSION SCHEDULES...
INPATIENT HOSPITAL REIMBURSEMENT
 HCRA CLAIMS PROCESSING Reimbursement: HCRA is not Medicaid; however, HCRA covered services are reimbursed at the hospital s outpatient or inpatient reimbursement rate allowed for Florida Medicaid. The
HCRA CLAIMS PROCESSING Reimbursement: HCRA is not Medicaid; however, HCRA covered services are reimbursed at the hospital s outpatient or inpatient reimbursement rate allowed for Florida Medicaid. The
Provider Preventable Conditions: Health Care Acquired Conditions and Present on Admission Policy
 Provider Preventable Conditions: Health Care Acquired Conditions and Present on Admission Policy Policy Number 2018F7002A Annual Approval Date 3/14/2018 Approved By Reimbursement Policy Oversight Committee
Provider Preventable Conditions: Health Care Acquired Conditions and Present on Admission Policy Policy Number 2018F7002A Annual Approval Date 3/14/2018 Approved By Reimbursement Policy Oversight Committee
North Carolina Inpatient Hospital Discharge Data - Data Dictionary FY2011 Standard Research File Alphabetic List of Variables and Attributes
 North Carolina Inpatient Hospital Discharge Data - Data Dictionary FY2011 Standard Research File Alphabetic List of Variables and Attributes One of these three variables must be suppressed (diag1, fac,
North Carolina Inpatient Hospital Discharge Data - Data Dictionary FY2011 Standard Research File Alphabetic List of Variables and Attributes One of these three variables must be suppressed (diag1, fac,
Inpatient Psychiatric Facility (IPF) Coverage & Documentation. Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016
 Coverage & Documentation. Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016") Inpatient Psychiatric Facility (IPF) Coverage & Documentation Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016 1 Disclaimer This information is current as of August
Inpatient Psychiatric Facility (IPF) Coverage & Documentation Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016 1 Disclaimer This information is current as of August
Table of Contents. 1.0 Description of the Procedure, Product, or Service Definitions Hospice Terminal illness...
 Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 1.1.1 Hospice... 1 1.1.2 Terminal illness... 1 2.0 Eligibility Requirements... 1 2.1 Provisions... 1 2.1.1
Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 1.1.1 Hospice... 1 1.1.2 Terminal illness... 1 2.0 Eligibility Requirements... 1 2.1 Provisions... 1 2.1.1
Chapter 9 Section 1. Ambulatory Surgical Center (ASC) Reimbursement
 Reimbursement") Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
Core Services Provided in Federally Clinical Coverage Policy No: 1D-4 Qualified Health Centers and Amended Date: October 1, 2015 Rural Health Clinics
 Qualified Health Centers and Amended Date: October 1, 2015 Rural Health Clinics Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Federally Qualified Health Centers... 1
Qualified Health Centers and Amended Date: October 1, 2015 Rural Health Clinics Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Federally Qualified Health Centers... 1
CAH SWING BED BILLING, CODING AND DOCUMENTATION. Lisa Pando, Sr. Consultant GPS Healthcare Consultants
 CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Facilities and Ancillaries This supplement of the Optima Health Provider Manual provides information of specific interest to Optima Health contracted
Optima Health Provider Manual Supplemental Information For Facilities and Ancillaries This supplement of the Optima Health Provider Manual provides information of specific interest to Optima Health contracted
Cotiviti Approved Issues List as of February 26, 2018
 Cotiviti Approved Issues List as of February 26, 2018 All physician/npp specialties 32 Ambulance Providers 34 Ambulatory Surgery Center (ASC), Outpatient Hospital 38 Inpatient Hospital 40 Inpatient Hospital,
Cotiviti Approved Issues List as of February 26, 2018 All physician/npp specialties 32 Ambulance Providers 34 Ambulatory Surgery Center (ASC), Outpatient Hospital 38 Inpatient Hospital 40 Inpatient Hospital,
Molina Healthcare of Ohio Nursing Facility and Assisted Living Provider Guide
 Molina Healthcare of Ohio Nursing Facility and Assisted Living Table of Contents General Information... 3 Definitions... 3 Verifying Eligibility... 5 Utilization Management/Authorizations... 5 Claims Management...
Molina Healthcare of Ohio Nursing Facility and Assisted Living Table of Contents General Information... 3 Definitions... 3 Verifying Eligibility... 5 Utilization Management/Authorizations... 5 Claims Management...
Best Practice Recommendation for
 Best Practice Recommendation for Submitting & Processing Claims (5010 version) WorkSMART A program of the Washington Healthcare Forum operated by OneHealthPort 1 For use with ASC X12N 837 (005010X222)
Best Practice Recommendation for Submitting & Processing Claims (5010 version) WorkSMART A program of the Washington Healthcare Forum operated by OneHealthPort 1 For use with ASC X12N 837 (005010X222)
LifeWise Reference Manual LifeWise Health Plan of Oregon
 11 UB-04 Billing Description This chapter contains participation, claims and billing information for providers who bill on a UB-04 (CMS 1450) claim form. This chapter supplements information contained
11 UB-04 Billing Description This chapter contains participation, claims and billing information for providers who bill on a UB-04 (CMS 1450) claim form. This chapter supplements information contained
TCS FAQ s. How will the implementation of national standard code sets reduce burden on the health care industry?
 TCS FAQ s What is a code set? Under HIPAA, a code set is any set of codes used for encoding data elements, such as tables of terms, medical concepts, medical diagnosis codes, or medical procedure codes.
TCS FAQ s What is a code set? Under HIPAA, a code set is any set of codes used for encoding data elements, such as tables of terms, medical concepts, medical diagnosis codes, or medical procedure codes.
Appeal Process Information
 First-Level Appeals Appeal Process Information Regulation 7 AAC 105.270 stipulates the length of time a provider has to submit a first-level appeal. Most firstlevel appeals must be filed within 180 days
First-Level Appeals Appeal Process Information Regulation 7 AAC 105.270 stipulates the length of time a provider has to submit a first-level appeal. Most firstlevel appeals must be filed within 180 days
Medicare Claims Processing Manual Chapter 11 - Processing Hospice Claims
 Medicare Claims Processing Manual Chapter 11 - Processing Hospice Claims Transmittals for Chapter 11 Table of Contents (Rev. 3326, 08-14-15) (Rev. 3378, 10-16-15) 10 - Overview 10.1 - Hospice Pre-Election
Medicare Claims Processing Manual Chapter 11 - Processing Hospice Claims Transmittals for Chapter 11 Table of Contents (Rev. 3326, 08-14-15) (Rev. 3378, 10-16-15) 10 - Overview 10.1 - Hospice Pre-Election
AWCC TABLE OF DATA REQUIREMENTS
 December 1, 2011 Advisory 2011-2 Billing for Provider Services (Rule 30) Effective January 1, 2012, to be considered a properly submitted medical bill, [Rule 30, I, F, 55; I, I, 7], all information submitted
December 1, 2011 Advisory 2011-2 Billing for Provider Services (Rule 30) Effective January 1, 2012, to be considered a properly submitted medical bill, [Rule 30, I, F, 55; I, I, 7], all information submitted
UPDATED Nursing/Intermediate Care Facility Providers
 December 2008 Provider Bulletin Number 8160 UPDATED Nursing/Intermediate Care Facility Providers Revenue Codes The revenue codes listed under field 42 for the UB-04 form were inadvertently deleted with
December 2008 Provider Bulletin Number 8160 UPDATED Nursing/Intermediate Care Facility Providers Revenue Codes The revenue codes listed under field 42 for the UB-04 form were inadvertently deleted with
Blue Membership as of November Penalty Due for Failure to Obtain Authorizations. Physician Anatomical Pathology Services Medicare Moratorium
 3rd/4th Quarter 2008 Blue News is a quarterly publication for hospital administrators from Blue Cross and Blue Shield of Louisiana Baton Rouge, New Orleans, Northshore area providers: Merle Francis Regional
3rd/4th Quarter 2008 Blue News is a quarterly publication for hospital administrators from Blue Cross and Blue Shield of Louisiana Baton Rouge, New Orleans, Northshore area providers: Merle Francis Regional
District of Columbia Medicaid Specialty Hospital Payment Method Frequently Asked Questions
 District of Columbia Medicaid Specialty Hospital Payment Method Frequently Asked Questions Version Date: July 20, 2017 Updates for October 1, 2017 Effective October 1, 2017 (the District s fiscal year
District of Columbia Medicaid Specialty Hospital Payment Method Frequently Asked Questions Version Date: July 20, 2017 Updates for October 1, 2017 Effective October 1, 2017 (the District s fiscal year
Observation Coding and Billing Compliance Montana Hospital Association
 Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Chapter 8 Section 2. Skilled Nursing Facility (SNF) Prospective Payment System (PPS)
 Prospective Payment System (PPS)") Skilled Nursing Facilities (SNFs) Chapter 8 Section 2 Skilled Nursing Facility (SNF) Prospective Payment System (PPS) Issue Date: April 1, 2002 Authority: 32 CFR 199.14(b); Sections 701 and 707 of NDAA
Skilled Nursing Facilities (SNFs) Chapter 8 Section 2 Skilled Nursing Facility (SNF) Prospective Payment System (PPS) Issue Date: April 1, 2002 Authority: 32 CFR 199.14(b); Sections 701 and 707 of NDAA
Local Educational Agency (LEA) Billing
 Billing") Local Educational Agency (LEA) Billing loc ed bil and Reimbursement Overview 1 This section contains information about reimbursable services for the Local Educational Agency (LEA) Medi-Cal Billing Option
Local Educational Agency (LEA) Billing loc ed bil and Reimbursement Overview 1 This section contains information about reimbursable services for the Local Educational Agency (LEA) Medi-Cal Billing Option
GIC Employees/Retirees without Medicare
 GIC Active Employees & Retirees without Medicare 7/1/18 GIC Employees/Retirees without Medicare HMO Summary of Benefits Chart This chart provides a summary of key services offered by your Health New England
GIC Active Employees & Retirees without Medicare 7/1/18 GIC Employees/Retirees without Medicare HMO Summary of Benefits Chart This chart provides a summary of key services offered by your Health New England
routine services furnished by nursing facilities (other than NFs for individuals with intellectual Rev
 4025.1 FORM CMS-2552-10 11-16 When an inpatient is occupying any other ancillary area (e.g., surgery or radiology) at the census taking hour prior to occupying an inpatient bed, do not record the patient
4025.1 FORM CMS-2552-10 11-16 When an inpatient is occupying any other ancillary area (e.g., surgery or radiology) at the census taking hour prior to occupying an inpatient bed, do not record the patient
LOUISIANA MEDICAID PROGRAM ISSUED: 08/15/12 REPLACED: 07/01/11 CHAPTER 25: HOSPITAL SERVICES SECTION 25.3: OUTPATIENT SERVICES PAGE(S) 11
 11") OUTPATIENT SERVICES Outpatient hospital services are defined as diagnostic and therapeutic services rendered under the direction of a physician or dentist to an outpatient in an enrolled, licensed and
OUTPATIENT SERVICES Outpatient hospital services are defined as diagnostic and therapeutic services rendered under the direction of a physician or dentist to an outpatient in an enrolled, licensed and
Connecticut Medical Assistance Program. CHC Service Provider Workshop
 Connecticut Medical Assistance Program CHC Service Provider Workshop Presented by: The Department of Social Services & HP for Billing Providers Agenda What s New in 2015 Electronic Messaging Re-Enrollment
Connecticut Medical Assistance Program CHC Service Provider Workshop Presented by: The Department of Social Services & HP for Billing Providers Agenda What s New in 2015 Electronic Messaging Re-Enrollment
Wyoming Medicaid- Provider Services Updates. Provider Workshops Summer 2017
 Wyoming Medicaid- Provider Services Updates Provider Workshops Summer 2017 Facilities Update TITLE 25- Involuntary Hospitalization Effective August 1, 2016- Wyoming Medicaid began processing Title 25 claims
Wyoming Medicaid- Provider Services Updates Provider Workshops Summer 2017 Facilities Update TITLE 25- Involuntary Hospitalization Effective August 1, 2016- Wyoming Medicaid began processing Title 25 claims
Provider-Based RHC Billing June 8, 2018
 Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
Provider-Based RHC Billing June 8, 2018 Sharon Shover, CPC, CEMC 502.992.3511 Provider-Based RHC Billing Agenda RHC Encounters Payment for RHC Services Same Day Visits Revenue Codes CG Modifier & QVL Non-RHC
Claims Operations Guide for Providers
 San Francisco Health Plan Claims Operations Guide for Providers November 2017 San Francisco Health Plan 50 Beale Street 12 th Floor San Francisco, CA 94105 Telephone: (415) 547-7818, Ext. 7115 Fax: (415)
San Francisco Health Plan Claims Operations Guide for Providers November 2017 San Francisco Health Plan 50 Beale Street 12 th Floor San Francisco, CA 94105 Telephone: (415) 547-7818, Ext. 7115 Fax: (415)
Facility-Based Behavioral Health Program Professional Fees Reimbursement Policy Annual Approval Date. Approved By
 Policy Number 2016RP505A Facility-Based Behavioral Health Program Professional Fees Reimbursement Policy Annual Approval Date 09/30/2016 Approved By Optum Behavioral Reimbursement Committee IMPORTANT NOTE
Policy Number 2016RP505A Facility-Based Behavioral Health Program Professional Fees Reimbursement Policy Annual Approval Date 09/30/2016 Approved By Optum Behavioral Reimbursement Committee IMPORTANT NOTE
Facility Name: Street Address: City: County: State: Zip: Web Site Address: Office Manager Name: Phone and Ext:
 FACILITY CREDENTIALING APPLICATION USI.V1.2010.01 FACILITY INFORMATION Please complete a separate application for each facility. Facility Name: Street Address: City: County: State: Zip: Phone: Fax: Federal
FACILITY CREDENTIALING APPLICATION USI.V1.2010.01 FACILITY INFORMATION Please complete a separate application for each facility. Facility Name: Street Address: City: County: State: Zip: Phone: Fax: Federal
Administrative Billing Data
 Administrative Billing Data Patient Identification and Demographic Information: From UB-04 Data or Medical Record Face Sheet. Note: When you go to enter data on this case, the information below will already
Administrative Billing Data Patient Identification and Demographic Information: From UB-04 Data or Medical Record Face Sheet. Note: When you go to enter data on this case, the information below will already
GUIDE TO BILLING HEALTH HOME CLAIMS
 GUIDE TO BILLING HEALTH HOME CLAIMS 1 GUIDE TO BILLING HEALTH HOME CLAIMS DEFINITIONS...1 BILLING TIPS...2 EDI TRANSACTIONS GUIDE...5 ATTACHMENT A SERVICE GRID...6 ATTACHMENT B FEE SCHEDULE...8 EXHIBIT
GUIDE TO BILLING HEALTH HOME CLAIMS 1 GUIDE TO BILLING HEALTH HOME CLAIMS DEFINITIONS...1 BILLING TIPS...2 EDI TRANSACTIONS GUIDE...5 ATTACHMENT A SERVICE GRID...6 ATTACHMENT B FEE SCHEDULE...8 EXHIBIT
MEDICAL POLICY No R2 TELEMEDICINE
 Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Summary of Changes Clarifications: Page 1, Section I. A 6, additional language added for clarification. Deletions: Additions Page 4, Section IV, Description, additional language added in regards to telemedicine.
Subject: 2009 Indiana Health Coverage Programs Provider Seminar
 INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 930 A U G U S T 2 7, 2009 To: All Providers Subject: 2009 Indiana Health Coverage Programs Provider Seminar Overview The Office
INDIANA HEALTH COVERAGE PROGRAMS P R O V I D E R B U L L E T I N B T 2 0 0 930 A U G U S T 2 7, 2009 To: All Providers Subject: 2009 Indiana Health Coverage Programs Provider Seminar Overview The Office
ICD-10 Frequently Asked Questions - AdvantX
 ICD-10 Frequently Asked Questions - AdvantX What Version of AdvantX is ICD-10 Compliant? Version 5.0.01 Where can I find ICD-10 Training Materials for AdvantX? 1. Visit our Client Portal (portal.sourcemed.net)
ICD-10 Frequently Asked Questions - AdvantX What Version of AdvantX is ICD-10 Compliant? Version 5.0.01 Where can I find ICD-10 Training Materials for AdvantX? 1. Visit our Client Portal (portal.sourcemed.net)
(a) The provider's submitted charge; or
 The provider's submitted charge; or") ACTION: Final DATE: 12/20/2013 11:35 AM 5101:3-1-60 Medicaid reimbursement. (A) The medicaid payment for a covered service constitutes payment in full and may not be construed as a partial payment when
ACTION: Final DATE: 12/20/2013 11:35 AM 5101:3-1-60 Medicaid reimbursement. (A) The medicaid payment for a covered service constitutes payment in full and may not be construed as a partial payment when
CONTRACT YEAR 2011 MEDICARE ADVANTAGE PRIVATE FEE-FOR-SERVICE PLAN MODEL TERMS AND CONDITIONS OF PAYMENT
 CONTRACT YEAR 2011 MEDICARE ADVANTAGE PRIVATE FEE-FOR-SERVICE PLAN MODEL TERMS AND CONDITIONS OF PAYMENT Table of Contents 1. Introduction 2. When a provider is deemed to accept Flexi Blue PFFS terms and
CONTRACT YEAR 2011 MEDICARE ADVANTAGE PRIVATE FEE-FOR-SERVICE PLAN MODEL TERMS AND CONDITIONS OF PAYMENT Table of Contents 1. Introduction 2. When a provider is deemed to accept Flexi Blue PFFS terms and
A County Organized Health System
 A County Organized Health System Presentation to Intermediate Care Facilities Paul Roberts, Director of Provider Relations and Contracting Pam Kapustay, RN, MSN, Director of Health Services Melanie Frampton,
A County Organized Health System Presentation to Intermediate Care Facilities Paul Roberts, Director of Provider Relations and Contracting Pam Kapustay, RN, MSN, Director of Health Services Melanie Frampton,
SNF Consolidated Billing Exclusions/Inclusions
 SNF Consolidated Billing Exclusions/Inclusions Under SNF consolidated billing rules, certain Part B services provided to SNF residents are to be billed directly by the SNF. The facility would bill the
SNF Consolidated Billing Exclusions/Inclusions Under SNF consolidated billing rules, certain Part B services provided to SNF residents are to be billed directly by the SNF. The facility would bill the
Chapter 9 Section 1. Ambulatory Surgical Center (ASC) Reimbursement
 Reimbursement") Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
If you want to subscribe to the provider only listserv, please with subscribe as the subject line.
 From: Sent: CMS ROCHI_Prov_Outreach Tuesday, March 06, 2012 1:48 PM Subject: CMS Medicare FFS Provider e News for Thu Mar 1 If you want to subscribe to the provider only listserv, please email: ROCHIFM@cms.hhs.gov
From: Sent: CMS ROCHI_Prov_Outreach Tuesday, March 06, 2012 1:48 PM Subject: CMS Medicare FFS Provider e News for Thu Mar 1 If you want to subscribe to the provider only listserv, please email: ROCHIFM@cms.hhs.gov
Florida Medicaid. Outpatient Hospital Services Coverage Policy. Agency for Health Care Administration. Draft Rule
 Florida Medicaid Agency for Health Care Administration Draft Rule Table of Contents Florida Medicaid 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal Authority... 1 1.3 Definitions... 1 2.0 Eligible
Florida Medicaid Agency for Health Care Administration Draft Rule Table of Contents Florida Medicaid 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal Authority... 1 1.3 Definitions... 1 2.0 Eligible