NHS East Surrey Clinical Commissioning Group Annual Report and Accounts
|
|
|
- Doreen Willis
- 5 years ago
- Views:
Transcription

1 NHS East Surrey Clinical Commissioning Group Annual Report and Accounts
2 Contents Section 1 Performance Report: an overview... 4 Welcome... 5 Who we are and what we do... 7 Our vision... 7 Our mission statement... 7 Our strategic objectives... 7 Our strategic priorities for 2017/ The local health picture... 7 Healthcare providers... 8 Other key partners... 9 Better Care Fund (BCF)... 9 Collaborative commissioner arrangement Our challenges Sustainability and Transformation Plan (STP) Our achievements for the year Clinical Engagement Patient and public engagement Our ambitions for the future Section 2 Performance Report: analysis Performance Overview Overview of the East Surrey CCG Corporate Performance Management Framework Outcomes: The NHS Outcomes Framework Outcomes: NHS England Outcomes Tool Lagging and leading indicators Improving quality Domain 1: Preventing people from dying prematurely Domain 2: Enhancing quality of life for people with long-term conditions Domain 3: enhancing quality of life for people with long-term conditions and helping people to recover from episodes of ill health or following injury Domain 4: Patient Experience Domain 5: Patient Safety NHS Constitution: ensuring patient access to timely treatment Clinical Priorities Sustainable development Health and wellbeing strategy Quality premium Reducing inequality Section 3 Accountability Report Corporate Governance Report Members Report
3 Composition of Governing Body Register of Interests Governance Statement Other sources of assurance Review of the effectiveness of governance, risk management and internal control Remuneration and Staff Report Remuneration Report Staff Report Exit packages, including special (non-contractual) payments Statement of Accountable Officer s responsibilities Parliamentary Accountability and Audit Report Section 4 Head of Internal Audit Opinion Section 5 Annual Accounts Section 6 Independent Auditor s Report
4 Section 1 Performance Report: an overview 4
5 Welcome As we reach the end of our fourth year as a Clinical Commissioning Group (CCG), I am pleased to say that we are making significant progress in many of our priority areas for commissioning high quality patient services. The past year has continued to be very challenging with stringent turnaround demands placed on the CCG as a result of the special measures regime ( Strengthening financial performance and accountability ) that the CCG was placed under by NHS England in July 2016, following the unplanned financial losses that emerged early in the 2016/17 financial year, mainly as a result of unidentified / undeliverable Quality, Improvement, Productivity and Prevention (QIPP) financial efficiencies. The CCG agreed with NHS England a financial recovery plan of 7.4m in August, following the appointment of a new Interim Accountable Officer (AO) and Interim Chief Financial Officer (CFO) While turnaround requirements put additional constraints onto us, they have also given us a unique opportunity to re-evaluate our priorities and look at how we can commission the best services for our patients, which deliver the right healthcare, at the right time, by the right healthcare professional, and in the right environment. We strive to make best use of public funds and take every opportunity to improve the quality of services for our patients. We have listened to, involved and acted on feedback to improve services which have directly benefitted people in our community. Despite our challenging financial position, we have continued our relentless focus on quality of care and the resilience of health and care services. Working with our federated GP member practices, we have developed four geographically-based networks to support the development of primary care services at scale and to act as the building block for integration with other community-based providers. Our member GP practices have been enthusiastic about shaping the development of the networks as they recognise these can be a great platform for building more robust primary care services for our population for the future. We worked closely with our local partners to develop health services and have enjoyed regional and national recognition. With Surrey and Sussex Hospitals NHS Trust (SASH) we have been shortlisted for a 2017 HSJ award for our Inflammatory Bowel Disease service and our nursing home service was shortlisted for the Kent, Surrey and Sussex Academic Health Science Network (KSSAHSN) Innovation Award. As a clinician, I am pleased to see that despite the huge financial pressures we face, the commitment of our CCG staff and those working within the services we commission continues to enable them to excel. This year has seen much change for our organisation. We ve seen a change in top leadership, with a new Accountable Officer, a new Chief Financial Officer and the appointment of our Chief Operating Officer. Under this fresh leadership we have reorganised our delivery structure and increased overall numbers of staff to ensure a more resilient commissioning structure. This enabled us to increase the capacity to support the transformation of our health service to ensure it continues to deliver high quality health and care for our changing population. While as a CCG we have continued to focus on the immediate turnaround plan, we have played an active role in shaping our future as part of the Sussex and East Surrey Sustainability and Transformation Plan (STP) to ensure the long term sustainability of the 5



6 health and care services we commission for our patients. I would like to thank all of our patients and local partners who have worked with us during the year and to all our dedicated staff - we would not have achieved so much without your commitment and support. Dr Elango Vijaykumar Clinical Chair NHS East Surrey CCG 6
7 Who we are and what we do NHS East Surrey Clinical Commissioning Group (CCG) has statutory responsibility for planning and commissioning hospital, community and mental health services across the districts of Tandridge, Redhill, Reigate and Horley. 7 We are a GP-led organisation with a local focus and have built on the established strengths of our 18 GP member practices, to ensure patients are at the heart of what we do - commissioning high quality and safe health services while making best use of our available resources. We know our local patients and we are responsive to their needs while ensuring that we are spending money wisely. We ensure that local people are involved and have their say when we make decisions about health services. In East Surrey, NHS England commissions primary care services, such as GP practices, dentists, community pharmacists and optometrists; and specialised services including renal (kidney), specialist women s and children s care and heart surgery. Surrey County Council has responsibility for Public Health and social care. Our vision We have embarked on an ambitious transformation journey, aiming to further raise the quality of services and patient satisfaction, while reducing the costs of healthcare. To support our ambitions, the Governing Body has reviewed and refreshed our mission statement, strategic objectives and priorities, to focus the CCG and our partner organisations on the things that really matter to us. Our mission statement To transform services in order to improve clinical care and outcomes. Our strategic objectives To deliver high quality, patient-centred services To deliver our statutory responsibilities To create a mature and vibrant organisation To create a financially sustainable health and social care economy in our geographical system Our strategic priorities for 2017/18 To increase our focus on prevention and self-care To continue to involve our patients in decision-making of transformation of services To shift care into the community To become an exemplar in the care of frail people Integration of service provision and pathways (health and social care). The local health picture East Surrey has a population of approximately 180,000 people in the districts of Tandridge, Redhill, Reigate and Horley, served by 18 GP member practices as shown below. In general, people are healthier than the national average. 7



8 8 Figure 1: Geographic area of East Surrey CCG showing member practices Healthcare providers We buy health services from a range of providers including: Surrey and Sussex Healthcare NHS Trust (SASH) which provides emergency and nonemergency services to the residents of East Surrey, north-east West Sussex, and South Croydon, including the major towns of Crawley, Horsham, Reigate, Redhill, Oxted and Caterham. In our area, the trust provides acute and complex services at East Surrey Hospital in Redhill. In addition, it provides a range of outpatient, diagnostic and less complex planned services at Caterham Dene Hospital and Oxted Health Centre, in Surrey. Surrey and Borders Partnership NHS Foundation Trust, provides health and social care services for people of all ages with mental health problems, drug and alcohol problems, and learning disabilities in Surrey and North East Hampshire. First Community Health and Care, a not-for-profit social enterprise that provides community healthcare services to people registered with GPs in East Surrey. South East Coast Ambulance Service NHS Foundation Trust responds to 999 calls from the public and urgent calls from healthcare professionals, and provides NHS 111 services across the region. 8
9 9 Our 18 GP member practices also provide health services to East Surrey s population, though these services are mainly commissioned by NHS England. Other key partners It is vital that we work closely with other NHS organisations and key partners, listening to what they have to say about the services we commission and working together to transform and improve services. Our key partners include: NHS Crawley CCG NHS Horsham and Mid Sussex CCG NHS Surrey Downs CCG Surrey CCG Collaborative (six CCGs across Surrey) NHS England Surrey County Council Tandridge District Council Reigate and Banstead Borough Council Voluntary and third sector organisations Patient groups Healthwatch Surrey Better Care Fund (BCF) It is widely recognised that improving outcomes for the public, providing better value for money and being more sustainable requires health and social care services working together to meet individuals needs. The BCF was created to provide an opportunity to transform local services so that people are provided with better integrated care and support. The BCF is a single pooled budget for health and social care services, of which we contributed million, to work more closely in local areas, based on a plan agreed between the NHS and local authorities. The BCF is designed to: Improve outcomes for people Drive closer integration between health and social care. Increase investment in preventative services in primary care, community health and social care Support the strategic shift from hospital based care to the community and to protect social care services. The Surrey Better Care Fund includes the following organisations: Surrey County Council NHS East Surrey CCG NHS Guildford and Waverley CCG NHS North West Surrey CCG NHS Surrey Heath CCG NHS Windsor, Ascot and Maidenhead CCG NHS Surrey Downs CCG NHS North East Hampshire and Farnham CCG 9
10 10 CCGs and councils, through Health and Wellbeing Boards, have identified their ambitions for improvement against the following metrics that provide evidence of better integrated care and support. These are highlighted in the table below: BCF Indicator Target Performance at Q3 (December 2012) Total non-elective admissions in to hospital (acute), all-age, per 100,000 population East Surrey CCG Quarterly planned rate: Q Q Q Q On track to meet target Estimated diagnosis rate for people with dementia 66.7% On track for improved performance, but not to meet full target See the performance analysis section of the report for actions taken to improve the CCG diagnosis rate. Residential admissions: Longterm support needs of older people (aged 65 and over) met by admission to residential and nursing care homes, per 100,000 population (Countywide data) Reablement: Proportion of older people (65 and over) who were still at home 91 days after discharge from hospital into reablement/ rehabilitation services (Countywide data) On track to meet target 71.2% On track to meet target Delayed transfers of care: Delayed transfers of care (delayed days) from hospital per 100,000 population (aged 18+) Q Q Q Q No improvement in performance Reasons for delays include: Awaiting completion of assessment Nursing Home placement 10
11 11 Patient or Family choice Awaiting Nursing home placement Awaiting care package in own home and Awaiting completion of assessment. This information is being fed back to the various Local Joint Commissioning groups within Surrey to address issues relevant to their Provider Organisations. Patient / Service User Experience Friends and Family Test (Inpatient) 94.2% On track to meet target Collaborative commissioner arrangement The main changes to these arrangements during include the following: Adults and children s safeguarding arrangements were bought together as a single team with retained specialist expertise The commissioning of mental health services across Surrey were aligned to support more local commissioning whilst retaining a Surrey wide oversight in areas of joint commissioning with Surrey County Council. The current shared commissioning arrangements are reflected below: Description of Collaborative Agreement 1. Support services from the safeguarding adult and children team Lead/host commissioner Guildford & Waverley CCG 2. Children s Services Commissioning Guildford & Waverley CCG 3. Mental health and learning disabilities services 5. Emergency Ambulance Services, NHS 111, Patient Transport Services (South East Coast Ambulance NHS Foundation Trust) Guildford and Waverley North West Surrey CCG 6. Continuing Health Care and NHS funded Surrey Downs CCG 11
12 Nursing care services 12 Our challenges Financial pressure Following the continued financial challenges and a significant cumulative deficit, NHS England placed our CCG under Legal Directions in December Further unplanned financial challenges materialised early in the 2016/17 financial year, mainly as a result of undelivered QIPP efficiencies NHS England placed us in Special Measures (strengthening financial performance and accountability) in July Resulting from the introduction of special measures a new Interim Accountable Officer (AO) and Interim Chief Financial Officer (CFO) were appointed. Subsequently we agreed new financial control totals and a Financial Recovery Plan (FRP) with NHS England in August 2016 of 7.4m, which represented the minimum level of financial performance against which the Governing Body must deliver for 2016/17 and for which the Interim AO and CFO would be held directly accountable. In December 2016, as a result of a predicted overheat in secondary care costs and the significant additional Funded Nursing Care costs ( 1m+) that materialised, we were granted a further increase in its control total of 5m by NHSE. Our CCG delivered its Financial Recovery Plan and additional QIPP efficiencies which enabled us to stay within its NHSE revised control total. The CCGs final actual out turn was 17.3m deficit rather than the 19.4m planned. As set out in the 2016/17 NHS Planning Guidance, CCGs were required to hold a 1 percent reserve uncommitted from the start of the year, created by setting aside the monies that CCGs were otherwise required to spend nonrecurrently. This was intended to be released for investment in Five Year Forward View transformation priorities to the extent that evidence emerged of risks not arising or being effectively mitigated through other means. In the event, the national position across the provider sector has been such that NHS England has been unable to allow CCGs 1% nonrecurrent monies to be spent. Therefore, to comply with this requirement, we have released our 1% reserve of 2.1m, resulting in the reduced deficit for the year of 17.3m. This additional surplus has been offset against other cost pressures from the current financial year. We now carry forward a cumulative deficit of 42m into the 2017/18 financial year. We have been allocated funds and control totals from NHS England for 2017/18 and 2018/19 and detailed financial plans have been submitted to the Governing Body and NHS England for both years as part of the CCGs two-year planning and contracting round. The recently introduced Capped Expenditure Programme (CEP) of NHS England and NHS Improvement requires the Sussex and East Surrey Health Economy to produce affordable operating plans during June 2017 and additional system wide planning work is presently underway to agree and ensure our planning alignment to the NHSE control totals for 2017/18 and 2018/19. 12
13 South Park Medical Practice 13 The health provider Malling Health (UK) Ltd informed NHS England in 2015 that they wished to end their contract with the NHS to run South Park Surgery. An agreement was then secured with them to continue running the surgery for a further year, so that NHSE and the CCG could use the extra time to explore if it would be possible to keep a GP surgery within the immediate area. The CCG explored a number of options including a branch surgery linked to a larger practice in Reigate, Redhill or Horley. Unfortunately, there were no other local GP practices who wished to open a branch surgery in the area, in addition to their existing services. NHSE convened a commissioning panel in November, which approved a recommendation that the surgery close and the list be dispersed to other practices, in order to give patients greater certainty about their long term care. Malling Health (UK) Ltd will continue to provide GP services at South Park Surgery until Friday 29 September In the meantime NHSE will work with other local GP practices to ensure a smooth transfer of patient care following the practice closure. Sustainability and Transformation Plan (STP) All NHS health organisations and local authorities that commission and provide health and care in Sussex and East Surrey are working across boundaries and come together to create an ambitious local plan to achieve a vision of a sustainable health and care system built around the needs of our local populations. We consider ourselves to be Sussex-facing and Surrey-connected: therefore we are working closely alongside two STP areas - Sussex and East Surrey STP and Surrey Heartlands STP. Sussex and East Surrey is one of the largest of 44 geographical Sustainability and Transformation Plan (STP) footprints in England that have been asked to produce a longterm plan outlining how local health and care services will evolve, improve and continue over the next five years. STP footprints are locally defined, based on natural communities, existing working relationships and patient flows. They take account of the scale needed to successfully deliver all health and care services. The team working on the STP is currently analysing data about how, why and where patients are treated in our hospitals, to better understand the ways the NHS and social care throughout Sussex and East Surrey could work better together to meet the huge demand from a growing population living with increasingly complex health and care needs. We need to do this local analysis to ensure our proposals are based on the priorities and challenges of our local communities. We are at a very early stage in the planning process and still establishing the clinical leadership required to drive the STP forward. When this is in place, it will be time to work alongside our patients, the public and NHS staff to develop and shape our NHS. No final decisions have been made about any services and will not be made without our patients and public being given the opportunity to be involved and voice their opinions. To ensure that STP developments are effective and relevant locally, we are also part of the Central Sussex and East Surrey Alliance (CSESA), which is one of three geographical planning units within the wider Sussex and East Surrey STP footprint. CSESA has developed a Place-Based Plan which sets out how the ambitions within the STP will be delivered locally. 13
14 14 We are actively working to develop service delivery models which fit the local ambition to develop a Multispecialty Community Provider (MCP). The Place-Based Plan sets out five key priorities which form the basis for our development of new models of care within the MCP, working with our local providers: Prevention and self-care: Empowerment and enablement of the whole population to stay healthy and well through prevention and education Long term conditions management : Care for long term conditions and end of life based largely in the community instead of an acute setting, reducing variation with a focus on self-management Coordinated care for frail and complex patients: Multidisciplinary, coordinated care for the frail and those patients with the most complex health and social needs including children and families Improved access to urgent care: An effective local network of urgent care, based on enhanced primary care services Cancer, Referral-to-Treatment (RTT) and A&E targets: Providing higher quality and more timely care across the system, as measured by consistently exceeding cancer RTT and A&E targets Our achievements for the year Integration of health and social care We have been focused on developing integration of our providers of community-based services and, since the agreement of the Central Sussex and East Surrey Alliance (CSESA) Place-Based Plan in October 2016, on progressing our plans for a local Multispecialty Community Provider (MCP) model. As mentioned above, we have developed networks of GP Practices to develop primary care at scale and established the building blocks for integrated care. Significant work was carried out during summer 2016 with primary care, community health, social care, mental health and ambulance services to develop the strategic intent for primary care and out of hospital services in East Surrey. The transformation of GP services provides the foundation for a wider, more joined up, sustainable out of hospital system that will support patients to remain in and/or return to their community or (with support) their homes, with improved health and wellbeing. Led by Primary Care, the NHS is working to an integrated Multidisciplinary Team (MDT) approach to delivery of care with improved access, which supports prevention and self-management; earlier identification; better continuity for people with long term conditions; and more coordinated care for people with the most complex needs. We have continued working to support East Surrey s GP Federation (Alliance for Better Care Limited) and establish it as a provider. The CCG awarded a contract to the Federation in September 2016 as Most Capable Provider for Enhanced Primary Care Services for East Surrey. The Federation was also successful in its application for one network to become a member of the wave two aspirant Primary Care Home Community of Practice. Work on the development of the MCP has been the focus for the latter part of the year. Governance arrangements are in place with the four key partners (the CCG, First Community Health and Care, Surrey County Council and Alliance for Better Care Limited) forming a Joint Executive, with a wider steering group involving other key organisations including mental 14
15 15 health, district and borough councils, St Catherine s Hospice and SECAmb. A joint programme team has been established including senior staff from each organisation, which are focusing on developing the programme and its three workstreams: New models of care Enablers including IT, estates, workforce, communications and public engagement MCP form, including legal, financial, contractual and organisational arrangements A wide range of staff from 10 community-based organisations across East Surrey are engaged in the programme, working together on developing the new models of care and beginning to work with local communities to develop a deeper understanding of the needs and aspirations of local people. Our ambition is to create the MCP in shadow form to operate from April 2018; the new models of care will be implemented as they are developed, with the full model in place from April Progress on interoperability FCHC and practices, across practices With new models of care emerging and evolving, there is a clear need for more effective information sharing between care settings, organisations and geographies, as well as between professionals and citizens, to optimise patient outcomes and quality of care. This relies on the ability of IT systems across health and care to interoperate with one another. In 2016/17 East Surrey CCG successfully secured funding for the development of an interoperability system that will be implemented during During 2016/17 interoperability was established, following a pilot, between all the GP Practices and our community service provider, FCHC, allowing information sharing between community health professionals. Financial We delivered the agreed 2016/17 NHS England Special Measures financial control totals and financial recovery plan, including QIPP at year end. Frailty Unit In October 2016, East Surrey CCG, in collaboration with Crawley, Horsham and Mid Sussex CCGs and East Surrey Hospital opened a new Frailty Unit at East Surrey Hospital. The Frailty Unit sits adjacent to the two care of the elderly wards in East Surrey Hospital. It has been fully refurbished to offer five daytime bays for patients attending for an extended visit to have a full assessment and investigations, where necessary. The bays offer comfortable chairs (and in exceptional circumstances, trolleys) for people and their carers to relax whilst their care and treatment plan is reviewed. The unit has been fully refurbished to offer a safe and inviting environment, which is dementia-friendly and opens out into a pleasant courtyard garden. The Frailty Unit accepts referrals directly from the A&E department or via GPs. In addition to the five bays, there are two consulting rooms, where GPs can book patients directly into appointments to see the multidisciplinary team. The team is made up of a Consultant Geriatrician, occupational therapists, nurses, physiotherapists, a pharmacist and a social worker. 15
16 16 The aim of the Frailty Unit is to provide early support to people, before their health or social care situation deteriorates into a crisis. Approximately 10-15% of people attending the Unit are admitted, meaning that the joint initiative results in the majority of people being supported to return to their usual place of residence. Care Homes The CCG has run a Care Home scheme for the last three years to address the issue that over 75s in care homes are three times more likely to be admitted to hospital than over 75s in their own homes. The Care Home scheme requires a GP-led comprehensive assessment within two weeks of admission to a care home, where past medical history and medication are reviewed. The patients, with their family and carers, agree a plan for emergency care including a Do Not Attempt Resuscitation (DNAR) form if appropriate now built in to the admissions process. Two care home matrons provide training for care home staff in appropriate circumstances for calling an ambulance, end of life care, and general up-skilling. A pharmacist also reviews patient medication, stopping unnecessary medicines and looks for potential iatrogenic illness i.e. complications related to diagnosis and treatment of a disease. Unique software developed with IC24 and SECAmb enables GP practices to upload the new patient care plan once and have it streamed automatically to the Out of Hours (OOH) service and to the ambulance database Intelligence Based Information System (IBIS). Should a care home call 999, IBIS triggers paramedic oversight of calls and grants the ambulance call centre access to the patient s emergency care plan, rendering them better equipped to respond quickly and appropriately and reducing unnecessary conveyances to hospital. Over three years the Care Homes project has delivered significant year on year reductions in both hospital admissions and associated costs for care home patients: Projected savings for : 1,308,000 This success has led to the application of a similar approach for patients at risk of admission and end of life care, meaning we now have 5000 specialised care plans on IBIS in East Surrey. Due to the success of this scheme, we were shortlisted as a finalist by the Kent Surrey Sussex Academic Health Science Network for the Excellence in Out of Hospital Care Award. In addition, a Medicines Optimisation Service in Care Homes project was commissioned to improve health outcomes and the well-being of elderly care home patients, reduce medicines waste and potentially reduce unplanned admissions. The project has been running since October 2015 and has been very successful. Evaluation indicates that the project to date has been self-funding, as the costs in reduction of inappropriate prescribing have paid for this service as well as improved the quality and safety of prescribing. Feedback from prescribers and care homes has also indicated that this dedicated resource to focus on medication review has been invaluable. 16
17 17 Carers NHS Guildford and Waverley CCG hosts the Partnership Manager for Carers for the Surrey CCGs. Together, we are committed to putting carers at the heart of everything we do. To support this commitment, a Surrey Carers Memorandum of Understanding (MoU) Together for Carers - was agreed between health and social care partners on 12 January Together for Carers defines an integrated approach to identifying, assessing and supporting carers health and wellbeing needs in Surrey, and looks to build on the already established inter-agency working to support carers across Surrey. A significant building block for delivering Together for Carers has been the Surrey Carers Prescription, which is a co-designed mechanism for delivering cost-effective, online, secure referrals ensuring fast track support to carers. It provides a trigger to statutory carers assessments and young carers assessments. More than 15,000 carers have received more than 20,000 carers services. The cost-effectiveness of this practical intervention was recognised by the Health Service Journal when it was shortlisted for the HSJ Value in Healthcare Award The CCGs participated in a joint procurement of a new independent carers support service across the whole of Surrey. The new service reflects priorities identified through co-design with carers, including benefits advice, support for young carers, independent information and advice, home-based breaks and learning and work for carers. The contract was awarded to Action for Carers Surrey, to commence 1 April The new service will allow carers to access support and advice through mechanisms such as webinars, social media and online counselling as well as face-to-face support. There will be an increased focus on supporting carers from black and minority ethnic groups and carers with mental health problems, and a Carers Support presence in all acute trusts in Surrey. We have focused on support for armed forces carers this year, which led to the establishment of the first national Military Young Carers Service in the country hosted by Surrey Young Carers. Following the success of further external funding applications this service will be expanded from 1 April 2017 to provide a whole family approach. We have held carer engagement events to help shape and improve our offer to marginalised groups, including the Nepalese and Gurkha Community and Young Carers of people with an alcohol/substance misuse problem. The Surrey CCGs were shortlisted for the Health Service Journal Commissioning for Carers Award in East Surrey CCG Quality of Antibiotic Prescribing 2016/17 During 2016/17 GP practices in East Surrey CCG were benchmarked against the Quality Premium antibiotic targets set by NHS England and given support, advice and patient information resources from the Medicines Management Team to improve the quality of antibiotic prescribing. Antibiotic training events were held for GPs and in depth practice audits on either general antibiotic prescribing or high risk broad spectrum antibiotic prescribing were undertaken in fourteen practices. During the course of the year both the overall number of antibiotic items and the high percentage risk broad spectrum antibiotics (co-amoxiclav, quinolones and cephlosporins) were successfully reduced. This should benefit patients by reducing the risk of drug resistance and reducing the incidence of multidrug resistant infections 17
18 18 such as MRSA and C.Difficile. The CCG should benefit from reductions in costly hospital admissions for resistant infections Rolling 12 month total antibacterial items per STAR PU EAST SURREY CCG National Quality Premium Target 2016/17 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 *STAR PU = Specific Therapeutic Group Age-Sex Related Prescribing Unit 13.00% 12.00% Rolling 12 months % high risk antibiotics 11.00% 10.00% 9.00% 8.00% 7.00% EAST SURREY CCG National Quality Premium Target 2016/17 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16 Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Medicines Incident Reporting Research shows that organisations which regularly report more patient safety incidents usually have a stronger learning culture where patient safety is paramount. To improve patient safety and prevent the reoccurrence of medication errors in primary care, we introduced a formal system for reporting medication incidents involving GP practices. As a result of introducing the formal process, our Medicines Management Team was able to analyse the incidents, identify and disseminate learning points in order to improve practice and help prevent reoccurrence at GP practice and CCG level. These incident reports have also contributed to national learning through submission to the online national reporting and learning system. 18
19 Primary care services 19 Primary care resilience and GPFV implementation plan: A key CCG priority is to support the development of primary care, in line with the national direction set out in the NHS Five Year Forward View (5YFV) and General Practice Forward View (GPFV). A comprehensive local implementation plan to address the sustainability and quality of general practice, including the key workstreams of workforce and workload, was submitted to NHSE in March 2017 and is one of the nine must-dos contained within the 2016/17 planning guidance. As part of the GPFV programme, five East Surrey practices were identified to receive resilience support in 2016/17. The resilience programme offers support to practices which are struggling and facing issues which could jeopardise the sustainability of the service. Current plans focus on supporting practices that are under additional pressures, and those whose patient list is currently capped. Funding was allocated by NHSE to support recruitment of additional clinical staff at two practices, and three practices received funding to undertake a diagnostic assessment to identify where change is needed and establish areas where further support may be required. GP in the Emergency Department: On average, there are approximately 90,000 visits to the A&E department of the East Surrey Hospital per year. The majority of these arrive during GP surgery opening hours. In 2016 East Surrey CCG piloted an initiative to develop a GP in ED service in East Surrey Hospital. The service aims to see those people who arrive in the A&E department (Emergency Department ED) who present with a condition that does not require a specialist emergency intervention. The pilot opened in August 2016 with two GPs on shift, seven days a week. Over winter, a third GP was added extending the hours from 10am 10.30pm. The service has been seeing approximately 350 people a month. In 2017/18, we are looking to work with the GPs and East Surrey Hospital to identify ways to build on this success and assist with alleviating the pressure on the A&E department. Extended Hours GP Service at Caterham Dene: As part of its plans for winter 2016/17, the CCG also worked with the GP Federation and First Community Health and Care to establish a walk-in GP service during weekday evenings and weekend and bank holidays, operating from the Minor Injuries Unit at Caterham Dene. The service operated from Christmas 2016 to the end of February. From March the service has been operating at weekends and bank holidays only in line with established demand, and will continue until the end of March 2018 when it is planned that GP access will be extended further in accordance with national guidance. Mental health Safe Haven: In partnership with Surrey and Borders Partnership NHS Foundation Trust (SABP), Richmond Fellowship and Reigate Stepping Stones, we launched the Safe Haven service in March The service supports clients to avoid crisis and maintain wellbeing and to signpost clients to other community services. The service is based in Redhill. 19
20 20 Since the launch, there have been on average 250 visits per month and approximately 20 new clients attending per month. There is evidence of good links across the system with clients reporting hearing about the service from their social networks, A&E, GP, other mental health services and the voluntary sector. Improving access to psychological therapies (IAPT): The IAPT service was re-procured last year and the new service, comprising four providers, was launched in July 2016, with the providers offering a range of opening times, face-to-face therapies, online therapies and group work in locations across East Surrey. We continue to work with our providers to increase public and clinical awareness of the services, encouraging self-referral as well as referrals from other health professionals. Currently self-referral accounts for 56% of all referrals. Recovery rates have improved from 45% to 49% since the service opened. New service leaflets will be published to promote the services across the area. Dementia: In collaboration with neighbouring CCGs, patient and carer groups, and providers we have developed a Surrey-wide Dementia Strategy. We are promoting the Well Pathway for Dementia. As a part of this, our main achievement has been to establish a Dementia Action Alliance with all providers and patient representatives to oversee the implementation of the strategy, and through training, we have been identified as an organisation with the status of dementia friendly. The Alliance is also working with GP practices and patient groups to develop dementia friendly status, including training to become dementia friends. To achieve this, the following steps have been taken: Appointment of a dementia champion. Workshop events held with practice staff to award them the status of being dementia friends. Educational events geared towards tier 2 dementia training. Dementia friendly community s pilots running across Surrey to test technologies which would offer support to dementia patients with the intention of enabling them to remain independent for longer. The dementia diagnosis rate in primary care now stands at 62.8% (improved from 61.5% in April 2016) against a 67.4% national target. Further work is on-going to improve the diagnosis rate to the national target, along with work to improve post-diagnostic services and support. We have a GP clinical lead for Dementia who is working with practices individually to improve their diagnosis rates as well as the post-diagnostic support services. Implementation of the Five Year Forward View for Mental Health (FYFVMH): The FYFVMH was published in February 2016 setting out the targets to be achieved by 2020/2021. Because the plan covers five years, there is a staged approach to starting the service developments to achieve the targets. 20
21 These are set out in the table below: 21 FYFVMH Priority 2016/17 plan Achievements 2017/18 plan Future in Mind : Increase access to high quality mental health services for an additional 70,000 children and young people per year Open a new children s and young people s mental health service (CAMHS) on 1 April The service opened in April Patients, carers and GPs are reporting higher levels of satisfaction. Achieve a 17% increase in children and young people s referrals to the new CAMH Service Increase access to evidence-based specialist perinatal mental health care. East Surrey will develop a bid for a new perinatal mental health service to commence in 2017/18 The CCG was successful in its bid and is developing the new service in partnership with Sussex Partnership Trust Open the Perinatal Mental Health Service Commission additional psychological therapies for people with anxiety and depression, with the majority of the increase integrated with physical healthcare. To achieve 15% access to psychological therapies and 50% recovery rate. Re-procure the services The new services commenced on 1 July The service is forecasting achieving 50% by the end of March. Action plans are in place with each of the 4 providers to continue progress to exceed 50%. To apply for NHS England s additional Transformation funding to support the development of the services to increase access to 17%. Expand capacity so that more than 50% of people experiencing a first episode of psychosis start treatment within two weeks of referral. Negotiations with the local mental health provider resulted in the standard being added into the contract from 1 April 2017 The access standard has been agreed within the contract At least 50% of people experiencing a first episode of psychosis will be seen within 2 weeks. Reduce suicides by 10%, with local government and other partners. East Surrey CCG is a member of the Surrey-wide Suicide Prevention Group. Local Citizen Advice Bureaus are contracted to provide a debt advisory service for people with a serious mental illness. Implementation of the Suicide Prevention Group action plan. 21
22 22 The Safe Haven has been opened to support people in crisis Commission effective 24/7 Crisis Response and Home Treatment Teams as an alternative to acute admissions. To open the Safe Haven as a replacement for the crisis house. The Safe Haven opened in April The crisis house will close to coincide with a new single point of access (24/7) for those in a crisis that will be integrated with the home treatment team. Eliminate out of area placements for non-specialist acute care by East Surrey has very low levels of out of area placements. The numbers vary over the year. There fewer than 10 out of area placements. A plan will be developed to eliminate out of area placements by 2020/21 Deliver integrated physical and mental health provision to people with severe mental illness Engage with stakeholders to define what the service will look like in GP practices A number of stakeholder events were held and workshops to design the new mental health support service that will work within GP practices. The business case for the new service was approved. Implement the new Primary Care Mental Health Service. By March 2018, all practices will have access to the service. Ensure that 50% of acute hospitals meet the core 24 standard for mental health liaison as a minimum, with the remainder aiming for this level Surrey and Sussex Hospital already has a 24/7 psychiatric liaison service, but the service does not currently meet the Core 24 standards. Within the FYFVMH, a new Transformation Fund has been announced to assist services to move to achieving the Core 24 standards. A working group has been established to develop a funding bid in October The Sustainability and Transformation Planning Board will identify the 50% of services in the area to meet the Core 24 standards. The working group will develop a bid for submission in October Increase access to Individual Placement Support (IPS) for people with severe mental illness East Surrey has an established IPS service. 13 IPS workers are employed by the Richmond Fellowship across Surrey. To continue to build on the existing service and review and increase access numbers. 22
23 CCGs will continue to meet a dementia diagnosis rate of at least two-thirds of the estimated number of people with dementia To meet the dementia diagnosis rate of 67.4% 23 East Surrey has a GP lead for Dementia who is working with GP practices to assist them with the identification of patients. In addition, we have established the first Dementia Action Alliance in Surrey and supported the development of a new dementia strategy. 1. Commence implementation of the strategy. 2. Achieve the dementia target Mazaars Review: A national report published in December 2015 following an independent review of deaths of people with a Learning Disability or Mental Health problem in contact with Southern Health NHS Foundation. In response to this report, Surrey CCGs and Surrey and Borders Partnership NHS Foundation Trust (SAPB) has developed an action plan which has led to the formation of a monthly review on deaths occurring among people with learning disabilities to ensure safe effective care is delivered. Learning Disabilities Services: In 2016, Bramdean Step Down Ward was decommissioned to release the funds to redevelop the community learning disability teams. A new intensive support team has been introduced to support people to remain in their usual place of residence and avoid admission. April Cottage, the Surrey admissions unit was relocated in 2016 to a more central base in Epsom. This will help integrate the unit with local community services and enable those admitted to retain contact with their friends and family. Patient Transport Services (PTS) Working with other CCGs in Surrey, North East Hampshire and Farnham and Hounslow, we have reviewed non-urgent NHS Patient Transport Services, with NHS North West Surrey CCG acting as the lead commissioner for the new Patient Transport Services contract, which started in April Together, we undertook a full review of service delivery, including input from patient groups to ensure the new service provider meets the needs of local people and will improve patients experience going forward. We believe the result of this project is an improved service that will better address the varying demands placed on PTS. 23
24 Long term conditions 24 Improving patients receiving first definitive treatment for cancer services across Surrey: Following the review of stroke services across Surrey in 2015/16 local health systems submitted proposals detailing plans to develop stroke care in line with the National Stroke Strategy and NHS Five Year Forward View. The proposals covered the whole stroke pathway from prevention to life after stroke. Following review of the proposals we have been working with NHS Crawley CCG to review the local stroke pathways with a focus on acute hospital care and community rehabilitation provision. Our review identified that whilst we have stroke services in East Surrey Hospital, community beds in Crawley and a community based neuro-rehabilitation team, the services could work more effectively by being better joined up. The national clinical guideline for Stroke states that hospital in-patients with Stroke who have mild to moderate disability should be offered early supported discharge, with treatment at home beginning within 24 hours of discharge. It further recommends early supported discharge (ESD) teams are in place to receive patients as early as 72 hours post stroke into the community to continue their rehabilitation. To maximise the effectiveness of our resources, we have been working with our community provider (First Community Health and Care) to redesign their existing services into one integrated Community Neuro-Rehabilitation Team. The new team will include an Early Supported Discharge team, as well as nurses offering support and a point of contact for people with complex neurological conditions; for example, Parkinson s Disease, Motor Neurone Disease, Huntingtons, Progressive Supranuclear Palsy (PSP) and Multiple Systems Atrophy (MSA). The new team will be in place in 2017/18. Cancer: We established a Cancer Steering Committee made up of representatives from the CCG and Public Health to work on ensuring our strategic priorities around prevention, improved and quicker diagnosis and living with and beyond cancer are delivered. Through this work, one of our achievements has been that East Surrey has been recruited onto a Cancer Research UK funded project to increase cervical screening rates. This is being led by University College London and will involve random selection of some of our practices to trial whether text messaging and tweaks to the follow-up letter encourage non-responders to take up screening. It is expected this will be delivered in the 2017/18 financial year. Diabetes NHS Diabetes Prevention Programme (NHS DPP)/Diabetes: Due to our being in a position of preparedness, we were selected by the South East Clinical Network Team to be part of tranche one of the NHS Diabetes Prevention Programme. We are currently delivering the programme, which seeks to identify through blood tests, people at risk of type 2 diabetes and refer them on to a 10-month course. On the course, they receive information on diet, exercise and living well alongside local peers, with the aim being to reduce their risk of developing diabetes. The programme is being delivered locally by Ingeus and has been designed by NHS England, Diabetes UK and Public Health England. So far, our practices have referred 327 patients 24
25 25 making us the top referrer in Surrey and third in all of Kent, Surrey and Sussex. There are 13 cohorts currently running locally. Hypoglycaemia /Diabetes: We are implementing the hypoglycaemia project in conjunction with SECAmb and the local Academic Health Science Networks (AHSN). The project seeks to reduce the number of acute inpatient admissions for hypoglycaemia by training paramedics to deal with hypoglycaemic incidents when they see and treat a patient with diabetes at home. The paramedics then pass the details over to the patient s GP who then invites the patient in for a review in order to understand why a hypo occurred and help avoid a repeat. Evidence has shown it was often the same patients who experienced hypoglycaemic incidents. There have been 12 incidents between March March 2017 of hypos following this pathway. Children s services Child and Adolescent Mental Health Services (CAMHS): In April 2016, the newly-procured Child and Adolescent Mental Health Service opened. The key change is that the service now has a single CAMHS Referral and Information Centre which helps navigate children and young people to the most appropriate service and through the system. This has proved a welcome introduction for both families and GPs. The operating hours have been extended to include Saturday mornings, and an employment support service has been introduced for young people. These changes have been made to increase the number of children and young people accessing help for their mental health needs. Children s Community Health Service reprocurement: Eight commissioning organisations committed to work together to jointly secure a provider for children s community health services across Surrey. These community services will focus on prevention of ill health, advising on child development and providing targeted and specialist medical, nursing or therapy services when needed (for example, because a child has a developmental delay, disability or significant health difficulties). Children and young people with special educational needs and disabilities (SEND) need integrated support to achieve their full potential. Through joint working with the local authority, a joint commissioning strategy for SEND has been produced and will be used to help plan and deliver priorities. This will include developing and delivering an integrated SEND offer with and for Surrey s children and families and developing and delivering an integrated early help offer for children and families in need. Clinical Engagement We have continued to engage with member practices principally through monthly meetings of the Practices Commissioning Committee attended by GPs and Practice Managers from all 18 member practices. At the meetings we discuss the vision for our strategic transformation as described elsewhere in this report, present our work in collaboration with our stakeholders, and consider a wide range of operational issues. This has meant a high level of transparency across our membership organisation which enables our primary care colleagues to be an intrinsic part of delivering our future model of care. 25
26 26 We now have 11 clinical leaders each with clear areas of clinical responsibility. This ensures that all transformation and development programmes are truly clinically-led. Regular meetings with GP and Consultants at East Surrey Hospital have been established to improve relationships and communications, and to provide a problem-solving forum to improve the quality of care for our patients. Patient and public engagement We have continued to engage with a wide range of patients, public and other local stakeholders to ensure that our vision for the future of local health services really meets local needs and reflect local views. We have continued to build relationships with key stakeholders including our two local MPs - Crispin Blunt (Reigate and Banstead) and Sam Gyimah (Tandridge) - members of Surrey County Council s Health and Wellbeing Board, Wellbeing and Health Scrutiny Board, and a range of health and social care partners, including across wider geographies such as the Sussex Urgent and Emergency Care Network and the South East Commissioning Assembly. In order to shape a shared vision for the future of local healthcare, we listen to, understand and act on what really matters to patients and people in our communities. Meaningful patient and public participation supports the development of targeted interventions, increases patient satisfaction, leads to a more effective use of resources and is a legal obligation of CCGs - as explained in Section 14Z2 of the Health and Social Care Act 2012 (amended). The following is an account demonstrating how we believe we have met the requirements of Section 14Z2 and have fulfilled the public involvement duty - for the public to be involved in (a) the planning of services, (b) the development and consideration of proposals for changes which, if implemented, would have an impact on services and (c) decisions which, when implemented, would have an impact on services. Engagement and involvement are both important elements of participation. For the purposes of this report the terms engagement and relationships will mean the same an on going and meaningful dialogue between interested parties, sharing information, opinions and ideas. The word involvement will be used when engaged parties become involved with the strategic planning, work and/or implementation of a specific project for CCG. How we use the messages that we have heard - The Engagement Cycle We use feedback gathered through engagement activities, views, comments and opinions to inform all stages of our work. The Engagement Cycle identifies five different stages when patients and the public can and should be engaged in commissioning decisions: 1. Community and stakeholder engagement to identify needs and aspirations. 2. Public engagement to develop priorities, strategies and plans. 3. Patient and carer engagement to improve services. 4. Patient, carer and public engagement to procure services. 26
27 27 5. Patient and carer engagement to monitor services We proactively seek the views and experiences of our local community, patients and carers, and especially of those less able to speak for themselves; the so-called seldom heard. Our main points of reference continue to be the CCG s Patient Reference Group, external community and health-orientated groups, patient representation and feedback collected when working on disease specific pathways. Most of our GP member practices (16 out of 18) have a Patient Participation Group (PPG). The role of these groups is primarily to support the practice - giving thoughts, ideas and opinions, helping with specific pieces of work that call for a patient perspective and acting as a communicator between the practice and their community. PPGs also represent their practice population on our Patient Reference Group (PRG). The Patient Reference Group The PRG is constituted of nominated representatives from individual Practice Participation Groups. It also, on occasions, extends an invitation to voluntary, community and faith sector organisations, support groups and individual representative patients. It is integral to our work and meets formally three times a year. The role of the PRG is to: help our Governing Body make decisions about the services they commission ensure that services reflect and meet the health needs of the local population ensure that we embrace the no decision about me without me promise actively promote the principles and values of the NHS Constitution. This year the PRG has: Helped PPGs develop by sharing good practice Worked to help redesign stroke pathways Become a Dementia Friendly Community Learnt more about the Frailty Unit, GP Federations and the Nursing Home Scheme Reviewed patient information and advised on readability and content Contributed evidence to CQC inspections and Supported and promoted; The development of Primary Care Networks Health and Well Being Advisors working in GP practices The Out of Hospital Strategy National Diabetes Self- Care programme Choosing Wisely Campaign - aims to avoid wasteful or unnecessary medical tests treatments and procedures The Integrated Health Management for Dementia trial The effective use of the NHS Accessible Information Standard The use of generic rather than branded drugs External community and health-orientated groups By engaging with existing groups, we listen to our community in environments that are convenient for them and in places where people feel safe and confident and are able to 27
28 28 express their views and give feedback. We are then able to build these views and experiences into our commissioning intentions and plans for service changes and improvements. Over the past year we have met with and heard from: Mental health service users Carers Mid and East Surrey Mental Health Stakeholder Group Tandridge Health and Wellbeing Board Disability Alliance Network Limpsfield Parish Council Headway (voluntary organisation for people with acquired brain injury) Young carers Motor Neurone Disease Association End of Life Care Forum Dementia summit East Surrey Domestic Abuse Service Arthritis Care Local Authority Health Partnership Board Surrey Gypsy and Travellers Forum Surrey Coalition of Disabled People Stroke Association Healthwatch Surrey We hold a record of engagement activities (such as those listed above). All our staff can view this, which includes detailed accounts and feedback. Feedback is then managed to inform commissioning decisions and activity. Patient Experience We use a wide range of activities and forums to make it as easy as possible for patients to feed back their experiences with our local healthcare providers. You can read more about these in depth in the Performance Analysis section of this report. Wider Stakeholder Engagement CCGs need to have strong relationships with a range of health and care partners in order to be successful commissioners within the local system. These relationships provide us with ongoing information, advice and knowledge to help them make the best possible commissioning decisions. We work collaboratively with the following key stakeholders in order to serve all of the people who live within our area; to help them look after themselves and to invest in and innovate the best possible health care. Engagement Strategy Our Engagement Strategy was approved by the Governing Body in January 2015 and is available on our website. Although the strategy envisages actions and plans until 2018, the ever changing NHS landscape suggests that a complete review and refresh is required. Our engagement plans will need to reflect those of the CSESA Place-Based Plans and the wider STP footprint communications. For these reasons it is also likely that the revised 28
29 29 Engagement Strategy will develop to become a joint Communication and Engagement Strategy. Communications: Communications is an integral element of good engagement. Without proper communication our public cannot make informed and considered decisions and we cannot inform them of how their contributions have changed/affected our plans. Our channels include: The website Your Health Matters quarterly newsletter for patients and the public. A monthly e-newsletter for member practices and for staff You Said/We Did In order to keep interested parties engaged, it is important to communicate any changes that they have helped to influence. We regularly publish examples of how the patient and public voice have contributed to improve services on our website and in Your Health Matters. The year ahead We have established some good relationships with key community groups, and need to ensure that others are developed further, particularly across the county borders in light of the emerging Sustainability and Transformation Plans. We will also be looking at opportunities to make contact with local businesses to try and engage one of our harder to reach groups; the working age adult. We are committed to reaching a wide range of people and will continue to focus efforts on those groups or individuals that may not ordinarily be reached by traditional routes such as formal meetings. We will continue to work closely with local Borough and District Councils, Surrey County Council and community, voluntary and faith sector organisations, which help us to reach many of the seldom heard communities. This partnership working makes engagement more appropriate (as more work involves co-commissioning), cost efficient and prevents so called consultation fatigue. Departmental heads will take more of a lead seeking engagement opportunities for their own projects, and there will be greater collaboration between the commissioning managers and engagement lead. The Patient Reference Group will become an increasingly important forum for us to explore more ways of engaging with and involving patients and for ensuring the public voice really contributes to our work over the next year. Through the continual development of relationships, we will continue to work together to support the vision of a truly patient-centred local health service. 29
30 30 Our ambitions for the future We aim to build on the good progress made operationally, achieve the planned and agreed financial outcomes and successfully address the following continuing challenges in 2017/18: Transformation of local services Our first priority is to transform local health services so that patients spend less time in hospital, and benefit from more targeted care and support in the community. This will ensure that patients are cared for more appropriately while also making local healthcare services financially sustainable in the longer term. Sustainability and Transformation Plan As outlined above we are working with Sussex and Surrey partners to develop a sustainable health system including working more locally on our place-based plan. Financial Sustainability Following the introduction of Special Measures, the CCG improved its underlying financial position. The CCG has been set challenging control totals for 2017/18 and 2018/19 and is preparing plans to deliver against these, supported by the Capped Expenditure Process and Sustainability and Transformation plans. This will further improve the underlying position and the achievement of future financial balance. Health system pressures Pressures on our local emergency department and hospital services generally were particularly intense over the 2016/17 winter period. We have worked with partners to do everything we can to alleviate pressure including ensuring that member practices were able to signpost patients to alternatives to A&E. 30
31 31 Section 2 Performance Report: analysis 31
32 Performance Overview 32 Overview of the East Surrey CCG Corporate Performance Management Framework 1. What are our statutory obligations for performance? The CCGs core purpose and key performance areas are determined by statute and various publications from NHS England. Our primary source of statutory guidance on performance reporting is the Health and Social Care Act The Health and Social Care Act Duty to improve the quality of services (Section 14R of the National Health Service Act 2006.) We have a duty to secure continuous improvement in the quality of services provided to patients. This means securing continuous improvement in the outcomes that are achieved from the provision of the services. The outcomes relevant include, in particular, outcomes which show: the clinical effectiveness of the services, the safety of the services, and the quality of the experience undergone by patients. Furthermore, regard must be had to the quality standards prepared by NICE. 2. Duty to deliver the requirements set out in the NHS Constitution (section 3 of the Health and Social Care Act 2012.) We must have regard to the NHS Constitution to ensure timely access to services for patients. Duty to reduce healthcare inequalities (Section 14T of the National Health Service Act 2006 (as amended). In exercising functions in relation to the health service, we must have regard to the need to reduce inequalities between people with respect to the benefits that they can obtain from the health service. Duty to involve and engage the public in commissioning (Section 14Z2 of the NHS Act 2006 (as amended). We must involve and engage patients and the public in planning, decision-making and proposals for change that will impact on individual or groups and how health services are provided to them. Duty to review the extent to which the CCG has contributed to the delivery of any joint health and wellbeing strategy in terms of (Section 116B (1)(b) of the Local Government and Public Involvement in Health Act 2007). Commissioning for Sustainable Development Commissioning for Sustainable Development is the process by which commissioners improve both the sustainability of an organisation and the way it provides services and interacts with people in the community. It is about striking the right balance between the three key areas of financial, social and environmental sustainability when making commissioning decisions. 32
33 33 Commissioning for Sustainable Development: Saves money Saves resources Benefits staff and patients. We have helped shape a more sustainable NHS, by: Developing a whole systems approach to commissioning - The CCG s definition of system sustainability includes health, social care and the resilience of local families, friends and communities that support those in need. It is not just about financial sustainability of health budgets The NHS in its planning guidance for 16/17 had requested systems to develop a STP (Sustainability and Transformation Plan) which were submitted in June The CCG is part of the Sussex and East Surrey STP. Using the commissioning cycle to increase sustainability. See the sustainable development section for more on how we ensure we make the most of our social, environmental and economic assets. Financial duties (section 27 of the Health and Social Care Act 2012.) We must, in respect of each financial year, perform our functions so as to ensure that its expenditure in that year does not exceed the amount allotted to it for that year. The duties in the Act relating to performance reporting may be summarised as follows): Purpose Key Performance Areas Improve outcomes Clinical Effectiveness Patient Safety Patient Experience Accessibility Waiting Times Reduce inequality Service variability Vulnerable groups Parity of Esteem Engagement and Involvement Governance processes embedding engagement and involvement Robust local community relationships Degree of engagement with seldom heard groups Holding providers to account Patient and public feedback Sustainable development Effective and efficient use of social, environmental and economic assets o spending public money well o smart and efficient use of natural resources and o building healthy, resilient communities Finance Surplus QIPP Savings Current Asset Management Better payment 33
34 34 Value for money The table above shows: Key Statutory Performance Areas In addition to the Health and Social Care Act requirements we also have to have regard to other documents such as: The CCG Improvement and Assessment Framework NHS Mandate The Five Year Forward View, GP Forward View, The Five Year Forward View for Mental Health and The Annual Planning Guidance for 2016/17 2. What are the key indicators monitored by the CCG to ensure delivery of our Core Purpose? We have implemented a robust corporate performance management framework to assess delivery of its statutory duties mentioned above, and for informing potential risk to delivery and the need for corrective action. The key measures for managing our performance against our core purpose, and the key performance areas are set out in key guidance documents prepared by NHS England, namely: Area to be measured Outcomes Accessibility (NHS Constitution Standards) Equality Engagement and Involvement Sustainable development Performance Framework used to Manage Performance Set of selected quantitative indicators from - CCG Improvement and Assessment Framework (CCG IAF) - The NHS Outcomes Framework - CCG Outcomes Indicator Set. Qualitative information from meetings, patient feedback and reports Set of nationally defined quantitative indicators Qualitative information from meetings and patient feedback The NHS Operational Planning measures for 2016/17 in relation to Mental Health and Learning Disabilities The Revised Equality Delivery System (EDS2) Qualitative information from meetings, patient feedback and reports Qualitative information from meetings, patient feedback and reports assessed against indicator 165a of the CCG IAF Qualitative narrative assessment of performance Finance Business rules in The Annual Planning Guidance: for 2016/17 The table above shows Performance Measure Guidance Documents Performance indicators provide a means for us to measure and assess the quality and productivity of the services we commission to ensure they are equitable, safe, accessible, effective, compassionate, well-led, responsive, and deliver a good patient experience. We know that services that deliver good quality care are more cost effective and efficient than 34
35 35 services that demonstrate poor quality. Performance indicators help us to know where our local services are performing well and where they are not. This information is used to identify and spread good practice ideas, as well as to inform us where to focus our attention to improve the care our patients receive in partnership with our service providers. The CCG quantitative indicator performance framework is an integration of key national frameworks that have been developed, namely, CCG Improvement and Assessment Framework (CCG IAF) NHS Outcomes Framework CCG Outcomes Indicator Set CCG Improvement and Assessment Framework (CCG IAF) The CCG Improvement and Assessment Framework (CCG IAF) is designed to supply indicators as markers of success and deliver improvements in our statutory responsibility. It is aligned to key CCG objectives and priorities. It is grouped into four key themes: Better Health, Better Care, Sustainability and a Well Led Organisation. The chart below highlights the key themes and the associated statutory responsibilities that are included. 1. Quality of Care 2. Parity of Esteem Prevention Inequality Better Health Better Care Well Led 1. Sustainability 2. Governance and probity 3. Workforce 4. Collaborative relationships 5. CCG leadership Sustainable Finance Right Care Transformation Digitilisation Estates An initial baseline assessment was undertaken by NHS England, across the whole spectrum. Further information on all these ratings can be found on the website MyNHS Within this CCG Improvement and Assessment Framework, NHSE identified six key clinical priorities, namely: cancer, dementia, diabetes, and learning disabilities, maternity and mental health. NHSE has provided more detailed review and feedback on our performance in these areas. 35
36 36 A summary of this review is provided under the Clinical Priorities section of this report. Further information on these ratings can be found on the website MyNHS. MyNHS MyNHS is a new comparison website tool that allows health and social care organisations to see how their services compare with those of others. It compares on a range of outcomes at both national and regional level and gives commissioners, providers and professionals a central snapshot of published data, to drive improvements in the quality of care. It has been developed by NHS England, together with the Department of Health, the Health and Social Care Information Service, the Care Quality Commission and Public Health England. Further information can be found here: Outcomes: The NHS Outcomes Framework The NHS Outcomes Framework sets out overarching indicators and improvement area measures across five domains, namely clinical effectiveness (three domains), patient experience (one domain) and patient safety (one domain). A more detailed description of the domains is as follows: Domain 1 - Preventing people from dying prematurely: This domain evidences how successful the NHS is in reducing the number of avoidable deaths Domain 2 - Enhancing quality of life for people with long-term conditions: This domain evidences how successful the NHS is supporting people with long-term conditions to live as normal a life as possible. Domain 3 - Helping people to recover from episodes of ill health or following injury: This domain evidences how people recover from ill health or injury and wherever possible how it can be prevented. Domain 4 - Ensuring that people have a positive experience of care: This domain evidences the degree to which the service delivered a positive experience of care for patients, service users and carers. Domain 5 - Treating and caring for people in a safe environment and protecting them from avoidable harm. This domain evidences areas for patient safety and the delivery better health outcomes. Outcomes: NHS England Outcomes Tool In 2016/17 there were 59 performance indicators reported in the NHS England Outcomes Tool that covered the five NHS Outcomes Framework domains. The NHS England Outcomes tool RAG rates CCGs according to their quartile positioning as follows: Green: in the upper (best) quartile (top 25%) 36
37 37 Amber: within the inter quartile range (within the 25% -75% range) Red: in the lowest (worst) quartile (worst 25%) In addition, the tables below also indicate how the CCG has performed relative to CCGs within its cluster, namely, Green: performing better than the cluster Red: performing worse than the cluster PAR: CCG performance on a par with the cluster performance. Lagging and leading indicators The outcomes framework and outcome tool indicators are by nature, mainly lagging indicators. Lagging indicators are measures focusing on results at the end of a time period, normally characterising historical performance. Leading indicators - early warning indicator - on the other hand, are measures that drive or lead to the performance of lag measures. This data enables proactive timely response to early signs of issues and risks. Lagging indicators could be impacted by current programmes work and are likely to impact on the next year s data when released. In addition to the indicators, to strengthen the CCG management of performance we review a range of information using national and local performance information to compare and triangulate performance standards between similar health service providers (benchmarking). We also receive reports from our patients and public, GPs and other organisations which have a role to play in assuring quality. Examples include the Care Quality Commission (CQC), NHS Improvement, Healthwatch, and via the East CCG web page Talk To East Surrey and Ask Carol. 37
38 38 Performance Analysis Report 38
39 Improving quality 39 This section gives an overview of performance against the five domains of the NHS Outcomes Framework. In addition to these indicators, to strengthen the CCG management of performance we review a range of information using national and local performance information to compare and triangulate performance standards between similar health service providers (benchmarking). We also use self-reports received from our patients and public, GPs and other organisations which have a role to play in assuring quality. Examples include the Care Quality Commission (CQC), NHS Improvements and Healthwatch. Clinical effectiveness Domain 1: Preventing people from dying prematurely Metric East Surrey CCG Value Cluster Value England Value Comparison to England Comparison to Cluster Year Potential Years of Life Lost amenable to healthcare - female Potential Years of Life Lost amenable to healthcare - male Under 75 Mortality from CVD Myocardial infarction, stroke and stage 5 kidney disease in people with diabetes Mortality within 30 days of hospital admission for stroke / /15 Under 75 Mortality from respiratory disease Under 75 Mortality from liver disease Emergency admissions for alcohol related liver disease /16 (Jul - Jun) Under 75 Mortality for Cancer One Year survival from all cancers combined Diagnosed 2012 One year survival from breast, lung and colorectal cancers Diagnosed 2011 Maternal smoking at delivery /17 Q1 Breast feeding prevalence at 6-8 weeks /16 Q1 Record of stage of cancer at diagnosis Percentage of cancers detected at stage 1 and 2 Record of lung cancer stage at decision to treat Mortality from breast cancer in females All-cause mortality - 12 months following a first emergency admission to hospital for heart failure in people aged 16 and over April March 2014 Hip fracture - incidence /16 (Jul - Jun) Neonatal mortality and stillbirths Low birth weight full-term babies Above table shows: East Surrey CCG Performance against NHS England Outcomes Tool Indicators Ambition 1 39
40 40 We were in the best quartile performance (RAG rated green) for ten of the 21 indicators in this domain and in the inter quartile range for the balance (RAG rated amber) except for Record of stage of cancer where the CCG was in the worse performing quartile. We also performed better than its comparative cluster in 14 of the 21 indicators, and performed better than the England average in 18 of the 21 indicators. The CCG performed well in the following areas: Improving the potential years of life lost for women Mortality within 30 days of hospital admission for stroke Under 75 mortality from cancer Hip fracture incidences Maternity, particularly smoking at delivery and breast feeding prevalence at six to eight weeks Emergency admissions for alcohol related liver disease. Key areas for improvement: Mortality from Cardiovascular, liver and respiratory disease Cancer, particularly around one-year survival rates and early diagnosis Maternity, particularly, neonatal mortality, stillbirths and low birth weight full term babies. Actions to improve performance We are working collaboratively with the host commissioner for Children's and Maternity, NHS Crawley CCG / NHS Horsham and Mid Sussex CCG, to support and implement the ambitions within the Better Births National Review published in March A successful bid for funding to improve perinatal mental health has been secured to take work forward. We have well established links with Guildford and Waverley CCG which is an early adopter site for the Better Births work stream to benefit from the learning arising from their work. Our clinical lead for women and children is aligned to the South East Clinical Networks which will inform the oversight of implementation of the national review. We have established a baseline position of the nine improvement areas within the better birth reviews with the local provider. From this work the priorities for improvement have been established. These are perinatal mental health, workforce and postnatal pathways. The CCG is actively engaged in the provider monthly commissioner meetings to better understand the service delivery and quality improvement actions. 40
41 Domain 2: Enhancing quality of life for people with longterm conditions Metric East Surrey CCG Value Cluster Value 41 England Value Comparison to England Comparison to Cluster Year Health related quality of life for people with long term conditons % of patients with long term conditions who feel supported to manage their condition People with diabetes dignosed less than a year referred to structured education / / /15 Unplanned hospitalisation for chronic ACS conditions Unplanned hospitalisation for asthma, diabetes and epilepsy in under 19s /16 (Jul - Jun) 2015/16 (Jul - Jun) Complications associated with diabetes /13 Access to community mental health services by people from Black and Minority Ethnicity (BME) groups Access to psychological therapies services by people from Black and Minority Ethnicity (BME) groups Percentage of referrals to IAPT services which indicated a reliable recovery following completion of treatment Percentage of referrals to IAPT services which indicated a reliable improvement following completion of treatment Percentage of referrals to IAPT services which indicated a reliable deterioration following completion of treatment Health-related quality of life for carers, aged 18 and above Health-related quality of life for people with long-term mental health conditions / / / /16 Above table shows: Our performance against Domain 2 of the NHS England Outcomes Tool Indicators. We were in the best quartile performance (RAG rated green) for seven of the 13 indicators in this domain, in the inter quartile range for three (RAG rated amber) and in the worst quartile (RAG rated red) for three. We performed better than its comparative cluster in eight of the 13 indicators. We performed better than the England average in 8 indicators. The CCG performed well in the following areas: Improving the health related quality of life for people with both physical and mental long term conditions, as well as for carers Reducing unplanned hospitalisation for patients with ambulatory care sensitive conditions (that is conditions that can be treated during the course of a day, without hospital admission) as well as patients under 19 years of age with asthma, diabetes and epilepsy. 41
42 Key areas for improvement 42 The proportion of people with diabetes who have been diagnosed less than a year, who are referred to structured education. Access to community mental health and Individual Access to Psychological Therapy (IAPT) for people from Black and Minority Ethnic (BME) groups. The recovery rates from IAPT is an issue that needs addressing Actions to improve performance The IAPT recovery target of 50% recovery rate has been achieved since January IAPT providers are collaborating to develop a marketing plan to support increased access for the whole population to achieve the 50% target. As part of the Five Year Forward View the target for for increased access will increase from 15-17%. Guildford & Waverley CCG has recently assumed lead commitment responsibilities for mental health including IAPT services. The quality monitoring processes are being fully reviewed and strengthened to ensure targets are met for 2017/18 and timely actions to address sub-optimal performance. A long term strategy for diabetes care is being developed that includes several interventions to prevent and manage diabetes. A key short term intervention is the implementation of a locally commissioned service scheme for identifying and managing those at high risk of type 2 diabetes during 2016/17. BME access issues will be addressed as part of the current Surrey-wide programme to transform mental health services. 42
43 43 Domain 3: enhancing quality of life for people with long-term conditions and helping people to recover from episodes of ill health or following injury Metric Emergency admissions for acute conditions that should not usually require hospital admission Emergency readmissions wihthin 30 days of discharge from hospital East Surrey CCG Value Cluster Value England Value Comparison to England Comparison to Cluster Year 2015/16 (Jul - Jun) /12 Elective Hip replacement (Primary) procedures (PROMS) Elective Knee replacement (Primary) procedures (PROMS) / /15 Elective groin hernia procedures (PROMS) /15 Elective varicose veins procedures (PROMS) n/a Emergency admission for children with lower respitory tract infections /16 (Jul - Jun) People who have had a stroke who are admitted to an acute stroke unit within 4 hours of arrival to hospital People who have had an acute stroke who receive thrombolysis People with stroke who are discharged from hospital with a joint health and social care plan People who have a follow-up assessment between 4 and 8 months after initial admission for stroke People who have had an acute stroke who spend 90% or more of their stay on a stroke unit Hip fracture: proportion of patients recovering to their previous levels of mobility/walking ability at 30 days Hip fracture: proportion of patients recovering to their previous levels of mobility/walking ability at 120 days / / / / / Hip fracture: collaborative orthogeriatric care Hip fracture: timely surgery Hip fracture: multifactorial falls risk assessment Alcohol-specific hospital admissions /16 (Jul - Jun) Emergency alcohol-specific readmission to any hospital within 30 days of discharge following an alcohol-specific admission Unplanned readmissions to mental health services within 30 days of a mental health inpatient discharge in people aged 17 and over Percentage of adults in contact with secondary mental health services in employment Hip fracture: care process composite indicator /16 (Jul - Jun) / /16 (Jul - Jun) Table above shows: Our Performance against Domain 3 of the NHS England Outcome Tool Indicators. 43
44 44 We were in the best quartile performance (RAG rated green) for nine of the 22 indicators in this domain, in the inter quartile range for nine (RAG rated amber) and in the worst quartile (RAG rated red) for four. We performed better than its comparative cluster in eleven of the 22 indicators and performed better than the England average in fourteen of the indicators. The CCG performed well in the following areas Reducing emergency admissions for acute conditions not usually requiring hospital admission Reducing emergency admissions for children with lower respiratory tract infections Reducing alcohol related hospital admissions with low readmission rates. Hip fracture surgery. Stroke patients with a care plan on discharge Key areas for improvement Emergency readmissions within 30 days of discharge (for both physical and mental health) Patient reported outcomes relating to specific elective procedures, namely hip replacement, knee replacement and groin hernia. All key areas relating to stroke but in particular, admission to a stroke unit within four hours and follow up assessment after the initial admission into hospital for a stroke. Actions to improve performance Emergency readmissions Robust personalised and collaborative care planning within primary, community and social care to enable an integrated planned discharge process Improved access to Musculoskeletal (MSK) and Integrated Clinical Assessment and Treatment (ICATS) service within the community setting Stroke pathway We have participated in the Surrey-wide development of commissioning for best practice stroke pathways from admission to post rehabilitation. We have developed a local model in partnership with our providers to strengthen the delivery of the community elements of the pathway to ensure seamless transitions across organisational pathways. This work will be taken forward in 2017/18 through a local whole system health economy task and finish group. The impact of this work will support the improvement of the overall Sentinel Stroke National Audit Programme (SSNAP) score which currently stands at D and the ambition to achieve a B rating. See more about our projects to review patients with Atrial Fibrillation in order to prevent strokes and the RightCare Cardiology project. 44
45 45 Domain 4: Patient Experience The drive to place quality at the heart of the NHS means that the patient and carers must be at the centre of everything the NHS does. There is evidence that patient experience is enhanced when the care provided is safe, effective and the outcomes of care are aligned with current best practice and evidence-based. Shared decision making and choice made in collaboration with the patient and their families is key to positive care experiences. Therefore understanding and responding to patient experience is one of the foundations for improving commissioning for quality and ensuring we have the right performance measures in place. Metric East Surrey CCG Value Cluster Value England Value Comparison to England Comparison to Cluster Year Patient experience of GP out-of-hours services /15 Patient experience of hospital care /16 Responsiveness to Inpatients' personal needs /16 Above table shows: Our Performance against Domain 4 of the NHS England Outcome Tool Indicators We performed better than our comparative cluster in 2 of the 3 indicators. We performed better than England average in 2 of the 3 indicators. We were in the best quartile performance (RAG rated green) for one of the three indicators in this domain, in the inter quartile range for one (RAG rated amber) and in the worst quartile (RAG rated red) for one (out of hours GP services). Areas for improvement The Out of Hours (OOH) service was procured in Recent data from the GP patient Survey reported in January 2016 is already reflecting improvements. National GP Patient Survey The GP Patient Survey (GPPS) is an England-wide survey, providing practice-level data about patients experiences of their GP practices. Ipsos MORI administers the survey on behalf of NHS England. The data published in January 2016 showed a response rate of 41% for our membership practices, which means that results were considered to be statistically significant. The GP Patient Survey (GPPS) measures patients experiences across a range of topics, including: Making appointments Waiting times Perceptions of care at appointments Practice opening hours Out-of-hours services 45

46 46 GPPS can be used as one element of evidence that can be triangulated with other sources of feedback, such as feedback from Patient Participation Groups, local surveys and the Friends and Family Test, to develop a fuller picture of patient experience. Overall positively reported experience for our membership practices was 86% against 85% nationally. For more information about the survey please visit How we hear about patient experiences We use a wide range of activities and forums to make it as easy as possible for patients to feed back their experiences with our local healthcare providers. Rant n Rave Our annual, open to all, agenda-less event in May aimed to listen to local views about health services or national policy and hear more about what people value most about the NHS; finding out what is working well and what we could do better. Key themes included concerns about the pressures on Primary Care (GP) services and appointments, feedback on the 111 service and waiting times/cancelled operations. Friends and Families Test Patients have an opportunity to routinely give their feedback following episodes of care through the Friends and Families Test (FFT). We have FFT running within community, inpatient, maternity, A&E, Primary Care (GP practices) and mental health services. 46
47 47 PALS and Complaints We seek to promote a culture of patient and public involvement throughout the organisation and there is a strong interface between Patient Advice and Liaison Service (PALS) and Complaints. Staff are empowered to manage issues before they escalate into something more serious. Feedback from service users, carers and relatives is welcomed and we approach all complaints in an honest and open way, with the principal aims of resolving the problem, satisfying the complainant s concerns and learning from the experience. Month PALS Total no. new Complaints no. new CCG Complaints Open/ Close d Total of CCG compla ints January open 1 February open 1 March open 3 April open 3 May open 3 June open 3 July open 4 August open 4 September None open 4 recorded* October open 4 November open 4 December open 4 Total It is still difficult to exactly quantify the number of PALS cases as receiving staff often judge a call business as usual rather than as a PALS enquiry. Although direct comparisons are of somewhat limited value, it would seem that the number of CCG PALS enquires is higher than for neighbouring CCGs (with a similar population), whilst the number of formal complaints is significantly lower. With such low numbers of complaints reported to us, it has not been possible to identify any themes. However, we receive regular complaints reports from providers, as complainants are far more likely to make a complaint directly to the service. Provider reports give us a clearer idea of the issues affecting patients and their families, and an opportunity to scrutinise and monitor associated action plans. PALS and Complaints data is reported to the Governing Body via the monthly Quality, Safety and Patient Experience Report and the Senior Management Team is notified of any immediate concerns or emerging themes. Our Complaints Policy accords with national requirements and also reflects the reforms to the health and social care system brought about by the Health and Social Care Act 2012, and embeds the recommendations contained in the Francis Enquiry report and other reports such as Berwick, Keogh, Clywd-Hart and My Expectations (PHSO) as well as the Government s response paper to the Francis Enquiry report. 47
48 48 Our PALS and Complaints services were subject to an internal audit in August 2016 and awarded a rating of Substantial Assurance. Soft Intelligence So called soft intelligence is referred to in the Francis report. It can provide valuable insight into the quality of services that our patients experience. Patients and members of the public are encouraged to report their experiences (good, bad or indifferent) through our website Talk to Carol. They can also use phone, text, letter or . Patient experiences reported in this way can sometimes show a very different picture to that reported through contract and performance management data. Patient choice We are fully engaged in offering choice to patients using the NHS e-referral Service (ERS). All the 18 GP Practices within our CCG are now using the electronic method of referring and referrers are being urged to send all referrals to first outpatient consultant led clinics using the NHS e-rs platform. We are progressively making ERS a mainstream function with a handful of GPs making their own ERS referrals, discussing and offering choice to patients during consultation. Some other referrers start off the ERS process by discussing the choice of service with the patient during consultation, and delegating their medical secretaries and other practice staff to complete the referral using ERS. In the majority of cases, patients are informed to come back and collect their appointment request letters with choices of hospitals, and are asked to go away and phone the national bookings telephone service, to book appointments with their hospitals of choice. We are also working with the local service provider (SASH) to offer the named clinical option, to make it part of patient choice. We are working to include all community services on the ERS menu, to provide a vehicle for making all referrals electronic, thereby streamlining the patient choice of place, date and time, regardless of service provider. We continue to monitor weekly bookings for each practice, and have appointed two clinical leads to engage with their colleagues in GP Practices to offer additional support and share experiences, lessons learned and best practice from high performing practices. 48
49 Domain 5: Patient Safety 49 Patient safety is a core duty for CCGs which we are committed to ensuring. Two areas for focus are infection control and serious incident management. Infection control Metric East Surrey CCG Value Cluster Value England Value Comparison to England Comparison to Cluster Year Incidence of healthcare-associated infection - MRSA April Sep 2016 Incidence of healthcare-associated infection - C.Difficile Above table shows: Our Performance against Domain 5 of the NHS England Outcome Tool Indicators We performed poorly in both domains when compared with both cluster and England performance. During the last year, robust systems have been established for investigating root cause analysis and learning from cases of MRSA blood stream infections and Clostridium difficile cases arising in primary, community and secondary care. There has been increased collaboration with experts in infection control across CCGs and providers that has informed a greater understanding of the root causes and contributory factors for infections. We have recruited an infection prevention and control nurse specialist to lead and support the implementation of our infection control action plans for 2016/17 as well as in depth learning accrued from root cause analysis and contributory factors from all cases investigated. Onwards root cause analysis for the reduced numbers for Clostridium difficile cases in 2016/2017 have again shown the at risk population as older people with multiple health conditions, long hospital prescribed antibiotic histories and people who are immunecompromised, where cases have been shown to be mostly unavoidable. Risk factors have been proton pump inhibitor usage, gastrointestinal surgery and steroid use. However there have only been two cases of inappropriately prescribed antibiotics and one case of an inappropriately requested repeat specimen which would suggest that that the learning from the previous year has had a positive effect. Regular assurance visits have been made to East Surrey Hospital following a peer review by another acute provider. A comprehensive action plan has been drawn up and agreed by provider and commissioner and is currently being implemented with learning embedded and ongoing monitoring arrangements established. Serious incidents management April Sep 2016 We have robust arrangements in place for serious incident management. During 16/17, the service was audited by TIAA internal auditors and was awarded substantial assurance. The below summarise the 2015 /16 and 2016/17 incidents per provider and the top three themes are summarised. Financial First South East Coast Surrey and Surrey and Total 49
50 Year 2015/2016 Quarter 1 Community Health and Care CIC 50 Ambulance Service NHS FT Borders Partnership NHS FT Sussex Healthcare NHS Trust Apr May Jun Quarter 2 Jul Aug Sep Quarter 3 Oct Nov Dec Quarter 4 Jan Feb Mar Total Financial Year 2016/2017 Quarter 1 First Community Health and Care CIC South East Coast Ambulance Service NHS FT Surrey and Borders Partnership NHS FT Surrey and Sussex Healthcare NHS Trust Apr May Jun Quarter 2 Jul Aug Sep Quarter 3 Oct Nov Dec Quarter 4 Jan Feb Mar Total Total 50
51 SI Themes 51 For all CCG registered patients across both financial years. First Community Health and Care CIC Pressure Ulcers meeting SI criteria Slips/Trips/F alls meeting SI criteria Accident (not slip/trip/fall) meeting SI criteria South East Coast Ambulance Service NHS FT Treatment delay meeting SI criteria Sub-optimal care of the deteriorating patient meeting SI criteria Accident e.g. collision/scald (not slip/trip/fall) meeting SI criteria Surrey and Borders Partnership NHS FT Apparent/actual/ suspected selfinflicted harm 149 of the 161 declared resulted in death Unauthorised absence meeting SI criteria Failure to obtain appropriate bed for child who needed it Surrey and Sussex Healthcare NHS Trust Slips/trips/falls meeting SI criteria Diagnostic incident including delay meeting SI criteria (including failure to act on test results) Sub-optimal care of the deteriorating patient meeting SI criteria In April 2016 to March 2017 there were 136 serious incidents which is an increase compared with the same time period 2015 /16, during which 85 incidents were reported. The reasons for the increase were discussed at our Clinical Quality Review Meetings in February and March and include changes in reporting requirements which incidents which occurred 1 year post discharge from services whereas previously it was 6 months, delayed submissions from last year as a consequence of increased number of coroners backlogs of reports. Following a deep dive into their governance and management processes around serious incidents SABP has strengthened oversight of SI s and there is now a dedicated Director of safety and Medical Director to oversee the improvements and embedded learning around safety. In conclusion, the reporting culture has improved, key themes have been identified and the commissioner and provider have worked in partnership to embed learning within and across organisations. Increased reporting is recognized as a proxy for a strong safety culture within an organisation. Together with our providers we have established robust arrangements to minimise the risk of recurrence of the same incident which reflects a culture of continuous quality improvements. 51
52 52 NHS Constitution: ensuring patient access to timely treatment The NHS Constitution targets ensure patients have timely access to elective care and diagnostics which in turn improves outcomes for patients and potentially avoids unnecessary costly emergency care. The target levels are mandated and can be clustered into three categories of care: elective, cancer and emergency. Our performance during 2016/17 for each category of care is highlighted in the tables below with a brief narrative. Elective Care and Diagnostic Access One of the key NHS Constitutional rights of patients is the right to be treated within no more than eighteen weeks from the date of referral. To allow for patient choice to delay treatment the target for the standard is set at 92%. The table below reflects our performance against the key NHS Constitution elective (planned) care standard - waiting time for patients on an incomplete pathway (i.e. patients currently waiting to be seen and treated). An integral part of that 18-week pathway is patient access to diagnostic services. The NHS Constitutional patient right for diagnostic services is that all patients should be seen within six weeks from their first consultant appointment. To allow for patient choice the target for the standard is that 99% of patients should be seen within six weeks. The tables below show our performance against the targets. Table below shows: Patient waiting times for Elective Care RTT Performance (%) - CCG View by Specialty by Month Incomplete Pathways APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH General Surgery 89.73% 89.31% 90.71% 89.71% 89.56% 91.25% 90.75% 90.24% 90.31% 90.15% 91.05% 91.55% Urology 93.93% 93.02% 93.49% 95.08% 94.12% 93.89% 94.19% 94.28% 94.49% 91.49% 91.42% 90.49% Trauma & Orthopaedics 93.72% 94.43% 95.47% 94.32% 93.71% 93.67% 94.58% 94.06% 91.65% 90.02% 89.84% 90.28% ENT 94.87% 95.10% 94.16% 95.87% 96.68% 97.39% 97.48% 96.80% 95.29% 96.41% 96.66% 96.86% Ophthalmology 91.70% 93.61% 90.85% 91.16% 90.00% 91.65% 93.85% 94.99% 93.30% 94.59% 92.61% 93.00% Oral Surgery % % Neurosurgery 76.09% 77.50% 56.52% 64.00% 64.29% 68.00% 64.29% 70.59% 53.33% 71.43% 60.00% 61.54% Plastic Surgery 89.25% 92.65% 95.45% 89.85% 90.78% 89.71% 91.55% 93.68% 94.15% 91.15% 89.53% 91.04% Cardiothoracic Surgery 85.71% 78.95% 80.00% 86.96% 84.62% 89.29% 86.67% 81.58% 71.79% 77.42% 77.27% 79.17% General Medicine 97.06% 93.75% 97.14% 97.14% 97.22% 95.56% 96.30% 92.86% 90.91% 93.75% 89.74% 87.50% Gastroenterology 94.50% 93.89% 95.79% 95.76% 95.28% 95.99% 95.75% 93.60% 94.55% 93.55% 94.87% 94.30% Cardiology 90.70% 91.88% 89.76% 91.16% 93.51% 94.35% 92.89% 94.59% 90.76% 91.11% 89.55% 88.61% Dermatology 91.88% 92.05% 92.12% 92.78% 93.53% 95.30% 94.05% 93.48% 90.56% 89.06% 89.78% 89.35% Thoracic Medicine 96.81% 97.07% 97.57% 97.87% 97.01% 97.21% 95.52% 97.18% 97.51% 97.34% 95.09% 96.00% Neurology 95.89% 95.22% 94.39% 89.51% 84.38% 81.29% 80.29% 81.91% 77.73% 79.78% 76.65% 73.19% Rheumatology 94.62% 94.46% 95.73% 91.41% 81.88% 83.15% 86.71% 93.11% 90.15% 93.01% 93.46% 94.91% Geriatric Medicine % % % 98.36% % 98.86% 97.30% 97.14% 95.92% 97.06% % % Gynaecology 95.42% 93.01% 92.98% 89.39% 92.66% 92.79% 93.62% 93.93% 91.90% 91.83% 91.18% 90.19% Other 92.67% 93.35% 92.24% 93.31% 92.93% 92.57% 90.87% 91.29% 89.72% 90.63% 88.66% 88.71% Total 92.85% 93.12% 93.05% 92.80% 92.37% 92.89% 92.87% 92.99% 91.44% 91.28% 90.59% 90.57% We met the incomplete pathway operating standard of 92% of patients on the waiting list having waited less than 18 weeks to be treated from April 2016 to November 2016; during this period there was particular pressure within General Surgery, Neurosurgery, Cardiothoracic Surgery and Cardiology. We breached the standard in from December 2016 to March 2017 with waiting time pressures across most specialties. 52
53 53 Table below shows: Patient waiting times for Diagnostic Services East Surrey CCG Diagnostic Performance (All Tests) Under 6 week waits Over 6 week waits Over 52 week waits Breach % April May June July August September October November December January February March % 0.6% 0.8% 0.6% 0.5% 0.6% 0.4% 0.2% 0.3% 0.5% 0.4% 0.3% 0.7% 0.6% 0.5% 0.7% 5.1% 6.4% 5.4% 5.2% 3.6% 1.0% 0.3% 0.2% We breached the diagnostic standard from August 2016 through to December Action plans were successfully implemented with our performance returning to the expected standard for the remainder of the financial year. Table below shows: Patient waiting list size APRIL MAY JUNE JULY AUGUST SEPTEMBER OCTOBER NOVEMBER DECEMBER JANUARY FEBRUARY MARCH 18 Week % < 18 Weeks % % % % % % % % % % % % % % % % % % % % % % % % Total Patients Weeks Despite provider data quality issues during September to November, the waiting list size has increased and was significantly higher in March 2017 (14,503) than at March 2016 (11,234). Consequently there is risk of continued breach in the future. Several providers exceed the safety norm of no more than 10 weeks to clear the waiting lists that exist at a point in time or the safety norm of 4 days to clear the backlog list. This would appear to be result of internal processes within the providers which could be compounded by increased referral rates. A review of the NHS England National RTT Pathway Monitoring Tool shows RTT pressure across most of East Surrey CCG main providers of elective care. Key issues affecting performance at Surrey and Sussex Healthcare NHS Trust (SaSH) Although we continue to manage referral demand through our Planned Care Locally Commissioned Service (LCS), the Trust is experiencing increased referrals from new areas, increasing pressure on capacity and hence the ability to deliver the standard. This is reflected in: Current underperformance against plan in elective activity and reduced numbers in completed admitted and non-admitted pathway activity. Provider staff shortages in key specialties. 53
54 54 Provider staff shortages in diagnostics reflected in under performance against plan in diagnostic activity. Reduced elective bed capacity through winter pressures, increased excess bed days and delays in discharging patients Ring fenced capacity for cancer patients to ensure compliance with cancer standards. Potential Impact Reduction in quality outcomes (effectiveness, patient experience and patient safety) Increase in costs if patients on the waiting list present themselves in an emergency admission. 25% reduction in the value of the 2016/17 Quality Premium received by us for failing to meet the incomplete pathway standard. Expectation and actions We will ensure all providers of care for East Surrey residents have a robust and achievable referral to treatment plan in place. A local system wide resilience plan is being developed through the newly created Planned Care Board working with the A&E Delivery Board and restructured Transformation Board. Joint demand and capacity modelling with our main acute provider (SASH) and Crawley CCG / Horsham and Mid Sussex CCG during the 2017/18 planning round to address demand and capacity issues. Our organisational restructure and increased staffing in the performance directorate has enabled the introduction of an improved and more robust performance management framework, which includes teams from finance, contracting and quality. Cancer In 2015/16 we had a cancer prevalence of 2.6%; this was slightly higher than the England prevalence 2.4%. Our performance for under 75 mortality rates is in the best 25%. However, we perform in the interquartile range for one-year survival from all cancers. To improve this performance requires early diagnosis (at Stage 1 and Stage 2) through nonemergency routes and early treatment. The NHS Constitutional cancer standards are in place to achieve this by: Requiring suspected cancer patients being seen by a consultant within two weeks from receiving a referral Patients receiving their first treatment within 31 days from date of diagnosis Patients receiving any subsequent treatment within 31 days and, The cancer pathway from referral to first definite treatment not exceeding 62 days 54
55 55 Currently we have a lower rate of patients diagnosed via emergency routes than the national average for all three tumor sites and 50.7% of cancers diagnosed at stage 1 or 2 which is above the cluster average and on a par with the national average. The growth rate in two-week urgent referrals has shown a significant increasing trend. However, the current conversion rate from two week wait referral to cancer diagnosis (occurrence) is approximately 14%. Performance against standards The table overleaf reflects our performance against the key NHS Constitution cancer waiting standards. It can be seen that there has been an improvement in cancer performance since September 2016, however, year to date we continue to breach one of the standards. 55
56 56 Access to Cancer Services E.B.6 : Percentage of patients seen within two weeks of an urgent GP referral for suspected cancer E.B.7 : Percentage of patients seen within two weeks of an urgent referralfor breast symptoms where cancer was not initially suspected. E.B.8 : Percentage of patients receiving first definitive treatment within one month (31-days) of a cancer diagnosis (measured from date of decision to treat ) Target April May June July August September October November December January February March YTD Last Year 93% 90.23% 92.99% 91.45% 96.11% 93.45% 95.76% 95.86% 94.95% 94.41% 94.70% 94.09% 94.23% 93.95% 93.39% 93% 81.03% 90.48% 80.00% 95.56% 97.96% 98.15% 97.83% 96.83% 89.83% 95.56% 93.65% % 93.26% 92.50% 96% 90.48% % 98.44% % 97.70% 94.74% 96.10% 98.80% % 95.95% 98.11% 97.22% 97.24% 97.22% E.B.9 : Percentage of patients receiving subsequent treatment for cancer within 31-days, where that treatment is Surgery E.B.10 : Percentage of patients receiving subsequent treatment for cancer within 31-days, where that treatment is an Anti-Cancer Drug Regimen E.B.11 : Percentage of patients receiving subsequent treatment for cancer within 31-days, where that treatment is a Radiotherapy Treatment Course E.B.12 : Percentage of patients receiving first definitive treatment for cancer within two months (62 days) of an urgent GP referral for suspected cancer. E.B.13 : Percentage of patients receiving first definitive treatment for cancer within 62-days of referral from an NHS Cancer Screening Service. E.B.14 : Percentage of patients receiving first definitive treatment for cancer within 62-days of a consultant decision to upgrade their priority status. Above table shows: Cancer waiting time performance 94% 98% 94% No patients in Month No patients in Month No patients in Month 92.86% % % 92.86% 90.00% % % % % % % 97.10% 98.05% % % % % % % % % % % % % 99.50% 94.12% 91.18% 96.67% % % % % % 95.83% % 93.10% 97.39% 97.13% 85% 80.65% 84.85% 89.47% 87.50% 82.50% 86.05% 75.00% 88.89% 85.71% 87.18% 82.14% 83.78% 84.63% 81.22% 90% 83.33% % 83.33% % % % % % % % 86% No patients in Month % No patients in Month No patients in Month % 96.97% 97.03% 75.00% 77.78% % % 66.67% % % % % 88.57% % 56
57 57 Patients receiving first definitive treatment for cancer within two months (62 days) of an urgent GP referral Our year-to-date performance of 84.6% is marginally below the 85% target for the standard. This is a consequence of: Performance by our main acute provider (SaSH) being below the target for April 2016 (81.5%) and October 2016 (80.7%). Due to changes in systems and processes implemented the Trust has exceeded the target of 85% from November 2016 to March 2017 with an average performance of 90.7% over this period. Although the number of patients is small, Royal Surrey County Hospital has consistently breached the target. The two continued areas of challenge for the RSCH are late referrals into the Trust and waits for Brachytherapy. The latter has a project improvement plan in place, and there is good progress to date. The late referrals are being addressed with a breach reallocation policy which is being considered by the Trusts Potential Impact: Reduction in quality outcomes (effectiveness, patient experience and patient safety). Increase in costs if patients on the waiting list present themselves in an emergency admission. 25% reduction in the value of the 2016/17 Quality Premium for failing to meet the 62 day cancer standard. Expectation and actions taken to date Providers have implemented plans to improve performance. Responsibility for delivery has been assigned to the local A&E Delivery Board. In the short term we are attending the Cancer Action Group and Cancer Patient Tracking List meetings with constant monitoring of performance by the quality team. In the long term, as Cancer is one of the national NHS England clinical priority areas, we are developing action plans to ensure compliance with the cancer standards and set trajectories to improve the one year survival rate. A Cancer Steering Group with a designated clinical lead, is in place to monitor implementation. Our organisational restructure and increased staffing in our performance directorate has enabled the introduction of an improved and more robust performance management framework, which includes teams from Finance, Contracting and Quality. 57


58 Emergency Care 58 The table below reflects our performance against the key NHS Constitution emergency care waiting standards. It can be seen that there have been continued incidences of breaches across all the standards indicating capacity issues at our main providers. Above Table shows: Emergency Care Standards: Accident and Emergency Accident and emergency Our main acute provider (SaSH) failed to meet the ED 4hr standard 95% of patients being seen within 4 hours in both December 2016 and January Reasons for this include: Although additional funding was provided from operational resilience monies, winter pressures resulted in increased ED attendances and growth in non-elective admissions. Discharge delays. Ambulance turnaround performance was significantly impacted in January 2017 with 66 breaches of the 1hr standard. Failure to maintain the emergency department standard due to lack of capacity in the health system has been included in the Trust s significant risk register with a risk score of 16; the standard was not achieved during 2016/17. Of concern is the current operational performance and pressure of surrounding acute providers in the region, particularly Brighton and Sussex which could result in patients being redirected and place our local acute trust under additional operational pressure. SaSH continues to meet the A&E Trolley Wait standard that patients should wait no longer than 12 hours before being admitted to a bed. Potential Impact Reduction in quality outcomes (effectiveness, patient experience and patient safety). 25% reduction in the value of the 2016/17 Quality Premium for failing to meet the ED four hour standards. 58
59 59 Expectation and actions taken to date We continue to monitor our main provider on a weekly basis, and the performance against national and locally agreed targets is a regular agenda item on the system wide local A&E Delivery Board. We have several schemes in place to improve patient discharge and reduce unnecessary attendances at A&E. Actions are in place to reduce handover delays (see Ambulance section below). Ambulance Performance continues to be a challenge with all national response rate standards being breached. A Unified Recovery Plan (URP) is in place and closely monitored by the lead commissioner (North West Surrey CCG). New improvement trajectories for the period October 2016 to March 2017 were agreed through the Strategic Partnership Group. See table below. SECAmb failed to meet these improvement trajectories from December 2016 as shown below: NHS Constitution Target Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 YTD Ambulance Performance East Surrey CCG 48.5% 60.0% 53.7% 47.1% 59.0% 48.7% 53.1% 62.3% 46.4% 59.3% 67.9% 52.4% 55.6% Red 1 NHS Surrey Total 75% 64.1% 62.3% 50.4% 45.9% 60.7% 56.7% 60.2% 60.0% 59.7% 62.8% 64.1% 60.5% 59.4% SECamb Commissioned 70.2% 66.4% 59.6% 62.1% 64.6% 62.6% 64.7% 65.6% 62.8% 65.5% 67.3% 65.7% 64.9% East Surrey CCG 49.3% 46.0% 49.3% 43.9% 44.5% 46.6% 45.6% 47.1% 45.3% 43.3% 46.3% 44.0% 45.8% Red 2 NHS Surrey Total 75% 49.0% 46.9% 44.2% 40.3% 42.7% 42.6% 45.0% 48.1% 45.9% 45.0% 45.8% 45.5% 45.0% SECamb Commissioned 60.0% 56.8% 51.4% 49.5% 52.5% 52.8% 53.7% 56.4% 51.6% 47.7% 50.0% 49.8% 52.6% East Surrey CCG 89.1% 88.6% 88.1% 85.2% 87.4% 87.8% 88.7% 90.7% 85.4% 83.2% 87.5% 87.4% 87.0% Cat A19 NHS Surrey Total 95% 91.6% 90.8% 86.3% 84.9% 89.6% 88.8% 89.1% 91.2% 88.4% 87.9% 88.9% 89.1% 88.7% SECamb Commissioned 93.5% 91.0% 88.8% 88.0% 89.7% 89.9% 89.9% 90.8% 87.8% 85.8% 88.3% 87.6% 89.1% Ambulance hours lost at hospital due to delayed handovers has contributed to this poor performance. January 2017 saw the worst ever month with 7,950 hours lost at hospital in spite of 1% fewer conveyances to hospital compared to the previous January. Potential Impact Reduction in quality outcomes (effectiveness, patient experience and patient safety). 25% reduction in the value of the 2016/17 Quality Premium for failing to meet the Red 1 response rate standard. 59


60 60 Actions taken to improve There are detailed actions within the URP that are beginning to show some positive step changes in R1, R2 and A19. In addition, provider organisation restructuring initiatives at both senior executive and operational level should contribute to improved performance. A system-wide action plan to introduce measures to address some of the underlying issues in handover delays is being finalised by NHS Improvement following input from SECAmb and other partner organisations. This will become part of the work plan for each of the A&E Delivery Boards and aims to address a number of issues across the pathway which have been identified as likely to smooth flow and reduce system bottlenecks. This will include an Emergency Handover Procedure. Commissioners and acute trusts are working with SECAmb to drive improvements. Mental Health Standards (Parity of Esteem) The table below highlights our performance against the national Parity of Esteem (Mental Health) standards. Our performance is described in more detail below. Improving Access to Psychological Therapies (IAPT) We failed to meet its annual target of 15% of the prevalent population accessing psychotherapy. However: Increased effort by practices and the introduction of self-referrals and referrals by other health professionals and Additional staff recruited and assigned to lead improvements 60
61 61 is having a positive effect. Performance in both February and March exceeded the monthly target of 1.25%. The prevalent population is the level of general need in the population; a local estimate of people who have depression and/or anxiety disorders based on the Adult Psychiatric Morbidity Survey, Both the six week and eighteen week waiting time standards were achieved. Meeting the recovery rate standards has proved a challenge for the CCG. Performance at M11 fell marginally short of the 50% target. Interventions by the South East Clinical Network in association with the Mental Health Intensive Support Team appear to have proved effective with recovery rates in February 17 (59%) and March 17 (52%) exceeding the standard. Consequently the CCG achieved the standard for the year. Dementia See the Mental Health/Dementia section under Our Achievements for the Year for details. Other standards We have consistently met the Early Intervention in Psychosis (EIP) standard and the Mental Health and Learning Disability Collaborative which oversees and manages performance, is confident targets will continue to be met. We have made progress throughout 2016/17 in reducing the number of inpatients who have either a learning disability and/or an autistic spectrum disorder (including Asperger s syndrome). The number of patients currently in inpatient beds has reduced to two with continuous reduction in the number of admissions zero admissions from June 2016 to January Furthermore, all learning disability patients: currently have a care coordinator are on a learning disability register have had a review in the last 26 weeks. East Surrey Mental Health and Learning Disability Collaborative performance CCG s Early Intervention in Psychosis During 2016 /17 good progress has been made to provide an integrated collaborative approach to effectively support people with learning disabilities and for people with learning disability and people with learning disability with autism and/or behaviour that challenges and mental health concerns. These services are commissioned by our host commissioner Guildford & Waverley CCG. We provide feedback and oversight from our local population into two key governance structures. These are the Learning Disability Programme Board and the Transformational Partnership Board. 1.0 The Learning Disability Programme Board In July 2016 the Learning Disability Programme Board was set up by our host commissioner Guildford & Waverley CCG with the aim to map current provision of services and identify gaps and provide oversight of the quality and developments across all commissioned services and work streams. 2.0 Transformational Partnership Board This board provides oversight for the delivery of the service model set out in national documents published to deliver the Transforming Care Plan 61
62 62 (January 2015). The national guidance issued in Building the Right Support - for people in Surrey with a learning disability and/or autism covers people with behaviour that challenges, and those with a mental health condition The Transforming Care Plan aims to enhance the current support people receive through the following objectives: A good and meaningful life. Choice and control. Support to my family and paid staff. Where I live and who I live with. Mainstream health services. Specialist multi-disciplinary health services in the community. Specialist social care support in the community. Hospital admissions to be support by a clear rationale of assessment and treatment. The Surrey plan was agreed at the Health and Wellbeing Board in April 2016 and was aligned with the 20:20 Vision for SEND (Special Educational Needs and Disabilities), to focus on life expectancy inequality as part of strategy across Surrey. 2.1 East Surrey Transforming Care During 2016/17 we made significant progress in delivering the requirements for Transforming Care. A weekly Transforming Care Response Group Meeting with health and social care teams. This tracks the progress and suitability of placements for this client group. A risk register is in place and is monitored at this meeting. We had nine individuals on the Transforming Care List. Seven individuals have been placed into settled accommodation with twice monthly oversight of their progress and the suitability of care support. Two individuals with very specialist complex needs are expected to transfer to a suitable community in 2017/18 when bespoke services can be procured. Proactive work is in place for identifying and working with younger people to prepare for community placements. 62
63 63 Clinical Priorities NHS England has provided the CCG with a formal assessment of the six priority clinical areas, namely, cancer, dementia, diabetes, learning disability, maternity and mental health. The outcome of this assessment is provided in the table below. Clinical Priority and Assessment Cancer Rating: Needs Improvement CCG IAF Indicator Number, Description and Performance Value 122a 122b 122c 122d Cancers diagnosed at early stage People with urgent GP referral having 1st definitive treatment for cancer within 62 days of referral One-year survival from all cancers Cancer patient experience Date of data Q ENGLAND 81.90% 70.20% 89.00% East Surrey and Sussex #N/A 79.00% #N/A 88.20% NHS East Surrey CCG 50.70% 78.40% 71.10% 87.40% 126a 126b Dementia Rating: Needs Improvement Estimated diagnosis rate for people with dementia Dementia care planning and post-diagnostic support Date of data Apr-16 #N/A ENGLAND 66.40% East Surrey and Sussex 63.30% #N/A NHS East Surrey CCG 61.50% #N/A 103a 103b Diabetes Rating: Needs Improvement Diabetes patients that have achieved all three of the NICErecommended treatment targets People with diabetes diagnosed less than a year who attend a structured education course Date of data ENGLAND 39.80% 5.70% East Surrey and Sussex 39.90% 4.30% NHS East Surrey CCG 37.80% 0.00% Learning Disbility 124a 124b 63
64 Clinical Priority and Assessment Rating: Needs Improvement 64 CCG IAF Indicator Number, Description and Performance Value People with a learning disability and/or autism receiving specialist inpatient care per million population Proportion of people with a learning disability on the GP register receiving an annual health check Date of data Mar ENGLAND % East Surrey and Sussex #N/A #N/A NHS East Surrey CCG % Maternity Rating: Needs Improvement 101a 125a 125b 125c Neonatal Women s Maternal mortality and experience of Choices in smoking at stillbirths per maternity maternity services delivery 1,000 births services Date of data Q ENGLAND 10.60% 7.1 East Surrey and Sussex 8.90% 5.7 #N/A #N/A NHS East Surrey CCG 7.30% % 123a 123b People with 1st episode of psychosis Mental Health Improving starting Rating: Performing Access to treatment with Well Psychological a NICErecommended Therapies recovery rate package of care treated within 2 weeks of referral Date of data Feb-16 Mar-16 ENGLAND 47.60% 62.90% East Surrey and Sussex 50.20% 72.30% NHS East Surrey CCG 53.90% 66.70% Actions to improve performance in these areas have been developed and implemented. Details thereof have been described elsewhere in this report. 64
65 Sustainable development Environment 65 What is Meant by Sustainability? Sustainability in this context is about the smart and efficient use of natural resources, to reduce both immediate and long-term social, environmental and economic risks. The cost of all natural resources is rising and there are increasing health and wellbeing impacts from the social, economic and environmental costs of natural resource extraction and use. The Mandate for Sustainability Reporting Sustainability has been recognised at a national level as an integral part of delivering high quality healthcare efficiently. The Department of Health Manual for Accounts states that all NHS bodies are required to produce a sustainability report as part of their wider annual report, to cover their performance on greenhouse gas emissions, waste management, and use of finite resources, following HM Treasury guidance. As an NHS organisation, and as a spender of public funds, we have an obligation to work in a way that has a positive effect on the communities for which we commission and procure healthcare services. Sustainability means spending public money well, the smart and efficient use of natural resources and building healthy, resilient communities. By making the most of social, environmental and economic assets we can improve health both in the immediate and long term even in the context of rising cost of natural resources. Spending money well and considering the social and environmental impacts is enshrined in the Public Services (Social Value) Act (2012). We acknowledge this responsibility to our patients, local communities and the environment by working hard to minimise our environmental footprint. As a part of the NHS, public health and social care system, it is our duty to contribute towards the level of ambition set in 2014 of reducing the carbon footprint of the NHS, public health and social care system by 34% (from a 1990 baseline) equivalent to a 28% reduction from a 2013 baseline by It is our aim to meet this target by reducing our carbon emissions. The CCG occupies office space situated on the first floor in the Tandridge District Council building. All building service contracts are managed by the Council, meaning that the CCG has not been in a position to implement a separate Sustainable Management Development Plan. We are working closely with the Council to ensure continuous improvements in terms of waste, utility consumption, water consumption and all other areas of building management in line with their ISO14001 Environmental Management System. Tandridge District Council has an Energy and Water Management Policy in place for staff and tenants. All the CCG s emissions are classed as Scope 3 using DEFRA foot printing methodology. This is due to the fact that the CCG occupies rented space in a shared building and neither owns nor leases vehicles. The largest areas of our corporate emissions are through our building energy use and travel. We have established 2013/14 as a baseline year for our organisation s emissions. 65
66 Summary of Performance Annual Energy Use Heating 66 Electricity (kwh) (kwh) Energy from Renewables 0% 50.0% Table above shows: Energy Usage Water consumption totals are unavailable as the floors are not individually metered. Policies In order to embed sustainability within our business it is important to explain where in our process and procedures sustainability features. Commissioning The largest area of emissions for our organisation is from our commissioned and procured services and products. Through developing sustainable procurement and low-carbon commissioning work, we aim to encourage carbon management and resource efficiency in our contracts with external suppliers and providers, contributing to building resilience and making reductions in the embodied carbon of our supply chain. With this we aim to reduce cost risk to the health sector, support services to minimise the potential for incidental public health impacts such as vehicle pollution, reduce environmental damage and improve the design of efficient local health services. We have already taken steps to encourage sustainable transport for patients accessing our commissioned services. We aim to commission services that provide care closer to patients homes; this helps to reduce carbon emissions by reducing the distance that patients need to travel to appointments. Travel We can improve local air quality and improve the health of our community by promoting active travel to our staff, through our providers and to the patients and public that use the services we commission. Every action counts and we are a lean organisation trying to realise efficiencies across the board for cost and carbon (CO2e) reductions. We support a culture for active travel to improve staff wellbeing and reduce sickness. Key environmental considerations for the CCG offices Our offices have movement light sensors in strategic points within the office, to trigger the lights, which saves on electricity when areas are not in use. The photocopier has defaulted passwords for each member of staff, to save on paper, reduce cartridge use and printing costs. Printing preferences have been defaulted to toner save, grey scale and double sided to reduce printing costs and paper use. The photocopier is leased from Konica Minolta, which includes use of recycle facilities for printer cartridges and toner waste. The CCG adheres to the Council policy which has been implemented for staff and all tenants, ensuring all staff turn off desktop computers at the end of the day. Confidential waste is shredded on site and recycled. Separate recycling receptacles are strategically placed in the office and kitchen, so that, as well as paper, we are also recycling cardboard, plastics and food waste. 66
67 67 For energy efficiency the building is only heated when it is in use, when seasonally required and to an agreed maximum temperature. The windows are coated, which insulates the office in the winter and restricts the heat from the sun in the summer. There is a hydro tap fitted in the kitchen, providing instant hot water for drinks, reducing electricity and saving on water. Conference phone facilities are available in the two meeting rooms and small offices, saving staff travelling time and reducing business mileage. Car sharing is encouraged when travelling to meetings. Floor space usage The CCG office space is fully utilised to include hot desking facilities, break out areas, three pods with network connections that can be used by staff when there is a need for a quiet area to work, and two meeting rooms with removable panels that can convert to one larger meeting room. This enables the CCG to maximise occupancy and to accommodate staff from other NHS organisations that we work closely with, including from South East CSU, South Central West CSU and the Medicines Management Team. The CCG works closely with Surrey County Council Public Health and Social Care teams and makes best use of the available hot desk facilities. The CCG hot desk procedure has resulted in greater efficiency of our desk usage on a weekly basis. 67
68 68 Health and wellbeing strategy We have a statutory responsibility to review in our Annual Report the extent to which we have has contributed to the delivery of the health and wellbeing strategy of its relevant Health and Wellbeing Board. The narrative below highlights the key priorities of the Surrey Health and Wellbeing Board and our contribution towards its implementation and delivery. Our CCG has carried out this self-assessment in consultation with Surrey County Council, via a process agreed between SCC and all Surrey CCGs. East Surrey CCG Annual Report 2016/17 - self assessment of 'contribution to the Surrey Heath and Wellbeing Strategy' Surrey Health and Wellbeing Strategy priority Contribution made by the CCG Improving children's health and wellbeing All CCGs have a collaborative commissioning arrangement for Surrey-wide children s services. NHS Guildford and Waverley CCG (GWCCG) isthe lead Commissioner for the Collaborative for both Surrey-wide Commissioning and Safeguarding for Children. In 2016/17 our priorities and achievements included: reducing inequity improving access to services and improving our data gathering and intelligence regarding need, demand, access and outcomes Children and Young People s Mental Health The new contracts for our jointly procured Surrey-wide Child and Adolescent Mental Health Service started on 1 April 2016 with GWCCG leading the contract management on behalf of the Surrey CCGs. The new service has already started to deliver the expected return on the significant additional investment made to support known areas of service gap. Key service improvements are: A single CAMHS Referral & Information Centre for all referrals; navigating children and young people to the most appropriate service and through the system. A no wrong door approach, ensuring all children, young people and families will be supported to find the right help at the right time. A reduction in the threshold criteria for acceptance into CAMHS resulting in a significant increase in numbers of people accessing services. 68
69 69 Extended operating hours: from 8am-8pm Monday to Friday and 9am - 12pm on Saturday. More accessible and user friendly services through convenient locations and online facilities. Automated clinical scheduling to ensure capacity, appointments and room availability is more transparent and easier to manage A new Behavioural Education and Neuro-disability (BEN) Pathway for children with Attention Deficit Hyperactivity Disorder (ADHD) and/or Autism Spectrum Disorder (ASD) offering pre and post diagnostic intervention Continued work with CAMHS Youth Advisors and the development of an employment pathway for young people that ensures user satisfaction To date, this has been largely successful with improvements in access and referrer satisfaction. However, delays in implementing an effective reporting system have limited our data intelligence and confidence in clarity of waiting times. This required a formal performance notice being issued. A positive response to the notice was received from the provider which has seen an improvement in data flows. In addition we successfully secured further CAMHS transformation funding to support the national priorities in Future in Mind. During 2016/17 we have been able to fund a number of projects, within both the statutory and voluntary sectors to transform services in emotional health and wellbeing. Examples of these services include: The Music to my ears programme is being implemented. This aims, through music, to run 1:1 and group work sessions targeted at those in greatest need and designed to help improve their levels of confidence. Mindfulness information to parents and training for teachers. across 18 schools for children up to Year 9 HOPE and Extended HOPE services: multi-agency services for CYP aged 11-18, being delivered from bases in Epsom and Guildford for the HOPE service and in the Guildford area for Extended HOPE. The services aim is to prevent acute admissions, out of county placements and Tier 4 admissions. Development of a Youth Safe Haven where children and young people can talk to someone in a safe place about the mental health issues that they face. The WeCare in Surrey video on youtube Introduction of Restore Rangers, a series of pop-up clubs that use local skills in the community to give young students with, or at risk of mental illness, a meaningful and satisfying education that will help them realise that their contribution is valuable to society. Introduction of Step by Step, a pilot service for those aged that includes six workshops to improve confidence, self-esteem and help reduce levels of anxiety. These services are monitored monthly through the CAMHS transformation 69
70 70 board which includes NHS England South membership and parent/carer and service user representation. As a sign of success, local GPs are reporting greater satisfaction ratings with the new service. Children and Young People s Developmental and Physical Health During 2016/17 we have been working with all CCGs, NHS England and Surrey County Council (SCC) in a procurement process to secure a single Surrey-wide Children s Community Health servicethat simultaneouslybuilds on the priorities reported to Health and Wellbeing Board last year. SEND (Special Educational Needs and Disabilities) Ensuring compliance with the Children and Families Act (2014) regarding children with Special Educational Needs and Disabilities (SEND). In particular: Delivering against our joint (SCC and CCG) commissioning principles to improve access and earlier intervention for speech and language therapy and occupational therapy Increasing uptake of personal health budgets from 2017 Developing a clear partnership strategy for SEND that places positive user experience at the heart of service planning and change Active involvement in the Surrey SEND Partnership, which has included the development of a clear SEND 2020 Strategy. Despite our ambitions for SEND, the Oct 2016 joint CQC/OFSTED inspection of SEND acknowledged the strength of the collaborative and leadership, but identified significant areas for improvement including that the experience of families remains poor. As a system we still have significant work to do to demonstrate our commitment to improve the experience of families in this area. We are working with the Director of Children s Services atscc, to develop the joint Written Statement of Action in response to the inspection and to work jointly with SCC support action and scrutiny with regard to the improvements required. Personal Health Budgets (PHB) Surrey wide, six children receive a personal health budget. Although low it is a 50% increase on 2015/16. To increase the numbers receiving a personal health budget, in April 2016, the choice to take a personal health budget was extended from including only people in receipt of Continuing Healthcare, to also include people with a long term health condition. To support this, from April 2017, we have allocated 3% of our Surrey spend on children s community services to personal health budgets. Maternity Better Births Smoking Cessation Although the numbers of pregnant women smoking is lower than the 70
71 71 average for the region, work continues to improve on this. SaSH (the CCG main acute provider trust) has adopted the South East Coast Strategic Clinical Network recommendations to reduce preterm birth and still birth. There has been joint work to collate a list of providers for referral to smoking cessation for pregnant women across Surrey and Sussex. Due to lack of funding, there has been no progress on Carbon Monoxide monitoring but plans are in place to implement this in 2017/18. Customised Growth Charts The trust established and embedded customised growth charts prior to the introduction of the national recommendations. Within the last year, the trust has obtained a one year software licence and participated in the strategic clinical network training to use the decision aid to assess risks of death in utero or weak baby at delivery. The outcome of this work has led to an increase in referrals to sonography to measure foetal growth. A business case has been submitted to increase the number of sonographers to 2 Whole Time Equivalent (WTE) as well as increasing the number of midwives to 0.5 WTE. This work has made a difference in identifying at risk pregnancy Benchmarking and audits have shown that SASH is performing well. Information for Parents Parental information on monitoring reduced foetal movements (RFM) at 24 weeks gestation, with routine discussion with the midwife, has long been established practice. Within the last year this has been reviewed and now includes use of stickers which are put into the hand held record as a prompt for the patient to record their foetal movements. Competency in Cardiotocograph (CTG) interpretation This is part of the maternity mandatory and statutory training. The Trust has won a bid to invest in an online training tool that tests competency in CTG. The trust will be using this assessment tool within the next financial year which will have a positive impact on CTG competency within the Trust. Improving older adults' health and wellbeing Overview During 2016/17, the CCG continued to build on the strategies designed in 2015/16, within the context of the wider Sustainability and Transformation Plan footprint. The focus in East Surrey has been to consistently work to develop schemes to support older adults. In particular, the key focus has been on supporting frail patients and those in Care Homes, striving to enable people to stay well for longer, recover more quickly when they experience ill health, and have the care they receive tailored to their wishes wherever possible. 71
72 72 Reducing admissions and promoting swift and integrated discharge Frailty (Pendleton) Unit: A key element of our plan in 2016/17 was the implementation of a Frailty Unit (Pendleton Unit) on the acute (SaSH) hospital site. The unit provides services for the assessment, diagnosis, observation, triage to treatment and rehabilitation service for complex older patients this supports rapid discharge and prevention of unnecessary acute admissions. The Frailty Unit establishes close working links with the local health economy partners, including social, voluntary, community and primary care services, to ensure a rapid discharge of patients back into community care with a robust and clearly defined package of care to support them back into their own home. The unit supports patients from the Surrey and Sussex locality. It is supported by and has been developed in conjunction with, SaSH, and Crawley CCG / Horsham and Mid Sussex CCG. A full review of clinical pathways is underway and will be used to inform future commissioning intentions for these schemes. Integrated multi-disciplinary teams (MDT) As part of the complex case management strategy the following steps have been taken to create integrated multi-disciplinary teams within the local health economy: Implementation of systems for risk stratification in primary care and case management by Community Matrons, supported by an extended Multi-Disciplinary Team (MDT). Introduction of Multi-Disciplinary Team meetings at Primary Care Network level Implementation of shared electronic care plans across East Surrey, with access available to Primary Care, Out of Hours, ambulance and community services professionals. New software and plans for further technological solutions to enable further sharing of clinical records and access to this information are being planned. This will support continuity of care and have far-reaching benefits for patients and staff. Signing of Data Sharing Agreements to ensure compliance with information governance duties and responsibilities. Primary Care Locally Commissioned Services (LCSs) We commission two schemes in Primary Care which focus specifically on improving the care coordination for older patients, and thereby reducing unnecessary urgent hospital activity. The benefits from these schemes have been: A growing recognition by practices of their frequent attenders and support mechanisms introduced at a practice level to target this group Almost 5,000 care plans written and uploaded to ShareMyCare/IBIS which are having a positive effect in reducing ambulance call-out rates and conveyances to hospital and improving patients experiences of 72
73 Promoting emotional wellbeing and mental health 73 care by addressing their preferences A&E attendances for Chronic Obstructive Pulmonary Disease (COPD) have reduced and overall, East Surrey CCG has defied the national rising trend in A&E attendances by remaining relatively flat over the period. In February 2017, the CCG was nominated as a finalist for its Multidisciplinary Care Homes Project in the Excellence in Out of Hospital Award category of the Kent Surrey Sussex Leadership & Innovation Awards (AHSN). This is an integral part of the broader Unplanned Care scheme. East Surrey CCGs success in ensuring high quality care for the elderly and frail is evidenced by East Surrey CCG being consistently ranked within the top ten performing CCGs nationally in controlling emergency admissions for conditions that would not ordinarily require an admission if the condition was appropriately managed. In addition, non-elective admissions have shown a consistent downward trend over the last three years. Dementia diagnosis See the Mental Health/Dementia section under Our Achievements for the Year for details. Newly Procured Child and Adolescent Mental Health Service See Children and Young People s mental health in the section Improving children's health and wellbeing above Mental Health Transformation Significant progress has been made during 16/17 to deliver the Mental Health Five Year Forward View. Key areas include: CAHMS: fully compliant with three of the five transformation criteria/indicators Crisis care: fully compliant with eleven of the fifteen transformation criteria/indicators Out of area placements: fully compliant with all the transformation criteria/indicators. The CCG is only non-compliant with two of the transformation criteria/indicators, namely, the commissioned liaison service routinely collecting outcome measures in line with the RCPsych standards for adults, and The CCG is not currently party/signatory to a joint s136 protocol with other local partners as per the Mental Health Act Code of Practice, which is regularly reviewed with a clear action plan to address any concerns This is being addressed through our Mental Health collaborative team. East Surrey Mental Health Safe Haven 73
74 74 See the Mental Health/Dementia section under Our Achievements for the Year for details. Improving Access to Psychological Therapies (IAPT) (Generally) During 16/17, to improve access to psychological therapy (IAPT) services for our registered population, East Surrey CCG increased access rates by supporting self-referral and referral by all registered health professional such as nurses, midwives and therapists, as well as GPs. Nationally Mandated Targets Plans are being developed collaboratively with other Surrey CCGs to ensure compliance with the nationally mandated targets to: Improve access rates to Children and Young People Mental Health services Improve waiting times for Children and Young People to access Eating Disorder Services. Improve Dementia diagnosis rates Increase Early Intervention in Psychosis Improve IAPT access and Recovery rates. Developing a preventative approach Signposting Wellbeing Prescription Following the successful expansion of the Well Being Prescription Service, ensuring that all Tandridge GP Practices have access to a dedicated Well Being Advisor, the service is now being rolled out in Redhill, Reigate and Horley. By the end of March 2017, 15 out of our 18 membership practices will have their own Wellbeing Advisor. This scheme is funded through the Better Care Fund and involves the Wellbeing Advisor taking referrals from GPs and working with patients to identify and address their wider health and wellbeing needs. York Health Economics Consortium undertook a cost-benefit evaluation of the Wellbeing Prescription Service and through this evaluation, generated an indicative return-on-investment (ROI) calculation based on two factors: reduced GP visits / and reduction in weight. Based on this calculation, the service appeared to demonstrate a positive ROI. However, this calculation of ROI may be limiting, as GPs get paid per head of practice population and not for patient attendance, so the benefits of reducing frequent attenders for the CCG and practices may relate more to an ability to contain demand and maintain practice resilience, rather than the generation of direct cost savings. It is however recognised that this demand reduction and additional practice capacity would have indirect long term cost saving opportunities for the wider health economy. This was an initial report and focussed on performance up until October We now have a new extended database in place so will be able to look at a much wider range of results when undertaking future analysis or ROI calculations. 74
75 Prevention 75 IRIS- Identification and Referral to Improve Safety (Domestic Abuse) 16 out of 18 ESCCG practices have either received IRIS training or signed up for training. Discussions are underway, to expand IRIS across the county. The Domestic Abuse Management Board (DAMB) is being asked to take this forward and look at funding opportunities. Diabetes Prevention: NHS Diabetes Prevention Programme See the Diabetes section under Our Achievements for the Year for details. In addition, we achieved 100 per cent compliance with the National Diabetes Audit (NDA), with all our eighteen practices submitting data for the 2016/17 audit. This data has been assessed and reported on by NHS Digital. The findings of the National Diabetes audit were disseminated to all practices to ascertain possible factors behind low compliance with some of the NICE guidance treatment targets. The NDA report and feedback from primary care has been used by the CCG to understand the current level of performance in diabetes care and this has informed our diabetes plans for 17/18 particularly in relation to implementing: the NICE diabetes best practice guidance relating to recommended treatment targets and the eight best practice care processes, and an improved and holistic diabetes pathway The recommendations are being implemented through the Clinical Governance Group and our Diabetes Forum. SASH Health and Wellbeing Commissioning for Quality and Innovation (CQUINs) payments framework This encourages sharing and continuous improvement to how care is delivered and to achieve transparency and overall improvement in healthcare. A Health and Wellbeing CQUIN is in place at SaSH to support workplace health Progress to date Physical activity scheme Scoping current range of physical activity available to staff and drawing a menu of options of internal and external programmes that can be accessed. This will be advertised on the intranet. National initiatives were being looked at to develop locally. Metrics include baseline sickness and absence Reviewing possibility of a health coach and promoting all activities and communication plan Work is in place to develop a SASH Active brand to support and promote physical activity programme being launched at the start of 75
76 76 January 2017 to coincide with New Year s Resolutions Access to physiotherapy Scoping work initiated to review current offer and then re-promote the service in Quarter 2 and review again in Quarter 3 to measure uptake and evaluate the musculoskeletal sickness rates. Mental health initiatives Scoping work in Quarter 1 to assess internal and external opportunities to access mental health support. Funding streams are being explored to provide relevant training (mindfulness, mental health awareness training) and source counselling services. Development of a health and wellbeing website to highlight support for mental health needs and services. Using mental health sickness rates as an indicator for measuring progress and effectiveness and establishing a baseline in relation thereto. Monitoring of website hits and take-up of mental health initiatives. Quarter 4 will report further on progress, however, updates at the Clinical Quality Review Meeting (CQRM) will be requested to monitor progress. Run the World The CCG is supporting the Run the World programme in local schools to promote physical activity in children. Active Surrey, the County Sports Partnership for Surrey, is challenging schools to run a route around the world over the course of this academic school year, visiting different sporting events on the way. Collectively schools should cover the 28,750 miles around the world The aim is for each child to be physically active every day so that he/she can become healthy and happy learners. Research Proposals Along with colleagues in public health, a research proposal is being developed that aims to increase cervical screening uptake through low cost interventions. Smoking Cessation, Health Checks, Alcohol and Contraception East Surrey GPs are signed up to deliver smoking cessation, NHS Health Checks, Alcohol Identification and Brief Advice (IBA)and Intrauterine Contraceptive Device and Implant fittings through public health agreements Weight Management Centre Public Health has commissioned a new WMC (Weight Management Centre) to deliver a Tier 2 weight management programme for children/young People and their families. It will be delivered throughout Surrey but will focus initially on East Surrey as this has been identified as an area of higher need. 76
77 Prevention Events 77 The Practices Commissioning Committee has held a pilot Prevention Event with public health and district/borough colleagues and is in the process of planning a series of these events. SafeguardingOverview the population It is our responsibility to ensure that its staff, providers and contractors are aware of and understand their responsibilities to safeguard and promote the welfare of children and adults. Guildford and Waverley CCG host the Surrey Wide Safeguarding Adult and Children services which include key posts in terms of Safeguarding Children, Safeguarding Adults, Child Death Overview Process (CDOP) and Looked After Children (LAC). Safeguarding Adults The CCG has recently recruited an integrated safeguarding vulnerable adult s manager post which covers both health and social care sectors. This post will strengthen our safeguarding infrastructure to ensure timely education, dissemination of learning and provide relevant monitoring and assurance across both health and social care providers. The Director of Quality and Nursing chairs the local East Surrey safeguarding adults group and is driving local improvements to ensure safeguarding processes are effectively implemented. We are working to a more proactive model with local authorities and the CQC to promote safe delivery of care within care homes and other registered providers. Currently all of our practices have a named GP safeguarding lead and all are up-to-date with level 3 safeguarding training. In addition over 53 participants across all 18 practices have attended the Mental Capacity Act (MCA) and Deprivation of Liberty (DoLs) training. This training was provided in response to learning from serious case reviews locally and nationally that reflected limited understanding, application and documentation of mental capacity. The Surrey Safeguarding Adults Board (SSAB) has six key priorities to meet its vision of everyone working together to enable people in Surrey to live a life free from fear, harm and abuse. These are: Communications Training To embrace a culture of learning To identify types of abuse and neglect that are frequently hidden from professionals or are hard to detect To work towards prevention of abuse and neglect Assurance of safeguarding practices We are a key stakeholder on the SSAB and is committed to working with all relevant partner agencies. During the CCG has: supported greater understanding of the Mental Capacity Act within primary care 77
78 78 promoted greater awareness within health of the importance of safeguarding adults at risk within society as a key stakeholder, contributed to the development of an integration and communication between the Safeguarding Children s Board Health and Child Safeguarding Group and the SSAB Adult Health Group jointly chaired with Adult Social Care, the SW Surrey SSAB Sub-group focusing on the safeguarding agenda within the locality contributed to the development of the Surrey County Council PREVENT Strategy (counter terrorism). Developing a Multi-Agency Safeguarding Hub for Surrey The CCG has worked on a joint project with Surrey County Council, and Surrey Police, to develop a Multi-Agency Safeguarding Hub (MASH). The MASH is the single point of contact for reporting concerns about the safety of a child, young person or adult. It aims to improve the safeguarding response for children and adults at risk of abuse or neglect through better information sharing and high-quality and timely responses. Safeguarding Children We are a member of the Surrey Safeguarding Children Board (SSCB) and Corporate Parenting Board (CPOG). The CCG contributes to work across the county to meet the safeguarding board core business objectives and priorities, stated in the SSCB Business Plan. The Core Business Objectives are to: Optimise the effectiveness of arrangements to safeguard and protect children and young people. Ensure clear governance arrangements are in place for safeguarding children and young people. Oversee serious case reviews (SCRs) and child death overview panel (CDOP) processes and ensure learning and actions are implemented as a result. Ensure that single-agency and multi-agency training is effective and contributes to a safe workforce. Raise awareness of the roles and responsibilities of the LSCB and promote agency and community roles and responsibilities in relation to safeguarding children and young people. The priorities are: To monitor and challenge the effectiveness of Early Help for children, young people and families who do not meet the thresholds for statutory intervention and support by Children s Social Care. To ensure professionals and the current child protection processes effectively protect those children identified as in need of protection and who are looked after (Looked After Children). To challenge and scrutinise the effectiveness of the response and impact of partners work to protect children and young people at risk of 78
79 79 Child Sexual Exploitation (CSE) To monitor and challenge the effectiveness and impact of the Domestic Abuse Services in reducing the incidences of Domestic Abuse and protecting children and young people from harm. Significant strands of work that the CCG have been involved with include: Learning from the Child Death Process, Serious Case Reviews and Safeguarding Inspections and ensure these lessons are embedded into practice across the Surrey health economy. Responding to local and national priorities which include, Domestic Abuse (DA), Female Genital Mutilation (FGM), Child Sexual Exploitation (CSE) and PREVENT Ongoing support of the MASH The Surrey Wide CCG Safeguarding team works closely with providers, including independent contractors, across the health economy to ensure there are robust monitoring systems to provide assurance that arrangements to safeguard children and to ensure the health needs of looked after children are robust. Transforming Care The CCG has established a Health and Social Care Group to provide operational and quality oversight for people who have learning disabilities or autism with challenging behaviours. These meetings have been held monthly. Now that the majority of people who were in inpatient care for assessment and treatment (7/11 people) have been placed in settled accommodation in the community, these meetings will be every two months. We contributed to the development of the five-year Surrey Transforming Care Plan. 79
80 80 Quality premium The Quality Premium is intended to reward clinical commissioning groups for improvements in the quality of the services that they commission and for associated improvements in health outcomes and reducing inequalities. The maximum quality premium payment for a CCG is 5 per head of population, potentially amounting to 875,000 for East Surrey CCG. The Quality Premium is based on achieving a series of select measures that cover a combination of national and local outcome priorities. Restrictions on receipt of Quality Premium NHS Constitution measures: A CCG will have its quality premium reduced if the providers from whom it commissions services do not meet the NHS Constitution requirements for certain patient rights or pledges. Quality gateway: The right to any quality premium payments to a CCG may be revoked by NHS England in cases of serious quality failure. Financial gateway: A CCG will not receive a quality premium if: in the view of NHS England, during 2015/16 the CCG has not operated in a manner that is consistent with the obligations and principles set out in Managing Public Money; or ends the 2015/16 financial year with an adverse variance against the planned surplus, breakeven or deficit financial position, or requires unplanned financial support to avoid being in this position; or it receives a qualified audit report in respect of 2015/16. If successful the Quality Premium is paid to the CCG in the October following the financial year under review 2015/16 Assessment (Due October 2016): The total potential value of the 15/16 Quality Premium for East Surrey CCG was of which the CCG received 203,000 for the 80
81 81 15/16. CCG performance is highlighted below. Potetential Value of Quality Premium 868,000 Step 1 Attainment of national and local goals Goals - Description Target % of QP Value Potential QP Value Result Actual Value National National Local Reducing potential years of lives lost through amenable mortality Reducing avoidable emergency admissions Delayed transfers of care which are an NHS responsibility Reduction in the number of patients attending an A&E department for a mental health-related needs who wait more than four hours to be treated and discharged, or admitted, together with a defined improvement in the coding of patients attending A&E. Improving Antibiotic Prescribing Part a: Reduction in number of antibiotics prescribed in primary care Payment weighting 50% of the total quality premium payment of 10% Improving Antibiotic Prescribing Part b: Reduction in proportion of co-amoxiclav, cephalosporins and quinolones Payment weighting 30% of the total quality premium payment of 10% Improving Antibiotic Prescribing Part c: Validation of secondary care prescribers total antibiotic prescription data Payment weighting 20% of the total quality premium payment of 10% 1.2% reduction in the average trend in the potential years of life lost (standardised for sex and age) from amenable mortality for the CCG population to be achieved over the period between the 2012 and 2015 calendar years. 0% 0 - Zero per cent change, or - Rate of admissions less than 1000 per population 16.7% 144,956 P 144,956 The total number of delayed days caused by delayed transfers of care in 2015/16 should be less than the number in 2014/ % 144,956 F 0 Data Quality Target The proportion of primary diagnosis codes at A&E with a valid 2 character A&E diagnosis or 3 digit ICD-10 code will be at least 90% 33% 289,044 F 0 Patient Target The proportion of patients with a primary diagnosis of mental health-related needs or poisoning that spend more than 4 hours in A&E is no greater than the average for all patients, or Reduction in the number of antibiotics prescribed in primary care by 1% (or greater) from each CCG s 2013/14 value. Target Value/Threshold % 48,174 P 48,174 Reduce by 10% from each CCG s 2013/14 value, or to be below the 2013/14 median Target Value/Threshold % Secondary care providers with 10% or more of their activity being commissioned by the relevant CCG have validated their total antibiotic prescribing data as certified by PHE Confirma-tion of data summited for validation to PHE 3.33% 28,904 F 0 2% 19,270 P 19,270 People with stroke who are discharged from hospital with Maintain the current rate of 85.7% 11.1% 96,348 P 96,348 a joint health and social care plan Alcohol: admissions Maintain the DSR per registered patients of % 96,348 P 96,348 Value of Quality Preium Achieved 100% 868, ,096 Step 2 Reduction for non-achievement of certain Patient Rights in terms of NHS Constitution % Reductio RAG NHS Constitution Right Reductio n in QP Rating n in Value Achieved Maximum 18 weeks from referral to treatment -92% Incomplete standard 30 P 0 Maximum four hour waits in A&E departments-95% standard 30 F 121,529 Maximum 14 day wait from an urgent GP referral for suspected cancer-93% standard 20 P 0 Maximum 8 minutes responses for Category A (Red 1) ambulance calls-75% standard 20 F 81,019 Reduction in value of QP 202,548 Net value of QP prior to application of overarching criteria 202,548 Step 3 Overarching Quality Criteria (Quality Gateway) One of a CCG s providers had experienced a serious quality failure and the assurance process had identified issues with the CCG s response in supporting resolution P Step 4 Overarching Financial Criteria (Financial Gateway) A CCG will not receive a quality premium if in the view of NHS England, during 2015/16 the CCG has not operated in a manner that is consistent with the obligations and principles set out in Managing Public Money A CCG will not receive a quality premium if it ends the 2015/16 financial year with an adverse variance against the planned surplus, breakeven or deficit financial position, or requires unplanned financial support to avoid being in this position A CCG will not receive a quality premium if it receives a qualified audit report in respect of 2015/16. P P P Outlook for 16/17 Quality Premium Assessment (Due October 2017) Due to the expected adverse variance in our deficit financial position for 16/17 it is unlikely that we will pass the financial gateway. As highlighted above, we are at risk of not meeting the key NHS Constitutional standards, namely: Maximum 18 weeks from referral to treatment for patients on the incomplete pathway waiting list standard (92%) Maximum four hour waits in A&E departments- standard (95%) Maximum two month (62-day) wait from urgent GP referral to first definitive treatment for cancer (85%) Maximum 8 minute response for Category A (Red 1) ambulance calls (75%) 81
82 82 Failure to meet each standard will reduce the value of the Quality Premium by 25%. The CCG is hence at risk that this could result in a 100% total reduction in the 2016/17 Quality Premium which becomes payable in October
83 83 Reducing inequality Equality This part of the report focuses on how we have met the three aims of the General Duties of the Equality Act We will demonstrate how we have commissioned services during 2016 whilst fulfilling the aims of the Equality Act 2010 and reducing health inequalities as required by Section 14T of the Health and Social Care Act The Equality Act 2010 provides a legal framework to strengthen and advance equality and human rights. The Act consists of general and specific duties. The general duty requires public bodies to show due regard to: Eliminating unlawful discrimination or any other conduct prohibited by or under the Act Advancing equality of opportunity between persons who share a protected characteristic and persons who do not share it. Fostering good relations between people who share a relevant protected characteristic and people who do not share it. There are nine protected characteristics covered by the Equality Act: Age, Disability, Gender re-assignment, Marriage and civil partnership, Pregnancy and maternity, Race including nationality and ethnic origin, Religion or belief, Sex (male/female), Sexual orientation. However, we have chosen to add two further groups which we feel may warrant special consideration. They are Carers and people living in rural/ socially isolated locations. The specific duties require public bodies to publish relevant, proportionate information showing how they meet the Equality Duty by 31 January each year. Our 2016 report can be accessed here. We are also required to set specific measurable equality objectives by 6 April every four years. Both general and specific duties are known as the Public Sector Equality Duties (PSED). Our Equality Strategy sets out our Equality Objectives. During 2016 we made the following progress against our Equality Objectives (which will be refreshed by 6 April 2017 and aligned to the priorities of the Health and Well Being Board); Embedding Quality, Equality and Privacy Impact Assessments (QEPIAs) For all new work and projects a Quality, Equality and Privacy Impact Assessment is required as part of the Business Case proposal. This assessment highlights and identifies engagement and involvement opportunities, which in turn help to shape and drive the project. Intelligence already received and recorded can also contribute to the assessment. The QEPIAs are undertaken at the start of new work, and regularly reviewed. Reviewing our own contracting, tendering and performance monitoring processes as a way of reducing health inequalities Ensuring the contracts and tendering process include specific requirements around equalities provides assurance that commissioners and providers are taking account of their responsibilities. It also enables the organisation to monitor how different communities access services and establish mechanisms to address any inequalities. By coupling this with effective performance measures, we are better able to monitor health outcomes for the population. 83
84 84 Anecdotally we believe that access to information and some services is still inequitable. One of our biggest challenges is to try and improve the monitoring of protected groups. Without data it is difficult to demonstrate if patient satisfaction/experience differs from group to group. The results of the Equality Delivery System baseline assessment and feedback from patient groups have shown that we still have much work to do with our provider organisations. Developing CQUINs (Commissioning for Quality and Innovation frameworks). The CQUIN payment framework supports improvements in the quality of services and the creation of new, improved patterns of care by enabling commissioners to reward excellence. The rewards are linked to a proportion of healthcare providers' income to the achievement of local quality improvement goals. Local CQUINs were aligned, where possible, between hospital and community providers with the common aim for reducing unnecessary admissions, reducing length of stay and improving communication and care planning. Achieving national recognition for Carers Commissioning The Surrey Clinical Commissioning Group Collaborative was shortlisted for this year s prestigious Health Services Journal Value Awards 2016 for Surrey Carers Prescription Service. The Carers Prescription provides professionals with a quick and easy solution to support Carers. The Carers Prescription is a secure, one-stop mechanism that passes the prescription on to a team who then make arrangements for the referral to be processed quickly and efficiently and passed to appropriate services and organisations across Surrey that help to support and care for Carers. Promoting the NHS Accessible Information Standard (NHSAIS) From 31 July 2016, all organisations that provide NHS care or adult social care are legally required to follow the Accessible Information Standard. The standard aims to make sure that people who have a disability, impairment or sensory loss are provided with information that they can easily read or understand with support so they can communicate effectively with health and social care services. Commissioners of NHS and publicly funded adult social care must also meet this standard, in that they must make sure that contracts, frameworks and performance management arrangements with provider bodies enable and promote the Standard s requirements. We have been raising awareness with partners and has sought assurance from providers (through contract and performance management and soft intelligence) regarding their compliance to NHSAIS. Becoming an official Dementia Friendly organisation. The Alzheimer s Society s Dementia Friends initiative was launched in March 2013 to give as many people as possible across England an understanding of Dementia and some of the actions we can all take to help those living with the condition. 84
85 85 We have a Dementia Champion and Clinical Lead who has trained staff within the CCG and partners practices so enable our staff to register and legitimately call ourselves part of a dementia friendly community. Improving services for people with mental health issues and learning disabilities Working with our member practices, Surrey Health and Welbeing Board and the Lead Commissioner for Mental Health and Learning Disabilities (Guildford and Waverley CCG), Surrey County Council and service providers, we identified a range of priorities which were progressed in 2016; Child and Adolescent Mental Health Services (CAMHS) Opening of the Safe Haven in Redhill See the Mental Health section under Our Achievements for the Year for details. Transforming stroke services The Surrey Collaborative are working together to transform the stroke pathway across Surrey. The programme of work has identified what good looks like for stroke care across the whole pathway. Following on from this, stroke services will be commissioned that deliver a high quality pathway for all. This will involve reconfiguring acute care so specialist services for hyper acute care are delivered by three hospitals in Surrey. See the Long Term Conditions section under Our Achievements for the Year for more. Undertaking a staff survey for the second year We took part in the National NHS Staff Survey, carried out at the end of 2016 and were pleased with the final response rate 80% Analysis of the results are not expected until February 2017 and will be shared with our teams. The Equality Delivery System (EDS2) The Equality Delivery System (EDS2) is a national toolkit which most NHS organisations use to self-assess their working environment, the decisions that they make and the services commissioned and provided for their local communities, while meeting the requirements of the Equality Act 2010 EDS2 has enabled us to: Analyse our performance against the EDS2 Goals and Outcomes Identify any gaps or areas that require improvement Identify any high risk areas as priorities for setting objectives EDS2 has four Goals: Better health outcomes Improved patient access and experience A representative and supported workforce Inclusive leadership We successfully completed the EDS2 process for Goals 1 and 2 during 2016 and chose to focus the EDS2 (in regard of their commissioning responsibilities for goals 1 and 2) on: 85
86 86 End of Life Care Neurological Rehabilitation in the Community We invited an external stakeholder grading panel to examine evidence, question and challenge the CCG and ultimately decide/score our performance. End of Life Care The Panel agreed the EDS2 Grade as DEVELOPING Neurological Rehabilitation in the community - The Panel agreed the EDS2 Grade as ACHIEVING Overall East Surrey CCG is assessed as DEVELOPING/ACHIEVING for EDS2 Goals 1 and 2. Work on Goal 3, a representative and supported workforce is dependent on analysis of result from staff survey (not expected until late February 2017) and Goal 4, Inclusive leadership, will progress and be reported in the Equality End of Year Summary Report (available on our website from 31 March 2017). The 2016 EDS2 Summary Report can be found on our website Given our work to date and our duties to evidence that; Equality impact analyses have been undertaken A wide range of information is taken into account when assessing impact and Engagement activity that has taken place Along with examples in the Annual PSED report that demonstrate how the CCG has been working during 2016 to: Eliminate unlawful discrimination Advance equality of opportunity Foster good relations We believe we are compliant with the Public Sector Equality Duties as set out in the 2010 Equality Act and has discharged its duty under Section 14T of the National Health Service Act 2006 (amended). Signed by Ian Ayres, Interim Accountable Officer Date 30 May
87 87 Section 3 Accountability Report 87
88 88 Corporate Governance Report Members Report Member practices The member practices, forming the membership body of the CCG We are a membership organisation made up of 18 local GP practices (with one branch surgery). Our member practices are: Birchwood Medical Practice (Horley) South Park Medical Centre (Reigate) Caterham Valley Medical Practice (Caterham) The Hawthorns Surgery (Redhill) Elizabeth House Medical Practice (Warlingham) The Moat House Surgery (Merstham) Greystone House Surgery (Redhill) The Wall House Surgery (Reigate) Holmhurst Medical Centre (Redhill) Townhill Medical Practice (Caterham) Lingfield Surgery (Lingfield) Warlingham Green Medical Practice (Warlingham) and Chaldon Road Surgery (Caterham) Oxted Health Centre (Oxted) Wayside Surgery (Horley) Pond Tail Surgery (Godstone) Whyteleafe Surgery (Whyteleafe) Smallfield Surgery (Smallfield) Woodlands Surgery (Redhill) Table above shows: Our member practices The CCG, as a corporate entity, is accountable to its member practices, acting on their behalf to commission health services in East Surrey. Composition of Governing Body The Governing Body oversees the work of the CCG by seeking and providing assurance that the CCG is properly fulfilling its duties, meeting its objectives and appropriately managing key risks. It comprises a GP Chair and four other GP members (known as Clinical Directors), a practice manager representative, an Accountable Officer, a Chief Finance Officer, a Board Nurse, a Secondary Care consultant (currently vacant) and four Lay Members with experience in governance and/or patient and public involvement. 88
89 89 The Governing Body members who have served during 2016/17 are as follows: Membership of the Governing Body 1 April May 2017 Voting Members Chair Dr Elango Vijaykumar GP members Dr Heidi Fahy Dr David Hill Dr Patrick Kerr Dr Richard Wright until 31 August 2016 Dr Thiruselvi Bangalore since 1 September 2016 Practice Manager Sue Latham Accountable Officer (AO) Elaine Jackson until 31 July 2016 Ian Ayres interim from 1 September 2016 Chief Finance Officer Richard Bates interim until 31 July 2016 Ray Davey interim from 18 July 2016 (handover period until 31 July 2016) Board nurse Avey Bhatia Secondary care doctor Vacancy Lay Members Graham Hanson (Governance) to 31 March 2017 David Congdon (Deputy CCG Chair) Nici Jupp (Patient and Public Involvement) Yvette Robbins Adrian Brown / Carol Pearson (Governance from 1 April 2017) Non-Voting Members Chief Operating Officer Peter Kottlar interim from 20 October 2016; permanent from 16 March 2017 Director of Quality and Nursing Karen Devanny 89
90 Director of Commissioning 90 Samantha Stanbridge Director of Delivery and Transformation Peter Kottlar until 19 October 2016 Director of Integration Caroline Farrar until 31 January 2017 Director of Out of Hospital Strategy Caroline Farrar from 01 February 2017 Director of Delivery Gareth Howells from 07 February 2017 Table above shows: East Surrey CCG s Governing Body membership You can find out more about the functions of the Governing Body in the East Surrey CCG Constitution Committee(s), including Audit Committee Membership body and Governing Body, committees and sub-committees The main committees are as follows. The terms of reference are available within our CCG Constitution, available at Detailed minutes are taken of all meetings. Practices Commissioning Committee The Practices Commissioning Committee is the formal component of our governance structure. It seeks to ensure all of our membership practices are actively involved, on a collaborative basis, in providing input and guidance to our activity as well as being a forum for feedback, reporting and communications back to our CCG. Governing Body The Governing Body has responsibility for ensuring that the CCG has appropriate arrangements in place to exercise its functions effectively, efficiently and economically and in accordance with our CCG s principles of good governance. Its work includes areas such as leading the setting of vision and strategy; approving commissioning plans; approving changes to allocation and use of funds; monitoring performance against plans; and providing assurance of strategic risk. Audit and Governance Committee The Audit and Governance Committee is established and constituted in line with the requirements of the NHS Audit Committee Handbook, NHS Codes of Conduct and Accountability, and the Higgs report, to provide the Governing Body with an independent and objective review on its financial systems, financial information and compliance with laws, guidance, and regulations governing the NHS. 90
91 91 Quality, Finance and Delivery Committee: The Committee is accountable to the Governing Body. It provides oversight of: the planning process and development of our Annual Operating Plan; performance and delivery against key performance indicators (KPIs), targets, finance, quality (including clinical quality) and contracting measures (including commissioning support organisations contract liaison and management); performance, key risks and actions relating to patient safety and quality. Remuneration Committee: The Remuneration Committee determines and approves all aspects of remuneration for our Chair and senior team (defined as at least the Chief Officer and their executive direct reports, plus other members of the executive management team), including interim appointments. It also makes recommendations to the Governing Body on determinations about the remuneration, conditions of service, fees and other allowances for CCG employees, and for people who provide services to the CCG. It also oversees other areas including the annual performance review, and annual pay review framework and timeframe. Information about any other committees, sub-committees and joint committees established by the clinical commissioning group s constitution. We also have a number of subgroups which report to the Quality, Finance and Delivery Committee. These are not established by our Constitution but are included here for completeness. Minutes are taken of all meetings, including details of decisions taken, membership and attendance records: Patient Reference Group The role of the Patient Reference Group (PRG) is to help our Governing Body make decisions about the services it commissions and to ensure that these services meet the health needs of the local population. The PRG is there to ensure that the voice of patients, their carers and the East Surrey public is embedded within our business. Membership is drawn from the patient participation groups of our GP Practices. Clinical Executive Team (CET) The CET is the combination of the Senior Management Team; the GP members of the Governing Body (including the Chair); and the Practice Manager representative. The CET is thus the senior committee of the CCG (rather than a committee of the Governing Body) and links to the Governing Body primarily via the Quality, Finance and Delivery (QFD) Committee. The CET ensures regular linkage between the CCG executive and the representatives of the GP members; and also provides core clinical input and assurance to the Quality Finance and Delivery Committee (QFD). Clinical Governance Group: Clinical governance is a systematic approach to maintaining and improving the quality of patient care within a health system (NHS). The overall objective of the Clinical Governance Group is to provide assurance to the Governing Body that the CCG is achieving recognisably 91
92 92 high standards of care; transparent responsibility and accountability for those standards; and a constant dynamic of improvement. This is achieved through: Providing expert advice and clinical input for discrete areas of the CCG s business and Overseeing the establishment and maintenance of procedures and systems of internal control designed to give reasonable assurance that all aspects of quality and clinical governance are in place. GP IT Steering Group The purpose of this group is to agree and implement a GP ICT strategy for East Surrey to monitor delivery of ICT services and recommend ICT solutions to support patient care pathways and other local priority developments, as defined in the strategic commissioning plan and within the overarching CCG IT Strategy. The forum has relevant ICT expertise and will act as the voice of primary care users within the CCG. Information Governance Steering Group: The Information Governance Steering Group is responsible for overseeing the assurance framework, management of risks and setting the priorities of the information governance and associated work plans. Quality and Safety Group The Quality and Safety Group provides assurance on the quality of services commissioned and promotes a culture of continuous improvement and innovation with respect to safety of services, clinical effectiveness and patient experience. The duties of the Quality Group are driven by the priorities for the clinical commissioning group and any associated risks or areas of quality improvement. Its programme of business is therefore flexible to new and emerging priorities and risks. Patient Participation Groups Most of our GP member practices have a patient participation group (PPG). The role of these groups is primarily to support the practice - giving thoughts, ideas and opinions, helping with specific pieces of work that call for a patient perspective and acting as a communicator between the practice and their community. PPGs also represent their practice population through East Surrey CCG's Patient Reference Group. QIPP (Quality, Innovation, Productivity and Prevention) Delivery Board The role of the QIPP Programme Board is to: Provide input into, review and oversee the development of the CCG s QIPP programme and Better Care Fund to ensure that the strategic, quality and financial objectives are delivered Monitor implementation and delivery of QIPP schemes Monitor the development of the QIPP scheme pipeline Discuss and agree how to manage key risks to delivery 92
93 Risk Management Group 93 The role of the Risk Management Group (RMG) is to look at risk management and mitigation, and to provide assurance to the Quality, Finance and Delivery (QFD) Committee that risks are being managed effectively. The Group is also responsible for the overall coordination of risk management activity. It ensures that the necessary processes are in place to achieve compliance with statutory requirements, to protect the CCG s staff and assets and, ultimately, the patients for whom East Surrey CCG commissions services. Membership of the Audit and Governance Committee 1 April May 17 The Audit and Governance Committee has a floating membership comprising Lay Members, GP members, the secondary care doctor, the practice manager representative and the board nurse. This is to ensure a broad range of input, and the widest possible involvement of all members in this work. This has been agreed as part of members professional development. Ahead of each meeting, specific members are invited to the meeting on a rotational basis. The Lay Member for Governance chairs the committee and attends all meetings. Name Role Changes Graham Hanson until 31 March 2017 Adrian Brown/Carol Pearson from 1 April 2107 Lay Member for Governance --- Floating membership (Please see note above) Lay Members; GP members; board nurse; secondary care doctor --- [Secondary care doctor post vacant] Table above shows: East Surrey CCG s Audit and Governance Membership Members of the Remuneration Committee 1 April May 2017 The Remuneration Committee has a floating membership comprising Lay Members, GP members, the practice manager representative, the secondary care doctor and the board nurse. At each meeting, a balance of members is invited, to ensure that sufficient members are present to reach a quorum, which does not have an interest in the matter under consideration. The Deputy CCG Chair, who is a Lay Member, chairs the Remuneration Committee and attends all meetings. Name Role Changes David Congdon Deputy Chair and Lay Member 93
94 Floating membership (Please see note above) 94 Lay Members; GP members; board nurse; secondary care doctor --- [Secondary care doctor post vacant] Table above shows: East Surrey CCG s Remuneration Committee Membership Members of the Quality, Finance and Delivery Committee 1 April May 2017 The membership of this committee includes all members of the Governing Body. This ensures that all members have oversight and assurance with regard to the CCG s quality, finance and delivery position. Members Dr Elango Vijaykumar CCG Clinical Chair --- Changes Dr Patrick Kerr GP member / Assistant Clinical Chair Elaine Jackson Accountable Officer Until 31 July 2016 Richard Bates Interim CFO Until 31 July 2016 Graham Hanson Lay Member for Governance --- David Congdon Lay Member (Deputy Chair) --- Karen Devanny Director of Quality and Nursing --- Samantha Stanbridge Director of Commissioning and Engagement --- Dr Heidi Fahy GP member / QFD Committee Chair Dr Richard Wright GP member Until 31 August 2016 Dr Thiruselvi Bangalore GP member Since 1 September 2016 Sue Latham Practice Manager --- Avey Bhatia Board Nurse --- Nicola Jupp Lay Member for Patient and Public Involvement (PPI)
95 95 Yvette Robbins Lay Member --- Peter Kottlar Director of Delivery and Transformation Until 19 October 2016 Chief Operating Officer Since 16 March 2017 (Interim from 20 Oct 15 March) Caroline Farrar Director of Integration Until 31 January 2017 Director of Out of Hospital Strategy Since 1 February 2017 Ray Davey Interim CFO From 18 July 2016 (handover to 31 July 2016) Ian Ayres Interim Accountable Officer From 1 September 2016 Gareth Howells Director of Delivery From 7 February 2017 Adrian Brown/Carol Pearson from 1 April 2107 Lay Member for Governance From 1 April 2017 Table above shows: Quality, Finance and Delivery Committee Membership Membership of the Practices Commissioning Committee (PCC) The Practices Commissioning Committee (PCC) is the formal component of our management structure that seeks to ensure all of the practices within the CCG are actively involved, on a collaborative basis, in providing input and guidance. It is also a forum for feedback, reporting and communications back from the CCG. When required, the PCC provides formal decisions on behalf of the member practices to the CCG, in line with the remit of the members as defined in the Constitution. The membership of the PCC is flexible in order to ensure the widest possible engagement and attendance, and support the individual needs of each practice. The practices agreed to nominate each practice s voting representative as being one of their regular attendees at the PCC. For its part, we also commit to ensure that if any matters will require formal approval at the PCC then at least one week s prior notice is given, and the nominated practice representative is expected to gain delegated approval from its practice principal(s), so that a decision is confirmed at the meeting. Each practice sends one voting member, but others are welcome to (and generally do) attend. In addition, members of the our Senior Management Team and Lay Members attend as guests and/or contributors. 95
96 Annual Performance of Committees 96 Governing Body Committee No. of meetings held 1 April March 2017 Attendance records maintained? Highlights of the Year 2016/17 Governing Body Five scheduled meetings during 2016/17: 14 April May 2016 (to approve annual report and accounts) 15 September September 2016 (AGM) 19 January 2017 Approved minutes with attendance recorded. Oversaw and approved key plans, policies and strategies. 2016/17 has been an extremely challenging year for the CCG, particularly in terms of financial performance being worse than the budgeted plan. The risks and mitigations have been reviewed and discussed in detail by the Governing Body and its committees. Four extraordinary meetings: 28 April July July October 2016 (Part 2) Audit and Governance Five meetings during 2016/17: 26 May 2016 (to approve the annual report and accounts) 9 June September December 2016 Approved minutes with attendance recorded. Detailed work plan which adheres to best practice governance guidance for the operation of Audit Committee It provides an independent and objective view of the CCG s financial systems, financial information and compliance with laws, regulations and directions governing the CGG, as they relate to finance. The Audit Committee has closely monitored and influenced the development of 96
97 97 9 March 2017 the CCG s risk and assurance arrangements. The Audit and Governance Committee independently monitored, reviewed and reported to the Governing Body on the processes of governance and, where appropriate, facilitated and supported, through its independence, the attainment of effective processes. Key activities included: Reviewing in detail the Annual Accounts for the CCG, including the audit completion report from external audit, and the annual audit letter, Assessing the Board Assurance Framework and ensuring that any highlighted risk areas were mitigated through reviews or other work streams, Considering the assurances on risk and control set out in Internal Audit s annual report and opinion, together with key assurances reported in individual reports. During its work, activities and areas of review throughout the year, the committee ensured that any areas of particular concern were brought to the Governing Body s attention. Approving the annual work plans for Internal and External Audit Remuneration Six meetings during 2016/17: 20 May July Aug Oct Jan March 2017 Approved minutes with attendance recorded. Reviewed Governing Body (Lay Member / GP member / independent member / SMT member) remuneration, following benchmarking with other local CCGs; time commitment and pay adjusted accordingly. (This required the withdrawal of the members from the meeting as appropriate, due to conflict of interests). 97
98 98 Cases for change and/or remuneration considered, e.g. to support recruitment/retention, taking into consideration business need, personal circumstances, etc. Quality, Finance and Delivery Eleven meetings during 2016/17: 5 May June June August September October November December February March March 2017 Approved minutes with attendance recorded. During the period of 1 April 2016 to 31 March 2017, the QFD Committee discussed and agreed the following items of business: Standing items: Quality, safety and patient experience reporting Engagement and delivery reporting Finance reporting Risk management reporting Patient Reference Group update As part of the above and where appropriate, in addition, the committee has reviewed and discussed: The planning process for the annual operating plan and commissioning intentions / plan Emerging arrangements for the Sustainability and Transformation Planning footprint Level of liaison with the commissioning support organisation (CSU) and any other relevant third party sources Progress on performance and actions against the annual financial plan (and specifically the Quality, Innovation, Productivity and Prevention; and Financial Recovery plans) Key risks and actions in relation to performance and 98
99 99 delivery against KPIs, targets, financial performance, and quality measures and performance; including actions relating to the Francis report and Winterbourne report, safeguarding children and adults, and a focus on concerns about stroke care and mental health. Key risks and actions in relation to performance and delivery of key contracts, particularly for acute contracts, and also including commissioning support organisation (CSU) contract liaison and management; Performance, key risks and actions relating to patient safety, and quality. As part of its role, the committee has approved (or recommended approval to the Governing Body as appropriate) of business cases for projects Register of Interests Full details about the Governing Body members registered interests can be found on our website: Personal data related incidents No personal data related incidents have taken place in 2016/17 which have required reporting via the Information Governance Toolkit or to the Information Commissioner as set out in the Health and Social Care Information Centre s guidance on serious incidents requiring investigation. Modern Slavery Act We fully support the Government s objectives to eradicate modern slavery and human trafficking. We do not meet the requirements for producing an annual Slavery and Human Trafficking Statement as set out in the Modern Slavery Act This is because our income/funding is earned from government sources and therefore is publicly funded and outside the scope of these reporting requirements. The duty to comply with the requirements of the Modern Slavery Act 2015 is enshrined within the CCG s Integrated Safeguarding Adults, Children and Young People Policy, available on our website. 99
100 Statement as to disclosure to auditors 100 Each individual who is a member of the Governing Body at the time the Members Report is approved confirms: so far as the member is aware, there is no relevant audit information of which the CCG s external auditor is unaware that he/she has taken all the steps that they ought to have taken as a member in order to make themselves aware of any relevant audit information and to establish that the CCG s auditor is aware of that information. Governance Statement Introduction and context We are a body established by NHS England on 1 April 2013 under the National Health Service Act 2006 (as amended). Our statutory functions are set out under the National Health Service Act 2006 (as amended). Our general function is arranging the provision of services for persons for the purposes of the health service in England. We are, in particular, required to arrange for the provision of certain health services to such extent as it considers necessary to meet the reasonable requirements of its local population. On 2 December 2015, as a result of the projected cumulated deficit of, in excess of 24m, and the continued financial challenges of the CCG we were placed under Legal Directions by NHSE, issued under Section 14Z21 of the National Health Service Act These may be accessed at: On 21 July 2016, following the emergence in quarter 1 of unplanned financial challenges that resulted from undeliverable QIPP efficiencies, we were placed in Special Measures by NHSE as part of a national reset financial plan designed to dramatically cut the annual trust deficit, and sharpen the direct accountability of trusts and CCGs to live within the public resources made available by Parliament and the Government in 2016/17. We delivered our Financial Recovery Plan and additional QIPP efficiencies which enabled the CCG to stay within its NHSE revised control total. As set out in the 2016/17 NHS Planning Guidance, CCGs were required to hold a 1 percent reserve uncommitted from the start of the year, created by setting aside the monies that CCGs were otherwise required to spend nonrecurrently. This was intended to be released for investment in Five Year Forward View transformation priorities to the extent that evidence emerged of risks not arising or being effectively mitigated through other means. In the event, the national position across the provider sector has been such that NHS England has been unable to allow CCGs 1% nonrecurrent monies to be spent. Therefore, to comply with this requirement, the CCG has released its 1% reserve of 2.1m, resulting in the reduced deficit for the year of 17.3m. Details of this programme are available on the NHSE website at 100
101 101 We are working closely with NHSE to address the issues identified, and achieve financial recovery. Accountable Officer s Scope of responsibility As Accountable Officer, I have responsibility for maintaining a sound system of internal control that supports the achievement of our policies, aims and objectives, whilst safeguarding the public funds and assets for which I am personally responsible, in accordance with the responsibilities assigned to me in Managing Public Money. I also acknowledge my responsibilities as set out under the National Health Service Act 2006 (as amended) and in my Clinical Commissioning Group Accountable Officer Appointment Letter. I am responsible for ensuring that the CCG is administered prudently and economically and that resources are applied efficiently and effectively, safeguarding financial propriety and regularity. I also have responsibility for reviewing the effectiveness of the system of internal control within the clinical commissioning group as set out in this governance statement. Governance arrangements and effectiveness The main function of the governing body is to ensure that the group has made appropriate arrangements for ensuring that it exercises its functions effectively, efficiently and economically and complies with such generally accepted principles of good governance as are relevant to it. The Members Report includes information about our Membership Body, Governing Body and Committees, including key responsibilities, membership, attendance records and highlights of their work over the year. UK Corporate Governance Code NHS Bodies are not required to comply with the UK Code of Corporate Governance. However, our Governing Body self-assessment has drawn upon best practice available, including those aspects of the UK Corporate Governance Code we consider to be relevant to the clinical commissioning group. This approach has been agreed in discussion with the CCG auditors, Grant Thornton. The self-assessment has generated several actions to improve governance during 2017/18. No substantial weaknesses in the CCG s governance were identified. Discharge of Statutory Functions In light of recommendations of the 1983 Harris Review, we have reviewed all of the statutory duties and powers conferred on it by the National Health Service Act 2006 (as amended) and other associated legislative and regulations. As a result, I can confirm that we are clear about the legislative requirements associated with each of the statutory functions for which it is responsible, including any restrictions on delegation of those functions. Responsibility for each duty and power has been clearly allocated to a lead Director. Directorates have confirmed that their structures provide the necessary capability and capacity to undertake all of the clinical commissioning group s statutory duties. Emergency Preparedness, Resilience and Response 101
102 102 We are a Category Two responder under the Civil Contingencies Act We have additional resilience responsibilities placed on us by NHS England through the EPRR Core Standards, which we are required to report on with Governing Body approval annually. In 2016/17 we participated fully in ensuring representation at both the Local Health Resilience Partnership (LHRP), A&E Delivery Board (A&EDB) Executive and Delivery groups responded fully to all information sharing requests with partner category one and two responders. It has also assisted NHS England in the production of a LHRP Risk register specifically for health to cover the SASH Health economy. During the course of 2016, we continued to operate in a collaboration agreement with Guildford and Waverley CCG to share emergency planning resource and expertise. This has ensured we continue to be resilience through consistency of approach going forward. The revised Incident Management Plan was approved on 5 December In meeting the need to have a plan to support arrangements to respond to risks on the community risk register and those that are prevalent, we held a training and awareness session around a Marauding Terrorist Firearms Attack, given the events in Brussels and Paris, on Monday 17 October The session was developed with the assistance of the South East Counter Terrorism Security Advisor and was delivered in partnership to ourselves and other system partners. The training session was followed by an exercise to test our current incident management plan and procedures based on this risk. This year s deep dive has been around business continuity. The additional resource from Guildford & Waverley CCG is developing our on-call capabilities and completion of our business continuity, which will strengthen our arrangements and embed the work across the organisation. Continuity has been incorporated into the incident management plan through a new more structured approach to responding to business disruption. There has been a range of training activity this financial year. Each NHS funded organisation must declare as part of their assurance their overall compliance with the NHS England core standards. We submitted a position of Substantial Assurance in 2016/17. Risk management arrangements and effectiveness The Board Assurance Framework (BAF) is the mechanism for managing the our strategic risks. It is aligned with our four strategic objectives. The contents of the BAF and risk register are subject to constant review, to ensure that they reflect our situation at all times. We hold quarterly meetings for board members, senior managers and risk owners to collectively and thoroughly review both the BAF and risk register to ensure they are robust in capturing all strategic and operational risks. Equality impact, quality impact and privacy impact assessments are conducted prior to any new project service review or redesign. This enables us to identify and mitigate potential risks. Any risks arising are then reflected in the risk register and/or Board Assurance Framework. Incident reporting is openly encouraged and handled. Members of the public and other stakeholders are encouraged to report incidents by phone, text, , post, or via face-to- 102
103 103 face visits and other events. We deal with individual incidents as appropriate, also ensuring that there are no performance or contractual elements that need addressing. Once incidents are resolved, they are followed up at the Clinical Quality Review meetings, to ensure that the relevant provider organisation has embedded the learning from the incident as appropriate. Our Engagement Strategy is currently being refreshed ahead of scheduled to reflect the changing strategic environment. We have a well-established ongoing programme of routine engagement activities, involving patients, district/borough councils, the voluntary sector, community and faith groups, and other public stakeholders. We risk assesses any concerns highlighted through these routes, and takes action if needed. Risk registers are routinely presented at Governing Body meetings held in public, and risks discussed at Governing Body committee meetings. Our risks also provide context for discussions at public engagement events. Our risk management policy was reviewed and revised during 2016/17, ahead of schedule, and the amendments were approved in January 2017 by the Governing Body. It provides a framework for the identification, evaluation and control of risk associated with the our commissioning functions and statutory responsibilities and facilitates a high-level of both management and Governing Body assurance that adequate processes are in place to ensure effective and efficient operations, financial stewardship, probity and compliance with laws and policies. The policy sets out clear roles and responsibilities for all staff and Governing Body members. The Governing Body agreed its Risk Appetite Statement in 2016 and this has been used to guide the development of the operating plan. Risks are identified from a number of sources, including but not limited to: Incident reports and trends (internal, and by monitoring incidents in commissioned services) Complaints monitoring in commissioned services Patient and staff surveys Inspections Key Performance Indicators Risk assessments Local risk registers External recommendations Strategic risks Strategic Objective 01: Deliver our Statutory Responsibilities Risk that the CCG will not deliver its revised financial recovery / QIPP plan 2016/17 and control total. Risk that the CCG will not be able to complete contract variations to bridge the 13m funding gap for the 2017/18 contract between ESCCG and SaSH s expectations for the year. Strategic Objective 02: Deliver High Quality, Patient-Centered Services 103
104 104 Risk that partner organisations (i.e.sash, FCHC, ABC Federation, neighbouring CCGs and SCC) and the Local Health Economy do not fully engage or support the CCG's strategic direction of establishing the Multi Community Provider (MCP) model. This is accentuated by lack of clarity around ESCCG's STP fit (Sussex vs. Surrey Heartlands) Risk that increasing demand coupled with the current level of investment in First Community Health and Care may lead to inadequate, reduced or insufficient capacity to effectively deliver services which would in turn, have an impact on our ability to achieve our objective To deliver high quality, patient-centred services." Risk that the South East Coast Ambulance Service (SECAMB) will fail to meet the required contractual obligation Delivery of the Clinical Navigation Hub (CNH) across 5 CCG s is complex. There are multiple dependencies with the potential to significantly impact upon the key design/development stages and ultimate delivery of the service. If these key areas are not effectively managed/supported then there is a significant risk that the CNH will not be delivered by March Stroke services in East Surrey are not meeting national and local best practice quality standards. This increases the risk of poor outcomes for patients in this cohort. SSNAP (Aug- Nov 2016) reports an overall score of D (lowest) for SaSH. Risk that internal operational and financial issues will constrain the pace of system and service transformation required for financial turnaround. Safeguarding Adults; Risk that the organisation may not have the capacity or capability to ensure that no harm is made to vulnerable adults Strategic Objective 03: SCCG 16/17-03 Create a Mature and Vibrant Organisation Risk that staff within the organisation may not have the capacity, capability and influence to cope with the scale and pace of change and the necessity to work in new ways required by Transformation Agenda. Strategic Objective 04: Create a Financially Sustainable Health and Social Care Economy Risk that move to new working arrangements as part of STP will have a negative impact on the substantial number of services currently delivered through the Surrey collaborative arrangements. " A risk that the South, Central and West CSU's working and delivery of the service will not be to the expected standard. Risk that inability to invest in Better Care Fund projects and wider out of hospital service model leads to failure to transform services and continued over-reliance on acute care. " Risk that cuts to adult social care and children's services, including decommissioning of some services, have a consequential financial impact on the wider system and increase costs for the CCG." Risk that changes to the IR35 ""disguised employee"" HMRC ruling sign off process scheduled for 1 April 2017 leads to disruption wherever interim staff are being used. This is 104
105 105 particularly significant for the CSU, who rely on interims for more than 80% of the services they currently provide to our CCG. We refresh, update and manages our operational and strategic risks through the following channels: Coordination of the risk management process. This was outsourced to South East Commissioning Support Unit during 2016/7 and taken in-house from 1 April Monthly meetings are held with individual directors and managers to review their allocated strategic and operational risks on a line-by-line basis. Clinical Executive Team meeting monthly collective line-by-line review of the clinical risks, as extracted from the strategic and operational risk registers. Senior Management Team monthly collective line-by-line review of the Strategic Risk Register. Heads of Service Group monthly collective line-by-line review of the Operational Risk Register. Quarterly overall sense check of the operational risk register. Risk Management Group (RMG) Quarterly line-by-line review and sense check of the Strategic Risk Register by a joint group of officers and Governing Body Members every quarter. The Risk Management Group reports to the Quality, Finance and Delivery Committee to give assurance. The overall Risk Management process is overseen by the Audit and Governance Committee, and audited by our Internal Auditor every year. In 2016/17 an internal audit opinion of Reasonable Assurance was awarded for Risk Management. Other sources of assurance Internal Control Framework A system of internal control is the set of processes and procedures in place in the clinical commissioning group to ensure it delivers its policies, aims and objectives. It is designed to identify and prioritise the risks, to evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively and economically. The system of internal control allows risk to be managed to a reasonable level rather than eliminating all risk; it can therefore only provide reasonable and not absolute assurance of effectiveness. Annual audit of conflicts of interest management The revised statutory guidance on managing conflicts of interest for CCGs (published June 2016) requires CCGs to undertake an annual internal audit of conflicts of interest management. To support CCGs to undertake this task, NHS England has published a template audit framework. Our auditors TIAA, carried out this review us in January 2017 as part of the planned internal audit work for 2016/17. Based on the work carried out an overall assessment of Reasonable Assurance was awarded, in relation to the overall adequacy of the arrangements to mitigate the key control risk areas Data Quality The last two years have seen significant improvement in provider contract reporting, ensuring commissioning organisations are able to report effectively around both quality and financial outcomes. Work continues with regard to the continuous development of high quality Board reports, with a move to automated bespoke production, enabling the CCG to meet the needs of its Governing Body. 105
106 106 Information Governance The NHS Information Governance Framework sets the processes and procedures by which the NHS handles information about patients and employees, in particular personal identifiable information. The NHS Information Governance Framework is supported by an information governance toolkit and the annual submission process provides assurances to the clinical commissioning group, other organisations and to individuals that personal information is dealt with legally, securely, efficiently and effectively. We self-assessed as compliant with all relevant aspects of the NHS Information Governance Toolkit before the national deadline of 31 March 2017 We place high importance on ensuring there are robust information governance systems and processes in place to help protect patient and corporate information. We have established an information governance management framework and have developed information governance processes and procedures in line with the information governance toolkit. We have ensured all staff undertake annual information governance training and maintain a staff information governance handbook to ensure staff are aware of their information governance roles and responsibilities. There are processes in place for incident reporting and investigation of serious incidents. We have developed information risk assessment and management procedures and a programme is being established to fully embed an information risk culture throughout the organisation against identified risks. Business Critical Models In line with best practice recommendations of the 2013 MacPherson review into the quality assurance of analytical models, an appropriate framework and environment is in place to provide quality assurance of business critical models. Third party assurances Where the CCG relies on third party providers, the arrangements are entered into either though a National Standard Contract (Long or Short Form) or a Grant all using the NHSE templates. Support services to the CCG are provided by the CSU under the Lead Provider Framework. Control Issues In the Month 9 Governance Statement return to NHS England, CCG identified the following control issues: CONTROL ISSUE CCG has been placed in Special Measures by NHSE, due to a failure to discharge its statutory financial duties CCG received a rating of Limited Assurance for an internal audit on its HR processes in November CCG received a rating of No Assurance for an internal audit on its processes for managing Off Payroll Appointments in June MITIGATING ACTIONS IN PLACE (AS OF MONTH NINE) Measures have been agreed with NHSE and are being implemented and monitored Action plan has been agreed with TIAA and is being implemented. TIAA will report on progress in the Annual Head of Internal Audit Opinion. Action plan was agreed with TIAA and all actions have now been closed. 106
107 The Surrey Collaborative received a rating of Limited Assurance in November 2016 for an internal audit on the Continuing Healthcare arrangements hosted by Surrey Downs CCG Action plan has been agreed with TIAA and is being implemented. TIAA will report on progress in the Annual Head of Internal Audit Opinion. As noted elsewhere in this report, the outstanding actions from the internal audits on HR and Continuing Healthcare have largely been closed, and no significant control issues are outstanding. We remain in Special Measures, due to a failure to discharge our statutory financial duties. Measures have been agreed with NHSE and are being implemented and monitored. The Special Measures indicate the gravity of our breach of its financial duties. NHSE has full oversight of our progress against its agreed plans to remedy this. Other than this, we have no significant control issues to report with regards to: organisational performance; failure to discharge statutory duties; lapses in control (breaches of conflicts of interest, fraud etc); information governance breaches; or any other serious concerns. Review of economy, efficiency & effectiveness of the use of resources During this last year we have made considerable progress in developing our Sustainability and Transformation Plan (Sussex and East Surrey STP). Our efforts have focused on developing and implementing our Financial Recovery Plan, agreed with NHS England, underpinned by robust benchmarking, data analysis and an identification of service transformation opportunities. The Governing Body has played a key role in approving and continuously monitoring and challenging the delivery of our Operating Plan and Financial Recovery Plan. The work of the Governing Body is supported by its committees, and rigorous annual internal and external work programmes. The Accountable Officer has overall responsibility for reviewing the effectiveness of the system of internal control within the clinical commissioning group. Our financial resources are split between programme (healthcare) and running costs (management costs). The running cost budget is nationally determined and for the CCG this is 3.8m, just over 21 per head of registered population. Expenditure reported at the end of 2016/17 is within the running cost budget. To deliver our deficit control total of 6.9m for 2016/17 we had an ambitious QIPP efficiency plan of 10.1m. In July 2016 the CCG revised the forecast QIPP delivery to 1.1m reflecting slippage on transformational investments, a lack of delivery on contractualised QIPP and delays to implementing pipeline schemes. In August the CCG developed a financial recovery plan of 7.4m to drive additional QIPP delivery in order to deliver the newly revised deficit control total of 14.4m. During December 2016 the deficit control total was revised to 19.4m following unexpected secondary care costs and a tariff increase in funded nursing care in excess of 1m. 107
108 108 We achieved total financial savings of 11.6m in 2016/17, which enabled the CCG to deliver its revised NHS England control total. As set out in the 2016/17 NHS Planning Guidance, CCGs were required to hold a 1 percent reserve uncommitted from the start of the year, created by setting aside the monies that CCGs were otherwise required to spend nonrecurrently. This was intended to be released for investment in Five Year Forward View transformation priorities to the extent that evidence emerged of risks not arising or being effectively mitigated through other means. In the event, the national position across the provider sector has been such that NHS England has been unable to allow CCGs 1% nonrecurrent monies to be spent. Therefore, to comply with this requirement, we have released its 1% reserve of 2.1m, resulting in the reduced deficit for the year of 17.3m. This additional surplus has been offset against other cost pressures from the current financial year. The CCG now carries forward a cumulative deficit of 42m into the 2017/18 financial year. In line with 2015/16, we anticipate an adverse economy, efficiency and effectiveness conclusion from external audit due to our in year and underlying deficit position. Moving forward we were allocated resources by NHS England for 2017/18 and 2018/19 as well as deficit control totals. Detailed financial plans were developed and submitted to the Governing Body and NHS England for both years and we are presently working with the Sussex and East Surrey health and care economy on establishing a balanced health economy through the newly introduced (by NHS England and NHS Improvement) Capped Expenditure Process in the very near future. We plan to continue to drive economic benefits through its preventative work and through service transformations with Multi Community Providers, etc. Efficiency, effectiveness and use of resources will also be improved further with all of our future contracts with providers. With the support of our contracts team, business analysis and commissioning collaborative colleagues we will continue to drive enhancements in this area. Delegation of functions We have continued to work with other Surrey and Sussex CCGs to manage contracts in a collaborative way and to ensure that the health economy remains viable and well managed. Our collaborative contracts with Surrey around Mental Health, Continuing Healthcare and Individual Funding Requests continue to meet our contractual requirements. We have strengthened our internal control, reporting and oversight of collaborative and hosted contracts to ensure we continue to meet our statutory responsibilities. Counter fraud arrangements Under the NHS Standard Contract all organisations providing NHS services are required to have appropriate anti-fraud arrangements in place. In 2015, NHS Protect published Standards for Providers: Fraud, Bribery and Corruption ( the Standards ) to assist organisations with this process. It incorporates a requirement that the Trust employs or contracts a qualified person or persons to undertake the full range of antifraud work, and that it produces a risk based work plan that details how it will approach antifraud and corruption work. We are committed to ensuring fraud, bribery and corruption does not proliferate within the organisation. The organisation is fully compliant with the directions issued by the Secretary of State in 1999, the NHS Standard Contract (2012) and the NHS Counter Fraud and Corruption Manual. 108
109 109 Our Counter Fraud Service is provided by TIAA Limited. The accredited Local Counter Fraud Specialist (LCFS) reports to the Chief Finance Officer and attends the Audit and Governance Committee meetings to report on the work achieved. The LCFS works to ensure that Counter Fraud is integrated into all our activity in a positive way. Throughout the past financial year there has been continued work to embed the counter fraud and anti-bribery culture. Work is undertaken against the Standards, comprising the area of Strategic Governance and the three key principals of Inform and Involve, Prevent and Deter, and Hold to Account. Reactive investigations comply with legislative requirements and with the NHS Counter Fraud and Corruption Manual. The LCFS liaises with other LCFS personnel and relevant external bodies for investigations, as appropriate. The LCFS is available to receive referrals and to report on the results of any investigations to the Chief Finance Officer and the Audit Committee. All sanctions available are considered following a reactive investigation, together with efforts to recover losses incurred. Internal Audit Internal audit primarily provides an independent and objective opinion to the Accountable Officer, the Board and the Audit Committee on the degree to which risk management, control and governance support the achievement of the organisation s agreed objectives. Internal audit also provides an independent and objective consultancy service specifically to help line management improve the organisation s risk management, control and governance. Review of the effectiveness of governance, risk management and internal control My review of the effectiveness of the system of internal control is informed by the work of the internal auditors, executive managers and clinical leads within the clinical commissioning group who have responsibility for the development and maintenance of the internal control framework. I have drawn on performance information available to me. My review is also informed by comments made by the external auditors in their annual audit letter and other reports. Our assurance framework provides me with evidence that the effectiveness of controls that manage risks to the clinical commissioning group achieving its principles objectives have been reviewed. Conclusion I have been advised on the implications of the result of internal audit s review of the effectiveness of the systems of internal control. As noted above, the auditors gave an overall opinion of Reasonable Assurance during 2016/17. As noted above, two opinions of Limited Assurance have been given during 2016/17 (one of which was for a hosted service). Action plans are in place for both areas, and both have been largely implemented at the time of writing this report. Otherwise, no significant internal control issues have been identified during 2016/17. Plans are in place to address minor weaknesses and ensure continuous improvement of the system is in place. 109
110 110 Annual Governance Statement Signed by Ian Ayres, Interim Accountable Officer Date 30 May
111 111 Remuneration and Staff Report Remuneration Report Introduction We are required, under guidance issued by the Department of Health, to include in its Annual Report a Remuneration Report that is subject to external audit opinion. The following contains all information referred to in the guidance and follows the same sequence in that document. There are some general items identified in the guidance that require audit opinion and many that do not. This report provides all of the necessary information and therefore may be audited as a whole. Definition of senior managers In accordance with the guidance, senior managers are defined as those persons in senior positions having authority or responsibility for directing or controlling the major activities of the CCG. This includes for the purpose of this report, executive, associate, clinical, advisory and Lay Members of the Governing Body. The Accountable Officer has confirmed that those persons cited in the Remuneration Report are those individuals in senior positions having authority or responsibility for directing or controlling the major activities of the CCG. This means those who influence the decisions of the entity as a whole rather than the decisions of individual directorates or departments. The Accountable Officer should be asked to confirm whether this covers more than the executive and non-executive directors. It is usually considered that the regular attendees of the entity s board meetings are its senior managers. The Accountable Officer has concurred with this definition of the senior manager for the purpose of this report. A full list is provided here. There is a presumption that all senior managers named above for whom disclosures are necessary have not objected to their details being disclosed or sought nondisclosure. A letter relating to disclosure of remuneration and pension details and the individuals right to seek non- disclosure has been issued to all parties to whom this report relates. Remuneration Committee report The Remuneration Committee is established in accordance with the CCG Constitution, Standing Orders and Scheme of Delegation. It has delegated authority from the Governing Body to ensure appropriate remuneration, allowances and terms of service for the CCG Chair and senior team (defined as at least the Chief Officer and their executive direct reports, plus other members of the executive management team), including interim appointments. The Remuneration Committee has a floating membership comprising Lay Members, GP members, the Secondary Care Doctor (this role is currently vacant) and the Board Nurse. At each meeting, a balance of members is invited to ensure that sufficient members are present to reach a quorum which does not have an interest in the matter under consideration. The Committee has met on six occasions during 2016/17 (20 May 2016, 9 June 2016; 18 July 2016, 2 Aug 2016, 20 Oct 2016, 17 March 2017). The Remuneration Committee quorum was met in all Remuneration Committee meetings for 2016/
112 112 The Chair of the committee is the CCG Deputy Chair, who is a Lay Member. A full list of members, their roles and the number of meetings each attended is below. Name of member Role Date joined committee Date left committee (if applicable) No. of committee meetings attended David Congdon Lay Member and RemCo Chair 1 November 2013 n/a 6 Dr Elango Vijaykumar Graham Hanson CCG Clinical Chair Lay Member Governance 1 April 2013 n/a 5 1 April March Nicola Jupp Lay Member 2 November 2015 n/a 1 Dr Patrick Kerr Susan Latham Clinical Director (GP Member) Practice Manager Representative 1 April 2013 n/a 1 1 July 2013 n/a 1 Yvette Robbins Lay Member 3 November 2015 n/a 4 In addition to the members listed above, the following CCG employees provided the committee with services and/or advice was material to the committee s deliberations. Name Role Service Elaine Jackson Chief Officer until 31 July May and 9 June 2016: present at meeting and provided advice. Ian Ayres Chief Officer from 1 September October 2016: present at meeting and Louise O Byrne Head of Governance and Assurance provided advice. All meetings except 16 March 2017: serviced the meeting and provided 112
113 113 advice. Peter Kottlar Chief Operating Officer 16 March 2017: present at meeting and provided advice. Ray Davey Richard Bates Interim Chief Finance Officer from 18 July 2016 (handover period until 31 July 2016). Interim Chief Finance Officer until 31 July March 2017: present at meeting and provided advice. 9 June 2016: present at meeting and provided advice. The following persons who are not employees of the CCG also provided services and/or advice to the committee, in their capacity as employees of the South East CSU. The HR service provided via South East CSU included advice on HR, employment and NHS terms and conditions matters, the interpretation of NHS Commissioning Board remuneration guidance for CCGs and the provision of benchmarking information relating to local and regional CCG Governing Bodies. Name Role Service Sarah Wainwright HR & OD Partner, South East CSU 20 May, 18 July, 2 August 2016: present at meeting (via phone on 18 July) and provided advice Policy on remuneration The Committee s deliberations are carried out within the context of national pay and remuneration guidelines, local comparability and taking account of independent advice regarding pay structures. In setting levels of remuneration, the Committee takes into account national guidance for CCGs; CCG benchmarking; locally prevailing employment conditions; and the levels of responsibility associated with each post. In addition the Committee has access to and takes advice from an HR specialist. The current remuneration policy does not specify performance related awards or targets and amendments to remuneration are to be considered and determined annually by the Committee. In determining the emoluments for office holders on the Governing Body, the Remuneration Committee considered the rates for previous and current NHS organisations and the specific NHS Commissioning Board (now NHS England) guidance as well as the best practice terms of appointment for Lay Members provided by the NHS Commissioning Board. In determining the pay and conditions for the senior employees, consideration was given to NHS very senior managers (VSM) and Agenda for Changes terms and conditions as well as CCG specific guidance in this area. 113
114 114 The performance of executive directors is monitored through an annual appraisal process based on organisational and individual objectives. A report on the appraisals and any recommendations for remuneration review would be submitted to the Remuneration Committee for consideration prior to any decision being taken on changes to a remuneration package. The performance of other Governing Body members is the responsibility of the CCG Clinical Chair and is based on an annual review process. No elements of the remuneration packages for the Chief Officer, Clinical Chair, Directors and other Governing Body members are directly linked to performance. Senior managers contracts The Chief Officer and Chief Finance Officer on the CCG Governing Body are interim employees. The Executive Directors have a permanent contract, which provides for a notice period of six months from the employee and six months from the employer. The contracts include the ability for the CCG to enact a pay in lieu of notice clause and there are no special contractual compensation provisions or any other form of termination payment. HM Treasury has issued specific guidance on severance payments (covering any payments that are not made under either legal or contractual obligation) and all such packages would require advance approval from the Treasury. The CCG has made no severance payment or provided any other non-contractual exit package during the year that fall within this requirement. The GP members, Lay Members and independent clinical members on the Governing Body are office holders and their terms of appointment provide that the individual may step down from office at any time with the expectation of three months notice. In the event of disqualification from holding office or a motion of no confidence from the membership, the CCG may terminate the appointment with no specified minimum notice period. There are no special contractual compensation provisions for early termination or any other form of termination payment. End dates of expired terms at a senior management level are contained within the Remuneration Table of this report; there have been no provisions awarded pertaining to early retirement or early terminations. (Please refer to note on Exit Packages). There have been no payments made for loss of office or other benefits in kind payable. One performance related bonus of 2,937 has been paid for satisfactory performance against 2015/16 deliverables. There have been no significant or other awards made to past senior managers within the definition of the guidance. Below are the contractual details of the Accountable Officer and Chief Finance Officer on the Governing Body who served in 2016/17: Elaine Jackson, Interim Accountable Officer until 31 July Interim contract Ian Ayres Interim Accountable Officer from 1 September This is a shared post with 114
115 NHS West Kent CCG. 115 Richard Bates, Interim Chief Finance Officer until 31 July Interim contract Ray Davey, Interim Chief Finance Officer from 18 July 2016 (handover period until 31 July 2016). Interim contract with 4 weeks notice. Below are the contractual details of the office holders on the Governing Body who served in 2016/17: Dr Patrick Kerr, Assistant Clinical Chair; GP member of the Governing Body. Appointed 1 April 2013, reappointed 6 April 2016 for three years; three months notice period; no special contractual compensation provisions for early termination. Dr Thiruselvi Banagalore, GP member of the Governing Body. Appointed 1 September 2017 for three years; three months notice period; no special contractual compensation provisions for early termination. Dr Elango Vijaykumar; Clinical Chair. Appointed as Chair 14 April 2015, term of office until 13 April 2018; three months notice period; no special contractual compensation provisions for early termination. Dr David Hill, Chair of the Practices Commissioning Committee; GP member of the Governing Body. Appointed 1 April 2013, reappointed 6 April 2016 for three years; three months notice period; no special contractual compensation provisions for early termination. Dr Heidi Fahy, GP member of the Governing Body. Appointed 1 April 2013; reappointed 6 April 2016 for eighteen months; three months notice period; no special contractual compensation provisions for early termination. Dr Richard Wright, GP member of the Governing Body. Appointed permanently 5 October 2015, resigned 31 August 2016; three months notice period; no special contractual compensation provisions for early termination. Sue Latham, Practice Manager Representative. Appointed 1 July 2013, reappointed 1 July 2016 to 30 June 2019; three months notice period; no special contractual compensation provisions for early termination. Avey Bhatia, registered nurse on the Governing Body. Appointed 1 May 2015 for three years; three months notice period; no special contractual compensation provisions for early termination. Graham Hanson, Lay Member on the Governing Body. Appointed 1 April 2013, term of office until 31 March 2016; extended to 30 June 2017; three months notice period; no special contractual compensation provisions for early termination. Yvette Robbins, Lay Member on the Governing Body. Appointed 3 November 2015, term of office until 2 November 2018; three months notice period; no special contractual compensation provisions for early termination. Nicola Jupp, Lay Member on the Governing Body. Appointed 3 November 2015, term of 115
116 116 office until 2 November 2018; three months notice period; no special contractual compensation provisions for early termination. David Congdon, Lay Member on the Governing Body. Appointed 1 November 2013, term of office until 31 October 2016; extended to 31 March 2018; three months notice period; no special contractual compensation provisions for early termination. The post of Secondary Care Doctor on the Governing Body has been vacant throughout the whole of 2016/7. Two new Lay Members have been appointed to the Governing Body from 1 st April 2017: Adrian Brown, Lay Member on the Governing Body. Appointed 1 April 2017, term of office until 31 March 2020; three months notice period; no special contractual compensation provisions for early termination Carol Pearson, Lay Member on the Governing Body. Appointed 1 April 2017, term of office until 31 March 2020; three months notice period; no special contractual compensation provisions for early termination Below are the contractual details of the executive members who supported the Governing Body during 2016/17: Karen Devanny, Director of Quality and Nursing. Permanent contract; six months notice period; no special contractual compensation provisions for early termination. Peter Kottlar, Chief Operating Officer. Permanent contract; six months notice period; no special contractual compensation provisions for early termination. Samantha Stanbridge, Director of Commissioning. Permanent contract; six months notice period; no special contractual compensation provisions for early termination. Caroline Farrar, Director of Out of Hospital Strategy. Permanent contract; six months notice period; no special contractual compensation provisions for early termination. Gareth Howells, Director of Delivery. Appointed 7 February Permanent contract; six months notice period; no special contractual compensation provisions for early termination. Salaries and Allowances All information required within the guidance has been provided where required. Where information is not available (either at present to the CCG, or not at all, whether due to previous records being unavailable, or where third party providers have not been able to provide information at the time of the Annual Report being produced), this position has been stated in the tables of the Remuneration Report. 116
117 117 Senior manager remuneration (including salary and pension entitlements) 09L - NHS EAST SURREY CCG SALARY & PENSION DISCLOSURES Salaries and allowances Name and title (a) (b) (c) (d) (e) (f) Salary Expense Payments (taxable) Performance Pay and bonuses Long-term Performance pay and bonuses All Pension Related Benefits TOTAL (a to e) Restated (bands of 5,000) (To nearest 100) (bands of 5,000) (bands of 5,000) (bands of 2,500) (bands of 5,000) (bands of 5,000) Dr Elango Vijaykumar, Clinical Chair - Note Dr David Hill, GP Member, PCC Chair and Clinical Director - Note Dr Heidi Fahy, GP Member and Clinical Director - Note Dr Patrick Kerr, GP member, Assistant Clinical Chair and Clinical Director - Note Dr Richard Wright, GP member and Clinical Director (to 31/08/16) - Note Dr Thiruselvi Bangalore, GP member and Clinical Director (from 01/09/16) - Note N/A Sue Latham, Practice Manager Representative - Note Dr Mike Baxter, Secondary Care Consultant (left 31/12/15) Avey Bhatia, Board Nurse Note Graham Hanson, Lay Member (Governance) David Congdon, Lay Member & Deputy Chair Yvette Robbins, Lay Member TOTAL Nicola Jupp, Lay Member Elaine Jackson, Accountable Officer (to 31/07/16) - Note 6 Ian Ayres, Accountable Officer (from 01/09/16) - Note 5 Karen McDowell, Chief Finance Officer (left 29/05/15) - Note 4 Richard Bates, Interim Chief Finance Officer (to 31/07/16) - Note 6 Ray Davey, Interim Chief Finance Officer (from 01/08/16) - Note 6 & Note 7 Samantha Stanbridge, Director of Commissioning & Engagement N/A N/A Karen Devanny, Director of Quality & Nursing Peter Kottlar, Director of Transformation & Delivery (to 19/10/16), Acting Chief Operating Officer (from 20/10/16), Chief Operating Officer (from 16/03/17) Caroline Farrar, Director of Integration (to 31/01/17), Director of Out of Hospital Strategy (from 01/02/17) Anouska Adamson-Parks, Interim Director of QIPP & Integration (to 15/05/15) Gareth Howells, Director of Delivery (from 07/02/17) N/A Note 1 - East Surrey CCG's GP Governing Body members' employment status is defined as 'Off Payroll' for NHS statutory accounting purposes. Compliance requires the CCG to include the employer pension contributions made to the NHS Pension Scheme in the salary column (a). Note 2 - The employing practice invoices the CCG for the contracted remuneration. Note 3 - Maidstone & Tunbridge Wells NHS Trust invoice the CCG for the contracted remuneration and employers national insurance and NHS pension contributions. Note 4 - This reflects NHS East Surrey CCG's share of the shared resource with NHS Guildford & Waverley CCG. Total benefits across both CCGs is within a band of 155, ,000. Note 5 - This reflects NHS East Surrey CCG's share of the shared resource with NHS West Kent CCG. Total benefits across both CCGs is within a band of 115, ,000. Note 6 - Interim appointment costs are generally higher, to reflect the fact that interim staff do not receive benefits such as employer pension contributions (14.3%), paid holiday, sick leave and bank holidays. The disclosed salaries also include VAT at 20%. Note 7 - The disclosed salaries also include agency commission and expenses. Expense Payments (Taxable) - Column (b) - This is the gross value of expenses allowances that are subject to UK income tax and paid or payable to the person in respect of qualifying services Where one or more senior managers of a CCG are paid more than 142,500 per annum, the CCG must satisfy itself that this remuneration is reasonable. Pay for a part time / part year senior manager should be compared against a pro rata of 142,500. In 2016/17 the CCG had three very senior managers that were paid pro rata more than 142,500 per annum; all posts were interim appointments. Interim appointment costs are generally higher, to reflect the fact that interim staff do not receive benefits such as employer pension contributions (14.3%), 117
118 118 paid holiday, sick leave and bank holidays. The disclosed salaries also include VAT at 20% and for one of the appointments an agency commission. Pension Benefits and liabilities Pension benefits are applicable to all executive senior managers employed by the CCG and the GP Governing Body members unless they wish to opt out of membership of the NHS Pension Scheme. Although the GP Governing Body members remuneration is pensionable, the CCG is not required to disclose GP pension benefits as their employment status with the CCG is on a contract for service basis and deemed to be off payroll. Other non-executive members do not contribute to the NHS Pension Scheme and are not subject to this disclosure. The pension information in the table is provided by the Greenbury Team at the NHS Business Services Authority (BSA) and is presented in accordance with reporting guidance. The pension information in the table below is calculated and provided by the NHS BSA and presented in accordance with the guidance. What is shown is the Cash Equivalent Transfer Value (CETV) for the past and present financial years, which demonstrates the actual increase in value for the individuals accrued pension benefits and the value of each individuals lump sum and pension at age sixty based on the previous and current year, again demonstrating the relevant increases. The calculations are based on records available at the time of publication. No Senior Managers were in receipt of Partnership or Stakeholder Pensions. Table below shows: Pension benefits as at 31 March
119 09L - NHS EAST SURREY CCG 119 PENSION DISCLOSURES Pension Benefits 2016/17 Name and title Real increase in pension at pension age Real increase in pension lump sum at pension age Total accrued pension at pension age at 31 March 2017 Lump sum at pension age related to accrued pension at 31 March 2017 Cash Equivalent Transfer Value at 1 April 2016 Real Increase in Cash Equivalent Transfer Value Cash Equivalent Transfer Value at 31 March 2017 Employers Contribution to Stake-holder Pension (bands of 2,500) (bands of 2,500) (bands of 5,000) (bands of 5,000) Samantha Stanbridge, Director of Commissioning & Engagement Karen Devanny, Director of Quality & Nursing Peter Kottlar, Director of Transformation & Delivery (to 19/10/16), Acting Chief Operating Officer (from 20/10/16), Chief Operating Officer (from 16/03/17) Caroline Farrar, Director of Integration (to 31/01/17), Director of Out of Hospital Strategy (from 01/02/17) Gareth Howells, Director of Delivery (from 07/02/17) Certain members do not receive officer pensionable remuneration therefore there will be no entries in respect of pensions for certain Members. Pension Benefits 2015/16 Restated Name and title Real increase in pension at pension age Real increase in pension lump sum at pension age Total accrued pension at pension age at 31 March 2016 Lump sum at pension age related to accrued pension at 31 March 2016 Cash Equivalent Transfer Value at 1 April 2015 Real Increase in Cash Equivalent Transfer Value Cash Equivalent Transfer Value at 31 March 2016 Employers Contribution to Stake-holder Pension (bands of 2,500) (bands of 2,500) (bands of 5,000) (bands of 5,000) Karen McDowell, Chief Finance Officer (to 29/05/15) * Samantha Stanbridge, Director of Commissioning & Engagement Karen Devanny, Director of Quality & Nursing Peter Kottlar, Director of Transformation & Delivery (from 01/10/15) Caroline Farrar, Director of Integration (from 08/02/16) Certain members do not receive officer pensionable remuneration therefore there will be no entries in respect of pensions for certain Members. * The pensions benefits for Karen McDowell represents her full accrued benefits to 31 March 2016 inclusive of all NHS organisations where she has worked, including NHS East Surrey CCG. Cash equivalent transfer values A cash equivalent transfer value (CETV) is the actuarially assessed capital value of the pension scheme benefits accrued by a member at a particular point in time. The benefits valued are the member s accrued benefits and any contingent spouse s (or other allowable beneficiary s) pension payable from the scheme. A CETV is a payment made by a pension scheme or arrangement to secure pension benefits in another pension scheme or arrangement when the member leaves a scheme and chooses to transfer the benefits accrued in their former scheme. The pension figures shown relate to the benefits that the individual has accrued as a consequence of their total membership of the pension scheme, not just their service in a senior capacity to which disclosure applies. The CETV figures and the other pension details include the value of any pension benefits in another scheme or arrangement which the individual has transferred to the NHS pension scheme. They also include any additional pension benefit accrued to the member as a result of their purchasing additional years of pension service in the scheme at their own cost. CETVs are calculated within the guidelines and framework prescribed by the Institute and Faculty of Actuaries. Real increase in CETV This reflects the increase in CETV effectively funded by the employer. It takes account of the increase in accrued pension due to inflation, contributions paid by the employee (including the value of any benefits transferred from another scheme or arrangement) and uses common market valuation factors for the start and end of the period. 119
120 Fair Pay Disclosure 120 Reporting bodies are required to disclose the relationship between the remuneration of the highest paid member in their organisation and the median remuneration of the organisation s workforce. The annualised banded remuneration of the highest paid director/member in East Surrey CCG in the financial year was 245k- 250k ( : k). This was 4.3 times ( , 4.6 times) the median remuneration of the workforce, which was 57k ( : 57k). In , nil ( : one) employees received remuneration in excess of the highest-paid director/member. Remuneration (excluding an Apprentice) ranged from 24k to 236k ( : 20k- 340k). Total remuneration includes salary, non-consolidated performance related pay, benefits-in-kind, but not severance payments. It does not include employer pension contributions and the cash equivalent transfer value of pensions. 120
121 121 Staff Report Number of senior managers Clinical Lead Governing Body Director Employee Grand Total Male Female Male Female Male Female Male Female Payband Total Band 2 1 Band 5 7 Band 7 2 Band 8 - Range A 7 Band 8 - Range B 4 Band 8 - Range C 6 Band 8 - Range D 5 Local Salary 14 Local VSM 1 Grand Total 47 Staff numbers and costs Fixed Term and Permanent Employees April 2016 March 2017 Average FTE Average Head Count 29 Staff Category Permanent Employees Other Staff Total Staff Average No. 000 Average No. 000 Average No. 000 ADMINISTRATIVE STAFF Senior manager ,550 Manager ,092 Clerical and administrative MEDICAL STAFF 121

122 122 GPs NURSING STAFF Manager TOTAL , , ,414 Staff composition The following tables are a profile of the CCG relating to the main protected characteristics. Tables do not include Governing Body membership / Clinical Leads (as at 31 March 2017). 122
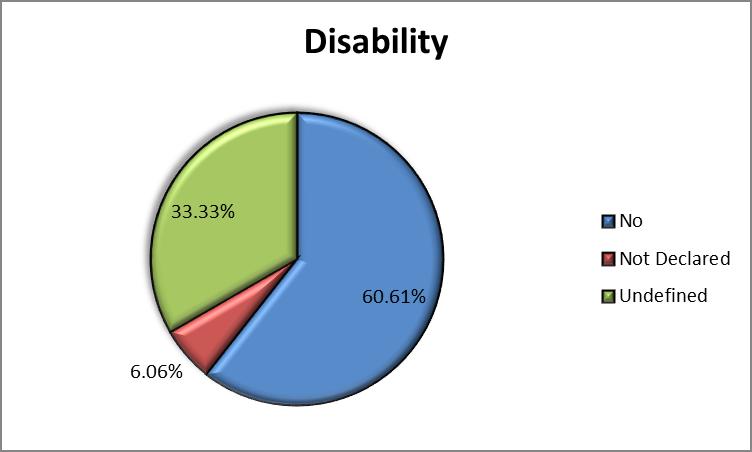
123
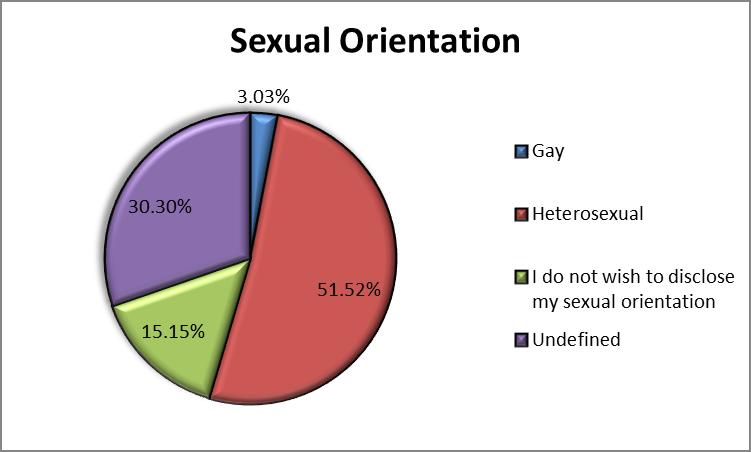
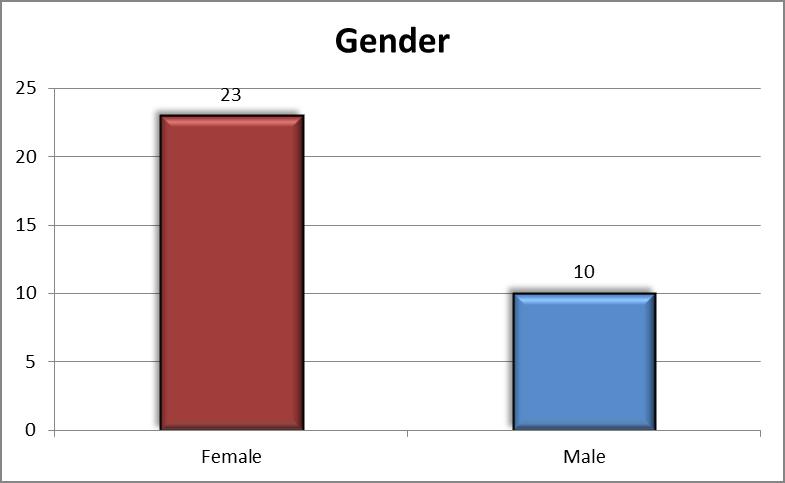
124
125 125 Sickness absence data April 2016 March 2017 Total Days Lost Total staff Years Average Working days lost Number of persons retiring on ill health grounds 0 Staff policies Communicating and Engaging There are a number of ways in which we communicate and engage with our staff. These include: Regular staff briefings Staff engagement forums Directorate staff meetings One to one meeting with managers for all staff. Participation in the national NHS Staff Survey in 2016 Policy on Disabled Employees Disabled employees are protected under the "protected characteristics" of the Equality Act 2010, one of which is disability. We ensure that the requirements and reasonable adjustments necessary for employees with disabilities are taken into account during their employment and that people with disabilities are not discriminated against on the ground of their disability at any stage of the recruitment process or in their employment with the CCG. Our Sickness Absence Policy confirms that where an employee becomes disabled as a result of sickness, we will make any necessary reasonable adjustments, as required, and in accordance with the Equality Act to enable the employee to return to work. The types of adjustments may include adjustments to work base, working hours, redeploying the employee 125
126 126 to another suitable position and providing any necessary equipment to assist the employee to perform their role. Equalities for Staff We promote a working environment in which all parties and procedures relating to recruitment, selection, training, promotion and employment are free from unfair discrimination, ensuring that no employee or prospective employee is discriminated against, whether directly or indirectly on the grounds of age; disability; gender reassignment; pregnancy and maternity; race including ethnic or national origins, colour or nationality; religion or belief; sex (gender); sexual orientation; marriage and civil partnership; trade union membership; responsibility for dependents or any other condition or requirement which cannot be shown to be justifiable. Expenditure on consultancy 2016/ / Off-payroll engagements Off payroll engagements are those where individuals, either self-employed or acting through a personal service company, are paid gross by the employer. Payments made in this way are therefore not subject to the usual deduction of income tax and national insurance. GP members of the Governing Body are disclosed as being off-payroll engagements but are paid through payroll. This is to satisfy HMRC as they deem long term contracts for service holders as office holders of the organisation, and require the organisation to deduct income tax and national insurance at source. This designation does not change their employment status with the CCG (as an off-payroll worker rather than an employee of the CCG) but is merely a route for HMRC to collect tax and national insurance in-year rather than ten months after the year end. In this situation the deduction of tax and national insurance is processed via ESR (the CCG s payroll system), and the resulting deduction paid over in the normal way. The individual remains an off-payroll worker. Table below shows: Off-payroll engagements longer than 6 months Off-payroll engagements as of 31 March 2017, for more than 220 per day and that last longer than six months: Number Number The total number that existed as of 31 March
127 127 - for less than one year at the time of reporting for between one and two years at the time of reporting for between 2 and 3 years at the time of reporting for between 3 and 4 years at the time of reporting 6 N/A Of the 13 off-payroll engagements identified, all are GPs or other practice staff who provide services to the CCG either on the Governing Body, on Committees or as Clinical Leads. All of these are paid through the CCG's payroll or by invoice from GP practices. All existing off-payroll engagements have at some point been subject to a risk based assessment as to whether assurance is required that the individual is paying the right amount of tax. Where necessary, we have sought assurance from the engagee. Table below shows: New Off-payroll engagements New off-payroll engagements between 1 April 2016 and 31 March 2017, for more than 220 per day and that last longer than six months: Number Number Number of new engagements, or those that reached six months in duration, between 1 April and 31 March - of the above, General Practitioners paid through the payroll with tax & NI contributions deducted Number of other new engagements which include contractual clauses giving the CCG the right to request assurance in relation to income tax and National Insurance obligations Nil Number for whom assurance has been requested N/A 1 Of which, the number: - assurance has been received 1 - assurance has not been received Nil - engagements terminated as a result of assurance not being received Nil 127
128 128 All contracts have been reviewed to ensure that they are compliant with IR35 rules. The CCG has sought assurance from all staffing agencies that all off-payroll engagements falling within IR35 are paid appropriately through umbrella arrangements. Table 3: Off-payroll Governing Body members / senior official engagements Off-payroll engagements of governing body members, and / or, senior officials with significant responsibility between 1 April 2016 and 31 March 2017: Number Number Number of off-payroll engagements of Governing Body members, and/or senior officers with significant financial responsibility, during the financial year (this includes all Governing Body GPs and the Practice Manager Representative) 9 8 Total number of individuals on payroll and off-payroll that have been deemed "Governing Body members, and/or senior officials with significant financial responsibility" during the financial year
129 129 Exit packages, including special (non-contractual) payments The CCG can report that there were no exit packages agreed in the year, and no costs related to departures accrued from previous years. There are no additional disclosures made that exceed contractual amounts outside of contractual and/or pension terms. There were no severance or special severance payments made. Severance payment accrued in year - This information has been audited by the CCG's external auditors Number of Payments Number Total value of payments 000s Made under contractual or statutory obligation 0 0 Made under contractual or statutory obligation, where the payment exceeds annual salary 0 0 Signed by Ian Ayres, Interim Accountable Officer Date 30 May
130 130 Statement of Accountable Officer s responsibilities The National Health Service Act 2006 (as amended) states that each Clinical Commissioning Group shall have an Accountable Officer and that Officer shall be appointed by the NHS Commissioning Board (NHS England). NHS England has appointed the Chief Executive Officer to be the Accountable Officer of the Clinical Commissioning Group. The responsibilities of an Accountable Officer, including responsibilities for the propriety and regularity of the public finances for which the Accountable Officer is answerable, for keeping proper accounting records (which disclose with reasonable accuracy at any time the financial position of the Clinical Commissioning Group and enable them to ensure that the accounts comply with the requirements of the Accounts Direction) and for safeguarding the Clinical Commissioning Group s assets (and hence taking reasonable steps for the prevention and detection of fraud and other irregularities), are set out in the Clinical Commissioning Group Accountable Officer Appointment Letter. Under the National Health Service Act 2006 (as amended), NHS England has directed each Clinical Commissioning Group to prepare annual financial statements as set out in the Accounts Direction. The financial statements are prepared on an accruals basis and must give a true and fair view of the state of affairs of the Clinical Commissioning Group and of its net expenditure, changes in taxpayers equity and cash flows for the financial year. In preparing the financial statements, the Accountable Officer is required to comply with the requirements of the Manual for Accounts issued by the Department of Health and in particular to: Observe the Accounts Direction issued by NHS England, including the relevant accounting and disclosure requirements, and apply suitable accounting policies on a consistent basis; Make judgements and estimates on a reasonable basis; State whether applicable accounting standards as set out in the Manual for Accounts issued by the Department of Health have been followed, and disclose and explain any material departures in the financial statements; and, Prepare the financial statements on a going concern basis. To the best of my knowledge and belief, and subject to the disclosures set out below, I have properly discharged the responsibilities set out under the National Health Service Act 2006 (as amended), Managing Public Money and in my Clinical Commissioning Group Accountable Officer Appointment Letter. Disclosures (as noted above): On 2 December 2015, we were placed under Legal Directions by NHSE, issued under Section 14Z21 of the National Health Service Act On 21 July 2016, we were placed in Special Measures by NHSE as part of a national reset plan As far as I am aware, there is no relevant audit information of which the CCG s auditors are unaware, and I have taken all the steps that I ought to have taken to make myself aware of any relevant information and to establish that the CCG s auditors are aware of that information 130
131 131 I confirm that the Annual Report and Accounts (ARA) as a whole is fair, balanced and understandable and that I take personal responsibility for the ARA and the judgments required for determining that it is fair, balanced and understandable. Signed by Ian Ayres, Interim Accountable Officer Date 30 May
132 132 Parliamentary Accountability and Audit Report East Surrey CCG is not required to produce a Parliamentary Accountability and Audit Report. Disclosures on remote contingent liabilities, losses and special payments, gifts, and fees and charges are included as notes in the Financial Statements of this report. Accountability Report Signed by Ian Ayres, Interim Accountable Officer Date 30 May
133 133 Section 4 Head of Internal Audit Opinion Following completion of the planned audit work for the financial year, the Head of Internal Audit issued an independent and objective opinion on the adequacy and effectiveness of our system of risk management, governance and internal control. The Head of Internal Audit concluded that: Reasonable assurance can be given that there are adequate and effective management and internal control processes to manage the achievement of the organisation s objectives. During the year, Internal Audit issued the following audit reports relating to our work areas: Area of Audit Management of serious incidents Review of complaints and FOI Requests Assurance Framework and Risk Management Critical Finance and Assurance NHS England Mandated Conflicts of Interest Review Service Transformation QIPP Review of HR Systems and Controls (including HR Workforce Training and Development) IG Toolkit v14 Review of Investments (including the Integrated Re-ablement and Frailty Units) Level of Assurance Given Substantial Assurance Substantial Assurance Reasonable Assurance Reasonable Assurance Reasonable Assurance Reasonable Assurance Limited Assurance Reasonable Assurance As agreed this was an Appraisal Review With regard to the Review of HR Systems and Controls, the key issues raised were: Personnel records were not maintained for all staff. Relevant records were not routinely maintained on employees files e.g. proof of identity; proof of right to work and evidence that employees had been subject to an occupational health check and clearance. The HR processes require to be strengthened The CCG does not have a policy covering training and development; and training completion rates by employees were low. An action plan was agreed and presented to the Audit and Governance Committee on 8 December TIAA carried out a follow-up visit in March The Final HOIA Opinion states: 133
134 134 From a total of 13 recommendations raised within the report nine out of the 10 recommendations have been implemented. The agreed implementation dates for the remaining recommendations (three) are not yet due. During the year, Internal Audit issued the following audit reports relating to Surrey-wide services hosted by other CCGs: Area of Audit Safeguarding Vulnerable Adults Governance Arrangements hosted by NHS Guildford and Waverley CCG Continuing Healthcare (Governance) hosted by Surrey Downs CCG Level of Assurance Given Reasonable Assurance Limited Assurance With regard to the Review of Continuing Healthcare (Governance), the key issues raised were: The CCG to review how the CHC Programme Board provides assurance to the CCG s Governing Body and the other CCGs within the collaborative. Most of the CHC contracts were not signed. The agenda for the CHC Programme Board does not include declaration of interests, and gifts and hospitality. Risk management e.g. the absence of an overarching CHC risk register which would incorporates the risks contained within the existing three risk registers i.e. CHC Risk Register, CHC Transforming Care Register and CHC QIPP Register. Adequacy and effectiveness of controls over Decision Support Tools (DSTs). Development of processes for managing nursing homes with adverse CQC inspection reports. An action plan has been agreed with. At the time of Surrey Downs CCG s February 2017 Audit Committee meeting, 22 of the 25 recommendations had been implemented and the remaining 3 were not yet due. 134

135 Internal Audit NHS East Surrey Clinical Commissioning Group Internal Audit Annual Report 2016/17 May 2017 FINAL
136 NHS East Surrey Clinical Commissioning Group Internal Audit Annual Report 2016/17 Internal Audit Annual Report INTRODUCTION This is the 2016/17 Annual Report by TIAA on the internal control environment at NHS East Surrey Clinical Commissioning Group. The annual internal audit report summaries the outcomes of the reviews we have carried out on the organisation s framework of governance, risk management and control. This report is designed to assist the Governing Body in making its Annual Governance Statement. HEAD OF INTERNAL AUDIT S ANNUAL OPINION I am satisfied that sufficient internal audit work has been undertaken to allow me to draw a reasonable conclusion as to the adequacy and effectiveness of East Surrey Clinical Commissioning Group s risk management, control and governance processes. In my opinion, except for the CCG s ability to deliver their planned financial control total (see Annex A), NHS East Surrey Clinical Commissioning Group has adequate and effective management, control and governance processes to manage the achievement of its objectives. Our formal Opinion is set out at Annex A. INTERNAL AUDIT PLANNED COVERAGE AND OUTPUT The 2016/17 Annual Audit Plan approved by the Audit and Governance Committee was for 118 days of internal audit coverage in the year. During the year there were changes to the Audit Plan and the changes were approved by the Audit Committee at their December 2016 meeting. The formal year-end Annual Opinion statement is set out in Annex A. All the planned work has been carried out and the reports have been issued (see Annex C). the Annual Audit Plan. ASSURANCE TIAA carried out 8 assurance reviews (excluding the two joint/collaborative reviews, and two other non-assurance audits), which were designed to ascertain the extent to which the internal controls in the system are adequate to ensure that activities and procedures are operating to achieve NHS East Surrey Clinical Commissioning Group s objectives. For each assurance review an assessment of the combined effectiveness of the controls in mitigating the key control risks was provided. Details of these are provided in Annexes B and C, and a summary is set out below. Assurance Assessments Number of Reviews Previous Year Substantial Assurance 2 1 Reasonable Assurance 5 6 Limited Assurance 1 1 No Assurance 0 1 The areas on which the assurance assessments have been provided can only provide reasonable and not absolute assurance against misstatement or loss and their effectiveness is reduced if the internal audit recommendations made have not been fully implemented. There was no work carried out which was in addition to the work set out in 137
137 NHS East Surrey Clinical Commissioning Group Internal Audit Annual Report 2016/17 We made the following total number of recommendations on our audit work carried out in 2016/17. AUDIT SUMMARY Urgent Important Routine Control weaknesses: There was one area reviewed by internal audit where it was assessed that the effectiveness of some of the internal control arrangements provided limited' assurance. Recommendations were made to further strengthen the control environment in this area and the management responses indicated that the recommendations had been accepted. Recommendations Made: We have analysed our findings/recommendations by risk area and these are summarised below. Risk Area Urgent Important Routine Directed Compliance Operational Reputational Operational Effectiveness Opportunities: One of the roles of internal audit is to add value and during the financial year we provided advice on opportunities to enhance the operational effectiveness of the areas reviewed and the number of these opportunities is summarised below. Operational 6 OTHER REVIEWS TIAA also carried out an appraisal Review of Investments (including the Integrated Re-ablement Unit). At the time of preparing this report, the review was at draft report stage and was being actively discussed with management. INDEPENDENCE AND OBJECTIVITY OF INTERNAL AUDIT There were no limitations or restrictions placed on the internal audit service which impaired either the independence or objectivity of the service provided. PERFORMANCE AND QUALITY ASSURANCE The following Performance Targets were used to measure the performance of internal audit in delivering the Annual Plan. Performance Measure Target Attained Completion of Planned Audits 100% 100% Audits Completed in Time Allocation 100% 100% Final report issued within 10 working days of receipt of responses Compliance with Public Sector Internal Audit Standards 95% 100% 100% 100% Ongoing quality assurance work was carried out throughout the year, and we continue to comply with ISO 9001 standards. An independent external review was carried out in 2016 of our compliance with Public Sector Internal Audit Standards (PSIAS) which met the requirement for an independent 5 year review. The outcome concluded that TIAA generally complies with all standards and requirements of the PSIAS. Our work also complies with the IIA-UK Professional Standards. During the last quarter of 2016/17 we undertook a perception survey across our clients. The results showed a generally high level of satisfaction and identified a number of areas where we will be looking to develop our service 138
138 NHS East Surrey Clinical Commissioning Group Internal Audit Annual Report 2016/17 further in 2017/18. RELEASE OF REPORT The table below sets out the history of this Annual Report. Date Report issued: 20 th April 2017 Date Final Report issued: 19 th May
139 140 Annexes Annex A Head of Internal Audit Opinion (HoIA) on the Effectiveness of the System of Internal Control for the Year Ended 31 March 2017 The purpose of my annual HoIA Opinion is to contribute to the assurances available to the Accountable Officer and the Governing Body which underpin the Governing Body s own assessment of the effectiveness of the organisation s system of internal control. This Opinion will in turn assist the Governing Body in the completion of its AGS. The Clinical Commissioning Group (CCG) closed 2015/16 with an in-year planned deficit of 9.3million. This deficit position was a 0.2million improvement from the 2014/15 in-year deficit position of 9.5million. The Finance Report presented by the Chief Finance Officer at the April 2017 meeting of the Governing Body stated the following in relation to the 2016/17 financial year: At month 11 the CCG is reporting a year to date deficit of 36.5m, 11.2m above the planned deficit of 25.3m. This is primarily due to the underachievement of QIPP and over performance on the SaSH and other acute contracts. TIAA notes that the CCG has been regularly reporting to its Governing Body and NHS England the financial position and also highlighting the unmitigated financial risks. Our opinion on the organisation s system of internal control has taken this factor into account. My opinion is set out as follows: Overall opinion; Basis for the opinion; and Commentary. My overall opinion is that except for the CCG s ability to deliver their planned financial control total, Reasonable assurance can be given that there is a generally sound system of internal control, designed to meet the organisation s objectives, and that controls are generally being applied consistently. However, some weakness in the design and/or inconsistent application of controls, put the achievement of particular objectives at risk.
140 141 The basis for forming my opinion is as follows: An assessment of the design and operation of the underpinning Assurance Framework and supporting processes; and An assessment of the range of individual opinions arising from risk-based audit assignments, contained within internal audit risk-based plans that have been reported throughout the year. This assessment has taken account of the relative materiality of these areas and management s progress in respect of addressing control weaknesses. Additional areas of work that may support the opinion will be determined locally but are not required for NHS England or Department of Health purposes e.g. any reliance that is being placed upon Third Party Assurances. COMMENTARY See Annexes B and C for a summary of completed internal audit work. Substantial Assurance reports: Management of serious incidents The key highlights from the review are summarised below: 1. There are effective systems for managing serious incidents, including processes for holding providers to account, and ensuring that learning from incidents is disseminated. 2. At the time of the audit the CCG was in the process of reviewing the Reporting and Learning from Serious Incidents Requiring Investigation Policy. This is scheduled to be presented to the Governing Body for approval on 6 October The revised reporting requirements be agreed with the CSU so as to highlight trends, actions required etc. in relation to serious incidents (SIs). Review of complaints and FoI Requests The key highlights from the review are summarised below: 4. The CCG has an up to date and compliant complaints policy. The CCG received 24 complaints during 2015/16, which were handled in accordance with the agreed policy. 5. The Governing Body via QFD Committee receives regular reports on Complaints. 6. South East CSU manages FOI requests on behalf of the CCG and 98% of the 258 requests received were handled in accordance with agreed timetable. 7. The Audit Committee has a standing agenda item on Information Governance which includes discussion of the quarterly reports. 8. Complaints are regularly reported to Quality Finance and Delivery Committee (QFD) ESCCG s good practice in maintaining and publishing a You Said We Did register was noted during this audit. Reasonable Assurance reports: Assurance Framework and Risk Management
141 142 The key highlights from the review are summarised below: 9. The CCG has a current Risk Management Policy and Strategy in place. 10. The CCG has recently reviewed its Risk Management Policy and Strategy and has re-invigorated the Risk Management Group. 11. The CCG has recently reviewed its Strategic Risk register and Board Assurance Framework, and updated them for the current situation the CCG finds itself in. 12. The Risk Management Group now brings together Executives, Heads of Service and Lay Members. Critical Finance and Assurance The key highlights from the review are summarised below: 1. The CCG has in place an up to date Constitution and Prime Financial Policies. 2. The controls over accounting, debt control, payroll and payments are operating satisfactorily. 3. The CCG is compliant with the guidance on off-payroll workers, however from January 2017 a number of Executive Directors and Senior Finance Staff will fall within the scope of the parameters set within the guidance. 4. Governance arrangements around the monitoring and reporting of the CCG's financial performance has been strengthened. The CCG also has a Turnaround Director in post. 5. The CCG's Scheme of Delegation does not match the arrangements in place for approval and authorisation under Special Directions. NHS England Mandated Audit - Conflicts of Interest Arrangements The CCG s compliance in relation to the five key areas reviewed are as below: 6. Governance arrangements - Partially Compliant. Process for appointing Lay Members is not in place. The Recruitment and Selection policy does not require conflicts to be declared until appointment 7. Declarations of interests and gifts and hospitality - Partially Compliant. Non declaration of nine donations by pharmaceutical companies reported by the APBI. 8. Registers of interests, gifts and hospitality and procurement decisions - Partially Compliant. Registers do not follow NHS England guidance. 9. Decision making processes and contract monitoring Fully Compliant. Procurement undertaken mainly in collaboration using NHS South of England Procurement Service (SoEPS). 10. Reporting concerns and identifying and managing breaches/ non-compliance Partially Compliant. Process largely in place and outlined within the Policy and no reported breaches at the time of the review. Service Transformation QIPP The key issues raised were:
142 The CCG did not achieve its QIPP Plan for 2015/16 achieving only 55% of plan, and as of M /17 the revised Financial Recovery Plan (FRP) is forecast to achieve the very challenging target of 75% of QIPP. 11. The Governance arrangements around the monitoring of delivery against the QIPP Plan were no robust from the start of the period under review until Month 5 of 2016/17 onwards when they were strengthened e.g. through the introduction of robust PIDs and business case approval process, QIPP monitoring process etc. 12. The CCG has changed its approach to the management of QIPP projects, retaining the PRINCE 2 approach but reintegrating the PMO and strengthening data and finance support. IG Toolkit v14 (Phase 2) This review was carried out in 2 Phases. An Assurance level was not provided for the Phase 1 review as this was an operational review. The key highlights from the Phase 2 review are summarised below: 13. Audit agreed with the current scoring of two of seven requirements reviewed. A further four were Unsubstantiated and one Overstated. 14. Overall the CCG was reporting Level 0 for three of the IGT requirements, three at Level 1, 16 at Level 2 (full compliance) and three at Level 3. Three were marked as Not Relevant. Action plans were in place to refresh evidence through to 31st March 2017 to seek to achieve Level 2 across all the requirements. 15. Owing to short-comings in services provided by the SCW CSU, considerable intervention was required by the CCG to ensure that evidence was made available to Internal Audit. 16. Evidence is awaited from NEL CSU for requirements outside the audit sample and there is a risk that achievement of Level 2 may not be able to be demonstrated if this is not received from NEL CSU by the submission date. 17. There have been no externally reportable IG incidents. TIAA notes that subsequent to the audit the CCG successfully submitted its evidence to support a level 2 assessment on the Toolkit v14 by the 31 st March 2017 deadline. Limited Assurance report: Limited assurance was provided for the following review: Review of HR Systems and Controls (including HR Workforce Training and Development) The key issues raised were: 18. Personnel records were not maintained for all staff. 19. Relevant records were not routinely maintained on employees files e.g. proof of identity; proof of right to work and evidence that employees had been subject to an occupational health check and clearance. 20. The HR processes require to be strengthened 21. The CCG does not have a policy covering training and development; and training completion rates by employees were low.
143 144 From a total of 13 recommendations raised within the report nine out of the 10 recommendations have been implemented. The agreed implementation dates for the remaining recommendations (three) are not yet due. Assurances across the CCG Collaborative: Continuing Healthcare (Governance) hosted by Surrey Downs CCG This review received only limited assurance, and the key issues raised were: The CCG to review how the CHC Programme Board provides assurance to the CCG s Governing Body and the other CCGs within the collaborative. Most of the CHC contracts were not signed. The agenda for the CHC Programme Board does not include declaration of interests, and gifts and hospitality. Risk management e.g. the absence of an overarching CHC risk register which would incorporates the risks contained within the existing three risk registers i.e. CHC Risk Register, CHC Transforming Care Register and CHC QIPP Register. Adequacy and effectiveness of controls over Decision Support Tools (DSTs). Development of processes for managing nursing homes with adverse CQC inspection reports. A follow up of the recommendations was carried out and 22 of the 25 recommendations have been implemented. TIAA confirmed that progress is being made towards implementing the remaining three recommendations.
144 145 Safeguarding Vulnerable Adults Governance Arrangements (hosted by NHS Guildford and Waverley CCG) The review received reasonable assurance and noted that progress has been made in implementing previous audit recommendations, and the integration of the Children s and Adults Services will strengthen the governance arrangements. However, at the time of the review, some of the processes being put in place were either at their infancy or being developed. The key issues raised were: 1. A review of all safeguarding risks across the collaborative be undertaken, including the development of a formal process through which all CCGs within the collaborative can be assured that all risks arising are consistently captured and mitigated. 2. All stakeholder CCGs within the collaborative be provided with sufficient assurance to demonstrate that overall capacity is sufficient, and that it will not impact on delivery of the children s service. 3. Develop and monitor an action plan to address the matters raised within the stakeholder survey. Other assurances from reviews TIAA have carried out across the CCG Collaborative: 4. The CCG is an Associate Commissioner for other provider contracts led by other CCGs within the collaborative. TIAA carried out an individual review of Contract Management and Monitoring (Provider Contracts) for North East Hampshire and Farnham CCG and Guildford and Waverley CCG and we were able to provide reasonable assurance and substantial assurance respectively that the lead CCGs had effective arrangements for performance managing and monitoring its healthcare providers, including those contracts where NHS East Surrey CCG is an Associate Commissioner Third Party Assurances: CSU s Service Auditor Report issued by their Internal Auditors i.e. 'Report on Internal Controls (Type II) Assurance regarding the maintenance of general ledger user access control is provided as part of the Service Auditor Report from the Internal Auditors of the CSU. The CSU s Service Auditor Report issued by their Internal Auditors i.e. 'Report on Internal Controls (Type II) Finance and Payroll (South London and Surrey) Reporting Period 1 March 2016 to 31 August 2016' qualified their opinion in respect of Control Objective A.3: CSU access to the payroll system is valid and appropriate. Apart from the areas qualified above, the audit opinion has concluded that the controls related to the objectives were suitably designed to provide reasonable assurance, and that the controls tested were operating with sufficient effectiveness. At the time of preparing this opinion the Service Auditor Report covering the period 1 st September 2016 to the 28 th February 2017 was yet to be issued.
145 146 Assurance Assessments Annex B System Status Substantial Assurance Reasonable Assurance Limited Assurance No Assurance Management of serious incidents Final Report Review of complaints and FoI Requests Final Report Assurance Framework and Risk Management Final Report Critical Finance and Assurance Final Report NHS England Mandated Conflicts of Interest Review Final Report Service Transformation QIPP Final Report Review of HR Systems and Controls (including HR Workforce Training and Development) Final Report IG Toolkit v14 (Phase 1) Final Report Assurance level was not provided for this review as this was an operational review IG Toolkit v14 (Phase 2) Final Report Review of Investments (including the Integrated Re-ablement and Frailty Units) Other Assurances Safeguarding Vulnerable Adults Governance Arrangements (final draft) hosted by NHS Guildford and Waverley CCG Continuing Healthcare (Governance) hosted by Surrey Downs CCG Final Report Final Report Final Report As agreed this was an Appraisal Review Actual against planned Internal Audit Work 2016/17 Annex C
146 147 System Planned Days Actual Days Assurance Assessment Status Comments Follow Up 8 8 N/A Completed Reported to every meeting of the Audit Committee. Additional follow up carried out on the limited assurance report on HR Review. Audit Needs Assessment (developing the 2017/18 Audit Plan) 2 2 N/A Completed Plan for 2017/18 completed Benchmarking and VFM Reviews 2 2 N/A Completed Various reports shared with the CCG e.g. IG Toolkit benchmarking report etc. Serious Incidents 7 7 Substantial Final Report Complaints and FOI Requests 7 7 Substantial Final Report HR Systems and Controls Review (Including HR/Work Force-Training and Development) Limited Final Report Continuing Healthcare (Hosted by Surrey Downs CCG) 2 2 Limited Final Report Assurance provided across Surrey CCGs Collaborative QIPP/Service Transformation Review Reasonable Final Report Assurance Framework and Risk Management 7 7 Reasonable Final Report Critical Financial Assurance Financial Accounting, Non-Pay Expenditure, Payroll and Budgetary Control Reasonable Final Report Investments/Service Transformation (mainly covering IRU and Frailty Unit; N/A-As agreed this was an Appraisal Review Final Report Safeguarding Adults (Hosted by Guildford and Waverley CCG) 2 2 Reasonable Final Report Assurance provided across Surrey CCGs Collaborative Information Management and Governance 8 8 Reasonable Final Report NHS England Mandated Audit Conflicts of Interest Reasonable Final Report System Planned Days Actual Days Assurance Assessment Status Management and planning (including meetings with management) etc. 8 8 N/A Completed Audit Committee-Attendance and preparing reports 5 5 N/A Completed Opinion Work and Filtering of Joint Assurances from 5 5 Overall assessment for 2016/17 Completed Draft Head of Internal Audit Opinion for
147 148 outsourced functions (CSU) etc. (Reasonable Assurance) 2016/17 presented to the March 2017 meeting of the CCG s Audit Committee. Annual Report to be presented to the May 2017 Audit Committee meeting
148 Section 5 Annual Accounts 149
149 Entity name: NHS East Surrey Clinical Commissioning Group This year This year ended 31 March 2017 This year commencing: 1 April 2016 Page 150
150 Contents Statement of Comprehensive Net Expenditure for the year ended 31 March Statement of Financial Position as at 31 March Statement of Changes In Taxpayers Equity for the year ended 31 March Statement of Cash Flows for the year ended 31 March Notes to the financial statements Accounting Policies Other Operating Revenue Revenue Employee benefits and staff numbers Operating expenses Better Payment Practice Code Operating Leases Property, plant and equipment Trade and other receivables Cash and cash equivalents Trade and other payables Provisions Contingencies Financial instruments Operating segments Pooled budgets Related party transactions Events after the end of the reporting period Losses and special payments Financial performance targets Notes on Financial performance targets Page 151
151 Statement of Comprehensive Net Expenditure for the year ended 31 March Note Income from sale of goods and services 2 (4,139) (6,871) Other operating income 0 (67) (29) Total operating income (4,206) (6,900) Staff costs 0 3,414 2,706 Purchase of goods and services 5 229, ,120 Depreciation and impairment charges Provision expense Other Operating Expenditure Total operating expenditure 233, ,341 Net Operating Expenditure 229, ,441 Comprehensive Expenditure for the year ended 31 March , ,441 Page 152
 (13,887)")
152 Statement of Financial Position as at 31 March Note Non-current assets: Property, plant and equipment Total non-current assets Current assets: Trade and other receivables 0 5,747 5,321 Cash and cash equivalents Total current assets 6,022 5,483 Total assets 6,171 5,621 Current liabilities Trade and other payables 0 (16,176) (13,887) Provisions 0 (133) (82) Total current liabilities (16,309) (13,969) Non-Current Assets less Net Current Liabilities (10,138) (8,348) Non-current liabilities Provisions 0 (114) (160) Total non-current liabilities (114) (160) Assets less Liabilities (10,252) (8,508) Financed by Taxpayers Equity General fund (10,252) (8,508) Total taxpayers' equity: (10,252) (8,508) The notes on pages 156 to 185 form part of this statement. The financial statements on pages 152 to 185 were approved by the Governing Body on 25 May 2017 and signed on its behalf by: Ray Davey Interim Chief Financial Officer Ian Ayres Accountable Officer Page 153
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Memorandum of understanding for shadow Accountable Care Systems
 Since Previously Discussed by BLMK CEOs: Memorandum of understanding for shadow Accountable Care Systems Dear Richard, As described in Next Steps on the NHS Five Year Forward View, we intend to name a
Since Previously Discussed by BLMK CEOs: Memorandum of understanding for shadow Accountable Care Systems Dear Richard, As described in Next Steps on the NHS Five Year Forward View, we intend to name a
Sussex and East Surrey STP narrative
 Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Meeting in Common of the Boards of NHS England and NHS Improvement. 1. This paper updates the NHS England and NHS Improvement Boards on:
 NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Council of Members. 20 January 2016
 Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Report to Patients. A summary of NHS Norwich Clinical Commissioning Group s Annual Report for 2014/15. Healthy Norwich. Patient
 Report to Patients A summary of NHS Norwich Clinical Commissioning Group s Annual Report for 2014/15 Healthy Norwich GP Care Patient Quality YourNorwich The work of the CCG, what it has achieved for patients,
Report to Patients A summary of NHS Norwich Clinical Commissioning Group s Annual Report for 2014/15 Healthy Norwich GP Care Patient Quality YourNorwich The work of the CCG, what it has achieved for patients,
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
WELCOME. To our first Annual General Meeting (AGM) Local clinicians working with local people for a healthier future
 Local clinicians working with local people for a healthier future") WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
NHS Trafford Clinical Commissioning Group (CCG) Annual General Meeting(AGM) 26th September
 Annual General Meeting(AGM) 26th September") RIGHT CARE RIGHT TIME RIGHT PLACE NHS Trafford Clinical Commissioning Group (CCG) Annual General Meeting(AGM) 26th September 2017 Introduction Matt Colledge Chair Introduction Trafford Clinical Commissioning
RIGHT CARE RIGHT TIME RIGHT PLACE NHS Trafford Clinical Commissioning Group (CCG) Annual General Meeting(AGM) 26th September 2017 Introduction Matt Colledge Chair Introduction Trafford Clinical Commissioning
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE. Purpose of Report: For Note
 Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
The Board is asked to note the report and to support the delivery of the Operational Plan and associated work programmes during 2017/18 and 2018/19.
 Subject: Reason for briefing note: Responsible officer(s): Senior leader sponsor: Windsor, Ascot & Maidenhead CCG Operating Plan 2017-19 Refresh To present the WAM CCG Operating Plan Refresh information
Subject: Reason for briefing note: Responsible officer(s): Senior leader sponsor: Windsor, Ascot & Maidenhead CCG Operating Plan 2017-19 Refresh To present the WAM CCG Operating Plan Refresh information
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Improvement and Assessment Framework Q1 performance and six clinical priority areas
 Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Governing Body 30 th September 2016 Improvement and Assessment Framework Q1 performance and six clinical priority areas Agenda item 16 Paper 10 Summariser: Authors and contributors: Executive Lead(s):
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS...
 CONTENTS EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS... 6 WHAT WE WILL CONTINUE TO ACHIEVE THROUGH THE HEALTH
CONTENTS EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS... 6 WHAT WE WILL CONTINUE TO ACHIEVE THROUGH THE HEALTH
New Savoy Conference Psychological Therapies in the NHS
 New Savoy Conference Psychological Therapies in the NHS Claire Murdoch CEO, Central and North West London NHS FT & National Mental Health Director, NHS England 21 March 2018 Mental Health Five Year Forward
New Savoy Conference Psychological Therapies in the NHS Claire Murdoch CEO, Central and North West London NHS FT & National Mental Health Director, NHS England 21 March 2018 Mental Health Five Year Forward
Longer, healthier lives for all the people in Croydon
 D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
General Practice 5 Year Forward View Operational Plan Leicester, Leicestershire and Rutland (LLR) STP
 STP") Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group East Leicestershire and Rutland Clinical Commissioning Group General Practice 5 Year Forward View Operational
Haringey and Islington
 Haringey and Islington Wellbeing Partnership Who we are Thoughts on system leadership and on leading within complex systems Observations from our experience Recognising where we are seeing and showing
Haringey and Islington Wellbeing Partnership Who we are Thoughts on system leadership and on leading within complex systems Observations from our experience Recognising where we are seeing and showing
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Melanie Craig NHS Great Yarmouth and Waveney CCG Chief Officer. Rebecca Driver, STP Communications and Jane Harper-Smith, STP Programme Director
 Agenda Item: 9 Governing Body Thursday 25 January 2018 Subject: Presented By: Prepared By: Submitted To: Purpose of Paper: Norfolk and Waveney Sustainability and Transformation Partnership Update Melanie
Agenda Item: 9 Governing Body Thursday 25 January 2018 Subject: Presented By: Prepared By: Submitted To: Purpose of Paper: Norfolk and Waveney Sustainability and Transformation Partnership Update Melanie
SUMMARY. Our progress in 2013/14. Eastbourne, Hailsham and Seaford Clinical Commissioning Group.
 Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme. Frequently Asked Questions Second Edition
 Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan. October 2016 submission to NHS England Public summary
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Update Report to Clinical Members. Quarter 3; what have we done so far
 Update Report to Clinical Members Quarter 3; what have we done so far Introduction: Dr Charlotte Canniff, Clinical Chair Following our Council of Members meeting in October we heard and recognised a clear
Update Report to Clinical Members Quarter 3; what have we done so far Introduction: Dr Charlotte Canniff, Clinical Chair Following our Council of Members meeting in October we heard and recognised a clear
INTEGRATION TRANSFORMATION FUND
 MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust
 Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
NHS Norwich CCG Operational Plan and
 NHS Norwich CCG Operational Plan 2017-18 and 2018-19 Commissioning NHS care for the people of Norwich 1 Release: V17 Final Date: 2016.01.11 Table of Contents Page 1 Introduction 4 2 National Background
NHS Norwich CCG Operational Plan 2017-18 and 2018-19 Commissioning NHS care for the people of Norwich 1 Release: V17 Final Date: 2016.01.11 Table of Contents Page 1 Introduction 4 2 National Background
Guideline scope Intermediate care - including reablement
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
NHS GRAMPIAN. Local Delivery Plan - Mental Health and Learning Disability Services
 NHS GRAMPIAN Board Meeting 01.06.17 Open Session Item 8 Local Delivery Plan - Mental Health and Learning Disability Services 1. Actions Recommended The Board is asked to: Note the context regarding the
NHS GRAMPIAN Board Meeting 01.06.17 Open Session Item 8 Local Delivery Plan - Mental Health and Learning Disability Services 1. Actions Recommended The Board is asked to: Note the context regarding the
Westminster Partnership Board for Health and Care. 17 January pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
A healthier Lancashire and South Cumbria
 A healthier Lancashire and South Cumbria Improving health and care for local people Published May 2017 Bay Health & Care Partners Pennine Lancashire Fylde Coast West Lancashire Central Lancashire Healthier
A healthier Lancashire and South Cumbria Improving health and care for local people Published May 2017 Bay Health & Care Partners Pennine Lancashire Fylde Coast West Lancashire Central Lancashire Healthier
Welcome to. Northern England and the Five Year Forward View for Mental Health. Thursday 2 February 2017 at the Radisson Blu, Durham
 Welcome to. Northern England and the Five Year Forward View for Mental Health Thursday 2 February 2017 at the Radisson Blu, Durham Introductions Chairs: Catherine Haigh, Chair of North East together and
Welcome to. Northern England and the Five Year Forward View for Mental Health Thursday 2 February 2017 at the Radisson Blu, Durham Introductions Chairs: Catherine Haigh, Chair of North East together and
Halton. Local system review report Health and Wellbeing Board. Background and scope of the local system review. The review team
 Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Northumberland Frail Elderly Pathway. Dr David Shovlin Fiona Brown
 Northumberland Frail Elderly Pathway Dr David Shovlin Fiona Brown What s special about the Frail Elderly Pathway Patient centered joint working across the entire health and social care system for over
Northumberland Frail Elderly Pathway Dr David Shovlin Fiona Brown What s special about the Frail Elderly Pathway Patient centered joint working across the entire health and social care system for over
NHS North West Surrey Clinical Commissioning Group
 NHS North West Surrey Clinical Commissioning Group Annual Report and Accounts 2016/17 North West Surrey CCG Annual Report 2016-17 2 Table of Contents 1. Introduction 5 About us 8 2. Performance Report
NHS North West Surrey Clinical Commissioning Group Annual Report and Accounts 2016/17 North West Surrey CCG Annual Report 2016-17 2 Table of Contents 1. Introduction 5 About us 8 2. Performance Report
Clinical Strategy
 Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
Clinical Strategy 2014-2018 Contents About the clinical strategy Page 2 About our Trust Page 3 What we stand for Page 6 Our clinical services Page 9 Supporting our staff Page 12 The five year plan Page
Norfolk and Waveney s Sustainability and Transformation Plan (June 2017)
") Norfolk and Waveney s Sustainability and Transformation Plan (June 2017) 1 Sustainability and Transformation Plans (STP) A national policy initiative that are part of the delivery of the NHS Five Year
Norfolk and Waveney s Sustainability and Transformation Plan (June 2017) 1 Sustainability and Transformation Plans (STP) A national policy initiative that are part of the delivery of the NHS Five Year
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Welcome. PPG Conference North and South Norfolk CCGs June 14 th 2018
 Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
Main body of report Integrating health and care services in Norfolk and Waveney
 Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
Item 18.73a ii Norfolk and Waveney Sustainability and Transformation Plan Update for governing bodies and trust boards September 2018 Purpose of report The purpose of this paper is to update members of
In this edition we will showcase the work of the development of a model for GP- Paediatric Hubs
 Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Approve Ratify For Discussion For Information
 NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
NHS North Cumbria CCG Governing Body Agenda Item 2 August 2017 10 Title: General Practice Update Report August 2017 Purpose of the Report This is the first report on General Practice since the CCG boundary
Sustainability and transformation plan (STP)
") Sustainability and transformation plan (STP) David Bowen-Cassie, Harrow CCG Alex Dewsnap, London Borough of Harrow Sanjay Dighe, Lay Member, Harrow CCG About Harrow A population of more than 239,000 people
Sustainability and transformation plan (STP) David Bowen-Cassie, Harrow CCG Alex Dewsnap, London Borough of Harrow Sanjay Dighe, Lay Member, Harrow CCG About Harrow A population of more than 239,000 people
Westminster Partnership Board for Health and Care. 21 February pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Summary two year operating plan 2017/18
 One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
Luton Borough Council: Reducing DTOC rates attributable to Social Care
 Briefing 17/20 May 2017 Insights into Social Care Practice Insights is a series of case studies, intended to promote and share the good practice among APSE member authorities in delivering adult social
Briefing 17/20 May 2017 Insights into Social Care Practice Insights is a series of case studies, intended to promote and share the good practice among APSE member authorities in delivering adult social
Mid and South Essex Success Regime Overview and next steps. Andy Vowles, Programme Director. 18 April 2016
 Mid and South Essex Success Regime Overview and next steps Andy Vowles, Programme Director 18 April 2016 What s in this briefing Part 1 overview Background to the Success Regime Action to date The challenge
Mid and South Essex Success Regime Overview and next steps Andy Vowles, Programme Director 18 April 2016 What s in this briefing Part 1 overview Background to the Success Regime Action to date The challenge
Developing Plans for the Better Care Fund
 Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
Annex to the NHS England Planning Guidance Developing Plans for the Better Care Fund (formerly the Integration Transformation Fund) What is the Better Care Fund? 1. The Better Care Fund (previously referred
REPORT 1 FRAIL OLDER PEOPLE
 REPORT 1 FRAIL OLDER PEOPLE Contents Vision f-3 Principles / Parameters f-4 Objectives f-6 Current Frail Older People Model f-8 ABMU Model for Frail and Older People f-11 Universal / Enabling f-12 Specialist
REPORT 1 FRAIL OLDER PEOPLE Contents Vision f-3 Principles / Parameters f-4 Objectives f-6 Current Frail Older People Model f-8 ABMU Model for Frail and Older People f-11 Universal / Enabling f-12 Specialist
Wolverhampton Clinical Commissioning Group 1
 Wolverhampton Clinical Commissioning Group 1 Introduction and Context In 2014, along with our partners, the CCG established our five year strategy for the Wolverhampton Health Economy. This set out our
Wolverhampton Clinical Commissioning Group 1 Introduction and Context In 2014, along with our partners, the CCG established our five year strategy for the Wolverhampton Health Economy. This set out our
Agenda Item No. 9. Key Information
 Key Information Name of footprint and no: Sussex and East Surrey (33) Region: NHSE South Nominated lead of the footprint including organisation/function: Michael Wilson, Chief Executive, Surrey and Sussex
Key Information Name of footprint and no: Sussex and East Surrey (33) Region: NHSE South Nominated lead of the footprint including organisation/function: Michael Wilson, Chief Executive, Surrey and Sussex
Newham Borough Summary report
 Newham Borough Summary report Item K1 September 2013 Prepared on 30/09/2013 by Support team GREEN Finance and Activity Millions AMBER RED Headlines M5 Financial position M4 activity data The QIPP net savings
Newham Borough Summary report Item K1 September 2013 Prepared on 30/09/2013 by Support team GREEN Finance and Activity Millions AMBER RED Headlines M5 Financial position M4 activity data The QIPP net savings
A new integrated model for Care Homes from Walsall CCG/Healthcare NHS Trust
 A new integrated model for Care Homes from Walsall CCG/Healthcare NHS Trust Sally Roberts - Director of Governance, Quality & Safety. Walsall CCG Katie Welborn Advanced Nurse Practitioner- Walsall Healthcare
A new integrated model for Care Homes from Walsall CCG/Healthcare NHS Trust Sally Roberts - Director of Governance, Quality & Safety. Walsall CCG Katie Welborn Advanced Nurse Practitioner- Walsall Healthcare
WEST HAMPSHIRE PERFORMANCE REPORT. Based on performance data available as at 11 th January 2018
 WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
Marginal Rate Emergency Threshold. Executive Summary
 Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
Part 1 meeting of the Castle Point and Rochford CCG Governing Body held on 29 th September 2016 Agenda item 16 Marginal Rate Emergency Threshold Submitted by: Prepared by: Status: Robert Shaw, Joint Director
South Yorkshire & Bassetlaw Health and Care Working Together Partnership
 South Yorkshire & Bassetlaw Health and Care Working Together Partnership Memorandum of Understanding Agreement Final Draft June 2017 1 Title Drafting coordinator Target Audience Version V 0.3 Memorandum
South Yorkshire & Bassetlaw Health and Care Working Together Partnership Memorandum of Understanding Agreement Final Draft June 2017 1 Title Drafting coordinator Target Audience Version V 0.3 Memorandum
Trust Board Meeting 05 May 2016
 Trust Board Meeting 05 May 2016 Title of the paper: Sustainability and Transformation Plan (STP) Update Agenda item: 15/37 Lead Executive: Trust objective: Purpose: Link to Board Assurance Framework (BAF)
Trust Board Meeting 05 May 2016 Title of the paper: Sustainability and Transformation Plan (STP) Update Agenda item: 15/37 Lead Executive: Trust objective: Purpose: Link to Board Assurance Framework (BAF)
Mental Health Social Work: Community Support. Summary
 Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Outcomes Based Commissioning. Update for Governing Body. 19 May 2015
 Outcomes Based Commissioning Update for Governing Body 19 May 2015 Background To enable the commissioning of the outcomes based contract (OBC) for out of hospital health and social care an outcomes framework
Outcomes Based Commissioning Update for Governing Body 19 May 2015 Background To enable the commissioning of the outcomes based contract (OBC) for out of hospital health and social care an outcomes framework
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
The operating framework for. the NHS in England 2009/10. Background
 the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
A guide to NHS Bexley Clinical Commissioning Group
 A guide to NHS Bexley Clinical Commissioning Group Everything you need to know about how local healthcare in Bexley is planned, bought and monitored. 1 Welcome to NHS Bexley Clinical Commissioning Group
A guide to NHS Bexley Clinical Commissioning Group Everything you need to know about how local healthcare in Bexley is planned, bought and monitored. 1 Welcome to NHS Bexley Clinical Commissioning Group
Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan
 Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan 2015-2020 1 Introduction 1.1 Welcome to the update on Warrington s Local Transformation Plan for Children and
Warrington Children and Young People s Mental Health and Wellbeing Local Transformation Plan 2015-2020 1 Introduction 1.1 Welcome to the update on Warrington s Local Transformation Plan for Children and
Appendix 1: Integrated Urgent Care Service Update. 1. Purpose
 Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
What will the NHS be like in 5 years, 20 years time?
 What will the NHS be like in 5 years, 20 years time? NHS Castle Point and Rochford Clinical Commissioning Group (CCG) and NHS Southend CCG are groups of local doctors and other health professionals who
What will the NHS be like in 5 years, 20 years time? NHS Castle Point and Rochford Clinical Commissioning Group (CCG) and NHS Southend CCG are groups of local doctors and other health professionals who
Summary annual report 2014/15
 1 Summary annual report 2014/15 2 Annual Report Summary 2014/15 3 St Thomas Hospital Guy s Hospital CATHEDRAL CHAUCER GRANGE RIVERSIDE ROTHERHITHE SURREY DOCKS Key facts about Southwark GP practices in
1 Summary annual report 2014/15 2 Annual Report Summary 2014/15 3 St Thomas Hospital Guy s Hospital CATHEDRAL CHAUCER GRANGE RIVERSIDE ROTHERHITHE SURREY DOCKS Key facts about Southwark GP practices in
DRAFT Service Specification GP-led Urgent Treatment Centre (UTC) Service
 Service") DRAFT Service Specification GP-led Urgent Treatment Centre (UTC) Service Executive summary: The Cornwall Sustainability and Transformation Plan known as Shaping our Future will describe a new model of
DRAFT Service Specification GP-led Urgent Treatment Centre (UTC) Service Executive summary: The Cornwall Sustainability and Transformation Plan known as Shaping our Future will describe a new model of
GP Forward View Operational Plan Draft Narrative December 2016 Subject to final approvals
 GP Forward View Operational Plan 2017-2019 Draft Narrative December 2016 Subject to final approvals Chairman s Foreword In March 2015 we published our Primary Care Strategy, which alongside its accompanying
GP Forward View Operational Plan 2017-2019 Draft Narrative December 2016 Subject to final approvals Chairman s Foreword In March 2015 we published our Primary Care Strategy, which alongside its accompanying
JOB DESCRIPTION. Joint Commissioning Manager for Older People s Residential Care and Nursing Homes
 JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
JOB DESCRIPTION Job Title: Grade: Team: Accountable to: Joint Commissioning Manager for Older People s Residential Care and Nursing Homes HAY 14 / AfC 8b (indicative) Partnership Commissioning Team Head
NHS ENGLAND BOARD PAPER
 NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
NHS ENGLAND BOARD PAPER Paper: PB.28.09.2017/07 Title: Update on Winter resilience preparation 2017/18 Lead Director: Matthew Swindells, National Director: Operations and Information Purpose of Paper:
Urgent Treatment Centres Principles and Standards
 Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Urgent Treatment Centres Principles and Standards July 2017 NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Richmond Clinical Commissioning Group
 Richmond Clinical Commissioning Group South west London five year forward plan Kathryn Magson, Chief Officer, Richmond CCG 7 December 2016 South West London Five Year Forward Plan Start well, live well,
Richmond Clinical Commissioning Group South west London five year forward plan Kathryn Magson, Chief Officer, Richmond CCG 7 December 2016 South West London Five Year Forward Plan Start well, live well,
GOVERNING BODY MEETING in Public 27 September 2017 Agenda Item 5.2
 GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
GOVERNING BODY MEETING in Public 27 September 2017 Paper Title Report Author Neil Evans Turnaround Director Referral Management s Contributors John Griffiths Date report submitted 20 September 2017 Dean
NHS Horsham and Mid Sussex Clinical Commissioning Group Annual Report and Accounts 2017/18
 NHS Horsham and Mid Sussex Clinical Commissioning Group Annual Report and Accounts 2017/18 NHS Horsham and Mid Sussex Clinical Commissioning Group ANNUAL REPORT 2017/18 1 2 ANNUAL REPORT 2017/18 NHS Horsham
NHS Horsham and Mid Sussex Clinical Commissioning Group Annual Report and Accounts 2017/18 NHS Horsham and Mid Sussex Clinical Commissioning Group ANNUAL REPORT 2017/18 1 2 ANNUAL REPORT 2017/18 NHS Horsham
Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk
 Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Midlothian Health and Social Care Partnership
 Midlothian Health and Social Care Partnership the right care the right support the right time This document is a draft, work in progress version. It includes current thinking on priorities / direction
Midlothian Health and Social Care Partnership the right care the right support the right time This document is a draft, work in progress version. It includes current thinking on priorities / direction
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 23 rd March 2017 Agenda No: 9.3 Attachment: 15 Title of Document: CCG Governing Body Assurance Report & Scorecards: Month 9 Quality &
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 23 rd March 2017 Agenda No: 9.3 Attachment: 15 Title of Document: CCG Governing Body Assurance Report & Scorecards: Month 9 Quality &
NHS Wirral CCG Operational Plan
 NHS Wirral CCG Operational Plan 2017-19 Contents 1 Introduction 3 1.1 Background 3 1.2 Strategic Context 3 1.3 Health Economy Profile 4 1.4 Deprivation 5 1.5 Complex Patients 5 1.6 Health Summary for Wirral
NHS Wirral CCG Operational Plan 2017-19 Contents 1 Introduction 3 1.1 Background 3 1.2 Strategic Context 3 1.3 Health Economy Profile 4 1.4 Deprivation 5 1.5 Complex Patients 5 1.6 Health Summary for Wirral