NHS NEWARK & SHERWOOD CLINICAL COMMISSIONING GROUP (CCG) CONSTITUTION. Version 22: Approved by NHS England on
|
|
|
- Domenic Brandon Lynch
- 5 years ago
- Views:
Transcription

1 NHS NEWARK & SHERWOOD CLINICAL COMMISSIONING GROUP (CCG) CONSTITUTION Version 22: Approved by NHS England on NHS England Effective Date: 27 January
2 [Page left intentionally blank] 2
3 Contents 1. INTRODUCTION AND COMMENCEMENT 5 2. AREA COVERED MEMBERSHIP MISSION STATEMENT, VISION, VALUES AND AIMS FUNCTIONS AND GENERAL DUTIES DECISION MAKING: THE GOVERNING STRUCTURE ROLES AND RESPONSIBILITIES STANDARDS OF BUSINESS CONDUCT AND MANAGING CONFLICTS OF INTEREST THE GROUP AS EMPLOYER TRANSPARENCY, WAYS OF WORKING AND STANDING ORDERS APPENDIX 1 LIST OF MEMBER PRACTICES APPENDIX 2 - NOLAN PRINCIPLES APPENDIX 3 NHS CONSTITUTION APPENDIX 4 - MEMORANDUM OF UNDERSTANDING IN RELATION TO GOVERNANCE ARRANGEMENTS WITH OTHER CCGs APPENDIX 5 - MEMORANDUM OF UNDERSTANDING IN RELATION TO COLLABORATIVE COMMISSIONING APPENDIX 6 - SCHEME OF DELEGATION APPENDIX 7 DEFINITIONS OF KEY DESCRIPTIONS USED IN THIS CONSTITUTION APPENDIX 8 PRIME FINANCIAL POLICIES APPENDIX 9 CONFLICTS OF INTEREST POLICY... Error! Bookmark not defined. APPENDIX 10 CCG STANDING ORDERS 146 3
4 FOREWORD The NHS Newark and Sherwood Clinical Commissioning Group was formed in April 2011 and we have always had an ambitious vision for healthcare in Newark and Sherwood. Achievement of this vision requires all of our practices to work together for the benefit of our population. We already have a strong track record of working together to improve care. As a Clinical Commissioning Group we have statutory duties to commission the best possible healthcare within our resource envelope to continuously improve quality and to achieve financial balance. Failure to do so has on-going consequences for our population. We therefore have to operate in a transparent and inclusive manner, so that the best possible decisions can be made. This constitution sets out how we govern ourselves and how we discharge our duties and responsibilities. It sets out our key processes for decision-making, including arrangements for transparency in the decision-making of the CCG and its governing body and provision for managing conflicts of interest. It also sets out the CCG s responsibilities in terms of commissioning services, arrangements in place to secure patient and public participation, collaborative working arrangements with local stakeholders and commitment to meeting the requirements set out in the Equality Act All of our member practices contributed to the development of this constitution and have been involved in its review. We commend this document which was updated in May 2016 setting out how we operate to serve our local population in the commissioning of healthcare services. Dr Mark Jefford, Clinical Chair Dr Amanda Sullivan, Chief Officer 1 Equality Act
5 1. INTRODUCTION AND COMMENCEMENT 1.1. Name The name of this clinical commissioning group is NHS Newark & Sherwood Clinical Commissioning Group Statutory Framework Clinical commissioning groups are established under the Health and Social Care Act 2012 ( the 2012 Act ) 2. They are statutory bodies which have the function of commissioning services for the purposes of the health service in England and are treated as NHS bodies for the purposes of the National Health Service Act 2006 ( the 2006 Act ) 3. The duties of clinical commissioning groups to commission certain health services are set out in section 3 of the 2006 Act, as amended by section 13 of the 2012 Act, and the regulations made under that provision NHS England is responsible for determining applications from prospective groups to be established as clinical commissioning groups 5 and undertakes an annual assessment of each established group 6. It has powers to intervene in a clinical commissioning group where it is satisfied that a group is failing or has failed to discharge any of its functions or that there is a significant risk that it will fail to do so Clinical commissioning groups are clinically led membership organisations made up of general practices. The members of the clinical commissioning group are responsible for determining the governing arrangements for their organisations, which they are required to set out in a constitution Status of this Constitution This constitution is made between the members of NHS Newark & Sherwood Clinical Commissioning Group and has effect from 1st day of April 2013, when NHS England established the group The Constitution is published on the group s website at Hardcopies can also be requested by writing to the Head of Corporate Governance at NHS Newark & Sherwood CCG, Balderton Primary Care Centre, Lowfield Lane, Balderton, Nottinghamshire, NG24 3HJ, or by calling See section 1I of the 2006 Act, inserted by section 10 of the 2012 Act 3 See section 275 of the 2006 Act, as amended by paragraph 140(2)(c) of Schedule 4 of the 2012 Act 4 Duties of clinical commissioning groups to commission certain health services are set out in section 3 of the 2006 Act, as amended by section 13 of the 2012 Act 5 See section 14C of the 2006 Act, inserted by section 25 of the 2012 Act 6 See section 14Z16 of the 2006 Act, inserted by section 26 of the 2012 Act 7 See sections 14Z21 and 14Z22 of the 2006 Act, inserted by section 26 of the 2012 Act 8 See in particular sections 14L, 14M, 14N and 14O of the 2006 Act, inserted by section 25 of the 2012 Act and Part 1 of Schedule 1A to the 2006 Act, inserted by Schedule 2 to the 2012 Act and any regulations issued 9 See section 14D of the 2006 Act, inserted by section 25 of the 2012 Act 5
6 1.4 Amendment and Variation of this Constitution This constitution can only be varied in two circumstances 10. a) where the group applies and that application is granted; b) where in the circumstances set out in legislation NHS England varies the group s constitution other than on application by the group. 10 See sections 14E and 14F of the 2006 Act, inserted by section 25 of the 2012 Act and any regulations issued 6

7 AREA COVERED 2.1. The geographical area covered by NHS Newark and Sherwood Clinical Commissioning Group includes the large market town of Newark and more rural small towns and villages, extending to the Sherwood area of Nottinghamshire and the A1 border with Lincolnshire The NHS Newark and Sherwood Clinical Commissioning Group is largely coterminous with the Newark and Sherwood District Council 7
8 3. MEMBERSHIP 3.1. Membership of the Clinical Commissioning Group The following practices comprise the members of NHS Newark & Sherwood Clinical Commissioning Group. Practice Name Address Balderton Primary Care Centre Lowfield Lane, Balderton, Nottinghamshire, NG24 3HG Barnby Gate Surgery 50 Barnby Gate, Newark, Nottinghamshire, NG24 1QD Bilsthorpe Surgery 35 Mickledale Lane, Bilsthorpe, Newark, Nottinghamshire, NG22 8QB Abbey Medical Group 59 Mansfield Road, Blidworth, Nottinghamshire, NG21 0RB Collingham Medical Centre High Street, Collingham, Nottinghamshire, NG23 7LB Fountain Medical Centre Sherwood Avenue, Newark, Nottinghamshire, NG24 1QH Hill View Surgery Kirklington Road, Rainworth, Nottinghamshire, NG21 0JP Hounsfield Surgery The Surgery, Hounsfield Way, Sutton on Trent, Nottinghamshire, NG23 6PX Lombard Medical Centre 2 Portland Street, Newark, Nottinghamshire, NG24 4XG Major Oak Surgery High Street, Edwinstowe, Nottinghamshire, NG21 9QS Middleton Lodge Practice Church Circle, New Ollerton, Nottinghamshire, NG22 9SZ Rainworth Health Centre Warsop Lane, Rainworth, Nottinghamshire, NG21 0AD Sherwood Medical Partnership including the following 2 sites: Crown Medical Centre Farnsfield Surgery Crown Farm Way, Forest Town, Mansfield, Nottinghamshire, NG19 0FW, Clipstone, Nottinghamshire, NG23 7LB and Station Lane, Farnsfield, Nottinghamshire, NG22 8LA, Southwell Medical Centre The Ropewalk, Southwell, Nottinghamshire, NG25 0AL All member practices have been involved in the development of this constitution and have formally agreed to its contents. They have received support and guidance from the Local Medical Committee (LMC) Eligibility Providers of primary medical services to a registered list of patients under a General Medical Services, Personal Medical Services or Alternative provider Medical Services contract, will be eligible to apply for membership of this group See section 14A(4) of the 2006 Act, inserted by section 25 of the Regulations to be made 8
9 4. MISSION STATEMENT, VISION, VALUES AND AIMS 4.1. Mission Statement NHS Newark & Sherwood Clinical Commissioning Group s mission statement is improve wellbeing and the health outcomes of our population Vision NHS Newark and Sherwood Clinical Commissioning Group has an ambitious vision for local health services. We want Newark and Sherwood residents to be proud of their local NHS. We want the local NHS to provide the safest and most effective services possible within available resources. We want patients to be treated with compassion and respect at all times. People will be able to take control and responsibility for their own and their loved ones health and care as far as possible. We want joined up services that are sensitive to the whole person. This includes mental health and social needs as well as physical health. We also want services to be accessible to all, based on individual needs. The group will promote good governance and proper stewardship of public resources in pursuance of its goals and in meeting its statutory duties Values Good corporate governance arrangements are critical to achieving the group s objectives The values that lie at the heart of the group s work are: a) working well together to serve local residents and to achieve the CCG goals b) valuing honesty, integrity, trust and transparency c) demonstrating the following behaviours: Showing respect for each other s views, even when we have very different perspectives Collaborating with others to improve patient care Sharing best practice and lessons to accelerate learning Striving for excellence in everything we do celebrate what works well and continually learn and improve Aims The group s aims are: a) Improving health through best quality within available resources (incorporating safety, effectiveness and patient experience); b) Improving health through system sustainability, service integration and 9
10 community provision; c) Improving health through partnership working to achieve the safest and most effective services within overall resources; d) Improving health through health outcomes. 4.5 Principles of Good Governance In accordance with section 14L(2)(b) of the 2006 Act 12, the group will at all times observe such generally accepted principles of good governance in the way it conducts its business. These include: a) the highest standards of propriety involving impartiality, integrity and objectivity in relation to the stewardship of public funds, the management of the organisation and the conduct of its business; b) The Good Governance Standard for Public Services 13 ; c) the standards of behaviour published by the Committee on Standards in Public Life (1995) known as the Nolan Principles 14 d) the seven key principles of the NHS Constitution 15 ; e) the Equality Act f) the standards for members of NHS Boards and Governing Bodies in England Accountability The group will demonstrate its accountability to its members, local people, stakeholders and NHS England in a number of ways, including by: a) publishing its constitution; b) appointing independent lay members and non GP clinicians to its governing body; c) holding meetings of its governing body and Primary Care Commissioning Committee in public (except where the group considers that it would not be in the public interest in relation to all or part of a meeting); d) publishing annually a commissioning plan; e) complying with local authority health overview and scrutiny requirements; f) meeting annually in public to publish and present its annual report (which must be published); g) producing annual accounts in respect of each financial year which must be externally audited; h) having a published and clear complaints process; i) complying with the Freedom of Information Act 2000; j) complying with the Health & Safety at Work etc Act 1974 k) providing information to NHS England as required. 12 Inserted by section 25 of the 2012 Act 13 The Good Governance Standard for Public Services, The Independent Commission on Good Governance in Public Services, Office of Public Management (OPM) and The Chartered Institute of Public Finance & Accountability (CIPFA), See Appendix 2 15 See Appendix 3 16 Seehttp:// 10
11 4.6.2 In addition to these statutory requirements, the group will demonstrate its accountability by: a) Adhering to the Better Together Agreement to support and enable the provision of integrated urgent, proactive, elective care, mental health and various social services b) producing an Interpractice Agreement for all member practices to adhere to c) producing an Integrated Governance Framework which details the committee accountability structure d) adhering to a Memorandum of Understanding in relation to integrated governance with other local Clinical Commissioning Groups 17 e) electing Governing Body GP constituency members to represent member practice views f) ensuring that clinical commissioning is clinically led g) ensuring an integrated risk management framework is embedded h) collaborating with key partners such as the Health & Well Being Board i) adhering to a Memorandum of Understanding in relation to collaborative commissioning 18 j) taking soundings from patients, public and community. This is through a variety of ways; through the Better Together Citizens Board; through the Stakeholder Reference Group, which is a sub- committee to the governing body made up of members of the community, Patient Participation Groups within each of the member practices, and other engagement activities The governing body of the group will throughout each year have an on-going role in reviewing the group s governance arrangements to ensure that the group continues to reflect the principles of good governance The governing body recognises and confirms that nothing in or referred to in this constitution (including in relation to the issue of any press release or other public statement or disclosure) will prevent or inhibit the making of any protected disclosure (as defined in the Employment Rights Act 1996, as amended by the Public Interest Disclosure Act 1998) by any member of the group, any member of its governing body, any member of any of its committees or sub-committees or the committees or sub-committees of its governing body, or any employee of the group or of any of its members, nor will it affect the rights of any worker (as defined in that Act) under that Act. 17 See Appendix 4 18 See Appendix 5 11
12 5 FUNCTIONS AND GENERAL DUTIES 5.1 Functions The functions that the group is responsible for exercising are largely set out in the 2006 Act, as amended by the 2012 Act. An outline of these appears in the Department of Health s Functions of clinical commissioning groups: a working document. They relate to: a) commissioning certain health services (where NHS England is not under a duty to do so) that meet the reasonable needs of: i) all people registered with member GP practices, and ii) people who are usually resident within the area and are not registered with a member of any clinical commissioning group; b) commissioning emergency care for anyone present in the group s area; c) paying its employees remuneration, fees and allowances in accordance with the determinations made by its governing body and determining any other terms and conditions of service of the group s employees; d) determining the remuneration and travelling or other allowances of members of its governing body In discharging its functions the group will: a) act 19, when exercising its functions to commission health services, consistently with the discharge by the Secretary of State and NHS England of their duty to promote a comprehensive health service 20 and with the objectives and requirements placed on NHS England through the mandate 21 published by the Secretary of State before the start of each financial year. The CCG will: i) delegate responsibility for complying with this duty to its Governing Body ii) develop the group s commissioning strategy and annual plan b) meet the public sector equality duty 22 by: i) selecting a governing body GP Equality and Diversity Champion ii) delegating responsibility to the Quality & Risk Sub Committee of the governing body and a lead individual to oversee its discharge iii) producing equality objectives through the Equality Delivery System toolkit iv) producing an Equality and Diversity Strategy to set out how the governing body will discharge its duties v) publishing at least annually information to demonstrate compliance vi) developing an equality and diversity plan vii) preparing and publishing specific and measurable equality objectives, revising these at least every four years viii) ensuring that patient participation involves all nine protected 19 See section 3(1F) of the 2006 Act, inserted by section 13 of the 2012 Act 20 See section 1 of the 2006 Act, as amended by section 1 of the 2012 Act 21 See section 13A of the 2006 Act, inserted by section 23 of the 2012 Act 22 See section 149 of the Equality Act 2010, as amended by paragraphs 184 and 186 of Schedule 5 of the 2012 Act 12
13 characteristics including age, disability, gender reassignment, pregnancy and maternity, race, religion or belief, sex, sexual orientation and for the elimination of discrimination element of the duty only marriage and civil partnership, where appropriate ix) ensuring equality and diversity is integral to business planning x) providing equality of opportunity c) work in partnership with its local authority[ies] to develop joint strategic needs assessments 23 and joint health and wellbeing strategies 24 by: i) being a member of the Nottinghamshire Health & Well Being Board ii) ensuring a senior clinician represents the governing body s views on the Health & Well Being Board iii) ensuring that member practices are consulted and their views and clinical insights are represented iv) ensuring that patients are engaged in the process and have an opportunity to provide feedback v) producing regular reports and updates to the governing body vi) ensuring that the joint health and wellbeing strategies integrate with the CCG commissioning intentions vii) take into account Newark District Council and Nottinghamshire County Council views viii) produce a Communication Engagement Experience Strategy to support effective partnership working ix) work with neighbouring local authorities to secure high quality health services for the CCG population x) work with both Healthwatch England and local Healthwatch to ensure that the views and experiences of patients, carers and other service users are taken into account. xi) Work with multiple partners to improve safeguarding for the population of Nottinghamshire. The work will be carried out by the Multi-Agency Safeguarding Hub (MASH) which will bring together colleagues from health, police, local authority, probation to improve safeguarding for the population of Nottinghamshire 5.2 General Duties - in discharging its functions the group will: Make arrangements to secure public involvement in the planning, development and consideration of proposals for changes and decisions affecting the operation of commissioning arrangements 25 by: a) Adhering to the NHS Newark & Sherwood CCG Statement of Principles: working in partnership with patients and the local community to secure the best care for them adapting engagement activities to meet the specific needs of the different patient groups and communities 23 See section 116 of the Local Government and Public Involvement in Health Act 2007, as amended by section 192 of the 2012 Act 24 See section 116A of the Local Government and Public Involvement in Health Act 2007, as inserted by section 191 of the 2012 Act 25 See section 14Z2 of the 2006 Act, inserted by section 26 of the 2012 Act 13
14 publishing information about health services on the group s website and through other media encouraging and acting on feedback ensuring that the Stakeholder Reference Group reports to the governing body in an advisory capacity producing the Communication Engagement Experience Strategy and Equality and Diversity strategy b) Make arrangements to secure that individuals to whom the services are being or may be provided are involved: in the planning of the commissioning arrangements by the group in the development of a rolling programme of activities to feed into the business planning cycle whether by being consulted or invited to comment in other ways in the development and consideration of proposals by the group for changes in the commissioning arrangements where the implementation of the proposals would have an impact on the manner in which services are delivered to the individuals or the range of service available to them and, in the decisions of the group affecting the operation of the commissioning arrangements where the implementation of the decisions would (if made) have such an impact proportionate to the changes being considered Promote awareness of, and act with a view to securing that health services are provided in a way that promotes awareness of, and have regard to the NHS Constitution 26 by: a) delegating responsibility to the group s governing body to monitor compliance b) ensuring the Chief Officer provides the Governing Body with an annual report regarding compliance with the duty Act effectively, efficiently and economically 27 by: a) the CCG determining the governing body duties to approve the Standing Orders, Scheme of Delegation and Reservation b) the CCG establishing an Activity and Finance Sub Committee to provide financial reassurance and review of member practice activity c) the CCG determining lead responsibilities for service commissioning with resource available d) establishing the Chief Officer to manage within financial resources e) establishing a committee governance structure which oversees the effective, efficient use of resources f) establishing lead responsibilities to commission the best services within budget to meet public need g) establishing lead responsibilities to review contracting activity and reviewing contract performance h) establishing lead responsibilities to monitor quality and patient safety activity carried out by provider organisations 26 See section 14P of the 2006 Act, inserted by section 26 of the 2012 Act and section 2 of the Health Act 2009 (as amended by 2012 Act) 27 See section 14Q of the 2006 Act, inserted by section 26 of the 2012 Act 14
15 i) establishing the Standing Financial Instructions and the system of financial control j) ensuring review of member practices activity across the CCG is carried out on a monthly basis to identify best practice and development of action plans where appropriate Act with a view to securing continuous improvement to the quality of services 28 by: a) working in collaboration with member practices, service users, provider organisations, other CCGs and the Local Authority to identify and implement continuous improvements to the quality of services for patients. The Governing Body has delegated responsibility for overseeing continuous improvement and the risk management to the Quality and Risk Sub Committee and overseeing safeguarding to the Safeguarding Adult Committee and Safeguarding Children Committee. b) being accountable to the CCG s Governing Body and providing assurances to both Newark and Sherwood and Mansfield and Ashfield CCGs that systems for the management and performance of all aspects of quality, patient safety, information technology, risk management and equality and diversity are properly established and remain effective. The Quality & Risk Sub Committee membership includes GPs, leads for quality and risk, lay representation and is chaired by the Governing Body s Chief Nurse. c) providing the governing body with information on improvements and areas of clinical risk in local provider services. Findings are presented to the governing body at each meeting through the Quality in Transition Dashboard and through presentation of minutes. d) analysing a number of data sources in order to determine the level of quality in provider services. To be carried out through: All Quality Scrutiny Panels, including those held monthly with Sherwood Forest Hospitals Foundation Trust and quarterly with the CCG out of hours provider, Central Nottinghamshire Clinical Services (CNCS) (Newark and Sherwood are the lead commissioner for quality in these two organisations). The findings from all these panels feed into the Quality Dashboards and provide our on-going scrutiny of quality and improvements. Review of feedback from member practices via our 'quality and contract feedback mechanism'. This is a simple form that provides practices with easy access to feedback issues relating to patient care Complaints and Patient Advisory Liaison (PALs) feedback both directly to the CCG and also through the Quality Scrutiny Panels. These sources are then analysed to give an overall picture of the level of quality and risk See section 14R of the 2006 Act, inserted by section 26 of the 2012 Act 15
16 e) delegating safeguarding vulnerable adults and children to the Safeguarding Adult Committee and Safeguarding Children Committee. The Safeguarding Committee is managed and chaired by NHS Newark and Sherwood CCG and provide assurance to five other CCGs within Nottinghamshire. It will ensure that systems and processes are in place to safeguard vulnerable adults and children respectively. The committees also oversee the implementation of action plans from serious case reviews and local audits. f) working in partnership to drive continuous improvements. The Multi- Agency Safeguarding Hub (MASH) brings together colleagues from health, police, local authority, probation to improve safeguarding for the population of Nottinghamshire Assist and support NHS England in relation to the Governing Body s duty to improve the quality of primary medical services 29 by: a) delegating strategic responsibility to the governing body for the oversight and improvement of primary care quality b) establishing responsibility for continuous improvements in primary care services c) assist and support NHS England in discharging its duties relating to individual GP performance management (medical performers list for GPs, appraisal and revalidation), administration of payments and list management d) working collaboratively with partner agencies and regulatory bodies e) ensuring the governing body and its member practices are engaged in production of the Joint Strategic Needs Assessment (JSNA) with local authority f) producing a primary care framework g) promoting compliance with the Care Quality Commission Standards h) promoting patient safety and sharing lessons learnt from incidents with Nottinghamshire CCGs and other partner agencies Carry out the functions relating to the commissioning of primary medical service under section 83 of the NHS Act, as outlined in the NHS Delegation Agreement: a) delegating the commissioning of primary medical services to the NHS Newark & Sherwood Primary Care Commissioning Committee b) promoting increased co-commissioning to ensure on-going quality, efficiency, productivity and value for money to remove administrative burdens c) monitoring of contracts, taking contractual action such as issuing branch/remedial notices d) designing local incentive schemes as an alternative to Quality Outcomes Framework (QOF) e) approving practice mergers f) undertaking reviews of primary care services g) managing the budget for commissioning of primary care services 29 See section 14S of the 2006 Act, inserted by section 26 of the 2012 Act 16
17 5.2.7 Have regard to the need to reduce inequalities 30 by: a) delegating strategic responsibility to the governing body to have due regard for reducing inequalities b) working in partnership with the local authority to identify health inequalities identified within the Joint Needs Assessment c) working with the Health & Well Being Board to maintain a holistic approach to reducing inequalities d) ensuring commissioning decisions taken include reducing inequalities Promote the involvement of patients, their carers and representatives in decisions about their healthcare 31 by: a) delegating strategic responsibility to the group s governing body to promote the involvement of patients, their carers and representatives in decisions about their healthcare b) establishing a Stakeholder Reference Sub Committee which is patient led c) ensuring a Better Together Citizens Board is established through the Better Together Alliance Agreement d) ensuring patient/carer representatives are involved in design/redesign of all services e) producing and actively working to a Communications Engagement Experience Plan f) producing and actively working to Equality and Diversity Objectives through the Equality Delivery Scheme toolkit g) producing an Equality and Diversity action plan h) reporting on progress to the governing body at regular intervals through the Patient and Public Involvement Governing Body Lay members i) establishing a schedule of engagement across the CCG area to discuss commissioning intentions, new services, patient pathways etc j) supporting member practices Patient Reference Groups k) ensuring the CCG website contains all up to date, relevant information for patients and carers l) working collaboratively with local third sector providers and other interest groups to understand the views and needs of their patients/carers Act with a view to enabling patients to make choices 32 by: a) delegating strategic responsibility to the governing body to ensure that patient choice is built into commissioning b) collaborative working with other CCGs and partner agencies to identify best practice to secure patient choice c) commissioning new services to facilitate patient choice d) developing commissioning/referral pathway ensuring that a suitable range of services are accessible to residents e) using a combination of procurement; introducing competition in a provider market Obtain appropriate advice 33 from persons who, taken together, have a broad 30 See section 14T of the 2006 Act, inserted by section 26 of the 2012 Act 31 See section 14U of the 2006 Act, inserted by section 26 of the 2012 Act 32 See section 14V of the 2006 Act, inserted by section 26 of the 2012 Act 33 See section 14W of the 2006 Act, inserted by section 26 of the 2012 Act 17
18 range of professional expertise in healthcare and public health by: a) delegating strategic responsibility to the governing body for gathering a broad range of professional expertise in healthcare and public health b) ensuring the governing body has membership which includes a range of professionals c) establishing strategic and operational committees and groups which include a range of professionals within its membership d) working with providers and the local authority to develop pathways through the Better Together Alliance Agreement e) delegating lead responsibility for pathway redesign to a range of healthcare professionals f) working collaboratively with partners including the Health & Well Being Board, public health, local authorities and provider organisations g) ensuring member practices are actively involved through various engagement methods including clinical protected learning time, clinical leadership development, workshops to review and discuss, for example, the CCG strategic objectives h) participating in healthcare networks to fully maximise a range of advice i) participating in the Clinical Executive j) participating in the Clinical Senates k) working with the Local Medical Committee (LMC) l) participating in the Commissioning Board assembly Promote innovation 34 by: a) delegating strategic responsibility to the governing body for the promotion of innovation b) collaborative working with local and regional research networks, such as the Academic Health Science Network and the Clinical Senate c) collaborative working with local organisations, including the local authority through the Better Together Alliance Agreement d) developing and implementing an Organisational Development Plan to assist innovative working and adoption of best practice e) communicating good practice/ideas via the internal member practice CCG newsletters f) encourage the adoption and diffusion of innovation through local meetings and forums g) engaging with patient/carers to seek new and innovative ways of working h) use contract levers to support innovation Promote research and the use of research 35 by: a) delegating strategic responsibility to the governing body to promote research and the use of research within the CCG b) establishing close links with the local National Institute for Health Research (NIHR) Networks including the Primary Care Research Network (PCRN), Comprehensive Local Research Network (CLRN) and Collaboration for Leadership in Applied Health Research and Care (CLAHRC). c) ensuring research activity is linked to CCG Quality, Innovation, Productivity and Prevention (QIPP) workstreams d) working collaboratively with CLAHRC to recruit patients through its Primary 34 See section 14X of the 2006 Act, inserted by section 26 of the 2012 Act 35 See section 14Y of the 2006 Act, inserted by section 26 of the 2012 Act 18
19 Care research projects and increase engagement with the local NIHR funded studies through co-production of recruitment strategies. e) engaging with CLAHRC to increase its research capacity through mechanisms such as Research into Practice awards f) working with CLAHRC, PCRN and CLRN to also provide research insight events for NHS staff research to improve the opportunities for patients to become aware of research activity g) capturing current research activity in the CCG area through use of links to the research networks h) influencing and promotion of research in the local area through intelligence gathered across the East Midlands network through meetings, conferences, research forums etc. i) Support trials on the basis of existing national guidance, our local priorities and on a case by case basis Have regard to the need to promote education and training 36 for persons who are employed, or who are considering becoming employed, in an activity which involves or is connected with the provision of services as part of the health service in England so as to assist the Secretary of State for Health in the discharge of his related duty 37 by: a) delegating strategic responsibility to the governing body for promotion of education and training b) providing development workshops for governing body members to support progression of strategic thinking and leadership skills c) providing development programmes for lay members of the governing body and its supporting committees d) commissioning developmental activities to support continued education and training for governing body members e) working collaboratively with other CCGs to provide joint training and education f) delegating operational responsibility to manage member practice learning and development to the Education Committee. The committee develops Protected Learning Time (PLT) events for all member practice employees g) delegating Education Committee chair responsibilities for PLT events to a member practice clinician h) ensuring that member practices have a feedback mechanism to report any areas of training and development needed to the Education Committee i) developing an Organisational Development Plan to support CCG staff progression j) providing staff development events and workshops k) ensuring talent management is fundamental to CCG development l) ensuring that all internal and external training and development opportunities are communicated via the CCG intranet and internal newsletters m) identifying any training and development needs during the redesign/design of new pathways/services n) working collaboratively with NHS England to identify clinical training needs through training and development mechanisms such as appraisals o) Ensuring processes are in place to monitor levels of compliance in relation to mandatory training 36 See section 14Z of the 2006 Act, inserted by section 26 of the 2012 Act See section 1F(1) of the 2006 Act, inserted by section 7 of the 2012 Act 19
20 p) Participating in the Nottinghamshire GP and Practice Staff Education and Training Board facilitated by the LMC Act with a view to promoting integration of both health services with other health services and health services with health-related and social care services where the group considers that this would improve the quality of services or reduce inequalities 38 by: a) delegating strategic responsibility to the governing body to have due regard for promotion of integration b) working in partnership with the local authority to identify integration of health and other services where the quality of services are improved and/or there is a reduction in inequalities c) ensuring commissioning decisions taken have included the potential of integration with other services d) establishing a Better Together Commissioning Committee which consists of members of the group and representatives from Nottinghamshire County Council and Mansfield & Ashfield CCG working in partnership to give strategic direction on aligning and commissioning integrated health and social care services. e) Establishing a Better Together Alliance Leadership Board with Membership, including Nottinghamshire County Council. 5.3 General Financial Duties details on how these will be met are set out in the Standing Orders and Standing Financial Instructions. In summary the group will perform its functions so as to: Ensure its expenditure does not exceed the aggregate of its allotments for the financial year 39 by a) delegating responsibility to the Chief Finance Officer b) establishing robust budget setting arrangements - the Chief Finance Officer will compile and submit to the governing body a Medium Term Plan which takes into account financial targets and forecast limits of available resources. The plan will contain: (i) (ii) a statement of the significant assumptions on which the plan is based; details of major changes in workload, delivery of services or resources required to achieve the plan. Prior to the start of the financial year the Chief Finance Officer will, on behalf of the Chief Officer, prepare and submit budgets for approval by the governing body. These will: (i) (ii) (iii) (iv) (v) be in accordance with the aims and objectives set out in the plan; accord with workload and manpower plans; be produced following discussion with appropriate budget holders; be prepared within the limits of available allotments and income; identify potential risks. 38 See section 223H(1) of the 2006 Act, inserted by section 27 of the 2012 Act 39 See section 14Z1 of the 2006 Act, inserted by section 26 of the 2012 Act 20
21 c) delegating authority appropriately - the governing body will delegate authority to spend to appropriately placed and trained budget holders who will be responsible and held to account for committing the resources. The role of the budget holder is specified in the Budget Management Framework. d) reporting and monitoring budget balances and taking remedial action - The Chief Finance Officer will produce a Budget Management Manual or equivalent which will describe the role and responsibilities of budget holders and managers and the budgetary control process. The Chief Finance Officer will monitor allotments, income and expenditure and produce a monthly monitoring report for the governing body. Such reports will be presented to an Activity & Finance Sub Committee or equivalent, which will be responsible for detailed perusal and understanding of the outcome of the monitoring reports. The report will then be presented to the governing body to focus on the key material issues as advised by the Activity & Finance Sub Committee. Budget Holders/Managers will identify variances and the reasons for them and inform the Chief Finance Officer of the remedial action they are taking. In the event that the Budget Manager cannot identify sufficient remedial action to bring the budget back into balance, the Budget Holder will identify further remedial action. This iterative process will be undertaken until the Chief Officer is assured that the total CCG budget is in balance and this can be reported to the governing body Ensure its use of resources (both its capital resource use and revenue resource use) does not exceed the amount specified by NHS England for the financial year 40 by a) the arrangements described in will also facilitate the meeting of any revenue and capital resource limits Take account of any directions issued by NHS England, in respect of specified types of resource use in a financial year, to ensure the group does not exceed an amount specified by NHS England 41 by a) the Chief Officer ensuring the governing body is aware of any directions issued by NHS England and will update the CCG plans/budgets accordingly so that any specified amounts are not exceeded Publish an explanation of how the group spent any payment in respect of quality made to it by NHS England 42 by a) providing a note on how the group spent any payment in respect of quality in the Annual Report 5.4 Other Relevant Regulations, Directions and Documents The group will 40 See sections 223I(2) and 223I(3) of the 2006 Act, inserted by section 27 of the 2012 Act 41 See section 223J of the 2006 Act, inserted by section 27 of the 2012 Act 42 See section 223K(7) of the 2006 Act, inserted by section 27 of the 2012 Act 21
22 a) comply with all relevant regulations; b) comply with directions issued by the Secretary of State for Health or NHS England; and c) take account, as appropriate, of documents issued by NHS England The group will develop and implement the necessary systems and processes to comply with these regulations and directions, documenting them as necessary in this constitution, its scheme of reservation and delegation and other relevant group policies and procedures. 22
23 DECISION MAKING: THE GOVERNING STRUCTURE 6.1 Authority to act The Clinical Commissioning Group is accountable for exercising the statutory functions of the group. It may grant authority to act on its behalf to: a) any of its members; b) its governing body; c) employees; d) a committee or sub-committee of the group The extent of the authority to act of the respective bodies and individuals depends on the powers delegated to them by the group as expressed through: a) the group s scheme of reservation and delegation; and b) for committees, their terms of reference. 6.2 Scheme of Reservation and Delegation The group s scheme of reservation and delegation sets out: a) those decisions that are reserved for the membership as a whole; b) those decisions that are the responsibilities of its governing body (and its committees), the group s committees and sub-committees, individual members and employees The clinical commissioning group remains accountable for all of its functions, including those that it has delegated. 6.3 General In discharging functions of the group that have been delegated to its governing body, its sub committees and joint committees and individuals must: a) comply with the group s principles of good governance, 43 b) operate in accordance with the group s scheme of reservation and delegation, c) comply with the group s standing orders, d) comply with the group s arrangements for discharging its statutory duties, 44 e) where appropriate, ensure that member practices have had the opportunity to contribute to the group s decision making process When discharging their delegated functions, subcommittees and joint committees must also operate in accordance with their approved terms of reference Where delegated responsibilities are being discharged collaboratively, the joint (collaborative) arrangements must: 43 See section 4.5 on Principles of Good Governance above 44 See chapter 5 above 23
24 a) identify the roles and responsibilities of those clinical commissioning groups who are working together; b) be specified within a Memorandum of Understanding c) identify any pooled budgets and how these will be managed and reported in annual accounts; d) specify under which clinical commissioning group s scheme of reservation and delegation and supporting policies the collaborative working arrangements will operate; e) specify how the risks associated with the collaborative working arrangement will be managed between the respective parties; f) identify how disputes will be resolved and the steps required to terminate the working arrangements; g) specify how decisions are communicated to the collaborative partners. 6.4 Sub Committees of the group The following sub committees have been established by the group: a) Clinical Executive Sub Committee, b) Activity & Finance Sub Committee c) Quality & Risk Sub Committee (joint committee with Mansfield and Ashfield CCG) d) Safeguarding Adult Committee (all county CCGs) e) Safeguarding Children Committee (all county CCGs) f) Audit and Governance Sub Committee g) Remuneration and Terms of Service Sub Committee h) Stakeholder Reference Group Sub Committee i) Commissioning Committee (joint committee with Mansfield and Ashfield CCG) j) Primary Care Commissioning Committee k) Affiliated Commissioning Committee l) Audit Panel (joint committee with Mansfield and Ashfield CCG) all of which are accountable to the governing body Committees and Sub Committees will only be able to establish their sub groups, to assist them in discharging their respective responsibilities, if this responsibility has been delegated to them by the group or the committee they are accountable to. 6.5 Joint Commissioning Arrangements with NHS England for the Exercise of CCG Functions The CCG may wish to work together with NHS England in the exercise of its commissioning functions The CCG and NHS England may make arrangements to exercise any of the CCG s commissioning functions jointly The arrangements referred to in paragraph [6.5.2] above may include other CCGs Where joint commissioning arrangements pursuant to [6.5.2] above are entered into, the parties may establish a joint committee to exercise the commissioning functions in question. 24
25 6.5.4 Arrangements made pursuant to [6.5.2] above may be on such terms and conditions (including terms as to payment) as may be agreed between NHS England and the CCG Where the CCG makes arrangements with NHS England (and another CCG if relevant) as described at paragraph [6.5.2] above, the CCG shall develop and agree with NHS England a framework setting out the arrangements for joint working, including details of: a) How the parties will work together to carry out their commissioning functions; b) The duties and responsibilities of the parties; c) How risk will be managed and apportioned between the parties; d) Financial arrangements, including, if applicable, payments towards a pooled fund and management of that fund; e) Contributions from the parties, including details around assets, employees and equipment to be used under the joint working arrangements The liability of the CCG to carry out its functions will not be affected where the CCG enters into arrangements pursuant to paragraph [6.5.2] above The CCG will act in accordance with any further guidance issued by NHS England on co-commissioning Only arrangements that are safe and in the interests of patients registered with member practices will be approved by the governing body The governing body of the CCG shall require, in all joint commissioning arrangements that the Accountable Officer of the CCG make a quarterly written report to the Governing Body and hold at least annual engagement events to review aims, objectives, strategy and progress and publish an annual report on progress made against objectives Should a joint commissioning arrangement prove to be unsatisfactory the governing body of the CCG can decide to withdraw from the arrangement, but has to give six months notice to partners, with new arrangements starting from the beginning of the next new financial year after the expiration of the six months notice period. 6.6 Joint Commissioning Arrangements with NHS England for the exercise of NHS England s functions The CCG may wish to work with NHS England and, where applicable, other CCGs, to exercise specified NHS England functions The CCG may enter into arrangements with NHS England and, where applicable, other CCGs to: a) Exercise such functions as specified by NHS England under delegated arrangements; Jointly exercise such functions as specified with NHS England. Where 25
26 arrangements are made for the CCG and, where applicable, other CCGs to exercise functions jointly with NHS England a joint committee may be established to exercise the functions in question Arrangements made between NHS England and the CCG may be on such terms and conditions (including terms as to payment) as may be agreed between the parties For the purposes of the arrangements described at paragraph [4.8.2] above, NHS England and the CCG may establish and maintain a pooled fund made up of contributions by the parties working together. Any such pooled fund may be used to make payments towards expenditure incurred in the discharge of any of the commissioning functions in respect of which the arrangements are made Where the CCG enters into arrangements with NHS England as described at paragraph [4.8.2] above, the parties will develop and agree a framework setting out the arrangements for joint working, including details of: a) How the parties will work together to carry out their commissioning functions; b) The duties and responsibilities of the parties; c) How risk will be managed and apportioned between the parties; d) Financial arrangements, including payments towards a pooled fund and management of that fund; e) Contributions from the parties, including details around assets, employees and equipment to be used under the joint working arrangements The liability of NHS England to carry out its functions will not be affected where it and the CCG enter into arrangements pursuant to paragraph [4.8.2] above The CCG will act in accordance with any further guidance issued by NHS England on co-commissioning Only arrangements that are safe and in the interests of patients registered with member practices will be approved by the Governing Body The Governing Body of the CCG shall require, in all joint commissioning arrangements that the Accountable Officer of the CCG make a quarterly written report to the Governing Body and hold at least annual engagement events to review aims, objectives, strategy and progress and publish an annual report on progress made against objectives Should a joint commissioning arrangement prove to be unsatisfactory the governing body of the CCG can decide to withdraw from the arrangement, but has to give six months notice to partners, with new arrangements starting from the beginning of the next new financial year after the expiration of the six months notice period. 6.7 Joint commissioning arrangements with other Clinical Commissioning Groups The clinical commissioning group (CCG) may wish to work together with other CCGs in the exercise of its commissioning functions. 26
27 6.7.2 The CCG may make arrangements with one or more CCG in respect of: delegating any of the CCG s commissioning functions to another CCG; exercising any of the commissioning functions of another CCG; or exercising jointly the commissioning functions of the CCG and another CCG For the purposes of the arrangements described at paragraph [6.7.2], the CCG may: make payments to another CCG; receive payments from another CCG; make the services of its employees or any other resources available to another CCG; or receive the services of the employees or the resources available to another CCG Where the CCG makes arrangements which involve all the CCGs exercising any of their commissioning functions jointly, a joint committee may be established to exercise those functions For the purposes of the arrangements described at paragraph [6.7.2] above, the CCG may establish and maintain a pooled fund made up of contributions by any of the CCGs working together pursuant to paragraph above. Any such pooled fund may be used to make payments towards expenditure incurred in the discharge of any of the commissioning functions in respect of which the arrangements are made Where the CCG makes arrangements with another CCG as described at paragraph [6.7.2] above, the CCG shall develop and agree with that CCG an agreement setting out the arrangements for joint working, including details of: How the parties will work together to carry out their commissioning functions; The duties and responsibilities of the parties; How risk will be managed and apportioned between the parties; Financial arrangements, including, if applicable, payments towards a pooled fund and management of that fund; Contributions from the parties, including details around assets, employees and equipment to be used under the joint working arrangements The liability of the CCG to carry out its functions will not be affected where the CCG enters into arrangements pursuant to paragraph [6.7.2] above The CCG will act in accordance with any further guidance issued by NHS 27
28 England on co-commissioning Only arrangements that are safe and in the interests of patients registered with member practices will be approved by the governing body The governing body of the CCG shall require, in all joint commissioning arrangements that the lead clinician and lead manager of the lead CCG make a quarterly written report to the governing body and hold at least annual engagement events to review aims, objectives, strategy and progress and publish an annual report on progress made against objectives Should a joint commissioning arrangement prove to be unsatisfactory the governing body of the CCG can decide to withdraw from the arrangement, but has to give six months notice to partners, with new arrangements starting from the beginning of the next new financial year The group has entered into joint arrangements with the following clinical commissioning groups: a) Rushcliffe, Nottingham North and East, Nottingham West, Mansfield and Ashfield CCGs in respect of the Safeguarding Adult Committee and Safeguarding Children Committee b) Rushcliffe, Nottingham North and East, Nottingham West, Mansfield and Ashfield CCGs in respect of the Individual Funding Request Panel c) Mansfield and Ashfield CCG in respect of the Quality & Risk Sub Committee d) Rushcliffe, Nottingham North and East, Nottingham West, Mansfield and Ashfield CCGs in respect of Information Governance and Information Management Sub Committee e) Mansfield and Ashfield CCG in respect of the Auditor Panel f) Southern Derbyshire CCG, North Derbyshire CCG, Erewash CCG, Hardwick CCG, Nottingham City CCG, Nottingham West CCG, Nottingham North and East CCG, Rushcliffe CCG, Mansfield and Ashfield CCG, Corby CCG, Nene CCG, West Leicestershire CCG, Leicester City CCG, East Leicestershire and Rutland CCG, Lincolnshire West CCG, South West Lincolnshire CCG, South Lincolnshire CCG in respect of the Affiliated Commissioning Committee. A joint Memorandum of Understanding in relation these arrangements has been developed (see Appendix 4) g) Bassetlaw CCG in respect of emergency planning and safeguarding h) A joint Memorandum of Understanding in relation to collaborative commissioning has been developed (see Appendix 5) i) Nottinghamshire County Council and Mansfield and Ashfield CCG in respect of the Better Together Commissioning Committee and programme board to ensure alignment and integration of health and social care services The group is a member of other partnership boards with the local councils: a. Nottinghamshire County Council in respect of the Mental Health, Learning Disability, Autism Joint Commissioning Group b. Nottinghamshire Adults Safeguarding Board where the CCG represents all five Nottinghamshire CCGs c. Nottinghamshire Children s Safeguarding Board where the CCG represents all five Nottinghamshire CCGs d. Rushcliffe, Nottingham North and East, Nottingham West and Mansfield and Ashfield in respect of prescribing. A mandate is in 28
29 place for Nottinghamshire Area Prescribing Committee. This committee also includes other organisations providing NHS services within the Nottinghamshire health community. 6.8 Joint Alliance Agreement with local commissioners and provider participants Joint Alliance Agreement with local commissioners and provider participants In 2013, leaders signed up to a system blueprint, Better Together setting out the services that will be needed in the future with a 5 year planning horizon to 2018/19. This set the foundations for how commissioners and providers work together across organisational boundaries to best match and manage projected population demand. A clear shared vision has been adopted across the system, with detailed plans to implement transformational interventions that impact on whole system quality, cost of provision and sustainability. The clinical commissioning group (CCG) has agreed to form an Alliance with local commissioners and provider participants to progress the work of the Better Together programme and wider system transformation and, in particular, to establish an improved financial, governance and contractual framework for the delivery of the services for mid-nottinghamshire. An independently chaired Board, the Alliance Leadership Board, is in place to oversee the delivery of the Better Together strategy. This collaboration comprises senior leaders who are empowered to make decisions and drive forward change in their constituent organisations. This is referred to as the Alliance in this constitution. Membership is as follows: Organisation Mansfield and Ashfield CCG Newark and Sherwood CCG NCC EMAS NHCT NUH SFHT NEMS Category Of Membership Full Alliance Member Full Alliance Member Full Alliance Member Full Alliance Member Full Alliance Member Full Alliance Member Full Alliance Member Full Alliance Member An Alliance Agreement has been approved by all participating organisations including the CCG Governing Body and will supplement and operate in conjunction with: a. The Services Contracts b. The Nottingham County Council Services Contracts c. Any other local partnering arrangements to the Services; and d. The joint commissioning arrangements between the mid-notts CCGs and Nottinghamshire County Council The Alliance Agreement came into force on 1 April 2016 with an Initial Period until 31 March 2019 with an option to extend for a period of 7 years from the expiry of the Initial 29
30 Period. From 1 April 2016 a transitional year will take place with participants agreeing to work together to develop and evolve the Alliance further As a Commissioner participant the CCG shall identify the health and social care needs and priorities of the mid-notts population, provide links to other relevant services such as housing and education and seek to put in place contractual arrangements with other third party providers to incentivise the Outcomes The Alliance Agreement sets out the Alliance governance, decision making, delegated authority and reserved matters, rectification, exclusion, termination and dispute resolution clauses. It also outlines the scope of services, outcomes and payment mechanisms The Alliance Agreement outlines the role the commissioner participants will undertake where a Change is proposed. The Commissioner participants will be entitled in their sole discretion to declare in the Notice of Change that a proposed change is a Mandatory Change and the date from which the Mandatory Change will be effective The CCG Governing Body has approved the CCG becoming a Full Member of the Alliance and, as such, will be entitled to vote at the Alliance Leadership Board. The CCG will nominate one member and one deputy member to join the Alliance Leadership Board from its Governing Body membership The CCG Governing Body has approved delegated authority to their nominated member and deputy member as set out within the CCG scheme of delegation The CCGs Commissioning Committee, a sub-committee of the CCG Governing Body, has the responsibility of carrying out the functions relating to the CCGs commissioning intentions except that of primary medical services. It will monitor the Alliance Leadership Board to ensure compliance with the requirements as set out in the Alliance Agreement is maintained. It will provide regular reporting to the CCG Governing Body. 6.9 The Governing Body Functions - the governing body has the following functions conferred on it by sections 14L(2) and (3) of the 2006 Act, inserted by section 25 the 2012 Act, together with any other functions connected with its main functions as may be specified in regulations or in this constitution The group reserves the right to confer additional responsibilities to the governing body in its role of co-ordinating commissioner of mental health/learning disabilities on behalf of five Nottinghamshire County CCGs. The group delegates responsibility to the governing body for the oversight of mental/learning disabilities/autism contract The governing body has responsibility for: a) oversight of safeguarding partnership arrangements and contributions to serious case reviews across the five Nottinghamshire CCGs b) ensuring that the group has appropriate arrangements in place to exercise its functions effectively, efficiently and economically and in accordance with the groups principles of good governance 46 (its main function); c) determining the remuneration, fees and other allowances payable to employees or other persons providing services to the group and the allowances payable under any pension scheme it may establish under paragraph 11(4) of Schedule 45 See section 14L(3)(c) of the 2006 Act, as inserted by section 25 of the 2012 Act 46 See section 4.4 on Principles of Good Governance above 30
31 1A of the 2006 Act, inserted by Schedule 2 of the 2012 Act; d) approving any functions of the group that are specified in regulations; 47 e) leading the setting of vision and strategy f) approving commissioning plans g) monitoring performance against plans h) Identifying and monitoring risks to the delivery of the strategic objectives i) Ensuring that the register of interest and register of decisions are reviewed regularly and updated as necessary Composition of the Governing Body - the governing body shall not have less than 16 and comprises of: a) The clinical chair; through a process of election and appointment b) Five clinical representatives of member practices, who must be nominated and elected by their peers, represent the following constituencies: i. Newark 1 Fountain Medical Centre, Barnby Gate Surgery and Hounsfield Surgery ii. Newark 2 Lombard Medical Centre, Balderton Primary Care Centre and Collingham Medical Centre iii. North West Sherwood Medical Partnership and Hillview iv. South Abbey Medical Group Surgery and Southwell Medical Centre v. North Central Major Oak Surgery, Middleton Lodge Practice and Bilsthorpe Surgery. c) One practice manager: who must be elected by their peers d) Four lay members: i. The vice chair of the CCG will lead on governance, audit, remuneration and conflict of interest matters and chair the Audit & Governance Sub Committee. This member must be appointed into this role ii. iii. Two to lead on patient and public participation matters. One of which will be the chair of the sub-committee One lay member to chair the Activity & Finance Sub Committee and Remuneration and Terms of Service Sub Committee. This member must be appointed to the role. The CCG may co-opt additional lay members to bring specific assurances e.g. audit. e) One registered nurse (the chief nurse); who fulfils the requirements of national guidance for the role and provides assurance on the quality of local services to the governing body f) One secondary care specialist doctor g) One governing body practice nurse 47 See section 14L(5) of the 2006 Act, inserted by section 25 of the 2012 Act 31
32 h) The chief officer i) The chief finance officer Other individuals are in attendance in an advisory capacity and non- voting members: i) Public Health Consultant ii) Director of Contracting and Urgent Care iii) Director of Procurement and Market Development iv) Director of Primary Care v) Director of Programme Delivery vi) Director of Transformation vii) County Council representative viii) Chair of the CCG Primary Care Commissioning Committee The Head of Corporate Governance will be in attendance in the role of governing body secretariat Sub Committees of the Governing Body - the governing body has appointed the following sub-committees: Audit & Governance Sub Committee the Audit & Governance Sub Committee, which is accountable to the group s governing body, provides the governing body with an independent and objective view of the group s financial systems, financial information and compliance with laws, regulations and directions governing the group in so far as they relate to finance. The sub-committee provides assurance on the effectiveness and management of risk through the CCG Assurance Framework 51 and other underlying assurance processes. The subcommittee will also review the establishment and maintenance of an effective system of integrated governance, risk management and internal control (both clinical and non-clinical). The governing body has approved and keeps under review the terms of reference for the Audit & Governance Sub Committee which includes information on the membership of the sub-committee. Remuneration and Terms of Service Sub Committee the Remuneration and Terms of Service Sub Committee, which is accountable to the group s governing body makes recommendations to the governing body on determinations about the remuneration, fees and other allowances for employees and for people who provide services to the group and on determinations about allowances under any pension scheme that the group may establish as an alternative to the NHS pension scheme. The governing body has approved and keeps under review the terms of reference for the Remuneration and Terms of Service Sub Committee which includes information on the membership of the subcommittee. Clinical Executive Sub Committee the Clinical Executive Sub- Committee which is accountable to the group s governing body ensures operational oversight to support the achievement of strategic objectives. This includes coordination of the development of commissioning plans, strategies and intentions, managing the investments and disinvestments decisions made by the group through the business case procurement process and by having an oversight of quality, QIPP, financial and contract performance, ensuring systems are in place to support the group s practice members, supporting the group s practice performance and primary care quality, championing redesign and innovation in 32
33 health care delivery, sharing knowledge, championing clinical research and development and collaborating with other clinical commissioning groups and partners. The Clinical Executive Sub Committee is also responsible for the reduction of health inequalities in access to and the outcome from healthcare. The governing body has approved and keeps under review the terms of reference for the Clinical Executive Sub Committee which includes information on the membership of the sub-committee. Activity & Finance Sub Committee the Activity & Finance Sub Committee, which is accountable to the group s governing body reviews financial reporting to ensure integrated planning with activity, service delivery and quality, reviews benchmarking information to ensure commissioning is cost effective and value for money, examines financial expenditure to support commissioning and decommissioning through the business case procurement process, drives key deliverables against the group s financial plan and year end targets, monitors performance against QIPP, monitors the group s risk model ensuring there are robust processes in place to manage risks and performance variance and reviews financial policies. The governing body has approved and keeps under review the terms of reference for the Activity and Finance Committee which includes information on the membership of the sub-committee Quality & Risk Sub Committee - the Quality & Risk Sub Committee which is accountable to the group s governing body, provides assurances to both NHS Newark and Sherwood CCG and NHS Mansfield and Ashfield CCG that systems for the management and performance of all aspects of quality, patient safety, risk management and equality and diversity are properly established and remain effective. The governing body has approved and keeps under review the terms of reference for the Quality & Risk Sub Committee which includes information on the membership of the sub-committee. Stakeholder Reference Group Sub Committee - the Stakeholder Reference Group Sub Committee, which is accountable to the group s governing body, is responsible for bringing together patients, carers, communities, the public and Newark and Sherwood commissioners to ensure patient views and experiences are taken into account in the planning, development and delivery of local health services. The governing body has approved and keeps under review the terms of reference of the Stakeholder Reference Group Sub Committee which includes information on the membership of the sub-committee. Safeguarding Adult Committee the Safeguarding Adult Committee, which is shared with other Nottinghamshire CCGs, is accountable to the group s governing body and is responsible for the promotion of and welfare of vulnerable adults across commissioned and contracted services and for monitoring compliance of those services, overseeing that processes are in place for implementing, monitoring and embedding safeguarding principles in service level agreements, monitoring key performance indicators, monitoring actions from serious case reviews affecting vulnerable adults and developing clear lines of accountability and reporting. The governing body has approved and keeps under review the terms of the reference for the Safeguarding Adult Committee which includes information on the membership of the committee. Safeguarding Children Committee the Safeguarding Children Committee, which is shared with other Nottinghamshire CCGs, is accountable to the group s governing body and is responsible for the promotion of and welfare of children 33
34 across commissioned and contracted services and for monitoring compliance of those services, overseeing that processes are in place for implementing, monitoring and embedding safeguarding principles in service level agreements, monitoring key performance indicators, monitoring actions from serious case reviews affecting vulnerable adults and developing clear lines of accountability and reporting. The governing body has approved and keeps under review the terms of reference for the Safeguarding Children Committee which includes information on the membership of the committee. Commissioning Committee the joint Mansfield & Ashfield CCG and Newark & Sherwood CCG Commissioning Committee, which is accountable to the group s governing bodies, provides assurance in relation to carrying out CCGs commissioning intentions except that of primary medical services. It ensures compliance with the requirements as outlined within the mid-notts Alliance Agreement, carries out the functions relating to the review and performance management of the CCGs membership of the Alliance and ensures compliance with public procurement regulations. The Committee receives regular reporting from the Alliance Leadership Board which is a collaboration of local commissioners and providers whose aim is to transform local services through partnership working. Primary Care Commissioning Committee - the Primary Care Commissioning Committee is accountable to the NHS Newark & Sherwood CCG CCG s governing body. The function of the committee is undertaken in the context of a desire to promote improved co-commissioning to increase quality, efficiency, productivity and value for money and to remove administrative barriers. The role of the Committee shall be to carry out the functions relating to the commissioning of primary medical services under section 83 of the NHS Act. East Midlands Affiliated Commissioning Committee (shared with other CCGs within the East Midlands) - The East Midlands Affiliated Commissioning Committee is accountable to the NHS Mansfield & Ashfield CCG s governing body. The function of the committee is to develop and maintain joint commissioning policies to maximise resources, reduce duplication and ensure the development of clinical and cost effective policies that improve the quality of care for patients. Auditor Panel (shared panel with Newark and Sherwood CCG) The function of the Auditor Panel is to advise the CCG Governing Body on the selection and appointment of external auditors In addition the Group has delegated certain functions to several joint committees comprising representatives from the CCG see paragraphs for further details. 34
35 ROLES AND RESPONSIBILITIES 7.1 Commissioning Practice Representatives i. Commissioning practice representatives represent their practice s views and act on behalf of the practice in matters relating to the group. Full details regarding the role of each member practice is set out in the NHS Newark & Sherwood CCG Interpractice Agreement. ii. A nominated commissioning practice representative is identified at each member practice. Their role is to work on behalf of the practice to ensure the following: dissemination of practice performance information to all staff at their practice; clinical commissioning is on the agenda of the practice meeting; monitoring and controlling their own commissioning budget share of all such data and information to assist the Group in monitoring the whole Group position against targets; capturing and analysing data needed to inform the audit and commissioning process; reviewing both their own practice-specific and Group-wide data on commissioning and referral activities and use these to inform and improve upon, so far as practicable, their own commissioning proposals; informing N&S CCG of their own commissioning needs and priorities in relation to patients to whom they provide services and relative to the wider population profile; following agreed referral activities and guidelines wherever clinically appropriate; making every effort to follow service redesign pathway guidelines; embracing medicines management advice and follow agreed prescribing guidelines wherever clinically appropriate; keeping accurate records of referrals to support analysis, validation and challenge data; co-operating and working with the Governing Body GP Constituency member Member practices are supported by their respective Governing Body GP Constituency member who facilitates the communication between the member practices and the governing body 7.2 Other GP and Primary Care Health Professionals In addition to the commissioning practice representatives identified in section 7.1 above, the group has identified a number of other GPs / primary care health professionals from member practices to either support the work of the group and / or represent the group rather than represent their own individual practices. These GPs and primary care health professional undertake the following roles on behalf of the group: 35
36 a. Clinical Advisor b. Public Health Consultant responsible for ensuring due regard for the need for health inequalities in access to and the outcome from healthcare c. Practice Manager the governing body practice manager is the link between the governing body and the practice manager s forum d. Pathway development and redesign clinical leads e. Clinical Executive Sub Committee clinical and non clinical membership f. Activity & Finance Sub Committee clinical and non clinical membership g. Quality & Risk Sub Committee clinical and non clinical membership 7.3 All Members of the Group s Governing Body Guidance on the roles of members of the group s governing body is set out in a separate document 48. In summary, each member of the governing body should share responsibility as part of a team to ensure that the group exercises its functions effectively, efficiently and economically, with good governance and in accordance with the terms of this constitution. Each brings their unique perspective, informed by their expertise and experience. 7.4 The Clinical Chair of the Governing Body The clinical chair of the governing body is responsible for: leading the governing body, ensuring it remains continuously able to discharge its duties and responsibilities as set out in this constitution; building and developing the group s governing body and its individual members; ensuring that the group has proper constitutional and governance arrangements in place; ensuring that, through the appropriate support, information and evidence, the governing body is able to discharge its duties; supporting the chief officer in discharging the responsibilities of the organisation; contributing to building a shared vision of the aims, values and culture of the organisation; leading and influencing to achieve clinical and organisational change to enable the group to deliver its commissioning responsibilities; Overseeing governance and particularly ensuring that the governing body and the wider group behaves with the utmost transparency and responsiveness at all times; 48 Draft clinical commissioning group Governing Body Members Roles Attributes and Skills, NHS England Authority, March
37 ensuring that public and patients views are heard and their expectations understood and, where appropriate as far as possible, met; ensuring that the organisation is able to account to its local patients, stakeholders and NHS England; ensuring that the group builds and maintains effective relationships, particularly with the individuals involved in overview and scrutiny from the relevant local authority(ies) Arranging the regular evaluation of the performance of the governing body, its sub committees and individual lay members Plan and conduct governing body meetings, with the Chief Officer. Facilitate the effective combination of all governing body members and ensure constructive relations within the organisation and constituent practices. Specific duties will include: Proactively direct and manage the development of major governing body decisions with complete consideration being given to all options during the process. Ensure that the governing body develops and oversees strategies, which will result in tangible improvements to the health of the population and clinical services. Ensure that the governing body establishes clear objectives to deliver agreed strategies and regularly review performance against these objectives. Ensure that the governing body maintains its responsibility for the effective governance of the organisation by making the best use of resources including the development of effective risk and performance management processes. Ensure that the governing body, and the organisation, observe the Secretary of State s policies and priorities, including the requirements of the Codes of Conduct and Accountability. Be aware of relevant, regulatory and Central Government policies. Ensure that the interests of all stakeholders, and influence of all advisers, are fairly balanced. Ensure that conflicts of interest are managed in a fair and transparent way The clinical chair of the governing body is also the senior clinical voice of the group. They will take the lead in interactions with stakeholders, including NHS England. 37
38 7.5 The Vice Lay Chair of the Governing Body The vice chair is a member of the governing body and deputises for the chair of the governing body where he or she has a conflict of interest or is otherwise unable to act The vice chair will lead on governance, audit, and conflict of interest matters 7.6 Role of the Joint Chief Officer/Accountable Officer The joint chief officer is a member of the governing body They carry out a joint chief officer role between NHS Newark & Sherwood CCG and NHS Mansfield & Ashfield CCG The role of chief officer has been summarised in a national document 49 as: being responsible for ensuring that the clinical commissioning group fulfils its duties to exercise its functions effectively, efficiently and economically thus ensuring improvement in the quality of services and the health of the local population whilst maintaining value for money; at all times ensuring that the regularity and propriety of expenditure is discharged, and that arrangements are put in place to ensure that good practice (as identified through such agencies as the Audit Commission and the National Audit Office) is embodied and that safeguarding of funds is ensured through effective financial and management systems. working closely with the chair of the governing body, the joint chief officer will ensure that proper constitutional, governance and development arrangements are put in place to assure the members (through the governing body) of the organisation s on-going capability and capacity to meet its duties and responsibilities. This will include arrangements for the on-going developments of its members and staff The joint chief officer role will be a shared position for NHS Newark & Sherwood and NHS Mansfield and Ashfield CCG. 7.7 Role of the Joint Chief Finance Officer The joint chief finance officer is a member of the governing body and is responsible for providing financial advice to the clinical commissioning group and for supervising financial control and accounting systems This role of joint chief finance officer has been summarised in a national 49 See the latest version of the NHS England Authority s Clinical commissioning group governing body members: Role outlines, attributes and skills 38
39 document 50 as: being the governing body s professional expert on finance and ensuring, through robust systems and processes, the regularity and propriety of expenditure is fully discharged; making appropriate arrangements to support, monitor on the group s finances; overseeing robust audit and governance arrangements leading to propriety in the use of the group s resources; being able to advise the governing body on the effective, efficient and economic use of the group s allocation to remain within that allocation and deliver required financial targets and duties; and producing the financial statements for audit and publication in accordance with the statutory requirements to demonstrate effective stewardship of public money and accountability to NHS England; oversees the development and execution of Quality, Innovation, Productivity and Prevention (QIPP) plans to ensure effective use of resources and value for money The role of joint chief finance officer will be a shared position for NHS Newark & Sherwood and NHS Mansfield and Ashfield CCG 7.8 Role of the Constituent GPs The Constituent GPs are members of the governing body They are formally elected to the governing body by member practices. This process is managed by the Local Medical Committee The Constituent GPs have the following responsibilities: Support to the chair/clinical lead to provide clinical leadership and to improve quality in primary care Provision of clinical advice to the governing body so that it is an effective commissioning body Liaison with constituent practices to gain their views and to keep them informed about Clinical Commissioning Group business Support to the Clinical Commissioning Group to deliver its commissioning objectives Support to the governing body to develop Quality, Innovation, Productivity and Prevention plans and to ensure financial balance Support the production and delivery of the Commissioning Strategic Plan Act as a corporate member of the governing body in line with the Nolan 50 See the latest version of the NHS England Authority s Clinical commissioning group governing body members: Role outlines, attributes and skills 39
40 principles of public life. 7.9 Role of the Governing Body Practice Manager The Governing Body Practice Manager is a member of the governing body They are formally elected to the governing body by their practice manager peers. This process is managed by the Local Medical Committee The Practice Manager has the following responsibilities: Support the governing body to improve quality in primary care Provide practice manager perspectives on commissioning issues Liaise with other practice managers to gain their views and to keep them informed about Clinical Commissioning Group business Support the governing body to develop QIPP plans and to ensure financial balance Support the production and delivery of the Commissioning Strategic Plan Act as a corporate member of the governing body in line with the Nolan principles of public life Fairly represent the range of practice manager views in relation to governing body business 7.10 Role of the Patient and Public Involvement Lay members The Patient and Public Involvement Lay members of the group are members of the governing body and are the voice of the patient They are appointed to the Governing Body in accordance with paragraph 2.2 of the Group s standing orders; They have a regular standing item on the governing body agenda to provide progress reports on Stakeholder Reference Group Sub Committee discussions. This also gives them the opportunity to reply to any questions or concerns the governing body has They will help to ensure that, in all aspects of the CCG s business the public voice of the local population is heard and that opportunities are created and protected for patient and public empowerment in the work of the CCG Role of the Activity & Finance Lay member The Activity & Finance Lay member is a member of the governing body They are appointed to the role by the governing body They will chair the Activity & Finance Sub Committee and the Remuneration and Terms of Service Sub Committee meeting which are sub-committees to the Governing Body They also attend joint committees on behalf of the governing body Role of Chief Nurse 40
41 The Chief Nurse is a member of the governing body They are appointed to the role by the governing body As well as sharing responsibility with the other members for all aspects of the CCG governing body business, the Chief Nurse will bring a broader view from their perspective as a Chief Nurse, on health and care issues to underpin the work of the CCG especially the contribution of nursing to patient care The Chief Nurse is the executive lead for Safeguarding Role of secondary care doctor The secondary care doctor is a member of the governing body They are appointed to the role by the governing body As well as sharing responsibility with the other members for all aspects of the CCG governing body business, the secondary care doctor will bring a broader view, on health and care issues to underpin the work of the CCG The secondary care doctor will, in particular, bring to the governing body an understanding of patient care in the secondary care setting Role of Governing Body Practice Nurse The Practice Nurse is a member of the Governing Body The Practice Nurse is elected to the role by their practice peers As well as sharing responsibility with the other members for all aspects of the CCG governing body business, the Practice Nurse will bring a broader view, on health and care issues to underpin the work of the CCG The Practice Nurse will, in particular, bring to the governing body an understanding of patient care in the primary care setting Joint Appointments with other Organisations The group has the following joint appointments with another organisation: Chief Officer/Accountable Officer and their team joint with NHS Mansfield and Ashfield CCG The Chief Nurse and their team which includes - Complaints team joint with NHS Mansfield and Ashfield CCG The Director of Contracting and Urgent Care and their team which includes Contracting team joint with NHS Mansfield and Ashfield CCG Finance team joint with NHS Mansfield and Ashfield CCG 41
42 The Assistant Director Mental Health and Learning Disabilities and their team joint with all five Nottinghamshire County CCGs The Chief Nurse and their Quality team - joint with NHS Mansfield and Ashfield CCG; and which includes Safeguarding Designated Nurse and GP trainer for safeguarding joint with all five Nottinghamshire County CCGs The Director of Primary Care and their team joint with NHS Mansfield and Ashfield CCG The Director of Programme Delivery and their Team joint with NHS Mansfield and Ashfield CCG The Director of Procurement and Market Development and their team - joint with NHS Mansfield and Ashfield CCG All these joint appointments are supported by a Memorandum of Understanding between the organisations who are party to these joint appointments. 42
43 8 STANDARDS OF BUSINESS CONDUCT AND MANAGING CONFLICTS OF INTEREST 8.1 Standards of Business Conduct Employees, members, committee and sub-committee members of the group and members of the governing body (and its committees) will at all times comply with this constitution and be aware of their responsibilities as outlined in it. They should act in good faith and in the interests of the group and should follow the Seven Principles of Public Life, set out by the Committee on Standards in Public Life (the Nolan Principles) The Nolan Principles are incorporated into this constitution at Appendix They must comply with the group s policy on business conduct, including the requirements set out in the policy for managing conflicts of interest. This policy will be available on the group s website at Hardcopies can also be requested by writing to the Head of Corporate Governance, at NHS Newark & Sherwood CCG, Balderton Primary Care Centre, Lowfield Lane, Balderton, Nottinghamshire, NG24 3HJ, or Individuals contracted to work on behalf of the group or otherwise providing services or facilities to the group will be made aware of their obligation with regard to declaring conflicts or potential conflicts of interest. This requirement will be written into their contract for services. 8.2 Conflicts of Interest Section 14O of the Health and Social Care Act 2012 sets out the minimum requirements in terms of what both NHS England and CCGs must do in terms of managing conflicts of interest. For the CCG, this means the following: Maintain appropriate registers of interests; Publish or make arrangements for the public to access those registers; Make arrangements requiring the prompt declaration of interests by the persons specified (members and employees) and ensure that these interests are entered into the relevant register; Make arrangements for managing conflicts and potential conflicts of interest (e.g. developing appropriate policies and procedures); and Have regard to guidance published by NHS England and Monitor in relation to conflicts of interest The CCG Conflicts of Interest Policy is available to view on the group s website at can also be requested by writing to the Head of Corporate Governance, at NHS Newark & Sherwood CCG, Balderton Primary Care Centre, Lowfield Lane, Balderton, Nottinghamshire, NG24 3HJ, or by calling
44 THE GROUP AS EMPLOYER 9.1 The group recognises that its most valuable asset is its people. It will seek to enhance their skills and experience and is committed to their development in all ways relevant to the work of the group. 9.2 The group will seek to set an example of best practice as an employer and is committed to offering all staff equality of opportunity. It will ensure that its employment practices are designed to promote diversity and to treat all individuals equally. 9.3 The group will ensure that it employs suitably qualified and experienced staff who will discharge their responsibilities in accordance with the high standards expected of staff employed by the group. All staff will be made aware of this constitution, the commissioning strategy and the relevant internal management and control systems which relate to their field of work. 9.4 The group will maintain and publish policies and procedures (as appropriate) on the recruitment and remuneration of staff to ensure it can recruit, retain and develop staff of an appropriate calibre. The group will also maintain and publish policies on all aspects of human resources management, including grievance and disciplinary matters 9.5 The group will ensure that its rules for recruitment and management of staff provide for the appointment and advancement on merit on the basis of equal opportunity for all applicants and staff. 9.6 The group will ensure that employees' behaviour reflects the values, aims and principles set out above. 9.7 The group will ensure that it complies with all aspects of employment law. 9.8 The group will ensure that its employees have access to such expert advice and training opportunities as they may require in order to exercise their responsibilities effectively. 9.9 The group will adopt a Code of Conduct for staff and will maintain and promote effective 'whistleblowing' procedures to ensure that concerned staff have means through which their concerns can be voiced Copies of this Code of Conduct, together with the other policies and procedures outlined in this chapter, will be available on the group s website at can also be requested by writing to the Head of Corporate Governance, at NHS Newark & Sherwood CCG, Balderton Primary Care Centre, Lowfield Lane, Balderton, Nottinghamshire, NG24 3HJ, or by calling
45 10 TRANSPARENCY, WAYS OF WORKING AND STANDING ORDERS 10.1 General The group will publish annually a commissioning plan and an annual report, presenting the group s annual report to a public meeting Key communications issued by the group, including the notices of procurements, public consultations, governing body and Primary Care Commissioning Committee meeting dates, times, venues, and certain papers will be published on the group s website at can also be requested by writing to the Head of Corporate Governance, at NHS Newark & Sherwood CCG, Balderton Primary Care Centre, Lowfield Lane, Balderton, Nottinghamshire, NG24 3HJ, or by calling The group may use other means of communication, including circulating information by post, or making information available in venues or services accessible to the public Financial Management and Governance Arrangements Manuals This constitution is also informed by Financial Management and Governance Arrangements Manuals which provide further details on how the group will operate. The manuals details the CCG financial duties, financial reporting, budget holder duties, sub- committee terms of reference and the CCG risk management policy. It also includes the following key financial documentation: Scheme of reservation and delegation which sets out those decisions that are reserved for the membership as a whole and those decisions that are the responsibilities of the group s governing body, the governing body s committees and sub-committees, the group s committees and sub-committees, individual members and employees; Standing orders which sets out the arrangements for meetings and the appointment processes to elect the group s representatives and appoint to the group s committees, including the governing body, which can be found at Annex 10; Prime financial policies - which sets out the group s control environment for managing the organisation s financial affairs. They enable sound administration; lessen the risk of irregularities and support commissioning and delivery of effective, efficient and economical services. 45
46 APPENDIX 1 LIST OF MEMBER PRACTICES Practice Name Balderton Primary Care Centre Barnby Gate Surgery Bilsthorpe Surgery Abbey Medical Group Collingham Medical Centre Fountain Medical Centre Hill View Surgery Hounsfield Surgery Lombard Medical Centre Major Oak Surgery Middleton Lodge Practice Rainworth Health Centre Sherwood Medical Partnership Southwell Medical Centre Address Lowfield Lane, Balderton, Nottinghamshire, NG24 3HG 50 Barnby Gate, Newark, Nottinghamshire, NG24 1QD 35 Mickledale Lane, Bilsthorpe, Newark, Nottinghamshire, NG22 8QB 59 Mansfield Road, Blidworth, Nottinghamshire, NG21 0RB High Street, Collingham, Nottinghamshire, NG23 7LB Sherwood Avenue, Newark, Nottinghamshire, NG24 1QH Kirklington Road, Rainworth, Nottinghamshire, NG21 0JP The Surgery, Hounsfield Way, Sutton on Trent, Nottinghamshire, NG23 6PX 2 Portland Street, Newark, Nottinghamshire, NG24 4XG High Street, Edwinstowe, Nottinghamshire, NG21 9QS Church Circle, New Ollerton, Nottinghamshire, NG22 9SZ Warsop Lane, Rainworth, Nottinghamshire, NG21 0AD Crown Farm Way, Forest Town, Nottinghamshire, NG19 0FW, and Station Lane, Farnsfield, Nottinghamshire, NG22 9DA The Ropewalk, Southwell, Nottinghamshire, NG25 0AL 46
47 APPENDIX 2 - NOLAN PRINCIPLES The Nolan Principles set out the ways in which holders of public office should behave in discharging their duties. The seven principles are: a) Selflessness Holders of public office should act solely in terms of the public interest. They should not do so in order to gain financial or other benefits for themselves, their family or their friends. b) Integrity Holders of public office should not place themselves under any financial or other obligation to outside individuals or organisations that might seek to influence them in the performance of their official duties. c) Objectivity In carrying out public business, including making public appointments, awarding contracts, or recommending individuals for rewards and benefits, holders of public office should make choices on merit. d) Accountability Holders of public office are accountable for their decisions and actions to the public and must submit themselves to whatever scrutiny is appropriate to their office. e) Openness Holders of public office should be as open as possible about all the decisions and actions they take. They should give reasons for their decisions and restrict information only when the wider public interest clearly demands. f) Honesty Holders of public office have a duty to declare any private interests relating to their public duties and to take steps to resolve any conflicts arising in a way that protects the public interest. g) Leadership Holders of public office should promote and support these principles by leadership and example. Source: The First Report of the Committee on Standards in Public Life (1995) 55 47
48 APPENDIX 3 NHS CONSTITUTION The NHS Constitution sets out seven key principles that guide the NHS in all it does: 1. the NHS provides a comprehensive service, available to all - irrespective of gender, race, disability, age, sexual orientation, religion or belief. It has a duty to each and every individual that it serves and must respect their human rights. At the same time, it has a wider social duty to promote equality through the services it provides and to pay particular attention to groups or sections of society where improvements in health and life expectancy are not keeping pace with the rest of the population 2. access to NHS services is based on clinical need, not an individual s ability to pay - NHS services are free of charge, except in limited circumstances sanctioned by Parliament. 3. the NHS aspires to the highest standards of excellence and professionalism - in the provision of high-quality care that is safe, effective and focused on patient experience; in the planning and delivery of the clinical and other services it provides; in the people it employs and the education, training and development they receive; in the leadership and management of its organisations; and through its commitment to innovation and to the promotion and conduct of research to improve the current and future health and care of the population. 4. NHS services must reflect the needs and preferences of patients, their families and their carers - patients, with their families and carers, where appropriate, will be involved in and consulted on all decisions about their care and treatment. 5. the NHS works across organisational boundaries and in partnership with other organisations in the interest of patients, local communities and the wider population - the NHS is an integrated system of organisations and services bound together by the principles and values now reflected in the Constitution. The NHS is committed to working jointly with local authorities and a wide range of other private, public and third sector organisations at national and local level to provide and deliver improvements in health and well-being 6. the NHS is committed to providing best value for taxpayers money and the most cost-effective, fair and sustainable use of finite resources - public funds for healthcare will be devoted solely to the benefit of the people that the NHS serves 7. the NHS is accountable to the public, communities and patients that it serves - the NHS is a national service funded through national taxation, and it is the Government which sets the framework for the NHS and which is accountable to Parliament for its operation. However, most decisions in the NHS, especially those about the treatment of individuals and the detailed organisation of services, are rightly taken by the local NHS and by patients with their clinicians. The system of responsibility and accountability for taking decisions in the NHS should be transparent and clear to the public, patients and staff. The Government will ensure that there is always a clear and up-to-date statement of NHS accountability for this purpose. Source: The NHS Constitution: The NHS belongs to us all (March 2012) 56 48
49 APPENDIX 4 - MEMORANDUM OF UNDERSTANDING IN RELATION TO GOVERNANCE ARRANGEMENTS WITH OTHER CCGs NHS Nottingham North and East Clinical Commissioning Group (1) NHS Nottingham West Clinical Commissioning Group (2) NHS Newark and Sherwood Clinical Commissioning Group (3) NHS Rushcliffe Clinical Commissioning Group (4) NHS Mansfield and Ashfield Clinical Commissioning Group (5) NHS Bassetlaw Clinical Commissioning Group (6) MEMORANDUM OF UNDERSTANDING IN RELATION TO COLLABORATIVE GOVERNANCE ARRANGEMENTS 49
50 Contents Introduction Objectives Joint Committees Safeguarding Committee Individual Funding Request Committee Information Governance and Information Management Committee NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Quality and Risk Committee NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Quality and Risk Committee General reporting arrangements for joint committees Oversight of joint committees Joint appointments and arrangements NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Chief Finance Officer and Deputy Finance Officer NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Director of Quality and Governance, Information and Performance and Directorate of Quality and Governance, Information and Performance NHS Mansfield and Ashfield CCG Executive Lead for Contracting and Directorate of Contracting (Acute) NHS Newark and Sherwood CCG Directorate of Contracting (Mental Health) NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Chief Finance Officer and Directorate of Finance NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Quality and Patient Safety and Directorate of Quality and Patient Safety NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Outcomes and Information and Directorate of Outcomes and Information NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Directorate of Contracting (Acute) NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Directorate of Contracting (Community Health Partnerships and non-acute contracts Funding of joint appointments Disputes between CCGs Review Termination or withdrawal Mutual termination Withdrawal from part Withdrawal from all General principles relating to termination or withdrawal Overriding principles 50
51 1. Introduction Developing clinical commissioning groups: Towards authorisation (DH: September 2011) set the clear expectation that CCGs will put in place: Collaborative arrangements for commissioning with other clinical commissioning groups, local authorities and NHS England, as well as the appropriate external commissioning support (Domain 5) The Health and Social Care Act 2012 (the 2012 Act ) encourages collaboration and makes provision to enable CCGs to establish appropriate collaborative arrangements with other CCGs and local authorities. This Memorandum of Understanding ( MOU ) establishes a framework for cooperation between NHS Nottingham North and East Clinical Commissioning Group, NHS Nottingham West Clinical Commissioning Group, NHS Newark and Sherwood Clinical Commissioning Group, NHS Rushcliffe Clinical Commissioning Group, NHS Mansfield and Ashfield Clinical Commissioning Group and NHS Bassetlaw Clinical Commissioning Group (the CCGs ). It sets out how the organisations will work together to maintain and strengthen collaborative governance working arrangements. This MOU shall come into effect on 1 April 2013 and shall continue until it is terminated in accordance with section 6. This MOU is a statement of intent for internal purposes and is not intended to create any legal obligations. This MOU sets out the principles which have been agreed between the CCGs in relation to: a. Joint committees (section 3); b. Joint appointments and arrangements (section 4); and c. CCG hosting arrangements (section 5) 2. Objectives The CCGs have decided to collaborate in order to achieve the following objectives: a. Clinical improvements Consistent, evidence based pathway development Effective and consistent performance management, clinical governance and risk management Service integration b. Efficiency Leverage with providers Keeping low transaction costs Sharing (potentially scarce) expertise and capacity c. Resilience and risk management 51
52 Managing financial risks Enabling diversity in CCG configuration and size Managing regulatory and legal change Managing extended absence of key staff Improved risk management and intelligence systems Business continuity arrangements These arrangements support each CCG s delivery of Quality, Innovation, Productivity and Prevention (QIPP), in both the clinical services commissioned and the commissioning process itself. Joint Committees Section 6.5 of the CCGs Constitutions and Section 14Z3 (2) (b) of the NHS Act 2006 (as inserted by 2012 Act) (the 2006 Act ) allows the CCGs to make arrangements with other clinical commissioning groups which may provide for the clinical commissioning groups to exercise any of their commissioning functions jointly. The CCGs have together established the following joint committee: Safeguarding Committee NHS Mansfield and Ashfield CCG, NHS Newark and Sherwood CCG, NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG have established the following joint committees: Individual Funding Request Committee; and Information Governance, Management & Technology Committee NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG have established the following joint committee: Quality and Risk Committee NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG have established the following joint committee: Quality and Risk Committee In accordance with the 2006 Act each of the CCGs have delegated authority in their respective scheme of reservation and delegation to members or employees participating in the aforementioned joint committees to make decisions on its behalf subject to the overriding principle that the CCG retains ultimate liability for any such decisions. a. The Safeguarding Committee The Safeguarding Committee has responsibility for overseeing strategy and policy development for children and adult safeguarding on behalf of NHS Mansfield and Ashfield CCG, NHS Newark and Sherwood CCG, NHS Nottingham North and East CCG, NHS Nottingham West CCG, NHS Rushcliffe CCG and NHS Bassetlaw CCG. NHS Newark and Sherwood CCG has responsibility to ensure that the committee meets its terms of reference and undertakes all of its defined duties. This includes (but is not limited to) meeting arrangements, chairing of meetings, minute taking at 52
53 meetings and governance arrangements relating to the administration and conduct of the committee. The Safeguarding Committee is constituted in accordance with the scheme of reservation and delegation of NHS Newark and Sherwood CCG. The applicable policies and procedures are owned and maintained by NHS Newark and Sherwood CCG. The Safeguarding Committee meetings shall be chaired by the Newark and Sherwood CCG and Mansfield and Ashfield CCG Director of Quality and Governance with executive responsibility for safeguarding at NHS Newark and Sherwood CCG and Mansfield and Ashfield CCG. The safeguarding lead or the Executive Nurse for safeguarding from each CCG (or their duly appointed deputy) shall attend each meeting of the Safeguarding Committee. The Safeguarding Committee shall meet on at least a quarterly basis. The Safeguarding Committee reports to the CCGs via submission of its minutes to the NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Quality and Risk Committee and the Governing Bodies of NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG. The Safeguarding Committee also submits an annual report to the Governing Bodies of NHS Mansfield and Ashfield CCG, NHS Newark and Sherwood CCG, NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG with a six monthly report on achievement against its objectives. Further the Safeguarding Committee submits reports on its activity to both the Children and Adult s local safeguarding boards. b. Individual Funding Request Committee The Individual Funding Request Committee ( IFRC ) considers all Individual Funding Requests ( IFR s ) and decides whether to support or not support these individual requests for funding where a service, intervention or treatment falls outside the relevant service agreements on behalf of NHS Mansfield and Ashfield CCG, NHS Newark and Sherwood CCG, NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG. The IFRC is administered by the Greater East Midlands Commissioning Support Organisation ( GEM ). GEM has responsibility for screening cases received before they are referred to the IFRC for consideration, independently reviewing the evidence submitted with the application for review and providing training of panel members GEM also provides administrative support to the IFRC which includes (but is not limited to) meeting arrangements, chairing of meetings, minute taking at meetings and governance arrangements relating to the administration and conduct of the committee. The IFRC is constituted in accordance with the scheme of reservation and delegation of NHS Nottingham West CCG. The applicable policies and procedures are owned and maintained by Nottingham West CCG. The IFRC is chaired by the lay member responsible for patient and public involvement 53
54 at NHS Mansfield & Ashfield CCG. The IFRC is attended by representatives from public health, the Chief Officers (or deputy) of the CCGs (including NHS Nottingham West) and CCG GP representatives. Other attendees include the Senior Prescribing Advisor, the IFR Manager and Health Economist. The IFRC shall meet on a monthly basis. The IFRC reports to the Governing Bodies of NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG and to the Quality and Risk Committee of NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG. The IFRC also provides an annual report to the Governing Bodies of NHS Mansfield and Ashfield CCG, NHS Newark and Sherwood CCG, NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG. c. Information Governance, Management & Technology Committee The Information Governance, Management & Technology Committee (the IGM&T Committee ) oversees information governance arrangements on behalf of NHS Mansfield and Ashfield CCG, NHS Newark and Sherwood CCG, NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG and its members have delegated authority from the CCGs to make decisions in respect of all matters relating to information governance and information management. NHS Rushcliffe CCG has responsibility for providing administrative support to the IG&IM Committee. This includes (but is not limited to) meeting arrangements, chairing of meetings, minute taking at meetings and governance arrangements relating to the administration and conduct of the committee. The IGM&T Committee is constituted in accordance with the scheme of reservation and delegation of NHS Rushcliffe CCG. The applicable policies and procedures are owned and maintained by NHS Rushcliffe CCG. The IGM&T Committee meetings shall be chaired by the NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Outcomes and Information. A representative from each CCG (or their duly appointed deputy) shall attend each meeting of the IG&IM Committee. The IGM&T Committee shall meet on a bi-monthly basis. The IGM&T Committee reports to the CCGs via submission of its minutes to each CCG governing body meeting. d. NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Quality and Risk Committee The NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Quality and Risk Committee has responsibility for ensuring that systems for the management and performance of all aspects of quality and patient safety are properly established and remain effective on behalf of NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG. NHS Newark and Sherwood CCG has responsibility for providing administrative 54
55 support to the NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Quality and Risk Committee. This includes (but is not limited to) meeting arrangements, chairing of meetings, minute taking at meetings and governance arrangements relating to the administration and conduct of the committee. NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Quality and Risk Committee is constituted in accordance with the scheme of reservation and delegation of NHS Newark and Sherwood CCG. The applicable policies and procedures are owned and maintained by Newark and Sherwood CCG The NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Quality and Risk Committee shall be chaired by a lay member from NHS Newark and Sherwood CCG. Representatives from NHS Newark and Sherwood CCG and NHS Mansfield and Ashfield CCG (or their duly appointed representatives) shall attend each meeting of the NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Quality and Risk Committee. The NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Quality and Risk Committee shall meet on a quarterly basis. The NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Quality and Risk Committee reports to NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG via submission of its minutes. The NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Quality and Risk Committee also submits an annual report to the Governing Bodies of NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG. The NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Quality and Risk Committee also shares its minutes with the NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Quality and Risk Committee to ensure that any opportunities for shared learning are identified. e. NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Quality and Risk Committee The NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Quality and Risk Committee has responsibility for ensuring that systems for the management and performance of all aspects of quality and patient safety are properly established and remain effective on behalf of NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG. NHS Nottingham North and East CCG has responsibility for providing administrative support to the NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Quality and Risk Committee. This includes (but is not limited to) meeting arrangements, chairing of meetings, minute taking at meetings and governance arrangements relating to the administration and conduct of the committee. NHS Nottingham North and East CCG has delegated responsibility for oversight and delivery of this function to the NHS Nottingham North and East CCG, NHS Nottingham 55
56 West CCG and NHS Rushcliffe CCG Director of Quality and Patient Safety and Directorate of Quality and Patient Safety. The NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Quality and Risk Committee is constituted in accordance with the scheme of reservation and delegation of NHS Nottingham North and East CCG. The applicable policies and procedures are maintained and owned by NHS Nottingham North and East CCG The NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Quality and Risk Committee is chaired by the lay member with responsibility for PPI at NHS Nottingham North and East CCG. Representatives from NHS Nottingham North and East CCG, NHS Rushcliffe CCG and NHS Nottingham West CCG (or their duly appointed representatives) shall attend each meeting of the NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Quality and Risk Committee. The NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Quality and Risk Committee shall meet on a bi-monthly basis. The NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Quality and Risk Committee reports to the NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG via submission of its minutes to their Governing Bodies. The NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Quality and Risk Committee also shares its minutes with the NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Quality and Risk Committee to ensure that any opportunities for shared learning are identified. The Committee receives all Quality Scrutiny Panel Minutes from all of the key providers of healthcare services to NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG to monitor their performance under their contract with the CCGs. This functions to provide an overview of quality for all providers f. General reporting and accountability principles for joint committees Each of the above joint committees shall ensure that they establish reporting and accountability structures which are in accordance with the Nolan principles of public life and such other principles of good governance as may be applicable to ensure there is adequate oversight of each joint committee to assure the CCGs that those functions which have been delegated are being carried out efficiently and effectively. Each committee will have regard to shared QIPP objectives across partner CCGs, and will identify and deliver opportunities for related improvements as relevant to its own remit and work programmes. g. Oversight of joint committees The CCGs will exercise oversight of the joint committees they are part of by: Signing and keeping under review the terms of reference of each committee; Monitoring the committee s compliance with their terms of reference; Requesting and 56
57 scrutinising further reports or assurances on specific matters as and when required; and Requiring attendance by one or more representatives of a committee to attend CCG Governing Body meetings to provide information on any matters within the remit of that committee as and when required. 3. Joint appointments and arrangements Sections 6.3 and 7.8 of the CCGs Constitutions and Section 14Z3 of the 2006 Act (as inserted by 2012 Act) allows a CCG to make joint appointments and arrangements with one or more of CCGs. NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG have made the following joint appointments: NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Chief Finance Officer, Deputy Finance Officer and Directorate of Finance; NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Director of Quality, Governance, Information and Performance and Directorate of Quality, Governance, Information and Performance; NHS Mansfield and Ashfield CCG Executive Lead for Contracting and Directorate of Contracting (Acute); and NHS Newark and Sherwood CCG Directorate of Contracting (Mental Health) NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG have made the following joint appointments: NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Chief Finance Officer and Directorate of Finance; NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Quality and Patient Safety and Directorate of Quality and Patient Safety; NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Outcomes and Information and Directorate of Outcomes and Information; NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Contracting and Directorate of Contracting (Acute); and NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Directorate of Contracting (Community Health Partnerships and nonacute contracts) NHS Mansfield and Ashfield CCG, NHS Newark and Sherwood CCG, NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG have made the following joint appointments: 57
58 NHS Mansfield and Ashfield CCG, NHS Newark and Sherwood CCG, NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Finance Healthcare Resources Team a. NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Chief Finance Officer and Deputy Finance Officer The NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Chief Finance Officer and Deputy Finance Officer are employed by NHS Mansfield and Ashfield CCG and shall work on behalf of NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG. The policies and procedures of NHS Mansfield and Ashfield CCG will apply in all matters concerning the employment of these individuals. Arrangements for the following shall be agreed between Mansfield and Ashfield CCG and the NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Chief Finance Officer and the Deputy Finance Officer: Approval of annual and special leave; Performance appraisal; and Disciplinary matters NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG shall bear the costs of any liability issues or redundancy/dismissal costs equally arising in connection with the employment of the NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Chief Finance Officer and the Deputy Finance Officer. b. NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG Director of Quality and Directorate of Quality, Governance, Information and Performance The Director of Quality and Governance and their team are employed by NHS Newark and Sherwood CCG and shall work on behalf of NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG. The policies and procedures of NHS Newark and Sherwood CCG will apply in all matters concerning the employment of the individual and their team. Arrangements for the following shall be agreed between NHS Newark and Sherwood CCG and the Director of Quality and Governance/employee in the team: Approval of annual and special leave; Performance appraisal; and Disciplinary matters NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG shall bear the costs of any liability issues or redundancy/dismissal costs equally arising in connection with the employment of the Director of Quality and Governance /any employee in their team. c. NHS Mansfield and Ashfield CCG Executive Lead for Contracting and Directorate of Contracting (Acute) The NHS Mansfield and Ashfield CCG Executive Lead for Contracting and their team 58
59 are employed by NHS Mansfield and Ashfield CCG. The Executive Lead for Contracting and their team shall also act on behalf of NHS Mansfield and Ashfield CCG, NHS Newark and Sherwood CCG, NHS Nottingham North and East CCG, NHSNottingham West CCG and NHS Rushcliffe CCG in respect of the contract management of Sherwood Forest Hospitals NHS Foundation Trust. The policies and procedures of NHS Mansfield and Ashfield CCG will apply in all matters concerning the employment of the individual and their team. Arrangements for the following shall be agreed between NHS Mansfield and Ashfield CCG and the Executive Lead for Contracting /the relevant employee in the team: Approval of annual and special leave; Performance appraisal; and Disciplinary matters NHS Mansfield and Ashfield CCG shall bear the costs of any liability issues or redundancy/dismissal costs equally arising in connection with the employment of the Executive Lead for Contracting /any employee in their team. a. NHS Newark and Sherwood CCG Directorate of Contracting (Mental Health) The NHS Newark and Sherwood CCG Directorate of Contracting (Mental Health) are employed by NHS Newark and Sherwood CCG. The NHS Mansfield and Ashfield Executive Lead for Contracting has responsibility for managing this team. The Directorate of Contracting (Mental Health)shall also act on behalf of NHS Mansfield and Ashfield CCG, NHS Newark and Sherwood CCG, NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG in respect of the contract management of Nottinghamshire Healthcare NHS Trust. The policies and procedures of NHS Newark and Sherwood CCG will apply in all matters concerning the employment of the team. Arrangements for the following shall be agreed between NHS Newark and Sherwood CCG and the relevant employee in the team: Approval of annual and special leave; Performance appraisal; and Disciplinary matters NHS Newark and Sherwood CCG shall bear the costs of any liability issues or redundancy/dismissal costs equally arising in connection with the employment of any employee in the team. b. NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Chief Finance officer and Directorate of Finance 59
60 The NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Chief Finance Officer and their team are employed by NHS Nottingham North and East CCG and shall work on behalf of NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG. The policies and procedures of NHS Nottingham North and East CCG will apply in all matters concerning the employment of the individual and their team. Arrangements for the following shall be agreed between NHS Nottingham North and East CCG and the NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Chief Finance Officer /the relevant employee in the team: Approval of annual and special leave; Performance appraisal; and Disciplinary matters NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG shall bear the costs of any liability issues or redundancy/dismissal costs equally arising in connection with the employment of the NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Chief Finance Officer /any employee in their team. c. NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Quality and Patient Safety and Directorate of Quality and Patient Safety The NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Quality and Patient Safety and their team are employed by NHS Nottingham North and East CCG and shall work on behalf of NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG. The Director of Quality and Patient Safety will perform the role of Caldicott Guardian. The policies and procedures of NHS Nottingham North and East CCG will apply in all matters concerning the employment of the individual and their team. Arrangements for the following shall be agreed between NHS Nottingham North and East CCG and the NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Quality and Patient Safety /the relevant employee in the team: Approval of annual and special leave; Performance appraisal; and Disciplinary matters NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG shall bear the costs of any liability issues or redundancy/dismissal costs equally arising in connection with the employment of the NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Quality and Patient Safety /any employee in their team. d. NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Outcomes and Information and Directorate of Outcomes and Information 60
61 The NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Outcomes and Information and their team are employed by NHS Rushcliffe CCG and shall work on behalf of NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG. The policies and procedures of NHS Rushcliffe CCG will apply in all matters concerning the employment of the individual and their team. Arrangements for the following shall be agreed between NHS Rushcliffe CCG and the NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Outcomes and Information /the relevant employee in the team: Approval of annual and special leave; Performance appraisal; and Disciplinary matters NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG shall bear the costs of any liability issues or redundancy/dismissal costs equally arising in connection with the employment of the NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Outcomes and Information /any employee in their team. e. NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Directorate of Contracting (Acute) The NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Contracting and their team are employed by Nottingham West CCG and shall work on behalf of NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG. The Directorate of Contracting shall also act on behalf of NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG in respect of the contract management of Nottingham University Hospitals NHS Trust. The policies and procedures of NHS Nottingham West CCG will apply in all matters concerning the employment of the individual and their team. Arrangements for the following shall be agreed between NHS Nottingham West CCG and the NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Contracting /the relevant employee in the team: Approval of annual and special leave; Performance appraisal; and Disciplinary matters NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG shall bear the costs of any liability issues or redundancy/dismissal costs equally arising in connection with the employment of the NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Contracting /any employee in their team. f. NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Directorate of Contracting (Community Health Partnerships and non-acute contracts) The NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS 61
62 Rushcliffe CCG Directorate of Contracting (Community Health Partnerships and nonacute contracts) are employed by Nottingham North and East CCG and shall work on behalf of NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG. The NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG shall have responsibility for managing this directorate. The Directorate of Contracting (Community Health Partnerships and nonacute contracts) shall also act on behalf of NHS Mansfield and Ashfield CCG and NHS Newark and Sherwood CCG in respect of the contract management of Community Health Partnerships and all non-acute contracts within Nottinghamshire. The policies and procedures of NHS Nottingham North and East CCG will apply in all matters concerning the employment of the team. Arrangements for the following shall be agreed between NHS Nottingham North and East CCG and the relevant employee in the team: Approval of annual and special leave; Performance appraisal; and Disciplinary matters NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG shall bear the costs of any liability issues or redundancy/dismissal costs equally arising in connection with the employment of the NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Contracting Team (Community Health Partnerships and non-acute contracts) g. The NHS Mansfield and Ashfield CCG, NHS Newark and Sherwood CCG, NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Finance Healthcare Resources Team The NHS Mansfield and Ashfield CCG, NHS Newark and Sherwood CCG, NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Finance Healthcare Resources Team are employed by NHS Mansfield and Ashfield CCG and shall work on behalf of NHS Mansfield and Ashfield CCG, NHS Newark and Sherwood CCG, NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG. The policies and procedures of NHS Mansfield and Ashfield will apply in all matters concerning the employment of the team. Arrangements for the following shall be agreed between NHS Mansfield and Ashfield CCG and the relevant employee in the team: Approval of annual and special leave; Performance appraisal; and Disciplinary matters NHS Mansfield and Ashfield CCG, NHS Newark and Sherwood CCG, NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG shall bear the costs of any liability issues or redundancy/dismissal costs equally arising in connection with the employment of the NHS Mansfield and Ashfield CCG, NHS Newark and Sherwood CCG, NHS Nottingham North and East CCG, NHS 62
63 Nottingham West CCG and NHS Rushcliffe CCG Finance Healthcare Resources Team. h. Funding of joint appointments The CCGs shall bear the remuneration and associated employee costs arising in connection with each of the joint posts referred to above, which include but are not limited to income tax and national insurance. For each of the above joint appointments (excluding the Directorates of Contracting) the funding shall be allocated on the basis of crude population for each CCG obtained from the Department of Health Exposition Book annually. Funding for the Directorates of Contracting shall be apportioned on the following basis: The funding for the NHS Mansfield and Ashfield CCG Directorate of Contracting is based activity for Sherwood Forest Hospitals NHS Foundation Trust. The funding for the NHS Newark and Sherwood CCG Directorate of Contracting is based on Nottinghamshire Healthcare NHS Trust contract values. The funding for The NHS Nottingham North and East CCG, NHS Nottingham West CCG and NHS Rushcliffe CCG Director of Contracting and Directorate of Contracting is based on the estimated contract activity for Community Health Partnerships and all non-acute contracts within Nottinghamshire for the relevant financial year. The estimate is calculated using the actual contract activity from the previous financial year and a financial evaluation of any known events or factors which are anticipated to have an impact on the annual contract activity. 4. Disputes between CCGs In the event of a dispute arising from or in connection with the interpretation or application of the functions referred to in this MOU between any two or more CCGs the following process will be adopted. a. Step 1 The issue in dispute shall be formally identified and raised with the appropriate senior manager within each CCG. The senior managers shall use all reasonable endeavors to resolve the dispute within 5 working days. b. Step 2 If the senior managers are unable to resolve the dispute within the timescales set out above they shall notify their respective Chief Officers. The Chief Officers shall use all reasonable endeavors to resolve the dispute within a further 5 working days. The Chief Officers shall notify the senior managers of their decision in writing. 63
64 c. Step 3 If the Chief Officers are unable to resolve the dispute within the timescales set out above they shall refer the matter to an independent arbitrator who shall be appointed by the Director of the Nottinghamshire and Derbyshire Local Area Team of the NHS Commissioning Team to determine the matter within 10 working days. The decision of the independent arbitrator is final. The parties shall ask the independent arbitrator to provide them with written notice of his/her decision including details of the rationale and any next steps which the parties are required to take. The parties will provide a joint report to their respective governing bodies on their progress in implementing the next steps referred to above at its next meeting. This report will summarise the parties progress and identify any relevant learning points. 5. Review This MOU may be reviewed annually as a minimum but may be reviewed and amended at any time on request. Any amendments must be agreed in writing by all of the CCGs. Where amendments to this MOU also require amendments to be made to one or more of the CCG s Constitutions such amendments shall only be effective once all of the relevant CCGs have received approval from NHS England in respect of the proposed amendment to their Constitutions. 6. Termination or withdrawal Termination of this Agreement shall not affect any rights or liabilities of the CCGs that have accrued prior to the date of termination. a. Mutual termination Subject to the general principles set out in section 7 of this MOU the CCGs may unanimously agree, in writing, to terminate this MOU in whole or in part at any time. b. Withdrawal from part Subject to the general principles set out in section 7 of this MOU a CCG may withdraw from one or more parts of the collaborative arrangements set out in this MOU: By giving the other CCGs not less than 3 month s written notice at any time; By giving the other CCGs not less than 3 month s written notice if any of the other CCGs are in persistent or repetitive breach or other material breach of any obligations under this MOU and the matter is not remedied following completion of the dispute resolution process set out above. c. Withdrawal from all Subject to the general principles set out in section 7 of this MOU a CCG may withdraw from all of the collaborative arrangements set out in this MOU: 64
65 By giving the other CCGs not less than 3 month s written notice at any time; By giving the other CCGs not less than 3 month s written notice if any of the other CCGs is in persistent or repetitive breach or other material breach of any obligations under this MOU and the matter is not remedied following completion of the dispute resolution process set out above. d. General principles relating to termination or withdrawal The following general principles shall apply in the event of termination or withdrawal (in whole or in part): Termination or withdrawal from the collaborative arrangements set out in this MOU by any one or more of the CCGs shall not affect the validity or enforceability of any of the other CCG s rights and responsibilities as set out in this MOU. Withdrawal from part of this MOU shall not affect the validity or enforceability of the withdrawing CCG s rights and responsibilities as set out in the remainder of the MOU to which they are a party. The CCGs will seek to agree the apportionment of any costs (whether directly or indirectly incurred) in connection with the withdrawal of one or more of the CCGs from all or part of these collaborative arrangements on a fair and equitable basis. 7. Overriding principles The CCGs agree to apply and interpret the terms of this MOU in accordance with the following general principles. The CCGs shall act: in the spirit of good faith; in the interests of minimising costs to themselves and to the other CCGs; in the interests of maintaining quality at all times; and in accordance with the terms of their Constitutions and any applicable statute, directions, orders, guidance or policy. Signed for and on behalf of NHS Bassetlaw CCG Signature: Name: Phil Mettam Position:Chief Officer Date:20 August
66 Signed for and on behalf of NHS Mansfield and Ashfield CCG Signature: Name: Deborah Jaines Position: Chief Operating Officer Date: 20 August 2012 Signed for and on behalf of NHS Newark and Sherwood CCG Signature: Name: Amanda Sullivan Position: Chief Officer Date: 20 August 2012 Signed for and on behalf of Nottingham North and East CCG Signature: Name: Sam Walters Position: Chief Officer Date:20 August


 NHS Newark and Sherwood Clinical")
 NHS Nottingham North and East")
 NHS Rushcliffe Clinical")
67 APPENDIX 5 - MEMORANDUM OF UNDERSTANDING IN RELATION TO COLLABORATIVE COMMISSIONING Memorandum of Understanding in relation to Collaborative Commissioning Arrangements within the Nottingham and Nottinghamshire Health Economy DATED 2012 (1) NHS Mansfield and Ashfield Clinical Commissioning Group (2) NHS Newark and Sherwood Clinical Commissioning Group (3) NHS Nottingham City Clinical Commissioning Group (4) NHS Nottingham North and East Clinical Commissioning Group (5) NHS Nottingham West Clinical Commissioning Group (6) NHS Rushcliffe Clinical Commissioning Group 67
68 TABLE OF CONTENTS Introduction Objectives for the Memorandum of Understanding Key Principles for Collaborative Commissioning The Collaborative Commissioning Process Overview of the Collaborative Commissioning Process Strategic Decision Making Joint Congress Contract Procurement and Management Process Reporting and Assurance Management of the MOU Procedures for review and variation of agreement terms Procedures for dealing with dispute resolution Procedures for full or partial termination of the MOU Signature page Appendix A Appendix B Appendix C1-C5 i ii iii- vii 68
69 INTRODUCTION 1. The Health and Social Care Act 2012 ( the Act ), and the consequent restructuring of responsibilities for commissioning health services to Clinical Commissioning Groups (CCGs) places a duty on commissioners to commission services effectively and efficiently, whilst remaining clinically led and keeping patients at the centre of the decision making process. 2. It is recognised by the six CCGs party to this Memorandum of Understanding ( the Parties ) in the Nottingham and Nottinghamshire health economy ( Nottinghamshire ) that best use of resources could be achieved by collaboratively commissioning a range of health services, especially where providers have a catchment wider than the boundaries of any one CCG. 3. The CCGs also recognise that, through effective collaboration for relevant commissioning activity, they may increase the robustness and quality of the overall commissioning process for each organisation by: 3.1. Effectively co-ordinating commissioning intentions and strategies to manage and share the budgeting and financial risks across the health economy as a whole; 3.2. Managing available commissioning resources across the area to ensure that best practice is shared, scarce resources are utilised effectively, good leadership is leveraged and information is made available to all CCGs in a timely and transparent manner; 3.3. Developing a whole system commissioning strategy to benefit patients whose clinical pathway entails a variety of providers across the Nottinghamshire health economy; 3.4. Developing a system-wide approach to the delivery of QIPP initiatives; 3.5. Allowing a more robust and wider geographical strategy for commissioning that may more effectively adapt to major service reconfigurations; and 3.6. Aligning CCG activity with the activities of their Local Authorities and NHS England Authority (NHS CBA). 4. The Act encourages collaboration between CCG organisations, and between CCGs and Local Authorities and the NHS CBA, and, where appropriate, supports them to develop and formalise approaches to collaborative commissioning. The CCGs have responded to this through their development and approval of this Memorandum of Understanding (MOU). 69
70 OBJECTIVES OF THE MEMORANDUM OF UNDERSTANDING 5. The primary objective of this (MOU) is to describe the framework for collaborative commissioning activity among the six CCGs within the Nottinghamshire health economy, namely: 5.1. NHS Mansfield and Ashfield Clinical Commissioning Group; 5.2. NHS Newark and Sherwood Clinical Commissioning Group; 5.3. NHS Nottingham City Clinical Commissioning Group; 5.4. NHS Nottingham North and East Clinical Commissioning Group; 5.5. NHS Nottingham West Clinical Commissioning Group; and 5.6. NHS Rushcliffe Clinical Commissioning Group. 6. This framework will be applied to the collaborative commissioning of five key contracts that exist for the provision of clinical services in Nottinghamshire. It is also intended to provide a basis that may be extended to further commissioning activities or CCG partners where appropriate in the future as agreed between the parties. The five key contracts referred to are as follows: 6.1. Nottingham University Hospital Trust; 6.2. Sherwood Forest Hospitals NHS Foundation Trust; 6.3. Nottinghamshire Healthcare NHS Trust; 6.4. County Health Partnership; and 6.5. Nottingham CityCare Partnerships CIC 7. The MOU will describe the process for the CCGs to present and align their commissioning strategies and it also describes the forums through which information on commissioning best practice can be shared and resources quality assured and co-ordinated. 8. The MOU will establish and formalise the key lines of accountability, reporting and assurance between the CCGs. 9. The MOU will describe the process through which the CCGs can obtain clarity and common purpose in their commissioning activities to best serve their communities. KEY PRINCIPLES FOR COLLABORATIVE COMMISSIONING 10. In establishing the terms of this MOU the CCGs have identified key principles that shall inform the collaborative commissioning arrangements. These are: Cooperation: The MOU is developed through and supported by co-operation between the CCGs, and also within their interactions with key stakeholders (patients, service providers, Local Authorities, NHS CBA and others) Strong clinical leadership and engagement: Clinical involvement will be embedded at all stages in the collaborative commissioning process Effective sharing and communication of information: The collaborative arrangements shall enable the effective sharing of information and assurance between CCGs to improve both clinical and contractual outcomes. The sharing and discussion of commissioning intentions and strategy between the CCGs will build clarity and common purpose within the health economy. 70
71 10.4. Efficient use of money and resources: The collaborative arrangements shall enable the efficient allocation and use of resources for commissioning activity and more widely across the health economy, in accordance with shared QIPP plans. It will ensure that there is an ongoing review of value for money, not only from service contracts but from commissioning resources provided by participating CCGs Innovation and robustness: The collaborative arrangements will enable the development of innovation in the commissioning process learning from best practice, and encourage proactive responsiveness to service redesign within the commissioning process and support the development of Quality Improvement Productivity and Prevention (QIPP) initiatives Combined perspective and local focus: The collaborative arrangements will enable the CCGs to benefit from economies of scale in interactions with service providers, however each CCG will ensure their local health needs inform collaborative commissioning decisions Accountability: Each participating CCG remains accountable to the population that they serve for services commissioned on their behalf. CCGs may delegate responsibility for procurement of contract monitoring activities but they retain overall commissioning accountability for their population. THE COLLABORATIVE COMMISSIONING PROCESS Overview of the Collaborative Commissioning Process 11. Based on the identified purposes and principles for collaborative commissioning the CCGs have sought to develop a clear process which will enable them to share their local commissioning strategies, identify commonalities in order to address strategic issues across the health community, delegate contracting responsibilities to a coordinating representative, whilst retaining oversight and accountability for service planning, quality and outcomes. It will allow for ongoing review of the initial analysis completed by CCGs that drove make share and buy decisions and ensure that the focus of commissioning at scale whilst retaining local ownership and local knowledge continue to provide quality and overall value for money. 12. To achieve this the MOU will expand upon the mechanisms for the three primary collaborative commissioning activities: The development of a collaborative commissioning strategy - the Joint Congress; The delegation of procurement and contract management to a co-ordinating organisation and team - the Contract Teams; and The ongoing requirements of reporting, assurance and accountability upon all the contracting CCGs - Reporting and Assurance. 13. Further details for each of these areas are set out in the sections below. The diagram at Appendix A provides an overview of this proposed collaborative commissioning structure. Strategic Decision Making Joint Congress 14. The purpose of the Joint Congress is to provide a platform for establishing and confirming the collaborative commissioning strategy of the CCGs, and to facilitate the ongoing review of the collaborative commissioning framework set out in this MOU. To achieve this, a number of required inputs, resources and outputs of the congress are defined here: 71
72 Inputs to the Joint Congress 15. Prior to the Joint Congress each CCG will have reviewed and/or updated their commissioning intentions, strategy and QIPP programmes. Each CCG shall take appropriate measures to ensure their commissioning intentions are informed by the perspectives of their own key stakeholders, including but not limited to patients, clinicians, Local Authority partners and the Health and Wellbeing Board. 16. Each CCG should be prepared to input their commissioning intentions into the Joint congress discussion so that commonalities can be identified and developed. Other key stakeholders in the Nottinghamshire health economy may also be asked to attend and share their perspectives to inform this process. These invitations will be agreed between the CCGs prior to the Congress. 17. It should be noted that the Joint Congress will not be the only forum for discussion of collaborative activity, for example, Chief Officers will meet more frequently to discuss operational issues. The Joint Congress is intended to be the formal platform for establishing a collaborative commissioning strategy for the CCGs and for the production of commissioning intentions. 18. There will be ongoing dialogue with providers as required. Procedures of Joint Congress Congress Chair 19. The Chairperson for the Joint Congress will rotate among the clinical leads of the CCGs. 20. The chair will be responsible for confirming the date of the forthcoming Congress and for ensuring that the appropriate individuals are invited to attend the Congress. 21. The Chair will also ensure that all parties contribute and inform the discussion regarding collaborative commissioning process and strategy. The Chair will also ensure that the outputs of the Joint Congress as agreed in this MOU are delivered. 22. The Chair will agree the agenda with the other CCG Chief Officers and Clinical Leads prior to the Congress. Attendance The following shall attend the Joint Congress as full members: 23. The Chief Officer of each the CCGs (or assigned deputy where they are unable to attend). 24. Finance, quality and contract leads for each of the five key contract teams. Other CCG leads in these areas may also be invited. 25. Clinical leads of each of the CCGs (or assigned deputy where they are unable to attend). Invited members The following may be invited members 26. Appropriate representatives from key partner organisations, for example NHS Erewash CCG, NHS Bassetlaw CCG, Nottingham City Local Authority and Nottinghamshire County Local Authority (Public Health, Director of Adult Services, Director of Children s Services); NHS England Local Area Team; commissioning support services; and major service providers. 27. All CCGs can nominate invited members from the above but invitations will be at the discretion of the Chair 28. Full members of the Congress will make decisions having taken into account the views and representations of any invited members. 72
73 Administration 29. NHS Rushcliffe will lead the administration for facilitating the Congress. All CCGs will provide resources as required and these will be agreed in advance. Timing 30. The Congress will take place bi-annually in January and July. The January Congress will be a half-day in length. The July Congress will be one day in length. Any CCG, in supporting the process for its commissioning plans, may request a meeting of the Congress. Output of Joint Congress Minutes and report of the Congress 31. The Chairperson shall ensure that minutes of the Congress are produced and made available to appropriate parties in a timely manner. The Chairperson shall ensure that appropriate resources are available for this task. In addition this document will confirm the following: The intentions and service strategy for collaborative commissioning for the coming period. The Chairperson shall ensure that the agreed scope (range of contracted services) of collaborative commissioning for the forthcoming year is confirmed by all CCGs and this is approved and evidenced; Clear guidance to Co-ordinating Chief Officers where commissioning intentions have been varied from previous periods (feeding into Process below). The relevant coordinating CCGs must ensure that they are satisfied that clear contracting intent has been agreed by each CCG, including expectations around the delivery of QIPP in each contract; Notes on any discussion regarding future service developments beyond the current year, for example anticipated changes in service configuration or changes in the requirements of local communities, and the assignment of any agreed additional actions; and The production of a document which can be used with providers to share the overall strategic commissioning intentions of the CCGs in relation to the local health system Contract Procurement and Management Process 32. Once the scope and intentions for collaborative commissioning have been confirmed by CCGs at the Joint Congress, responsibility for procurement and monitoring of the contracts with service providers will devolve to the relevant Contract Team, led by the appointed Co-ordinating Chief Officer. 33. The following processes will be implemented for each contract to be procured collaboratively: Roles and Responsibilities 34. In order to provide assurance to the CCGs regarding due process at a minimum each Contract Team must have an identified individual, able to fulfil the following roles: Coordinating Chief Officer 35. The Coordinating Chief Officer is responsible for: 73
74 35.1. Ensuring the contract negotiation and sign-off is in line with the intentions of the collaborating CCGs, as specified at the Joint Congress 57 One individual can be nominated to fulfil more than one role e.g. contract lead and information lead may be the same person: 58 Deputies can be assigned to any of these roles where the leads are unable to fulfil them for a period of time. Deputising arrangements must be communicated to Chief Officers in all CCGs Ensuring all appropriate policies and procedures are in place (and communicated with the contract team and provider) to effectively manage the contract; Ensuring availability of and overseeing the resources required to deliver and manage the contract and communicating the named individual for each role to the provider. Where these resources are provided by a CCG(s) other than the Coordinating Chief Officers own, the Co-ordinating Chief Officer must ensure that appropriate lines of communication are maintained to line management within the supporting CCG(s) in order to ensure the team members have time and resources to support the contract delivery; Ensure that processes are established to quality assure the commissioning support arrangements into the contract using a process analogous to the commissioning support services business review process Where a performance issue is identified new or ongoing, the co-ordinating Chief Officer will be responsible for identifying a lead (through negotiation with the other CCGs). It is likely that where the issue is being driven by one CCG (e.g. through demands of their population or referral activity by partner practices) they will resource the role. Any actions required to resolve the performance issue (as it relates to the provider) will be agreed with the co-ordinating Chief Officer; and Agreeing any projects that will be developed directly between the provider and one of the collaborating CCGs on a standalone basis Ensuring that there is effective communication with each CCG party to this agreement, and with those fulfilling named roles (contract lead, quality lead, information lead and performance) such that they are made aware of all material issues relating to the performance and management of the contract (issue of remedial breach notices etc). Contract Manager 36. The Contract Manager will act as the day to day point of contact with the Service Provider to ensure the delivery of contracted services; Using professional knowledge, understanding and judgement to escalate issues as appropriate to the Chief Officer; Managing communication to and from the provider including any changes to the contracting terms and conditions (variations) requested by the service provider back to the collaborating Chief Officers and subsequently obtaining follow-up agreements of the provider s amendments from them; The co-ordination of all administrative activities relevant to the procurement and ongoing management of the contract, including the facilitation of key meetings relevant to the contracting process. The confirming and communication of key dates. The maintenance and updating of key contract documentation including the Contract Terms and Conditions, minutes of meetings and other information as required They will support the Co-ordinating Chief Officer in the contract negotiation process; 74
75 and The management of other contributing team members to ensure appropriate resource are available to deliver and manage the contract. Clinical Lead 37. The Clinical Lead is responsible for providing clinical oversight and insight into the contract negotiations and ongoing contract performance. Where appropriate this will includeinforming the contract reporting process and supporting the assurance provided to the CCGs; Representing the views of the constituent GP membership within their own CCG, and liaising with the Clinical Leads of the CCGs to ensure views of their constituent CCGs are accounted for in the commissioning process; and Providing a link, through the transfer of information and communication between primary healthcare providers, and the Co-ordination Chief Officer and Contract Team. Finance Lead 38. The Finance Lead is responsible for the gathering, assessment and analysis of financial information relating to the commissioning process and ongoing contract; Using professional knowledge, understanding and judgement to escalate issues as appropriate to the co-ordinating Chief Officer; The appropriate monitoring and accounting for financial management of the contract on behalf of the CCGs; The timely and clear communication of financial information and concerns to the Co-ordinating Chief Officer, and via the Co-ordinating Chief Officer to other impacted CCGs where appropriate. This includes participation in the contract reporting process; The management of other contributing team members to ensure appropriate resource is available to deliver and manage the service contract; and Co-ordinating the payment of the contract on behalf of the collaborating CCGs Quality Lead 39. The Quality Lead is responsible for the gathering, assessment and analysis of quality information relating to the commissioning process; Using professional knowledge, understanding and judgement to escalate issues as appropriate to the co-ordinating Chief Officer; The development of CQIN indicators and monitoring of their in year performance; The escalation of quality concerns within the contract management processes; Co-ordinating the activity of infection control and safeguarding with respect to delivering the contract and acting as the first point of contact for the provider; The appropriate monitoring and accounting for the quality management of the contract on behalf of the collaborating CCGs; The timely and clear communication of information and concerns regarding quality to the Co-ordinating Chief Officer, and via the Co-ordinating Chief Officer to other 75
76 impacted CCGs where appropriate. This includes participation in the contract reporting process; and The management of other contributing team members to ensure appropriate resource is available to deliver and manage the service contract with respect to quality. Information Lead 40. Information Lead is responsible for the maintenance and ongoing monitoring of the reporting process relating to the contract; Using professional knowledge, understanding and judgement to escalate issues as appropriate to the co-ordinating Chief Officer; They are responsible for the co-ordination and delivery of the contract reporting on behalf of the co-ordinating Chief Officer. This includes ensuring that the timeliness, frequency and quality of reporting is maintained; The Information Lead will act as the key point of contact for requests for information regarding the contract from interested parties, including collaborating CCGs and service providers where the point of contact is otherwise not clear, and also other stakeholders such as NHS CBA, the Local Authorities and others; and The management of other contributing team members to ensure appropriate resource is available to deliver and manage the service contract. Performance Lead 41. Monitoring of contract performance against the agreed standards / targets laid out in the contract; Liaison and contact with equivalent Subject Matter Experts (SMEs) in the provider organisations to gain understanding of underlying issues Generating draft Contract Query / Performance Notices / other communications for sign-off by the co-ordinating Chief Officer Discuss and, where necessary challenge, providers on proposed Remedial Action Plans Recommend the agreement (or otherwise) of Remedial Actions Plans on behalf of the Commissioners for sign-off by the co-ordinating Chief Officer Provide Statements of Assurance to the Information Lead to include in reports to individual CCGs as part of their internal performance reporting / management processes Ensure that the progress of individual actions and milestones in Remedial Actions Plans is monitored along with the impact on the required improvement of the performance standard Produce Contract Query / Performance Notice Closure Reports for consideration by the Contract Executive Board. 42. The key roles for the five main contracts have been allocated among the participating CCGs. This allocation is set out in the table at Appendix B. These arrangements will be reviewed annually as part of the review and variations procedure as set out below. 76
77 43. Beyond these defined contract roles the structure of the contract delivery and monitoring team may vary from contract to contract depending on the scope and nature of activities, the nature of the service provider and other factors. The Coordinating Chief Officer remains responsible for ensuring the structure in place is sufficient to deliver and monitor the contract appropriately and for ensuring that the contract structure is communicated annually and on review to all CCG Chief Officers party to this agreement. The currentstructures for each contract covered by this agreement are set out in Appendix C along with the names of each lead role. Accountability for delivery of collaborative contracting 44. Each CCG remains accountable to their local populations for the affordability and quality of services, through the setting of the parameters of the contract envelope and commissioning framework. They will delegate responsibility for contract negotiation, delivery and management to the Co-ordinating Chief Officer who will operate only within the confines of the parameters set. The Co-ordinating Chief Officer will then engage themselves and the Contract Team in such activities (meetings, monitoring, information gathering and so forth) as they deem necessary to deliver the commissioning intentions of the CCGs. 45. Through the ongoing processes of communication with service providers, the service provider intentions should be also be understood, and discussed and reflected by all CCGs in the development of collaborative commissioning strategy. Where, during the procurement of contracts, the Co-ordinating Chief Officer becomes aware the contract scope or terms are likely to vary materially from the expressed intentions of the collaborating CCGs (or in the absence of these intentions, from the previous contracted terms) they shall communicate this to the CCGs and seek agreement to continue before contracting on their behalf. Reporting and Assurance Reporting 46. As specified in the Contract Team roles and responsibilities, the Finance, Quality, Performance and Information Leads are responsible for generating required contract reporting on behalf of the Co-ordinating Chief Officer. The Co-ordinating Chief Officer remains responsible for the timely distribution of reports to the CCGs and other relevant stakeholders. The Co-ordinating Chief Officer must also ensure appropriate measures are in place to ensure the quality and clarity of reported information. 47. For each contract a contract update report will be produced and distributed on a monthly basis. 48. The reports for each contract will cover the following sections and information: Contract performance including year to date activity levels (absolute and in comparison to prior year and plan, broken down by CCG and category of contracted service); Summary of areas of over/underperformance during the month, including thresholds for defining this. Summary of follow-up to areas of over/underperformance in the previous month; Summary update on progress of QIPP schemes; Summary of other activities, for example CQC reviews, ongoing service reconfigurations and so forth; and For each of the forthcoming areas the report will specify any identified issues; explain the impact for the overall health economy; explain the impact for specific 77
78 CCGs; put forward follow-up and mitigating actions, and responsible parties. 49. The overall aim of the reporting process will be timeliness and clarity. To achieve this each contract will use the same reporting structure in order to aid understanding for all users. Ongoing assurance obligations of Coordinating Chief Officer to the partner CCGs 50. As has been set out, the Co-ordinating Chief Officer takes responsibility for monitoring contract performance. They may delegate aspects of this to appropriate members of the Contract Team; however the Co-ordinating Chief Officer retains responsibility for the effective monitoring and communicating of concerns related to the contract to relevant partner CCGs and to those fulfilling named roles (quality lead etc). This remains the case even where an aspect of the contract management (e.g. finance, quality and so forth) is resourced by another partner CCG. 51. The Co-ordinating Chief Officer must ensure the timely escalation of contract issues and the timely production of routine reporting in line with the process specified for the contract. Where an issue arises requiring an urgency of action beyond that afforded through the reporting processes, the Co-ordinating Chief Officer is responsible for communicating the issue to partner CCGs in the most appropriate and timely manner in addition to the formal reporting. 52. Where key dates and milestones in a contract procurement and management processes have been agreed by all CCGs the Co-ordinating Chief Officer shall communicate any potential failure to meet such milestones as soon as it becomes apparent that this may occur. Reporting of failures/potential failures be made in writing and sent to the Chief Officers and clinical leads in each member CCG. They shall also be minuted at official contract meetings and form part of the standard report to CCG Governing Bodies. 53. Where the Co-ordinating Chief Officer relies on members of the Contracting Team who sit outside their own CCG, they must also communicate any concerns (for example, regarding performance or quality of work, or over or under-resourcing) to the line management within the supporting CCG. Supporting CCGs will retain line management responsibilities, including personal development and training, for their own staff Ongoing assurance obligations of the partner CCGs to the Co-ordinating Chief Officer 54. As has been stated, although the partner CCG may delegate responsibility to the Coordinating Chief Officer to act as an agent on their behalf for a collaboratively commissioned contract, each CCG remains accountable to their populations for the quality and performance of commissioned services. 55. As such the Accountable Office remains responsible for identifying (through reporting), understanding and ensuring appropriate follow-up and mitigating activity occurs for all contract issues impacting their population and must assist the Coordinating Chief Officer to resolve any issues identified. 56. Additionally, where partner CCGs are contributing resources to a mixed contract team led by another Chief Officer, the partner CCG must ensure that they can adequately provided the agreed support, and provide appropriate time, staff resources and management support to assist the co-ordinating Chief Officer in their efforts. Ongoing assurance role of the Commissioning Assurance Panel 57. On a quarterly basis the Commissioning Assurance Panel will convene to discuss all contracts in the scope of this MOU. The panel will include all Chief Officers from the CCGs and all Contract Managers. 78
79 58. The purpose of the Panel will be: To monitor the ongoing reporting of all collaborative commissioning activity and identify and areas of concern in the commissioning process or contract performance for each contract that are not being effectively tackled and to indentify issues that may be similarly affecting a range of contracts; and To highlight any areas where due reporting and assurance activities for each contract are not being performed appropriately Agree a programme of review for shared commissioning support arrangements To review the quality and value for money of shared commissioning support arrangements (in line with the scheduled review programme) and confirm the continuation of such arrangements or agree any further benchmarked review required or market testing. 59. The Panel will be facilitated and chaired by the incumbent Chair of the Joint Congress and will communicate findings to each CCG Governing Body in a written report. MANAGEMENT OF THE MOU Procedures for the review and variation of the MOU Review 60. This MOU will be reviewed at the Joint Congress on an annual basis as a minimum. The process of review will be undertaken by all CCGs and attending Contract Team members to ensure that it is fit for purpose, incorporates best practice, and accurately represents the procedures undertaken within the collaborative commissioning framework. Variation 61. The process for variation of the terms of the MOU are as follows: 62. Variation may be made to the terms of this MOU, either as a result of the review process explained above, or at any other time with the agreement of all participating CCGs; 63. Where a variation is requested, any amendment or addition to the MOU must be agreed in writing by all of the CCGs. 64. Where amendments to this MOU also require amendments to be made to one or more of the collaboratively commissioned service contracts, such amendments shall only be effective once the relevant co-ordinating Chief Officer has received corresponding agreement from the relevant service provider; and 65. Should an amendment or agreement not be confirmed by all CCGs, the dispute resolution process set out below will be enacted. Procedures for dealing with dispute resolution 66. In the event of a dispute arising from or in connection with the interpretation or application of the functions referred to in this MOU between any two or more CCGs the following process will be adopted. 67. Step The issue in dispute shall be formally identified and raised with the appropriate Contract Manager. The Contract Manager shall use all reasonable endeavours to resolve the dispute within 5 working days. 79
80 68. Step If the relevant Contract Manager is unable to resolve the dispute within the timescales set out above, or is a party in the dispute, then both parties shall notify their respective Chief Officers The Chief Officers shall use all reasonable endeavours to resolve the dispute within a further 5 working days The Chief Officers shall notify the Contract Manager of their decision in writing; 69. Step If the Chief Officers are unable to resolve the dispute within the timescales set out above, unless a further extension of timescale or process is agreed by both Chief Officers, they shall refer the matter to the Managing Director of the Local Area Team of the NHS CBA who shall determine the matter within 10 working days The decision of the Managing Director of the Local Area Team of the NHS CBA is final. The incumbent Chair of the Joint Congress will co-ordinate this process with the NHS CBA Director, and write to the parties notifying them of the decision, the rationale and setting out any next steps which the parties are required to take The parties will provide a joint report to their respective CCG Governing Bodies regarding their progress in implementing the next steps referred to above at its next meeting. This report will summarise the parties progress and identify any relevant learning s. Procedures for full or partial termination of the MOU 70. Termination of this Agreement shall not affect any rights or liabilities of the CCGs that have accrued prior to the date of termination. 71. Mutual termination of the agreement by all CCGs CCGs may unanimously agree, in writing, to terminate this MOU in whole or in part at any time. Such mutual termination may be initiated through the Joint Congress, or through other protocols as required. All CCGs will confirm this termination in writing, and the Chair of the Joint Congress will also inform the impacted service providers and the NHS CBA. 72. Withdrawal by a CCG from a part of this agreement. A CCG may withdraw from one or more parts of the collaborative arrangements set out in this MOU: By giving the other CCGs not less than 3 month s written notice and not less than 3 months prior to the annual contracting renewal /renegotiation date By giving the other CCGs not less than 1 month s written notice if any of the other CCGs are in persistent or repetitive breach or other material breach of any obligations under this MOU and the matter is not remedied following completion of the dispute resolution process set out above. 73. Withdrawal by a CCG from all part of this agreement. A CCG may withdraw from all of the collaborative arrangements set out in this MOU: By giving the other CCGs not less than 3 month s written notice and not less than 3 months prior to the annual contracting renewal /renegotiation date. 80
81 73.2. By giving the other CCGs not less than 1 month s written notice if any of the other CCGs are in persistent or repetitive breach or other material breach of any obligations under this MOU and the matter is not remedied following completion of the dispute resolution process set out above. 74. General principles relating to termination or withdrawal. The following general principles shall apply in the event of termination or withdrawal (in whole or in part): Termination or withdrawal from the collaborative arrangements set out in this MOU by any one or more of the CCGs shall not affect the validity or enforceability of any of the other CCG s rights and responsibilities as set out in this MOU The CCGs will seek to agree the apportionment of any costs (whether directly or indirectly incurred) in connection with the withdrawal of one or more of the CCGs from all or part of these collaborative arrangements on a joint and equitable basis. Approval of the Memorandum of Understanding The following parties accept and approve these documents NHS Mansfield and Ashfield Clinical Commissioning Group Signed Date 20 August 2012 NHS Newark and Sherwood Clinical Commissioning Group Signed Date 20 August 2012 NHS Nottingham City Clinical Commissioning Group Signed Date 20 August 2012 NHS Nottingham North and East Clinical Commissioning Group Signed Date 20 August
82 NHS Nottingham West Clinical Commissioning Group Signed Date 20 August 2012 NHS Rushcliffe Clinical Commissioning Group Signed Vicky Bailey Date 20 August
83 m i s s i o n i n g A s s u r a n c e P a n 83
84 APPENDIX 6- SCHEME OF DELEGATION There are 3 tables in this Appendix: Table 1 covers the matters reserved or delegated for decision to the Membership, Governing Body, Accountable/Chief Officer, Chief Finance Officer, Audit and Governance Sub Committee, Remuneration and Terms of Service Sub Committee, Activity and Finance Sub Committee and Quality and Risk Sub Committee and Primary Care Commissioning Committee Table 2 covers the matters reserved or delegated for decision to the Clinical Executive Sub Committee, Better Together Committee, Stakeholder Reference Group Sub Committee, Safeguarding Adult Committee and Safeguarding Children Committee. Table 3 covers the ratification and approvals by the relevant Body, Committee or Sub Committees within the CCG. Table 1: Policy area Decision Reserved to the Member- ship Reserved/ delegated to Governing Body Accountable Officer/Chief Officer Chief Finance Officer Audit &Governance Sub Committee Remuneration and Terms of Service Sub Committee Activity & Finance Sub Committee Quality &Risk Sub Committee Primary Care Commis- sioning Committee REGULATION AND CONTROL Determine the arrangements by which the members of the group approve those decisions that are reserved for the membership. REGULATION AND CONTROL Approving any functions of the group specified in regulations REGULATION AND CONTROL Consideration and approval of applications to NHS England on any matter concerning changes to the group s core constitution including terms of reference for the group s governing body and. the overarching scheme of reservation and delegated powers. REGULATION Consideration and approval of 84
85 Policy area Decision Reserved to the Member- ship Reserved/ delegated to Governing Body Accountable Officer/Chief Officer Chief Finance Officer Audit &Governance Sub Committee Remuneration and Terms of Service Sub Committee Activity & Finance Sub Committee Quality &Risk Sub Committee Primary Care Commis- sioning Committee AND CONTROL the constitution and making recommendations to the group membership thereon REGULATION AND CONTROL Consideration and approval of the Terms of Reference (to be contained in the Financial Management and Governance Manual) and membership for Committees/Sub Committees of the Governing Body set out in the constitution REGULATION AND CONTROL Consideration and approval of arrangements for taking urgent decisions REGULATION AND CONTROL Consideration and approval of prime financial policies REGULATION AND CONTROL Exercise or delegation of those functions of the clinical commissioning group which have not been retained as reserved by the group, delegated to the governing body or other committee or subcommittee or [specified] member or employee REGULATION AND CONTROL In emergency or urgency to exercise with the Clinical Chair 85
86 Policy area Decision Reserved to the Member- ship Reserved/ delegated to Governing Body Accountable Officer/Chief Officer Chief Finance Officer Audit &Governance Sub Committee Remuneration and Terms of Service Sub Committee Activity & Finance Sub Committee Quality &Risk Sub Committee Primary Care Commis- sioning Committee REGULATION AND CONTROL of the governing body, the powers of the governing body having consulted with at least two other governing body members and provided it is reported to the next meeting of the governing body. If the event of the Clinical Chair being conflicted, the Accountable Officer will consult with the Vice Chair of the governing body and one other non- conflicted governing body GP member. If all members of the governing body GP members are conflicted, the Accountable Officer will consult with the Vice Chair and one other voting member Prepare the group s overarching scheme of reservation and delegation, which sets out those decisions of the group reserved to the membership and those delegated to the o group s governing body o committees and subcommittees of the group, or o its members or employees and sets out those decisions of in conjunc tion with GB member s as stated 86
87 Policy area Decision Reserved to the Member- ship Reserved/ delegated to Governing Body Accountable Officer/Chief Officer Chief Finance Officer Audit &Governance Sub Committee Remuneration and Terms of Service Sub Committee Activity & Finance Sub Committee Quality &Risk Sub Committee Primary Care Commis- sioning Committee Commissioning & Contracting within an Alliance the governing body reserved to the governing body and those delegated to the o governing body s committees and subcommittees, o members of the governing body, an individual who is member of the group but not the governing body or a specified person o for inclusion in the group s constitution. All matters relating to the work of the Alliance Leadership Board as set out in the Alliance Agreement dated 1 st April 2016 and the Alliance Leadership Board Terms of reference dated 19 th May 2016 with the exception of: a) Matters reserved for governing bodies as outlined in clause 11.4 of the Alliance Agreement dated 1 st April 2016 b) Other key strategic matters as listed below: Risk share Payment mechanisms Outcomes Proposed Chief Officer/C CG Clinical Chair 87
88 Policy area Decision Reserved to the Member- ship Reserved/ delegated to Governing Body Accountable Officer/Chief Officer Chief Finance Officer Audit &Governance Sub Committee Remuneration and Terms of Service Sub Committee Activity & Finance Sub Committee Quality &Risk Sub Committee Primary Care Commis- sioning Committee changes to the governance arrangements of the Alliance REGULATION AND CONTROL Approval of the group s overarching scheme of reservation and delegation. REGULATION AND CONTROL Prepare the group s operational scheme of delegation, which sets out those key operational decisions delegated to individual employees of the clinical commissioning group, not for inclusion in the group s constitution REGULATION AND CONTROL Approval of the group s operational scheme of delegation that underpins the group s overarching scheme of reservation and delegation as set out in its constitution. REGULATION AND CONTROL Approve arrangements for managing exceptional funding requests. REGULATION AND CONTROL Set out who can execute a document by signature/use of the seal. REGULATION AND CONTROL Authority to sign documents on behalf of the group o r Chair or Chair of 88
89 Policy area Decision Reserved to the Member- ship Reserved/ delegated to Governing Body Accountable Officer/Chief Officer Chief Finance Officer Audit &Governance Sub Committee Remuneration and Terms of Service Sub Committee Activity & Finance Sub Committee Quality &Risk Sub Committee Primary Care Commis- sioning Committee REGULATION AND CONTROL PRACTICE MEMBER REPRESENT- ATIVES & MEMBERS OF THE GOVERNING BODY PRACTICE MEMBER REPRESENT- ATIVES & MEMBERS OF THE GOVERNING BODY PRACTICE MEMBER REPRESENT- ATIVES & MEMBERS OF THE Authority to execute documents using the group s Seal Approve the arrangements for o identifying practice members to represent practices in matters concerning the work of the group; and o appointing clinical leaders to represent the group s membership on the group s governing body, for example through election (if desired). Approve and ratify the appointment of elected membership. Approve the process for recruiting and removing nonelected members and PPI lay members to the governing body (subject to any regulatory requirements) and succession of the GB or Chair of the GB the GB or Chair of the GB 89
90 Policy area GOVERNING BODY Decision planning. Reserved to the Member- ship Reserved/ delegated to Governing Body Accountable Officer/Chief Officer Chief Finance Officer Audit &Governance Sub Committee Remuneration and Terms of Service Sub Committee Activity & Finance Sub Committee Quality &Risk Sub Committee Primary Care Commis- sioning Committee PRACTICE MEMBER REPRESENT- ATIVES & MEMBERS OF THE GOVERNING BODY Approve arrangements for identifying the group s proposed accountable officer. STRATEGY & PLANN-ING Agree the vision, values and overall strategic direction of the group. STRATEGY & PLANN-ING Approval of the group s operating structure. STRATEGY & PLANNING Approval of operational changes with regard to the group s operating structure STRATEGY & PLANNING Approval of the group s commissioning plans STRATEGY & PLANNING Approval of the group s corporate budgets that meet the financial duties as set out in section 5.3 of the main body of the constitution. STRATEGY & PLANNING Approval of variations to the approved budget where variation would have a significant impact on the overall 90
91 Policy area Decision Reserved to the Member- ship Reserved/ delegated to Governing Body Accountable Officer/Chief Officer Chief Finance Officer Audit &Governance Sub Committee Remuneration and Terms of Service Sub Committee Activity & Finance Sub Committee Quality &Risk Sub Committee Primary Care Commis- sioning Committee ANNUAL REPORTS & ACCOUNTS approved levels of income and expenditure or the group s ability to achieve its agreed strategic aims. Approval of the group s annual report and annual accounts. ANNUAL REPORTS & ACCOUNTS Approval of the arrangements for discharging the group s statutory financial duties. HUMAN RESOURCES Approve the terms and conditions, remuneration and travelling or other allowances for governing body members, including pensions and gratuities. HUMAN RESOURCES Approve terms and conditions of employment for all employees of the group including, pensions, remuneration, fees and travelling or other allowances payable to employees and to other persons providing services to the group. HUMAN RESOURCES Approve any other terms and conditions of services for the group s employees HUMAN RESOURCES Advise the governing body on the terms and conditions of employment for all employees 91
92 Policy area Decision of the group including allowances, any bonuses, pensions and/or termination arrangements Reserved to the Member- ship Reserved/ delegated to Governing Body Accountable Officer/Chief Officer Chief Finance Officer Audit &Governance Sub Committee Remuneration and Terms of Service Sub Committee Activity & Finance Sub Committee Quality &Risk Sub Committee Primary Care Commis- sioning Committee HUMAN RESOURCES Advise the governing body on pensions, remuneration, fees and allowances payable to other persons providing services to the group. HUMAN RESOURCES Approve disciplinary arrangements for employees, including the accountable officer (where he/she is an employee or member of the clinical commissioning group) and for other persons working on behalf of the group. HUMAN RESOURCES Review disciplinary arrangements where the accountable officer is an employee or member of another clinical commissioning group HUMAN RESOURCES Approval of the arrangements for discharging the group s statutory duties as an employer QUALITY & SAFETY Approve arrangements to minimise clinical risk, maximise patient safety and to secure continuous improvement in quality and patient outcomes. QUALITY & SAFETY Approve arrangements for supporting NHS England in 92
93 Policy area Decision Reserved to the Member- ship Reserved/ delegated to Governing Body Accountable Officer/Chief Officer Chief Finance Officer Audit &Governance Sub Committee Remuneration and Terms of Service Sub Committee Activity & Finance Sub Committee Quality &Risk Sub Committee Primary Care Commis- sioning Committee discharging its responsibilities in relation to securing continuous improvement in the quality of general medical services OPERATION- AL & RISK MANAGE- MENT Prepare and recommend an operational scheme of delegation that sets out who has responsibility for operational decisions within the group. OPERATION- AL & RISK MANAGE- MENT Approve and oversee the group s counter fraud and security management arrangements. OPERATION- AL & RISK MANAGE- MENT Approval of the group s risk management arrangements. OPERATION- AL & RISK MANAGE- MENT Approve arrangements for risk sharing and or risk pooling with other organisations (for example arrangements for pooled funds with other clinical commissioning groups or pooled budget arrangements under section 75 of the NHS Act 2006) OPERATION- AL & RISK MANAGE- MENT Approval of a comprehensive system of internal control, including budgetary control, that underpin the effective, efficient and economic operation of the group. 93
94 Policy area Decision Reserved to the Member- ship Reserved/ delegated to Governing Body Accountable Officer/Chief Officer Chief Finance Officer Audit &Governance Sub Committee Remuneration and Terms of Service Sub Committee Activity & Finance Sub Committee Quality &Risk Sub Committee Primary Care Commis- sioning Committee OPERATION- AL & RISK MANAGE- MENT Approve proposals for action on litigation against or on behalf of the clinical commissioning group. OPERATION- AL & RISK MANAGE- MENT Approve the group s arrangements for business continuity and emergency planning INFORM- ATION GOVER- NANCE Approve the group s arrangements for handling complaints. INFORM- ATION GOVER- NANCE Approval of the arrangements for ensuring appropriate and safekeeping and confidentiality of records and for the storage, management and transfer of information and data INFORM- ATION GOVER- NANCE Approval of the supporting policies for ensuring appropriate and safekeeping and confidentiality of records and for the storage, management and transfer of information and data TENDERING & CONTRACT- ING Approval of the group s contracts for any commissioning support in line with financial limits set out in the in line with financial limits set out in the operation al 94
95 Policy area Decision Reserved to the Member- ship Reserved/ delegated to Governing Body Accountable Officer/Chief Officer Chief Finance Officer Audit &Governance Sub Committee Remuneration and Terms of Service Sub Committee Activity & Finance Sub Committee Quality &Risk Sub Committee Primary Care Commis- sioning Committee TENDERING & CONTRACT- ING PARTNER- SHIP WORKING PARTNER- SHIP WORKING Approval of the group s contracts for corporate support (for example finance provision). Approve decisions that individual members or employees of the group participating in joint arrangements on behalf of the group can make. Such delegated decisions must be disclosed in this scheme of reservation and delegation. Approve arrangements for delegation to joint committees established under section 75 of the 2006 Act. operatio nal scheme of delegati on in line with financial limits set out in the operation al scheme of delegatio n scheme of delegation in line with financial limits set out in the operatio n al scheme of delegation N.B. approval of decisions will be the Joint Commissioning 95
96 Policy area COMMISSION -ING & CONTRACT- ING FOR CLINICAL SERVICES COMMISSION -ING & CONTRACT- ING FOR GP PRACTICE SERVICES COMMISSION -ING & CONTRACT- ING FOR CLINICAL SERVICES Decision groups Approval of the arrangements for discharging the group s statutory duties associated with its commissioning functions, including but not limited to promoting the involvement of each patient, patient choice, reducing inequalities, improvement in the quality of services, obtaining appropriate advice and public engagement and consultation. Approval of the arrangements for discharging the group s statutory duties associated with its GP practice commissioning functions, including but not limited to promoting the involvement of each patient, patient choice, reducing inequalities, improvement in the quality of services, obtaining appropriate advice and public engagement and consultation. Approve arrangements for coordinating the commissioning of services with other groups and or with the local authority(ies), where appropriate. (detailed within a Memorandum of Understanding) Reserved to the Member- ship Reserved/ delegated to Governing Body Accountable Officer/Chief Officer Chief Finance Officer Audit &Governance Sub Committee Remuneration and Terms of Service Sub Committee Activity & Finance Sub Committee Quality &Risk Sub Committee Primary Care Commis- sioning Committee 96
97 Policy area Decision Reserved to the Member- ship Reserved/ delegated to Governing Body Accountable Officer/Chief Officer Chief Finance Officer Audit &Governance Sub Committee Remuneration and Terms of Service Sub Committee Activity & Finance Sub Committee Quality &Risk Sub Committee Primary Care Commis- sioning Committee COMMUNI- CATIONS COMMUNI- CATIONS Approving arrangements for handling Freedom of Information requests. Determining arrangements for handling Freedom of Information requests. 97
98 Table 2 Policy Area Decision Accountabl- e Officer/ Chief Officer Chief Finance Officer Clinical Executive Better Together Committee Stakeholder Reference Group Safeguarding Adult Committee Safeguarding Children Committee OPERA- TIONAL AND RISK MANAG MENT Authorise practice budgets with clear focus on clinical implications OPERA- TIONAL AND RISK MANAG MENT Approve annual reports for CCG relating to safeguarding vulnerable adults OPERA- TIONAL AND RISK MANAG MENT Approve annual reports for CCG relating to safeguarding children 98
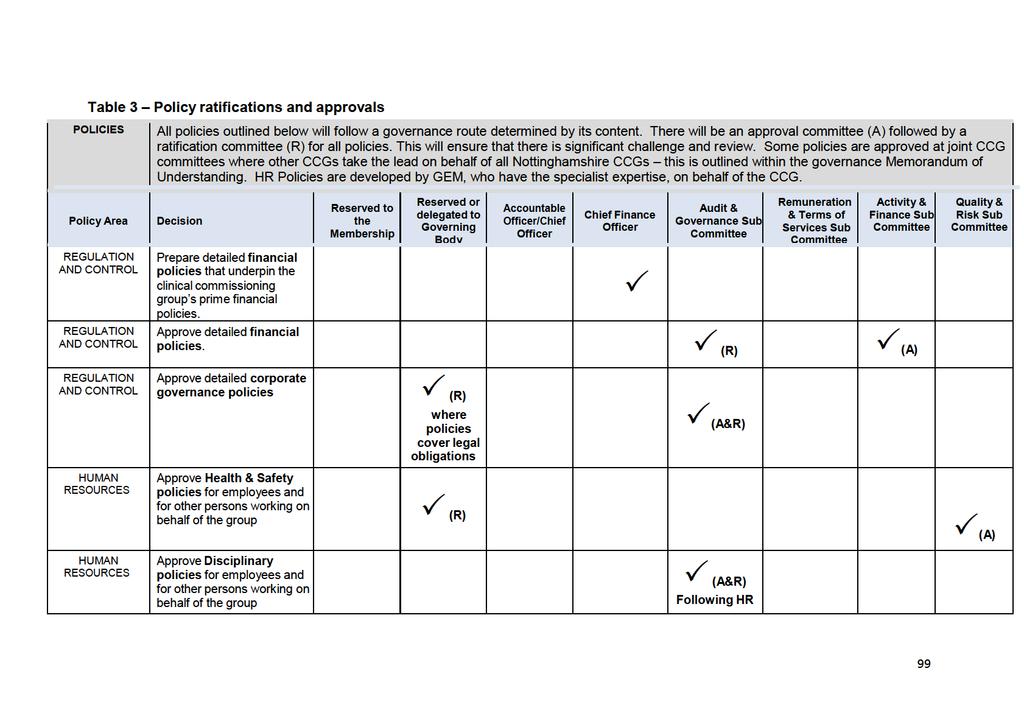
99
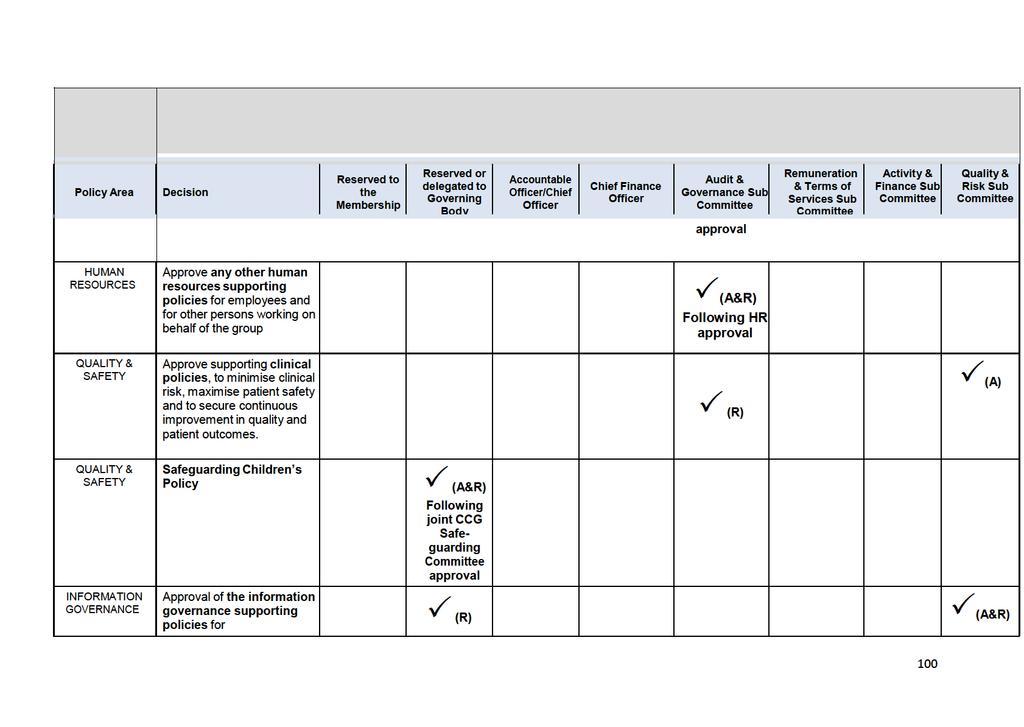
100
101 POLICIES All policies outlined below will follow a governance route determined by its content. There will be an approval committee (A) followed by a ratification committee (R) for all policies. This will ensure that there is significant challenge and review. Some policies are approved at joint CCG committees where other CCGs take the lead on behalf of all Nottinghamshire CCGs this is outlined within the governance Memorandum of Understanding. HR Policies are developed by GEM, who have the specialist expertise, on behalf of the CCG. Policy Area Decision Reserved to the Membership Reserved or delegated to Governing Body Accountable Officer/Chief Officer Chief Finance Officer Audit & Governance Sub Committee Remuneration & Terms of Services Sub Committee Activity & Finance Sub Committee Quality & Risk Sub Committee ensuring appropriate and safekeeping and confidentiality of records and for the storage, management and transfer of information and data where policies cover legal obligations Following joint CCG IGM&T Sub Committee
102 APPENDIX 7 DEFINITIONS OF KEY DESCRIPTIONS USED IN THIS CONSTITUTION 2006 Act National Health Service Act Act Health and Social Care Act 2012 (this Act amends the 2006 Act) Chief officer an individual, as defined under paragraph 12 of Schedule 1A of the 2006 Act (as inserted by Schedule 2 of the 2012 Act), appointed by NHS England, with responsibility for ensuring the group: complies with its obligations under: o sections 14Q and 14R of the 2006 Act (as inserted by section 26 of the 2012 Act), o sections 223H to 223J of the 2006 Act (as inserted by section 27 of the 2012 Act), o paragraphs 17 to 19 of Schedule 1A of the NHS Act 2006 (as inserted by Schedule 2 of the 2012 Act), and o any other provision of the 2006 Act (as amended by the 2012 Act) specified in a document published by the Board for that purpose; exercises its functions in a way which provides good value for money. Area Chair of the governing body Chief finance officer Clinical commissioning group Committee Financial year Group Governing body the geographical area that the group has responsibility for, as defined in Chapter 2 of this constitution the individual appointed by the group to act as chair of the governing body the qualified accountant employed by the group with responsibility for financial strategy, financial management and financial governance a body corporate established by NHS England in accordance with Chapter A2 of Part 2 of the 2006 Act (as inserted by section 10 of the 2012 Act) a committee or sub-committee created and appointed by: the membership of the group a committee / sub-committee created by a committee created / appointed by the membership of the group a committee / sub-committee created / appointed by the governing body this usually runs from 1 April to 31 March, but under paragraph 17 of Schedule 1A of the 2006 Act (inserted by Schedule 2 of the 2012 Act), it can for the purposes of audit and accounts run from when a clinica commissioning group is established until the following 31 March NHS Newark & Sherwood NHS Clinical Commissioning Group, whose constitution this is the body appointed under section 14L of the NHS Act 2006 (as inserted by section 25 of the 2012 Act), with the main function of ensuring that a clinical commissioning group has made appropriate arrangements for ensuring that it complies with: its obligations under section 14Q under the NHS Act 2006 (as inserted by section 26 of the 2012 Act), and 102
103 Governing member body such generally accepted principles of good governance as are relevant to it. any member appointed to the governing body of the group Lay member Member Practice representatives Registers interests of a lay member of the governing body, appointed by the group. A lay member is an individual who is not a member of the group or a healthcare professional (i.e. an individual who is a member of a profession regulated by a body mentioned in section 25(3) of the National Health Service Reform and Health Care Professions Act 2002) or as otherwise defined in regulations a provider of primary medical services to a registered patient list, who is a members of this group (see tables in Chapter 3 and Appendix B) an individual appointed by a practice (who is a member of the group) to act on its behalf in the dealings between it and the group, under regulations made under section 89 or 94 of the 2006 Act (as amended by section 28 of the 2012 Act) or directions under section 98A of the 2006 Act (as inserted by section 49 of the 2012 Act) registers a group is required to maintain and make publicly available under section 14O of the 2006 Act (as inserted by section 25 of the 2012 Act), of the interests of: the members of the group; the members of its governing body; the members of its committees or sub-committees and committees or sub-committees of its governing body; and its employees. 103
104 Appendix 8 PRIME FINANCIAL POLICIES OF NEWARK AND SHERWOOD CCG 1. INTRODUCTION 1.1. General PRIME FINANCIAL POLICIES Updated on 10 March These Prime Financial Policies and any supporting policies or procedures issued from time to time by or on behalf of the Chief Finance Officer shall have effect as if incorporated into the CCG s constitution The Prime Financial Policies are part of the CCG s control environment for managing the organisation s financial affairs. They contribute to good corporate governance, internal control and managing risks. They enable sound administration; lessen the risk of irregularities and support commissioning and delivery of effective, efficient and economical services. They also help the Accountable Officer and Chief Finance Officer to effectively perform their responsibilities. They should be used in conjunction with the scheme of Delegation within Constitution (see Appendix E of the Constitution) Number not used These Prime Financial Policies identify the financial responsibilities which apply to everyone working for the CCG and its constituent organisations. They do not provide detailed procedural advice and should be read in conjunction with any detailed financial policies issued by or on behalf of the Chief Finance Officer from time to time. The Chief Finance Officer is responsible for approving all detailed financial policies A list of the CCG s detailed financial policies will be published and maintained on the CCG s website at and on Hard copies can also be requested by writing to the Corporate Governance Team at: NHS Mansfield and Ashfield CCG. Hawthorn House, Ransomwood Business Park, Southwell Road, Mansfield, NG21 0HJ NHS Newark and Sherwood CCG, Balderton Primary Care Centre, Lowfield Lane, Balderton, Nottinghamshire, NG24 3HJ Or ruth.lloyd@mansfieldandashfieldccg.nhs.uk or call Should any difficulties arise regarding the interpretation or application of the Prime Financial Policies or any other supporting financial policies or procedures then the advice of the Accountable Officer must be sought before acting. The user should also be familiar with and comply with the provisions of the CCG s Constitution, Standing Orders and Scheme of Delegation Failure to comply can in certain circumstances be regarded as a disciplinary matter that could result in dismissal. 104
105
106
107
108
109
110
111
112
113
114 Conflicts of Interest Policy NHS Mansfield and Ashfield and NHS Newark and Sherwood Clinical Commissioning Groups Based on the national guidance and recommended framework from NHS England this information builds/strengthens the CCGs existing conflicts of interest policy January
115 VERSION DATE: January 2016 VERSION NUMBER: 3.0 STATUS: DEVELOPED BY: POLICY SPONSOR: Approved Corporate Governance Team Chief Officer APPROVED BY: Governing Body REVIEW DATE: January 2016 TARGET AUDIENCE: All CCG Staff and Governing Body Members 115
116 Contents Introduction 3 What are Conflicts of Interest? 4 Legislative Framework 4 Principles and General Safeguards 5 Maintaining a Register of Interests and a Register of Decisions 6 Register of Procurement Decisions 7 Governance and Decision-making Processes 8 Procurement 8 Decision-making when a Conflict of Interest Arises: Primary Medical Care 10 Record Keeping 11 Role of Commissioning Support 11 Transparency 11 Breaches of this policy (Including Counter Fraud guidance) 12 Annexes: 1. NHS Clinical Commissioners, Royal College of General Practitioners and British Medical Association - Shared principles on conflicts of interest when CCGs are commissioning from member practices Declaration of Conflict of Interest Template for Bidders/Contractors Declaration of Interest Template for Members/Employees Procurement Template
117 Introduction Clinical commissioning groups (CCGs) manage conflicts of interest as part of their day-to-day activities. Effective handling of such conflicts is crucial for the maintenance of public trust in the commissioning system. Importantly, it also serves to give confidence to patients, providers, Parliament and tax payers that CCG commissioning decisions are robust, fair, transparent and offer value for money. In May 2014, NHS England offered CCGs the opportunity to take on an increased responsibility for the commissioning of primary care. In light of this new development, NHS England, in consultation with national stakeholders, developed strengthened guidance for the management of conflicts of interest and this policy reflects this strengthened guidance. Equality and diversity are at the heart of the CCGs values. Throughout the development of the policies and processes cited in this document, the CCGs have given due regard to the need to: Reduce health inequalities in access and outcomes of healthcare services Integrate services where this might reduce health inequalities Eliminate discrimination, harassment and victimisation Advance equality of opportunity and foster good relations between people who share a relevant protected characteristic (as cited in under the Equality Act 2010) and those who do not share it. This policy also reflects the seven principles of public life promulgated by the Nolan Committee. These include: Selflessness Integrity Objectivity Accountability Openness Honesty Leadership The policy states that when the CCGs are seeking to take on delegated or joint commissioning responsibilities, their audit committee chair and accountable officer will be required to provide direct formal attestation to NHS England that the CCGs have complied with their guidance. Subsequently, this attestation will form part of an annual certification. CCG approaches to management of conflicts of interest will also be considered on an ongoing basis as part of CCG assurance. Further details will be issued early in 2015 as to the forms that the initial attestation, the annual certification and on-going assurance will take. 117
118 What are conflicts of interest? A conflict of interest occurs where an individual s ability to exercise judgment, or act in a role, is or could be impaired or otherwise influenced by his or her involvement in another role or relationship. The individual does not need to exploit his or her position or obtain an actual benefit, financial or otherwise, for a conflict of interest to occur: For the purposes of Regulation 6 [National Health Service (Procurement, Patient Choice and Competition) (No.2) Regulations 20137], a conflict will arise where an individual s ability to exercise judgment or act in their role in the commissioning of services is impaired or influenced by their interests in the provision of those services. Monitor - Substantive guidance on the Procurement, Patient Choice and Competition Regulations (December 2013) As well as direct financial interests, conflicts can arise from an indirect financial interest (e.g. payment to a spouse) or a non-financial interest (e.g. reputation). Conflicts of loyalty may arise (e.g. in respect of an organisation of which the individual is a member or with which they have an affiliation). Conflicts can arise from personal or professional relationships with others, e.g. where the role or interest of a family member, friend or acquaintance may influence an individual s judgment or actions, or could be perceived to do so. Depending upon the individual circumstances, these factors can all give rise to potential or actual conflicts of interest. For a commissioner, such as the CCGs, a conflict of interest may therefore arise when their judgment as commissioners could be, or be perceived to be, influenced and impaired by their own concerns and obligations as a provider. In the case of a GP involved in commissioning, an obvious example is the award of a new contract to a provider in which the individual GP has a financial stake. However, the same considerations, and the approaches set out in this policy, apply when deciding whether to extend a contract. NHS Clinical Commissioners have carried out a review of current guidance on conflicts of interest management and, together with the Royal College of General Practitioners and the British Medical Association, have developed a set of key principles that apply in this context. These principles are set out in Annex 1. Legislative Framework The UK Bribery Act 2010 has revised the legal framework for combating bribery and corruption in the public and private sectors. This act makes it a criminal offence to offer, give or receive a financial or other advantage as a reward for an improper act such as the award of a contract. The Act also introduced a corporate offence (which can lead to an unlimited fine) where an organisation has failed to tackle bribery. The Conflicts of Interest Policy is a key tool to demonstrate that the CCG has appropriate arrangements in place to meet their responsibilities in protecting both staff and the organisation against any suggestion of impropriety or inappropriate behaviour. Section 14O of the Health and Social Care Act 2012 sets out the minimum requirements in terms of what both NHS England and CCGs must do in terms of managing conflicts of interest. For CCGs, this means that they: Maintain appropriate registers of interests; Publish or make arrangements for the public to access those registers; Make arrangements requiring the prompt declaration of interests by the persons specified (members and employees) and ensure that these interests are entered into the relevant register; Make arrangements for managing conflicts and potential conflicts of interest (e.g. 118
119 developing appropriate policies and procedures); and Have regard to guidance published by NHS England and Monitor in relation to conflicts of interest. Section 14O is supplemented by the procurement specific requirements set out in the National Health Service (Procurement, Patient Choice and Competition) (No.2) Regulations 20139; in particular, regulation 6 requires the following: CCGs must not award a contract for the provision of NHS health care services where conflicts, or potential conflicts, between the interests involved in commissioning such services and the interests involved in providing them affect, or appear to affect, the integrity of the award of that contract; and CCGs must keep a record of how it managed any such conflict in relation to NHS commissioning contracts it enters into. (As set out in section 8 below, details of this should also be published by the CCG.) An interest is defined for the purposes of regulation 6 as including an interest of the following: a member of the commissioner organisation; a member of the governing body of the commissioner; a member of its committees or sub-committees or committees or sub-committees of its governing body; or an employee. As with section 14O, regulation 6 sets out the basic framework within which CCGs must operate. The detailed requirements are set out in the guidance issued by Monitor (Substantive guidance on the Procurement, Patient Choice and Competition Regulations) and, in particular, section 7 of that statutory guidance. Monitor s view is that care must be taken to ensure that conflicts do not affect, or appear to affect, the integrity of the award of commissioning contracts. It is important to ensure that the management of conflicts of interest includes the management of perceived conflicts and that there is an appropriate record of how such issues are managed, particularly in the context of specific procurement decisions. Principles and General Safeguards The general safeguards that will be needed to manage conflicts of interest will vary to some extent, depending on at what stage in the commissioning cycle decisions are being made. The following principles are integral to the commissioning of all services, including decisions on whether to continue to commission a service, such as by contact extension, and will be applied at all stages of the CCGs commissioning and decision making processes: Doing business appropriately. If commissioners get their needs assessments, consultation mechanisms, commissioning strategies and procurement procedures right from the outset, then conflicts of interest become much easier to identify, avoid and/or manage, because the rationale for all decision-making will be clear and transparent and should withstand scrutiny; Being proactive, not reactive. Commissioners should seek to identify and minimise the risk of conflicts of interest at the earliest possible opportunity, for instance by: considering potential conflicts of interest when electing or selecting individuals to join the governing body or other decision-making bodies; ensuring individuals receive proper induction and training so that they understand their obligations to declare conflicts of interest. They should establish and maintain registers of interests, and agree in advance how a 119
120 range of possible situations and scenarios will be handled, rather than waiting until they arise; Assuming that individuals will seek to act ethically and professionally, but may not always be sensitive to all conflicts of interest. Rules should assume people will volunteer information about conflicts and, where necessary, exclude themselves from decision-making, but there should also be prompts and checks to reinforce this; Being balanced and proportionate. Rules should be clear and robust but not overly prescriptive or restrictive. They should ensure that decision-making is transparent and fair, but not constrain people by making it overly complex or cumbersome; Openness. Ensuring early engagement with patients, the public, clinicians and other stakeholders, including local Healthwatch and Health and Wellbeing Boards, in relation to proposed commissioning plans; Responsiveness and best practice. Ensuring that commissioning intentions are based on local health needs and reflect evidence of best practice securing buy in from local stakeholders to the clinical case for change; Transparency. Documenting clearly the approach taken at every stage in the commissioning cycle so that a clear audit trail is evident; Securing expert advice. Ensuring that plans take into account advice from appropriate health and social care professionals, e.g. through clinical senates and networks, and draw on commissioning support, for instance around formal consultations and for procurement processes; Engaging with providers. Early engagement with both incumbent and potential new providers over potential changes to the services commissioned for a local population. Creating clear and transparent commissioning specifications that reflect the depth of engagement and set out the basis on which any contract will be awarded; Following proper procurement processes and legal arrangements, including even- handed approaches to providers; Ensuring sound record-keeping, including up to date registers of interests; and A clear, recognised and easily enacted system for dispute resolution. Maintaining a Register of Interests and a Register of Decisions The CCG maintains a register of interest of: members of the governing body and subcommittees of the governing body; and all CCG employees. The register is placed on the CCG website and is available in hard copy form upon request to the Head of Corporate Governance. Individuals have an obligation to declare any conflict or potential conflict in relation to a decision to be made by the Committee or sub committee as soon as they become aware of it, and in any event within 28 days. Whenever interests are declared, they will be reported to the Head of Corporate Governance, who will then update the register accordingly. The register of interests will also be updated whenever a new or revised interest is declared. 120
121 The register includes the interests of all relevant individuals within their own organisations (e.g. partners in a GP practice), who have a relationship with the CCGs and who would potentially be in a position to benefit from the CCGs decisions. The register will include sufficient information about the nature of the interest and the details of those holding the interest. The register will be regularly confirmed or updated: On appointment: Applicants for any appointment to the CCGs or their governing bodies will be asked to declare any relevant interests. When an appointment is made, a formal declaration of interests will again be made and recorded. At meetings: All attendees will be asked to declare any interest they have in any agenda item before it is discussed or as soon as it becomes apparent. Even if an interest is declared in the register of interests, it will be declared in meetings where matters relating to that interest are discussed. Declarations of interest will be recorded in minutes of meetings. Quarterly: The CCGs will have systems in place to satisfy themselves on a quarterly basis that their registers of interests are accurate and up to date. On changing role or responsibility: Where an individual changes role or responsibility within a CCG or its governing body, any change to the individual s interests will be declared. On any other change of circumstances: Wherever an individual s circumstances change in a way that affects the individual s interests (e.g. where an individual takes on a new role outside the CCGs or sets up a new business or relationship), a further declaration should be made to reflect the change in circumstances. This could involve a conflict of interest ceasing to exist or a new one materialising. Where an individual fails to comply with this policy on managing conflicts of interest, the Head of Corporate Governance will initially review the circumstances and escalate for further investigation where appropriate. The Audit Chairs/Clinical Chairs and the Chief Executive will undertake this investigation and report their findings to the CCGs Audit Committees and Governing Bodies. See Annexes 2 and 3 for declaration of interest templates. Register of Procurement Decisions The CCGs will also maintain a register of procurement decisions taken, including: the details of the decision; who was involved in making the decision (i.e. governing body or committee members and others with decision-making responsibility); and a summary of any conflicts of interest in relation to the decision and how this was managed by the CCGs. The register will be updated whenever a procurement decision is taken. 121
122 In the interests of transparency, each register of interests and the register of decisions will be placed on the CCGs websites; and will be available on request from the Head of Corporate Governance. Procurement The CCGs will manage conflicts and potential conflicts of interests when awarding a contract by prohibiting the award of a contract where the integrity of the award has been, or appears to have been, affected by a conflict; and will keep appropriate records of how they have managed any conflicts in individual cases. Other issues to be considered include: Competitive tender Where the CCGs are commissioning a service through competitive tender (i.e. seeking to identify the best Provider or set of providers for a service), a conflict could arise where GP practices or other providers in which CCG members have an interest are among those bidding. Any Qualified Provider (AQP) If the CCGs are commissioning a service through the AQP, then a conflict could arise where one or more GP practices (or other providers in which the CCG members have an interest) are amongst the qualified providers from whom our patients can choose. In these circumstances (and more generally), the CCGs should demonstrate that GP practices have offered fully their informed choice at the point of referral and for auditing and publishing referral patterns. Where appropriate, out of area GPs/clinicians on procurement panels will be used. Out of hospital services This is a particular area where consideration should be given as to whether GP practices are potential providers. Managing (bidders) contracts If a party has a conflict of interest relating to a contract, they must not be involved in the procuring, tendering, managing or monitoring of this contract. Monitoring arrangements for such contracts will include provisions for an independent challenge of bills and invoices, and termination of the contract if the relationship is unsatisfactory. These will build on wellestablished procedures for declaring interests when GPs or other clinicians make a referral. Designing service requirements It is good practice to engage relevant providers, especially clinicians, in confirming that the design of service specifications will meet patient need. Such engagement, done transparently and fairly, is entirely legal. However, conflicts of interest can occur if a commissioner engages selectively with only certain providers (be they incumbent or potential new providers) in developing a service specification for a contract for which they may later bid. Principles The CCGs will follow good practice when engaging relevant providers, especially clinicians, in confirming that the design of service specifications will meet patient need. The CCGs will seek, as far as possible, to specify the outcomes that it wishes to see delivered through a new service, rather than the process by which these outcomes are to be achieved. As well as supporting innovation, this helps prevent bias towards particular providers in the specification of services. 122
123 Such engagement will follow the three main principles of procurement law, namely equal treatment, non-discrimination and transparency. This includes ensuring that the same information is given to all. In Summary the CCGs will: advertise the fact that a service design/re-design exercise is taking place widely and invite comments from any potential providers and other interested parties (ensuring a record is kept of all interactions); as the service design develops, engage with a wide range of providers on an on-going basis to seek comments on the proposed design, e.g. via the commissioner s website or via workshops with interested parties; use engagement to help shape the requirement to meet patient need but take care not to gear the requirement in favour of any particular provider(s); if appropriate, engage the advice of an independent clinical adviser on the design of the service; be transparent about procedures; ensure at all stages that potential providers are aware of how the service will be commissioned; and maintain commercial confidentiality of information received from providers. The CCGs will ensure that conflicts of interest are managed on an on-going basis. The Procurement template at Annex 4 will be used by the CCGs when drawing up their plans to commission services. Governance and Decision-making Processes The CCGs shall consider whether conflicts of interest should exclude individuals from being appointed to the Governing Bodies or to a committee or sub-committee of the CCGs. Such consideration shall be made on a case by case basis depending on the nature and extent of the interest, in particular whether the individual (or a family member) could benefit from any decision the Governing Body might make and whether the interest relates to such a significant area of business that the individual would be unable to make a full and proper contribution to the Governing Body. Any individual who has a material interest in an organisation which provides or is likely to provide substantial business to a CCG (either as a provider of healthcare or commissioning support services) shall not be a member of the Governing Body. Decision-making when a conflict of interest arises: Where members of the Governing Body, its committees or sub-committees, or a committee or sub-committee of the CCG have a material interest, they will either be excluded from relevant parts of meetings, or join in the discussion but not participate in the decision-making itself (i.e. not have a vote). The Chair of the meeting has responsibility for deciding whether there is a conflict of interest and the appropriate course of corresponding action. In making such decisions, the chair will consult the Head of Corporate Governance. All decisions, and details of how any conflict of interest issue has been managed, will be recorded in the minutes of the meeting and published in the registers. Where the Chair of any meeting of the CCGs, including committees, sub-committees, or the Governing Body and the Governing Body s committees and sub-committees, has a personal interest, previously declared or otherwise, in relation to the scheduled or likely business of the meeting, they must make a declaration and the deputy Chair will act as Chair for the relevant part of the meeting. Where arrangements have been confirmed for the 124
124 management of the conflict of interests or potential conflicts of interests in relation to the 125
125 Chair, the meeting must ensure these are followed. Where no arrangements have been confirmed, the deputy Chair may require the Chair to withdraw from the meeting or part of it. Where there is no deputy Chair, the members of the meeting will select one. Where GPs have a material interest, they shall be excluded from relevant parts of meetings, or join in the discussion but not participate in the decision-making itself (i.e. not have a vote). If all of the GPs or other practice representatives on a decision-making body could have a material interest in a decision, particularly where the CCGs are proposing to commission services on a single tender basis from all GP practices in the area, or where it is likely that all or most practices would wish to be qualified providers for a service under AQP. The CCG shall: refer the decision to the Governing Body and exclude all GPs or other practice representatives with an interest from the decision-making process; consider co-opting individuals from a Health and Wellbeing Board or from another CCG onto the Governing Body, or inviting the Health and Wellbeing Board or another CCG to review the proposal, to provide additional scrutiny (though the voting rights of any invitees shall be in accordance with the provisions of the CCG s constitution); ensure that rules on being quorate at meetings (set out in the CCG s constitution) enable decisions to be made; and plan ahead to recognise when items on meeting agendas that require decisions to be made are coming up that the agreed processes for ensuring they remain quorate are implemented. The Chair (or their deputy where relevant) may, depending on the nature of the conflict, allow GPs or other practice representatives to join in the Governing Body s discussion (but not vote) about the proposed decision. Where more than 50% of the members of a meeting are required to withdraw from a meeting or part of it, owing to the arrangements agreed for the management of conflicts of interests or potential conflicts of interests, the Chair (or deputy) will determine whether or not the discussion can proceed. In making this decision the Chair will consider whether the meeting is quorate, in accordance with the number and balance of membership set out in the relevant terms of reference. Where the meeting is not quorate, owing to the absence of certain members, the discussion will be deferred until such time as a quorum can be convened. Where a quorum cannot be convened from the membership of the meeting, owing to the arrangements for managing conflicts of interest or potential conflicts of interests, the Chair of the meeting shall consult with the Head of Corporate Governance on the action to be taken. Decision-making when a Conflict of Interest Arises: Primary Medical Care Procurement decisions relating to the commissioning of primary medical services will be made by a sub- committee of the CCGs Governing Bodies. This will in the case of delegated commissioning, be a committee established by Mansfield & Ashfield CCG and the Newark & Sherwood CCG (the Mid Nottinghamshire CCGs). The membership of the committee will be constituted so as to ensure that the majority is held by lay and executive members, with the Chair and Vice Chair being lay members. In addition to existing CCG lay members, members will be drawn from the CCGs executive members, except where these members may themselves have a conflict of interest (e.g. if they are GPs or have other conflicts of interest). Provision will be made for the committee to have the ability to call on additional lay members or CCG members when required, for example where the committee is not quorate because of conflicts of interest. It could also include GP representatives from other CCG areas and non-gp clinical representatives (such as the CCGs secondary care specialists and/or governing body nurse leads). 126
126 Any conflicts of interest issues will be considered on an individual basis. The CCGs will have a reciprocal arrangement with other local CCGs in order to support effective clinical representation within the committee. A standing invitation will be made to the CCGs local Healthwatch and Health and Wellbeing Board to appoint representatives to attend commissioning committee meetings, including, where appropriate, for items where the public is excluded from a particular item or meeting for reasons of confidentiality. These representatives will not form part of the membership of the committee. The meetings of these committees, including the decision-making and the deliberations leading up to the decision, will be held in public (unless the CCGs have concluded it is appropriate to exclude the public). To note: the above arrangements for primary medical care decision making do not preclude GP participation in strategic discussions on primary care issues, subject to appropriate management of conflicts of interest. They apply to decision-making on procurement issues and the deliberations leading up to the decision. Record Keeping As set out above a clear record of any conflicts of interest will be kept by the CCGs in their register of interests. It will record procurement decisions made, and will detail any conflicts that arise in the context of the decision and how they are managed. These registers will be available for public inspection as detailed above. Details of all contracts, including the contract value, are published on the CCGs websites as soon as contracts are agreed. All services commissioned through Any Qualified Provider (AQP), will also be published on the website along with the type of services they are commissioning and the agreed price for each service. Role of Commissioning Support The CCGs cannot sub-delegate commissioning decisions to an external provider of commissioning support. However, the CCGs shall ensure that it seeks and receives appropriate technical support to decide the most appropriate procurement route, undertake procurements and manage contracts in ways that manage conflicts of interest and preserve integrity of decision-making. Where another CCG or a commissioning support service undertake procurement activity on behalf of the CCGs, the CCGs shall ensure that they are compliant with requirements of the regulations in the same way the CCGs must be themselves. Transparency In line with commitments on transparency of GP earnings, there will be a new contractual requirement for GP practices to publish on their practice website by 31 March 2016, the mean net earnings of GPs in their practice (to include contractor and salaried GPs) relating to 2014/15 financial year. The figure will include earnings from NHS England, CCGs and local authorities for the provision of GP services that relate to the contract and which would have previously been commissioned by PCTs. 127
127 Breaches of this policy Breaches of this policy will be managed in the following way: Incidents of any perceived breach of this policy should be sent directly to the Head of Corporate Governance The Head of Corporate Governance to investigate the perceived breach and to report the findings to the Chair of the Audit Committee in the first instance Where breaches are confirmed further discussion between the Audit Chair, the Chief Officer / Accountable Officer and/or CCG Chair should take place, where necessary, to agree on the most appropriate cause of action The Audit Committee should receive a formal report on the investigations and actions, and where appropriate provide full information to the Governing Body through usual governance reporting arrangements Where a serious breach of this policy takes place the Governing Body will be asked to approve appropriate cause of action Both the Mansfield and Ashfield CCG and the Newark and Sherwood CCG will view instances where this policy is not followed as extremely serious and may take disciplinary action against individuals as a result, which may in turn result in dismissal. Both CCGs will also automatically and immediately refer all cases of potential fraud, corruption and bribery to the CCGs NHS Counter Fraud Specialist for consideration of criminal investigation and potential prosecution as required by the CCGs Counter Fraud, Bribery and Corruption Policy. Referrals will also be made where appropriate, to the pertinent professional regulatory body such as the GMC and NMC. The CCGs will always seek to use the most effective means to recover any taxpayer funding lost due to fraud, corruption or bribery. This may include action via the criminal courts using the Proceeds of Crime Act, or civil recovery. Fraud, Corruption and Bribery Fraud The Fraud Act 2006 came into force on the 15 January 2007 and introduced the general offence of fraud. This is broken down into a number of key areas in terms of criminal offences including; Fraud by false representation Fraud by failing to disclose information Fraud by abuse of position Possession and making or supplying articles for use in fraud Obtaining services dishonestly Corruption and Bribery The UK Bribery Act 2010 has replaced previous Prevention of Corruption Acts and created two general offences of bribery: Offering or giving a bribe to induce someone to behave, or to reward someone for behaving, improperly and; Requesting or accepting a bribe in exchange for acting improperly, or where the request or acceptance is itself improper A new corporate offence has also been introduced Negligent failing by a company or limited liability partnership to prevent bribery being given or offered by an employee or agent on behalf of that organisation. 128
128 All staff working for both groups are required to be aware of the UK Bribery Act 2010 and should also refer to both group s Fraud, Bribery and Corruption Policies for further details. Individuals who fail to disclose relevant interests, outside employment or receipts of gifts or hospitality as required by this policy or the group s Standing Orders and other related financial policies such as the Gifts and Hospitality Policy may be subject to the varying forms of criminal, disciplinary and regulatory actions listed above on page 12 regarding policy breaches. Reporting Suspicions All cases of suspected fraud, corruption, or bribery must be investigated by an accredited NHS Counter Fraud Specialist appointed by both groups. The CCGs appointed Counter Fraud Specialist is Ian Morris, telephone ian.morris@360assurance.nhs.uk or reports can be made directly through the Assistant Chief Officer and Corporate Director. The Raising Concerns at Work (Whistleblowing Policy) details the procedure for individuals to follow if they have concerns about any malpractice connected with the CCGs, without fear of adverse repercussions. Public Concern at Work a registered charity can be contacted for help and advice by UK advice line: whistle@pcaw.org.uk or phone - Whistleblowing Advice Line: The Head of Governance is responsible for maintaining the Register of Interests, holding the Gifts and Hospitality Register and reviewing the implementation of this policy. The Accountable Officer The Chief Officer for both groups has ultimate accountability for the strategic and operational management of both organisations, including ensuring all policies are adhered to. The CCG Governing Bodies will ratify this policy for use throughout the groups. Both groups encourage all individuals to raise any concerns that they may have about the conduct of others in the CCGs or the way in which they are run. The groups are committed to the principle of public accountability and will investigate genuine and reasonable concerns expressed by individuals relating to malpractice within the groups. Individuals will not be discriminated against or suffer a detriment as a result of making such a disclosure, as laid down by the Public Interest Disclosure Act 1998 (PIDA). Annexes Annex 1: NHS Clinical Commissioners, Royal College of General Practitioners and British Medical Association principles on conflicts of interest Annex 2: Declaration of conflict of interests for bidders/contractors template Annex 3: Declaration of interests for members/employees template Annex 4: Procurement template 129
129 Annex 1: NHS Clinical Commissioners, Royal College of General Practitioners and British Medical Association - Shared principles on conflicts of interest when CCGs are commissioning from member practices December Introduction The ability for CCGs to become involved in co-commissioning General Practice and primary care services has the potential to bring many benefits but it also brings with it the potential for perceived and actual conflicts of interest. NHS Clinical Commissioners (NHSCC), the Royal College of General Practitioners (RCGP) and the British Medical Association (BMA) have decided to collectively outline their high level starting principles in managing conflicts of interest when CCGs commission from member practices. In large part this has brought together principles articulated in previous lines/guidance/steer from the above organisations and NHS England. Our principles are applicable to each of the three primary care commissioning models open to CCGs and should not be seen as being directive or be interpreted to mean that we prefer one model over another. These decisions need to remain a local, professionally led, decision. In developing these shared principles we would like them to sit alongside NHS England s updated guidance on Managing Conflicts of Interest (December 2014). We are on a journey regarding the co-commissioning of primary care and we will review these principles when needed and as CCGs work through the guidance. It should be noted that this paper is not designed to address the issue of perceived or actual conflicts of interest in CCGs holding and performance managing GP contracts under cocommissioning arrangements 2. Our headline shared principles around conflicts of interest We collectively agree the following in relation to managing conflicts of interest when CCGs commission from member practices: If CCGs are doing business properly (needs assessments, consultation mechanisms, commissioning strategies and procurement procedures), then the rationale for what and how they are commissioning is clearer and easier to withstand scrutiny. Decisions regarding resource allocation should be evidence-based, and there should be robust mechanisms to ensure open and transparent decision making. CCGs must have robust governance plans in place to maintain confidence in the probity of their own commissioning, and maintain confidence in the integrity of clinicians. CCGs should assume that those making commissioning decisions will behave ethically, but individuals may not realise that they are conflicted, or lack awareness of rules and procedures. To mitigate against this, CCGs should ensure that formal prompts, training and checks are implemented to make sure people are complying with the rules. As a rule of thumb, if in doubt, disclose CCGs should anticipate many possible conflicts when electing/selecting individuals to commissioning roles, and where necessary provide commissioners with training to ensure individuals understand and agree in advance how different scenarios will be dealt with. It is important to be balanced and proportionate the purpose of these tools is not to constrain decision-making to be complex or slow. 130
130 3. Addressing perceived as well as actual conflicts of interest Conflicts of interest in the NHS are not new and they are not always avoidable. The documents we reviewed to produce this paper were all clear that the existence of a conflict is not the same as impropriety and focus on how to avoid potential or perceived wrongdoing. Most importantly all acknowledge that perceived wrongdoing can be as detrimental as actual wrongdoing, and risks losing confidence in the probity of CCGs and the integrity of wider clinicians such as GPs in networks/federations, individual practices and partners. The RCGP/NHS Confederation also notes evidence from the BMJ that people think they aren t biased by potential conflicts but often are so the common theme is - if in any doubt it s important to disclose. The RCGP/NHS Confederation and NHS England Guidance identify four types of potential conflict of interest: direct financial; indirect financial (for example a spouse has a financial interest in a provider); non-financial (i.e. reputation) and; loyalty (i.e., to professional bodies). The BMA recognises that for CCGs there will be situations where the best decision for the population and taxpayers is not in the best interest of individual patients (for whom GPs are required to advocate) and that this can create a perceived conflict. The RCGP/NHS Confederation paper acknowledges this but in terms of the governance when commissioning services. 4. Planning for populations CCGs must always demonstrate that their commissioned services meet the needs of their local populations, as such CCGs will need to work with their Health and Wellbeing Boards or other local strategic bodies to ensure there is alignment to local strategic plans. What is clear from all the existing guidance is that CCGs will need to identify the situations where they are involving their governing body clinicians to strategically plan for their population, and situations where their governing body clinicians need to be separated from procurement, planning and decision-making processes. In the former it is critically important to secure clinical expertise. In the latter, the CCGs will need to manage risks around perceived and actual conflicts in relation to the tendering of services. The BMA outlines that decisions regarding resource allocation should be evidence based, and there should be robust mechanisms to ensure open and transparent decision making. As such, GP involvement must be agreed at each stage of the commissioning and procurement process so that potential risks of conflicts are appropriately defined and mitigated early on. 5. Good practice for CCGs All the guidance suggests CCGs must have robust governance plans in place to maintain confidence in the probity of their own commissioning, and maintain confidence in the integrity of clinicians. 131
131 The RCGP/NHS Confederation suggests using existing NHS guidance as a starting point: Identify potential conflicts Declare interests in a register Exclude individuals from discussion or decision making if financial interest exceeds 1% equity in the provider organisation - depending on the nature of the discussion (we would also add that includes considering the share of the contract value to make sure there are no loopholes, this might also apply to practices with profit sharing arrangements) Continue to manage conflicts post-decision i.e. contract managing (carefully separating overall strategy development for populations from individual procurement processes. The former will be important for CCG lay involvement and include secondary care clinicians and non-executive board nurses, the latter can be managed by managers) NHS England guidance also says that an individual with a material interest in an organisation which provides or is likely to provide significant business should not be a member of CCG Governing Bodies. The BMA suggests anything above 5% equity is a material interest. The RCGP/NHS Confederation reference this threshold but also say that something lower than a 1% stake could also be a material interest (if the size of the bid is significant). Clearly these thresholds need to be considered in relation to individual practices and GP partners once co-commissioning is in place. The perceived risks must be recognised early on and we feel some worked case study examples would be helpful for CCGs as they work through the updated guidance. NHSCC, the RCGP and the BMA are planning to work with NHS England and Monitor to identify these examples. NHSCC believe that CCG lay members, secondary care doctors and nurses on governing bodies play a vital role in the design, implementation, leadership and monitoring of conflicts of interest systems and processes. They can provide robust challenge and ultimately a protection for GPs working in both the commissioning and provision of health care. Enabling them to carry out their roles in this regard is vital. CCGs should also be proactive in their approach when considering conflicts when electing/selecting people, doing a proper induction (i.e. include continuous training and review at both Governing Body and membership (assembly level) and ensuring understanding from individuals, and agree in advance how different scenarios will be dealt with. The CCGs should ensure individuals are prompted to declare an interest but not absolved from their responsibility to declare as well. Again, CCG lay members, secondary care doctors and nurse members of the Governing Body have a critical role in this process, as an independent arbiter and as those providing appropriate scrutiny and oversight. NHS England s Code of Conduct guidance specifically explores when CCGs are commissioning services from their own GP member practices. W hen CCGs are commissioning from federations of practices, the same guidance should apply. As practical support NHS England have also produced an updated code of conduct template for use when drawing up local plans (see their updated guidance). The template asks a series of questions to provide assurance to Health and W ellbeing Boards that the service meets local needs, and to the Audit Committee or external auditors that robust process was used to commission the service, select the appropriate procurement route and address potential conflicts of interest. 132
132 6. Good practice - for individuals The current guidance suggests that individuals making decisions in CCGs do so with the Nolan principles of public life in mind: selflessness, integrity, objectivity, accountability, openness, honesty, and leadership. They also refer to the guidance the General Medical Council (GMC) has produced for doctors including: You must not allow any interests you have to affect the way you prescribe for, treat, refer or commission services for patients. If you are faced with a conflict of interest, you must be open about the conflict, declaring your interest informally, and you should be prepared to exclude yourself from decision making. You must not try to influence patients choice of healthcare services to benefit you, someone close to you, or your employer. If you plan to refer a patient for investigation, treatment or care at an organization in. NHS England guidance indicates that individuals must declare an interest as soon as they come aware of it, and within 28 days. More informally, the RCGP/NHS Confederation also suggested the simple Paxman test - whether explaining the situation to an investigative reporter/journalist like Jeremy Paxman would cause embarrassment. W e think it would be helpful to develop this type of text into a tool for CCGs to use locally. Finally, the BMA suggested that commissioner doctors: Declare all interests, even if they are potential conflicts or the individual is unsure whether it counts as a conflict, as soon as possible. Update a register of interests every three months. Doctors must be familiar with their organisation s formal guidance. If individual doctors have any questions, they should seek advice from colleagues, err on the side of being open about conflicts of interest, or seek external advice from professional or regulatory bodies. In addition to the above, the RCGP suggests there should also be a requirement to update the register of interests if a material difference arises in the circumstances of an individual at any point. 7. Procurement processes CCGs and member practices According to the BMA guidance, when CCGs are procuring community level services, these contracts are often below threshold requiring a competitive tender process. There are a number of procurement options for CCGs in this situation for example a few may include: 1. Competitive tender where GP practices are likely to bid 2. AQP where GP providers are likely to be among the qualified providers 3. Single tender from GP practices. From the guidance that exists different questions arise around conflicts of interest when the above procurement processes are used. For example: Identifying whether approaches such as AQP are being used with the safeguards to ensure 133
133 that patients are aware of the choices available to them. 134
134 If single tender is the route used, CCGs will need to demonstrate a few things depending on the nature of the procurement. For example that there are no other capable providers, why the successful bid was preferred to the others and the impact of disproportionate tendering costs. (Monitor s procurement guidance provides many useful steers on what CCGs will need to demonstrate). For primary care co-commissioning, NHSCC believes one of the elements to include on procurement processes are the issues around standing financial orders and schemes of delegation which should not allow CCGs to divide primary care budgets into smaller budgets to circumvent the procurement process. NHSCC s lay member network will have examples/steer on the correct wording to use from previous local experiences. Regardless of what is the local application, the most important part of this process is transparency. NHS England says to set out the details, including the value of all contracts on the CCGs websites. If they are using AQP, the types and prices of services they are commissioning should be on the websites. All of this information should also be in the CCGs annual reports. When making procurement decisions, the current guidance suggests that anyone with a perceived or material conflict should be excluded from decision making, either both excluded from voting or from discussion and voting. W hat is not clear in the guidance is how far back this rule goes i.e. to the planning stage or just the development of the specification and procurement. CCGs will need to agree that line locally. According to the reviewed guidance if all GPs and practice representatives due to make a decision are conflicted, then the CCGs should be: Referring decisions to the governing body, so that lay members / the nurse / the secondary care doctor can make the final decision. However this may weaken GP clinical input into decision making. Co-opting individuals from the HW B or another CCG onto the governing body, or invite the HW B / another CCG to review the proposal to provide additional scrutiny (these individuals would only be able to participate in decision making if this was set out in the CCGs constitution) Ensure that quoracy rules enable decisions to be made in this circumstance Plan ahead to ensure that agreed processes are followed Use an appropriately constituted arms-length external scrutiny committee to ensure probity (recommended by the BMA). CCGs can use commissioning support services (CSS) to reduce potential conflicts, for example a CSS can help select the best procurement route and prepare bids etc. However, this cannot completely eliminate the conflict as CCGs are responsible for signing off specification and evaluation criteria, signing off which providers to invite to tender, and making the final decision on the selection of the provider. The CCGs are responsible for ensuring that their CSS or other third parties are compliant with regulations in the same way that the CCGs must be. NHS England also suggest any questions about the service going beyond the scope of the GP contract should be discussed with NHS England area teams, clearly that would need review in light of new delegated co-commissioning arrangements. 135
135 Networks and Federations We note that the increasing number of GP networks and federations could potentially present an added complication to local procurement processes. If most or all CCG member practices are part of the local federation, then this could mean that a practice not part of the federation/excluded from a federation may not have the opportunity to win contracts through competitive tender because the process is more suited to federated organisations. One way to mitigate this would be for the CCGs to always design and procure service specifications according to best practice (with openness and transparency), thereby supporting all practices to bid. One area to be careful about is when all the GPs on a governing body have a declared interest in local federations this makes decision making and accountability complex and the CCGs will need to work that through carefully with the input of its lay members and wider clinicians on the governing body. Again, an external scrutiny committee with non-conflicted clinicians such as from a neighbouring CCG may be helpful. 8. Local engagement Separately, the BMA suggests that LMCs should be involved in CCGs either by formal consultation, a non-voting seat on governing body, or as an observer on governing body. They indicate that a non-voting governing body seat would be the best option. Neither of the other two papers we reviewed address this. 9. Other conflicts of interest issues for consideration Personal conflict The RCGP/NHS Confederation highlight that in CCG governing bodies a personal conflict can arise because CCG leaders are elected by their constituent GP members. There could be a perception that CCG governing bodies are favouring the most vocal or influential of their GP practice members. Related to this is the potential indirect interest for elected GPs to build a constituency of supporters within their CCG. The CCGs are responsible for ensuring that their CSS or other third parties are compliant with regulations in the same way that the CCGs must be. NHS England guidance suggests that in the case of every GP governing body member being conflicted, the lay members, registered nurse and secondary care doctor make the decision (and that the constitution is written so that this is quorate). This could however mean that decisions would be taken without a GP perspective. Alternatively, CCGs may bring in members of the Health and W ellbeing Board or another CCG to provide oversight, or as the BMA suggests use an external scrutiny committee to make decisions. Use of primary care incentive schemes In its guidance, the BMA highlights its concerns about the professional and ethical implications of CCGs applying incentive schemes to reduce referral or prescribing activity. The BMA urges any doctor, whether commissioner or provider, to consider the schemes carefully and ensure that scheme is based on clinical evidence. NHSCC suggests that one solution is to ensure that the expertise of secondary care clinicians and nurses on governing bodies plays an important part in providing clinical input and lay members can scrutinize commercial/ financial and performance data. The RCGP acknowledge that it is not ethical to under-treat or under-refer for financial gain, but is not unethical to review and reflect on variations in referral/prescribing rates and try to reduce referrals in line with evidence or best practice. 136
136 Note to the reader: This paper has been developed from a review of three guidance documents and brings together previous lines/guidance from NHSCC, NHS England, the RCGP and the BMA. BMA Conflicts of interest in the new commissioning system: Doctors in commissioning roles April 2013 RCGP/NHS Confederation Managing conflicts of interest in clinical commissioning groups September 2011 NHS England Managing conflicts of interest: guidance for clinical commissioning groups. March 2013 (includes Commissioning Board Document that precedes it). We have also read across the paper to the new version of this document published December NHSCC have also supplemented the principles raised in this paper with some points for steer that have been raised by members of its lay member network. 137
137 Annex 2: Declaration of Conflict of Interests for Bidders/Contractors Template NHS Mansfield and Ashfield Clinical Commissioning Group and NHS Newark and Sherwood Clinical Commissioning Group bidders/potential contractors/service providers declaration form: financial and other interests This form is required to be completed in accordance with the CCGs Constitutions, and s140 of the NHS Act 2006 (as amended by the Health and Social Care Act 2012) and the NHS (Procurement, Patient Choice and Competition) (No2) Regulations 2013 and related guidance Notes: All potential bidders/contractors/service providers, including sub-contractors, members of a consortium, advisers or other associated parties (Relevant Organisation) are required to identify any potential conflicts of interest that could arise if the Relevant Organisation were to take part in any procurement process and/or provide services under, or otherwise enter into any contract with, the CCG, or with NHS England in circumstances where the CCGs are jointly commissioning the service with, or acting under a delegation from, NHS England. If any assistance is required in order to complete this form, then the Relevant Organisation should contact the Head of Corporate Governance. The completed form should be sent to the Head of Corporate Governance. Any changes to interests declared either during the procurement process or during the term of any contract subsequently entered into by the Relevant Organisation and the CCGs must be notified to the CCGs by completing a new declaration form and submitting it to the Head of Corporate Governance. Relevant Organisations completing this declaration form must provide sufficient detail of each interest so that the CCGs, NHS England and also a member of the public would be able to understand clearly the sort of financial or other interest the person concerned has and the circumstances in which a conflict of interest with the business or running of the CCG or NHS England (including the award of a contract) might arise. If in doubt as to whether a conflict of interests could arise, a declaration of the interest should be made. Interests that must be declared (whether such interests are those of the Relevant Person themselves or of a family member, close friend or other acquaintance of the Relevant Person), include the following: the Relevant Organisation or any person employed or engaged by or otherwise connected with a Relevant Organisation (Relevant Person) has provided or is providing services or other work for the CCGs or NHS England a Relevant Organisation or Relevant Person is providing services or other work for any other potential bidder in respect of this project or procurement process the Relevant Organisation or any Relevant Person has any other connection with the CCGs or NHS England, whether personal or professional, which the public could perceive may impair or otherwise influence the CCGs or any of their members or employees judgements, decisions or actions. 138
138 Declarations: Name of Relevant Organisation: Interests Type of Interest Provision of services or other work for the CCGs or NHS England Details Provision of services or other work for any other potential bidder in respect of this project or procurement process Any other connection with the CCGs or NHS England, whether personal or professional, which the public could perceive may impair or otherwise influence the CCGs or any of their members or employees judgements, decisions or actions Name of Relevant Person Interests [complete for all Relevant Persons] Type of Interest Details Personal interest or that of a family member, close friend or other acquaintance? Provision of services or other work for the CCG or NHS England 139
139 Provision of services or other work for any other potential bidder in respect of this project or procurement process Any other connection with the CCG or NHS England, whether personal or professional, which the public could perceive may impair or otherwise influence the CCGs or any of their members or employees judgements, decisions or actions To the best of my knowledge and belief, the above information is complete and correct. I undertake to update as necessary the information. Signed: On behalf of: Date: 140
140 Annex 3: Declaration of Interests for Members/Employees Template NHS Mansfield and Ashfield Clinical Commissioning Group and NHS Newark and Sherwood Clinical Commissioning Group member / employee/ governing body member / committee or sub-committee member (including committees and subcommittees of the governing body) [delete as appropriate] declaration form: financial and other interests This form is required to be completed in accordance with the CCGs Constitutions and section 14O of The National Health Service Act 2006, the NHS (Procurement, Patient Choice and Competition) regulations 2013 and the Substantive guidance on the Procurement, Patient Choice and Competition Regulations Notes: Each CCG must make arrangements to ensure that the persons mentioned above declare any interest which may lead to a conflict with the interests of the CCGs and /or NHS England and the public for whom they commission services in relation to a decision to be made by the CCGs and/or NHS England or which may affect or appear to affect the integrity of the award of any contract by the CCGs and/or NHS England. A declaration must be made of any interest likely to lead to a conflict or potential conflict as soon as the individual becomes aware of it, and within 28 days. If any assistance is required in order to complete this form, then the individual should contact the Head of Corporate Governance. The completed form should be sent by both and signed hard copy to the Head of Corporate Governance. Any changes to interests declared must also be registered within 28 days by completing and submitting a new declaration form. The register will be published on the CCG s websites and will be made available in hard copy upon request to the Head of Corporate Governance. Any individual and in particular members and employees of the CCGs and/or NHS England must provide sufficient detail of the interest, and the potential for conflict with the interests of the CCG and/or NHS England and the public for whom they commission services, to enable a lay person to understand the implications and why the interest needs to be registered. If there is any doubt as to whether or not a conflict of interests could arise, a declaration of the interest must be made. Interests that must be declared (whether such interests are those of the individual themselves or of a family member, close friend or other acquaintance of the individual) include: roles and responsibilities held within member practices; directorships, including non-executive directorships, held in private companies or PLCs ownership or part-ownership of private companies, businesses or consultancies likely or possibly seeking to do business with the CCGs and /or with NHS England shareholdings (more than 5%) of companies in the field of health and social care; a position of authority in an organisation (e.g. charity or voluntary organisation) in the field of health and social care; any connection with a voluntary or other organisation (public or private) contracting for NHS services; 141
141 research funding/grants that may be received by the individual or any organisation in which they have an interest or role; any other role or relationship which the public could perceive would impair or otherwise influence the individual s judgment or actions in their role within the CCGs. If there is any doubt as to whether or not an interest is relevant, a declaration of the interest must be made. Declaration: Name: Position within or relationship with, the CCGs or NHS England: Interests Type of Interest Details Personal interest or that of a family member, close friend or other acquaintance? Roles and responsibilities held within member practices Directorships, Including nonexecutive directorships, held in private companies or PLCs Ownership or partownership of private companies, businesses or consultancies likely or possibly seeking to do business with the CCGs and/or with NHS England Shareholdings (more than 5%) of companies in the field of health and social care 142
142 Positions of authority in an organisation (e.g. charity or voluntary organisation) in the field of health and social care Any connection with a voluntary or other organisation contracting for NHS services Research funding/grants that may be received by the individual or any organisation they have an interest or role in [Other specific interests?] Any other role or relationship which the public could perceive would impair or otherwise influence the individual s judgment or actions in their role within the CCGs and/or with NHS England. To the best of my knowledge and belief, the above information is complete and correct. I undertake to update as necessary the information provided and to review the accuracy of the information provided regularly and no longer than annually. I give my consent for the information to be used for the purposes described in the CCGs Constitutions and published accordingly. Signed: Date: 143
143
144
NHS WOLVERHAMPTON CLINICAL COMMISSIONING GROUP CONSTITUTION
 NHS WOLVERHAMPTON CLINICAL COMMISSIONING GROUP CONSTITUTION Version: [78] NHS England Effective Date: 1 December 2015 April 2017 CONTENTS Part Description Page Foreword 1 1 Introduction and Commencement
NHS WOLVERHAMPTON CLINICAL COMMISSIONING GROUP CONSTITUTION Version: [78] NHS England Effective Date: 1 December 2015 April 2017 CONTENTS Part Description Page Foreword 1 1 Introduction and Commencement
NHS HALTON CLINICAL COMMISSIONING GROUP CONSTITUTION. Version: 4
 NHS HALTON CLINICAL COMMISSIONING GROUP CONSTITUTION Version: 4 Approved by NHS Halton Clinical Commissioning Group Members Forum and Governing Body on 5 th November 2015 NHS England Effective Date: 16
NHS HALTON CLINICAL COMMISSIONING GROUP CONSTITUTION Version: 4 Approved by NHS Halton Clinical Commissioning Group Members Forum and Governing Body on 5 th November 2015 NHS England Effective Date: 16
Collaborative Agreement for CCGs and NHS England
 RCCG/GB/15/164 Collaborative Agreement for CCGs and NHS England East Midlands Collaborative Commissioning Oversight Group (EMCCOG) 1. Particulars 1.1. This Agreement records the particulars of the agreement
RCCG/GB/15/164 Collaborative Agreement for CCGs and NHS England East Midlands Collaborative Commissioning Oversight Group (EMCCOG) 1. Particulars 1.1. This Agreement records the particulars of the agreement
Agreeing the methodology used to calculate weighted rates for CCG GP practice reporting
 Agreeing the methodology used to calculate weighted rates for CCG GP practice reporting Introduction The mid-nottinghamshire analytics team are currently reviewing the reporting methodology used to support
Agreeing the methodology used to calculate weighted rates for CCG GP practice reporting Introduction The mid-nottinghamshire analytics team are currently reviewing the reporting methodology used to support
Quality and Governance Committee. Terms of Reference
 Quality and Governance Committee Terms of Reference 1. Constitution 1.1 The Clinical Commissioning Group s Governing Body hereby resolves to establish a Committee of the Governing Body known as the Quality
Quality and Governance Committee Terms of Reference 1. Constitution 1.1 The Clinical Commissioning Group s Governing Body hereby resolves to establish a Committee of the Governing Body known as the Quality
Patient Experience Strategy
 Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Reservation of Powers to the Board & Delegation of Powers
 Reservation of Powers to the Board & Delegation of Powers Status: Draft Next Review Date: March 2014 Page 1 of 102 Reservation of Powers to the Board & Delegation of Powers Issue Date: 5 April 2013 Document
Reservation of Powers to the Board & Delegation of Powers Status: Draft Next Review Date: March 2014 Page 1 of 102 Reservation of Powers to the Board & Delegation of Powers Issue Date: 5 April 2013 Document
Cambridgeshire and Peterborough Sustainability and Transformation Partnership
 Cambridgeshire and Peterborough Sustainability and Transformation Partnership Governance Framework November 2017 Page 1 of 28 Contents 1. Introduction 2. Sustainability and Transformation Partnership 3.
Cambridgeshire and Peterborough Sustainability and Transformation Partnership Governance Framework November 2017 Page 1 of 28 Contents 1. Introduction 2. Sustainability and Transformation Partnership 3.
Putting Barnsley People First. Quality and Patient Safety Committee Terms of Reference
 Putting Barnsley People First Quality and Patient Safety Committee Terms of Reference 1. Introduction NHS Barnsley Clinical Commissioning Group Quality and Patient Safety Committee 1.1 The Clinical Commissioning
Putting Barnsley People First Quality and Patient Safety Committee Terms of Reference 1. Introduction NHS Barnsley Clinical Commissioning Group Quality and Patient Safety Committee 1.1 The Clinical Commissioning
Joint framework: Commissioning and regulating together
 With support from NHS Clinical Commissioners Regulation of General Practice Programme Board Joint framework: Commissioning and regulating together A practical guide for staff January 2018 Publications
With support from NHS Clinical Commissioners Regulation of General Practice Programme Board Joint framework: Commissioning and regulating together A practical guide for staff January 2018 Publications
Mental Health Social Work: Community Support. Summary
 Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
MEMORANDUM OF UNDERSTANDING
 MEMORANDUM OF UNDERSTANDING Memorandum of Understanding Co-Commissioning Between NHS England Lancashire And South Cumbria And Clinical Commissioning Groups 1 Memorandum of Understanding (MoU) for Primary
MEMORANDUM OF UNDERSTANDING Memorandum of Understanding Co-Commissioning Between NHS England Lancashire And South Cumbria And Clinical Commissioning Groups 1 Memorandum of Understanding (MoU) for Primary
Overarching Section 75 Agreement Adults Integrated Health and Social Care Services. Subject. Cabinet Member
 ACTION TAKEN BY CABINET MEMBER (EXECUTIVE FUNCTION) Subject Cabinet Member Overarching Section 75 Agreement Adults Integrated Health and Social Care Services Cabinet Member for Adults Cabinet Member for
ACTION TAKEN BY CABINET MEMBER (EXECUTIVE FUNCTION) Subject Cabinet Member Overarching Section 75 Agreement Adults Integrated Health and Social Care Services Cabinet Member for Adults Cabinet Member for
Quality of Care Approach Quality assurance to drive improvement
 Quality of Care Approach Quality assurance to drive improvement December 2017 We are committed to equality and diversity. We have assessed this framework for likely impact on the nine equality protected
Quality of Care Approach Quality assurance to drive improvement December 2017 We are committed to equality and diversity. We have assessed this framework for likely impact on the nine equality protected
Health and Safety Strategy
 NHS Newcastle Gateshead Clinical Commissioning Group Health and Safety Strategy Document Status Equality Impact Assessment Document Ratified/Approved By Final No impact Quality, Safety and Risk Committee
NHS Newcastle Gateshead Clinical Commissioning Group Health and Safety Strategy Document Status Equality Impact Assessment Document Ratified/Approved By Final No impact Quality, Safety and Risk Committee
BOARD PAPER - NHS ENGLAND. Internal Delegation arrangements for Greater Manchester Devolution
 Paper: PB.31.03.16/08 BOARD PAPER - NHS ENGLAND Title: Internal Delegation arrangements for Greater Manchester Devolution Lead Director: Paul Baumann, Chief Financial Officer Karen Wheeler, National Director:
Paper: PB.31.03.16/08 BOARD PAPER - NHS ENGLAND Title: Internal Delegation arrangements for Greater Manchester Devolution Lead Director: Paul Baumann, Chief Financial Officer Karen Wheeler, National Director:
Quality Assurance Framework Adults Services. Framework. Version: 1.2 Effective from: August 2016 Review date: June 2017
 Quality Assurance Framework Adults Services Framework Version: 1.2 Effective from: August 2016 Review date: June 2017 Signed off by: Sharon Gogan Title: Head of Adult Social Care Date: 20 th May 2014 Quality
Quality Assurance Framework Adults Services Framework Version: 1.2 Effective from: August 2016 Review date: June 2017 Signed off by: Sharon Gogan Title: Head of Adult Social Care Date: 20 th May 2014 Quality
NHS Equality Delivery System for Isle of Wight NHS Trust. Interim baseline assessment against the
 Interim baseline assessment against the NHS Equality Delivery System for Isle of Wight NHS Trust The NHS Isle of Wight has adopted the NHS Equality Delivery System as the framework to achieve compliance
Interim baseline assessment against the NHS Equality Delivery System for Isle of Wight NHS Trust The NHS Isle of Wight has adopted the NHS Equality Delivery System as the framework to achieve compliance
Cabinet Member for Education, Children and Families
 Meeting Cabinet Resources Committee Date 24 September 2013 Subject Provision of therapies to Children with Special Educational Needs and placements to children in care Report of Summary Cabinet Member
Meeting Cabinet Resources Committee Date 24 September 2013 Subject Provision of therapies to Children with Special Educational Needs and placements to children in care Report of Summary Cabinet Member
Equality Objectives
 Equality Objectives 2015 2019 This document is available in alternative community languages and formats upon request, such as large print and electronically. Please contact the Equality, Diversity and
Equality Objectives 2015 2019 This document is available in alternative community languages and formats upon request, such as large print and electronically. Please contact the Equality, Diversity and
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
Delegated Commissioning Updated following latest NHS England Guidance
 Delegated Commissioning Updated following latest NHS England Guidance 13th August 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England (Direct
Delegated Commissioning Updated following latest NHS England Guidance 13th August 2015 Croydon, Kingston, Merton, Richmond, Sutton and Wandsworth NHS Clinical Commissioning Groups and NHS England (Direct
COMMISSIONING FOR QUALITY FRAMEWORK
 This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version COMMISSIONING FOR QUALITY FRAMEWORK Document Title: Commissioning for Quality Framework
This document is uncontrolled once printed. Please check on the CCG s Intranet site for the most up to date version COMMISSIONING FOR QUALITY FRAMEWORK Document Title: Commissioning for Quality Framework
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD
 BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD") INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
EXECUTIVE MEDICAL DIRECTOR JOB DESCRIPTION. Medical Education Leads Clinical Directors (professional leadership) Director of Clinical Audit
 Director of Clinical Audit") EXECUTIVE MEDICAL DIRECTOR JOB DESCRIPTION Job Title: Accountable to: Responsible for: Executive Medical Director Chief Executive Director of Research & Development Medical Education Leads Clinical Directors
EXECUTIVE MEDICAL DIRECTOR JOB DESCRIPTION Job Title: Accountable to: Responsible for: Executive Medical Director Chief Executive Director of Research & Development Medical Education Leads Clinical Directors
QUALITY COMMITTEE. Terms of Reference
 QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
QUALITY COMMITTEE Terms of Reference This Committee will report to NHS Halton CCG Governing Body on the development, improvement and monitoring of all areas of quality. This will include clinical effectiveness,
Sources of evidence [note: you may reference other sources of evidence] Quarterly National Reporting Systems to the SHA on Waiting Times.
![Sources of evidence [note: you may reference other sources of evidence] Quarterly National Reporting Systems to the SHA on Waiting Times.](/thumbs/78/77117024.jpg "Sources of evidence [note: you may reference other sources of evidence] Quarterly National Reporting Systems to the SHA on Waiting Times.") PATIENT RIGHTS/PLEDGES Rights/pledges/Actions 1. The NHS commits to provide convenient, easy access to services within waiting times set out in the Handbook to the. The Primary Care Trust has a process
PATIENT RIGHTS/PLEDGES Rights/pledges/Actions 1. The NHS commits to provide convenient, easy access to services within waiting times set out in the Handbook to the. The Primary Care Trust has a process
Leeds West CCG Governing Body Meeting
 Agenda Item: LW2015/115 FOI Exempt: N Leeds West CCG Governing Body Meeting Date of meeting: 4 vember 2015 Title: Delegated Commissioning of Primary Medical Services Lead Governing Body Member: Dr Simon
Agenda Item: LW2015/115 FOI Exempt: N Leeds West CCG Governing Body Meeting Date of meeting: 4 vember 2015 Title: Delegated Commissioning of Primary Medical Services Lead Governing Body Member: Dr Simon
Report to the Merton Clinical Commissioning Group Board
 Merton CCG Board 13.06 12 Pt1 : 3.3 : Att 03 : 01 of 03 Report to the Merton Clinical Commissioning Group Board Date of Meeting: Wednesday 13 th June 2012 Agenda No: 3.3 ATTACHMENT 03 Title of Document:
Merton CCG Board 13.06 12 Pt1 : 3.3 : Att 03 : 01 of 03 Report to the Merton Clinical Commissioning Group Board Date of Meeting: Wednesday 13 th June 2012 Agenda No: 3.3 ATTACHMENT 03 Title of Document:
Equality and Diversity
 Equality and Diversity Vision Statement Yasmin Mahmood Senior Associate Equality and Diversity May 2016 page 1/9 Introduction NHS Merton CCG is committed to ensuring equality, diversity and inclusion are
Equality and Diversity Vision Statement Yasmin Mahmood Senior Associate Equality and Diversity May 2016 page 1/9 Introduction NHS Merton CCG is committed to ensuring equality, diversity and inclusion are
Delegated Commissioning of Primary Medical Services Briefing Paper
 Appendix One Delegated Commissioning of Primary Medical Services Briefing Paper 1.0 Introduction Swindon CCG has been jointly commissioning Primary Medical Services with NHS England under co-commissioning
Appendix One Delegated Commissioning of Primary Medical Services Briefing Paper 1.0 Introduction Swindon CCG has been jointly commissioning Primary Medical Services with NHS England under co-commissioning
Framework for managing performer concerns NHS (Performers Lists) (England) Regulations 2013
 (England) Regulations 2013") Framework for managing performer concerns NHS (Performers Lists) (England) Regulations 2013 Information reader box NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information
Framework for managing performer concerns NHS (Performers Lists) (England) Regulations 2013 Information reader box NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information
Birmingham, Sandwell and Solihull Eligibility Criteria Policy for NHS Non-Emergency Patient Transport (NEPT)
") Birmingham, Sandwell and Solihull Eligibility Criteria Policy for NHS Non-Emergency Patient Transport (NEPT) Version: 0.1 Ratified by: Date ratified: 1 st June 2016 Name of originator/author: Name of responsible
Birmingham, Sandwell and Solihull Eligibility Criteria Policy for NHS Non-Emergency Patient Transport (NEPT) Version: 0.1 Ratified by: Date ratified: 1 st June 2016 Name of originator/author: Name of responsible
Application Pack: Applicants for Transformation Manager
 Application Pack: Applicants for Transformation Manager Contents 1.0 Information about NHS Eastern Cheshire Clinical Commissioning Group and the Eastern Cheshire Healthcare Economy 2.0 Job Description
Application Pack: Applicants for Transformation Manager Contents 1.0 Information about NHS Eastern Cheshire Clinical Commissioning Group and the Eastern Cheshire Healthcare Economy 2.0 Job Description
4 Year Patient and Public Involvement Strategy
 4 Year Patient and Public Involvement Strategy 2015-18 Contents Page(s) 1. Introduction - 2. Summary of the patient and public involvement strategy 2015-18 - 3. Definitions of involvement and best practice
4 Year Patient and Public Involvement Strategy 2015-18 Contents Page(s) 1. Introduction - 2. Summary of the patient and public involvement strategy 2015-18 - 3. Definitions of involvement and best practice
Direct Commissioning Assurance Framework. England
 Direct Commissioning Assurance Framework England NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning Development Finance Human Resources
Direct Commissioning Assurance Framework England NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning Development Finance Human Resources
North East Hampshire and Farnham Clinical Commissioning Group Safeguarding Framework
 North East Hampshire and Farnham Clinical Commissioning Group Safeguarding Framework North East Hampshire and Farnham Clinical Commissioning Group Safeguarding Strategic Framework Page 3 of 27 Contents
North East Hampshire and Farnham Clinical Commissioning Group Safeguarding Framework North East Hampshire and Farnham Clinical Commissioning Group Safeguarding Strategic Framework Page 3 of 27 Contents
SPONSORSHIP AND JOINT WORKING WITH THE PHARMACEUTICAL INDUSTRY
 SPONSORSHIP AND JOINT WORKING WITH THE PHARMACEUTICAL INDUSTRY 1 SUMMARY This document sets out Haringey Clinical Commissioning Group policy and advice to employees on sponsorship and joint working with
SPONSORSHIP AND JOINT WORKING WITH THE PHARMACEUTICAL INDUSTRY 1 SUMMARY This document sets out Haringey Clinical Commissioning Group policy and advice to employees on sponsorship and joint working with
Trust Board Meeting in Public: Wednesday 18 January 2017 TB Equality, Diversity and Inclusion Progress Report
 Trust Board Meeting in Public: Wednesday 18 January 2017 Title Equality, Diversity and Inclusion Progress Report Status History For noting Further to receipt of the Equality, Diversity and Inclusion, Annual
Trust Board Meeting in Public: Wednesday 18 January 2017 Title Equality, Diversity and Inclusion Progress Report Status History For noting Further to receipt of the Equality, Diversity and Inclusion, Annual
1. Introduction. 2. Purpose of the Ethical Framework
 Ethical Decision-Making Framework for Individual Funding Requests (IFRs) v1.1 1. Introduction 1.1 This Ethical Framework sets out the values that South London IFR Panels and South London CCGs will apply
Ethical Decision-Making Framework for Individual Funding Requests (IFRs) v1.1 1. Introduction 1.1 This Ethical Framework sets out the values that South London IFR Panels and South London CCGs will apply
IT ALL STARTS WITH YOU
 Email: jo.curtis@nhs.net IT ALL STARTS WITH YOU Tell us about your experience Help us improve NHS services This guide takes you through the different ways you can tell the NHS about your experiences, so
Email: jo.curtis@nhs.net IT ALL STARTS WITH YOU Tell us about your experience Help us improve NHS services This guide takes you through the different ways you can tell the NHS about your experiences, so
Communication & Engagement Strategy Stoke-on-Trent & North Staffordshire Clinical Commissioning Groups
 Communication & Engagement Strategy Stoke-on-Trent & North Staffordshire Clinical Commissioning Groups 2017 2021 The NHS belongs to all of us. It is there to improve our health and wellbeing, supporting
Communication & Engagement Strategy Stoke-on-Trent & North Staffordshire Clinical Commissioning Groups 2017 2021 The NHS belongs to all of us. It is there to improve our health and wellbeing, supporting
Update on co-commissioning of primary care: guidance for CCG member practices and LMCs
 Update on co-commissioning of primary care: guidance for CCG member practices and LMCs British Medical Association bma.org.uk This paper is an update of previous GPC (general practitioners committee) guidance
Update on co-commissioning of primary care: guidance for CCG member practices and LMCs British Medical Association bma.org.uk This paper is an update of previous GPC (general practitioners committee) guidance
Enhanced service specification. Avoiding unplanned admissions: proactive case finding and patient review for vulnerable people
 Enhanced service specification Avoiding unplanned admissions: proactive case finding and patient review for vulnerable people 1 Enhanced service specification Avoiding unplanned admissions: proactive case
Enhanced service specification Avoiding unplanned admissions: proactive case finding and patient review for vulnerable people 1 Enhanced service specification Avoiding unplanned admissions: proactive case
WORKING WITH THE PHARMACEUTICAL INDUSTRY
 WORKING WITH THE PHARMACEUTICAL INDUSTRY Page 1 of 11 WORKING WITH THE PHARMACEUTICAL INDUSTRY CCG Policy Reference: SuttonCCG/SLCSU/GOV/099 THIS POLICY WILL BE APPROVED BY THE CLINICAL COMMISSIONING GROUP
WORKING WITH THE PHARMACEUTICAL INDUSTRY Page 1 of 11 WORKING WITH THE PHARMACEUTICAL INDUSTRY CCG Policy Reference: SuttonCCG/SLCSU/GOV/099 THIS POLICY WILL BE APPROVED BY THE CLINICAL COMMISSIONING GROUP
ACTION TAKEN UNDER DELEGATED POWERS BY OFFICER 27 th March Contracts Award for Accommodation and Support Services (Lot 1 Support at Home)
") ACTION TAKEN UNDER DELEGATED POWERS BY OFFICER 27 th March 2017 Title Contracts Award for Accommodation and Support Services (Lot 1 Support at Home) Report of Dawn Wakeling, Adults & Health Commissioning
ACTION TAKEN UNDER DELEGATED POWERS BY OFFICER 27 th March 2017 Title Contracts Award for Accommodation and Support Services (Lot 1 Support at Home) Report of Dawn Wakeling, Adults & Health Commissioning
Wandsworth CCG. Continuing Healthcare Commissioning Policy
 Wandsworth CCG Continuing Healthcare Commissioning Policy Document Control Title Originator/author: Approval Body Wandsworth CCG Continuing Healthcare Commissioning Policy Alison Kirby / Munya Nhamo Wandsworth
Wandsworth CCG Continuing Healthcare Commissioning Policy Document Control Title Originator/author: Approval Body Wandsworth CCG Continuing Healthcare Commissioning Policy Alison Kirby / Munya Nhamo Wandsworth
Policy and Resources Committee 13 February 2018
 Policy and Resources Committee 13 February 2018 Title Public Health Nursing 0-19 Report of Wards Status Urgent Key Councillor Richard Cornelius All Public No Yes Enclosures None Officer Contact Details
Policy and Resources Committee 13 February 2018 Title Public Health Nursing 0-19 Report of Wards Status Urgent Key Councillor Richard Cornelius All Public No Yes Enclosures None Officer Contact Details
CCG authorisation: the role of medicines management
 May 2012 The NHS medicines bill for 2010 was 12.9 billion, of which secondary care costs accounted for 32%. Prescribing inflation in 2010 ran at 4.8% and it is estimated that around 14% of total CCG budgets
May 2012 The NHS medicines bill for 2010 was 12.9 billion, of which secondary care costs accounted for 32%. Prescribing inflation in 2010 ran at 4.8% and it is estimated that around 14% of total CCG budgets
BIRMINGHAM CITY COUNCIL
 BIRMINGHAM CITY COUNCIL PUBLIC REPORT Report to: CABINET Report of: Strategic Director for People Date of Decision: 28 th June 2016 SUBJECT: STRATEGY AND PROCUREMENT PROCESS FOR THE PROVISION OF EARLY
BIRMINGHAM CITY COUNCIL PUBLIC REPORT Report to: CABINET Report of: Strategic Director for People Date of Decision: 28 th June 2016 SUBJECT: STRATEGY AND PROCUREMENT PROCESS FOR THE PROVISION OF EARLY
Primary Care Commissioning Next Steps to Delegated Commissioning September Board Paper. 2.0 Delegated Opportunities, Benefits and Risks
 Primary Care Commissioning Next Steps to Delegated Commissioning September Board Paper 1.0 Introduction This paper provides a briefing to the Wandsworth CCG Board on our progress in developing a Primary
Primary Care Commissioning Next Steps to Delegated Commissioning September Board Paper 1.0 Introduction This paper provides a briefing to the Wandsworth CCG Board on our progress in developing a Primary
NHS England (Wessex) Clinical Senate and Strategic Networks. Accountability and Governance Arrangements
 Clinical Senate and Strategic Networks. Accountability and Governance Arrangements") NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
NHS England (Wessex) Clinical Senate and Strategic Networks Accountability and Governance Arrangements Version 6.0 Document Location: This document is only valid on the day it was printed. Location/Path
Equality and Health Inequalities Strategy
 Equality and Health Inequalities Strategy 1 Schematic of the Equality and Health Inequality Strategy Improving Lives: People and Patients Listening and Learning Gaining Knowledge Making the System Work
Equality and Health Inequalities Strategy 1 Schematic of the Equality and Health Inequality Strategy Improving Lives: People and Patients Listening and Learning Gaining Knowledge Making the System Work
TRUST BOARD TB(16) 44. Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals
 44. Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals") TRUST BOARD TB(16) 44 Title: Action: Meeting: Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals FOR NOTING Date of meeting Purpose: The purpose
TRUST BOARD TB(16) 44 Title: Action: Meeting: Summary of Lord Carter recommendations Operational productivity and performance in English acute hospitals FOR NOTING Date of meeting Purpose: The purpose
Central Alerting System (CAS) Policy
 Policy") Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified By Central Alerting System (CAS) Policy NTW(O)17 Gary O Hare Executive Director of Nursing and Operations Tony Gray
GCP Training for Research Staff. Document Number: 005
 GCP Training for Research Staff Document Number: 005 Version: 1 Ratified by: RFL Committee Date ratified: 03.06.2014 Name of originator/author: Directorate: Department: Name of responsible individual:
GCP Training for Research Staff Document Number: 005 Version: 1 Ratified by: RFL Committee Date ratified: 03.06.2014 Name of originator/author: Directorate: Department: Name of responsible individual:
Looked After Children Annual Report
 Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
Looked After Children Annual Report Reporting period April 2016 March 2017 Authors Maxine Lomax - Designated Nurse for Child Protection & Looked After Children Dr. Bin Hooi Low - Designated Doctor for
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Primary Care Commissioning Committee. Terms of Reference. FINAL March 2015
 Primary Care Commissioning Committee Terms of Reference FINAL March 2015 1. Introduction 1.1. Simon Stevens, the Chief Executive of NHS England, announced on 1 May 2014 that NHS England was inviting Clinical
Primary Care Commissioning Committee Terms of Reference FINAL March 2015 1. Introduction 1.1. Simon Stevens, the Chief Executive of NHS England, announced on 1 May 2014 that NHS England was inviting Clinical
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
Document Title: Document Number:
 including Document Title: Document Number: Version: 2.0 Ratified by: Committee Date ratified: 25/01/2018 Name of originator/author: Directorate: Department: Name of responsible individual: Rachel Fay Corporate
including Document Title: Document Number: Version: 2.0 Ratified by: Committee Date ratified: 25/01/2018 Name of originator/author: Directorate: Department: Name of responsible individual: Rachel Fay Corporate
Wig and Hair Replacement Policy
 Leeds CCGs Wigs and Hair Replacement Policy 2016-19 Wig and Hair Replacement Policy Version: 2016-19 Ratified by: NHS Leeds West CCG Assurance Committee on; 16 vember 2016 NHS Leeds rth CCG Governance
Leeds CCGs Wigs and Hair Replacement Policy 2016-19 Wig and Hair Replacement Policy Version: 2016-19 Ratified by: NHS Leeds West CCG Assurance Committee on; 16 vember 2016 NHS Leeds rth CCG Governance
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Primary Care Comissioning Committee Report. 3. Key Messages: The Clinical Commissioning Group is required to invest 3 per head
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Primary Care Comissioning Committee Report. 3. Key Messages: The Clinical Commissioning Group is required to invest 3 per head
Clinical Commissioning Group Governing Body Paper Summary Sheet For: PUBLIC session PRIVATE session. Date of Meeting: 24 March 2015
 Clinical Commissioning Group Governing Body Paper Summary Sheet For: PUBLIC session PRIVATE session Date of Meeting: 24 March 205 For: Decision Discussion Noting Agenda Item and title: Author: GOV/5/03/20
Clinical Commissioning Group Governing Body Paper Summary Sheet For: PUBLIC session PRIVATE session Date of Meeting: 24 March 205 For: Decision Discussion Noting Agenda Item and title: Author: GOV/5/03/20
Central Bedfordshire Council. Determination of Proposal to Commission New Middle School Places in Leighton Buzzard
 Central Bedfordshire Council EXECUTIVE 6 October 2015 Determination of Proposal to Commission New Middle School Places in Leighton Buzzard Report of: Cllr Mark Versallion, Executive Member for Education
Central Bedfordshire Council EXECUTIVE 6 October 2015 Determination of Proposal to Commission New Middle School Places in Leighton Buzzard Report of: Cllr Mark Versallion, Executive Member for Education
How NICE clinical guidelines are developed
 Issue date: January 2009 How NICE clinical guidelines are developed: an overview for stakeholders, the public and the NHS Fourth edition : an overview for stakeholders, the public and the NHS Fourth edition
Issue date: January 2009 How NICE clinical guidelines are developed: an overview for stakeholders, the public and the NHS Fourth edition : an overview for stakeholders, the public and the NHS Fourth edition
Review of Terms of Reference of Quality Assurance Committee
 Review of Terms of Reference of Quality Assurance Committee Governing Body meeting 3 May 2018 H Author(s) Sponsor Director Purpose of Paper Sue Laing, Corporate Services Risk and Governance Manager Mandy
Review of Terms of Reference of Quality Assurance Committee Governing Body meeting 3 May 2018 H Author(s) Sponsor Director Purpose of Paper Sue Laing, Corporate Services Risk and Governance Manager Mandy
Standards conduct, accountability
 Standards of conduct, accountability and openness Standards of conduct, accountability and openness Throughout this document: members refers to all members of a board the Chair, the non-executives, the
Standards of conduct, accountability and openness Standards of conduct, accountability and openness Throughout this document: members refers to all members of a board the Chair, the non-executives, the
Minutes of the Patient Participation Group Thursday 2 nd February 2017
 Minutes of the Patient Participation Group Thursday 2 nd February 2017 Present: David Green, Sue Ashton, Michael Reilly, Richard Hayward, Debbie Swain and Kathryn Clark 1. Apologies: Mary Hodgeon and Ernie
Minutes of the Patient Participation Group Thursday 2 nd February 2017 Present: David Green, Sue Ashton, Michael Reilly, Richard Hayward, Debbie Swain and Kathryn Clark 1. Apologies: Mary Hodgeon and Ernie
Impact Assessment Policy. Document author Assured by Review cycle. 1. Introduction Policy Statement Purpose or Aim Scope...
 Impact Assessment Policy Board library reference Document author Assured by Review cycle P132 Quality Impact Assessment Policy Quality and Standards Committee 3 Years This document is version controlled.
Impact Assessment Policy Board library reference Document author Assured by Review cycle P132 Quality Impact Assessment Policy Quality and Standards Committee 3 Years This document is version controlled.
City Integrated Commissioning Board
 Meeting-in-common of the City & Hackney Clinical Commissioning Group and City of London Corporation City Integrated Commissioning Board Meeting on Tuesday 23 May, 09:30-11:30 Tomlinson Centre, Queensbridge
Meeting-in-common of the City & Hackney Clinical Commissioning Group and City of London Corporation City Integrated Commissioning Board Meeting on Tuesday 23 May, 09:30-11:30 Tomlinson Centre, Queensbridge
EUROPEAN STRUCTURAL INVESTMENT FUNDS (ESIF) ESF SEaMLESS Programme
 ESF SEaMLESS Programme") Central Bedfordshire Council EXECUTIVE 7 February 2017 EUROPEAN STRUCTURAL INVESTMENT FUNDS (ESIF) ESF SEaMLESS Programme Report of Cllr Steven Dixon, Executive Member for Education and Skills steven.dixon@centralbedfordshire.gov.uk
Central Bedfordshire Council EXECUTIVE 7 February 2017 EUROPEAN STRUCTURAL INVESTMENT FUNDS (ESIF) ESF SEaMLESS Programme Report of Cllr Steven Dixon, Executive Member for Education and Skills steven.dixon@centralbedfordshire.gov.uk
Document Details Title
 Document Details Title Quality and Equalities Impact Assessment (QEIA) Process Guidance Trust Ref No 2046-45852 Local Ref (optional) Main points the document This document explains the process for QEIA,
Document Details Title Quality and Equalities Impact Assessment (QEIA) Process Guidance Trust Ref No 2046-45852 Local Ref (optional) Main points the document This document explains the process for QEIA,
A meeting of NHS Bromley CCG Governing Body 25 May 2017
 South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
South East London Sector A meeting of NHS Bromley CCG Governing Body 25 May 2017 ENCLOSURE 4 SOUTH EAST LONDON 111 AND GP OUT OF HOURS MEMORANDUM OF UNDERSTANDING SUMMARY: The NHS England Commissioning
Ethical framework for priority setting and resource allocation
 Ethical framework for priority setting and resource allocation UNIQUE REF NUMBER: CD/XX/083/V2.0 DOCUMENT STATUS: Approved - Commissioning Development Committee 16 August 2017 DATE ISSUED: August 2017
Ethical framework for priority setting and resource allocation UNIQUE REF NUMBER: CD/XX/083/V2.0 DOCUMENT STATUS: Approved - Commissioning Development Committee 16 August 2017 DATE ISSUED: August 2017
CCG Involvement Strategy and 2016/19 action plan
 CCG Involvement Strategy and 2016/19 action plan 1 Contents 1. Introduction and purpose of document 5 2. Our commitment to effective involvement 5 3. Legislation our statutory obligations 7 4. Aims of
CCG Involvement Strategy and 2016/19 action plan 1 Contents 1. Introduction and purpose of document 5 2. Our commitment to effective involvement 5 3. Legislation our statutory obligations 7 4. Aims of
Sharing the Learning Implementing the Equality Delivery System for the NHS EDS/EDS2
 Sharing the Learning Implementing the Equality Delivery System for the NHS EDS/EDS2 Organisation: Name and type of organisation Job title: Contact details: Name, telephone, email Your details Southern
Sharing the Learning Implementing the Equality Delivery System for the NHS EDS/EDS2 Organisation: Name and type of organisation Job title: Contact details: Name, telephone, email Your details Southern
Quality Strategy. CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July Head of Clinical Quality & Patient Safety
 Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
Document Title: GCP Training for Research Staff. Document Number: SOP 005
 Document Title: GCP Training for Research Staff Document Number: SOP 005 Version: 2 Ratified by: Version 2, 04/10/2017 Page 1 of 13 Committee Date ratified: 26/10/2017 Name of originator/author: Directorate:
Document Title: GCP Training for Research Staff Document Number: SOP 005 Version: 2 Ratified by: Version 2, 04/10/2017 Page 1 of 13 Committee Date ratified: 26/10/2017 Name of originator/author: Directorate:
JOB DESCRIPTION DIRECTOR OF SCREENING. Author: Dr Quentin Sandifer, Executive Director of Public Health Services and Medical Director
 JOB DESCRIPTION DIRECTOR OF SCREENING Author: Dr Quentin Sandifer, Executive Director of Public Health Services and Medical Director Date: 1 November 2017 Version: 0d Purpose and Summary of Document: This
JOB DESCRIPTION DIRECTOR OF SCREENING Author: Dr Quentin Sandifer, Executive Director of Public Health Services and Medical Director Date: 1 November 2017 Version: 0d Purpose and Summary of Document: This
Specialised Services: CPL-008 Referral Management Policy
 Specialised Services: CPL-008 Referral Management Policy 2017 Version 2.0 Document information Document purpose Document name Policy Referral Management Policy Author Welsh Health Specialised Services
Specialised Services: CPL-008 Referral Management Policy 2017 Version 2.0 Document information Document purpose Document name Policy Referral Management Policy Author Welsh Health Specialised Services
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust
 Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
BUSINESS CONTINUITY MANAGEMENT POLICY
 BUSINESS CONTINUITY MANAGEMENT POLICY UNIQUE REFERENCE NUMBER: AC/XX/068/V1.1 DOCUMENT STATUS: Approved by Audit & Gov Committee - 20 July 2017 DATE ISSUED: August 2017 DATE TO BE REVIEWED: August 2020
BUSINESS CONTINUITY MANAGEMENT POLICY UNIQUE REFERENCE NUMBER: AC/XX/068/V1.1 DOCUMENT STATUS: Approved by Audit & Gov Committee - 20 July 2017 DATE ISSUED: August 2017 DATE TO BE REVIEWED: August 2020
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Interim Process and Methods of the Highly Specialised Technologies Programme
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Principles Interim Process and Methods of the Highly Specialised Technologies Programme 1. Our guidance production processes are based on key principles,
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Principles Interim Process and Methods of the Highly Specialised Technologies Programme 1. Our guidance production processes are based on key principles,
JOB DESCRIPTION. CHC/Complex Care Administrator. Continuing Healthcare/Complex Care. Operational Lead. Administration CHC/Complex Care
 JOB DESCRIPTION Job Title CHC/Complex Care Administrator Pay Band Band 3 Base Department/ Team Responsible to Accountable to Responsible For 1829 Building, Countess of Chester Health Park, Chester Continuing
JOB DESCRIPTION Job Title CHC/Complex Care Administrator Pay Band Band 3 Base Department/ Team Responsible to Accountable to Responsible For 1829 Building, Countess of Chester Health Park, Chester Continuing
CCG: CO01 Access and Choice Policy
 Corporate CCG: CO01 Access and Choice Policy Version Number Date Issued Review Date V2 21 January 2016 January 2018 Prepared By: Consultation Process: NECS Commissioning Manager CCG Head of Corporate Affairs.
Corporate CCG: CO01 Access and Choice Policy Version Number Date Issued Review Date V2 21 January 2016 January 2018 Prepared By: Consultation Process: NECS Commissioning Manager CCG Head of Corporate Affairs.
Safeguarding Children Policy Sutton CCG
 Sutton Clinical Commissioning Group Safeguarding Children Policy Sutton CCG DA Whole Organisation Approach to Safeguarding Safeguarding is Everyone s Business Author- Carol Lambe, Assistant Director Commissioning
Sutton Clinical Commissioning Group Safeguarding Children Policy Sutton CCG DA Whole Organisation Approach to Safeguarding Safeguarding is Everyone s Business Author- Carol Lambe, Assistant Director Commissioning
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Implementation Policy for NICE Guidelines
 The Newcastle upon Tyne Hospitals NHS Foundation Trust Implementation Policy for NICE Guidelines Version No.: 5.3 Effective From: 08 May 2017 Expiry Date: 02 March 2019 Date Ratified: 23 February 2017
The Newcastle upon Tyne Hospitals NHS Foundation Trust Implementation Policy for NICE Guidelines Version No.: 5.3 Effective From: 08 May 2017 Expiry Date: 02 March 2019 Date Ratified: 23 February 2017
Safeguarding Adults Policy
 Safeguarding Adults Policy Ratified Status Quality and Patient Safety Committee V2 Issued November 2015 Approved By Consultation Equality Impact Assessment Quality and Patient Safety Committee Safeguarding
Safeguarding Adults Policy Ratified Status Quality and Patient Safety Committee V2 Issued November 2015 Approved By Consultation Equality Impact Assessment Quality and Patient Safety Committee Safeguarding
A Participation Standard for the NHS in Scotland Standard Document
 A Participation Standard for the NHS in Scotland Standard Document Scottish Health Council Scottish Health Council 2010 Published August 2010 ISBN 1-84404-916-7 You can copy or reproduce the information
A Participation Standard for the NHS in Scotland Standard Document Scottish Health Council Scottish Health Council 2010 Published August 2010 ISBN 1-84404-916-7 You can copy or reproduce the information
NHS Continuing Healthcare Service Provider and Local Authority NHS Continuing Healthcare Inter-agency Disputes Policy
 NHS Continuing Healthcare Service Provider and Local Authority NHS Continuing Healthcare Inter-agency Disputes Policy Reference No: CG056 Version: Version 0. 6 Ratified by: SWL CCG Governing Body Date
NHS Continuing Healthcare Service Provider and Local Authority NHS Continuing Healthcare Inter-agency Disputes Policy Reference No: CG056 Version: Version 0. 6 Ratified by: SWL CCG Governing Body Date
Integration Scheme. Between. Glasgow City Council. and. NHS Greater Glasgow and Clyde
 Integration Scheme Between Glasgow City Council and NHS Greater Glasgow and Clyde December 2015 Page 1 of 60 1. Introduction 1.1 The Public Bodies (Joint Working) (Scotland) Act 2014 (the Act) requires
Integration Scheme Between Glasgow City Council and NHS Greater Glasgow and Clyde December 2015 Page 1 of 60 1. Introduction 1.1 The Public Bodies (Joint Working) (Scotland) Act 2014 (the Act) requires
How CQC monitors, inspects and regulates NHS GP practices
 How CQC monitors, inspects and regulates NHS GP practices March 2018 Updates to this guidance since October 2017: NEW annual provider information collection (for practices rated as good and outstanding)
How CQC monitors, inspects and regulates NHS GP practices March 2018 Updates to this guidance since October 2017: NEW annual provider information collection (for practices rated as good and outstanding)
CO33: Policy for commissioning of a care provision within the continuing healthcare pathway
 CO33: Policy for commissioning of a care provision within the continuing healthcare pathway Page 1 of 30 Contents 1. Introduction... 3 2. Definitions... 5 3. Mental capacity & Representation... 6 4. Identification
CO33: Policy for commissioning of a care provision within the continuing healthcare pathway Page 1 of 30 Contents 1. Introduction... 3 2. Definitions... 5 3. Mental capacity & Representation... 6 4. Identification
Framework Agreement for Care Homes in Central Bedfordshire
 Meeting: Executive Date: 5 November 2013 Subject: Framework Agreement for Care Homes in Central Bedfordshire Report of: Summary: Cllr Carole Hegley, Executive Member for Social Care, Health and Housing
Meeting: Executive Date: 5 November 2013 Subject: Framework Agreement for Care Homes in Central Bedfordshire Report of: Summary: Cllr Carole Hegley, Executive Member for Social Care, Health and Housing
Calderdale CCG - Governing Body Job Description Registered Nurse
 Calderdale CCG - Governing Body Job Description Registered Nurse Function Specific Responsibilities Individual members of the Governing Body bring a range of perspectives, drawn from their different professions,
Calderdale CCG - Governing Body Job Description Registered Nurse Function Specific Responsibilities Individual members of the Governing Body bring a range of perspectives, drawn from their different professions,
Medicines Optimisation Strategy
 Medicines Optimisation Strategy 2014-2017 Contents Section Page 1 Foreword 3 2 Strategic Principles for Medicines Optimisation 4 3 Introduction 4 4 Trust Vision and Values 5 5 Strategy Development 5 6
Medicines Optimisation Strategy 2014-2017 Contents Section Page 1 Foreword 3 2 Strategic Principles for Medicines Optimisation 4 3 Introduction 4 4 Trust Vision and Values 5 5 Strategy Development 5 6
Safeguarding Adults Reviews Protocol
 Staffordshire and Stoke on Trent Adult Safeguarding Partnership Board Safeguarding Adults Reviews Protocol July 2016 SAR Process July 2014 (revised July 2016) Page 1 Contents 1. Introduction 2. Criteria
Staffordshire and Stoke on Trent Adult Safeguarding Partnership Board Safeguarding Adults Reviews Protocol July 2016 SAR Process July 2014 (revised July 2016) Page 1 Contents 1. Introduction 2. Criteria
NHS CONSTITUTION (MARCH 2013) RIGHTS AND PLEDGES TO PATIENTS AND THE PUBLIC
 RIGHTS AND PLEDGES TO PATIENTS AND THE PUBLIC") NHS CONSTITUTION (MARCH 2013) RIGHTS AND PLEDGES TO PATIENTS AND THE PUBLIC APPENDIX A Access to Health Services o Receive NHS services free of charge, apart from certain limited exceptions sanctioned
NHS CONSTITUTION (MARCH 2013) RIGHTS AND PLEDGES TO PATIENTS AND THE PUBLIC APPENDIX A Access to Health Services o Receive NHS services free of charge, apart from certain limited exceptions sanctioned