Improving outcomes, cutting costs: Procuring NIA innovations via the NHS Innovation and Technology Tariff
|
|
|
- Dylan Pierce
- 5 years ago
- Views:
Transcription
1 Improving outcomes, cutting costs: Procuring NIA innovations via the NHS Innovation and Technology Tariff
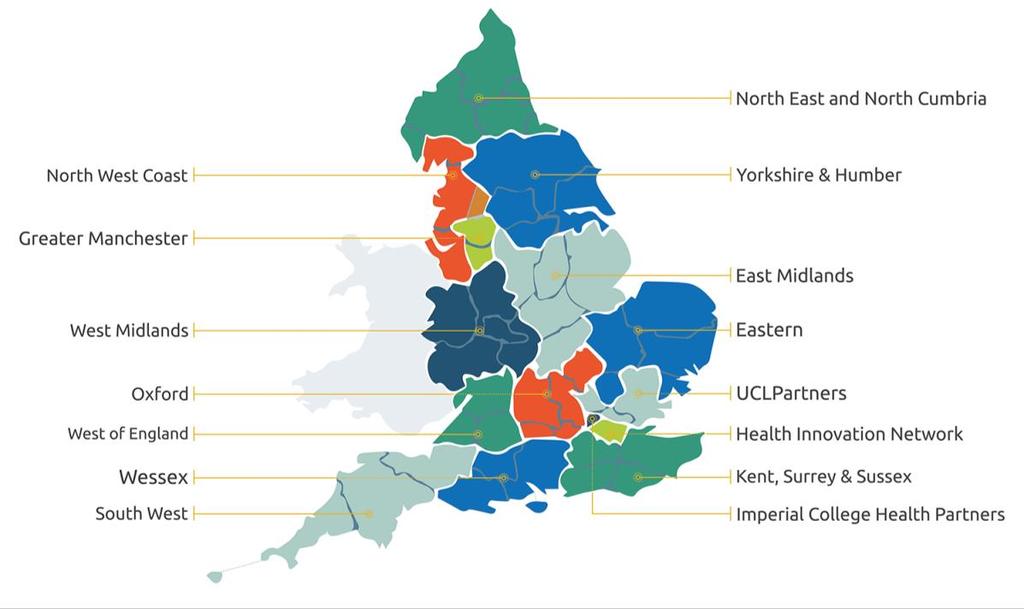
2 The role of England s 15 AHSNs in supporting and spreading innovation Dr Chris Parker CBE Managing Director, West Midlands AHSN
3
4 How England s 15 AHSNs make a difference We connect: bringing together academics, NHS, researchers and industry to accelerate innovation and facilitate the adoption and spread of proven ideas We are catalysts: helping facilitate change across whole health and social care economies - with a focus on improving outcomes for patients We create: the right environment for relevant industries to work with the NHS and other parts of the healthcare sector
5 Since April M people have benefited from AHSN activity 226 innovations have been adopted via significant AHSN involvement Over 330M in innovation funding has been leveraged by AHSNs AHSN-enabled innovations have been implemented in over 11,400 sites
6 The NHS Innovation Accelerator NHS England initiative delivered in partnership with the country s 15 AHSNs, hosted by UCLPartners Supporting delivery of FYFV by accelerating uptake of high impact, evidence-based innovations for patient, population and NHS staff benefit Currently supporting 25 Fellows representing 26 innovations aimed at: activating people to selfmanage; earlier intervention; long term conditions management; improving safety 469 additional NHS commissioners and providers now using NIA innovations; 28.6m in external funds secured; 14 awards won; 10 selling internationally Impact data demonstrates earlier intervention, reductions in complications and emergency admissions, cost savings
7 Introducing NHS England s Innovation and Technology Tariff Rob Chesters Senior Innovation and Research Manager, NHS England
8 Accessing the zero cost NHS Innovation and Technology Tariff ITT was introduced to incentivise the adoption and spread of transformational innovation in the NHS. It aims to remove the need for multiple local price negotiations and guarantee automatic reimbursement when an approved innovation is used. At the same time the ITT allows NHS England to optimise its purchasing power and negotiate national bulk buy price discounts where applicable on behalf of the NHS. For as the first year of the ITT this is a pathfinder year and 6 themes have been identified which could provide innovation benefits to the NHS at scale.
9 Theme Example product How will it operate (currency) 1) Guided mediolateral episiotomy to minimise the risk of Episcissors-60 Incentive based on activity. The price per use. obstetric anal sphincter injury 2) Reduction of bacterial contamination and accidental administration of medication Non-injectable arterial connector (NIC) Provided under the zero cost model. The value of this device per patient is 2. 3) Prevention of ventilated associated pneumonia in critically ill patients Pnuex Provided under the zero cost model. NHS England is covering the cost of the tubes valued at 150 each. 4) Applications for the self-management of Chronic Obstructive Pulmonary Disease mycopd Provided under the zero cost model. NHS England is covering the cost of licences valued at per patient. 5) Frozen Faecal microbiota transplantation (FMT) for recurrent Clostridium difficile infection rates Frozen Faecal Microbiota Transplants for Chronic C.difficile Infections Provided under the zero cost model. NHS England is covering the cost of FMT aliquots valued at per patient. 6) Management of Benign prostatic hyperplasia as a day case Urolift Re-imbursement automated via tariff recoded under a new OPCS code. In parallel, but separately from the ITT, NHS England is centrally funding a 7th theme Identification and measurement of atrial fibrillation through mobile ECG technology. Further information on this programme of work will be published in due course.

10 Accessing the zero cost NHS Innovation and Technology Tariff Themes Guided mediolateral episiotomy to minimise the risk of obstetric anal sphincter injury and The Management of Benign prostatic hyperplasia as a day case operate under separate arrangements.
11 Accessing the zero cost NHS Innovation and Technology Tariff For 5 of the 6 themes require the completion of a Minimum Data Set to NHS via Arden Gem CSU. Theme 6:- Prostatic urethral lift systems to treat benign prostatic hyperplasia is covered by National Tariff. Data about use of the procedure will be collected through National Tariff audit processes and specific data reporting requirements are not included in the ITT.
12 Accessing the zero cost NHS Innovation and Technology Tariff For further information please contact the NHS England Innovation and Research Unit here
13 mycopd Ian Thompson, Strategic Director, my mhealth (Representing NIA Fellow, Dr Simon Bourne)

14 (C) my mhealth limited Not for distribution outside agreements

 my mhealth limited 2017 - Not for")
15 mycopd Patient Interface Simple registration Symptoms Collections Self management Rehab Inhaler videos Comprehensive education Mindfulness Chest clearance Notifications..and much more (C) my mhealth limited Not for distribution outside agreements
16 System wide integration Management Application EMIS System 1 Vision Hospital EHR Patient Application Clinician Application Wearables Equipment (C) my mhealth limited Not for distribution outside agreements
 my mhealth limited 2017 - Not for distribution outside agreements")
17 Example inhaler videos Only your device shown Every device Correct education any time Inhalers, nebulisers, spacers Correct 98% of inhaler errors (C) my mhealth limited Not for distribution outside agreements

 my mhealth limited 2017 - Not for distribution")
18 Education Anatomy of the lungs and what is COPD Exercise Smoking cessation Breathlessness part 1 & 2 Medication and treatment Pacing Part 1 & 2 Oxygen Chest Clearance Exacerbations Anxiety and depression Nutrition Travelling Benefits Sex and breathlessness Self-management Weather Pollution (C) my mhealth limited Not for distribution outside agreements

 my mhealth limited 2017 - Not for")
19 Rehabilitation Full 6 week course Maintenance class Full exercise instruction Coming soon exercise prescribing! (C) my mhealth limited Not for distribution outside agreements
 my mhealth limited 2017 - Not")
20 6 MWT CAT 6 MWT Class Online Class Online (C) my mhealth limited Not for distribution outside agreements
 my mhealth limited 2017 - Not for")
21 -2.6 Weight Reduction Kg -4.7 Class Online (C) my mhealth limited Not for distribution outside agreements

 my")

22 Examples where mhealth products are being used? L B NL D D P L (C) my mhealth limited Not for distribution outside agreements
 my mhealth limited 2017 - Not for distribution outside")
23 Business Model COPD Example Based on an average CCG with 5000 patient with COPD 25% reduction in exacerbations and hospital admissions Delivery of evidence based PR at scale with reduced costs In year savings of > 200k (C) my mhealth limited Not for distribution outside agreements



24 Diabetes COPD Heart failure Cardiac Rehabilitation Asthma Co morbidities are present in 25% of patients with long-term conditions Each patient receives on average just 15mins clinician time/yr/morbidity (C) my mhealth limited Not for distribution outside agreements
25 Episcissors-60 Alex Fisher, Director, Advanced Global Health Ltd (Representing NIA Fellow, Dr Dharmesh Kapoor)
26 Achieving Innovation at Scale in the NHS: EPISCISSORS-60 ALEX FISHER DIRECTOR, ADVANCED GLOBAL HEALTH LTD


27 EPISCISSORS-60 FIRST SCISSORS DESIGNED TO GIVE AN ACCURATE MEDIOLATERAL EPISIOTOMY; PATENT OWNED BY PLYMOUTH HOSPITALS NHS TRUST
28 OBSTETRIC ANAL SPHINCTER INJURIES (OASIS) Incidence 30,000 new cases each year in UK 6% in first vaginal births Leading cause of anal incontinence in women (9:1 F:M) Direct costs 1625 per case for repair + postoperative care million each year Indirect costs 25% of women choose elective caesarean delivery (extra 1100 per birth; 4.9 million each year) 2500 per year/person for fecal incontinence

29 LITIGATION COSTS o PERINEAL TRAUMA IS THE 4 TH HIGHEST REASON FOR CLAIMS MADE IN OBSTETRICS OVER 10 YEARS. o 31MILLION IN LEGAL PAYOUTS ALONE o OASIS BEING MOOTED AS A PATIENT SAFETY INDICATOR o 1.6 MILLION DAMAGES FOR OASIS DUE TO AN ACUTELY ANGLED EPISIOTOMY.
30 WHERE EPISIOTOMY IS INDICATED, THE MEDIOLATERAL TECHNIQUE IS RECOMMENDED, WITH CAREFUL ATTENTION TO ENSURE THE ANGLE IS 60 DEGREES AWAY FROM THE MIDLINE WHEN THE PREINEUM IS DISTENDED. (D)
31 SUMMARY OF CURRENT PRACTICE: HOW GOOD ARE WE AT EYEBALLING EPISIOTOMY ANGLES? Draw on paper 1/3 rd doctors & midwives drew episiotomies>40 0 (Tincello 2003) Cut on paper 15% cut degrees 37% cut when asked to cut at % cut below or above this range(naidu 2014) Actual patients No midwife & 22% doctors performed episiotomies with suture angle >40 0 (Andrews 2005) 43% episiotomies were not mediolateral/lateral (Fodstad 2014)

32 SPECIAL SCISSORS DESIGNED TO ENSURE AN INCISION ANGLE OF 60 DEGREES HAVE BEEN SHOWN TO BE EFFECTIVE IN ACHIEVING THE CORRECT ANGLE 29,30. EVIDENCE LEVEL 3
33 RESULTS FROM UK HOSPITALS THAT COMPLETELY REPLACED ALL OLD EPISIOTOMY SCISSORS WITH EPISCISSORS-60 o 20% REDUCTION IN CHILDBIRTH ANAL SPHINCTER INJURIES (OASIS) AT POOLE AND HINCHINGBROOKE HOSPITALS (VAN ROON ET AL. 2015) o 40-50% REDUCTION AT CROYDON UNIVERSITY HOSPITAL (LOU, 2016) o 40-50% REDUCTION AT ROYAL FREE AND BARNET HOSPITALS (MYERS, 2016, UNPUBLISHED AUDIT).
34 EPISCISSORS-60 BY NHS ACUTE TRUSTS PURCHASED/LOOKING TO PURCHASE = 63 TRIALLING AND DISCUSSING INTERNALLY = 15 DECLINED = 34 NO RESPONSE = 31
35 BARRIERS TO ADOPTION - 1 DIFFICULT IN MAKING A COGENT BUSINESS CASE - SINCE THESE INJURIES ATTRACT REIMBURSEMENT VIA PAYMENT BY RESULTS, THE HOSPITAL WOULD LOSE INCOME IF THE INJURY RATE WENT DOWN. SOLUTION - ITT TO PROVIDE FUNDS TO BUY SCISSORS - MAKING CCG S AWARE OF THE COST IMPLICATIONS TO THEM OF CONTINUED HIGH RATES OF OASIS (DETAILED IN THE UNIVERSAL GUIDANCE FROM NHS ENGLAND)
36 BARRIERS TO ADOPTION 2 SINGLE USE INSTRUMENTATION - ONE-THIRD OF ENGLISH TRUSTS USE SINGLE-USE BIRTH PACKS - HAVE OFF-SITE SHARED STERILISATION FACILITIES - REPORT A 40% REUSABLE INSTRUMENT LOSS RATE OVER 5 YEARS FROM THESE FACILITIES SOLUTION -?
37 BARRIERS TO ADOPTION 3 MIDWIVES CONCERNS ABOUT IT LEADING TO RISING EPISIOTOMY RATES SOLUTION - STRESSING THAT OVERALL PERINEAL BURDEN REMAINS UNCHANGED; I.E. WE ARE SWAPPING FIRST AND SECOND DEGREE TEARS THAT OCCUR ANYWAY IF EPISIOTOMIES ARE NOT PERFORMED - EPISIOTOMIES DO NOT LEAD TO MORE PAIN, BLEEDING IN HEAD-TO-HEAD COMPARISONS
38 BARRIERS TO ADOPTION - 4 CLINICAL APATHY - STATUS QUO IS SATISFACTORY - NOT ENOUGH ROBUST EVIDENCE ABOUT THE SCISSORS - NEED A RANDOMISED CONTROL TRIAL (RCT) SOLUTIONS - CCG S SHOULD CHALLENGE TRUSTS TO COME UP WITH OASIS REDUCTION PLANS BY 20-50% OTHERWISE PBR PAYMENTS SHOULD BE CURTAILED BY THIS LEVEL - USE ANY OTHER VALIDATED MEANS TO PERFORM 60 DEGREE ANGLED EPISIOTOMIES (AS PER RCOG RECOMMENDATION) - RCT WOULD COMPARE EPISCISSORS-60 WITH WHAT? NO OTHER PROVEN METHOD EXISTS - RCT WOULD COST MORE THAN REPLACING ALL EPISIOTOMY SCISSORS IN ENGLAND WITH EPISCISSORS-60
39 WHY HINCHINGBROOKE DECIDED TO ADOPT EPISCISSORS-60 A 60 DEGREE EPISIOTOMY WAS RECOMMENDED AS A WAY TO PREVENT CHILDBIRTH ANAL INJURIES BY THE RCOG EPISCISSORS-60 WERE MENTIONED IN THAT GUIDANCE AS BEING A FIXED ANGLE DEVICE THAT TAKES AWAY THE GUESSWORK AND HUMAN ERROR IN TRYING TO ESTIMATE THE ANGLE AT THE TIME OF BIRTH NO-BRAINER TO PREVENT AVOIDABLE HARM
40 BARRIERS TO ADOPTION MAKING THE CASE INTERNALLY FOR INVESTMENT - WHICH BUDGET TO DIP INTO FOR FUNDS? CAPITAL OR OPERATIONAL? - HOSPITALS WOULD LOSE INCOME IF INJURY RATE IS REDUCED - NO INCENTIVE TO REDUCE INJURY RATE CHANGING CLINICAL PRACTICE - INTRODUCING THE COMPREHENSIVE SUPPORT TRAINING PROGRAMME LED TO BUY-IN FROM THE MIDWIFERY AND MEDICAL STAFF - REPLACEMENTS OF ALL EPISIOTOMY SCISSORS WITH EPISCISSORS-60
41 BENEFITS SEEN BY THE TRUST POST- IMPLEMENTATION - 20% REDUCTION IN CHILDBIRTH ANAL SPHINCTER INJURIES WITHIN 5 MONTHS OF INTRODUCTION - CORRESPONDING INCREASE IN NUMBER OF EPISIOTOMIES PERFORMED DUE TO INCREASED CONFIDENCE AMONG DOCTORS AND MIDWIVES - NOW IT HAS BECOME THE NORM - HAS INFLUENCED NEIGHBOURING TRUSTS LIKE CAMBRIDGE TO ADOPT EPISCISSORS-60 - FUNDING REMAINS A HUGE OBSTACLE - INNOVATION TARIFF WILL GREATLY HELP.
42 Non-injectable arterial connector (NIC) Dr Maryanne Mariyaselvam, NIA Fellow
43 NIC Non-injectable arterial connector

44 Inadvertant injection into the arterial line Never give medication into the arterial line
45 Inadvertant injection into the arterial line As common as 1:3400 procedures 1 Since 2008 NPSA Arterial safety alert >150 incidents 2 ~ 2/month in the NHS Catastrophic error Patients suffer Nurses suffer 1. Complications after unintentional intra-arterial injection of drugs: Risks, Outcomes and Management Strategies Mayo Clinic Proceedings, June 2005; 80(6): Reported incidence of arterial line errors Personal correspondance, Medical Director, NHS England
46 Need a solution that always allows: Take a blood sample Never inject
47 NIC: Non-injectable arterial connector Arterial connector One way valve Prevents accidental injection bacterial contamination blood spillage during sampling
48 NIC: Non-injectable arterial connector Arterial connector One way valve Prevents accidental injection bacterial contamination blood spillage during sampling Safety innovation STOPS the problem Safety innovation PROTECTS patients & staff


49 Simple to implement 1. Use NIC instead of standard arterial connector 2. NIC stays on for the life time of the arterial line (3-7 days)

50 NIC use blood conserving sampling 1. Aspirate at the transducer port
51 NIC use blood conserving sampling 2. If desired, withdraw 0.2 ml deadspace from sampling port
52 NIC use blood conserving sampling 3. Aspirate ABG sample from the NIC

53 NIC use blood conserving sampling 4. Replace waste syringe, flush both NIC and arterial line by pinching the transducer
54 NIC: Studies Laboratory study 0% bacterial contamination of the arterial line Simulation study 10/15 gave medication into the arterial line (standard systems) Clinical evaluation (250 healthcare staff) 98% believe it is important to use the NIC 26% had personally seen an incident which could have been prevented by the NIC
55 NIC: Studies Health Economic Analysis - cost saving for the NHS 2 per unit Patient feedback (NHS England Citizen Senate): 100% (13/13) agreed the NIC should be used in hospitals Excellent idea, feel confident this would benefit my family, myself and the NHS making mistakes impossible keeps people alive and reduces cost per episode
56 Awards Winner: National Patient Safety and Care Award (2012) Winner: Innovation Prize, Association of Anaesthetists of Great Britain and Ireland (2015)

57 The non-injectable arterial connector (NIC) is a great patient safety device and is an easily implementable solution, which makes wrong route drug administration into the arterial line impossible. For the safety and best practice for our patients, I heartily recommend this device should be used on all arterial lines in the NHS Professor Sir Bruce Keogh, Medical Director NHS England
58
59 Innovation and Technology Tariff Full reimbursement for the NIC starts 1 April 2017
60 NHS Innovation and Technology Tariff Starts 1 st April 2017 for 2 years Order from Amdel Medical Ltd Soon available on the NHS supply chain
61 Peter Young Maryanne Mariyaselvam
62 PneuX Peter Young, NIA Fellow
63 PneuX Pneumonia Prevention System

64 PneuX System Preventing VAP Ventilation Tube
65 Ventilator Associated Pneumonia (VAP) Leading cause of infective hospital-acquired mortality in ICU Affects up to 20,000 patients per year in the UK Up to 30% of these patients will die from VAP = 6,000 people Patient contracts VAP increases Complications Length of mechanical ventilation Length of stay Antibiotic use 1 episode of VAP costs the NHS 10,000 to 20,000
66 Case Study Intubated patient transferred to our ICU

67 Oral Cavity Full of Bacterial Laden Fluid Videolaryngoscopy of larynx
68 Patient was transferred to our ICU Standard leaky cuff in place Patient had developed a pneumonia On arrival: Growth of staph aureus, coliforms and candida From both mouth and the lungs Tube exchange to PneuX PneuX care plan instituted Patient recovered in 7 days
69 Pathophysiology: after intubation Rapid colonisation with pathogenic bacteria of oropharynx Gastric contents reflux into the oropharynx Secretions accumulate above the cuff Standard tubes allow aspiration of secretions Leads to microbial colonisation of the lungs Ventilator-associated Pneumonia The presence and sequence of endotracheal tube colonization. Eur Respir J 1999,13:546-51



70 Standard leaky cuffs v PneuX Standard Cuffs PneuX
71 Leakage of bacteria past ALL ICU tube cuffs University of Wales, Cardiff Endotracheal tubes and fluid aspiration. BMC Anaesthesiology 2017; 17(1):36
72 Leakage of bacteria past ALL ICU tube cuffs University of Wales, Cardiff EXCEPT ONE Endotracheal tubes and fluid aspiration. BMC Anaesthesiology 2017; 17(1):36
73 Ability of five endotracheal tube cuffs to prevent leaks Massachusetts General Hospital Microcuff SealGuard TaperGuard Mallinckrodt HiLo PneuX Leak ml/hr Performance of the PneuX system: a bench study comparison with 4 other endotracheal tube cuffs. Respiratory Care 2017;62:102 12
74 Ability of five endotracheal tube cuffs to prevent leaks Massachusetts General Hospital Microcuff SealGuard TaperGuard Mallinckrodt HiLo EXCEPT ONE PneuX Leak ml/hr p< Performance of the PneuX system: a bench study comparison with 4 other endotracheal tube cuffs. Respiratory Care 2017;62:102 12
75 LoVAP study New Cross Hospital PneuX halves Post-Operative Pneumonia rates 1 p = 0.03 Independent Cost Evaluation (RCS & University of Birmingham) 700 saving per PneuX used 2 1. Significant reduction in ventilator-associated pneumonia with the Venner-PneuX System in high-risk patients undergoing cardiac surgery. Eur J Cardiothorac Surg. 2015;47(3):e VAP cost effectiveness study. Presented at the 29 th European Association for Cardio-Thoracic Surgery. 2015, Amsterdam
76 LoVAP study New Cross Hospital PneuX halves Post-Operative Pneumonia rates 1 p = 0.03 Independent Cost Evaluation (RCS & University of Birmingham) 700 saving per PneuX used 2 1. Significant reduction in ventilator-associated pneumonia with the Venner-PneuX System in high-risk patients undergoing cardiac surgery. Eur J Cardiothorac Surg. 2015;47(3):e VAP cost effectiveness study. Presented at the 29 th European Association for Cardio-Thoracic Surgery. 2015, Amsterdam
77 Multi-Drug Resistance with leaky cuffs ICUs breed MDR bacteria Repeated antibiotics and re-infection drives resistance Tracheal colonisation in 87% of ventilated ICU patients with standard tubes 1 50% of all antibiotics administered in ICU are for treatment of VAP 2 14 months use of PneuX showed: zero colonisation zero VAP zero antibiotics used for new lung infection or colonisation 3 1. Implications of Endotracheal Biofilm in VAP. Critical Care (3):R93 2. Ventilator-associated Pneumonia in the ICU. Critical Care : The incidence of VAP using the PneuX System. BMC Res Notes ;4:92

78 Optimising the design

79 PneuX : Protect the lungs, larynx & trachea

80 Tubes with one subglottic drainage port don t work effectively Suck tracheal mucosa into channel Investigating the failure to aspirate subglottic secretions. Anesth Analg (4):1083-5

81 PneuX Triple ports prevent unopposed suction on the tracheal wall

82 PneuX subglottic suction

83 Subglottic irrigation is only possible with the PneuX
84 TSM maintains the cuff pressure at all times
85 Citizens Senate: Patient s Perspective We are hugely impressed with the benefits to patient safety We urge organisations to ensure the PneuX system is adopted This is an opportunity that cannot be ignored Having reviewed the costs & benefits, we are keen for wide scale adoption 100% approval. Data collected: NHS England Citizen Senate 2015
86 The Most Disturbing Slide You May Ever See

87 Barriers Perverse Financial Incentives we generate an income from patients that develop VAP because of their increased length of stay The CCG pay if we shorten the time that patients spend in ICU this will reduce the income..150 bed days so a loss of income of 199, Managerial response to business case in a hospital with a clinical request for the PneuX. NHS 2016
88 Innovation and Technology Tariff Full reimbursement for the PneuX starts 1 April 2017
89 NHS Innovation and Technology Tariff Starts 1 st April 2017 for 2 years Order from Qualitech Healthcare Ltd Order directly from the company Ordering set up through normal procurement process 0 cost to you (company paid by NHS England) You will need 24 ETT per TSM
90 Peter Young Maryanne Mariyaselvam
91 LOCAL AHSN LOGOS HERE AliveCor s Kardia Francis White, NIA Fellow

92 Kardia Mobile A pulse check with a difference? 2017 AliveCor 92


93 Healthcare costs a crisis Healthcare costs Technology 2017 AliveCor 93

94 A Major Cause of Stroke 1 in 4 over 40 will have AF* AF effects >2m in UK Leading cause of stroke *Atrial Fibrillation 2017 AliveCor 94


95 How do you find AF? Two appointments? More? 2017 AliveCor 95


 2017")
96 Why not just 1? Make diagnosis Rhythm strip PDF ( Cardiologist if uncertain) 2017 AliveCor 96

97 Who says this is OK? European Society of Cardiology Guidelines/Atrial-Fibrillation-Management 2017 AliveCor 97


98 The future: Self-Care 2017 AliveCor 98
99 UroLift Justin Hall, General Manager of NeoTract
100

")

101 The LUTS / BPH Cycle Burden of Care Primary Care (Medication / GP Consultations) Post-operative Complications Emergency Admission Surgery
 = 80 mins")

102 Current situation Men with moderate or severe symptoms are generally offered a surgical procedure (TURP or laser) TURP and laser involves cutting away or removing existing tissue Length of stay = 2-3 days Theatre time (general anaesthetic) = 80 mins (significantly longer for HoLEP laser) Excellent disobstruction Serious adverse events Lengthy recovery TURP: Complex and persistent complications, including: Bleeding Infection Incontinence Prolong length of stay and place further burden on the NHS Sexual dysfunction
103 1. Health and Social Care Information Centre 2014; 2. Kirby R et al. ProState of the Nation report. A call to action: delivering more effective care for BPH patients in the UK ; Speakman M et al. BJU Int 2015; 115: ; Health Episode Statistics. Cost based on national Tariff; 5. Health Economic Statistics. For every patient who had BPH surgery (OPCS M65) in 2009, an analysis of complications (listed by ICD10) for each of the 5 years following the procedure. Numbers of spells and costs (based on tariff) for this activity. 6. Lukacs B et al. Eur Urol. 2013; 64: LUTS due to BPH Cost burden to the NHS BPH drug treatment Million/yr PRIMARY CARE BPH/bladder drug use after TURP: 6 At 1 yr: 23% At 5 yrs: 40% Primary Care Consultations 1.6 million consultations 2 44 Million/yr 3 BPH-related hospital episodes Million/yr Average length of stay: 9 days 50% of acute care is non-elective Elective BPH surgery 4 43 Million/yr 20,000 TURP procedures/yr 60,000 inpatient bed days/yr 27,000 theatre hours/yr Surgery-related complications 5 * 109 Million 70,000 hospital spells *cumulative over 5 year pathway 55 Million in Year 1 ACUTE CARE BPH-related hospital episodes ACUTE CARE Surgery
104 1. Health and Social Care Information Centre 2014; 2. Kirby R et al. ProState of the Nation report. A call to action: delivering more effective care for BPH patients in the UK ; Speakman M et al. BJU Int 2015; 115: ; Health Episode Statistics. Cost based on national Tariff; 5. Health Economic Statistics. For every patient who had BPH surgery (OPCS M65) in 2009, an analysis of complications (listed by ICD10) for each of the 5 years following the procedure. Numbers of spells and costs (based on tariff) for this activity. 6. Lukacs B et al. Eur Urol. 2013; 64: LUTS due to BPH Cost burden to the NHS National E & W Midlands BPH drug treatment Million/yr PRIMARY CARE BPH drug treatment Million/yr BPH/bladder drug use after TURP: 6 At 1 yr: 23% At 5 yrs: 40% Primary Care Consultations 1.6 million consultations 2 44 Million/yr 3 BPH-related hospital episodes Million/yr Average length of stay: 9 days 50% of acute care is non-elective ACUTE CARE Primary Care Consultations 305,000 consultations 2 7 Million/yr 3 BPH-related hospital episodes 4 61 Million/yr BPH-related hospital episodes Elective BPH surgery 4 43 Million/yr 20,000 TURP procedures/yr 60,000 inpatient bed days/yr 27,000 theatre hours/yr Surgery-related complications 5 * 109 Million 70,000 hospital spells *cumulative over 5 year pathway 55 Million in Year 1 ACUTE CARE Surgery Elective BPH surgery Million/yr 3,200 TURP procedures/yr 9,600 inpatient bed days/yr 4,200 theatre hours/yr Surgery-related complications 5 * 15.4 Million 9,400 hospital spells *cumulative over 5 year pathway 8 Million in Year 1

105 1. Health and Social Care Information Centre 2014; 2. Kirby R et al. ProState of the Nation report. A call to action: delivering more effective care for BPH patients in the UK ; Speakman M et al. BJU Int 2015; 115: ; Health Episode Statistics. Cost based on national Tariff; 5. Health Economic Statistics. For every patient who had BPH surgery (OPCS M65) in 2009, an analysis of complications (listed by ICD10) for each of the 5 years following the procedure. Numbers of spells and costs (based on tariff) for this activity. 6. Lukacs B et al. Eur Urol. 2013; 64: LUTS due to BPH Cost burden to the NHS National E & W Midlands BPH drug treatment Million/yr PRIMARY CARE BPH drug treatment Million/yr BPH/bladder drug use after TURP: 6 At 1 yr: 23% At 5 yrs: 40% Primary Care Consultations 1.6 million consultations 2 44 Million/yr 3 Complications (hospital episodes) from current surgical procedures 5 BPH-related hospital episodes Million/yr Average length of stay: 9 days 50% of acute care is non-elective Elective BPH surgery 4 43 Million/yr 20,000 TURP procedures/yr 60,000 inpatient bed days/yr 27,000 theatre hours/yr Surgery-related complications 5 * 109 Million 70,000 hospital spells *cumulative over 5 year pathway 55 Million in Year 1 ACUTE CARE 4,800 per patient over 5 years BPH-related hospital episodes > 2,500 costs in Year 1 ACUTE CARE Surgery Primary Care Consultations 305,000 consultations 2 7 Million/yr 3 BPH-related hospital episodes 4 61 Million/yr Elective BPH surgery Million/yr 3,200 TURP procedures/yr 9,600 inpatient bed days/yr 4,200 theatre hours/yr Surgery-related complications 5 * 15.4 Million 9,400 hospital spells *cumulative over 5 year pathway 8 Million in Year 1


106 The Key Patients & Urologists Are Seeking Straightforward Procedure Quick, reliable, reproducible Local anesthesia Day case Safe No complex and persistent complications Rapid Relief Patients quickly return to normal living Preserve Function Bladder function Sexual function Durable Years of relief Cost Effective Less expensive for system

107 A NEW View: What is BPH, really? BPH is a mechanical problem. Benign Prostate Hyperplasia is, by definition, benign tissue. Pressure Removing or destroying this benign tissue can cause complications. Hyperplastic tissue takes more work to open Why not just move it out of the way?
 Ambulatory day-case treatment patients return home within a few hours Permanent intra-prostatic UroLift implants are delivered to separate encroaching lateral prostate lobes and")

108 Enter Prostatic Urethral Lift! (The Urolift System) Ambulatory day-case treatment patients return home within a few hours Permanent intra-prostatic UroLift implants are delivered to separate encroaching lateral prostate lobes and expand the urethral lumen Minimally invasive Does not cause tissue injury Avoids the complex and persistent complications associated with removing tissue, and also avoids permanent side effects, such as sexual dysfunction. 1-6 Short, <30-min procedure, performed under local anaesthetic or occasionally light sedation Patients return home after a few hours without a catheter, and follow-up can be by telephone The treatment effect of Urolift has been shown to be durable, with published data out to 5 years 1,6 1. Roehrborn CG. Urol Clin N Am 2016; 43: Sonksen J et al. J Urol 2016;195(4S):e Perera M et al. Eur Urol 2015;67: NICE Medical Technology Guidance, MTG26, Sept 2015; Roehrborn CG. Abstract presented at EAU, London 2017
109 Minimally Invasive Safety Profile Most common AE were mild to moderate, typically resolve by 2-4 weeks: PUL Subjects Control Subjects Dysuria 34% 17% Hematuria 26% 5% Pelvic pain 18% 5% Urgency 7% 0% Urge Incontinence 4% 2% UTI 3% 2% No incidence (0%) of de novo sustained ejaculatory or erectile dysfunction. Roehrborn et al. Can J Urol 2015

110 Recovered (QoR VAS) Satisfied Patients* Improved Quality of Care UroLift patients recover more quickly TURP catches up only between 6 to 12 months UroLift patients satisfied sooner and to greater extent 100% 90% 80% 70% 60% 50% 40% 30% 20% 85% 80% 75% p< % 65% p<0.05 PUL 60% TURP 55% Months Sonksen et al. Eur Urol 2015; 68; PUL randomized to TURP [gold standard surgery] 95% 90% PUL TURP Months *would recommend procedure
 MAC00226-01")

111 Recently- 5-year durability data (confidential) MAC Rev A Roehrborn CG. Abstract presented at EAU, London In press

112 NICE Guidance Aug - Nov 2016 Jan 2014 IPG Established safety and efficacy. Recommended with normal arrangements for clinical governance, consent and audit Sept 2015 MTG Established value to NHS. Recommended as a cost saving alternative to current surgical options Nov 2015 Adoption Support Health technology adoption programme: Provided practical information and advice on the adoption of Urolift by the NHS NICE Shared Learning Case studies showcasing the adoption experience at 3 NHS Trusts

113 Implementation and Activity Urolift is an easy and rapidly deployable technology True day case procedure that does not rely on capital purchase, infrastructure or staff changes Patients return home and can be followed up by telephone Eligible patients can be recruited from the urology waiting list or from outpatient clinics At least 40% patients currently being treated with TURP or laser would be clinically eligible for Urolift

114 Prostatic Urethral Lift is included in the National Tariff Prostatic Urethral Lift (Urolift) OPCS National Tariff 2017/18 Average tariff used for comparative purposes M68.3 Endoscopic Insertion of prosthesis to compress lobe of prostate 2,107-2,538 depending on CC 2,354 TURP / laser M65.1 / M65.3 / M65.4 2,127-2,893 depending on CC Best Practice Day Case Tariff 2,271 For comparative purposes, in 2015/16: 43% of TURP/laser procedures had no CC 56% of TURP laser procedures had intermediate CC 1% of TURP/laser procedures had major CC Comparable price to Best Practice Tariff for current standard of surgical care

115 Benefits - Patients Compared with the current standard of surgical care, Urolift offers: Rapid and sustained improvement in symptoms and flow Durable benefits, with published data out to 5 years Improved safety and side effect profile Preservation of sexual function Significantly reduced post-operative complications - more rapid return to daily living 1. Roehrborn CG. Urol Clin N Am 2016; 43: Sonksen J et al. J Urol 2016;195(4S):e Perera M et al. Eur Urol 2015;67: NICE Medical Technology Guidance, MTG26, Sept 2015
116 Benefits - NHS Improved safety and reduced risk of complex and persistent complications Efficiency and productivity savings Estimated savings of at least 2,400 per patient over 5 years ( 1,200 in year 1) in reduced complications requiring hospital care 1 Improved bed capacity and no risk of delayed transfer of care No overnight stay compared with 3 bed days with TURP Reduced re-admission rates Not associated with any of the persistent or complex complications seen with current surgical treatments 2-5 Reduced catheterisationassociated urinary tract infection (CAUTI) Patients are rarely catheterised, compared with routine catheterisation for many days following a TURP procedure. Reduced requirement for outpatient follow-up A Urolift procedure follow-up can be by telephone, reducing pressure on outpatients clinics 1. Health Economic Statistics. For every patient who had BPH surgery (OPCS M65) in 2009, an analysis of complications (listed by ICD10) for each of the 5 years following the procedure. Numbers of spells and costs (based on tariff) for this activity. Based on conservative estimate of 50% reduction in complications (based on clinical evidence and NHS users) and 40% adoption in patients who would otherwise undergo a TURP procedure; 2. Roehrborn CG. Urol Clin N Am 2016; 43: Sonksen J et al. J Urol 2016;195(4S):e Perera M et al. Eur Urol 2015;67: NICE Medical Technology Guidance, MTG26, Sept 2015

 for this activity. 6. Lukacs B et al. Eur Urol. 2013; 64: 493 501.")

117 1. Health and Social Care Information Centre 2014; 2. Kirby R et al. ProState of the Nation report. A call to action: delivering more effective care for BPH patients in the UK ; Speakman M et al. BJU Int 2015; 115: ; Health Episode Statistics. Cost based on national Tariff; 5. Health Economic Statistics. For every patient who had BPH surgery (OPCS M65) in 2009, an analysis of complications (listed by ICD10) for each of the 5 years following the procedure. Numbers of spells and costs (based on tariff) for this activity. 6. Lukacs B et al. Eur Urol. 2013; 64: Cost impact across East & West Midlands* National E & W Midlands BPH drug treatment Million/yr Near cost neutral tariff compared with current BPH/bladder drug use Primary Care Consultations surgery after TURP: million consultations 2 At 1 yr: 44 Million/yr 3 23% For each annual cohort of patients treated: At 5 yrs: 40% BPH-related hospital episodes 4 Saving 3.1 Million over 5 years PRIMARY CARE 321 Million/yr treatment ACUTE CARE ( 1.6 Million saving in Year 1) in surgery related complications that require hospital Average length of stay: 9 days 50% of acute care is non-elective BPH-related hospital episodes Per patient Elective saving BPH surgery = 2,400 over 5 years 4 ( 1,300/patient saving in Year 1) 43 Million/yr 20,000 TURP procedures/yr 60,000 inpatient bed days/yr 27,000 theatre hours/yr Saving 3,900 inpatient bed days/year Surgery-related complications 5 * 109 Million 70,000 hospital spells *cumulative over 5 year pathway 55 Million in Year 1 ACUTE CARE Surgery BPH drug treatment Million/yr Primary Care Consultations 305,000 consultations 2 7 Million/yr 3 BPH-related hospital episodes 4 61 Million/yr Elective BPH surgery Million/yr 3,200 TURP procedures/yr 9,600 inpatient bed days/yr 4,200 theatre hours/yr Surgery-related complications 5 * 15.4 Million 9,400 hospital spells *cumulative over 5 year pathway 8 Million in Year 1



118 Summary Benefits of Urolift are in line with: Five year forward view and STP objectives around addressing: Care & quality gap Improved safety and reduced burden of care Durable benefit Funding and efficiency gap No delayed transfer of care In-year cost savings Accelerated Access Review: an innovative medical technology with cost saving potential Innovation & Technology Tariff Affordability: cost and net cost to the NHS based on estimated demand, potential savings and procurement routes Return on Investment: based on scale, likelihood and time taken to realise Suitability for Tariff: The potential tariff routes Impact: Scalability, including feasibility and speed of realisation of benefit Strategic fit with NHS England priorities
119 Thank you
120 Q&A
121 Thank you for your participation in Improving outcomes, cutting costs For more information about the innovations showcased at today s event: NIA@uclpartners.com For more information about the NHS Innovation and Technology Tariff (ITT): innovation.england@nhs.net LOCAL AHSN LOGOS HERE
Non-Injectable Arterial Connector (NIC)
") NHS Innovation Accelerator Implementation Toolkit Non-Injectable Arterial Connector (NIC) Introduction NHS England s Innovation and Technology Tariff (ITT) went live on 1 April 2017. This new Tariff was
NHS Innovation Accelerator Implementation Toolkit Non-Injectable Arterial Connector (NIC) Introduction NHS England s Innovation and Technology Tariff (ITT) went live on 1 April 2017. This new Tariff was
NHS Innovation Accelerator. Implementation Toolkit. mycopd
 NHS Innovation Accelerator Implementation Toolkit mycopd Introduction NHS England s Innovation and Technology Tariff (ITT) went live on 1 April 2017. This new Tariff was introduced to incentivise the adoption
NHS Innovation Accelerator Implementation Toolkit mycopd Introduction NHS England s Innovation and Technology Tariff (ITT) went live on 1 April 2017. This new Tariff was introduced to incentivise the adoption
NHS Innovation Accelerator. Economic Impact Evaluation Case Study: PneuX TM 1. BACKGROUND
 NHS Innovation Accelerator Economic Impact Evaluation Case Study: PneuX TM 1. BACKGROUND The PneuX Pneumonia Prevention System is an endotracheal/tracheostomy tube system for airway management, designed
NHS Innovation Accelerator Economic Impact Evaluation Case Study: PneuX TM 1. BACKGROUND The PneuX Pneumonia Prevention System is an endotracheal/tracheostomy tube system for airway management, designed
This is the second version of this Implementation Support Pack (September 2017)
") Contents Introduction... 2 Overview of Implementation Process... 3 Step 1: Engage Clinical Team... 3 Key Points... 3 Summary Overview PneuX System... 4 PowerPoint Presentation... 7 Step 2: Business Case...
Contents Introduction... 2 Overview of Implementation Process... 3 Step 1: Engage Clinical Team... 3 Key Points... 3 Summary Overview PneuX System... 4 PowerPoint Presentation... 7 Step 2: Business Case...
NHS Innovation Accelerator Evaluation
 NHS Innovation Accelerator Evaluation March 2018 @NHSAccelerator www.nhsaccelerator.com What is the NHS Innovation Accelerator (NIA)? NHS England initiative delivered in partnership with the Country s
NHS Innovation Accelerator Evaluation March 2018 @NHSAccelerator www.nhsaccelerator.com What is the NHS Innovation Accelerator (NIA)? NHS England initiative delivered in partnership with the Country s
Healthcare-Associated Infections
 Healthcare-Associated Infections A healthcare crisis requiring European leadership Healthcare-associated infections (HAIs - also referred to as nosocomial infections) are defined as an infection occurring
Healthcare-Associated Infections A healthcare crisis requiring European leadership Healthcare-associated infections (HAIs - also referred to as nosocomial infections) are defined as an infection occurring
4.4 Finance your future: What role can the NHS play in growing local economies?
 4.4 Finance your future: What role can the NHS play in growing local economies? Lord Andrew Mawson, Chair of Well North and social entrepreneur Duncan Selbie, Chief Executive Officer of Public Health England
4.4 Finance your future: What role can the NHS play in growing local economies? Lord Andrew Mawson, Chair of Well North and social entrepreneur Duncan Selbie, Chief Executive Officer of Public Health England
Delivering on A Promise to Learn A Commitment to Act. The National Patient Safety Collaborative learning event
 Delivering on A Promise to Learn A Commitment to Act The National Patient Safety Collaborative learning event Dr Mike Durkin NHS National Director of Patient Safety NHS Improvement Aidan Fowler Director
Delivering on A Promise to Learn A Commitment to Act The National Patient Safety Collaborative learning event Dr Mike Durkin NHS National Director of Patient Safety NHS Improvement Aidan Fowler Director
CYSTOSCOPY AND URETHRAL BULKING INJECTIONS
 CYSTOSCOPY AND URETHRAL BULKING INJECTIONS Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association
CYSTOSCOPY AND URETHRAL BULKING INJECTIONS Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association
CYSTOSCOPY AND DILATATION (IN WOMEN)
") Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
LAPAROSCOPIC RADICAL REMOVAL OF THE KIDNEY AND URETER
 Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
MEATAL/URETHRAL DILATATION
 Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
INSPECTION/EXAMINATION OF THE URETER ± BIOPSY
 Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
INFORMATION FOR PATIENTS
 The British Association of Urological Surgeons 35-43 Lincoln s Inn Fields London WC2A 3PE Phone: Fax: Website: E- mail: +44 (0)20 7869 6950 +44 (0)20 7404 5048 www.baus.org.uk admin@baus.org.uk INFORMATION
The British Association of Urological Surgeons 35-43 Lincoln s Inn Fields London WC2A 3PE Phone: Fax: Website: E- mail: +44 (0)20 7869 6950 +44 (0)20 7404 5048 www.baus.org.uk admin@baus.org.uk INFORMATION
SURGERY FOR A CONGENITAL HYDROCELE/HERNIA
 SURGERY FOR A CONGENITAL HYDROCELE/HERNIA Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association
SURGERY FOR A CONGENITAL HYDROCELE/HERNIA Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association
LAPAROSCOPIC SIMPLE REMOVAL OF THE KIDNEY
 Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
RADICAL REMOVAL OF THE KIDNEY AND URETER
 Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
BLADDER INSTILLATION FOR PAINFUL BLADDER CONDITIONS
 BLADDER INSTILLATION FOR PAINFUL BLADDER CONDITIONS Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association
BLADDER INSTILLATION FOR PAINFUL BLADDER CONDITIONS Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association
COPD Management in the community
 COPD Management in the community Anne Jones Independent Respiratory Nurse Consultant RN,BSc(Hons),PGDip(RespMed)/MA Content of session Will consider the impact of COPD COPD Strategy recommendations and
COPD Management in the community Anne Jones Independent Respiratory Nurse Consultant RN,BSc(Hons),PGDip(RespMed)/MA Content of session Will consider the impact of COPD COPD Strategy recommendations and
Laparoscopic Radical Nephrectomy
 Urology Department Laparoscopic Radical Nephrectomy Information Aims of this leaflet To give information on the intended benefits and potential risks of kidney surgery To guide you in the decisions you
Urology Department Laparoscopic Radical Nephrectomy Information Aims of this leaflet To give information on the intended benefits and potential risks of kidney surgery To guide you in the decisions you
Post-operative "Fast-Track" pathways for lung resection. Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic
 Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic
Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic Surgery Mayo Clinic Post-operative "Fast-Track" pathways for lung resection Dennis A. Wigle Division of Thoracic
@ncepod #tracheostomy
 @ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
@ncepod #tracheostomy 1 Introduction Tracheostomy: Remedy upper airway obstruction Avoid complications of prolonged intubation Protection & maintenance of airway The number of temporary tracheostomies
Welcome to the Anaesthesia and Perioperative Care Prioritisation Survey
 Welcome to the Anaesthesia and Perioperative Care Prioritisation Survey We want you to nominate the most important topics for future research in anaesthesia and perioperative care. We are therefore asking
Welcome to the Anaesthesia and Perioperative Care Prioritisation Survey We want you to nominate the most important topics for future research in anaesthesia and perioperative care. We are therefore asking
Clinical guideline Published: 23 April 2008 nice.org.uk/guidance/cg65
 Hypothermia: prevention ention and management in adults having surgery Clinical guideline Published: 23 April 2008 nice.org.uk/guidance/cg65 NICE 20. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Hypothermia: prevention ention and management in adults having surgery Clinical guideline Published: 23 April 2008 nice.org.uk/guidance/cg65 NICE 20. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
SACRAL NERVE STIMULATION (NEUROMODULATION)
") SACRAL NERVE STIMULATION (NEUROMODULATION) Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association
SACRAL NERVE STIMULATION (NEUROMODULATION) Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association
Integrated respiratory action network for patients with COPD
 Integrated respiratory action network for patients with COPD In this Future Hospital Programme case study Dr Helen Ward describes how a team from The Royal Wolverhampton NHS Trust established a respiratory
Integrated respiratory action network for patients with COPD In this Future Hospital Programme case study Dr Helen Ward describes how a team from The Royal Wolverhampton NHS Trust established a respiratory
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement Programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement Programme aims to support organisations to become more transparent and consistent in publishing safety, experience
CONSENT FORM UROLOGICAL SURGERY
 CONSENT FORM for UROLOGICAL SURGERY (Designed in compliance with consent form 1) PATIENT AGREEMENT TO INVESTIGATION OR TREATMENT Patient Details or pre-printed label Patient s NHS Number or Hospital number
CONSENT FORM for UROLOGICAL SURGERY (Designed in compliance with consent form 1) PATIENT AGREEMENT TO INVESTIGATION OR TREATMENT Patient Details or pre-printed label Patient s NHS Number or Hospital number
NHS England Innovation and Technology Payment 2018 to 2019 Technical Notes
 NHS England Innovation and Technology Payment 2018 to 2019 Technical Notes NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp.
NHS England Innovation and Technology Payment 2018 to 2019 Technical Notes NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp.
Patient copy. Periurethral bulking agent for stress urinary incontinence. Patient Information to be retained by patient
 PLEASE PRINT WHOLE FORM DOUBLE SIDED ON YELLOW PAPER Patient Information to be retained by patient affix patient label Who is this leaflet for? This leaflet provides information about having an injection
PLEASE PRINT WHOLE FORM DOUBLE SIDED ON YELLOW PAPER Patient Information to be retained by patient affix patient label Who is this leaflet for? This leaflet provides information about having an injection
SHOCKWAVE LITHOTRIPSY FOR STONES
 Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
INTRAVESICAL INSTILLATION OF DMSO
 Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
FREEING OF FORESKIN ADHESIONS
 Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
INTRODUCING THE NHS INNOVATION ACCELERATOR
 INTRODUCING THE NHS INNOVATION ACCELERATOR 2 High impact, evidence-based healthcare solutions for patient, population and NHS staff benefit. Foreword from Professor Sir Bruce Keogh I am delighted to introduce
INTRODUCING THE NHS INNOVATION ACCELERATOR 2 High impact, evidence-based healthcare solutions for patient, population and NHS staff benefit. Foreword from Professor Sir Bruce Keogh I am delighted to introduce
THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY
 CONDITIONS IN THE COMMUNITY") THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY An Economic Assessment of the South Eastern Trust Virtual Ward Introduction and Context Chronic (long-term)
THE VIRTUAL WARD MANAGING THE CARE OF PATIENTS WITH CHRONIC (LONG-TERM) CONDITIONS IN THE COMMUNITY An Economic Assessment of the South Eastern Trust Virtual Ward Introduction and Context Chronic (long-term)
C-GALL PATIENT INFORMATION LEAFLET
 C-GALL PATIENT INFORMATION LEAFLET The purpose of this study is to compare keyhole gall bladder surgery (laparoscopic cholecystectomy) with watchful waiting in people who suffer from pain due to gallstones
C-GALL PATIENT INFORMATION LEAFLET The purpose of this study is to compare keyhole gall bladder surgery (laparoscopic cholecystectomy) with watchful waiting in people who suffer from pain due to gallstones
Collaborating to improve safety and quality of care
 Collaborating to improve safety and quality of care Our plan 2017 2018 Innovation Agency North West Coast Patient Safety Collaborative Contents Introduction... 1 National workstreams... 2 Regional programmes...
Collaborating to improve safety and quality of care Our plan 2017 2018 Innovation Agency North West Coast Patient Safety Collaborative Contents Introduction... 1 National workstreams... 2 Regional programmes...
DORSAL SLIT OF THE FORESKIN
 Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
LAPAROSCOPIC RECONSTRUCTION OF THE PELVIS OF THE KIDNEY
 Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
Procedure Specific Information What is the evidence base for this information? This publication includes advice from consensus panels, the British Association of Urological Surgeons, the Department of
INNOVATION, HEALTH AND WEALTH A SCORECARD
 INNOVATION, HEALTH AND WEALTH A SCORECARD Page 2 CONTENTS 4 EXECUTIVE SUMMARY 6 INTRODUCTION 7 3 MILLION LIVES 9 INTRA-OPERATIVE FLUID MANAGEMENT/OESOPHAGEAL DOPPLER MONITORING 11 CHILD IN A CHAIR IN A
INNOVATION, HEALTH AND WEALTH A SCORECARD Page 2 CONTENTS 4 EXECUTIVE SUMMARY 6 INTRODUCTION 7 3 MILLION LIVES 9 INTRA-OPERATIVE FLUID MANAGEMENT/OESOPHAGEAL DOPPLER MONITORING 11 CHILD IN A CHAIR IN A
CARDIFF AND VALE NHS TRUST YMDDIRIEDOLAETH GIG CAERDYDD A R FRO CARDIAC SURGERY PATIENT INFORMATION BOOKLET
 CARDIFF AND VALE NHS TRUST YMDDIRIEDOLAETH GIG CAERDYDD A R FRO CARDIAC SURGERY PATIENT INFORMATION BOOKLET Welcome / Croeso Welcome to the Cardiothoracic Department unit at the University Hospital of
CARDIFF AND VALE NHS TRUST YMDDIRIEDOLAETH GIG CAERDYDD A R FRO CARDIAC SURGERY PATIENT INFORMATION BOOKLET Welcome / Croeso Welcome to the Cardiothoracic Department unit at the University Hospital of
BUGS BE GONE: Reducing HAIs and Streamlining Care!
 BUGS BE GONE: Reducing HAIs and Streamlining Care! SUSAN WHITNEY, RN, PCCN, MM, BME FLORIDA HOSPITAL ORLANDO, FL SUWHIT@AOL.COM LEARNING OUTCOMES 1. Describe HAI s and the impact disposable ECG leads have
BUGS BE GONE: Reducing HAIs and Streamlining Care! SUSAN WHITNEY, RN, PCCN, MM, BME FLORIDA HOSPITAL ORLANDO, FL SUWHIT@AOL.COM LEARNING OUTCOMES 1. Describe HAI s and the impact disposable ECG leads have
Patient Safety Course Descriptions
 Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Commissioning for Quality & Innovation (CQUIN)
") Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Best Practice Guidelines BPG 5 Catheter Care
 Best Practice Guidelines BPG 5 Catheter Care BGP 5 1 DOCUMENT STATUS: Reviewed DATE ISSUED: March 2014 DATE TO BE REVIEWED: 13.10.17 AMENDMENT HISTORY VERSION DATE AMENDMENT HISTORY V1 March 2014 New Guideline
Best Practice Guidelines BPG 5 Catheter Care BGP 5 1 DOCUMENT STATUS: Reviewed DATE ISSUED: March 2014 DATE TO BE REVIEWED: 13.10.17 AMENDMENT HISTORY VERSION DATE AMENDMENT HISTORY V1 March 2014 New Guideline
Reducing HCAI- What the Commissioner needs to know.
 Reducing HCAI- What the Commissioner needs to know. Sarah Mantle HCAI/AMR project lead NHS England #NHSEngAMR Do Tweet Introduction Healthcare Associated Infections (HCAI) can develop as a result of direct
Reducing HCAI- What the Commissioner needs to know. Sarah Mantle HCAI/AMR project lead NHS England #NHSEngAMR Do Tweet Introduction Healthcare Associated Infections (HCAI) can develop as a result of direct
Assessment. Repair Longitudinal. PErineal (PEARLS): Study. Can we improve perineal assessment and repair? Professor Christine Kettle
: Study. Can we improve perineal assessment and repair? Professor Christine Kettle") PErineal Assessment Repair Longitudinal Study (PEARLS): Can we improve perineal assessment and repair? Professor Christine Kettle University Hospital of North Staffordshire Overview Background Informing
PErineal Assessment Repair Longitudinal Study (PEARLS): Can we improve perineal assessment and repair? Professor Christine Kettle University Hospital of North Staffordshire Overview Background Informing
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Linking the LAS with Health & Social Care. 6 th December 2016
 Linking the LAS with Health & Social Care 6 th December 2016 Outline: About me.. LAS Context Integrating LAS with H&SC London Ambulance Service NHS Trust 2 LAS context London Ambulance Service NHS Trust
Linking the LAS with Health & Social Care 6 th December 2016 Outline: About me.. LAS Context Integrating LAS with H&SC London Ambulance Service NHS Trust 2 LAS context London Ambulance Service NHS Trust
HOSPITAL ACQUIRED COMPLICATIONS. Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program
 HOSPITAL ACQUIRED COMPLICATIONS Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program HOSPITAL ACQUIRED COMPLICATIONS (HACS) A medical condition or complication that a patient develops during
HOSPITAL ACQUIRED COMPLICATIONS Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program HOSPITAL ACQUIRED COMPLICATIONS (HACS) A medical condition or complication that a patient develops during
Medical technologies guidance Published: 21 March 2018 nice.org.uk/guidance/mtg37
 Thopaz+ portable digital system for managing chest drains Medical technologies guidance Published: 21 March 2018 nice.org.uk/guidance/mtg37 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Thopaz+ portable digital system for managing chest drains Medical technologies guidance Published: 21 March 2018 nice.org.uk/guidance/mtg37 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Position within the Organisation GP Research Lead
 Document Description Document Type Standard Operating Procedure C-Reactive Protein (CRP) Testing Service Application General Practitioners, Version 1.0 Ratification date August 2016 Review date March 2018
Document Description Document Type Standard Operating Procedure C-Reactive Protein (CRP) Testing Service Application General Practitioners, Version 1.0 Ratification date August 2016 Review date March 2018
Imperial College Health Partners - at a glance
 Imperial College Health Partners - at a glance Imperial College Health Partners - at a glance Our vision and purpose This document is intended to provide an introduction to Imperial College Health Partners
Imperial College Health Partners - at a glance Imperial College Health Partners - at a glance Our vision and purpose This document is intended to provide an introduction to Imperial College Health Partners
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Specialised Services Service Specification. Adult Congenital Heart Disease
 Specialised Services Service Specification Adult Congenital Heart Disease Document Author: Executive Lead: Approved by: Issue Date: Review Date: Document No: Specialised Planner Director of Planning Insert
Specialised Services Service Specification Adult Congenital Heart Disease Document Author: Executive Lead: Approved by: Issue Date: Review Date: Document No: Specialised Planner Director of Planning Insert
Research from the Health Protection Agency
 Changing wound care protocols to reduce postoperative caesarean section infection and readmission KEY WORDS Caesarean section Infection Diabetes Obesity PICO Opsite Post-Op Visible Due to concern centring
Changing wound care protocols to reduce postoperative caesarean section infection and readmission KEY WORDS Caesarean section Infection Diabetes Obesity PICO Opsite Post-Op Visible Due to concern centring
Marianne Chulay is a critical care nursing/clinical research consultant in Chapel Hill, NC. The author has no financial relationships to disclose.
 VAP is a common and potentially fatal complication of ventilator care. Following the latest CDC recommendations is the best defense you can offer your patients. Marianne Chulay, RN, DNSC, FAAN Marianne
VAP is a common and potentially fatal complication of ventilator care. Following the latest CDC recommendations is the best defense you can offer your patients. Marianne Chulay, RN, DNSC, FAAN Marianne
Guidelines for patients undergoing surgery as part of an Enhanced Recovery Programme (ERP)
") Guidelines for patients undergoing surgery as part of an Enhanced Recovery Programme (ERP) Summary Helping you to get better sooner after surgery June 2012 Foreword These guidelines have been produced
Guidelines for patients undergoing surgery as part of an Enhanced Recovery Programme (ERP) Summary Helping you to get better sooner after surgery June 2012 Foreword These guidelines have been produced
Quick guide: planning for increased seasonal demand in respiratory illness
 Quick guide: planning for increased seasonal demand in respiratory illness Published by NHS England and NHS Improvement December 2017 The British Thoracic Society is pleased to endorse this quick guide,
Quick guide: planning for increased seasonal demand in respiratory illness Published by NHS England and NHS Improvement December 2017 The British Thoracic Society is pleased to endorse this quick guide,
Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery
 CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
CLINICAL GUIDELINE Perioperative management of the higher risk surgical patient with an acute surgical abdomen undergoing emergency surgery CG10214-2 For use in (clinical areas): For use by (staff groups):
Your care in the best place At home, in your community and in our hospitals
 Draft V3 for Joint Committee as at 23 Nov 2017 All content in this document is subject to change prior to the approval of the STP Joint Committee of CCGs on 29 Nov 2017 Your care in the best place At home,
Draft V3 for Joint Committee as at 23 Nov 2017 All content in this document is subject to change prior to the approval of the STP Joint Committee of CCGs on 29 Nov 2017 Your care in the best place At home,
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms
 Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
Psychological Therapies for Depression and Anxiety Disorders in People with Longterm Physical Health Conditions or with Medically Unexplained Symptoms Guide for setting up IAPT-LTC services 1. Aims The
The Pulmonary Hypertension Service Specification (Adult)
") Understanding the management of Pulmonary Hypertension in adults in the UK Short guide 2: The Pulmonary Hypertension Service Specification (Adult) This project was jointly developed by PHA UK and Actelion
Understanding the management of Pulmonary Hypertension in adults in the UK Short guide 2: The Pulmonary Hypertension Service Specification (Adult) This project was jointly developed by PHA UK and Actelion
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Patient Information. Having a Laparoscopy
 Patient Information Having a Laparoscopy This information has been written to explain your operation, and the benefits and risks. The medical and nursing staff will be happy to answer any questions you
Patient Information Having a Laparoscopy This information has been written to explain your operation, and the benefits and risks. The medical and nursing staff will be happy to answer any questions you
COPD SERVICE RE-DESIGN
 COPD SERVICE RE-DESIGN Dr Mukesh Singh GP Principal & GPwSI Respiratory Medicine, Horse Fair Practice, Rugeley Clinical Lead LTC & Governing Body member Cannock Chase CCG COPD DRIVERS FOR RE-DESIGN DOH
COPD SERVICE RE-DESIGN Dr Mukesh Singh GP Principal & GPwSI Respiratory Medicine, Horse Fair Practice, Rugeley Clinical Lead LTC & Governing Body member Cannock Chase CCG COPD DRIVERS FOR RE-DESIGN DOH
Collaborative Working to reduce hospital admissions. Dr Firdaus Adenwalla Annette Davies Beth Griffiths
 Collaborative Working to reduce hospital admissions Dr Firdaus Adenwalla Annette Davies Beth Griffiths Ageing population A third of babies born in the UK in 2013 are expected to live to be a 100. (Office
Collaborative Working to reduce hospital admissions Dr Firdaus Adenwalla Annette Davies Beth Griffiths Ageing population A third of babies born in the UK in 2013 are expected to live to be a 100. (Office
Out of tariff high cost drug / technology business case template
 Out of tariff high cost drug / technology business case template Out of tariff high cost drug / technology business case template Please read all the criteria before completing any of the template For
Out of tariff high cost drug / technology business case template Out of tariff high cost drug / technology business case template Please read all the criteria before completing any of the template For
Medicare Value Based Purchasing August 14, 2012
 Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
THE ROY CASTLE LUNG CANCER FOUNDATION
 Surgery for lung cancer How will it be decided if I am suitable for surgery? Successful surgery for lung cancer, with the chance of cure, may only be possible after the surgeon has considered the following
Surgery for lung cancer How will it be decided if I am suitable for surgery? Successful surgery for lung cancer, with the chance of cure, may only be possible after the surgeon has considered the following
Performance Scorecard 2013
 NORTHWESTERN LAKE FOREST HOSPITAL Performance Scorecard 2013 updated May 2013 Northwestern Lake Forest Hospital is committed to providing the communities we serve the highest quality health care through
NORTHWESTERN LAKE FOREST HOSPITAL Performance Scorecard 2013 updated May 2013 Northwestern Lake Forest Hospital is committed to providing the communities we serve the highest quality health care through
SCHEDULE 2 THE SERVICES Service Specifications
 SCHEDULE 2 THE SERVICES Service Specifications Service Specification No Service ParaDoc Commissioner City and Hackney CCG Commissioner Lead Leah Herridge Provider CHUHSE Provider Lead Date of Review September
SCHEDULE 2 THE SERVICES Service Specifications Service Specification No Service ParaDoc Commissioner City and Hackney CCG Commissioner Lead Leah Herridge Provider CHUHSE Provider Lead Date of Review September
Evaluation Tool* Clinical Standards ~ March 2010 Chronic Obstructive Pulmonary Disease** Services
 Evaluation Tool* Clinical Standards ~ March 2010 Chronic Obstructive Pulmonary Disease** Services *Formerly known as Self-Assessment Framework ** Chronic Obstructive Pulmonary Disease (COPD) Standard 1:
Evaluation Tool* Clinical Standards ~ March 2010 Chronic Obstructive Pulmonary Disease** Services *Formerly known as Self-Assessment Framework ** Chronic Obstructive Pulmonary Disease (COPD) Standard 1:
Telehealth for Acute and Urgent Care
 Telehealth for Acute and Urgent Care the Andrew Waring, Consultant, Serengeti Projects Ltd Agenda Individual and workshop introductions and objectives Benefits Chronic Telehealth Benefits Acute and Urgent
Telehealth for Acute and Urgent Care the Andrew Waring, Consultant, Serengeti Projects Ltd Agenda Individual and workshop introductions and objectives Benefits Chronic Telehealth Benefits Acute and Urgent
Kingston Primary Care commissioning strategy Kingston Medical Services
 Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Kingston Primary Care commissioning strategy Kingston Medical Services Kathryn MacDermott Director of Planning and Primary Care Kathryn.macdermott@kingstonccg.nhs.uk kmacdermott@nhs.net 1 Contents 1. Introduction...
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Lorenzo for clinical outcomes transformation? Ben Bridgewater
 Lorenzo for clinical outcomes transformation? Ben Bridgewater Global Trends - Outcomes and Transformation: The Landscape The problems The obstacles The solutions Ageing population and consumerism Increasing
Lorenzo for clinical outcomes transformation? Ben Bridgewater Global Trends - Outcomes and Transformation: The Landscape The problems The obstacles The solutions Ageing population and consumerism Increasing
Addressing ambulance handover delays: actions for local accident and emergency delivery boards
 Addressing ambulance handover delays: actions for local accident and emergency delivery boards Published by NHS England and NHS Improvement November 2017 Contents Foreword... 2 Actions to be taken now,
Addressing ambulance handover delays: actions for local accident and emergency delivery boards Published by NHS England and NHS Improvement November 2017 Contents Foreword... 2 Actions to be taken now,
We plan. We achieve.
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
Continence & Catheter Training For Nursing Homes For Jan-June 2016
 Continence & Catheter Training For Nursing Homes For Jan-June 2016 To secure your place Please fax or email the booking form on the back to susan.eley1@nhs.net Or fax to Fax: 01782 652724 The Continence
Continence & Catheter Training For Nursing Homes For Jan-June 2016 To secure your place Please fax or email the booking form on the back to susan.eley1@nhs.net Or fax to Fax: 01782 652724 The Continence
UNIVERSITY OF MASSACHUSETTS MEDICAL SCHOOL ANESTHESIOLOGY RESIDENCY PROGRAM GOALS AND OBJECTIVES
 UNIVERSITY OF MASSACHUSETTS MEDICAL SCHOOL ANESTHESIOLOGY RESIDENCY PROGRAM GOALS AND OBJECTIVES CA-2/CA-3 REQUIRED ROTATIONS IN PEDIATRIC ANESTHESIOLOGY The Department of Anesthesiology has established
UNIVERSITY OF MASSACHUSETTS MEDICAL SCHOOL ANESTHESIOLOGY RESIDENCY PROGRAM GOALS AND OBJECTIVES CA-2/CA-3 REQUIRED ROTATIONS IN PEDIATRIC ANESTHESIOLOGY The Department of Anesthesiology has established
NHS North Yorkshire and York
 CASE STUDY NHS North Yorkshire and York Managing long term conditions through redesigning the care pathways and integrating telehealth North Yorkshire and York The challenge Strategic plans NHS North Yorkshire
CASE STUDY NHS North Yorkshire and York Managing long term conditions through redesigning the care pathways and integrating telehealth North Yorkshire and York The challenge Strategic plans NHS North Yorkshire
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Mohamad Fakih, MD, MPH
 Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Neurosurgery. Themes. Referral
 06 04 Neurosurgery The following recommendations were produced by the British Society of Neurological Surgeons to highlight where resources could be released in NHS neurological services, while maintaining
06 04 Neurosurgery The following recommendations were produced by the British Society of Neurological Surgeons to highlight where resources could be released in NHS neurological services, while maintaining
Advance Health Care Planning: Making Your Wishes Known. MC rev0813
 Advance Health Care Planning: Making Your Wishes Known MC2107-14rev0813 What s Inside Why Health Care Planning Is Important... 2 What You Can Do... 4 Work through the advance health care planning process...
Advance Health Care Planning: Making Your Wishes Known MC2107-14rev0813 What s Inside Why Health Care Planning Is Important... 2 What You Can Do... 4 Work through the advance health care planning process...
Standards for insertion, follow up and explant of implantable loop recorders [ILRs] by non-medical staff
![Standards for insertion, follow up and explant of implantable loop recorders [ILRs] by non-medical staff](/thumbs/84/89530524.jpg "Standards for insertion, follow up and explant of implantable loop recorders [ILRs] by non-medical staff") Standards for insertion, follow up and explant of implantable loop recorders [ILRs] by non-medical staff August 2018 First edition 1. Introduction This document has been produced by a group of arrhythmia
Standards for insertion, follow up and explant of implantable loop recorders [ILRs] by non-medical staff August 2018 First edition 1. Introduction This document has been produced by a group of arrhythmia
NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION
 NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION DR AHMAD SHALTUT OTHMAN JAB ANESTESIOLOGI & RAWATAN RAPI HOSP SULTANAH BAHIYAH ALOR SETAR, KEDAH Nosocomial infection Nosocomial or hospital
NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION DR AHMAD SHALTUT OTHMAN JAB ANESTESIOLOGI & RAWATAN RAPI HOSP SULTANAH BAHIYAH ALOR SETAR, KEDAH Nosocomial infection Nosocomial or hospital
Surgical Treatment for Cancer of the Oesophagus
 Oxford Oesophagogastric Centre Surgical Treatment for Cancer of the Oesophagus Information for patients This leaflet gives you information about your planned operation, possible risks and complications,
Oxford Oesophagogastric Centre Surgical Treatment for Cancer of the Oesophagus Information for patients This leaflet gives you information about your planned operation, possible risks and complications,
N: Emergency Nursing. Alberta Licensed Practical Nurses Competency Profile 135
 N: Emergency Nursing Alberta Licensed Practical Nurses Competency Profile 135 Competency: N-1 Multi-Systems Assessment N-1-1 N-1-2 N-1-3 N-1-4 Demonstrate knowledge and ability to apply critical thinking
N: Emergency Nursing Alberta Licensed Practical Nurses Competency Profile 135 Competency: N-1 Multi-Systems Assessment N-1-1 N-1-2 N-1-3 N-1-4 Demonstrate knowledge and ability to apply critical thinking
HOSPITAL QUALITY MEASURES. Overview of QM s
 HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
STATEMENT OF PURPOSE August Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008)
") 1. Trust Profile STATEMENT OF PURPOSE August 2015 Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008) 1.1 Worcestershire Acute Hospitals NHS Trust was formed on 1
1. Trust Profile STATEMENT OF PURPOSE August 2015 Provided to the Care Quality Commission to comply with The Health & Social Care Act (2008) 1.1 Worcestershire Acute Hospitals NHS Trust was formed on 1
INFORMATION FOR PATIENTS WHO ARE PREPARING FOR LUNG RESECTION SURGERY
 St James s Hospital Department of Cardiothoracic Surgery INFORMATION FOR PATIENTS WHO ARE PREPARING FOR LUNG RESECTION SURGERY R 255 JULY 2014 CONTENTS Your lungs and how they work...1 Why do I need surgery?...1
St James s Hospital Department of Cardiothoracic Surgery INFORMATION FOR PATIENTS WHO ARE PREPARING FOR LUNG RESECTION SURGERY R 255 JULY 2014 CONTENTS Your lungs and how they work...1 Why do I need surgery?...1
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support The Open and Honest Care: Driving Improvement organisations to become more transparent
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support The Open and Honest Care: Driving Improvement organisations to become more transparent
A prospectus of opportunities: how our plans can support your plans. Business plan
 A prospectus of opportunities: how our plans can support your plans Business plan 2018-2019 West of England AHSN Business Plan 2018-19 Contents Introduction...4 Outline plan...5 Building on our success
A prospectus of opportunities: how our plans can support your plans Business plan 2018-2019 West of England AHSN Business Plan 2018-19 Contents Introduction...4 Outline plan...5 Building on our success
National Primary Care Cluster Event ABMU Health Board 13 th October 2016
 National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
ANTERIOR RESECTION WHAT ARE THE BENEFITS OF HAVING AN ANTERIOR RESECTION?
 WHAT IS AN ANTERIOR RESECTION? ANTERIOR RESECTION This is an operation that is designed to remove part of your lower large bowel and then join the bowel ends back together again. This is called an anastamosis.
WHAT IS AN ANTERIOR RESECTION? ANTERIOR RESECTION This is an operation that is designed to remove part of your lower large bowel and then join the bowel ends back together again. This is called an anastamosis.
Extracorporeal Shock Wave Lithotripsy (ESWL) An information guide
 An information guide") TO PROVIDE THE VERY BEST CARE FOR EACH PATIENT ON EVERY OCCASION Extracorporeal Shock Wave Lithotripsy (ESWL) An information guide Extracorporeal Shock Wave Lithotripsy (ESWL) What does the procedure involve?
TO PROVIDE THE VERY BEST CARE FOR EACH PATIENT ON EVERY OCCASION Extracorporeal Shock Wave Lithotripsy (ESWL) An information guide Extracorporeal Shock Wave Lithotripsy (ESWL) What does the procedure involve?
SIMULATION COURSE PROGRAMME
 SIMULATION COURSE PROGRAMME 2016-2017 1 Contents PAGE Foundation Training.. 3 General Internal Medicine Regional Training. 4 ROBuST - RCOG Operative Birth Simulation Training. 5 Trauma Team Member Courses
SIMULATION COURSE PROGRAMME 2016-2017 1 Contents PAGE Foundation Training.. 3 General Internal Medicine Regional Training. 4 ROBuST - RCOG Operative Birth Simulation Training. 5 Trauma Team Member Courses