Creating a No Wait ED
|
|
|
- Janel Patterson
- 5 years ago
- Views:
Transcription
1 This presenter has nothing to disclose Creating a No Wait ED Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Process Improvement & Hospital Operations Kaiser South Sacramento April 5, 2016

2 Case Study: Kaiser South Sacramento

3 Our Past: Impending Disaster! (c) Murrell 2015
4 Kaiser South Sacramento ED The County Hospital for Sacramento Busiest ED In Sacramento Kaiser Facility Serves mixed payer/socioeconomic population (almost 40% Medi-Cal/Uninsured) Level 2 Trauma Center UC Davis ED residency teaching On pace for 130,000 visits this year Up 20% in volume in 2015, continued increases in 2016 (c) Murrell 2015

5 Space Constrained 49 ED bays Lose 3 for Trauma 4 dedicated to psych Over 2500 patients per ED bay!

6 Our Past State
7 Prior Baseline Data 450 hours of diversion annually LWOT rates 6.6% on average, but over 12% some months Average door to doctor: 55 minutes Total time in ED on average 4 ½ hours for discharged patients 8 hours for admitted patients But wide variability day to day with much longer times some days (c) Murrell 2015

8 MD perspective May work a 12 hour shift and only see 8 patients with 30 or more patients in the waiting room Poor flow made it impossible to see patients Doctors were frustrated, complaining to administration about ED function Patients angry, staff angry, chaos! Unnecessary tests ordered (c) Murrell 2015
 Murrell")
9 For our patients Waits of 5-6 hours to see a doctor patients in the waiting room every night at 11pm Calls to see if I could get them in quicker (c) Murrell 2015

10 We saw the crisis coming Volume going up from 67,000 in 2008 to 130,000 in 2016 Trauma started Aug 2009 County psychiatric failures Hospital space constraints: 180 IP beds
 Murrell")
11 Worried it could have been us (c) Murrell 2015
")
12 Our Current State (c) Murrell 2015
13 Our Current State Time to Physician 19 minutes LWOT: 0.4% all of last year Diversion hours: Zero! Length of Stay Down ESI Level 4,5: 43 minutes Discharged patients: 2 hours 9 minutes Rare inpatient holds in the ED!
14 2015 Year End Totals: 80% of patients are out of the ED in under 4 hours, and 55% are done in under 2 hours Frequency Totals 0-2 Hours 55.0 Percent 2-4 Hours 25.2 Percent 4-6 Hours 9.1 Percent 6-10 Hours 5.0 Percent > 10 Hours 5.7 Percent
15 Current State: Patient Side March, 2011: our ED 3 year old girl, brought in by mom vomiting and diarrhea for 3 days, no fever Quickly evaluated by MD who said she just doesn t look right LP showed >7000 white cells, culture grows out meningococcus (c) Murrell 2015

16 (c) Murrell 2015
17 Recap Measure Before After Hours on Divert per year Percent LWOBS 6.6% 0.4% Door-to-Doc (minutes) LOS Treat & Release (hours) LOS Treat & Admit (hours) So, how is it possible to go from Before to After? (c) Murrell 2015
18 A little about Kaiser Prepaid integrated health system No financial incentive to admit patients Similar acuity to other ED s, but good follow-up and available testing allows discharge of many patients Examples: stable chest pain, atrial fibrillation, TIA, deep vein thrombosis, diverticulitis So, not only do we diagnose our patients, we treat as many as possible to send them home But remember almost half of our patients are non-kaiser (c) Murrell 2015
19 Acuity In a comparison study, had the same acuity as most Level 2 Trauma Centers Because of systems that are in place we only admit 11% of patients vs 18% typically As an example, only 10% of chest pain patients are admitted, 75% of GI bleeds are scoped and sent home- a different mindset Best clinical outcomes- nationally recognized (c) Murrell 2015


20 How to even get started? Two key elements: Process Culture (c) Murrell 2015
21 Amazing cultural change over time Worked to empower all employees to own the change and think about process improvement in their everyday life. Told all new hires if you don t like change you probably don t want to work here Gave all physicians leadership books and challenged them to do projects that would help the department Is precedent- Toyota got over 80,000 suggestions from employees and implemented 99% of them. Easier said then done! (c) Murrell 2015
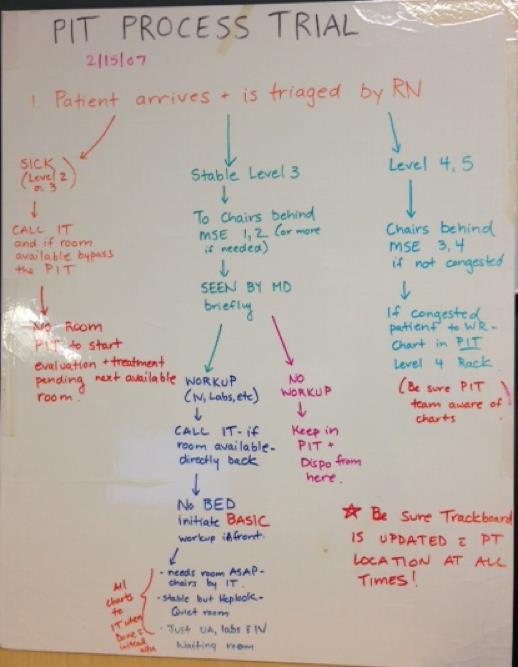
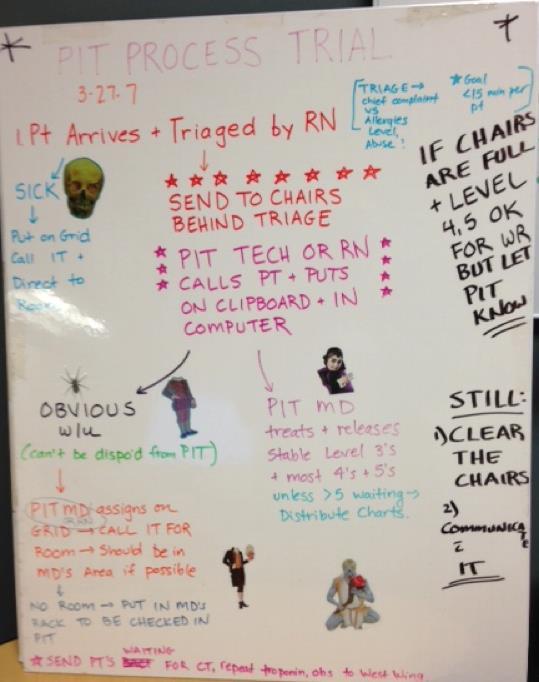
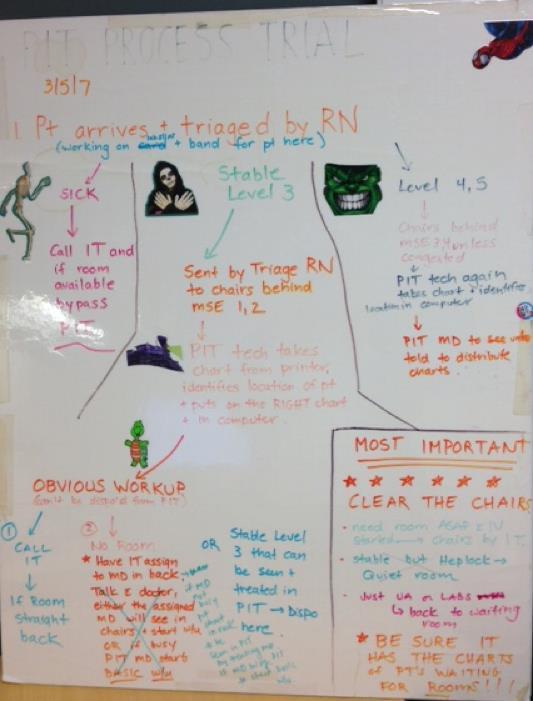
22 Flow Prior To Changes Flow was controlled by the IT RN. Same MD could own patients on opposite sides of the ED! Internal Triage RN Waiting Room Often 30 or more patients in the waiting room at 11pm. Medical Screening Exam (c) Murrell 2015 Patient Arrives
 Murrell")
23 What we discovered: Key Principles: Small reductions in service time can really make an impact in times of high utilization Decreasing length of stay is the most key metric for dramatic improvement quickly (c) Murrell 2015
24 We live on the high end of the curve (c) Murrell 2015
")
25 Building Blocks to Improve Flow: Rapid Care Hospital Partnership Team Assignment System Vertical 3 Area Clinical Decision Area Open Data Staffing for Volumes (c) Murrell 2015

26 Lets start at the beginning
27 Leadership & Perseverance Set a Vision Look at every process critically Goal: better for patients, easier for staff Involve the frontline staff Continuous improvement Open data with clear metrics Have fun!
28 Pearls Set a vision with the staff our patients do not wait, we want to be the best emergency department in America Take risks: ask forgiveness later a few hours of time for the staff in a Kaizen event will pay off in spades later Small tests of change everyone is willing to try something for a day, week, month especially if their voice is heard when making changes
29 Improving Flow in the ED High volume ED: different patient streams based on acuity Low Medium High All with very clear & different workflows with the goal of decreasing length of stay to create capacity.
30 Triage Remember, a non-value added necessity in many cases Eliminate when possible Directly pull into an area: if you guessed wrong just shift the patient! 90% of the time, first impression is the right one (c) Murrell 2015
31 Process Improvement Doesn t need to be fancy to work

32 Rapid Care Our first project Low acuity patients were triaged to home 30% of our patients fit in this category after healthcare reform

33 Rapid Care: Low Acuity Flow Started us thinking in a new way Think triage to home Small constrained area Well defined teams that work well together One Contact as much as possible Minimize movement Uniform work stations & stocking
 Murrell")
34 That was our first project- Many failures along the way (c) Murrell 2015
 Murrell 2015")
35 % LWBS Immediate Results (c) Murrell 2015
36 Low Acuity Flow Low Acuity Treatment Area Triage only if delays Patient Arrives
 (c) Murrell")
37 Streamlined Low Acuity (Video) (c) Murrell 2015





38 No repeat work Goal arrival to discharge in under one hour Patient MD RN All sitting in close proximity and working toward rapid dischargeminimal movement by everyone! (c) Murrell 2015

39 (c) Murrell 2015
 Murrell")
40 Consider every step Minimize movement for everyone (c) Murrell 2015
41 The System Makes It Easy Before Process Change After Process Change
42 Mid-Acuity Flow Area to treat healthy patients who need more testing Goal to save high acuity beds in the main ED Patients like it better, improves the system
43 Key Points: KEEP VERTICAL PATIENTS VERTICAL! PO meds instead of IV meds: patients like it better! Never change your diagnostics Partner with radiology to eliminate contrast Have a phlebotomist if possible Results waiting room for patients who need testing Partner with the Main ED if more treatment or admission is needed

44 Mid Acuity Flow MD/RN team in the front eliminates waste Immediate communication between the team members

45 Mid Acuity Patients: no one in extremis! Abdominal pain Back pain- <40 years Chest pain-< 30 years DVT rule out Flank pain-<40 years Headache with migraine history Pelvic pain (stable r/o ectopic) Pediatric fever over 6 months Gastroenteritis
46 What you need to start Streamlined area for intake similar to low acuity area Pelvic Room Phlebotomist Partner nurse & treatment nurse Results waiting room

47 Our Intake Results Patients with the same chief complaint had an hour cut off of their length of stay Abdominal pain diagnosed in under 2 hours

48 Main ED

49 Need to make the main ED more manageable

50 Main ED Teams Team composed of a doctor and two RN s Each team gets six rooms in the main ED with 2 flex beds when needed Manage your own area Code rooms flexible for any team
51 Team Assignment System Patients are assigned to a color coded team in the main ED on arrival! This created ownership for patients and decreased our time to MD dramatically Started at 55 minutes: now average 19 minutes arrival to MD start (over 350 patients a day) MD s like it because they are front loaded with patients, then tapered at the end of their shift

52 Team Assignment System Brief Triage Green Team Beds Patient Arrives

53 Starts with the vision! The job is easier if everyone lifts a little
54 Other ED best practices Portal System: Front end rooms where MD s meet their patients and order testing with a dedicated phlebotomist (decrease order turnaround time) Rocket start : Frontload a number of patients when MD is fresh Merry-go-round : when capacity a problempatients enter an area and meet MD, have EKG s, labs, radiology done- when room available in main ED, testing complete

55 Hospital Capacity- The same principles apply Decrease arrivals Decrease length of stay Standardize care when possible
56 Start at the Front: Observation Unit Decreases arrivals to the hospital Standardizes care Procedure Room: better for patients, easier for doctors (MD s can scope twice as many patients- no down time)
57 Observation Unit Example Eight Rooms Staffed with ED MD s/rn s with a focus on flowallows for Trauma, Pediatrics, Gyne A Flexible Unit Observation with more testing: GI bleed, chest pain, TIA, syncope, pyelonephritis Procedures: Transfusion, dialysis certain disposition: mild DKA, early sepsis, asthma
58 GI Bleed: a case study for flow Elderly patient arrives in ED with lower GI bleed complaint Vital signs checked, istat hemoglobin done, other labs drawn and sent Immediate transfer to CDA Message left on the GUT phone if afterhours Standardized bowel prep begun, transfused if needed, serial labs Scope in the AM in a procedure room IN THE CDA (minimal movement) 75% are discharged home after recovery


59 Happy Doctor/Happy Patient
60 Is it working for us? Trial was done with CDA, closed for three months then reopened When CDA was closed admission percentage rapidly climbed to 13% Hospital became impacted Now, consistently admission percentage down to around 10%

61 Better Patient Satisfaction than ED or Hospital
62 Protocols Chest pain GI bleed DKA Abdominal pain Asthma Pyelonephritis Head injury Plus many others

63 For everything to work: Staffing for our volumes Refining our staffing we did not match our staffing to the demand! (c) Murrell 2015
64 12:00 AM 1:00 AM 2:00 AM 3:00 AM 4:00 AM 5:00 AM 6:00 AM 7:00 AM 8:00 AM 9:00 AM 10:00 AM 11:00 AM 12:00 PM 1:00 PM 2:00 PM 3:00 PM 4:00 PM 5:00 PM 6:00 PM 7:00 PM 8:00 PM 9:00 PM 10:00 PM 11:00 PM Nursing Staffing: Before Nursing Staffing Kaiser South Sacramento ED Arrivals by Hour of the Day Kaiser South Sacramento 2008
65 12:00 AM 1:00 AM 2:00 AM 3:00 AM 4:00 AM 5:00 AM 6:00 AM 7:00 AM 8:00 AM 9:00 AM 10:00 AM 11:00 AM 12:00 PM 1:00 PM 2:00 PM 3:00 PM 4:00 PM 5:00 PM 6:00 PM 7:00 PM 8:00 PM 9:00 PM 10:00 PM 11:00 PM Nursing Staffing Post Change Nursing Staffing- Kaiser South Sacramento ED Arrivals by Hour of the Day Kaiser South Sacramento
66 Physician Staffing: Before Aggregate Physicians - Demand vs Staffed Capacity Projected Aggregate Physician Demand Current Aggregate Physician Staffing (c) Murrell 2015
67 Physician Staffing: Post Aggregate Physicians - Demand vs Staffed Capacity Projected Aggregate Physician Demand Current Aggregate Physician Staffing (c) Murrell 2015
 Murrell")
68 After Health Care Reform Looking at Staffing at Least Monthly (c) Murrell 2015
69 Not just the assignments: Team Work! Team composed of a doctor and two RN s Each team gets six rooms in the main ED with 2 flex beds when needed Manage your own area Code rooms flexible for any team Liked because loaded with 3 patients initially, but tapered at the end so home on time See many more patients than a traditional system (c) Murrell 2015
70 Team Assignment System Brief Triage Green Team Beds (c) Murrell 2015 Patient Arrives
71 Open Data First we met together as a group and decided goals Then, worked on systems so MD s could reach goals without heroics Staff meeting discussed efficiency tips and shared our best practices Efficiency balanced with quality, patient satisfaction (c) Murrell 2015
 Murrell")
72 Open data Metrics are not random: chosen to CREATE THE CAPACITY we need to see our patients and eliminate waiting times (c) Murrell 2015
73 Results: standard deviation narrowed, length of stay decreased
74 Results No push-back MD s requesting more data Want to add nursing and tech data in as well (c) Murrell 2015
")
75 Open Data Results (c) Murrell 2015

76 Open Data Impact Studied
 Murrell")
77 Many Hospitals: War between ED & Inpatient (c) Murrell 2015


78 What we want Teamwork Smooth Flow
79 Solution: ED presence to improve hospital flow Found a partner on the floor who wanted to make things better Wanted to go beyond the traditional meetings without many results The two of us decided to sponsor a series of Kaizen events with ED/Floor participation (c) Murrell 2015

")
80 Bed Hub An assigned person who focused on placement of patients (c) Murrell 2015
81 Same Vision: Patients Do Not Wait Daily bed huddle with ED and Floor Nursing leadership MD participation when beds are tight Use a predictive model to anticipate admissions: we know they are coming, we just don t know their names RN/PCC s predict the discharges Main result: ownership for the patients waiting in the ED
 Murrell 2015")
82 Look at Every Step Improving the report to the floor Kaizen event to standardize the reporting process and prevent repeat calls Frontline staff helping to drive the process (c) Murrell 2015
83 Example of Improvement (c) Murrell 2015
84 Other Possibilities Intermediate Medicine Observation Unit Standardized Protocols for the 48 hour patient Congestive heart failure COPD exacerbation Non-critical Sepsis

85 Rapid Surgical Unit Created in six weeks after a winter summit Same principles: standardize care, decrease length of stay But better for patients, easier for staff


86
 Murrell")
87 What to do when there is just not enough room (c) Murrell 2015
 Murrell")
88 We don t have to be surprised (c) Murrell 2015

89 The Unexpected Will Always Happen (c) Murrell 2015
")
90 Standardized Overcrowding Score (c) Murrell 2015
")
91 Visible to all employees (c) Murrell 2015
 Murrell")
92 Linked to a surge plan (c) Murrell 2015
93 Technology Now linked to a phone app Automatically sends updates Monitors if actions are completed Creates transparency & accountability
94 Other Ideas The Scheduled Hospital Stay Improved Discharge Process Prepped the day before Pharmacy delivers to room Discharge lounge Medical Directors for Each Unit

95 Our Final Truths! The longer they stay the more work they are The deeper they get the longer they stay (c) Murrell 2015
")
96 Most of all a culture of patient centered innovation and flow (c) Murrell 2015

97 (c) Murrell 2015
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
How can we provide the same world class care to patients with psychiatric disorders? 11/27/2016. Dec 2016 Orlando, FL
 The presenters have nothing to disclose Transforming Emergency Psychiatry Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Hospital
The presenters have nothing to disclose Transforming Emergency Psychiatry Karen Murrell, MD, MBA, FACEP Physician Lead-Emergency Medicine, Kaiser Northern California Assistant Physician in Chief- Hospital
Improving ED Flow through the UMLN II
 Improving ED Flow through the UMLN II Good Samaritan Hospital Medical Center West Islip, NY 437 beds, 50 ED beds http://www.goodsamaritan.chsli.org Good Samaritan Hospital Medical Center, a member of Catholic
Improving ED Flow through the UMLN II Good Samaritan Hospital Medical Center West Islip, NY 437 beds, 50 ED beds http://www.goodsamaritan.chsli.org Good Samaritan Hospital Medical Center, a member of Catholic
Emergency Department Patient Flow Strategies. University of Maryland Medical Center
 Emergency Department Patient Flow Strategies University of Maryland Medical Center Medical Admitting Officer Attending Hospitalist Hours: 9a 11p Mon Friday Goal to partner with ED team and provide oversight
Emergency Department Patient Flow Strategies University of Maryland Medical Center Medical Admitting Officer Attending Hospitalist Hours: 9a 11p Mon Friday Goal to partner with ED team and provide oversight
Publication Year: 2013
 THE INITIAL ASSESSMENT PROCESS ST. JOSEPH'S HEALTHCARE HAMILTON Publication Year: 2013 Summary: The Initial Assessment Process (IAP) was developed collaboratively by the emergency physicians, nursing,
THE INITIAL ASSESSMENT PROCESS ST. JOSEPH'S HEALTHCARE HAMILTON Publication Year: 2013 Summary: The Initial Assessment Process (IAP) was developed collaboratively by the emergency physicians, nursing,
Fast Track Development at Aultman Hospital
 Fast Track Development at Aultman Hospital Academy for Excellence in Healthcare IAP C-12 Aultman Jan. 17, 2018 fisher.osu.edu 1 Fast Track Development Aultman Hospital improves ED turnaround times, patient
Fast Track Development at Aultman Hospital Academy for Excellence in Healthcare IAP C-12 Aultman Jan. 17, 2018 fisher.osu.edu 1 Fast Track Development Aultman Hospital improves ED turnaround times, patient
Observation Unit. Romil Chadha
 Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
An academic medical center is practicing wasteology to pare time, expense,
 Quality improvement Practicing wasteology in the OR An academic medical center is practicing wasteology to pare time, expense, and hassle from its OR processes. Using lean thinking, the center is streamlining
Quality improvement Practicing wasteology in the OR An academic medical center is practicing wasteology to pare time, expense, and hassle from its OR processes. Using lean thinking, the center is streamlining
Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA
 These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, Mike Williams, MPH/HSA The Abaris Group
 NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
NEW INNOVATIONS TO IMPROVE PATIENT FLOW IN THE ED AND HOSPITAL OCTOBER 12, 2010 Mike Williams, MPH/HSA The Abaris Group Outline Page 2 1. Top Innovations ED and Hospital 2. Top Barriers 3. Steps to Eliminate
Brent Treichler, M.D., FACEP Assistant Professor, UT Southwestern Department of Surgery, Division of Emergency Medicine Chief of Emergency Services,
 Brent Treichler, M.D., FACEP Assistant Professor, UT Southwestern Department of Surgery, Division of Emergency Medicine Chief of Emergency Services, Parkland Health and Hospital System September 13, 2010
Brent Treichler, M.D., FACEP Assistant Professor, UT Southwestern Department of Surgery, Division of Emergency Medicine Chief of Emergency Services, Parkland Health and Hospital System September 13, 2010
Healthcare Finance Management Association: Continuous Improvement Foundations
 Like us on Facebook and enjoy some helpful downloads and connections Continuous Improvement Solutions, LLC 8801 Bethnal Rd., Bella Vista, AR 72714 479.685.8380 cisolutionsllp@gmail.com Chad Smith: Trainer,
Like us on Facebook and enjoy some helpful downloads and connections Continuous Improvement Solutions, LLC 8801 Bethnal Rd., Bella Vista, AR 72714 479.685.8380 cisolutionsllp@gmail.com Chad Smith: Trainer,
San Diego County 4 th Annual Overcrowding Summit. Roneet Lev, MD, FACEP
 San Diego County 4 th Annual Overcrowding Summit Roneet Lev, MD, FACEP Agenda Purpose of this conference Improve ED Care in San Diego County Inspire Ideas Learn from each others to improve care Collegiality
San Diego County 4 th Annual Overcrowding Summit Roneet Lev, MD, FACEP Agenda Purpose of this conference Improve ED Care in San Diego County Inspire Ideas Learn from each others to improve care Collegiality
South Warwickshire s Whole System Approach Transforms Emergency Care. South Warwickshire NHS Foundation Trust
 South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS Foundation Trust South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS
South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS Foundation Trust South Warwickshire s Whole System Approach Transforms Emergency Care South Warwickshire NHS
9/15/2017 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE LEARNING OBJECTIVES
 THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
THROUGHPUT. IT S NOT JUST AN EMERGENCY DEPARTMENT ISSUE D O N N A C R I M M I N S - B O N N E L L, B S N, M H S M, C P H Q, L S S G B LEARNING OBJECTIVES 1) Define who is affected by inefficiency in throughput
LWOT Reduction Plan Success Story: Advocate Trinity Hospital
 LWOT Reduction Plan Success Story: Advocate Trinity Hospital Draft Submitted Jan. 6, 2011 Jacquelyn Whitten, DNP, RN Kimberly McIntyre, EdD(c), MSN, RN Julian M. Magdaleno, MS February 19, 2012 The Leaving
LWOT Reduction Plan Success Story: Advocate Trinity Hospital Draft Submitted Jan. 6, 2011 Jacquelyn Whitten, DNP, RN Kimberly McIntyre, EdD(c), MSN, RN Julian M. Magdaleno, MS February 19, 2012 The Leaving
IHI Open School Advanced Case Study October 14, 2010 Clemson University
 IHI Open School Advanced Case Study October 14, 2010 Clemson University Catherine Simmons 1, Drew Sargent 1, and Kate Wright 1 Public Health Science Hallie Bagnal 2 and Megan Hohenberger 2 Biological Science
IHI Open School Advanced Case Study October 14, 2010 Clemson University Catherine Simmons 1, Drew Sargent 1, and Kate Wright 1 Public Health Science Hallie Bagnal 2 and Megan Hohenberger 2 Biological Science
EMERGENCY DEPARTMENT CASE MANAGEMENT
 EMERGENCY DEPARTMENT CASE MANAGEMENT By Linda Sallee, Haley Rhodes, Sapna Patel, Cathleen Trespasz Healthcare consumers are becoming more empowered to have healthcare on their terms. With telemedicine,
EMERGENCY DEPARTMENT CASE MANAGEMENT By Linda Sallee, Haley Rhodes, Sapna Patel, Cathleen Trespasz Healthcare consumers are becoming more empowered to have healthcare on their terms. With telemedicine,
Improving Pain Center Processes utilizing a Lean Team Approach
 Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
ED crowding: Causes, Consequences, Solutions
 ED crowding: Causes, Consequences, Solutions Jesse M. Pines, MD, MBA, MSCE Associate Professor of Emergency Medicine and Health Policy George Washington University Urgent Matters Webinar April 23, 2010
ED crowding: Causes, Consequences, Solutions Jesse M. Pines, MD, MBA, MSCE Associate Professor of Emergency Medicine and Health Policy George Washington University Urgent Matters Webinar April 23, 2010
"Pull Don't Push A Paradigm Shift for Patient Throughput" Elizabeth Carlton, RN, MSN, CCRN-K, CPHQ The University of Kansas Hospital
 "Pull Don't Push A Paradigm Shift for Patient Throughput" Elizabeth Carlton, RN, MSN, CCRN-K, CPHQ The University of Kansas Hospital The University of Kansas Hospital Leading the Nation in Caring, Healing,
"Pull Don't Push A Paradigm Shift for Patient Throughput" Elizabeth Carlton, RN, MSN, CCRN-K, CPHQ The University of Kansas Hospital The University of Kansas Hospital Leading the Nation in Caring, Healing,
Engaging Frontline Staff in Real-Time Improvement
 Engaging Frontline Staff in Real-Time Improvement Sharon Mann and Jennifer Phillips Session Code C6 These presenters have nothing to disclose Institute for Healthcare Improvement December 2013 2012 2013
Engaging Frontline Staff in Real-Time Improvement Sharon Mann and Jennifer Phillips Session Code C6 These presenters have nothing to disclose Institute for Healthcare Improvement December 2013 2012 2013
10 Things To Know About
 10 Things To Know About Nurse Call 100% Nurse Approved 10 Things to Know About Nurse Call in 2016 Nurse call systems have evolved. Today s nurse call systems provide front-line nurses with critical communications
10 Things To Know About Nurse Call 100% Nurse Approved 10 Things to Know About Nurse Call in 2016 Nurse call systems have evolved. Today s nurse call systems provide front-line nurses with critical communications
Building a Smarter Healthcare System The IE s Role. Kristin H. Goin Service Consultant Children s Healthcare of Atlanta
 Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Building a Smarter Healthcare System The IE s Role Kristin H. Goin Service Consultant Children s Healthcare of Atlanta 2 1 Background 3 Industrial Engineering The objective of Industrial Engineering is
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Real Time Demand Capacity Surge Planning
 This presenter has nothing to disclose. Real Time Demand Capacity Surge Planning Katharine Luther, RN, MPM April 6, 2016 Theoretical Frameworks P2 Queuing Theory Compression wave Framework P3 Resar,, Roger
This presenter has nothing to disclose. Real Time Demand Capacity Surge Planning Katharine Luther, RN, MPM April 6, 2016 Theoretical Frameworks P2 Queuing Theory Compression wave Framework P3 Resar,, Roger
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
TEAM ASSESSMENT PULL PROCESS CHILDREN S HEALTHCARE OF ATLANTA AT SCOTTISH RITE
 Publication Year: 2011 TEAM ASSESSMENT PULL PROCESS CHILDREN S HEALTHCARE OF ATLANTA AT SCOTTISH RITE Summary: The Team Assessment Pull Process (TAPP) is a technique to redesign emergency department patient
Publication Year: 2011 TEAM ASSESSMENT PULL PROCESS CHILDREN S HEALTHCARE OF ATLANTA AT SCOTTISH RITE Summary: The Team Assessment Pull Process (TAPP) is a technique to redesign emergency department patient
University of Michigan Emergency Department
 University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
Same day emergency care: clinical definition, patient selection and metrics
 Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Perfecting Emergency Department Operations
 These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
These presenters have nothing to disclose Perfecting Emergency Department Operations Kirk Jensen, MD, MBA, FACEP Jody Crane, MD, MBA, FACEP Karen Murrell, MD, MBA Kevin, MStat, MA April 28-29, 2015 Cambridge,
Looking at Patient Flow in Hours and Days
 This presenter has nothing to disclose Looking at Patient Flow in Hours and Days Getting Patients to the Right Level of Care at the Right Time October 23, 2014 Session Objectives Understand the differences
This presenter has nothing to disclose Looking at Patient Flow in Hours and Days Getting Patients to the Right Level of Care at the Right Time October 23, 2014 Session Objectives Understand the differences
The Nuts and Bolts of Setting Up an ED Observation Unit
 The Nuts and Bolts of Setting Up an ED Observation Unit Michael A. Ross MD FACEP Professor of Emergency Medicine Emory University School of Medicine Medical Director Observation Medicine Atlanta, Georgia
The Nuts and Bolts of Setting Up an ED Observation Unit Michael A. Ross MD FACEP Professor of Emergency Medicine Emory University School of Medicine Medical Director Observation Medicine Atlanta, Georgia
Eliminating Common PACU Delays
 Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
Results from Contra Costa Regional Medical Center
 Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
Results from Contra Costa Regional Medical Center Karin Stryker, MBA DSRIP Manager, Health Services Administrator Chris Farnitano, MD Medical Director, Ambulatory Care High Impact Interventions Sepsis
The Use of a Clinical Decision Area in the Emergency Managing ED Observation with Clinical Decision Areas Department to Reduce Length of Stay
 The Use of a Clinical Decision Area in the Emergency Managing ED Observation with Clinical Decision Areas Department to Reduce Length of Stay Rose Colangelo Manager, ED Scripps Memorial Hospital Objectives
The Use of a Clinical Decision Area in the Emergency Managing ED Observation with Clinical Decision Areas Department to Reduce Length of Stay Rose Colangelo Manager, ED Scripps Memorial Hospital Objectives
MERCY MEDICAL CENTER. Mercy Medical Center Improves Patient Care, Lowers Costs with the Hospital Operating System
 MERCY MEDICAL CENTER Mercy Medical Center Improves Patient Care, Lowers Costs with the Hospital Operating System Success Snapshot Reduced acute LOS from 4.6 to 3.74 and observation LOS from 1.51 to 1.31
MERCY MEDICAL CENTER Mercy Medical Center Improves Patient Care, Lowers Costs with the Hospital Operating System Success Snapshot Reduced acute LOS from 4.6 to 3.74 and observation LOS from 1.51 to 1.31
Chest Pain Accredited. Transplant Program-Heart, Kidney, Liver. Hear Transplant Program serving San Antonio area for 25 years
 PUTTING THE PATIENT FIRST IN PATIENT PLACEMENT 8 Hospital System, 1 Freestanding ED Provide healthcare to 26 surrounding counties within South Texas International Transfer Services Methodist Healthcare
PUTTING THE PATIENT FIRST IN PATIENT PLACEMENT 8 Hospital System, 1 Freestanding ED Provide healthcare to 26 surrounding counties within South Texas International Transfer Services Methodist Healthcare
Partnerships- Cooperation with other care providers that is guided by open communication, trust, and shared decision-making.
 1 E P 7: Describe and demonstrate the structure(s) and process(es) used to engage internal experts and external consultants to improve care in the practice setting. When Riverside nurses from any level
1 E P 7: Describe and demonstrate the structure(s) and process(es) used to engage internal experts and external consultants to improve care in the practice setting. When Riverside nurses from any level
Building healthy communities. together. San Joaquin Valley Insurance Authority. Anthem Blue Cross
 Building healthy communities together San Joaquin Valley Insurance Authority Anthem Blue Cross San Joaquin Valley Insurance Authority Medical-Health & Wellness Summary Findings and Recommendations Findings
Building healthy communities together San Joaquin Valley Insurance Authority Anthem Blue Cross San Joaquin Valley Insurance Authority Medical-Health & Wellness Summary Findings and Recommendations Findings
Flex Care : An Integrated Care Delivery Approach for Low Acuity Patients Presenting to the ED
 Flex Care : An Integrated Care Delivery Approach for Low Acuity Patients Presenting to the ED Stuart M. Levine, MD, FACP President and Chief Medical Officer MedStar Harbor Hospital 1 Introduction CY17
Flex Care : An Integrated Care Delivery Approach for Low Acuity Patients Presenting to the ED Stuart M. Levine, MD, FACP President and Chief Medical Officer MedStar Harbor Hospital 1 Introduction CY17
The Impact of Emergency Department Use on the Health Care System in Maryland. Deborah E. Trautman, PhD, RN
 The Impact of Emergency Department Use on the Health Care System in Maryland Deborah E. Trautman, PhD, RN The Future of Emergency Care in the United States Health System Institute of Medicine June 2006
The Impact of Emergency Department Use on the Health Care System in Maryland Deborah E. Trautman, PhD, RN The Future of Emergency Care in the United States Health System Institute of Medicine June 2006
Objectives. Emergency Medicine Risk Factors
 The Uniqueness of Emergency Medicine Risk Management W. Peter Vellman, MD, FACEP Serio Physician Management, LLC Littleton, CO Objectives Recognize key areas impacting the provision of emergency medical
The Uniqueness of Emergency Medicine Risk Management W. Peter Vellman, MD, FACEP Serio Physician Management, LLC Littleton, CO Objectives Recognize key areas impacting the provision of emergency medical
SFGH. Management System. Components. SFGH Management System. Improvement. Time. Strategic Planning True North. Value Streams: Rapid Improvement Events
 SFGH Management System 1 SFGH Management System Components Strategic Planning True North Improvement Management System Value Streams: Rapid Improvement Events Time 2 1 Refining our Strategic Planning PATIENT
SFGH Management System 1 SFGH Management System Components Strategic Planning True North Improvement Management System Value Streams: Rapid Improvement Events Time 2 1 Refining our Strategic Planning PATIENT
Chat with a Doctor: On-Demand, Asynchronous Physician Advice
 Chat with a Doctor: On-Demand, Asynchronous Physician Advice Session 189: March 7, 2018 Ari Melmed, MD, FACEP Assistant Regional Director for Telehealth, Colorado Permanente Medical Group 1 Conflict of
Chat with a Doctor: On-Demand, Asynchronous Physician Advice Session 189: March 7, 2018 Ari Melmed, MD, FACEP Assistant Regional Director for Telehealth, Colorado Permanente Medical Group 1 Conflict of
Riverside s Vigilance Care Delivery Systems include several concepts, which are applicable to staffing and resource acquisition functions.
 1 EP8: Describe and demonstrate how nurses used trended data to formulate the staffing plan and acquire necessary resources to assure consistent application of the Care Delivery System(s). Riverside Medical
1 EP8: Describe and demonstrate how nurses used trended data to formulate the staffing plan and acquire necessary resources to assure consistent application of the Care Delivery System(s). Riverside Medical
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE
 EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
EXPANDING MENTAL HEALTH SERVICES AND THE BOTTOM LINE Theresa Hyer, Rideout Health Eric Zeller, M.D., CEP America Moderated by Sheree Lowe, California Hospital Association TOPICS FOR TODAY Overview of the
DIVISION OF EMERGENCY MEDICINE DEPARTMENT OF ACUTE MEDICINE
 DIVISION OF EMERGENCY MEDICINE DEPARTMENT OF ACUTE MEDICINE Ambulatory Care Unit Standard Operational Policy Document Control Reference No: First published: November 2014 Version: 004 Current Version Published:
DIVISION OF EMERGENCY MEDICINE DEPARTMENT OF ACUTE MEDICINE Ambulatory Care Unit Standard Operational Policy Document Control Reference No: First published: November 2014 Version: 004 Current Version Published:
Capital Zone Emergency Services Council CZESC
 Capital Zone Emergency Services Council CZESC Quarterly Report Quarter 4 (October to December 2015) With focus on the Emergency Departments of Cobequid Community Health Centre And Hants Community Hospital
Capital Zone Emergency Services Council CZESC Quarterly Report Quarter 4 (October to December 2015) With focus on the Emergency Departments of Cobequid Community Health Centre And Hants Community Hospital
Consultation Paper. Distributed Medical Imaging in the new Royal Adelaide Hospital Central Adelaide Local Health Network
 Consultation Paper Distributed Medical Imaging in the new Royal Adelaide Hospital Central Adelaide Local Health Network Issued: April 2016 TABLE OF CONTENTS TABLE OF CONTENTS 2 1. INTRODUCTION 3 2. PURPOSE
Consultation Paper Distributed Medical Imaging in the new Royal Adelaide Hospital Central Adelaide Local Health Network Issued: April 2016 TABLE OF CONTENTS TABLE OF CONTENTS 2 1. INTRODUCTION 3 2. PURPOSE
Capital Zone Emergency Services Council CZESC
 Capital Zone Emergency Services Council CZESC Quarterly Report Quarter 4 (October to December 2016) With focus on the Emergency Departments of Cobequid Community Health Centre And Hants Community Hospital
Capital Zone Emergency Services Council CZESC Quarterly Report Quarter 4 (October to December 2016) With focus on the Emergency Departments of Cobequid Community Health Centre And Hants Community Hospital
Observation Coding and Billing Compliance Montana Hospital Association
 Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
UW MEDICINE PATIENT EDUCATION. Angiography: Kidney Exam. How to prepare and what to expect. What is angiography? DRAFT. Why do I need this exam?
 UW MEDICINE PATIENT EDUCATION Angiography: Kidney Exam How to prepare and what to expect This handout explains how to prepare and what to expect when having a kidney exam using angiography. What is angiography?
UW MEDICINE PATIENT EDUCATION Angiography: Kidney Exam How to prepare and what to expect This handout explains how to prepare and what to expect when having a kidney exam using angiography. What is angiography?
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING
 JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
JULY 2012 RE-IMAGINING CARE DELIVERY: PUSHING THE BOUNDARIES OF THE HOSPITALIST MODEL IN THE INPATIENT SETTING About The Chartis Group The Chartis Group is an advisory services firm that provides management
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health
 REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
Enhancing Efficiency and Communication in Perioperative Services Through Technology
 Enhancing Efficiency and Communication in Perioperative Services Through Technology Linda Yoder, RN, BSN, MBA, Clinical Director, Perioperative Services, GI Lab, Cross Creek Ambulatory Center Every driver
Enhancing Efficiency and Communication in Perioperative Services Through Technology Linda Yoder, RN, BSN, MBA, Clinical Director, Perioperative Services, GI Lab, Cross Creek Ambulatory Center Every driver
PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November 2017
 Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Report Contents: PATIENT CARE SERVICES REPORT Submitted to the Joint Conference Committee, November By: Terry Dentoni, MSN, RN, CNL - ZSFG Chief Nursing Officer 1. Professional Nursing.....1 2. Emergency
Increase Your Bottom Line by Eliminating Physician Driven Denials. Olakunle Olaniyan MD President Case Management Covenants
 Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
The Path to Sustainable Improvements
 What Do You Do When Your Improvement Project FAILS? The Path to Sustainable Improvements Thursday, March 3, 2016 10:00 AM Reza Ziaee, MA, MSE, MBB, PhD, FHIMSS - Antelope Valley Hospital James Bologna
What Do You Do When Your Improvement Project FAILS? The Path to Sustainable Improvements Thursday, March 3, 2016 10:00 AM Reza Ziaee, MA, MSE, MBB, PhD, FHIMSS - Antelope Valley Hospital James Bologna
Secure Texting. and Care Alerts. CCN Member Resource Briefing II July 2017
 Secure Texting u and Care Alerts CCN Member Resource Briefing II July 2017 1 What We ll Cover After this module, you ll know more about: 1. What secure texting is, and how you and your practice can get
Secure Texting u and Care Alerts CCN Member Resource Briefing II July 2017 1 What We ll Cover After this module, you ll know more about: 1. What secure texting is, and how you and your practice can get
Using Lean Principles to Decrease Outpatient Registration Wait Times. It s a Journey not a Destination
 Using Lean Principles to Decrease Wait Times It s a Journey not a Destination 533 Bed Acute Care System 461 Beds at AnMed Health Medical Center 72 Beds at AnMed Health Women s and Children's Hospital 45
Using Lean Principles to Decrease Wait Times It s a Journey not a Destination 533 Bed Acute Care System 461 Beds at AnMed Health Medical Center 72 Beds at AnMed Health Women s and Children's Hospital 45
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
QAPI Making An Improvement
 Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
Managing Queues: Door-2-Exam Room Process Mid-Term Proposal Assignment
 Concept/Objectives Managing Queues: Door--Exam Process Mid-Term Proposal ssignment Children s Healthcare of tlanta (CHO has plans to build a new facility that will be over 00,000 sq. ft., and they are
Concept/Objectives Managing Queues: Door--Exam Process Mid-Term Proposal ssignment Children s Healthcare of tlanta (CHO has plans to build a new facility that will be over 00,000 sq. ft., and they are
Clinical and Financial Successes at Advocate Health Care Utilizing our
 Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program June 2, 2016 Cindy Welsh, RN, MBA, FACHE VP for Critical Care and Medical Professional Affairs Advocate Health Care
LAC+USC Healthcare Network 1707 E Highland, Suite North State Street
 Proceedings of the 2008 Winter Simulation Conference S. J. Mason, R. R. Hill, L. Mönch, O. Rose, T. Jefferson, J. W. Fowler eds. DISCRETE EVENT SIMULATION: OPTIMIZING PATIENT FLOW AND REDESIGN IN A REPLACEMENT
Proceedings of the 2008 Winter Simulation Conference S. J. Mason, R. R. Hill, L. Mönch, O. Rose, T. Jefferson, J. W. Fowler eds. DISCRETE EVENT SIMULATION: OPTIMIZING PATIENT FLOW AND REDESIGN IN A REPLACEMENT
Improve the Efficiency and Service of the Emergency Room at North Side Hospital
 Improve the Efficiency and Service of the Emergency Room at North Side Hospital John Melton, VP and CEO Washington County Operations meltonjw@msha.com Kerry Vermillion, CFO Washington County Operations
Improve the Efficiency and Service of the Emergency Room at North Side Hospital John Melton, VP and CEO Washington County Operations meltonjw@msha.com Kerry Vermillion, CFO Washington County Operations
Putting It All Together: Strategies to Achieve System-Wide Results
 1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
1 Putting It All Together: Strategies to Achieve System-Wide Results Katharine Luther, Lloyd Provost, Pat Rutherford Hospital Flow Professional Development Program April 4-7, 2016 Cambridge, MA Session
TeleCardiology Platform
 TeleCardiology Platform Michael GeRue MSN, COO Parkview Heart Institute October 21, 2017 Disclosures None TeleCardiology Telehealth fits into the IHI Triple Aim: Patient experience Less travel time, easier
TeleCardiology Platform Michael GeRue MSN, COO Parkview Heart Institute October 21, 2017 Disclosures None TeleCardiology Telehealth fits into the IHI Triple Aim: Patient experience Less travel time, easier
Pearls for Swing and night shifts
 Pearls for Swing and night shifts Swing Attending Physicans Swing 1: 12p-11p. To help ATP and Swing 2 with admissions, ICU transfers and staff APP admissions. Will get the cross-cover pager (4951) at 7pm
Pearls for Swing and night shifts Swing Attending Physicans Swing 1: 12p-11p. To help ATP and Swing 2 with admissions, ICU transfers and staff APP admissions. Will get the cross-cover pager (4951) at 7pm
APPLICATION OF SIMULATION MODELING FOR STREAMLINING OPERATIONS IN HOSPITAL EMERGENCY DEPARTMENTS
 APPLICATION OF SIMULATION MODELING FOR STREAMLINING OPERATIONS IN HOSPITAL EMERGENCY DEPARTMENTS Igor Georgievskiy Alcorn State University Department of Advanced Technologies phone: 601-877-6482, fax:
APPLICATION OF SIMULATION MODELING FOR STREAMLINING OPERATIONS IN HOSPITAL EMERGENCY DEPARTMENTS Igor Georgievskiy Alcorn State University Department of Advanced Technologies phone: 601-877-6482, fax:
Psychiatric Patient Boarding Problems in the Emergency Department
 Psychiatric Patient Boarding Problems in the Emergency Department IMPROVING TIMELINESS, ACCESS, AND QUALITY LOWERING COSTS AND RE-HOSPITALIZATIONS Scott Zeller, MD Chief, Psychiatric Emergency Services
Psychiatric Patient Boarding Problems in the Emergency Department IMPROVING TIMELINESS, ACCESS, AND QUALITY LOWERING COSTS AND RE-HOSPITALIZATIONS Scott Zeller, MD Chief, Psychiatric Emergency Services
ED Facility Design and Informatics. Disclosure Information. Stock Ownership Forerun. Objectives. A Must Have Book. Estimating Treatment Spaces
 ED Facility Design and Informatics Cambridge Health Alliance Harvard Medical School Cambridge, MA Disclosure Information Stock Ownership Forerun Objectives A Must Have Book! Review planning considerations
ED Facility Design and Informatics Cambridge Health Alliance Harvard Medical School Cambridge, MA Disclosure Information Stock Ownership Forerun Objectives A Must Have Book! Review planning considerations
Grand River Hospital and St Mary s General Hospital Increases Throughput, Cuts Costs using Lean
 LEAN CASE STUDY: Grand River Hospital and St Mary s General Hospital Increases Throughput, Cuts Costs using Lean In healthcare today, having to do more with less goes with the territory. Volumes are increasing
LEAN CASE STUDY: Grand River Hospital and St Mary s General Hospital Increases Throughput, Cuts Costs using Lean In healthcare today, having to do more with less goes with the territory. Volumes are increasing
Julie Kelley, MSW, MPH Program Chief, Mental Heath/Psychiatry Contra Costa Regional Medical Center Martinez, CA
 Julie Kelley, MSW, MPH Program Chief, Mental Heath/Psychiatry Contra Costa Regional Medical Center Martinez, CA Patients and Families as Care Partners April 20, 2011 Little about us Contra Costa Regional
Julie Kelley, MSW, MPH Program Chief, Mental Heath/Psychiatry Contra Costa Regional Medical Center Martinez, CA Patients and Families as Care Partners April 20, 2011 Little about us Contra Costa Regional
Part 4. Change Concepts for Improving Adult Cardiac Surgery. In this section, you will learn a group. of change concepts that can be applied in
 Change Concepts for Improving Adult Cardiac Surgery Part 4 In this section, you will learn a group of change concepts that can be applied in different ways throughout the system of adult cardiac surgery.
Change Concepts for Improving Adult Cardiac Surgery Part 4 In this section, you will learn a group of change concepts that can be applied in different ways throughout the system of adult cardiac surgery.
Using Quality Improvement to Optimize Pediatric Discharge Efficiency
 This presenter has nothing to disclose Using Quality Improvement to Optimize Pediatric Discharge Efficiency Christine White MD, MAT Associate Professor-Hospital Medicine Cincinnati Children s Hospital
This presenter has nothing to disclose Using Quality Improvement to Optimize Pediatric Discharge Efficiency Christine White MD, MAT Associate Professor-Hospital Medicine Cincinnati Children s Hospital
The Impact of Pre Hospital Blood Collection on Time to Laboratory Test Results and Emergency Department Length of Stay
 The Impact of Pre Hospital Blood Collection on Time to Laboratory Test Results and Emergency Department Length of Stay Improving the Odds on Quality Las Vegas, Nevada January 25 27, 2012 Principal Investigator:
The Impact of Pre Hospital Blood Collection on Time to Laboratory Test Results and Emergency Department Length of Stay Improving the Odds on Quality Las Vegas, Nevada January 25 27, 2012 Principal Investigator:
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring
 Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Capital Zone Emergency Services Council CZESC
 Capital Zone Emergency Services Council CZESC Quarterly Report Quarter 2 (April to June 2016) With focus on the Emergency Department of Dartmouth General Hospital and Collaborative Emergency Centres of
Capital Zone Emergency Services Council CZESC Quarterly Report Quarter 2 (April to June 2016) With focus on the Emergency Department of Dartmouth General Hospital and Collaborative Emergency Centres of
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
VENICE FAMILY CLINIC: Improving capacity and managing patient lead times
 CASE STUDY, 4/12 VENICE FAMILY CLINIC: Improving capacity and managing patient lead times PREPARED BY Professor Kumar Rajaram, UCLA Anderson School of Management Karen Conner, MD, UCLA David Geffen School
CASE STUDY, 4/12 VENICE FAMILY CLINIC: Improving capacity and managing patient lead times PREPARED BY Professor Kumar Rajaram, UCLA Anderson School of Management Karen Conner, MD, UCLA David Geffen School
Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance?
 Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance? Betty Bibbins, MD, CHC, CPEHR, CPHIT President & Chief Medical Officer Website:
Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance? Betty Bibbins, MD, CHC, CPEHR, CPHIT President & Chief Medical Officer Website:
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program
 Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program April 30, 2016 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate Health
Clinical and Financial Successes at Advocate Health Care Utilizing our Tele-ICU Program April 30, 2016 Michael Ries, MD, MBA, FCCM, FCCP, FACP Medical Director Adult Critical Care and eicu Advocate Health
BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL
 Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Publication Year: 2004 BEDSIDE REGISTRATION CAPE CANAVERAL HOSPITAL Summary: Cape Canaveral hospital implemented a streamlined bedside registration process in order to reduce the time patients spent waiting
Thinking of Going Lean? A 360-degree view of changing the culture of a healthcare system through a Lean Transformation
 Thinking of Going Lean? A 360-degree view of changing the culture of a healthcare system through a Lean Transformation AHA Leadership Summit Thursday, July 27, 2017 Please note that the views expressed
Thinking of Going Lean? A 360-degree view of changing the culture of a healthcare system through a Lean Transformation AHA Leadership Summit Thursday, July 27, 2017 Please note that the views expressed
Definitions and Regulatory Considerations
 Observation Medicine Mark G. Moseley, MD, MHA, FACEP Associate Professor of Emergency Medicine Medical Director for Emergency Services Department of Emergency Medicine The Ohio State University Medical
Observation Medicine Mark G. Moseley, MD, MHA, FACEP Associate Professor of Emergency Medicine Medical Director for Emergency Services Department of Emergency Medicine The Ohio State University Medical
Ascom GRADY MEMORIAL LEVERAGES ASCOM TO IMPROVE HCAHPS SCORES
 Customer: Grady Health System Solution: Ascom i62 VoWiFi handsets, Medamax GRADY MEMORIAL LEVERAGES ASCOM TO IMPROVE HCAHPS SCORES Questions About Ascom Wireless Solutions? Learn more about dependable
Customer: Grady Health System Solution: Ascom i62 VoWiFi handsets, Medamax GRADY MEMORIAL LEVERAGES ASCOM TO IMPROVE HCAHPS SCORES Questions About Ascom Wireless Solutions? Learn more about dependable
ED Care Triage: Linkage to Primary Care
 ED Care Triage: Linkage to Primary Care BEST PRACTICES SUMMARY Updated 4/17/2017 ONECITY HEALTH SERVICES 199 Water Street, 31st Floor, New York, NY 10038 EXECUTIVE SUMMARY The goal of the ED Care Triage
ED Care Triage: Linkage to Primary Care BEST PRACTICES SUMMARY Updated 4/17/2017 ONECITY HEALTH SERVICES 199 Water Street, 31st Floor, New York, NY 10038 EXECUTIVE SUMMARY The goal of the ED Care Triage
Improving Patient Experience, Safety and Progression through Care Model Redesign & Lean Management
 Improving Patient Experience, Safety and Progression through Care Model Redesign & Lean Management Michelle Cline, RN, MSN, Care Model Redesign Manager Donna Litwinski, PT, Master Lean Fellow April 2018
Improving Patient Experience, Safety and Progression through Care Model Redesign & Lean Management Michelle Cline, RN, MSN, Care Model Redesign Manager Donna Litwinski, PT, Master Lean Fellow April 2018
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Decrease Doc-to-Decision Times for Major EMS Patients at Mount Carmel East
 Decrease Doc-to-Decision Times for Major EMS Patients at Mount Carmel East Academy for Excellence in Healthcare IAP C-08 MCE Sept. 14, 2016 fisher.osu.edu 1 Decrease Doc-to-Decision Times for Major EMS
Decrease Doc-to-Decision Times for Major EMS Patients at Mount Carmel East Academy for Excellence in Healthcare IAP C-08 MCE Sept. 14, 2016 fisher.osu.edu 1 Decrease Doc-to-Decision Times for Major EMS
Predictive Analytics and the Impact on Nursing Care Delivery
 Predictive Analytics and the Impact on Nursing Care Delivery Session 2, March 5, 2018 Whende M. Carroll, MSN, RN-BC - Director of Nursing Informatics, KenSci, Inc. Nancee Hofmeister, MSN, RN, NE-BC Senior
Predictive Analytics and the Impact on Nursing Care Delivery Session 2, March 5, 2018 Whende M. Carroll, MSN, RN-BC - Director of Nursing Informatics, KenSci, Inc. Nancee Hofmeister, MSN, RN, NE-BC Senior
ABC s of PES. Greg Miller, MD MBA CMO Unity Center for Behavioral Health
 ABC s of PES Greg Miller, MD MBA CMO Unity Center for Behavioral Health Content Outline Overview of Unity Services Emergency Psychiatry: Historical Perspective Emergency Psychiatry: Current Service Delivery
ABC s of PES Greg Miller, MD MBA CMO Unity Center for Behavioral Health Content Outline Overview of Unity Services Emergency Psychiatry: Historical Perspective Emergency Psychiatry: Current Service Delivery
Improving Patient Flow & Reducing Emergency Department (ED) Crowding
 Crowding") February 2010 URGENT MATTERS LEARNING NETWORK II ISSUE BRIEF 1 Improving Patient Flow & Reducing Emergency Department (ED) Crowding Robert Wood Johnson Foundation-Supported Learning Network of Hospitals
February 2010 URGENT MATTERS LEARNING NETWORK II ISSUE BRIEF 1 Improving Patient Flow & Reducing Emergency Department (ED) Crowding Robert Wood Johnson Foundation-Supported Learning Network of Hospitals
BETHESDA HEALTH. Commitment to Care: Partnering with Care Logistics to Adopt a Patient-First System for Care
 BETHESDA HEALTH Commitment to Care: Partnering with Care Logistics to Adopt a Patient-First System for Care Success Snapshot Commitment to Care transformation initiative has driven $11 million in annual
BETHESDA HEALTH Commitment to Care: Partnering with Care Logistics to Adopt a Patient-First System for Care Success Snapshot Commitment to Care transformation initiative has driven $11 million in annual
Moving the Needle on Hospital Throughput: Breaking Through the Status Quo. Session ID: 325
 Moving the Needle on Hospital Throughput: Breaking Through the Status Quo Session ID: 325 Objectives Objective 1: Demonstrate how two common strategies can be deployed to maximum benefit to support improvements
Moving the Needle on Hospital Throughput: Breaking Through the Status Quo Session ID: 325 Objectives Objective 1: Demonstrate how two common strategies can be deployed to maximum benefit to support improvements
MnCHOICES Assessment and Support Plan
 MnCHOICES Assessment and Support Plan 11/01/2017 Minnesota Department of Human Services mn.gov/dhs 1 Beyond Assessment: Integration of assessment and support plan application State and federal requirements
MnCHOICES Assessment and Support Plan 11/01/2017 Minnesota Department of Human Services mn.gov/dhs 1 Beyond Assessment: Integration of assessment and support plan application State and federal requirements
LEAN Transformation Storyboard 2015 to present
 LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,