Improving the safety of medication dispensing in primary care by combining human factors and quality improvement sciences
|
|
|
- Eustacia Garrison
- 5 years ago
- Views:
Transcription

1 Improving the safety of medication dispensing in primary care by combining human factors and quality improvement sciences Programme delivery team; Tony Jamieson, Y&H AHSN Improvement Academy. Gerry Armitage University of Bradford. Noshaba Anwar Improvement Academy. John Bibby Improvement Academy. Judith Dyson Hull University. Maureen McGeorge - Improvement Academy. Correspondence to Objective This paper describes a quality improvement programme in patient safety within community (primary care) pharmacies in England. Dispensing medicines in community pharmacy is a process which is required to be highly reliable. The pharmacy team must combine clinical, technical and non-technical skills in order to accurately supply medicines which are safe and effective for patients. Research estimates that up to 3.32% of dispensed items include an error (James et al., 2009). Although this level of accuracy could be considered to be very high, errors can have serious consequences for patients and for the responsible pharmacists. Pharmacy professionals have a recognised role in patient safety (Royal Pharmaceutical Society, 2010). They have developed systems to guard against error; however, there is still a need to reduce errors further. This project made use of structured education on patient safety based on human factors theory and a facilitated quality improvement methodology. Its objectives were to: Build an awareness, in the members of the pharmacy teams, of the common causes of error in community pharmacy Increase knowledge and skills of how to undertake an improvement project Improve systems that minimise the occurrence of dispensing errors Increase the accuracy of dispensing in the participating teams Context and setting The delivery of healthcare is by its nature complex and error prone. We know that there is an error in the prescribing process of 5 to 7% of prescriptions, dependent on the setting (Avery et al., 2013) (Lewis et al., 2009). Of the medication error reports to the UK s National Reporting and Learning System between 2005 and 2010 (the majority of which are reported by hospitals), 16% reported actual patient harm, and 0.9% resulted in death or severe harm (Cousins et al., 2012). Unintended discrepancies in patients medicines after discharge from hospital frequently occur, affecting 43% of repeat prescriptions in primary care and more
2 than half of all patients discharged (Garfield et al. 2009). Problems with medicines after hospital discharge are particularly associated with adverse health consequences. The dispensing error rate in hospitals has been estimated as % of dispensed medicines and in community pharmacies, the estimate is % of dispensed medicines (James et al., 2009). In 2007 over 748 million prescriptions were prescribed and dispensed in primary care and this resulted in just 5,223 medication error reports being submitted to the National Reporting and Learning System (NRLS) by community pharmacies (National Patient Safety Agency, 2009), a figure far lower than would be expected from the research in error rates. Factors such as mental workload, distraction and dispensing with divided attention have been highlighted as conditions which increase the dispensing error rate (Family, 2013) (Harvey, 2015) and these conditions highlight the importance of human factors in community pharmacy practice. Human factors in healthcare is an approach to enhancing clinical performance through an understanding of the effects of teamwork, tasks, equipment, workspace, culture and organisation has on human behaviour and abilities. It has foundations in psychology, sociology, physiology, design and engineering and is the key to understanding why errors are made and how to prevent them. The NHS has been slow to follow the lead of other safety critical industries in the adoption of human factors, particularly so in primary care and so the National Quality Board (2013) published a concordat on human factors in which it describes the commitment of leadership organisations in the NHS to increase the understanding and use of human factors to improve safety. Community Pharmacies, being the setting for this project, are private organisations that contract with the NHS. They are recognised to be isolated in primary care as a consequence of their contractual obligations. Pharmacists are subject to specific requirements relating to medicines governance that severely restrict the amount of time they can leave the pharmacy premises for which they are responsible whilst it is open to the public. Design The programme adopted the Training & Action for Patient Safety (TAPS) methodology as described by Slater et at. (2012). This methodology had been used successfully on previous local projects led by the core team. The core elements of the TAPS approach, which were considered by the core team to be advantageous, are: a 20-week programme of involvement; participation of between 7-15 multi-disciplinary teams; a requirement on participating teams to attend an orientation session and three workshops (Table 1); a requirement on participating teams to complete a case study log and to regularly report measures of their success; availability of support to the participating teams by telephone or face-toface, as required, from the core team.
3 The TAPS approach shares similarities with a clinical community of improvement as it offers an organised structure for supporting and securing improvements in health systems across multiple sites (The Health Foundation, 2013). The structure itself is a simple one, comprising: a core team to provide high-level leadership, direction, coordination and organisational support site teams in participating organisations that make change happen locally. The core team enables the community to be vertically integrated (focused on shared goals) and the site teams in participating organisations allow horizontal integration (thus activating peer influence and knowledge-sharing). The core team consisted of: An experienced senior pharmacist with professional credibility. An experienced Quality improvement programme manager. A project manager/improvement facilitator. Patient safety and quality improvement educators. To provide a clinical community of improvement for community pharmacy teams Table 1 TAPS workshop programme Orientation Event (1/2 day) (week 0) Workshop 1 (1-day) (week 4) Workshop 2 (1/2 day)(week 12) Workshop 3 (evening session)(week 20) Description of TAPS approach. 1 st Educational intervention on Human Factors. Introduction of the improvement measure. 2 nd Educational Intervention on Human factors. Education on IHI improvement model. Education on run-charts. Demonstration of methods of improving safety. Peer review. 3 rd Educational intervention on Human Factors. Education on annotating run charts Peer review. Presentation of results. Programme Measures Primary measure In order to ensure consistency of meaning and therefore measurement of outcome, a definition for a dispensing error medication incident in this programme was agreed with the participants: Any unintended or unexpected incident which led to harm or could have led to harm which arose from an act or omission by a member of the pharmacy team. This focussed the improvement activity within the participating teams on things that were in the power of the team to change.
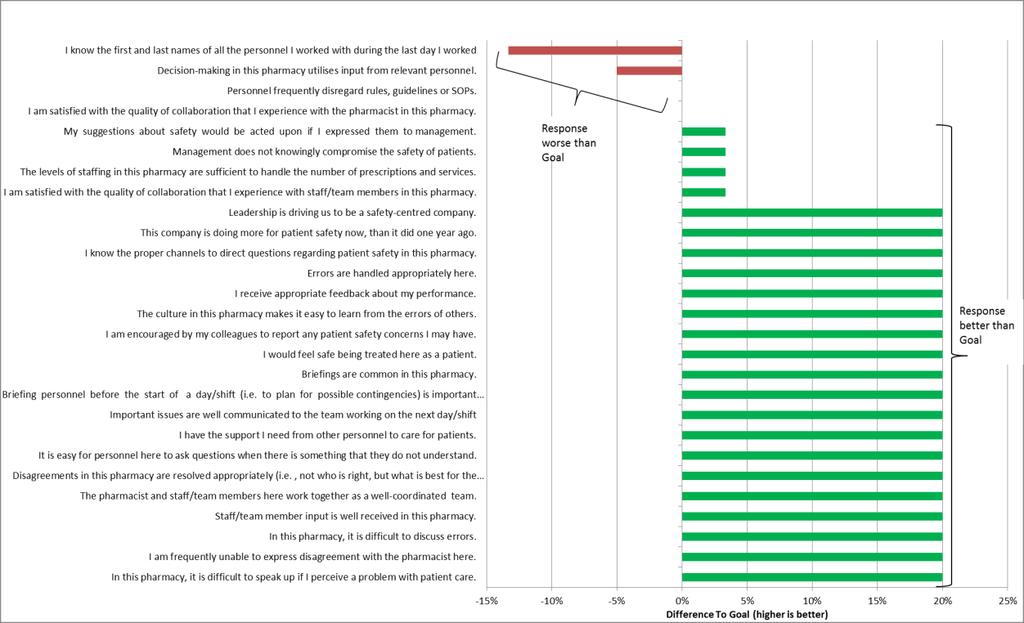
4 Due to the relatively small number of actual errors occurring (and the potential severity of associated consequences), the teams agreed to focus on the measurement of near misses. The improvement measure of dispensing safety was therefore agreed with the participating teams as: The number of prescription items identified at the final check which required referral back into the dispensing process for whatever reason (near misses) as a proportion of the number of items dispensed that day. Near misses Daily item count In addition the teams completed an anonymous safety culture and teamwork survey based upon the work of Sexton, et al. (2006). This was done prior to the commencement of the improvement programme and was repeated at the end of the programme. Recruitment of site teams The task of recruiting teams was therefore complex and used a number of routes, including recruitment through local pharmaceutical committees, superintendents of pharmacy chains, Local Professional Networks for Pharmacy, and the Royal Pharmaceutical Society Local Pharmacy Forum. Nine teams signed up to the programme. Two teams did not complete the 20-week programme due to insurmountable staffing issues. The participating teams were from a range of pharmacy settings: 1 GP practice dispensary (working over 2 sites) 3 independent pharmacies (1 of which withdrew from the programme) 5 pharmacies from across 3 large multiple pharmacy chains (1 of which withdrew from the programme). These included high-street, GP practice and hospital outpatient based dispensaries Improvement Methods The Institute for Healthcare Improvement s Model for Improvement was used by the participating teams throughout the programme (Figure 1) (Langley et al 2009). The participating teams were supported by the core team to populate and annotate runcharts (Perla et al., 2011) using the improvement measure. Orientation Event (week 0) This half day event brought teams together to learn about the TAPS methodology and have an introduction to human factors and improvement science, including a discussion of the proposed programmes measures. Teams also completed the safety culture and teamwork survey and took away multiple copies for completion by their pharmacy colleagues.
5 First visit In the fortnight following the Orientation Event, each team was visited by the Project Team. The purpose of the visit included: meeting others team members collecting the completed safety culture and teamwork surveys supporting teams to work out best ways of gathering their measures agreeing a day of the week when the daily measures would be submitted clarifying any outstanding matters Workshop 1 (week 4) This full-day event provided a more in-depth understanding of how to apply the Model for Improvement, including use of run charts, and introduction to a range of patient safety improvement tools. There were: Process mapping A template for significant event audit derived from the NPSA guidance on Significant Event Audit in general Practice (National Patient Safety Agency, 2008) and the Yorkshire Contributory Factors Framework (Lawton et al., 2012) Achieving Behaviour Change for Patient Safety toolkit. (Taylor et al., 2013) Safety briefings incorporating elements of the Patient Safety WalkRound (Frankle et al., 2003) Guidance from NPSA (2007) on Design for patient safety design of the dispensing environment SBAR structured communication tool. (NHS Institute, 2008) Workshop 2 (week 12) This half-day workshop offered detailed input on patient safety and human factors, and gave teams the opportunity to begin to annotate their run charts with details of the various interventions that had effected their measures. Workshop 3 (week 20) The final event brought teams together to share stories of their improvement journey and to celebrate their successes. Interim supports The participating teams were contacted or visited by the Project Team at least every 2 weeks. Teams were offered encouragement and a range of advice on improvement methods including the PDSA cycles and measures. They also facilitated transfer of intelligence (shared learning) between the participating teams.

6 Figure 1 IHI model for improvement Findings of initial measurement Culture Survey Baseline Safety Culture and Teamwork surveys were received from five of the teams. The results showed high scores across the determinants when compared to teams in other settings (for example acute trust wards. [Local data on file]) with some variation across team members (Appendix 1). Notably it could be seen that the most senior person in each team (being the main pharmacist or GP lead for dispensing), scored lower confidence in the safety of their organisations than the rest of the teams. Primary Measure Six out of the eight sites were able to establish a baseline for the improvement measure. One pharmacy had a much lower denominator (daily number of dispensed items) than the other participating pharmacies and this impacted on the numerator (near misses). This necessitated a different improvement measure of, Days between a near miss. A baseline was established for this pharmacy on this basis. One pharmacy (Pharmacy D) did not record, on a daily basis, the number of items it dispensed. As a result the run chart displayed the number of near misses per 100 items based upon an average of 400 items per day. Seven participating teams (eight sites) produced annotated run-charts, with support form the core team, by the end of the programme. All the teams undertook PDSA cycles as part of the programme and utilised a range of the tools provided. The participating teams also
7 tested interventions they had designed themselves that were directed at addressing human factors. Interventions included: Management of distractions Debriefing Enhanced Significant Event Audit Changes to process. (e.g. crosschecking documentation) Changes to task allocation (e.g. who answers the telephone) Environmental management (e.g. dispensary lay-out, arrangement of shelves) Changes to responsibility (e.g. improved self-checking) Encouraging a culture of incident reporting Use of the SBAR tool Case studies of the interventions can be found in Appendix 2 One pharmacy (Pharmacy D) implemented an intervention which was not associated with the management of human factors. The intervention was to take staff members off dispensing duties if they made 3 errors identified at the final check. Findings of successive measurement Primary Measure Pharmacy A (Figure 2) achieved a reduction in the mean number of near misses per 100 items identified by 8 consecutive data points below the baseline. Figure 2 Pharmacy A
8 Pharmacy B (Figure 3) saw an increase in the mean number of near misses per 100 items which then decreased back to baseline. The run-chart was not annotated with the interventions made by the team. Figure 3 Pharmacy B Pharmacy C (Figure 4) did not achieve a change in the baseline during the programme. The pharmacy did identify a recurring spike in the data which was used to identify special cause type variation. Figure 4 Pharmacy C
9 Pharmacy D (Figure 5) generated a run chart based upon an average number of prescriptions rather than the actual number dispensed. No changes in baseline were achieved. Figure 5 Pharmacy D Pharmacy E (Figure 6) achieved a reduction in the baseline median number of near misses per 100 items following a clearly annotated intervention. The revised median was sustained for the rest of the programme. Figure 6 Pharmacy E
10 Pharmacy F (Figure 7). The run chart showed an early reduction in the baseline. However this was attributed to a period when near misses were not recorded by the pharmacy. Towards the end of the programme an annotated intervention was followed by a reduction in the mean number of near misses per 100 items (as demonstrated by 8 consecutive data points below the previous average). Figure 7 Pharmacy F Pharmacy G (Figure 8) achieved 2 reductions in the mean number of near misses per 100 items. The run chart was not annotated with the interventions. Figure 8 Pharmacy G
11 Pharmacy H generated a run chart based upon the number of days between near misses. No change in the baseline was identified. Figure 9 Pharmacy H Safety Culture and Teamwork survey Three pharmacy teams repeated the Safety Culture and Teamwork Survey at the end of the programme. The response rate was lower than the baseline, preventing direct comparison. Three of the participating teams also provided feedback on their experience of being involved in the programme in the form of video testimonials. The interview questions were based on value creation stories described by (Wenger et al., 2011). The testimonials from the teams ( that participation in the programme was informative, practical and rewarding. Analysis Recruitment of teams was successful despite the necessity to accommodate the contractual and legal requirements for pharmacists to remain on the pharmacy premises for which they are responsible. This was achieved by providing the workshop sessions on a Sunday when most of the participating team s premises were closed to the public and by the core team visiting the teams at their place of work. Six of the seven participating teams engaged with the TAPS approach and adopted the IHI methodology readily. Common traits of these participating teams, noted by the core team, were:
12 High motivation for improving safety Camaraderie within the team; Participative leadership and A past history of making changes for improvement Participating teams had not previously received training in the avoidance of error or human factors, however all except one of the interventions that the teams put into place demonstrated that they had understood the human factors theory and were able to translate it into practice. The TAPS approach requires the participating teams to come out of their work environment for the training and peer support elements of the programme. Attendance at the workshops was variable across the teams with some teams were unable to attend all four events with some bringing a larger number of delegates than others. The provision of interim supports by the core team was therefore important in maintaining momentum throughout the programme. The application of improvement methodology using PDSA cycles was incorporated into the participating teams daily activities. However, not all interventions tried by the teams were tested using PDSA cycles and in most cases it was difficult to attribute causality to a particular intervention, when a change in the average on the run charts was achieved. The ease with which the teams were able to update their run charts and the visual impact the charts had in the participating teams allowed for continuous monitoring of improvements. Unfortunately, annotation was less consistent and this may have led to some interventions being poorly evaluated for their effectiveness. The results of the safety culture and teamwork survey which was done at the start of the programme reflected well on the participating teams relative to findings from teams in other service areas. Indeed, the results fostered open dialogue within the teams and provided insight into what behaviours are manifest in a strong safety culture. It is arguable that the close quarters working (restricted work space) in pharmacy dispensaries necessitates a greater level of co-operation than other environments where interaction between the team is less frequent. It is not possible from the returns of the repeat survey to draw any definitive conclusions. Pharmacy D did not share all the traits of the other participating teams. This pharmacy did not engage as strongly with the core team and it did not record its daily number of items dispensed which was necessary for the calculation of the primary improvement measure. It was slow to start its first PDSA cycle and chose an intervention which appeared to be a punishment for human failure without consideration of the human factors involved. Conclusion The programme has shown that statistically significant reductions in dispensing errors can be achieved in community pharmacies though a combination of training and action in
13 human factors and quality improvement. The participating teams demonstrated that quality improvement methodologies can be accommodated into the busy dispensary routine and that measuring for patient safety in a dispensary is effective in monitoring the effects of change. The TAPS approach was also effective at embedding human factors and quality improvement into community dispensaries. It could be argued that the participating teams, being volunteers for a novel approach to safety improvement, were not representative of pharmacy in the UK. It is possible that, to be successful in using this quality improvement methodology to improve patient safety, pharmacy teams may need to share some of the characteristics that the core team observed in the participating teams; motivation for improving safety, camaraderie within the team, participative leadership, adequate staffing (being that the teams did not consider staffing levels to require increasing) and a past history of making changes for improvement. It may be possible to use the Safety Culture & Teamwork Survey to identify pharmacies that are likely to succeed in completing a quality improvement programme such as this one. However this would need to be tested on a larger cohort of pharmacies than were involved in this programme. The success of the approach taken in this programme suggests that there are significant opportunities to improve patient safety through training in human factors and quality improvement methodologies. Inclusion of these elements into undergraduate and post graduate education programmes for pharmacists and pharmacy technicians may prove beneficial in particular in embedding continuous quality improvement into every-day practice. References Avery, A. J., Ghaleb, M., Barber, N., Dean Franklin, B., Armstrong, S. J., Serumaga, B., Dhillon, S., Freyer, A., Howard, R., Talabi, O. and Mehta, R. L. (2013) The prevalence and nature of prescribing and monitoring errors in English general practice: a retrospective case note review. British Journal of General Practice, 63 (613), Cousins, DH. Gerrett, D. Warner, B. (2012) A review of medication incidents reported to the National Reporting and Learning System in England and Wales over 6 years ( ). Br J Clin Pharmacol 74(4): Family, H. (2013) The effects of mental workload on medicines safety in a community pharmacy setting. University of Bath, department of Pharmacy and Pharmacology. (accessed 05/11/ Frankel, A. Graydon-Baker, E. Neppl, C. Simmonds, T. Gustafson, M. Gandhi, T.K. (2003) Patient Safety Leadership WalkRounds. Joint Commission on Quality and Safety. 29: 1 Garfield, S. Barber, N. Walley, P. (2009) Quality of medication use in primary care-mapping the problem, working to a solution: a systematic review of the literature. BMC Med. 50.
14 Harvey, J., Avery, A. J., Ashcroft, D., Boyd, M., Phipps, D. L., & Barber, N. (2015). Exploring safety systems for dispensing in community pharmacies: Focusing on how staff relate to organizational components. Research in Social & Administrative Pharmacy, 11(2), Langley, GL. Moen, R. Nolan, KM. Nolan, TW. Norman, CL. Provost, LP. (2009) The Improvement Guide: A Practical Approach to Enhancing Organizational Performance (2nd edition). San Francisco: Jossey-Bass Publishers. Lawton, R., McEachan, R. R. C., Giles, S. J., Sirriyeh, R., Watt, I. S. and Wright, J. (2012) Development of an evidence-based framework of factors contributing to patient safety incidents in hospital settings: a systematic review. BMJ Quality & Safety, 21 (5), Lewis, PJ. Dornan, T. Taylor, D. (2009). Systematic review of the prevalence, incidence and nature of prescribing errors in hospital inpatients. Drug Safety, 32(5) National Patient Safety Agency. (2007) Design for patient safety; A guide to the design of the dispensing environment. Edition 1. (Accessed 5/11/2015http:// ) National Patient Safety Agency. (2008) Significant Event Audit. (accessed 5/11/ National Patient Safety Agency. (2009) Safety in Doses, Improving the use of medicines in the NHS. National Quality Board. (2013). Human Factors in Healthcare -A Concordat from the National Quality Board. NHS Institute. (2008) SBAR- Situation-Background-Assessment-Recommendation. (Accessed 5/11/ ment_tools/sbar_-_situation_-_background_-_assessment_-_recommendation.html ) NPA National Pharmacy Association. (2012) (accessed 5/11/ Perla, RJ. Provost, LP. Murray, SK. (2011) The run chart: a simple analytical tool for learning from variation in healthcare processes. BMJ Qual Saf 20: Royal Pharmaceutical Society. (2010) Patient Safety - A briefing for Parliamentarians participating in the debate on the Health Select Committee report on Patient Safety. (Accessed 5/11/ The Health Foundation (2013) Using Clinical Communities to improve Quality (Accessed 5/11/ Sexton, JB. Helmreich, RL. Neilands, TB. Rowan, K. Vella, K. Boyden, J. Roberts, PR. Thomas, EJ. (2006) The Safety Attitudes Questionnaire: Psychometric Properties, Benchmarking Data, and Emerging Research. BMC Health Services Research, 6: 44.
15 Slater, B. L., Lawton, R., Armitage, G., Bibby, J. and Wright, J. (2012), Training and action for patient safety: Embedding interprofessional education for patient safety within an improvement methodology. J. Contin. Educ. Health Prof., 32: Taylor, N. Slater, B. Lawton, R. Wright, J. Robins, V. (2013) Using behaviour change and implementation science to embed National Patient Safety Agency guidance within NHS organisations. Bradford Institute for Health Research. (Accessed 5/11/ aviour%20change%20taylor%20et%20al%202013%20final%20rif%20report.pdf) Wenger, E., Trayner, B., and de Laat, M. (2011) Promoting and assessing value creation in communities and networks: a conceptual framework. Rapport 18, Ruud de Moor Centrum, Open University of the Netherlands (Accessed 3/12/ ) Acknowledgements. The Improvement Academy would like to acknowledge the following people and organisations for their invaluable contributions to the development and delivery of this programme. The participating team members. The programme delivery team. David Alldred Leeds University Jaspal Bagral Improvement Academy Louise Barber Improvement Academy Alison Blenkinsopp Bradford University John Evans - ASDA Pharmacy Hannah Family Bath University Rebecca Lawton Leeds University & Bradford Institute of Heath Research Graham Prestwich Lay adviser to Improvement Academy Michael Rooney Improvement Academy Kirstie Samuel Lay adviser to Improvement Academy Beverly Slater Improvement Academy Rachel Urban Community Pharmacy West Yorkshire.
16 Appendix 1 Safety Culture & Teamwork Survey Baseline results
17
18
19 Appendix 2 Case Studies. Pharmacy C The team wanted to reduce the number of near misses occurring daily in the dispensing process of their dispensary. They identified that as a team, they work well together, however there was a desperate need to streamline the dispensing process and collect measures to identify any pitfalls During the first Learning Workshop, the team completed a process map of their dispensing process. The team identified some necessary changes that they felt would improve the dispensing process. The team had many big plans in place to streamline the whole dispensing process. They decided to improve the near misses recording sheet and collect measures from both sites. They also decided to re-arrange the reception and dispensary workspace so that dispensers had more space to work and concentrate in. Pharmacy D The team wanted to reduce the number of near misses occurring daily in the dispensing process of their pharmacy. They identified that as a team, they work well together, however there were some small changes that they could make to allow for a smoother run of the pharmacy. One issue regarding auto-repeat system they had in place caused confusion to staff and patients alike. The confusion was linked to where in the dispensary prescriptions and completed medication bags were placed. The team felt that organising this area well will reduce stress levels within staff members and increase their confidence. During the first Learning Workshop, the team completed a process map of their dispensing process. The team identified some necessary changes that they felt would increase patient satisfaction and reduce stress on work colleagues. They identified that if they explained the auto-repeat process accurately and created laminate cards to give to patients regarding their auto-repeats, both staff and patients would have more clarity and control in their monthly medicines supply. The main priority for the team was a need to reduce the number of calls and unnecessary visits they were getting from patients expecting medicines to be ready. This was very time consuming for staff to explain to patients the day their medicines will be ready for collection, and frustrating for patients alike. The team identified that the way they collected their near misses was not effective and not a true reflection of the actual number of near misses occurring daily. As the near miss log was electronic, and the team only had two computers between them, the computer was hardly available to input near miss data at the time of the event. This led to forgetting to update the log, and as a result not having reliable measures to work from. On a visit, we suggested having a paper log of near miss entries which would be available all the time and can be accessed to update near misses as they occur. This was successfully implemented and the team realised that this allowed them to record near miss data easily, providing reliable measures to work with. Pharmacy F The team wanted to reduce the number of near misses occurring daily in the dispensing process of their pharmacy. They identified that as a team, they work well together, however the dispensing layout caused many distractions and thus increased the level of near misses occurring. They felt that
20 due to close working within colleagues, and an open-view layout of the dispensary, the distraction level was the main cause of lack of concentration. Repetitive tasks also increased the error rate. During the first Learning Workshop, the team completed a process map of their dispensing process. The team identified some necessary changes that they felt would increase patient satisfaction and reduce stress on work colleagues. The main priority for the team was a need to change the dispensary layout. As dispensers were working next to each other, paperwork was getting mixed and sometimes labels were put on wrong medications. To avoid this from occurring, the two computers used for dispensing were moved further away from each other and dispensing assistants managing the paperwork were stood further away from each other using the computer as a useful obstacle. Furthermore as the team worked closely together and identified that communication between them was a major distraction to work, they decided to change this by informing other colleagues that they were concentrating so not to talk. As they were very friendly with each other and wanting the signal to be quiet, to be subtle, they decided to put their index finger on their lip, to signal no talking please, I am concentrating. The team found this worked extremely well and did not hinder their working relationship too. Other changes included minimal multi-tasking. If a dispenser is busy dispensing medication, they should not leave their work for other reasons e.g. answer the telephone, handle the reception desk. Rather, they should leave dispensing if the reception desk needs cover or if they have to answer the phone, they need to go back to dispensing and start from the beginning with the prescription sheet. The team found that this reduced work pressure and allowed them time to concentrate on dispensing fully. Pharmacy H The team wanted to reduce the number of near misses occurring daily in the dispensing process of their pharmacy. They identified that as a team, they work well together, however effective communication regarding Prescription Collection Service (PCS) was an issue. They felt that patients would arrive to collect a prescription and often prescriptions had not been ordered or were not ready. This led to low patient satisfaction and an increase in stress on the team. During the first Learning Workshop, the team completed a process map of their dispensing process. The team identified some necessary changes that they felt would increase patient satisfaction and reduce stress on work colleagues. The main priority for the team was a need to streamline the PCS. They introduced a clearly labelled basket for any prescription that required faxing to the relevant GP Practice. Any prescriptions in the basket were the responsibility of the individual who placed it there and an agreement was in place that no-one should finish their shift with incomplete tasks relation to the PCS. The document used to pick up any repeat prescriptions from neighbouring GP practices was amended. Rather than having a list of patients with GP Practices on a table (in no particular order), the table was split into the different GP Practices. This ensured that no patient was missed out when dispensing assistants went to collect repeat prescriptions on their behalf. See also
UKMi and Medicines Optimisation in England A Consultation
 UKMi and Medicines Optimisation in England A Consultation Executive Summary Medicines optimisation is an approach that seeks to maximise the beneficial clinical outcomes for patients from medicines with
UKMi and Medicines Optimisation in England A Consultation Executive Summary Medicines optimisation is an approach that seeks to maximise the beneficial clinical outcomes for patients from medicines with
East Gippsland Primary Care Partnership. Assessment of Chronic Illness Care (ACIC) Resource Kit 2014
 Resource Kit 2014") East Gippsland Primary Care Partnership Assessment of Chronic Illness Care (ACIC) Resource Kit 2014 1 Contents. 1. Introduction 2. The Assessment of Chronic Illness Care 2.1 What is the ACIC? 2.2 What's
East Gippsland Primary Care Partnership Assessment of Chronic Illness Care (ACIC) Resource Kit 2014 1 Contents. 1. Introduction 2. The Assessment of Chronic Illness Care 2.1 What is the ACIC? 2.2 What's
Medicines Optimisation: Helping patients to make the most of medicines
 Medicines Optimisation: Helping patients to make the most of medicines Good practice guidance for healthcare professionals in England May 2013 Endorsed by Foreword The NHS Constitution establishes the
Medicines Optimisation: Helping patients to make the most of medicines Good practice guidance for healthcare professionals in England May 2013 Endorsed by Foreword The NHS Constitution establishes the
Initial education and training of pharmacy technicians: draft evidence framework
 Initial education and training of pharmacy technicians: draft evidence framework October 2017 About this document This document should be read alongside the standards for the initial education and training
Initial education and training of pharmacy technicians: draft evidence framework October 2017 About this document This document should be read alongside the standards for the initial education and training
RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT SAFETY
 RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT SAFETY medicalprotection.org +44 (0)113 241 0359 or +44 (0)113 241 0624 RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT
RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT SAFETY medicalprotection.org +44 (0)113 241 0359 or +44 (0)113 241 0624 RISK MANAGEMENT EXPERT SUPPORT TO MANAGE RISK AND IMPROVE PATIENT
The Yorkshire & Humber Improvement Academy Clinical Leadership Training Programme
 The Yorkshire & Humber Improvement Academy Clinical Leadership Training Programme The Improvement Academy (IA) is one of the leading quality and safety improvement networks in the UK. The IA works across
The Yorkshire & Humber Improvement Academy Clinical Leadership Training Programme The Improvement Academy (IA) is one of the leading quality and safety improvement networks in the UK. The IA works across
Safer use of anticoagulants: the NPSA patient safety alert Steve Chaplin MSc, MRPharmS
 Safer use of anticoagulants: the NPSA patient safety alert Steve Chaplin MSc, MRPharmS Steve Chaplin describes the NPSA s anticoagulant patient safety alert and the measures it recommends for making the
Safer use of anticoagulants: the NPSA patient safety alert Steve Chaplin MSc, MRPharmS Steve Chaplin describes the NPSA s anticoagulant patient safety alert and the measures it recommends for making the
Information shared between healthcare providers when a patient moves between sectors is often incomplete and not shared in timely enough fashion.
 THE DISCHARGE MEDICINES REVIEW SERVICE Introduction During a stay in hospital a patient s medicines may be changed. Studies show that many patients may experience an error or problem with their medicines
THE DISCHARGE MEDICINES REVIEW SERVICE Introduction During a stay in hospital a patient s medicines may be changed. Studies show that many patients may experience an error or problem with their medicines
Safety Huddles: Bringing fun to the frontline and reducing harm
 Safety Huddles: Bringing fun to the frontline and reducing harm Alison Lovatt Clinical Network Director, Improvement Academy Ali Cracknell Consultant Medicine For Older People, Leeds Teaching Hospitals
Safety Huddles: Bringing fun to the frontline and reducing harm Alison Lovatt Clinical Network Director, Improvement Academy Ali Cracknell Consultant Medicine For Older People, Leeds Teaching Hospitals
Reconciliation of Medicines on Admission to Hospital
 Reconciliation of Medicines on Admission to Hospital Policy Title State previous title where relevant. State if Policy New or Revised Policy Strand Org, HR, Clinical, H&S, Infection Control, Finance For
Reconciliation of Medicines on Admission to Hospital Policy Title State previous title where relevant. State if Policy New or Revised Policy Strand Org, HR, Clinical, H&S, Infection Control, Finance For
NATIONAL PATIENT SAFETY AGENCY DRAFT PATIENT SAFETY ALERT. Safer Use of Injectable Medicines In Near-Patient Areas
 NATIONAL PATIENT SAFETY AGENCY DRAFT PATIENT SAFETY ALERT Safer Use of Injectable Medicines In Near-Patient Areas Wide Stake Holder Consultation January March 2006 The NPSA is undertaking a wide stake
NATIONAL PATIENT SAFETY AGENCY DRAFT PATIENT SAFETY ALERT Safer Use of Injectable Medicines In Near-Patient Areas Wide Stake Holder Consultation January March 2006 The NPSA is undertaking a wide stake
Integrating quality improvement into pre-registration education
 Integrating quality improvement into pre-registration education Jones A et al (2013) Integrating quality improvement into pre-registration education. Nursing Standard. 27, 29, 44-48. Date of submission:
Integrating quality improvement into pre-registration education Jones A et al (2013) Integrating quality improvement into pre-registration education. Nursing Standard. 27, 29, 44-48. Date of submission:
Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING
 Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING Contents Page 1.0 Purpose 2 2.0 Definition of medication error
Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING Contents Page 1.0 Purpose 2 2.0 Definition of medication error
Supervising pharmacist independent
 Supervising pharmacist independent prescribers in training Summary of responses to the discussion paper Introduction 1. Two of the General Pharmaceutical Council s core activities are setting standards
Supervising pharmacist independent prescribers in training Summary of responses to the discussion paper Introduction 1. Two of the General Pharmaceutical Council s core activities are setting standards
W e were aware that optimising medication management
 207 QUALITY IMPROVEMENT REPORT Improving medication management for patients: the effect of a pharmacist on post-admission ward rounds M Fertleman, N Barnett, T Patel... See end of article for authors affiliations...
207 QUALITY IMPROVEMENT REPORT Improving medication management for patients: the effect of a pharmacist on post-admission ward rounds M Fertleman, N Barnett, T Patel... See end of article for authors affiliations...
EVALUATION OF THE COMMUNITY PHARMACY RESEARCH READY ACCREDITATION PROGRAMME
 EVALUATION OF THE COMMUNITY PHARMACY RESEARCH READY ACCREDITATION PROGRAMME 2016 Contents 1 Executive Summary... 3 1.1 What is Research Ready... 3 1.2 Purpose of the Evaluation... 3 1.3 Results of the
EVALUATION OF THE COMMUNITY PHARMACY RESEARCH READY ACCREDITATION PROGRAMME 2016 Contents 1 Executive Summary... 3 1.1 What is Research Ready... 3 1.2 Purpose of the Evaluation... 3 1.3 Results of the
GUIDANCE ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY
 ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
THE USE OF SMARTPHONES IN CLINICAL PRACTICE
 Art & science The synthesis of art and science is lived by the nurse in the nursing act JOSEPHINE G PATERSON THE USE OF SMARTPHONES IN CLINICAL PRACTICE Sally Moore and Dharshana Jayewardene look at the
Art & science The synthesis of art and science is lived by the nurse in the nursing act JOSEPHINE G PATERSON THE USE OF SMARTPHONES IN CLINICAL PRACTICE Sally Moore and Dharshana Jayewardene look at the
High level guidance to support a shared view of quality in general practice
 Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
How can I make safety huddles work in my area?
 How can I make safety huddles work in my area? Safety Huddles: How can I make patient safety huddles work for my area? Dr Ali Cracknell Consultant in Medicine for Older People (Leeds Teaching Hospitals
How can I make safety huddles work in my area? Safety Huddles: How can I make patient safety huddles work for my area? Dr Ali Cracknell Consultant in Medicine for Older People (Leeds Teaching Hospitals
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine
 Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Who s s on What? Latest Experience with the Framework Challenges and Successes. November 29, Margaret Colquhoun Project Leader ISMP Canada
 Who s s on What? Latest Experience with the Framework Challenges and Successes November 29, 2005 Margaret Colquhoun Project Leader ISMP Canada 1 Outline ISMP Canada Partnership with SHN The Canadian Getting
Who s s on What? Latest Experience with the Framework Challenges and Successes November 29, 2005 Margaret Colquhoun Project Leader ISMP Canada 1 Outline ISMP Canada Partnership with SHN The Canadian Getting
Consultation on initial education and training standards for pharmacy technicians. December 2016
 Consultation on initial education and training standards for pharmacy technicians December 2016 The text of this document (but not the logo and branding) may be reproduced free of charge in any format
Consultation on initial education and training standards for pharmacy technicians December 2016 The text of this document (but not the logo and branding) may be reproduced free of charge in any format
National Programme to Prevent Central-Line Associated Bacteraemia. Project Charter October 2011 to April 2013
 National Programme to Prevent Central-Line Associated Bacteraemia Project Charter October 2011 to April 2013 1. Overview Central-Line Associated Bacteraemia (CLAB) prevention is one of the most important
National Programme to Prevent Central-Line Associated Bacteraemia Project Charter October 2011 to April 2013 1. Overview Central-Line Associated Bacteraemia (CLAB) prevention is one of the most important
Recommendations for safe trainee changeover
 Recommendations for safe trainee changeover Introduction Doctors in training in the UK have historically started new six-monthly rotations in February and August, with the majority of junior doctors rotating
Recommendations for safe trainee changeover Introduction Doctors in training in the UK have historically started new six-monthly rotations in February and August, with the majority of junior doctors rotating
Improving harm from falls as part of the Patient safety initiative
 Improving harm from falls as part of the Patient safety initiative The story so far. 1. CONTEXT 1.1. Since January 2011, 2gether NHS Foundation Trust has been involved in the NHS South West Quality and
Improving harm from falls as part of the Patient safety initiative The story so far. 1. CONTEXT 1.1. Since January 2011, 2gether NHS Foundation Trust has been involved in the NHS South West Quality and
Safety in Mental Health Collaborative
 NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
Improving teams in healthcare
 Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Improving compliance with oral methotrexate guidelines. Action for the NHS
 Patient safety alert 13 Alert Immediate action Action Update Information request Ref: NPSA/2006/13 Improving compliance with oral methotrexate guidelines Oral methotrexate is a safe and effective medication
Patient safety alert 13 Alert Immediate action Action Update Information request Ref: NPSA/2006/13 Improving compliance with oral methotrexate guidelines Oral methotrexate is a safe and effective medication
Standards for the initial education and training of pharmacy technicians. October 2017
 Standards for the initial education and training of pharmacy technicians October 2017 The text of this document (but not the logo and branding) may be reproduced free of charge in any format or medium,
Standards for the initial education and training of pharmacy technicians October 2017 The text of this document (but not the logo and branding) may be reproduced free of charge in any format or medium,
Quality Management in Pharmacy Pre-registration Training: Current Practice
 Pharmacy Education, 2013; 13 (1): 82-86 Quality Management in Pharmacy Pre-registration Training: Current Practice ELIZABETH MILLS 1*, ALISON BLENKINSOPP 2, PATRICIA BLACK 3 1 Postgraduate Academic Course
Pharmacy Education, 2013; 13 (1): 82-86 Quality Management in Pharmacy Pre-registration Training: Current Practice ELIZABETH MILLS 1*, ALISON BLENKINSOPP 2, PATRICIA BLACK 3 1 Postgraduate Academic Course
Registrant Survey 2013 initial analysis
 Registrant Survey 2013 initial analysis April 2014 Registrant Survey 2013 initial analysis Background and introduction In autumn 2013 the GPhC commissioned NatCen Social Research to carry out a survey
Registrant Survey 2013 initial analysis April 2014 Registrant Survey 2013 initial analysis Background and introduction In autumn 2013 the GPhC commissioned NatCen Social Research to carry out a survey
Literature review: pharmaceutical services for prisoners
 Author: Rosemary Allgeier, Principal Pharmacist in Public Health. Date: 08 October 2012 Version: 1a Publication and distribution: NHS Wales (intranet and internet) Public Health Wales (intranet and internet)
Author: Rosemary Allgeier, Principal Pharmacist in Public Health. Date: 08 October 2012 Version: 1a Publication and distribution: NHS Wales (intranet and internet) Public Health Wales (intranet and internet)
Surgical Safety Checklist:
 Implementing the Surgical Safety Checklist: the journey so far... Introduction This document summarises the experience and reflections of NHS Trusts about their progress in implementing the World Health
Implementing the Surgical Safety Checklist: the journey so far... Introduction This document summarises the experience and reflections of NHS Trusts about their progress in implementing the World Health
Patient Safety. At the heart of all we do
 Patient Safety At the heart of all we do Introduction from our Medical Director Over the last 15 years it has been recognised that patient safety problems exist throughout the NHS as they do in every health
Patient Safety At the heart of all we do Introduction from our Medical Director Over the last 15 years it has been recognised that patient safety problems exist throughout the NHS as they do in every health
Guidance on supporting information for revalidation
 Guidance on supporting information for revalidation Including specialty-specific information for medical examiners (of the cause of death) General introduction The purpose of revalidation is to assure
Guidance on supporting information for revalidation Including specialty-specific information for medical examiners (of the cause of death) General introduction The purpose of revalidation is to assure
Public Health Skills and Career Framework Multidisciplinary/multi-agency/multi-professional. April 2008 (updated March 2009)
") Public Health Skills and Multidisciplinary/multi-agency/multi-professional April 2008 (updated March 2009) Welcome to the Public Health Skills and I am delighted to launch the UK-wide Public Health Skills
Public Health Skills and Multidisciplinary/multi-agency/multi-professional April 2008 (updated March 2009) Welcome to the Public Health Skills and I am delighted to launch the UK-wide Public Health Skills
NMC programme of change for education Prescribing and standards for medicines management
 NMC programme of change for education Prescribing and standards for medicines management This response form relates to our consultation on nurse and midwifery prescribing competency proposals, programme
NMC programme of change for education Prescribing and standards for medicines management This response form relates to our consultation on nurse and midwifery prescribing competency proposals, programme
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014
 Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Improvement Fellows Spring Networking event
 Improvement Fellows Spring Networking event Wednesday 1 st March 2017 Leeds e: academy@yhahsn.nhs.uk / t: 01274 383966 www.improvementacademy.org Our # for the event #ImprovementFellows @improvementacademy
Improvement Fellows Spring Networking event Wednesday 1 st March 2017 Leeds e: academy@yhahsn.nhs.uk / t: 01274 383966 www.improvementacademy.org Our # for the event #ImprovementFellows @improvementacademy
Step by step measurement guide
 Step by step measurement guide The guide has been produced under a creative commons license please use the symbols shown for guidance if you wish to use or adapt the material This edited presentation has
Step by step measurement guide The guide has been produced under a creative commons license please use the symbols shown for guidance if you wish to use or adapt the material This edited presentation has
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013
 Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME
 Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
Dr Natalie Taylor. The impact of a behavioural change approach to the implementation of national patient safety guidelines
 The impact of a behavioural change approach to the implementation of national patient safety guidelines 2014 AIHI Research Symposium Dr Natalie Taylor Prof. Rebecca Lawton Beverley Slater Prof. John Wright
The impact of a behavioural change approach to the implementation of national patient safety guidelines 2014 AIHI Research Symposium Dr Natalie Taylor Prof. Rebecca Lawton Beverley Slater Prof. John Wright
Supporting Leadership for Quality Improvement and Safety. AN ATTRIBUTES FRAMEWORK for HEALTH AND SOCIAL CARE
 Supporting Leadership for Quality Improvement and Safety AN ATTRIBUTES FRAMEWORK for HEALTH AND SOCIAL CARE This Attributes Framework was developed in partnership with key stakeholders within Health and
Supporting Leadership for Quality Improvement and Safety AN ATTRIBUTES FRAMEWORK for HEALTH AND SOCIAL CARE This Attributes Framework was developed in partnership with key stakeholders within Health and
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU. Change Package.
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Quality Improvement Strategy
 Quality Improvement Strategy 2018-2021 2WORCESTERSHIRE ACUTE HOSPITALS NHS TRUST QUALITY IMPROVEMENT STRATEGY 2017-2020 Contents Introduction 3 How we define quality 4 What are we trying to accomplish?
Quality Improvement Strategy 2018-2021 2WORCESTERSHIRE ACUTE HOSPITALS NHS TRUST QUALITY IMPROVEMENT STRATEGY 2017-2020 Contents Introduction 3 How we define quality 4 What are we trying to accomplish?
Managing the Transition to Electronic Repeat Dispensing
 Managing the Transition to Electronic Repeat Dispensing 1 Executive Summary The volume of medicines issued as repeat medicines to patients managing long term conditions grows each year. 77% of the over
Managing the Transition to Electronic Repeat Dispensing 1 Executive Summary The volume of medicines issued as repeat medicines to patients managing long term conditions grows each year. 77% of the over
Management of Reported Medication Errors Policy
 Management of Reported Medication Errors Policy Approved By: Policy & Guideline Committee Date of Original 6 October 2008 Approval: Trust Reference: B45/2008 Version: 4 Supersedes: 3 February 2015 Trust
Management of Reported Medication Errors Policy Approved By: Policy & Guideline Committee Date of Original 6 October 2008 Approval: Trust Reference: B45/2008 Version: 4 Supersedes: 3 February 2015 Trust
Document Details Clinical Audit Policy
 Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
JOB DESCRIPTION. Pharmacy Technician
 JOB DESCRIPTION Pharmacy Technician Issued by AT Medics Primary Care Pharmacy Technician Job Description Job Title: Reporting to: Location: Salary: Job status: Contract: Notice Period: Primary care pharmacy
JOB DESCRIPTION Pharmacy Technician Issued by AT Medics Primary Care Pharmacy Technician Job Description Job Title: Reporting to: Location: Salary: Job status: Contract: Notice Period: Primary care pharmacy
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report
 Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Alert. Patient safety alert. Actions that can make anticoagulant therapy safer. 28 March Action for the NHS and the independent sector
 Patient safety alert 18 Alert 28 March 2007 Immediate action Action Update Information request Ref: NPSA/2007/18 Actions that can make anticoagulant therapy safer Anticoagulants are one of the classes
Patient safety alert 18 Alert 28 March 2007 Immediate action Action Update Information request Ref: NPSA/2007/18 Actions that can make anticoagulant therapy safer Anticoagulants are one of the classes
Disclosure Statement. Learning Objectives 4/11/2017. Practical Improvement Science in Medication Safety. Jason Timothy Wong, PharmD
 // Practical Improvement Science in Medication Safety Jason Timothy Wong, PharmD PGY Health-System Pharmacy Administration Resident Oregon Health and Science University OSHP Annual Seminar DATE: April,
// Practical Improvement Science in Medication Safety Jason Timothy Wong, PharmD PGY Health-System Pharmacy Administration Resident Oregon Health and Science University OSHP Annual Seminar DATE: April,
Medicines Reconciliation: Standard Operating Procedure
 Clinical Medicines Reconciliation: Standard Operating Procedure Document Control Summary Status: Version: Author/Owner/Title: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation
Clinical Medicines Reconciliation: Standard Operating Procedure Document Control Summary Status: Version: Author/Owner/Title: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation
YORKSHIRE AND HUMBER CLINICAL PHARMACY BENCHMARKING
 YORKSHIRE AND HUMBER CLINICAL PHARMACY BENCHMARKING Chris Acomb BSc MPharm FRPharmS Clinical Pharmacy Manager (Professional Development) Leeds Teaching Hospitals With thanks to all my fellow Clinical Pharmacy
YORKSHIRE AND HUMBER CLINICAL PHARMACY BENCHMARKING Chris Acomb BSc MPharm FRPharmS Clinical Pharmacy Manager (Professional Development) Leeds Teaching Hospitals With thanks to all my fellow Clinical Pharmacy
Final Report ALL IRELAND. Palliative Care Senior Nurses Network
 Final Report ALL IRELAND Palliative Care Senior Nurses Network May 2016 FINAL REPORT Phase II All Ireland Palliative Care Senior Nurse Network Nursing Leadership Impacting Policy and Practice 1 Rationale
Final Report ALL IRELAND Palliative Care Senior Nurses Network May 2016 FINAL REPORT Phase II All Ireland Palliative Care Senior Nurse Network Nursing Leadership Impacting Policy and Practice 1 Rationale
Provide Safe and Effective Medicines Management in Primary Care
 Primary Drivers Secondary Drivers Aim Safe and reliable prescribing, monitoring and administration of high risk medications that require systematic monitoring Implement systems for reliable prescribing
Primary Drivers Secondary Drivers Aim Safe and reliable prescribing, monitoring and administration of high risk medications that require systematic monitoring Implement systems for reliable prescribing
Improving the prevention, early detection and management of Acute Kidney Injury (AKI) in Wessex
 in Wessex") Improving the prevention, early detection and management of Acute Kidney Injury (AKI) in Wessex The case for change AKI is recognised as a major public health and patient safety concern nationally and
Improving the prevention, early detection and management of Acute Kidney Injury (AKI) in Wessex The case for change AKI is recognised as a major public health and patient safety concern nationally and
Supporting Leadership for Quality Improvement and Safety. An Attributes Framework for Health and Social Care
 Supporting Leadership for Quality Improvement and Safety An Attributes Framework for Health and Social Care November 2014 In 2011, Charlotte McArdle and Dr Anne Kilgallen, the then Co-chairs of the Quality
Supporting Leadership for Quality Improvement and Safety An Attributes Framework for Health and Social Care November 2014 In 2011, Charlotte McArdle and Dr Anne Kilgallen, the then Co-chairs of the Quality
North School of Pharmacy and Medicines Optimisation Strategic Plan
 North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
Disability Discrimination Act 1995; Equality Act 2010; and Multicompartment
 Contract and IT January 2016 PSNC Briefing 01/16: Equality Act 2010 This briefing updates PSNC Briefing 084/13: Equality Act 2010 on the Equality Act 2010 (incorporating its predecessor legislation the
Contract and IT January 2016 PSNC Briefing 01/16: Equality Act 2010 This briefing updates PSNC Briefing 084/13: Equality Act 2010 on the Equality Act 2010 (incorporating its predecessor legislation the
Dr. Emily Cooper Leadership Fellow, Improvement Academy Alison O Halloran Compliance Manager, Roche Healthcare Kirsty Smith Team Leader, Fieldhead
 Dr. Emily Cooper Leadership Fellow, Improvement Academy Alison O Halloran Compliance Manager, Roche Healthcare Kirsty Smith Team Leader, Fieldhead Court Nursing Home, Roche Healthcare One of the UK s leading
Dr. Emily Cooper Leadership Fellow, Improvement Academy Alison O Halloran Compliance Manager, Roche Healthcare Kirsty Smith Team Leader, Fieldhead Court Nursing Home, Roche Healthcare One of the UK s leading
Story Street Walk-in Service
 Story Street Walk-in Service Service User Engagement www.hullccg.nhs.uk NHSHullCCG @NHSHullCCG Page 2 Story Street Walk-in Service Service User Engagement Introduction The Walk-in Service is based in the
Story Street Walk-in Service Service User Engagement www.hullccg.nhs.uk NHSHullCCG @NHSHullCCG Page 2 Story Street Walk-in Service Service User Engagement Introduction The Walk-in Service is based in the
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
Who Cares About Medication Reconciliation? American Pharmacists Association American Society of Health-system Pharmacists The Joint Commission Agency
 The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
4. Hospital and community pharmacies
 4. Hospital and community pharmacies As FIP is the international professional organisation of pharmacists, this paper emphasises the role of the pharmacist in ensuring and increasing patient safety. The
4. Hospital and community pharmacies As FIP is the international professional organisation of pharmacists, this paper emphasises the role of the pharmacist in ensuring and increasing patient safety. The
Maryland Patient Safety Center s Call for Solutions Submission. Organization: Atlantic General Hospital
 Maryland Patient Safety Center s Call for Solutions Submission Organization: Atlantic General Hospital Solution Title: Using the Evolution of Data Collection Methods 2 Drive Revolution in the Reduction
Maryland Patient Safety Center s Call for Solutions Submission Organization: Atlantic General Hospital Solution Title: Using the Evolution of Data Collection Methods 2 Drive Revolution in the Reduction
Supporting information for appraisal and revalidation: guidance for Supporting information for appraisal and revalidation: guidance for ophthalmology
 FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
Supporting information for appraisal and revalidation: guidance for psychiatry
 Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
The Search for Best Practice in Medication Reconciliation
 The Search for Best Practice in Medication Reconciliation National Medicines Forum November 2013 Marie Kehoe O Sullivan Director, Safety and Quality Improvement HIQA HIQA Collaboration with IHI Open School
The Search for Best Practice in Medication Reconciliation National Medicines Forum November 2013 Marie Kehoe O Sullivan Director, Safety and Quality Improvement HIQA HIQA Collaboration with IHI Open School
Improving medical handover at the weekend: a quality improvement project
 BMJ Quality Improvement Reports 2015; u207153.w2899 doi: 10.1136/bmjquality.u207153.w2899 Improving medical handover at the weekend: a quality improvement project Emma Michael, Chandni Patel Broomfield
BMJ Quality Improvement Reports 2015; u207153.w2899 doi: 10.1136/bmjquality.u207153.w2899 Improving medical handover at the weekend: a quality improvement project Emma Michael, Chandni Patel Broomfield
Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02
 Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02 V02 issued Issue 1 May 11 Issue 2 Dec 11 Planned review May
Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02 V02 issued Issue 1 May 11 Issue 2 Dec 11 Planned review May
Improving the reporting of medication-related safety incidents
 Rationale Improving the reporting of medication-related safety incidents Research shows that organisations which regularly report more patient safety incidents usually have a stronger learning culture
Rationale Improving the reporting of medication-related safety incidents Research shows that organisations which regularly report more patient safety incidents usually have a stronger learning culture
EXPERIENCE OF THE ERADICATION OF PRESSURE ULCERS IN PRIMARY CARE
 EXPERIENCE OF THE ERADICATION OF PRESSURE ULCERS IN PRIMARY CARE HAMISH LAING Consultant plastic and reconstructive surgeon ABM University Health Board, Wales UK Terminology 2 Pressure sores Bed sores
EXPERIENCE OF THE ERADICATION OF PRESSURE ULCERS IN PRIMARY CARE HAMISH LAING Consultant plastic and reconstructive surgeon ABM University Health Board, Wales UK Terminology 2 Pressure sores Bed sores
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1)
 Medication Chart implementation and training guide (version 1.1)") Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
 Trust Monitored Dosage System 0115 949 5421 email: mds@boots.co.uk 104628 12/05 Boots Monitored Dosage Service Group home service offer Trust contents Summary of offer 3 Monitored Dosage System 5 The Boots
Trust Monitored Dosage System 0115 949 5421 email: mds@boots.co.uk 104628 12/05 Boots Monitored Dosage Service Group home service offer Trust contents Summary of offer 3 Monitored Dosage System 5 The Boots
AIMS Rehab Annual Report Editors: Hannah Rodell and Kanza Raza. Published: May Publication Number: CCQI 230
 AIMS Rehab Annual Report 2016 Editors: Hannah Rodell and Kanza Raza Published: May 2016 Publication Number: CCQI 230 Contents Foreword... 5 Introduction... 6 Network Activity... 7 Membership... 7 Accreditation...
AIMS Rehab Annual Report 2016 Editors: Hannah Rodell and Kanza Raza Published: May 2016 Publication Number: CCQI 230 Contents Foreword... 5 Introduction... 6 Network Activity... 7 Membership... 7 Accreditation...
School of Nursing and Midwifery. MMedSci / PGDip General Practice Advanced Nurse Practitioner (NURT101 / NURT102)
") School of Nursing and Midwifery MMedSci / PGDip General Practice Advanced Nurse Practitioner (NURT101 / NURT102) Programme Outline 2017 1 Programme lead Dr Ian Brown. Lecturer Primary Care Nursing 0114
School of Nursing and Midwifery MMedSci / PGDip General Practice Advanced Nurse Practitioner (NURT101 / NURT102) Programme Outline 2017 1 Programme lead Dr Ian Brown. Lecturer Primary Care Nursing 0114
Emergency Medicine Programme
 Emergency Medicine Programme Implementation Guide 8: Matching Demand and Capacity in the ED January 2013 Introduction This is a guide for Emergency Department (ED) and hospital operational management teams
Emergency Medicine Programme Implementation Guide 8: Matching Demand and Capacity in the ED January 2013 Introduction This is a guide for Emergency Department (ED) and hospital operational management teams
Introduction of EPMA in paediatric practice in UK:
 Introduction of EPMA in paediatric practice in UK: REALISING THE CLINICAL BENEFITS AND ENGAGING CLINICAL STAFF Stephen Marks Consultant Paediatric Nephrologist and EPMA lead Great Ormond Street Hospital
Introduction of EPMA in paediatric practice in UK: REALISING THE CLINICAL BENEFITS AND ENGAGING CLINICAL STAFF Stephen Marks Consultant Paediatric Nephrologist and EPMA lead Great Ormond Street Hospital
Tackling the challenge of non-adherence
 Tackling the challenge of non-adherence 2 How is adherence defined? WHO definition: the extent to which a person s behaviour taking medication, following a diet and/or executing lifestyle changes corresponds
Tackling the challenge of non-adherence 2 How is adherence defined? WHO definition: the extent to which a person s behaviour taking medication, following a diet and/or executing lifestyle changes corresponds
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Medicines optimisation: the safe and effective use of medicines to enable the best possible outcomes 1.1 Short title Medicines
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Medicines optimisation: the safe and effective use of medicines to enable the best possible outcomes 1.1 Short title Medicines
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Engaging clinicians in improving data quality in the NHS
 Engaging clinicians in improving data quality in the NHS Key findings and recommendations from research conducted by the Royal College of Physicians ilab September 2006 Summary This document summarises
Engaging clinicians in improving data quality in the NHS Key findings and recommendations from research conducted by the Royal College of Physicians ilab September 2006 Summary This document summarises
WAITING TIMES 1. PURPOSE
 Agenda Item Meeting of Lanarkshire NHS Board 28 April 2010 Lanarkshire NHS board 14 Beckford Street Hamilton ML3 0TA Telephone 01698 281313 Fax 01698 423134 www.nhslanarkshire.org.uk WAITING TIMES 1. PURPOSE
Agenda Item Meeting of Lanarkshire NHS Board 28 April 2010 Lanarkshire NHS board 14 Beckford Street Hamilton ML3 0TA Telephone 01698 281313 Fax 01698 423134 www.nhslanarkshire.org.uk WAITING TIMES 1. PURPOSE
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Health and Social Care Directorate Quality standards Process guide
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health and Social Care Directorate Quality standards Process guide December 2014 Quality standards process guide Page 1 of 44 About this guide This guide
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health and Social Care Directorate Quality standards Process guide December 2014 Quality standards process guide Page 1 of 44 About this guide This guide
Standards for the provision and use of Medicines Administration Record (MAR) charts
 charts") Standards for the provision and use of Medicines Administration Record (MAR) charts Background The MAR chart is the formal record of administration of medicines and may be required to be used as evidence
Standards for the provision and use of Medicines Administration Record (MAR) charts Background The MAR chart is the formal record of administration of medicines and may be required to be used as evidence
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages. This SPSRN work is funded by
 Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Transnational Skill Standards Pharmacy Assistant
 Transnational Skill Standards Pharmacy Assistant REFERENCE ID: HSS/ Q 5401 Mapping for Pharmacy Assistant (HSS/ Q 5401) with UK SVQ level 2 Qualification Certificate in Pharmacy Service Skills Link to
Transnational Skill Standards Pharmacy Assistant REFERENCE ID: HSS/ Q 5401 Mapping for Pharmacy Assistant (HSS/ Q 5401) with UK SVQ level 2 Qualification Certificate in Pharmacy Service Skills Link to
The Pharmacist in Primary Care An Introduction. Project Report Executive summary
 The Pharmacist in Primary Care An Introduction Project Report Executive summary Professor John Campbell, Mark Healey, Dr Laura Sims, Dr Anna Sansom, Dr Jo Butterworth Overview An NHS Education South West
The Pharmacist in Primary Care An Introduction Project Report Executive summary Professor John Campbell, Mark Healey, Dr Laura Sims, Dr Anna Sansom, Dr Jo Butterworth Overview An NHS Education South West
Learning from Deaths Policy
 Learning from Deaths Policy Version: 3 Approved by: Board of Directors Date Approved: October 2017 Lead Manager: Associate Medical Director for Patient Safety and Clinical Risk Responsible Director: Medical
Learning from Deaths Policy Version: 3 Approved by: Board of Directors Date Approved: October 2017 Lead Manager: Associate Medical Director for Patient Safety and Clinical Risk Responsible Director: Medical
Corporate Induction: Part 2
 Corporate Induction: Part 2 Identification of preventable Adverse Drug Reactions from a regulatory perspective March 1 st 2013, EMA Workshop on Medication Errors Presented by Almath Spooner, Pharmacovigilance
Corporate Induction: Part 2 Identification of preventable Adverse Drug Reactions from a regulatory perspective March 1 st 2013, EMA Workshop on Medication Errors Presented by Almath Spooner, Pharmacovigilance
Foundation Pharmacy Framework
 Association of Pharmacy Technicians UK Foundation Pharmacy Framework A framework for professional development in foundation across pharmacy APTUK Foundation Pharmacy Framework The Professional Leadership
Association of Pharmacy Technicians UK Foundation Pharmacy Framework A framework for professional development in foundation across pharmacy APTUK Foundation Pharmacy Framework The Professional Leadership
JOB DESCRIPTION. 2. To participate in the delivery of medicines administration depending on local need and priorities.
 JOB DESCRIPTION JOB TITLE: Clinical Pharmacy Technician PAY BAND: 5 DEPARTMENT/DIVISION: BASED AT: REPORTS TO: PHARMACY/A5 University Hospitals Birmingham Pharmacy Support Manager PROFESSIONALLY RESPONSIBLE
JOB DESCRIPTION JOB TITLE: Clinical Pharmacy Technician PAY BAND: 5 DEPARTMENT/DIVISION: BASED AT: REPORTS TO: PHARMACY/A5 University Hospitals Birmingham Pharmacy Support Manager PROFESSIONALLY RESPONSIBLE
NHS WORKFORCE RACE EQUALITY STANDARD 2017 DATA ANALYSIS REPORT FOR NATIONAL HEALTHCARE ORGANISATIONS
 NHS WORKFORCE RACE EQUALITY STANDARD 2017 DATA ANALYSIS REPORT FOR NATIONAL HEALTHCARE ORGANISATIONS Publication Gateway Reference Number: 07850 Detailed findings 3 NHS Workforce Race Equality Standard
NHS WORKFORCE RACE EQUALITY STANDARD 2017 DATA ANALYSIS REPORT FOR NATIONAL HEALTHCARE ORGANISATIONS Publication Gateway Reference Number: 07850 Detailed findings 3 NHS Workforce Race Equality Standard
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
What does governance look like in homecare?
 What does governance look like in homecare? Dr David Cousins PhD FRPharmS Head of Pa)ent Safety, Healthcare at Home Ltd This Satellite is sponsored by Healthcare at Home Ltd Definitions Clinical governance
What does governance look like in homecare? Dr David Cousins PhD FRPharmS Head of Pa)ent Safety, Healthcare at Home Ltd This Satellite is sponsored by Healthcare at Home Ltd Definitions Clinical governance
Medicines Optimisation Strategy
 Medicines Optimisation Strategy 2014-2017 Contents Section Page 1 Foreword 3 2 Strategic Principles for Medicines Optimisation 4 3 Introduction 4 4 Trust Vision and Values 5 5 Strategy Development 5 6
Medicines Optimisation Strategy 2014-2017 Contents Section Page 1 Foreword 3 2 Strategic Principles for Medicines Optimisation 4 3 Introduction 4 4 Trust Vision and Values 5 5 Strategy Development 5 6
TRUST BOARD TB(16) 44. Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals
 44. Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals") TRUST BOARD TB(16) 44 Title: Action: Meeting: Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals FOR NOTING Date of meeting Purpose: The purpose
TRUST BOARD TB(16) 44 Title: Action: Meeting: Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals FOR NOTING Date of meeting Purpose: The purpose