Mobile Medical Review Team Observation Services & the 2 Midnight Rule. The Audio and/or Video Recording of this Educational Session is Prohibited
|
|
|
- Melvin Gaines
- 5 years ago
- Views:
Transcription

1 Mobile Medical Review Team Observation Services & the 2 Midnight Rule The Audio and/or Video Recording of this Educational Session is Prohibited

2 National Government Services, Inc. Medicare Part A & Part B Jurisdiction K Maine Vermont New Hampshire Massachusetts New York Connecticut Rhode Island NGS Part A & B Jurisdiction K
3 Medicare Part A/B Differentiation Part A Inpatient** Hospital Skilled Nursing Facilities Part B Outpatient Hospitals Clinics Ambulatory Surgery Centers 3
4 Mobile Medical Review Team Jurisdiction K --Part A Medical Directors: Laurence Clark, MD Stephen Boren, MD J/K Operational Manager: Julia Meehan, MBA Senior Medical Review Nurses: Cindy Mancill BSN, RN, CCM, CPHM Nancy Krupka BSN, MS Kay Osadchey RN, CCM, CPHM Jan Sawyer BSN Shelly Bernardini RN, CPHM Mandy Zinger-Gutchess RN, CPHM


5 Mobile Medical Review Team Onsite Visits The Notification Letter includes10 original medical records that were originally DENIED by the Medical Review Staff for Not Reasonable & Necessary Inpatient Services 5
6 Mobile Medical Review Team Current Focus & Goals Current Focus: Medical Necessity of Short-Stay Inpatient Admissions Onsite Visit Goals: Provide an interactive educational opportunity for hospital clinicians. Identify and report facility best practices. Review & discussion of denied claims to assist in comprehension of the new 2 Midnight Rule from CMS Provide resources to assist facility in addressing areas of concern. Provide a contact person for questions pertaining to proper utilization of Part A inpatient admissions. 6
7 Observation Definition: Set of specific, clinically appropriate services which include ongoing short term treatment, assessment and reassessment before a decision can be made regarding whether patients will require further treatment as hospital inpatients or if they are able to be discharged from the hospital. Medicare Benefit Policy Manual Chapter 20.6, B Coverage of Outpatient Observation Services
8 Observation Services Documentation for Observation Services and Inpatient Admissions must support medically reasonable and necessary care Medicare does not provide payment for custodial care Observations may span up to 2 Midnights When the patient is stable and/or improving and the physician is excluding diagnosis/diagnoses- consider observation services When evaluating the patient and the treatment plan includes monitor and/or observe - consider observation services Medicare has no rule about designated observation beds - any bed may be assigned Transfer s received should be evaluated upon arrival and a decision to admit as an inpatient or place in observation is based on the evaluation - not just the status of the patient from the transferring facility Apply screening criteria at the time the status decision is made - not necessarily upon presentation to the ED The physician may convert from Observation to Inpatient Admission at any time during the hospital stay when the patient s condition requires increasing services over a longer period of time
9 Skilled Nursing Facility Stays The beneficiary must have a stay of 3 inpatient admission days before they qualify for the Skilled Nursing admission. Outpatient observation services do not count towards the three day qualifying hospital stay This rule has not changed in light of the new two midnight rule.
10 Outpatient Procedures Comorbid conditions have been successfully managed prior to scheduled outpatient procedure dates. Many of these patients have specialty clearance allowing for outpatient procedures. Outpatient surgery from the emergency room does not automatically mean the patient is admitted as an inpatient. Remember: Outpatient procedures that are billed as inpatient should have documentation to support the need for inpatient status. 10
11 General Rule for 0-1 Midnight Stays When a patient enters a hospital for a surgical procedure (not specified by Medicare as inpatient only under 42 C.F.R (n), diagnostic test, or any other treatment) and the physician expects to keep the patient in the hospital for 0-1 midnights, the services are generally inappropriate for inpatient admission and inpatient payment under Medicare part A, regardless of the hour that the patient came to the hospital or whether the patient used a bed. CMS directs Contractors to deny these inappropriate admissions unless unforeseen circumstances shortened the stay or there are other rare or unusual circumstances that necessitate an inpatient admission.
12 In Brief: Outpatient surgical procedures do not support inpatient admission, unless there is documented evidence of clinical complications The hour of the patient s arrival or the location in which the patient was treated do not play a role in supporting inpatient status.
13 Appropriate Short Inpatient Hospital Stays If an unforeseen circumstance results in a shorter beneficiary stay than the physicians reasonable expectation of at least 2 midnights, the patient may be considered to be appropriately treated on an inpatient basis and hospital inpatient payment may be made under Medicare Part A. Such circumstances must be documented in the medical record in order to be considered upon medical review. Examples include: Death Transfer to another hospital Departure against medical advice Clinical improvement where the patient stayed less than the expected 2 midnights
14 In Brief: The physician s admitting note may correctly describe and support inpatient admission, even in circumstances that change and result in faster improvement and discharge than originally anticipated. The key factor here is an admission note that supports a reasonable and medically necessary plan of care, over an estimated timeframe of a period exceeding beyond 2 Midnights
15 Inappropriate Short Inpatient Hospital Stays Situations that do not represent instances in which an inpatient admission would be appropriate without an expectation of a 2 midnight hospital stay: CMS does not believe that the use of telemetry, by itself, is the type of rare and unusual circumstance that would justify an inpatient admission in the absence of a 2 midnight expectation. We note that telemetry is neither rare nor unusual, and that it is commonly used by hospitals on outpatients (ER and observation patients) and on patients fitting the historical definition of outpatient observation; that is, patients for whom a brief period of assessment or treatment may allow the patient to avoid a hospital stay.
16 Inappropriate-- Short Inpatient Hospital Stays Situations that do not represent instances in which an inpatient admission would be appropriate without an expectation of a 2 midnight hospital stay: Beneficiaries admitted to Intensive Care Unit (ICU). As CMS specified in the final rule, the use of an ICU, by itself, would not be the type of rare and unusual circumstance that would justify an inpatient admission in the absence of a 2 midnight expectation. An ICU label is applied to a wide variety of facilities providing a wide variety of services. Due to the wide variety of services, that can be provided in different areas of a hospital, CMS does not believe that a patient assignment to a specific hospital location, such as a certain unit or location, would justify an inpatient admission in the absence of a 2-midnight expectation.
17 In Brief Use of telemetry services, or placing a patient in an ICU environment for care, do not, as isolated factors, support medical necessity for inpatient admission.
18 CMS Directive to Contractors for Patient Status Reviews Documentation Requirements Do not review any Procedure on Inpatient-Only List Evaluate whether, at the time of the admission order, it was reasonable for the admitting practitioner to expect the beneficiary to require medically necessary services (incl. inpatient & outpatient services) over a period of time spanning at least 2 midnights. The beneficiary s medical necessity assessment is whether clinical presentation, prognosis, and expected treatment support the expectation of the need for hospital care spanning 2 or more midnights Severity of Illness and intensity of services are complex medical factors to consider when assessing whether the physician was reasonable in forming his or her expectation that a beneficiary required hospital services for 2 or more midnights. It is not necessary for a beneficiary to meet inpatient level of care as defined by a commercial screening tool, in order for Part A payment to be appropriate. Just because a beneficiary meets inpatient level of care as defined by a commercial screening tool, this does not mean that a DRG Part A payment is appropriate.
19 CMS Directive to Contractors for Patient Status Reviews Documentation Requirements The 2 Midnight Benchmark is based upon the physician s expectation of the required duration of medically necessary hospital services at the time the inpatient order is written and the formal admission begins. Consider all documented complex medical factors that support a reasonable expectation of the needed duration of the stay relative to the 2 midnight benchmark, including all of the following: Patient History/Co-morbidities Severity of signs and symptoms Current Medical Needs Risk/Probability of an adverse event occurring during the time period for which hospitalization is considered
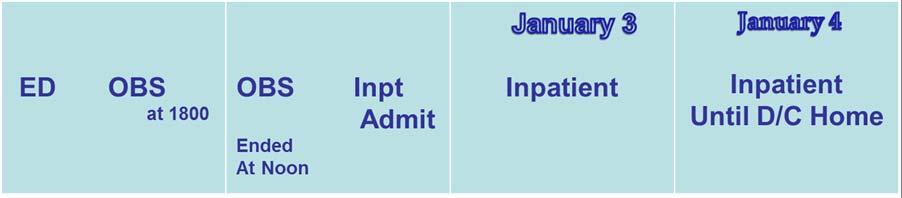
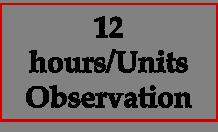
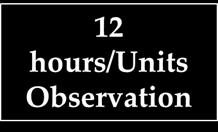
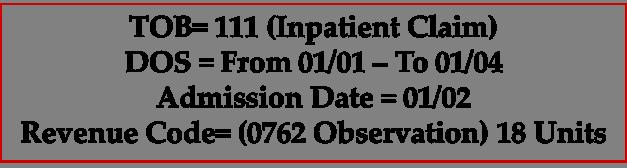
20 CMS Directive to Contractors for Patient Status Reviews 2 Midnight Benchmark 2 Midnight Benchmark Time the beneficiary spent receiving outpatient services within the hospital prior to inpatient admission, in addition to the postadmission duration of care. This pre-admission time may include services such as: Observation services Treatment in the emergency department Procedures provided in the operating room or other treatment areas If the beneficiary arrives through the emergency room the clock starts ticking when the beneficiary starts receiving care. For other methods of arrival, the starting point is when the beneficiary starts receiving services following arrival to the hospital. Wait times prior to the initiation of care (ex: ED waiting room) and triaging activities will not be considered.
21 In Brief MACs will not review claims for Inpatient-Only services Medical necessity drives these reviews: does the clinical picture correlate with the physician s estimate for care beyond 2 Midnights? We are awaiting final instructions from CMS on whether billable diagnostic services OR initiation of care by a physician or NPP starts the count toward 2 Midnights CMS has already established that triage and subsequent time in the waiting room are not to be included in this time assessment
22 Claims for Admissions that Span 2 or More Midnights 2 Midnight Presumption Hospital stays spanning 2 or more midnights after beneficiary formally admitted as inpatient pursuant to physician order will be presumed to be reasonable & necessary for inpatient status as long as the stay at the hospital is medically necessary CMS has directed Contractors NOT to focus medical review efforts on stays spanning at least 2 midnights after admission absent evidence of systemic gaming, abuse, or delays in the provision of care, in an attempt to qualify for the 2 midnight presumption. Contractors may review these claims as part of routine monitoring activity or as part of other targeted reviews
23 Claims For Hospital Admissions That Span 0-1 Midnight Inpatient stays spanning 0-1 midnight after the beneficiary is formally admitted as an inpatient are not subject to the presumption and may be selected for review. If total time in the hospital receiving medically necessary care (including pre-admission outpatient time from the time care is initiated in the hospital) spans 2 or more midnights, the 2- midnight benchmark for inpatient admission will be met and payment supported upon medical review.
24 In Brief Inpatient stays of 2 Midnight duration after the decision for admission will carry a presumption of medical necessity Inpatient stays of 0-1 Midnight duration after the decision for admission will not carry a presumption of medical necessity and may be subject to review Hospitals need to avoid unusual delays in providing care, which may infer an abusive gaming pattern
25 Status Decision Making A TWO-STEP Process Step One: Is there medical necessity for facility services or can this patient be discharged home? Step Two: Beyond the ensuing two-midnights, refer the patient to Inpatient Admission, based on a full assessment of care requirements and anticipated time frames. Reminder: Apply inpatient guidelines at the time of patient status decision, not at the point of arrival
26 Two Step Process STEP ONE: STEP TWO: Establish a probable or differential diagnosis and treatment plan The determination- Can the patient be discharged home? YES = Release Home NO= Proceed to Step Two Definitive Diagnosis-Patient requires definitive multi day diagnostics &/or therapeutic treatments (longer than twomidnights ) = INPATIENT Patient remains unstable= INPATIENT **Refer to Handout 26
27 Observation to Inpatient Admission Claims
28 Condition Code 44 Changing an Inpatient Admission to an Outpatient Observation Status Must occur prior to patient discharge The beneficiary should be notified in writing of status change and fiscal responsibilities that correlate with Medicare Part B observation Admitting Physician & Utilization Review Physician must concur and both document appropriately the reason for the status change The beneficiary has appeal rights to the QIO
29 Orders for Observation Status and Inpatient Admissions Place in Observation or Refer to Observation When outpatient observation services is the physician s intent. Admit to Inpatient When inpatient admission is the physician s intent. 29
30 Practitioner Orders A Medicare beneficiary is considered an inpatient of a hospital if formally admitted as an inpatient pursuant to an order for inpatient admission by a physician or other qualified practitioner. All of the following will be considered in an effort to reinforce the policy that the physician should be involved in the determination of patient status and to improve clarity among hospitals, beneficiaries, and ordering practitioners regarding whether the beneficiary is being treated as a hospital inpatient or hospital outpatient: CONTENT specify admission for inpatient services QUALIFICATION OF THE ORDERING/ADMITTING PRACTITIONER Discussed in further detail on slide #32 Verbal/Telephone orders must be authenticated by the ordering practitioner (or another practitioner with the required admitting qualification in his/her own right) in the medical record prior to discharge unless the hospital or state requires an earlier time frame. KNOWLEDGE OF THE PATIENT Discussed in further detail on slide #32 TIMING The order must be furnished at or before the time of the inpatient admission. Medicare does not permit retroactive orders or the inference of orders. Authentication of the order is required prior to discharge and may be performed and documented as part of the physician certification. SPECIFICITY OF THE ORDER Must be present in the medical record Must specify the admitting practitioner s recommendation to admit to inpatient, or as an inpatient for inpatient services. ***
31 Referring to Observation When a patient status decision determines that the patient will be placed in Observation Status the patient should be notified via signed consent about his/her status. This is mandatory in NY state & must occur within the first 24 hours of the time the order for observation is written. Beneficiary appeal rights do not apply
32 Patient Status Appeals Remember: Observation is an outpatient status order that is billed on an outpatient Part B claim. Currently the beneficiary has no avenue for appeal of an order written for outpatient observation services.
33 Certification of Orders When conducting a patient status review, CMS instructs the contractor to assess the hospital s compliance with the admission order, the two midnight benchmark and the certification requirements. The physician certification, which includes the practitioner order, is considered along with other documentation in the medical record as evidence that hospital inpatient services were reasonable and medically necessary. Medicare considers only the following physicians, podiatrists or dentists to have sufficient knowledge of the case to serve as the certifying physician: The admitting physician of record ( attending ) or a physician on call for him/her A surgeon responsible for a major surgical procedure on the beneficiary or a surgeon on call for him/her A dentist functioning as the admitting physician of record or as the surgeon responsible for a major dental procedure And, in the specific case of a non-physician, non-dentist admitting practitioner who is licensed by the state and has been granted privileges by the facility, a physician member of the hospital staff (such as a physician member of the utilization review committee) who has reviewed the case and who also enters into the record a complete certification statement that specifically contains all of the content elements discussed above.
34 Physician Certification Requirements Content Timing Authorization to Sign the Certification Format Default Methodology for Initial Certification Authentication of the practitioner order Reason for inpatient services Estimated time the beneficiary requires hospitalization Plans for post hospital care, if appropriate Certification begins with the order for inpatient admission Certification must be completed, signed, dated and documented in the medical record prior to discharge Outlier cases must be certified and recertified as provided in 42 CFR A Physician who is a doctor of Medicine or osteopathy, dentist in the circumstances specified in 42 CFR (d), and a doctor of podiatric medicine if his/or her certification is consistent with the functions her or she is authorized to perform under state law. Must be signed by the physician responsible for the case, or by another physician who has knowledge of the case and who is authorized to do so by the responsible physician or by the hospitals medical staff **See previous slide for specific information regarding authorization** As specified in 42 CFR , no specific procedures or forms are required for certification and recertification statements. The provider may adopt any method that permits verification. The certification and recertification statements may be entered on forms, notes, or records that the appropriate individual signs, or on a separate form. Except as provided for delayed certifications, there must be a separate signed statement for each certification or recertification. In the absence of specific certification forms or certification statements, CMS and its contractors will look for the following medical record elements in order to meet the initial inpatient certification requirements: The authentication requirement for the practitioner order will be met by the signature or countersignature of the inpatient admission order by the certifying physician. The requirement to certify the reasons that hospital inpatient services are or were medically required will be met either by the diagnosis and plan documented in the inpatient assessment or by the inpatient admitting diagnosis and orders. The estimated time requirement will be met by the inpatient admission order written in accordance with the 2 Midnight benchmark, supplemented by the physician notes and discharge planning instructions. The post hospital care plan requirement will be met either by physician notes or by discharge planning instructions.
35 Plan of Care & Progress Notes The expectation is that all documentation within a medical record will be legible, as sequential as possible; and that the detailed events (including dates, times, and data) will correspond accordingly. The Plan of Care & Progress Notes Should Include: Specifically whether services are Outpatient/Observation or Inpatient at the time of the documentation. Date, time, diagnosis, plan, & legible signature. The anticipated time-frame for completion of the defined treatment plan. Any & all rationale or events that precipitated any change in patient status from Observation to Inpatient Services. 35
36 Probe & Educate Program Centers for Medicaid & Medicare Directive to Contractors Admissions on or after October 1, 2013 thru March 31, 2014 Patient status reviews for claims submitted by acute care inpatient facilities, long term care hospitals, and inpatient psychiatric facilities Determine hospital compliance with CMS-1599-F which focuses on the appropriateness of an inpatient admission versus treatment on an outpatient basis INCLUDING: Admission Order Requirements ( ) Certification Requirements (http;// 2 Midnight Benchmark
37 Initial Probe Reviews Admissions on or after 10/1/13 Contractor to select 10 claims for prepayment review (25 claims for large hospitals) & based on results of these Deny claims found to be out of compliance with CMS 1599-F Based on results Contractor to conduct educational outreach efforts during the next 3 months.
38 Initial Probe Reviews Educational Outreach Efforts Providers with moderate/significant or major denial/non-compliance issues/concerns will be offered education from the Contractor via 1:1 telephone conferencing Educational Call: Discuss reasons for denials Provide education Deliver reference materials Answer any questions
39 Additional Probe Reviews Those providers identified as having moderate/significant or major concerns will be placed on additional probe reviews on claims with dates of admission between January and March additional claims (25 for large facilities) for providers with moderate/significant concerns 100 additional claims (250 for large facilities) for providers with major concerns
40 # Of Claims In A Sample That Did NOT Comply With Policy (Dates of Admission 10/13 3/14) No or Minor Concerns Moderate to Significant Concerns Major Concerns 10 Claims Reviewed 0-1 Concerns 2-6 Concerns 7+ Concerns 25 Claims Reviewed 0-2 Concerns 3-13 Concerns 14+ Concerns Action Contractor Direction from CMS: Deny Non Compliant Claims Send Summary Letter Indicating Claims Denied & Reason for Denials Explain that no more reviews will be conducted under the Probe & Educate process Explain that the provider will be subjected to the normal data analysis and review process Contractor Direction from CMS: Deny Non Compliant Claims Send detailed review results letters explaining each denial Send summary letter offering 1:1 telephone call to discuss and indicate the contractor will repeat Probe & Educate process with 10 or 25 claims Repeat Probe & Educate of 10 or 25 claims with dates of admission 1/14 3/14 Contractor Direction from CMS: Deny Non Compliant Claims Send detailed review results letters explaining each denial Send summary letter offering 1:1 telephone call to discuss and indicate the contractor will repeat Probe & Educate process with 10 or 25 claims Repeat Probe & Educate of 10 or 25 claims with dates of admission 1/14 3/14 IF PROBLEM CONTINUES REPEAT PROBE & EDUCATE WITH INCREASED CLAIM VOLUME OF CLAIMS
41 Gaming Contractors are instructed to monitor inpatient hospital claims spanning 2 or more midnights after admission for evidence of systematic gaming, abuse or delays in the provision of care in an attempt to qualify for the 2 midnight presumption. Contractors must identify such trends through probe reviews and through its data sources, such as that provided by the CERT (Comprehensive Error Rate Testing) contractor, First-look Analysis for Hospital Outlier Monitoring (FATHOM) and PEPPER reports (Program for Evaluating Payment Patterns Electronic Report).
42 CMS Monitoring The Centers for Medicaid & Medicare will be monitoring provider billing trends for the purpose of avoiding Contractor prepayment probe audits during this initial probe & educate period. They will monitor for variances indicative of: Abuse Gaming Systemic delays in submission of claims
43 National Government Services Inpatient Provider Resources Tools & Materials (upper right hand corner of web page) Self-Help Inpatient Provider Resources CMS Ruling 90-1 Provide education regarding medical necessity of inpatient admission, role of physician documentation, and provider responsibility in providing economic & medically necessary care. 43
44 Thank You! DISCLAIMER: National Government Services, Inc. has produced this material as an informational reference for providers furnishing services in our contract jurisdiction. National Government Services employees, agents, and staff make no representation, warranty, or guarantee that this compilation of Medicare information is error-free and will bear no responsibility or liability for the results or consequences of the use of this material. Although every reasonable effort has been made to assure the accuracy of the information within these pages at the time of publication, the Medicare Program is constantly changing, and it is the responsibility of each provider to remain abreast of the Medicare Program requirements. Any regulations, policies, and/or guidelines cited in this publication are subject to change without further notice. Current Medicare regulations can be found on the Centers for Medicare & Medicaid Services (CMS) Web site at
Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015)
") 7 Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015) Medical Review of Inpatient Hospital Claims Starting on October 1, 2015, the
7 Reviewing Short Stay Hospital Claims for Patient Status: Admissions On or After October 1, 2015 (Last Updated: 11/09/2015) Medical Review of Inpatient Hospital Claims Starting on October 1, 2015, the
2014 Hospital Admission Criteria
 2014 Hospital Admission Criteria Created on 11/20/2013 Audio and/or Video Recording of this Educational Session is Prohibited Agenda Inpatient vs. observation 2-midnight benchmark and presumption Admission
2014 Hospital Admission Criteria Created on 11/20/2013 Audio and/or Video Recording of this Educational Session is Prohibited Agenda Inpatient vs. observation 2-midnight benchmark and presumption Admission
LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN
 LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN Created on 6/2/2014 DISCLAIMER DISCLAIMER: WPS Medicare has produced this material as an informational reference. Every reasonable
LESSONS LEARNED FROM THE PROBE AND EDUCATE AUDIT K. CHEYENNE SANTIAGO, RN Created on 6/2/2014 DISCLAIMER DISCLAIMER: WPS Medicare has produced this material as an informational reference. Every reasonable
CMS New Standards for Hospital Inpatient Admissions October Physician Admission Order Check List Detail
 Providing technologically supported physician advisory and case management services to healthcare providers and payors CMS New Standards for Hospital Inpatient Admissions October 2013 Physician Admission
Providing technologically supported physician advisory and case management services to healthcare providers and payors CMS New Standards for Hospital Inpatient Admissions October 2013 Physician Admission
In this course, we will cover: The Two Midnight Rule and the rule s documentation requirements Medical Necessity standards Inpatient Order and
 In this course, we will cover: The Two Midnight Rule and the rule s documentation requirements Medical Necessity standards Inpatient Order and Certification requirements for physicians Outpatient Observation
In this course, we will cover: The Two Midnight Rule and the rule s documentation requirements Medical Necessity standards Inpatient Order and Certification requirements for physicians Outpatient Observation
Documentation Updates for Physicians
 Documentation Updates for Physicians CMS IPPS 2014 Final Rule AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
Documentation Updates for Physicians CMS IPPS 2014 Final Rule AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
FY 2014 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy
 FY 2014 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014,
FY 2014 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014,
Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy
 Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014, the Centers
Changes to Medicare Inpatient Admission and Reimbursement Standards: CMS s Two Midnight Rule and the Revised Part A to Part B Rebilling Policy Mark Polston King & Spalding In Fiscal Year 2014, the Centers
AAPC Webinar 3/28/2016
 Short Stays for the Coder Where Are We Now? Heather Greene, MBA, RHIA, CPC, CPMA AHIMA Approved ICD-10 CM/PCS Trainer Copyright 2016 AAPC Agenda The Two-Midnight Rule Supportive documentation Observation
Short Stays for the Coder Where Are We Now? Heather Greene, MBA, RHIA, CPC, CPMA AHIMA Approved ICD-10 CM/PCS Trainer Copyright 2016 AAPC Agenda The Two-Midnight Rule Supportive documentation Observation
CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule
 CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule John Zelem, MD, FACS Executive Medical Director Audit, Compliance and Education (ACE) AHA Solutions, Inc., a subsidiary
CMS IPPS 2014 Final Rule: Physician Education on Observation Status and 2-Midnight Rule John Zelem, MD, FACS Executive Medical Director Audit, Compliance and Education (ACE) AHA Solutions, Inc., a subsidiary
Inpatient Hospital Services Billing, Denials and Reimbursement: Evolving Regulatory and Legal Landscape
 Presenting a live 90-minute webinar with interactive Q&A Inpatient Hospital Services Billing, Denials and Reimbursement: Evolving Regulatory and Legal Landscape Navigating the Interplay of Inpatient and
Presenting a live 90-minute webinar with interactive Q&A Inpatient Hospital Services Billing, Denials and Reimbursement: Evolving Regulatory and Legal Landscape Navigating the Interplay of Inpatient and
CMS -1599F. The 2 Midnight Rule Effective October 1, 2013
 Joseph Nitti, M.D. Medical Director/Physician Advisor Continuum of Care Dept. Morristown Medical Center 973-971-4004 CMS -1599F The 2 Midnight Rule Effective October 1, 2013 Determination of Inpatient
Joseph Nitti, M.D. Medical Director/Physician Advisor Continuum of Care Dept. Morristown Medical Center 973-971-4004 CMS -1599F The 2 Midnight Rule Effective October 1, 2013 Determination of Inpatient
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
AHLA. Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions
 AHLA Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions Timothy P. Blanchard Blanchard Manning LLP Orcas, WA Joan C. Ragsdale CEO MedManagement LLC Vestavia,
AHLA Z. New Rules: Hospital Patient Status, Observation, Part B Billing for Denied Inpatient Admissions Timothy P. Blanchard Blanchard Manning LLP Orcas, WA Joan C. Ragsdale CEO MedManagement LLC Vestavia,
Benefit Criteria for Outpatient Observation Services to Change for Texas Medicaid
 Benefit Criteria for Outpatient Observation Services to Change for Texas Medicaid Information posted on October 8, 2010 Effective for dates of service on or after December 1, 2010, the benefit criteria
Benefit Criteria for Outpatient Observation Services to Change for Texas Medicaid Information posted on October 8, 2010 Effective for dates of service on or after December 1, 2010, the benefit criteria
The In and Out of the Medicare Two Midnight Rule. Disclaimer. Objectives 3/31/2014
 The In and Out of the Medicare Two Midnight Rule Brenda Keeling, RN, CPHQ, CCM Patient Response, Inc. 1 Disclaimer Information enclosed was current at the time it was presented. Medicare policy changes
The In and Out of the Medicare Two Midnight Rule Brenda Keeling, RN, CPHQ, CCM Patient Response, Inc. 1 Disclaimer Information enclosed was current at the time it was presented. Medicare policy changes
Executive Summary, December 2015
 CMS Revises Two-Midnight Rule to Allow An Exception for Part A Payment for Hospital Services Provided to Patients Requiring Inpatient Care for Less Than Two Midnights Executive Summary, December 2015 Sponsored
CMS Revises Two-Midnight Rule to Allow An Exception for Part A Payment for Hospital Services Provided to Patients Requiring Inpatient Care for Less Than Two Midnights Executive Summary, December 2015 Sponsored
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
Complex Challenges/Financial Impact Medical Necessity Compliance Role of the Physician Advisor. NJHFMA Finance for Clinicians Session March 24, 2016
 1 Complex Challenges/Financial Impact Medical Necessity Compliance Role of the Physician Advisor NJHFMA Finance for Clinicians Session March 24, 2016 Complex Challenges 2 Declining Inpatient Admissions
1 Complex Challenges/Financial Impact Medical Necessity Compliance Role of the Physician Advisor NJHFMA Finance for Clinicians Session March 24, 2016 Complex Challenges 2 Declining Inpatient Admissions
The Two-Midnight Rule: Practical Strategies for Hospital Compliance Officers
 AIS s Management Insight Series The Two-Midnight Rule: Practical Strategies for Hospital Compliance Officers Adapted from an AIS webinar presented by Abby Pendleton, Esq. Founding Partner The Health Law
AIS s Management Insight Series The Two-Midnight Rule: Practical Strategies for Hospital Compliance Officers Adapted from an AIS webinar presented by Abby Pendleton, Esq. Founding Partner The Health Law
CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations. Agenda
 CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations Ralph Wuebker, MD, MBA Chief Medical Officer AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for
CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations Ralph Wuebker, MD, MBA Chief Medical Officer AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for
Medical Necessity Certification 3/4/2014. CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations. Agenda. Valid Admissions What Changed?
 CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations Ralph Wuebker, MD, MBA Chief Medical Officer AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for
CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations Ralph Wuebker, MD, MBA Chief Medical Officer AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for
August 14, 2013 COF Bi- Monthly Call. Questions or comments? Contact Ivy Baer: or
 August 14, 2013 COF Bi- Monthly Call Questions or comments? Contact Ivy Baer: ibaer@aamc.org or 202-828-0499 OPPS Comment Period Is NOW Comments Due 9/6 Hospital Outpatient Services Proposal (OPPS) On
August 14, 2013 COF Bi- Monthly Call Questions or comments? Contact Ivy Baer: ibaer@aamc.org or 202-828-0499 OPPS Comment Period Is NOW Comments Due 9/6 Hospital Outpatient Services Proposal (OPPS) On
Inpatient Psychiatric Facility (IPF) Coverage & Documentation. Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016
 Coverage & Documentation. Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016") Inpatient Psychiatric Facility (IPF) Coverage & Documentation Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016 1 Disclaimer This information is current as of August
Inpatient Psychiatric Facility (IPF) Coverage & Documentation Presented by Palmetto GBA JM A/B MAC Provider Outreach and Education September 7, 2016 1 Disclaimer This information is current as of August
New Medical Review Strategy: Targeted Probe and Educate 1928_0917
 New Medical Review Strategy: Targeted Probe and Educate 2017 1928_0917 Today s Presenters J6 and JK Provider Outreach & Education Consultants Jean Roberts, RN, BSN, CPC Nathan L. Kennedy, Jr., CHC, CPC,
New Medical Review Strategy: Targeted Probe and Educate 2017 1928_0917 Today s Presenters J6 and JK Provider Outreach & Education Consultants Jean Roberts, RN, BSN, CPC Nathan L. Kennedy, Jr., CHC, CPC,
Comprehensive Observation Services and the 2-Midnight Rule Part 1 June 13, 2014
 Comprehensive Observation Services and the 2-Midnight Rule Part 1 June 13, 2014 Mary Guyot Principal mguyot@stroudwater.com 207-650-5830 (cell) Presentation Sources & Disclaimer This presentation was prepared
Comprehensive Observation Services and the 2-Midnight Rule Part 1 June 13, 2014 Mary Guyot Principal mguyot@stroudwater.com 207-650-5830 (cell) Presentation Sources & Disclaimer This presentation was prepared
Medicare General Information, Eligibility, and Entitlement
 Medicare General Information, Eligibility, and Entitlement Chapter 4 - Physician Certification and Recertification of Services Transmittals for Chapter 4 Table of Contents (Rev. 50, 12-21-07) 10 - Certification
Medicare General Information, Eligibility, and Entitlement Chapter 4 - Physician Certification and Recertification of Services Transmittals for Chapter 4 Table of Contents (Rev. 50, 12-21-07) 10 - Certification
Review of Claims Affected by Temporary Suspension of BFCC-QIO Short Stay Reviews Q&As
 Review of Claims Affected by Temporary Suspension of BFCC-QIO Short Stay Reviews Q&As INTRODUCTION On May 4, 2016, the Centers for Medicare & Medicaid Services (CMS) temporarily paused the Beneficiary
Review of Claims Affected by Temporary Suspension of BFCC-QIO Short Stay Reviews Q&As INTRODUCTION On May 4, 2016, the Centers for Medicare & Medicaid Services (CMS) temporarily paused the Beneficiary
Observation Coding and Billing Compliance Montana Hospital Association
 Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Today s Presenters & Agenda
 EHR s Accelerated Compliance Training (ACT) Series: Updates on Regulatory Developments and Audit Activity February 25, 2015 Today s Presenters & Agenda Presenters: Ralph Wuebker, MD, MBA, Chief Medical
EHR s Accelerated Compliance Training (ACT) Series: Updates on Regulatory Developments and Audit Activity February 25, 2015 Today s Presenters & Agenda Presenters: Ralph Wuebker, MD, MBA, Chief Medical
PATIENT STATUS DEFINITIONS, 2 MIDNIGHT RULE AND 96 HOUR RULE
 PURPOSE It is the policy of Mason General Hospital and Family of Clinics (MGH&FC) that based on the Patient Status Definitions, all placements concerning the use of observation beds, or placements made
PURPOSE It is the policy of Mason General Hospital and Family of Clinics (MGH&FC) that based on the Patient Status Definitions, all placements concerning the use of observation beds, or placements made
HFMA WEBINAR. CMS s Two-Midnight Rule: How Will It Impact Short-Stay Cases?
 HFMA WEBINAR CMS s Two-Midnight Rule: How Will It Impact Short-Stay Cases? Date: September 24, 2013 Time: 2:00 3:30 p.m. Central (12:00 1:30 pm Pacific/1:00 2:30 pm Mountain/3:00 4:30 pm Eastern) Follow
HFMA WEBINAR CMS s Two-Midnight Rule: How Will It Impact Short-Stay Cases? Date: September 24, 2013 Time: 2:00 3:30 p.m. Central (12:00 1:30 pm Pacific/1:00 2:30 pm Mountain/3:00 4:30 pm Eastern) Follow
Outpatient Observation Services
 Outpatient Observation Services Presented by: Gina Hobert, MBA, CHC, CPC-I, CPMA, CEMC, CRC Sr. Manager, Baker Newman Noyes Definition MCR Benefit Policy Manual, CMS 100-02, Chapter 6, 20.6 A. Outpatient
Outpatient Observation Services Presented by: Gina Hobert, MBA, CHC, CPC-I, CPMA, CEMC, CRC Sr. Manager, Baker Newman Noyes Definition MCR Benefit Policy Manual, CMS 100-02, Chapter 6, 20.6 A. Outpatient
Cigna Medical Coverage Policy
 Cigna Medical Coverage Policy Subject Observation Care Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 4 References... 5 Effective Date... 10/15/2014 Next Review
Cigna Medical Coverage Policy Subject Observation Care Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 4 References... 5 Effective Date... 10/15/2014 Next Review
Learning Objectives. It Starts With an Order and an Expectation
 1 Under What Condition: Understanding Condition Codes 44 and W2 Debbie Mackaman, RHIA, CPCO, CCDS Regulatory Specialist HCPro, an H3.Group Brand Middleton, MA Learning Objectives At the completion of this
1 Under What Condition: Understanding Condition Codes 44 and W2 Debbie Mackaman, RHIA, CPCO, CCDS Regulatory Specialist HCPro, an H3.Group Brand Middleton, MA Learning Objectives At the completion of this
50938 Federal Register / Vol. 78, No. 160 / Monday, August 19, 2013 / Rules and Regulations
 50938 Federal Register / Vol. 78, No. 160 / Monday, August 19, 2013 / Rules and Regulations The quality, utility, and clarity of the information to be collected. Recommendations to minimize the information
50938 Federal Register / Vol. 78, No. 160 / Monday, August 19, 2013 / Rules and Regulations The quality, utility, and clarity of the information to be collected. Recommendations to minimize the information
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Adapting Your Medical Necessity Compliance Program In An Evolving Regulatory Environment
 Adapting Your Medical Necessity Compliance Program In An Evolving Regulatory Environment Joydip Roy MD Vice President of Compliance and Physician Education Adapting Your Medical Necessity Compliance Program
Adapting Your Medical Necessity Compliance Program In An Evolving Regulatory Environment Joydip Roy MD Vice President of Compliance and Physician Education Adapting Your Medical Necessity Compliance Program
CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations
 CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations Ralph Wuebker, MD, MBA Chief Medical Officer AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for
CMS IPPS 2014 Final Rule: Overview & Best Practice Recommendations Ralph Wuebker, MD, MBA Chief Medical Officer AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for
See page 16. Drug diversion in healthcare facilities, Part 1: Identify and prevent. Erica Lindsay
 Compliance TODAY May 2015 a publication of the health care compliance association www.hcca-info.org From the courtroom to Compliance one lawyer s journey and the lessons learned an interview with Tracy
Compliance TODAY May 2015 a publication of the health care compliance association www.hcca-info.org From the courtroom to Compliance one lawyer s journey and the lessons learned an interview with Tracy
Medicare Part C Medical Coverage Policy
 Clinical Trial Services Origination: June 28, 1999 Review Date: April 18, 2018 Next Review: April, 2020 Medicare Part C Medical Coverage Policy DESCRIPTION OF PROCEDURE Clinical trials (or clinical research
Clinical Trial Services Origination: June 28, 1999 Review Date: April 18, 2018 Next Review: April, 2020 Medicare Part C Medical Coverage Policy DESCRIPTION OF PROCEDURE Clinical trials (or clinical research
TORRANCE MEMORIAL MEDICAL STAFF
 BYLAWS COMMITTEE: APPROVED WITH NO CHANGES 10/3/2017 Dates Approved: Medical Executive Committee 09/14/2010; 12/9/2014 PATIENT ATTRIBUTION PLAN: This Attribution Plan assures that all staff are able to
BYLAWS COMMITTEE: APPROVED WITH NO CHANGES 10/3/2017 Dates Approved: Medical Executive Committee 09/14/2010; 12/9/2014 PATIENT ATTRIBUTION PLAN: This Attribution Plan assures that all staff are able to
Central Ohio HFMA Fall Education Hot Topics: Maintaining Compliance in Times of Change. November 22, 2013
 Central Ohio HFMA Fall Education Hot Topics: Maintaining Compliance in Times of Change November 22, 2013 Agenda IPPS Final rule inpatient status changes Proposed OPPS changes to reporting hospital evaluation
Central Ohio HFMA Fall Education Hot Topics: Maintaining Compliance in Times of Change November 22, 2013 Agenda IPPS Final rule inpatient status changes Proposed OPPS changes to reporting hospital evaluation
Care Plan Oversight Services and Physician Services for Certification
 Education Makes the Difference Care Plan Oversight Services and Physician Services for Certification and Recertification of Medicare-Covered Home Health Services A CMS CONTRACTED INTERMEDIARY CARRIER The
Education Makes the Difference Care Plan Oversight Services and Physician Services for Certification and Recertification of Medicare-Covered Home Health Services A CMS CONTRACTED INTERMEDIARY CARRIER The
MEDICARE FINAL RULE Related to INPATIENT Hospital Status Effective
 MEDICARE FINAL RULE Related to INPATIENT Hospital Status Effective 10-1-13 TIMELINE August 2, 2013 Final rule published August 19, 2013 CMS holds open door forum. Many questions raised Sept 5, 2013 CMS
MEDICARE FINAL RULE Related to INPATIENT Hospital Status Effective 10-1-13 TIMELINE August 2, 2013 Final rule published August 19, 2013 CMS holds open door forum. Many questions raised Sept 5, 2013 CMS
Inpatient orders and Physician Certification MUST BE authenticated PRIOR to discharge No EXCEPTIONS.
 2 Midnight Rule for InPatient Admission On August 2, 2013 the Centers for Medicare & Medicaid Services (CMS) issued a final rule (CMS- 1599-F) updating Medicare payment policies which modifies and clarifies
2 Midnight Rule for InPatient Admission On August 2, 2013 the Centers for Medicare & Medicaid Services (CMS) issued a final rule (CMS- 1599-F) updating Medicare payment policies which modifies and clarifies
Passport Advantage Provider Manual Section 5.0 Utilization Management
 Passport Advantage Provider Manual Section 5.0 Utilization Management Table of Contents 5.1 Utilization Management 5.2 Review Criteria 5.3 Prior Authorization Requirements 5.4 Organization Determinations
Passport Advantage Provider Manual Section 5.0 Utilization Management Table of Contents 5.1 Utilization Management 5.2 Review Criteria 5.3 Prior Authorization Requirements 5.4 Organization Determinations
MLN Matters Number: MM6699 Related Change Request (CR) #: 6699
 #: 6699") News Flash Medicare will cover immunizations for H1N1 influenza also called the "swine flu." There will be no coinsurance or copayment applied to this benefit, and beneficiaries will not have to meet their
News Flash Medicare will cover immunizations for H1N1 influenza also called the "swine flu." There will be no coinsurance or copayment applied to this benefit, and beneficiaries will not have to meet their
POLICY SUBJECT: POLICY:
 POLICY SUBJECT: Healthcare Provider Documentation and Compliance Standards Business: Madonna Rehabilitation Hospital - Omaha Date of Origin: 7/1/2016 System: Quality & Risk Management Review Date: 07/25/2016
POLICY SUBJECT: Healthcare Provider Documentation and Compliance Standards Business: Madonna Rehabilitation Hospital - Omaha Date of Origin: 7/1/2016 System: Quality & Risk Management Review Date: 07/25/2016
POLICY AND REGULATIONS MANUAL TITLE: HOSPITALIZATION & MEDICAL NECESSITY REVIEW
 Page Number: 1 of 21 TITLE: HOSPITALIZATION & MEDICAL NECESSITY REVIEW PURPOSE: To provide guidelines for the hospitalization of patients and for assignment of the appropriate Status to patients in the
Page Number: 1 of 21 TITLE: HOSPITALIZATION & MEDICAL NECESSITY REVIEW PURPOSE: To provide guidelines for the hospitalization of patients and for assignment of the appropriate Status to patients in the
MEDICARE CONDITIONS OF PARTICIPATION (CoPs) SPECIFIC TO THE HOSPITAL MEDICAL STAFF
 SPECIFIC TO THE HOSPITAL MEDICAL STAFF") 482.12 CONDITION OF PARTICIPATION: GOVERNING BODY There must be an effective governing body that is legally responsible for the conduct of the hospital. If a hospital does not have an organized governing
482.12 CONDITION OF PARTICIPATION: GOVERNING BODY There must be an effective governing body that is legally responsible for the conduct of the hospital. If a hospital does not have an organized governing
CMSA Connecticut Chapter 2014 IPPS Rule
 CMSA Connecticut Chapter 2014 IPPS Rule EAST PENNSYLVANIA ACMA MARCH 1, 2014 THE 2014 IPPS: WHAT YOU NEED TO KNOW ABOUT THE 2 MIDNIGHT RULE June 7, 2014 STEVEN J. MEYERSON, M.D. Senior Vice President Regulations
CMSA Connecticut Chapter 2014 IPPS Rule EAST PENNSYLVANIA ACMA MARCH 1, 2014 THE 2014 IPPS: WHAT YOU NEED TO KNOW ABOUT THE 2 MIDNIGHT RULE June 7, 2014 STEVEN J. MEYERSON, M.D. Senior Vice President Regulations
State of Montana. Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES
 State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT January 31, 2013 Children s Mental Health
State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT January 31, 2013 Children s Mental Health
ATTACHMENT I. Outpatient Status: Solicitation of Public Comments
 ATTACHMENT I The following text is a copy of the Federation of American Hospitals ( FAH ) comments in response to the solicitation of public comments on outpatient status that was contained in CMS-1589-P;
ATTACHMENT I The following text is a copy of the Federation of American Hospitals ( FAH ) comments in response to the solicitation of public comments on outpatient status that was contained in CMS-1589-P;
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability
 Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
Using PEPPER and CERT Reports to Reduce Improper Payment Vulnerability Cheryl Ericson, MS, RN, CCDS, CDIP CDI Education Director, HCPro Objectives Increase awareness and understanding of CERT and PEPPER
Medicare Inpatient Admission Standards: Two Midnight and Physician Certification Rules
 Ohio Hospital Association Medicare Inpatient Admission Standards: Two Midnight and Physician Certification Rules Christa Nordlund cfn1@fuse.net Jeri Rose West Chester Hospital 7700 University Drive West
Ohio Hospital Association Medicare Inpatient Admission Standards: Two Midnight and Physician Certification Rules Christa Nordlund cfn1@fuse.net Jeri Rose West Chester Hospital 7700 University Drive West
Home Health Certification/Recertification Michigan Home Care & Hospice Association
 Certification/Recertification Michigan Home Care & Hospice Association May 3, 2017 Disclaimer National Government Services, Inc. has produced this material as an informational reference for providers furnishing
Certification/Recertification Michigan Home Care & Hospice Association May 3, 2017 Disclaimer National Government Services, Inc. has produced this material as an informational reference for providers furnishing
Regulatory Compliance Risks. September 2009
 Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Rehabilitation Regulatory Compliance Risks September 2009 1 Agenda - Rehabilitation Compliance Risks Understand the basic requirements for Inpatient Rehabilitation Facilities (IRFs) and Outpatient Rehabilitation
Health Management Policy
 Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
Health Management Policy Policy Number: 0101 Effective Date: 4/1/18 Policy Title: Circumvention of PPS/Readmission Review Applies To: Generations Advantage Purpose: The Martin s Point Health Care Medicare
AMBULATORY SURGERY FACILITY GENERAL INFORMATION
 AMBULATORY SURGERY FACILITY GENERAL INFORMATION I. BCBSM s Ambulatory Surgery Facility Programs Traditional BCBSM s Traditional Ambulatory Surgery Facility Program includes all facilities that are licensed
AMBULATORY SURGERY FACILITY GENERAL INFORMATION I. BCBSM s Ambulatory Surgery Facility Programs Traditional BCBSM s Traditional Ambulatory Surgery Facility Program includes all facilities that are licensed
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review
 UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
UnitedHealthcare Medicare Readmission Review Program for Medicare Advantage Plans General Clinical Guidelines for Payment Review Introduction The UnitedHealthcare Medicare Readmission Review Program is
CAH PREPARATION ON-SITE VISIT
 CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
KDHE-DHCF: Kansas Department of Health and Environment - Division of Health Care Finance. UM Retrospective Review Services.
 KDHE-DHCF: Kansas Department of Health and Environment - Division of Health Care Finance UM Retrospective Review Services Provider Manual August 2017 This page intentionally blank Table of Contents KDHE-DHCF:
KDHE-DHCF: Kansas Department of Health and Environment - Division of Health Care Finance UM Retrospective Review Services Provider Manual August 2017 This page intentionally blank Table of Contents KDHE-DHCF:
Using Clinical Criteria for Evaluating Short Stays and Beyond
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford I. History A. Social Security Act Medical Necessity and Utilization Review 1. Items or services necessary for the diagnosis
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford I. History A. Social Security Act Medical Necessity and Utilization Review 1. Items or services necessary for the diagnosis
Chapter 11 Section 3. Hospice Reimbursement - Conditions For Coverage
 Hospice Chapter 11 Section 3 Issue Date: February 6, 1995 Authority: 32 CFR 199.4(e)(19) 1.0 APPLICABILITY This policy is mandatory for reimbursement of services provided by either network or nonnetwork
Hospice Chapter 11 Section 3 Issue Date: February 6, 1995 Authority: 32 CFR 199.4(e)(19) 1.0 APPLICABILITY This policy is mandatory for reimbursement of services provided by either network or nonnetwork
Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care
 Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care Marc Tucker, DO Senior Director Audit, Compliance & Education AHA Solutions, Inc.,
Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care Marc Tucker, DO Senior Director Audit, Compliance & Education AHA Solutions, Inc.,
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: observation_room_services 2/1997 3/2013 3/2014 3/2013 Description of Procedure or Service Observation services
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: observation_room_services 2/1997 3/2013 3/2014 3/2013 Description of Procedure or Service Observation services
Ambulance Services: New Policy and Review Updates (A/B) July 11, 2018
 July 11, 2018") Ambulance Services: New Policy and Review Updates (A/B) July 11, 2018 Presented By First Coast Service Options, Inc. Provider Outreach & Education Robert Lewis, CPC Provider Relations Representative 1
Ambulance Services: New Policy and Review Updates (A/B) July 11, 2018 Presented By First Coast Service Options, Inc. Provider Outreach & Education Robert Lewis, CPC Provider Relations Representative 1
Advanced Evaluation and. AAPC Regional Conference Chicago 10/27/12
 Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
Advanced Evaluation and Management AAPC Regional Conference Chicago 10/27/12 Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practiceintegrity.com Disclaimer Information
CHAPTER 13 SECTION 6.5 HOSPITAL REIMBURSEMENT - TRICARE/CHAMPUS INPATIENT MENTAL HEALTH PER DIEM PAYMENT SYSTEM
 TRICARE/CHAMPUS POLICY MANUAL 6010.47-M DEC 1998 PAYMENTS POLICY CHAPTER 13 SECTION 6.5 HOSPITAL REIMBURSEMENT - TRICARE/CHAMPUS INPATIENT MENTAL HEALTH PER DIEM PAYMENT SYSTEM Issue Date: November 28,
TRICARE/CHAMPUS POLICY MANUAL 6010.47-M DEC 1998 PAYMENTS POLICY CHAPTER 13 SECTION 6.5 HOSPITAL REIMBURSEMENT - TRICARE/CHAMPUS INPATIENT MENTAL HEALTH PER DIEM PAYMENT SYSTEM Issue Date: November 28,
Course Module Objectives
 Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of
Course Module Objectives CM100-18: Scope of Services, Practice, and Education CM200-18: The Professional Case Manager Case Management History, Regulations and Practice Settings Case Management Scope of
Private Duty Nursing. May 2017
 Private Duty Nursing May 2017 Overview Provider Enrollment Member Eligibility Private Duty Nursing Services Specialized Private Duty Nursing Services Billing Additional Information 2 Provider Enrollment
Private Duty Nursing May 2017 Overview Provider Enrollment Member Eligibility Private Duty Nursing Services Specialized Private Duty Nursing Services Billing Additional Information 2 Provider Enrollment
Let s Chat: Hospice Notice of Election Timely Filing
 Let s Chat: Notice of Election Timely Filing January 2016 1700_0116 Today s Presenter Corrinne Ball, RN, CPC, CAC, CACO Provider Outreach and Education Consultant 2 Disclaimer National Government Services,
Let s Chat: Notice of Election Timely Filing January 2016 1700_0116 Today s Presenter Corrinne Ball, RN, CPC, CAC, CACO Provider Outreach and Education Consultant 2 Disclaimer National Government Services,
Observation Services Tool for Applying MCG Care Guidelines
 In the event of a conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include
In the event of a conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include
Community Health Network, Inc. MEDICAL STAFF POLICIES & PROCEDURES
 Community East Community South Community North TITLE: Medical Record Chart Requirements The medical record of care comprises all the data and information about a patient s visit. It functions as both a
Community East Community South Community North TITLE: Medical Record Chart Requirements The medical record of care comprises all the data and information about a patient s visit. It functions as both a
Short Stay Reviews Update September 19, 2016 Page 1 of 12
 Event Title: Short Stay Review Update Event Date: 9/19/2016 Speaker Operator Scott Fortin Cheryl Cook Transcript Today's conference is scheduled to begin momentarily. Until that time your lines will be
Event Title: Short Stay Review Update Event Date: 9/19/2016 Speaker Operator Scott Fortin Cheryl Cook Transcript Today's conference is scheduled to begin momentarily. Until that time your lines will be
State of Montana. Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES
 State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT October 1, 2012 Children s Mental Health
State of Montana Department of Public Health and Human Services CHILDREN S MENTAL HEALTH BUREAU PROVIDER MANUAL AND CLINICAL GUIDELINES FOR UTILIZATION MANAGEMENT October 1, 2012 Children s Mental Health
Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC Disclaimer
 Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
Advanced Evaluation and Management More than a roll of the dice? History Exam Medical Decision Making Jaci Johnson, CPC,CPMA,CEMC,CPC H,CPC I President, Practice Integrity, LLC jaci@practieintegrity.com
Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN:
 Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN:") Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN: 909207 Welcome to Medicare Learning Network Podcasts at the Centers for Medicare
Audio Title: Revised and Clarified Place of Service (POS) Coding Instructions Audio Date: 6/3/2015 Run Time: 16:03 Minutes ICN: 909207 Welcome to Medicare Learning Network Podcasts at the Centers for Medicare
Chapter 7 Section 1. Hospital Reimbursement - TRICARE Inpatient Mental Health Per Diem Payment System
 Mental Health Chapter 7 Section 1 Hospital Reimbursement - TRICARE Inpatient Mental Health Per Diem Payment System Issue Date: November 28, 1988 Authority: 32 CFR 199.14(a) 1.0 APPLICABILITY This policy
Mental Health Chapter 7 Section 1 Hospital Reimbursement - TRICARE Inpatient Mental Health Per Diem Payment System Issue Date: November 28, 1988 Authority: 32 CFR 199.14(a) 1.0 APPLICABILITY This policy
Discharge Planning/ Transition of Care: What s Hot in the 20-teens CMSANJ - July 24, 2014
 Discharge Planning/ Transition of Care: What s Hot in the 20-teens CMSANJ - July 24, 2014 Jackie Birmingham, RN, BSN, MS VP, Emerita, Clinical Leadership Curaspan Health Group jbirmingham@curaspan.com
Discharge Planning/ Transition of Care: What s Hot in the 20-teens CMSANJ - July 24, 2014 Jackie Birmingham, RN, BSN, MS VP, Emerita, Clinical Leadership Curaspan Health Group jbirmingham@curaspan.com
Patient Placement Getting it Right the First Time
 Patient Placement Getting it Right the First Time Union Hospital Who we are! 300 bed Acute Care Hospital Average Daily Census (adult &peds) 203 ED Visit 51,741 Medical Necessity Why it is so important?
Patient Placement Getting it Right the First Time Union Hospital Who we are! 300 bed Acute Care Hospital Average Daily Census (adult &peds) 203 ED Visit 51,741 Medical Necessity Why it is so important?
Justifying Medicare Inpatient Admissions RAC Response and Appeals Tactics
 Justifying Medicare Inpatient Admissions RAC Response and Appeals Tactics Gregory Palega, MD JD MedManagement LLC Medical Director of Regulatory Affairs gpalega@medmanagementllc.com Objectives Learn the
Justifying Medicare Inpatient Admissions RAC Response and Appeals Tactics Gregory Palega, MD JD MedManagement LLC Medical Director of Regulatory Affairs gpalega@medmanagementllc.com Objectives Learn the
Using the Inpatient Psychiatric Facility (IPF) PEPPER to Support Auditing and Monitoring Efforts: Session 1
 PEPPER to Support Auditing and Monitoring Efforts: Session 1") Using the Inpatient Psychiatric Facility (IPF) PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER IPF PEPPER target
Using the Inpatient Psychiatric Facility (IPF) PEPPER to Support Auditing and Monitoring Efforts: Session 1 March, 2016 Kimberly Hrehor Agenda Session 1: History and basics of PEPPER IPF PEPPER target
Inpatient Psychiatric Services for Under Age 21 Arkansas Medicaid Regulations and Documentation
 Inpatient Psychiatric Services for Under Age 21 Arkansas Medicaid Regulations and Documentation Presented by: Shelly Rhodes Shelly.Rhodes@beaconhealthoptions.com Disclaimer Disclaimer: This presentation
Inpatient Psychiatric Services for Under Age 21 Arkansas Medicaid Regulations and Documentation Presented by: Shelly Rhodes Shelly.Rhodes@beaconhealthoptions.com Disclaimer Disclaimer: This presentation
Evaluation and Management Auditing Back to the Basics. Objectives. Audit Start with the benchmarks CMS MEDPAR by specialty 4/22/2013
 Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Evaluation and Management Auditing Back to the Basics E&M Audit Sonda Kunzi, CPC, CPMA, CPPM, CPC-I Associate Director, Cohen Healthcare Consulting Ltd. Objectives Discuss good basic audit techniques Review
Payment Policy: 30 Day Readmission Reference Number: CC.PP.501 Product Types: ALL
 Payment Policy: 30 Day Readmission Reference Number: CC.PP.501 Product Types: ALL Effective Date: 01/01/2015 Last Review Date: 04/28/2018 Coding Implications Revision Log See Important Reminder at the
Payment Policy: 30 Day Readmission Reference Number: CC.PP.501 Product Types: ALL Effective Date: 01/01/2015 Last Review Date: 04/28/2018 Coding Implications Revision Log See Important Reminder at the
AMENDATORY SECTION (Amending WSR , filed 8/27/15, effective. WAC Inpatient psychiatric services. Purpose.
 AMENDATORY SECTION (Amending WSR 15-18-065, filed 8/27/15, effective 9/27/15) WAC 182-550-2600 Inpatient psychiatric services. Purpose. (1) The medicaid agency, on behalf of the mental health division
AMENDATORY SECTION (Amending WSR 15-18-065, filed 8/27/15, effective 9/27/15) WAC 182-550-2600 Inpatient psychiatric services. Purpose. (1) The medicaid agency, on behalf of the mental health division
RULES OF TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT WORKERS COMPENSATION DIVISION
 RULES OF TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT WORKERS COMPENSATION DIVISION CHAPTER 0800-02-25 WORKERS COMPENSATION MEDICAL TREATMENT TABLE OF CONTENTS 0800-02-25-.01 Purpose and Scope
RULES OF TENNESSEE DEPARTMENT OF LABOR AND WORKFORCE DEVELOPMENT WORKERS COMPENSATION DIVISION CHAPTER 0800-02-25 WORKERS COMPENSATION MEDICAL TREATMENT TABLE OF CONTENTS 0800-02-25-.01 Purpose and Scope
Chapter 6 Section 3. Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment)
") Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
Diagnostic Related Groups (DRGs) Chapter 6 Section 3 Hospital Reimbursement - TRICARE DRG-Based Payment System (Basis Of Payment) Issue Date: October 8, 1987 Authority: 32 CFR 199.14(a)(1) 1.0 APPLICABIITY
Hospital Inpatient Quality Reporting (IQR) Program
 Program") Clinical Episode-Based Payment (CEBP) Measures Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives, and Quality Reporting (VIQR) Outreach
Clinical Episode-Based Payment (CEBP) Measures Questions & Answers Moderator Candace Jackson, RN Project Lead, Hospital IQR Program Hospital Inpatient Value, Incentives, and Quality Reporting (VIQR) Outreach
A Review of Current EMTALA and Florida Law
 A Review of Current EMTALA and Florida Law South Carolina Hospital Fined $1.28 Million for EMTALA violations Doctor fined $40,000 for not showing up at Emergency Room Chicago Hospital and Docs settle EMTALA
A Review of Current EMTALA and Florida Law South Carolina Hospital Fined $1.28 Million for EMTALA violations Doctor fined $40,000 for not showing up at Emergency Room Chicago Hospital and Docs settle EMTALA
Observation Services Tool for Applying MCG Care Guidelines Policy
 In the event of conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include,
In the event of conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include,
CMS Local Coverage Determination (LCD) of Psychiatric Partial Hospitalization Programs for Massachusetts, New York, and Rhode Island
 of Psychiatric Partial Hospitalization Programs for Massachusetts, New York, and Rhode Island") CMS Local Coverage Determination (LCD) of Psychiatric Partial Hospitalization Programs for Massachusetts, New York, and Rhode Island L33626 Coverage Indications and Limitations Psychiatric partial hospitalization
CMS Local Coverage Determination (LCD) of Psychiatric Partial Hospitalization Programs for Massachusetts, New York, and Rhode Island L33626 Coverage Indications and Limitations Psychiatric partial hospitalization
ALABAMA MEDICAID AGENCY ADMINISTRATIVE CODE CHAPTER 560-X-5 PSYCHIATRIC FACILITIES FOR INDIVIDUALS 65 OR OVER TABLE OF CONTENTS
 Medicaid Chapter 560-X-5 ALABAMA MEDICAID AGENCY ADMINISTRATIVE CODE CHAPTER 560-X-5 PSYCHIATRIC FACILITIES FOR INDIVIDUALS 65 OR OVER TABLE OF CONTENTS 560-X-5-.01 560-X-5-.02 560-X-5-.03 560-X-5-.04
Medicaid Chapter 560-X-5 ALABAMA MEDICAID AGENCY ADMINISTRATIVE CODE CHAPTER 560-X-5 PSYCHIATRIC FACILITIES FOR INDIVIDUALS 65 OR OVER TABLE OF CONTENTS 560-X-5-.01 560-X-5-.02 560-X-5-.03 560-X-5-.04
The following is a summary of each of the updates from the meeting.
 This week, National Government Services (NGS) conducted a home health advisory meeting in the Centers for Medicare and Medicaid Services (CMS ) Region V office in Chicago for the State Associations in
This week, National Government Services (NGS) conducted a home health advisory meeting in the Centers for Medicare and Medicaid Services (CMS ) Region V office in Chicago for the State Associations in
Presented by: Arlene Maxim, RN-Founder A.D. Maxim Consulting, LLC.
 Presented by: Arlene Maxim, RN-Founder A.D. Maxim Consulting, LLC. On January 24, 2013, the U. S. District Court for the District of Vermont approved a settlement agreement in the case of Jimmo v. Sebelius,
Presented by: Arlene Maxim, RN-Founder A.D. Maxim Consulting, LLC. On January 24, 2013, the U. S. District Court for the District of Vermont approved a settlement agreement in the case of Jimmo v. Sebelius,
Outpatient Hospital Facilities
 Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
ABOUT FLORIDA MEDICAID
 Section I Introduction About eqhealth Solutions ABOUT FLORIDA MEDICAID THE FLORIDA AGENCY FOR HEALTH CARE ADMINISTRATION The Florida Agency for Health Care Administration (AHCA or Agency) is the single
Section I Introduction About eqhealth Solutions ABOUT FLORIDA MEDICAID THE FLORIDA AGENCY FOR HEALTH CARE ADMINISTRATION The Florida Agency for Health Care Administration (AHCA or Agency) is the single
Mississippi Medicaid Inpatient Services Provider Manual
 Mississippi Medicaid Inpatient Services Provider Manual Effective Date: November 2015 Revised: June 2016 Inpatient Services Provider Manual Introduction eqhealth Solutions (eqhealth) is the Utilization
Mississippi Medicaid Inpatient Services Provider Manual Effective Date: November 2015 Revised: June 2016 Inpatient Services Provider Manual Introduction eqhealth Solutions (eqhealth) is the Utilization