Training Bulletin. December Emergency Health Services Branch Ministry of Health and Long-Term Care. Issue Number 111 version 1.
|
|
|
- Martha Booker
- 5 years ago
- Views:
Transcription
1
2
3 Training Bulletin Deceased Patient Standard December 2010 Issue Number 111 version 1.0 Emergency Health Services Branch Ministry of Health and Long-Term Care
4
5 Training Bulletin, Issue Number 111 version 1.0 Deceased Patient Standard Introduction Paramedics are often called to respond to situations where a death, either expected or unexpected, occurs outside of a Health Care Facility. At times, these cases have resulted in prolonged scene attendance for paramedics if the death is not accepted as a coroner s investigation and there is difficulty in contacting or identifying a primary care physician to attend the scene to complete the Medical Certificate of Death (MCOD). Prolonged scene attendance at these types of calls may impact the ability for paramedics to respond to other emergency calls. In 2007, the Deceased in the Home Working Group (DHWG) was formed in the City of Toronto. The DHWG was tasked with developing and trialing alternate solutions for situations when an at home death occurred in an effort to reduce scene times for emergency personnel and reduce possible anxiety experienced by family members of the deceased due to delayed transfer of the deceased from the scene of the death. A trial of an alternate approach to dealing with deaths that occur outside of Health Care Facilities was implemented in the City of Toronto in June Following the success of this trial, it was decided that the new process would be implemented province-wide. This has lead to the development of a new Deceased Patient Standard for paramedics that will be integrated into the Basic Life Support Patient Care Standards (BLS PCS). This new standard will direct the practice of all paramedics in the province in cases where they are called to respond to a death occurring outside of a Health Care Facility. The Deceased Patient Standard will replace the existing Patients with Vital Signs Absent (Transportation) Standard found in Section 1 of the current version of the BLS PCS. This Training Bulletin has been developed to introduce paramedics to the new Deceased Patient Standard and to highlight the major differences between this new standard and the outgoing Patients with Vital Signs Absent (Transportation) Standard. A rationale for the changes, where applicable, has been included. A copy of the new Deceased Patient Standard has been included as an appendix to this bulletin (Appendix A) as a reference. As well, a copy of the Investigating Coroners Best Practice Guideline #5 Interaction of Investigating Coroners with Emergency Medical Services, Police, Body Removal Services and Funeral Services Arising from Death Investigations (Appendix B) has been included. This document will provide paramedics with information regarding the procedures that will be undertaken by Investigating Coroners in situations where death has occurred outside of a Health Care Facility. Deceased Patient Standard 1 December 2010 Issue Number 111-version 1.0
6 Explanations for Selected Definitions in the New Standard Definitions for terms relevant to the Deceased Patient Standard have been enhanced and organized into a specific section at the beginning of the Standard. The consolidation of the definitions in alphabetical order into a specific section at the beginning of the document will make it easier for paramedics to quickly find a definition should they require clarification of a term used in other sections of the standard. A more detailed definition for Deceased Patient has been included in the Standard. The definition takes into account several criteria that were not included in the Patients with Vital Signs Absent (Transportation) Standard, including; patients without vital signs and the subject of a Do Not Resuscitate Confirmation Form, patients without vital signs and the subject of a Termination of Resuscitation Order and patients without vital signs and the subject of a Withhold Resuscitation Order. This definition, along with the definition for Obviously Dead replaces the Criteria for Presuming Death section of the previous Standard. Several new definitions have been added to the Deceased Patient Standard to provide clarity. These include: Palliative Care Team Responsible Person Termination of Resuscitation Order Withhold Resuscitation Order Palliative Care Team means a team of health care professionals who provide palliative care to a terminally ill patient. Responsible Person means an adult who, in the reasonable belief of the paramedic, is capable to remain with the Deceased Patient and assume responsibility for the Deceased patient (i.e. an individual who can secure and control access to the scene until the coroner or the coroner s delegate arrives on the scene). Termination of Resuscitation Order means an order given by a physician, including a Base Hospital Physician, to a paramedic to stop resuscitation measures. Withhold Resuscitation Order means an order given by a physician, including a Base Hospital Physician, to a paramedic to not initiate resuscitation measures. Paramedics are obligated to initiate resuscitation for all patients except those who meet the criteria of obviously dead, patients who are the subject of a Do Not Resuscitate Confirmation Form or in cases where the paramedics are presented with a valid Medical Certificate of Death (MCOD). There may be some circumstances however, where a patient may be the subject of a Withhold Resuscitation Order and resuscitation is not initiated. Examples where resuscitation may be withheld include: a physician on the scene licensed to practice medicine in Ontario who has assumed responsibility for patient care gives a direct order not to initiate resuscitation; a distraught relative on the scene does not want the patient resuscitated and impedes access to the patient (paramedics should contact the Base Hospital Physician for direction in these cases). Deceased Patient Standard 2 December 2010 Issue Number 111-version 1.0
7 Explanations for Selected Procedures in the New Standard In All Cases of Death This area has been expanded within the Deceased Patient Standard to provide additional direction to paramedics in all cases of death. This area has also been moved forward in the Procedures Section of the standard to a more logical position reflecting the fact that it applies in all cases where death occurs whether it is expected or not. If termination of resuscitation occurs in the ambulance enroute to a health care facility, the crew will advise dispatch to contact the coroner, and continue to the destination unless otherwise directed by dispatch. Paramedics should follow any local policies with regard to specifically where in the health care facility the deceased patient is to be taken on their arrival (e.g. Morgue vs. ER). Paramedics should also be aware that in all cases of death where the coroner has assumed jurisdiction, all directions issued by the coroner or a person appointed by a coroner or to whom a coroner has delegated any powers are to be followed. In Cases of Obvious or Unexpected Death This area has been expanded to include direction to paramedics regarding procedures they must follow in cases where a coroner or police services are not on the scene of an obvious or unexpected death. In such cases, paramedics are to advise dispatch of the death and dispatch will notify the police or coroner. If dispatch is told that neither the police nor coroner can attend the scene in a timely fashion, dispatch will immediately seek further direction from the coroner concerning the responsibilities of the paramedics including whether they may leave the scene. Paramedics are to remain on the scene until they receive further notification from dispatch. In Cases of Expected Death Palliative Care Team members have now been included as a contact (in addition to the primary care physician) in cases where a patient has been receiving palliative care in the home. This change reflects current practice of providing care and support to terminally ill patients by a multidisciplinary Palliative Care Team. If the primary care physician or Palliative Care Team member cannot be contacted or if they are not able to attend the scene, or there is no Responsible Person who can remain on the scene until the primary care physician or Palliative Care Team member arrives, the paramedic crew must advise dispatch of the situation in which case, dispatch will notify the police or coroner of the death and that there is no one at the scene who can take responsibility for the deceased patient. If requested by the coroner, paramedics will provide the coroner with the circumstances of the death. Based on the circumstances, the Investigating Coroner will either release the paramedic crew from the scene or instruct the crew to remain on the scene until the coroner or their designate can attend the scene and assume responsibility for the deceased patient. This process will allow for a quicker release of paramedic crews from the scene in circumstances where the coroner determines that their continued attendance is not necessary. Deceased Patient Standard 3 December 2010 Issue Number 111-version 1.0
8 Process on Scene In the event that the coroner or their designate has not arrived on scene within a reasonable period of time, paramedics should contact dispatch and request an update on their estimated time of arrival. Summary It is anticipated that the implementation of the Deceased Patient Standard for paramedics in conjunction with the release of the Investigating Coroners Best Practice Guidelines #5 by the Office of the Chief Coroner will result in: Increased utilization of MCODs by primary care practitioners; Decreased utilization of MCODs by Investigating Coroners; Earlier release of EMS personnel and police from scenes where a death has occurred. Paramedics need to review and become familiar with the new Deceased Patient Standard. Paramedics are also encouraged to review the Investigating Coroners Best Practice Guideline #5 to familiarize themselves with the procedures that will be undertaken by Investigating Coroners in circumstances where death has occurred outside of a Health Care Facility. It should be noted that Section 1-General Standard of Care- of the Basic Life Support Patient Care Standards will be updated to include the new Deceased Patient Standard at a later date. Paramedics who have any questions regarding the Deceased Patient Standard should direct them to the ambulance service management or training division for clarification. Deceased Patient Standard 4 December 2010 Issue Number 111-version 1.0
9 Appendix A Deceased Patient Standard
10
11 Emergency Health Services Branch, Ontario Ministry of Health and Long-Term Care Deceased Patient Standard APPENDIX A All patients will be deemed to be viable and will be treated as living persons and provided with the care and transportation required, unless they are Deceased Patients as defined in this standard. Definitions: For the purposes of this Standard, the following definitions shall apply: Deceased Patient means a patient who is: a) Obviously dead; b) the subject of a medical certificate of death, presented to the paramedic crew, in the form that is prescribed by the Vital Statistics Act and that appears on its face to be completed and signed in accordance with that Act; c) without vital signs and the subject of a Do Not Resuscitate Confirmation Form; d) without vital signs and the subject of a Termination of Resuscitation Order given by a physician, including a Base Hospital Physician; or e) without vital signs and the subject of a Withhold Resuscitation Order given by a physician, including a Base Hospital Physician. Expected Death means a death that was imminently anticipated generally as a result of a progressive end stage terminal illness. Obviously Dead means death has occurred if gross signs of death are obvious, including by reason of: a) decapitation, transection, visible decomposition, putrefaction; or b) absence of vital signs and: i) a grossly charred body; ii) an open head or torso wounds with gross outpouring of cranial or visceral contents; iii) gross rigor mortis (i.e. limbs and/or body stiff, posturing of limbs or body); or iv) lividity (i.e. fixed, non-blanching purple or black discolouration of skin in dependent area of body). Palliative Care Team means a team of health care professionals who provides palliative care to a terminally ill patient. Responsible Person means an adult who, in the reasonable belief of the paramedic, is capable to remain with the Deceased Patient and assume responsibility for the Deceased Patient. Termination of Resuscitation Order means an order given by a physician, including a Base Hospital Physician, to a paramedic to stop resuscitation measures. Basic Life Support Patient Care Standards January 2011 Section 1 General Standard of Care A-1
12 Emergency Health Services Branch, Ontario Ministry of Health and Long-Term Care Unexpected Death means a death that was not imminently anticipated, including traumatic deaths, deaths related to the environment, accidental deaths, and medical deaths not imminently anticipated. Withhold Resuscitation Order means an order given by a physician, including a Base Hospital Physician, to a paramedic to not initiate resuscitation measures. Procedure In All Cases of Death The procedures in this section are to be followed once a patient is considered to be a Deceased Patient. 1. Document the history, patient assessment and patient care procedures (including the results of all such procedures) on the Ambulance Call Report. 2. Each paramedic will ensure that the Deceased Patient is treated with respect and dignity. 3. In cases of suspected foul play, follow the directions set out in the Police Notification Standard. 4. If applicable, follow all directions issued by a coroner or a person appointed by a coroner or to whom a coroner has delegated any powers or authority pursuant to the Coroners Act (Ontario). 5. If termination of resuscitation occurs in the ambulance enroute to a health care facility, the paramedic crew will advise dispatch to contact the coroner, and continue to the destination unless otherwise directed by dispatch. In Cases of Obvious or Unexpected Death 1. In the absence of police or a coroner on scene, advise dispatch of the death, in which case dispatch shall notify the police or coroner. 2. If a coroner indicates that he or she will attend at the scene, then the paramedic crew shall remain at the scene until the coroner arrives and assumes custody of the Deceased Patient. If the coroner indicates that he or she will not attend at the scene, paramedics will remain on the scene until the arrival of a person appointed by a coroner or to whom a coroner has delegated any powers or authority pursuant to the Coroners Act (Ontario). 3. Where dispatch notifies the police or coroner under Paragraph 1 and at any time dispatch is told that neither police nor coroner can attend the scene in a timely fashion, dispatch shall immediately, a) seek further direction from the coroner concerning the responsibilities of the paramedics, including whether they may leave the scene, and b) advise the paramedics to remain on the scene until further notification by dispatch. Where at any time the paramedics have not received any further direction under Subparagraph 3(a) above, the paramedics may request that dispatch seek direction from the coroner concerning their responsibilities, including whether they may leave the scene. A-2 Basic Life Support Patient Care Standards January 2011 Section 1 General Standard of Care
13 Emergency Health Services Branch, Ontario Ministry of Health and Long-Term Care In Cases of Expected Death 1. Advise dispatch of the death. 2. Make a request of a Responsible Person, if one is present, to notify the primary care physician or a member of the Palliative Care Team (if any) of the patient and request their attendance at the scene. 3. If the Responsible Person is unable to provide the notice in Paragraph 2 above, advise dispatch of the death, in which case dispatch shall attempt to notify the primary care physician or member of the Palliative Care Team (if any) of the Deceased Patient, and request their attendance at the scene. 4. If the Deceased Patient s primary care physician or Palliative Care Team member is contacted and indicates that he or she will attend at the scene, then the paramedic crew shall remain at the scene until their arrival. 5. Notwithstanding Paragraph 4 above, if there is a Responsible Person present, and the paramedics reasonably believe that the Responsible Person will remain until the primary care physician or Palliative Care Team arrives, then the paramedics may depart as soon as documentation has been completed or they are assigned to another call. If the police are at the scene and are willing to remain until the arrival of the physician or Palliative Care Team member, the paramedics may leave the scene. 6. If the primary care physician or Palliative Care Team member cannot be contacted or if none of them are able to attend, or there is no Responsible Person on scene, the paramedic crew shall so advise dispatch, in which case dispatch shall notify the police or coroner of the death and that there is no one else at the scene who can take responsibility for the Deceased Patient. 7. If requested by the coroner, paramedics will provide the coroner with the circumstances of the death. Paramedics will either be released from the scene or instructed to remain with the Deceased Patient until the coroner or a person appointed by a coroner or to whom a coroner has delegated any powers or authority pursuant to the Coroners Act (Ontario) or a Responsible Person can attend the scene and assume responsibility for the Deceased Patient. Basic Life Support Patient Care Standards January 2011 Section 1 General Standard of Care A-3
14
15 Appendix B Investigating Coroners Best Practice Guideline #5
16
17 Best Practice Guideline #5 Interaction of Investigating Coroners with Emergency Medical Services, Police, Body Removal Services, and Funeral Services Arising from Death Investigations Introduction Emergency Medical Services (EMS) personnel and police officers are most often the first to respond to a death that occurs outside of a Health Care Facility (e.g. private residence). In many cases, the practice is for the first responders to contact the on-call Investigating coroner to ascertain whether or not the death meets criteria set out in Section 10 of the Coroners Act. The police and/or EMS personnel must carefully consider such matters as scene integrity, investigative issues, family concerns and disposition of the body. These matters may be further complicated for EMS personnel and/or police if the death is not accepted as a coroner's investigation. At times, this has resulted in prolonged scene attendance for EMS personnel and police, particularly where there is no identified primary care practitioner, or he/she cannot be reached to complete the Medical Certificate of Death (MCOD). Prolonged scene attendance, not only ties up the availability of EMS personnel and police to respond to other calls, but it may cause additional anxiety to the family of the deceased, as the transfer of the deceased from the death scene is also delayed. In 2007, the Deceased in the Home Working Group (DHWG) was formed in the City of Toronto to develop and trial alternate solutions for situations when an "at home" death occurred and: 1. It was expected; and 2. It was not accepted by the coroner for investigation; and 3. The primary care practitioner was not available to complete the MCOD (i.e. because one did not exist, or would not attend, or could not be located). The DHWG was comprised of members from: EMS, the College of Physicians and Surgeons of Ontario, the Toronto Police Service, Investigating coroners, the Office of the Chief Coroner, Body Removal Services, Toronto Funeral Services, and the Sunnybrook Osler Centre for Pre-Hospital Care. Processes were developed for unexpected deaths, expected deaths (see flowcharts), and obvious deaths. The principles discussed by the DHWG included the following: 1. Coroners do not have legislative authority to investigate all deaths; their jurisdiction arises 'from Sections 10 and 15 of the Coroners Act. Best Practice Guideline #5: 1of 12 Interaction of Investigating Coroners with Emergency Medical Services, Police, Body Removal Services, and Funeral Services Arising from Death Investigations Issued: Date for review:
18 2. Coroners ate not an appropriate default for death certification with respect to lack of available primary care practitioners or refusal of primary care practitioners to attend in natura,1 death circumstances. 3. Primary care practitioners have a duty of care to a patient prior to his/her death; "When death of the patient at home is the expected outcome, the health care professional responsible for signing the MCaD is to be designated in advance. It is not acceptable to rely on the coroner to certify the death".1 4. Police and EMS personnel have encountered situations illustrated in #3 above with increasing frequency, and their involvement can be unnecessarily prolonged as processes do not exist for their timely release from expected natural death scenes, even when advanced directives such as outlined in the "Do Not Resuscitate Confirmation Form To Direct the Practice of Paramedics and Firefighters after February 1,2008,,2 existed. 5. Customarily, body removal and funeral services will not transport decedents in the absence of a Coroner's Warrant for Post Mortem Examination, a Warrant to Bury the Body of a Deceased Person, or a MCaD. The DHWG proposed alternate solutions included the following: 1. Body removal services and funeral services agreed to accept bodies and tra,nsport to the funeral home of the family's choice, where the death was an expected natural death in the home (and therefore not a coroner's case) in the absence of the documents cited in #5 above, provided that: A. A primaty care practitioner existed and temporarily could not be located; or, B. A primary care practitioner existed, but could not attend at the time of death; c. and, An Investigating coroner directed the tra,nsport of the deceased to the funeral home. This transport would occur at the family's expense. 2. The funeral director, working cooperatively with the family, police and the Investigating coroner, would contact the primary care practitioner at the eatliest time possible and request that the MCaD be completed. 3. If completion of the MeOD could not be achieved within a reasonable period of time, (generally within 24 hours, or earlier, if there are pressing plans for burial or cremation), the coroner would then accept the death for investigation. 1 Decision making for the End of Life, Policy #1-06, The College of Physicians and Surgeons of Ontario, July 2006, pg Verbeek Rand Sherwood C, End-of-Life care in the home; how a new procedure for Ontario paramedics and fire 'nghters may affect your patients and your practice, Ontario Medical Review, November 2007, pg. 43. Best Practice Guideline #5: 2 of 12 Interaction of Investigating Coroners with En1ergency Medical Services, Police, Body Removal Services, and Funeral Services Arising from Death Investigations Issued: Date for review:
19 4. If the death was an expected death, but there was no primary care practitioner, the coroner would accept the case immediately. Two consensus solutions that allowed the alternate approach to develop were: 1. The willingness of body removal services and funeral services to transport and accept bodies in the absence of a Coroner's Warrant for Post Mortem Examination, a Warrant to Bury the Body of a Deceased Person, or a MCaD. 2. The agreement by the Chief Coroner that if a body has been transferred to a funeral home and the prima,ry care practitioner could not be located to complete the MCaD, the case would be accepted by a coroner for investigation. A project implementing the alternate approach was launched in the City of Toronto in June 2009 and was trialed successfully. The anticipated outcomes of this project were that there would be: Increasing acceptance by primary care practitioners to complete MCaDs; Decreased utilization of Investigating coroners to complete MCaDs; Earlier release of police and EMS personnel from death scenes. Given the success of the DHWG project in Toronto, it will now be implemented province-wide. Purpose 1. To create a uniform provincial policy for management of death scenes where Investigating coroners interact with EMS personnel and police. 2. To provide Investigating coroners with new tools to assist in timely disposition of decedents, particularly where the deaths are expected and/or anticipated and therefore outside of the coroner's jurisdiction. 3. To streamline EMS and police approaches at death scenes following the direction of the Investigating coroner and therefore, reduce the time commitment at death scenes by emergency first responders. 4. To provide unifying principles to manage decedents where the death is accepted as a coroner's case throughout the province. Best Practice Guideline #5: 3 of 12 Interaction of Investigating Coroners with Emergency Medical Services, Police, Body Ren10val Services, and Funeral Services Arising from Death Investigations Issued: Date for review:
20 Legislative Authority Police assistance 9. (1) The police force having jurisdiction in the locality in which a coroner has jurisdiction shall make available to the coroner the assistance of such police officers as are necessary for the purpose of carrying out the coroner's duties. 2009, c. 15, s. 5 Interference with body 11. No person who has reason to believe that a person died in any of the circumstances mentioned in Section 10 shall interfere with or alter the body or its condition in any way until the coroner so directs by a warrant. R.S.O. 1990, c. C.37, s. 11. Investigative powers 16. (1) A coroner may, (a) examine or take possession of any dead body, or both; and (b) enter and inspect any place where a dead body is and any place from which the coroner has reasonable grounds for believing the body was removed. R.S.O. 1990, c. C.37, s. 16 (1); 2009, c. 15, s. 8. (2) A coroner who believes on reasonable and probable grounds that to do so is necessary for the purposes of the investigation may, (a) inspect any place in which the deceased person was, or in which the coroner has reasonable grounds to believe the deceased person was, prior to his or her death; (b) inspect and extract information from any records or writings relating to the deceased or his or her circumstances and reproduce such copies there from as the coroner believes necessary; (c) seize anything that the coroner has reasonable grounds to believe is material to the purposes of the investigation. R.S.O. 1990, c. C.37, s. 16 (2). Guiding Principle The patient will be deceased as per the Deceased Patient Standard within the Basic Life Support Patient Care Standards (BLS). The BLS states the Ministry of Health and Long-Term Care expectations with respect to how paramedics will interact with their patients, and constitute the minimum standards for patient care for all levels of paramedics in Ontario. (See Appendix A) Best Practice Guideline #5: 4 of 12 Interaction of Investigating Coroners with Enlergency Medical Services, Police, Body Renloval Services, and Funeral Services Arising from Death Investigations Issued: Date for review:

21 Cases of Unexpected Deaths These cases will generally be referred to the coroner by the police, or at times, EMS personnel pursuant to Section 10 of the Coroners Act. Possible outcomes are: A. Coroner accepts the case for investigation 1. If the coroner accepts the case for investigation, the police service will be asked to remain and EMS personnel will generally be released from the scene. 2. If the police are not present, the EMS personnel will remain on the scene until it has been secured by the police, or alternatively, until the Investigating coroner directs that EMS personnel may be released from the scene. 3. Patient care documentation will be provided to the Investigating coroner by EMS personnel, pursuant to Section 16 of the Coroners Act, upon request. Completion of a Coroner's Authority (or Delegated Authority) to Seize During an Investigation is unnecessary. 4. EMS personnel will communicate with the Investigating coroner regarding the disposition of any records. EMS personnel may leave documentation at the scene with the Investigating coroner, his/her delegate or the responsible caregiver, including the Ambulance Call Reporl (ACR) or Patient Care Record. Where the documentation is left with a caregiver, it will be placed in a sealed envelope, wherever possible. The ambulance service may also provide this documentation to the Investigating coroner via electronic transmission or fax. 5. The Investigating coroner will attend the scene, examine the body, and provide further direction regarding disposition of the decedent. B. Coroner does not accept the case for investigation While many deaths outside of health care facilities are perceived as sudden and unexpected from the perspective of family members or first responders, careful scrutiny by the experienced physician coroner will often determine that the death does not meet Section 10 criteria and therefore does not require investigation. An illustrative case example is of a 62 year old man who was observed by his spouse to collapse in his kitchen. He had a pacemaker and was being treated for congestive heart failure. The five year mortality for congestive heart failure in men is 50%. 3 Information indicated that his death appeared clearly arrhythmogenic and therefore his death was not unexpected to the Investigating coroner. However, it is unlikely that a plan for a health care professional to attend at the home to certify death would have been discussed/arranged given the decedent had been apparently well and relatively mobile prior to collapse. 3 Best Practice Guideline #5: 5 of 12 Interaction of Investigating Coroners with Emergency Medical Services, Police, Body Ren10val Services, and Funeral Services Arising from Death Investigations Issued: Date for review:

22 In these situations, the following should occur: 1. The Investigating coroner on call will be contacted by EMS personnel or police to discuss the circumstances following verification of death. 2. EMS personnel will remain on the scene until the police arrive, or may depart if a responsible person is present and with the knowledge of the Investigating Coroner on call. 3. The Investigating coroner on call will attempt to contact the primary care practitioner with the assistance of the police. 4. The Investigating coroner on call may utilize the Case Selection Data Form for Natural Deaths to guide his/her case selection decision. 4 The Investigating coroner would utilize and complete the form. The completed form and an invoice would be submitted within one business day to the Regional Supervising Coroner, when not accepting it as a case for investigation. 5. If the death was an expected death, but there was no primary care practitioner involved or their practice is not within reasonable proximity, the Investigating coroner will accept the case immediately. 6. If the primary care practitioner cannot be located in a reasonable period of time, or is unwilling to attend the scene in a timely manner, the Investigating coroner can direct a funeral service provider to transfer the body to the funeral home of the family's choice. The family will incur the expense of the transport as part of the funeral costs. 7. The Investigating coroner will be responsible to arrange a plan for the funeral home in the event that the primary care practitioner does not complete the MCOD within 24 hours. This may include providing the funeral home a contact method to reach the initial Investigating coroner or alternatively, the Investigating coroner will provide the case data to the next scheduled Investigating coroner and will ensure that the funeral home is aware of the contact method. 8. The primary care practitioner can then attend at the funeral home to complete the MCOD within a reasonable time period. The Investigating coroner on call will not accept the case for investigation. If the desired funeral home is not within reasonable proximity, there should be consideration for immediate involvement of the Investigating coroner. 9. If the primary care practitioner does not complete the MCOD within 24 hours, the funeral home will contact the Investigating coroner on call, who will then accept the case for investigation and complete the MCOD. If the funeral process is to be expedited to accommodate religious or conscience-based beliefs, the Investigating coroner on call may be contacted earlier. 4 See Investigating Coroners Best Practice Guideline #4 Investigating Coroners' Acceptance of Natural Deaths for Investigation. Best Practice Guideline #5: 6 of 12 Interaction of Investigating Coroners with Emergency Medical Services, Police, Body Removal Services, and Funeral Services Arising from Death Investigations Issued: Date for review:
23 Unexpected Death: A death that was not imminently anticipated. e.g. traumatic deaths, deaths related to the environment, accidental deaths, and medical deaths not imminently anticipated, such as sudden cardiac arrest. (NB: This definition is for the purposes of paramedics, and not necessarily coroners.) Investigating coroner On Call Contacted NO Coroner Investigation Coroner Investigation Coroner attempts to Contact Primary MD EMS Clears if Body Remains in Custody of Police until Coroner Attends Primary MD WILL ATTEND In Timely Fashion Primary MD CANNOT be contacted or WILL NOT ATTEND or WILL BE DELAYED EMS Clears if Body remains in custody of Police or Family Coroner Contacts Funeral Service Provider Primary MD Completes Death Certificate EMS Clears if Body remains in custody of Police or Family Funeral Service Provider Called by Family Funeral Service Provider Retrieves Body Coroner Completes Medical Certificate of Death if Primary MD NOT AVAILABLE Best Practice Guideline #5: 7 of 12 Interaction of Investigating Coroners with Emergency Medical Services l Police l Body Removal Services l and Funeral Services Arising from Death Investigations Issued: Date for review:
24 Cases of Expected Deaths Paramedics and firefighters are expected to honour a DNR Confirmation Form, and all other first responders are encouraged to do so as well. 1. EMS personnel will remain on the scene until the police arrive, or may depart if a responsible person is present. 2. EMS personnel will request that the family notify the primary care practitioner or palliative care team to request their attendance to complete a MeOD. 3. If the family cannot comply, EMS personnel will discuss with their dispatch and request that a primary care practitioner or palliative team member be contacted to attend. 4. If the primary care practitioner or the palliative care team member cannot be located or cannot attend, the police or dispatch will notify the Investigating coroner on call. 5. The Investigating coroner on call will attempt to contact the primary care practitioner with the assistance of the police. 6. The Investigating coroner on call may utilize the Case Selection Data Form for Natural Deaths to guide his/her case selection decision. 5 The Investigating coroner on call would utilize and complete the form. The completed form and an invoice would be submitted within one business day to the Regional Supervising Coroner, when not accepting it as a case for investigation. 7. If the death was an expected death, but there was no primary care practitioner involved or their practice is not within reasonable proximity, the Investigating coroner will accept the case immediately. 8. If the primary care practitioner can not be located in a reasonable period of time, or is unwilling to attend the scene in a timely manner, the Investigating coroner can direct a funeral service provider to transfer the body to the funeral home of the family's choice. The family will incur the expense of the transport as part of the funeral costs. 5 See Investigating Coroners Best Practice Guideline #4 Investigating Coroners' Acceptance of Natural Deaths for Investigation. Best Practice Guideline #5: 8 of 12 Interaction of Investigating Coroners with Emergency Medical Services, Police, Body Removal Services, and Funeral Services Arising from Death Investigations Issued: Date for review:
25 9. The Investigating coroner will be responsible to arrange a plan for the funeral home in the event that the primary care practitioner does not complete the MCOD within 24 hours. This may include providing the funeral home a contact method to reach the initial Investigating coroner or alternatively, the Investigating coroner will provide the case data to the next scheduled coroner and will ensure that the funeral home is aware of the contact method. 10. The primary care practitioner can then attend at the funeral home to complete the MCOD within a reasonable time period. The Investigating coroner on call will not accept the case for investigation. If the desired funeral home is not within reasonable proximity, there should be consideration for immediate involvement of the Investigating coroner. 11. If the primary care practitioner does not complete the MCOD within 24 hours, the funeral home will contact the Investigating coroner on call who will then accept the case for investigation and complete the MCOD. If the funeral process is to be expedited to accommodate religious or conscience-based beliefs, the Investigating coroner on call may be ca,lled earlier. Best Practice Guideline #5: 9 of 12 Interaction of Investigating Coroners with Emergency Medical Services, Police, Body Removal Services, and Funeral Services Arising from Death Investigations Issued: Date for review:
26 Expected Death: A Death that was imminently anticipated generally as a result of a progressive end stage terminal illness, such as cancer. (NB: This definition is for the purposes of paramedics, and not necessarily coroners.) \. Family or EMS Contacts Primary MD or Palliative Care Nurse I / Primary MD/Nurse WILL ATTEND EMS Clears if Body Remains in Custody of Police or Family," ' Primary MD/Nurse CANNOT be contacted or Primary MD/Nurse WILL NOT ATTEND or WILL BE DELAYED [ Contact Coroner 1 / EMS Clears if Body Remains in Custody of Police or FarTlily \. Coroner calls Primary MD INurse or Funeral Service Provider as per Unexpected Death Protocol Best Practice Guideline #5: 10 of 12 Interaction of Investigating Coroners with Emergency Medical Services, Police, Body Removal Services, and Funeral Services Arising from Death Investigations Issued: Date for review:
 may not occur unless directed by the coroner.")
27 Transport Decisions When Termination of Resuscitation is Ordered Principles 1. As outlined in Section 11 of the Coroners Act, if there is reason to believe that the death may require involvement of a coroner, interference with the body (i.e. movement or alteration of medical equipment) may not occur unless directed by the coroner. This authority supersedes any standard, policy or regulation in any other Act. 2. A deceased person should generally not be returned to a residence from which he/she has been removed. 3. Effective communication between the Investigating coroner, the police and the paramedics is of the utmost importance. Case specific plans should take into account operational issues for both the coroner and the EMS, 4. Coroners prefer that the body of the deceased person remain at the death scene. There have been instances in Ontario where removal of a deceased person has seriously hampered a death investigation. 5. The above noted procedures (Cases of Unexpected Deaths and Cases of Expected Deaths) are applicable in these cases (i.e. termination of resuscitation may occur in a natural death at home that after discussion with the Coroner does not require an investigation). Procedure 1. When an order for termination of resuscitation arising from the Deceased Patient Standard is received in the field, and the deceased person has not been removed from the place of death, paramedics should not remove the body. The applicable procedure (Cases of Unexpected Deaths and Cases of Expected Deaths) will be followed. 2. If the deceased has been moved to the ambulance, and the ambulance has not yet departed the scene, dispatch must be notified and contact with the coroner 6 will be made to determine the appropriate next steps prior to departure from the scene. The paramedics should apprise the coroner of any operational concerns regarding ambulance service/coverage issues that may arise by maintaining the body in the ambulance and holding the ambulance at the scene. The coroner should facilitate appropriate next steps to allow a rapid return of the ambulance to service. The paramedics and the coroner should discuss each case in which there was a Termination of Resuscitation Death. The ultimate decisions regarding disposition of the deceased should be documented. 6 Contact with the Coroner can be made by paramedics or dispatch according to established local protocols. Best Practice Guideline #5: 11 of 12 Interaction of Investigating Coroners with Emergency Medical Services Police, Body Removal Services, and Funeral Services l Arising from Death Investigations Issued: Date for review:
28 3. If the ambulance is in motion when resuscitation is terminated, paramedics should continue to the nearest hospital emergency department as the family will most likely be en-route concurrently. The body shall be transferred to an appropriate hospital area that will allow family attendance with the decedent in a dignified manner. Paramedics must notify the coroner of the death and location of the decedent. The paramedics should discuss with the Investigating coroner where the patient care documentation (e.g. ACR) will be left for the coroner. Such documentation may also be provided to the Investigating coroner via electronic transmission or fax. Appropriate documentation of the identity of the decedent should be affixed to the body, where possible, by the paramedics. Bibliography 1. Verbeek R and Sherwood C, End-of-Life care in the home; how a new procedure for Ontario paramedics and fire fighters may affect your patients and your practice, Ontario Medical Review, November The Coroners Act R.S.O Decision making for the End of Life, Policy #1-06, The College of Physicians and Surgeons of Ontario, July Investigating Coroners Best Practice Guideline #4 Investigating Coroners' Acceptance of Natural Deaths for Investigation 5. Basic Life Support Patient Care Standards, Ministry of Health and Long-Term Care. Deceased Patient Standard Best Practice Guideline #5: 12 of 12 Interaction of Investigating Coroners with Emergency Medical Services, Police, Body Removal Services, and Funeral Services Arising from Death Investigations Issued: Date for review:
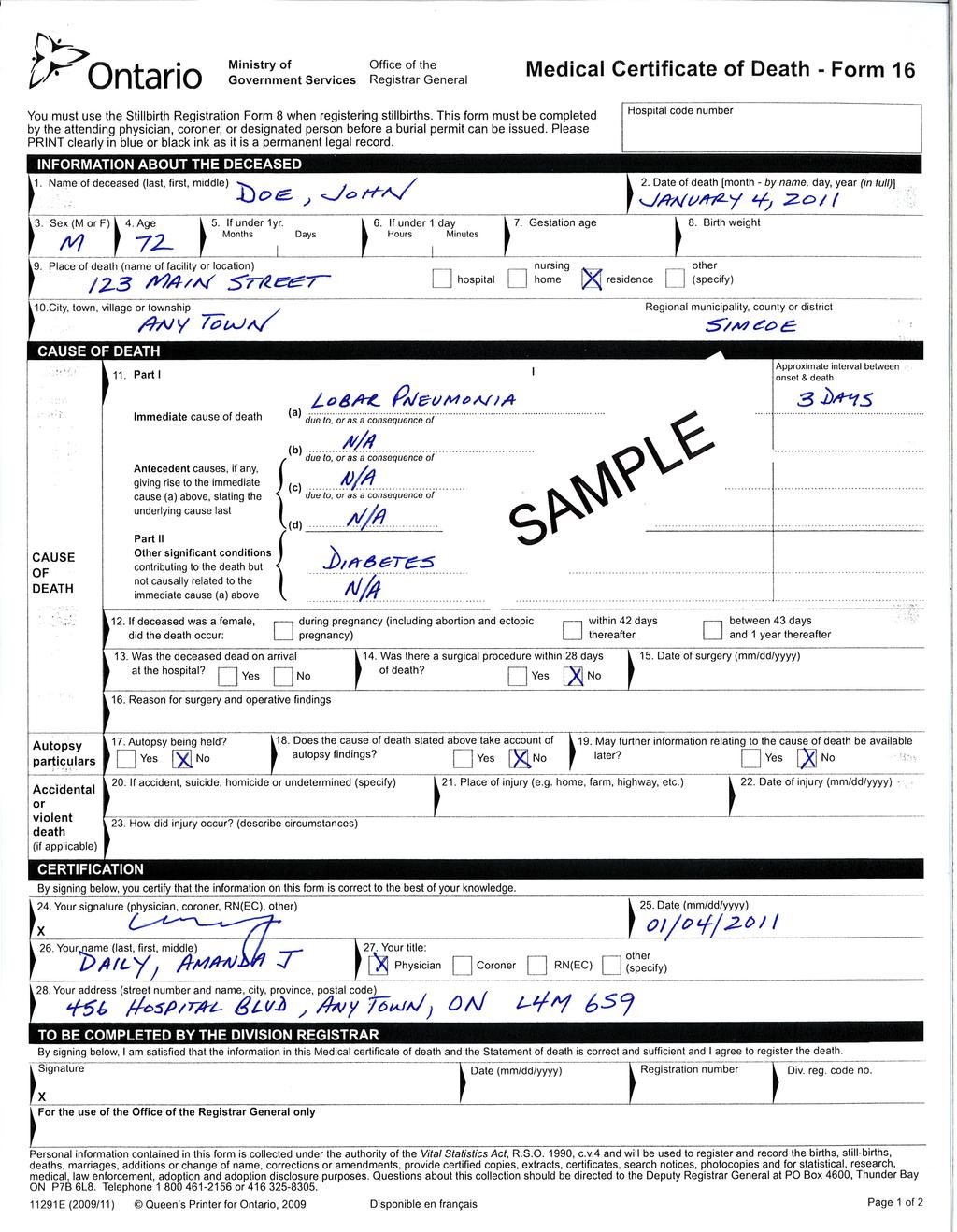
29 Appendix C Sample of Completed Medical Certificate of Death
30
31
32
33
Office of the Chief Coroner bureau du Coroner en Chef 26 Grenville Street 26 Rue Grenville Toronto ON. M7A 2G9
 Office of the Chief Coroner bureau du Coroner en Chef 26 Grenville Street 26 Rue Grenville Toronto ON. M7A 2G9 Toronto ON. M7A 2G9 Telephone: (416) 314-4000 Telephone: (416) 314-4000 Facsimile: (416) 314-4030
Office of the Chief Coroner bureau du Coroner en Chef 26 Grenville Street 26 Rue Grenville Toronto ON. M7A 2G9 Toronto ON. M7A 2G9 Telephone: (416) 314-4000 Telephone: (416) 314-4000 Facsimile: (416) 314-4030
Best Practice Guideline #5. Management of Deaths Occurring Outside of Health Care Facilities
 Best Practice Guideline #5 Management of Deaths Occurring Outside of Health Care Facilities Introduction Emergency Medical Services (EMS) personnel and police officers are most often the first to respond
Best Practice Guideline #5 Management of Deaths Occurring Outside of Health Care Facilities Introduction Emergency Medical Services (EMS) personnel and police officers are most often the first to respond
Determination of Death in the Prehospital Setting
 Determination of Death in the Prehospital Setting Supersedes: 02-03-09 Effective: 12-01-16 PURPOSE The purpose of this procedure is to establish guidelines for the withholding or termination of resuscitation
Determination of Death in the Prehospital Setting Supersedes: 02-03-09 Effective: 12-01-16 PURPOSE The purpose of this procedure is to establish guidelines for the withholding or termination of resuscitation
CONNECTICUT STATE BLS GUIDELINES GUIDELINES FOR WITHHOLDING RESUCITATION ADULT - AGE 18 AND OVER
 CONNECTICUT STATE BLS GUIDELINES GUIDELINES FOR WITHHOLDING RESUCITATION ADULT - AGE 18 AND OVER Purpose: To provide specific instruction regarding the protocols used to withhold or withdraw resuscitation
CONNECTICUT STATE BLS GUIDELINES GUIDELINES FOR WITHHOLDING RESUCITATION ADULT - AGE 18 AND OVER Purpose: To provide specific instruction regarding the protocols used to withhold or withdraw resuscitation
DEATH IN THE FIELD. Escambia County, Florida - ALS/BLS Medical Protocol
 This protocol is divided into separate sections that cover the different situations of death in the field that the paramedic will be presented with. All patients found in cardiac arrest will receive cardiopulmonary
This protocol is divided into separate sections that cover the different situations of death in the field that the paramedic will be presented with. All patients found in cardiac arrest will receive cardiopulmonary
South Cook County Policies and Procedures. September, 2015
 South Cook County Policies and Procedures September, 2015 Objectives Upon completion of the program, the participant will be able to: 1.Understand the transport guidelines for emotionally disturbed patients
South Cook County Policies and Procedures September, 2015 Objectives Upon completion of the program, the participant will be able to: 1.Understand the transport guidelines for emotionally disturbed patients
Municipal EMS Directors and Managers CAOs of Upper Tier Municipalities and Designated Delivery Agents Ornge
 Ministry of Health and Long-Term Care Emergency Health Services Branch 5700 Yonge Street, 6 th Floor Toronto ON M2M 4K5 Tel.: 416-327-7909 Fax: 416-327-7879 Toll Free: 800-461-6431 Ministère de la Santé
Ministry of Health and Long-Term Care Emergency Health Services Branch 5700 Yonge Street, 6 th Floor Toronto ON M2M 4K5 Tel.: 416-327-7909 Fax: 416-327-7879 Toll Free: 800-461-6431 Ministère de la Santé
Medical Assistance in Dying
 POLICY STATEMENT #4-16 Medical Assistance in Dying APPROVED BY COUNCIL: REVIEWED AND UPDATED: PUBLICATION DATE: KEY WORDS: RELATED TOPICS: LEGISLATIVE REFERENCES: REFERENCE MATERIALS: OTHER RESOURCES:
POLICY STATEMENT #4-16 Medical Assistance in Dying APPROVED BY COUNCIL: REVIEWED AND UPDATED: PUBLICATION DATE: KEY WORDS: RELATED TOPICS: LEGISLATIVE REFERENCES: REFERENCE MATERIALS: OTHER RESOURCES:
Many who are interested in medicine, palliative care and hospice and bioethics have been
 NEW "DNR" RULES WENT INTO EFFECT MAY 20, 1999 Many who are interested in medicine, palliative care and hospice and bioethics have been carefully following the progress of the legislation on "portable DNR"
NEW "DNR" RULES WENT INTO EFFECT MAY 20, 1999 Many who are interested in medicine, palliative care and hospice and bioethics have been carefully following the progress of the legislation on "portable DNR"
A PERSONAL DECISION
 A PERSONAL DECISION Practical information about determining your future medical care including declaration, powers of attorney for health care and organ donation Determining Your Medical Care is Your
A PERSONAL DECISION Practical information about determining your future medical care including declaration, powers of attorney for health care and organ donation Determining Your Medical Care is Your
Expected Death in the Home Protocol EDITH. Guidelines for Implementation
 EDITH Guidelines for Implementation Hospice Palliative Care Teams for Champlain Champlain Community Care Access Centre Centre d accès aux soins communautaires de Champlain Table of Contents 1. Overview...
EDITH Guidelines for Implementation Hospice Palliative Care Teams for Champlain Champlain Community Care Access Centre Centre d accès aux soins communautaires de Champlain Table of Contents 1. Overview...
Medical Assistance in Dying
 College of Physicians and Surgeons of Ontario POLICY STATEMENT #4-16 Medical Assistance in Dying APPROVED BY COUNCIL: REVIEWED AND UPDATED: PUBLICATION DATE: KEY WORDS: RELATED TOPICS: LEGISLATIVE REFERENCES:
College of Physicians and Surgeons of Ontario POLICY STATEMENT #4-16 Medical Assistance in Dying APPROVED BY COUNCIL: REVIEWED AND UPDATED: PUBLICATION DATE: KEY WORDS: RELATED TOPICS: LEGISLATIVE REFERENCES:
Expected Death in the Home Protocol EDITH. Guidelines
 EDITH Hospice Palliative Care Teams for Central LHIN Sep 2015 Table of Contents 1. Overview... 3 2. Legislation... 3 3. Process... 4 Appendix 1 Do Not Resuscitate Confirmation Form... 6 Appendix 2 Do Not
EDITH Hospice Palliative Care Teams for Central LHIN Sep 2015 Table of Contents 1. Overview... 3 2. Legislation... 3 3. Process... 4 Appendix 1 Do Not Resuscitate Confirmation Form... 6 Appendix 2 Do Not
HEALTH CARE POWER OF ATTORNEY
 HEALTH CARE POWER OF ATTORNEY NOTE: YOU SHOULD USE THIS DOCUMENT TO NAME A PERSON AS YOUR HEALTH CARE AGENT IF YOU ARE COMFORTABLE GIVING THAT PERSON BROAD AND SWEEPING POWERS TO MAKE HEALTH CARE DECISIONS
HEALTH CARE POWER OF ATTORNEY NOTE: YOU SHOULD USE THIS DOCUMENT TO NAME A PERSON AS YOUR HEALTH CARE AGENT IF YOU ARE COMFORTABLE GIVING THAT PERSON BROAD AND SWEEPING POWERS TO MAKE HEALTH CARE DECISIONS
WESTCHESTER REGIONAL
 WESTCHESTER REGIONAL EMERGENCY MEDICAL SERVICES COUNCIL POLICY STATEMENT Supersedes/Updates: New Policy No. 11-02 Date: February 8, 2011 Re: EMS System Resource Utilization Pg(s): 5 INTRODUCTION The Westchester
WESTCHESTER REGIONAL EMERGENCY MEDICAL SERVICES COUNCIL POLICY STATEMENT Supersedes/Updates: New Policy No. 11-02 Date: February 8, 2011 Re: EMS System Resource Utilization Pg(s): 5 INTRODUCTION The Westchester
ADVANCE DIRECTIVE FOR A NATURAL DEATH ("LIVING WILL")
") ADVANCE DIRECTIVE FOR A NATURAL DEATH ("LIVING WILL") NOTE: YOU SHOULD USE THIS DOCUMENT TO GIVE YOUR HEALTH CARE PROVIDERS INSTRUCTIONS TO WITHHOLD OR WITHDRAW LIFE-PROLONGING MEASURES IN CERTAIN SITUATIONS.
ADVANCE DIRECTIVE FOR A NATURAL DEATH ("LIVING WILL") NOTE: YOU SHOULD USE THIS DOCUMENT TO GIVE YOUR HEALTH CARE PROVIDERS INSTRUCTIONS TO WITHHOLD OR WITHDRAW LIFE-PROLONGING MEASURES IN CERTAIN SITUATIONS.
Northwest Community EMS System POLICY MANUAL
 Policy Title: ILLINOIS POLST forms and Advance Directive Guidelines No. D - 5 Board approval: 11/10/16 Effective: 12/1/16 Supersedes: 1/30/15 Page: 1 of 9 References: Public Act 094-0865 that amends the
Policy Title: ILLINOIS POLST forms and Advance Directive Guidelines No. D - 5 Board approval: 11/10/16 Effective: 12/1/16 Supersedes: 1/30/15 Page: 1 of 9 References: Public Act 094-0865 that amends the
ADVANCE MEDICAL DIRECTIVES
 Advance Directives ADVANCE MEDICAL DIRECTIVES The "Montana Rights of the Terminally Ill Act" (also known as the Montana Living Will Act") allows individuals the maximum possible control over their own
Advance Directives ADVANCE MEDICAL DIRECTIVES The "Montana Rights of the Terminally Ill Act" (also known as the Montana Living Will Act") allows individuals the maximum possible control over their own
SUDDEN DEATH POLICY Includes notification form for Sudden Unexplained Death in Infancy
 SUDDEN DEATH POLICY Includes notification form for Sudden Unexplained Death in Infancy First Issued January 2007 Issue Version One Purpose of Issue/Description of Change Outlines the process that staff
SUDDEN DEATH POLICY Includes notification form for Sudden Unexplained Death in Infancy First Issued January 2007 Issue Version One Purpose of Issue/Description of Change Outlines the process that staff
Ethics in EMS. Presented by: Dwayne Cottel ACP Jeff Conway ACP, LLB
 Ethics in EMS Presented by: Dwayne Cottel ACP Jeff Conway ACP, LLB Objectives Define Ethics, Morals and Ethical Dilemmas Review of Legal and Ethical Accountability in EMS Describe common Ethical Dilemmas
Ethics in EMS Presented by: Dwayne Cottel ACP Jeff Conway ACP, LLB Objectives Define Ethics, Morals and Ethical Dilemmas Review of Legal and Ethical Accountability in EMS Describe common Ethical Dilemmas
UK LIVING WILL REGISTRY
 Introduction A Living Will sets out clearly and legally how you would like to be treated or not treated if you are unable to make, participate in or communicate decisions about your medical care in the
Introduction A Living Will sets out clearly and legally how you would like to be treated or not treated if you are unable to make, participate in or communicate decisions about your medical care in the
VERIFICATION OF LIFE EXTINCT POLICY DECEMBER Verification of Life Extinct Policy December 2009 Page 1 of 18
 VERIFICATION OF LIFE EXTINCT POLICY DECEMBER 2009 Page 1 of 18 POLICY TITLE: Verification of Life Extinct Policy POLICY REFERENCE NUMBER: Med01/009 IMPLEMENTATION DATE: December 2009 REVIEW DATE: December
VERIFICATION OF LIFE EXTINCT POLICY DECEMBER 2009 Page 1 of 18 POLICY TITLE: Verification of Life Extinct Policy POLICY REFERENCE NUMBER: Med01/009 IMPLEMENTATION DATE: December 2009 REVIEW DATE: December
Directive to Physicians and Family or Surrogates Advance Directives Act (see , Health and Safety Code) Directive
 Directive") Directive to Physicians and Family or Surrogates Advance Directives Act (see 166.033, Health and Safety Code) This is an important legal document known as an Advance Directive. It is designed to help you
Directive to Physicians and Family or Surrogates Advance Directives Act (see 166.033, Health and Safety Code) This is an important legal document known as an Advance Directive. It is designed to help you
Policy for: The Verification of Expected Death
 Policy for: The Verification of Expected Death Document Reference: SCH Serco CP Version: 2 Status: For approval Type: Document applies to (area): Suffolk Community Healthcare Serco Document applies to
Policy for: The Verification of Expected Death Document Reference: SCH Serco CP Version: 2 Status: For approval Type: Document applies to (area): Suffolk Community Healthcare Serco Document applies to
Medical Aid in Dying (MAID) Update July 14, 2016
 Update July 14, 2016") Medical Aid in Dying (MAID) Update July 14, 2016 The federal government gave Royal Assent to Bill C-14, An Act to amend the Criminal Code and to make related amendments to other Acts (medical assistance
Medical Aid in Dying (MAID) Update July 14, 2016 The federal government gave Royal Assent to Bill C-14, An Act to amend the Criminal Code and to make related amendments to other Acts (medical assistance
Issue Date: June 2003 Review Date: October 2015
 Title: Preamble Number: 4.1 Category: 4.0 Certification Policies Page 1 of 1 In the evolution of the Base Hospital system a balance between consistency and necessary variation in practice has been sought.
Title: Preamble Number: 4.1 Category: 4.0 Certification Policies Page 1 of 1 In the evolution of the Base Hospital system a balance between consistency and necessary variation in practice has been sought.
College of Physicians and Surgeons of Newfoundland & Labrador STANDARD OF PRACTICE
 College of Physicians and Surgeons of Newfoundland & Labrador STANDARD OF PRACTICE Medical Assistance in Dying (MAiD) APPROVED BY COUNCIL: March 12, 2016 REVIEWED AND UPDATED: July 27, 2016 TO BE REVIEWED
College of Physicians and Surgeons of Newfoundland & Labrador STANDARD OF PRACTICE Medical Assistance in Dying (MAiD) APPROVED BY COUNCIL: March 12, 2016 REVIEWED AND UPDATED: July 27, 2016 TO BE REVIEWED
Local Health Integration Network Authorities under the Local Health System Integration Act, 2006
 Purpose This document outlines principles that guide the potential use of the new Local Health Integration Network (LHIN) directive, investigatory and supervisory authorities ( statutory authorities )
Purpose This document outlines principles that guide the potential use of the new Local Health Integration Network (LHIN) directive, investigatory and supervisory authorities ( statutory authorities )
Re: Feedback on Interim Guidance Document on Physician-Assisted Death. Re: Response to Request for Stakeholder Feedback on Physician-Assisted Dying
 Via email: interimguidance@cpso.on.ca College of Physicians and Surgeons of Ontario 80 College Street Toronto, Ontario M5G 2E2 January 13, 2016 Re: Feedback on Interim Guidance Document on Physician-Assisted
Via email: interimguidance@cpso.on.ca College of Physicians and Surgeons of Ontario 80 College Street Toronto, Ontario M5G 2E2 January 13, 2016 Re: Feedback on Interim Guidance Document on Physician-Assisted
Do Not Attempt Resuscitation Policy
 Do Not Attempt Resuscitation Policy PROV 27 March 2009 1 Document Management Title of document Do Not Attempt Resuscitation Policy Type of document Policy PROV 27 Description To ensure that do not resuscitate
Do Not Attempt Resuscitation Policy PROV 27 March 2009 1 Document Management Title of document Do Not Attempt Resuscitation Policy Type of document Policy PROV 27 Description To ensure that do not resuscitate
ARTICLE XIV DEATH Do Not Resuscitate Policy
 ARTICLE XIV DEATH 14.1 Pronouncement of Death Pronouncement of death of a patient in the Hospital is the responsibility of the attending physician or his Physician designee. Such judgment shall not be
ARTICLE XIV DEATH 14.1 Pronouncement of Death Pronouncement of death of a patient in the Hospital is the responsibility of the attending physician or his Physician designee. Such judgment shall not be
Advance Care Planning In Ontario. Judith Wahl B.A., LL.B. Advocacy Centre for the Elderly 2 Carlton Street, Ste 701 Toronto, Ontario M5B 1J3
 Advance Care Planning In Ontario Judith Wahl B.A., LL.B. Advocacy Centre for the Elderly 2 Carlton Street, Ste 701 Toronto, Ontario M5B 1J3 wahlj@lao.on.ca www.advocacycentreelderly.org What is Advance
Advance Care Planning In Ontario Judith Wahl B.A., LL.B. Advocacy Centre for the Elderly 2 Carlton Street, Ste 701 Toronto, Ontario M5B 1J3 wahlj@lao.on.ca www.advocacycentreelderly.org What is Advance
REGISTERED NURSE VERIFICATION OF EXPECTED DEATH POLICY & PROCEDURE
 REGISTERED NURSE VERIFICATION OF EXPECTED DEATH POLICY & PROCEDURE Unique ID: NHSL. Author (s): F Cook / I Lavery / A McGibbon Category/Level/Type: 1 Version: 1 Status: Published Authorised by: Clinical
REGISTERED NURSE VERIFICATION OF EXPECTED DEATH POLICY & PROCEDURE Unique ID: NHSL. Author (s): F Cook / I Lavery / A McGibbon Category/Level/Type: 1 Version: 1 Status: Published Authorised by: Clinical
Oswego County EMS. Multiple-Casualty Incident Plan
 Oswego County EMS Multiple-Casualty Incident Plan Revised December 2013 IF this is an actual MCI THEN go directly to the checklist section on page 14. 2 Index 1. Purpose 4 2. Objectives 4 3. Responsibilities
Oswego County EMS Multiple-Casualty Incident Plan Revised December 2013 IF this is an actual MCI THEN go directly to the checklist section on page 14. 2 Index 1. Purpose 4 2. Objectives 4 3. Responsibilities
Dear Colleague. MANAGEMENT OF DEATHS IN THE COMMUNITY (In hours and out of hours) Purpose
 Purpose") Directorate of Chief Medical Office Crown Agent and Chief Executive of Crown Office and Procurator Fiscal Service Dear Colleague MANAGEMENT OF DEATHS IN THE COMMUNITY (In hours and out of hours) Purpose
Directorate of Chief Medical Office Crown Agent and Chief Executive of Crown Office and Procurator Fiscal Service Dear Colleague MANAGEMENT OF DEATHS IN THE COMMUNITY (In hours and out of hours) Purpose
PATIENT SERVICES POLICY AND PROCEDURE MANUAL
 SECTION Patient Services Manual Multidiscipline Section NAME Patient Rights and Responsibilities PATIENT SERVICES POLICY AND PROCEDURE MANUAL EFFECTIVE DATE 8-1-11 SUPERSEDES DATE 7-20-10 I. PURPOSE To
SECTION Patient Services Manual Multidiscipline Section NAME Patient Rights and Responsibilities PATIENT SERVICES POLICY AND PROCEDURE MANUAL EFFECTIVE DATE 8-1-11 SUPERSEDES DATE 7-20-10 I. PURPOSE To
Professional Standard Regarding Medical Assistance in Dying
 Suite 5005 7071 Bayers Road Halifax, Nova Scotia Canada B3L 2C2 Phone: (902) 422 5823 Toll free: 1 877 282 7767 Fax: (902) 422 5035 www.cpsns.ns.ca February 8, 2018 1 Professional Standard Regarding Medical
Suite 5005 7071 Bayers Road Halifax, Nova Scotia Canada B3L 2C2 Phone: (902) 422 5823 Toll free: 1 877 282 7767 Fax: (902) 422 5035 www.cpsns.ns.ca February 8, 2018 1 Professional Standard Regarding Medical
ADVANCE MEDICAL DIRECTIVES
 ADVANCE MEDICAL DIRECTIVES Health Care Declaration (Living Will) and Medical Power of Attorney What is an Advance Directive? Many people are concerned about what would happen if, due to a mental or physical
ADVANCE MEDICAL DIRECTIVES Health Care Declaration (Living Will) and Medical Power of Attorney What is an Advance Directive? Many people are concerned about what would happen if, due to a mental or physical
1. Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) Decisions Guideline
 Decisions Guideline") 1. Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) Decisions Guideline 1.1 Part A - Patient admitted into Acute Care... 2 1.1.1 Special Points... 2 1.1.2 Further Guidelines for Assessment and DNACPR
1. Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) Decisions Guideline 1.1 Part A - Patient admitted into Acute Care... 2 1.1.1 Special Points... 2 1.1.2 Further Guidelines for Assessment and DNACPR
Durable Power of Attorney for Health Care and Health Care Directive
 Durable Power of Attorney for Health Care and Health Care Directive and HIPAA Privacy Authorization Form Frequently Asked Questions and Answers, Instructions, and Forms Distributed as a public service
Durable Power of Attorney for Health Care and Health Care Directive and HIPAA Privacy Authorization Form Frequently Asked Questions and Answers, Instructions, and Forms Distributed as a public service
Replaces: 5/20/2016 Formulated: 3/85 Reviewed:10/17 PROCEDURE TO BE FOLLOWED IN CASES OF OFFENDER DEATH
 Page 1 of 7 PURPOSE: POLICY: To outline procedures to be followed in the event of an offender s death. Pronouncement of offender deaths will be consistent with Chapter 671of the Texas Health and Safety
Page 1 of 7 PURPOSE: POLICY: To outline procedures to be followed in the event of an offender s death. Pronouncement of offender deaths will be consistent with Chapter 671of the Texas Health and Safety
Assembly Bill No. 199 Assemblywomen Woodbury and Titus. Joint Sponsor: Senator Hardy
 Assembly Bill No. 199 Assemblywomen Woodbury and Titus Joint Sponsor: Senator Hardy CHAPTER... AN ACT relating to health care; authorizing a physician assistant or advanced practice registered nurse to
Assembly Bill No. 199 Assemblywomen Woodbury and Titus Joint Sponsor: Senator Hardy CHAPTER... AN ACT relating to health care; authorizing a physician assistant or advanced practice registered nurse to
ILLINOIS Advance Directive Planning for Important Health Care Decisions
 ILLINOIS Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
ILLINOIS Advance Directive Planning for Important Health Care Decisions CaringInfo 1731 King St., Suite 100, Alexandria, VA 22314 www.caringinfo.org 800/658-8898 CaringInfo, a program of the National Hospice
Planning For (And Dealing With) Incapacity
 Incapacity") CHAPTER NINE Planning For (And Dealing With) Incapacity Much of the material is drawn from the Residents Health Care Decision Making chapter of the Nursing Home Companion, published by Bet Tzedek Legal
CHAPTER NINE Planning For (And Dealing With) Incapacity Much of the material is drawn from the Residents Health Care Decision Making chapter of the Nursing Home Companion, published by Bet Tzedek Legal
End of Life Care Policy. Document author Assured by Review cycle. 1. Introduction Purpose Scope Definitions...
 End of Life Care Policy Board library reference Document author Assured by Review cycle P011 Lead Nurse Quality and Standards Committee 3 Years Contents 1. Introduction...3 2. Purpose...3 3. Scope...3
End of Life Care Policy Board library reference Document author Assured by Review cycle P011 Lead Nurse Quality and Standards Committee 3 Years Contents 1. Introduction...3 2. Purpose...3 3. Scope...3
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE DISCLOSURE OF HARM SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND NUMBER
TITLE DISCLOSURE OF HARM SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND NUMBER
INQUEST INTO THE DEATH OF: MARIE TANNER
 INQUEST INTO THE DEATH OF: MARIE TANNER Details Name of Deceased: Marie Tanner Date of Death: January 21, 2002 Place of Death: Peterborough Regional Health Centre Cause of Death: Cardiac Arrest Caused
INQUEST INTO THE DEATH OF: MARIE TANNER Details Name of Deceased: Marie Tanner Date of Death: January 21, 2002 Place of Death: Peterborough Regional Health Centre Cause of Death: Cardiac Arrest Caused
THE CODE 1000 PLAN. for ST. LOUIS COUNTY AND MUNICIPAL LAW ENFORCEMENT AGENCIES. January 2013
 THE CODE 1000 PLAN for ST. LOUIS COUNTY AND MUNICIPAL LAW ENFORCEMENT AGENCIES January 2013 1 of 12 Table of Contents SECTION 1.0 GENERAL... 1 1.1 Definition - Purpose - Applicability...1 1.2 Authority...1
THE CODE 1000 PLAN for ST. LOUIS COUNTY AND MUNICIPAL LAW ENFORCEMENT AGENCIES January 2013 1 of 12 Table of Contents SECTION 1.0 GENERAL... 1 1.1 Definition - Purpose - Applicability...1 1.2 Authority...1
PRIVACY BREACH MANAGEMENT GUIDELINES. Ministry of Justice Access and Privacy Branch
 Ministry of Justice Access and Privacy Branch December 2015 Table of Contents December 2015 What is a privacy breach? 3 Preventing privacy breaches 3 Responding to privacy breaches 4 Step 1 Contain the
Ministry of Justice Access and Privacy Branch December 2015 Table of Contents December 2015 What is a privacy breach? 3 Preventing privacy breaches 3 Responding to privacy breaches 4 Step 1 Contain the
PHILADELPHIA FIRE DEPARTMENT EMS PROCEDURE #10 JUNE, 2008
 PHILADELPHIA FIRE DEPARTMENT EMS PROCEDURE #10 SUBJECT: MEDICAL COMMAND COMMUNICATIONS 1. PURPOSE To establish and set forth the procedure for a Philadelphia Fire Department (PFD) paramedic or firefighter
PHILADELPHIA FIRE DEPARTMENT EMS PROCEDURE #10 SUBJECT: MEDICAL COMMAND COMMUNICATIONS 1. PURPOSE To establish and set forth the procedure for a Philadelphia Fire Department (PFD) paramedic or firefighter
ADVANCE DIRECTIVE INFORMATION
 ADVANCE DIRECTIVE INFORMATION NOTE: This Advance Directive Information and the form Living Will and Durable Power of Attorney for Health Care on the Arkansas Bar Association s website are being provided
ADVANCE DIRECTIVE INFORMATION NOTE: This Advance Directive Information and the form Living Will and Durable Power of Attorney for Health Care on the Arkansas Bar Association s website are being provided
Notification of a Death Record of Death C Cremation cert
 Notification of a Death Record of Death C120002 Cremation cert Notification; the registered nurse is responsible for notifying family, medical staff, telephone officer and mortality coordinator or the
Notification of a Death Record of Death C120002 Cremation cert Notification; the registered nurse is responsible for notifying family, medical staff, telephone officer and mortality coordinator or the
SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY DOCUMENTATION, EVALUATION AND NON-TRANSPORTS
 SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY DOCUMENTATION, EVALUATION AND NON-TRANSPORTS Policy Reference No.: 4040 Review Date: February 1, 2011 Supersedes: August 1, 2008 TABLE OF CONTENTS I. PURPOSE
SAN FRANCISCO EMERGENCY MEDICAL SERVICES AGENCY DOCUMENTATION, EVALUATION AND NON-TRANSPORTS Policy Reference No.: 4040 Review Date: February 1, 2011 Supersedes: August 1, 2008 TABLE OF CONTENTS I. PURPOSE
ILLINOIS ASSOCIATION OF CHIEFS OF POLICE FUNERAL PROTOCOLS RETIRED OFFICER DEATH
 ILLINOIS ASSOCIATION OF CHIEFS OF POLICE FUNERAL PROTOCOLS RETIRED OFFICER DEATH I. Purpose: This is a guide to Law Enforcement Officers Retiree Death General Protocols. Law Enforcement is a Quasi-Military
ILLINOIS ASSOCIATION OF CHIEFS OF POLICE FUNERAL PROTOCOLS RETIRED OFFICER DEATH I. Purpose: This is a guide to Law Enforcement Officers Retiree Death General Protocols. Law Enforcement is a Quasi-Military
PATIENT RIGHTS, PRIVACY, AND PROTECTION
 REGIONAL POLICY Subject/Title: ADVANCE CARE PLANNING: GOALS OF CARE DESIGNATION (ADULT) Approving Authority: EXECUTIVE MANAGEMENT Classification: Category: CLINICAL PATIENT RIGHTS, PRIVACY, AND PROTECTION
REGIONAL POLICY Subject/Title: ADVANCE CARE PLANNING: GOALS OF CARE DESIGNATION (ADULT) Approving Authority: EXECUTIVE MANAGEMENT Classification: Category: CLINICAL PATIENT RIGHTS, PRIVACY, AND PROTECTION
The Halachic Medical Directive
 The Halachic Medical Directive ADVANCE DIRECTIVE WITH RESPECT TO HEALTH CARE DECISIONS AND POST- MORTEM DECISIONS FOR USE IN NEW JERSEY The Halachic Medical Directive is designed to help ensure that all
The Halachic Medical Directive ADVANCE DIRECTIVE WITH RESPECT TO HEALTH CARE DECISIONS AND POST- MORTEM DECISIONS FOR USE IN NEW JERSEY The Halachic Medical Directive is designed to help ensure that all
DAVIS POLICE DEPARTMENT
 Index as: Trauma and Grief Support Program TAGS DAVIS POLICE DEPARTMENT TRAUMA & GRIEF SUPPORT PROGRAM Policy and Procedure 1.44-A DEPARTMENT MANUAL I. POLICY Members of the Davis Police and Fire Departments
Index as: Trauma and Grief Support Program TAGS DAVIS POLICE DEPARTMENT TRAUMA & GRIEF SUPPORT PROGRAM Policy and Procedure 1.44-A DEPARTMENT MANUAL I. POLICY Members of the Davis Police and Fire Departments
Policy Document Control Page
 Policy Document Control Page Title: Section 17 (Leave of Absence) Policy Version: 9 Reference Number: CL7 Supersedes Supersedes: Section 17 (Leave of Absence) Policy V8 Description of Amendment(s): Updated
Policy Document Control Page Title: Section 17 (Leave of Absence) Policy Version: 9 Reference Number: CL7 Supersedes Supersedes: Section 17 (Leave of Absence) Policy V8 Description of Amendment(s): Updated
Dementia and End-of-Life Care
 Dementia and End-of-Life Care Part IV: What practical information should I know? About this resource The needs of people with dementia at the end of life* are unique and require special considerations.
Dementia and End-of-Life Care Part IV: What practical information should I know? About this resource The needs of people with dementia at the end of life* are unique and require special considerations.
Determination of Death In The Field, Termination of Resuscitative Efforts in the Field, and Do Not Resuscitate (DNR) Policy
 Policy") Determination of Death In The Field, Termination of Resuscitative Efforts in the Field, and Do Not Resuscitate (DNR) Policy Purpose: To provide guidance for determining when prehospital resuscitation attempts
Determination of Death In The Field, Termination of Resuscitative Efforts in the Field, and Do Not Resuscitate (DNR) Policy Purpose: To provide guidance for determining when prehospital resuscitation attempts
Community Transportation Pilot Grant Program Application Guidelines and Requirements
 Community Transportation Pilot Grant Program Application Guidelines and Requirements 2014-2015 Issued: November 2014 Ministry of Transportation Municipal Transit Policy Office, Transit Policy Branch 1
Community Transportation Pilot Grant Program Application Guidelines and Requirements 2014-2015 Issued: November 2014 Ministry of Transportation Municipal Transit Policy Office, Transit Policy Branch 1
Medical Advance Directives
 Chapter 24 Medical Advance Directives Michael A. Kirtland, Esq. Kirtland & Seal, L.L.C. SYNOPSIS 24-1. Living Wills 24-2. CPR Directives and DNR Orders 24-3. Medical Orders for Scope of Treatment 24-4.
Chapter 24 Medical Advance Directives Michael A. Kirtland, Esq. Kirtland & Seal, L.L.C. SYNOPSIS 24-1. Living Wills 24-2. CPR Directives and DNR Orders 24-3. Medical Orders for Scope of Treatment 24-4.
MARYLAND ADVANCE DIRECTIVE PLANNING FOR FUTURE HEALTH CARE DECISIONS
 MARYLAND ADVANCE DIRECTIVE PLANNING FOR FUTURE HEALTH CARE DECISIONS A guide to Maryland Law on Health Care Decisions (Forms Included) State of Maryland Office of the Attorney General Dear Fellow Marylander:
MARYLAND ADVANCE DIRECTIVE PLANNING FOR FUTURE HEALTH CARE DECISIONS A guide to Maryland Law on Health Care Decisions (Forms Included) State of Maryland Office of the Attorney General Dear Fellow Marylander:
SOUTH CAROLINA HEALTH CARE POWER OF ATTORNEY
 SOUTH CAROLINA HEALTH CARE POWER OF ATTORNEY INFORMATION ABOUT THIS DOCUMENT THIS IS AN IMPORTANT LEGAL DOCUMENT. BEFORE SIGNING THIS DOCUMENT, YOU SHOULD KNOW THESE IMPORTANT FACTS: 1. THIS DOCUMENT GIVES
SOUTH CAROLINA HEALTH CARE POWER OF ATTORNEY INFORMATION ABOUT THIS DOCUMENT THIS IS AN IMPORTANT LEGAL DOCUMENT. BEFORE SIGNING THIS DOCUMENT, YOU SHOULD KNOW THESE IMPORTANT FACTS: 1. THIS DOCUMENT GIVES
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE ADVANCE CARE PLANNING AND GOALS OF CARE DESIGNATION SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Seniors Health PARENT DOCUMENT TITLE, TYPE AND NUMBER Not Applicable
TITLE ADVANCE CARE PLANNING AND GOALS OF CARE DESIGNATION SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Seniors Health PARENT DOCUMENT TITLE, TYPE AND NUMBER Not Applicable
Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) Policy
 Policy") Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) Policy 1 Policy Title: Executive Summary: Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) Policy Cardiopulmonary resuscitation (CPR) can be attempted
Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) Policy 1 Policy Title: Executive Summary: Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) Policy Cardiopulmonary resuscitation (CPR) can be attempted
PHYSICIAN S GUIDELINES FOR WRITING DO NOT RESUSCITATE ORDERS
 PHYSICIAN S GUIDELINES FOR WRITING DO NOT RESUSCITATE ORDERS THE PURPOSE OF CPR IS THE PREVENTION OF SUDDEN UNEXPECTED DEATH. CPR IS NOT INDICATED IN CERTAIN SITUATIONS SUCH AS CASES OF TERMINAL IRREVERSIBLE
PHYSICIAN S GUIDELINES FOR WRITING DO NOT RESUSCITATE ORDERS THE PURPOSE OF CPR IS THE PREVENTION OF SUDDEN UNEXPECTED DEATH. CPR IS NOT INDICATED IN CERTAIN SITUATIONS SUCH AS CASES OF TERMINAL IRREVERSIBLE
Printed from the Texas Medical Association Web site.
 Printed from the Texas Medical Association Web site. Medical Power of Attorney Patient and Health Care Provider Information September 1999 General Information To be read by the Patient and Health Care
Printed from the Texas Medical Association Web site. Medical Power of Attorney Patient and Health Care Provider Information September 1999 General Information To be read by the Patient and Health Care
SAN LUIS OBISPO CITY FIRE EMERGENCY OPERATIONS MANUAL E.O MULTI-CASUALTY INCIDENTS Revised: 8/14/2015 Page 1 of 10. Purpose.
 Revised: 8/14/2015 Page 1 of 10 Purpose The establishment of these procedures is designed to provide an organized, coordinated and expandable resource management approach to be utilized by the numerous
Revised: 8/14/2015 Page 1 of 10 Purpose The establishment of these procedures is designed to provide an organized, coordinated and expandable resource management approach to be utilized by the numerous
Review Date 01/07/2014 Director of Nursing, Midwifery and Quality Expiry Date 10/07/2015 Withdrawn Date
 Policy No: OP35 Version: 2.0 Name of Policy: Rapid Release of Bodies Effective From: 21/08/2012 Date Ratified 11/07/2012 Ratified SafeCare Committee Review Date 01/07/2014 Sponsor Director of Nursing,
Policy No: OP35 Version: 2.0 Name of Policy: Rapid Release of Bodies Effective From: 21/08/2012 Date Ratified 11/07/2012 Ratified SafeCare Committee Review Date 01/07/2014 Sponsor Director of Nursing,
LOUISIANA ADVANCE DIRECTIVES
 LOUISIANA ADVANCE DIRECTIVES Legal Documents To Make Sure Your Choices for Future Medical Care or the Refusal of Same are Honored and Implemented by Your Health Care Providers ADVANCE DIRECTIVES INTRODUCTION
LOUISIANA ADVANCE DIRECTIVES Legal Documents To Make Sure Your Choices for Future Medical Care or the Refusal of Same are Honored and Implemented by Your Health Care Providers ADVANCE DIRECTIVES INTRODUCTION
This Annex describes the emergency medical service protocol to guide and coordinate actions during initial mass casualty medical response activities.
 A N N E X C : M A S S C A S U A L T Y E M S P R O T O C O L This Annex describes the emergency medical service protocol to guide and coordinate actions during initial mass casualty medical response activities.
A N N E X C : M A S S C A S U A L T Y E M S P R O T O C O L This Annex describes the emergency medical service protocol to guide and coordinate actions during initial mass casualty medical response activities.
South Central Region EMS & Trauma Care Council Patient Care Procedures
 South Central Region EMS & Trauma Care Council Patient Care s Table of Contents PCP #1 Dispatch PCP #2 Response Times PCP #3 Triage and Transport PCP #4 Inter-Facility Transfer PCP #5 Medical Command at
South Central Region EMS & Trauma Care Council Patient Care s Table of Contents PCP #1 Dispatch PCP #2 Response Times PCP #3 Triage and Transport PCP #4 Inter-Facility Transfer PCP #5 Medical Command at
REVISED 2005 EDITION. A Personal Decision
 REVISED 2005 EDITION A Personal Decision Practical information about determining your future medical care, including living wills, powers of attorney for health care, mental health treatment preference
REVISED 2005 EDITION A Personal Decision Practical information about determining your future medical care, including living wills, powers of attorney for health care, mental health treatment preference
Advance Care Planning The Legal Issues. Judith Wahl B.A., LL.B. Advocacy Centre for the Elderly 1 2 Carlton Street, Ste 701 Toronto, Ontario M5B 1J3
 Advance Care Planning The Legal Issues Judith Wahl B.A., LL.B. Advocacy Centre for the Elderly 1 2 Carlton Street, Ste 701 Toronto, Ontario M5B 1J3 wahlj@lao.on.ca www.advocacycentreelderly.org What is
Advance Care Planning The Legal Issues Judith Wahl B.A., LL.B. Advocacy Centre for the Elderly 1 2 Carlton Street, Ste 701 Toronto, Ontario M5B 1J3 wahlj@lao.on.ca www.advocacycentreelderly.org What is
REGULATORY DOCUMENTS. The main classes of regulatory documents developed by the CNSC are:
 Canadian Nuclear Safety Commission Commission canadienne de sûreté nucléaire REGULATORY GUIDE Emergency Planning at Class I Nuclear Facilities and Uranium Mines and Mills G-225 August 2001 REGULATORY DOCUMENTS
Canadian Nuclear Safety Commission Commission canadienne de sûreté nucléaire REGULATORY GUIDE Emergency Planning at Class I Nuclear Facilities and Uranium Mines and Mills G-225 August 2001 REGULATORY DOCUMENTS
DURABLE POWER OF ATTORNEY FOR HEALTH CARE
 DURABLE POWER OF ATTORNEY FOR HEALTH CARE (Please print or type required information) I. Appointment of Patient Advocate I, your name of full legal address hereby appoint name of your designated patient
DURABLE POWER OF ATTORNEY FOR HEALTH CARE (Please print or type required information) I. Appointment of Patient Advocate I, your name of full legal address hereby appoint name of your designated patient
Title 18-A: PROBATE CODE. Article 5: PROTECTION OF PERSONS UNDER DISABILITY AND THEIR PROPERTY
 Title 18-A: PROBATE CODE Article 5: PROTECTION OF PERSONS UNDER DISABILITY AND THEIR PROPERTY Part 8: UNIFORM HEALTH-CARE DECISIONS ACT HEADING: PL 1995, C. 378, PT. A, 1 (NEW) 5-801. Definitions As used
Title 18-A: PROBATE CODE Article 5: PROTECTION OF PERSONS UNDER DISABILITY AND THEIR PROPERTY Part 8: UNIFORM HEALTH-CARE DECISIONS ACT HEADING: PL 1995, C. 378, PT. A, 1 (NEW) 5-801. Definitions As used
E m e rgency Health S e r v i c e s Syste m M o d e r n i zation
 E m e rgency Health S e r v i c e s Syste m M o d e r n i zation Briefing Paper on Legislative Amendments to the Ambulance Act July 2017 Enhancing Emergency Services in Ontario (EESO) Ministry of Health
E m e rgency Health S e r v i c e s Syste m M o d e r n i zation Briefing Paper on Legislative Amendments to the Ambulance Act July 2017 Enhancing Emergency Services in Ontario (EESO) Ministry of Health
Land Ambulance Service Certification Standards
 Land Ambulance Service Certification Standards Ministry of Health and Long-Term Care Emergency Health Services Branch June 2008 I Application Content: An application to be certified or re-certified to
Land Ambulance Service Certification Standards Ministry of Health and Long-Term Care Emergency Health Services Branch June 2008 I Application Content: An application to be certified or re-certified to
GUIDELINES TO DOCTORS ON REPORTING DEATHS TO THE CORONER
 Directorate of Clinical and Quality Assurance & Trust Secretary GUIDELINES TO DOCTORS ON REPORTING DEATHS TO THE CORONER Reference: CQG001 Version: 1.4 This version issued: 10/04/14 Result of last review:
Directorate of Clinical and Quality Assurance & Trust Secretary GUIDELINES TO DOCTORS ON REPORTING DEATHS TO THE CORONER Reference: CQG001 Version: 1.4 This version issued: 10/04/14 Result of last review:
Living Standard Project
 Living Standard Project Change Request Form v1.0 Emergency Health Services Branch Ministry of Health and Long-Term Care Document Control Version Number (status) Date of Issue Brief Description of Change
Living Standard Project Change Request Form v1.0 Emergency Health Services Branch Ministry of Health and Long-Term Care Document Control Version Number (status) Date of Issue Brief Description of Change
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS
 ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version
ALLOCATION OF RESOURCES POLICY FOR CONTINUING HEALTHCARE FUNDED INDIVIDUALS APPROVED BY: South Gloucestershire Clinical Commissioning Group Quality and Governance Committee DATE Date of Issue:- Version
ADVANCE HEALTH CARE DIRECTIVE HEALTH CARE POWER OF ATTORNEY AND LIVING WILL
 ADVANCE HEALTH CARE DIRECTIVE A HEALTH CARE POWER OF ATTORNEY AND LIVING WILL INSIDE: LEGAL DOCUMENTS AND INSTRUCTIONS TO ASSIST YOU WITH IMPORTANT HEALTH CARE DECISIONS Health Care Decision Making Modern
ADVANCE HEALTH CARE DIRECTIVE A HEALTH CARE POWER OF ATTORNEY AND LIVING WILL INSIDE: LEGAL DOCUMENTS AND INSTRUCTIONS TO ASSIST YOU WITH IMPORTANT HEALTH CARE DECISIONS Health Care Decision Making Modern
AKRON POLICE DEPARTMENT PROPOSED EMERGENCY MENTAL ILLNESS PROCEDURE INTRODUCTION
 INTRODUCTION AKRON POLICE DEPARTMENT Police officers are often called upon to respond to incidents involving persons who are known to be or suspected of suffering from a mental illness. The degree of police
INTRODUCTION AKRON POLICE DEPARTMENT Police officers are often called upon to respond to incidents involving persons who are known to be or suspected of suffering from a mental illness. The degree of police
Base Hospital Advanced Life Support Program for Durham Region
 Title: Purpose and Goals of the Base Hospital Program Number: 2.1 Category: 2.0 Base Hospital Roles and Responsibilities Written By: M. Epp Approved By: Dr. R. Vandersluis Issue Date: October 2002 Review
Title: Purpose and Goals of the Base Hospital Program Number: 2.1 Category: 2.0 Base Hospital Roles and Responsibilities Written By: M. Epp Approved By: Dr. R. Vandersluis Issue Date: October 2002 Review
NO TALLAHASSEE, June 30, Mental Health/Substance Abuse
 CFOP 155-52 STATE OF FLORIDA DEPARTMENT OF CF OPERATING PROCEDURE CHILDREN AND FAMILIES NO. 155-52 TALLAHASSEE, June 30, 2017 Mental Health/Substance Abuse USE OF DO NOT RESUSCITATE (DNR) ORDERS IN STATE
CFOP 155-52 STATE OF FLORIDA DEPARTMENT OF CF OPERATING PROCEDURE CHILDREN AND FAMILIES NO. 155-52 TALLAHASSEE, June 30, 2017 Mental Health/Substance Abuse USE OF DO NOT RESUSCITATE (DNR) ORDERS IN STATE
MEDICAL ASSISTANCE IN DYING
 CMA POLICY MEDICAL ASSISTANCE IN DYING RATIONALE The legalization of medical assistance in dying (MAiD) raises a host of complex ethical and practical challenges that have implications for both policy
CMA POLICY MEDICAL ASSISTANCE IN DYING RATIONALE The legalization of medical assistance in dying (MAiD) raises a host of complex ethical and practical challenges that have implications for both policy
North Carolina College of Emergency Physicians Standards Policy Table of Contents
 Policy North Carolina College of Emergency Physicians Standards Policy Table of Contents Disposition Policy Section 1. Criteria for Death or Withholding Resuscitation 2. Deceased Subjects 3. Discontinuation
Policy North Carolina College of Emergency Physicians Standards Policy Table of Contents Disposition Policy Section 1. Criteria for Death or Withholding Resuscitation 2. Deceased Subjects 3. Discontinuation
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health
 CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health Manual: Subject: Emergency Medical Services Administrative Policies and Procedures Multi-Casualty
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health Manual: Subject: Emergency Medical Services Administrative Policies and Procedures Multi-Casualty
TERMS OF ENGAGEMENT FOR AGENCY WORKERS (CONTRACT FOR SERVICES) Assignment Details Form
 Assignment Details Form") TERMS OF ENGAGEMENT FOR AGENCY WORKERS (CONTRACT FOR SERVICES) 1. DEFINITIONS AND INTERPRETATION 1.1. In these Terms the following definitions apply: Actual Rate of Pay Actual QP Rate of Pay Actual QP
TERMS OF ENGAGEMENT FOR AGENCY WORKERS (CONTRACT FOR SERVICES) 1. DEFINITIONS AND INTERPRETATION 1.1. In these Terms the following definitions apply: Actual Rate of Pay Actual QP Rate of Pay Actual QP
North Dakota: Advance Directive
 North Dakota: Advance Directive NOTE: This form is being provided to you as a public service. The attached forms are provided as is and are not the substitute for the advice of an attorney. By providing
North Dakota: Advance Directive NOTE: This form is being provided to you as a public service. The attached forms are provided as is and are not the substitute for the advice of an attorney. By providing
Region III STEMI Plan
 Region III STEMI Plan I. Plan Goals A. To develop a Region III STEMI System that when implemented, will result in decreased mortality and morbidity in the MIEMSS Region III. In order to accomplish this,
Region III STEMI Plan I. Plan Goals A. To develop a Region III STEMI System that when implemented, will result in decreased mortality and morbidity in the MIEMSS Region III. In order to accomplish this,
Fairfax Surgical Center. Statement of Patient Rights and Responsibility
 Fairfax Surgical Center Statement of Patient Rights and Responsibility PATIENT RIGHTS The Fairfax Surgical Center (ASC) respects the dignity and pride of each individual we serve. Every patient has the
Fairfax Surgical Center Statement of Patient Rights and Responsibility PATIENT RIGHTS The Fairfax Surgical Center (ASC) respects the dignity and pride of each individual we serve. Every patient has the
State of North Carolina Department of Correction Division of Prisons
 State of North Carolina Department of Correction Division of Prisons POLICY & PROCEDURES Chapter: F Section:.0400 Title: Emergency Leave Issue Date: 10/03/05 Supersedes: 08/26/02.0401 General This policy
State of North Carolina Department of Correction Division of Prisons POLICY & PROCEDURES Chapter: F Section:.0400 Title: Emergency Leave Issue Date: 10/03/05 Supersedes: 08/26/02.0401 General This policy
DNACPR. Maire O Riordan 14 th January 2015
 DNACPR Maire O Riordan 14 th January 2015 Objectives NHS Scotland DNACPR policy Decision making framework and the forms DNACPR within ACP context Communicationwith patients, relatives and colleagues Background
DNACPR Maire O Riordan 14 th January 2015 Objectives NHS Scotland DNACPR policy Decision making framework and the forms DNACPR within ACP context Communicationwith patients, relatives and colleagues Background
Maryland MOLST FAQs. Maryland MOLST Training Task Force
 Maryland MOLST FAQs Maryland MOLST Training Task Force October 2017 Frequently Asked Questions About Maryland MOLST What does MOLST stand for? MOLST is an acronym that stands for Medical Orders for Life-Sustaining
Maryland MOLST FAQs Maryland MOLST Training Task Force October 2017 Frequently Asked Questions About Maryland MOLST What does MOLST stand for? MOLST is an acronym that stands for Medical Orders for Life-Sustaining
Ambulance Response 90th Percentile Times
 Time Perth County Paramedic Services Perth County EMS Provincial Response Time Reporting: Prior to the downloading of land ambulance services in 2000 to the upper tier municipalities (UTM) and Designated
Time Perth County Paramedic Services Perth County EMS Provincial Response Time Reporting: Prior to the downloading of land ambulance services in 2000 to the upper tier municipalities (UTM) and Designated
L e g a l I s s u e s i n H e a l t h C a r e
 Page 1 L e g a l I s s u e s i n H e a l t h C a r e Tutorial #6 January 2008 Introduction Patients have the right to accept or refuse health care treatment. For a patient to exercise that right, he or
Page 1 L e g a l I s s u e s i n H e a l t h C a r e Tutorial #6 January 2008 Introduction Patients have the right to accept or refuse health care treatment. For a patient to exercise that right, he or
Adult: Any person eighteen years of age or older, or emancipated minor.
 Advance Directives Policy and Procedure Purpose To provide an atmosphere of respect and caring and to ensure that each patient's ability and right to participate in medical decision making is maximized
Advance Directives Policy and Procedure Purpose To provide an atmosphere of respect and caring and to ensure that each patient's ability and right to participate in medical decision making is maximized