NHS Stockport Clinical Commissioning Group Governing Body Part 1 A G E N D A
|
|
|
- Regina Sarah Waters
- 5 years ago
- Views:
Transcription

1 001 Chair: Enquiries to: Ms J Crombleholme Laura Latham Laura.latham1@nhs.net NHS Stockport Clinical Commissioning Group Governing Body Part 1 A G E N D A The next meeting of the NHS Stockport Clinical Commissioning Group Governing Body will be held at Regent House, Stockport at 10.00am on 23 May 2018 Agenda item Report Action Indicative Timings Lead 1 Apologies Verbal To receive and note J Crombleholme 2 Declarations of Interest Verbal To receive and note 3 Approval of the draft Minutes of the meeting held on 28 March 2018 Attached To receive and approve J Crombleholme 4 Actions Arising Attached To comment and note J Crombleholme 5 Notification of Items for Any Other Business Verbal To note and consider J Crombleholme 6 Chair s Report Verbal To note J Crombleholme 7 Patient Story Video J Crombleholme 8 CCG Annual Report and Accounts 2017/18 Written Report To approve M Chidgey and Audit Committee Representative 9 Statement Of Involvement Written Report To approve T Ryley 10 Chief Operating Officer s Report Written To note G Mullins Report 11 Any Other Business Verbal To note J Crombleholme Date, Time and Venue of Next meeting The next NHS Stockport Clinical Commissioning Group Governing Body meeting will be held on 25 July at 10am at Regent House, Stockport. Potential agenda items should be notified to stoccg.gb@nhs.net by 3 July 2018
2 002
3 003 NHS STOCKPORT CLINICAL COMMISSIONING GROUP MINUTES OF THE GOVERNING BODY MEETING HELD AT REGENT HOUSE, STOCKPORT ON WEDNESDAY 28 MARCH 2018 PART 1 PRESENT Mrs J Crombleholme Mrs G Mullins Mr M Chidgey Mrs A Rolfe Dr D Kendall Ms C Morgan Mr J Greenough Dr V Owen Smith Dr R Gill Dr S Woodworth Lay Member (Chair) Chief Operating Officer Chief Finance Officer Executive Nurse Secondary Care Consultant Lay Member for Primary Care Lay Member for Finance and Audit Clinical Director Public Health Chief Clinical Officer Interim Medical Director IN ATTENDANCE Mr T Ryley Dr D Jones Mrs L Latham Mrs S Carroll Director of Strategy and Performance Director of Service Reform Associate Director Corporate Governance Healthwatch Stockport 83/17 APOLOGIES Apologies were received from Dr L Hardern and Dr A Johnson. 84/17 DECLARATIONS OF INTEREST There were no declarations of interest on this occasion. 85/17 APPROVAL OF THE DRAFT MINUTES OF THE GOVERNING BODY MEETING HELD ON 28 JANUARY 2018 The minutes of the meeting held on 28 January 2018 were approved as a correct record. 86/17 ACTIONS ARISING Patient Story Action completed and to be removed from the log Performance Report Action completed and to be removed from the log Safeguarding Report Action still to be completed. 87/17 ANY OTHER BUSINESS There were no items on this occasion. 88/17 PATIENT STORY 1
4 004 The Governing Body heard from a patient who had recently engaged in the Man Vs Fat Football initiative. He explained the support available on and off the pitch and the motivation of the league based activities based on exercise and weightloss goals. He noted how goals were scored on and off the pitch and the overall sense of team achievement He shared his passion for football and the benefits to his health and explained how the team spirit off the pitch was as motivating as the football itself. The Governing Body commented on the following elements of the story: The patient had accessed the initiative outside Stockport and V Owen Smith would investigate provision for the scheme or similar within Stockport. The importance of providing a range of activities for those in harder to reach groups. GPs present were aware of the scheme and signposting to it but noted the importance of easy access to social prescribing schemes and awareness raising of available options. The need to understand the motivations of individuals and the focus on behavioural coaching. Resolved: That Governing Body: 1. Note the Patient Story and express thanks to the patient for sharing their experience. 89/17 CORPORATE PERFORMANCE REPORTS (a) Finance M Chidgey provided an overview of the CCG s financial position as at Month 11 of the 2017/18 financial year. He confirmed that the outturn position was in line with the CCG s planned surplus and confirmed the NHS England technical financial adjustments which would be made. He confirmed that the 0.5% financial reserve as part of the NHS England Risk Share arrangements could now be released. He confirmed the financial variances in the areas of acute treatment, Continuing and Complex Healthcare and Prescribing. The Governing Body was informed that the CCG would be carrying a recurrent deficit forward into the 2018/19 year. The Governing Body noted the importance of clarity of message regarding the requirements placed on the CCG by NHS England for the technical adjustments. On behalf of the Governing Body, J Greenough expressed thanks to M Chidgey and the Finance Team for controlling expenditure within the year. Resolved: That Governing Body: (i) Notes the year-to-date position is in line with plan. (ii) Notes that an outturn breakeven position is forecast to be delivered. (iii) Notes a NIL net risk position is now being reported. (iv) Notes that the position includes provision in full of the 0.5% non-recurrent uncommitted reserve as required by NHS England business rules. (v) Notes that the Mental Health financial performance target is forecast to be achieved. (vi) Notes that a recurrent deficit of c 3.10m is currently forecast to be carried forward into 18/19 and the consequent impact on the CIP target for 2018/19. (b) Performance M Chidgey provided an overview of current performance noting in particular the three key areas of Urgent Care Emergency Department Performance, Ambulance Reporting and the Elective Care Referral to Treatment Standard. With regard to urgent care performance he informed the governing body performance was significantly below the required standard and this had continued. He explained that no statistical variances could be identified in terms of activity or demand levels at system level. The Governing Body was informed that performance over Winter was significantly below the trajectory agreed with the Greater Manchester Health and Social Care Partnership. The Governing Body considered the commissioning approach to additional capacity for the Winter period including winter resilience beds at NHS Stockport Foundation Trust, 2
5 005 community beds and wider schemes which had been commissioned as part of system transformation including 7 Day GP Services and Pathfinder. Challenges regarding recruitment and staffing were noted. M Chidgey noted the significant number of 12 hour breaches which had been reported at NHS Stockport Foundation Trust in January. He confirmed that medical staffing levels within the Emergency Department had been increased over night and that patients were seen by a senior clinician in many cases much earlier as part of their patient journey. It was noted that the Urgent Care Improvement Plan implementation and monitoring remained a significant focus for the CCG and its system partners. The Governing Body was informed that as a result of local performance against new measures for ambulance reporting, the CCG had formally escalated the matter to NHS Blackpool CCG as the lead commissioner. Cancellation of elective surgery during the Winter Period in line with national policy was noted to have impacted on Elective Care Referral to Treatment times. In considering the report the Governing Body noted the following: Impact on time taken to admit patients at NHS Stockport Foundation Trust who arrived by ambulance and the impact of delayed handovers on ambulance capacity. Review of North West Ambulance Service (NWAS) in terms of fluctuations in performance and the size constraints of the Emergency Department. Importance of Community Services providing prompt responses to patient discharge in order to facilitate effective flow. R Gill confirmed that information was being gathered across the system to try and gauge demand in primary care services. The role of the Finance and Performance Committee in considering key performance areas was noted. Plans in place to respond to mixed sex breaches at Pennine Care and the role of Quality Committee in seeking assurance in terms of the impact on quality and patient experience. Specialties particularly impacted on by performance against the 18 week Referral to Treatment requirement were orthopaedics, ophthalmology, general surgery and ENT. Excellent performance in the areas of cancer and mental health were noted. Resolved: That the Governing Body: 1. Notes the format and timing of performance reporting in transitioning to a quarterly integrated performance report. 2. Notes the performance issues highlighted to the Governing Body, in particular the continued levels of urgent care performance. 3. Requests that future performance reporting include Referral To Treatment narrative in terms of distribution of waiting list including breakdown by speciality on admitted and none-admitted. 90/17 STOCKPORT TOGETHER HIGHLIGHT REPORT T Ryley provided an update on the recent activity of the Stockport Together Transformation Programme and drew the Governing Body s attention to progress made in terms of the implementation of service delivery, the complexity and issues associated on delivering substantial large scale change and the focus on delivery in Quarter 1 of the 2018/19 year. He highlighted the following key elements: Progress had been good in implementing a number of significant elements of the new models of care. Some had been delayed in initial implementation and taking a service to fully optimised and operationally effectively was critical. Delay in implementation had impacted on timescales for benefit delivery. IM&T delivery to support change had continued to progress although the reduction in the national Digital Fund allocation to Greater Manchester would impact on Stockport. The establishment of the Leadership Team and Chief Executive of Stockport Neighbourhood Care had accelerated the organisation s development. 3
6 006 Greater integration could be demonstrated in the neighbourhoods. The Governing Body considered the issues where greatest resource was being focused in terms of implementation and in particular the pace in mobilising the GP Federation, Viaduct Care to which a contract had been negotiated for the delivery of 7 Day Services. The Benefits Realisation Plan would be reported to a future meeting of the Governing Body and the CCG would review a re-negotiated Investment Agreement with Greater Manchester Health and Social Care Partnership in Quarter 1 as was happening across all Localities. In response to the report the Governing Body considered the following issues: The upcoming system review visit by the Care Quality Commission (CQC) and commissioner support and input to the process. The importance of ensuring cultural and behavior change across the system in terms of future commissioning and provision in order to realise the benefits of transformation. The importance of the Benefits Realisation Plan providing measures which were both qualitative and quantitative and in particular, the tiered approach to tracking delivery noting that Tier 4 focussed on what was experienced or felt differently on the ground. The Governing Body noted the delay in implementation and therefore benefits delivery. D Jones confirmed that the independent evaluation of the Stockport Together Programme was underway and would consider the impact at both system and person level of change. Resolved: That Governing Body note the report. 91/17 LOCALITY CHAIRS UPDATE S Woodworth provided a brief overview of practice based work including engagement through Viaduct Care in the implementation of 7 Day Services and work with district nursing in Victoria Neighbourhood. He acknowledged the pressures which had been felt across General Practice during Winter and expressed thanks to GP colleagues for supporting the population and continuing to deliver high quality services to their patients. He commended the efforts of GPs in terms of flu vaccination rates across Stockport. Resolved: That Governing Body note the update. 98/17 REPORT OF THE CHAIR J Crombleholme confirmed that a Part 2 meeting would take place on the rising of the Part 1 meeting. 99/17 REPORT OF THE CHIEF OPERATING OFFICER G Mullins introduced the report and the following updates on key elements were provided: Care Quality Commission System Review Visit Upcoming CCG Quarter Four Assurance Meeting Relocation of the CCG s Headquarters to Stopford House The Governing Body was informed of the CCG s work to commission effective urgent care, including understanding of demand and required service and capacity responses. She noted that additional leadership level capacity had been deployed in this area and a significant amount of wider team resource would focus on ensuring delivery of the Urgent Care Plan and CCG s approach to commissioning urgent care. In response to questioning, the Governing Body was informed that: A number of contractual notices had been issued to NHS Stockport Foundation Trust in response to performance issues relating to delivery of Urgent Care. 4
7 007 Financial penalties had been applied in line with contractual provisions with money being reinvested into improvements including additional winter capacity and funding for the acute interface service. A review of commissioning of urgent care would take place in the coming months. Changes in leadership at NHS Stockport Foundation Trust had recently taken place and lack of change earlier had impacted on the pace of cultural and behavior change. Commissioners were aligning support for NHS Stockport Foundation Trust with regulators. The Trust did deliver high quality outcomes for patients in many areas including orthopedics, stroke and neurology. Resolved: That Governing Body note the report. 100/17 REFRESH AND UPDATE OF CCG OPERATIONAL PLAN 2018/19 M Chidgey provided an overview of the CCG Operational Plan highlighting the recently issued planning guidance and areas requiring specific review. He confirmed that the final version would be submitted to Greater Manchester Health and Social Care Partnership at the end of April He noted the distance from financial target for both the region and Stockport and the basis on which the CCG s budget and plans had been developed. He confirmed the CIP requirement for the CCG in 2018/19 and the risk share in place across the Locality relating to system investment and return in transformation. The plan was noted to include 2.5m unidentified CIP. The Governing Body was informed of the activity elements of the plan, including position of no growth as aligned to delivery of new models of care. Benefits assumed in 2017/18 would be carried forward in 2018/19. In particular requirements around prescribing costs were highlighted, including national work to reduce level of price concessions. Investments in mental health were noted and in particular previous proposed commitments around commissioning of new services including stroke rehabilitation. M Chidgey confirmed that all contracts for the coming year had been agreed and signed and mobilisation of Stockport Together was underway. A compliant trajectory regarding urgent care performance had been submitted to regulators by the Urgent and Emergency Care Delivery Board (UECDB) however this continued to pose a significant performance risk for the system. In considering the report the following elements were noted by the Governing Body: The need as part of delivery planning to consider development of clinical priorities for focus in the coming year. Capacity to deliver the requirements of the Plan in 2018/19 was highlighted, in particular the importance of ensuring commissioner leadership in the commissioning of new models of care and related services. Focus on neighbourhoods as a key mechanism for delivery. The development of Viaduct as a lead partner in delivering key elements of the CCG Plans including 7 Day Services. Additional focus in plans required on how patient experience had informed the focus. The need for plans to recognise the significant workforce challenges which existed across the system. In response to questioning about unidentified CIP, M Chidgey confirmed that in response to submitting a plan including unidentified CIP, the CCG would be required to undertake a financial risk assessment on non-delivery. Resolved: That Governing Body: 1) Approves the refresh of the Operational Plan, specifically the financial Plan for 2018/19 (appendices 1-3 attached) and to confirm that in approving the plan the level of financial risk of the CCG is understood. 2) Approves the stated investments and CIP schemes. 5
8 008 3) Notes the significant level of agreement of contracts with providers and that this includes a contract with the GP Federation. 4) Delegates to the CFO the ability to vary this plan resulting from:- Final contract negotiation outcome. Further revisions to national guidance or GMHSCP agreement. Further progress on CIP and Investment Plans 5) Note that a system wide urgent care plan is required to be submitted in April. 101 /17 REPORTS FROM COMMITTEES (a) Quality Committee A Rolfe provided an overview of the recent work of the Committee including highlighting to Governing Body the areas in which greater assurance could be provided. These included Safe Staffing, Safeguarding and issues relating to NHS Stockport Foundation Trust. Resolved: That Governing Body notes the report. (b) Finance and Performance Committee V Owen Smith confirmed that as part of the Committee s work they had considered delivery of 2017/18 CIP, planning for 2018/19 and considered a benchmarking report on prescribing in order to provide further assurance locally. Resolved: That Governing Body notes the report. (c) Primary Care Commissioning Committee J Crombleholme provided an overview of the recent work of the Committee noting in particular the approval of the merger of Eastholme Surgery and Heaton Moor Medical Group. Resolved: That Governing Body notes the report. 6
9 009 NHS Stockport Clinical Commissioning Group 28 March 2018 Actions arising from Governing Body Part 1 Meetings NUMBER ACTION MINUTE DUE DATE OWNER AND UPDATE 3 Safeguarding Annual Report Notes that C Morgan and J Greenough would meet with J Parker to review the work which had been undertaken in 2017/18 and would inform the Annual Report. 81/18 April 2018 C Morgan, J Greenough and J Parker 4 Patient Story 1. Note the Patient Story and express thanks to the patient for sharing their experience. 88/17 April 2018 L Latham 5 Performance Report 1. Requests that future performance reporting include Referral To Treatment narrative in terms of distribution of waiting list including breakdown by speciality on admitted and none-admitted. 89 (b) July 2018 M Chidgey
10 010

11 011 Draft CCG Annual Report 2017/18 and Draft Audit findings Report. NHS Stockport Clinical Commissioning Group will allow people to access health services that empower them to live healthier, longer and more independent lives. NHS Stockport Clinical Commissioning Group 7th Floor Regent House Heaton Lane Stockport SK4 1BS Tel: Fax: Text Relay: Website: Page 1 of 3
12 012 Executive Summary What decisions do you require of the Governing Body? The Governing Body are requested to:- Approve the draft Annual report and Accounts for 2017/18. Consider the report of the independent auditors. Confirm that the Accountable Officer should sign the letter of representation. Delegate to the Chief Finance officer authority to amend the draft report and accounts for:- o any changes recommended by the external auditors in their final report. o any immaterial formatting or content changes identified prior to finalisation of the report. and to agree with the chair how any such changes should be recorded and reported. Please detail the key points of this report The reports cover:- Annual Report and Accounts This is a statutory report, it is confirmed that in regard to form and content it meets the nationally mandated standards. The accounts of the CCG are consistent with the forecast financial position reported to the Governing Body in March 2018 with the exception of the following changes required by NHSE:- o Increase in surplus of 2m due to release of the national risk reserve. o Increase in surplus of 0.5m due to rebate of Category M drug charges. Audit Findings Report The Audit Findings report highlights any significant findings arising from the audit for the benefit of those charged with governance, as required by International Standard on Auditing (UK & Ireland) 260, the Local Audit and Accountability Act 2014 and the National Audit Office Code of Audit Practice. What are the likely impacts and/or implications? Individually and in combination, these documents are a fundamental part of both the CCG s statutory reporting requirements and the system of internal control. How does this link to the Annual Business Plan? These are mandated reporting requirements. What are the potential conflicts of interest? None Where has this report been previously discussed? Audit Committee 16 th May 2018 Page 2 of 3
13 013 Clinical Executive Sponsor: Ranjit Gill Presented by: Mark Chidgey Rob Jones (KPMG) Annual Report and Accounts Audit Findings Report Meeting Date: 22 nd May 2018 Agenda item: 6 Page 3 of 3
14 014

15 015 Annual Report & Accounts
16 016 BLANK PAGE 2
17 017 NHS Stockport Clinical Commissioning Group Annual Report and Accounts 2017/18 Presented to Parliament pursuant to Schedule 15 of the NHS Act
18 018 Contents Title Page 1. Performance Report Overview 5 a. Welcome from Chief Operating Officer and Chair 5 b. About NHS Stockport CCG 7 c. Vision and Values Performance Analysis 18 a. Performance Summary 18 b. Key performance highlights 20 c. Performance Report 21 d. Key risks and issues 24 e. Financial summary 26 f. Sustainability 27 g. Improving quality 28 h. Engaging people and communities 31 i. Reducing health inequalities 39 j. Health and wellbeing strategy Accountability Report Corporate Governance Report 43 a. Members Report 43 b. Statement of Accountable Officers Responsibilities 51 c. Governance Statement Remuneration and Staff Report Parliamentary Accountability and Audit Report Financial Statements and Notes 79 4
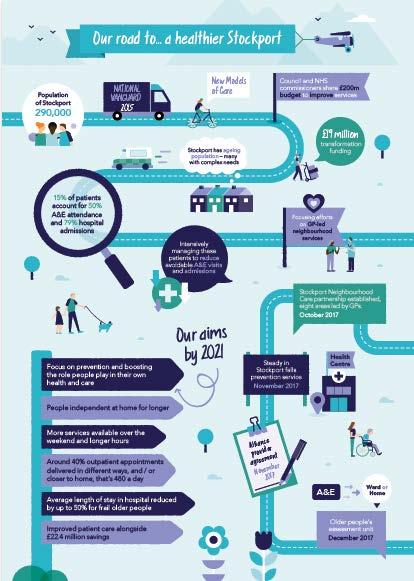
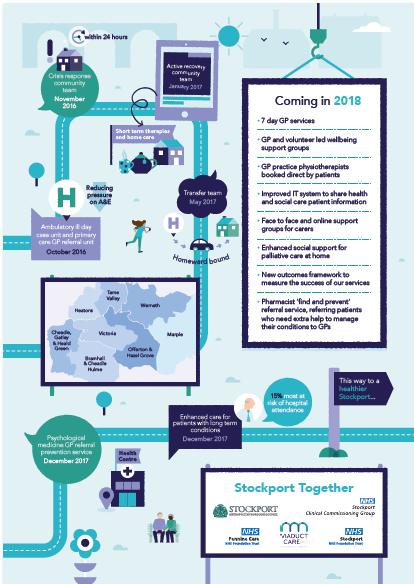
19 PERFORMANCE REPORT 1.1 Overview This performance overview provides a summary of: The purpose of NHS Stockport Clinical Commissioning Group The key risks to achieving our objectives How the CCG has performed during the year Further detail can be found within the annual report and accounts. a Welcome from Chief Clinical Officer and Chair The last year has seen residents across Stockport continue to receive the high quality of care, despite the very challenging financial climate facing the NHS - a fact that is recognised by local communities. Overall patient satisfaction with their GP surgery is rated amongst the highest across the whole of Greater Manchester. Add to that, the recorded high levels of satisfaction patients have with their hospital and community health services, and we really have much to be proud of. However we continue to face a number of complex challenges and consequently we are working in greater collaboration with partners, including social care, to change the way services are delivered. Our local Accident and Emergency (A&E) performance continues to be the most difficult issue we face. Despite on-going initiatives and support, Stockport NHS Foundation Trust A&E is still rated as one of the lowest at achieving its 4-hour wait targets in England. A range of complex issues have combined resulting in these difficulties but it is an area we are determined to improve. One positive step was the introduction of shared access to patients health records, enabling staff within A&E to easily view a patient s General Practice (GP) record so speeding up treatment and care. The challenging financial climate for both health and social care over the past few years, combined with increasing demand from a growing and ageing population, have put services under enormous pressure. It has been clear for some time that we simply cannot carry on with our current hospitalbased model of care. Instead, the NHS needs to work differently, based on the needs of the population we serve, by providing more care in people s homes and the community whilst breaking down barriers between services. This means co-ordinating the work of general practices, community services and hospitals to meet the needs of people requiring care. This is particularly important for the growing numbers of people with several medical conditions who receive care and support from a variety of health and social care staff. 5
20 020 Over the last 12 months we have engaged with a large number of specialist interest groups, patients, carers and local communities to help shape the future of health and social care across the area as part of our Stockport Together Programme. Through a year-long listening project and formal consultation more than 30,000 people were represented by local organisations and groups in providing feedback on plans to meet the future challenges. Over the last year, as part of our Stockport Together programme we have begun to see the delivery of more joined-up health and social care services across our communities and have introduced a number of new services to keep patients safe and avoid hospital admissions. To support the developments within the community, Stockport is the only locality within Greater Manchester to have successfully implemented GP Extended Access to every practice and has a scheduled rolling introduction of 8am-8pm GP coverage by June A new GP Home Visiting service is being launched, to ensure that vulnerable patients are seen much quicker, helping to keep them out of hospital and supporting a faster discharge to get them home safely if they are admitted. With Mental Health becoming an increasing area for demand, over 1m has been invested in a new community based Psychological Medicine service in Primary Care. The service will work with people who have complex mental health issues to ensure they are supported in the community. In doing so, we can improve people s health and wellbeing, deliver a better patient journey and reduce demand on our urgent care services. In addition a number of other services have been successfully introduced including the Steady in Stockport falls and bone health service, Crisis Response Team and a new Urgent Treatment Centre and Frailty Unit at Stepping Hill Hospital. Finally, another significant success was the amazing work by our GPs, District Nurses, Midwives, School Health and other community teams to help Stockport to achieve the highest level of flu vaccination in England, with more than 85,000 people immunised, which is a huge achievement. Whilst we have more challenges ahead, none of the improvements that have taken place over the last year would have been possible without the hard work and commitment of staff to deliver the changes. This is now transforming the way care is delivered, in the interest of the patients we serve. There is much we should be proud of from this past year and in the years ahead we will continue to improve, innovate, and re-shape health care services around our local communities. Dr Ranjit Gill Chief Clinical Officer Jane Crombleholme Chair of the Governing Body 6
21 021 b. About NHS Stockport Clinical Commissioning Group NHS Stockport Clinical Commissioning Group ( The CCG ) was formed on 1 April The CCG was licensed without conditions by NHS England. The CCG is an NHS clinical commissioning group made up of the 39 General Practices in Stockport (as of March 2018). The CCG commissions (buys) health and care services on behalf of patients registered with Stockport GPs. The services that the CCG is responsible for include: Planned hospital care Urgent and emergency care Rehabilitation care Community health services Mental health and learning disability services The CCG is also a level 3 delegated commissioner of primary care services, which means the organisation is responsible for managing the contracts with GP Practices. The organisation works closely with patients and health and social care partners (for example, hospitals, the Local Authority and patient groups) to ensure services meet local health needs. The GP practices have appointed a Governing Body to discharge the CCG responsibilities on their behalf. How the CCG operates NHS Stockport CCG is responsible for making sure that the 300,000 people registered with a Stockport GP have access to the healthcare services they need. The CCG recognises that our decisions, policies and services have a major impact on the lives and wellbeing of the local people and actively seeks to engage with all sectors of the community to ensure that everyone has an equal chance to have their say before any major decisions are made. Stockport continues to be one of the healthiest places to live in the North West, resulting in a generally older population than the rest of Greater Manchester. However, this is not the experience of all of our residents. Local communities experience varying levels of affluence and have significantly different health needs, in the least affluent areas life expectancy is 10 years lower than in the most affluent. Stockport, like other local areas across the country, faces a number of challenges in the delivery of existing health and social care services. These issues include: The success of an ageing population leads to increasingly complex care needs for individuals who are at higher risk of isolation and loneliness. This is because more people live on their own without direct family support; A population where birth rates have risen, especially in areas of deprivation. This has lead to more children and young people living in low income households where health outcomes are poorer; 7
22 022 Changes in the most common health issues experienced by the population, to those linked to lifestyles or are otherwise preventable; A period of economic challenge that affects the incomes and entitlement of the most vulnerable people in Stockport; Fragmented services which are complicated to access, has duplications and are not as focussed on the individual s needs as they could be; A system where too many people are admitted to hospital when many could be better and more appropriately cared for at home; Increasing financial pressures with deficits forecasts for Stockport as demand growth continues if service delivery is not improved. Stockport s population has a wide range of health needs. Stockport has the oldest age profile in Greater Manchester and the population of the area continues to age. Currently 19.4% people are aged 65+ and this is likely to rise to 21.8% by 2024, with an additional 9,681 people. On average each year our local health and social care activity includes: 98,000 A&E attendances 89,00 hospital admissions 543,000 community contacts 8,500 adult social care clients 700,000 GP practice visits 11,000 people in touch with Pennine Care Children and Young People Almost 1 in 4 children in Stockport are overweight or obese by the age of 4 rising to almost 1 in 3 by the age of 10. Almost 1 in 4 of 5 year olds suffered tooth decay. 8,500 children and young people are estimated to live in poverty. Over 70% of young adults are not active enough. Anxiety is the major long term condition affecting young people in Stockport with more than 2,700 cases reported. Self-harm hospital admissions in those aged are higher than the national average. Adults and Older People 1 in 4 of adults are overweight or obese putting them at greater risk of liver disease, heart disease and diabetes. Cancer is the major cause of premature death with 45% of deaths under 75 years. Stockport s population is older than the England average, with an increasing number of older people living with dementia and other long term conditions. Half the older population of Stockport has a long term health problem or disability and 1 in 5 has 2 or more long term conditions. 1 in 3 older people live alone. 2,700 older residents suffer with Dementia. 8
23 023 c. Vision and Values Vision The CCG s vision is We exist so that Stockport people will access high quality health services that empower them to live healthier, longer and more independent lives and underpins the organisations approach to everything it does to help improve the health and services across the borough. Values The values that lie at the heart of our work are: Being quality obsessed - by putting the patient at the centre of decision-making we will continually improve services. Keeping a primary and community focus - we will deliver care as close to home as possible, with general practice at the heart of care. Innovation we will continually look for better and more cost effective ways of delivering care. Working collaboratively - we will look to work constructively with others to shape the future. Patient responsibility - we will work with patients and carers, empowering them to take responsibility for their own health and use NHS resources wisely. Distributive leadership - we will devolve decision making and resources to those best placed to meet the needs of our community. Behaving Professionally - we will be trustworthy, evidence-based, systematic and disciplined. The CCG s values inspire the organisation to design and commission high quality services for patients. The organisation aims to meet local needs, deliver improved health outcomes and demonstrate best practice with partners. The same spirit is driving the organisation to continue to widen our partnership working, with the goal of transforming the whole health and social care system in Stockport as part of the devolution of Greater Manchester. The CCG strongly believe that as an integrated commissioner it will be in an ideal position to continue to deliver this transformation, by focusing on self-care and prevention, reducing dependence on hospital care and delivering more services closer to home. This Annual Report details the work in the 2017/18 financial year and celebrates the dedication and hard work of staff. 9
24 024 Improving health and social care in Stockport Like many areas across the country, health and social care services in Stockport are subject to growing demand from an ageing population with increasingly complex care needs. In its current fragmented form, the health and social care system is financially unsustainable. Our vision is to provide a truly joined-up, high quality, sustainable health and care system with partners across health and social care services in both Stockport and Greater Manchester. Strategic objectives: In collaboration with our GP members, local people and partners the CCG has identified four strategic objectives: 1 Transform the experience and care of adults with long term and complex conditions; 2 Increase the clinical cost effectiveness of elective treatment and prescribing; 3 Improve the quality, safety and performance of local health services in line with local and national expectations; 4 Ensure better prevention of disease and early identification of disease leading to reduced inequalities. These objectives will help the CCG to focus on ensuring that people living in Stockport will receive integrated health and social care services that are designed to keep them well, rather than focusing on treating their symptoms when they become ill. The effective use of technology and data will help us to understand people and their health and care needs better and to provide the right advice and support to help them stay healthy for as long as possible. People will be at the heart of the system and care will wrap around them. However everyone will understand the part they can play in preserving health and care services for future generations by using available resources wisely and well. GPs will be pivotal as the first point of contact for many people needing access to health and care. They will take responsibility for working with other care providers who will all make use of technology to ensure that every individual in Stockport receives the best care for their needs delivered as close to home as possible. Integrated teams of primary, community, mental health and social care professionals will provide a single service, close to home, that focuses on the needs of the individual. Professionals will work with people to help them remain at home and independent without requiring a visit to or stay in hospital or residential care. The CCG will implement an approach which will ensure that service users are connected to others with similar health conditions so that they can share emotional and practical support. Routine services will be available for more days of the week, offering a much wider range of proactive and responsive services that meet the needs of patients in a modern society. 10
25 025 When ill, or experiencing an escalation in conditions, people will have access to high quality hospital services, working together across the South of Greater Manchester to ensure general and specialist care of the highest standards 24 hours per day, seven days per week are available when people really need it. People will have access to high quality elective surgical and medical services from a choice of providers with a greater emphasis on day case treatment using the most modern techniques with after care provided closer to home. So whilst some people may travel further for their initial treatment, their follow up care such as out-patients appointments will be provided within their local community or even within their own homes via Skype, texting or other means of communication. The CCG will improve access to mental health services to ensure that mental wellbeing is treated as well as physical health. As a result of these improvements, the health and care system will ensure that the people of Stockport receive the best quality care available with more personal control over both their care budget and their own health. Ultimately, less people in Stockport will die of preventable diseases, adding 1,000 years of life to the population and reducing health inequalities in the borough. Delivering our vision The CCG recognises that the vision requires a collaborative approach to deliver the best outcomes for local people. The CCG is an active partner is Greater Manchester s devolved Health and Social Care Partnership, working with health and social care partners across the metropolitan boroughs to improve health and increase the quality of services. Locally, the vehicle for change is Stockport Together, which brings together local health and social care partners with GPs and voluntary organisations to improve services across the borough. The organisation is also delivering change in other ways, including the Healthier Together collaboration. Strategic Commissioning Ever since NHS Stockport CCG was established in 2013, it has continued to evolve and find better, more collaborative ways of working with partners. Nationally, and indeed locally, there has been good progress on greater integration of front line services, with health and social care coming together and in the commissioning of services. Stockport has also developed a local health outcomes framework that will change the way in which services are commissioned and have a far greater emphasis on local population needs. Commissioners from health and care have been working even more closely together since 2016 and have pooled approximately 200m of money, underpinned by a Section 75 legal agreement, in order to commission services from a collaborative position. This is overseen by the Health and Care Integrated Commissioning Board which is comprised of Clinical and Council Leaders and meets in public. 11
26 026 In 2017/18 the focus for the Board has been on: Developing the Outcomes Framework; Working collaboratively to further improve quality in care settings, including care and residential homes; Taking a systems approach to planning and contracting; and Concluding the procurement for the Multi-Specialty Community Provider (MCP). As a result of the CCG s ambition to become an integrated strategic commissioner working with Stockport Council, there are two levels of commissioning that are emerging within health and social care and Stockport will continue to evolve to ensure it is able to meet the needs of local communities. Strategic Commissioning Strategic Commissioning will be the system-wide leadership and planning across Stockport. The overall function will be to deliver improvements over the longer term in the way the local health and care system operates, ensuring that has a clear understanding of needs and requirements across the area and at a neighbourhood level. It will also monitor the local system performance as well as redesigning and repositioning services to better meet local needs. Tactical Commissioning Tactical Commissioning will continue to provide a focused partnership with providers, organising: The procurement of some services; Contracting and sub-contracting Day-to-day management of the provider performance, against key criteria, including the new outcomes framework. This tactical commissioning function would normally focus on the short-term and annual cycles and in most cases will operate at locality level. Viaduct Care The CCG signed a ground-breaking agreement in March 2018 with Stockport GPs to deliver a range of new services that will increase access to high quality primary and urgent care. All the GP Practices have formally joining together to form a new GP Community Interest Company, Viaduct Care, that aims to improve and expand access to local services. The planned new services will be delivered in each of the eight neighbourhoods across Stockport. One of the new services to be launched, Clinical Triage and Home Visiting, will include GPs, Paramedics and Advanced Nurse Practitioners delivering urgent care home visits 7- days a week for patients clinically assessed by their own GP as too ill to leave home. The aims will be to support patients in the community, avoid unnecessary admissions, and where a patient requires admission, this is co-ordinated. 12
27 027 Patients will be able to give consent for the visiting clinician to have full access to their electronic GP record at their bedside, which will improve the quality of care and mean that repeat prescriptions can be ordered more quickly. The new service should also reduce the volume of additional home visits for local GPs, reducing the pressure on already busy practices. In addition, Stockport GP Practices have led the way in expanding access to local services, which has included GPs supporting the busy A&E at Stepping Hill Hospital by either re-directing non-emergency patients or providing treatment to those with non-urgent conditions 12-hours a day, every day. Viaduct Care will also be launching an expanded 7-day GP Service, with pre-booked, longer routine GP and nurse-led appointments available between 9am-1pm on a Saturday and Sunday in each neighbourhood. Plans are already underway for more new GP-led services that will help patients receive the best quality healthcare and continually improve access to services across local communities. This includes increasing direct access in GP practices to Physiotherapy, Pharmacy and Mental Health and Well Being Services to support social prescribing. Greater Manchester Health & Social Care Partnership In April 2016 Greater Manchester took charge of its health and care system as one Partnership spanning NHS and local government, commissioners and providers of both physical and mental health. In doing so, we embarked upon the most radical health and care transformation programme in the country. We are now approaching the third year of the delivery of our strategy Taking Charge. Two years into our journey, we can see a health and care landscape in Greater Manchester that looks fundamentally different. Our approach to this change has been guided by a core principle: identifying who contributes to health creation and how they can be better connected. Through our programme of reform and investment we now see our way to the system architecture in GM that will be in place as a legacy of Taking Charge. This will comprise these recognisable and consistent features: The establishment of 10 Local Care Organisations (LCOs) integrating provision; Pooled health and social care resources into a single budget, managed through an integrated Single Commissioning Function in all ten localities; New models of hospital provision seeing hospitals working together in Greater Manchester at a much greater scale than ever before to a set of consistent quality standards; A Greater Manchester-wide architecture where it makes sense to do things at greater scale including the GM Commissioning Hub, Health Innovation Manchester, a Digital Collaborative, a Workforce Collaborative and a one public service estate strategy. To find out more go to: 13
28 028 Stockport CCG has led the development of a framework for evaluation of locality care organisations in Greater Manchester to ensure that the GMH&SCP are able to evaluate the success of the devolution programme. Stockport have been the first LCO to commence local evaluation and will share the findings from this work at the earliest possible point to support decision making and future planning within Stockport and across the region. Stockport Together Locally, our plan to deliver these changes is Stockport Together, bringing together health and social care partners with GPs and voluntary organisations to improve services across the borough. This new model of care is built around eight Neighbourhood Teams, which bring together primary and social care, physical and mental health services to meet the needs of local people 7 days a week. They are supported to do this by an integrated Intermediate Tier providing essential community crisis response, intermediate care, reablement and home care services 24/7 to avoid unnecessary admissions to hospital and support sustainable early discharge. Changes to Urgent Care will optimise how people with ambulatory care-sensitive conditions are managed in the community, rather than as a hospital admission. The CCG will roll out alternative approaches to traditional Outpatient models that deliver more effective solutions outside of a hospital setting, using technology to enable communications, advice and treatment between patients, GPs and specialists. These improvements will deliver: Improved health and wellbeing with an emphasis on independence; A financially sustainable health and care system; A reduction in premature mortality from causes preventable by healthcare, with healthy life expectancy increasing fastest in the most deprived areas of Stockport; A reduction in the number of people reporting social isolation; More people feeling supported to manage their condition; Fewer working adults with long-term sickness; More people / carers who would recommend the service; More people at end of life die in their preferred place of choice; Meeting the NHS constitutional standards. More information is available via: 14
29 029 15
30 030 16
31 Performance Analysis a. Performance Summary In December 2016, NHS Stockport agreed its two-year operational plan for 2017/ /19. Our commissioning intentions for 20171/18 prioritised: Providing stability for General Practice whilst developing Primary Care at scale; Significantly investing in mental health and community services to enable a sustainable shift in service provision from reactive acute care to preventative and proactive integrated care out of hospital; Delivering on key national standards with assurance that there is sufficient acute care capacity to meet need; Developing Stockport Together s new model of care. Investing in Change Over 2017/18 the CCG has seen significant progress in a number of areas, including: An additional 2m was invested into General Practice above the 2016/17 funding to increase contract values, deliver the GP Forward View, to improve estates, IM&T and continue to support the GP development scheme; A further 0.43m of non-recurrent funding was invested in development of the GP federation, roll-out of the EMIS web patient record system, training care navigators and medical assistants for all practices and the GP resilience programme; An additional 2.8m was invested into neighbourhoods to build Primary Care at scale, including additional pharmacy advisors working in General Practice, mental health liaison and direct access physiotherapy; An additional 0.95m was invested into Mental Health services, supporting increased capacity in CAMHS, IAPT, RAID and Early Intervention in Psychosis services; post-diagnostic dementia care; and community eating disorder teams; The CCG commissioned extra elective activity in hospital to reduce backlogs and waiting times; The CCG reached agreement to provide 6m of GP investment with Viaduct Care; The CCG signed off business cases investing an additional 9m into neighbourhood based services, the benefits of which people will start to see in Delivering New Models of Care Commissioned the Greater Manchester standards for primary care; Established a GP Streaming service in A&E, taking 20 patients a day out of the emergency department; Implemented post-diagnostic care and support for dementia; Recruited a specialist nurse in primary care to improve uptake of annual health checks among people with a learning disability; Launched a new community falls service Steady in Stockport; Development of a Provider Alliance, bringing together partners in shadow form; 17
32 032 Cross-economy agreement of Stockport Together s detailed transformation plans for the next 5 years. Improving Quality and Meeting National Standards Major improvements have been seen in managing Delayed Transfers of Care rates through increased discharge to assess, weekend working and care home development. However there is more to do to ensure patients are not waiting longer than necessary in an acute setting; Rated as Outstanding nationally for cancer services, with local patients more likely to be diagnosed early (54.4% compared to 52.4% nationally) and one-year survival rates among the highest in the country at 71.9%; Rated as Outstanding nationally for dementia services, with one of the highest diagnosis rates in the country (73.5% compared to the national standard of 66.7%); Improved our national ratings for Mental Health and Diabetes care; Investment over recent years has resulted in notable improvements in mental health performance, meeting all national standards for the year and improving our clinical rating under the CCG Integrated Assurance Framework; Patients in Stockport are more likely to receive all the NICE-recommended treatment targets for diabetes, with performance 4.7% higher than the national average; CCG achievement of the NHS financial business rules. Whilst the care provided in regard to high risk general surgery at Stepping Hill Hospital is already good, Stockport CCG is committed to the development and delivery of a single service for general surgery across the South East Sector of Greater Manchester. The new service will mean that Stepping Hill becomes a hub site and as such will see patients that would previously have been cared for at Tameside Integrated Care Foundation Trust. 18
33 033 b. The key performance highlights 2017/18 Performance of the CCG is monitored by NHS England, devolved to the Greater Manchester Health and Social Care Partnership, who regularly reviews our progress against: The CCG Improvement and Assessment Framework NHS Constitutional Standards. Our latest CCG assessment, which was published by NHS England in the summer of 2017, rated NHS Stockport CCG s annual performance as good, reflecting in particular significant improvements in financial performance and mental health services. The 2017/18 rating will be published in the summer of The latest Improvement and Assessment Framework (IAF) published by NHS England also highlighted areas where Stockport s performance is among the best in the country: Children aged in Stockport are less likely to be classified as overweight or obese; Diabetes Patients in Stockport are more likely to receive all NICE-recommended treatment targets; Stockport GPs have among the best rates for appropriate prescribing of broad spectrum antibiotics; Stockport patients are among the most likely to have cancers diagnosed at early stage; Over 90% of Stockport patients referred into cancer services start treatment within 62 days; One-year survival from all cancers is among the highest in the country at 71.9%; Patient experience of cancer services in Stockport is among the best nationally; Patient experience of maternity services in Stockport is among the best in the country at 82.5%; Post-diagnostic support for dementia patients amongst best in England at 80.5%; Patient experience of GP services in Stockport remains very high with 90% rating their care positively. 19
34 034 c. Performance report The CCG Improvement and Assessment Framework (CCG IAF): Over 2017/18 the CCG has made significant improvements in performance, remaining top rated across the country for cancer and dementia care, and improving our performance in mental health and diabetes. Clinical Priority 2016 Rating Progress made 2017 rating Cancer Top Performing Greater Manchester has established a Cancer Vanguard site, which will implement the findings of the cancer task force report. Outstanding Dementia Top Performing Investment made in dementia support for care homes and in neighbourhood teams. Outstanding Diabetes Greatest Need for Improvement Improved local Practice participation in the national diabetes audit to over 60%. Strong, positive outcomes above the England average. Investments made in patient education. Requires Improvement Maternity Needs Improvement Work is underway at Stockport NHS Foundation Trust to implement the national maternity services review. No rating to date Mental Health Greatest Need for Improvement Invested in additional mental health services to improve access, quality and safer staffing levels. There has been real progress on Mental Health targets and plan to improve further. Requires Improvement Learning Disabilities Needs Improvement Work is underway to improve uptake of LD Health Checks in Stockport including recruiting an LD nurse to support General Practice and all GP Practices are now signed up to the DES. The CCG are working with Greater Manchester on a common LD strategy across the city region. No rating to date As noted above, Stockport s performance is rated among the best in the country for 12 indicators, covering cancer, dementia, diabetes, primary care and patient satisfaction. As at the January 2018 national ratings, improvements remain to be made in: Attendance at structured education courses for patients diagnosed with diabetes additional Xpert patient courses have been commissioned to support this challenge; The rate of injuries from falls has improved across the year thanks to investment in a Steady in Stockport community falls prevention service, however work remains to bring performance in line with peers; The continued roll-out of Stockport s neighbourhood teams and improvements in the management of ambulatory care sensitive conditions will support improvements in urgent care performance and continued improvements in Delayed Transfers of Care. Adult social care improvements in line with Adult Social Care policy and focused quality improvements in nursing and residential care homes. 20
35 035 NHS Constitutional Standards Stockport s performance remains strong on cancer standards and mental health performance has consistently improved. Urgent Care Whilst the system has delivered a significant reduction in Delayed Transfers of Care (DTOC) waiting times for the Emergency Department (ED) remain significantly below the national constitution standard of four hours. Our main provider Trust, Stockport NHS Foundation Trust, has also reported a considerable increase in the number of people waiting over 12 hours in the ED department as part of to a very challenging winter period. New ambulance performance metrics were introduced part way through the year. Our ambulance provider North West Ambulance Service is not achieving response time expectations. In response, the CCG continues to work in partnership with providers to ensure that pathways are clear and services are resilient and safe. National funding secured in December is being used for schemes in Primary Care, Mental Health and Acute services as approved by the Stockport Urgent Care Delivery Board. Examples include additional medical staffing overnight within the Emergency Department, additional Mental Health beds within Stockport and enhanced case management within primary care. Alongside these additional interventions the Stockport Together new models of care continue to be implemented. The Acute Interface has been implemented with additional ambulatory care capacity in place on the Stepping Hill site and GPs reviewing patients within the Emergency Department. The neighbourhood model of care, including 7-day GP access, acute home visiting and multi-disciplinary review of patients has been launched with full mobilisation to be realised by the end of Elective Care The waiting time for diagnostic tests (6 week waits) is consistently close to the national standards but cumulatively fell short of the required levels. Performance for patients waiting at Stockport NHS Foundation Trust are consistently above the national standard with the majority of long waits for those patients accessing care at Manchester University Hospitals NHS Trust (formerly UHSM and CMFT). Cancelled operations increased over the winter period as a consequence of the nationally led prioritisation of urgent care over elective procedures. Where possible our providers have looked to minimise cancellations and day case procedures in particular have been relatively unaffected. There have been a number of 52 week waits with the main themes being: Administrative processes in providers - additional training is being provided to staff; 21
36 036 At Manchester University Hospitals NHS Trust, long waiting list issues are being addressed, but continue to delay care. In addition there is a very specialist plastic surgery service which is one of a very small number of services offering a specialist breast construction procedure. Demand for this procedure is very high and hence referrals are exceeding available capacity. Quality Indicators The CCG has had three confirmed MRSA infections identified against a zero tolerance policy and has also narrowly failed against the trajectory of total number of patients with a Clostridium Difficile diagnosis. The quality team continues to work with providers on analysis of cases and consolidated learning to improve infection control. The number of reported mixed sex accommodation breaches has increased during 2017/18. It is believed that this is predominantly greater awareness of the standards resulting in improved reporting at both Pennine Care and Stockport FT. A business case to alter the ward layout of inpatient facilities at Pennine Care is currently under review. Code NHS Constitution Indicator National Standard 2017/2018 Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar 2017/18 YTD to March 18 A&E Waits Patients should be admitted, transferred or discharged within 4hours of their E.B.5 arrival at an A&E department 95% 86.95% 88.22% 86.69% 81.99% 84.63% 81.99% 86.89% 80.41% 75.23% 74.34% 75.89% 70.11% 81.21% E.B.S.5 No waits from decision to admit to admission (trolley waits) over 12 hours Ambulance (Performance at Ambulance Trust Level) ARP.01 Category 1 (life-threatening) calls - 90th centile appropriate response time 00:15:00 #N/A #N/A #N/A #N/A 00:15:59 00:16:21 0:15:36 00:16:14 00:18:37 00:16:44 00:14:53 00:14:43 ARP.02 Category 1 (life-threatening) calls mean time taken for a response to arrive 00:07:00 #N/A #N/A #N/A #N/A 00:10:07 00:09:50 00:09:29 00:09:44 00:11:17 00:09:51 00:08:51 08:40:00 ARP.03 Category 2 (emergency) calls 90th centile appropriate response time 00:40:00 #N/A #N/A #N/A #N/A 00:55:54 00:56:11 00:57:41 01:10:18 01:43:58 01:31:33 01:12:05 01:14:15 ARP.04 Category 2 (emergency) calls mean time taken for an appropriate response to arrive 00:18:00 #N/A #N/A #N/A #N/A 00:24:20 00:25:04 00:25:55 00:30:34 00:44:49 00:39:59 00:31:59 00:32:34 ARP.05 Category 3 (urgent) calls 90th centile appropriate response time 02:00:00 #N/A #N/A #N/A #N/A 01:37:27 01:58:21 02:01:58 02:02:02 02:54:47 03:14:16 03:02:00 03:14:19 Category 4 (non-urgent assess, treat, transport calls only) 90th centile ARP.06 appropriate response time Category A calls resulting in an emergency response arriving within 8minutes E.B.15.i Red 1 Category A calls resulting in an emergency response arriving within 8minutes E.B.15.ii Red 2 Category A calls resulting in an ambulance arriving at the scene within 19 E.B.16 minutes Referral To Treatment Waiting Patients on incomplete non-emergency pathways waiting no more than 18 E.B.3 weeks from referral 03:00:00 #N/A #N/A #N/A #N/A 02:34:21 02:40:28 02:28:47 02:36:00 03:33:35 03:16:31 03:10:54 03:26:02 75% 70.08% 65.92% 62.50% 64.67% #N/A #N/A #N/A #N/A #N/A #N/A #N/A #N/A 75% 68.94% 64.43% 64.67% 64.17% #N/A #N/A #N/A #N/A #N/A #N/A #N/A #N/A 95% 92.54% 90.08% 89.39% 89.80% #N/A #N/A #N/A #N/A #N/A #N/A #N/A #N/A 92% 92.47% 92.89% 92.52% 92.41% 91.97% 91.61% 91.83% 92.18% 91.63% 91.31% 90.76% 89.35% 91.73% E.B.S.4 Zero tolerance of over 52 week waiters Diagnostic test waiting times Patients waiting for a diagnostic test should have been waiting no more than 6 E.B.4 weeks from referral Cancelled Operations 99% 99.2% 99.2% 98.8% 98.6% 98.0% 98.4% 99.1% 99.2% 98.9% 99.3% 99.5% 98.5% 99.0% E.B.S.6 Urgent operations cancelled a second time Number of patients not treated within 28 days of last minute elective cancellation. E.B.S.2 (Quarterly Measure) Cancer Waits Maximum two-week wait for first outpatient appointment for patients referred E.B.6 urgently with suspected cancer by a GP Maximum two-week wait for first outpatient appointment for patients referred E.B.7 urgently with breast symptoms (where cancer was not initially suspected) Maximum one month (31-day) wait from diagnosis to first definitive treatment for E.B.8 all cancers 0 #N/A #N/A 6 #N/A #N/A 2 #N/A #N/A 1 #N/A #N/A % 97.17% 97.95% 97.05% 97.95% 98.83% 97.57% 97.20% 97.65% 95.99% 96.47% 98.14% 96.13% 97.35% 93% 93.62% 96.84% 94.85% 98.57% 97.44% 94.92% 98.37% 97.89% 96.95% 99.23% % 98.03% 97.21% 96% 99.15% % 98.45% 99.17% 98.54% 98.26% 99.25% % 98.33% % % 99.25% 99.22% E.B.9 Maximum 31-day wait for subsequent treatment where that treatment is surgery 94% 95.83% % % % % 93.55% % % % % % 96.55% 98.77% E.B.10 Maximum 31-day wait for subsequent treatment where that treatment is an anticancer 98% % % % % % % % % % % % % % drug regimen E.B.11 Maximum 31-day wait for subsequent treatment where the treatment is a course 94% % % 97.30% % % % % % % % % % 99.78% of radiotherapy E.B.12 Maximum two month (62-day) wait from urgent GP referral to first definitive 85% 91.67% 77.05% 82.00% 90.91% 89.71% 87.50% 91.89% 84.29% 89.47% 84.48% 85.48% 92.86% 87.43% treatment for cancer E.B.13 Maximum 62-day wait from referral from an NHS screening service to first 90% % 82.35% % % % % % % % % % % 97.27% definitive treatment for all cancers E.B.14 Maximum 62-day wait for first definitive treatment following a consultant's No National Standard 84.21% 85.00% 95.83% 69.23% 82.61% 90.91% 88.46% 80.00% 79.17% 84.62% 80.00% 77.78% 83.33% decision to upgrade the priority of the patient Mental Health (February & March IAPT Performance based on Local data) Care Programme Approach - % of people followed up within 7 days of dischrage 95% % % % 92.00% % % 94.00% % 93.00% % 83.00% % 97.25% from psychiatric inpatinet care Percentage of people experiencing first episode of psychosis accessing 50% 0% 89% 83% 80% 100% 60% 60% 50% 67% 33% 80% 100% 70% treatment within two weeks. Percentage of people referred to the IAPT programme treated within 6 weeks of 75% 81.63% 86.67% 86.27% 84.00% 87.72% 87.76% 87.23% 93.22% 93.75% 88.37% 94.35% 90.45% 89.29% referral Percentage of people referred to the IAPT programme treated within 18 weeks of 95% 97.96% % 98.04% % % 97.96% 97.87% % % % % % 99.69% referral IAPT Recovery rate - the percentage of people who are moving to recovery 50% 51.11% 50.00% 46.81% 54.35% 52.83% 45.65% 52.38% 49.12% 52.27% 48.78% 62.84% 51.32% 52.39% during the reporting period. IAPT access 1.25% 1.20% 1.70% 1.79% 1.48% 1.59% 1.13% 1.55% 2.33% 1.50% 1.65% 1.78% 1.67% 1.61% Healthcare Acquired Infections E.A.S.4 HCAI measure (MRSA) E.A.S.5 HCAI measure (Clostridium difficile infections) 86 for the year Mixed Sex Accommodation Breaches E.B.S.1 Mixed Sex Accommodation Breaches
37 037 d. Key Risks and Issues The continued focus for the CCG in 2017/18 has been continuing to commission high quality health care services for the patients of Stockport whilst leading complex system wide transformation of the health and care system through the Stockport Together Programme. The CCG has aligned resource to ensure collaborative transformation work at Locality and Greater Manchester level has continued to progress in year alongside the delivery of the organisation s statutory duties including performance against the NHS Constitutional indicators. Performance in key areas has remained challenging and this has impacted on the risk profile of the CCG. The CCG s Governing Body has continued to monitor closely the organisation s financial position including its Cost Improvement Plan (CIP) Programme and the requirement for benefit delivery anticipated through the implementation of the Stockport Together Programme. The CCG ended the year delivering its agreed financial plan which included an in-year planned surplus of 3.82m. As a result of activity being above planned levels, non-delivery of recurrent CIP and an increase in the number of CHC placements, a 3.10m forecast recurrent deficit will be carried forward into 2018/19. System financial sustainability across health and care has been a priority for the CCG working collaboratively with partners. The CCG s financial and performance risks are reflected in the Board Assurance Framework and Operational Risk Register. In addition to the CCG s financial position, the CCG has continued to closely monitor the achievement of the NHS Constitutional target relating to Emergency Department performance and has ensured continued senior clinical and managerial leadership through the Urgent and Emergency Care Delivery Board and related sub-boards and governance structures. Those leaders have continued to focus on implementing detailed plans agreed with system partners and worked to ensure activity, where possible, can be deflected into alternative and appropriate settings, Delayed Transfers of Care (DToC) figures have been reduced successfully in-year. Risks relating to the urgent care system have featured heavily in strategic and operational risk registers with a particular focus on quality and safety of commissioned services. Mitigations have been monitored through a system wide Urgent Care Plan. The CCG has continued its current cycle of bi-monthly reporting of the Board Assurance Framework in year to reflect the scale, pace and complexity of the transformation programme underway and the increased risk profile of the organisation. It is also reflective of the increased requirement for risk leadership required at Governing Body level given the increased level of strategic and operational risk being mitigated. The Governing Body has continued to accept that, in delivering the benefits of New Care Models across health and care, the organisation s exposure to necessary risks is increased. Proactive risk management and oversight of mitigations has remained constant throughout the year with a particular focus on risks graded extreme and high. The continuous focus on system and partnership is reflected in the reporting of strategic and operational risks within the CCG. The innovation and organisational development 23
38 038 themes capture those risks, which linked to the system-wide transformation programme will create and deliver a sustainable health and care system for Stockport including system financial balance. System-wide and commissioner capacity and capability to deliver the strategy and operational requirements of transformation, and the CCG s routine business, have been reviewed closely in year. The CCG s leadership capacity has been flexed to ensure sufficient leadership and quality is in place in priority areas as aligned to the delivery of the CCG s Strategy and Operational Plan. Countering Fraud, Bribery and Corruption As part of ensuring the proper use of public funds, NHS Stockport CCG is committed to countering fraud, bribery and corruption. The CCG has a nominated Anti-Fraud Specialist (AFS), provided via Mersey Internal Audit Agency (MIAA), who is operationally accountable to the CCG Chief Finance Officer and reports on risks and progress to the Audit Committee. The CCG takes a proactive approach to reducing the risk of fraud. Regular information is circulated to staff to raise awareness of the latest fraud alerts and how to identify and report suspected fraud. The organisation has policies in place for staff, including declarations of interests and the Anti-Fraud, Bribery and Corruption and Response Plan Policy, which reinforce the commitment of the organisation to maintain an embedded counter fraud culture and to take robust action where allegations of fraud, bribery and corruption are received. During 2017/18, the NHS Counter Fraud Authority (NHS CFA) conducted a focussed assessment inspection at the CCG, against the NHS Standards for Commissioners, covering all standards under Strategic Governance and Inform & Involve. The CCG was awarded a green rating by the Inspector, for all the standards assessed, demonstrating a high level of compliance. 24

39 039 e. Financial Summary Stockport CCG received an allocation of 461.1m in ( 447.2m This is one of the lowest levels of funding for any of the Greater Manchester CCGs and is c 16m below the level that NHS England calculates is required to meet the health needs of the Stockport population. We have achieved all of the financial requirements of the CCG including our in-year target surplus of 3.82m. The CCG Governing Body has placed particular emphasis on increasing investment into Mental Health and it is confirmed that the Mental Health Investment standard has been achieved. Planned investments into Primary, Community and Mental Health have been maintained despite unplanned increases in expenditure with acute providers. The CCG has delivered marginally in excess of the required 17.4m Cost Improvement Programme (CIP) and has underspent against the allocation of 6.4m that we receive for management and administration resources. The chart below shows how, on average, the CCG spends the c 1,400 that we receive to meet the health needs each person within Stockport. For the CCG will receive a recurrent allocation of 459.1m with a target surplus of 0.0m and the CCG is planning to achieve this target. 25
40 040 f. Sustainability The CCG recognises that as a large employer and consumer of goods, services and resources in the delivery of its work and has the potential to impact on the environment and our community significantly. As a responsible organisation it aims to reduce the impact on the environment and use resources efficiently and wisely to improve health outcomes, for the benefit of the local community. As an NHS organisation and as a spender of public funds, there is an obligation to work in a way that has a positive effect on the communities when commissioning and procuring healthcare services. Sustainability means spending public money well, the smart and efficient use of natural resources and building healthy, resilient communities. By making the most of social, environmental and economic assets the organisation can improve health both in the immediate and long term even in the context of the rising cost of natural resources. The CCG has adopted a Sustainability Policy which recognises its obligations as a local employer. The CCG recognises that the decisions it takes on a daily basis have a major impact on its staff, on the local economy and on the environment. This policy uses as its foundation the Good Corporate Governance Assessment Model and therefore looks at ten areas where the organisation can improve sustainability: energy and carbon management, procurement and food, low carbon travel, transport and access, water, waste, the estate, corporate citizenship (organisation and workforce development), working with partners to reduce environmental impact, governance, commissioning and procurements (buying green) and finance. The policy sets out some practical steps which the CCG can and has taken to improve its work on sustainability. These include becoming an agile workforce and enabling staff to work from home and from partner locations which has resulted in a 22% reduction in the office space requirement over the past three years. A current review has resulted in a planned move to shared accommodation with the Local Authority which, as well as reducing expenditure on rent, has an associated reduction in power and heat that contributes to cost and carbon savings. The current policies and the planned office move will reduce further the amount of commuting by staff to the office and to meetings with partner organisations, which when added to the support given to staff with the purchase of annual rail tickets, subsidised bus passes and the cycle to work scheme contributes to reduced vehicle journeys, improved air quality and reduction carbon emissions. When commissioning services, the CCG and their partners will take account of their accessibility by public transport and other environmental and social impacts of their decisions. The move to a paper-lite working environment continues to provide benefits in both resource and savings, with a continued reduction in the amount of paper waste and associated costs. 26
41 041 g. Improving quality The CCG monitors performance and quality in a number of ways, through an early warning system, through the contract and performance framework and through the quality assurance schedule, each reporting through to the Quality and Performance Meeting and Quality board. The systems are used in order to identify where quality or performance is sub-standard; where it has been identified that this is the case a collaborative quality improvement plan is put into place to support improvement. The CCG has a range of mechanisms such as KPIs and quality schedules that are used to monitor quality and performance. The CCG Quality Team uses comprehensive clinical and quality information as part of the real time quality assurance framework within the early warning system and to inform future quality improvement projects. The data required is predominantly focused on our main provider Stockport NHS Foundation Trust; however the team also have a comprehensive set of minimum quality standards, which are applied to all providers and services within Stockport and that can be effectively monitored. The CCG recognise that in all services there are areas for improvement and relish the opportunity to ensure that the services within Stockport are of the highest standard. Whilst in some areas work is in progress and areas for development have been highlighted, the organisation can always use these opportunities to grow in order to assure excellence. This approach ensures that services really are better, using what communities, national guidance and clinical quality standards define as better quality and not just relying on finance or contractual targets. The CCG has excellence at our core and has a vision of unsurpassed care across our services. The CCG expects providers to work in an open and transparent way with commissioners, to have a forensic pursuit of improvement, to deliver care to the standards of the 6Cs, in safely staffed organisations, 7-days a week. Providers must also evidence a zero harm culture and fulfil their duty of candour responsibilities with rigour in a culture of learning with clearly accountable leadership. The CCG has worked collaboratively with all partners during the recent winter period and associated demands on the Emergency Department and urgent care delivery systems. Additional support was provided to ensure that patient flow was assisted by a number of services to reduce DTOC and move patients through the urgent care system. The support to the smaller providers including care homes with nursing has been greatly improved since the Designated Nurse for Safeguarding Adults commenced work in October The collaborative work with the newly appointed Quality Improvement Nurse in the Local Authority Enhanced Quality Team has proved effective and responsive when safeguarding concerns have been raised. This partnership working is improving outcomes for adults at risk. Supporting staff to understand their role in mental capacity assessment has been a focus for the Safeguarding Team this year following recommendations in a CQC review and from the serious adult reviews. A comprehensive policy is being drafted to include simple assessment templates. Easy access coaching and supervision is fundamental, as issues present, so that staff feel confident to assess and plan for any best interest decisions. 27
42 042 There has been a drive to ensure that staff understand how the learning from previous serious case reviews involving children applies to their own practice. A series of 7 minute briefings have been used, which have evaluated well, as a means to disseminate learning. The Designated Nurse and Designated Doctor for Safeguarding Children worked closely with the Safeguarding Children Board to present at a well-attended serious case review learning event. This was recorded and uploaded for staff to access and use in their own teams and across GM. Sharing learning across GM is a priority and will promote consistency of safeguarding practice with those families who transfer in and out of areas. The Named GP for Safeguarding has worked on supporting GP's to apply read codes to their patients who have vulnerabilities and associated risks which will impact on children. Audit has demonstrated that GP's are recognising risk and intervening to prevent harm. The impact of an increasing amount of children becoming looked after in Stockport and nationally, is significant across all provider services. The Designated Nurse for Looked After Children continues to escalate and support the specialist provider team where the quality of health assessments could be improved. Focus in 2018/19 will be around the commissioned services for this vulnerable cohort of children to determine how to meet increasing demand. The CCG has a robust procedure in place for monitoring and recording serious incidents that are reported on the STEIS system. Through working collaboratively with the Governance Team at Stockport NHS Foundation Trust and Pennine Care NHS Foundation Trust to tighten up the reporting, reviewing and finalising reports and have reduced the number of overdue reports significantly, currently standing at no overdue reports (in line with the 60 day protocol). Themes and trends are monitored via the CCG Quality Committee via a process of SIRI reports and deep dives/quality reviews. The CCG will continue to monitor serious incidents for all providers through the appropriate reporting and monitoring mechanisms. The CCG monitor the Harm Free Care data reports and updates Quality Committee on performance around the HFC agenda, The Quality Team has a representative on the Falls Steering Group and the Wound Care Steering Group at SFT, and also on the Greater Manchester Quality Collaborative, Pressure Ulcer Collaborative and IPC Collaborative. The CCG has carried out a number of quality assurance visits to numerous sites, which have included Stockport FT (A&E/urgent care; medicine; The Meadows); Pennine Care adult and older age units and The Priory; community homes; local hospice etc. A programme of visits is being devised for the coming year which will include FT; intermediate care; paediatrics; community homes. These visits focus on the delivery of safe and effective care, and provide the CCG with assurances that the services commissioned are effectively monitored. The CCG continues to work closely with care homes and home care agencies to ensure that there is a holistic provision and range of care across Stockport. Successful collaborative working with Stockport Metropolitan Borough Council has realised the implementation of a joint quality and support team to enable nursing and care standards 28
43 043 across Stockport to improve. The organisations also celebrated the very best of care home and home care practice at the Stockport Star Awards event in February. The Continuing and Complex Healthcare (CCHC) team continues to follow the National Framework for NHS Continuing Healthcare and NHS-funded Nursing Care Guidance, which assist in determining if someone is eligible to receive NHS CHC funding and assess an individual to determine whether they have a 'primary health need'. This is a national process followed by every CCG to assist in ensuring there is no variation in access, and the assessment process is consistent across the NHS. All CCGs complete the bench-marking figures on a quarterly basis and Stockport CCG s performance within the conversion rate for people who are eligible for NHS CHC continues to be low in comparison to other CCGs. This is due to the effective management of the available pathways that people can follow. To ensure that the team is managing the threshold, there continues to be peer review with other CCGs to give assurance in relation to the delivering of the process. NHS England (NHSE) has also introduced a directive that states that there needs to be a reduction of assessments taking place in the hospital. Therefore, the team actively changed the approach within the hospital to ensure that there is a reduction in the number of completed assessments in hospital. There are dedicated nurses who work alongside the social work and discharge team within the hospital to support this process. The regional NHS CHC teams of NHS England need assurance that arrangements are in place to meet the overall strategic challenges for NHS CHC. From the Assurance Framework review, the emphasis is to share good practice and to aid a consistent approach to the eligibility of the NHS CHC Framework throughout England. Stockport CCHC team has been fully engaged in the Assurance Framework process. The CHC team report performance against standards to the CCG quality committee bi-monthly and audit internal processes to ensure lessons are learnt and processes are as effective as they can be. The CCG works in collaboration with the Local Authority with a joint quality meeting for providers of care for our CHC patients in Stockport. This can often lead to packages of joint support for a provider or care home between CHC and the local authority quality team and monitors providers through the contractual process. 29
44 044 h. Engaging people and communities The CCG aims to work with local partners to improve health outcomes and secure high quality healthcare for the people of Stockport, now and for future generations. It is important that everyone is able to have greater control of their health and wellbeing and to be supported to live longer, healthier lives with high quality health and care services that are compassionate, inclusive and constantly improving. Our ambition is to place patients, public and our local communities at the heart of everything the CCG does. To achieve this, genuine patient and public participation is essential. The NHS Five Year Forward View (2014) and Next steps on the NHS Five year Forward View (2017) describes a new relationship between the NHS, patients and the public, including a commitment to engage communities and citizens in decisions about the future of health. Public involvement helps us to understand people s needs, and to prioritise those people who experience the poorest health outcomes enabling us to improve access and reduce health inequalities. It provides opportunities to see things differently and to be innovative, leading to a better use of our limited resources. In addition, the CCG has a legal duty under Section 14Z2 of the National Health Service Act 2006 (as amended) to make arrangements to involve the public in the commissioning of services for NHS patients. Within the CCG s constitution there is a commitment to ensure that there is meaningful public involvement in the planning, development and shaping of local services. These are governed by the following principles: Working in partnership with patients and the local community to secure the best care for them; Adapting engagement activities to meet the specific needs of the different patient groups and communities; Publishing information about health services on the CCG website and through other media; Encouraging and acting on feedback; Identifying how the CCG will monitor and report its compliance against this statement of principles. The CCG works with a range of partners across the voluntary and third sector and has always worked closely with patient groups, including Healthwatch, in order to engage as wide an audience as possible and to involve them in decision making. The CCG s Chief Operating Officer holds regular meetings with the Healthwatch Chair, who also sits as a representative on the Governing Body and the Citizen s Representation Panel. In addition, where developments are being planned, Commissioners attend Healthwatch briefing sessions to ensure local involvement in shaping plans. Members and officers of Healthwatch are also regularly involved at a formal CCG committees and workshops. 30
45 045 Our approach to public involvement is to make sure that a wide variety of different mechanisms, methods and approaches are used to engage with people. The CCG uses a number of methods to involve and engaged with our communities and to listen to their views and needs. Some of these approaches include: Citizens Representation Panel; Citizen Space have your say ; Public meetings; Social media surveys/polls and general comments; Prevention and screening events; Focus groups; Information stalls at supermarkets and events; Presentations at local groups; Patient story podcasts; Healthwatch attendance at governing body and committees. The CCG has also led the development of Public Voice, a patient and public participation group for the South East Sector of Greater Manchester which focuses on the development of Healthier Together. The group includes lay representation from Stockport, Tameside and Glossop, North Derbyshire and East Cheshire and is led by an appointed Lay Chair, Lesley Surman. Lesley is also a member of the South East Sector Healthier Together Programme Board to ensure lay views are represented. The group have, in the last year: Developed a patient and public led design ethos to ensure that the views of lay people are adopted within service change; Undertaken a review of public transport links across the sector and a set of recommendations regarding public transport to support patient access; Been involved in numerous workshops with clinicians to further develop the plans for Healthier Together; Observed and provided comments on a mock multi-disciplinary team meeting to support the development the sector Multi-Disciplinary Team. To ensure that patient views are heard at every level of the organisation, the CCG has appointed lay members to sit on our committees and present a patient perspective to discussions and decisions: The Governing Body has appointed three independent lay members, who in addition to being full governing body members have additional specialist roles: Jane Crombleholme is the designated lead for patient and public involvement but in late 2017 commenced transfer of the portfolio to assume responsibility for primary care commissioning. It is the CCG s intention for formally ratify this change at the Annual General Meeting in July John Greenough who leads on audit, remuneration and conflict of interest matters. Christine Morgan who is the lay member for primary care commissioning and chair of the Primary Care Commissioning Committee. She informally assumed responsibility for patient and public involvement in late It is the CCG s intention for formally ratify this change at the Annual General Meeting in July
46 046 The Governing Body has a representative from Healthwatch Stockport and the Chair of the Health and Wellbeing Board in attendance at all meetings to feed in local views. The Finance and Performance Committee includes the Lay Member responsible for audit and finance. The Quality Committee includes the Lay Member with a remit for public involvement and a Healthwatch member. The Audit Committee is chaired by the lay member responsible for audit and finance. The Remuneration committee is chaired by the lay member responsible for audit and finance. The Primary care commissioning committee is chaired by the lay member for primary care. i. What our patients and communities tell us about local services In the CCG received a wide range of queries, compliments, comments and complaints from local communities. In addition, the CCG s manage requests for information submitted under the Freedom of information Act. All of these contacts from the public are monitored and analysed so that trends in requests or issues are fed into the Governing Body and the relevant commissioning team to ensure that improvements are made as a result of local contacts. Over , NHS Stockport received: 69 Complaints 134 Compliments and enquiries 23 MP letters 242 Freedom of Information requests Friends and Families Test The Friends and Family Test (FFT) is a single question survey which asks patients whether they would recommend the NHS service they have received to friends and family who need similar treatment or care. Since it was initially launched in April 2013, the FFT has been rolled out in phases to most NHS funded services in England, giving patients the opportunity to leave feedback on their care and treatment. Friends and Family Test results for 2016/17 across the borough can are summarised below and the data relates to the most recent national publication in January 2018: GP Services: Overall satisfaction with GPs services across Stockport remains high and over 90% of patients would recommend them. Although this is slightly lower than the 92% in 2017, this is above the England average rate of 89%. The percentage of respondents who would not recommend GP services across Stockport is below the England average range at 4% compared with almost 6% nationally. 32
47 047 Accident and Emergency: The percentage of patients who would recommend Stockport A&E services as a place to receive care has remained the same compared to 2016/17 (with 87% in Jan 2017 and 87% in Jan 2018). There has been a slight increase in the percentage of respondents who would not recommend the A&E service from 6% in January 2017 to 7% to January It is likely that this change is reflective of the challenging performance seen in A&E departments. The percentage of patients who would recommend A&E services in Stockport is also just above the England average of 86% in January Inpatients: On average 94% of respondents would recommend Stockport as a place to receive inpatient care, which is slightly lower than the rate of 95% reported in January This is just below the England average rate of 95%. The percentage of respondents who would not recommend inpatient services across Stockport is also within the England average range of 2%. Outpatients: On average in January % of respondents would recommend outpatient services, which is the same as the previous year and slightly below the England average of 94%. The proportion of respondents stating they would not recommend outpatient services are also within the England average range at 2%. Maternity: The percentage of patients who would recommend Stockport Maternity services as a place to receive care has remained the same when compared to 2016/17 (with 98% in Jan 2017 and 98% in Jan 2018). This is higher than the national England average of 96%. The proportion of respondents stating they would not recommend maternity services has also increased slightly from 1% to 2%, which is in line with the England average. ii. Public involvement priorities and impact over the last year Over the last 12 months the CCG has worked with a range of communities and local partners to involve and engage patients and the public. One major element was a large formal consultation on the proposals to transform health and social care services across Stockport in a system wide partnership, which includes Stockport Council, NHS Stockport Foundation Trust, Viaduct Health and NHS Pennine Care Foundation Trust. When the partners formed Stockport Together, they pledged to provide, A safe, affordable and integrated health and social care system to meet the needs of Stockport. What this means in reality is transforming the way that healthcare is managed and organised in Stockport so the services our communities rely on are fit for purpose in the 21st century. In setting up Stockport Together, there was the understanding about the rising number of older people in Stockport, and the greater need for health and social care support both in the short and long term. Our assumptions are that if the health and wellbeing of the older generation can be improved, then their quality of life should greatly improve and the need for inpatient and outpatient care (health services provided in a hospital setting) should be reduced. 33
48 048 The CCG knows these are big changes and as a result, it was essential that the organisation engaged and involved local people to have their say on the proposals for change. During the summer of 2017 a series of listening events with the public and organisations was launched, which included an active interest in delivering health and care services in Stockport. Initially one event per neighbourhood was scheduled, with additional events held upon request in additional locations or with specific groups, meaning 12 sessions were held in total with varying attendance levels. A total of 287 people attended the events during the listening phase and there were an additional 195 people in attendance at other forums. The aim of the exercise was to provide the public with the opportunity to receive information, take part in discussions, and provide feedback on: The case for change (the reasons why the changes need to be made); Some of the changes that have already been made (i.e. Transfer to Assess service); The plans being developed for the future; What impacts (positive and negative) the public think the changes will have on them, their family and friends. Each meeting was two hours long, and upon arrival all attendees were given an issues document which outlined the above information. The format was to begin with a presentation, then work in groups to discuss a series of scenarios supplied. Questions were then invited from attendees, which were answered at the time whenever possible. Presenters varied each time but included clinicians, leaders and directors from the partner organisations. Clinicians worked with the engagement officers to develop the scenarios and questions. They were designed to show examples of some of the problems people commonly face in the current system. The topics are shown the below: Repeat prescriptions; Recovery after a hospital episode; Outpatients; Mental health; Falls; Alternatives to a GP appointment; Pneumonia care. The scenario format was used to help focus the mind on a few key areas. Stockport Together covers such a wide remit of services therefore it was not assumed that these would address everything included in the plans and were intended to provide some context to some of the proposed plans. 34
49 049 Write ups from each session formally captured the discussions on the day, along with all of the information provided by members of the public during the scenarios exercise. These were fed into the central Stockport Together team, and the scenario responses were distributed to the relevant programme teams for consideration. Following on from these events, the CCG together with the Local Authority with support of partners in the Stockport Together Programme agreed to proceed with a formal public consultation. This was designed to further develop our assessment of local needs and strengthen action plans that had been created to: Change the way services are planned and organised; The plans to organise health, social care, and mental health services in teams that work in eight neighbourhoods; and Ensuring hospital services are in place for those that need them while reducing pressure on those services. The consultation was launched on 10 October 2017 and concluded on 30 November It consisted of street surveys in neighbourhoods, on-line and postal surveys, discussion groups and public meetings. In addition to the over 500 responses from individuals, organisations representing around 38,000 people also submitted responses. In addition, a wide range of protected groups, as defined by the Equalities Act 2010, were contacted and encouraged to feedback. Simultaneously, reports were presented (Equality Impact Assessments) that considered the impact of changes on these groups. Throughout the consultation process, the CCG took advice from the Consultation Institute and through this organisation, commissioned an independent analysis of the public s feedback to the consultation. The analysis showed that the main thrust of the proposals to create and invest in a more integrated and community-based health and social care system delivered in neighbourhoods was strongly supported by the public. However, there were greater concerns and scepticism around the potential decommissioning of hospital beds and the tests to ensure that the CCG had fundamentally altered the need for these beds. The public and key stakeholders also made a number of important comments and suggestions relating to ways that would strengthen implementation of plans. During February 2018, both the CCG Governing Body and Stockport Council Cabinet approved the proposed plans, subject to these recommendations being built-in to their implementation. These recommendations included: More frequent and effective involvement of local people in shaping health and social care services; More collaborative working between patients and clinicians; Checks and balances to ensure equal and fair representation for people who often do not have their voices heard; Remove complexity when presenting financial information; 35
50 050 Adopt close-working with Neighbourhoods (GPs) to ensure more effective local engagement; Build on networks established with protected groups to ensure greater involvement; Develop a more formal position for the third sector in our partnership arrangements; Greater integration of mental health services into neighbourhood teams; Greater alignment of housing, leisure and education relating to the wider determinants of health; Create a more robust and comprehensive workforce plan that embraces a system approach to health and social care. Through a variety of approaches, including focus groups, representative groups, street surveys, online surveys and public events, the consultation reached an estimated 38,000 residents, meaning that over 10% of local residents were able to have their say on how decisions for the future are made. iii. The Impact of involving our communities in decision-making. Feedback from involvement exercises is reported to the CCG s Governing Body. It is used as a key piece of evidence for consideration in decisions and showing how the views of communities are translated into commissioning decisions. One of the key tools for feeding back to local people is the CCG s engagement website: For those without access to the internet, write-ups of events are also sent out to local groups after they have met with the NHS. Sign-up sheets are also taken at all public events so people who wish to receive a write-up of the event can have this sent to them in their preferred format. Articles summarising formal consultations are included in the local council publication that is delivered to all households in Stockport. In addition, feedback reports are sent to Healthwatch for inclusion in their regular newsletter and targeted feedback articles are also included in a wide range of local newsletters. iv. Future Plans The recent Stockport Together public consultation has highlighted issues in how to engage and involve local communities. As a direct result of feedback, the CCG has developed five guiding principles that should be adopted by providers of Health and Social Care Services across Stockport as a partnership. They are: Increase citizens knowledge about the issues to address as a Health and Social Care System; Encourage citizens to contribute additional knowledge and use that knowledge to inform how services are developed; 36
51 051 Encourage citizens to collaborate in both policy and funding decision making involvement in designing work plans/funding rather than early view of drafted plans; Create opportunities for citizens to engage with each other; Ask people What Matters to You as a person centred approach to care. As Stockport adopt a neighbourhood approach to delivering health and social care services, similarly, it is essential to consider a neighbourhood approach to engagement and involvement. Through GP practices and our new neighbourhood leads, there is a key role for the localised model in partnership working with local people using an asset based approach and maximizing connections between existing groups and/or organisations.. Moving forward, more detailed planning is required between commissioners and providers to determine the appropriate levels of engagement. These considerations will include: The statutory requirement of the Joint Commissioner to engage with local populations to assess the overall health and social care needs of that population; The advantaged position of neighbourhood leads - having frequent contact with local people through GP practice or specialist services; The access to people (including hard to reach and seldom heard groups) that the third sector open up in promoting population health messages and increased levels of engagement and involvement. Stockport CCG is tasked with a number of different roles: from directly commissioning and buying services, to ensuring that local health and care plans are designed to meet the need of local communities. The CCG wants to work closely with patients, carers and citizens who have experience of using health and care support or services to make improvements in how that care is planned, organised and delivered. The CCG know that people share our ambition to continually improve services into the future. Although there have been significant changes in the NHS, in Stockport there is a continued commitment to improve the way people are involved to shape better health and care services. The intention is to strengthen this work and to get better at demonstrating the difference that can be made by increasing how communities can be involved in shaping services and decision-making. As the needs of local communities and population change, the CCG will continue to work with them together to establish how best to meet new challenges. Over the next year will the focus will be on further improvements in engagement and act on what patients and the public are telling the organisation. 37
52 052 i. Reducing health inequality The CCG has been designing new models of care, as part of Stockport Together, to develop services and approaches that aim to reduce health inequalities. In the Find and Prevent programme, the prime rationale is to reduce the long term level of disease, providing a better quality of life for patients and their families, and increasing healthy life expectancy, to close the health and wellbeing gap. Another rationale is to address the variation in health outcomes (inequalities) and care provision (quality gap) across Stockport. It has been shown that improving the health of the population in our most deprived populations to levels experienced in other parts of the Borough, would significantly reduce the burden of disease in the borough. Stockport generally has a high quality of care in General Practice, with many examples of innovation and excellence. There is however still variation between practices. The programme will enable the standardisation of prevention and the sharing of good practice, reducing variation and enabling the lower performing areas to level up to the best. The Healthy Communities Programme aims to contribute to the transformation of the relationship between people, services and communities, through delivery of person and community centred care. This wide range of programmes particularly focuses on self-care, promoting emotional wellbeing, addressing loneliness and supporting community connections. Unfortunately the life expectancy differences between our most deprived and least deprived areas in Stockport are not showing an improvement and deaths in women under 75 years (premature deaths) are a particular cause for concern. The CCG values diversity and is committed to reducing inequalities in the workplace, in health outcomes, in access to, and experience of, local services. Challenging discrimination and addressing inequalities are essential to achieving our vision of high quality healthcare for Stockport. Each year the CCG publishes an annual equality report, setting out information on diversity within our population and our workforce, as well as the work undertaken throughout the year to reduce inequalities. Below are some examples of how the CCG has reached out to different groups and diverse communities within the population group covered, so that their voices are heard. There are also examples of where staff are being developed to support people from diverse communities which can be found on the CCG s website at: As a public sector organisation there is a legal duty under the Equality Act (2010) to ensure equal access to services for all diverse communities. This includes making adjustments so that for those whose first or preferred language is not English or who use sign language as their main means of communication can receive the same level of service as other patients. The CCG continues to manage the interpretation budget for local Primary Care services on behalf of NHS England, who now commission these services. The service provides 38
53 053 interpretation at medical appointments in General Practice; NHS dentistry; NHS pharmacy and NHS optometry. NHS Stockport CCG holds interpreting contracts with: Stockport Interpreting Unit, for the provision of face-to-face for foreign language interpreters in over 30 languages; The Big Word, for the provision of 24/7 phone interpretation services in over 200 languages; Language Empire for the provision of face-to-face British Sign Language interpreters; Sign Video for the provision of Skype based British Sign Language interpreters. Over the financial year 2017/18 interpretation was used for 2,882 healthcare appointments (an increase of 477 compared to ). A total of 65 languages were used, in addition to sign language, with Farsi was the most commonly used language, followed by Polish, Arabic, Urdu, Kurdish, and British Sign Language. 39
54 054 j. Health and wellbeing strategy The delivery of the Joint Health and Wellbeing Strategy requires the contributions and involvement of all members of the Stockport Health and Wellbeing Board and its partner organisations. Stockport CCG has four senior representatives on the local Health and Wellbeing Board to ensure strong CCG involvement and clinical leadership. The CCG worked with our local partners to develop Stockport s Health and Wellbeing Strategy, which reflects local health and wellbeing needs and influences the direction of our Strategic Plans. Stockport, like other local areas across the country, is facing a number of issues which mean there is a need to change how health and social care services are delivered. In response to this, the key themes of the strategy are to deliver a health and care system which is: Prevention focussed; Community asset based; Person centred; Integrated; Delivered through neighbourhoods; Financially sustainable. This vision is complex and cannot be delivered through a single plan. Instead, a range of programmes including Stockport Together, Stockport Family and Greater Manchester Devolution, as well as many topic themed strategies and partnership approaches, will help the systems in Stockport evolve. The strategy sets out the ways in which the CCG will develop the health and social care system in Stockport to meet these needs and vision over the next three years. This strategy has been produced jointly by Stockport Council, NHS Stockport CCG, Stockport Healthwatch and many other contributors from partners, other professionals and voluntary and community sector representatives. It has been approved by the Health and Wellbeing Board. Dr Ranjit Gill Chief Clinical Officer Date: 40
55 Accountability Report Overview The accountability report is required to have three sections as detailed below: Corporate Governance Report: the purpose of the corporate governance report is to explain the composition and organisation of the entity s governance structures, how these support the achievement of the entity s objectives and how they reflect the generally accepted principles of good governance as stated in the National Health Service Act Remuneration and staff report: the remuneration and staff report sets out the organisation s remuneration policy for directors and senior managers, reports on how that policy has been implemented and sets out the amounts awarded to directors and senior managers. In addition, the report provides details on remuneration and staff that users of the accounts see as key to accountability. Parliamentary Accountability and Audit Report: this is not mandatory for the CCG, however the CCG has opted to include relevant disclosures within the appropriate sections of the annual report. 2.1 Corporate Governance Report a. Members Report Member practices Practice GP Member Representative ADSHALL ROAD MEDICAL PRACTICE Dr Anna Gillott ADSWOOD ROAD SURGERY Dr Lydia Hardern ALVANLEY FAMILY PRACTICE Dr Jaweeda Idoo ARCHWOOD MEDICAL PRACTICE Dr Graham Parker BEECH HOUSE MEDICAL PRACTICE Dr Simon Woodworth BRACONDALE MEDICAL CENTRE Dr Adam Firth BRAMHALL HEALTH CENTRE Dr Javid Ali BRAMHALL PARK MEDICAL CENTRE Dr Alexander Bayes BREDBURY MEDICAL CENTRE Dr Robert Beardsell BRINNINGTON HEALTH CENTRE Dr James Higgins CALE GREEN SURGERY Dr Rachel Tomalin CARITAS GENERAL PRACTICE PARTNERSHIP Dr Abigail Webster CHADSFIELD MEDICAL PRACTICE Dr Rachel Kilroy CHEADLE HULME HEALTH CENTRE Dr Ruth Seabrook HULME HALL MEDICAL GROUP Dr Steve Hastings CHEADLE MEDICAL PRACTICE Dr Tariq Shah DR H LLOYD'S PRACTICE Dr Hazem Lloyd FAMILY SURGERY Dr Ian Dickie 41
56 056 GATLEY MEDICAL CENTRE HEALD GREEN HEALTH CENTRE 1 HEALD GREEN HEALTH CENTRE 2 HEATON MERSEY MEDICAL PRACTICE HEATON MOOR GROUP PRACTICE HEATON NORRIS HEALTH CENTRE 1 HIGH LANE MEDICAL CENTRE MANOR MEDICAL PRACTICE MARPLE BRIDGE SURGERY MARPLE COTTAGE SURGERY MARPLE MEDICAL PRACTICE PARK VIEW GROUP PRACTICE SOUTH REDDISH MEDICAL CENTRE 2 SPRINGFIELD SURGERY STOCKPORT MEDICAL GROUP THE GUYWOOD PRACTICE THE SURGERY 3 THE SURGERY 1 THE VILLAGE SURGERY VERNON PARK SURGERY BENTS LANE MEDICAL PRACTICE WOODLEY HEALTH CENTRE 2 Dr Peter Carne Dr Penelope Owen Dr Carmel Morris Dr Jeremy Wynn Dr Rebecca Locke Dr Christopher Marshall Dr Robert Mathewson Dr Martin Leahy Dr Morag Needham Dr Andrew Johnson Dr Howard Sunderland Dr Sasha Johari Dr Geeta Gupta Dr Ameer Aldabbagh Dr Naomi Lalloo Dr Raina Patel Dr Abdul Ghafoor Dr Hany Azmy Dr Daniel Goldspink Dr Suvajit Chattergee Dr Abdul Ghafoor Dr Amjad Choudry Composition of Governing Body Meet the Governing Body The Governing Body has been delegated by its council of GP members the power to conduct the overall management of the CCG. They meet regularly to conduct their formal business. The papers and minutes of these meetings are published on the CCG website Members of the public or other interested parties are invited to notify attendance in advance either by telephoning or ing the CCG reception on or ccg.reception@nhs.net. The Governing Body is mainly made up of local GPs and includes clinical representatives such as a nurse, public health specialist and hospital consultant. There are also three lay representatives including a lay member chair, a lay finance member and a lay member for primary care. Jane Crombleholme - Lay Chair I am Chair of the Governing Body for the CCG. I have a long record of public service serving as an NHS non-executive director on several NHS organisations since I have been a foundation trust governor, charity trustee, chair of my local primary school and a school governor at my children s high school. In my professional life, I am Head of Executive Education at Alliance Manchester Business School, part of the University of Manchester where I have worked for almost 20 years. 42
57 057 I feel very proud to work for the NHS. I know it is not perfect but I want to do my bit to make sure that the service we all pay for as taxpayers is high-quality, responsive and fit for purpose. I feel that this is best done locally - Stockport is where I was born and live along with a very large extended family. Stockport s NHS and wider public services have got to be good enough for all of us and I want to do my bit to make that happen. Dr Ranjit Gill Chief Clinical Officer I ve been a GP in Stockport since 1991 at Stockport Medical Group, in Edgeley and Great Moor. Stockport s population now live longer and healthier lives than ever before. But in that time Stockport s NHS has not been modernised fast enough to provide the type of care to match the current and future needs of Stockport s people. Our population needs to have access to the advances in health and social care which predict and prevent ill health and relapse, and provide consistently excellent care. Being a practicing GP in today s NHS remains extremely rewarding, but is becoming increasingly difficult. All NHS staff are working really hard but in an NHS designed for the last century. With the changes we re making we can we make Stockport s NHS one of the best places to work in, anywhere in the UK. Stockport now has a chance to change its health and care system. With 19m of funding from the Greater Manchester Transformation Fund we can invest in General Practice, Community, Social Care and Mental Health Services to provide the care that people actually need. I hope that Devolution for Greater Manchester will continue to try and address the root causes of the poor health in much of Greater Manchester. By helping people to look after themselves better and modernising our NHS, we can we make sure that Stockport s people have some of the best health in the world, and the best care every time its needed. Gaynor Mullins Chief Operating Officer I am Chief Operating Officer which is the most senior manager of the CCG. I am responsible for ensuring that arrangements are in place so that the CCG can successfully deliver its business objectives. I ensure that effective management systems are in place and I am responsible for the daily operations of the CCG and its staff. During 2017/18 I took responsibility for developing future integrated commissioning arrangements across health and social care, acting as the Director of Integrated Commissioning. I am also the lead CCG Chief Operating Officer for primary care on behalf of Greater Manchester CCGs Dr Andy Johnson GP Locality Chair I am the GP locality chair for the Marple & Werneth locality committee, the vice chair of the Governing Body, a member of the audit committee and the clinical cancer lead for the CCG. In addition to this I am a GP at Marple Cottage surgery. Dr Peter Carne GP Locality Chair (in post until January 2018) I am the GP locality chair for Cheadle and Bramhall, Chair of the Finance & Performance 43
58 058 Committee, a member of the Governing Body and the Remuneration committee. From April 2017 I will also commence the role of Cheadle Neighbourhood Lead. I have been a GP partner at Gatley Medical Centre since 1992 and Locality Chair for Cheadle & Bramhall since I also work regular sessions for Mastercall, the local out-of-hours GP service. Prior to taking up my CCG Locality Chair role I worked at St Ann s Hospice for 19 years. I feel that my wealth of primary care experience can contribute to an improvement in cost effective patient care in Stockport. Dr Lydia Hardern - GP Locality Chair I am the GP locality chair for Stepping Hill & Victoria as well as a member of the Governing Body and Chair of STAMP (Stockport Area Medicines Panel). I currently work as a GP at Adswood Road Surgery in Stockport. Prior to this, during my training, I worked as a junior doctor at Stepping Hill Hospital. I have a special interest in child heath, women s health and cancer care. As a GP who has lived in Stockport throughout my childhood and professional life, I am passionate about the future of the NHS in Stockport and deeply committed to ensuring the quality of services meets the needs of our community in the coming years despite the current challenges. Dr James Higgins - GP Locality Chair (in post until January 2018) I am the GP locality chair for Heatons and Tame Valley and a member of the Governing Body as well as the Named GP for Safeguarding for Stockport CCG. Born and brought up around South Manchester, I left to study medicine at the University of Birmingham, graduating in After completing my foundation programme in Birmingham I spent a year working in Auckland, New Zealand before returning to my home town to commence my GP training. Following completion of this in 2010, I took up my current post as a GP partner at Brinnington Surgery where I take a lead role within the practice for cancer care, mental health and dementia and safeguarding children and vulnerable adults. I also have a role in training junior doctors within the practice. I consider myself to be in a very privileged position in my CCG role as it gives me the opportunity to help shape services within Stockport using my clinical experience and insight to implement changes that are practical, achievable and most importantly, that will make a real difference to the health of the patients we serve. Dr Vicci Owen-Smith - Clinical Director of Public Health I am the Clinical Director for Public Health within the CCG and I also work as a Deputy Director of Public Health for Stockport. Before working in Public Health, I was a GP in Stockport. 44
59 059 I am passionate about improving inequalities in health across Stockport, in enthusing people about the considerable health and well-being benefits of incorporating physical activity into their day to day lives, of drinking and eating healthily as well as not smoking. Dr Catherine Briggs Clinical Director for Quality and Provider Management (in post until December 2017) I am Clinical Director for Quality and Provider Management. This means that I take a clinical lead on looking at quality of services in local hospitals and other places where people receive care in Stockport. I chair a number of committees, and am especially involved in ensuring that people receive high quality emergency and planned treatments in a timely manner and in line with national targets. I am also actively involved, from a clinical perspective, in the Stockport Together transformation work. I have a deep passion for the NHS and am proud to work within this as a GP partner at Bracondale Medical Centre in Heaviley in Stockport. The work I do in the CCG enables me to take a much broader view of the care we deliver at the practice and hopefully means that patients receive better care as a result. I have previously worked as a GP with special interest in Urology. I also live in Stockport and have 2 children who are growing up quickly. I am keen that the NHS in Stockport and nationally continues to deliver improvements in patient care in a sustainable way that guarantees that all Stockport residents receive high quality care for the foreseeable future. Dr Viren Mehta - Clinical Director of GP Member Development (on secondment from October 2016 to present) I am the Clinical Director on the Governing Body for GP Member Development in addition to my role as a GP at Cheadle Medical Practice. My responsibility is for the engagement and development of GP member practices of the CCG. From October 2016 I have been on secondment as Medical Director for Viaduct Health. John Greenough Lay Member I am the lay member responsible for finance and governance and in this capacity I take the lead on matters of finance, audit, remuneration and conflict of interest. I am also the chair of the Audit and Remuneration Committees. I was previously a partner at the financial services firm, KPMG, where I obtained considerable experience of public sector finance. Christine Morgan Lay Member I am the lay member with special responsibility for primary care and chair of the Primary Care Commissioning Committee. My full-time career was in education and I now work part-time in non-executive, lay member and patient expert roles. 45
60 060 I am an advocate of patient/carer involvement and partnership working in all aspects of health and care in order to ensure that decision-making is based on what really matters to people. Mark Chidgey Chief Finance Officer I was appointed as the Chief Finance Officer (CFO) for NHS Stockport CCG in March I have worked in the NHS for 28 years and as a qualified accountant for 22 of those years. My NHS career started at the MRI before moving to The Christie Hospital, and then to Stockport PCT in I have worked for Stockport CCG since its inception in My finance role covers three main areas. Firstly being the principal financial adviser on all issues that the Governing Body considers. Secondly ensuring that the CCG meets its statutory financial duties and finally making sure that the CCG has strong controls and processes in place to ensure that the budget we hold on behalf of our population is spent in the most effective and appropriate way. As well as the traditional CFO duties I work with healthcare provider organisations to ensure that the people of Stockport receive the high quality, effective healthcare that they need. Together with my team we identify the appropriate provider(s) for each service and agree contracts with the providers that set out the standards we expect for our patients. Dr Deborah Kendall Secondary Care Consultant I am the secondary care consultant for the Governing Body. This is in addition to my role as a consultant paediatrician at Lancashire Teaching Hospitals NHS Foundation Trust (Royal Preston Hospital). Anita Rolfe Executive Nurse I am the Executive Nurse at the CCG and have responsibilities for quality and safety of care, safeguarding and continuing health care across Stockport. Making sure that the healthcare that people of all ages receive is good, safe and timely is the core function of my role. As a nurse leader, I work closely with nursing and care colleagues from Stockport NHS Foundation Trust, Pennine Care NHS Foundation Trust, Stockport Metropolitan Borough Council, care homes and home care agencies to develop a confident, capable nursing, allied health professional and care workforce to meet the demands of the 21 st century NHS. A key interest of mine is making sure that older people in the care system have a good experience in their later life. In order for this to happen, all of us whether we are in a care role or not need to think how we might help someone who is older to be less lonely, feel valued, be cared for, feel looked after, enjoy themselves. My experience of being a District Nurse and lead nurse of community services made me realise how people recover better in their own home out of a hospital setting, where their surroundings are familiar. I work closely with all the partners across Stockport to support people who have needed a hospital stay to get home as soon as they can. I am aware of 46
61 061 and appreciate the essential role that families and friends play in assisting people to get home as soon as possible and would like to thank each and every one of you for your continued support. As a patient, a mother, a daughter, a sister, a wife, and an aunt, I am thankful what the NHS has done for us as a family and I am very proud to be part of the NHS in Stockport. Directors in attendance Tim Ryley Director of Strategic Planning and Performance Dr Diane Jones Director of Service Reform Roger Roberts Director of General Practice Development Committee(s), including Audit Committee Council of Members Governing Body Health and Care Integrated Commissioning Board Remuneration Committee Primary Care Commissioning Committee Marple and Werneth Locality Committee Quality Committee Finance and Performance Committee Heatons and Tame Valley Locality Committee Cheadle and Bramhall Locality Committee Stepping Hill and Victoria Locality Committee Governing Body Committees which operated during the financial year were: Audit Committee John Greenough (Chair) - Lay Member Bernard Braiden Member David Swift Member Dr Andy Johnson Locality Council Chair Remuneration Committee John Greenough (Chair) Lay Member Jane Crombleholme Lay Member, Chair of NHS Stockport CCG Dr Peter Carne Locality Council Chair 47
62 062 Dr Viren Mehta Clinical Director for General Practice Development on secondment Finance and Performance Committee Vacant (Chair) Dr Vicci Owen Smith Clinical Director Public Health (Vice Chair) Gaynor Mullins Chief Operating Officer Dr Ranjit Gill Chief Clinical Officer Dr Viren Mehta Clinical Director General Practice Development on secondment from October 2016 John Greenough Lay Member Quality Committee Anita Rolfe: Executive Nurse member of the Governing Body (clinical) Dr Simon Woodworth (Medical Director): Clinical Director for Quality & Provider Management (clinical) Dr James Higgins (TBC): Locality Council Committee Chair (clinical) Jane Crombleholme: Lay Member, Chair of NHS Stockport CCG (non-clinical) Julie Parker: Safeguarding Lead Nurse (clinical) Sandra Walker (Quality Lead): Senior Commissioning Quality and Performance Lead (clinical) Susan Parker (but is CCG employee): A Nurse or Allied Healthcare Professional who is not an employee of NHS Stockport CCG nor a member of the Governing Body (clinical) Sue Carroll: A Healthwatch committee representative (non-clinical) Vicci Owen-Smith: The Clinical Director, Public Health (clinical) Register of Interests The Governing Body Register of Interests is available on the CCG website at: Personal data related incidents There were no Serious Untoward Incidents relating to data security breaches reported in 2017/18. Statement of Disclosure to Auditors Each individual who is a member of the CCG at the time the Members Report is approved confirms: So far as the member is aware, there is no relevant audit information of which the CCG s auditor is unaware that would be relevant for the purposes of their audit report The member has taken all the steps that they ought to have taken in order to make him or herself aware of any relevant audit information and to establish that the CCG s auditor is aware of it. Modern Slavery Act 48
63 063 NHS Stockport Clinical Commissioning Group fully supports the Government s objectives to eradicate modern slavery and human trafficking but does not meet the requirements for producing an annual Slavery and Human Trafficking Statement as set out in the Modern Slavery Act
64 064 b. Statement of Accountable Officer s Responsibilities The National Health Service Act 2006 (as amended) states that each Clinical Commissioning Group shall have an Accountable Officer and that Officer shall be appointed by the NHS Commissioning Board (NHS England). NHS England has appointed the Chief Operating Officer to be the Accountable Officer of NHS Stockport Clinical Commissioning Group. The responsibilities of an Accountable Officer are set out under the National Health Service Act 2006 (as amended), Managing Public Money and in the Clinical Commissioning Group Accountable Officer Appointment Letter. They include responsibilities for: The propriety and regularity of the public finances for which the Accountable Officer is answerable; For keeping proper accounting records (which disclose with reasonable accuracy at any time the financial position of the Clinical Commissioning Group and enable them to ensure that the accounts comply with the requirements of the Accounts Direction); For safeguarding the Clinical Commissioning Group s assets (and hence for taking reasonable steps for the prevention and detection of fraud and other irregularities); The relevant responsibilities of accounting officers under Managing Public Money, Ensuring the CCG exercises its functions effectively, efficiently and economically (in accordance with Section 14Q of the National Health Service Act 2006 (as amended)) and with a view to securing continuous improvement in the quality of services (in accordance with Section14R of the National Health Service Act 2006 (as amended)); Ensuring that the CCG complies with its financial duties under Sections 223H to 223J of the National Health Service Act 2006 (as amended). Under the National Health Service Act 2006 (as amended), NHS England has directed each Clinical Commissioning Group to prepare for each financial year financial statements in the form and on the basis set out in the Accounts Direction. The financial statements are prepared on an accruals basis and must give a true and fair view of the state of affairs of the Clinical Commissioning Group and of its net expenditure, changes in taxpayers equity and cash flows for the financial year. In preparing the financial statements, the Accountable Officer is required to comply with the requirements of the Group Accounting Manual issued by the Department of Health and in particular to: Observe the Accounts Direction issued by NHS England, including the relevant accounting and disclosure requirements, and apply suitable accounting policies on a consistent basis; Make judgements and estimates on a reasonable basis; 50
65 065 State whether applicable accounting standards as set out in the Group Accounting Manual issued by the Department of Health have been followed, and disclose and explain any material departures in the financial statements; and Prepare the financial statements on a going concern basis. To the best of my knowledge and belief, I have properly discharged the responsibilities set out under the National Health Service Act 2006 (as amended), Managing Public Money and in my Clinical Commissioning Group Accountable Officer Appointment Letter. I also confirm that: as far as I am aware, there is no relevant audit information of which the CCG s auditors are unaware, and that as Accountable Officer, I have taken all the steps that I ought to have taken to make myself aware of any relevant audit information and to establish that the CCG s auditors are aware of that information. that the annual report and accounts as a whole is fair, balanced and understandable and that I take personal responsibility for the annual report and accounts and the judgments required for determining that it is fair, balanced and understandable... Date... Dr Ranjit Gill Chief Clinical Officer 51
66 066 c. Governance Statement Introduction and Context NHS Stockport Clinical Commissioning Group (CCG) was licensed from 1 April 2013 under provisions enacted in the Health and Social Care Act 2012, which amended the National Health Service Act As at 1 April 2013 the CCG was licensed without conditions and has continued to be responsible since through to for meeting health needs within the available budget for the Stockport population. The CCG does this through the commissioning of local health and care services including those for elective hospital care, rehabilitation care, urgent and emergency care, most community health services and mental health and learning disability services. The CCG has agreed a constitution with its members which sets out how the organisation carries out its duties and makes decisions. The CCG is a membership organisation; all GP practices in Stockport must be members of the CCG and each GP practice nominates a GP member representative who has voting rights. The Member Representatives are collectively known as the Council of Members. The CCG has established and maintained its purpose as being Because of us people will access health services that empower them to live healthier, longer and more independent lives. The CCG s vision is to be known and respected for the consistent achievement of national and local quality objectives, for an increase proportion of care being delivered in primary and community settings, for the reduction of inequalities in health outcomes, for developing a strong sense of personal responsibility for the health among our population and for having lean, agile and innovative leadership. The CCG s values are to be primary and community focussed, quality obsessed, innovative, collaborative, reliable, empowering and professional. Scope of Responsibility As Accountable Officer, I have responsibility for maintaining a sound system of internal control that supports the achievement of the CCG s policies, aims and objectives whilst safeguarding the public funds and assets for which I am personally responsible, in accordance with my responsibilities assigned through Managing Public Money. I also acknowledge the responsibilities as set out in my CCG Accountable Officer Appointment Letter. I am responsible for ensuring that the CCG is administered prudently and economically and that resources are applied efficiently and effectively, safeguarding financial propriety and regularity. Compliance with the UK Corporate Governance Code The detailed provisions of the UK Corporate Governance Code are not mandatory for public sector bodies. However the CCG continues to manage and report on its corporate governance arrangements by drawing upon best practice available, including relevant aspects of the Code the CCG deems to be relevant to its business. 52
67 067 The CCG Governance Framework The National Health Service Act 2006 (as amended) at paragraph 14L (2)(b) states: The main function of the Governing Body is to ensure that the Group has made appropriate arrangements for ensuring that it complies with such generally accepted principles of good governance as are relevant to it. Robust, well communicated and understood and embedded corporate governance arrangements are critical to achieving the CCG s objectives. In accordance with paragraph 14L (2)(b) of the 2006 Act, the CCG will at all times observe such generally accepted principles of good governance in the way it conducts its business. These include: The highest standards of propriety involving impartiality, integrity and objectivity in relation to the stewardship of public funds, the management of the organisation and the conduct of its business; The Good Governance Standard for Public Services; The standards of behaviour published by the Committee on Standards in Public Life (1995) known as the Nolan Principles ; The key principles of the NHS Constitution; The Equality Act 2010; Standards for Members of NHS Boards and Governing Bodies in England. The CCG Council of Members is accountable for exercising the CCG s statutory functions. It may delegate authority to act on its behalf to any of its Members, its Governing Body, to a Committee or Sub-Committee of the Group or to any of its employees. The extent of the authority to act depends on the powers delegated by the Council of Members as expressed through the Constitution, the CCG s Scheme of Reservation and Delegation and for Committees and Sub-Committees, through their Terms of Reference. The CCG s Scheme of Reservation and Delegation sets out those decisions that are reserved for the membership as a whole, acting through the Council of Members and those decisions that are the responsibilities of its Governing Body of the Group s Committees and Sub-Committees and of individual members and of its employees. The Council of Members remains accountable for all of its functions, including those that it has delegated. In discharging the functions of the CCG that have been delegated to them, the Governing Body any Committees, Joint Committees and Sub-Committees of the CCG and individuals must: Comply with the CCG s principles of good governance; Operate in accordance with the CCG s scheme of Reservation and Delegation; Comply with the CCG s arrangements for discharging its statutory duties; Where appropriate, ensure that Member Practices have had the opportunity to contribute to the CCG s decision-making processes. 53
68 068 When a Committee, Sub-Committee or Joint Committee discharges delegated functions, it must also operate in accordance with its approved Terms of Reference. These are approved by the Governing Body and can be found on the CCG s website. The diagram on page 47 shows the structure of the CCG s Committees. The CCG has been operating with revised governance arrangements following implementation of recommendations arising from a review in January The Council of Members has approved a number of required changes to the CCG s Constitution during 2017/18 which were administrative in nature and reflected minor changes in the designation of CCG clinical roles reflective of current leadership arrangements. The Audit Committee provides the Governing Body with an independent and object view of the CCG s financial systems, financial information and compliance with laws, regulations and directions governing the CCG in so far as they relate to finance. It supports the Governing Body in discharging its duties to effectively, efficiently and economically manage its resources and to adhere to the principles of good governance. The Quality Committee is accountable to the CCG s Governing Body for providing assurance of patient safety, patient experience and clinical effectiveness of commissioned services in line with the CCG s Quality Strategy. It provides leadership for the quality agenda in Stockport and ensures commissioned services are continuously improving, achieving and exceeding national and local standards. The Remuneration Committee makes recommendations to the Governing Body on determinations about the remuneration, fees and other allowances for employees and for people who provide services to the CCG and on determinations about allowances under any pension scheme that the CCG may establish as an alternative to the NHS Pension Scheme. The Finance and Performance Committee is responsible for the development and monitoring of the CCG s Operational Plan and priority areas as linked to the CCG s delivery of financial and performance targets and for making recommendations to the CCG s Governing Body in respect of those areas. The Primary Commissioning Committee is responsible for carrying out the functions relating to the commissioning of primary medical services under Section 83 of the NHS Act which were delegated to the CCG from NHS England under delegated commissioning arrangements. The Health and Care Integrated Commissioning Board (HCICB) was established as part of the Section 75 Agreement between the CCG and Stockport Metropolitan Borough Council. The HCICB is accountable and responsible on behalf of both Commissioners for the deployment and management of the pooled budget and the commissioning of services from the pool. The Committees reported the following highlights for 2017/18: Quality Committee The Quality Committee meeting has reviewed a number of quality reports from a range of providers and areas, in line with the quality assurance framework managed by the quality 54
69 069 and safeguarding teams. During the last financial year, the Quality Committee has focused deep dives on St Ann s Hospice, Diabetes, Maternity and Safe Staffing. Key areas reviewed by the Committee were: Patient safety; Quality dashboards; Consideration of the revised Statement of Commitment for all partners of the Stockport Safeguarding Children Board; Commissioner responsibilities in relation Provider CQC reports; Mortality; Mixed Sex Accommodation; SEND - Special Educational Needs and Disabilities audit; Assurance Framework 2017/18; Quality & Performance reports on Mental Health; Transforming Care for People with Learning Disabilities. Audit Committee Overall opinion of significant assurance given by Internal Audit in 2017/18; Unqualified audit opinion received from External Audit in 2016/17; Implemented a risk-based work programme for the full financial year; Appointed and inducted new External Auditors re Stockport Together Programme in line with Governing Body recommendation; Monitored progress against the Internal Audit Plan and received and considered the detailed findings of specific reports; Provided assurance to the Governing Body on the management of the CCG s Operational Risks through regular review of the Operational Risk Register; Reviewed and provided assurance to the Governing Body on anti-fraud matters and organisational compliance. Remuneration Committee Recommended changes to the remuneration of a number of CCG Executive Members. Finance and Performance Committee Oversaw the development and approval of the 2017/18 Better Care Fund, CIP (Cost Improvement Plan) for 2018/19, NHS Rightcare Plan for Wave 2 and the CCG s Operational Plan refresh for 2018/19; Reviewed the CCG s financial position and oversaw the development of an in year Recovery Plan; Monitored activity against the Operational Plan on a monthly basis; Oversaw a full review of performance reporting in the CCG and the development of a new framework; Reviewed requested updates on the Mental Health Parity of Esteem Investment Plan, Transformation Fund spend, UHSM Contract performance in 2017/18 and a trends analysis of ED attendances at Stockport NHS Foundation Trust; Received updates from the Stockport Area Medicines Panel (STAMP); Monitored assurance activity through reporting on the CCG Improvement and Outcomes Framework and NHS Rightcare Benchmarking. 55
70 070 Primary Care Commissioning Committee Continually reviewed and maintained overview of quality issues across General Practice including Care Quality Commission Inspection outcomes; Managed applications relating to practice mergers and boundary changes; Oversaw the commissioning and contracting of GP Seven Day Services; Considered safeguarding compliance across General Practice. Health and Care Integrated Commissioning Board Overseen the financial management of the pooled budget on behalf of Joint Commissioners; Reviewed and provided challenge on health and care performance indicators and patient outcomes in Stockport in particular focussing on urgent care performance and the interface between health and care services; Remained sighted on the procurement of the MCP and the wider work of integrated commissioning; Considered progress updates on the development of the Outcomes Framework. Locality Committees Undertaken the constitutional requirement for an annual meeting at which an overview of the activity within the previous year was considered along with required governance matters; In order to manage the finite clinical leadership resource available within the economy, resource and capacity available for Localities has been focussed in year focussed on supporting the development of the Neighbourhoods. The CCG s 3 Year Board Development Programme commissioned by the Chair to support her in continuing to enhance the role and effectiveness of the Governing Body and its members was extended into 2017/18 in order to enable continuity of support at a critical time in system and organisational transformation. In year members spend time focussed outside formal meetings reviewing their performance, setting the strategic direction on key internal and external matters and considering their role as leaders across the wider system. Areas of strategy which have been the focus of their work have included the future of strategic commissioning, clinical leadership, integrated commissioning and continued development of General Practice and Primary Care. The Clinical Commissioning Group Risk Management Framework The CCG s Risk Management Strategy has been in place since and provides the framework in which the organisation works proactively to minimise exposure to unnecessary risks, provides mitigation against those risks which cannot be avoided and maximise opportunities presented to the most benefit. The Strategy takes into account the complex environment in which the CCG continues to operate and the significant amount, and pace, of change which the organisation continues to experience. It uses a theme-based approach to categorising risk as a reflection of the cross cutting nature of the organisation s work and includes risk appetites for individual elements in order to guide behaviours at operational and leadership level. A target likelihood score and timescale was added in the previous year in order to enable more accurate tracking of the implementation and impact of the mitigations on the 56
71 071 likelihood of the risk materialising. The approach in place continues to ensure the management of opportunity is undertaken. The implementation of the strategy includes bi-monthly live risk updating and moderation sessions to ensure a consistent approach is taken to the scoring and understanding of risk by the CCG. Themes such as partnership and innovation risk demonstrate that the CCG s risk management approach is reflective of the collaborative work of the Stockport Together Partnership and Greater Manchester Health and Social Care Partnership. The continued development of the approach to managing risk by the CCG demonstrates a commitment by the organisation to managing risk in a mature manner which is reflective of the complex internal and external environments. The approach is one of proactive risk and opportunity management. Further alignment across the wider Locality will be a priority in the coming year, in particular to ensure alignment to the risk approach of the Greater Manchester Health and Social Care Partnership. Risk Assessment The CCG s strategic risk profile is detailed within the Board Assurance Framework. Each strategic risk is reviewed by the Executive Director Risk owner on a monthly basis to determine the likelihood of the risk arising, to consider the effectiveness of the controls and to identify any future events which may impact on the area of risk in either a positive or negative way. The reviews are undertaken in line with the risk appetite agreed for each theme which is reviewed by the theme owner as a whole on a bi-monthly basis. The same process of review is undertaken for those elements of the Framework shown as opportunities. The Board Assurance Framework is reported regularly to the Governing Body and also alongside the Operational Risk Register to the CCG s Audit Committee. Reporting frequency to Governing Body was increased to bi-monthly in 2016/17 to take into account the requirement for increased risk leadership and scrutiny of the information at a time of significant transformation and increased risk exposure for the organisation. This frequency has been maintained. Both documents are aligned under the same thematic areas and risk appetite measures and have been considered regularly throughout the year. Risks impact has remained under continued review and where environmental factors have changed significantly, impact scores have been altered to reflect increased impact. The Board Assurance Framework contains a number of extreme risks which have been present at more than one reporting cycle per year. These are: 02. The CCG fails to commission and design new models of care as part of the Stockport Together Programme; 03. The CCG does not fully maximise the opportunities for membership engagement in the development of its Strategy and priorities; 06. Providers' capacity and capability fails to deliver in line with the CCG strategy and quality expectations; 07. The CCG fails to remain within financial balance and operate within the Business Rules as required by NHS England; 57
72 The capability, capacity and skill mix of the primary care workforce fails to align to the strategic direction of the Stockport economy. The CCG has detailed mitigations in place against each of the risks which are reviewed bimonthly and over which the Chair of the Governing Body and the Chief Operating Officer maintain strategic oversight. The CCG has a number of areas deemed as high risk on the Framework, which demonstrates the complex partnership environment in which the organisation is working and the significant transformation programmes underway. These are: 05. The organisation's capacity, capability and/or internal engagement are inadequate. (Including commissioned support services); 09. The CCG fails to meet its statutory duties for compliance (including procurement); 10. The CCG fails to deliver improvements in health inequalities within the borough of Stockport; 12. The CCG fails to play a key leadership role in the Stockport Together Partnership and ensure the views of primary care are incorporated; 14. General Practice fails to reform to deliver the requirements of transformation. All have specific mitigations against them to demonstrate continuing management of the strategic risks. The risk appetite for the Compliance Theme was increased from low to moderate in the previous year to reflect the need to adjust behaviour and organisational exposure to risk to achieve the strategic intention to procure a Multi-Specialty Community Provider (MCP.) This risk remained a continual focus of the CCG s Executive Team until the decision to conclude the procurement approach was reached. The Governing Body routinely receives a compliance dashboard which sets out the CCG s performance against its areas of statutory requirement. This has been included in the Performance Report which is presented by the Chief Operating Officer. This is complemented by the Strategic Impact Report which combined provide the Governing Body with an oversight of the CCG s performance as well as some deep dive detailed reporting of specific areas of concern to Members. The Governing Body has also reviewed the output of the NHS England Quarterly assurance meetings which has provided an independent assessment of the CCG s performance. Meetings of the Governing Body are held in public and are minuted, allowing the patients and public of Stockport are able to ascertain for themselves the degree of rigour of the Governing Body s review of the CCG s performance. The Clinical Commissioning Group Internal Control Framework A system of internal control is the design of processes and procedures to ensure that the CCG delivers its policies, aims and objectives. It is designed to identify and prioritise the 58
73 073 risks, to evaluate the likelihood of those risks being realised and the impact should they be realised and to manage them efficiently, effectively and economically. The system of internal control allows risk to be managed to a reasonable level rather than eliminating all risks entirely. It can therefore only provide reasonable and not absolute assurance of effectiveness. The Governing Body is responsible for setting the strategic direction of the CCG and in support of this, approves the annual operational plan. At each Governing Body meeting there is a Resilience and Compliance Report which sets out the CCG s progress against its constitutional requirements and statutory compliance indicators. The report details progress and identifies those areas of underperformance or of significant challenge and sets out the actions being taken by the Executive to improve performance. The Governing Body also receives a Strategic Impact Report which provides a strategic overview of the performance against key indicators in the CCG s Operational Plan. A key component of the CCG s Performance Reporting is the Board Assurance Framework. The Framework provides a view of the organisation s performance from the perspective of its strategic risk profile. Each of the strategic themes and individual strategic risks has an Executive Director as its risk owner. Information Governance The NHS Information Governance Framework sets the processes and procedures by which the NHS handles information about patients and employees, in particular patient identifiable information. The NHS Information Governance Framework is supported by an information governance toolkit and the annual submission process provides assurances to the clinical commissioning group, other organisations and to individuals that personal information is dealt with legally, securely, efficiently and effectively. In year a full review of the CCG s Information Asset Register was undertaken with relevant Information Asset Owners and Administrators. This included a review of the information assets held by the organisation, the form in which they are stored and for which purpose and the risk rating associated with potential loss or damage. The CCG places high importance on ensuring there are robust information governance systems and processes in place to help protect patient and corporate information. We have established an information governance management framework and submitted the Information Governance Toolkit Self-Assessment at Level 2 on 31 March The CCG agreed an Information Governance Action Plan for 2017/18 against which progress could be demonstrated in year. The Information Governance Framework was reviewed and re-confirmed at the end of the financial year in order to reflect changes to established information governance practices. Review of Economy, Efficiency and Effectiveness of the Use of Resources 59
74 074 The Governing Body has received a monthly Finance Report which includes details of the CCG s achievement against surplus targets, its year to date financial position and the key challenges to its financial position. The Governing Body has been supported in its financial oversight and challenge by the Finance and Performance Committee. The CCG s Audit Committee maintains oversight of the organisation s financial processes. It is supported in its work by both internal and external auditors with internal audit providing significant assurance for the CCG s key financial systems. Feedback from delegation chains regarding business, use of resources and responses to risk The CCG has a defined scheme of reservation and delegation in the CCG s constitution approved by its GP members, the Council of Members. This identifies which functions are reserved for the Council of Members and Governing Body and which are delegated for discharge across the CCG in line with effective use of resources and risk management processes. In support of this the CCG has Financial Operational Arrangements which identify what financial responsibilities the following levels of authority have: Level 1 Accountable Officer; Level 2 CCG Governing Body; Level 3 Chief Operating Officer / Chief Finance Officer; Level 4 Budget holders, in accordance with specific levels of authority granted to individuals; Level 5 All other officers. The Governing Body receives regular reports from all its Committees to provide assurance regarding the arrangements for the discharge of delegated functions, including those relating to finance and risk. Internal Audit provides independent assurance on the processes in place as part of the annual internal audit plan which is supplemented by the oversight of the assurance of the CCG s value for money, economy, efficiency and effectiveness by the External Auditors. Review of Effectiveness of Governance, Risk Management and Internal Control As Accountable Officer I have responsibility for reviewing the effectiveness of the system of internal control within the clinical commissioning group. Capacity to Handle Risk The CCG s processes and procedures for risk management are overseen by the Associate Director Corporate Governance and Organisational Effectiveness. The CCG s Risk Management Strategy remains fit for purpose in order to ensure that the organisation s arrangements and capacity for handling and managing risk are appropriate and continue to reflect the complex partnership environment in which the CCG is operating and the significant amount and pace of change underway. Training has been provided to Theme and Risk Owners and resources made available to ensure knowledge of the strategy and associated risk best practice remains current. 60
75 075 Moderation has been built into established processes for reviewing and updating the CCG s strategic and operational risk documents and staff regularly engage in discussions about the proactive management of risk within their work areas. Embedding risk leadership was a priority in 2017/18 and will continue to be so in 2018/19. The staff and managers of the CCG are able to approach the Associate Director Corporate Governance and Organisational Effectiveness for support with identifying, assessing and managing their areas of risk. The Audit Committee reviews the effectiveness and operation of the CCG s risk management processes; this is led by the Governing Body s Lay Member for Audit and Governance who is the Chair of the Audit Committee. Review of Effectiveness My review of the effectiveness of the system of internal control is informed by the work of the internal auditors and the executive manages and clinical leads within the clinical commissioning group who have responsibility for the development and maintenance of the internal control framework. I have drawn on the performance information available to me. My review is also informed by comments made by the external auditors in their annual audit letter and other reports. The Board Assurance Framework itself provides me with evidence that the effectiveness of the controls that manage risks to the clinical commissioning group achieving its principle objectives have been reviewed. I have been advised on the implications of the result of my review of the effectiveness of the system of internal control by the Governing Body and the Audit Committee and a plan to ensure continuous improvement of the system, is in place. Head of Internal Audit Opinion Following completion of the planned audit work for the financial year for the CCG, the Head of Internal Audit issued an independent and objective opinion on the adequacy and effectiveness of the CCG s system of risk management, governance and internal control. The Head of Internal Audit concluded that: Substantial Assurance, can be given that that there is a good system of internal control designed to meet the organisation s objectives, and that controls are generally being applied consistently. The overall opinion is underpinned by the work conducted through the risk based internal audit plan, including key financial systems, QIPP and PMO Effectiveness. This opinion is provided in the context that the Clinical Commissioning Group like other organisations across the NHS is facing a number of challenging issues and wider organisational factors: Financial Position QIPP CCG Annual The YTD and forecast outturn positions were reported to Governing Body in March 2018 to be in line with the planned in year surplus. The savings target for 2017/18 was 17.4m with 16.4m achieved as at month 11. The CCG is anticipating full delivery. The CCG has been rated as Green by NHS England in its annual 61
76 076 Assessment Senior Management Changes Provider Performance Greater Manchester Health & Social Care Partnership assessment of performance against key performance indicators. Senior management within the CCG has remained stable during 2017/18. The CCG has continued to regularly report providers performance against a range of targets. The CCG s primary provider, Stockport NHS FT has consistently met targets for cancer waiting times, but has struggled to maintain required performance levels to meet the 4 and 12 hour urgent care waiting time standards, but also acknowledge that this is a national issue. The health and social care landscape in England is changing, with huge funding pressures across all public services. The Trust creation and direction is underpinned by Taking charge of our Health and Social Care in Greater Manchester, The Manchester Agreement. The Stockport Together programme is coming to the end of the second year of its 5-year plan and the second year of the 3-year Greater Manchester Partnership Investment Agreement. During 2018/19 the emphasis will be on optimising the services already mobilised and completing mobilisation of those under development. The Health and Care Integrated Commissioning Board is a Joint Committee of NHS Stockport Clinical Commissioning Group and Stockport Metropolitan Borough Council and continue to monitor Section 75 agreement to establish a pooled budget between Social Care and Health with the aim of cutting across organisational boundaries, improving the health and well-being of people in Stockport and providing better value for money. In providing this opinion I, The Head of Internal Audit, can confirm continued compliance with the definition of internal audit (as set out in your Internal Audit Charter), code of ethics and professional standards. I also confirm organisational independence of the audit activity and that this has been free from interference in respect of scoping, delivery and reporting. Tim Crowley Director of Audit, MIAA March 2018 During the year, Internal Audit issued the following audit reports SIGNIFICANT ASSURANCE: There are some weaknesses in the design and/or operation of controls which could impair the achievement of the objectives of the system, function or process. However, either their impact would be minimal or they would be unlikely to occur. Key Financial Systems QIPP To assess the robustness of the CCG s key financial systems and to confirm that the key controls in place are operating effectively. To assess the robustness of the CCG s identification and implementation of QiPP Schemes. 62
77 077 Programme Management Office Effectiveness Information Governance Toolkit To evaluate the effectiveness of the PMO function and the established processes to drive delivery and reporting on the Stockport Together programme work streams. To provide an opinion on: The policies, systems and operational activities in place to complete, approve and submit the IG Toolkit scores; The function and attendance of key committees/ groups; Departmental spot checks to assess staff understanding and implementation of IG guidance; and The validity of the scores of a sample of proposed 2017/18 IG toolkit final submission. Medicines Optimisation To provide assurance that the CCG has put in place arrangements to ensure that Practice Based Medicines Coordinators deliver the previously defined outcomes expected and to compare the value of this provision with that of employed medicines co-ordinators. LIMITED ASSURANCE: There are weaknesses in the design and / or operation of controls which could have a significant impact on the achievement of the key system, function or process objectives but should not have a significant impact on the achievement of organisational objectives. Performance Management (2016/17 cfwd) Continuing & Complex Healthcare To examine the arrangements for managing the performance of the CCG (and its constituent parts) and also the arrangements for managing the performance of the CCG s healthcare providers. To provide an assurance opinion on the arrangements in place for determining eligibility and provision of NHS continuing healthcare in compliance with the National Framework through evaluation of local procedures and arrangements. The review also considered contractual and performance management, quality and financial monitoring mechanisms. The full Director of Audit Opinion and Annual Report is available at the following link (insert link following approval). Data Quality The Governing Body is presented with different types of data from a number of sources. Much of the data is provided to the CCG by specialist analysts at the Greater Manchester Shared Services (part of the North West Commissioning Support Unit.) Oversight of the data provided is given by the CCG s Head of Strategic Business Intelligence and the Finance and Contracts Lead. The CCG has launched a Primary Care Dashboard with a view to providing individual practices and localities with data about key areas of performance so they can better benchmark and understand activity levels with a view to flat-lining performance in areas such as referrals and prescribing. This supplements existing dashboards which cover Secondary and Urgent Care. 63
78 078 The Governing Body also receives information which is more of a narrative form including the assurance reports from its Committees. A key element of the CCG s internal control systems is the Governing Body s effectiveness in triangulating these different sources and types of information. During the year the Governing Body has continued to review the level of type of data it requires to carry out its role effectively and similarly, that required by the wider CCG in support. This has led to continued improvements and refinement in reporting and in response to recommendations arising from a review of performance management by the CCG s Internal Auditors. A performance framework, to be underpinned by revised reporting and governance arrangements is under development. Business Critical Models The CCG uses only those models prescribed by NHS England. Data Security The CCG has submitted a satisfactory level of compliance with the Information Governance Toolkit Assessment which has resulted in a self-assessment at Level 2. Discharge of Statutory Functions Arrangements put in place by the CCG, and explained within the corporate governance framework, have been developed with extensive expert external legal input to ensure compliance with all relevant legislation. That legal advice also informed the matters reserved for the Council of Members and Governing Body s decision and the Scheme of Delegation. In light of the Harris Review, the CCG has reviewed all of the statutory duties and powers conferred on it by the National Health Service Act 2006 (as amended) and other associated legislation and regulations. As a result, I can confirm that the CCG is clear about the legislative requirements associated with each of the statutory functions for which it is responsible, including any restrictions on delegation of those functions. Responsibility for each duty and power has clearly been allocated to a Lead Director. Directorates have confirmed that their structures provide the necessary capability and capacity to undertake all of the CCG s statutory duties. As part of integrated commissioning work, the CCG has been reviewing its statutory functions in order to plan the future strategic direction of commissioning. Conclusion No significant internal control issues have been identified throughout the year and up until the approval of the annual accounts. Dr Ranjit Gill Accountable Officer DATE: 64
79 079 65
80 Remuneration and Staff Report Remuneration Report Remuneration Committee Membership of the remuneration committee can be found on page 47. Policy on the remuneration of senior managers The CCG as a membership organisation is responsible for agreeing its own remuneration with all the duties and freedoms that that implies. There are a small number of pieces of national guidance that exist to guide the CCG in developing its Remuneration Policy which include: 1. Remuneration Guidance for Chief Officers (where the senior manager also undertakes the accountable officer role) and Chief Finance Officers; 2. Greater Manchester commissioned guidance from Hay on the remuneration of clinical leadership; 3. Nationally set pay rates for all those organisations using Agenda for Change as the basis of employment for staff. The CCG uses the relevant national guidance and local benchmarking information to continually review its approach to Remuneration for directors and senior managers. It has available to it expertise from Human Resources professionals through the Greater Manchester Shared Service and from an external and independent strategic Human Resources Adviser. The CCG is committed to an open and transparent approach to remuneration and has established a Remuneration Committee in accordance with its constitution to discharge its relevant duties. The Committee, in reviewing and applying the CCGs Remuneration Policy, makes recommendations to Governing Body for approval Remuneration of Very Senior Managers The CCG has three senior managers who would have been paid more than 150,000 per annum had they worked on a full time basis. All senior managers provided clinical leadership and the CCG has satisfied itself that the remuneration is reasonable through the application of its remuneration policy. Senior manager remuneration (including salary and pension entitlements) The CCG is required to disclose the remuneration and benefits of senior managers who have held office during the year. The definition used for a Senior Manager is those persons in senior positions having authority or responsibility for directing or controlling the major activities of the Commissioning Group. This has been applied as those who regularly attend the Governing Body meetings. 66
81 081 For each member of the Governing Body who has served during the financial year 2017/18 their remuneration and pension benefits are shown below together with prior year comparatives. These figures are subject to audit. Name and Title 2017/18 (a) (b) (c) (d) (e) (f) Salary (bands of 5,000) Expense payments (taxable) to nearest 100 Performance pay and bonuses (bands of 5,000) Long term performance pay and bonuses (bands of 5,000) All pensionrelated benefits (bands of 2,500) TOTAL (a to e) (bands of 5,000) Dr Ranjit Singh Gill Chief Clinical Officer Ms Jane Marie Crombleholme** Lay Member and Chair Mr John Greenough** Lay Member Miss Christine Morgan** Lay Member Primary Care Gaynor Dawn Mullins Chief Operating Officer Mark Gerard Chidgey Chief Finance Officer Dr Catherine Helen Briggs Clinical Director of Quality and Provider Management (Resigned December 2017) Dr Viren Mehta Clinical Director for General Practice Development Dr Peter Carne** Chair of Cheadle and Bramhall Locality Council Committee (resigned January 2018) Dr Lydia Hardern** Chair of Stepping Hill and Victoria Locality Council Committee Dr James Higgins** 67
82 082 Chair of Heatons and Tame Valley Locality Council Committee (resigned January 2018) Named GP Safeguarding Dr Andrew Johnson** Chair of Marple and Werneth Locality Council Committee Clinical Lead for Cancer Dr Diane Lesley Jones Director of Service Reform Roger Ian Roberts Director of General Practice Development Timothy Patrick Ryley Director of Strategic Planning And Performance Anita Rolfe Executive Nurse Dr Deborah Kendal*** Secondary Care Consultant Dr Vicci Owen Smith**** Director for Public Health Note The total figure is expressed in bandings of 5,000 based on the actual remuneration values and therefore may vary to the total of salary bands added together. * All pension related benefits represents the annual increase in pension entitlement based on the assumption that pension entitlements will be paid for 20 years from the date of retirement. ** Non-executive members do not receive pensionable remuneration; therefore there are no disclosures in respect of pension related benefits for non-executive members *** Members whose pension benefits are held and disclosed by another employing authority **** Dr Vicci Owen-Smith is employed by Stockport Metropolitan Borough Council and the work undertaken in her role as Clinical Director for Public Health is provided in-kind Name & Title Salary & Fees Taxable Benefits Annual Long-term All Pension TOTAL Performance Performance Related Benefits* (rounded to Related Bonuses Related Bonuses (bands of 5,000) nearest 00) (bands of 5,000) (bands of 5,000) (bands of 2,500) (bands of 5,000) Dr Ranjit Singh Gill Chief Clinical Officer Ms Jane Marie Crombleholme** Lay Member and Chair
83 083 Mr John Greenough** Lay Member Miss Christine Morgan** Lay Member Primary Care Gaynor Dawn Mullins Chief Operating Officer Mark Gerard Chidgey Chief Finance Officer Dr Catherine Helen Briggs Clinical Director of Quality and Provider Management Dr Viren Mehta Clinical Director for General Practice Development Dr Peter Carne** Chair of Cheadle and Bramhall Locality Council Committee Dr Lydia Hardern** Chair of Stepping Hill and Victoria Locality Council Committee Dr James Higgins** Chair of Heatons and Tame Valley Locality Council Committee Named GP Safeguarding Dr Andrew Johnson** Chair of Marple and Werneth Locality Council Committee Clinical Lead for Cancer Dr Diane Lesley Jones Director of Service Reform Roger Ian Roberts Director of General Practice Development Timothy Patrick Ryley Director of Strategic Planning And Performance Anita Rolfe 69
84 084 Executive Nurse Dr Deborah Kendal*** Secondary Care Consultant Dr Vicci Owen Smith**** Director for Public Health Senior Employee Salaries (subject to audit) NHS Stockport CCG has made a commitment in its Constitution to disclose the salaries of all senior employees. The definition of a senior employee is anyone with a salary of 50,000 or above if they were to be paid on a whole time equivalent basis (WTE) (a) (a) Name & Title Salary Salary (bands of 5,000) (bands of 5,000) Aaron Atkinson Head of Strategic Business Intelligence (commenced November 2017) N/A Mrs Elizabeth Bailey Medicines Optimisation Lead Mrs Susan Jane Brett Head of Continuing and Complex Healthcare (retired October 2017) James Brown Head of Communications & Business Support (commenced December 2017) N/A Mrs Lesley Brown Programme Manager (commenced June 2017) N/A Daniel William Byrne Head of Performance Information (retired October 2017) Sean Capper Associate Director of IM & T Mrs Angela Dawber Head of Planning & Performance N/A David Andrew Dolman Deputy Chief Finance Officer Mrs Gina Erlander Evans Joint Commissioning Lead Mrs Louise Hayes Head of Communications & Business Support (left September 2017) N/A Ms Laura Janda Associate Director of Planning & Performance (commenced August N/A 70
85 ) Mrs Laura Latham Associate Director Corporate Governance and Organisational Effectiveness Mrs Gillian Suzanne Miller Deputy Director of Provider Management Mrs Karen Moran Senior Service Reform Manager Mrs Julie Parker Head of Safeguarding/Designated Nurse Safeguarding Children Mrs Julie Ryley Head of Primary Care Development Dr Adam Firth GP Digital Champion and Advisor (WTE 0.006) Dr Ruth Seabrook Vice - Chair of Cheadle and Bramhall Locality Council Committee (WTE 0.015) Mrs Sarah Williamson Associate Director (Continuing & Complex Healthcare) (commenced December 2017) N/A Dr Simon Woodworth Clinical Lead for Urgent Care (WTE 0.2) GP IT Advisor (WTE 0.006) Susan Parker Clinical Lead for Ophthalmology Dr Nijabat Hussain Clinical Lead for Mental health (WTE 0.117) Dr Karen McEwan McMillan GP Lead (WTE 0.222) Clinical Lead for Planned Care (WTE 0.2) Dr Alan Gilman Chief Clinical Information Lead (WTE 0.2) Dr Heather Proctor Clinical Lead for Prescribing (WTE 0.2) (Finished June 2016) N/A 5-10 Pension benefits as at 31 March 2018 (subject to audit) For each Senior Manager who served during the year, their pension benefits are shown below: (a) (b) (c) (d) (e) (f) (g) (h) Real Real increase Total Lump sum at Cash Real Cash Employers increase in in pension accrued pension age Equivalent Increase in Equivalent Contribution pension at lump sum at pension at related to Transfer Cash Transfer to pension pension age pension accrued Value at 1 Equivalent Value at 31 partnership age (bands of (bands of 2,500) age at 31 March 2018 pension at 31 March 2018 April 2017 Transfer Value March 2018 pension 2,500) (bands of (bands of ,000)
86 086 Name and title Dr Ranjit Singh Gill Chief Clinical Officer Mrs Gaynor Dawn Mullins Chief Operating Officer Dr Catherine Helen Briggs Clinical Director of Quality and Provider Manangement Dr Viren Mehta Clinical Director of General Practice Development Mark Gerard Chidgey Chief Finance Officer Dr Diane Lesley Jones Director of Service Reform Roger Ian Roberts Director of General Practice Development Timothy Patrick Ryley Director of Strategic Planning and Performance Anita Rolfe Executive Nurse Cash equivalent transfer values A cash equivalent transfer value (CETV) is the actuarially assessed capital value of the pension scheme benefits accrued by a member at a particular point in time. The benefits valued are the member s accrued benefits and any contingent spouse s (or other allowable beneficiary s) pension payable from the scheme. A CETV is a payment made by a pension scheme or arrangement to secure pension benefits in another pension scheme or arrangement when the member leaves a scheme and chooses to transfer the benefits accrued in their former scheme. The pension figures shown relate to the benefits that the individual has accrued as a consequence of their total membership of the pension scheme, not just their service in a senior capacity to which disclosure applies. The CETV figures and the other pension details include the value of any pension benefits in another scheme or arrangement which the individual has transferred to the NHS pension scheme. They also include any additional pension benefit accrued to the member as a result of their purchasing additional years of pension service in the scheme at their 72
87 087 own cost. CETVs are calculated within the guidelines and framework prescribed by the Institute and Faculty of Actuaries. Real increase in CETV This reflects the increase in CETV that is funded by the employer. It does not include the increase in accrued pension due to inflation or contributions paid by the employee (including the value of any benefits transferred from another scheme or arrangement). Compensation on early retirement of for loss of office The CCG made no payments during the financial year 2017/18 to any Senior Manager or other employee as compensation on early retirement or loss of office. Payments to past members There were no payments made during the financial year 2017/18 to any previous Senior Manager. Pay multiples (subject to audit) Reporting bodies are required to disclose the relationship between the remuneration of the highest-paid director/member in their organisation and the median remuneration of the organisation s workforce. The annualised full time equivalent banded remuneration of the highest paid Member at NHS Stockport CCG in the financial year 2017/18 was 167,500 (2016/17: 167,500). This was 4.71 times (2016/17: 4.69) the median remuneration of the workforce, which was 35,577 (2016/17: 35,738). In 2017/18, no employees received remuneration in excess of the highest-paid Member. Remuneration mid-point bandings ranged from 17,500 to 167,500 (2016/17: 12,500 to 167,500). The increase in the pay multiple is a reflection of the 2017/18 NHS pay award. Total remuneration includes salary, non-consolidated performance-related pay, benefits-inkind, but not severance payments. It does not include employer pension contributions and the cash equivalent transfer value of pensions. Staff Report As at 31 st March 2018 the CCG employed 142 ( ) individuals which equates to ( WTE) whole time equivalents (WTE). Number of Governing Body Members Employed by Band The table below outlines the number of Governing body Members employed by band: Number of Governing Body Members Employed by Band Payscale Description Headcount Non-Agenda for Change 15 Total 15 73
88 088 Staff composition In common with most health organisations, women make up the majority of our workforce, with 69.12% of our employees being female, which is slightly lower when compared to 71.77% in Gender breakdown by roles: Directors Employees Total Employees Female = 46.7% Female = 71.9% Female = 69.1% Male = 53.3% Male = 28.1% Male = 30.9% Sickness absence data Sickness absence is reported at organisational level each month to the senior management team as part of the Workforce Performance Report. Monthly reports at individual employee level are shared with line managers and the Human Resource Advisor works closely with managers to proactively manage sickness cases in line with the Sickness Absence Policy. Further information on staff sickness & absence can be found within note 4.3 of the Financial Statements section of the Annual Accounts published as part of this Annual Report. Staff sickness absence and ill health retirements Number Total Days Lost 1,144 Total Staff Years 109 Average working Days Lost 10.5 Staff sickness absence data is based on a calendar year (January-December) due to current financial year data not being available for inclusion within the accounts. Staff policies In line with our public sector equality duty, our annual equality and diversity report published in outlines our approach to equality and diversity including how this relates to our workforce. For more information visit 74
89 089 75
90 090 Staff numbers and costs [Remove Bracket Info] ADMIN PROGRAMME TOTAL Permanent Employees Other Total Permanent Employees Other Total Permanent Employees Other '000 '000 '000 '000 '000 '000 '000 '000 '000 N4A N4B N4C N4D N4E N4F N4G N4H N4I Total Salaries and wages 2, ,950 1, ,199 4, ,149 Social security costs Employer contributions to the NHS Pension Scheme Other pension costs Apprenticeship Levy Termination benefits Gross Employee Benefits Expenditure 3, ,673 2, ,591 5, ,264 Less: Recoveries in respect of employee benefits (note 4.1.2) Net employee benefits expenditure including capitalised costs , ,673 2, ,591 5, ,264 Less: Employee costs capitalised Net employee benefits expenditure excluding capitalised costs 3, ,673 2, ,591 5, ,264 Staff Numbers Average number of people employed
91 091 Staff numbers and costs ADMIN PROGRAMME TOTAL Permanent Employees Other Total Permanent Employees Other Total Permanent Employees Other Total '000 '000 '000 '000 '000 '000 '000 '000 '000 N4A N4B N4C N4D N4E N4F N4G N4H N4I Salaries and wages 2, ,979 1, ,078 4, ,057 Social security costs Employer contributions to the NHS Pension Scheme Other pension costs Apprenticeship Levy Termination benefits Gross Employee Benefits Expenditure 3, ,687 1, ,408 5, ,095 Less: Recoveries in respect of employee benefits (note 4.1.2) Net employee benefits expenditure including capitalised costs , ,687 1, ,408 5, ,095 Less: Employee costs capitalised Net employee benefits expenditure excluding capitalised costs 3, ,687 1, ,408 5, ,095 Staff Numbers Average number of people employed
92 092 Expenditure on consultancy During 2017/18 the CCG spent 52,000 (2016/17 782,000) on consultancy services. This related to the public consultation as part of the Stockport Together Programme. Off-payroll engagements Following the Review of Tax Arrangements of Public Sector Appointees published by the Chief Secretary to the Treasury on 23 May 2012, the CCG must publish information on their highly paid and/or senior manager s off-payroll engagements For all off-payroll engagements as at 31 March 2018, for more than 245 per day and that last longer than six months: Number Number of existing engagements as of 31 March Of which, the number that have existed: for less than one year at the time of reporting for between one and two years at the time of reporting 1 for between 2 and 3 years at the time of reporting for between 3 and 4 years at the time of reporting for 4 or more years at the time of reporting 1 The existing off-payroll engagements have been subject to risk assessment as to whether assurance is required that the individual is paying the correct amount of tax and, where necessary, that assurance has been sought New off-payroll engagements The Government has reformed the Intermediaries legislation, introducing Chapter 10 Part 2 Income Taxes (Earnings and Pensions) Act 2003 (ITEPA 2003) supporting Chapter 8 Part 2 ITEPA 2003, often known as IR35. The legislation for the off-payroll working rules within the public sector applies to payments made on or after 6 April Under the reformed off-payroll working rules, Departments must determine whether the rules apply when engaging a worker through a Personal Service Company (PSC). Where the reformed public sector rules apply, entities must disclose all new off-payroll engagements, or those that reached six months in duration, between 1 April 2017 and March 2018, for more than 245 per day and that last for longer than six months Number Number of new engagements, or those that reached six months in duration, between 1 April 2017 and 31 March Number assessed as caught by IR35 0 Number assessed as not caught by IR35 1 Number engaged directly (via PSC contracted to department) are on the departmental payroll 0 Number of Engagements reassessed for consistency / assurance purposes during the year 0 78
93 093 Number of engagements that saw a change to IR35 Status following the consistency review. 0 Off-payroll engagements / senior official engagements For any off-payroll engagements of Board members and / or senior officials with significant financial responsibility, between 01 April 2017 and 31 March 2018: Number of off-payroll engagements of board members, and/or senior officers with significant financial responsibility, during the financial year Total no. of individuals on payroll and off-payroll that have been deemed board members, and/or, senior officials with significant financial responsibility, during the financial year. This figure should include both on payroll and off-payroll engagements Exit packages, including special (non-contractual) payments Table 1: Exit Packages (subject to audit) Exit package cost band (inc. any special payment element Number of compulsory redundancies WHOLE NUMBERS ONLY s Cost of compulsory redundancies Number of other departures agreed WHOLE NUMBERS ONLY s Cost of other departures agreed Less than 10, ,029 10,000-25, ,369 25,001-50,000 50, , , , , ,000 > 200,000 TOTALS Agrees to A below Total number of exit packages WHOLE NUMBERS ONLY s Total cost of exit packages Number of departures where special payments have been made WHOLE NUMBERS ONLY s Cost of special payment element included in exit packages Redundancy and other departure cost have been paid in accordance with the provisions of NHS Stockport CCG policy. Exit costs in this note are accounted for in full in the year of departure. 79
94 094 Table 2: Analysis of Other Departures (subject to audit) Voluntary redundancies including early retirement contractual costs Mutually agreed resignations (MARS) contractual costs Early retirements in the efficiency of the service contractual costs Contractual payments in lieu of notice* Exit payments following Employment Tribunals or court orders Non-contractual payments requiring HMT approval** Agreements Total Value of agreements Number 000s TOTAL 0 0 The Remuneration Report includes disclosure of exit packages payable to individuals named in that Report. 80
95 Parliamentary Accountability and Audit Report NHS Stockport CCG is not required to produce a Parliamentary Accountability and Audit Report but has opted to include disclosures on remote contingent liabilities, losses and special payments, gifts, and fees and charges in this Accountability Report from page 42. An audit certificate and report is also included in this Annual Report at page
96 Financial Statements and Notes to the Annual Accounts Please see attached financial statements and notes to the Annual Accounts. Dr Ranjit Gill Accountable Officer [x] May/June
97 097 NHS Stockport CCG - Annual Accounts CONTENTS Page Number (tbc) Foreword to the Accounts Contents The Primary Statements: Statement of Comprehensive Net Expenditure for the year ended 31st March 2018 Statement of Financial Position as at 31st March 2018 Statement of Changes in Taxpayers' Equity for the year ended 31st March 2018 Statement of Cash Flows for the year ended 31st March 2018 Notes to the Accounts Note 1. Accounting policies Note 2. Other operating revenue Note 3. Revenue Note 4. Employee benefits and staff numbers Note 5. Operating expenses Note 6. Better payment practice code Note 7. Operating leases Note 8. Property, plant and equipment Note 9. Trade and other receivables Note 10. Cash and cash equivalents Note 11. Trade and other payables Note 12. Provisions Note 13. Financial instruments Note 14. Operating segments Note 15. Pooled budgets Note 16. Related party transactions Note 17. Events after the end of the reporting period Note 18. Financial performance targets
98 098 NHS Stockport CCG - Annual Accounts Statement of Comprehensive Net Expenditure for the year ended 31 March Note '000 '000 Income from sale of goods and services 2 (1,121) (2,312) Other operating income 2 (620) (344) Total operating income (1,741) (2,656) Staff costs 4 6,264 6,095 Purchase of goods and services 5 445, ,572 Depreciation and impairment charges Provision expense 5 (174) (63) Other Operating Expenditure Total operating expenditure 452, ,823 Comprehensive Expenditure for the year ended 31 March , ,167
99 099 NHS Stockport CCG - Annual Accounts Statement of Financial Position as at 31 March Note '000 '000 Non-current assets: Property, plant and equipment Total non-current assets 0 4 Current assets: Trade and other receivables 9 1,203 2,048 Cash and cash equivalents Total current assets 1,463 2,106 Total assets 1,463 2,110 Current liabilities Trade and other payables 11 (23,048) (23,831) Provisions 12 0 (201) Total current liabilities (23,048) (24,032) Non-Current Assets plus/less Net Current Assets/Liabilities (21,585) (21,922) Financed by Taxpayers Equity General fund (21,585) (21,922) Revaluation reserve 0 0 Other reserves 0 0 Charitable Reserves 0 0 Total taxpayers' equity: (21,585) (21,922) The notes on pages [ ] to [ ] form part of this statement The financial statements on pages [ ] to [ ] were approved by the Governing Body on 23 May 2018 and signed on its behalf by: Chief Accountable Officer Dr Ranjit Gill
100 100 NHS Stockport CCG - Annual Accounts Statement of Changes In Taxpayers Equity for the year ended 31 March 2018 Changes in taxpayers equity for Revaluation Other Total General fund reserve reserves reserves '000 '000 '000 '000 Balance at 01 April 2017 (21,922) 0 0 (21,922) Transfer between reserves in respect of assets transferred from closed NHS bodies Adjusted NHS Clinical Commissioning Group balance at 31 March 2018 (21,922) 0 0 (21,922) Changes in NHS Clinical Commissioning Group taxpayers equity for Net operating expenditure for the financial year (450,351) (450,351) Total revaluations against revaluation reserve Net funding 450, ,688 Balance at 31 March 2018 (21,585) 0 0 (21,585) Changes in taxpayers equity for Revaluation Other Total General fund reserve reserves reserves '000 '000 '000 '000 Balance at 01 April 2016 (21,265) 0 0 (21,265) Transfer of assets and liabilities from closed NHS bodies as a result of the 1 April 2013 transition Adjusted NHS Clinical Commissioning Group balance at 31 March 2017 (21,265) 0 0 (21,265) Changes in NHS Clinical Commissioning Group taxpayers equity for Net operating costs for the financial year (440,167) (440,167) Total revaluations against revaluation reserve Net funding 439, ,510 Balance at 31 March 2017 (21,922) 0 0 (21,922) The notes on pages x to xx form part of this statement
101 101 NHS Stockport CCG - Annual Accounts Statement of Cash Flows for the year ended 31 March Note '000 '000 Cash Flows from Operating Activities Net operating expenditure for the financial year (450,351) (440,167) Depreciation and amortisation (Increase)/decrease in trade & other receivables (291) Increase/(decrease) in trade & other payables 11 (783) 1,194 Provisions utilised 12 (27) (206) Increase/(decrease) in provisions 12 (174) (63) Net Cash Inflow (Outflow) from Operating Activities (450,485) (439,528) Net Cash Inflow (Outflow) from Investing Activities 0 0 Net Cash Inflow (Outflow) before Financing (450,485) (439,528) Cash Flows from Financing Activities Grant in Aid Funding Received 450, ,510 Net Cash Inflow (Outflow) from Financing Activities 450, ,510 Net Increase (Decrease) in Cash & Cash Equivalents (18) Cash & Cash Equivalents at the Beginning of the Financial Year Cash & Cash Equivalents (including bank overdrafts) at the End of the Financial Year The notes on pages x to xx form part of this statement
102 102 NHS Stockport CCG - Annual Accounts Notes to the financial statements 1 Accounting Policies NHS England has directed that the financial statements of clinical commissioning groups shall meet the accounting requirements of the Group Accounting Manual issued by the Department of Health and Social Care. Consequently, the following financial statements have been prepared in accordance with the Group Accounting Manual issued by the Department of Health and Social Care. The accounting policies contained in the Group Accounting Manual follow International Financial Reporting Standards to the extent that they are meaningful and appropriate to clinical commissioning groups, as determined by HM Treasury, which is advised by the Financial Reporting Advisory Board. Where the Group Accounting Manual permits a choice of accounting policy, the accounting policy which is judged to be most appropriate to the particular circumstances of the clinical commissioning group for the purpose of giving a true and fair view has been selected. The particular policies adopted by the clinical commissioning group are described below. They have been applied consistently in dealing with items considered material in relation to the accounts. 1.1 Going Concern These accounts have been prepared on the going concern basis Public sector bodies are assumed to be going concerns where the continuation of the provision of a service in the future is anticipated, as evidenced by inclusion of financial provision for that service in published documents. Where a clinical commissioning group ceases to exist, it considers whether or not its services will continue to be provided (using the same assets, by another public sector entity) in determining whether to use the concept of going concern for the final set of Financial Statements. If services will continue to be provided the financial statements are prepared on the going concern basis. 1.2 Accounting Convention These accounts have been prepared under the historical cost convention modified to account for the revaluation of property, plant and equipment, intangible assets, inventories and certain financial assets and financial liabilities. 1.3 Acquisitions & Discontinued Operations Activities are considered to be acquired only if they are taken on from outside the public sector. Activities are considered to be discontinued only if they cease entirely. They are not considered to be discontinued if they transfer from one public sector body to another. 1.4 Movement of Assets within the Department of Health and Social Care Group Transfers as part of reorganisation fall to be accounted for by use of absorption accounting in line with the Government Financial Reporting Manual, issued by HM Treasury. The Government Financial Reporting Manual does not require retrospective adoption, so prior year transactions (which have been accounted for under merger accounting) have not been restated. Absorption accounting requires that entities account for their transactions in the period in which they took place, with no restatement of performance required when functions transfer within the public sector. Where assets and liabilities transfer, the gain or loss resulting is recognised in the Statement of Comprehensive Net Expenditure, and is disclosed separately from operating costs. Other transfers of assets and liabilities within the Department of Health and Social Care Group are accounted for in line with IAS 20 and similarly give rise to income and expenditure entries. 1.5 Pooled Budgets Where the clinical commissioning group has entered into a pooled budget arrangement under Section 75 of the National Health Service Act 2006 the clinical commissioning group accounts for its share of the assets, liabilities, income and expenditure arising from the activities of the pooled budget, identified in accordance with the pooled budget agreement. If the clinical commissioning group is in a jointly controlled operation, the clinical commissioning group recognises: The assets the clinical commissioning group controls; The liabilities the clinical commissioning group incurs; The expenses the clinical commissioning group incurs; and, The clinical commissioning group s share of the income from the pooled budget activities. If the clinical commissioning group is involved in a jointly controlled assets arrangement, in addition to the above, the clinical commissioning group recognises: The clinical commissioning group s share of the jointly controlled assets (classified according to the nature of the assets); The clinical commissioning group s share of any liabilities incurred jointly; and, The clinical commissioning group s share of the expenses jointly incurred. 1.6 Critical Accounting Judgements & Key Sources of Estimation Uncertainty In the application of the clinical commissioning group s accounting policies, management is required to make judgements, estimates and assumptions about the carrying amounts of assets and liabilities that are not readily apparent from other sources. The estimates and associated assumptions are based on historical experience and other factors that are considered to be relevant. Actual results may differ from those estimates and the estimates and underlying assumptions are continually reviewed. Revisions to accounting estimates are recognised in the period in which the estimate is revised if the revision affects only that period or in the period of the revision and future periods if the revision affects both current and future periods Critical Judgements in Applying Accounting Policies The following are the critical judgements, apart from those involving estimations (see below) that management has made in the process of applying the clinical commissioning group s accounting policies that have the most significant effect on the amounts recognised in the financial statements: Contributions to the NHS continuing healthcare risk pool scheme are accounted for in accordance with the mechanism set out in the letter to clinical commissioning Accountable Officers and Chief Finance Officers dated 12 September 2014 (Gateway reference 02252) Key Sources of Estimation Uncertainty The following are the key estimations that management has made in the process of applying the clinical commissioning group s accounting policies that have the most significant effect on the amounts recognised in the financial statements: Prescribing Liability
103 103 NHS Stockport CCG - Annual Accounts Notes to the financial statements The clinical commissioning group receives financial information from NHS Business Services Authority relating to the costs of drugs prescribed by clinical commissioning group prescribers (independent GPs). The information available for actual drug costs prescribed in the year is provided two month in arrears, therefore the actual data received at the Statement of Financial Position date is to 31 January 2018, and an estimate for February and March is required. Two months of prescribing activity totalling 7,845,558 ( ,972,672) has been estimated. 1.7 Revenue Revenue in respect of services provided is recognised when, and to the extent that, performance occurs, and is measured at the fair value of the consideration receivable. Where income is received for a specific activity that is to be delivered in the following year, that income is deferred. 1.8 Employee Benefits Short-term Employee Benefits Salaries, wages and employment-related payments are recognised in the period in which the service is received from employees, including bonuses earned but not yet taken. The cost of leave earned but not taken by employees at the end of the period is recognised in the financial statements to the extent that employees are permitted to carry forward leave into the following period Retirement Benefit Costs Past and present employees are covered by the provisions of the NHS Pensions Scheme. The scheme is an unfunded, defined benefit scheme that covers NHS employers, General Practices and other bodies, allowed under the direction of the Secretary of State, in England and Wales. The scheme is not designed to be run in a way that would enable NHS bodies to identify their share of the underlying scheme assets and liabilities. Therefore, the scheme is accounted for as if it were a defined contribution scheme: the cost to the clinical commissioning group of participating in the scheme is taken as equal to the contributions payable to the scheme for the accounting period. For early retirements other than those due to ill health the additional pension liabilities are not funded by the scheme. The full amount of the liability for the additional costs is charged to expenditure at the time the clinical commissioning group commits itself to the retirement, regardless of the method of payment. 1.9 Other Expenses Other operating expenses are recognised when, and to the extent that, the goods or services have been received. They are measured at the fair value of the consideration payable. Expenses and liabilities in respect of grants are recognised when the clinical commissioning group has a present legal or constructive obligation, which occurs when all of the conditions attached to the payment have been met Property, Plant & Equipment Recognition Property, plant and equipment is capitalised if: It is held for use in delivering services or for administrative purposes; It is probable that future economic benefits will flow to, or service potential will be supplied to the clinical commissioning group; It is expected to be used for more than one financial year; The cost of the item can be measured reliably; and, The item has a cost of at least 5,000; or, Collectively, a number of items have a cost of at least 5,000 and individually have a cost of more than 250, where the assets are functionally interdependent, they had broadly simultaneous purchase dates, are anticipated to have simultaneous disposal dates and are under single managerial control; or, Items form part of the initial equipping and setting-up cost of a new building, ward or unit, irrespective of their individual or collective cost. Where a large asset, for example a building, includes a number of components with significantly different asset lives, the components are treated as separate assets and depreciated over their own useful economic lives Valuation All property, plant and equipment are measured initially at cost, representing the cost directly attributable to acquiring or constructing the asset and bringing it to the location and condition necessary for it to be capable of operating in the manner intended by management. All assets are measured subsequently at valuation. Land and buildings used for the clinical commissioning group s services or for administrative purposes are stated in the statement of financial position at their re-valued amounts, being the fair value at the date of revaluation less any impairment. Revaluations are performed with sufficient regularity to ensure that carrying amounts are not materially different from those that would be determined at the end of the reporting period. Fair values are determined as follows: Land and non-specialised buildings market value for existing use; and, Specialised buildings depreciated replacement cost. HM Treasury has adopted a standard approach to depreciated replacement cost valuations based on modern equivalent assets and, where it would meet the location requirements of the service being provided, an alternative site can be valued. Properties in the course of construction for service or administration purposes are carried at cost, less any impairment loss. Cost includes professional fees but not borrowing costs, which are recognised as expenses immediately, as allowed by IAS 23 for assets held at fair value. Assets are re-valued and depreciation commences when they are brought into use. Fixtures and equipment are carried at depreciated historic cost as this is not considered to be materially different from current value in existing use. An increase arising on revaluation is taken to the revaluation reserve except when it reverses an impairment for the same asset previously recognised in expenditure, in which case it is credited to expenditure to the extent of the decrease previously charged there. A revaluation decrease that does not result from a loss of economic value or service potential is recognised as an impairment charged to the revaluation reserve to the extent that there is a balance on the reserve for the asset and, thereafter, to expenditure. Impairment losses that arise from a clear consumption of economic benefit are taken to expenditure. Gains and losses recognised in the revaluation reserve are reported as other comprehensive income in the Statement of Comprehensive Net Expenditure.
104 104 NHS Stockport CCG - Annual Accounts Notes to the financial statements Subsequent Expenditure Where subsequent expenditure enhances an asset beyond its original specification, the directly attributable cost is capitalised. Where subsequent expenditure restores the asset to its original specification, the expenditure is capitalised and any existing carrying value of the item replaced is written-out and charged to operating expenses Depreciation, Amortisation & Impairments Freehold land, properties under construction, and assets held for sale are not depreciated. Otherwise, depreciation and amortisation are charged to write off the costs or valuation of property, plant and equipment and intangible noncurrent assets, less any residual value, over their estimated useful lives, in a manner that reflects the consumption of economic benefits or service potential of the assets. The estimated useful life of an asset is the period over which the clinical commissioning group expects to obtain economic benefits or service potential from the asset. This is specific to the clinical commissioning group and may be shorter than the physical life of the asset itself. Estimated useful lives and residual values are reviewed each year end, with the effect of any changes recognised on a prospective basis. Assets held under finance leases are depreciated over their estimated useful lives. At each reporting period end, the clinical commissioning group checks whether there is any indication that any of its tangible or intangible noncurrent assets have suffered an impairment loss. If there is indication of an impairment loss, the recoverable amount of the asset is estimated to determine whether there has been a loss and, if so, its amount. Intangible assets not yet available for use are tested for impairment annually. A revaluation decrease that does not result from a loss of economic value or service potential is recognised as an impairment charged to the revaluation reserve to the extent that there is a balance on the reserve for the asset and, thereafter, to expenditure. Impairment losses that arise from a clear consumption of economic benefit are taken to expenditure. Where an impairment loss subsequently reverses, the carrying amount of the asset is increased to the revised estimate of the recoverable amount but capped at the amount that would have been determined had there been no initial impairment loss. The reversal of the impairment loss is credited to expenditure to the extent of the decrease previously charged there and thereafter to the revaluation reserve Leases Leases are classified as finance leases when substantially all the risks and rewards of ownership are transferred to the lessee. All other leases are classified as operating leases The Clinical Commissioning Group as Lessee Operating lease payments are recognised as an expense on a straight-line basis over the lease term. Lease incentives are recognised initially as a liability and subsequently as a reduction of rentals on a straight-line basis over the lease term Cash & Cash Equivalents Cash is cash in hand and deposits with any financial institution repayable without penalty on notice of not more than 24 hours. Cash equivalents are investments that mature in 3 months or less from the date of acquisition and that are readily convertible to known amounts of cash with insignificant risk of change in value. In the Statement of Cash Flows, cash and cash equivalents are shown net of bank overdrafts that are repayable on demand and that form an integral part of the clinical commissioning group s cash management Provisions Provisions are recognised when the clinical commissioning group has a present legal or constructive obligation as a result of a past event, it is probable that the clinical commissioning group will be required to settle the obligation, and a reliable estimate can be made of the amount of the obligation. The amount recognised as a provision is the best estimate of the expenditure required to settle the obligation at the end of the reporting period, taking into account the risks and uncertainties. Where a provision is measured using the cash flows estimated to settle the obligation, its carrying amount is the present value of those cash flows using HM Treasury s discount rate as follows: Timing of cash flows (0 to 5 years inclusive): Minus 2.420% (previously: minus 2.70%) Timing of cash flows (6 to 10 years inclusive): Minus 1.85% (previously: minus 1.95%) Timing of cash flows (over 10 years): Minus 1.56% (previously: minus 0.80%) When some or all of the economic benefits required to settle a provision are expected to be recovered from a third party, the receivable is recognised as an asset if it is virtually certain that reimbursements will be received and the amount of the receivable can be measured reliably. A restructuring provision is recognised when the clinical commissioning group has developed a detailed formal plan for the restructuring and has raised a valid expectation in those affected that it will carry out the restructuring by starting to implement the plan or announcing its main features to those affected by it. The measurement of a restructuring provision includes only the direct expenditures arising from the restructuring, which are those amounts that are both necessarily entailed by the restructuring and not associated with on-going activities of the entity Clinical Negligence Costs The NHS Resolution operates a risk pooling scheme under which the clinical commissioning group pays an annual contribution to the NHS Resolution which in return settles all clinical negligence claims. The contribution is charged to expenditure. Although the NHS Resolution is administratively responsible for all clinical negligence cases the legal liability remains with the clinical commissioning group Non-clinical Risk Pooling The clinical commissioning group participates in the Property Expenses Scheme and the Liabilities to Third Parties Scheme. Both are risk pooling schemes under which the clinical commissioning group pays an annual contribution to the NHS Resolution and, in return, receives assistance with the costs of claims arising. The annual membership contributions, and any excesses payable in respect of particular claims are charged to operating expenses as and when they become due Continuing healthcare risk pooling In a risk pool scheme was been introduced by NHS England for continuing healthcare claims, for claim periods prior to 31 March Under the scheme clinical commissioning group contribute annually to a pooled fund, which is used to settle the claims Contingencies
105 105 NHS Stockport CCG - Annual Accounts Notes to the financial statements A contingent liability is a possible obligation that arises from past events and whose existence will be confirmed only by the occurrence or nonoccurrence of one or more uncertain future events not wholly within the control of the clinical commissioning group, or a present obligation that is not recognised because it is not probable that a payment will be required to settle the obligation or the amount of the obligation cannot be measured sufficiently reliably. A contingent liability is disclosed unless the possibility of a payment is remote. A contingent asset is a possible asset that arises from past events and whose existence will be confirmed by the occurrence or non-occurrence of one or more uncertain future events not wholly within the control of the clinical commissioning group. A contingent asset is disclosed where an inflow of economic benefits is probable. Where the time value of money is material, contingencies are disclosed at their present value Financial Assets Financial assets are recognised when the clinical commissioning group becomes party to the financial instrument contract or, in the case of trade receivables, when the goods or services have been delivered. Financial assets are derecognised when the contractual rights have expired or the asset has been transferred. Financial assets are classified into the following categories: Financial assets at fair value through profit and loss; Held to maturity investments; Available for sale financial assets; and, Loans and receivables. The classification depends on the nature and purpose of the financial assets and is determined at the time of initial recognition Financial Assets at Fair Value Through Profit and Loss Embedded derivatives that have different risks and characteristics to their host contracts, and contracts with embedded derivatives whose separate value cannot be ascertained, are treated as financial assets at fair value through profit and loss. They are held at fair value, with any resultant gain or loss recognised in calculating the clinical commissioning group s surplus or deficit for the year. The net gain or loss incorporates any interest earned on the financial asset Held to Maturity Assets Held to maturity investments are non-derivative financial assets with fixed or determinable payments and fixed maturity, and there is a positive intention and ability to hold to maturity. After initial recognition, they are held at amortised cost using the effective interest method, less any impairment. Interest is recognised using the effective interest method Available For Sale Financial Assets Available for sale financial assets are non-derivative financial assets that are designated as available for sale or that do not fall within any of the other three financial asset classifications. They are measured at fair value with changes in value taken to the revaluation reserve, with the exception of impairment losses. Accumulated gains or losses are recycled to surplus/deficit on de-recognition Loans & Receivables Loans and receivables are non-derivative financial assets with fixed or determinable payments which are not quoted in an active market. After initial recognition, they are measured at amortised cost using the effective interest method, less any impairment. Interest is recognised using the effective interest method. Fair value is determined by reference to quoted market prices where possible, otherwise by valuation techniques. The effective interest rate is the rate that exactly discounts estimated future cash receipts through the expected life of the financial asset, to the initial fair value of the financial asset. At the end of the reporting period, the clinical commissioning group assesses whether any financial assets, other than those held at fair value through profit and loss are impaired. Financial assets are impaired and impairment losses recognised if there is objective evidence of impairment as a result of one or more events which occurred after the initial recognition of the asset and which has an impact on the estimated future cash flows of the asset. For financial assets carried at amortised cost, the amount of the impairment loss is measured as the difference between the asset s carrying amount and the present value of the revised future cash flows discounted at the asset s original effective interest rate. The loss is recognised in expenditure and the carrying amount of the asset is reduced through a provision for impairment of receivables. If, in a subsequent period, the amount of the impairment loss decreases and the decrease can be related objectively to an event occurring after the impairment was recognised, the previously recognised impairment loss is reversed through expenditure to the extent that the carrying amount of the receivable at the date of the impairment is reversed does not exceed what the amortised cost would have been had the impairment not been recognised. 1.2 Financial Liabilities Financial liabilities are recognised on the statement of financial position when the clinical commissioning group becomes party to the contractual provisions of the financial instrument or, in the case of trade payables, when the goods or services have been received. Financial liabilities are de-recognised when the liability has been discharged, that is, the liability has been paid or has expired Financial Guarantee Contract Liabilities Financial guarantee contract liabilities are subsequently measured at the higher of: The premium received (or imputed) for entering into the guarantee less cumulative amortisation; and, The amount of the obligation under the contract, as determined in accordance with IAS 37: Provisions, Contingent Liabilities and Contingent Assets Financial Liabilities at Fair Value Through Profit and Loss Embedded derivatives that have different risks and characteristics to their host contracts, and contracts with embedded derivatives whose separate value cannot be ascertained, are treated as financial liabilities at fair value through profit and loss. They are held at fair value, with any resultant gain or loss recognised in the clinical commissioning group s surplus/deficit. The net gain or loss incorporates any interest payable on the financial liability Other Financial Liabilities
106 106 NHS Stockport CCG - Annual Accounts Notes to the financial statements After initial recognition, all other financial liabilities are measured at amortised cost using the effective interest method, except for loans from Department of Health and Social Care, which are carried at historic cost. The effective interest rate is the rate that exactly discounts estimated future cash payments through the life of the asset, to the net carrying amount of the financial liability. Interest is recognised using the effective interest method Value Added Tax Most of the activities of the clinical commissioning group are outside the scope of VAT and, in general, output tax does not apply and input tax on purchases is not recoverable. Irrecoverable VAT is charged to the relevant expenditure category or included in the capitalised purchase cost of fixed assets. Where output tax is charged or input VAT is recoverable, the amounts are stated net of VAT Third Party Assets Assets belonging to third parties (such as money held on behalf of patients) are not recognised in the accounts since the clinical commissioning group has no beneficial interest in them Losses & Special Payments Losses and special payments are items that Parliament would not have contemplated when it agreed funds for the health service or passed legislation. By their nature they are items that ideally should not arise. They are therefore subject to special control procedures compared with the generality of payments. They are divided into different categories, which govern the way that individual cases are handled. Losses and special payments are charged to the relevant functional headings in expenditure on an accruals basis, including losses which would have been made good through insurance cover had the clinical commissioning group not been bearing its own risks (with insurance premiums then being included as normal revenue expenditure) Accounting Standards That Have Been Issued But Have Not Yet Been Adopted The DHSC Group accounting manual does not require the following Standards and Interpretations to be applied in These standards are still subject to FREM adoption and early adoption is not therefore permitted. IFRS 9: Financial Instruments ( application from 1 January 2018) IFRS 14: Regulatory Deferral Accounts ( not applicable to DH groups bodies) IFRS 15: Revenue for Contract with Customers (application from 1 January 2018) IFRS 16: Leases (application from 1 January 2019) IFRS 17: Insurance Contracts (application from 1 January 2021) IFRIC 22: Foreign Currency Transactions and Advance Consideration (application from 1 January 2018) IFRIC 23: Uncertainty over Income Tax Treatments (application from 1 January 2019) The application of the Standards as revised would not have a material impact on the accounts for , were they applied in that year.
107 107 NHS Stockport CCG - Annual Accounts Other Operating Revenue Total Admin Programme Total '000 '000 '000 '000 Education, training and research Non-patient care services to other bodies 1, ,067 2,270 Other revenue Total other operating revenue 1, ,540 2,656 Revenue in this note does not include cash received from NHS England, which is drawn down directly into the bank account of the CCG and credited to the General Fund. The majority of 'Non-patient care services revenue to other bodies' relates to contributions made by Stockport Metropolitan Borough Council to the Stockport health and social care transformation programme "Stockport Together'. The reduction reflects a change in the flow of funding rather than a reduction in investment in the programme in Revenue Total Admin Programme Total '000 '000 '000 '000 From rendering of services 1, ,539 2,642 From sale of goods Total 1, ,540 2,656
108 108 NHS Stockport CCG - Annual Accounts Employee benefits and staff numbers Employee benefits Total Total Permanent Employees Other '000 '000 '000 Employee Benefits Salaries and wages 5,149 4, Social security costs Employer Contributions to NHS Pension scheme Other pension costs Apprenticeship Levy Termination benefits Gross employee benefits expenditure 6,264 5, Less recoveries in respect of employee benefits (note 4.1.2) Total - Net admin employee benefits including capitalised costs 6,264 5, Less: Employee costs capitalised Net employee benefits excluding capitalised costs 6,264 5, Employee benefits Total Total Permanent Employees Other '000 '000 '000 Employee Benefits Salaries and wages 5,057 4, Social security costs Employer Contributions to NHS Pension scheme Other pension costs Apprenticeship Levy Termination benefits Gross employee benefits expenditure 6,095 5, Less recoveries in respect of employee benefits (note 4.1.2) Total - Net admin employee benefits including capitalised costs 6,095 5, Less: Employee costs capitalised Net employee benefits excluding capitalised costs 6,095 5, The increase in employee benefits is reflective of the NHS pay award and increase in the average number of staff employed as detailed in note 4.2.
109 109 NHS Stockport CCG - Annual Accounts Employee benefits and staff numbers Employee benefits Total Total Permanent Employees Other Total '000 '000 '000 '000 Employee Benefits Salaries and wages 5,149 4, ,950 Social security costs Employer contributions to the NHS Pension Scheme Other pension costs Apprenticeship Levy Other post-employment benefits Other employment benefits Termination benefits Gross employee benefits expenditure 6,264 5, ,673 Less recoveries in respect of employee benefits (note 4.1.2) Total - Net admin employee benefits including capitalised costs 6,264 5, ,673 Less: Employee costs capitalised Net employee benefits excluding capitalised costs 6,264 5, , Employee benefits Total Total Permanent Employees Other Total '000 '000 '000 '000 Employee Benefits Salaries and wages 5,058 4, ,980 Social security costs Employer contributions to the NHS Pension Scheme Other pension costs Apprenticeship Levy Other post-employment benefits Other employment benefits Termination benefits Gross employee benefits expenditure 6,095 5, ,687 Less recoveries in respect of employee benefits (note 4.1.2) Total - Net admin employee benefits including capitalised costs 6,095 5, ,687 Less: Employee costs capitalised Net employee benefits excluding capitalised costs 6,095 5, ,687
110 110 NHS Stockport CCG - Annual Accounts Average number of people employed Total Permanently employed Other Total Number Number Number Number Total Of the above: Number of whole time equivalent people engaged on capital projects The increase in staff numbers reflects an Increase in investment into the Medicines Optimisation Team across a range of disciplines as part of the mobilisation of the Stockport Together programme. 4.3 Staff sickness absence and ill health retirements Number Number Total Days Lost 1,144 1,049 Total Staff Years Average working Days Lost Exit packages agreed in the financial year Compulsory redundancies Other agreed departures Total Number Number Number Less than 10, , ,029 10,001 to 25, , ,369 25,001 to 50, ,001 to 100, ,001 to 150, ,001 to 200, Over 200, Total 3 20, , Compulsory redundancies Other agreed departures Total Number Number Number Less than 10, ,001 to 25, ,001 to 50, ,001 to 100, ,001 to 150, ,001 to 200, Over 200, Total Redundancy and other departure costs have been paid in accordance with the provisions of the [require scheme name]. Exit costs are accounted for in accordance with relevant accounting standards and at the latest in full in the year of departure. Where entities has agreed early retirements, the additional costs are met by NHS Entities and not by the NHS Pension Scheme, and are included in the tables. Ill-health retirement costs are met by the NHS Pension Scheme and are not included in the tables. The individuals to which these payments relate, do not require a disclsoure in the renumeration report.
111 111 NHS Stockport CCG - Annual Accounts Pension costs Past and present employees are covered by the provisions of the two NHS Pension Schemes. Details of the benefits payable and rules of the Schemes can be found on the NHS Pensions website at Both are unfunded defined benefit schemes that cover NHS employers, GP practices and other bodies, allowed under the direction of the Secretary of State in England and Wales. They are not designed to be run in a way that would enable NHS bodies to identify their share of the underlying scheme assets and liabilities. Therefore, each scheme is accounted for as if it were a defined contribution scheme: the cost to the NHS body of participating in each scheme is taken as equal to the contributions payable to that scheme for the accounting period. In order that the defined benefit obligations recognised in the financial statements do not differ materially from those that would be determined at the reporting date by a formal actuarial valuation, the FReM requires that the period between formal valuations shall be four years, with approximate assessments in intervening years. An outline of these follows: Accounting valuation A valuation of scheme liability is carried out annually by the scheme actuary (currently the Government Actuary s Department) as at the end of the reporting period. This utilises an actuarial assessment for the previous accounting period in conjunction with updated membership and financial data for the current reporting period, and is accepted as providing suitably robust figures for financial reporting purposes. The valuation of the scheme liability as at 31 March 2018, is based on valuation data as 31 March 2017, updated to 31 March 2018 with summary global member and accounting data. In undertaking this actuarial assessment, the methodology prescribed in IAS 19, relevant FReM interpretations, and the discount rate prescribed by HM Treasury have also been used. The latest assessment of the liabilities of the scheme is contained in the report of the scheme actuary, which forms part of the annual NHS Pension Scheme Accounts. These accounts can be viewed on the NHS Pensions website and are published annually. Copies can also be obtained from The Stationery Office Full actuarial (funding) valuation The purpose of this valuation is to assess the level of liability in respect of the benefits due under the schemes (taking into account recent demographic experience), and to recommend contribution rates payable by employees and employers. The last published actuarial valuation undertaken for the NHS Pension Scheme was completed for the year ending 31 March The Scheme Regulations allow for the level of contribution rates to be changed by the Secretary of State for Health, with the consent of HM Treasury, and consideration of the advice of the Scheme Actuary and employee and employer representatives as deemed appropriate. The next actuarial valuation is to be carried out as at 31 March 2016 and is currently being prepared. The direction assumptions are published by HM Treasury which are used to complete the valuation calculations, from which the final valuation report can be signed off by the scheme actuary. This will set the employer contribution rate payable from April 2019 and will consider the cost of the Scheme relative to the employer cost cap. There are provisions in the Public Service Pension Act 2013 to adjust member benefits or contribution rates if the cost of the Scheme changes by more than 2% of pay. Subject to this employer cost cap assessment, any required revisions to member benefits or contribution rates will be determined by the Secretary of State for Health after consultation with the relevant stakeholders. For , employers contributions of 601,339 were payable to the NHS Pensions Scheme ( : 579,820) were payable to the NHS Pension Scheme at the rate of 14.3% of pensionable pay. The scheme s actuary reviews employer contributions, usually every four years and now based on HMT Valuation Directions, following a full scheme valuation. The latest review used data from 31 March 2012 and was published on the Government website on 9 June These costs are included in the NHS pension line of note 4.1.
112 112 NHS Stockport CCG - Annual Accounts Operating expenses Total Total '000 '000 Gross employee benefits Employee benefits excluding governing body members 5,604 5,433 Executive governing body members Total gross employee benefits 6,264 6,095 Other costs Services from other CCGs and NHS England 1,413 1,680 Services from foundation trusts 268, ,227 Services from other NHS trusts 14,233 13,850 Sustainability Transformation Fund 0 0 Services from other WGA bodies 0 1 Purchase of healthcare from non-nhs bodies 64,378 61,920 Purchase of social care 1 1 Chair and Non Executive Members Supplies and services clinical 954 1,111 Supplies and services general 7,147 5,869 Consultancy services Establishment Transport Premises 2,446 2,092 Depreciation 5 5 Audit fees Prescribing costs 48,840 48,431 GPMS/APMS and PCTMS 36,534 34,845 Other professional fees excl. audit Legal fees Grants to Other bodies 0 90 Education and training Provisions (174) (63) CHC Risk Pool contributions Non cash apprenticeship training grants 0 0 Total other costs 445, ,728 Total operating expenses 452, ,823 The 4.3m (1.%) increase in expenditure for services from foundation trusts is due to the transfer of 3.5m of specialised commissioning services from NHS England in relaton to Christies NHS Foundation Trust, together with a general increase in the level of activity commissioned by the CCG from Stockport Foundation Trust, Central Manchester Foundation Trust, University Hospital South Manchester Foundation Trust and Salford Royal Foundation Trust.
113 113 NHS Stockport CCG - Annual Accounts Better Payment Practice Code Measure of compliance Number '000 Number '000 Non-NHS Payables Total Non-NHS Trade invoices paid in the Year 13, ,029 12, ,892 Total Non-NHS Trade Invoices paid within target 12, ,043 12, ,584 Percentage of Non-NHS Trade invoices paid within target 96.99% 98.23% 96.90% 98.75% NHS Payables Total NHS Trade Invoices Paid in the Year 3, ,165 3, ,170 Total NHS Trade Invoices Paid within target 2, ,974 3, ,521 Percentage of NHS Trade Invoices paid within target 95.82% 99.58% 96.09% 99.41% The Better Payment Practice Code requires the CCG to pay all valid invoices by the due date or within 30 days of receipt of a valid invoice, whichever is later.
114 114 NHS Stockport CCG - Annual Accounts Operating Leases 7.1 As lessee The CCG occupies property owned and managed by NHS Property Services Limited. There is currently no formal leases in place however the arrangements with NHS Property Services Limited fall within the definition of an IAS 17 operating lease and are therefore reported within this note Payments recognised as an Expense Land Buildings Other Total Land Buildings Other Total '000 '000 '000 '000 '000 '000 '000 '000 Payments recognised as an expense Minimum lease payments 0 2, , , ,078 Contingent rents Sub-lease payments Total 0 2, , , ,078 Whilst our arrangements with Community Health Partnership's Limited and NHS Property Services Limited fall within the definition of operating leases, rental charge for future years has not yet been agreed. Consequently this note does not include future minimum lease payments for the arrangements only Future minimum lease payments Land Buildings Other Total Land Buildings Other Total '000 '000 '000 '000 '000 '000 '000 '000 Payable: No later than one year Between one and five years After five years Total
115 115 NHS Stockport CCG - Annual Accounts Property, plant and equipment Assets under Land Buildings excluding dwellings Dwellings construction and payments on account Plant & machinery Transport equipment Information technology Furniture & fittings Total '000 '000 '000 '000 '000 '000 '000 '000 '000 Cost or valuation at 01 April Cost/Valuation at 31 March Depreciation 01 April Charged during the year Depreciation at 31 March Net Book Value at 31 March (0) (0) Purchased (0) (0) Total at 31 March (0) (0) Asset financing: Owned (0) (0) Total at 31 March (0) (0)
116 116 NHS Stockport CCG - Annual Accounts Trade and other receivables Current Non-current Current Non-current '000 '000 '000 '000 NHS receivables: Revenue NHS receivables: Capital NHS prepayments NHS accrued income Non-NHS and Other WGA receivables: Revenue Non-NHS and Other WGA receivables: Capital Non-NHS and Other WGA prepayments Non-NHS and Other WGA accrued income Provision for the impairment of receivables VAT Total Trade & other receivables 1, ,048 0 Total current and non current 1,203 2,048 Included above: Prepaid pensions contributions 0 0 The majority of the receivables are with other government bodies, therefore the risk of non payment is considered to be remote. 9.1 Receivables past their due date but not impaired '000 '000 '000 DH Group Bodies Group Bodies All receivables prior years By up to three months By three to six months By more than six months Total of the amount above has been recovered post the statement of financial position date.
117 117 NHS Stockport CCG - Annual Accounts Cash and cash equivalents '000 '000 Balance at 01 April Net change in year 202 (18) Balance at 31 March Made up of: Cash with the Government Banking Service Cash with Commercial banks 0 0 Cash in hand 0 0 Current investments 0 0 Cash and cash equivalents as in statement of financial position Bank overdraft: Government Banking Service 0 0 Bank overdraft: Commercial banks 0 0 Total bank overdrafts 0 0 Balance at 31 March
118 118 NHS Stockport CCG - Annual Accounts Trade and other payables Current Non-current Current Non-current '000 '000 '000 '000 NHS payables: revenue 2, ,851 0 NHS accruals 1, ,110 0 NHS deferred income Non-NHS and Other WGA payables: Revenue 1, ,594 0 Non-NHS and Other WGA accruals 17, ,233 0 Non-NHS and Other WGA deferred income Tax Other payables and accruals Total Trade & Other Payables 23, ,831 0 Total current and non-current 23,048 23,831 Other payables include 58k outstanding pension contributions at 31 March 2018
119 119 NHS Stockport CCG - Annual Accounts Provisions Current Non-current Current Non-current '000 '000 '000 '000 Continuing care Other Total Total current and non-current Continuing Care Other Total '000 '000 '000 Balance at 01 April Arising during the year Utilised during the year (9) (18) (27) Reversed unused (142) (32) (174) Balance at 31 March Expected timing of cash flows: Within one year Between one and five years After five years Balance at 31 March Of the provisons of 201k made made in , only 27k was utilised.
120 120 NHS Stockport CCG - Annual Accounts Financial instruments 13.1 Financial risk management Financial reporting standard IFRS 7 requires disclosure of the role that financial instruments have had during the period in creating or changing the risks a body faces in undertaking its activities. Because NHS clinical commissioning group is financed through parliamentary funding, it is not exposed to the degree of financial risk faced by business entities. Also, financial instruments play a much more limited role in creating or changing risk than would be typical of listed companies, to which the financial reporting standards mainly apply. The clinical commissioning group has limited powers to borrow or invest surplus funds and financial assets and liabilities are generated by day-to-day operational activities rather than being held to change the risks facing the clinical commissioning group in undertaking its activities. Treasury management operations are carried out by the finance department, within parameters defined formally within the NHS clinical commissioning group standing financial instructions and policies agreed by the Governing Body. Treasury activity is subject to review by the NHS clinical commissioning group and internal auditors Currency risk The NHS clinical commissioning group is principally a domestic organisation with the great majority of transactions, assets and liabilities being in the UK and sterling based. The NHS clinical commissioning group has no overseas operations. The NHS clinical commissioning group therefore has low exposure to currency rate fluctuations Interest rate risk The CCG does not borrow money and therefore has no exposure to interest rate risk Credit risk Because the majority of the NHS clinical commissioning group and revenue comes parliamentary funding, NHS clinical commissioning group has low exposure to credit risk. The maximum exposures as at the end of the financial year are in receivables from customers, as disclosed in the trade and other receivables note Liquidity risk NHS clinical commissioning group is required to operate within revenue and capital resource limits, which are financed from resources voted annually by Parliament. The NHS clinical commissioning group draws down cash to cover expenditure, as the need arises. The NHS clinical commissioning group is not, therefore, exposed to significant liquidity risks.
121 121 NHS Stockport CCG - Annual Accounts Financial instruments cont'd 13.2 Financial assets At fair value through profit and loss Loans and Receivables Available for Sale Total '000 '000 '000 '000 Receivables: NHS Non-NHS Cash at bank and in hand Total at 31 March , ,246 At fair value through profit and loss Loans and Receivables Available for Sale Total '000 '000 '000 '000 Receivables: NHS Non-NHS Cash at bank and in hand Total at 31 March , , Financial liabilities At fair value through profit and loss Other Total '000 '000 '000 Payables: NHS 0 3,483 3,483 Non-NHS 0 19,444 19,444 Total at 31 March ,927 22,927 At fair value through profit and loss Other Total '000 '000 '000 Payables: NHS 0 2,961 2,961 Non-NHS 0 20,870 20,870 Total at 31 March ,831 23,831
122 122 NHS Stockport CCG - Annual Accounts Operating segments The CCG has one operating segment which is the commmissioning of healthcare services
123 123 NHS Stockport CCG - Annual Accounts Pooled budgets Section 75 of the NHS Act 2006 allows NHS organisations and local authorities to make contributions to a pooled budget. The purpose of a pooled budget is to improve partnership working between organisations and provide integrated and improved services for patients. The CCG has entered into a pooled budget with Stockport Metropolitan Borough Council (SMBC) who host the pooled budget. In resources totalling 203.0m were pooled. Whilst the provisions contained within the section 75 agreement indicate that joint control exists the fund operates through lead commissioner arrangements whereby the nominated lead commissioner enters into legal contract with providers and the non lead commissioner cedes control over the end-contract. Under lead commissioning arrangements an organisation acting as a lead commissioner accounts for its own transactions without recognising its interest in its share of total assets, liabilities, revenue and expenditure that relate to the whole Fund. The total expenditure on pooled budget activities in by the CCG is 117.4m ( m) which is the expenditure on those services commissioned by the CCG in the table, plus 14.3m ( m) contribution to services commissioned by Stockport MBC. The CCG received no income for pooled budget activities. The NHS clinical commissioning group shares of the income and expenditure handled by the pooled budget in the financial year were: '000 '000 Income 0 0 Expenditure (117,402) (114,873) Pooled Budget for statement of accounts 2017/18 Prevention Boroughwide Community / Acute Total Out of Funding provided to the Pooled Budget Stockport Council (21,236) (7,224) (72,199) 0 (100,659) * Stockport CCG (136) (4,586) (27,059) (70,588) (102,369) Total (21,372) (11,810) (99,258) (70,588) (203,028) Expenditure met from the Pooled Budget Stockport Council 21,023 6,996 73, ,153 Stockport CCG 136 4,596 26,906 71, ,055 Total 21,159 11, ,040 71, ,208 Net (surplus) / deficit arising from the pooled budget in year (213) (218) ,180 Net (surplus) / deficit split by each partner: Stockport Council (213) (228) Stockport CCG 0 10 (153) Total (213) (218) ,180 * Includes 14.3m contributed by the CCG to enable SMBC to fulfil its lead commissioner role under the section 75 agreement Pooled Budget for statement of accounts 2016/17 Prevention Boroughwide Community / Out of Acute Total Hospital Funding provided to the Pooled Budget Stockport Council (22,159) (7,277) (69,556) (98,992) ** Stockport CCG (368) (2,884) (29,393) (67,478) (100,123) Total (22,527) (10,161) (98,949) (67,478) (199,115) Expenditure met from the Pooled Budget Stockport Council 21,752 6,579 71,309 99,640 Stockport CCG 368 2,884 27,753 69, ,673 Total 22,120 9,463 99,062 69, ,313 Net (surplus) / deficit arising from the pooled budget in year (407) (698) 113 2,190 1,198 Net (surplus) / deficit split by each partner: Stockport Council (407) (698) 1, Stockport CCG 0 0 (1,640) 2, Total (407) (698) 113 2,190 1,198 ** Includes 14.2m contributed by the CCG to enable SMBC to fulfil its lead commissioner role under the section 75 agreement
124 124 NHS Stockport CCG - Annual Accounts Related party transactions Details of related party transactions with individuals are as follows: The following individuals were members of the CCG's Governing Body during the financial year and the CCG has transacted with other organisations to which the members are connected. Details of these relationships and transactions are set out below: Amounts owed Amounts due Amounts owed Amounts due Payments to Related Party Receipts from Related Party to Related Party from Related Party Payments to Related Party Receipts from Related Party to Related Party from Related Party '000 '000 '000 '000 '000 '000 '000 '000 Dr Ranjit Singh Gill, Chief Clinical Officer Senior Partner at Stockport Medical Group 2, , Member of Viaduct Health via Stockport Medical Group Jane Marie Crombleholme, Chair of the Governing Body Sister in law is a Manager at Stockport NHS Foundation Trust 175, , Brother in law is a Clinician at Pennine Care NHS Foundation Trust 28, , Dr Catherine Helen Briggs, Clinical Director of Quality and Provider Management (Resigned December 2017) GP Partner at Bracondale Medical Centre Husband is a Consultant Anaesthetist at University Hospital of South Manchester NHS Foundation Trust 14, , Merged with Central Manchester UHNHSFT 1/10/2017 to form Manchester Hospitals NHS Foundation Trust 25, Member of Viaduct Health via Bracondale Medical Practice Dr Viren Mehta, Clinical Director for General Practice Development GP Partner at Cheadle Medical Practice 1, , Member of Viaduct Health via Cheadle Medical Practice & also a Director Dr Lydia Hardern, Chair of Stepping Hill Victoria Locality Council Committee GP Partner Adswood Road Surgery Stockport LMC Member Representative Member of Viaduct Health via Adswood Road Surgery Dr Peter Carne, Chair of Cheadle and Bramhall Locality Council Committee (Resigned January 2018) GP at Gatley Medical Centre 1, , Director of ELR Locum Ltd which provides Out of hours GP cover to Mastercall Healthcare 4, , Stockport LMC Officer Member of Viaduct Health via Gatley Medical Centre and Neighbourhood GP Lead for Cheadle Dr James Higgins, Chair of Heatons and Tame Valley Locality Council Committee (Resigned January 2018) GP Principal at Brinnington Health Centre 1, , Out of hours GP with Mastercall Healthcare 4, , Ex-wife is employed by University Hospital of South Manchester NHS Foundation Trust 14, , Merged with Central Manchester UHNHSFT 1/10/2017 to form Manchester Hospitals NHS Foundation Trust 25, Member of Viaduct Health via Brinnington Health Centre. GP representative for Tame Valley on Viaduct Health Leadership Council and subsequently Neighbourhood GP Lead for Tame Valley Member of Viaduct Care Dr Andrew Johnson, Chair of Marple and Werneth Locality Council Committee GP Partner of Marple Cottage Surgery 1, Member of Viaduct Health via Marple Cottage Surgery and Neighbourhood GP Lead for Marple Dr Diane Lesley Jones, Director of Service Reform Brother is HR Director at University Hospitals Birmingham NHS Foundation Trust Dr Deborah Kendall, Secondary Care Consultant Consultant Paediatrician, Lancashire Teaching Hospital NHS Foundation Trust Self emplyoed private medical consultant at Spire Hospital Dr Vicci Owen-Smith, Clinical Director for Public Health Deputy Director of Public Health at Stockport Metropolitan Borough Council 31, , ,855 2,037 2, Trustee of the Together Trust Associate Medical Director (honorary) Stockport NHS Foundation Trust 175, , Anita Rolfe, Executive Nurse Provides coaching services to Executive Nurse at NHS Oldham CCG 2, , Daughter is employedby Stockport NHS Foundation Trust 175, , Sister-in-law is employed by Pennine Care NHS Foundation Trust 28, , Tim Ryley, Director of Strategic Planning and Performance Wife is seconded to Viaduct Health from her role of Head of Primary Care Development at NHS Stockport CCG The Department of Health is regarded as a related party. During the year the CCG has had a significant number of material transactions with entities for which the Department is regarded as the parent Department. Details of these transactions are set out below: Amounts owed to Related Party Amounts due from Related Party Amounts owed to Related Party Amounts due from Related Party Payments to Related Party Receipts from Related Party Payments to Related Party Receipts from Related Party '000 '000 '000 '000 '000 '000 '000 '000 Stockport NHS Foundation Trust 175, , Manchester Hospitals NHS Foundation Trust 25, University Hospital South Manchetser NHS Foundation Trust 14, , Central Manchester University Hospitals NHS Foundation Trust 10, , Pennine Care NHS Foundation Trust 28, , North West Ambulance Services NHS Trsut 10, , Salford Royal NHS Foundation Trust 8, , NHS Oldham CCG 2, , East Cheshire NHS Trust 2, , The Christie NHS Foundation Trust 3, NHS Property Services 2, , Stockport Metropolitan Borough Council 31, , ,855 2,037 2,
125 125 NHS Stockport CCG - Annual Accounts Events after the end of the reporting period There are no post balance sheet events which will have a material effect on the financial statements of the CCG 18 Financial performance targets The CCG has a number of financial duties under the NHS Act 2006 (as amended). The CCG's performance against those duties are as follows: Target Performance Target Performance Expenditure not to exceed income 455, , , ,823 Capital resource use does not exceed the amount specified in Directions Revenue resource use does not exceed the amount specified in Directions 454, , , ,167 Capital resource use on specified matter(s) does not exceed the amount specified in Directions Revenue resource use on specified matter(s) does not exceed the amount specified in Directions Revenue administration resource use does not exceed the amount specified in Directions 6,434 5,160 6,450 5,307 The CCG achieved a surplus of 3.8m for the financial year ended 31 March Of this 1.3m represents the planned surplus of NHS Stockport CCG and 2.5m is nationally mandated changes relating to 0.5% system risk reserve ( 2.0m) and prescribing charges ( 0.5m). As a result of an amended calculation methodology from NHS England, the 2017/18 in year revenue allocation has been calculated on the basis of the total allocation exclusive of any historic financial surpluses carried forward from ( 7m). In 2016/17 the figure was recorded as the total in year allocation. As set out in the 2017/18 NHS Planning Guidance, CCGs were required to hold a 0.5% reserve uncommitted from the start of the year, created by setting aside the monies that CCGs were otherwise required to spend non-recurrently. This was intended to be released for investment in Five Year Forward View transformation priorities to the extent that evidence emerged of risks not arising or being effectively mitigated through other means. In the event, the national position across the provider sector has been such that NHS England has been unable to allow CCGs 0.5% non-recurrent monies to be spent. Therefore, to comply with this requirement, NHS Stockport CCG has released its 0.5% reserve to the bottom line, resulting in an additional surplus for the year of 2.0m. This additional surplus has been offset against other national cost pressures from the current financial year.

126 126 Statement of Involvement Annual Statement April 2017 to March 2018 NHS Stockport Clinical Commissioning Group will allow people to access health services that empower them to live healthier, longer and more independent lives. NHS Stockport Clinical Commissioning Group 7th Floor Regent House Heaton Lane Stockport SK4 1BS Tel: Fax: Text Relay: Website:
127 127 What decisions do you require of the Governing Body? To note and review the activity and methods used for public engagement during Please detail the key points of this report The CCG has a duty to involve and consult patients, local communities and stakeholders in the planning and development of services. The leadership of the CCG is committed to ensuring that patient views are at the heart of everything the organisation does. Between 1 April 2017 to the 31 March 2018 NHS Stockport Clinical Commissioning Group delivered 54 engagement events and through the formal Stockport Together Consultation reached over 30,000 people about a range of topics, including: Changing the way we plan and organise services; Organise health, social care, and mental health services in teams that work in eight neighbourhoods; and Ensure hospital services are in place for those that need them while reducing pressure on those services. A wide variety of communication methods were used to reach people and different groups within local communities and give the CCG a better understanding of local views on the health service and priorities for change. What are the likely impacts and/or implications? Local people influencing strategic priorities and being involved in decisions that affect their health and social care. People more empowered to take control of their own health. How does this link to the Annual Business Plan? The statement of involvement is a statutory duty. What are the potential conflicts of interest? None Where has this report been previously discussed? N/A Clinical Executive Sponsor: R Gill Presented by: Tim Ryley Meeting Date: 23 May 2018 Agenda item: 8 Reason for being in Part 2 (if applicable) N/A
128 128 Statement of Patient & Public Involvement 1 P age

129 Foreword There is no doubt that there are major challenges facing health and care not only here in Stockport and Greater Manchester but which are seen nationally and globally too. It is acknowledged that new and different ways of thinking and working are needed to create some new solutions and improve quality of health and care. As well as professionals, patients, carers and the public can, and do, provide critical insight, experience and expertise into this work and the NHS Constitution states that : The patient will be at the heart of everything the NHS does. 1 NHS Stockport Clinical Commissioning Group, and partner organisations 2 is committed to working more closely with the people it serves in order to make improvements to health and care and the quality of people s lives. How it is currently doing this is described in this report. Working directly with patients, carers and the public is increasingly being seen and understood as critical to effective working across health and care and to sustainable solutions. What matters to people must be valued and used as an underpinning principle of any health and care commissioning or provider organisation s way of working. The challenge is to build this way of working into processes and systems so that it becomes essential to design, delivery and assessment of care. NHS Stockport Clinical Commissioning Group intends to build on achievements to date and has ambition and plans to increase and renew the involvement of patients, carers and the public, working alongside its partners, so that it is systematic and consistent in its approach. We hope to hear from you so we will know What Matters to You. 3 Christine Morgan John Houghton James Brown Chair Deputy Chair Head of Communications Citizen Representation Panel Citizen Representation Panel NHS Stockport CCG References: 1. The NHS Constitution for England 2. Stockport Together 3. What Matters To You Scotland. 2 P age
130 Introduction The purpose of this report is to outline the work NHS Stockport Clinical Commissioning Group (CCG) has undertaken during the financial year from 1 April 2017 up to 31 March 2018 to engage and involve local people and communities. Stockport CCG is responsible for making sure that the 300,000 people living in the borough have access to the healthcare services they need. We recognise that our decisions, policies, and services have a major impact on the lives and wellbeing of the local people, so we actively seek to engage with all sectors of the community to ensure that everyone has an equal chance to have their say before we make major decisions. Stockport continues to be one of the healthiest places to live in the North West, but we know that this is not the experience of all of our residents. Local communities experience varying levels of affluence and have significantly different health needs. Similar to other local areas across the country Stockport faces a number of challenges in the delivery of existing health and social care services. These issues include: An ageing population with increasingly complex care needs and at higher risk of isolation and loneliness. This is because more people live on their own without direct family support; A population where birth rates have risen, especially in areas of deprivation. This has led to more children and young people living in low income households where health outcomes are poorer; Changes in the most common health issues experienced by the population, to those which are linked to lifestyles or are otherwise preventable; A period of economic challenge that affects the incomes and opportunities of the most vulnerable people in Stockport; Fragmented services which are complicated to access, have duplications and are not as focussed on the individual s needs as could be; A system where too many people are admitted to hospital. This is when they would be better and more appropriately cared for at home; Increasing financial pressures with deficits forecasts for Stockport as demand growth continues if service delivery is not improved. Stockport s population has a wide range of health needs, and has the oldest age profile in Greater Manchester. Currently 19.4% people are aged 65+, likely to rise to 21.8% by 2024, an additional 9,681 people. There are significant health inequalities in Stockport, with life expectancy varying by 10 years between the most and least deprived areas. Smoking cessation rates are improving, but smoking rates are more than twice as high as average in areas of deprivation. Children and Young People Almost 1 in 4 children in Stockport are overweight or obese by the age of 4 rising to almost 1 in 3 by the age of 10. Almost 1 in 4 of 5 year olds have suffered tooth decay 8,500 children and young people are estimated to live in poverty. Over 70% of young adults are not active enough Anxiety is the major long term condition affecting young people in Stockport with more than 2,700 cases reported. Self-harm hospital admissions in those aged are higher than the national average Adults and Older People 3 P age
131 131 1 in 4 adults are overweight or obese putting them at greater risk of liver disease, heart disease and diabetes. Cancer is now the major cause of premature death with 45% of deaths under 75 years. Stockport s population is older than the England average, with around 55,600 residents aged 65 and over. Of these, 7,400 are aged 85 or over. By 2025 these age groups are projected to grow to 66,500 and 11,000 respectively. Half the older population of Stockport has a long term health problem or disability and 1 in 5 has 2 or more long term conditions 1 in 3 older people live alone 2,700 older residents suffer with Dementia 3. Who we are and what we do NHS Stockport Clinical Commissioning Group (CCG) is a group of GPs from every practice in Stockport with responsibility for planning, designing, buying and monitoring the health services for the local population. These services include: Planned hospital care; Rehabilitation care; Urgent and emergency care; Most community health services; Mental health and learning disability services. 3.1 Our vision The CCG s vision is We exist so that Stockport people will access high quality health services that empower them to live healthier, longer and more independent lives and underpins the organisations approach to everything it does to help improve the health and services across the borough.. 4. Placing patients and communities at the heart of what we do The CCG aims to work with local partners to improve health and secure high quality healthcare for the people of Stockport, now and for future generations. We want everyone to have greater control of their health and their wellbeing, and to be supported to live longer, healthier lives with high quality health and care services that are compassionate, inclusive and constantly improving. Our ambition is to place patients, public and our local communities at the heart of everything we do. To achieve this, genuine patient and public participation is essential. The NHS Five Year Forward View (2014) and Next steps on the NHS Five year Forward View (2017) describes a new relationship between the NHS, patients and the public, including a commitment to engage communities and citizens in decisions about the future of health. Public involvement helps us to understand people s needs, and to prioritise those people who experience the poorest health outcomes enabling us to improve access and reduce health inequalities. It provides opportunities to see things differently and to be innovative, leading to a better use of our limited resources. In addition the CCG has a legal duty under Section 14Z2 of the National Health Service Act 2006 (as amended) to make arrangements to involve the public in the commissioning of services for NHS patients. 4 P age
132 132 Within the CCG s constitution we have made the commitment to ensure that there is meaningful public involvement in the planning, development and shaping of local services. These are governed by the following principles: Working in partnership with patients and the local community to secure the best care for them; Adapting engagement activities to meet the specific needs of the different patient groups and communities; Publishing information about health services on the CCG website and through other media; Encouraging and acting on feedback; Identifying how the group will monitor and report its compliance against this statement of principles. The CCG works with a range of partners across the voluntary and third sector and have always worked closely with patient groups, including Healthwatch, in order to engage as wide an audience as possible and to involve them in decision making. The CCG s Chief Operating Officer holds regular meetings with the Healthwatch Chair, who also sits as a representative on the Governing Body.. Healthwatch is also represented on the the Citizen s Representation Panel. In addition, where developments are being planned, commissioners attend Healthwatch briefing sessions to ensure local involvement in shaping plans. Members and officers of Healthwatch are also regularly involved in formal CCG committees and workshop Our approach to public involvement is to make sure that we use a wide variety of different mechanisms, methods and approaches to engage with people. The CCG uses a number of methods to involve and engaged with our communities and to listen to their views and needs. Some of these approaches include: Citizens Representation Panel The Citizens Representation Panel has continued to meet during 2017/18 and as plans for the implementation of the Stockport Together Programme matured the frequency of meetings moved to a 6 weekly cycle. Detail of the work the panel was involved in collectively and individually is contained in section 7. Patient Panel In last year s report 2016/17 it had been noted that the Citizen and Patient Panels were overlapping in content and input so it was decided to close the Patient Panel formally in December Members were thanked for their past involvement and invited to consider joining the Citizen Panel in order to ensure that patient and carer voice was strongly represented on the newly refreshed Citizen Panel. Citizen Space Citizen Space have your say is the CCG s online consultation database where members of the public can take part in surveys and keep up to date with the engagement work the CCG is undertaking. This year includes a total of 53 events and surveys. Public meetings Across the year Stockport CCG ran a total of 24 public Listening Events which included organisations such as: Stockport Mind Stroke organisation Carers of Adults with a Learning Disability Bramhall & Shaw Health PPG Bramhall U3A 5 P age
133 133 Cheadle Medical Practice PPG Rescare Heaton Moor Residents Group Stroke Support Group Stockport Homes Stepping Hill staff Stockport Care Homes Forum PIE group Healthwatch Heald Green PG Carers Forum Home Support Providers Forum Carers Voice Forum Signpost Information Day As a result and after taking into account what had been heard at the listening events, 13 pubic consultation events were run as part of the formal Stockport Together Consultation. This included: Marple PPG Cheadle PPG Breathe Easy Group Poets Corner Action Group Walthew House NHS Watch Disability Stockport Mental Health Carers Group Alvanley PPG Bredbury PPG Healthwatch Walthew House (two separate events) Patient story Patient story videos and podcasts are shown at the beginning of each Governing Body meeting. Topics covered this year have included; bowel cancer, a patient who chose to make a number of lifestyle changes which resulted in him no longer needing diabetes medication, a patient who wanted to voice her concerns about the lack of respect she felt she had received from NHS services and an overweight patient who has taken up playing football with other overweight men and is now successfully losing weight Governing Body composition To ensure that patient views are heard at every level of the organisation, the CCG has appointed lay members to sit on our committees and present a patient perspective to discussions and decisions. The CCG has also led the development of Public Voice, a patient and public participation group for the South East Sector of Greater Manchester which focuses on the development of Healthier Together. The group includes lay representation from Stockport, Tameside and Glossop, North Derbyshire and East Cheshire and is led by an appointed Lay Chair, Lesley Surman. Lesley is also a member of the South East Sector Healthier Together Programme Board to ensure lay views are represented. The group have, in the last year: Developed a patient and public led design ethos to ensure that the views of lay people are adopted within service change; Undertaken a review of public transport links across the sector and a set of recommendations regarding public transport to support patient access; Been involved in numerous workshops with clinicians to further develop the plans for Healthier Together; 6 P age
134 134 Observed and provided comments on a mock multi-disciplinary team meeting to support the development the sector Multi-Disciplinary Team. The Governing Body has appointed three independent lay members, who in addition to being full governing body members have additional specialist roles: Jane Crombleholme chairs the CCG Governing Body and from January 2018 chairs the Primary Care Commissioning Committee. John Greenough leads on audit, remuneration and conflict of interest matters. Christine Morgan is the lay member and from late 2017 took the lead for patient and public involvement. The Governing Body has also co-opted a representative of Healthwatch Stockport and the Chair of the Health and Wellbeing Board to attend all meetings and feed in local views. The Finance and Performance Committee includes the Lay Member responsible for audit and finance The Quality Committee includes the Lay Member with a remit for public involvement and a Healthwatch member The Audit Committee is chaired by the lay member responsible for audit and finance The Remuneration committee is chaired by the lay member responsible for audit and finance The Primary care commissioning committee is chaired by the lay member for primary care 5. Promoting Equality and Reducing Health Inequality NHS Stockport values diversity and is committed to reducing inequalities in the workplace, in health outcomes, in access to and experience of local services. Challenging discrimination and addressing inequalities are key to achieving our vision of high quality healthcare for Stockport. Each year the CCG publishes an annual equality report, setting out information on diversity within our population and our workforce, as well as the work we have undertaken throughout the year to reduce inequalities. Below are some examples of how we have reached out to different groups and diverse communities within the population group covered, so that their voices are heard. There are also examples of where we are developing staff to support people from diverse communities: The full range of reports can be found on the CCG s website at: As a public sector organisation, we have a legal duty under the Equality Act (2010) to ensure equal access to our services for all our diverse communities. This includes making adjustments so that for those whose first or preferred language is not English or who use sign language as their main means of communication can receive the same level of service as other patients. The CCG continues to run the interpretation budget for local Primary Care services on behalf of NHS England, who now commission these services. The service provides interpretation at medical appointments in General Practice; NHS dentistry; NHS pharmacy and NHS optometry. NHS Stockport CCG holds interpreting contracts with: Stockport Interpreting Unit, for the provision of face-to-face for foreign language interpreters in over 30 languages. 7 P age
135 135 The Big Word, for the provision of 24/7 phone interpretation services in over 200 languages. Language Empire for the provision of face-to-face British Sign Language interpreters. Sign Video for the provision of Skype based British Sign Language interpreters. Over the financial year interpretation was used for 2,882 healthcare appointments (an increase of 477 compared to ). A total of 65 languages were used, in addition to sign language, Farsi was the most commonly used language, followed by Polish, Arabic, Urdu, Kurdish, and British Sign Language. 6. What our patients and communities tell us about local services The Friends and Family Test (FFT) is a single question survey which asks patients whether they would recommend the NHS service they have received to friends and family who need similar treatment or care. Since it was initially launched in April 2013, the FFT has been rolled out in phases to most NHS funded services in England, giving patients the opportunity to leave feedback on their care and treatment. Friends and Family Test results for 2016/17 across the borough are summarised below and the data relates to the most recent national publication in January 2018: GP Services: Overall satisfaction with GPs services across Stockport remains high with over 90% of patients who would recommend them, although this is slightly lower than the 92% in This is just above the England average rate of 89%. The percentage of respondents who would not recommend GP services across Stockport is also below the England average range at 4% compared with almost 6% nationally. Accident & Emergency: The percentage of patients who would recommend Stockport A&E services as a place to receive care has remained the same compared to 2016/17 (with 87% in Jan 17 and 87% in Jan 18). There has been a slight increase in the percentage of respondents who would not recommend the A&E service from 6% in January 2017 to 7% to January It is likely that this change is reflective of the challenging performance seen in A&E departments. The percentage of patients who would recommend A&E services in Stockport is also just above the England average of 86% in January Inpatients: On average 94% of respondents would recommend Stockport as a place to receive inpatient care, which is slightly lower than the rate of 95% reported in January This is just below the England average rate of 95%. The percentage of respondents who would not recommend inpatient services across Stockport is also within the England average range of 2%. Outpatients: On average in January % of respondents would recommend outpatient services, which is the same as the previous year and slightly below the England average of 94%. The proportion of respondents stating they would not recommend outpatient services is also within the England average range at 2%. Maternity: The percentage of patients who would recommend Stockport Maternity services as a place to receive care has remained the same when compared to 2016/17 (with 98% in Jan 17 and 98% in Jan 18). This is higher than the national England average of 96%. The 8 P age
136 136 proportion of respondents stating they would not recommend maternity services has also increased slightly from 1% to 2%. This is in line with the England average. In the CCG received a wide range of queries, compliments, comments and complaints from local communities. In addition, the CCG s manage requests for information submitted under the Freedom of information Act. All of these contacts from the public are monitored and analysed so that trends in requests or issues are fed into the Governing Body and the relevant commissioning team to ensure that improvements are made as a result of local contacts. Over , NHS Stockport received: 69 Complaints 134 Compliments and enquiries 23 MP letters 242 Freedom of Information requests 7. Public involvement priorities and impact over the last year Over the last 12 months the CCG has worked with a range of communities and local partners to involve and engage patients and the public. One major element was a large formal consultation on the proposals to transform health and social care services across Stockport in a system wide partnership, which includes Stockport Council, NHS Stockport Foundation Trust, Viaduct Health and NHS Pennine Care Foundation Trust. Citizen Panel Final business plans that have been scrutinised by the panel during 2017/18 included: Ambulatory Care; Intermediate Tier; Neighbourhood model of care, including Healthy Communities; Outpatients. Clinicians and senior staff led the presentation of these plans and key questions and comments by the panel were noted and taken back to programme teams for consideration. In addition the panel was interested in the wider issues that have an impact on people s health and wellbeing and enjoyed a session presented by Tanya King from Stockport Homes and learned about the support for individual tenant s quality of life. The stage of development of the Outcomes framework was discussed with the panel as a group and two members of the panel attend the Expert reference groups working with clinicians, staff and the Voluntary sector to agree objectives and measures for Clinical and Social Outcome Measures and Personal and Social Outcome Measures. The Citizen panel advised, questioned and commented on the process and evaluation of the Listening Events detailed in section 7.1 and the subsequent formal consultation. In December 2017 when the Citizen panel was joined by members of the previous patient panel an interactive, market place style session was held with staff from Viaduct Health, Stepping Hill Hospital Outpatients team, Stockport Council and the Empowering People and Communities stand of the Neighbourhood model of care. The Citizen panel both as a collective group and as individuals are strengthening the ambition of the CCG and its system wide partners to develop working partnerships which lean more towards 9 Page
137 137 co-design and coproduction on the participation ladder. (See Appendix A Participation ladder). In this way members can have a strategic view and also work in coproduction on operational strands such as the Outcomes framework, the Red Bag initiative, the new Falls strategy and Empowering People and Communities. 7.1 Stockport Together Public Involvement When the partners formed Stockport Together, they pledged to provide, A safe, affordable and integrated health and social care system to meet the needs of Stockport. What this means in reality is transforming the way that healthcare is managed and organised in Stockport so the services you rely on are fit for purpose in the 21st century. In setting up Stockport Together, there was the understanding about the rising number of older people in Stockport, and the greater need for health and social care support both in the short and long term. Our assumptions are, if we can improve the health and wellbeing of the older generation, then their quality of life should greatly improve, and the need for in and outpatient care (health services provided in a hospital setting) should be reduced. We know these are big changes and, as a result, we also know that early on, we needed to engage and involve local people to have their say on our proposals for change. During the summer of 2017, we launched a series of listening events with the public and organisations that have an active interest in delivering health and care services in Stockport. Initially one event per neighbourhood was scheduled, with additional events held upon request in additional locations or with specific groups, meaning 13 sessions were held in total with varying attendance levels. 287 people attended the events during the listening phase and there were an additional 195 people spoken to in other forums. The aim of the exercise was to provide the public with the opportunity to receive information take part in discussions and provide feedback on: The case for change (the reasons why the changes need to be made); Some of the changes that have already been made (i.e. transfer to assess service); The plans being developed for the future; What impacts (positive and negative) the public think the changes will have on them, their family and friends. Each meeting was two hours long, and upon arrival all attendees were given an issues document which outlined the above information. The format was to begin with a presentation, then work in groups to discuss a series of scenarios we supplied. Questions were then invited from attendees, which were answered at the time whenever possible. Presenters varied each time but included clinicians, leaders and directors from the partner organisations. Clinicians worked with the engagement officers to develop the scenarios and questions. They were designed to show examples of some of the problems people commonly face in the current system. The topics are shown the below: Repeat prescriptions Recovery after a hospital episode Outpatients Mental health 10 P age
138 138 Falls Alternatives to a GP appointment Pneumonia care The scenario format was used to help focus the mind on a few key areas. Stockport Together covers such a wide remit of services therefore it was not assumed that these would address everything included in the plans, and were intended to provide some context to some of the proposed plans. Write ups from each session formally captured the discussions on the day, along with all of the information provided by members of the public during the scenarios exercise. These were fed into the central Stockport Together team, and the scenario responses were distributed to the relevant programme teams for consideration. Following on from these events, partners in the Stockport Together Programme decided to proceed with further, more detailed consultation. This was designed to further develop our assessment of local needs and strengthen action plans we had created to: Change the way we plan and organise services; Organise health, social care, and mental health services in teams that work in eight neighbourhoods; and Ensure hospital services are in place for those that need them while reducing pressure on those services. The consultation was launched on October 10 th and lasted until November 30 th It consisted of street surveys in neighbourhoods, on-line and postal surveys, discussion groups and public meetings. In addition to the over 500 responses from individuals, organisations representing around 38,000 people also submitted responses. In addition, a wide range of protected groups as defined by the Equalities Act 2010 were contacted and encouraged to feedback. Simultaneously, we presented reports (Equality Impact Assessments) that considered the impact of changes on these groups. Throughout the consultation process, NHS Stockport CCG took advice from the Consultation Institute and, through this organisation, commissioned an independent analysis of the public s feedback to the consultation. The analysis showed that the main thrust of the proposals to create and invest in a more integrated and community based health and social care system delivered in neighbourhoods was strongly supported by the public. However, there were greater concerns and skepticism around one of the ways to fund this investment, (the decommissioning of hospital beds), and the tests to ensure that we had fundamentally altered the need for these beds. The public and key stakeholders also made a number of important comments and suggestions relating to ways that would strengthen implementation of plans. During February 2018, both the CCG Governing Body and Stockport Council Cabinet approved the proposed plans, subject to these recommendations being built-in to their implementation. These recommendations included: More frequent and effective involvement of local people in shaping health and social care services; More collaborative working between patients and clinicians; Checks and balances to ensure equal and fair representation for people who often do not have their voices heard; 11 P age
139 139 Remove complexity when we present financial information; Adopt close-working with Neighbourhoods (GPs) to ensure more effective local engagement; Build on networks established with protected groups to ensure greater involvement; Develop a more formal position for the third sector in our partnership arrangements; Greater integration of mental health services into neighbourhood teams; Greater alignment of housing, leisure and education relating to the wider determinants of health; Create a more robust and comprehensive workforce plan that embraces a system approach to health and social care. Through a variety of approaches, including focus groups, representative groups, street surveys, online surveys and public events, the consultation reaches an estimated 30,000 residents, meaning that over 10% of local residents were able to have their say on how we make decisions for the future. Stockport Together Outcomes Framework - Expert Reference Groups The Stockport Together Outcomes Framework is integral to delivering the benefits of the Stockport Together programme. The outcomes will define what matters most to Stockport population groups (segments) in respect of health and social care. The Outcomes Framework will take the form of a set of measures (clinical, social and patient reported) and will form part of the new MCP contract. A set of outcome measures exists as a long list compiled from the work already undertaken by Stockport Together patient groups, existing outcomes frameworks and national measures e.g. PROMs. The Expert Reference Groups (ERGs) will bring together key stakeholders to review this list. The Groups will validate, prioritise and weight outcome measures for the population segment they represent. There are 4 ERGs comprised of clinicians, providers, commissioners and patient representatives. Each ERG represents a key population groups/segments as shown below: Healthy & Acutely ill but curable Chronic Disease Short Period of decline and dying Older people living with Frailty and or Dementia 100 Day Challenge Nationally an Elective Care Transformation Programme was set up with the aim of using coproduction to develop high impact interventions that would help reduce referrals. Local health and care systems would be able to develop and test interventions aimed at reducing referrals and improving outpatient arrangements in just 100 days. The principles for the 100-day challenge process is to: Work with local health systems and national clinical leaders to identify the challenges related to a particular specialty; Work with clinicians and managers in local systems to agree the interventions to be tested to improve patient care, reduce waiting times and improve efficiency; Share the learning of the 100 day challenge in handbooks. Stockport s rapid testing projects to date have been: Cardio-Respiratory Breathlessness Clinic Orthopaedics OA knee Gastroenterology IBD and fatty liver pathways Diabetes Upskilling primary care and patient education workshops 12 P age
140 140 Dermatology One Stop Clinics, Virtual Transfer of Images (Advice and Guidance), Direct Listing from Dermatology to ENT Ophthalmology -Virtual Glaucoma clinics within primary care optometry practices. Stockport began each project by identifying the problem we wanted to solve. These included: Multiple hospital appointments, long time to definitive diagnosis, duplicated diagnostics for patients with symptom of breathlessness; High percentage of patients referred for hip and knee replacement surgery not fit or not appropriate for surgery; Long wait to diagnosis for patients with new diagnosis of, or flare up of IBD; Increasing numbers of patients with type 2 diabetes being referred in to secondary care system under extreme pressure. Poor uptake of Expert Patient Diabetes structured education. A number of stakeholders from primary care, secondary care, social care, voluntary sector and patients came together to work on the projects. These projects have produced a number of successes to date, these include the Breathlessness Clinic continuing to run twice monthly clinics, these are based on a Leicester model and have been presented at best practice nationally. In Orthopaedics 40% of patients are now being referred more appropriately, patient education workshops are being delivered empowering patients to better manage their symptoms and a patient passport has been developed. Time for diagnosis for new IBD patients has been reduced from 29 weeks to around 9 and a telephone advice clinic is now available for patients. GPs are now able to contact consultants directly for advice for patients presenting in surgery. In Diabetes care consultants now hold virtual clinics with GP practices to discuss case studies and there is now a patient education workshop My Diabetes, My Life. All stakeholders involved in the projects have found benefits in this new way of working as they have been able to build relationships and collaborate with other colleagues and are now working in a more patient-centred approach. Ensuring the groups were fully empowered and involved to try something different has been found to be a liberating experience and has produced quick results. Alvanley GP Practice A special event, run by Greater Manchester Health and Social Care Partnership, was set up to celebrate the vital role practice nurses play in providing patients with the very best care. One focus was on how practice nurses are innovatively using social prescribing to help patients, particularly those who are lonely and feel isolated. Social prescribing is a different way of dealing with health problems and research has shown it massively improves a person s well-being and consequently reduces their need for medication and doctor appointments. It includes setting up things like local walking and singing groups, creating community allotments for local people to look after and use, or running other befriending activities. Alvanley Family Medical Practice, based in Woodley, is spearheading this sort of imaginative work and won the GM Nursing Team of the Year as a result. The practice s head nurse Katherine Parker also picked up the impressive title of Practice Nurse Innovator of the Year for leading the winning team with commitment and enthusiasm. Earlier in the year the Alvanley Practice also won a prestigious apprenticeship award hailing it as the best small business in the region. The National Apprenticeship Service challenged the nation s top apprenticeship employers to show how apprenticeships have made a real difference to them. 13 P age
141 141 In the Small Business of the Year category for Greater Manchester, Cheshire and Staffordshire region, Alvanley Family Practice fought off tough competition to win. The practice succeeded after showing how it is growing its own talent with apprenticeships and how their apprentices are making a significant difference to their workplace. 8. The Impact of involving our communities in decision-making. Feedback from involvement exercises is reported to the CCG s Governing Body. It is used as a key piece of evidence for consideration in decisions and showing how the views of communities are translated into commissioning decisions. One of the key tools for feeding back to local people is the CCG s engagement website: For those without access to the internet, write-ups of events are also sent out to local groups after they have met with the NHS. Sign-up sheets are also taken at all public events so people who wish to receive a write-up of the event can have this sent to them in their preferred format. Articles summarising formal consultations are included in the local Council publication that is delivered to all households in Stockport. In addition, feedback reports are sent to the Healthwatch for inclusion in their regular newsletter and targeted feedback articles are also included in a wide range of local newsletters. A full breakdown of engagement events, surveys and activities can be found in Appendix 1 which outlines: What we did; When; How many local people were consulted; What we did as a result of local feedback; and Where to go to get a full write-up of the consultation and results. 9. Future Plans The recent Stockport Together public consultation has highlighted issues in the way we engage and involve local communities. As a direct result of feedback, the CCG has developed five guiding principles that should be adopted by providers of Health and Social Care Services across Stockport as a partnership. They are: Increase citizens knowledge about the issues we need to address as a Health and Social Care System; Encourage citizens to contribute additional knowledge and use that knowledge to inform how we shape services; Encourage citizens to collaborate in both policy and funding decision making involvement in designing work plans/funding rather than early view of drafted plans; Create opportunities for citizens to engage with each other; Ask people What Matters to You as a person centred approach to care. 9.1 Shaping the way we engage and involve communities. As Stockport adopt a neighbourhood approach to delivering health and social care services, similarly, we need to consider a neighbourhood approach to engagement and involvement. 14 P age
142 142 Through GP practices and our new neighbourhood leads, there is a key role for working with local people and maximizing connections between existing groups and organisations. Moving forward, more detailed planning is required between Commissioners and Providers to determine the appropriate levels of engagement. These considerations will include: The statutory requirement of the Joint Commissioner to engage with local populations to assess the overall health and social care needs of that population; The advantaged position of neighbourhood leads - having frequent contact with local people through GP practice or specialist services; The access to people (including hard to reach and seldom heard groups) that the third sector open up in promoting population health messages and increased levels of engagement and involvement. 9.2 What Matters to You Since the Stockport Together consultation, the CCG has considered an approach to Engagement and Involvement that both responds to feedback from the consultation on the future of Health and Social Care Services in Stockport, as well as take an approach to Engagement and Involvement that takes a more person-centred approach. What matters to you? was developed by NHS Scotland to encourage and support meaningful conversations between people who provide health and social care and the people, families and carers who receive such care. We know from experience and evidence that focusing on what really matters to people can lead to big improvements for people and communities, and the quality and effectiveness of care. We also know that this approach is empowering for the people who provide support and care, enabling them to work to their values and bringing deeper satisfaction to daily work. What matters to you? is a simple question that can deepen the connection between patients and caregivers and is an approach that Commissioners are keen to encourage as we meet the challenges of integrating our services and working closer with patients, their families and the wider local populations. Asking What matters to you? has the potential to enhance the care experience for patients, and contribute to the population health and cost pressure aspects of our future challenges. For example, you may assume a patient wants aggressive treatment, but when you ask them what matters to them, you may find out that their priority is to go home. You discuss the pros and cons and risks of all the options, and it becomes clear that the patient wants to be comfortable at home with their family in the environment they know best. Finding out what matters can also help address how we engage with our staff. Ask staff What matters to you? Take a moment to find out how they re doing and what they re dealing with, as a person this can go a long way to empowering staff for future changes. During a pilot project will be developed to launch What Matters into some of the neighbourhood teams to ensure that patients can influence the direct level of care they receive. 15 P age
143 Conclusion Stockport CCG is tasked with a number of different roles: from directly commissioning and buying services, to ensuring that local health and care plans are designed to meet the need of local communities. We hope that this review has provided a range of examples of how we have worked in partnership with patients and communities in carrying out our responsibilities. We want to work closely with patients, carers and citizens who have experience of using health and care support or services to make improvements in how that care is planned, organised and delivered. We know that people share our ambition to continually improve services into the future. Although we have seen significant changes in the NHS this review demonstrates our continued commitment to improve the way we involve people to shape better health and care services. However, our intention is to strengthen this work and to get better at demonstrating the difference we can really make, by increasing how communities can be involved in shaping services and decision-making. As the needs of our local communities and population change, we will continue to work with them together to establish how best to meet new challenges. Over the next year we will focus on further improvements in how we engage and act on what patients and the public are telling us. Finally we would like to thank all of our patients, staff and community partners who have worked with us in to help achieve our goals. 16 P age
 17 P")
144 144 Appendix A - Ladder of Participation (Adapted by New Economics Foundation and Think Local Act Personal from Sherry Arnstein s model of participation) 17 P age

145 145 Appendix B - Co-production model NHS England/Coalition for Collaborative Care 18 P age
NHS Stockport Clinical Commissioning Group Governing Body Part 1 A G E N D A
 Chair: Enquiries to: Ms J Crombleholme Laura Latham 07827 239332 Laura.latham1@nhs.net NHS Stockport Clinical Commissioning Group Governing Body Part 1 A G E N D A The next meeting of the NHS Stockport
Chair: Enquiries to: Ms J Crombleholme Laura Latham 07827 239332 Laura.latham1@nhs.net NHS Stockport Clinical Commissioning Group Governing Body Part 1 A G E N D A The next meeting of the NHS Stockport
NHS Stockport Clinical Commissioning Group Governing Body Part 1 A G E N D A
 Chair: Enquiries to: Ms J Crombleholme Laura Latham 07827 239332 Laura.latham1@nhs.net NHS Stockport Clinical Commissioning Group Governing Body Part 1 A G E N D A The next meeting of the NHS Stockport
Chair: Enquiries to: Ms J Crombleholme Laura Latham 07827 239332 Laura.latham1@nhs.net NHS Stockport Clinical Commissioning Group Governing Body Part 1 A G E N D A The next meeting of the NHS Stockport
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Health and Care Integrated Commissioning Board AGENDA. Tuesday 27 February pm. To be held in Town Hall, Edward Street, Stockport
 Health and Care Integrated Commissioning Board AGENDA Tuesday 27 February 2018 2pm To be held in Town Hall, Edward Street, Stockport Joint Commissioning Board Stockport Council and NHS Stockport CCG 1.
Health and Care Integrated Commissioning Board AGENDA Tuesday 27 February 2018 2pm To be held in Town Hall, Edward Street, Stockport Joint Commissioning Board Stockport Council and NHS Stockport CCG 1.
NHS Stockport Clinical Commissioning Group Governing Body Part 1 A G E N D A
 Chair: Enquiries to: Ms J Crombleholme Laura Latham 07827 239332 Laura.latham1@nhs.net NHS Stockport Clinical Commissioning Group Governing Body Part 1 A G E N D A The next meeting of the NHS Stockport
Chair: Enquiries to: Ms J Crombleholme Laura Latham 07827 239332 Laura.latham1@nhs.net NHS Stockport Clinical Commissioning Group Governing Body Part 1 A G E N D A The next meeting of the NHS Stockport
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Sussex and East Surrey STP narrative
 Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Sussex and East Surrey STP narrative What is the STP? The Sussex and East Surrey Sustainability and Transformation Partnership (STP) outlines how the NHS and social care will work together to improve and
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan. October 2016 submission to NHS England Public summary
 Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
Bedfordshire, Luton and Milton Keynes Sustainability and Transformation Plan October 2016 submission to NHS England Public summary 15 November 2016 Contents 1 Introduction what is the STP all about?...
MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE. Purpose of Report: For Note
 Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
Meeting in Common of the Boards of NHS England and NHS Improvement. 1. This paper updates the NHS England and NHS Improvement Boards on:
 NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
NHS Improvement and NHS England Meeting in Common of the Boards of NHS England and NHS Improvement Meeting Date: Thursday 24 May 2018 Agenda item: 03 Report by: Matthew Swindells, National Director: Operations
Health and Care Integrated Commissioning Board AGENDA. Tuesday 28 November pm start. To be held in Boardroom, Regent House, Stockport
 Health and Care Integrated Commissioning Board AGENDA Tuesday 28 November 2017 1.30pm start To be held in Boardroom, Regent House, Stockport Joint Commissioning Board Stockport Council and NHS Stockport
Health and Care Integrated Commissioning Board AGENDA Tuesday 28 November 2017 1.30pm start To be held in Boardroom, Regent House, Stockport Joint Commissioning Board Stockport Council and NHS Stockport
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8
 DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
DRAFT BUSINESS PLAN AND CORPORATE OBJECTIVES 2017/8 West London Clinical Commissioning Group This document sets out a clear set of plans and priorities for 2017/18 reflecting West London CCGs ambition
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS...
 CONTENTS EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS... 6 WHAT WE WILL CONTINUE TO ACHIEVE THROUGH THE HEALTH
CONTENTS EXECUTIVE SUMMARY... 1 HEALTH AND WELLBEING STRATEGY VISION... 2 ULTIMATE AIM... 3 DELIVERING THE VISION AND THE PRIORITIES... 4 FOCUS... 6 WHAT WE WILL CONTINUE TO ACHIEVE THROUGH THE HEALTH
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary
 Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
Northumberland, Tyne and Wear, and North Durham Draft Sustainability and Transformation Plan A summary This summary has been prepared to aid understanding of the draft STP technical submission. Copies
SWLCC Update. Update December 2015
 SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
SWLCC Update Update December 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England Working together to improve the quality of care in South West
Our vision. Ambition for Health Transforming health and social care services in Scarborough, Ryedale, Bridlington and Filey
 Ambition for Health Transforming health and social care services in Scarborough, Ryedale, Bridlington and Filey Our vision www.ambitionforhealth.co.uk Contents 1.0 Introduction: A shared ambition for health
Ambition for Health Transforming health and social care services in Scarborough, Ryedale, Bridlington and Filey Our vision www.ambitionforhealth.co.uk Contents 1.0 Introduction: A shared ambition for health
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Health and care in South Yorkshire and Bassetlaw. Sustainability and Transformation Plan a summary
 Health and care in South Yorkshire and Bassetlaw Sustainability and Transformation Plan a summary Introduction This is the summary version of the South Yorkshire and Bassetlaw Sustainability and Transformation
Health and care in South Yorkshire and Bassetlaw Sustainability and Transformation Plan a summary Introduction This is the summary version of the South Yorkshire and Bassetlaw Sustainability and Transformation
Cranbrook a healthy new town: health and wellbeing strategy
 Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Cranbrook a healthy new town: health and wellbeing strategy 2016 2028 Executive Summary 1 1. Introduction: why this strategy is needed, its vision and audience Neighbourhoods and communities are the building
Bolton s 5 Year Plan for Reform (Locality Plan)
") Bolton s 5 Year Plan for Reform (Locality Plan) Moving from Planning to Delivery Final Draft Version 1.2 31 st October 2016 Page 1 Contents Section Section Title Page 1.0 Executive Summary 4 2.0 Bolton
Bolton s 5 Year Plan for Reform (Locality Plan) Moving from Planning to Delivery Final Draft Version 1.2 31 st October 2016 Page 1 Contents Section Section Title Page 1.0 Executive Summary 4 2.0 Bolton
Melanie Craig NHS Great Yarmouth and Waveney CCG Chief Officer. Rebecca Driver, STP Communications and Jane Harper-Smith, STP Programme Director
 Agenda Item: 9 Governing Body Thursday 25 January 2018 Subject: Presented By: Prepared By: Submitted To: Purpose of Paper: Norfolk and Waveney Sustainability and Transformation Partnership Update Melanie
Agenda Item: 9 Governing Body Thursday 25 January 2018 Subject: Presented By: Prepared By: Submitted To: Purpose of Paper: Norfolk and Waveney Sustainability and Transformation Partnership Update Melanie
Improving General Practice for the People of West Cheshire
 Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Improving General Practice for the People of West Cheshire Huw Charles-Jones (GP Chair, West Cheshire Clinical Commissioning Group) INTRODUCTION There is a growing consensus that the current model of general
Westminster Partnership Board for Health and Care. 21 February pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 21 February 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Council of Members. 20 January 2016
 Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
Council of Members 20 January 2016 Feedback on election process: Council of Members Chair and Deputy Chair Malcolm Hines, Chief Financial Officer Minutes of last meeting: 14 October 2015 Dr. Richard Proctor,
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Oxfordshire Clinical Commissioning Group: Annual Public meeting
 Oxfordshire Oxfordshire Clinical Commissioning Group: Annual Public meeting Dr Joe McManners Clinical Chair 28 September 2017 Agenda Oxfordshire Review of the year: 2016 / 2017 Financial Accounts Bicester
Oxfordshire Oxfordshire Clinical Commissioning Group: Annual Public meeting Dr Joe McManners Clinical Chair 28 September 2017 Agenda Oxfordshire Review of the year: 2016 / 2017 Financial Accounts Bicester
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT
 NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Welcome. PPG Conference North and South Norfolk CCGs June 14 th 2018
 Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
Welcome PPG Conference North and South Norfolk CCGs June 14 th 2018 Housekeeping Packed Agenda! Quick feedback on the national patient participation conference Primary care general update and importance
High level guidance to support a shared view of quality in general practice
 Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
The Oldham Locality Plan for Health & Social Care Transformation. April 2016-March 2021
 The Oldham Locality Plan for Health & Social Care Transformation April 2016-March 2021 1 Contents Foreword... 3 How the plan works... 6 Section 1: Strategic direction... 9 1.1 Our vision... 9 1.2 The challenges
The Oldham Locality Plan for Health & Social Care Transformation April 2016-March 2021 1 Contents Foreword... 3 How the plan works... 6 Section 1: Strategic direction... 9 1.1 Our vision... 9 1.2 The challenges
Longer, healthier lives for all the people in Croydon
 D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
D R A F T Croydon Clinical Commissioning Group Prospectus 2013/14 Longer, healthier lives for all the people in Croydon (Version TL) 1 Contents Foreword from the chair 3 Introduction 4 Who we are our Governing
Trafford. Local system review report. Background and scope of the local system review. The review team. Health and wellbeing board
 Trafford Local system review report Health and wellbeing board Date of review: 16-20 October 2017 Background and scope of the local system review This review has been carried out following a request from
Trafford Local system review report Health and wellbeing board Date of review: 16-20 October 2017 Background and scope of the local system review This review has been carried out following a request from
SUMMARY. Our progress in 2013/14. Eastbourne, Hailsham and Seaford Clinical Commissioning Group.
 Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Eastbourne, Hailsham and Seaford Clinical Commissioning Group SUMMARY Our progress in 2013/14 www.eastbournehailshamandseafordccg.nhs.uk 1 Welcome NHS is a membership organisation made up of the 21 GP
Manchester. Local system review report. Background and scope of the local system review. The review team. Health and Wellbeing Board
 Manchester Local system review report Health and Wellbeing Board Date of review: 16 20 October 2017 Background and scope of the local system review This review has been carried out following a request
Manchester Local system review report Health and Wellbeing Board Date of review: 16 20 October 2017 Background and scope of the local system review This review has been carried out following a request
NICE guideline Published: 22 September 2017 nice.org.uk/guidance/ng74
 Intermediate care including reablement NICE guideline Published: 22 September 2017 nice.org.uk/guidance/ng74 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Intermediate care including reablement NICE guideline Published: 22 September 2017 nice.org.uk/guidance/ng74 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
North School of Pharmacy and Medicines Optimisation Strategic Plan
 North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
Shaping Future Care. A sustainability and transformation plan for Devon.
 Shaping Future Care A sustainability and transformation plan for Devon www.devonstp.org.uk October 2014 Who is involved? Foreword: what is the STP? Delivering a Sustainability and Transformation Plan (STP)
Shaping Future Care A sustainability and transformation plan for Devon www.devonstp.org.uk October 2014 Who is involved? Foreword: what is the STP? Delivering a Sustainability and Transformation Plan (STP)
Integrating Health & Social Care in Kirklees
 Integrating Health & Social Care in Kirklees The case for change DRAFT v3.1 June 2017 Integrated Commissioning - Building on Existing Approaches Some example Children s services Mental health Hospital
Integrating Health & Social Care in Kirklees The case for change DRAFT v3.1 June 2017 Integrated Commissioning - Building on Existing Approaches Some example Children s services Mental health Hospital
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Please indicate: For Decision For Information For Discussion X Executive Summary Summary
 Governing Body 22 March 2017 Details Part 1 X Part 2 Agenda Item No. 10 Title of Paper: Board Member: Author: Presenter: PAHT Quality Improvement Plan Catherine Jackson, Executive Nurse Catherine Jackson,
Governing Body 22 March 2017 Details Part 1 X Part 2 Agenda Item No. 10 Title of Paper: Board Member: Author: Presenter: PAHT Quality Improvement Plan Catherine Jackson, Executive Nurse Catherine Jackson,
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme. Frequently Asked Questions Second Edition
 Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Cambridgeshire and Peterborough Sustainability and Transformation Plan / Fit for the Future Programme Frequently Asked Questions Second Edition Contents Introduction to the Sustainability and Transformation
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION THE BUDGET NUMBERS
 BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
BIRMINGHAM CITY COUNCIL SERVICE REVIEWS GREEN PAPER UPDATE: ADULTS SOCIAL CARE INTRODUCTION Birmingham City Council is facing a big challenge, having to cut the budget we can control by half over seven
Health and care services in Herefordshire & Worcestershire are changing
 Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
Health and care services in Herefordshire & Worcestershire are changing An update on a five year plan to provide safe, effective and sustainable care in our area www.yourconversationhw.nhs.uk Your Health
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
Suffolk & North East Essex STP Implementation Plan. 20 th October Draft
 Suffolk & North East Essex STP Implementation Plan 20 th October 2016 Draft 1 Executive Summary In Suffolk and North East Essex, the NHS, general practice and local government have come together to develop
Suffolk & North East Essex STP Implementation Plan 20 th October 2016 Draft 1 Executive Summary In Suffolk and North East Essex, the NHS, general practice and local government have come together to develop
Improving Healthcare Together : NHS Surrey Downs, Sutton and Merton clinical commissioning groups Issues Paper
 Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Improving Healthcare Together 2020-2030 NHS Surrey Downs, Sutton and Merton CCGs Improving Healthcare Together 2020-2030: NHS Surrey Downs, Sutton and Merton clinical commissioning groups Surrey Downs
Strategic Plan for Fife ( )
") www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
Richmond Clinical Commissioning Group
 Richmond Clinical Commissioning Group South west London five year forward plan Kathryn Magson, Chief Officer, Richmond CCG 7 December 2016 South West London Five Year Forward Plan Start well, live well,
Richmond Clinical Commissioning Group South west London five year forward plan Kathryn Magson, Chief Officer, Richmond CCG 7 December 2016 South West London Five Year Forward Plan Start well, live well,
A guide to NHS Bexley Clinical Commissioning Group
 A guide to NHS Bexley Clinical Commissioning Group Everything you need to know about how local healthcare in Bexley is planned, bought and monitored. 1 Welcome to NHS Bexley Clinical Commissioning Group
A guide to NHS Bexley Clinical Commissioning Group Everything you need to know about how local healthcare in Bexley is planned, bought and monitored. 1 Welcome to NHS Bexley Clinical Commissioning Group
Review of Local Enhanced Services
 Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
Review of Local Enhanced Services 1. Background and context 1.1 CCGs are required to prepare for the phasing out of LESs by April 2014 by reviewing the existing LES portfolio and developing commissioning
grampian clinical strategy
 healthfit caring listening improving consultation grampian clinical strategy 2016 to 2021 1 summary version NHS Grampian Clinical Strategy 2016 to 2021 Purpose and aims 5 Partnership working and the changing
healthfit caring listening improving consultation grampian clinical strategy 2016 to 2021 1 summary version NHS Grampian Clinical Strategy 2016 to 2021 Purpose and aims 5 Partnership working and the changing
Norfolk and Waveney STP - summary of key elements
 Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Our Vision Norfolk and Waveney STP - summary of key elements 1. We have agreed our vision: To support more people to live independently at home, especially the frail elderly and those with long term conditions.
Primary Care Strategy. Draft for Consultation November 2016
 Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
Primary Care Strategy Draft for Consultation November 2016 1 Introduction Welcome to the Isle of Wight CCG s draft Primary Care Strategy. The CCG is required to develop and publish a strategy that sets
WELCOME. To our first Annual General Meeting (AGM) Local clinicians working with local people for a healthier future
 Local clinicians working with local people for a healthier future") WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
WELCOME To our first Annual General Meeting (AGM) AGM agenda 1:00pm TIME ITEM LEAD Welcome and Governing Body introductions Liz Wise, Chief Officer 1:05pm 1:25pm 1:35pm 1:50pm Presentation of the Annual
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
This will activate and empower people to become more confident to manage their own health.
 Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
Mid Nottinghamshire Self Care Strategy 2014-2019 Forward The Mid Nottinghamshire Self Care Strategy will be the vehicle which underpins our vision to deliver an increased understanding of and knowledge
INTEGRATION TRANSFORMATION FUND
 MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
MEETING DATE: 12 December 2013 AGENDA ITEM NUMBER: Item 6.6 AUTHOR: JOB TITLE: DEPARTMENT: Caroline Briggs Director of Commissioning NHS North Lincolnshire Clinical Commissioning Group REPORT TO THE CLINICAL
A consultation on the Government's mandate to NHS England to 2020
 A consultation on the Government's mandate to NHS England to 2020 October 2015 You may re-use the text of this document (not including logos) free of charge in any format or medium, under the terms of
A consultation on the Government's mandate to NHS England to 2020 October 2015 You may re-use the text of this document (not including logos) free of charge in any format or medium, under the terms of
Item No. 9. Meeting Date Wednesday 6 th December Glasgow City Integration Joint Board Finance and Audit Committee
 Item No. 9 Meeting Date Wednesday 6 th December 2017 Glasgow City Integration Joint Board Finance and Audit Committee Report By: Contact: Sharon Wearing, Chief Officer, Finance and Resources Allison Eccles,
Item No. 9 Meeting Date Wednesday 6 th December 2017 Glasgow City Integration Joint Board Finance and Audit Committee Report By: Contact: Sharon Wearing, Chief Officer, Finance and Resources Allison Eccles,
NHS Norwich CCG Operational Plan and
 NHS Norwich CCG Operational Plan 2017-18 and 2018-19 Commissioning NHS care for the people of Norwich 1 Release: V17 Final Date: 2016.01.11 Table of Contents Page 1 Introduction 4 2 National Background
NHS Norwich CCG Operational Plan 2017-18 and 2018-19 Commissioning NHS care for the people of Norwich 1 Release: V17 Final Date: 2016.01.11 Table of Contents Page 1 Introduction 4 2 National Background
GM Devolution. Darren Banks Executive Director of Strategy
 GM Devolution Darren Banks Executive Director of Strategy Ground to be covered Greater Manchester The Devolution Journey What we are doing and the governance Manchester s Locality Plan 2 Greater Manchester:
GM Devolution Darren Banks Executive Director of Strategy Ground to be covered Greater Manchester The Devolution Journey What we are doing and the governance Manchester s Locality Plan 2 Greater Manchester:
North West London Sustainability and Transformation Plan Summary
 North West London Sustainability and Transformation Plan Summary Being well, living well: a sustainability and transformation plan for North West London November 2016 Have your say We want to hear your
North West London Sustainability and Transformation Plan Summary Being well, living well: a sustainability and transformation plan for North West London November 2016 Have your say We want to hear your
Agenda Item No. 9. Key Information
 Key Information Name of footprint and no: Sussex and East Surrey (33) Region: NHSE South Nominated lead of the footprint including organisation/function: Michael Wilson, Chief Executive, Surrey and Sussex
Key Information Name of footprint and no: Sussex and East Surrey (33) Region: NHSE South Nominated lead of the footprint including organisation/function: Michael Wilson, Chief Executive, Surrey and Sussex
Manchester Health and Care Commissioning Board. A partnership between Manchester. City Council and NHS Manchester Clinical Commissioning Group
 Manchester Health and Care Commissioning Board A partnership between Manchester City Council and NHS Manchester Clinical Commissioning Group Agenda Item: Report Title: Date: Strategic Commissioning Prepared
Manchester Health and Care Commissioning Board A partnership between Manchester City Council and NHS Manchester Clinical Commissioning Group Agenda Item: Report Title: Date: Strategic Commissioning Prepared
Shaping the best mental health care in Manchester
 Clinical Transformation Plans Manchester Shaping the best mental health care in Manchester Meeting the needs of our communities Improving Lives OUR SHARED WAY AHEAD... Clinical Service Transformation in
Clinical Transformation Plans Manchester Shaping the best mental health care in Manchester Meeting the needs of our communities Improving Lives OUR SHARED WAY AHEAD... Clinical Service Transformation in
Annual Report Summary 2016/17
 Annual Report Summary 2016/17 Making sure you get the healthcare you need Annual Report summary 2016/17 Introduction by our Clinical Chair and Chief Executive Officer Dr Chris Ritchieson Clinical Chair
Annual Report Summary 2016/17 Making sure you get the healthcare you need Annual Report summary 2016/17 Introduction by our Clinical Chair and Chief Executive Officer Dr Chris Ritchieson Clinical Chair
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL
 DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
DELIVERING THE LEFT SHIFT IN ACUTE ACTIVITY THE COMMUNITY MODEL 1. Introduction The Strategic Outline Case (SOC) and subsequent developing Outline Business Case (OBC) for the reconfiguration of acute hospital
LEARNING FROM THE VANGUARDS:
 LEARNING FROM THE VANGUARDS: STAFF AT THE HEART OF NEW CARE MODELS This briefing looks at what the vanguards set out to achieve when it comes to involving and engaging staff in the new care models. It
LEARNING FROM THE VANGUARDS: STAFF AT THE HEART OF NEW CARE MODELS This briefing looks at what the vanguards set out to achieve when it comes to involving and engaging staff in the new care models. It
System Leadership. What do System Leaders need to improve flow by 2020? Helen Kilgannon & Cathy Sloan
 System Leadership What do System Leaders need to improve flow by 2020? Helen Kilgannon & Cathy Sloan Outcomes of the session Increased understanding of the principles of system leadership Increased understanding
System Leadership What do System Leaders need to improve flow by 2020? Helen Kilgannon & Cathy Sloan Outcomes of the session Increased understanding of the principles of system leadership Increased understanding
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Looked After Children Annual Report
 Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
The operating framework for. the NHS in England 2009/10. Background
 the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
the voice of NHS leadership briefing DECEMBER 2008 ISSUE 172 The operating framework for the NHS in England 2009/10 Key points No new national targets. National priorities are the same as last year. but
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS
 CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
CLINICAL STRATEGY IMPLEMENTATION - HEALTH IN YOUR HANDS Background People across the UK are living longer and life expectancy in the Borders is the longest in Scotland. The fact of having an increasing
Westminster Partnership Board for Health and Care. 17 January pm pm Room 5.3 at 15 Marylebone Road
 Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Westminster Partnership Board for Health and Care 17 January 2018 4.30pm - 6.00pm Room 5.3 at 15 Marylebone Road Agenda Item # Item and discussion points Lead Papers Timing 1 Preliminary business Welcome
Summary annual report 2014/15
 1 Summary annual report 2014/15 2 Annual Report Summary 2014/15 3 St Thomas Hospital Guy s Hospital CATHEDRAL CHAUCER GRANGE RIVERSIDE ROTHERHITHE SURREY DOCKS Key facts about Southwark GP practices in
1 Summary annual report 2014/15 2 Annual Report Summary 2014/15 3 St Thomas Hospital Guy s Hospital CATHEDRAL CHAUCER GRANGE RIVERSIDE ROTHERHITHE SURREY DOCKS Key facts about Southwark GP practices in
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Agenda for the next Government
 Agenda for the next Government General election 2017 The Richmond Group of Charities We are the Richmond Group of Charities and we help people of all ages who have serious long term physical and mental
Agenda for the next Government General election 2017 The Richmond Group of Charities We are the Richmond Group of Charities and we help people of all ages who have serious long term physical and mental
Sustainability and transformation plan (STP)
") Sustainability and transformation plan (STP) David Bowen-Cassie, Harrow CCG Alex Dewsnap, London Borough of Harrow Sanjay Dighe, Lay Member, Harrow CCG About Harrow A population of more than 239,000 people
Sustainability and transformation plan (STP) David Bowen-Cassie, Harrow CCG Alex Dewsnap, London Borough of Harrow Sanjay Dighe, Lay Member, Harrow CCG About Harrow A population of more than 239,000 people
August Planning for better health and care in North London. A public summary of the NCL STP
 August 2017 Planning for better health and care in North London A public summary of the NCL STP Planning for better health and care in North London North London NHS organisations are working together with
August 2017 Planning for better health and care in North London A public summary of the NCL STP Planning for better health and care in North London North London NHS organisations are working together with
NHS Providers Strategy Directors Network meeting Five Year Forward View and Vanguards - Birmingham Community Healthcare NHS Trust our story
 NHS Providers Strategy Directors Network meeting Five Year Forward View and Vanguards - Birmingham Community Healthcare NHS Trust our story Lorraine Thomas Director of Business and Organisational Development
NHS Providers Strategy Directors Network meeting Five Year Forward View and Vanguards - Birmingham Community Healthcare NHS Trust our story Lorraine Thomas Director of Business and Organisational Development
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
04c. Clinical Standards included in the Strategic Outline Care part 1, published in December 216
 0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published
0c Clinical s included in the Strategic Outline Care part, published in December 6 Clinical standards The following clinical standards were included in the Strategic Outline Case part (SOC), published