2. Introduction and Aims Document purpose, context and aims The strategic planning process...13
|
|
|
- Morris Richard
- 5 years ago
- Views:
Transcription
1
2 Contents 1. Executive Summary Purpose and scope Context and objectives Summary of clinical models Risks and mitigations Strategic implementation plan Next steps Introduction and Aims Document purpose, context and aims The strategic planning process Strategic Context National and regional context Local context Quality, patient and staff context Financial position and case for change Vision and Summary Objectives Clinical Model Current and Future Unplanned care Planned care Children s services Risks and Mitigations Strategic Implementation Plan Next Steps Appendix Appendix A - KGH floor plans (indicative) Appendix B - ISTC floor plan Appendix C - Current and future state of services...59
3 1. Executive Summary 1.1 Purpose and scope 1. Barking, Havering and Redbridge University Hospitals NHS Trust is one of the largest acute trusts in England, and provides services for over 700,000 people across two sites - Queen s Hospital (QH) and King George Hospital (KGH). 2. For six successive years it has been unable to breakeven, and the Trust is therefore targeting recurrent cost savings of 100.1m over the five year period to FY17/18. In October of 2012, the Trust Board discussed a high level Clinical Strategy Options paper which proposed how the Trust s financial difficulties could be addressed through productivity improvements, reconfiguring services, reductions in the size of the estate and additional income support. 3. The Board s preference for progression was a reconfiguration option. In December 2012 the Board agreed on the high level option to take forward. Work has been on-going on the Clinical Strategy, covering the detailed split of services across the sites and supporting patient pathways covering the Trust as a whole. This work has been clinically led; all Clinical Directors have been involved and have consulted widely within their departments. The results of this work are summarised in this document. 4. This strategy sits alongside and complements a number of other strategies, reports and plans for BHRUT, particularly those working towards improving quality, reducing clinical risk and driving up performance. These include the annual Quality Account, setting out quality objectives for the coming year and reporting on performance, the Quality Strategy, currently in preparation, the Trust s Patient Experience Strategy, and detailed plans for managing and boosting performance, such as those on the Emergency care pathway, financial recovery or addressing external reviews such as the Francis and Berwick reviews. To avoid duplication, the Clinical Strategy focuses on the implementation of the service change programme set out in the Health for north east London plans, and paves the way for the more detailed business cases on the major capital works and the long term financial model (LTFM). 1.2 Context and objectives 5. The national context drives the rationale for strategic change at BHRUT: NHS Trusts throughout England are facing on-going financial challenges as they strive to make efficiency savings of 4-5% per annum as a minimum Trusts across England are encountering increasing operational pressures, particularly through escalating A&E attendances and unplanned admissions to hospital There is ever increasing scrutiny of trusts, hospitals, departments and individual healthcare professionals. Rolling CQC inspections, the Francis report, and more recently the Keogh Review, are increasing pressure to maintain high standards of care at all times, requiring changes to health service culture and working practices in the context of a constrained funding environment.
4 6. Health for North East London (HfNEL) is a commissioner and clinicial led sector wide industry reconfiguration programme to improve health care provision across the region. The drivers for change were put forward in The Case for Change in North East London 1. A 16 week public consultation then followed which resulted in the proposals below being agreed by the Joint Committee of Primary Care Trusts in December The plans were reviewed by the Independent Reconfiguration Panel, and the Secretary of State signed off the plans, subject to certain safeguards, in October The safeguards sought to ensure that capacity was increased at Queen s before being reduced at King George, that services at Queen s and at other local health services are of a high standard, and that a vision for the future of King George has been presented prior to full implementation of the programme. The main elements of the programme are: A&E, medical and surgical inpatient care and critical care to be provided at five hospitals in north east London - Queen's, Whipps Cross, The Royal London, Homerton and Newham Develop a campus model of maternity care with maternity delivery at five hospitals - Queen s, Whipps Cross, The Royal London, Homerton and Newham. A new midwifery-led unit at Queen s and expanded capacity at other hospitals (now implemented) Planned surgery to move from Queen s to King George Hospital except where there are benefits in co-locating services or on the basis of clinical need. Develop a kidney dialysis service at King George Hospital (kidney dialysis at KGH has now been implemented) Provide more specialist care for children at Queen s and The Royal London and improve the services available at other hospitals Improve rehabilitation and out-of-hosptial care, so that patients are cared for in the appropriate setting Improve performance and quality of healthcare provided This clinical strategy contains amongst other modifications, the agreed HfNEL changes 7. BHRUT currently has an emergency department (ED) and urgent care centre (UCC) on both the Queen s Hospital site and the King George Hospital sites. The ED on the Queen s Hospital site is under immense pressure with an overload of patients. This was noted in the Care Quality Commission s (CQC) whole trust investigation in autumn 2011, and the Secretary of State signed off the plans subject to the improvements recommended by the CQC being made. Following a 2012 inspection, the CQC has told BHRUT that it must make urgent improvements to Queen s Hospital after it failed to meet two of the three national standards for Emergency Departments. Implementation of the strategy is closely connected with the delivery of improved performance on the emergency care pathway. Some elements of the clinical strategy will help deliver these improvements, such as the capital works to redesign the Queen s Emergency departments. Importantly, some other elements of the strategy, such as the reduction in capacity of King George to provide a full emergency department, should not be implemented until there is improved capacity and performance at Queen s. 1 The Case for Change in North East London, Feb 2009, Health for North East London. 2 Why change is needed in North East London, 2009, Health for North East London
5 1.3 Summary of clinical models 8. BHRUT is committed to the provision of high quality patient care and financial sustainability, enabled by HfNEL, the changes agreed by the Trust Board in December 2012, and a need to address ED performance on the Queen s site. This in turn is underpinned by the strategic interventions proposed in this document. The key components of the Clinical Strategy are highlighted in the tables below. Unplanned care Move all emergency medicine and surgery to Queen s Hospital by mid 2015 as planned Maintain and develop 24/7 urgent care centres on both sides as per HfNEL Radically redevelop the Queen s ED to address the current performance issues and address the forecast additional demand. Key changes are: o Introduce a Senior Streamer o Route patients arriving at the ED to the UCC, ED area, four-speciality assessment centres and short stay beds as appropriate o Physically remodel the existing ED to accommodate the four speciality assessment areas, cope with the increased demand and support the proposed clinical model o Provide dedicated facilities for children, including a paediatric specific entrance Radical redevelopment of the Queen s ED 8. All adult patients will enter the emergency care pathway through the Big Front Door. The exceptions are ambulance patients requiring immediate access to resuscitation. For adults, the Senior Streamer at the front door of the ED will triage the patient s optimum treatment location as opposed to the patient being served at ED by default. The patient will be referred to any one of the ED Areas: 1. ED majors / resuscitation 2. Adult UCC Or to three of the four Speciality Assessment Areas: Or to: 1. Medical Assessment Unit 2. Elders Receiving Unit 3. Surgery and ENT Note: The fourth area is the Paediatric Assessment Unit 1. Eye casualty 2. Operating theatre 3. Gynaecology/EPAU currently on Cornflower B ward 4. Urology receiving room Or transferred out to the community response service, or referred back to their GP.
6 9. All paediatric patients will enter the paediatric emergency department through a dedicated paediatric entrance. Once again, the exceptions are ambulance patients requiring immediate access to resuscitation. 10. For children, the Senior Streamer at the front door of the paediatric ED will triage the patient s optimum treatment location as opposed to the patient being served at ED by default. The patient will be referred to any one of the ED Areas: 1. Paediatric ED majors/resuscitation/ucc Or to one of the Speciality Assessment Areas: 1. Paediatric Assessment Unit (PAU) Or to: 1. Special Surgery (Trauma & Orthopaedics / Max Fax) 2. Specialist Medicine (Haematology / Oncology) These children, if admitted would be accommodated within Tropical Lagoon (Paediatric) Ward irrespective of the lead speciality. Alternatively, they can be discharged home from either the ED or PAU, or referred back to their GP. Planned Care Maximise use of the Queen s site for complex inpatient activity Maximise the use of KGH for day case, short stay elective and diagnostic activity Place intermediate care and rehabilitation at KGH specifically including orthogeriatrics, stroke, neurosurgical (rehabilitation proposed new service), and grades I & II elderly patients (intermediate care) who do not need the support of a major acute hospital. This will: 1. Decompress the Queen s site to improve patient experience, cope with winter pressures, allow the space to systemically focus on reducing LoS 2. Provide a ready pool of patients to be addressed through the on-going development of integrated care and community interventions 3. Allow capacity for further community services on the KGH site, should this be required in the future. Centralise all breast services into a dedicated unit located on the KGH site with colocalised breast histopathology at KGH Move critical care beds from KGH, supporting the strategy of complex inpatient activity at Queen s Utilise sufficient space at KGH to provide a high quality of patient care across both sites. This will be the subject of detailed capacity modelling and is subject to assumptions on likely LoS improvement and impact of integrated care initiatives, but initial estimates place this at around 55-60% Implement new services on the space liberated on the KGH site (BHRUT), or provide alternative uses for the space, through a range of identified opportunities Implement the dedicated BHRUT Cancer Strategy to place excellence in patient care at the centre of caring for and serving the community.
7 Maximise use of the Queen s site for complex inpatient activity & maximise use of KGH for day case, short stay elective and diagnostic activity Services moved to Queen s Hospital General surgery IP centralised at QH Cardiology IP centralised at QH Diabetes and Endocrinoloy transferred to QH Renal OPD transferred to QH All Medical Speciality IP transferred to QH Critical Care transferred to QH Neonatal unit transferred to QH All Paediatric inpatients to move to QH Pathology centralised to QH Colorectal IP centralised at QH Oncology OP seen exclusively at QH Complex urology transferred to QH Services moved to King George Hospital Majority of day cases to move to KGH Paediatric day cases transferred to KGH Intermediate care to be placed at KGH Specialised commissioned pain services to be established at KGH Non complex spinal services extended to KGH All breast services centralised into a dedicated centre on the KGH site with co-localised breast histopatholoy Dermatology day case and routine OPD transferred to KGH Orthodontics moved to KGH Rheumatology day case & OPD transferred to KGH Maintenance and development of antenatal and associated services at KGH Potential to provide a neuro rehabilitation service at KGH Place intermediate care and rehabilitation at KGH 11. BHRUT embraced 7/7 working, with consultant presence on all the medial specialty wards from September BHRUT is now developing enhanced diagnostic support, along with the physiotherapy support that is necessary to fully realise the Length of Stay (LoS) reductions required. BHRUT recognises that there are problems in discharging patients due to delays in transfers and provision of medication. BHRUT will be setting up a working group to significantly improve performance in this area, which is recognised as an issue. 12. The Trust welcomes work by our partners in primary care, social services and social care to improve access to out-of-hospital care and pathways for patinets pre-admission and post-discharge, particulary in seven day provision of services. This will complement the BHRUT strategy and maximise the benefits to the local population. 13. The Trust is committed to develop models of integrated care with partners, particularlyfor elders. To this end, work with the Integrated Care Coalition has led to plans to implement a Joint Discharge Team from April 2014, and the Frailty service of BHRUT are now working closely with the Community Treatment Team (NELFT CTT) to manage patients in a more integrated fashion. This will include the post acute care of the elderly services, both bedded and in the community. 14. As stated in the case for change for integrated care in Barking and Dagenham, Havering and Redbridge 3, Implementation of the Barking, Havering and Redbridge University Hospitals reconfiguration (which is essential if services are to improve) relies on improvement of intermediate care services. Coupled with the fact that the Trust has consistently over-performed over the past few years (despite 5.7m of in-plan QIPP for 13-14), it would be prudent to assume that the local health economy is unlikely to be in a position to deliver this model of care in a way that will deliver material reductions in demand by the summer of 2015, when the ED closes at KGH and acute beds are removed. 3 Integrated care in Barking and Dagenham, Havering and Redbridge: The case for change, August 2012, pg11
8 15. The achievement of moving LoS in all HRGs to national upper quartile performance will be extremely challenging and thus a number of intermediate care and acute rehabilitation beds (orthogeriatric and stroke) will be needed in the medium term, whilst the system undergoes the very necessary changes.these beds are listed below: Medium stay for elderly patients: following acute assessment, some patients will need the benefit of a longer period of care, often they will be patients with more than one condition. 30 beds are available for these patients. The LoS should be no longer than 3-5 days when patients will be discharged home or to the community Enhanced intermediate care and acute rehabilitation:by providing enhanced intermediate care at the less acute and pressurised setting of KGH, the pressure on the acute admission beds at Queen s will be reduced. Ortho-geriatrics patients:following trauma patients will be transferred to KGH for acute rehabilitation, if fit, 72 hours after surgery. Acute stroke rehabilitation:this will remain at KGH on a reduced bed base, given the recent introduction of early supportive discharge. Neuro-Rehabilitation: the proposal to provide an enhanced neuro-rehabilitation service for patients who are at present experiencing long delays in the system in accessing rehabilitation following head injuries and neurosurgery is to be worked up. This service could be centred at the KGH site. Centralise all breast services into a dedicated unit located on the KGH site 16. BHRUT symptomatic and asymptomatic breast services are currently provided at KGH in Ilford, Victoria Hospital in Romford and Harold Wood Polyclinic. All breast surgical services were centralised at KGH as part of a Vascular/Breast reconfiguration plan in February Outpatient clinics are undertaken at KGH and Victoria Hospital with screening taking place on each site. 17. In centralising all breast services at KGH the breast histopathologists would relocate from Queen s to KGH, including a triple-assessment clinic. A small co-located working laboratory would be created in which operative specimens could be reviewed at the time of the procedure being undertaken. This would result in: real time advice as to whether further tissue resection would be required; minimise the number of returns to theatres for those requiring a wider excision of the tumour; negate the need for tissue to be transferred between sites that has the inherent risk of a specimen being misplaced or lost; support a quicker turnaround of results for the one-stop diagnostic outpatient clinics. BHRUT to implement new services on the space liberated on the KGH site, or provide alternative uses for the space 18. Potential options are: Pregnancy Advisory Service Brentwood blood transfusion Unit BHRUT/UCLP research Unit for the LIFE longitudinal study ISTC activity Pharmacy dispensary/pre-packaging TTA production unit / store Neuroscience rehab Specialised commissioned pain services to include psychotherapy Short stay spinal elective surgery Community paediatric mental health service Community rehabilitation beds
9 UCC Medical records move from current site Breast screening move from current site NELFT use of outpatient services Agreement on the set of new services to be placed on the KGH site, and precise location, will be reached with commissioners (and third parties as required). Children Community rehabilitation beds (Heronwood and Galleon, Gray s Court etc Complete the vision for paediatric services, as per HfNEL. Specifically: o UCC SCBU to move toqueen s o Medical Paediatric records inpatients move to from move current to Queen s site o Paediatric day case and elective and planned diagnostics at KGH (emergency Breast diagnostics screening at Queen s) move from current site Complete the vision for paediatric services % of the current catchment is aged under 16 and there is significant population growth in young couples and children. 30% of A&E attendances are children, and there are nogps with a special interest in paediatrics in the local area. The key issues to be addressed in children s services are therefore the growth in demand for these services, as well as the need for continued provision of high quality care. 20. In the last three years, the demand for specialist neonatal care has increased by 9%. Additionally, it is expected that 8,000 8,300 births will occur at QH. Currently, the established neonatal nursing levels are below the recommended staffing levels recommended by the British Association of Perinatal Medicine, but support from agency staff means that safe staffing levels are maintained and are flexible dependent on demand and capacity fluctuations. 21. The strategy consists of implementation of HfNEL, coupled with implementation of further opportunities for continuous improvement, specifically: SCBU to be relocated to Queen s Hospital to ensure efficiencies in medical and nursing establishments alongside timely attendance to labour ward emergencies and neonatal care Paediatric inpatient to move to Queen s to maximise the use of the Queen s site for complex inpatient activity as per HfNEL. This will ensure the children do benefit from the support given by the Paediatric Specialist surgeons Paediatric day case and elective and planned diagnostics at KGH maximising short stay elective and diagnostic activity. Note: paediatric outpatients will remain on both sites Extension of the existing Hot Line providing direct access to advice and guidance for GPs to paediatric consultants to KGH as well as the Queen s site Changes to the paediatric ED as covered in the Unplanned Care section of this Executive Summary 1.4 Risks and mitigations 22. The risks to successfully delivering a major restructuring programme must be carefully monitored and mitigated. The table below shows the identified red and amber risks to restructuring of the clinical services across the two sites. These have been divided into internal risks to delivery that the Trust has the ability to influence, and external risks over which the Trust has limited influence.
10 23. Risks will also be mitigated through the external assurance process that will be undertaken before major service moves are given final approval to be implemented. This process will be overseen by local and national commissioners, reporting to NHS England, to ensure there is robust and sustainable system readiness before major changes are made, such as the closure of the King George Emergency department. Contextual risks within the Trusts control ID Description Impact Likelihood Total Mitigation Failure to build the additional critical care R1 beds at Queen s due to a failure to obtain approval and agreement on the funding (PDC Robust business case documentation development funded) Robust programme management processes to ensure that changes to clinical services are appropriately risk Efficiency increases through theatre utilisation assessed and emerging risks R2 and LoS are not fully delivered in expected timescales, leading to a requirement to use are emphasised and managed greater than expected space at KGH Options for adittional temporary bed capacity being considered and maintaining a presence on the KGH site to enable flexibility R3 The non-delivery of CIP plans (productivity savings rather than reconfiguration savings) affects the overall affordability of the Trust and consequently the delivery of transformational programme Robust programme management processes to minimise the risk of nondelivery of CIPs, with nonrecurrent measures being used to close any in-year shortfalls R4 Failure to agree additional service delivery by BHRUT from the space liberated on the KGH site Reach CCG agreement promptly on use of the space Ensure development of robust links with community services R5 Failure to deliver reductions in LoS through failure to deliver an integrated care strategy with a single point of access Engagement with and support for the integrated joint health and social steering group Contextual risks outside of Trust control Likelihood ID Description Impact Total Level of non-elective activity may be more than planned as a result of the non-delivery R of Commissioner QIPP, meaning that additional capacity may be required Mitigation The Trust will collaborate with commissioners to deliver QIPP plans. If reductions are not delivered, further
11 improvements in LoS to reduce the beds requirement or utilisation of additional beds at the KGH sire will be needed R12 Changes in strategic commissioning intentions due to a change in the political environment Scenario modelling to identify the range of possible outcomes. Strong commissioner engagement Strategic implementation plan 24. A high level strategic implementation plan by clinical directorate has been developed and is outlined below. Key milestones / dependencies are: 1. Intermediate care beds to be established at KGH inspring2014.this will free up space on the QH site to support reconfiguration 2. Renal dialysis to be moved off the QH siteinsummer2014 to allow work on the Queen s Hospital ED to commence as soon the full business case is approved in August Emergency department redevelopment and critical care bed provision at QH to be completed in autumn 2015, allowing the majority of the day case activity to move to the KGH site, and majority of the IP activity to move to the QH site in early Note: Access to the ISTC by BHRUT has not been assumed within this clinical strategy. A decision on the ISTC at the external reconfiguration group would enable earlier transfer of non complex surgical cases from QH to KGH. Floor plans for the ISTC are given in appendix B.
12 Intermediate care at KGH Renal dialysis off-site KGH ED closes and critical care beds move to QH Majority of DCs at KGH & surgical IP at QH Emergency Care ED business case approvals Full business case approval (Aug 14) QH UCC made 24/7 QH UCC 24/7 (Spring 14) Senior streamer at QH KGH UCC made 24/7 KGH UCC 24/7 (Summer 14) Renal dialysis off-site (June 14) Physically remodel QH ED KGH ED closes to blue light ambulances (earliest Summer 15) ED transferred to QH KGH ED closes (end 15) Acute Medicine Cath lab business case Intermediate care at KGH Catheter laboratory business case approval (Jan 14) Cathlab developed Cardiology IP to QH Intermediate care at KGH Catheter laboratory complete (July 14) KGH cardiology closes (Aug 14) Diabetes & Endo to QH Medical speciality IP to QH Anaesthetics Children Neuro- Sciences Critical care bed business case approvals OBC/FBC post natal beds business case Pain services to KGH Post natal beds at QH complete (Aug 14) at QH SCBU built SCBU business case approvals Neonatal at QH complete (Feb 15) at QH Paediatric inpatients to QH Paediatric DC to KGH Neurosciences to transfer activity from QH to KGH Pain services at KGH (Summer 14) Combined OBC/FBC approved (Feb 14) Post natal Full business case approval (Aug 14) Build critical care capacity at QH Critical care beds moved to QH (October 15) Pathology Breast screening at KGH Hot lab to support breast services established at KGH (May 14) Pathology centralised at QH Pathology centralised at QH site (Feb 15) Radiology Breast screening business case Breast facility Breast facility established at KGH (May 14) Develop Radiology services within ED Increased utilisation of advanced practice reporting radiographers Specialist Medicine Dermatology DC/OPD to KGH Rheumatology OPD to KGH Dermatology at KGH (Spring 15) Rheumatology OPD at KGH (Spring 15) Specialist Surgery Ophthalmology cross site ENT cross site Orthodontics moved to KGH Specialist surgery reconfiguration complete (June 14) Surgery Colorectal IP to QH Majority of DCs to KGH Complex urology to QH General surgical IP to QH Majority of DCs at KGH & surgical IP at QH (Spring 16) Women Sexual Health / GUM off site Gynaecology day cases at KGH Estates Capital Build / refurbishment works at KGH (BHRUT) New services / new tenants on KGH Queen s hospital infrastructure QH infrastructure complete (June 15) upgrades Ophthalmic theatres complete (Jan 14) Renal dialysis off-site (June 14) Catheter laboratory complete (July 14) Post natal beds at QH complete (Aug 14) Neonatal at QH complete (Feb 15) Pathology centralised at QH site (Feb 15) ED and critical care build complete (Oct 15)
13 1.7 Next steps 26. This clinically led qualitative strategy will be further refined in three stages: 1. The quantitative impact of this strategy will be assessed using a capacity planning model and Trust LTFM through November 2013 to test a range of scenarios 2. The quantitative clinical strategy will complete at the end of November 2013 to feed into the Outline Business Case (OBC)for the proposed changes 3. The strategy will be operationalisedthrough the transformation programmeandby individual Clinical Directorates through their operational business plans
14 2. Introduction and Aims 2.1 Document purpose, context and aims 27. Barking, Havering and Redbridge University Hospitals NHS Trust (the Trust) is one of the largest acute Trusts in England and provides services for over 700,000 people across two sites - Queen s Hospital (QH) and King George Hospital (KGH). 28. For six consecutive years it has been unable to breakeven,and the Trust is required to implement recurring cost reductions of c 110m over a five year period.in October of 2012, the Trust Board discussed a high level Clinical Strategy Options paper which proposed how the Trust s financial difficulties could be addressed through productivity improvements, reconfiguring services, reductions in the size of the estate and additional income support. The Board s preference for progression was a reconfiguration option. In December 2012 the Board agreed on the high level option to take forward. This document provides the clinically led strategy covering the next level of detail below the agreed high level option for the Trust. 2.2 The strategic planning process 29. Following the Board decision at the end of 2012, work has been on-going on the Clinical Strategy, covering the detailed split of services across the sites and supporting patient pathwayscovering the Trust as a whole. This work has been clinically led; all Clinical Directors have been involved and have consulted widely within their departments. The results of this work are summarised in this document. 30. In parallel with this clinically led strategy development, work has been underway on a capacity and financial model of the Trust. This work covers both LTFM development and refinement, and development of a detailed capacity and workforce model. 31. Both areas of work are scheduled to complete at the end of October, with Trust Board review and agreement to the clinical strategy. 32. Throughout November, scenario modelling combining the clinical strategy with the capacity and financial modelling will be undertaken to refine the strategy. 33. This is expected to complete at the end of November when it will feed into the Outline Business Case (OBC) for the proposed changes. 34. The summary timeline is shown below: October Qualitative Clinical Strategy 2013 November Quantitative Clinical Strategy December OBC submission to TDA Clinically Led Strategy Development Capacity and financial modelling Scenario modelling and refinement Integration with OBC
15 3. Strategic Context 3.1 National and regional context 35. The national context breaks down into three areas which drive the rationale for strategic change at BHRUT: On-going financial challenge. NHS Trusts throughout England are required to deliver efficiency savings of circa 4-5% per annum as a minimum. Increasingly it is recognised traditional CIP schemes alone will no longer deliver the required savings. Trusts will be expected to engage in wider transformational change and service reconfiguration with other agencies and providers in order to deliver the savings required. Increasing operational pressures. Trusts across England are encountering increasing demand for acute services, particularly through escalating A&Eattendances and unplanned admissions to hospital. An ageing population with associated long-term conditions will demand more from health care providers year on year. Increasing quality expectations. There is ever increasing scrutiny of Trusts, hospitals, departments and individual healthcare professionals. Rolling CQC inspections, the Francis report, and more recently the Keogh Review, are increasing pressure to maintain high standards of care at all times, requiring changes to health service culture and working practices in the context of a constrained funding environment. 36. Health for North East London (HfNEL) 4 is a commissioner and clinician led sector wide reconfiguration programme aiming to improve health care provision for the people of north east London. The main drivers for the change were highlighted in The Case for Change in North East London publication 5, produced by the local PCTs in This highlighted six main reasons why change was needed: The need to improve the health of people in north east London and ensure healthcare services are meeting public expectations; The population of north east London is rising rapidly leading to greater demand on health services; Patients benefit from care closer to home and more care can be delivered in community settings than ever before - so hospital treatment is not always the answer; Current services are under severe pressure and there are staffing challenges which prevent the NHS delivering the best quality care; The need to adopt new models of care and best practice which can deliver better outcomes for patients; and The need to make best use of taxpayers money. 37. Following this publication, local clinicians from across the sector worked together to develop proposals to improve the quality and sustainability of services. As the proposals developed, patients, the public and local groups were involved to understand their views on health services and the ideas from the clinicians. 38. A 16 week public consultation followed, which resulted in the proposals below being agreed. 6 The plans were further reviewed rby the Independent Reconfiguration Panel, and the Secretary of State signed off the plans, subject to certain safeguards, in October The safeguards sought to ensure that capacity was increased at Queen s before being reduced at King George, that services at Queen s and at other local health services are of a high standard, and that a vision for the future of King George has been presented prior to full implementation of the programme. The plans include the following: 4 Health for North East London: 5 The Case for Change in North East London, Feb 2009, Health for North East London. 6 Why change is needed in North East London, 2009, Health for North East London
16 A&E, medical and surgical inpatient care and critical care to be provided at five hospitals in north east London - Queen's, Whipps Cross, The Royal London, Homerton and Newham. Urgent care to be enhanced at all hospitals with better and quicker access to tests, consultants and specialist advice. King George Hospital to provide 24/7 urgent care, and short stay assessment and treatment services. Develop a campus model of maternity care with maternity delivery at five hospitals - Queen s, Whipps Cross, The Royal London, Homerton and Newham. A new midwifery-led unit at Queen s and expanded capacity at other hospitals (now implemented). Planned surgery to move from Queen s to King George Hospital except where there are benefits in co-locating services or on the basis of clinical need. Develop a kidney dialysis service at King George Hospital (Kidney dialysis at KGH is now implemented). Provide more specialist care for children at The Royal London and Queen s and improve the services available at other hospitals. Improve rehabilitation and out-of-hosptial care, so that patients are cared for in the appropriate setting Improve performance and quality of healthcare provided. This clinical strategy contains amongst other modifications, the agreed HfNEL changes. 3.2 Local context 39. The Trust provides services to a population located across three areas, Havering, Redbridge, and Barking and Dagenham, and general and emergency services to the population of West Essex. The three areas have diversepopulations. Havering has a population of around 232,000 and low levels of deprivation, Redbridge has around 264,000 people and average levels of deprivation, and Barking and Dagenham has around 172,000 people and high levels of deprivation. Queen s Hospital in Romford is the main hospital for people in the Havering area, while King George Hospital is in Ilford, and mainly serves people in Redbridge and Barking and Dagenham. 40. The Trust provides elective and non-elective services in an inpatient and outpatient setting across its two main sites. Most services are provided at both sites, with some specialist services (e.g. Trauma, Vascular Surgery) only provided on one site. There iscurrently a total of 1,254 beds across both sites, of which 855 are located on the Queen s site and 399 on the King George site. Of these, 744 are inpatient beds on the Queen s site, and 341 are inpatient beds on the King George site. The remainder are day case and assessment beds. There are a total of 22 theatres across both sites that operate on a two session per day model, over 5 days a week (with some weekend lists). Analysis against national benchmarks has shown that there is an opportunity to reduce the beds and theatre requirement which will help to create the necessary capacity for any reconfiguration.
17 3.3 Quality, patient and staff context 41. The Secretary of State approved the HfNEL plans subject to certain safeguards to ensure that implementation did not take place until it would be safe to do so. The safeguards required services at Queen s and other local health services to be of a high standard, with concerns raised by the Care Quality Commission, including in their investigation of autumn 2011 addressed. BHRUT has been working to address the need for improved performance, particularly on the emergency care pathway, and this strategy sets out the wider context behind this work and the planned redevelopment of the Queen s Emergency department, which will facilitate this improved performance. 42. BHRUT currently has an emergency department (ED) and urgent care centre (UCC) on both the Queen s Hospital site and the King George Hospital sites. The ED on the Queen s Hospital site is under immense pressure with an overload of patients. The Care Quality Commission (CQC) has told BHRUT that it must make urgent improvements to Queen s Hospital. An inspection in December 2012 found it failed to meet two of the three national standards for Emergency Departments. 43. A further inspection carried out by CQC in May 2013, showed that patients are still spending too long in the ED at Queen s Hospital. On occasions patients who needed to be admitted to the hospital had waited for more than 14 hours in the department. National standards state that 95% of patients should be seen within four hours and no patient should be in the department for more than 12 hours. These delays increase the risk of poor clinical outcomes for patients. In March and April % of patients arriving at Queen s by emergency ambulance were assessed within 43 minutes and 45 minutes respectively. The quality indicator for this measure is 15 minutes, and the maximum time any patient should wait is 20 minutes. 44. Futhermore, a patient survey carried out in April 2013 of patients who had visited BHRUT, showed that patients felt they were not given enough privacy when being examined or treated and not given enough information about their condition or treatment within the A&E department. 45. Recruitment of consultant and middle grade staff for BHRUT has been an issue for the previous 2 years; this, alongside recent staff departures, has left both sites understaffed at these key levels. Both sites are therefore currently highly dependant upon locum doctors. This issue is reflected in the 2012 NHS Staff Survey, which shows how BHRUT compares with other acute trusts on an overall indicator of staff engagement. The trust's score of 3.56 was in the lowest (worst) 20% when compared with trusts nationwide. Specific areas on concern where BHRUT scored in the bottom 20% nationally include; staff suffering from work-related stress, low job satisfaction, staff recommendation of the trust as a place of work or to receive treatment and effective team working within the trust. 3.4 Financial position and case for change 46. BHRUT Trust needs to move from its 2012/ m deficit position, to a sustainable financial position. This will require annual cost reductions of around 5% of cost base per year to FY17/18, with recurrent savings of at least 100m over this 5 year period. This suggests that significant service reconfiguration will be needed to achieve cost reductions of this level. A proportion of these savings can be realised through implementing HfNEL s reconfiguration plan, and the remainder through the clincial strategy changes agreed by the board. Major reconfiguration will be needed to services across both sites to achieve the step change in cost levels required to reach the desired surplus position. 47. The current DoH policy is for all Trusts to reach Foundation Trust status. Should the Trust be unable to demonstrate financial viability then entry into the Unsustainable Providers Regime is a potential outcome.
18 4. Vision and Summary Objectives 48. BHRUT is committed to the provision of high quality patient care and financial sustainability, enabled byhfnel,the changes agreed by the Trust Board in December 2012, and a need to address ED performance on the Queen s site. This in turn is underpinned by the strategic interventions proposed in this document. Strategic Objectives Deliver safe, quality, effective care Enablers Address poor performance in the Queen s ED Decompress the Queen s site and promote integrated care Implement HfNEL Base Case BHRUT Clinical Strategy Radically redevelop the Queen s ED and address the forecast additional demand (3) Place intermediate care and rehabilitation at KGH (6) Utilise sufficient space at KGH to provide a high quality of patient care across both sites (9) Complete the vision for paediatric services (11) Move all emergency medicine and surgery to Queen s Hospital (1) Maintain an urgent care centre on both sites (2) Ensure BHRUT is financially secure Implement Extension to HfNEL(Option 2) Maximise usage of Queen s site Develop an elective centre on KGH site Move critical care beds from KGH (8) BHRUT to implement new services from the space liberated on the KGH site (10) Maximise the use of KGH for day case, short stay elective and diagnostic activity (5) Maximise the use of the Queen s site for complex inpatient activity (4) Centralise all breast services into a dedicated unit located on the KGH site (7) 49. In summary, the key components of the BHRUT clinical strategy are: 1. Move all emergency medicine and surgery to Queen s Hospital by mid 2015, as planned 2. Increase the quality of care and usage ofthe urgent care centre on both sites, as per HfNEL, making them both 24/7 3. Radically redevelop the Queen s ED to address the current performance issues and address the forecast additional demand. Key changes are: Introduce a Senior Streamer Route patients arriving at the ED to the UCC, ED area, four-speciality assessment centres and short stay beds as appropriate
19 Physically remodel the existing ED to accommodate the fourspeciality assessment areas, cope with the increased demand and support the proposed clinical model Provide dedicated facilities for children, including a paediatric specific entrance 4. Maximise use of the Queen s site for complex inpatient activity as per HfNEL, using detailed and agreed split of service provision across the two sites 5. Maximise the use of KGH for day case, short stay elective and diagnostic activity with or without the ISTC activity / building 6. Place intermediate care and rehabilitation at KGH specifically including orthogeriatrics, stroke, neurosurgical (rehabilitation proposed new service), and grades I & II elderly patients (intermediate care) who do not need the support of a major acute hospital. This will: 1. Decompress the Queen s site to improve patient experience, cope with winter pressures, allow the space to systemically focus on reducing LoS 2. Provide a ready pool of patients to be addressed through the on-going development of integrated care and community interventions 3. Allow capacity for further community services on the KGH site, should this be required in the future. 7. Centralise all breast services into a dedicated unit located on the KGH site with colocalised breast histopathology at KGH 8. Move critical care beds from KGH,supporting the strategy of complex inpatient activity at Queen s 9. Utilise sufficient space at KGH to provide a high quality of patient care across both sites. This will be the subject of detailed capacity modelling and is subject to assumptions on likely LoS improvement and impact of integrated care initiatives, but initial estimates place this at around 55-60% 10. Implement new services on the space liberated on the KGH site (BHRUT), or provide alternative uses for the space, through a range of identified opportunities 11. Complete the vision for paediatric services, as per HfNEL. Specifically: 1. SCBU to move to the Queen s site 2. Paediatric inpatients to move to Queen s 3. Paediatric day case and elective and planned diagnostics at KGH (emergency diagnostics at Queen s)
20 5. Clinical Model Current and Future 50. The description of the clinical model and service split across sites is divided into three areas: 5.1 Unplanned care Unplanned care, covering ED, UCC and assessment areas Planned care, covering Acute Medicine s, Neuro-Sciences, Surgery, Specialist Surgery, Anaesthetics, Specialist Medicine, Pathology, Women s services and Radiology Children s services 51. BHRUT currently has an emergency department (ED) and urgent care centre (UCC) on both the Queen s Hospital site and the King George Hospital sites. In support of the overall strategy to centralise complex and acute care at the Queen s Hospital site, the ED at the KGH site will close, whilst increasing the usage ofthe UCC on both sites. 52. However, the ED on the Queen s Hospital site is under immense pressure. The ED department at QH has approximately 130,000 referrals per year; the hospital is designed for 90,000.A number of concerns around the quality and safety of patient care in the department have been raised by both the Trust and the CQC, including a warning notice that was issued in May 2013 in relation to care and welfare to patients. There has also been poor performance in the 95% four hour wait standard for emergency care and major delays in finding beds at Queen s Hospital. 53. A number of specific issues currently exist at the Queen s Hospital site relating to unplanned care: 1. Inadequate staffing levels with a high dependency on locum doctors at both consultant and middle grades. The Trust has found it difficult to recruit to consultant and middle grade staff and there have been 4 recent resignations from the consultant team 2. Queen s UCC is under-utilised and does not meet London Quality Standards 3. There are opportunities to improve clinical governance 4. Poor patient flow, with: a. Delays in getting speciality input in the acute pathway b. There is a high proportion of ED patients in Majors requiring admission to speciality c. There are multiple unnecessary duplications occurring within the pathway 5. Forecast increase in workload of 30%, following the agreed closure of the KGH ED 54. ED performance is a key area of concern for BHRUT, and a programme of interventions is planned to address them. The clinical strategy addresses each of these issues in turn, but some issues are difficult to manage and require a wider health economy approach to combat them: 1. Inadequate staffing levels Recruit middle grades and consultants, including international recruitment. Introduce joint consultant posts with Barts Health and innovative A&E / speciality consultant posts. The Trust will recruit through a specialist recruitment agency as required Develop nurse skill mix and numbers. Recruit six emergency nurse practitioners, with the potential of ten new posts Enhance the basic skills of nurses, physician s assistants and HCAs, through training in phlebotomy and cannulation Maximise support to the medical workforce. Specifically, ensure direct support from physician s assistants on basic tasks and administrative support from wider medical workforce, together with exploration of opportunities to recruit from other relevant professional groups
21 Introduce four Speciality Assessment Areas to increase reliance on acute medical teams, and reduce reliance on A&E consultant and middle grade staff 2. Queen s UCC is under-utilised and does not meet London Quality Standards Streaming to the UCC to be increased (using the Senior Streamer as described in the patient flow intervention described below) Review of current UCC services to ensure services are commissioned and provided in line with quality standardsand directly align to London Quality Standards. BHRUT fully embraces all London Quality standards and is committed to directly aligning with them 3. There are opportunities to improve Clinical Governance Medical and Nursing Directors of the Trust to timetable regular meetings to improve communication, involvement and ownership of staff at all levels in the decision making process of the Trust Hold regular meetings and audits of key actions to support a multidisciplinary clinical governance structure within A&E. Document learnings from serious incidents and complaints Undertake an audit to analyse categories for emergency readmissions in order to take action and reduce current rate 4. Poor patient flow:changesin patient flow are underpinned by a more fundamental re-classification of the Trust as a whole into three functions: Assessment, Short Stay and Long Stay. This restructuring of the organisation will support the ED and facilitate the delivery of effective and time conscious care. Assessment is defined as immediate or near immediate decision making by a senior doctor and the facility to do observations and give lifesaving treatments in a timely manner. The service delivered in ED Resus, Majors, Urgent Care, Speciality Assessment Areas, and Paediatric ED.The assessment period is 6-8 hours, during which a decision will be made on whether they are discharged home, or admitted to short stay or to a long stay ward. Short Stay will consist of patients being under the Trust s care for between hours. This stay will be associated with Surgery,Elders Receiving Unit (ERU) and Medical Assessment Unit. Long stay is defined as the patient receiving care by the trust for a period of over 48 hours. This is associated with Medical, Surgical,Orthopaedics and Paediatrics being located in the main body of the hospital. 5. Forecast increase in workload of 30%, following the agreed closure of the KGH ED.This is in line with the HfNELDecision Making Business Case in relation to ED. It assumes 65% of current ED activity will be staying at KGH in the 24/7 UCC, of which 5% will be lost through attrition and the 30% remaining of true ED activity will travel to QH. 55. It should be noted that Medical GP unit on MAU B will close as a result of the development of the four Speciality Assessment Areaswhich will include these services. 56. A decision is needed from commissioners as to the requirement for a GP Out of Hours service on the Queen s site when the UCC moves to 24/7 working, and if this service should be re-provided at QH or elsewhere within the local health economy. 57. A summary of the specific changes is: Radically redevelop the Queen s ED to address the current performance issues and address the forecast additional demand. Introduce a Senior Streamer Route patients arriving at the ED to the UCC, ED area,speciality assessment centres and short stay beds as appropriate, hence admitting patients directly to the medical assessment unit (to be under the care of acute medical teams)
22 Physically remodel the existing ED to accommodate the speciality assessment areas, cope with the increased demand and support the proposed clinical model Provide dedicated facilities for children, including a paediatric specific entrance Complete a review of the availability of pathology reports, particularly radiology, to reduce the delays caused to patients to be discharged directly from A&E Establish a system of regular joint review (ward/board rounds) by the floor consultant and nurses in charge of the Queen s Hospital department Work with social services and community services to support 7 day consultant working and expedite safe patient discharge 58. In the current model, (Figure 1) ambulances and walk-ins arrive straight into the ED, where inadequate staffing and capacity leads to the issues identified above. Figure 1 Current Model ED Areas Ambulance and walk in patients Over burdened ED Department Delayed ambulance unloading Results in duplication 59. The change is service delivery is illustrated in Figure 2, which emphasises how implementation of a Senior Streamer at the front door can act as a guide to ensure patients receive the services they require by the appropriate utilisation of the hospital service offerings. Figure 2 Future Model ED Areas Resus Majors Ambulance and Walk In patients Senior Streamer At front door Four-Specialist Assessment Areas Urgent Care Centre Minors 60. Improved use of other roles, including the Community Treatment Team, will enable patients to receive the most appropriate care. This may include care from the community teams avoiding the need for hospital admission.
23 61. A breakdown of the flow of patients entering the hospital to receiving the required service is provided below. The description integrates the proposed changes to the patient experience and to the way the unplanned services are offered. 62. Entry into the emergency care pathway occurs through: 1. Arrival by ambulance 2. Self-referral or walk in 3. GP referral, either to ED or direct referral to the appropriate assessment area 63. All adult patients will enter the emergency care pathway through the Big Front Door. The exceptions are ambulance patients requiring immediate access to resuscitation. 64. For adults, the Senior Streamer at the front door of the ED will triage the patient s optimum treatment location as opposed to the patient being served at ED by default. Patient will be referred to any one of the ED Areas: 1. ED majors / resuscitation 2. Adult UCC 65. Or to three of the four Speciality Assessment Areas: Or to: 1. Medical Assessment Unit 2. Elders Receiving Unit 3. Surgery and ENT Note: The fourth area is the Paediatric Assessment Unit 1. Eye casualty 2. Operating theatre 3. Gynaecology/EPAU currently on Cornflower B ward 4. Urology receiving room Or be transferred out again to the community response service. 66. Patients can be discharged home at any point or referred back to their GP. 67. BHRUT fully embrace the concept of ambulatory care, and are developing the necessary pathways. Over the next 18 months this will be further developed in consultation with commissioners. 68. BHRUT has a good track record of working with the London Ambulance Service (LAS). Joint working with the LAS will continue, for example with LAS presence in the ED commencing in November.
24 Figure 3 Proposed model for adults Proposed Model - Adult Adult patients from walk in or ambulance or GP referral Senior Streamer Community Response Service ED Areas (including orthopaedic assessment 4 hrs) Majors Resuscitation Speciality Assessment Areas (6-8 hrs) Surgery and ENT General Medicine Elders Receiving Unit (ERU) Urgent Care Centre Minors Elders Receiving Unit (Unit A) (24-36 hours) 10 assessment beds 20 short stay elderly care beds Surgical & ENT (24-36 hours) 10 assessment beds Medical Assessment (Unit B) (24 36 hrs) 10 assessment beds 20 medical short stay beds Main body of Hospital (Long-Stay Wards) > 36 hours 69. All paediatric patients will enter the paediatric emergency department through a dedicated paediatric entrance. Once again, the exceptions are ambulance patients requiring immediate access to resuscitation. As currently undertaken when capacity issues occur on either site, Treat & Transfer will take place to move children from the KGH UCC to the QH ED, with children being blue lighted to Queen's as currently. Children will not be routinely blue lighted between sites. 70. As shown in figure 4, for children, the Senior Streamer at the front door of the paediatric ED will triage the patient s optimum treatment location as opposed to the patient being served at ED by default. Patient will be referred to any one of the ED Areas: 1. Paediatric ED majors/resuscitation/ UCC 71. Or to one of the Speciality Assessment Areas: Or to: 1. Paediatric Assessment Unit (PAU) 1. Special Surgery (Trauma & Orthopaedics / Max Fax) 2. Specialist Medicine (Haematology / Oncology)
25 These children, if admitted would be accommodated within Tropical Lagoon (Paediatric) Ward irrespective of the lead speciality. Alternatively, they can be discharged home at any point or referred back to their GP. Figure 4 Proposed model for children Proposed Model - Children Blue light ambulance Children from walk in or ambulance or GP referral Senior Streamer ED Resuscitation Area Paediatric ED Area (4 hrs) Majors UCC Paediatric Assessment Unit (0-23 hrs) 10 beds Surgical Patients Medical patients Tropical Lagoon (Paediatric Long Stay Wards) > 24 hours Outline of service received from ED majors, Adult UCC and Paediatric ED/UCC 72. Patients will be assessed by an ED doctor, ENP, UCC practitioner, or a speciality doctor. Any speciality referral will receive a response within 30 minutes of the request. 73. In the event that the senior streamer was unable to classify the likely end speciality, patients will be managed in ED with a 4 hour turn around. 74. Patients may be: Discharged home using their own transport. Discharged home or to community by hospital transport. Social care support may be required.
26 75. A decision will be made to admit either to speciality ward or to assessment unit for further assessment and diagnostics. Outline of service received from Assessment Units 76. The clinical strategy has been developed with two overriding principles in mind: That these are assessment and not admissions units. Patients will be assessed and decisions regarding on going care will be made within 6-8 hours of arrival there. KPIs for rapid diagnostic testing and results will be in place. This means that each bed/trolley will turn over 2-3 times within a 24 hour period. That there are very significant clinical benefits in having medical, frail elders, surgical and paediatric areas in close proximity to one another and the supporting diagnostic facilities. Each assessment area will have consultants and senior decision makers for 12 hours a day, 7 days a week (probably to 22.00). Senior speciality opinion will be aided with this model of care. In particular, this will enable improved care of the elderly input into surgical cases, easier surgical assessment of paediatric cases and surgical to medical and medical to surgical review.furthermore, BHRUT will look to extend on-site consultant cover to 16 hours per day, 7 days a week once the existing significant recruitment challenge is overcome. 77. The adult speciality assessment areas will have a dedicated triage area, and an administration and welcoming help desk. Patients will receive junior speciality input within 30 minutes and consultation input within 4 hours. The standard is that the different specialist units will have a 4 hour turn around. Specialities will manage patients requiring attention of their speciality and be responsible for the outcome. The unit will be governed solely by Speciality Consultants and no referral will be required to be seen by speciality (as the decision is made by the streamer). Orthopaedic trauma 78. The orthopaedic assessment, including patients suffering orthopaedic trauma, will take place within the ED providing advice to the UCC as required. Patients with Fractured Neck of Femur (NOF) will be fast tracked to the NOF unit. Elderly patients suffering from fractured neck of femur will be directed to the NOF stabilisation unit on the orthopaedic ward (operating on 24 hours, 7 days a week) for assessment by the ortho-geriatrician and anaesthetist, and stabilised as necessary. Acute stroke 79. Patient will be fast tracked to Hyper-Acute Stroke Unit (HASU), following the pathway currently in place. Gynaecology and early pregnancy patients 80. Patients will be referred from triage directly to the Gynaecology/EPAU assessment currently on Cornflower B. Urology 81. Patients with urological conditions such as acute urinary retention will be directed to the urology receiving room at Queen s Hospital in the future (post ED closure at KGH) Elders Receiving Unit 82. The Elders Receiving Unit (ERU) will help manage older patients that are over the age of 80 years. The ERU is a multifaceted integration of Comprehensive Geriatric Assessment (CGA) into existing Emergency Department practice, consisting of: Care pathways embedded into ED documentation raising awareness of key issues such as cognition, falls, continence, and safeguarding etc. and directing ED staff to relevant resources
27 Two bays and two side rooms within the MAU staffed by geriatricians, primary care coordinators, nurses and therapists, all of whom work in a seamless integrated manner to initiate CGA In-reach into ED offering advice, support and management of older people in ED Robust links with community services through a Single Point of Access (SPA) jointly owned by BHRUT &Community Treatment Team (CTT)& Psychiatric Liaison Team ERU outreach service (offering CGA to patients at high risk of adverse outcomes on discharge from the unit) Robust links with GPs, for example supporting care pathways relating to admissions to community hospitals through direct conversations with GPs using the SPA, working with CTT/Psychiatric Liaison Team Education and training of clinicians and students - Joint governance meetings involving geriatricians, ED staff and community staff and CTT/Psychiatric Liaison Team Paediatrics Children will be assessed within a unit sited in close proximity to the paediatric ED/UCC. This Paediatric Assessment Unit will have facilities for assessment and observation. It is expected that most assessments will be complete within 4 hours. There will be a group of patients who may need observation up to 23 hours maximum. After that the child will either be discharged or admitted to Tropical Lagoon ward. Acute Oncology Service 83. The Acute Oncology Service (AOS) within BHRUT is supported by clinicians and 3 dedicated AOS Nurses, all of which work an 8am 8pm rota. This is set to become a 7 day a week service with the recruitment of 2 further nurses. All patients attending the ED are flagged by the A&E staff to the AOS service. The Trust is currently looking at extending the use of the A&E Symphony system to introduce an electronic flag. 84. Clear guidelines are in place in ED on the management of neutropenic sepsis and metastatic spinal cord compression. A patient Passport System has been in situ for some time within the Trust for those who are undergoing or have undergone treatments within the last 6 weeks. The AOS is also in the process of developing inpatient beds into a 24/7 assessment unit so that acute oncology patients do not have to attend A&E and can be fasted tracked straight to the Oncology ward for assessment. Short Stay Beds 85. The adultspeciality Assessment Areas will serve General Medicine, Elderly Care and Surgical specialities.paediatrics will have a combined assessment and observation facility within the Paediatric Assessment Unit.There will be an incremental 20 assessment beds. The current MAU A& B capacity of 60 beds will remain, but there will be an additional area (formally renal) for the surgical assessment area and Paediatric Assessment and Short Stay Paediatric beds with 10 beds each. General Medicine 86. There will be short stay beds for patients who need a longer period of assessment than 6-8 hours, but for whom the need for admission to a speciality ward, rehabilitation or discharge is still unclear. The LoS for these beds will be limited to hours only. Elders Receiving Unit
28 87. There will be a need for some patients having been assessed in the Elders receiving Unit (ERU) to have need of a further period of assessment. In the main the patients will be suffering from a single condition only. These beds will be part of the medicine short stay beds. Surgery 88. Following assessment on the SAU, some patients may need a further period of assessment (less than 48 hours) or need minor emergency surgery. The short stay beds will be part of the overall surgical bed base on the surgical floor. Paediatrics 89. The introduction of the 4-hour target in Emergency Department has driven a need for decisions about admission or discharge to be made quickly. This partly explains the rise in paediatric inpatient admissions since 2007.In the early stages of minor illness and in the very young, it is not always possible to make safe decisions within a 4-hour period and children and young people may benefit from a further period of observation and treatment. 90. BHRUT will convert the current PAU model (10am 9pm) and develop a model of care open 24/7 that shifts management of minor illness away from an inpatient setting to provide safe, rapid access to assessment, observation and appropriate intervention by clinicians with paediatric expertise. It will consist of 10 beds and a seating treatment area co located or adjacent to Paediatric ED for when assessment of up to 23 hours is required. 91. In addition, the requirement to make a clinical decision about the child s continuing care within 4 hours in the emergency department can mean that some children who need only a short (less than 24 hours) period of observation and further treatment are unnecessarily admitted into an inpatient bed. 92. Generally within paediatrics (locally and nationally) it is identified that length of stay is low and a significant number of children have a zero (less than 24 hours) length of stay. There is also a national consensus amongst both parents / carers and professionals alike, that children are best cared for in the home environment and kept out of hospital when at all possible. 93. Experience has consistently shown that the opening of a short stay PAU leads to a reduction in both inpatient demand and cost.
29 5.2 Planned care 94. BHRUT has directorates covering Emergency care, Acute Medicine, Neuro-Sciences, Surgery, Specialist Surgery, Anaesthetics, Specialist Medicine, Pathology,Women s, Children s and Radiology. This section of the strategy is focussed on areas excludingemergency care and Children s services which are covered in sections 5.1 and 5.3 of the document. 95. The key elements of the strategy for planned care are: 1. Maximise use of the Queen s site for complex inpatient activity as per HfNEL, using detailed and agreed split of service provision across the two sites 2. Maximise the use of KGH for day case, short stay elective and diagnostic activity with or without the ISTC activity / building 3. Place intermediate care and rehabilitation at KGH specifically including orthogeriatrics, stroke, neurosurgical (rehabilitation proposed new service), and grades I & II elderly patients (intermediate care) who do not need the support of a major acute hospital.this will: 1. Decompress the Queen s site to improve patient experience, cope with winter pressures, allow the space to systemically focus on reducing LoS 2. Provide a ready pool of patients to be addressed through the on-going development of integrated care and community interventions 3. Allow capacity for further community services on the KGH site, should this be required in the future. 4. Centralise all breast services into a dedicated unit located on the KGH site with colocalised breast histopathology at KGH 5. Move critical care beds from KGH, supporting the strategy of complex inpatient activity at Queen s 6. Utilise sufficient space at KGH to provide a high quality of patient care across both sites. This will be the subject of detailed capacity modelling and is subject to assumptions on likely LoS improvement and impact of integrated care initiatives, but initial estimates place this at around 55-60% 7. Implement new services on the space liberated on the KGH site (BHRUT), or provide alternative uses for the space, through a range of identified opportunities, this is to be address as part of capacity modelling Maximise use of the Queen s site for complex inpatient activity, and maximise use of KGH for day case, short stay elective and diagnostic activity 96. The breakdown of proposed service changes and proposed split by site is given below by specialty. For completeness, the service split for Emergency Care and Children s has also been included below. Acute Medicines 97. List of changes: Cardiology IP centralised at Queen s Diabetes and Endocrinology transferred to Queen s Renal OPD transferred to Queen s
30 All medical speciality IP (respiratory/ endocrine/ gastro/ nephrology) transferred to Queen s NB: Care of the Elderly to remain at Queen s Current state Care of the Elderly IP Cardiac IP / DC Queen s Hospital Medical speciality IP (respiratory / gastro / nephrology) Endoscopy Clinical Diagnostic unit Virtual ward Clinical assessment unit King George Hospital Orthogeriatric IP Intermediate care IP Cardiology IP / diagnostics Endoscopy Medical speciality IP / (endocrine/ nephrology) Cardiac angio lab Cardiac IP Medical specialties OPD cross site Future state Queen s Hospital Acute care of the Elderly IP Cardiac cath lab Cardiac IP All medical speciality IP (respiratory / endocrine / gastro / nephrology) Endoscopy Clinical Diagnostic unit Virtual ward Clinical assessement unit Cardiology IP / diagnostics King George Hospital Orthogeriatric IP Intermediate care IP Endoscopy All Medical specialties OPD cross site
31 Anaesthetics 98. List of changes: Critical Care transferred to Queen s Specialised commissioned pain services to be established at KGH (potential new service) Current state Queen s Hospital Anaesthetics Critical Care general and neuro Theatres Critical Care outreach Admissions administration Day surgery unit Pre assessment OPD Pain services DC and OPD King George Hospital Anaesthetics Day surgery unit Theatres Admissions administration Critical Care general Pre assessemnt OPD Cross site pre assessment OPD Future state Queen s Hospital Anaesthetics Critical Care general and neuro Theatres including some day surgery Critical Care outreach Anaesthetics Day surgery unit Theatres King George Hospital Admissions administration Pain services DC and OPD Specialised commissioned outpatient pain services including psychology (potential new service) Pre assessment OPD
32 Children 99. List of changes: Neonatal Unit transferred to Queen s All Paediatric inpatients to move to Queen s Paediatric DC (excluding max fax) transferred to KGH Note: Paediatric outpatients will remain on both sites Current state Queen s Hospital Neonatal Unit Paediatric IP / DC /oncology Paediatric A&E and short stay assessment unit Paediatric medicine Paediatric surgery King George Hospital Paediatric DC surgery Paediatric diagnostic day unit Neonatal Unit Paediatric medicine short stay Paediatric A&E Paediatric OPD Future state Queen s Hospital Neonatal Unit Paediatric IP / DC oncology Paediatric A&E and short stay assessment unit Paediatric emergency surgery King George Hospital Paediatric Day cases (all day cases excl Maxillofacial) Paediatric diagnostic and surgical day unit Paediatric OPD
33 Emergency care 100. List of changes: The emergency department service will be transferred to Queen s exclusively Urgent Care Centres to be made 24/7 Radically redevelop the Queen s ED to address the current performance issues and address the forecast additional demand, including: o o o o Introduce a senior streamer Route patients arriving at the ED to the UCC, ED area, speciality assessment areas and short stay beds as appropriate Physically remodel the existing ED to accommodate multiple speciality assessment areas, cope with the increased demand and support the proposed clinical model (medical, elders receiving unit, paediatric assessment unit, surgical assessment unit) The ED model set out in this strategy is yet to be agreed with commissioners. It is under review following CQC visits and the CCG commissioned review of the ED at BHRUT Current state Emergency Department Queen s Hospital Urgent Care Centre ( ) Emergency Department King George Hospital Urgent Care Centre (0800-MDN) Future state Emergency Department Urgent Care centre 24/7 Queen s Hospital Urgent Care Centre 24/7 King George Hospital
34 Neuro-Sciences 101. List of changes: Potential to provide a neuro-science rehabilitation service at KGH (new) Extend non complex spinal services to KGH Current state Queen s Hospital Neurology IP Hyper Acute Stroke unit Acute stroke rehab IP Stroke OPD Neurosurgery IP / OPD / DC Neuro critical care Stroke rehab King George Hospital Cross site Neuro OPD Future state Queen s Hospital Neurology IP Hyper Acute Stroke unit Acute stroke rehab IP Stroke OPD Neurosurgery IP / OPD / DC Neuro critical care King George Hospital Stroke rehab Neurosurgical Rehab (potential new service) Day case/short stay spinal list Spinal OPD cross site
35 Pathology 102. List of changes: Pathology centralised to Queen s Centralise all breast services into a dedicated centre on the KGH site with co-localised breast histopathology Current state Pathology Services Mortuary Queen s Hospital Mortuary Pathology Services King George Hospital Future state Pathology services Mortuary Queen s Hospital Small mortuary store King George Hospital Breast Histopathologists co-located with breast services to support one stop diagnostics
36 Radiology 103. List of changes: Breast screening on the KGH site to centralise all breast services into a dedicated centre on the KGH site with co-localised breast histopathology Addition of a PET scanner as a potential new service Current state Queen s Hospital Interventional radiology- theatres and diagnostics Interventional and radiology on call provision Nuclear medicine MRI Fluoroscopy Radiology General King George Hospital Interventional radiology Breast screening MRI Radiology General Nuclear medicine Future state Queen s Hospital Interventional radiology- theatres and diagnostics Interventional and radiology on call provision Nuclear medicine MRI Fluoroscopy Radiology General PET Scanner (potential new service) King George Hospital Interventional radiology support Breast screening including service transferred from Victoria Hospital MRI Radiology General
37 Specialist Medicine 104. List of changes: Dermatology day case and routine OPD transferred to KGH Rheumatology day cases and OPD transferred to KGH Oncology OP exclusively seen at Queen s Changes to pharmacy service provision in the 2 sites Current state Queen s Hospital Oncology IP / OPD Oncology Day unit Radiotherapy Clinical Haematology IP / DC / OPD Dermatology day cases and routine OPD Rheumatology day cases / OPD and diagnostics Haemaglobinopathy DVT service OPD Pharmacy King George Hospital Oncology Day Unit/OPD Rheumatology,day cases and diagnostics DVT service OPD Pharmacy Haemaglobinopathy Future state Queen s Hospital Oncology IP / OPD Oncology Day unit Radiotherapy Clinical Haematology IP / DC / OPD Haemaglobinopathy DVT service OPD Pharmacy IP / dispensary / robot / store Thrombosis OPD King George Hospital Oncology day unit / OPD Rheumatology OPD Rheumatology day cases and diagnostics Dermatology day cases and routine OPD Pharmacy dispensary / pre-packing TTA production unit / store 105. Specialist Medicine includes a dedicated Cancer Strategy with the vision of placing excellence in patient care at the centre of BHRUT s work in caring for and serving the community. The goals are as follows: Prevention and early diagnosis Enhancing patient experience Improving clinical outcomes Developing world class care
38 Promoting cancer research Being the provider of choice for cancer services Maintaining quality, efficiency, productivity and innovation Striving to be a first class employer Promoting collaborative working Prevention, Early Diagnosis and Reducing Inequalities 106. The aim is to improve not just on the low one-year survival of our patients but improve the overall survival across the North East London and Essex and eventually to have comparable survival rates to those in Europe. In order to achieve a reduction in mortality rates and improve survival it is essential to prevent cancers developing initially and to ensure that if they do develop they are diagnosed at an early stage BHRUT is currently working with London Cancer and a number of tumour groups to ensure that optimal pathways following diagnosis can be achieved. There will be a phased approach to reduce any surplus follow-up capacity identified as a result Improving outcomes and some of the factors that affect survival fall outside of the direct control of BHRUT; it is our role to support and influence those providers that are responsible for providing prevention, early detection, and screening Tackling inequalities will be fundamental to this. In order to achieve this BHRUT is committed to the following: Working with Primary Care partners to promote healthier lifestyles To work with the Health and Wellbeing Board to promote healthier lifestyles to prevent secondary cancers from developing and to assist patients to deal with the impact of side effects of treatment Extend screening, including age extension and improving access to the national screening programmes. Queen's is already a bowel screening provider, and BHRUT are in the process of attaining JAG acreditation for the KGH Endoscopy Unit in order to support B&D and Redbridge more locally. The Trust is now almost ready to implement the Breast age extension, with planned change before the end of the financial year. To implement best practice early diagnosis pathways next year, as part of the plans for wider implementation across London Working on increasing endoscopy capacity in order to meet the likely needs of the colorectal ED pathway The London Cancer Radiotherapy ERG will be assessing the number of brachytherapy patients and provide recommendations regarding where brachytherapy ought to be provided. This is being addressed in BHRUT s Peer Review work programme Ensure the Trust is involved with pilots and projects for the screening of other cancers such as Prostate cancer and Ovarian cancer Continue working with the Local Authority on the National Awareness Early Detection Initiatives projects Improve access to diagnostic tests, including chest x-rays, non-obstetric ultra-sound scanning, flexible sigmoidoscopy/ colonoscopy and MRI Continue to work with the Local Authority to educate GPs on cancer issues
39 Improve the year on year survival rates for one, three and five year survival for all tumour sites and monitor these. These will be monitored by the Cancer Strategy Implementation Group Continue to collect staging data in a minimum of 95% of all stageable cancers and thus contributing to the monitoring of the changes in survival rates and late presentations Improve the quality of data that is published on external websites and in National Audits By 2016 have the most improved survival rates across London Enhancing Patient Experience 110. The major London Cancer Centres have all received poor reviews in the National Cancer Patient Survey released in August BHRUT are determined to improve patient experience; patients will experience high quality care in a safe and pleasant environment and betreated with dignity and respect. Thestrategic objective is for patients to have the highest standard of care. Key to this is ensuring that patients are involved in the decision making process relating to their cancer journey, have a seamless transition between provider organisations, have help in understanding the relevant information for all points of their journey and have the support of a key worker throughout their pathway to achieve this.bhrut fully embrace the principles of enhanced recovery across all major cancer surgical areas in order to improve patient experience and outcomes and also reduce LOS Ultimately, the ambition of BHRUT is to have the best cancer survey results in England. Measurement of progress towards these objectives will be against the following: From 2013/14 ensure that each Multi-Disciplinary Team (MDT) undertakes a detailed review of their national cancer patient survey results, and produces an action plan for improvement To maintain a year-on-year reduction in patient complaints and concerns From 2013/14 ensure that every MDT can demonstrate the quality of their patient s experience through locally agreed indicators such as reduced LOS, reduced readmission rates, access to Clinical Nurse Specialists (CNS s), and CQC compliance By the end of 2013/14 ensure that the 62-day target is achieved and maintained, so that waiting times are kept to an absolute minimum Discharge summaries to be sent to GP surgeries within 24 hours to ensure seamless transfer of information between primary and secondary care All patients to be offered a permanent record of their consultation Ensure that patients are seen within a maximum of 30 minutes of their appointment time, less for patients receiving their first treatment Ensure that patients receive their chemotherapy treatment within 60 minutes of their appointment time From 2013 ensure that all patients requiring an emergency admission are admitted to the Oncology ward From 2014 establish a plan for the provision of Bereavement Services Ensure all members of an MDT have undergone Advanced Communication Skills training Ensure participation in the National Cancer Survivorship Initiative, particularly the introduction of end of treatment summaries and Health and Well-Being clinics Ensure roll out of the Electronic Holistic Needs Assessment (EHNA) tool to all tumour sites Implement individual end of life care plans for patients who are in the dying phase
40 Work in partnership with MacMillan who will be supporting these efforts, funding project managers to drive forward these improvements Developing World Class Care 112. BHRUT wants to continue to develop its Cancer Centre to be one of the key providers of cancer care within London, providing sustainable care and treatment that is recognised as the best in London and comparable to other world class cancer care providers. To achieve this, BHRUT will work in partnership with UCLP / London Cancer, with whom it has a shared vision to provide the latest surgical, radiotherapy and drug treatments forpatients Measurement of progress towards these objectives will be against the following: From 2013/14 continue to improve access to diagnostic services, including direct access By 2013 have the required capacity to deliver the number of radiotherapy fractions as set out in the National Radiotherapy Advisory Group s (NRAG) report and submit data for the Radiotherapy Dataset (RTDS) By 2015 implement, or have plans to implement, the latest treatment technologies such as extended laparoscopic, robotic, image-guided and laser surgery By 2014 implement, or have plans to implement, up-to-date radiotherapy treatment techniques From 2013 review the provision of PET CT services, with the aim of establishing a local service From 2013 review the provision of supportive services such as OT, physio, dietetics and clinical psychology developing these as part of the drive to improve outcomes and patient experience Ensure that all MDT Leads are clinically engaged in the implementation of the proposed Models of Care through London Cancer By 2013/14 demonstrate that we are following Best Practice Cancer Commissioned Pathways for the appropriate tumour sites From 2013/14 implement on-going support for older people following the successful Macmillan s Older Persons Pilot By 2013/14 ensure that all chemotherapy is prescribed using the electronic prescribing system From 2013 submit data for the Systemic Anti-Cancer Therapy (SACT) dataset Improve patients access to SACT by utilising the Cancer Drugs Fund Continue to develop the role of an Acute Oncology Service (AOS). BHRUT arealready fully compliant with peer review measures for acute oncology, including 5 dedicated consultant PAs per week for the service, such that there is a consultant lead AOS service daily Monday - Friday, with the weekend covered by the consultant oncologist on call and 4 dedicated AOS Clinical Nurse Specialists. From 2013/14 review the use of oncology inpatient beds to support admission avoidance and rapid assessment for acute oncology patients Develop a program of real-time patient feedback to ensure continual evaluation and improvement of services Promoting Cancer Research 114. BHRUT s research programme has greatly improved over the past year, with a vision to be a leader for the cancer research programme across London. Working with partners at UCLP BHRUT
41 arerecruiting more patients into clinical trials and making the latest effective treatments available in clinical practice.this will include introducing early phase clinical trials into theportfolio Measurement of progress towards these objectives will be against the following: From 2013 raise the profile of the research provided by BHRUT By 2013/14 enter at least a third of all patients each year into National Cancer Research Networks (NCRN) approved studies From 2013/14 improve uptake of patients into Radiotherapy clinical studies From 2013/14 increase total research income by 250,000 per annum From 2014/15 open early phase clinical trials Work with London Cancer to give patients access to the most novel and exciting new therapies before they are adopted by the wider NHS, including research into survivorship Being the Provider of Choice for Cancer Services 116. As the largest cancer centre within London Cancer BHRUT will establish a local and London-wide reputation to become the provider of choice for local and peripheral patients and referrers. BHRUT willplay a leading role in developing safe, high quality care as documented in the Case for Change for London, the Cancer Reform Strategy and Improving Outcomes A Strategy for Cancer, demonstrating objective improvements in outcomes and in patient and survivorship experience Measurement of progress towards these objectives will be against the following: From 2013 ensure continued compliance of 100% with all IOGs Ensure that all MDTs continue to participate in the annual Peer Review self assessment, internal validation and external visitation programme From 2013/14 publish cancer performance data and information to enable patients and referrers make an informed choice on where to be treated Develop a cancer specific BHRUT website Ensure full participation in all National Cancer Audits By 2014/15 improve the overall scores for the National Cancer Patients Experience survey Maintaining Quality, Efficiency, Productivity and Innovation 118. BHRUT want to show services at the forefront of excellent clinical quality and with excellent financial management. This objective works closely with ensuring that patients have a positive experience at a challenging time in their lives Measurement of progress towards these objectives will be against the following: From 2013/14 ensure that all MDTs achieve at least 85% compliance with National Cancer Peer Programme; Manual for Cancer Services By the end of 2013/14 ensure that the 62-day target is achieved and maintained By 2014/15 implement service line reporting to closely monitor our income and expenditure By 2013/14 implement a 7-day a week nurse led AOS From 2013/14 review the use of oncology inpatient beds to support admission avoidance and rapid assessment for acute oncology patients
42 From 2013/14 publish all articles and presentations, innovations and audit oucomes on the BHRUT website By 2014/15 improve the overall scores for the National Cancer Patients Experience survey. Specialist Surgery 120. List of changes: Ophthalmology to become cross site ENT DC/ OPD to become cross site Orthodontics moved to KGH Current state Queen s Hospital ENT IP / OPD Maxillofacial DC / IP / OPD Dental Ophthalmology DC/ Eye casualty / OPD Orthodontics diagnostics/opd Orthopaedic trauma IP / DC ENT assessment unit Orthopaedics EL & DC King George Hospital Cross site Orthopaedics/Ophthalmology OPD Future state Queen s Hospital ENT IP / OPD Maxillofacial DC / IP/ OPD Dental Ophthalmology DC / Eye casualty Orthopaedic trauma IP / DC ENT / Max Fax Assessment Unit King George Hospital ENT day surgery Orthodontics diagnostics / OPD Ophthalmology LA cataracts Orthopaedics EL & DC Cross site ENT/Ophthalmology/Orthopaedic OPD Surgery 121. List of changes: Colorectal IP centralised at Queen s Hospital Majority of Day Cases will move to KGH
43 General surgical IP from KGH to Queen s Centralise all breast services into a dedicated centre on the KGH site with co-localised breast histopathology Complex urology to Queen s NB: Upper GI IP/ OPD to remain at Queen s Hospital Current state Queen s Hospital Vascular IP EL/NEL DC /diagnostics Colorectal IP / DC Upper GI IP / OPD General Surgery IP / DC / short stay Surgical Assessment Unit King George Hospital Urology DC / short stay IP Urology diagnostics and bladder chemotherapy Urology receiving room General surgery DC / short stay Breast surgery/opd Colorectal IP/DC Cross site Vascular/colorectal/urology/surgery Future state Queen s Hospital Urology Cancers / Complex TURPs & BTs Vascular IP EL/NEL/diagnostics Colorectal IP / OPD Upper GI IP/ OPD General Surgery IP Surgical Assessment Unit Urology receiving room King George Hospital Urology DC / short stay IP (including non complex TURPs & BTs) Urology diagnostics and bladder chemotherapy Breast IP/ DC/ OPD/ diagnostics / all screening (including Victoria Hospital screening) Vascular DC Colorectal DC General surgery DC / short stay Cross site Vascular/colorectal/urology/surgery Women s Services 122. List of changes: Maintenance and development of antenatal and associated services at KGH Exploration of the portfolio of day case gynaecological services to be developed at KGH Sexual Health / GUM to move off-site into a community setting NB: Maternity to remain at Queen s Hospital exclusively
44 Current state Queen s Hospital Obstetrics Gynaecology IP and oncology Maternity Antenatal screening Sexual health / GUM Antenatal screening King George Hospital Future state Queen s Hospital Obstetrics Gynaecology IP and oncology Maternity Antenatal screening Gynaecology DC Antenatal screening King George Hospital Sexual health / GUM off site Maternity Services 123. BHRUTprovides a spectrum of maternity services offering a range of midwifery, obstetric,fetal medicine, neonatal, anaesthetic and other associated services. The birth rate is rising within BHRUT s catchment area, and for 2012/13 the number of births across both sites was 8, Theprior provision of maternity services across two sites was associated with several issues. In particular, choices for the local population were limited, with an unbalanced delivery of obstetric care for women as a result of more emphasis being placed on QH site for obstetric care compared to KGH. A co-located Midwifery Led Unit, The Queen s Birth Centre, has proven to be a popular and safe choice for low risk women, with almost 50% of those births being water births. Maintenance and development of antenatal services at KGH planned 125. The services supporting Antenatal Care are well developed and work is underway to consider what further specialist support can be developed to support the delivery of community based antenatal services to this population. Exploration of the portfolio of gynaecological services to be developed at KGH planned 126. Given advances in gynaecological medicine and increasing use of minimally invasive techniques a review of services will be undertaken to evaluate the scope for moving services from Queen s to KGH as treatments move from inpatient to ambulatory care, to day case, to the outpatient setting. Such approaches are now becoming the first choice for most women. Sexual Health / GUM to move off-site 127. Subject to business case approval, sexual health / GUM will move fully off the QH site and into a community setting. This will both free-up space on the QH site and make the service more accessible for service users.
45 Implementation of a campus model of maternity services - already complete 128. Improvements were implemented and planned at QH site to improve the quality of maternity services. The crucial areas where improvements have been made are: Implementation of a new triage system Funding and recruiting additional midwives to maintain a staff ratio of 1:29 Recruiting additional nurses and support staff Maintenance of a Maternity HDU facility. Achieving a ratio of 1:1 midwife care in labour for more than 95% of women Improving medical staffing including senior anaesthetic presence Improving systems for engagement and feedback from women and families Increasing usage of the midwifery-led unit, promoting normality for low-risk women 129. Successful implementation of the campus model provides a choice of place of birth: Obstetric Led Unit at Queen s Hospital: The unit offers care for women with complex needs and includes a range of pain relief, anaesthetics, intensive and high dependency care, blood transfusion and neonatal services. Co-located Midwifery Led Unit: Organised and managed by midwives, with a senior midwife responsible for service operation. Provision of care for women with low risk complications and based in the same building as the obstetric unit, with a close enough proximity to enable rapid transfer if appropriate. Home Birth: Organised and managed by midwives to support women with low risk of complications. Where an emergency situation occurs, formal local multidisciplinary arrangements will be arranged including transfer in labour and midwives referring directly to the most senior obstetrician on obstetric unit and/or the paediatrician. The midwife is responsible for transfer and must remain to care both for the woman and the baby during the transfer and continuing on in the transferred unit, if the capability exists. Placement of intermediate care and rehabilitation at KGH 130. As stated in the case for change for integrated care in Barking and Dagenham, Havering and Redbridge 7, Implementation of the Barking, Havering and Redbridge University Hospitals reconfiguration (which is essential if services are to improve) relies on improvement of intermediate care services. Coupled with the fact that the Trust has consistently over-performed over the past few years(despite 5.7m of in-plan QIPP for 13-14), it would be prudent to assume that the local health economy is unlikely to be in a position to deliver this model of care in a way that will deliver material reductions in demand by the summer of 2015, when the ED closes at KGH and acute beds are removed. The achievement of moving LOS in all HRGs to national upper quartile performance will also be extremely challenging and thus a number of intermediate care and acute rehabilitation beds (ortho-geriatric and stroke) will be needed in the medium term, whilst the system undergoes the very necessary changes. These proposed changes are detailed below. They will: Decompress the Queen s site to improve patient experience, cope with winter pressures, allow the space to systemically focus on reducing LOS Provide a ready pool of patients to be addressed through the on-going development of integrated care and community interventions 7 Integrated care in Barking and Dagenham, Havering and Redbridge: The case for change, August 2012, pg11
46 Reducing Length of Stay (LoS) 131. BHRUT embraced 7/7 working, with consultant presence on all the medial specialty wards from September BHRUT is now developing enhanced diagnostic support, along with the physiotherapy support that is necessary to fully realise the LoS reductions required. BHRUT recognises that there are problems in discharging patients due to delays in transfers and provision of medication. BHRUT will be setting up a working group to significantly improve performance in this area, which is recognisedas an issue Greater co-ordination and a lead clinician approach to complex cases might speed up LoS. BHRUT have therefore developed the medical specialty units as co-terminus in order to allow rapid access to different specialties. If patients are formally referred to see another specialty this will be organised within 24 hours by a senior clinician, and if clinically required it will be organised sooner. Developing models of integrated care 133. The Trust is committed with partners to develop models of integrated care, particularly for elders. To this end, work with the Integrated Care Coalition has led to plans to implement a Joint Discharge Team from April 2014 and the Frailty service of BHRUT are now working more closely with the Community Treatment Team (NELFT) to manage patients in a more integrated fashion. This will include the post-acute care of the elderly services, both bedded and in the community BHRUT will develop services for frail elders with partners to enable all frail elders to have timely access to specialist support and opinion, both in hospital and in the community. This will include developing further current work which aims to assess those appropriate emergency elder patients in a more dedicated space away from the Emergency department, as well as alternatives to Hospital admission. It will also offer appropriate assessment to frail elderly patients in other pathways (orthopaedic, surgery, cancer). BHRUT will look to: Implement real-time senior specialist review (7/7) Ensure daily senior decision capability on each ward Work in partnership with NELFT, to facilitate the assessment at home at the point at which acute hospital setting is no longer benefiting patient Move Consultants from post-take to on-take 135. BHRUT have a joint working group with NELFT, which is chaired by the NELFT Executive Director of integrated services, and attended by the BHRUT COO, to meet and develop joint strategies and have joint responses to operational issues. This includes operationally excellent working with NELFT s Community Treatment Team(CTT). All NELFT s community hospitals have input from BHRUT geriatricians BHRUT recognise that bedded medical assessment units are potentially unnecessary for the majority of geriatric medical patients. Medium Stay Beds for elderly patients 137. Following acute assessment, some patients will need the benefit of a longer period of care. Often they will be patients with more than one condition. 30 beds are available for these patients.these are presently located on Sky A ward. The LoS on this unit will be no longer than 3-5 days. Patients will be then discharged home or to the community. Some however, will need a further period of care and will require transfer to a care of the elderly ward.
47 Enhanced Intermediate Care and Acute rehabilitation a.medical and care of elderly patients Many patients do not necessarily need the backup and support of a major acute hospital, such as Queen s, but do need enhanced intermediate care, that at the present time is not easily provided out of hospital. This type of care can be provided, in a less acute and pressurised setting at KGH. In doing so, there will be a reduction in the pressure on the acute admission beds at Queen s. Admission for some patients could occur immediately after acute assessment or even triage. b. Ortho-geriatrics patients 139. Following trauma patients will be transferred to KGH for acute rehabilitation, if fit, 72 hours after surgery. This existing and successful pathway will be continued. c. Acute stroke rehabilitation 140. Acute rehabilitation of some patients recovering from an acute stroke takes place at KGH. Although the number of beds is being reduced following the introduction of early supportive discharge, beds will remain at KGH for acute rehabilitation. d. Neuro-rehabilitation 141. Proposals for a new service will be worked up to provide an enhanced neuro-rehabilitation service for patients who are at present experiencing long delays in the system in accessing rehabilitation following head injuries and neurosurgery. These patients currently experience long delays and prevent the efficient use of neurosurgical beds. This service could be centred on the KGH site. It could be used by, and would be helpful to, other NHS care providers who have similar issues. Support from specialised commissioners will be sought for this service e. Improved intermediate care and community rehabilitation Barking and Dagenham, Havering and Redbridge CCGs are working together with BHRUT, local authorities and other providers to improve intermediate care and community rehabilitation. The BHRUT clinical strategy sits alongside and complements these plans. The CCGs currently have a high number of intermediate care beds, reflecting a history of lack of investment in intermediate care services in the community and at home. Current inpatient provision includes: Borough Barking and Dagenham Redbridge Havering Name of facility Grays Court, Dagenham Heronwood & Galleon unit, Wanstead Foxglove ward, King George Hospital The CCGs strategy is to improve care patients own homes or closer to home, shifting activity away from hospitals and into the community, moving away from relying on institutional (bed based) services as the default option and instead considering individual needs, choice and ability to return home. This will also seek to reduce the number of hospital admissions for preventable causes and reduce length of stay and discharge to institutional beds rather than community faciliites. In order to deliver this, two new services are being trialled by the CCGs: community treatment team (CTT): consisting of doctors, nurses, occupational therapists, physiotherapists, social workers, and support workers. It provides short term intensive care and support to people experiencing health and/or social care crisis to help them be cared for in their own home, rather than be referred to hospital. It supports people to return home as soon as possible following an acute/community inpatient stay where this is required/appropriate and provides a single point of access to intensive rehabilitation at home or a bed in a community inpatient unit if necessary. intensive rehabilitation service (IRS) at home: a team of nurses, occupational therapy staff, physiotherapy staff and rehabilitation assistants with access to a geriatrician as required, accessed via the via CTT. The CTT and IRS schemes will be reviewed, alongside existing inpatient provision, and patient and public feedback taken into account by the CCGs when planning the way forward for improved intermediate care and community rehabilitation.
48 Centralise all breast services into a dedicated unit located on the KGH site 143. BHRUT symptomatic and asymptomatic breast services are currently provided at KGH in Ilford, Victoria Hospital in Romford and Harold Wood Polyclinic. All breast surgical services were centralised at KGH as part of a Vascular/Breast reconfiguration plan in February Outpatient clinics are undertaken at KGH and Victoria Hospital with screening taking place on each site It is planned to locate all the outpatient activity with the surgical centre. The patient will have all services provided from one site and will have increased access to the support services provided by the specialist nurses. There will be greater cross cover during leave and increased flexibility with clinic slot times. Outpatient services will be moved from the general outpatient areas at KGH into thespecialistarea In centralising all breast services (including a triple-assessment clinic)at KGH the breast histopathologists would relocate from Queen s to KGH. A small co-located working laboratory would be created in which operative specimens could be reviewed at the time of the procedure being undertaken. This would result in:real time advice as to whether further tissue resection would be required; minimise the number of returns to theatres for those requiring a wider excision of the tumour; negate the need for tissue to be transferred between sites that has the inherent risk of a specimen being misplaced or lost; support a quicker turnaround of results for the one-stop diagnostic outpatient clinics Subject to activity modelling, Block 6 of KGH could accommodate all of breast services and it is planned that gynaecology day cases, children s day unit for diagnostics, medical and elective procedures, antenatal screening and all outpatients related to these services would be in this block. A dedicated Women s and Children s unit would be established. Utilise sufficient space at KGH to provide a high quality of patient care across both sites This will be the subject of detailed capacity modelling and is subject to assumptions on likely LoS improvement and impact of integrated care initiatives, but initial estimates place this at around 55-60%. The estimate of the BHRUT estate requirement is based upon the transfer of services as described in this clinical strategy, and conservative assumptions on the floor area required for the various services to be placed on the KGH site. This will be further refined as part of detailed capacity modelling in November. The services included in this 55-60% are listed below. Note that it does not include the UCC at KGH, which may or may not be provided by BHRUT in the future BHRUT fully recognise the impact of the changes of service on other providers and will be transparent in sharing analysis on the impact of the changes with other providers The Redbridge CCG Clinical Director for the KGH Vision Steering Group is currently meeting with key clinical stakeholders to get their views on the future configuration of services at KGH. This on-going dialogue will continue to inform the Primary Care Vision for KGH. Potential location of services at KGH 150. Block 6 Women and Children s Unit All breast services + mini pathology lab + all screening services from Victoria and radiology Paediatric day unit and outpatients Gynae short stay elective and outpatients Antenatal screening Potential area for UCL / BHRUT neonatal research centre 151. Block 5 & part of Block 4 Surgical and Diagnostic unit Radiology
49 Endoscopy Theatres Day unit surgical and medical Ophthalmology Urology diagnostics Orthopaedic elective Outpatients Redbridge polyclinic institution Pain services Orthodontic services Cardiology diagnostics Pre assessment Pharmacy Pathology 24/7 short stay ward Admissions 152. Block 3 Potential area for Pregnancy advisory service in vacated angio suite Potential area for office / secretarial space on ground floor 4 wards empty 153. Block 2- Rehabilitation Unit Barts Health Institute Therapies Orthogeriatrics Stroke and neuroscience rehab Intermediate care (NELFT instate x1 ward) 154. Block 1 Service yard Mortuary store Restaurant Potential area for Brentwood transfusion service BHRUT to implement new services on the space liberated on the KGH site 155. Agreement on the set of new services to be placed on the KGH site, and precise locations, will be reached with commissioners (and 3rd parties as required) over the next six months, and subject to detailed capacity modelling. This will include agreement on relocating the current services at Loxford and Kenwood Gardens into KGH, with the exact site and timelines to be decided. BHRUT is supportive of NELFT relocating services, and the Trustis conscious of the need to resolve this speedily as the lease for Kenwood Gardens is due to expire at the end of September 2014.Any decision to centralise community rehabilitation beds at KGH, and their location, will be subject to formal consultation in early Identified opportunities are:
50 Potential New Services for King George Hospital Opportunity Pregnancy Advisory Service (currently using obstetric suite at KGH would require 1 theatre per week and separate OPD) Brentwood blood transfusion Unit (size approximately equivalent to 2 wards) BHRUT/UCLP research Unit for the LIFE longitudinal study (UCL Partners and Institute of Child Health (size approximately equivalent to 1 ward) ISTC activity Pharmacy dispensary/pre-packaging TTA production unit / store (subcontracted) Neuroscience rehab (neurology and neurosurgery) Specialised commissioned pain services to include psychotherapy Short stay spinal elective surgery Community paediatric mental health service Further community rehabilitation beds UCC Medical records move from current site Breast screening move from current site NELFT use of outpatient services Potential Service Provider BHRUT (future provider subject to retender) National Blood Transfusion Service UCLP / BHRUT BHRUT BHRUT BHRUT BHRUT BHRUT NELFT Commissioners / NELFT/BHRUT Commissioners / BHRUT BHRUT BHRUT NELFT 157. In addition to all the above, there is: Continuation of the renal unit Continuation of NELFT intermediate care ward (Foxglove) 5.3 Children s services % of the current catchment is aged under 16 and there is significant local population growth in young couples and children. Demand on women s and children s services is forecast to rise substantially in the coming years. Currently 30% of A&E attendances are children, and there are no GPs with a special interest in in paediatrics in the local area. Neonatal Care 159. Inherently, neonatal care is highly technical and,have improved systematically due to advances over the past three decades, the outcomes for sick and very premature babies. In the last three years, the demand for specialist neonatal care has increased by 9% due to increases in fertility rates in women under 20 and over 40, the availability of assisted conception and a30% increase in women admitted at 25 weeks of gestation or less whose babies require specialist care The BHRUT service belongs to the North East London Neonatal Network and is supported by the neonatal transport service 24/7. QH is the main level 2 unit, consequently it requires a separate medical rota to provide for the level of activity it incurs. However, KGH incurs less intensity as it
51 provides only level 1. The Unit is developing clinical skills to include Nitric Oxygen therapy and Cooling, which will enable the unit to reduce transfers out of the unit where clinically appropriate Babies requiring neonatal care are expected to receive their initial package of care at units located outside of BHRUT. Neonatal care can be required for several days and/or weeks, when it is safe babies should be transferred back to a unit more local to their family s place of residence. Currently, the KGH SCBU is predominantly utilised as a NICU Step down facility for babies from Queen s NICU or repatriation from other NICU units in the region A requirement to split the nursing and medical rotas exists until the neonatal unit becomes centralised to QH. Additionally, it is expected that 8,000 8,300 births will occur at QH. Currently, the established neonatal nursing levels are below the recommended staffing levels recommended by the British Association of Perinatal Medicine, but support from agency means that safe staffing levels are maintained and are flexible dependent on demand and capacity fluctuations The key issues to be addressed in women s and children s services are therefore the growth in demand for these services, as well as the need for continued provision of high quality care The strategy consists of implementation ofhfnel, coupled with implementation of further opportunities for continuous improvement, specifically: SCBU to Queen s to complement the overall strategy of moving complex inpatient activity to the Queen s site Move paediatric inpatients to Queen s Move paediatric day case and elective and planned diagnostics to KGH (with emergency diagnostics at Queen s). Note: Paediatric outpatients will be retained on both sites. Roll out of Hot Clinics in support of the emergency care stream at KGH, as currently undertaken at Queen s Develop the Paediatric Emergency Department clinical pathway as described in the Unplanned Care section of this document Relocate SCBU to Queen s- planned 165. Centralisation of the SCBU to one site will ensure efficiencies in medical and nursing establishments and better nurse / cot ratios, while ensuring timely attendance to labour ward emergencies and neonatal care in addition to facilitating postnatal discharged Centralisation of the neonatal care to Queen s will open an opportunity to improve the senior medical cover for the unit. Centralisation of the neonatal consultant rota will enable the team to extend the consultant presence on the unit to include weekends and supporting the postnatal care pathways in maternity, hence preventing unnecessary admissions. Paediatric inpatients to move to Queen shospital - planned 167. This supports the strategy to maximise the use of the Queen s site for complex inpatient activity as per HfNEL.This will ensure optimal usage of Consultant Paediatricians supported by the clinical specialties. Whilst the Trust does not have Specialist Paediatric surgeons, children do benefit from a team of experts with paediatric interest. Paediatric day case and elective and planned diagnostics at KGH - planned 168. This supports the strategy to maximise the use of KGH for day case, short stay elective and diagnostic activity. This will be aligned to the proposed changes of clinical services described elsewhere. Roll out of Hot Clinics - planned 169. Extension of the existing Hot Line providing direct access to advice and guidance for GPs to paediatric consultants to KGH as well as the Queen s site.
52 Develop thepaediatric Emergency Department clinical pathway - planned 170. As covered in the Unplanned Care section of this strategy, with provision of dedicated facilities for children including a paediatric specific entrance. 6. Risks and Mitigations 171. Restructuring clinical services across the 2 sites entails a variety of risks. The table below summarises key risks and mitigations. The risk register is split into risks that are primarily within Trust control and can therefore be directly addressed, and contextual risks that are primarily outside of Trust control and can therefore only indirectly addressed. Risk rating matrix Risks within Trust control ID Description Impact Likelihood Total Mitigation Failure to build the additional critical care R1 beds at Queen s due to a failure to obtain approval and agreement on the funding Robust business case documentation development (PDC funded) Robust programme management processes to ensure that changes to clinical R2 Efficiency increases through theatre utilisation and LoS are not fully delivered in expected timescales, leading to a services are appropriately risk assessed and emerging risks are emphasised and managed requirement to use greater than expected space at KGH Options for additional temporary bed capacity being considered and maintaining a presence on the KGH site to enable flexibility R3 The non-delivery of CIP plans (productivity savings rather than reconfiguration savings) affects the overall affordability of the Trust and consequently the delivery of transformational programme Robust programme management processes to minimise the risk of nondelivery of CIPs, with nonrecurrent measures being used to close any in-year shortfalls R4 Failure to agree additional service delivery by BHRUT from the space liberated on the KGH site Reach CCG agreement promptly on use of the space Ensure development of robust links with community services R5 Failure to deliver reductions in LoS through failure to deliver an integrated care strategy with a single point of access Engagement with and support for the integrated joint health and social steering group
53 R6 Higher than forecast demand at Queen s Hospital ED post closure of KGH Development of a flexible design Robust development of assumptions to underpin the modelling R7 Inaccurate assumptions leading to errors in capacity modelling Development of a range of scenarios to assess the range of likely outcomes Development of a flexible design to accommodate uncertainty Utilise spare capacity on the Queen s and KGH sites Implement programme Context ual risks outside of Trust control R8 Clinical quality will not be maintained during major clinical service reconfiguration management to ensure that all changes to the clinical services are appropriately risk assessed and emerging risks are emphasised and managed in robust way Use of specialist recruitment agency if required R9 Failure to recruit and / or retain staff in ED Increase reliance on acute medicial team R10 Loss of activity from centralising all breast services on KGH site and hence reducing catchment ID Description Impact R11 R12 Level of non-elective activity may be more than planned as a result of the non-delivery of Commissioner QIPP, meaning that additional capacity may be required Changes in strategic commissioning intentions due to a change in the political environment Enhance skills of nurses, assistants and HCOs Review of referral patterns ate has been developed and is outlined below. Key milestones / dependencies are: Likelihood Total Mitigation The Trust will collaborate with commissioners to deliver QIPP plans. If reductions are not delivered, further improvements in LoS to reduce the beds requirement or utilisation of additional beds at the KGH site will be needed Scenario modelling to identify the range of possible outcomes. Strong commissioner engagement 7. Strate gic Imple menta tion Plan 172. A high level strategic impleme ntation plan by clinical director
54 1. Intermediate care beds to be established at KGH inspring2014.this will free up space on the QH site to support reconfiguration 2. Renal dialysisto be moved off the QH siteinsummer2014 to allow work on the Queen s Hospital ED to commence as soon the full business case is approved in August Emergency department redevelopment and critical care bed provision at QH to be completed in autumn 2015, allowing the majority of the day case activity to move to the KGH site, and majority of the IP activity to move to the QH site in early Note: Access to the ISTC by BHRUT has not been assumed within this clinical strategy.a decision on the ISTC at the external reconfiguration group would enable earlier transfer of non complex surgical cases from QH to KGH. Floor plans for the ISTC are given in appendix B.
55 Intermediate care at KGH Renal dialysis off-site KGH ED closes and critical care beds move to QH Majority of DCs at KGH & surgical IP at QH Emergency Care ED business case approvals Full business case approval (Aug 14) QH UCC made 24/7 QH UCC 24/7 (Spring 14) Senior streamer at QH KGH UCC made 24/7 KGH UCC 24/7 (Summer 14) Renal dialysis off-site (June 14) Physically remodel QH ED KGH ED closes to blue light ambulances (earliest Summer 15) ED transferred to QH KGH ED closes (end 15) Acute Medicine Cath lab business case Intermediate care at KGH Catheter laboratory business case approval (Jan 14) Cathlab developed Cardiology IP to QH Intermediate care at KGH Catheter laboratory complete (July 14) KGH cardiology closes (Aug 14) Diabetes & Endo to QH Medical speciality IP to QH Anaesthetics Children Neuro- Sciences Critical care bed business case approvals OBC/FBC post natal beds business case Pain services to KGH Post natal beds at QH complete (Aug 14) at QH SCBU built SCBU business case approvals Neonatal at QH complete (Feb 15) at QH Paediatric inpatients to QH Paediatric DC to KGH Neurosciences to transfer activity from QH to KGH Pain services at KGH (Summer 14) Combined OBC/FBC approved (Feb 14) Post natal Full business case approval (Aug 14) Build critical care capacity at QH Critical care beds moved to QH (October 15) Pathology Breast screening at KGH Hot lab to support breast services established at KGH (May 14) Pathology centralised at QH Pathology centralised at QH site (Feb 15) Radiology Breast screening business case Breast facility Breast facility established at KGH (May 14) Develop Radiology services within ED Increased utilisation of advanced practice reporting radiographers Specialist Medicine Dermatology DC/OPD to KGH Rheumatology OPD to KGH Dermatology at KGH (Spring 15) Rheumatology OPD at KGH (Spring 15) Specialist Surgery Ophthalmology cross site ENT cross site Orthodontics moved to KGH Specialist surgery reconfiguration complete (June 14) Surgery Colorectal IP to QH Majority of DCs to KGH Complex urology to QH General surgical IP to QH Majority of DCs at KGH & surgical IP at QH (Spring 16) Women Sexual Health / GUM off site Gynaecology day cases at KGH Estates Capital Build / refurbishment works at KGH (BHRUT) New services / new tenants on KGH Queen s hospital infrastructure QH infrastructure complete (June 15) upgrades Ophthalmic theatres complete (Jan 14) Renal dialysis off-site (June 14) Catheter laboratory complete (July 14) Post natal beds at QH complete (Aug 14) Neonatal at QH complete (Feb 15) Pathology centralised at QH site (Feb 15) ED and critical care build complete (Oct 15)
56 8. Next Steps 174. This clinically led qualitative strategy will be further refined in three stages: 1. The quantitative impact of this strategy will be assessed usinga capacity planning modeland Trust LTFM through November 2013 to test a range of scenarios 2. The quantitative clinical strategy will complete at the end of November 2013 to feed into the Outline Business Case (OBC)for the proposed changes 3. The strategy will be operationalisedthrough the transformation programmeandby individual Clinical Directorates through their operational business plans

57 9. Appendix 9.1 Appendix A - KGH floor plans (indicative)
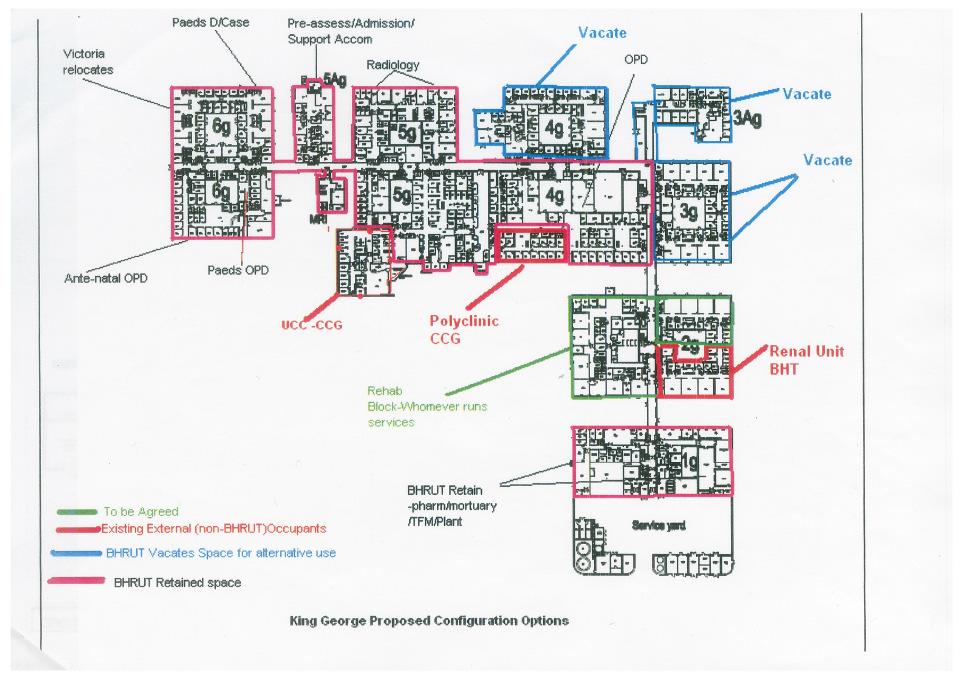
58
The Royal Wolverhampton NHS Trust & Wolverhampton CCG consultation on proposals to deliver planned care at Cannock Chase Hospital
 The Royal Wolverhampton NHS Trust & Wolverhampton CCG consultation on proposals to deliver planned care at Cannock Chase Hospital Introduction Supplementary Briefing Paper This paper provides more detailed
The Royal Wolverhampton NHS Trust & Wolverhampton CCG consultation on proposals to deliver planned care at Cannock Chase Hospital Introduction Supplementary Briefing Paper This paper provides more detailed
CLINICAL SERVICES STRATEGY
 CLINICAL SERVICES STRATEGY DECEMBER 2016 contents 01 About Our Trust Introduction to our Trust 03 The PRIDE Way 04 Our overall strategic direction 05 Our key strategic challenges 05 02 Strategic Context
CLINICAL SERVICES STRATEGY DECEMBER 2016 contents 01 About Our Trust Introduction to our Trust 03 The PRIDE Way 04 Our overall strategic direction 05 Our key strategic challenges 05 02 Strategic Context
Statement of Purpose. June Northampton General Hospital NHS Trust
 Statement of Purpose June 2016 Northampton General Hospital NHS Trust The statement of purpose is made in compliance with Care Quality Commission (Registration) Regulations 2009: Regulation 12 and Schedule
Statement of Purpose June 2016 Northampton General Hospital NHS Trust The statement of purpose is made in compliance with Care Quality Commission (Registration) Regulations 2009: Regulation 12 and Schedule
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
NHS Board Workforce Projections 2017 NHS LANARKSHIRE. Table of Contents
 NHS Board Workforce Projections 2017 NHS LANARKSHIRE Table of Contents 1. Overall 1.1 Comments / Data Quality Issues / Direction of Travel 1.2 Brief Information on Workforce Cost Savings (non-staff) i.e.
NHS Board Workforce Projections 2017 NHS LANARKSHIRE Table of Contents 1. Overall 1.1 Comments / Data Quality Issues / Direction of Travel 1.2 Brief Information on Workforce Cost Savings (non-staff) i.e.
Briefing on the first stage of the Acute Services Review the clinical recommendations
 Briefing on the first stage of the Acute Services Review the clinical recommendations Introduction Over 100 clinicians from our four main hospitals, GPs, NHS managers and patient representatives have been
Briefing on the first stage of the Acute Services Review the clinical recommendations Introduction Over 100 clinicians from our four main hospitals, GPs, NHS managers and patient representatives have been
STATEMENT OF PURPOSE August Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008)
") 1. Trust Profile STATEMENT OF PURPOSE August 2015 Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008) 1.1 Worcestershire Acute Hospitals NHS Trust was formed on 1
1. Trust Profile STATEMENT OF PURPOSE August 2015 Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008) 1.1 Worcestershire Acute Hospitals NHS Trust was formed on 1
DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES
 Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
Enclosure I DELIVERING THE LONDON QUALITY STANDARDS AND 7 DAY SERVICES Trust Board Meeting Item: 13 Date: 25 th May 2016 Purpose of the Report: Enclosure: I To update the Board on the Trust s current performance
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Our achievements of 2009/10 l Our plans for 2010/11
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Our achievements of 2009/10 l Our plans for 2010/11 PAGE 2 WE PLAN. WE ACHIEVE We achieve 2009/10 was another great year
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Our achievements of 2009/10 l Our plans for 2010/11 PAGE 2 WE PLAN. WE ACHIEVE We achieve 2009/10 was another great year
Redesign of Front Door
 Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
Redesign of Front Door Transforming Acute and Urgent Care Strategic Background and Context Our Change and Improvement Programme What have we achieved and how? What did we learn? Ian Aitken, General Manager
8.1 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CLINICAL SERVICES REVIEW CONSULTATION OPTIONS. Date of the meeting 18/05/2016
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CLINICAL SERVICES REVIEW CONSULTATION OPTIONS Date of the meeting 18/05/2016 Author Sponsoring Clinician Purpose of Report Recommendation
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING CLINICAL SERVICES REVIEW CONSULTATION OPTIONS Date of the meeting 18/05/2016 Author Sponsoring Clinician Purpose of Report Recommendation
Board of Directors Meeting
 Board of Directors Meeting Date: 30 July 2008 Agenda item: 10.2, Part 1 Title: Prepared by: Presented by: Action required: Elaine Hobson, Director of Operations Elaine Hobson, Director of Operations The
Board of Directors Meeting Date: 30 July 2008 Agenda item: 10.2, Part 1 Title: Prepared by: Presented by: Action required: Elaine Hobson, Director of Operations Elaine Hobson, Director of Operations The
TRANSFORMING ACUTE SERVICES FOR THE ISLE OF WIGHT. Programme Report to the Governing Body 1 st February 2018
 TRANSFORMING ACUTE SERVICES FOR THE ISLE OF WIGHT Programme Report to the Governing Body 1 st February 2018 1 TABLE OF CONTENTS EXECUTIVE SUMMARY 3 1.0 PURPOSE AND SCOPE 7 1.1 The Case for Change 7 1.2
TRANSFORMING ACUTE SERVICES FOR THE ISLE OF WIGHT Programme Report to the Governing Body 1 st February 2018 1 TABLE OF CONTENTS EXECUTIVE SUMMARY 3 1.0 PURPOSE AND SCOPE 7 1.1 The Case for Change 7 1.2
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April Ipswich Hospital NHS Trust NHS East of England Department of Health
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
Summary two year operating plan 2017/18
 One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
Craigavon Area Hospital Profile
 Craigavon Area Hospital Profile 2012 Craigavon Area Hospital Profile Craigavon Area Hospital is located in Craigavon, County Armagh and is an essential part of the hospital network provided by the Southern
Craigavon Area Hospital Profile 2012 Craigavon Area Hospital Profile Craigavon Area Hospital is located in Craigavon, County Armagh and is an essential part of the hospital network provided by the Southern
Barking, Havering and Redbridge University Hospitals NHS Trust
 Update on investigation report Barking, Havering and Redbridge University Hospitals NHS Trust Queen s Hospital King George Hospital June 2012 Contents Page 1.1 The Trust 3 1.2 Regulatory background 3 1.3
Update on investigation report Barking, Havering and Redbridge University Hospitals NHS Trust Queen s Hospital King George Hospital June 2012 Contents Page 1.1 The Trust 3 1.2 Regulatory background 3 1.3
University Hospitals Bristol NHS Foundation Trust
 University Hospitals Bristol NHS Foundation Trust University Hospitals Bristol Main Site Quality Report Upper Maudlin Street Bristol BS2 8HW Tel: 0117 923 0060 Website: www.uhbristol.nhs.uk Date of inspection
University Hospitals Bristol NHS Foundation Trust University Hospitals Bristol Main Site Quality Report Upper Maudlin Street Bristol BS2 8HW Tel: 0117 923 0060 Website: www.uhbristol.nhs.uk Date of inspection
Burton Hospitals NHS Foundation Trust
 Statement of purpose Health and Social Care Act 2008 Statement of Purpose Health and Social Care Act 2008 Version : 10 Date : July 2017 Date of Next Review : 12 months Service Provider Full name: Address:
Statement of purpose Health and Social Care Act 2008 Statement of Purpose Health and Social Care Act 2008 Version : 10 Date : July 2017 Date of Next Review : 12 months Service Provider Full name: Address:
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust
 Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Business Case Authorisation Cover Sheet
 Business Case Authorisation Cover Sheet Section A Business Case Details Business Case Title: Directorate: Division: Sponsor Name Consultant in Anaesthesia and Pain Medicine Medicine and Rehabilitation
Business Case Authorisation Cover Sheet Section A Business Case Details Business Case Title: Directorate: Division: Sponsor Name Consultant in Anaesthesia and Pain Medicine Medicine and Rehabilitation
Better Healthcare in Barnet, Enfield and Haringey
 Better Healthcare in Barnet, Enfield and Haringey Purpose: To provide an update on the changes that will be implemented across Barnet, Enfield and Haringey from autumn 2013 To describe how Finchley Memorial
Better Healthcare in Barnet, Enfield and Haringey Purpose: To provide an update on the changes that will be implemented across Barnet, Enfield and Haringey from autumn 2013 To describe how Finchley Memorial
Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome:
 TRUST BOARD Date of Meeting: Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome: For noting For information For decision Title of Report: Update on Clinical Strategy Aims: To brief Trust Board
TRUST BOARD Date of Meeting: Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome: For noting For information For decision Title of Report: Update on Clinical Strategy Aims: To brief Trust Board
West Hertfordshire Hospitals NHS Trust. Operational Plan 2016/17. Summary
 West Hertfordshire Hospitals NHS Trust Operational Plan 2016/17 Summary 22 August 2016 Contents 1. Introduction........................... 3 2. Your Care, Your Future and WHHT clinical and organisational
West Hertfordshire Hospitals NHS Trust Operational Plan 2016/17 Summary 22 August 2016 Contents 1. Introduction........................... 3 2. Your Care, Your Future and WHHT clinical and organisational
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Statement of Purpose
 Statement of Purpose Contents as set out in Schedule 3, The Care Quality Commission (Registration) Regulations 2009. Guy's and St Thomas' NHS Foundation Trust provides integrated hospital and community
Statement of Purpose Contents as set out in Schedule 3, The Care Quality Commission (Registration) Regulations 2009. Guy's and St Thomas' NHS Foundation Trust provides integrated hospital and community
TRUST BOARD SEPTEMBER Surgical Services Reconfiguration
 def Agenda item: 8 (i) TRUST BOARD SEPTEMBER 2011 Surgical Services Reconfiguration PURPOSE: PREVIOUSLY CONSIDERED BY: To provide the Trust Board with an update on plans to reconfigure the Trust s surgical
def Agenda item: 8 (i) TRUST BOARD SEPTEMBER 2011 Surgical Services Reconfiguration PURPOSE: PREVIOUSLY CONSIDERED BY: To provide the Trust Board with an update on plans to reconfigure the Trust s surgical
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Better Healthcare in Bucks Reconfiguring acute services
 service redesign case study March 2013 No. 3 Reconfiguring acute services Key points Reach a shared understanding of the case for change across the local health economy. Start public engagement as early
service redesign case study March 2013 No. 3 Reconfiguring acute services Key points Reach a shared understanding of the case for change across the local health economy. Start public engagement as early
Stewart Mason, Emergency Planning and Resilience Officer Tom Jones, Clinical Programme Manager
 Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to RECEIVE and APPROVE the Emergency Department Service Continuity Plan (Princess Royal Hospital site). Trust Board Date Thursday
Paper 8 Recommendation DECISION NOTE Reporting to: The Trust Board is asked to RECEIVE and APPROVE the Emergency Department Service Continuity Plan (Princess Royal Hospital site). Trust Board Date Thursday
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST
 EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS MEETING DATE: 29 JANUARY 2015 SUBJECT: REPORT FROM: PURPOSE: CQC ACTION PLAN CHAIR OF IMPROVEMENT PLAN DELIVERY BOARD Discussion
EAST KENT HOSPITALS UNIVERSITY NHS FOUNDATION TRUST REPORT TO: BOARD OF DIRECTORS MEETING DATE: 29 JANUARY 2015 SUBJECT: REPORT FROM: PURPOSE: CQC ACTION PLAN CHAIR OF IMPROVEMENT PLAN DELIVERY BOARD Discussion
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
SBAR Report phase 1 Maternity, Gynaecology & Neonatal services
 North Wales Maternity, Gynaecology, Neonatal and Paediatric service review SBAR Report phase 1 Maternity, Gynaecology & Neonatal services Situation The Minister for Health and Social Services has established
North Wales Maternity, Gynaecology, Neonatal and Paediatric service review SBAR Report phase 1 Maternity, Gynaecology & Neonatal services Situation The Minister for Health and Social Services has established
Five Reconfiguration Tests Self-assessment (Path to Excellence Phase 1a)
") Appendix 5.2: Five Reconfiguration Tests Self-assessment (Path to Excellence Phase 1a) Version 1.0 March, 2017 Draft to be updated post-consultation to inform final decision Five tests self-assessment
Appendix 5.2: Five Reconfiguration Tests Self-assessment (Path to Excellence Phase 1a) Version 1.0 March, 2017 Draft to be updated post-consultation to inform final decision Five tests self-assessment
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Barnet Health Overview and Scrutiny Committee 6 October 2016
 Barnet Health Overview and Scrutiny Committee 6 October 2016 Title Health Tourism Report of Wards Status Urgent Key Enclosures Officer Contact Details Barnet Clinical Commissioning Group All Public No
Barnet Health Overview and Scrutiny Committee 6 October 2016 Title Health Tourism Report of Wards Status Urgent Key Enclosures Officer Contact Details Barnet Clinical Commissioning Group All Public No
Estates Infrastructure
 DRAFT POLICY IN DEVELOPMENT NORTH EAST LONDON SUSTAINABILITY & TRANSFORMATION PLAN Transformation underpinned by system thinking and local action Delivery Plan 5 of 8: Estates Infrastructure Contents No.
DRAFT POLICY IN DEVELOPMENT NORTH EAST LONDON SUSTAINABILITY & TRANSFORMATION PLAN Transformation underpinned by system thinking and local action Delivery Plan 5 of 8: Estates Infrastructure Contents No.
RTT Recovery Planning and Trajectory Development: A Cambridge Tale
 RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
Transforming Clinical Services. Our developing clinical strategy
 Transforming Clinical Services Our developing clinical strategy Transforming clinical services A developing clinical strategy for the new Foundation Trust Since 1 April 2011, County Durham and Darlington
Transforming Clinical Services Our developing clinical strategy Transforming clinical services A developing clinical strategy for the new Foundation Trust Since 1 April 2011, County Durham and Darlington
SAFE STAFFING GUIDELINE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline title SAFE STAFFING GUIDELINE SCOPE 1. Safe staffing for nursing in accident and emergency departments Background 2. The National Institute for
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Vanguard Programme: Acute Care Collaboration Value Proposition
 Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Kingston Hospital NHS Foundation Trust Length of stay case study. October 2014
 Kingston Hospital NHS Foundation Trust Length of stay case study October 2014 The hospital has around 520 beds and provides acute medical services for a population of around 320,000 in Kingston, Richmond,
Kingston Hospital NHS Foundation Trust Length of stay case study October 2014 The hospital has around 520 beds and provides acute medical services for a population of around 320,000 in Kingston, Richmond,
Community and Mental Health Services High Level Market Research PROSPECTUS
 and Mental Health Services High Level Market Research PROSPECTUS February 2014 Supporting people in Dorset to lead healthier lives NHS DORSET CLINICAL COMMISSIONING GROUP PROSPECTUS FOR COMMUNITY AND MENTAL
and Mental Health Services High Level Market Research PROSPECTUS February 2014 Supporting people in Dorset to lead healthier lives NHS DORSET CLINICAL COMMISSIONING GROUP PROSPECTUS FOR COMMUNITY AND MENTAL
Item E1 - Bart s Health Quality Indicators
 Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Debbie Vogler, Director of Business & Enterprise. Kate Shaw, Associate Director of Service Transformation
 Reporting to: Trust Board 24 September 2015 Paper 5 Title Sponsoring Director Author(s) Future Configuration of Hospital Services - Post-Project Evaluation Debbie Vogler, Director of Business & Enterprise
Reporting to: Trust Board 24 September 2015 Paper 5 Title Sponsoring Director Author(s) Future Configuration of Hospital Services - Post-Project Evaluation Debbie Vogler, Director of Business & Enterprise
We plan. We achieve.
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
TRUST BOARD MEETING 24 JULY 2013 PERFORMANCE REPORT MONTH 3 DIRECTOR OF OPERATIONS DIRECTOR OF OPERATIONS DIRECTOR OF OPERATIONS
 TRUST BOARD MEETING 24 JULY 2013 PERFORMANCE REPORT MONTH 3 def Agenda Item: 10c PURPOSE PREVIOUSLY CONSIDERED BY Objective(s) to which issue relates * Risk Issues (Quality, safety, financial, HR, legal
TRUST BOARD MEETING 24 JULY 2013 PERFORMANCE REPORT MONTH 3 def Agenda Item: 10c PURPOSE PREVIOUSLY CONSIDERED BY Objective(s) to which issue relates * Risk Issues (Quality, safety, financial, HR, legal
Seven day hospital services: case study. South Warwickshire NHS Foundation Trust
 Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Seven day hospital services: case study South Warwickshire NHS Foundation Trust March 2018 We support providers to give patients safe, high quality, compassionate care within local health systems that
Ayrshire and Arran NHS Board
 Paper 12 Ayrshire and Arran NHS Board Monday 26 March 2018 Financial Management Report for the 11 months to 28 February 2018 Author: Bob Brown, Assistant Director of Finance Governance and Shared Services
Paper 12 Ayrshire and Arran NHS Board Monday 26 March 2018 Financial Management Report for the 11 months to 28 February 2018 Author: Bob Brown, Assistant Director of Finance Governance and Shared Services
STATEMENT OF PURPOSE
 STATEMENT OF PURPOSE This is the Statement of Purpose for Hull and East Yorkshire Hospitals NHS Trust as required by the Health and Social Care Act 2008 (regulated Activities) Regulations 2014 Schedule
STATEMENT OF PURPOSE This is the Statement of Purpose for Hull and East Yorkshire Hospitals NHS Trust as required by the Health and Social Care Act 2008 (regulated Activities) Regulations 2014 Schedule
Improving Healthcare Together : NHS Surrey Downs, Sutton and Merton clinical commissioning groups Issues Paper
 Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Community urgent care consultation Frequently asked questions
 Community urgent care consultation Frequently asked questions How will services change at Loxford Polyclinic? Are you reducing or downgrading the service at Loxford Polyclinic? Are you already making the
Community urgent care consultation Frequently asked questions How will services change at Loxford Polyclinic? Are you reducing or downgrading the service at Loxford Polyclinic? Are you already making the
Title Open and Honest Staffing Report April 2016
 Title Open and Honest Staffing Report April 2016 File location WILJ2102 Meeting Board of Directors Date 25 th May 2016 Executive Summary This paper provides a stocktake on the position of South Tyneside
Title Open and Honest Staffing Report April 2016 File location WILJ2102 Meeting Board of Directors Date 25 th May 2016 Executive Summary This paper provides a stocktake on the position of South Tyneside
Aneurin Bevan Health Board. Improving Theatre Performance
 Aneurin Bevan Health Board Improving Theatre Performance 1 Introduction This report provides an overview on actions being taken to improve theatre performance within the Health Board. The report provides
Aneurin Bevan Health Board Improving Theatre Performance 1 Introduction This report provides an overview on actions being taken to improve theatre performance within the Health Board. The report provides
How CQC monitors, inspects and regulates NHS trusts. June 2017
 How CQC monitors, inspects and regulates NHS trusts June 2017 CONTENTS MONITORING AND INFORMATION SHARING... 2 How we monitor and inspect NHS trusts... 2 CQC Insight... 2 Provider information request...
How CQC monitors, inspects and regulates NHS trusts June 2017 CONTENTS MONITORING AND INFORMATION SHARING... 2 How we monitor and inspect NHS trusts... 2 CQC Insight... 2 Provider information request...
Central Adelaide Local Health Network Clinical Directorate Structures
 Central Adelaide Local Health Network Clinical Directorate Structures Consultation Paper February 2014 Version 2 Document Information and Revision History 1. Version 2. Date 3. Comment 1.0 12 February
Central Adelaide Local Health Network Clinical Directorate Structures Consultation Paper February 2014 Version 2 Document Information and Revision History 1. Version 2. Date 3. Comment 1.0 12 February
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
THE FUTURE OF YOUR HOSPITALS: Planned Care site
 THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
Worcestershire Acute Hospitals NHS Trust
 Worcestershire Acute Hospitals NHS Trust Worcestershire Royal Hospital Quality Report Charles Hastings Way Worcester WR5 1DD Tel: 01905 763333 Website: www.worcsacute.nhs.uk Date of inspection visit: 12,
Worcestershire Acute Hospitals NHS Trust Worcestershire Royal Hospital Quality Report Charles Hastings Way Worcester WR5 1DD Tel: 01905 763333 Website: www.worcsacute.nhs.uk Date of inspection visit: 12,
Question 1 a) What is the Annual net expenditure on the NHS from 1997/98 to 2007/08 in Scotland? b) Per head of population
 What is the Annual net expenditure on the NHS from 1997/98 to 2007/08 in Scotland? b) Per head of population") NHS SPENDING - SCOTLAND Question 1 a) What is the Annual net expenditure on the NHS from 1997/98 to 2007/08 in Scotland? b) Per head of population Question 2 a) Annual real (GDP deflated) increase in net
NHS SPENDING - SCOTLAND Question 1 a) What is the Annual net expenditure on the NHS from 1997/98 to 2007/08 in Scotland? b) Per head of population Question 2 a) Annual real (GDP deflated) increase in net
The operating framework for. the NHS in England 2009/10. Background
 the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
Westminster Partnership Board for Health and Care. 17 January pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Royal National Orthopaedic Hospital NHS Trust Integrated Business Plan
 Section 1: Executive Summary 1.1 Vision and Strategy RNOH Vision - A World Class Centre of Excellence Summary The RNOH is a world renowned specialist hospital for the diagnosis and treatment of complex
Section 1: Executive Summary 1.1 Vision and Strategy RNOH Vision - A World Class Centre of Excellence Summary The RNOH is a world renowned specialist hospital for the diagnosis and treatment of complex
Best Care Clinical Strategy Principles for the next 10 years of Best Care. Dr Caroline Allum, Executive Medical Director
 Best Care Clinical Strategy 2017 2027 Principles for the next 10 years of Best Care Produced By: Produced For: Dr Caroline Allum, Executive Medical Director NELFT Board Date Produced: 17 th July 2017 Version:
Best Care Clinical Strategy 2017 2027 Principles for the next 10 years of Best Care Produced By: Produced For: Dr Caroline Allum, Executive Medical Director NELFT Board Date Produced: 17 th July 2017 Version:
Overall rating for this trust Good. Inspection report. Ratings. Are services safe? Requires improvement. Are services effective?
 Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018
 Produced in February 2018") 6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
Shetland NHS Board. Board Paper 2017/28
 Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Board Paper 2017/28 Shetland NHS Board Meeting: Paper Title: Shetland NHS Board Capacity and resilience planning - managing safe and effective care across hospital and community services Date: 11 th June
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
South Warwickshire s Whole System Approach Transforms Emergency Care. South Warwickshire NHS Foundation Trust
 South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS Foundation Trust South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS
South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS Foundation Trust South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS
NHS England (London) Assurance of the BEH Clinical Strategy
 Assurance of the BEH Clinical Strategy") NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
Purpose of the Report: Update to the Trust Board on the clinically-led Trauma and Orthopaedic GIRFT review. Information Assurance X
 Item 9.4 To: Trust Board From: Mark Brassington Date: 18 th May 2018 Healthcare Standard Title: Trauma and Orthopaedic GIRFT Author: Richard James, General Manager Responsible Director/s: Mark Brassington
Item 9.4 To: Trust Board From: Mark Brassington Date: 18 th May 2018 Healthcare Standard Title: Trauma and Orthopaedic GIRFT Author: Richard James, General Manager Responsible Director/s: Mark Brassington
Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May 2016
 Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May RAG Dark green Light green Amber Red White Definition Action complete and assurance gained Action
Royal College of Paediatrics and Child Health Service Review Action Plan and Progress Report 26 th May RAG Dark green Light green Amber Red White Definition Action complete and assurance gained Action
Paper 5.0 SHAPING A HEALTHIER FUTURE PAEDIATRIC TRANSITION: ANTICIPATED BENEFITS OF THE TRANSITION AND PROPOSED MODEL OF CARE.
 SHAPING A HEALTHIER FUTURE PAEDIATRIC TRANSITION: ANTICIPATED BENEFITS OF THE TRANSITION AND PROPOSED MODEL OF CARE December 2015 Version 2.2 Paper 5.0 1 Purpose This document sets out the proposed new
SHAPING A HEALTHIER FUTURE PAEDIATRIC TRANSITION: ANTICIPATED BENEFITS OF THE TRANSITION AND PROPOSED MODEL OF CARE December 2015 Version 2.2 Paper 5.0 1 Purpose This document sets out the proposed new
Operational Plan Burton Hospitals NHS Foundation Trust
 Operational Plan 2014-16 Burton Hospitals NHS Foundation Trust 1 BOARD STATEMENT... 4 2 EXECUTIVE SUMMARY... 5 3 THE SHORT TERM CHALLENGE... 7 3.1 Background... 7 3.2 Commissioner Challenges... 7 3.3 Quality
Operational Plan 2014-16 Burton Hospitals NHS Foundation Trust 1 BOARD STATEMENT... 4 2 EXECUTIVE SUMMARY... 5 3 THE SHORT TERM CHALLENGE... 7 3.1 Background... 7 3.2 Commissioner Challenges... 7 3.3 Quality
Aneurin Bevan University Health Board Stroke Services Redesign Programme
 Aneurin Bevan University Health Board Services Redesign Programme 1 Introduction This report aims to update the Health Board on progress with the Services Redesign Programme of work which commenced in
Aneurin Bevan University Health Board Services Redesign Programme 1 Introduction This report aims to update the Health Board on progress with the Services Redesign Programme of work which commenced in
Delivering Improvement in Practice
 v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
North West London Accident and Emergency Performance Report for the winter of 2016/17. North West London Joint Health Overview and Scrutiny Committee
 North West London Accident and Emergency Performance Report for the winter of 2016/17 North West London Joint Health Overview and Scrutiny Committee 20 April 2017 1 This paper will summarise the performance
North West London Accident and Emergency Performance Report for the winter of 2016/17 North West London Joint Health Overview and Scrutiny Committee 20 April 2017 1 This paper will summarise the performance
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
Mid and South Essex Success Regime Overview and next steps. Andy Vowles, Programme Director. 18 April 2016
 Mid and South Essex Success Regime Overview and next steps Andy Vowles, Programme Director 18 April 2016 What s in this briefing Part 1 overview Background to the Success Regime Action to date The challenge
Mid and South Essex Success Regime Overview and next steps Andy Vowles, Programme Director 18 April 2016 What s in this briefing Part 1 overview Background to the Success Regime Action to date The challenge
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017
 Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
NEL Sustainability and Transformation Plan (STP) Communications and engagement plan (phase 2) Contents
 Communications and engagement plan (phase 2) Contents") NEL Sustainability and Transformation Plan (STP) Communications and engagement plan (phase 2) Contents 1. Aims... 2 1.1 Purpose... 2 1.2 Out of scope... 2 2. Background... 2 3. NEL STP main objectives...
NEL Sustainability and Transformation Plan (STP) Communications and engagement plan (phase 2) Contents 1. Aims... 2 1.1 Purpose... 2 1.2 Out of scope... 2 2. Background... 2 3. NEL STP main objectives...
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
WAITING TIMES AND ACCESS TARGETS
 NHS Board Meeting Tuesday 17 December 2013 Lead Director (Acute Services Division) Board Paper No 13/60 Recommendation: WAITING TIMES AND ACCESS TARGETS The NHS Board is asked to note progress against
NHS Board Meeting Tuesday 17 December 2013 Lead Director (Acute Services Division) Board Paper No 13/60 Recommendation: WAITING TIMES AND ACCESS TARGETS The NHS Board is asked to note progress against
SUMMARY. Our progress in 2013/14. Eastbourne, Hailsham and Seaford Clinical Commissioning Group.
 Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Reducing Elective Waits: Delivering 18 week pathways for patients. Programme Director NHS Elect Caroline Dove.
 Reducing Elective Waits: Delivering 18 week pathways for patients Programme Director NHS Elect Caroline Dove What I will cover 1. Why 18 Weeks is different 2. Where are we now 3. New models of delivery
Reducing Elective Waits: Delivering 18 week pathways for patients Programme Director NHS Elect Caroline Dove What I will cover 1. Why 18 Weeks is different 2. Where are we now 3. New models of delivery
THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS
 THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS ICCHNR SYMPOSIUM University of Kent at Canterbury 15 th -16 th September 2016 Dr John M Ribchester GP Chair and Clinical Lead for Encompass MCP
THE EMERGING PICTURE OF NEW CARE MODELS IN THE ENGLISH NHS ICCHNR SYMPOSIUM University of Kent at Canterbury 15 th -16 th September 2016 Dr John M Ribchester GP Chair and Clinical Lead for Encompass MCP
Urgent Treatment Centres Principles and Standards
 Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
The future of Barking, Havering and Redbridge University Hospitals NHS Trust
 The future of Barking, Havering and Redbridge University Hospitals NHS Trust Westminster Hall, Wednesday15 July (4.30pm) Debate initiated by Mike Gapes This pack provides general background material relating
The future of Barking, Havering and Redbridge University Hospitals NHS Trust Westminster Hall, Wednesday15 July (4.30pm) Debate initiated by Mike Gapes This pack provides general background material relating
Presentation to the Care Quality Commission. Dr. Lucy Moore, CEO 15 September 2015
 Presentation to the Care Quality Commission Dr. Lucy Moore, CEO 15 September 2015 Our Improvement Journey- Key Messages We have Board, Executive and Divisional leadership teams now in place with serious
Presentation to the Care Quality Commission Dr. Lucy Moore, CEO 15 September 2015 Our Improvement Journey- Key Messages We have Board, Executive and Divisional leadership teams now in place with serious