Efficiency Review of The Welsh Ambulance Services NHS Trust
|
|
|
- Ursula Haynes
- 5 years ago
- Views:
Transcription
1 Efficiency Review of The Welsh Ambulance Services NHS Trust Undertaken by Lightfoot Solutions in association with Lis Nixon Associates And Baker Tilly on behalf of Health Commission Wales and The Welsh Ambulance Services NHS Trust Final Report
2 Contents 1. Executive summary Background to the Review Introduction The EMS Service in Wales The structure of the review The emerging role of ambulance services in the delivery of unscheduled care Emerging best practice in ambulance services Establishing equitable and appropriate standards of response across the community The Category A 8 minute response process Response areas and achievable response standards The Category A and Category B 14/18/21 minute response standard The 14/18/21 minute response process Emerging clinical best practice The impact of technology Implications of the model Findings Benchmarking Achieving the Category A 8 minute AOF target The implications of extended travel times and hospital delays Calculating resource requirements for WAST Unit hour requirements Ambulance staff requirement Adjusting for overtime and relief Overtime Relief Achievable performance levels and additional resource requirements under different scenarios Achievable performance levels with existing resources Additional resource requirements to meet the 14/18/21 minute performance standards Financial analysis Income Fully absorbed cost model Financial summary Other findings Control room processes Clinical procedures Organisational issues Conclusions and recommendations Conclusions Recommendations Appendix 1 Suggested benchmarking measures Appendix 2 - Recommended deployment locations by LHB area Appendix 3 Cost model methodology
3 1. Executive summary This report is the result of a project commissioned jointly by Health Commission Wales (HCW) and the Welsh Ambulance Services NHS Trust (WAST) to review the adequacy of the funding of WAST in order to meet its current performance targets and at the same time to establish whether there were opportunities for WAST to improve the efficiency of its operations. In Section 3 of the report we outline emerging best practice in the delivery of ambulance services and the role that the ambulance service can play in the delivery of an integrated urgent care service. WAST is the only organisation that provides urgent care services on a day to day basis across the whole of Wales and as such is uniquely well placed to play a central role in the development of this new model of service delivery. Moreover, we believe that by adopting this new model it should be possible for WAST to achieve significantly improved standards of response and patient care relative to the standards that are currently being achieved. In Section 4 we set out the findings of our analysis of the efficiency and effectiveness of WAST and our assessment of the additional resource and funding that WAST will need if it is to meet all its key performance targets. Section 5 of the report sets out our conclusions and our recommendations in relation to the actions that we believe are required by the key stakeholders to enable WAST to provide a service that compares favourably with the best performing ambulance trusts in the rest of the United Kingdom. The principal findings from our analysis are as follows. WAST s performance in relation to the Category A 8 minute target has improved significantly since the beginning of However there has been little or no improvement during this period in relation to the Category A and Category B 14/18/21 minute standards Although Wales covers a larger geographical area than other ambulance trusts in the UK, the proportion of EMS activity that occurs in towns and cities in Wales is similar to that of comparable ambulance trust areas in England Wales experiences a relatively high number of 999 calls per head of population and a relatively high proportion of these calls result in a patient being transported to hospital. This results in pressure being placed on WAST and on hospitals in Wales that we believe could be alleviated if suitable call triage and assessment procedures were used and alternative care pathways were available for patients We estimate that the total cost that WAST incurred in providing the EMS service in was mil. WAST received 95.6 mil of funding for the EMS service in from HCW, NLIAH and the Air Ambulance Charity. The difference was funded by income for other purposes e.g. ARRP 3
4 Hospital delays have a significant impact on the ability of WAST to meet its performance targets. During the reference period for our review, WAST would have required an additional 900 ambulance hours per week in order to compensate for the delays in handing over patients at hospital at an annualised cost of 2.3 mil per year. This effect is of particular significance in the South East region of the Trust. WAST s performance with respect to the initial phase of allocating a vehicle to a 999 call compares poorly with other ambulance trusts in England. A significant contributory factor to this performance gap is the lack of an Automated Vehicle Location System (AVLS) and related mobile data systems on EMS vehicles in Wales. This makes it difficult for WAST reliably to locate and deploy the most appropriate vehicle to respond to a 999 call. Once the benefits of its investment in AVLS and mobile data are available, WAST could meet the current Category A 8 minute targets both at a national and LHB level with its current staffing levels and overtime rates and with the level of hospital delays that occurred during the reference period for this review. In order to do this WAST would need to accelerate the implementation of a deployment strategy that o o o o is based on 7 minute deployment areas in the more densely populated areas matches resource more precisely to the location of activity relies more extensively on the use of single manned response vehicles, and makes more extensive use of Community First Response schemes in less densely populated areas as the initial response to Category A incidents. The current level of staffing does not allow WAST to meet the 14/18/21 minute standards and also requires a reliance on high levels of overtime to fill core shifts. In addition, the shortage of staff in certain areas is preventing WAST from undertaking sufficient ongoing professional training. Based on WAST s current levels of overtime and planned level of relief, we estimate that the cost of the additional staff required to meet the current 14/18/21 minute performance standards would be 3,744,000. This would rise to 8,647,000 if WAST were to operate with no reliance on overtime to cover shifts and with the level of cover for holidays, sickness, training and other lost hours that was recommended in a Department of Health paper published in April 2007 setting out best practices in managing ambulance trusts. If it were fully resourced in accordance with the recommendations in this report, WAST should be able to achieve a Category A 8 minute performance target of at least 70% for the whole of Wales as well as meeting all the 14/18/21 minute standards. The current practice with respect to the 14/18/21 minute standards means that WAST sends more double staffed ambulances in response to lower acuity 999 calls than occurs at some other ambulance trusts. As advocated in this report, an alternative approach which distinguishes more clearly between the requirement for an appropriate initial assessment of the patient s requirements and the subsequent 4
5 provision of transportation once it has been determined that the patient needs transporting to hospital could significantly reduce the number of ambulance hours that WAST requires and also reduce the number of cases where the patient is transported to hospital. It should be noted however that a change of this type will require a significant change in practice within WAST as well as actions by other stakeholders to ensure that alternative pathways are available for patients. Consequently the benefits from this change are likely to take between 3 and 5 years to be fully realised. If WAST were able to match the levels of ambulance attendance and transportation that are achieved in some trusts in England it could reduce the number of ambulance hours required by around 410 per week by comparison with the level that was planned in 2008/9. This would save around 1,025,000 per year in staff costs If hospital handover times were improved so that only 10% of hospital handovers took longer than 15 minutes this would reduce the number of ambulance hours required by comparison with the reference period for this review by 710 per week. This would save a further 1,966,000 per year. If WAST were able to obtain the full benefits from lower ambulance attendance rates and reduced hospital delays it should be possible for the Trust to meet both the AOF Category A 8 minute targets and the 14/18/21 minute standards with a staff cost that would be 1,876,000 lower than the level in 2008/9 based on the current overtime and planned relief levels and would be 2,497,000 higher than the 2008/9 levels based on the lower overtime and higher relief scenario. If WAST were to change its operating model in the way that is advocated in this report and was also able to obtain the full benefits of lower ambulance attendances and reduced hospital delays outlined above, it should also be able to realise savings of up to 280,000 in fleet costs as a result of greater use of cars and less use of double staffed ambulances. WAST may also be able to realise additional savings in the following areas o o reducing its administrative overheads reducing the number of operating centres and control rooms It should however be noted that we have not examined these areas in any detail during this review. In addition to the detailed findings of our analysis set out above, we have also identified a number of organisational issues which we believe need to be addressed if WAST is to achieve a successful transition to the new approach to the delivery of its services that is advocated in the report. In particular The challenges of agreeing a common vision between WAST and its many stakeholders about the role that WAST should play in the delivery of urgent care across Wales has previously made it difficult for the Trust to plan its future direction with any certainty and to communicate this to its staff. At the time of this review, 5
6 WAST has submitted a vision statement to NHS Wales for comment and consideration and is also working with the seven new LHBs to include key objectives within the LHBs own Urgent Care Plans. This offers an opportunity to establish a jointly agreed role for WAST that will form the basis for the implementation of the recommendations in this report The geographical spread of the Trust, the requirement for senior management to be located in three different regional centres and the amount of change in the senior management team has made it difficult to establish a stable management structure. The new management structure that has recently been introduced provides a framework within which WAST can create the senior management team that will be required to implement the strategy that is recommended in this report The quality of clinical oversight, supervision and training has not had sufficient focus at a time when the Trust has been under pressure to deliver performance. This has been recognised by WAST and a number of initiatives are currently under way to address these issues. However, the pressure on resource and the low levels of relief continue to make it difficult for the Trust to release staff to undertake appropriate levels of clinical training The funding arrangements for WAST have been unclear in the past and require clarification in the new NHS structure so that the link between funding and service delivery can be made transparent The current commissioning and performance management arrangements for WAST do not facilitate clear lines of accountability between WAST and its commissioners and performance managers for the delivery of the EMS service Although WAST could achieve the AOF Category A 8 minute target for the initial attendance at life threatening incidents with its current resource based on best practice call cycle performance and the current levels of overtime and relief, the current level of recurring funding that WAST receives is insufficient to enable it to achieve the 14/18/21 minute standards. We therefore believe that WAST will require additional funding in the short term in order to provide a fully effective EMS service that delivers appropriate levels of clinical care to patients From our discussions with both WAST and HCW we understand that many of the issues that we have highlighted in this report arise from the previous structure of the NHS in Wales and are already being addressed. In particular, the new structure for the LHBs provides a significant opportunity to establish a jointly agreed strategy and role for WAST within the urgent care system in Wales. We are confident that the implementation of the approach that is recommended in this report will enable WAST to provide the people of Wales with standards of care from their ambulance service that are comparable with the best standards that are achieved elsewhere in the United Kingdom. 6
7 2. Background to the Review 2.1. Introduction Since its establishment in 1998 there has been a history of performance issues at WAST. In 2006, as a result of widespread concerns about the way in which the Trust was being managed and its failure to meet the performance targets set for it by the Welsh Assembly Government, the Wales Audit Office was commissioned to produce a report into the problems that the Trust was facing and a new Chief Executive - Mr Alan Murray - was appointed to run the Trust. The Audit Office Report which was published in December 2006 identified a large number of areas of concern relating to the way that the Trust had previously been managed and made a number of recommendations for improvements. Following the publication of this report, a significant number of changes were successfully introduced by the new management team and a follow up review by the Audit Office published in June 2008 found that significant progress that had been made in a number of areas resulting in clear improvements in performance against the required targets and standards. In particular performance with respect to the Category A 8 minute target had improved by around 10 percentage points and performance in relation to GP Urgent journeys had also improved. However, there had been litlle or no improvement in performance with respect to the standards for attendance by an ambulance within 14/18/21 minutes. Subsequent to the publication of the follow up report, there have been further discussions between WAST and HCW about the actions that the Trust needs to take in order to address the issues identified by the Audit Commission and the resources that it requires to meet the current performance standards on a consistent basis. In particular WAST expressed concerns that its current level of funding was insufficient to allow it to maintain the level of resource that would be required to meet the current performance standards in view of the particular challenges that it faces as a Trust including in particular the problems caused by extended hospital delays in certain parts of Wales. At the same time Heath Commission Wales was concerned to establish whether WAST was adopting best practice with respect to the effectiveness and efficiency of its operational, clinical and financial processes. Consequently HCW and WAST agreed to jointly commission this review to establish how WAST s performance and cost efficiency compares with that of other comparable ambulance trusts in the rest of the United Kingdom the level of resource that WAST requires in order to meet the required AOF targets and performance standards, the potential for obtaining cost savings from operating in a more efficient way, and the opportunities that might exist for WAST to contribute to a more efficient and effective delivery of unscheduled care services from adopting emerging best practices in the delivery of ambulance services as seen elsewhere in the United Kingdom. 7
8 2.2. The EMS Service in Wales The role of the EMS service at WAST has three components To respond within the required time to 999 calls received by the Trust To respond to requests from doctors to transport to hospital patients whose doctor has determined that they need admission To transport patients from hospital or between hospitals where the hospital determines that the patient requires a double staffed ambulance for the joiurney in question On average in 2008/9 WAST responded to emergency incidents, 1020 urgent incidents and 210 transfers each week. At the outset, 999 calls are categorised into three categories of urgency by the calltaker using a telephone based triage system called the Advanced Medical Priority Dispatch System (AMPDS) as follows Category A - immediately life threatening condition/injury Category B - serious but not life threatening condition/injury Category C - neither life threatening or serious condition / injury In the first quarter of 2009 the percentage of 999 incidents to which WAST responded in each category were as follows Category A 41% Category B - 43% Category C - 16%, The response to an emergency incident has the following two components, an initial response to provide immediate attention and to establish what the patient s requirements are and if appropriate the provision of transportation to hospital in most cases in a fully equipped double staffed emergency ambulance. In Wales in the first quarter of 2009, 72% of all 999 incidents resulted in a patient being transported to hospital. With effect from 1 April 2009, WAST is required to meet the following performance targets in relation to its EMS service, as detailed in the Annual Operating Framework (AOF) 1. 65% of all Category A incidents across Wales must be responded to by a suitable responder within eight minutes of the chief complaint being verified by the calltaker and a minimum level of 60% must be achieved in every LHB area. This target has to 8
9 be met on a month-by-month basis as well as on a year-to-date basis. This response target is important in cases such as heart attacks where early resuscitation is provided. The type of response can be a fully equipped ambulance, a Rapid Response Vehicle (RRV), an emergency services co-responder, for instance Fire and Rescue Service and the Police, or a Community First Responder scheme. In addition to these AOF targets there are standards which were set for Wales in 1999 for the response times of ambulance crews capable of transporting the patient to hospital, where the first responder was not an ambulance crew. Whilst these are not AOF targets they are standards that are aimed at in order to ensure that there is a suitably equipped ambulance at the scene of the incident to support on scene care and transport appropriate patients to hospital or other services. These standards are 2. 95% of all Category A incidents must also be attended by a fully equipped emergency ambulance within a specified time of the start of the incident which is set at 14 minutes in Cardiff, 21 minutes in Powys, Ceredigion, Gwynned and Anglesey and 18 minutes elsewhere in Wales 3. 95% of all Category B incidents must be attended by a fully equipped emergency ambulance within the 14/18/21 minute time period from the start of the incident 4. 95% of all Urgent calls must be in hospital within 15 minutes of the time when the doctor specified that the patient should arrive Over the year to 31 March 2009, WAST achieved a performance level of 60.7% across Wales for Category A performance at 8 minutes, 85.07% for Category A performance at the 14/18/21 minute standard and % for Category B performance at the 14/18/21 minute standard. The rest of this report analyses the factors that affect WAST s ability to meet these targets and standards, identfies the resources that would be required to achieve these goals and suggests how WAST might be able to change its practices in a manner that delivers better results for patients in Wales while enabling WAST to adopt a more cost effective operating model 9
10 2.3. The structure of the review Our review consisted of the following four complementary work streams: 1. A benchmarking exercise that compared WAST s performance and efficiency based on a number of selected indicators with two broadly comparable English ambulance trusts South Western Ambulance Service Trust and East of England Ambulance Service Trust 2. An analysis of the demand profile to which WAST is required to respond together with a review of the deployment strategy and rota structure by comparison with best practice in other ambulance trusts to assess the extent to which performance could be improved by enhanced operating procedures and the extent to which additional resource might be required in order to meet the performance standards. The reference period for this analysis was a 13 week period from 3 November 2008 to 2 February A review based on structured interviews of the effectiveness of WAST s processes and systems, and current operational and clinical procedures together with a review of the current commissioning practices. 4. An analysis of the fully loaded costs that WAST incurs in providing the EMS service, an analysis of the way in which WAST uses its income to fund the EMS service and a comparison of the current cost model with good practice both in ambulance trusts and in other organisations. 10
11 3. The emerging role of ambulance services in the delivery of unscheduled care 3.1. Emerging best practice in ambulance services The ambulance service is an integral part of a healthcare system that exists to meet patients needs when they have an unplanned medical emergency. In order to provide this service in the best interests of the patient it is highly desirable that ambulance services are planned and delivered in the context of an overall plan for the provision of unscheduled care services. In this context, the provision of both ambulance response and other elements of the unscheduled care system have been the subject of a number of reviews in recent years with a view to making the provision of care more appropriate, more responsive to patients needs and more efficient. In Wales this includes the Delivering Emergency Care Strategy that was announced in February 2008 A key theme in these initiatives is the recognition that the current system of providing unscheduled care is inefficient and in many cases does not meet the patient s needs in the most effective way. In particular, they recognise that addressing the patient s needs in a timely and appropriate manner whilst at the same time preventing unnecessary admissions to hospital should be a high priority for a well managed unscheduled care system. In this context they also recognise that appropriate assessment and triage of the patient s needs at the point at which the patient accesses the healthcare system is key to the delivery of the most appropriate service and the best outcome for the patient. In recognition of this fact, there has been a significant change in the past three to four years in the way in which ambulance trusts in England respond to 999 emergency calls. At the core of this is the recognition of the need for a separation between the response to the initial emergency and the assessment of the patient s needs from the subsequent process of transporting the patient to hospital once it has been determined that this is the most appropriate response. This has led to an increase in the number of cases where a single staffed response car staffed by a paramedic attends an incident prior to a decision to deploy an ambulance. There has also been an upskilling in the capabilities of the staff employed by ambulance trusts to enable them to assess the needs of the patient and - where appropriate - to treat the patient at home or at the scene of the incident. As a result, in trusts that have adopted this model of response there has been a significant reduction in the proportion of patients who are transported to hospital with rates of transportation to hospital now below 55% in some cases by comparison with the 72% transportation rate that is seen in Wales. In parallel with the trend to place more reliance on the use of single responders for the initial assessment of the patient s needs, the English ambulance trusts are also required to meet a significantly higher standard of initial response to life threatening Category A incidents than currently applies in Wales. The response standard that applies to the English trusts is to attend 75% of all Category A incidents within 8 minutes from the time that the caller is connected to the trust s switchboard. This compares with the AOF target that applies in 11
12 Wales which requires that WAST responds to 65% of Category A incidents within 8 minutes from the time that the calltaker has determined the nature of the emergency. The effect of this is that the response time in relation to Category A incidents in Wales is around 80 seconds longer than it is in England as shown in Figure 1 below. It should be noted however, that the move to the new Call Connect performance standard in England has required significant investment in both resources and technology and took over two years to achieve. The benefits that the English trusts have obtained from this investment in terms of their ability to respond quickly to incoming calls also makes it difficult to undertake a direct comparisons of their performance with WAST. Figure 1 The Category A 8 minute response standards The overall effect of these changes has been that English trusts are now placing a significantly greater reliance on single staffed vehicles to provide the initial response to Category A calls and are also experiencing an increasing number of cases where a single staffed vehicle is the only response that is required for Category B and Category C incidents. By contrast in Wales double staffed ambulances still constitute the initial response for 70% of all 999 calls. The issues associated with the greater use of single staffed response vehicles are discussed in more detail below Establishing equitable and appropriate standards of response across the community A key consideration when determining the most appropriate way for an ambulance service to meet its performance targets is the need to establish equitable standards of response across the whole community whilst at the same time recognising the implications of the standards that are agreed in terms of both practicability and cost effectiveness. The overarching consideration in determining the achievability of the performance targets is the way in which geography, demography, transport, road and health infrastructures influence the amount of resource that is required to achieve the target in question. This is 12
13 materially different when considering the response to the Category A 8 minute target and the Category A and Category B 14/18/21 minute standard The Category A 8 minute response process The primary purpose of the Category A 8 minute target is to provide lifesaving services to a patient who has suffered a heart attack within a timeframe that carries a reasonable chance of resuscitation. In this context the response can consist of any suitably trained person who has access to a defibrillator which they have been trained to use and does not have to consist of a vehicle capable of transporting the patient. (The provision of suitable transportation for a Category A incident is is covered by the 14/18/21 minute standard). In order to meet this standard, a trust has to plan with a high level of certainty to have a suitable level of response resource available that is capable of attending these life threatening incidents within the time that is allowed for the response. The amount of resource that is required to deliver this standard of response is determined by the likely location of the incident and the amount of time that the responder has available to travel to the incident. The time that is available for the responder to travel to the scene of the incident is the time that remains within the 8 minute response window once the response vehicle has been identified by the dispatch centre the responder has been notified of the incident and the responder is in the response vehicle and beginning to travel to the scene of the incident. In the case of WAST, the time that is available for the responder to travel to the scene of the incident - assuming best practice processes and technology - is 7 minutes as summarised in Figure 2 below Figure 2 The components of the Category A response process 13

14 The implication of this is that it is only possible to reach a Category A incident within the 8 minute window where there is a response resource that is already available and positioned within a 7 minute drive time of the incident at the time that the 999 call is received. Consequently in determining the amount of resource that is required to meet the standard it is necessary to identify the locations where Category A incidents are most likely to occur and to plan the deployment of the Trust s response resource within those areas Response areas and achievable response standards A typical area that could be covered within a 7 minute drive time is shown in Figure 3 below Figure 3 A 7 minute deployment area in Caerphilly By identifying those areas where Category A incidents are most likely to occur it is then possible to identify the optimal location of response vehicles within 7 minute drivezones to maximise the likelihood that the incident will receive a response within the 8 minute response window. Deployment planning of this type has played a very significant role in enabling English trusts to meet the new Call Connect standard. A similar approach is already utilised by WAST in North Wales and is under development within the South East and Central and West regions. It should be noted however that WAST s current technology systems do not support a technological solution similar to that which is used by the English ambulance trusts and they are therefore using paper based systems to support this approach to deployment. Where adequate resource is available and it is deployed in this way, a high level of Category A performance is often achieved in some cases in excess of 85%. However, it is clear that this approach to deployment, which requires the provision of a dedicated response resource which is fully funded by the ambulance trust, will only be cost effective in those more densely populated areas where there is a sufficiently high level of activity to ensure that the response vehicle undertakes a reasonable level of activity. 14
15 Typically urban area activity of this type, where there is a high probablility of 2 or more category A incidents occurring in any 24 hour period within a drivezone, accounts for between 70% and 80% of the activity within the area of an ambulance trust. This leaves between 20% and 30% of the Category A incidents where an alternative model is required for the provision of initial response. The areas outside the more densely populated urban areas fall into three groupings as follows Mid sized market towns where there is a predictable level of daily activity, but there are less than 2 Category A incidents on average per day Smaller towns and large village communities where there is occasional activity but there is less than 1 Category A incident on average per day and Sparsely populated rural areas where activity is widely spread and there are no material concentrations of population In the mid sized market towns, it is not realistic or cost effective for the ambulance trust to provide a dedicated resource solely to respond to Category A incidents within the 8 minute response window. However, it is possible for the ambulance trust to establish a retained (paid for) response scheme in collaboration with the local health community and possibly also involving the Fire and Rescue Service and the Police which can provide an appropriate level of initial response for that community. In these cases it is realistic to expect that an initial response provided by a scheme of this type will meet or exceed the 65% Category A standard. In the smaller towns and larger villages, it is more difficult for an ambulance trust to provide an assurance of a suitable level of initial response without the involvement of volunteer responders. In many parts of the United Kingdom there are a large number of communities of this type which are more than a 7 minute drive from the nearest town and where typically there will be at most one or two Category A incidents per week. The only practical way of providing an initial response in these areas within the 8 minute window is through a voluntary Community Responder scheme. Where such schemes exist they can provide a high level of initial response to their local community, but the development of schemes of this type is time consuming and requires a high level of commitment from the local community. It should be recognised, however, that although the community responders are volunteers, the infrastructure necessary to support, manage and deploy community responders has its own cost that has to be borne by the ambulance trust. In the sparsely populated areas, which are outside the reach of a community response scheme, it is unrealistic for an ambulance trust to plan to achieve any sustained level of category A 8 minute performance and in general ambulance trusts find it difficult to achieve levels of Category A performance above 40-50% outside the urban areas and the larger market towns. 15
16 The Category A and Category B 14/18/21 minute response standard The 14/18/21 minute Category A and Category B standards in Wales require that a fully equipped ambulance attends the incident within the specified time window measured from the start time of the incident. This corresponds to similar 19 minute standard that applies to ambulance trusts in England. This standard exists in order to address three separate requirements as follows In the case of a Category A incident where the initial response has been by a community responder or another responder that is not provided directly by the ambulance trust the standard ensures that this lay response is backed up within an appropriate time by a suitably trained responder provided by the ambulance trust In the case of a Category B incident the standard ensures that there is an appropriate initial response to the incident by a suitably trained responder provided by the ambulance trust In the situation where it is determined that the patient requires urgent transportation to hospital the standard ensures that a suitable transportation resource will be made available within an appropriate time. It is however particularly important for the efficiency and effectiveness of the ambulance service that the performance standards for the initial response and for the subsequent transportation of the patient are addressed separately. Indeed, if this distinction is not recognised within the performance standard, it will not be possible to obtain the benefits that would otherwise be available from the more extensive use of single staffed response vehicles to undertake the initial assessment of the patient s requirements. The reason for this is that in those cases where it is appropriate to send a single staffed vehicle to an incident it will take a minimum of 10 minutes from the start of the incident before it is clear whether transportation is required. In most cases this leaves insufficient time for a double staffed ambulance to travel to the scene within the available time window should this be required. Moreover in many cases where transportation to hospital is required it will not be necessary for this to be provided immediately in a fully equipped emergency ambulance. However, if the performance standards are interpreted to apply to both the initial response and also to the arrival of the transportation resource it is necessary to send a double staffed ambulance to every Category A and Category B incident whether or not a single staffed response car has also been dispatched to respond to the incident. This has two effects. Firstly it significantly reduces the potential benefits of any investment in single staffed response vehicles in terms of their potential to reduce the ambulance attendance and transportation rates. Secondly it requires the Trust to maintain a level of resource in the form of double staffed emergency ambulances which is higher than it would otherwise need to be. As a result, it is increasingly being recognised that a more appropriate approach is to establish separate performance standards for the initial response to incidents and for the 16
17 subsequent transport requirement. This means that the standard for the initial response relates to the attendance by a fully equipped response vehicle. A second standard can then be established for emergency transportation which requires that where an urgent request has been received for transport by an emergency ambulance, the transporting vehicle arrives at the scene within the appropriate time window measured from the time at which the request for transportation is received. The current position with respect to the appropriate interpretation of the 14/18/21 minute response standards in Wales is unclear. The standards which were drafted in 1999 are clearly response standards rather than transportation standards. However, the standards predated the wider use of single staffed response vehicles and therefore refer to the response provided by WAST taking the form of a fully equipped ambulance rather than a fully equipped response vehicle as is the case in England. As a result it is open to interpretation whether a single staffed response vehicle is a suitable initial response to meet the 14/18/21 minute standard for both Category A and Category B incidents and at the time of our review this issue remained unresolved The 14/18/21 minute response process Unlike the case with the Category A 8 minute target it is possible to develop a deployment strategy that will ensure that all of the regions within Wales have a response by a fully equipped emergency vehicle within the 14/18/21 minute standard. In order to be able to meet this standard, however, WAST requires sufficient transportation resource to be able to respond not only to the normal daily levels of activity, but also to peak levels of activity and to provide the required level of cover and transporting capacity across all the geographic regions in Wales. The factors that determine the amount of resource that is required to meet this standard are The predicted average and peak level of activity at each hour for each day of the week The volume of activity and the geographic area that can be covered by an ambulance operating in more rural areas The percentage of incidents that require transportation to hospital The length of time that it takes an ambulance to complete a job, including in particular o o o the time taken to reach the hospital the time taken to return from hospital and the time taken to hand over the patient to the care of the hospital staff. In calculating this resource requirement it is also important to recognise that the same double staffed ambulance resource is also required to meet the performance standards for Urgent incidents as well as responding to Category C incidents and Hospital Transfers. In 17
18 this context, ambulance trusts are examining options for providing transport to hospital in cases where the patient s condition does not require them to be accompanied by a paramedic or in a double staffed vehicle. This includes the more extensive use of an intermediate tier of high dependency vehicles that can be staffed by two intermediate staff or the use of patient transport service vehicles in the same way as is provided for patients who are attending hospital for planned appointments Emerging clinical best practice Ambulance services are increasingly recognising that in order to meet patients clinical needs in the most appropriate way they need to reconsider all aspects of their activities. This extends from the initial way that calls are triaged through to the range of alternative treatments that can be offered to the patient at the patient s home as well as the alternatives that exist to hospitalisation. At the level of callhandling, there are significant differences between ambulance trusts in the way that calls are classified by call takers. There are a number of factors that affect the rate of classification which make benchmarking of this measure difficult. In WAST at the time of our review Category A call classification was around 40%. In other trusts it ranges from as high as 45% to below 30%. One key consideration that influences the percentage of calls that are classified as Category A is the calltaker s knowledge of the call triage system and in particular the extent to which supplementary questions are used to clarify the nature of the incident. We understand that WAST has been working hard recently to ensure that calltakers are trained in the use of the supplementary questions and that the proportion of calls classified as Category A had fallen to 37% in the course of June In trusts with the lower rates of Category A calls, effective use of the supplementary questions is often combined with a clinical desk where a caller may be passed from the calltaker to a nurse or paramedic who continues to talk to the patient whilst at the same time a vehicle is travelling to the incident. This may result in the incident being downgraded to a lower categorisation. In the case of Category C incidents in particular this also provides opportunities for rerouting patients to alternatives to an ambulance. This may be NHS Direct or an Out of Hours service or may result in the patient attending a minor injuries unit without the need for an ambulance. An appropriately resourced clinical desk also allows paramedics who are on scene to discuss suitable treatments with a colleague and provides information about the alternatives that are available. We understand that WAST has already trialled the use of clinical nurse advisers to triage Category C emergency calls by telephone and is keen to extend the use of this service. A further development which WAST is also discussing is the provision of an information hub. This can involve a bed bureau function that maintains a central information source that can identify where there are available beds for patients. It can also be a source of information about the available resources to meet patients needs including information about services provided by social services and voluntary services as an alternative to taking the patient to hospital. This can also provide a more integrated link between the ambulance service, NHS 18
19 Direct and Out of Hours services something that WAST is particularly well placed to do because both the EMS service and NHS Direct Wales are now within a single trust. In this context we understand that WAST has submitted an expression of interest in accordance with the Assembly s Invest to Save initiative to implement NHS Pathways jointly with health and Social Care partners in Wales. In addition, WAST already has a relatively high proportion of its front line staff who are paramedics which provides a good starting point for the transition to the alternative response model. However there will be a requirement for a change in working practices from the current position where the majority of paramedics work primarily on double staffed ambulances and are currently accustomed to receiving backup in almost all cases when they are working on single staffed response vehicles. The future model will put significantly greater emphasis on paramedics being able to work alone in the first instance and spending a larger proportion of their time in single staffed response vehicles. An additional issue that will need to be addressed is the number of incidents that are attended by a single staffed vehicle. The new model will require paramedics to act as first responders in areas where activity is relatively low. In some cases - notably in towns where the expected level of activity is less than two Category A calls per day - it may be more appropriate for these staff to become part of a community medical team and to provide support for admissions avoidance and long term conditions management rather than requiring them to act solely as a response resource to 999 calls. In this context, it will also be appropriate for WAST to consider more extensive use of Specialist Practitioners. Different trusts have developed different practices towards the use of schemes of this type and in a number of cases these schemes have proved to be very effective in treating the patient at home or providing support for minor injury units and so helping to reduce the number of cases where Category B and Category C incidents require ambulance attendance or transportation. The introduction of Specialist Practitioners is part of WAST s five year workforce plan and we understand that recruitment is currently under way to fill these roles. A further possibility in terms of the development of clinical services that can be provided by ambulance trusts is demonstrated by the fact that some ambulance trusts in England have begun to set up and operate minor injury units themselves as part of an admissions avoidance strategy. Clearly developments of the type outlined above cannot be achieved without careful planning. But they are indicative of the changes that are under way within the ambulance service and they will lead to ambulance trusts which are very different organisations from what they have been in the past. This requires them to be more closely integrated in to the unscheduled care system with a different range of clinical capabilities and skills and with a very different leadership from the traditional ambulance service. This is fully recognised by WAST and the trust is working hard with its partners in health and social care to achieve these outcomes. 19
20 3.4. The impact of technology The ability of an ambulance service to deliver a high quality service to patients in its area is critically influenced by the technology that the trust has at its disposal. There are a number of key components to this technology which affect the ability of the trust to operate at the highest levels of performance. These are Computer aided dispatch (CAD) systems which manage the deployment of vehicles and their dispatch to individual incidents Automatic vehicle location systems (AVLS) which are able to identify at all times the exact location of vehicles and to provide this information to the CAD system. This enables the CAD to track vehicles throughout the day to optimise the way in which vehicles are deployed and dispatched to incidents and to calculate the exact times that are taken by vehicles to mobilise and travel to the scene of an incident Mobile data systems that allow the dispatch centre to communicate automatically with response vehicles and which provide sat nav guidance to the crew to find the quickest route to the incident Automated caller line identification systems which speed up the process of identifying the location of an incident by showing the calltaker the address of a landline from which a call is being made An electronic patient record system in the form of a handheld device that can be used by ambulance crews to speed up the recording of the details of an incident and provide an electronic record of these details for subsequent use Historically WAST s technology infrastructure has been a significant hindrance to its ability to perform at a level comparable with other ambulance trusts. In particular the absence of a suitable radio system in Wales prevented the introduction of AVLS with the result that it was only possible to identify where a vehicle was by contacting the crew by phone and asking them to confirm their location. WAST estimate that the absence of AVLS has resulted in a level of Category A performance that is 5 percentage points below where it would otherwise have been. We understand that the business case for mobile data and AVLS has now been approved and these benefits are likely to be introduced during The majority of ambulance trusts in England either have introduced or are currently planning to introduce the current generation of CAD systems and it is on these systems that CAD providers are currently focusing their development efforts. WAST currently operates with a legacy CAD system that has been superseded by a more up to date system from the CAD provider. As a result, although the system will be maintained, it will not benefit from the enhancements that will be applied to the later system and over time the performance of the current system will lag behind. Consequently the system will have to be upgraded or replaced in the near future if WAST is to maintain a level of performance that is comparable with other Trusts. We understand that WAST is currently developing a plan to replace the current CAD system during 2009/10. 20
21 The limitations of the current CAD and the lack of a mobile data system also means that WAST cannot obtain the full benefits of an automated caller line identification system. Although as shown in Figure 1, the current performance standard does not include the time taken to answer the call and identify the location of the incident, nevertheless the absence of this technology is delaying the response to the patient and will become a key requirement if WAG were to decide to change the performance standards to start from the time that the call is answered Implications of the model There are significant benefits in terms of efficiency and effectiveness for WAST to move in the direction outlined in this Section. These include Impoved patient experience More effective and efficient use of operational resources Leverage on the investment that has already been undertaken Better and more fulfilling roles for staff both in front line and support roles Greater integration with the rest of the NHS in Wales in the delivery of urgent care In many ways WAST is well placed to move in this direction. It is the only organisation within the NHS in Wales that has an overview on a day to day basis of the pattern of demand for unscheduled care. In addition, WAST has the considerable advantage relative to ambulance trusts in England of already having completed a merger with NHS Direct Wales and it also provides the support for the Out of Hours in part of the region. Furthermore it already has a relatively high proportion of its staff who are paramedics. However it would also pose significant challenges and would require change in organisation and practices. In particular it would require Willingness of staff and the public to accept the change to single staffed response Further upskilling of staff in control Further upskilling of clinical staff Further upskilling of financial/support staff Investment in appropriate technology to support the change The rest of this report assesses the current position of the Trust in relation to its existing mandate, its current performance effectiveness and its readiness to move in this direction. 21

22 4. Findings 4.1. Benchmarking Appendix 1 sets out a proposed set of benchmarking data which if it were collected for different ambulance trusts - would allow a full comparison to be made of the effectiveness and efficiency of WAST in comparison with other ambulance services. Currently a subset of this data is available from different trusts and based on the available data we have prepared the following comparisons between WAST and two high performing English trusts with a similar geographical pattern of activity to that seen in Wales South Western Ambulance Service and East of England Ambulance Service Table 1 Selected Benchmarking data 22

23 The main conclusions from these figures are as follows: 999 calls per head of population WAST receives one call per year for every 6.2 people in Wales by comparison with one call per 6.5 people in the case of South Western Ambulance Service and one call per 9.9 people in the case of East of England Ambulance Service 23
24 Average income per call received WAST receives 9% less income per call received than South Western Ambulance Service and 22% less than East of England Ambulance Service. WAST receives 8% more EMS calls than South Western Ambulance Service but 14% fewer calls than East of England Ambulance Service. Dividing the EMS income by the number of calls gives the following figures. o o o WAST per call South Western Ambulance Service per call East of England Ambulance Service per call Average income per head of population WAST receives 6% less income per head of population in EMS funding than South Western Ambulance Service and 24% more per head of population than East of England Ambulance Service. Dividing the EMS income by the population headcount gives the following figures o o o WAST per head of population South Western Ambulance Service per head of population East of England Ambulance Service per head of population Headcount WAST has a whole time equivalent headcount that is 11% more than South Western Ambulance Service total headcount and that is 30% less than East of England Ambulance Service. However for frontline services WAST has a headcount that is 6% lower than South Western Ambulance Service and 39% lower than East of England Ambulance Service. EMS Vehicles WAST has 5% more EMS vehicles than South Western Ambulance Service and 29% fewer vehicles than East of England Ambulance Service. Area covered with an area of 20,640 Square KM in which to operate WAST covers 15% more area than South Western Ambulance Service and 6% more than East of England Ambulance Service. The comparisons above demonstrate the difficulty of basing a comparison of the efficiency of an ambulance trust on any one benchmarking measure. Under the measure of funding per 999 call, WAST received a lower level of funding than either South Western Ambulance Service or East of England Ambulance Service in 2007/8. However, under the measure of funding per head of population WAST received a lower level of funding than South Western Ambulance Service but a higher level of funding than East of England Ambulance Service. It is therefore necessary to consider a range of complementary measures in order to gain a full understanding of the external factors that affect the ambulance service as well as the efficiency with which the service is operated Table 2 below provides a further ranking for the three trusts using certain publicly available indicators. 24

25 Table 2. Comparison of WAST with benchmark trusts on selected benchmark metrics As can be seen from the rankings above the indicator where WAST scores highest is the number of incidents responded to per member of front line staff and the measurement of income per member of frontline staff. This reflects the fact that WAST is currently operating with high levels of overtime and low levels of relief thereby running the service with fewer frontline staff than would be recommended. Table 3 compares WAST s performance in relation to key call cycle measures with the performance of an area within the East of England Ambulance Trust consisting of Essex, Norfolk, Suffolk and Cambridgeshire a geographic area that is highly comparable with Wales in terms of the proportion of activity that occurs in sparsely populated areas. 25

26 Table 3 WAST call cycle performance against East of England benchmark area This underlines that the key difference in the management of the call cycle between WAST and East of England Ambulance Service lies in the initial phase of call handling, the allocation of a vehicle to an incident and the time it takes for the vehicle to arrive at the scene of the incident. This reflects the availability of resources, the investment in technology that is available to support the call handling and dispatch processes and the effectiveness with which the deployment plan and other Control room processes are managed. WAST compares well with East of England Ambulance Service with respect to the remainder of the call cycle once a vehicle has arrived at the scene of the incident. The table also highlights the fact that in trusts such as East of England Ambulance Service which have lower hospital transportation ratios the amount of time spent at the scene of the incident by the attending vehicle increases Achieving the Category A 8 minute AOF target Our analysis of the distribution of Category A activity within Wales has confirmed that, with the appropriate resource and infrastructure, it is possible for WAST to meet and even to exceed the current 65% target by adopting a structured approach to response based on the principles of separating initial response from transportation. Our analysis is based on the following assumptions WAST will provide a dedicated response resource to respond to at least 75% of Category A incidents within 8 minutes in any area ( Urban areas) where there are 4 26
 where there are between 2 and 4 Category A and Category B incidents per day within a 7 minute drivezone area.")
27 or more Category A and Category B incidents per day within a 7 minute drivezone area WAST will ensure that there is a suitable response resource available to respond to at least 70% of all Category A incidents within 8 minutes in any area ( semi urban areas) where there are between 2 and 4 Category A and Category B incidents per day within a 7 minute drivezone area. This may be a dedicated trust resource or may be a response scheme developed jointly with the local health community WAST will seek to develop appropriate community response schemes in other areas ( rural areas) where there are less than 2 Category A and Category B incidents per day within any 7 minute drivezone area. Category A performance in these areas is currently 40%, and WAST should aspire to raise performance in these areas to 50% by developing additional schemes WAST has fully deployed AVLS and mobile data The urban and semi urban areas we have identified in each of the LHB areas where we recommend that WAST should locate its deployment points for its vehicles are listed in Appendix 2. Based on these assumptions, the levels of activity in these three areas in each of the LHB areas and the possible levels of performance in each of the LHB areas and across WAST is as follows Table 4 Category A activity and potential performance by LHB area This shows that Wales does not have an unusually large proportion of its activity in rural areas by comparison with English trusts of comparable size. Moreover, with the exception of Powys, no LHB area has a level of rural activity which is out of line with similar geographical areas in England which already achieve Category A performance at levels which are at least as good and in many cases higher than the performance levels indicated in Table 4. 27
28 Consequently it should be possible for WAST to achieve the levels of performance indicated with a suitably resourced response model of this type. In order to achieve these levels of performance, however, WAST will have to place greater emphasis on the use of single staffed response vehicles which are the key resource that is required in order to achieve a reliable and consistent level of Category A performance with at least 50% of all Category A calls in the urban areas being attended in the first instance by a single staffed response vehicle. In addition, focused attention is required to ensure that there is an appropriate initial response resource either in the form of a double staffed ambulance on a standby point or an appropriately funded first responder scheme in all the semi urban areas that have been identified. In addition to these initiatives, WAST also needs to increase the use of Community Responder schemes and on-site static defibrillators at locations where Category A incidents are likely to occur. The existence of schemes of this type are an important contributory factor to the overall level of the initial response to Category A incidents, particularly in rural areas. In a number of English ambulance trusts initial response of this type contributes up to ten percentage points of the overall Category A 8 minute performance. By contrast in Wales this type of response currently contributes only around five percentage points to overall category A performance, with Community Response schemes contributing less than two percentage points to overall Category A performance in the first quarter of We understand that WAST plans to appoint a National First Responder manager with the objective of significantly improving the contribution from these types of scheme The implications of extended travel times and hospital delays The length of time for which an ambulance is committed to any incident before it is available to attend a subsequent incident is a key factor in determining the amount of resource that an ambulance trust requires. Where ambulances are committed to incidents for longer than expected this has a significant impact on the ability of an ambulance trust to meet its performance targets. The two factors that have the greatest influence on the variability of the job cycle time for an ambulance are extended travel times to hospital and delayed handovers at hospital. In ambulance services which achieve relatively high levels of utilisation of their ambulance resource, the average time for which an ambulance is committed to an incident in a highly populated urban area with a local hospital in the vicinity is around 62 minutes as summarised in Figure 4 below 28
.")

29 Figure 4 The best practice ambulance call cycle in urban areas This incident cycle time enables an ambulance trust to plan on the basis that an ambulance will complete its involvement in any incident in one hour (this is referred to as one unit hour ). However, when the time taken to travel to the hospital or to hand over the patient is extended, the unit hour has to be increased to take into account this additional time. In the case of an extended travel time to hospital, the effect on the incident cycle time is further compounded by the fact that the vehicle in question has to travel a longer distance both on the inward journey to the hospital and on the return journey. This can have a significant effect on the availability of ambulances and consequently the number of vehicles that are required to respond to a given level of activity. In the same way, when the handover of the patient at the hospital takes longer than 15 minutes, this also has an effect on the amount of resource that the trust needs as the vehicle is unavailable to attend a subsequent incident The overall impact of extended travel times and hospital delays is shown in Table 5 below which indicates that additional resource is required to compensate for these effects in each of the new LHB areas. Table 5 Extended travel times and hospital handover times by LHB area 29

30 4.4. Calculating resource requirements for WAST Unit hour requirements In order to meet the Category A 8 minute AOF target, as well as preparing for the change towards the response model outlined in Section 3.2 above, WAST needs to be able to provide sufficient single staffed response vehicles to respond to a minimum of 50% of the anticipated Category A incidents in all the urban areas identified. In addition, in order to meet the 14/18/21 minute standards, WAST also has to plan to have sufficient double staffed ambulances to attend all the Category A and Category B incidents that may require an ambulance to transport the patient to hospital as well as having sufficient ambulances to respond to Category C, Doctors Urgent and Hospital Transfers incidents in a timely fashion. As outlined in Section above, the interpretation of the Category A and Category B 14/18/21 minutes standards has a significant effect on our findings. At present WAST is interpreting these standards on the basis that a double staffed ambulance is required to attend a Category A or a Category B incident within the 14/18/21 minute time window in 95% of cases where an ambulance arrives on scene. As a result, WAST is currently sending ambulances to a high proportion of all 999 incidents even where a single staffed response vehicle has also been sent to the incident. Moreover, since it is not clear at the start of an incident whether an ambulance will be required, the only way in which the standard could be met consistently and reliably would be to send an ambulance immediately to every incident where a vehicle attends. This requires WAST to increase still further the number of ambulances that are sent to incidents Based on this interpretation of the 14/18/21 minute standard (the Base case scenario), Table 3 sets out our estimate of the average number of rapid response vehicle ( RRV ) and ambulance hours that WAST would require per week to meet all the performance targets and standards in each LHB area in 2009/10. This shows that WAST would require an additional 1100 RRV hours per week together with a further 1118 ambulance unit hours by comparison with the current planned rotas to deliver the 14/18/21 minute standards as well as the AOF targets. Table 6 Unit hours required - Base case scenario 30

31 If this interpretation of the 14/18/21 minute performance standards is used, any additional investment in RRVs would be extremely inefficient as RRVs would be accompanied by ambulances to all incidents whether or not the ambulance was required as a transport resource. This would preclude WAST from gaining the potential benefit of the reduction in ambulance unit hours that would otherwise be available from the more effective use of single staffed response vehicles. Moreover, the current operating procedures in WAST result in a significantly higher proportion of ambulances attending 999 incidents than occurs in comparable English trusts and also results in a materially higher proportion of patients being transported to hospital. As Table 4 shows, WAST s overall ambulance attendance ratio for 999 calls would be 93% if double staffed ambulances were required to meet the 14/18/21 minute standard in all cases. This compares with 81% achieved in the East of England Ambulance Service. Similarly, the ambulance transportation ratio in Wales in Q was 70% by comparison with 52% in East of England Ambulance Service. This results in WAST utilising 1745 more ambulance hours per week and transporting 1108 more patients per week to hospital than would be the case at the East of England Ambulance Service.. Table 7 Ambulance attendance and transportation ratios By contrast, if the alternative interpretation of the 14/18/21 minute response standards were used which would allow the increased use of single staffed response vehicles to undertake an initial assessment of patients as is the case in England, 410 fewer ambulance hours would be required to meet the performance standards by comparison with the current rotas and in addition there could be a significantly different outcome for patients by avoiding unnecessary attendances at hospital. At the same time, however, there would also be an increase in the time that was spent at the scene of the incident assessing the patient s needs which would have to be taken into consideration in determining the overall adjustment to the required resource In should also be noted that the total recommended unit hours for ambulances in Table 6 includes an adjustment of 900 hours per week to reflect the effect of extended hospital turnaround time as set out in Table 2. If the pattern of extended hospital delays that has been observed over the past year could be addressed, this would result in a further reduction in the amount of ambulance resource that WAST requires. However, it should also 31

32 be noted that any change in operating practice towards a greater reliance on single staffed response vehicles as the initial response to incidents will involve significant changes in working practices and will require careful planning by WAST. It would also require the availability of alternative pathways for patients who would otherwise be taken to hospital Ambulance staff requirement The staff resources required to fill the recommended rotas and the associated cost is dependent on a number of factors The number of hours that are assumed to be available per week once factors such as sickness, holidays, training time and other anticipated non availability (collectively referred to as Relief ) has been taken into account The amount of overtime that is required to cover shift overruns and other unanticipated hours worked ( Core overtime ) The amount of overtime that is assumed to be worked in addition to contracted hours to fill planned shifts ( Additional overtime ) The additional payments that are required over and above base salary to cover items such as unsocial hours and pension contributions ( Add on costs ) The proportion of staff of different levels of qualification that are required to cover shifts on different types of vehicle The position with respect to the availability and use of front line ambulance resource in WAST in 2008/9 is set out in Table 5 below Table 8 Front line staff resource, cost and available hours to fill rotas This shows that in 2008/9 WAST had a total of 1301 front line staff with a total direct cost of 53.6mn and an overtime rate of around 19%. Based on the 2008/9 overtime rates and the assumption of a relief factor of 26.8% this would have produced a total of 42,522 hours 32
33 available to man vehicles which matches almost exactly the total of 42,502 rota hours that were planned by WAST Adjusting for overtime and relief The implications of this increase for the additional number of staff that WAST would require and the associated cost of those staff depends critically on the assumptions that are made for 2009/10 about the rate of additional overtime that it is acceptable to plan for and also the appropriate level of relief that WAST should build into its planning Overtime In our calculations, we have assumed that the amount of overtime that WAST requires to cover shift overruns and other unanticipated extractions is 5%. This compares with an actual rate of payment for shift overruns in 2008/9 of 4%. Based on this planning assumption the level of additional overtime (ie overtime paid to fill core shifts) was particularly high in 2008/9 at around 14%. This is a relatively inexpensive way for WAST to increase the available hours to fill its shifts, but it depends on the willingness of staff to work additional hours and as such does not provide a robust mechanism for managing rosters. It also raises issues about the extent to which a planned reliance on overtime is an appropriate HR policy. It would therefore be imprudent for WAST to plan to continue to rely on these levels of overtime in 2009/10 as a means of filling core rota lines. The actual figure for additional overtime in any year will be dependent on the extent to which vacancies are filled and other extractions are in line with plan. Our calculations of the resource requirements that are required to meet the existing performance standards therefore show the resource requirement under two different scenarios a current scenario where WAST continues to operate with the levels of overtime employed in 2009/10 and an alternative calculation where overtime is used solely to cover unplanned extra hours at the end of shifts or to cover occasional unanticipated peaks in sickness etc Relief The level of relief that WAST builds into its plans is also a critical factor affecting staff numbers and costs. A level of relief has to be built in to resource planning to cover factors such as holidays, sickness, training and other planned and unplanned absence. The main components of relief are Annual Leave Public holidays and time off in lieu Sickness Training Maternity leave Other (including staff management duties, internal meetings, union representation etc) 33
34 It is generally recognised that best practice staff management in ambulance trusts would apply a relief factor of 35% to cover these factors - a level recommended in a Department of Health paper released in April In practice, there is considerable variation in the relief factors that ambulance trusts apply in their resource planning. For example, whilst WAST plans at 26.8% in the case of the services used for comparative purposes the South Western Ambulance Service uses a 35% relief planning assumption, whilst the East of England Ambulance Service plans at a level of 28%. However, since most of the other factors resulting in staff being unavailable for work such as holidays and sickness are non discretionary and the resulting absence has to be covered from the relief factor, it is typically the ongoing training component which suffers when trusts are unable to operate at a sufficiently high level of relief and this is currently the case in WAST based on the current relief factor of 26.8%. It is therefore highly desirable from a staff management perspective that WAST should increase its relief factor from its current low rate as soon as it is able in order to be able to plan for appropriate ongoing professional training for staff. The precise level of relief that WAST needs to incorporate into its planning depends on the detailed training requirements of its staff. We have not undertaken an analysis of the training days that WAST needs to set aside to ensure that its staff maintain the appropriate levels of ongoing training and we have therefore undertaken our analysis of the resource implications of adjusting the relief factor based on the 35% rate that is included in the Department of Health publication Achievable performance levels and additional resource requirements under different scenarios Achievable performance levels with existing resources As Table 9 shows, if WAST continued to operate with its current levels of staff and current overtime and relief factors, but was also able to match the best practice call cycle management processes that are operational in the high performing English trusts, we believe that it would be possible for WAST to meet the 65% Category A 8 minute AOF target in 2009/10 and to meet the 60% standard in each of the LHB areas under each of the following three scenarios. 1 Hospital delays continue at the level observed during the reference period for this study 2 70% of hospital handovers are achieved within 15 minutes 3 90% of hospital handovers are achieved within 15 minutes. 34

35 Table 9 Achievable performance levels with current establishment However, Table 9 also confirms that - based on the current operating model - WAST would not be able to meet either the Category A or Category B 14/18/21 minutes standards or the standard for Urgent journeys under any of these three scenarios based on the current operating model. In addition, if WAST were to operate with a lower level of overtime and a higher relief factor it would only be able to meet the Category A 8 minute performance targets if hospital delays were reduced significantly below the levels observed during our review Additional resource requirements to meet the 14/18/21 minute performance standards Based on the analysis outlined in Section 4.4 above, we have analysed the additional staff requirement and the associated costs for WAST under the following scenarios with respect to the 14/18/21 minute standards 1 WAST sends a double staffed ambulance to all Category A and Category B incidents which requires a vehicle to attend (The Base Case scenario) 2 WAST continues to send double staffed ambulances to the majority of Category A and Category B incidents as at present (the Current response scenario) 3 WAST reduces its ambulance attendance at all categories of incidents to the best standards achieved by English trusts (the Reduced attendance scenario) 4 WAST reduces its ambulance attendance rate to the English benchmark and 90% of hospital handovers are achieved within 15 minutes (the Full benefits scenario) 35
36 As Table 10 shows, in order to meet all the performance standards under the Base Case scenario, WAST would require a minimum further 99 staff to enable it to produce the necessary hours to fill the rotas. This calculation is based on the assumptions that the Trust continues to operate with its current rates of overtime and planned relief and that hospital delays remain at the level observed during the reference period for this report. If the Trust reduces its reliance on overtime to the level that is required to cover frictional factors such as overruns at end of shifts and occasional unexpected sickness a further 163 staff would be required and this would add a further 1,679,000 to the cost base. Moreover, increasing the relief factor from 26.8% to 35% would require WAST to employ a further 82 staff and would add a further 3,206,000 to the total cost bringing the total additional cost of filling the new rotas to 8,647,000 Table 10 - Staff requirement Base Case scenario Table 11 shows the potential reductions in the ambulance hours and the related financial savings that could be achieved relative to the Base Case Scenario if WAST were able to operate based on a different interpretation of the 14/18/21 minute standards and was also able to reduce the number of cases where an ambulance attendance was required at Category B and Category C calls. This shows that the number of ambulance hours required could be reduced by a total of 1524 per week from these initiatives. Moreover Table 12 also shows that the required hours could be reduced by a further a further 710 hours per week if 90% of hospital handovers could be achieved within 15 minutes. 36


37 Table 11 Savings in unit hours and cost relative to Base case scenario The staffing and financial implications of these different scenarios relative to the position in 2008/9 is summarised in Table 12. Table 12 Staff requirement and costs under alternative scenarios 37
38 This shows that under the Current Response model where WAST is not required to send an ambulance to every Category A and Category B incident to meet the 14/18/21 minute standards, but where the full benefits of the new response model have not yet been realised, WAST would require 57 more staff at an additional cost of 2,370,000 in order to meet all its performance targets on the assumption that it maintained its current levels of overtime and relief. The staff requirement would increase to 224 at an additional cost of 4,017,000 if WAST were to reduce its reliance on overtime to cover core shifts. The staff requirement would increase further to 305 staff at an additional cost of 7,144,000 if WAST were to increase its planned relief factor from 26.8% to 35%. Table 12 also shows that if WAST were able to obtain all the potential benefits of lower attendance rates and reduced delays at hospital, it would be able to meet all its performance targets and standards with 33 fewer staff and at a cost that was 1,876,000 lower than in 2008/9 based on the current levels of overtime and relief. The staff requirement under this scenario would increase to 110, but the overall cost would still be 386,000 lower than in 2008/9 if WAST were to operate without relying on overtime to fill core shifts. The staff requirement under this scenario would increase further to 184 at an additional cost of 2,497,000 if WAST were to increase its planned relief factor from 26.8% to 35% Financial analysis Our financial analysis consisted of the following four distinct work streams: The identification of the income streams for WAST for the year 2008/09, The development of a fully absorbed cost model identifying the cost of delivering EMS in Wales based upon 2008/09 figures,and A financial summary of the impacts of the various proposed changes within the report. 38

39 Income Based upon the information provided by WAST, the Trust received the following income in 2008/9: Table 11 WAST sources of income 2008/ Fully absorbed cost model In order to ascertain the costs of delivering EMS within Wales we have produced a cost model which aims to identify the fully absorbed cost of the services using the methodology set out in Appendix 3. For the purpose of this exercise, the Air Ambulance Service was included within the analysis of the cost of providing the EMS service The results from the summary cost model for the year 2008/9 are as follows: 39

40 Table 12 Fully allocated cost by service line By comparing the income in Table 11 with the fully absorbed costs of each of the service lines we can see that based upon the model developed there was a shortfall in EMS funding in 2008/9 of 5,747,000. However it must be noted that the cost model has not been built on a detailed analysis of cost consumption, rather on an agreed approach to allocating overheads, the result of which is that there could be a margin of error in the allocation of overheads Financial summary Whilst the work we have performed relating to income and fully absorbed costs highlights a potential shortfall in EMS income of 5.7m we believe that further activity analysis is required in order to identify the true costs associated with delivering each of the activities undertaken by WAST. Clearly there is an element of cross-funding within the Trust and therefore the Trust should consider ways in which to bring each of its service lines into a recurrent breakeven position. We were also asked if the achievement of a 2m costs saving for EMS was possible. There are a number of areas where we believe further investigation may result in opportunities for significant savings. These include: Control & Administration - Based upon the comparison table above we believe that there may be potential savings within the back office functions at WAST and this is an area that needs further examination. For example WAST has over 100 more members of staff in either the Control & Manager and Administrative roles than SWAST. Furthermore the comparison of numbers is not on a like for like basis with the numbers for WAST being based upon whole time equivalents and the numbers for South Western Ambulance Service being based upon total people employed. The cost of staff and directors at WAST is 91,098,000 with an average costs per whole time equivalent of 33,678. The average cost of staff employed at South Western Ambulance Service WAST is 31,945 but as mentioned before the numbers are not wholly comparable. However what is clear is that the number of staff employed by WAST in these non frontline roles is significantly higher than the number employed by South Western Ambulance Service The possible savings 40
41 would depend upon how many of these non frontline roles are indeed excessive, below we summarise the potential savings: 5% of roles could be removed - 168,390 10% of roles could be removed - 336,780 25% of roles could be removed - 841,000 50% of roles could be removed - 1,683,900 We have not undertaken any analysis in the course of this review to validate the extent to which these activities might be streamlined and savings realised. Moreover, the above numbers assume a linear relationship which may not be true. Nevertheless, they serve as an indication as to the potential savings that might be available. Fleet Costs - A further area of potential cost savings would arise if WAST moves towards a model that utilises more RRV s and fewer double staffed ambulances. The scope for such savings in the fleet running costs is suggested by a comparison of fleet costs with South Western Ambulance Service. The average fleet cost per vehicle at South Western Ambulance Service is 20,554 which is 18% lower than the average fleet cost at WAST of 24,182. Based on the assumption that the average cost of an RRV for WAST is 10,000 per year and the average cost of a double staffed ambulance is 30,000 per year, WAST would obtain savings of 280,000 per year from the change in the mix of vehicles that would result under the Full Benefits scenario Operating centres and control rooms - One factor that has a significant effect on the cost base of WAST is the number of operating centres and control rooms that the Trust currently supports. At present WAST operates from three operational centres in St Asaph, Cwmbran and Swansea and operates five control rooms including both the EMS and NHS Direct locations. In the course of this review we have not undertaken any analysis of the potential opportunities that might exist for reducing costs through a reduction in the number of control rooms and operating centres and therefore we can not provide any estimate of the potential savings that might be available from this area. However, this is an area which should be examined in the context of any detailed review of the Trust s cost base. At the same time, the additional resources that WAST requires in order to meet its performance targets will increase the Trust s cost base. The tables below summarise the financial impact of the proposed changes to the operating model. Table 15 shows the financial impact of funding the Base Case operating model based on the changes to staffing levels that are required to fill the new rosters, the costs of reducing overtime from the current level of 19% to 5% and an adjustment to change relief from the current 26.8% to 35%. Table 16 shows the associated costs of moving to the new model using more RRV s and fewer double staffed ambulances and assuming that all the benefits identified in Section 4.5 in terms of reduced ambulance hours have been realised. (Please 41
 Table 15 Funding requirements for the Base Case operating model Table 16 Funding requirement for the Full Benefits operating model Based upon the information above it is clear that if WAST were to")

42 note that these costs relate simply to the costs of frontline staff and do not reflect any savings associated with the change of fleet.) Table 15 Funding requirements for the Base Case operating model Table 16 Funding requirement for the Full Benefits operating model Based upon the information above it is clear that if WAST were to start to change its operating model in line with the recommendations in this report at the same time as reducing the levels of overtime worked and increasing the relief factor by the full amounts indicated there will be a significant level of investment required. However against this investment there should also be savings in fleet costs and other operating efficiencies associated with changing the model which have not been quantified at this stage. It should also be noted that the additional staff required to fill the new rosters are to deliver a 95% performance against the 14/18/21 minute standard, not the Category A 8 minute AOF targets, which as stated earlier can be met from existing resources under the conditions identified In terms of the question of what level of cash releasing CIP the Trust can achieve, based upon the above and assuming that both relief and overtime are operated at the levels specified, it is clear that under the current operating model the Trust is not able to operate a 42
43 cash releasing CIP whilst at the same time delivering its AOF performance targets. Moreover, the Trust will require additional funding if it is to meet the 14/18/21 minute standards. However, if the full benefits of the new operating model could be obtained the Trust would require an additional funding of only 2.5mil, and offset against this could be the potential savings highlighted above Other findings In the course of our work we also reviewed WAST s operational readiness to adopt the practices that are advocated in this report in comparison with best practice at other ambulance trusts. These included a review of Control room processes, Clinical practices and the overall organisational structure of the Trust. Our findings in respect of these considerations are set out below Control room processes WAST currently operates three Control Rooms, one based in each of the three regions. Each of the control rooms is managed by a Utilisation Manager and performance management takes place within the regional management structure. At the time of our review, control practices varied across the different regions and we identified a number of areas where there were opportunities for improving the efficiency and effectiveness of the control processes. Across all the three control rooms the dispatch process was slower than we would have expected despite the fact that the information from the call takers was available to dispatchers almost immediately. The approach to vehicle deployment relied heavily on the use of double staffed ambulances and was inhibited by the absence of system status planning software, mobile data and vehicle location technology which the Trust plans to introduce later this year. In addition, we believe that there is potential for improved utilisation of community and static responders with appropriate investment in the necessary infrastructure to support this. The Trust s proposed new structure which includes a Trust wide head of the Control should serve to improve and coordinate operational practices across the three Control Rooms and accelerate the work that is already underway within the Trust s National Control Steering Group to standardise control processes and systems. Moreover, further improvement in the effectiveness and efficiency of Control Staff should be possible through consolidating the performance management arrangements that WAST has recently put in place. In this context, the Trust is currently working with Landmark Consulting to implement a structured approach to performance management that will apply across the three control rooms and the managers in the South East have already received training in this process. The Trust has also recognised the need to improve its deployment and utilisation of Rapid Response Vehicles (RRVs) and has been in discussion with Staff Side Organisations concerning the introduction of modern operational procedures. The current operating model predominantly uses double staffed ambulances and therefore any change in the model so as 43
44 to make greater use of Rapid Response Vehicles would require a material change in organisational culture and behaviour. There is also significant scope for WAST to leverage the benefits of the co-location of NHS Direct within the Control Centres and to increase the proportion of Category C calls that are handled by means of telephone triage. In particular, the move to Vantage Point House in the South East Region provides a control room that, with the appropriate technology, would be capable of providing an integrated single point of contact for the local health economy. We understand that WAST is developing a Clinical Contact Strategy for the advancement of its Control Centres and discussion is taking place with some Out of Hours GP providers about further opportunities that exist for integrated working. Systems for managing Category C calls are also being developed in conjunction with WAG and we understand that WAST have worked closely with WAG to establish alternative pathway of care for low acuity calls which draws on similar work that has been undertaken elsewhere in the UK. A number of PDSA cycles have been used to establish the benefits of providing telephone nurse triage for Category C calls. Based on this work we have been informed that the Clinical Desk model is currently operational in both Central and West and the South East regions and is an integral part of the new Clinical Control Centre strategy. The Trust has also included within the LDP submission its intention to link CAS (the NHS Direct Software) and the Alert 2000 CAD (the Ambulance software) so as to widen the availability of Category C triage to all Nurses in NHS Direct Wales. The Trust has also submitted an Invest to Save bid in collaboration with health partners to implement NHS Pathways as a single clinical triage platform within Wales Clinical procedures From our review we believe that there is scope for further improvements in clinical practice at each stage of the patient pathway. In this context it is essential that a common vision is agreed for WAST among all the key stakeholders which can then be communicated clearly to staff. This vision should be of a clinical service with a huge role to play in the delivery of the unscheduled care agenda both nationally and locally as outlined in this report rather than solely as an emergency response and transportation service. Moreover, the clinical strategy needs to be understood within the Trust as clearly complementing the delivery of performance standards. As research demonstrates, clear clinical gains can be made from early intervention by trained health professionals. In the control rooms we believe that significant opportunities exist for greater integration with NHS Direct and Out of hours providers and that these opportunities should be maximized. In particular, the clinical advice that is already available to callers to NHS Direct could be made available more extensively to EMS callers as well as to paramedics and other ambulance staff. There is also an opportunity to better influence the management of patients across the system by capacity managing ambulances going to the various A & E departments and in time beginning to develop other alternative points of access. We also believe that the clinical supervision and support available to operations teams could be enhanced. During our review we saw little evidence of any input from the control room for front line staff if they have a problem and it was also difficult to ascertain the 44
45 numbers of paramedics, technicians and clinical team leaders at each station. Moreover, there was little evidence of sharing best practice either within or between Regions. We also understand that, although WAST has now established a clear plan for providing clinical training for staff at all levels, there have been difficulties in releasing staff to undertake the training at the current levels of overtime and relief. A further issue is that turnaround times at hospitals vary widely. There is currently limited understanding of what factors influence these times and little sharing across Wales of best practice developments used at local level. WAST is working towards alleviating the delays and the use of the touch screens at the hospitals to record handover times is a very positive initiative, but this is mitigated by poor processes in the hospitals which need to be addressed in order to solve the ongoing problems caused for WAST by extended hospital delays. WAST recognises the need to strengthen its clinical processes and a number of initiatives are currently under way that are designed to address these issues. We understand that a draft clinical strategy and vision document has recently been developed which is underpinned by various other strategies e.g paramedicine, nursing, clinical effectiveness and Partners in Health. The Clinical Contact Strategy is also in final draft. Both documents will now be taken through a consultation process to ensure wide and meaningful stakeholder engagement and input before the documents are presented to the Trust Board. In addition, the current implementation of the new role of Clinical Team Leader should ensure that paramedics have clinical leadership at a local level. WAST is also introducing a new role of Specialist Practitioner which will take paramedics/nurses through the novice to expert framework and will complement the role of the Clinical Team Leaders. The development of these new roles and indeed the CCS is dependent on the development of robust clinical supervision and mentorship networks throughout WAST. Regional Professional Advisory Groups and the National Clinical Advisory Group will ensure professional issues are addressed, action taken and lessons learnt and shared across the Trust Organisational issues The fact that WAST operates from three regional offices and the senior management team are spread across these three locations makes the management of the Trust a particular challenge. A new organisation structure has recently been introduced with the objective of streamlining the management structure and a number of senior appointments have been made or are currently planned, including a new Director of Human Resources and a new Regional Director in Central and West. However at the time of our review the Trust did not have a substantive Operations Director, two of the three Regional Directors had only recently been appointed and there was no head of control for the Trust as a whole. It will therefore be important that the Trust ensures that the new management structure is implemented effectively and that there is a strong focus on the effectiveness of the senior management team. A further issue for WAST is the current arrangement for funding and performance management. HCW is the principal funding organisation for the EMS service in WAST, but it does not have responsibility for commissioning other elements of the urgent care system. However, WAST also receives funding from a number of other sources including NLIAH and WAG. As a result, there is currently no one organisation that is responsible for funding the 45
46 fully loaded cost of providing the EMS service. The basis on which funding is currently being provided and will be provided in the future (whether on the basis of journeys, attendances or incidents that are responded to) is also unclear due to the current reorganisation of the NHS. The arrangements for the performance management of WAST are currently through the North Wales Regional Office and it is unclear how this process holds the two parties to account for the delivery of their respective responsibilities. The establishment of the new LHB structure provides the opportunity to revisit this structure possibly through the appointment of a nominated LHB to act as the lead commissioner and performance manager for WAST. 5. Conclusions and recommendations 5.1. Conclusions WAST has made significant progress since the original Audit Office report in There have been a number of positive developments in the way that the Trust is now operating and Category A performance in particular has improved significantly during this time. However, the results of this review show that that there are still some fundamental issues that are preventing WAST from performing at a level that is comparable with similar organisations elsewhere in the UK. As a result patients in Wales are not receiving a level of service that is commensurate with that achieved by other ambulance trusts elsewhere in the United Kingdom.. The key findings from our benchmarking analysis and our asessment of the the current efficiency and effectiveness of WAST are as follows WAST s performance in relation to the Category A 8 minute target has improved significantly since the beginning of However there has been little or no improvement during this period in relation to the Category A and Category B 14/18/21 minute standards. Although Wales covers a larger geographical area than other ambulance trusts in the UK, the proportion of EMS activity that occurs in towns and cities in Wales is similar to that of comparable ambulance trust areas in England Wales experiences a relatively high number of 999 calls per head of population and a relatively high proportion of these calls result in a patient being transported to hospital. This results in pressure being placed on WAST and on hospitals in Wales that we believe could be alleviated if suitable call triage and assessment procedures were used and alternative care pathways were available for patients We estimate that the total cost that WAST incurred in providing the EMS service in was mil. WAST received 95.6 mil of funding for the EMS service in 46
47 from HCW, NLIAH and the Air Ambulance Charity. The difference was funded by income for other purposes e.g. ARRP. Hospital delays have a significant impact on the ability of WAST to meet its performance targets. During the reference period for our review, WAST would have required an additional 900 ambulance hours per week in order to compensate for the delays in handing over patients at hospital at an annualised cost of 2.3 mil per year. This effect is of particular significance in the South East region of the Trust. WAST s performance with respect to the initial phase of allocating a vehicle to a 999 call compares poorly with other ambulance trusts in England. A significant contributory factor to this performance gap is the lack of an Automated Vehicle Location System (AVLS) and related mobile data systems on EMS vehicles in Wales. This makes it difficult for WAST reliably to locate and deploy the most appropriate vehicle to respond to a 999 call. Once the benefits of its investment in AVLS and mobile data are available, WAST could meet the current Category A 8 minute targets both at a national and LHB level with its current staffing levels and overtime rates and with the level of hospital delays that occurred during the reference period for this review. In order to do this WAST would need to accelerate the implementation of a deployment strategy that o o o o is based on 7 minute deployment areas in the more densely populated areas matches resource more precisely to the location of activity relies more extensively on the use of single manned response vehicles, and makes more extensive use of Community First Response schemes in less densely populated areas as the initial response to Category A incidents. The current level of staffing does not allow WAST to meet the 14/18/21 minute standards and also requires a reliance on high levels of overtime to fill core shifts. In addition, the shortage of staff in certain areas is preventing WAST from undertaking sufficient ongoing professional training. Based on WAST s current levels of overtime and planned level of relief, we estimate that the cost of the additional staff required to meet the current 14/18/21 minute performance standards would be 3,744,000. This would rise to 8,647,000 if WAST were to operate with no reliance on overtime to cover shifts and with the level of cover for holidays, sickness, training and other lost hours that was recommended in a Department of Health paper published in April 2007 setting out best practices in managing ambulance trusts If it were fully resourced in accordance with the recommendations in this report, WAST should be able to achieve a Category A 8 minute performance target of at least 70% for the whole of Wales as well as meeting all the 14/18/21 minute standards. The current practice with respect to the 14/18/21 minute standards means that WAST sends more double staffed ambulances in response to lower acuity 999 calls than occurs at some other ambulance trusts. As advocated in this report, an 47
48 alternative approach which distinguishes more clearly between the requirement for an appropriate initial assessment of the patient s requirements and the subsequent provision of transportation once it has been determined that the patient needs transporting to hospital could significantly reduce the number of ambulance hours that WAST requires and also reduce the number of cases where the patient is transported to hospital. It should be noted however that a change of this type will require a significant change in practice within WAST as well as actions by other stakeholders to ensure that alternative pathways are available for patients. Consequently the benefits from this change are likely to take between 3 and 5 years to be fully realised. If WAST were able to match the levels of ambulance attendance and transportation that are achieved in some trusts in England it could reduce the number of ambulance hours required by around 410 per week by comparison with the level that was planned in 2008/9. This would save around 1,025,000 per year in staff costs If hospital handover times were improved so that only 10% of hospital handovers took longer than 15 minutes this would reduce the number of ambulance hours required by comparison with the reference period for this review by 710 per week. This would save a further 1,966,000 per year. If WAST were able to obtain the full benefits from lower ambulance attendance rates and reduced hospital delays it should be possible for the Trust to meet both the AOF Category A 8 minute targets and the 14/18/21 minute standards with a staff cost that would be 1,876,000 lower than the level in 2008/9 based on the current overtime and planned relief levels and would be 2,497,000 higher than the 2008/9 levels based on the lower overtime and higher relief scenario. If WAST were to change its operating model in the way that is advocated in this report and was also able to obtain the full benefits of lower ambulance attendances and reduced hospital delays outlined above, it should also be able to realise savings of up to 280,000 in fleet costs as a result of greater use of cars and less use of double staffed ambulances. WAST may also be able to realise additional savings in the following areas o o reducing its administrative overheads reducing the number of operating centres and control rooms It should however be noted that we have not examined these areas in any detail during this review. In addition to the detailed findings of our analysis set out above, we have also identified a number of organisational issues which we believe need to be addressed if WAST is to achieve a successful transition to the new approach to the delivery of its services that is advocated in the report. In particular The challenges of agreeing a common vision between WAST and its many stakeholders about the role that WAST should play in the delivery of urgent care 48
49 across Wales has previously made it difficult for the Trust to plan its future direction with any certainty and to communicate this to its staff. At the time of this review, WAST has submitted a vision statement to NHS Wales for comment and consideration and is also working with the seven new LHBs to include key objectives within the LHBs own Urgent Care Plans. This offers an opportunity to establish a jointly agreed role for WAST that will form the basis for the implementation of the recommendations in this report The geographical spread of the Trust, the requirement for senior management to be located in three different regional centres and the amount of change in the senior management team has made it difficult to establish a stable management structure. The new management structure that has recently been introduced provides a framework within which WAST can create the senior management team that will be required to implement the strategy that is recommended in this report The quality of clinical oversight, supervision and training has not had sufficient focus at a time when the Trust has been under pressure to deliver performance. This has been recognised by WAST and a number of initiatives are currently under way to address these issues. However, the pressure on resource and the low levels of relief continue to make it difficult for the Trust to release staff to undertake appropriate levels of clinical training The funding arrangements for WAST have been unclear in the past and require clarification in the new NHS structure so that the link between funding and service delivery can be made transparent The current commissioning and performance management arrangements for WAST do not facilitate clear lines of accountability between WAST and its commissioners and performance managers for the delivery of the EMS service Although WAST could achieve the AOF Category A 8 minute target for the initial attendance at life threatening incidents with its current resource based on best practice call cycle performance and the current levels of overtime and relief, the current level of recurring funding that WAST receives is insufficient to enable it to achieve the 14/18/21 minute standards. We therefore believe that WAST will require additional funding in the short term in order to provide a fully effective EMS service that delivers appropriate levels of clinical care to patients. Nevertheless, our review has confirmed that, following the merger with NHS Direct, WAST is uniquely placed to contribute to the delivery of a high quality urgent care service in Wales. Moreover, there are significant opportunities for WAST to change the way that it operates so that it is able to deliver an improved and more cost effective service. Indeed we see no reason why these standards should not be comparable to those that are achieved in England. In particular we believe that, based on the resources that we have recommended, WAST should be able to achieve a performance standard of at least 70% for Category A performance and also to meet suitably defined 14/18/21 minutes response and transportation standards for both Category A and Category B incidents. It should also be 49
50 possible for WAST to reduce significantly the current reliance on emergency ambulances for transportation to hospital and also to reduce the overall number of patients who are transported to hospital by a combination of suitable initial assessment and the availability of alternatives to hospital for patients to access. However, for these benefits to be achieved WAST needs to work closely with the rest of the urgent care system in Wales and to operate within a more clearly defined planning and performance management structure than has occurred previously. The new LHB structure which becomes operational on 1 October 2009 provides a unique opportunity to establish an agreed strategy and a new governance and operating framework for WAST based on these findings and our recommendations which are set out below Recommendations In line with our findings and conclusions set out above we would like to make the following specific recommendations with respect to the future direction of the Welsh Ambulance Service WAST s vision of its future direction needs to be based on the principles set out in this report, agreed with the Welsh Assembly Government, the new LHBs and other key stakeholders and communicated to its staff WAST should establish with WAG and the LHBs a clear interpretation of the 14/18/21 minute standards that apply to both Category A and Category B incidents WAST should agree with the LHBs a plan to significantly reduce the ambulance attendance and transportation ratios for Category B and Category C calls. WAST should ensure that the structured approach to the deployment of RRVs and other initial response vehicles set out in Section above is implemented effectively WAST should ensure that the benefits of the new management structure are realised as soon as possible The Director of Operations should ensure that the Trust s performance management and performance improvement processes are reinforced, deliver consistency of performance and are used to enable the changes that are recommended in this report. This should include a mechanism for defining and sharing best practice for operations staff across the three Regions The National Control Development Lead should establish common operational and clinical practices that will operate in each of the control rooms and develop training programmes and performance management methodologies for control room staff 50
51 WAST should improve the clinical input that is provided from the Control rooms for both patients and front line staff and make better use of the potential that exists from the co-location of ambulance control and NHS Direct through the implementation of the Clinical Control Room Strategy WAST should continue with its plans for the introduction of Specialist Practitioners and Clinical Team Leaders WAST in partnership with the LHBs should proactively seek to increase the number of co-responder schemes and community responder schemes that operate in the semi urban and rural areas and should ensure that there is an appropriate support and deployment infrastructure to support this. WAST should establish a clear staff development plan and agree with the LHBs a level of relief that will allow staff to undertake the training that is required to maintain their ongoing professional development WAST should proceed with its plan for the implementation of a new CAD system as soon as possible. This is necessary to enable WAST to improve service resilience by allowing the sharing of information across the control rooms as well as enabling the Trust to benefit from additional functionality that is not available in the current legacy CAD system WAST and the LHBs should review the Trust s current regional configuration in the context of the proposals for communications hubs and the need to deliver a cost effective control function. In preparation for establishing new funding contracts, WAST should complete a review of the fully loaded cost of providing the EMS and PCS services in order to establish a sound basis for establishing the funding requirements and the contract currency for the two services. WAST should agree with the LHBs an appropriate subset of the measures outlined in this report that can be used to benchmark its performance on a regular basis against similar ambulance trusts elsewhere in the United Kingdom WAG in conjunction with the new LHB s should develop and agree the future planning and delivery arrangements for WAST, ensuring a clarity and focus upon outcomes and performance WAST should undertake a strategic review of its support services to establish whether there are alternative ways in which these services could be provided at lower cost WAST and the LHBs should develop a fully costed plan to implement the actions required to deliver the new delivery model and should establish a joint programme management farmework to oversee the implementation of the plan 51

52 Appendix 1 Suggested benchmarking measures 52
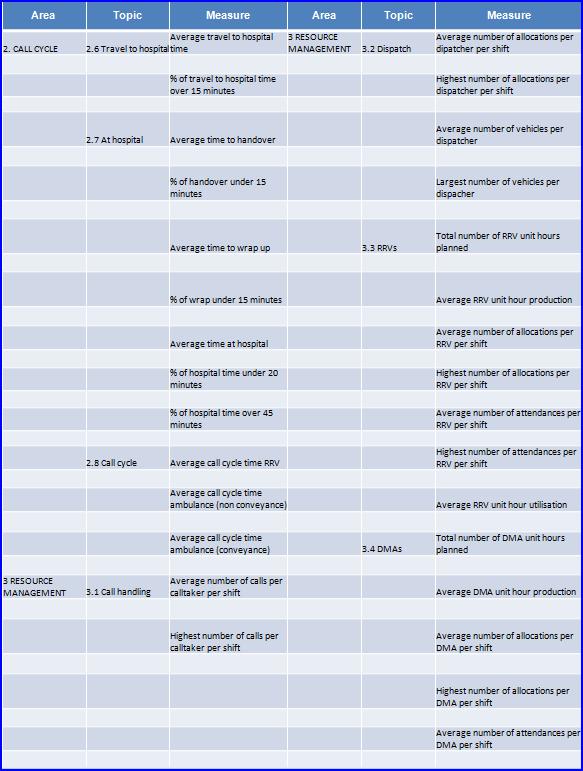
53 53
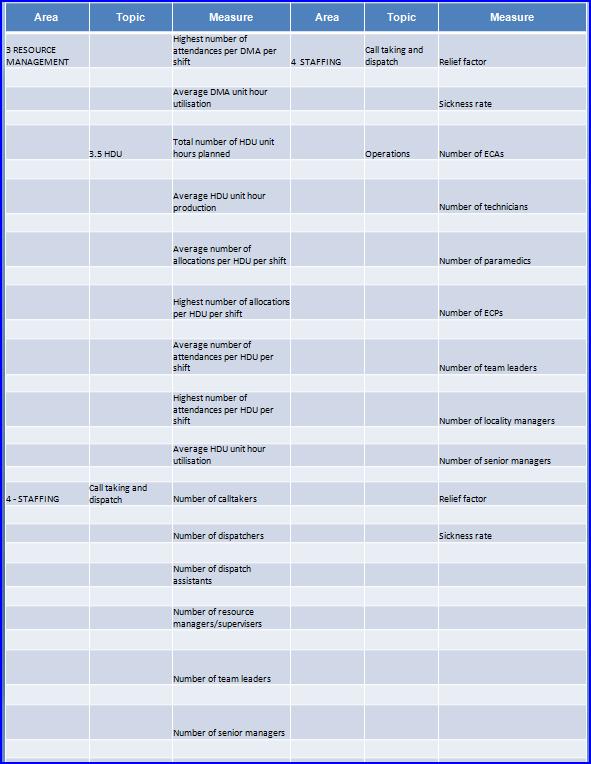
54 54
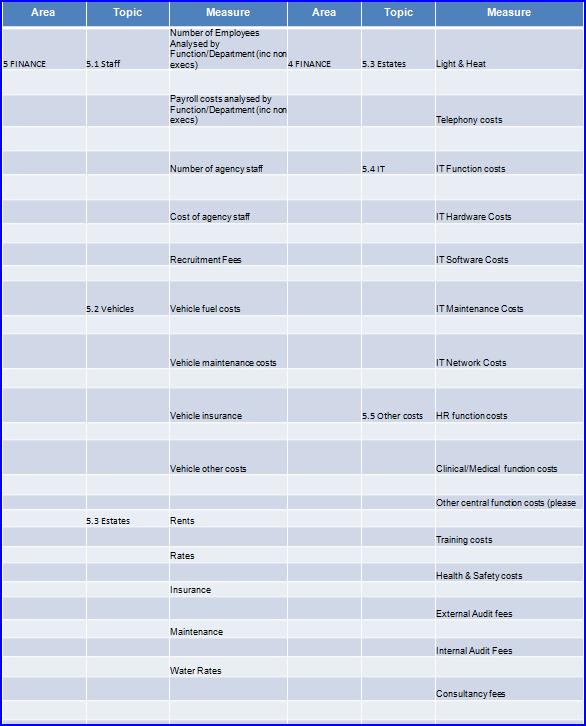
55 55
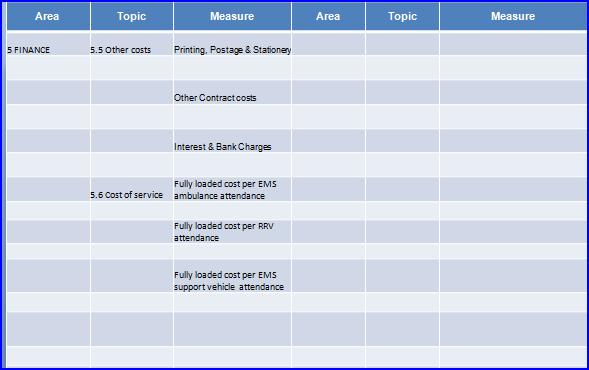
56 56

57 Appendix 2 - Recommended deployment locations by LHB area 57
Pre-hospital emergency care key performance indicators for emergency response times
 Pre-hospital emergency care key performance indicators for emergency response times Item Type Report Authors (HIQA) Publisher (HIQA) Download date 05/09/2018 21:43:37 Link to Item http://hdl.handle.net/10147/324297
Pre-hospital emergency care key performance indicators for emergency response times Item Type Report Authors (HIQA) Publisher (HIQA) Download date 05/09/2018 21:43:37 Link to Item http://hdl.handle.net/10147/324297
NHS Ambulance Services
 Report by the Comptroller and Auditor General NHS England NHS Ambulance Services HC 972 SESSION 2016-17 26 JANUARY 2017 4 Key facts NHS Ambulance Services Key facts 1.78bn the cost of urgent and emergency
Report by the Comptroller and Auditor General NHS England NHS Ambulance Services HC 972 SESSION 2016-17 26 JANUARY 2017 4 Key facts NHS Ambulance Services Key facts 1.78bn the cost of urgent and emergency
Transforming NHS ambulance services
 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1086 SESSION 2010 2012 10 JUNE 2011 Department of Health Transforming NHS ambulance services 4 Summary Transforming NHS ambulance services Summary 1 In
REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1086 SESSION 2010 2012 10 JUNE 2011 Department of Health Transforming NHS ambulance services 4 Summary Transforming NHS ambulance services Summary 1 In
IMPROVING UNSCHEDULED CARE IN WALES - UPDATE
 AGENDA ITEM No. 10 MEETING : TRUST BOARD DATE : 22 APRIL 2009 REPORT OF : CLINICAL DIRECTORATE Contact : Grayham McLean, Unscheduled Care Lead Officer Tel: 01792 562900 Email: grayham.mclean@ambulance.wales.nhs.uk
AGENDA ITEM No. 10 MEETING : TRUST BOARD DATE : 22 APRIL 2009 REPORT OF : CLINICAL DIRECTORATE Contact : Grayham McLean, Unscheduled Care Lead Officer Tel: 01792 562900 Email: grayham.mclean@ambulance.wales.nhs.uk
Analysis Method Notice. Category A Ambulance 8 Minute Response Times
 AM Notice: AM 2014/03 Date of Issue: 29/04/2014 Analysis Method Notice Category A Ambulance 8 Minute Response Times This notice describes an Analysis Method that has been developed for use in the production
AM Notice: AM 2014/03 Date of Issue: 29/04/2014 Analysis Method Notice Category A Ambulance 8 Minute Response Times This notice describes an Analysis Method that has been developed for use in the production
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report
 Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Recommendation 1. The Committee recommends that:
 Written Response by the Welsh Government to the report of the Petitions Committee entitled Mandatory Welsh legislation to ensure Defibrillators in all public places - Report on the Consideration of a Petition
Written Response by the Welsh Government to the report of the Petitions Committee entitled Mandatory Welsh legislation to ensure Defibrillators in all public places - Report on the Consideration of a Petition
INFORMATION STANDARDS GOVERNANCE PROCESS INFORMATION STANDARD DEVELOPMENT PROPOSAL FOR NEW OR CHANGED INFORMATION STANDARD
 INFORMATION STANDARDS GOVERNANCE PROCESS INFORMATION STANDARD DEVELOPMENT PROPOSAL FOR NEW OR CHANGED INFORMATION STANDARD Emergency Ambulance to A&E Handover Monitoring Information February 2008 DRAFT
INFORMATION STANDARDS GOVERNANCE PROCESS INFORMATION STANDARD DEVELOPMENT PROPOSAL FOR NEW OR CHANGED INFORMATION STANDARD Emergency Ambulance to A&E Handover Monitoring Information February 2008 DRAFT
Scottish Ambulance Service. Our Future Strategy. Discussion with partners
 Discussion with partners Our values Glossary of terms We will: put the patient at the heart of everything we do. treat each and every person well, with respect and dignity. always be open, honest and fair.
Discussion with partners Our values Glossary of terms We will: put the patient at the heart of everything we do. treat each and every person well, with respect and dignity. always be open, honest and fair.
Review of pre-hospital emergency care services to ensure high quality in the assessment, diagnosis, clinical management and transporting of acutely
 Review of pre-hospital emergency care services to ensure high quality in the assessment, diagnosis, clinical management and transporting of acutely ill patients to appropriate healthcare facilities 2 December
Review of pre-hospital emergency care services to ensure high quality in the assessment, diagnosis, clinical management and transporting of acutely ill patients to appropriate healthcare facilities 2 December
Note performance against the 30 minute standard for SAS call outs broken down by category of calls across NHS Highland Board area
 Argyll & Bute CHP Committee Date of Meeting: 27 October 2010 Item No: 11.3 UPDATE ON STRATEGIC OPTIONS FRAMEWORK FOR EMERGENCY AND URGENT RESPONSE IN REMOTE AND RURAL COMMUNITIES AND MEMORANDUM OF UNDERSTANDING
Argyll & Bute CHP Committee Date of Meeting: 27 October 2010 Item No: 11.3 UPDATE ON STRATEGIC OPTIONS FRAMEWORK FOR EMERGENCY AND URGENT RESPONSE IN REMOTE AND RURAL COMMUNITIES AND MEMORANDUM OF UNDERSTANDING
Ambulance Response Programme (ARP) Impact Assessment
 Impact Assessment") Ambulance Response Programme (ARP) Impact Assessment Executive Summary In 2015 the Ambulance Response Programme (ARP) commenced as a component of the Urgent and Emergency Care Review under the leadership
Ambulance Response Programme (ARP) Impact Assessment Executive Summary In 2015 the Ambulance Response Programme (ARP) commenced as a component of the Urgent and Emergency Care Review under the leadership
National Audit Office value for money study on NHS ambulance services
 National Audit Office value for money study on NHS ambulance services Robert White 7 February 2017 Introduction (1) Some key facts on the financial environment NHS 1.85bn net deficit of NHS bodies (NHS
National Audit Office value for money study on NHS ambulance services Robert White 7 February 2017 Introduction (1) Some key facts on the financial environment NHS 1.85bn net deficit of NHS bodies (NHS
Sponsoring director: Purpose: Decision Assurance For information Disclosable X Non-disclosable
 TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
NHS Wales Review of the 111 Pathfinder In Association with Janette Turner, University of Sheffield Final Report November 2017
 NHS Wales Review of the 111 Pathfinder In Association with Janette Turner, University of Sheffield Final Report November 2017 THE POWER OF BEING UNDERSTOOD AUDIT TAX CONSULTING TABLE OF CONTENTS NHS WALES
NHS Wales Review of the 111 Pathfinder In Association with Janette Turner, University of Sheffield Final Report November 2017 THE POWER OF BEING UNDERSTOOD AUDIT TAX CONSULTING TABLE OF CONTENTS NHS WALES
This paper explains the way in which part of the system is changing to become clearer and more accessible, beginning with NHS 111.
 Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
Unscheduled care in Haringey 1. Introduction There have been many changes to urgent, unscheduled and unplanned care over recent years. To begin with Casualty departments became Accident and Emergency departments,
Transforming Welsh Ambulance Service: scrapping times, supporting patients!
 Transforming Welsh Ambulance Service: scrapping times, supporting patients! Dr Brendan Lloyd Medical Director Welsh Ambulance Services Trust Founding Senior Fellow FMLM Dr John Kotter: Leading Change 8-stage
Transforming Welsh Ambulance Service: scrapping times, supporting patients! Dr Brendan Lloyd Medical Director Welsh Ambulance Services Trust Founding Senior Fellow FMLM Dr John Kotter: Leading Change 8-stage
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Centre for Health Technology Evaluation
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Centre for Health Technology Evaluation Increasing capacity within Technology Appraisals Consultation comments proforma Name Role Organisation E-Mail Address
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Centre for Health Technology Evaluation Increasing capacity within Technology Appraisals Consultation comments proforma Name Role Organisation E-Mail Address
NHS 111. Introduction. Background
 NHS 111 Introduction The NHS 111 service is being introduced to make it easier for the public to access healthcare services when they need medical help fast, but it s not a lifethreatening situation. The
NHS 111 Introduction The NHS 111 service is being introduced to make it easier for the public to access healthcare services when they need medical help fast, but it s not a lifethreatening situation. The
The management of chronic conditions by NHS Wales. 4 December
 The management of chronic conditions by NHS Wales 4 December 2008 www.wao.gov.uk I have prepared this report for presentation to the National Assembly under the Government of Wales Acts 1998 and 2006.
The management of chronic conditions by NHS Wales 4 December 2008 www.wao.gov.uk I have prepared this report for presentation to the National Assembly under the Government of Wales Acts 1998 and 2006.
Review of Emergency Ambulance Services Commissioning Arrangements
 Review of Emergency Ambulance Services Commissioning Arrangements Date issued: July 2017 Document reference: 261A2017 Status of report I have prepared and published this report under section 61 of the
Review of Emergency Ambulance Services Commissioning Arrangements Date issued: July 2017 Document reference: 261A2017 Status of report I have prepared and published this report under section 61 of the
National Collaborative Commissioning: Quality & Delivery Framework
 Frequently Asked Questions National Collaborative Commissioning: Quality & Delivery Framework Emergency Ambulance Services PREFACE Emergency Ambulance Services have a critical role to play in the provision
Frequently Asked Questions National Collaborative Commissioning: Quality & Delivery Framework Emergency Ambulance Services PREFACE Emergency Ambulance Services have a critical role to play in the provision
Supporting the acute medical take: advice for NHS trusts and local health boards
 Supporting the acute medical take: advice for NHS trusts and local health boards Purpose of the statement The acute medical take has proven to be a challenge across acute hospital trusts and health boards
Supporting the acute medical take: advice for NHS trusts and local health boards Purpose of the statement The acute medical take has proven to be a challenge across acute hospital trusts and health boards
Vanguard Programme: Acute Care Collaboration Value Proposition
 Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Response to NHS England s consultation on Supporting research in the NHS on excess treatment costs and clinical research set-up January 2018
 Response to NHS England s consultation on Supporting research in the NHS on excess treatment costs and clinical research set-up January 2018 Summary The Academy welcomes NHS England s proposals to better
Response to NHS England s consultation on Supporting research in the NHS on excess treatment costs and clinical research set-up January 2018 Summary The Academy welcomes NHS England s proposals to better
Prescription for Rural Health 2011
 Foreword Prescription for Rural Health is the Welsh NHS Confederation s contribution to the debate on health in rural Wales. This document has been published alongside Prescription for Health 2011, which
Foreword Prescription for Rural Health is the Welsh NHS Confederation s contribution to the debate on health in rural Wales. This document has been published alongside Prescription for Health 2011, which
The Welsh NHS Confederation s response to the inquiry into cross-border health arrangements between England and Wales.
 Welsh Affairs Committee. Purpose: The Welsh NHS Confederation s response to the inquiry into cross-border health arrangements between England and Wales. Contact: Nesta Lloyd Jones, Policy and Public Affairs
Welsh Affairs Committee. Purpose: The Welsh NHS Confederation s response to the inquiry into cross-border health arrangements between England and Wales. Contact: Nesta Lloyd Jones, Policy and Public Affairs
Explanatory Memorandum to the Mental Health (Secondary Mental Health Services) (Wales) Order 2012
 (Wales) Order 2012") Explanatory Memorandum to the Mental Health (Secondary Mental Health Services) (Wales) Order 2012 This Explanatory Memorandum has been prepared by the Department for Health, Social Services and Children
Explanatory Memorandum to the Mental Health (Secondary Mental Health Services) (Wales) Order 2012 This Explanatory Memorandum has been prepared by the Department for Health, Social Services and Children
National Ambulance Service (NAS) Workforce Support Policy. Protection of Lone Workers. Document developed by NASWS Document approved by
 Workforce Support Policy. Protection of Lone Workers. Document developed by NASWS Document approved by") National Ambulance Service (NAS) Workforce Support Policy Protection of Lone Workers Document reference number NASWS011 Document developed by Chief Ambulance Officer HR Revision number Approval date 4
National Ambulance Service (NAS) Workforce Support Policy Protection of Lone Workers Document reference number NASWS011 Document developed by Chief Ambulance Officer HR Revision number Approval date 4
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Surge Management. Prepared by NEAS Resilience,
 Surge Management Prepared by NEAS Resilience, 13.09.2017 Plans for Winter 2017/18 Overview of system within locality The Strategic principles of the NEAS Surge Management Plan are to ensure: Response standards
Surge Management Prepared by NEAS Resilience, 13.09.2017 Plans for Winter 2017/18 Overview of system within locality The Strategic principles of the NEAS Surge Management Plan are to ensure: Response standards
CT Scanner Replacement Nevill Hall Hospital Abergavenny. Business Justification
 CT Scanner Replacement Nevill Hall Hospital Abergavenny Business Justification Version No: 3 Issue Date: 9 July 2012 VERSION HISTORY Version Date Brief Summary of Change Owner s Name Issued Draft 21/06/12
CT Scanner Replacement Nevill Hall Hospital Abergavenny Business Justification Version No: 3 Issue Date: 9 July 2012 VERSION HISTORY Version Date Brief Summary of Change Owner s Name Issued Draft 21/06/12
Control: Lost in Translation Workshop Report Nov 07 Final
 Workshop Report Reviewing the Role of the Discharge Liaison Nurse in Wales Document Information Cover Reference: Lost in Translation was the title of the workshop at which the review was undertaken and
Workshop Report Reviewing the Role of the Discharge Liaison Nurse in Wales Document Information Cover Reference: Lost in Translation was the title of the workshop at which the review was undertaken and
Conveyance of Patients S6 Mental Health Act (Replaces Policy No. 182.Clinical)
") (Replaces Policy No. 182.Clinical) POLICY NUMBER TPMHA&MCA/103 VERSION NUMBER V.4 RATIFYING COMMITTEE Pan Sussex MHA Monitoring Committee DATE OF EQUALITY & HUMAN 01 August 2015 RIGHTS IMPACT ASSESSMENT
(Replaces Policy No. 182.Clinical) POLICY NUMBER TPMHA&MCA/103 VERSION NUMBER V.4 RATIFYING COMMITTEE Pan Sussex MHA Monitoring Committee DATE OF EQUALITY & HUMAN 01 August 2015 RIGHTS IMPACT ASSESSMENT
Recommendations of the NH Strategy
 Urgent care Newark Hospital should continue to provide sub-acute care1, based on the existing ambulance diversion protocol. Refine the ambulance protocol to include additional sub-acute presentations that
Urgent care Newark Hospital should continue to provide sub-acute care1, based on the existing ambulance diversion protocol. Refine the ambulance protocol to include additional sub-acute presentations that
Cardiff & Vale of Glamorgan Community Health Council
 MONITORING VISIT REPORT Service/ward monitored: Date/time: Monitoring team: UHB/Trust staff: Purpose of visit Brief description of area visited: Cardiff East Ambulance Station 14 th January 2015 2.00pm
MONITORING VISIT REPORT Service/ward monitored: Date/time: Monitoring team: UHB/Trust staff: Purpose of visit Brief description of area visited: Cardiff East Ambulance Station 14 th January 2015 2.00pm
Patient Pathway Guidelines:
 Welsh Ambulance Services NHS Trust: Patient Pathway Guidelines: For Fallers, Resolved Hypoglycaemia and Resolved Epileptic Seizures aged 18 years and over Version 1.7 DOCUMENT CONTROL SHEET Document Version
Welsh Ambulance Services NHS Trust: Patient Pathway Guidelines: For Fallers, Resolved Hypoglycaemia and Resolved Epileptic Seizures aged 18 years and over Version 1.7 DOCUMENT CONTROL SHEET Document Version
NHS 111 urgent care service
 NHS 111 urgent care service Frequently Asked Questions (FAQs) Contents Background 2 Operational 3 NHS Direct 5 999 5 101 6 Training 7 Service Impact 7 Telephony 8 Marketing 8 1 Background Why are you introducing
NHS 111 urgent care service Frequently Asked Questions (FAQs) Contents Background 2 Operational 3 NHS Direct 5 999 5 101 6 Training 7 Service Impact 7 Telephony 8 Marketing 8 1 Background Why are you introducing
NORTH WALES CLINICAL STRATEGY. PRIMARY CARE & COMMUNITY SERVICES SBAR REPORT February 2010
 NORTH WALES CLINICAL STRATEGY PRIMARY CARE & COMMUNITY SERVICES SBAR REPORT February 2010 Situation The Primary Care & Community Services workstream had been tasked with answering the following question:
NORTH WALES CLINICAL STRATEGY PRIMARY CARE & COMMUNITY SERVICES SBAR REPORT February 2010 Situation The Primary Care & Community Services workstream had been tasked with answering the following question:
Headline consensus statement
 Consensus Statement on Saving Lives and Improving Health and Wellbeing between the Association of Ambulance Chief Executives (AACE) and the Chief Fire Officers Association (CFOA) 17 th March 2016 1. This
Consensus Statement on Saving Lives and Improving Health and Wellbeing between the Association of Ambulance Chief Executives (AACE) and the Chief Fire Officers Association (CFOA) 17 th March 2016 1. This
Consultation on proposals to introduce independent prescribing by paramedics across the United Kingdom
 Patient and public summary for: Consultation on proposals to introduce independent prescribing by paramedics across the United Kingdom The full consultation document is available on the NHS England consultation
Patient and public summary for: Consultation on proposals to introduce independent prescribing by paramedics across the United Kingdom The full consultation document is available on the NHS England consultation
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
Evaluation of NHS111 pilot sites. Second Interim Report
 Evaluation of NHS111 pilot sites Second Interim Report Janette Turner Claire Ginn Emma Knowles Alicia O Cathain Craig Irwin Lindsey Blank Joanne Coster October 2011 This is an independent report commissioned
Evaluation of NHS111 pilot sites Second Interim Report Janette Turner Claire Ginn Emma Knowles Alicia O Cathain Craig Irwin Lindsey Blank Joanne Coster October 2011 This is an independent report commissioned
Transforming Mental Health Services Formal Consultation Process
 Project Plan for the Transforming Mental Health Services Formal Consultation Process June 2017 TMHS Project Plan v6 21.06.17 NOS This document can be made available in different languages and formats on
Project Plan for the Transforming Mental Health Services Formal Consultation Process June 2017 TMHS Project Plan v6 21.06.17 NOS This document can be made available in different languages and formats on
INVESTIGATION UNDER SECTION 17 OF THE WELSH LANGUAGE ACT Hywel Dda University Health Board
 INVESTIGATION UNDER SECTION 17 OF THE WELSH LANGUAGE ACT 1993 Hywel Dda University Health Board October 2014 Background The principal aim of the Welsh Language Commissioner, an independent body established
INVESTIGATION UNDER SECTION 17 OF THE WELSH LANGUAGE ACT 1993 Hywel Dda University Health Board October 2014 Background The principal aim of the Welsh Language Commissioner, an independent body established
Committee of Public Accounts
 Written evidence from the NHS Confederation AMBULANCE SERVICE NETWORK/NATIONAL AMBULANCE COMMISSIONING GROUP KEY LINES ON FUTURE MODELS FOR AMBULANCE SERVICE COMMISSIONING Executive Summary Equity and
Written evidence from the NHS Confederation AMBULANCE SERVICE NETWORK/NATIONAL AMBULANCE COMMISSIONING GROUP KEY LINES ON FUTURE MODELS FOR AMBULANCE SERVICE COMMISSIONING Executive Summary Equity and
cc: Emergency Ambulance Services Committee Members EMERGENCY AMBULANCE SERVICES COMMITTEE ANNUAL GOVERNANCE STATEMENT 2015/16
 EASC Agenda Item 4.5 Appendix 1 To: Mrs Allison Williams, Chief Executive, Cwm Taf University Health Board cc: Emergency Ambulance Services Committee Members EMERGENCY AMBULANCE SERVICES COMMITTEE ANNUAL
EASC Agenda Item 4.5 Appendix 1 To: Mrs Allison Williams, Chief Executive, Cwm Taf University Health Board cc: Emergency Ambulance Services Committee Members EMERGENCY AMBULANCE SERVICES COMMITTEE ANNUAL
Written Response by the Welsh Government to the report of the Health, Social Care and Sport Committee entitled Primary Care: Clusters
 Written Response by the Welsh Government to the report of the Health, Social Care and Sport Committee entitled Primary Care: Clusters I am grateful to the Committee for its inquiry into primary care. Clusters
Written Response by the Welsh Government to the report of the Health, Social Care and Sport Committee entitled Primary Care: Clusters I am grateful to the Committee for its inquiry into primary care. Clusters
GOVERNANCE REVIEW. Contact Details for further information: Pam Wenger, Committee Secretary.
 Joint Committee Meeting 26 January 2016 Title of the Committee Paper GOVERNANCE REVIEW Executive Lead: Chair Author: Committee Secretary Contact Details for further information: Pam Wenger, Committee Secretary.
Joint Committee Meeting 26 January 2016 Title of the Committee Paper GOVERNANCE REVIEW Executive Lead: Chair Author: Committee Secretary Contact Details for further information: Pam Wenger, Committee Secretary.
Independent Mental Health Advocacy. Guidance for Commissioners
 Independent Mental Health Advocacy Guidance for Commissioners DH INFORMATION READER BOX Policy HR / Workforce Management Planning / Performance Clinical Estates Commissioning IM&T Finance Social Care /
Independent Mental Health Advocacy Guidance for Commissioners DH INFORMATION READER BOX Policy HR / Workforce Management Planning / Performance Clinical Estates Commissioning IM&T Finance Social Care /
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Consultation on fee rates and fee scales
 Consultation on fee rates and fee scales 2016-17 Consultation on fee rates and fee scales 2016-17 Overview This consultation invites views and comments on the Wales Audit Office s proposals for: fee rates
Consultation on fee rates and fee scales 2016-17 Consultation on fee rates and fee scales 2016-17 Overview This consultation invites views and comments on the Wales Audit Office s proposals for: fee rates
Improving Healthcare Together : NHS Surrey Downs, Sutton and Merton clinical commissioning groups Issues Paper
 Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Future of Respite (Short Breaks) Services for Children with Disabilities
 Services for Children with Disabilities") Future of Respite (Short Breaks) Services for Children with Disabilities Consultation Feedback Report 2014 Foreword from the Director of Children s Services Within the Northern Trust area we know that
Future of Respite (Short Breaks) Services for Children with Disabilities Consultation Feedback Report 2014 Foreword from the Director of Children s Services Within the Northern Trust area we know that
NHS GRAMPIAN. Grampian Clinical Strategy - Planned Care
 NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
NHS GRAMPIAN. Local Delivery Plan - Section 2 Elective Care
 NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
Together for Health A Delivery Plan for the Critically Ill
 Together for Health A Delivery Plan for the Critically Ill 2013-2016 March 2015 Approved at CPG Board 25 th March 2015 1. BACKGROUND AND CONTEXT Together for Health a Delivery Plan for the Critically Ill
Together for Health A Delivery Plan for the Critically Ill 2013-2016 March 2015 Approved at CPG Board 25 th March 2015 1. BACKGROUND AND CONTEXT Together for Health a Delivery Plan for the Critically Ill
NHS GRAMPIAN. Clinical Strategy
 NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
The NHS Employers submission to the Migration Advisory Committee (MAC) call for evidence
 call for evidence") The NHS Employers submission to the Migration Advisory Committee (MAC) call for evidence Our organisation represents the whole range of views from across employing organisations in the NHS in England on
The NHS Employers submission to the Migration Advisory Committee (MAC) call for evidence Our organisation represents the whole range of views from across employing organisations in the NHS in England on
Primary Care Workforce Survey Scotland 2017
 Primary Care Workforce Survey Scotland 2017 A Survey of Scottish General Practices and General Practice Out of Hours Services Publication date 06 March 2018 An Official Statistics publication for Scotland
Primary Care Workforce Survey Scotland 2017 A Survey of Scottish General Practices and General Practice Out of Hours Services Publication date 06 March 2018 An Official Statistics publication for Scotland
Developing. National Service Frameworks
 Developing National Service Frameworks A guide for policy colleagues developing National Service Frameworks for Healthcare services in Wales 1 Background 1. National Service Frameworks (NSF) were originally
Developing National Service Frameworks A guide for policy colleagues developing National Service Frameworks for Healthcare services in Wales 1 Background 1. National Service Frameworks (NSF) were originally
UCAS. Welsh language scheme
 UCAS Welsh language scheme 2010-2013 Prepared under the Welsh Language Act 1993 Preface This is the Welsh language scheme (the scheme) presented by the Universities and Colleges Admissions Service (UCAS),
UCAS Welsh language scheme 2010-2013 Prepared under the Welsh Language Act 1993 Preface This is the Welsh language scheme (the scheme) presented by the Universities and Colleges Admissions Service (UCAS),
Capacity Plan. incorporating the Resourcing Escalatory Action Plan. (copy for external circulation)
") Capacity Plan incorporating the Resourcing Escalatory Action Plan (copy for external circulation) Index No: Capacity Plan (REAP) Page 1 of 8 1. BACKGROUND 1.1. For many years the London Ambulance Service
Capacity Plan incorporating the Resourcing Escalatory Action Plan (copy for external circulation) Index No: Capacity Plan (REAP) Page 1 of 8 1. BACKGROUND 1.1. For many years the London Ambulance Service
NHS Emergency Planning Guidance
 NHS Emergency Planning Guidance Planning for the development and deployment of Medical Emergency Response Incident Teams in the provision of advanced medical care at the scene of an incident NHS Emergency
NHS Emergency Planning Guidance Planning for the development and deployment of Medical Emergency Response Incident Teams in the provision of advanced medical care at the scene of an incident NHS Emergency
Internal Audit. Healthcare Governance. October 2015
 October 2015 Report Assessment G A G G G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted or
October 2015 Report Assessment G A G G G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted or
Briefing April 2017 Nuffield Winter Insight Briefing 3: The ambulance service
 Briefing April 2017 Nuffield Winter Insight Briefing 3: Prof. John Appleby and Mark Dayan has come to be a totemic symbol of the NHS in England, free at the point of use and available to all. It represents
Briefing April 2017 Nuffield Winter Insight Briefing 3: Prof. John Appleby and Mark Dayan has come to be a totemic symbol of the NHS in England, free at the point of use and available to all. It represents
Allied Health Review Background Paper 19 June 2014
 Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
Allied Health Review Background Paper 19 June 2014 Background Mater Health Services (Mater) is experiencing significant change with the move of publicly funded paediatric services from Mater Children s
Performance Evaluation Report Pembrokeshire County Council Social Services
 Performance Evaluation Report 2013 14 Pembrokeshire County Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Pembrokeshire County Council
Performance Evaluation Report 2013 14 Pembrokeshire County Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Pembrokeshire County Council
STEP 1: STEP 2: STEP 3: STEP 4: STEP 5: Version: 1.0 Document Reference: 7716
 Welsh Ambulance Services NHS Trust National Collaborative Commissioning: Quality and Delivery Framework Ambulance Quality Indicators: October - December 2017 STEP 1: STEP 2: STEP 3: STEP 4: STEP 5: AQI
Welsh Ambulance Services NHS Trust National Collaborative Commissioning: Quality and Delivery Framework Ambulance Quality Indicators: October - December 2017 STEP 1: STEP 2: STEP 3: STEP 4: STEP 5: AQI
Quarterly Reporting Template - Guidance
 Quarterly Reporting Template - Guidance Notes for Completion The data collection template requires the Health & Wellbeing Board to track through the high level metrics and deliverables from the Health
Quarterly Reporting Template - Guidance Notes for Completion The data collection template requires the Health & Wellbeing Board to track through the high level metrics and deliverables from the Health
SBAR Report phase 1 Maternity, Gynaecology & Neonatal services
 North Wales Maternity, Gynaecology, Neonatal and Paediatric service review SBAR Report phase 1 Maternity, Gynaecology & Neonatal services Situation The Minister for Health and Social Services has established
North Wales Maternity, Gynaecology, Neonatal and Paediatric service review SBAR Report phase 1 Maternity, Gynaecology & Neonatal services Situation The Minister for Health and Social Services has established
Medical and Clinical Services Directorate Clinical Strategy
 www.ambulance.wales.nhs.uk Medical and Clinical Services Clinical Strategy Unique reference No: Version: 1.4 Title of author: Medical and Clinical Services No of Pages: 11 Implementation date: Next review
www.ambulance.wales.nhs.uk Medical and Clinical Services Clinical Strategy Unique reference No: Version: 1.4 Title of author: Medical and Clinical Services No of Pages: 11 Implementation date: Next review
Provision of Adult Thoracic Surgery in South Wales Mid-Point Review
 Provision of Adult Thoracic Surgery in South Wales Mid-Point Review Status For Review Version Number 1.0 Publication Date 27th July 2018 V1.0 27 rd July 2018 2018 Contents 1. Introduction... 3 2. Context...
Provision of Adult Thoracic Surgery in South Wales Mid-Point Review Status For Review Version Number 1.0 Publication Date 27th July 2018 V1.0 27 rd July 2018 2018 Contents 1. Introduction... 3 2. Context...
Appendix 1: Integrated Urgent Care Service Update. 1. Purpose
 Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Introduction. The Care Quality Commission (CQC) monitors,
 monitors,") 1 2 Introduction The Care Quality Commission (CQC) monitors, inspects and regulates services to make sure they meet fundamental standards of quality and safety. It has a legal duty to listen to the things
1 2 Introduction The Care Quality Commission (CQC) monitors, inspects and regulates services to make sure they meet fundamental standards of quality and safety. It has a legal duty to listen to the things
Methods: Commissioning through Evaluation
 Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service E08/S/b Neonatal Intensive Care Transport Commissioner Lead Provider Lead Period Date of Review 12 Months 1. Population
SCHEDULE 2 THE SERVICES A. Service Specifications Service Specification No. Service E08/S/b Neonatal Intensive Care Transport Commissioner Lead Provider Lead Period Date of Review 12 Months 1. Population
Emergency Medicine Programme
 Emergency Medicine Programme Implementation Guide 8: Matching Demand and Capacity in the ED January 2013 Introduction This is a guide for Emergency Department (ED) and hospital operational management teams
Emergency Medicine Programme Implementation Guide 8: Matching Demand and Capacity in the ED January 2013 Introduction This is a guide for Emergency Department (ED) and hospital operational management teams
NATIONAL AMBULANCE SERVICE ONE LIFE PROJECT
 February 2015 NATIONAL AMBULANCE SERVICE ONE LIFE PROJECT Improving patient outcomes from Out Of Hospital Cardiac Arrest David Hennelly AP MSc Jan 2015 THE ONE LIFE PROJECT IS BEING LED BY THE NATIONAL
February 2015 NATIONAL AMBULANCE SERVICE ONE LIFE PROJECT Improving patient outcomes from Out Of Hospital Cardiac Arrest David Hennelly AP MSc Jan 2015 THE ONE LIFE PROJECT IS BEING LED BY THE NATIONAL
Sussex and East Surrey STP narrative
 Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Management of surge and escalation in critical care services: standard operating procedure for adult respiratory extra corporeal membrane oxygenation
 Management of surge and escalation in critical care services: standard operating procedure for adult respiratory extra corporeal membrane oxygenation 1 NHS England INFORMATION READER BOX Directorate Medical
Management of surge and escalation in critical care services: standard operating procedure for adult respiratory extra corporeal membrane oxygenation 1 NHS England INFORMATION READER BOX Directorate Medical
Policy Fire Services First Responder Schemes. National Ambulance Service (NAS)
") Policy Fire Services First Responder Schemes National Ambulance Service (NAS) Document reference number Revision number NASCG008 Document developed by 2 Document approved by Gearóid Oman, Paramedic Supervisor
Policy Fire Services First Responder Schemes National Ambulance Service (NAS) Document reference number Revision number NASCG008 Document developed by 2 Document approved by Gearóid Oman, Paramedic Supervisor
Mental Health (Wales) Measure Implementing the Mental Health (Wales) Measure Guidance for Local Health Boards and Local Authorities
 Measure Implementing the Mental Health (Wales) Measure Guidance for Local Health Boards and Local Authorities") Mental Health (Wales) Measure 2010 Implementing the Mental Health (Wales) Measure 2010 Guidance for Local Health Boards and Local Authorities Januar y 2011 Crown copyright 2011 WAG 10-11316 F6651011 Implementing
Mental Health (Wales) Measure 2010 Implementing the Mental Health (Wales) Measure 2010 Guidance for Local Health Boards and Local Authorities Januar y 2011 Crown copyright 2011 WAG 10-11316 F6651011 Implementing
The National Programme for IT in the NHS: an update on the delivery of detailed care records systems
 Report by the Comptroller and Auditor General HC 888 SesSIon 2010 2012 18 may 2011 Department of Health The National Programme for IT in the NHS: an update on the delivery of detailed care records systems
Report by the Comptroller and Auditor General HC 888 SesSIon 2010 2012 18 may 2011 Department of Health The National Programme for IT in the NHS: an update on the delivery of detailed care records systems
REABLEMENT SERVICE FOR NORTHERN IRELAND REGIONAL REABLEMENT PATHWAY. (for use by Health and Social Care Trusts)
") REABLEMENT SERVICE FOR NORTHERN IRELAND REGIONAL REABLEMENT PATHWAY (for use by Health and Social Care Trusts) July 2016 INDEX Section 1: Introduction - Regional Definition for Reablement - Regional Reablement
REABLEMENT SERVICE FOR NORTHERN IRELAND REGIONAL REABLEMENT PATHWAY (for use by Health and Social Care Trusts) July 2016 INDEX Section 1: Introduction - Regional Definition for Reablement - Regional Reablement
RESPONSE TO RECOMMENDATIONS FROM THE HEALTH & SOCIAL CARE COMMITTEE: INQUIRY INTO ACCESS TO MEDICAL TECHNOLOGIES IN WALES
 Recommendations 1, 2, 3 1. That the Minister for Health and Social Services should, as a matter of priority, identify means by which a more strategic, coordinated and streamlined approach to medical technology
Recommendations 1, 2, 3 1. That the Minister for Health and Social Services should, as a matter of priority, identify means by which a more strategic, coordinated and streamlined approach to medical technology
Performance Evaluation Report Gwynedd Council Social Services
 Performance Evaluation Report 2013 14 Gwynedd Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Gwynedd Council Social Services for the year
Performance Evaluation Report 2013 14 Gwynedd Council Social Services October 2014 This report sets out the key areas of progress and areas for improvement in Gwynedd Council Social Services for the year
Investment Committee: Extended Hours Business Case (Revised)
") PAPER 06 Investment Committee: Extended Hours Business Case (Revised) OVERALL STRATEGY 1. SaHF Care Closer to Home This Extended Hours Business Case is developed within the context of Shaping a Healthier
PAPER 06 Investment Committee: Extended Hours Business Case (Revised) OVERALL STRATEGY 1. SaHF Care Closer to Home This Extended Hours Business Case is developed within the context of Shaping a Healthier
North School of Pharmacy and Medicines Optimisation Strategic Plan
 North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
Cylchlythyr Circular
 Tŷ Afon, Heol Bedwas Bedwas, Caerffili, CF83 8WT Tŷ Afon, Bedwas Road Bedwas, Caerphilly CF83 8WT 029 2085 9696 www.hefcw.ac.uk Cylchlythyr Circular Global Challenges Research Fund: Institutional three-year
Tŷ Afon, Heol Bedwas Bedwas, Caerffili, CF83 8WT Tŷ Afon, Bedwas Road Bedwas, Caerphilly CF83 8WT 029 2085 9696 www.hefcw.ac.uk Cylchlythyr Circular Global Challenges Research Fund: Institutional three-year
Business Case Advanced Physiotherapy Practitioners in Primary Care
 1 Business Case Advanced Physiotherapy Practitioners in Primary Care 1.0 Introduction This scheme supports the sustainability of primary care and the move towards a first line prudent multi-professional
1 Business Case Advanced Physiotherapy Practitioners in Primary Care 1.0 Introduction This scheme supports the sustainability of primary care and the move towards a first line prudent multi-professional
Integrated Performance Report
 To provide a safe and effective healthcare service to all our communities in the East of England Integrated Performance Report Meeting Date: July 2016 Data: The month of June (May for Clinical & HART)
To provide a safe and effective healthcare service to all our communities in the East of England Integrated Performance Report Meeting Date: July 2016 Data: The month of June (May for Clinical & HART)
Care home services for older people
 Care home services for older people Procurement strategy - engagement report September 2017 1 CONTENTS: 1. Introduction.... 3 2. Language... 3 3. Survey analysis... 4 a) People living in care homes....
Care home services for older people Procurement strategy - engagement report September 2017 1 CONTENTS: 1. Introduction.... 3 2. Language... 3 3. Survey analysis... 4 a) People living in care homes....
Delivering surgical services: options for maximising resources
 Delivering surgical services: options for maximising resources THE ROYAL COLLEGE OF SURGEONS OF ENGLAND March 2007 2 OPTIONS FOR MAXIMISING RESOURCES The Royal College of Surgeons of England Introduction
Delivering surgical services: options for maximising resources THE ROYAL COLLEGE OF SURGEONS OF ENGLAND March 2007 2 OPTIONS FOR MAXIMISING RESOURCES The Royal College of Surgeons of England Introduction
Review of Voluntary Sector Support
 Executive Committee 25 th March 2014 Agenda Item No. Review of Voluntary Sector Support Report by: Michael Enston, Executive Director, Corporate Services Wards Affected: All Fife wards Purpose This report
Executive Committee 25 th March 2014 Agenda Item No. Review of Voluntary Sector Support Report by: Michael Enston, Executive Director, Corporate Services Wards Affected: All Fife wards Purpose This report
Implementing the Mental Health (Wales) Measure 2010
 Measure 2010") Implementing the Mental Health (Wales) Measure 2010 Guidance for Local Health Boards and Local Authorities on the Establishment of Joint Schemes for the Delivery of Local Primary Mental Health Support
Implementing the Mental Health (Wales) Measure 2010 Guidance for Local Health Boards and Local Authorities on the Establishment of Joint Schemes for the Delivery of Local Primary Mental Health Support
: Geraint Davies, Director of Commercial Services
 Report to : Trust Board of Directors Date of Report: 15/05/2015 Agenda Item: 0/15 Date of Meeting : 28 May 2015 Subject Report from Purpose : Report on Corporate Risk Register : Geraint Davies, Director
Report to : Trust Board of Directors Date of Report: 15/05/2015 Agenda Item: 0/15 Date of Meeting : 28 May 2015 Subject Report from Purpose : Report on Corporate Risk Register : Geraint Davies, Director
Facing the Future Audit 2017: Facing the Future: Standards for acute general paediatric services Facing the Future: Together for child health
 : Facing the Future: Standards for acute general paediatric services Facing the Future: Together for child health April 28 These Standards were audited with involvement from &US Young Inspectors For more
: Facing the Future: Standards for acute general paediatric services Facing the Future: Together for child health April 28 These Standards were audited with involvement from &US Young Inspectors For more
JOB DESCRIPTION DIRECTOR OF SCREENING. Author: Dr Quentin Sandifer, Executive Director of Public Health Services and Medical Director
 JOB DESCRIPTION DIRECTOR OF SCREENING Author: Dr Quentin Sandifer, Executive Director of Public Health Services and Medical Director Date: 1 November 2017 Version: 0d Purpose and Summary of Document: This
JOB DESCRIPTION DIRECTOR OF SCREENING Author: Dr Quentin Sandifer, Executive Director of Public Health Services and Medical Director Date: 1 November 2017 Version: 0d Purpose and Summary of Document: This